
Rationale and design of the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An...
9
Clinical Trial Design Rationale and design of the CONFIRM ( COronary CT Angiography Evaluatio N For Clinical Outcomes: An Inte Rnational Multicenter) Registry James K. Min, MD a,b, * ,†,‡ , Allison Dunning, MS c,‡ , Fay Y. Lin, MD a , Stephan Achenbach, MD d , Mouaz H. Al-Mallah, MD, MSc e , Daniel S. Berman, MD f,† , Matthew J. Budoff, MD g , Filippo Cademartiri, MD h , Tracy Q. Callister, MD i , Hyuk-Jae Chang, MD, PhD j , Victor Cheng, MD f , Kavitha M. Chinnaiyan, MD k , Benjamin Chow, MD l , Augustin Delago, MD m , Martin Hadamitzky, MD n , Jorg Hausleiter, MD n , Ronald P. Karlsberg, MD o , Philipp Kaufmann, MD p , Erica Maffei, MD h , Khurram Nasir, MD q , Michael J. Pencina, PhD r , Gilbert L. Raff, MD k , Leslee J. Shaw, PhD s,† , Todd C. Villines, MD t Departments of a Medicine; b Radiology; c Public Health, Weill Cornell Medical College and the New York Presbyterian Hospital, 520 E 70th Street, Starr Pavilion, K415, New York, NY 10021, USA; d Department of Medicine, University of Ehrlangen, Ehrlangen, Germany; e Department of Medicine, Wayne State University, Henry Ford Hospital, Detroit, MI, USA; f Department of Imaging, Cedars-Sinai Medical Center, Los Angeles, CA, USA; g Department of Medicine, Harbor UCLA Medical Center, Los Angeles, CA, USA; h Department of Radiology, University Hospital of Parma, Parma, Italy; i Tennessee Heart and Vascular Institute, Hendersonville, TN, USA; j Division of Cardiology, Severance Cardiovascular Hospital, Seoul, Korea; k Department of Cardiology, William Beaumont Hospital, Royal Oak, MI, USA; l Department of Medicine and Radiology, University of Ottawa, ON, Canada; m Capital Cardiology Associates, Albany, NY, USA; n Division of Cardiology, University of Munich, Munich, Germany; o Cardiovascular Research Foundation, David Geffen School of Medicine UCLA, Beverly Hills, CA; p University Hospital, Zurich, Switzerland; q Yale University School of Medicine, Conflict of interest: S.A. has received grant support from Siemens and Bayer Schering Pharma and is a consultant for Servier. M.A.-M. has received support from AHA, BCBS Foundation of Michigan, and Astellas. M.J.B. has received modest compensation from the speakers bureau of GE Healthcare. F.C. has received grant support from GE Healthcare. K.C. has received grant support from Bayer Pharma, Blue Cross Blue Shield Blue Care MI. B.C. has received research and fellowship support from GE Healthcare and research support from Pfizer and AstraZeneca and educational support from TeraRecon. J.H. has received research support from Siemens Medical Systems. P.K. has received institutional research support from GE Healthcare and grant support from Swiss National Science Foundation. E.M. has received grant support from GE Healthcare. J.K.M. has received modest compensation from the speakers bureau and medical advisory board and significant research support from GE Healthcare. G.L.R. has received grant support from Siemens, Blue Cross Blue Shield Blue Care MI, and Bayer Pharma. The other authors report no conflicts of interest. * Corresponding author. E-mail address: [email protected] † Member of CONFIRM Executive Steering Committee. ‡ Member of Data Coordinating Center. Submitted September 13, 2010. Accepted for publication January 12, 2011. 1934-5925/$ - see front matter Ó 2011 Society of Cardiovascular Computed Tomography. All rights reserved. doi:10.1016/j.jcct.2011.01.007 Journal of Cardiovascular Computed Tomography (2011) 5, 84–92
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Rationale and design of the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An...

Journal of Cardiovascular Computed Tomography (2011) 5, 84–92
Clinical Trial Design
Rationale and design of the CONFIRM (COronary CTAngiography EvaluatioN For Clinical Outcomes: AnInteRnational Multicenter) Registry
James K. Min, MDa,b,*,†,‡, Allison Dunning, MSc,‡, Fay Y. Lin, MDa,Stephan Achenbach, MDd, Mouaz H. Al-Mallah, MD, MSce, Daniel S. Berman, MDf,†,Matthew J. Budoff, MDg, Filippo Cademartiri, MDh, Tracy Q. Callister, MDi,Hyuk-Jae Chang, MD, PhDj, Victor Cheng, MDf, Kavitha M. Chinnaiyan, MDk,Benjamin Chow, MDl, Augustin Delago, MDm, Martin Hadamitzky, MDn,Jorg Hausleiter, MDn, Ronald P. Karlsberg, MDo, Philipp Kaufmann, MDp,Erica Maffei, MDh, Khurram Nasir, MDq, Michael J. Pencina, PhDr, Gilbert L. Raff, MDk,Leslee J. Shaw, PhDs,†, Todd C. Villines, MDt
Departments of aMedicine; bRadiology; cPublic Health, Weill Cornell Medical College and the New York PresbyterianHospital, 520 E 70th Street, Starr Pavilion, K415, New York, NY 10021, USA; dDepartment of Medicine, University ofEhrlangen, Ehrlangen, Germany; eDepartment of Medicine, Wayne State University, Henry Ford Hospital, Detroit, MI,USA; fDepartment of Imaging, Cedars-Sinai Medical Center, Los Angeles, CA, USA; gDepartment of Medicine, HarborUCLA Medical Center, Los Angeles, CA, USA; hDepartment of Radiology, University Hospital of Parma, Parma, Italy;iTennessee Heart and Vascular Institute, Hendersonville, TN, USA; jDivision of Cardiology, Severance CardiovascularHospital, Seoul, Korea; kDepartment of Cardiology, William Beaumont Hospital, Royal Oak, MI, USA; lDepartment ofMedicine and Radiology, University of Ottawa, ON, Canada; mCapital Cardiology Associates, Albany, NY, USA; nDivisionof Cardiology, University of Munich, Munich, Germany; oCardiovascular Research Foundation, David Geffen Schoolof Medicine UCLA, Beverly Hills, CA; pUniversity Hospital, Zurich, Switzerland; qYale University School of Medicine,
Conflict of interest: S.A. has received grant support from Siemens and Bayer Schering Pharma and is a consultant for Servier. M.A.-M. has received
support from AHA, BCBS Foundation of Michigan, and Astellas. M.J.B. has received modest compensation from the speakers bureau of GE Healthcare. F.C.
