
Adaptive dose finding based ont-statistic for dose–response trials
Upload
universityofsydneyCategory
view
1download
0
Rationale for National and Local Dose Reference Levels and CollectiveEffective Dose in CT
Francis Zarb, MSc,a,* Louise Rainford, PhD,b Shane Foley, BSc,b and Mark F. McEntee, PhDb
a Institute of Health Care, University of Malta, Maltab School of Medicine & Medical Science, Health Science Centre, Belfield, Dublin, Ireland
Journal of Medical Imaging and Radiation Sciences 40 (2009) 109-115
Journal of Medical Imaging and Radiation Sciences
Journal de l’imagerie médicaleet des sciences de la radiation
www.elsevier.com/locate/jmir
ABSTRACT
Purpose: This article is intended as a review of the methods of estab-lishing dose reference levels (DRLs) in relation to computerized
tomography (CT) and their role in the standardization and auditingof radiation dose in CT.
Discussion: CT is considered a high radiation dose examination.The potential for dose reduction resulting from the establishmentof DRLs is discussed. The rationale for the use of DRLs in relation
to the use of appropriate radiation measurements and CT dose de-scriptors are discussed. The estimation of the radiation risk to the ir-radiated individual is given by the effective dose, which takes into
consideration the type of radiation and the radiosensitivity of the ir-radiated tissues. The collective dose is used to describe the radiationexposure of a population from low doses of different sources of
radiation.
Conclusion: Dose comparison between individual imaging sites is
a vital part of DRL establishment and facilitates standardization ofradiation dose levels for patients attending for a CT examination.Measurements of both effective and collective dose are difficult toachieve in practice. CT dose descriptors such as CT dose index
and dose length product provide the means of comparing and mon-itoring the effect of optimized CT scanning protocols on the radia-tion dose.
Introduction
The aim of radiation protection in computed tomography(CT), as for all modes of imaging employing ionizing radia-tion, is to provide an appropriate standard of protection topatients against the harmful effects of radiation without re-ducing the diagnostic efficacy of the examination. The aimof justified CT examinations is to obtain CT images of suffi-cient image quality using minimal radiation dose following
* Corresponding author. University of Malta, Institute of Health Care,
Division of Radiography Studies, Msida, Malta. Tel: 00356-23401833
E-mail address: [email protected] (F. Zarb).
1939-8654/09/$ - see front matter � 2009 Elsevier Inc. All rights reserved.
doi: 10.1016/j.jmir.2009.06.001
RESUME
Objet : Le present document se veut un examen des methodes d’eta-blissement des niveaux de reference diagnostiques (NRD) en tomoden-
sitometrie et de leur role dans la normalisation et la verification de la dosede rayonnement en tomodensitometrie.
Discussion : La tomodensitometrie est consideree comme un exa-men dont la dose de rayonnement est elevee. On aborde la possibilitede reduire la dose a l’aide de l’etablissement de NRD et la raison
d’etre de l’utilisation des NRD par rapport a l’utilisation de mesuresde rayonnement et de descripteurs de dose appropries pour la tomo-densitometrie. L’evaluation du risque de rayonnement du patient est
donnee par la dose efficace (E) qui tient compte du type de rayonne-ment et de la radiosensibilite des tissus irradies. La dose collective (S)est utilisee pour decrire la radioexposition d’une population prove-
nant de faibles doses de sources de rayonnement differentes.
Conclusion : La comparaison des doses entre des sites d’imagerie in-
dividuels est une partie essentielle de l’etablissement des NRD et fa-cilite la normalisation des niveaux des doses de rayonnement pour lespatients subissant un examen de tomodensitometrie. Les mesures dela dose effective et collective sont difficiles a effectuer en pratique. Les
descripteurs de dose de tomodensitometrie tels que l’indice de dosetomodensitometrique et le produit dose-longueur (PDL) offrent lemoyen de comparer et de surveiller l’effet de l’optimisation des pro-
tocoles de tomodensitometrie sur la dose de rayonnement.
the As Low As Reasonably Possible principle. The aim of ra-diation protection in diagnostic imaging is preventing deter-ministic effects and limiting stochastic effects of radiation.Deterministic (nonstochastic) radiation effects are thosewhich result if a threshold radiation dose is exceeded. Stochas-tic radiation effects are those effects, the probability of whichincreases with an increase in radiation dose [1].
