Ratios of Nine Risk Factors in Children With Recurrent Febrile Seizures
6
Ratios of Nine Risk Factors in Children With Recurrent Febrile Seizures Ayse Tosun, MD*, Guldane Koturoglu, MD † , Gul Serdaroglu, MD † , Muzaffer Polat, MD ‡ , Zafer Kurugol, MD † , Sarenur Gokben, MD † , and Hasan Tekgul, MD † Febrile seizures are the most common convulsive disorder of childhood, with a recurrence probability of 33%. The aim of the study was to determine the risk factors for re- currence of febrile seizures in children. In this descriptive, cross-sectional study, nine risk factors of recurrence of febrile seizures were investigated in 259 children with febrile seizures: (1) sex; (2) domicile; (3) income level; (4) family history of febrile seizures; (5) family history of epilepsy; (6) level of fever; (7) duration of fever; (8) type of seizure, simple vs complex; and (9) age at seizure onset. The risk factors were compared for 119 children with isolated febrile seizures (45.9% of the total) and 140 children with two or more febrile seizure recurrences (54.1%). Among the patients with and without recurrent febrile seizures, 32% and 18% were domiciled in nonur- ban areas, respectively (P = 0.012). There was a family his- tory of febrile seizures in 57% and 44% of cases with and without recurrent febrile seizures, respectively (P = 0.031). According to the logistic regression analysis, a fam- ily history of febrile seizures was a risk factor that affected recurrence (P = 0.018; odds ratio OR = 1.933; 95% confi- dence interval CI = 1.121-3.333). We also found that domi- cile (P = 0.001) and income (P = 0.013) were risk factors for recurrence. A family history of epilepsy was not a sig- nificant risk factor (P = 0.129; OR = 2.110; 95% CI = 0.804-5.539). Ó 2010 by Elsevier Inc. All rights reserved. Tosun A, Koturoglu G, Serdaroglu G, Polat M, Kurugol Z, Gokben S, Tekgul H. Ratios of nine risk factors in children with recurrent febrile seizures. Pediatr Neurol 2010;43:177- 182. Introduction Epidemiologic studies have demonstrated the importance of environmental and personal factors, particularly genetic factors, in the development of first febrile seizures in chil- dren, as well as recurrent febrile convulsions [1-8]. Although febrile seizures are generally benign, they remain important, based on the risk of developing epilepsy (a relatively low risk) but especially on risk of recurrence, seen in 23-42% of cases [1,5,9-11]. The decision to initiate prophylaxis and determining the prognosis of febrile seizures are important issues for the clinician. A family history of febrile seizures, early age at onset, lower temperature at the time of febrile seizures, and shorter duration of fever before the febrile seizures are the significant risk factors for recurrent febrile seizures [1,9,10,12,13]. Although a family history of epilepsy, seizures with complex features, and neurodevelopmental abnormality are known risk factors for developing epilepsy, their status as risk factors for recurrent febrile seizures remains controversial [1,4,8,10,13,14]. For two of the generally accepted risk factors for recurrent febrile seizures (i.e., for the level of fever required to diagnose febrile seizure and for the duration of fever prior to the seizure), different definitions have been used in different studies [1,7,9,10,12]. The objective of the present study was to determine the ratios of nine generally accepted risk factors for recurrent febrile seizures in a sample of children with and without recurrent febrile seizures. Methods and Patients Risk Factors, Study Population, and Methods The study was designed to address nine generally accepted risk factors for recurrent febrile seizures: (1) sex; (2) domicile of family, urban vs non- urban; (3) income level of family, relative to subsistence; (4) family history of febrile seizures; (5) family history of epilepsy; (6) level of fever causing seizures, (7) duration of fever before seizures, (8) type of seizure, simple vs complex; and (9) age at seizure onset. From the *Department of Pediatrics, Adnan Menderes University Medical Faculty, Aydin, Turkey; the † Department of Pediatrics, Ege University Medical Faculty, Izmir, Turkey; and the ‡ Department of Pediatrics, Celal Bayar University Medical Faculty, Manisa, Turkey. Communications should be addressed to: Dr. Koturoglu; Department of Pediatrics; Ege University Medical School; 35040 Bornova-Izmir, Turkey. E-mail: [email protected] Received December 31, 2009; accepted May 3, 2010. Ó 2010 by Elsevier Inc. All rights reserved. doi:10.1016/j.pediatrneurol.2010.05.007 0887-8994/$—see front matter Tosun et al: Risk Factors in Febrile Seizures 177
