PROPOSAL FORM ROLLING CONTINUATION CHANNEL ...
166
PROPOSAL FORM ROLLING CONTINUATION CHANNEL (CCM AND SUB-CCM APPLICANTS) Applicant Name Namibia Coordinating Committee for AIDS, Tuberculosis (TB) and Malaria (NaCCATuM) Country Republic of Namibia Applicant Type Country Coordinating Mechanism (CCM) Income Level Lower-middle Income Country Disease HIV Expiring Grant Number NMB-202-G01-00 Round 2 Other same disease grants that have links to this proposal: None Currency X USD or EURO RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 1/160
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of PROPOSAL FORM ROLLING CONTINUATION CHANNEL ...

PROPOSAL FORM ROLLING CONTINUATION CHANNEL (CCM AND SUB-CCM APPLICANTS)
Applicant Name Namibia Coordinating Committee for AIDS, Tuberculosis (TB) and Malaria (NaCCATuM)
Country Republic of Namibia
Applicant Type Country Coordinating Mechanism (CCM)
Income Level Lower-middle Income Country
Disease HIV
Expiring Grant Number NMB-202-G01-00 Round 2
Other same disease grants that have links to this proposal:
None
Currency X USD or EURO
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 1/160
INDEX OF SECTIONS AND KEY ATTACHMENTS FOR PROPOSALS Page
1. Funding Summary and Contact Details ................................................ 2 2. Applicant Summary (including eligibility) ............................................ 6
+ Attachment C: Membership details of CCM 3. Proposal Summary ................................................................................ 15 4. Program Description ............................................................................. 20 5. Funding Request ................................................................................. 104
+ Attachment A: Performance Framework (Indicators and targets)
+ Attachment B: Preliminary List of Pharmaceutical and other Health Products
+ Detailed Proposal Budget: Quarterly for years 1 and 2 and annual details for years 3
to 6
+ Detailed Work plan: Quarterly for years 1 and 2 and annual details for years 3 to 6
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 2/160
LIST OF TABLES AND FIGURES TABLES Table 1: Relevant New Stakeholders/Potential Service Delivery Organisations Represented on
NaCCATuM Table 2: NaCCATuM Governance Tools Table 3: HIV Prevalence Rate by Age Group and Year of Survey Table 4: Population sizes of the most affected population groups in 2001/02 (Round 2) and in
2008/09 Table 5: Availability of Key Health Professionals in the Public Sector Table 6: Actions Taken to Address TRP Comments on Round 5 HIV Proposal Table 7: Actions Taken to Address TRP Comments on Round 6 HIV Proposal Table 8: CCM Response to TRP Comments on Round 8 HIV Proposal Table 9: Minimum Package of Outreach Services Table 10: Current HRH Vacancies, Posts Filled by Funding Source and Gaps Still to Be Filled FIGURES Figure 1: HIV Prevalence by Year of Survey Figure 2: Shift in Age-specific HIV Prevalence Among Pregnant Women Between 2000 and
2008 Figure 3: HIV prevalence by Youth, Adult Age Groups and Year Figure 4: Total Number of Patients on ARV Nationwide in Public Health System Between
March 2004 and March 2009 Figure 5: Number of Women Attending Maternity Wards at PMTCT Sites: a Comparison
Between 2004/05, 2005/06, 2006/07 and 2007/08 Figure 6: HIV Prevalence by District (2008) and the Distribution of PLHIV on ART (March 2009) Figure 7: Health Sector Funding Allocation Breakdown by Financing Source, 2001/02−2006/07 Figure 8: Breakdown by Financing Source Figure 9: MOHSS Allocation vs. Actual Expenditure 2001/02 – 2006/07 Figure 10: Total Number of New HIV Infections in Children and Adults, 2000/01 to 2015/16 Figure 11: Deaths Due to AIDS-related Illness and New HIV Infections over Time Figure 12: MOHSS PMU Management Structure Figure 13: Proposed NANASO Organogram Figure 14: CMS Distribution Channels Figure 15: HIS Boundaries Among Existing Applications
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 3/160
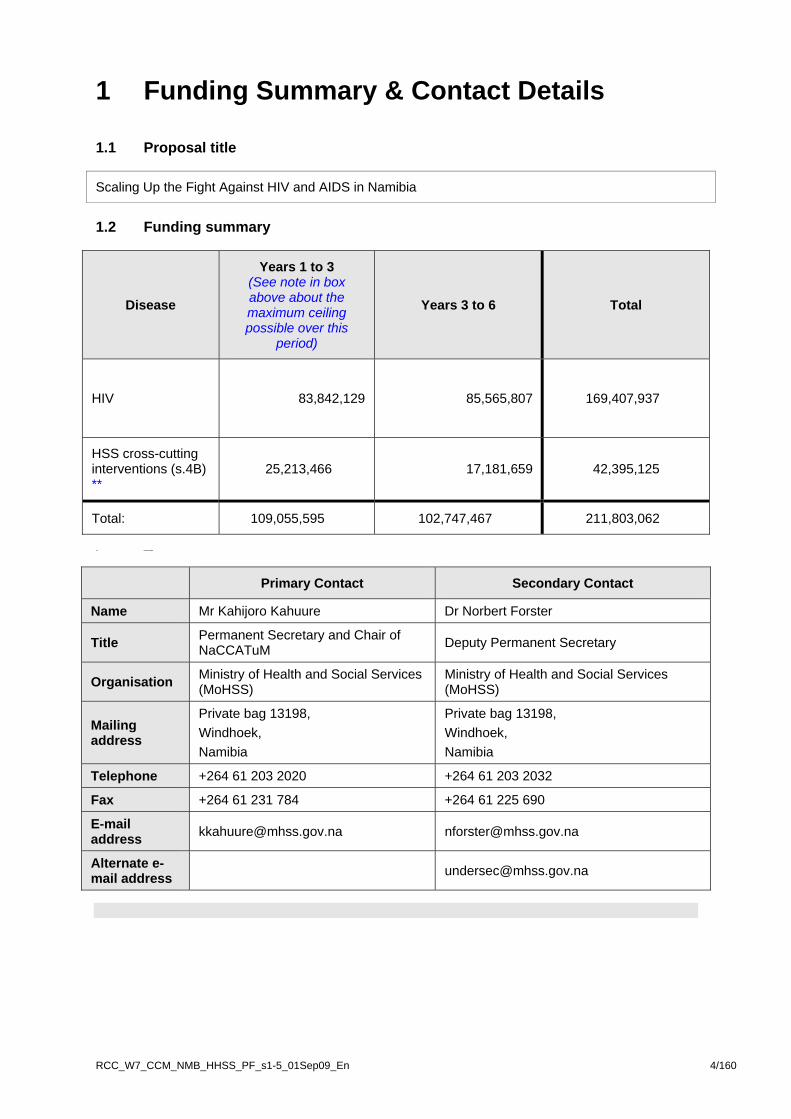
1 Funding Summary & Contact Details 1.1 Proposal title
Scaling Up the Fight Against HIV and AIDS in Namibia
1.2 Funding summary
Disease
Years 1 to 3 (See note in box above about the maximum ceiling possible over this
period)
Years 3 to 6 Total
HIV
83,842,129
85,565,807 169,407,937
HSS cross-cutting interventions (s.4B) **
25,213,466 17,181,659 42,395,125
Total: 109,055,595 102,747,467 211,803,062
1.3
Contact details
Primary Contact Secondary Contact
Name Mr Kahijoro Kahuure Dr Norbert Forster
Title Permanent Secretary and Chair of NaCCATuM Deputy Permanent Secretary
Organisation Ministry of Health and Social Services (MoHSS)
Ministry of Health and Social Services (MoHSS)
Mailing address
Private bag 13198, Windhoek, Namibia
Private bag 13198, Windhoek, Namibia
Telephone +264 61 203 2020 +264 61 203 2032
Fax +264 61 231 784 +264 61 225 690
E-mail address [email protected] [email protected]
Alternate e-mail address [email protected]
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 4/160

1.4 List of Abbreviations and Acronyms used by the Applicant Acronym/
Abbreviation Meaning
ADR Adverse drug reaction ADT Anti-retroviral dispensing tool AIDS Acquired immunodeficiency syndrome AIS AIDS Indicator Survey AMICAAL Alliance of Mayors Initiative for Community Action on AIDS at the Local Level ANC Antenatal care ART Anti-retroviral therapy; anti-retroviral treatment ARV Anti-retrovirals BCC Behaviour change communication BSS Behavioural surveillance survey CACOC Constituency AIDS Coordinating Committee CBHC Community-based health care CBO Community-based organisation CBS Central Bureau of Statistics CCCW Constituency child care worker CCE-CC Community Capacity Enhancement through Community Conversations CCM Country Coordinating Mechanism CDC Center for Disease Control (US) CED Centre for Entrepreneurial Development (Polytechnic of Namibia) CHBC Community and home-based care CMS Central medical stores CoHeNa Advanced Community Health Care Services Namibia COMBI Communication for behaviour impact CPT Cotrimoxazole preventive therapy CSO Civil society organisation CSS Community system strengthening CT Counselling and testing DACOC District AIDS Coordinating Committee DBS Dry blood spot DED Deutscher Entwicklungsdienst (German Development Service) DHIS District health information system DHS Demographic and health survey DNA Deoxyribo nucleic acid DOTS Directly observed treatment DSP Directorate for Special Programmes (MOHSS) EID Early infant diagnosis (of HIV) EPI Expanded programme of immunisation EPMS Electronic patient monitoring system (for ART) EPP Estimates and projections package ETR Electronic TB Register EU European Union FBO Faith-based organisation FP Family planning GAMET Global AIDS Monitoring and Evaluation Team of the World Bank GBV Gender-based violence GF Global Fund GFATM Global Fund to Fight AIDS, Tuberculosis and Malaria GDP Gross domestic product GRN Government of the Republic of Namibia GTZ
Deutsche Gesellschaft für Technische Zusammenarbeit (German Development Cooperation)
HBC Home-based care HCT HIV counselling and testing HDI Human development index HIS Health information system HISPN Health Information System Programme Network
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 5/160
HIV Human immunodeficiency virus HMIS Health management information system HRD Human resource development HRH Human resource for health HRM Human resource management HSS Health systems strengthening HTC HIV counselling and testing IEC Information, education and communication IGA Income generating activity ILO International Labour Organisation IMAI Integrated management of adolescent and adult illness IMR Infant mortality rate IPT Isoniazid preventive therapy IT Information technology JICA Japanese International Cooperation Agency KAPB Knowledge, attitude, practices and behaviour KIT Royal Tropical Institute LAC Legal Assistance Centre LAN Local area network LFA Local Fund Agent LSE(P) Life skills education (programme) M&E Monitoring and evaluation MARP Most at risk population MCH/FP Maternal and child health/family planning MCP Multiple and concurrent partnerships MDG Millennium Development Goal MDR Multi-drug resistant (TB) MGECW Ministry of Gender Equality and Child Welfare MICT Ministry of Information and Communication Technology MOE Ministry of Education MOF Ministry of Finance MoHSS Ministry of Health & Social Services MOSS Ministry of Safety and Security MOWT Ministry of Works and Transport MOYNSSC Ministry of Youth, National Service, Sports and Culture MRLGHRD Ministry of Regional and Local Government, Housing and Rural Development MSH Management Sciences for Health MSM Men having sex with men MTCT Mother to child transmission MTEF Medium-term expenditure framework MTP III National HIV/AIDS Strategic Medium Term Plan III (on HIV and AIDS) MTP IV National HIV/AIDS Strategic Medium Term Plan IV (on HIV and AIDS) NABCOA Namibian Business Coalition on HIV and AIDS NaCCATuM Namibia Coordinating Committee for AIDS, Tuberculosis and Malaria NAC National AIDS Committee NAEC National AIDS Executive Committee NAMACOC National Multi-sectoral AIDS Coordination Committee NAMDEB Namibia Diamond Corporation NANASO Namibian Network of AIDS Service Organisations NASOMA National Social Marketing Programme Namibia NCCI Namibia Chamber of Commerce & Industry NDP III National Development Plan III NEF Namibia Employers Federation NHA National health accounts NHIES Namibia Household and Income Expenditure Survey NIP Namibia Institute of Pathology NGO Non-governmental organisation NPA National Plan of Action NPC National Planning Commission NSF National Strategic Framework
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 6/160

NYC National Youth Council OI Opportunistic infection OPM Office of the Prime Minister OVC Orphans and vulnerable children PC&I Pharmaceutical Control & Inspections PCR Polymerase chain reaction PEP Post-exposure prophylaxis PEPFAR US President’s Emergency Plan for AIDS Relief PHC Primary health care PITC Provider-initiated testing and counselling PLWHA People Living with HIV and AIDS PMC Programme Management Committee PMIS Pharmaceutical management information system PMS Performance management system PMTCT Prevention of mother to child transmission PMU Programme management unit PPP Public-private partnerships PP&HRD Policy and Planning and Human Resource Development Directorate PR Principal Recipient QSL Quality Surveillance Laboratory RACOC Regional AIDS Coordinating Committee RH Reproductive health RM&E Response Monitoring & Evaluation (MOHSS/DSP subdivision) RMS Regional medical store SCMS Supply chain management system SDA Service delivery area SMA Social Marketing Association SME Small and medium-sized enterprises SOP Standard operating procedures SR Sub-recipient SRH Sexual and reproductive health SSR Sub sub-recipient STI Sexually transmitted infection SW Sex worker TA Technical assistance TAC Technical Advisory Committee TB Tuberculosis TBA Traditional birth attendant TCC Technical Coordinating Committee TCE Total control of the epidemic TIPC Therapeutics Information and Pharmacovigilance Centre TOR Terms of reference TRP Technical Review Panel TTR Treat, Train and Retain TWG Technical Working Group UN United Nations UNAIDS United Nations Joint Programme on HIV/AIDS UNAM University of Namibia UNDP United Nations Development Programme UNFPA United Nations Population Fund UNGASS United Nations General Assembly on HIV/AIDS Special Session UNICEF United Nations Children’s Fund UNODC United Nations Office on Drugs and Crime USAID United States Agency for International Development UNCRC United Nations Convention for Rights of the Child USAID United States Agency for International Development USG United States Government VCT Voluntary counselling and testing WAN Wireless area network WFP World Food Programme
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 7/160

WHO World Health Organisation WPP Workplace programme WSN Women’s Solidarity Namibia XDR-TB Extreme drug resistant tuberculosis
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 8/160
2. Applicant Summary (including eligibility)
MB_HHSS_PF_s1-5_01Sep09_En 9/160
2.1 Members and Operations
2.1.1 Membership Summary Clarified Section 2.1.1
The current CCM membership is set out in Annex A2.
2.1.2 Member Knowledge and Experience in Cross-cutting Issues
Health Systems Strengthening (HSS)
(a) Describe the capacity and experience of the applicant to consider how health system issues impact programmes and outcomes for the three diseases.
The profile of the CCM includes members with experience, capacity and knowledge in HSS from the Government, multi- and bilateral donors and NGOs. They bring a wide range of competencies that have been utilised to address gaps and weaknesses in the health system relevant to the country context and to the development of this proposal so that the response is integrated and recognises the interdependence of each part of the health system on the three diseases.
Of the 31 CCM members, the following have considerable experience in HSS:
• The United Nations Joint Programme on HIV/AIDS (UNAIDS) and the World Health Organisation (WHO) – at the Policy, Health Infrastructure and Service Delivery levels;
• The US President’s Emergency Plan for AIDS Relief (PEPFAR) – at the Management level;
• The NGO Advanced Community Health Care Services Namibia (CoHeNa) – at the Service Delivery level;
• The Ministry of Regional and Local Government, Housing and Rural Development (MRLGHRD) – this Ministry is responsible for decentralisation and therefore also for the Regional AIDS Coordinating Committees (RACOCs ) who deal with Management and
Sector Representation Number of Members
X Academic/educational sector 1
X Government 10
X Non-government organisations (NGOs)/community-based organisations (CBOs) 8
X People living with the diseases 2
X Other 1
X Private sector 3
X Faith-based organisations (FBOs) 1
X Multilateral and bilateral development partners in country 5
Total Number of Members: 31
RCC_W7_CCM_N

Service Delivery; and • The MoHSS – in Service Delivery, Policy Design and Management.
More specifically: • WHO brings technical guidance to CCM deliberations based on its mandate to member
states to assist them in facing the challenge of developing a more systematic and sustainable approach to health that responds to the needs of the country. WHO is also the author of the publication ‘Everybody’s Business: Strengthening health systems to improve health outcomes. WHO’s Framework for Action’ (commonly known as the six building blocks) which is now used as the cornerstone for the development of Global Fund HSS interventions; hence WHO brings expertise on all aspects of the six building blocks to the CCM;
• The representative of the Office of the Prime Minister (OPM) is a specialist in human resource issues. As such, the CCM has been able to call upon this in-house expertise with regard to advice on the human resources and manpower planning for the three diseases;
• PEPFAR has been key to the development of HSS interventions, especially in the area of laboratories and diagnostics, through support to the Namibia Institute for Pathology (NIP), and medical products and technologies;
• The MoHSS Deputy Permanent Secretary, also the focal point for the Global Fund (GF) grants, and until very recently the chair of the Programme Management Committee (PMC) which provides direction on all matters pertaining to the implementation of GF grants, is the former Director of the Policy Planning and Human Resources Directorate and has provided invaluable advice to the CCM in matters pertaining to HSS. He provides mentorship in the area of leadership and governance;
• The Chairman of the CCM is an economist and as such brings an understanding of health financing issues; and
• The involvement of the FBOs and other NGOs in CCM discussions on HSS has changed the paradigm from the usual manner of working – getting messages from above – to a more representative approach of bringing messages from below, thus ensuring a better recognition of the needs of communities and the individual in terms of the management and delivery of HSS issues at this critical level.
To support the development of the proposal, the CCM designated certain of its members to form a Technical Coordinating Committee (TCC), ensuring that each TCC member brought expertise in a particular area. Care was taken to ensure that Community System Strengthening (CSS), Gender, HSS and Private Sector representatives were designated as TCC members, involved in every aspect of proposal development and assessment. Where appropriate these experts were co-opted onto the Core Team (responsible for drafting the proposal) to help prepare relevant sections of the proposal pertaining to their area of expertise. In addition, to assist with the development of the HIV proposal, technical working groups (TWGs) for more than 42 key areas, including those mentioned above, were established (Annex C.14, List of Technical Experts, and Annex C.15, List of Stakeholder Meetings/Technical Working Groups). These multi-disciplinary teams not only led the discussions for the identification of technically appropriate areas for scaling up but helped in the development of specific goals, indicators, activities and budgets.
Gender Awareness
(b) Describe the capacity and experience of the applicant ion gender issues including the number of members with requisite knowledge and skills.
Through their involvement in the country’s planning process for a multi-sectoral HIV and AIDS response, all the CCM members have provided inputs on the depth and complexity of gender issues in relation to the development and implementation of the National HIV/AIDS Strategic
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 10/160
Medium Term Plan III on HIV and AIDS 2004-2009 (MTP III) and the forthcoming MTP IV. Most of the CCM members have either had sensitisation and training in relation to the drivers of the epidemic as they relate to gender-disaggregated issues or are directly involved in professional work with a significant gender-related dimension. For example:
• Three-quarters of the members have had gender sensitisation awareness through two major conferences: (a) the 1st National HIV/AIDS Male Leaders Conference 2008 which was attended by both men and women from a cross-section of the Namibian population (politicians, civil servants, church leaders, NGOs, private sector and people living with HIV and AIDS); most of the issues dealt with during this conference were gender related; and (b) in May 2008 there was a similar conference entitled ‘Women and HIV’. The attendance was almost similar to the earlier one that targeted men and the issues covered were also gender-related (Annex J.19, Report of the 1St National HIV/AIDS Male Leaders Conference and Annex J.37, Women and HIV – May 2008)
In addition, there are two organisations represented on the CCM whose focus of work is gender-based: • Women’s Solidarity Namibia (WSN), which has a manual used for training women on gender
linked to issues that are a barrier to women accessing HIV and sexual and reproductive health (SRH) services, such as some cultural norms and practices, gender violence and abuse. Plans are also underway to train men using the same manual. Consultations held with men have enabled WSN to adapt its approach and manual to involve men in scaling up and strengthening male involvement in increasing access to services such as voluntary counselling and testing (VCT), participation in couple discussions on the prevention of mother to child transmission (PMTCT) and post-delivery management for a family-centred approach. Furthermore, this expertise will be brought to bear during the implementation of RCC with its focus on scaling up the response through strengthening community-level interventions. WSN’s representative on the CCM is also a Member of Parliament and is influential with regard to issues relating to both gender and orphans and vulnerable children (OVC), which has contributed towards raising the profile of both these topics within the CCM; and
• The Ministry of Gender Equality and Child Welfare (MGECW) coordinates the high level strategic Inter-Ministerial Committee on Gender-based Violence (GBV) and violence against women in general, highlighting these topics within the CCM. The Ministry held a conference on GBV in June 2007 and one of the Inter-Ministerial Committee’s roles is to advise on the appropriate implementation of recommendations drawn from this conference. Its role is also to advise Cabinet and other key stakeholders on the implementation of policy, legislation and other actions to combat and prevent GBV. The Committee brings together representatives from government, civil and private sectors, almost all of whom are CCM members, as well as other relevant stakeholders.
• CCM members from UN organisations work within an explicitly gender-focused approach cogniscent of the relationship between gender inequality and vulnerability to HIV and STI.
Other strengths in gender issues among CCM members include the fact that multilateral and bilateral CCM members have also received gender sensitisation training within their respective institutions and all these agencies have adopted gender as an integral cross-cutting issue within their work. Both the proposed Principal Recipients (PRs), the MoHSS and the Namibian Network of AIDS Service Organisations (NANASO), have conducted gender mainstreaming training and have used this knowledge in their work in HIV and AIDS, as well as in their work with partners, affiliated organisations and others.
Multi-sectoral Planning
(c) Describe the capacity and experience of the applicant in multi-sectoral programme design.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 11/160

The CCM has a strong track record of multi-sectoral programme design, implementation and monitoring, with all 31 members having the requisite experience in multi-sectoral planning, and most having been and/or continuing to be involved in GF programme development, service delivery and assessment. The success of the implementation of the Round 2 GF grant, where 19 of the 21 indicator targets were met or exceeded by the 25 Sub-recipients (SRs) covering a wide range of public, private and community organisations, is a testament to the strength of the CCM in designing and managing a multi-sectoral programme.
Beyond their involvement in Global Fund proposal planning, development, implementation and oversight, all the CCM members have a distinguished record of participation in the country’s highest multi-sectoral HIV and AIDS planning processes. The development of both the current MTP III and the forthcoming MTP IV (over a period of 18 months for the latter) has entailed a considerable amount of consultation at all levels and across all sectors. All CCM members have been actively involved in one way or another, culminating in the MTP IV Stakeholder Consultations held on 1 July 2009. Individual CCM members also have experience in multi-sectoral programme planning and management through participation in PEPFAR’s annual multi-sectoral Country Operational Plans. CCM members from UN organisations and programmes are very familiar with developing technical support and programme implementation strategies that are multi-sectoral as well as involving civil society and public and private sector at national and decentralised levels.
Finally, the proposed civil society PR, NANASO, has strong links with the health system as it revises community-based policies and standards for improving the quality of services at various levels of the health and social service system.
2.2 Eligibility 2.2.1 Application History
X Applied for funding in Round 6 and/or Round 7 and was determined as having met the minimum eligibility requirements.
Complete all of s.2.2.2 to s.2.2.8 below
2.2.2 Broad and Inclusive Membership
Since the last time you applied to the Global Fund and were determined compliant with the minimum requirements:
(a) Have non-government sector members (including any new members since the last application) continued to be transparently selected by their own sector; and
X Yes
(b) Is there continuing active membership of people living with and/or affected by the diseases? X Yes
2.2.3 Processes to Select Principal Recipients for Programme Implementation during the
Rolling Continuation Channel Term
(a) Describe the process used to transparently select each of the Principal Recipient(s) nominated in this proposal.
For the Round 2 HIV proposal, the MoHSS was proposed as the PR and was unanimously endorsed by the CCM based on its available infrastructure, presence, involvement and experience in managing donor funds. The CCM also noted that the Government of Namibia
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 12/160

had been ranked second in Africa by Transparency International in terms of overall accountability. When the decision was taken for Namibia to apply for Round 8 funding, the CCM felt that the implementation arrangements for the next round of funding should be strengthened through expanding programme delivery and improving programme management among different groups. This was to be achieved through selecting additional PRs to support the public sector PR, the MoHSS, in accordance with the GF’s guiding principle of dual track financing. The selection of a second PR was therefore the direct outcome of the decision recorded at the governance workshop held for members in October 2007. The workshop was facilitated by a CCM expert from Geneva, among others. During the workshop, the importance of dual track financing was emphasised. The dual track financing issue then became one of the major recommendations of the workshop report, which was eventually endorsed by the entire CCM membership (Annex A7, Governance Workshop Report, and Annex A10, Minutes of CCM Meeting 10 April 2008 and 6 June 2008). When NaCCATuM decided to submit an HIV proposal under Round 8, one of the first issues that came up was the selection of a second or more PR(s). Information on dual track financing was presented in the form of a Fact Sheet on the subject and the premise that it was a strong recommendation for the Round 8 proposal development process. The idea was unanimously endorsed by the CCM and a process was put in place to take the matter forward; in February 2008, an Ad Hoc Sub-committee was established to select additional PRs. The Sub-committee represented all the stakeholders on the CCM. The Ad Hoc Sub-committee developed Terms of Reference (TOR) which were circulated to the CCM (Annex A.13, NaCCATuM R8 PR Committee TOR and membership list) and endorsed by the CCM membership. The Sub-committee then drafted a call for expressions of interest that was placed in three local newspapers and appeared on 21, 23 and 25 April 2008 (Annex A14, NaCCATuM Call for Expression of Interest for PRs of Round 8). The announcement informed interested applicants about the process to apply for selection as a PR, and where to obtain the application form. The advertisement provided two contact names (members of the Ad Hoc Sub-committee) and telephone numbers, with a deadline date for submission of applications. The announcement stated the minimum key competency requirements as follows:
• Legal status as recognised by Namibian laws; • Programme management capacity (organisational structure, sufficient and
appropriately qualified staff); • Experience in managing SRs; • Experience in financial management and systems (qualified finance staff and audited
financial statements for the last three years compliant with audit requirements); and • Competence in monitoring and evaluation (M&E) systems.
The announcement was also sent to the entire CCM membership, via e-mail, to ensure its wide distribution to constituents and contacts. Additionally, the announcement was sent to the MRLGHRD, also via e-mail, to disseminate to all relevant structures within all 13 regions. The Ad Hoc Sub-committee developed comprehensive templates for application forms and review forms with a score sheet. These were shared with a few technical people to ensure robustness. The application forms were then made available to interested parties (Annex A15, PR Application and review forms). The Ad Hoc Sub-committee reviewed the submissions against the review forms and made recommendations to the CCM at its meeting on 6 June 2008. In this way an additional PR, representing civil society groups, was selected. During this meeting the CCM also unanimously decided that in view of its good track record the current public sector PR should continue under Round 8 (Annex A10, NaCCATuM minutes of 6 June 2008). The CCM Secretariat sent letters to all the applicants, confirming the nomination of the successful applicant. Those who were unsuccessful were given reasons for their failure to be chosen.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 13/160

N/A.
When Namibia was invited to apply for the Rolling Continuation Channel (RCC) in April 2009 (Annex A8), discussions were held at the NaCCATuM meeting of 8 April 2009 concerning the potential scope and scale up of Round 2 activities (Annex A10 NaCCATuM minutes of 8 April 2009). It had already been agreed under the previous discussions concerning Round 8 that implementation arrangements would be strengthened through the appointment of a second non-public sector PR. It was also evident that, following new research on the drivers of the epidemic (discussed later in section 4.1.2), activities initiated under Round 2 would have to be scaled up and expanded to encompass new target groups and most at risk populations (MARPs), such as prison inmates, men who have sex with men (MSM), sex workers (SW) and mobile populations (seasonal farm workers and labourers, tourists, police and armed forces, migrants, etc.) currently underserved by Round 2. It was clear to the CCM that the umbrella civil society organisation (CSO) proposed as PR for Round 8 was equally essential for a RCC submission which would strive to broaden the service delivery base through partnering with civil society sub-recipients with a track record in working with marginalised groups. Accordingly, at its meeting of 5 June 2009, NaCCATuM unanimously agreed to re-endorse the PRs for the failed Round 8, the MoHSS and NANASO, as PRs for the RCC proposal (Annex A10 NaCCATuM Minutes of 5 June 2009). This decision was reaffirmed at the 38th NaCCATuM meeting on 9 July 2009. The Namibia CCM understands that civil society and other sectors can play a vital role in widening the base for the HIV and AIDS response and in implementing grants. The CCM is also aware of the capacities of various sectors and is, therefore, encouraged by the willingness of NANASO to review and take steps to strengthen its organisational capacity and functioning. As was argued during the selection process, the current PR (the MoHSS) was in a similar situation when the grants for Round 2 were awarded in 2004, but has been able to effectively and successfully manage all the five GF grants. The country is confident that, with the appropriate mechanisms in place to assist, which will include support to NANASO from the current experienced MoHSS Global Fund Programme Management Unit (PMU) and technical and financial support from UNAIDS and WHO, NANASO will be able to build its capacity to become a formidable implementing agency and in turn build the capacity of its member organisations. More details on these processes are to be found in section 2.2.6 below.
(b) Attach the signed and dated minutes of the meeting(s) at which the CCM (or Sub-CCM) decided on the Principal Recipient(s) for this proposal.
Annex A10: 9 July 2009
2.2.4 Principal Recipients
Name Sector
Ministry of Health and Social Services (MoHSS) HIV
Namibia Network of AIDS Service Organisations (NANASO) HIV
2.2.5 Non-implementation of Dual Track Financing
2.2.6 Transparent Proposal Development Processes
A If this proposal continues/scales-up the interventions from the expiring grant, describe in detail the transparent process used by the CCM (or Sub-CCM) to ensure that:
(a) a broad group of stakeholders (including CCM, or Sub-CCM, members and non-members) were involved in evaluating the appropriateness of continuing the interventions; and
(b) the decision to continue relevant interventions was made after discussion among the
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 14/160

stakeholders consulted.
Considerable effort has been made to undertake a comprehensive, painstakingly transparent and fully participatory path in order to ensure the development of a RCC proposal that addresses the concerns of the widest possible array of stakeholders. This is described below. Phase 1 In its 34th Meeting on 8 April 2009, NaCCATuM endorsed the decision that Namibia should submit a proposal for the RCC (Round 2) for HIV, TB and Malaria. At the 35th Meeting on 12 May 2009, NaCCATuM reaffirmed this decision and not to apply for Round 9 for HIV because: firstly, funding for Namibia’s Round 2 Phase 2 for HIV and AIDS was due to end in 2009 and continued support is deemed to be of the utmost necessity in the current phase of the epidemic; and, secondly, since Namibia had performed well under Round 2, many successful interventions were in place which could form the platform on which to continue current efforts to build, expand and scale up activities. Phase 2 During its meeting on 10 April 2008 (Annex A10), NaCCATuM established an Ad Hoc Sub-committee for the selection of a second PR for the Round 8 proposal in accordance with the dual tracking recommendation by Global Fund. Discussions were widespread, intense and inclusive, and culminated in the endorsement of the key civil society umbrella organisation NANASO as the second PR. As noted in section 2.2.3 above, the MoHSS was endorsed to retain its PR status (Annex A10, Minutes of NaCCATuM Meeting 16 June 2008). NANASO was also tasked to address capacity issues in consultation with the GF Namibia secretariat. Capacity strengthening would be essential to enable the organisation to reach its full potential in widening the scope of service delivery outside the public sector, and this would be recognised in the RCC Proposal. At the NaCCATuM meeting on 5 June 2009 (Annex A10), CCM members were asked to reaffirm the decision on the two PRs. Phase 3 NaCCATuM had already established a TCC to coordinate the development of the proposal for Round 8; TORs were prepared (Annex A16) and members selected to represent a broad spectrum of interests and thematic expertise from the CCM. It was agreed by both the National AIDS Executive Committee (NAEC) and NaCCATuM that this Committee should continue its role during the RCC development and application process. The TCC met weekly, and sometimes more often, throughout the process (Annex C11) and briefed the relevant constituents on a regular basis, as well as reporting back to the CCM as necessary. The Minutes and attendance lists are available for all meetings and are attached in Annex C11. Phase 4 A National Stakeholders Meeting was called for 13 May 2009 to announce NaCCATuM’s decision to apply for the GF RCC Wave 7 application for all three diseases. This invitation was also advertised prior to the meeting through three national daily newspapers (Annex B2, Minutes of Stakeholder Consultation 13 May 2009 and Annex B2 List of participants). All attendees were encouraged to share ideas and raise concerns. It was clearly stated that the process of consultation was ongoing and that TWGs would be established to ensure the close involvement of all actors representing the service delivery areas (SDAs) as well as other technical and thematic interests. Participants from existing SRs and other interested individuals/organisations were invited to share and contribute. At this well attended meeting, participants received information on the progress of all Global Fund Rounds; the various SDAs and those SRs active in each SDA intervention; and guidelines and comparisons between Round-based applications versus RCC applications. The RCC process was explained in depth, and the expected timeline was discussed. Phase 5 A Concept Paper was produced (see Annex C2) to assist stakeholders to understand the gaps and
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 15/160
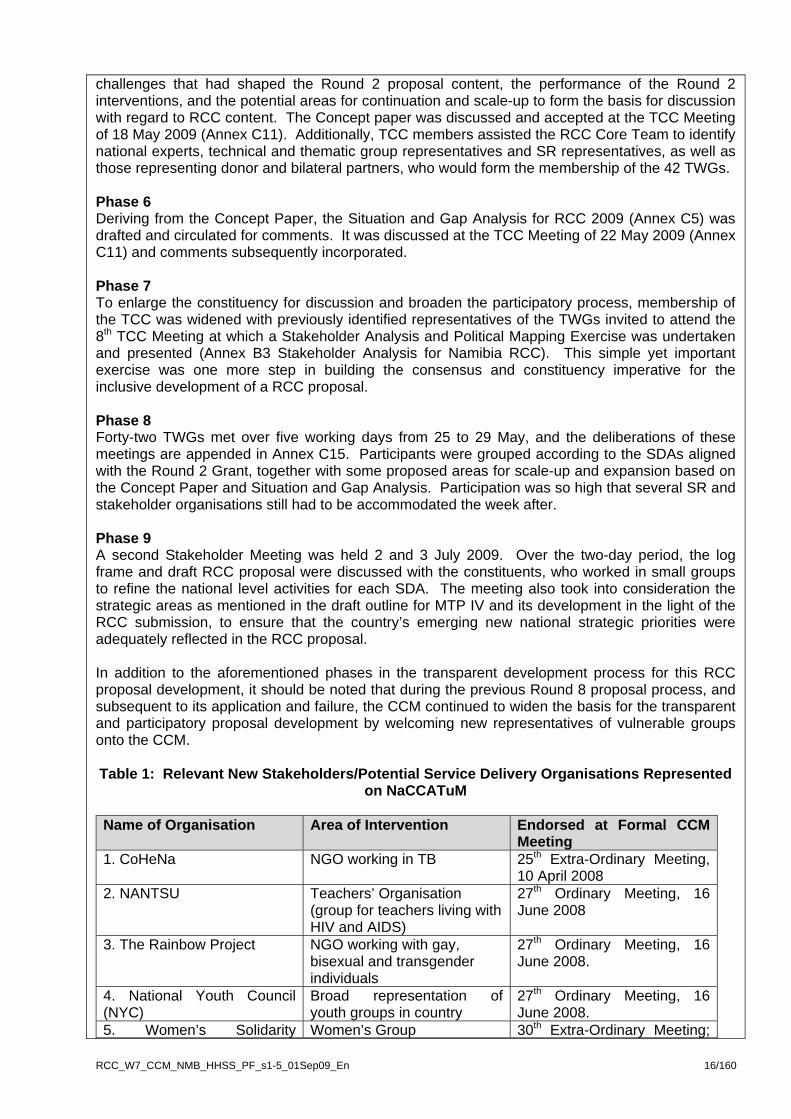
challenges that had shaped the Round 2 proposal content, the performance of the Round 2 interventions, and the potential areas for continuation and scale-up to form the basis for discussion with regard to RCC content. The Concept paper was discussed and accepted at the TCC Meeting of 18 May 2009 (Annex C11). Additionally, TCC members assisted the RCC Core Team to identify national experts, technical and thematic group representatives and SR representatives, as well as those representing donor and bilateral partners, who would form the membership of the 42 TWGs. Phase 6 Deriving from the Concept Paper, the Situation and Gap Analysis for RCC 2009 (Annex C5) was drafted and circulated for comments. It was discussed at the TCC Meeting of 22 May 2009 (Annex C11) and comments subsequently incorporated. Phase 7 To enlarge the constituency for discussion and broaden the participatory process, membership of the TCC was widened with previously identified representatives of the TWGs invited to attend the 8th TCC Meeting at which a Stakeholder Analysis and Political Mapping Exercise was undertaken and presented (Annex B3 Stakeholder Analysis for Namibia RCC). This simple yet important exercise was one more step in building the consensus and constituency imperative for the inclusive development of a RCC proposal. Phase 8 Forty-two TWGs met over five working days from 25 to 29 May, and the deliberations of these meetings are appended in Annex C15. Participants were grouped according to the SDAs aligned with the Round 2 Grant, together with some proposed areas for scale-up and expansion based on the Concept Paper and Situation and Gap Analysis. Participation was so high that several SR and stakeholder organisations still had to be accommodated the week after. Phase 9 A second Stakeholder Meeting was held 2 and 3 July 2009. Over the two-day period, the log frame and draft RCC proposal were discussed with the constituents, who worked in small groups to refine the national level activities for each SDA. The meeting also took into consideration the strategic areas as mentioned in the draft outline for MTP IV and its development in the light of the RCC submission, to ensure that the country’s emerging new national strategic priorities were adequately reflected in the RCC proposal. In addition to the aforementioned phases in the transparent development process for this RCC proposal development, it should be noted that during the previous Round 8 proposal process, and subsequent to its application and failure, the CCM continued to widen the basis for the transparent and participatory proposal development by welcoming new representatives of vulnerable groups onto the CCM.
Table 1: Relevant New Stakeholders/Potential Service Delivery Organisations Represented
on NaCCATuM Name of Organisation Area of Intervention Endorsed at Formal CCM
Meeting 1. CoHeNa NGO working in TB 25th Extra-Ordinary Meeting,
10 April 2008 2. NANTSU Teachers’ Organisation
(group for teachers living with HIV and AIDS)
27th Ordinary Meeting, 16 June 2008
3. The Rainbow Project NGO working with gay, bisexual and transgender individuals
27th Ordinary Meeting, 16 June 2008.
4. National Youth Council (NYC)
Broad representation of youth groups in country
27th Ordinary Meeting, 16 June 2008.
5. Women’s Solidarity Women’s Group 30th Extra-Ordinary Meeting;
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 16/160
Namibia 8 October 2008
(c) Attach documents that show the transparent, broadly inclusive processes used to decide whether to continue (and if so, most probably, scale-up) some or all of the interventions from the expiring grant.
B1, B2, B3
2.2.7 Managing Conflicts of Interest
(a) Are the Chair and/or Vice-Chair of the CCM (or Sub-CCM) from the same entity as any of the nominated Principal Recipient(s) in this proposal?
X Yes
(b) If yes, attach the plan for the management of actual and potential conflicts of interest. A6
Chairmanship of the CCM In November 2007 a capacity building workshop for CCM members was held. CCM members from Zambia and Zimbabwe came to share experiences, and expertise was provided by a CCM specialist from GF Geneva (Annex J36 Waterberg Workshop Report). At this meeting, management of conflicts of interest was discussed.
In the CCM meeting of 8 April 2008, members revisited the issue of the chair of the CCM also being the PR’s Accounting Officer. It was decided to maintain the current status for the moment, until the application and successful award of the next Global Fund Round. Thus the current incumbent would remain until the end of 2008 and, upon feedback of the results of the application for Round 8 the CCM would select another chair (Annex A10, NaCCATuM Minutes 8 April 2008). When it was announced that the country had been unsuccessful in Round 8, it was agreed that the Chair would remain until the results of the RCC application were announced.
Prior to the development of the governance documents this year (March–June 2009), the old Conflict of Interest Policy did not state how long CCM office bearers could hold office. A new governance policy was adopted by the CCM in June 2009 and addresses the issue of tenure; a Chair cannot hold office for more than two years. The implementation of the Policy has not yet started; however, a dissemination workshop is planned for September 2009 during which actions that need to occur will be prioritised, including the election of the new Chair. Following this, the implementation of the new policy will start.
However, it should be noted that, under the existing and new Conflict of Interest Policy and Procedures, if a matter under discussion is viewed as creating a potential conflict of interest then the members have the power to request a member to leave the room. If the person required to leave is the Chair, then the Vice Chair from the private sector takes over chairing the meeting.
Establishment of separate secretariat for NaCCATuM Another step that the CCM has taken to avoid conflicts of interest has been the establishment of an independent Secretariat – the Polytechnic of Namibia. Previously the PMC, comprised of PMU and senior PR officials, had fulfilled this role. However, after months of deliberations by a NaCCATuM sub-committee, tender procedures and interviews, the Polytechnic of Namibia’s Centre for Entrepreneurial Development (CED) was appointed as the Secretariat. The outsourcing of this important function is a vital step in ensuring a transparent process and avoiding conflicts of interest. NaCCATuM’s improved governance and oversight Namibia is one of the GF’s pilot countries for the Dashboard M&E Tool whose primary role is to provide a snapshot of the programmatic and financial delivery of priority grant indicators and targets. Although still in its pilot phase, the Tool has already been used to reorient CCM members to better oversee the implementation of the current GF grants and permit new parameters to be
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 17/160

set. It is anticipated that the development and implementation of this and other vital CCM tools such as the CCM Constitution and Governance Manual will result in the strengthening of CCM members to be able to better operate in a transparent and accountable manner. At the NaCCATuM Meeting on 5 June 2009 (Annex A10, op. cit.), the following NaCCATuM governance documents/tools were tabled:
Table 2: NaCCATuM Governance Tools
Name of Tool/Document Status of
Tool/Document Decision Taken Annex
1. Dash Board Pilot Work in Progress To train newly selected Secretariat and transfer functions
In progress
2. NaCCATuM Constitution Completed Endorsed with minor corrections
A1
3. Governance Manual Completed Endorsed A4 4.Oversight Plan; Work Plan and Budget.
Completed Endorsed A5
5. TORs for M&E; Finance/Audit and Conflict of Interest sub-committees
Work in Progress To be referred to a future NaCCATuM meeting for further discussion.
In progress
2.2.8 Proposal Endorsement by Members
Attachment C – Membership information and Signatures
Has 'Attachment C' been completed with the numbers of all members of the CCM (or Sub-CCM)
Yes
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 18/160
3. Proposal Summary
3.1 Duration of proposal
Planned start date To
Month and year: July 2010 June 2016
3.2 Consolidation of Grants
(a) Does the CCM (or Sub-CCM) wish to consolidate any existing same disease Global Fund grant(s) with part or all of this RCC proposal? X No
3.3 Alignment of Planning and Fiscal Cycles
Describe how the start date:
(a) contributes to alignment with the national planning, budgeting and fiscal cycle; and/or
(b) in grant consolidation cases, increases alignment of planning, implementation and reporting efforts.
3.3.1 Namibia’s national planning and fiscal cycle runs from 1 April to 31 March. Based on the experience of the previous TB Round 5 and Malaria Round 6 grants, it is expected that detailed contractual negotiations would last from November 2009 until mid-2010, and that Phase 1 would commence in July 2010. 3.3.2 Given this assumption, the programme managers will instruct the independent auditors that the financial year-end of the Global Fund RCC HIV programme shall be 31 March, in line with the Namibian fiscal cycle. The first statutory accounts would be produced for the nine months to 31 March 2011, and for five twelve-month periods thereafter, finishing on 31 March 2016. The final statutory report would cover the three months ending 30 June 2016.
3.4 Programme-based Approach?
3.4.1 Does planning and funding for the country's response to the disease occur through a programme-based approach?
No
3.5 Summary of Rolling Continuation Channel Proposal
Provide a summary of the proposal described in detail in section 4.
3.5.1 Namibia is one of the top five worst HIV and AIDS affected countries in the world. The epidemic is generalised, with most HIV infections transmitted heterosexually. HIV prevalence peaked at 22 percent in 2002; however, since then a declining trend is observed with a fall in prevalence to 17.8 percent according to 2008 data.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 19/160
3.5.2 At the start of the epidemic, the country was largely unprepared to manage the disease. Although Namibia is a low-middle income country with the eleventh highest Human Development Index (HDI) in Africa, it also has one of the largest income disparities in the world as evidenced by the Gini Coefficient of 0.6, according to the 2003/4 Namibia Household Income and Expenditure Survey (NHIES). The high burden of disease from HIV and TB has placed an additional strain on the nation’s available resources, a situation which is exacerbated by the high levels of unemployment placed at 36.4 percent in 2004 as stated in the country’s Third National Development Plan (Annex J16, NDPIII) and poverty at 27.6 percent (Central Bureau for Statistics (CBS) (2008). A Review of Poverty and Inequality in Namibia. National Planning Commission: Windhoek). 3.5.3 On a positive note, the HIV and AIDS epidemic in Namibia has seen dynamic changes during the last few years. These include: (a) increased levels of funding through a strong relationship between the GF, the Government of the Republic of Namibia (GRN) and PEPFAR in terms of aligning and allocating funds to priority interventions; (b) the engagement of growing numbers of organisations and partners from public, private and civil society sectors; and (c) expanding geographical coverage of services and programmes implemented. The GF 2 programme has undoubtedly contributed significantly towards the country’s ability to scale up its response. The RCC proposal is based on a rigorous gap analysis, best practice and lessons learned to improve the consolidation of the response, as well as focus on scaling up, new interventions aimed at recently identified most at risk populations (MARP), and on the sustainability of programme interventions. 3.5.4 The proposal targets the entire country’s population, with specific emphasis on key affected populations such as: people living with HIV and AIDS who make up 9.8 percent of the population; pregnant women and their infants at risk; men, who are less willing to test or access treatment than women; youth (approximately 431,356 or 21.7 percent of the population aged between 15 and 24); and orphans and vulnerable children (OVC) who make up 12.6 percent of the population. In addition, MARP will be targeted, including sex workers (SW), men who have sex with men (MSM), prison inmates and mobile groups such as truckers, SWs, miners, migrants and seasonal farm workers. 3.5.5 The proposal includes a HSS section (4B) that addresses some cross-cutting health systems weaknesses, which have significant impact on HIV, Malaria and TB programming and service delivery outcomes. 3.5.6 The Global Fund is being requested for a total amount of USD 211,803,062 over six years, which is approximately 15 percent of the annual average cost of the Namibian HIV and AIDs and RB response. Of this amount, USD169,407,937 is for the HIV and AIDS component, while USD 42,395,125 is for HSS 3.5.7 The total funding request under this RCC proposal is summarised in the table below:
US$ Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Total
HIV 29,336,605
26,421,034
28,084,490
27,161,219
29,905,910
28,498,680
169,407,937
HSS 9,189,387
8,825,758
7,198,321
6,881,173
6,038,017
4,262,469
42,395,125
Total 38,525,992
35,246,792
35,282,811
34,042,392
35,943,927
32,761,149
211,803,062
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 20/160

3.5.8 The overarching goal of the Round 2 programme remains the same under the RCC: - To reduce the prevalence of HIV and AIDS morbidity and mortality, and mitigate the socioeconomic impact of the HIV and AIDS epidemic in Namibia. 3.5.9 The proposal’s four objectives mirror those of the Round 2, and are aligned with the four thematic strategic areas under the forthcoming National HIV/AIDS Strategic Plan Medium Term Plan IV (MTP IV) 2011-2015. The impact indicators remain the same. The body of the proposal itself shows the linkage of each service delivery area (SDA) under Round 2 to those under the RCC. 3.5.10 The key objectives, SDAs, activities and timeframes under this proposal are as follows: Objective 1: Reduce new HIV, TB and other STI infections 3.5.11 A major portion of this proposal will be used to conduct mass media and community outreach campaigns for the general population, both in and out of school youths, uniformed services and MARP. Condom distribution national targets are 35 million in 2010 rising to 38.6 million by 2016 (with GRN funding). This proposal however only requests support for 21 million condoms per annum. National targets for voluntary counselling and testing (VCT) are gradually scaled-up towards 2016 of which the proposal requests funds for about 30-40 percent coverage of all clients per annum. The PMTCT target for the percentage of pregnant women receiving a complete course of prophylaxis is 75 percent for 2010, with an additional scale-up towards 90 percent annually. With regard to sexually transmitted infection (STI), this previously neglected SDA is addressed in the RCC through scaling up diagnosis and treatment, training health care workers, facility-level mentoring and monitoring and evaluation (M&E). Objective 2: Reduce morbidity and mortality through universal access to comprehensive HIV/TB/STI treatment, care and support services 3.5.12 A key component of this proposal will be to build on the successes of Round 2 through expanding the scope and scale of proven interventions to reach grater numbers of people through decentralised, better quality and more accessible antiretroviral (ART), community home-based care (CHBC) and integrated management of TB/HIV services at the community level. ART roll-out, which started in 2003, has been scaled up as follows: all 34 hospitals covered by 2006 (100 percent) and 32 health centres, bigger clinics and outreach points (by 2009), and will reach an additional number of 78 health centres, clinics and outreach point by 2016. This strategy will increase ART accessibility and is expected to increase coverage for adults and children in need from 81 percent in June 2009 to 87 percent by 2015/16. 3.5.13 Other interventions include improving the continuum of care and support through strengthening referral systems between facilities and CHBC, addressing concerns about treatment adherence and HIV prevention, as well as the SRH needs of people living with HIV and AIDS. To improve treatment adherence, funds are requested for nutritional support for poor clients in rural areas. RCC interventions will build on Round 2 to continue and expand case management for the chronically ill, adapting existing activities to increase community-based organisation (CBO) service delivery, including support groups for people living with HIV and AIDS and to improve geographical coverage. Regarding, TB and HIV collaborative activities, the proposal aims at improving the screening of people with HIV for TB symptoms, and vice versa. Objective 3: Reduce the impact of HIV/TB/STIs on infected and affected individuals, families and communities 3.5.14 The country target is to reach 130,000 OVC by 2010 and going up to 250,000
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 21/160
(100%) coverage of OVC by 2015. The RCC proposal aims to support on average 17 percent of those in need per annum with the provision of a comprehensive package of basic care and support (including educational assistance, shelter, nutritional, psychosocial and material support), support to caregivers and improvement of coordination and referral mechanisms between different levels of service delivery at the community level. Objective 4: Strengthen the leadership and governance required for the scale up of the national HIV and AIDS response 3.5.15 Regarding engendered workplace programmes (WPP), the proposal aims to scale up peer education and VCT in workplaces, in particular through mobile testing. It is envisaged that sector policy development will be supported through strengthening gender and human rights components. Currently WPP are being supported on a large scale by the private sector in selected districts. However, there is a need to expand the package of services. Meanwhile, in both private and public sector, the capacity of WPP service providers to manage and implement WPP will be enhanced. 3.5.16 The selection of a CSO umbrella organisation as the second non-public sector Principal Recipient (PR) highlights the RCC proposal’s increased emphasis on community systems strengthening (CSS) for programme sustainability. 3.5.17 Activities will include the provision of capacity building to strengthen community organisations offering HIV and AIDS and TB care and support. 3.5.18 Under the SDA for programme management and administration, the PRs will be equipped with the necessary M&E tools and capacity building to help them manage the expanded response, to improve coordination and management of decentralised HIV and AIDS activities at provincial and district levels, develop best practice and information sharing mechanisms and strengthen gender responsive M&E activities related to programme management. 3.5.19 The requested HIV budget is broken down into major objectives as follows:
Major Objective % of Total Cost
Reduce new HIV, TB and other STI infections. 33 Reduce morbidity and mortality through universal access to comprehensive HIV/TB/STI treatment, care and support services.
50
Reduce the impact of HIV/TB/STI on infected and affected individuals, families and communities. 5
Strengthen the leadership and governance required for the scale up of the national HIV and AIDS response. 12
Total 100 3.5.20 This proposal includes HSS cross-cutting interventions as follows: Objective 1a: Strengthen the availability and accessibility of quality HIV, TB and Malaria services (Service Delivery) 3.5.21 Interventions under this objective will focus on: (a) provision of equipment (mobile clinic vans) to strengthen coordination and delivery of mobile and outreach health services in the public sector; (b) provision of transport to strengthen referral and
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 22/160

supervisory services, delivery of samples, management of district hospitals, health education and condom distribution; (c) provision of adequate space for VCT, ART and PHC service delivery (35 renovations should be completed by 2015); and (d) improving services for people with disabilities. Objective 2a: Strengthen human resources to improve the effective management of HIV, TB and Malaria (Health Workforce) 3.5.22 The need for a stronger human resources system has been identified as a key constraint to be addressed both for HIV and AIDS and for the health system as a whole. Key aspects of the activities under this component are as follows: (a) rretention of currently employed health workers for HIV and AIDS, TB and malaria service delivery; (b) rrecruitment of additional staff to cope with scaling up HIV and AIDS, TB and malaria services and the decentralisation of services to health centres and clinics; (c) provision of full bursaries for the pre-service and in-service training of health workers; and (d) expansion and upgrading of national health training institutions by providing additional staff and equipment. The global fund contribution for scaling-up human resources for strengthening health systems will come to a total of 67 health professionals. Objective 3a: To sstrengthen M&E systems to ensure evidence-based decisions (Health information Systems [HIS]) 3.5.23 Interventions under this component include: (a) harmonisation of the management and coordination of the national M&E programme, including that for HIV and AIDS, TB and malaria, by installing and maintaining an integrated national database; (b) provision of pre-service and in-service M&E capacity building; and (c) ccontributions to the implementation of relevant national surveys for impact assessment. Objective 4a: To sstrengthen systems that provide equitable access to quality essential pharmaceutical and health products and technologies (Pharmaceutical and health products) 3.5.24 Activities include: (a) procurement of vehicles to distribute medicines and other supplies, and (b) procurement of equipment for the Quality Surveillance Laboratory (QSL). Objective 5a: To Strengthen systems that provide equitable financing for health 3.5.25 An analytical study will be conducted of medical insurance funds used for designing health finance reforms. 3.5.26 The requested HIV budget is broken down in major objectives as follows:
Major Objective % of Total Cost
1a. Strengthen the availability and accessibility of quality HIV, TB and malaria services. (Service Delivery) 29 2a. Strengthen human resources to improve the effective management of HIV, TB and malaria programmes. (Health Workforce)
45
3a. Strengthen M&E systems to ensure evidence-based decision-making. (HIS) 13.5
4a. Strengthen systems that provide equitable access to quality essential pharmaceutical and health products and technologies. (Pharmaceutical and Health Products)
12.5
5a. Strengthen systems that provide equitable financing Nil
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 23/160

for health
Total 100
MB_HHSS_PF_s1-5_01Sep09_En 24/160
4. Programme Description
4.1. Key Changes in the Stage or Dynamics of the Disease
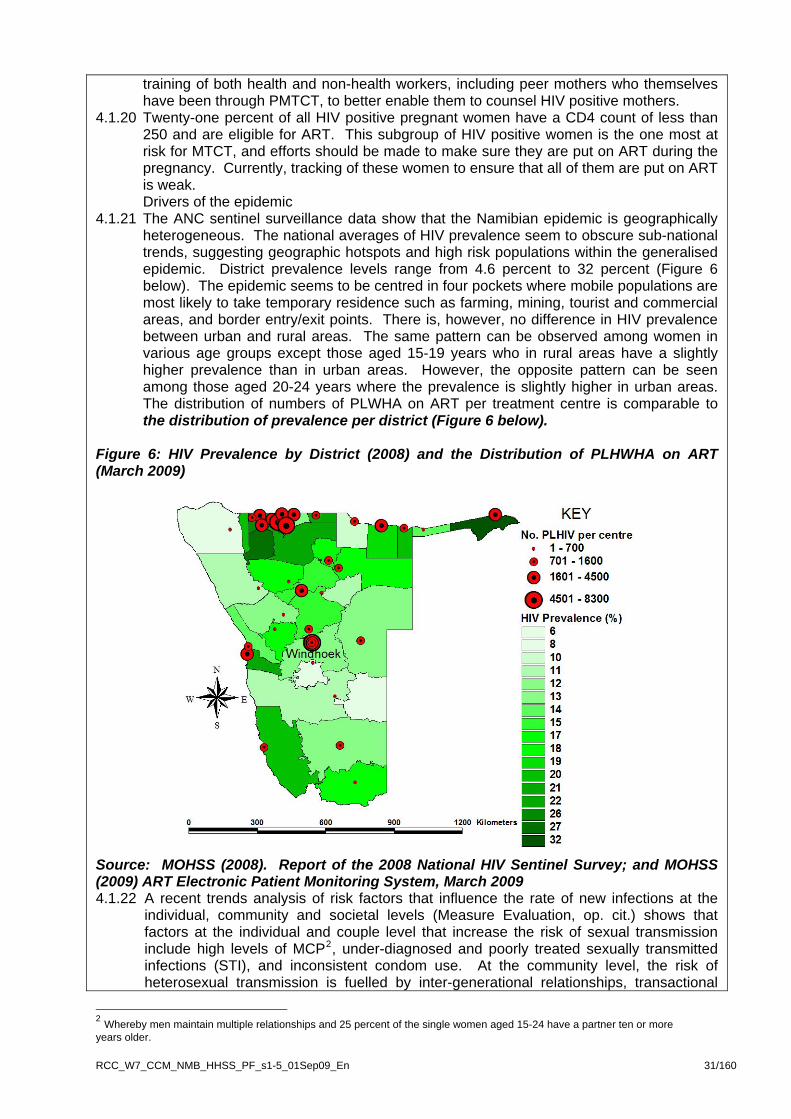
Summarise the main changes in the stage or dynamics of the disease, including any changes in the most affected population group(s) between when the original proposal for the expiring grant was submitted, and now. Introduction 4.1.1 A rapid epidemiological synthesis of the HIV and AIDS epidemic in Namibia shows that
the country has a generalised HIV epidemic with most HIV infections transmitted heterosexually and from mother to child. HIV continues to be a major public health concern and a risk for Namibia’s socioeconomic development, particularly when coupled with the high prevalence of TB, affecting all socioeconomic groups and all sectors. In the more populous Northern regions of Namibia, where 40 percent of the population lives, the situation is further aggravated by the high prevalence of Malaria.
4.1.2 The transmission dynamics of the HIV and AIDS epidemic in Namibia have become clearer since the implementation of the Round 2 Grant. Following extensive research conducted in late 2008, the drivers of the epidemic were finally identified; the most important include: (i) high levels of multiple and concurrent partnerships (MCP) with inconsistent condom use; (ii) inter-generational sex; and (iii) transactional sex (Measure Evaluation: 2008. HIV/AIDS in Namibia: Behavioural and Contextual Factors Driving the Epidemic, Macro). Given that 11.8 percent of infants were found to be HIV positive (MOHSS: 2009. Annual Progress Report, April 2007 to March 2008), it is estimated that mother to child transmission (MTCT) contributes over 1,000 new HIV infections annually and therefore is another important driver of the epidemic Main changes in the stage and dynamics of the disease
4.1.2 The national trends in HIV prevalence, using HIV sero-prevalence data from antenatal clinics (ANC), show that the epidemic appears to be stabilising and seems to be at the start of a declining trend following the drop in prevalence to 17.8 percent in 2008 compared with 19.9 percent in 2006 and 22.0 percent in 2002 (Figure 1 below). However, an ANC prevalence of 17.8 percent is still high and MTCT will continue to be a major contributor to new infections if effective PMTCT strategies are not implemented. Although Namibia is yet to conduct a population-based HIV prevalence survey, the Spectrum estimate for adult HIV prevalence in 2008 is 15.4 percent (Namibia Spectrum Model Projections and Estimates 2009).
4.1.3 These improvements in the prevalence rate can be attributed to considerably increased levels of funding, including the Round 2 HIV Grant, the engagement of growing numbers of organisations and partners from the public, private and civil society sectors, expanding geographical coverage of services and programmes implemented, and an increasing coverage of needs and beneficiary demand.
RCC_W7_CCM_N

Figure 1: HIV Prevalence by Year of Survey
4.2
8.4
15.4
17.4
19.317.8
19.9
22.0
19.7
0
5
10
15
20
25
1992 1994 1996 1998 2000 2002 2004 2006 2008
Year
%H
IV P
reva
lenc
e
Source: MOHSS (2008). Report of the 2008 National HIV Sentinel Survey. October 2008. 4.1.4 Comparing the age specific prevalence data between 2000 and 2008 shows how the
HIV epidemic has matured over time (Table 3 and Figure 2 below). Mean HIV prevalence has dropped among ANC clients over the past six years, with the largest decreases in HIV prevalence observed among pregnant women aged 15-19 and 20-24. The overall HIV prevalence for the age group 15-24 years is 10.6 percent. While the prevalence in adult age groups (35-44 years) appears to be increasing, the prevalence in the younger age groups (15-19, 20–24 years) is decreasing, from 12.0 to 5.1 percent and 20.0 to 14.0 percent respectively between 2000 and 2008. As a result, the MTP III targets for the younger adult population (aged 15-19) have been exceeded while those for the older adults are yet to be achieved. The peak prevalence has shifted to older ages, probably due to the aging of cohorts and a decline in infection levels among young women.
Table 3: HIV Prevalence Rate by Age Group and Year of Survey
Age Group
1994
1996
1998
2000
2002 2004 2006 2008
% HIV prevalence target (MTP III)
Progress towards achieve
ment
15-19 6 11 12 12 11 10 10.2 5.1 9 Exceeded
target
20-24 11 18 20 20 22 18 16.4 14.0 15 Exceeded
target
25-29 9 17 22 25 28 26 26.9
23..8 21
Target not
achieved
30-34 9 18 19 21 27 24 29.5 27.2 20
Target not
achieved
35-39 3 8 12 15 21 24 24.1 26.0 16
Target not
achieved
40-44 1 12 14 9 16 12 16.9 17.7 14
Target not
achieved
45-49 12 1 13 8 12 13 9.1 13.8 No target
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 25/160

set
ource: MOHSS (2008). Report of the 2008 National HIV Sentinel Survey. October 2008;
igure 2: Shift in Age-specific HIV Prevalence Among Pregnant Women Between 2000
Sand MOHSS (2004) Medium Term Plan (MTP III) 2004-2009 Fand 2008
0
5
10
15
20
25
30
15-19 20-24 25-29 30-34 35-39 40-44 45-49Age Group
HIV
% P
reva
lenc
e
2000
2008
Source: MOHSS (2008), ibid.
.1.6 HIV prevalence among young women aged 15 to 24 years, a proxy for recent infections,
4.1.7 (aged between
igure 3: H
4
has dropped considerably from 15.2 percent in 2004 and 14.2 percent in 2006 to 10.6 percent in 2008 (Ibid, p.15). This is probably attributable to the country’s behaviour change interventions that emphasise consistent preventive behaviour particularly amongst the younger age group (15-19 year olds) where prevalence has dropped by half since 2002 (from 11 to 5.1 percent). However, based on the Estimates and Projections Package (EPP) and Spectrum Model of 2008, it was estimated that 15-24 year olds would continue to account for 44 percent of all new infections every year (Namibia Spectrum Model Projections and Estimates 2008). The apparent increase in prevalence among the older pregnant women
IV prevalence by Youth, Adult Age Groups and Year
30-49 years) is probably due to the ageing cohort effect as HIV-infected women are living longer with provision of antiretroviral therapy (ART). In addition, condom use is higher among youth (DHS 2006), but this is primarily due to the fact that they are less likely to be married. Among respondents that had sex with a non-marital, non-cohabitating partner, condom use varies little by age.
F
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 26/160

