
Molecular Basis of Impaired Glycogen Metabolism during Ischemic Stroke and Hypoxia
Upload
independentCategory
view
0download
0
REVIEW
Recanalization therapy for acute ischemic stroke, part 2:mechanical intra-arterial technologies
Saeed Ansari & Maryam Rahman &
Douglas J. McConnell & Michael F. Waters &
Brian L. Hoh & J. Mocco
Received: 28 March 2010 /Accepted: 29 August 2010 /Published online: 24 November 2010# Springer-Verlag 2010
Abstract Stroke therapy has been revolutionized in the pasttwo decades with the widespread implementation of chemicalthrombolysis for acute stroke. However, chemical thrombolysiscontinues to be limited in its efficacy secondary to relativelyshort time windows and a high associated risk of hemorrhage.In an attempt to minimize hemorrhagic complications andextend the available therapeutic window, mechanical devicesdesigned specifically for thrombus removal, clot obliteration,and arterial revascularization have experienced a recent surge indevelopment and utilization. As such, chemical thrombolyticsnow represent only one ofmany options in acute stroke therapy.These new mechanical devices have extended the potentialtreatment window and now provide alternatives to patients whodo not respond to conventional intravenous thrombolysis. Thisreview will discuss the development of these devices, support-ing literature, and the individual strengths that each engenderstowards a life-saving therapy for stroke.
Keywords Mechanical instrument . Stroke . Thrombolysis .
Stents . Review
Introduction
Stroke is the third most common cause of death in theUnited States, following heart diseases and cancer, resulting
in over 150,000 deaths annually [1]. Stroke treatment anddisability costs between $15 and $30 billion of annualhealth care expenses in the United States alone [2].However, since the introduction of thrombolytic therapyin acute ischemic stroke in late 1950s [3], functionaloutcomes and burden of disability have improved consid-erably [4, 5]. The success of intravenous thrombolytictherapy has led to advances in intra-arterial (IA) thrombol-ysis and mechanical recanalization for the treatment ofacute stroke. The continued development of new mechan-ical methods of recanalization pose potential advantages inimproving outcomes compared with intravenous thrombo-lytic agents alone [6]. Additionally, sophisticated imagingcombined with mechanical recanalization has extended thetime window for treatment of acute stroke beyond the3- and 6-h limit of intraveneous (IV) and intra-arterialthrombolysis [4, 5, 7]. The focus of this paper is to reviewthe data regarding the currently available endovascularmechanical instruments used in acute ischemic stroke.
Clot removal
While chemical thrombolysis has been an encouragingavenue of stroke therapy development, treatment failureshave led to investigation of alternatives, including mechan-ical thrombectomy for embolic ischemic stroke. Thesestrategies were initially tested on patients with contra-indications to pharmacologic thrombolysis [8] or whopresented late after the onset of symptoms [9, 10].Mechanical device trials included a variety of methods todissociate clot including clot maceration with the micro-catheter or microwire [11, 12], thrombectomy [13], embo-lectomy [7], and balloon angioplasty [14]. Unfortunately,despite enthusiasm, early studies using these methods did
S. Ansari :M. Rahman :D. J. McConnell :B. L. Hoh :J. Mocco (*)Department of Neurosurgery, University of Florida,Gainesville, FL, USAe-mail: [email protected]
M. F. WatersDepartment of Neurology, University of Florida,Gainesville, FL, USA
Neurosurg Rev (2011) 34:11–20DOI 10.1007/s10143-010-0294-1

not significantly improve recanalization rates compared todirect chemical thrombolysis [15] and were associated withnot insignificant symptomatic intracranial hemorrhage ratesof 5% to 7% [7, 13, 14, 16]. However, mechanicalthrombectomy has recently been revived, first by the useof embolectomy devices, and now by promising data withother technologies.
Embolectomy devices maybe used to entangle, incor-porate, or interdigitate the thrombus and extract itthrough the guide catheter or sheath. The use ofsuccessful embolectomy retrieval of foreign bodies fromcerebral vessels had been described previously [17, 18].Subsequently, Chopko et al. [19] reported the retrieval ofintra-arterial middle cerebral artery (MCA) clot using asnare in 2000. They described a patient with a clot lodged inthe middle cerebral artery (M1–M2 junction) with persistentarterial occlusion, despite treatment with urokinase, systemicheparin, systemic abciximab, and mechanical guidewiremaceration. Successful clot retrieval was performed with a4-mm gooseneck snare in two separate maneuvers, andreconstitution of normal flow was seen in immediatepostoperative angiography. Nesbit et al. [20] have describedusing Microsnare (Microvena, Minneapolis, MN) (n=6) andNeuronet (Guidant, Temecula, CA) (n=5) to treat acutestroke in 11 patients. They achieved recanalization inapproximately 50% of subjects with both devices with noadverse effects related to devices.
Mechanical thrombectomy was mostly experimentalfor acute embolic stroke until the Merci clot retriever(Concentric Medical, Mountain View, CA) was approvedby FDA in 2004. This device is a flexible nitinol wirewith coil loops that is used in combination with amicrocathether and a balloon-guided catheter [10]. TheMerci retriever was first studied in a phase I multicentertrial that enrolled 30 patients who were ineligible for IVrt-PA or who fail IV rt-PA therapy [7]. Successfulrecanalization of occluded vessels was demonstrated in43% of patients treated with mechanical thrombolysisalone and in 64% with the addition of IA rt-PA. Nine of 18revascularized subjects and zero of 10 non-revascularizedsubjects had achieved significant recovery (modifiedRankin scale [mRS] score, ≤3) at 1 month of follow-up.Thirty-six percent of patients died within 1 month oftreatment, although no deaths were directly related totreatment with the device.
