
different kinds of trees, transplanted when young by himself. In ...
Upload
independentCategory
view
2download
0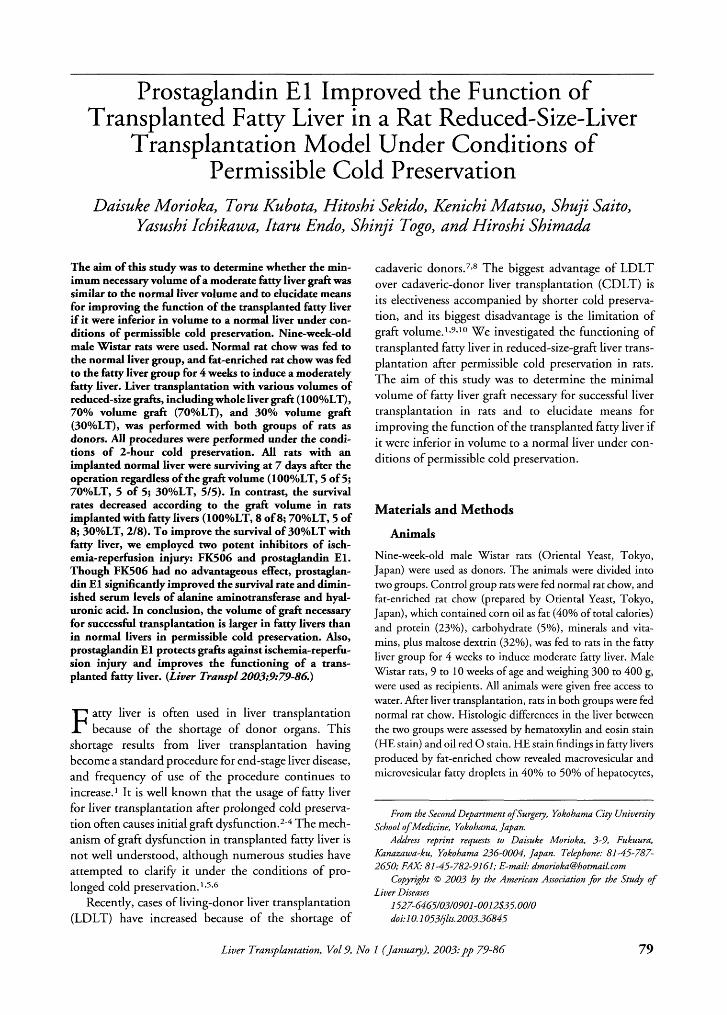
Prostaglandin E l Improved the Function of Transplanted Fatty Liver in a Rat Reduced-Size-Liver
Transplantation Model Under Conditions of Permissible Cold Preservation
Duisuke Morioku, Toru Kubotu, Hitosbi Sekido, Kenicbi Mutsuo, Sbuji Suito, Yausbi Ichikuwa, Itmu Endo, Sbinji Togo, and Hirosbi Sbimudu
The aim of this study was to determine whether the min- imum necessary volume of a moderate fatty liver graft was similar to the normal liver volume and to elucidate means for improving the function of the transplanted fatty liver if it were inferior in volume to a normal liver under con- ditions of permissible cold preservation. Nine-week-old male W ~ s t a r rats were used. Normal rat chow was fed to the normal liver group, and fat-enriched rat chow was fed to the fatty liver group for 4 weeks to induce a moderately fatty liver. Liver transplantation with various volumes of reduced-size grafts, including whole liver graft (lOO%LT), 70% volume graft (7Oo/oLT), and 30% volume graft (30%LT), was performed with both groups of rats as donors. All procedures were performed under the condi- tions of 2-hour cold preservation. All rats with an implanted normal liver were surviving at 7 days after the operation regardless of the graft volume (1 OOYoLT, 5 of 5; 7o0/oLT, 5 of 5; 30°/oLT, 9 5 ) . In contrast, the survival rates decreased according to the graft volume in rats implanted with fatty livers (lOOYoLT, 8 of 8; 70%LT, 5 of 8; 30%LT, 218). To improve the survival of 30%LT with fatty liver, we employed two potent inhibitors of isch- emia-reperfusion injury: FK506 and prostaglandin El. Though FK506 had no advantageous effect, prostaglan- din El significantly improved the survival rate and dimin- ished serum levels of alanine aminotransferase and hyal- uronic acid. In conclusion, the volume of graft necessary for successful transplantation is larger in fatty livers than in normal livers in permissible cold preservation. Also, prostaglandin El protects grafts against ischemia-reperfu- sion injury and improves the functioning of a trans- planted fatty liver. (Liver Transpl2003;9:79-86)
F atty liver is often used in liver transplantation because of the shortage of donor organs. This
shortage results from liver transplantation having become a standard procedure for end-stage liver disease, and frequency of use of the procedure continues to increase.' It is well known that the usage of fatty liver for liver transplantation after prolonged cold preserva- tion often causes initial graft dy~function.~-* The mech- anism of graft dysfunction in transplanted fatty liver is not well understood, although numerous studies have attempted to clarify it under the conditions of pro- longed cold preservation. 1,5,6
Recently, cases of living-donor liver transplantation (LDLT) have increased because of the shortage of
Liver Transplantation, VoL 9,
cadaveric don0rs.7.~ The biggest advantage of LDLT over cadaveric-donor liver transplantation (CDLT) is its electiveness accompanied by shorter cold preserva- tion, and its biggest disadvantage is the limitation of graft v0lume.1~9~'~ We investigated the functioning of transplanted fatty liver in reduced-size-graft liver trans- plantation after permissible cold preservation in rats. The aim of this study was to determine the minimal volume of fatty liver graft necessary for successful liver transplantation in rats and to elucidate means for improving the function of the transplanted fatty liver if it were inferior in volume to a normal liver under con- ditions of permissible cold preservation.