15.2 14.2
10.6
23.9
26.524.7
0
5
10
15
20
25
30
2004 2006 2008
Year
HIV
% P
reva
lenc
e
15-24
25-49
2004 2006 2008 Source: Ibid. Changes in the most affected population groups between Round 2 and by 2008 4.1.8 There have been changes in most of the affected population groups between 2001/02
and 2008/09 (Table 4 below). There has been an increase in the numbers of PLWHA from 178,000 in 2001/02 to 195,270 in 2008/09 (Namibia Spectrum Model Projections and Estimates 2009). However, while HIV prevalence has dropped from 18 percent to 15 percent over the same period with a fall by one-half among young (15-24) men and women, the number of children living with HIV and AIDS has doubled from 7,360 to slightly more than 16,000 due to increased survival rates as a result of high antiretroviral (ARV) coverage for those in need. Similarly, HIV prevalence among children has doubled. The increase in the numbers of PLWHA exacerbates the need to provide care, treatment and support services for both infected and affected populations. The questions that need to be addressed include: how will the ART roll-out be decentralised to meet these needs? How will the health system cope with the growing numbers? And how can civil society be mobilised to assist in providing care and support, as well as influence the requisite increase in access?
4.1.9 The total number of new HIV infections has reduced greatly since the Round 2
application (2001/02) by approximately one-half, indicating that there have been successful HIV prevention interventions (Table 4 below). This could be because in almost all 13 regions condom use among non-marital and non-cohabitating partners has significantly increased over time among both women and men, as indicated by a comparison of the 2000 DHS with those of the 2006 DHS (Measure Evaluation: 2008, op. cit.). Among women, condom at the last sex with a non-marital/cohabitating partner increased from 43 percent in 2000 to 62 percent in 2006; for men, the corresponding increase was from 67 percent in 2000 to 78 percent in 2006 (DHS, 2000 and 2006). In both instances, these increases were statistically significant.
4.1.10 The number of total annual AIDS deaths is almost the same since the Round 2
application at approximately 11,000 (Table 4). However, there has been an increase of about 1,000 in AIDS deaths among adults, while among children there has been a reduction by one-half. The difference in trends between adults and children may largely be due to an aging cohort of adults on treatment and a higher coverage of ARVs among children.
4.1.11 People in need of ART have increased from approximately 43,500 in 2001/02 to about
79,700 by 2008/09, most probably because more PLWHA have advanced in their stage of infection and more of them are surviving as a result of the rapid scale-up of the ART
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 27/160
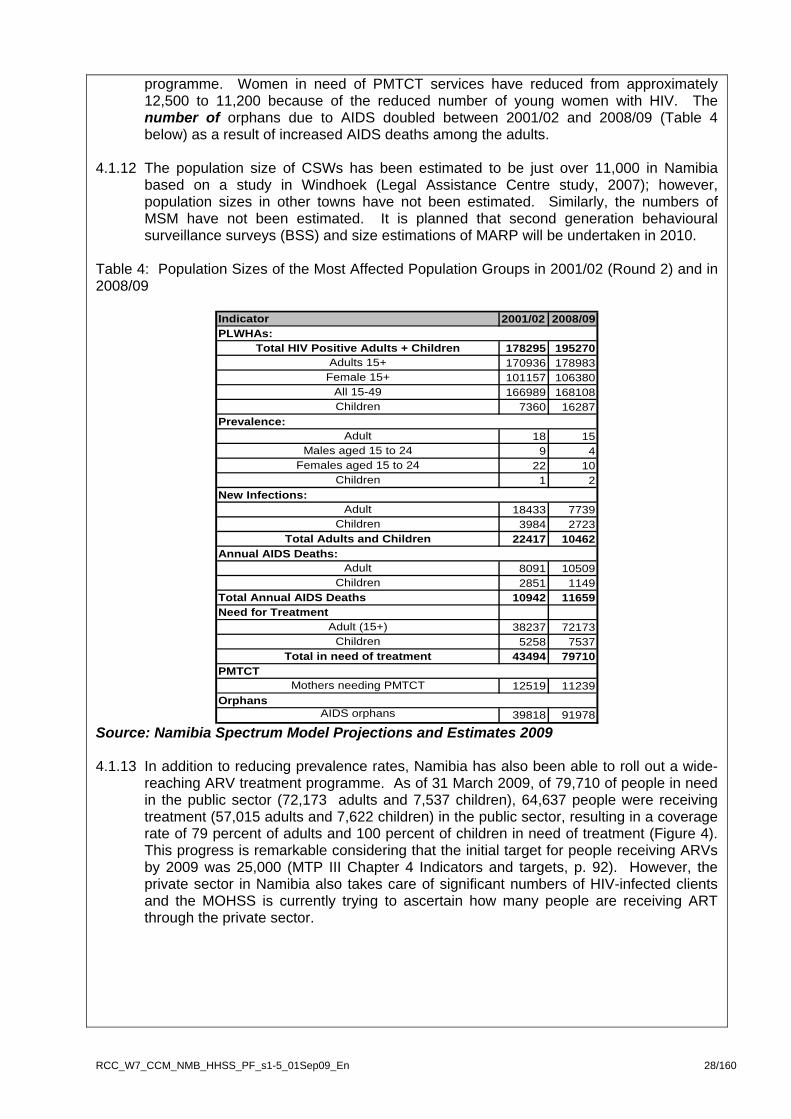
programme. Women in need of PMTCT services have reduced from approximately 12,500 to 11,200 because of the reduced number of young women with HIV. The number of orphans due to AIDS doubled between 2001/02 and 2008/09 (Table 4 below) as a result of increased AIDS deaths among the adults.
4.1.12 The population size of CSWs has been estimated to be just over 11,000 in Namibia
based on a study in Windhoek (Legal Assistance Centre study, 2007); however, population sizes in other towns have not been estimated. Similarly, the numbers of MSM have not been estimated. It is planned that second generation behavioural surveillance surveys (BSS) and size estimations of MARP will be undertaken in 2010.
Table 4: Population Sizes of the Most Affected Population Groups in 2001/02 (Round 2) and in 2008/09
Indicator 2001/02 2008/09
Total HIV Positive Adults + Children 178295 195270Adults 15+ 170936 178983
Female 15+ 101157 106380All 15-49 166989 168108Children 7360 16287
Adult 18 15Males aged 15 to 24 9 4
Females aged 15 to 24 22 10Children 1 2
Adult 18433 7739Children 3984 2723
Total Adults and Children 22417 10462
Adult 8091 10509Children 2851 1149
Total Annual AIDS Deaths 10942 11659Need for Treatment
Adult (15+) 38237 72173Children 5258 7537
Total in need of treatment 43494 79710
Mothers needing PMTCT 12519 11239
AIDS orphans 39818 91978
Annual AIDS Deaths:
PMTCT
Orphans
PLWHAs:
Prevalence:
New Infections:
Source: Namibia Spectrum Model Projections and Estimates 2009 4.1.13 In addition to reducing prevalence rates, Namibia has also been able to roll out a wide-
reaching ARV treatment programme. As of 31 March 2009, of 79,710 of people in need in the public sector (72,173 adults and 7,537 children), 64,637 people were receiving treatment (57,015 adults and 7,622 children) in the public sector, resulting in a coverage rate of 79 percent of adults and 100 percent of children in need of treatment (Figure 4). This progress is remarkable considering that the initial target for people receiving ARVs by 2009 was 25,000 (MTP III Chapter 4 Indicators and targets, p. 92). However, the private sector in Namibia also takes care of significant numbers of HIV-infected clients and the MOHSS is currently trying to ascertain how many people are receiving ART through the private sector.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 28/160
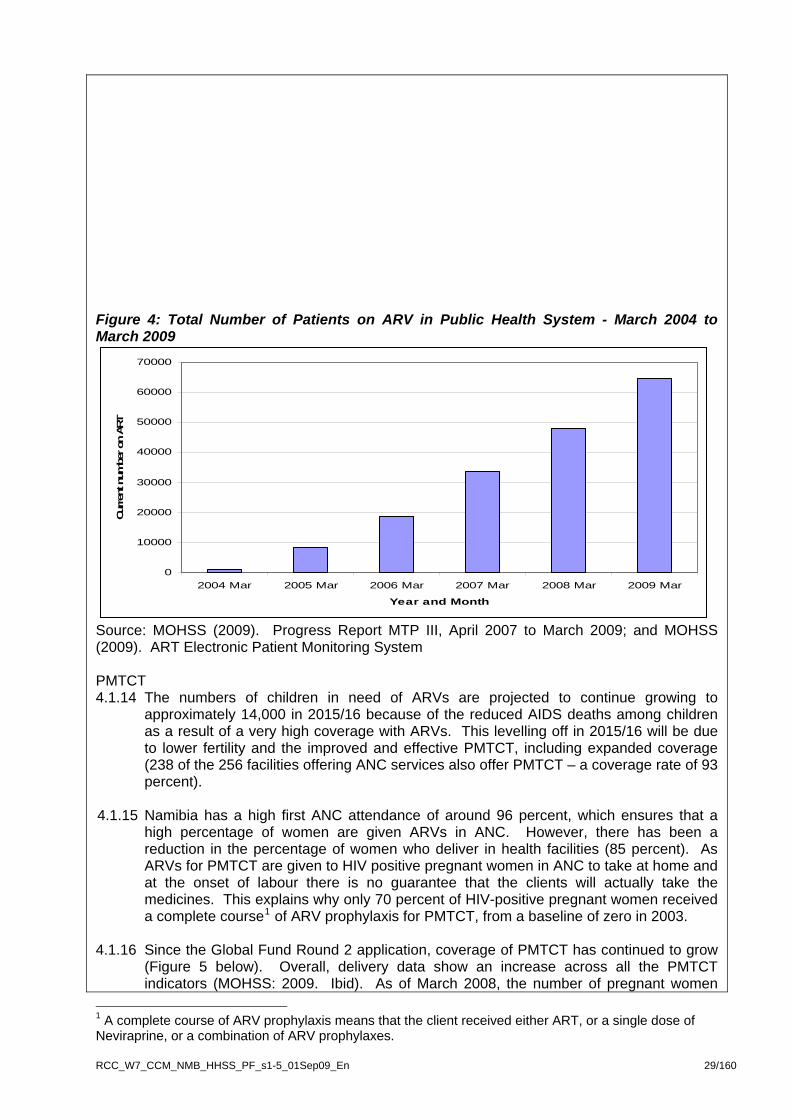
Figure 4: Total Number of Patients on ARV in Public Health System - March 2004 to March 2009
0
10000
20000
30000
40000
50000
60000
70000
2004 Mar 2005 Mar 2006 Mar 2007 Mar 2008 Mar 2009 Mar
Year and Month
Curren
t num
ber o
n AR
T
Source: MOHSS (2009). Progress Report MTP III, April 2007 to March 2009; and MOHSS (2009). ART Electronic Patient Monitoring System PMTCT 4.1.14 The numbers of children in need of ARVs are projected to continue growing to
approximately 14,000 in 2015/16 because of the reduced AIDS deaths among children as a result of a very high coverage with ARVs. This levelling off in 2015/16 will be due to lower fertility and the improved and effective PMTCT, including expanded coverage (238 of the 256 facilities offering ANC services also offer PMTCT – a coverage rate of 93 percent).
4.1.15 Namibia has a high first ANC attendance of around 96 percent, which ensures that a
high percentage of women are given ARVs in ANC. However, there has been a reduction in the percentage of women who deliver in health facilities (85 percent). As ARVs for PMTCT are given to HIV positive pregnant women in ANC to take at home and at the onset of labour there is no guarantee that the clients will actually take the medicines. This explains why only 70 percent of HIV-positive pregnant women received a complete course1 of ARV prophylaxis for PMTCT, from a baseline of zero in 2003.
4.1.16 Since the Global Fund Round 2 application, coverage of PMTCT has continued to grow
(Figure 5 below). Overall, delivery data show an increase across all the PMTCT indicators (MOHSS: 2009. Ibid). As of March 2008, the number of pregnant women
1 A complete course of ARV prophylaxis means that the client received either ART, or a single dose of Neviraprine, or a combination of ARV prophylaxes.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 29/160

who delivered at PMTCT sites was 44,226. Of these women, 87 percent delivered with a known HIV status compared to 80 percent in 2006/07 and 58 percent in 2005/06. Twenty percent of the women were HIV positive in 2007/08 compared to 21.0 and 23.0 percent in 2006/07 and 2005/06 respectively. In 2007/08 about 70 percent of positive mothers delivering received complete ARV prophylaxis based on the national guidelines (MOHSS: 2008. Guidelines for the Prevention of Mother to Child Transmission of HIV) compared with 64 percent in 2006/07 and 58 percent in 2005/06.
Figure 5: Number of Women Attending Maternity Wards at PMTCT Sites: A Comparison Between 2004/05, 2005/06, 2006/07 and 2007/08
Women delivering at PMTCT sites a comparison between FY 2004/05, 2005/06, 2006/07 & 2007/08
5437 475945766276
185111211884
7844
21885
3154
24185
41382
7145
34740
43711
38668
766054817851
44226
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
WOMENDELIVERED
KNOWN HIVSTATUS
TOTAL HIV+ TOTAL RECEIVINGARV
PROPHYLAXIS
TOTALBREASTFEEDING
Num
ber o
f pre
gnan
t wom
en
2004/052005/062006/072007/08
Source: MOHSS (2009). Progress Report MTP III, April 2007 to March 2009; and MOHSS (2009). ART Electronic Patient Monitoring System 4.1.17 In comparison, 98 percent of HIV-exposed babies received ARV prophylaxis, provided to
the infant within the health facility. This high percentage is due to the fact that the provision of infant ARV prophylaxis for PMTCT is entirely in the hands of the health care workers in the health facility, and this minimises the chance of the baby missing the doses.
4.1.18 Namibia has a programme for the early infant diagnosis (EID) of HIV and hence has the possibility of testing all HIV-exposed infants from six weeks after delivery; however, not all HIV-exposed babies present for follow-up at exactly six weeks. The mean age at HIV testing for HIV through deoxyribo nucleic acid polymerase chain reaction (DNA PCR) is currently 22 weeks. To date, more than 200 health facilities submit dried blood spot (DBS) samples for HIV DNA PCR. All positive infants diagnosed through HIV DNA PCR are eligible to commence ART, as recommended in the April 2008 WHO guidelines for treating HIV positive infants less than 12 months.
4.1.19 The majority (98 percent) of HIV positive mothers in Namibia express the intention to exclusively breastfeed, although it is not clear if this intention is always translated into practice. Infant feeding counselling and support needs to be stepped up through the
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 30/160
training of both health and non-health workers, including peer mothers who themselves have been through PMTCT, to better enable them to counsel HIV positive mothers.
4.1.20 Twenty-one percent of all HIV positive pregnant women have a CD4 count of less than 250 and are eligible for ART. This subgroup of HIV positive women is the one most at risk for MTCT, and efforts should be made to make sure they are put on ART during the pregnancy. Currently, tracking of these women to ensure that all of them are put on ART is weak. Drivers of the epidemic
4.1.21 The ANC sentinel surveillance data show that the Namibian epidemic is geographically heterogeneous. The national averages of HIV prevalence seem to obscure sub-national trends, suggesting geographic hotspots and high risk populations within the generalised epidemic. District prevalence levels range from 4.6 percent to 32 percent (Figure 6 below). The epidemic seems to be centred in four pockets where mobile populations are most likely to take temporary residence such as farming, mining, tourist and commercial areas, and border entry/exit points. There is, however, no difference in HIV prevalence between urban and rural areas. The same pattern can be observed among women in various age groups except those aged 15-19 years who in rural areas have a slightly higher prevalence than in urban areas. However, the opposite pattern can be seen among those aged 20-24 years where the prevalence is slightly higher in urban areas. The distribution of numbers of PLWHA on ART per treatment centre is comparable to the distribution of prevalence per district (Figure 6 below).
Figure 6: HIV Prevalence by District (2008) and the Distribution of PLHWHA on ART (March 2009)
Source: MOHSS (2008). Report of the 2008 National HIV Sentinel Survey; and MOHSS (2009) ART Electronic Patient Monitoring System, March 2009 4.1.22 A recent trends analysis of risk factors that influence the rate of new infections at the
individual, community and societal levels (Measure Evaluation, op. cit.) shows that factors at the individual and couple level that increase the risk of sexual transmission include high levels of MCP2, under-diagnosed and poorly treated sexually transmitted infections (STI), and inconsistent condom use. At the community level, the risk of heterosexual transmission is fuelled by inter-generational relationships, transactional
2 Whereby men maintain multiple relationships and 25 percent of the single women aged 15-24 have a partner ten or more years older.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 31/160
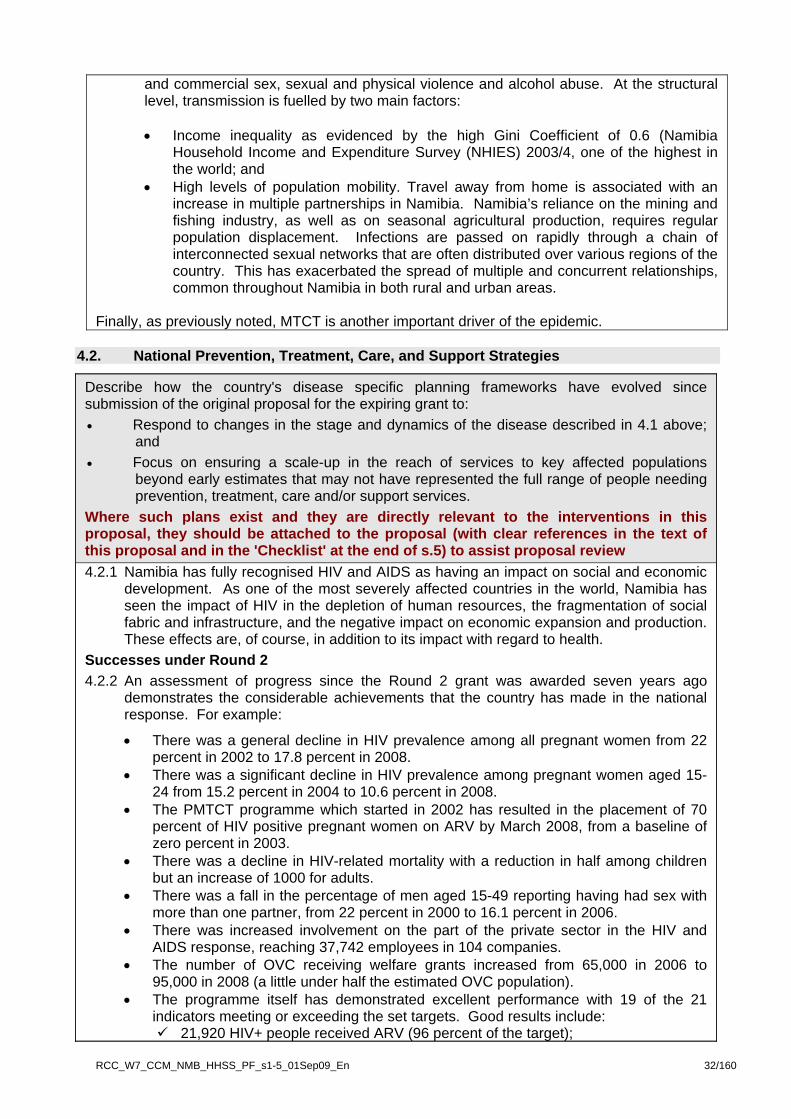
and commercial sex, sexual and physical violence and alcohol abuse. At the structural level, transmission is fuelled by two main factors:
• Income inequality as evidenced by the high Gini Coefficient of 0.6 (Namibia
Household Income and Expenditure Survey (NHIES) 2003/4, one of the highest in the world; and
• High levels of population mobility. Travel away from home is associated with an increase in multiple partnerships in Namibia. Namibia’s reliance on the mining and fishing industry, as well as on seasonal agricultural production, requires regular population displacement. Infections are passed on rapidly through a chain of interconnected sexual networks that are often distributed over various regions of the country. This has exacerbated the spread of multiple and concurrent relationships, common throughout Namibia in both rural and urban areas.
Finally, as previously noted, MTCT is another important driver of the epidemic.
4.2. National Prevention, Treatment, Care, and Support Strategies
Describe how the country's disease specific planning frameworks have evolved since submission of the original proposal for the expiring grant to: • Respond to changes in the stage and dynamics of the disease described in 4.1 above;
and • Focus on ensuring a scale-up in the reach of services to key affected populations
beyond early estimates that may not have represented the full range of people needing prevention, treatment, care and/or support services.
Where such plans exist and they are directly relevant to the interventions in this proposal, they should be attached to the proposal (with clear references in the text of this proposal and in the 'Checklist' at the end of s.5) to assist proposal review 4.2.1 Namibia has fully recognised HIV and AIDS as having an impact on social and economic
development. As one of the most severely affected countries in the world, Namibia has seen the impact of HIV in the depletion of human resources, the fragmentation of social fabric and infrastructure, and the negative impact on economic expansion and production. These effects are, of course, in addition to its impact with regard to health.
Successes under Round 2 4.2.2 An assessment of progress since the Round 2 grant was awarded seven years ago
demonstrates the considerable achievements that the country has made in the national response. For example:
• There was a general decline in HIV prevalence among all pregnant women from 22 percent in 2002 to 17.8 percent in 2008.
• There was a significant decline in HIV prevalence among pregnant women aged 15-24 from 15.2 percent in 2004 to 10.6 percent in 2008.
• The PMTCT programme which started in 2002 has resulted in the placement of 70 percent of HIV positive pregnant women on ARV by March 2008, from a baseline of zero percent in 2003.
• There was a decline in HIV-related mortality with a reduction in half among children but an increase of 1000 for adults.
• There was a fall in the percentage of men aged 15-49 reporting having had sex with more than one partner, from 22 percent in 2000 to 16.1 percent in 2006.
• There was increased involvement on the part of the private sector in the HIV and AIDS response, reaching 37,742 employees in 104 companies.
• The number of OVC receiving welfare grants increased from 65,000 in 2006 to 95,000 in 2008 (a little under half the estimated OVC population).
• The programme itself has demonstrated excellent performance with 19 of the 21 indicators meeting or exceeding the set targets. Good results include:
21,920 HIV+ people received ARV (96 percent of the target);
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 32/160
45,207 people received VCT (251 percent of the target); 5,391 HIV+ pregnant women received a PMTCT prophylaxis course (134 percent
of the target); 40,069 chronically ill people received home-based care (HBC) (133 percent of
the target); and 54,426 OVC received either material support or psycho-social care (155 percent
of the target).
HIV and AIDS Interventions 2002-2009 4.2.3 Since the initiation of the implementation of the Round 2 Grant major strategies and
programmes have centred on the following:
• Enabling environment; • Prevention; • Treatment, care and support; • Impact mitigation; and • Health system strengthening (HSS).
Enabling Environment 4.2.4 Strengthening the decentralised response and mainstreaming HIV and AIDS: The
National Development Plan (NDP III) developed in 2007 guides the Government’s annual planning and budgeting process. It clearly states that HIV and AIDS represents a significant challenge to the achievement of national goals of food security, poverty reduction, macroeconomic growth, sustainable development and the realisation of Vision 2030, the country’s aspirations for its future. The epidemic has the potential to reverse human development gains achieved since independence and deepening poverty. A 2007 UNDP report on trends in human development and human poverty in Namibia clearly establishes the principal reason for the reduction of life expectancy and increased mortality caused by the HIV and AIDS epidemic. It also indicates that the epidemic through its negative impacts on survival can intensify a long-term deterioration in human poverty3. The key result area 9, Quality of Life, outlines HIV and AIDS as a development issue reversing economic growth, therefore needing comprehensive efforts to deal with the pandemic across all sub sectors.
4.2.5 To address this, efforts are being made to develop sector-based approaches for the internal and external mainstreaming of HIV and AIDS into sector strategies, such as the National Policy on HIV and AIDS for the Education Sector. The 2008 ‘Guide to HIV and AIDS Mainstreaming’ is intended to ensure that all stakeholders implement holistic responses to HIV and AIDS. Mainstreaming activities are also supported through German Development Cooperation (GTZ) and the German Development Service (DED). The former supports workplace programmes (WPP) in specific sectors such as transport, agriculture and tourism, both through the ministries and the Government-owned parastatals; the latter provides technical assistance to support decentralised Government initiatives in the regions. Also supporting the decentralised response, Community Capacity Enhancement through Community Conversations (CCE-CC) was introduced in Namibia in 2007 subsequent to a consultative process with UNDP, the Government of Namibia through the Ministry of Regional Local Government, Housing and Rural Development (MRLGHRD), the National Planning Commission and AMICAAL. The CCE-CC approach creates safe, interactive spaces for communities to address the challenges posed by the HIV and AIDS epidemic. This transformational participatory methodology was adopted by the MRLGHRD to strengthen local responses to HIV and AIDS in line with MTPIII sub-section 4.1.
4.2.6 A National HIV and AIDS Policy was ratified and published in 2007 (Annex J1) National HIV and AIDS Policy). The policy still needs to be fully disseminated and a consensus built for full implementation by all stakeholders and partners. In addition, there are now several laws in place to protect women’s inheritance, PLWHA rights (through the Labour
3 Trends in Human Development and Human Poverty in Namibia; Background Paper to the Namibia HDR
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 33/160
Law), and that deal with issues of statutory rape. 4.2.7 The National HIV/AIDS Strategic Plan – Medium Term Plan III (MTP III) 2004-2009
was developed in 2003, and serves as the guide for the national and sub-national responses to HIV and AIDS, including the structures for response coordination and management. It has been extended to 2010 to allow for the development of the MTP IV. MTP III has five main components covering (i) Enabling Environment; (ii) Prevention; (iii) Treatment, Care and Support; (iv) Impact Mitigation; and (v) Integrated and Coordinated Programme Management.
4.2.8 Over the past years higher quality and more accessible epidemiological data and other
information on the HIV and AIDS epidemic have become available (for example, the Mid Term Review of the MTPIII, the study on the Drivers of the Epidemic and the process of the development of MTP IV, including the situation and gap analysis). As a result, current strategies have become more focused and refined, but are still aligned with the MTP III. More emphasis has recently been put on the following:
Prevention 4.2.9 While the high prevalence rate means that the sheer numbers of those with HIV implies
increasing attention to treatment, care and support services, Namibia recognises that prevention is the cornerstone of an HIV and AIDS control management strategy to halt and reverse the epidemic. Combined and interactive strategies for prevention include:
• Technical Advisory Committee (TAC) for HIV Prevention established in 2008 to provide
guidance and coordination on the development and implementation of the draft National Strategy for the Prevention of Sexual Transmission of HIV 2009-2014;
• Strengthening mass media campaigns targeting the public in general and youth in particular (Take Control Initiative). They also include more targeted face-to-face behaviour change communication (BCC) interventions aiming at youth and key affected populations (CSW, MSM and mobile populations) through Communication for Behaviour Impact (COMBI) and Total Control of the Epidemic (TCE) officers;
• Scaling up of counselling and testing (CT), including a recent move towards provider-initiated testing and counselling (PITC) to encourage more clients to be tested and to reduce stigma and discrimination; and increasing awareness of VCT through annual National Testing Days (two to date), plus increasing access to VCT through the introduction of rapid testing at static, outreach and mobile sites;
• Targeting men to increase male involvement in prevention efforts through the 1st National HIV/AIDS Male Leaders Conference in 2008;
• Promoting male circumcision through the Draft Male Circumcision Policy and the Draft National Strategy for the Prevention of Sexual Transmission of HIV 2009-2014, with interventions to be covered by PEPFAR;
• Strengthening the control, prevention and treatment of STIs (2007/2008 MOHSS STI Annual Report);
• PMTCT has been substantially increased under the Round 2 Grant, from a baseline of zero pregnant HIV positive women on ARVs in 2002 to 70 percent by 2008. Namibia has a total number of health facilities of 335, of which 256 facilities have ANC services. Of these, 238 offer PMTCT services (a coverage of 93 percent). Efforts are ongoing to equip all 256 sites with ANC services to enable them to offer PMTCT. Thereafter, the 79 sites which do not offer ANC (and therefore no PMTCT services) will be upgraded to provide this service. In this way, coverage for PMTCT will be increased to minimise the number of HIV positive women who are unable to access PMTCT services. The PMTCT programme has been further strengthened by the introduction of a more effective and efficient ARV prophylaxis regimen from August 2008 and concerted efforts to put all eligible HIV positive pregnant women on ART (2008 MOHSS PMTCT Guidelines);
4.2.10 The aforementioned strategies and policy developments have already had a positive
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 34/160
impact on the national response’s ability to better tailor prevention interventions to meet current needs. Some examples include the identification of new target groups since Round 2, as follows:
• The MTP IV status report (Annex J2) reports prison inmates, previously not identified as a vulnerable group under Round 2, as a priority group for prevention interventions that may reduce incidence rates in prisons to below the epidemic threshold. Namibia currently ranks among the top five African countries with the highest per capita rates of imprisonment, with 267 per 100,000 currently serving sentences or in pre-trial detention. The Ministry of Safety and Security (MOSS) estimates that there are over 4,000 prison inmates in Namibia of whom 494 are known to be HIV–positive, according to official records and recent research conducted by the Legal Assistance Centre (LAC), the AIDS Law Unit and the University of Wyoming College of Law. The report further states there have been recent efforts to increase HIV and AIDS staff training for new prison wardens but significant problems still exist. These problems include: risks faced by inmates (for example, having to share a razor); violence throughout the country’s prisons and detention centres is common and widespread, with instances of violence to assert power or dominance or violence to ward off sexual advances. The United Nations Office on Drugs and Crime (UNODC) is partnering with the MOSS and the following activities are being implemented and/or are planned: (i) review of legislation relating to HIV and AIDS prevention and care in prisons; (ii) a review of studies conducted on HIV and AIDS in Namibian prisons; (iii) creation of a National Steering Committee and TWGs; (iv) distribution of materials on HIV and AIDS in prisons to the Prison Services Department, the National Steering Committee and TWG members; (v) development of a regional prison assessment tool; (vi) familiarisation visits to all 13 prisons to foster the development of sensitisation workshops for policy and decision-makers; (vii) mapping of training needs for prisoners and prison staff and subsequent development of curricula; (viii) identification of a local NGO to conduct training in prisons; (ix) joint planning with the Center for Disease Control (CDC), MOHSS and MOSS for the National Prison Awareness and HIV Testing Week; and other activities are in the pipeline.
• Using World Bank computation data and qualitative estimates by LAC in its research report Prostitution in Windhoek the number of CSWs is estimated to be in the order of 11,000. About half of all CSWs are to be found in Windhoek and its suburbs; the balance of CSWs are largely distributed at the coastal towns of Lüderitz, Swakopmund, and Walvis Bay, and the regional boarder towns/transit route of Namibian’s north i.e. Katima Mulilo, Ondangwa, Oshakati, Oshikango and Rundu.
• More recent strategies are aimed at improved outcomes in the area of prevention, leading to key affected populations (including MSM, CSW, mobile populations (temporary farm and migrant workers, truckers, fishermen, armed forces, and tourists) and youth) increasingly accessing comprehensive SRH, STI and HIV services and programmes. This will reduce high-risk behaviour and ultimately reduce HIV transmission and HIV prevalence among young women and men aged 15-24.
Treatment, Care and Support 4.2.11 In the past six years, treatment has included ART management of OIs and palliative
care in general. The decentralisation of ART and PMTCT services, through the delivery of the Integrated Management of Adolescent and Adult Illnesses (IMAI) approach, has expanded the scope of treatment. All district hospitals now provide ART services. By 2009 an additional 32 health centres, bigger clinics, and outreach point were established.
4.2.12 The ART scale up plan (Annex J38) aims to extend ART services to more health centres and clinics, with the goal of decentralising ART to at least three sites per quarter and to have 78 additional sites providing ART services by 2016. To support the scale up of ART services, the following activities are being or will be undertaken:
• Training of new personnel and retraining of existing personnel in all aspects of HIV
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 35/160

and AIDS management including but not limited to Standard Treatment Guidelines, and SOPs for ART, warehouse inventory and IMAI;
• Training of PLWHA and counselling staff to support people on ART; • Renovation of health facilities to accommodate increasing numbers of patients on
ART; • Procurement and maintenance of vehicles for outreach services; • Recruitment of health care workers where needed for ART/IMAI sites; • Procurement of equipment for ART sites; • M&E for the implementation of the ART scale-up plan; • Decentralisation of the National Institute of Pathology’s (NIP) services to the
peripheral health facilities; • Increased government expenditure on ARVs as required; • Increasing storage infrastructure and transport for HIV and AIDS commodities; • Increasing human resources for HIV and AIDS case management; • Training of personnel in supply chain management at all levels; and • Capacity building for pharmaceutical control and inspections (PC & I) and quality
surveillance laboratory (QSL). 4.2.13 Part of the complementary strategy to facility-based care is community outreach and
HBC through interventions such as:
• An increase in mobile centres and community health workers; • An increase in quality community services such as community home-based care
(CHBC), support to PLWHA support groups and the standardisation of services aligned with national service standards and the needs of the community;
• The revision of the National Community-Home based Care (CHBC) Policy and the adoption of the recently finalised CHBC standards booklet;
• Strengthening of regional and local response coordination (RACOCs, DACOCs and CACOCs) for quality assurance and linkages between health facilities and community-based service providers;
• Integrating food assistance and income generating activities (IGA) into community level support;
• Collaboration between TB and HIV for improving services to the co-infected patient; and
• Greater coverage of family and community support services for OVC as well as the increased coverage of comprehensive and quality community-based care services for adults, particularly in the most rural regions, and targeting the poorest segments of society, through FBOs, CBOs and others.
4.2.14 One of the ways in which this will be achieved is through the greater involvement of CSOs, in particular the 13 SRs to be managed by the umbrella CSO PR, NANASO, who brings together more than 400 NGOs, CSOs and FBOs working in the HIV and AIDS field. NANASO will be responsible for civil society strengthening and this will be undertaken through a capacity building needs assessment to form the basis of the development of a capacity building short-, medium- and long-term training strategy and operational plan.
4.2.15 In implementing treatment strategies, more people from traditionally underserved communities are expected to be better able to access treatment, and be better informed patients with regard to treatment literacy.
Impact Mitigation 4.2.16 Mitigating the impact of HIV and AIDS is central to reversing the vicious cycle of
additional HIV infections, exacerbating food insecurity and poverty, and the increased vulnerabilities of women and children resulting in more infections. The impact of HIV and AIDS has contributed to children not being able to access critical services: Out of
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 36/160
the 250,000 OVCs in Namibia, 16.5 percent are accessing free basic external support, with 41 percent possessing three basic material needs. Birth registration rates have decreased to 67 percent, and access to education at secondary level is decreasing. Improving service delivery for OVC is central to mitigating the impact of HIV and AIDS. Mitigation strategies have recognised the central role of Government to coordinate the national response to OVC through service delivery mechanisms. This approach facilitates a sustainable coordinated response that simultaneously enables government sectors to deliver services together with NGOs, while ensuring adequate monitoring and evaluation feedback mechanisms for continued improved service delivery. A number of initiatives have been put in place to mitigate the effect of the epidemic:
• The 2006-2010 OVC National Plan of Action (NPA), launched by the Prime Minister, articulates the Government’s multi-sectoral commitments to mitigate the impact of HIV for OVC. The Plan was piloted in three regions with local Regional Councils developing their work plans to achieve the NPA goals. A progress report for 2007-2008 published in early 2009 maps out progress made, and identifies gaps that need to be addressed to ensure that the NPA goals are met.
• The OVC Permanent Task Force mandated by the Cabinet to coordinate the implementation of the NPA has met quarterly between 2006 and 2009. This has brought together over 50 Government, civil society and development stakeholders to coordinate implementation.
• OVC Forums at regional and constituency level have been established and strengthened with five out of 13 regions, and 35 out of 107 constituencies, functioning. They coordinate the OVC response at constituency and regional level, and link up communities to service providers.
• A human resource and capacity gap analysis of the MGECW identified gaps to address to ensure the Ministry is able to fulfil their social welfare obligations. As a result the OPM has approved 100 social worker posts, and 112 Constituency Child Care Worker (CCCW) posts. In 2006, 18 social workers were recruited, and in June 2009, 43 more. Four CCCW have been recruited.
• Initiatives to support OVC are being implemented by public, private and civil society sectors reaching over 52,000 OVC as of end 2008 with primary and supplementary direct support.
• Child Welfare Grants, including foster care and maintenance grants for poor guardians, have increased from 40,685 in January 2006, to 56,778 in January 2008, and to 99,490 in January 2009, to 105,140 in June 2009.
• A major blockage to children accessing Child Welfare Grants or educational exemptions is the frequent lack of birth registration documentation. The Government has prioritised registered children and registered over 13,000 children in 2008 in a mobile birth registration campaign. A birth registration facility was also set up at a high volume birth hospital, and the Government is scaling up this initiative countrywide.
• Namibia has an OVC Policy, which was approved in 2005, and is in the process of finalising the Child Care and Protection Bill, which deals with foster and alternative care, adoptions, child abuse, trafficking, child court procedures and grants.
• After 16 years of development, the States Party Report for the Convention on the Rights of the Child has been finalised by the Government. It is to be submitted to the United Nations Convention for Rights of the Child (UNCRC) by October 2009.
4.2.17 Other impact mitigation interventions include:
• Workplace programmes which have been scaled up under Round 2, mainly through the private sector reaching 104 large, medium and small companies with workplace policies, peer education, condom distribution, and recently mobile wellness clinics reaching 40,973 people.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 37/160
In addition, the following achievements should be noted: HSS 4.2.18 The orientation of the public health services is towards the provision of PHC which is
delivered through outreach points, clinics, health centres and district hospitals. T he provision of quality health and social care services can only be achieved if there are qualified human resources, uninterrupted supply of medicines and pharmaceuticals, well constructed and maintained health facilities, good information systems, and sufficient health financing, among others. The Government has done fairly well in improving and maintaining health facilities; 37 new clinics were constructed compared with the target of 15 and 16 district hospitals renovated compared with the target of 15. However, only six health were centres renovated out of a target of 15 (NDP III, Volume 1, p 178). With regard to human resources 140 sub–professional cadres (pharmacist assistants, environmental assistants, and medical laboratory technicians) were trained compared with the target of 100, while 15 medical doctors and 30 health inspectors were trained. All (100 percent) regions and districts have a decentralised computerised health information system (HIS). The essential medicines used in public hospitals are procured through the Government’s Central Medical Stores (CMS) and distributed from there to the two regional medical stores where the stocks are maintained.
4.2.19 Despite these achievements, the burden of disease still requires efforts to construct and
renovate health facilities to provide more space and access to services. Disease monitoring and surveillance is a necessity and, although the District Health Information System (DHIS) is in place, the infrastructure technology to support it and expertise in data analysis at the point of collection is lacking. Furthermore, the service provision suffers from a lack of personnel in all cadres at all levels.
Issues relating to HSS are covered in more detail in section 4.4.2.
Monitoring and Evaluation (M&E) 4.2.20 There has been considerable effort towards the development and implementation of one
unified national multi-sectoral M&E system. To address the provision of efficient, high quality, standardised and timely information that will foster an environment of data sharing and maximise its utilisation, a national multi-level M&E infrastructure has been developed. The Plan for National Multi-sectoral Monitoring and Evaluation of HIV/AIDS 2006/7 to 2008/9 (Annex J4) was developed in 2006 and aims to establish an effective coordinated national M&E system for HIV and AIDS. The objectives of the M&E plan include assessment of the epidemic’s impact by monitoring trends and explaining changes in the levels of HIV and AIDS prevalence over time. In this way, the M&E plan will respond to changes in the stage and dynamics of the disease as described in 4.1. The M&E plan defines a list of core indicators that will enable progress to be tracked. National HIV and TB Targets (Annex J5) for the indicators in the M&E work plan were set in 2008. These will ensure planned, quantified scale up in the reach of services to key affected populations beyond early estimates that may not have represented the full range of people needing prevention, treatment, care and/or support services; and thus of particular importance to this proposal that focuses on those key groups.
4.2.21 The key implementation strategies of the National Plan are:
• To coordinate HIV and AIDS surveillance and research, and programme monitoring and evaluation;
• Establish an institutional network with key line ministries, civil society and private sector and development partners towards one national M&E system,
• Systematically collect and use data to track progress on key interventions; • Assess the impact by monitoring trends; • Ensure a platform for partnership, networking and collaboration between national
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 38/160

level and local levels; and • Build consensus on data sources and methods of data collection methods for the
core set of national indicators that focus on the impact and outcomes of the national response, and integrate HIV, AIDS and TB routine data collection.
4.2.22 To address inadequate human resources, technical capacity and institutional
capabilities, sectoral M&E officers were recruited and deployed to three strategic sectors: NANASO (civil society), the private sector Namibian Business Coalition on HIV and AIDS (NABCOA), and MRLGHRD and OPM (public sector) to improve the quality of data captured. Partnerships across and within sectors have been strengthened through monthly national M&E committee meetings. Biannual ANC surveillance for pregnant women attending ANC has been undertaken to estimate the prevalence of HIV infection in pregnant women aged 15-49 years, to identify geographic and socio-demographic characteristics associated with higher prevalence and to monitor infection trends over time. Regular supportive supervisory visits are conducted in all districts providing ART services. To assist in compiling and analysing data, tools were developed and/or reviewed. The VCT programme revised the tools for data collection and developed a new register which is being piloted.
Scaling up the National Response 4.2.23 The HIV and AIDS MTP IV is currently under development and builds on the most recent
epidemiological data, the MTP III revised costing and mid-term review, the MTP III Progress Report of May 2009, the Gap and Situation Analysis for Global Fund Round 8, and the NDP III. It identifies four critical areas to be addressed in the forthcoming programme:
• Prevention: (i) Focus on the key drivers of the epidemic and MARPs, and continue roll-out of the
existing male circumcision, PMTCT and VCT programmes.
(ii) Develop a regional focus, taking into account prevalence and incidence rates, and balancing this with the focus on key drivers and MARPs.
• Treatment, Care and Support: (iii) Scale up ART roll out and change the scope of the CHBC and PLWHA support
programmes by focusing on prevention and ART adherence.
• Impact Mitigation: (iv) Strengthen the community response for support to OVC and poverty reduction, and
enhance the evidence-based and strategic management of the national response, including HSS.
4.2.24 The MTP IV strategic framework is comprised of the following five Strategic Interventions:
1. Prevention 2. Treatment, care and Support 3. Impact Mitigation 4. Enabling Environment 5. Coordination and Management
4.2.25 The RCC proposal follows the MTP IV strategic framework and recommendations as
stated in the Report on the Status of MTP III and Recommendations for MTP IV (Second Draft), 1 July 2009 (Annex J2)
Conclusion
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 39/160

4.2.26 Thus the policy requirements are in place to support the enabling environment
necessary for scaling up the response. Together with the solid base for expansion provided by the achievements under Round 2 detailed above, along with substantial mobilisation of the requisite organisations at public, private and civil society level (comprising some 400 + CSOs and 30,000 volunteers), the country is well poised to build on these successes and take the national response to its next logical steps.
4.3. Population and Epidemiological Background to Proposal
4.3.1 Geographic Reach of this Proposal
Activities will be implemented:
X Across the whole country
4.3.2 Size of Population Group(s) Covered by this Proposal
Population Group(s) Population Size Source of Data Year of Estimate
Total country population (all ages) 1,991,746
Central Bureau of Statistics (CBS)/National Planning
Commission (NPC), 2006, Population Projections 2001-2031. National and regional
figures. Windhoek: CBS/NPC, January, medium variant, p.24
Year of estimate: 2006, projected from 2001 population census,
medium variant.
Girls 0–14 years 373,652 See above See above
Women 15–19 years 116,713 See above See above
Women 20–24 years 101,918 See above See above
Women > 25 years 428,848 See above See above
Women 15-49 years 528,652 See above See above
Boys 0–14 years 370,951 See above See above
Men 15–19 years 113,651 See above See above
Men 20–24 years 99,074 See above See above
Men > 25 years 386,940 See above See above
Men 15-49 years 504,541 See above See above
People living on less than US$1 per day 700,000 NHIES 2003/04
Women giving birth, per year 61,100
MOHSS/Directorate of Special Programmes (DSP) (2008), Estimates and Projections of
the Impact of HIV/AIDS in Namibia [Spectrum model
data]
2008
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 40/160
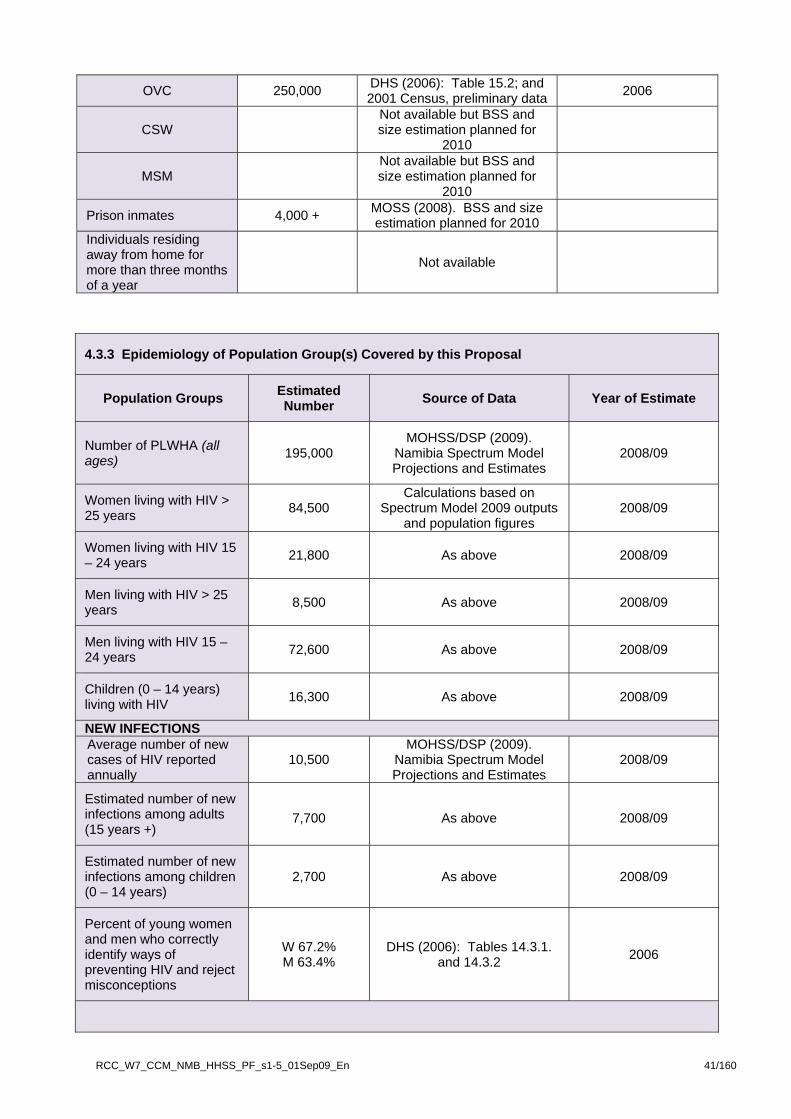
OVC 250,000 DHS (2006): Table 15.2; and 2001 Census, preliminary data 2006
CSW Not available but BSS and size estimation planned for
2010
MSM Not available but BSS and size estimation planned for
2010
Prison inmates 4,000 + MOSS (2008). BSS and size estimation planned for 2010
Individuals residing away from home for more than three months of a year
Not available
4.3.3 Epidemiology of Population Group(s) Covered by this Proposal
Population Groups Estimated Number Source of Data Year of Estimate
Number of PLWHA (all ages) 195,000
MOHSS/DSP (2009). Namibia Spectrum Model Projections and Estimates
2008/09
Women living with HIV > 25 years 84,500
Calculations based on Spectrum Model 2009 outputs
and population figures 2008/09
Women living with HIV 15 – 24 years 21,800 As above 2008/09
Men living with HIV > 25 years 8,500 As above 2008/09
Men living with HIV 15 – 24 years 72,600 As above 2008/09
Children (0 – 14 years) living with HIV 16,300 As above 2008/09
NEW INFECTIONS Average number of new cases of HIV reported annually
10,500 MOHSS/DSP (2009).
Namibia Spectrum Model Projections and Estimates
2008/09
Estimated number of new infections among adults (15 years +)
7,700 As above 2008/09
Estimated number of new infections among children (0 – 14 years)
2,700 As above 2008/09
Percent of young women and men who correctly identify ways of preventing HIV and reject misconceptions
W 67.2% M 63.4%
DHS (2006): Tables 14.3.1.
and 14.3.2
2006
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 41/160

KEY POPULATIONS AT HIGHER RISK
Sex workers reached with comprehensive HIV and SRH services (including CT, STI screening and family planning (FP) health services)
Not available
Men who have sex with men reached with comprehensive HIV and sexual and reproductive health services (CT, STI screening and sexual health)
Not available
Mobile persons reached with HIV and SRH services
Not available
Prison inmates reached with HIV and SRH services
Not available
TESTING AND COUNSELING
Percent of males 15-49 years who report having been tested and received results in past 12 months
18% DHS (2006): Table 14.10.2 (p. 212) 2006
Percent of females 15-49 years who report having been tested and received results in past 12 months
29% DHS (2006): Table 14.10.2 2006
Estimated annual number of women 15-49 with unmet need for contraception
35,420
Derived from DHS 2006, Table 7.3.1, and 2001 Census
– calculated as 6.7%*2006 female population projection
(medium) 15-49 years)
2006
Percent of births assisted by skilled birth assistants per year
81.4% DHS (2006): Table 10.7 2006
Women in need of 10,850 MOHSS/DSP (2009).
Namibia Spectrum Model Projections and Estimates
2008/09
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 42/160
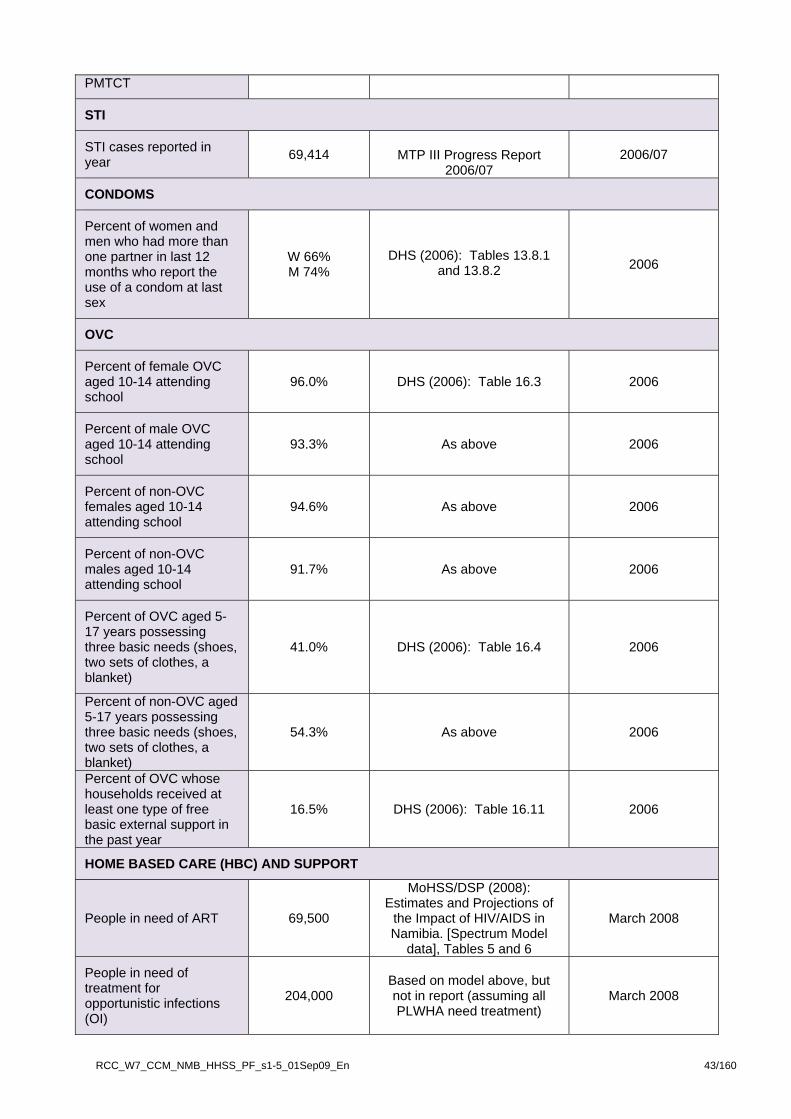
PMTCT
STI
STI cases reported in year 69,414 MTP III Progress Report
2006/07 2006/07
CONDOMS
Percent of women and men who had more than one partner in last 12 months who report the use of a condom at last sex
W 66% M 74%
DHS (2006): Tables 13.8.1 and 13.8.2 2006
OVC
Percent of female OVC aged 10-14 attending school
96.0% DHS (2006): Table 16.3 2006
Percent of male OVC aged 10-14 attending school
93.3% As above 2006
Percent of non-OVC females aged 10-14 attending school
94.6% As above 2006
Percent of non-OVC males aged 10-14 attending school
91.7% As above 2006
Percent of OVC aged 5-17 years possessing three basic needs (shoes, two sets of clothes, a blanket)
41.0% DHS (2006): Table 16.4 2006
Percent of non-OVC aged 5-17 years possessing three basic needs (shoes, two sets of clothes, a blanket)
54.3% As above 2006
Percent of OVC whose households received at least one type of free basic external support in the past year
16.5% DHS (2006): Table 16.11 2006
HOME BASED CARE (HBC) AND SUPPORT
People in need of ART 69,500
MoHSS/DSP (2008): Estimates and Projections of
the Impact of HIV/AIDS in Namibia. [Spectrum Model
data], Tables 5 and 6
March 2008
People in need of treatment for opportunistic infections (OI)
204,000 Based on model above, but not in report (assuming all PLWHA need treatment)
March 2008
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 43/160
4.4. Major Ongoing Weaknesses and Gaps that Affect Outcomes
4.4.1 National Disease Programme
Describe: • The main weaknesses of the current disease programme and how these weaknesses affect
achievement of planned national program outcomes; • Existing gaps in the delivery of services to target populations; and • Main weaknesses of and/or gaps in the health system that affect disease programme outcomes. 4.4.1.1 The weaknesses and challenges in the implementation of the current HIV strategies and
programmes are described below by thematic area. The analysis is based on the Concept Paper (Annex C2) which compared the challenges and gaps at the time of the design of the Round 2 proposal with the challenges and gaps which are prominent today, and on the Situation and Gap Analysis prepared for the RCC (Annex C5).
Enabling Environment.
4.4.1.2 The legislative environment for the optimum development and expansion of services targeting specific groups is not as conducive as it could be; for example, sodomy is still illegal.
4.4.1.3 Although the OPM has an HIV and AIDS Unit and there is apparent strong political support from
Government, HIV is not placed at the highest level of the Government structure (e.g. in the President’s Office) and there is no Cabinet level accountability mechanism for ensuring and monitoring line ministry budget allocation and implementation of sectoral activities in support of the national response to HIV and AIDS. With the exception of the Minister for Health and Social Services, there is limited sustained and visible high level political leadership for the national response to HIV and AIDS and limited engagement with people living with HIV to counter high levels of stigma and discrimination.
4.4.1.4 While private sector involvement in HIV and AIDS has increased significantly as a result of
Round 2 activities, there has been inconsistent management commitment and interest and workplace programmes (WPP) have not been institutionalised. There is a lack of allocated budgets for WPP, and lack of capacity to manage and implement WPP among most businesses.
4.4.1.5 Civil society remains largely dependent upon international financial support, particularly at
regional and constituency levels, where CSOs are being called upon by affected communities to play a much stronger and expanded role in supporting access to prevention and treatment, as well as linking health facilities with the community.
4.4.1.6 There is no effective integration between HIV and RH, for example, through a standing
committee on integration that would bridge the policy and service delivery gap that currently exists between the HIV and RH programmes. However, creating this linkage would improve coverage and strengthen the healthcare system.
Prevention
4.4.1.7 While IEC interventions have resulted in high levels of awareness in the population countrywide (Annex J8 2006/7 Demographic and Health Survey (DHS)), they have not achieved the desired level of impact on behaviour change. The DHS shows that young people aged 15-24 years are using condoms more, have fewer multiple concurrent partnerships and are exposed to more education about HIV and condoms than their elders. However, they do not use condoms consistently and have the highest infection rates; 44 percent of new HIV infections in Namibia are in young men and women between the age of 15 and 24. There is thus an ongoing need to intensify efforts to address behaviour change.
4.4.1.8 Availability and accessibility has increased significantly (25 million in 2007 compared with five
million condoms in 2002). However, demand still outstrips supply, especially for the female condom, and there is therefore an unmet need for both male and female condoms countrywide, including in the remotest areas of the country.
4.4.1.9 To date prevention activities have largely been implemented through a ‘blanket approach’ rather
than targeting specific populations, risk behaviours and vulnerabilities. The national prevention strategy is being developed and, when finalised, will assist in coordinating prevention efforts in
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 44/160
Namibia. At present, however, activities geared to the different rural and urban settings as well as key population groups at increased risk to HIV infection (i.e. young people, CSW, mobile populations such as migrant workers and other groups, MSM and prison inmates) and the behavioural factors that fuel the epidemic (such as high levels of MCP, inconsistent condom use, inter-generational sex, and transactional sex), are not well coordinated. The poor targeting of interventions to tackle the drivers of the epidemic and to reach key affected populations has resulted in programmes that have not significantly reversed the epidemic;
4.4.1.10 There is weak integration of SRH with HIV and AIDS programmes, especially into PMTCT, STI,
WPP, condom, BCC, and ART. For those that are already integrated, they are not user-friendly for clients of all age groups, especially men. Neither have the opportunities and community linkages of the SRH programme been effectively used to reach at-risk populations with HIV prevention interventions;
4.4.1.11 While many organisations claim to work with youth, funding for activities targeting this critical age
group is inadequate and the proposed activities are not innovative, interactive or entertaining enough to appeal to young people.
4.4.1.12 The lack of recreational activities in rural areas is a major problem, leading to use of alcohol and
subsequent risky behaviour, especially but not only among young people. Not enough has been done to link messages of alcohol abuse with increased vulnerability to HIV and other STIs.
4.4.1.13 Adolescent-friendly health services are not provided as a standalone service but are incorporated
into maternal and child health/family planning (MCH/FP) services and do not receive the dedicated attention that is necessary if this group’s high vulnerability needs are to be addressed. Hence existing adolescent SRH services are inadequate, not only because of this but because there is minimal support towards establishing adolescent SRH care guidelines and for the appropriate training of health care workers. Yet specific SRH services for adolescents are critical for reinforcing messages to facilitate positive sexual behaviour;
4.4.1.14 While social mobilisation around VCT and PMTCT means that some progress has been made in
encouraging people to be tested, much remains to be done; there is insufficient acknowledgement of the cultural factors that inhibit people, especially men, and this needs to be addressed.
4.4.1.15 Male involvement in PMTCT remains low (with only four percent of men accepting to be tested
through ANC); and yet men are the decision-makers in the home and strongly influence health-seeking behaviour and acceptability of services within communities. Failure to fully engage men has implications on disclosure and follow-up, and could potentially contribute to inciting GBV. Enhancement of linkages at the community level in PMTCT and the implementation of innovative strategies to improve mother-baby pair follow-up in PMTCT are needed.
4.4.1.16 There is limited availability of information on the key populations at increased risk to HIV infection
such as CSW and MSM. One recent study in Katutura, a suburb of Windhoek, suggested that 70 percent of CSW tested were HIV positive (WID 2006).
4.4.1.17 There is inadequate access to VCT in remote and marginalised communities, limited referral to
community services for those who test positive and lack of post-test clubs to help those who test negative to stay negative.
4.4.1.18 Levels of stigma and discrimination remain high, especially among women; few women are
willing to share their status with their partners and men are less willing to be tested than women. 4.4.1.19 There is inadequate capacity and willingness among political, traditional, church and corporate
leaders to provide sustained and visible support to the national response to HIV and AIDS to counter stigma and discrimination and to support the mainstreaming of HIV and AIDS.
4.4.1.20 Socio-cultural norms that are obstacles to effective prevention still prevail and have not been
challenged; for example, the perceived desirability for a man to have several partners and for a young woman to bear children. There is little understanding of the connections between gender and socio-cultural issues, and HIV and AIDS, and this limits the ability of service providers to effectively deliver BCC interventions.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 45/160
4.4.1.21 Little is being done with regard to intergenerational sex, one of the main drivers of the epidemic; the dynamics of the relationships between young girls and older, usually married, men, are not well understood and as a result interventions are not appropriately targeted.
4.4.1.22 There are gaps in the coordination of various prevention sub-components, e.g. poor coordination
and management capacity to guide stakeholders involved in mass media and community outreach. HIV prevention efforts are also currently fragmented and uncoordinated, within and among all sectors (public, civil and private). As a result of these gaps, there is unnecessary duplication of efforts and poor synergies between the various sectors and partners, and among the diverse prevention sub-components.
Treatment
4.4.1.23 During the time period covering the Round 2 grant, Namibia has made major progress in improving access to ART for people in need of treatment (with June 2009 ART coverage at 75%). However, management structures and accompanying human resources have not matched the rapid scale up of ART. Other weaknesses that lower the quality of treatment services, with the risk of HIV drug resistance emerging, are noted in the following paragraphs.
4.4.1.24 Outreach services by treatment teams from hospitals and health centres have commenced, but
there remains limited access to treatment in some of the remote rural areas. 4.4.1.25 Momentum in areas that have made good progress, such as HIV care and treatment, including
counselling, have not yet been fully taken advantage of so as to facilitate the acceleration of prevention efforts.
4.4.1.26 While Namibia has done very well with paediatric AIDS treatment, there are challenges in
addressing HIV-infected adolescents and in follow up of HIV-infected babies from PMTCT. Through its PMTCT HIV Guidelines, Namibia has adopted the WHO Four Prongs of PMTCT; the fourth prong, which deals with comprehensive care for the HIV positive woman and her family, is weak. After an HIV positive mother has delivered she needs to be enrolled into a continuum of care but the tracking system in this regard needs to be strengthened. In addition, her partner and other members of her family need to be tested and enrolled into care and/or treatment.
4.4.1.27 While the country has good testing rates with PCR, ongoing and continued follow-up of HIV-
exposed children through to 18 months (when final HIV infection status should be determined) has been challenging. While Namibia has high ANC attendance and institution delivery coverage, there are still women who either do not come to the ANC, do not deliver in the health facilities or do not come for the postnatal visits. Accordingly, community mobilisation efforts are needed to make sure these missed opportunities are minimised. The reproductive health needs of HIV positive pregnant women are not fully addressed and access to reproductive health commodities is rather limited.
4.4.1.28 There has been slow integration of nutrition services in HIV and AIDS management. 4.4.1.29 Treatment adherence data are available; however, there are constraints in addressing defaulters. 4.4.1.30 Significantly fewer men are accessing VCT and, as a result, ART services (only 38 percent
compared to 62 percent for women); and there has been no movement to pilot home-based VCT as in nearby countries, including Botswana, Lesotho, Zambia and Uganda.
4.4.1.31 There is inadequate integration of treatment services with community level services and weak
collaboration and referrals to provide comprehensive services (including TB/HIV) and to reach an adequate geographical and target group coverage.
4.4.1.32 The HIV programme has not utilised the existing SRH community channels (e.g. CBDs, TBAs,
RH peer educators) to improve treatment literacy, adherence support, psychosocial support, HBC and referral for facility-based testing and treatment.
Care and Support
4.4.1.33 There are three main weaknesses with respect to care and support. First, there is inadequate coordination and collaboration within and between the public sector (coordination and quality
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 46/160
assurance) and civil society (main implementers of services and PLWHA networks), especially at the decentralised levels. Moreover, in most of the regions referral systems are also not well developed, for example, between health facilities, CHBC providers and PLWHA support groups.
4.4.1.34 Second, while there is increased demand for CHBC support groups, little is being done to
formally sustain such groups. Standardised quality community support services (PLWHA support groups, CHBC, and OVC support) are not available throughout the country, especially at community level. Currently, work is being done to standardise a minimum package of HBC/palliative care services at community level as well as better integrate HIV/TB, SRH and PHC issues that have been inadequately represented in the past. Psychosocial support, medical and legal services are not readily available at community level.
4.4.1.35 Third, there is inadequate nutritional support integrated into the comprehensive package of
services, including food security and/or other material support for PLWHA and OVC. This affects, for example, adherence to ART and/or school attendance and performance.
4.4.1.36 There is also inadequate community mobilisation to increase utilisation of the available services. Impact Mitigation 4.4.1.37The economic downturn gives rise to increasing poverty and food insecurity. Poor and severely
poor are estimated in 28 percent and 14 percent of households respectively. 40 percent rises in food prices, crop failures from recurrent floods, and increasing food insecurity are exacerbating the mitigating efforts because of decreased livelihoods and increased associated vulnerabilities. These affect ART adherence for PLWHA who do not have the means to cover transport and food.
4.4.1.38 Multi-sectoral coordination directed through the MGECW is not able to secure sufficiently high
level participation from multi-sectoral line ministries (such as MOE and MoHSS) in coordination forums, such as the OVC Permanent Task Force.
4.4.1.39 Child Welfare Grants are benefiting over 105,000 OVC in Namibia (42 percent of the total
number of OVC). However, grant administration functions are deleteriously affecting the social workers’ abilities to fulfil their therapeutic functions. It is also becoming apparent that children who are benefiting from the grants are being forced to pay school fees, which defeats the purpose of the grants.
4.4.1.40 The retention and remuneration of volunteers has proved to be a great challenge, especially in
the absence of monetary and other incentives. The implications of sustaining programmes are also of concern if incentives are given and not sustained.
4.4.1.41 Some of the smaller civil society organisations providing care and support to OVC and other
vulnerable groups have weak capacity. 4.4.1.42 If the foregoing weaknesses (paragraphs 4.4.1.2-4.4.1.54) are not addressed, especially to
ensure adequate coverage of poor and underserved communities (particularly in the northeast, northwest and south), the overall efforts to mitigate the impact of the epidemic will be severely hampered and national goals and objectives are unlikely to be achieved.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 47/160

