Psychological functioning of partners of Australian combat veterans: Contribution of veterans’...
14
Psychological Functioning of Partners of Australian Combat Veterans: Contribution of Veterans’ PTSD Symptoms and Partners’ Caregiving Distress [DRAFT COPY ONLY] Gail V MacDonell, Einar B Thorsteinsson*, Navjot Bhullar*, and Donald W Hine University of New England, Armidale, Australia *Equal contributors. In press, Australian Psychologist Manuscript accepted for publication June 28, 2014 Journal site: http://onlinelibrary.wiley.com/journal/10.1111/(ISSN)1742-9544 Please address correspondence to: Dr Navjot Bhullar Psychology School of Behavioural, Cognitive and Social Sciences University of New England, Armidale, NSW, Australia [email protected]
Transcript of Psychological functioning of partners of Australian combat veterans: Contribution of veterans’...

Psychological Functioning of Partners of Australian Combat Veterans: Contribution of
Veterans’ PTSD Symptoms and Partners’ Caregiving Distress
[DRAFT COPY ONLY]
Gail V MacDonell, Einar B Thorsteinsson*, Navjot Bhullar*, and Donald W Hine
University of New England, Armidale, Australia
*Equal contributors.
In press, Australian Psychologist
Manuscript accepted for publication June 28, 2014
Journal site: http://onlinelibrary.wiley.com/journal/10.1111/(ISSN)1742-9544
Please address correspondence to:
Dr Navjot Bhullar
Psychology
School of Behavioural, Cognitive and Social Sciences
University of New England, Armidale, NSW, Australia

PARTNERS OF COMBAT VETERANS 2
Abstract
Previous research has found Posttraumatic Stress Disorder (PTSD) symptoms in combat veterans to be associated with impaired psychological functioning in their partners. However, little is known about possible mediators of this association. The present study investigated the mediational properties of six dimensions of the revised Partners of Veterans’ Distress Scale (MacDonell, Marsh, Hine, & Bhullar, 2010). Participants were 181 female partners of Australian combat veterans, age ranging from 43 and 83 years (M = 60.47, SD = 4.96), who completed measures assessing their caregiving distress levels, dyadic adjustment, mental health and satisfaction with life. The combat veterans also completed a scale measuring their PTSD symptoms. Our results indicated that higher scores of veterans’ PTSD were associated with lower levels of dyadic adjustment, mental health, and satisfaction with life in their partners. Partners reported distress related to exhaustion and intimacy problems significantly mediated the relationship between veterans’ PTSD symptoms and their partners’ satisfaction with life, whereas partners’ distress associated with intimacy problems was the sole significant mediator for their dyadic adjustment, and exhaustion was the only significant mediator for partners’ mental health. Implications for programs designed to address the significant needs of the partners of combat veterans are discussed. Key words: caregiving distress; combat veterans; dyadic adjustment; mental health; partners of veterans; PTSD.

PARTNERS OF COMBAT VETERANS 3
Living and caring for a person with a mental health disorder such as depression or Posttraumatic Stress Disorder (PTSD) may serve as a chronic stressor placing caregivers at risk for psychological, emotional and physical problems (Lev-Wiesel & Amir, 2001; Pearlin, Mullan, Semple, & Skaff, 1990). Much of the research that has been done in this area refers to wives and partners as caregivers (Calhoun, Beckham, & Bosworth, 2002), who have been shown to be the most vulnerable group. In other populations, spouses/intimate others are more likely to give three to five times more care than other family members (Frederick & Fast, 1999) and have been shown to be far more intensely involved in the caregiving process (Dupuis & Smale, 2004) than other non-family or secondary caregivers.
Research suggests that partners of veterans constitute a high-risk population with serious implications for their mental and physical health, emotional well-being and marital problems (Alessi, Ray, Ray, & Stewart, 2001). Dekel and Monson (2010) found a link between veterans’ deployment stressors, including exposure to combat, and their poorer family functioning. Previous studies have established that combat veterans have a significantly higher rate of depression and PTSD (Hoge, Castro, Messer, McGurk, Cotting, & Koffman, 2004; Miliken, Auchterlonie, & Hoge, 2007; Sayers, Farrow, Ross, & Oslin, 2008; Westerink & Giarratano, 1999) than the general population. In turn, veterans’ mental health problems tend to negatively impact on their family members (Beckham, Lytle, Kudler, Feldman, & Palmer, 1997; Calhoun et al., 2002). Findings from the United States, Israel, Holland, Croatia and Iran (Calhoun et al., 2002; Dekel, Goldblatt, Keidar, Solomon, & Polliack, 2005; Dirkzwager, Bramsen, Adèr, & van der Ploeg, 2005; Frančikovišć, Stevanovic, Jelušić, Roganović, Klarić, & Grković, 2007; Salimi, Azad-Marazbadi, Karaminia, Mirzamani, & Hosseini-Sangtrashani, 2006) and Australia (MacDonell et al., 2010; Outram, Hansen, MacDonell, Cockburn, & Adams, 2009; Westerink & Giarratano, 1999) suggest that partners of combat veterans have a significantly higher risk of developing psychological problems as a result of living and caring for their veterans, than the general population (Alessi et al., 2001).
