
Raisen District, Madhya Pradesh Field Visit Report
17
Raisen District, Madhya Pradesh Field Visit Report By: Dr. Arpana Kullu, Consultant NRHM-I MoHFW
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Raisen District, Madhya Pradesh Field Visit Report
Raisen District, Madhya Pradesh Field Visit Report
By: Dr. Arpana Kullu, Consultant
NRHM-I MoHFW
Introduction
For the Action based Monitoring of High Focused Districts, first visit was made to the district
of Raisen in Madhya Pradesh from 26th April 2010 to 30th April 2010. The facilities visited and key
persons visited for monitoring are enumerated in the Table 1 shown below. The monitoring visit, out
of 7 blocks, visit was made to 4 blocks and it included interaction with the Health staff including the
Medical Officers, Block Programme Managers , Nursing Staff and few ASHA’s , to gain a better
understanding of the processes and difficulties in functioning.
Table 1: Showing the Blocks and Persons visited for monitoring.
Methodology
Secondary Data was collected for the structured format from the state and district HMIS
data format that was already available at the respective Programme Management Unit. The primary
data was collected for the qualitative responses in the format through interactions with the health
staff during the visits to the health facilities.
In addition to the State Program Management Unit, the District Program Management Unit and the
Block Program Management Unit, facilities from all the three level were randomly selected to
conduct the monitoring. From the tertiary level the District Hospital was covered, from the
secondary level , CHC Mandideep, Block PHC(Obdullaganj), CHC Bareilly, CHC Sanchi and CHC Silwani
and from the primary level PHC Salamatpur and SC Itkhedi. And during these community visits the
frontline workers including the ASHA’s, LHV and ANM’s were also interviewed.
DATE DISTRICT/BLOCK PLACE VISITED PERSONS VISITED
27.04.10 Raisen SPMU, Bhopal District Health Office, Raisen
SPM- Mr. Kumar Sourav ASO- Mr. Raikward IEC Consultant- Mr.Amit Sharma
28.04.10 1).Obdullaganj 2).Bareilly
CHC Mandideep & Block PHC(Obdullaganj) CHC Bareilly
BMO- Dr.K.P.Yadav BPM- Mr.Sunil & Mr.Soni BMO- Dr.B.D.Khare
29.04.10 Raisen (Sanchi) CHC Sanchi & PHC Salamatpur District Hospital
BMO- Dr.Das BPM- Ms. Rashmi MO
30.04.10 Silwani CHC Silwani SC Itkhedi
BMO-Dr. Manre BPM- Deepak Singh LHV- Sulochana

District Profile: Raisen , Madhya Pradesh
The district caters to a population of 14 lakhs. The neighbouring districts are Vidisha, Sehore and
Hoshangabad. Besides Bhopal, Vidisha district provides medical care to the patients referred out
from Raisen block. The terrain in the district is plain and it has a good connectivity by roadways as
shown in the map below. The distict is divided into 7 blocks namely, Sanchi-Raisen, Obdullaganj-
Gohaganj, Silwani, Bareilly, Udaipura, Gairatganj and Begamganj.
Figure 1: Road Map of Raisen District showing boundaries and road routes.

District, Raisen Madhya Pradesh is one of the closest districts to the state capital of Bhopal.
According to the Ranking and Mapping of Districts done by IIPs in 2006 the rank given to Raisen was
359 out of the total of 593 districts. The further elaboration of the indicators of the district is given in
Figure 2 shown below.
Figure 2: Rank of Raisen District, Source: Jansankhya Sthirta Kosh
District Programme Management unit
The DPMU at Raisen is headed by Dr. Chaubey, CDHO. The DPMU is stationed approximately
60kms from the State Programme Management Unit in Bhopal. It mainly monitors and supervises
the functioning of the whole district. But the lack of staff being one of the universal problems across
districts, Raisen is no different.
Currently the position of District Programme Manager lies vacant since last one year hence
the currently staff in position mainly the ASO and the IEC Consultant who have been working in the
DPMU manage the responsibilities of the DPM, which often results in multi tasking by them. More
over the DPMU as well as BPMU’s also lack data entry operator staff hence the burden falls on the
existing staff. In addition, due to the non-availability and incomplete data leaves very limited
baseline information to plan further. Thus lack of skilled staff results in compromised state of
available data for any monitoring and evaluation. Hence forth there was a lot of information in the
format that was unavailable.
