Race-based differences in length of stay among patients undergoing pancreatoduodenectomy
10
Race-based differences in length of stay among patients undergoing pancreatoduodenectomy Eric B. Schneider, PhD, a Keri L. Calkins, BA, b Matthew J. Weiss, MD, a Joseph M. Herman, MD, c Christopher L. Wolfgang, MD, PhD, a Martin A. Makary, MD, MPH, a Nita Ahuja, MD, a Adil H. Haider, MD, MPH, a and Timothy M. Pawlik, MD, MPH, PhD, a Baltimore, MD Background. Race-based disparities in operative morbidity and mortality have been demonstrated for various procedures, including pancreatoduodenectomy (PD). Race-based differences in hospital length- of-stay (LOS), especially related to provider volume at the surgeon and hospital level, remain poorly defined. Methods. Using the 2003–2009 Nationwide Inpatient Sample, we determined year-specific PD volumes for surgeons and hospitals and grouped them into terciles. Patient race (white, black, or Hispanic), age, sex, and comorbidities were examined. Median length of stay was calculated, and multivariable logistic regression was used to examine factors associated with increased LOS. Results. Among 4,319 eligible individuals, 3,502 (81.1%) were white, 423 (9.8%) were black, and 394 (9.1%) were Hispanic. Overall median LOS was 12 days (range, 0–234). Median annual surgeon volume was 8 (interquartile range [IQR], 2–19; range, 1–54). Annual hospital volume ranged from 1 to 129 (median, 19; IQR, 7–55). White patients were more likely to have been treated at medium- to high-volume hospitals (odds ratio [OR] 1.53, P < .001) and by medium- to high-volume surgeons (OR 1.62, P < .001) than black or Hispanic patients. After PD, white, black, and Hispanic patients demonstrated similar in-hospital mortality (5.1%, 5.7% and 7.2% respectively P = .250). After adjustment, black (OR 1.36, P = .010) and Hispanic (OR 1.68, P < .001) patients were more likely to have a greater LOS after PD. Conclusion. Black and Hispanic PD patients were less likely than white patients to be treated at higher- volume hospitals and by higher-volume surgeons. Proportional mortality and LOS after PD were greater among black and Hispanic patients. (Surgery 2014;j:j-j.) From the Department of Surgery, a Johns Hopkins School of Medicine; Department of Epidemiology, b Johns Hopkins Bloomberg School of Public Health; and Department of Radiation Oncology, c Johns Hopkins School of Medicine, Baltimore, MD REDUCING HOSPITAL LENGTH OF STAY (LOS) among pa- tients undergoing complex operative procedures has been proposed as a possible mechanism for reducing health care–related costs. 1 LOS has also been suggested as a possible indicator of quality of care among patients undergoing complex oper- ative procedures. 2 Reducing LOS may reduce overall costs, as well as decrease patient exposure to nosocomial infection by getting patients out of the hospital faster. 3,4 In turn, substantial efforts have been made to reduce LOS among patients undergoing various operative procedures. 4-6 Previ- ous reports including data from our own group have demonstrated that both provider and patient factors impact hospital LOS. 7 LOS may be particu- larly important for complex operations that are associated with prolonged hospital stays such as pancreatoduodenectomy (PD). As such, our group previously examined inpatient hospital LOS after PD. While hospital and provider volume impacted LOS of patients, patient-specific factors, including age and comorbidity status, also were associated with prolonged LOS. 7 Although a substantial amount of literature has focused on the effect of volume on perioperative outcomes such as mortal- ity, 8 less attention has been focused on other Presented at the 9th Annual Academic Surgical Congress in San Diego, CA, February 4–6, 2014. Accepted for publication April 2, 2014. Reprint requests: Timothy M. Pawlik, MD, MPH, PhD, Professor Surgery and Oncology, John L. Cameron Professor of Alimen- tary Tract Surgery, Chief, Division of Surgical Oncology, Johns Hopkins Hospital, 600 N. Wolfe Street, Blalock 665, Baltimore, MD 21287. E-mail: [email protected]. 0039-6060/$ - see front matter Ó 2014 Mosby, Inc. All rights reserved. http://dx.doi.org/10.1016/j.surg.2014.04.004 SURGERY 1 ARTICLE IN PRESS
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Race-based differences in length of stay among patients undergoing pancreatoduodenectomy

ARTICLE IN PRESS
PresenteDiego, C
Accepte
ReprintSurgerytary TraHopkinMD 212
0039-60
� 2014
http://d
Race-based differences in length ofstay among patients undergoingpancreatoduodenectomyEric B. Schneider, PhD,a Keri L. Calkins, BA,b Matthew J. Weiss, MD,a Joseph M. Herman, MD,c
Christopher L. Wolfgang, MD, PhD,a Martin A. Makary, MD, MPH,a Nita Ahuja, MD,a
Adil H. Haider, MD, MPH,a and Timothy M. Pawlik, MD, MPH, PhD,a Baltimore, MD
Background. Race-based disparities in operative morbidity and mortality have been demonstrated forvarious procedures, including pancreatoduodenectomy (PD). Race-based differences in hospital length-of-stay (LOS), especially related to provider volume at the surgeon and hospital level, remain poorlydefined.Methods. Using the 2003–2009 Nationwide Inpatient Sample, we determined year-specific PD volumesfor surgeons and hospitals and grouped them into terciles. Patient race (white, black, or Hispanic), age,sex, and comorbidities were examined. Median length of stay was calculated, and multivariable logisticregression was used to examine factors associated with increased LOS.Results. Among 4,319 eligible individuals, 3,502 (81.1%) were white, 423 (9.8%) were black, and394 (9.1%) were Hispanic. Overall median LOS was 12 days (range, 0–234). Median annualsurgeon volume was 8 (interquartile range [IQR], 2–19; range, 1–54). Annual hospital volume rangedfrom 1 to 129 (median, 19; IQR, 7–55). White patients were more likely to have been treated at medium-to high-volume hospitals (odds ratio [OR] 1.53, P < .001) and by medium- to high-volume surgeons(OR 1.62, P < .001) than black or Hispanic patients. After PD, white, black, and Hispanic patientsdemonstrated similar in-hospital mortality (5.1%, 5.7% and 7.2% respectively P = .250). Afteradjustment, black (OR 1.36, P = .010) and Hispanic (OR 1.68, P < .001) patients were more likely tohave a greater LOS after PD.Conclusion. Black and Hispanic PD patients were less likely than white patients to be treated at higher-volume hospitals and by higher-volume surgeons. Proportional mortality and LOS after PD were greateramong black and Hispanic patients. (Surgery 2014;j:j-j.)
