
Predictors of depressive symptomatology among low-income adolescent mothers
Upload
independentCategory
view
5download
0
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [CDL Journals Account]On: 2 November 2009Access details: Access Details: [subscription number 794532497]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Vulnerable Children and Youth StudiesPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t724921266
Rates and predictors of anxiety and depressive disorders in adolescents ofparents with HIVPatricia Lester a; Mary Jane Rotheram-Borus a; Sung-Jae Lee a; Scott Comulada a; Suzi Cantwell a; Nancy Wua; Ying Ying Lin a
a Center for Community Health, Department of Psychiatry, University of California, Los Angeles, USA
Online Publication Date: 21 July 2006
To cite this Article Lester, Patricia, Rotheram-Borus, Mary Jane, Lee, Sung-Jae, Comulada, Scott, Cantwell, Suzi, Wu, Nancy and Lin,Ying Ying(2006)'Rates and predictors of anxiety and depressive disorders in adolescents of parents with HIV',Vulnerable Childrenand Youth Studies,1:1,81 — 101
To link to this Article: DOI: 10.1080/17450120600659028
URL: http://dx.doi.org/10.1080/17450120600659028
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
Vulnerable Children and Youth Studies, April 2006; 1(1): 81–101
ISSN 1745-0128 print/ISSN 1745-0136 online © 2006 Taylor & FrancisDOI: 10.1080/17450120600659028
RVCH1745-01281745-0136Vulnerable Childern and Youth Studies, Vol. 1, No. 1, March 2006: pp. 0–0Vulnerable Children and Youth StudiesRates and predictors of anxiety and depressive disorders in adolescents of parents with HIV
Anxiety and depressive disorders in adolescents of parents with HIVP. Lester et al.PATRICIA LESTER, MARY JANE ROTHERAM-BORUS, SUNG-JAE LEE, SCOTT COMULADA, SUZI CANTWELL, NANCY WU, & YING YING LIN
Center for Community Health, Department of Psychiatry, University of California, Los Angeles, USA
AbstractChildren with a parent with HIV (PWH) are expected to be at increased risk for anxiety and depres-sive disorders because of the potential impact of parental HIV illness and death. PWH and theiradolescent children were initially recruited in the context of a randomized intervention trial, withmore than 60% of adolescents experiencing death of a parent prior to assessment. Using the Com-posite International Diagnostic Interview, lifetime and recent anxiety and depressive disorders weremeasured 4 years following enrollment. Adolescents of PWH had high rates of any lifetime and recentanxiety disorders. In particular, both lifetime and recent rates of post-traumatic stress disorder werehigh. Lifetime anxiety disorders were significantly associated with older age, baseline emotionaldistress and prior traumatic exposure, while lifetime depressive disorders were associated with femalegender, parental bereavement and prior traumatic exposure. These findings demonstrate the need forappropriate screening and treatment of adolescents of PWH.
Keywords: Adolescence, parents with HIV, anxiety disorder, depressive disorder, trauma, bereavement
Introduction
Confronting chronic illness and potential death in a parent is a major challenge to a child’sadjustment at any age. In the developed world, about 4–5% of children experience a par-ent’s death before reaching adulthood (Lutzke et al., 1997), while another 5–15% livewith a chronically ill parent (Stanton et al., 2001). The AIDS epidemic has increasedthese rates, with about 36 000 to 65 000 adolescents losing at least one parent to AIDS,and an estimated 350 000 children now living with a parent with HIV in the United States(Drucker & Vermund, 1989; Michaels & Levine, 1992; Schuster et al., 2000). Interna-tionally, an estimated 40 million adults, most of them parents, are now living with HIV(UNAIDS, 2002), and about 13 million children have been orphaned by AIDS(UNAIDS, 2002). As improved treatment strategies continue to prolong the lives of par-ents with HIV, more children are living with a chronically ill parent (Eron et al., 1995;Kinloch-de Loes & Perrin, 1995). While the impact of living with and possibly losing aparent with HIV (PWH) on adolescent adjustment remains unclear, the children of PWHare expected to be at greater risk for both anxiety and depressive disorders. Thus, this
Correspondence: Patricia Lester, MD, Center for Community Health, 10920 Wilshire Blvd, Suite 350, Los Angeles, CA 90024-6521,USA. Tel: 310 794 3227. Fax: 310 794 8297. E-mail: [email protected]
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
82 P. Lester et al.
study evaluates the rates and predictors of adolescent anxiety and depressive disordersfollowing parental HIV diagnosis.
Adolescents living with a chronically ill parent face daily challenges related to their par-ent’s emotional and physical health. In previous studies, childhood anxiety and depressionhave been associated with having a physically ill parent (Brech, 1996; Compas et al., 1994,1996; Lutzke et al., 1997; Romer et al., 2002; Stanton et al., 2001). Children of terminallyill parents report adjustment problems at twice the rate of other children while the parent isliving (Siegel et al., 1996). Parental physical illness may alter family functioning in multipleways, including the disruption of routines, inhibition of parental support and monitoringand heightened fears over parental death (Rosenheim & Reicher, 1986; Saldinger et al.,2003). For families most often run by a single HIV-infected parent, there are added con-cerns for the adolescent child. Adolescent children of chronically ill parents are oftenexpected to assume adult roles within the family (Compas et al., 1996; Stein et al., 1999),with caretaking responsibilities for younger siblings (Rotheram-Borus et al., 2001b). Theymay also tend to their parents’ needs during periods of parental physical illness or hospital-ization (Rotheram-Borus et al., 1997). Attempting to meet their parent’s increased physicaland emotional needs may result in lost developmental opportunities for these adolescents,particularly the chance to establish autonomy and obtain parental guidance (Parkes &Weiss, 1983; Rosenheim & Reicher, 1986; Rotheram-Borus et al., 2002).
In addition, adolescents of PWH often confront multiple adversities that may influencetheir risk for anxiety and depressive disorders over time. In the United States, HIV differ-entially affects families already affected by poverty, substance abuse, and community viol-ence (Centers for Disease Control and Prevention [CDC], 1996; Rotheram-Borus et al.,2001a). Adolescent children of PWH are raised predominantly in single-parent Latino orAfrican American households (CDC, 2001). HIV illness carries the potential burden ofsocial stigma for these families, creating the strain of balancing the risk of illness disclosureand the need for social support. Previous reports on this population indicate that most ado-lescents are aware of their parent’s HIV status relatively soon after serostatus identification,potentially sharing the parent’s concerns regarding disclosure and social stigma (Lee &Rotheram-Borus, 2001). The risk for social isolation for these adolescents is particularlysalient during a period when peer support is central to developmental progression (Frierson &Lippmann, 1987; Herek & Capitanio, 1993; Herek et al., 2002; Romer et al., 2002). Giventhese multiple stressors, we expected an increased risk for anxiety and depressive disordersamong adolescents of PWH.
In addition to higher overall rates of anxiety and depressive disorders, we anticipated thata number of parental factors would heighten the risk for adolescent anxiety and depressivedisorders. Parental emotional distress and active substance use have been related to poorchild adjustment in other contexts (Anderson & Henry, 1994; Biederman et al., 2000;Kumpfer et al., 1996; Pandina & Johnson, 1989; Rotunda et al., 1995). Parents with HIVhave high rates of emotional distress, as well as substance use (Rotheram-Borus & Stein,1999), increasing the chances that their children will be depressed (Cummings & Davies,1994). Parents with HIV who are more affected by their illness will be less available to pro-vide parental monitoring and care to their adolescent children, thus increasing the risk foradjustment problems. Thus, we anticipated that parental emotional distress, substance useand physical illness status would predict greater rates of anxiety and depressive disorders intheir adolescent children.
Clinically recognized as one of the most potentially stressful life events for a child, paren-tal death is a risk for adjustment problems in the children of PWH (American PsychiatricAssociation, 1987). Parentally bereaved children have been found to have increased rates
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Anxiety and depressive disorders in adolescents of parents with HIV 83
of depression (Balk, 1983; Harris et al., 1986; Raphael et al., 1990; Siegel et al., 1992;West et al., 1991). Other studies have shown that more than a third of bereaved childrenhave been found to meet criteria for psychiatric disorders (Sanchez et al., 1994; Siegelet al., 1996). Thus, we anticipated that prior parental loss would increase the risk fordepression and anxiety in adolescents of PWH.
In addition, a number of other child factors have been proposed to be related toincreased anxiety and depressive disorders during adolescence, including older child age,ethnicity, female gender, prior traumatic exposure and substance use. In facing the illnessand potential death of a parent, older children may be at greater risk for adjustment diffi-culties, as they have greater awareness of the meaning and consequences of parental illnessand death (Lewandowski, 1992; Raveis et al., 1999). Gender differences were also antici-pated in children’s responses to parental illness and death, with children’s roles within fam-ilies strongly related to their gender (Bornstein, 1995; Lee et al., 2002).
Prior exposure to traumatic events in addition to parental loss was also expected toincrease the risk for anxiety and depressive disorders for these youth. Traumatic exposureis associated with lifelong neurobiological alterations, resulting in susceptibility to drug andalcohol abuse (Post et al., 2001), as well as the likelihood of later anxiety (Heim &Nemeroff, 2001) and depressive disorder (Kaufman & Charney, 2001). We anticipatedthat these factors would be associated with increased risk for anxiety and depressive disor-ders in adolescents of PWH.
The current study was conducted with families of PWH recruited in New York City andfollowed prospectively over 6 years. These families participated in a randomized family-based intervention trial for parents with HIV and their adolescent children. The interven-tion was designed to enhance adolescent adjustment in the setting of parental HIV diseaseand death. Previous reports from the intervention trial have shown benefits in reducing prob-lem behaviors and emotional distress for both parents and children in the interventiongroup at 2-year follow-up (Rotheram-Borus et al., 2001a); however, at 4-year follow-up,the intervention and control parents and adolescents no longer showed differences in emo-tional distress or multiple problem behaviors (Rotheram-Borus et al., 2003). Given that thecurrent study assessment was conducted at about 4 years following recruitment and deliv-ery of the intervention, intervention status was not anticipated to predict adolescent anxietyand depressive disorders in the current analyses.
In summary, we anticipated that given the profound social and personal stressors affectingfamilies affected by parental HIV illness, rates of anxiety and depressive disorders in theiradolescent children would be higher than the general population. We anticipated that rates ofdisorder would be predicted by parental mental and physical health status, parental death, aswell as adolescent age, ethnicity, gender, prior traumatic exposure and substance use.