Besides the existing difficulties what is commendable is that the district is still able to upload
their data within its limited capacities. The deputation of Block Program Managers also requires due
appreciation since they are contributing immensely in providing managerial support for tracking
funds and monitoring activities under the mission at the block level. But to further utilise their skills
and capacities more effectively they need even more clear and focused guidelines on their roles and
responsibilities, as told by them
.
Health Facilities in the District
Health Facility Number
District Hospital 1
Community Health Centre 9
Primary Health Centre 19
Sub Health Centre 176
Currently the number of health facilities in the district is not sufficient to meet the needs the
whole population of 14lakhs. And there hasn’t been any proposal in the district health plan within
last year for construction of any PHC or CHC.
Capacity Building
Along with ensuring availability of the health staff in the facilities NRHM focuses on build on the
capacities of the existing staff. For which there are provisions for trainings at all levels. As mentioned
in the monitoring format the trainings for doctors in EmOC, LSAS, Abdominal Tubectomy (Minilap)
and IMNCI in the last one year has been nil.
Human Resource
The problem of shortage of specialists in the districts is not any different to Raisen. Currently in the district, there are 40 regularly employed MBBS doctors and there are another 40 MBBS doctors who are deputed on contractual positions. For specialists there are 20 specialists available in the whole district.
And even with the ones available the services provided are not adequate. For example, the number Of caesareans performed in 2009-2010 in the District hospital: 48. Moreover when combined with other problems of lack of supportive staff it becomes even more difficult to provide essential care also.
The area under the field staff on average is 7-8 villages which in terms of population
constitutes a population of up to 600 people. There has been a significant addition of ANM’s in the
district. A total of 216 ANM’s were added in the year 2009-2010.
The current state of vacant and filled positions of ASHA’s and AWW’s is given in the
following table.( Source: State HMIS data, updated till Feb 2010)

ASHA’s
Filled Vacant
AWW
Filled Vacant
Total No of
Villages
Bareilly 145 108 260 -7 253
Sanchi 173 24 197 53 262
Silwani 120 129 112 137 249
Obdullaganj 145 108 195 58 253
Udaipura 137 30 157 8 155
Gairatganj 85 77 98 64 162
Begumganj 118 78 116 80 196
Communitization Process: Community participation is an important component of NRHM for which
many strategies have been incorporated in the programme so as to ensure that the health mission
reaches the underserved communities and involve people in planning process also. Broadly these
strategies include Selection of ASHA’s, Rogi Kalyan Samiti and Village Health and Sanitation
Committee. Even after five years of NRHM the programme has not been able to reach completely up
till the community level.
(i). ASHA’s
The observations and concerns regarding ASHAs’s that were found out in the district are as follows:
There are a total of 940 ASHA’s in the district against the sanctioned positions of 1477.
Hence a huge need of almost 537 ASHA’s still remains unmet. For which strategies like making the
eligibility criterion more flexible needs to be adopted.
On interactions with the DPMU staff it was told that 625 drug kits given to ASHA’s was
supplied only once in the year 2007, hence the newly selected ASHA’s in the last couple year did not
receive these drug kits. Whereas, the data shows that all the 940 ASHA’s have received drug kits.
This information requires further probing at the PHC and Sub Centre levels.
Moreover the ASHA’s when inducted in the system they were supposed to be the between
the beneficiaries and the providers, and support the system to generate demand for the services
amongst the people, hence they were chosen as voluntary workers and not regular employees. But
now they have become a part of the system, this was substantiated when the ASHA’s who were
interviewed and asked about their roles and responsibilities they would reply that they are expected
to get all the pregnant women in their village to the health facility for delivery.
(ii). RKS
To upgrade facilities in the public health system and with a purpose to provide sustainable
quality care with accountability and people’s participation along with total transparency. The RKS is
in place in all the health facilities as per the guidelines in the framework. But their meetings do not
happen regularly as told by one of the Block Medical Officers and thus utilization of funds for which
the RKS was formed is very difficult to mobilise. Therefore currently the funds are not utilised with
complete efficiency.
