
Relation of chronic and episodic stressors to psychological distress, reactivity, and health...
21
INTERNATIONALJOURNAL OF BEHAVIORAL MEDICINE. 4(1), 39-59 Copyright 9 1997. Lawrence Erlbaum Assocmtes, Inc. Relation of Chronic and Episodic Stressors to Psychological Distress, Reactivity, and Health Problems Stephen J. Lepore, Heather J. Miles, and Jodi S. Levy This study tested the hypothesis that exposure to chronic stressor,s, which reflect persistent, negative life situations, would have greater physiological, psychological, and physical health costs than exposure to episodic or intermediate-length stressors, which reflect relatively transient, negative life situations. We also tested whether cardiovascular reactivity, conceptualized as a marker of underlying pathophysiologi- cal states, would mediate the relation between chronic stress and psychological distress and illness. Participants were 75 male and 75 female coIlege students. Compared with students experiencing few chronic life stressors, students experienc- ing many chronic life sttessors had exaggerated cardiovascular responses to acute challenges, delayed recovery to resting levels of cardiovascular functioning after the acute challenges, elevated psychological distress levels, and they reported more illnesses. None of the outcomes was associated with the number of episodic or intermediate-length life stressors students experienced. Cardiovascular reactivity did not mediate the stress-distress or stress-iI)ness ,associations. The results suggest that ongoing stressors that are static are more detrimental to health and well-being than are episodic or change-related stressors. Key words: cardiovascular reactivity, chronic stress, psychophysiology, life events A central assumption of psychological stress research is that life events, particularly those that signify transitions (e.g., divorce, job loss), can trigger biological re- sponses that can increase illness susceptibility. The theoretical underpinnings of this research are traceable to Selye's (1956) notion that nonspecific environmental Stephen .[, Lepore, Carnegie Mellon University, PitL~burgh, PA, USA; Heather J. Miles, Stanford t ril~c~il.~,,Palo AIhL CA, lISA; ]c~dl S L,c,v~, Michigan Stale t lm~e~lty. F,t.~t I~lnc;in[. MI, L SA Th.~ rc~ear~;hIx.'ncfittedfrom the diLgent and careful n.-~carcha.~.,l~tanceol'Ju~e Klernmcr, Mtehelr Mr Laurie Modelt, Holly Tt~k, and Andy White, to whom we am most grateful. We thank G:~ry Evans and Sheldon Cohen for their comments on an earlier draft oF this re'title. Corre.~pondenc~ concerning this a.,'ticle slmuId be addre.~,~d to Stephen J. Lepom, Department .of Psychology. Carnegie Mellon University. Pittsburgh. PA 15213-3890. E-mail: sleporc@=Lndrcw.cmu. edu
Transcript of Relation of chronic and episodic stressors to psychological distress, reactivity, and health...

INTERNATIONAL JOURNAL OF BEHAVIORAL MEDICINE. 4(1), 39-59 Copyright �9 1997. Lawrence Erlbaum Assocmtes, Inc.
Relation of Chronic and Episodic Stressors to Psychological Distress,
Reactivity, and Health Problems
Stephen J. Lepore, Heather J. Miles, and Jodi S. Levy
This study tested the hypothesis that exposure to chronic stressor,s, which reflect persistent, negative life situations, would have greater physiological, psychological, and physical health costs than exposure to episodic or intermediate-length stressors, which reflect relatively transient, negative life situations. We also tested whether cardiovascular reactivity, conceptualized as a marker of underlying pathophysiologi- cal states, would mediate the relation between chronic stress and psychological distress and illness. Participants were 75 male and 75 female coIlege students. Compared with students experiencing few chronic life stressors, students experienc- ing many chronic life sttessors had exaggerated cardiovascular responses to acute challenges, delayed recovery to resting levels of cardiovascular functioning after the acute challenges, elevated psychological distress levels, and they reported more illnesses. None of the outcomes was associated with the number of episodic or intermediate-length life stressors students experienced. Cardiovascular reactivity did not mediate the stress-distress or stress-iI)ness ,associations. The results suggest that ongoing stressors that are static are more detrimental to health and well-being than are episodic or change-related stressors.
Key words: cardiovascular reactivity, chronic stress, psychophysiology, life events
A central assumption of psychologica l stress research is that l ife events, part icularly
those that s ignify transitions (e.g., divorce, j o b loss), can tr igger b iological re-
sponses that can increase il lness susceptibility. The theoretical underpinnings o f
this research are t raceable to Se lye ' s (1956) notion that nonspeci f ic envi ronmenta l
Stephen .[, Lepore, Carnegie Mellon University, PitL~burgh, PA, USA; Heather J. Miles, Stanford t ril~c~il.~,, Palo AIhL CA, lISA; ]c~dl S L,c,v~, Michigan Stale t lm~e~lty. F,t.~t I~lnc;in[. MI, L SA
Th.~ rc~ear~;h Ix.'ncfitted from the diLgent and careful n.-~carch a.~.,l~tance ol'Ju~e Klernmcr, M tehelr Mr Laurie Modelt, Holly Tt~k, and Andy White, to whom we am most grateful. We thank G:~ry Evans and Sheldon Cohen for their comments on an earlier draft oF this re'title.
Corre.~pondenc~ concerning this a.,'ticle slmuId be addre.~,~d to Stephen J. Lepom, Department .of Psychology. Carnegie Mellon University. Pittsburgh. PA 15213-3890. E-mail: sleporc@=Lndrcw.cmu. edu
40 LEPORE, MILES. LEVY
changes can evoke a sequence of biological responses that directly and indirectly contribute to disease processes. Although there has been some debate as to whether illness is provoked by any life change or primarily by undesirable and uncon- troIlable life change (see Thoits, 1983), the emphasis on change-related stress has remai ned strong to this day. A central problem with this approach is that it provides no information on the duration of stressor exposure, thereby limiting investigators" abilities to examine the independent and possibly unique effects of chronic versus episodic life stressors on disease susceptibility (Lepore, 1995).
The need to distinguish chronic from episodic life stress is becoming increas- ingly obvious. Population surveys reveal that chronic stressors are a pervasive part of everyday life (Mattli,, Wethington. & Kessler, 1990). We also know that typical events on life events measures can vary considerably in duration (e.g., job loss) or they may be proxies for enduring stressful situations (e.g., divorce as a marker of ongoing marital strains; Lepore, 1995). Inve~igators who have compared the relative effects of episodic and chronic stressors agree that chronic stress may be more strongly related to mental and physical disorders (e.g., Brown & Harris, 1989; Eckenrode, t984). Finally, it appears that chronic stressors may deplete biological, psychological, and social coping resources, thereby increasing risk for illnesses and undermining people's ability to cope with novel challenges (Lepore. 1997; Lepore & Evans, 1996; Lepore, Evans, & Schneider, 1991 ).
One reason that chronic stress is believed to have inimical effects on health is that it can alter the physiological state of an organism, as well as its bodily integrity. When behavioral and psychological demands are chronic, the body will respond with a persistently high level of activation (cf. McEwen & Stellar, 1993). The continuous arousal signals resulting from chronic stress may contribute to an underlying pathophysiologieal state. For instance, the heightened state of arousat induced by chronic stress may read to sensitiration, or hyperrespoBsiveness, to environmental challenges and a decreased capacity to adjust levees of arousal upon the cessation of the challenges (Fleming, Baum, Davidson, Rectanus, & McArdle, 1987). Thus, chronic stress may interfere with physiological mechanisms that enable organisms to regulate their physiological responses to stressors, thereby sustaining arousal. In describing the impact ofchronic stressors on health, McEwen and Stellar (I 993) argued that "the strain on the body produced by repeated ups and downs of the physiologic response, as well as by the elevated activity of physiologic systems under challenge, and the changes in metabolism and the impact of wear and tear on a number of organs and tissues, can predispose the organism to disease'" (p. 2094). Sterling and Eyer (1988) also noted that chronic arousal associated with ongoing behavioral or psychological demands produces bodily changes, such as immunosuppression, which could increase susceptibility to illness.