To date, very few studies have specifically examined the relationship between veterans’ PTSD and their partners’ psychological functioning. One of such studies by Dekel, Solomon, and Bleich (2005) explored the relative impact of the veterans’ impairment along with the partners’ distress related to partners’ marital adjustment. They found that the partners’ distress mediated the relationship between the veterans’ level of impairment and the partners’ marital adjustment. That is, veterans’ level of impairment was related to greater distress in their partners, which in turn reduced well-being outcomes in partners (Dekel, Solomon, et al., 2005). However, this study used more of a global indicator (Caregiver Burden Inventory [CBI]), originally developed for caregivers of patients with Alzheimer’s disease, as a measure of partners’ distress or sense of burden related to caregiving. Though the CBI evaluates feelings and responses of caregivers to their spouses’ needs, it does not specifically identify and measure the precise stressors of partners of combat veterans.
A range of scales, such as the Burden Interview (BI) and the Symptom Checklist-90- Revised (SCL-90-R) have been used to assess the psychosocial impacts associated with caring for veterans (Beckham, Lytle, & Feldman, 1996). However, these measures did not assess specific indices of psychological distress faced by partners of combat veterans. To that end, MacDonell et al. (2010) developed a first of its kind measure assessing the specific realms implicated in the experience of distress related to caregiving role in partners of Australian combat veterans. This resulted in the Partners of Veterans Distress Scale (POV-DS), a new scale that exclusively measures the specific stressors that are common to partners of veterans and the degree of distress that each of these stressors may cause. The item pool for POV-DS was based on 12 thematic themes obtained from focus groups. These themes include financial difficulties, social problems with family, social problems with friends,

PARTNERS OF COMBAT VETERANS 4
difficulty in coping with veterans’ changes in mood and behavior, worrying about the future, problems associated with their children, despair at the lack of support from outside the veteran community, emotional and psychological problems, lack of intimacy, sense of isolation, feeling overwhelmed, and physical health problems. Further details about scale development and validation can be found in MacDonell et al. (2010). The authors found that partners in their study reported significantly poorer levels of mental and physical health than the comparative norms. In addition, higher scores on partner distress dimensions were significantly related with poorer physical and mental health and lower satisfaction in life outcomes in partners. Specifically, distress related to exhaustion explained unique variance in physical health (3%), mental health (3%) and satisfaction in life (2%).
Previous research has also suggested a link between caregiving distress dimensions and a number of caregiver outcomes such as psychological disorders (e.g., depression, anxiety, low self-esteem see Beckham et al., 1996; Braithwaite, 1996; Westerink & Giarratano, 1999) and marital problems (Calhoun et al., 2002; Evans, McHugh, Hopwood, & Watt, 2003; Renshaw, Rodrigues, & Jones, 2008). Braithwaite (1996) found that ‘dysfunctional caregiving’ distress dimension, similar to Lawton, Moss, Kleban, Glicksman, and Rovine (1991) ‘burden’ dimension, was related to negative caregiving outcomes such as negative affect and minor psychiatric symptoms (depression and anxiety). Thus, it provides evidence that caregiving distress dimensions are related to caregiver outcome variables in a predictable fashion and at the same time add to our understanding of underlying mechanisms of these outcomes. Moreover, while some studies have explored the clusters of PTSD symptoms of the veteran with intimate dysfunction, (Evans et al., 2003; Solomon, Dekel, & Mikulincer, 2008), none have really examined the identified factors found from the partners’ perspective, on their own well-being. Aims
The present study extends previous research of (Dekel, Solomon, et al., 2005), one of the few systemic investigations of factors contributing to distress in partners of trauma victims. This study used male Israeli veterans who had been diagnosed with PTSD. They used structural equation modelling and examined the relative contribution of the level of impairment of the veteran and the wife’s level of distress, to examine if there was a mediated or direct effect through the wife’s sense of caregiving burden. Though using cross-sectional data, Dekel, Solomon, et al. (2005) provided a framework of a model with direction of relationships between the variables under investigation. Using this model, our study examined the role of distinctive dimensions of partners’ distress (as measured by POV-DS; MacDonell et al., 2010) in the relationship between the veterans’ level of impairment (PTSD symptoms) and the partners’ psychological functioning (marital adjustment, mental health and satisfaction with life). We predicted that greater levels of PTSD symptoms experienced by veterans would be associated with higher levels of distress appraisal related to caregiving demands in their partners, which in turn would result in poorer psychological functioning in partners of combat veterans.