Later, The Mechanical Embolus Removal in CerebralIschemia (MERCI) trial was designed to test the safety andefficacy of the Merci clot retrieval device to restore thepatency of intracranial arteries within the first 8 h of anacute stroke [10]. This was a prospective single-armmulticenter trial in which 151 patients were treated withthe Merci device due to ineligibility for IV rt-PA.Recanalization was achieved in 46% (69/151) of patients
on intention to treat analysis and in 48% (68/141) ofpatients in whom the device was deployed. The outcomeswere significantly better than that expected compared to thecontrol arm of the PROACT II study (P<0.0001) [5]. Theoverall rate of good outcome (mRS score,≤2) was 27.7%,and mortality at 3 months was 43.5%. Good neurologicoutcomes at 90 days were more frequent (46% versus10%), and mortality rates were lower (32% versus 54%) inpatients who were successfully recanalized compared tothose with unsuccessful recanalization. The Multi MERCItrial was a prospective, multicenter, single-arm trial ofpatients with large vessel stroke treated within 8 h ofsymptom onset [9, 21]. The study design was similar toMERCI trial with an additional objective to evaluate thesafety and technical efficacy data on a newer generation (L5Retriever) (Fig. 1) device. The device was deployed in 164patients out of 1,088 patients who were screened with asuccessful recanalization rate of 55% using the retrieveralone and 68% after adjunctive therapy (mechanical deviceand IA rt-PA). Overall rates of good outcome (36%) andmortality (34%) at 3 months were substantially improved incomparison with those in MERCI trial [9]. A recent study,similar to MERCI and multi MERCI trials, by Devlin et al.[22] on 25 consecutive patients with acute ischemic strokeusing Merci retriever demonstrated a successful reperfusionrate of 56% in target vessels. The mortality rate at 90 days
Fig. 1 Schematic pictures of Merci and Penumbra clot retrievers. aMerci clot retriever is torqued to ensnare the thrombus; the L5 devicehas a series of monofilaments that attach proximal and distal to thehelical nitinol coils and differs from the X5/X6 family of devices. bPenumbra reperfusion catheters and separators in three differentgauges. Courtesy of Penumbra, Inc., Alameda, CA
12 Neurosurg Rev (2011) 34:11–20
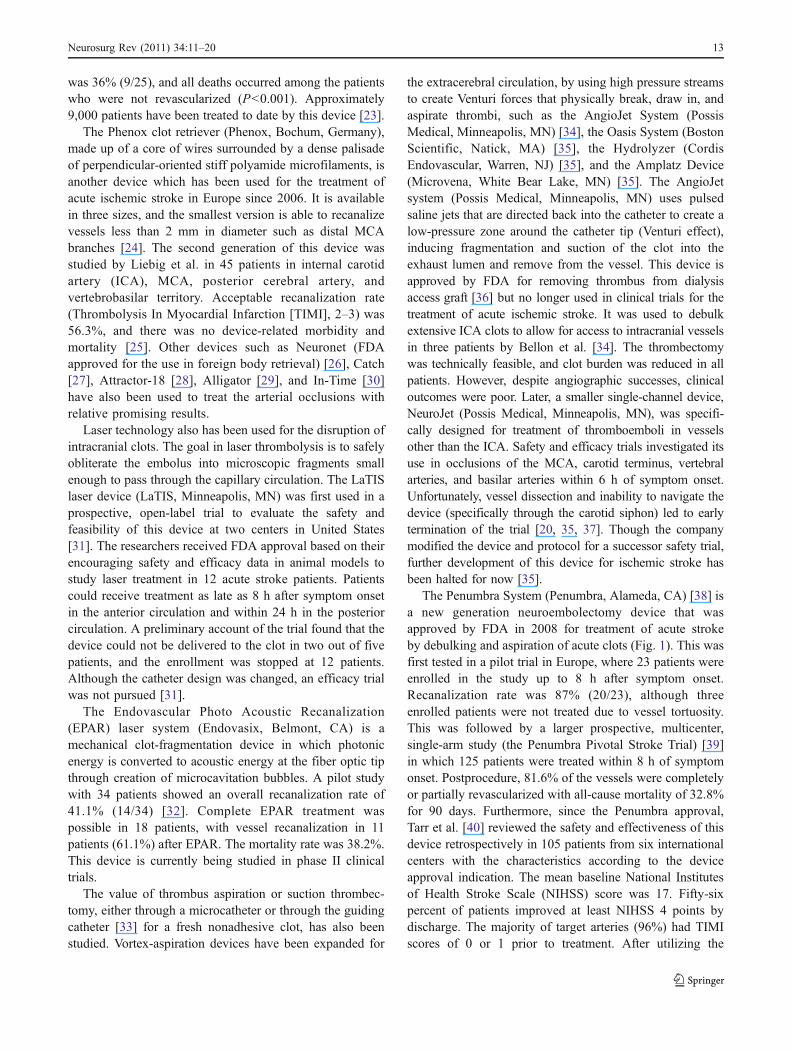
was 36% (9/25), and all deaths occurred among the patientswho were not revascularized (P<0.001). Approximately9,000 patients have been treated to date by this device [23].
The Phenox clot retriever (Phenox, Bochum, Germany),made up of a core of wires surrounded by a dense palisadeof perpendicular-oriented stiff polyamide microfilaments, isanother device which has been used for the treatment ofacute ischemic stroke in Europe since 2006. It is availablein three sizes, and the smallest version is able to recanalizevessels less than 2 mm in diameter such as distal MCAbranches [24]. The second generation of this device wasstudied by Liebig et al. in 45 patients in internal carotidartery (ICA), MCA, posterior cerebral artery, andvertebrobasilar territory. Acceptable recanalization rate(Thrombolysis In Myocardial Infarction [TIMI], 2–3) was56.3%, and there was no device-related morbidity andmortality [25]. Other devices such as Neuronet (FDAapproved for the use in foreign body retrieval) [26], Catch[27], Attractor-18 [28], Alligator [29], and In-Time [30]have also been used to treat the arterial occlusions withrelative promising results.
Laser technology also has been used for the disruption ofintracranial clots. The goal in laser thrombolysis is to safelyobliterate the embolus into microscopic fragments smallenough to pass through the capillary circulation. The LaTISlaser device (LaTIS, Minneapolis, MN) was first used in aprospective, open-label trial to evaluate the safety andfeasibility of this device at two centers in United States[31]. The researchers received FDA approval based on theirencouraging safety and efficacy data in animal models tostudy laser treatment in 12 acute stroke patients. Patientscould receive treatment as late as 8 h after symptom onsetin the anterior circulation and within 24 h in the posteriorcirculation. A preliminary account of the trial found that thedevice could not be delivered to the clot in two out of fivepatients, and the enrollment was stopped at 12 patients.Although the catheter design was changed, an efficacy trialwas not pursued [31].
The Endovascular Photo Acoustic Recanalization(EPAR) laser system (Endovasix, Belmont, CA) is amechanical clot-fragmentation device in which photonicenergy is converted to acoustic energy at the fiber optic tipthrough creation of microcavitation bubbles. A pilot studywith 34 patients showed an overall recanalization rate of41.1% (14/34) [32]. Complete EPAR treatment waspossible in 18 patients, with vessel recanalization in 11patients (61.1%) after EPAR. The mortality rate was 38.2%.This device is currently being studied in phase II clinicaltrials.
The value of thrombus aspiration or suction thrombec-tomy, either through a microcatheter or through the guidingcatheter [33] for a fresh nonadhesive clot, has also beenstudied. Vortex-aspiration devices have been expanded for
the extracerebral circulation, by using high pressure streamsto create Venturi forces that physically break, draw in, andaspirate thrombi, such as the AngioJet System (PossisMedical, Minneapolis, MN) [34], the Oasis System (BostonScientific, Natick, MA) [35], the Hydrolyzer (CordisEndovascular, Warren, NJ) [35], and the Amplatz Device(Microvena, White Bear Lake, MN) [35]. The AngioJetsystem (Possis Medical, Minneapolis, MN) uses pulsedsaline jets that are directed back into the catheter to create alow-pressure zone around the catheter tip (Venturi effect),inducing fragmentation and suction of the clot into theexhaust lumen and remove from the vessel. This device isapproved by FDA for removing thrombus from dialysisaccess graft [36] but no longer used in clinical trials for thetreatment of acute ischemic stroke. It was used to debulkextensive ICA clots to allow for access to intracranial vesselsin three patients by Bellon et al. [34]. The thrombectomywas technically feasible, and clot burden was reduced in allpatients. However, despite angiographic successes, clinicaloutcomes were poor. Later, a smaller single-channel device,NeuroJet (Possis Medical, Minneapolis, MN), was specifi-cally designed for treatment of thromboemboli in vesselsother than the ICA. Safety and efficacy trials investigated itsuse in occlusions of the MCA, carotid terminus, vertebralarteries, and basilar arteries within 6 h of symptom onset.Unfortunately, vessel dissection and inability to navigate thedevice (specifically through the carotid siphon) led to earlytermination of the trial [20, 35, 37]. Though the companymodified the device and protocol for a successor safety trial,further development of this device for ischemic stroke hasbeen halted for now [35].