-
Upload
adnanmenderes -
Category
Documents
-
view
0 -
download
0
Transcript of Ratios of Nine Risk Factors in Children With Recurrent Febrile Seizures

Ratios of Nine Risk Factors in Children With
Recurrent Febrile SeizuresAyse Tosun, MD*, Guldane Koturoglu, MD†, Gul Serdaroglu, MD†, Muzaffer Polat, MD‡,
Zafer Kurugol, MD†, Sarenur Gokben, MD†, and Hasan Tekgul, MD†
Febrile seizures are the most common convulsive disorderof childhood, with a recurrence probability of 33%. Theaim of the study was to determine the risk factors for re-currence of febrile seizures in children. In this descriptive,cross-sectional study, nine risk factors of recurrence offebrile seizures were investigated in 259 children withfebrile seizures: (1) sex; (2) domicile; (3) income level;(4) family history of febrile seizures; (5) family historyof epilepsy; (6) level of fever; (7) duration of fever; (8)type of seizure, simple vs complex; and (9) age at seizureonset. The risk factors were compared for 119 childrenwith isolated febrile seizures (45.9% of the total) and140 children with two or more febrile seizure recurrences(54.1%). Among the patients with and without recurrentfebrile seizures, 32% and 18% were domiciled in nonur-ban areas, respectively (P = 0.012). There was a family his-tory of febrile seizures in 57% and 44% of cases with andwithout recurrent febrile seizures, respectively (P =0.031). According to the logistic regression analysis, a fam-ily history of febrile seizures was a risk factor that affectedrecurrence (P = 0.018; odds ratio OR = 1.933; 95% confi-dence interval CI = 1.121-3.333). We also found that domi-cile (P = 0.001) and income (P = 0.013) were risk factorsfor recurrence. A family history of epilepsy was not a sig-nificant risk factor (P = 0.129; OR = 2.110; 95% CI =0.804-5.539). � 2010 by Elsevier Inc. All rights reserved.
Tosun A, Koturoglu G, Serdaroglu G, Polat M, Kurugol Z,
Gokben S, Tekgul H. Ratios of nine risk factors in children
with recurrent febrile seizures. Pediatr Neurol 2010;43:177-
182.
Introduction
Epidemiologic studies have demonstrated the importance
of environmental and personal factors, particularly genetic
From the *Department of Pediatrics, Adnan Menderes University MedicalFaculty, Aydin, Turkey; the †Department of Pediatrics, Ege UniversityMedical Faculty, Izmir, Turkey; and the ‡Department of Pediatrics, CelalBayar University Medical Faculty, Manisa, Turkey.
� 2010 by Elsevier Inc. All rights reserved.doi:10.1016/j.pediatrneurol.2010.05.007 � 0887-8994/$—see front matter
factors, in the development of first febrile seizures in chil-
dren, as well as recurrent febrile convulsions [1-8].
Although febrile seizures are generally benign, they
remain important, based on the risk of developing
epilepsy (a relatively low risk) but especially on risk of
recurrence, seen in 23-42% of cases [1,5,9-11].
The decision to initiate prophylaxis and determining the
prognosis of febrile seizures are important issues for the
clinician. A family history of febrile seizures, early age at
onset, lower temperature at the time of febrile seizures,
and shorter duration of fever before the febrile seizures
are the significant risk factors for recurrent febrile seizures
[1,9,10,12,13]. Although a family history of epilepsy,
seizures with complex features, and neurodevelopmental
abnormality are known risk factors for developing
epilepsy, their status as risk factors for recurrent febrile
seizures remains controversial [1,4,8,10,13,14].
For two of the generally accepted risk factors for
recurrent febrile seizures (i.e., for the level of fever required
to diagnose febrile seizure and for the duration of fever
prior to the seizure), different definitions have been
used in different studies [1,7,9,10,12]. The objective of
the present study was to determine the ratios of nine
generally accepted risk factors for recurrent febrile
seizures in a sample of children with and without
recurrent febrile seizures.
Methods and Patients
Risk Factors, Study Population, and Methods
The study was designed to address nine generally accepted risk factors
for recurrent febrile seizures: (1) sex; (2) domicile of family, urban vs non-
urban; (3) income level of family, relative to subsistence; (4) family history
of febrile seizures; (5) family history of epilepsy; (6) level of fever causing
seizures, (7) duration of fever before seizures, (8) type of seizure, simple vs
complex; and (9) age at seizure onset.