has received grant support from GE Healthcare. K.C. has received grant support from Bayer Pharma, Blue Cross Blue Shield Blue Care MI. B.C. has received
research and fellowship support from GE Healthcare and research support from Pfizer and AstraZeneca and educational support from TeraRecon. J.H. has
received research support from Siemens Medical Systems. P.K. has received institutional research support from GE Healthcare and grant support from Swiss
National Science Foundation. E.M. has received grant support from GE Healthcare. J.K.M. has received modest compensation from the speakers bureau and
medical advisory board and significant research support from GE Healthcare. G.L.R. has received grant support from Siemens, Blue Cross Blue Shield Blue
Care MI, and Bayer Pharma. The other authors report no conflicts of interest.
* Corresponding author.
E-mail address: [email protected]
† Member of CONFIRM Executive Steering Committee.
‡ Member of Data Coordinating Center.
Submitted September 13, 2010. Accepted for publication January 12, 2011.
1934-5925/$ - see front matter � 2011 Society of Cardiovascular Computed Tomography. All rights reserved.
doi:10.1016/j.jcct.2011.01.007
Min et al Rationale and design of the CONFIRM Registry 85
New Haven, CT; rHarvard Clinical Research Institute, Boston, MA; SDepartment of Medicine, Emory University School ofMedicine, Atlanta, GA, USA and tCardiology Service, Department of Internal Medicine, Walter Reed Army MedicalCenter, Washington, DC, USA
KEYWORDS:Computed tomography;Atherosclerosis;Prognosis;Coronary disease;Nonobstructive
BACKGROUND: Coronary computed tomographic angiography (CCTA) of 64-detector rows or greaterrepresents a novel noninvasive anatomicmethod for evaluation of patients with suspected coronary arterydisease (CAD). Early studies suggest a potential for prognostic risk assessment by CCTA findings butwere limited by small patient cohorts or single centers. TheCONFIRM (COronaryCTAngiographyEval-uatioN For Clinical Outcomes: An InteRnational Multicenter) registry is a large, prospective, multina-tional dynamic observational study of patients undergoing CCTA. The primary aim of CONFIRM is todetermine the prognostic value of CCTA findings for the prediction of future adverse CAD events.
METHODS: The CONFIRM registry currently represents 27,125 consecutive patients at 12 clustersites in 6 countries in North America, Europe, and Asia. CONFIRM sites were chosen on the basis of ad-equateCCTAvolume, siteCCTAproficiency, and local demographic characteristics andmedical facilitiesto ensure a broad-based sample of patients. Patients comprising the present CONFIRM cohort includethose with suspected but without known CAD, with known CAD, or asymptomatic persons undergoingCAD evaluation. A data dictionary comprising a wide array of demographic, clinical, and CCTA findingswas developed by theCONFIRM investigators and is uniformly used for all patients. Patients are followedup after CCTA performance to identify adverse CAD events, including death, myocardial infarction,unstable angina, target vessel revascularization, and CAD-related hospitalization.
CONCLUSIONS: From a number of countries worldwide, the information collected from the CON-FIRM registry will add incremental and important insights into CCTA findings that confer prognosticvalue beyond demographic and clinical characteristics. The results of the CONFIRM registrywill providevaluable information about the optimal methods for using CCTA findings.� 2011 Society of Cardiovascular Computed Tomography. All rights reserved.
Introduction
Coronary computed tomographic angiography (CCTA) of64-detector rows or greater has been recently introduced as anovel noninvasive anatomic method for evaluating coronaryartery disease (CAD), showing high diagnostic accuracy fordetection and exclusion of obstructive CAD.1–3 Several re-cent reports have also examined the prognostic value ofCCTA findings for prediction of future adverse CAD events,but they were generally limited to single centers and by smallpatient cohorts.4–14 Further, prior studies examining riskstratification by CCTA findings have been primarily re-stricted to measures of obstructive CAD bymaximal luminaldiameter stenosis severity on a per-patient or per-vessel basis,with other plaque characteristics visualized by CCTA, in-cluding location, distribution, extent, and composition, andnoncoronary cardiac findings, including left ventricularsystolic function, volume, and regional wall motion, largelyneglected within development of prognostic models.
To date, no large multicenter study has examined thetotality of coronary plaque characteristics and noncoronarycardiac findings as detected by CCTA for optimal refine-ment of prognostic risk stratification. In this regard,CONFIRM (COronary CT Angiography EvaluatioN ForClinical Outcomes: An InteRnational Multicenter) registryhas been developed to provide a vehicle by which CCTAfindings could be identified to optimize risk assessment.This report describes the rationale and design features ofthe CONFIRM registry.
Overall study design
CONFIRM is a prospective, open-label, international, mul-ticenter dynamic observational registry designed to evaluateassociations between CCTA imaging findings and clinicalpresentation (cross-sectional) and their ability to predict mor-tality and major adverse cardiac events (MACEs; longitudinal)in patients with chronic CAD. The registry uses a novelcollaborative design with contribution and merger of similarprospectively enrolled cohorts from 12 sites around the world.Qualifying sites with complete risk factor, clinical presentationandCCTAdata recording, and follow-up for all-causemortalityandMACEs contributed data for common analysis, with phase1 of the CONFIRM registry closed as of September 1, 2010.
