
Induction immunotherapy in pediatric heart transplant recipients: a multicenter study
Upload
independentCategory
view
2download
0
Reactive Antibodies Against BacillusCalmette-Guerin Heat-Shock Protein-65Potentially Predict the Outcome ofImmunotherapy for High-Grade TransitionalCell Carcinoma of the BladderPeter U. Ardelt, MD1; Burkhard Kneitz, MD1; Patrick Adam, MD2; Cora Reiss, PhD3; Arkadius Kocot, MD1;
Joachim Fensterle, PhD4; Limor Chen, PhD5; Renata Pasqualini, PhD6; Wadih Arap, MD, PhD6; Elmar W. Gerharz, MD1;
and Hubertus Riedmiller, MD1
BACKGROUND: Intravesical immunotherapy with Mycobacterium bovis (M. bovis) bacillus Calmette-Guerin (BCG) is
the current standard of care against superficial, high-grade transitional cell carcinoma (TCC) of the urinary bladder
(carcinoma in situ and pathologic T1, grade 3 disease). However, individual patient outcome is barely predictable
because of the lack of serum markers. Consequently, progression to muscle-invasive bladder cancer and critical delay
of treatments (such as neoadjuvant combination chemotherapy and/or radical cystectomy) often occur. The objec-
tives of this study were to identify a marker for measuring the BCG-induced immune response and to predict the out-
comes and potential improvements of BCG immunotherapy. METHODS: Because host immunoresponse mediates
BCG activity, the authors screened a combinatorial random peptide library on the circulating pool of immunoglobu-
lins (Igs) purified from an index patient after successful BCG immunotherapy to identify the corresponding target
antigen(s). RESULTS: An immunogenic peptide motif was selected, isolated, and validated from M. bovis BCG heat-
shock protein 65 (HSP-65) as a dominant epitope of the humoral response to treatment. Increasing IgA and IgG anti-
HSP-65 titers specifically predicted a positive patient outcome in a cohort of patients with bladder cancer relative to
several cohorts of control patients. CONCLUSIONS: The current results indicated that antibody production against M.
bovis BCG HSP-65 can serve as a serologic marker for the predictive outcome of BCG immunotherapy. Subsequent
studies will determine the value of this candidate marker to modify BCG-based treatment for individual patients with
bladder cancer. Cancer 2010;116:600–9. VC 2009 American Cancer Society.
KEYWORDS: bacillus Calmette-Guerin, immunotherapy, heat-shock proteins, transitional cell carcinoma.
Intravesically administeredMycobacterium bovis bacillus Calmette-Guerin (M. bovis BCG) has become the treat-ment of choice against superficial, high-grade transitional cell carcinoma (TCC) (carcinoma in situ [Cis] and pathologicT1 [pT1], grade 3 tumors). Repeated intravesical instillations induce a complex immunologic response that results in tu-mor eradication in �75% after the induction cycle1-3 and long-term remission in 50% to 75% of patients.4,5 Evidenceexists that, primarily, a cellular immune response is necessary for successful BCG immunotherapy.6,7 Interferon c andinterleukin 12, both mediators of a T-helper cell 1 (TH1)-mediated immune response, essentially are necessary for a posi-tive BCG effect in vivo.7 However, it also has been demonstrated that intravesical application ofM. bovis BCG results inthe activation of both TH-1-mediated and TH-2-mediated pathways and that separation is less strict.7,8
Patients who do not respond to BCG (�30%) are at increased risk of progression to muscle-invasive disease andmetastasis. Delays in starting more aggressive treatments, such as neoadjuvant combination chemotherapy and/or radical
DOI: 10.1002/cncr.24770, Received: February 24, 2009; Revised: May 19, 2009; Accepted: May 26, 2009, Published online December 2, 2009 in Wiley
InterScience (www.interscience.wiley.com)
Corresponding author: Peter U. Ardelt, MD, Department of Urology and Pediatric Urology, Bavarian Julius Maximilians-University Medical School,
Oberdurrbacher Strasse 6, 97080 Wurzburg, Germany; Fax: (011) 49-931-201-32013; [email protected]
1Department of Urology and Pediatric Urology, Bavarian Julius Maximilians-University Medical School, Wurzburg, Germany; 2Institute of Pathology, Bavarian Julius
Maximilians-University Medical School, Wurzburg, Germany; 3Department of Physiological Chemistry I, Bavarian Julius Maximilians-University Medical School,
Wurzburg, Germany; 4Institute of Medical Radiology and Cell Research, Bavarian Julius Maximilians-University Medical School, Wurzburg, Germany; 5Teva Pharma-
ceutical Industries, Jerusalem, Israel; 6David H. Koch Center, The University of Texas M. D. Anderson Cancer Center, Houston, Texas
600 Cancer February 1, 2010
Original Article

cystectomy, may lead to potentially worse outcomes.Thus, it is paramount to identify nonresponders to BCGimmunotherapy as early as possible in their clinical courseso that these individuals may be considered for moreaggressive therapeutic strategies. Several adverse factorsfor the outcome of BCG immunotherapy are known,such as age, incomplete tumor resection, and tumorsize.9,10 A second resection before BCG immunotherapyis associated with an improved outcome.10 However, cur-rently, the success of BCG immunotherapy is determinedonly indirectly according to the presence or absence of tu-mor at the time of re-evaluation, and the induced immuneresponse cannot be measured directly during or afterinduction.
Because the immune response has an establishedrole as a predictive biomarker in cancer therapy for manytumors,11-14 including human bladder cancer, and cer-tainly in the setting of BCG therapy,3,8 we attempted toidentify candidate serum markers for measuring theimmune response and, thus, the outcome of BCG immu-notherapy through combinatorial epitope mapping (‘‘fin-gerprinting’’) of the antibody response to BCG. In thisreport, we describe a peptide from M. bovis BCG heat-shock protein 65 (HSP-65) that elicits a strong and spe-cific humoral response to treatment. Reactive serum titersafter BCG treatment predicted a positive outcome for acohort of patients with bladder cancer. If these results areconfirmed in larger, prospective, follow-up studies, thenthis approach and finding will lead to an antibody-basedassay for measuring BCG-induced antitumor response.This assay should allow for the early detection of nonres-ponding patients and an immunotherapy designed specif-ically for each patient.