Communications should be addressed to:Dr. Koturoglu; Department of Pediatrics; Ege University Medical School;35040 Bornova-Izmir, Turkey.E-mail: [email protected] December 31, 2009; accepted May 3, 2010.
Tosun et al: Risk Factors in Febrile Seizures 177

Table 1. Risk factors in 259 febrile seizure patients with (Positive)
and without (Negative) recurrence
Patients, no. (%)*Risk Factors Negative Positive P value
Sample size n = 119 n = 140
Sex
Male 67 (56) 80 (57) 0.892
Female 52 (44) 60 (43)
Domicile
Urban 97 (82) 95 (68) 0.012
Nonurban 22 (18) 45 (32)
Income level
# Subsistence wage 26 (22) 13 (9) 0.005
> Subsistence wage 93 (78) 127 (91)
Family history of febrile seizure
Positive 52 (44) 80 (57) 0.031
Negative 67 (56) 60 (43)
Family history of epilepsy
Positive 7 (6) 20 (14) 0.027
Negative 112 (94) 120 (86)
Level of fever
#39�C 69 (58) 75 (54) 0.747
>39�C 50 (42) 59 (42)
Duration of fever before seizure
#1 hour 38 (32) 28 (20) 0.046
>1 hour 81 (68) 106 (79)
Complex febrile seizure
Positive 16 (13) 17 (12) 0.754
Negative 103 (87) 123 (88)
Age at seizure onset
#18 months 61 (51) 87 (62) 0.078
Included in the present study were 259 children admitted to the Ege
University Medical School Department of Pediatrics, Division of Child
Neurology, and the Emergency Department between January 2004 and
January 2008 with a history of a febrile seizure and normal findings on
neurologic examination. Children with seizures during fever with an
axillary temperature of 37.8�C or higher were categorized as febrile seizure
patients [12,15].
Children who had their first febrile seizure between 3 months and 5
years of age and who presented with recurrent seizures after the age of 5
years were eligible for inclusion. Excluded from the study were children
who had evidence of intracranial infections or head trauma, history of neo-
natal seizures, afebrile seizures, developmental retardation, or pathologic
findings on the neurologic examination prior to admission.
Level of fever was recorded as axillary temperature measured by the
medical staff at admission to the emergency department during the time
of the febrile seizure, or axillary temperature measured by the family prior
to admission. An axillary temperature of 39�C or less was defined as low
fever.
The following sociodemographic characteristics and clinical data were
recorded on previously designed forms: domicile (urban vs nonurban), pa-
rental education (primary school vs lower-secondary school or higher),
family income (relative to the subsistence wage level, defined as 500
Turkish liras), type of family (nuclear vs extended), family history of con-
sanguinity, family history of febrile seizures, family history of epilepsy,
level of fever during the seizure (#39�C vs >39�C), seizure duration
(#15 minutes vs >15 minutes), type of seizure (generalized tonic-clonic,
focal, or atonic), classification of the seizure (complex [i.e., focal, pro-
longed than 15 minutes, and recurrences in 24 hours or within the same fe-
brile illness] vs simple), time from onset of fever to seizure (#1 hour vs >1
hour, or #24 hours vs <24 hours), cause of fever (upper respiratory tract
infection, lower genital tract infection, urinary tract infection, or postvacci-
nation), total number of febrile seizures at admission, and the history and
reason for any hospitalization in the neonatal unit.
>18 months 58 (49) 53 (38)
* Column percentage.
Statistical AnalysisThe data were evaluated using the SPSS statistical package, version 11
(SPSS, Chicago, IL). The percentage and mean � standard deviation
values were calculated for descriptive statistics. A chi-square test was
used for intergroup comparisons, and logistic regression analysis (back-
ward method) was used for multivariate analysis. The risk was presented
as the odds ratio (OR) and 95% confidence interval (CI). The level of
statistical significance was set at P < 0.05.
Results
This cross-sectional descriptive study included 259 chil-
dren, of whom 147 (57%) were male, for a male:female ra-
tio of 1.3:1. The mean age overall was 33.08 � 18.97
months (range, 6-84 months). The mean age of the 140 chil-
dren with recurrent febrile seizures was 38.22 � 19.44
months. Of these 140 children, 80 (57%) were male, for
a male:female ratio of 1.2:1.
Sociodemographic features and the distribution of risk
factors for children with and without recurrent febrile sei-
zures are presented in Table 1.