Materials and Methods
Animals
Nine-week-old male Wistar rats (Oriental Yeast, Tokyo, Japan) were used as donors. The animals were divided into two groups. Control group rats were fed normal rat chow, and fat-enriched rat chow (prepared by Oriental Yeast, Tokyo, Japan), which contained corn oil as fat (40% of total calories) and protein (23%), carbohydrate (5%), minerals and vita- mins, plus maltose dextrin (32%), was fed to rats in the fatty liver group for 4 weeks to induce moderate fatty liver. Male Wistar rats, 9 to 10 weeks of age and weighing 300 to 400 g, were used as recipients. All animals were given free access to water. After liver transplantation, rats in both groups were fed normal rat chow. Histologic differences in the liver between the two groups were assessed by hematoxylin and eosin stain (HE stain) and oil red 0 stain. H E stain findings in fatty livers produced by fat-enriched chow revealed macrovesicular and microvesicular fatty droplets in 40% to 50% of hepatocytes,
From the Second Department o f Surgery, Yokohama City University School o f Medicine, Yokohama, Japan.
Address reprint requests to Daisuke Morioka, 3-9, Fukuura, Gnazawa-ku, Yokohama 236-0004, Japan. Telephone: 81-45-787- 2650; FAX 81-45-782-9161; E-mail: [email protected]
Copyright 0 2003 by the American Association f . r the Study of
I527-6465/03/090I -OOI2$35.00/0 doi: IO. 1053~lts.2003.36845
Liver Diseases
N o l (Janua y), 2003: pp 73-86 79
80 Morioka et a1
Figure 1. Liver histology of donor rats. (A) Fatty liver stained by HE stain. Macro-micro fatty droplets were detected in 40% to 50% of hepatocytes. (Original magni- fication: X40). (B) Fatty liver stained by oil red 0 stain. Oil red 0 well-stained droplets were seen in 40% to 50% of hepatocytes. (x 100). (C) Normal liver stained by oil red 0 stain. No fatty droplets were seen. ( x 100)
and these droplets were well stained by oil red 0. Little fatty droplets were seen in the livers of the control group (Fig. 1). Animals received humane care in compliance with the guide- lines for the use of experimental animals of the Yokohama
City University Institutional Animal Care and Use Commit- tee.
Liver Transplantation Procedure
The rats were anesthetized with ether, and liver transplanta- tion was performed with the technique described by Kamada and Calne" with minor modification. Briefly, heparin (300 U) in 2 mL of saline solution was injected into the penile vein, and a 4-mm long stent prepared from a polyethylene tube was inserted into the common bile duct and secured with 6-0 sutures. In whole liver transplantation (lOO%LT), the graft liver was not resected at all. In 70% volume liver transplanta- tion (70%LT), the left lobe was resected, and in 30% volume liver transplantation (30%LT), the left and middle lobes were resected, as described by Kubota.10 Livers were flushed in situ with proper amounts of histidine-tryptophan-ketoglutarate (HTK) solution at 4°C according to graft volume (lOO%LT, 15 mL; 7o%LT, 10 mL; 30%LT, 5 mL). Venous cuffs pre- pared from 14- and 12-gauge intravenous catheters were placed in the portal vein and infrahepatic vena cava, respec- tively, and grafts were stored in H T K solution at 4°C. For transplantation, the liver of the recipient was removed after clamping the suprahepatic vena cava, the portal vein, and the infrahepatic vena cava. Just before the grafts were implanted, they were flushed with proper amounts of Ringer's lactate at 4°C according to graft volume (lOO%LT, 10 mL; 7o%LT, 7 mL; 30%LT, 3 mL). Grafts were transplanted by connecting the suprahepatic vena cava with a running suture, then insert- ing a cuff into the appropriative vessels and securing them with 6-0 sutures. The bile duct was anastomosed with an intraluminal stent. The transplantation procedure required less than 60 minutes, during which time the portal vein was clamped for 17 to 22 minutes.
To elucidate the permissible preservation time for fatty liver in this study, lOO%LT with livers explanted from fatty liver rats after 2- and 6-hour periods of cold preservation were performed as a preliminary investigation.
Experiment 1
T o evaluate the graft function after transplantation, we exam- ined the following: 1. animal survival at 7 days, 2. serum levels of alanine aminotransferase (ALT) and hyaluronic acid (HA) at 24 and 48 hours after reperfusion, and 3. histologic changes in the liver at 24 and 48 hours after reperfusion assessed by H E stain. (Items 2 and 3 were examined only in lOO%LT and 3o%LT.)
Experiment 2
Rats with fatty livers were divided into three groups: In Group 1, 0.5 pglkglmin of prostaglandin E l (PGE1) (aloprostadil alfadex, O n o Pharmaceutical, Osaka, Japan) was given to rats with fatty livers via a tail vein during donation, and HTK solution and Ringer's lactate both containing 1 pglmL of PGEl were used as the preservation rinse and washout fluid, respectively. Group 2 received 0.3 mglkg of FK506 (tacroli- mus hydrate, Fujisawa Pharmaceutical, Osaka, Japan) 24
PGEI for Reduced-Sized Fatty Liver Gray5 81
1; 1 2-hour-cold-preserved group
2o l
(n=5) l
l p < 0.01
I 6-hour-cold-preserved group
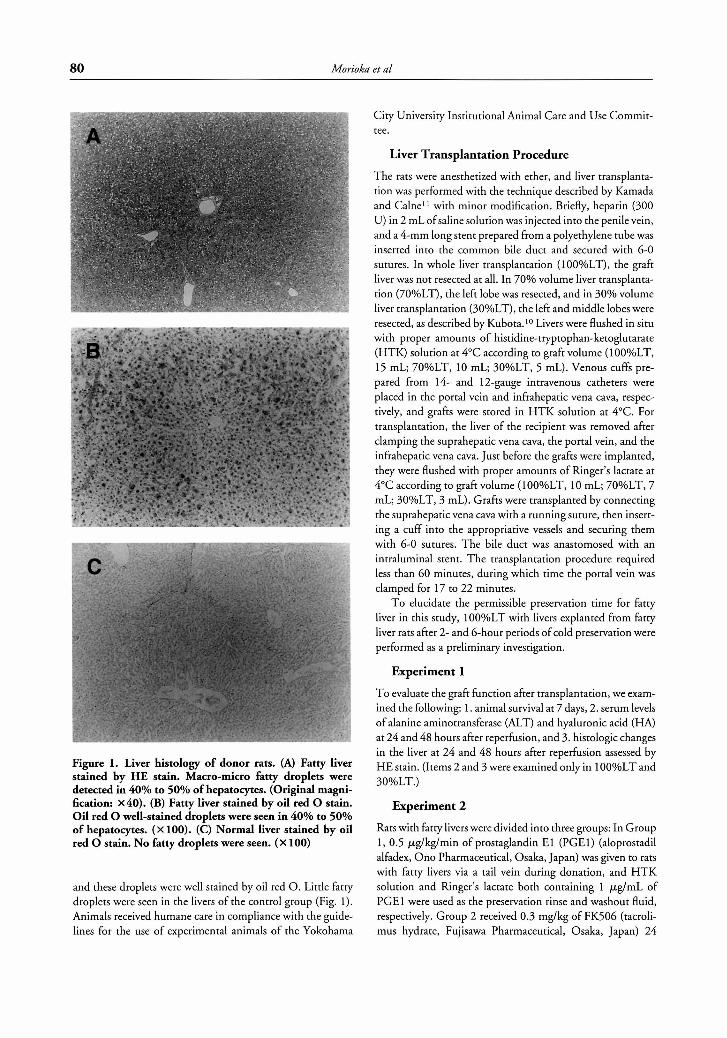
Figure 2. Survival rates after whole liver transplantation with 2-hour-cold-preserved fatty liver and 6-hour-cold- preserved fatty liver. Survival rates of rats implanted with 2-hour-cold-preserved fatty livers were significantly better than those of rats implanted with 6-hour-cold-preserved fatty livers.