MATERIALS AND METHODS
Collection of Patient Serum Samples
All experiments were reviewed and approved by the Insti-tutional Review Board of the Bavarian Julius Maximili-ans-University Medical School, Wurzburg, Germany.Written informed consent was obtained from all patients.Sera samples were collected and immediately frozen at�80�C after centrifugation from patients who werereceiving BCG therapy (n¼ 16) for superficial high-gradeTCC (Cis or pT1/grade 3 tumors) at the time of initial di-agnosis, after the induction cycle, and at the first follow-up. Control samples were obtained from patients whohad other stages of TCC (Ta, T2-T4; n ¼ 38), patientswho had prostate cancer (n ¼ 40), and age-matched
healthy volunteers (n ¼ 40). Standard exclusion criteriafor BCG immunotherapy were applied, and only patientswho had not received previous intravesical therapies forurothelial tumors were eligible.
Screening of the Phage-Display RandomPeptide Library
We used a random peptide phage-display library based onthe vector fUSE5, displaying inserts with the generalarrangement CX7C (C, cysteine; X, any residue).15 Aninsertless phage clone served as a negative control. For allexperiments, IgGs were immobilized and/or purified onprotein G-agarose beads (Sigma-Aldrich, Taufkirchen,Germany). Screening was performed as described previ-ously.15 Briefly, 109 transducing units (TU) of the CX7Crandom peptide phage-display library were precleared for60 minutes at 4�C on pooled, immobilized IgG fromhealthy control volunteers. After centrifugation, equalamounts of the supernatant were added to immobilizedIgGs from patients with bladder cancer and from healthycontrol volunteers. After incubation for 2 hours at 4�C,the beads were washed 5 times with phosphate-bufferedsaline (PBS). Bound phages were eluted with 0.1 M gly-cine buffer, pH 2.2, and were neutralized with 1 M Tris/HCl, pH 7.0. Reinfection was performed with 1 mLof log-phase Escherichia coli (E. coli) K91. Sequentialrounds of phage amplification were performed asdescribed previously.15 Serial dilutions were plated intriplicate to determine the ratio of bound phage after eachscreening round.
DNA Amplification and Sequencing
After the second selection round, serial dilutions wereplated for single bacterial colony isolation. IndividualDNA corresponding to the peptide inserts of randomlypicked phage clones (n ¼ 30) was amplified with the pri-mers 50-AGGTTGGTGCCTTCGTAGTG-30 and 50-GTTTAGTACCGCCACCCTCA-30 and was purifiedwith EXO SAP IT, (USB, Cleveland, Ohio). Sequencingwas performed with the primer 50-CCCTCATAGTTAGCGTAACGATCT-30, the CEQ 2000 Dye Termi-nator Cycle Sequencing Kit, and a CEQ 2000 automatedsequencer (both from Beckmann Coulter, Fullerton,Calif). Sequences were aligned and compared with onlineprotein databases of the National Center for Biotechnol-ogy Information (available at: http://ncbi.nlm.nih.gov/blast/Blast.cgi accessed January 2008).
Predicting BCG Immunotherapy Outcome/Ardelt et al
Cancer February 1, 2010 601

Phage Binding Assay and CompetitiveBinding Inhibition
For phage binding assays, 1 lg of purified IgG was immo-bilized on Nunc Maxisorp plates (Nunc, Wiesbaden,Germany) overnight at 4�C. After blocking wells withPBS that contained 0.1% Tween-20 and 1% nonfat driedmilk (NFDM) for 2 hours at room temperature (RT), weadded 108 TU of either amplified phage clones or controlphage for 2 hours at RT. For inhibition assays, increasingamounts of corresponding glutathione-S-transferase(GST)-fused peptides or wild-type (negative control)GST were preincubated for 30 minutes at RT before theaddition of phages. Unbound phages were removed bywashing 5 times with PBS that contained 0.1% Tween-20and 1% NFDM. Bound phages were recovered with 200lL log-phase E. coli K91 and were plated in serial dilu-tions (triplicate plates for each dilution).
Enzyme-Linked Immunoadsorbent Assay andPatient Screening
For the enzyme-linked immunoadsorbent assay (ELISA),1 lg of purified M. bovis BCG HSP-65 (StressGen Bio-technologies Corp., Victoria, British Columbia, Canada)per well was immobilized on Maxisorp plates (Nunc)overnight at 4�C. Wells were blocked with PBS that con-tained 0.1% Tween-20 and 1% NFDM for 2 hours atRT. Next, 100 lL of 1:200 diluted serum was added over-night at 4�C. After 5 washes with PBS that contained0.5% NFDM, bound antibodies were detected with per-oxidase-coupled rabbit-antihuman IgG (diluted 1:5.000)or with goat-antihuman IgA secondary antibody (diluted1:5.000) for 1 hour at RT (both from Sigma-Aldrich).The substrate tetramethylbenzidine (Sigma-Aldrich) wasadded for 20 minutes, and absorbance at 620 nm wasdetermined in an automated ELISA plate reader (LabSys-tems, Vantaa, Finland). For competitive inhibition, se-rum samples were preincubated with HIGAEGR-GSTfor 20 minutes at RT.
Western Blot Analysis
In total, 150 ng of M. bovis BCG HSP-65 were resolvedby electrophoresis on a 12.5% sodium dodecyl sulfate-polyacrylamide gel, and proteins were electrotransferredonto a polyvinylidene fluoride membrane. After blockingof the membrane with PBS that contained 7% NFDM,100 lL of patient serum (1:200) were added at 4�C over-night. After washing with PBS that contained 7%powdered milk, bound IgGs were detected with a peroxi-dase-coupled rabbit-antihuman IgG secondary antibody
(Sigma-Aldrich). Detection was performed with the Roti-Lumin reagent (Roth, Karlsruhe, Germany). A monoclo-nal mouse IgM anti-human HSP-65 (anti-huHSP-65)antibody (StressGen Biotechnologies Corp.) served as apositive control.
Immunohistochemistry
HSP detection was performed on archived, formalin-fixed, paraffin-embedded tissue sections (1 lm) with amonoclonal mouse IgG anti-huHSP-65 antibody (Stress-Gen Biotechnologies Corp.). The secondary antibody wasa horseradish peroxidase, polymerized IgG antibody.Detection was performed with Liquid DABþ SubstrateChromogen System (DAKO, Glostrup, Denmark), andslides were counterstained with hematoxylin. The inten-sity of HSP-65 (from 0 to 3 arbitrary units) was graded bya pathologist using similarly treated slides of breast cancertissue as a positive control.