Method Participants
Participants were 181 female members of the Partners of Veterans Association of Australia (PVA), membership in this association is open to any person whose current or former partner served in a theatre of war or campaign, or is currently serving in any peacekeeping/peacemaking duties or any other military operational service), and their veteran spouses, respectively. Age of female partners ranged from 43 to 83 years (M = 60.47, SD = 4.96), while their veterans’ age ranged from 49 to 88 (M = 63.89, SD = 4.56). The length of marriage for the couples ranged from 2 to 60 years (M = 35.58, SD = 9.77). Majority of the female partners (89%) identified themselves as carers for their veteran, while 85% of the

PARTNERS OF COMBAT VETERANS 5
veterans indicated that they had a Carer. Eighty five per cent of the partners belonged to a support group, while 90% of the veterans indicated that they belonged to a support group or Ex-Service organisation. In terms of service type, 10% of veterans indicated they had served in the Airforce, 84% in the Army, and 5% in the Navy. Just over half (54%) were long-term service-personnel (those that have served over two years) with 43% were National Conscripts (soldiers who were under compulsory Military service and were conscripted under Australian legislation of 1965 with new powers that allowed them to be sent to serve overseas and served two years), while 3% where National Conscripts who stayed on to become long term service personnel. Just under 4% indicated they had fought in World War II or Korea, 13% Malaya/Borneo, 80% in Vietnam, 2% in Somalia, Kashmir, Gulf War 1 or Operation Catalyst (Australia’s contribution to the US-led Multinational Force effort to develop a secure and stable environment in Iraq and assist national recovery programs), and 1% indicated ‘other’ as their first conflict. Of those who indicated that they had been deployed in an active service zone more than once, 68% had been deployed twice, 9% three times, 9% four times and 4% five times. Measures
Participants answered questions pertaining to age, gender and other demographics. All measures used were relatively brief assessments to minimize any burden on this population. They completed the following questionnaires:
The Partners of Veterans-Distress Scale Revised (POV-DSR) was used to measure distress in partners of combat veterans. Participants were asked if a potential stressor applied to them: Yes/No, such as ‘the term walking on eggshells applies to my relationship with my husband/partner’ and ‘I get enough sleep at night’ and ‘I know I can ask any friend or relative over to our home any time I please’ and, if so, how much personal distress it caused. Degree of distress was assessed using a 5-point Likert-type response scale of 0 (does not cause me distress), 1 (mild distress), 2 (moderate distress), 3 (severe distress), and 4 (extremely severe distress) and distress ratings were averaged to obtain a (sub) scale score. Respondents who indicated that a stressor did not apply to them were also assigned a distress score of 0 for that item.
The POV-DSR is shorter version (35 items) of the 45-item Partners of Veterans-Distress Scale (POV-DS; MacDonell et al., 2010) and assesses six (Social isolation, Hyper-vigilance, Financial problems, Intimacy problems, Social isolation, Poor sleep, and Exhaustion) of the seven POVS-DS indices of the partners’ distress. This measure’s indices give scope for a more detailed analysis than a generalised or global approach, thus improve practical significance.
The POV-DSR excludes the negative affect subscale, comprising two items pertaining to being diagnosed with anxiety and depression, thus preventing duplication of mental health construct as both distress subscale (mediator) and outcome measure (DV). Pearson’s correlation between the POV-DS and the POV-DSR for each index (based on data collected for the present study) was also high (> .90), thus suggesting good convergent validity. Respective items pertaining to the POV-DSR were averaged to compute six indices POV-DSR, with a higher score indicating greater distress. Internal reliabilities as assessed by Cronbach’s α of the POV-DSR indices ranged from good to excellent in the present study: .83 for sleep problems, .93 for hyper-vigilance, .79 for social isolation, .89 for financial problems, .94 for exhaustion, and .93 for intimacy problems.
The Dyadic Adjustment 7-item Scale (DAS-7; Hunsley, Pinsent, Lefebvre, James-Tanner, & Vito, 1995). This self-report scale is used to assess marital functioning. The DAS-7 comprises seven items, six of which are rated on a six-point Likert–type scale, from 0 (always disagree) to 5 (always agree) to questions pertaining to the extent of their agreement or disagreement on ‘philosophy of life’, ‘aims, goals,

PARTNERS OF COMBAT VETERANS 6
and things believed important’ and ‘amount of time spent together’. Next three items ‘have a stimulating exchange of ideas’, ‘ calmly discuss something together’, and ‘worked together on a project’ were assessed on a 6-point scale, from 0 (never) to 5 (more often than once a day). One remaining item ‘degree of happiness in their relationship’ was rated on a 7-point scale, from 0 (extremely unhappy) to 6 (perfectly happy). The scores are summed with higher score indicating greater dyadic or marital adjustment, thus a better relationship. Cronbach’s α in the present study was .90.
The Mental Health Inventory (MHI-5; Berwick, Murphy, Goldman, Ware, Barsky, & Weinstein, 1991) comprises 5 items to assess mental health. It assesses psychological well-being as well as symptoms of psychological distress. It is suitable for non-psychiatric populations. For each of the five questions, participants are asked to rate on a 6-point scale, ranging from 1 (all of the time) to 6 (none of the time). Sample items include ‘How much of the time in the previous month (i) been a very nervous person, (ii) felt peaceful and calm’. Two items were reverse scored. MHI-5 scores range from 5 to 30, with higher score indicating greater mental health. Cronbach’s α in the present study was .91.
The Satisfaction with Life Scale (SWLS; Diener, Emmons, Larson, & Griffin, 1985) is a 5-item scale that assesses the cognitive-judgmental component of subjective well-being known as global life satisfaction. Participants are asked to rate on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree). Sample items include ’In most ways my life is close to ideal’, ‘I am satisfied with my life’. Higher scores indicate greater satisfaction with life. Cronbach’s α for this present study was .91.