Study objectives
Primary objective
The primary objective of the CONFIRM registry is toidentify, quantify, and integrate coronary and noncoronarycardiac findings byCCTAwith demographic and clinical datafor refinement of risk stratification of persons with suspectedor known CAD. Specifically, we will determine CCTAfindings that predict intermediate-term (2-year) mortalityevents, with incremental improvement over traditional riskassessment of symptomatic (Morise Score) and asymptom-atic (Framingham Risk Score) persons suspected of CAD.

86 Journal of Cardiovascular Computed Tomography, Vol 5, No 2, March/April 2011
Secondary objectives
The secondary objectives of the CONFIRM registryinclude the following: (1) to determine optimal methods ofscoring CCTA to allow for the most accurate risk stratifica-tion; (2) to examine prognostic risk assessment of CCTAcoronary and noncoronary cardiac findings in specific sub-groups, including but not limited to diabetics, women, anddifferent ethnic groups; (3) to determine the incrementalvalueofCCTAfindings beyondcoronary artery calciumscore(CACS) for prediction of incident adverse CAD events; (4) toassociate clinical symptoms and demographic data to CCTAcoronary artery findings with an aim at refining estimates oflikelihood of CAD for symptomatic persons with suspectedCAD; (5) to associate CCTA coronary and noncoronarycardiac findings with clinical risk factors and symptoms fordevelopment of a CCTA global risk score for symptomaticpersons with suspected CAD; (6) to examine post-CCTAresource utilization, particularly as related to rates of down-stream invasive coronary angiography; and (7) to identifyspecific coronary artery plaque characteristics identified onCCTA that are associated with ‘‘culprit’’ lesions at the time ofincident presentation of acute myocardial infarction.
Targeted population
The targeted population for the CONFIRM registry wasa large and representative sample of adults R 18 years ofage who have undergone CCTA by physician referral. Todo so, we invited sites that had collected cohorts of CCTApatients with risk factors, symptoms, CCTA findings, andoutcomes to contribute data for a merged database. Thissample includes patients with suspected but without knownCAD, with known CAD, and asymptomatic persons under-going risk stratification through atherosclerosis identifica-tion by CCTA to evaluate the significance of CCTAfindings in different clinical contexts.
Study endpoints
The primary endpoint of the CONFIRM registry ismortality by all causes. Secondary endpoints of CONFIRMinclude MACEs, inclusive of death, myocardial infarction,unstable angina requiring hospitalization, and target vesselrevascularization and rates of downstream invasive coronaryangiography.
Eligibility criteria
Patient eligibility criteria
All consecutive patients at cluster sites meeting allinclusion criteria undergoing CCTA of 64-detector rows orgreater are included within the CONFIRM registry. Patient
inclusion criteria include the following: (1) ageR 18 years,(2) evaluation by CCTAwith 64-detector rows or greater forCAD evaluation, (3) interpretable CCTA; and (4) prospectivedata collection for CAD risk factors. No explicit patientexclusion criteria were defined.
Site eligibility criteria
Each participating site that contributed patient-level datato the CONFIRM registry meets the following site require-ments: (1) .200 patients per annum undergoing CCTA by64-detector rows or greater, (2) incorporation of CCTA intodaily clinical practice by members of the medical centerother than those involved with the CCTA performance andinterpretation, and (3) director of laboratory possessinglevel III-equivalent expertise in CCTA.
Study sites/participating centers
During the initial phase of the CONFIRM registry, 12cluster sites contributed data from patients undergoingCCTA of 64-detector rows or greater (Fig. 1). Six countriesin North America, Europe, and Asia are presently repre-sented in this multinational effort, including the UnitedStates, Canada, Germany, Switzerland, Italy, and SouthKorea. Data collection activities began in 1 center in 2003and at most centers in 2005, with a goal of collecting dataon approximately 30,000 patients. Participating sites repre-sent a mixture of academic university-based medical centersand private practice sites (Table 1).
The initial geographic clusters were chosen to representpatient populations with diverse demographic and clinicalcharacteristics, medical centers of different sizes and withdifferent diagnostic capabilities, and sites where CCTA hasbeen incorporated into daily clinical cardiac practice. Whenrequired, each site principal investigator representing acluster site obtained approval from the local ethics com-mittee or institutional review board.
Sites were eligible for merger into the CONFIRM registryif they performed prospective cohort collection of CCTAfindings with .80% overlap with the predefined datadictionary. Databases had to include uniform collection ofmajor categories of patient data, including demographics,prior CAD and revascularization history, Framingham riskfactors, symptom indication for CCTA, codedCCTA stenosisseverity over a Society of Cardiovascular Computed Tomog-raphy (SCCT) coronary model, and obtained follow-up forall-cause mortality forR1 year with,5% loss to follow-up.Sites were allowed to provide both previously published andunpublished data.
Patient recruitment and evaluation
All current CONFIRM study patients underwent CCTAby order of a physician. At the time of the CCTA

Figure 1 Distribution of follow-up time over CONFIRM sites. DF, Diamond Forrestor, WRAMH, Walter Reed Army Medical Hospital;WBH, William Beaumont Hospital; CSMC, Cedars-Sinai Medical Center; THVI, Tennessee Heart and Vascular Institute.
Min et al Rationale and design of the CONFIRM Registry 87
examination, information was prospectively collected relat-ing to demographics, targeted medical history, cardiovascu-lar risk factor profiles and was recorded in site-specific casereport forms (CRFs) (Table 2). Standardized definitions forcardiovascular risk factors were used. Indication for CCTAperformancewas also recorded and classified into the follow-ing seven categories: anginal equivalent (including pain,tightness, pressure), dyspnea, asymptomatic, preoperativeevaluation, electrophysiologic indication (eg, pulmonaryvein mapping, left atrial appendage evaluation), congenitalheart disease evaluation, or other.