The hypothesized relation between chronic stress exposure and increased disease susceptibility due to underlying physiological alterations is compelling, but empiri- cal supporl for this model still is limited. Even basic data on the relative effects of

CHRONIC AND EPISODIC STRESSORS ~1
chronic versus episodic stressors on psychological, physiological, and health outcomes is lacking. This study was designed to ( ! ) provide descriptive data on the relation between strcssors of different durations and a range of outcomes (psycho- logical symptoms, psychobiologic reactivity, and reports of physical health prob- lems) and (2) examine whether psychobioIogic reactivity mediates the association between chronic stress and reported health problems. We hypothesized that if chronic stress exposure results in exaggerated physiological responses to environ- mental challenges and interferes with adjustment processes, individuals exposed to chronic stressors should exhibit increased psychobiologic reactivity (e.g., height- ened cardiovascular responses) when exposed to novel challenges and they should take longer to recover to baseline levels of functioning when the challenge is removed. Wc further hypothesized that if these physiological alterations increase illness susceptibility.--either because sustained arousal directly damages bodily systems and organs or because it can suppress immune functions that protects people from invading agents--then people exhibiting higher reactivity to chal- lenges also should report more health problems.
Previous research provides some empirical support for these predictions. First, it is plausible that chronic stress exposure can increase cardiovascular responses to acute challenges. At least a dozen studies have examined how individual differences in background stress levels relate to cardiovascular responses to laboratory stressors (see Lcpore & Evans, 1996). The results of these studies have been quite mixed: Some studies indicate no association between life stress and cardiovascular re- sponse to challenge (e.g., Cohen, Simons, Rose, McGowan, & Zclson, 1986), some indicate a positive relation (e.g., Evans, Allen, Tafalla, & O'Meara, 1996), and some indicate a negative relation (e.g., Schaubroeck & Ganstcr, 1993). Although it is difficult to account for these diverse findings, it appears that null findings have been reported in studies examining episodic life cvents (Cohen, Simons, et aL., 1986; Jorgensen & Houston, 1989; Pardine & Napoli, 1983; Vingerhocts, Ratliff-Crain, Jabaaij, Menges, & Bantu, 1996) and both positive (Fleming et al., I987) and negative (Schaubrocck & Ganster, ] 993) associations have been observed in studies of chronic strcssors (e.g., crowding, work stress). To our knowledge, this study is the first to directly compare the relative effects of chronic versus episodic stress exposure on cardiovascular reactivity.
Second, thcrc is evidcnce that individuals with extreme increases in heart rate and diastolic blood pressure during a laboratory challenge report more frequent minor illnesses (e.g., colds, infections) than do individuals with moderate to low increases (Dembroski, MacDougall, Slaats, Eliot, & Buell, 198 t ). Dembroski et at. ( 1981) argued that cardiovascuIar reactivity per sc is not responsible for the illness episodes their participants experienced. Instead, they suggest that reactivity reflects underlying differences in individuals' sympathetic and neuroendocrine activity that may have immunosuppresive effects that increase illness susceptibility. Results from two recent studies indicate that stress4nduced sympathetic arousal (i.e.,
42 LEPORE, MILES, LEVY
heightened catecholamine and cardiovascular responses) is associated with immu- nosuppression (Manuck, Cohen. Rabin, Muldoon, & Bachen, 1991; Zakowski, McAllister, Deal, & Baum, 1992). Moreover, prolonged elevations in neuroendo- crine and hemodynamic activity have been implicated in chronic degenerative diseases, such as hypertension and other cardiovascular-related dise~LSeS (Manuck, Kaplan, & Matthews, I986; Manuck, Kasprowicz, & Muldoon, 1990). Thus, cardiovascular reactivity may be a vulnerability factor in cardiovascular health, as well as a marker of an underlying pathophysiologieal state that may compromise host resistance and increase acute illness onset (also see Boyce et al., 1995). In addition to extreme reactivity, slowed recovery to prechallenge levels of arousal could be an important mediator in the chronic stress-health relation. If chronically stressed individuals take longer to recover from challenges they will experience sustained arousal even when exposed to nonchronic stressors. Health risks could increase if the sustained arousal incurred from slow recovery is directly damaging to bodily systems and organs or if it suppresses immune system functioning.
METHOD
Participants
The participants were 75 men and 75 women enrolled at Carnegie Mellon Univer- sity. They received class credit and $10. Their mean age was 19.45 years ( S D =
1.99 years) and the racial distribution was 69% White, 21% Asian, 3% African American, and 7% other races.
Procedures
Data were collected from participants individually during two laboratory sessions and one follow-up interview. The day before Session I, participants were instructed to abstain from alcohol consumption for 24 hr and to abstain from exercise, caffeine, and nicotine for at least 3 hr before their lab visit.
Session I: The acute stress challenge. Participants completed a ques- tionnaire on background characteristics and were asked to describe any "health problems, minor or major, such as a cold, infection, asthma, headaches, or an injury" they had in the prior month. The acute stress challenge ,,vas then administered ir~ the following sequence: Rest I (6 min), Stressor I (8 min of mental arithmetic), Rest 2 (6 min). Stressor 2 (8 rain speech), and Recovery (6 rain). During the resting and recovery phases, participants watched a nature video with relaxing music.
In the mental arithmetic task, participants were required to count backward and aloud at a rate equal to or faster than an audiotaped tone, which was emitted every 2 sec. Participants counted backward by 7 sec (from 4,562) for 4 rain and then
CHRONIC AND EPISODIC STRESSORS 43
backward by 9 sec (from 2,785) for 4 min. Participants who lost their place or stopped counting were instructed via intercom to restart at the beginning number. In the speech task, participants had 4 rain to argue for and 4 min to argue against the use of animals by humans for sport, food, and research. They were given a page o f notes to support their arguments and were told that their speech would be observed via closed-circuit television and judged for its quality. Participants who prematurely stopped talking were instructed via intercom to continue their argu- ments.
We assessed systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) using an automated blood pressure monitor (A & D Medical UA-751, Milpitas, CA). Readings were taken every 2 min during each of the five phases.
Session Ih The interview. One week after Session I, participants returned to the laboratory to complete measures of psychological distress symptoms, expo- sure to life stressors, and neuroticism.
Follow-up contact. Two to 3 months after Session II, we contacted partici- pants to gather follow-up information on illnesses. Participants were reminded of when they were in the study and asked whether between that time and 2 months later they had "experienced any health problems, minor or major, such as a cold, infection, asthma, headaches, or an injury." They also were asked to describe their health problems.
Measures
SCL-gO-R Symptom scale. Psychological distress was measured with the Depressive and Anxious symptoms subscales of the SCL-90-R, which have been shown to have adequate internal characteristics and convergent validity (Derogatis, 1983). Scores from the two scales were averaged to form a singte distress index because the scales were highly intercorrelated (r = .77, p .001 ).
