Psychological Distress in Men during the COVID-19 Pandemic ...
19
Citation: de Sousa, A.R.; Teixeira, J.R.B.; Palma, E.M.S.; Moreira, W.C.; Santos, M.B.; de Carvalho, H.E.F.; Almeida, É.S.; Florencio, R.M.S.; de Queiroz, A.M.; Merces, M.C.d.; et al. Psychological Distress in Men during the COVID-19 Pandemic in Brazil: The Role of the Sociodemographic Variables, Uncertainty, and Social Support. Int. J. Environ. Res. Public Health 2022, 19, 350. https://doi.org/ 10.3390/ijerph19010350 Academic Editor: Paul B. Tchounwou Received: 22 November 2021 Accepted: 18 December 2021 Published: 29 December 2021 Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affil- iations. Copyright: © 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/ 4.0/). International Journal of Environmental Research and Public Health Article Psychological Distress in Men during the COVID-19 Pandemic in Brazil: The Role of the Sociodemographic Variables, Uncertainty, and Social Support Anderson Reis de Sousa 1 , Jules Ramon Brito Teixeira 2 , Emanuel Missias Silva Palma 3 , Wanderson Carneiro Moreira 4,5 , Milena Bitencourt Santos 1 , Herica Emilia Félix de Carvalho 6 , Éric Santos Almeida 1 , Raíssa Millena Silva Florencio 7 , Aline Macêdo de Queiroz 8 , Magno Conceição das Merces 9 , Tilson Nunes Mota 10 , Isabella Félix Meira Araújo 1 , Josielson Costa da Silva 1 , Sélton Diniz dos Santos 2 , Emerson Lucas Silva Camargo 11 , Luciano Garcia Lourenção 12 , Richardson Augusto Rosendo da Silva 13 , Evanilda Souza de Santana Carvalho 2 , Iracema Lua 14 ,Sônia Barros 4 , Tânia Maria de Araújo 2 ,Márcia Aparecida Ferreira de Oliveira 4,15 , Álvaro Pereira 1 , Wilson Abreu 16 and Carlos Alberto da Cruz Sequeira 16, * 1 Escola de Enfermagem, Universidade Federal da Bahia, Salvador 40231-300, BA, Brazil; [email protected] (A.R.d.S.); [email protected] (M.B.S.); [email protected] (É.S.A.); [email protected] (I.F.M.A.); [email protected] (J.C.d.S.); [email protected] (Á.P.) 2 Departamento de Saúde, Universidade Estadual de Feira de Santana, Feira de Santana 44001-970, BA, Brazil; [email protected] (J.R.B.T.); [email protected] (S.D.d.S.); [email protected] (E.S.d.S.C.); [email protected] (T.M.d.A.) 3 Escola Bahiana de Medicina e Saúde Pública, Salvador 40290-000, BA, Brazil; [email protected] 4 Escola de Enfermagem, Universidade de São Paulo, Sao Paulo 05403-000, SP, Brazil; [email protected] (W.C.M.); [email protected] (S.B.); [email protected] (M.A.F.d.O.) 5 Coordenação de Saúde do Adolescente, Jovem e Homem, Diretoria Técnica, Secretaria de Saúde, Prefeitura Municipal de Ananindeua, Ananindeua 67130-600, PA, Brazil 6 Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, Ribeirao Preto 14040-902, SP, Brazil; [email protected] 7 Faculdade Estácio de Alagoinhas, Alagoinhas 48010-970, BA, Brazil; raissafl[email protected] 8 Faculdade de Enfermagem, Universidade Federal do Pará, Belem 66075-110, PA, Brazil; [email protected] 9 Departamento de Ciências da Vida, Universidade do Estado da Bahia, Salvador 1150-000, BA, Brazil; [email protected] 10 Secretaria de Ciência, Tecnologia e Inovação, Salvador 41745-004, BA, Brazil; [email protected] 11 Curso de Psicologia, Campus Ribeirão, Universidade de Ribeirão Preto, Ribeirao Preto 11440-003, SP, Brazil; [email protected] 12 Escola de Enfermagem, Universidade Federal do Rio Grande, Rio Grande 96201-900, RS, Brazil; [email protected] 13 Departamento de Enfermagem, Universidade Federal do Rio Grande do Norte, Natal 59012-300, RN, Brazil; [email protected] 14 Instituto de Saúde Coletiva, Universidade Federal da Bahia, Salvador 40110-040, BA, Brazil; [email protected] 15 Programa de Pós-Graduação em Enfermagem, Centro de Ciências da Saúde, Universidade Federal de Santa Maria, Santa Maria 97105-900, RS, Brazil 16 Centro de Investigação em Tecnologias e Serviços de Saúde, Escola Superior de Enfermagem do Porto, 4200-072 Porto, Portugal; [email protected] * Correspondence: [email protected] Abstract: Objective: To analyze the relationships between sociodemographic variables, intolerance to uncertainty (INT), social support, and psychological distress (i.e., indicators of Common Mental Disorders (CMDs) and perceived stress (PS)) in Brazilian men during the COVID-19 pandemic. Methods: A cross-sectional study with national coverage, of the web survey type, and conducted with 1006 Brazilian men during the period of social circulation restriction imposed by the health authorities in Brazil for suppression of the coronavirus and control of the pandemic. Structural equation modeling analysis was performed. Results: Statistically significant direct effects of race/skin color (λ = 0.268; p-value < 0.001), socioeconomic status (SES) (λ = 0.306; p-value < 0.001), household composition Int. J. Environ. Res. Public Health 2022, 19, 350. https://doi.org/10.3390/ijerph19010350 https://www.mdpi.com/journal/ijerph
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Psychological Distress in Men during the COVID-19 Pandemic ...

�����������������
Citation: de Sousa, A.R.; Teixeira,
J.R.B.; Palma, E.M.S.; Moreira, W.C.;
Santos, M.B.; de Carvalho, H.E.F.;
Almeida, É.S.; Florencio, R.M.S.; de
Queiroz, A.M.; Merces, M.C.d.; et al.
Psychological Distress in Men during
the COVID-19 Pandemic in Brazil:
The Role of the Sociodemographic
Variables, Uncertainty, and Social
Support. Int. J. Environ. Res. Public
Health 2022, 19, 350. https://doi.org/
10.3390/ijerph19010350
Academic Editor: Paul B.
Tchounwou
Received: 22 November 2021
Accepted: 18 December 2021
Published: 29 December 2021
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2021 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
International Journal of
Environmental Research
and Public Health
Article
Psychological Distress in Men during the COVID-19 Pandemicin Brazil: The Role of the Sociodemographic Variables,Uncertainty, and Social SupportAnderson Reis de Sousa 1, Jules Ramon Brito Teixeira 2 , Emanuel Missias Silva Palma 3,Wanderson Carneiro Moreira 4,5 , Milena Bitencourt Santos 1 , Herica Emilia Félix de Carvalho 6 ,Éric Santos Almeida 1 , Raíssa Millena Silva Florencio 7 , Aline Macêdo de Queiroz 8,Magno Conceição das Merces 9 , Tilson Nunes Mota 10, Isabella Félix Meira Araújo 1, Josielson Costa da Silva 1 ,Sélton Diniz dos Santos 2 , Emerson Lucas Silva Camargo 11 , Luciano Garcia Lourenção 12 ,Richardson Augusto Rosendo da Silva 13 , Evanilda Souza de Santana Carvalho 2, Iracema Lua 14, Sônia Barros 4,Tânia Maria de Araújo 2 , Márcia Aparecida Ferreira de Oliveira 4,15 , Álvaro Pereira 1, Wilson Abreu 16
and Carlos Alberto da Cruz Sequeira 16,*
1 Escola de Enfermagem, Universidade Federal da Bahia, Salvador 40231-300, BA, Brazil;[email protected] (A.R.d.S.); [email protected] (M.B.S.); [email protected] (É.S.A.);[email protected] (I.F.M.A.); [email protected] (J.C.d.S.);[email protected] (Á.P.)
2 Departamento de Saúde, Universidade Estadual de Feira de Santana, Feira de Santana 44001-970, BA, Brazil;[email protected] (J.R.B.T.); [email protected] (S.D.d.S.); [email protected] (E.S.d.S.C.);[email protected] (T.M.d.A.)
3 Escola Bahiana de Medicina e Saúde Pública, Salvador 40290-000, BA, Brazil; [email protected] Escola de Enfermagem, Universidade de São Paulo, Sao Paulo 05403-000, SP, Brazil;
[email protected] (W.C.M.); [email protected] (S.B.); [email protected] (M.A.F.d.O.)5 Coordenação de Saúde do Adolescente, Jovem e Homem, Diretoria Técnica, Secretaria de Saúde,
Prefeitura Municipal de Ananindeua, Ananindeua 67130-600, PA, Brazil6 Escola de Enfermagem de Ribeirão Preto, Universidade de São Paulo, Ribeirao Preto 14040-902, SP, Brazil;
[email protected] Faculdade Estácio de Alagoinhas, Alagoinhas 48010-970, BA, Brazil; [email protected] Faculdade de Enfermagem, Universidade Federal do Pará, Belem 66075-110, PA, Brazil; [email protected] Departamento de Ciências da Vida, Universidade do Estado da Bahia, Salvador 1150-000, BA, Brazil;
[email protected] Secretaria de Ciência, Tecnologia e Inovação, Salvador 41745-004, BA, Brazil; [email protected] Curso de Psicologia, Campus Ribeirão, Universidade de Ribeirão Preto, Ribeirao Preto 11440-003, SP, Brazil;
[email protected] Escola de Enfermagem, Universidade Federal do Rio Grande, Rio Grande 96201-900, RS, Brazil;
[email protected] Departamento de Enfermagem, Universidade Federal do Rio Grande do Norte, Natal 59012-300, RN, Brazil;
[email protected] Instituto de Saúde Coletiva, Universidade Federal da Bahia, Salvador 40110-040, BA, Brazil;
[email protected] Programa de Pós-Graduação em Enfermagem, Centro de Ciências da Saúde,
Universidade Federal de Santa Maria, Santa Maria 97105-900, RS, Brazil16 Centro de Investigação em Tecnologias e Serviços de Saúde, Escola Superior de Enfermagem do Porto,
4200-072 Porto, Portugal; [email protected]* Correspondence: [email protected]
Abstract: Objective: To analyze the relationships between sociodemographic variables, intoleranceto uncertainty (INT), social support, and psychological distress (i.e., indicators of Common MentalDisorders (CMDs) and perceived stress (PS)) in Brazilian men during the COVID-19 pandemic.Methods: A cross-sectional study with national coverage, of the web survey type, and conducted with1006 Brazilian men during the period of social circulation restriction imposed by the health authoritiesin Brazil for suppression of the coronavirus and control of the pandemic. Structural equation modelinganalysis was performed. Results: Statistically significant direct effects of race/skin color (λ = 0.268;p-value < 0.001), socioeconomic status (SES) (λ = 0.306; p-value < 0.001), household composition
Int. J. Environ. Res. Public Health 2022, 19, 350. https://doi.org/10.3390/ijerph19010350 https://www.mdpi.com/journal/ijerph
Int. J. Environ. Res. Public Health 2022, 19, 350 2 of 19
(λ = 0.281; p-value < 0.001), PS (λ = 0.513; p-value < 0.001), and INT (λ = 0.421; p-value < 0.001) wereevidenced in the occurrence of CMDs. Black-skinned men with higher SES, living alone, and withhigher PS and INT levels presented higher prevalence values of CMDs. Conclusions: High levels ofPS and INT were the factors that presented the strongest associations with the occurrence of CMDsamong the men. It is necessary to implement actions to reduce the stress-generating sources as wellas to promote an increase in resilience and the development of intrinsic reinforcements to deal withuncertain threats.