(iii). Village and Health Sanitation Committee
There are 664 VHSC’s in the district and the target for the next year is 736 which are still less
when we equate them to the number of Gram Panchayats in the district. The committees are
formed wherever there are ASHA’s thus places where an ASHA is not there VHSC’s are also absent.
The VHSC’s that are already in place they have a joint bank account in the name of ASHA and the
Women representative from the PRI. And the fund utilized only requires the signatory to produce a
utilization certificate, there is no monitoring mechanism to ensure that the money is utilized for the
purpose it is released.
In addition since there is no incentive for the members of the VHSC to actively conduct meetings and
organise for activities and further the community presence of the health providers is also low there
is very little motivation for them to initiate and participate in its functioning.
(iv). IEC activities
IEC is one of the important activities which the health system adopts in order to ensure that
people are informed about the preventive health measures they can adopt in order to avoid any
kind of health hazard. In addition IEC activities are also helpful in communicating about the health
services available and to create a demand for the same. These activities are implemented through
many ways like through patient-doctor interaction during diseased hospital visit, through ASHA’s
while motivating women for ANC, PNC check ups, Institutional Deliveries etc., through posters
displayed in the health facility as well as in the villages etc. Also there is a provision of separate head
for IEC activities in the programme plan and funds are released under the same.
But currently this is not getting its due importance in the districts, very few poster were
observed in the facility also their content included a lot of written matter hence it was difficult for an
illiterate person to understand them. Also when the ASHA’s were asked about the information
during their field visits it was very limited to institutional delivery whereas the scope of them
dispensing information can easily be scaled up by including PNC check up, RTI, STI and other
preventable diseases. The patient doctor interaction was also just limited to symptom- prescription
level, where patient enumerates his chief complaint and the doctor writes the prescription and tells
him how to and where to take the medicine from.

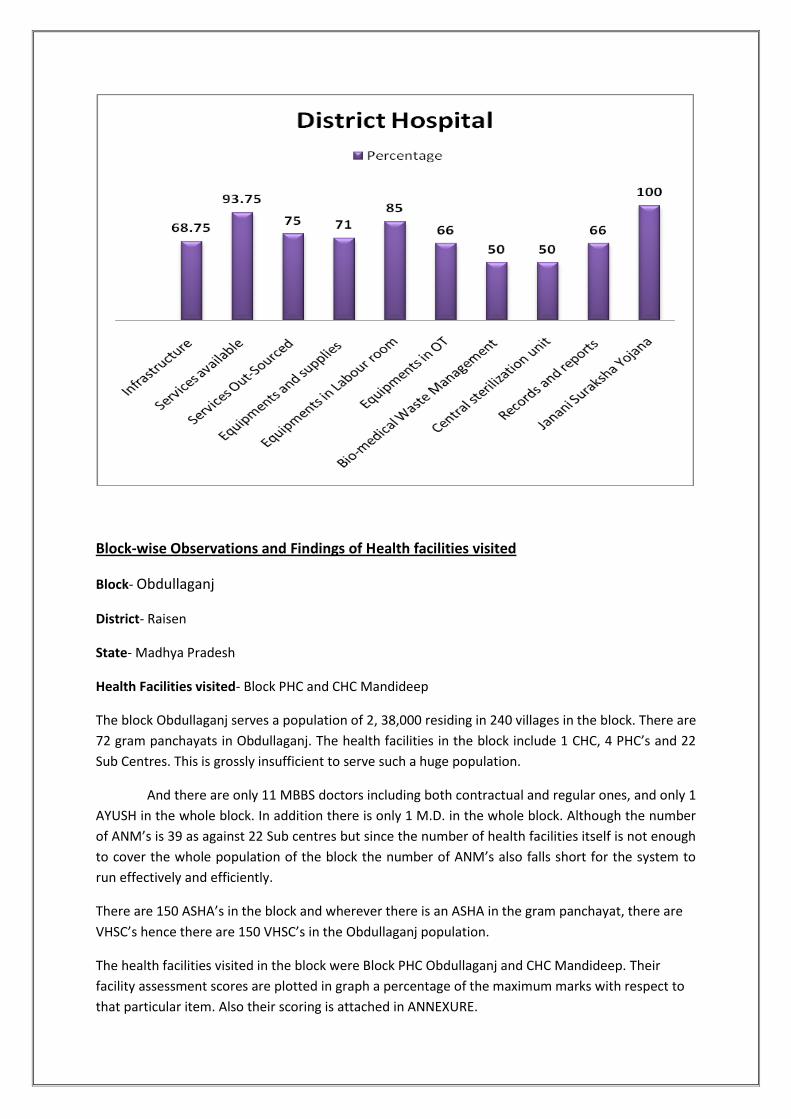
Inspection of Health Facilities

District Hospital, Raisen
The District Hospital at Raisen is 200 bedded hospital (recently upgraded from 100,
in past couple of years) catering to a population of 14lakhs. The Services provided at the
hospital range from regular OPD and IPD services, emergency care, basic laboratory services
including blood, urine and sputum examination, radiological examination. The average
number of OPD patients seen per day at the hospital is 300.