Neuroticism. Individuals high in neuroticism may exaggerate physical and psychological distress symptoms or their exposure to stressors on self-report measures. Therefore, we included the neuroticism subscale of the Eysenck Person- ality Inventory (EPI-N; Eysenck & Eysenck, 1975)as a covariate in analyses. The measure has adequate reliability and convergent validity.
Stressors, w e constructed a 42-item stress measure appropriate for cotlege students using items from the Inventory of College Students' Recent Life Experi- ences (ICSRLE; Kohn, Lafreniere, & Gurevich, 1990), a measure of social hassles and stressors used with college students (Lepore, Evans. & Palsane, 1991 ; Lepore,
44 LEPORE, MILES. LEVY
1996), and several major life event items. Both the ICSRLE and the social hassles measures have adequate reliability and predictive validity. The measure fsee Appendix) covers stressors related to school, work, finances, and relationships. Participants also reported any additional life stressors they experienced.
Respondents examined the list and marked all stressors that they had experienced in the prior year. We used a semistructured interview procedure to estimate the duration of the stressors. To facilitate recall, a calendar was available and respon- dents were prompted to think about what other things were going on when they experienced a stressor (e.g., the season, a holiday). Three indices of cumulative stressor exposure were computed from the duration data: episodic stressors (number of stressors lasting less than I month), intermediate-length stressors (number of stressors lasting 1 to 8 months), and chronic stressors (number of stressors lasting 9 or more months). We attempted to have an equivalent number of stressors in each duration category, so we chose cutoff dates based on the distribution of event durations: 34% of the stressors lasted less than a month, 38% lasted 1 to 8 months. and 28% lasted 9 or more months. We also calculated a total stressor score, which was the sum of stressors experienced over the I-year period.
We assessed reliability by administering the interview to 24 college students ( 12 men and 12 women) twice over a 2-month period. Reliability was assessed for the I 0-month overlapping period of the two interviews. Most of the events reported in the first interview were reported again 2 months later (M = 90.50%, SD = 10.20%). The correlation between number of episodic events recalled in both interviews was r = .92, for intermediate-length events it was r = .94, and for chronic events it was r = .94 (all ps < .(301). The overall mean proportion of agreement on the time frame of events (i.e., same start and end dates) was 79.40% (SD = 10.20%). The mean proportion of agreement on the time frame for episodic stressors was 74.30% (SD = 18.40%), for intermediate-length stressors it was 72.80% fSD = 23.70%), and for chronic stressors it was 85.40% (SD = 12.00%).
Math and speech performance. Math and speech performance were vide- otaped to test for internal validity threats. Trained observers counted the number of calculations and restarts made during the math task, and timed the number of seconds participants spoke during the speech task. An independent observer coded the same behaviors on 50% of the participants. The interobserver correlations were all high (number of calculations r = .99, number of restarts r= .97, speaking duration r = .85; all ps < .001).
Othercovariates. Body mass and cigarette smoking were measured to use as covariates in the blood pressure analyses. The Body Mass Index (BMI: a method for comparing weight across height groups) was calculated using the following formula: kgtm:. The smoking variable was the number of cigarettes participants reported to smoke on a typical day.
CHRONIC AND EPISODIC STRESSORS 4 5
RESULTS
The main goal of tile analyses was to compare the relative effects of stressors of different durations on psychological distress, cardiovascular reactivity and recov- ery, and illnesses. Each analysis started with an examination of the relation between total stressor exposure and the outcome. We then examined the associations between the number of stressors of different durations and the outcome. Appropri- ate covariates were included in analyses as indicated in the following sections. Gender did not moderate any of the relations between the variables.
Cardiovascular Functioning
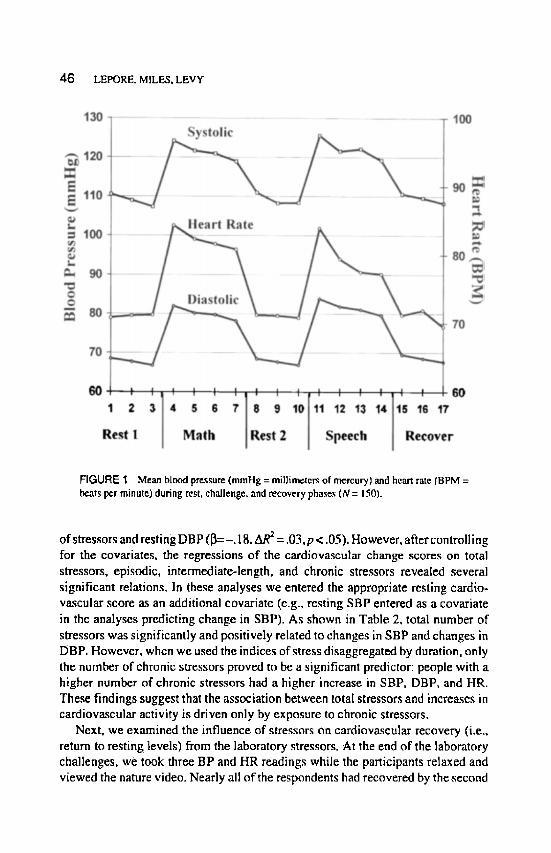
Figure 1 shows the mean SBP, DBP, and HR at each measurement period across the five phases. Repeated measures analyses of variance (ANOVA) revealed no significant differences in participants' mean BP and HR responses across the two resting phases and two challenge phases, respectively. Pearson correlations indi- cated that the cardiovascular responses were highly stable across the two resting phases (SBP r = .87, DBP r = .80, HR r = .89; all ps < .001 ) and across the two stressor phases (SBP r = .84, DBP r = .74, HR r - .83; all ps < .001). We calculated cardiovascular change scores using aggregated responses to the math and speech challenges (i.e., average of the four math and four speech scores minus average of last two premath and last two prespeech resting scores) for SBP, DBP, and HR, respectively (aggregation improves the reliability of cardiovascular measures; see Kamarck et al., 1992). The aggregated cardiovascular change scores had high internal consistency (Cronbach alpha's ranged from .91 to .96). From resting to task, the average increases in SBP, DBP, and HE all were significant (alI ps < .001). The number of math calculations and restarts were not correlated with the aggre- gated cardiovascular change scores or the change scores during the math task (all ps .05). Speaking duration was not correlated with the aggregated cardiovascular change scores or with the change scores during the speech (all ps > .05). Thus, the challenge manipulation worked and was not confounded by performance on the tasks.
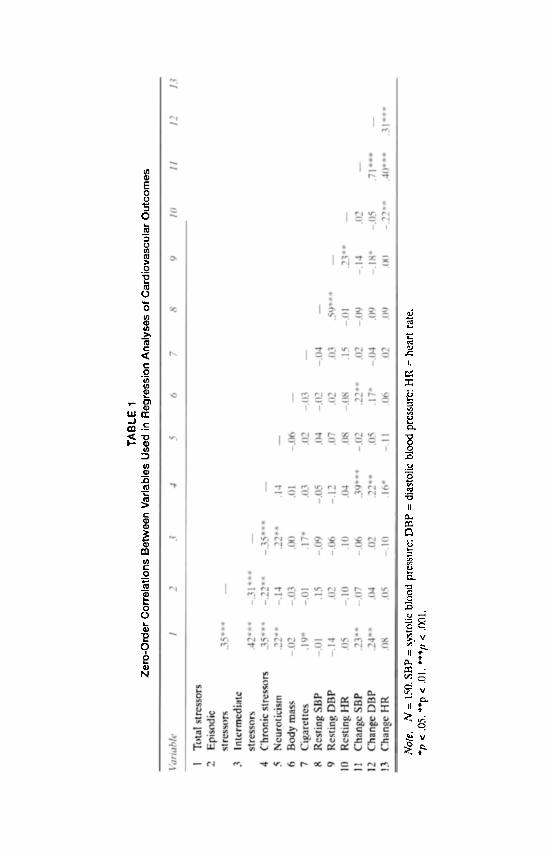
Our first analysis examined the associations between the stressor variables and the resting and change scores for SBP, DBP, and HR. We examined these relations using regression analyses, which allowed us to covary neuroticism, BMI, and number of cigarettes smoked per day. Covariates were entered as a single block. Table 1 shows the zero-order correlations between the variables used in the regression analyses.
