mca-degree-programme-2018-2019.pdf - Thiagarajar College ...
Upload
khangminh22Category
view
3download
0
North Wales Clinical Psychology Programme
PROGRAMME MANUAL 2019
PROGRAMME MANUAL / 2019
CONTENTS
1. Introduction Content Page
Programme Team 1 Team Structure 2 Programme Approval and Accreditation 3 Programme Overview 4 - 40 Programme Specification 41 - 55 Service User and Carer Involvement 56 - 59
2. Curriculum
Content Page Academic Syllabus 61 - 120 Research/Study Time 121
3. Clinical Experience
Content Page Allocating Clinical Placements 123 - 174 BPS Guidelines on Clinical Supervision 175 - 181 Client Consent Form for Audio/Video Recording Of Psychology Session for Academic Assessment
182
Long Term Clinical Work Record Form 183 - 184 Sample Placement Agreement 185 - 188 Initial Placement Review Training Co-Ordinator Checklist
189 - 192
Mid-Placement Review Training Co-Ordinator Checklist
193 - 198
Evaluation of Clinical and Professional Competence: Assessment Form
199 - 213
Placement Quality Checklist 214 - 217 How to Use the Clinical Practice Portfolio 218 - 221 Clinical Practice Portfolio 222 - 237 Supervisor Authentication of Portfolio Form
238
PROGRAMME MANUAL / 2019
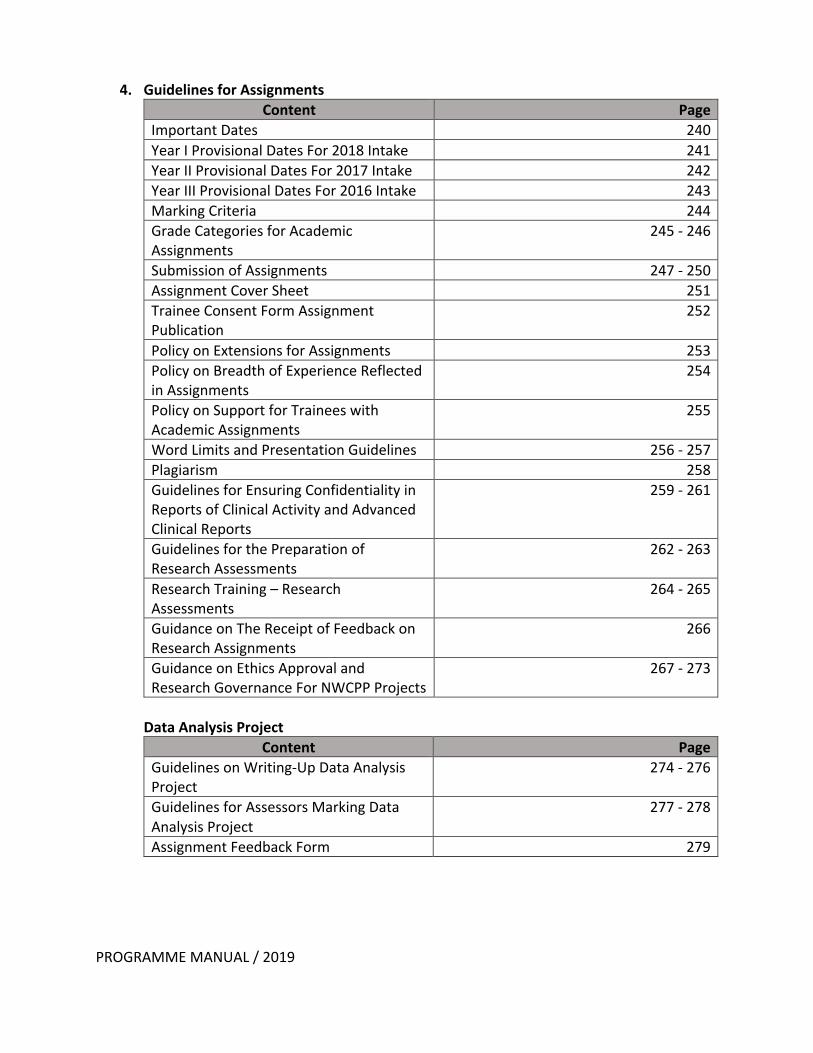
4. Guidelines for Assignments
Content Page Important Dates 240 Year I Provisional Dates For 2018 Intake 241 Year II Provisional Dates For 2017 Intake 242 Year III Provisional Dates For 2016 Intake 243 Marking Criteria 244 Grade Categories for Academic Assignments
245 - 246
Submission of Assignments 247 - 250 Assignment Cover Sheet 251 Trainee Consent Form Assignment Publication
252
Policy on Extensions for Assignments 253 Policy on Breadth of Experience Reflected in Assignments
254
Policy on Support for Trainees with Academic Assignments
255
Word Limits and Presentation Guidelines 256 - 257 Plagiarism 258 Guidelines for Ensuring Confidentiality in Reports of Clinical Activity and Advanced Clinical Reports
259 - 261
Guidelines for the Preparation of Research Assessments
262 - 263
Research Training – Research Assessments
264 - 265
Guidance on The Receipt of Feedback on Research Assignments
266
Guidance on Ethics Approval and Research Governance For NWCPP Projects
267 - 273
Data Analysis Project
Content Page Guidelines on Writing-Up Data Analysis Project
274 - 276
Guidelines for Assessors Marking Data Analysis Project
277 - 278
Assignment Feedback Form 279
PROGRAMME MANUAL / 2019
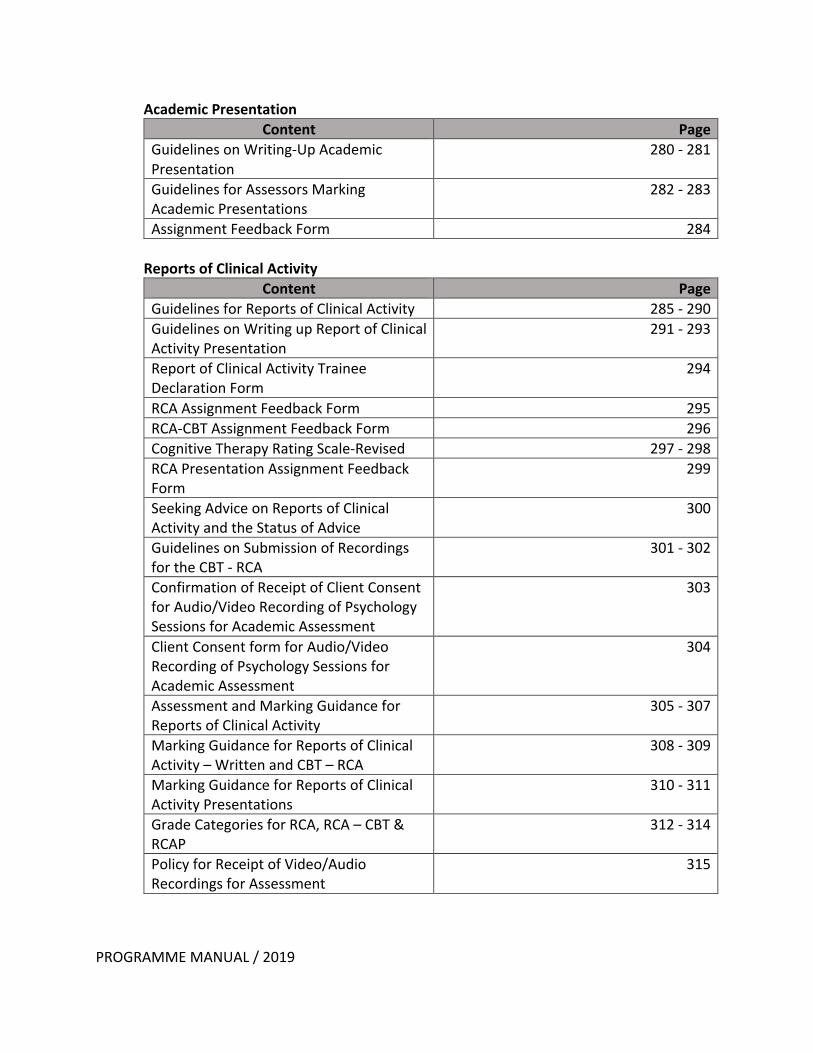
Academic Presentation Content Page
Guidelines on Writing-Up Academic Presentation
280 - 281
Guidelines for Assessors Marking Academic Presentations
282 - 283
Assignment Feedback Form 284 Reports of Clinical Activity
Content Page Guidelines for Reports of Clinical Activity 285 - 290 Guidelines on Writing up Report of Clinical Activity Presentation
291 - 293
Report of Clinical Activity Trainee Declaration Form
294
RCA Assignment Feedback Form 295 RCA-CBT Assignment Feedback Form 296 Cognitive Therapy Rating Scale-Revised 297 - 298 RCA Presentation Assignment Feedback Form
299
Seeking Advice on Reports of Clinical Activity and the Status of Advice
300
Guidelines on Submission of Recordings for the CBT - RCA
301 - 302
Confirmation of Receipt of Client Consent for Audio/Video Recording of Psychology Sessions for Academic Assessment
303
Client Consent form for Audio/Video Recording of Psychology Sessions for Academic Assessment
304
Assessment and Marking Guidance for Reports of Clinical Activity
305 - 307
Marking Guidance for Reports of Clinical Activity – Written and CBT – RCA
308 - 309
Marking Guidance for Reports of Clinical Activity Presentations
310 - 311
Grade Categories for RCA, RCA – CBT & RCAP
312 - 314
Policy for Receipt of Video/Audio Recordings for Assessment
315

PROGRAMME MANUAL / 2019
Evidence Based Briefing
Content Page Guidelines on Writing-up Evidence Based Briefing
316 - 317
Guidelines for Assessors Marking Evidence Based Briefings
318 - 319
Assignment Feedback Form 320 Service Related Research Projects
Content Page Guidelines on Writing-up Service Related Research Projects
321 - 323
Service Related Research Projects Proposals
324 - 325
Research Supervision Agreement 326 - 327 Research Supervision Form 328 Research Submission Form 329 Research Timetable for Service Related Research Projects
330
Guidelines for Assessors Marking SRRP Posters
331 - 332
Assignment Feedback form for SRRP Posters
333 - 334
Final Resources for SRRP 335
Professional issues Content Page
Guidelines on Writing-up Professional Issues Assignment
336 - 337
Guidelines for Assessors Marking Professional Issues Assignments
338 - 339
Assignment Feedback Form 340
PROGRAMME MANUAL / 2019
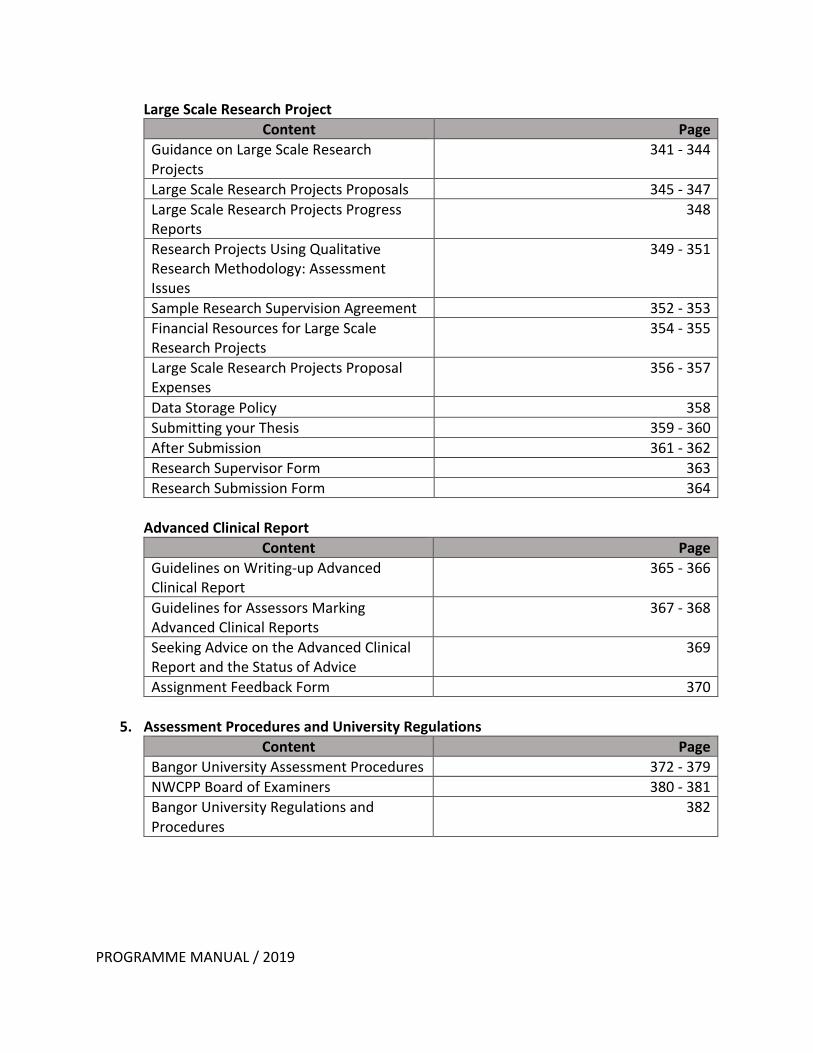
Large Scale Research Project Content Page
Guidance on Large Scale Research Projects
341 - 344
Large Scale Research Projects Proposals 345 - 347 Large Scale Research Projects Progress Reports
348
Research Projects Using Qualitative Research Methodology: Assessment Issues
349 - 351
Sample Research Supervision Agreement 352 - 353 Financial Resources for Large Scale Research Projects
354 - 355
Large Scale Research Projects Proposal Expenses
356 - 357
Data Storage Policy 358 Submitting your Thesis 359 - 360 After Submission 361 - 362 Research Supervisor Form 363 Research Submission Form 364
Advanced Clinical Report
Content Page Guidelines on Writing-up Advanced Clinical Report
365 - 366
Guidelines for Assessors Marking Advanced Clinical Reports
367 - 368
Seeking Advice on the Advanced Clinical Report and the Status of Advice
369
Assignment Feedback Form 370
5. Assessment Procedures and University Regulations Content Page
Bangor University Assessment Procedures 372 - 379 NWCPP Board of Examiners 380 - 381 Bangor University Regulations and Procedures
382
PROGRAMME MANUAL / 2019
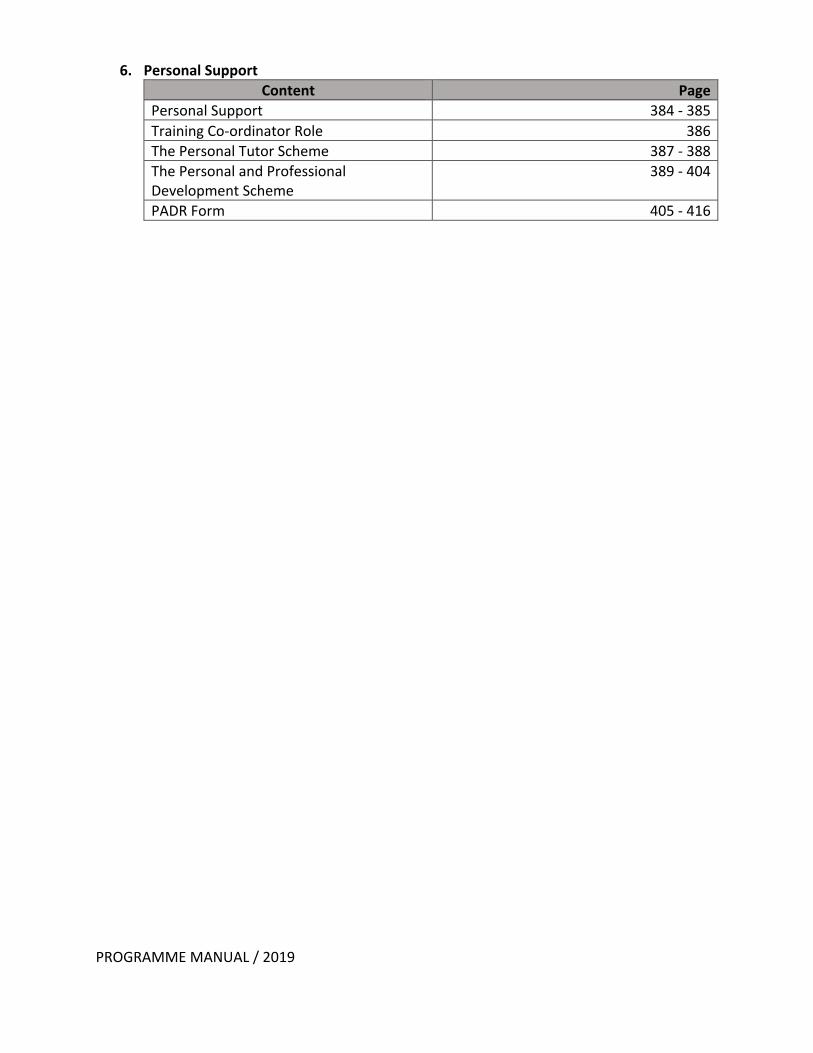
6. Personal Support Content Page
Personal Support 384 - 385 Training Co-ordinator Role 386 The Personal Tutor Scheme 387 - 388 The Personal and Professional Development Scheme
389 - 404
PADR Form 405 - 416
SECTION 1
INTRODUCTION
SECTION 1
PROGRAMME MANUAL / 2019
North Wales Clinical Psychology Programme School of Psychology, Bangor University Brigantia Building (1st Floor), College Road, Bangor, Gwynedd, North Wales, LL57 2AS Tel: 01248 382205 PROGRAMME TEAM: Programme Director: Professor Robert Jones
01248 382627 [email protected]
Deputy Programme Director, Reader in Clinical Psychology & Chair of the Board of Examiners: Dr Michaela Swales (Monday, Tuesday)
01248 382552 [email protected]
Academic Director: Dr Elizabeth Burnside (Monday, Tuesday, Thursday)
01248 382204 [email protected]
Research Director: Dr Mike Jackson (Monday, Tuesday, Friday)
01248 388746 [email protected]
Clinical Director: Dr Renee Rickard (Monday, Tuesday, Thursday)
01248 383778 [email protected]
Programme Manager: Ms Donna Pierce
01248 383654 [email protected]
Admissions Tutor: Dr Carolien Lamers (Monday, Tuesday, Thursday)
01248 388068 [email protected]
Clinical Tutor: Dr Katie Bigham
01248 388842 [email protected]
Academic Tutor: Dr Christine Blincoe (Monday, Tuesday, Thursday)
01248 383890 [email protected]
Research Tutor: Dr Christopher Saville
01248 388740 [email protected]
Senior Administrator & PA to the Programme Director: Ms Fiona Greenly-Jones
01248 388059 [email protected]
Administrative Assistant (Research, Finance & Selection): Miss Mared Williams
01248 388365 [email protected]
Administrative Assistant (Curriculum & Clinical): Mrs Debbie Jones (Monday, Tuesday, Wednesday)
01248 382205 [email protected]
Administrative Assistant (Curriculum & Clinical): Mrs Anna Roberts (Thursday, Friday)
01248 382205 [email protected]
SHARED Curriculum & Clinical email: [email protected]
1
SECTION 1
PROGRAMME MANUAL / 2019
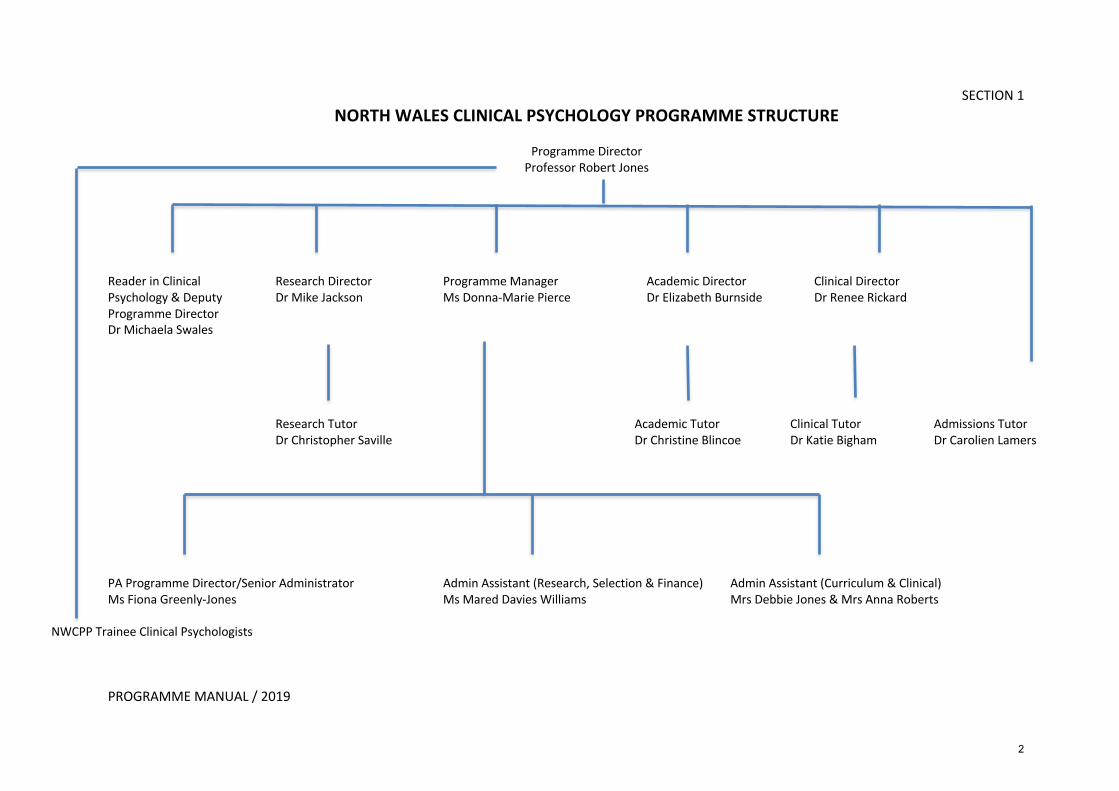
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME STRUCTURE
Programme Director
Professor Robert Jones
Reader in Clinical Research Director Programme Manager Academic Director Clinical Director Psychology & Deputy Dr Mike Jackson Ms Donna-Marie Pierce Dr Elizabeth Burnside Dr Renee Rickard Programme Director Dr Michaela Swales Research Tutor Academic Tutor Clinical Tutor Admissions Tutor Dr Christopher Saville Dr Christine Blincoe Dr Katie Bigham Dr Carolien Lamers
PA Programme Director/Senior Administrator Admin Assistant (Research, Selection & Finance) Admin Assistant (Curriculum & Clinical) Ms Fiona Greenly-Jones Ms Mared Davies Williams Mrs Debbie Jones & Mrs Anna Roberts
NWCPP Trainee Clinical Psychologists
2
SECTION 1
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME APPROVAL AND ACCREDITATION
The Programme is approved by the Health & Care Professions Council, the statutory regulator for practitioner psychologists in the UK. It is a legal requirement that anyone who wishes to practise using a title protected by the Health Professions Order 2001 (e.g. Clinical Psychologist) is on the HCPC Register. For more information please see the HCPC website at: https://www.hcpc-uk.org . The Programme is also accredited by the British Psychological Society https://www.bps.org.uk . The Society is the professional body responsible for developing and supporting the discipline of psychology and disseminating psychological knowledge to the public and policy makers. It is the key professional body for psychology and psychologists, with numerous benefits of membership. Please see www.bps.org.uk/membership for further information. Successful completion of the Programme confers eligibility to apply for Chartered Membership of the Society and full membership of the Division of Clinical Psychology. The Programme is validated by Bangor University https://www.bangor.ac.uk who award the degree of Doctorate of Clinical Psychology.