Biostatistics
The optical density (OD) of antibody reactions measuredin ELISAs and phage binding were compared with 2-sidedStudent t tests. Standard deviations are reported as stand-ard errors of the mean.
RESULTS
Combinatorial Screening on IgG From aBCG-Responding Bladder Cancer Patient
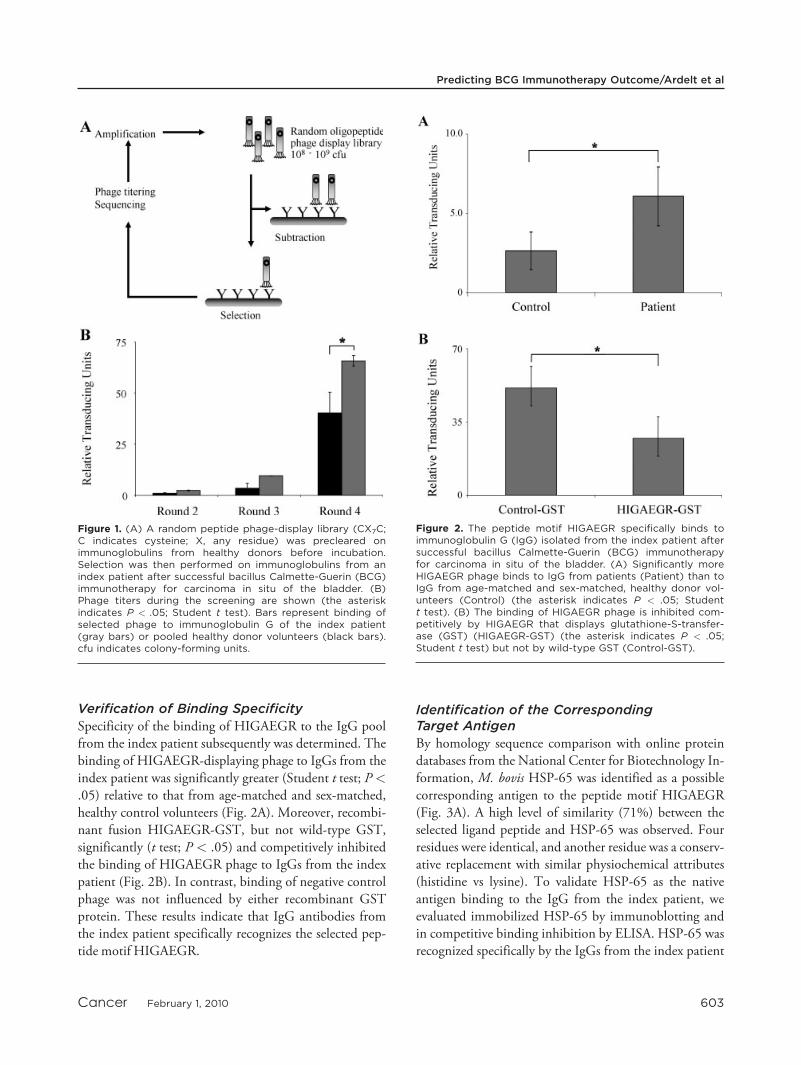
A bladder cancer patient with Cis and concomitantT1/grade 2 disease who had a positive clinical outcomeafter BCG immunotherapy served as the index patient(Patient 2). The circulating antibody pool from thisindex patient was probed according to a previousreport from a sample that was obtained 3 months afterinitial diagnosis and 2 weeks after the last weekly BCGinstillation.11 Successive rounds of screening of a 7-mer, cyclic, random peptide phage-display library wereperformed on IgGs that were isolated in serum fromthis index patient after the induction cycle of BCGimmunotherapy. During the screening, we observed aserial and marked increase in phage binding to the im-mobilized IgG from the index patient compared withcontrol IgG obtained from healthy volunteers (Fig. 1).This results indicated binding of the selected ligandpeptides displayed on the phage to the IgG from thepatient. Sequencing the DNA corresponding to theinserts of individually selected phage clones identifiedan enrichment of the peptide motif HIGAEGR.
Original Article
602 Cancer February 1, 2010
Verification of Binding Specificity
Specificity of the binding of HIGAEGR to the IgG poolfrom the index patient subsequently was determined. Thebinding of HIGAEGR-displaying phage to IgGs from theindex patient was significantly greater (Student t test; P<
.05) relative to that from age-matched and sex-matched,healthy control volunteers (Fig. 2A). Moreover, recombi-nant fusion HIGAEGR-GST, but not wild-type GST,significantly (t test; P < .05) and competitively inhibitedthe binding of HIGAEGR phage to IgGs from the indexpatient (Fig. 2B). In contrast, binding of negative controlphage was not influenced by either recombinant GSTprotein. These results indicate that IgG antibodies fromthe index patient specifically recognizes the selected pep-tide motif HIGAEGR.
Identification of the CorrespondingTarget Antigen
By homology sequence comparison with online proteindatabases from the National Center for Biotechnology In-formation, M. bovis HSP-65 was identified as a possiblecorresponding antigen to the peptide motif HIGAEGR(Fig. 3A). A high level of similarity (71%) between theselected ligand peptide and HSP-65 was observed. Fourresidues were identical, and another residue was a conserv-ative replacement with similar physiochemical attributes(histidine vs lysine). To validate HSP-65 as the nativeantigen binding to the IgG from the index patient, weevaluated immobilized HSP-65 by immunoblotting andin competitive binding inhibition by ELISA. HSP-65 wasrecognized specifically by the IgGs from the index patient
Figure 1. (A) A random peptide phage-display library (CX7C;C indicates cysteine; X, any residue) was precleared onimmunoglobulins from healthy donors before incubation.Selection was then performed on immunoglobulins from anindex patient after successful bacillus Calmette-Guerin (BCG)immunotherapy for carcinoma in situ of the bladder. (B)Phage titers during the screening are shown (the asteriskindicates P < .05; Student t test). Bars represent binding ofselected phage to immunoglobulin G of the index patient(gray bars) or pooled healthy donor volunteers (black bars).cfu indicates colony-forming units.