Posttraumatic Stress Disorder Scale (PTSD; Breslau, Peterson, Kessler, & Schultz, 1999). Veterans completed a short 7-item screening scale for PTSD symptoms designed for all trauma survivors. It consists of five avoidance and numbing symptom cluster items such as ‘Do you avoid being reminded of the experience by staying away from certain places, people or activities?’ and two hyper-arousal symptom cluster items, such as ‘Do you become jumpy or easily startled by ordinary noise or movement?’ Respondents answer each item as either ‘yes’ or ‘no’. Items are scored by adding the number of ‘yes’ responses (Breslau et al., 1999), with a score of four or above is symptomatic of having PTSD providing an optimal cut-off point for separating individuals with and without PTSD. This screening tool can also be used as predictor for the probability of having PTSD. Majority of the veteran respondents (77%) scored four or above on this scale. Cronbach’s α of this scale used in the present study was .67. Procedure
Participants were recruited via a PVA magazine circulated among partners of Australian combat veterans. Participants (partners of combat veterans), who were in a dyadic relationship, were invited to participate along with their veteran spouses. Those who agreed to participate were sent a questionnaire with a reply-paid envelope. Ethics approval was given by Human Research Ethics Committee of the university at which the researchers work. Statistical Analysis
To determine whether the relationship between veterans’ PTSD (IV) and partners’ marital adjustment, mental health, and satisfaction with life (DVs) was mediated by the six dimensions of partners’ distress assessed by the POV-DSR (mediators), three multiple mediation analyses were conducted using an SPSS Macro developed by Hayes, Preacher, and Myers (2011). This macro includes bootstrapped confidence intervals (CIs) for assessing the significance of the three indirect paths. These bootstrapped CIs have been shown to be less biased than the Sobel’s test (Preacher & Hayes, 2008). Bootstrap is a preferred method for mediation analysis over approaches such as those of Baron and Kenny’s (1986) causal steps approach, and the Sobel’s test, because of criticisms for low statistical power and increased chance of a Type II error (Preacher & Hayes, 2008). A detailed description of bootstrapped
PARTNERS OF COMBAT VETERANS 7
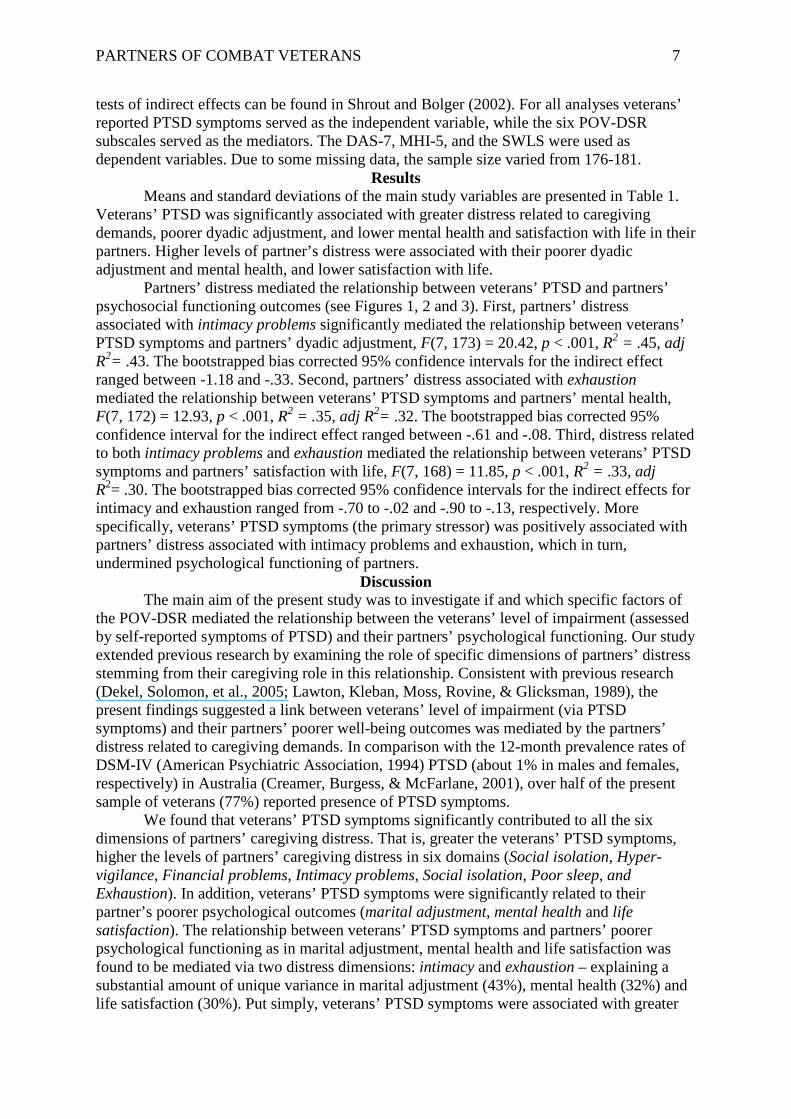
tests of indirect effects can be found in Shrout and Bolger (2002). For all analyses veterans’ reported PTSD symptoms served as the independent variable, while the six POV-DSR subscales served as the mediators. The DAS-7, MHI-5, and the SWLS were used as dependent variables. Due to some missing data, the sample size varied from 176-181.
Results Means and standard deviations of the main study variables are presented in Table 1.
Veterans’ PTSD was significantly associated with greater distress related to caregiving demands, poorer dyadic adjustment, and lower mental health and satisfaction with life in their partners. Higher levels of partner’s distress were associated with their poorer dyadic adjustment and mental health, and lower satisfaction with life.