At some centers, additional information was obtainedrelated to chest pain quality, including presence of chestpain, pressure, or tightness; worsening of chest pain withexertion; relief of chest pain with rest or nitroglycerin;number of episodes of chest pain per week; and presence of
Table 1 Sites in the CONFIRM registry
Site no. Site (reorder to group by continent)
1 Severance Cardiovascular Hospital, Seoul, Sou2 University of Munich, Munich, Germany3 University Hospital of Parma, Parma, Italy4 University Hospital Zurich, Zurich, Switzerland5 Ottawa Heart Institute, ON, Canada6 Cedars-Sinai Medical Center, Los Angeles, CA7 Capital Cardiology Associates, Albany, NY8 Harbor UCLA Medical Center, Los Angeles, CA9 Tennessee Heart and Cardiovascular Institute,
Hendersonville, TN10 Walter Reed Army Medical Center, Washington11 Wayne State University, Henry Ford Hospital,12 William Beaumont Hospital, Royal Oak, MI
dyspnea (Fig. 1). Similarly, selected centers recorded lipidlevels, serum creatinine, and creatinine clearance. Patientswere further identified as having versus not having priorknown CAD. Prior known CAD status included patientswith history of myocardial infarction, prior percutaneouscoronary intervention, and prior coronary artery bypassgraft (CABG). A subset of patients underwent concurrentcoronary artery calcium scoring. Completed CRFs weremaintained by sites until being merged with the other inves-tigative CONFIRM sites.
Patient follow-up
Patient follow-up was performed by each local institu-tion by a dedicated physician or research nurse or both(Fig. 2). All CONFIRM study patients were followed for a
Location N
th Korea Asia 4912Europe 1785Europe 1895Europe 736North America 2171North America 2477North America 499North America 2116North America 4807
, DC North America 626Detroit, MI North America 935
North America 4166
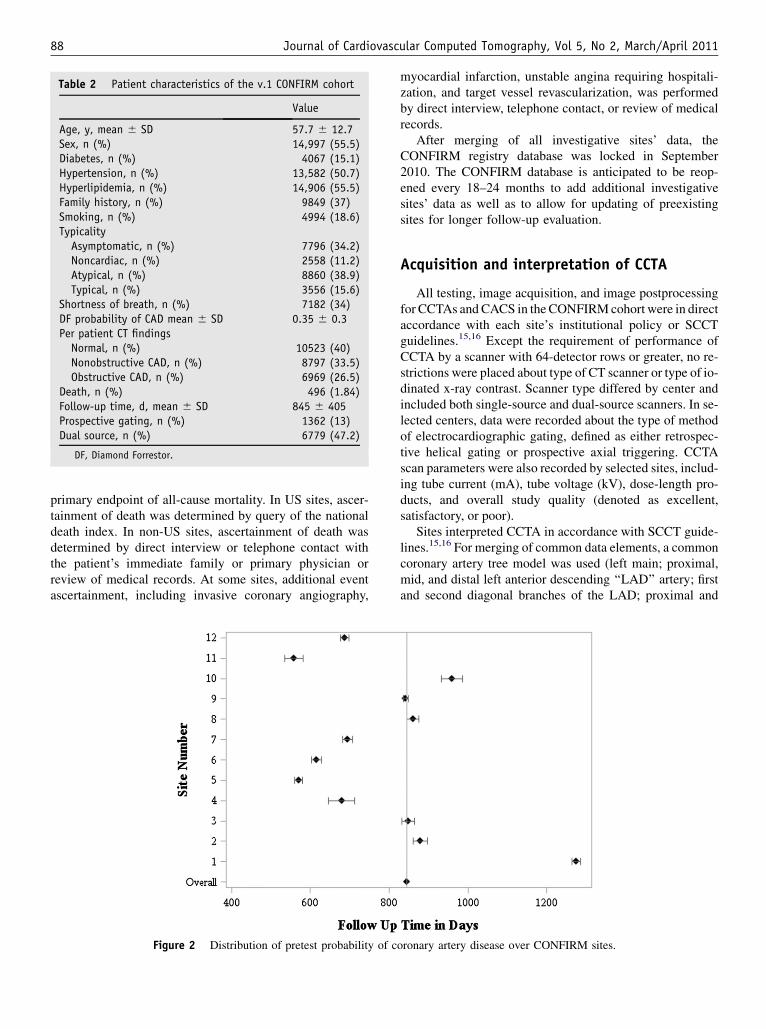
Table 2 Patient characteristics of the v.1 CONFIRM cohort
Value
Age, y, mean 6 SD 57.7 6 12.7Sex, n (%) 14,997 (55.5)Diabetes, n (%) 4067 (15.1)Hypertension, n (%) 13,582 (50.7)Hyperlipidemia, n (%) 14,906 (55.5)Family history, n (%) 9849 (37)Smoking, n (%) 4994 (18.6)TypicalityAsymptomatic, n (%) 7796 (34.2)Noncardiac, n (%) 2558 (11.2)Atypical, n (%) 8860 (38.9)Typical, n (%) 3556 (15.6)
Shortness of breath, n (%) 7182 (34)DF probability of CAD mean 6 SD 0.35 6 0.3Per patient CT findingsNormal, n (%) 10523 (40)Nonobstructive CAD, n (%) 8797 (33.5)Obstructive CAD, n (%) 6969 (26.5)
Death, n (%) 496 (1.84)Follow-up time, d, mean 6 SD 845 6 405Prospective gating, n (%) 1362 (13)Dual source, n (%) 6779 (47.2)
DF, Diamond Forrestor.
88 Journal of Cardiovascular Computed Tomography, Vol 5, No 2, March/April 2011
primary endpoint of all-cause mortality. In US sites, ascer-tainment of death was determined by query of the nationaldeath index. In non-US sites, ascertainment of death wasdetermined by direct interview or telephone contact withthe patient’s immediate family or primary physician orreview of medical records. At some sites, additional eventascertainment, including invasive coronary angiography,
Figure 2 Distribution of pretest probability of c
myocardial infarction, unstable angina requiring hospitali-zation, and target vessel revascularization, was performedby direct interview, telephone contact, or review of medicalrecords.