Keywords: men’s health; COVID-19; mental disorders; stress; psychological; social support
1. Introduction
The health crisis caused by COVID-19 exerted a negative impact on the mental healthof the world’s population. The experience of unknown situations and the fear of contam-ination imposed by the burden of the disease and its repercussions produced new dailystressors and exacerbated previous ones already structurally present in societies [1–4].Together, these factors generate continuous situations of suffering and contribute to theincrease in psychological distress, as evidenced by indicators of Common Mental Disorders(CMDs) and perceived stress [5–7]. While the former refer to a set of symptoms, such asfatigue, insomnia, irritability, problems concentrating, and somatizations [5–8], the latterinvolves feelings about the uncontrollable and unpredictable nature of everyday eventsand the individual assessment of the ability to face such questions [4,5].
It is estimated that nearly one billion people are affected by some mental disorder dueto the pandemic, with an emphasis on symptoms of anxiety, anguish and depression, anddisorders resulting from alcohol use and substance abuse in addition to the increase insuicide rates [1–6]. The deleterious effects caused by the pandemic have been measured andshow a reduction in life expectancy at birth, in the ability to work, and in absenteeism andpresentism in addition to growth in unemployment and informality. Jointly, these situationsinstall contexts that culminate in massive mental ailments in the male population [9–13].
The rapid spread of COVID-19, associated with the need for social distancing, forcedquarantine, and blockades across the world, has placed imposed high stress levels onpeople [14,15], and sustaining these measures has increased the prevalence of CMDs in thepopulations [16,17], contributing to the increase in depressive and anxiety disorders, identi-fied by the WHO as the most common psychiatric diseases in the world’s population [18,19].Studies carried out prior to the COVID-19 pandemic identified high prevalences of CMDin men in Brazil, which ranged from 11.1% [20,21].
Consequently, the COVID-19 pandemic resulted in a psychologically chaotic and dis-mal setting. The radical changes in the individuals’ daily routines and the general context offear and insecurity converge to unfamiliar situations and significant uncertainties that, dueto their persistence over time, also provoke reactions of intolerance to this uncertainty [5,7].Intolerance to uncertainty is described as the predisposition of an individual to consider thepossibility of a negative event occurring regardless of the possibility of its actual occurrenceas unacceptable [1,2].
Thus, intolerance to uncertainty is considered as one of the main underlying compo-nents of anxiety disorders [22], obsessive compulsive disorder (OCD) [23], post-traumaticstress disorder in depression [24], depression [25], and panic disorder [26]. Thus, inabilityto cope with uncertainty can be a negative predictor for well-being [27].
Social support is a basic human need and an important moderator of the impactsof the high psychological demands related to the COVID-19 pandemic. High social sup-port has a protective effect and mitigates the negative impacts of stress on physical andpsychological well-being [28]. Thus, the social support received during the pandemic isable to provide positive reinforcement to deal with stressful situations and prevent theoccurrence/worsening of CMD.
Int. J. Environ. Res. Public Health 2022, 19, 350 3 of 19
In addition, there is evidence that CMDs are associated with social inequalities, asindividuals in unfavorable socioeconomic conditions (e.g., black individuals, low income,and low level of education) are in a situation of greater vulnerability due to the constantexperience of the feeling of insecurity, hopelessness, and risk of violence [29–31]. Thesesensations were possibly exacerbated by the COVID-19 pandemic, which supports theneed to verify this association in men in Brazil, a country known to be marked by socialinequalities and inequities.
Similarly, higher prevalence of CMD has been observed in people who live alone [32].Overall, the loneliness of living alone largely explains the association with CMD [32]. Dueto the need for social isolation to prevent and control COVID-19, people who live alone areeven more susceptible to loneliness, which represents an increase in the potential risk forthe development of CMD.
Epidemiological indicators, such as the number of new cases, the rates and lengthof hospital stay, the unfavorable outcomes of the disease, and the number of deaths haveshown that the male population has been more impacted, evidencing that being a man is arisk factor for COVID-19 [33,34]. However, these results are restricted to the physical dimen-sion of the disease and hardly advance the analysis of the mental health dimension [35,36].
In addition to that, population-based studies investigating the mental health situationin the context of the pandemic have included predominantly female samples [37–39],which limits a more comprehensive identification of the magnitude of the problem and,consequently, restricts the adoption of coping measures to a specific audience. In thiscontext, this study contributes to overcoming this gap in scientific knowledge based on theresearch and appreciation of aspects related to the male population, which permeate thesubjectivities and the social, symbolic, psychological, and psycho-emotional constructionsof the population and their repercussions on health [40,41].
Given the above, it is considered crucial to give visibility to the mental health ofmale populations and to the aspects associated with the occurrence of mental disorders tostrengthen the confrontation of the life dimensions affected by the pandemic in addition tocontributing to overcoming this moment of profound health and social crisis generated bythe dissemination of COVID-19.
Thus, this study aimed at analyzing the relationships between sociodemographicvariables, intolerance to uncertainty (INT), social support, and psychological distress, thatis, indicators of Common Mental Disorders (CMDs) and perceived stress (PS), in Brazilianmen during the COVID-19 pandemic.
2. Methods2.1. Type of Study
A cross-sectional study with national coverage, of the web survey type, and carriedout during the period of social circulation restriction imposed by the health authorities inBrazil for suppression of the coronavirus and control of the pandemic.
2.2. Sample and Participants
The sample was estimated at 923 participants, considering the population of64,520,660 Brazilian men with Internet access [42], 50% prevalence estimate, 95% con-fidence level, 5% precision, 80% power, effect of study design of two, and a 20% increasefor losses.
The snowball technique [43] was used to recruit the participants through digital socialnetworks (Facebook®, Instagram®, WhatsApp®, Grindr®). This is a non-probabilisticsampling technique performed by means of reference chains, where the first eligible andrecruited participants invite new participants from their network of contacts (family, friendsand acquaintances) who, in turn, indicate new participants and so on successively, until theestimated sample is minimally reached.
Initially, 25 participants were recruited, five from each of the Brazilian regions, whowere called seeds. These participants were encouraged to send the research link to other
Int. J. Environ. Res. Public Health 2022, 19, 350 4 of 19
men from their contact networks. At the end, 27 seeds were recorded, one from each of theBrazilian states.
The inclusion criteria adopted were as follows: being digitally literate to access theInternet and being at least 18 years old. The individuals excluded were those non-residents,in Brazil, or who were in the country at the time of data collection.
2.3. Procedures, Measurements, Variables and Outcome
For data collection, a questionnaire that was structured in blocks was used, includingthe following:
(a) Sociodemographic characteristics: sexual identity, age, schooling, self-reportedrace/skin color, house-sharing or not, work situation, and use of health plans;
(b) Common Mental Disorders (CMDs): the Self-Reporting Questionnaire (SRQ-20)was used to screen CMDs. SRQ-20 is validated for use in Brazil with satisfactory per-formance indicators [44–46]. It consists of 20 items with dichotomous answer categories(0—no; 1—yes). The cutoff point for men is at least five positive answers [47];
(c) Perceived Stress level: the ten-item version of the Perceived Stress Scale (PSS-10) [47], cross-culturally adapted [48] and validated for use in the Brazilian population [49],was used. The items have five-point Likert-type answer options (0 = never, 1 = almost never,2 = sometimes, 3 = almost always, 4 = always) and are distinguished in questions withpositive and negative connotations, thus inverting the score of the positive questions. Theperceived stress score is calculated by the sum of the scores obtained in the ten items [47,48].The levels were categorized as low (from zero to 13 points), moderate (from 14 to 26 points),and high (27 points or more) [50];
(d) Level of intolerance to uncertainty: the Intolerance of Uncertainty Scale (IUS) [51],12-item version (IUS-12) [52], cross-culturally adapted [53] and validated for use in theBrazilian population [54], was applied. The items contain answer options arranged in aLikert scale, varying from one (not at all characteristics) to five (very characteristic) andassessing two dimensions: prospective IU (seven items) and inhibitory IU (five items). Thevalidation study in Brazil evidenced a two-factor structure with high correlation betweenthem (0.83) [55], which can indicate the existence of a higher-order factor (intolerance touncertainty) [24,56]. The literature published to the present day indicates diverse evidenceof the one-factor solution of intolerance to uncertainty as well as the use of its overallscore [57,58]. The higher the score, the greater the level of intolerance to uncertainty. TheIUS-12 latent construct showed adequate internal consistency (α = 0.89;ω = 0.89);
(e) Level of social support: the instrument used was the 2-Way Social Support Scale(2-WSSS) [58], 20-item version, transculturally adapted and validated in Brazil [59]. 2-WSSSassesses four social support dimensions: (1) receiving emotional support (seven items);(2) receiving instrumental support (four items); (3) offering emotional support (four items);and (4) offering instrumental support (five items). The items are answered in a Likert scale,varying from zero (it never applies) to five (it always applies). Higher scores indicate higherlevels of social support. In this study, 2-WSSS presented satisfactory internal consistency(α = 0.85;ω = 0.96).
The self-reporting questionnaire was elaborated in a specific data-collection platformand made available through the Internet. From then onwards, it was widely publicizedon Facebook®, Instagram®, WhatsApp®, and Grindr® digital social networks by fivetrained researchers for autonomous and voluntary adherence as well as by making adirect invitation to the individuals who met the eligibility criteria. The data were collectedbetween May and September 2020. The participants had access to the questionnaire afterreading and signing the free and informed consent form and thus agreeing to participate inthe study. Before each block of questions, the necessary information to answer them weremade available as well as the option not to answer any question. The instructions aboutthe recall period for each instrument were clarified.
Int. J. Environ. Res. Public Health 2022, 19, 350 5 of 19
2.4. Conceptual Framework and Study Hypotheses
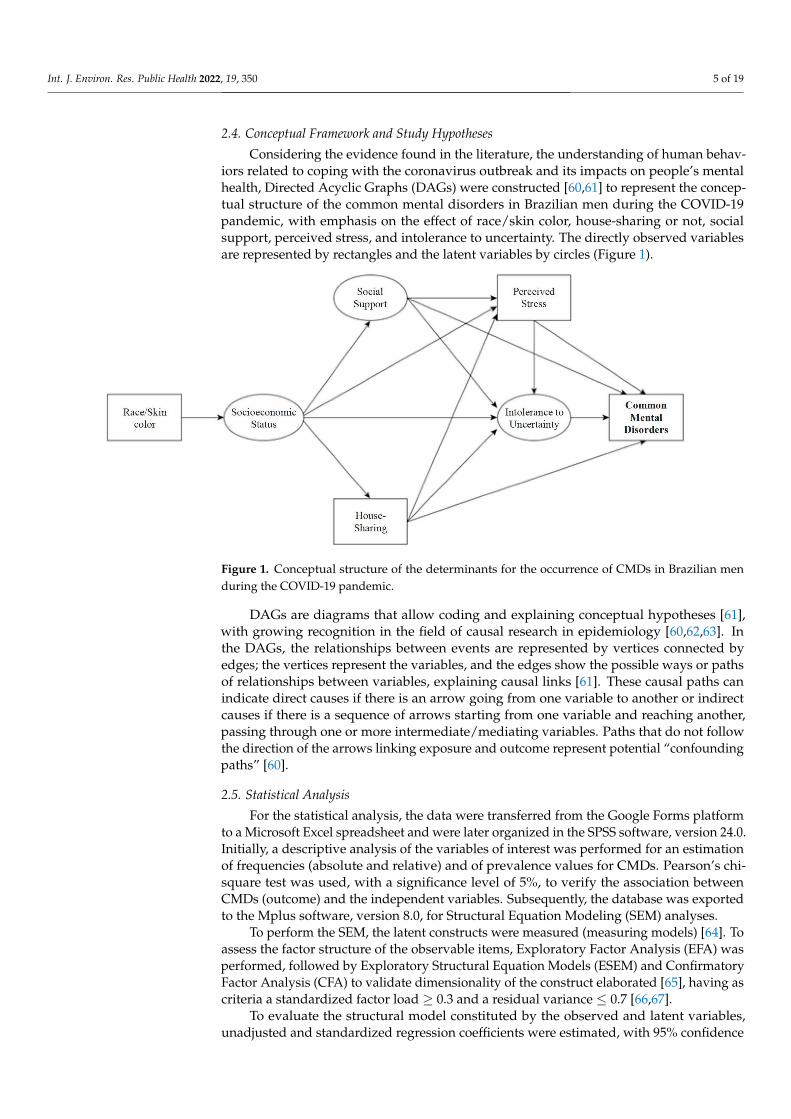
Considering the evidence found in the literature, the understanding of human behav-iors related to coping with the coronavirus outbreak and its impacts on people’s mentalhealth, Directed Acyclic Graphs (DAGs) were constructed [60,61] to represent the concep-tual structure of the common mental disorders in Brazilian men during the COVID-19pandemic, with emphasis on the effect of race/skin color, house-sharing or not, socialsupport, perceived stress, and intolerance to uncertainty. The directly observed variablesare represented by rectangles and the latent variables by circles (Figure 1).