Method
Participants
The assessment of adolescent anxiety and depressive psychiatric disorders took placewithin the context of a family-based intervention trial and longitudinal follow-up. FromAugust 1993 to March 1995, a consecutive series of referrals to the Division of AIDS Serv-ices of PWH with adolescent children was identified for the intervention trial. The NewYork City HIV/AIDS Services Administration provides enhanced welfare benefits and casemanagement services to 95% of PWH who meet income criteria (similar to eligibility forMedicaid) (New York City Human Resources Division of AIDS Services, 1993). Case
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
84 P. Lester et al.
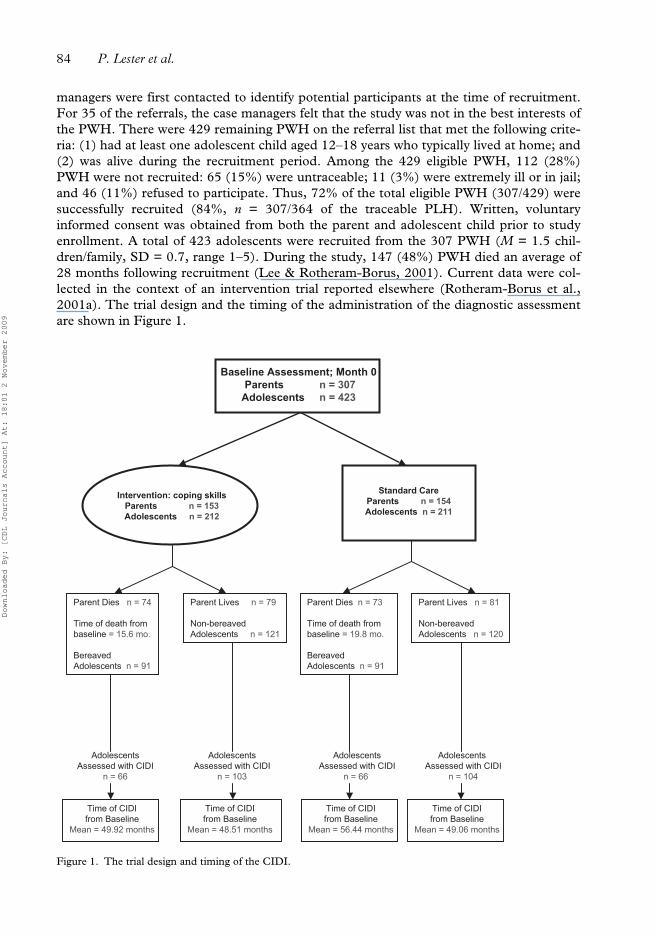
managers were first contacted to identify potential participants at the time of recruitment.For 35 of the referrals, the case managers felt that the study was not in the best interests ofthe PWH. There were 429 remaining PWH on the referral list that met the following crite-ria: (1) had at least one adolescent child aged 12–18 years who typically lived at home; and(2) was alive during the recruitment period. Among the 429 eligible PWH, 112 (28%)PWH were not recruited: 65 (15%) were untraceable; 11 (3%) were extremely ill or in jail;and 46 (11%) refused to participate. Thus, 72% of the total eligible PWH (307/429) weresuccessfully recruited (84%, n = 307/364 of the traceable PLH). Written, voluntaryinformed consent was obtained from both the parent and adolescent child prior to studyenrollment. A total of 423 adolescents were recruited from the 307 PWH (M = 1.5 chil-dren/family, SD = 0.7, range 1–5). During the study, 147 (48%) PWH died an average of28 months following recruitment (Lee & Rotheram-Borus, 2001). Current data were col-lected in the context of an intervention trial reported elsewhere (Rotheram-Borus et al.,2001a). The trial design and the timing of the administration of the diagnostic assessmentare shown in Figure 1.
Figure 1. The trial design and timing of the CIDI.
Baseline Assessment; Month 0
Parents n = 307
Adolescents n = 423
Intervention: coping skills
Parents n = 153
Adolescents n = 212
Adolescents
Assessed with CIDI
n = 66
Adolescents
Assessed with CIDI
n = 103
Time of CIDI
from Baseline
Mean = 49.92 months
Time of CIDI
from Baseline
Mean = 48.51 months
Standard Care
Parents n = 154
Adolescents n = 211
Adolescents
Assessed with CIDI
n = 66
Adolescents
Assessed with CIDI
n = 104
Time of CIDI
from Baseline
Mean = 56.44 months
Time of CIDI
from Baseline
Mean = 49.06 months
Parent Dies n = 74
Time of death from
baseline = 15.6 mo.
Bereaved
Adolescents n = 91
Parent Dies n = 73
Time of death from
baseline = 19.8 mo.
Bereaved
Adolescents n = 91
Parent Lives n = 81
Non-bereaved
Adolescents n = 120
Parent Lives n = 79
Non-bereaved
Adolescents n = 121
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Anxiety and depressive disorders in adolescents of parents with HIV 85
Intervention
At the time of the baseline interview, families (PWH and all adolescent children) wereassigned randomly to the intervention (n = 153 PLH, n = 212 youth) or the standard carecondition (n = 154 PWH, n = 211 youth; Rotheram-Borus et al., 2001a). Similar numbersof PWH died in the intervention (n = 74) and standard care (n = 73) conditions over thefollow-up period (Rotheram-Borus et al., 1997).
The intervention was delivered in three modules. Intervention sessions were held on Sat-urdays at a central location with two sessions each day. Lunch, childcare and transporta-tion were provided. Module 1 comprised eight sessions for parents only, and addressedillness disclosure, decision making, adjustment to disease status and parenting skills. Mod-ule 2 comprised 12 sessions for both parents and youth; the sessions focused on custodyplanning, reduction of risk acts and parent–youth communication. Module 3 comprisedeight sessions for bereaved youth and new caregivers after parental death. These sessionsfocused on grieving, setting life goals and establishing a positive relationship with theguardian. Complete intervention manuals are available at http://chipts.ucla.edu/interven-tions/manuals/index.html
Assessments
Timing. Adolescents were followed longitudinally starting in 1993–95 until 2000 (M =50.4 months, similar across intervention conditions and bereavement status). They werereassessed at 3-month intervals for the first 2 years (follow-up rate: 95% reassessed at leastonce annually; mean follow-up rate per assessment, 83%) and then at 6-month intervals(follow-up rate: 96% reassessed at least once annually, mean follow-up rate, 84%). If chil-dren within the family became 12 years of age during the follow-up period, these childrenwere recruited with informed consent of both the parent and adolescent and added to thecohort. From 1995–2000, 50 youth aged into the study, resulting in about 12% of adoles-cents being followed longitudinally for less than 2 years. The 50 adolescents who aged intothe study after the initial recruitment of the parent were no different than those recruitedearlier on gender, ethnicity or parent’s level of emotional distress.
For this analysis, an assessment of anxiety and depressive disorders was scheduledbetween January 1998 and January 2000 using the Composite International DiagnosticInterview (CIDI); 339 (80%) of the adolescents from 226 families completed this specialassessment. Of note, the CIDI assessment was conducted 4 years following enrollment, onaverage (SD = 1 year).
Interviewers. Interviewers were predominantly African American and Latino (62%);40% were bilingual in Spanish and English. A certified CIDI trainer provided extensivetraining of interviewers, which included a review of the fourth Diagnostic and StatisticalManual of Mental Disorders version IV (DSM-IV) diagnostic categories, modeling ofeffective interviews, practice interviews and ongoing clinical supervision and monitoringfrom audiotapes.
Parent and adolescent assessments
Sociodemographic characteristics. Adolescent gender, age and ethnicity were recorded.In addition, whether the adolescent lived with one or both parents was documented atbaseline.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
86 P. Lester et al.
Brief Symptom Inventory (BSI). The BSI (Derogatis, 1993) is a 53-item self-report inven-tory of mental health symptoms. Parent and adolescent participants self reported thedegree of distress for each symptom during the past week on a scale from 0 (not at all) to 4(extremely). The BSI is a highly reliable (α = 0.97) index of mental health symptoms.Parental baseline BSI scores were used in analyses, adolescent baseline and current BSIscores. For adolescents, current assessments were those matched assessments measuredwithin a 12-month window of the administration of the CIDI.
Substance use. This was reported for a variety of specific substances, including street namesfor alcohol, marijuana or hard drug use (crack, cocaine, heroin, barbiturates, inhalants, hal-lucinogens and methamphetamines). Both parents’ and adolescents’ lifetime and currentsubstance use was summarized in indices as yes (1) or no (0) for each of the following: (1)abstinence from alcohol and drugs; (2) use of alcohol; (3) use of marijuana; and (4) harddrug use.
Parental death. Adolescents reported a history of parental death at baseline. Death ofthe study HIV positive parent after baseline was recorded by routinely contacting thefamily and monitoring state records. In addition, information on non-study parentaldeath was collected during follow-up assessment. Death dates were only available forstudy parents.
Parental HIV illness status. At baseline, parents self-reported their HIV diagnostic status(asymptomatic, symptomatic or AIDS).
Adolescent anxiety and depressive disorders
Composite International Diagnostic Interview (CIDI). At follow-up assessment, the CIDI(World Health Organization, 1998) was administered to the adolescents to assess both life-time and recent (during the prior year) anxiety and depressive disorders. A computerizedscoring system was used to provide anxiety and depression diagnostic categories accordingto the DSM-IV. The CIDI has been found to have excellent inter-rater reliability, test–retest reliability, be internally consistent with kappas of 0.41 (generalized anxiety disorder)to 0.84 (panic disorder) and to be valid in a series of large international field trials (forreviews see Andrews & Peters, 1998; Wittchen, 1994).
We scored both lifetime and recent occurrence of (1) any unipolar depressive disorders,including major depressive disorder and dysthymic disorder; and (2) any anxiety disor-ders, including panic disorder with or without agoraphobia, phobias (agoraphobia,specific or social), obsessive–compulsive disorder, generalized anxiety disorder and post-traumatic stress disorder (PTSD). Summary depressive or anxiety disorder measures con-sisted of the presence (1) or absence (0) of any depressive disorders, any anxiety disordersand (PTSD).
Traumatic exposure. Adolescents in the study were also asked about potentially traumaticexposures during their lifetime as part of the CIDI protocol assessment of PTSD. Thelist of traumatic exposures consisted of 11 events (e.g., ‘Were you ever involved in a life-threatening accident?’; ‘Were you ever seriously physically attacked or assaulted?’; ‘Didyou ever witness someone being badly injured or killed?’). Traumatic exposure level wasdetermined by summing the number of events that adolescents reported (range 0–11events).