Of the 259 children, 33 (12.7%) were diagnosed with
complex febrile seizures. The incidence of complex febrile
seizures was as follows: seizures lasting less than 15 min-
utes occurred in 34 cases; focal seizures occurred in 13
cases; and two or more seizures within the same day
occurred in 8 cases. Seizures recurred in 140 of the 259
cases (54%).
178 PEDIATRIC NEUROLOGY Vol. 43 No. 3
There was no statistically significant difference between
children with and without recurrent febrile seizures with
respect to sex, level of fever during the seizure, whether
the seizure was complex, and age at first seizure (Table
1). There was also no significant difference for parental
education, consanguinity, type of family, cause of fever,
any history of hospitalization in the neonatal intensive
care unit, and duration of seizure (data not shown).
In the present study, having a seizure with a low fever oc-
curred in 75 of 140 cases with recurrent febrile seizures
(54%) and in 69 of 119 cases without recurrent febrile
seizures (58%) (P = 0.747).
Among the cases with recurrent febrile seizures, 22% had
a seizure within the first hour of the febrile episode and
78% had a seizure after the first hour of the febrile episode.
The first seizure occurred at #18 months of age in 87 of
140 cases with recurrent febrile seizures (62%) and in 61 of
119 cases without recurrence (51%) (P = 0.078).
There were no statistically significant differences be-
tween the cases with and without recurrent febrile seizures
with respect to the seizures that had focal characteristics
(P = 0.558), lasted more than 15 minutes (P = 0.431), or
recurred during the same illness (P = 0.626). Among the
140 patients with recurrent febrile seizures, 17 (12%)

0
5
10
15
20
25
30
35
40
45
50
3 4 5 6 7 8
Number of risk factors
Number of cases
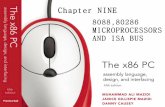
Figure 1. Distribution of multiple risk factors among 140 cases ofrecurrent febrile seizures. The maximum number of risk factors is nine(listed in Table 1).
Table 2. The nine risk factors for recurrence of febrile seizures
according to logistic regression analysis
Risk Factors P value Odds Ratio
95%
Confidence
Interval
Sex: Female* vs Male 0.627 1.144 0.665-1.968
Domicile: Urban* vs Nonurban 0.001 2.942 1.516-5.709
Income level: # Subsistence wage*
vs > Subsistence wage
0.013 2.766 1.234-6.197
Family history of febrile seizures:
Negative* vs Positive
0.018 1.933 1.121-3.333
Family history of epilepsy:
Negative* vs Positive
0.129 2.110 0.804-5.539
Level of fever: #39�C* vs >39�C 0.653 1.132 0.659-1.945
Duration of fever before seizure:
#1 hour* vs >1 hour
0.054 1.876 0.988-3.563
Complex febrile seizure: Positive*
vs Negative
0.553 1.281 0.565-2.906
Age at seizure onset: #18 months
vs >18 months*
0.105 1.565 0.910-2.691
* Reference category.
had complex febrile seizures. There was no significant
difference between patients with and without recurrent
febrile seizures with respect to complex febrile seizures
(P = 0.754).
Of the 140 patients with recurrent febrile seizures, 41
(55%) had 3 or more recurrences (range, 3-12). The sex
ratio for this subset was the same as for the full sample of
140 (i.e., a male:female ratio of 1.2:1).
Recurrent febrile seizures were significantly higher in
cases with nonurban domicile, compared with urban domicile
(P = 0.012). The recurrence rate in the children of families
with an income level greater than the subsistence wage level
(91%) was significantly higher than for those with a family
income level below the subsistence level (9%) (P = 0.005).
The recurrence rate of febrile seizures was significantly
higher in children with a positive family history of febrile
seizures (57%), compared with those without such a family
history (44%) (P = 0.031) (Table 1). For those with a his-
tory of febrile seizures among first degree relatives, the
rates were 36% for cases with recurrent febrile seizures
and 27.2% for cases without, respectively, whereas the
rates were 21% and 20% among second degree relatives,
respectively (P = 0.581). In addition, the recurrence rate
of febrile seizures was 58% in cases with a family history
of febrile seizures in one relative, and 65.9% in those with
a family history of febrile seizures in two or more rela-
tives (P = 0.378).
A positive family history of epilepsy was significantly
higher in children with recurrent febrile seizures, compared
with those without recurrent febrile seizures (P = 0.027).