Figure 1. Conceptual structure of the determinants for the occurrence of CMDs in Brazilian menduring the COVID-19 pandemic.
DAGs are diagrams that allow coding and explaining conceptual hypotheses [61],with growing recognition in the field of causal research in epidemiology [60,62,63]. Inthe DAGs, the relationships between events are represented by vertices connected byedges; the vertices represent the variables, and the edges show the possible ways or pathsof relationships between variables, explaining causal links [61]. These causal paths canindicate direct causes if there is an arrow going from one variable to another or indirectcauses if there is a sequence of arrows starting from one variable and reaching another,passing through one or more intermediate/mediating variables. Paths that do not followthe direction of the arrows linking exposure and outcome represent potential “confoundingpaths” [60].
2.5. Statistical Analysis
For the statistical analysis, the data were transferred from the Google Forms platformto a Microsoft Excel spreadsheet and were later organized in the SPSS software, version 24.0.Initially, a descriptive analysis of the variables of interest was performed for an estimationof frequencies (absolute and relative) and of prevalence values for CMDs. Pearson’s chi-square test was used, with a significance level of 5%, to verify the association betweenCMDs (outcome) and the independent variables. Subsequently, the database was exportedto the Mplus software, version 8.0, for Structural Equation Modeling (SEM) analyses.
To perform the SEM, the latent constructs were measured (measuring models) [64]. Toassess the factor structure of the observable items, Exploratory Factor Analysis (EFA) wasperformed, followed by Exploratory Structural Equation Models (ESEM) and ConfirmatoryFactor Analysis (CFA) to validate dimensionality of the construct elaborated [65], having ascriteria a standardized factor load ≥ 0.3 and a residual variance ≤ 0.7 [66,67].
To evaluate the structural model constituted by the observed and latent variables,unadjusted and standardized regression coefficients were estimated, with 95% confidence
Int. J. Environ. Res. Public Health 2022, 19, 350 6 of 19
intervals (95%CI) and p-value < 0.05. The size of the direct, indirect, and total effects wereclassified as follows: weak/small (around 0.10), moderate/medium (close to 0.30), andstrong/big (>0.50) [68].
The Weighted Least-Squares Means and Variance Adjusted (WLSMV) estimator wasused as a function of the modeling with categorical data. To re-specify the model, theModification Indices (MI ≥ 10) and the Expected Parameter Changes (EPC ≥ 0.25) wereassessed [69]. To assess fit of the models, the Root Mean-Square Error of Approximation(RMSEA > 0.06—exceptionally < 0.08, with a 90% confidence interval below 0.08) [69],the Comparative Fit Index (CFI ≥ 0.95), and the Tucker–Lewis Index (TLI ≥ 0.95) wereadopted [68].
2.6. Ethical Considerations
Ethical approval regarding this study was obtained from the institutional ethics com-mittee (decision: 4,087,611; CAAE: 32889420.9.0000.5531). All the participants in this studywere only included after informed consent had been obtained from them. All proceduresperformed in this study were compatible with the ethical standards of the institutionalresearch committee and with those of the Declaration of Helsinki and its comparableethical standards.
3. Results
The study participants were 1006 men. The predominant profile included non-heterosexuals (54.1%), aged from 29 to 39 years old (45.1%), higher education (73.8%),black-skinned individuals (59.2%), without a partner (67.3%), with monthly income up totwo minimum wages (41.6%), living with family members/friends (76.6%), and workers(75.0%). A high proportion of people depending exclusively on SUS care and services wasobserved (41.9%) (Table 1).
Table 1. Sociodemographic and occupational characteristics and prevalence of CMD in Brazilian menduring the COVID-19 pandemic. Brazil, 2020. (N = 1.006).
Variables N % N p p-Value
Sexual identity (N = 945)Heterosexual 434 45.9 228 52.5 0.785
Non-heterosexual 511 54.1 273 53.4Age group
18 to 28 years old 314 31.2 197 62.7 <0.00129 years old to 39 years old 454 45.1 257 56.6
40 years or more 238 23.7 92 38.7Education
Elementary/high school 264 26.2 146 55.3 0.696University education 742 73.8 400 53.9
Race/color (N = 1.001)White 376 37.4 197 52.4 0.247Yellow 19 1.9 11 57.9Brown 397 39.5 211 53.1Black 196 19.5 116 59.2
Indigenous 13 1.3 10 76.9Marital statusWith partner 329 32.7 152 46.2 <0.001No partner 677 67.3 394 58.2
Monthly income *Up to 2 salaries 418 41.6 203 56.4 0.0833 to 4 salaries 228 22.7 109 47.8
5 salaries or more 360 35.8 234 56.0Who they reside with (N = 1.005)
Int. J. Environ. Res. Public Health 2022, 19, 350 7 of 19
Table 1. Cont.
Variables N % N p p-Value
Family/Friend(s) 770 76.6 409 53.1 0.163Alone 235 23.4 137 59.3
Work situationIt works 755 75.0 397 52.6 0.062
Does not work 251 25.0 149 59.4Use of health planExclusively SUS 376 37.4 207 55.1 0.040
SUS and private plan 369 36.7 214 58.0Exclusively private plan 261 25.9 125 47.9
Perceived stressLow 223 22.2 26 11.7 <0.001
Moderate 613 60.9 363 59.2High 170 16.9 157 92.4
Uncertainty intoleranceLow 327 32.5 79 24.2 <0.001
Moderate 317 31.5 169 53.3High 362 36.0 298 82.3
Receive social supportHigh 371 36.9 160 43.1 <0.001
Moderate 309 30.7 167 54.0Low 326 32.4 219 67.2
Give social supportLow 334 33.2 186 55.7 0.765
Moderate 275 27.3 145 52.7High 397 39.5 215 54.2
p, prevalence; SUS, public health system. * Minimum wage in force in the period of data collection: R$ 1045,00.
The overall prevalence of CMDs was 54.3%. Higher prevalence of CMDs was observedamong the youngest individuals (62.7%), those with lower schooling (55.3%), black-skinned(55.1%), without a partner (58.2%), and among those who lived alone (58.3%), did not work(59.4%), had high levels of stress (92.4%), intolerance to uncertainty (82.3%), and receivedlow social support (67.2%). The moderate stress levels reached 60.9%, while 36.0% reportedhigh levels of intolerance to uncertainty. Receiving high social support was mentioned by36.9% and offering high social support by 39.5% (Table 1).
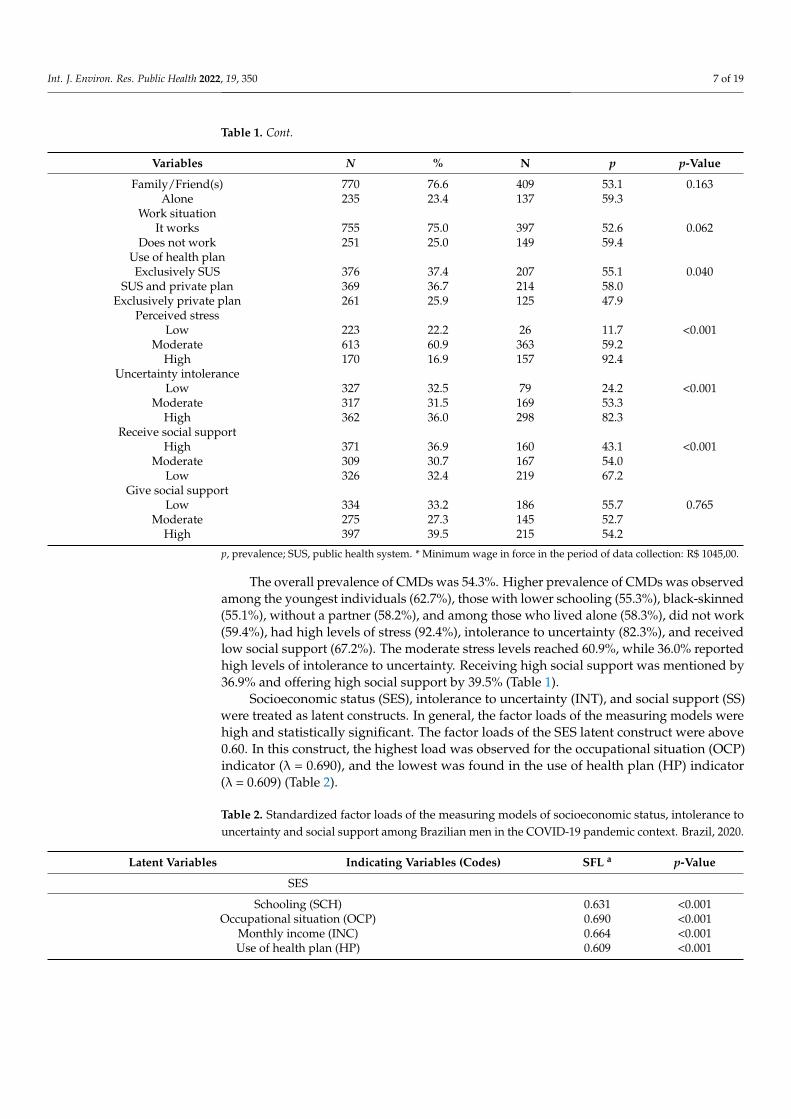
Socioeconomic status (SES), intolerance to uncertainty (INT), and social support (SS)were treated as latent constructs. In general, the factor loads of the measuring models werehigh and statistically significant. The factor loads of the SES latent construct were above0.60. In this construct, the highest load was observed for the occupational situation (OCP)indicator (λ = 0.690), and the lowest was found in the use of health plan (HP) indicator(λ = 0.609) (Table 2).
Table 2. Standardized factor loads of the measuring models of socioeconomic status, intolerance touncertainty and social support among Brazilian men in the COVID-19 pandemic context. Brazil, 2020.
Latent Variables Indicating Variables (Codes) SFL a p-Value
SES
Schooling (SCH) 0.631 <0.001Occupational situation (OCP) 0.690 <0.001
Monthly income (INC) 0.664 <0.001Use of health plan (HP) 0.609 <0.001
Int. J. Environ. Res. Public Health 2022, 19, 350 8 of 19
Table 2. Cont.