3

SECTION 1
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME PROGRAMME OVERVIEW
CRITERIA FOR ADMISSION Before applying, candidates should have already obtained a single or joint honours first or upper
second-class psychology degree or conversion degree and be eligible for the Graduate Basis for
Membership with the British Psychological Society. There is no Accreditation of Prior Learning
mechanism. Candidates are required to have gained at least one year's relevant clinical or research
experience as paid employment. Clinically relevant experience should have given the candidate
opportunity for substantial interaction with people with significant health or psychological
difficulties, similar to the clients seen by clinical psychologists. Research experience should involve
the investigation of psychological phenomenon within a clinical population. Because the Programme
covers a large geographical area, it is an advantage for trainees to hold a full driving licence. The
Programme is subject to the Equal Opportunities policies of Betsi Cadwaladr University Health Board
(BCUHB) and Bangor University. We are pleased to accept applications from candidates from a wide
range of backgrounds. The Programme welcomes enquiries from candidates with disabilities and
operates the Double Tick system.
A significant proportion of the population in North Wales speaks Welsh as their first language. Welsh
speaking candidates are strongly encouraged to apply for this Programme.
All applications to the Programme are processed by the Clearing House for Postgraduate Courses in
Clinical Psychology. Any queries about entry requirements or the application process can be found
on the Clearing House website. Further information about the Programme, the selection criteria and
procedures can be found at http://nwcpp.bangor.ac.uk/ or applicants can contact our Admissions
Tutor, Dr Carolien Lamers ([email protected]).
CRITERIA FOR PROGRESSION
The only outcome from this Programme is the Doctorate in Clinical Psychology. There are no lower
level exit qualifications for unsuccessful candidates or aegrotat degrees. Progression through the
Programme is contingent on achieving an appropriate standard in academic, clinical and research
domains. In Part I, assignments receiving a fail grade must be resubmitted. Only one resubmission
is allowed. If the assignment still fails the assignment is considered a substantive fail. In circumstances where the reduction in grade is the result of a significant breach of confidentiality the candidate will not be allowed to resubmit the assignment. Trainees will normally be excluded on the third substantive failed assignment (including placements)
or two failed placements. Full details of assessment procedures and failure criteria are provided in
Section 5 of the Programme Manual. Trainees must pass both Parts I and II of the Programme; Part I
consists of those assessments normally undertaken in Years 1 and 2 of the Programme, and Part II
consists of the Large-Scale Research Project, Advanced Clinical Report and evaluation of clinical
competence on a specialist clinical placement. Trainees may undertake Part II before having
successfully completed Part I, but both Parts must be completed satisfactorily for the award of
DClinPsy. This confers eligibility to apply for registration with the Health and Care Professions
Council and confers eligibility for chartered status with the British Psychological Society.
4
SECTION 1
PROGRAMME MANUAL / 2019
AIMS The main aim of the Programme is to meet the needs of the NHS for Chartered Clinical Psychologists
registered with the Health Professions Council (HCPC), who have a wide range of clinical,
organisational and research skills and who have developed standards of high professional integrity
and an internalised model of reflective practice flexible enough to accommodate change. The
Programme aims to select trainees for their commitment to clinical psychology and potential to
develop a high level of clinical and academic competence. It aims to foster this approach by
encouraging the development of skills, knowledge and values that underpin research, evaluation,
clinical and professional competence. This approach takes place within a supportive structure that
facilitates personal and professional growth and uses the close links that exist in North Wales
between the academic and clinical communities. Developments in the delivery of clinical psychology
training are agreed between the Programme staff, trainees, stakeholders in BCUHB, and the
University. This is done through discussion and decision-making within the Programme Training
Committee (where all stakeholders are represented) and its sub-committees.
PROCESS
Achievement of these aims will entail the following:
1. "A Registered Clinical Psychologist with a wide range of clinical, organisational and research
skills".
1.1 A curriculum that emphasises the integration of practical skills with a rigorous
theoretical and evidence base, following a scientist-practitioner model.
1.2 Placements that reflect a wide range of clients, service delivery systems and types of
work, as is appropriate in three years.
1.3 Project work that addresses practical research questions, and focuses on integrating
research skills into everyday clinical practice.
2. “A Registered Clinical Psychologist with standards of high professional integrity".
2.1 From the outset, identification and discussion of the ethical value base of
professional practice including aspects such as power, respect and control.
2.2 Exploration of the legal and practical issues likely to be encountered within the
profession.
2.3 A clear exposition of the HCPC – Standards of conduct, performance and ethics, the
HCPC - Guidance on conduct and ethics for students, the BPS - Code of Conduct, the
DCP statement of the Core Purpose and Philosophy of the profession and the
Professional Practice Guidelines of the Division of Clinical Psychology of the BPS.
3. "A Registered Clinical Psychologist with an internalised model of reflective practice flexible
enough to accommodate change".
3.1 The presentation and discussion of a range of models of practice by skilled and
experienced practitioners in Clinical Psychology.
3.2 An exploration of the current status of Health Care Provision and the implications
for the delivery and development of Psychology Services.
3.3 Attention to issues of personal responsibility and personal needs throughout the
Programme, to enable trainees to enrich their training with their own experience.
3.4 The provision of opportunities throughout the Programme for each trainee to reflect
on and monitor their own development, and to identify their own learning and
training needs.
5
SECTION 1
PROGRAMME MANUAL / 2019
SPECIFIC OBJECTIVES
1. To meet the local, regional and national need for trained Clinical Psychologists to
work within the National Health Service, with special emphasis on attracting Welsh
speaking staff.
2. To adapt the content of the training, where possible, to the skills and experience of
individual trainees.
3. To support and develop the skills of practising Clinical Psychologists as teachers,
supervisors and researchers.
4. To act as a resource for practising Clinical Psychologists seeking post qualification
training.
5. To act as a bridge between the practical demands of health care delivery and
current research findings in Psychology.
EVIDENCE OF SUCCESS
As evidence that the Programme is achieving its aims the trainees will be able to:
1. Assess and formulate clinical problems, to deliver a clinical service and to evaluate
outcomes.
2. Show flexibility and reflectiveness in their approach to clinical, research and service
development issues.
3. Show evidence of well-rounded professional development over time.
In addition, through its annual Open Meeting, the Programme will examine whether it is successfully
training clinical psychologists who between them adequately meet the needs of the Clinical
Psychology Services in North Wales. This will include the need to increase the proportion of clinical
psychologists who speak Welsh.
SPECIFIC STRENGTHS Clinical Supervisors
No training programme in clinical psychology can exist without the support of the clinical
psychologists in the NHS. In North Wales, we have a dedicated group of clinical psychologists who
provide not only a high standard of placements for our trainees but also teach on academic blocks,
supervise research, act as Personal Tutors to trainees, sit on Programme committees, act as
assessors for assignments, and assist in the shortlisting and interviewing of candidates. The Heads
of Services and Specialities in North Wales show an unstinting commitment to the training of clinical
psychologists locally, and the Programme is greatly indebted to them for their continued support.
Support for trainees
The Programme has a long tradition of providing both practical and emotional support to trainees.
The staff recognise the way in which clinical training is both emotionally and physically demanding
and attempt to provide as much support as possible. In material terms, trainees may obtain a lease
car if they wish and they have a generous study leave allowance. For emotional support, each
trainee has access to a Training Co-ordinator, a Personal Tutor, and a Personal and Professional
Development Psychological Therapist. The Programme approves the Personal and Professional
Development Psychological Therapists but thereafter does not know which trainee seeks counselling
or from whom. The independence of this support system is much valued by trainees. More
information on this is contained in the current Programme Manual.
6

SECTION 1
PROGRAMME MANUAL / 2019
Theory-Practice Integration
All teaching sessions aim to assist trainees to recognise the links between clinical experience and the
development of theoretical/research issues and from this to the development of clinical services.
Teaching quality
Teaching on the Programme in the main areas of Adult Mental Health, Older Adults, Child and
Adolescent Psychology, Intellectual Disability, Forensic Clinical Psychology, Health Clinical Psychology
and Neuropsychology is delivered to a high standard by practising clinicians who are able to use
illustrations from their own clinical practice to facilitate learning. Teaching receives consistently
good feedback.
‘Vision’
The Programme regularly reviews, with its stakeholders, areas for further development. The Staff
team meet annually to develop and refine the vision for the programme using themes from this day
to inform programme delivery and development.
Welsh/English bi-lingual placements
As part of a strategy to meet the needs of Welsh speakers using the local health services and who
wish to have services delivered in Welsh, there is now a strong group of Welsh-speaking clinical
psychologists who provide Welsh/English bi-lingual placements so that Welsh speaking trainees on
the Programme can develop their skills in offering a clinical psychology service in Welsh. Some
placements take place in locations where the majority of meetings are conducted through the Welsh
language and in these circumstances, simultaneous translation is typically available to non-Welsh
speaking team members, including trainees.
Service User involvement
The Programme’s Service User and Carer Involvement Group is referred to as the People Panel. The
panel was established in 2008 with the specific aim of enhancing trainee learning from a Service
User /Carer perspective. The panel comprises individuals who have had involvement with Adult
Mental Health Services, Health Clinical Psychology, Older Adult Services and Intellectual Disability
Services. The panel is involved in a number of different aspects of the training programme from the
development of client consent guidelines for trainees on placement to the development of forms for
service user feedback to be completed at the end of placement. Service users also play a key role in
our Selection procedures and are actively involved with a number of teaching sessions on the
programme. Trainee feedback on these sessions is always extremely positive and highly valued.
Trainees are encouraged to consult with Service users for advice regarding potential research topics,
use of questionnaires and outcome measures. Furthering this involvement between trainees and
Service Users and Carers is a key developmental area for our programme.
At the last BPS and HCPC accreditation visit in 2012 the Programme’s People Panel was commended
as follows; ‘The programme enjoys the support and contribution of a committed and engaged group of service users who feel valued in their role and spoke of a positive and well- supported experience. This aspect of the programme’s provision has developed well since the previous BPS visit (2007) and continues to go from strength to strength, having now become a tangible and embedded part of the programme with a direct impact on the training experience’
7
SECTION 1
PROGRAMME MANUAL / 2019
LIMITATIONS Opportunities for placements in specific specialist areas is more limited than in city-based
Programmes in the UK. However, in recent years there has been a greater variety of 3rd year
specialist placement options including autism spectrum disorders, DBT, ACT, Schema Therapy, early
intervention in psychosis, and a greater range of Health Clinical Psychology options including child
health, in addition to placements in specific specialist services such as the North Wales Brain Injury
Service, the North Wales Adolescent Service and Forensic Clinical Psychology Services.
The North Wales Clinical Psychology Programme covers a very wide geographical area, which means
that trainees are sometimes on placement at some distance from the Programme base. Some NHS
Psychology departments are also distant from the Programme base. In recognition of this, and to
ensure that geographical distance from the Programme does not lead to isolation from the
Programme, the Programme ensures that:
• trainees attend the University for teaching sessions at frequent and regular
intervals whilst on placement
• placements in year 1 receive three placement visits and in years 2 and 3,
placements receive at least one placement visit with the option for
additional visits from training co-ordinators
• most key Programme meetings are held in a central location rather than at
the Programme base.
Due to the small size of the clinical training Programme and of the clinical psychology community in
North Wales, many Clinical Psychologists hold dual roles e.g. supervisor, assessor of trainees
submitted work, Programme Team member. In order to avoid role conflict, the following practices
are in place:
• Programme Team members do not provide clinical supervision to trainees
for whom they are the Training Co-ordinator
• trainee assignments are not assessed by a Clinical Psychologist involved in
the supervision of that assignment.
EDUCATIONAL AIMS
By the end of the Programme trainees will have the knowledge, values and skills to:
I. develop working alliances with clients, including individuals, carers and/or
services, in order to:
• carry out psychological assessment
• develop a formulation based on psychological theories and knowledge
• carry out a range of psychological interventions
• evaluate their work
II. communicate effectively with clients, referrers and others, orally,
electronically and in writing.
III. work effectively with clients from a diverse range of backgrounds,
understanding and respecting the impact of difference and diversity upon
their lives.
8
SECTION 1
PROGRAMME MANUAL / 2019
IV. work effectively with systems relevant to clients, including for example
statutory and voluntary services, self-help and advocacy groups, user-led
systems and other elements of the wider community.
V. work in a range of indirect ways to improve psychological aspects of health
and healthcare.
VI. conduct research that enables the profession to develop its knowledge base
and to monitor and improve the effectiveness of its work
VII. manage a personal learning agenda and self-care
VIII. apply critical reflection and self-awareness that enables the transfer of
knowledge and skills to new settings and problems
TEACHING, LEARNING AND ASSESSMENT METHODS USED TO ENABLE LEARNING OUTCOMES TO BE ACHIEVED To enable trainees to achieve the outcomes listed in the Programme Specification, a variety of
teaching and learning methods are used:
• teaching sessions conducted at the Programme base in the School of
Psychology where adult learning methods are adopted. Learning occurs
through a variety of teaching formats. Whilst some amount of didactic
teaching is important, much of the teaching is workshop-based
concentrating on both skills training and experiential methods. Given the
small cohort size we are well placed to be able to use small group format
teaching.
• private study, including reading, writing reports and academic assignments,
with guidance and feedback from clinical supervisors and Training Co-
ordinators.
• clinical placements over the three years covering a range of specialist
settings supervised by experienced local clinicians during which trainees
learn to apply the knowledge gained to a wide range of clinical problems.
• supervised research – small and larger scale research projects under the
supervision of clinical psychologists and/or academics in applied psychology.
Assessment of learning outcomes occurs through a range of different formats:
• Three academic assignments (presentation, evidence-based briefing and
professional issues assignment) covering specialist areas and professional
issues completed in the first two years of the Programme. These assess
knowledge and understanding of psychological theory and the evaluation of
evidence across a range of specialist areas, and the ability to report this in a
suitable format.
• Four Reports of Clinical Activity completed in the first two years of the
Programme and covering the four core clinical areas undertaken. These
reports assess the ability to understand and describe clinical processes with
a range of clients in a range of settings and to provide an account of this
incorporating the scientist-practitioner and reflective-practitioner models.