After merging of all investigative sites’ data, theCONFIRM registry database was locked in September2010. The CONFIRM database is anticipated to be reop-ened every 18–24 months to add additional investigativesites’ data as well as to allow for updating of preexistingsites for longer follow-up evaluation.
Acquisition and interpretation of CCTA
All testing, image acquisition, and image postprocessingfor CCTAs and CACS in theCONFIRMcohort were in directaccordance with each site’s institutional policy or SCCTguidelines.15,16 Except the requirement of performance ofCCTA by a scanner with 64-detector rows or greater, no re-strictions were placed about type of CT scanner or type of io-dinated x-ray contrast. Scanner type differed by center andincluded both single-source and dual-source scanners. In se-lected centers, data were recorded about the type of methodof electrocardiographic gating, defined as either retrospec-tive helical gating or prospective axial triggering. CCTAscan parameters were also recorded by selected sites, includ-ing tube current (mA), tube voltage (kV), dose-length pro-ducts, and overall study quality (denoted as excellent,satisfactory, or poor).
Sites interpreted CCTA in accordance with SCCT guide-lines.15,16 For merging of common data elements, a commoncoronary artery tree model was used (left main; proximal,mid, and distal left anterior descending ‘‘LAD’’ artery; firstand second diagonal branches of the LAD; proximal and
oronary artery disease over CONFIRM sites.
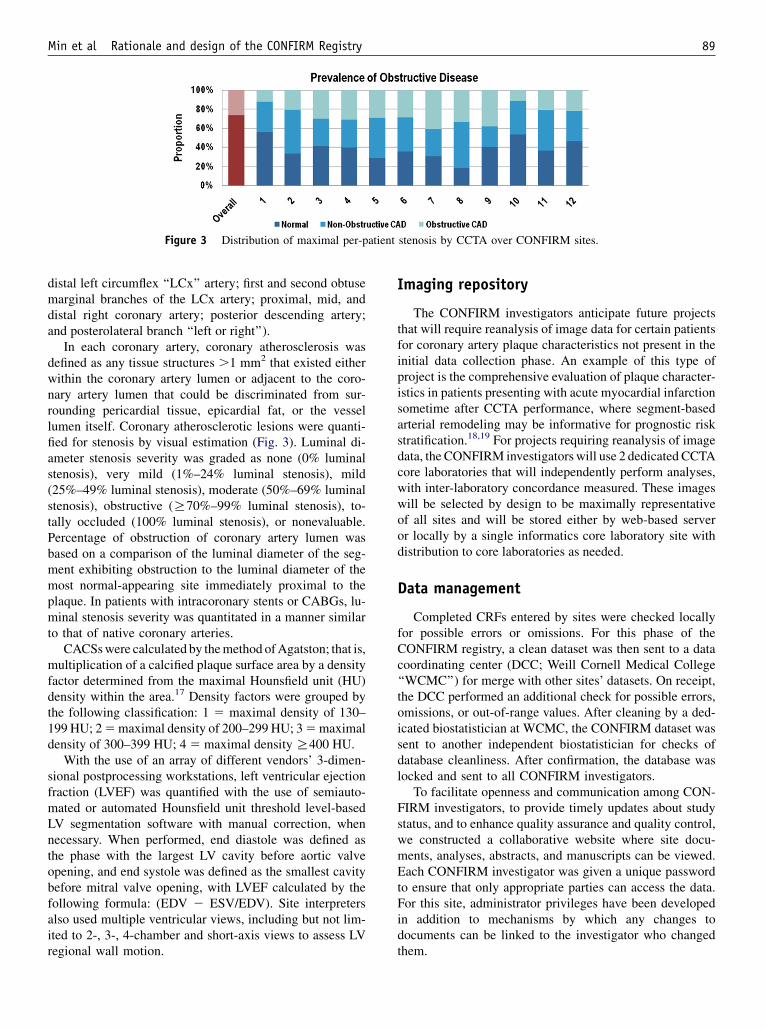
Figure 3 Distribution of maximal per-patient stenosis by CCTA over CONFIRM sites.
Min et al Rationale and design of the CONFIRM Registry 89
distal left circumflex ‘‘LCx’’ artery; first and second obtusemarginal branches of the LCx artery; proximal, mid, anddistal right coronary artery; posterior descending artery;and posterolateral branch ‘‘left or right’’).
In each coronary artery, coronary atherosclerosis wasdefined as any tissue structures .1 mm2 that existed eitherwithin the coronary artery lumen or adjacent to the coro-nary artery lumen that could be discriminated from sur-rounding pericardial tissue, epicardial fat, or the vessellumen itself. Coronary atherosclerotic lesions were quanti-fied for stenosis by visual estimation (Fig. 3). Luminal di-ameter stenosis severity was graded as none (0% luminalstenosis), very mild (1%–24% luminal stenosis), mild(25%–49% luminal stenosis), moderate (50%–69% luminalstenosis), obstructive (R70%–99% luminal stenosis), to-tally occluded (100% luminal stenosis), or nonevaluable.Percentage of obstruction of coronary artery lumen wasbased on a comparison of the luminal diameter of the seg-ment exhibiting obstruction to the luminal diameter of themost normal-appearing site immediately proximal to theplaque. In patients with intracoronary stents or CABGs, lu-minal stenosis severity was quantitated in a manner similarto that of native coronary arteries.
CACSswere calculated by themethod ofAgatston; that is,multiplication of a calcified plaque surface area by a densityfactor determined from the maximal Hounsfield unit (HU)density within the area.17 Density factors were grouped bythe following classification: 1 5 maximal density of 130–199 HU; 25maximal density of 200–299 HU; 35maximaldensity of 300–399 HU; 4 5 maximal densityR400 HU.
