
Psychosocial and neuropsychological outcomes in two high-functioning males 20 years after traumatic...
20
This article was downloaded by: [The University Of Melbourne Libraries] On: 24 February 2015, At: 21:01 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Neurocase: The Neural Basis of Cognition Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/nncs20 Psychosocial and neuropsychological outcomes in two high-functioning males 20 years after traumatic brain injury Fiona J. Bardenhagen a b , Stephen C. Bowden a b , Robert B. Shields c , Vanessa McKay a , Peter J. Smith d , Simon Vogrin b , Steven J. Collins b & Mark J. Cook b a School of Behavioural Sciences, University of Melbourne , Parkville, 3052 b Department of Clinical Neurosciences , St Vincent's Hospital , Melbourne, 3065 c Central East Area Mental Health Service, Northwestern Healthcare Service Mental Health Program , Melbourne, 3001 d Department of Medical Imaging , St Vincent's Hospital , Melbourne, 3065, Australia Published online: 17 Jan 2008. To cite this article: Fiona J. Bardenhagen , Stephen C. Bowden , Robert B. Shields , Vanessa McKay , Peter J. Smith , Simon Vogrin , Steven J. Collins & Mark J. Cook (1999) Psychosocial and neuropsychological outcomes in two high- functioning males 20 years after traumatic brain injury, Neurocase: The Neural Basis of Cognition, 5:4, 325-343, DOI: 10.1080/13554799908411986 To link to this article: http://dx.doi.org/10.1080/13554799908411986 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http:// www.tandfonline.com/page/terms-and-conditions
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Psychosocial and neuropsychological outcomes in two high-functioning males 20 years after traumatic...

This article was downloaded by: [The University Of Melbourne Libraries]On: 24 February 2015, At: 21:01Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Neurocase: The Neural Basis of CognitionPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/nncs20
Psychosocial and neuropsychological outcomesin two high-functioning males 20 years aftertraumatic brain injuryFiona J. Bardenhagen a b , Stephen C. Bowden a b , Robert B. Shields c , VanessaMcKay a , Peter J. Smith d , Simon Vogrin b , Steven J. Collins b & Mark J. Cook ba School of Behavioural Sciences, University of Melbourne , Parkville, 3052b Department of Clinical Neurosciences , St Vincent's Hospital , Melbourne, 3065c Central East Area Mental Health Service, Northwestern Healthcare Service MentalHealth Program , Melbourne, 3001d Department of Medical Imaging , St Vincent's Hospital , Melbourne, 3065, AustraliaPublished online: 17 Jan 2008.
To cite this article: Fiona J. Bardenhagen , Stephen C. Bowden , Robert B. Shields , Vanessa McKay , Peter J. Smith ,Simon Vogrin , Steven J. Collins & Mark J. Cook (1999) Psychosocial and neuropsychological outcomes in two high-functioning males 20 years after traumatic brain injury, Neurocase: The Neural Basis of Cognition, 5:4, 325-343, DOI:10.1080/13554799908411986
To link to this article: http://dx.doi.org/10.1080/13554799908411986
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”)contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensorsmake no representations or warranties whatsoever as to the accuracy, completeness, or suitabilityfor any purpose of the Content. Any opinions and views expressed in this publication are the opinionsand views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy ofthe Content should not be relied upon and should be independently verified with primary sources ofinformation. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands,costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial orsystematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution inany form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Neurocase (1999) Vol. 5 , pp. 325-343 0 Oxford Universih Press 1999
Psychosocial and Neuropsychological Outcomes in Two High-functioning Males 20 Years After Traumatic Brain Injury
Fiona J. Bardenhagen112, Stephen C. Bowden1g2, Robert B. Shields3, Vanessa McKayl, Peter J. Smith4, Simon Vogrin2, Steven J. Collins2 and Mark J. Cook2
'School of Behavioural Sciences, University of Melbourne, Parkville, 3052, *Department of Clinical Neurosciences, St Vincent's Hospital, Melbourne, 3065, 3Central East Area Mental Health Service, Northwestern Healthcare Service Mental Health Program, Melbourne, 3001 and 4Department of Medical Imaging, St Vincent's Hospital, Melbourne, 3065, Australia
Abstract
Researchers have emphasized a need for ongoing rehabilitation and support for individuals with traumatic brain injury FBI), yet there are few detailed descriptions of long-term outcome, and many people with long-standing TBI do not or cannot access support services. HB and NL, two men who sustained severe TBI, presented for neuropsychological consultation for the first time more than 20 years post-injury. Referral was prompted by significant mood and relationship disturbances, and ongoing mnemonic and cognitive symptoms. Structural imaging showed a very large lesion involving the orbitofrontal and dorsolateral regions of NL's left frontal lobe, while HB had a smaller lesion involving cortical and subcortical matter in the dorsolateral region of the left frontal lobe. Results from a range of neuropsychological tests indicated residual weakness in memory and variable impairments on two experimental tests of prefrontal working memory: Delayed Alternation and Object Alternation. The Minnesota Multiphasic Personality Inventory-2 highlighted a pattern of severe psychological disturbance in HB which improved in response to antidepressant medication. Measures of emotional empathy and adaptive functioning suggested significant changes attributable to disruption of prefrontal aspects of the limbic system.
Introduction
The importance of early identification and rehabilitation of traumatic brain injury (TBI) is well established (Lishman, 1998). However, rehabilitation often ceases after acute physical and neuropsychological symptoms have resolved. Long-term outcome research is rare, with the majority of follow-up research focusing on the first 2 years after injury. Searches of the Medline and PsycLIT databases for TBI follow-up studies published up to December 1998 indicate more than 50 publications up to 5 years post-injury, but only 19 follow-up studies with post-injury intervals of 5 years or more (see Table 1). Significant and ongoing long-term difficulties were identified by researchers who investigated a broad range of psychological and physical symptoms after adult or paediatric TBI. The persistence of emotional, cognit- ive and somatic sequelae many years after TBI indicates the need for ongoing access to support, education and rehabilitation programmes.
Identification and treatment of psychosocial disorders after TBI is an important aspect of care which has often been neglected (Emilien and Waltregny, 1996; van Reekum et a/.,
1996). There is evidence of increased cognitive, emotional and behavioural changes 5 years post-injury, and increases in unemployment between 2 and 5 years post-injury (Olver et al., 1996). Ongoing psychosocial rehabilitation for at least a number of years after the injury has been strongly recommended (Morton and Wehman, 1995; Emilien and Waltregny, 1996; Olver et al., 1996; van Reekum et a/., 1996); however, such services are rarely available, especially for rural populations (Fyffe and McCubbery, 1996). The potentially disruptive effects of TBI on social relationships and leisure activities, with resultant anxiety and depression, create greater demands on the family or care givers (Morton and Wehman, 1995). Depressive symptoms, inappropri- ateness, indifference and difficulties with the pragmatics of communication after TBI have recently been identified as significant contributors to family functioning, care-giver stress and patient unemployment (Groom et al., 1998).
The measurement, monitoring and active treatment of neurobehavioural symptoms is an important rehabilitative goal after TBI (Groom et a/., 1998). Eslinger and colleagues
Correspondence to: Fiona J . Bardenhagen, Department of Clinical Neurosciences, St Vincent's Hospital, 41 Victoria Parade, Fitzroy, Victoria. 3065. Australia, Tel: 61-3-9288-3559; Fax: 61-3-9288-3350; e-mail: [email protected]
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