One Report of Clinical Activity takes the form of a presentation and is
delivered towards the end of the second year of the Programme. Another
9
SECTION 1
PROGRAMME MANUAL / 2019
Report of Clinical Activity focuses on the use of Cognitive Behavioural
Therapy (CBT). Trainees are encouraged to submit this report based on work
undertaken during the Adult Mental Health placement. Under
circumstances when this is not possible trainees are required to submit the
RCA(CBT) in relation to work undertaken during another first or second year
placement.
• One Advanced Clinical Report to be submitted towards the end of the final
year of training. This assesses issues relating to the process of clinical
practice, and in particular, reflective practice and personal / professional
development.
• Evaluations of Clinical and Professional Competence completed at the end
of each clinical placement by the placement supervisor. These evaluations
assess the subject-specific clinical skills of interviewing and observational
skills, assessment, formulation & reformulation, intervention/evaluation,
communication, teaching, professional and ethical behaviour,
organisational, leadership and MDT working, self-development and
feedback from others.
• One Service Related Research Project (e.g. audit project, small scale
evaluation), which assesses the ability to conduct research mainly in the
context of service evaluation and development using appropriate methods
for the research question.
• One Data Analysis Project, completed in the first year of training. This
assesses the ability to develop clear research questions and to flexibly and
creatively apply statistical skills in the analysis of large datasets and ‘real
world’ clinical data.
• One Large-Scale Research project; a substantial piece of research of a
theoretical nature and of clinical relevance and presented in ‘journal paper’
form, namely a literature review and an empirical paper reporting the main
findings of a piece of original research. This assesses the ability to formulate,
develop and carry out a research project based on a theoretically based
research question and to present the findings in an appropriate manner for
a professional academic/clinical readership.
Please see the Learning Assessment Outcomes Table for full details of how these
assessments are related to learning outcomes.
In addition, there are several (informal) formative assessments such as the WAIS pass out,
in-class statistics tests, CBT skills development workshops and research project proposals.
Whilst on clinical placement, trainees are required to maintain an up-to-date Clinical
Practice Portfolio detailing their clinical and professional experiences. This is to enable
trainees, supervisors and Programme staff to monitor the range of clinical work experienced
in relation to the stated learning outcomes. On completion of each placement an up to date
electronic version of the Portfolio has to be submitted to the Programme office together
with a hard copy of the ‘Supervisor Authentication of Portfolio’ form.
10

SECTION 1
PROGRAMME MANUAL / 2019
Details of the requirements for each piece of assessed work are contained in the Programme
Manual.
Formative feedback is also provided through the CBT skills development workshops, clinical
supervision, annual appraisals, and placement visits as well as through reading drafts of
academic assignments.
11
SECTION 1
PROGRAMME MANUAL / 2019
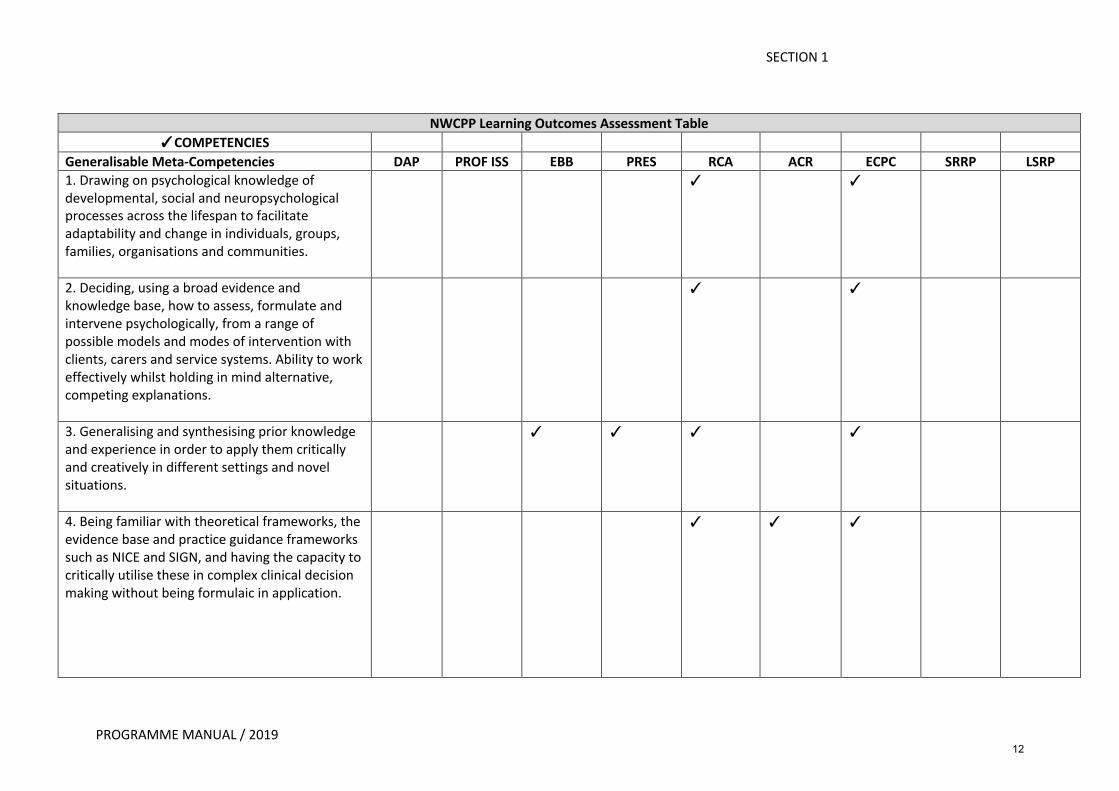
NWCPP Learning Outcomes Assessment Table
�COMPETENCIES Generalisable Meta-Competencies DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP 1. Drawing on psychological knowledge of developmental, social and neuropsychological processes across the lifespan to facilitate adaptability and change in individuals, groups, families, organisations and communities.
� �
2. Deciding, using a broad evidence and knowledge base, how to assess, formulate and intervene psychologically, from a range of possible models and modes of intervention with clients, carers and service systems. Ability to work effectively whilst holding in mind alternative, competing explanations.
� �
3. Generalising and synthesising prior knowledge and experience in order to apply them critically and creatively in different settings and novel situations.
� � � �
4. Being familiar with theoretical frameworks, the evidence base and practice guidance frameworks such as NICE and SIGN, and having the capacity to critically utilise these in complex clinical decision making without being formulaic in application.
� � �
12
SECTION 1
PROGRAMME MANUAL / 2019
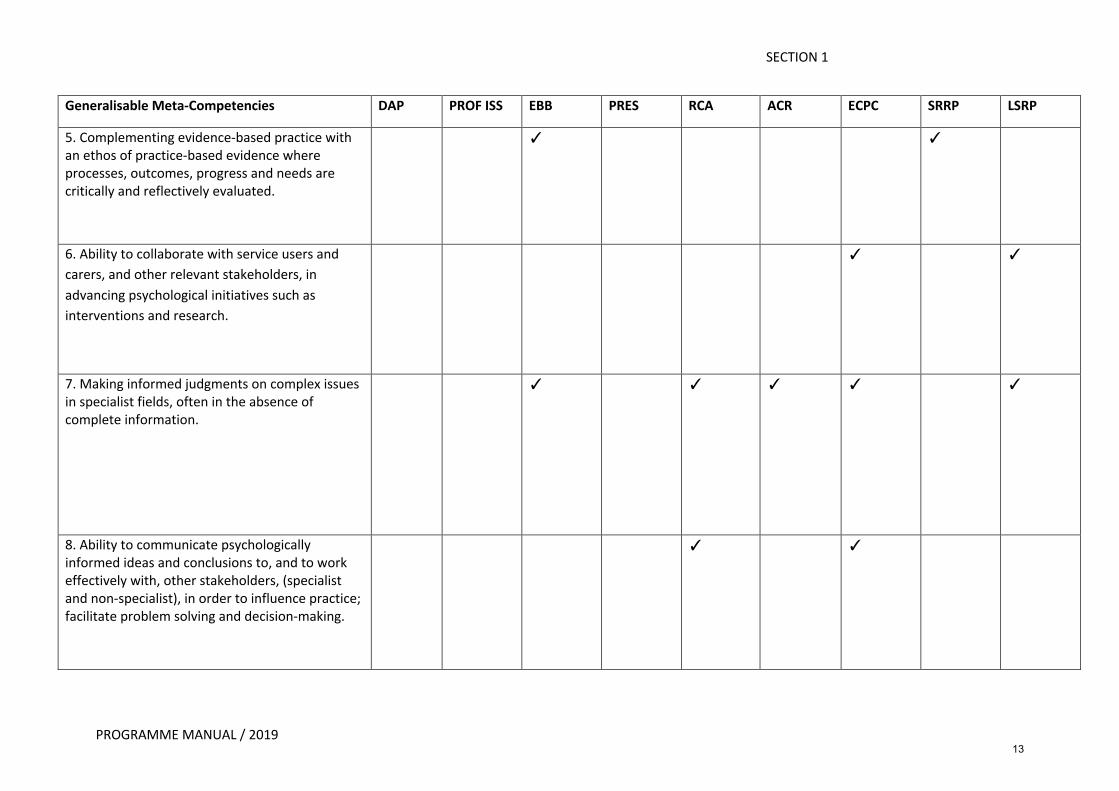
Generalisable Meta-Competencies DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
5. Complementing evidence-based practice with an ethos of practice-based evidence where processes, outcomes, progress and needs are critically and reflectively evaluated.
� �
6. Ability to collaborate with service users and
carers, and other relevant stakeholders, in
advancing psychological initiatives such as
interventions and research.
� �
7. Making informed judgments on complex issues in specialist fields, often in the absence of complete information.
� � � � �
8. Ability to communicate psychologically informed ideas and conclusions to, and to work effectively with, other stakeholders, (specialist and non-specialist), in order to influence practice; facilitate problem solving and decision-making.
� �
13
SECTION 1
PROGRAMME MANUAL / 2019
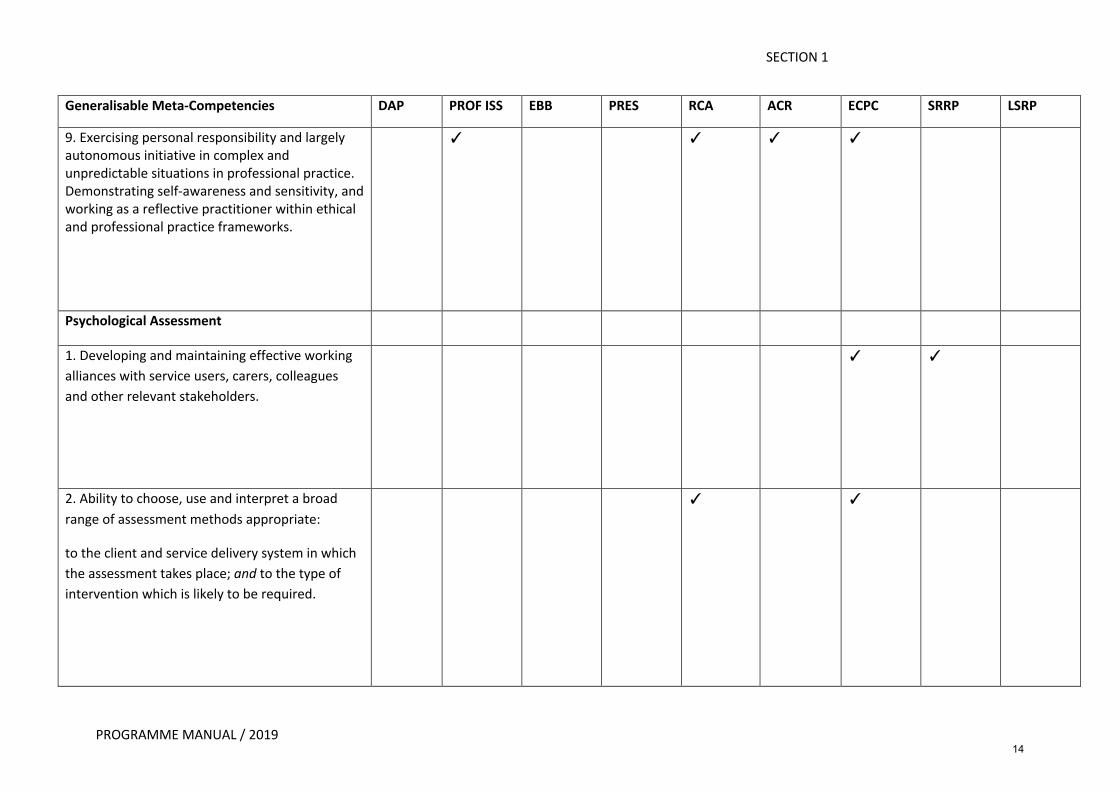
Generalisable Meta-Competencies DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
9. Exercising personal responsibility and largely autonomous initiative in complex and unpredictable situations in professional practice. Demonstrating self-awareness and sensitivity, and working as a reflective practitioner within ethical and professional practice frameworks.
� � � �
Psychological Assessment
1. Developing and maintaining effective working
alliances with service users, carers, colleagues
and other relevant stakeholders.
� �
2. Ability to choose, use and interpret a broad
range of assessment methods appropriate:
to the client and service delivery system in which
the assessment takes place; and to the type of
intervention which is likely to be required.
� �
14
SECTION 1
PROGRAMME MANUAL / 2019
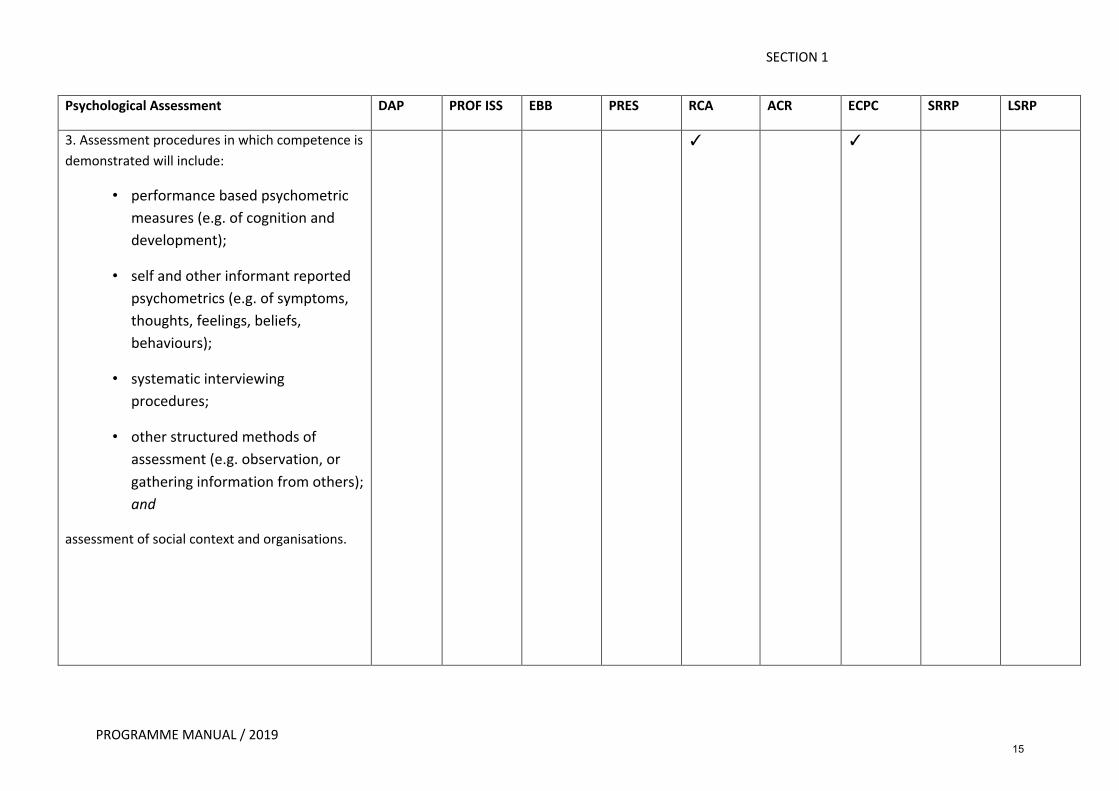
Psychological Assessment DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
3. Assessment procedures in which competence is
demonstrated will include:
• performance based psychometric
measures (e.g. of cognition and
development);
• self and other informant reported
psychometrics (e.g. of symptoms,
thoughts, feelings, beliefs,
behaviours);
• systematic interviewing
procedures;
• other structured methods of
assessment (e.g. observation, or
gathering information from others);
and
assessment of social context and organisations.
� �
15
SECTION 1
PROGRAMME MANUAL / 2019
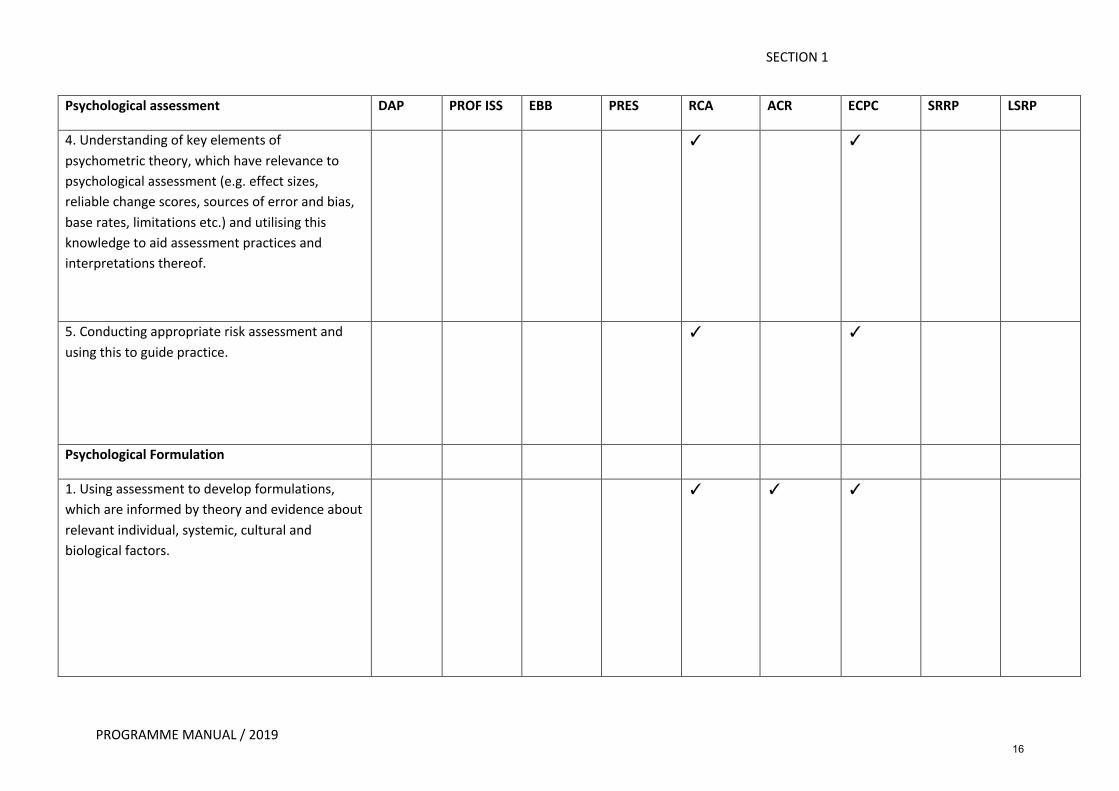
Psychological assessment DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
4. Understanding of key elements of
psychometric theory, which have relevance to
psychological assessment (e.g. effect sizes,
reliable change scores, sources of error and bias,
base rates, limitations etc.) and utilising this
knowledge to aid assessment practices and
interpretations thereof.