The measurement of dose values in CT is necessary to es-tablish whether doses require some specified action or reduc-tion and is often helpful in the management of radiationprotection. These values are known as dose reference levels(DRLs) or reference values (RV). The European Council Di-rective (97/43/EURATOM) [2] defines DRLs, emphasizing
the importance of their implementation and use. The objec-tive of DRLs is to avoid radiation dose to the patient thatdoes not contribute to the production of diagnostic informa-tion [3].The establishment of DRLs is mandated in Euro-pean Union (EU) member states. DRLs are a reflection ofgood practice in standard situations. If exceeded withoutproper justification, intervention or remedial action shouldbe considered [3]. Remedial action is recommended to iden-tify the cause and rectify consistently observed dose valueshigher than the selected DRL values, which should not beexceeded. Without DRLs, no level for remedial action isknown [4–6].
Radiation risk is measured in terms of the effective dose (E),which enables comparison of the average amount of radiationreceived by the entire body from a specific radiological exam-ination with that from background radiation [7, 8]. The prod-uct of the average E for an individual within a populationand the number of persons exposed give the collective effectivedose (S) for that population. These dose quantities are usedin comparing the risk from ionizing radiation between differ-ent examinations and the population risk between differentcountries [7, 8].
CT radiation doses vary between different clinical sitesboth nationally and internationally. Patient dose surveys indi-cate that variations in the doses for the same CT examinationare too great to be solely attributed to differences in patientsize, but may also be due to a number of other factors suchas different types of equipment, or use of different scanningprotocols and procedures [9]. To evaluate fully the impactof the factors influencing patient dose an investigation ofa broad range of CT examinations, scanning protocols, andscanner technology is required. A collective dose assessmentincluding different types of CT scanners is also necessary. Ac-cording to the ALARA principle, diagnostic quality imagesshould be obtained with the least possible dose. Hence, itwould be unjustified to produce CT images of the same qual-ity using different radiation doses. If similar CT exams areperformed with different radiation doses, then there is a poten-tial for dose reduction. Investigations to standardize and lowerradiation doses in CT are always encouraged [9–13].
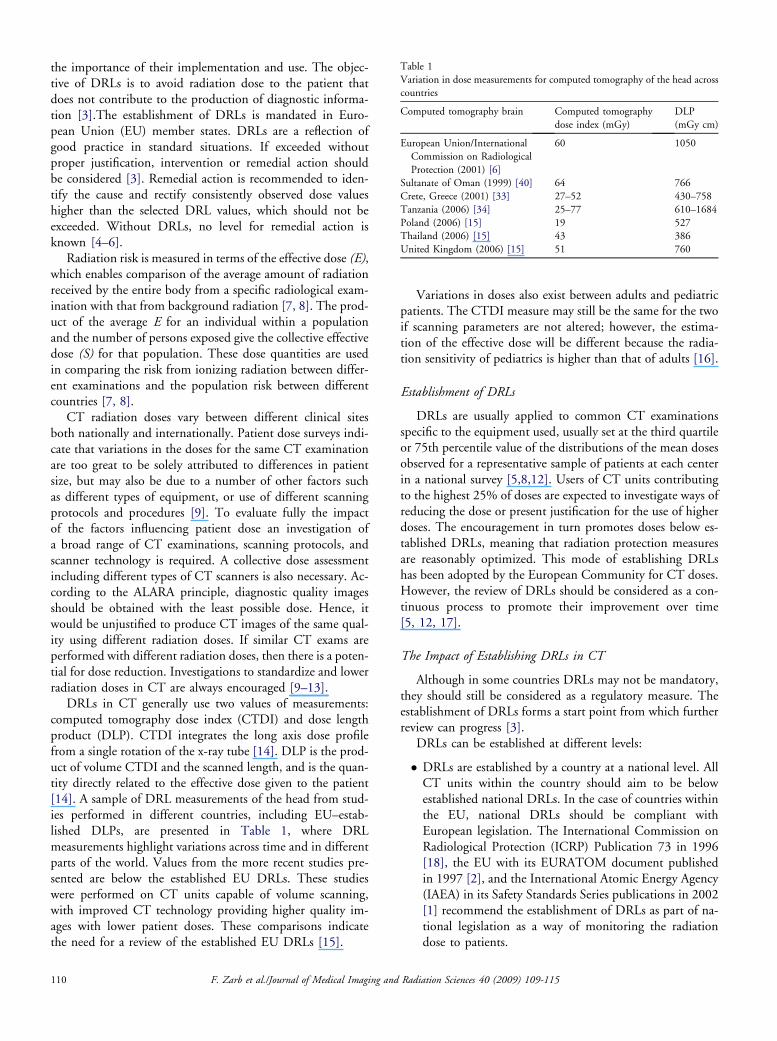
DRLs in CT generally use two values of measurements:computed tomography dose index (CTDI) and dose lengthproduct (DLP). CTDI integrates the long axis dose profilefrom a single rotation of the x-ray tube [14]. DLP is the prod-uct of volume CTDI and the scanned length, and is the quan-tity directly related to the effective dose given to the patient[14]. A sample of DRL measurements of the head from stud-ies performed in different countries, including EU–estab-lished DLPs, are presented in Table 1, where DRLmeasurements highlight variations across time and in differentparts of the world. Values from the more recent studies pre-sented are below the established EU DRLs. These studieswere performed on CT units capable of volume scanning,with improved CT technology providing higher quality im-ages with lower patient doses. These comparisons indicatethe need for a review of the established EU DRLs [15].