From the Department of Surgery,a Johns Hopkins School of Medicine; Department of Epidemiology,b JohnsHopkins Bloomberg School of Public Health; and Department of Radiation Oncology,c Johns Hopkins Schoolof Medicine, Baltimore, MD
REDUCING HOSPITAL LENGTH OF STAY (LOS) among pa-tients undergoing complex operative procedureshas been proposed as a possible mechanism forreducing health care–related costs.1 LOS has alsobeen suggested as a possible indicator of qualityof care among patients undergoing complex oper-ative procedures.2 Reducing LOS may reduce
d at the 9th Annual Academic Surgical Congress in SanA, February 4–6, 2014.
d for publication April 2, 2014.
requests: Timothy M. Pawlik, MD, MPH, PhD, Professorand Oncology, John L. Cameron Professor of Alimen-ct Surgery, Chief, Division of Surgical Oncology, Johnss Hospital, 600 N. Wolfe Street, Blalock 665, Baltimore,87. E-mail: [email protected].
60/$ - see front matter
Mosby, Inc. All rights reserved.
x.doi.org/10.1016/j.surg.2014.04.004
overall costs, as well as decrease patient exposureto nosocomial infection by getting patients out ofthe hospital faster.3,4 In turn, substantial effortshave been made to reduce LOS among patientsundergoing various operative procedures.4-6 Previ-ous reports including data from our own grouphave demonstrated that both provider and patientfactors impact hospital LOS.7 LOS may be particu-larly important for complex operations that areassociated with prolonged hospital stays such aspancreatoduodenectomy (PD). As such, our grouppreviously examined inpatient hospital LOS afterPD. While hospital and provider volume impactedLOS of patients, patient-specific factors, includingage and comorbidity status, also were associatedwith prolonged LOS.7 Although a substantialamount of literature has focused on the effect ofvolume on perioperative outcomes such as mortal-ity,8 less attention has been focused on other
SURGERY 1

ARTICLE IN PRESSSurgeryj 2014
2 Schneider et al
metrics such as LOS. Furthermore, the effect ofcertain patient-specific factors, such as race, onLOS remains poorly defined.
Understanding race disparities in health care hasbeen emphasized as an area of national impor-tance.9,10Most research on the topic of racial dispar-ities has focused on differences in access andutilization of health services and operative proce-dures.8 Other studies have examined variations insurgical mortality.11 These previous data haveconsistently demonstrated substantial race-baseddisparities in the use of specialty surgical services,as well as worse outcomes among blacks after awide range of operative procedures.8,11 Race-baseddifferences in mortality after pancreatic cancerresection have also been demonstrated; however,differences in other postoperative outcomes suchas LOS have not been examined previously.8,12
Given the increasing importance of LOS ashospital- and provider-based metrics, improvedunderstanding of the factors impacting LOS iscritical. Although we focused previously on otherpatient-specific factors as related to LOS after PD,the impact of race on LOS was not examined.7
Therefore, we sought to examine the specific rela-tionship between race and LOS by using nationaldata from the Agency for Healthcare Researchand Quality Healthcare Costs and Utilization Proj-ect Nationwide Inpatient Sample (NIS) database.In particular, we examined the impact of race onLOS relative to other patient (eg, comorbidity sta-tus) and perioperative (eg, complications), as wellas provider and hospital level (eg, PD volume)factors.
METHODS
A retrospective, cross-sectional study was per-formed using the NIS dataset, which is based on a20% sample of all discharges from acute hospital-ization collected on an annual basis.13 All patientswho underwent PD (identified using the Interna-tional Classification of Diseases, 9th Revision, ClinicalModification procedure codes) for any reason be-tween 2003 and 2009 were identified. The studysample was restricted to patients with a reportedrace or ethnicity of white, black, or Hispanic.Race is known to be missing in the NIS for approx-imately one-fifth of all patients, and these missingvalues do not occur at random. For these reasons,we relied upon a complete case analysis (CCA),where only patients with reported race wereincluded in the final study cohort. The CCAmethod may introduce moderate bias; however,in experimental analyses using NIS data CCA intro-duced only moderate bias, especially for samples in
which missing values for race were in the range of20%.14 The study dataset was restricted further tocontain only patients with available data for age,sex, LOS, hospital teaching status, hospital vol-ume, surgeon volume, and comorbidities, asmeasured with the Elixhauser comorbidity score,which was calculated for each study subject basedon the International Classification of Diseases, 9th
Revision, Clinical Modification procedure codes.15
The outcomes of interest, including inpatientLOS, morbidity, and in-hospital mortality, wereascertained with the use of the NIS records. MedianLOS for all patients was defined as ‘‘prolonged’’based on the median LOS (ie, #12 days vs >12days). Complications examined included place-ment of a percutaneous drain, postoperative hem-orrhage, postoperative hemorrhagic anemia,postoperative infection, failure to thrive (malnutri-tion), respiratory complication, operative re-exploration, accidental laceration, anestheticreaction, liver abscess, peritonitis, gastrointestinalhemorrhage, biliary fistula, intestinal fistula,stomach-duodenal fistula, paralytic ileus pressureulcer, deep-vein thrombosis, pulmonary embolism,aspiration, central line infection, cardiac complica-tions, postoperative shock, nonhealing surgicalwound, and urinary complications. For descriptiveand analytical purposes, providers and hospitalswere grouped into terciles by annual, PD proce-dure–specific volume.