� �
5. Conducting appropriate risk assessment and
using this to guide practice.
� �
Psychological Formulation
1. Using assessment to develop formulations,
which are informed by theory and evidence about
relevant individual, systemic, cultural and
biological factors.
� � �
16
SECTION 1
PROGRAMME MANUAL / 2019
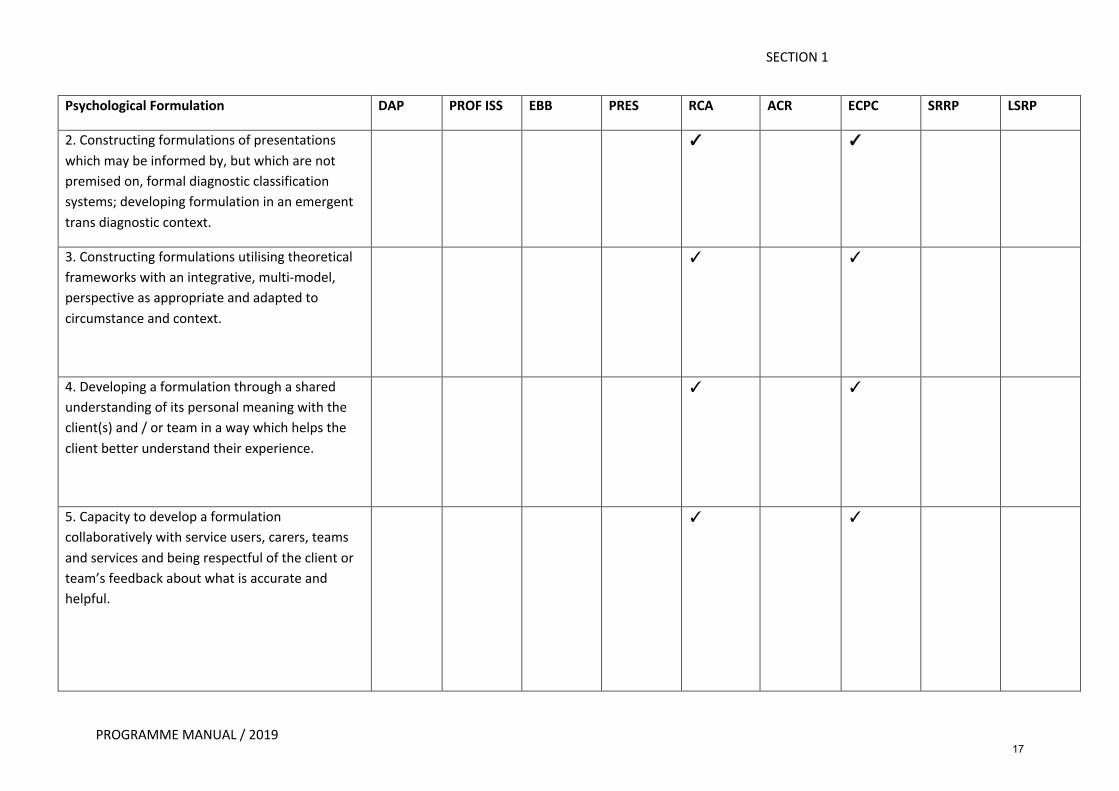
Psychological Formulation DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
2. Constructing formulations of presentations
which may be informed by, but which are not
premised on, formal diagnostic classification
systems; developing formulation in an emergent
trans diagnostic context.
� �
3. Constructing formulations utilising theoretical
frameworks with an integrative, multi-model,
perspective as appropriate and adapted to
circumstance and context.
� �
4. Developing a formulation through a shared
understanding of its personal meaning with the
client(s) and / or team in a way which helps the
client better understand their experience.
� �
5. Capacity to develop a formulation
collaboratively with service users, carers, teams
and services and being respectful of the client or
team’s feedback about what is accurate and
helpful.
� �
17
SECTION 1
PROGRAMME MANUAL / 2019
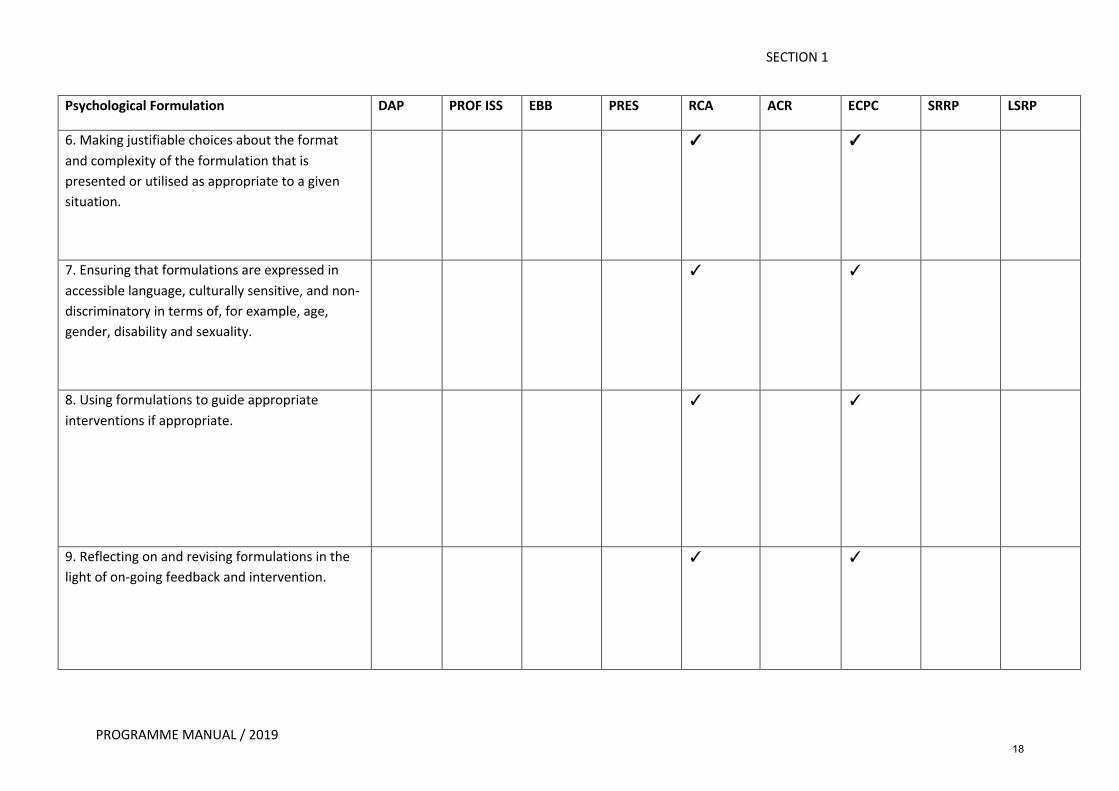
Psychological Formulation DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
6. Making justifiable choices about the format
and complexity of the formulation that is
presented or utilised as appropriate to a given
situation.
� �
7. Ensuring that formulations are expressed in
accessible language, culturally sensitive, and non-
discriminatory in terms of, for example, age,
gender, disability and sexuality.
� �
8. Using formulations to guide appropriate
interventions if appropriate.
� �
9. Reflecting on and revising formulations in the
light of on-going feedback and intervention.
� �
18
SECTION 1
PROGRAMME MANUAL / 2019
Psychological Formulation DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
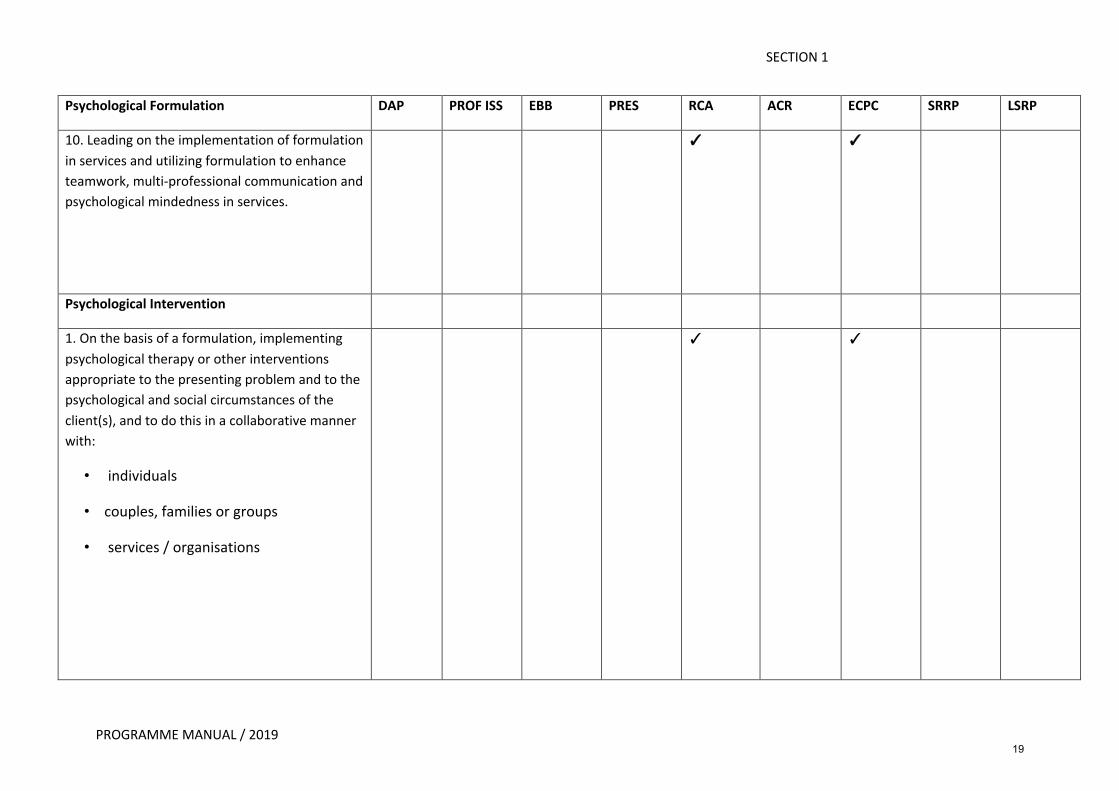
10. Leading on the implementation of formulation
in services and utilizing formulation to enhance
teamwork, multi-professional communication and
psychological mindedness in services.
� �
Psychological Intervention
1. On the basis of a formulation, implementing
psychological therapy or other interventions
appropriate to the presenting problem and to the
psychological and social circumstances of the
client(s), and to do this in a collaborative manner
with:
• individuals
• couples, families or groups
• services / organisations
� �
19
SECTION 1
PROGRAMME MANUAL / 2019
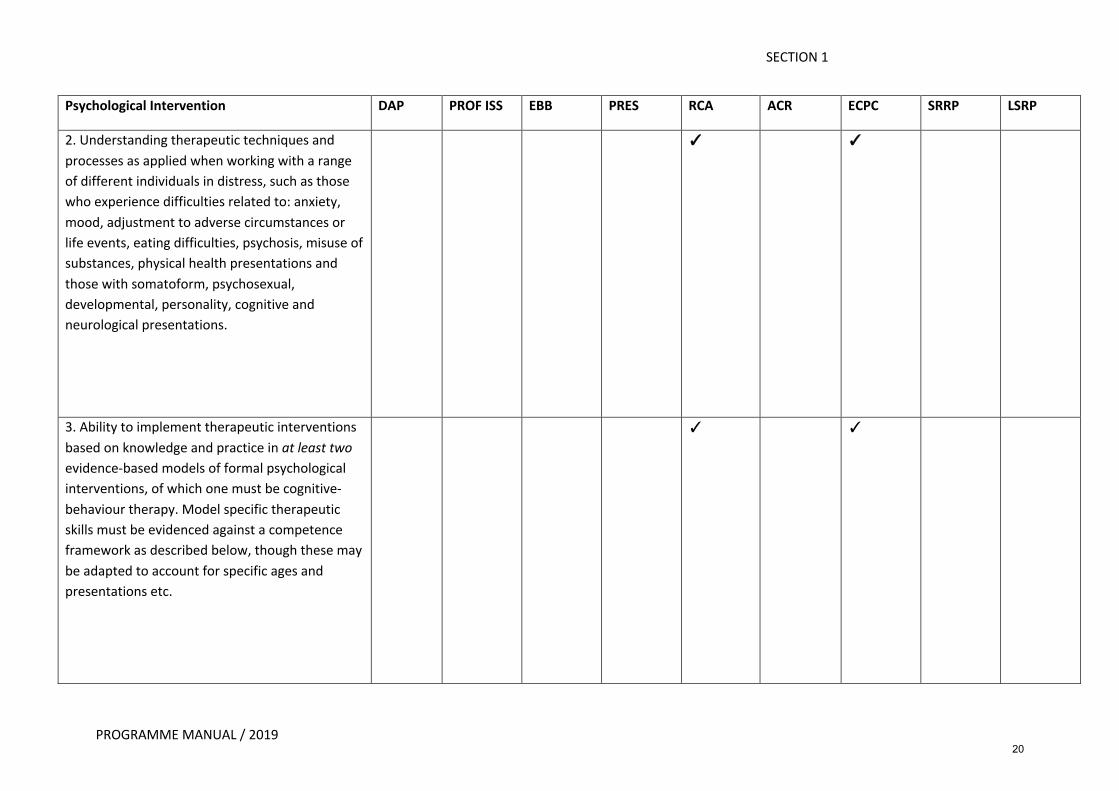
Psychological Intervention DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
2. Understanding therapeutic techniques and
processes as applied when working with a range
of different individuals in distress, such as those
who experience difficulties related to: anxiety,
mood, adjustment to adverse circumstances or
life events, eating difficulties, psychosis, misuse of
substances, physical health presentations and
those with somatoform, psychosexual,
developmental, personality, cognitive and
neurological presentations.
� �
3. Ability to implement therapeutic interventions
based on knowledge and practice in at least two evidence-based models of formal psychological
interventions, of which one must be cognitive-
behaviour therapy. Model specific therapeutic
skills must be evidenced against a competence
framework as described below, though these may
be adapted to account for specific ages and
presentations etc.
� �
20
SECTION 1
PROGRAMME MANUAL / 2019
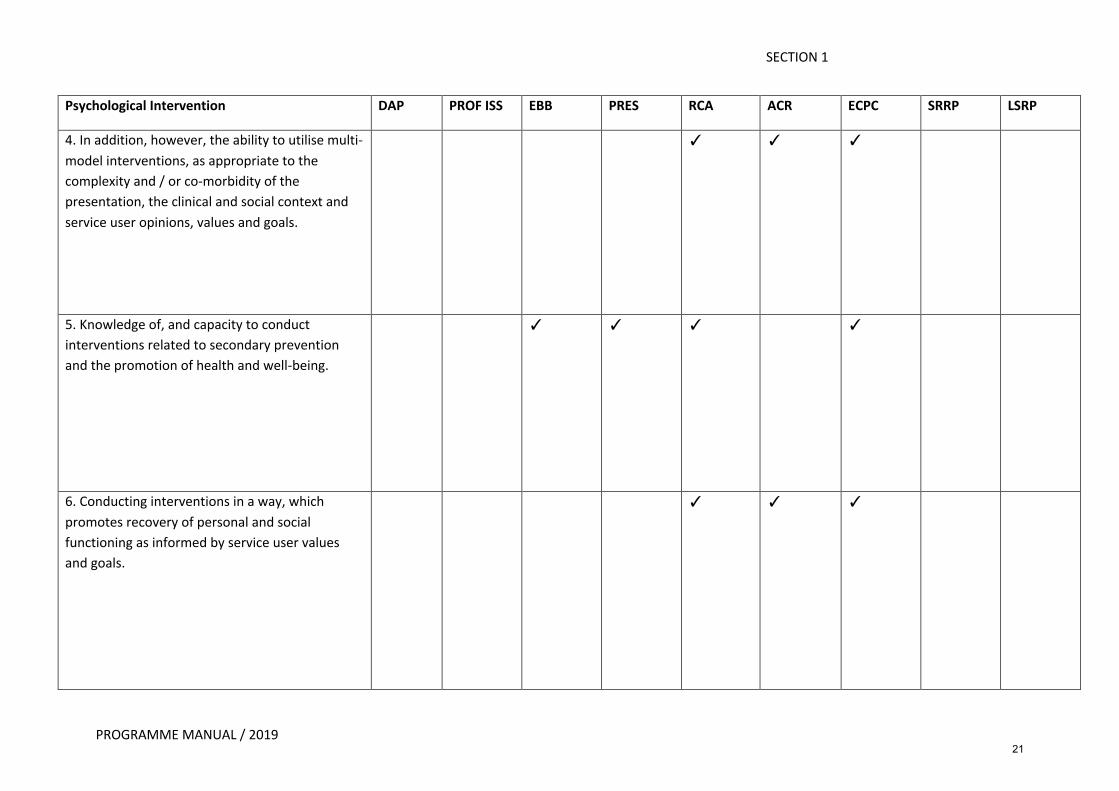
Psychological Intervention DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
4. In addition, however, the ability to utilise multi-
model interventions, as appropriate to the
complexity and / or co-morbidity of the
presentation, the clinical and social context and
service user opinions, values and goals.
� � �
5. Knowledge of, and capacity to conduct
interventions related to secondary prevention
and the promotion of health and well-being.
� � � �
6. Conducting interventions in a way, which
promotes recovery of personal and social
functioning as informed by service user values
and goals.