hours before harvesting, and group 3 rats were naive rats with fatty livers. Also in groups 2 and 3, an amount of saline equal to that in group 1 was given during donation. Then 30%LT with livers explanted from each group was performed by the method described above. We examined the following items to evaluate the transplanted livers explanted from each group: 1. animal survival at 7 days after operation in each group, 2. serum levels of ALT and HA at 24 and 48 hours after reper- fusion in groups 1 and 3, 3. histologic changes in the liver at 24 and 48 hours after reperfusion assessed by hematoxylin eosin stain in groups 1 and 3. The extent of necrosis was assessed in 8 sections of each liver sample by examining the center sections of the anterior and posterior caudate lobes and 3 sections at equal intervals within the right and square lobes. The extent of necrosis of the liver slices was determined by projecting slides of the slices onto a digitizing board, tracing around necrotic areas, and expressing these as a percentage of the total area with digitizing s o h a r e (National Institutes of Health Image 1.52.)
Statistical Analysis
All results were expressed as the mean ? standard deviation (SD). The statistical significance of differences was deter- mined by Student's t-test or log rank test in the Kaplan-Meyer survival curve. A P value of less than .05 was considered statistically significant.
Results
Preliminary Investigation to Determine the Permissible Cold Preservation for Fatty Liver in This Study
Survival after transplantation was significantly better in rats transplanted with 2-hour-cold-preserved fatty liv- ers than rats transplanted with 6-hour-cold-preserved
fatty livers. Based on this result, we selected 2-hour cold preservation as permissible cold preservation; therefore, the following experiments were all performed under the conditions of 2-hour cold preservation (Fig. 2).
Experiment 1 Survival afier liver transplantation. In the control
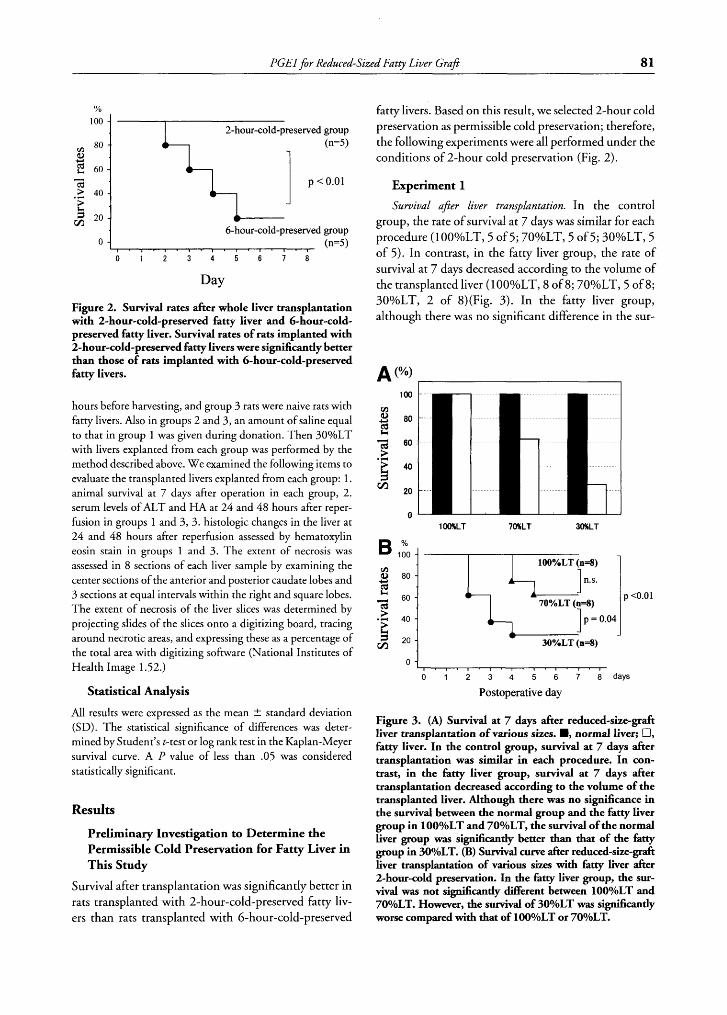
group, the rate of survival at 7 days was similar for each procedure (1 OO%LT, 5 of 5; 70%LT, 5 of 5; 30%LT, 5 of 5) . In contrast, in the fatty liver group, the rate of survival at 7 days decreased according to the volume of the transplanted liver (lOOYoLT, 8 of 8; 70%LT, 5 of 8; 30%LT, 2 of 8)(Fig. 3). In the fatty liver group, although there was no significant difference in the sur-
1 OOSCLT 70KLT 30KLT
100%LT (n=8)
70%LT @=8)
c, I p = 0.04 I JO%LT(n=8)
J
o I 2 3 4 5 6 7 a d a y s
Postoperative day
Figure 3. (A) Survival at 7 days after reduced-size-graft liver transplantation of various sizes. M, normal liver; cl, fatty liver. In the control group, survival at 7 days after transplantation was similar in each procedure. In con- trast, in the fatty liver group, survival at 7 days after transplantation decreased according to the volume of the transplanted liver. Although there was no significance in the survival between the normal group and the fatty liver group in 100YoLT and 7O%LT, the survival of the normal liver group was significantly better than that of the htty group in 3o0/oLT. (B) Survival curve after reduced-size-graft liver transplantation of various sizes with htty liver after 2-hour-cold preservation. In the htty liver group, the sur- vival was not significantly different between 1OOYoLT and 7OYoLT. However, the survival of 30°/oLT was Significantly worse compared with that of 1OOYoLT or 70YoLT.