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Anxiety and depressive disorders in adolescents of parents with HIV 87
Data analysis
Selection bias was examined among adolescents and parents for demographics, sub-stance use and emotional distress on the Brief Symptom Inventory (BSI). χ2 and t-testswere used for categorical and continuous variables, respectively. Comparisons weremade for: (1) adolescents who completed the CIDI interview and non-completers; (2)adolescent and parent responses on the baseline interview among those who were laterbereaved and those non-bereaved; and (3) those in the intervention and standard careconditions.
Univariate analyses compared summary lifetime and recent disorders on adolescent mea-sures, including demographics and background characteristics. Random-intercept logisticregressions (Bryk & Raudenbush, 1992) of four primary outcomes (lifetime and recentsummary depressive or anxiety disorders) were examined for the proposed predictors.Those predictors found to be significant (p < 0.05) in univariate analyses were included ina predictor set for multivariate models. As there were 339 adolescents in 226 families in ourstudy, all models included family-random intercepts to account for the non-independentnature of sampling 339 adolescents from 226 families. The following predictors were notincluded in our multivariate final models because they were not significantly associatedwith either lifetime or recent depression and anxiety disorders on univariate analysis: ado-lescent ethnicity, parental substance use, parental illness status, adolescent interventionstatus and living with one parent. Despite its lack of significance as a predictor, we consid-ered including ethnicity in our final models because it was hypothesized to have an effecton outcomes. However, most participants were of ethnic minority (37% African Americanand 51% Latino), resulting in little variability to be included as a meaningful covariate inthe model. Therefore, ethnicity was not included in our final models. We also examinedthe following two-way interactions: bereavement by parent BSI and trauma by interven-tion. Neither interaction was significant; therefore, they were not included in our finalmodels.
Results
Population
Overall, adolescents of PWH completing the CIDI had a mean age of 18.9 years; about halfwere male (45%) and most were either Latino (51%) or African American (37%). Only 3%of adolescents were Caucasian, and 1% were Asian/Other. Sixty percent were parentallybereaved prior to the CIDI (n = 204/339). About half (46%) the adolescents reported life-time abstinence for any alcohol or drug use and low rates of hard drug use at baseline (4%).
Potential selection bias at recruitment
Regarding potential selection effects in the sample at the time of recruitment, the adoles-cents who completed the CIDI interview and those who did not were similar at baseline,with only two exceptions. The CIDI was completed by a higher proportion of females thanmales (χ2 = 5.14, d.f. = 1, p = 0.02) and relatively more Latinos compared to other ethnicgroups (χ2 = 6.02, d.f. = 2, p = 0.05). The age, living situation (with both or a singleparent), intervention condition, current substance use and emotional distress (BSI) weresimilar at the time of recruitment among those who completed the CIDI and those who didnot. The parents of adolescents who completed the CIDI were also comparable on all par-ent assessments.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
88 P. Lester et al.
Parental bereavement
In our study we had 204 parental deaths, consisting of 132 study and 72 non-study par-ent deaths. For adolescents bereaved from study parents (n = 132), the average timefrom parental death to the CIDI assessment was 37.4 months. The time from study par-ent’s death to administration of the CIDI was more than 48 months for 27% of youth,37–48 months for 32% of youth, 25–36 months for 25% of youth and less than 25months for 16% of the youth. Child age, intervention status and living situation weresimilar at baseline among the adolescents who were later bereaved compared to the non-bereaved youth.
Traumatic exposure
Adolescents reported a mean of 1.39 lifetime traumatic exposures, SD = 1.65. About40% reported no traumatic exposures, 24% reported one traumatic exposure, 14%reported two traumatic exposures and 21% reported more than two traumatic exposuresout of 11 types of traumatic exposures. Of these, the most common traumatic exposurereported was witnessing someone being badly injured or killed (33.3%). Notably, about18% of these adolescents reported a history of serious physical assault, as well as beingthreatened with a weapon, held captive or kidnapped. About 12% reported a history ofsexual molestation.
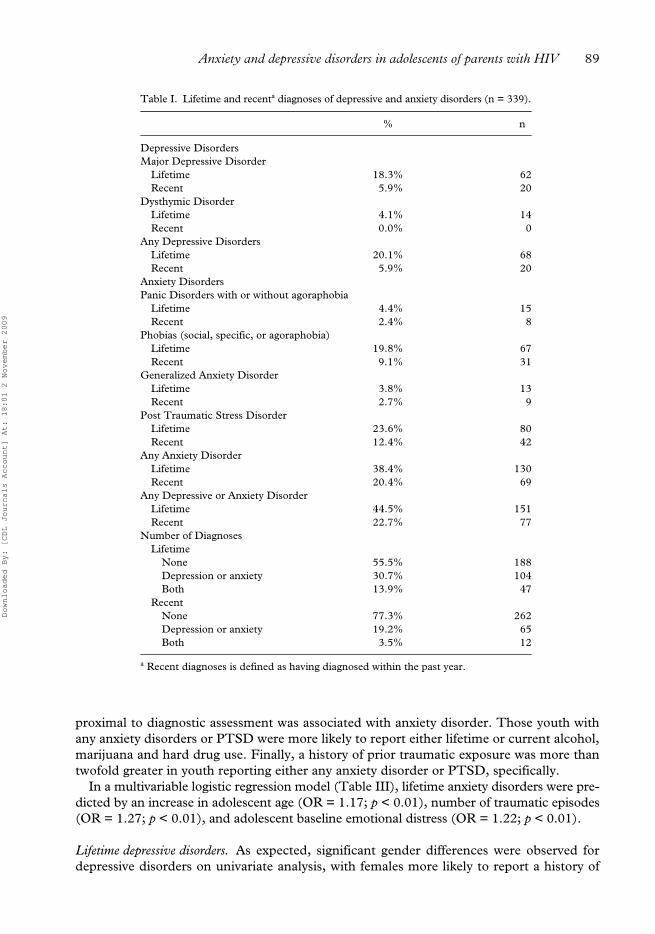
Rates of lifetime and recent disorders (Table I)
Anxiety disorders. Overall, adolescents of PWH had high rates of both lifetime (38.4%) andrecent (20.4%) anxiety disorders. Most of the anxiety disorders were accounted for by spe-cific phobias (19.8% lifetime, 9.1% recent) and PTSD (23.6% lifetime, 12.4% recent). Forthose with lifetime PTSD, youth reported a mean number of 2.75 traumatic exposures, SD= 1.65, compared to only 0.97 reported by those not meeting criteria for PTSD. Similarly,those meeting criteria for recent PTSD reported a mean of 2.22, SD = 2.13 traumaticexposures. Of those reporting a lifetime diagnosis of PTSD (n = 80/339), 26% reportedwitnessing someone being badly injured or killed, 9% had been seriously physicallyattacked or assaulted, 9% had been threatened with a weapon, held captive or kidnappedand 14% had been sexually molested. A similar distribution of traumatic exposures wasreported for those meeting criteria for recent PTSD.
Depressive disorder. Overall, 18.3% of the youth met criteria for a major depressive disorderduring their lifetime, and 5.9% reported a recent episode. Almost half the youth hadexperienced at least one anxiety or depressive disorder (44.5%), while 22.7% of adoles-cents had at least one recent disorder.
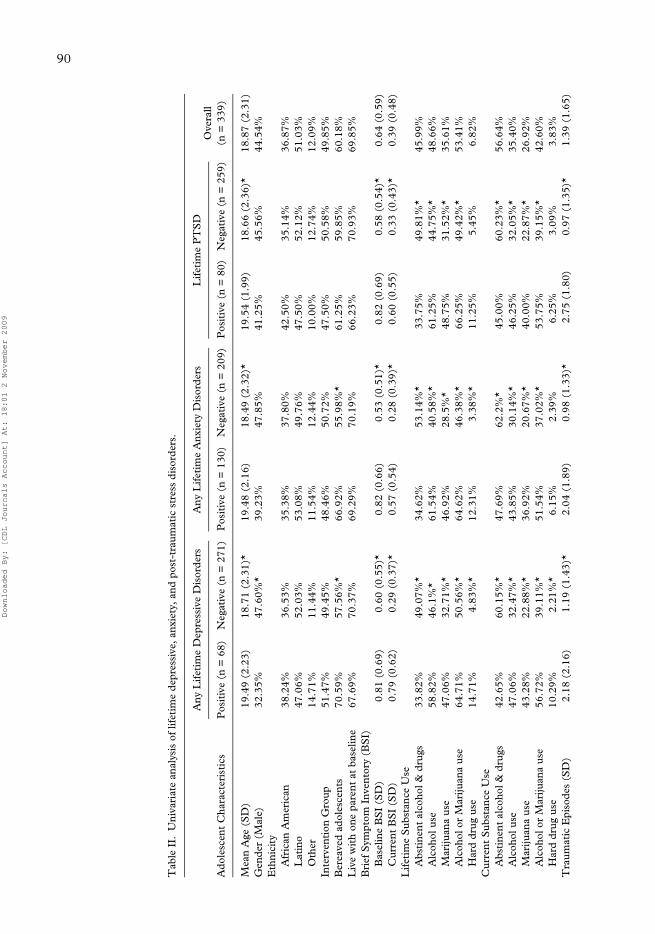
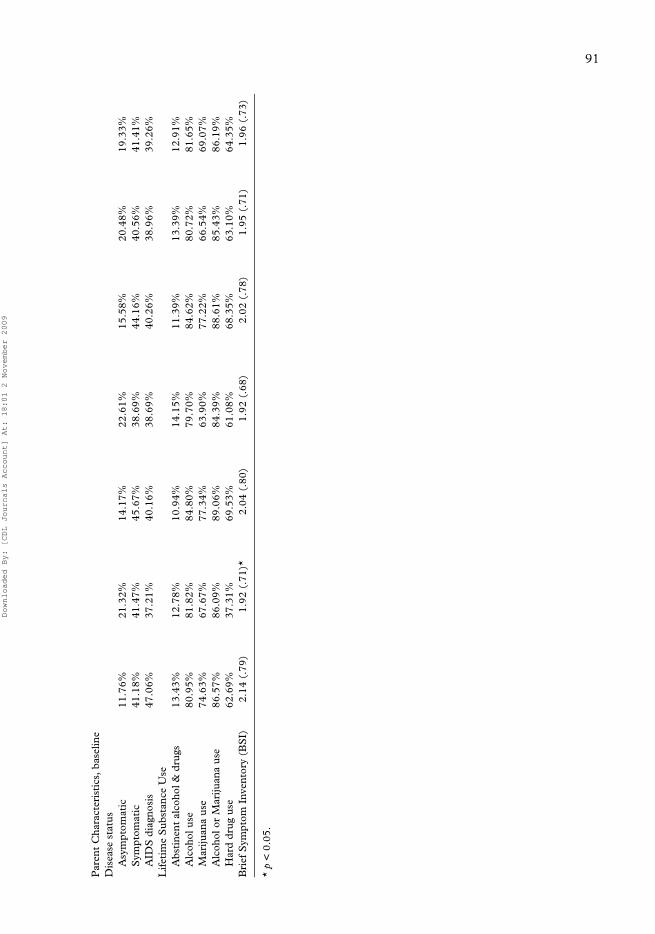
Univariate predictors of lifetime depressive and anxiety disorders (Table II)
Lifetime anxiety disorders. Compared to those without a history of anxiety disorders, youthmeeting criteria for any lifetime anxiety disorder were older. Surprisingly, males andfemales reported anxiety disorders and PTSD at similar rates in this high-risk group.Ethnicity was not correlated with anxiety disorders. Those youth reporting a history of anyanxiety disorder during their lifetime were significantly more likely to have experiencedparental death (67% vs. 56%). Greater emotional distress measured both at baseline and
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Anxiety and depressive disorders in adolescents of parents with HIV 89
proximal to diagnostic assessment was associated with anxiety disorder. Those youth withany anxiety disorders or PTSD were more likely to report either lifetime or current alcohol,marijuana and hard drug use. Finally, a history of prior traumatic exposure was more thantwofold greater in youth reporting either any anxiety disorder or PTSD, specifically.