Latent Variables Indicating Variables (Codes) SFL a p-Value
INT
Uncertainty prevents me from living a full life (I1) 0.747 <0.001I profoundly loathe unforeseen events (I2) 0.710 <0.001
I feel frustrated when I don’t have all the information I need (I3) 0.669 <0.001It is necessary to think about the future to avoid surprises (I4) 0.393 <0.001
A small unforeseen event can ruin everything, even with the best planning (I5) 0.749 <0.001When it’s time to act, uncertainty paralyzes me (I6) 0.620 <0.001
Uncertainty makes me vulnerable (I7) 0.754 <0.001I always want to know what the future will bring me (I8) 0.611 <0.001
I hate to be taken by surprise (I9) 0.610 <0.001The slightest sign of doubt dissuades me from acting (I10) 0.678 <0.001I should be able to organize everything beforehand (I11) 0.634 <0.001
Uncertainty does not allow me to sleep well (I12) 0.694 <0.001
Receiving
I have someone I can talk to about the pressures in my life (S1) 0.838 <0.001There is at least one person with whom I can share most of the things (S2) 0.838 <0.001
When I’m feeling down, there’s someone I can count on (S3) 0.907 <0.001I have someone in my life who offers me emotional support (S4) 0.899 <0.001
There is at least one person in whom I feel I can trust (S5) 0.820 <0.001There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001
I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS
If I’m in trouble, someone will help me (S13) 0.845 <0.001I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS
I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001I seek to encourage people when they’re feeling down (S9) 0.723 <0.001
People close to me tell me their deepest concerns (S10) 0.710 <0.001I comfort other people in difficult times (S11) 0.867 <0.001
People trust me when they have problems (S12) 0.737 <0.001
OES
I help others when they are too busy (S17) 0.685 <0.001I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001
I provided help when someone who lived with me was ill (S19) 0.588 <0.001I’m a person whom others ask for help with tasks (S20) 0.401 <0.001
RS a
RES b 0.882 <0.001RIS b 0.949 <0.001
Offering
OIS b 0.857 <0.001OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emo-tional support; RIS, receiving instrumental support; OIS, offering instrumental support; OES, offering emotionalsupport; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
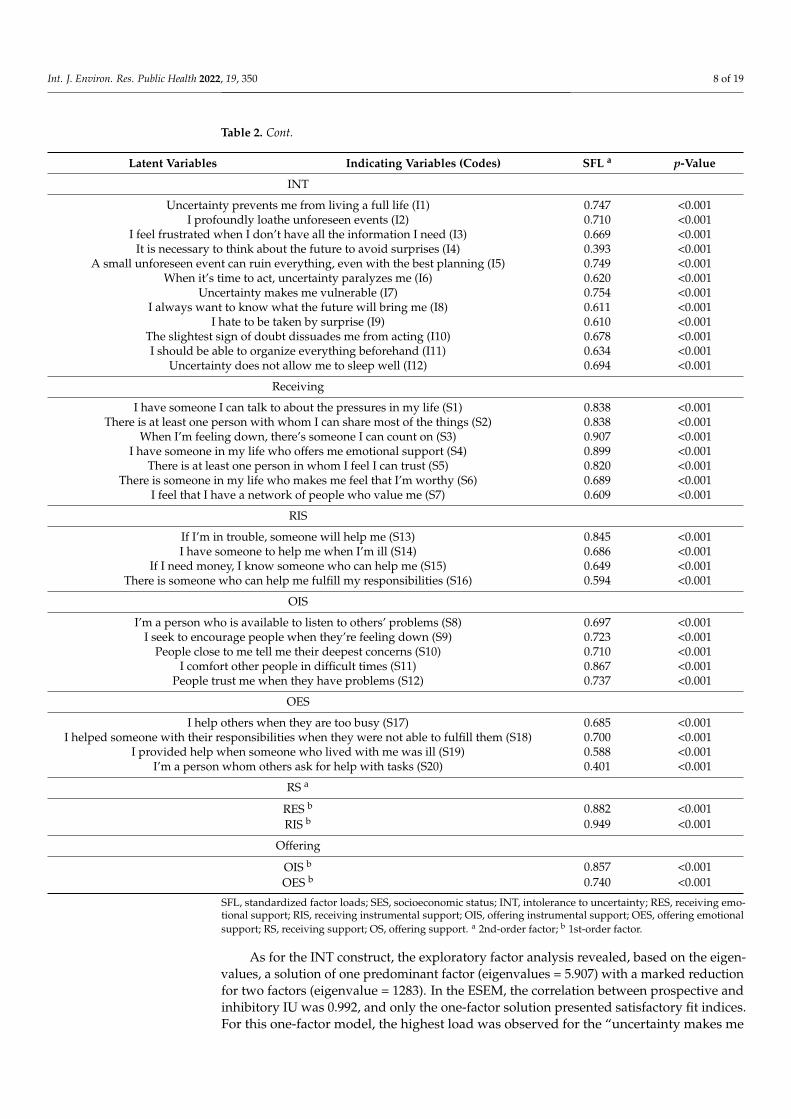
As for the INT construct, the exploratory factor analysis revealed, based on the eigen-values, a solution of one predominant factor (eigenvalues = 5.907) with a marked reductionfor two factors (eigenvalue = 1283). In the ESEM, the correlation between prospective andinhibitory IU was 0.992, and only the one-factor solution presented satisfactory fit indices.For this one-factor model, the highest load was observed for the “uncertainty makes me

Int. J. Environ. Res. Public Health 2022, 19, 350 9 of 19
vulnerable” item (I7) (λ = 0.754) and the lowest one for “it is necessary to think about thefuture to avoid surprises” (I4) (λ = 0.393) (Table 2).
The SS measuring model was initially evaluated by the indicators of the first-orderfactors: receiving emotional support (RES), receiving instrumental support (RIS), offeringemotional support (OES), and offering instrumental support (OIS), all with high factorloads and statistically significant. For RES and RIS, the highest loads were observed for theitems “when I’m feeling down, there’s someone I can count on” (S3) (λ = 0.907) and “if I’min trouble someone will help me” (S13) (λ = 0.845) and the lowest ones for “I feel I have anetwork of people who value me” (S7) (λ = 0.609) and “there’s someone who can help mefulfill my responsibilities” (S16) (λ = 0.594), respectively. For GES and GIS, greater burdenswere verified for “I helped someone with their responsibilities when they were not able tofulfill them” (S18) (λ = 0.700) and “I comfort other people in difficult times” (S11) (λ = 0.867)and lower ones for “I’m a person whom others ask for help with tasks” (S20) (λ = 0.401) and“I’m a person available to listen to others’ problems” (S8) (λ = 0.697), respectively. The highcorrelation between the constructs of receiving (r = 0.832) and offering (r = 0.864) supportendorsed the existence of the respective second-order factors called receiving support (RS)and offering support (OS), without a significant residual correlation (r = 0.430) (Table 2).
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-orderfactors of the SS model and in the model considering the correlations between all the latentvariables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
OS) CMM
RMSEAIndex 0.038 0.049 0.046 0.046
90% CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048p-Value 0.671 0.518 0.939 0.998
CFI 0.997 0.992 0.959 0.976TLI 0.991 0.986 0.950 0.974R a
RS
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
OS - - 0.430 -SES
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
INT - - - −0.098SES
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
RS - - - −0.019SES
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
OS - - - −0.033INT
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
RS - - - −0.325INT
Int. J. Environ. Res. Public Health 2022, 18, x FOR PEER REVIEW 9 of 20
I have someone in my life who offers me emotional support (S4) 0.899 <0.001 There is at least one person in whom I feel I can trust (S5) 0.820 <0.001
There is someone in my life who makes me feel that I’m worthy (S6) 0.689 <0.001 I feel that I have a network of people who value me (S7) 0.609 <0.001
RIS If I’m in trouble, someone will help me (S13) 0.845 <0.001 I have someone to help me when I’m ill (S14) 0.686 <0.001
If I need money, I know someone who can help me (S15) 0.649 <0.001 There is someone who can help me fulfill my responsibilities (S16) 0.594 <0.001
OIS I’m a person who is available to listen to others’ problems (S8) 0.697 <0.001
I seek to encourage people when they’re feeling down (S9) 0.723 <0.001 People close to me tell me their deepest concerns (S10) 0.710 <0.001
I comfort other people in difficult times (S11) 0.867 <0.001 People trust me when they have problems (S12) 0.737 <0.001
OES I help others when they are too busy (S17) 0.685 <0.001
I helped someone with their responsibilities when they were not able to fulfill them (S18) 0.700 <0.001 I provided help when someone who lived with me was ill (S19) 0.588 <0.001
I’m a person whom others ask for help with tasks (S20) 0.401 <0.001 RS a
RES b 0.882 <0.001 RIS b 0.949 <0.001
Offering OIS b 0.857 <0.001 OES b 0.740 <0.001
SFL, standardized factor loads; SES, socioeconomic status; INT, intolerance to uncertainty; RES, receiving emotional support; RIS, receiving instrumental support; OIS, offering instrumental sup-port; OES, offering emotional support; RS, receiving support; OS, offering support. a 2nd-order factor; b 1st-order factor.
The SES, INT, and SS measuring models obtained satisfactory fit indices. The evalu-ation of the correlations between these latent constructs, both between the second-order factors of the SS model and in the model considering the correlations between all the latent variables, evidenced adequate discriminant validity (r < 0.90) (Table 3).
Table 3. Fit indicators of the measuring models, using CMDs as response variable, Brazil, 2020.
Indices SES INT SS (RS OS) CMM RMSEA
Index 0.038 0.049 0.046 0.046 90%CI 0.000–0.078 0.040–0.059 0.041–0.050 0.043–0.048
p-Value 0.671 0.518 0.939 0.998 CFI 0.997 0.992 0.959 0.976 TLI 0.991 0.986 0.950 0.974 R a
RS OS - - 0.430 - SES INT - - - −0.098 SES RS - - - −0.019 SES OS - - - −0.033 INT RS - - - −0.325 INT OS - - - −0.067
OS - - - −0.067
SES, socioeconomic status; INT, intolerance to uncertainty; SS, social support; RS, receiving social support; OS,offering social support; CMM, Correlated Measuring Models; RMSEA, Root Mean Square Error of Approximation;90% CI, 90% confidence interval; TLI, Tucker–Lewis Index; CFI, Comparative Fit Index. a Residual correlations(1) between the latent variables.
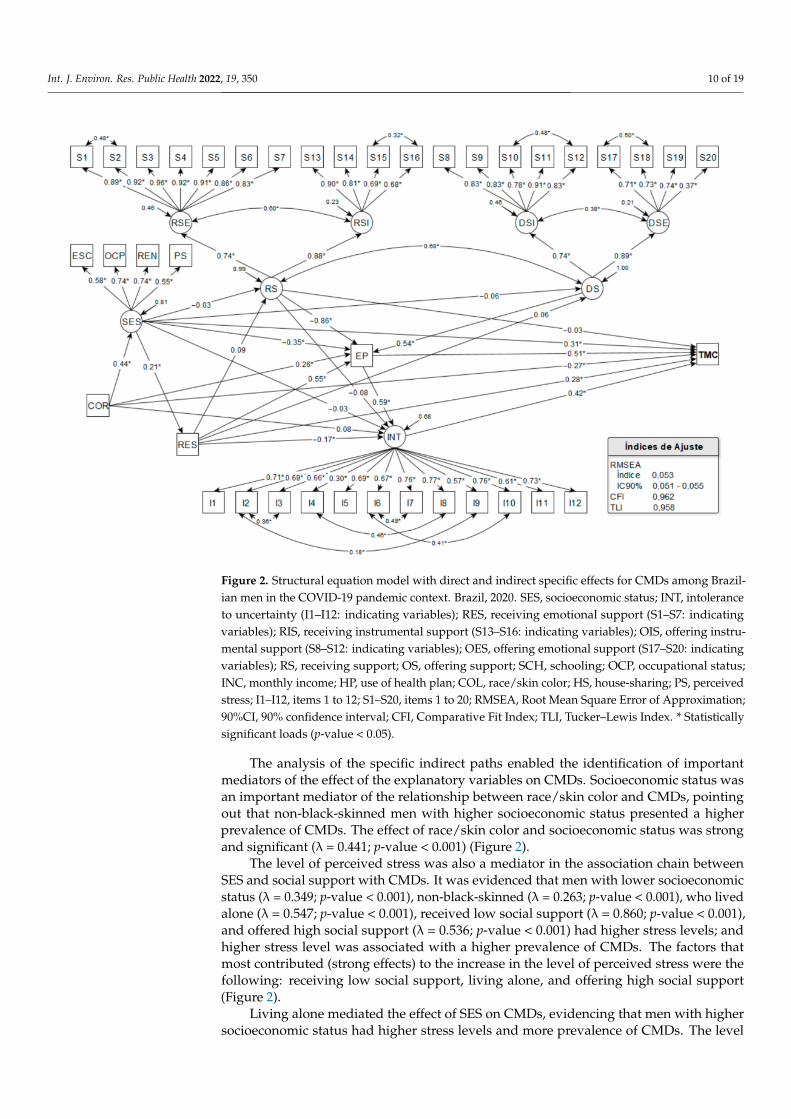
In the structural model, CMDs was considered as response variable. The SES, RS, OS,and INT latent variables and the self-reported race/color (COL), house-sharing (HS), andperceived stress (PS) observed variables were used as explanatory variables. The directeffects for CMDs were assessed for all the variables of the model, with the exception ofOS, and their structural inter-relationships were considered in the paths of specific indirecteffects. The estimated structural equation model presented adequate fit indices (Figure 2).