4.4.2 Health System Health System Weaknesses/Gaps
a) Describe the main weaknesses of and/or gaps in the health system that affect
outcomes for the disease. The description should, in addition to explaining health system issues that impact outcomes for this disease, also include a discussion of issues that impact outcomes for other diseases where the weaknesses/gaps are common ONE PAGE MAXIMUM
b) Describe what is already being done, and by whom [not what is planned in this
proposal], to respond to health system weaknesses and gaps that affect outcomes for this disease.
ONE PAGE MAXIMUM
4.4.2.1 The delivery of services for HIV and AIDS, TB and malaria interventions requires substantial investments in the underlying health systems, more especially in the health workforce, medicines and logistics, diagnostic capacities, infrastructure and health information system. The main gaps are described below.
Service Delivery
4.4.2.2 While healthcare providers consistently aim to provide high quality care, limited resources such as staffing, infrastructure and equipment make the provision of health and social services a challenge. The recent Health and Social Services Review (Annex J7) has revealed that the essential national health package is yet to be finalised.
4.4.2.3 Most basic health services are delivered through the PHC system as envisaged in the Health
Policy Framework (see Annex J39). HIV and AIDS, TB and malaria interventions are integrated into PHC; hence in theory all PHC facilities should be able to offer care and treatment for both communicable and non-communicable diseases. However, geographical access to PHC is a constraint in Namibia. According to the Medium-term Expenditure Framework 2008-2012, out of a population of around two million people, 37 percent live more than 20km from a public health facility (Annex J12). The situation is further compounded by weaknesses in the diagnostic service system; for example, laboratory and X-ray services are only offered at hospitals, meaning that patients or samples often need to be transported to the nearest hospital for examination, causing diagnostic delays and long waiting times for results to be provided to the client. In some regions, people have to travel for more than 300km to reach the nearest hospital (Health and Social Services Review 2008, Annex J6.). Most regions report that no transport is available to help patient’s access services at hospitals.
4.4.2.4 In most regions, support supervision from the regional levels to health facilities is generally weak (ibid).
4.4.2.5 Physical infrastructure is inadequate to meet the required service delivery needs and the existing infrastructure is inequitably distributed. Those who are most affected are those in the lowest socioeconomic quintiles (Annex J13, Basic Income Grant report 2009). Moreover, the existing infrastructure is unable to cope with the scale and volume of services that stem from an increased case load as a result of HIV and AIDS/TB co-infection. The lack of space is not only detrimental for efficient laboratory diagnosis, infection control and storage of supplies but also means that clients do not have the privacy needed for HIV and AIDS consultations.
4.4.2.6 The MoHSS has its own fleet of vehicles, including ambulances and trucks for medical supplies. However, only 67 percent of vehicles are in good running condition and this affects the delivery of supplies to regional medical stores and health facilities. The frequent breakdown of critical equipment and machines coupled with the absence of replacement parts are severe constraints to the delivery of quality services. Existing infrastructure is maintained by the MOHSS as well
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 48/160
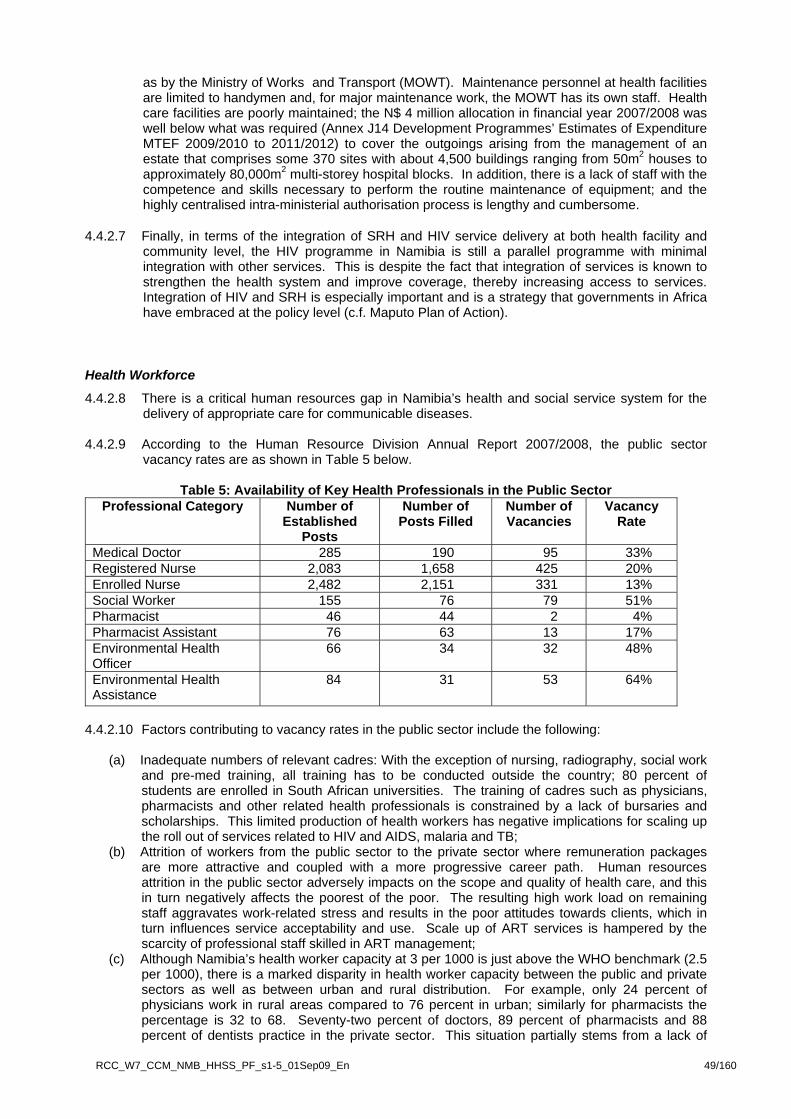
as by the Ministry of Works and Transport (MOWT). Maintenance personnel at health facilities are limited to handymen and, for major maintenance work, the MOWT has its own staff. Health care facilities are poorly maintained; the N$ 4 million allocation in financial year 2007/2008 was well below what was required (Annex J14 Development Programmes’ Estimates of Expenditure MTEF 2009/2010 to 2011/2012) to cover the outgoings arising from the management of an estate that comprises some 370 sites with about 4,500 buildings ranging from 50m2 houses to approximately 80,000m2 multi-storey hospital blocks. In addition, there is a lack of staff with the competence and skills necessary to perform the routine maintenance of equipment; and the highly centralised intra-ministerial authorisation process is lengthy and cumbersome.
4.4.2.7 Finally, in terms of the integration of SRH and HIV service delivery at both health facility and community level, the HIV programme in Namibia is still a parallel programme with minimal integration with other services. This is despite the fact that integration of services is known to strengthen the health system and improve coverage, thereby increasing access to services. Integration of HIV and SRH is especially important and is a strategy that governments in Africa have embraced at the policy level (c.f. Maputo Plan of Action).
Health Workforce
4.4.2.8 There is a critical human resources gap in Namibia’s health and social service system for the delivery of appropriate care for communicable diseases.
4.4.2.9 According to the Human Resource Division Annual Report 2007/2008, the public sector
vacancy rates are as shown in Table 5 below.
Table 5: Availability of Key Health Professionals in the Public Sector Professional Category Number of
Established Posts
Number of Posts Filled
Number of Vacancies
Vacancy Rate
Medical Doctor 285 190 95 33% Registered Nurse 2,083 1,658 425 20% Enrolled Nurse 2,482 2,151 331 13% Social Worker 155 76 79 51% Pharmacist 46 44 2 4% Pharmacist Assistant 76 63 13 17% Environmental Health Officer
66 34 32 48%
Environmental Health Assistance
84 31 53 64%
4.4.2.10 Factors contributing to vacancy rates in the public sector include the following:
(a) Inadequate numbers of relevant cadres: With the exception of nursing, radiography, social work and pre-med training, all training has to be conducted outside the country; 80 percent of students are enrolled in South African universities. The training of cadres such as physicians, pharmacists and other related health professionals is constrained by a lack of bursaries and scholarships. This limited production of health workers has negative implications for scaling up the roll out of services related to HIV and AIDS, malaria and TB;
(b) Attrition of workers from the public sector to the private sector where remuneration packages are more attractive and coupled with a more progressive career path. Human resources attrition in the public sector adversely impacts on the scope and quality of health care, and this in turn negatively affects the poorest of the poor. The resulting high work load on remaining staff aggravates work-related stress and results in the poor attitudes towards clients, which in turn influences service acceptability and use. Scale up of ART services is hampered by the scarcity of professional staff skilled in ART management;
(c) Although Namibia’s health worker capacity at 3 per 1000 is just above the WHO benchmark (2.5 per 1000), there is a marked disparity in health worker capacity between the public and private sectors as well as between urban and rural distribution. For example, only 24 percent of physicians work in rural areas compared to 76 percent in urban; similarly for pharmacists the percentage is 32 to 68. Seventy-two percent of doctors, 89 percent of pharmacists and 88 percent of dentists practice in the private sector. This situation partially stems from a lack of
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 49/160

sufficient incentives for health professionals to encourage them to work in rural areas; and (d) The formal structure of the health system ends at the clinic level and outreach points.
Community-based health is emphasised by the MoHSS as a means to improving access to basic health care. However, there are no clear structures to support community-based health care services. The volunteer community health workers have few incentives and are inadequately supported by communities and health workers (2008 Health and Social Services Review, op. cit)
Health Information Systems (HIS) 4.4.2.11 Although the various information systems are in place, there is a lack of capacity at all levels
both in the management and coordination of information systems as well as in data generation and processing. The information technology (IT) set up at the MOHSS is weak, with only four supporting staff members. This makes it difficult to support the regions efficiently and effectively, and there is no provision for IT at sub-national levels. The Health Management Information System (HMIS) is computerised at the level of regional health teams, hospitals and health centres; however, at clinics it is paper-based. At sub-national levels there are no dedicated human resources to manage data collection and entry; consequently, this is managed by nurses on top of their clinical duties. Information and telecommunication technology is inadequate and expertise in designing, operating and maintaining IT systems is lacking. Capacity to implement relevant surveys is low and there is a lack of an active surveillance system to monitor the safety of ARVs, TB, and malaria medicines. Furthermore, there is no central repository of data to ensure the ready availability and accessibility of relevant knowledge.
4.4.2.12 In a nutshell, at the facility level the data are collected but not systematically; they are not
analysed and, as a consequence, are not fed back into the system. Data collection, analysis and dissemination are currently too weak to be used to develop interventions to meet evidence-based needs, required if scale up is to be achieved.
Vaccines and Technology
4.4.2.13 The introduction in recent years of new medicines and technologies (ART, VCT, new malaria and TB treatment regimens) into the pharmaceutical supply and distribution system has resulted in a relatively large number of additional medicines and other supply items, some of which are required in large volume. This has led to constraints related to physical space and transport capacity in and between the Central and Regional Medical Stores and various health facility pharmacies, respectively. Similarly, hospital pharmacies do not have the physical space for storing ARVs and drugs related to TB, malaria and other diseases.
4.4.2.14 Furthermore, the Integrated Financial Management System, required to ensure the prompt
payment of supplies, is not operational at regional and district level. In some cases, non-payment results in the non-delivery of services by suppliers. The distribution supply for non-facility based commodities such as condoms is also weak.
Health Financing
4.4.2.15 The Namibian health care system is comprised of a mix of public and private financing. The public system provides universal coverage and is predominantly funded through general taxation, while the private health care system, which provides either comprehensive or partial health care coverage, is funded largely through employee and employer contributions. For the period 2000–2005, the health sector was financed by government, private and external resources, with the Government being the greatest source of financing (Figure 7).
4.4.2.16 However, the proportion of health financing from both public and private sectors has been on
the decline (Figure 8). 4.4.2.17 The government allocation to health has been increasing in absolute terms as indicated in the
figure below. However, of the total amount of funds spent on health in 2006/07, 44.0 percent came from public sources, 24.7 percent from households (largely through insurance), 22.4 percent from donors, and 8.9 percent from companies. The public sources declined from the 63 in 2001/02 to the levels of 44%. It is further to be indicated the level of donor support to the MoHSS increased from 4% in 2001/02 to 13.9% in 2006/07(National Health Accounts 2001/02 -
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 50/160
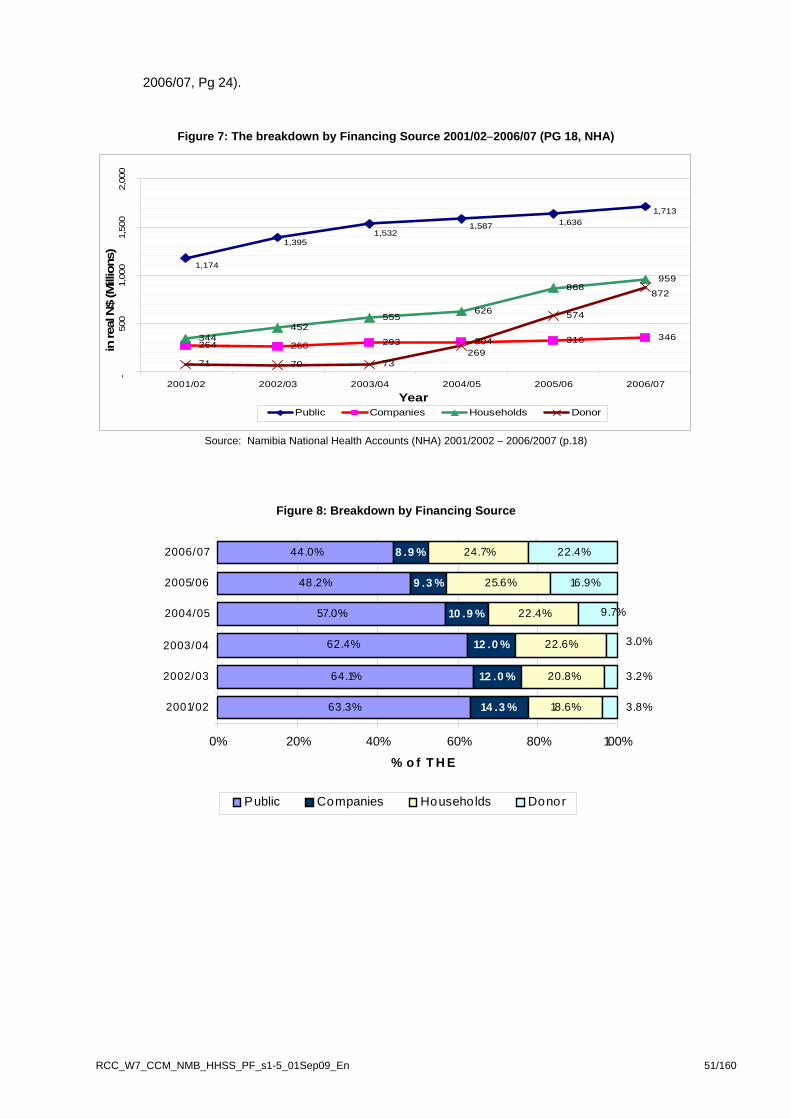
2006/07, Pg 24).
Figure 7: The breakdown by Financing Source 2001/02−2006/07 (PG 18, NHA)
264 260 293 304 316 346344452
555626
868959
71 70 73
574
1,174
1,3951,532
1,587 1,6361,713
269
872
-50
01,
000
1,50
02,
000
2001/02 2002/03 2003/04 2004/05 2005/06 2006/07
Year
in re
al N
$ (M
illio
ns)
Public Companies Households Donor
Source: Namibia National Health Accounts (NHA) 2001/2002 – 2006/2007 (p.18)
Figure 8: Breakdown by Financing Source
63.3%
64.1%
62.4%
57.0%
48.2%
44.0%
14 .3 %
12 .0 %
12 .0 %
10 .9 %
9 .3 %
8 .9 %
18.6%
20.8%
22.6%
22.4%
25.6%
24.7%
16.9%
22.4%
3.8%
3.2%
3.0%
9.7%
0% 20% 40% 60% 80% 100%
2001/02
2002/03
2003/04
2004/05
2005/06
2006/07
% o f T H E
Public Companies Households Donor
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 51/160

4.4.2.18 Figure 9 compares the Government’s budget allocation for health with actual expenditure.
Figure 9 A: MOHSS Allocation vs. Actual Expenditure 2001/02 – 2006/07
1,000,000,000
1,100,000,000
1,200,000,000
1,300,000,000
1,400,000,000
1,500,000,000
1,600,000,000
1,700,000,000
1,800,000,000
2001
/200
2
2002
/200
3
2003
/200
4
2004
/200
5
2005
/200
6
2006
/200
7
Financial Year
Nam
ibia
n D
olla
rs
AllocationExpenditure
Source: Health and social Services Review, p.120.
Fig. 9 B: MOHSS allocation vs Expenditure for FY 2007/2008
Programme Budget Allocation Expenditure % Variance
Tertiary 650,455,204.00 629,320,414-01 3,3 % Regional & District 994,423,896.00 1,001,430,127-71 -0,7% Disease Control 23,732,320.00 23,148,638-91 2,5% Social Protection 14,304,508.00 13,541,012-80 5,3% Total 1,682,916,000.00 1,667,440,194-94 0,9%
4.4.2.19 The MoHSS provides public health care for 85 percent of the Namibian population who are poor
and low-income earners, while private health care provides for the remaining 15 percent in the middle and high-income bracket. The resources used by the private sector are almost half that of the Government and this illustrates inequities in resources in terms of populations served. The budgeting and reporting of expenditure are based on line item budgeting and this makes it problematic with regard to reporting on financial expenditure for communicable and non-communicable diseases.
4.4.2.20 The MoHSS charges user fees at health facilities in Namibia according to the policy framework as articulated in Ministerial Circular 8 of 2001. However, in spite of this, certain services are classified as free-of-charge such as any well-baby, ANC and post–natal, FP or immunisation services which are part of preventative care. Likewise patients who are admitted to a state hospital or health facility because they suffer from, or have been in contact with a person who suffers from, a notifiable disease is treated free-of-charge. The policy asserts that no person shall be turned away or denied services because of their inability to pay. The MOHSS is revising the user fees schedules and in the current draft it is recommended that, for diseases of public health concern such as TB and HIV and AIDS, patients are to be exempted from fees. Furthermore, the revision is looking at the exemption of user fees for OVC, pensioners and the disabled, as per the Ministerial directive of the enlarged ministerial management meeting in February 2009.
4.4.2.21 The ministerial allocation from central government for FY 2007/2008 was N$ 1,7 billion (Pg 7 Minister of Health, Budget Motivation Vote 13, FY 2008/2009), for FY 2008/2009 the allocation was N$ 2.1 billion while for the FY 2009/2010 the allocation is N$ 2.4 billion (Pg. 10 Minister of Health, Motivation for budget Vote 13, FY 2009/2010). Therefore over the years the budget
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 52/160

RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 53/160
allocation has been increasing in absolute terms. Due to the economic downturn the development budget allocation is anticipated to decrease to N$ 259 million in the FY 2010/2011 from the current N$ 334 million (Pg 3, Development Programme Estimates of Expenditures, MTEF 2009/2010 – 2011/2012).
Leadership and Governance 4.4.2.22 The national and regional institutional framework for the management and coordination of HIV
and AIDS has been put in place to ensure the coordination, full representation, coverage and sustainability of the response. This is described in detail in the Concept Paper (Concept Paper, op. cit.) and so shall not be repeated here except to note that, with the exception of NAEC, the national, regional and district coordinating mechanisms in place meet rarely or sporadically, although this frequency varies between sectors.
4.4.2.23 The MTP III is linked to national long- and medium-term plans (Vision 2030, NDP, the National HIV/AIDS Policy 2007 and the TB Medium-term Plan). Mechanisms for ongoing multi-sectoral partnerships, governance and collaboration with the academic sector are also laid out in MTP III.
4.4.2.24 In order to improve public health leadership and systems performance, the Government has launched an initiative aimed at the MOHSS’ most senior leadership team. The African Public Health Leadership and Systems Innovation Initiative is creating a replicable model for improving public health leadership and systems performance, beginning in Namibia. The newly launched Initiative is being implemented by Synergos and aims to improve public health service throughout the country. It invests in a strategic set of national health leaders including senior government officials, clinical technicians, community health providers and representatives from business and civil society. Health leadership cohorts are guided through an intensive two year process, involving leadership capacity building as well as the creation of innovation projects that address urgent health challenges. The initiative is working to significantly improve the performance and capacity of the Namibian Ministry of Health’s senior most leadership team.
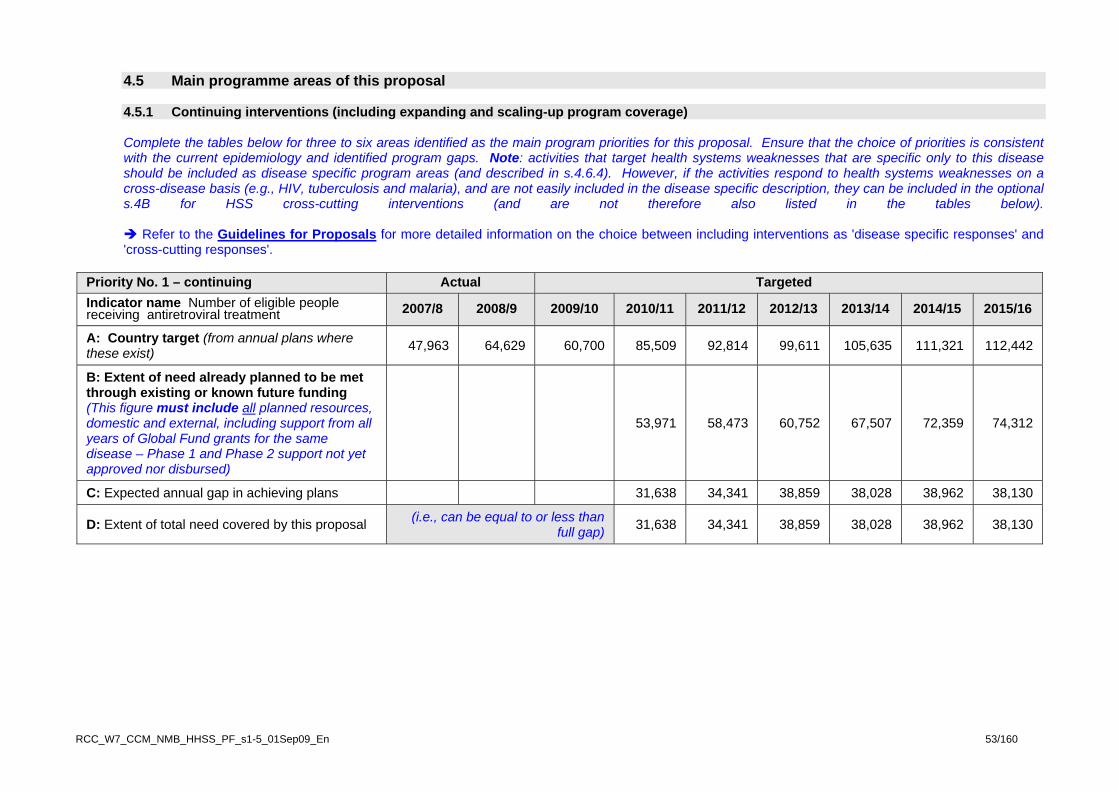
4.5 Main programme areas of this proposal 4.5.1 Continuing interventions (including expanding and scaling-up program coverage) Complete the tables below for three to six areas identified as the main program priorities for this proposal. Ensure that the choice of priorities is consistent with the current epidemiology and identified program gaps. Note: activities that target health systems weaknesses that are specific only to this disease should be included as disease specific program areas (and described in s.4.6.4). However, if the activities respond to health systems weaknesses on a cross-disease basis (e.g., HIV, tuberculosis and malaria), and are not easily included in the disease specific description, they can be included in the optional s.4B for HSS cross-cutting interventions (and are not therefore also listed in the tables below).
Refer to the Guidelines for Proposals for more detailed information on the choice between including interventions as 'disease specific responses' and 'cross-cutting responses'.
Priority No. 1 – continuing Actual Targeted Indicator name Number of eligible people receiving antiretroviral treatment 2007/8 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16
A: Country target (from annual plans where these exist) 47,963 64,629 60,700 85,509 92,814 99,611 105,635 111,321 112,442
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
53,971 58,473 60,752 67,507 72,359 74,312
C: Expected annual gap in achieving plans 31,638 34,341 38,859 38,028 38,962 38,130
D: Extent of total need covered by this proposal (i.e., can be equal to or less than full gap) 31,638 34,341 38,859 38,028 38,962 38,130
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 53/160
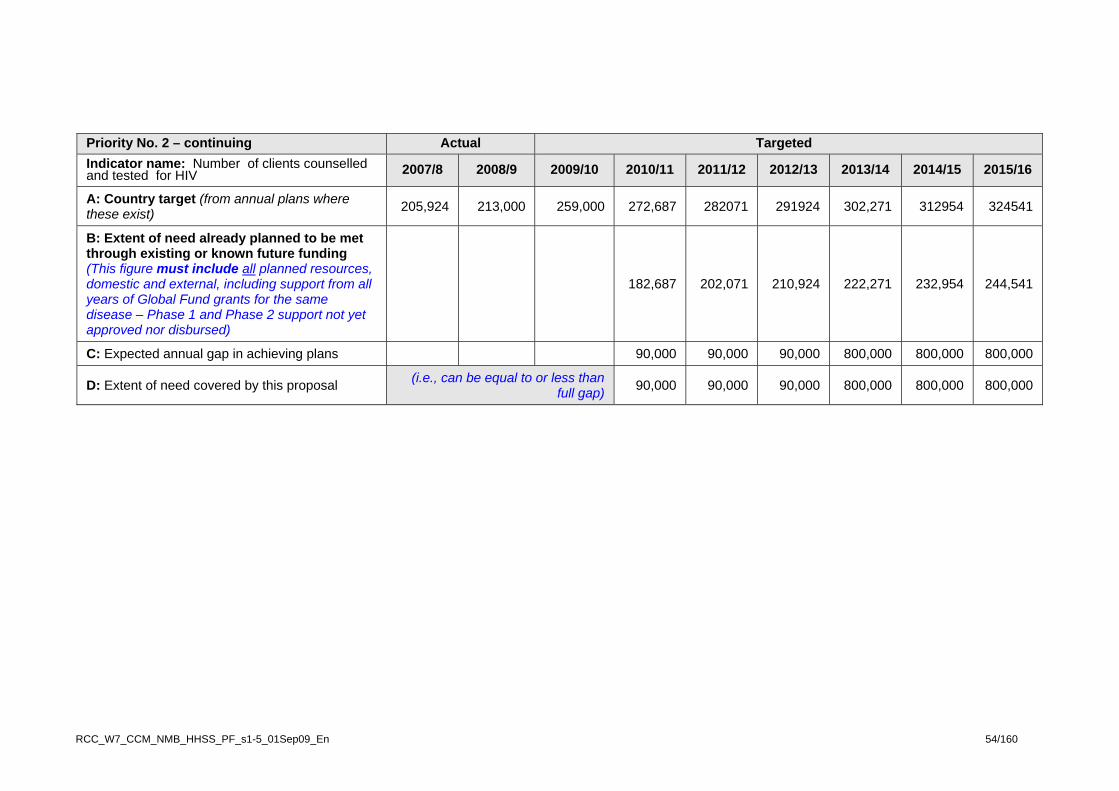
Priority No. 2 – continuing Actual Targeted Indicator name: Number of clients counselled and tested for HIV 2007/8 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16
A: Country target (from annual plans where these exist) 205,924 213,000 259,000 272,687 282071 291924 302,271 312954 324541
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
182,687 202,071 210,924 222,271 232,954 244,541
C: Expected annual gap in achieving plans 90,000 90,000 90,000 800,000 800,000 800,000
D: Extent of need covered by this proposal (i.e., can be equal to or less than full gap) 90,000 90,000 90,000 800,000 800,000 800,000
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 54/160
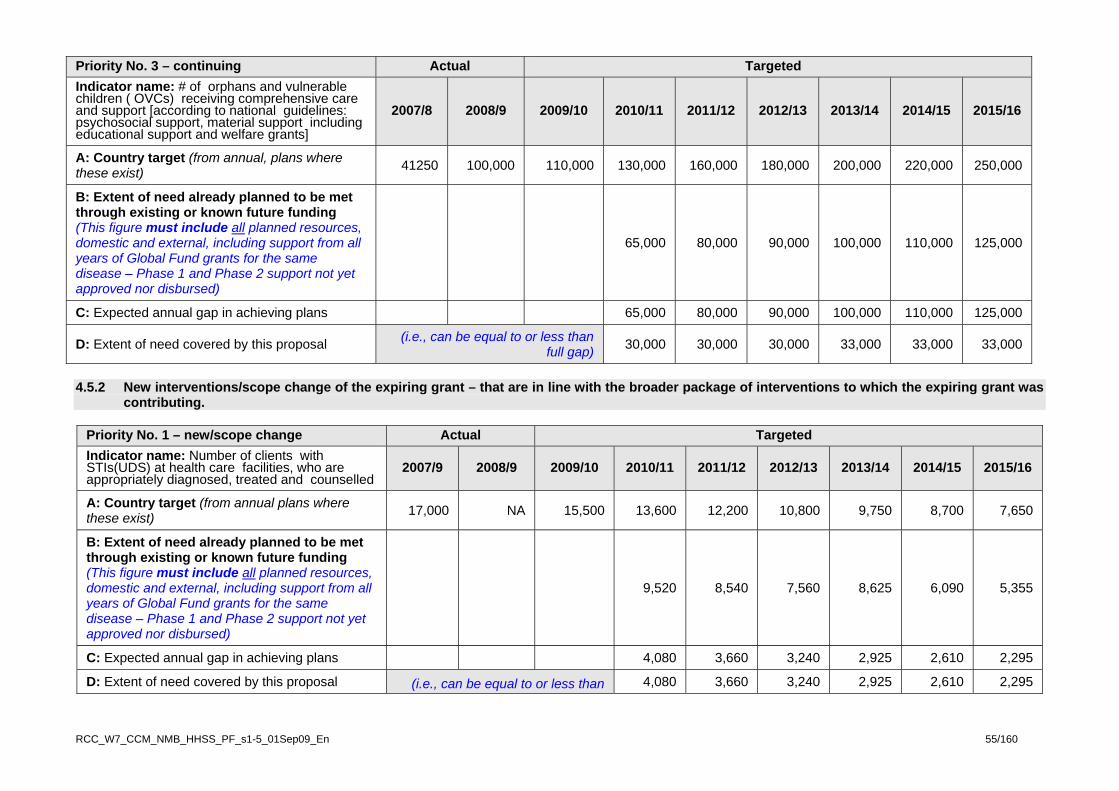
4.5.2 New interventions/scope change of the expiring grant – that are in line with the broader package of interventions to which the expiring grant was
contributing.
Priority No. 1 – new/scope change Actual Targeted Indicator name: Number of clients with STIs(UDS) at health care facilities, who are appropriately diagnosed, treated and counselled
2007/9 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16
A: Country target (from annual plans where these exist) 17,000 NA 15,500 13,600 12,200 10,800 9,750 8,700 7,650
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
9,520 8,540 7,560 8,625 6,090 5,355
C: Expected annual gap in achieving plans 4,080 3,660 3,240 2,925 2,610 2,295
D: Extent of need covered by this proposal (i.e., can be equal to or less than 4,080 3,660 3,240 2,925 2,610 2,295
Priority No. 3 – continuing Actual Targeted Indicator name: # of orphans and vulnerable children ( OVCs) receiving comprehensive care and support [according to national guidelines: psychosocial support, material support including educational support and welfare grants]
2007/8 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16
A: Country target (from annual, plans where these exist) 41250 100,000 110,000 130,000 160,000 180,000 200,000 220,000 250,000
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
65,000 80,000 90,000 100,000 110,000 125,000
C: Expected annual gap in achieving plans 65,000 80,000 90,000 100,000 110,000 125,000
D: Extent of need covered by this proposal (i.e., can be equal to or less than full gap) 30,000 30,000 30,000 33,000 33,000 33,000
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 55/160

Priority No. 1 – new/scope change Actual Targeted
2010/11 2011/12 2013/14 2014/15 Indicator name: Number of clients with STIs(UDS) at health care facilities, who are appropriately diagnosed, treated and counselled
2007/9 2008/9 2009/10 2012/13 2015/16
full gap)
Priority No. 2 – new/scope change Actual Targeted Indicator name: Number of sex workers reached with comprehensive HIV and sexual and reproductive health services.
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16
A: Country target (from annual plans where these exist) NA NA 150 300 1,000 2000 3,000 4,000 5,000
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
60 200 400 600 800 1,000
C: Expected annual gap in achieving plans 240 800 1,600 2,400 3,200 4,000
D: Extent of need covered by this proposal (i.e., can be equal to or less than full gap) 240 800 1,600 2,400 3,200 4,000
Priority No. 3 – new/scope change Actual Targeted Indicator name: Number of men who have sex with men reached with comprehensive HIV and sexual and reproductive health services
2006 2007 2008 2009 2010 2011 2012 2013 2014
A: Country target (from annual plans where these exist) NA NA 150 300 600 1,500 2,000 2,500 3,000
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
120 240 600 800 1000 1,200
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 56/160
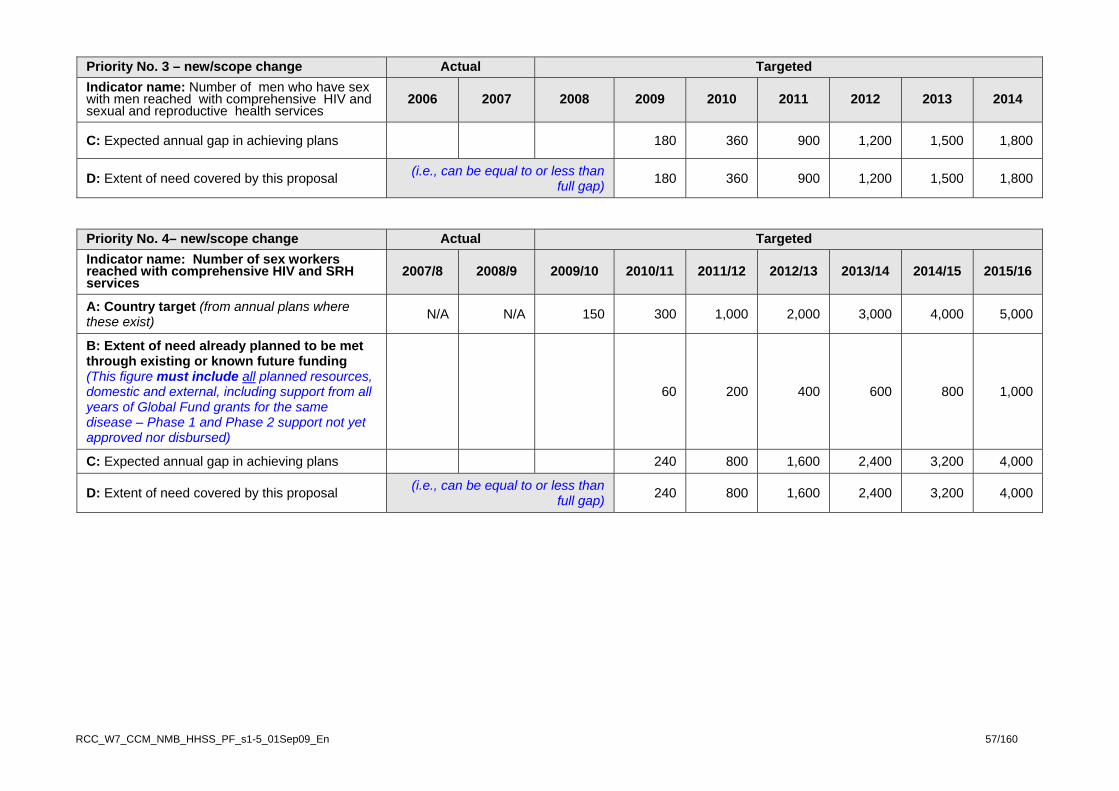
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 57/160
Priority No. 3 – new/scope change Actual Targeted Indicator name: Number of men who have sex with men reached with comprehensive HIV and sexual and reproductive health services
2006 2007 2008 2009 2010 2011 2012 2013 2014
C: Expected annual gap in achieving plans 180 360 900 1,200 1,500 1,800
D: Extent of need covered by this proposal (i.e., can be equal to or less than full gap) 180 360 900 1,200 1,500 1,800
Priority No. 4– new/scope change Actual Targeted Indicator name: Number of sex workers reached with comprehensive HIV and SRH services
2007/8 2008/9 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16
A: Country target (from annual plans where these exist) N/A N/A 150 300 1,000 2,000 3,000 4,000 5,000
B: Extent of need already planned to be met through existing or known future funding (This figure must include all planned resources, domestic and external, including support from all years of Global Fund grants for the same disease – Phase 1 and Phase 2 support not yet approved nor disbursed)
60 200 400 600 800 1,000
C: Expected annual gap in achieving plans 240 800 1,600 2,400 3,200 4,000
D: Extent of need covered by this proposal (i.e., can be equal to or less than full gap) 240 800 1,600 2,400 3,200 4,000

4.6 Analysis of priorities for Rolling Continuation Channel proposal Scope and Scale Considerations
4.6.1 Continuation of Expiring Grant’s strategy
(a) Does this proposal continue the same objectives, same service delivery areas, and same focus and range of interventions as the expiring grant without any changes to program scale (i.e., no substantial increase in coverage) or scope (e.g., increasing the population groups covered, or the range of services offered?
No
4.6.2 Programme scale adjustments in this proposal
(a) Does this proposal include a significant planned scale adjustment (whether a scale up by substantially increasing coverage for existing interventions, or, if relevant to the current disease profile, a reduction in interventions) compared to the expiring grant’s planned focus and outcomes?
Yes
(b) If yes to (a), summarise the planned scale adjustments, and why this change will create more effective and sustained strategies for greater health outcomes and impact.
4.6.2.1 This proposal will continue the same objectives, same service delivery areas, and same focus and range of interventions as the expiring grant with changes to programme scale. It is important to note that the service delivery areas mentioned below are scaling up to increase geographical and target group coverage which will receive increasing government financial support. Prevention
4.6.2.2 SDA: BCC Mass Media: National capacity will be strengthened in order to better enhance the mass media coordination through the “Take Control” initiative. The initiative will be responsible for all visual, audio and print mass media materials development targeting all segments of the general population. The Take Control initiative coordinates all relevant organisations working on mass media and HIV/AIDS and TB. This initiative is supported by many development partners but PEPFAR and Global Fund are contributing the most significant financial resources in addition to the government resources of the Ministry of Information, Communication and Technology (MICT). Round 2 contributed to the relationship campaign “Be There to Care” and will also contribute to the new campaign on Multiple Concurrent Partnerships. The latter is addressing one of the main drivers of the HIV epidemic. During Round 2 comprehensive HIV knowledge among 15-24 years old increased from 38.9% among females and 50.7% among males to 64.9% and 61.9% respectively. Through scale up of institutional capacity building of Take Control initiative and mass production, the mass media on HIV, SRH and TB needs to become less fragmented and more communities will receive better behaviour change communication materials. This will increase
Note to applicants: The tables in s.4.5.1 (continuing interventions/scale-up) and s.4.5.2 (new interventions/scope change) highlight the main priorities. These priorities and all other activities should be very clearly described in the questions in s.4.6 below to ensure that the Technical Review Panel has a clear understanding of the planned work, and outcomes, over the proposal term. Applicants are strongly encouraged to describe all activities in the RCC proposal in a detailed way, including who will implement the activities. Applicants should not assume that the TRP will read the earlier qualifying proposal at the sa me time as reading this proposal.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 59/160

comprehensive knowledge through social mobilisation and awareness interventions thereby sustainably empowering the people to make informed prevention and care decisions and change behaviour (e.g. limiting the number of sexual partners). More emphasis is being placed on ensuring that messages are based on information about the drivers of the epidemic i.e. MCP and transactional sex, trans-generational sex, alcohol use, gender violence, MTCT etc. Message content will also be amplified to include SRH and gender issues. 4.6.2.3 SDA: PMTCT: The PMTCT scaled up through increased funding from PEPFAR and Global Fund, and funding is well aligned in terms of co-funding training. Under Round 2, Global Fund contributed to the PCR test but from 2010 PEPFAR and GRN co-finance the tests. Information and education on PMTCT will be given to women and girls of reproductive age even before they fall pregnant. Information on sexual and reproductive health will be given to women of reproductive age to help prevent unwanted pregnancies; before and after the pregnancy, especially in the vulnerable postnatal period when they present for the scheduled postnatal visit 6 weeks after delivery. This service will be scaled-up using outreach and client education and prevention strategies especially through mobile clinics and CHBC services which are already well established in Namibia. Collaboration with programmes such as reproductive health, family planning and ANC would be scaled-up to reach the remaining HIV uninfected populations. 4.6.2.4 As more women become aware of PMTCT, more of them will receive a complete course of ARVs for prophylaxis and the percentage coverage of women receiving a complete course of ARV prophylaxis for PMTCT will continue to increase from the current 70% to an estimated 85% by 2014/15; this, coupled with Namibia’s use of combination ARV prophylaxis for PMTCT will lead to fewer children being born HIV infected, with reduction of MTCT risk from 11.8% to 6% by the end of the RCC period). Provision of counselling and testing to male partners of women attending ANC will be scaled-up through male involvement campaigns; thus ANC and PMTCT services will be entry points to care and treatment for male partners of pregnant women, should they turn out to be HIV infected. 4.6.2.5 After delivery the present situation is that women/mothers do return for post-natal services where emphasis on adherence to ARV treatment, infant feeding, nutrition and family planning education will be reinforced. However, to increase tracking of women post-natal additional support will be given to community based organizations to support, supervise mothers and families in the home. HIV infected pregnant women need on-going psychosocial care and support. To this end, peer mothers (HIV positive mothers who themselves have passed through PMTCT) will be used to provide support for other HIV infected mothers to help them follow through with the continuum of HIV care. The HIV infected mothers will receive support to enable them and their families to continue coming for follow-up even after delivery as they will need CD4 count monitoring and prophylaxis (cotrimoxazole and INH); in addition to early infant diagnosis of HIV infection in their HIV exposed infants in whom PMTCT failed, provision of Cotrimoxazole prophylaxis to all HIV exposed infants, disclosure to partners as well as support for infant feeding. This will help with minimizing drop-out and loss to follow-up rates for the mother-baby pair from PMTCT. 4.6.2.6 Namibia has adopted the April 2008 WHO recommendations to initiate all HIV positive infants on ART at the time they are definitively diagnosed as HIV positive, preferably in the first 12 weeks of life. The HIV DNA PCR algorithm for Namibia recommends testing all HIV exposed infants at 6 weeks of age; conveniently scheduled to coincide with the 6 weeks postnatal visit for the mother as well as the 6 weeks immunization for the baby. With the high attendance (> 90%) for first immunization visit, greater harmonization of infant HIV testing with primary health care that includes immunization and growth promotion will lead to high rates of PMTCT follow-up for HIV exposed babies. Concerted efforts will be made in the next few years to fully integrate infant HIV testing and Cotrimoxazole prophylaxis within MCH services. This activity is already in-process as Namibia is undertaking a process to incorporate information on maternal HIV status on the under-5 Child Health Card. This will facilitate identification of HIV exposed babies, and lead to appropriate care and follow up being administered to eligible children 4.6.2.7 SDA: Condoms: The promotion and distribution of both female and male condoms will be scaled up. During Round 2, and annual average of 18 million condoms were procured (roughly 18/25..of the total condoms distributed). PEPFAR contribute in 2008 & 2009 with 4.5 million condoms annually and the government is increasingly stepping in with additional funding. During the RCC time frame annually 21 million condoms will be procured and the increasing demand will be covered by the GRN contribution. The RCC foresees a study to estimate the condom need in order to strengthen the procurement and distribution forecasts. Youth will be specifically targeted through IEC/BCC messages as one of the main
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 60/160

drivers is multiple concurrent partnerships and sexual and reproductive health messages (“dual protection”) have been inadequate. . Therefore, condom usage in high risk sex among adults of 66% (Women) and 74% (men) recorded in 2006 (DHS 2006) will increase to a target of 81% and 89% respectively by 2014/15. The female condom distribution scale up will result in increased condom usage among the females that is currently much lower than among the males. 4.6.2.8 SDA: HIV Counselling and Testing (HTC): The scale up through public and private sector outreach and mobile clinics make the counselling and testing services, as well as a link to ART services more accessible in the hard to reach places. Men will be specifically targeted through community mobilisation. It is expected that the percentage of adults counselled and tested in the past 12 months will increase from 18 percent among men and 29 percent among women to 34 percent and 47 percent respectively by 2014/15. In 2008, the MoHSS counselling and testing programme initiated national testing days (NTDs) and for 2009 more than 80,000 clients showed up during a period of 4 days (roughly one-fifth of the target population). Therefore, the programme wishes to continue with this intervention and improve geographical coverage as well through starting with mobile testing. The Namibian Business Coalition (NABCOA) started with mobile testing, in collaboration with PharmAccess, under Round 2 in 2009. In addition, Namibia aims to increase the number of men enrolled into care and treatment as currently there is a significant difference with the female counter parts. PEPFAR is the main financial contributor (rapid test, training and salaries lay counsellors), Global funds contributes between 30-40% (mobile testing, training, community mobilisers), and the Government and private sector are increasing contributors. Treatment
4.6.2.9 SDA: ARV Treatment and Monitoring: The ART roll out to the 34 hospitals in Namibia was completed under Round 2. The scale up towards increase geographical coverage has started in phase II of Round 2 by rolling out the ART programme to health centres and the bigger clinics, as well as through outreach (currently at 66 in 2009). During the RCC time frame the programme plans to roll-out ART to at least 3 additional sites per quarter (12 sites per year). This scale-up is possible as the MOHSS officially adopted the WHO IMAI strategy in 2005 which allows nurses to conduct clinical consultations for HIV/AIDs patients more than one year on ART treatment without serious complications (estimated that 80% of the patients more than one year on ART can be seen by registered nurses) as well as those enrolled for care and not eligible for ART. In addition it is important to note that the Government contribution to ART drugs is increasing from 47% (2010) to 59% (2015) over the RCC time frame. The PEPFAR and Global Fund contribution is expected to decrease from respectively 16 to 6%, and 37% to 34%. This strategy will increase the accessibility to ART and is expected to increase ART coverage of those adults and children in need from 81% (June 09 Spectrum) to 87% by 2014/15. However, this will depend on future guidelines of WHO and UNAIDS related to the eligibility criteria on CD4 count. This will further reduce AIDS deaths. The growing concern related to ART adherence needs to be addressed through community home based care (see section 4.6.3). 4.6.2.10 In decentralising care, the HIV programme will, as much as possible, use existing systems rather than creating a parallel system of service delivery. Clinics that provide maternal and child health (MCH), for example, are distributed throughout the country. These clinics will be assessed for provision of comprehensive HIV care, their capacity improved, staff trained and services integrated. Decentralisation will further look into ways to integrate treatment, care and support at the community level. Hence, existing health workers in the community including those who have traditionally provided SRH services only will be trained and linked up with clinics to provide treatment literacy, adherence support, psychosocial support, nutritional counselling and HBC. They will also be important channels for referral from community to the clinics. Impact Mitigation 4.6.2.11 SDA: Support for OVC: The national OVC Policy which is supported through an Action Plan 2006 – 2010 has been developed outlining a comprehensive package of strategies and interventions for OVCs. However, the DHS 2006, as well as two programme evaluations of civil society organisations (Catholic AIDS Action and the Namibian Red Cross Society) supporting OVCs strongly indicate that a minimum comprehensive service package for OVC is lagging behind. Therefore scaling-up support to OVCs through standardised and quality training of community volunteers and material and psychosocial support, as well as increased monitoring support is foreseen under the RCC proposal. The expected
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 61/160

outcome of these interventions is an increase of the percentage of OVCs whose households receive at least one type of free basic external support in caring for the child from 16.5% in 2006 to 65% (too high) by 2014/15. The Government is a major contributor to OVC support as the OVC welfare grants are entirely financed by domestic resources, and the public service commission approved in 2008 the “less qualified” Community Child care workers to address the shortage of social workers (task shifting) and strengthen the outreach to OVC in communities. Both Global Fund and PEPFAR (through USAID) are co-financing civil society organisations, roughly about 50% each. 4.6.2.12 The expanded regional monitoring framework, which will underpin the work of NANASO regional workers, will also include monitoring activities at the individual OVC level. The expected outcome of these interventions is an increase of the percentage of OVCs whose households receive at least one type of free basic external support in caring for the child from 16.5 percent in 2006 to 65 percent by 2014/15. 4.6.2.13 SDA: Workplace Policy and Programmes: Under Round 2 public (local authorities) and private sector workplace programmes have been scaled-up. Although it has proven not be easy to convince senior and middle management of the benefits of workplace programme, the interventions of IEC/BCC and counselling and testing are gaining ground. It is expected that this will be an effective strategy for the scale up of workplace programmes to reach more workers, and especially men. It is expected that men with means contributed to the driver on multiple concurrent partnerships. Data of prevalence surveys in some private sector companies tested (2007) by PharmAccess showed the following results:
1. Mining Sector: 805 people tested. 724 men. HIV Prevalence – 21% 2. Services Sector: 383 people tested. 311 men. HIV Prevalence – 17% 3. Manufacturing Sector: 400 people tested. 332 men. HIV Prevalence 22%
Workplace programmes in both private and public sectors will be scaled up, including PEP and VCT linked to SRH services in the workplace with follow up support for behaviour change and referral to ensure the continuum of care. Workplace programmes, linked to the mobile clinics, will also be linked to home testing. This is expected to increase the proportions of both sexes - but especially men - being tested, to reduce the opportunities for GBV (since both partners will have been tested together), and to facilitate the development of a family-centred approach to care if needed – or, if the couple is negative, enable messages to reinforce positive health-seeking behaviours to be delivered to both partners by the same person, thus ensuring a shared understanding of the information received. 4.6.2.14 Linkages between services: The scale up of services will include the strategy of improving the linkages between various services for synergy and sustainability. Examples of services that will be strengthened through improved linkages are: PHC, SRH, MCH/FP, STIs, HIV and AIDS and TB. 4.6.2.15 In particular, efforts will be made to improve the integration of SRH with HIV and AIDS. Existing community SRH channels will be mapped out and their capacity assessed and improved so that they participate effectively in comprehensive HIV prevention. The channels include those used for distribution of contraceptives, pregnancy care (e.g. TBAs), sex education (through both traditional and modern channels – school and out-of-school peer education system, etc). The channels will then be used to pass prevention messages, mobilise for HIV testing, PMTCT, condom distribution and other forms of prevention.
4.6.3 Programme Scope Change Planned in this Proposal
(a) Does this proposal include a proposed change in scope as compared to the expiring grant’s scope? (e.g., by adding new population groups, or incorporating, as a hypothetical example, treatment to complement prevention services under the expiring grant)
Yes
(b) If yes to (a), summarise the planned scope change and why this change will improve the national response to the disease, for greater health outcomes and impact.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 62/160

4.6.3.1 This proposal will continue the same objectives, cover the same service delivery areas, and have the same focus and range of interventions as the expiring grant but with changes to the programme scope. The planned scope of the programme will change as described in paragraphs 4.6.3.2- 4.6.3.8 below. 4.6.3.2 SDA: BCC Community Outreach and Schools: As a result of recent research on the drivers of the epidemic and the national prevention strategy, which is under development, interventions targeting the Most at Risk Populations (MARPs) need to start as soon as possible. Small scale initiatives of civil society organisations need substantial support to address the target group coverage and risk behaviour. Currently no funding from Government, PEPFAR or Global Fund (Round 2) have been directed to addressing MARP interventions. The MARPs identified for this proposal are the newly identified vulnerable groups such as CSWs, inmates of correctional services, and MSM. The main interventions proposed are behaviour studies, development of targeted IEC material and peer education, as well as mobile outreach to address the identified MARPs. 4.6.3.3 The RCC will continue to address uniformed services but will reinforce interventions for out-of school and in-school youth. Life skills education is currently being mainstreamed into the school curricula with support of UNICEF. This ensures that the life skills subjects become examinable. In addition, the Ministry of Education wishes to reinstate full-time life skills teachers to ensure that student needs are adequately addressed by qualified teachers. Therefore life skills education funded under round 2 for in-school youth will continue with out-of-school youth only. The results of (OVC) counselling of in-school youth through teachers trained in counselling have not been as successful as hoped. Although an impact assessment is ongoing, the Ministry of Education is proceeding with the integration of both life skills as well as counselling into the pre-service teacher training curriculum. In regions where progress was made, counselling support groups need to be established and trained. Successful intervention by civil society organisations for both youth (OYO – drama tours) and the general population (DAPP) interventions are sustained but need to change focus from IEC to BCC addressing the drivers of the epidemic. 4.6.3.4 SDA: STI: Another change in the prevention scope has been to broaden it to include STI. There will be integration of STI services in all clinic services, including those providing SRH. This will offer, and increase, the opportunity for providing HIV services as well. STI treatment following the syndromic approach will be scaled up. Research will be conducted on factors affecting partner notification as this is one of the major barriers to STI treatment success. Following this study, partner notification will be strengthened to ensure treatment success rates. Condom distribution will target those presenting with STIs. Information and education will be tailored towards promoting positive health seeking behaviour in relation to STI. An etiological study will conducted to inform treatment protocols. Mobile clinics, currently testing for syphilis and Hepatitis B, will offer condoms and FP information and referral. 4.6.3.5 SDA: Care and Support to Chronically lll: As a lot more patients access ARTs, the scope of care previously needed under this SDA by community home based care volunteers has changed. The successful roll-out of ART resulted in very few bedridden patients (programme evaluation: Catholic AIDS Action and the Namibian Red Cross Society (2008). To address this change, the draft CHBC policy and standards will be updated and disseminated. CBHC givers need to refocus their tasks in the areas of prevention, including positive prevention, adherence to ART drugs by PLHIV, community directly observed treatment (DOTS) at rural community level as well care to OVCs. In order to scale-up these changed scope of services, all the primary and secondary care givers will retrained using the newly developed standardised training manuals. A mapping is required to ensure adequate geographical and target groups coverage (main target group remains HIV/AIDS and TB (around 90% of chronic disease clients)) and enhance monitoring and evaluation. To increase adherence nutritional support and food IGAs need to be initiated or scaled up, and referral systems between health facilities and CHBC and PLWHAs support groups needs to be strengthened. PEPFAR (through USAID) and Global fund are the main funders of the civil society organisations and contribute roughly 50% each. 4.6.3.6 SDA: HIV/TB integration: Due to the high burden of TB in Namibia and the ensuing HIV/TB co-infection, the integration currently undertaken under the Round 5 TB grant as an entry point includes case finding in PLHIV, testing and counselling, TB patients receiving CPT and HIV-positive TB patients
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 63/160
who started on and continued on ART during or at the end of TB treatment. In this proposal, the change in scope is the use of isoniazid Preventive Therapy, as an entry point for HIV/TB co-infection. The integration of the two diseases will be strengthened through a Committee established by stakeholders of the two diseases for purposes of coordination. Finally, mobile clinics will also start to offer TB testing on site. 4.6.3.7 Improved Integration of HIV and AIDS with SRH: Integration of services, especially integration of HIV and SRH, will be strengthened both at clinic and community levels to strengthen health system capacity and improve access. 4.6.3.8 SDA: Strengthening of Civil Society and Institutional Strengthening: The selection of a CSO as a PR has necessitated a change in scope of the services for strengthening of civil society and institutional strengthening. NANASO, selected as the second PR, will need strengthening through institutional capacity building. In terms of programme management and administration, NANASO will need resources that allow it to play an effective managerial and fiduciary role, to be able to advise its constituents in this regard, and to play a much stronger role at the regional level in coordinating civil society efforts generally and focusing it towards the changes and scope outlined in these SDAs. 4.6.3.9. SDA: Programme Management and Administration: Namibia’s response on duel tracking was to select NANASO as second PR. It will need strengthening through institutional capacity building through the current programme management unit of the public sector PR, envisaged through one year on the job training of newly recruited civil society PMU staff. 4.6.3.10 Surveys and surveillance: Under Round 2, funding was provided for some national surveys. Under the RCC, the focus is on all relevant national surveys (DHS, AIS, HFS, Sentinel Surveys), as well as streamlined M&E processes on established a national research agenda and joint HIV/AIDS reviews. The PEPFAR contribution is estimated to be 50% to the national surveys cost to be covered by development partners. The Government is contributing as well with logistical support. In the RCC, there is provision for funding of an AIDS Indicator survey (AIS) as it will provide HIV status and other biological indicators of all respondents who have been interviewed in addition to behavioural data. This change in scope will firstly enable secondary analysis to determine the association between HIV prevalence and behaviour. Secondly, it will enable Namibia to obtain for the first time a more accurate estimate of the adult general population HIV prevalence because AIS is a population based survey. Second generation behavioural surveys will provide data on HIV prevalence, behaviour and population size of most at risk populations such as CSWs and MSMs that has been lacking.
4.6.4 Detailed description of activities relevant to scale and scope changes Below the description is listed in a table listing the goal, divided into the four objectives, and also highlighting the relevant impact and outcome indicators for that particular SDA area.
GOAL: TO REDUCE THE PREVALENCE OF HIV AND AIDS INFECTION AND MORTALITY, AND MITIGATE THE SOCIOECONOMIC IMPACTS OF THE HIV AND AIDS EPIDEMIC IN NAMIBIA
Major Strategies Major Activities Potential
partner Target Populations
Objective 1: To reduce new HIV, TB and other STI infections
1.1: Prevention: Behaviour Change Communication - Mass Media
Indicator: # of HIV/AIDS radio and television programmes produced and aired
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 64/160

1.1.1 Develop and disseminate IEC messages targeting the major drivers of the epidemic and MARPS
This activity builds on R2 with an increased emphasis on harmonising and scaling-up BCC messages to increase effectiveness, based on recent information from new research on the drivers of the epidemic. There will be a renewed focus on strengthened coordination and evidenced-based media campaigns through 3 main activities: • Develop and disseminate national standards and
guidelines for IEC materials; • Update and adapt IEC messages to target the
major drivers of the epidemic and MARPs; and • Scale up targeted messages through researching,
producing, translating and disseminating information through print, radio and TV media.
MICT General population
1.2: Prevention: Behaviour Change Communication – Community Outreach and Schools
Indicators: # of people reached by HIV/AIDS awareness outreach services
1.2.1 Strengthen BCC interventions for MARPs, youth and communities.
The interventions for in-school youth as funded under Round 2 were adapted under the RCC applying lessons learned. The interventions for MARPs are new and a crucial component of the overall prevention strategy under development. Lessons learned from previous experiences will be brought to bear, such as integrating SRH, STI, gender in interventions as well as targeting BCC focusing on drivers, key affected populations, including new groups identified recently such as inmates of correctional services. Specific activities will include: • Expand support for youth programmes for out of
school youth, including outreach programmes on HIV, SRH and STI, plus related issues such as alcohol and gender concerns;
• Strengthen (mainstreaming) BCC interventions in primary and secondary schools;
• Target CSWs, prison inmates, MSM and mobile populations with BCC interventions;
• Target drivers of the epidemic and communities through the TCE programme and other proven interventions;
• Conduct a MTR of the national BCC programme; and
• Conduct a national impact evaluation study.
SMA, OYO, DAPP, NAPPA, MoE. MoSS, Rainbow
MARPS, Youth General Population
1.3: Prevention: Condoms
Indicator: # of condoms distributed through social marketing and free through the public sector 1.3.1 Increase uptake and correct use of condoms.
The RCC continues with an emphasis on promoting consistent use of condoms, procurement of male and female condoms, and expansion of outlets. Activities will include: • Conduct operational research on condom use,
including a national survey of the existing programme;
• Procurement and packaging of condoms for free distribution;
• Public distribution of condoms including though logistics officers and community volunteers; and
• Support condom social marketing.
Commodity Exchange, Nasoma, MoHSS-condoms
Population of Reproductive age
1.4: Prevention : Testing and Counselling
Indicator: # of people counselled and tested for HIV who received their results
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 65/160
1.4.1 Increase access to a comprehensive package of VCT services.
Activity 3 of R2 will continue, focusing on increasing geographical and target group coverage through mobile and outreach testing and community mobilisation in public and private sector. Increased support to the National testing day will be provided as the last two years the number of people counselled and tested showed the cost-effectiveness of this intervention. Findings from studies on male involvement will be used to develop services targeting men at community level and in workplaces. The private sector has gained experience on male involvement through mobile outreach services and this will be used as a model for the public sector to scale up through development of public sector mobile clinics. Activities will include: • Increase uptake of VCT through mass media;
campaigns, and social mobilisation • Train lay counsellors and other community
caregivers on HIV testing and counselling ; • Procure rapid test kits, demonstration models and
consumables for VCT; and • Increase access to VCT through community
volunteer programme, mobile units and workplace VCT programmes.
MoHSS – VCT, NABCOA
General Population
1.5: Prevention: PMTCT
Indicator: # of pregnant women receiving complete course of ARV prophylaxis
1.5.1 Increase access to comprehensive PMTCT services, including SRH
The RCC will continue with the Round 2 interventions but the focus is on integrating SRH services and integration with community services, as well as scaling-up post-natal support for mother and baby. There is also a need to increase access to PMTCT services in the hard-to-reach areas and to link these with campaigns for people of reproductive age. Health facility data collection forms are presently easy to collect but, as the programmes scale-up outreach, community and home care services, a system for collecting post-delivery and infant feeding data is necessary. Activities will include the following: • Update and disseminate PMTCT policy and
guidelines, with particular emphasis on integrating SRH to the extent possible;
• Train and retrain various cadres of healthcare providers on PMTCT services including post-delivery services and SRH;
• Increase social mobilisation to improve uptake of PMTCT services in hard to reach areas;
• Support the delivery of integrated PMTCT and SRH services;
• Train support groups to encourage HIV-infected mothers on infant feeding issues and other concerns; and
• Undertake operational research on infant and young child feeding.
MoHSS - PMTCT
Pregnant women and their partners
1.6: Prevention: STI Diagnosis and Treatment
Indicator: # of clients with STIs at health care facilities who are appropriately diagnosed treated and counselled
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 66/160

1.6.1 Expand access to STI/SRH services to targeted groups
This SDA is new under the RCC but it is now recognised that addressing STIs is an essential component to expanding HIV prevention and achieving success. The RCC focuses on newly developed policy guidelines and strengthening diagnosis and treatment of STI by health care workers through mentoring and training, and increased monitoring and supervision. To date support (human and financial) to the national STI programmes has been limited and the failure to adequately diagnose and treat STIs has contributed to their increase and potential for exacerbating the spread of HIV. Activities will include: • Support the establishment of training and
mentoring programmes for service providers at PHC facilities, SRH and HIV clinics and within youth-friendly health care and social services;
• Develop and disseminate STI messages through IEC brochures and wall charts;
• Undertake operational research on the best mechanisms for reaching vulnerable target groups (youth, CSWs, MSM, prison inmates, mobile populations) with SRH/STI services;
• Strengthen quality of SRH/STI services.
MoHSS-STI Population of Reproductive age
Objective 2. To reduce morbidity and mortality through universal access to comprehensive HIV/TB/STI treatment, care and support services 2.1: Treatment: ART
Indicator: # of adults and children with advanced HIV infection receiving ART 2.1.1 Contribute to universal coverage of adults and children in need of ART
This activity continues to be scaled up through decentralising the ART provision to health centres and bigger clinics, and outreach. The Government contribution is more than 50% and will slightly increase as the contributions from GF and PEPFAR scale down. In terms of lab test, the GF will cover the national cost of HIV Elisa tests only. PEPFAR contributes substantially to bio-clinical test and PCR but decreases over time, which teh GRN will take up again. There is an urgent need to enhance the capacity of all cadres of health care providers in various sectors (NGO, CBO, FBO, etc.) at the district level to deliver quality services. The monitoring system for the present ARV services needs to be improved in order to be better able to measure adherence through quality assurance. Activities will include: • Support training and retraining on ART
management for various cadres of healthcare providers;
• Update and disseminate IEC materials on ART; • Procure drugs for adults and children on ART; • Procure and perform bio-clinical tests for people on
ART; and • Provide quality assurance at all ART sites.
MoHSS Case Management
Adults and children in need of treatment
2.2: Care and Support: Care and Support for Chronically Ill People
Indicators: 1. # of chronically ill persons receiving home-based care 2. # of PLHIV receiving care and support, including ongoing psycho-social support
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 67/160