Statistical analysis. Numerical variables werereported as medians and interquartile ranges,whereas categorical variables were described astotals and frequencies. Bivariate comparisonswere assessed with the Student t test, Wilcoxonrank-sum test, analysis of variance, Kruskal Wallistest, or the v2 test, as appropriate. Surgeon andhospital volumes were modeled as fixed effects(as terciles of PD volume) to explore their associa-tion with LOS. We used logistic regression modelsto adjust for patient demographic characteristics,patient comorbidities, and relevant hospital char-acteristics when examining patient LOS, account-ing for clustering by hospital. We conductedsensitivity analyses to explore possible colinearitybetween surgeon and hospital volume tercileswith logistic regression models, controlling forphysician and hospital volume terciles separately;in addition, a combined logistic regression model,which included both physician and hospital vol-ume terciles, was explored. Furthermore, the cor-relation between surgeon and hospital volumeterciles was examined with Spearman’s correlationcoefficient. An additional sensitivity analysis wasperformed to examine LOS as actual counts of
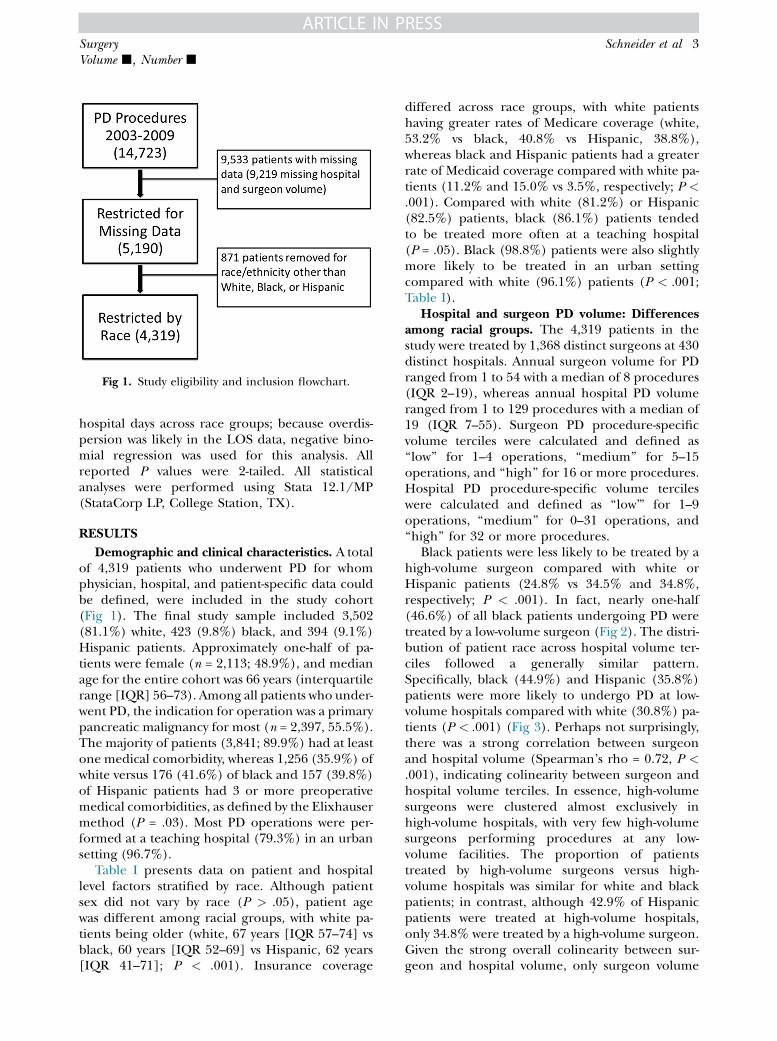
Fig 1. Study eligibility and inclusion flowchart.
ARTICLE IN PRESSSurgeryVolume j, Number j
Schneider et al 3
hospital days across race groups; because overdis-persion was likely in the LOS data, negative bino-mial regression was used for this analysis. Allreported P values were 2-tailed. All statisticalanalyses were performed using Stata 12.1/MP(StataCorp LP, College Station, TX).
RESULTS
Demographic and clinical characteristics. A totalof 4,319 patients who underwent PD for whomphysician, hospital, and patient-specific data couldbe defined, were included in the study cohort(Fig 1). The final study sample included 3,502(81.1%) white, 423 (9.8%) black, and 394 (9.1%)Hispanic patients. Approximately one-half of pa-tients were female (n = 2,113; 48.9%), and medianage for the entire cohort was 66 years (interquartilerange [IQR] 56–73). Among all patients who under-went PD, the indication for operation was a primarypancreatic malignancy for most (n = 2,397, 55.5%).The majority of patients (3,841; 89.9%) had at leastone medical comorbidity, whereas 1,256 (35.9%) ofwhite versus 176 (41.6%) of black and 157 (39.8%)of Hispanic patients had 3 or more preoperativemedical comorbidities, as defined by the Elixhausermethod (P = .03). Most PD operations were per-formed at a teaching hospital (79.3%) in an urbansetting (96.7%).
Table I presents data on patient and hospitallevel factors stratified by race. Although patientsex did not vary by race (P > .05), patient agewas different among racial groups, with white pa-tients being older (white, 67 years [IQR 57–74] vsblack, 60 years [IQR 52–69] vs Hispanic, 62 years[IQR 41–71]; P < .001). Insurance coverage
differed across race groups, with white patientshaving greater rates of Medicare coverage (white,53.2% vs black, 40.8% vs Hispanic, 38.8%),whereas black and Hispanic patients had a greaterrate of Medicaid coverage compared with white pa-tients (11.2% and 15.0% vs 3.5%, respectively; P <.001). Compared with white (81.2%) or Hispanic(82.5%) patients, black (86.1%) patients tendedto be treated more often at a teaching hospital(P = .05). Black (98.8%) patients were also slightlymore likely to be treated in an urban settingcompared with white (96.1%) patients (P < .001;Table I).
Hospital and surgeon PD volume: Differencesamong racial groups. The 4,319 patients in thestudy were treated by 1,368 distinct surgeons at 430distinct hospitals. Annual surgeon volume for PDranged from 1 to 54 with a median of 8 procedures(IQR 2–19), whereas annual hospital PD volumeranged from 1 to 129 procedures with a median of19 (IQR 7–55). Surgeon PD procedure-specificvolume terciles were calculated and defined as‘‘low’’ for 1–4 operations, ‘‘medium’’ for 5–15operations, and ‘‘high’’ for 16 or more procedures.Hospital PD procedure-specific volume tercileswere calculated and defined as ‘‘low’’’ for 1–9operations, ‘‘medium’’ for 0–31 operations, and‘‘high’’ for 32 or more procedures.
