
RBANS neuropsychological profiles within schizophrenia samples recruited from non-clinical settings
11
RBANS neuropsychological profiles within schizophrenia samples recruited from non-clinical settings Carmel M. Loughland a,b, ⁎ , Terry J. Lewin a,b,c , Vaughan J. Carr a,b , Jim Sheedy a,d , Anthony W. Harris a,d a Neuroscience Institute of Schizophrenia and Allied Disorders (NISAD) 384 Victoria Street Darlinghurst NSW 2010, Australia b Centre for Mental Health Studies University of Newcastle NSW 2308, Australia c Hunter New England Mental Health PO Box 833 Newcastle NSW 2300, Australia d The Brain Dynamics Centre, Westmead Hospital and the University of Sydney, Australia Received 2 June 2006; received in revised form 18 August 2006; accepted 31 August 2006 Available online 17 October 2006 Abstract Background: This paper examines the potential impact of recruitment source differences in schizophrenia research by comparing the neuropsychological performance of volunteers from the NISAD Schizophrenia Research Register with recently published schizophrenia normative data for the Repeatable Battery for Neuropsychological Status (RBANS). Methods: The Register sample comprised 285 volunteers with schizophrenia or schizoaffective disorder. Their RBANS performance was compared with US data from 575 predominantly outpatient-recruited schizophrenia patients. Results: The Register sample displayed impairments in immediate and delayed memory, but near-normal language, attention and visuospatial-constructional performance (mean RBANS total score = 88.72, SD = 16.35). By contrast, health service-recruited schizophrenia patients displayed impairments on all RBANS scales (mean RBANS total score = 70.54, SD = 14.80). Within the Register sample, volunteers with low levels of current functioning had immediate and delayed memory performance comparable to the US schizophrenia sample. Gender and school completion status were also associated with different RBANS profiles. Conclusions: These findings reinforce the notion that a severity/functioning gradient exists across schizophrenia recruitment sources, which has important implications for research design and generalizability. Memory impairments have emerged as a central feature of schizophrenia. © 2006 Elsevier B.V. All rights reserved. Keywords: Neuropsychological tests; Patient selection; Repeatable Battery for Neuropsychological Status (RBANS); Schizophrenia; Selection bias 1. Introduction Schizophrenia is associated with a broad range of cognitive impairments across several domains (Hein- richs and Zakzanis, 1998) including memory, particu- larly verbal (Brebion et al., 2004; Tracy et al., 2001; Tuulio-Henriksson et al., 2004) and working memory (Fuller et al., 2005; Lee and Park, 2005; Silver et al., 2003), attention (Gold et al., 1994, 2003), visuo-spatial Schizophrenia Research 89 (2007) 232 – 242 www.elsevier.com/locate/schres ⁎ Corresponding author. Neuroscience Institute of Schizophrenia and Allied Disorders (NISAD), Centre for Mental Health Studies, PO Box 833 Newcastle 2300, Australia. Tel.: +61 4924 6611; fax: +61 4924 6608. E-mail address: [email protected] (C.M. Loughland). 0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2006.08.022
Transcript of RBANS neuropsychological profiles within schizophrenia samples recruited from non-clinical settings
89 (2007) 232–242www.elsevier.com/locate/schres
Schizophrenia Research
RBANS neuropsychological profiles within schizophreniasamples recruited from non-clinical settings
Carmel M. Loughland a,b,⁎, Terry J. Lewin a,b,c, Vaughan J. Carr a,b,Jim Sheedy a,d, Anthony W. Harris a,d
a Neuroscience Institute of Schizophrenia and Allied Disorders (NISAD) 384 Victoria Street Darlinghurst NSW 2010, Australiab Centre for Mental Health Studies University of Newcastle NSW 2308, Australia
c Hunter New England Mental Health PO Box 833 Newcastle NSW 2300, Australiad The Brain Dynamics Centre, Westmead Hospital and the University of Sydney, Australia
Received 2 June 2006; received in revised form 18 August 2006; accepted 31 August 2006Available online 17 October 2006
Abstract
Background: This paper examines the potential impact of recruitment source differences in schizophrenia research by comparingthe neuropsychological performance of volunteers from the NISAD Schizophrenia Research Register with recently publishedschizophrenia normative data for the Repeatable Battery for Neuropsychological Status (RBANS).Methods: The Register sample comprised 285 volunteers with schizophrenia or schizoaffective disorder. Their RBANSperformance was compared with US data from 575 predominantly outpatient-recruited schizophrenia patients.Results: The Register sample displayed impairments in immediate and delayed memory, but near-normal language, attention andvisuospatial-constructional performance (mean RBANS total score=88.72, SD=16.35). By contrast, health service-recruitedschizophrenia patients displayed impairments on all RBANS scales (mean RBANS total score=70.54, SD=14.80). Within theRegister sample, volunteers with low levels of current functioning had immediate and delayed memory performance comparable tothe US schizophrenia sample. Gender and school completion status were also associated with different RBANS profiles.Conclusions: These findings reinforce the notion that a severity/functioning gradient exists across schizophrenia recruitmentsources, which has important implications for research design and generalizability. Memory impairments have emerged as a centralfeature of schizophrenia.© 2006 Elsevier B.V. All rights reserved.
Keywords: Neuropsychological tests; Patient selection; Repeatable Battery for Neuropsychological Status (RBANS); Schizophrenia; Selection bias
⁎ Corresponding author. Neuroscience Institute of Schizophreniaand Allied Disorders (NISAD), Centre for Mental Health Studies, POBox 833 Newcastle 2300, Australia. Tel.: +61 4924 6611; fax: +614924 6608.
E-mail address: [email protected](C.M. Loughland).
0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2006.08.022
1. Introduction
Schizophrenia is associated with a broad range ofcognitive impairments across several domains (Hein-richs and Zakzanis, 1998) including memory, particu-larly verbal (Brebion et al., 2004; Tracy et al., 2001;Tuulio-Henriksson et al., 2004) and working memory(Fuller et al., 2005; Lee and Park, 2005; Silver et al.,2003), attention (Gold et al., 1994, 2003), visuo-spatial
233C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
ability (Takahashi et al., 2004) and learning (Kurtz et al.,2001). Deficits in memory and attention are observed tobe present at illness onset (Hill et al., 2004), areassociated with earlier disease onset (Tuulio-Henrikssonet al., 2004), and remain relatively stable throughout thecourse of the illness until old age, where furtherdeterioration is observed (Fitzgerald et al., 2004; Harveyet al., 1999). Deficits in memory and attention have beenreported in first-degree relatives of schizophreniaprobands (Sponheim et al., 2004), suggesting a familialtransmission component for these deficits.
Cognitive impairment also appears to be relativelyindependent of symptomatology in schizophrenia(Cornblatt et al., 1999; Goldberg et al., 1995) andresponds minimally even to second generation anti-psychotics (Blyler and Gold, 2000), with ongoingnegative impacts on social and occupational function-ing, despite treatment (Goldberg et al., 1995; Green,1996). For this reason, cognitive deficits may be ofconsiderable prognostic importance in schizophreniaand routine cognitive assessment should be part of goodclinical practice (Gold et al., 1999). However, whilebrief, reliable and easily administered neuropsycholog-ical assessment tools are available, many are notsufficiently sensitive for use in schizophrenia patients(e.g., Mini-Mental State; Gold et al., 1999), or else thereis insufficient normative data available to interpretperformance (Wilk et al., 2004).
The Repeatable Battery for Assessment of Neuro-psychological Status (RBANS; Randolph, 1998) is a USstandardised adult (20–89 years) cognitive screeninginstrument that assesses five cognitive domains: imme-diate memory, visual-constructional ability, language,attention, and delayed memory, as well as a globalmeasure, the RBANS total score. While originallydeveloped as a brief, individually administered neuro-psychological assessment for dementia patients (Ran-dolph et al., 1998), the utility of the RBANS as aneffective screening instrument for schizophrenia hasalso been demonstrated (Dickerson et al., 2004; Goldet al., 1999; Hobart et al., 1999; Wilk et al., 2002).