� � �
21
SECTION 1
PROGRAMME MANUAL / 2019
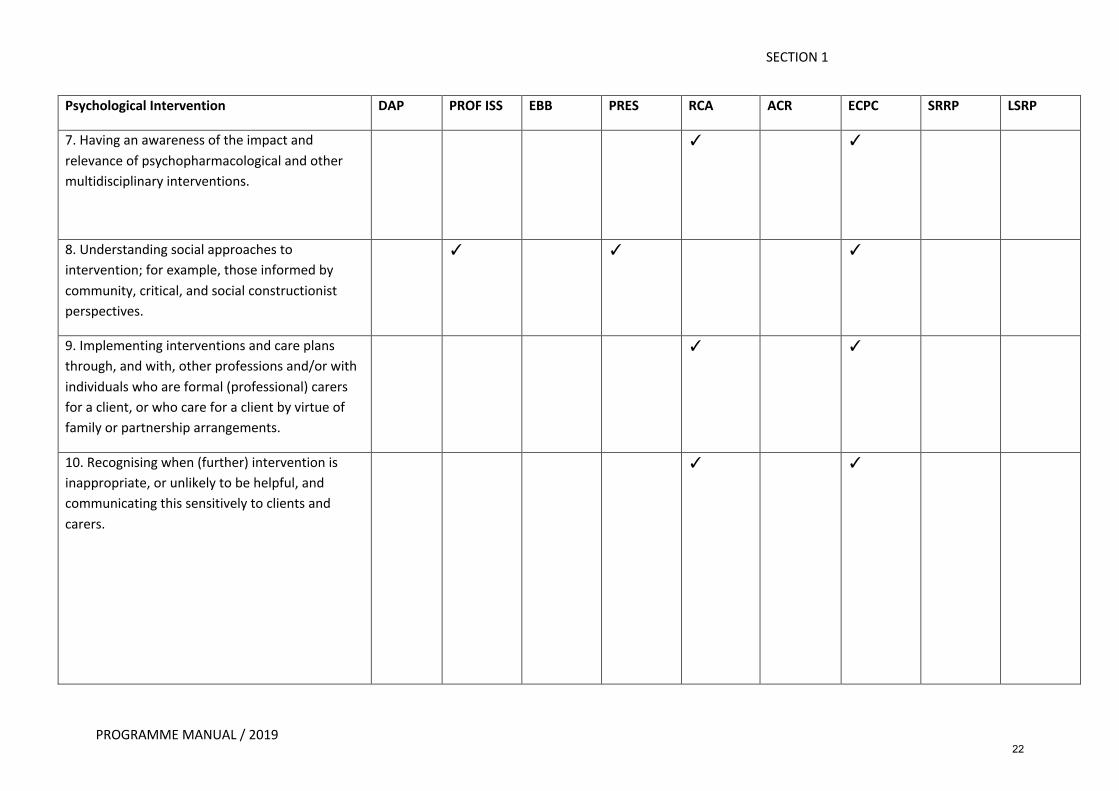
Psychological Intervention DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
7. Having an awareness of the impact and
relevance of psychopharmacological and other
multidisciplinary interventions.
� �
8. Understanding social approaches to
intervention; for example, those informed by
community, critical, and social constructionist
perspectives.
� � �
9. Implementing interventions and care plans
through, and with, other professions and/or with
individuals who are formal (professional) carers
for a client, or who care for a client by virtue of
family or partnership arrangements.
� �
10. Recognising when (further) intervention is
inappropriate, or unlikely to be helpful, and
communicating this sensitively to clients and
carers.
� �
22
SECTION 1
PROGRAMME MANUAL / 2019
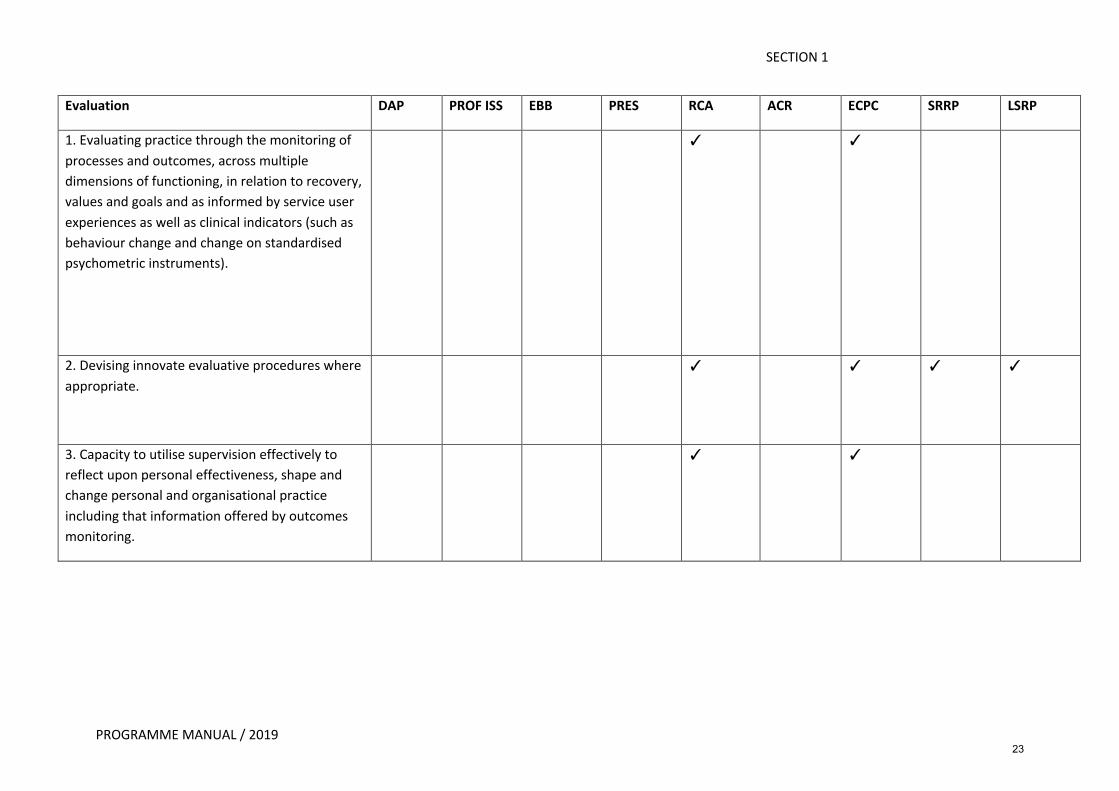
Evaluation DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
1. Evaluating practice through the monitoring of
processes and outcomes, across multiple
dimensions of functioning, in relation to recovery,
values and goals and as informed by service user
experiences as well as clinical indicators (such as
behaviour change and change on standardised
psychometric instruments).
� �
2. Devising innovate evaluative procedures where
appropriate.
� � � �
3. Capacity to utilise supervision effectively to
reflect upon personal effectiveness, shape and
change personal and organisational practice
including that information offered by outcomes
monitoring.
� �
23
SECTION 1
PROGRAMME MANUAL / 2019
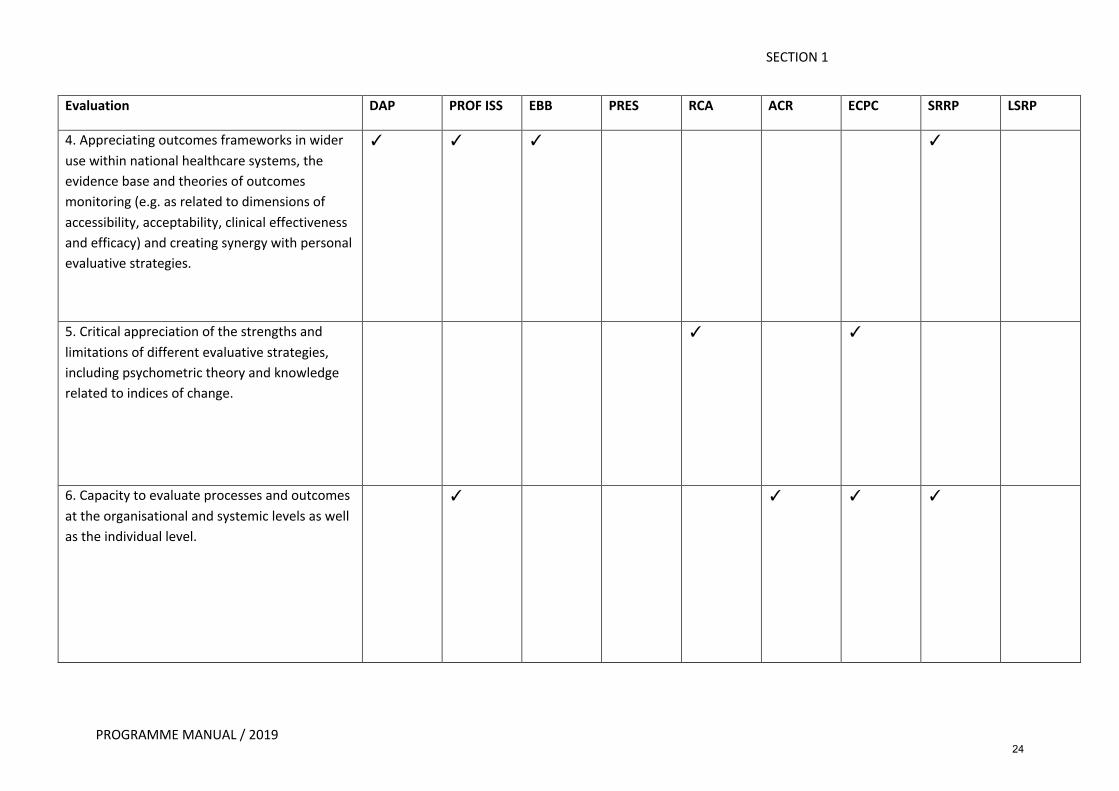
Evaluation DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
4. Appreciating outcomes frameworks in wider
use within national healthcare systems, the
evidence base and theories of outcomes
monitoring (e.g. as related to dimensions of
accessibility, acceptability, clinical effectiveness
and efficacy) and creating synergy with personal
evaluative strategies.
� � � �
5. Critical appreciation of the strengths and
limitations of different evaluative strategies,
including psychometric theory and knowledge
related to indices of change.
� �
6. Capacity to evaluate processes and outcomes
at the organisational and systemic levels as well
as the individual level.
� � � �
24
SECTION 1
PROGRAMME MANUAL / 2019
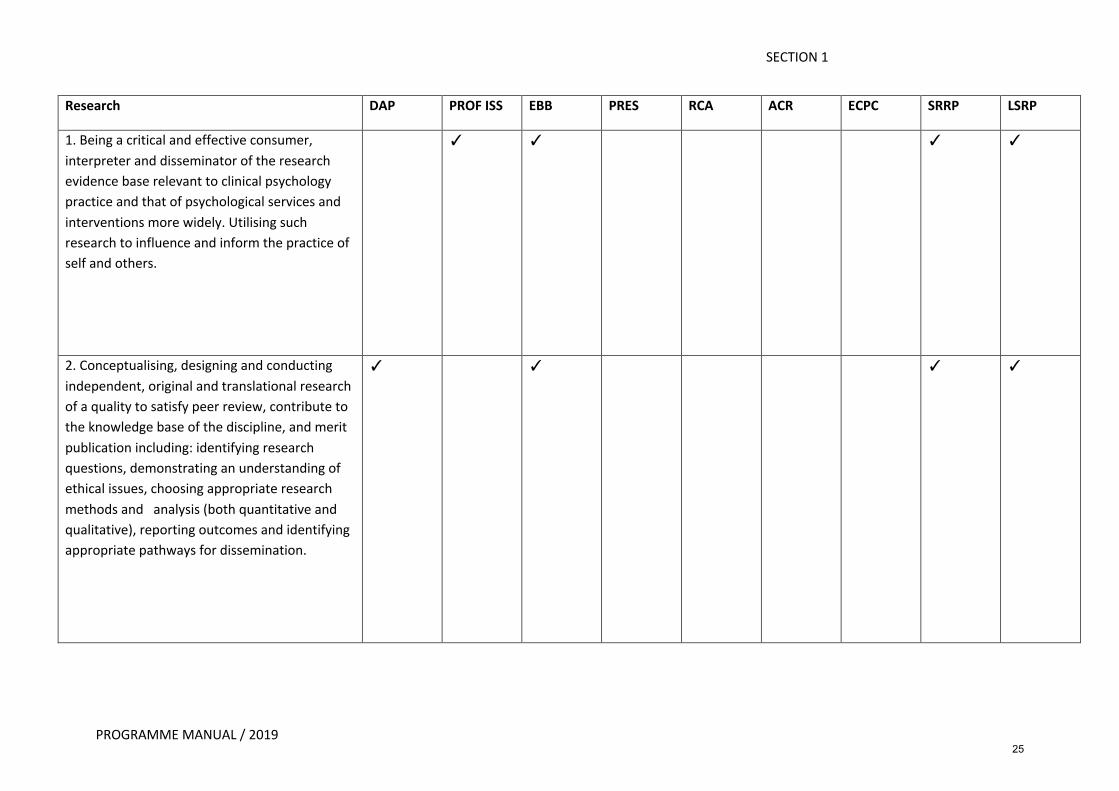
Research DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
1. Being a critical and effective consumer,
interpreter and disseminator of the research
evidence base relevant to clinical psychology
practice and that of psychological services and
interventions more widely. Utilising such
research to influence and inform the practice of
self and others.
� � � �
2. Conceptualising, designing and conducting
independent, original and translational research
of a quality to satisfy peer review, contribute to
the knowledge base of the discipline, and merit
publication including: identifying research
questions, demonstrating an understanding of
ethical issues, choosing appropriate research
methods and analysis (both quantitative and
qualitative), reporting outcomes and identifying
appropriate pathways for dissemination.
� � � �
25
SECTION 1
PROGRAMME MANUAL / 2019
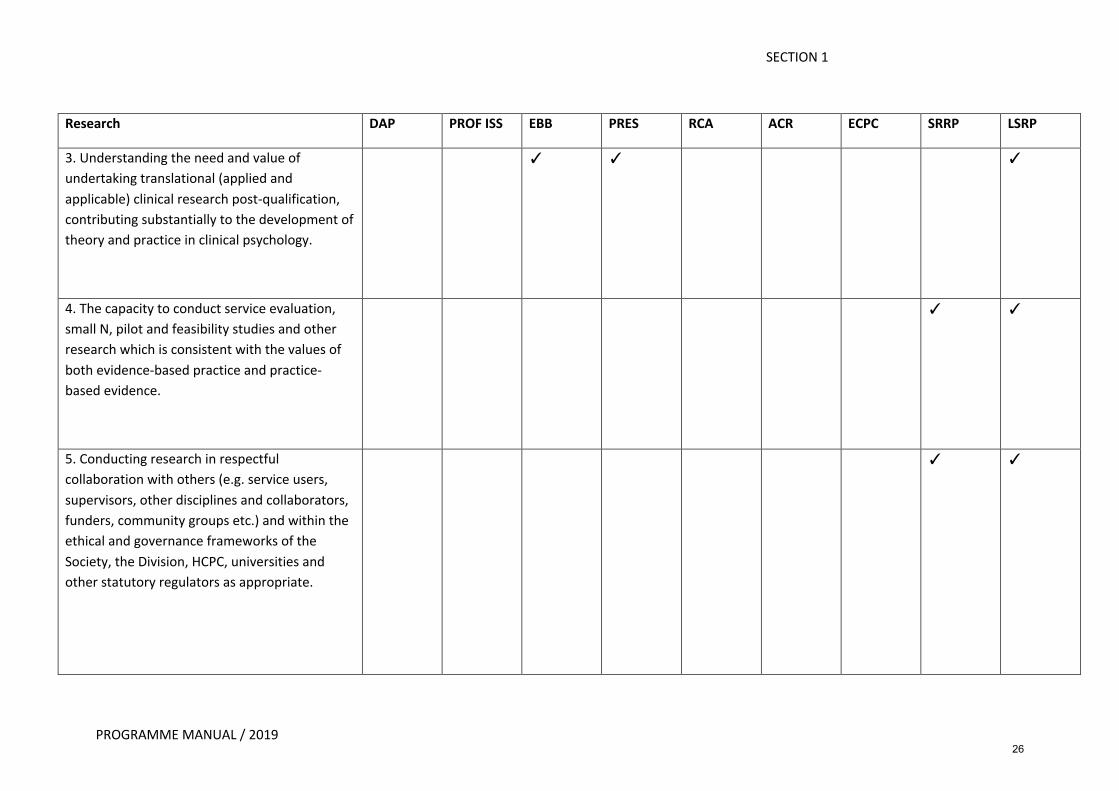
Research DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
3. Understanding the need and value of
undertaking translational (applied and
applicable) clinical research post-qualification,
contributing substantially to the development of
theory and practice in clinical psychology.
� � �
4. The capacity to conduct service evaluation,
small N, pilot and feasibility studies and other
research which is consistent with the values of
both evidence-based practice and practice-
based evidence.
� �
5. Conducting research in respectful
collaboration with others (e.g. service users,
supervisors, other disciplines and collaborators,
funders, community groups etc.) and within the
ethical and governance frameworks of the
Society, the Division, HCPC, universities and
other statutory regulators as appropriate.
� �
26
SECTION 1
PROGRAMME MANUAL / 2019
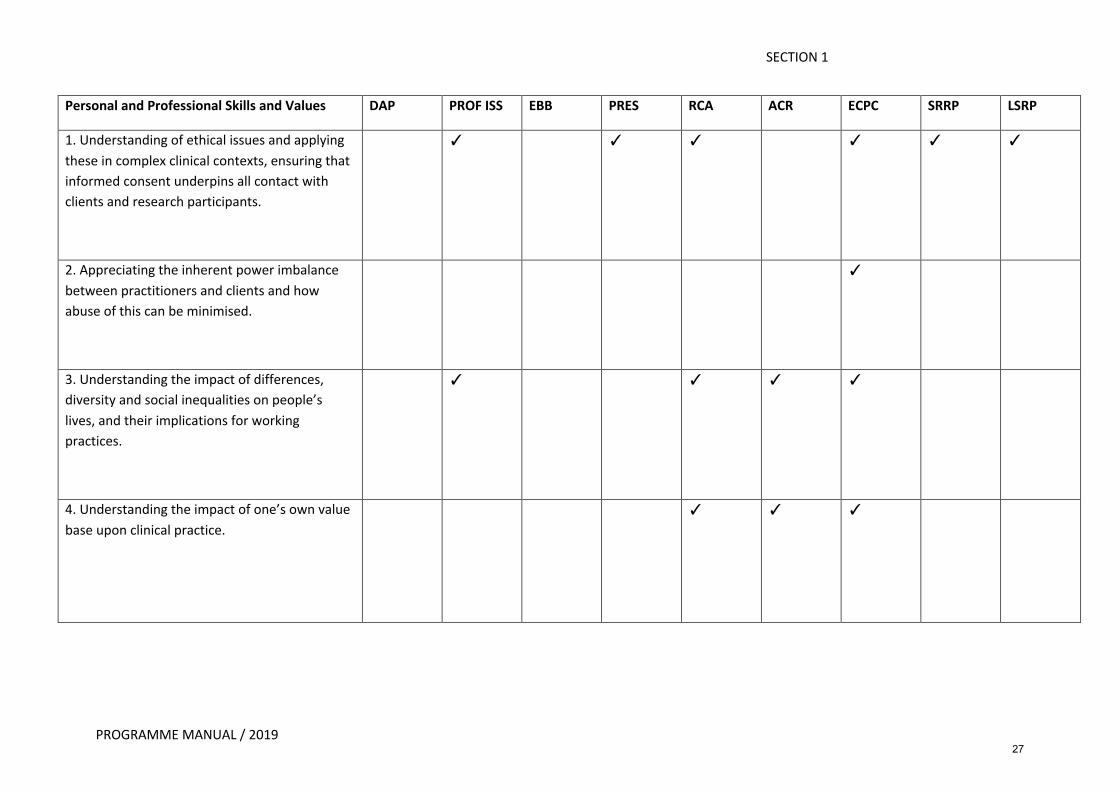
Personal and Professional Skills and Values DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
1. Understanding of ethical issues and applying
these in complex clinical contexts, ensuring that
informed consent underpins all contact with
clients and research participants.