Black patients were less likely to be treated by ahigh-volume surgeon compared with white orHispanic patients (24.8% vs 34.5% and 34.8%,respectively; P < .001). In fact, nearly one-half(46.6%) of all black patients undergoing PD weretreated by a low-volume surgeon (Fig 2). The distri-bution of patient race across hospital volume ter-ciles followed a generally similar pattern.Specifically, black (44.9%) and Hispanic (35.8%)patients were more likely to undergo PD at low-volume hospitals compared with white (30.8%) pa-tients (P < .001) (Fig 3). Perhaps not surprisingly,there was a strong correlation between surgeonand hospital volume (Spearman’s rho = 0.72, P <.001), indicating colinearity between surgeon andhospital volume terciles. In essence, high-volumesurgeons were clustered almost exclusively inhigh-volume hospitals, with very few high-volumesurgeons performing procedures at any low-volume facilities. The proportion of patientstreated by high-volume surgeons versus high-volume hospitals was similar for white and blackpatients; in contrast, although 42.9% of Hispanicpatients were treated at high-volume hospitals,only 34.8% were treated by a high-volume surgeon.Given the strong overall colinearity between sur-geon and hospital volume, only surgeon volume

Table I. Demographic, hospital, and surgeon characteristics by patient race
Non-Hispanic white3,502
Non-Hispanic black423
Hispanic394 P value
Sex — — — .450Female 1,797 (51.3%) 204 (48.2%) 205 (52.0%) —Male 1,705 (48.7%) 219 (51.8%) 189 (48.0%) —
Age, years — — — —Median (IQR) 67 (57-74) 60 (52-69) 62 (51-71) —<65 1,861 (53.1%) 150 (35.5%) 158 (40.1%) <.00165+ 1,641 (46.9%) 273 (64.5%) 236 (59.9%) —
Elixhauser comorbidities — — — .0292 or less 2,246 (64.1%) 247 (58.4%) 237 (60.2%) —3+ 1,256 (35.9%) 176 (41.6%) 157 (39.8%) —
Primary expected payer* — — — <.001Medicare 1,863 (53.2%) 171 (40.8%) 153 (38.8%) —Medicaid 121 (3.5%) 47 (11.2%) 59 (15.0%) —Private insurer 1,356 (38.7%) 162 (38.7%) 121 (30.7%) —Self-pay 88 (2.5%) 25 (6.0%) 35 (8.9%) —No charge 10 (0.3%) 6 (1.4%) 18 (4.6%) —Other 64 (1.8%) 8 (1.9%) 8 (2.0%) —
Hospital teaching status — — — .050No 657 (18.8%) 59 (13.9%) 69 (17.5%) —Yes 2,845 (81.2%) 364 (86.1%) 325 (82.5%) —
Location of hospital — — — <.001Rural 136 (3.9%) 5 (1.2%) 2 (0.5%) —Urban 3,366 (96.1%) 418 (98.8%) 392 (99.5%) —
Region of hospital — — — <.001Northeast 1,024 (29.2%) 110 (26.0%) 66 (16.8%) —Midwest 520 (14.8%) 55 (13.0%) 3 (0.8%) —South 1,435 (41.0%) 241 (57.0%) 272 (69.0%) —West 523 (14.9%) 17 (4.0%) 53 (13.5%) —
Annual hospital volume — — — <.001Low 1–9 1,077 (30.8%) 190 (44.9%) 141 (35.8%) —Medium 10–31 1,203 (34.4%) 121 (28.6%) 84 (21.3%) —High 32+ 1,222 (34.9%) 112 (26.5%) 169 (42.9%) —
Annual surgeon volume — — — <.001Low 1–4 1,175 (33.6%) 197 (46.6%) 171 (43.4%) —Medium 5–15 1,120 (32.0%) 121 (28.6%) 86 (21.8%) —High 16+ 1,207 (34.5%) 105 (24.8%) 137 (34.8%) —
*Missing payer information for four non-Hispanic black patients.IQR, Interquartile range.
ARTICLE IN PRESSSurgeryj 2014
4 Schneider et al
was used in subsequent multivariable logisticregression models.
Morbidity, mortality, and LOS: Impact of race.Complications were frequent after PD (Table II).Overall, 1,943 (45.0%) patients experienced at leastone postoperative complication. Themost commontype of complication was gastrointestinal in nature,with 388 (9.0%) patients experiencing some typeof surgical-site complication, including postopera-tive hemorrhage, accidental laceration, or wounddehiscence, and a similar numberdeveloping apost-operative infection 385 (8.9%). Although the over-all number of complications were distributedevenly between white versus nonwhite patients
(white, 44.2% vs black, 48.7% vs Hispanic, 48.0%;P = .10), specific complication types weremore com-mon among black patients. For example, woundcomplications were more frequent among black(11.1%) and Hispanic (10.4%) patients comparedwith white (7.9%) patients (P = .02). In contrast,the incidence of more severe morbidity such as res-piratory (white, 3.7% vs black, 3.1% vs Hispanic,3.6%; P = .77) or gastrointestinal (white, 12.6% vsblack, 11.1% vs Hispanic, 12.4%; P = .69) complica-tions did not differ across race groups. The propor-tional likelihoodof any complicationwas greater forpatients treated by low-volume (58.8%) versus mid-volume (49.3%) or high-volume (38.7%) surgeons

Fig 2. Annual PD surgeon volume tercile stratified by racial group.
Fig 3. Annual PD hospital volume tercile stratified by racial group.
ARTICLE IN PRESSSurgeryVolume j, Number j
Schneider et al 5
(P< .001) with the following specific complicationsassociatedwith increasedproportional likelihoodofLOS above the median: central line infection(93%), pneumonia (88.5%), surgical-site infection(82.3%), acute renal failure (78.3%), pulmonaryfailure (77.5%) venous thromboembolism(66.7%), and myocardial infarction (63.9%).