110 F. Zarb et al./Journal of Medical Imaging a
Variations in doses also exist between adults and pediatricpatients. The CTDI measure may still be the same for the twoif scanning parameters are not altered; however, the estima-tion of the effective dose will be different because the radia-tion sensitivity of pediatrics is higher than that of adults [16].
Establishment of DRLs
DRLs are usually applied to common CT examinationsspecific to the equipment used, usually set at the third quartileor 75th percentile value of the distributions of the mean dosesobserved for a representative sample of patients at each centerin a national survey [5,8,12]. Users of CT units contributingto the highest 25% of doses are expected to investigate ways ofreducing the dose or present justification for the use of higherdoses. The encouragement in turn promotes doses below es-tablished DRLs, meaning that radiation protection measuresare reasonably optimized. This mode of establishing DRLshas been adopted by the European Community for CT doses.However, the review of DRLs should be considered as a con-tinuous process to promote their improvement over time[5, 12, 17].
The Impact of Establishing DRLs in CT
Although in some countries DRLs may not be mandatory,they should still be considered as a regulatory measure. Theestablishment of DRLs forms a start point from which furtherreview can progress [3].
DRLs can be established at different levels:
� DRLs are established by a country at a national level. AllCT units within the country should aim to be belowestablished national DRLs. In the case of countries withinthe EU, national DRLs should be compliant withEuropean legislation. The International Commission onRadiological Protection (ICRP) Publication 73 in 1996[18], the EU with its EURATOM document publishedin 1997 [2], and the International Atomic Energy Agency(IAEA) in its Safety Standards Series publications in 2002[1] recommend the establishment of DRLs as part of na-tional legislation as a way of monitoring the radiationdose to patients.
Table 1
Variation in dose measurements for computed tomography of the head across
countries
Computed tomography brain Computed tomography
dose index (mGy)
DLP
(mGy cm)
European Union/International
Commission on Radiological
Protection (2001) [6]
60 1050
Sultanate of Oman (1999) [40] 64 766
Crete, Greece (2001) [33] 27–52 430–758
Tanzania (2006) [34] 25–77 610–1684
Poland (2006) [15] 19 527
Thailand (2006) [15] 43 386
United Kingdom (2006) [15] 51 760
nd Radiation Sciences 40 (2009) 109-115

� Local DRLs are established by a hospital or group of hospi-tals to monitor local practice, providing feedback on optimi-zation programs and ensuring good practice is harmonizedand maintained at national and international levels.