� � � � � �
2. Appreciating the inherent power imbalance
between practitioners and clients and how
abuse of this can be minimised.
�
3. Understanding the impact of differences,
diversity and social inequalities on people’s
lives, and their implications for working
practices.
� � � �
4. Understanding the impact of one’s own value
base upon clinical practice.
� � �
27
SECTION 1
PROGRAMME MANUAL / 2019
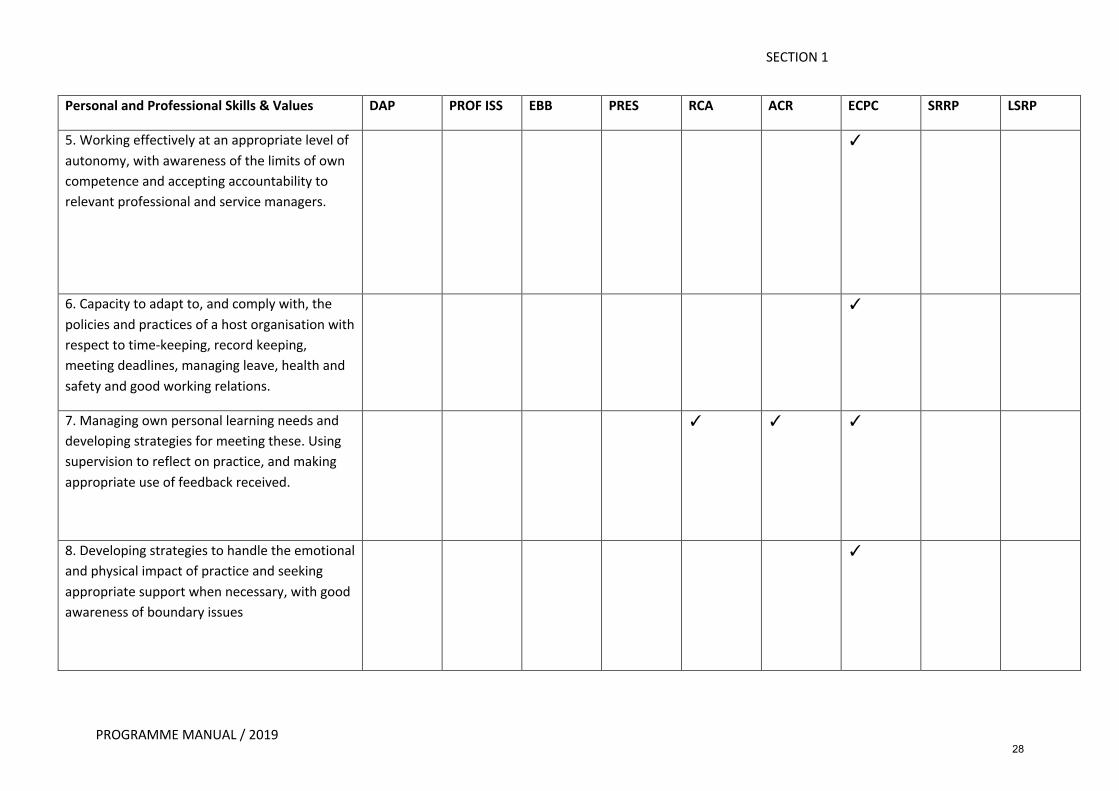
Personal and Professional Skills & Values DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
5. Working effectively at an appropriate level of
autonomy, with awareness of the limits of own
competence and accepting accountability to
relevant professional and service managers.
�
6. Capacity to adapt to, and comply with, the
policies and practices of a host organisation with
respect to time-keeping, record keeping,
meeting deadlines, managing leave, health and
safety and good working relations.
�
7. Managing own personal learning needs and
developing strategies for meeting these. Using
supervision to reflect on practice, and making
appropriate use of feedback received.
� � �
8. Developing strategies to handle the emotional
and physical impact of practice and seeking
appropriate support when necessary, with good
awareness of boundary issues
�
28
SECTION 1
PROGRAMME MANUAL / 2019
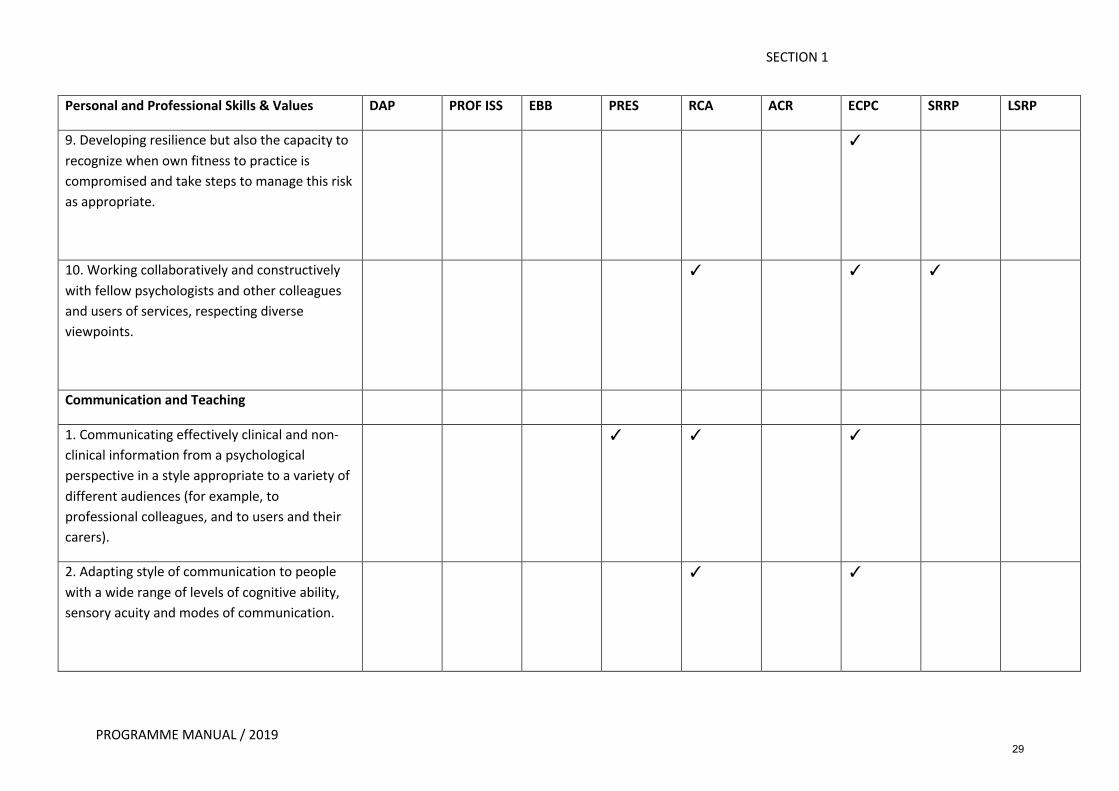
Personal and Professional Skills & Values DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
9. Developing resilience but also the capacity to
recognize when own fitness to practice is
compromised and take steps to manage this risk
as appropriate.
�
10. Working collaboratively and constructively
with fellow psychologists and other colleagues
and users of services, respecting diverse
viewpoints.
� � �
Communication and Teaching
1. Communicating effectively clinical and non-
clinical information from a psychological
perspective in a style appropriate to a variety of
different audiences (for example, to
professional colleagues, and to users and their
carers).
� � �
2. Adapting style of communication to people
with a wide range of levels of cognitive ability,
sensory acuity and modes of communication.
� �
29
SECTION 1
PROGRAMME MANUAL / 2019
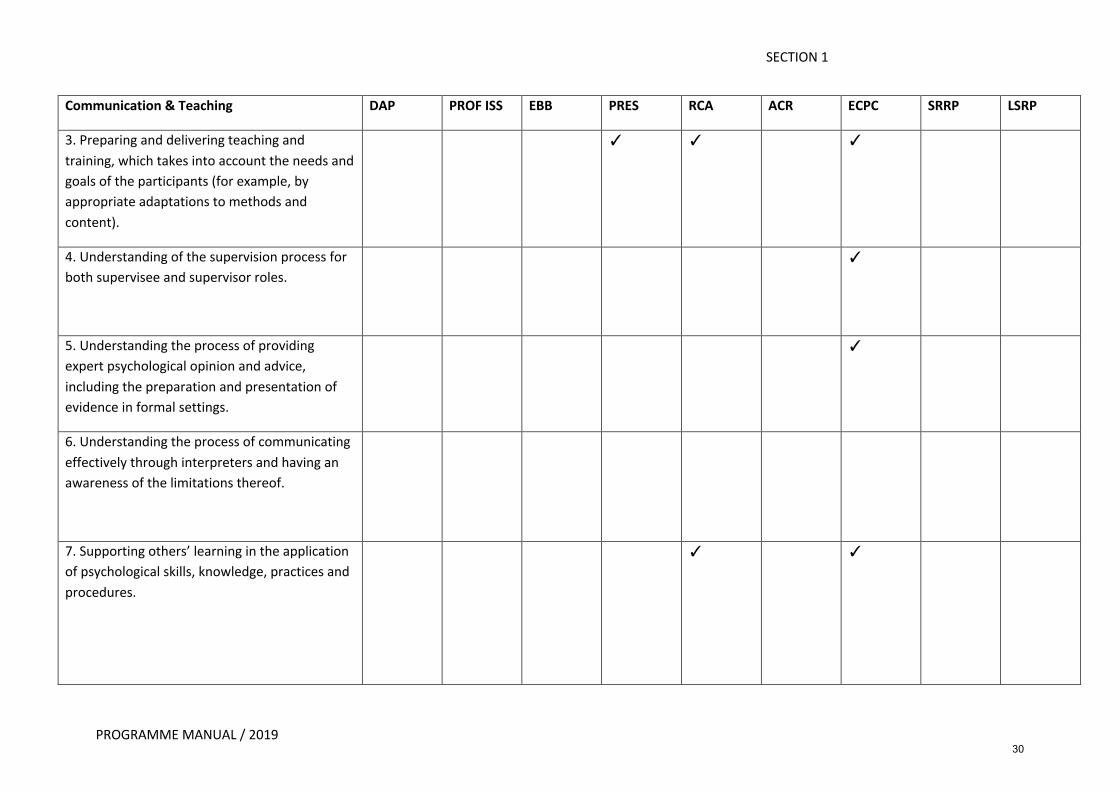
Communication & Teaching DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
3. Preparing and delivering teaching and
training, which takes into account the needs and
goals of the participants (for example, by
appropriate adaptations to methods and
content).
� � �
4. Understanding of the supervision process for
both supervisee and supervisor roles.
�
5. Understanding the process of providing
expert psychological opinion and advice,
including the preparation and presentation of
evidence in formal settings.
�
6. Understanding the process of communicating
effectively through interpreters and having an
awareness of the limitations thereof.
7. Supporting others’ learning in the application
of psychological skills, knowledge, practices and
procedures.
� �
30
SECTION 1
PROGRAMME MANUAL / 2019
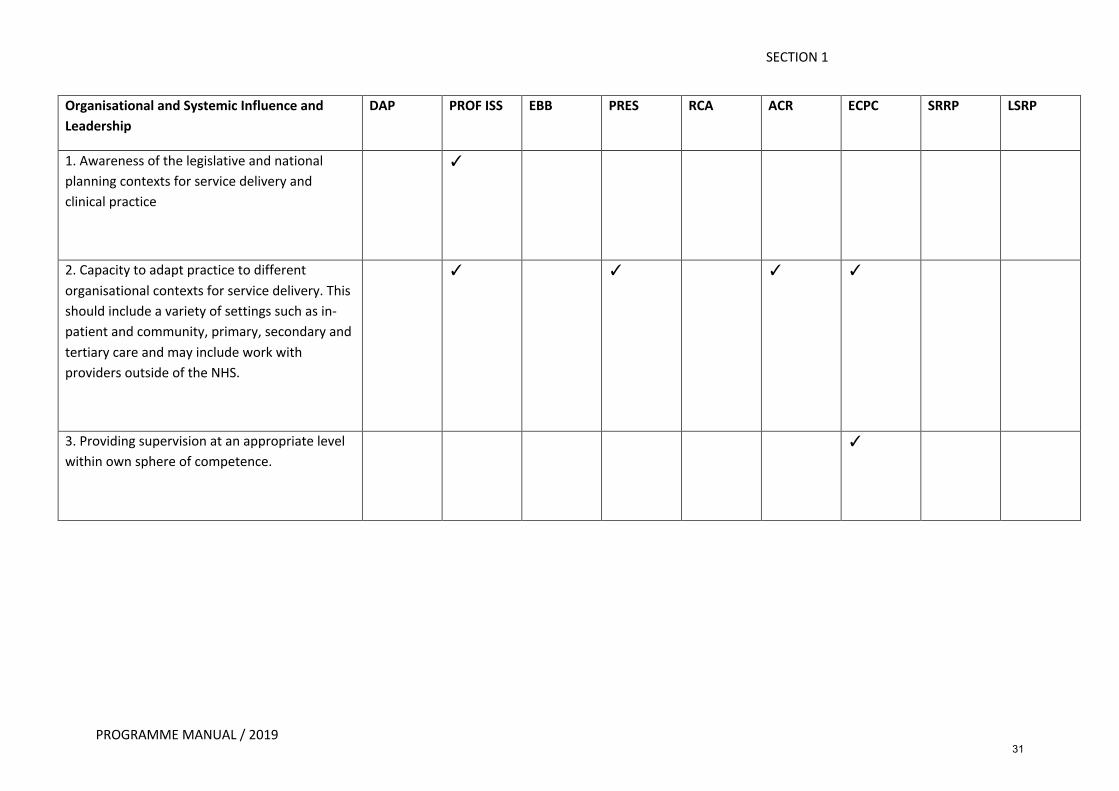
Organisational and Systemic Influence and Leadership
DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
1. Awareness of the legislative and national
planning contexts for service delivery and
clinical practice
�
2. Capacity to adapt practice to different
organisational contexts for service delivery. This
should include a variety of settings such as in-
patient and community, primary, secondary and
tertiary care and may include work with
providers outside of the NHS.
� � � �
3. Providing supervision at an appropriate level
within own sphere of competence.
�
31
SECTION 1
PROGRAMME MANUAL / 2019
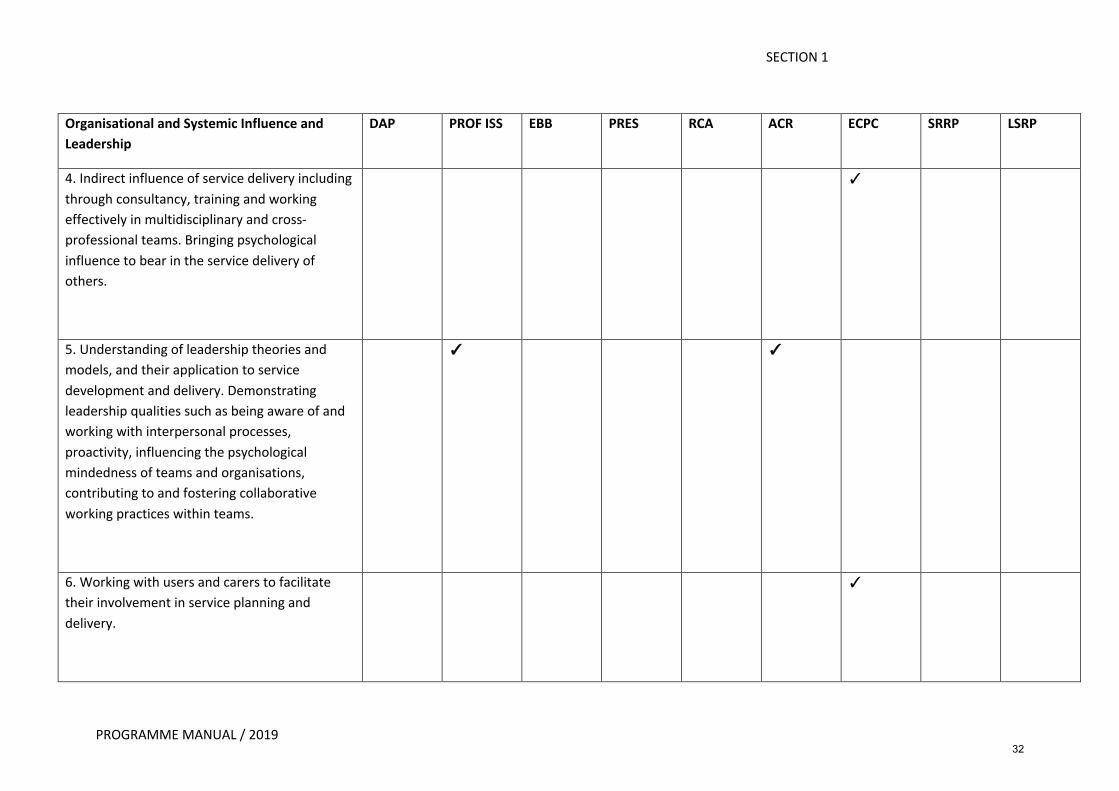
Organisational and Systemic Influence and Leadership
DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
4. Indirect influence of service delivery including
through consultancy, training and working
effectively in multidisciplinary and cross-
professional teams. Bringing psychological
influence to bear in the service delivery of
others.
�
5. Understanding of leadership theories and
models, and their application to service
development and delivery. Demonstrating
leadership qualities such as being aware of and
working with interpersonal processes,
proactivity, influencing the psychological
mindedness of teams and organisations,
contributing to and fostering collaborative
working practices within teams.
� �
6. Working with users and carers to facilitate
their involvement in service planning and
delivery.