After controlling for the covariates, the respective regressions of resting SBP. DBP, and HR on total stressors, episodic, h~termediate-length, and chronic stressors revealed only one significant relation: a negative association between total number
46 LEPORE. MILES, LEVY
FIGURE "[ Mean blood pre.~te (mmHg = millimeters of mercury) and heart rate fBPM = beats per minute) during rest, challenge, and recovery phases (N= 150).
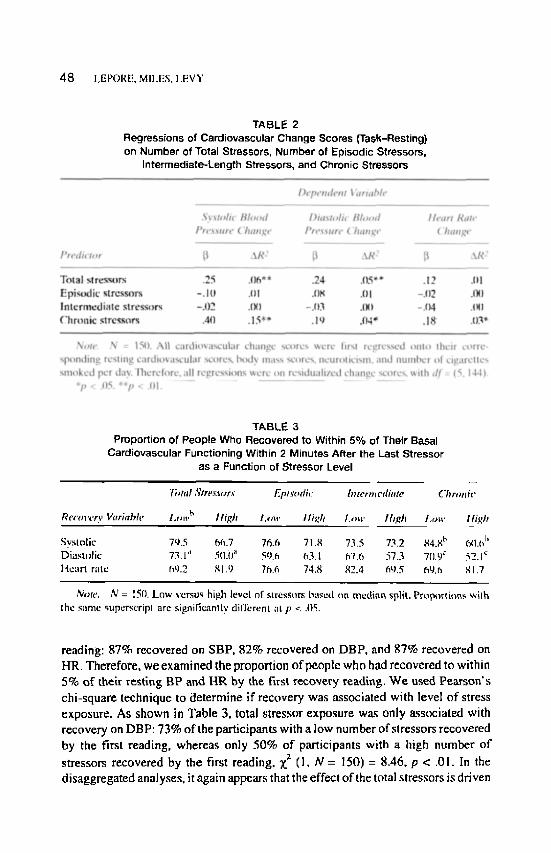
of stressors and resting DBP (]3=-. 18, AR 2 = .03,p < .05). However, after controlling for the covariates, the regressions of the cardiova~ular change ~ores on total stressors, episodic, intermediate-length, and chronic stressors revealed several significant relations. In these analyses we entered the appropriate resting cardio- vascular score as an additional covariate (e.g., resting SBP entered as a covariate in the analyses predicting change in SBP). As shown in Table 2, total number of stressors was significantly and positively related to changes in SBP and changes in DBP. However, when we used the indices of stress disaggregated by duration, only the number of chronic stressors proved to be a significant predictor: people with a higher number of chronic stressors had a higher increase in SBP, DBP, and HR. These findings suggest that the association between total stressors and increases in cardiovascular activity is driven only by exposure to chronic stressors.
Next, we examined the influence of stressors on cardiovascular recovery (i.e.. return to resting levels) from the laboratory stressors. At the end of the laboratory challenges, we took three BP and HR readings while the participants relaxed and viewed the nature video. Nearly all of the respondents had recovered by the second
t~
E 0
0
t~
O
r~ c :
E ._(2
, r - ~ 1 Q~
L U E
. ?
" E
{:
~J r Q
. m c~
O
0
~J
N
IJ
r l
II
r ~
r~
CJ
, o
~ . V
~.rLi V
o. ~ v
48 LEPORE. MILES. LEVY
TABLE 2 Regressions of Cardiovascular Change Scores (Task-Resting) on Number of Total Stressors, Number of Episodic Stressors,
Intermediate-Length Stressors, and Chronic Stressors
TABLE 3 Proportion of People Who Recovered to Within 5% of Thetr Basal
Cardiovascular Functioning Within 2 Minutes After the Last Stressor as a Function of .~tressor Level
T, ttd ,~tre.~'.~rsts Episodh"
Recovery Vttriahte l.,~v "~ I ligh Low I ligh
Systolic 79.5 ~ .7 76.6 71.8 Diastolic 73.1" 50.i~ ;~ 59.e, ~'~3. l Heart rate h~J.2 gl .U 7h.6 74.8
hTterm edittte (.'11r~ m it"
Low Ihgh Low l f igh
73.5 73.2 ,~4./,l t' t"A].f~ I '
fi7.6 57.3 7[1.9 ~" 52.1 c 82.4 69.5 fig.h ,q 1.7
Note; N = 150. Low versos high level of strcssors baxed on mcdia~ split. Prop~wtit~ns ~igh the s~mc superscripl are significaalty difl;erent a lp < .I}5.
reading: 87% recovered on SBP, 82% recovered on DBP, and 87% recovered on HR. Therefore, we examined the proportion of people who had recovered to within 5% of their resting BP and HR by the first recovery reading. W e used Pear son ' s chi-square technique to determine if recovery was associated with level o f stress exposure. As shown in Table 3, total stressor exposure was only a.ssociated with recovery on DBP: 73% of the participants with a low number of slressors recovered by the first reading, whereas only 50% of participants with a high number o f
stressors recovered by the first reading, Z z (I , N = 1501 = 8,46, p < .01. In the disaggregated analyses, it again appears that the effect of the total stressors is driven
CHRONIC AND EPISODIC STRF.S$ORS 4 9
by the chronic stressors. As shown in Table 3, exposure to episodic and intermedi- ate-length stressors had no relation to recovery, but exposure to chronic stressors
was associated with slower SBP and DBP recovery, Z: (I , N = 150) = I 1.24, p < .001, and 5.59, p < .05, respectively.
Because speed of recovery is inversely related to level of reactivity, the chi- square results might just reflect the extreme reactivity in people who have many chronic stressors. To rule out this possibility, we used logistic regression analyses to examine the relation between stressor exposure and recovery controlling for level o f reactivity (change scores). The recovery and stressor variables were dichoto- mized. The results paralleled those of the chi-square analysis. Relative to people with few total stressors, people with many total stressors were less likely to have recovered to their basal DBP on the first recovery reading (odds ratio = 2.49; Wald [df= 1 ] = 10.24, p < .0t), even after controlling for DBP change scores. In addition, relative to people with few chronic stressors, people with many chronic stressors were less likely to have recovered to their basal level of SBP (odds ratio = 2.35; Wald [d f= ] ] = 3.84, p < .05) and DBP (odds ratio = 2.06; Wald [d f= l] = 4.16, p < .05), even after controlling for SBP and DBP change scores, respectively.