326 F. J . Bardenhagen et al.
Table 1. Results of Medline and PsycLIT database search for abstracts detailing follow-up of TBI cases more than 5 years post-injury
Authors Fo l low-~p
Patients N interval Summary of selected major tindings and recommendations
Olver C I d. , 1996
Kaitaro d., 1995
Hillier r / d.. 1997
Asikainen ('I (I/., 1996
Vogunthaler rr d., 1989
Wood and Yurdakul. 1997 Schalen er ti/., 1991
Hetherington P I d.. 1996
Wilson, 1992
Wilson. I994
Bellus c'/ d.. 1996
Eiimes er d., 1996
Jordan P I d.. 1992
Shordone or (I/.. 1995
Dawson and Chipman, 1095
Leichtman. 1992
Klonoff rr d,, 1993
Virkkunen rr d.. 1976
TBI 254 103
Severe TBI 19
TB I 67
Head injuries I76 ( I 14 minor. 35 moderate, and 27 severe). compared with 64 lower limb injured
TBI
TBI ( 3 3 mild, 24 moderate, I8 severe)
TBI Severe TBI
TBI and controls
TBI
Encephalitis (n = 2); head injury (n = 3 ) ; and stroke ( n = 2 ) Unspecified brain injury patients in a state psychiatric hospital 55 brain-injured adults
Children with mild TBI and matched controls Severe TBI
TBI survey respondents
Brain-injured child
Mild head injuries sustained during childhood
Open head injuries sustained in World war 11
508
75
131 I06
26
7
2
55
14
20
454
I
159
507
2 years 5 years
5 years
5 years
5 years
5 t years
4 7 years
5-8 years 5-8 years
5-1 0 years
5-10 years
6-10 years
4 and 17 years
19 months to 8 years 10 years
10 years
Mean of 13 years
15 years
23 years
30 years
Comparison of outcomes 2 and 5 years post-injury. Higher incidence of cognitive. behavioural and emotional changes reponed at 5 years. 32% of those working at 2 years were not employed at 5 years. Need for intermittent lifelong intervention following TBI Effects of long-term disabilities on everyday life i n patients and relative\. Rel;itiw\ emphasized changes in personality and emotional reactions Main focus on neurophysical symptoms. 50% of case3 were reliant o n welfare system. The most common residual physical problems were headaches. halance difficulties, and fatigudweakness. However, 5 7 6 felt they had improved in iill art% Reviewed and compared on cognitive. behavioural and somatic impairments. No difference in prevalence of headaches. dizziness or anxiety with type of HI sewrity. Memory problems, depressed mood and frequency of cognitive impairments increased with injury severity. Improvement is needed i n long-term management of certain patients due to misunderstanding of somatic. hehavioural antl cognitive impairments Review of social and professional outcomes in scvere and mild TBI. Those with severe injury sustained i n childhood or early teens and lower levels of education had poorer social and vocational outcome than those who sustained injury in late teem or early adulthood Telephone interview with significant other. Generally. more severe injuries resulted in
more dependent and less productive patients at follow-up. although some patients with mild injuries had poor outcomes, and several severely impaired patient\ had relatively good outcomes 49% of patients divorced or separated in 5-8 years following TBI Questionnaires, interviews and neurophysical examinations of patients initially judged as good recovery/moderate disability 6 months post-injury. 40-50% had coordination disturbances, >20% had speech disorders and cranial nerve deficits. 28% had psychiatric symptoms in need of treatment; 40% had interpersonal problems, and 2&30% had difticulties with leisure activities. Relatives reported problems with hostile feelings (71%). failing memory ( 5 2 % ) and fatiguability (18% ).
Improvements in facilities for rehabilitation may positively affect psychosocial adjustment Comparison of performance on reaction time tasks hetween S and 10 years post-TB1 and controls. No difference in reaction time between groups, although intergroup variability was greater in the 5-year post-injury group than in either the 10-year or control groups Review of memory impairments: 58% showed no change, 31% improved. 1 1 % deteriorated. Patients were using more memory aids and strategies than at the end of a memory therapy program 5-10 years earlier Review of recovery after various forms of acquired dyslexia
Lithium, in the context of an intensive behavioural rehabilitation programme, found to he an effective agent in management of aggressive and/or self-injurious behaviours
Rehabilitation resulted in iniprovements in functional skills antl social hehaviour that affected the type of placement possible and improved quality of life No difference in language functioning between TBI children and controls
Psychosocial, cognitive, physical and emotional status retrospectively rated through interviews with relatives and significant others. Ratings for pre-niorhid. I , 2 . 5 and ;I mean 10.3 years post-injury indicated significant gains after 2 years post-injury. antl gradual improvements in functioning for at least 10 years post-injury. Recovery process does not appear to end I or 2 years post-injury Survey based on disablement framework by WHO. 66% of respondents reported need for ongoing assistance with some activities of daily living, 75% were not working and 90% reported some limitations or dissatisfaction with their social integration Exploration of the efficacy of psychotherapy with neurologically impaired childreii and their families, and the importance of follow-up contacts Found 'Significant relationships between subjective sequelae and objective, psychosocial measures of adaptation including educational lag. uneniployment. current psychologicaVpsychiatric problems. and relationships with family memhers.. Continuity of complaints elicited during 5-year follow-up and long-term sequelx'. Social adaptability of brain-injured people, using long-term criminal development a3
a criterion. 'Criminal acts were often very accidental and had happened o n l y after several decades following the head injury'. 5.7% of patients were imprisoned for criminal acts. No relationship between criminality and location of lesions
Medline search terms for the period 1966 to December 1998 were: 'brain damage, chronic/psychologicaI' and 'follow-up studies'. PsycLIT search term3 for the period 1887 to December 1998 were: 'brain damage' and 'follow-up studies'. There were 54 abstracts reporting follow-up intervals of up to S years. Of these. I6 publications covered a 6-month follow-up interval, 19 described a 12-month interval, 10 detailed a 2-year post-injury interval. six studies covered ii
3-year interval and three publications described 4-year follow-up intervals.
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5
Long-term outcomes in TBI 327
have recently used questionnaire measures of empathy to examine the socio-emotional sequelae of brain injury (Eslinger et al., 1996; Eslinger, 1998). Changes in empathic processing occur after a range of focal cerebral lesions, with non-frontal patients endorsing items suggesting low social self-confidence, while patients with frontal lesions indicated difficulty in unstructured, unpredictable social situations where it is important to perceive, interpret and interact appropriately with others (Eslinger, 1998). A strong relation- ship between cognitive flexibility and empathy measures was found in patients with dorsolateral frontal lesions, but not in those with orbitofrontal lesions. Eslinger ef al. (1 996) suggest that deficits in ‘social executors’ involving social self-regula- tion, self-awareness, empathy and an appreciation of social salience may account for many behavioural and personality changes post-injury.
Dramatic changes in emotion and personality following injury to the frontal cortex were made famous by the case of Phineas Gage (e.g. Stuss et a/., 1992; Damasio et al., 1994). Reconstruction of the injury caused to Gage’s brain indicated damage to the ventromedial frontal region, an area postulated to be crucial in social reasoning and processing of emotion (Damasio et a/., 1994). Impairments in socio- emotional processing may be complex, ranging from auto- nomic responses and contingency-based learning to cognitive and emotional aspects of empathy. For example, patients with damage to the ventromedial region may show abnormal autonomic responses to socially meaningful stimuli, even though their autonomic responses to unconditioned stimuli are normal (Damasio et al., 1990). Impairments in the ability to modify responses on contingency-based learning tasks in patients with ventral frontal lesions may partly explain inappropriate and disinhibited behaviours (Rolls et a/., 1994). People with ventral frontal damage also show impairments in the identification of facial and vocal emotional expression (Hornak et al., 1996), impairments which may contribute to inappropriate responses in social situations. These patients may be aware of their behavioural problems, but may not be able to control their responses to others, even with the benefit of past negative experiences or the knowledge of appropriate behaviours (Hornak et al., 1996; Eslinger, 1998). Other research suggests that patients with ventromedial lesions are insensitive to the future consequences of their actions, and tend to be guided by immediate demands only (Bechara et al., 1994). These patients may also have reduced ability to feel negative emotions and to empathize with others (Hornak et a/., 1996). Impaired integration of emotional and social experiences, combined with poor control of behaviour, including self-monitoring and self-correcting, may therefore account for the complex personality and behavioural changes following ventral and ventromedial frontal lesions (Stuss et al., 1992).
Deficits in emotional processing following prefrontal injury are thought to arise from the interconnections between the orbital and medial prefrontal cortex and the autonomic systems involved in normal visceral responses to affective
stimuli. Excellent reviews of the neuroanatomical systems underlying emotional processing are provided by Barbas (1995) and Price et al. (1996). The orbitofrontal cortex has extensive connections with the limbic system and basal forebrain, and Barbas (1995) argues that the posterior basal and medial parts of the prefrontal cortex are, in fact, cortical components of the limbic system. The orbital and medial prefrontal limbic cortices receive input from each of the sensory systems and also from polymodal areas (Barbas, 1995). Affect-related responses to this sensory input are thought to arise through interactions with the amygdala (Price et al., 1996). Limbic cortices in the posterior orbitofrontal region also receive projections from premotor cortices, and are involved in autonomic responses (Barbas, 1995). The posterior orbitofrontal region is therefore well placed to integrate information from both the internal and external environment. The orbital and medial prefrontal cortex also have indirect connections with the basal ganglia via the amygdala and other limbic structures (Price et a/., 1996). Disruption of these connections results in difficulty sup- pressing previously learned stimulus-reward associations (Price et al., 1996) which may contribute to disturbed emotional or social behaviours. Finally, the orbitofrontal cortex is implicated in mnemonic processes through its involvement with other limbic regions (Barbas, 1995).
There is a growing body of magnetic resonance imaging (MRI) evidence reflecting hippocampal volume loss and related memory impairments in individuals with TBI ( e g Bigler et al., 1996). Comparative neuropsychological tests such as Delayed Matching to Sample (DMTS) and Delayed Non-Matching to Sample (DNMTS) have contributed to knowledge about the limbic system and its role in associative memory (e.g. Mishkin and Appenzeller, 1987). Similar research using delayed reaction tests such as Delayed Alternation (DA), Object Alternation (OA) and Delayed Response (DR) has provided experimental evidence to support a model of prefrontal working memory (for reviews, see Goldman-Rakic, 1987, 1995; Fuster, 1989; Oscar-Berman and Bardenhagen, 1998). While DR is a simple measure of the ability to maintain an inner representation and respond appropriately after time has passed, DA and OA have more complex rule-induction components (Bardenhagen and Bowden, 1998). Research using these tests in non-human primates has provided some support for the functional division of the frontal lobes into orbitofrontal and dorsolateral systems (Oscar-Berman et al., 1991, 1992). The extremely close connections between the prefrontal cortex and limbic systems may account for the overlapping sensitivity of DA, DR, DMTS and DNMTS to prefrontal and limbic damage in non- human primates (e.g. Mahut, 1971; Bauer and Fuster, 1976; Isseroff et al., 1982; Bachevalier and Mishkin, 1986). While there is evidence of DA and OA impairments in patients with TBI (Gansler et al., 1996), there has been no published research to date examining TBI patients on both delayed reaction and DMTS paradigms. Given the common symptom of memory impairments in TBI, and the damage to temporal
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

328 F. J . Bardenhagen et id.
and prefrontal areas, deficits on DMTS may be expected in addition to impairments on DA and OA.
This article presents the cases of two men, HB and NL, who sustained severe TBIs in the mid-1970s. Structural imaging more than 20 years post-injury showed that HB had a lesion in the dorsolateral region of the left frontal lobe, while NL had a very large lesion involving cortical and subcortical tissue in the orbitofrontal and dorsolateral regions of the left frontal lobe. High pre-morbid functioning was reflected in the later presentation of both cases, but neither man had regained pre-injury vocational status. Both men had experienced relationship difficulties, although they described these differently. They also experienced psychosocial prob- lems that had been exacerbated by a lack of early identification and education post-injury, combined with little ongoing support. Their performances on a variety of cognitive tests more than 20 years post-injury were less striking than the difficulties described by both patients and their families. The long-term sequelae of severe TBI in the cases of HB and NL are presented and compared with respect to the different injuries received. Performances on a variety of cognitive, affective and experimental tests, and the implications for long-term interventions, are discussed. Given the paucity of long-term follow-up studies in TBI, and the evolution of our understanding of the role of the interconnections between the orbitofrontal cortex and limbic system in emotion and social behaviour, examination of these two cases offers insights into the role of orbitofrontal and dorsolateral pre- frontal cortex in adaptive behaviours many years after TBI.
Materials and methods
The patients were initially seen for routine neuropsycho- logical assessment at St Vincent’s Hospital, Melbourne, Australia. To maintain confidentiality, representative demo- graphic details have been substituted. Informed consent to participate in this study was obtained from both patients.
Cognitive and emotional assessment included the Wechsler Adult Intelligence Scale-Revised (WAIS-R; Wechsler, 1981), Wechsler Memory Scale-Revised (WMS-R; Wechsler, 1987), Boston Naming Test (BNT; Kaplan et al., 1993), Controlled Oral Word Association Test (COWAT; Spreen and Strauss, 1991). Beck Depression Inventory (BDI; Beck, 1987), State- Trait Anxiety Inventory (STAI; Speilberger, 1983), Minnesota Multiphasic Personality Inventory-2 (MMPI-2; Butcher et al., I 989), National Adult Reading Test (NART; Nelson, 1982), Wisconsin Card Sorting Test (WCST; Heaton et al., 1993), Short Category Test (Wetzel and Boll, 1987), Trail Making Test (Reitan and Wolfson, 1985) and the Pushbutton Maze test of visuospatial memory (Bowden et al., 1992). Both patients were reviewed approximately 14 months later using the WAlS-111 and WMS-111 (Wechsler, 1997a,b). All clinical tests were administered in a standardized manner according to published instructions where available.
A number of experimental tests of frontal and limbic function were administered, as follows:
1. Delayed Alternation was given in the manner described previously (Freedman and Oscar-Berman, 1986; Barden- hagen, 1997). The participant sat opposite the experimenter. A curtain suspended from a frame was between them, hiding a black stimulus board with two circular stimulus wells, each well covered by identical black square plaques. A standard set of instructions was used (Oscar-Berman et al.. 1982; Freedman and Oscar-Berman, 1986). Participants were required to learn that the side on which a 5 cent piece was located was alternated after each correct response. This rule was not explained in the task instructions. The first trial was initiated when the experimenter raised the curtain and reminded the participant to try to get a coin every time the curtain went up, because they would be paid the value of all the coins they collected. For the first trial of DA, a coin was put under each plaque. For the second trial, the coin was put under the side not chosen on the preceding trial. When an incorrect choice was made, the coin remained in the same position while the curtain was lowered for 20 s and then raised again for the participant to make another choice. If the incorrect side was chosen again, this was counted as a perseverative error. The trial was completed when the correct side was chosen. On the trial following a correct response, the opposite side was baited. There was a 20 s intertrial interval, and the learning criterion was 12 consecutive correct responses. The failure criterion was 50 trials. 2. Object Alternation was administered as described elsewhere (Freedman, 1990, 1994; Bardenhagen, 1997; Bardenhagen and Bowden, 1998). The apparatus used for DA was also used in OA, with three-dimensional stimulus objects (a plastic clothes peg and a metal key) on each black stimulus plaque. Participants were told they would see two objects, and that there would always be a 5 cent coin under one of the objects. Participants were told to try to find the coin every time the curtain was raised because they would be paid the value of the coins they had collected at the end of the test. They were not told of the object alternation rule, rather, they had to induce it through doing the task (Bardenhagen and Bowden, 1998). The participants had to learn that the coin was alternated between the objects after each correct response. The objects were placed in left and right positions after each correct response according to a random schedule. On the first trial of OA, each object was baited with a coin. There was an intertrial interval of 20 s, then for the second trial, a coin was put under the object not chosen on the preceding trial. For the next trial, after another 20 s intertrial interval, the other object was baited. Baiting of the objects and any alterations to their positions occurred after the curtain was lowered. A correction procedure was used as in DA, and continued until the participant chose correctly. Perseverative errors were defined as for DA. Testing ceased at 12 consecutive correct responses, or a failure criterion of 50 trials. 3. Delayed Matching to Sample was administered on an IBM-compatible computer according to a procedure described previously (Bardenhagen and Bowden, 1995; Bardenhagen,
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