Among the 4,319 patients undergoing PD, therewere 232 deaths for an overall in-hospital mortalityof 5.4%. Mortality after PD among low-volumehospitals (9.6%) and low-volume surgeons (9.3%)was greater than mortality among high-volumehospitals (2.3%) and high-volume surgeons(2.4%) (both P < .001). Mortality after PD was

Table II. Operative complications
Complications
Non-Hispanicwhite (n = 3,502)
Non-Hispanicblack (n = 423)
Hispanic(n = 394)
P valueNo. % No. % No. %
Percutaneous drain 158 4.5 16 3.8 35 8.9 <.001Postoperative hemorrhage 162 4.6 34 8 27 6.9 .003Postoperative hemorrhagic anemia 345 9.9 59 13.9 50 12.7 .012Postoperative infection 304 8.7 36 8.5 45 11.4 .185Failure to thrive 300 8.6 39 9.2 28 7.1 .526Respiratory complication 132 3.8 13 3.1 14 3.6 .765Any complication* 1,548 44.2 206 48.7 189 48 .098
*The following complications not included in the table are included in ‘‘Any complication’’: operative re-exploration, accidental laceration, anestheticreaction, liver abscess, peritonitis, gastrointestinal hemorrhage, biliary fistula, intestinal fistula, stomach-duodenal fistula, paralytic ileus pressure ulcer,deep-vein thrombosis, pulmonary embolism, aspiration, central line infection, cardiac complications, postoperative shock, nonhealing surgical wound,urinary complication.
Table III. Logistic regression examining in-patient mortality, clustered across 430 hospitals (n = 4,319*)
In-hospital mortality Odds ratio 95% confidence interval P value
Age (per additional year) 1.03 1.01–1.06 .001Female sex 0.68 0.51–0.92 .0122 or less Elixhauser comorbidities (ref) — —3 or more Elixhauser comorbidities 1.16 0.89–1.51 .260Low surgeon volume (1–4) (ref) — —Medium surgeon volume (5–15) 0.50 0.36–0.70 <.001High surgeon volume (16+) 0.34 0.21–0.55 <.001Any complication 10.92 7.02–16.96 <.001Teaching hospital 0.85 0.59–1.22 .378Northeast region (ref) — —Midwest region 0.78 0.51–1.21 .275South region 1.14 0.76–1.72 .528West region 1.14 0.72–1.82 .581White (ref) — —Black 1.10 0.71–1.70 .684Hispanic 1.27 0.81–1.99 .300Rural (ref) — —Urban 1.87 0.71–4.89 .204Medicare (ref) — —Medicaid 0.95 0.39–2.29 .909Private 0.63 0.41–0.98 .041Self-pay 1.28 0.59–2.78 .536No charge 0.87 0.16–4.66 .871Other 2.07 0.84–5.08 .113
*Four non-Hispanic black patients missing payer information were excluded.
ARTICLE IN PRESSSurgeryj 2014
6 Schneider et al
not associated with race (white, 5.1% vs black,5.7%, Hispanic, 7.1%; P = .25). Among patientstreated only by a high-volume surgeon, PD mortal-ity was 2.2% for whites versus 5.7% for blacksversus 0.7% for Hispanic patients (P = .03). Incontrast, among patients treated by a low-volumesurgeon, PD mortality was 9.0% for whites versus7.7% for blacks versus 13.5% for Hispanic patients(P = .12). On multivariable regression, race was notassociated with the odds of in-hospital PD mortal-ity; however, treatment by a high- (odds ratio
[OR] 0.30, 95% confidence interval [95% CI]0.20–0.45, P < .001) or mid-volume (OR 0.48,95% CI 0.34–0.68, P < .001) surgeon remainedstrongly associated with a lesser odds of in-hospital death compared with PD patients by alow-volume surgeon (Table III).
After PD, the overall median LOS during theindex admission was 12 days. Median LOS was leastat high-volume hospitals (11 days [IQR, 8–16]) andgreatest at low-volume hospitals (16 days [IQR, 11–23]) (P < .001). In fact, patients undergoing PD at
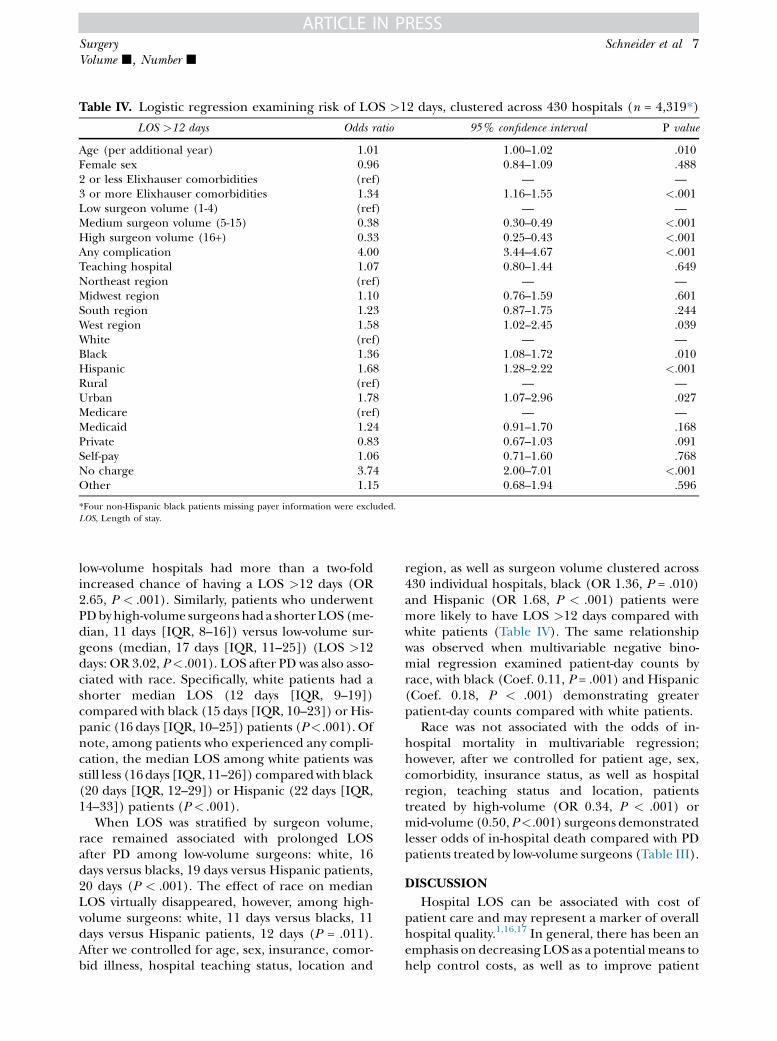
Table IV. Logistic regression examining risk of LOS >12 days, clustered across 430 hospitals (n = 4,319*)
LOS >12 days Odds ratio 95% confidence interval P value
Age (per additional year) 1.01 1.00–1.02 .010Female sex 0.96 0.84–1.09 .4882 or less Elixhauser comorbidities (ref) — —3 or more Elixhauser comorbidities 1.34 1.16–1.55 <.001Low surgeon volume (1-4) (ref) — —Medium surgeon volume (5-15) 0.38 0.30–0.49 <.001High surgeon volume (16+) 0.33 0.25–0.43 <.001Any complication 4.00 3.44–4.67 <.001Teaching hospital 1.07 0.80–1.44 .649Northeast region (ref) — —Midwest region 1.10 0.76–1.59 .601South region 1.23 0.87–1.75 .244West region 1.58 1.02–2.45 .039White (ref) — —Black 1.36 1.08–1.72 .010Hispanic 1.68 1.28–2.22 <.001Rural (ref) — —Urban 1.78 1.07–2.96 .027Medicare (ref) — —Medicaid 1.24 0.91–1.70 .168Private 0.83 0.67–1.03 .091Self-pay 1.06 0.71–1.60 .768No charge 3.74 2.00–7.01 <.001Other 1.15 0.68–1.94 .596
*Four non-Hispanic black patients missing payer information were excluded.LOS, Length of stay.