Figure 2. The peptide motif HIGAEGR specifically binds toimmunoglobulin G (IgG) isolated from the index patient aftersuccessful bacillus Calmette-Guerin (BCG) immunotherapyfor carcinoma in situ of the bladder. (A) Significantly moreHIGAEGR phage binds to IgG from patients (Patient) than toIgG from age-matched and sex-matched, healthy donor vol-unteers (Control) (the asterisk indicates P < .05; Studentt test). (B) The binding of HIGAEGR phage is inhibited com-petitively by HIGAEGR that displays glutathione-S-transfer-ase (GST) (HIGAEGR-GST) (the asterisk indicates P < .05;Student t test) but not by wild-type GST (Control-GST).
Predicting BCG Immunotherapy Outcome/Ardelt et al
Cancer February 1, 2010 603

and by the IgGs from another patient after successfulBCG immunotherapy, but not by IgGs from healthy con-trol volunteers (Fig. 3B). Binding of the IgGs from theindex patient was augmented over binding to the controlIgGs; moreover, binding was inhibited competitively bythe cognate HIGAEGR-GST, but not by wild-type GST(Fig. 3C). Binding of control IgG was not influenced byany recombinant GSTs. Together, these results indicatethat M. bovis BCG HSP-65 is the native antigen corre-sponding to the peptide sequence HIGAEGR. Thus, thehumoral immune response from the index patient specifi-cally targetsM. bovis BCGHSP-65.
Humoral Immune Response AgainstHSP-65
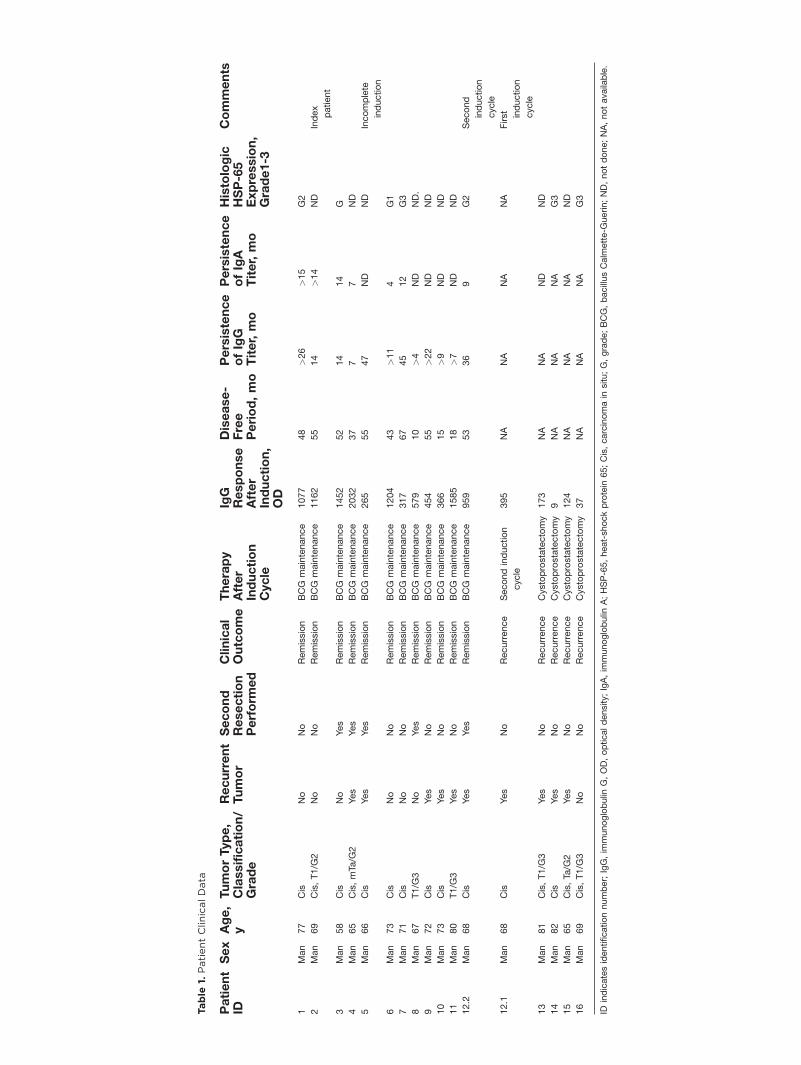
We determined the predictive value of IgG and IgA anti-bodies against M. bovis BCG HSP-65 in a panel ofpatients who were receiving BCG immunotherapy for su-perficial, high-grade TCC (n ¼ 16). Antibody titersagainst M. bovis BCG HSP-65 were measured at initialdiagnosis, after the induction cycle, and at the first follow-up (Table 1).
Eleven patients responded to BCG immunotherapyand remained tumor-free for up to 67 months. Fourpatients did not respond and underwent radical cystecto-mies. Another patient required a second induction cycleafter an initial clinical failure. Data from the failed andsuccessful induction cycles were added to the nonrespond-ing group and the responding group, respectively.