Long-term outcomes in TBI 329
1997). DMTS is a forced-choice recognition memory test in which participants are shown one, two, four or eight target stimuli and then asked to choose the stimulus they think is correct whenever they see a set of two after a short delay. The stimuli were rectangular, randomly shaded, 6x6 monochrome matrices. After learning to match to sample in an acquisition training phase, participants are tested on lists of one, two, four and eight stimuli. There were 10 trials of each list length, resulting in a total of 40 trials. Stimulus presentation and delay durations were as described before (Bardenhagen and Bowden, 1995). Participants were given 5 cents for every correct answer at the end of the test. 4. The 6-Elements Risk was administered according to the protocol used by Levine et al. ( 1 998), and was based on the Six Element Test described by Shallice and Burgess ( 199 I ). It consists of six groups of simple pencil and paper items, divided into two sets of three categories (naming, arithmetic and simple copying). Some of the items are marked as being worth more points than others. Participants are given 5 min to complete as many items and to earn as many points as possible, following certain rules. Performance was measured by the proportion of high-point items completed (Levine et al.. 1998). 5 . Three self-report questionnaires were given for the patients and a significant other to complete: the Hogan Empathy Scale provides an indication of role-taking and perspective-taking ability (Hogan, 1969); the Questionnaire Method of Emotional Empathy (QMEE) examines the sensit- ivity to others’ emotions and emotional responsiveness (Mehrabian and Epstein, 1972; Eslinger, 1998); the Brock Adaptive Functioning Questionnaire (BAFQ) allows patients and families to describe the behavioural sequelae of brain injury (Dywan and Segalowitz, 1993).
Case histories
Case 1
HB was a 26-year-old customs officer when he was involved in a motor vehicle accident, 20 years before he presented for neuropsychological assessment. He sustained a depressed compound skull fracture involving the left frontal bone, a fractured right scapula and multiple internal injuries. He was admitted to a country hospital for the first 2 weeks then transferred to a tertiary metropolitan hospital where his skull fracture and tom dura mater were surgically treated. He was discharged home after 10-12 weeks. Education about TBI and ongoing rehabilitation were not provided. HB does not recall the accident at all. His hospital records were unobtainable and he could not give specific details of the duration of loss of consciousness. He describes a retrograde amnesia of approximately 15-20 min, and just under a day of post-traumatic amnesia, but was not certain of the exact duration. There have been no lasting physical disabilities from the accident, but he reports occasional feelings of dizziness, and headaches every 2-3 weeks.
HB attempted to return to work about 6 months after the accident, but was asked to leave after 2 months. He was told he was aggressive and having black-outs, but was unaware of these symptoms himself, although he said his memory was very bad at the time. Although he has held a number of positions since, none have been up to the standard of his pre-morbid occupation. He went back to his civilian trade as an automotive mechanic for a while, then became a camping- ground caretaker for about 18 months before enrolling in a Bachelor of Social Work. He was unable to complete the course due to separation from his first wife and difficulty coping with the pressures of assignments and exams. He then worked as a maintenance man at a special school for 6 years. He resigned from that position when he became uncomfortable with the increasing responsibilities he was expected to take for the children’s care on school excursions. He now helps his second wife with computer work. He has received a Workers Compensation pension since leaving the Customs Service.
Personal history. There is no reported family history of psychiatric or neurological disorder. HB was born at term without complication and his early childhood development appears to have been somewhat advanced. His early childhood was spent in a large city. His father was a career soldier and when HB was 5 or 6 years old the family moved to a rural army base. His father was a heavy drinker and the parental relationship was conflictual, but HB denies any significant childhood abuse or neglect. His parents separated after he left home at 17 years of age. He attended state primary and secondary schools, where he was an above-average student. He completed his trade-school apprenticeship as an auto- motive mechanic in 4 years, gaining dux of his class of 50, and with final results in the upper 1% for the state enrolment of 500. He then worked for several years with a major automotive manufacturer, gaining additional trade certificates, before deciding on a career change. He joined the Australian Customs Service 2.5 years before the accident and had been working with the promise of promotion when he sustained the TBI.
HB mamed his first wife when he was 22, 4 years before the accident. They remained married for 10 years after the accident, then she departed, leaving him with the care of their four children. HB said that the cognitive and psychological sequelae of the accident were a major factor in the marital breakdown, although his wife’s unrelated personal problems and extra-marital affairs, some of which pre-dated his TBI, also contributed. His children ranged in age from 6 to 13 when the marriage broke down. HB said it was ‘not easy’ looking after them by himself, and that he probably paid less attention to them than he should. He married his second wife 18 months after his first wife left him, and they describe a strong and mutually supportive relationship. He remains in contact with his first wife, and continues to express sincere concern for her well-being.
HB is a non-smoker and non-drinker. He denied ever using recreational drugs. He said his social activities are limited
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

330 F. J. Bardenhagen et id.
because people do not understand his disability, nor why he receives a Worker’s Compensation pension. His main activit- ies are fishing and helping his wife with computer work.
Presenting symptoitis. HB reported that his main problem was his very short temper. He confessed to feeling guilty and hating himself for his inability to control it. He described a tendency to fly into a rage with minimal provocation, accompanied by a sense of loss of control. He said he feels afraid and knows he is being irrational when he loses his temper, but that ‘It’s like I’m watching someone else’. Removing himself from the situation was the best way for h i m to avoid losing his temper. On one occasion, 20 years post-injury, HB punched a hole in a wall and broke a chair, then found himself on the floor gasping for breath and with his heart pounding. The police arrived after a neighbour reported a domestic dispute, and HB and his wife had to reassure then1 that things were okay. This incident led him to seek advice from his general practitioner. He was very afraid that he might become violent towards others, and that his marriage might deteriorate. His wife confirmed this paltern of behaviour and expressed concern about the anxiety hia temper caused him. She felt helpless when he became enraged, and was frightened that they would lose each other.
HB also described difficulties with attention, concentration and memory which have persisted in the 20 years since the accident. He complained of being easily distracted, and often forgetting where he is driving, the reason for his trip and directions. He relies on notes, lists and repetition in order to learn and recall daily information, and often has to re-read material in order to understand it. He blames his inability to work in regular employment and to succeed in academic work on his distractibility and need for repetition. He has enjoyed learning to use computers ‘Because they do not mind if you make mistakes, they do not mind how many times you do the same thing, and they allow you to learn’. He freely expresses his disappointment at the loss of his career. and his ongoing frustration over the changes to his life.
Neirrologicwl e.rumintrtion and neuroimaging. HB was referred for a neurological consultation by his general practi- tioner, 20 years post-injury, when he became concerned about his increasing lack of control of his explosive temper. Clinical neurological examination was normal, although brief cognitive screening suggested difficulties with learning and memory. and issues of current depression and unresolved grief over the loss of his career. He was commenced on the selective serotonin reuptake inhibitor (SSRI) antidepressant medication Sertraline (Zoloft), 50 mg daily. Neuropsycho- logical assessment was requested to investigate problems with memory and learning, poor impulse control and lowered frustration tolerance.
A cerebral computed tomograph (CT) was reported as revealing an area of decreased attenuation of cortex and underlying white matter in the left frontal lobe. The anterior horn of the left lateral ventricle was dilated. Appearances were reported as consistent with contusion and subsequent
gliosis from the prior head injury. No further abnormalities were evident.
Cerebral MRI images obtained on a 1.5 T Siemens system revealed a wedge-shaped area of encephalomalacia in the left frontal region, involving the cortex and adjacent white matter, extending down to the level of the frontal horn of the left lateral ventricle (Fig. I ) . The frontal horn was mildly dilated, consistent with volume loss in the left frontal lobe. A linear area of TI hypointensity was noted adjacent to the atrium of the left lateral ventricle. This was hyperintense on T2- and proton density-weighted imaging, and may represent an old shear injury. No blood products were identitied to indicate an old haematoma. Other small foci of T:! hyperintensity in the deep white matter were reported as consistent with either old shear injuries or small-vessel ischaemic changes from hypertension and/or atherosclerosis: however, there is no known history of hypertension or other cerebrovascular risk factors. There was no abnormality in the brainstem.
Hippocampal volumes were measured according to a published protocol (Cook et nl., 1992) and were found to be in the normal range for males. The left and right hippocampi were 3.3664 and 3.4575 cm3, respectively (control values. mean t 1 SD: left: 3.349 ? 0.357 cm3; right: 3.422 f 0.338 cm”.
Neurops?,chological a,s.ses.rment. ( I ) Mood arid personulit?: HB was extremely anxious when first seen for neuropsycho- logical assessment, 20 years after his TBI. He revealed high state and trait anxiety on the STAI (state and trait anxiety were at the 85th and 99th percentiles, respectively, for his age). His score of 25 on the BDI was in the moderate to severe depression range. He acknowledged thoughts of killing himself, but said he would never act on these thoughts because of the effect on his family.
The MMPI-2 was administered to allow a more conipre- hensive delineation of his symptoms (see Table 2). His profile was valid, and suggested a pattern of chronic psychological maladjustment with extreme psychological distress at the time of assessment. There were elevations on six of the clinical scales (Scales I , 2, 3, 4, 7 and 8), confirming his anxiety and depression. This pattern of elevations highlights the difficulties in standard codetype interpretations (Butcher et al., 1989). In addition to prominent features of anxiety and depression, he showed symptoms of anger, poor impulse control, unusual ideation and somatization. He felt he deserved to be punished, and felt hopeless, regretful and unhappy about his life. He was plagued by anxiety, pessiniism and worry about the future. He reported problems with his physical health and numerous somatic concerns. He felt that life was no longer worthwhile and that he was losing control of his thought processes. He wanted relief from his suffering. HB reported feelings of guilt and remorse about his poor control of his temper, attributing it to his head injury.
(2) Cognition and memory. Scores on standardized neuro- psychological tasks are presented in Table 3. His scores on the WAIS-R were in the high average to superior range, and
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

Long-term outcomes in TBI 331
Fig. 1. Case HB. (a) Three-dimensional reconstruction of a 1.5 T MRI scan taken 21 years after the accident. The arrow points to a depression in the cortex corresponding to the major lesion site. (b) Sagittal section showing area of encephalomalacia involving cortex and underlying white matter. (c) and (d) Corresponding transverse and coronal sections. (e) Coronal section showing encephalomalacia extending to frontal horn of left lateral ventricle. (f) Linear area of TI hypointensity adjacent to the atrium of the left lateral ventricle.
were consistent with pre-morbid estimates based on the NART, but were somewhat higher than predicted by demo- graphic variables. The Profile Variability Index (PVI) analysis was non-significant (McLean et a/., 1990). Examination of WAIS-R factor scores (Atkinson, 199 1 b) revealed a signifi- cant strength on Verbal Comprehension. There were no clinically significant differences between any of his WAIS- R factor scores (base rates > 5%; Atkinson, 1991b).
HB achieved average to above average scores on the WMS-R (see Table 3 ) . There were no significant differences between any of his WMS-R memory indices. His Attention/ Concentration index (ACI) was commensurate with general intellectual abilities, while his Visual Memory and Delayed Recall indices were significantly lower than his full-scale intelligence quotient (FSIQ) ( P < 0.05; Atkinson, 1991a). His performance on the Pushbutton Maze (Bowden et a/., 1992), a test of visuospatial memory, was between the 50th and 75th percentiles corrected for WAIS-R Block Design age-scaled score.
Language screening revealed superior confrontational nam-
ing and verbal fluency for his age and education (Spreen and Strauss, 1998, pp. 437457). His scores on parts A and B of the Trail Making Test were above the 70th percentile for his age (Spreen and Strauss, 1998, p. 540).
Neiiropsychological review. HB was reviewed 17 months after the initial assessment. He and his wife were happily settling into a new home in the city, but had ongoing concerns about his explosive temper. Although a psychiatric referral had been made after the first assessment, he had been lost to follow-up during relocation. At the eventual review, he said he had been more worried about things in general over the previous year. He described it as a ‘nebulous general anxiety’, and said that efforts to overcome it made him tired. His state (8 1 st percentile) and trait (100th percentile) anxiety were unchanged from the first assessment, and his BDI score (22) again indicated moderate to severe depression. He was in good spirits and cooperated well with the review assessment, however, and did not appear as overtly anxious as during the initial assessment.
Table 3 shows HB’s performance on the WAIS-111 in
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