The Penumbra System (Penumbra, Alameda, CA) [38] isa new generation neuroembolectomy device that wasapproved by FDA in 2008 for treatment of acute strokeby debulking and aspiration of acute clots (Fig. 1). This wasfirst tested in a pilot trial in Europe, where 23 patients wereenrolled in the study up to 8 h after symptom onset.Recanalization rate was 87% (20/23), although threeenrolled patients were not treated due to vessel tortuosity.This was followed by a larger prospective, multicenter,single-arm study (the Penumbra Pivotal Stroke Trial) [39]in which 125 patients were treated within 8 h of symptomonset. Postprocedure, 81.6% of the vessels were completelyor partially revascularized with all-cause mortality of 32.8%for 90 days. Furthermore, since the Penumbra approval,Tarr et al. [40] reviewed the safety and effectiveness of thisdevice retrospectively in 105 patients from six internationalcenters with the characteristics according to the deviceapproval indication. The mean baseline National Institutesof Health Stroke Scale (NIHSS) score was 17. Fifty-sixpercent of patients improved at least NIHSS 4 points bydischarge. The majority of target arteries (96%) had TIMIscores of 0 or 1 prior to treatment. After utilizing the
Neurosurg Rev (2011) 34:11–20 13

Penumbra System, revascularization was achieved in 83.3%of patients with TIMI 2 and 3 in 52% and 31.3% ofpatients, respectively. ICH occurred in 6 (5.7%) patients at24 h, and the mortality rate was 21% (22/105). Thesestudies suggest that the experience of Penumbra System ina “real world” is consistent with that from its preapprovaltrial in the rate of revascularization, procedural side effects,and all cause mortality.
Angioplasty and stents
Angioplasty has been a traditional mechanical treatmentof arterial thrombosis or plaque. Using a balloon, theatherosclerotic plaque is disrupted into the intima andmedia of the vessel. This leads to subintimal fissuringand desquamation. After several weeks, healing withintimal retraction and neointima formation leads to asmooth intimal surface [41, 42]. Dotter and Judkins [43]published their experience in the use of percutaneoustransluminal angioplasty (PTA) for treatment of high-grade atherosclerotic lesions of the peripheral arteries forfirst time in 1964.
Because of the technical problems in accessing intracra-nial arteries and also the potential complication of inducingstroke due to embolization of debris at the angioplasty site,the study of PTA for cerebral vessels lagged behind that forother vessels. In 1993, Higashida et al. [44] reported astudy of PTA in 274 patients with symptomatic atheroscle-rotic lesions involving both extracranial and intracranialvessels. PTA of intracranial vessels was performed in 18cases; stroke occurred in six cases (33%), which includedthree deaths (17%), and transient cerebral ischemiaoccurred in four cases (22%). In all three patients whodied, systemic anticoagulation and medical therapy hadbeen unsuccessful, and all had progressive neurologicdeterioration with evidence of severe brain stem ischemiaat the time of treatment.
In a pilot study by Nakono et al. [45], successfulrecanalization was achieved with percutaneous angioplas-ty (PTA) in 8/10 patients with MCA occlusion. Theinvestigators then compared PTA to IA thrombolysis alonein patients with acute MCA trunk occlusion. Thirty-sixpatients were treated with IA thrombolytic therapy alone(control group) and 34 patients underwent PTA. Recana-lization rate was significantly higher in the PTA group,91.2% versus 63.9% in controls, and the incidence ofsymptomatic intracranial hemorrhage was reduced in thePTA group (2.9% versus 19.4% controls). Since then,other studies have also supported these findings with highrates of recanalization, low rates of ICH or systemicbleeding, and significant improvement in neurologicfunction with combined angioplasty and thrombolysis
[46, 47]. In addition, many investigations have shownthe technical feasibility and high efficacy of PTA in acuteischemic stroke [14, 48, 49], and it seems to beparticularly useful in cases of atherothrombotic disease,in which the residual stenosis may reduce flow sufficientlyto lead to rethrombosis [50].
For improved durability, angioplasty research led tointerest in stents for the treatment and prevention ofstroke. Stents either are permanently deployed or can beused in conjunction with thrombolytics for immediatereperfusion and retrieved at the end of the procedure.The 1990s saw stents move into the neurovascular arenafor the management of a variety of cerebrocasculardiseases including arterial and venus sinus stenosis,arterial aneurysm, and arterial dissection [51]. An earlycase report in 2006 by Levy et al. [52] reported the use ofstents to treat acute ischemic stroke. The authorssuccessfully used balloon-mounted stents to recanalize aproximal left MCA occlusion. This case report wasfollowed by a larger retrospective series the same year,in which balloon-mounted stents were used in 19 patients[13]. Stenting was only performed as a rescue procedureafter other interventions had failed to recanalize occludedarteries. An overall TIMI score of 2 or 3 was achieved in79% of patients. Encouraged by this early data, once self-expanding stents (SES) became available, considerationbegan to occur for their use in acute stroke. TheNeuroform SES (Boston Scientific, Natick, MA),designed