The District hospital is coming up with a Sick Newborn Care unit which is under construction
and is planned to be fully functional by the month of June 2010.The hospital also has a
blood bank in its premises but the state of the blood bank does not seem that it is utilised
regularly.
Clogged drain immediately outside the labour room and the state of toilets was very
unhealthy and unhygienic for the beneficiaries availing services at the hospital.
There was insufficient light and ventilation in the wards. Cleanliness and infection control
were unsatisfactory. Absence of patient amenities like screens in wards for patient privacy
stools for attendants, sufficient seating arrangements for patients was also observed.
Waste disposal and universal precautions for infection control were also not followed;
disposable gloves were being washed and reused.
In the last year only 35 C-sections were done in the district hospital even when they have a
gynaecologist in the health facility. And with the blood storage not in use the district
hospital
Block-wise Observations and Findings of Health facilities visited
Block- Obdullaganj
District- Raisen
State- Madhya Pradesh
Health Facilities visited- Block PHC and CHC Mandideep
The block Obdullaganj serves a population of 2, 38,000 residing in 240 villages in the block. There are
72 gram panchayats in Obdullaganj. The health facilities in the block include 1 CHC, 4 PHC’s and 22
Sub Centres. This is grossly insufficient to serve such a huge population.
And there are only 11 MBBS doctors including both contractual and regular ones, and only 1
AYUSH in the whole block. In addition there is only 1 M.D. in the whole block. Although the number
of ANM’s is 39 as against 22 Sub centres but since the number of health facilities itself is not enough
to cover the whole population of the block the number of ANM’s also falls short for the system to
run effectively and efficiently.
There are 150 ASHA’s in the block and wherever there is an ASHA in the gram panchayat, there are
VHSC’s hence there are 150 VHSC’s in the Obdullaganj population.
The health facilities visited in the block were Block PHC Obdullaganj and CHC Mandideep. Their
facility assessment scores are plotted in graph a percentage of the maximum marks with respect to
that particular item. Also their scoring is attached in ANNEXURE.