332 F. J . Bardenhagen et al.
Table 2. Case HB: Minnesota Multiphasic Personality Inventory-2 T-scores at initial neuropsychological assessment ( T I : 20 years post-TBI) and I9 months later (Tz: 47 days after the increase in Sertraline from 50 to 100 mg daily)
L F K F(B) VRIN TRIN Hs D
HY
Pd
DI D2 D3 D4 D5
HYl HY2 HY3 HY4 HY5
Pd 1 Pd2 Pd3 Pd4 Pd5
48 58 47 71 54 50 71 99 103 59 75 104 96 74 56 47 93 67 40 79 51 61 52 62 82
53 61 49 79 54 64 53* 89* 90* 70 51* 96 85* 67 61 51 79* 52* 48 66* 45 61 64 57 67*
Pa
Pt s c
Ma
Si
ANX
64 Pal 58 Pa2 75 Pa3 41
99 81
Scl 55 Sc2 78 Sc3 96 Sc4 87 Sc5 82 Sc6 70
62 Ma1 42 Ma2 53 Ma3 53 Ma4 56
56 Sil 42 Si2 54 Si3 74
85
60 52 61* 46 85* 65 * 41 69 78* 82 68* 55* 59 50 53 59 50 61 39 67 68 82
FRS
OBS DEP
HEA
BIZ
ANG
WRK CYN
37 FRSl 44 FRS2 32
83 87
DEPl 90 DEP2 94 DEP3 70 DEP4 63
12 HEAl 57 HEA2 74 HEA3 81
49 BIZ1 44 BIZ2 54
69 ANGI 65 ANG2 67
84 47
CYNl 47 CYN2 48
37 44 32 70* 89 95 85 77 63 54* 44* 54* 49* 41 44 41 57* 52 62 80 43 44 44
ASP
TPA
LSE
SOD
FAM
TRT
50 ASPI 49 ASP2 53
55 TPAl 57 TPA2 51
82 LSEl 80 LSE2 62
49 SOD1 5 1 SOD2 47
52 FAMl 56 FAM2 58
83 TRTl 90 TRT2 68
50 49 53 47 52 46 74 85 4X 53 60 42 49 4h 67 75 X4 6X
~~
Decreased scores on retest of I SD or more are marked with an asterisk.
Table 3. HB: Neuropsychological abilities at initial assessment, 20 years after TBI ( T I : WAIS-R, WMS-R) and review 17 months later (Tz: WAIS-111. WMS-111)
Verbal IQ Performance IQ
WAIS-R Fuctor Scores Verbal Comprehension Perceptual Organization Freedom from Distractibility
WAIS-WWAIS-III age-scaled scores Information Digit Span Vocabulary Arithmetic Comprehension Similarities Letter Number Sequencing
WMS-R Indices Verbal Memory Visual Memory General Memory
Delayed Recall Attention/Concentration
I24 110
I29 111 I l l
16 13 15 I 1 15 13
114 100 112
98 118
National Adult Reading Test (predicted WAIS-R FSIQ) Controlled Oral Word Association Test (CFL) Category Fluency (animals) Boston Naming Test (total correct) Pushbutton Maze (errors over 10 trials)
130 121
14 I 1 16 15 18 13 14
Full Scale IQ
WAIS-III Factor Scores Verbal Comprehension Perceptual Organization Working Memory Processing Speed
Picture Completion Picture Arrangement Block Design Object Assembly Digit Symbol Matrix Reasoning Symbol Search
WMS-III Indices Auditory Immediate Visual Immediate Immediate Memory Auditory Delayed Visual Delayed General Memory Working Memory Auditory Recognition Delayed
119 12x
10 9 14 IS I I 16 13 12 7 I I - 14 - I I
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

Long-term outcomes in TBI 333
comparison with his WAIS-R scores from 17 months before. There were no clinically significant differences between any of the WAIS-I11 IQ or Factor scores. His WAIS-I11 IQ scores were better than expected given his WAIS-R scores, using the 95% confidence interval based on the standard error of prediction (Dudek, 1979) and information provided in the WAIS-111 - WMS-111 Technical Manual (The Psychological Corporation, 1997, pp. 79-80). The reason for this improve- ment is unclear. One possibility could be a subtle improve- ment in mood, because although HB remained anxious and depressed on objective measures, he did seem less anxious about the review assessment.
Memory abilities, as measured by the WMS-111, ranged from the 14th percentile (Visual Immediate) to the 63rd percentile (Auditory Immediate; see Table 3). WMS-111 Working Memory was at the 84th percentile. There were no clinically significant differences between any of the WMS-I11 memory indices; however, his Immediate, Visual Immediate and Visual Delayed Memory indices were significantly lower than predicted from his WAIS-111 FSIQ (base rates < 5%; The Psychological Corporation, 1997).
Psychiatric evaluation. After the neuropsychological review, HB was referred for psychiatric evaluation regarding his ongoing mood concerns. He had had no previous psychiat- ric assessment. He described recurrent episodes of dysphoria involving symptoms of depression, anxiety and tension. During these episodes, he was extremely irritable and sensit- ive, and could lose his temper very easily. These episodes were either spontaneous or triggered by some frustration and lasted from days to weeks, leaving him exhausted for a few days. Occasionally during these dysphoric episodes, anxiety symptoms reach the severity of panic attacks. Such episodes were usually triggered by a distressing episode of forgetting, such as going into town and forgetting the reason for his trip. He said that the episodes had occurred at least every couple of months since the accident. Since commencing Sertraline 1 year before the psychiatric evaluation, he had not had any bad episodes of dysphoria or accompanying dyscontrol, although he still had episodes of bad temper.
On mental state examination, HB presented as a middle- aged man of neat and clean appearance, dressed in casual clothes. He was polite and cooperative throughout interview, and maintained good eye contact. He conveyed a relaxed and friendly manner. His speech was lucid and fluent, his mood was euthymic and he conveyed a broad range of appropriate affects. His conversation was rational and appro- priate. He gave a straightforward account of his symptoms as described. There were no pathological abnormalities of mood, thought or perception.
An organic mood disorder due to TBI was diagnosed, taking the form of episodic dysphoria occasionally accompanied by emotional dyscontrol with explosive rage. It was significant and promising that his symptoms had responded partially to a low dose of Sertraline, so he was advised to increase his regular daily dose from 50 to 100 mg (50 mg twice daily). This was expected to have further benefit in preventing
episodes and diminishing the severity of those that may still occur.
Several weeks later, HB attended St Vincent’s Hospital one last time to complete experimental tests for the current research. He reported feeling much calmer and less volatile since increasing his dose of Sertraline. His wife verified the improvement, saying he was always a caring and kind husband, but was now even more caring and loving than before. She said his mood seemed more stable and he was less anxious about having explosive outbursts. The MMPI-2 was readministered 8 weeks after the neuropsychological review, and 47 days after the psychiatric consultation. Table 2 shows reductions of up to 3 SD in previously elevated scales, consistent with the improvement reported by HB and his wife.
Summary of rzeuropsychological results. HB’s major pre- senting complaint was related to his explosive temper. Initial assessment on the MMPI-2 indicated a pattern of severe and long-standing psychological disturbance related to TBI. Psychiatric evaluation resulted in a diagnosis of organic mood disorder and a therapeutic improvement in symptoms after an increase in the dose of his SSRI antidepressant medication. His performance on the initial and review cogni- tive assessments, prior to the medication increase, revealed a man of above-average intellect with relative weaknesses in visual memory and delayed recall on the WMS-R and WMS-111, but no scores approached an impaired range. Given that subtest scatter increases with IQ level (Matarazzo et al., 1988), the lack of significant scatter in HB’s profile may indicate a general decrease in intellectual abilities from pre-morbid levels. Above-average scores on measures of attentional abilities were not consistent with his complaints of distractibility and concentration problems, which may indicate insensitivity of the Wechsler Memory and Intelli- gence scales to attentional problems in TBI (Crossen and Wiens, 1988; Schmidt er al., 1994), or subjective misinter- pretation of symptoms of depression and anxiety.
Case 2
NL, a right-handed man, was involved in a serious collision between his car and a truck at the age of 24. He sustained multiple skull fractures and other orthopaedic injuries. He has been told he was unconscious for the first 5 days with a post-traumatic amnesia of at least 4 weeks. He was managed in an acute-care medical centre for 4 weeks, then spent 2 months as an in-patient at a rehabilitation hospital. He continued to attend out-patient rehabilitation for the next 3 years. He said he was profane and inappropriate after the accident, and that his rehabilitation stopped once this behaviour improved. No follow-up services were otherwise provided. Accident compensation was awarded in an out-of- court settlement 2 years after the accident, and the money was spent paying off his house.
NL made an almost full recovery from his orthopaedic injuries, apart from a slight residual problem in supination of his left arm. Neurological sequelae were more persistent
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

334 F. J . Bardenhagen et ril .
with seizures beginning some 2-3 years after the accident. During these fits, he would initially experience himself pivoting to the left and would then lose consciousness. None were accompanied by loss of bladder control and all lasted less than 5 min. He bit his tongue on one occasion. He had about six seizures before he was seen by a neurologist, investigated with EEG, and commenced on Phenytoin, on which he has remained ever since. His last seizure was 12 years after the accident, when he forgot to take his medication. He has been on a stable dose of Phenytoin (200 mg mane, 300 mg nocte) since then, with no seizures for 10 years.
NL's first marriage ended within 1 year of the accident. He said his first wife was unable to cope with the way he had changed. He married again soon after and had three children. When rehabilitation ceased 3 years after the TBI, NL attempted to return to work in the computer industry. He initially had difficulty keeping any position for more than a few months at a time, but he persevered and eventually entered the management field. Over the next 13 years, he was employed and dismissed by six different companies. His highest position after the accident was as second in charge of the computer room of a large utility service. He held this position for 5 years, but resigned after being demoted by a new manager. He moved to the country with his wife and children, and experienced a period of mild depression, which seems to have been reactive to various work frustrations and other stressors at that time. He began to study for a technical certificate in information technology, but said he was unable to complete the course because it was difficult to remember things between classes. He was employed for only 3 months out of the 6 years that he lived in the country, but earned some money over that time through providing computer installation and support to several local businesses.
Serious marital problems began when NL and his family moved to the country. His continued unemployment and his wife's frustration at his cognitive impairments compounded the disharmony over the next 5 years, until separation was contemplated. Marriage counselling at a regional hospital provided education about the effects of TBI, which helped his wife understand him better and reduced some of the stress. His first neuropsychological assessment at St Vincent's Hospital, 22 years post-injury, also provided specific informa- tion and strategies which helped NL deal with his difficulties. Around this time, NL successfully applied for a disability pension. The marital situation deteriorated again after a few months. NL said his wife thought he had lapsed back into bad behaviours, while she told us her husband's cognitive state had worsened. She was upset by his forgetfulness, general inefficiency and tendency to isolate himself in his room rather than mixing with the family. She said he had 'given up' and alleged that he must be depressed. She terminated their relationship 12 months after the initial neuropsychological assessment. He moved to the nearest city to live with relatives and began to work for his brother in a computer business. NL was re-examined 14 months after the initial assessment to monitor his progress.
Personal hisrory NL is the youngest of four siblings. There is no family history of neurological or psychiatric disorder. He was born at term without complication and his early development was entirely normal. He seems to have had a reasonably happy childhood despite the death of his father when he was 4 years old. He attended a private boys' school, attaining high grades and subsequently enrolling in a law degree course at a prestigious university. He became very ill with glandular fever at the end of the tirst year of his course, then attempted the second year before he was fully recovered, gaining poorer marks than usual. He took leave of absence after the second year, but never returned to his course, finding that he preferred work as a computer programmer. He worked successfully for ii number of com- panies as a qualified computer systems analyst and program- mer until the time of the accident. NL's brother said that N L was a highly intelligent, skilled and competent person prior to the accident.
NL is a light drinker, an ex-smoker and denies using any other recreational drugs. He describes his personality iis
extroverted and sociable. His major hobbies and interests are computers and watching motor sports.
Cognitive svmproms. A consistent account of his cognitive difficulties was obtained from NL, his wife and his brother at the initial neuropsychological assessment and 14 month review. They reported that he has difficulty maintaining i1
logical train of thought over multiple steps and performing sequential tasks. He has to write down the steps of a task in order to remember and complete them in the correct order. but even then tends to omit important steps. He has trouble breaking tasks down into steps without assistance. He has difficulty recommencing interrupted tasks, often needing to start over again, saying he can focus attention on only one task at a time. He cannot attend to a conversation or task i f there is too much background noise. NL finds i t difficult to get himself ready for work in the mornings. has trouble allocating priorities at work, and tends to get distracted by interesting but unnecessary tasks and errands. such as leaving work to drive across town to purchase a new gadget which he might need in the future.
NL and his informants also described trouble with learning and retention of information, stating that he needs to rely on notes and lists. He forgets to do important things, like turning off heating appliances, locking doors and collecting his children from their activities. He realized that fatiguability, and loss of concentration when tired, have hindered his work in the past, and has found he can only do any kind of mental work for approximately 20 h per week.
NL reported that he was very short tempered for several years after the accident, and although this has improved over time, he has ongoing concerns about irritability. He said that up until 4 years before the neuropsychological assessment, he had occasional rages in frustration at not being able to perform tasks, but that these had not been directed at property or other people. His wife said he became frustrated and angry when asked to do things which were too difficult. Their
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