Several studies provide evidence that the RBANS hasgood sensitivity for detecting cognitive impairments inpeople with schizophrenia. Randolph (1998), in additionto the original RBANS standardisation sample, collecteddata from small clinical samples with various disorders,including a sample of 59 individuals with schizophrenia.The schizophrenia sample had amean RBANS total scoreof 72.8 (SD=16.6), almost 2 SDs below the standardisa-tion (non-clinical or normal population) mean(Mean=100, SD=15 per scale). Patients performedpoorest on indices of immediate memory (Mean=73.8,
SD=18.3), delayed memory (Mean=74.9, SD=19.1)and attention (Mean=77.2, SD=17.5), relative to lan-guage (Mean=83.5, SD=17.5) and visual-constructional(Mean=82.5, SD=21.1) indices. This pattern of perfor-mance in schizophrenia has been replicated in largersamples (Dickerson et al., 2004; Gold et al., 1999; Hobartet al., 1999; Wilk et al., 2002), although, until recently(Wilk et al., 2004), normative data for schizophrenia werenot available. Schizophrenia patients have also beenreported to show marked impairment on the RBANSrelative to patients with bipolar disorder (Hobart et al.,1999; Dickerson et al., 2004).
The RBANS normative data reported by Wilk et al.(2004) is based predominantly on outpatients with adiagnosis of schizophrenia or schizoaffective disorder(N=575: 301 males, 184 females) recruited from twoUS mental health treatment facilities. These data mirrorprevious RBANS findings in that the RBANS totalscore (Mean=70.54, SD=14.80) was approximately 2SDs below the standardisation sample, with the greatestdeficits observed again in memory and attention.Education, but not age, was significantly associatedwith all RBANS index scores, so that better RBANSperformance was associated with higher education level.The authors concluded that their normative dataprovides a useful tool for clinicians to compare thepattern or severity of cognitive impairment in schizo-phrenia patients, and for researchers wanting to relatecognitive performance in their samples to that of a largernormative group.
However, previous research by our group (Lough-land et al., 2004) demonstrates that schizophreniasamples derived from various recruitment sources differon a number of variables of potential relevance (e.g.,illness onset, relationships and supports, current func-tioning, illness course). Therefore, it is unclear as towhat extent poor performance on the RBANS, asreported byWilk et al. (2004) and others, represents coredeficits in cognitive functioning or the consequences ofsampling from treatment settings. Arguably, schizo-phrenia samples recruited from non-clinical (i.e., non-mental health service) and community settings mayhave less cognitive impairment relative to thoserecruited from clinical services. To date, no studieshave reported on RBANS performance in samplesrecruited predominantly from non-clinical and commu-nity settings or in groups outside of the United States.
The NISAD Schizophrenia Research Register is anAustralian volunteer research database of people withschizophrenia and their families who have responded topublic recruitment campaigns to participate in schizophre-nia research projects at a future date (Loughland et al.,
234 C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
2001). This Register provided an opportunity to examineRBANS profiles in a volunteer community sample.Consequently, the purpose of this paper is two-fold: 1) tocompare the neuropsychological performance of Registervolunteers with the schizophrenia normative RBANS dataof Wilk et al. (2004); and 2) to examine RBANSdifferences within subgroups of the current sample definedon the basis of their general functioning. This is the firstpaper to report RBANS data in a large Australiancommunity sample of individuals with schizophrenia.Because there is evidence that the Register samplecomprises a more highly functioning and motivatedschizophrenia group (Loughland et al., 2004), it waspredicted that they would have less cognitive impairmenton the RBANS relative to schizophrenia samples recruitedfrom treatment services (e.g., Wilk et al., 2004), but that thelower functioning Register subgroup would perform at alevel similar to that of the normative RBANS sample.
2. Methods
2.1. Register sample
The NISAD Schizophrenia Research Register is anactive, evolving database of volunteers prepared toparticipate in research projects (Loughland et al., 2001).Register members may be at different stages of theassessment cycle (e.g., initial intake, clinical andneuropsychological assessment, participation in approvedexternal projects supported by the Register, etc.). At thetime of preparation of the current paper, 285 volunteers(147 males, 138 females) with a confirmed ICD-10diagnosis of schizophrenia (N=278) or schizoaffectivedisorder (N=7) had completed an RBANS as part of theircore Register assessments, with 87.4% (N=249) of theseneuropsychological assessments being completed by asingle interviewer. All volunteers were aged 18 years orolder and English speaking. Although none of thevolunteers were hospitalised at the time of assessment,almost all reported using antipsychotic medication.
2.2. Measures
The Diagnostic Interview for Psychosis (DIP; Castleet al., 2006; Jablensky et al., 2000) was used to confirmtheir ICD-10 diagnosis and to collect socio-demographicdata, drug and alcohol usage, and medical and familyhistory information. Neuropsychological performancewas measured using the RBANS (Randolph, 1998) andthe National Adult Reading Test (NART; Nelson, 1982),a measure of premorbid intelligence. Both instrumentshave been found to have good reliability and validity for
use in schizophrenia (Gold et al., 1999; Hobart et al.,1999; Wilk et al., 2002). Current psychopathology wasrated using the Positive and Negative Syndrome Scales(PANSS; Kay et al., 1997), while general functioningwas rated using the Global Assessment of Functioning(GAF) scale (American Psychiatric Association, 1994).Although the psychometric properties of the GAF werenot assessed in the current study, it has been documentedas having satisfactory interrater reliability (Startup et al.,2002), discriminant validity (Greenberg and Rosenheck,2005), and sensitivity to treatment effects (Haddocket al., 2003) in other schizophrenia studies.
As detailed elsewhere (Loughland et al., 2004),selected questions from the World Health OrganizationDisability Assessment Schedule (DAS; WHO, 1988)were used to derive twomeasures of disability: a personaldisability score (range: 0–10) based on five DAS items(participation in household activities, interests, self-care,occupational performance and overall socializing) and asocial disability score (range: 0–6) based on three DASitems (intimate relationships, deterioration in relation-ships and social withdrawal). A measure of face-to-facefamily support was derived from interview items (range0–5), following Carr et al. (2003), while course ofdisorder was measured on a 5-point ordinal scale (singleepisode with good or unknown recovery, multipleepisodes and good recovery, multiple episodes and partialrecovery, chronic illness and little or no deterioration,chronic illness and clear deterioration). Qualified psy-chologists conducted the neuropsychological assessmentsand clinical interviews, and written informed consent wasobtained from all volunteers. To reduce potential fatigueeffects, the neuropsychological assessments were con-ducted prior to the clinical interviews.
2.3. Comparison sample
RBANS normative data for a predominantly outpatientsample of schizophrenia patients has recently beenpublished by Wilk et al. (2004). This sample comprised575 patients (391 males, 184 females) with a DSM-IVdiagnosis of schizophrenia or schizoaffective disorder, whowere recruited from two largeUSAbased treatment settings(i.e.,Maryland Psychiatric ResearchCentre, Sheppard PrattHealth System/Chestnut LodgeHospital). RBANS profilesfor this normative sample are reported later, together withcomparisons with the Register sample (see Table 3).
2.4. Data analysis
Data were analysed using SPSS statistical software(version 12.0). Analyses of variance (ANOVAs) and

235C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
chi-square tests were used to examine differencesbetween subgroups for the continuous and categoricaloutcome variables, respectively, with Scheffé follow-uptests, as appropriate. To facilitate comparisons withother studies, RBANS neuropsychological functioningscores are reported in terms of their standardiseddiscrepancy from the original, non-clinical populationnorms (Mean=100, SD=15 per scale) of Randolph(1998). In this instance, ZN refers to the standardiseddifference (Z-score) between the observed score or meanand the normal population; that is, observed value minus100, and divided by 15. As a partial control for thenumber of statistical tests, the threshold for significancewas set at pb0.01.