for use in the cerebrovascular aneurysm, wasused to treat an occlusion of the left MCA in a 57-year-old woman after unsuccessful thrombolysis treatment[53]. The stent immediately restored flow through theMCA without incident. A year later, Levy et al. [54]published the results of another retrospective series, thistime utilizing SES. Of 19 occlusions in 18 patients, 15were successfully recanalized, again yielding a recanali-zation rate of 79%. In this trial, stent placement was theprimary intervention in six cases, although the authorsnoted that the most successful strategy was multi-modal,incorporating pharmacological and mechanical interven-tion. The encouraging results of these two studies led to aprospective trial (SARIS), featuring the Wingspan SES(Boston Scientific, Natick, MA) as the primary interven-tion for 20 cases of acute stroke [55]. All twenty patientsachieved TIMI scores of either 2 or 3, constituting anoverall recanalization rate of 100%. This study alsoincluded the use of the Enterprise stent (EnterpriseVascular Reconstruction Device, Codman Neurovascular,Raynham, MA), used in two cases in which theWingspan could not be navigated through especiallytortuous vasculature. The potential relevance of theEnterprise stent was further supported by a retrospectiveseries of 20 patients, in which the Enterprise stent
14 Neurosurg Rev (2011) 34:11–20
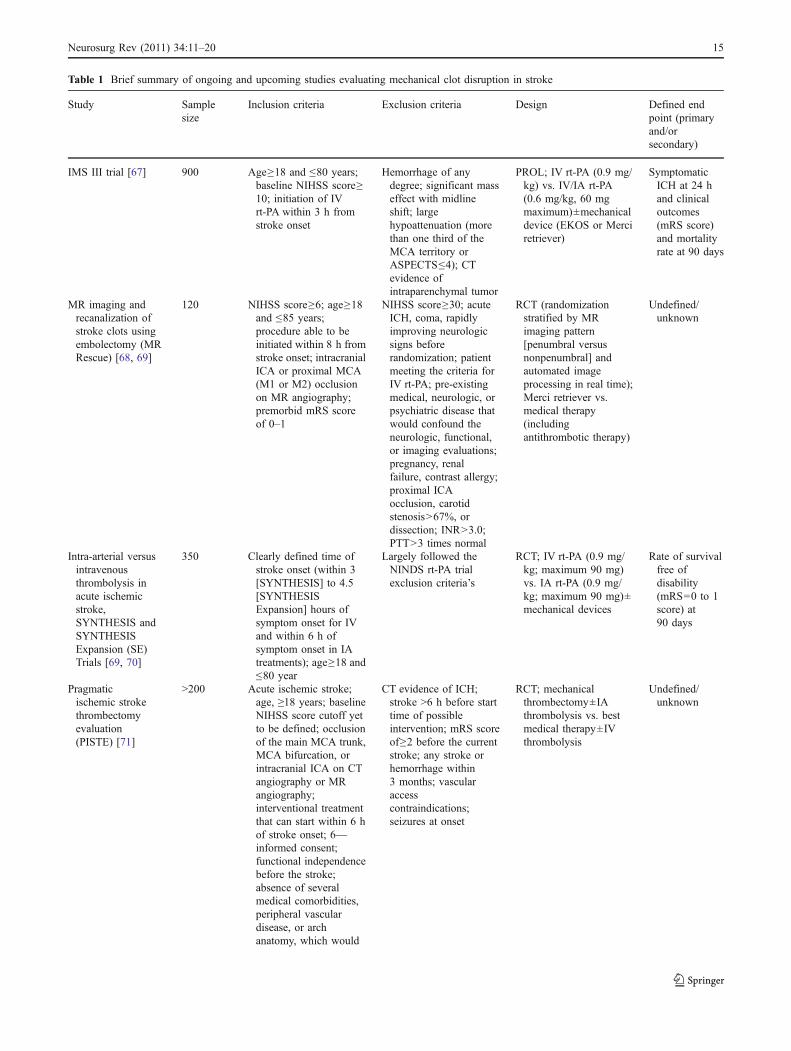
Table 1 Brief summary of ongoing and upcoming studies evaluating mechanical clot disruption in stroke
Study Samplesize
Inclusion criteria Exclusion criteria Design Defined endpoint (primaryand/orsecondary)
IMS III trial [67] 900 Age≥18 and ≤80 years;baseline NIHSS score≥10; initiation of IVrt-PA within 3 h fromstroke onset
Hemorrhage of anydegree; significant masseffect with midlineshift; largehypoattenuation (morethan one third of theMCA territory orASPECTS≤4); CTevidence ofintraparenchymal tumor
PROL; IV rt-PA (0.9 mg/kg) vs. IV/IA rt-PA(0.6 mg/kg, 60 mgmaximum)±mechanicaldevice (EKOS or Merciretriever)
SymptomaticICH at 24 hand clinicaloutcomes(mRS score)and mortalityrate at 90 days
MR imaging andrecanalization ofstroke clots usingembolectomy (MRRescue) [68, 69]
120 NIHSS score≥6; age≥18and ≤85 years;procedure able to beinitiated within 8 h fromstroke onset; intracranialICA or proximal MCA(M1 or M2) occlusionon MR angiography;premorbid mRS scoreof 0–1
NIHSS score≥30; acuteICH, coma, rapidlyimproving neurologicsigns beforerandomization; patientmeeting the criteria forIV rt-PA; pre-existingmedical, neurologic, orpsychiatric disease thatwould confound theneurologic, functional,or imaging evaluations;pregnancy, renalfailure, contrast allergy;proximal ICAocclusion, carotidstenosis>67%, ordissection; INR>3.0;PTT>3 times normal
RCT (randomizationstratified by MRimaging pattern[penumbral versusnonpenumbral] andautomated imageprocessing in real time);Merci retriever vs.medical therapy(includingantithrombotic therapy)
Undefined/unknown
Intra-arterial versusintravenousthrombolysis inacute ischemicstroke,SYNTHESIS andSYNTHESISExpansion (SE)Trials [69, 70]
350 Clearly defined time ofstroke onset (within 3[SYNTHESIS] to 4.5[SYNTHESISExpansion] hours ofsymptom onset for IVand within 6 h ofsymptom onset in IAtreatments); age≥18 and≤80 year
Largely followed theNINDS rt-PA trialexclusion criteria’s
RCT; IV rt-PA (0.9 mg/kg; maximum 90 mg)vs. IA rt-PA (0.9 mg/kg; maximum 90 mg)±mechanical devices
Rate of survivalfree ofdisability(mRS=0 to 1score) at90 days
Pragmaticischemic strokethrombectomyevaluation(PISTE) [71]
>200 Acute ischemic stroke;age, ≥18 years; baselineNIHSS score cutoff yetto be defined; occlusionof the main MCA trunk,MCA bifurcation, orintracranial ICA on CTangiography or MRangiography;interventional treatmentthat can start within 6 hof stroke onset; 6—informed consent;functional independencebefore the stroke;absence of severalmedical comorbidities,peripheral vasculardisease, or archanatomy, which would
CT evidence of ICH;stroke >6 h before starttime of possibleintervention; mRS scoreof≥2 before the currentstroke; any stroke orhemorrhage within3 months; vascularaccesscontraindications;seizures at onset
RCT; mechanicalthrombectomy±IAthrombolysis vs. bestmedical therapy±IVthrombolysis
Undefined/unknown
Neurosurg Rev (2011) 34:11–20 15

achieved an overall recanalization rate (TIMI 2–3) of100% [56].
It has been suggested that with the development of anewer generation of stents with better navigability, the rateof successful stent deployment and overall safety havegreatly improved, potentially furthering the value of stent-based therapies for acute stroke [57, 58]. Novel interven-tional treatment techniques and devices such as “tempo-rary endovascular bypass” [59, 60] and “stent-platform-based thromboembolectomy devices” [61, 62] representnew options in acute stroke treatment. They seem to betechnically feasible with high success rate of recanaliza-tion. Disadvantages such as post-interventional antiplatelettherapy and in-stent stenosis are minimized with theseapproaches. However, it should be stressed that stentingfor cerebral vessels is not without limitations with the
current technology, and the long-term sequelae are notknown. Prospective, randomized trials are necessarybefore the role of stents in the treatment of acute ischemicstroke can be defined.
Is mechanical recanalization of value?