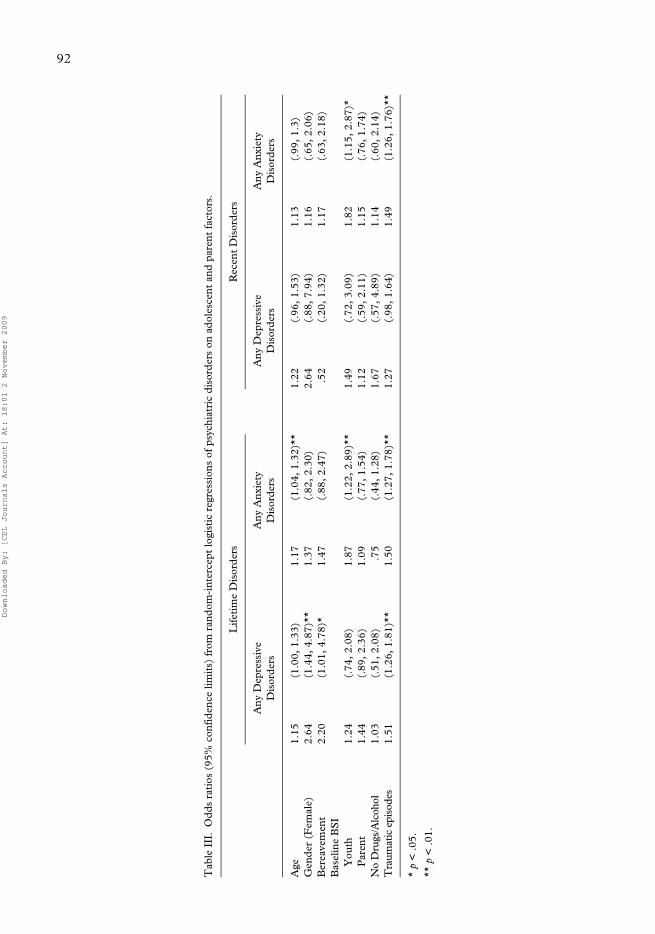
In a multivariable logistic regression model (Table III), lifetime anxiety disorders were pre-dicted by an increase in adolescent age (OR = 1.17; p < 0.01), number of traumatic episodes(OR = 1.27; p < 0.01), and adolescent baseline emotional distress (OR = 1.22; p < 0.01).
Lifetime depressive disorders. As expected, significant gender differences were observed fordepressive disorders on univariate analysis, with females more likely to report a history of
Table I. Lifetime and recenta diagnoses of depressive and anxiety disorders (n = 339).
% n
Depressive DisordersMajor Depressive Disorder
Lifetime 18.3% 62Recent 5.9% 20
Dysthymic DisorderLifetime 4.1% 14Recent 0.0% 0
Any Depressive DisordersLifetime 20.1% 68Recent 5.9% 20
Anxiety DisordersPanic Disorders with or without agoraphobia
Lifetime 4.4% 15Recent 2.4% 8
Phobias (social, specific, or agoraphobia)Lifetime 19.8% 67Recent 9.1% 31
Generalized Anxiety DisorderLifetime 3.8% 13Recent 2.7% 9
Post Traumatic Stress DisorderLifetime 23.6% 80Recent 12.4% 42
Any Anxiety DisorderLifetime 38.4% 130Recent 20.4% 69
Any Depressive or Anxiety DisorderLifetime 44.5% 151Recent 22.7% 77
Number of DiagnosesLifetime
None 55.5% 188Depression or anxiety 30.7% 104Both 13.9% 47
RecentNone 77.3% 262Depression or anxiety 19.2% 65Both 3.5% 12
a Recent diagnoses is defined as having diagnosed within the past year.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
90
Tab
le I
I.U
niva
riat
e an
alys
is o
f lif
etim
e de
pres
sive
, anx
iety
, and
pos
t-tr
aum
atic
str
ess
diso
rder
s.
Ado
lesc
ent
Cha
ract
eris
tics
Any
Lif
etim
e D
epre
ssiv
e D
isor
ders
Any
Lif
etim
e A
nxie
ty D
isor
ders
Lif
etim
e P
TS
DO
vera
ll(n
= 3
39)
Pos
itiv
e (n
= 6
8)N
egat
ive
(n =
271
)P
osit
ive
(n =
130
)N
egat
ive
(n =
209
)P
osit
ive
(n =
80)
Neg
ativ
e (n
= 2
59)
Mea
n A
ge (
SD
)19
.49
(2.2
3)18
.71
(2.3
1)*
19.4
8 (2
.16)
18.4
9 (2
.32)
*19
.54
(1.9
9)18
.66
(2.3
6)*
18.8
7 (2
.31)
Gen
der
(Mal
e)32
.35%
47.6
0%*
39.2
3%47
.85%
41.2
5%45
.56%
44.5
4%E
thni
city
Afr
ican
Am
eric
an38
.24%
36.5
3%35
.38%
37.8
0%42
.50%
35.1
4%36
.87%
Lat
ino
47.0
6%52
.03%
53.0
8%49
.76%
47.5
0%52
.12%
51.0
3%O
ther
14.7
1%11
.44%
11.5
4%12
.44%
10.0
0%12
.74%
12.0
9%In
terv
enti
on G
roup
51.4
7%49
.45%
48.4
6%50
.72%
47.5
0%50
.58%
49.8
5%B
erea
ved
adol
esce
nts
70.5
9%57
.56%
*66
.92%
55.9
8%*
61.2
5%59
.85%
60.1
8%L
ive
wit
h on
e pa
rent
at
base
line
67.6
9%70
.37%
69.2
9%70
.19%
66.2
3%70
.93%
69.8
5%B
rief
Sym
ptom
Inv
ento
ry (
BS
I)B
asel
ine
BS
I (S
D)
0.81
(0.
69)
0.60
(0.
55)*
0.82
(0.
66)
0.53
(0.
51)*
0.82
(0.
69)
0.58
(0.
54)*
0.64
(0.
59)
Cur
rent
BS
I (S
D)
0.79
(0.
62)
0.29
(0.
37)*
0.57
(0.
54)
0.28
(0.
39)*
0.60
(0.
55)
0.33
(0.
43)*
0.39
(0.
48)
Lif
etim
e S
ubst
ance
Use
Abs
tine
nt a
lcoh
ol &
dru
gs33
.82%
49.0
7%*
34.6
2%53
.14%
*33
.75%
49.8
1%*
45.9
9%A
lcoh
ol u
se58
.82%
46.1
%*
61.5
4%40
.58%
*61
.25%
44.7
5%*
48.6
6%M
ariju
ana
use
47.0
6%32
.71%
*46
.92%
28.5
%*
48.7
5%31
.52%
*35
.61%
Alc
ohol
or
Mar
ijuan
a us
e64
.71%
50.5
6%*
64.6
2%46
.38%
*66
.25%
49.4
2%*
53.4
1%H
ard
drug
use
14.7
1%4.
83%
*12
.31%
3.38
%*
11.2
5%5.
45%
6.82
%C
urre
nt S
ubst
ance
Use
Abs
tine
nt a
lcoh
ol &
dru
gs42
.65%
60.1
5%*
47.6
9%62
.2%
*45
.00%
60.2
3%*
56.6
4%A
lcoh
ol u
se47
.06%
32.4
7%*
43.8
5%30
.14%
*46
.25%
32.0
5%*
35.4
0%M
ariju
ana
use
43.2
8%22
.88%
*36
.92%
20.6
7%*
40.0
0%22
.87%
*26
.92%
Alc
ohol
or
Mar
ijuan
a us
e56
.72%
39.1
1%*
51.5
4%37
.02%
*53
.75%
39.1
5%*
42.6
0%H
ard
drug
use
10.2
9%2.
21%
*6.
15%
2.39
%6.
25%
3.09
%3.
83%
Tra
umat
ic E
piso
des
(SD
)2.
18 (
2.16
)1.
19 (
1.43
)*2.
04 (
1.89
)0.
98 (
1.33
)*2.
75 (
1.80
)0.
97 (
1.35
)*1.
39 (
1.65
)
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
91
Par
ent
Cha
ract
eris
tics
, bas
elin
eD
isea
se s
tatu
sA
sym
ptom
atic
11.7
6%21
.32%
14.1
7%22
.61%
15.5
8%20
.48%
19.3
3%S
ympt
omat
ic41
.18%
41.4
7%45
.67%
38.6
9%44
.16%
40.5
6%41
.41%
AID
S d
iagn
osis
47.0
6%37
.21%
40.1
6%38
.69%
40.2
6%38
.96%
39.2
6%L
ifet
ime
Sub
stan
ce U
seA
bsti
nent
alc
ohol
& d
rugs
13.4
3%12
.78%
10.9
4%14
.15%
11.3
9%13
.39%
12.9
1%A
lcoh
ol u
se80
.95%
81.8
2%84
.80%
79.7
0%84
.62%
80.7
2%81
.65%
Mar
ijuan
a us
e74
.63%
67.6
7%77
.34%
63.9
0%77
.22%
66.5
4%69
.07%
Alc
ohol
or
Mar
ijuan
a us
e86
.57%
86.0
9%89
.06%
84.3
9%88
.61%
85.4
3%86
.19%
Har
d dr
ug u
se62
.69%
37.3
1%69
.53%
61.0
8%68
.35%
63.1
0%64
.35%
Bri
ef S
ympt
om I
nven
tory
(B
SI)
2.14
(.7
9)1.