ARTICLE IN PRESSSurgeryVolume j, Number j
Schneider et al 7
low-volume hospitals had more than a two-foldincreased chance of having a LOS >12 days (OR2.65, P < .001). Similarly, patients who underwentPDbyhigh-volume surgeonshad a shorter LOS (me-dian, 11 days [IQR, 8–16]) versus low-volume sur-geons (median, 17 days [IQR, 11–25]) (LOS >12days: OR 3.02, P< .001). LOS after PD was also asso-ciated with race. Specifically, white patients had ashorter median LOS (12 days [IQR, 9–19])compared with black (15 days [IQR, 10–23]) or His-panic (16 days [IQR, 10–25]) patients (P<.001). Ofnote, among patients who experienced any compli-cation, the median LOS among white patients wasstill less (16days [IQR, 11–26]) comparedwithblack(20 days [IQR, 12–29]) or Hispanic (22 days [IQR,14–33]) patients (P < .001).
When LOS was stratified by surgeon volume,race remained associated with prolonged LOSafter PD among low-volume surgeons: white, 16days versus blacks, 19 days versus Hispanic patients,20 days (P < .001). The effect of race on medianLOS virtually disappeared, however, among high-volume surgeons: white, 11 days versus blacks, 11days versus Hispanic patients, 12 days (P = .011).After we controlled for age, sex, insurance, comor-bid illness, hospital teaching status, location and
region, as well as surgeon volume clustered across430 individual hospitals, black (OR 1.36, P = .010)and Hispanic (OR 1.68, P < .001) patients weremore likely to have LOS >12 days compared withwhite patients (Table IV). The same relationshipwas observed when multivariable negative bino-mial regression examined patient-day counts byrace, with black (Coef. 0.11, P = .001) and Hispanic(Coef. 0.18, P < .001) demonstrating greaterpatient-day counts compared with white patients.
Race was not associated with the odds of in-hospital mortality in multivariable regression;however, after we controlled for patient age, sex,comorbidity, insurance status, as well as hospitalregion, teaching status and location, patientstreated by high-volume (OR 0.34, P < .001) ormid-volume (0.50,P<.001) surgeons demonstratedlesser odds of in-hospital death compared with PDpatients treated by low-volume surgeons (Table III).
DISCUSSION
Hospital LOS can be associated with cost ofpatient care and may represent a marker of overallhospital quality.1,16,17 In general, there has been anemphasis on decreasing LOS as a potentialmeans tohelp control costs, as well as to improve patient

ARTICLE IN PRESSSurgeryj 2014
8 Schneider et al
outcomes. In addition to the potential cost savingsassociated with shorter LOS, patients dischargedsooner from inpatient care have been shown tohave a decreased risk of exposure to nosocomialinfection.18 In fact, although some clinicians haveexpressed concern about decreasing LOS, shorterLOS has not been associated with adverse healthoutcomes for a variety of patients undergoing awide range of procedures.17,19 In contrast, ourgroup previously reported that patients with a lesserLOS after colorectal operation had better outcomesthan those patients with a prolonged LOS.4 Otherinvestigators have similarly noted that a shorterLOS after operation is associated with comparable,or better, outcomes.20 PD is an operation that typi-cally is associated with a longer LOS comparedwith other gastrointestinal procedures. To optimizeLOS after PD, it is important for providers to under-stand the factors associated with LOS.
Although our previous work focused exclusivelyon clinical patient factors as well as provider andhospital volume, other factors may play an impor-tant role in LOS. Race has been shown to impactreceipt of specialty care, as well as postoperativemortality8; however, the impact of race on LOS ispoorly defined. The current paper is importantbecause we were able to characterize and quantifythe relationship between race andLOS. Specifically,we identified race-based differences in LOS andfound that white patients have a median LOS thatis 3 days less than black patients and 4 days lessthan Hispanic patients. Interestingly, even amongpatients who had a complication, this difference inLOS not only persisted but was slightly more pro-nounced (median LOS: white, 16 days vs black, 20vsHispanic, 22 days;P<.001). Furthermore, even af-ter we controlled for other competing risk factors,black and Hispanic patients remained at a 37%and65% increased risk, respectively, of having a pro-longed LOS after PD compared with white patients.
The reason for patient variability in perioperativequality indicators, such as mortality, LOS, andreadmission, are undoubtedly multifactorial. Varia-tions in LOS, specifically, may be related to differ-ences in underlying patient comorbidity status. Forexample, our group noted previously that patientswithmore comorbid illness weremore likely to havea prolonged duration of stay after PD.7 As noted byRooks et al, black and Hispanic patients, in general,aremore affected by chronicmedical comorbiditiessuch as hypertension, cardiac disease, and dia-betes.21-23 Although in the current study, blackand Hispanic patients were younger than white pa-tients, black and Hispanic patients were more likelyto have at least one medical comorbidity (white,
88.5% vs black, 92.2% vs Hispanic, 89.1%,P = .01), as well as three or more medical comorbid-ities (white, 35.9% vs black, 41.6% vs Hispanic,39.8% P = .03). It is unlikely, therefore, that any dis-parities in LOS were attributable entirely to differ-ences in patient comorbidity among white andnonwhite patients. These findings regarding LOSare consistent with the report by Lucas et al,24 whonoted that adjusting for patient characteristicssuch as morbidity status had no effect on the oddsratio of mortality by race.