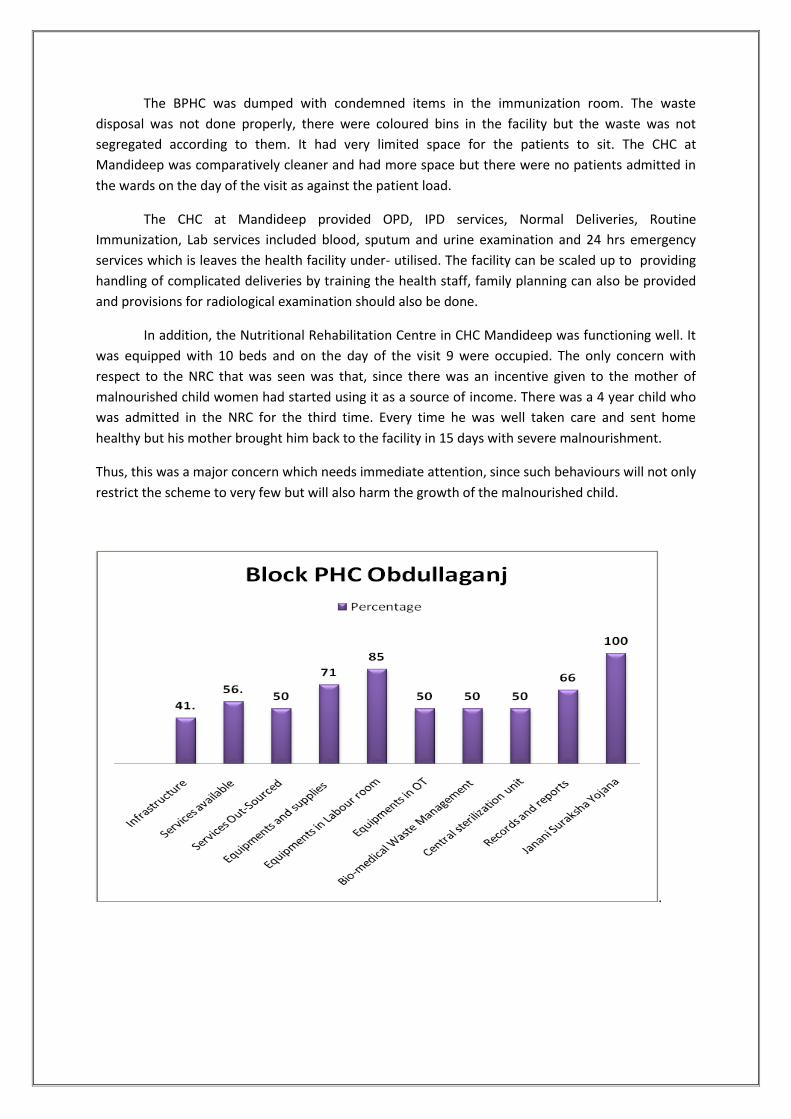
The BPHC was dumped with condemned items in the immunization room. The waste
disposal was not done properly, there were coloured bins in the facility but the waste was not
segregated according to them. It had very limited space for the patients to sit. The CHC at
Mandideep was comparatively cleaner and had more space but there were no patients admitted in
the wards on the day of the visit as against the patient load.
The CHC at Mandideep provided OPD, IPD services, Normal Deliveries, Routine
Immunization, Lab services included blood, sputum and urine examination and 24 hrs emergency
services which is leaves the health facility under- utilised. The facility can be scaled up to providing
handling of complicated deliveries by training the health staff, family planning can also be provided
and provisions for radiological examination should also be done.
In addition, the Nutritional Rehabilitation Centre in CHC Mandideep was functioning well. It
was equipped with 10 beds and on the day of the visit 9 were occupied. The only concern with
respect to the NRC that was seen was that, since there was an incentive given to the mother of
malnourished child women had started using it as a source of income. There was a 4 year child who
was admitted in the NRC for the third time. Every time he was well taken care and sent home
healthy but his mother brought him back to the facility in 15 days with severe malnourishment.
Thus, this was a major concern which needs immediate attention, since such behaviours will not only
restrict the scheme to very few but will also harm the growth of the malnourished child.
.

Block- Bareilly
District- Raisen
State- Madhya Pradesh
Health Facilities visited- CHC Bareilly and Sub Centre Itkhedi
The block Bareilly serves a population of 2, 45,000 residing in 248 villages in the block. There are 103
gram panchayats in Bareilly. The health facilities in the block include 2 CHC, 4 PHC’s and 43 Sub
Centres.
And there are only 10 MBBS doctors including both contractual and regular ones, and only 1 AYUSH
in the whole block. In addition there are 3 specialists in the block, 1 M.D. Medicine, 1 Paediatrician
and 1 Gynaecologist in the whole block. There are 43 ANM’s in the whole block hence one for each
Sub Centre.
There are 175 ASHA’s in the block and 81 VHSC hence every ASHA in the block is not a member of a
VHSC.