Local DRLs may be lower than national DRLs; even so,these still require regular review, especially if changes in proto-cols, procedures, or equipment are affected. Equipmentchanges can especially affect local DRLs. Over the last decade,there has been an influx of CT scanners with volume scanningcapabilities, especially multislice CT units, replacing conven-tional ones. The impact of this new technology on establishedDRLs needs to be investigated [3, 5, 6].
In the United Kingdom, the concept of national and localDRLs is well established and has served as a catalyst in theoptimization of radiation doses in CT. National surveys [19]comparing radiation doses in CT over time show the reduc-tion of doses with the optimization measures undertaken(Table 2). One such measure involved the replacementof all conventional CT units by single or multislice volumescanners. The latest doses in the UK 2005 survey can serveas templates of reference for future studies.
DRLs should be estimated through dose quantities andtechniques that are easy to measure using a percentile pointon the observed distribution for patients that are specific tothe country or region. It is for these reasons that DRLs shouldreflect the dose and associated risk, be simple to understand,translatable, and allow comparisons to be made [5, 12].
CT Dose Quantities
EU directives require the assessment of patient doses in CTusing dose quantities that are simple to obtain and can cor-rectly reflect the patient dose, allowing the assessment of theassociated risk in CT examinations. Dose quantities shouldgive a meaningful indication of patient dose, consideringthe details of the scanning. Dose quantities should be applica-ble to all current and new types of CT scanners includingmultislice CT techniques. CT dose measurements need tobe consistent with other reference doses and dose descriptorsalready in use allowing comparison of the CT doses withother imaging examinations [2, 8, 20].
Table 2
United Kingdom computed tomography dose survey data [6,19]
Computed tomography
examination 1993 2003
Total scanners 360 471
Sample size
(Geographically spread
across United Kingdom)
75 126
Manufacturers GE/Siemens/Philips GE/Siemens/Philips
Toshiba
DLP (mGy cm) DLP (mGy cm)
Head 1050 760
Chest 650 430
Abdomen 780 510
F. Zarb et al./Journal of Medical Imaging an
The complexity of dose descriptors is exemplified by thenumber of radiation dose measurement methods in CT. Theirpurpose is mainly to test compliance with dose limits anddose constraints and provide a practical means for assessingthe doses received. The collective effective dose (S) is usedfor relative comparisons of the exposures of populations as re-quired by Article 12 of EURATOM council directive [2,8].The effective dose (E) is the dose quantity measure used forregulatory purposes to limit the occurrence of stochasticeffects of radiation and can be used for comparison purposesas long as the patient populations are similar [8, 21].
Collective Effective Dose
S is used in describing the radiation exposure from lowdoses of radiation of different sources of radiation of a popu-lation or group. S is given by the product of the average E ofan individual belonging to the exposed population and thenumber of persons exposed [7]. The person-sievert (personmSv) or man-sievert (man-mSv) is the unit expressing S,which is related to the total adverse health consequences of ra-diation exposure of a population [7, 8].
Effective Dose
The E estimates the whole-body dose required to producethe same stochastic risk as the partial-body dose actually deliv-ered in a localized radiological procedure. This measure allowscomparison of the radiation risk of CT with other diagnosticionizing radiation examinations, [22] taking into account therelative radio sensitivities of the body regions examined[4, 8, 13, 23].
Table 3 gives a comparison of CT doses in terms of E, withthe corresponding radiographic examination of the same ana-tomical region [24]. It can be noted that the doses in CT aremuch higher than their corresponding plain radiographyexaminations, indicating that the increase in diagnostic infor-mation in CT is obtained at a higher dose. This is justified aslong as this information is actually required for diagnosis [25].