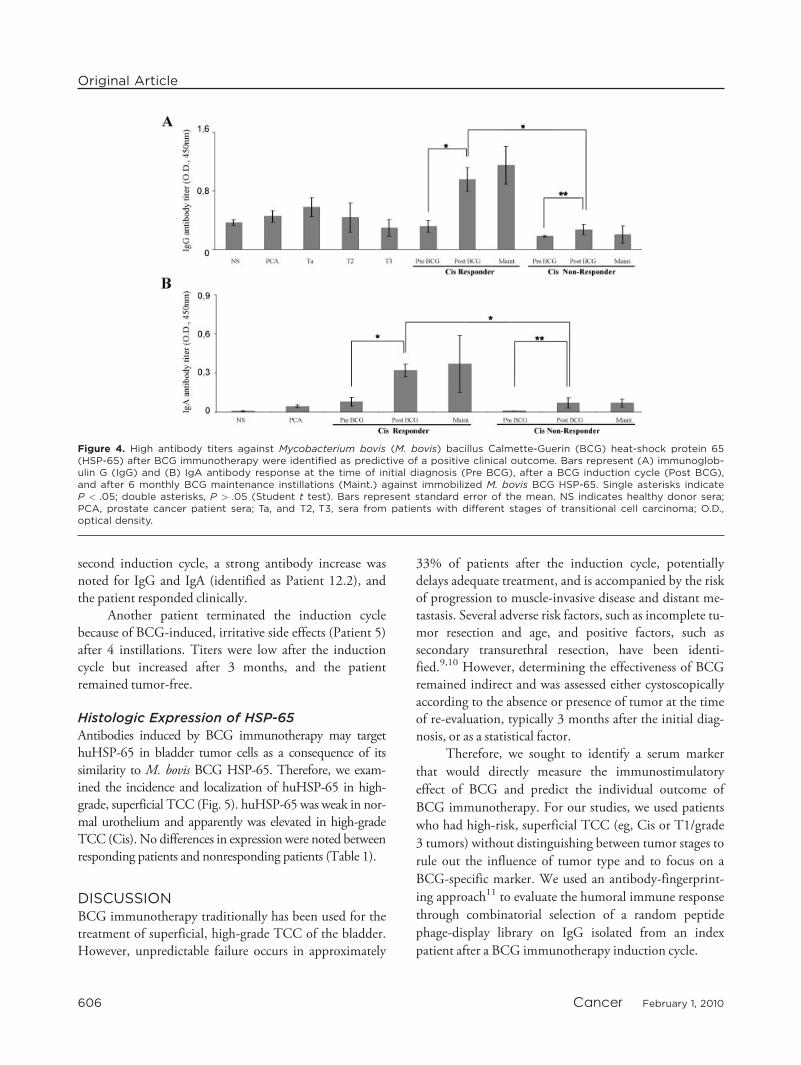
No significant correlation of the clinical outcomewith the following clinical features was observed in thissmall population: age (IgG titer vs age; P¼ .19), status ofthe tumor as recurrent or primary (IgG titer vs tumor sta-tus; P ¼ .17), and restaging resection before BCG immu-notherapy (IgG titer vs status of resection; P ¼ .16). IgGand IgA antibody titers against M. bovis BCG HSP-65were low in prostate cancer patients and healthy controlvolunteers. Similarly, titers in patients with bladder cancerother than superficial, high-grade TCC were low. Allpatients who were receiving BCG immunotherapy hadlow titers before therapy, regardless of their later clinicaloutcome (Figs. 4A and 4B) (OD for responders: IgG,0.32 � 0.08; IgA, 0.08 � 0.03; OD for nonresponders:IgG, 0.18 � 0.01; IgA, 0.01 � 0.0). In clinically nonres-ponding patients, anti-HSP-65-specific antibody titersdid not change detectably after the induction cycle (OD:IgG, 0.27 � 0.12; IgA, 0.07 � 0.04). In contrast, bothIgG and IgA antibody titers rose significantly (pre-BCGvs post-BCG: IgG, P < .01; IgA, P < .05) in clinicallyresponding patients (OD: IgG, 0.95 � 0.16; IgA, 0.32 �0.05) and were significantly higher than titers in nonres-ponding patients (responders vs nonresponders: IgG, P<
.01; IgA, P < .05). Furthermore, titers remained elevatedthroughout maintenance therapy and declined after up to47 months and 15 months for IgG and IgA, respectively.These results demonstrate that increasing IgG and IgAantibody titers against M. bovis BCG HSP-65 after aBCG induction cycle exhibit a positive predictive valuefor clinical outcome.
Patient 12 initially failed BCG immunotherapy(identified as Patient 12.1). Here, no significant increasein either antibody titer was observed. However, after a
Figure 3. Mycobacterium bovis (M. bovis) bacillus Calmette-Guerin (BCG) heat-shock protein (HSP)-65 is the antigencorresponding to the peptide HIGAEGR. (A) The selected oli-gopeptide HIGAEGR exhibits a strong similarity to the N-ter-minal sequence of M. bovis BCG HSP-65. (B) Western blotanalysis demonstrated that, after BCG immunotherapy, 2patients, but not healthy controls, had immunoglobulin G(IgG) directed against M. bovis BCG HPS-65. (C) Binding ofthe index patient’s IgG (Patient) to M. bovis BCG HSP-65 wascompetitively inhibited by HIGAEGR/glutathione-S-transfer-ase (GST) (light gray bars) but not by wild-type GST (darkgray bars). The binding of healthy donor IgG (Control) wassignificantly lower and was not influenced by HIGAEGR/GST(the asterisk indicates P < .05; Student t test). KD indicateskilodaltons; O.D., optical density.
Original Article
604 Cancer February 1, 2010
Table
1.PatientClinicalData
Patient
IDSex
Age,
yTumorType,
Classification/
Grade
Recurrent
Tumor
Second
Resection
Perform
ed
Clinical
Outcome
Therapy
After
Induction
Cycle
IgG
Response
After
Induction,
OD
Disease-
Free
Period,mo
Persistence
ofIgG
Titer,mo
Persistence
ofIgA
Titer,mo
Histologic
HSP-65
Expression,
Grade1-3
Comments
1Man
77
Cis
No
No
Remission
BCG
maintenance
1077
48
>26
>15
G2
2Man
69
Cis,T1/G
2No
No
Remission
BCG
maintenance
1162
55
14
>14
ND
Index
patient
3Man
58
Cis
No
Yes
Remission
BCG
maintenance
1452
52
14
14
G
4Man
65
Cis,mTa
/G2
Yes
Yes
Remission
BCG
maintenance
2032
37
77
ND
5Man
66
Cis
Yes
Yes
Remission
BCG
maintenance
265
55
47
ND
ND
Incomplete
induction
6Man
73
Cis
No
No
Remission
BCG
maintenance
1204
43
>11
4G1
7Man
71
Cis
No
No
Remission
BCG
maintenance
317
67
45
12
G3
8Man
67
T1/G
3No
Yes
Remission
BCG
maintenance
579
10
>4
ND
ND.