Multiple risk factors for recurrent febrile seizures in chil-
dren occurred as follows (these data are also presented
graphically in Fig 1): three of the nine risk factors in 12
cases (8.6%), four risk factors in 29 cases (20.7%), five
risk factors in 43 cases (30.7%), six risk factors in 36 cases
(25.7%), seven risk factors in 16 cases (11.4%), and eight
risk factors in 4 cases (2.9%).
In the present study, according to the results of multi-
variate logistic regression analysis, nonurban domicile
(OR = 2.942; 95% CI = 1.516-5.709), having an
income over the subsistence wage (OR = 2.766; 95%
CI = 1.234-6.197), and a family history of febrile seizures
(OR = 1.933; 95% CI = 1.121-3.333) were significant
risk factors for recurrent febrile seizures. However, a fam-
ily history of epilepsy (OR = 2.110; 95% CI = 0.804-
5.539) and having the seizure after the first hour of the
febrile illness (OR = 1.876; 95% CI = 0.988-3.563)
were not a significant risk factor (Table 2).
Five risk factors (nonurban domicile, income greater than
the subsistence wage, a positive family history of febrile
seizures, a positive family history of epilepsy, and having
the seizure after the first hour of the febrile illness) contrib-
uted to a statistically significant difference in cases with re-
current febrile seizures, compared with those without
a recurrence (Table 1), but did not contribute to a significant
difference between cases with a single recurrence and those
with two or more recurrences (Table 3).
Discussion
The course of febrile seizures in childhood is usually be-
nign, and the long term prognosis is good; however, febrile
seizures recur in one third of cases, and three or more recur-
rences are observed in approximately 10% of cases. Many
risk factors have been studied and identified for recurrence
[1,3,7,8,16]. The most frequently reported risk factors are
a family history of febrile seizures, young age at seizure
onset, having seizures with a relatively low fever, and
shorter duration of fever before the seizures. A family
history of epilepsy and the peak temperature during the
febrile seizure are still controversial risk factors [1,7,10].
From a large number of international studies, it has been
reported that a family history of febrile seizures is a power-
ful prognostic risk factor for recurrent febrile seizures,
and the risk increases with the number of relatives
who have that history [4,6,7,9,10,17-20]. Approximately
Tosun et al: Risk Factors in Febrile Seizures 179

Table 3. Risk factors in recurrent febrile seizures patients by
number of recurrences
Risk Factors
Patients with
1 recurrence,
no. (%)*
Patients with $2
recurrences,
no. (%)* P-value
Sample size n = 66 n = 74
Sex
Male 38 (58) 42 (57) 0.922
Female 28 (42) 32 (43)
Domicile
Urban 49 (70) 49 (66) 0.660
Nonurban 25 (30) 25 (34)
Income level
# Subsistence wage* 5 (8) 8 (11) 0.510
> Subsistence wage 61 (92) 66 (90)
Family history of febrile seizures†
Positive (n = 132) 41 (62) 39 (53) 0.261
Negative (n = 127) 25 (38) 35 (47)
Family history of epilepsy
Positive 11 (17) 9 (12) 0.447
Negative 55 (83) 65 (88)
Level of fever
#39�C 35 (53) 40 (54) 0.631
>39�C 30 (45) 29 (39)
Duration of fever before seizure
# 1 hour 10 (16) 18 (24) 0.151
> 1 hour 54 (84) 52 (66)
Complex febrile seizure
Positive 9 (14) 8 (11) 0.609
Negative 57 (86) 66 (89)
Age at seizure onset
#18 months 37 (56) 50 (68) 0.161
>18 months 29 (44) 24 (32)
* Reference category.† Sample size given is the total number of family members in that
category, excluding the patient cohort.
25-40% of children with febrile seizures had a positive
family history of febrile seizures, and the risk of
developing febrile seizures among their siblings was
reported as 9-22% [4,7,19]. In accord with similar reports
[5,10,17,18,21,22], in the present study a positive family
history of febrile seizures was significantly higher in
children with recurrent febrile seizures, compared with
those without recurrent febrile seizures (P = 0.031).
Rantala and Uhari [23] reported that a family history of
febrile seizures was not a risk factor for recurrent febrile
seizures, whereas a history of febrile seizures among the
first degree relatives was significant. Van Esch et al. [19]
reported that a history of febrile seizures among the first de-
gree relatives increased the risk of recurrent febrile seizures;
however, the presence of febrile seizures among second de-
gree relatives was not a significant risk factor for recurrent
febrile seizures. In the present study, the rates of febrile sei-
zures among first degree and second degree relatives were
similar, at 62.5% and 58%, respectively; however, a positive
history of febrile seizures among first degree relatives was
not a significant risk factor (P = 0.581). The recurrence
rate of febrile seizures increased with the increase in the
180 PEDIATRIC NEUROLOGY Vol. 43 No. 3
number of family members with a history of febrile sei-
zures; however, the difference was not statistically signifi-
cant (P = 0.378). The present findings indicate that
a family history of febrile seizures is the most important
risk factor (OR = 1.933; 95% CI = 1.121-3.333).