E is the sum of absorbed doses to individual organsweighted for their radiation sensitivity measured in Sv. Theorgan weighting factors depend on the biological radiationsensitivities of the organs and the scanned range. In 2006,ICRP updated their calculation of radiation doses by includ-ing new organ models and adopting organ-specific elementcomposition densities resulting in slightly higher effectivedoses than those presented under ICRP Publication 60 in
Table 3
Comparison of computed tomography doses with conventional radiography
doses in the United Kingdom [24]
Examination
Conventional x-ray
imaging effective dose
E (mSv)
Computed tomography
scanning effective dose
E (mSv)
Chest (anteroposterior) 0.02 8.0
Abdomen (anteroposterior) 1.0 10.0
Head (anteroposterior,
posteroanterior, lateral)
0.07 2.0
Pelvis (anteroposterior) 0.7 10.0
d Radiation Sciences 40 (2009) 109-115 111
1990. Although a reduction in tissue weighting was imple-mented for the gonads, a major factor contributing to the in-crease in dose was the higher weighting of 0.12 given to breasttissue in 2006 [26] as opposed to 0.05 given in 1990 [4], to-gether with the inclusion in the 2006 update of more organsand tissues. The new tissue weighting factors result in a signif-icant increase in the effective dose for examinations of thehead but also significant dose reductions for the pelvis. Thechanges in tissue weighting factors should be consideredwhen comparing effective doses not to confuse differencesdue to these changes with changes due to differences in prac-tice [8, 21, 26].
E is the most appropriate measure available as a radiationdose descriptor where radiation levels are below thresholds re-quired to induce deterministic (nonstochastic) effects. Themagnitude of E is related to the stochastic radiation risk ofcancer induction and the production of genetic effects. Thelimitation of E is that it represents the radiation risk for theindividual but not of the general population; hence, the S isnecessary to assess this risk [8]. From estimations of E, theestimation of the S, and hence, the population risk, can beobtained [4, 5, 8, 23, 26–29].
Because it is not practically possible to measure the exact ra-diation dose absorbed by the patient, a reliable measure of thedose can be obtained from estimates of E. There are severalways of estimating E. One way is by measuring the doses in an-thropomorphic phantoms or by calculating E using publishedconversion factors [20]. Another way of estimating E is throughCTDI and DLP measurements in conjunction with conversioncoefficients. Special software programs using Monte Carlo cal-culations are based on the simulation of the passage of largenumbers of x-ray photons through a patient’s body. ImPACT(Image Performance Assessment of CT Scanners) group in theUnited Kingdom and CT-Expo group in Germany have devel-oped such software, and these are the ones commonly used forthe estimation of E [5, 8, 10, 11, 30, 31].
The radiation risk associated with CT examinations isavailable on CT scanners by data derived from such measure-ments made in head and body phantoms. These data are dis-played on the CT units as CTDI and DLP [4, 5, 28, 32].Weighted CTDI (CTDIw) for single slice and DLP for
a complete examination have been proposed in the EuropeanGuidelines as appropriate dose measures for the establishmentof DRLs in CT [8, 32, 33, 34]. These will now be discussed.
CTDI
CTDI is the main dose descriptor in CT, integrating theradiation dose for a single slice delivered both within and be-yond the scanned volume. The average CTDI of all the slicesacross the field of view from periphery to center, known asCTDIw, takes into account variations in the absorbed doseacross the field. CTDIw represents the average dose for a singleslice in the scanned volume for contiguous scans and is a moreaccurate descriptor for the radiation dose per slice within thescanned volume. CTDIw can be obtained from measurementsof CTDI100 obtained using a 100-mm ionization chamber(Figure 1) placed both in the center and at the periphery ofa 16-cm Lucite phantom for the head and a 32-cm Lucitephantom for the body (Figure 2). CTDIw is given by[5, 28, 29, 31–35]:
CTDIw ¼ 1=3 CTDI 100 ðcenterÞþ 2=3 CTDI 100 ðperipheryÞ
A limitation for the use of CTDIw is that it cannot be usedfor the estimation of doses to organs lying partially or totallyoutside the body region under examination. However, Hida-jat et al [20] concluded that because the highest organ dosesoccur for those organs within the scanned region, CTDIwcan still be used as a good estimate of E, especially wheninstruments for measurements of E in anthropomorphicphantoms and conversion factors are not available.
In cases where there are gaps between the slices and involume scanning, CTDIw must account for these gaps oroverlaps within the scans, resulting in the dose descriptor-volume CTDI (CTDIvol) given by:
CTDIvol ¼ ðmAsÞ eff X CTDIw
where (mAs)eff is indicated on the CT user console [29, 31].For volume scanning, CTDIw is divided by the pitch to
give a mean dose CTDIvol along the z-axis [8, 27, 31]:
Figure 1. A 100-mm ionization chamber used for computed tomography dose index (CTDI) measurements.