With the use of an array of different vendors’ 3-dimen-sional postprocessing workstations, left ventricular ejectionfraction (LVEF) was quantified with the use of semiauto-mated or automated Hounsfield unit threshold level-basedLV segmentation software with manual correction, whennecessary. When performed, end diastole was defined asthe phase with the largest LV cavity before aortic valveopening, and end systole was defined as the smallest cavitybefore mitral valve opening, with LVEF calculated by thefollowing formula: (EDV 2 ESV/EDV). Site interpretersalso used multiple ventricular views, including but not lim-ited to 2-, 3-, 4-chamber and short-axis views to assess LVregional wall motion.
Imaging repository
The CONFIRM investigators anticipate future projectsthat will require reanalysis of image data for certain patientsfor coronary artery plaque characteristics not present in theinitial data collection phase. An example of this type ofproject is the comprehensive evaluation of plaque character-istics in patients presenting with acute myocardial infarctionsometime after CCTA performance, where segment-basedarterial remodeling may be informative for prognostic riskstratification.18,19 For projects requiring reanalysis of imagedata, the CONFIRM investigators will use 2 dedicated CCTAcore laboratories that will independently perform analyses,with inter-laboratory concordance measured. These imageswill be selected by design to be maximally representativeof all sites and will be stored either by web-based serveror locally by a single informatics core laboratory site withdistribution to core laboratories as needed.
Data management
Completed CRFs entered by sites were checked locallyfor possible errors or omissions. For this phase of theCONFIRM registry, a clean dataset was then sent to a datacoordinating center (DCC; Weill Cornell Medical College‘‘WCMC’’) for merge with other sites’ datasets. On receipt,the DCC performed an additional check for possible errors,omissions, or out-of-range values. After cleaning by a ded-icated biostatistician at WCMC, the CONFIRM dataset wassent to another independent biostatistician for checks ofdatabase cleanliness. After confirmation, the database waslocked and sent to all CONFIRM investigators.
To facilitate openness and communication among CON-FIRM investigators, to provide timely updates about studystatus, and to enhance quality assurance and quality control,we constructed a collaborative website where site docu-ments, analyses, abstracts, and manuscripts can be viewed.Each CONFIRM investigator was given a unique passwordto ensure that only appropriate parties can access the data.For this site, administrator privileges have been developedin addition to mechanisms by which any changes todocuments can be linked to the investigator who changedthem.

90 Journal of Cardiovascular Computed Tomography, Vol 5, No 2, March/April 2011
Data analysis
Descriptive, univariate, and multivariate analyses wereconducted. For the primary objective, the proportionalhazards assumptions were tested for each CCTA findingin relation to mortality, and a multivariate Cox proportionalhazards model is used to evaluate the association of CCTAfindings with the risk of death from all causes. Regressionmodels were adjusted for demographic and clinical varia-bles and symptoms, and likelihood ratio tests are used todetermine a multivariable P value. Backward stepwise re-gression was used to select an independently predictiveset of CCTA findings. Receiver operating curves were plot-ted for models with clinical data alone and in conjunctionwith CCTA findings, and a C statistic was calculated todetermine the discriminatory ability of CCTA findings. Inaddition to the secondary analyses described above,CONFIRM investigators were also encouraged to proposeanalyses with prespecification of hypotheses and statisticalplans. To address multiple hypothesis testing, statistical sig-nificance accounted for false discovery rates.
The primary analysis was multivariate Cox regression formortality risk of obstructive (R50% intraluminal stenosis ona per-patient basis) disease adjusting for 8 covariates (age,sex, hypertension, hyperlipidemia, smoking, family historyof CAD, typicality of angina, and interaction of age and sex).On the basis of a 1.7% rate of all cause-mortality, a 25%prevalence of obstructive CAD, and an R2 of 0.24 with theuse of preliminary data, 24,152 patients would be requiredto detect a 30% excess hazard for obstructive CAD with90% power and an a of 0.05 with 8-way Bonferroni correc-tion for multiple hypothesis testing.
CONFIRM investigative sites have and will performstatistical analyses with the use of local site statisticians orelse will submit statistical analysis plans to the DCC forperformance. In the former case, the DCC confirms find-ings by replication of analyses, whereas, in the latter case,the DCC findings are confirmed by an independent third-party biostatistician.
Given the multiple sites in CONFIRM, an importantconsideration for analysis is heterogeneity of data. Analy-ses with inclusion of exposures, outcomes, or covariateswith significant heterogeneity will be performed with arandom-effects model by site and confirmed with sensitiv-ity analysis, removing each site sequentially from analysisto estimate the standard error of the mean.
Patients with incomplete CCTA or outcome reportingare excluded from CONFIRM analyses, as are patients withmissing age and sex. For patients with other missing-at-random covariate values, multiple imputation procedureswill be performed by site. Patients with missing demo-graphics such as age and sex will be excluded.
For sites that did not collect one entire category of riskfactors such as family history, a dummy value for ‘‘missingby site’’ are assigned as a covariate. Sites that did notcollectR1 entire category of risk factors are excluded from
the CONFIRM dataset. For each primary analysis, sensi-tivity analysis is performed with Monte Carlo simulationsof 100 imputations to estimate the standard error of themean.
Discussion
Since the introduction of 64-detector row CCTA in 2005,several prospective multicenter studies have shown highdiagnostic performance of CCTA for detection and exclusionof obstructive CAD.1–3 However, data relating CCTA find-ings to prognostic risk stratification have been primarily lim-ited to single centers with large-scale data lacking.4–14 Assuch, uncertainty remains about the precise role of CCTAin clinical evaluation of persons with suspected CAD. Thislimitation is not specific to CCTA, but it has been presentfor other noninvasive cardiac imaging methods, with singlecenters generally taking long periods of time to accrueenough data to formulate large patient cohort analyses.