Comparing different reperfusion studies is fraught witherror, as widely varying methodology and patientselection criteria are used in various studies. However,while overall mechanical revascularization trials demon-strate effective recanalization rates, these studies doreport lower rates of good outcome and higher mortalitycompared to IV and/or IA thrombolytic studies. Impor-tantly, mechanical embolectomy studies have used
Table 1 (continued)
Study Samplesize
Inclusion criteria Exclusion criteria Design Defined endpoint (primaryand/orsecondary)
preclude safe cerebralangiography
Safety and efficacy ofneuroflotechnology inischemic stroke(SENTIS) [69]
≤488 Acute ischemic stroke;5≥NIHSS≥18
Undefined/unknown RCT; standard medicalmanagement+NeuroFlodevice vs. standardmedical managementalone
90 daysneurologicaland functionalassessment
Safety and efficacy ofNeuroFlo in 8–24 hstroke patients(FLO-24) [69]
26 18≥age≥85 years; 4≥NIHSS≥20; patientwith last known timesymptom-free between8 and 24 h; discernibleperfusion–diffusionmismatch on MRimaging
Undefined/unknown POL; NeuroFlo device All adverseeventsoccurringfrom baselinethrough30 dayspost-treatment
Feasibility and safetyof NeuroFlo instroke patientsreceiving rt-PA [69]
26 Patients with acuteischemic strokes whoqualify for and haveundergone IV rt-PAtherapy; 5≥NIHSS≥22;who can begin theNeuroFlo procedurewithin 3 h of initiationof IV rt-PA
Undefined/unknown POL; IV rt-PA+NeuroFlodevice (in patients withminimal clinicalimprovement followinginitiation of IV rt-PA)
Undefined/unknown
Randomized trial ofendovasculartreatment of acuteischemic strokeversus medicalmanagement(RETRIEVE) [69]
Undefined/unknown
Acute ischemic stroke;patient who can betreated within 8 h fromstroke onset (the exactprotocol details arecurrently being defined)
Undefined/unknown RCT; Merci retriever vs.best medical therapy±IV thrombolysis
Undefined/unknown
PROL indicates prospective randomized open-label study, POL prospective open-label study, RCT randomized controlled trial, EKOS EKOSMicroLys US infusion catheter, IA intra-arterial, IV intravenous, NIHSS National Institutes of Health Stroke Scale, mRS modified Rankin Scale,ICH intracranial hemorrhage, ICA intra cranial artery, MCA middle cerebral artery, MR angiography magnetic resonance angiography, CTangiography computerized tomography angiography, rt-PA recombinant tissue plasminogen activator, ASPECTS [72] Alberta Stroke ProgramEarly CT Score
16 Neurosurg Rev (2011) 34:11–20

recanalization as their primary end point withoutexcluding patients with poor functional baseline. Sub-group analysis of the NINDS data showed that patientswith severe strokes had only an 8% likelihood ofachieving clinically significant improvement with rt-PA[63]. Chemical thrombolysis trials typically excludedpatients with poor baseline functional status, potentiallyexplaining the discrepancy between chemical and me-chanical thrombolytic studies. Differences in clot locationand burden and time from symptom onset to treatment inthese studies are also potential explanations for thedifferences between recanalization and clinical outcomes.Recently, Josephson et al. [64] compared the results ofMERCI and multi MERCI trial with PROACT II toidentify the patients in MERCI and multi MERCI trialswho would have been eligible for PROACT II. Rates ofgood outcome (mRS score, ≤2) and mortality at 90 dayswere subsequently compared, adjusting for differences inbaseline NIHSS score and age. Sixty-eight patientsenrolled in MERCI and 81 enrolled in multi MERCIwere eligible for PROACT II. In both unadjusted andadjusted analyses, PROACT II-eligible patients withthrombectomy showed a trend toward better clinicaloutcomes and non-significant mortality rates (adjustedanalysis: MERCI, 29.1%; multi MERCI, 18.0%; PRO-ACT II control, 27.1%) compared with the PROACT IIcontrol arm. In comparison with the PROACT IItreatment subjects, thrombectomy patients showed similarrates of good outcome and mortality rates. They conclud-ed that the differences in the rates of mortality and goodoutcome between the MERCI/multi MERCI trials and thePROACT II trial are explained by differences in studydesign and baseline patient characteristics. Rha and Saver[65] performed a meta-analysis on 53 studies between1985 and 2002 encompassing 2066 patients to assessvessel recanalization, either spontaneous or therapeutical-ly induced in acute ischemic stroke. Higher recanalizationrates with mechanical devices (83.6%) were seen in theirstudy compared with combined IV–IA thrombolysis(67.5%), IA fibrinolytic (63.2%), IV fibrinolytic(46.2%), and spontaneous (24.1%) recanalization. Fur-thermore, a recent study evaluated the cost and effective-ness of mechanical thrombectomy compared withstandard medical therapy in patients who are ineligibleto receive rt-PA [66]. The authors demonstrated thattreatment of acute ischemic stroke with mechanical throm-bectomy increased survival time compared with standardmedical therapy (2.37 versus 1.83 quality-adjusted life years).Their sensitivity analysis showed that mechanical thrombec-tomy remained cost-effective for all model inputs varied overa reasonable range, except for age at stroke treatment. Forsubjects older than 82 years of age, the treatment was onlyborderline cost-effective.
Future directions
The endovascular treatment of acute ischemic stroke is anactively evolving field with new pharmacological agents andmechanical devices to recanalize occluded vessels developingat a rapid pace (Table 1). Regardless of what approach isused, time to treatment and proper selection of the patientsremain critical. As continued technologic advances occur tomeet the special needs of navigating tortuous cerebralcirculation, we can anticipate continued improvements inoutcomes. Currently, only two devices are FDA approved,the Merci device and Penumbra System; however, nomechanical device has been assessed in a randomized trial,and true evidence-based efficacy has yet to be shown. Untilhigh quality prospective randomized trials are performed,these data will remain promising suggestions of futurepotential, rather than actualized contributions to a newstandard of care.
Acknowledgements The authors wish to thank David Peace for hisdrawing and invaluable helps in this article.