112 F. Zarb et al./Journal of Medical Imaging and Radiation Sciences 40 (2009) 109-115

Figure 2. Computed tomography dose index (CTDI) head and body phantom.
CTDIvol ¼ CTDw=pitch
The CTDIvol can be determined by both of the above for-mulas depending on which scanning parameters are availablefor calculation. CTDI as DRL may be specified as eitherCTDIw or CTDIvol; in this case, the distinction is madedepending on the type of scanner being used (conventional/sequential scans vs. volume scans).
CTDIvol represents the average dose within a scan volumerelative to a standardized CT phantom. CTDIvol is not thedose specific to the patient but a standardized index of the av-erage dose delivered from the scanning series. However, itdoes not correlate very well with E because it does not takeinto account the number of scans or the length of the scannedregion [20, 32, 36]. Another dose measurement commonlyused in CT is DLP.
Dose Length Product
A complete CT examination consists of a number of scansthrough the anatomical region. A longer scan length employsa greater number of slices and longer anatomical lengthadministering a higher radiation dose. The CTDIvol multi-plied by the total scan length in centimeters is given as theDLP in milligray cm (mGy cm) [5, 27, 31, 32, 5, 36].
DLP ðmGy cmÞ ¼ CTDIvol ðmGyÞX total scan length ðcmÞ
DLP correlates better with E than CTDIvol, and can easilybe used as a measure of E. There is a linear relationship be-tween DLP and E and a linear relationship between E andthe stochastic risk; hence, as DLP increases with the numberof scans, E also increases. DLP can thus be used to comparethe stochastic risk between different CT examinations [20].
DLP is a more realistic measure of E and in calculating theDLP the measure of CTDIvol is still necessary. Although
F. Zarb et al./Journal of Medical Imaging
CTDIvol is estimated on the selected scanning parameters be-fore scanning, DLP is calculated after the scanning has takenplace and so is more accurate in the estimation of E. DLP andCTDIvol are now required by EURATOM council directiveto be displayed on the CT console. After the displayed valuesare tested for their functionality and reliability during accep-tance tests, they may be recorded for use in population CTdose surveys [8, 31].
The Purpose of Establishing DRLs in CT
The establishment of CT DRLs in terms of CTDIw,CTDIvol, and DLP aids in the identification of those exam-inations with protocols resulting in high doses. DRLs formthe baseline for optimization to reduce the dose given forthese CT examinations in identified clinical sites [37].DRLs also monitor how radiation dose is affected by changesin CT protocols and techniques [32].
The main purposes of establishing DRLs in CT are to limitthe number of unjustifiably high-dose examinations by promot-ing good practice and implementing the ALARA principle. Phy-sicians and radiographers should be made aware to optimizeradiation protection in CT. Identification of an optimal rangeof dose values for specific CT scanning protocols thus improvesthe management of patient dose in medical imaging [6, 38].
Recommendations for Dose Reduction in CT
Optimization for dose reduction can be effected in differ-ent ways. Colang et al [16] highlight their recommendationsfor optimizing dose reductions in CT by the following:
� Using automatic exposure control when available, auto-matically changing the mA setting according to the sizeof the anatomical region scanned� Limiting the scanning region to the minimum required,
reducing the number of images obtained and irradiatingless body tissue
and Radiation Sciences 40 (2009) 109-115 113

� Developing guidelines comparing dose indictors withstandards� Educating imaging professionals in optimization of expo-
sure settings to help them choose the correct parametersfor the particular clinical situation� Educating imaging professionals, referrers, and patients
about the risks and benefits of CT so that requests are jus-tified and limited� Continuous research improving the clinical applications
of CT
Continuous monitoring of DRLs helps in the effectiveevaluation of these implementations so that further changesand adjustments may be carried out to continuously optimizeradiation doses.