Based on many studies, a positive family history of
epilepsy is still controversial as a risk factor for recurrent fe-
brile seizures. From a few studies, it was reported that a fam-
ily history of epilepsy moderately increases in the risk of
febrile seizure recurrence [5,14]. In contrast, other studies
revealed no difference in recurrence risk between children
with and without a family history of epilepsy [1,9-11,21].
In yet other reports, a family history of epilepsy is listed
either among probable or among certain risk factors for
recurrent febrile seizures [1,8,9,12,24]. In the present
study, a positive family history of epilepsy was found in
greater proportion among children with recurrent febrile
seizures than among those without recurrence (P =
0.027). Nonetheless, family history of epilepsy in cases
with recurrent febrile seizures was not a significant risk
factor according to multivariate logistic regression
analysis (P = 0.129; OR = 2.110; 95% CI = 0.804-5.539).
A relationship has been reported between age at onset of
febrile seizures and recurrence of febrile seizures
[2,3,9,12,17,25]. In the meta-analysis by Berg et al. [17],
it was demonstrated in 12 of 14 studies that febrile seizures
at early ages increase rates of recurrence. A first febrile sei-
zure at less than 18 months of age and a family history of
febrile seizures are reported to be the strongest and the
most consistent risk factors for recurrent febrile seizures
[1,5,9,12,17,21]. Berg et al. [12] reported the risk of recur-
rence within 1 year as 30% for cases with the first febrile
seizure at less than 18 months of age, and as 18% for those
with their first febrile seizure later than that.
Some authors consider young age to be associated with
a lower threshold for febrile seizures [25], whereas others
explain the association on the basis of the potential for
more febrile disease at this age [12,20,23,26]. Uran
et al. [27] reported that the onset of febrile seizures before
the age of 1 year was a significant risk factor for recur-
rence. However, in the present study, and similar to the
findings of Rantala and Uhari [23] and Tarkka et al.
[11], age at onset of febrile seizures was not a significant
risk factor for recurrent febrile seizures (P = 0.078).
Although the definition of febrile seizures includes the
presence of fever, there is no current evidence on the
level of fever required for a diagnosis of febrile seizures
[4]. Most febrile seizures occur either early or late in the
course of illness, and may be the primary cause for
hospital admission in approximately 25-50% of cases
[4,7,13,24]. Despite the common belief that the rate of
rise in temperature is more important for the development
of a febrile seizure than the level of fever as such, there is
no evidence to support this hypothesis [4,7,24,28].
From many studies, it has been reported that a relatively
low temperature increases the rate of recurrent febrile
seizures [1,9,10,12,18,29]. Methodologic problems remain,

however, including the degree of fever defined for febrile
seizures, the measurements of fever (axillary or rectal), the
time of temperature measurement (before the seizure or at
the time of seizure), measuring the temperature at home or
in the emergency department, interventions (e.g.,
antipyretics or warm baths) to lower the fever performed
prior to hospital admission, and recording the temperature
accurately (�F or �C units) [4,7,9]. It has been suggested
that a diagnosis of febrile seizures should be based on
medical history and physical examination findings alone,
because it is not practical to determine of the level of fever
required to diagnose a febrile seizure. This suggestion is in
accord with the recommendations of the National Institutes
of Health [15].
In the present study, low fever was defined as axillary
temperature of 39�C or less. Low fever at the initial febrile
seizure was observed in 75 of the 140 cases with recurrence
of febrile seizure (54%) and in 69 of the 119 cases without
recurrence (58%); the difference was not significant
(P = 0.747). Although much of the literature does indicate
some association between fever and recurrence of febrile
seizures, results from several studies support the present
negative findings [11,14,18,23].
The duration of fever before a febrile seizure is an impor-
tant risk factor for recurrence of febrile seizures. The shorter
the duration of fever prior to the seizure, the greater the risk
for recurrence [1,3,13]. Berg et al. [12] reported febrile sei-
zure recurrence rates as follows: 44% in cases with a fever
duration of less than 1 hour before a febrile seizure, 23% in
cases with a fever duration of 1-24 hours, and 13% in sub-
jects with a fever duration greater than 24 hours. Pavlidou
et al. [10] found that recurrence rates of febrile seizures
were significantly higher for cases with a febrile seizure
within the first 12 hours of the febrile episode, compared
with a seizure between hours 12 and 24 hours; this signifi-
cance disappeared as the number of recurrences increased.