82 Mo rio ka et al
A (mU/ml)
1000
800
p < 0.01
Time after reperfusion
3000 p = 0.01 4 2500 1 , , a 2000
p < 0.01
n 1500 4
Time after reperfusion
B P c 0.01 (mU/ml) 1-1
- . ..
1400 1
p < 0.01
n
I 24hr 48hr
Time after reperfusion
p < 0.01 I
4000 -
I 1 24hr 48hr
Time after reperfusion
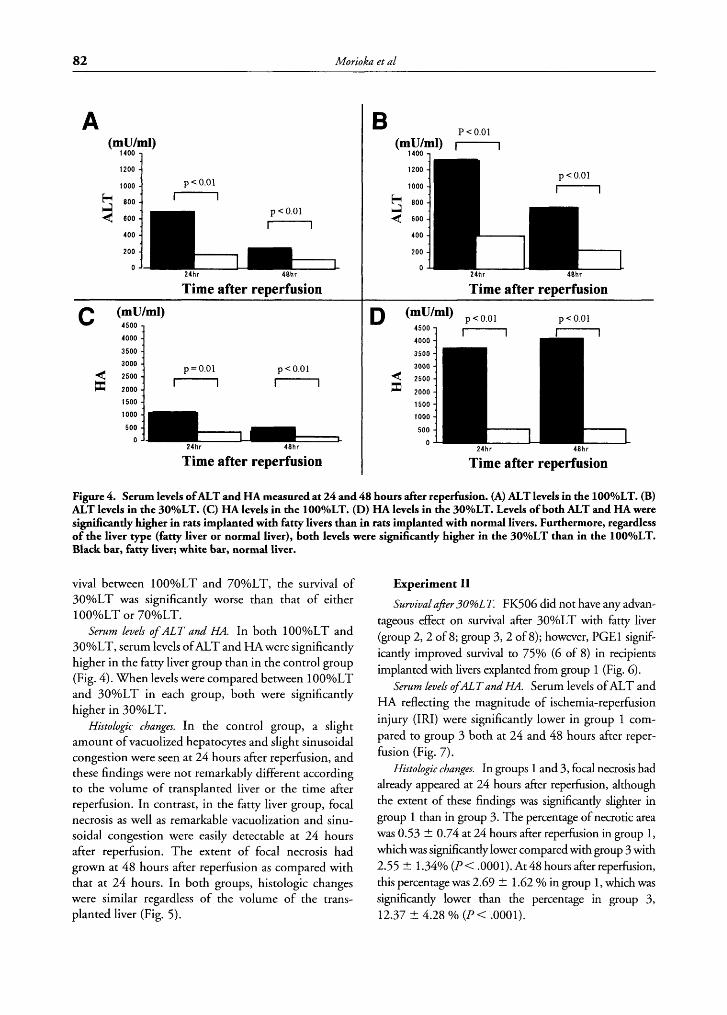
Figure 4. Serum levels ofALT and HA measured at 24 and 48 hours after reperfusion. (A) ALT levels in the 100YoLT. (B) ALT levels in the 3o0/oLT. (C) HA levels in the 100°/oLT. (D) HA levels in the 3O%LT. Levels of both ALT and HA were significantly higher in rats implanted with fatty livers than in rats implanted with normal livers. Furthermore, regardless of the liver type (fatty liver or normal liver), both levels were significantly higher in the 30%LT than in the lOO%LT. Black bar, fatty liver; white bar, normal liver.
viva1 between 100YoLT and 70%LT, the survival of 30%LT was significantly worse than that of either 100%LT or 70YoLT.
Serum levels of A L T and HA. In both 1 OO%LT and 30%LT, serum levels of ALT and HA were significantly higher in the fatty liver group than in the control group (Fig. 4). When levels were compared between 1 OO%LT and 30%LT in each group, both were significantly higher in 30%LT.