A few unique exceptions of collaboration have permittedacceleration of prognostic risk assessment of noninvasivecardiac imaging findings by combining data from multiplecenters to form very large patient cohorts; these registrieshave served as prototypes for CONFIRM. As an example,Shaw et al20,21 examined prognosis of 4728 patients at 5centers undergoing exercise and adenosine myocardialperfusion scintigraphy (MPS) imaging in the MyoviewMulticenter registry and 11,372 patients undergoing MPSor invasive coronary angiography at 7 centers in the Eco-nomics of Noninvasive Diagnosis registry. A similar typeof registry at 3 hospitals in 11,132 patients undergoing ex-ercise or dobutamine echocardiography identified highlyimpactful findings about echo findings and prognosis.22
The CONFIRM registry shares many similar strengthsand limitations to the aforementioned registries. The collab-orative spirit among all the CONFIRM investigators hasresulted in the acquisition and assembly of a large database toexamine the prognostic value of CCTA findings in a shorttime. The current dataset is geographically diverse, repre-sentative of persons who are presently undergoing clinicallyindicated CCTA, and uses uniform methods of scoring.Further, the CONFIRM dataset includes both cross-sectionalfindings as well as longitudinal follow-up. The cross-sectional findings will be helpful to relate CCTA angio-graphic findings tomeasures of CAD likelihood, whereas thelongitudinal follow-up data may be useful for enhanced riskstratification by summary measures, including global symp-tomatic risk scores. The CONFIRM study represents a novelapproach that affords multiple advantages. As participantscontribute data, core laboratory services, administrative andanalysis time in parallel, this study structure allows rapid andwell-powered investigation of important medical researchquestions. Thus, a collaborative studymay be performedwithsimilar sample size to a largegovernment- or industry-fundedstudy with much smaller expense. Note that the collaborative

Min et al Rationale and design of the CONFIRM Registry 91
spirit by which CONFIRM was developed has thus requiredno outside funding and, thus,may serve as an example of howfuture registries may be constructed.
Patients were not excluded on the basis of appropriate-use criteria from the American College of Cardiology/American Heart Association, reflecting international pat-terns of CCTA referral and to preserve the ability to examinethe interaction of CT findings with context for outcomes.Future studies may be able to test whether net reclassifica-tion by CCTA differs by appropriateness of indication.
Despite its strengths, the CONFIRM registry possesses allof the intrinsic limitations of observational open-label reg-istries. These include selection biases for patients referredfor CCTA imaging, potential heterogeneity between sites,interobserver and intersite variability in CCTA diagnosis,differential post-CCTA treatment patterns, as well as otherunobserved confounders. In common to all registries, theCONFIRM registry cannot accomplish the uniformity ofascertainment of prospective observational studies such asMulti-Ethnic Study of Atherosclerosis or the causal associ-ation of randomized controlled trials. We have aimed tomitigate some of these limitations by use of standardizeddata definitions, inclusion of sites only where CCTA hasbeen incorporated into general clinical care, and inclusion ofsites where performance and interpretation of CCTA are ledby persons with adequate proficiency. Future aims of theCONFIRM registry will be to increase the numbers ofpatients enrolled, the duration of follow-up, the number ofcenters involved, and geographic diversity (eg, SouthAmerica and Australia). However, the strength of the CON-FIRM registry is rapid, low-cost provision of hypothesis-generating data in a large ‘‘real-world’’ registry, with manyquestions requiring large-scale randomized controlled trialsfor validation of findings.
Conclusion
The CONFIRM registry will enable association of CCTAfindings to downstream risk of mortality and MACEs in aglobal fashion with the use of current generation CCTAtechnology. The unique ability of CCTA to examine plaquecharacteristics beyond stenosis severity alone, includingplaque burden, distribution, location, composition, andremodeling, will provide unique epidemiologic insightsinto CAD risk in a manner previously not possible. Further,the continually updating data collection of CONFIRM willallow for the generation of numerous hypothesis about short-,intermediate-, and long-term risk. These observations willbe valuable for the design of future randomized controlledtrials as well as the construction of future registries aimed atmore-focused patient subsets. Most importantly, the findingsfrom CONFIRM may be valuable to identify deficiencies inthe knowledge about CCTA findings and risk and, in thisregard, foster optimal patient care.
References
1. Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E,
Scherer M, Bellinger R, Martin A, Benton R, Delago A, Min JK:
Diagnostic performance of 64-multidetector row coronary computed to-
mographic angiography for evaluation of coronary artery stenosis in in-
dividuals without known coronary artery disease: results from the
prospective multicenter ACCURACY (Assessment by Coronary Com-
puted Tomographic Angiography of Individuals Undergoing Invasive
Coronary Angiography) trial. J Am Coll Cardiol. 2008;52:1724–32.
2. Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van
Mieghem CA, Nieman K, van Werkhoven JM, Pundziute G,
Weustink AC, de Vos AM, Pugliese F, Rensing B, Jukema JW, Bax JJ,
Prokop M, Doevendans PA, Hunink MG, Krestin GP, de Feyter PJ:
Diagnostic accuracy of 64-slice computed tomography coronary
angiography: a prospective, multicenter, multivendor study. J Am Coll
Cardiol. 2008;52:2135–44.
3. Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H,
Gottlieb I, Paul N, Clouse ME, Shapiro EP, Hoe J, Lardo AC, Bush DE,
de Roos A, Cox C, Brinker J, Lima JA: Diagnostic performance of coro-
nary angiography by 64-row CT. N Engl J Med. 2008;359:2324–36.
4. Min JK, Shaw LJ, Devereux RB, Okin PM, Weinsaft JW, Russo DJ,
Lippolis NJ, Berman DS, Callister TQ: Prognostic value of multide-
tector coronary computed tomographic angiography for prediction of
all-cause mortality. J Am Coll Cardiol. 2007;50:1161–70.
5. Min JK, Feignoux J, Treutenaere J, Laperche T, Sablayrolles J: The
prognostic value of multidetector coronary CT angiography for the
prediction of major adverse cardiovascular events: a multicenter obser-
vational cohort study. Int J Cardiovasc Imaging. 2010;26:721–8.