Previous studies have demonstrated that blackpatients were more likely than white patients topresent for surgical treatment at smaller hospi-tals.8,25 In addition, black patients undergo a vari-ety of operative procedures by surgeons who havenot undergone advanced or specialized trainingor who have less overall and procedure-specificexperience.16 Hispanic patients have the samepattern of proportionally more care by low-volume hospitals and providers.8 Liu et al8
reported race-based disparities in access to high-volume operative care for a variety of complexoperative procedures for both black patients andindividuals of Hispanic origin compared with simi-larly treated white patients.
In the current study, we noted similar disparitiesin the pattern of care among patients seeking PD.Specifically, black patients were less likely to betreated by a high-volume surgeon compared withwhite or Hispanic patients (24.8% vs 34.5% and34.8%, respectively; P < .001). In fact, nearly one-half (46.6%) of all black patients undergoing PDwere treated by low-volume surgeons (Fig 2). Inter-estingly, even though black and Hispanic patientswere more likely to be treated by low-volume sur-geons and at low-volume hospitals, we failed to iden-tify any significant difference in overall morbidity(white, 44.2% vs black, 48.7% vs Hispanic, 48.0%;P = .10) ormortality (white, 5.1% vs black, 5.7%,His-panic, 7.1%; P = .25). In contrast, morbidity andmortality were associated with PD volume---with pa-tients treated at low-volume hospitals being at riskfor greater morbidity and mortality.
Regarding LOS, both black and Hispanic pa-tients were significantly more likely to experience aprolonged LOS after PD compared with whitepatients. Overall the median LOS after PD was 12days, which was also the median LOS among whitepatients. In contrast, median LOS among black(15 days) or Hispanic (16 days) patients was consid-erably (z25–30%) greater in duration. On multi-variable analysis, after controlling for competingpatient- and hospital-level factors, race remainedstrongly associated with LOS. In fact, black and

Table V. LOS and race by annual hospital and surgeon volume
Volume Non-Hispanic white Non-Hispanic black Hispanic P value
Low surgeon (1–4) 1,175 197 171 .001LOS #12 days 435 (37.0%) 58 (29.4%) 41 (24.0%) —LOS >12 days 740 (63.0%) 139 (70.6%) 130 (76.0%) —
Medium surgeon (5–15) 1,120 121 86 .015LOS #12 days 671 (59.9%) 68 (56.2%) 38 (44.2%) —LOS >12 days 449 (40.1%) 53 (43.8%) 48 (55.8%) —
High surgeon (16+) 1,207 105 137 .004LOS #12 days 797 (66.0%) 59 (56.2%) 74 (54.0%) —LOS >12 days 410 (34.0%) 46 (43.8%) 63 (46.0%) —
Low hospital (1–9) 1,077 190 141 <.001LOS #12 days 413 (38.35%) 59 (31.0%) 32 (22.7%) —LOS >12 days 664 (61.65%) 131 (69.0%) 109 (77.3%) —
Medium hospital (10–31) 1,203 121 84 <.001LOS #12 days 678 (56.4%) 60 (49.6%) 25 (29.8%) —LOS >12 days 525 (43.6%) 61 (50.4%) 59 (70.2%) —
High hospital (32+) 1,222 112 169 .019LOS #12 days 812 (66.45%) 66 (58.9%) 96 (56.8%) —LOS >12 days 410 (33.55%) 46 (41.4%) 73 (43.2%) —
LOS, Length of stay.
ARTICLE IN PRESSSurgeryVolume j, Number j
Schneider et al 9
Hispanic patients remained at a 37% and 65%increased risk, respectively, of having a prolongedLOS after PD compared with white patients. LOSwas also strongly impacted by PD procedural vol-ume, with patients operated on by low-volumesurgeons having the greatest LOS (Table V).
The interaction of PD volume and race was ofparticular interest. Specifically, although race re-mained associated with prolonged LOS after PDamong low-volume surgeons (white, 16 days vsblacks, 19 days vs Hispanic patients, 20 days), theeffect of race on LOS virtually disappeared amonghigh-volume surgeons (white, 11 days vs blacks, 11days vs Hispanic patients, 12 days). These datasuggest that increasing access to greater-volumeproviders may decrease the LOS associated withundergoing PD among black and Hispanic pa-tients. The reason why LOS was more comparableamong white, black, and Hispanic patients is com-plex. For example, it is possible that social andcultural factors that could not be accounted for inNIS may underlie, at least in part, some of theobserved difference in LOS across racialgroups.17,19,23 As with readmission, the factors asso-ciated with LOS are multifaceted and may includepre-admission factors, health care factors and hos-pital course, as well as postdischarge factors such associal characteristics like socioeconomic status, thedischarge environment, availability of caregivers,and health care self-efficacy.24
The current study had several limitations. Theclinical course of specific patients beyond the
index hospitalization could not be ascertained,because the NIS database does not provide patientidentifiers. Therefore, we could not assess otherimportant perioperative metrics such as readmis-sion. It is possible that sample size among theblack and Hispanic patients may limit our abilityto assess adequately the independent effects ofrace and surgeon volume on the incidence ofsome complications, as well as the specific effect ofthese complications on patient LOS, particularlyfor less common complications. Because of theadministrative nature of the NIS, robust data oncancer-specific factors such as stage were notavailable for those patients with a diagnosis ofcancer. Previous studies have noted that blackpatients with cancer tend to present later in thecourse of their disease26; we were not able to ac-count for the possibility that cancer stage mighthave affected LOS. Also, approximately one fifthof individual records had data missing for raceand reliance on CCA may introduce some bias.Finally, as is the case for any study that employslarge administrative datasets, our study may havebeen affected by the possibility of coding inaccur-acies.27 It is likely, however, that any reporting biaswas random in nature and would not change theunderlying findings.