Conclusion
Over the past three decades, CT has been established as anessential tool for diagnosis. The overwhelming benefits accruedto patients from justified and optimized CT examinations haveincreased the widespread use of CT in medical radiology[6, 36, 39]. CT is a high-dose examination, implying the needto protect the patient from unnecessary or high radiation dosesby justifying every exam and optimizing each procedure usingDRLs and collective dose studies for this purpose. The use ofDRLs as a comparison of the dose given for specific CT exam-inations is an effective way of monitoring and limiting CT doseto patients as given in the UK example. Dose surveys have dem-onstrated that where the concept of DRLs was applied, dosereductions in CT did take place; hence, the emphasis of estab-lishing DRLs nationwide. The establishment of collective dosefrom manmade exposures is a legal and ethical requirement thathas been implemented in EU directives requiring member statesto establish collective doses and implement DRLs for optimiza-tion purposes [2, 36].
The S obtained from estimations of the average E basedon CT dose descriptors serve as an indication of the radiationdose in CT [35]. Although CTDIw or CTDIvol are a simpleand effective way of relating to E in CT, DLP is linearly cor-related to E and hence a better dose descriptor. DRLs arenormally presented as both CTDIw or CTDIvol and DLP to-gether with an estimate of E.
Acknowledgments
The authors would like to thank the following colleaguesfor providing scientific material and other support: M. Borgand P. Bezzina.
References
[1] IAEA. (2002). Radiological protection for medical exposure to ionizing
radiation. Safety guide. Safety standards series No. RS-G-1.5. Vienna,
Austria; IAEA.
[2] Council directive. In: European Union. 97/43/EURATOM. June 1997.
[3] Vano, E., & Gonzalez, L. (2000). Patient dosimetry and reference doses:
practical considerations. Radiat Protect Dosim 90, 85–88.
114 F. Zarb et al./Journal of Medical Imaging
[4] ICRP. (1991). Annals of the ICRP Publication 60: 1990 recommendations
of the ICRP on radiological protection. Oxford, UK: Pergamon Press.
[5] European Commission. European guidelines on quality criteria for com-
puted tomography, 1999.
[6] ICRP. (2001). Diagnostic reference levels in medical imaging: review
and additional advice. A web module produced by Committee 3 of
the ICRP.
[7] Sherer, M., Visconti, P., & Ritenour, E. (2002). Radiation protection in
medical radiography. Philadelphia, PA: Mosby.
[8] European Commission. European guidance on estimating population
doses from medical x-ray exposures, 2008.
[9] Faulkner, K., & Corbett, R. (1998). Commentary: reference doses and
quality in medical imaging. Br J Radiol 71, 1001–1002.
[10] Jurik, A., Jessen, K., & Hansen, J. (1997). Image quality and dose in
computed tomography. Eur Radiol 7, 77–81.
[11] Shrimpton, P., & Edyvean, S. (1998). Commentary: CT scanner do-
simetry. Br J Radiol 71, 1–3.
[12] Seeram, E., & Brennan, P. (2006). Diagnostic reference levels in radiol-
ogy. Radiol Technol 77, 373–384.
[13] Hall, E., & Brenner, D. (2008). Cancer risks from diagnostic radiology.
Br J Radiol 81, 362–378.
[14] Huda, W., Nickoloff, E., & Boone, J. (2008). Overview of patient do-
simetry in diagnostic radiology in the USA for the past 50 years. Med
Phys 35, 5713–5728.
[15] Tsapaki, V., Aldrich, J., Sharma, R., Staniszewska, M.,
Krisanachinda, A., & Rehani, M., et al. (2006). Dose reduction in
CT while maintaining diagnostic confidence: diagnostic reference levels
at routine head, chest and abdominal CT - IAEA coordinated research
project. Radiology 240, 828–834.
[16] Colang, J., Killion, J., & Vano, E. (2007). Patient dose from CT: a lit-
erature review. Radiol Technol 79, 17–26.
[17] Clarke, J., Cranley, K., Robinson, J., Smith, P., & Workman, A.
(2000). Application of draft European Commission reference levels to
a regional CT dose survey. Br J Radiol 73, 43–50.
[18] ICRP. (1996). ICRP. Radiological protection and safety in medicine.
ICRP Publication 73. Ann ICRP 26, 2.
[19] Shrimpton, P., Hillier, M., Lewis, M., & Dunn, M. (2005). Doses from
computed tomography (CT) examinations in the UK - 2003 review.