2.2.1 Strengthen the continuum of care and support through community-based responses
As a result of the ART Roll-out, the number of bedridden patients has decreased substantially and therefore CHBC has shifted towards support for treatment adherence, psycho-social support and prevention (including SRH and TB). The strengthening of referrals services between health facilities and community services is a focus area under the RCC. The Tusano project under Round 2 showed excellent results in linking PLHIV support groups to existing CHBC or other organisations and this can be enhanced for further roll out. There is a need to start training all CHBC providers in the national standardised training curriculum to improve the quality of services. Improved reporting, supervising and coordinating with other community services is envisaged. The National standards for CHBC were recently developed and will be printed with support of the RCC. Standardisation of training for PLHIV support groups is also needed. There is a need to ensure that labour laws and volunteer policy regarding the remuneration of CHBC providers are implemented and enforced. CHBC kits, however substantially reduced, must meet national standards and refills must be available at health care facilities. Finally, all service delivery sites coordinated by various partners should use standardised surveillance and monitoring tools. The Mapping will enhance improved geographical coverage. Activities will include: • Review, update and disseminate national policy
and standards for CHBC; • Train trainers, volunteers and supervisors on
national CHBC curriculum, including adherence support;
• Training PLHIV support groups on standardised counselling and IGAs;
• Deliver CHBC services, including prevention, treatment and care and support; and
• Improve treatment adherence to ART using patient advocates linked to PHC facilities.
MoHSS –HBC; Catholic AIDS Action, CCN, AIDS Care Trust, Namibian Red Cross Society, SMA/Tusano project, Positive Vibes, Lironga Eparu
PLHIV
2.2.2 Provide package of support for PLHIV who are most in need
Interventions under R2 will be scaled up; incorporating IGAs as vegetable gardens to foster sustainability. Training of lay-counsellors will be supported through an NGO specialised in accredited counselling training. Increased geographical coverage is foreseen through a additional network of PLHIV. Activities will include; • Provide nutritional support to PLHIV who are ill or
malnourished; • Conduct training for PLHIV, including on managing
support groups and positive living; • Provide social support services to PLHIV, including
support groups, counselling, IGAs, and material assistance; and
• Provide psychosocial support to volunteers and other carers.
Lironga Eparu, Positive Vibes, SMA/Tusano
PLHIV
2.3: Collaborative Activities: TB/HIV.
Indicator: # of eligible PLHIVs provided with IPT
2.3.1 Strengthen the diagnosis and treatment of TB and HIV co-infection
Activity 5 of R2 has been expanded to include links with TB. Activities will include: • Strengthen TB/HIV collaborative interventions with
a focus on community level services
MoHSS Case Management
HIV/TB co-infected adults and children
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 68/160
Objective 3: Reduce the impact of HIV/TB/STIs on infected and affected individuals, families and communities. 3.1: Care and Support: Support for OVC
Indicator: # of OVC whose households received at least one type of free basic external support in caring for the child 3.1.1 Expand quality and coverage of services for OVC
Activity 8 of R2 is continued under this intervention. The Programme will be adapted to increase CBO service delivery to OVC according to the minimum package of services as per national OVC plan and to improve coverage in priority areas. Many organisations provide help to OVC but only a few provide comprehensive support. Monitoring the present programmes needs to done systematic and standardised training to community volunteers will enhance quality services. Proposed activities include: • Undertake regional mapping exercise on existing
OVC services; • Train care givers and social workers supporting
OVC on psychosocial support; • Based on regional OVC business plans, provide a
comprehensive package of support services to OVC, including psychosocial, nutritional, educational and material support;
• Implement IGA for OVC households; and • National, regional, and local coordination of OVC
programme
MGCEW, CAA, NRCS, ACT, CCN
OVC
Objective 4. Strengthen the leadership and governance required for the scale up of the national HIV and AIDS response 4.1: Supportive Environment: Policy Development, Including Workplace Policy and Programmes
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 69/160

Indicators: 12. # of people reached through HIV/AIDS workplace programmes
4.1.1 Strengthen policy development and workplace programmes
Activity 7 of R2 will be continued. Currently the development of work place programmes are being supported by the private sector or large and small & medium sized companies and in the public sector at the level of local authorities. The components of work place programmes on peer education and BCC, as well as testing is being enhanced,. Activities will encompass: • Develop and disseminate policies related
to HIV and AIDS • Develop and disseminate IEC materials
for the workplace; • Train and support peer educators in the
workplace; • Support capacity within private sector
organisations to manage and implement workplace programmes;
• Support capacity within public sector organisations to manage and implement workplace programmes; and
•
NABCOA, AMICAALL
Employees and their families
4.2: Strengthen civil society and institutional capacity building Indicators: 1. # of CSOs providing public health services at community level that receive support for organisational and systems development 4.2.1 Strengthen CSOs to support the scale up the national HIV response
Although this was not specified as a planned core activity in R2, interventions under this SDA continue those started under R2 but integrated into other SDAs at that time. However, increased emphasis on Community Systems Strengthening for sustainability over the last five years means that such activities have to be visibly scaled up through a standalone SDA with measurable indicators. Activities will include the provision of training assistance to strengthen community organisations offering HIV and AIDS and TB care and support.
NANASO Civil society NGOs
4.3: Response Management & M&E Indicator: # of surveys completed 4.3.1 Strengthen the management and coordination of the national response
Not specified as a planned core activity in R2 but implied continuation. Introduction of a civil society PR for duel track financing necessitates capacity building • Strengthen capacity for the management
of the national programme • Support the operations of the civil society
PR; • Support the operations of the government; • and • Support the M&E function of the
government PR.
PRs (MoHSS, NANASO)
General Population
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 70/160

4.6.5 Incorporation of lessons learned into this proposal Describe below: (a) how this proposal addresses and resolves weaknesses or bottlenecks encountered during implementation of the
expiring grant (including through the selection of additional PR(s) from appropriate sectors); and
(b) how this proposal has taken into account weaknesses identified by the TRP in a recent review of a same disease proposal from the country.
Applicants are encouraged to comment on any significant levels of undisbursed funds under earlier Global Fund grants (including 'Phase 2' amounts anticipated to become available).
(a) Lessons Learned: Addressing and Resolving Weaknesses and Bottlenecks from the Implementation of Round 2 Activities
Prevention
4.6.5.1 Life skills education programme (LSEP) in-school: The MTP III Mid-term Review (2007) revealed that the impact of the MOE’s LSEP was limited because it was not integrated into the curriculum and therefore not attended by all students. The PMU also conducted an assessment of the MOE’s LSEP and concluded that: (i) teachers do not teach the programme because they have already heavy workloads and the LSEP is not an examinable subject; (ii) there are no supervision mechanisms in place to ensure that teachers actually do teach the programme; and (iii) integrating SRH will be critical to reduce the number of adolescent pregnancies as well as HIV infections.
4.6.5.2 Under the RCC, therefore:
• There will be Full integration of the LSEP into the school curriculum through a three-pronged approach:
(i) sensitisation and training of teachers; (ii) matching community counsellors and peer educators with schools (so that these trained staff can provided support to the LSEP through coming into schools and assisting in, or delivering, the LSEP); and (iii) developing indicators to assess the performance of teachers with regard to teaching the LSEP.
4.6.5.3 Out-of-school youth: According to the 2006/2007 DHS, in the 12 months preceding the survey 65.6 percent of young men and 74 percent of young women aged 15 –19 years were unemployed. Out-of-school youth therefore cannot be neglected. School drop-outs and those that fail Grade 10 are of special concern and need special attention. From past programme experience we have learned that this age group is very difficult to reach. This therefore emphasises the importance of providing LSE, grants for vocational training, and IGA training to prevent the marginalisation of out-of-school youth. Football clubs and other social centres, where these young people are likely to congregate, have already proved to be effective vehicles for getting information across, especially if such information is provided by their peers. Such information must also include information on alcohol use and the role it plays in increasing vulnerability. Condom promotion and distribution must also be provided, together with information on where and how to access services.
4.6.5.4 BCC: While the interventions under Round 2 have had an impact on the level of knowledge (over 80
percent for the age group 15–19 years, according to the DHS 2006/2007), this has not translated into sufficient behaviour change for the same age group (only an insignificant decrease in prevalence rates of 2 percent according to 2007 sero-surveillance). This means, therefore, that the country needs to improve its BCC strategy which would include:
a) Designing appropriate messages and targeting the information: Evaluations of mass media
campaigns and information shared at Take Control review meetings have suggested that messages must be better linked to the key drivers of the epidemic. Messages in earlier years targeted the general population and assumed that the audience was homogenous; yet BCC needs to be age- and region-specific and targeted to appropriate audiences. Youth aged 10-14 need to be targeted with messages to delay age at first intercourse, and abstinence, while young people aged 15-24 should be targeted with messages on reducing partners, using condoms, and family planning. Multiple campaigns have been implemented simultaneously but the messages were often not harmonised; in general this strategy was not cost-effective. In this proposal, the activities include strategies to align communication efforts through the Take Control mechanisms. For both the strategies on key affected populations and
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 71/160
through the Take Control mechanism, coordination is scheduled to align messages of communication material and campaigns from the interpersonal level up to mass media level to increase exposure to consistent messaging and thus reach the drivers of the epidemic.
b) Addressing MARPs: The MTP III Mid-term Review also indicated the urgent need to address sex
workers and MSM with appropriate interventions, a finding substantiated by the research on the drivers of the epidemic in late 2008. The MTPIV Status Report also highlights the importance of reaching vulnerable prison inmates. However, only a few small-scale initiatives by CSOs are currently targeting key affected populations; and these efforts, which are mainly in Windhoek, have thus far not yielded the desired results. A recent small-scale survey suggests that HIV prevalence is very high among sex workers and yet there are no significant and efficient interventions targeting this vulnerable group. As a result of illegality and stigma and discrimination, these populations have difficulties in accessing services. Therefore, this proposal includes interventions to support and strengthen the work of current NGOs and FBOs (such as Social Marketing Association and the Rainbow Project for MSM) working with these populations to collect more quantitative and qualitative information to assess the size and behaviours of these groups and to create outreach services to meet their needs.
4.6.5.5 The integration of SRH with HIV is paramount as women who are living with HIV need to be able to
make informed choices about their fertility. Women often state that their partners do not want to use condoms, which in their case would be for dual protection. Yet full integration of SRH into HIV goes far beyond RH and PMTCT. Collaboration between the PHC Division, where SRH services are traditionally offered, and the DSP, the main custodian of HIV and AIDS, must be scaled up. In recognition of the need to integrate SRH into HIV programmes a draft consolidated national reproductive and child health policy has been developed and is pending approval.
4.6.5.6 In Namibia PMTCT is already provided at ANC and maternity care services. Although the prescribed package of services for PMTCT includes elements of SRH screening, prevention and treatment of STIs, counselling and support on infant feeding and family planning, the emphasis is more on counselling and testing for HIV and the provision of single dose Nevarapine to those who are HIV positive as well as their new born babies. According to the Ministerial Circular dated 8 June 2009, emergency contraception has been declared safe and should be made available to all women, including those living with HIV and AIDS. Also, regardless of the chosen method, condom use should be an integral part of contraceptive counselling for all clients as this is the only method that prevents STIs/HIV transmission between partners. This is of particular importance for women and adolescents who are HIV positive.
4.6.5.7 A challenge, however, is the limited availability of funds for SRH compared with HIV and AIDS; yet the two are inextricably linked. Under this RCC proposal, SRH will, when and where possible, be integrated with all training, informational material development and counselling.
4.6.5.8 Condoms: Programme data and supervisory visits reveal that condom availability (including the female condom) needs to be scaled up across the country. Programme reports from rural areas suggest that condoms are still difficult to access in some rural areas.. The programme data also showed that the unit cost of the socially marketed condom was higher than the free of charge, widely accepted and popular ‘Smile’ condom. Therefore the socially marketed condoms will be phased out but the logistical officers responsible for condom distribution will be maintained. Targeted messages promoting condom use, including dual use for dual protection, will be developed for the various vulnerable target groups through the Take Control initiative. For hard-to-reach areas, condoms will be made available at non-traditional outlets such as kuka shops (shebeens).
4.6.5.9 WPP: It is crucial to prevention efforts to reach as many employees as possible through peer education and condom promotion and distribution at the workplace. Through the roll-out of WPP, both NABCOA and the OPM have learned that WPPs need to be kept as simple as possible. The interventions described in 4.6.4 are focused on external BCC technical support to standardise and scale up peer education. Skilled educators are needed to be able to get across sensitive messages on the main drivers of the epidemic (alcohol use, MCP, inconsistent condom use/unprotected sex, transactional and inter-generational sex, lack of knowledge of status/HIV testing and other SRH issues), and in particular leaders and managers need to be reached if political commitment and capacity for WPP is to be scaled up and referral to VCT established.. The skilled educators should also set up referral systems to company clinics for other services, where these exist, and to public sector services.
4.6.5.10 VCT: Namibia organised its first national testing day in May 2008. While the turnout was overwhelming, it
also raised concerns about the accessibility of VCT services. The differential between male and female testing behaviour shows the importance of targeting men with these services, and this will be addressed in the expanded scope of the RCC proposal. Scaling up rapid testing and assuring the quality of counselling
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 72/160

by community counsellors is increasingly needed, while the missing link with SRH needs to be addressed, such as the referral of HIV positive women to ANC and RH services. The MoHSS approved mobile testing through the Guidelines for Outreach Counselling and Testing (CT), launched in 2008. The first initiative under these Guidelines was put in place by the private sector with GF resources. This initiative is already showing good results in the increased uptake of VCT. The country would like to build on this initiative by extending mobile testing to the public sector, where the major challenges have been the distance from health facilities and issues of accessibility, particularly by men. Accordingly, under the RCC the Global Fund is requested to co-finance the expansion of mobile testing. The proposal also includes the recruitment of social mobilisers for the communities, a large part of their tasks being to mobilise men.
Treatment
4.6.5.11 ART: Although Namibia has done very well in improving the uptake of ART in general, scaling up of these services at the clinic level is needed in order to sustain the Government’s universal access targets. This proposal has interventions related to scaling up biomedical tests, procurement of first-line ARVs, and staff retention at the national coordination and health services delivery levels to ensure continuation and scale up of services. A recent Local Fund Agent (LFA) study undertaken in Okahandja indicated a non-adherence rate of 20 percent; hence efforts with regard to adherence need to be reinforced by reinforcing strong linkages with CHBC workers at the community level.
4.6.5.12 Nutrition: Lack of adherence to treatment has been attributed in part to poor nutrition (food has been identified as a commonly cited reason for not taking medication). This RCC proposal includes interventions for vitamin-enriched dry food assistance for the poorest segment of clients on ART. In addition, and for reasons of sustainability, the establishment of kitchen gardens will also be encouraged for civil society groups. In the long term, however, the country will have to look at the broader issue of food security.
Care and Support
4.6.5.13 OVC: The MGECW recognises that it requires capacities to fulfil its social welfare functions for the burgeoning number of OVC. As a result a human resource and capacity gap analysis was undertaken in 2007, which identified gaps requiring scaled-up service delivery. One of the gaps included the need for a comprehensive human resource development strategy, and scholarships for social workers. These activities are currently underway in 2009, with an HR analysis being conducted, and scholarships being provided for a limited number of social worker students. The role of civil society in assisting with implementing complementary services is crucial. Through the involvement of civil society in the preparation of this proposal, it was learned that there is a significant variance in the quality of service packages provided to OVC and that there is insufficient coordination between CSOs and the public sector at the community level. The interventions in this proposal focus on standardising quality of services and on recruiting and training more social workers, while ensuring that national, regional and constituency level coordination take place through Government systems.
4.6.5.14 CHBC: With the rapid uptake of ART, the role of CHBC has changed over the course of the years as many of those on ART are healthier and do not need the level of care previously required. This has led the MoHSS, through the Directorate of Primary Health, to formulate the National Policy on Community Based Care (2008), which was recently strengthened by the National Community Home–based Care Standards in 2009. The goal of these standards is to provide a benchmark for the provision of quality CHBC for the chronically and terminally ill, including at risk groups and other vulnerable persons in the home community. Many services are provided by a large number of CSOs in order to improve the capacity of households to manage chronic and terminal illnesses and to be more self-sustaining. However, these services are not delivered in a coordinated and structured manner, nor are they comprehensive in a way that addresses the holistic needs of the client and family. During the discussions with CHBC providers to develop the CHBC policy, a number of key issues were raised, such as the standardisation and quality of services and the need for a career path, to improve the retention of CHBC providers. A training curriculum has been developed and this proposal includes provision of training for CHBC providers on the new standards of service and for career development.
4.6.5.15 PLWHA support groups need institutional and technical support to deliver the appropriate counselling services. Although the number of support groups is increasing, there is insufficient geographical and target group coverage (e.g. related to key affected populations, and women to women, men to men support groups) and there is no one umbrella organisation that is universally accepted and which can organise these support groups in terms of the local response. This means that PLWHA support groups function in a fragmented manner and so do not maximise their joint strengths. This proposal includes interventions that will strengthen their capacity at the institutional level and also strengthen the capacity of
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 73/160

members. Staff capacity will be strengthened through the recruitment of additional staff as well as training of some of the existing staff. The training will be critical, particularly in the light of the newly adopted CHBC policy and standards which apply to critical services such as treatment adherence and psychosocial support, roles that PLWHA must take on board if they are to be at the centre of the national response. These PLWHA will also need to be at the heart of discussions on SRH for HIV positive individuals. In order to reduce stigma and discrimination, it will be important to increase the number of PLWHA and sexual minorities working as health professionals. The selection of the second PR from civil society is intended to stimulate CSOs to play an important role in delivering these activities. It is hoped that CSO PR will ensure that collaboration and coordination between different PLWHA organisations will also be strengthened for maximum impact.
Human Resources
4.6.5.16 Experience in rolling out expanded services and regular site visits has shown that scaling up quality services cannot happen without addressing the shortage of human resources and the limited budget and capacity to renovate infrastructures. Therefore, the recruitment of additional staff as a short-term strategy and training through more scholarships for a greater number of health professions as a long-term strategy is included in this proposal within the cross-cutting HSS component. In terms of renovation, some resources will be built into this proposal for conducting minor renovations but also to contribute to the GRN’s planned capital expenditure.
Renovations
4.6.5.17 The GRN and donor funds have renovated a number of facilities and this has tremendously helped to improve the uptake of various HIV and AIDS services. However, physical infrastructure still remains inadequate to meet the required service delivery needs and the existing infrastructure is inequitably distributed. Those who are most affected are those in the lowest socioeconomic quintiles. Moreover, the existing infrastructure is unable to cope with the scale and volume of services that stem from an increased case load as a result of HIV and AIDS/TB co-infection. The lack of space is not only detrimental for efficient laboratory diagnosis, infection control and storage of supplies but also means that clients do not have the privacy needed for HIV and AIDS consultations. Under this RCC additional facilities will be renovated alongside construction of new facilities by GRN under its capital projects plan.
Integration of Activities
4.6.5.18 Lastly, the main lessons learned related to training and BCC were that a more integrated approach is needed, including attention to gender issues, SRH and improvement in the necessary referrals between various services. The initial decision to train all health staff resulted in a high annual absence of health care workers from their duties due to the high number of training courses being conducted. Therefore, training needs to be rationalised, regionalised and integrated where feasible. The provision of information and education, especially through campaigns, needs to become more integrated and standard messages need to address the key drivers of the epidemic based on the research from 2008. Furthermore, at the community level, staff needs to provide more comprehensive behaviour change messages, and not only relating to one SDA area (such as condom promotion or PMTCT) alone. This implies considerably more work with staff on how to get across messages concerning behaviour change in more intimate areas of people’s lives. Through this process we have learned to integrate more effectively medical training and to coordinate the production and distribution of BCC material.
(b) Weaknesses Identified by TRP Comments on Previous Rounds
4.6.5.19 Unfortunately, Namibia has failed to secure a Global Grant in the three previous Rounds for which it has applied (Rounds 5, 6 and 8). An analysis was undertaken of TRP comments for Rounds 5, 6 and 8, and WHO Peer Review comments for Round 8; (attached as Annex J 40).
4.6.5.20 The concerns of the TRP and Peer Review have been addressed in the current RCC proposal as follows
(c.f. Tables 6, 7 and 8 below): Table 6: Actions taken to Address TRP Comments on Round 5 HIV Proposal
Weaknesses identified by TRP Remedial Actions
• The financial gap analysis is based on an administration and overhead charge of 20 percent. We believe that this percentage is excessive. There
• Since the submission of the Round 5 proposal, the country through the current PR has undertaken a costing study of the various HIV intervention areas
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 74/160

was no gap between the original cost needs and available resources.
and a funding database has been established. These have facilitated improved planning and proposal development.
• The above gap analysis needs were increased by 25 percent across the board without detailed explanation based on the comments from the IMF. This is excessive and inappropriate.
• Please see the comment above.
• Additionality of further GFATM funds to existing funds already in country is not clearly demonstrated.
• Since the submission of Round 5, the country conducted joint reviews of HIV interventions as well as planning during proposal development. For example, under the failed Round 8, the other key funder, PEPFAR, extensively participated in the stakeholder consultations including facilitating some of the technical working groups and working on different thematic areas. In the same vein, all HIV stakeholders have been participating in PEPFAR’s annual Country Operational Planning sessions since 2007. All of the above has been put in place to enable the country to maximise the use of available resources.
• Capacity to absorb new funds in the light of all the substantial other funds that are going into the country has not been clearly demonstrated.
• Although the CCM resubmitted the failed Round 5 under Round 6, it desisted from submitting a proposal under Round 7 in order for the country to monitor the absorptive capacity of the implementers under Round 2. The CCM has been doing this through monitoring on a quarterly basis by assessing the SRs’ presentation of quarterly reports and examining the expenditure patterns against the burn rate percentage set for any specific quarter. Where an SR is not performing both programmatically and financially, a recommendation is made to reallocate funds to an SR that is performing well under the similar thematic area. Since 2007, the absorptive capacity of the Round 2 implementers has significantly improved and the programme performance is almost in tandem with financial performance.
• Further involvement of civil society in the implementation would strengthen a subsequent proposal.
• As described under Section 2 of the Wave 7 HIV RCC proposal, NANASO was selected as a second PR in 2008. NANASO is the umbrella organisation for the AIDS CSOs in Namibia. It is to be noted that NANASO is currently an SR under Round 2 HIV grant. With its selection as PR, it is anticipated that the role of the CSOs at every level, particularly at the grass roots level, will be enhanced to allow for their increased involvement in the national response.
Table 7: Actions taken to Address TRP Comments on Round 6 HIV Proposal
Weaknesses identified by TRP Remedial Actions
• Despite a prior TRP request, there is no gap analysis that takes into account the major increase in funding from PEPFAR for 2007 (US $50 million 2006 to US$70 million). Nor does the proposal take into account specific activities that will increase due to funding available from the Round 2 Grant. The absence of these analyses makes it very difficult for the TRP to evaluate the additionality of the services to be supported by the newly requested funds.
• Since 2007, the country has undertaken a costing study for key intervention areas as well as establishing a funding database. Both PEFAR and the GF PR attend all national programme reviews, national target setting exercises, programmatic and funding gap analysis (such as the one recently undertaken for MTP IV/NSF), planning for GF rounds-based proposals and PEPFAR’s annual Country Operational Plan. The PEPFAR Coordinator is also a member of the CCM. In this way the country ensures there is no duplication. For example, PEPFAR no longer undertakes renovations but GF resources are used for these; both PEPFAR
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 75/160
and GF contribute proportionately to the ART drugs but PEPFAR solely focuses on most of the diagnostics and lab requirements; and so on.
• Difficult to evaluate the strength of specific interventions as information on many activities only appear in the detailed budget, and not in the proposal narrative in sufficient detail.
• Since the submission of the Round 6 HIV proposal, there have been several evaluations of the various interventions. These include project level thematic evaluations such OVC, CHBC, WPPs within municipalities, impact of training assessment study; as well as a nationwide DHS. All these have informed the development of the RCC HIV proposal. In addition, several guidelines have been revised to make facility-based interventions more comprehensive, i.e. PMTCT (move from single dose Nevarapine to AZT + 3TC, follow up of positive mothers, etc.); VCT (to increase uptake through mobile units); ART (move from D40 to AZT) and adoption of WHO policy of task shifting to make ART more accessible); study on male circumcision; and development of a prevention strategy that clearly identifies the drivers of the epidemic.
• Considering the existence of the nursing school, the rationale behind seeking funds for external training of a cadre of new nurses is not provided.
• The GRN has increased the intake of students at the national nursing school. In the meantime, to fill vacancies, the GRN, using its own resources, has been recruiting nurses from other Sub–Saharan African countries. It is to be noted that those recruited had no jobs in their countries of origin.
4.6.5.21 With regard to the TRP comments on Round 8, the CCM wrote separately to the GF in Geneva on 10
November 2008, outlining their concerns regarding the comments which were felt to be inconsistent and inaccurate with regard to the information provided in the body of the proposal. The comments and the CCM’s response are detailed below in Table 8. No answer was received from the Global Fund.
Table 8: CCM Response to TRP Comments on Round 8 HIV Proposal
• The proposal lacks details on activities (who will conduct the activities, where and what exactly will be done).
Attachment D clearly lists the main activity, details the activity (Column J) and lists the implementer (Column L). In column K of the budget spreadsheet entitled “Responsible for Implementation”, the implementing agencies for every activity are specifically identified where known, or broadly identified where only the sector is currently known, (e.g. “NGOs to be identified”). In the current RCC proposal, the table completed in section 4.6.4 contains a broad description of the major activities to be undertaken under each SDA, their relevance with regard to Round 2 (continued, expanded or new), and lists the implementing partners/SRs. This table is drawn directly from the attached log frame and work plan. The latter contains sub-activity detail on content.
• No clear definition of some of the target population, e.g. reference to mobile populations without defining who they are
Section 3.1.2 of the Gap Analysis lists vulnerable populations as female and male CSWs; mobile and migrant workers; PLWHA; prison inmates and MSM. Sections 4.5.1, and 4.2.1 and 4.2.2 and Attachment A) also listed the priority target populations. The country conceded that mobile groups were not clearly defined and should have been clarified as including truck drivers and migrant workers as clients of sex workers. However, this was not seen as a substantial flaw in the proposal, since the activities and budget for this target population were a relatively small element. Care has been taken in this RCC proposal to ensure that all target groups are clearly defined, including mobile populations, in several sections as appropriate.
• There is lack of quantitative information on what The quantitative information was clearly contained in
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 76/160

would be achieved through potential Round 8 funding Attachment A, the Performance Framework, and Section 4.5.1 referred to the specific indicators.
• A large proportion of the budget is allocated to purchasing commodities such as cars, office furniture, and equipment at the expense of direct benefits to persons living with HIV or AIDS
The CCM felt that the TRP had failed to review in detail the attachments to the proposal, which contained the following information.
The total amount under “infrastructure” over five years was USD 13.0m (8%), and of this amount, USD 7.0m (4.3%), was for renovation of ART and VCT facilities, which clearly do provide a direct benefit to PLWHA. The remaining amount, USD 6.0m (3.7%), was largely for the aforementioned commodities; however, the CCM did not feel that 3.7% could be considered to constitute a “large proportion of the budget”.
Over Phase 1, the “non-renovation” proportion is 9.1% which, at a stretch, could be considered large, but certainly not unusual given that capital costs have to be incurred up front in any programme. The Round 8 proposal introduced a new civil society PR and a large number of new civil society NGOs focusing on PLWHA and key affected population/vulnerable groups, all of whom would have had to build up their infrastructure if they were to be able to deliver the services needed for PLWHA. It was also noted that the proposal did not include any pharmaceutical products, health products and only limited health equipment.
• A large number of new staff positions are being created to be funded by the Global Fund grant including general administration staff such as drivers. There is no mention how this expansion of personnel will be sustained
By sorting the HR lines in the budget into New and Existing positions, it could be seen that the total number of new positions amounted to 700, of which 300 are Health or Programme Management specialists and 400 are administrative positions, of which there are very few drivers. Of the 400 new administrative positions over 50 percent would have been employed by the new CSOs (key affected populations and PLWHA support groups), and the new Civil Society PR, and that a large proportion of the remainder were attributed to new or expanded public sector SRs and not with existing SRs. It was felt that the main focus of the proposal, to scale up prevention and the community response), required a significant number of human resources, especially within CSOs. As discussed in Sections 4.7.1 and 5.1.3 of the proposal, NGOs are currently heavily donor dependent, and rarely have material IGA to absorb personnel costs. As soon as activities begin to show a demonstrable impact (for example, a lowering of the prevalence rate), staffing and funding could be scaled down. The Round 8 proposal also noted that the MoHSS had committed to gradually absorb donor-funded staff, as had been indicated in the work plan and budget from Year Three onwards (see Section 4.7.1 on sustainability).
4.6.6 Risks arising from disease specific responses to health systems weaknesses and gaps
If the activities described in s.4.6.4 include responses to health systems weaknesses and gaps through a disease-specific programme approach, describe how the programming for this support has sought to mitigate any risks or unintended consequences of that support (compared responses that are undertaken on a cross-disease basis).
N/A.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 77/160

Programme Linkages
4.6.7 Links to Other Grants or Programmes
(a) Describe:
• any programme or operational links between the focus of this proposal and the activities or interventions supported through: (i) an existing Global Fund grant (including new proposals recently approved) or (ii)
• Whether this proposal is asking for support for the same programme areas or interventions as another existing same disease Global Fund grant, and if so, why this is not a request for duplicative funding.
4.6.7.1 For this proposal, the programmatic and financial gap analysis took into account
contributions from the successful Round 2 of the Global Fund. An analysis was undertaken of the usage of disbursed funds, issues surrounding implementation and the achievements made to date.
4.6.7.2 Namibia was granted USD 17,204,526 (Phase 1: USD 5,264,225; and Phase II: USD
11,940,301) for TB from the Global Fund in Round 5. Links with TB Round 5 have been taken into account in the SDA covering HIV/TB collaborative activities. Funding for the TB component is included in this RCC proposal under a separate disease component section.
4.6.7.3 Due to the high burden of TB in Namibia and the ensuing HIV/TB co-infection, the integration
of the two disease areas currently undertaken under the Round 5 TB grant include, as an entry point: case finding in PLWHA, HTC for TB patients, TB patients receiving cotrimoxazole prevention therapy (CPT) and HIV positive TB patients who started on and continued on ART during or at the end of TB treatment. In this proposal the entry point will be isoniazid preventive therapy (IPT), so there will be provision of IPT to PLWHA with TB under this RCC proposal. Integration will be strengthened and maintained through a Committee established by the stakeholders of the two diseases.
4.6.7.4 HIV and AIDS Round 2 will come to an end in December 2009. There is no other Global
Fund support for HIV and AIDS in Namibia. Hence this proposal does not seek to support parallel activities funded by another Global Fund grant; rather, it will continue and intensify successful activities under Round 2.
Other Partner Contributions 4.6.7.5 In addition, this RCC proposal supports and complements interventions supported by other
donors as follows: • Community Home-based Care: According to the Status Report on the National HIV and
AIDS Response, funding levels from other programmes in 2007/8 will remain constant for the fiscal year 2009/10 at 74 percent. Other partners in CHBC are: USG/PEPFAR, multilateral partners and GRN. GRN supports the community health care unit. PEPFAR supports the standardization of services through the new guidelines and development of training manuals and career development. PEPFAR also supports civil society in the provision of C&HBC services complementary to GF support. GF support is sought to continue TA in MOHSS, enhance coordination and technical support among CSO, food assistance to PLWHA and lactating HIV positive women and newly weaned babies, procurement of HBC kits, supporting remunerations for community HBC providers and rolling out of standardized basic package of services training.
• OVCs: Other Partners: USG/PEPFAR, multilaterals and GRN. GRN is financing the entire OVC grants programme and provides staff at national and regional levels. The Government is also the major financier of the school feeding programme. PEPFAR is supporting the standardization of quality services, monitoring and evaluation systems, OVC database, direct service delivery of material and psychosocial support, IGAs for OVC and TA to MGECW for
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 78/160

systems strengthening. GF support is requested to support additional Social Workers for Social grants, operationalise standards of services for care providers, and strengthen civil society and public sector service delivery.
• Condoms: GRN and GF resources finance the condom programme at 90%. There is a limited contribution of 10% from PEPFAR and UNFPA.
• PMTCT: Combined current level of support of 48% by PEPFAR/CDC and UNICEF is expected to remain constant in the coming years. GF Resources are required for follow up of positive mothers, technical support (continued from round 2) and for the production of informational and behaviour change materials.
• STI: GRN is currently contributing substantially. GF resources are requested for the strengthening diagnosis and adequate treatment of STIs as a matter of urgency. The RCC also proposes to update the STI guidelines, for mentoring and training health care workers, producing wall charts (job aides) and strengthening M&E. Research will be conducted on factors affecting partner notification as this is one of the major barriers to STI treatment success. Following this study, partner notification will be strengthened to ensure treatment success rates. Condom distribution will target those presenting with STIs as well. Information and education will be tailored towards promoting positive health seeking behaviour in relation to STI. An etiological study will conducted to inform treatment protocols. WHO will provide Technical Assistance.
• VCT: Current level of Support through PEPFAR /CDC is expected to remain constant at 55%
covering technical support, guidelines development and provision of testing kits and procurement of some mobile units. GF resources are needed to continue the support to the technical assistance in the national coordination unit, strengthen M&E, and co-finance the roll-out of mobile testing and community mobilization and creation of linkages with civil society organisations.
• ART: GRN provides a substantial portion of HR and hospital services and will continue to contribute to medicines and laboratories supply. PEPFAR/CDC is expected to support medicine procurement and currently supports bio-clinical monitoring tests, laboratory TA, and retention of current medical health personnel. In this proposal GF is expected to procure 50% of paediatric first line drugs and 45%of adult first line drugs. In addition it is important to note that the government contribution to ART drugs will be increasing from 47% (2010) to 59% (2015) over the RCC time frame. The GF resources will also cover retention of current medical staff and the recruitment of additional staff, with support to these staff progressively reverting to the GRN (please refer to the HSS budget); The RCC also provides for procurement of equipment. Ref: Status Report National HIV/AIDS Response.
• Prevention: Mass Media: GRN contributes to staffing, infrastructure and logistics at national and regional levels. PEPFARCDC/USAID and UNICEF will continue to support ‘Take Control campaign’, development and production of the HIV and AIDS mass media campaign for the general public. GF resources are requested for mass media to support the drivers of the epidemic, curriculum development for in school life skills.
• Prevention: Community Outreach: PEPFAR and UNICEF will contribute about 10% to this SDA. Funding from GF is needed to institutionally strengthen the three public sector ministries and civil society to deliver youth targeted campaigns and peer education for out of school youth.
• Workplace programmes: GRN is increasingly contributing full-time staff to workplace programmes and allocating budget. PEPFAR/DOD supports the Ministry of Defence, police force, Ministry of Education, Office of the Prime Minister and to a very small extent NABOCOA. GTZ/DED supports the Ministry of Transport, five other ministries and NABCOA. UNDP supports the OPM with impact studies and provides small scale support for high level meetings. GF resources are required to provide additional support to OPM for scaling –up
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 79/160

peer education, TA on BCC, and to scale up workplace activities, including mobile VCT units.
4.7 Enhancing In-country Capacity and Equality
4.7.1. Partnerships with the private sector to support increased coverage and services
a) The private sector may be co-investing in the activities in this proposal, or participating in a way that contributes to outcomes (even if not a specific activity). If so, summarize the main contribution anticipated over the proposal term, and how these contributions are important to achievement of the planned outcomes and outputs.
(Refer to the Guidelines for Proposals for a definition of Private Sector and some examples of the types of financial and non-financial contributions from the Private Sector in the framework of a co-investment partnership).
4.7.1.1 In 2003, the Namibian Business Coalition on AIDS (NABCOA) was set up through a collaboration
between the Namibian Chamber of Commerce and Industry (NCCI) and UNAIDS. Its purpose is to mobilise the private sector response in line with the priorities set out in the national strategic framework.
4.7.1.2 With regard to developing, implementing and monitoring specific partnerships with the private sector in
Namibia, NABCOA collaborates with various development partners and business entities. These typically include:
a) DED, primarily through capacity building and technical assistance through the various private sector stakeholders and the relevant Ministries;
b) Namibian Employers Federation (NEF) and the Ministry of Labour, through the International Labour Organisation (ILO) approach to workplace programmes;
c) PharmAccess Namibia (an international development NGO working in affordable and accessible medical products and wellness screening at workplaces);
d) World Bank, through a public-private partnerships (PPP) initiative with institutional development funding to build capacity among the NPC, NABCOA and Lironga Eparu (PLWHA organisation);
e) AWISA (programme for HIV and AIDS interventions for small and medium-sized enterprises (SMEs);
f) UNAIDS through technical support and capacity building; and g) BizAids (implementation programme for HIV and AIDS interventions for the informal sector).
4.7.1.3 DED has a full-time private sector/WPP expert as well as a co-funding programme for PPP and
corporate social responsibility. NEF has recently added a full-time staff member solely dedicated to Occupational Health and Safety at the workplace. In cooperation with these two organisations, NABCOA is planning the following innovative approaches with the private sector (including both financial and non-financial contributions from businesses):
Public Private Partnerships
4.7.1.4 Employee Wellness Programmes. Employee wellness programmes take the concept of workplace programmes one step further. The latter focuses solely on HIV and AIDS; the former includes HIV and AIDS within a holistic approach to public health. This enables better integration of key issues such as reproductive health and STIs. This new approach to WPP is being gradually expanded throughout some of the bigger business in Namibia.
4.7.1.5 Combating HIV and AIDS in Supply Chains. This activity fosters collaboration between small scale and
large scale companies doing business together. Two major business groups in Windhoek assess HIV-related issues within suppliers and distributors in their supply chains, and put in place strategies to address these issues. For example, they might train company employees to become peer educators, share IEC/BCC materials, encourage VCT and treatment initiatives, and assist access to affordable medical aid products. Financial contributions from the companies include costs for promotional material, support to World AIDS Day, and family health days, including testing. Non-financial contributions include mentoring smaller companies’ HIV staff.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 80/160
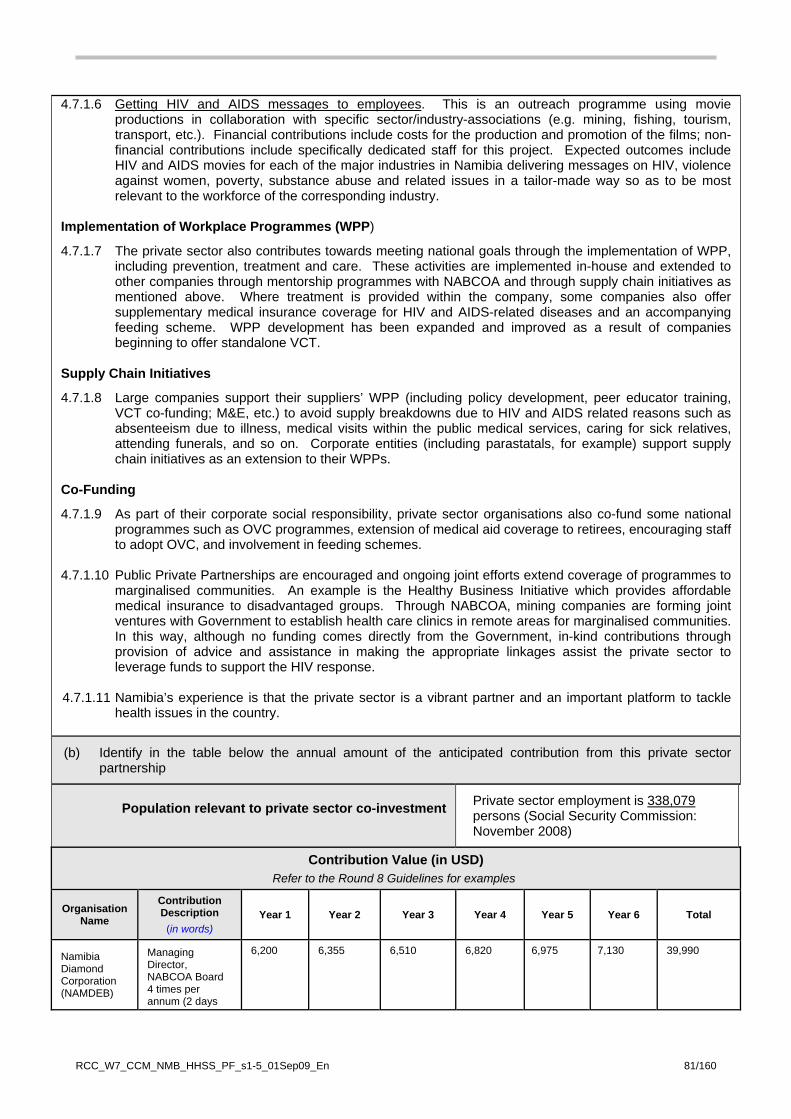
4.7.1.6 Getting HIV and AIDS messages to employees. This is an outreach programme using movie productions in collaboration with specific sector/industry-associations (e.g. mining, fishing, tourism, transport, etc.). Financial contributions include costs for the production and promotion of the films; non-financial contributions include specifically dedicated staff for this project. Expected outcomes include HIV and AIDS movies for each of the major industries in Namibia delivering messages on HIV, violence against women, poverty, substance abuse and related issues in a tailor-made way so as to be most relevant to the workforce of the corresponding industry.
Implementation of Workplace Programmes (WPP)
4.7.1.7 The private sector also contributes towards meeting national goals through the implementation of WPP, including prevention, treatment and care. These activities are implemented in-house and extended to other companies through mentorship programmes with NABCOA and through supply chain initiatives as mentioned above. Where treatment is provided within the company, some companies also offer supplementary medical insurance coverage for HIV and AIDS-related diseases and an accompanying feeding scheme. WPP development has been expanded and improved as a result of companies beginning to offer standalone VCT.
Supply Chain Initiatives
4.7.1.8 Large companies support their suppliers’ WPP (including policy development, peer educator training, VCT co-funding; M&E, etc.) to avoid supply breakdowns due to HIV and AIDS related reasons such as absenteeism due to illness, medical visits within the public medical services, caring for sick relatives, attending funerals, and so on. Corporate entities (including parastatals, for example) support supply chain initiatives as an extension to their WPPs.
Co-Funding
4.7.1.9 As part of their corporate social responsibility, private sector organisations also co-fund some national programmes such as OVC programmes, extension of medical aid coverage to retirees, encouraging staff to adopt OVC, and involvement in feeding schemes.
4.7.1.10 Public Private Partnerships are encouraged and ongoing joint efforts extend coverage of programmes to
marginalised communities. An example is the Healthy Business Initiative which provides affordable medical insurance to disadvantaged groups. Through NABCOA, mining companies are forming joint ventures with Government to establish health care clinics in remote areas for marginalised communities. In this way, although no funding comes directly from the Government, in-kind contributions through provision of advice and assistance in making the appropriate linkages assist the private sector to leverage funds to support the HIV response.
4.7.1.11 Namibia’s experience is that the private sector is a vibrant partner and an important platform to tackle
health issues in the country.
(b) Identify in the table below the annual amount of the anticipated contribution from this private sector partnership
Population relevant to private sector co-investment
Private sector employment is 338,079 persons (Social Security Commission: November 2008)
Contribution Value (in USD) Refer to the Round 8 Guidelines for examples
Organisation Name
Contribution Description
(in words) Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Total
Namibia Diamond Corporation (NAMDEB)
Managing Director, NABCOA Board 4 times per annum (2 days
6,200
6,355
6,510
6,820
6,975
7,130
39,990
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 81/160
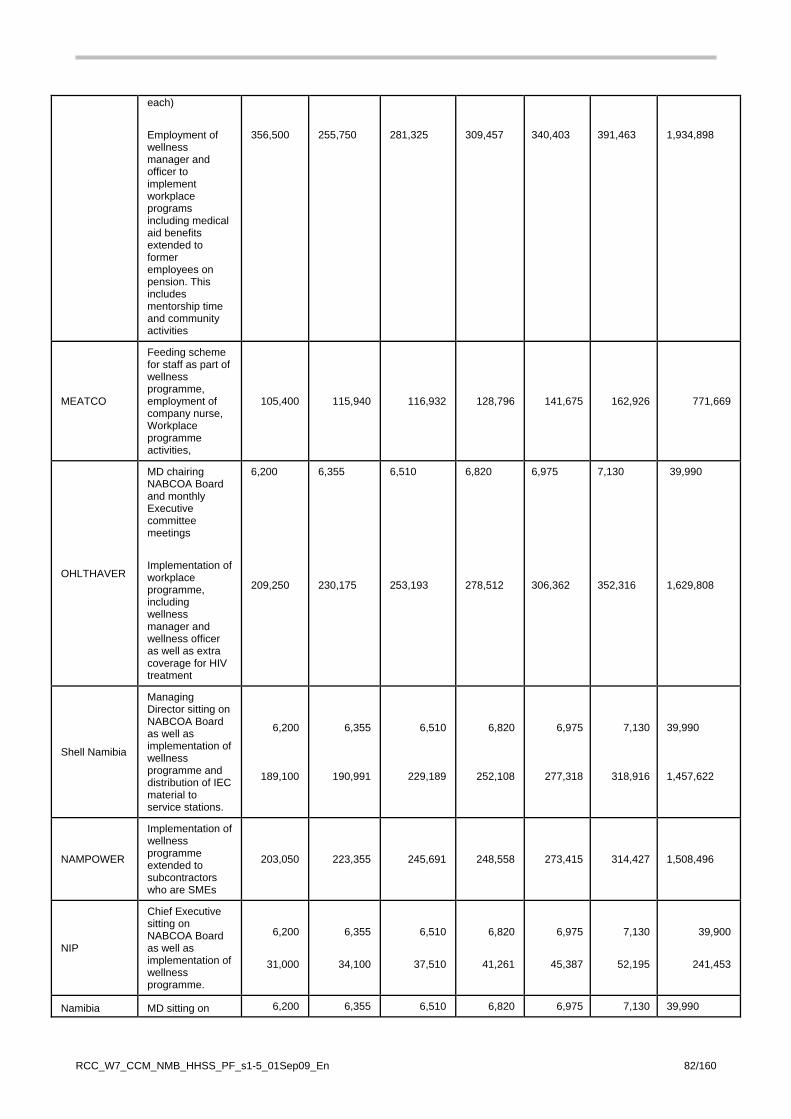
each) Employment of wellness manager and officer to implement workplace programs including medical aid benefits extended to former employees on pension. This includes mentorship time and community activities
356,500
255,750
281,325
309,457
340,403
391,463
1,934,898
MEATCO
Feeding scheme for staff as part of wellness programme, employment of company nurse, Workplace programme activities,
105,400 115,940 116,932 128,796 141,675 162,926 771,669
OHLTHAVER
MD chairing NABCOA Board and monthly Executive committee meetings Implementation of workplace programme, including wellness manager and wellness officer as well as extra coverage for HIV treatment
6,200 209,250
6,355 230,175
6,510 253,193
6,820 278,512
6,975 306,362
7,130 352,316
39,990 1,629,808
Shell Namibia
Managing Director sitting on NABCOA Board as well as implementation of wellness programme and distribution of IEC material to service stations.
6,200
189,100
6,355
190,991
6,510
229,189
6,820
252,108
6,975
277,318
7,130
318,916
39,990 1,457,622
NAMPOWER
Implementation of wellness programme extended to subcontractors who are SMEs
203,050 223,355 245,691 248,558 273,415 314,427 1,508,496
NIP
Chief Executive sitting on NABCOA Board as well as implementation of wellness programme.
6,200
31,000
6,355
34,100
6,510
37,510
6,820
41,261
6,975
45,387
7,130
52,195
39,900
241,453
Namibia MD sitting on 6,200 6,355 6,510 6,820 6,975 7,130 39,990
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 82/160

Beverages (Coca Cola)
NABCOA Board as well as implementation of wellness programme. And distribution of material to customers.
206,150
226,765
249,442
274,386
301,824
347,098
1,605,665
Additional 50 known companies who are members of NABCOA
Implementation of WPP. Treatment is mostly by way of medical aid with focal persons
193,750 213,125 234,438 257,881 283,669 326,219 1,509,081
TOTALS 1,525,200 1,521,976 1,680,270 1,825,058 2,004,928 2,301,210 10,858,642
4.7.2 Enhancing Social and Gender Equality
Gender equality
4.7.2.1 One of the key factors in the spread of the HIV epidemic in Namibia is the traditional norms that maintain women’s lower status in society. Differential power between men and women at household and community level influences access to information, services, goods and treatment, including HIV and AIDS, TB and malaria programmes. In Namibian society, as in many others, women are socialised into becoming mothers although, unusually, many women bear children outside marriage. Nonetheless, in spite of the fact that the median age for first sexual intercourse is relatively high for women at 19.3 years and 18.2 years for men (2006/07 NDHS, op. cit.), cultural and traditional norms still hold sway. Women are thus placed in positions where they are unable to negotiate safe sex.
4.7.2.2 A number of factors contribute to the high levels of HIV in Namibia - high levels of multiple and
concurrent partnerships with inconsistent condom use, inter-generational sex and transactional sex – and all these are significantly influenced by gender differentials (Macro International (2008), op. cit.).
4.7.2.3 Inter-generational sex exposes adolescents and young adults to partners who, by virtue of their
age, are more likely to be HIV positive. Among women aged 15 to 24, seven percent of single women and 26 percent of married women have a partner ten or more years older. Inter-generational sex in Namibia is associated with higher levels of STIs and with having multiple partners. These partnerships introduce the virus into the younger generation, where it quickly spreads as a result of rapid partner turnover (among men) and common concurrent partnerships.
4.7.2.4 It is likely that multiple and concurrent partnerships are contributing to the rapid spread of HIV
throughout the country. In 2006, 16 percent of sexually active men and three percent of sexually active women reported more than one partner over the previous 12 months. Having multiple partners is not common, nor apparently a major risk factor for HIV for the majority of women. However, the widespread practice, among men, of maintaining multiple relationships is contributing to the high levels of HIV infection among young women (2006/07 NDHS, op. cit.; VCT data). Concurrent partnerships, occurring within a month of each other, are particularly problematic due to elevated rates of transmission within the first weeks of infection. Several studies have recorded high levels of concurrent partnerships throughout Namibia, although nationally representative data are not available. Pervasive alcohol abuse and low levels of HIV risk perception serve to foster multiple and concurrent partnerships, and may discourage consistent condom use.
4.7.2.5 When these inter-generational and multiple or concurrent partnerships occur in a context, such as
Namibia, where condom use is inconsistent, male circumcision rare, STIs under-diagnosed and under-treated, and approximately 1 in 7 adults is already infected with HIV, the results are a devastating epidemic.
4.7.2.6 Transactional sex appears to be common, even expected in many sectors of Namibia, although
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 83/160
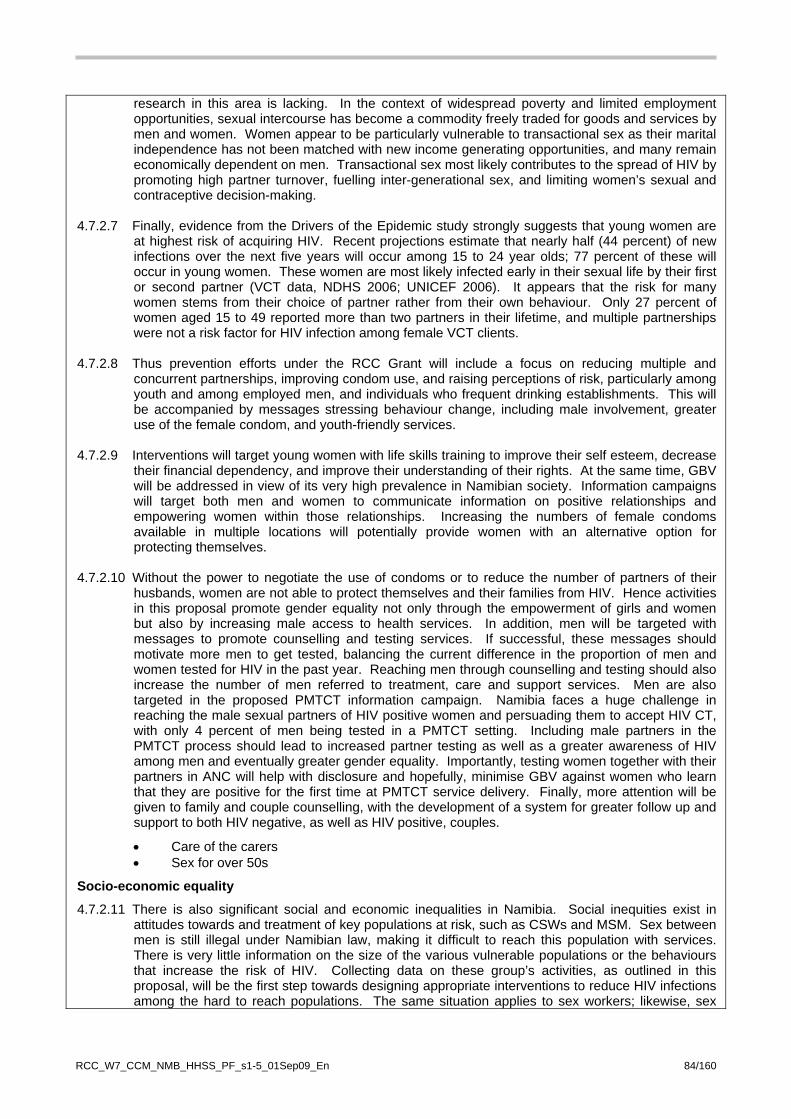
research in this area is lacking. In the context of widespread poverty and limited employment opportunities, sexual intercourse has become a commodity freely traded for goods and services by men and women. Women appear to be particularly vulnerable to transactional sex as their marital independence has not been matched with new income generating opportunities, and many remain economically dependent on men. Transactional sex most likely contributes to the spread of HIV by promoting high partner turnover, fuelling inter-generational sex, and limiting women’s sexual and contraceptive decision-making.
4.7.2.7 Finally, evidence from the Drivers of the Epidemic study strongly suggests that young women are
at highest risk of acquiring HIV. Recent projections estimate that nearly half (44 percent) of new infections over the next five years will occur among 15 to 24 year olds; 77 percent of these will occur in young women. These women are most likely infected early in their sexual life by their first or second partner (VCT data, NDHS 2006; UNICEF 2006). It appears that the risk for many women stems from their choice of partner rather from their own behaviour. Only 27 percent of women aged 15 to 49 reported more than two partners in their lifetime, and multiple partnerships were not a risk factor for HIV infection among female VCT clients.
4.7.2.8 Thus prevention efforts under the RCC Grant will include a focus on reducing multiple and
concurrent partnerships, improving condom use, and raising perceptions of risk, particularly among youth and among employed men, and individuals who frequent drinking establishments. This will be accompanied by messages stressing behaviour change, including male involvement, greater use of the female condom, and youth-friendly services.
4.7.2.9 Interventions will target young women with life skills training to improve their self esteem, decrease
their financial dependency, and improve their understanding of their rights. At the same time, GBV will be addressed in view of its very high prevalence in Namibian society. Information campaigns will target both men and women to communicate information on positive relationships and empowering women within those relationships. Increasing the numbers of female condoms available in multiple locations will potentially provide women with an alternative option for protecting themselves.
4.7.2.10 Without the power to negotiate the use of condoms or to reduce the number of partners of their
husbands, women are not able to protect themselves and their families from HIV. Hence activities in this proposal promote gender equality not only through the empowerment of girls and women but also by increasing male access to health services. In addition, men will be targeted with messages to promote counselling and testing services. If successful, these messages should motivate more men to get tested, balancing the current difference in the proportion of men and women tested for HIV in the past year. Reaching men through counselling and testing should also increase the number of men referred to treatment, care and support services. Men are also targeted in the proposed PMTCT information campaign. Namibia faces a huge challenge in reaching the male sexual partners of HIV positive women and persuading them to accept HIV CT, with only 4 percent of men being tested in a PMTCT setting. Including male partners in the PMTCT process should lead to increased partner testing as well as a greater awareness of HIV among men and eventually greater gender equality. Importantly, testing women together with their partners in ANC will help with disclosure and hopefully, minimise GBV against women who learn that they are positive for the first time at PMTCT service delivery. Finally, more attention will be given to family and couple counselling, with the development of a system for greater follow up and support to both HIV negative, as well as HIV positive, couples.
• Care of the carers • Sex for over 50s
Socio-economic equality
4.7.2.11 There is also significant social and economic inequalities in Namibia. Social inequities exist in attitudes towards and treatment of key populations at risk, such as CSWs and MSM. Sex between men is still illegal under Namibian law, making it difficult to reach this population with services. There is very little information on the size of the various vulnerable populations or the behaviours that increase the risk of HIV. Collecting data on these group’s activities, as outlined in this proposal, will be the first step towards designing appropriate interventions to reduce HIV infections among the hard to reach populations. The same situation applies to sex workers; likewise, sex
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 84/160

work is illegal in Namibia and it is extremely difficult to reach this vulnerable group or their clients with prevention and treatment services for HIV and other STIs. Activities in this RCC programme should help reduce the HIV risk for these key affected populations, as well as their clients.
4.7.2.12 Despite Namibia’s classification as a lower middle-income country, it has one of the highest Gini
coefficients in the world. Economic inequities are well documented and need to be addressed. There is currently no evidence that HIV has infected poorer Namibians more than richer Namibians. In fact, evidence from neighbouring countries would suggest that the wealthy population is more likely to be living with HIV. However, we do know that the less advantaged population is more vulnerable to the consequences of HIV infection.
4.7.2.13 Activities in this proposal will lead to mitigation of the impact of the HIV epidemic on the poorest
populations through multiple channels. The proposed activities will provide food and other support to OVC in and out of school. This will help children stay in school and have the nutrition required to grow and learn. Activities will also encourage long-term sustainability through vocational training to OVC who might have dropped out of school due to financial constraints or the need to take care of ill family members. Peer group clubs, such as girls’ clubs, and after school clubs, will also play a significant role in supporting this group. OVC will be targeted according to age groups rather than clustered together without any differential.
4.7.2.14 Coordinated service delivery will be achieved through strengthened social welfare systems that
facilitate OVC Forums at regional, and constituency level, and at national level through the OVC Permanent Task Force.
4.7.2.15 PLWHA will also be supported through a two-tiered approach. The first priority is to provide food
assistance as well as home based care to those in need. A referral system will be put in place to guide PLWHA to community services that will be able to help them find work or access other social services.
4.8 Planning for Sustainability and Impact
4.8.1 Potential for Sustainability (a) Strengthening national capacity and processes
Describe how this proposal makes an important contribution to the strengthening and/or further development of national systems and institutional capacity (including the capacity of the public, private and NGO sectors, and communities affected by the disease). Refer to country evaluation reviews, if available.
4.8.1.1 Namibia is a large country with a small and widely distributed population. Distances between
services are huge, many people live in remote and/or hard to reach areas, and segments of the population are somewhat mobile which also challenges the consistent provision of services.
4.8.1.2 The community level in Namibia is seen as a crucial level for scaling up HIV interventions, engaging
key affected groups in participatory and creative ways which are tailored to the local situation, addressing the indirect determinants of HIV (such as social and gender inequalities) and establishing strong partnerships between the public, private and non-governmental sectors. Consequently, this proposal has been developed in close collaboration with the stakeholders of these communities to ensure that consultations identified the weaknesses in community systems and developed a shared vision of how these systems can be enhanced to support the continuation and scaling up of improved interventions under Round 2, while integrating new interventions based on recent evidence concerning drivers of the epidemic and MARPs.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 85/160

4.8.1.3 A number of activities described in this proposal are derived from concerted efforts to strengthen community systems in line with a common understanding of how the local response must be delivered:
• The most important is the selection of a non-governmental institution, NANASO, as the second PR.
As an umbrella organisation working with a plethora of small local NGOs (as well as bigger national ones), it will be able to put the appropriate mechanisms in place to support its constituents to develop their capacity at the local level.
• It will also address weaknesses, especially in the areas of CHBC and OVC support through civil society, related to geographical coverage (Mapping exercises), meeting the needs of key affected groups, access to capacity building and technical support, and maximising the comparative advantages of different types of NGOs.
• From the operational perspective, activities have been designed to address issues of health system strengthening through expanding service delivery through widening the service delivery base (PPP through building on the private sector and CSO delivery), capacity building, strengthening referral systems, information sharing, advocacy and coordination: all these activities are calculated to contribute towards community system strengthening, as well as the increased effectiveness of the programmatic interventions described under Objectives 1-4 of this proposal.
Government of Namibia 4.8.1.4 As the MTP III mid-term review suggested, the governance of the national HIV and AIDS response
needs strengthening at the management level. Increased political commitment and capacity is needed to strengthen the governance structure (inter-ministerial coordination and collaboration) and the overall multi-sectoral response. This proposal includes:
1. The strengthening of relevant units and directorates with key ministries to assist the National
response (MICT, MOE, Ministry of Youth, National Service, Sports and Culture (MOYNSSC), OPM, MGECW etc.) to scale up coordination on programme activities.
2. The involvement of leaders in mass media campaigns and main events. On the last National Testing Day, the Prime Minister, the Minister of Health and Social Services, and one of the 13 regional governors publicly went for an HIV test. These were significant examples to persuade others to be tested. PLWHA became increasingly visible and, together with popular artists and leaders, they can combat stigma and discrimination.
3. The GRN is already contributing largely to the OVC support (all social welfare grants (MGECW)) and health systems (staffing, infrastructure), and coordination at national and regional level (MoHSS). However it is important to reiterate that currently the MoHSS is co-financing ART drugs for about 50% and this is projected to be scaled-up, which allows a more sustainable approach.
Civil Society 4.8.1.5 CSOs have been strengthened with support from Global Fund, PEPFAR and other donors, but only
a few, larger organisations have sufficient capacity to deal with the management and administration issues related to donor requirements and delivery of services with adequate geographical and target group coverage. Civil society currently depends heavily on donor funding; hence mechanisms need to be developed for more sustainable financing. This proposal supports community systems strengthening through professionalising community services (CHBC, OVC support, and PLWHA support groups). This will be done by: standardisation of quality services; standardised training curricula; better coordination among civil society organisations and between civil society and the public sector (RACOC, CACOC, etc.); putting in place quality assurance; ensuring proper referral structures between community civil society services and public sector services; and NGOs/CBOs management training. In addition, this submission proposes to build human resource and infrastructure capacity, and by providing technical support and training, we propose to strengthen the CSOs involved in implementing the programmes funded by the RCC. The appointment of a PR for the non-government sector will contribute to the strengthening not only of the PR itself but also other CSOs working with the PR on programme implementation.
Private Sector
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 86/160

4.8.1.6 The private sector suffers, as does the public sector, from limited political commitment at middle management and senior management level. NABCOA and Lironga Eparu need to put stronger emphasis on advocating the social responsibilities and the potential role of co-investment of the private for profit sector.
(b) Alignment with Broader Developmental Frameworks Describe how this proposal’s strategy integrates within broader developmental frameworks such as Poverty Reduction Strategies, the Highly-Indebted Poor Country (HIPC) Initiative and the Millennium Development Goals. Also include an overview of any links to international initiatives, e.g. as the WHO/UNAIDS ‘Universal Access Initiative’ or the 'Global Plan to Stop Tuberculosis 2006-2015' for HIV/TB collaborative active ties, or the 'Roll Back Malaria Global Strategic Plan’).
4.8.1.7 Namibia is a signatory to a wide range of international and regional agreements, treaties,
declarations and commitments. Of particular relevance for HIV are the 200 UN Millennium Development Goals (MDGs), the UNGASS Declaration and Commitment on HIV/AIDS (2001, 2006), and the African Union Ministerial Meeting on Universal Access (2007). Namibia is strongly committed to achieving the Universal Access targets. In February 2008, a national target setting was held, which reflects the universal access targets for the health sector programmes (Annex J5 National HIV and TB targets).
4.8.1.8 At the national level, various policies and plans ensure that the RCC proposal is aligned with broader
development frameworks. These include:
• Vision 2030, which provides the overall guiding framework for all the country’s development policies;
• Third National Development Plan 2007/08-2011/12, which highlights cross-cutting areas for development – and HIV and AIDS is one of them;
• Plan for Multi-sectoral Monitoring and Evaluation of HIV and AIDS 2006/07-2008/09; • National HIV and AIDS Policy 2007, which addresses the situation in Namibia and incorporate
most of the current international policy principles (such as the UNAIDS/WHO ‘Universal Access Initiative’);
• National HIV and AIDS Strategic Medium Term Plan III (2004-2009); • Draft National Strategy for the Prevention of Sexual Transmission of HIV 2009-2014; • Draft National HIV and AIDS Strategic Medium Term Plan IV (2010-2015); • 2008 Guide to HIV and AIDS Mainstreaming, designed to ensure an holistic response to HIV and
AIDS; • National OVC Plan of Action; • National Policy on HIV/AIDS for the Education Sector; • Strategic Plan for Rolling Back Malaria in Namibia 2003-2007; • Human Resources for Health Strategy, the application of which is critical for the sustainability of
staff in the health sector; • National Medicine Policy; • National Pharmaceutical Master Plan; and • Medium Term Expenditure Framework 2008-2012.
4.8.2 Evidence of impact/potential for impact
For the questions below, the concept of 'impact' refers to whether there is clear evidence of impact on the relevant disease epidemic or influence of planned interventions on disease prevalence, incidence, mortality and/or averted infections.
(a) Potential for demonstrating impact How will the additional support provided by this proposal increase the capacity of the country to demonstrate that its national disease strategy will have, or has the potential to have, a measurable impact on the burden of the disease (whether expressed in terms of overall morbidity and/or mortality and/or averted infections).
4.8.2.1 The RCC proposal is expected to consolidate and build on the achievements realised under
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 87/160