92 (
.71)
*2.
04 (
.80)
1.92
(.6
8)2.
02 (
.78)
1.95
(.7
1)1.
96 (
.73)
* p
< 0
.05.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
92
Tab
le I
II.
Odd
s ra
tios
(95
% c
onfi
denc
e lim
its)
fro
m r
ando
m-i
nter
cept
logi
stic
reg
ress
ion
s of
psy
chia
tric
dis
orde
rs o
n ad
oles
cent
and
par
ent
fact
ors.
Lif
etim
e D
isor
ders
Rec
ent
Dis
orde
rs
Any
Dep
ress
ive
Dis
orde
rsA
ny A
nxie
ty
Dis
orde
rsA
ny D
epre
ssiv
e D
isor
ders
Any
Anx
iety
D
isor
ders
Age
1.15
(1.0
0, 1
.33)
1.17
(1.0
4, 1
.32)
**1.
22(.
96, 1
.53)
1.13
(.99
, 1.3
)G
ende
r (F
emal
e)2.
64(1
.44,
4.8
7)**
1.37
(.82
, 2.3
0)2.
64(.
88, 7
.94)
1.16
(.65
, 2.0
6)B
erea
vem
ent
2.20
(1.0
1, 4
.78)
*1.
47(.
88, 2
.47)
.52
(.20
, 1.3
2)1.
17(.
63, 2
.18)
Bas
elin
e B
SI
You
th1.
24(.
74, 2
.08)
1.87
(1.2
2, 2
.89)
**1.
49(.
72, 3
.09)
1.82
(1.1
5, 2
.87)
*P
aren
t1.
44(.
89, 2
.36)
1.09
(.77
, 1.5
4)1.
12(.
59, 2
.11)
1.15
(.76
, 1.7
4)N
o D
rugs
/Alc
ohol
1.03
(.51
, 2.0
8).7
5(.
44, 1
.28)
1.67
(.57
, 4.8
9)1.
14(.
60, 2
.14)
Tra
umat
ic e
piso
des
1.51
(1.2
6, 1
.81)
**1.
50(1
.27,
1.7
8)**
1.27
(.98
, 1.6
4)1.
49(1
.26,
1.7
6)**
* p
< .0
5.
** p
< .0
1.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009

Anxiety and depressive disorders in adolescents of parents with HIV 93
any depressive disorder than males. Older youth were more likely to have met criteria for adepressive disorder over a lifetime. Youth reporting more symptoms of emotional distressat baseline and proximal to the diagnostic assessment were more likely to have a depressivedisorder, indicating the ongoing risk of distress in this group over time. As anticipated,those youth reporting a history of depressive disorder during their lifetime were more likelyto be parentally bereaved (71%) than those without a history of depression (59%). Also asexpected, adolescents reporting any depressive disorders during their lifetime had almostdouble the rate of prior traumatic episodes. We also found a high association between thepresence of current or lifetime alcohol, marijuana and hard drug use and the presence oflifetime depression. Ethnicity was not a predictor of depressive disorders.
In a multivariate logistic regression model (Table III) lifetime depressive disorders werepredicted by female gender (OR = 2.64; p < 0.01), number of traumatic episodes (OR =1.26; p < 0.01) and parental bereavement (OR = 1.01; p = 0.05).
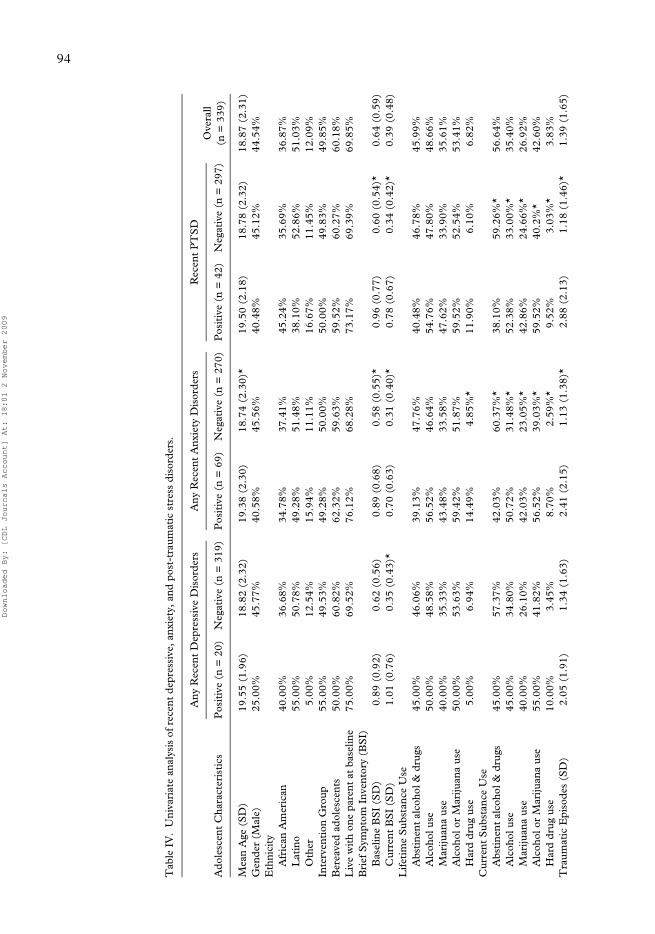
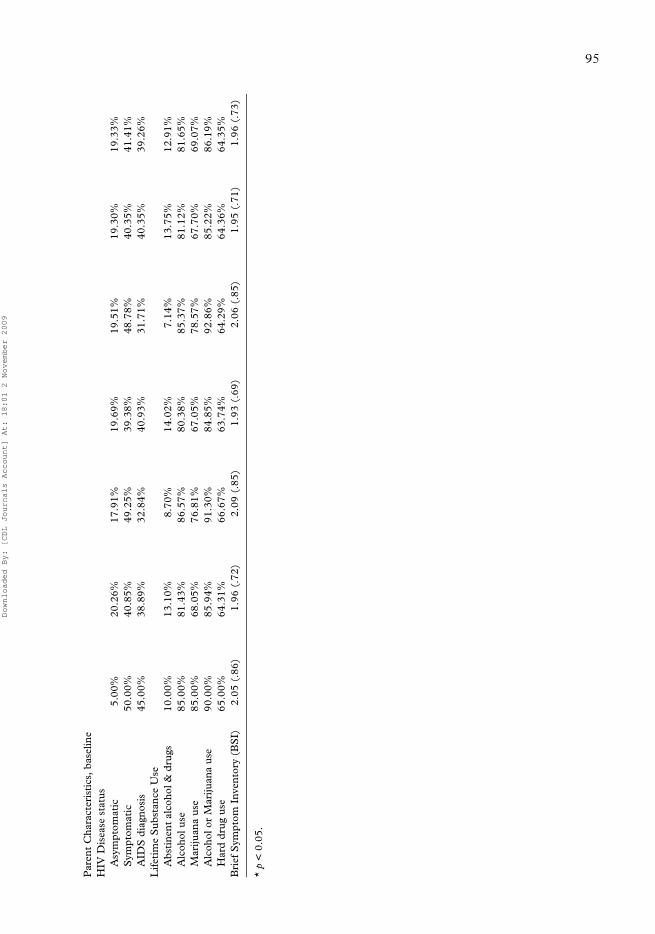
Univariate predictors of recent depressive and anxiety disorders (Table IV)
Recent anxiety disorders. Youth reporting more symptoms of emotional distress at baselineand proximal to the diagnostic assessment were more likely to meet criteria for a recentanxiety disorder, as well as PTSD. Recent anxiety disorders were predicted by the presenceof lifetime hard drug use, and were associated with current alcohol, marijuana and harddrug use. Similar patterns of association were found for PTSD and substance use. Greaterfrequency of traumatic exposure predicted both recent PTSD and any anxiety disorder. Ina multivariable logistic regression model (Table III), recent anxiety disorders were pre-dicted by an increase in the number of traumatic episodes (p = 0.05) and adolescent emo-tional distress at baseline (p = 0.01).
Recent depressive disorders. Youth reporting more recent symptoms of emotional distressimmediately prior to the CIDI were more likely to have a recent depressive disorder (TableIV). In the multivariable logistic regression model (Table III), none of the predictors weresignificant. Random effects were problematic for model fitting due to the small number ofreported cases of recent depressive disorders (n = 20) relative to the number of predictors.
Discussion
A central finding from this study is that adolescents with PWH have high rates of both life-time and recent anxiety disorders. Lifetime rates of any anxiety disorder for these youth arealmost four times those reported for other samples of children before the age of 20 years(Bernstein & Borchardt, 1991; Fonagy et al., 2002). In adolescents, anxiety disorders arerelatively common, with 13 of every 100 children and adolescents ages 9–17 experiencingsome kind of anxiety disorder (US Department of Health and Human Services, 2003).Similar high rates of anxiety disorders have been found for other youth affected by a paren-tal illness and death (Bernstein & Borchardt, 1991; Fonagy et al., 2002; Gibbs, 1989;Goenjian et al., 1995). In particular, rates of PTSD are elevated for these youth, withalmost one in four youth meeting criteria for PTSD during their lifetimes. Comparativedata record lifetime rates of PTSD of 4.4% among adult men and 10.4% among womenwhen trauma occurs to a loved one (Giaconia et al., 1995) and rates of 14.5% among ado-lescents who have experienced a prior traumatic event (Sack et al., 1996). Notably, PTSDrates found in this population are similar to adolescents who are refugees of the Cambodianwar (Sack et al., 1996) or survivors of ethnic cleansing in Bosnia (Weine et al., 1995).
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
94
Tab
le I
V.
Uni
vari
ate
anal
ysis
of
rece
nt d
epre
ssiv
e, a
nxie
ty, a
nd p
ost-
trau
mat
ic s
tres
s di
sord
ers.