The CHC Bareilly was a 30 bedded health facility and it is a CemOC institution but it did not have a
blood storage facility in place and the position of the anaesthetist was vacant. Hence although the
institution was a CemOC institution on paper it wasn’t functioning like one. All the complicated cases
were referred out to either the District Hospital or to Bhopal.
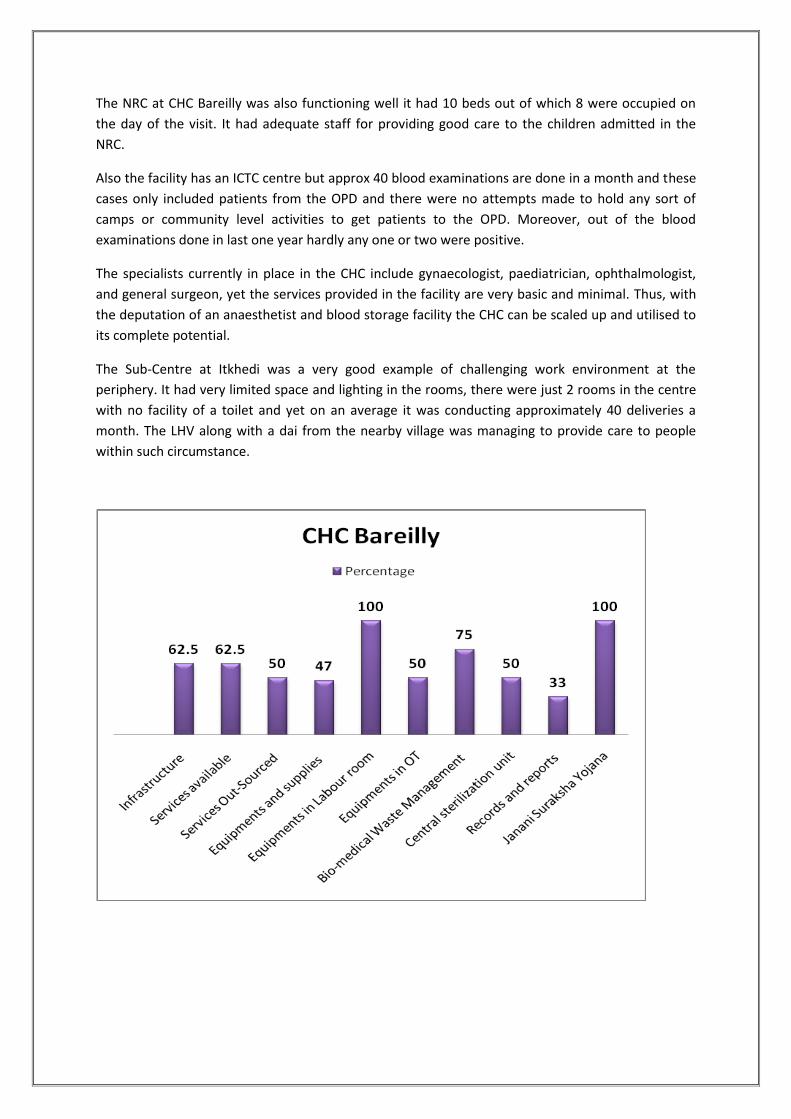
The NRC at CHC Bareilly was also functioning well it had 10 beds out of which 8 were occupied on
the day of the visit. It had adequate staff for providing good care to the children admitted in the
NRC.
Also the facility has an ICTC centre but approx 40 blood examinations are done in a month and these
cases only included patients from the OPD and there were no attempts made to hold any sort of
camps or community level activities to get patients to the OPD. Moreover, out of the blood
examinations done in last one year hardly any one or two were positive.
The specialists currently in place in the CHC include gynaecologist, paediatrician, ophthalmologist,
and general surgeon, yet the services provided in the facility are very basic and minimal. Thus, with
the deputation of an anaesthetist and blood storage facility the CHC can be scaled up and utilised to
its complete potential.
The Sub-Centre at Itkhedi was a very good example of challenging work environment at the
periphery. It had very limited space and lighting in the rooms, there were just 2 rooms in the centre
with no facility of a toilet and yet on an average it was conducting approximately 40 deliveries a
month. The LHV along with a dai from the nearby village was managing to provide care to people
within such circumstance.