Partners’ distress mediated the relationship between veterans’ PTSD and partners’ psychosocial functioning outcomes (see Figures 1, 2 and 3). First, partners’ distress associated with intimacy problems significantly mediated the relationship between veterans’ PTSD symptoms and partners’ dyadic adjustment, F(7, 173) = 20.42, p < .001, R2 = .45, adj R2= .43. The bootstrapped bias corrected 95% confidence intervals for the indirect effect ranged between -1.18 and -.33. Second, partners’ distress associated with exhaustion mediated the relationship between veterans’ PTSD symptoms and partners’ mental health, F(7, 172) = 12.93, p < .001, R2 = .35, adj R2= .32. The bootstrapped bias corrected 95% confidence interval for the indirect effect ranged between -.61 and -.08. Third, distress related to both intimacy problems and exhaustion mediated the relationship between veterans’ PTSD symptoms and partners’ satisfaction with life, F(7, 168) = 11.85, p < .001, R2 = .33, adj R2= .30. The bootstrapped bias corrected 95% confidence intervals for the indirect effects for intimacy and exhaustion ranged from -.70 to -.02 and -.90 to -.13, respectively. More specifically, veterans’ PTSD symptoms (the primary stressor) was positively associated with partners’ distress associated with intimacy problems and exhaustion, which in turn, undermined psychological functioning of partners.
Discussion The main aim of the present study was to investigate if and which specific factors of
the POV-DSR mediated the relationship between the veterans’ level of impairment (assessed by self-reported symptoms of PTSD) and their partners’ psychological functioning. Our study extended previous research by examining the role of specific dimensions of partners’ distress stemming from their caregiving role in this relationship. Consistent with previous research (Dekel, Solomon, et al., 2005; Lawton, Kleban, Moss, Rovine, & Glicksman, 1989), the present findings suggested a link between veterans’ level of impairment (via PTSD symptoms) and their partners’ poorer well-being outcomes was mediated by the partners’ distress related to caregiving demands. In comparison with the 12-month prevalence rates of DSM-IV (American Psychiatric Association, 1994) PTSD (about 1% in males and females, respectively) in Australia (Creamer, Burgess, & McFarlane, 2001), over half of the present sample of veterans (77%) reported presence of PTSD symptoms.
We found that veterans’ PTSD symptoms significantly contributed to all the six dimensions of partners’ caregiving distress. That is, greater the veterans’ PTSD symptoms, higher the levels of partners’ caregiving distress in six domains (Social isolation, Hyper-vigilance, Financial problems, Intimacy problems, Social isolation, Poor sleep, and Exhaustion). In addition, veterans’ PTSD symptoms were significantly related to their partner’s poorer psychological outcomes (marital adjustment, mental health and life satisfaction). The relationship between veterans’ PTSD symptoms and partners’ poorer psychological functioning as in marital adjustment, mental health and life satisfaction was found to be mediated via two distress dimensions: intimacy and exhaustion – explaining a substantial amount of unique variance in marital adjustment (43%), mental health (32%) and life satisfaction (30%). Put simply, veterans’ PTSD symptoms were associated with greater

PARTNERS OF COMBAT VETERANS 8
level of partners’ distress associated with intimacy problems and feelings of exhaustion, which in turn, resulted in poorer psychological functioning in partners.
In particular, our findings suggested that disruption of intimacy explained the relationship between veterans’ PTSD symptoms and their partners’ poorer dyadic adjustment, whereas the effect of veterans’ impairment on their partners’ mental health was due to the feelings of exhaustion experienced by partners. Interestingly, both intimacy problems and exhaustion were the significant mediators for partners’ satisfaction of life. One possible explanation for experiencing distress related to exhaustion might be due to the arduous task of continuously interpreting the needs of their veterans, along with feeling responsible for all family matters. Adding to that, the experience of emotional alienation by not being able to share thoughts and feelings with their veteran spouses leads to intimacy problems. Seemingly, the cumulative effect of these two caregiving distress dimensions undermines partner’ satisfaction with life, which is a global cognitive-judgmental evaluation of life (Diener et al., 1985).
The present findings suggest that an intervention or program should aim at addressing key distress indices related to caregiving demands, which may in turn improve psychological functioning. For example, increase respite services for those partners experiencing distress related to exhaustion and/or provision of couple counselling services for the ones experience intimacy issues. It has been recognised that in most cases, the spouse/partner is crucial to the health of the veteran couple (Orthner & Rose, 2009). Therefore, programs addressing family issues rather than singling out only the veteran for ‘treatment’ of mental health problems might prove useful. Future research might also investigate the roles of partners’ primary and secondary stress appraisal models (Lawton et al., 1989; Lazarus & Folkman, 1984), sense of mastery (Folkman, Lazarus, Gruen, & DeLongis, 1986), and social support (Calhoun et al., 2002; Folkman et al., 1986) to further reveal the underlying mechanisms of caregiving role overload, specifically in partners of combat veterans. Limitations and Future Research Directions
There are several limitations that should be noted when interpreting the findings from the present study. First, the present sample is not representative of partners of combat veterans and do not generalise to the entire Australian partner population or to partners of combat veterans in other countries. Future research could examine the relationships explored in the present study using a younger cohort of partners as well as partners of current serving members of Australian defense services, thus providing further evidence of the robustness of the current findings. Second, this study used a cross sectional design. It has provided a snapshot of these couples at a single point in time. Future research could explore these relationships longitudinally to ascertain the cyclic nature of the relationship between veterans’ level of impairment and their partners’ poorer well-being outcomes (Lazarus & Folkman, 1984; Pearlin et al., 1990). Such type of longitudinal analysis will also help to delineate an overlap between distress dimensions and outcome measures.