Long-term outcomes in TBI 335
children learnt to be very quiet in the house and car because of his inability to concentrate if they were noisy. Mrs NL felt he had become more easily agitated over the previous 6 years. She said he was short tempered and sometimes aggressive, though his brother believed he had never been physically aggressive, only verbally so. Mrs NL complained that her husband was not aware of the problems within their family. His brother said NL had always been very aware of other people before his accident, e.g. by being aware of people standing alone at parties and trying to help them fit in, but has been less aware of social contexts since then.
These difficulties caused his wife significant frustration and distress. She complained that she had to tell him how to do 'everything' because he could not seem to work things out for himself. His brother finds that NL needs to be monitored and guided throughout the working day. He has found that urgent tasks do not suit NL because he does not work quickly, and often does unnecessary extra tasks without thinking about the inconvenience this might cause the client. He said NL used to be conscientious, reliable, thoughtful and able to reason things through logically, but that all these characteristics have now changed. NL's brother was keen to accommodate NL's forgetfulness and inefficiency in a flexible and supportive workplace, but began to lose patience with him after a few months. Referral to a vocational rehabilitation service was arranged to assist with defining NL's responsibilit- ies and maintaining a good working relationship between the brothers. This involved identification of problems NL was having at work, provision of structure, checklists and diaries, and education of other employees about NL's needs. Four months later, the rehabilitation case manager reported improvements in his workplace performance through use of the tools and strategies provided.
Neurological examination and neuroimaging. A neurolo- gical consultation was requested 22 years after the accident to review the need for continuing anticonvulsant prophylaxis. Clinical neurological examination was normal. EEG was reported as showing 'a modest increase in non-specific slow- wave components with a left temporal emphasis of uncertain significance'. A cerebral CT was requested and was reported to show extensive decreased attenuation in the subcortical matter of the left frontal lobe, with dilatation of the left frontal horn of the lateral ventricle and atrophy of the overlying cortex consistent with long-standing head injury. No further abnormalities were noted. After discussion of EEG and neuroimaging results, NL eventually decided to continue taking Phenytoin to avoid possible recurrence of seizures which would prevent him from driving. Neuro- psychological assessment was arranged to assist with the development of strategies for dealing with his cognitive difficulties.
MRI scans taken 24 years after the injury indicated a large area of hypointensity occupying almost the entire subcortical region of the left frontal lobe (Fig. 2). T1 images showed left frontal hypointensity consistent with encephalomalacia. The lesion involved the rostral-inferior aspects of the left
frontal cortex. Thinning of the corpus callosum anteriorly was consistent with atrophy and Wallerian degeneration. Mild ex vacuo enlargement of the frontal horn of the left lateral ventricle was also present. There were also bilateral small areas of gliosis or encephalomalacia in the postero-superior aspects of the parietal lobes, consistent with contracoup injuries.
Hippocampal volumes were measured according to the same protocol used for HB (Cook et al., 1992) and were found to be reduced relative to the male control values reported above for HB. The left hippocampus was 1.94 SD below the mean, at 2.6554 cm3, while the right hippocampus was 1.57 SD below the mean, at 2.8897 cm3.
Neuropsychological assessment. NL was well motivated and cooperative with neuropsychological testing 22 years after his TBI. His affect was friendly, mood was euthymic, and his responses to pencil and paper tests of mood and anxiety were asymptomatic (his BDI score was 5, and STAI state and trait anxiety were at the 9th and 14th percentiles, respectively, for his age). His general intellectual abilities (Table 4) were in the high average to superior range, consistent with pre-morbid estimates based on the NART and demographic information. The difference between his verbal IQ and performance IQ was not clinically significant (two-tailed base rate > 5%; Kaufman, 1990). The Profile Variability Index analysis was normal (McLean et al., 1990), and there were no significant differences between the WAIS- R factor scores (Atkinson, 1991b).
All WMS-R Memory Indices (Table 4), except the ACI, were significantly lower than his WAIS-R FSIQ ( P < 0.05; Atkinson, 1991a). Despite his complaints of poor concentra- tion, NL's score on the WMS-R ACI was commensurate with his general intellectual abilities. His performance on the Pushbutton Maze (Bowden et al., 1992) was between the 10th and 25th percentile relative to his Block Design age- scaled score of 17.
NL's performance on confrontational naming and verbal fluency tasks was average to above average (Spreen and Strauss, 1998). His performance on Trails A was between the 20th and 30th percentiles for his age, and Trails B was between the 80th and 90th percentiles (Spreen and Strauss, 1998, p. 540).
Fourteen month review. NL was reviewed 14 months after the initial assessment, 1 week after his marriage ended. He was sad but philosophical about the breakdown of his marriage, and no depressive symptoms were elicited on clinical interview. His affect was peculiarly flat and subdued, however, and he said he could not remember how he had been feeling over the preceding weeks. The MMPI-2 was administered to investigate his mood and other symptoms (see Table 5) . The obtained MMPI-2 profile was valid, with no significant elevations on the clinical scales. His responses suggested that he considered his present adjustment to be adequate, although there were a number of personality traits which may result in maladaption under conditions of stress.
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

336 F. J . Bardenhagen et al.
Fig. 2. Case NL. (a) Three-dimensional reconstruction of a 1.5 T MRI scan taken 24 years after the accident. Note the large area of disruption i n the left frontal region, (b) Sagittal section showing hypointensity consistent with encephalomalacia, involving the antero-inferior region of the left frontal lobe. (c ) and (dl Corresponding transverse and coronal sections. (e) Transverse section showing thinning of the anterior portion of the corpus callosum. (fJ Transverse section showing bilateral small areas of gliosis or encephalornalacia in the postero-superior aspects of the parietal lobes.
These traits include pessimism, dissatisfaction, self-puni- tiveness, tension and a tendency towards low moods.
On the review assessment, the difference between his WAIS-111 VIQ and PIQ was not significant (Table 4). The only difference between the various WAIS-111 factor scores that approached a clinically significant base rate of less than 5% was in the Perceptual Organizatioflrocessing Speed contrast, with a frequency of 8.7%. His WAIS-111 IQ scores were not significantly different from his WAIS-R IQs, using the 95% confidence intervals based on the standard error of prediction for his WAIS-R scores (Dudek, 1979) and the information provided in the WAIS-111 - WMS-111 Technical Manual (The Psychological Corporation, 1997).
NL's WMS-111 scores were similar to the WMS-R memory indices obtained 14 months earlier, and indicated average memory abilities (Table 4). There were no clinically signific- ant differences between any of the WMS-111 memory indices, nor between any of the WMS-111 indices and the scores predicted from his WAIS-111 FSIQ.
Summary of neuropsychological results. NL's performances
on standardized neuropsychological tests were reasonably consistent across the initial and review assessments. His general intellectual and attentional abilities were consistent with pre-morbid estimates of high average to superior intellec- tual functioning, although the lack of significant scatter in NL's profile, as in HB's, may indicate a general decrease in intellectual abilities from pre-morbid levels (Matorazzo et (11.. 1988). Scores on tests of memory, language and psychomotor speed were not obviously impaired, other than a low average performance on the Pushbutton Maze. Although the differ- ences between his WMS-R memory indices and his WAIS-R FSIQ were statistically significant, contrasts between his WMS-111 memory indices and WAIS-111 FSIQ were not statistically or clinically significant. Therefore, reports ol forgetfulness in NL were most strongly supported by poor visuospatial memory on the Pushbutton Maze relative to his very high score on WAIS-R Block Design (Bowden et (11.. 1992). However, given his level of intelligence, the severity of his brain injury, including reduced bilateral hippocanipal volumes, and the possibility that his current level of intellec-
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5
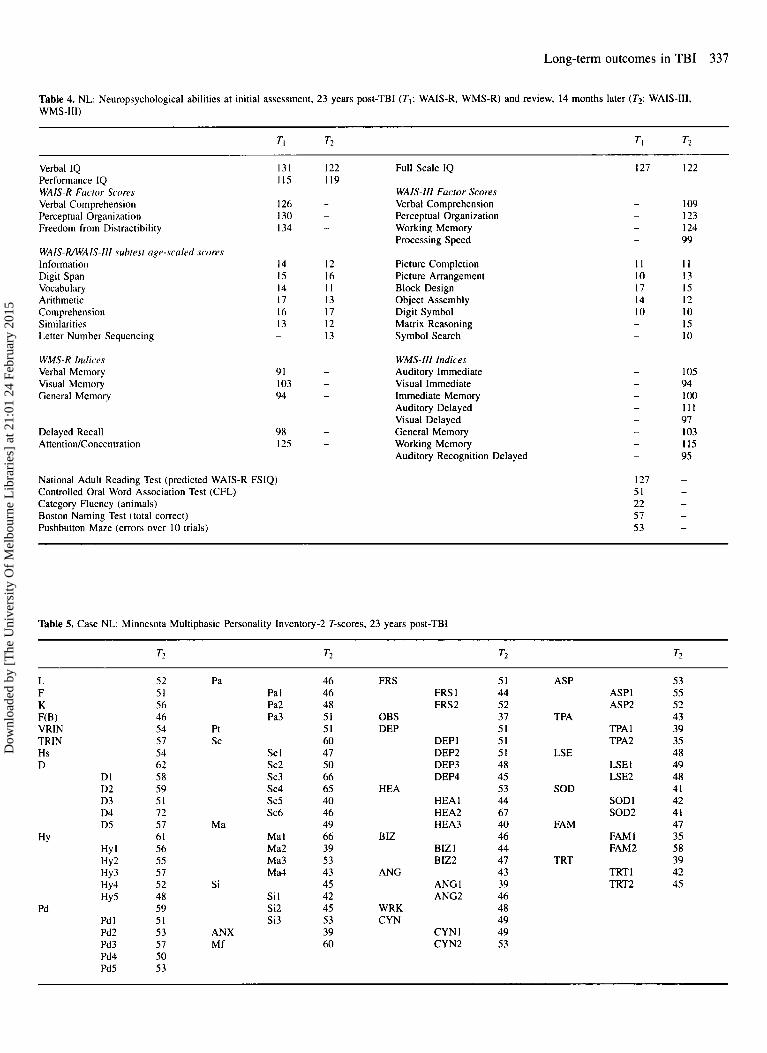
Long-term outcomes in TBI 337
Table 4. NL: Neuropsychological abilities at initial assessment, 23 years post-TBI ( T I : WAIS-R, WMS-R) and review, 14 months later (T?: WAIS-111, WMS-111)
TI T2 TI T?
Verbal IQ Performance IQ WAIS-R Factor Scores Verbal Comprehension Perceptual Organization Freedom from Distractibility
131 115
126 I30 I34
WAIS-WWAIS-Ill subtest age-scaled scores Information 14
Vocabulary 14 Arithmetic 17 Comprehension 16 Similarities 13 Letter Number Sequencing -
Digit Span 15
WMS-R Indices Verbal Memory Visual Memory General Memory
91 103 94
Delayed Recall AttentiodConcentration
98 I25
National Adult Reading Test (predicted WAIS-R FSIQ) Controlled Oral Word Association Test (CFL) Category Fluency (animals) Boston Naming Test (total correct) Pushbutton Maze (errors over 10 trials)
I22 119
- -
-
12 16 I I 13 17 12 13
-
- -
- -
Full Scale IQ
WAIS-Ill Factor Scores Verbal Comprehension Perceptual Organization Working Memory Processing Speed
Picture Completion Picture Arrangement Block Design Object Assembly Digit Symbol Matrix Reasoning Symbol Search
WMS-Ill Indices Auditory Immediate Visual Immediate Immediate Memory Auditory Delayed Visual Delayed General Memory Working Memory Auditory Recognition Delayed
127 I22
- 109 - 123 - 124 - 99
1 1 1 1 10 13 17 15 14 I2 10 10 - 15 - 10
- 105 - 94 - 100 - 111 - 97 - I03 - I15 - 95
127 - 51 - 22 - 57 - 53 -
Table 5. Case NL: Minnesota Multiphasic Personality Inventory-2 T-scores, 23 years post-TBI
L F K F(B) VRIN TRIN Hs D
DI D2 D3 D4 DS
HY
Pd
HY I Hy2
HY4 HY 5
Hy3
Pd 1 Pd2 Pd3 Pd4 PdS
52 51 56 46 54 57 54 62 58 59 51 72 57 61 56 55 57 52 48 59 51 53 57 50 53
Pa Pa I Pa2 Pa3
Pt s c
s c 1 sc2 sc3 s c 4 sc5 Sc6
Ma I Ma2 Ma3 Ma4
Si 1 Si2 Si3
Ma
Si
ANX Mf
46 46 48 51 51 60 47 50 66 65 40 46 49 66 39 53 43 45 42 45 53 39 60
FRS FRS 1 FRS2
OBS DEP
DEP 1 DEP2 DEP3 DEP4
HEA
BIZ
ANG
HEA 1 HEA2 HEA3
BIZ I B 122
ANGl ANG2
WRK CYN
CYNl CYN2
51 44 52 37 51 51 51 48 45 53 44 67 40 46 44 47 43 39 46 48 49 49 53
ASP ASPI ASP2
TPA 1 TPA2
LSEl LSE2
SOD1 SOD2
FAM 1 FAM2
TRTl TRT2
TPA
LSE
SOD
FAM
TRT
53 55 52 43 39 35 48 49 48 41 42 41 47 35 58 39 42 45
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