9Man
72
Cis
Yes
No
Remission
BCG
maintenance
454
55
>22
ND
ND
10
Man
73
Cis
Yes
No
Remission
BCG
maintenance
366
15
>9
ND
ND
11
Man
80
T1/G
3Yes
No
Remission
BCG
maintenance
1585
18
>7
ND
ND
12.2
Man
68
Cis
Yes
Yes
Remission
BCG
maintenance
959
53
36
9G2
Second
induction
cycle
12.1
Man
68
Cis
Yes
No
Recurrence
Secondinduction
cycle
395
NA
NA
NA
NA
First induction
cycle
13
Man
81
Cis,T1/G
3Yes
No
Recurrence
Cystoprostatectomy
173
NA
NA
ND
ND
14
Man
82
Cis
Yes
No
Recurrence
Cystoprostatectomy
9NA
NA
NA
G3
15
Man
65
Cis,Ta
/G2
Yes
No
Recurrence
Cystoprostatectomy
124
NA
NA
NA
ND
16
Man
69
Cis,T1/G
3No
No
Recurrence
Cystoprostatectomy
37
NA
NA
NA
G3
IDindicatesidentificationnumber;IgG,im
munoglobulin
G,OD,opticaldensity;IgA,im
munoglobulin
A;HSP-65,heat-shockprotein
65;Cis,carcinomain
situ;G,grade;BCG,bacillusCalm
ette-G
uerin;ND,notdone;NA,notavailable.
second induction cycle, a strong antibody increase wasnoted for IgG and IgA (identified as Patient 12.2), andthe patient responded clinically.
Another patient terminated the induction cyclebecause of BCG-induced, irritative side effects (Patient 5)after 4 instillations. Titers were low after the inductioncycle but increased after 3 months, and the patientremained tumor-free.
Histologic Expression of HSP-65
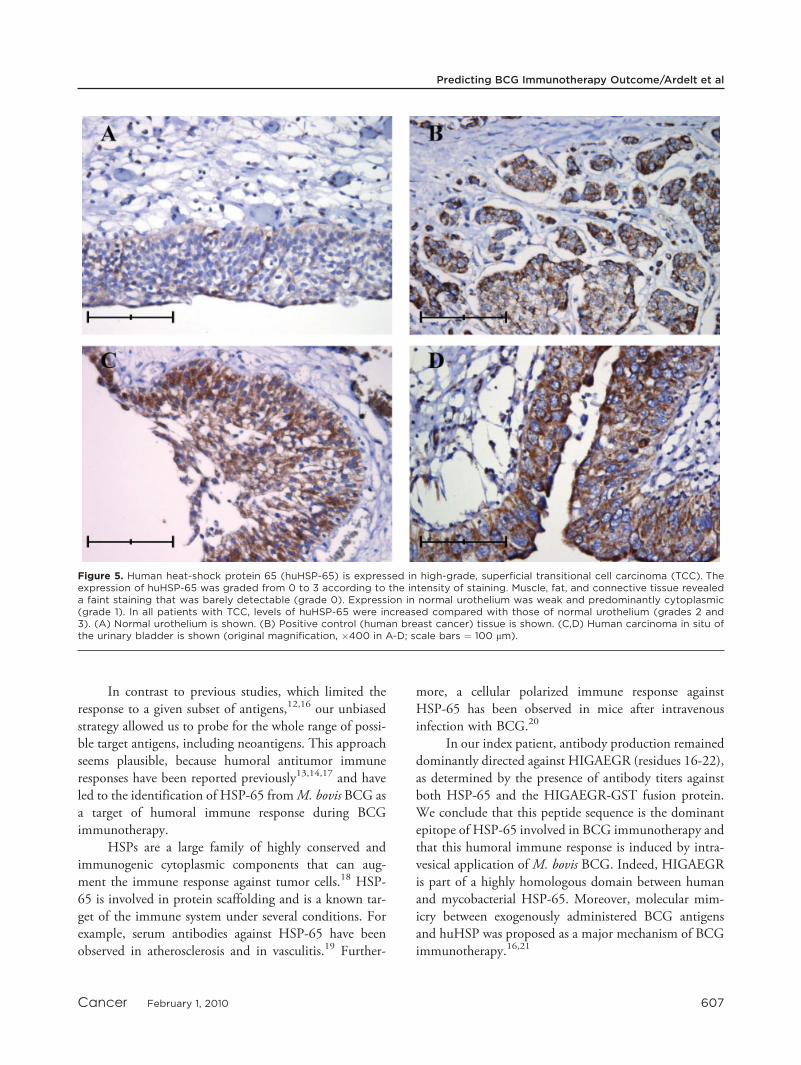
Antibodies induced by BCG immunotherapy may targethuHSP-65 in bladder tumor cells as a consequence of itssimilarity to M. bovis BCG HSP-65. Therefore, we exam-ined the incidence and localization of huHSP-65 in high-grade, superficial TCC (Fig. 5). huHSP-65 was weak in nor-mal urothelium and apparently was elevated in high-gradeTCC (Cis). No differences in expression were noted betweenresponding patients and nonresponding patients (Table 1).
DISCUSSIONBCG immunotherapy traditionally has been used for thetreatment of superficial, high-grade TCC of the bladder.However, unpredictable failure occurs in approximately
33% of patients after the induction cycle, potentiallydelays adequate treatment, and is accompanied by the riskof progression to muscle-invasive disease and distant me-tastasis. Several adverse risk factors, such as incomplete tu-mor resection and age, and positive factors, such assecondary transurethral resection, have been identi-fied.9,10 However, determining the effectiveness of BCGremained indirect and was assessed either cystoscopicallyaccording to the absence or presence of tumor at the timeof re-evaluation, typically 3 months after the initial diag-nosis, or as a statistical factor.
Therefore, we sought to identify a serum marker
that would directly measure the immunostimulatory
effect of BCG and predict the individual outcome of
BCG immunotherapy. For our studies, we used patients
who had high-risk, superficial TCC (eg, Cis or T1/grade
3 tumors) without distinguishing between tumor stages to
rule out the influence of tumor type and to focus on a
BCG-specific marker. We used an antibody-fingerprint-
ing approach11 to evaluate the humoral immune response
through combinatorial selection of a random peptide
phage-display library on IgG isolated from an index
patient after a BCG immunotherapy induction cycle.
Figure 4. High antibody titers against Mycobacterium bovis (M. bovis) bacillus Calmette-Guerin (BCG) heat-shock protein 65(HSP-65) after BCG immunotherapy were identified as predictive of a positive clinical outcome. Bars represent (A) immunoglob-ulin G (IgG) and (B) IgA antibody response at the time of initial diagnosis (Pre BCG), after a BCG induction cycle (Post BCG),and after 6 monthly BCG maintenance instillations (Maint.) against immobilized M. bovis BCG HSP-65. Single asterisks indicateP < .05; double asterisks, P > .05 (Student t test). Bars represent standard error of the mean. NS indicates healthy donor sera;PCA, prostate cancer patient sera; Ta, and T2, T3, sera from patients with different stages of transitional cell carcinoma; O.D.,optical density.