Psychological Distress
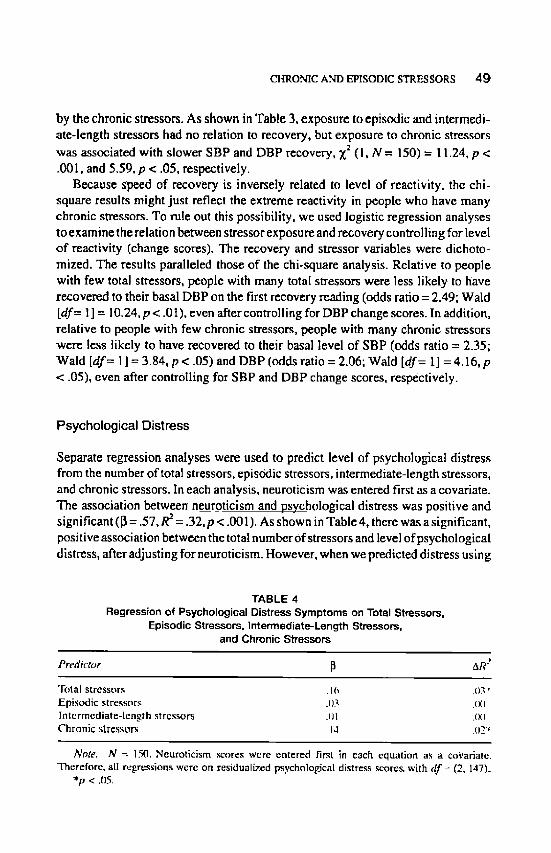
Separate regression analyses were used to predict level o f psychological distress from the number of total stressors, episodic stressors, intermediate-length stressors, and chronic stressors. In each analysis, neuroticism was entered first as a covariate. The association between neuroticism and psychological distress was positive and significant ([3 = .57, R z = .32, p < .001). As shown in Table 4, there was a significant, positive association between the total number of stressors and level of psychological distress, after adjusting for neuroticism. However, when we predicted distress using
TABLE 4 Regression of Psychological Distress Symptoms on Total Stressors,
Episodic Stressors. Intermediate-Length Stressom, and Chronic Stressors
Predictor ~ AR~'
Total s t ressors .16 .()3:'
E p i s o d i c s t ressors .1)3 .I X) I m c r m c d i a t e - l c n g t h s t rcssors +(J[ .Ix) C h r o n i c stre.,isors .14 _()2 "~
Note, N = ].50. Neuro t ic i sm ~ o r e s were en te red first in each equa t ion as a coVariatc. Therefore , al l regress ions were on residualiz.ed psychological distress ~ores . wi th df ~ (2, 147).
*p < .05.
50 LEPORE, MILES, LEV'~
the indices of stress disaggregated by duration, the only significant predictor was the number of chronic stressors: Higher chronic stress was associated with a higher level of psychological distress. These results suggest that chronic stressors account for the positive association between the total number of stressors and psychological distress,
To test whether cardiovascular reactivity accounted for any of the covariation between chronic stress and psychologicaldistress symptoms, we first examined the association between the cardiovascular change scores and symptoms. The change scores must be significantly related to symptoms to qualify as potential mediators. Zero-order correlations revealed that distress was correlated only with DBP change scores (Pearson's r = .16, p < .05). To test if DBP reactivity accounted for the association between chronic stress and distress, we entered participants' DBP change scores into the regression equation used to predict distress from chronic stress, controlling for neuroticism. When DBP change scores were entered into the equation prior to chronic stress scores, the chronic stress-distress association
became marginal (~i = .1 I, AR 2 = .01, p < .10). However, we also observed that when chronic stress scores were entered into the equation prior to DBP change
scores, the DBP reactivity-distress association became marginal (~ -=. 11, fiR" = .01, p < .10). Thus, although higher DBP reactivity was associated with higher distress, it does not appear to have mediated the relation between chronic stress and distress.
Illnesses
To test whether stress was related to reports of any illness and particular illnesses (e.g., cold), we used logistic regression techniques with illness outcomes dichoto- mized (absent-present). For these analyses, the stressor variables were categorized on the basis of whether the number of stressors reported was in the lower tertile (low), middle tertile (medium), or upper tertile (high). Using the lower tertile of stressors as our reference level, we estimated the odds ratio, or relative risk, of reporting an illness in people who had a medium or high level of stressors. All analyses included neuroticism and prior illness (reported during Session I) as covariates.
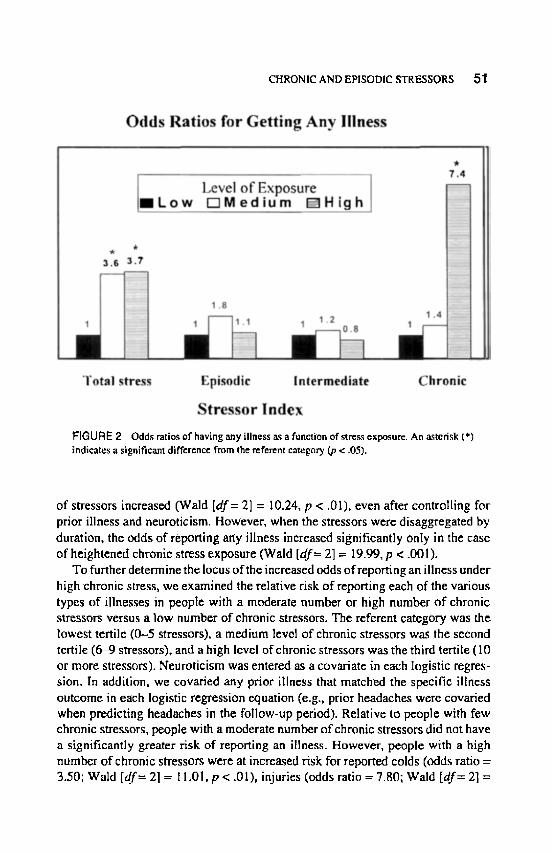
Several illness categories were derived from the self-report data. One category was whether or not any illness was reported. Other categories included injury, headache, cold, allergy, asthma, and infection (other than upper respiratory). Nearly half of the sample reported at least one illness during the first and follow-up interview (52.7% and 45.3%, respectively). In the first analysis, we examined whether people reporting a moderate or high number of stressors were more likely to report an illness than were people experiencing a low number of stressors. As Figure 2 illustrates, the odds of reporting any illness increased as the total number
CHRONIC AND EPISODIC STRF_.SSORS 5"[
FIGURE 2 Odds ratios of having any illness a.s a function of ~rc~ exposure. An a.~terisk (*) indicates a significant difference from the referent category (p < .05).
of stressors increased (Wald [df= 2] = 10.24, p < .01), even after controlling for prior illness and neuroticism. However, when the stressors were disaggregated by duration, the odds of reporting any illness increased significantly onIy in the case of heightened chronic stress exposure (Wald [df= 2] = 19.99, p < .001).
To further determine the locus of the increased odds of reporting an illness under high chronic stress, we examined the relative risk of reporting each of the various types of illnesses in people with a moderate number or high number o f chronic stressors versus a low number of chronic stressors. The referent category was the lowest tertile (0-5 stressors), a medium level of chronic stressors was the second tertile (6~9 stressors), and a high level of chronic stressors was the third tertite (10 or more stressors). Neuroticism was entered as a covariate in each logistic regres- sion. In addition, we covaried any prior illness that matched the specific illness outcome in each logistic regression equation (e.g., prior headaches were covaried when predicting headaches in the follow-up period). Relative to people with few chronic stressors, people with a moderate number of chronic stressors did not have a significantly greater risk of reporting an illness. However, people with a high number of chronic stressors were at increased risk for reported colds (odds ratio = 3.50; Wald [d.f= 2] = l l . 0 1 , p < .01), injuries (odds ratio = 7.80; Wald [df= 2] =

5 2 LEPORE, MILES. LEVY
10.71 p < .01), and headaches (odds ratio = 10.20; Wald [dr= 2] = 4.23, p < .05) relative to people with few chronic stressors.