References
1. Kung HC, Hoyert DL, Xu J, Murphy SL (2008) Deaths: final datafor 2005. Natl Vital Stat Rep 56:1–120
2. Dobkin B (1995) The economic impact of stroke. Neurology 45:S6–S9
3. Sussman BJ, Fitch TS (1958) Thrombolysis with fibrinolysin incerebral arterial occlusion. J Am Med Assoc 167:1705–1709
4. The NINDS t-PA Stroke Study Group (1995) Tissue plasminogenactivator for acute ischemic stroke. The National Institute ofNeurological Disorders and Stroke rt-PA Stroke Study Group. NEngl J Med 333:1581–1587
5. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C,Pessin M, Ahuja A, Callahan F, Clark WM, Silver F, Rivera F(1999) Intra-arterial prourokinase for acute ischemic stroke. ThePROACT II study: a randomized controlled trial. Prolyse in acutecerebral thromboembolism. JAMA 282:2003–2011
6. Weaver WD, Simes RJ, Betriu A, Grines CL, Zijlstra F, Garcia E,Grinfeld L, Gibbons RJ, Ribeiro EE, DeWood MA, Ribichini F(1997) Comparison of primary coronary angioplasty and intrave-nous thrombolytic therapy for acute myocardial infarction: aquantitative review. JAMA 278:2093–2098
7. GobinYP, Starkman S,Duckwiler GR, Grobelny T,Kidwell CS, JahanR, Pile-Spellman J, Segal A, Vinuela F, Saver JL (2004) MERCI 1: aphase 1 study of mechanical embolus removal in cerebral ischemia.Stroke 35:2848–2854 (a journal of cerebral circulation)
8. Nogueira RG, Smith WS (2009) Safety and efficacy of endovas-cular thrombectomy in patients with abnormal hemostasis: pooledanalysis of the MERCI and multi MERCI trials. Stroke 40:516–522 (a journal of cerebral circulation)
9. Smith WS, Sung G, Saver J, Budzik R, Duckwiler G,Liebeskind DS, Lutsep HL, Rymer MM, Higashida RT,Starkman S, Gobin YP, Frei D, Grobelny T, Hellinger F,Huddle D, Kidwell C, Koroshetz W, Marks M, Nesbit G,Silverman IE (2008) Mechanical thrombectomy for acuteischemic stroke: final results of the multi MERCI trial. Stroke39:1205–1212 (a journal of cerebral circulation)
Neurosurg Rev (2011) 34:11–20 17

10. Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, GobinYP, Lutsep HL, Nesbit GM, Grobelny T, Rymer MM, SilvermanIE, Higashida RT, Budzik RF, Marks MP (2005) Safety andefficacy of mechanical embolectomy in acute ischemic stroke:results of the MERCI trial. Stroke 36:1432–1438 (a journal ofcerebral circulation)
11. Barnwell SL, Clark WM, Nguyen TT, O’Neill OR, Wynn ML,Coull BM (1994) Safety and efficacy of delayed intraarterialurokinase therapy with mechanical clot disruption for thrombo-embolic stroke. Ajnr 15:1817–1822
12. Sorimachi T, Fujii Y, Tsuchiya N, Nashimoto T, Harada A, Ito Y,Tanaka R (2004) Recanalization by mechanical embolus disrup-tion during intra-arterial thrombolysis in the carotid territory. Ajnr25:1391–1402
13. Levy EI, Ecker RD, Horowitz MB, Gupta R, Hanel RA,Sauvageau E, Jovin TG, Guterman LR, Hopkins LN (2006)Stent-assisted intracranial recanalization for acute stroke: earlyresults. Neurosurgery 58:458–463, discussion 458–463
14. Nakano S, Iseda T, Yoneyama T, Kawano H, Wakisaka S (2002)Direct percutaneous transluminal angioplasty for acute middlecerebral artery trunk occlusion: an alternative option to intra-arterial thrombolysis. Stroke 33:2872–2876 (a journal of cerebralcirculation)
15. del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA,Gent M (1998) PROACT: a phase II randomized trial ofrecombinant pro-urokinase by direct arterial delivery in acutemiddle cerebral artery stroke. PROACT Investigators. Prolyse inAcute Cerebral Thromboembolism. Stroke 29:4–11 (a journal ofcerebral circulation)
16. Mahon BR, Nesbit GM, Barnwell SL, Clark W, Marotta TR, WeillA, Teal PA, Qureshi AI (2003) North American clinicalexperience with the EKOS MicroLysUS infusion catheter for thetreatment of embolic stroke. Ajnr 24:534–538
17. Standard SC, Chavis TD, Wakhloo AK, Ahuja A, Guterman LR,Hopkins LN (1994) Retrieval of a Guglielmi detachable coil afterunraveling and fracture: case report and experimental results.Neurosurgery 35:994–998, discussion 999
18. Watanabe A, Hirano K, Mizukawa K, Kamada M, Okamura H,Suzuki Y, Ishii R (1995) Retrieval of a migrated detachable coil—case report. Neurol Med Chir (Tokyo) 35:247–250
19. Chopko BW, Kerber C, Wong W, Georgy B (2000) Transcathetersnare removal of acute middle cerebral artery thromboembolism:technical case report. Neurosurgery 46:1529–1531
20. Nesbit GM, Luh G, Tien R, Barnwell SL (2004) New and futureendovascular treatment strategies for acute ischemic stroke. J VascInterv Radiol 15:S103–S110
21. Smith WS (2006) Safety of mechanical thrombectomy andintravenous tissue plasminogen activator in acute ischemic stroke.Results of the multi Mechanical Embolus Removal in CerebralIschemia (MERCI) trial, part I. Ajnr 27:1177–1182
22. Devlin TG, Baxter BW, Feintuch TA, Desbiens NA (2007) Themerci retrieval system for acute stroke: the Southeast RegionalStroke Center experience. Neurocrit Care 6:11–21
23. Nogueira RG, Schwamm LH, Hirsch JA (2009) Endovascularapproaches to acute stroke, part 1: drugs, devices, and data. Ajnr30:649–661
24. Henkes H, Reinartz J, Lowens S, Miloslavski E, Roth C, Reith W,Kuhne D (2006) A device for fast mechanical clot retrieval fromintracranial arteries (Phenox clot retriever). Neurocrit Care 5:134–140
25. Liebig T, Reinartz J, Guethe T, Roth C, Miloslavski E (2008)Early clinical experiences with a new thrombectomy device forthe treatment of ischemic stroke (abstract). Stroke 39:608 (ajournal of cerebral circulation)
26. Mayer TE, Hamann GF, Brueckmann HJ (2002) Treatment ofbasilar artery embolism with a mechanical extraction device:
necessity of flow reversal. Stroke 33:2232–2235 (a journal ofcerebral circulation)
27. Chapot R (2005) First experience with the catch, a new device forcerebral thrombectomy. Interv Neuroradiol 11(suppl 2):58
28. Schumacher HC, Meyers PM, Yavagal DR, Harel NY, Elkind MS,Mohr JP, Pile-Spellman J (2003) Endovascular mechanicalthrombectomy of an occluded superior division branch of the leftMCA for acute cardioembolic stroke. Cardiovasc Interv Radiol26:305–308
29. Kerber CW, Wanke I, Bernard J Jr, Woo HH, Liu MW, Nelson PK(2007) Rapid intracranial clot removal with a new device: thealligator retriever. Ajnr 28:860–863
30. Bergui M, Stura G, Daniele D, Cerrato P, Berardino M, BradacGB (2006) Mechanical thrombolysis in ischemic stroke attribut-able to basilar artery occlusion as first-line treatment. Stroke37:145–150 (a journal of cerebral circulation)
31. Clark WM, Buckley LA, Nesbit GM, Lutsep HL, Barnwell SL,Doherty AJ, Gregory KW (2000) Intraarterial laser thrombolysistherapy for clinical stroke: a feasibility study (abstract). Stroke31:307 (a journal of cerebral circulation)