Third, only one measure of veteran’s level of impairment (e.g., PTSD symptoms) was used in the present study. Future research might also investigate additional factors such as veterans’ functional disability and other mental health problems (e.g., depression). Fourth, we used a revised version of original POV-DS, labeled as POV-DSR in the present study. The POV-DSR was developed to exclude the negative affect subscale, thus preventing duplication of mental health construct as both distress subscale (mediator) and outcome measure (DV). In addition, previous research suggested that poor sleep might be a symptom of mental illness (Miller, 2010), suggesting using this subscale (poor sleep) may be a confound for the mental health outcome (DV). However, El-Sheikh, Kelly, and Rauer (2013) highlighted the importance of sleep, in relationship processes (with couples) and mental health. It may seem plausible that sleep problems may increase the risk of developing mental health issues,

PARTNERS OF COMBAT VETERANS 9
therefore we retained this subscale as an independent distress index predicting mental health outcomes in partners of combat veterans. Although these two versions of the partner distress scale exhibited high convergent validity, more studies are needed to replicate the present findings. Finally, future research might examine the possible mediating roles of partner’s perceptions of PTSD symptoms (e.g., Renshaw & Caska, 2012) and attributions of veteran’s mental health (e.g., Renshaw et al., 2008) in the relationship between veteran’s level of impairment and their partner’s psychological functioning. Conclusion
The most important contribution of the present study is to empirically demonstrate the integral role of caregiving distress in understanding mechanisms impacting on psychological functioning of partners of Australian combat veterans. The clinical implications of the present study underline the importance of assisting partners of combat veterans. Negative dyadic and family relationships may in fact impede the treatment of veterans, which, in turn, tend to hinder positive outcomes for veterans and their family unit (Tarrier, Sommerfield, & Pilgrim, 1999). By identifying and addressing the cumulative impact of the specific indices of partners’ distress associated with intimacy problems and exhaustion, could in fact improve functioning of the family unit as a whole and subsequently lead to better outcomes for veterans. What is already known on this topic
1. Posttraumatic stress disorder (PTSD) symptoms in combat veterans are known to be associated with impaired psychological functioning in their partners.
2. Partners of combat veterans have a significantly higher risk of developing psychological problems as a result of living and caring for their veterans, than the general population.
3. Currently there has been limited examination of the link between veterans' PTSD symptoms and their partners' poorer psychological functioning..
What this paper adds
1. This study examined the role of specific dimensions of partners' distress in the relationship between veteran's level of impairment (via PTSD symptoms) and the psychological functioning of their partners.
2. Partners reported that distress related to exhaustion and intimacy problems significantly mediated the relationship between veteran's PTSD symptoms and their partners' satisfaction with life, whereas, partners' distress associated with intimacy problems was the sole significant mediator for their dyadic adjustment, and exhaustion was the only significant mediator for partners' mental health.
3. This study provides new insights into the relative contributions of distinctive dimensions of caregiving distress partners of combat veterans.

PARTNERS OF COMBAT VETERANS 10
References Alessi, M. W., Ray, J. W., Ray, G. E., & Stewart, S. J. (2001). Personality and psychopathology profiles of
veterans' wives: Measuring distress using the MMPI-2. Journal of Clinical Psychology, 57, 1535-1542. doi:10.1002/jclp.1115
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology, 51, 1173-1182. doi:10.1037/0022-3514.51.6.1173
Beckham, J., Lytle, B. L. E., Kudler, S. K., Feldman, M. E., & Palmer, S. (1997). Minnesota multiphasic personality profiles of Vietnam veterans with posstraumatic stress disorder and their children. Journal of Clinical Psychology, 53, ss847-852. doi:10.1002/(SICI)1097-4679(199712)53:8<847::AID-JCLP9>3.0.CO;2-C
Beckham, J. C., Lytle, B. L., & Feldman, M. E. (1996). Caregiver burden in partners of Vietnam war veterans with posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 64, 1066-1072. doi:10.1037/0022-006X.64.5.1068
Berwick, D. M., Murphy, J. M., Goldman, P. A., Ware, J. E. J., Barsky, A. J., & Weinstein, M. C. (1991). Performance of a five-item mental health screening test. Med Care. doi:10.1097/00005650-199102000-00008
Braithwaite, V. (1996). Between stressors and outcomes: Can we simplify caregiving process variables. The Gerentologist, 36, 42-53. doi:10.1093/geront/36.1.42
Breslau, N., Peterson, E. L., Kessler, R. C., & Schultz, L. R. (1999). Short screening scale for DSM-IV Posttraumatic Stress Disorder. American Journal of Psychiatry, 156, 908-911. doi:156:908-911.