Ado
lesc
ent
Cha
ract
eris
tics
Any
Rec
ent
Dep
ress
ive
Dis
orde
rsA
ny R
ecen
t A
nxie
ty D
isor
ders
Rec
ent
PT
SD
Ove
rall
(n =
339
)P
osit
ive
(n =
20)
Neg
ativ
e (n
= 3
19)
Pos
itiv
e (n
= 6
9)N
egat
ive
(n =
270
)P
osit
ive
(n =
42)
Neg
ativ
e (n
= 2
97)
Mea
n A
ge (
SD
)19
.55
(1.9
6)18
.82
(2.3
2)19
.38
(2.3
0)18
.74
(2.3
0)*
19.5
0 (2
.18)
18.7
8 (2
.32)
18.8
7 (2
.31)
Gen
der
(Mal
e)25
.00%
45.7
7%40
.58%
45.5
6%40
.48%
45.1
2%44
.54%
Eth
nici
tyA
fric
an A
mer
ican
40.0
0%36
.68%
34.7
8%37
.41%
45.2
4%35
.69%
36.8
7%L
atin
o55
.00%
50.7
8%49
.28%
51.4
8%38
.10%
52.8
6%51
.03%
Oth
er5.
00%
12.5
4%15
.94%
11.1
1%16
.67%
11.4
5%12
.09%
Inte
rven
tion
Gro
up55
.00%
49.5
3%49
.28%
50.0
0%50
.00%
49.8
3%49
.85%
Ber
eave
d ad
oles
cent
s50
.00%
60.8
2%62
.32%
59.6
3%59
.52%
60.2
7%60
.18%
Liv
e w
ith
one
pare
nt a
t ba
selin
e75
.00%
69.5
2%76
.12%
68.2
8%73
.17%
69.3
9%69
.85%
Bri
ef S
ympt
om I
nven
tory
(B
SI)
Bas
elin
e B
SI
(SD
)0.
89 (
0.92
)0.
62 (
0.56
)0.
89 (
0.68
)0.
58 (
0.55
)*0.
96 (
0.77
)0.
60 (
0.54
)*0.
64 (
0.59
)C
urre
nt B
SI
(SD
)1.
01 (
0.76
)0.
35 (
0.43
)*0.
70 (
0.63
)0.
31 (
0.40
)*0.
78 (
0.67
)0.
34 (
0.42
)*0.
39 (
0.48
)L
ifet
ime
Sub
stan
ce U
seA
bsti
nent
alc
ohol
& d
rugs
45.0
0%46
.06%
39.1
3%47
.76%
40.4
8%46
.78%
45.9
9%A
lcoh
ol u
se50
.00%
48.5
8%56
.52%
46.6
4%54
.76%
47.8
0%48
.66%
Mar
ijuan
a us
e40
.00%
35.3
3%43
.48%
33.5
8%47
.62%
33.9
0%35
.61%
Alc
ohol
or
Mar
ijuan
a us
e50
.00%
53.6
3%59
.42%
51.8
7%59
.52%
52.5
4%53
.41%
Har
d dr
ug u
se5.
00%
6.94
%14
.49%
4.85
%*
11.9
0%6.
10%
6.82
%C
urre
nt S
ubst
ance
Use
Abs
tine
nt a
lcoh
ol &
dru
gs45
.00%
57.3
7%42
.03%
60.3
7%*
38.1
0%59
.26%
*56
.64%
Alc
ohol
use
45.0
0%34
.80%
50.7
2%31
.48%
*52
.38%
33.0
0%*
35.4
0%M
ariju
ana
use
40.0
0%26
.10%
42.0
3%23
.05%
*42
.86%
24.6
6%*
26.9
2%A
lcoh
ol o
r M
ariju
ana
use
55.0
0%41
.82%
56.5
2%39
.03%
*59
.52%
40.2
%*
42.6
0%H
ard
drug
use
10.0
0%3.
45%
8.70
%2.
59%
*9.
52%
3.03
%*
3.83
%T
raum
atic
Epi
sode
s (S
D)
2.05
(1.
91)
1.34
(1.
63)
2.41
(2.
15)
1.13
(1.
38)*
2.88
(2.
13)
1.18
(1.
46)*
1.39
(1.
65)
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
95
Par
ent
Cha
ract
eris
tics
, bas
elin
eH
IV D
isea
se s
tatu
sA
sym
ptom
atic
5.00
%20
.26%
17.9
1%19
.69%
19.5
1%19
.30%
19.3
3%S
ympt
omat
ic50
.00%
40.8
5%49
.25%
39.3
8%48
.78%
40.3
5%41
.41%
AID
S d
iagn
osis
45.0
0%38
.89%
32.8
4%40
.93%
31.7
1%40
.35%
39.2
6%L
ifet
ime
Sub
stan
ce U
seA
bsti
nent
alc
ohol
& d
rugs
10.0
0%13
.10%
8.70
%14
.02%
7.14
%13
.75%
12.9
1%A
lcoh
ol u
se85
.00%
81.4
3%86
.57%
80.3
8%85
.37%
81.1
2%81
.65%
Mar
ijuan
a us
e85
.00%
68.0
5%76
.81%
67.0
5%78
.57%
67.7
0%69
.07%
Alc
ohol
or
Mar
ijuan
a us
e90
.00%
85.9
4%91
.30%
84.8
5%92
.86%
85.2
2%86
.19%
Har
d dr
ug u
se65
.00%
64.3
1%66
.67%
63.7
4%64
.29%
64.3
6%64
.35%
Bri
ef S
ympt
om I
nven
tory
(B
SI)
2.05
(.8
6)1.
96 (
.72)
2.09
(.8
5)1.
93 (
.69)
2.06
(.8
5)1.
95 (
.71)
1.96
(.7
3)
* p
< 0
.05.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
96 P. Lester et al.
These findings underscore the importance of appropriate assessment and intervention pro-tocols for post-traumatic stress in children of PWH.
Unexpectedly, these youth report only modestly elevated rates of recent and lifetimedepressive disorders compared to nationally representative samples. The National Insti-tutes of Mental Health has reported that one in 20 teens, or 5%, have moderately severe tosevere depression (Essau & Dobson, 1999; National Institutes of Mental Health, 2005).Among ethnic minority families without an HIV-infected parent, the rates of currentdepressive disorder are reported as 3.1% for African Americans (Brown et al., 1995) and3.3% for Latinos (Kessler et al., 1995) compared to the 5.9% found for youth of PWH.
Rather than clinical models that focus primarily on a vulnerability for depression in theyouth of PWH, these findings suggest that traumatic stress models may better illuminatethe experience of living with a chronically ill parent, as well as experiencing their untimelydeath (McCloskey & Walker, 2000). Consistent with previous studies on risk for anxiety(Heim & Nemeroff, 2001) and depressive disorders (Kaufman & Charney, 2001), priortraumatic exposure was found to increase the likelihood of both anxiety and depressivedisorders for these youth, even when all significant univariate predictors had beenincluded in a multivariable regression model. For adolescents of PWH, living under theshadow of potential or actual parental death may present a particular vulnerability toadjustment problems following traumatic exposure. These youth are often exposed tomultiple stressors as they contend with the vulnerability and helplessness associated withtheir parent’s HIV illness, including episodic bouts of a parent’s physical and, in somecases, neurological deterioration, intrusive medical interventions, parental emotional dis-tress and parental substance use. All of these factors may erode important domains ofparental functioning, especially the parent’s capacity to maintain or rebuild a sense of pro-tection and safety for their children, which is central to recovery from trauma (Pynooset al., 1999). This loss of parental functioning may inhibit recovery from prior traumaticexposures, and leave the adolescent at higher risk for both community and interpersonaltrauma. Of note, this study did not specifically assess potentially traumatic events relatedto a parent’s HIV illness, which may have further elucidated the relationship of parentalHIV illness and its risk for PTSD.
Not surprisingly, this study also demonstrates an expected association between bothlifetime and current substance use and anxiety and depressive disorders for children ofPWH, as have been found in other contexts (Clark et al., 2003; Hovens et al., 1994;Kandel et al., 1997; Minkoff, 2001; Rohde et al., 1996; Rounsaville, 2004). A lifetimediagnosis of depressive disorder was significantly correlated with both lifetime and currentsubstance use of alcohol, marijuana, and hard drugs. Studies on the temporal order ofdepression and substance abuse in adolescents have found depression to occur before,after, and concurrent with the onset of substance abuse (Duncan et al., 1997; Rao et al.,2000; Rohde et al., 1996). A diagnosis of recent anxiety disorders, including PTSD, wasalso significantly associated with current use of alcohol, marijuana and hard drugs. Due tothe timing of the CIDI diagnostic interview, the temporal order of lifetime anxiety anddepressive disorders in relation to substance use cannot be determined. However, a base-line report of hard drug use predicted later anxiety disorder, suggesting an early or sharedvulnerability for anxiety disorder in those youth using hard drugs during adolescence.Notably, in all of the multivariable models, substance use (alcohol, marijuana or harddrug) was not found to be independently associated with lifetime or current disorders inthese youth. Similar to earlier studies showing an increased risk for substance abuse withprior trauma exposure, these findings provide indirect support for traumatic exposure as acommon risk factor for the presence of substance use and anxiety and depressive disorder
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009

Anxiety and depressive disorders in adolescents of parents with HIV 97
(Kilpatrick et al., 2000). Most importantly, these findings underscore the need for ongoingmental health and substance abuse screening and treatment services in youth affected byparental HIV illness.
Based on prior research we anticipated that parental distress, whether reflected in thestage of HIV illness, emotional distress or substance use, would predict anxiety anddepressive disorders in their children (Garber et al., 1997). However, the influence ofparental distress on psychiatric disorder in the youth several years later appeared lim-ited. Parental emotional distress did predict lifetime depression in the youth in univari-ate analysis. We propose that parental BSI, a dimensional measure of distress, measuredseveral years prior to the diagnostic assessment of youth did not adequately capture thepresence of parental anxiety or depression. Similarly, parental substance use and illnesslevel reported at baseline did not predict lifetime or recent disorders many years later inthe youth.
Adolescent’s emotional distress on the BSI at recruitment and proximal to the diagnosticassessment was associated with both lifetime and current anxiety and depressive disorders.Certainly, the presence of increased emotional distress proximal to the presence of disorder inthe youth was anticipated and serves to confirm the findings of this study. The finding thatemotional distress at baseline predicts both lifetime and current disorders also demonstratesthe ongoing risk for symptoms of adjustment difficulties across the course of development.
With increasing age, Rost (1992) has asserted that the impact of parental bereavementwould decrease as youth age and have more personal resources. This was not observed.Across diagnostic disorders, adolescents report higher rates of lifetime disorder withincreasing age. We saw a similar pattern for recent diagnoses, with older age as a significantpredictor for recent anxiety disorders in the youth. With age, adolescents are much morelikely to realize the implications and carry the burden of parental illness and death. Adoles-cents are less likely to be taken care of by others when their parent becomes impaired or, insome cases, dies. For example, custody plans were made less often for adolescents com-pared to children aged 6–12 years (Rotheram-Borus et al., 2002).