Round 2 and to further impact upon the programme’s overarching goal through more effective and efficient strategies in the service delivery areas that are guided by evidence. The goal for the RCC remains the same as that of the Round 2 application which is “To reduce the prevalence of HIV infection and HIV/AIDS morbidity and mortality, with subsequently mitigated social and economic impact of the HIV/AIDS epidemic in Namibia”. The impact indicators which the RCC proposal will use to assess achievement of the goal are as follows:
1. HIV prevalence among pregnant woman. 2. Prevalence of HIV infection among pregnant woman aged 15-24 years. 3. Percentage of infants born to HIV infected mothers who are HIV infected. 4. Percentage of people still alive and on therapy at six and 12 months after initiation of treatment.
4.8.2.2 In a joint consensus workshop for the RCC draft proposal review and the HIV and AIDS National
Strategic Framework (NSF) for 2010 to 2015 held in July 2009, it was agreed by stakeholders that the RCC application was aligned to the planned impact level results of the NSF (Report of the First National Consensus Workshop for the MTP IV Development). The planned impact level results of the NSP are as follows:
1. The rate of HIV incidence is reduced by 0.5 percent in 2010 to 0.3 percent by 2015. 2. The percentage of young people aged 15-24 who are HIV infected is reduced from 10.6 percent
in 2008 to five percent by 2015. 3. The percentage of adults and children (0-14) with HIV still alive at 12 months after the initiation
of ART is increased from 69 percent (adults) and 82 percent (children) in 2007 to 90 percent (adults) and 95 percent (children) by 2015.
4. Percentage men and women 18-59 yrs, who have been very sick or who died within the past 12 months after being very sick, whose households received at least one type of free basic external support to care for them within the past year is increased, from 15.8 percent in 2007 to 25 percent in 2015.
5. The coordination and management of the multi-sectoral response is efficient and effective at all levels – national, sectoral, regional and community - as measured by NCPI.
4.8.2.3 Therefore, the RCC will contribute to averting new infections and reduction of morbidity and mortality as well as improvement of livelihoods of the affected. Some of the key linkages between the proposed service delivery areas of the RCC and the expected impact are described here.
Averting Infections
4.8.2.4 With maintenance of the intensity of prevention efforts under Round 2, it is estimated that new infections will continue to reduce from 10,400 in 2008/09 to 7,500 in 2015/16 (Figure 7) (Namibia Spectrum Model Projections and Estimates 2009). The success of reducing HIV infection among pregnant women aged 15 to 24 years attending ANC from 17.9 percent in 2002 to 10.4 percent in 2008 is expected to continue and to have reduced to five percent by 2015 (see Figure 10).
Figure 10: Total Number of New HIV Infections in Children and Adults
2000/01 - 2015/16
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 88/160
0
5000
10000
15000
20000
25000
30000
2000
/01
2001
/02
2002
/03
2003
/04
2004
/05
2005
/06
2006
/07
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
2013
/14
2014
/15
2015
/16
Year
Num
ber o
f New
HIV
Infe
ctio
ns
Adult
Children
TOTAL Adults andChildren
Source: Namibia Spectrum Model Projections and Estimates 2009
4.8.2.5 Without the RCC, there would be a risk of not being able to continue this trend. With the RCC,
efforts to reduce new HIV infections are expected to be more intense since interventions will be evidence-based, founded on new knowledge of the epidemic (Measure Evaluation (2008), op. cit.). The SDA BCC Mass Media will not only be scaled up but will design messages and target audiences guided by the evidence on the drivers of the epidemic. The BCC community outreach and school SDA will use the proven approach of peer education and interpersonal communication to ensure behaviour change addressing drivers such as MCP, low condom usage and misconceptions of risk, with all messages being disseminated within a holistic approach that also touches on issues of alcohol and drug use, gender concerns and SRH. The RCC plans to procure and distribute 12 million condoms annually and promote their usage. During the RCC period, condom usage in high risk sex among adults (currently 66 percent of women and 74 percent of men, according to the 2006 DHS) will increase to a target of 81 percent and 89 percent respectively by 2014/15. The planned further decentralisation of ART services, including services for PMTCT, will ensure that more HIV infected mothers have access to ARVs and therefore MTCT will reduce from 11.8 percent in 2007/08 to six percent by the end of the RCC period.
Reduction in Morbidity and Mortality 4.8.2.6 One other major success story of Round 2 was the ART scale-up that resulted in the initial
reduction in AIDS deaths. However, there is a danger that AIDS mortality may begin to rise again due to an aging cohort of persons on ART as depicted in Figure 8 below (Namibia Spectrum Model Projections and Estimates 2009). The RCC aims at reducing this effect. The RCC ART SDA will further impact upon AIDS-related mortality and morbidity by increasing the numbers of people on ART through supporting the decentralisation of ART services and procuring ARVs. This strategy will increase accessibility to ART and is expected to increase ART coverage of those in need from 82 percent to 90 percent among adults by 2014/15. As a result, the percentage of adults and children with HIV still alive at 12 months after initiation of ART will increase from 69 percent (adults) and 82 percent (children) in 2007 to 90 percent (adults) and 95 percent (children) by 2015 (Figure 11). Therefore, as the size of the treatment population increases, the absolute number of deaths will grow though patients would have lived longer.
Figure 11: Deaths Due to AIDS-related Illness and New HIV Infections Over Time
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 89/160

0
5000
10000
15000
20000
25000
30000
2000
/01
2001
/02
2002
/03
2003
/04
2004
/05
2005
/06
2006
/07
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
2013
/14
2014
/15
2015
/16
Year
Num
ber
AIDS related deathsNew HIV Infections
Source: Namibia Spectrum Model Projections and Estimates 2009
4.8.2.7 Morbidity and mortality due to HIV and AIDS will also be further reduced through the SDA on
Care and Support to the Chronically Ill. An expansion of outreach services will bring interventions closer to the community and therefore increase accessibility and use of care services. More people will be enrolled into care and treatment through scaling up the service delivery area on HIV Counselling and Testing through public and private sector mobile clinics by making these services more accessible in the hard to reach places. It is expected that the percentage of adults counselled and tested in the past 12 months will increase from 18 percent among men and 29 percent among women to a target of 34 percent and 47 percent respectively by 2014/15.
4.8.2.8 Support to HSS will have a wider impact than that that due to HIV and AIDS services alone.
The RCC will contribute to the reduction in under 5 child mortality from 69 per 1,000 live births by 2007 to 45 by 2015 (Millennium Development Goals Report, Namibia, 2008 Annex J 41 ) through supporting human resources and the infrastructural development of the health sector.
Socio-economic Impact 4.8.2.9 The SDA for support for OVC will increase the percentage of OVCs whose households receive
at least one type of free basic external support in caring for the child from 16.5 percent in 2006/7 to 65 percent by 2015. Welfare grants provided by the public sector will be scaled up through hiring of CCCW under the aegis of the RCC grant.
4.8.2.10 The RCC support to conduct an AIS during the first and sixth year as well as the BSS and the
ANC sentinel surveillance will present an excellent opportunity to assess the expected impact of the grant application. A mid-term review and final end evaluation of the HIV and AIDS NSF will be facilitated by the findings of these surveys, and in turn these results will foster the development of further evidence-based interventions based on best practice.
(b) Impact Measurement Systems (IMS)
Describe the strengths and weaknesses of in-country systems and organisation(s)/team(s) that evaluate potential for health impact, determine country impact measurement indicators, and track/monitor achievements towards national goals.
4.8.2.11 The National Response is monitored through mid-term evaluations (MTP II (2003) and MTP III
(2007)) and the NAEC which has quarterly review meetings that address the multi-sectoral response. The health sector also conducts annual TB/HIV review meetings to manage the cross-ranging aspects of the two diseases.
4.8.2.12 Data sources and information systems that are used to collect routine data include the ART
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 90/160

electronic patient monitoring system (ePMS), the District Health Information System (DHIS which collects PMTCT, Maternity and ANC, and CT data), Early Infant Diagnosis-Dried Blood Spot Database (DBS), and the Electronic TB Register (ETR).
4.8.2.13 The main data sources for the key HIV and AIDS impact and outcome indicators include the bi-
annual HIV Sentinel Surveillance surveys that monitor HIV prevalence among pregnant women attending ANC clinics and the DHS which measure trends in key demographic and health indicators, particularly those related to behaviour change. Since 2006, Namibia has used the EPP and Spectrum (v 3.14) model for national HIV estimates and projections. The national health information system (HIS) provides routine data for output indicators where interventions lead to reduced prevalence over the longer term, for instance the PMTCT and VCT indicators.
4.8.2.14 Namibia’s other data sources for measuring impact include the AIDS Indicator Survey (a sub-set
of the DHS) which will be conducted in 2009, and for the first time will collect nationally representative HIV prevalence data. Other evaluation activities include a Health Facility Survey (data collection ongoing and expected to be completed in September 2009), the mid-term review of the national HIV and AIDS strategic plan, semi- and annual reports from the GRN Ministries, the improved NANASO M&E annual monitoring study of CSO activity, and routine Knowledge, Attitude, Behaviour and Practice (KABP) surveys undertaken by key civil society partners and other donors. Currently, protocols for an HIV Drug Resistance Survey and an ART Adherence Survey are under review and are scheduled to be implemented in early 2009.
4.8.2.15 Currently there is a national Monitoring and Evaluation Committee which meets quarterly to
discuss data and surveillance issues. This committee is comprised of officials from various Ministries, development partners, civil society, NGO partners and other stakeholders, and is led by the MOHSS. Although strategic impact analysis has not been done to date, a new national data triangulation TWG, with technical support from the University of California San Francisco and CDC, is being established and will meet regularly to use these various data sources to answer larger impact questions in a timely and methodical manner. The first analysis was completed in June 2009.
4.8.2.16 Furthermore, there are national task forces for different substantive areas which are responsible
for reviewing outcome and impact data. Recently, the Prevention TWG completed various analyses on the drivers of the epidemic and presented these data at the National Prevention Consultation in November 2008. During this meeting, data analyses at the national and regional levels were presented to determine Namibia’s key drivers of the epidemic. This work has been a key step to the development of the national prevention priorities for the MTP IV (2010-2014).
4.8.2.17 Additionally, the MoHSS conducts an annual programme review meeting to review various data
as a means to assess progress toward goals and objectives and to identify areas for improvement.
4.8.2.18 In late 2006, both Measure Evaluation and UNAIDS/GAMET (the Global AIDS Monitoring and
Evaluation Team of the World Bank) conducted assessments of the HIV M&E system in Namibia. Both assessments found: (a) a lack of skilled human capacity to carry out the required functions of an M&E system; (b) a need for a strengthened organisational structure for M&E; (c) a need for a more decentralised data flow; and (d) the need for timely reporting.
Strengths
4.8.2.19 In the last 18 months since these assessments were carried out, there have been numerous improvements to the M&E system.
Organisational structure 4.8.2.20 Funding from Round 2 has allowed the four major sectoral partners (MRLGHRD, NABCOA,
NANASO and OPM) to hire M&E officers; another 13 were placed in each region to support the Regional Councils. Additional data clerks were recruited to speed up the access to data which are collected from the HIS. Through other donor funding, two M&E officers were also recruited to assist the Response Monitoring and Evaluation subdivision in the DSP (RM&E) with their
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 91/160
activities of rolling out a programme monitoring system and creating an evaluation agenda. 4.8.2.21 To address some of the concerns of the organisational structure, the MOHSS subdivision for
RM&E structure was reviewed. The context of RM&E’s mandate and the activities of the integrated action plan assigned to the RM&E sub-division were used as a basis to define the functions of the RM&E sub-division. This reorganisation is still in progress as staff members adjust to the revised job descriptions.
Data collection systems
4.8.2.22 The country is currently rolling out the system for programme monitoring which routes all data on non-clinical HIV activities through the regional offices. This will allow the RACOCs to have immediate access to the data coming from their region. The data will then be routed to the RM&E for collation and regular reporting.
4.8.2.23 In addition the RM&E sub-division is currently rolling out a new ePMS. The ePMS system is
designed to provide health facilities with immediate data on their ART patients, before sending to the national level.
Data use
4.8.2.24 Namibia recently completed a report on Estimates and Projections of the Impact of HIV in Namibia (Annex J9). This report provides useful data on the number of people infected, the number needing treatment, the number who will die of AIDS-related causes, and so on, to help design and plan programmes. In addition, the country recently completed a target setting exercise where M&E officers and programme officers worked together to determine what results are feasible over the next five years.
Weaknesses Organisational structure
4.8.2.25 Very few CSOs have M&E officers or structures in place. At the national level M&E officers lack M&E, management and research skills.
Data collection systems
4.8.2.26 The sentinel surveillance provides limited information on trends but does not provide a solid measure of HIV prevalence in the general population as it only focuses on pregnant women. A nationally-representative household survey which measures HIV prevalence is needed to calibrate the ANC surveillance to the national prevalence. There is no biological surveillance on key populations at higher risk of becoming infected.
4.8.2.27 For behavioural data, the DHS is only conducted every five or six years, hindering the routine
monitoring of risky behaviours. A smaller nationally-representative household survey specifically for HIV related behavioural data is needed in-between the DHS surveys to provide more routine measures.
4.8.2.28 There is no central database to maintain the data related to HIV services. Data collected
through the HIS are not easily available for monitoring and management purposes. Reporting to the HIS from the health facilities is often delayed and is not necessarily disaggregated as needed for evidence-based responses.
4.8.2.29 Lastly, the new ePMS as well as the pharmaceutical patient based systems are currently
separate from the HIS (currently operated by a different MOHSS Directorate). The PMTCT and the PCR patient monitoring systems are also handled separately from the HIS. The PMTCT data from ANC and maternity departments are captured in the HIS but the EID PCR patient monitoring system runs separately from the HIS being under the DSP’s M&E Unit. As a result, it is difficult to monitor or track if the 21 percent of HIV positive pregnant women who are eligible to receive ART actually receive it. It is also difficult to track if all the HIV-exposed infants from PMTCT actually receive early testing with HIV DNA PCR and, if they do, if they are all put on ART in time. There is therefore need to have an integrated monitoring system that harmonises
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 92/160
these data bases to make them compatible and communicating with each other and to facilitate the tracking of patients throughout the continuum of care for HIV-infected mothers and their HIV-exposed babies.
Data use
4.8.2.30 Dissemination of routine data collected in the M&E system is still weak. Plans are in place to produce a quarterly bulletin; however the human resources are not yet available for this activity.
(c) Strengthening monitoring and evaluation systems What improvements to the M&E systems in the country (including those of the Principal Recipients and Sub-Recipients) are included in this proposal to overcome gaps and/or strengthen reporting into the national impact measurement systems framework?
4.8.2.31 Approximately 7 percent of the proposal is intended for monitoring and evaluation activities.
These funds will focus on key areas for improvement including human capacity, conducting surveys required for monitoring the epidemic, and producing data for decision-making.
Organisational structure
4.8.2.32 Resources from this proposal will contribute toward staffing the national offices mandated with monitoring and evaluating HIV (RM&E Sub-division, Management Information and Research Sub-division, and the HIS Sub-division) as well as other sectors. Under the RCC, specific efforts will be made to enhance the skills of service delivery providers in monitoring, evaluation and reporting skills. At the national and regional level coordination will be enhanced through training on project cycle management and developing a comprehensive cost work plan. These activities will improve the M&E systems in both civil society and the public sector (which already has changes to its annual M&E studies in the pipeline directed towards better impact assessment). Human capacity building for M&E requires a wide range of activities, including formal training, in-service training, mentorship, coaching and internships. M&E capacity building under the RCC will focus not only on the technical aspects of M&E, but also address skills in management, supervision, advocacy and communication.
Data collection systems
4.8.2.33 The routine community-based monitoring system (system for programme monitoring) will provide programme activity data to monitor progress. While some resources exist from the Government and development partners to implement this system, resource gaps remain. Global Fund RCC funding will be used for the ongoing training for all HIV service providers on system for programme monitoring.
4.8.2.34 Biological and behavioural surveillance and surveys are essential to determine the drivers and
the spread of the HIV epidemic in each country. Surveillance and surveys provide data to support the construction of the standardized national indicators defined in the national M&E plan. Many partners contribute towards conducting surveys but most contribute towards providing technical assistance; therefore there is often a lack of resources for in-country activities such as data collection and processing. Additional support from the RCC is needed to complete the funding for the AIDS Indicator Survey 2010 and the DHS 2011, which will both include HIV testing. In addition support is needed to continue the HIV Sentinel Surveillance for years 2010, 2012, and 2014, the Health Facility Surveys, and biological and behavioural surveillance of key populations at increased risk to HIV.
4.8.2.35 For sound decision-making, it is important to be confident about data quality. Regular data
quality checks and provision of feedback are important mechanisms to improve or sustain data quality. Data auditing needs to be done on a quarterly basis to check for accuracy and completeness of reports submitted and to compare the reports with the source documents at service provision level. The proposal will cover monitoring and support visits to assure quality data.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 93/160
Data use
4.8.2.36 The most important reason for conducting M&E is to provide the data needed for guiding policy formulation and programme operations. As mentioned earlier, the proposal will cover activities to encourage data use, such as workshops to discuss the implications of M&E data for programme planning and improvement, ensuring dissemination of good quality data in a timely manner and developing appropriate information products for different users.
4.9 Implementation Capacity
4.9.1 Principal Recipient Capacities Describe the respective technical, managerial and financial capacities of each PR in this proposal (continuing and new) to
manage and oversee implementation of the program (or their proportion) having regard to the proposed changes in scale and/or scope identified in section 4.6.
What plan(s) exist to strengthen the PR(s)' capacity to absorb these changes into their implementation management framework, and ensure strong performance? Also discuss any anticipated barriers to strong performance, and how they will be addressed, referring to any assessments of the PR(s) undertaken either for the Global Fund or other donors (e.g., capacity-building, staffing and training requirements, etc.).
PR 1: Ministry of Health and Social Services (MOHSS)
4.9.1.1 The MOHSS, selected as the sole PR in 2002 by NaCCATuM, is the current PR for the Round 2 grants. Due to issues related to capacity, the MOHSS did not start implementing the Round 2 grants until January 2005, following the establishment of the PMU. Initially, the PMU was not managed directly by the MOHSS but was outsourced to a consortium consisting of a national consulting firm, NEDICO, in partnership with two international institutions, the Royal Tropical Institute (KIT) and the Malaria Consortium of Liverpool (NEDICO Consortium). The NEDICO Consortium recruited and managed all the staff, both national and international, and to a certain extent the consortium was accountable for the performance of the grant on behalf of the PR. The initial staff workforce comprised:
• Four international senior Managers: Programme Director, Operations Manager, Finance Manager and M&E Manager;
• Three national Managers headed the Operations, Finance and M&E units respectively; and
• The other staff complement consisted of officers and support staff for M&E, Operations, Procurement and Administration.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 94/160

4.9.1.2 The arrangement with the NEDICO Consortium lasted for a period of two years (the duration of Round 2 Phase I). The MOHSS, on the advice of the GF, absorbed all the PMU staff into its staff establishment and signed direct contacts with all 13 PMU staff. The PMU is now an integral part of the Directorate of Special Programmes (DSP), the MOHSS directorate that is responsible for the management of external resources for the three diseases funded by GFATM and other donors. The PMU staff complement has increased over time. With the award of Round 5, there was an increase in the number of Sub–recipients to over 40 from the initial 27 under the Round 2 grants. The PR was requested to propose the number of additional staff needed to manage the increase workload. The proposal was presented to GFATM and, following an assessment by the Local Fund Agent (LFA), a recommendation was made to increase the PMU staff by an additional four persons to strengthen the Finance Unit (2), M&E Unit (1) and Operations Unit (1), bringing the total number of PMU staff to 17. Figure 12 below depicts the current organisation structure of the PMU.
Figure 12: MOHSS PMU Management Structure
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 95/160
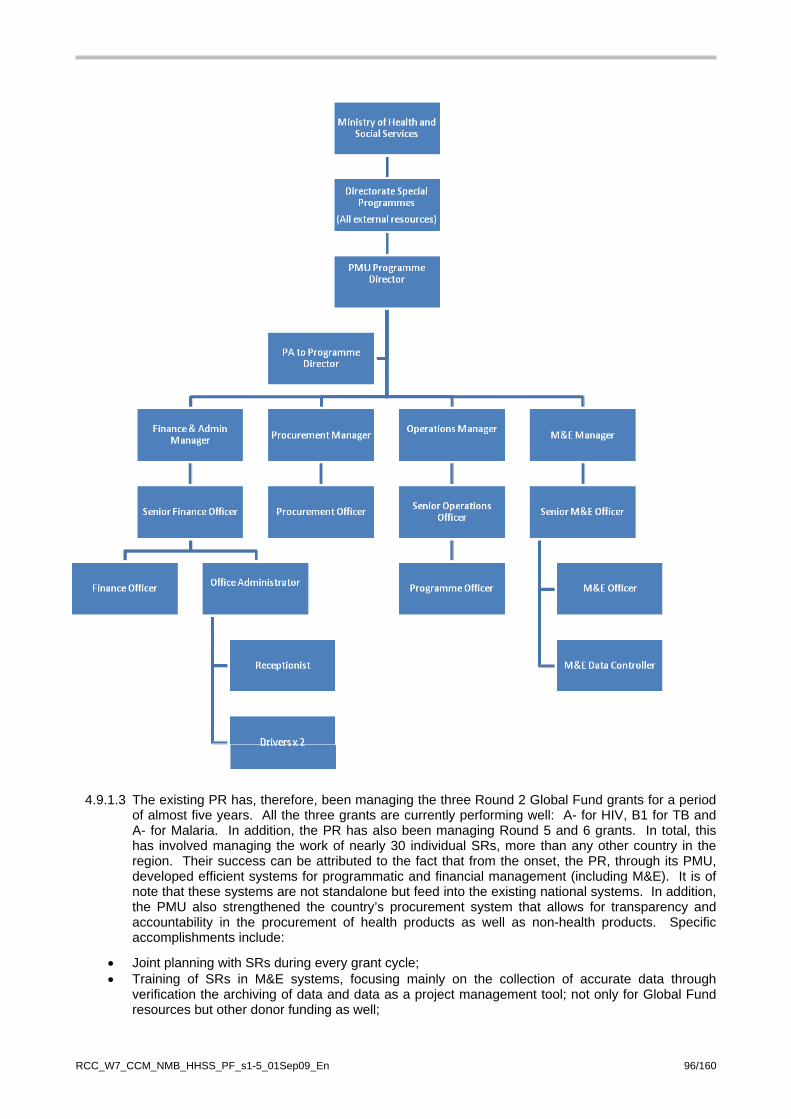
4.9.1.3 The existing PR has, therefore, been managing the three Round 2 Global Fund grants for a period of almost five years. All the three grants are currently performing well: A- for HIV, B1 for TB and A- for Malaria. In addition, the PR has also been managing Round 5 and 6 grants. In total, this has involved managing the work of nearly 30 individual SRs, more than any other country in the region. Their success can be attributed to the fact that from the onset, the PR, through its PMU, developed efficient systems for programmatic and financial management (including M&E). It is of note that these systems are not standalone but feed into the existing national systems. In addition, the PMU also strengthened the country’s procurement system that allows for transparency and accountability in the procurement of health products as well as non-health products. Specific accomplishments include:
• Joint planning with SRs during every grant cycle; • Training of SRs in M&E systems, focusing mainly on the collection of accurate data through
verification the archiving of data and data as a project management tool; not only for Global Fund resources but other donor funding as well;
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 96/160

• Regular monitoring of SRs for verification of secondary data and assisting SRs with implementation challenges;
• Training of SRs in financial systems and assisting them to establish these systems; • Training SRs in some of the thematic areas for a better understanding of comprehensive
interventions; • Handling procurement of large quantities of equipment and commodities through the procurement
sub-unit and a specially constituted tender committee for the Global Fund resources; • Compiling accurate quarterly and six-monthly financial and programmatic reports and defending
these during NaCCATuM sub-committees and full meetings; and • Compiling annual reports.
4.9.1.4 The management of these grants has not been without challenges:
• The sheer number of sub–grants make it impossible for the current PMU to devote enough time to each and every SR; and
• The constant staff turnover has meant that the PMU is continually trying to balance the training of new staff with consistent support to the SRs.
4.9.1.5 Nonetheless, as a PR the MOHSS has sufficient capacity, a good knowledge of Global Fund
guidelines and an excellent track record in receiving and managing a large amount of funds. It has made efficient arrangements for disbursement of these funds to the SRs and for implementation and overseeing SR programme activities.
4.9.1.6 It is for all the above reasons that the Namibia CCM endorsed the decision to retain the MOHSS as
one of the PRs for the public sector programmes for a subsequent Round application (Annex A10, Minutes of NaCCATuM Meeting 6 June 2008) and this was reaffirmed at the CCM meetings for the RCC of 5 June and 9 July 2009 (Annexes A10), Minutes of NaCCATuM dated 5 June and 9 July 2009)
4.9.1.7 As the country moves into dual track financing system, it will be critical for the current PR
arrangement to remain intact for at least the first phase of the RCC, for the following reasons:
PR 2: Namibian Network of AIDS Service Organisations (NANASO) Criteria for selection as a second PR 4.9.1.8 Through a transparent selection process, NANASO was chosen as the second PR; and
the Namibian CCM endorsed this selection on 5 June 2008 (see sections 2.2.3 on Processes to Select Principal Recipients for Programme Implementation during the Rolling Continuation Channel Term and 2.2.5 Transparent Proposal Development Processes). During the period 2006 up to mid-2007, NANASO undertook a review of its strategic plan and an organisational assessment (Annex K2, NANASO Capacity Assessment Report), followed by a consultative process in 2008 (Annex K4). The first two exercises were accomplished in collaboration with the MOHSS, the current PR. One of the major objectives of the review of the strategic plan and the organisational assessment was to strengthen NANASO as a ‘shadow PR’ that would fully assume the role of a PR in subsequent Global Fund Rounds that Namibia would apply for. This decision was based on several facts:
1. Since its establishment in 1991, NANASO has acted as an umbrella organisation that
brings together most of the NGOs, FBOs and CBOs working on HIV and AIDS in Namibia. Its membership base comprises over 400 grassroots organisations.
2. In this capacity, NANASO has been responsible for monitoring the contribution of the civil sector in the multilateral response to HIV and AIDS and therefore is conversant with the strengths and weaknesses of the civil society. This M&E function for CSOs provides an alternative way of monitoring and evaluating sector performance which can either validate
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 97/160
or provide an additional perspective to the Government’s response with regard to policy development and intervention.
3. NANASO has a proven track record in effectively representing vulnerable individuals and families through its support to grassroots organisations who are the first line of defence. Its understanding of the community needs means that capacity building can be tailored to meet the localised needs of its constituents and this is NANASO’s key comparative advantage.
4. Although NANASO as yet does not have specific experience in grant management, it is preparing for their role in managing SRs through the development of a small grant policy and accompanying structure, waiting to be rolled out. However, NANASO already has prior experience in small grant processes through its involvement in the UNAIDS Small Grants Fund review panel, participation of the pre-assessment of potential grantees, and monitoring of the recipients.
5. It sees its grant management role as complementary to its network support role. Feedback from its strengthened network support activities and its M&E role enables it to: • Work with the civil society SRs to ensure that their interventions are closely linked to
and are consistent with the bigger picture of CSO activity on the ground; • Identify where additional SR activity would be justified, and how; • Strengthen community interventions through the implementation of a Small Grants
programme, • Encourage outsourcing by SRs to sub-sub-recipients (SSR) where local circumstances
suggest this; and • Work with the MOHSS to identify where CSOs can be used as SSRs, again according
to local circumstances. 4.9.1.9 NANASO’s real strength lies in its convening capacity, being able to bring disparate and often
competing organisations together to discuss issues and to assist in putting organisations in touch with each other through its extensive network of affiliates. National conferences for all the NGOs have been held in 2006, 2007, 2008 and 2009 with over 200 participants at each conference, to provide constituents with an overview of GF process and instil in them the importance of civil society participation. All conferences were unanimous in supporting the need for a civil society PR, and that this PR should be NANASO (Annexes K6).
4.9.1.10 NANASO’s current staff capacity is:
• Executive Director • Advocacy Officer • Financial Administrative Officer and assistant, plus Admin/HR Officer • M&E Officer • Network and Member Support Officer • Training Officer and assistant • Information Officer and assistant • IT assistant • Logistical support staff
4.9.1.11 This staffing structure will change under the RCC and is discussed below in the section on
proposed changes in NANASO’s reorganisation under the RCC. Meanwhile, in preparation for assuming the role of the second PR, NANASO has been strengthened by additional international and national technical capacity in the following areas:
• Organisational development, governance and leadership, M&E, research and development, data and financial management;
• Fund raising, resource mobilisation, partnership development, business strategy development; and • Project management.
4.9.1.12 The international expertise has come from the private sector which was a deliberate effort by
NANASO to bring the best principles of the private sector to NANASO’s programme delivery.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 98/160
NANASO within the RCC 4.9.1.13 NANASO will scale up its ability to improve CSO activity through:
(a) Improving the coordination of civil society activities at a regional level and below through the deployment of seven regional officers in three regional offices to cover all 13 regions. These will specifically seek to improve the interface between community level activities and regional agencies, with specific aims to improve community-based responses and community involvement in decision-making; improve coordination among agencies (as highlighted across this RCC proposal); strengthen the interface between community level responses and health care systems; and strengthen the work of CSOs vis-à-vis marginalised groups. NANASO will be aided in this by strengthened database and M&E systems for CSOs at the regional level;
(b) Strengthening the CSO interface between HIV and AIDS, Malaria and TB programmes, the integration of HIV and AIDS and SRH programmes among CSOs and developing programmes relating to nutrition among CSOs, by establishing a small programme control unit that develops programme interventions for CSOs in the light of M&E findings;
(c) Securing better coverage in relation to HIV and AIDS programmes in Ohangwena in particular, and in Omusati and Oshikoto, where levels of CSO activity appear to be lower than is needed;
(d) Building capacity among CSOs through the use of national institutional and service standards, which will be integrated into the national vocational and education training programme of unit standards and through specific capacity building interventions among CSOs covering HIV and AIDS management, GBV, BCC, financial management, M&E and reporting and resource mobilisation; and
(e) Developing further HIV and AIDS resource centres to support the strengthened regional operation. Proposed changes in NANASO’s organisation under the RCC 4.9.1.14 NANASO already has existing Administration and Finance Units (the latter with an accountant), conversant with the Global Fund Secretariat reporting requirements. As a result of the organisational assessment, a new organogram for NANASO was drawn up (Figure 13) to reflect the following changes:
• A Deputy Director who will also be a Public Health Advisor; • A Finance Manager to represent the substantially strengthened finance function; • Creation of a Grants’ Management Unit together with a Grants’ Manager; and • An M&E Manager to support the existing M&E Officer.
4.9.1.15 NANASO has a functioning Executive Committee, to be renamed Board of Directors, which
provides effective strategic direction and management oversight and will guide NANASO in its new role. Changes in the Board of Directors are being made to widen the scope of advice and mentorship currently available to the organisation, and support the greatly expanded role that NANASO will play.
4.9.1.16 In addition, NANASO has a financial policy, human resource policy, grant management policy and
a fund raising policy (Annex K3, NANASO Policies). All these documents have been developed as a result of recommendations made during the organisational assessment.
4.9.1.17 Finally, the intention is to establish regional offices over an incremental period of time so that by
the end of the programme period NANASO will be able to provide the tailored service delivery support as described above, and will be able to bring back feedback from the grassroots level to feed into central-level policy and management decisions. These offices will be established on a priority basis according to criterion such as HIV prevalence.
Figure 13: Proposed NANASO Organogram
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 99/160
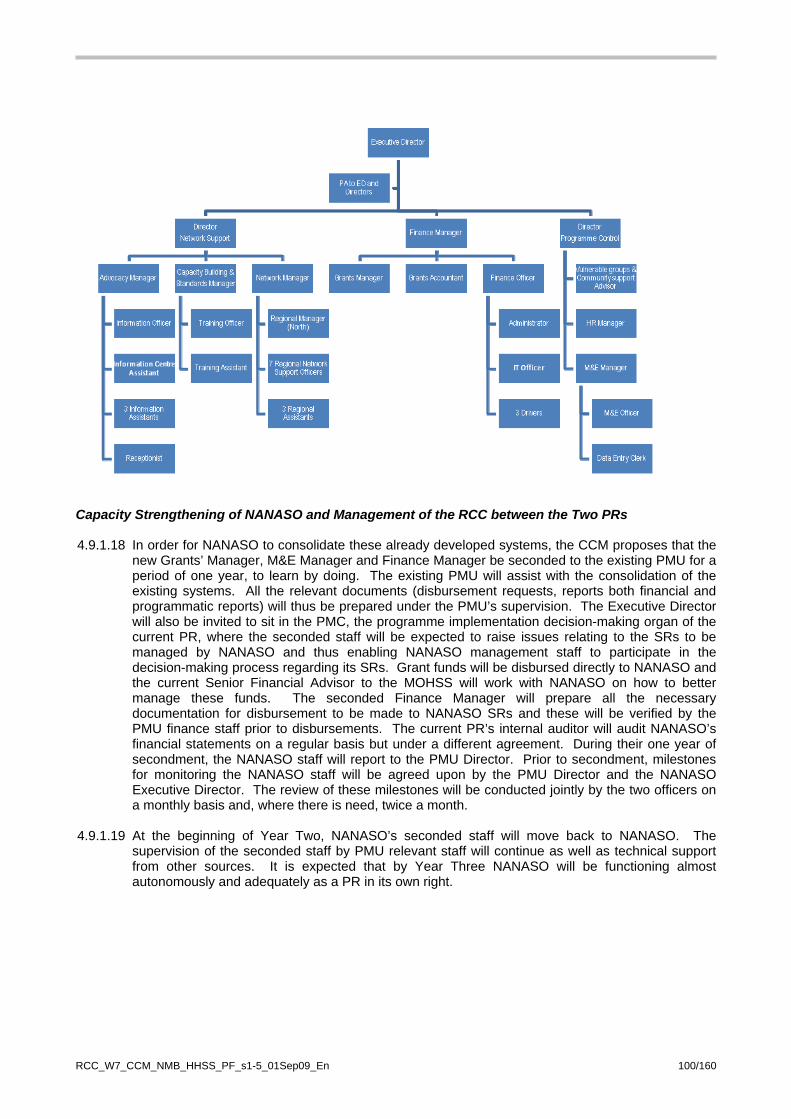
Capacity Strengthening of NANASO and Management of the RCC between the Two PRs 4.9.1.18 In order for NANASO to consolidate these already developed systems, the CCM proposes that the
new Grants’ Manager, M&E Manager and Finance Manager be seconded to the existing PMU for a period of one year, to learn by doing. The existing PMU will assist with the consolidation of the existing systems. All the relevant documents (disbursement requests, reports both financial and programmatic reports) will thus be prepared under the PMU’s supervision. The Executive Director will also be invited to sit in the PMC, the programme implementation decision-making organ of the current PR, where the seconded staff will be expected to raise issues relating to the SRs to be managed by NANASO and thus enabling NANASO management staff to participate in the decision-making process regarding its SRs. Grant funds will be disbursed directly to NANASO and the current Senior Financial Advisor to the MOHSS will work with NANASO on how to better manage these funds. The seconded Finance Manager will prepare all the necessary documentation for disbursement to be made to NANASO SRs and these will be verified by the PMU finance staff prior to disbursements. The current PR’s internal auditor will audit NANASO’s financial statements on a regular basis but under a different agreement. During their one year of secondment, the NANASO staff will report to the PMU Director. Prior to secondment, milestones for monitoring the NANASO staff will be agreed upon by the PMU Director and the NANASO Executive Director. The review of these milestones will be conducted jointly by the two officers on a monthly basis and, where there is need, twice a month.
4.9.1.19 At the beginning of Year Two, NANASO’s seconded staff will move back to NANASO. The
supervision of the seconded staff by PMU relevant staff will continue as well as technical support from other sources. It is expected that by Year Three NANASO will be functioning almost autonomously and adequately as a PR in its own right.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 100/160

4.9.2 Sub-Recipient information
(a) Are the majority of sub-recipients (SRs) from the expiring grant, continuing their roles and responsibilities in this proposal?
Yes Go to s.4.9.3
No answer (b) before
completing s.4.9.3
(b) If no, explain why, and for new SRs who will either receive a substantial proportion of the funding for this proposal or will be involved in funding to sub-sub-recipients:
(i) describe the transparent process by which new SRs were identified and the criteria that were applied in the identification process.
(ii) summarize the past implementation experience of these new SRs
4.9.3 Sub-Recipient capacities What plans exists to strengthen the capacity of the major SR(s) to absorb the continuing and/or expanded responsibilities under this proposal, and ensure strong performance? Please also discuss any anticipated barriers to strong performance, and how they will be addressed, referring to any evaluations by the existing PR(s) of SR capacities (e.g., capacity-building needs, staffing and training requirements, etc.).
4.9.3.1 Through 19 SRs and seven Sub-SRs, the MOHSS will be responsible for the public sector, private sector and the PLHIV network SRs. The MOHSS has been allocated the PLHIV network because the CCM decided it would be inappropriate to place another network under the new PR, NANASO, which is also a network. For activities falling under the PLHIV network that it cannot undertake, these will be sub-granted to other NGOs working with PLHIV in specialised areas. 4.9.3.2 The public sector SRs will be those that are involved in service delivery at health facilities such as ART, PMTCT, STI and CT. However, there are other non-facility based services covered by the public sector, where the target population is big and the intervention is regulated by policies developed by the public sector. This is the case of youth (BCC for in-school as well as for out-of -school youth), food assistance, coordination of OVC, and workplace which is shared between the public, private, and academic sectors. 4.9.3.3 The civil society SRs under NANASO will undertake the majority of implementation at the community level and for key affected populations. These will include HBC and care and support for OVC and PLHIV. There will be 10 relatively big NGO SRs and six smaller ones to which some of the main SRs will sub-grant. 4.9.3.4 The majority of the pre-identified SRs have been involved in the implementation of HIV programmes including the Round 2 grant implementation. Thus valuable experience has been gained by most of the SRs throughout the duration of the current Round 2 implementation. Some examples include:
• MOHSS condom SR – through development of a comprehensive distribution strategy, this SR has been able to distribute large quantities of condoms, thus meeting its targets and surpassing those targets;
• MOHSS ART SR – through the strengthening of its human capacity, it has managed to put large numbers on people on treatment; and
• Some of the civil society SRs in the area of OVC, through the review of quality of OVC services, have managed to provide care and support to OVC and reached their targets.
4.9.3.5 After almost five years of implementation, most of these SRs now have adequate capacity to continue implementation without major challenges. However, since most interventions will be scaled up, capacity challenges should be expected, which will be addressed through budgetary allocations to recruit additional staff for some of the SDA areas. For a few of the SRs that have been facing challenges in implementation (such as the PLHIV network), capacity building plans are underway to strengthen the organisation to enhance its performance. As for the new SRs, identified for new SDAs, an assessment will
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 101/160

be conducted to identify weaknesses and funds will build into their sub-grants to address these weaknesses through technical assistance support. 4.9.3.6 Some SRs have not been identified for some of the activities under the new SDAs. The number of SRs to be identified is not expected to exceed five. Since these SDAs are few and the remaining activities identified through the work of the TWGs, established by the CCM, are also few, calls for submissions detailing the activities will be made by the CCM. On receipt of notification that the RCC CCP has been accepted, these submissions will then be reviewed by the same TWGs that worked on the new SDAs. Following selection, the newly identified SRs will be assessed and, for any weaknesses identified, technical assistance support will be built into their sub-grant agreements. Should there be a delay, as was the case under Round 2 grant, mechanisms to accelerate implementation will be put in place.
4.10 Management of Pharmaceuticals and Health Products
4.10.1 Overview of changes to the management of pharmaceutical and health products
(a) Does this proposal involve the management of pharmaceuticals and other health products?
X Yes answer question (b)
(b) If yes to (a), does this proposal give rise to any change(s) in the roles and responsibilities for management of pharmaceuticals and health products compared to the expiring grant?
X No Complete section 4.10.2 and then complete s.4B if relevant to
this proposal, and/or go to section 5 and Attachment B (detailing quantities and unit costs for health products)
4.10.2 Management of pharmaceuticals and health products for continuing PR(s) involving a
scale-up of ongoing activities Describe: (a) how implementation arrangements relevant to this proposal have been planned to ensure (including, as
relevant, plans to obtain necessary additional technical assistance, training or other capacity building assistance) that continuing PR(s) have sufficient capacity to absorb the increased responsibilities in respect to the management of pharmaceuticals and health products for the planned scale-up; and
(b) the extent to which the ongoing management of pharmaceuticals and health products under this proposal will be coordinated with other procurement and supply management actions in support of the national disease prevention and control program to ensure greater impact on the disease.
(a) Planned interventions to support the scale up of activities under the RCC
Policy Changes 4.10.2.1 Notable policy changes that will support the proposed scale up of activities under the RCC include:
• The review and launching of the National Medicine Policy and subsequent introduction of the National Pharmaceutical Master Plan which outlines a road map for the implementation of the National Medicine Policy;
• The planned introduction of a training curriculum for Pharmaceutical Technicians and provision for these staff in staff establishments. This will strengthen HR provision for pharmaceutical service delivery and improve the retention of sub-professional pharmacy staff; and
• The Pharmacy Management Information System is being implemented to monitor and evaluate pharmaceutical service delivery.
IMAI Roll out and Management 4.10.2.2 IMAI was introduced in 2007 to increase access to ART and improve adherence to therapy by bringing treatment facilities closer to the people. Through IMAI, clients who have been stabilised on treatment and whose adherence is proven to be satisfactory are able to collect their ARV refills from the nearest health centres and clinics. To sustain the successful roll out and continue to work towards
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 102/160

achieving the programme’s aims which will contribute towards meeting the RCC’s objectives, the following planned interventions will be undertaken:
• Provision of transport facilities: o to supply distant health centres and clinics with ARV refills; o for outreach (i.e. mobile ART clinics); and o for monitoring and evaluation;
• Training and retraining of health centre and clinic nurses in Standard Treatment Guidelines, ART counselling, ARV medicines counselling, recognition of danger signs from medications, Medicine-Medicine and Medicine-Food interactions, pharmaceutical inventory control and reporting;
• Upgrading of storage infrastructure in health centres and clinics to accommodate the secure storage and dispensing of ARVs and the increase in volume of medicines stored at clinics (discussed further below); and
• M&E of IMAI roll out. Infrastructure
4.10.2.3 One of the scale-up strategies for ART provision is the decentralisation of services to the clinics and health centres in the outlying and/or rural areas. As such, the storage infrastructure in health centres and clinics needs to be upgraded to provide adequate and secure storage of medicines.
4.10.2.4 Another consequence of the scale-up is that the volume of HIV and AIDS-related commodities
has increased exponentially, thereby significantly increasing the need for upgrading secure storage facilities for pharmaceuticals and related health products across all levels of the supply chain. With support from PEPFAR through the Supply Chain Management System (SCMS), a racking installation project in the CMS, has increased ARV pallet capacity by 73 percent and floor area for ARV storage by 100 percent, creating 960m² of storage space and 767 additional pallet bays. Cold chain data logging and cooling systems were installed to ensure optimum storage conditions for the stored pharmaceuticals and health products. Similar interventions are planned for the RMS. However, despite this effort, storage at CMS remains a problem. The Government plans to construct a new purpose-built Central Medical Store (CMS) during the next five years. Additionally, renovations to increase storage space are required at the two RMS, and various hospitals, clinics and health centres, and this will be supported by PEPFAR.
4.10.2.5 In addition a bigger fleet of medicine distribution trucks is required to ensure timely
transportation of pharmaceuticals and other health products in appropriate conditions. 4.10.2.6 Strengthening the infrastructure for pharmaceutical and health product delivery not only
benefits the HIV Programmes but also those of malaria and TB. Therefore pharmaceutical strengthening infrastructure has been included under the cross-cutting HSS section of this proposal. The Pharmaceutical Division will prioritise the most immediate requirements with regard to the necessary infrastructure to support the scale up and expansion of activities under the RCC. However, the Division plans to undertake a needs assessment and facility storage mapping exercise in autumn 2009, to supplement the information which will be provided by the facility mapping currently underway, due to be completed in September 2009. This will provide a comprehensive and detailed situation analysis to be used as the evidence base for advocating for support under future Rounds.
Human Resources
4.10.2.7 In view of the increasing number of chronically ill HIV patients, the volume of pharmaceuticals and health products will increase exponentially over the next few years. Additional human resources will be required to ensure proper management of these medicines and health products while ensuring their appropriate use.
4.10.2.8 The Government is in the process of reviewing its staff establishment. An important aspect of
this revision is the creation of positions for all pharmaceutical personnel that are currently supported by development partners. The aim is for the Government to be able to absorb all staff currently funded by development partners. Until the staffing establishment review is
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 103/160

finalised and adopted, the Global Fund is requested to continue to support the current pharmacy personnel.
4.10.2.9 Another important aspect of strengthening human resources is training. Pharmacy personnel
have been trained and retrained on the inventory control of pharmaceuticals and other health products. Standard Operating Procedures (SOPs) have been put in place and regular supervisory support visits are carried out by Regional Pharmacists to improve adherence to SOPs. The Government plans to introduce a training curriculum for Pharmaceutical Technicians and is making provision for this in the MoHSS staff establishment plan; this will strengthen the management of pharmaceuticals and health supplies. Furthermore there is ongoing training of health centre and clinic nurses on appropriate National Treatment Guidelines and the IMAI standard operating procedures on the management of ARV medicines. This will ensure proper management of pharmaceuticals and other supplies as ART service delivery and management continues to be decentralised to these smaller health facilities.
4.10.2.10 Pre-service and post-graduate training is important to ensure the ongoing and sustainable
availability of suitably qualified personnel. The Government provides bursaries for both pre-service and post-graduate training.
4.10.2.11 Human resource strengthening does not benefit the HIV programme only but the Malaria and
Tuberculosis Control Programmes as well. Therefore interventions with regard to human resource strengthening have been put under the cross cutting HSS section of this proposal.
Financing of ARV Medicines
4.10.2.12 The sustained availability of ARVs is critical to the success of Namibia’s ART programme. As the number of patients receiving ART continues to increase, so does the cost of providing ART. Some of the factors that affect the scale and provision of ARVs are as follows:
• There has been an increase in the number of clients on ART since 2005 from 14,500 in
December 2005 to 65,000 by March 2009; • Switching clients from first line ART regimens to second line and salvage regimens, which
are more expensive than the first line regimens; • Changes in treatment guidelines have resulted in the replacement of regimens containing
Stavudine- with those containing Zidovudine; and it is likely that there will be a change in adult first line ART regimen from Zidovudine to Tenofovir; and
• Change in guidelines to initiate ART at a higher CD4 count.
4.10.2.13 The Government currently funds about 35 percent of the total cost of ARVs. The Clinton Foundation and PEPFAR, through CDC, contribute approximately five and 25 percent respectively, and the remaining 35 percent is supplied by the Global Fund. However, as the quantity of ARVs and OI drugs will need to be scaled up to support the increasing numbers of chronically ill and the expanded ART programme proposed under the RCC, a gap in funding for ARVs will become apparent. Moreover, as the cooperative agreement between the Government and the Clinton Foundation ends in December 2009, the funding gap will become greater. The situation is further exacerbated by the fact that PEPFAR/CDC announces the available funds for ARV medicines on an annual basis and the committed amounts will decrease by 10% annually beyond 2011.
4.10.2.14 In order to sustain the availability of ARV medicines, the Global Fund is requested to continue
co-financing the procurement of ARV medicines. Under the RCC, the Global Fund would fund the following for new and existing clients:
• 45 percent of the cost of the adult first line ARV medicines used by the majority of the adult population on ART; and
• The full cost of the top six (highest total cost) paediatric first line ARV medicines used by the majority of the paediatric population on ART.
4.10.2.15 CDC will fund second line treatment for new and existing clients. The Government will fund the rest of the ARV medicines, including those that cannot be paid for using GF or CDC. Please
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 104/160
refer to the ARV funding plan (Annex J38). Other System Strengthening Interventions
4.10.2.16 A comprehensive quality assurance system is crucial for ensuring that the public receives quality, efficacious and safe medicines. Apart from ensuring that all pharmaceuticals procured meet the Global Fund quality criteria, MoHSS’ Quality Surveillance Laboratory (QSL) performs tests to ensure that all pharmaceuticals delivered to the CMS meet the minimum quality standards before distribution. The QSL also performs post marketing surveillance by testing products from health facilities and the public that have queried quality. The QSL needs to be strengthened through the provision of equipment that is critical to perform these important tests. The equipment needs are as outlined in the HSS section of this proposal, since strengthening the QSL benefits all three diseases.
Other Capacity Building Assistance
4.10.2.17 Ensuring the rational use of pharmaceutical and other health products is important for the success of the HIV, TB and malaria programmes. The MOHSS, through the Therapeutics Information and Pharmacovigilance Centre (TIPC), provides broad-based medicine safety monitoring (pharmacovigilance) services. The TIPC also provides unbiased therapeutics information to health workers and the general public in Namibia.
4.10.2.18 In addition to the existing passive surveillance, the TIPC needs to further strengthen
pharmacovigilance by establishing an active surveillance system. This will allow the investigation of signals (reported cases of serious adverse effects) with significant public health importance. Further details on strengthening pharmacovigilance are given in the HSS section, where it has been included as part of the cross-cutting components benefitting all three diseases.
(b) Coordination of Ongoing Management of Pharmaceutical and Health Products with Other
Partners
4.10.2.19 The Government’s CMS procures all pharmaceuticals and health products for the public sector. CMS is responsible for the coordination of the distribution of all procured pharmaceuticals and health products through its well established distribution system. The PR ensures that all procured pharmaceuticals and health products meet the Global Fund quality criteria. Furthermore the PR ensures that the Global Fund price and quality report is completed for all pharmaceuticals and health products.
4.10.2.20 PEPFAR, through the PEPFAR-funded SCMS, procures some HIV and AIDS-related
commodities, of which a portion are supplied to the public sector through CMS and others to CSOs augmenting public sector service provision. It is not anticipated that the current coordination of procurement activities will change as a result of expanded interventions under the RCC.
4.11 Management of Pharmaceuticals and Health Products
New PR(s) and/or Newly Introduced Activities
4.11.1 Table of Amended Roles and Responsibilities Describe the amended roles and responsibilities for pharmaceutical and health products management under this proposal.
Activity Which organisations and/or departments are responsible for this function?
In this proposal what is the role of the organisation responsible for this function?
Does this proposal request funding for additional staff or technical assistance
Procurement policies & systems MoHSS PR No
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 105/160
Intellectual property rights Ministry of Trade and Industry None No
Quality assurance and quality control MoHSS PR No
Management and coordination More details required in s.4.11.3
MoHSS PR No
Product selection MoHSS PR No
Management Information Systems (MIS) MoHSS PR No
Forecasting MoHSS PR No
Procurement and planning MoHSS PR No
Storage and inventory management More details required in s.4.11.4
MoHSS PR No
Distribution to other stores and end-users More details required in s.4.11.4
MoHSS PR No
Ensuring rational use and patient safety (pharmacovigilance)
MoHSS PR No
4.11.2 Procurement Capacity
(a) Will management of pharmaceutical and health products be carried out (or managed under a sub-contract) exclusively by the Principal Recipient(s) or will sub-recipients also procure these products?
PR only
4.11.3 Alignment with Existing Systems Describe the extent to which ongoing management of pharmaceutical and health products under this proposal will be coordinated, to the extent possible and appropriate having regard to country contextual considerations, with other pharmaceutical and health product management actions undertaken in support of the national disease prevention and control program.
4.11.3.1 All pharmaceuticals and related products are procured through the MoHSS Pharmaceutical Services
sub-division, the CMS, and are stored and distributed through their normal channels. As a result there is no differentiation at the operational level between supplies purchased with funds from different development partners and those purchased by the MoHSS. This avoids parallel systems and minimises changes in product presentation (that might lead to reduced adherence by clients). In addition, sustainability is optimised by the avoidance of parallel systems.
4.11.3.2 Quality of pharmaceuticals is assured through the functions of another sub-division of the MoHSS
Pharmaceutical Services, Pharmaceutical Inspection and Control. Quality assurance is a result of the combination of a rigorous registration process and current good manufacturing practices, including inspection of manufacturing facilities and testing of samples and supplied products at the Quality Surveillance Laboratory.
4.11.3.3 The TIPC was established in 2007. The Centre serves as a reference unit with regard to collecting
pharmacovigilance information, monitoring and disseminating information on adverse drug reactions. The Medicines and Related Substance Control Act of 2003 requires that manufacturers and their representatives in Namibia keep records of all adverse reactions reported to them and submit these to the Namibian Medicines Regulatory Council. The Act further stipulates that the prescriber has to inform the Namibian Medicines Regulatory Council of any adverse effects of any of the medicines prescribed.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 106/160
4.11.4 Storage and Distribution Systems
(a) Will the same organisation as in the expiring grant provide the supply management (storage and distribution) functions for pharmaceutical and health products during the proposal term?
Yes
(b) Indicate which types of organisations will be involved in the supply management of pharmaceutical and health products during the proposal term. If more than one of the adjacent boxes is checked, also briefly describe the inter-relationships between these entities when answering (c) and (d) below.
National medical store, the CMS
(c) Describe each organisation's current storage capacity for pharmaceutical and health products, and indicate how a possible scaling up of interventions and increased requirements under this proposal will be transparently and effectively managed.
Capacity 4.11.4.1 CMS: The CMS serves as the Ministry's central agency for procurement, storage and distribution of
essential medicines and related clinical supplies for the entire public health sector. Medicines procured, stored and distributed are those approved by the MOHSS and are specified in the Namibian Essential Medicines List (Nemlist). The CMS manages about 1,600 items sourced from some 75 suppliers.
4.11.4.2 The CMS manages annual procurement to the value of around US$34 million. Currently it has a total
warehouse area of 4,000 m² and of this one-third is occupied by ARV medicines. Clearly, available storage space is a major constraint. Some work has been undertaken using PEPFAR funding through the Supply Chain Management System (SCMS) to renovate and reorganise storage in the CMS. This has resulted in a doubling of capacity to store ARVs. However, there is an urgent need to construct a new, purpose-built CMS; and this is planned as part of Namibia’s National Development Plan III.
4.11.4.3 In addition to the CMS there are two Regional Medical Stores in Oshakati and Rundu. These two
stores receive supplies directly from the CMS and supply health facilities in their vicinity with pharmaceuticals and related supplies. Other hospitals receive their supplies directly from the CMS. The storage floor space at the Regional Medical Stores is 550m² in Oshakati and 420 m² in Rundu. Both Regional Stores currently only have storage on one level but a proposal is in the pipeline to strengthen the flooring and introduce a mezzanine floor for ARV storage.
(d) Describe each organisation's current distribution capacity for pharmaceutical and health products. In your
response, indicate how any increased responsibility for distribution of pharmaceutical and health products under this proposal will be managed, and potential challenges addressed. In addition, provide an indicative estimate of the percentage of the country and/or population covered by pharmaceutical and health product management services under this proposal, and the relative percentage increase (if any) this represents on existing distribution arrangements for the nominated distribution partners.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 107/160

4.11.4.4 The CMS distribution channels are described in Figure 14 below.
Figure 14: CMS Distribution Channels
Rehoboth Health Centre
2 Health Centres (Katutura & Khomasdal) and 8 Clinics
12 Health Centres and 61 Clinics
Oshakati Regional Medical Store
6 District Hospitals: Okahao, Outapi, Tsandi, Okongo, Eenhana and Engela
Partners eg SCMS & CHAI
3 Intermediate Hospitals: Katutura, Oshakati and Rundu
Commercial Suppliers Central Medical Stores
26 District HospitalsEach District hospital supplies Health Centers and Clinics in
its District
Procurement Committee5 Catholic Health Services
Hospitals: Oshikuku, St Marys, Aroab, Nyangana and Andara
Rundu Regional Medical Store7 Health Centres & 15 Clinics
in Rundu district
National Referral Hospital: Windhoek Central Hospital
Nankudu Hospital which supplies its Clinics and Health
Centres
1 Lutheran Medical Services Hospital: Onandjokwe
4.11.4.5 The CMS runs its own fleet, with four 20-ton trucks and one 5-ton truck. This fleet supplies the two
Regional Medical Stores and 29 public hospitals countrywide, as well as five health centres, ten clinics and 15 school hostels in Khomas Region. It delivers supplies to these sites every six weeks, according to a delivery schedule. Due to an increase in patient enrolment in the HIV, TB and malaria programmes, in addition to the normal distribution carried out by the CMS there has been an increase of about 33 percent in the level of activities that the fleet has to handle.
4.11.4.6 The challenges experienced with the current distribution system are as follows:
1. The fleet is aging; two of the trucks are nearly 20 years old. This results in frequent breakdowns and high maintenance costs. When any of the large trucks are off the road, deliveries have to be sent using the Nampost courier which is not cost effective.
2. The greatly increased volume of supplies to be delivered to hospitals means that the current fleet is inadequate to meet demand. There are reduced possibilities for combined deliveries due to the increased volume being delivered to each hospital.
3. Loading and unloading the trucks is very labour intensive and often the trucks are delayed at a delivery point while the hospital finds staff to assist with unloading. This problem will be addressed by palletising deliveries. However, to manage the trucks will have to be equipped with
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 108/160

mechanical tail lifts and pallet movers, and all receiving health facilities will also require manual pallet movers.
4. The implementation of palletised deliveries will also improve the security of goods in transit as the pallets will be wrapped, so any tampering will be immediately evident.
5. Only two of the current large trucks have temperature control facilities. This is far from ideal in the Namibian climate where temperatures frequently exceed 40°C and the distances to be covered by the trucks are very far. It is therefore planned to purchase trucks with temperature control facilities, plus cold storage compartments.
4.11.4.7 The CMS distribution system supplies medicines for the entire public health system that caters for the
health needs of approximately 95 percent of the Namibian population. The remaining five percent receive their health care from private providers. With regard to provision of ART services, the MoHSS currently has over 65,000 clients receiving ARVs. This figure is expected to increase to approximately 110,000 by 2015 – an increase of almost 70 percent. Obviously this will have a significant impact on the demands placed upon the CMs’ distribution system.
4.11.4.8 The Regional Medical Stores also deliver scheduled orders to their clients. These stores experience
similar problems to the CMS. Therefore there is an urgent need to procure new, temperature controlled delivery trucks for both Regional Stores.
4.11.4.9 Ideally the CMS will, in the future, also be responsible for the distribution of HBC kits. Currently, the
HBC programme is utilising hired trucks to transport the kits with support from SCMS, a PEPFAR-implementing partner that also helps in the forecasting and pipeline monitoring of the flow of the kits. However, CMS cannot take this function over until its current transport crisis has been addressed.
4.11.5 Pharmaceutical and Health Products Selection • Complete 'Attachment B' to this Proposal Form for the relevant disease, to list all of the pharmaceutical and
health products that are requested to be funded in this proposal. Also include the expected costs per unit, and information on the existing 'Standard Treatment Guidelines ('STGs').
• If the pharmaceutical products included in ‘Attachment B’ are not included in the current national, institutional or World Health Organisation STGs, or Essential Medicines Lists ('EMLs'), describe below the STGs that are planned to be utilized, and the rationale for their use.
N/A
4.11.6 Multi-drug-resistant tuberculosis (HIV and tuberculosis proposals only)
Is the provision of treatment of multi-drug-resistant tuberculosis included in this HIV proposal as part of HIV/TB collaborative activities?
No
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 109/160