338 F. J . Bardenhagen ef al.
Table 6. Perfommances on clinical and experimental tests of frontal function by HB and NL, and performance on comparative neuropsychological tests by HB. NL iind I5 male controls
HB NL H B NI
M/i,YCO/lSi/l c(lrd ,%J~IiJlg TeSl Correct Errors Perseverative responses
%Or/ COlf'KO/? Te.Vl ( T-score)
Si r E l P / / I ~ ~ ) I I S Z,Sl Number of parts attempted Maximum time on any one step 15-point itenis Naming errors Copying errors Accuracy score
62 80 10 48 5 19
43 32
616 616 65 s 70 s 67 61 0 1 I 0 -134s -27 s
Non-perseverative errors Perseverative errors Categories
Number of steps Rule violations 1-point items Arithmetic errors No. of check marks Time estimation rating
5 5 6
6 0 0 0 7 4
30 18 2
6 0 0 2 4 2.5
HB NL Controls Mean SD
Ilrltr,viv/ Altrrnrrtiori Trials to criterion Non-perseverative errors Perseverative errors
0hjrc.f A/lrr~~cltiori Trials to criterion Non-perseverative errors Perseverative errors
I)rlo,vrcl Miitching I O Sortrplu Acquisition ('36 correct) Liht of I (%' correct) List of 2 ( % correct) List of 4 (94 correct) List of 8 (% correct)
25 44 6 7 2 2
50 29 27 5 0 0
I00 I00 I00 90 90 90 75 65 62.5 51.3
16.93 7 17 I .h7 2.06 0.47 0.74
31.87 I4,h-I 9.00 9.07 I .XO 1.7x
95.33 9.15 78.00 13.20 64.67 9.01 61.42 8.89
The WCST was performed on initial assessment for both men (20 years post-TBI for HB, 23 years post-TBI for NL). All other tests were administered on review appointments ( I9 months after initial assessment for HB, 14 months for NL). DA, OA, DMTS Controls: age mean = 36.07 years (SD = 10.32). education mean = 12.27 years (SD = 2.06), WAIS-R FSlQ mean = 106.86 (SD = 16.88).
tual functioning was lower than pre-morbidly, it is also possible that scores in the average range on the WMS-R and WMS-111 memory indices may reflect a loss of efficiency from his pre-morbid memory levels.
Clinical and experimental measures of frontal and limbic function
Performances of HB and N L on a range of measures thought to be sensitive to frontal and limbic functions are presented in Table 6. HB had no problems whatsoever on the WCST. N L was less successful with total errors at the 6th percentile for his age and education, non-perseverative errors at the 3rd percentile and categories at the 5th percentile (Heaton et al., 1993); however, interpretation of the WCST requires caution in view of the wide confidence intervals associated with these scores (Paolo et a / . , 1996). Neither man was impaired on the Short Category Test, although HB approached the recommended cut-off T-score of 46 for people aged 45 and
above (Wetzel and Boll, 1987). Neither man had significant difficulties on the 6-Elements Test, both approached the task in an organized fashion with no rule breaks, and attempted only 15-point items in the allocated time.
HB and NL's performances on DA, OA and DMTS were compared with those of a control group tested previously (see Table 6; Bardenhagen, 1997). On DA, N L took signitic- antly more trials to reach criterion than the control group [t(14) = 3.66, P < 0.051 and made more non-perseverative errors [ t ( 14) = 1.94, P < 0.051 [statistical procedure described by Crawford and Howell (1999)l. NL's performance on OA was not significantly different from controls, and his two perseverative errors on DA were not abnormal, given the highly skewed nature of perseverative errors on this task, and that 13.3% of the controls made two perseverative errors. HB made significantly more non-perseveralive errors on OA than the control group [ t ( 14) = 1.92, P < 0.051. but did not differ significantly on other OA or DA measures. On DMTS, performance was measured by the mean per cent correct on
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

Long-term outcomes in TBI 339
Table 7. Brock Adaptive Functioning Questionnaire Protiles. tilled in by Mr and Mrs HB, and by NL and his brother
Domain
HB NL
Awareness Change Awareness Change
Self Other Self Other Self Other Self Other
Planning Initiation Flexibility Excess Caution Attention Memory Arousal Level Emotionality Impulse Control Aggressiveness Social Monitoring Empathy
51 80 60 82 73 73 46 60 37 50 49 48
57 80 70 64 57 68 60 45 29 44 51 40
50 I00 25 80 86 75 40 50 14 20 42 60
37 50 85 84 71 65 68 45 40 28 43 52
63 5s 55 76 s1 58 56 50 57 40 49 52
43 5 0 I00 I00 71 75 8 0 I00 71 I00 71 I00
71 7s I00 80 71 63 80 SO 43 30 43 60
A high score indicates that the person may he having difticulty in the domain. Mrs HB did not complete the change items because she did not know him before his injury
each list length; no significant differences were found between the cases and the controls on any of the DMTS measures. The apparent lack of impairment on DMTS in either man may be due to lack of test sensitivity in people with average memory. Alternatively, the average range performance on DMTS may reflect real loss from higher levels of pre-morbid function, particularly since the control group had IQ scores in the average range, whereas HB and NL had high average to superior scores on the WAIS-R and WAIS-111.
Self-report measures
On the BAFQ, HB and his wife indicated difficulties in excess caution, initiation, attention, memory and flexibility (Table 7). HB indicated significant change in all of these areas, and was more aware of his problems than his wife in all areas except for flexibility. NL and his brother noted difficulties in flexibility, excess caution, attention, arousal level and memory. NL‘s brother indicated greater planning and impulse control difficulties than were reported by NL. NL indicated change in every area except planning, while his brother indicated greater changes than NL in planning and initiation.
On the QMEE, HB’s score of 43 was nearly 1 SD higher than the men tested by Mehrabian and Epstein (1972). His wife’s ratings gave him a score of 20, which was closer to the mean value for men of 23 (SD = 22). NL‘s self-rating of 36 was much higher than the score of zero given by his brother. This suggests that although NL rates his emotional empathy as normal, he may not appear as empathic to others. This may explain his wife’s frustration with his lack of responsiveness to their marital situation. HB scored 34 on Hogan’s empathy scale (his wife did not complete the questionnaire), while NL scored 37 and his brother rated him at 31. All scores on Hogan’s scale were within normal limits, compared to a mean empathy score for a sample of normal adults of 34.75 (SD = 3.68; Grattan and Eslinger, 1989).
Discussion
HB and NL‘s cases illustrate the range and severity of long- term neuropsychological outcomes after TBI. Both men had been awarded compensation soon after their injuries and therefore continuing litigation issues did not contribute to their symptoms. At the time of our long-term follow-up assessments, 22-24 years after injury, both were normal on clinical neurological examination, despite large left frontal lesions and other signs of cerebral damage consistent with TBI. Pharmacologically responsive sequelae of their TBIs included an organic mood disorder with explosive temper which responded well to Sertraline in the case of HB. and post-traumatic epilepsy which has been managed with Phenytoin in the case of NL. Both men complained of difficulties with memory and attention, and coping with the demands of work and study, but neuropsychological assessment revealed a pattern of average to superior scores on almost all measures and no severe impairments on experimental measures of executive functions. While HB and NL‘s performances on delayed reaction tests illustrate the sensitivity of these tests to prefrontal lesions, they failed to support the specificity of DA and OA to dorsolateral and orbitofrontal lesions, respectively (Freedman, 1990; Oscar- Berman, 1991). This may be because the abilities underlying performance on DA and OA, like other abilities, may have recovered to some extent, or because DA and OA are sensitive to deficits in inductive reasoning (Bardenhagen and Bowden, 1998), which might rely on distributed neural networks (Jonides, 1996). Unlike Grafman et a/. (1986), who reported greater cognitive impairments in Vietnam veterans with left dorsofrontal lesions than those with left orbitofrontal lesions, HB and NL had patterns of cognitive impairment which were not obviously different. This may be because the neuropathological effects of their TBIs were more diffuse than the penetrating injuries studied by Grafman et al. ( 1986).
The difficulty in quantifying mnemonic and cognitive
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