In conclusion, both black and Hispanic patientswho underwent PD were less likely than whitepatients to have been treated either at a greater-volume hospital or by a greater-volume surgeon.Although morbidity and mortality after PD were
ARTICLE IN PRESSSurgeryj 2014
10 Schneider et al
comparable among black and Hispanic patientscompared with white patients, LOS was longer innonwhite patients. The difference in LOS couldnot be explained by differences in patient comor-bidity status, or incidence of postoperative compli-cations, among the different racial groups. Rather,the largest effect of LOS seemed to be related todifferences in access to high- versus low-volumehospitals and providers. As such, efforts to improveaccess and referral of nonwhite patients to high-volume institutions and surgeons for complexoperative procedures such as PD should remain apoint of emphasis, although it seems unlikely thateven universal treatment by high-volume providerswould abrogate completely the race-based differ-ences observed in this study.
REFERENCES
1. Taheri PA, Butz DA, Greenfield LJ. Length of stay has min-imal impact on the cost of hospital admission. J Am CollSurg 2000;191:123-30.
2. Keller DS, Chien HL, Hashemi L, Senagore AJ, Delaney CP.The HARM score: a novel, easy measure to evaluate qualityand outcomes in colorectal surgery. Ann Surg 2013 Sep 16.[Epub ahead of print].
3. Kiran RP, Delaney CP, Senagore AJ, Steel M, Garafalo T, Fa-zio VW. Outcomes and prediction of hospital readmissionafter intestinal surgery. J Am Coll Surg 2004;198:877-83.
4. Schneider EB, Hyder O, Brooke BS, Efron J, Cameron JL,Edil BH, et al. Patient readmission and mortality after colo-rectal surgery for colon cancer: impact of length of stay rela-tive to other clinical factors. J Am Coll Surg 2012;214:390-8.
5. Kelly M, Sharp L, Dwane F, Kelleher T, Comber H. Factorspredicting hospital length-of-stay and readmission after colo-rectal resection: a population-based study of elective andemergency admissions. BMC Health Serv Res 2012;12:77.
6. KehletH,WilmoreDW. Evidence-based surgical care and theevolution of fast-track surgery. Ann Surg 2008;248:189-98.
7. Schneider EB, Hyder O, Wolfgang CL, Dodson RM, HaiderAH, Herman JM, et al. Provider versus patient factors im-pacting hospital length of stay after pancreaticoduodenec-tomy. Surgery 2013;154:152-61.
8. Liu JH, Zingmond DS, McGory ML, SooHoo NF, Ettner SL,Brook RH, et al. Disparities in the utilization of high-volume hospitals for complex surgery. JAMA 2006;296:1973-80.
9. Agency for Healthcare Research and Quality. Nationalhealthcare disparities report. Rockville (MD): Agency forHealthcare Research and Quality; 2003.
10. Smedley B, Stith A, Nelson A. Unequal treatment: confront-ing racial and ethnic disparities in health care. Washington(DC): National Academies Press; 2003.
11. Lucas FL, Stukel TA, Morris AM, Siewers AE, Birkmeyer JD.Race and surgical mortality in the United States. Ann Surg2006;243:281-6.
12. Abraham A, Al-Refaie WB, Parsons HM, Dudeja V, VickersSM, Habermann EB. Disparities in pancreas cancer care.Ann Surg Oncol 2013;20:2078-87.
13. HCUP Nationwide Inpatient Sample (NIS). HealthcareCost and Utilization Project (HCUP). 2007-2009. Agencyfor Healthcare Research and Quality, Rockville, MD. Avail-able from: www.hcup-us.ahrq.gov/nisoverview.jsp.
14. Henry AJ, Hevelone ND, Lipsitz S, Nguyen LL. Comparativemethods for handling missing data in large databases. J VascSurg 2013;58:1353-9.
15. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbiditymeasures for use with administrative data. Med Care 1998;36:8-27.
16. Donabedian A. The quality of care. How can it be assessed?JAMA 1988;260:1743-8.
17. Clarke A. Why are we trying to reduce length of stay? Eval-uation of the costs and benefits of reducing time in hospitalmust start from the objectives that govern change. QualHealth Care 1996;5:172-9.
18. Barnett AG, Page K, Campbell M, Martin E, Rashleigh-RollsR, Halton K, et al. The increased risks of death and extralengths of hospital and ICU stay from hospital-acquiredbloodstream infections: a case-control study. BMJ Open2013;3:e003587.
19. Pearson SD, Kleefield SF, Soukop JR, Cook EF, Lee TH.Critical pathways intervention to reduce length of hospitalstay. Am J Med 2001;110:175-80.
20. Lawrence JK, Keller DS, Samia H, Ermlich B, Brady KM, No-bel T, et al. Discharge within 24 to 72 hours of colorectal sur-gery is associated with low readmission rates when usingEnhancedRecovery Pathways. J AmColl Surg2013;216:390-4.
21. Rooks RN, Simonsick EM, Klesges LM, Newman AB, Ayo-nayon HN, Harris TB. Racial disparities in health care ac-cess and cardiovascular disease indicators in black andwhite older adults in the Health ABC Study. J Aging Health2008;20:599-614.
22. Davis AM, Vinci LM, Okwuosa TM, Chase AR, Huang ES.Cardiovascular health disparities: a systematic review ofhealth care interventions (review). Med Care Res Rev2007;64(5 Suppl):29S-100S.
23. McWilliams JM, Meara E, Zaslavsky AM, Ayanian JZ. Differ-ences in control of cardiovascular disease and diabetes byrace, ethnicity, and education: U.S. trends from 1999 to2006 and effects of medicare coverage. Ann Intern Med2009;150:505-15.
24. Lucas DJ, Haider A, Haut E, Dodson R, Wolfgang CL, AhujaN, et al. Assessing readmission after general, vascular, andthoracic surgery using ACS-NSQIP. Ann Surg 2013;258:430-9.
25. Schneider EB, Hyder O, Wolfgang CL, Hirose K, Choti MA,Makary MA, et al. Patient readmission and mortality aftersurgery for hepato-pancreato-biliary malignancies. J AmColl Surg 2012;215:607-15.
26. Fitzgerald TL, Bradley CJ, Dahman B, Zervos EE. Gastroin-testinal malignancies: when does race matter? J Am CollSurg 2009;209:645-52.
27. Nathan H, Pawlik TM. Limitations of claims and registrydata in surgical oncology research. Ann Surg Oncol 2008;15:415-23.