Original Article
606 Cancer February 1, 2010
In contrast to previous studies, which limited theresponse to a given subset of antigens,12,16 our unbiasedstrategy allowed us to probe for the whole range of possi-ble target antigens, including neoantigens. This approachseems plausible, because humoral antitumor immuneresponses have been reported previously13,14,17 and haveled to the identification of HSP-65 fromM. bovis BCG asa target of humoral immune response during BCGimmunotherapy.
HSPs are a large family of highly conserved andimmunogenic cytoplasmic components that can aug-ment the immune response against tumor cells.18 HSP-65 is involved in protein scaffolding and is a known tar-get of the immune system under several conditions. Forexample, serum antibodies against HSP-65 have beenobserved in atherosclerosis and in vasculitis.19 Further-
more, a cellular polarized immune response againstHSP-65 has been observed in mice after intravenousinfection with BCG.20
In our index patient, antibody production remaineddominantly directed against HIGAEGR (residues 16-22),as determined by the presence of antibody titers againstboth HSP-65 and the HIGAEGR-GST fusion protein.We conclude that this peptide sequence is the dominantepitope of HSP-65 involved in BCG immunotherapy andthat this humoral immune response is induced by intra-vesical application of M. bovis BCG. Indeed, HIGAEGRis part of a highly homologous domain between humanand mycobacterial HSP-65. Moreover, molecular mim-icry between exogenously administered BCG antigensand huHSP was proposed as a major mechanism of BCGimmunotherapy.16,21
Figure 5. Human heat-shock protein 65 (huHSP-65) is expressed in high-grade, superficial transitional cell carcinoma (TCC). Theexpression of huHSP-65 was graded from 0 to 3 according to the intensity of staining. Muscle, fat, and connective tissue revealeda faint staining that was barely detectable (grade 0). Expression in normal urothelium was weak and predominantly cytoplasmic(grade 1). In all patients with TCC, levels of huHSP-65 were increased compared with those of normal urothelium (grades 2 and3). (A) Normal urothelium is shown. (B) Positive control (human breast cancer) tissue is shown. (C,D) Human carcinoma in situ ofthe urinary bladder is shown (original magnification, �400 in A-D; scale bars ¼ 100 lm).
Predicting BCG Immunotherapy Outcome/Ardelt et al
Cancer February 1, 2010 607

There is evidence that a mainly cellular immuneresponse is required for successful BCG immunotherapy.6
However, it has been demonstrated that intravesical appli-cation of M. bovis BCG induces TH-2–mediated path-ways. Therefore, it is tempting to speculate that BCGimmunotherapy activates both cellular and humoralimmune effector mechanisms.8 It is uncertain whether theproduction of this antibody is therapeutically effective.We propose that it reflects activation of the immune sys-tem, and, in contrast to cellular activation, titers can bemeasured serially to determine the state of immune activa-tion during and after BCG immunotherapy. It is note-worthy that a patient with BCG-induced urosepsis didnot exhibit an increase in anti-HSP-65 IgG titers, a resultindicating that this immunologic phenomenon is notmerely a sign of nonspecific stress (data not shown).
Our findings are consistent with those of otherinvestigators. Lamm et al demonstrated a positive clinicaloutcome in patients who had an increase in anti-BCGIgG antibodies after BCG immunotherapy.22 Therefore,it was not entirely surprising that an increase in both IgAand IgG titers after immunotherapy had a positive predic-tive value. However, our findings are in contrast withthose of Zlotta et al12 and van der Meijden et al23; bothgroups have reported antibody production against myco-bacterial components as a negative prognostic marker forthe outcome of BCG immunotherapy. However, the dif-ferences in patient selection could explain the diametri-cally opposed results: The patients recruited by Zlottaet al had a history of repeated recurrence and repeated fu-tile intravesical therapies (eg, mitomycin). Because 16 of17 reported patients had low and presumably less aggres-sive grades (from 1 to 2), we propose that these patientshad a high tendency for recurrence.12,23 In our cohort, allpatients had grade 3 disease and had received no priorintravesical therapies. Thus, it is likely that that additionalfactors are determining the high aggressiveness of sometumors. A more extensive study with more patients shouldidentify reasons for the opposing results.
In addition, the data reported here raise questionsabout the optimal BCG immunotherapy regimen. Typi-cally, the induction cycle comprises 6 weekly instillations.In 1 patient, BCG immunotherapy was terminated after 4instillations because of severe side effects. IgG titersagainst HSP-65 increased moderately after 3 months butwere high at the next follow-up after 3 months, and thepatient remained tumor-free. Another patient did notexhibit a significant increase in titers after 6 weekly instil-lations, and that patient developed a clinical recurrence.
After a second induction cycle, his titers increased, and hehas remained tumor-free since that time. Therefore, wepropose an ‘‘individually tailored’’ induction cycle to beachieved by the monitoring of anti-M. bovis BCG HSP-65 titers. In the case of an insufficient increase in titers,additional cycles might be helpful before routine transure-thral biopsy after 3 months. This treatment would be con-sistent with the common clinical practice—in case offailure, a second induction cycle may be performed.24
The histologic expression of huHSP-65 was heterogene-ous; it was elevated in high-grade, superficial TCC, and itwas not suitable as a predictive marker of clinical outcomeafter BCG therapy.
A potential weakness of this study is that it repre-sents results from a single institution and from a relativelysmall number of patients. However, the results were statis-tically significant. Because of the rarity of the disease and atendency toward early cystectomy for T1/grade 3 disease,the patient numbers were low. Therefore, a larger andmulticentric study would be desirable to further verifythese results. This type of study also can rule out the possi-ble influence of results from a single institution, such assurgical factors. Furthermore, such a study would allow aclear multivariate analysis of additional influencing fac-tors, such as age and second transurethral resection beforeBCG immunotherapy.