3. Results
3.1. Sample characteristics and GAF subgroups
The left-hand columns of Table 1 summarise thedemographic and clinical characteristics of the Registersample. Unlike other studies, the current sample wasdivided equally on several key variables, with approx-imately half of the volunteers being male (51.6%),having a secondary school education or higher (52.9%),being single (i.e., never married, 47.7%), unemployed(53.6%), and having a history of substance abuse ordependence (53.3%). On average, Register volunteerswere almost 40 years of age, with a typical illness onsetaround the age of 21 years. The profile of mean scoresacross the six measures of current functioning reportedin Table 1 is consistent with the moderate overall GAFscore for the sample (Mean=59.49, SD=10.91), whichis above that for schizophrenia samples recruitedthrough mental health services (e.g., medication non-responders; Mean=39.4, SD=10.6) (Christensen et al.,2005) but below that observed for community recruitedpatients participating in substance abuse treatmentstudies (Mean=68.75, SD=12.80) (Baker et al., 2006).
To facilitate an examination of relationships betweencurrent functioning and demographic, clinical andneuropsychological characteristics, the Register samplewas divided into three subgroups based on current levelof functioning: Low (GAF≤50, N=49, 17.2%), Medi-um (GAF 51 to 60,N=120, 42.1%) and High (GAFN60,N=116, 40.7%); the mean GAF scores for these threesubgroups were, respectively, 44.41, 55.71 and 69.78.As shown in the right-hand columns of Table 1, therewere no significant differences between the GAFsubgroups in age, gender, marital status, age at illnessonset, premorbid stressors prior to onset, family historyof psychosis, history of substance abuse or dependence,
or levels of family support. The high functioning GAFsubgroup had a lower proportion of unemployed peoplethan the two other subgroups and there was a statisticallynon-significant trend for a greater proportion of the highfunctioning subgroup to have completed secondaryschool compared to the other two subgroups. The lowand medium GAF subgroups had significantly lowerpremorbid IQs (NART) and a more chronic course ofillness than the high functioning subgroup, but did notdiffer from each other on either of these variables. Interms of the DAS measures of functioning, the low,medium and high GAF subgroups differed significantlyfrom each other in personal disability in the expecteddirection, and the low functioning subgroup showedgreater social disability than the medium and highfunctioning subgroups, which did not differ from eachother. On the PANSS measures of symptomatology,severity of negative symptoms differed significantlybetween each GAF subgroup in the expected direction,as did the general psychopathology measure. Positivesymptomswere higher in the lowGAF subgroup than themedium and high functioning subgroups, which did notdiffer from each other. PANSS total scores differedsignificantly between each subgroup, with symptomseverity decreasing from low through medium to highGAF score subgroups.
3.2. Properties of RBANS subtests and scales
As a check on the likely utility of the RBANSmeasure for Australian, community-recruited schizo-phrenia samples, we undertook a brief review of some ofits psychometric properties. Table 2 reports RBANSsubtest profiles for the Register sample, while thecorresponding scale (or index) scores are summarised inthe left-hand columns of Table 3. An examination of thedistributional characteristics of the 12 RBANS subtests(as reflected in the medians in Table 2) revealed that fourof the subtests were insufficiently challenging for thecurrent sample (i.e., displayed ‘ceiling effects’): figurecopy (with 62.8% scoring 19 or 20); picture naming(with 85.6% scoring 10); digit span (with 43.9% scoring15 or 16); and list recognition (with 60.0% scoring 19 or20). As a consequence, the reliability coefficients(Cronbach alphas) for several of the RBANS scaleswere poor: immediate memory (α=0.73); visual-constructional (α=0.37); language (α=0.07); attention(α=0.22); and delayed memory (α=0.75). However, thefour subtests with ceiling effects were distributed acrossfour of the RBANS scales, and there were still moderateto strong correlations between these scales (rangingfrom r=0.33 to 0.72). The overall reliability of the
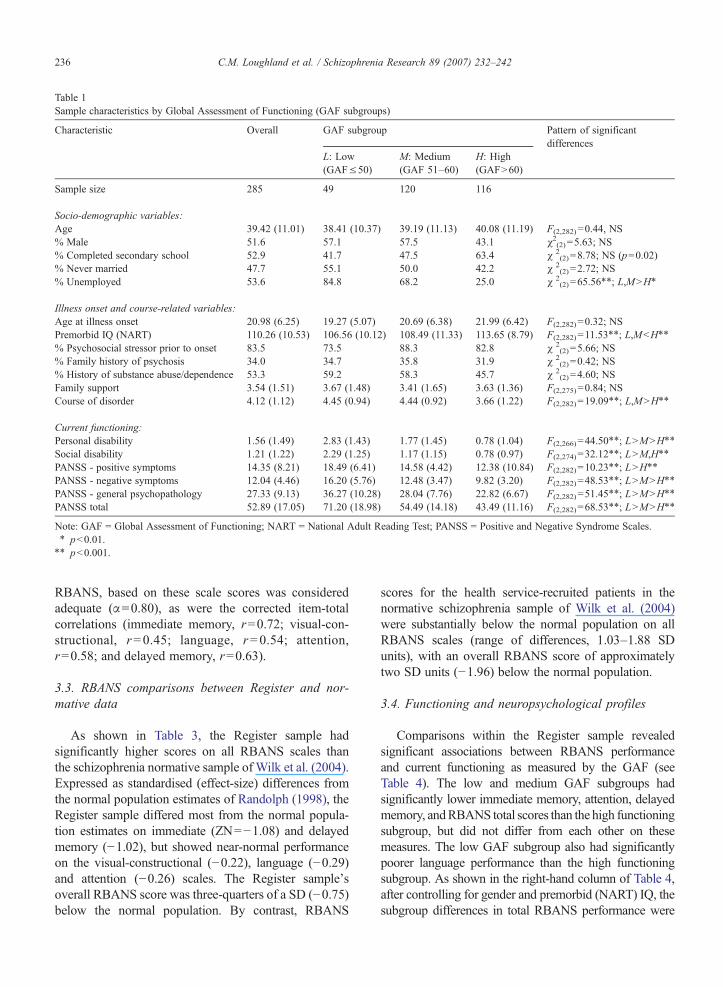
Table 1Sample characteristics by Global Assessment of Functioning (GAF subgroups)
Characteristic Overall GAF subgroup Pattern of significantdifferences
L: Low(GAF≤50)
M: Medium(GAF 51–60)
H: High(GAFN60)
Sample size 285 49 120 116
Socio-demographic variables:Age 39.42 (11.01) 38.41 (10.37) 39.19 (11.13) 40.08 (11.19) F(2,282)=0.44, NS% Male 51.6 57.1 57.5 43.1 χ2(2)=5.63; NS% Completed secondary school 52.9 41.7 47.5 63.4 χ 2
(2)=8.78; NS (p=0.02)% Never married 47.7 55.1 50.0 42.2 χ 2
(2)=2.72; NS% Unemployed 53.6 84.8 68.2 25.0 χ 2
(2)=65.56⁎⁎; L,MNH⁎
Illness onset and course-related variables:Age at illness onset 20.98 (6.25) 19.27 (5.07) 20.69 (6.38) 21.99 (6.42) F(2,282)=0.32; NSPremorbid IQ (NART) 110.26 (10.53) 106.56 (10.12) 108.49 (11.33) 113.65 (8.79) F(2,282)=11.53⁎⁎; L,MbH⁎⁎
% Psychosocial stressor prior to onset 83.5 73.5 88.3 82.8 χ 2(2)=5.66; NS
% Family history of psychosis 34.0 34.7 35.8 31.9 χ 2(2)=0.42; NS
% History of substance abuse/dependence 53.3 59.2 58.3 45.7 χ 2(2)=4.60; NS
Family support 3.54 (1.51) 3.67 (1.48) 3.41 (1.65) 3.63 (1.36) F(2,275)=0.84; NSCourse of disorder 4.12 (1.12) 4.45 (0.94) 4.44 (0.92) 3.66 (1.22) F(2,282)=19.09⁎⁎; L,MNH⁎⁎
Current functioning:Personal disability 1.56 (1.49) 2.83 (1.43) 1.77 (1.45) 0.78 (1.04) F(2,266)=44.50⁎⁎; LNMNH⁎⁎
Social disability 1.21 (1.22) 2.29 (1.25) 1.17 (1.15) 0.78 (0.97) F(2,274)=32.12⁎⁎; LNM,H⁎⁎
PANSS - positive symptoms 14.35 (8.21) 18.49 (6.41) 14.58 (4.42) 12.38 (10.84) F(2,282)=10.23⁎⁎; LNH⁎⁎
PANSS - negative symptoms 12.04 (4.46) 16.20 (5.76) 12.48 (3.47) 9.82 (3.20) F(2,282)=48.53⁎⁎; LNMNH⁎⁎
PANSS - general psychopathology 27.33 (9.13) 36.27 (10.28) 28.04 (7.76) 22.82 (6.67) F(2,282)=51.45⁎⁎; LNMNH⁎⁎
PANSS total 52.89 (17.05) 71.20 (18.98) 54.49 (14.18) 43.49 (11.16) F(2,282)=68.53⁎⁎; LNMNH⁎⁎
Note: GAF = Global Assessment of Functioning; NART = National Adult Reading Test; PANSS = Positive and Negative Syndrome Scales.⁎ pb0.01.⁎⁎ pb0.001.