COPY AND AND INSERT HERE THE OPTIONAL HEALTH SYSTEMS STRENGTHENING CROSS-CUTTING SECTION 4.B IF RELEVANT TO STRATEGY OF
ROLLING CONTINUATION CHANNEL PROPOSAL
4B. Program Description - HSS Cross-cutting Interventions
4B.1 Description of 'HSS cross-cutting intervention'
Title: Intervention 1 Improving equitable access to affordable and quality health care
Beneficiary Diseases: HIV, TB, Malaria
WHO "Building Block" category Service Delivery
(a) Description of rationale for and linkages to improved/increased outcomes in respect of HIV, tuberculosis and/or malaria:
The first HSS component on service delivery is based on the Namibian MOHSS strategic plan for 2009-2013 (Annex J7), which articulates the concerns of the extensive 2008 MOHSS Health and Social Services Systems Review (Annex J6) undertaken to highlight the service delivery gaps. Various technical policies and reports that provide guidance for service implementation are available on the website – http://www.healthnet.org.na The national health system’s needs, including public sector, NGO, FBO, private sector and community systems, are integrated and described in this HSS component below. This HSS request primarily strengthens Namibia’s regional and district health services programme whose objective is to promote, protect and improve the health of families, especially women and children, with the specific aim of reducing maternal and infant deaths, as well as malnutrition among under-fives; to increase coverage and access of FP and RH health services at the primary and secondary health care level within the health districts; the strengthening of outreach mobile services. Improve public health education, environmental health in rural areas and the provision of HIV Rapid Testing, ART and PMTCT services. 1.1. Inadequate mobile diagnostic/treatment and outreach services in the public sector Given the vast distances and the sparsely populated regions within the country (Annex J8, Demographic and Health Survey, 2006/07), outreach/mobile services are essential for areas where it would be inefficient to construct static facilities (Annex E4, Health Facility Inventory). The country’s small population is widely dispersed and there is no public transportation in very remote rural areas. The population is very poor. Village level participatory poverty assessment studies show that, while people understand the importance of using a condom, they cannot access them easily. For example, the nearest MOHSS clinic where free condoms are available may be as much as 75 km away, and few can afford to buy condoms from the local shops or shebeens. Moreover, in the absence of mobile services, district-level programmes such as DOTS, malaria education, VCT, ART, and immunisation cannot be effectively delivered. In the public sector, PHC outreach is based on a roster whereby communities are visited on a six-week schedule. The PHC Programme serves all 13 regions (health directorates) via 34 health districts, 44 health centres, 265 clinics and 1,150 outreach points across the country. Through these established structures the MOHSS provides comprehensive outreach in partnership with CSOs. The MOHSS Systems Review (op. cit., p. 4) identified that the formal structure for health extension work
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 110/160

in communities ends at clinics and outreach points. Although the MOHSS prioritises CBHC implementation and has trained about 5,000 community health workers, there are no clear formal structures to support CBHC. The Review (ibid, p.9) found that most regions had no vehicles for outreach: this adversely affects a number of health indicators such as coverage for the expanded programme of immunisation (EPI) and infant mortality rates (IMR). Communities are informed beforehand when to gather at the outreach points. However, with the considerable constraints arising due to the lack of fully equipped vans, the ageing fleet of district and regional vehicles, inadequate organisation and poor linkages with community structures, the messages sometimes reach the communities very late, and not enough people present for outreach services. The MOHSS has Draft National Guidelines for Outreach Services (Annex 5.2) and elements of these were incorporated into the Guidelines for Outreach Counseling and Testing (CT) which was launched towards the end of 2007 (Annex E5.1). These two documents highlight the MOHSS’ aims and management of outreach activities. In 2008, the MOHSS conducted a successful National HIV Testing event for the first time in Namibia to encourage testing, particularly through use of outreach services. Examples from the private sector through the two NABCOA mobile units launched earlier this year show that mobile outreach clinics have the potential to offer more than just VCT. The scaled up package that will be offered by the mobile outreach service is summarised in Table 10A below.
Table 10A: Minimum Package for Outreach Services
Compulsory HCT Services currently offered using the available vehicles
Additional services to be offered using mobile vans to be brought in with CDC and Global Fund resources
• Health information and education on HIV and AIDS (group sessions, pamphlets, leaflets, posters etc).
• Individual or couple pre-test counselling.
• HIV Rapid Testing. • Individual or couple post-test
counselling. • Condom demonstrations and
distribution. • Referrals for HIV treatment,
care and support services.
• Case management: Malaria, TB and ART clinics. • Health information and education sessions on TB,
STI, FP and ART. • Health information and education sessions on
seasonal health risks applicable to the specific community such as risk of waterborne diseases and malaria.
• TB screening and referral. • STI screening and referral. • SRH services, including FP. • Weight measurements, cholesterol checks, blood
pressure checks. • Baby clinics.
The minimum package integrates SRH services with HIV, and MCH integration with HIV services for pregnant women. The aforementioned NABCOA mobile vans for the WPP were donated by the GF and PharmAccess, and they are working very well. However, only six months after their launch the uptake has been so great that demand has far outstripped availability; hence NABCOA requires two additional vans which will be provided under the HIV disease component of this proposal. Annex E6 shows a photo of van, and Annexes E6.1 and E6.2 its interior. The aim is to expand and improve outreach in the public sector, by procuring a total of 13 vans, one per region, to replicate this private sector success story in the public sector. Thus CDC will provide seven mobile clinics, to be maintained by the GRN, and GF support is needed to fill the gap of six vans, including their maintenance. These will be purchased in Year 1. To improve planning, delivery integration, coordination and reporting on all the outreach services in the public sector there is a need to recruit 1 National Health Extension Coordinator to be based in the PHC Directorate, while the regions would be advised to select an Extension Task Manager from among existing staff. The National Coordinator would be responsible for liaising with all MOHSS directorates and the regions to ensure better scheduling, and improved community preparation both for the interventions and also for follow up after mobile interventions. The mobile clinics would be based in the
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 111/160

regions, and allocated one per region, but their utilisation would be nationally coordinated, thus the National Coordinator would be able to deploy the mobile vans to regions facing challenges like flood disaster in the north of the country, and also prioritise regions with rougher terrain, larger geographical distances and poorer infrastructure. The Coordinator working with the M&E Unit would update M&E forms to reflect this activity, and would prepare a section on this activity in the MOHSS Annual Report that synthesises the number of outreach activities, number and type of diagnosis/treatment provided, type of vehicle and personnel used in outreach, management and coordination of outreach at national, regional and district levels, and the successes, challenges and lessons learned. The expected outcome is not just in terms of the Iv programme; this intervention would also result in improved EPI, decreased IMR, and better RH outcomes, including a decrease in unwanted pregnancies. 1.2. Inadequate logistics Inadequate transportation affects service delivery because it is difficult to plan and implement supervisory and technical backstopping from region to district and from the district to the rural clinics and outreach sites. The current fleet of vehicles bought between 2005-2008 is ageing, not so much in terms of the number of years they have been in use, but in terms of their high mileage. Diagnostic services and referral to higher levels of care are central to the management of HIV, TB and Malaria. Hospitals offer a comprehensive range of diagnostic and clinical services. Samples and/or patients are transported from lower level facilities to the NIP based at district hospitals. This system works reasonably well but is constrained by the lack of functional transport at health centres and clinics (Annex J6, op. cit. 2008). This makes it difficult to collect and deliver samples to the laboratories and also affects referral services. By 2016, many of the vehicles purchased between 2005 and 2008 will have exceeded the manufacturing warranty mileage due to their extensive use. Cars that have exceeded an economically useful life are more inefficient because of increased operational and maintenance costs. Twenty vehicles in the current fleet will therefore need to be replaced between 2010 and 2013 (Annex E7, Fleet Inventory). This investment is substantial but essential for addressing the transport-related constraints to service delivery. In order to secure as well as improve the control and management of the fleet and other assets, a computerised software system linked to sequenced barcodes on the equipment and vehicles will be installed. This system will also be linked to the Accounting and Finance Department for purposes of reinforcing accountability. Three officers will be trained on the latest version of computer software asset tracking and the drivers will also be trained on safe driving techniques, vehicle maintenance and how to make their inputs in the effective use of the fleet management computer software. The drivers would be trained in Years 1, 3 and 6. Supervision Supportive supervision and technical backstopping from the regional level to district level and from the district to health facilities has not only been affected by lack of vehicles, but also due to the inadequate linkage of supervision to the Performance Management System (PMS). The United States Agency for International Development (USAID) will provide support for the PMS review and the Government will provide more funds to cover the costs of routine supervision particularly from July 2012, when funds in the existing Global Fund Round 5 TB and Round 6 Malaria grants to support this activity will cease. Beyond the support requested for the additional vehicles which enhances supervision, no other support for supervision is required from the Global Fund in this RCC, as the government and USAID will provide additional funds for this activity. Government would be supported by USAID to train the health workforce on supervisory skills and mentorship of subordinates, and the staff would be assessed on how well they discharge this vital responsibility in their annual performance reviews. The enhanced transport logistics and provision of the replacement vehicles to be supported by the Global Fund would improve supervision. 1.3. Inadequate infrastructure for service delivery and staff accommodation As previously noted, existing health facilities are inadequate to cope with the increased case load related to the epidemic of HIV and TB and Malaria, which have bought greater numbers of outpatients to the health facilities. The early effects of the rapid population growth rate (Annex J10, Population Projections 2001-2031) also contributes to service overload, and health facilities must have adequate space for SRH services including FP and STI, critical to slowing down the population growth rate as well as STI
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 112/160

infection rates. It is apparent that, in spite of a small population, the constrained ability of the health system to provide SRH services is reflected in adverse health outcomes such as high maternal mortality and morbidity. The socio-economic consequences of rapid population growth have resulted in the rural-urban migration of youths accompanied by a proliferation of informal settlements around cities, high youth unemployment and crime. These trends are escalating, with the capital city of Windhoek growing at 4.3 percent annually. There is therefore a clear requirement for the RCC HSS request to recognise the importance of dealing with SRH within health system needs. Attainment of the SRH goals and targets, as outlined in the Millennium Development Goals (MDGs), also directly affect achievement of the HIV MDG as well as the education and gender MDGs. The Government has made considerable efforts to improve the availability of ART; in FY 2006/07 ART was only available in 34 hospitals (Annex J12, MTEF 2009/10 – 2011/12, p. 317) but by 2008 the number had increased to 58 facilities, including health centres and clinics. However, space at facilities is inadequate and has been improvised by converting outpatient waiting rooms into consulting rooms to provide for ART and TB services. The facilities are currently overwhelmed, with inadequate space for privacy during consultations, particularly for VCT and counselling for GBV. Examination rooms for FP and pregnant women are insufficient. Hospital wards are inadequate for TB-MDR treatment, given the lack of infection control and densely populated waiting rooms. Rural communities lack adequate staff housing, so it is difficult to retain staff in the rural clinics. Moreover, the budget allocated to maintenance in the public sector is low and public health facilities are therefore often poorly maintained (Annex J6, op. cit.). The response has consisted of building temporary shelters outside clinics, and implementing clinic expansion and staff accommodation in hard-to-reach communities through GRN remodelling of hospitals and clinics to provide more wards, including for TB. PEPFAR has remodelled ART/ANC sites in hospitals and clinics, including some of the facilities of the Ministry of Defence.
Lessons have been learned and renovations are now better managed, as discussed in earlier sections of this proposal. The GRN and its partners are now ready to undertake the essential renovations and constructions needed to ensure privacy, improve quality of care, infection control and patient satisfaction and to retain staff in remote areas with better accommodation. Thus the GF is required to renovate 20 health facilities to create space for VCT and integrated services that include TB and Malaria; expand and renovate eight hospitals and 13 clinics to accommodate ART facilities; and meet infection control standards due to the high rate of TB/HIV co-infection in the country (~60%). Clinics in remote locations will be upgraded to include staff accommodation. 1.4. Inadequate services for people with Disabilities People with disabilities are not adequately served by existing HIV and AIDS, TB and Malaria services. Many disabled adolescents are unable to access SRH services, and are also more likely to be exposed to sexual abuse and violence. When deaf people present in clinics, given the overcrowding and pressure of work, they are forced to wait until after all other patients have been attended to, and are treated last. Other reasons for poor service delivery for the disabled are the lack of sign language interpreters and material in Braille. A consultant will be engaged to assist the public, private and NGO sectors including NANASO, the various associations for the disabled, and the National Disability Council to develop a protocol/guide for managing the disabled in the health care system, to be printed and widely disseminated in the aforementioned sectors. However, only the guide will be printed under the HSS component. All other IEC/BCC materials for the disabled will be produced under the specific disease component. The MOHSS will improve services for the disabled by setting up regular monthly clinic for the disabled linked to interpreter services for the deaf disabled. Transport and incentives for the Interpreters will be provided. Special outreach through the mobile clinics described under 1.1 will also be offered in collaboration with the associations for the disabled. All these interventions described under sections 1.1 to 1.4 above are in line with the MOHSS Strategic Plan as follows:
1. Service Provision includes “improved fleet management”.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 113/160
2. Infrastructure Development and Management states “The minimum District Service Packages will be defined, sufficient extension of health services at community level will be implemented. Adequate development and maintenance strategies for health facilities will be effected and the often unnecessary and expensive referral system will be optimised”.
3. Governance: “Address problems of inadequate/inappropriate information and communication
technologies coordination, delayed payment of suppliers, poor record keeping, poor communication and coordination, bureaucracy, outdated legislation, policies, guidelines”.
HSS Service Delivery Objective 1a: Strengthen the availability and accessibility of quality HIV, TB and Malaria services (Service Delivery)
Detailed Activities
1.1 Provision of personnel and equipment (mobile clinic vans) to strengthen coordination and delivery of mobile and outreach health services in the public sector-(continuation and scale-up of Round 2).
1.1.1 Procure 6 4x4 special vehicles equipped for mobile diagnostic and treatment. 1.1.2 Provide for fuel & maintenance for 6 vans for the public sector at 40,000 kms per year, including insurance. 1.1.3 Recruit 1 National Coordinator in PHC Directorate to liaise with regions to manage mobile health services and their linkage with PHC and community health extension workers.
1.2 Provision of transport to strengthen referral and supervisory services, delivery of samples, management of district hospitals, health education and condom distribution (continuation and scale–up of Round 2).
1.2.1 Procure 20 4x4 Double Cabin Flatbed Jeeps for district hospitals. 1.2.2 Provide for fuel and maintenance for 20 DC's at 40,000 kms per year. 1.2.3 Insure 20 4x4 Double Cabin Flatbed Jeeps annually. 1.2.4 Contribute to the procurement, instalment and maintenance of fleet management software either from MoHSS or from a subcontractor, including training 3 staff on the use of the software. 1.2.5. Train drivers on safe driving techniques, vehicle maintenance and use of fleet management computer software in Years 1, 3 and 6.
1.3 Provide adequate space for service provision and staff accommodation (continuation and scale–up of Round 2).
1.3.1 Utilise in-house Architects for site-specific assessment and to collate documentation, including that on community participation arranged by the MOHSS PHC Directorate. 1.3.2 Renovate 20 health facilities to create space for VCT and other integrated services, (including pharmacy dispensaries and storage areas). This would be implemented as follows: 2 in Year 1, 8 in Year 2, 8 in Year 3 and 2 in Year 4. 1.3.3 Renovate 8 hospitals, 4 per annum (Aranos, Grootfontein, Keetmanshoop, Luderitz, Okaho, Opuwo, Rundu and Swakopmund) to accommodate ART, (including waiting area, pharmacy dispensaries and storage areas) and other facilities. 1.3.4 Build 13 clinics in remote communities (2 in Year 1, and 3 in subsequent years) to accommodate ART and other facilities (including pharmacy dispensaries and storage areas). 1.3.5 Convert old clinic buildings to staff accommodation for 13 remote communities.
1.4 Improve services for people with disabilities (continuation and scale–up under Round 2).
1.4.1 Hire 1 Consultant to assist organisations for the disabled (Deaf, Blind, etc ) to establish a database of sign language interpreters, Braille material, etc. and develop a protocol for the employment of interpreters; secure material in Braille in collaboration with NANASO and MOHSS DSP and PHC directorates. 1.4.2. Print copies of the protocol for use as guidelines in facilities and as training material. 1.4.3. Conduct a dissemination workshop to communicate database and protocols to relevant stakeholders ( including the private sector) for further dissemination and use. 1.4.4. Employ and compensate (transport and incentives) interpreters as and when required by clients with hearing disabilities (health facility Social Workers arrange for Deaf Sign Language Interpreters ahead of clinic appointments for deaf people). 1.4.5. Organise special outreach using diagnostic vans above to offer services to deaf, blind,
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 114/160
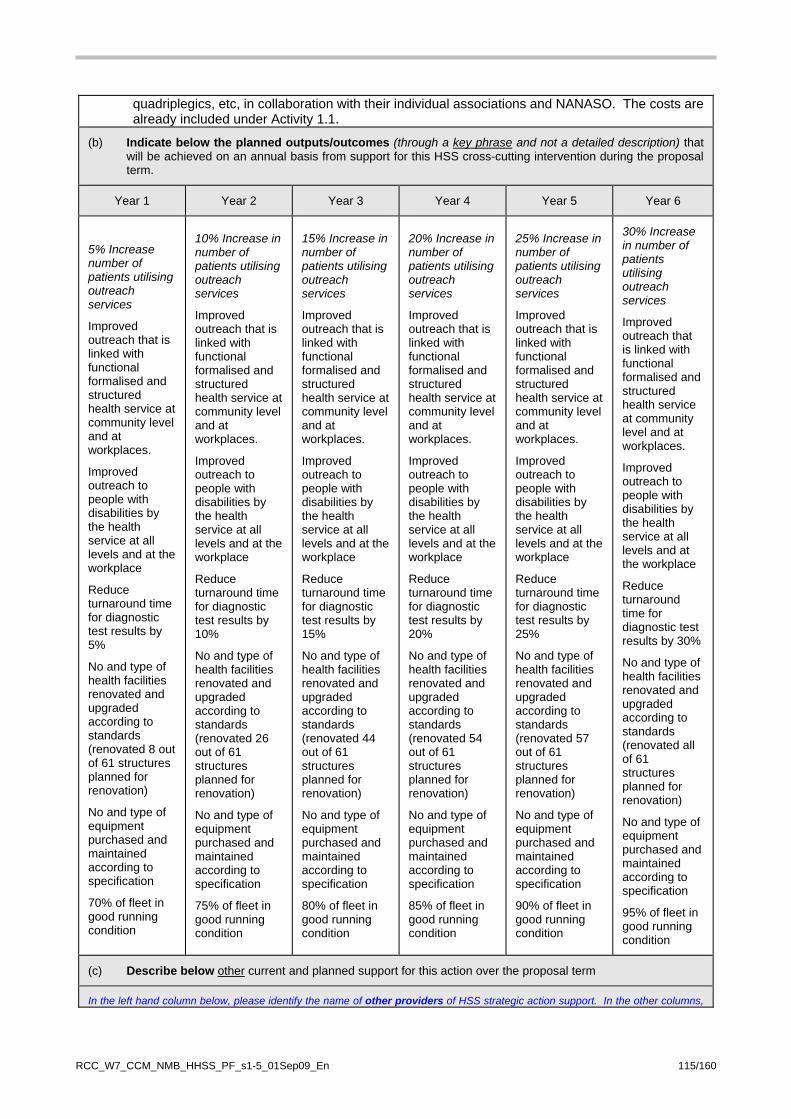
quadriplegics, etc, in collaboration with their individual associations and NANASO. The costs are already included under Activity 1.1.
(b) Indicate below the planned outputs/outcomes (through a key phrase and not a detailed description) that will be achieved on an annual basis from support for this HSS cross-cutting intervention during the proposal term.
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
5% Increase number of patients utilising outreach services
Improved outreach that is linked with functional formalised and structured health service at community level and at workplaces.
Improved outreach to people with disabilities by the health service at all levels and at the workplace
Reduce turnaround time for diagnostic test results by 5%
No and type of health facilities renovated and upgraded according to standards (renovated 8 out of 61 structures planned for renovation)
No and type of equipment purchased and maintained according to specification
70% of fleet in good running condition
10% Increase in number of patients utilising outreach services
Improved outreach that is linked with functional formalised and structured health service at community level and at workplaces.
Improved outreach to people with disabilities by the health service at all levels and at the workplace
Reduce turnaround time for diagnostic test results by 10%
No and type of health facilities renovated and upgraded according to standards (renovated 26 out of 61 structures planned for renovation)
No and type of equipment purchased and maintained according to specification
75% of fleet in good running condition
15% Increase in number of patients utilising outreach services
Improved outreach that is linked with functional formalised and structured health service at community level and at workplaces.
Improved outreach to people with disabilities by the health service at all levels and at the workplace
Reduce turnaround time for diagnostic test results by 15%
No and type of health facilities renovated and upgraded according to standards (renovated 44 out of 61 structures planned for renovation)
No and type of equipment purchased and maintained according to specification
80% of fleet in good running condition
20% Increase in number of patients utilising outreach services
Improved outreach that is linked with functional formalised and structured health service at community level and at workplaces.
Improved outreach to people with disabilities by the health service at all levels and at the workplace
Reduce turnaround time for diagnostic test results by 20%
No and type of health facilities renovated and upgraded according to standards (renovated 54 out of 61 structures planned for renovation)
No and type of equipment purchased and maintained according to specification
85% of fleet in good running condition
25% Increase in number of patients utilising outreach services
Improved outreach that is linked with functional formalised and structured health service at community level and at workplaces.
Improved outreach to people with disabilities by the health service at all levels and at the workplace
Reduce turnaround time for diagnostic test results by 25%
No and type of health facilities renovated and upgraded according to standards (renovated 57 out of 61 structures planned for renovation)
No and type of equipment purchased and maintained according to specification
90% of fleet in good running condition
30% Increase in number of patients utilising outreach services
Improved outreach that is linked with functional formalised and structured health service at community level and at workplaces.
Improved outreach to people with disabilities by the health service at all levels and at the workplace
Reduce turnaround time for diagnostic test results by 30%
No and type of health facilities renovated and upgraded according to standards (renovated all of 61 structures planned for renovation)
No and type of equipment purchased and maintained according to specification
95% of fleet in good running condition
(c) Describe below other current and planned support for this action over the proposal term
In the left hand column below, please identify the name of other providers of HSS strategic action support. In the other columns,
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 115/160
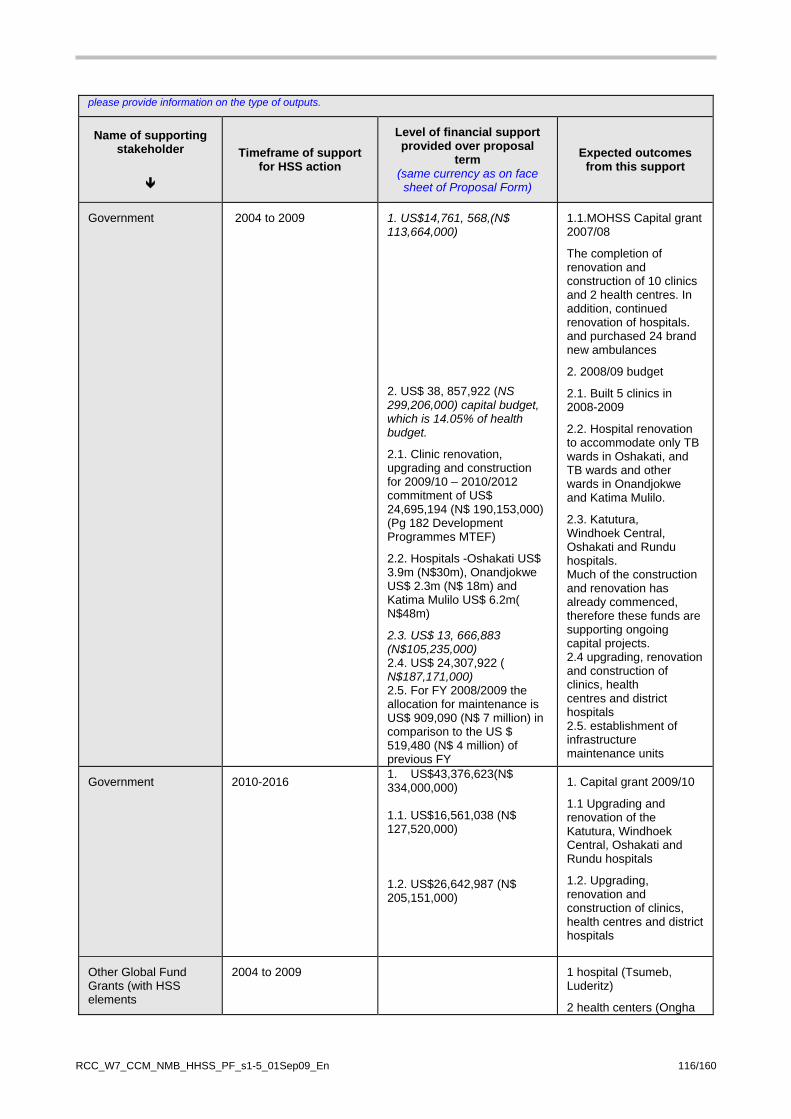
please provide information on the type of outputs.
Name of supporting stakeholder
Timeframe of support for HSS action
Level of financial support provided over proposal
term (same currency as on face sheet of Proposal Form)
Expected outcomes from this support
Government 2004 to 2009 1. US$14,761, 568,(N$ 113,664,000)
2. US$ 38, 857,922 (NS 299,206,000) capital budget, which is 14.05% of health budget.
2.1. Clinic renovation, upgrading and construction for 2009/10 – 2010/2012 commitment of US$ 24,695,194 (N$ 190,153,000) (Pg 182 Development Programmes MTEF)
2.2. Hospitals -Oshakati US$ 3.9m (N$30m), Onandjokwe US$ 2.3m (N$ 18m) and Katima Mulilo US$ 6.2m( N$48m)
2.3. US$ 13, 666,883 (N$105,235,000) 2.4. US$ 24,307,922 ( N$187,171,000) 2.5. For FY 2008/2009 the allocation for maintenance is US$ 909,090 (N$ 7 million) in comparison to the US $ 519,480 (N$ 4 million) of previous FY
1.1.MOHSS Capital grant 2007/08
The completion of renovation and construction of 10 clinics and 2 health centres. In addition, continued renovation of hospitals. and purchased 24 brand new ambulances
2. 2008/09 budget
2.1. Built 5 clinics in 2008-2009
2.2. Hospital renovation to accommodate only TB wards in Oshakati, and TB wards and other wards in Onandjokwe and Katima Mulilo.
2.3. Katutura, Windhoek Central, Oshakati and Rundu hospitals. Much of the construction and renovation has already commenced, therefore these funds are supporting ongoing capital projects. 2.4 upgrading, renovation and construction of clinics, health centres and district hospitals 2.5. establishment of infrastructure maintenance units
Government 2010-2016 1. US$43,376,623(N$ 334,000,000) 1.1. US$16,561,038 (N$ 127,520,000) 1.2. US$26,642,987 (N$ 205,151,000)
1. Capital grant 2009/10
1.1 Upgrading and renovation of the Katutura, Windhoek Central, Oshakati and Rundu hospitals
1.2. Upgrading, renovation and construction of clinics, health centres and district hospitals
Other Global Fund Grants (with HSS elements
2004 to 2009
1 hospital (Tsumeb, Luderitz)
2 health centers (Ongha
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 116/160

and Otavi)
2 clinics (Okuryangava, Kasheshe
Renovated 18 ART/VCT facilities
HIV/AIDS Round 2 grant-bought a total of 61 vehicles, 34 in Phase 1 and 27 in Phase 2
CDC 2004 to 2009 Vehicles- $3,003,690
Clinical and laboratory equipment- $4,705,603
Health facility renovations-$3,880,810
31 Vehicles, 19 bought in 2005, 12 in 2006 and 2 in 2007)
Clinical and laboratory equipment
Renovation of 9 ART/ANC Sites- 6 hospitals (Eenhana, Engela, Okongo, Oshakati, Otjiwarongo, Gobabis)
1 Clinic (Kuisebmund – Walvis Bay)
CDC 2010-2016 Reduce by !0% annually Vehicles, Clinical and laboratory equipment
Clinton Foundation 2007-2009 US$230,896 (N $1,777,900)
1. Renovated TB/ART Clinic at Katutura Health Centre
I-TECH 2004-2009 Equipment/renovations $ 150,000
Equipment/renovations Ministry of Defense lab equipment Ministry of Defense renovations for Counselling and Testing Sites Ministry of Defense renovations for ART site Ministry of Defense renovations for lab National Institute of Pathology labs renovations
National Institute of Pathology renovations of resource center
I-TECH 2010-2016 Equipment/renovations $300,000
Equipment/renovations Ministry of Defense renovations for additional Counseling and Testing Sites
Ministry of Defense renovations for 1 additional ART site
Dutch Foreign Ministry implemented by PharmAccess
2004-2009 Approximately 10—15%, 30,000 Euros of total Okambilimbili programme
Mobile VCT and wellness screening services in the private sector consisting
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 117/160
cost €3,000,000 of 1 Mobile Clinic
4B.1 Description of 'HSS cross-cutting intervention'
Title: Intervention 2 To reduce vacancy rates among health workers and providing a conducive environment for health workers (with emphasis on hard to reach areas)
Beneficiary Diseases: HIV, TB, Malaria
WHO "Building Block" category Health Workforce
(a) Description of rationale for and linkages to improved/increased outcomes in respect of HIV, tuberculosis and/or malaria:
The interventions proposed under this intervention are in line with the MOHSS Strategic Plan, which under Human Resource Management, states “Recruitment, remuneration and retention policies and strategies will be reviewed and upgraded, decision-making will be devolved to appropriate levels and staff shortages will be vigorously addressed.” Scaling up access to HIV, TB and malaria diagnosis and treatment is reliant on an adequate supply of appropriately trained human resources for health (HRH). Although overall the proportion of health workers, at 3.0 per 1000, is above the 2.5/1000 population recommended by WHO international guidelines, there is in general a wide disparity between the private and public sectors as well as the rural and urban areas. Within the public sector, there are chronic shortages for frontline workers (particularly doctors and pharmacists) which if addressed could reach the 2.5 WHO benchmark in the public sector. There is also a marked disparity in health worker capacity between the public and private sectors as well as according to urban and rural distribution. A factor which contributed to this in the past was the lack of incentives and enhancements to ensure a more equitable distribution of the workforce. While low remuneration contributes to attrition from the public sector, the low production of health workers from training institutions, the lack of appropriate incentives and the high demand for health services created by the three diseases have also contributed significantly to vacancy rates in the health sector in Namibia. 2.1 Initiatives To Retain Health Workers In The Public Sector The GRN has responded to the above challenges by developing a HRH strategy, which is critical for sustainability once the foreign workforce leaves (as it will when expatriates from Kenya, Nigeria and Zimbabwe, where the bulk of the foreign workforce come from, leave as conditions improve in their countries). If the HRH strategy is implemented as planned, the identified vacancies should be filled, even taking into consideration the 5 percent attrition in the public sector. To minimise this attrition, one year of mandatory community service will be enforced for all students financed by both national and development partners. The MOE, which oversees the Namibia Financial Assistance Fund in collaboration with the MOHSS, and other relevant institutions are working out details on the bonding of students to the public service. The deprivation package to attract health workers had been abolished because it was found to be ineffective. However, an incentive package that includes an increase in salary adjustment of 28 percent for lower categories and 24 percent for higher categories, as well as housing benefits, has been approved for implementation in financial year 2009/2010, as contained in Annex E25, PSM Circular No of 2009 - General Salary Adjustment and Annex E26, Housing Allowance For Staff Members Below The Management Cadre. For health workers undertaking post-graduate studies, the MOHSS supports staff members with tuition fees and living allowances on top of their salaries. With regard to medical officers, the MOHSS has a policy which allows for limited private practice. Finally, the OPM is coordinating a committee which aims at setting the norms for the provision of incentives for health workers in rural and hard-to-reach areas; and through the NDP III a considerable amount of renovation and building of staff accommodation is being implemented, particularly in remote areas. While some health workers will undoubtedly be lost to both the global market and the private sector,
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 118/160
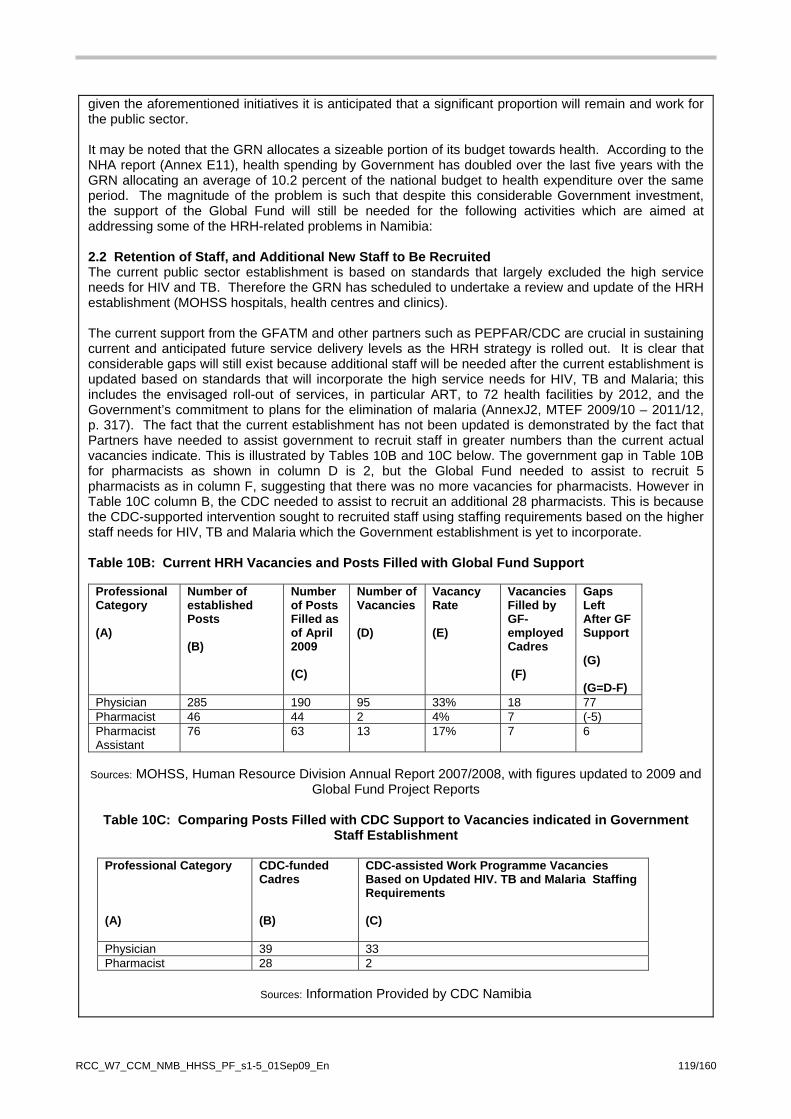
given the aforementioned initiatives it is anticipated that a significant proportion will remain and work for the public sector. It may be noted that the GRN allocates a sizeable portion of its budget towards health. According to the NHA report (Annex E11), health spending by Government has doubled over the last five years with the GRN allocating an average of 10.2 percent of the national budget to health expenditure over the same period. The magnitude of the problem is such that despite this considerable Government investment, the support of the Global Fund will still be needed for the following activities which are aimed at addressing some of the HRH-related problems in Namibia: 2.2 Retention of Staff, and Additional New Staff to Be Recruited The current public sector establishment is based on standards that largely excluded the high service needs for HIV and TB. Therefore the GRN has scheduled to undertake a review and update of the HRH establishment (MOHSS hospitals, health centres and clinics). The current support from the GFATM and other partners such as PEPFAR/CDC are crucial in sustaining current and anticipated future service delivery levels as the HRH strategy is rolled out. It is clear that considerable gaps will still exist because additional staff will be needed after the current establishment is updated based on standards that will incorporate the high service needs for HIV, TB and Malaria; this includes the envisaged roll-out of services, in particular ART, to 72 health facilities by 2012, and the Government’s commitment to plans for the elimination of malaria (AnnexJ2, MTEF 2009/10 – 2011/12, p. 317). The fact that the current establishment has not been updated is demonstrated by the fact that Partners have needed to assist government to recruit staff in greater numbers than the current actual vacancies indicate. This is illustrated by Tables 10B and 10C below. The government gap in Table 10B for pharmacists as shown in column D is 2, but the Global Fund needed to assist to recruit 5 pharmacists as in column F, suggesting that there was no more vacancies for pharmacists. However in Table 10C column B, the CDC needed to assist to recruit an additional 28 pharmacists. This is because the CDC-supported intervention sought to recruited staff using staffing requirements based on the higher staff needs for HIV, TB and Malaria which the Government establishment is yet to incorporate. Table 10B: Current HRH Vacancies and Posts Filled with Global Fund Support
Professional Category (A)
Number of established Posts (B)
Number of Posts Filled as of April 2009 (C)
Number of Vacancies (D)
Vacancy Rate (E)
Vacancies Filled by GF-employed Cadres (F)
Gaps Left After GF Support (G) (G=D-F)
Physician 285 190 95 33% 18 77 Pharmacist 46 44 2 4% 7 (-5) Pharmacist Assistant
76 63 13 17% 7 6
Sources: MOHSS, Human Resource Division Annual Report 2007/2008, with figures updated to 2009 and
Global Fund Project Reports
Table 10C: Comparing Posts Filled with CDC Support to Vacancies indicated in Government Staff Establishment
Professional Category (A)
CDC-funded Cadres (B)
CDC-assisted Work Programme Vacancies Based on Updated HIV. TB and Malaria Staffing Requirements (C)
Physician 39 33 Pharmacist 28 2
Sources: Information Provided by CDC Namibia
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 119/160
Thus the number of existing staff to be retained and new additional staff to be supported by Global Fund, composed mainly of doctors and pharmacists, is shown under Activities 2.1 and 2.2 below. The GRN will begin to bear an increasing burden of the salary costs of the doctors, pharmacists and pharmacist assistants from Year 3 by contributing 10 percent in Year 3, 20 percent in Year 4, 30 percent in Year 5 and 40 percent in Year 6. While this is a good move towards sustainability, it is important to note that the salaries paid for posts funded by partners are much higher than those paid by the Government; if the pay structures were similar there would be no problem with the drive towards sustainability. Thus there is also a need for consensus on a policy decision on the top ups allowed by partners. Some partners are already concerned about this, as well as the disparity between salaries paid even among the partners. However, in the absence of higher government wages, a uniform top up paid by all donors is the interim solution. An important fact is that this dialogue is beginning, and the key actors are the CCM/Global Fund, MOHSS and USG/PEPFAR. It should be noted that there is no request for nurses because the GRN has invested heavily in training nurses using the existing schools of nurses in the country and has absorbed the trained personnel as well as being supported by bilateral partners, in particular the Kenyan Government. With regard to other cadres, a total of 375 health-related students completed their training at the Ministry's Health Training Centres at the end of 2008. This number includes 345 enrolled nurse midwifes, 10 environmental health assistants, nine pharmacy assistants and 11 medical laboratory technicians. 2.3 Improvement of Health Worker Capacity Through Training and Upgrading Training Facilities The five-year HR strategy (2009-2013), which is line with the NDP III, has committed to train 225 physicians, 90 pharmacists, 1,025 nurses, 200 social workers and 1,350 nurses/midwifes (NDP III, Annex J16). A Medical School is in the process of being established at the University of Namibia and will soon be operational. The cost of establishing the Medical School is supported by the GRN and donations from the Finnish and Cuban governments. However, even when the Medical School is up and running, there will be a time lag before the locally trained physicians are available for employment. Training abroad is therefore necessary as an interim strategy to meet HR requirements by 2013. Resources, albeit inadequate, are available from the national budget, thus leaving gaps to be filled by donors. Therefore this HSS component requests support for additional bursaries for the various cadres as detailed in Activity 2.3 below to contribute to meeting HR targets in support of the scale–up of required services for HIV, TB and Malaria in a timely manner. National and regional health training centres lack lecture rooms, furniture and the requisite training audiovisual equipment. Increasing the intake of students also necessitates the rehabilitation of existing lecture rooms as well as the provision of more books for the library. The expansion will create additional space to increase enrolment at these training centres. The GRN will renovate training centres in Oshakati and Otjiwarongo as per NDP III; Global Fund support is required to fill the gaps detailed in Annexes E23 (Summary Needs for Human Resources, Equipment and Renovation), E23.1 (List of Books), E23.2 (List of Demonstration Models), E23.3 (Layout of Areas for Renovation) and E23.4 (Functions and Space Requirements for Environmental Laboratory), outlined in Activity 2.4 below. Objective 2a: Strengthen human resources to improve the effective management of HIV, TB and Malaria Detailed Activities 2.1 Retain currently employed health workers for HIV/AIDS, TB and Malaria service delivery (continuation of Round 2):
2.1.1 Retain 20 Medical Officers in Years 1 and 2, reducing in percentage of salary in Years 3-6 as GRN takes over.
2.1.2 Retain 1 Senior Medical Officer in Years 1 and 2, reducing in percentage of salary in Years 3-6 as GRN takes over.
2.1.3. Retain 11 Pharmacists in Years 1 and 2, reducing in percentage of salary in Years 3-6 as GRN takes over.
2.1.4. Retain 16 Pharmacist Assistants in Years 1 and 2, reducing in percentage of salary in Years 3-6 as GRN takes over.
2.1.5. Retain 1 Tutor Pharmacist in Years 1 and 2, reducing in percentage of salary in Years 3-6
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 120/160
as GRN takes over. 2.1.6. Retain 1 Architect in MOHSS DSP to facilitate renovation of health facilities 2.1.7. Provide currently employed medical officers pharmacists and pharmacist assistants with
travel allowances as per contract (one annual home leave with round trip air ticket, etc) 2.2 Recruit additional staff to cope with scaling up HIV and AIDS (based on Integrated Management of Adolescent and Adult Illnesses (IMAI) and Treat, Train and Retrain (TTR) adopted concepts), TB and Malaria services and decentralisation (continuation and scale-up of Round 2):
2.2.1 Provide advertising and other recruitment costs. 2.2.2 Recruit 20 Pharmacist Assistants., 5 in Quarter 5, 5 in Quarter 6, 5 in Quarter 7 and 5 in Quarter 8). 2.2.3 Recruit 4 Psychologists, 1 in each Quarter in Year 2. 2.2.4 Procure desktop computers and office furniture for newly recruited office based staff. 2.2.5 Provide newly recruited staff with travel allowances as per contract (one annual home leave, with round trip air ticket, etc)
2.3 Provide full bursaries for pre service and in-service training of health workers (continuation of Round 2):
2.3.1 Provide bursaries to 25 students to achieve entry requirements for medical and pharmacy 2-year courses. 2.3.2 Provide bursaries to 15 student doctors, for a 6-year course. 2.3.3 Provide bursaries to 7 student pharmacists, for a 4-year course. 2.3.4 Provide bursaries to 7 student pharmacist assistant for a 2-year course . 2.3.5 Provide bursaries to 7 student social workers, for a 4-year course. 2.3.6 Provide bursaries to 5 student Psychologists, for a 4-year course. 2.3.7 Provide bursaries to 5 student Nutritionists/Dieticians, for a 4-year course. 2.3.8 Provide bursaries for 3 staff to undergo masters degree at a foreign University, 2 in Year 1 and 1 in Year 3.
2.4 Expand and upgrade national health training institutions by providing additional staff and equipment (continuation of Round 2):
2.4.1. One Medical Laboratory Technician Programme Tutor. 2.4.2. One Medical Laboratory Technician Clinical Tutor. 2.4.3. One Research/Technology and Information Systems Officer (HPA, 3BL2). 2.4.4. TwoEnvironmental Health Assistant Programme Tutor. 2.4.5. Two Radiographic Assistant Programme Tutor. 2.4.6. Five Enrolled Nurse/Midwife Programme Tutor (one for each of the five regional training
centres). 2.4.7. Renovation of 1 lecture theatre 2.4.8. Renovation of 13 offices. 2.4.9. Renovation of 1 Multipurpose Environmental Health Training Laboratory/Simulation Room to perform functions as in Annex E23.4. 2.4.10. Teaching demonstration models as in Annex E23.2. 2.4.11. Journals and selected texts as in Annex E23.1. 2.4.12. IT Equipment for Training-10 Computers. 2.4.13. 7 LCD Projector. 2.4.14. 5 Digital cameras. 2.4.15. 20 USB sticks. 2.4.16. 60-seater bus to convey students to practicum sites
(b) Indicate below the planned outputs/outcomes (through a key phrase and not a detailed description) that will be achieved on an annual basis from support for this HSS cross-cutting intervention during the proposal term.
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
0% Increased percentage of Salaries of Global Fund supported health workers
0% Increase in the percentage of Salaries of Global Fund supported health workers
10% Increase in the percentage of Salaries of Global Fund supported health workers
20% Increase in the percentage of Salaries of Global Fund supported health workers
30% Increase in the percentage of Salaries of Global Fund supported health workers
40% Increase in the percentage of Salaries of Global Fund supported
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 121/160
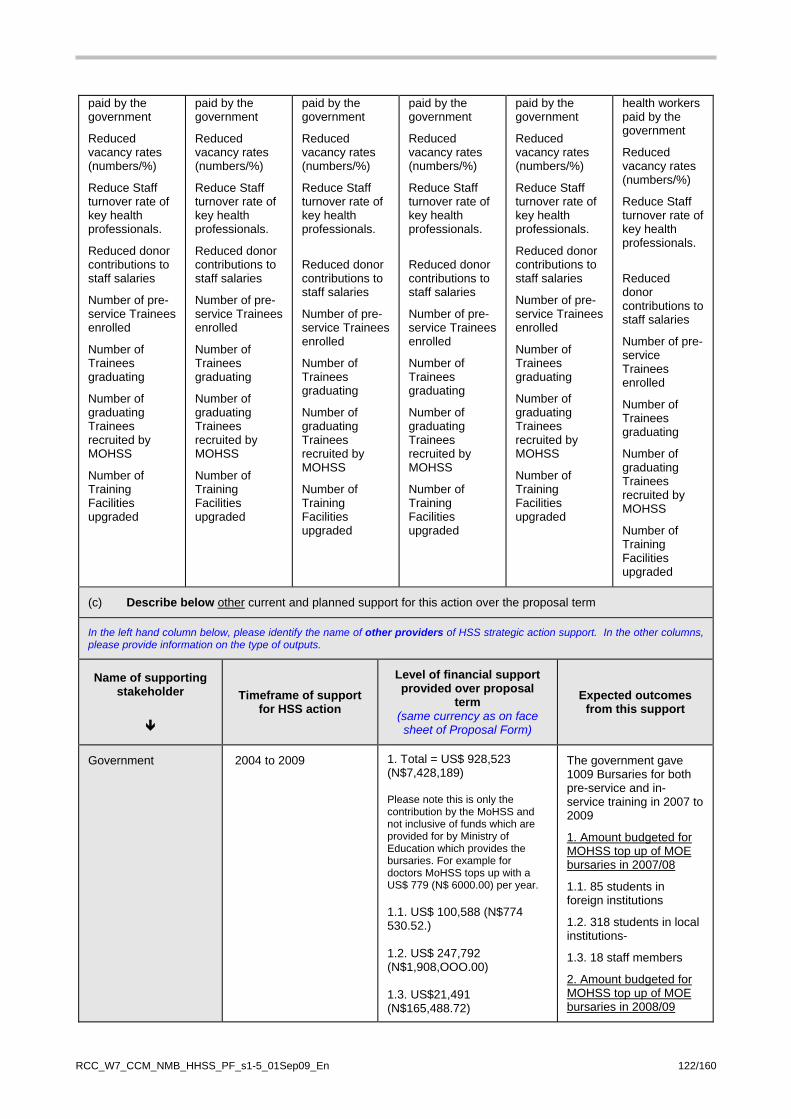
paid by the government
Reduced vacancy rates (numbers/%)
Reduce Staff turnover rate of key health professionals.
Reduced donor contributions to staff salaries
Number of pre-service Trainees enrolled
Number of Trainees graduating
Number of graduating Trainees recruited by MOHSS
Number of Training Facilities upgraded
paid by the government
Reduced vacancy rates (numbers/%)
Reduce Staff turnover rate of key health professionals.
Reduced donor contributions to staff salaries
Number of pre-service Trainees enrolled
Number of Trainees graduating
Number of graduating Trainees recruited by MOHSS
Number of Training Facilities upgraded
paid by the government
Reduced vacancy rates (numbers/%)
Reduce Staff turnover rate of key health professionals.
Reduced donor contributions to staff salaries
Number of pre-service Trainees enrolled
Number of Trainees graduating
Number of graduating Trainees recruited by MOHSS
Number of Training Facilities upgraded
paid by the government
Reduced vacancy rates (numbers/%)
Reduce Staff turnover rate of key health professionals.
Reduced donor contributions to staff salaries
Number of pre-service Trainees enrolled
Number of Trainees graduating
Number of graduating Trainees recruited by MOHSS
Number of Training Facilities upgraded
paid by the government
Reduced vacancy rates (numbers/%)
Reduce Staff turnover rate of key health professionals.
Reduced donor contributions to staff salaries
Number of pre-service Trainees enrolled
Number of Trainees graduating
Number of graduating Trainees recruited by MOHSS
Number of Training Facilities upgraded
health workers paid by the government
Reduced vacancy rates (numbers/%)
Reduce Staff turnover rate of key health professionals.
Reduced donor contributions to staff salaries
Number of pre-service Trainees enrolled
Number of Trainees graduating
Number of graduating Trainees recruited by MOHSS
Number of Training Facilities upgraded
(c) Describe below other current and planned support for this action over the proposal term
In the left hand column below, please identify the name of other providers of HSS strategic action support. In the other columns, please provide information on the type of outputs.
Name of supporting stakeholder
Timeframe of support for HSS action
Level of financial support provided over proposal
term (same currency as on face sheet of Proposal Form)
Expected outcomes from this support
Government 2004 to 2009 1. Total = US$ 928,523 (N$7,428,189) Please note this is only the contribution by the MoHSS and not inclusive of funds which are provided for by Ministry of Education which provides the bursaries. For example for doctors MoHSS tops up with a US$ 779 (N$ 6000.00) per year. 1.1. US$ 100,588 (N$774 530.52.) 1.2. US$ 247,792 (N$1,908,OOO.00) 1.3. US$21,491 (N$165,488.72)
The government gave 1009 Bursaries for both pre-service and in-service training in 2007 to 2009
1. Amount budgeted for MOHSS top up of MOE bursaries in 2007/08
1.1. 85 students in foreign institutions
1.2. 318 students in local institutions-
1.3. 18 staff members
2. Amount budgeted for MOHSS top up of MOE bursaries in 2008/09
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 122/160

2.1. US$ 279,098 (N$ 2,149,062.59) 2.2. US$ 288,116 (N$2,218,500.00) 2.3 US$ 27,611 (N$212,609.34) 3. Exact amounts not easily ascertained
2.1. 165 students in foreign institutions
2.2. 382 students in local institutions-
2.3 41 staff members
3, 2008/09 budget improvement of conditions of services for employees of mission hospitals.
Government 2010-2016 Approx USD 1m
Other Global Fund Grants (with HSS elements (if applicable)
2004 to 2009
Recruited 21 Doctors, 11 Pharmacists, 16 Pharmacist Assistants, 1 Tutor Pharmacist, 6 PMTCT Tutors, and 1 Training/Nursing Coordinator.
CDC 2004 to 2009 1. Bursaries -$2,122,573
2. Health workers emoluments- $55,945, 607
3. Training-$5,391,400
4. Support for the establishment of an accredited MPH programme
1. 947 Bursaries
2. Recruited 1,138 health workers
3. In service training of 27,903 participants
4. Grant to the University of Washington to support the establishment of an accredited MPH programme in UNAM
CDC Projected for 2010-2016 Bursaries $1m annually
Health workers emoluments- reduce by 10% annually
Training would remain constant from 2009 level of $1,395,150
Clinton Foundation 2004-2009 US$ 104,611 (N $805,512) Training of primary health care workers (incl adaptation of IMCI materials and printing of materials)
Clinton Foundation 2010-2016
WHO 2004-2009 1. Stress Management Trainings provided to Health Workers and VCT Community Counsellors,
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 123/160
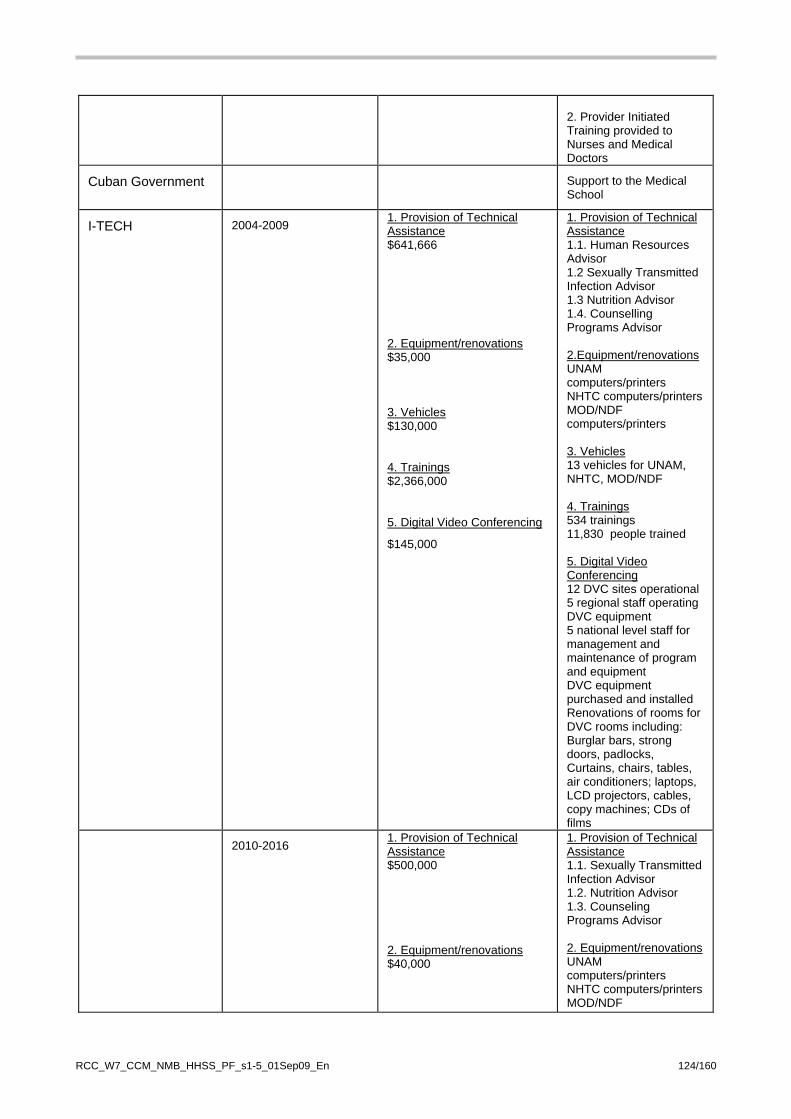
2. Provider Initiated Training provided to Nurses and Medical Doctors
Cuban Government Support to the Medical School
I-TECH 2004-2009 1. Provision of Technical Assistance $641,666
2. Equipment/renovations $35,000 3. Vehicles $130,000 4. Trainings $2,366,000 5. Digital Video Conferencing
$145,000
1. Provision of Technical Assistance 1.1. Human Resources Advisor 1.2 Sexually Transmitted Infection Advisor 1.3 Nutrition Advisor 1.4. Counselling Programs Advisor 2.Equipment/renovations UNAM computers/printers NHTC computers/printers MOD/NDF computers/printers 3. Vehicles 13 vehicles for UNAM, NHTC, MOD/NDF 4. Trainings 534 trainings 11,830 people trained 5. Digital Video Conferencing 12 DVC sites operational 5 regional staff operating DVC equipment 5 national level staff for management and maintenance of program and equipment DVC equipment purchased and installed Renovations of rooms for DVC rooms including: Burglar bars, strong doors, padlocks, Curtains, chairs, tables, air conditioners; laptops, LCD projectors, cables, copy machines; CDs of films
2010-2016 1. Provision of Technical Assistance $500,000
2. Equipment/renovations $40,000
1. Provision of Technical Assistance 1.1. Sexually Transmitted Infection Advisor 1.2. Nutrition Advisor 1.3. Counseling Programs Advisor 2. Equipment/renovations UNAM computers/printers NHTC computers/printers MOD/NDF
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 124/160
3. Vehicles $150,000 4. Trainings: $3,126,000 5. Digital Video Conferencing $277,000
computers/printers 3. Vehicles 10 vehicles for UNAM, NHTC, MOD/NDF 4. Trainings: 890 trainings 15,630 people trained 5. Digital Video Conferencing Continued support of 12 current sites and opening of 3 new sites Continued support of 5 regional staff and 3 new ones Continued support of 5 national level staff for management and maintenance of program and equipment Additional DVC equipment purchased and installed at 3 new sites
Renovations of rooms for DVC including: Burglar bars, strong doors, padlocks, Curtains, chairs, tables, air conditioners; laptops, LCD projectors, cables, copy machines; CDs of films
4B.1 Description of 'HSS cross-cutting intervention'
Title: Intervention 3 Strengthening timeliness and quality of data to ensure evidence informed decisions
Beneficiary Diseases HIV, TB and Malaria
WHO "Building Block" category Health Information Systems
(a) Description of rationale for and linkages to improved/increased outcomes in respect of HIV, tuberculosis and/or malaria:
Background The interventions proposed are in line with the MOHSS Strategic Plan under which, in the section on Governance, the Ministry intends to “Address problems of inadequate/inappropriate information and communication technologies coordination, delayed payment of suppliers, poor record keeping, poor communication and coordination, bureaucracy, outdated legislation, policies, guidelines”. They are also covered in the NDP III (Annex J16), and, more specifically, the “national database” is covered in the MTP III (Annex J20, Subcomponent 5.4, surveillance and operational research, 5.4.1 multi-sectoral
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 125/160
HV/AIDS research coordination, p. 82) and in the Plan for Multi-sectoral Monitoring and Evaluation for HIV/AIDS, 2006/7 and 2008/9 (Annex J4, section 5.4, Information System Development, p. 26). The details of the system are further described in “The System Boundary Document for the Collection of HIV/AIDS. TB and Malaria Programme Monitoring and Evaluation, Annex E12, pages 2 and 8-9. Earlier evaluations done by the UNAIDS/World Bank-Gamet in 2005 (Annex J25) and USAID Measure (Annex E13) in 2006, as well as the more recent MOHSS System Review of 2008 outline M&E weakness and proposed solutions; all these assessments made similar recommendations. Thus no additional M&E assessments are needed, and the focus of this HSS request is on filling the identified gaps by using Global Fund resources to make the investments agreed by the Government and all key stakeholders. Fragmented HMIS Function in Different Directorates and Lack of Professional HMIS/M&E cadre The MOHSS System Review, Annex J6 page 3 says “the MOHSS has many standalone information systems managed by different divisions in different directorates. This fragmented structure has created overlaps and duplications between the various systems”; and on page 4 it recommended the development of an integrated M&E system for all programmes (research, MIS, HIS, epidemiology and M&E) under one roof. This was then stated as an objective in the MOHSS Strategic Plan (Annex J7, p. 15,) which targets the integrated MIS to be 100% in place by 2012. A major challenge related to the structural and organisational deficiency described above is the inadequate numbers of the professional cadre of HMIS/M&E staff composed of epidemiologists, medical demographers, statisticians, M&E officers, data clerks/Statistical assistants, IT staff, etc. Thus there is a need for: (a) the creation of the new directorate as above; and (b) the need to professionalise the HMIS/M&E cadre, who should be employed to work solely on the HMIS/M&E and related functions. Presently health staff such as nurses combine HMIS/M&E functions with their clinical work at facility and district levels. One of the hospital nursing staff plays the role of the HIS focal officer for each district and is responsible for the collection and data entry of the summary forms received from the health facilities. However, they are also responsible for other clinical duties within the district hospital and, once those trained and experienced in this task are posted away, the quality of data and reporting suffers. This continues until a capable replacement is found or the incumbent is trained. It would therefore be difficult for an efficient M&E system to be build using the existing workforce and organisational structure. Consequently, there is hardly any analysis at the point of data generation i.e. clinics, health centres and hospitals, where data is merely forwarded to the next level. This limits the opportunity for use of this data to inform decisions at point of use in a timely manner . It also misses out on the opportunity to validate data that has been collected. The result is that there are delays in generating evidence that would inform decisions on the programmatic and service delivery management of HIV, TB and Malaria. Occasionally, reports are produced on this data. Ad hoc data requested by national level programme managers and others are also provided by the epidemiology division. The Government is already working proactively to meet the recommendation on creating a professional HMIS/M&E cadre along with an HMIS directorate that would rationalise the HMIS/M&E function currently shared between three directorates. The 6 professional M&E staff from the Round 2 Global Fund to be retained under the HIV and AIDS disease component and the 1 M&E Officer supported under the TB Round 6 grant would continue to support the MOHSS while these HSS initiatives are implemented. Moreover, the M&E capacity building to be undertaken in-service and pre-service training as proposed in Activity 3.3 below will contribute to improving the efficiency of the existing workforce and also increase the pool of potential candidates to staff the envisaged directorate. 3.1 Harmonise the management and coordination of the national M&E programme by establishing the National Integrated Database Representative high quality and timely data is essential for monitoring health sector, including grant, performance. Since the HMIS was introduced in 1989, progress has been made in establishing the various components of the HMIS including finances, service delivery and human resources. The computerised HIS is widely used throughout the country at national, regional and district level. Revision of the system took place in 1994, 2000 and again during 2007/2008. During these revisions, the MOHSS adopted the DHIS from the Health Information Systems Programme Network (HISPN) .
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 126/160
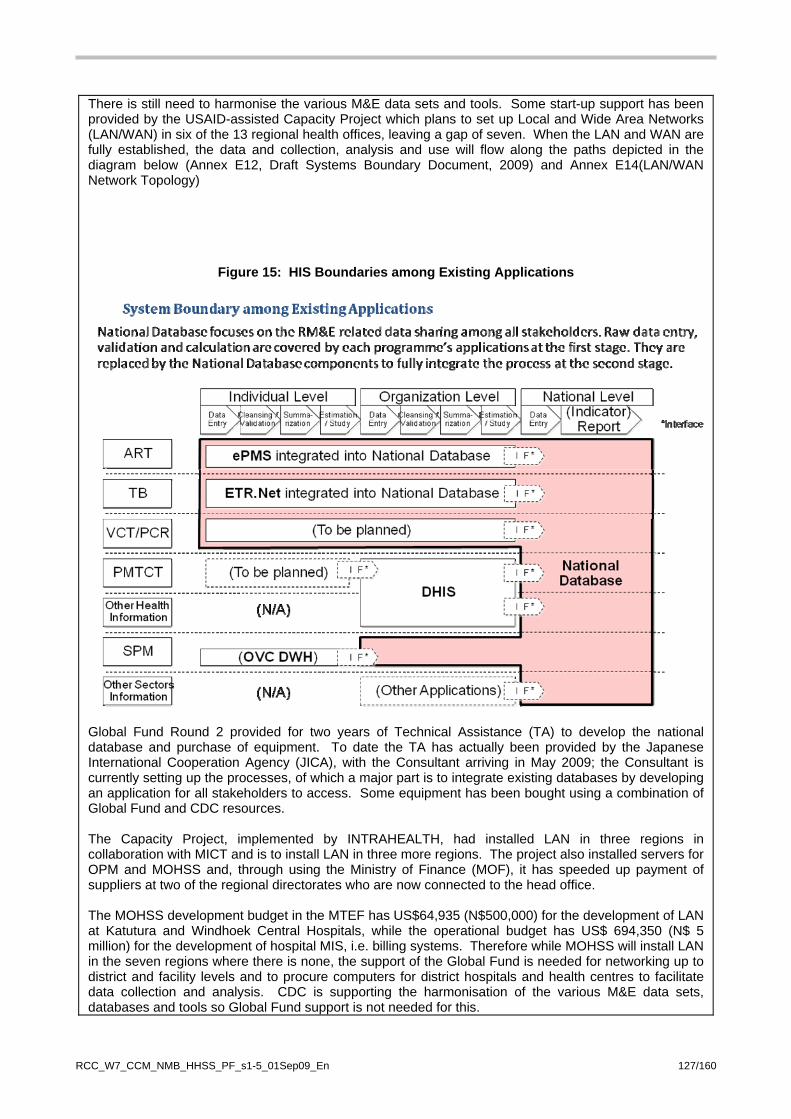
There is still need to harmonise the various M&E data sets and tools. Some start-up support has been provided by the USAID-assisted Capacity Project which plans to set up Local and Wide Area Networks (LAN/WAN) in six of the 13 regional health offices, leaving a gap of seven. When the LAN and WAN are fully established, the data and collection, analysis and use will flow along the paths depicted in the diagram below (Annex E12, Draft Systems Boundary Document, 2009) and Annex E14(LAN/WAN Network Topology)
Figure 15: HIS Boundaries among Existing Applications
Global Fund Round 2 provided for two years of Technical Assistance (TA) to develop the national database and purchase of equipment. To date the TA has actually been provided by the Japanese International Cooperation Agency (JICA), with the Consultant arriving in May 2009; the Consultant is currently setting up the processes, of which a major part is to integrate existing databases by developing an application for all stakeholders to access. Some equipment has been bought using a combination of Global Fund and CDC resources. The Capacity Project, implemented by INTRAHEALTH, had installed LAN in three regions in collaboration with MICT and is to install LAN in three more regions. The project also installed servers for OPM and MOHSS and, through using the Ministry of Finance (MOF), it has speeded up payment of suppliers at two of the regional directorates who are now connected to the head office. The MOHSS development budget in the MTEF has US$64,935 (N$500,000) for the development of LAN at Katutura and Windhoek Central Hospitals, while the operational budget has US$ 694,350 (N$ 5 million) for the development of hospital MIS, i.e. billing systems. Therefore while MOHSS will install LAN in the seven regions where there is none, the support of the Global Fund is needed for networking up to district and facility levels and to procure computers for district hospitals and health centres to facilitate data collection and analysis. CDC is supporting the harmonisation of the various M&E data sets, databases and tools so Global Fund support is not needed for this.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 127/160
Formal active surveillance systems for adverse drug reaction (ADR)-Pharmacovigilance The building of an active pharmacovigilance system, which includes the creation of a database and its IT infrastructure to enable reporting of adverse drug reactions by facilities, would be incorporated into the building of the integrated national database described above, to avoid the creation of another standalone database and M&E system. If possible the same ADSL lines to be used by the integrated national database would be used by the active pharmacovigilance database. However, since the pharmacovigilance database may be constructed faster than the national database, provisions would be made for it to use dial up phone lines with the purchase of 3G modems only for 2010 to 2011; from 2012 onwards it would be incorporated into the ADSL line or which ever line is used by the national database. Also to be incorporated into the national database are the plans to build an electronic dispensing system, not only for ART but for all medicines, and this would be linked with the pharmacy section in the health facilities. It would also aid forecasting, procurement and pharmacovigilamce for all medicines. The justification for, and the earlier work done leading to the development of the formal active surveillance systems for ADR, is discussed below. The TIPC was established in 2007 to provide broad-based medicine safety monitoring services and the provision of unbiased therapeutics information to health workers and the general public in Namibia. Pharmacovigilance is even more necessary nowadays, and in future years, given the increased number of patients on multiple drug therapy schedules. The TIPC, which operates as a unit within the secretariat of the Namibia Medicines Regulatory Council, has clearly defined structures, systems, and roles. MOHSS with support from development partners has successfully developed the basic institutional capacity for the TIPC to fulfil its mandate by providing staffing, infrastructure, training and tools for the centre, including electronic databases (VigiFlow, Micromedex, Cochrane library), reference texts and high impact journals.
The TIPC has developed a spontaneous reporting system in Namibia. The reports obtained through this passive reporting are evaluated for causality and attribution.
Although routine reporting of adverse events is important for early detection of unknown ADR, the data obtained are often incomplete to reliably calculate risks. Therefore, if an unknown ADR occurs or there is an unusual change in the severity or frequency of reporting of a known reaction, further evaluation of these events and identification of risk factors may be required. Proper quantification of prevalence (risk) of serious ADR requires further collection of information through active surveillance (cohort event monitoring) which provides a complete ADR profile for the medicines of interest. It is planned that signals of significant public health importance will be further investigated using formal active surveillance systems. However, there is currently no system in place for active surveillance activities. Therefore funds are requested to establish the formal active surveillance systems in Namibia. 3.2. Pre-service and In-service capacity building for M&E/HMIS In order to manage the HMIS and the structural improvements necessary, it is vital to have officers with the commensurate skills. Currently, there is no systematic training in M&E by the tertiary institutions in Namibia, and there is also no training suitable for the various cadres, for example data clerks and middle level M&E Officers. Earlier initiatives include the GF-supported partnership between MOHSS and UNAM, under which two 5-day orientation courses on M&E were organised. JICA, working with the University of Pretoria in South Africa, funded participation in a 5-day orientation course on M&E, developed a curriculum in 2007 and 1 Lecturer from UNAM attended a 3-day M&E Management course in Pretoria. UNAIDS/World Bank had recommended partnership with the University of Addis Ababa, Ethiopia, which through its partnership with Tulane University, USA, is running a Masters programmes in M&E. CDC is funding the University of Washington to create an accredited Masters in Public Health programme in UNAM; activities include training of teachers, curriculum development, and visiting professors/mentors. All these resources will be leveraged with the additional support of the UN system to ensure the availability of sustainable M&E training, suitable for the different cadres of health and non-health workers in Namibia. To ensure availability of M&E cadres for employment, a Certificate Course (three weeks) in M&E will be supported at UNAM, the Polytechnic and national health training centres, where graduates or individuals with commensurate qualifications would be eligible for the training. This activity will improve the
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 128/160