32. Berlis A, Lutsep H, Barnwell S, Norbash A, Wechsler L, JungreisCA, Woolfenden A, Redekop G, Hartmann M, Schumacher M(2004) Mechanical thrombolysis in acute ischemic stroke withendovascular photoacoustic recanalization. Stroke 35:1112–1116(a journal of cerebral circulation)
33. Lutsep HL, Clark WM, Nesbit GM, Kuether TA, Barnwell SL(2002) Intraarterial suction thrombectomy in acute stroke. Ajnr23:783–786
34. Bellon RJ, Putman CM, Budzik RF, Pergolizzi RS, Reinking GF,Norbash AM (2001) Rheolytic thrombectomy of the occludedinternal carotid artery in the setting of acute ischemic stroke. Ajnr22:526–530
35. Molina CA, Saver JL (2005) Extending reperfusion therapy foracute ischemic stroke: emerging pharmacological, mechanical,and imaging strategies. Stroke 36:2311–2320 (a journal ofcerebral circulation)
36. Lee MS, Singh V, Wilentz JR, Makkar RR (2004) AngioJetthrombectomy. J Invasive Cardiol 16:587–591
37. Lutsep HL. Mechanical Thrombolysis in Acute Stroke. eMedicinefrom WebMD. Updated May 26, 2009. Available at: http://emedicine.medscape.com/article/1163240-overview. AccessedNovember 19, 2010
38. Bose A, Henkes H, Alfke K, Reith W, Mayer TE, Berlis A,Branca V, Sit SP (2008) The Penumbra system: a mechanicaldevice for the treatment of acute stroke due to thromboembolism.Ajnr 29:1409–1413
39. Penumbra Pivotal Stroke Trial Investigators (2009) The PenumbraPivotal stroke trial: safety and effectiveness of a new generation ofmechanical devices for clot removal in intracranial large vesselocclusive disease. Stroke 40:2761–2768 (a journal of cerebralcirculation)
40. Tarr R, Alfke K, Stingele R, Jansen O, Frei D, Bellon R, MadisonM, Struffert T, Dorfler A, Grunwald IQ, Reith W, Haass A (2009)Initial post-market experience of the Penumbra System: revascu-larization of large vessel occlusion in acute ischemic stroke in theUnited States and Europe [abstract]. Stroke journal cerebralcirculation 40:48
41. Block PC, Baughman KL, Pasternak RC, Fallon JT (1980) Trans-luminal angioplasty: correlation of morphologic and angiographicfindings in an experimental model. Circulation 61:778–785
42. Castaneda-Zuniga WR, Formanek A, Tadavarthy M, Vlodaver Z,Edwards JE, Zollikofer C, Amplatz K (1980) The mechanism ofballoon angioplasty. Radiology 135:565–571
43. Dotter CT, Judkins MP (1964) Transluminal treatment of arterio-sclerotic obstruction. Description of a new technic and a preliminaryreport of its application. Circulation 30:654–670
18 Neurosurg Rev (2011) 34:11–20

44. Higashida RT, Tsai FY, Halbach VV, Dowd CF, Hieshima GB(1993) Cerebral percutaneous transluminal angioplasty. Heart DisStroke 2:497–502
45. Nakano S, Yokogami K, Ohta H, Yano T, Ohnishi T (1998) Directpercutaneous transluminal angioplasty for acute middle cerebralartery occlusion. Ajnr 19:767–772
46. Qureshi AI, Siddiqui AM, Suri MF, Kim SH, Ali Z, Yahia AM,Lopes DK, Boulos AS, Ringer AJ, Saad M, Guterman LR,Hopkins LN (2002) Aggressive mechanical clot disruption andlow-dose intra-arterial third-generation thrombolytic agent forischemic stroke: a prospective study. Neurosurgery 51:1319–1327, discussion 1327–1319
47. Yoneyama T, Nakano S, Kawano H, Iseda T, Ikeda T, Goya T,Wakisaka S (2002) Combined direct percutaneous transluminalangioplasty and low-dose native tissue plasminogen activatortherapy for acute embolic middle cerebral artery trunk occlusion.Ajnr 23:277–281
48. Abou-Chebl A, Bajzer CT, Krieger DW, Furlan AJ, Yadav JS(2005) Multimodal therapy for the treatment of severe ischemicstroke combining GPIIb/IIIa antagonists and angioplasty afterfailure of thrombolysis. Stroke 36:2286–2288 (a journal ofcerebral circulation)
49. Ueda T, Sakaki S, Nochide I, Kumon Y, Kohno K, Ohta S (1998)Angioplasty after intra-arterial thrombolysis for acute occlusion ofintracranial arteries. Stroke 29:2568–2574 (a journal of cerebralcirculation)
50. Qureshi AI, Siddiqui AM, Kim SH, Hanel RA, Xavier AR,Kirmani JF, Suri MF, Boulos AS, Hopkins LN (2004) Reocclu-sion of recanalized arteries during intra-arterial thrombolysis foracute ischemic stroke. Ajnr 25:322–328
51. Horowitz MB, Purdy PD (2000) The use of stents in the managementof neurovascular disease: a review of historical and present status.Neurosurgery 46:1335–1342, discussion 1342–1333
52. Levy EI, Ecker RD, Hanel RA, Sauvageau E, Wehman JC,Guterman LR, Hopkins LN (2006) Acute M2 bifurcation stentingfor cerebral infarction: lessons learned from the heart: technicalcase report. Neurosurgery 58:E588, discussion E588
53. Fitzsimmons BF, Becske T, Nelson PK (2006) Rapid stent-supportedrevascularization in acute ischemic stroke. Ajnr 27:1132–1134
54. Levy EI, Mehta R, Gupta R, Hanel RA, Chamczuk AJ, Fiorella D,Woo HH, Albuquerque FC, Jovin TG, Horowitz MB, Hopkins LN(2007) Self-expanding stents for recanalization of acute cerebro-vascular occlusions. Ajnr 28:816–822
55. Levy EI, Siddiqui AH, Crumlish A, Snyder KV, Hauck EF,Fiorella DJ, Hopkins LN, Mocco J (2009) First food and drugadministration-approved prospective trial of primary intracranialstenting for acute stroke: SARIS (stent-assisted recanalization inacute ischemic stroke). Stroke 40:3552–3556 (a journal ofcerebral circulation)
56. Mocco J, Hanel RA, Sharma J, Hauck EF, Snyder KV, NatarajanSK, Linfante I, Siddiqui AH, Hopkins LN, Boulos AS, Levy EI(2009) Use of a vascular reconstruction device to salvage acuteischemic occlusions refractory to traditional endovascular recan-alization methods. J Neurosurg 2(3):557–562
57. SSYLVIA Study Investigators (2004) Stenting of symptomaticatherosclerotic lesions in the vertebral or intracranial arteries(SSYLVIA): study results. Stroke 35:1388–1392 (a journal ofcerebral circulation)
58. Schumacher HC, Khaw AV, Meyers PM, Gupta R, Higashida RT(2004) Intracranial angioplasty and stent placement for cerebralatherosclerosis. J Vasc Interv Radiol 15:S123–S132
59. Hauck EF, Mocco J, Snyder KV, Levy EI (2009) Temporaryendovascular bypass: a novel treatment for acute stroke. Ajnr30:1532–1533
60. Kelly ME, Furlan AJ, Fiorella D (2008) Recanalization of anacute middle cerebral artery occlusion using a self-expanding,
reconstrainable, intracranial microstent as a temporary endovas-cular bypass. Stroke 39:1770–1773 (a journal of cerebralcirculation)
61. Henkes H, Liebig T, Miloslavski E, Guethe T, Schmid E,Wiethoelter H (2009) Endovascular acute ischemic stroke treat-ment using the self-expanding and fully retrievable Solitaire stent.Stroke 40:144 (a journal of cerebral circulation)
62. Jahan R (2008) A novel, self expanding, fully retractablemechanical thromboembolectomy device for treatment of acuteischemic stroke. In: 5th Annual Meeting of the Society ofNeuroInterventional Surgery (SNIS). Lake Tahoe, California