236 C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
RBANS, based on these scale scores was consideredadequate (α=0.80), as were the corrected item-totalcorrelations (immediate memory, r=0.72; visual-con-structional, r=0.45; language, r=0.54; attention,r=0.58; and delayed memory, r=0.63).
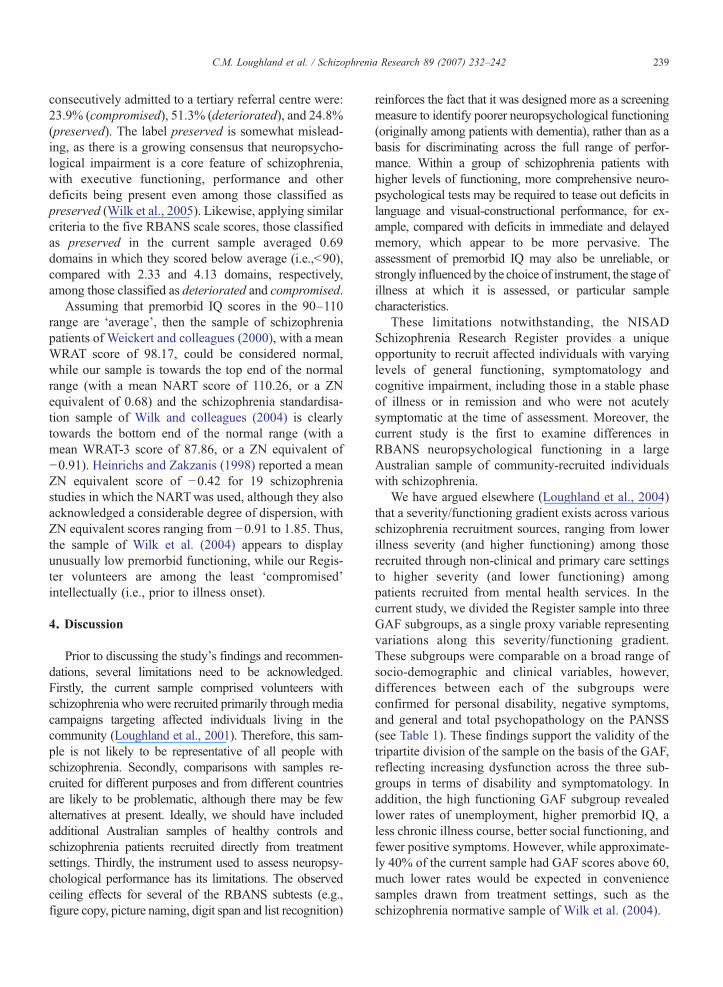
3.3. RBANS comparisons between Register and nor-mative data
As shown in Table 3, the Register sample hadsignificantly higher scores on all RBANS scales thanthe schizophrenia normative sample of Wilk et al. (2004).Expressed as standardised (effect-size) differences fromthe normal population estimates of Randolph (1998), theRegister sample differed most from the normal popula-tion estimates on immediate (ZN=−1.08) and delayedmemory (−1.02), but showed near-normal performanceon the visual-constructional (−0.22), language (−0.29)and attention (−0.26) scales. The Register sample'soverall RBANS score was three-quarters of a SD (−0.75)below the normal population. By contrast, RBANS
scores for the health service-recruited patients in thenormative schizophrenia sample of Wilk et al. (2004)were substantially below the normal population on allRBANS scales (range of differences, 1.03–1.88 SDunits), with an overall RBANS score of approximatelytwo SD units (−1.96) below the normal population.
3.4. Functioning and neuropsychological profiles
Comparisons within the Register sample revealedsignificant associations between RBANS performanceand current functioning as measured by the GAF (seeTable 4). The low and medium GAF subgroups hadsignificantly lower immediate memory, attention, delayedmemory, andRBANS total scores than the high functioningsubgroup, but did not differ from each other on thesemeasures. The low GAF subgroup also had significantlypoorer language performance than the high functioningsubgroup. As shown in the right-hand column of Table 4,after controlling for gender and premorbid (NART) IQ, thesubgroup differences in total RBANS performance were
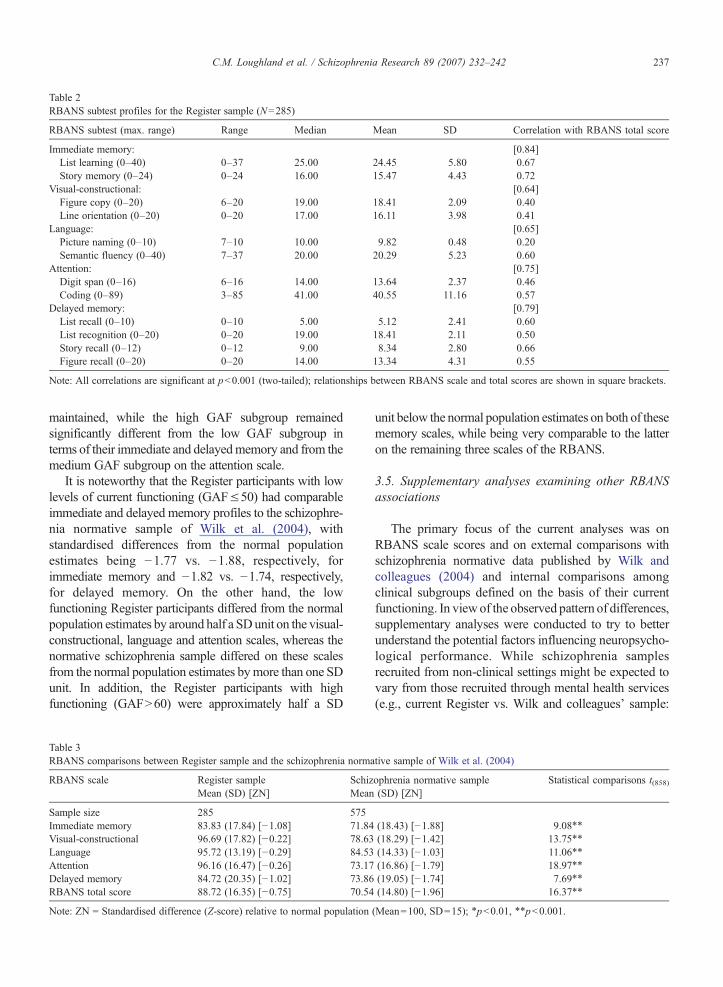
Table 2RBANS subtest profiles for the Register sample (N=285)
RBANS subtest (max. range) Range Median Mean SD Correlation with RBANS total score
Immediate memory: [0.84]List learning (0–40) 0–37 25.00 24.45 5.80 0.67Story memory (0–24) 0–24 16.00 15.47 4.43 0.72
Visual-constructional: [0.64]Figure copy (0–20) 6–20 19.00 18.41 2.09 0.40Line orientation (0–20) 0–20 17.00 16.11 3.98 0.41
Language: [0.65]Picture naming (0–10) 7–10 10.00 9.82 0.48 0.20Semantic fluency (0–40) 7–37 20.00 20.29 5.23 0.60
Attention: [0.75]Digit span (0–16) 6–16 14.00 13.64 2.37 0.46Coding (0–89) 3–85 41.00 40.55 11.16 0.57
Delayed memory: [0.79]List recall (0–10) 0–10 5.00 5.12 2.41 0.60List recognition (0–20) 0–20 19.00 18.41 2.11 0.50Story recall (0–12) 0–12 9.00 8.34 2.80 0.66Figure recall (0–20) 0–20 14.00 13.34 4.31 0.55
Note: All correlations are significant at pb0.001 (two-tailed); relationships between RBANS scale and total scores are shown in square brackets.