6. Min JK, Lin FY, Dunning AM, Delago A, Egan J, Shaw LJ,
Berman DS, Callister TQ: Incremental prognostic significance of
left ventricular dysfunction to coronary artery disease detection by
64-detector row coronary computed tomographic angiography for
the prediction of all-cause mortality: results from a two-centre study
of 5330 patients. Eur Heart J. 2010;31:1212–9.
7. Chow BJ, Wells GA, Chen L, Yam Y, Galiwango P, Abraham A,
Sheth T, Dennie C, Beanlands RS, Ruddy TD: Prognostic value of
64-slice cardiac computed tomography severity of coronary artery dis-
ease, coronary atherosclerosis, and left ventricular ejection fraction.
J Am Coll Cardiol. 2010;55:1017–28.
8. Hadamitzky M, Meyer T, Hein F, Bischoff B, Martinoff S, Schomig A,
Hausleiter J: Prognostic value of coronary computed tomographic angi-
ography in asymptomatic patients. Am J Cardiol. 2010;105:1746–51.
9. Hadamitzky M, Hein F, Meyer T, Bischoff B, Martinoff S, Schomig A,
Hausleiter J: Prognostic value of coronary computed tomographic an-
giography in diabetic patients without known coronary artery disease.
Diabetes Care. 2010;33:1358–63.
10. Hadamitzky M, Freissmuth B, Meyer T, Hein F, Kastrati A, Martinoff S,
Schomig A, Hausleiter J: Prognostic value of coronary computed tomo-
graphic angiography for prediction of cardiac events in patients with sus-
pected coronaryartery disease. JACCCardiovasc Imaging. 2009;2:404–11.
11. Ostrom MP, Gopal A, Ahmadi N, Nasir K, Yang E, Kakadiaris I,
Flores F, Mao SS, Budoff MJ: Mortality incidence and the severity
of coronary atherosclerosis assessed by computed tomography angiog-
raphy. J Am Coll Cardiol. 2008;52:1335–43.
12. van Werkhoven JM, Schuijf JD, Gaemperli O, Jukema JW, Kroft LJ,
Boersma E, Pazhenkottil A, Valenta I, puncziute G, de Roos A,
van der Wall EE, Kaufmann PA, Bax JJ: Incremental prognostic value
of multi-slice computed tomography coronary angiography over coro-
nary artery calcium scoring in patients with suspected coronary artery
disease. Eur Heart J. 2009;30:2622–9.
13. van Werkhoven JM, Schuijf JD, Gaemperli O, Jukema JW, Boersma E,
Wijns W, Stolzmann P, Alkadhai H, Valenta I, Stokkel MP, Kroft LJ, de
Roos A, Pundziute G, Scholte A, van der Wall EE, Kaufmann PA,
Bax JJ: Prognostic value of multislice computed tomography and gated

92 Journal of Cardiovascular Computed Tomography, Vol 5, No 2, March/April 2011
single-photon emission computed tomography in patients with sus-
pected coronary artery disease. J Am Coll Cardiol. 2009;53:623–32.
14. van Werkhoven JM, Cademartiri F, Seitun S, Maffei E, Palumbo A,
Martini C, Tarantini G, Kroft LJ, de Roos A, Weustink AC,
Jukema JW, Ardissino B, Mollet NR, Schuijf JD, Bax JJ: Diabetes:
prognostic value of CT coronary angiography–comparison with a non-
diabetic population. Radiology. 2010;256:83–92.
15. Abbara S, Arbab-Zadeh A, Callister TQ, Desai MY, Mamuya W,
Thomson L, Weigold WG: SCCT guidelines for performance of cor-
onary computed tomographic angiography: a report of the Society
of Cardiovascular Computed Tomography Guidelines Committee.
J Cardiovasc Comput Tomogr. 2009;3:190–204.
16. Raff GL, Abidov A, Achenbach S, Berman DS, Boxt LM, Budoff MJ,
Cheng V, DeFrance T, Hellinger JC, Karlsberg RP: Society of Cardi-
ovascular Computed Tomography: SCCT guidelines for the interpreta-
tion and reporting of coronary computed tomographic angiography.
J Cardiovasc Comput Tomogr. 2009;3:122–36.
17. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr.,
Detrano R: Quantification of coronary artery calcium using ultrafast
computed tomography. J Am Coll Cardiol. 1990;15:827–32.
18. Motoyama S, Kondo T, Sarai M, Sugiura A, Harigaya H, Sato T,
Inoue K, Okumura M, Ishii J, Anno H, Virmani R, Ozaki Y,
Hishida H, Narula J: Multislice computed tomographic characteristics
of coronary lesions in acute coronary syndromes. J Am Coll Cardiol.
2007;50:319–26.
19. Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T,
Naruse H, Ishii J, Hishida H, Wong ND, Virmani R, Kondo T,
Ozaki Y, Narula J: Computed tomographic angiography characteristics
of atherosclerotic plaques subsequently resulting in acute coronary
syndrome. J Am Coll Cardiol. 2009;54:49–57.
20. Shaw LJ, Hendel RC, Heller GV, Borges-Neto S, Cerqueira M,
Berman DS: Prognostic estimation of coronary artery disease risk
with resting perfusion abnormalities and stress ischemia on myocar-
dial perfusion SPECT. J Nucl Cardiol. 2008;15:762–73.
21. Shaw LJ, Hachamovitch R, Heller GV, Marwick TH, Travin JI,
Iskandrian AE, Kesler K, Lauer MS, Hendel R, Borges-Neto S,
Lewin HC, Berman DS, Miller D: Noninvasive strategies for the
estimation of cardiac risk in stable chest pain patients. The Econom-
ics of Noninvasive Diagnosis (END) Study Group. Am J Cardiol.
2000;86:1–7.
22. Shaw LJ, Vasey C, Sawada S, Rimmerman C, Marwick TH: Impact of
gender on risk stratification by exercise and dobutamine stress echo-
cardiography: long-term mortality in 4234 women and 6898 men.
Eur Heart J. 2005;26:447–56.




