Statistically significant direct effects were evidenced with COL (λ = −0.268;p-value < 0.001), SES (λ = 0.306; p-value < 0.001), HS (λ = 0.281; p-value < 0.001), PS(λ = 0.513; p-value < 0.001), and INT (λ = 0.421; p-value < 0.001) for the CMDs. Thus,black-skinned men, those with higher socioeconomic status, living alone, and with higherlevels of stress and intolerance to uncertainty presented higher prevalence values of CMDs.There were strong effects of PS and INT and medium effects of the other variables, showingthat high levels of stress and intolerance to uncertainty were the factors with the strongestdirect associations with the prevalence of CMDs (Figure 2).
Int. J. Environ. Res. Public Health 2022, 19, 350 10 of 19
Figure 2. Structural equation model with direct and indirect specific effects for CMDs among Brazil-ian men in the COVID-19 pandemic context. Brazil, 2020. SES, socioeconomic status; INT, intoleranceto uncertainty (I1–I12: indicating variables); RES, receiving emotional support (S1–S7: indicatingvariables); RIS, receiving instrumental support (S13–S16: indicating variables); OIS, offering instru-mental support (S8–S12: indicating variables); OES, offering emotional support (S17–S20: indicatingvariables); RS, receiving support; OS, offering support; SCH, schooling; OCP, occupational status;INC, monthly income; HP, use of health plan; COL, race/skin color; HS, house-sharing; PS, perceivedstress; I1–I12, items 1 to 12; S1–S20, items 1 to 20; RMSEA, Root Mean Square Error of Approximation;90%CI, 90% confidence interval; CFI, Comparative Fit Index; TLI, Tucker–Lewis Index. * Statisticallysignificant loads (p-value < 0.05).
The analysis of the specific indirect paths enabled the identification of importantmediators of the effect of the explanatory variables on CMDs. Socioeconomic status wasan important mediator of the relationship between race/skin color and CMDs, pointingout that non-black-skinned men with higher socioeconomic status presented a higherprevalence of CMDs. The effect of race/skin color and socioeconomic status was strongand significant (λ = 0.441; p-value < 0.001) (Figure 2).
The level of perceived stress was also a mediator in the association chain betweenSES and social support with CMDs. It was evidenced that men with lower socioeconomicstatus (λ = 0.349; p-value < 0.001), non-black-skinned (λ = 0.263; p-value < 0.001), who livedalone (λ = 0.547; p-value < 0.001), received low social support (λ = 0.860; p-value < 0.001),and offered high social support (λ = 0.536; p-value < 0.001) had higher stress levels; andhigher stress level was associated with a higher prevalence of CMDs. The factors thatmost contributed (strong effects) to the increase in the level of perceived stress were thefollowing: receiving low social support, living alone, and offering high social support(Figure 2).
Living alone mediated the effect of SES on CMDs, evidencing that men with highersocioeconomic status had higher stress levels and more prevalence of CMDs. The level

Int. J. Environ. Res. Public Health 2022, 19, 350 11 of 19
of intolerance to uncertainty was also an important effect mediator: men who lived withfamily members/friends (λ = 0.170; p-value = 0.021), notably non-black-skinned and thosewith higher socioeconomic status, had a higher level of intolerance to uncertainty andhigher prevalence of CMDs. Intolerance to uncertainty also mediated the effect of perceivedstress on CMDs, indicating that men with higher stress levels, especially those with lowersocioeconomic status, non-black-skinned, who lived alone and with low levels of receivingsocial support, and high levels of offering social support, had higher levels of intoleranceto uncertainty (λ = 0.592; p-value < 0.001), resulting in a higher prevalence of CMDs. Thefactor that most contributed to the increase in intolerance to uncertainty was the high levelof perceived stress, with a strong and significant effect (Figure 2).
The greatest total effects in CMDs were observed for higher level of perceived stress(λ = 0.763; p-value < 0.001), receiving low social support (λ = 0.716; p-value < 0.001), livingalone (λ = 0.587; p-value < 0.001), high intolerance to uncertainty (λ = 0.421; p-value < 0.001),and high social support (λ = 0.409; p-value < 0.001), all strong and significant. There wasa small overall effect of socioeconomic status (λ = 0.183; p-value < 0.001), but the indirecteffects, mediated by high levels of perceived stress and intolerance to uncertainty, wererobust and significant (Table 4).
Table 4. Standardized total and indirect effects of the structural equation model, using CMDs asresponse variable among Brazilian men in the COVID-19 pandemic context. Brazil, 2020.
Paths SFL SE Est/SE a p-Value b
Total Effects
INT→ CMDs 0.421 0.047 8.87 <0.001RS→ CMDs −0.716 0.051 −14.12 <0.001OS→ CMDs 0.409 0.021 19.11 <0.001SES→ CMDs 0.183 0.043 4.21 <0.001PS→ CMDs 0.763 0.039 19.46 <0.001
COL→ CMDs −0.021 0.040 −0.53 0.595HS→ CMDs 0.587 0.035 16.75 <0.001
Specific indirect effects
RS
RS→ PS→ CMDs −0.442 0.039 −11.46 <0.001RS→ INT→ CMDs −0.032 0.025 −1.31 0.190
RS→ PS→ INT→ CMDs −0.214 0.037 −5.84 <0.001
OS
OS→ PS→ CMDs 0.275 0.012 23.48 <0.001OS→ PS→ INT→ CMDs 0.134 0.022 5.97 <0.001
SES
SES→ HS→ CMDs 0.060 0.014 4.22 <0.001SES→ PS→ CMDs −0.179 0.036 −4.96 <0.001
SES→ INT→ CMDs 0.021 0.027 0.79 0.429SES→ RS→ CMDs 0.001 0.002 0.38 0.701
SES→ HS→ PS→ CMDs 0.060 0.014 4.22 <0.001SES→ RS→ PS→ CMDs 0.012 0.025 0.48 0.629SES→ OS→ PS→ CMDs −0.015 0.015 −1.00 0.318
SES→ HS→ INT→ CMDs −0.015 0.008 −1.88 0.060SES→ PS→ INT→ CMDs −0.087 0.022 −3.96 <0.001SES→ RS→ INT→ CMDs 0.001 0.002 0.49 0.625SES→ HS→ RS→ CMDs 0.001 0.001 −0.42 0.673
SES→ HS→ RS→ PS→ CMDs −0.008 0.006 −1.37 0.170SES→ HS→ OS→ PS→ CMDs 0.003 0.003 0.93 0.351SES→ HS→ PS→ INT→ CMDs 0.029 0.009 3.31 0.001
Int. J. Environ. Res. Public Health 2022, 19, 350 12 of 19
Table 4. Cont.
Paths SFL SE Est/SE a p-Value b
SES→ RS→ PS→ INT→ CMDs 0.006 0.012 0.48 0.629SES→ OS→ PS→ INT→ CMDs −0.007 0.008 −0.99 0.325SES→ HS→ RS→ INT→ CMDs −0.001 0.001 −1.06 0.289
SES→ HS→ RS→ PS→ INT→ CMDs −0.004 0.003 −1.37 0.171SES→ HS→ OS→ PS→ INT→ CMDs 0.002 0.002 0.92 0.356
PS
PS→ INT→ CMDs 0.249 0.040 6.22 <0.001
COL
COL→ PS→ CMDs 0.135 0.006 20.80 <0.001COL→ INT→ CMDs −0.034 0.019 −1.78 0.075COL→ SES→ CMDs 0.135 0.006 20.80 <0.001
COL→ SES→ HS→ CMDs 0.026 0.006 4.21 <0.001COL→ SES→ PS→ CMDs −0.079 0.016 −4.93 <0.001COL→ PS→ INT→ CMDs 0.066 0.011 5.92 <0.001
COL→ SES→ INT→ CMDs 0.009 0.012 0.79 0.429COL→ SES→ RS→ CMDs 0.000 0.001 0.38 0.702
COL→ SES→ HS→ PS→ CMDs 0.026 0.006 4.21 <0.001COL→ SES→ RS→ PS→ CMDs 0.005 0.011 0.48 0.629COL→ SES→ OS→ PS→ CMDs −0.007 0.007 −1.00 0.319
COL→ SES→ HS→ INT→ CMDs −0.007 0.004 −1.88 0.060COL→ SES→ PS→ INT→ CMDs −0.038 0.010 −3.95 <0.001COL→ SES→ RS→ INT→ CMDs 0.000 0.001 0.49 0.625COL→ SES→ HS→ RS→ CMDs 0.000 0.001 −0.42 0.673
COL→ SES→ HS→ RS→ PS→ CMDs −0.004 0.003 −1.37 0.170COL→ SES→ HS→ OS→ PS→ CMDs 0.001 0.002 0.93 0.351COL→ SES→ HS→ PS→ INT→ CMDs 0.013 0.004 3.30 0.001COL→ SES→ RS→ PS→ INT→ CMDs 0.003 0.005 0.48 0.629COL→ SES→ OS→ PS→ INT→ CMDs −0.003 0.003 −0.99 0.325COL→ SES→ HS→ RS→ INT→ CMDs 0.000 0.000 −1.06 0.289
COL→ SES→ HS→ RS→ PS→ INT→ CMDs −0.002 0.001 −1.37 0.171COL→ SES→ HS→ OS→ EP→ INT→ CMDs 0.001 0.001 0.92 0.356
HS
HS→ PS→ CMDs 0.281 0.012 23.79 <0.001HS→ INT→ CMDs −0.071 0.033 −2.17 0.030HS→ RS→ CMDs −0.002 0.006 −0.43 0.668
HS→ RS→ PS→ CMDs −0.038 0.026 −1.45 0.146HS→ OS→ PS→ CMDs 0.015 0.016 0.97 0.334HS→ PS→ INT→ CMDs 0.136 0.023 5.93 <0.001HS→ RS→ INT→ CMDs −0.003 0.003 −1.10 0.273
HS→ RS→ PS→ INT→ CMDs −0.019 0.013 −1.46 0.144HS→ OS→ PS→ INT→ CMDs 0.007 0.008 0.96 0.338
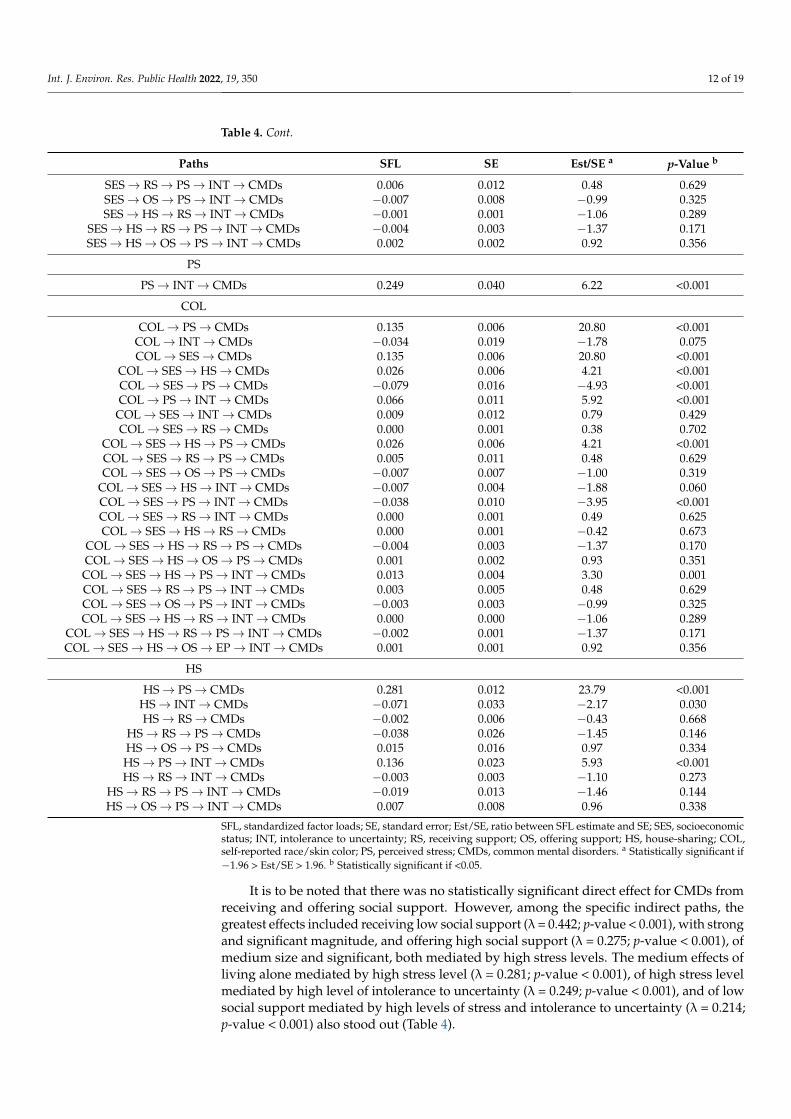
SFL, standardized factor loads; SE, standard error; Est/SE, ratio between SFL estimate and SE; SES, socioeconomicstatus; INT, intolerance to uncertainty; RS, receiving support; OS, offering support; HS, house-sharing; COL,self-reported race/skin color; PS, perceived stress; CMDs, common mental disorders. a Statistically significant if−1.96 > Est/SE > 1.96. b Statistically significant if <0.05.