Block- Raisen, Sanchi
District- Raisen
State- Madhya Pradesh
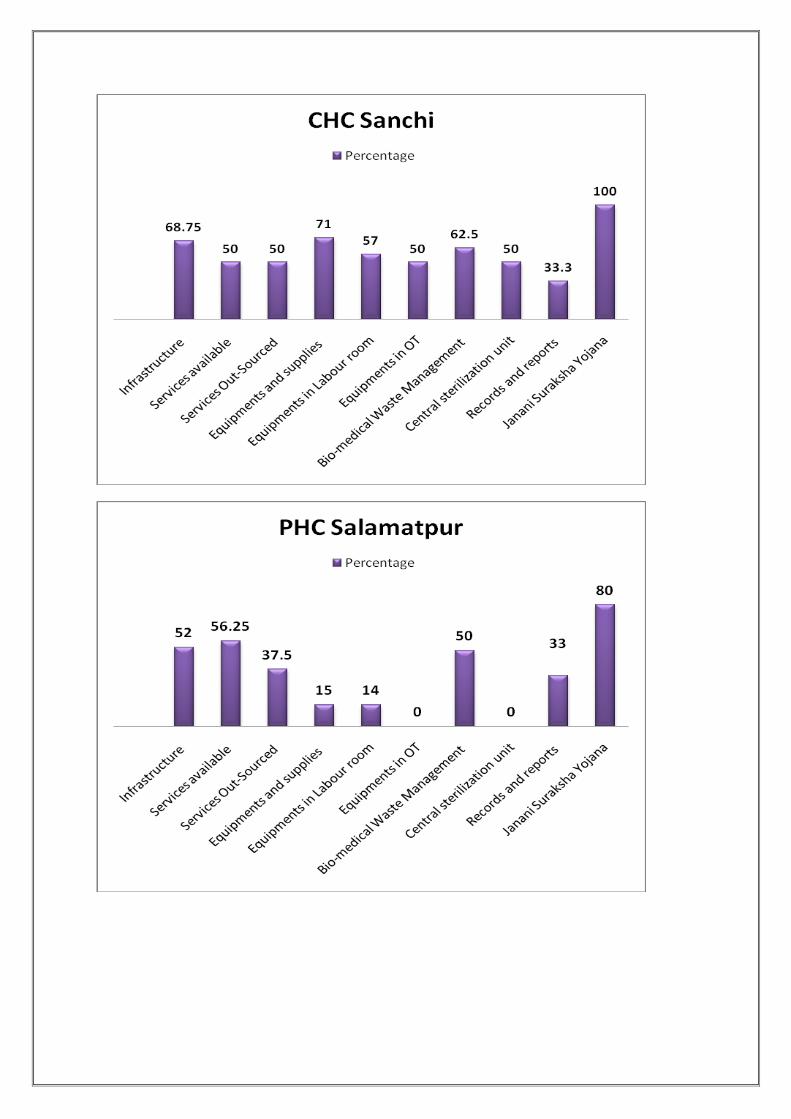
Health Facilities visited- Block CHC, Sanchi and PHC Salamatpur.
Block Raisen has its headquarters at Sanchi hence it is also called as Block Sanchi. It covers a
population of approximately 1,80,000 The health facilities available for the population in the block
are 1 CHC, 3 PHC’s and 30 Sub Centers. There are no specialists in the block. There are approximately
250 villages in the block out of which 110 has VHSC that are functional in terms that they have a
bank account in their name and they are utilising the funds. There are on paper 146 ASHA’s in the
block but only 136 of them are currently are actively working.
There are RKS at all the facilities and at every level but their functioning is not monitored or
supervised as there is no format to ensure that. The meetings for RKS are held at the discretion of
the chairman, the SDM hence it often gets delayed and are not held at regular intervals.
Block CHC, Sanchi- the Block CHC located at Sanchi which is approximately < 1Km away from the
famous historic monument Sanchi Stupa. The new building for the CHC is currently under
construction since last 6 months and is planned to be functional in another 6 months or so. It has a
daily OPD of approximately 150 per day. And for 24 hrs health services the doctor is on call and the
nursing staffs is stationed at the CHC.