In the present study, the recurrence rate was significantly
higher in cases with a fever duration of less than 1 hour prior
to the febrile seizure (P = 0.017). No significant difference
could be established in terms of a single recurrence and
multiple recurrences of febrile seizures. Similarly, Chung
et al. [18] did not find a significant relationship between
the duration of fever prior to the febrile seizure and
recurrence of febrile seizures.
In the present study, nonurban domicile was one of the
risk factors for recurrence of febrile seizures (P = 0.012),
probably due to due to difficulties in reaching a health cen-
ter during the febrile episode. In addition, the level of ma-
ternal education was primary school or lower in 36% of
the cases with recurrence of febrile seizures (and in 20%
of the cases, for paternal education), but this was not statis-
tically significant. Similarly, for nonurban domicile the ma-
ternal of education was primary school or lower in 54% of
the cases (and 36%, for paternal education). This finding
may reflect the inadequate knowledge of parents about mea-
suring, evaluating, and lowering the child’s temperature
during the course of a febrile episode.
In the present study, the recurrence rate was significantly
higher in the children of families with an income level
above the subsistence wage, compared with those with an
income level below the subsistence wage (91% and 9%, re-
spectively) (P = 0.005). These findings may be explained by
fewer hospital admissions for patients with income level be-
low subsistence, and by the absence of social security, and
also by more hospital admissions for patients with income
above subsistence wage (influenced by, for example, avail-
ability of private cars, as well as a high economic status and
consciousness about the disease).
Aydin et al. [30] found that socioeconomic status and the
level of paternal education were significantly lower in
patients with febrile seizures, Forsgren et al. [31] reported
the level of maternal education as a risk factor. In the present
study, the level of maternal education was primary school or
lower in 43% of the cases with multiple recurrence of febrile
seizures, but this was not statistically significant.
Sex, ethnic origin, complex febrile seizures, and patho-
logic findings on neurologic examination were not among
the risk factors for recurrence of febrile seizures identified
by Shinnar and Glauser [1]. In the present study, both fe-
brile seizure and recurrence were more frequent in male
than in female cases (male:female ratios of 1.3:1 and
1.2:1, respectively). This finding is in accord with many
other studies [10,11,18,22]. The sex ratio for cases with
recurrence did not vary between isolated recurrence and
three or more recurrences, but remained constant at 1.2:1.
Recurrence of febrile seizures is more frequently encoun-
tered in children who had complex febrile seizures [32].
Nonetheless, and in accord with the present findings, there
are also studies demonstrating no relationship between
complex febrile seizures and the risk for recurrence of fe-
brile seizures [12,23].
Thus, although febrile seizures are the most frequently
observed seizures of childhood and have a good prognosis,
it is important for clinicians to know the potential risk factors
for recurrence. The present cross-sectional study determined
the risk ratios for recurrence of febrile seizures in a Turkish
population. Additional studies should be designed using the
defined risk ratios in a scoring model for children with
febrile seizures in a longitudinal prospective study.
References
[1] Shinnar S, Glauser TA. Febrile seizures. J Child Neurol 2002;
17(Suppl. 1):S44-52.
[2] Jones T, Jacobsen SJ. Childhood febrile seizures: overview and
implications. Int J Med Sci 2007;4:110-4.
[3] Leung AK, Robson WL. Febrile seizures. J Pediatr Health Care
2007;21:250-5.
[4] Waruiru C, Appleton R. Febrile seizures: an update. Arch Dis
Child 2004;89:751-6.
[5] Annegers JF, Blakley SA, Hauser WA, Kurland LT. Recurrence of
febrile convulsions in a population-based cohort. Epilepsy Res 1990;5:209-16.
[6] Berg AT, Shinnar S, Shapiro ED, Salomon ME, Crain EF,
Hauser WA. Risk factors for a first febrile seizure: a matched case-
control study. Epilepsia 1995;36:334-41.
[7] Fetveit A. Assessment of febrile seizures in children. Eur J Pediatr
2008;167:17-27.
Tosun et al: Risk Factors in Febrile Seizures 181

[8] Millar JS. Evaluation and treatment of the child with febrile sei-
zure. Am Fam Physician 2006;73:1761-4.