Finally, we used regression analyses to examine the associations between stressor exposures and total number of illnesses reported, as well as the potential mediating effects of cardiovascular reactivity. In each regression, neuroticism scores and nu tuber of prior illnesses were entered first as covariates. The covariates accounted for a significant proportion of the variance in the reports of illnesses, F(2, 147) = 5.03, p < .01. As shown in Table 5, after adjusting for neuroticism and prior illness, there was a significant, positive association between total stressor exposure and number of reported illnesses. However, in the disaggregated analyses only the number of chronic stressors was significantly related to the number of reported illnesses: People with a high number of chronic stressors reported more illnesses than did people with a relatively low number of chronic stressors.
To test whether cardiovascular reactivity accounted fo r any of the covariation between chronic stressors and illnesses, we first examined whether SBP, DBP, and HR change scores were related to number of illnesses reported. To qualify as mediators, these cardiovascular variables would have to be significantly related to both the number of chronic stressors and the number of illnesses. From the results presented in Table 2, we know that chronic stress predicts cardiovascular reactivity. Zero-order correlations revealed that of the three f e s t iv i ty measures, only SBP reactivity was significantly correlated with total number of illnesses (Pearson's r = .24,p < .01 ). Thus, we limited the mediation analyses to SBP reactivity. When SBP change scores were entered prior to chronic stress scores in the equations predicting illnesses, the chronic stress-illness association was diminished slightly and re-
mained statistically significant ([3 = .33, p <.001). Moreover, when we repeated these analyses reversing the order of entry of chronic stress and SBP change scores (i.e., entering chronic stress prior to SBP change scores), the SBP reactivity-illness association was nonsignificant (13 = .09). Thus. although higher SBP reactivity was
TABLE 5 Regression of Total Number of Illnesses on Total S t m s s o r s , Episodic
Stressors, Intermediate-Length Stressors, and Chronic Stmssors
I ' rcdwlor l~ .~,R:
Total stressors .23 .05" Episodic stressors -.04 .002 Intermediate-length stressors -.08 .(XJ6 Chronic stressors .37 .13*"
No~e. N -~ 15(1. Number o( ~rinr ;.llnes~s a~d neuro~,icLsm ~ o ~ s ~vere entered firs!, in each equation as ~ cavari~te. Therefore, all rcgre~ions were on residualized illness scorer~ with a [ = (3, ~4~).
*/7 < All. **p < .~IL
CHRONIC AND EPISODIC STRESSOR5 53
associated with number of illnesses, it did not appear to mediate the relation between chronic stress and number of illnesses.
DISCUSSION
The results showed that exposure to chronic stressors---but not episodic or inter- mediate-length stressors--appears to have physiological, psychological, and so- matic costs. These findings are consistent with theories of chronic stress (cf. Gotttieb, I997; Lepore & Evans, 1996; Sterling & Eyer, 1988; McEwen & Stellar, 1993). However, the results also indicated that cardiovascular reactivity does not mediate the negative association between chronic stress and acute psychological distress or reports of physical health problems. The failed mediation effects suggest that cardiovascular reactivity is not a useful marker of potential pathophysiological processes underlying the relation between chronic stress and acute illnesses. Overall. these findings challenge some time-worn notions about the relation between life stress and illness, yet at the same time, they beg the question of why chronic stress is associated with such diverse and negative outcomes.
Implications of the Comparative Analyses
In nearly all analyses, the total number of stressors was negatively related to the outcomes. Compared with people with relatively few strcssors, people with a high number of life stressors had exaggerated SBP and DBP responses during the laboratory challenges, had delayed recovery to baseline DBP after the challenges ended, and had elevated psychological distress symptoms and illness reports. The traditional account of these effects would be that people with more life stressors are suffering from the cumulative effects of life changes. However, this account is not supported by the results relating stressors of different durations to the outcomes. When the total number of life s~essors was disaggregated by duration, only the chronic stress index was related to the outcomes. Furthermore, the chronic sucss
index was rclatcd to some outcomes that had no relation to the total stress index,
such as SBP recovery from challenge and HR reactivity. These findings are not
consistent with a simple change-based model of stress. One implication of these
findings is that psychological stress researchers should devote more effort to studying chronic stressors, which reflect persistent demands and a lack of chaagc.
There are several other noteworthy aspects of our comparative analyses. One is that the relation between Chronic stress and health problems could not be explained by self-report biases due to neuroticism. In studies by McGonagle and Kessler (1990) and Avison and Turner 0988) chronic stressors were more strongly related to psychological distress than were acute strcssors. However, these results could be explained by underlying biases in reporting of both events and distress symptoms.
54 LEPORE, MILES, LEVY
In this study we statistically controlled for neuroticism, which should control for this major alternative explanation of the findings. In addition, we found that chronic stress was associated with physiological outcomes, which would not be subject to the same biases underlying self-reports of psychological distress and illness. Moreover. the relation between chronic stress exposure and cardiovascular responses to challenge in our study could not be attributed to behavioral factors, such as task performance. smoking, and obesity. Of course, because of the correlational research design, it is possible that some other nonspecified factor (e.g,, social interaction patterns) caused both exposure to chronic stress and the negative outcomes.
In many studies of stress and illness, there lurks a possibility that chronic illness can account for the association between stress and subsequent illness. As Depue and Monroe (t986) noted, chronic disorders are quite common and, in longitudinal studies; the level of prior disorder is often the most powerful predictor of subsequent disorder. It is conceivable that chronic disorders, such as frequent headaches, colds, and injuries, could increase chronic stress. For example, people who frequently are ill may have less time or ability to respond to everyday demands, which will make the demands persist. In this study, we did not have a measure of chronic illness. However, we did measure illnesses experienced near the time of the experimental sessions and statistically controlled for these when predicting illnesses in the 2-month follow-up period. Prior illness was associated with subsequent illness, suggesting that some people are prone to chronic disorders. Nevertheless, chronic stress was a significant predictor of number of illnesses and specific illnesses after adjusting for prior illnesses. These findings suggest that the associations between chronic stress and illnesses in the folIow-up period were not an artifact of chronic disorders.
The Pathways Linking Chronic Stress and Health Problems
A second focus of our research was to test whether the relations between chronic stress, acute illness, and psychological distress could be attrihuted to a pathophysi- ological state induced by chronic stress. Several of the prerequisite conditions in the proposed mediation model were met. First, there was a positive association between chronic stress exposure and cardiovascular reactivity to acute challenges. Second. extreme DBP reactivity was associated with a high level of psychological distress; extreme SBP reactivity was associated with a high number of illnesses, Yet, the regression-based mediation analyses suggested that the increased reactiv- ity, psychological distress, and iIlnesses were just independent correlates of chronic stress exposure.