237C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
maintained, while the high GAF subgroup remainedsignificantly different from the low GAF subgroup interms of their immediate and delayedmemory and from themedium GAF subgroup on the attention scale.
It is noteworthy that the Register participants with lowlevels of current functioning (GAF≤50) had comparableimmediate and delayed memory profiles to the schizophre-nia normative sample of Wilk et al. (2004), withstandardised differences from the normal populationestimates being −1.77 vs. −1.88, respectively, forimmediate memory and −1.82 vs. −1.74, respectively,for delayed memory. On the other hand, the lowfunctioning Register participants differed from the normalpopulation estimates by around half a SDunit on the visual-constructional, language and attention scales, whereas thenormative schizophrenia sample differed on these scalesfrom the normal population estimates bymore than one SDunit. In addition, the Register participants with highfunctioning (GAFN60) were approximately half a SD
Table 3RBANS comparisons between Register sample and the schizophrenia norma
RBANS scale Register sampleMean (SD) [ZN]
SchizMean
Sample size 285 575Immediate memory 83.83 (17.84) [−1.08] 71.84Visual-constructional 96.69 (17.82) [−0.22] 78.63Language 95.72 (13.19) [−0.29] 84.53Attention 96.16 (16.47) [−0.26] 73.17Delayed memory 84.72 (20.35) [−1.02] 73.86RBANS total score 88.72 (16.35) [−0.75] 70.54
Note: ZN = Standardised difference (Z-score) relative to normal population
unit below the normal population estimates on both of thesememory scales, while being very comparable to the latteron the remaining three scales of the RBANS.
3.5. Supplementary analyses examining other RBANSassociations
The primary focus of the current analyses was onRBANS scale scores and on external comparisons withschizophrenia normative data published by Wilk andcolleagues (2004) and internal comparisons amongclinical subgroups defined on the basis of their currentfunctioning. In viewof the observed pattern of differences,supplementary analyses were conducted to try to betterunderstand the potential factors influencing neuropsycho-logical performance. While schizophrenia samplesrecruited from non-clinical settings might be expected tovary from those recruited through mental health services(e.g., current Register vs. Wilk and colleagues' sample:
tive sample of Wilk et al. (2004)
ophrenia normative sample(SD) [ZN]
Statistical comparisons t(858)
(18.43) [−1.88] 9.08⁎⁎
(18.29) [−1.42] 13.75⁎⁎
(14.33) [−1.03] 11.06⁎⁎
(16.86) [−1.79] 18.97⁎⁎
(19.05) [−1.74] 7.69⁎⁎
(14.80) [−1.96] 16.37⁎⁎
(Mean=100, SD=15); ⁎pb0.01, ⁎⁎pb0.001.

Table 4RBANS comparisons between the Register sample Global Assessment of Functioning (GAF) subgroups
RBANS scale GAF subgroup Pattern of subgroup differences
L: Low (≤50)Mean (SD) [ZN]
M: Medium (51–60)Mean (SD) [ZN]
H: High (N60)Mean (SD) [ZN]
WithoutcovariatesF(2,282)
Controlling forgender andpremorbid IQF(2,280)
Sample size 49 120 116Immediate memory 73.45 (17.57) [−1.77] 81.43 (17.88) [−1.24] 90.70 (15.06) [−0.62] 20.44⁎⁎ L,MbH⁎⁎ 10.38⁎⁎ LbH⁎⁎
Visual-constructional 93.16 (19.24) [−0.46] 94.97 (18.41) [−0.34] 99.96 (16.13) [0.00] 3.53, NS 0.94, NSLanguage 90.27 (17.47) [−0.65] 94.97 (12.67) [−0.34] 98.80 (10.63) [−0.08] 7.92⁎⁎ LbH⁎⁎ 3.80, NSAttention 91.73 (15.01) [−0.55] 91.99 (18.23) [−0.53] 102.34 (12.91) [0.16] 15.15⁎⁎ L,MbH⁎⁎ 6.47⁎⁎ MbH⁎
Delayed memory 72.65 (21.56) [−1.82] 82.32 (19.96) [−1.18] 92.29 (17.05) [−0.51] 19.79⁎⁎ L,MbH⁎⁎ 11.60⁎⁎ LbH⁎⁎
RBANS total score 80.02 (15.80) [−1.33] 85.48 (16.25) [−0.97] 95.75 (13.77) [−0.28] 23.15⁎⁎ L,MbH⁎⁎ 11.80⁎⁎ L⁎⁎,M⁎bH
Note: ZN = Standardised difference (Z-score) relative to normal population (Mean=100, SD=15); ⁎pb0.01, ⁎⁎pb0.001 (Overall ANOVAs orANCOVAs, with Scheffé follow-up tests).
238 C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
51.6% vs. 68.0% male; 0.0% vs. 20.3% inpatients; andmean premorbid IQ, 110.26 vs. 87.86), both sources mayprovide useful insight into the factors associated withcurrent neuropsychological functioning.
In the Register sample, females (N=138) displayedhigher performance than males (N=147) on both theRBANS memory scales: mean immediate memory, 86.79(SD=18.06) vs. 81.05 (SD=17.23), F(1,283) =7.55,pb0.01; mean delayed memory, 88.11 (SD=19.22) vs.81.53 (SD=20.93),F(1, 283)=7.61,pb0.01; correspondingto standardised (ZN) differences of 0.38 to 0.44 units.However, there were no gender effects for the other scalesor RBANS total scores. Conversely, secondary schoolcompleters (N=147) did not differ from non-completers(N=131) on either of the memory scales, but displayedhigher performance on each of the other scales and overall:mean visual-constructional, 99.94 (SD=17.02) vs. 92.46(SD=17.68), F(1,276)=12.90, pb0.001; mean language,97.35 (SD=12.47) vs. 93.50 (SD=13.75), F(1,276)=6.01,p=0.02; mean attention, 100.00 (SD=15.47) vs. 91.64(SD=16.79), F(1,276) = 18.66, pb0.001; and meanRBANS total, 91.63 (SD=15.79) vs. 84.98 (SD=16.34),F(1,276)=11.89, pb0.001; with the latter also being theequivalent of a standardised (ZN) difference of 0.44 units.Or framed differently, even among the subgroup ofsecondary school completers, who displayed normalperformance on the RBANS visual-constructional, lan-guage and attention scales, there were clear memorydeficits: mean immediate memory, 85.78 (SD=16.77);mean delayed memory, 85.33 (SD=19.80).
There was a moderate correlation between RBANStotal scores and premorbid (NART) IQ in the Registersample (r=0.52, pb0.001), which was identical to thatreported by Wilk et al. (2004) for the relationship withpremorbid (WRAT-3) IQ. Moreover, the simple rawscore regression equation linking NART and RBANS
scores in the Register sample was: RBANS=(0.813×NART)+ (−0.955). By plugging the meanWRAT-3 score from the Wilk et al. (2004) sample (of87.86) into this equation, the predicted mean RBANSscore for the US sample would have been 70.48, whichis very close to the published value (of 70.54). In short,the overall difference in RBANS total scores betweenthe two samples appears to be largely proportionate tothe difference in premorbid IQ scores.