NRPB W67.
[20] Hidajat, N., Maurer, J., Schroder, R., Nunnemann, A. W. M.,
Pauli, K., & Felix, R. (1999). Relations between physical dose quantities
and patient dose in CT. Br J Radiol 72, 556–561.
[21] Harrison, J., & Streffer, C. (2007). The ICRP protection quantities,
equivalent and effective dose: Their basis and application. Radiat Protect
Dosim 127, 12–18.
[22] Huda, W., Atherton, J., Ware, D., & Cumming, W. (1997). An ap-
proach for the estimation of effective radiation dose at CT in pediatric
patients. Radiology 203, 417–422.
[23] Ware, D., Huda, W., Mergo, P., & Litwiller, A. (1999). Radiation ef-
fective doses to patients undergoing abdominal CT examinations. Radi-
ology 210, 645–650.
[24] Dawson, P. (2004). Patient dose in multislice CT: Why is it increasing
and does it matter? Br J Radiol 77, S10–S13.
[25] IAEA. (2006). Applying radiation safety standards in diagnostic radiol-
ogy and interventional procedures using x-rays. IAEA Safety report se-
ries 39:1–96.
[26] Lee, C., Lee, C., Han, E., & Bolch, W. (2007). Consideration of ICRP
2006 revised tissue weighting factors on age dependent values of effec-
tive dose for external photons. Phys Med Biol 52, 41–58.
[27] McNitt-Gray, M. (2002). AAPM/RSNA physics tutorial for residents:
topics in CT - Radiation dose in CT. RadioGraphics 22, 1541–1553.
[28] Mayo, J., Aldrich, J., & Muller, N. (2003). Radiation exposure at chest
CT: a statement of the Fleischner Society. Radiology 228, 15–21.
[29] Flohr, T., & Ohnesorge, B. (2006). Developmens in CT. Imaging 18,
45–61.
[30] Martin, C., Sutton, D., & Sharp, P. (1999). Balancing patient dose and
image quality. Appl Radiat Isotopes 50, 1–19.
and Radiation Sciences 40 (2009) 109-115

[31] ICRU. (2005). Patient dosimetry for X-Rays Used In Medical Imaging.
J ICRU 5, 2.
[32] Hatziioannou, K., Papanastassiou, E., Delichas, M., & Bousbouras, P.
(2003). A contribution to the establishment of diagnostic reference
levels in CT. Br J Radiol 76, 541–545.
[33] Tsapaki, V., Kottou, S., & Papadimitriou, D. (2001). Application of
European Commission reference dose levels in CT examinations in
Crete, Greece. Br J Radiol 74, 836–840.
[34] Ngaile, J., Msaki, P., & Kazema, R. (2006). Towards establishment of
the national reference dose levels from computed tomography examina-
tions in Tanzania. J Radiol Protect 26, 213–225.
[35] McNitt-Gray, M. (2002). Radiation dose in CT. RadioGraphics 22,
1541–1553.
F. Zarb et al./Journal of Medical Imaging
[36] Kalra, M., Maher, M., Toth, T., Hamberg, L., Blake, M., & Shepard, J., et al.
(2004). Strategies for CT radiation dose optimization. Radiology 230,
619–628.
[37] Johnston, D., & Brennan, P. (2000). Reference dose levels for patients
undergoing common diagnostic X-ray examinations in Irish hospitals.
Br J Radiol 73, 396–402.
[38] Veit, R., Bauer, B., Bernhardt, H., & Lechel, U. (1998). Proposed pro-
cedure for the establishment of diagnostic reference levels in Germany.
Radiat Protect Dosim 80, 117–120.
[39] United Nations Scientific Committee on the Effects of Atomic Radia-
tion. Sources of ionizing radiation. UNSCEAR 2000;1.
[40] Goddard, C., & Al-Farsi, A. (1999). Radiation doses from CT in the
Sultanate of Oman. Br J Radiol 72, 1073–1077.
and Radiation Sciences 40 (2009) 109-115 115
Copyright © 2022 FDOKUMEN




