In summary, to our knowledge, this report is thefirst to demonstrate a humoral immune response againstHSP-65 at the time of re-evaluation after the inductioncycle as a positive predictive marker for individual patientoutcomes from BCG immunotherapy. IgA and IgG titersmeasured before and after the induction cycle predictedthe success of treatment. We propose that monitoringanti-HSP-65 titers during the induction cycle would ena-ble the development of an early assay for the detection ofnonresponders and would lead to a treatment regimendesigned on an individual basis.
CONFLICT OF INTEREST DISCLOSURESThis study was supported by a grant from the InterdisciplinaryCenter for Clinical Research, University of Wurzburg (to P.U.A.).
REFERENCES1. Murakami T, Ebara S, Saika T, et al. Routine transurethral
biopsy of the bladder is not necessary to evaluate theresponse to bacillus Calmette-Guerin therapy. Acta MedOkayama. 2007;61:341-344.
2. Morales A, Eideger D, Bruce A. Intracavitary bacillus Calm-ette-Guerin in the superficial bladder tumor. J Urol.1976;116:180-183.
Original Article
608 Cancer February 1, 2010

3. Sharma P, Old LJ, Allison JP. Immunotherapeutic strategiesfor high-risk bladder cancer. Semin Oncol. 2007;34: 165-172.
4. Herr HW, Schwalb DM, Zhang ZF, et al. Intravesical bacillusCalmette-Guerin therapy prevents tumor progression and deathfrom superficial bladder cancer: ten-year follow-up of a pro-spective randomized trial. J Clin Oncol. 1995;13:1404-1408.
5. Alexandroff AB, Jackson AM, O’Donnell MA, James K.BCG immunotherapy of bladder cancer: 20 years on.Lancet. 1999;353:1689-1694.
6. Saint F, Patard JJ, Maille P, et al. T helper 1/2 lymphocyteurinary cytokine profiles in responding and nonrespondingpatients after 1 and 2 courses of bacillus Calmette-Guerinfor superficial bladder cancer. J Urol. 2001;166:2142-2147.
7. Bohle A, Brandau S. Immune mechanisms in bacillus Calm-ette-Guerin immunotherapy for superficial bladder cancer. JUrol. 2003;170:964-969.
8. Atkins H, Davies BR, Kirby JA, Kelly JD. Polarisation of aT-helper cell immune response by activation of dendriticcells with CpG-containing oligonucleotides: a potential ther-apeutic regime for bladder cancer immunotherapy. Br JCancer. 2003;89:2312-2319.
9. Herr HW. Age and outcome of superficial bladder cancertreated with bacille Calmette-Guerin therapy. Urology.2007;70:65-68.
10. Herr HW. Restaging transurethral resection of high risk su-perficial bladder cancer improves the initial response to bacil-lus Calmette-Guerin therapy. J Urol. 2005;174:2134-2137.
11. Mintz PJ, Kim J, Do KA, et al. Fingerprinting the circulat-ing repertoire of antibodies from cancer patients. Nat Bio-technol. 2003;21:57-63.
12. Zlotta AR, Drowart A, Huygen K, et al. Humoral responseagainst heat shock proteins and other mycobacterial antigensafter intravesical treatment with bacille Calmette-Guerin(BCG) in patients with superficial bladder cancer. Clin ExpImmunol. 1997;109:157-165.
13. Hansson Y, Paulie S, Larsson A, Lundblad ML, Perlmann P,Naslund I. Humoral and cellular immune reactions against tu-mor cells in patients with urinary bladder carcinoma. Correla-tion between direct and antibody-dependent cell-mediatedcytotoxicity. Cancer Immunol Immunother. 1983;16:23-29.
14. Studer UE, deKernion JB, Lovrekovich H, Lovrekovich L.Quantitative measurements of humoral immune response in
mice to a FANFT induced bladder tumor. Urol Res.1985;13:123-130.
15. Pasqualini R, Arap W, Rajotte D, Ruoslahti E. In vivoselection of phage-display libraries. In: Barbas CF 3rd, Bur-ton DR, Scott JK, Silverman GJ, eds. Phage Display: ALaboratory Manual. Cold Spring Harbor, NY: Cold SpringHarbor Laboratory Press; 2000:1-24.
16. Zlotta AR, Van Vooren JP, Denis O, et al. What are theimmunologically active components of bacille Calmette-Guerin in therapy of superficial bladder cancer? Int J Can-cer. 2000;87:844-852.
17. Troye M, Hansson Y, Paulie S, Perlmann P, Blomgren H,Johansson B. Lymphocyte-mediated lysis of tumor cells invitro (ADCC), induced by serum antibodies from patientswith urinary bladder carcinoma or from controls. Int J Can-cer. 1980;25:45-51.
18. Fuller KJ, Issels RD, Slosman DO, Guillet JG, Soussi T,Polla BS. Cancer and the heat shock response. Eur J Cancer.1994;30A:1884-1891.
19. Schett G, Metzler B, Kleindienst R, et al. Myocardial injuryleads to a release of heat shock protein (hsp) 60 and a sup-pression of the anti-hsp65 immune response. Cardiovasc Res.1999;42:685-695.
20. Charo J, Geluk A, Sundback M, et al. The identification of acommon pathogen-specific HLA class I A*0201-restricted cy-totoxic T cell epitope encoded within the heat shock protein65. Eur J Immunol. 2001;31:3602-3611.
21. Bruno S, Machi AM, Semino C, et al. Phenotypic, func-tional and molecular analysis of lymphocytes associated withbladder cancer. Cancer Immunol Immunother. 1996; 42:47-54.
22. Lamm DL, Thor DE, Winters WD, Stogdill VD, RadwinHM. BCG immunotherapy of bladder cancer: inhibition oftumor recurrence and associated immune responses. Cancer.1981;48:82-88.
23. van der Meijden AP, Steerenberg PA, van Hoogstraaten IM,et al. Immune reactions in patients with superficial bladdercancer after intradermal and intravesical treatment with ba-cillus Calmette-Guerin. Cancer Immunol Immunother.1989;28:287-295.
24. van der Meijden AP, Sylvester R, Oosterlinck W, et al.EAU guidelines on the diagnosis and treatment of urothelialcarcinoma in situ. Eur Urol. 2005;48:363-371.
Predicting BCG Immunotherapy Outcome/Ardelt et al
Cancer February 1, 2010 609
Copyright © 2022 FDOKUMEN




