The magnitude of the difference between premorbidIQ and RBANS total scores provides a rough guide toeach patient's overall level of deterioration. In the Wilket al. (2004) sample, there was a mean difference of17.96 points (for the 242 patients with WRAT-3 data).By comparison, the mean (NART minus RBANS) dif-ference in the current sample was 21.54 points(SD=14.06), which was statistically significant(F(1,282)=645.96, pb0.001). There was also a lessmarked reduction among the high functioning GAFsubgroup (17.90 points, SD=12.37) than either themedium (23.02 points, SD=14.84; F(1,282) = 8.20,pb0.01) or the low GAF subgroups (26.53 points,SD=13.95; F(1,282)=13.64, pb0.001), reinforcing theassociation between cognitive and general functioning.
Viewed from the cognitive impairment perspectivedescribed by Weickert et al. (2000), patterns ofintellectual functioning within the current samplecould be divided into three categories: intellectuallycompromised (N=15, 5.3%, those with premorbid IQscores below 90); and, among those with premorbid IQscores in the average or above average range (i.e.,≥90),intellectually deteriorated (N=208, 73.0%, those with aNART–RBANS differenceN10 points), or intellectuallypreserved (N=62, 21.8%, those with a difference≤10points). The corresponding rates in Weickert andcolleagues (2000) study of 117 schizophrenia patients
239C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
consecutively admitted to a tertiary referral centre were:23.9% (compromised), 51.3% (deteriorated), and 24.8%(preserved). The label preserved is somewhat mislead-ing, as there is a growing consensus that neuropsycho-logical impairment is a core feature of schizophrenia,with executive functioning, performance and otherdeficits being present even among those classified aspreserved (Wilk et al., 2005). Likewise, applying similarcriteria to the five RBANS scale scores, those classifiedas preserved in the current sample averaged 0.69domains in which they scored below average (i.e.,b90),compared with 2.33 and 4.13 domains, respectively,among those classified as deteriorated and compromised.
Assuming that premorbid IQ scores in the 90–110range are ‘average’, then the sample of schizophreniapatients of Weickert and colleagues (2000), with a meanWRAT score of 98.17, could be considered normal,while our sample is towards the top end of the normalrange (with a mean NART score of 110.26, or a ZNequivalent of 0.68) and the schizophrenia standardisa-tion sample of Wilk and colleagues (2004) is clearlytowards the bottom end of the normal range (with amean WRAT-3 score of 87.86, or a ZN equivalent of−0.91). Heinrichs and Zakzanis (1998) reported a meanZN equivalent score of −0.42 for 19 schizophreniastudies in which the NARTwas used, although they alsoacknowledged a considerable degree of dispersion, withZN equivalent scores ranging from −0.91 to 1.85. Thus,the sample of Wilk et al. (2004) appears to displayunusually low premorbid functioning, while our Regis-ter volunteers are among the least ‘compromised’intellectually (i.e., prior to illness onset).
4. Discussion
Prior to discussing the study's findings and recommen-dations, several limitations need to be acknowledged.Firstly, the current sample comprised volunteers withschizophrenia who were recruited primarily through mediacampaigns targeting affected individuals living in thecommunity (Loughland et al., 2001). Therefore, this sam-ple is not likely to be representative of all people withschizophrenia. Secondly, comparisons with samples re-cruited for different purposes and from different countriesare likely to be problematic, although there may be fewalternatives at present. Ideally, we should have includedadditional Australian samples of healthy controls andschizophrenia patients recruited directly from treatmentsettings. Thirdly, the instrument used to assess neuropsy-chological performance has its limitations. The observedceiling effects for several of the RBANS subtests (e.g.,figure copy, picture naming, digit span and list recognition)
reinforces the fact that it was designed more as a screeningmeasure to identify poorer neuropsychological functioning(originally among patients with dementia), rather than as abasis for discriminating across the full range of perfor-mance. Within a group of schizophrenia patients withhigher levels of functioning, more comprehensive neuro-psychological tests may be required to tease out deficits inlanguage and visual-constructional performance, for ex-ample, compared with deficits in immediate and delayedmemory, which appear to be more pervasive. Theassessment of premorbid IQ may also be unreliable, orstrongly influenced by the choice of instrument, the stage ofillness at which it is assessed, or particular samplecharacteristics.
These limitations notwithstanding, the NISADSchizophrenia Research Register provides a uniqueopportunity to recruit affected individuals with varyinglevels of general functioning, symptomatology andcognitive impairment, including those in a stable phaseof illness or in remission and who were not acutelysymptomatic at the time of assessment. Moreover, thecurrent study is the first to examine differences inRBANS neuropsychological functioning in a largeAustralian sample of community-recruited individualswith schizophrenia.
We have argued elsewhere (Loughland et al., 2004)that a severity/functioning gradient exists across variousschizophrenia recruitment sources, ranging from lowerillness severity (and higher functioning) among thoserecruited through non-clinical and primary care settingsto higher severity (and lower functioning) amongpatients recruited from mental health services. In thecurrent study, we divided the Register sample into threeGAF subgroups, as a single proxy variable representingvariations along this severity/functioning gradient.These subgroups were comparable on a broad range ofsocio-demographic and clinical variables, however,differences between each of the subgroups wereconfirmed for personal disability, negative symptoms,and general and total psychopathology on the PANSS(see Table 1). These findings support the validity of thetripartite division of the sample on the basis of the GAF,reflecting increasing dysfunction across the three sub-groups in terms of disability and symptomatology. Inaddition, the high functioning GAF subgroup revealedlower rates of unemployment, higher premorbid IQ, aless chronic illness course, better social functioning, andfewer positive symptoms. However, while approximate-ly 40% of the current sample had GAF scores above 60,much lower rates would be expected in conveniencesamples drawn from treatment settings, such as theschizophrenia normative sample of Wilk et al. (2004).

240 C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
With respect to cognitive functioning, the Registersample was 0.75 SD below the normal population on theRBANS total score, due primarily to their poorerperformance on each of the immediate memory anddelayed memory scales. In contrast, the normativeschizophrenia sample was approximately 2 SDs belowthe normal population on the RBANS total score, andthis was more-or-less uniform across all of the scales.The Register sample was clearly less cognitivelyimpaired overall than the normative schizophreniasample, particularly on the visual-constructional, lan-guage and attention scales, but was comparatively closerto the normative schizophrenia sample on the immediatememory and delayed memory scales. These findingsconfirm the expected higher level of cognitive function-ing in the Register sample, but also identify substantialimmediate and delayed memory deficits as prominentfeatures of schizophrenia regardless of sampling sources.
Within the Register sample, and controlling forgender and premorbid IQ, cognitive functioning wasclearly associated with different levels of generalfunctioning as measured by the GAF (see Table 4).The high GAF subgroup was clearly less cognitivelyimpaired than the medium and low GAF subgroups onRBANS total score, and similarly less cognitivelyimpaired than the low GAF subgroup on immediateand delayed memory. Notwithstanding this lesser degreeof cognitive impairment, the high GAF subgroup stilldiffered from the normal population estimates by morethan half a SD on immediate and delayed memory, whilebeing comparable to the normal population on all othersubscales, as well as differing by only 0.28 SD on theRBANS total score. On the other hand, the low GAFsubgroup showed the closest similarity in cognitiveprofile to the normative schizophrenia sample, particu-larly in relation to immediate and delayed memory.However, the differences between them on the visual-constructional, language and attention subscales (SDdifferences of 0.96, 0.38 and 1.24, respectively) are moredifficult to explain, except to suggest that these cognitivefunctions may relate to premorbid functioning, illnessacuity, medication effects or to other influences notcaptured in the datasets, such as socio-economic factors.
The supplementary analyses examining RBANSassociations with gender, school completion and pre-morbid IQ further highlighted the key role played bymemory deficits. Gender and school completion wereassociated differently with neuropsychological perfor-mance. Females displayed less marked memory deficitsthan males, possibly indicative of a less severe form ofschizophrenia (Leung and Chue, 2000), while schoolcompleters displayed clear memory deficits but normal
visual-constructional, language and attentional perfor-mance, suggestive of either a post-school illness onset orpositive impacts on these cognitive domains associatedwith school attendance. Observed sample differences inoverall RBANS performance were also consistent withthe magnitude of differences in premorbid functioning.Moreover, three-quarters of the Register sample dis-played evidence of intellectual deterioration (Weickertet al., 2000), which was comparable in scale to thatreported by Wilk et al. (2004).