As anticipated, the family-based intervention was not found to predict fewer recent anxi-ety and depressive disorders several years after the intervention, either directly or throughinteraction effects. As noted earlier, the intervention has been associated with significantlyfewer symptoms of emotional distress, as well as reductions in multiple problem behaviorsfor the adolescents 2 years following intervention delivery (Rotheram-Borus et al., 1997;Rotheram-Borus et al., 2001a), but did not persist in measures of emotional adjustment at4 and 6 years of follow-up. Notably, intervention benefits did emerge for the youth in otherkey functional outcomes 6 years following intervention delivery, including later childbear-ing, greater enrollment in school or work and less dependency on social subsidies(Rotheram-Borus et al., 2004). However, it appears that the initial and later benefits of theintervention are not reflected in decreased anxiety and depressive disorders during thisassessment window. Current intervention models do not adequately plan for ways to sus-tain intervention effects over time. Future interventions must recognize the ongoing chal-lenges faced by the children and families of PWH over time, and incorporate the need forongoing support, or booster sessions, into their designs.
Strengths and limitations of the study
This study provides diagnostic information and longitudinal risk factors in high risk, ethnicminority youth, a historically understudied group. The study design includes both youthand parent assessments, providing the opportunity to evaluate the relationship between
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009

98 P. Lester et al.
parental factors and youth outcomes. Because New York City had a centralized referralservice for all persons entering the Division of AIDS Services, we were able to recruit a rep-resentative sample of PWH. From a consecutive series of PLH, 72% were recruited (84% ifuntraceable were excluded). The follow-up rates were also high over several years and ran-domization to the intervention resulted in highly similar subgroups, both of parents and ofyouth. More than 80% of the youth completed the CIDI and there did not appear to beany selection bias among those who completed the assessment. The unexpected survival ofmore than half the HIV infected parents allowed us to examine the impact of bereavementon the rates of psychiatric disorders among their adolescent children, as well as the impactof living with a chronically ill, HIV-infected parent.
Despite these strengths, this study has a number of limitations. First, we do not have com-prehensive information on the timing of important stressful events in relationship to the diag-nostic assessment. For example, our assessment did not collect detailed information about thetiming of traumatic exposure in the adolescent’s life history. Further, we lack importantinformation about the timing and type of death of the non-study parents. Future studies ofchildren of HIV-infected parents should include detailed information about potentially stress-ful life events and their relationship with onset of psychiatric disorders in these youth. Suchinformation will help better target assessment and intervention to high-risk periods for theyouth of PWH.
Another limitation is that this study did not have a control group of adolescents withoutan HIV-infected parent in order to compare the base rates of psychiatric diagnoses in high-risk youth from comparable neighborhoods. Future studies of adolescents of PWA wouldbenefit from inclusion of a neighborhood control group.
Conclusion
The results of this study provide the first detailed report on anxiety and depressive disor-ders in youth affected by parental HIV illness and death. These findings highlight the highprevalence of PTSD in youth of PWH, underscoring the importance of trauma-focusedassessment and intervention strategies in children of PWH. In addition, these findingsindicate the risk of prior traumatic exposure for both anxiety and depressive disorders inadolescents of PWH, suggesting potential pathways for vulnerability in youth negotiatingadolescence with a seriously ill parent. Perhaps the most striking finding of this study is thateven facing the ongoing challenges of parental HIV illness and death, more than half (56%)of the adolescents did not report a history of any anxiety or depressive disorders over theirlifetime. Future investigation may better elucidate risk and protective factors related todevelopmental trajectory and psychopathology in adolescents facing parental illness anddeath, and provide further information about the timing of risk in these youth.
References
American Psychiatric Association (1987). Diagnostic and statistical manual of mental disorders (3rd edn, revised).Washington, DC: American Psychiatric Association.
Anderson A. R., & Henry, C. S. (1994). Family system characteristics and parental behaviors as predictors of ado-lescent substance use. Adolescence, 29, 405–420.
Andrews, G., & Peters, L. (1998). The psychometric properties of the Composite International Diagnostic Inter-view. Social Psychiatry and Psychiatric Epidemiology, 33, 80–88.
Balk, D. (1983). Effects of sibling death on teenagers. Journal of Scholarly Health, 53, 14–18.Bernstein, G. H., & Borchardt, C. M. (1991). Anxiety disorders in childhood and adolescents: A critical review.
Journal of the American Academy of Child and Adolescent Psychiatry, 30, 518–532.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Anxiety and depressive disorders in adolescents of parents with HIV 99
Biederman, J., Faraone, S. V., Monuteaux, M. C., & Feighner, J. A. (2000). Patterns of alcohol and drug use inadolescents can be predicted by parental substance use disorders. Pediatrics, 106, 792–797.
Bornstein, M. H. (1995). Handbook of parenting, Vol. 1. Children and parenting. Hillsdale, NJ: Lawrence ErlbaumAssociates.
Brech, C. (1996). Die Bedeutung der Beziehungserfahrungen adoleszenter Maedchen und junger Frauen fuer ihre weibli-che Identitaetsfindung vor dem Hintergrund der Brustrebserkrankung der Mutter. Unpublished PsychologischeDiplomarbeit, Universitat Hamburg, Hamburg, Germany.
Brown, D. R., Ahmed, F., Gary, L. E., & Milburn, N. G. (1995). Major depression in a community sample ofAfrican Americans. American Journal of Psychiatry, 152, 373–378.
Bryk, A. S., & Raudenbush, S. W. (1992). Hierarchical Linear Models, Applications and data Analysis Methods.Newbury Park, CA: Sage Publications.
Centers for Disease Control and Prevention. (1996). US HIV and AIDS cases reported through June 1996. HIV/AIDS surveillance report, 8. Atlanta, GA: Centers for Disease Control and Prevention.
Centers for Disease Control and Prevention. (2001). US HIV and AIDS cases reported through June 2001. HIV/AIDS surveillance report, 13. Atlanta, GA: Centers for Disease Control and Prevention.
Clark, D. B., Wood, D. S., Cornelius, J. R., Bukstein, O. G., & Martin, C. S. (2003). Clinical practices in thepharmacological treatment of comorbid psychopathology in adolescents with alcohol use disorders. Journal ofSubstance Abuse Treatment, 25, 293–295.
Compas, B., Worsham, N., Epping-Jordan, J., Howell, D., Grant, K., Mireault, G., et al. (1994). When mom ordad has cancer: Markers of psychological distress in children of cancer patients, spouses, and children. HealthPsychology, 13, 507–515.
Compas, B., Worsham, N., Ey, S., & Howell, D. (1996). When mom or dad has cancer: II. Coping, cognitiveappraisals, and psychological distress in children of cancer patients. Health Psychology, 15, 167–175.
Cummings, E. M., & Davies, P. T. (1994). Maternal depression and child development. Journal of Child Psychologyand Psychiatry, 35, 73–112.
Derogatis, L. R. (1993). Brief Symptom Inventory: Administration, scoring and procedures manual. Minneapolis, MN:National Computer Systems.
Drucker, E., & Vermund, S. H. (1989). Estimating population prevalence of human immunodeficiency virusinfection in urban areas with high rates of intravenous drug use: A model of the Bronx in 1988. AmericanJournal of Epidemiology, 130, 133–142.
Duncan, S. C., Alpert, A., Duncan, T. E., & Hops, H. (1997). Adolescent alcohol use development and youngadult outcomes. Drug and Alcohol Dependence, 49, 39–48.
Eron, J. J., Benoit, S. L., Jemsek, J., MacArthur, R. D., Santana, J., Quinn, J. B., et al. (1995). Treatment withlamivudine, zidovudine, or both in HIV-positive patients with 200 to 500 CD4+ cells per cubic millimeter.North American HIV Working Party. New England Journal of Medicine, 333, 1662–1669.
Essau, C., & Dobson, K. (1999). Epidemiology of depressive disorders. In C. A. Essau, & F. Petermann (Eds),Depressive disorders in children and adolescents: Epidemiology, risk factors, and treatment (pp. 69–103). Northvale,NJ: Jason Aronson, Inc.
Fonagy, P., Target, M., Cottrell, D., Phillips, J., & Kurtz, Z. (2002). What works for whom? A critical review oftreatments for children and adolescents (xiii, pp. 577). New York: Other Press.
Frierson, R. L., & Lippmann, S. B. (1987). Psychologic implications of AIDS. American Family Physician, 35, 109–116.Garber, J., Robinson, N. S., & Valentiner, D. (1997). The relation between parenting and adolescent depression:
Self-worth as a mediator. Journal of Adolescent Research, 12, 12–33.Giaconia, R., Reinherz, H., Silverman, A., Pakiz, B., Frost, A., & Cohen, E. (1995). Traumas and posttraumatic
stress disorder in a community population of older adolescents. Journal of the American Academy of Child andAdolescent Psychiatry, 34, 1369–1380.
Gibbs, J. T. (1989). Black American adolescents. In J. T. Gibbs, L. N. Huang, & Associates (Eds), Children ofcolor: Psychological interventions with minority youth (pp. 179–223). San Francisco: Jossey-Bass.
Goenjian, A. K., Pynoos, R. S., Steinberg, A. M., Najarian, L. M., Asarnow, J. R., Karayan, I., et al. (1995). Psy-chiatric co-morbidity in children after the 1988 earthquake in Armenia. Journal of the American Academy ofChild and Adolescent Psychiatry, 34, 1174–1184.
Harris, T., Brown, G. W., & Bifulco, A. (1986). Loss of parent in childhood and adult psychiatric disorder: Therole of lack of adequate parental care. Psychological Medicine, 16, 641–659.
Heim, C., & Nemeroff, C. B. (2001). The role of childhood trauma in the neurobiology of mood and anxiety dis-orders: Preclinical and clinical studies. Biological Psychiatry, 49, 1023–1039.
Herek, G. M., & Capitanio, J. P. (1993). Public reactions to AIDS in the United States: A second decade ofstigma. American Journal of Public Health, 83, 574–577.
Herek, G. M., Capitanio, J. P., & Widaman, K. F. (2002). HIV-related stigma and knowledge in the UnitedStates: Prevalence and trends, 1991–1999. American Journal of Public Health, 92, 371–377.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
100 P. Lester et al.
Hovens, J. G. F. M., Cantwell, D. P., & Kiriakos, R. (1994). Psychiatric comorbidity in hospitalized adolescentsubstance abusers. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 476–483.