There are several plausible explanations for the failed mediation. First, we might have been mistaken in our assumption that cardiovascular reactivity is a good proxy for other pathophysiol ogical processes (e.g., i mmu ne suppression, increased circu- lation of catecholamines) that could potentially increase individuals' risk for
CHRONIC AND EPISODIC STRFe..SSOP, S 55
psychological and physical health problems (see Cohen & Manuck, 1995). Al- though cardiovascular, immune, and neuroendocrine systems may all be influenced by a central mediator, the extent to which alterations in these systems relate to illness may depend on the type of illness in question, the time course of the illness, and other individual factors (e.g., genetics). For example, heightened cardiovascular reactivity may be an important mediator in the relation between chronic stress and risk for vascular or Coronary heart diseases among individuals with a family history of such diseases. In addition, the influence of cardiovascular reactivity on vascular and coronary disease processes may be observable only in experimental animal studies or in very long-term prospective studies with humans. In contrast, the association between chronic stress and the onset of acute illnesses, such as viral infections, may depend on exposure to an infectious agent, host resistance to the agent due to genetic factors or prior exposure, and the degree to which chronic stress diminishes immune system functioning. Thus, although it may be fruitful to examine the mediating role of cardiovascular reactivity in the link between chronic stress and vascular or coronary disease outcomes, investigations of infectious illnesses should examine more plausible and proximal psychobiologic mediators, such as immune reactivity.
Another potential explanation for the failed mediation is that the relation between chronic stress and illness outcomes was due to cognitive and behavioral factors rather than underlying pathophysiological processes. For example, chronic stress may increase social support seeking, which could increase exposure to infectious agents and risk for catching a cold. Chronic stress also may lead to attention narrowing, which could increase accidents and risk for having an injury. Finally, chronic stress could have increased individuals" psychological distress by diminishing their self-concept or increasing feelings of helplessness. Other inves- tigators have referred to the unhealthy consequences of individuals' behavioral, cognitive, and emotional responses to stressors as a cost of coping (cf. Cohen, Evans, Stokols, & Krantz, 1986). The costs of coping may be particularly high, or damaging to health and well-being, when stressors are chronic.
Interpretations and Limitations
Although our analyses emphasized the predictive power of chronic stress over episodic and intermediate-length stressors, we do not wish to convey that retatively short-term stressors are of no importance to stress and illness processes. It is possible that episodic stressors could trigger specific illnesses and catastrophic events such as heart attacks in people who are already predisposed to such illnesses (Kamarck & Jennings, 199t). In addition, some short-lived stressors may cause people to experience chronic stressors. Norris and Uhl (1993) found that in the aftermath of a hurricane, acute hurricane-related stressors, such as material losses

5 6 LEPORE, MILES. LEVY
and personal injuries, produced long-term psychological distress by increasing chronic stress in various life domains, including marriage, finances, and personal relationships. Traumatic, short-lived events also can trigger chronic stress reactions in people who experience persistent and unbidden intrusive thoughts about the events (e.g., Lepore, Silver, Wortman, & Wayment, 1996). Thus, we believe that research on episodic stress should continue; but, simultaneously, empirical tests of emerging models of chronic stress and their unique effects on illness processes must be increased.
In light of the limitations of this study, we are cautious in our interpretation of the patterns of as.~ociations. However, the patterns are noteworthy for their strength and reliability in predicting a wide range of negative outcomes. The strength of the associations is impressive because the chronic stressors facing this sample appear to be relatively minor in magnitude. For most of the sample, the chronic stressors they encountered--social isolation, extreme workload, conflicts with room- mates--stem from being students in a competitive college environment, located far away from family and friends. These stressors will eventually come to an end, as students leave college. In community samples, chronic stressors might be more enduring and severe, such as caring for a chronically ill relative, being chronically unemployed, or living in a violent neighborhood. When stressors are more severe and enduring than the ones reported by participants in this study, they may have even stronger and more pervasive effects on health than those documented herein.
In summary, our comparative analyses suggest that chronic stress exposure, but not exposure to episodic or intermediate-length stressors, was associated with (I) higher levels of psychological distress; (2) exaggerated cardiovascular responses to acute challenges; (3) slower recovery to basal cardiovascular functioning at the cessation of acute challenges; (4) a greater number of reported illnesses; and (5) a higher risk for reporting a cold, a headache, or an injury. The comparative analyses included various statistical controls for potential confounds (e.g., smoking, neuroti- cism), as well as controls for resting cardiovascular scores in the reactivity analyses and prior illnesses in the illness analyses. The hypothesis that cardiovascular reactivity would act as a mediator of the relations between chronic stress and psychological distress and physical illness was not supported by the data. Overall, the findings suggest that change-based models of stress do not adequately account for the negative effects of stress. It appears that investigators need to develop or adopt new conceptualizations of stress processes to account for the negative effects of chronic stress.
REFERENCES
Avison, W. R.. & Turner, R. 1. (1988). $tr~.~ful life event,~ and deprc~.~ive symp4oms: Di~ggregating the r of acute strCssors and chronic strains. Journal of Health and Social Behavior. 29.
253-264.
CHRONIC AND EPISODIC STRESSORS 57
Boyce. W T., Chesr~y, M., Alkon, A., Tschann, J. M., A dan'Ls, S., Cheslefman, B.. Cohen. 0., Kaiser, P., Folkn-,an, S,, & Wara, D. (1995). Psychobio]o~c reactivity to stre.~s and childhood respiratory [llnesse.~: RcsulL~ of two prospective studies. Psychosomatic Medicine, 57, 411-422.
Brown, G. W., & Harris, T, O. (F_As.). (1989). ore events az~d illness. New York: Guilford. Cohen, L. H., Simons, R. F., Rose, S. C., MeGowan, L, & Zclson, M. A. 0986). Relationships among
negative llfe events, physiological reactivity, and health syrnnptornatology. Journal of Huma~ Stress. 12, 142-148.
Cohen, S., Evans, G. W.. Stokols, D., & Kmntz, D. $. (1986). Behavior, health, mldenvironmental stre~s. New York: Plenum.
Cohen, $., & Manuck, S. B. (1995). Strc.q.% ~activity, and disease. P,D,cho.mmatfr Medicine, 5Z 423.~426.
Dembroski, T. M., MacDougall, J. M.. Slaats, S., Eliot. R. S., & Buell, J. C. ( 1981 ). C-'haltenge-induced cardiovascular response as a predictor of minor illnessc.~. Journal of Human Stress, Z 2-.~.
I~pur R. A., & Monroe. S. M. (1986). Conceptualization and measurement of human disorder in life stress mse..atch: The problem of chronic disturbance. P~chological Bulletin, 90, 36-5 I.
Derogatis. L. R. (1983). The SCL-90-R: Admini.Tfrafion, scoring, and procedures manual-l/(2nd ed.). Towson, MD: Clinical Psychometric Re,arch.
Eckenrode, J. (1984). Tic impact of chronic and acute strcssors on daily reports of mood. Journal r~ PersonallY. and Social P.w. ctmlogy, 46. 907-918.
Evans. G. W., Allen. K. M., Tafalia, R., & O'Meaxa. T. (1996). Multiple xtmssor~: Performance, psychophysiological and affective responses. Jourr~al qfEnvironmental P.~.chology, 16, 147-154.
Eyscnck. H. J., & Ey~nek, S. B. G. (1975). Mane t of the E.vsenck Personality Questionnaire. San Diego, CA: Educational and Industrial Testing Service.
Fleming, I., Baum, A., Davidson, L. M.. Rec~anus. E., & McArdle, S. (1987). Chronic swess as a factor in physiological w~tiviW to challenge. Health P,D, chology. 6. 221-23"/.