63. The NINDS t-PA Stroke Study Group (1997) Generalized efficacy oft-PA for acute stroke. Subgroup analysis of the NINDS t-PA StrokeTrial. Stroke 28:2119–2125 (a journal of cerebral circulation)
64. Josephson SA, Saver JL, Smith WS (2009) Comparison ofmechanical embolectomy and intraarterial thrombolysis in acuteischemic stroke within the MCA: MERCI and multi MERCIcompared to PROACT II. Neurocrit Care 10:43–49
65. Rha JH, Saver JL (2007) The impact of recanalization on ischemicstroke outcome: a meta-analysis. Stroke 38:967–973 (a journal ofcerebral circulation)
66. Patil CG, Long EF, Lansberg MG (2009) Cost-effectivenessanalysis of mechanical thrombectomy in acute ischemic stroke. JNeurosurg 110:508–513
67. Khatri P, Hill MD, Palesch YY, Spilker J, Jauch EC, CarrozzellaJA, Demchuk AM, Martin R, Mauldin P, Dillon C, Ryckborst KJ,Janis S, Tomsick TA, Broderick JP (2008) Methodology of theinterventional management of stroke III trial. Int J Stroke 3:130–137
68. Becker KJ, Brott TG (2005) Approval of the MERCI clotretriever: a critical view. Stroke 36:400–403 (a journal of cerebralcirculation)
69. Nogueira RG, Yoo AJ, Buonanno FS, Hirsch JA (2009) Endovas-cular approaches to acute stroke, part 2: a comprehensive review ofstudies and trials. AJNR 30:859–875. doi:10.3174/ajnr.A1604
70. (2008) Major ongoing stroke trials. Stroke 39:e51–e60 (a journalof cerebral circulation)
71. Molyneux A, Rothwell P (2009) Pragmatic ischaemic strokethrombectomy evaluation (PISTE): mechanical thrombectomy orrevascularisation for acute ischaemic stroke—plans for a prospec-tive randomised trial [abstract]. In: Proceedings of the 29th ABC-WIN Seminar. Val d'Isere, France
72. Barber PA, Demchuk AM, Zhang J, Buchan AM (2000) Validityand reliability of a quantitative computed tomography score inpredicting outcome of hyperacute stroke before thrombolytictherapy. ASPECTS study group. Alberta Stroke Programme EarlyCT Score. Lancet 355:1670–1674
Comments
Carlo Schaller, Geneva, SwitzerlandThis is part 2 of a review concerning the treatment of acute stroke.
Whereas in part 1 the authors had focussed on techniques ofintravenous and intra-arterial thrombolyisis, here they summarize thejoint evolution of imaging technology and the development ofinterventional neuroradiological techniques for the mechanical retriev-al of intra-arterial clots, placement of stents, and local administrationof thrombolytic agents. It is a very helpful and clear description ofstate-of-the-art technology and related trials. Whereas mechanical clotremoval, e.g., by microwires proved not very effective, and evenhazardous during its beginnings about a decade ago, recent advanceswith miniaturization of steerable endovascular tools caused a newinterest for their application in the treatment of acute stroke. The
Neurosurg Rev (2011) 34:11–20 19

authors refer to a number of recent such studies, e.g., the MERCI trial.They highlight the different mechanical approaches from retrievingdevices to Laser fragmentation, saline pressure stream, or aspiration-fragmentation of the thrombus. They discuss the potential benefits ofangioplasty in combination with deployment of stents and localadministration of thrombolytic agents. As they point out clearly: onlyfew devices have made it through FDA approval already, andpromising results from single small studies have to be looked atcautiously, as, e.g., patient selection differs between the studies. It isobvious that there is a multitude of experimental devices formechanical clot destruction and/or retrieval, and that here are moreto come. And, there is a certain danger that technologically drivenspecialists as neuroradiologists and neurosurgeons would jump onnew and mechanically appealing tools. It is our obligation within thecommunity of clinical neuroscientists that these tools shall beevaluated in the same strict and prospective and controlled manneras it applies for the more conservative approaches of intra-arterial andintravenous thrombolysis. Again, it is quite clear: the limits betweenour fields are less demarcated than ever before in the treatment ofstroke, and each of the involved specialists, may it be a neurologist, aneuroradiologist, or a neurosurgeon, respectively, has to play his/herrole, and needs to be updated concerning recent developments in themanagement of these patients, as each of us may have something tocontribute, and as the sequence of treatment steps needs to becoordinated in a reasonable manner (e.g., placement of ICP probes orperformance of hemicraniectomy prior to stenting and anticoagulationetc.). This does also speak in favor of further development of jointemergency admission centers and of neuro-intensive care settings,which does require quite some lobbying still with the respective healthcare authorities in most countries.
Atos Alves de Sousa, Belo Horizonte, BrazilThis is a very good and relevant literature review on mechanical
intra-arterial technologies for recanalization in acute ischemicstroke. First of all, we must say that the subject is very relevant,as acute ischemic stroke is one of the most common causes ofdeath in developed countries. Besides, the window for thetreatment of acute stroke by intravenous and intra-arterial throm-bolysis is very short—from 3 to 6 h—so the mechanical intra-arterial recanalization could be a rather important option to savelives and avoid neurological damage. The present state-of-the-art ofthe endovascular treatment of acute ischemic stroke and theconstant development of new endovascular technologies is verypromising, and neuroscientists will probably find papers like thisone very helpful for their daily practice.
Giuseppe Lanzino, Rochester, USAIn this well-written review of current endovascular mechanical
therapies, the authors provide a state-of-art summary of currenttherapeutic strategies. Recently, there has been an explosion ofinterest in the endovascular management of acute stroke. Several ofthe strategies utilized are theoretically appealing and oftenaccompanied by excellent angiographic results. However, thestrength of the evidence supporting the use of these therapies isnot of the highest quality. Despite widespread utilization of thesetherapies, there are no randomized trial documenting their efficacyand the data supporting their use are often based on comparisonswith historical controls with all of the inherent limitations relatedto such comparisons. Hopefully, the results of some of the ongoingrandomized studies will clarify the real role and efficacy of this(theoretically appealing) approach.
20 Neurosurg Rev (2011) 34:11–20
Copyright © 2022 FDOKUMEN




