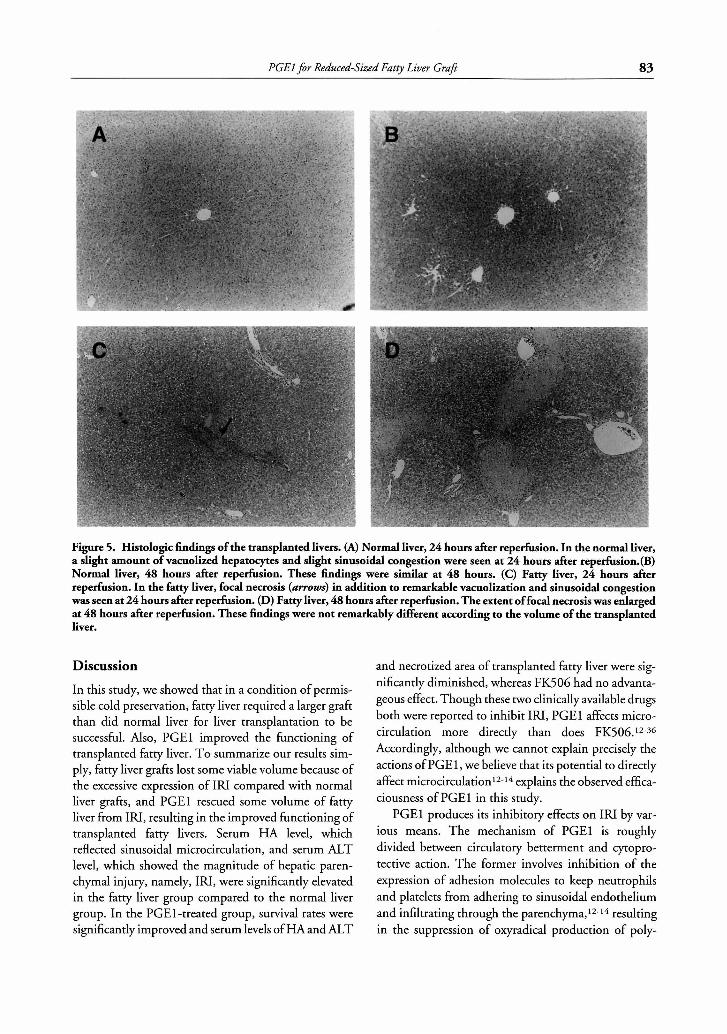
Histologic changes. In the control group, a slight amount of vacuolized hepatocytes and slight sinusoidal congestion were seen at 24 hours after reperfusion, and these findings were not remarkably different according to the volume of transplanted liver or the time after reperfusion. In contrast, in the fatty liver group, focal necrosis as well as remarkable vacuolization and sinu- soidal congestion were easily detectable at 24 hours after reperfusion. The extent of focal necrosis had grown at 48 hours after reperfusion as compared with that at 24 hours. In both groups, histologic changes were similar regardless of the volume of the trans- planted liver (Fig. 5).
Experiment I1 Survivalafter 3 0 % ~ ~ . FK506 did not have any advan-
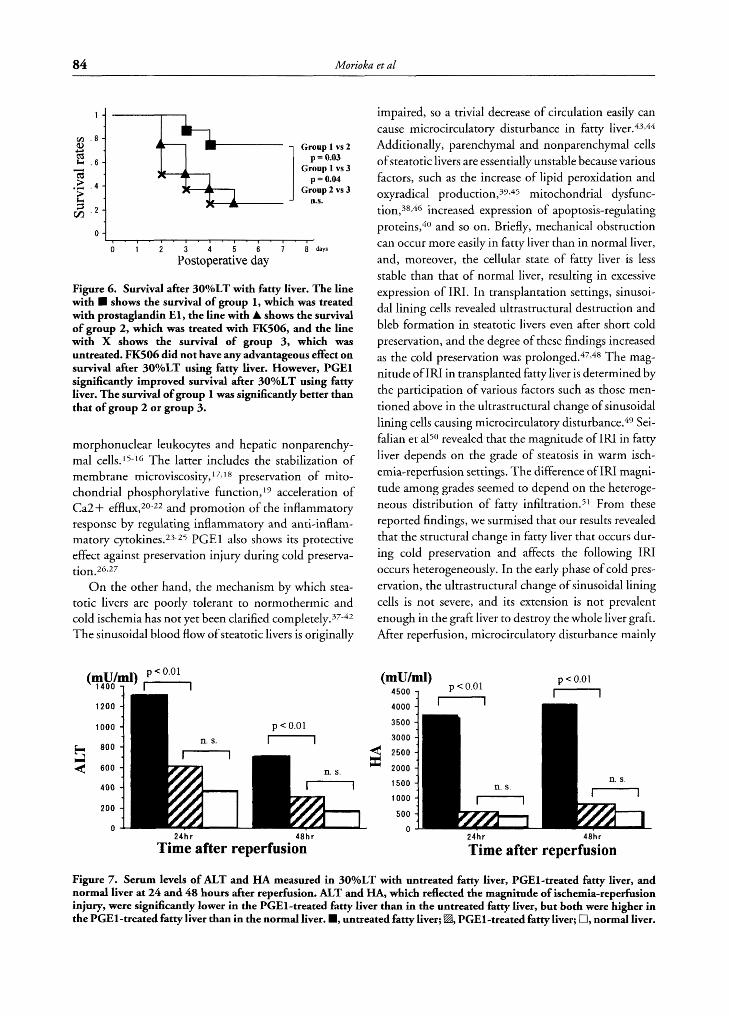
tageous effect on survival after 30%LT with fatty liver (group 2 ,2 of 8; group 3 ,2 of 8); however, PGEl signif- icantly improved survival to 75% (6 of 8) in recipients implanted with livers explanted from group 1 (Fig. 6).
Serum levels ofAL T and HA. Serum levels of ALT and HA reflecting the magnitude of ischemia-reperfusion injury ( IN) were significantly lower in group 1 com- pared to group 3 both at 24 and 48 hours after reper- fusion (Fig. 7).
Histologic changes. In groups 1 and 3, focal necrosis had already appeared at 24 hours after reperfusion, although the extent of these findings was significantly slighter in group 1 than in group 3. The percentage of necrotic area was 0.53 ? 0.74 at 24 hours &er reperfusion in group 1, which was significantly lower compared with group 3 with 2.55 -t 1.34% (P < .OOOl). At 48 hours after reperfusion, this percentage was 2.69 ? 1.62 Yo in group 1, which was significantly lower than the percentage in group 3, 12.37 5 4.28 % (P< ,0001).
PGEl $r Reduced-Sized Fatty Liver Graft 83
Figure 5. Histologic findings of the transplanted livers. (A) Normal liver, 24 hours after reperfusion. In the normal liver, a slight amount of vacuolized hepatocytes and slight sinusoidal congestion were seen at 24 hours after reperfusion.(B) Normal liver, 48 hours after reperfusion. These findings were similar at 48 hours. (C) Fatty liver, 24 hours after reperfusion. In the fatty liver, focal necrosis (arrows) in addition to remarkable vacuolization and sinusoidal congestion was seen at 24 hours after reperfusion. (D) Fatty liver, 48 hours after reperfusion. The extent of focal necrosis was enlarged at 48 hours after reperfusion. These findings were not remarkably different according to the volume of the transplanted liver.