340 F. J. Bardenhagen et a/.
effects of TBI in high-functioning individuals is highlighted by these cases, where memory scores in the average range may actually reflect a decrease from pre-morbid functioning in above-average individuals. Although their IQ scores were broadly consistent with pre-morbid estimates, the lack of significant scatter in their scores may reflect a general diminution of intellectual abilities (Matarazzo, 1972, 1988; Silverstein, 1993). The discrepancy between self-reported attentional problems and the high scores obtained by HB and N L on attentional indices drawn from the Wechsler scales may be due to the insensitivity of these measures (Crossen and Wiens, 1988; Schmidt et a/., 1994). Alternatively, subjective perceptions of attention and concentration difficulties are a common accompaniment of mood disorders (Lishman, 1998). The prominence of these features in the symptoms of both men may thus be related to dysthymia or anxiety, features of which were prominent in the post-TB1 course of both HB and NL.
The men and their respective informants also indicated a variety of difticulties in behaviour and emotional functioning since their brain injuries. Although HB's general practitioner had originally attributed his explosive temper to 'acting out behaviour', psychiatric consultation resulted in a diagnosis of organic mood disorder and an increased dose of SSRI antidepressant medication. The MMPI-2 demonstrated the extent of HB's distress and illustrated his recovery in response to the increased medication. In the case of NL, an MMPI-2 profile and self-reported empathy in the normal range con- trasted with a variety of neurobehavioural changes reported by his brother and wife. These discrepancies underscore the difficulty in characterizing personality and emotional processing after TBI. Not surprisingly, there have been significant and ongoing psychological adjustment issues for each case, particularly in terms of employment, relationships and self-esteem. According to all the available evidence, including detailed informant reports, these difficulties are attributable to the effects of their cerebral injuries on complex cognitive and regulatory processes.
The functional connectivity of the limbic and frontal regions. and the role of these networks in social and emotional behaviour, may assist in understanding the outcomes in these two cases. In NL, diffuse neuropathological changes included a large left prefrontal lesion, abnormal left temporal interictal EEG and reduced hippocampal volumes bilaterally. This massive disruption of frontal and limbic systems resulted in a range of social, emotional and behavioural disturbances which persisted more than 20 years post-TBI. These difficul- ties included a lack of emotional responsiveness, a decrease i n awareness of other's feelings and distractibility at work despite feedback from his brother. The disparity between his self-perceptions and that of his brother on the QMEE provides empirical support for deficient emotional empathy in NL. This discrepancy may also account for his strangely flat, vague and philosophical presentation shortly after the breakdown of his second marriage. The BAFQ indicates that NL is aware of multiple changes since his injury, including changes in
empathy. However, this awareness was not reflected in his responses to the QMEE. NL perceives his emotional perceptions and reactions to be normal, but his reactions t o emotional situations do not appear entirely normal to others. This behavioural disturbance may be amenable to family education and a skills acquisition programme focusing on improving NL's adaptive reactions to a range of emotional and situational cues (Rolls er a/., 1994; Hornak c'r rrl . , 1996; Eslinger, 1998).
There are similarities between NL's presentation and that of Vietnam veterans with penetrating left orbitofrontal lesions studied approximately IS years after injury (Grafinan c r l r l . .
1986). These veterans presented themselves in an 'angelic' light. and reported a greater interest in philosophical issue\, also reporting few distressing behaviours and feelings, and a more cavalier attitude towards interpersonal problems (Grafman et a / . , 1986). NL also appears to have impairments in the four social executors described by Eslinger o r r r l . (1996). Impaired social self-regulation is evident in his l ow frustration tolerance and resulting irritability, anger and aggressiveness, and his appearance of apathy to his wife. Impairment in social self-awareness, or knowledge and insight about oneself in social situations, was evident in the BAFQ scores. His brother indicated that NL frequently makes inappropriate or tactless comments, often makes sexually inappropriate remarks, and that NL had changed i n these areas. NL was also aware of these changes. but reported that he did these things less frequently than suggested by his brother. Although NL perceives normal levels of emotional empathy, he appears to have difticulty communicating his feelings to others. His brother noted a change in NL's social sensitivity, though scores on the BAFQ Social Monitoring scale indicated this was not a major issue. Finally, impaired social salience may be inferred from his wife's description of his under-responsiveness to the breakdown in their mar- riage, and her belief that he had just 'given up'.
HB differed from NL in his more restricted left dorsolateral frontal lesion, the prominence of a pharmacologically responsive organic mood disorder, and maintenance of il
supportive and mutually fulfilling marital relationship. His emotional dyscontrol and explosive rage are consistent with reported disinhibition of mood states that reflect increased anger and hostility reported from the Vietnam veteran sample with left dorsofrontal lesions (Grafman er ( I / . , 1986). HB's tirst marriage broke down several years after the accident, and although he takes some responsibility for the failure of the relationship, i t is clear that his wife's intidelity and personal issues pre-dated his TBI and were significant contrib- uting factors. HB's scores on the empathy measures indicate greater than average emotional empathy. Similar results have been found in a small proportion ( 5 % ) of brain-injured patients, where heightened emotional empathy sometimes causes more symptoms of anxiety (Eslinger, 1998). With successful treatment of his organic mood disorder. his great sensitivity to others' feelings seems to be ii positive aspect in his marital relationship. In terms of the social executors
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5
Long-term outcomes in TBI 341
described by Eslinger et al. (1996), HB’s social self- awareness. sensitivity and salience appear to be unimpaired. Difficulties with social self-regulation were apparent in his affective instability, but this responded well to SSRI antide- pressant medication.
Research reviewed in the Introduction highlights the role of orbitofrontal cortex in the integration of emotional stimuli and behaviour. Deficits in the ability to learn from social-emotional experience are thought to arise from impairments in autonomic reactivity, contingency-based learning and emotional pro- cessing (Damasio et d., 1990; Rolls et d., 1994; Hornak et d., 1996). While it is conceivable that the social and emotional sequelae of TBI in NL‘s case are results of similar impairments, these aspects of emotional processing and learning were not assessed in this study. However, NL‘s tendency to be distracted by irrelevant tasks and details while at work suggests a diffi- culty perceiving the consequences of his actions and a tendency to be guided by immediate goals, which has also been noted in patients with ventromedial lesions (Bechara et nl., 1994). This tendency contributed to difficulties in his relationship with his wife and brother, but, fortunately, it seems that provision of structure in his workplace by the vocational rehabilitation ser- vice has helped NL organize himself during working hours and avoid distractions.
Recognition that parts of orbital and medial frontal cortex are limbic cortex helps clarify the complex behavioural changes seen in many cases of TBI. Disruption of the frontal aspect of the limbic system results in emotional and behavioural changes which are beyond the scope of many neuropsycho- logical tests. Even though the MMPI-2 was sensitive to HB’s distress and organic mood disorder, the kind of emotional and interpersonal changes seen in NL and other cases of orbitofron- tal injury may be best detected by measures of empathy and social behaviour which are also rated by relatives. Such meas- ures are still being developed, but show great promise for the characterization and treatment of sociakmotional problems in TBI populations (e.g. Groom er al., 1998).
Education about the effects of TBI reportedly came late for both men and their families. Both HB and NL said education had helped them to understand and accept the changes that had occurred. Although education also helped their families, it did not save NL‘s marriage. He said he had been ‘grumpy, self- centred, and upset with the world’ after his injury, and was told he would get better. He said he had expected to be able to do things as before, and was upset that he could not. He said that his growing awareness and acceptance of his limitations may have contributed to his wife’s perception of deterioration over the past 6 years, but that their close proximity in the house due to his unemployment may have also made her more aware of his difficulties. HB said he still gets anxious, but not as often as he did prior to prescription of Sertraline and TBI education. With the help of further investigations and education he had received over the last 2 years, he said ‘A lot of things had fallen into place that hadn’t before. Ignorance can be frightening sometimes’.
These cases illustrate that significant needs for support,
rehabilitation and intervention may exist more than 20 years after severe TBI. Provision of education about the effects of TBI, even though it was provided over 20 years after their injuries, helped HB and NL come to terms with their difficult- ies. Referral to vocational rehabilitation services may help establish and maintain flexible and realistic work arrangements where difficulties in employment are noted. Education, pharm- acotherapy and vocational interventions had therapeutic effects in these cases. HB’s good response to antidepressant medica- tion indicates that mood disturbance, including dysphoria, irrit- ability and explosive rage, should not be regarded as an untreatable consequence of TBI without a thorough psycholo- gical and psychiatric investigation. The persistence of person- ality and behavioural changes more than 20 years after TBI highlights the need for a more holistic approach to neuro- psychological assessment, incorporating psychosocial meas- ures, including emotional behaviour and empathy, along with the more usual measures of attention, memory, cognition, lan- guage, mood and personality. Many patients with mood dis- turbance secondary to an organic condition may benefit from active management, regardless of time since injury.
Acknowledgements
We gratefully acknowledge the participation of HB, NL and their families in this research. We are also indebted to Paul Eslinger for his encouragement, advice and support. This art- icle was supported in part by an Australian Research Council grant to S. B. and M. C.
References
Asikainen I. Kaste M, Sarner S. Patients with traumatic brain injury referred to a rehabilitation and re-employment programme: social and professional outcome for 508 Finnish patients 5 or more years after injury. Brain Injury 1996; 10: 883-99.
Atkinson L. Concurrent use of the Wechsler Memory Scale-Revised and the WAIS-R. British Journal of Clinical Psychology 1991a; 30: 87-90.
Atkinson L. Some tables for statistically based interpretation of WAIS-R factor scores. Psychological Assessment: A Journal of Consulting and Clinical Psychology 1991b; 3: 288-91.
Bachevalier J, Mishkin M. Visual recognition impairment follows ventromedial but not dorsolateral prefrontal lesions in monkeys. Behavioural Brain Research 1986; 20: 249-61.
Barbas H. Anatomic basis of cognitive emotional interactions in the primate prefrontal cortex. Neurosciences and Behavioral Reviews 1995; 19: 499-5 10.
Bardenhagen FJ. An investigation of comparative neuropsychological tests in alcohol-dependent people. PhD Dissertation, University of Melbourne, Victoria, Australia, 1997.
Bardenhagen FJ, Bowden SC. Does knowledge of the response rule determine human performance on an animal test of amnesia? Neuropsychology 1995; 9: 573-9.
Bardenhagen FJ, Bowden SC. Cognitive components of perseverative errors on the object alternation task. Brain and Cognition 1998; 37: 224-36.
Bauer RH, Fuster JM. Delayed-matching and delayed-response deficit from cooling dorsolateral prefrontal cortex in monkeys. Journal of Comparative and Physiological Psychology 1976; 90: 293-302.
Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994: 50: 7-15.
Beck AT. Beck Depression Inventory: manual. San Antonio, TX: The Psychological Corporation. 1987.
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

342 F. J. Bardenhagen et 01.
Bellus SB. Stewart D. Vergo JG, Kost PP, Grace J, Barkstrom SR. The use of lithium in the treatment of aggressive behaviors with two brain-injured individuals in a state psychiatric hospital. Brain Injury 1996; 10: 849-60
Bigler ED, Johnson SC. Anderson CV, Blatter DD, Gale SD, Russo AA el 01. Traumatic brain injury and memory: The role of hippocampal atrophy. Neuropsychology 1996; 10: 33342.
Bowden SC. Dumendzic J, Clifford C, Hopper J, Tucker A. Kinsella G. Normal performance on the Austin Maze. The Clinical Neuropsychologist 1992; 6: 43-52.
Butcher JN. Dahlstroin WG, Graham JR, Tellegen A, Kaemmer 9 . Minnesota Multiphasic Personality Inventory-2 (MMPI-2): Manual for administration and scoring. Minneapolis: University of Minnesota Press, 1989.
Cook MJ, Fish DR. Shorvon SD, Straughan K, Stevens JM. Hippocampal volumetric and morphoinetric studies in frontal and temporal lobe epilepsy. Brain 1992; I 15: 1001-15.
Crawford JR. Howell DC. Comparing an individual's test score against norms derived from small samples. The Clinical Neuropsychologist 1999; in press.
Crossen JR. Wiens AN. Residual neuropsychological deficits following head- injury on the Wechsler Memory Scale-Revised. The Clinical Neuropsychologist 1988; 2: 393-9.
Damasio AR, Tranel D, Damasio H. Individuals with sociopathic behavior caused by frontal damage fail to respond autonomically to social stimuli. Behavioral Brain Research 1990; 41: 81-94.
Damasio H, Grabowski T, Randall F, Galaburda AM, Damasio AR. The return of Phineas Gage: Clues about the brain from the skull of a famous patient. Science 1994; 264: 1102-5.
Dawson DR. Chipman M. The disablement experienced by traumatically brain- in,jured adults living in the community. Brain Injury 1995; 9; 339-53.
Dudek FJ. The continuing misinterpretation of the standard error of measurement. Psychological Bulletin 1979; 86: 335-7.
Dywan J, Segalowirz SJ. Electrophysiological correlates of family-reported hehaviour after traumatic brain injury. Journal of Clinical and Experimental Neuropsychology 1993: 15: 106.
Eames P, Cotterill G, Kneale T, Storrar AL. Outcome of intensive rehabilitation after severe brain injury: A long-term follow up study. Brain Injury 1996; 10: 63 1-50,
Eniilien G. Waltregny A. Traumatic brain injury, cognitive and emotional dysfunction. Impact of clinical neuropsychology research. Acta Neurologica Belgica 1996; 96: 89-101.
Eslinger PJ. Neurological and neuropsychological bases of empathy. European Neurology 1998; 39: 193-9.
Eslinger PJ, Grattan LM. Geder L. Neurologic and neuropsychologic aspects of frontal lobe impairments in postconcussive syndrome. In: Rizzo M, Tranel D. editors. Head injury and postconcussive syndrome. New York: Churchill Livingstone, 1996: 41540.
Freedman M. Object alternation and orbitofrontal system dysfunction in Alzheimer's and Parkinson's disease. Brain and Cognition 1990; 14: 134-43.
Freedman M. Frontal and parietal lobe dysfunction in depression: delayed alternation and tactile learning deficits. Neuropsychologia 1994; 32: 1015-25.
Freedinan M. Oscar-Berman M. Bilateral frontal lobe disease and selective delayed response deficits in humans. Behavioural Neuroscience 1986: 100: 33742.
Fuster JM. The prefrontal cortex. Anatomy. physiology. and neuropsychology of the frontal lohe. 2nd ed. New York: Raven Press, 1989.
Fyffe C. McCubhery J . 'If only we had somewhere to tu rn...' the service needs of people with acquired brain injury in a rural community. Australian Journal o f Rural Health 1996; 4: 232-6.
Ciansler DA. Covall S. McGrath N, Oscar-Berman M. Measures of prefrontal dysfunction after closed head injury. Brain and Cognition 1996; 30: 194-204.
Coldman-Rakic PS. Circuitry of primate prefrontal cortex and regulation of hehaviour hy representational memory. In: Mountcastle VB, Plum F, editors. Handbook of physiology: The nervous system. V. Higher functions of the hrain. Part 1. Bethesda. MD: American Physiological Society, 1987: 373417.
Goldman-Rakic PS. Anatomical and functional circuits in prefrontal cortex of nonhuman primates. In: Jasper HH, Riggio S, Goldman-Rakic PS, editors. Epilepsy and the functional anatomy of the frontal lobe. New York: Raven Press, 199.5: 51-65.
Grafman J. Vance SC, Weingarter H. Salazar AM, Amin D. The effects of lateralized frontal lesions in mood regulation. Brain 1986; 109: 1127-48.
Grattan LM. Eslinger PJ. Higher cognition and social behavior: Changes in cognitive flexibility and empathy after cerebral lesions. Neuropsychology
Groom KN, Shaw TG, O'Connor ME, Howard NI, Pickens A. Neurobehavioral symptoms and family functioning in traumatically brain-injured adults. Archives of Clinical Neuropsychology 1998; 13: 695-71 I .
1989; 3: 175-85.
Heaton RK, Chelune GJ, Talky JL, Kay GG, Curtiss G. Wisconsin Card Sorting Test manual: Revised and expanded. Odessa, FL: Psychological Assessment Resources, 1993.
Hetherington CR. 'No longer Gage': frontal lobe dysfunction and emotional changes. Journal of Consulting and Clinical Psychology 1992; 60: 349-59
Hetherington CR. Stuss DT, Finlayson MA. Reaction time and variability S and 10 years after traumatic brain injury. Brain Injury 1996: 10: 473-86.
Hillier SL, Sharpe MH, Metzer J. Outcomes 5 years post traumatic brain injury (with further reference to neurophysical impairment and disability). Brain Injury 1997; I I : 661-75.
Hogan, R. Development of an empathy scale. Journal of Consulting and Clinical
Hornak J, Rolls ET, Wade D. Face and voice expression identification in patients with emotional and behavioral changes following ventral lobe damoge. Neuropsychologia 1996; 34: 24741.
lsseroff A, Rosvold HE, Galkin TW. Goldman-Rakic PS. Spatial memory itnpairments following damage to the mediodorsal nucleus of the thalamus in rhesus monkeys. Brain Research 1982; 232: 97-1 13.
Jonides J. Working memory and thinking. In: Smith EE. Osherson DN. editors. Thinking: An invitation to cognitive science. Vol. 3. 2nd ed. Cambridge. MA: MIT Press, 1996: 21545.
Jordan FM, Cannon A, Murdoch BE. Language ahilities of mildly closed head injured (CHI) children 10 years post injury. Brain Injury 1992: 6: 39-14,
Kaitaro T, Koskinen S , Kaipio ML. Neuropsychological problems in everyday life: a five year follow up study of young severely closed-head-injured patients. Brain Injury 1995; 9: 713-27.
Kaplan EF, Goodglass H. Weintraub S. The Boston Naming Test. 2nd ed. Philadelphia: Lea and Febiger, 1993.
Kaufman AS. Assessing adolescent and adult intelligence. Boston: Allyn and Bacon, 1990.
Klonoff H, Clark C. Klonoff Processing Speed. Long-term outcome of head injuries: a 23 year follow up study of children with head injuries. Journal of Neurology, Neurosurgery and Psychiatry 1993; 56: 4 10-5.
Leichtman M. Psychotherapeutic interventions with brain injured children and their families: 11 Psychotherapy. Bulletin of the Menninger Clinic 1902; SO: 33840.
Levine 9. Stuss DT, Milberg WP, Alexander MP. Schwutz M. MacDonald R. The effects of focal and diffuse brain damage on strategy application: Evidcncc from focal lesions, traumatic brain injury, and normal aging. Journal i i f the International Neuropsychological Society 1998; 4: 247-64.
Psychology 1969; 33: 307-16.
Lishman WA. Organic psychiatry. 3rd ed. Oxford: Blackwell Science. 19YX. Mahut H. Spatial and object reversal learning in monkeys with partial temporol
lobe ablations. Neuropsychologia 197 I ; 9: 409-24. Masson F, Maurette P, Salmi LR, Dartigues JF. Vecsey J, Destaillats J M r f 0 1 .
Prevalence of impairments 5 years after a head injury, and their relationship with disabilities and outcome. Brain Injury 1996; 10: 487-97.
Matarazzo JD. Wechsler's measurement and appraisal of adult intelligence. 5th ed. Baltimore, MD: Williams and Wilkins, 1972.
Matarazzo JD, Daniel MH, Prifitera A, Herman DO. Inter-subtest scatter in the WAIS-R standardization sample. Journal of Clinical Psychology 19x8; 44: 94G50.
McLean JE, Reynolds CR. Kaufman AS. WAIS-R suhtest scatter using the profile variability index. Psychological Assessment: A Journal o f Consulting and Clinical Psychology 1990; 2: 289-92.
Mehrabian A, Epstein N. A measure of emotional empathy. Journal o f Personality 1972; 40: 52543.
Mishkin M, Appenzeller T. The anatomy of memory. Scientific American 1987;
Morton MV, Wehman P. Psychosocial and emotional sequelae of individuals with traumatic brain injury: a literature review and recommendations. Brain Injury 1995; 9: 81-92.
Nelson HE. National Adult Reading Test (NART): test manual. Windsor. 1JK: NFER Nelson, 1982.
Olver JH. Ponsford JL, Curran CA. Outcome following traumatic brain injury: AcomparisonbetweenZand5 yearsafterinjury. BrainInjury 1996: 10: X41-X.
Oscar-Berman M. Clinical and experimental approaches to varieties of memory. International Journal of Neuroscience I99 I ; 58: 135-50.
Oscar-Berman M, Bardenhagen FJ. Nonhuman animal models of memory dysfunction in neurodegenerative disease. In: Troster A, editor. Memory i n neurodegenerative disease: Biological, cognitive, and clinical perspectives. Cambridge: Cambridge University Press, 1998: 3-20.
Oscar-Berman M, Zola-Morgan S, Oberg RGE, Bonner RT. Comparatiw neuropsychology and Korsakoff's syndrome. I l l d e l a y e d response, delayed alternation and DRL performance. Neuropsychologia 1982; 20: 187-202.
256: 62-7 I .
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5