The most parsimonious explanation for the pattern ofresults reported here and by Wilk et al. (2004) is thatmemory deficits are a central feature of schizophrenia,whose severity largely parallels current functioning(which also tends to be poorer among males). Otherneuropsychological deficits are either less pervasive,influenced more by sampling source or characteristics,or phase of illness, or they are simply more difficult toassess reliably, particularly in higher or lower function-ing samples. It could also be the case that differentillness trajectories are associated with different neuro-psychological and functioning profiles (e.g., earlieronset with more marked attentional, language andvisual-constructional deficits and, consequently, poorerschool performance and higher unemployment).
In the absence of comprehensive RBANS normativedata for schizophrenia across the full range of cognitivefunctioning (i.e., including samples recruited from non-clinical settings), it may be appropriate to consult theRBANS subtest profiles for the different levels of educationreported byWilk et al. (2004, Table 5). Such a suggestion isreinforced by the fact that Wilk et al. (2004) foundsignificant associations between education and each of theRBANS index and subtest scores. By way of illustration,theRegister recruited sample fell between the 50th and 75thpercentile on the “educationNhigh school” norms reportedby Wilk et al. (2004) across the twelve RBANS subtests,averaging around the 66th percentile; or alternatively, forthe “education=high school” norms, the current sampleaveraged around the 77th percentile. While level ofeducation is a useful proxy for some aspects of cognitivefunctioning, it is still essential to develop a more completeset of norms for the RBANS.
In conclusion, it is evident that variation in source ofrecruitment can significantly influence the observedlevels of cognitive impairment in schizophrenia, as mea-sured by a standardised neuropsychological test battery.Cognitive impairment is also associated with degree offunctional disability, but immediate and delayedmemorydeficits remain prominent regardless of recruitmentsource and level of functional disability. These findingsare compatible with an expanding set of studies that
241C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
consistently report memory dysfunction as a centralfeature of schizophrenia (Brebion et al., 2004; Fulleret al., 2005; Lee and Park, 2005; Lencz et al., 2006;Silver et al., 2003; Takahashi et al., 2004; Wilk et al.,2005), including among patients in the prodromal stagesof first episode schizophrenia (Lencz et al., 2006; Wilket al., 2005). The other cognitive abnormalities that havebeen observed in schizophrenia samples may arise as aresult of other, non-core factors (e.g., phase of illness,medication side effects).
We have previously reported that source of patientrecruitment is associated with wide differences in illnessonset factors, relationship and support factors, levels offunctioning and illness course (Loughland et al., 2004).The present study demonstrates that source of recruit-ment can also influence the degree and pattern ofcognitive deficits. Schizophrenia research publicationsrarely take sampling sources into account, there being“an implicit assumption that … one schizophreniasample should be pretty similar to another” (Craddocket al., 2006), and many research findings are likely to bebased on non-representative schizophrenia samples thatdiffer from each other in important ways. We suggestthat this may bias research findings in ways that arerarely discussed. However, the role of differing ascer-tainment procedures has been acknowledged in thecontext of genetic studies by Craddock et al. (2006),who state that these procedures are likely to lead tosamples differing in severity, chronicity and treatment –and, we would add, cognitive functioning – that may beinfluenced by genes that do not increase the risk of thedisorder. We acknowledge that the Register sample isskewed towards more highly functioning and less cog-nitively impaired individuals. However, we would alsoargue that the sample recruited from treatment settingsby Wilk et al. (2004) is not representative of the popula-tion of people with schizophrenia either, being skewedtowards more disabled and more cognitively impairedindividuals.
In addition to the above, recent Australian data (Carret al., 2002) suggests that, in any given year, almost two-thirds (63.2%) of patients with schizophrenia are not indirect contact with community or inpatient mentalhealth services, receiving the majority of their carefrom general practitioners. Since patients recruitedthrough the Register tend to be similar to those recruitedthrough general practice (Loughland et al., 2004), itcould be argued that representative samples would needto recruit a minimum of half of their participants throughsources such as the Register, general practice, or othergeneral community settings. A truly representative sam-ple of people with schizophrenia needs to encompass
both ends of the spectrum and recruit from a wider rangeof sources than is currently usual practice in schizo-phrenia research.
Acknowledgements
The authors thank the NISAD Schizophrenia Re-search Register, Australia, and its volunteers withschizophrenia for providing the data used in thisresearch. NISAD is supported by infrastructure fundingfrom New South Wales Health.
References
American Psychiatric Association, 1994. Diagnostic Criteria from DSM-IV-TR. American Psychiatric Association Inc., Arlington, VA.
Baker, A., Bucci, S., Lewin, T.J., Kay-Lambkin, F., Constable, P.M.,Carr, V.J., 2006. Cognitive-behaviour therapy for substance usedisorders in people with psychotic disorders: randomised con-trolled trial. Br. J. Psychiatry 188, 439–448.
Blyler, C.R., Gold, J.M., 2000. Cognitive effects of typical antipsychotictreatment: another look. In: Sharma, T., Harvey, P.D. (Eds.), Cognitionin Schizophrenia. Oxford University Press, New York.
Brebion, G., David, A.S., Jones, H., Pilowsky, L.S., 2004. Semanticorganization and verbal memory efficiency in patients withschizophrenia. Neuropsychology 18, 378–383.
Carr, V.J., Lewin, T.J., Barnard, R.E., Walton, J.M., Allen, J.L.,Constable, P.M., Chapman, J.L., 2002. Comparisons betweenschizophrenia patients recruited from Australian general practicesand public mental health services. Acta Psychiatr. Scand. 105,346–355.
Carr, V.J., Johnston, P.J., Lewin, T.J., Rajkumar, S., Carter, G.L.,Issakidis, C., 2003. Patterns of service use among persons withschizophrenia and other psychotic disorders. Psychiatr. Serv. 54,226–235.
Castle, D.J., Jablensky, A., McGrath, J.J., Carr, V., Morgan, V.,Waterreus, A., Valuri, G., Stain, H., McGuffin, P., Farmer, A.,2006. The diagnostic interview for psychoses (DIP): development,reliability and applications. Psychol. Med. 36, 69–80.
Christensen, A.F., Poulsen, J., Nielsen, C.T., Bork, B., Christensen, A.,Christensen, M., 2005. Patients with schizophrenia treated witharipiprazole: a multicentre naturalistic study. Acta Psychiatr.Scand. 113, 148–153.
Cornblatt, B., Obuchowski, M., Roberts, S., Pollack, S., Erlenmeyer-Kimling, L., 1999. Cognitive and behavioural precursors ofschizophrenia. Dev. Psychopathol. 11, 487–508.
Craddock, N., Owen, M.J., O'Donovan, M.C., 2006. The catechol-O-methyl transferase (COMT) gene as a candidate for psy-chiatric phenotypes: evidence and lessons. Mol. Psychiatry 11,446–458.
Dickerson, F., Boronow, J.J., Stallings, C., Origoni, A.E., Cole, S.K.,Yolken, R.H., 2004. Cognitive functioning in schizophrenia andbipolar disorder: comparison of performance on the RepeatableBattery for the Assessment of Neuropsychological Status.Psychiatry Res. 129, 45–53.
Fitzgerald, D., Lucas, S., Redoblado, M.A., Winter, V., Brennan, J.,Anderson, J., Harris, A., 2004. Cognitive functioning in youngpeople with first episode psychosis: relationship to diagnosis andclinical characteristics. Aust. N. Z. J. Psychiatry 38, 501–510.
242 C.M. Loughland et al. / Schizophrenia Research 89 (2007) 232–242
Fuller, R.L., Luck, S.J., McMahon, R.P., Gold, J.M., 2005. Workingmemory consolidation is abnormally slow in schizophrenia. J.Abnorm.Psychology 114, 279–290.