Discussion
In this study, we showed that in a condition of permis- sible cold preservation, fatty liver required a larger graft than did normal liver for liver transplantation to be successful. Also, PGEl improved the functioning of transplanted fatty liver. To summarize our results sim- ply, fatty liver grafts lost some viable volume because of the excessive expression of IN compared with normal liver grafts, and PGEl rescued some volume of fatty liver from I N , resulting in the improved functioning of transplanted fatty livers. Serum HA level, which reflected sinusoidal microcirculation, and serum ALT level, which showed the magnitude of hepatic paren- chymal injury, namely, I N , were significantly elevated in the fatty liver group compared to the normal liver group. In the PGEl-treated group, survival rates were significantly improved and serum levels of HA and ALT
and necrotized area of transplanted fatty liver were sig- nificantly diminished, whereas FK506 had no advanta- geous effect. Though these two clinically available drugs both were reported to inhibit IRI, PGEl affects micro- circulation more directly than does FK506.12-36 Accordingly, although we cannot explain precisely the actions of PGEl, we believe that its potential to directly affect microcir~ulation~~-~* explains the observed effica- ciousness of PGEl in this study.
PGEl produces its inhibitory effects on IN by var- ious means. The mechanism of PGEl is roughly divided between circulatory betterment and cytopro- tective action. The former involves inhibition of the expression of adhesion molecules to keep neutrophils and platelets from adhering to sinusoidal endothelium and infiltrating through the parenchyma,12-14 resulting in the suppression of oxyradical production of poly-
84 Mo rio ka et a L
4 +-,
~:~~~~~~ Group p = 0.03 1 vs 2
e Group l vs 3 p = 0.04
Group 2 vs 3 . 4 : g . 2 -
n.s.
0 - , ~ I . , . I ' , . , . , . ,
0 1 2 3 4 5 6 7 8 d a y s
Postoperative day
Figure 6. Survival after 30°/oLT with fatty liver. The line with W shows the survival of group 1, which was treated with prostaglandin El , the line with A shows the survival of group 2, which was treated with FK506, and the line with X shows the survival of group 3, which was untreated. FK506 did not have any advantageous effect on survival after 30°/oLT using fatty liver. However, PGEl significantly improved survival after 30%LT using fatty liver. The survival of group 1 was significantly better than that of group 2 or group 3.
morphonuclear leukocytes and hepatic nonparenchy- mal ce11s.15-16 The latter includes the stabilization of membrane mi~roviscosity,~7~~8 preservation of mito- chondrial phosphorylative function, l 9 acceleration of Ca2+ efflux,20-22 and promotion of the inflammatory response by regulating inflammatory and anti-inflam- matory ~ytokines.~3-~5 PGEl also shows its protective effect against preservation injury during cold preserva-
O n the other hand, the mechanism by which stea- totic livers are poorly tolerant to normothermic and cold ischemia has not yet been clarified ~ompletely.37-~~ The sinusoidal blood flow of steatotic livers is originally
impaired, so a trivial decrease of circulation easily can cause microcirculatory disturbance in fatty l i ~ e r . ~ ~ , ~ ~ Additionally, parenchymal and nonparenchymal cells of steatotic livers are essentially unstable because various factors, such as the increase of lipid peroxidation and oxyradical production,39,45 mitochondrial dysfunc- ti0n,38,4~ increased expression of apoptosis-regulating
and so on. Briefly, mechanical obstruction can occur more easily in fatty liver than in normal liver, and, moreover, the cellular state of fatty liver is less stable than that of normal liver, resulting in excessive expression of IRI. In transplantation settings, sinusoi- dal lining cells revealed ultrastructural destruction and bleb formation in steatotic livers even after short cold preservation, and the degree of these findings increased as the cold preservation was prol0nged.~7,~~ The mag- nitude of IRI in transplanted fatty liver is determined by the participation of various factors such as those men- tioned above in the ultrastructural change of sinusoidal lining cells causing microcirculatory d i~ tu rbance .~~ Sei- falian et a150 revealed that the magnitude of IRI in fatty liver depends on the grade of steatosis in warm isch- emia-reperfusion settings. The difference of IRI magni- tude among grades seemed to depend on the heteroge- neous distribution of fatty infiltrati0n.5~ From these reported findings, we surmised that our results revealed that the structural change in fatty liver that occurs dur- ing cold preservation and affects the following IRI occurs heterogeneously. In the early phase of cold pres- ervation, the ultrastructural change of sinusoidal lining cells is not severe, and its extension is not prevalent enough in the graft liver to destroy the whole liver graft. After reperfusion, microcirculatory disturbance mainly
(mU/ml) 4500 7 p < 0.01 - p < 0.01
n p < 0.01 (mU/ml) , ,
1 4 0 0 7
p < 0.01
1 24hr 48hr 24hr 48hr
Time after reperfusion Time after reperfusion
Figure 7. Serum levels of ALT and HA measured in 3o0/oLT with untreated fatty liver, PGEl-treated fatty liver, and normal liver at 24 and 48 hours after reperfusion. ALT and HA, which reflected the magnitude of ischemia-reperfusion injury, were significantly lower in the PGEl-treated fatty liver than in the untreated fatty liver, but both were higher in the PGEl-treated fatty liver than in the normal liver. W, untreated fatty liver; H, PGEl-treated fatty liver; U, normal liver.

PGEl for Reduced-Sized Fatty Liver Graj? 85
occurs in the lesion in which the ultrastructural change is present, causing focal necrosis. However, lesions in which the ultrastructural change is slight or nonexistent are not necrotized or remain viable. In a whole liver graft, a viable lesion can be sufficiently abundant to let an individual live. In contrast, in 30%LT, the original volume is small, and the destruction caused by IRI decreased the viable lesion, resulting in transplanted liver failure. In addition, although the mechanism of the dysfunction of transplanted fatty liver involves sev- eral processes, PGEl can affect each process and inhibit IRI, leading to improved functioning of the trans- planted fatty liver. If we employ other agents such as a vasodilator or an antiplatelet or anti-inflammatory agent, we might be able to clarify the mechanism of the dysfunction of transplanted fatty liver and the efficacy of PGEl observed in this study.