It is to be noted that there was no statistically significant direct effect for CMDs fromreceiving and offering social support. However, among the specific indirect paths, thegreatest effects included receiving low social support (λ = 0.442; p-value < 0.001), with strongand significant magnitude, and offering high social support (λ = 0.275; p-value < 0.001), ofmedium size and significant, both mediated by high stress levels. The medium effects ofliving alone mediated by high stress level (λ = 0.281; p-value < 0.001), of high stress levelmediated by high level of intolerance to uncertainty (λ = 0.249; p-value < 0.001), and of lowsocial support mediated by high levels of stress and intolerance to uncertainty (λ = 0.214;p-value < 0.001) also stood out (Table 4).
Int. J. Environ. Res. Public Health 2022, 19, 350 13 of 19
4. Discussion
The study evidenced a high prevalence of CMDs in men, which corroborates otherfindings on the high rates of mental illness in the Brazilian population during the COVID-19pandemic [70,71]. In the pandemic context, no studies analyzing CMDs were identified,hindering comparisons. However, high prevalence values of sadness/depression, anxi-ety/nervousness, worsening of sleep problems, and panic syndrome were observed inBrazil during the pandemic [70,71]. These feelings experienced by men can be evokedto understand the high prevalence of CMD among them in the pandemic context sincethe instrument used to assess these minor mental disorders allows the identification ofsymptoms of anxious and depressive behavior, decreased energy, somatic symptoms, anddepressive mood [44–46].
In this study, the high prevalence of CMDs is more pronounced among black-skinnedmen, higher socioeconomic status, living alone, and higher levels of PS and INT, and theselast two factors are the ones most strongly associated with CMDs. Although OS has notpresented any direct effect, specific indirect effects, such as receiving low social supportand offering high social support, both mediated by high stress levels, were associatedwith CMDs.
The socioeconomic differences seem to exert an effect on the development of CMDsalthough the underlying mechanisms of that association are not yet well understood. Theeffect of higher socioeconomic status on the higher occurrence of CMDs is apparentlycontroversial to what is documented in the literature [72,73], but some aspects can beevoked to understand this finding in this context of the COVID-19 pandemic: (a) the studywas carried out in a virtual environment, which contributed to the lower access of men withlow socioeconomic status and possible underestimation of CMDs in this stratum; (b) menwith higher socioeconomic status may have a better perception of their mental healthstatus due to a better schooling level [72], reflecting higher CMDs rates in a self-reportingquestionnaire; (c) due to the restrictions imposed by the COVID-19 pandemic, men withhigher socioeconomic status may be experiencing, abruptly and suddenly, more financialdeprivation related to business and work, in social relationships, and in their life dynamics,situations that are already part of the daily lives of those with lower socioeconomic statuseven before the pandemic, and due to the absence of intrinsic reinforcement, they endup in mental distress; and (d) greater fear of poverty is associated with higher stress andanxiety levels among people with higher socioeconomic status during the pandemic, andmaintenance of these levels reflects in mental illness [74]. Thus, this finding needs to beresearched longitudinally in order to explore the possibilities of the causal link.
The “living alone” factor mediated the effect of SES on the CMDs so that those withhigher socioeconomic status presented higher stress levels and higher prevalence of CMDs.These two factors, mediated by the high PS and INT levels, presented considerable indirecteffects for CMDs. Living with family members/friends was related to a higher level ofintolerance to uncertainty and to more prevalence of CMDs. In this context, althoughmeasures of social distancing and quarantine of the population are important for reducingmorbidity and mortality due to COVID-19, their effects on the health of the population areundeniable. Regarding mental health, feelings and emotions, such as boredom, loneliness,anger, and sadness, can emerge not only because of the precautionary and control measuresimposed but also because of the perception of vulnerability to contagion and risk of illness,especially among those who live alone [75].
The PS and INT factors are very inter-related so that men with higher PS levels hadhigher INT levels, resulting in greater prevalence of CMDs. The PS level was influenced byseveral factors, such as lower socioeconomic status, non-black-skinned people, living alone,receiving low social support, and offering high social support. A study carried out withBrazilian parents also identified that PS was the variable most strongly related to the CMDsymptoms, showing that the higher the level of perceived stress, the greater the suspicionof these disorders [76]. Several factors have been associated with the occurrence of stressduring the pandemic, which include concern about physical health and precautionary and
Int. J. Environ. Res. Public Health 2022, 19, 350 14 of 19
disease control measures [76], anger and confusion arising from quarantine and socialdistancing [75], income reduction [75–77], fear of infection [75], and being part of a riskgroup for COVID-19 [77].
Regarding the socioeconomic situation of the men, the excess of demands, the fear ofincome loss, and the holding of the capital power may have contributed to increased stresslevels and, consequently, to a higher prevalence of CMDs. This association is an importantwarning sign to be included in the global public health agenda, in a commitment to promoteactions to reduce stress, increase literacy in male mental health for the perception of stress,and self-management of mental health care [78].
INT is a vulnerability factor associated with the development and maintenance ofmental disorders [79]. Uncertainty about the future is a potentially stressful condition [80],hence the strong association with the occurrence of CMDs. The study evidenced that INTis negatively associated with mental well-being, especially when mediated by lonelinessand fear of COVID-19, which are feelings intensely experienced during the pandemic [81].Thus, it is necessary to implement actions to promote increased resilience and develop-ment and/or strengthening of intrinsic reinforcements to deal with the impacts of regularexposure to uncertain threats.
It is also highlighted that, although there are groups at higher risk, COVID-19 ends upaffecting different social segments, and men tend to adhere less to the care measures and toneglect their health [82]. The occurrence and extension of this scenario can be even moreimpactful when considering social support, whether from the perspective of receiving oroffering emotional and instrumental support. Thus, it is indispensable to formulate andstrengthen already existing actions to promote psychosocial and emotional support formen in an exercise of citizenship and health care promotion that strengthens socio-affectivenetworks, enabling men to have someone to count on in critical moments like a pandemic.
In addition to the categories of psychological disorders such as stress, other structuralcategories need to be analyzed in the scenario of impacts on male mental health, such asrace/skin color and territory (geographic location and area of residence), since our findingsidentified that black-skinned men, those with higher socioeconomic status, who lived alone,and with higher levels of stress and intolerance to uncertainty had a higher prevalence ofCMDs. Thus, an intersectional perspective needs to be employed as a way of explaining thevulnerabilities, inequalities, inequities, and necropolitics that promote overlapping impactson the health, quality of life, and well-being of men who belong to marginalized groups, anaspect confirmed in our study when we identified the disparity in economic status amongnon-black-skinned men.
Although knowledge about the disease is advanced, there are still many gaps. Com-monly, guided behaviors are based on scientific evidence, protocols, and guidelines. How-ever, the recommendations themselves present certain degree of uncertainty, which gener-ates doubts and discomfort in the face of the unknown on the part of authorities, healthprofessionals, and the population [83]. Given this scenario, it is necessary to accept theexistence of these uncertainties, limitations, and incompleteness in current knowledge.Transparency regarding these issues is a strategy to deal with the unknown in a rational andethical way. In addition, the relevance of providing information and guidelines as recom-mended by the health authorities is emphasized as a way to avoid excessive simplificationsand the dissemination of easy answers if they do not exist. Thus, gaining trust becomesone of the greatest challenges and ends up fighting mistrust and fake news [84], whichintensify the emergence of conspiracy theories, misinformation, and “infodemic” [85–90].
Our study adopted a cross-sectional design and a sampling technique with recruitmentby non-probabilistic methods, which limit the causal inference and external validity of theresults. In addition to that, participation of men with no access to the interview via theInternet was excluded, which may have over- or under-estimated the prevalence of CMDsin the strata evaluated.

Int. J. Environ. Res. Public Health 2022, 19, 350 15 of 19
5. Conclusions
The results of this study point out the high prevalence of CMDs in men in the pandemiccontext and reinforce the need to assess the factors that precede this disease and to replicatethe study with women. In addition to that, they endorse the importance of constructinglatent variables to measure subjective aspects since three important latent constructs wererevealed to be better studied, namely socioeconomic status, intolerance to uncertainty, andsocial support.
In addition to that, the study allowed identifying a higher prevalence of CMDs amongyounger men, with lower schooling, black-skinned, without a partner, who lived alone,did not work, with high levels of stress and intolerance to uncertainty, and who receivedlow social support. It was also evidenced that the high levels of stress and intoleranceto uncertainty were the factors that presented the strongest direct associations with theoccurrence of CMDs.
These findings indicate that stress and intolerance to uncertainty are important factorsin understanding mental suffering among men. Dealing with unexpected situations, withthe loss of close people and future life perspectives accentuates stress levels, with theconsequence of the occurrence and/or worsening of CMD. This situation is even worse inthe presence of receiving low social support from close people and/or the government, asthis support has an important mitigating effect on mental suffering, being able to resolve theharmful impacts of high psychological demand and the low control over adverse situations.
Thus, the importance of developing mental health promotion policies and actions formale populations is highlighted, considering that intervening in the aspects associated withthe occurrence of CMDs is crucial to facing the impacts of the COVID-19 pandemic in thedifferent life dimensions.
Author Contributions: Conceptualization, A.R.d.S. and Á.P.; methodology, validation, formal analy-sis, investigation, data curation, writing—original draft preparation, writing—review and editing,and visualisation, A.R.d.S., J.R.B.T., E.M.S.P., W.C.M., M.B.S., H.E.F.d.C., É.S.A., R.M.S.F., A.M.d.Q.,M.C.d.M., T.N.M., I.F.M.A., J.C.d.S., S.D.d.S., E.L.S.C., L.G.L., R.A.R.d.S., E.S.d.S.C., I.L., S.B., T.M.d.A.,M.A.F.d.O., Á.P., W.A. and C.A.d.C.S. All authors have read and agreed to the published version ofthe manuscript.