[9] Offringa M, Bossuyt PM, Lubsen J, et al. Risk factors for seizure
recurrence in children with febrile seizures: a pooled analysis of individual
patient data from five studies. J Pediatr 1994;124:574-84.
[10] Pavlidou E, Tzitiridou M, Kontopoulos E, Panteliadis CP. Which
factors determine febrile seizure recurrence? A prospective study. Brain
Dev 2008;30:7-13.
[11] Tarkka R, Rantala H, Uhari M, Pokka T. Risk of recurrence and
outcome after the first febrile seizure. Pediatr Neurol 1998;18:218-20.
[12] Berg AT, Shinnar S, Hauser WA, et al. A prospective study of
recurrent febrile seizures. N Engl J Med 1992;327:1122-7.
[13] Sadleir LG, Scheffer IE. Febrile seizures. BMJ 2007;334:307-11.
[14] Al-Eissa YA. Febrile seizures: rate and risk factors of recurrence.
J Child Neurol 1995;10:315-9.
[15] Armon K, Stephenson T, MacFaul R, Hemingway P,
Werneke U, Smith S. An evidence and consensus based guideline for the
management of a child after a seizure. Emerg Med J 2003;20:13-20.
[16] Knudsen FU. Febrile seizures: treatment and prognosis. Epilep-
sia 2000;41:2-9.
[17] Berg AT, Shinnar S, Hauser WA, Leventhal JM. Predictors of re-
current febrile seizures: a metaanalytic review. J Pediatr 1990;116:329-37.
[18] Chung B, Wat LC, Wong V. Febrile seizures in southern Chinese
children: incidence and recurrence. Pediatr Neurol 2006;34:121-6.
[19] van Esch A, Steyerberg EW, van Duijn CM, Offringa M, Derk-
sen-Lubsen G, van Steensel-Moll HA. Prediction of febrile seizures in sib-
lings: a practical approach. Eur J Pediatr 1998;157:340-4.
[20] Offringa M, Derksen-Lubsen G, Bossuyt PM, Lubsen J. Risk
factors for the occurrence of recurrent convulsions following an initial
febrile convulsion [In Dutch]. Ned Tijdschr Geneeskd 1992;136:516-21.
182 PEDIATRIC NEUROLOGY Vol. 43 No. 3
[21] Berg AT, Shinnar S, Darefsky AS, et al. Predictors of recurrent
febrile seizures: a prospective cohort study. Arch Pediatr Adolesc Med
1997;151:371-8.
[22] Gururaj AK, Bener A, Al-Suweidi EK, Al-Tatari HM,
Khadir AE. Predictors of febrile seizure: a matched case-control study. J
Trop Pediatr 2001;47:361-2.
[23] Rantala H, Uhari M. Risk factors for recurrences of febrile con-
vulsions. Acta Neurol Scand 1994;90:207-10.
[24] Trainor JL. Evaluating and treating the child with a febrile sei-
zure. Clin Pediatr Emerg Med 1999;1:13-20.
[25] van Stuijvenberg M, Steyerberg EW, Derksen-Lubsen G,
Moll HA. Temperature, age, and recurrence of febrile seizure. Arch Pediatr
Adolesc Med 1998;152:1170-5.
[26] Al-Ossaimi S, Jawad NH. Recent advances in febrile seizures.
Kuwait Med J 2001;33:7-12.
[27] Uran N, Mengucuk O, Gulez P. Evaluation of febrile
convulsions retrospectively [In Turkish]. T Klin J Pediatr 1997;6:
108-13 [Available at http://tipdizini.turkiyeklinikleri.com/download_pdf.
php?Fid=D42210].
[28] Berg AT. Are febrile seizures provoked by a rapid rise in temper-
ature? Am J Dis Child 1993;147:1101-3.
[29] el-Radhi AS, Banajeh S. Effect of fever on recurrence rate of fe-
brile convulsions. Arch Dis Child 1989;64:869-70.
[30] Aydin A, Ergor A, Ozkan H. Effects of sociodemographic factors
on febrile convulsion prevalence. Pediatr Int 2008;50:216-20.
[31] Forsgren L, Sidenvall R, Blomquist HK, Heijbel J, Nystrom L.
An incident case-referent study of febrile convulsions in children: genetical
and social aspects. Neuropediatrics 1990;21:153-9.
[32] Berg AT, Shinnar S. Complex febrile seizures. Epilepsia 1996;
37:126-33.