sustainability and numbers of those with a M&E skill set and numbers, because it will eventually lead to the provision of various training programmes suitable for the different cadres at the participating training institutions. It is estimated that 25-50 participants will be trained each year and Global Fund support is required under this HSS to fund scholarships for 20 candidates each year from Years 4-6 (2012/3-2015/16). The first two years 2010/11-2011/12 would be spent building on the earlier initiatives described above, aimed at assisting the training institutions to institutionalise the course; however, this would be funded by other partners such as PEPFAR, the UN System and bilateral donors. The Global Fund would assist to send currently employed M&E staff to the training in the first two years, as part of in-service training, but this would not include payment of tuition fees, as the MOHSS would be organising the course in collaboration with the UN system and the training institutions. The further development of the institutionalisation of these courses would be supported by the UN System (UNAIDS, UNFPA, UNICEF and WHO,) in Namibia. The UN would support International Experts who would facilitate and lead the training, while the MOHSS and the University, Polytechnic and national health training centres would select the Lecturers who would be their National Counterparts. Every effort would be made to select committed Lecturers who would not emigrate. Risks would be identified and sustainability assured by building the capacity at the University, Polytechnic and national health training centres, so that at least one if not all of these institutions would organise the subsequent courses. The UN would also cover the costs of sending the Lecturers to UN-organised regional M&E courses. The first course would be held with the national team understudying the external consultants; the second course would be organised solely by the national team. The Global Fund would support the transport and per diems of the course participants for the first two courses, and if deemed cost effective some of the courses could be held in the regions. The three Training Institutions would collaborate and pool resources to organise the first two courses with the support of MOHSS and the UN system. It is envisaged that the training institutions would by then have acquired enough capacity to organise subsequent course with their institutions regular curriculum, for which tuition fees would be paid. This approach also allows enough time for the institutions to redesign the curriculum and have it approved by their relevant academic authorities and accredited by the Namibia Qualifications Authority (NQA). It is hoped that through this initiative the University would eventually develop a Masters programme in M&E, the Polytechnic a Diploma course, while the national health training centres, with the support of both the Polytechnic and the University, would be able to organise training for data clerks and also organise in-service training in M&E for other cadres of health workers. This investment would also provide a pool of National Consultants in M&E, as the lecturers would be available to undertake consulting assignments. Also, as the MOHSS implements the creation of the single HMIS/Research/Epidemiology Directorate, this in-country capacity would increase the pool of candidates to staff this directorate. M&E Officers working in the public, civil society and private sector have a high turnover and there are usually modifications in the existing M&E systems. Therefore there is a need for the bi-annual training of M&E officers to ensure quality provision. There are 13 Regional and seven Sectoral M&E Officers. In addition to these, another 15 M&E Officers from partner organisations will be expected to attend the training, which would be supported by the Global Fund. 3.3 Impact Assessment The improved routine HIS captures most of the relevant information for grant M&E and other sector performance. After more than five years of investment from the Government, GFATM and other partners, it is pertinent to conduct an impact assessment to evaluate the programme. Global Fund support is requested to contribute towards the Demographic Health and Health Facility Surveys; the cost would be equally shared between the Government, Global Fund and PEPFSAR/USAID. An HSS component would be added to the DHS, so that the impact of this Global Fund-supported HSS, and those of Government and other partners, could be tracked through the production of the relevant indicators. 3.4 Poor Data Quality and Inadequate Supervision The problem of spotty reports and unverified data would be rectified partly by the training activities described above but, since training alone will not resolve this, M&E supervision and data quality
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 129/160

incentives/checks will also be done. The current staff performing the HMIS/M&E tasks would be made more efficient by inviting and acknowledging the District Coordinators from the three best Districts with full M&E reports to the Quarterly MoHSS M&E review, organised for MoHSS and its partners, to review AIDS, TB and Malaria and other M&E issues. Also an award to honour the best reporting district/region would be awarded annually based on a league for regions and districts. The logistics to improve supervision are captured in the activity regarding vehicles requested under Objective 1, and the staff and the required training are captured above. Thus new funds are needed only for the data quality incentives/checks. Objective 3a: Strengthen M&E systems to ensure evidence-based decision-making Detailed Activities 3.1 Harmonise the management and coordination of the national M&E programme, including M&E for HIV and AIDS, TB and Malaria by installing and maintaining an integrated national database (continuation of Round 2):
3.1.1 Establish WAN connecting all hospitals to regional offices (outsourced HR computer experts/consultants would install the systems over a 2 year period).
3.1.2 Establish LAN in 32 Hospitals and 1 health centre (install the system over 2 years), this includes payment for leased commercial phone line (ADSL) over 4 years.
3.1.3 Development of national database to fully integrate existing program databases by purchasing equipment, including servers to be based in MOHSS (4 computers, etc).
3.1.4 Recruit 2 computer experts as System Administrators to maintain the systems over 4 years (Yr 3-6). 3.1.5 Maintenance of database and equipment per annum. 3.1.6 Details of Pharmacovigilance database whose development and maintenance is to be integrated into that of the national database:
• Establish formal active surveillance systems - establish database for active surveillance including central database and the facility based user interface
• Provide training to key staff at national and regional level. • Procure 3G modem and use for 2 years only. • Desktop Computer for sentinel sites • Laptops and statistical software • Broad band internet for two years only, after which migrate to national database IT infrastructure
3.2 Pre-service and in-service capacity building for M&E (continuation of Round 2):
3.2.1 Hold bi-annual M&E Refresher Training for 30 M&E officers from all stakeholders, for 5 Days using 3 facilitators
3.2.2 Hold one training on Project Management and Cycle for 10 senior staff for 5 days, repeated every 2nd year
3.2.3 Train Technical Staff on database programming and proper data management (Data Manager, Systems Analyst, M&E officers)
3.2.4 Train M&E Data Entry clerks (refresher training and new recruits each year) 3.2.5 Provide support (transport and per diems only) for 25 candidates each per year for first
two years to attend training courses to be organised by MOHSS, UN System, UNAM, the Polytechnic and national health training centres, for 21 days.
3.2.6 Provide support in terms of scholarships covering (tuition fees, transport and per diems) for 20 candidates each per year for last 3 (year 4-6) years to attend certificate and other training courses to be organised by UNAM, the Polytechnic and national health training centres, for 21 days.
3.3 Contribute to the Implementation of relevant national surveys for impact assessment (continuation of Round 2):
3.3.1 Demographic Health Survey in 2011/12 3.3.2 Health Facility Survey in 2014
3. Improve coordination and supervision for M&E (continuation of Round 2):
3.4.1 Quarterly MOHSS M&E review, for MOHSS and partners. (4 meetings of 30 people per
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 130/160
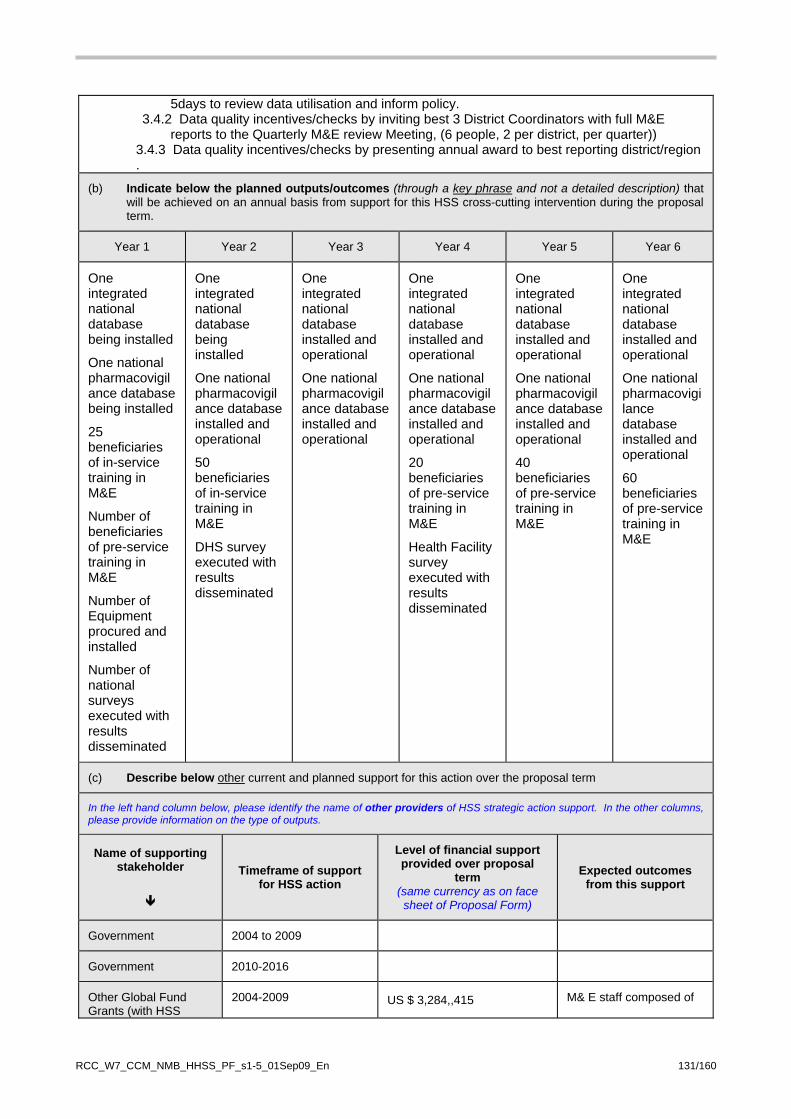
5days to review data utilisation and inform policy. 3.4.2 Data quality incentives/checks by inviting best 3 District Coordinators with full M&E
reports to the Quarterly M&E review Meeting, (6 people, 2 per district, per quarter)) 3.4.3 Data quality incentives/checks by presenting annual award to best reporting district/region .
(b) Indicate below the planned outputs/outcomes (through a key phrase and not a detailed description) that will be achieved on an annual basis from support for this HSS cross-cutting intervention during the proposal term.
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
One integrated national database being installed
One national pharmacovigilance database being installed
25 beneficiaries of in-service training in M&E
Number of beneficiaries of pre-service training in M&E
Number of Equipment procured and installed
Number of national surveys executed with results disseminated
One integrated national database being installed
One national pharmacovigilance database installed and operational
50 beneficiaries of in-service training in M&E
DHS survey executed with results disseminated
One integrated national database installed and operational
One national pharmacovigilance database installed and operational
One integrated national database installed and operational
One national pharmacovigilance database installed and operational
20 beneficiaries of pre-service training in M&E
Health Facility survey executed with results disseminated
One integrated national database installed and operational
One national pharmacovigilance database installed and operational
40 beneficiaries of pre-service training in M&E
One integrated national database installed and operational
One national pharmacovigilance database installed and operational
60 beneficiaries of pre-service training in M&E
(c) Describe below other current and planned support for this action over the proposal term
In the left hand column below, please identify the name of other providers of HSS strategic action support. In the other columns, please provide information on the type of outputs.
Name of supporting stakeholder
Timeframe of support for HSS action
Level of financial support provided over proposal
term (same currency as on face sheet of Proposal Form)
Expected outcomes from this support
Government 2004 to 2009
Government 2010-2016
Other Global Fund Grants (with HSS
2004-2009 US $ 3,284,,415 M& E staff composed of
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 131/160
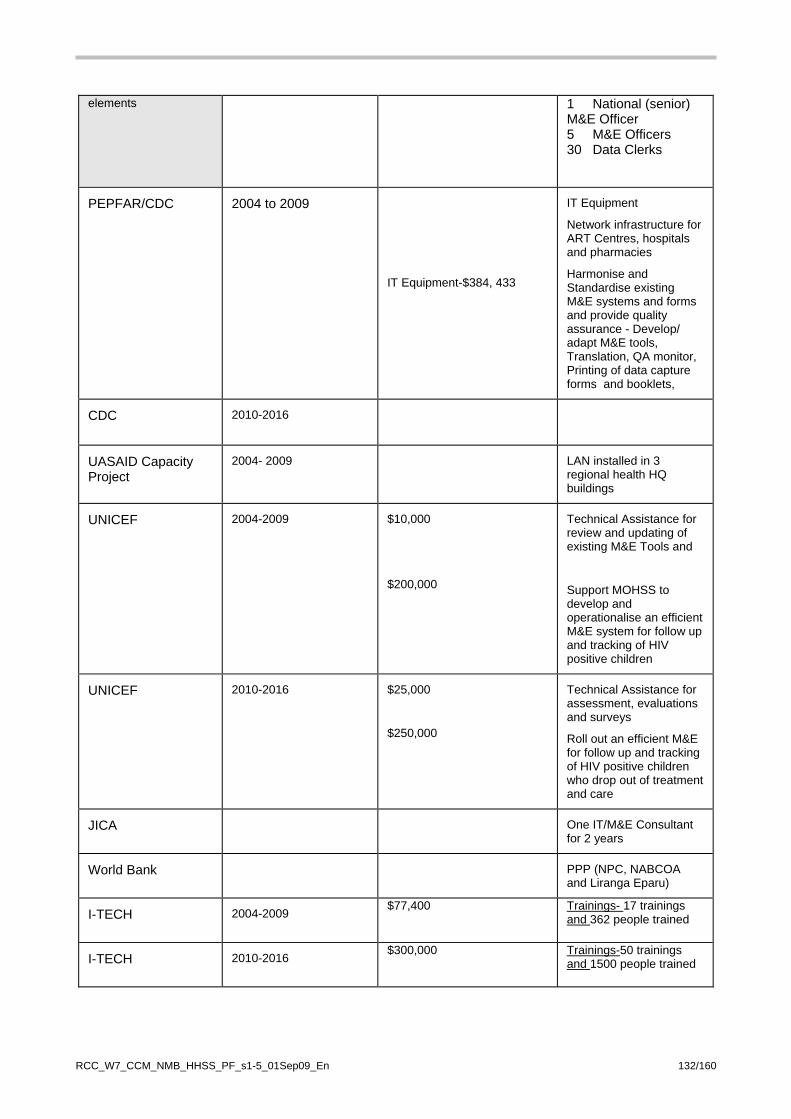
elements 1 National (senior) M&E Officer 5 M&E Officers 30 Data Clerks
PEPFAR/CDC 2004 to 2009
IT Equipment-$384, 433
IT Equipment
Network infrastructure for ART Centres, hospitals and pharmacies
Harmonise and Standardise existing M&E systems and forms and provide quality assurance - Develop/ adapt M&E tools, Translation, QA monitor, Printing of data capture forms and booklets,
CDC
2010-2016
UASAID Capacity Project
2004- 2009 LAN installed in 3 regional health HQ buildings
UNICEF 2004-2009 $10,000
$200,000
Technical Assistance for review and updating of existing M&E Tools and
Support MOHSS to develop and operationalise an efficient M&E system for follow up and tracking of HIV positive children
UNICEF 2010-2016 $25,000
$250,000
Technical Assistance for assessment, evaluations and surveys
Roll out an efficient M&E for follow up and tracking of HIV positive children who drop out of treatment and care
JICA One IT/M&E Consultant for 2 years
World Bank PPP (NPC, NABCOA and Liranga Eparu)
I-TECH 2004-2009 $77,400
Trainings- 17 trainings and 362 people trained
I-TECH 2010-2016 $300,000
Trainings-50 trainings and 1500 people trained
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 132/160

4B.1 Description of 'HSS cross-cutting intervention' Refer to the RCC Guidelines for information completing this section.
Title: Intervention 4 (Change number for each intervention)
Strengthen systems that provide equitable access to quality essential pharmaceutical and health products and technologies
Beneficiary Diseases: (e.g., HIV, tuberculosis,
and malaria?) HIV, TB, Malaria
WHO "Building Block" category (Refer to the RCC
Guidelines)
Systems that provide equitable access to quality essential pharmaceutical and health products and technologies
(a) Description of rationale for and linkages to improved/increased outcomes in respect of HIV, tuberculosis and/or malaria:
Background In the MOHSS Strategic Plan, under Governance, the Ministry aims to “address problems of inadequate/inappropriate information and communication technologies co-ordination, delayed payment of suppliers, poor record keeping, poor communication and co-ordination, bureaucracy, outdated legislation, policies, guidelines”
The existing health facilities are inadequate to cope with the increased case load related to storage of the bulky medicines. While the budget allocated to maintenance in the public sector is low, government with the support of donors like PEPFAR /CDC is renovating and expanding stores in health facilities, thus this support is not required from the Global Fund. Inadequate Number Of Distribution Trucks With increase in patients on ART and TB space along the whole supply chain is overburdened. The volume of supplies that need to be distributed to the different levels of care are increased and the Central Medical Stores (CMS) has had to undertake more trips with the current fleet it has which is inefficient. Two trucks were procured under the Global Fund in round 2, and CDC also provided 1 truck, some of the fleet is ageing, and the vast distances is also a challenge. Additional temperature controlled trucks can improve the efficiency of the distribution system, as well as a van for distribution. The requirements are detailed in activity 4.1 below.
Inadequate capacity of the Quality Surveillance Laboratory The Quality Surveillance Laboratory (QSL) receives an average of about 400 samples of which just over 200 samples are ARVs and TB medicines and the rest are other generic medicines. QSL analyses about 250 samples leaving a backlog of 150 samples not analyzed. Of the samples analyzed about 150 are ARVs and TB medicines and 100 generic medicines. The major constraint has been the limited equipment in the laboratory. ARVs are analyzed using HPLC whilst the generic medicines in addition to the use of HPLC are also analyzed using UV-Vis spectrophotometer. The other pieces of equipment are required for other tests in the monographs the optical rotation, moisture in tablets, hardness in tablets etc. which we currently cannot do because of the constraints in equipment. If we can get another HPLC and UV-Vis spectrophotometer this will increase our output by 100-150 samples and lower the backlog of samples to very low levels which are manageable. The QSL therefore needs to be strengthened with the equipment detailed in activity 4.2 below. OBJECTIVE 4: Strengthen systems that provide equitable access to quality essential
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 133/160
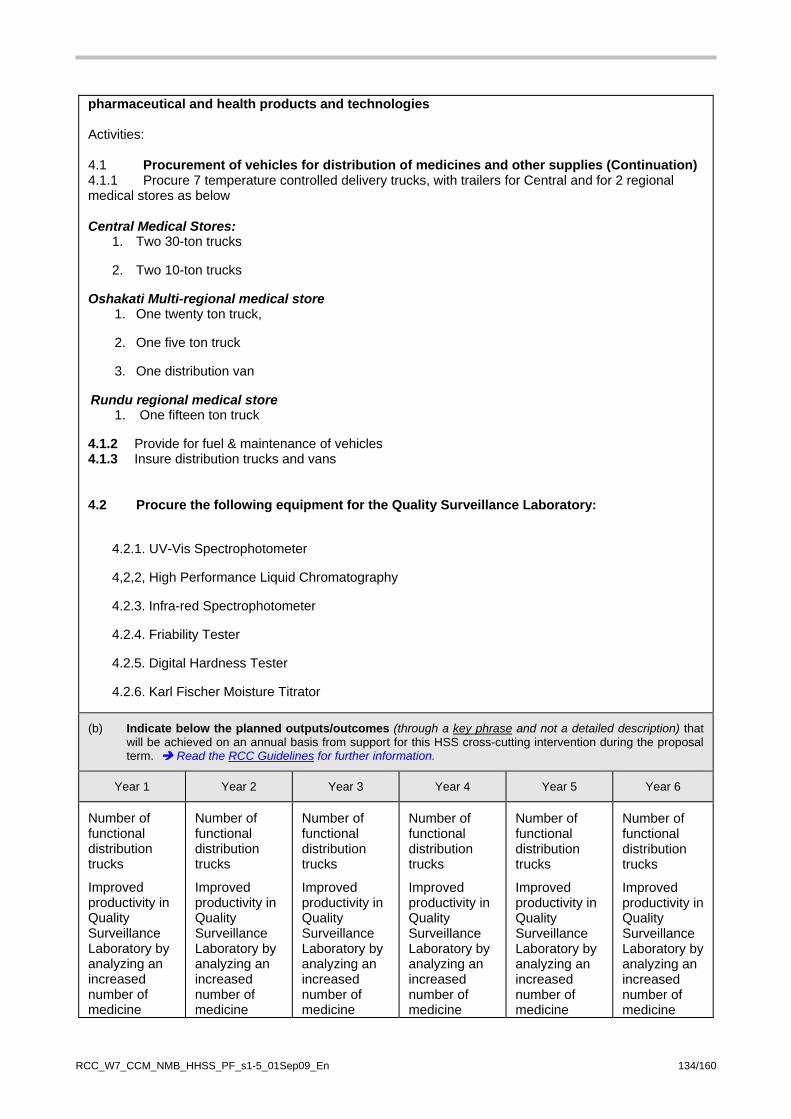
pharmaceutical and health products and technologies Activities: 4.1 Procurement of vehicles for distribution of medicines and other supplies (Continuation) 4.1.1 Procure 7 temperature controlled delivery trucks, with trailers for Central and for 2 regional medical stores as below Central Medical Stores:
1. Two 30-ton trucks
2. Two 10-ton trucks
Oshakati Multi-regional medical store 1. One twenty ton truck,
2. One five ton truck
3. One distribution van
Rundu regional medical store 1. One fifteen ton truck
4.1.2 Provide for fuel & maintenance of vehicles 4.1.3 Insure distribution trucks and vans 4.2 Procure the following equipment for the Quality Surveillance Laboratory:
4.2.1. UV-Vis Spectrophotometer
4,2,2, High Performance Liquid Chromatography
4.2.3. Infra-red Spectrophotometer
4.2.4. Friability Tester
4.2.5. Digital Hardness Tester
4.2.6. Karl Fischer Moisture Titrator
(b) Indicate below the planned outputs/outcomes (through a key phrase and not a detailed description) that will be achieved on an annual basis from support for this HSS cross-cutting intervention during the proposal term. Read the RCC Guidelines for further information.
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
Number of functional distribution trucks
Improved productivity in Quality Surveillance Laboratory by analyzing an increased number of medicine
Number of functional distribution trucks
Improved productivity in Quality Surveillance Laboratory by analyzing an increased number of medicine
Number of functional distribution trucks
Improved productivity in Quality Surveillance Laboratory by analyzing an increased number of medicine
Number of functional distribution trucks
Improved productivity in Quality Surveillance Laboratory by analyzing an increased number of medicine
Number of functional distribution trucks
Improved productivity in Quality Surveillance Laboratory by analyzing an increased number of medicine
Number of functional distribution trucks
Improved productivity in Quality Surveillance Laboratory by analyzing an increased number of medicine
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 134/160
samples annually
samples annually
samples annually
samples annually
samples annually
samples annually
(c) Describe below other current and planned support for this action over the proposal term
In the left hand column below, please identify the name of other providers of HSS strategic action support. In the other columns, please provide information on the type of outputs.
Name of supporting stakeholder
Timeframe of support for HSS action
Level of financial support provided over proposal
term (same currency as on face sheet of Proposal Form)
Expected outcomes from this support
Government 2004 to 2009
Government 2010-2016
Other Global Fund Grants (with HSS elements (if applicable)
2004 to 2009
Two Distribution Trucks
Other: CDC)
2004 to 2009 US$ 213,595
(N$ 1,644,689.75)
One 30 Ton Distribution Truck bought in 2005
Other: (CDC)
2010-2016
USAID MSH
USAID SCMS Renovation of Central Medical Stores
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 135/160
4B.1 Description of 'HSS cross-cutting intervention' Refer to the RCC Guidelines for information completing this section.
Title: Intervention 5 (Change number for each intervention)
Strengthen systems that provide equitable financing for health
Beneficiary Diseases: (e.g., HIV, tuberculosis,
and malaria?) HIV, TB, Malaria
WHO "Building Block" category (Refer to the RCC
Guidelines)
Health Financing
(a) Description of rationale for and linkages to improved/increased outcomes in respect of HIV, tuberculosis and/or malaria:
MAXIMUM ONE PAGE FOR EACH ACTION
Improving the private sector insurance and risk protection of the poor by expanding the workplace health insurance cover for low income groups that can include other diseases and not only stand alone HIV/AIDS insurance cover. The very robust private sector in Namibia are capable to invest in the well being of its workforce (when convinced) by contributing substantial monthly premiums of medical insurance policies for its low income workers. This can be done by executing Cost Benefit Analysis (CBA’s) at the company level to convince company executives/managers about costs to company and long terms productivity losses as a result of sick employees. Establishing strong Private/Private; Public/Private and Public/Private/Union partnerships are starting to bear fruit, as the union movement (NUNW) in Namibia has joined the efforts of private sector to assist in the development, design and implementation of affordable medical aid (insurance) products as a means to ensure access to Treatment (ARV); Care and Support for its workers and hence more people in Namibia. To support this initiative, the NUNW embarked on an initiative to also (just like private sector) develop its own medical insurance to ensure workplaces will take care of its employees. This obviously will also have benefits for spouses/other family members. The following Low Cost Options came to light during the last 4 years:
1. Vitality – US$5 (N$ 39) [comprehensive HIV/AIDS Cover only] 2. Vital Care - US$27 (N$ 211) [comprehensive HIV/AIDS Cover PLUS PHC cover] 3. Blue Diamond – US$21 (N$ 168) [comprehensive HIV/AIDS PLUS PHC cover] 4. NHP Economic Plan – US$37 (N$286) [comprehensive HIV/AIDS Cover PLUS PHC cover]
There is a need for analytic study to inform policy options, for example: should NUNW create another medical insurance scheme or should it be trying to expand an existing one. Towards this One Consultant would be hired for 45 days to do the following activities: (a) Actuarial review and organizational review of the existing funds (b) Feasibility of NUNW creating another medical insurance scheme or trying to merge with/expand an existing one. (c) Provide strategic plan to reform the funds and engage stakeholder consultations. (c) Execute scoping exercise to obtain buy-in from relevant stakeholders i.e. Private Sector Corporates; Unions; Government and Others. The aim being to be able to use the results of the analysis to support Health financing reforms in the
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 136/160

future Global Fund proposals and in discussions and policy dialogue between the Government of Namibia and other partners, Objective 5: Strengthen systems that provide equitable financing for health Activities 5.1.1. Hire One Consultant for 45 days to do Analytic Study of Medical Insurance Funds
(b) Indicate below the planned outputs/outcomes (through a key phrase and not a detailed description) that will be achieved on an annual basis from support for this HSS cross-cutting intervention during the proposal term. Read the RCC Guidelines for further information.
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
Consultancy executed
Report used for Stakeholder Consultations
Report of Analytic Study of Medical Insurance Funds used for designing Health Finance Reforms Funding sought for Health Finance Reforms from Global Fund and other sources
Funding sought for Health Finance Reforms from Global Fund and other sources
(c) Describe below other current and planned support for this action over the proposal term
In the left hand column below, please identify the name of other providers of HSS strategic action support. In the other columns, please provide information on the type of outputs.
Name of supporting stakeholder
Timeframe of support for HSS action
Level of financial support provided over proposal
term (same currency as on face sheet of Proposal Form)
Expected outcomes from this support
Government 2004 to 2009
Government 2010-2016
Other Global Fund Grants (with HSS elements (if applicable)
2004 to 2009
4B.2 Engagement of HSS Key Stakeholders in Proposal Development
(a) Briefly describe which and how important HSS stakeholders (e.g., ministries of planning, finance etc) have been involved in the identification and development of appropriate HSS cross-cutting interventions for this RCC proposal, and how coordination of the proposed HSS cross-cutting interventions has been ensured across the three diseases (and, where relevant, beyond).
Involvement of HSS Stakeholders and Coordination across Malaria, HIV/AIDS and TB, (and, where
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 137/160
relevant, beyond).
The development of the MoHSS strategic plan (Annex J7) was a highly collaborative process that drew upon a comprehensive and participatory health and social systems review, (Annex J6) that was supported by WHO, UNFPA, USAID etc and engaged many stakeholders. Consequently, the Strategic Plan truly represents a national direction for Health Systems Strengthening. This was the take off point of this HSS request.
These was then consolidated through a series of meetings and consultations detailed below:
1. Meetings in NaCCATuM on which National Planning Commission, PEPFAR and the UN are all members. See minutes in Annex A10
2. Stakeholder Meeting on RCC attended by NGOs, Donors etc. See Annex B2
3. Meetings of TCC, 13 meetings in total, see minutes in Annex C11, TCC diagrammatic composition Annex C7 and membership Annex C9
4. Deliberations on HSS at two consultative meetings at Hotel Thule, attended by stakeholders/participants, Annex C13, see minutes in Annex C15
5. Review meeting of the HSS on Friday 17 July attended by HSS task managers from NGOs, donors, UN and the MOHSS. See minutes in Annex E18.
6. Meeting with National Planning Commission and Ministries of Finance and Works and Transport to ensure speedier renovation of health facilities and staff accommodation.
7. Meeting with HSS Proposal drafting team and TB and Malaria Proposal drafting teams to harmonise, Monday 20 July, TB/Malaria Conference Room, Annex E19
8. Review meeting of the HSS M&E objective on Tuesday 21 July, at Global Fund PMU attended by M&E task managers from NGOs, donors, UN and the MOHSS. See minutes in Annex E20
9. Meeting with Associations for the Disabled to improve access and quality of care, Annex E21
10. HSS M&E meeting on Friday 23 July to finalise HSS Performance Framework Attachment A
11. HSS Budget meeting on Saturday 24 July to finalise HSS budget and eliminate any overlap with the disease specific budgets
Involvement of National Planning Commission and Ministries of Finance and Works and Transport
Beyond participation in above meetings. The government development planning and budgetary mechanism ensure involvement of and coordination between these key ministries.
MOHSS, Directorate of Policy and Planning, the National Planning Commission and other stakeholders, including the Ministry Works and Transport developed the five year NDP 3, covering 2007/8- 20011/12. NDP 3 includes all capital projects. NDP 3 is currently being implemented and monitored. Donor support, PEPFAR etc are all captured in the NDP 3, see Annex J16, so there is donor coordination, and avoidance of duplication and overlap.
MOF, NPC and MOHSS implement and fund NDP 3 via 3 year MTEF. The current MTEF 2009/10- 2011/12, (Annex J12) shows the facilities that government plans to renovate in this time frame.
MOHSS did a Health Systems Review in 2008, (see report as Annex J6), a MOHSS Strategic Plan, covering 2009-2013; (MOHSS Annex J7) was derived from this. The planned outputs and outcomes used in this HSS request are derived from the MOHSS SP.
So government and donor funded capital projects captured in NDP 3 are not duplicated in this HSS requests, only gaps are filled.
(b) Has the CCM (or Sub-CCM) ensured that:
(i) the HSS cross-cutting interventions in this proposal do not repeat any request for funding under any of the specific disease components (section 4.6 of each disease)?; and
X
Yes
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 138/160

RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 139/160
(ii) the detailed work plan** and the 'Performance Framework'** (Attachment A) for this disease includes separate worksheets which clearly identify the HSS cross-cutting interventions by objective, SDA, and activity for the initial two years of the proposal?
** Applicants may prepare a separate work plan for the HSS cross-cutting interventions and a separate 'Performance Framework' (Attachment A) if they prefer.
X Yes
4B.3 Strategy to mitigate initial unintended consequences
If there are some perceived initial disruptive consequences of the planned investment in any or all of the HSS cross-cutting interventions set out in section 4B.1 above (e.g., human resource movement or loss for other services):
What were the factors considered when deciding to proceed with the request for the financial support in any event?
What is the country's proposed strategy for mitigating these potential disruptive consequences?
Health facility Social Workers arranging for Deaf Sign language Interpreters ahead of appointments of deaf people could promote a stigma among health providers, and to ensure this does not have adverse effects, advocacy and orientation sessions would be done to the health workers
There would be disruption of services during renovation of health facilities. This would be managed through prior advocacy to the facility staff and users. Steps would be taken to improve patient flow, use temporary spaces etc and reduce waiting time. Additional staff would be deployed to facilities being renovated so that clients/patients do not suffer unduly.
Ensure that renovations are fast. This possible with improved MOHSS payment system and the fact that the health facilities renovation work plan is aligned with the government financial cycle of 1st April to 31st March, along with all the other improvement in the procurement process described earlier.
Government intends to renovate and maintain facilities during the MTEF, these are mostly expansion to existing facilities, thus future maintenance of the 46 Health Facilities which the Global Fund would be supporting in this HSS would not be a burden on the government’s budget.
Payment for the leased commercial phone line for the maintenance of the Integrated National Database in future years would also not be a burden on the government’s budget, as it intends to introduce a centralised procurement system under the OPM. Under this system, government would bundle and negotiate one telecommunications carrier for several ministries, thereby reducing the cost, as opposed to the current situation in the early days of the development of these IT systems under which various ministries have contracted different carriers.

5. Funding request 5.1 Financial gap analysis
Summary Information provided in the table below should be explained further in sections 5.1.1 – 5.1.3 below. Clarified Section Table 5.1
Financial gap analysis (USD$) Note Adjust headings (as necessary) in tables from calendar years to financial years (e.g., FY ending 2007; etc) to align with national planning and fiscal periods
Actual Expected Planned Estimated
2008 2009 2010 2011 2012 2013 2014 2015
HIV program funding needs to deliver comprehensive prevention, treatment and care and support services to target populations
Line A Provide annual amounts 209,529,073 226,933,404 255,262,831 276,547,151 293,323,709 310,923,132 329,578,519 349,353,231
Line A.1 Total need over length of RCC Funding Request (combined total need over RCC proposal term) 1,814,988,573
Current and future resources to meet financial need
Domestic source B1: Loans and debt relief N/A N/A N/A N/A N/A N/A N/A N/A
Domestic source B2 National funding resources 88,811,796 92,541,893 106,687,082 131,653,338 158,670,978 166,950,376 169,222,364 171,140,900
Domestic source B3 Private Sector contributions (national) 1,525,200 1,521,976 1,680,270 1,825,058 2,004,928 2,301,210
Total of Line B entries Total current & planned DOMESTIC
(including debt relief) resources: 88,811,796 92,541,893 108,212,282 133,175,314 160,351,248 168,775,434 171,227,292 173,442,110
External source C 1 (MULTI-LATERALS) 988,141 882,323 882,323 882,323 882,323 882,323 882,323 882,323
External source C2 (BI-LATERALS)
73,722,379 72,247,931 70,802,973 69,386,913 67,999,175 66,639,192 65,306,408 64,000,280
External source C3 Private Sector contributions
(International)
N/A
N/A
N/A
N/A
N/A
N/A
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 139/160
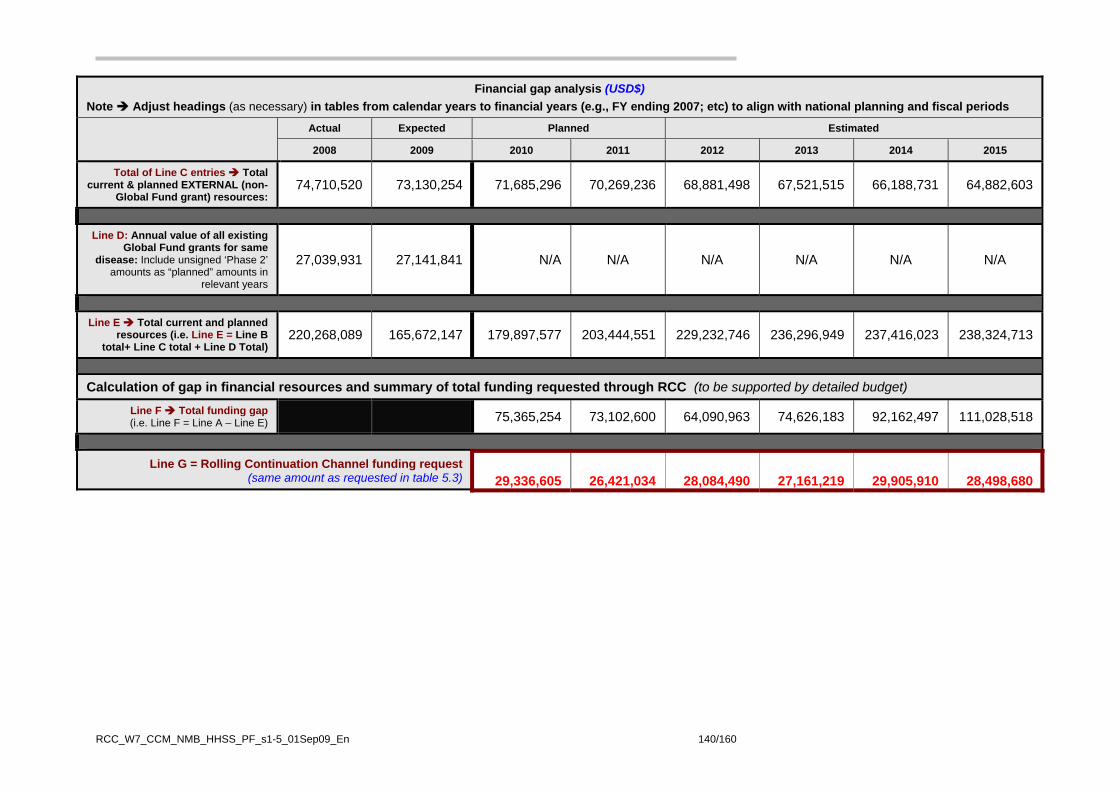
Financial gap analysis (USD$) Note Adjust headings (as necessary) in tables from calendar years to financial years (e.g., FY ending 2007; etc) to align with national planning and fiscal periods
Actual Expected Planned Estimated
2008 2009 2010 2011 2012 2013 2014 2015
Total of Line C entries Total current & planned EXTERNAL (non-
Global Fund grant) resources: 74,710,520 73,130,254 71,685,296 70,269,236 68,881,498 67,521,515 66,188,731 64,882,603
Line D: Annual value of all existing Global Fund grants for same
disease: Include unsigned ‘Phase 2’ amounts as “planned” amounts in
relevant years
27,039,931 27,141,841 N/A N/A N/A N/A N/A N/A
Line E Total current and planned resources (i.e. Line E = Line B
total+ Line C total + Line D Total) 220,268,089 165,672,147 179,897,577 203,444,551 229,232,746 236,296,949 237,416,023 238,324,713
Calculation of gap in financial resources and summary of total funding requested through RCC (to be supported by detailed budget)
Line F Total funding gap (i.e. Line F = Line A – Line E) 75,365,254 73,102,600 64,090,963 74,626,183 92,162,497 111,028,518
Line G = Rolling Continuation Channel funding request (same amount as requested in table 5.3) 29,336,605 26,421,034 28,084,490 27,161,219 29,905,910 28,498,680
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 140/160
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 141/160
Part H – 'Cost Sharing' calculation for Lower-middle income and Upper-middle income applicants
In this RCC proposal, the total maximum funding request for in Line G is: (a) For Lower-Middle income countries, an amount that results in the Global Fund's overall contribution (all grants) to the national program reaching not more than 65% of
the national disease program funding needs over the proposal term; and (b) For Upper-Middle income countries, an amount that results in the Global Fund overall contribution (all grants) to the national program reaching not more than 35% of
the national disease program funding needs over the proposal term.
Line H Cost Sharing calculation as a percentage (%) of overall funding from Global Fund
Cost sharing = (Total of Line D entries over 2010-2015 period + Line G Total) X 100 Line A.1
11.67 %
Cost sharing = (0 + 211,803,062) X 100 1,814,988,573

5.1.1 Explanation of financial needs – LINE A in table 5.1
Explain how the annual amounts were:
• developed (e.g., through costed national strategies, a Medium Term Expenditure Framework [MTEF], or other basis); and
• budgeted in a way that ensues that government, non-government and community needs were included to ensure fully implementation of country's disease program strategies.
For additional information and verification, please see “Revised Costing of Namibia’s 3rd HIV/AIDS Medium Term Plan (MTP III); technical report, MoHSS, October 2007 (Annex I.4) and updated costing for MTP IV available from MoHSS.
An extensive costing exercise was conducted in Namibia in 2007 in view of the development of the National Development Plan III (NDPIII) and the HIV/AIDS Strategic Plan (MTP IV). This costing was updated end 2008. The NAEC decided that the Rourse Needs Estimation (RNE) Model is updated every two years to allow to incorporate strategies and interventions, as well as changing unit cost, inflation and exchange rates. The RNE model is comprised of 21 HIV and AIDS programme areas covering the entire multi-sectoral response. The multi-sectoral response includes public sector, civil society and the private for profit sector. The civil society is the main implementer of community support services (OVC, PLWHA, and CHBC, as well as BCC-out reach). The private for profit sector is mainly involved through work place programmes. The costing followed the UNAIDS resource needs methodology based on four basic criteria: the size of the population being targeted by the intervention or service, the coverage of the target population (fiscal year 2006/07 was used as baseline), the target coverage, and the unit cost of providing the intervention or service. The costing covered the period 2007/08 up to 2014/2015. The model was presnetd at the recent implementers meeting, held in June 09 in Windhoek, and was well received. The costing exercise has some limitations. The IEC and BCC programme area is still estimated too low as data were lacking of BCC out reach sevices. The cost related to enabling environment, including legal assistance, could not be done due to lack of time. Overall, this costing exercise was done in a rather conservative manner, taking into account the perspective of sustainability. It did not take into account external technical assistance, which is rather costly compared to local technical assistance. Therefore, the final results are estimated to be still on the lower side compared to the current actual cost. The cost of the national HIV and AIDS response is estimated to be around 5% of the GDP (2005). The per capita average annual resource need is estimated to be between US$106. The annual cost of ART drugs and related laboratory tests alone is around US$306 per patient or US$ 537 if including HR and overhead cost. The revised costing revealed that focusing on preventing new infections is key for the financial sustainability, and that we should not underestimate the importance of continued external donor funding in this regard. The costing exercise conducted in 2007 was done in such a way that each programme area could choose from three scenarios. Following the target setting exercise in February 2008, the scenarios were selected and the figures in Line A of Table 5.1 indicate the compilation of the selected scenario cost that were updated end 2008. Regarding the annual budgeting for HIV and AIDS, the Government medium-term expenditure framework (MTEF) is following the NDPII and therefore the budget only reflects HIV and AIDS budgets of the public sector.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 142/160
5.1.2 Domestic funding – 'LINE B' entries in table 5.1
Explain the processes used to:
• prioritize domestic financial contributions to the national disease program (including HIPC [Heavily Indebted Poor Country] and other debt relief, and grant or loan funds that are contributed through the national budget); and
• ensure that domestic resources are utilized efficiently, transparently and equitably, to help implement treatment, prevention, care and support strategies at the national, sub-national and community levels.
Prioritisation is done through the annual planning and budgeting process guided by the NDP III and Vision 2030. As explained earlier, HIV and AIDS is one of the five cross-cutting areas throughout the NDP III, as well as a stand alone component for the multi-sectoral HIV and AIDS response. The current MTEF (2008/09 to 2010/11) is based on results-based budgeting. The budget allocation is based on costed activity plans of all Government Offices, Ministries and Agencies (OMAs) and all regional councils. The Government works with two budgets, a recurrent and a development budget. The development budget is allocated by the National Planning Commission (NPC) and directed towards poverty reduction. The recurrent budget is allocated by the Ministry of Finance (MoF) to the OMAs and regional councils. The national budget cycle runs from June to February (preparation), March/April (approval), and 1 April until 31 March (implementation). Ensuring proper use of domestic resources happens by monitoring the quarterly reports submitted by OMAs to NPC and MoF. However, these reports do not specifically track all expenditure on HIV and AIDS activities mainstreamed throughout the OMAs. Therefore, the Resource Mobilisation and Development Coordination (RMDC) subdivision of the Directorate for Special Programmes within MoHSS, collects annual data on HIV and AIDS related budgets and expenditure. The most substantial budget allocations and expenditure towards HIV and AIDS concern: Prevention: the Ministry of Education for life skills training and school feeding; the Ministry of Information and Communication Technology for mass media campaigns; and the Ministry of Safety and Security for the Women and Child Protection Units and programmes with inmates of correctional services. Almost all OMAs have budgets for work place programmes. Care and Support: the Ministry of Gender Equality and Child Welfare and the Ministry of Labour and Social Welfare, for OVC and disability grants (eligible PLWHs can benefit from the latter); and the Ministry of Regional and Local Government, Housing and Rural Development for regional coordination and management of HIV response. Treatment: the MoHSS for the health sector programmes (including increasing share of ART drugs and laboratory cost) and health systems The allocations to regional level are done through the thirteen Regional Councils and regional sections of the OMAs, following the decentralization process.
Other domestic contributions are monitored by NABCOA, for the private sector, and by NANASO, for civil society.
5.1.3 External funding excluding Global Fund – 'LINE C' entries in table 5.1
Explain any changes in contributions anticipated over the proposal term (and the reason for any identified reductions in external resources over time). Any current delays in accessing the external funding identified in table 5.1 should be explained (including the reason for the delay, and plans to resolve the issue(s)).
The changes expected over the course of the proposal regarding funding are summarized below. Government funding: with the commitment of taking on a substantial part of the ART drugs and fully financing the OVC grants (notably, these are the biggest HIV and AIDS programmes in terms of cost), the Government contribution is expected to rise on an annual basis as is projected in table 5.1. The Government funds are generally accessed with a delay of three months (June instead of April) due the parliamentary approval process. Multi-lateral funding: The UN system allocates funding on an annual or bi-annual basis. There is an expected decrease as UNICEF decreases operational funding towards the life skills programme.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 143/160

RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 144/160
The majority of the funding of the UN is allocated to technical and strategic support and little funding goes into direct programme implementation. Bi-lateral funding: Many bilateral donors have already left Namibia or are in the process of doing so. The European donor countries are channelling their funds to the Global Fund at the global level. The EU is retreating from HIV and AIDS funding for the same reason. Therefore the bi-lateral funding is expected to decrease. The accessibility of funds varies. PEPFAR funding: This has decreased slightly for 2010 and as PEPFAR will provide a large part of the contribution as well to the Global Fund at the global level, the funding is expected to decrease over time (10% decrease already from 2011 on ART drugs and laboratory equipment). The Country Operational Plans (COP) are prepared a year in advance and funding for implementation is only accessible one year later (COP 09 is approved in November 08 and funding disbursed to implementers beginning 2010). PEPFAR contributes to the following Global Fund SDA areas: BCC-Mass media & Outreach (co-funding national campaign & faith based organizations); Condoms (procurement condoms (4.5 million on total of estimated need of 35 million); C&T (significant contribution around 60% of total estimated needs); PMTCT (idem as C&T); ART (drugs (15%), biomedical test, staffing (about 70% of estimated needs) etc.); Care and support chronically ill & OVC support (50%); WPP (focusing on MoE and OPM); TB/HIV (TB-CAP technical assistance); strengthening of civl society (USAID/PACT focusing on faith based organizations); and M&E (50% of total estimated needs). The partnership between global Fund, PEPFAR, and Government is strong and funding is well aligned with priorities and is additional and complementary. Funding from private sector: This is expected to increase slightly as more companies will invest in workplace programmes. However, social contribution as defined by the Global Fund guidelines as relatively low.
The civil society is heavily donor dependent and the contribution is not expected to change.

5.2 Detailed Budget Suggested steps in budget completion: 1. Submit a detailed proposal budget in Microsoft Excel format as a clearly numbered Annex D: HIV
Annex E: HSS
Wherever possible, use the same numbering for budget line items as the program description. 2. From that detailed budget, prepare a 'Summary by Objective and Service Delivery Area'
(section 5.3) 3. From the same detailed budget, prepare a 'Summary by Cost Category' (section 5.4); and 4. Ensure the detailed budget is consistent with the detailed workplan of program activities. 5. Do not include any CCM (or Sub-CCM or RCM) operating costs in this proposal. This support is now
available through a separate application for funding made direct to the Global Fund (and not funded through grant funds). The application is available on the Global Fund's website.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 145/160

5.3 Summary of detailed budget by objective and service delivery area
Objective Number
Service delivery area (Use the same numbering as in program description in s. 4.6.4)
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Total
1 1.1 BCC Mass Media 692,864 788,959 844,380 792,953 840,530 890,962 4,850,649
1 1.2 BCC - Community & Schools 5,168,394 3,024,430 3,376,672 2,997,995 5,565,038 3,158,120 23,290,649
1 1.3 Condoms 2,914,504 3,188,447 2,429,258 3,390,220 2,730,919 2,894,774 17,548,123
1 1.4 Counselling and Testing 1,108,827 1,123,092 1,030,365 1,086,776 1,058,875 1,242,848 6,650,782
1 1.5 PMTCT 830,653 616,606 613,293 604,534 697,617 679,254 4,041,957
1 1.6 STI Diagnosis & Treatment 310,281 251,434 343,761 70,468 120,540 79,178 1,175,662
2 2.1 Anti Retroviral Therapy 9,335,200 8,567,434 10,642,467 9,620,477 10,061,178 10,390,726 58,617,483
2 2.2 Care and Support for the Chronically Ill 3,928,983 3,895,058 3,755,366 3,010,628 3,189,504 3,269,668 21,049,206
2 2.3 TB/HIV 222,676 176,686 164,028 173,870 184,302 195,360 1,116,922
3 3.1 Support services to OVC 1,268,158 1,459,615 1,405,436 1,557,055 1,662,629 1,762,387 9,115,281
4 4.1 Policy development including workplace policy 934,337 776,283 820,065 1,006,660 906,173 957,281 5,400,798
4 4.2 Strengthening of civil society and institutional capacity building
628,624 582,765 547,522 581,715 495,978 521,862 3,358,466
4 4.3 Response Management, M&E and Surveillance 1,993,104 1,970,226 2,111,876 2,267,868 2,392,625 2,456,258 13,191,957
Total requested from the Global Fund: 29,336,605 26,421,034 28,084,490 27,161,219 29,905,910 28,498,680 169,407,937
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 146/160
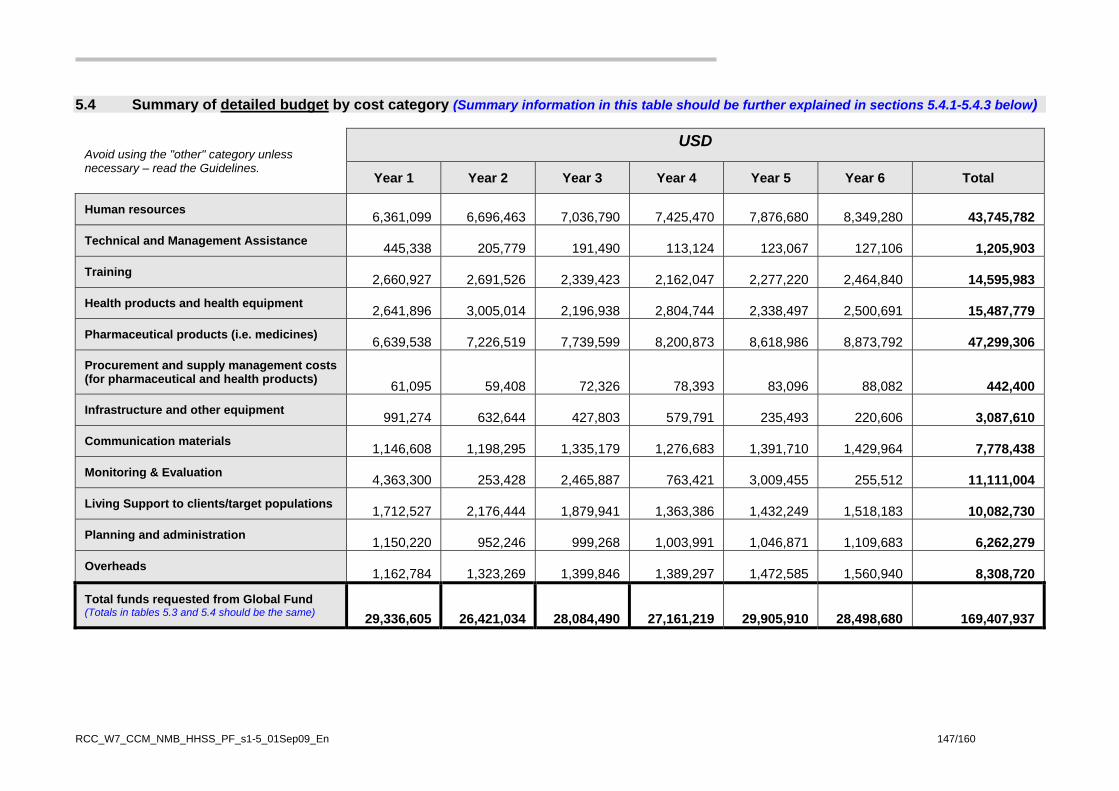
5.4 Summary of detailed budget by cost category (Summary information in this table should be further explained in sections 5.4.1-5.4.3 below)
Avoid using the "other" category unless necessary – read the Guidelines.
USD
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Total
Human resources 6,361,099 6,696,463 7,036,790 7,425,470 7,876,680 8,349,280
43,745,782 Technical and Management Assistance 445,338 205,779 191,490 113,124 123,067 127,106
1,205,903
Training 2,660,927 2,691,526 2,339,423 2,162,047 2,277,220 2,464,840
14,595,983 Health products and health equipment 2,641,896 3,005,014 2,196,938 2,804,744 2,338,497 2,500,691
15,487,779
Pharmaceutical products (i.e. medicines) 6,639,538 7,226,519 7,739,599 8,200,873 8,618,986 8,873,792
47,299,306 Procurement and supply management costs (for pharmaceutical and health products) 61,095 59,408 72,326 78,393 83,096 88,082
442,400
Infrastructure and other equipment 991,274 632,644 427,803 579,791 235,493 220,606
3,087,610 Communication materials 1,146,608 1,198,295 1,335,179 1,276,683 1,391,710 1,429,964
7,778,438
Monitoring & Evaluation 4,363,300 253,428 2,465,887 763,421 3,009,455 255,512
11,111,004 Living Support to clients/target populations 1,712,527 2,176,444 1,879,941 1,363,386 1,432,249 1,518,183
10,082,730
Planning and administration 1,150,220 952,246 999,268 1,003,991 1,046,871 1,109,683
6,262,279 Overheads 1,162,784 1,323,269 1,399,846 1,389,297 1,472,585 1,560,940
8,308,720
Total funds requested from Global Fund (Totals in tables 5.3 and 5.4 should be the same) 29,336,605 26,421,034 28,084,490 27,161,219 29,905,910 28,498,680 169,407,937
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 147/160
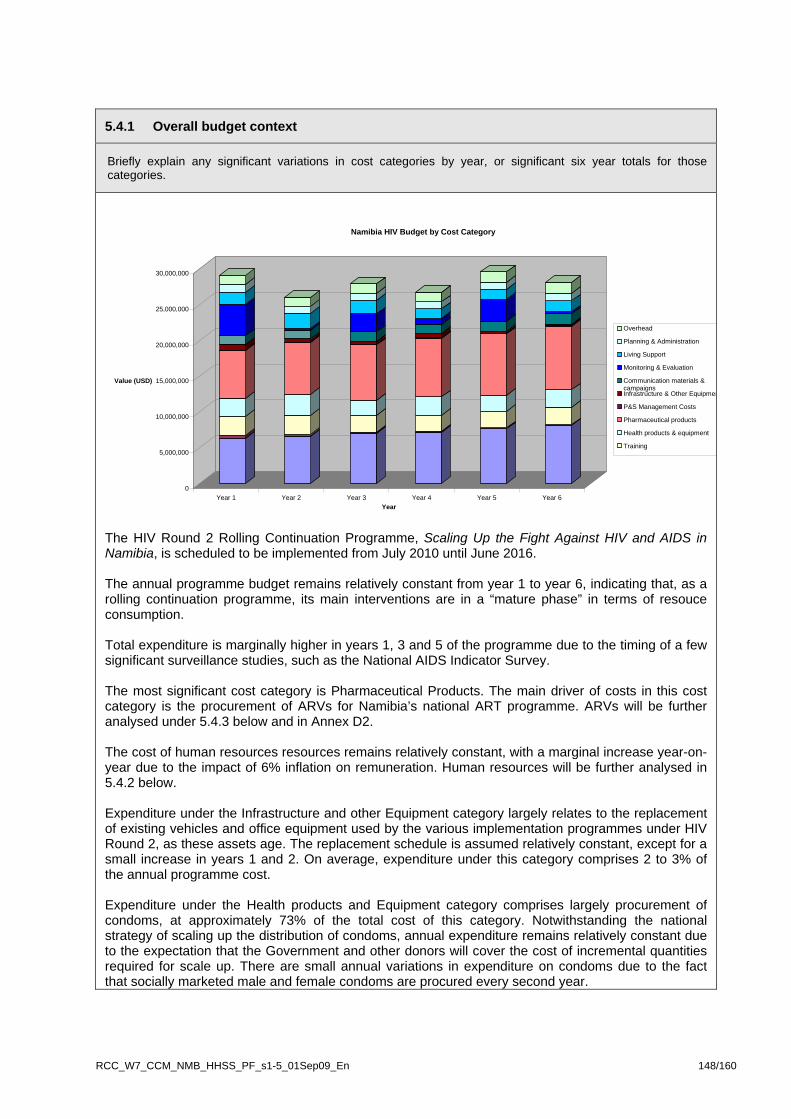
5.4.1 Overall budget context
Briefly explain any significant variations in cost categories by year, or significant six year totals for those categories.
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
Value (USD)
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6Year
Namibia HIV Budget by Cost Category
Overhead
Planning & Administration
Living Support
Monitoring & Evaluation
Communication materials &campaignsInfrastructure & Other Equipmen
P&S Management Costs
Pharmaceutical products
Health products & equipment
Training
The HIV Round 2 Rolling Continuation Programme, Scaling Up the Fight Against HIV and AIDS in Namibia, is scheduled to be implemented from July 2010 until June 2016. The annual programme budget remains relatively constant from year 1 to year 6, indicating that, as a rolling continuation programme, its main interventions are in a “mature phase” in terms of resouce consumption. Total expenditure is marginally higher in years 1, 3 and 5 of the programme due to the timing of a few significant surveillance studies, such as the National AIDS Indicator Survey. The most significant cost category is Pharmaceutical Products. The main driver of costs in this cost category is the procurement of ARVs for Namibia’s national ART programme. ARVs will be further analysed under 5.4.3 below and in Annex D2. The cost of human resources resources remains relatively constant, with a marginal increase year-on-year due to the impact of 6% inflation on remuneration. Human resources will be further analysed in 5.4.2 below. Expenditure under the Infrastructure and other Equipment category largely relates to the replacement of existing vehicles and office equipment used by the various implementation programmes under HIV Round 2, as these assets age. The replacement schedule is assumed relatively constant, except for a small increase in years 1 and 2. On average, expenditure under this category comprises 2 to 3% of the annual programme cost. Expenditure under the Health products and Equipment category comprises largely procurement of condoms, at approximately 73% of the total cost of this category. Notwithstanding the national strategy of scaling up the distribution of condoms, annual expenditure remains relatively constant due to the expectation that the Government and other donors will cover the cost of incremental quantities required for scale up. There are small annual variations in expenditure on condoms due to the fact that socially marketed male and female condoms are procured every second year.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 148/160
5.4.2 Human resources In cases where 'human resources' represents an important share of the budget, summarize: (i) the basis for the budget calculation over the initial three years; (ii) the method of calculating the anticipated costs over years four to six; and (iii) to what extent human resources spending will strengthen service delivery. Useful information to support the assumptions to be set out in the detailed budget includes: a list of the proposed positions that is consistent with assumptions on hours, salary etc included in the detailed budget; and the proportion (in percentage terms) of time that will be allocated to the work under this proposal.
Attach supporting information as a clearly named and numbered annex
The Human Resources cost category is the second largest cost category after Pharmaceutical Products. The Human Resources category contributes 26% of the total cost of the 6-year programme.
The methodology used to budget for Human Resources was largely underpinned by an activity-based costing approach, except for programme management positions. The following assumptions supported the costing of human resources:
• Where existing positions were funded under the Round 2 HIV grant, the same salary scales have been applied to the Rolling Continuation programme.
• Where existing Round 2 positions were funded, a 10% inflationary increase was factored in to arrive at year 1 prices, and thereafter a steady 6% inflation rate was applied to annual salaries year-on-year. The inflation factoring is in line with official inflation forecasting by the Government of Namibia.
• Where positions are full time, the full “cost-to-company” remuneration package is provided for, including medical aid and social security.
• Remuneration scales of civil society positions have been based on remuneration of actual positions funded by participating organizations in Round 2. However, to ensure consistency and cost-effectiveness, the remuneration scales of civil society positions under the RCC programme have been standardized, using the Civil Society Salary Survey (published by NANGOF Trust, 2009) as the main reference point. Remunerations for civil society positions can be found on sheet 5 and sheet 6 of Annex D1, Namibia HIV Budget Tool. A summary of human resources deployed are listed below.
o Distribution staff for managing the roll out of mass media campaigns and IEC production
o School counsellors and assistant school counsellors participating in schools-based life skills and counselling programme. Schools in Namibia do not have full time life skills teachers or school based counsellors to address the high needs of OVCs in the education sector. School Counsellors will therefore fill the gap of providing psychosocial support to OVCs. They work with schools at the regional and district level.
o Regional and district co-ordinators & project officers for regional peer education and outreach programmes. This cadre will ensure appropriate peer education at the grass roots level and well as establishing effective referral systems to health facilities
o Co-ordinators and support staff for outreach centres servicing various vulnerable groups and well as supporting groups of outreach workers operating from centres
o BCC Field workers undertaking comprehensive behaviour change interventions, focusing on the drivers of the epidemic
o Logistical support officers and distribution resources for condoms. These staff will ensure the availability and accessibility through out all the 13 regions of Namibia, as the condom distribution programme is scaled up.
o Mobile Counselling and Testing teams. These teams will ensure increased outreach services to workplaces and hard to reach areas of the country.
o Data clerks for data management for PMTCT, ART, VCT programmes. These clerks will be crucial to fulfilling the roles of primary data entry, management and reporting due to the shortage of staff within these divisions
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 149/160

o Project officers & co-ordinators to support cadres of community workers under for CHBC programme, PLHIV and OVC programmes in all 13 regions and to stregthen integration of community and PHC services
o Nutritionist and assistants to guide roll-out of nutritional support programme at ART sites
o Full time and further part time lay counsellors to support PLHIV and OVC
o Mentors for workplace programmes
o Regional support officers and assistants for civil society responses and capacity building
o Programme management teams for approx imately 15 non-government sub recipients and 10 public sector recipients. These teams include a project manager, account officer and project officer or M&E officer. Larger programmes have provision for a driver and part-time inputs from financial manager. Please see detailed budget note Annex D1, Namibia HIV Budget Tool.
o Programme Management Units for a civil society PR and a government PR. Both PMUs have provision for grant managers, finance managers, accounts assistants, M&E officers and M&E assistants. The government PMU has provision for a procurement service and IT support, as well as administrative support staff. Please see detailed budget note Annex D1, Namibia HIV Budget Tool.
The pie graph below below provides an indication of the human resource cost associated with each service delivery area.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 150/160
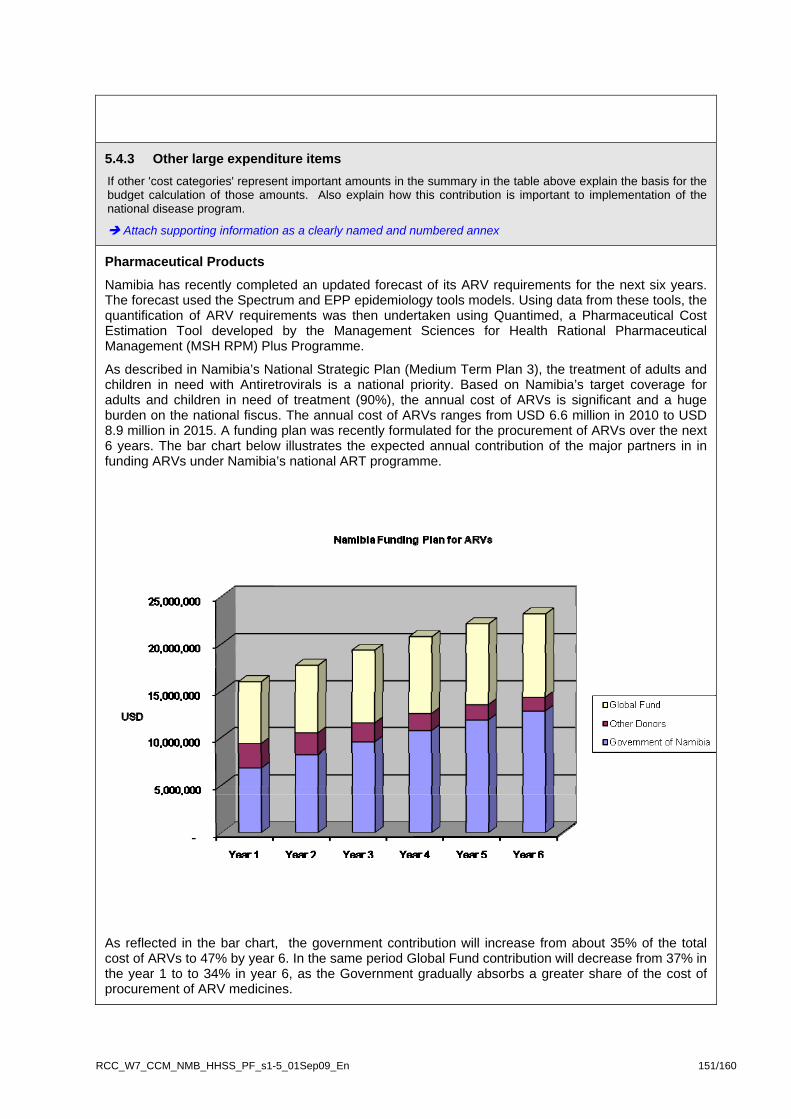
5.4.3 Other large expenditure items If other 'cost categories' represent important amounts in the summary in the table above explain the basis for the budget calculation of those amounts. Also explain how this contribution is important to implementation of the national disease program.
Attach supporting information as a clearly named and numbered annex
Pharmaceutical Products
Namibia has recently completed an updated forecast of its ARV requirements for the next six years. The forecast used the Spectrum and EPP epidemiology tools models. Using data from these tools, the quantification of ARV requirements was then undertaken using Quantimed, a Pharmaceutical Cost Estimation Tool developed by the Management Sciences for Health Rational Pharmaceutical Management (MSH RPM) Plus Programme.
As described in Namibia’s National Strategic Plan (Medium Term Plan 3), the treatment of adults and children in need with Antiretrovirals is a national priority. Based on Namibia’s target coverage for adults and children in need of treatment (90%), the annual cost of ARVs is significant and a huge burden on the national fiscus. The annual cost of ARVs ranges from USD 6.6 million in 2010 to USD 8.9 million in 2015. A funding plan was recently formulated for the procurement of ARVs over the next 6 years. The bar chart below illustrates the expected annual contribution of the major partners in in funding ARVs under Namibia’s national ART programme.
As reflected in the bar chart, the government contribution will increase from about 35% of the total cost of ARVs to 47% by year 6. In the same period Global Fund contribution will decrease from 37% in the year 1 to to 34% in year 6, as the Government gradually absorbs a greater share of the cost of procurement of ARV medicines.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 151/160
Please see Annexure D2, National Funding Plan for ARVs, Quantification Forecast Methodology and Schedule of Pharmaceuticals, for a more detailed review of the ARV forecast and funding plan.
Monitoring and evaluation
The monitoring and evaluation cost category comprises the development and production of M&E tools, routine monitoring and evaluation field visits periodic operational research studies and national surveys. Although the cost of most of the national studies is reduced due to the expectation of co-funding, they do, nevertheless, remain significant cost drivers. That said, the research and surveys selected for the RCC programme are seen as indispensable in guiding Namibia’s responses to the HIV AIDS epidemic. The main surveys under the programme are:
• KAP surveys for vulnerable groups • Behavioural surveillance surveys (BSS) for Most at Risk Populations in 7 regions (year 1 & 4) • AIDS Indicator Survey (AIS) (year 1 & 5) • HIV sentinel Survey (years 3 & 5) • National Condom Need Estimation Survey (year 1 & 4) • Infant and young child feeding research (year 1) • STI etiologic study to determine the etiologies of the three common syndromes (year 3) • ART adherence and resistance survey (year 1 & 3) • National Survey of Workplace Programmes (year 1 & 4)
5.5 Funding requests in the context of a common funding mechanism In this section, common funding mechanism refers to situations where all funding is contributed into a common fund for distribution to implementing partners. Do not complete this section if the country pools, for example, procurement efforts, but all other funding is managed separately.
5.5.1 Operational status of common funding mechanism
Briefly summarize the main features of the common funding mechanism, including the fund's name, objectives, governance structure and key partners.
Attach, as clearly named and numbered annexes to your proposal, the memorandum of understanding, joint Monitoring and Evaluation procedures, the latest annual review, accountability procedures, list of key partners, etc.
5.5.2 Measuring performance How often is program performance measured by the common funding mechanism? Explain whether program performance influences financial contributions to the common fund.
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 152/160
5.5.3 Additionality of Global Fund request Explain how the funding requested in this proposal (if approved) will contribute to the achievement of outputs and outcomes that would not otherwise have been supported by resources currently or planned to be available to the common funding mechanism.
If the focus of the common fund is broader than the disease program, applicants must explain the process by which they will ensure that funds requested will contribute towards achieving impact on the disease outcomes during the proposal term.
COPY HERE AN OPTIONAL SECTION 5B THAT IS TO BE INSERTED INTO THIS
PROPOSAL HERE IF THE PROPOSAL INCLUDES S.4B
Section 5B – Health System Strengthening cross-cutting interventions
OPTIONAL ADDITIONAL SECTION TO BE INSERTED IN THE ROLLING CONTINUATION CHANNEL PROPOSAL Copy sections 5B.1 to 5B.4 inclusive below into the applicant's Rolling Continuation Channel proposal form after s.5.5. SECTION 5B CAN ONLY BE INCLUDED IF:
The applicant has identified gaps and constraints in the health system that have an impact on HIV, tuberculosis and malaria outcomes;
The interventions required to respond to these gaps and constraints are 'cross-cutting' and benefit more than one of the three diseases;
Section 4B is included in after s.4.11.6 of the Rolling Continuation Channel Proposal Form.
Read the RCC Guidelines to consider including HSS cross-cutting interventions
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 153/160
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 154/160
5B.1 Detailed Budget Steps in budget completion: 1. Submit a detailed budget of the HSS cross-cutting interventions in Microsoft Excel format
using the same numbering for budget line items as in the description of HSS cross-cutting interventions in section 4B.1.
The detailed budget must be submitted as a clearly numbered annex.
The HSS cross-cutting interventions may be prepared as a separate Excel worksheet of the disease budget, or a separate file (Excel workbook) at the applicant's election.
For guidance on the level of detail required refer to the detailed budget guidance in
section 5.2 of the RCC Guidelines. (i.e., same instructions as for the disease budget preparation)
2. From that detailed budget, prepare a 'Summary by Objective and Service Delivery Area'
(section 5B.2). (Note – 'SDAs' for the purpose of HSS cross-cutting interventions are not the same as the SDAs for the diseases. Refer to s.5B.2 of the RCC Guidelines for more information).
3. From the same detailed budget, prepare a 'Summary by Cost Category' (section 5B.3); and 4. Ensure the detailed budget is consistent with the detailed workplan for HSS cross-cutting
interventions, and the 'Performance Framework' for HSS cross-cutting interventions (Attachment A).
READ THE RCC GUIDELINES FOR MORE INFORMATION