�
32
SECTION 1
PROGRAMME MANUAL / 2019
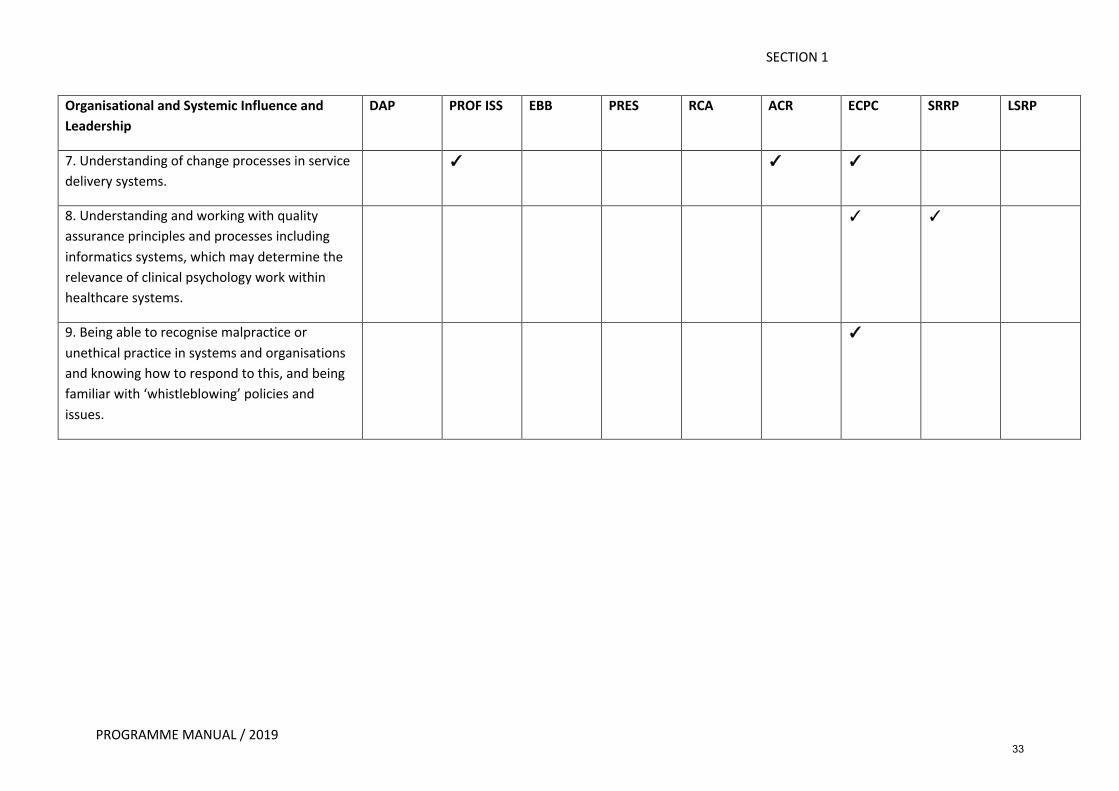
Organisational and Systemic Influence and Leadership
DAP PROF ISS EBB PRES RCA ACR ECPC SRRP LSRP
7. Understanding of change processes in service
delivery systems. � � �
8. Understanding and working with quality
assurance principles and processes including
informatics systems, which may determine the
relevance of clinical psychology work within
healthcare systems.
� �
9. Being able to recognise malpractice or
unethical practice in systems and organisations
and knowing how to respond to this, and being
familiar with ‘whistleblowing’ policies and
issues.
�
33
PROGRAMME MANUAL / 2019
SECTION 1
PROGRAMME STRUCTURE The Programme is full time over three years. At least 50% of the time, excluding annual leave, is spent in clinical practice and up to 10% of the time is designated as private study time. The rest of the time is spent in academic teaching and research. Attendance at teaching is compulsory and is viewed by the Programme as part of trainees’ work duties as salaried NHS staff.
Academic component
Teaching is organised within 29 teaching strands that reflect the core competencies outlined in the BPS accreditation standards. These include sessions that are directly relevant to clinical work; Psychological Theory, Principles of Formulation and Assessment, therapies and interventions as well as those that reflect essential supporting skills of Clinical Psychology; Professional Issues and Personal Development, Leadership and Research. The organisation of the syllabus is also designed to provide trainees with materials most relevant to their placements and stage of training. The programme begins with a five-week induction block that provides an introduction to the programme as a whole and to key concepts and theories. Although delivered with a lifespan perspective, in year one, clinically based sessions focus particularly on the application to work in older adult and adult mental health services. In year two, teaching sessions build on materials already covered in year one, and focus on their application to working with children and adolescents, and people with intellectual disabilities. Each of the Client/Services foci covers the features, prevalence and incidence of the major needs and problems arising, together with issues of difference and diversity and the influences of life-span factors. Psychological theories and models, including experimental investigations, of these needs and problems and their causes, vulnerability and maintaining factors are discussed. Assessment, formulation and intervention approaches relevant to the client group are discussed in detail, and the evaluation of interventions considered in relation to the evidence-base. Therapies and Interventions are also taught incrementally. Year one begins with strong focus on the acquisition and development of Cognitive Behaviour Therapy (CBT) theory and skills, including opportunities for formative assessment within the timetabled syllabus. This continues into year two, and in year three Schema Focused Therapy is introduced as part of the CBT stream. The introduction of third wave approaches begins at the start of training with an 8-week mindfulness course. Partway through year 1, trainees receive an experiential introduction to Acceptance and Commitment Therapy (ACT), followed by ongoing ACT skills sessions. In year two trainees receive training in Applied Behavioural Analysis and Dialectical Behaviour Therapy (DBT). In year three, training in Compassion Focused Therapy (CFT) is introduced. In addition to sessions aimed at skills development, theoretical sessions introduce the principles of Psychodynamic Approaches, Systemic Family Therapy and Cognitive Analytic Therapy. Third year academic sessions pursue a range of topics at a more specialist and advanced level and focus mainly on Therapies and Interventions, Leadership and Professional Issues and Personal Development.
A robust Research training component is delivered across the three years. This encourages the development of critical analytical skills as well as applied research skills to directly support the research assignments required by the programme. The Professional and Ethical Working and Leadership strands are directed at the professional basis of clinical psychology and the evolving role of the clinical psychologist in the NHS (such as the increasing importance placed on the development of leadership skills). Similarly, the wider context
34
PROGRAMME MANUAL / 2019
SECTION 1
of psychological contributions to the organisation and management of health care services, is inter-woven across the three years of the Programme. Regular, timetabled specific sessions on social inclusion and diversity and reflective practice encourage trainees to routinely consider issues of diversity and equality and to develop and hone their skills as reflective practitioners. In years one and two, teaching takes place in academic blocks, followed by regular 'College Days' to further encourage theory-research practice links and to ensure that trainees maintain contact with the Programme base. In year three teaching is delivered in five evenly spaced week-long blocks.
While the majority of the teaching is undertaken by clinical and academic psychologists within North Wales, psychologists from outside the area are also invited to contribute where appropriate. There is also a small contribution from other professions such as Psychiatry, Nursing, Pharmacy, 3rd sector and Service Users. Clinical Component
Clinical experience starts in November of Year 1 and extends over the three years of the Programme. In the first year of the Programme, trainees complete placements in adult mental health and older adults. In the second-year, trainees complete placements in child and adolescent mental health services and intellectual disabilities. In the third-year, trainees are able to exercise more choice about their clinical experience basing their choice on their own interests, training needs and placement availability. Placements available at the time of writing include: adult mental health, older adults, specialist CAMHS, intellectual disabilities, specialist child development services, neuropsychology/brain injury, psychiatric rehabilitation, substance misuse services, Tier 4 adolescent in-patient service, forensic services, DBT interventions, CBT for psychosis, ACT interventions, Schema Therapy, renal medicine, pain management, child health and other health clinical psychology services. In addition to these, trainees may explore the possibility of other third year placements within North Wales.
Clinical experience gained covers the range of problems, clients, settings and modes laid down by the Health and Care Professions Council and the British Psychological Society and includes:
Clients:
• clients with problems acute to enduring, and from mild to severe • clients with problems ranging from those with mainly biological and/or
neuropsychological causation, to those emanating mainly from psychological factors • clients with problems of coping/adaptation and problems of resilience to adverse
circumstances, trauma and life events including bereavement and other chronic physical and mental health conditions
• clients from a range of backgrounds reflecting the demographic characteristics of the population. Trainees are encouraged to reflect on the impact of difference and diversity on people’s lives (including sexuality, disability, ethnicity, culture, faith, cohort differences of age, socio-economic status), and their implications for working practices
• clients with significant levels of challenging behaviour • clients with a range of levels of intellectual functioning over a range of ages,
specifically to include experience with clients with developmental learning disabilities and acquired cognitive impairment
35
PROGRAMME MANUAL / 2019
SECTION 1
• clients whose disability makes it difficult for them to communicate • carers and families.
Settings:
• inpatient, or other residential facilities for individuals with high dependency needs, both acute and long term
• primary, secondary, and community health care. Modes:
• direct work • indirect work, through staff and/or carers • work within multi-disciplinary teams and specialist service systems, including some
observation or other experience of change and planning in service systems • work (practice, teach, advise) in at least two evidence-based models of formal
psychological therapy. This includes CBT and third wave therapies as a minimum, plus opportunities to pursue other evidence-based models within placements
Trainees are also encouraged to:
• work with complexity across a range of perspectives, demonstrating flexibility in application of whichever approach is most appropriate for the client or system; and
• be critical of their own approach, and aware of how to practise in the absence of reliable evidence, as well as being able to contribute from their work to the evidence base.
The Welsh and UK context
Trainees’ work is informed by a substantial appreciation of the legislative and organisational contexts within which clinical practice is undertaken, including for example:
• Government policy statements and legislation relevant to Wales, England and the other devolved nations (e.g. Mental Health Measure (Wales), Mental Health Act, Mental Capacity Act, Children Act, Disability Discrimination Act, Health and Social Care Act, Data Protection Act, employment legislation, etc.);
• organisation of the NHS and social care in Wales, England and the other devolved nations
Research Component
The Programme at Bangor is nested firmly within the scientist-practitioner tradition and the research component of the Programme reflects the emphasis on evidence-based practice within the NHS. The Programme places special emphasis on the research role of the clinical psychologist and in developing the links between general psychological theory and clinical phenomena. The primary aim of the Programme is to provide the trainee with a thorough academic, clinical and professional training in clinical psychology to meet the requirements of clinical psychologists in the National Health Service. This is reflected in the content of the research curriculum offered on the Programme. In general, the research training offered is an integral part of the attempt ensure that trainees acquire skills from a wide theoretical spectrum. A key strategy in this training is to ensure that all trainees are exposed to a wide range of research methods and strategies. It is regarded as
36

PROGRAMME MANUAL / 2019
SECTION 1
particularly important that the research training remains flexible and relevant to the changing needs of the modern NHS. As such, the curriculum may change over time optimally to prepare trainees for any developments within the research needs of the profession.
The focus of the research training on the Bangor Programme is twofold. First, there is a curriculum relating to research design, methodology and the analysis of research data. These are some of the skills that clinical psychologists need to conduct research in their jobs either alone or in a team. Second, the completion of three pieces of research work throughout the Programme (one data analysis project, a service related research project, and one large-scale research project) helps to develop research skills within different contexts. As with many clinical skills, trainees may have a good understanding of what they should try to accomplish in broad terms but may have only a limited idea of how to proceed moment by moment. Working under supervision of experienced supervisors (NHS psychologists and University academics) is an excellent way of learning about the research process through direct experience
The overall aim of the research component of the Programme incorporates both skill and confidence building in addition to the teaching of the knowledge base necessary to conduct research. By the end of the Programme the trainee should be equipped with the knowledge to critically evaluate existing research, and with the skill and experience to successfully participate in the full-life cycle of a research project that responds to the demands of the workplace, employs rigorous research methods, and furthers the body of research evidence in clinical psychology.
Research Curriculum and Teaching Methods The research curriculum includes a number of formal teaching sessions mainly in the first year of training but also during the second and third year. Sessions on psychometric principles, statistics, data analysis, the use of SPSS, literature review, and qualitative methodologies are included. In addition, there are one-off sessions on choosing and planning research projects and writing the thesis. A range of research supervision is available across BCUHB and also in the School of Psychology. Research supervisors are selected by the Programme for their successful previous supervision experience, and, in the absence of prior experience, supervisors are teamed with more experienced research supervisors, either from the School of Psychology or the BCUHB. While a percentage of the research training on this programme takes place through workshops, seminars, lectures and tutorials, the majority of research training takes place at a one-to-one or small group level. This includes assistance from the research team and supervisors in the planning and completion of the Data Analysis Project and the Service Related Research Project through to intensive supervision of the Large-Scale Research Project. Throughout the three years, the emphasis is both on doing research and learning more formally about research methods and therefore the research teaching and the research assignments are explicitly linked. Similarly, through the Service Related Research Project trainees will get an understanding of research in an applied clinical context. This involves the trainee in issues to do with time planning; collaborating with practicing clinical psychologists and researchers to formulate research questions; assessing the feasibility of different methodological approaches to answering research questions; monitoring ongoing research investigations and making adjustments for unforeseen circumstances; developing skills in different formats of dissemination.
Finally, through the Large-Scale Research Project, the trainees will get experience of planning and undertaking an investigation of psychological questions relevant to clinical settings and/or clinical
37
PROGRAMME MANUAL / 2019
SECTION 1
populations. The emphasis for this project is on integrating research experience with theoretical knowledge in clinical psychology to develop a clinically relevant research project, encouraging trainees to expand their skills as autonomous researchers. The thesis will typically involve more complex methodological and design training and this will typically be given on an individual basis, in the context of group meetings, individual meetings and supervision. Methods for evaluating the quality of teaching, learning and support Trainees have the opportunity to provide feedback on the quality of the Programme in the following ways:
• individual trainee feedback on all teaching sessions, which is collated by the year co-ordinator and sent on to individual teachers.
• individual feedback on each placement the trainee undergoes. • meetings with Training Co-ordinators to provide informal feedback. • individual trainee annual appraisal (PADR) meetings where trainees are
invited to feedback on all aspects of their experience of training. • trainee representation at all Programme committees (Training, Supervisors,
Selection, Curriculum and the People Panel (service user group) • an annual anonymised review of the Personal Development Scheme. • an annual anonymised audit of placement quality • annual Postgraduate Research Experience Survey
The ways in which the quality of the Programme is checked, both inside and outside the University, are:
External mechanisms:
• External Examiners moderate and review academic components of the programme and provide an Annual Report for Bangor University. Our External Examiners meet the criteria specified by the Health and Care Professions Council. They are appropriately experienced and qualified and are from the Health and Care Professions Council’s Register of Practitioner Psychologists.
• Annual monitoring by the Health and Care Professions Council and five-
yearly accreditation by the British Psychological Society Committee for Training in Clinical Psychology.
• The Programme is subject to Bangor University Quality Assurance
Procedures, including annual quality reports and periodic internal quality reviews of the whole of the School of Psychology’s teaching and learning provision.
• The Welsh Assembly Government who commission clinical psychology
training in Wales hold an annual contract review with the School of Psychology and the Programme Team.
38
PROGRAMME MANUAL / 2019
SECTION 1
Internal Mechanisms:
• A Programme Training Committee which oversees the Programme, including the work of the Programme Team, and gives strategic direction to the development of the Programme. All major stakeholders are represented on this committee. It has three sub-Committees that report to the Training Committee. These are: The Supervisors Committee, Curriculum Committee and the Selection Committee. There are trainee representatives on all of these four committees.
• An Examining Board, which exists to oversee the implementation of the
assessment procedures of the NWCPP in line with the University regulations, HCPC and BPS standards.
• An annual Stakeholders Meeting. This is open to all qualified clinical
psychologists and trainees. At this meeting staff are updated on developments in the last twelve months and matters such as examiners reports, recruitment and retention and strategic developments may be considered.
• Regular Programme Team meetings where issues to do with the day-to-day
running of the Programme and individual trainee progress are monitored. Support for Student Learning The Programme is based within one of the leading schools of psychology within the UK. In the 2014 Research Exercise Framework the School of Psychology ranked in the top 20 in the UK with 89% of its research considered either 'Internationally Excellent' or 'World leading'. In 2017, Bangor University was awarded a Gold Award in the Teaching Excellence Framework and was the only University in Wales to achieve this. Bangor is also in the Top 5 in the UK for Student Support (WhatUni? Student Choice Awards 2018). Within this context, there are a variety of systems available to support learning on the Programme:
• All trainees are allocated a Training Co-ordinator at the start of the Programme. The Training Co-ordinators are all members of the Programme Team and they are trainees' first points of contact. Training Co-ordinators will undertake placement visits and give formative feedback on draft assignments but will also be able to advise on a range of issues related to training as well as providing pastoral care. In addition, they can monitor and oversee trainee progress and development over the three years of the Programme and help tailor individual training plans to individual training needs. Training Co-ordinators also conduct the annual appraisal of their own trainees.
• At the start of the Programme trainees are issued with vouchers for the Personal
and Professional Development Scheme. This enables them to see a Psychological Therapist who is approved by, yet totally independent of, the Programme, to discuss and explore the impact clinical training has on them both personally and professionally. Full confidentiality and anonymity is preserved within this process.
39
PROGRAMME MANUAL / 2019
SECTION 1
• All trainees are encouraged to identify a Personal Tutor (from a list of names of local clinicians provided by the Programme) in order to have an opportunity to discuss, amongst other matters, professional and other issues arising out of clinical training.
• Trainees receive two manuals at the start of the Programme. The Programme
Manual specifies clearly and in detail the entire relevant academic, clinical and research guidelines and requirements. In addition, an Administrative Handbook outlines procedure for issues such as travel claims, lease cars and study leave.
• A clinical psychology library that comprises books ordered specifically for trainees on
the Programme. Trainees have priority access to these books. • Full access to electronic journals and the larger Psychology library collection in
Bangor University.
• Clinical and research supervisors based within both the local NHS and the School of Psychology who bring to the Programme an impressive level of expertise and dedication.
• School of Psychology computing and laboratory facilities.
• School of Psychology research participant panels.
• The Trainee Resource room with networked computers and plug-in workspaces for
laptops as well a networked NHS computer.
• An extensive Psychological Test library for the use of trainees.
• In addition, BCUHB have their own Occupational Health department with a range of services available to trainees and the University has a full range of student support services (including disability support) available to trainees.
40
SECTION 1
PROGRAMME MANUAL / 2019
Programme Specification
Section A. Programme Details
1. Title of Programme
English Clinical Psychology
Welsh Seicoleg Glinigol
2. Name and level of award E.g. BA, MSc, Cert HE, PG Dip Doctorate in Clinical Psychology - DClinPsy
3. List of Intermediate or
exit-point qualifications
English n/a
Welsh
4. Mode of Study (FT/PT/DL) Full-time
5. Duration of the course Full-time 3 years
Part-time n/a
Section B. Programme Specification
1. Awarding Institution Bangor University
2. Teaching Institution Bangor University
3. External accreditation body (where appropriate)
Health and Care Professions Council (HCPC) & British Psychological
Society (BPS)
4. Final Award Doctorate in Clinical Psychology
5. UCAS/Programme Code
(where known)
C8AG
DLINPSY/PSY
6. Name of appropriate QAA Benchmarking Group
Committee on Training in Clinical Psychology (CTCP) of the British
Psychological Society (BPS);
HCPC standards of Education and Training
QAA Framework for Higher Education Qualifications
QAA Doctoral Degree Characteristics
7. Date when Programme Specification was produced or updated
November 2002. Updated 2006, 2007, 2009. Further revised and ratified 15th July 2014 by NWCPP Training
Committee. Revised by the Programme Team in line with BPS
Accreditation standards published 2015. Further revised
October 2018.