A very good practice that was observed in the CHC Sanchi that the BPM had very well
organised detailed immunization schedule in the block, which included the name of the health staff
and the village they are suppose to visit in a month, as a result of which there were hardly any
sessions dropped in last one year. Also there was a format for the Village Health Plan that is
supposed to be filled up by the ASHA’s was also an appreciable effort made for ensuring
contributions from the beneficiaries in the village health plan and then eventually in the District
Health plan. A copy of the format is attached in the ANNEXURE towards the end of the report.
The PHC at Salamatpur was located very near to the road but was slightly uphill in position.
It was a six bedded facility and provided regular and basic services to the people coming to the
facility. It usually had an OPD of approximately 50 per day and family planning included NSVT and
IUD insertions. And conducted somewhere around 350 deliveries per year which only included
normal deliveries and the complicated deliveries are referred out to District Hospital or Bhopal.
The facility did not have a boundary wall since the land on which the health facility was built
was disputed and due to absence of a boundary wall people residing nearby had started encroaching
in which was a concern since the security of the staff was compromised. There was no vehicle hence
field visits were a tedious exercise for the field staff. VHSC’s were formed in most of the villages and
guidelines were given to each one of them and were functioning independently but none of them
had undergone any training as to how exactly it has to be operationalised and specific roles and
responsibilities of its members.

Block- Silwani
District- Raisen
State- Madhya Pradesh
Health Facilities visited- CHC Silwani
There are 246 villages and there are 68 Gram Panchayats covering a population of 1,34,000. The
health facilities in the block include 1 CHC, 2 PHC and 20 Sub Centres. Out of the 20 sub centres only
9 have a building and 1 is under construction and 2 more are proposed in the District Health Plan,
rest of them are rented.
The human resource in the block includes 3 M.B.B.S doctors and there are no specialists. In addition
there is 1 AYUSH doctor and there are 27 ANM’s. There are a total of 130 ASHA’s in the block which
is short by 116 when corroborated with the number of villages in the block.
This block was one of the ignored blocks in the district. It did not have sufficient number of health
facilities to meet the needs of the people. And since half of the sub-centres in the block did not have
a building of their own the staff faced difficulties.
CHC Silwani is a 30 bedded health facility and was in a very deteriorating condition. There
were wards and structures in place but were being used as it is. Cleanliness was not properly
maintained. Sheets were not laid over the beds in the wards. No screens for patient’s privacy. An
overall assessment of the facility is presented through the graph below and the scores as per the
monitoring format is attatched in the ANNEXURES.
Actionable Points
Deputation of District Programme Manager at the DPMU with immediate effect so
as to ensure the processes of planning, organizing and monitoring are carried out in
the district.
Recruitment of data analyst at the DPMU’s and BPMU’s to ensure the quality of data
and regular updating.
Trainings for doctors in EmOC, LSAS, Abdominal Tubectomy (Minilap) and IMNCI. Also the
ANM trainings in IMNCI should be taken up as soon as possible.
Cleanliness and hygiene in the health facilities to ensure infection control and not to
harm the patients should be the objective.
Segregation of waste into infectious and non-infections substances in separate color
coded bins need to be implemented with immediate effect to avoid hospital
acquired infections of both the beneficiaries as well as the providers.
The health facilities in the district are dumped with unused and broken/condemned
equipments which occupy space and further add to the space constraint. Hence
adequate protocols and mechanisms have to be adopted for scrap management.
ASHA’s need to be recognized as messengers of health information in the
community and not as mere assistance to the ANM’s. They also need to be
representatives of their villages instead of the health provider and generate demand
for the health services in the community.
VHSC’s need to be monitored and supervised. Producing utilization certificate and
account numbers should not be the only criterion for assessing the functioning of the
committee. The villagers need to be active part and should be able to relate to the
objective of the VHSC which can be done slowly and gradually by more effective IEC
activities through ASHA’s.
Interventions in the incentive scheme for the mothers of the malnourished children
in the Nutritional Rehabilitation Centre




