Funding: National Funds through FCT—Fundação para a Ciência e Tecnologia, I.P., within CINTESIS,R&D Unit (reference UIDB/4255/2020) and Escola Superior de Enfermagem do Porto UIDB/4255/2020.
Institutional Review Board Statement: The study was conducted according to the guidelines ofthe Declaration of Helsinki and the study was approved by the Research Ethics Committee atUniversidade Federal da Bahia (decision: 4,087,611; CAAE: 32889420.9.0000.5531) on 8 April 2020.
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study.
Data Availability Statement: The datasets generated during the current study are not publiclyavailable but are available from the corresponding author on reasonable request.
Acknowledgments: To the men who participated in the study. All participants agreed to participatein the study by signing the Informed Consent Form.
Conflicts of Interest: The authors declare no conflict of interest.
References1. Dal’Bosco, E.B.; Floriano, L.S.M.; Rangel, A.G.S.S.; Ribas, M.C.; Cavalheiro, A.P.G.; Silva, C.L.D.; Cabral, L.P.A. Coping in mental
health during social isolation: Analysis in light of Hildegard Peplau. Rev. Bras. Enferm. 2021, 75, e20201207. [CrossRef]2. Sousa, A.R.; Teixeira, J.R.B.; Mota, T.N.; Santana, T.D.S.; Santos, S.D.D.; Merces, M.C.D.; Carvalho, E.S.S.; Sousa, Á.F.L. Coping
strategies, concerns, and habits of Brazilian men in the COVID-19 context. Rev. Bras. Enferm. 2021, 74, e20210040. [CrossRef]3. Faro, A.; Bahiano, M.A.; Nakano, T.C.; Reis, C.; Silva, B.F.P.; Vitti, L.S. COVID-19 e saúde mental: A emergência do cuidado. Estud.
De Psicol. (Campinas) 2020, 37, 1–14. [CrossRef]4. Mari, J.J.; Oquendo, M.A. Mental health consequences of COVID-19: The next global pandemic. Trends Psychiatr. Psychother 2020,
42, 219–220. [CrossRef]
Int. J. Environ. Res. Public Health 2022, 19, 350 16 of 19
5. Moreira, W.C.; Sousa, A.R.; Nóbrega, M.D.P.S.S. Mental illness in the general population and health professionals duringCOVID-19: A scoping review. Texto Contexto Enferm. 2020, 29, e20200215. [CrossRef]
6. Paiano, M.; Jaques, A.E.; Nacamura, P.A.B.; Salci, M.A.; Radovanovic, C.A.T.; Carreira, L. Mental health of healthcare professionalsin China during the new coronavirus pandemic: An integrative review. Rev. Bras. Enferm. 2020, 73, e20200338. [CrossRef][PubMed]
7. Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J.Psychiatr. 2020, 42, 232–235. [CrossRef] [PubMed]
8. Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirusoutbreak is urgently needed. Lancet Psychiat. 2020, 7, 228–229. [CrossRef]
9. Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possiblesuicide prevention strategies. Asian J. Psychiatr. 2020, 51, 102073. [CrossRef]
10. Goyal, K.; Chauhan, P.; Chhikara, K.; Gupta, P.; Singh, M.P. Fear of COVID 2019: First suicidal case in India. Asian J. Psychiatr.2020, 49, 101989. [CrossRef]
11. Gonzalez-Diaz, J.M.; Cano, J.F.; Pereira-Sanchez, V. Psychosocial impact of COVID-19-related quarantine: Reflections after thefirst case of suicide in Colombia. Cad Saúde Pública 2020, 36, e00117420. [CrossRef]
12. Gonçalves Júnior, J.; de Sales, J.P.; Moreno, M.M.; Rolim-Neto, M.L. The Impacts of SARS-CoV-2 Pandemic on Suicide: A LexicalAnalysis. Front. Psychiatr. 2021, 10, 593918. [CrossRef]
13. Sousa, A.R.; Moreira, W.C.; Queiroz, A.M.; Rezende, M.F.; Teixeira, J.R.B.; Merces, M.C.; Silva, A.V.; Camargo, E.L.S. COVID-19pandemic decrease men’s mental health: Background and consequence analysis. J. Bras. Psiquiatr. 2021, 70, 141–148. [CrossRef]
14. Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395,e37–e38. [CrossRef]
15. Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19.Diabetes Metab. Syndr. 2020, 14, 779–788. [CrossRef]
16. Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: Asystematic review and meta-analysis. J. Affect. Disord. 2021, 15, 91–98. [CrossRef] [PubMed]
17. Cui, L.; Wang, X.; Wang, H. Challenges facing coronavirus disease 2019: Psychiatric services for patients with mental disorders.Psychiatr. Clin. Neurosci. 2020, 74, 371–372. [CrossRef]
18. World Health Organization (WHO). Depression and Other Common Mental Disorders: Global Health Estimates. 2017. Avail-able online: www.who.int/mental_health/management/depression/prevalence_global_health_estimates/en/ (accessed on30 April 2021).
19. Souza, I.M.; Sousa, J.P.M. Brazil: World leader in anxiety and depression rates. Rev. Bras. De Psiquiatr. 2017, 39, 384. [CrossRef]20. Smolen, J.R.; Araújo, E.M.; Oliveira, N.F.; Araújo, T.M. Intersectionality of Race, Gender, and Common Mental Disorders in
Northeastern Brazil. Ethn. Dis. 2018, 28, 207–214. [CrossRef] [PubMed]21. Morriss, J.; Christakou, A.; van Reekum, C.M. Nothing is safe: Intolerance of uncertainty is associated with compromised fear
extinction learning. Biol. Psychol. 2016, 121, 187–193. [CrossRef] [PubMed]22. Holaway, R.M.; Heimberg, R.G.; Coles, M.E. A comparison of intolerance of uncertainty in analogue obsessive-compulsive
disorder and generalized anxiety disorder. J. Anxiety Disord. 2006, 20, 158–174. [CrossRef]23. Hollingsworth, D.W.; Gauthier, J.M.; McGuire, A.P.; Peck, K.R.; Hahn, K.S.; Connolly, K.M. Intolerance of uncertainty mediates
symptoms of PTSD and depression in African American veterans with comorbid PTSD and substance use disorders. J. BlackPsychol. 2018, 44, 667–688. [CrossRef]
24. McEvoy, P.M.; Mahoney, A.E.J. Achieving certainty about the structure of intolerance of uncertainty in a treatment-seeking samplewith anxiety and depression. J. Anxiety Disord. 2011, 25, 112–122. [CrossRef] [PubMed]
25. Tolin, D.F.; Abramowitz, J.S.; Brigidi, B.D.; Foa, E.B. Intolerance of Uncertainty in obsessive-compulsive disorder. J. Anxiety Disord.2003, 17, 233–242. [CrossRef]
26. Satici, B.; Saricali, M.; Satici, S.A.; Griffiths, M.D. Intolerance of Uncertainty and Mental Wellbeing: Serial Mediation by Ruminationand Fear of COVID-19. Int. J. Ment. Health Addict. 2020, 15, 1–12. [CrossRef]
27. Anselmi, L.; Barros, F.C.; Minten, G.C.; Gigante, D.P.; Horta, B.L.; Victora, C.G. Prevalência e determinantes precoces dostranstornos mentais comuns na coorte de nascimentos de 1982, Pelotas, RS. Rev. De Saúde Pública 2008, 42, 26–33. [CrossRef]
28. Mattos, A.I.S.; de Araújo, T.M.; de Almeida, M.M.G. Almeida Interaction between demand-control and social support in theoccurrence of common mental disorders. Rev. De Saúde Pública 2017, 51, 48. [CrossRef]
29. Ribeiro, I.B.d.S.; Correa, M.M.; Oliveira, G.; Cade, N.V. Common mental disorders and socioeconomic status in adolescents ofERICA. Rev. De Saúde Pública 2020, 54, 4. [CrossRef] [PubMed]
30. Patel, V.; Kleinman, A. Poverty and common mental disorders in developing countries. Bull. World Health Organ. 2003, 81,609–615.
31. Coutinho, L.M.S.; Matijasevich, A.; Scazufca, M.; Meneses, P.R. Prevalência de transtornos mentais comuns e contexto social:Análise multinível do São Paulo Ageing & Health Study (SPAH). Cad. Saude Publica 2014, 30, 1875–1883. [CrossRef]
32. Jacob, L.; Haro, J.M.; Koyanagi, A. Relationship between living alone and common mental disorders in the 1993, 2000 and 2007National Psychiatric Morbidity Surveys. PLoS ONE 2019, 14, e0215182. [CrossRef] [PubMed]
Int. J. Environ. Res. Public Health 2022, 19, 350 17 of 19
33. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/(accessed on 14 September 2021).
34. Brasil Ministério da Saúde (BR). Boletim Epidemiológico Especial. Doença Pelo Coronavírus COVID-19. Brasília, DF (BR): MS,2021. Available online: https://www.gov.br/saude/pt-br/media/pdf/2021/outubro/01/boletim_epidemiologico_covid_82.pdf(accessed on 14 September 2021).
35. Brasil Ministério da Saúde (BR). Boletim Epidemiológico Especial. Doença Pelo Coronavírus COVID-19. Brasília, DF (BR): MS,2020. Available online: http://saude.gov.br/images/pdf/2020/July/15/Boletim-epidemiologico-COVID-22.pdf (accessed on30 April 2021).
36. Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T.Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 1–10.[CrossRef] [PubMed]
37. Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Ziebuhr, J. The species Severe acute respiratorysyndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [CrossRef]
38. Windsor, L.C.; Reinhardt, G.Y.; Windsor, A.J.; OstergardI, R.; Allen, S.; Burns, C.; Giger, J.; Wood, R. Gender in the time ofCOVID-19: Evaluating national leadership and COVID-19 fatalities. PLoS ONE 2020, 15, e0244531. [CrossRef]
39. Tibubos, A.N.; Otten, D.; Ernst, M.; Beutel, M.E. A Systematic Review on Sex- and Gender-Sensitive Research in Public MentalHealth during the First Wave of the COVID-19 Crisis. Front. Psychiatr. 2021, 12, 712492. [CrossRef]
40. Seidler, Z.E.; Dawes, A.J.; Rice, S.M.; Oliffe, J.L.; Dhillon, H.M. The role of masculinity in men’s help-seeking for depression: Asystematic review. Clin. Psychol. Rev. 2016, 49, 106–118. [CrossRef]
41. Sousa, A.R.; Santana, T.S.; Moreira, W.C.; Sousa, Á.F.L.; Carvalho, E.S.S.; Craveiro, I. Emoções e estratégias de coping de homensà pandemia da covid-19 no Brasil. Texto E Contexto Enferm. 2020, 29, e20200248. [CrossRef]
42. Núcleo de Informação e Coordenação do Ponto BR (NIC. br). Pesquisa Sobre O Uso Das Tecnologias De Informação E Comuni-cação: Pesquisa TIC Domicílios, ano 2019: Tabelas. São Paulo: 2020. Available online: http://cetic.br/pt/arquivos/domicilios/2019/individuos/#tabelas (accessed on 30 April 2021).