Calhoun, P. S., Beckham, J. C., & Bosworth, H. B. (2002). Caregiver burden and psychological distress in partners of veterans with chronic posttraumatic stress disorder. Journal of Traumatic Stress, 15, 205-212 doi:10.1023/A:1015251210928
Creamer, M., Burgess, P., & McFarlane, A. C. (2001). Post-traumatic stress disorder: Findings from the Australian National Survey of Mental Health and Well-being. Psychological Medicine, 31, 1237-1247. doi:10.1017/S0033291701004287
Dekel, R., Goldblatt, H., Keidar, M., Solomon, Z., & Polliack, M. (2005). Being a wife of a veteran with posttraumatic stress disorder. Family Relations, 54, 24-36. doi:10.1111/j.0197-6664.2005.00003.x
Dekel, R., & Monson, C. M. (2010). Military-related post-traumatic stress disorder and family relations: Current knowledge and future directions. Aggression and Violent Behavior, 15, 303-309. doi:10.1016/j.avb.2010.03.001
Dekel, R., Solomon, Z., & Bleich, A. (2005). Emotional distress and marital adjustment of caregivers: Contribution of level of impairment and appraised burden. Anxiety, Stress & Coping, 18, 71-82. doi:10.1080/10615800412336427
Diener, E., Emmons, R. A., Larson, R. J., & Griffin, S. (1985). The Satisfaction with Life Scale. Journal of Personality Assessment, 49, 71-76s. doi:10.1207/s15327752jpa4901_13
Dirkzwager, A. J. E., Bramsen, I., Adèr, H., & van der Ploeg, H. M. (2005). Secondary Traumatization in partners and parents of Dutch peacekeeping soldiers. Journal of Family Psychology, 19, 217-226. doi:10.1037/0893-3200.19.2.217
Dupuis, S., & Smale, B. (2004). Caregivers of person with dementia: Roles, experiences, supports and coping. A literature review. Ontario: University of Waterloo.
El-Sheikh, M., Kelly, R., & Rauer, A. (2013). Quick to berate, slow to sleep: Interpartner psychological conflict, mental health, and sleep. Health Psychology, 32, 1057-1066. doi:10.1037/a0031786
Evans, L., McHugh, T., Hopwood, M., & Watt, C. (2003). Chronic posttraumatic stress disorder and family functioning of Vietnam veterans and their partners. Australian and New Zealand Journal of Psychiatry, 37, 765-772. doi:10.1111/j.1440-1614.2003.01267.x
Folkman, S., Lazarus, R. S., Gruen, R. J., & DeLongis, A. (1986). Appraisal, coping, health status, and psychological symptoms. Journal of Personality and Social Psychology, 50, 571-579. doi:10.1037/0022-3514.50.3.571
Frančikovišć, T., Stevanovic, A., Jelušić, I., Roganović, B., Klarić, M., & Grković, J. (2007). Secondary traumatization of wives of war veterans woth posttraumatic stress disorder. Croatian Medical Journal, 48, 177-184.
Frederick, J. A., & Fast, J. E. (1999). Eldercare in Canada: Who does how much? (No. 11-008-XPE). Ottawa, Ontario, Canada: Statistics Canada. Retrieved from http://publications.gc.ca/Collection-R/Statcan/11-008-XIE/0029911-008-XIE.pdf.

PARTNERS OF COMBAT VETERANS 11
Hayes, A. F., Preacher, K. J., & Myers, T. A. (2011). Mediation and the estimation of indirect effects in political communication research. In E. P. Bucy & R. L. Holbert (Eds.), Sourcebook for Political Communication Research: Methods, measures and analytical techniques. New York: Routledge.
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat Duty in Iraq and Afghanistan, mental health problems, and barriers to care. The New England Journal of Medicine, 351, 13-22. doi:10.1056/NEJMoa040603
Hunsley, J., Pinsent, C., Lefebvre, M., James-Tanner, S., & Vito, D. (1995). Construct validity of the short forms of the Dyadic Adjustment Scale. Family Relations, 44, 231-237. doi:10.2307/585520
Lawton, M. P., Kleban, M. H., Moss, M., Rovine, M., & Glicksman, A. (1989). Measuring caregiving appraisal. Journal of Gerentology, 44, 61-71. doi:10.1093/geronj/44.3.P61
Lawton, M. P., Moss, M., Kleban, M. H., Glicksman, A., & Rovine, M. (1991). A two-factor model of caregiving appraisal and psychological well-being. Journal of Gerentology, 46, 181-189. doi:10.1093/geronj/46.4.p181
Lazarus, R. S., & Folkman, S. (1984). Stress, Appraisal and Coping. New York: Springer Publishing Company. Lev-Wiesel, R., & Amir, A. (2001). Secondary traumatic stress, psychological distress, sharing of traumatic
reminiseces, and marital quality among spouses of holocaust child survivors. Journal of Marital and Family Therapy, 27, 433-444. doi:10.1111/j.1752-0606.2001.tb00338.x
MacDonell, G. V., Marsh, N. V., Hine, D. W., & Bhullar, N. (2010). The development and psychometric evaluation of a measure to assess distress in partners of Australian combat veterans. Australian and New Zealand Journal of Psychiatry, 44, 839-845.