The usage of moderate or severe fatty liver for trans- plantation after prolonged cold preservation often causes graft dysfunction. Fatty livers should be refused for transplantation if other grafts are available,l but the shortage of donor organs accompanied by the preva- lence of liver transplantations needed sometimes com- pels physicians to use fatty livers for transplantation. Numerous studies have been performed to clarify the mechanism of graft dysfunction of fatty liver under the conditions of whole liver transplantation performed after prolonged cold preservation, as occurs with CDLT. Recently, the number of cases of LDLT has increased. Therefore, we have investigated the usage of reduced-size grafts of fatty liver for transplantation after permissible cold preservation. We have described some of the useful aspects of fatty liver in transplantation, even ifwe could only remark slightly on its mechanism. Further investigations are needed to confirm and fur- ther elucidate the findings of this study.
References Urena MAG, Moreno Gonzalez E, Romero CJ, Ruiz-Delgado FC, Moreno Sanz C. An approach to the rational use of steatotic donor livers in liver transplantation. Hepatogastroenterol 1999;
Todo S, Demetris AJ, Makowka L, Teperman L, Podesta L, Shaver T, et al. Primary nonfunction of hepatic allografts with preexisting fatty infiltration. Transplantation 1989;47:903-305. Adam R, Reynes M, Johann M, Morino M, Astarcioglu I, Kaf- etzis I, et al. The outcome of steatotic grafts in liver transplanta- tion. Transplant Proc 199 1;23: 1538-1 540. D’Alessandro A M , Kalayoglu M, Sollinger HW, Hoffmann RM, Reed A, Knechtle SJ, et al. The predictive value of donor liver biopsies for the development of primary non function after orthotopic liver transplantation. Transplantation 1991;5 1: 157- 163.
46~1164-1173.
5.
6 .
7 / .
8.
C).
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Hayashi M, Tokunaga Y, Fujita T, Tanaka K, Yamaoka Y, Ozawa K. The effects of cold preservation on steatotic graft viability in rat liver transplantation. Transplantation 1993;56: 282-287. Husberg BS, Genyk YS, Klintmalm GB. A new rat model for studies of the ischemic injury after transplantation of fatty livers: Improvement after postoperative administration of prostaglan- din. Transplantation 1994;57:457-458. Kawasaki S, Makuuchi M, Matsunami H, HashikuraY, Ikegami T, Nakazawa Y, et al. Living related liver transplantation in adults. Ann Surg 1998;227:269-274. Kawasaki S, Makuuchi M, Matsunami H, Hashikura Y, Ikegami T, Nakazawa Y, et al. Living related liver transplantation: A wider application. Transplant Proc 1995;27: 1170-1 172. Kawasaki S, Makuuchi M, Ishizone S, Matsunami H, Terada M, Kawarazaki H. Liver regeneration in recipients and donors after transplantation. Lancet 1992;339:580-58 1. Kubota T, Takabe K, Yang M, Sekido H, Endo I, Ichikawa Y, et al. Minimum sizes for remnant and transplanted livers in rats. J Hep Bil Pancr Surg 1997;4:398-404. Kamada N, Calne RY. A surgical experience with five hundred thirty liver transplants in the rat. Surgery 1983;93:64-69. Natori S, Fujii Y, Kurosawa H, Nakano A, Shimada H. Prosta- glandin El protects against ischemia-reperfusion injury of the liver by inhibition of neutrophil adherence to endothelial cells. Transplantation 1997;64:15 14-1520. Lou J, Buhler L, Deng S, Mentha G, Montesano R, Grau GE, Morel P. Inhibition of leukocyte adherence and transendothelial migration in cultured human liver vascular endothelial cells by prostaglandin El. Hepatology 1998;27:822-828. Iwata K, Shimazu M, Wakabayashi G, Ohshima A, Yoshida M, l tajima M. Intraportal perfusion of prostaglandin El attenuates hepatic postischemic microcirculatory impairments in rats. J Gastroenterol Hepatol 1999; 14:634-641. Shirabe K, Kin S, Shinagawa Y, Chen S, Payne WD, Sugimachi K. Inhibition of thromboxane A2 activity during warm ischemia of the liver. J Surg Res 1996;61:103-107. Itasaka H, Suehiro T, Wakiyama S, Yanaga K, Shimada M, Sugimachi K. The mechanism of hepatic graft protection against reperfusion injury by prostaglandin El. Jpn J Surg 1999;29:526- 532. Masaki N, Ohta Y, Shirataki H, Ogata I, Hayashi S, Yamada S, et al. Hepatocyte membrane stabilization by prostaglandin El and E2: Favorable effects on rat liver injury. Gastroenterology 1992;102:572-576. Hanazaki K, KurodaT, Kajikawa S, Shinohara E, Haba Y, Iida F. Prostaglandin El protects liver from ischemic damage. J Surg Res 1994;57:380-384. Ueda Y, Matsuo K, Kamei T, Kayashima K, Konomi K. Protec- tive effect of prostaglandin E l (PGEl) on energy metabolism and reticuloendothelial function in the ischemically damaged canine liver. Liver 1989;9:6-13. Kurosawa H, Shimada H, Nakano A, Natori S, Fujii Y. The role of intracellular calcium in the production of superoxide anion by Kuppfer cells stimulated by lipopolysaccharide and the efficacy of prostaglandin El. Int Hepatol Corn 1996;4:326-333. Sikujara 0, Monden M, Toyoshima K, Okamura J, Kosaki G. Cytoprotective effect of prostaglandin I2 on ischemia-induced hepatic cell injury. Transplantation 1983;36:238-243. Kishimoto S, Sakon M, Umeshita K, Miyoshi H, Taniguchi K, Meng W, et al. The inhibitory effect of prostaglandin El on

86 Morioka et al
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