Gold, J., Hermann, B., Wyler, A., Goldberg, T., Weinberger, D., 1994.Schizophrenia and temporal lobe epilepsy: a neurological analysis.Arch. Gen. Psychiatry 51, 265–272.
Gold, J., Queern, B., Iannone, V.N., Buchanan, R.W., 1999.Repeatable Battery for the Assessment of NeuropsychologicalStatus as a screening test in schizophrenia, I: sensitivity, reliabilityand validity. Am. J. Psychiatry 156, 1944–1950.
Gold, J.M., Wilk, C.M., McMahon, R.P., Buchanan, R.W., Luck, S.J.,2003. Working memory for visual features and conjunctions inschizophrenia. J. Abnorm. Psychology 112, 61–71.
Goldberg, T.E., Torrey, E.F., Gold, J.M., Bigelow, L.B., Ragland, R.D.,Taylor, E.,Weinberger, D.R., 1995. Genetic risk of neuropsychologicalimpairment in schizophrenia: a study of monozygotic twins discordantand concordant for the disorder. Schizophr. Res. 17, 77–84.
Green,M.F., 1996.What are the functional consequences of neurocognitivedeficits in schizophrenia? Am. J. Psychiatry 153, 321–330.
Greenberg, G.A., Rosenheck, R.A., 2005. Using the GAF as a nationalmental health outcome measure in the Department of VeteransAffairs. Psychiatr. Serv. 56, 420–426.
Haddock, G., Barrowclough, C., Tarrier, N., Moring, J., O'Brien, R.,Schofield, N., Quinn, J., Palmer, S., Davies, L., Lowens, I.,McGovern, J., Lewis, S., 2003. Cognitive-behavioural therapy andmotivational intervention for schizophrenia and substance misuse:18-month outcomes of a randomised controlled trial. Br. J.Psychiatry 183, 418–426.
Harvey, P.D., Silverman, J.M., Mobs, R.C., Parrella, M., White, L.,Powchik, P., Davidson, M., Davis, K.L., 1999. Cognitive declinein late-life schizophrenia: a longitudinal study of geriatricchronically hospitalised patients. Biol. Psychiatry 45, 32–40.
Heinrichs, R.W., Zakzanis, K.K., 1998. Neurocognitive deficit inschizophrenia: a quantitative review of the evidence. Neuropsychology12, 426–445.
Hill, S.K., Schuepbach, D., Herbener, E.S., Keshavan, M.S., Sweeney,J.A., 2004. Pretreatment and longitudinal studies of neuropsycho-logical deficits in antipsychotic-naïve patients with schizophrenia.Schizophr. Res. 68, 49–63.
Hobart, M., Goldberg, R., Bartko, J., Gold, J., 1999. RepeatableBattery for the Assessment of Neuropsychological Status as ascreening test in schizophrenia, II: convergent/discriminantvalidity and diagnostic group comparisons. Am. J. Psychiatry156, 1952–1957.
Jablensky, A., McGrath, J., Herrman, H., Castle, D., Gureje, O., Evans,M., Carr, V., Morgan, V., Korten, A., Harvey, C., 2000. Psychoticdisorders in urban areas: an overview of the study on lowprevalence disorders. Aust. N. Z. J. Psychiatry 34, 221–236.
Kay, S.R., Fiszbein, A., Opler, L.A., 1997. The Positive and NegativeSyndrome Scale (PANSS) for schizophrenia. Schizophr. Bull. 13,261–276.
Kurtz, M., Moberg, P., Mozley, L., Hickey, T., Arnold, S., Biller, W.,Gurr, R., 2001. Cognitive impairment and functional status inelderly institutionalised patients with schizophrenia. Int. J. Geriatr.Psychiatry l16, 631–638.
Lee, J., Park, S., 2005. Working memory impairments in schizophre-nia: a meta-analysis. J. Abnorm. Psychology 114, 599–611.
Lencz, T., Smith, W.C., McLaughlin, D., Auther, A., Nakayama, E.,Hovey, L., Cornblatt, B.A., 2006. Generalized and specific
neurocognitive deficits in prodromal schizophrenia. Biol. Psychiatry59, 863–871.
Leung, A., Chue, P., 2000. Sex differences in schizophrenia: a reviewof the literature. Acta Psychiatr. Scand., Suppl. 401, 3–38.
Loughland, C.M., Carr, V.J., Lewin, T.J., 2001. The NISADSchizophrenia Research Register: why do we need a database ofschizophrenia volunteers? Aust. N. Z. J. Psychiatry 35, 660–667.
Loughland, C.M., Carr, V.J., Lewin, T.J., Barnard, R.E., Chapman, J.L.,Walton, J.M., 2004. Potential sampling and recruitment sourceimpacts in schizophrenia research. Psychiatry Res. 125, 117–127.
Nelson, H.E., 1982. National Adult Reading Test (NART): TestManual. NFER-Nelson, Windsor.
Randolph, C., 1998. Repeatable Battery for the Assessment ofNeuropsychological Status (RBANS): Test Manual. HarcourtBrace and Company, San Antonio.
Randolph, C., Tierney, M., Mohr, E., Chase, T., 1998. The RepeatableBattery for the Assessment of Neuropsychological Status(RBANS): preliminary clinical validity. J. Clin. Exp. Neuropsy-chol. 20, 310–319.
Silver, H., Feldman, P., Bilker, W., Gur, R.C., 2003. Working memorydeficit as a core neuropsychological dysfunction in schizophrenia.Am. J. Psychiatry 160, 1809–1816.
Sponheim, S.R., Steele, V.R., McGuire, K.A., 2004. Verbal memoryprocesses in schizophrenia patients and biological relatives ofschizophrenia patients: intact implicit memory, impaired explicitrecollection. Schizophr. Res. 71, 339–348.
Startup, M., Jackson, M.C., Bendix, S., 2002. The concurrent validityof the Global Assessment of Functioning (GAF). Br. J. Clin.Psychol. 41, 417–422.
Takahashi, H., Iwase, M., Nakahachi, T., Sekiyama, R., Tabushi, K.,Kajimoto, O., Shimizu, A., Takeda, M., 2004. Spatial workingmemory deficit correlates with disorganization symptoms andsocial functioning in schizophrenia. Psychiatry Clin. Neurosci. 59,453–460.
Tracy, J., Mattson, R., King, C., Bundick, T., Celenza, M., Glosser, G.,2001. A comparison of memory for verbal and non-verbal materialin schizophrenia. Schizophr. Res. 50, 199–211.
Tuulio-Henriksson, A., Partonen, T., Suvisaari, J., Haukka, J.,Lonnqvist, J., 2004. Age at onset and cognitive functioning inschizophrenia. Br. J. Psychiatry 185, 215–219.
Weickert, T.W., Goldberg, T.E., Gold, J.M., Bigelow, L.B., Egan, M.F.,Weinberger, D.R., 2000. Cognitive impairments in patients withschizophrenia displaying preserved and compromised intellect.Arch. Gen. Psychiatry 57, 907–913.
Wilk, C.M., Gold, J.M., Bartko, J.J., Dickerson, F., Fenton, W.S.,Knable, M., Randolph, C., Buchanan, R.W., 2002. Test–reteststability of the Repeatable Battery for the Assessment ofNeuropsychological Status in schizophrenia. Am. J. Psychiatry159, 838–844.
Wilk, C.M., Gold, J.M., Humber, K., Dickerson, F., Fenton, W.S.,Buchanan, R.W., 2004. Brief cognitive assessment in schizophrenia:normative data for the Repeatable Battery for the Assessment ofNeuropsychological Status. Schizophr. Res. 70, 175–186.
Wilk, C.M., Gold, J.M., McMahon, R.P., Humber, K., Iannone, V.N.,Buchanan, R.W., 2005. No, it is not possible to be schizophrenicyet neuropsychologically normal. Neuropsychology 19, 778–786.
World Health Organization,1998. WHO Psychiatric Disability As-sessment Schedule (WHO/DAS). World Health Organization,Geneva.




