Miliken, C. S., Auchterlonie, J. L., & Hoge, C. W. (2007). Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. Journal of American Medical Association, 298, 2141- 2148. doi:10.1001/jama.298.18.2141
Miller, M. (2010). Sleep and mental health. Norwalk: Belvoir Media Group, LLC. , Retrieved from: http://search.proquest.com.ezproxy.une.edu.au/docview/1370178728?accountid=17227
Orthner, D. K., & Rose, R. (2009). Work separation demands and spouse psychological well-being. Family Relations, 58, 392-403. doi:10.1111/j.1741-3729.2009.00561.x
Outram, S., Hansen, V., MacDonell, G., Cockburn, J., & Adams, J. (2009). Still living in a war zone: Perceived health and wellbeing of partners of Vietnam veterans attending partners’ support groups in NSW, Australia. Australian Psychologist, 44, 128-135. doi:10.1080/00050060802630353
Pearlin, L., Mullan, J., Semple, S., & Skaff, M. (1990). Caregiving and the stress process: An overview of concepts and their measures. The Gerontologist, 30, 583-594. doi:10.1093/geront/30.5.583
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879-891. doi:10.3758/brm.40.3.879
Renshaw, K. D., & Caska, C. M. (2012). Relationship distress in partners of combat veterans: The role of partners’ perceptions of posttraumatic stress symptoms. Behavior Therapy, 43, 416-426. doi:10.1016/j.beth.2011.09.002
Renshaw, K. D., Rodrigues, C. S., & Jones, D. H. (2008). Psychological symptoms and marital satisfaction in spouses of Operation Iraqi Freedom veterans: Relationships with spouses’ perceptions of veterans’ experiences and symptoms. Journal of Family Psychology, 22, 586-594. doi:10.1037/0893-3200.22.3.586
Salimi, S. H., Azad-Marazbadi, E., Karaminia, R., Mirzamani, S. M., & Hosseini-Sangtrashani, S. (2006). Being a wife of a veteran with psychiatric problem or chemical warfare exposure: A preliminary report from Iran. Iranian Journal Psychiatry, 1, 65-69.
Sayers, S. L., Farrow, V. A., Ross, J., & Oslin, D. W. (2008). Family problems among recently returned Military veterans reffered for a mental health evaluation. Journal of Clinical Psychiatry, e1-e8. doi:10.4088/JCP.07m03863
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychological Methods, 7, 422-445. doi:10.1037//1082-989x.7.4.422
Solomon, Z., Dekel, R., & Mikulincer, M. (2008). Complex trauma of war captivity: a prospective study of attachment and post-traumatic stress disorder. Psychological Medicine, 38, 1427-1434. doi:10.1017/S0033291708002808
Tarrier, N., Sommerfield, C., & Pilgrim, H. (1999). Relatives' expressed emotion (EE) and PTSD treatment outcomes. Psychology Medicine, 29, 801-881.
Westerink, J., & Giarratano, L. (1999). The impact of posttraumatic stress disorder on partners and children of Australian Vietnam veterans. Australian and New Zealand Journal of Psychiatry, 33, 841-847. doi:10.1046/j.1440-1614.1999.00638.x

PARTNERS OF COMBAT VETERANS 12
Table 1 Correlations, Means and Standard Deviations of the Main Study Variables Measure 1 2 3 4 5 6 7 8 9 10 M SD 1. DAS - .57** .63** -.22** -.51** -.36** -.32** -.66** -.52** -.17* 18.18 6.90 2. MHI - .67** -.35** -.50** -.41** -.49** -.44** -.56** -.24** 18.66 5.28 3. SWLS - -.23** -.49** -.37** -.36** -.52** -.54** -.19* 17.76 8.10 4. Sleepa - .57** .52** .48** .46** .54** .15* 1.34 1.07 5. Hyper-vigilancea - .70** .56** .78** .79** .29** 2.32 1.27 6. Social isolationa - .48** .64** .65** .32** 1.14 1.06 7. Financial problemsa - .53** .69** .27** 0.98 1.01 8. Intimacy problemsa - .77** .30** 1.54 1.25 9. Exhaustiona - .31** 2.03 1.34 10. Veterans’ PTSD - 4.91 1.82
Notes. SWLS = Satisfaction with Life Scale; MHI = Mental Health Inventory; DAS = Dyadic Adjustment Scale; and PTSD = Posttraumatic Stress Disorder Scale. Unless otherwise noted variables are based on partners’ assessments. a Subscales of the POV-DSR. * p < .05, ** p < .01.

PARTNERS OF COMBAT VETERANS 13
Figure 1. POV-DSR subscales as potential mediators of the relationship between veterans’ PTSD levels and partners’ dyadic adjustment. The model indicates that the relationship is mediated by partners’ distress associated with intimacy problems. All reported path coefficients are unstandardised. * p < .05, ** p < .01, *** p < .001
Figure 2. POV-DSR subscales as potential mediators of the relationship between veterans’ PTSD levels and partners’ mental health. The model indicates that the relationship is mediated by partners’ distress associated with exhaustion. All reported path coefficients are unstandardised. ** p < .01, *** p < .001

PARTNERS OF COMBAT VETERANS 14
Figure 3. POV-DSR subscales as potential mediators of the relationship between veterans’ PTSD levels and partners’ satisfaction with life. The model indicates that the relationship between veterans’ PTSD levels and partners’ satisfaction with life is mediated by partners’ distress associated with intimacy problems and exhaustion. All reported path coefficients are unstandardised. * p < .05, ** p < .01, *** p < .001