Long-term outcomes in TBI 343
Oscar-Berman M, McNamara P. Freedman M. Delayed-Response tasks: parallels between experimental ablation studies and findings in patients with frontal lesions. In: Levin H. Eisenberg HM. Benton AL, editors. Frontal lobe function and dysfunction. New York: Oxford University Press, 1991: 230-55.
Oscar-Berman M, Hutner N, Bonner RT. Visual and auditory spatial and nonspatial delayed-response performance by Korsakoff and non-Korsakoff alcoholic and aging individuals. Behavioural Neuroscience 1992; 106: 613- 22.
Paolo AM, Axelrod BN. Troster AI. Test-retest stability of the Wisconsin Card Sorting Test. Assessment 1996; 3: 13743.
Price JL, Carmichael ST. Drevets WC. Networks related to the orbital and medial prefrontal cortex; a substrate for emotional behavior. Progress in Brain Research 1996; 107: 523-36.
The Psychological Corporation. WAIS-111 - WMS-I11 technical manual. San Antonio, TX: Harcourt Brace and Co., 1997.
Reitan RM. Wolfson D. The Halstead-Reitan Neuropsychological Test Battery. Tucson, AZ: Neuropsychology Press, 1985.
Rolls ET, Hornak J, Wade D. McGrath J. Emotion related learning in patients with social and emotional changes associated with frontal lobe damage. Journal of Neurology, Neurosurgery and Psychiatry 1994; 57: 15 18-24.
Sbordone RJ. Liter JC, Pettler-Jennings P. Recovery of function following severe traumatic brain injury: a retrospective 10 year follow-up. Brain Injury 1995; 9: 285-99.
Schalen W. Hansson L, Nordstom G. Nordstrom CH. Psychosocial outcome 5- 8 years after severe traumatic brain lesions and the impact of rehabilitation services. Brain Injury 1994; 8: 49-64.
Schmidt M, Trueblood W, Merwin M, Durham RL. How much do 'Attention' tests tell us'? Archives of Clinical Neuropsychology 1994; 9: 383-94.
Shallice T. Burgess PW. Deficits in strategy application following frontal lobe damage in man. Brain 1991; 114: 72741,
Silverstein AB. Type I . Type 11. and other types of errors in pattern analysis. Psychological Assessment 1993; 5 : 7 2 4 .
Speilberger CD. State-Trait Anxiety Inventory. Paolo Alto, CA: Mind Garden, 1983.
Spreen 0, Strauss E. A compendium of neuropsychological tests: Administration. norms, and commentary. New York: Oxford University Press, 199 I .
Spreen 0, Srrauss E. A compendium of neuropsychological tests: Administration. norms, and commentary. New York: Oxford University Press, 1998.
Stuss DT, Gow CA, Hetherington CR. 'No longer Gage': Frontal lobe dysfunction and emotional changes. Journal of Consulting and Clinical
van Reekum R. Bolago 1. Finlayson MA, Garner S, Links PS. Psychiatric disorders after traumatic brain injury. Brain Injury 1996; 10: 319-27.
Virkkunen M, Nuutila A, Huusko S. Effect of brain injury on social adaptability: Longitudinal study on frequency of criminality. Acta Psychiatrica Scandinavica 1976: 53: 168-72.
Vogenthaler DK, Smith KR Jr, Goldfader P. Head injury, a multivariate study: predicting long term productivity and independent living outcome. Brain Injury 1989; 3: 369-85.
Wechsler D. Manual for the Wechsler Adult Intelligence Scale-Revised. New York: Psychological Corporation, 198 I .
Wechsler D. Manual for the Wechsler Memory Scale-Revised. New York: Psychological Corporation, 1987.
Wechsler D. Wechsler Adult Intelligence Scale. 3rd ed. San Antonio, TX: The Psychological Corporation, 1997a.
Wechsler D. Wechsler Memory Scale. 3rd ed. San Antonio, TX: The Psychological Corporation, I997b.
Wetzel L, Boll TJ. Short Category Test, booklet format. Los Angeles, CA: Western Psychological Services, 1987.
Wood RL, Yurdakul LK. Change in relationship status following traumatic brain injury. Brain Injury 1997; I I : 491-501.
Wilson B. Recovery and compensatory strategies in head injured memory impaired people several years after insult. Journal of Neurology, Neurosurgery and Psychiatry 1992; 55: 177-80.
Wilson BA. Syndromes of acquired dyslexia and patterns of recovery: a 6- to 10 year follow-up study of seven brain injured people. Journal of Clinical and Experimental Neuropsychology 1994; 16: 354-7 I .
Psychology 1992: 60: 349-59.
Received on 19 October; 1998: resubmitted and accepted on 18 March, 1999
Psychosocial and neuropsychological outcomes in two high-functioning males 20 years after traumatic brain injury
F. J. Bardenhagen, S. C. Bowden, R. B. Shields, V. McKay, P. J. Smith, S. Vogrin, S. J. Collins and M. J. Cook Abstract Researchers have emphasized a need for ongoing rehabilitation and support for individuals with traumatic brain injury (TBI), yet there are few detailed descriptions of long-term outcome, and many people with long-standing TBI do not or cannot access support services. HB and NL, two men who sustained severeTBI, presented for neuropsychological consultation for the first time more than 20 years post-injury. Referral was prompted by significant mood and relationship disturbances, and ongoing mnemonic and cognitive symptoms. Structural imaging showed a very large lesion involving the orbitofrontal and dorsolateral regions of NL's left frontal lobe, while HB had a smaller lesion involving cortical and subcortical matter in the dorsolateral region of the left frontal lobe. Results from a range of neuropsychological tests indicated residual weakness in memory and variable impairments on two experimental tests of prefrontal working memory: Delayed Alternation and Object Alternation. The Minnesota Multiphasic Personality Inventory-2 highlighted a pattern of severe psychological disturbance in HB which improved in response to antidepressant medication. Measures of emotional empathy and adaptive functioning suggested significant changes attributable to disruption of prefrontal aspects of the limbic system.
Journal
Neurocase Reference Number:
Primary diagnosis of interest
Author's designation of case
Key theoretical issue
Neurocase 1999; 5 : 3 2 5 4 3
0162
Traumatic brain injury
HB, NL
0 Orbitofrontal function and outcome after traumatic brain injury
Key words: traumatic brain injury; neuropsychology; personality
Scan, EEG and related measures
Standardized assessment CT, MRI, EEG
Wechsler Adult Intelligence Scale-Revised, Wechsler Memory Scale-Revised, Boston Naming Test, Controlled Oral Word Association Test. Beck Depression Inventory, State-Trait Anxiety Inventory, Minnesota Multiphasic Personality Inventory-2, National Adult Reading Test, Wisconsin Card Sorting Test. Short Category Test, Trail Making Test, Pushbutton Maze, WAIS-III and WMS-111
Other assessment Delayed Alternation, Object Alternation, Delayed Matching to Sample, 6-Elements Task, Hogan's empathy scale, the QMEE, Brock Adaptive Functioning Questionnaire
Lesion location 0 Case HB: large left dorsolateral lesion and small white matter lesions
consistent with old shear injuries 0 Case NL: large left antero-inferior lesion, thinning of the genu of the corpus
callosum, small bilateral lesions in the postero-superior aspects of the parietal lobes
Lesion type Encephalomalacia in frontal lobe lesions, shear injuries in case HB, and Wallerian degeneration and contracoup injuries in case NL
Language English
Dow
nloa
ded
by [
The
Uni
vers
ity O
f M
elbo
urne
Lib
rari
es]
at 2
1:01
24
Febr
uary
201
5




