43. Biernacki, P.; Waldorf, D. Snowball sampling: Problems and techniques of chain referral sampling. Sociol. Methods Res. 1981, 10,141–163. [CrossRef]
44. Mari, J.J.; Williams, P. A validity study of a psychiatric screening questionnaire (SRQ-20) in primary care in the city of Sao Paulo.Br. J. Psychiatr. 1986, 148, 23–26. [CrossRef]
45. Santos, K.O.B.; Araújo, T.M.; Sousa Pinho, P.; Silva, A.C.C. Avaliação de um instrumento de mensuração de morbidade psíquica:Estudo de validação do Self-Reporting Questionnaire (SRQ-20). Rev. Baiana De Saúde Pública 2010, 34, 544. [CrossRef]
46. Santos, K.O.B.; Carvalho, F.M.; Araújo, T.M. Consistência interna do self-reporting questionnaire-20 em grupos ocupacionais. Rev.Saude Publica 2016, 50, 6. [CrossRef]
47. Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [CrossRef][PubMed]
48. Luft, C.D.; Sanches, S.O.; Mazo, G.Z.; Andrade, A. Versão brasileira da Escala de Estresse Percebido: Tradução e validação paraidosos. Rev. Saúde Pública 2007, 41, 606–615. [CrossRef] [PubMed]
49. Machado, W.L.; Damásio, B.F.; Borsa, F.C.; Silva, J.P. Dimensionalidade da Escala de Estresse Percebido (Perceived Stress Scale,PSS10) em uma amostra de professores. Psicol. Reflex. Crit. 2014, 27, 38–43. [CrossRef]
50. Ma, Y.; Rosenheck, R.; He, H. Psychological stress among health care professionals during the 2019 novel coronavirus diseaseOutbreak: Cases from online consulting customers. Intensive Crit. Care Nurs. 2020, 61, 102905. [CrossRef]
51. Freeston, M.H.; Rheaume, J.; Letarte, H.; Dugas, M.J.; Ladouceur, R. Why Do People Worry? Personal. Individ. Differ. 1994, 17,791–802. [CrossRef]
52. Carleton, R.N.; Norton, M.A.; Asmundson, G.J. Fearing the unknown: A short version of the Intolerance of Uncertainty Scale. J.Anxiety Disord. 2007, 21, 105–117. [CrossRef] [PubMed]
53. Kretzmann, R.P. Intolerance of Uncertainty Scale (IUS-12) Para Uso No Brasil: Adaptação Transcultural E Propriedades Psi-cométricas. Ph.D. Thesis, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil, 2018.
54. Kretzmann, R.P.; Gauer, G. Psychometric properties of the Brazilian Intolerance of Uncertainty Scale–Short Version (IUS-12).Trends Psychiatr. Psychother 2020, 42, 129–137. [CrossRef] [PubMed]
55. Norton, P.J. A psychometric analysis of the Intolerance of Uncertainty Scale among four racial groups. J. Anxiety Disord. 2005, 6,699–707. [CrossRef]
56. Yao, N.; Qian, M.; Jiang, Y.; Elhai, J.D. The Influence of Intolerance of Uncertainty on Anxiety and Depression Symptoms inChinese-speaking Samples: Structure and Validity of The Chinese Translation of The Intolerance of Uncertainty Scale. J. Pers.Assess. 2021, 103, 406–415. [CrossRef] [PubMed]
57. Bottesi, G.; Noventa, S.; Freeston, M.H.; Ghisi, M. Seeking certainty about Intolerance of Uncertainty: Addressing old and newissues through the Intolerance of Uncertainty Scale-Revised. PLoS ONE 2019, 14, e0211929. [CrossRef]
58. Shakespeare-Finch, J.; Obst, P.L. The development of the 2-Way Social Support Scale: A measure of giving and receiving emotionaland instrumental support. J. Pers. Assess. 2011, 93, 483–490. [CrossRef] [PubMed]
Int. J. Environ. Res. Public Health 2022, 19, 350 18 of 19
59. Bastianello, M.R. Implicações Do Otimismo, Autoestima E Suporte Social Percebido Na Qualidade De Vida De Mulheres ComCâncer De Mama [Implications of Optimism, Self Esteem and Perceived Social Support on Quality of Life of Women with BreastCancer]. Ph.D. Thesis, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil, 2015.
60. Glymour, M.M.; Greenland, S. Causal diagrams. Ch. 12. In Modern Epidemiology, 3rd ed.; Rothman, K.J., Greenland, S., Lash, T.L.,Eds.; Lippincott: Philadelphia, PA, USA, 2008.
61. Hernán, M.A.; Robins, J.M. Causal Inference: What If ; Chapman & Hall/CRC: Boca Raton, FL, USA, 2020.62. Cortes, T.R.; Faerstein, E.S.; Claudio, J. Utilização de diagramas causais em epidemiologia: Um exemplo de aplicação em situação
de confusão. Cad. Saúde Pública 2016, 32, e00103115. [CrossRef] [PubMed]63. Werneck, G.L. Diagramas causais: A epidemiologia brasileira de volta para o futuro. Cad. De Saúde Pública 2016, 32, e00120416.
[CrossRef]64. Marôco, J. Análise De Equações Estruturais-Fundamentos Teóricos, 2nd ed.; Software e Aplicações: Lisboa, Portugal, 2014.65. Marsh, H.W.; Muthén, B.; Asparouhov, T.; Lüdtke, O.; Robitzsch, A.; Morin, A.J.S.; Trautwein, U. Exploratory structural equation
modeling, integrating CFA and EFA: Application to students’ evaluations of university teaching. Struct. Equ. Modeling 2009, 16,439–476. [CrossRef]
66. Hair, J.F.J.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Análise Multivariada De Dados, 6th ed.; Bookman: Porto Alegre,RS, Brazil, 2009.
67. Reichenheim, M.E.; Hökerberg, Y.H.M.; Moraes, C.L. Assessing construct structural validity of epidemiological measurementtools: A seven-step roadmap. Cad. Saúde Pública 2014, 30, 927–939. [CrossRef]
68. Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2015.69. Brown, T.A. Methodology in the social sciences. In Confirmatory Factor Analysis for Applied Research, 2nd ed.; Guilford Press:
New York, NY, USA, 2015.70. Barros, A.J.D.; Victora, C.G.; Menezes, A.M.B.; Horta, B.L.; Hartwig, F.; Victora, G.; Pellanda, L.C.; A Dellagostin, O.; Struchiner,
C.J.; Burattini, M.N.; et al. Social distancing patterns in nine municipalities of Rio Grande do Sul, Brazil: The Epicovid19/RSstudy. Rev. Saúde Pública 2020, 54, 75. [CrossRef]
71. Lipp, M.E.N.; Lipp, L.M.N. Stress e transtornos mentais durante a pandemia da COVID-19 no Brasil. Rev. Da Acad. Paul. DePsicol. 2020, 40, 180–191.
72. Dorner, T.E.; Mittendorfer-Rutz, E. Socioeconomic inequalities in treatment of individuals with common mental disordersregarding subsequent development of mental illness. Soc. Psychiatr. Psychiatr. Epidemiol. 2017, 52, 1015–1022. [CrossRef][PubMed]
73. Jokela, M.; Batty, G.; Vahtera, J.; Elovainio, M.; Kivimäki, M. Socioeconomic inequalities in common mental disorders andpsychotherapy treatment in the UK between 1991 and 2009. Br. J. Psychiatr. 2013, 202, 115–120. [CrossRef]
74. Salameh, P.; Hajj, A.; A Badro, D.; Selwan, C.A.; Aoun, R.; Sacre, H. Mental Health Outcomes of the COVID-19 Pandemic and aCollapsing Economy: Perspectives from a Developing Country. Psychiatr. Res. 2020, 294, 113520. [CrossRef]
75. Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact ofquarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [CrossRef]
76. Riter, H.S.; Almeida, M.L.; Vescovi, G.; Marques, F.M.; Pedrotti, B.G.; Mallmann, M.Y.; Pieta, M.A.M.; Frizzo, G.B. Symptoms ofCommon Mental Disorders in Brazilian Parents During the COVID-19 Pandemic: Associated Factors. Psychol. Stud. 2021, 66,270–279. [CrossRef] [PubMed]
77. Duarte, M.Q.; Santo, M.A.S.; Lima, C.P.; Giordani, J.P.; Trentini, C.M. COVID-19 e os impactos na saúde mental: Uma amostra doRio Grande do Sul, Brasil. Cien Saude Colet 2020, 25, 3401–3412. [CrossRef] [PubMed]
78. Sousa, A.R.; Alves, G.V.; Queiroz, A.M.; Florêncio, R.M.S.; Moreira, W.C.; Nóbrega, M.D.P.S.S.; Teixeira, E.; Rezende, M.F. Men’smental health in the COVID-19 pandemic: Is there a mobilization of masculinities? Rev. Bras. Enferm. 2021, 74, e20200915.[CrossRef]
79. Angehrn, A.; Krakauer, R.L.; Carleton, R.N. The Impact of Intolerance of Uncertainty and Anxiety Sensitivity on Mental HealthAmong Public Safety Personnel: When the Uncertain is UnavoidableInt. J. Cogn. 2020, 44, 919–930. [CrossRef]
80. Giusti, L.; Salza, A.; Mammarella, S.; Bianco, D.; Ussorio, D.; Casacchia, M.; Roncone, R. Everything Will Be Fine. Duration ofHome Confinement and “All-or-Nothing” Cognitive Thinking Style as Predictors of Traumatic Distress in Young UniversityStudents on a Digital Platform During the COVID-19 Italian Lockdown. Front. Psychiatr. 2020, 11, 574812. [CrossRef]
81. Rehman, S.U.; Ullah, R.; Imran, M.; Iqbal, K.; Saleem, Z.; Khattak, S.R. Intolerance of Uncertainty and Mental Well-being:Important Role of Loneliness and Fear of COVID-19: Evidence from Higher Educational Institutions. Multicult. Educ. 2021, 7,147–154. [CrossRef]
82. Alves, A.A.M.; Rodrigues, N.F.R. Determinantes sociais e econômicos da Saúde Mental. Rev. Port. Saúde Pública 2010, 28, 127–131.[CrossRef]
83. Sousa, A.R.; Araújo, I.F.M.; Borges, C.C.L.; Oliveira, J.A.; Almeida, M.S.; Caribé, W.; Junior, F.J.N.S. Men’s health in the covid-19pandemic: Brazilian panorama. Rev. Baiana Enferm. 2021, 35, e38683. [CrossRef]
84. Botton, A.; Cúnico, S.D.; Strey, M.N. Diferenças de gênero no acesso aos serviços de saúde: Problematizações obrigatórias.Mudanças-Psicol. Da Saúde 2017, 25, 67–72. [CrossRef]
85. Sousa, A.R.; Queiroz, A.M.; Florêncio, R.M.S.; Alves, G.V.; Pedreira, L.C.; Teixeira, E. Sentidos e significados atribuídos porhomens ao vivido na pandemia da Covid-19. Rev. Esc. Enferm. USP 2021, 55, e03763. [CrossRef]

Int. J. Environ. Res. Public Health 2022, 19, 350 19 of 19
86. Moreira, W.C.; Sousa, K.H.J.F.; Sousa, A.R.; Santana, T.S.; Zeitoune, R.C.G.; Nóbrega, M.P.S.S. Mental health interventionsimplemented in the COVID-19 pandemic: What is the evidence? Rev. Bras. Enferm. 2021, 74, e20200635. [CrossRef]
87. Moreira, W.C.; Nóbrega, M.P.S.S.; Lima, F.P.S.; Lago, E.C.; Lima, M.O. Effects of the association between spirituality, religiosityand physical activity on health/mental health: A sistematic review. Rev. Esc. Enferm. USP 2020, 54, e03631. [CrossRef] [PubMed]
88. Romiti, G.F.; Talerico, G. Embracing the Uncertainty: An Important Lesson from COVID-19. J. Gen. Intern. Med. 2021, 36,3562–3564. [CrossRef] [PubMed]
89. Vasconcellos-Silva, P.R.; Castiel, L.D. COVID-19, as fake news e o sono da razão comunicativa gerando monstros: A narrativa dosriscos e os riscos das narrativas. Cad. Saúde Pública 2020, 36, e00101920. [CrossRef] [PubMed]
90. de Sousa, F.L.; Teixeira, J.R.B.; Lua, I.; Souza, F.D.O.; Ferreira, A.J.F.; Schneider, G.; de Carvalho, H.E.F.; de Oliveira, L.B.; Lima,S.V.M.A.; de Sousa, A.R.; et al. Determinants of COVID-19 Vaccine Hesitancy in Portuguese-Speaking Countries: A StructuralEquations Modeling Approach. Vaccines 2021, 9, 1167. [CrossRef]