Goltlieb, B. H. (Ed.). (1997). Coping with chronic stres.v. New York: Plenum, Jorgen~n. R. S., & Houston, B. K. 0989). Reporting of life evenLy, family history of hypertension, and
cardiovascular activity at rest and during psychological stm~s. Biological P.~chefo~,, 2R, 13Y,-148. Kamatck, T. W., & Jennings, J. R. ( 1991 ). Biobchavioral factors in sudden cardiac death. Psy. chelogical
Bulletin, 109. 42-75. Kamarck. T. W., Jennings, J. R., Debski. T. T.. Glickrnan-Weiss, E., Johnson, P. S., Eddy, M..f., &
Manuck, S, B. f 1992). Reliable measures of behaviorally-evoked cardioVtL~culat reactivity from a PC-b~.~.d test battery: Results from student and community samples. P.vychophysiolog?,.., 29, [7-2B.
Kohn. P. M,, Lafteniere, K., & Gupcvich, M. (1990). The Inventow of College StudenL~" Recent Life Experiences: A decontaminated h~slcs scale for a special population. Journal of Befm~,iorat Medicine, I3, 619--.630.
Lcporc, S. J. (1995). Measurement of chronic stressor. In S. Cohen, R. C. Ke.~ler, & L. U. Gordon (Eds.). Me~L~uring .~tress: A guide for health and social scientist.~ (pp. 102-121 ). New York: Oxford Univer~i~y P ~ .
Lepom, S. J. (1995). [ Dally strcsso~s among coileg~ Students]. Unpublished raw data, Lcpo~c, S. J. (1997). Social--~nvironmcntal influences on the chronic stress process. In B. H. Gottlieb
(Ed.), Coping with chronic .vtre.vs (pp. 133-160). New York: Plenum. Lcporr S. J., & Evans, G. W. (1996). Coping with rnuItiple s~rcssors in the environment. In M. Zcidner
& N. S. Endler (Ed~)., Handbook q[coping: Theoo,, research, opplicatior~, (pp. 350-380). New York: Wiley.
Lcporc, S. ~., Evans, G. W., & Palsanr M. N. (1991). Social hassles and psychological health in the context of chronic crowding. Journal of Health & Social Belu~'viar, 32, 3.57-367.
LcpOrc, S..l., Evans, G. W., & Schneider, M. (1992). Dynamic role of social support in the [ink between chronic stress and psychological distress. Journal of Per.~onality and Social Psychology, 61. 899-909.
�9 ~ LEPORE. MILES. LEVY
Lepom, S ,I. Silver, R. C. Worlman. C. B., & Waymcnt, H. A. [ J996"]. Social constrain|s, inzrUsivc thoughts, and depressive symptoms among bereaved molhers. Journal n[Per.tonat{~., anti Social P~.chotogy, 70, 2"/1-2R2.
Manuck, S. B.. Cohen, S., Rabin, B. S., Muidoon, M. F., & Bachen, E. A. { 1991 ). Individual diffcrcnce.~ in cellular immune response to stress. P.rveholagical Sciem'e. 2, 11 I - ! 15.
Manuck, S. B., Kaplan, J. R., & Matthews, K. A. (1986). Behavioral antecedents of coronary hcaJr disease and athcrosclcrosi.r Arterio.r162 6, 2-14.
Manuck, S. B., Ka,~mwicz. A. L.. & Muldo~n. M. P. 119q6). ~havlorally-evoked cardiova.~cular reactivity and hypertension: Conceptual issues and pOtential a.<~soCiations, Annal.q o[ BehaVioral Medicine, 12, 17-29,
Ma~tlin, J. A., Wethington, E., & Kessler, R. C. (Ig90). Situational determinants of coping a~d coping effectiveness. Journal of Health and Se~cial Behavior, 31, 162-172.
MeEwen, B. S., & Stellar, E, ( [993~, Stress and the, iod~,,~id~-~: M~chanisms ~eading to disease. Archives of Internal Medicine, 153. 2093-2 IOI.
McGonag]c, K. A.. & Kessler, R. C. (1990). Chronic ~tress, acute stress, and depressive symptoms. American Journal of Communi~ P.r)~'hology, I ~, 681-706.
Norris, F. H., & Uhl, G. A. (1993). Chronic stress a.,~ a mediator of acute stress- The ca.~ of Hurricane Hugo. Journal of Applied Social P.~'che~logy. 233, 1263-1284.
Pardinc, P., & Napoli, A. (1983). Physiological r~activity and Ncent llfe-stres.,; experience. Jaurnat of CorLrulting and Clinical P.cyehotogy, M, 467-469.
Schaubrocck, ,~., & Gan.~ter, D. C. H~3) . Chronic demands and re.~pon,~ivity Io challenge. Journal r Applied P,~chology, 7& 7.'3-85.
Sclyc, H. (1956). The stress ofhfe. New York: McGraw-Hi[L Sterling, P., & E,yer, J. (1988). Allo.~.~i.~: A new paradigm to explain arousal pathology, In J, Fi.~l",cr &
J. Reason (Eds.), Handbook of life stress, cognitian, andhealth (pp, 629---649). New York: Wiley. Thoits, P. A. ~,1983). [)irncnsions of 1i[r events that int'lucnce psychological disl~.'~s: An evaluation and
synlhesis of the literature. In H. B. Kaplan (~d.l, Pxvchasocial stress: Trends in theoo' and research (pp. 33~103). New York: Academic.
Vingcfhoels, A. J. 1. M., Ratliff-Crain, J., Jaba~dj, L., Menges, L. L, & Baum, A. 0996). Self-reported sttcssors, symptom complaints and psychobiologicaJ functioning: I. Cardiovascular ~mms reactivity. louma~ of P.~,che)samatic Research, 40, 177-t90.
Zakowski, S. G., McAIlister, C. G., Deal, M., & Baum, A. (1992). St~ss, reactivity, and immune function in hcahhy males. Health P.wcholagy II, 223-232.

Friend o r roc,rnmilfc was strcssed out or dcprersrd' Rejucted from a friend or loverh Had your trust betrayedh Involvcd in :$ long-distance relationship" No1 enoush time l o mccl ohlignlionsh Problem with the law (arrcaled. lickelrd, deraincd. e1c.p (.ml.lirl with fricnd. roommate, or loverh Struggling l a keep up in school' Tension will, ;I friend. roommstc, or luvcr" Diff iculty wilh writing or m;lthh Left out o f social nctivity' Prolrlrms with rwmma l r " Prohlcrnr with lransportalion. gcttinp whrrc yon nrcd to" Scparaletl f r r m people you care a h d 1)ifficully wi lh pirllhoylricnd's parents" 'Enre rcl;uionship with T.4 o r pnrfcssor" Didn' l rcceirc cllcck on time (c.g.. from work, parents. or financial aid)" 'lbrned down for a rlatr" Difficulty wi lh scvual periwmancc' Dea l t o f a friend or relali\.cC Smnconc close to y w had serious illness o r accidml' H;d nn unwanlrrd visilor" Psrenls had financial prnhlcms or crises" Diff icully communicating with a parenl' Connicl hetwocn members of your family" Had prrronal money prol,lcms (c.g.. difficulty paying hills or huyinc food ic ln lh inp~ Trrruhle iinding or kccping n jnh" Could not find adequalc living arrangement" Diifioully with landlord' Strugplinp t o meel the academic standards of dhc r$ p . lam-out .. or par sick from alcohol or drug consumption" Somrnnr c l u ~ l o yoo h;$d alcohol or drug n,hloma R Slruppling l o mcel own academic standards Kcquircrl l o ma le class presentation' Vicl im or witnchs In n crimc' Friend or relative was victim of a crime' l iw many things to do at uncr" Socially isolated"




