oxidative stress-induced hepatocyte injury evaluated by cal- pain-p activation. Transplantation 2000;69:23 14-23 19. Parry GC, Mackrnan N. Role of cyclic AMP response element- binding protein in cyclic AMP inhibition of NF-KB-mediated transcription. J Immunol 1997;159:5450. Haraguchi S, Good RA, Day NK. Immunosuppressive retroviral peptides: CAMP and cytokine patterns. Immunol Today 1995; 16:595. Perrot MD, Fischer S, Liu M, Jin R, Bai X-H, Waddell TK, Keshavjee S. Prostaglandin E l protects lung transplants from ischemia-reperfusion injury: A shift from pro- to anti-inflamma- tory cytokines. Transplantation 2001;72: 1505-1 5 12. Takahashi K, Yamamoto N, Egawa H, Takeuchi T, Yamaguchi T, Takada Y, et al. Effect of prostaglandin El on preservation injury of canine liver grafts preserved in UW solution. Trans- plant Int 1993;6:245-250. Cywes R, Harvey PRC, Packham MA, Cameron R, Strasberg SM. The influence of prostaglandin El on platelet adherence and injury in preserved rat liver allografts. Liver Transplant Surg
Sakr MF, Zetti GM, Hassanein TI, Farghali H, Nalesnik MA,
Gavaler JS, et al. FK506 ameliorates the hepatic injury associated with ischemia and reperfusion in rats. Hepatology 199 1; 13:947- 951. Dhar K, Nagasue N, Kimoto T, Uchida M, Takemoto Y, Naka- mura T. The salutary effect of FK506 in ischemia-reperfusion injury of the canine liver. Transplantation 1992;54:583-588. Sakr MF, McClain CJ, Gavaler JS, Tetti GM, Starzl TE, Van Thiel DH. FK506 pre-treatment is associated with reduced levels of tumor necrosis factor and interleukin 6 following hepatic ischemia/reperfusion. J Hepatol 1993; 17:301-307. Suzuki S, Toledo-Peleyra LH, Rodriguez FJ, Cejalvo D. Neutro- phil infiltration as an important factor in liver ischemia and reperfusion injury. Modulating effects of FK506 and cyclospor- ine. Transplantation 1993;55:1265-1272. Suzuki S, Toledo-Pereyra LH. Interleukin l and tumor necrosis factor production as the initial stimulates pf liver ischemia and reperfusion injury. J Surg Res 1994;57:253-258. Dhar DK, Teramoto Y, Nagasue N, Uchida M, Ono T, Naka- mura T. FK506 maintains cellular calcium homeostasis in isch- emia-reperfusion injury of the canine liver. J Surg Res 1996;60:
Garcia-Criado FJ, Palma-Vargas JM, Valdunciel-Garcia JJ, Toledo AH, Misawa K, Gomez-Alonzo A, et al. Tacrolimus (FK506) down-regulates free radical tissue levels, serum cyto- kines, and neutrophil infiltration after severe liver ischemia. Transplantation 1997;64:594-598. Matsuda T, Yamaguchi Y, Matsumura F, Akizuki E, Okabe K, Lian J, et al. Immunosuppressants decrease neutrophil chemoat- tractantand attenuate ischemia/reperfusion injury of the liver in rats. J Trauma 1998;44:475-484.
1996;2:23-36.
142-146.
36. Kaibori M, Inoue T, Tu W, Oda M, Kwon AH, Kamiyama Y, et al. FK506, but not cyclosporin A, prevents mitochondrial dys- function during hypoxia in rat hepatocytes. Life Sci 2001;69: 17- 26.
37. Hui A-M, Kawasaki S, Makuuchi M, Nakayama J, Ikegami T, Miyagiwa S. Liver injury following normothermic ischemia in steatotic rat liver. Hepatology 1994;20: 1287-1293.
38. Koneru B, Reddy M, Torre A, Patel D, Ippolito T, Ferrante RJ. Studies of hepatic warm ischemia in the obese Zucker rat. Trans- plantation 1995;59:942-946.
39. Nardo B, Domenicali M, Caraceni P, Dall’Agata M, Mazziotti A, Bernardi M, Cavallari A. Ischemia-reperfusion injury in the diet-induced rat fatty liver. Transplant Proc 1998;30:2317.
40. Rashid A, Wu T-C, Huang C-C, Chen C-H, Lin HZ, Yang SQ, et al. Mitochondrial proteins that regulate apoptosis and necrosis are induced in mouse fatty liver. Hepatology 1999;29: 1 131- 1138.
41. Caraceni P, Nardo B, Dmenicali M, Turi P, Vici M, Simoncini M, et al. Ischemia-reperfusion injury in the rat fatty liver: Role of nutritional status. Hepatology 1999;29:1139-1146.
42. Hakamada K, Sasaki M, Takahashi K, Umehara Y, Konn M. Sinusoidal flow block after warm ischemia in rats with diet- induced fatty liver. J Surg Res 1997;70: 12-20.
43. Ohara K. Study of microcirculatory changes in experimental dietary fatty liver. Hokkaido Igaku Zasshi 1989;64: 177-185.
44. Day C, James 0. Hepatic steatosis: Innocent bystander or guilty party? Hepatology 1998;27:1463-1466.
microvesicular steatosis. J Hepatol 1997;26:43-53. 46. Fukumori T, Ohkohchi N, Tsukamoto S, Satomi S. The mech-
anism of injury in a steatotic liver graft during cold preservation. Transplantation 1999;67: 195-200.
47. Fukumori T, Ohkohchi N, Tsukamoto S, Satomi S. Why is a liver with steatosis susceptible to cold ischemic injury? Trans- plant Proc 1999;31:548-549.
48. Carles J, Fawaz R, Neaud V, Hamoudi NE, Bernard PH, Bala- baud BSP. Ultrastructure of human liver grafts preserved with UW solution: Comparison between patients with low and high postoperative transaminases levels. J Submicrosc Cytol Pathol
45. Fromenty B, Pessayre D. Impaired mitochondrial function in
1994;26:67-73. 49. Hatsugai K, Ohkohchi N, Fukumori T, Akamatsu Y, Satomi S.
Mechanism of primary non-function in a rat model for fatty liver transplantation. Transplant Int 2000;13:583-590.
50. Seifalian AM, Piasecki C, Aganval A, Davidson BR. The effect of graded steatosis on flow in the hepatic parenchymal microcircu- lation. Transplantation 1999;68:780-784.
5 1. Sun C-K, Zhang X-Y, Zimmermann A, Davis G, Wheatley AM. Effect of ischemia-reperfusion injury on the microcirculation of the steatotic liver of the Zucker rat. Transplantation 2001;72: 1625-1631.
Copyright © 2022 FDOKUMEN




