5B.2 Summary of detailed budget for HSS cross-cutting interventions by objective and service delivery area
Table 5B.2 – Summary of detailed budget by objective and service delivery area
Budget breakdown by SDA
Objective Number
Service delivery area (Use the same numbering as the detailed
work plan for HSS cross-cutting interventions)
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Total
1 HSS: Service delivery 2,658,135 2,930,604 2,228,699 2,499,224 1,181,090 656,312 12,154,065
2 HSS: Health workforce 3,405,274 3,502,267 3,578,062 3,340,036 2,838,686 2,435,463 19,099,788
3 HSS: Information Systems 1,310,113 1,759,798 720,485 330,574 1,264,221 371,433 5,756,623
4 HSS: Medical Products, Vaccines and Technology 1,789,877 633,089 671,075 711,339 754,019 799,260 5,358,659
5 HSS: Financing 25,989 0 0 0 0 0 25,989
Total funds requested from Global Fund for HSS cross-cutting interventions (i.e., total for all the interventions described on a programmatic basis in s.4B.1, where included in the RCC proposal)
9,189,387 8,825,758 7,198,321 6,881,173 6,038,017 4,262,469 42,395,124
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 155/160
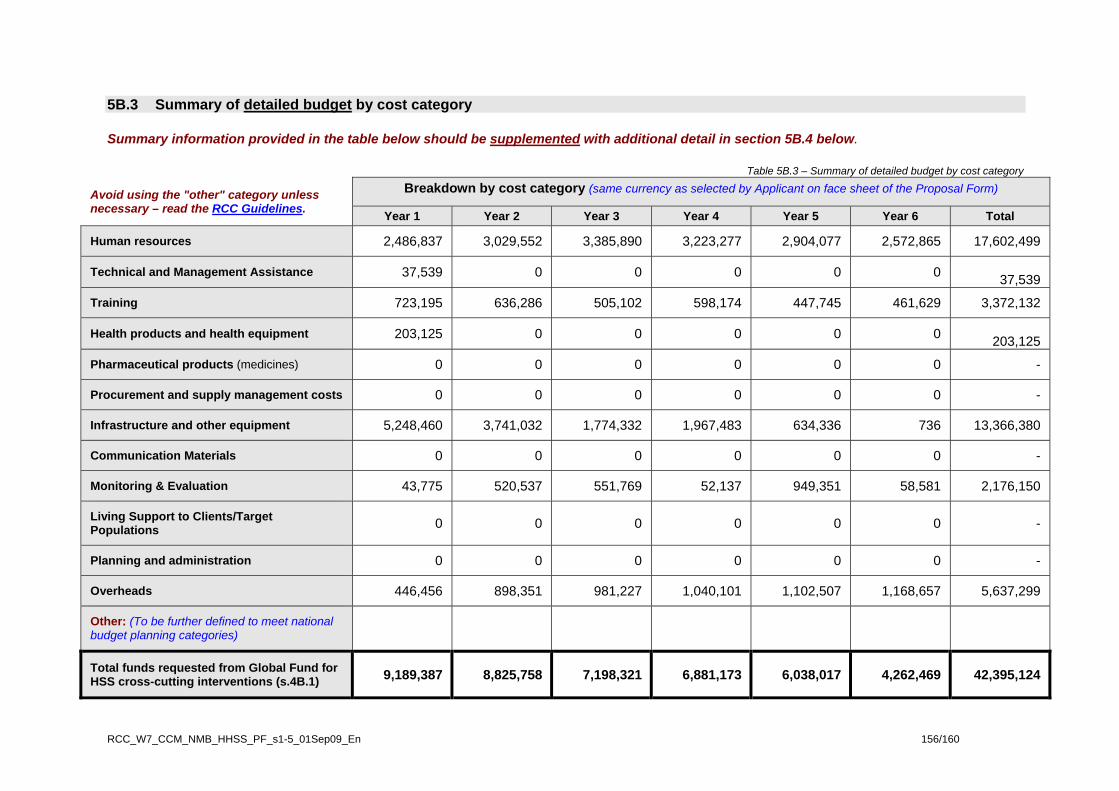
5B.3 Summary of detailed budget by cost category
Summary information provided in the table below should be supplemented with additional detail in section 5B.4 below.
Table 5B.3 – Summary of detailed budget by cost category
Avoid using the "other" category unless necessary – read the RCC Guidelines.
Breakdown by cost category (same currency as selected by Applicant on face sheet of the Proposal Form)
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Total
Human resources 2,486,837 3,029,552 3,385,890 3,223,277 2,904,077 2,572,865 17,602,499
Technical and Management Assistance 37,539 0 0 0 0 0 37,539
Training 723,195 636,286 505,102 598,174 447,745 461,629 3,372,132
Health products and health equipment 203,125 0 0 0 0 0 203,125
Pharmaceutical products (medicines) 0 0 0 0 0 0 -
Procurement and supply management costs 0 0 0 0 0 0 -
Infrastructure and other equipment 5,248,460 3,741,032 1,774,332 1,967,483 634,336 736 13,366,380
Communication Materials 0 0 0 0 0 0 -
Monitoring & Evaluation 43,775 520,537 551,769 52,137 949,351 58,581 2,176,150
Living Support to Clients/Target Populations 0 0 0 0 0 0 -
Planning and administration 0 0 0 0 0 0 -
Overheads 446,456 898,351 981,227 1,040,101 1,102,507 1,168,657 5,637,299
Other: (To be further defined to meet national budget planning categories)
Total funds requested from Global Fund for HSS cross-cutting interventions (s.4B.1) 9,189,387 8,825,758 7,198,321 6,881,173 6,038,017 4,262,469 42,395,124
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 156/160

5B.4.1 Briefly explain any significant variations in cost categories by year, or significant six year totals for those categories.
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Value
Thousands
1 2 3 4 5 6Years
Namibia R2 RCC Cost by CategoryOther
Overheads
Planning and Administration
Living Support to Clients/TargetPopulationMonitoring and Evaluation (M&E)
Communication Materials
Infrastructure and Other Equipment
Procurement and Supply ManagementCosts (PSM)Pharmaceutical Products (Medicines)
Health Products and Health Equipment
Training
Technical & Management Assistance
Human Resources
The two biggest cost categories, throughout the budget period, comprise Human Resources (HR) and Infrastructure and other Equipment (I&OE). A brief explanation of the trends of these categories is presented below. Human Resources ($17.6 million over 6 years) HR is the biggest cost category over the 6 year period and comprises mainly he costs attached to retaining components of the existing health workforce, the recruitment of additional health workers and teaching staff for the National Health Training Center. The increasing trend in HR is caused by the recruitment of new staff during the first three years i.e. not all recruitments take place in year 1. The subsequent decline in HR from year 3 to Year 6 results from the fact that the GF contribution to certain health workforce positions is reduced by 10% per annum. In year 6 the GF request therefore comprises 60% of the total cost for these positions. The increased contribution from the GRN underpins a commitment to improving the sustainability of these interventions. Infrastructure and equipment ($13.4 million over 6 years) It becomes apparent from the graph above that the expenditure on I&OE is highest in year1, declines in years 2 to 5 with no expenditure in year 6. Significant items in I&OE comprise extension and renovation of clinics for ART and other services (both extension of stand alone clinics and within hospitals), procurement of vehicles for distribution and service delivery and the establishment of a national data base. I&OE costs are high in year one because the large refrigerated trucks (for distribution of drugs) are procured in year one and all other facility based vehicles are procured over years 1 and 2. The development and operationalisation of the national IT networks and integrated database also takes place over the first 2 years. Extension and renovation of clinics takes place reasonably evenly over the first 4 years with a decline in year 5. (See annex E 3-2 and E 3-3 for clinic construction costs and estimate of per square meter rate of hospital clinic extension / renovation).
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 157/160
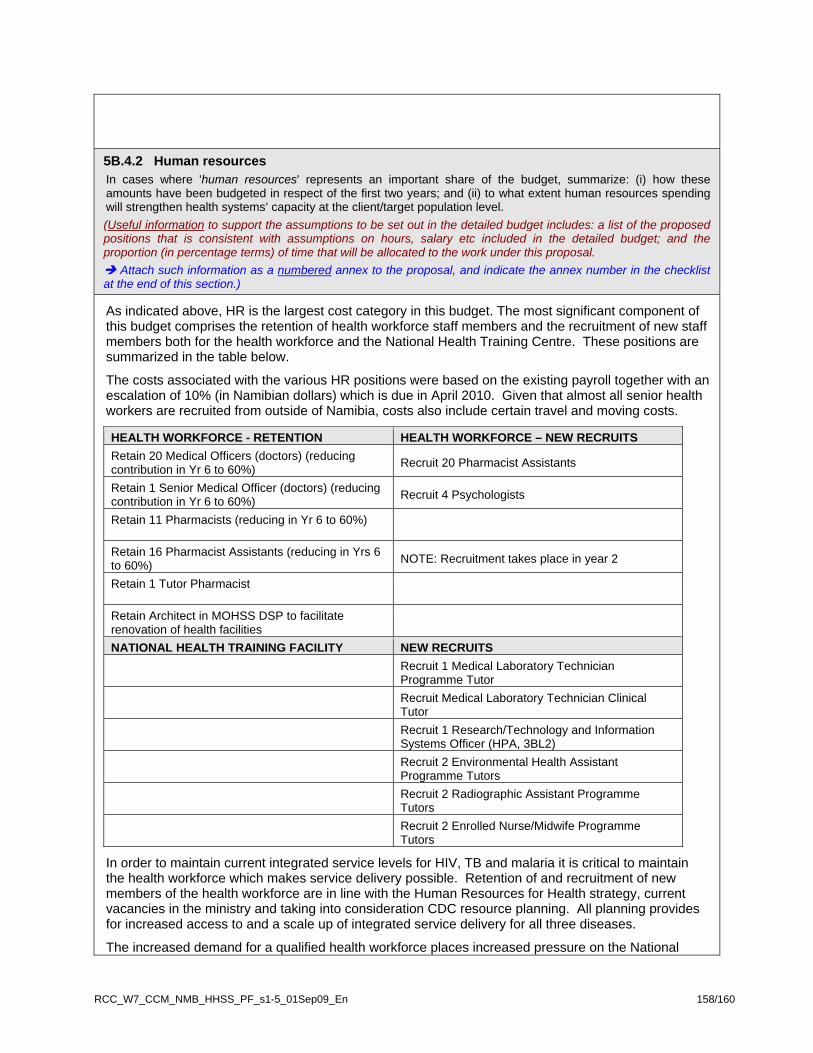
5B.4.2 Human resources In cases where 'human resources' represents an important share of the budget, summarize: (i) how these amounts have been budgeted in respect of the first two years; and (ii) to what extent human resources spending will strengthen health systems’ capacity at the client/target population level. (Useful information to support the assumptions to be set out in the detailed budget includes: a list of the proposed positions that is consistent with assumptions on hours, salary etc included in the detailed budget; and the proportion (in percentage terms) of time that will be allocated to the work under this proposal.
Attach such information as a numbered annex to the proposal, and indicate the annex number in the checklist at the end of this section.)
As indicated above, HR is the largest cost category in this budget. The most significant component of this budget comprises the retention of health workforce staff members and the recruitment of new staff members both for the health workforce and the National Health Training Centre. These positions are summarized in the table below.
The costs associated with the various HR positions were based on the existing payroll together with an escalation of 10% (in Namibian dollars) which is due in April 2010. Given that almost all senior health workers are recruited from outside of Namibia, costs also include certain travel and moving costs.
HEALTH WORKFORCE - RETENTION HEALTH WORKFORCE – NEW RECRUITS Retain 20 Medical Officers (doctors) (reducing contribution in Yr 6 to 60%) Recruit 20 Pharmacist Assistants
Retain 1 Senior Medical Officer (doctors) (reducing contribution in Yr 6 to 60%) Recruit 4 Psychologists
Retain 11 Pharmacists (reducing in Yr 6 to 60%)
Retain 16 Pharmacist Assistants (reducing in Yrs 6 to 60%) NOTE: Recruitment takes place in year 2
Retain 1 Tutor Pharmacist
Retain Architect in MOHSS DSP to facilitate renovation of health facilities
NATIONAL HEALTH TRAINING FACILITY NEW RECRUITS
Recruit 1 Medical Laboratory Technician Programme Tutor
Recruit Medical Laboratory Technician Clinical Tutor
Recruit 1 Research/Technology and Information Systems Officer (HPA, 3BL2)
Recruit 2 Environmental Health Assistant Programme Tutors
Recruit 2 Radiographic Assistant Programme Tutors
Recruit 2 Enrolled Nurse/Midwife Programme Tutors
In order to maintain current integrated service levels for HIV, TB and malaria it is critical to maintain the health workforce which makes service delivery possible. Retention of and recruitment of new members of the health workforce are in line with the Human Resources for Health strategy, current vacancies in the ministry and taking into consideration CDC resource planning. All planning provides for increased access to and a scale up of integrated service delivery for all three diseases.
The increased demand for a qualified health workforce places increased pressure on the National
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 158/160
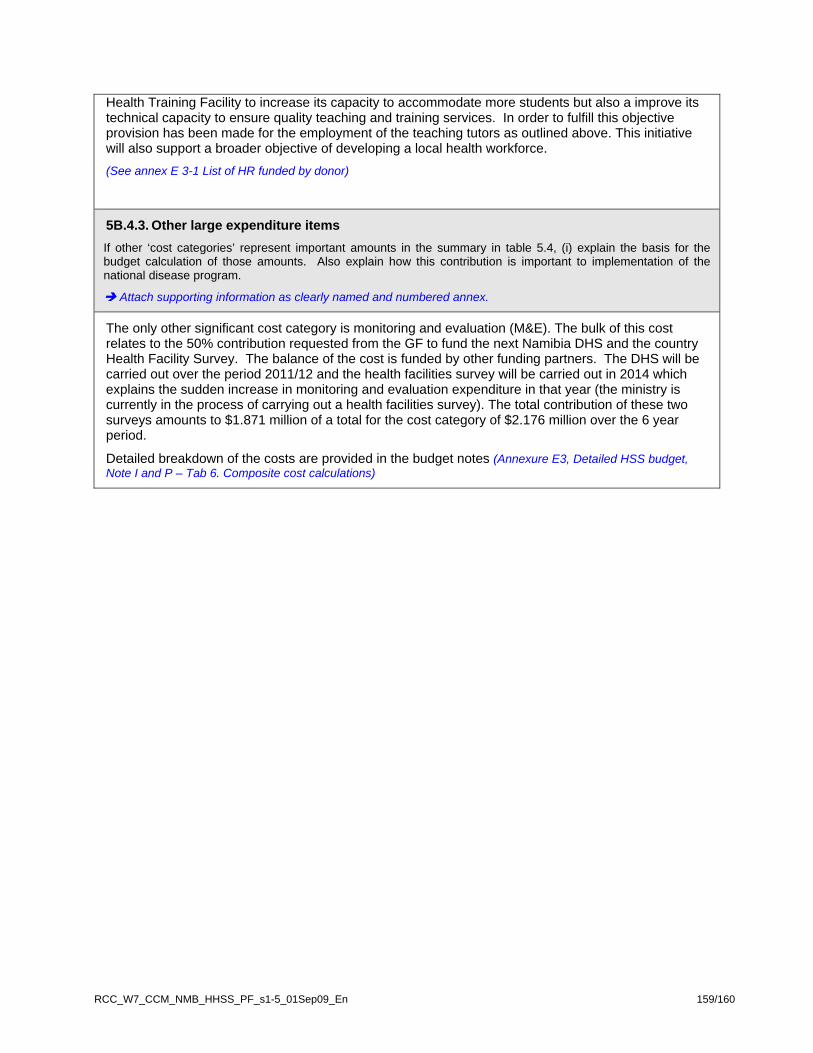
RCC_W7_CCM_NMB_HHSS_PF_s1-5_01Sep09_En 159/160
Health Training Facility to increase its capacity to accommodate more students but also a improve its technical capacity to ensure quality teaching and training services. In order to fulfill this objective provision has been made for the employment of the teaching tutors as outlined above. This initiative will also support a broader objective of developing a local health workforce. (See annex E 3-1 List of HR funded by donor)
5B.4.3. Other large expenditure items If other ‘cost categories’ represent important amounts in the summary in table 5.4, (i) explain the basis for the budget calculation of those amounts. Also explain how this contribution is important to implementation of the national disease program.
Attach supporting information as clearly named and numbered annex.
The only other significant cost category is monitoring and evaluation (M&E). The bulk of this cost relates to the 50% contribution requested from the GF to fund the next Namibia DHS and the country Health Facility Survey. The balance of the cost is funded by other funding partners. The DHS will be carried out over the period 2011/12 and the health facilities survey will be carried out in 2014 which explains the sudden increase in monitoring and evaluation expenditure in that year (the ministry is currently in the process of carrying out a health facilities survey). The total contribution of these two surveys amounts to $1.871 million of a total for the cost category of $2.176 million over the 6 year period.
Detailed breakdown of the costs are provided in the budget notes (Annexure E3, Detailed HSS budget, Note I and P – Tab 6. Composite cost calculations)
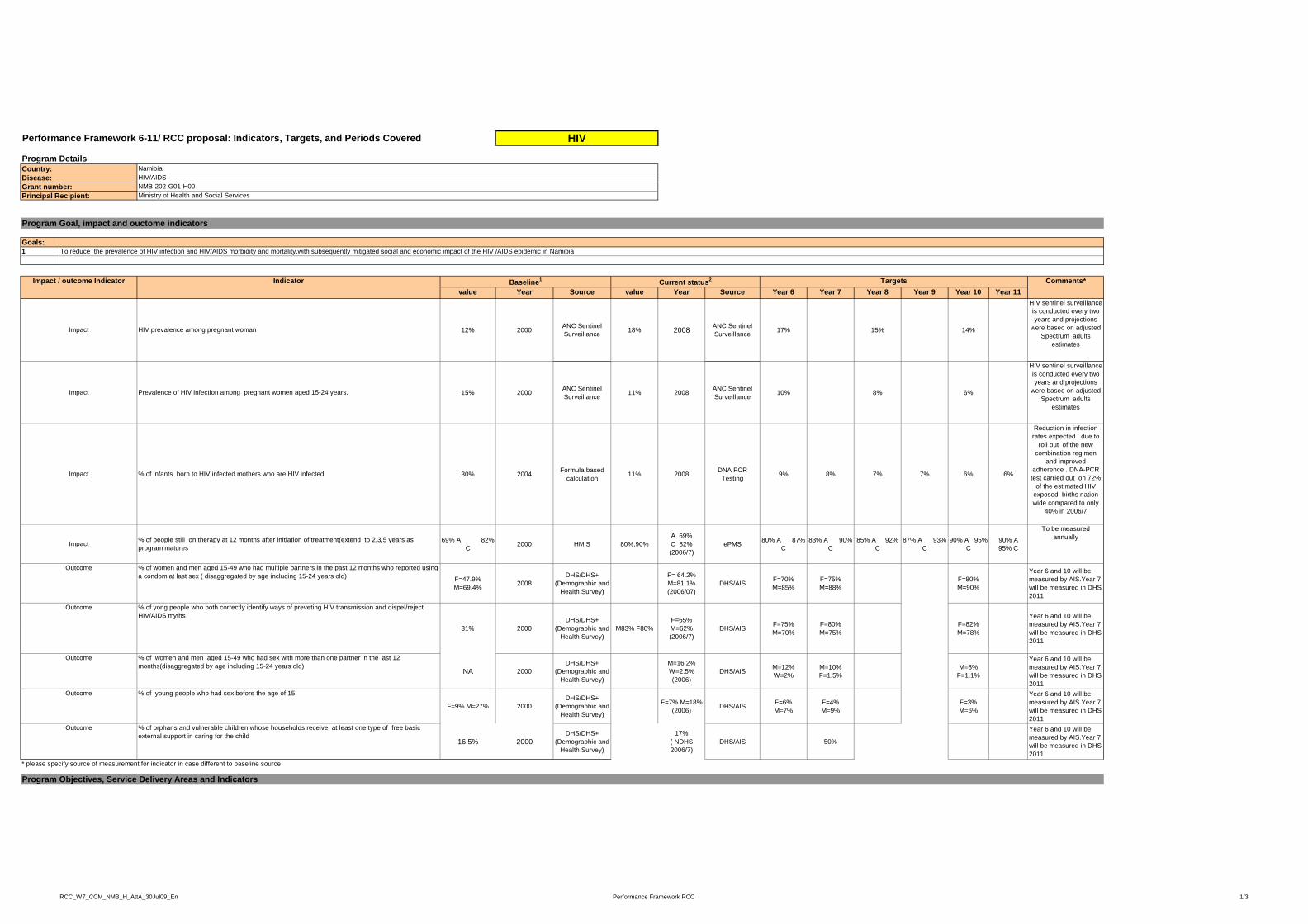
Principal Recipient:
HIV/AIDSNMB-202-G01-H00Ministry of Health and Social Services
Performance Framework 6-11/ RCC proposal: Indicators, Targets, and Periods Covered
Program DetailsCountry:Disease:Grant number:
Namibia
HIV
Goals:1
value Year Source value Year Source Year 6 Year 7 Year 8 Year 9 Year 10 Year 11
12% 2000 ANC Sentinel Surveillance 18% 2008 ANC Sentinel
Surveillance 17% 15% 14%
HIV sentinel surveillance is conducted every two years and projections
were based on adjusted Spectrum adults
estimates
15% 2000 ANC Sentinel Surveillance 11% 2008 ANC Sentinel
Surveillance 10% 8% 6%
HIV sentinel surveillance is conducted every two years and projections
were based on adjusted Spectrum adults
estimates
HIV prevalence among pregnant woman
Prevalence of HIV infection among pregnant women aged 15-24 years.
Comments*
To reduce the prevalence of HIV infection and HIV/AIDS morbidity and mortality,with subsequently mitigated social and economic impact of the HIV /AIDS epidemic in Namibia
Impact
Program Goal, impact and ouctome indicators
Impact
Indicator Baseline1Impact / outcome Indicator TargetsCurrent status2
30% 2004 Formula based calculation 11% 2008 DNA PCR
Testing 9% 8% 7% 7% 6% 6%
Reduction in infection rates expected due to
roll out of the new combination regimen
and improved adherence . DNA-PCR test carried out on 72%
of the estimated HIV exposed births nation wide compared to only
40% in 2006/7
69% A 82% C 2000 HMIS 80%,90%
A 69% C 82% (2006/7)
ePMS 80% A 87% C
83% A 90% C
85% A 92% C
87% A 93% C
90% A 95% C
90% A 95% C
To be measured annually
F=47.9% M=69.4% 2008
DHS/DHS+ (Demographic and
Health Survey)
F= 64.2% M=81.1% (2006/07)
DHS/AIS F=70% M=85%
F=75% M=88%
F=80% M=90%
Year 6 and 10 will be measured by AIS.Year 7 will be measured in DHS 2011
31% 2000DHS/DHS+
(D hi d M83% F80%F=65% M 62% DHS/AIS F=75% F=80% F=82%
Year 6 and 10 will be measured by AIS.Year 7
Outcome
Impact
% of infants born to HIV infected mothers who are HIV infectedImpact
% of yong people who both correctly identify ways of preveting HIV transmission and dispel/reject HIV/AIDS myths
% of people still on therapy at 12 months after initiation of treatment(extend to 2,3,5 years as program matures
% of women and men aged 15-49 who had multiple partners in the past 12 months who reported using a condom at last sex ( disaggregated by age including 15-24 years old)
Outcome
31% 2000 (Demographic and Health Survey)
M83% F80% M=62% (2006/7)
DHS/AIS %M=70%
%M=75%
%M=78%
ywill be measured in DHS 2011
NA 2000DHS/DHS+
(Demographic and Health Survey)
M=16.2% W=2.5% (2006)
DHS/AIS M=12% W=2%
M=10% F=1.5%
M=8% F=1.1%
Year 6 and 10 will be measured by AIS.Year 7 will be measured in DHS 2011
F=9% M=27% 2000DHS/DHS+
(Demographic and Health Survey)
F=7% M=18% (2006) DHS/AIS F=6%
M=7%F=4% M=9%
F=3% M=6%
Year 6 and 10 will be measured by AIS.Year 7 will be measured in DHS 2011
16.5% 2000DHS/DHS+
(Demographic and Health Survey)
17% ( NDHS 2006/7)
DHS/AIS 50%
Year 6 and 10 will be measured by AIS.Year 7 will be measured in DHS 2011
Outcome % of orphans and vulnerable children whose households receive at least one type of free basic external support in caring for the child
% of women and men aged 15-49 who had sex with more than one partner in the last 12 months(disaggregated by age including 15-24 years old)
% of young people who had sex before the age of 15
Outcome
Program Objectives, Service Delivery Areas and Indicators
Outcome
* please specify source of measurement for indicator in case different to baseline source
RCC_W7_CCM_NMB_H_AttA_30Jul09_En Performance Framework RCC 1/3
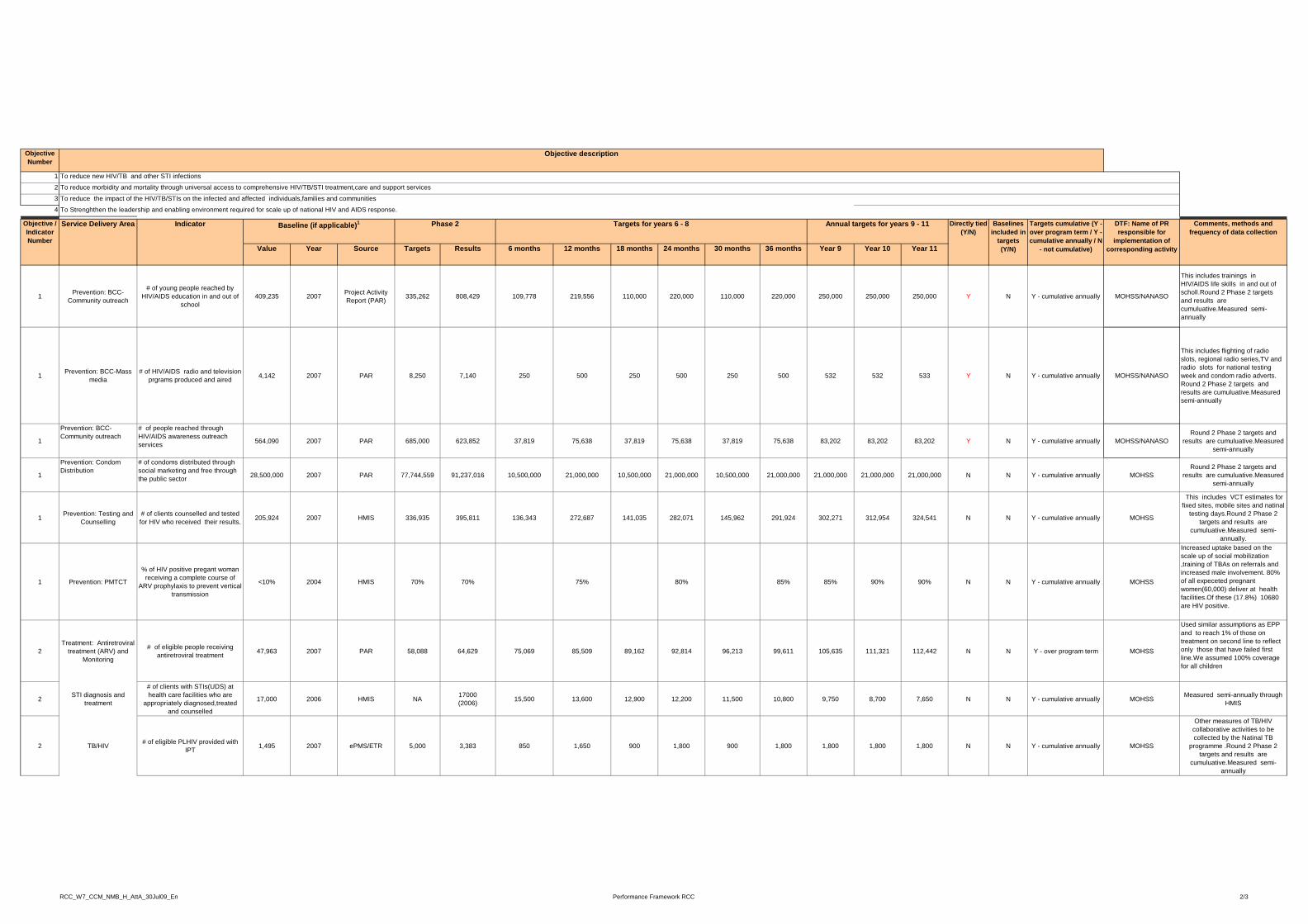
Objective Number
1
2
3
4
Objective description
To reduce new HIV/TB and other STI infections
To reduce morbidity and mortality through universal access to comprehensive HIV/TB/STI treatment,care and support services
To reduce the impact of the HIV/TB/STIs on the infected and affected individuals,families and communities
To Strenghthen the leadership and enabling environment required for scale up of national HIV and AIDS response4
Value Year Source Targets Results 6 months 12 months 18 months 24 months 30 months 36 months Year 9 Year 10 Year 11
1 Prevention: BCC- Community outreach
# of young people reached by HIV/AIDS education in and out of
school409,235 2007 Project Activity
Report (PAR) 335,262 808,429 109,778 219,556 110,000 220,000 110,000 220,000 250,000 250,000 250,000 Y N Y - cumulative annually MOHSS/NANASO
This includes trainings in HIV/AIDS life skills in and out of scholl.Round 2 Phase 2 targets and results are cumuluative.Measured semi-annually
1 Prevention: BCC-Mass media
# of HIV/AIDS radio and television prgrams produced and aired 4,142 2007 PAR 8,250 7,140 250 500 250 500 250 500 532 532 533 Y N Y - cumulative annually MOHSS/NANASO
This includes flighting of radio slots, regional radio series,TV and radio slots for national testing week and condom radio adverts. Round 2 Phase 2 targets and results are cumuluative.Measured semi-annually
DTF: Name of PR responsible for
implementation of corresponding activity
Directly tied (Y/N)
Targets for years 6 - 8 Comments, methods and frequency of data collection
Service Delivery Area Indicator Phase 2Baseline (if applicable)1 Targets cumulative (Y - over program term / Y - cumulative annually / N
- not cumulative)
Baselines included in
targets (Y/N)
Annual targets for years 9 - 11
To Strenghthen the leadership and enabling environment required for scale up of national HIV and AIDS response.
Objective / Indicator Number
1
Prevention: BCC- Community outreach
# of people reached through HIV/AIDS awareness outreach services 564,090 2007 PAR 685,000 623,852 37,819 75,638 37,819 75,638 37,819 75,638 83,202 83,202 83,202 Y N Y - cumulative annually MOHSS/NANASO
Round 2 Phase 2 targets and results are cumuluative.Measured
semi-annually
1
Prevention: Condom Distribution
# of condoms distributed through social marketing and free through the public sector 28,500,000 2007 PAR 77,744,559 91,237,016 10,500,000 21,000,000 10,500,000 21,000,000 10,500,000 21,000,000 21,000,000 21,000,000 21,000,000 N N Y - cumulative annually MOHSS
Round 2 Phase 2 targets and results are cumuluative.Measured
semi-annually
1 Prevention: Testing and Counselling
# of clients counselled and tested for HIV who received their results. 205,924 2007 HMIS 336,935 395,811 136,343 272,687 141,035 282,071 145,962 291,924 302,271 312,954 324,541 N N Y - cumulative annually MOHSS
This includes VCT estimates for fixed sites, mobile sites and natinal
testing days.Round 2 Phase 2 targets and results are
cumuluative.Measured semi-annually.
1 Prevention: PMTCT
% of HIV positive pregant woman receiving a complete course of
ARV prophylaxis to prevent vertical transmission
<10% 2004 HMIS 70% 70% 75% 80% 85% 85% 90% 90% N N Y - cumulative annually MOHSS
Increased uptake based on the scale up of social mobilization ,training of TBAs on referrals and increased male involvement. 80% of all expeceted pregnant women(60,000) deliver at health facilities.Of these (17.8%) 10680 are HIV positive.
Used similar assumptions as EPP
2Treatment: Antiretroviral
treatment (ARV) and Monitoring
# of eligible people receiving antiretroviral treatment 47,963 2007 PAR 58,088 64,629 75,069 85,509 89,162 92,814 96,213 99,611 105,635 111,321 112,442 N N Y - over program term MOHSS
Used similar assumptions as EPP and to reach 1% of those on treatment on second line to reflect only those that have failed first line.We assumed 100% coverage for all children
2 STI diagnosis and treatment
# of clients with STIs(UDS) at health care facilities who are
appropriately diagnosed,treated and counselled
17,000 2006 HMIS NA 17000 (2006) 15,500 13,600 12,900 12,200 11,500 10,800 9,750 8,700 7,650 N N Y - cumulative annually MOHSS Measured semi-annually through
HMIS
2 TB/HIV # of eligible PLHIV provided with IPT 1,495 2007 ePMS/ETR 5,000 3,383 850 1,650 900 1,800 900 1,800 1,800 1,800 1,800 N N Y - cumulative annually MOHSS
Other measures of TB/HIV collaborative activities to be collected by the Natinal TB
programme .Round 2 Phase 2 targets and results are
cumuluative.Measured semi-annually
RCC_W7_CCM_NMB_H_AttA_30Jul09_En Performance Framework RCC 2/3
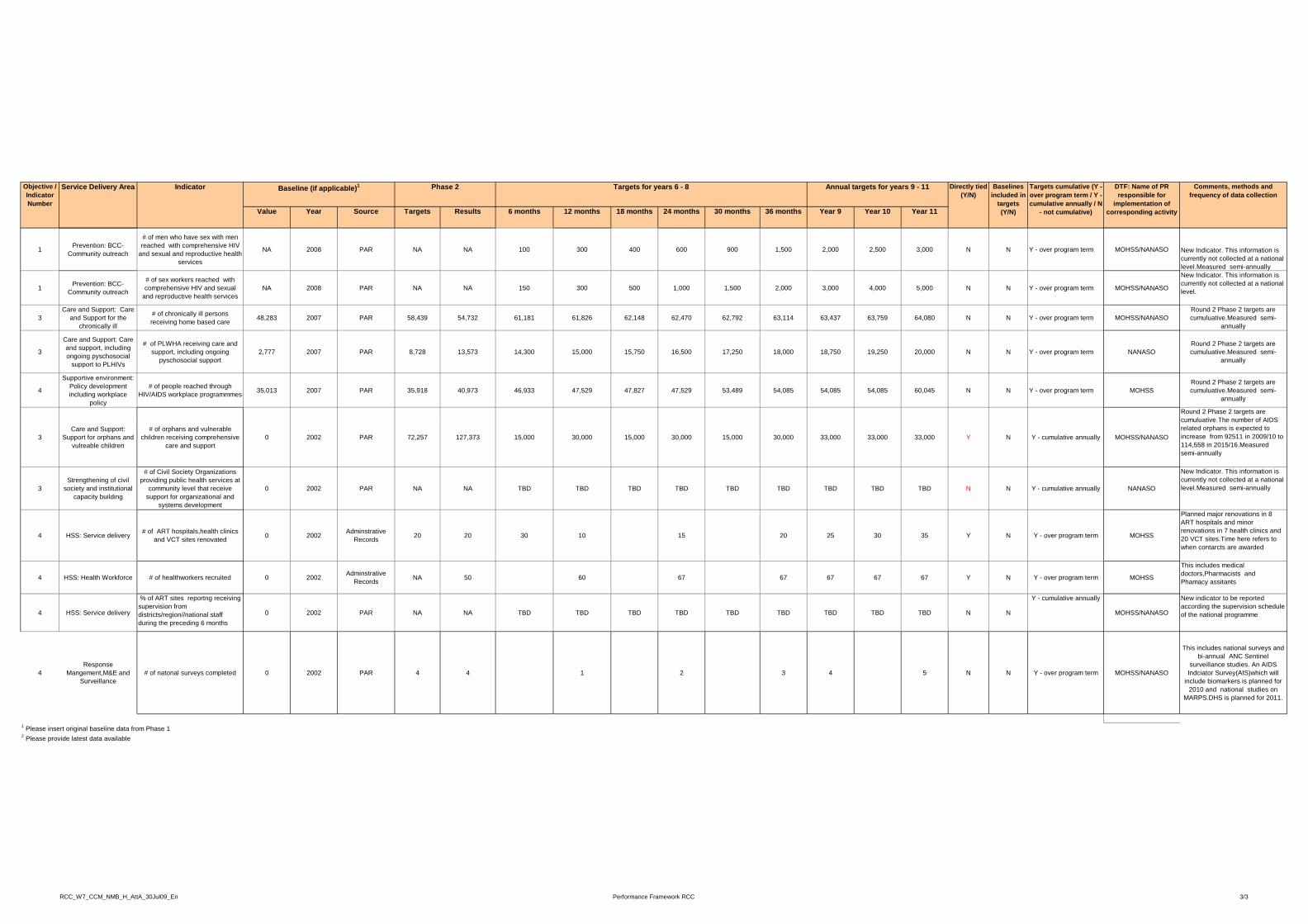
V l Y S T t R lt 6 th 12 th 18 th 24 th 30 th 36 th Y 9 Y 10 Y 11
DTF: Name of PR responsible for
implementation of
Directly tied (Y/N)
Targets for years 6 - 8 Comments, methods and frequency of data collection
Service Delivery Area Indicator Phase 2Baseline (if applicable)1 Targets cumulative (Y - over program term / Y - cumulative annually / N
Baselines included in
targets
Annual targets for years 9 - 11Objective / Indicator Number
Value Year Source Targets Results 6 months 12 months 18 months 24 months 30 months 36 months Year 9 Year 10 Year 11 corresponding activity- not cumulative)(Y/N)
1 Prevention: BCC- Community outreach
# of men who have sex with men reached with comprehensive HIV
and sexual and reproductive health services
NA 2008 PAR NA NA 100 300 400 600 900 1,500 2,000 2,500 3,000 N N Y - over program term MOHSS/NANASO New Indicator. This information is currently not collected at a national level.Measured semi-annually
1 Prevention: BCC- Community outreach
# of sex workers reached with comprehensive HIV and sexual
and reproductive health servicesNA 2008 PAR NA NA 150 300 500 1,000 1,500 2,000 3,000 4,000 5,000 N N Y - over program term MOHSS/NANASO
New Indicator. This information is currently not collected at a national level.
3Care and Support: Care
and Support for the chronically ill
# of chronically ill persons receiving home based care 48,283 2007 PAR 58,439 54,732 61,181 61,826 62,148 62,470 62,792 63,114 63,437 63,759 64,080 N N Y - over program term MOHSS/NANASO
Round 2 Phase 2 targets are cumuluative.Measured semi-
annually
3
Care and Support: Care and support, including ongoing pyschosocial
support to PLHIVs
# of PLWHA receiving care and support, including ongoing
pyschosocial support2,777 2007 PAR 8,728 13,573 14,300 15,000 15,750 16,500 17,250 18,000 18,750 19,250 20,000 N N Y - over program term NANASO
Round 2 Phase 2 targets are cumuluative.Measured semi-
annually
4
Supportive environment: Policy development including workplace
policy
# of people reached through HIV/AIDS workplace programmmes 35,013 2007 PAR 35,918 40,973 46,933 47,529 47,827 47,529 53,489 54,085 54,085 54,085 60,045 N N Y - over program term MOHSS
Round 2 Phase 2 targets are cumuluative.Measured semi-
annually
Round 2 Phase 2 targets are l ti Th b f AIDS
3Care and Support:
Support for orphans and vulreable children
# of orphans and vulnerable children receiving comprehensive
care and support 0 2002 PAR 72,257 127,373 15,000 30,000 15,000 30,000 15,000 30,000 33,000 33,000 33,000 Y N Y - cumulative annually MOHSS/NANASO
cumuluative.The number of AIDS related orphans is expected to increase from 92511 in 2009/10 to 114,558 in 2015/16.Measured semi-annually
3Strengthening of civil
society and institutional capacity building
# of Civil Society Organizations providing public health services at
community level that receive support for organizational and
systems development
0 2002 PAR NA NA TBD TBD TBD TBD TBD TBD TBD TBD TBD N N Y - cumulative annually NANASO
New Indicator. This information is currently not collected at a national level.Measured semi-annually
4 HSS: Service delivery # of ART hospitals,health clinics and VCT sites renovated 0 2002 Adminstrative
Records 20 20 30 10 15 20 25 30 35 Y N Y - over program term MOHSS
Planned major renovations in 8 ART hospitals and minor renovations in 7 health clinics and 20 VCT sites.Time here refers to when contarcts are awarded
4 HSS: Health Workforce # of healthworkers recruited 0 2002 Adminstrative Records NA 50 60 67 67 67 67 67 Y N Y - over program term MOHSS
This includes medical doctors,Pharmacists and Phamacy assitants
4 HSS: Service delivery
% of ART sites reportng receiving supervision from districts/region//national staff during the preceding 6 months
0 2002 PAR NA NA TBD TBD TBD TBD TBD TBD TBD TBD TBD N N
Y - cumulative annually
MOHSS/NANASO
New indicator to be reported according the supervision schedule of the national programme
g g
4Response
Mangement,M&E and Surveillance
# of natonal surveys completed 0 2002 PAR 4 4 1 2 3 4 5 N N Y - over program term MOHSS/NANASO
This includes national surveys and bi-annual ANC Sentinel
surveillance studies. An AIDS Indciator Survey(AIS)which will
include biomarkers is planned for 2010 and national studies on
MARPS.DHS is planned for 2011.
2 Please provide latest data available
1 Please insert original baseline data from Phase 1
RCC_W7_CCM_NMB_H_AttA_30Jul09_En Performance Framework RCC 3/3
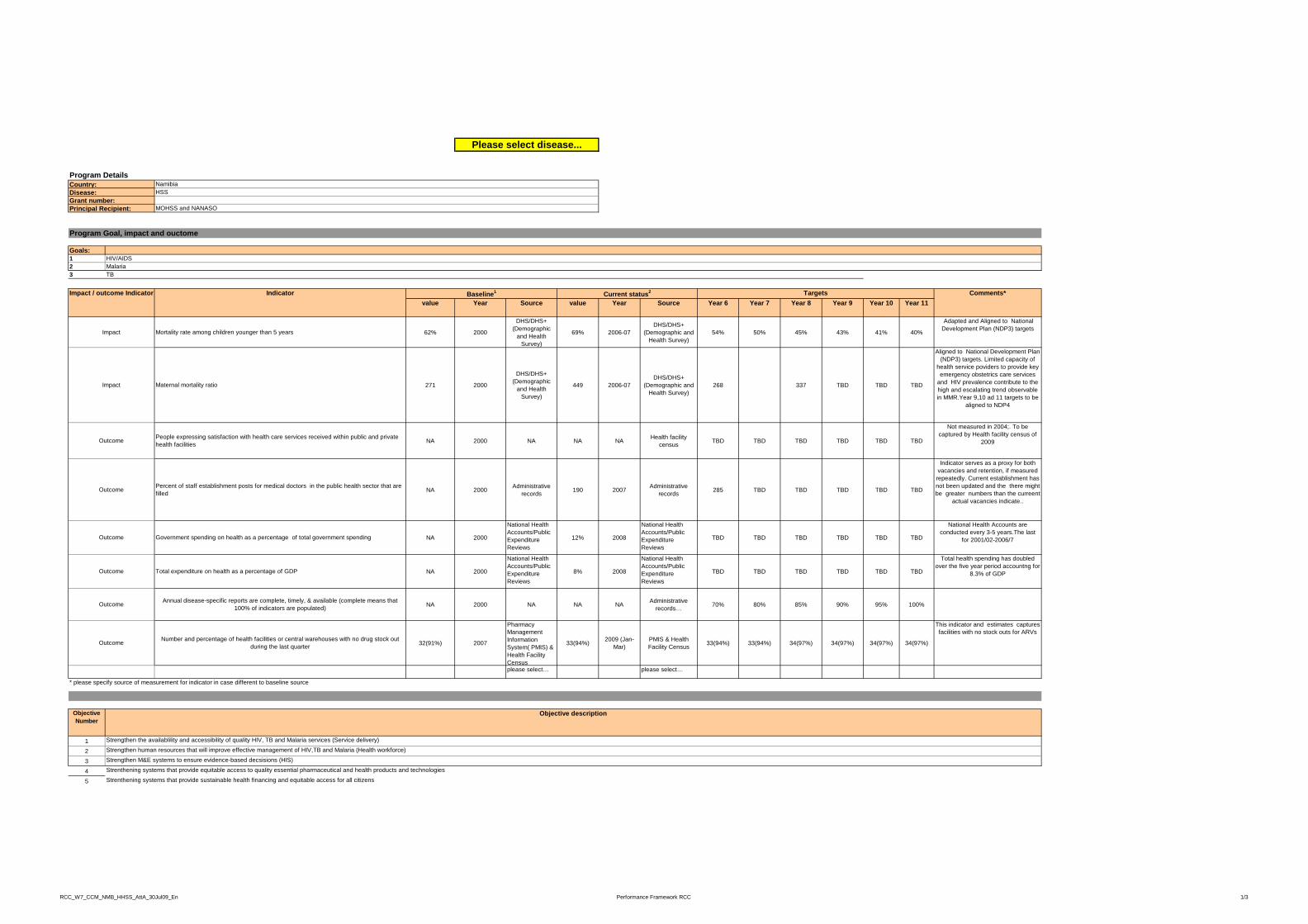
Program DetailsCountry:Disease:Grant number:Principal Recipient:
NamibiaHSS
MOHSS and NANASO
Please select disease...
Goals:123 TB
value Year Source value Year Source Year 6 Year 7 Year 8 Year 9 Year 10 Year 11
62% 2000
DHS/DHS+ (Demographic
and Health Survey)
69% 2006-07DHS/DHS+
(Demographic and Health Survey)
54% 50% 45% 43% 41% 40%
Adapted and Aligned to National Development Plan (NDP3) targets
271 2000
DHS/DHS+ (Demographic
and Health Survey)
449 2006-07DHS/DHS+
(Demographic and Health Survey)
268 337 TBD TBD TBD
Aligned to National Development Plan (NDP3) targets. Limited capacity of
health service poviders to provide key emergency obstetrics care services
and HIV prevalence contribute to the high and escalating trend observable in MMR.Year 9,10 ad 11 targets to be
aligned to NDP4
Impact
Impact
Baseline1
Principal Recipient:
HIV/AIDSMalaria
Comments*
Program Goal, impact and ouctome
Indicator Current status2 TargetsImpact / outcome Indicator
MOHSS and NANASO
Maternal mortality ratio
Mortality rate among children younger than 5 years
NA 2000 NA NA NA Health facility census TBD TBD TBD TBD TBD TBD
Not measured in 2004;. To be captured by Health facility census of
2009
NA 2000 Administrative records 190 2007 Administrative
records 285 TBD TBD TBD TBD TBD
Indicator serves as a proxy for both vacancies and retention, if measured repeatedly. Current establishment has not been updated and the there might be greater numbers than the curreent
actual vacancies indicate..
NA 2000
National Health Accounts/Public Expenditure Reviews
12% 2008
National Health Accounts/Public Expenditure Reviews
TBD TBD TBD TBD TBD TBD
National Health Accounts are conducted every 3-5 years.The last
for 2001/02-2006/7
NA 2000
National Health Accounts/Public Expenditure Reviews
8% 2008
National Health Accounts/Public Expenditure Reviews
TBD TBD TBD TBD TBD TBD
Total health spending has doubled over the five year period accountng for
8.3% of GDP
NA 2000 NA NA NA Administrative records… 70% 80% 85% 90% 95% 100%
Pharmacy This indicator and estimates captures
Outcome People expressing satisfaction with health care services received within public and private health facilities
Outcome Percent of staff establishment posts for medical doctors in the public health sector that are filled
Outcome Total expenditure on health as a percentage of GDP
Outcome Government spending on health as a percentage of total government spending
Annual disease-specific reports are complete, timely, & available (complete means that 100% of indicators are populated)Outcome
32(91%) 2007
yManagement Information System( PMIS) & Health Facility Census
33(94%) 2009 (Jan-Mar)
PMIS & Health Facility Census 33(94%) 33(94%) 34(97%) 34(97%) 34(97%) 34(97%)
pfacilities with no stock outs for ARVs
please select… please select…
Objective Number
12345
* please specify source of measurement for indicator in case different to baseline source
Objective description
Outcome
Strengthen the availablility and accessibility of quality HIV, TB and Malaria services (Service delivery)
Strenthening systems that provide sustainable health financing and equitable access for all citizens
Number and percentage of health facilities or central warehouses with no drug stock out during the last quarter
Strenthening systems that provide equitable access to quality essential pharmaceutical and health products and technologies
Strengthen M&E systems to ensure evidence-based decsisions (HIS)Strengthen human resources that will improve effective management of HIV,TB and Malaria (Health workforce)
RCC_W7_CCM_NMB_HHSS_AttA_30Jul09_En Performance Framework RCC 1/3

Value Year Source Targets Results 6 months 12 months 18 months 24 months 30 months 36 months Year 9 Year 10 Year 11
1.1 Service Delivery
# of functional mobile diagnostic vehicles in public and private sector 0 2004 Project Activity
Report(PAR) 2 2 2 7 10 10 10 10 10 10 10 Y Y Y - over program term MOHSS & NABCOA
Two vehicles procured for NABCOA by GF and Dutch Government are included. CDC
vehicles are not included, as when they would be bought is to be determined
1.2 Service Delivery
# of functional additional operational vehicles bought by Global Fund
0 2004 Project Activity Report(PAR) 61 61 10 10 20 20 20 20 20 20 20 Y N Y - over program term MOHSS These are only the 20 additional vehicles to be
bought under this RCC
# of health care facilities renovated and upgraded to Health Facility 41 Facilitie-20 VCT sites 13 clinics 8 hospitals
Comments, methods and frequency of data collection
Service Delivery Area Indicator
Phase 2Baseline (if applicable)1 Targets cumulative (Y - over program term / Y - cumulative annually / N - not cumulative)
Directly tied (Y/N)
Targets for years 6 - 8 Baselines included in
targets (Y/N)
Annual targets for years 9 - 11 DTF: Name of PR responsible for
implementation of corresponding activity
Objective / Indicator Number
1.3 Service Delivery renovated and upgraded to meet national standards 0 2004
Health Facility Management
report60 29 6 15 23 30 35 41 Y N Y - over program term MOHSS
41 Facilitie-20 VCT sites,13 clinics, 8 hospitals to be renovated. Time here refers to when
contracts are awarded
1.4 Service Delivery
# of staff accomodation renovated and upgraded to meet national standards 0 2004
Health Facility management
reportNA NA 2 5 8 11 13 Y Y Y - over program term MOHSS 13 Staff quarters to be renovated. Time here
refers to when contarcts are awarded
1.5 Service Delivery
% of health facilities reporting receiving supervision from districts/regional/national staff during the preceding 6 months.
0 2004 Supervisory Reports NA NA TBD TBD TBD TBD TBD TBD TBD TBD TBD Y N Y - over program term MOHSS To be reported according to the supervision
schedule of the national programme.
1.6 Service Delivery# of disabled persons
accessing health-facility services
0 2004 Project report TBD TBD TBD TBD TBD TBD TBD TBD TBD TBD TBD Y N Y - over program term MOHSS
Associations for disabled to collaborate with MOHSS to ensure functional rooster of
resource persons. Desk analysis to determine baseline & size of disabled population
2.1 Health Workforce
# of existing workers retained 0 2004 Project payroll
report 118 118 70 70 70 70 70 70 70 70 70 Y N Y - over program term MOHSS
2.2 Health Workforce
# of new workers employed0 2004 Project payroll
report NA NA TBD TBD TBD TBD TBD TBD TBD 24 Y N Y - over program term MOHSS
# of student bursaries 2.3 Health
Workforceawarded 0 2004 Project Activity
report 10 10 12 24 36 50 65 74 Y N Y - over program term MOHSS
RCC_W7_CCM_NMB_HHSS_AttA_30Jul09_En Performance Framework RCC 2/3
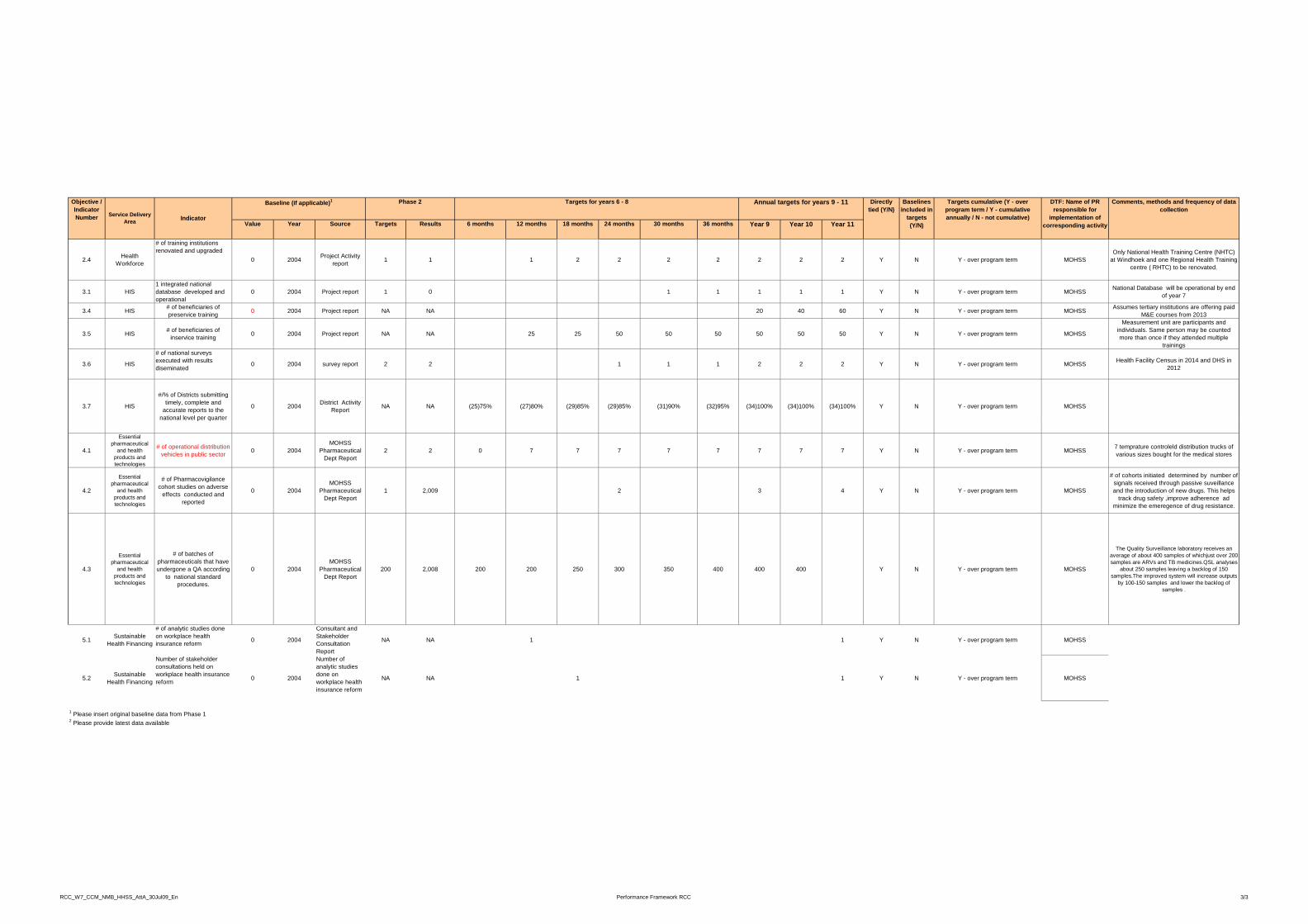
Comments, methods and frequency of data collection
Phase 2Baseline (if applicable)1 Targets cumulative (Y - over program term / Y cumulative
Directly tied (Y/N)
Targets for years 6 - 8 Baselines included in
Annual targets for years 9 - 11 DTF: Name of PR responsible for
Objective / Indicator
Value Year Source Targets Results 6 months 12 months 18 months 24 months 30 months 36 months Year 9 Year 10 Year 11
collection Service Delivery
Area Indicator program term / Y - cumulative annually / N - not cumulative)
tied (Y/N) included in targets (Y/N)
responsible for implementation of
corresponding activity
Indicator Number
2.4 Health Workforce
# of training institutions renovated and upgraded
0 2004 Project Activity report 1 1 1 2 2 2 2 2 2 2 Y N Y - over program term MOHSS
Only National Health Training Centre (NHTC) at Windhoek and one Regional Health Training
centre ( RHTC) to be renovated.
3.1 HIS1 integrated national database developed and operational
0 2004 Project report 1 0 1 1 1 1 1 Y N Y - over program term MOHSS National Database will be operational by end of year 7
3.4 HIS # of beneficiaries of preservice training 0 2004 Project report NA NA 20 40 60 Y N Y - over program term MOHSS Assumes tertiary institutions are offering paid
M&E courses from 2013
3.5 HIS # of beneficiaries of inservice training 0 2004 Project report NA NA 25 25 50 50 50 50 50 50 Y N Y - over program term MOHSS
Measurement unit are participants and individuals. Same person may be counted more than once if they attended multiple
trainings
3.6 HIS
# of national surveys executed with results diseminated
0 2004 survey report 2 2 1 1 1 2 2 2 Y N Y - over program term MOHSS Health Facility Census in 2014 and DHS in 2012
3.7 HIS
#/% of Districts submitting timely, complete and
accurate reports to the national level per quarter
0 2004 District Activity Report NA NA (25)75% (27)80% (29)85% (29)85% (31)90% (32)95% (34)100% (34)100% (34)100% Y N Y - over program term MOHSS
national level per quarter
4.1
Essential pharmaceutical
and health products and technologies
# of operational distribution vehicles in public sector 0 2004
MOHSS Pharmaceutical
Dept Report2 2 0 7 7 7 7 7 7 7 7 Y N Y - over program term MOHSS 7 temprature controleld distribution trucks of
various sizes bought for the medical stores
4.2
Essential pharmaceutical
and health products and technologies
# of Pharmacovigilance cohort studies on adverse
effects conducted and reported
0 2004MOHSS
Pharmaceutical Dept Report
1 2,009 2 3 4 Y N Y - over program term MOHSS
# of cohorts initiated determined by number of signals received through passive suveillance and the introduction of new drugs. This helps
track drug safety ,improve adherence ad minimize the emeregence of drug resistance.
4.3
Essential pharmaceutical
and health products and technologies
# of batches of pharmaceuticals that have undergone a QA according
to national standard procedures.
0 2004MOHSS
Pharmaceutical Dept Report
200 2,008 200 200 250 300 350 400 400 400 Y N Y - over program term MOHSS
The Quality Surveillance laboratory receives an average of about 400 samples of whichjust over 200 samples are ARVs and TB medicines.QSL analyses
about 250 samples leaving a backlog of 150 samples.The improved system will increase outputs
by 100-150 samples and lower the backlog of samples .
# f l ti t di d C lt t d
5.1 Sustainable Health Financing
# of analytic studies done on workplace health insurance reform 0 2004
Consultant and Stakeholder Consultation Report
NA NA 1 1 Y N Y - over program term MOHSS
5.2 Sustainable Health Financing
Number of stakeholder consultations held on workplace health insurance reform 0 2004
Number of analytic studies done on workplace health insurance reform
NA NA 1 1 Y N Y - over program term MOHSS
2 Please provide latest data available
1 Please insert original baseline data from Phase 1
RCC_W7_CCM_NMB_HHSS_AttA_30Jul09_En Performance Framework RCC 3/3