Kaufman, J., & Charney, D. (2001). Effects of early stress on brain structure and function: Implications forunderstanding the relationship between child maltreatment and depression. Developmental Psychopathology,13, 451–471.
Kandel, D. B., Johnson, J. G., Bird, H. R., Canino, G., Goodman, S. H., Lahey, B. B., et al. (1997). Psychiatricdisorders associated with substance use among children and adolescents: findings from the Methods for theEpidemiology of Child and Adolescent Mental Disorders (MECA) Study. Journal of Abnormal Child Psychol-ogy, 25, 121–132.
Kessler, R., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. (1995). Posttraumatic stress disorder in theNational Comorbidity Survey. Archives of General Psychiatry, 52, 1048–1060.
Kilpatrick, D. G., Acierno, R., Saunders, B., Resnick, H. S., Best, C. L., & Schnuur, P. P. (2000). Risk factors foradolescent substance abuse and dependence: data from a national sample. Journal of Consulting and ClinicalPsychology, 68, 19–30.
Kinloch-de Loes, S., & Perrin, L. (1995). Therapeutic interventions in primary HIV infection. Journal of AcquiredImmune Deficiency Syndrome and Human Retrovirology, 10, S69–S76.
Kumpfer, K. L., Molgaard, V., & Spoth, R. (1996). The Strengthening Families Program for the prevention ofdelinquency and drug use. In R. D. V. Peters, & R. J. McMahon (Eds), Banff international behavioral scienceseries: Vol. 3. Preventing childhood disorders, substance abuse, and delinquency (pp. 241–267). Thousand Oaks,CA: Sage.
Lee, M. B., Lester, T., & Rotheram-Borus, M. J. (2002). The relationship between the adjustment of motherswith HIV and their adolescent daughters. Journal of Clinical Child Psychology and Psychiatry, 7, 71–84.
Lee, M., & Rotheram-Borus, M. J. (2001). Challenges associated with increased survival among parents livingwith HIV. American Journal of Public Health, 91, 1303–1309.
Lewandowski, L. (1992). Needs of children during the critical illness of a parent or sibling. Critical Care NursingClinics of North America, 4, 57–85.
Lutzke, J. R., Ayers, T. S., Sandler, I. N., & Barr, A. (1997). Risks and interventions for the parentally bereavedchild. In S. A. Wolchik & I. N. Sandler (Eds), Handbook of children's coping: Linking theory and intervention(pp. 215–243). New York, NY: Plenum Press.
McCloskey, L. A., & Walker, M. (2000). Posttraumatic stress in children exposed to family violence and single-event trauma. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 108–115.
Michaels, D., & Levine, C. (1992). Estimates of the number of motherless youth orphaned by AIDS in theUnited States. Journal of the American Medical Association, 268, 3456–3461.
Minkoff, K. (2001). Best practices: Developing standards of care for individuals with co-occurring psychiatric andsubstance use disorders. Psychiatric Services, 52, 597–599.
National Institutes of Mental Health. (2005). Brief notes on the mental health of children and adolescents. Avail-able at: http://www.medhelp.org/NIHlib/GF-233.html (accessed 30 July 2005).
New York City Human Resources Division of AIDS Services. (1993). Report: New York City Division of AIDSServices. New York City, NY: New York City Human Resources Division of AIDS Services.
Pandina, R. J., & Johnson, V. (1989). Familial drinking history as a predictor of alcohol and drug consumptionamong adolescent children. Journal of Studies on Alcohol, 50, 245–253.
Parkes, C. M., & Weiss, R. S. (1983). Recovery from bereavement. New York: Basic Books.Post, R. M., Leverich, G. S., Xing, G., & Weiss, R. B. (2001). Developmental vulnerabilities to the onset and
course of bipolar disorder. Developmental Psychopathology, 13, 581–598.Pynoos, R. S., Steinberg, A. M., & Piacentini, J. C. (1999). A developmental psychopathology model of child-
hood traumatic stress and intersection with anxiety disorders. Biological Psychiatry, 46, 1542–1554.Rao, U., Daley, S. E., & Hammen, C. (2000). Relationship between depression and substance use disorders in
adolescent women during the transition to adulthood. Journal of the American Academy of Child and AdolescentPsychiatry, 39, 215–222.
Raphael, B., Cubis, J., Dunne, M., & Lewin, T. (1990). The impact of parental loss on adolescents’ psychosocialcharacteristics. Adolescence, 25, 689–700.
Raveis, V. H., Siegel, K., & Karus, D. (1999). Children’s psychological distress following the death of a parent.Journal of Youth and Adolescence, 28, 165–180.
Rohde, P., Lewinsohn, P. M., Seely, J. R. (1996). Psychiatric comorbidity with problematic alcohol use in highschool students. Journal of the American Academy of Child Adolescent Psychiatry, 35, 101–109.
Romer, G., Barkmann, C., Schulte-Markwort, M., Thomalla, G., Behrendt, M., & Riedesser, P. (2002). Childrenof somatically ill parents: A methodological review. Journal of Clinical Child Psychology and Psychiatry, 7, 17–38.
Rosenheim, E., & Reicher, R. (1986). Children in anticipatory grief: The lonely predicament. Journal of ClinicalChild Psychology, 15, 115–119.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Anxiety and depressive disorders in adolescents of parents with HIV 101
Rost, R. (1992). Psychosoziale Probleme von Kindern körperlich kranker Eltern - ein Literaturüberblick. UnpublishedMedizinische Dissertation, Albert-Ludwigs-Universität Freiburg, Germany.
Rotheram-Borus, M. J., Lee, M. B., Gwadz, M., & Draimin, B. (2001a). An intervention for parents with AIDSand their adolescent children. American Journal of Public Health, 91, 1294–1302.
Rotheram-Borus, M. J., Lee, M., Leonard, N. L., Lin, Y., Franzke, L., Turner, E., et al. (2003). Four-yearbehavioral outcomes of an intervention for parents living with HIV and their adolescent children. AIDS, 17,1217–1225.
Rotheram-Borus, M. J., Lee, M., Lin, Y. Y., & Lester, P. (2004). Six-year intervention outcomes for adolescentchildren of parents with the human immunodeficiency virus. Archives of Pediatrics and Adolescent Medicine,158, 742–748.
Rotheram-Borus, M. J., Leonard, N. L., Lightfoot, M., Franzke, L. H., Tottenham, N., & Lee, S. (2002). Pickingup the pieces: Caregivers of adolescents bereaved by parental AIDS. Journal of Clinical Child Psychology andPsychiatry, 7, 115–124.
Rotheram-Borus, M. J., Murphy, D. A., Miller, S., & Draimin, B. H. (1997). An intervention for adolescentswhose parents are living with AIDS. Journal of Clinical Child Psychology Psychiatry, 2, 201–219.
Rotheram-Borus, M. J., & Stein, J. A. (1999). Problem behavior of adolescents whose parents are living withAIDS. American Journal of Orthopsychiatry, 69, 228–239.
Rotheram-Borus, M. J., Stein, J. A., & Lin, Y. Y. (2001b). Impact of parent death and an intervention on theadjustment of adolescents whose parents have HIV/AIDS. Journal of Consulting and Clinical Psychology, 69,763–773.
Rotunda, R., Scherer, D., & Imm, P. (1995). Family systems and alcohol misuse: Research on the effects of alco-holism on family functioning and effective family interventions. Professional Psychology: Research and Practice,26, 95–104.
Rounsaville, B. J. (2004). Treatment of cocaine dependence and depression. Biological Psychiatry, 56, 803–809.Sack, W., Clarke, G., & Seeley, J. (1996). Multiple forms of stress in Cambodian adolescent refugees. Child Devel-
opment, 67, 107–116.Saldinger, A., Cain, A., & Porterfield, K. (2003). Managing traumatic stress in children anticipating parental
death. Psychiatry, 66, 168–181.Sanchez, L., Fristad, M., Weller, R. A., & Weller, E. B. (1994). Anxiety in acutely bereaved prepubertal children.
Annals of Clinical Psychiatry, 6, 39–43.Schuster, M. A., Kanouse, D. E., Morton, S. C., Bozzette, S. A., Miu, A., Scott, G. B., et al. (2000). HIV-
infected parents and their children in the United States [see comments]. American Journal of Public Health,90, 1074–1081.
Siegel, K., Karus, D., & Raveis, V. H. (1996). Adjustment of children facing the death of a parent due to cancer.Journal of the American Academy of Child and Adolescent Psychiatry, 35, 442–450.
Siegel, K., Mesagno, F. P., Karus, D., Christ, G., Banks, K. B., & Moynihan, R. (1992). Psychosocial adjustmentof children with a terminally ill parent. Journal of the American Academy of Child and Adolescent Psychiatry, 31,327–333.
Stanton, A. L., Collins, C. A., & Sworowski, L. A. (2001). Adjustment to chronic illness: Theory and research. InA. Baum, T. A. Revenson, & C. E. Singer (Eds), Handbook of health psychology (pp. 387–399). Mahwah, NJ:Erlbaum.
Stein, J. A., Riedel, M., & Rotheram-Borus, M. J. (1999). Parentification and its impact on adolescent children ofparents with AIDS. Family Process, 38, 193–208.
UNAIDS (2002). AIDS Epidemic Update: December 2002. Available at: http://www.who.int/hiv/pub/epidemiology/epi2002/en (accessed 10 December 2004).
US Department of Health and Human Services (2003). Children’s mental health facts. Children and adolescents withanxiety disorders. Available at: http://www.mentalhealth.samhsa.gov/publications/allpubs/CA-0007/ (accessed23 July 2005).
Weine, S., Becker, D., McGlashan, T., Vojvoda, D., & Hartman S. (1995). Adolescent survivors of ‘ethniccleansing’: Observations on the first year in America. Journal of the American Academy of Child and AdolescentPsychiatry, 34, 1153–1159.
West, S. G., Sandler, I., Pillow, D. R., Baca, L., & Gersten, C. (1991). The use of structural equation modelingin generative research: Toward the design of a preventive intervention for bereaved children. American Journalof Community Psychology, 19, 459–480.
Wittchen, H. U. (1994). Reliability and validity studies of the WHO – Composite International Diagnostic Inter-view (CIDI): A critical review. Journal of Psychiatric Research, 28, 57–84.
World Health Organization. (1998). Composite International Diagnostic Interview: Data entry and scoring manual.Geneva, Switzerland: World Health Organization.
Downloaded By: [CDL Journals Account] At: 18:01 2 November 2009
Copyright © 2022 FDOKUMEN




