8. Main educational aims of
the programme
The Programme recognises that Clinical Psychology is a caring
profession with a number of distinctive features. Chief among these
are the close interdependence between research and practice, and
41
PROGRAMME MANUAL / 2019
the importance of the systematic application of psychological
models, theories, and evidence in a reflective manner that respects
difference and diversity in the lives of clients and colleagues. At the
forefront of the profession of clinical psychology are the needs of
clients and recognition of the importance of organisational and
systemic contexts within which psychological difficulties occur. The
main aim of the Programme is to meet the needs of the NHS and its
Service Users for Health and Care Professions Council registered
Clinical Psychologists. This staff group have a wide range of clinical,
organisational and research skills, and have developed standards of
high professional integrity and an internalised model of reflective
practice flexible enough to accommodate change.
The Programme aims to select trainees for their potential to develop
a high level of academic, clinical, professional and leadership
competence. It aims to foster this potential by incorporating the
philosophy outlined above in its training, encouraging the
development of skills, knowledge and values underpinning research
and evaluation, clinical and professional competence. This approach
takes place within a supportive structure that facilitates personal
and professional growth and uses the close links that exist in North
Wales between the academic community and clinical services.
There are two official languages in Wales (Welsh and English) with a
significant number of the population who speak Welsh as a first
language (ranging from 14% to 69% depending on area). The
Programme is keen to better meet the needs of the Welsh speaking
community by aiming to increase the numbers of Welsh speaking
trainees on the programme.
9. Intended programme outcomes for each of the categories
(the outcomes must be numbered sequentially)
The Programme provides a holistic experience of training enabling students to achieve an integrated
set of learning outcomes.
Generalisable meta-
competencies
1.1 Drawing on psychological knowledge of developmental, social
and neuropsychological processes across the lifespan to
facilitate adaptability and change in individuals, groups,
families, organisations and communities.
1.2 Deciding, using a broad evidence and knowledge base, how
to assess, formulate and intervene psychologically, from a
range of possible models and modes of intervention with
clients, carers and service systems. Ability to work effectively
whilst holding in mind alternative, competing explanations.
1.3 Generalising and synthesising prior knowledge and
experience in order to apply them critically and creatively in
different settings and novel situations.
1.4 Being familiar with theoretical frameworks, the evidence
base and practice guidance frameworks such as NICE and
SIGN, and having the capacity to critically utilise these in
42
PROGRAMME MANUAL / 2019
complex clinical decision making without being formulaic in
application.
1.5 Complementing evidence-based practice with an ethos of
practice-based evidence where processes, outcomes,
progress and needs are critically and reflectively evaluated.
1.6 Ability to collaborate with service users and carers, and other
relevant stakeholders, in advancing psychological initiatives
such as interventions and research
1.7 Making informed judgments on complex issues in specialist
fields, often in the absence of complete information
1.8 Ability to communicate psychologically-informed ideas and
conclusions to, and to work effectively with, other
stakeholders, (specialist and non-specialist), in order to
influence practice, facilitate problem solving and decision
making
1.9 Exercising personal responsibility and largely autonomous
initiative in complex and unpredictable situations in
professional practice. Demonstrating self-awareness and
sensitivity, and working as a reflective practitioner within
ethical and professional practice frameworks.
Psychological assessment
2.1 Developing and maintaining effective working alliances
with service users, carers, colleagues and other relevant
stakeholders
2.2 Ability to choose, use and interpret a broad range of
assessment methods appropriate:
• to the client and service delivery system in which
the assessment takes place; and
• to the type of intervention which is likely to be
required.
2.3 Assessment procedures in which competence is
demonstrated will include:
• performance-based psychometric measures (e.g. of
cognition and development);
• self and other informant reported psychometrics
(e.g. of symptoms, thoughts, feelings, beliefs,
behaviours);
• systematic interviewing procedures; • other structured methods of assessment (e.g.
observation, or gathering information from others); and • assessment of social context and organisations.
2.4 Understanding of key elements of psychometric theory which have relevance to psychological assessment (e.g. effect sizes, reliable change scores, sources of error and bias, base rates, limitations etc.) and utilising this knowledge to aid assessment practices and interpretations thereof.
2.5 Conducting appropriate risk assessment and using this to guide practice.
43
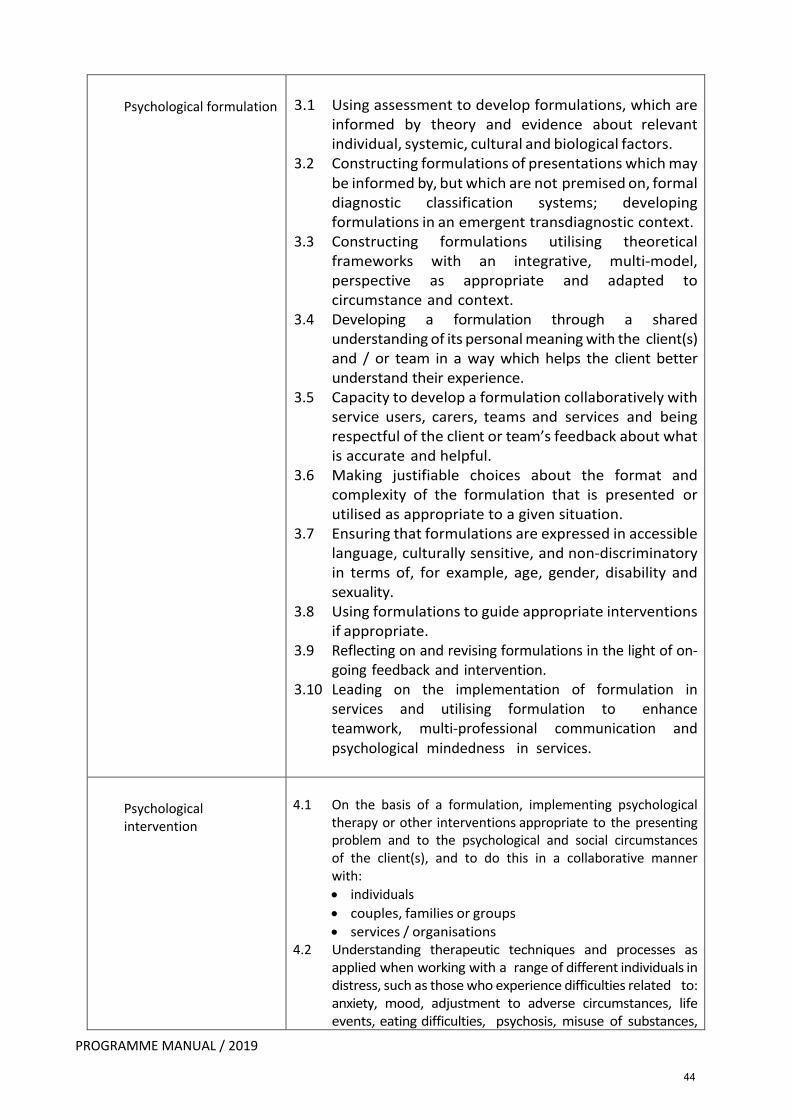
PROGRAMME MANUAL / 2019
Psychological formulation
3.1 Using assessment to develop formulations, which are
informed by theory and evidence about relevant
individual, systemic, cultural and biological factors.
3.2 Constructing formulations of presentations which may
be informed by, but which are not premised on, formal
diagnostic classification systems; developing
formulations in an emergent transdiagnostic context.
3.3 Constructing formulations utilising theoretical
frameworks with an integrative, multi-model,
perspective as appropriate and adapted to
circumstance and context.
3.4 Developing a formulation through a shared
understanding of its personal meaning with the client(s)
and / or team in a way which helps the client better
understand their experience.
3.5 Capacity to develop a formulation collaboratively with
service users, carers, teams and services and being
respectful of the client or team’s feedback about what
is accurate and helpful.
3.6 Making justifiable choices about the format and
complexity of the formulation that is presented or
utilised as appropriate to a given situation.
3.7 Ensuring that formulations are expressed in accessible
language, culturally sensitive, and non-discriminatory
in terms of, for example, age, gender, disability and
sexuality.
3.8 Using formulations to guide appropriate interventions
if appropriate.
3.9 Reflecting on and revising formulations in the light of on-
going feedback and intervention.
3.10 Leading on the implementation of formulation in
services and utilising formulation to enhance
teamwork, multi-professional communication and
psychological mindedness in services.
Psychological
intervention
4.1 On the basis of a formulation, implementing psychological
therapy or other interventions appropriate to the presenting
problem and to the psychological and social circumstances
of the client(s), and to do this in a collaborative manner
with:
• individuals
• couples, families or groups
• services / organisations
4.2 Understanding therapeutic techniques and processes as
applied when working with a range of different individuals in
distress, such as those who experience difficulties related to:
anxiety, mood, adjustment to adverse circumstances, life
events, eating difficulties, psychosis, misuse of substances,
44
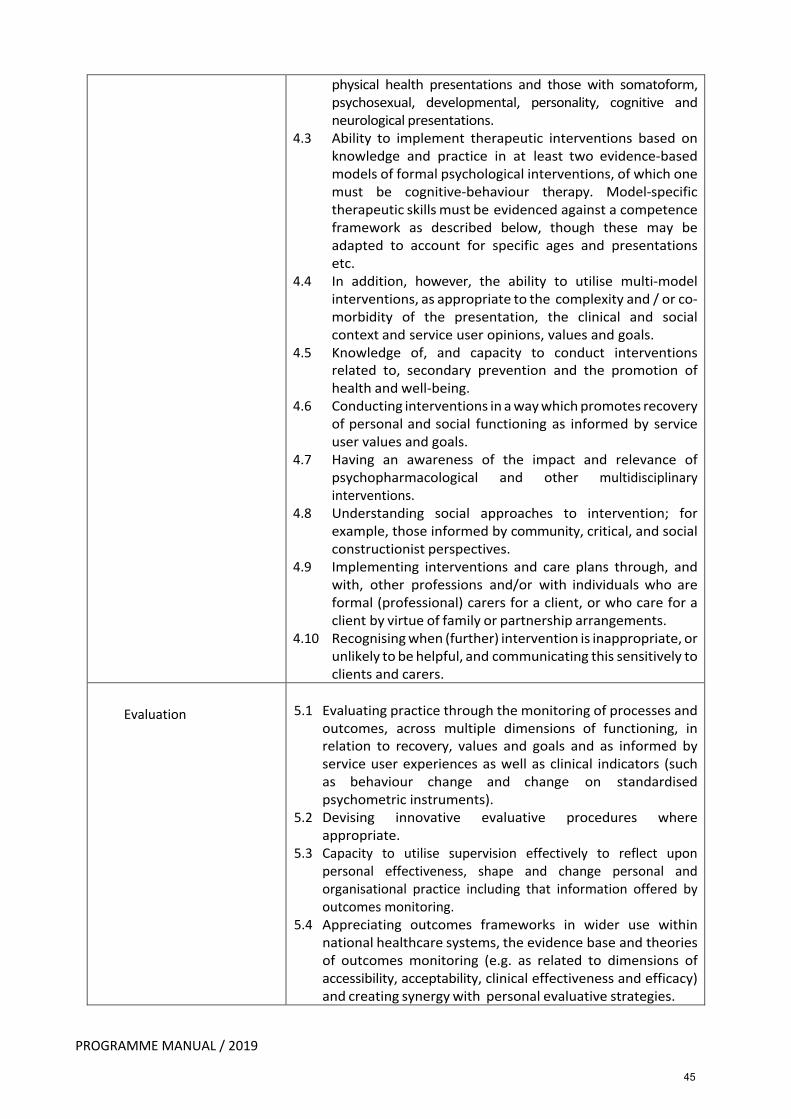
PROGRAMME MANUAL / 2019
physical health presentations and those with somatoform,
psychosexual, developmental, personality, cognitive and
neurological presentations.
4.3 Ability to implement therapeutic interventions based on
knowledge and practice in at least two evidence-based
models of formal psychological interventions, of which one
must be cognitive-behaviour therapy. Model-specific
therapeutic skills must be evidenced against a competence
framework as described below, though these may be
adapted to account for specific ages and presentations
etc.
4.4 In addition, however, the ability to utilise multi-model
interventions, as appropriate to the complexity and / or co-
morbidity of the presentation, the clinical and social
context and service user opinions, values and goals.
4.5 Knowledge of, and capacity to conduct interventions
related to, secondary prevention and the promotion of
health and well-being.
4.6 Conducting interventions in a way which promotes recovery
of personal and social functioning as informed by service
user values and goals.
4.7 Having an awareness of the impact and relevance of
psychopharmacological and other multidisciplinary
interventions.
4.8 Understanding social approaches to intervention; for
example, those informed by community, critical, and social
constructionist perspectives.
4.9 Implementing interventions and care plans through, and
with, other professions and/or with individuals who are
formal (professional) carers for a client, or who care for a
client by virtue of family or partnership arrangements.
4.10 Recognising when (further) intervention is inappropriate, or
unlikely to be helpful, and communicating this sensitively to
clients and carers.
Evaluation
5.1 Evaluating practice through the monitoring of processes and
outcomes, across multiple dimensions of functioning, in
relation to recovery, values and goals and as informed by
service user experiences as well as clinical indicators (such
as behaviour change and change on standardised
psychometric instruments).
5.2 Devising innovative evaluative procedures where
appropriate.
5.3 Capacity to utilise supervision effectively to reflect upon
personal effectiveness, shape and change personal and
organisational practice including that information offered by
outcomes monitoring.
5.4 Appreciating outcomes frameworks in wider use within
national healthcare systems, the evidence base and theories
of outcomes monitoring (e.g. as related to dimensions of
accessibility, acceptability, clinical effectiveness and efficacy)
and creating synergy with personal evaluative strategies.
45
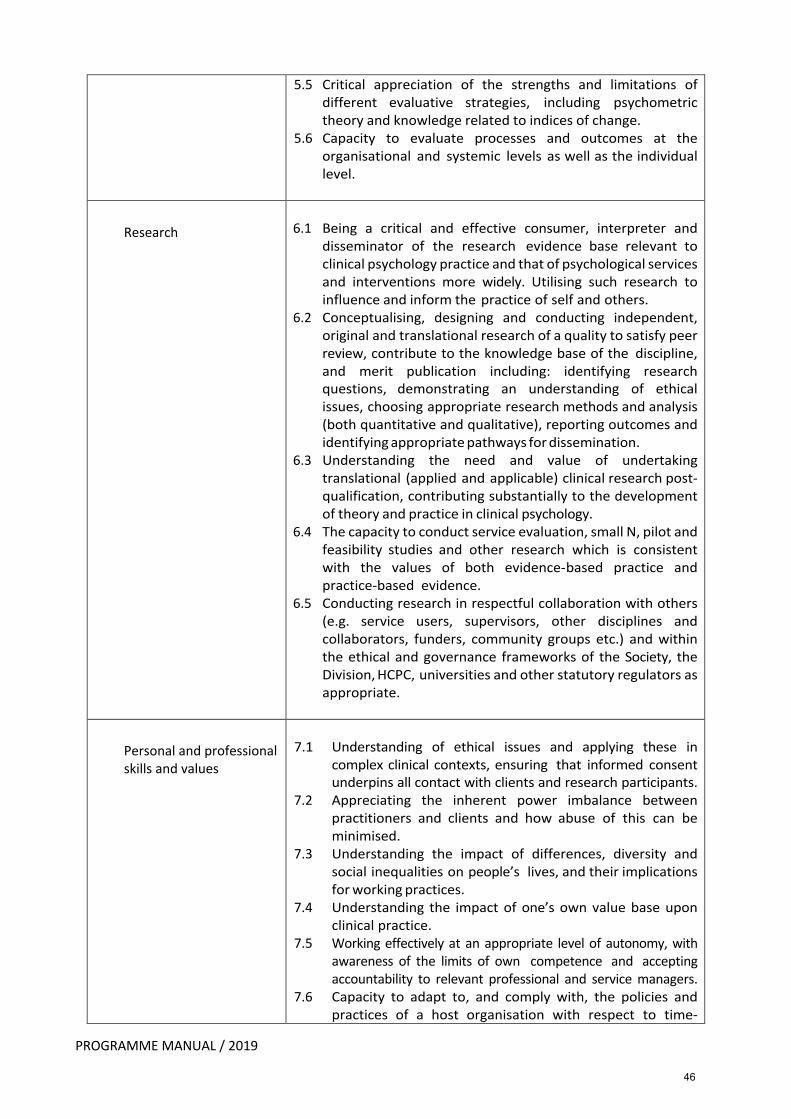
PROGRAMME MANUAL / 2019
5.5 Critical appreciation of the strengths and limitations of
different evaluative strategies, including psychometric
theory and knowledge related to indices of change.
5.6 Capacity to evaluate processes and outcomes at the
organisational and systemic levels as well as the individual
level.
Research
6.1 Being a critical and effective consumer, interpreter and
disseminator of the research evidence base relevant to
clinical psychology practice and that of psychological services
and interventions more widely. Utilising such research to
influence and inform the practice of self and others.
6.2 Conceptualising, designing and conducting independent,
original and translational research of a quality to satisfy peer
review, contribute to the knowledge base of the discipline,
and merit publication including: identifying research
questions, demonstrating an understanding of ethical
issues, choosing appropriate research methods and analysis
(both quantitative and qualitative), reporting outcomes and
identifying appropriate pathways for dissemination.
6.3 Understanding the need and value of undertaking
translational (applied and applicable) clinical research post-
qualification, contributing substantially to the development
of theory and practice in clinical psychology.
6.4 The capacity to conduct service evaluation, small N, pilot and
feasibility studies and other research which is consistent
with the values of both evidence-based practice and
practice-based evidence.
6.5 Conducting research in respectful collaboration with others
(e.g. service users, supervisors, other disciplines and
collaborators, funders, community groups etc.) and within
the ethical and governance frameworks of the Society, the
Division, HCPC, universities and other statutory regulators as
appropriate.
Personal and professional
skills and values
7.1 Understanding of ethical issues and applying these in
complex clinical contexts, ensuring that informed consent
underpins all contact with clients and research participants.
7.2 Appreciating the inherent power imbalance between
practitioners and clients and how abuse of this can be
minimised.
7.3 Understanding the impact of differences, diversity and
social inequalities on people’s lives, and their implications
for working practices.
7.4 Understanding the impact of one’s own value base upon
clinical practice.
7.5 Working effectively at an appropriate level of autonomy, with
awareness of the limits of own competence and accepting
accountability to relevant professional and service managers.
7.6 Capacity to adapt to, and comply with, the policies and
practices of a host organisation with respect to time-
46
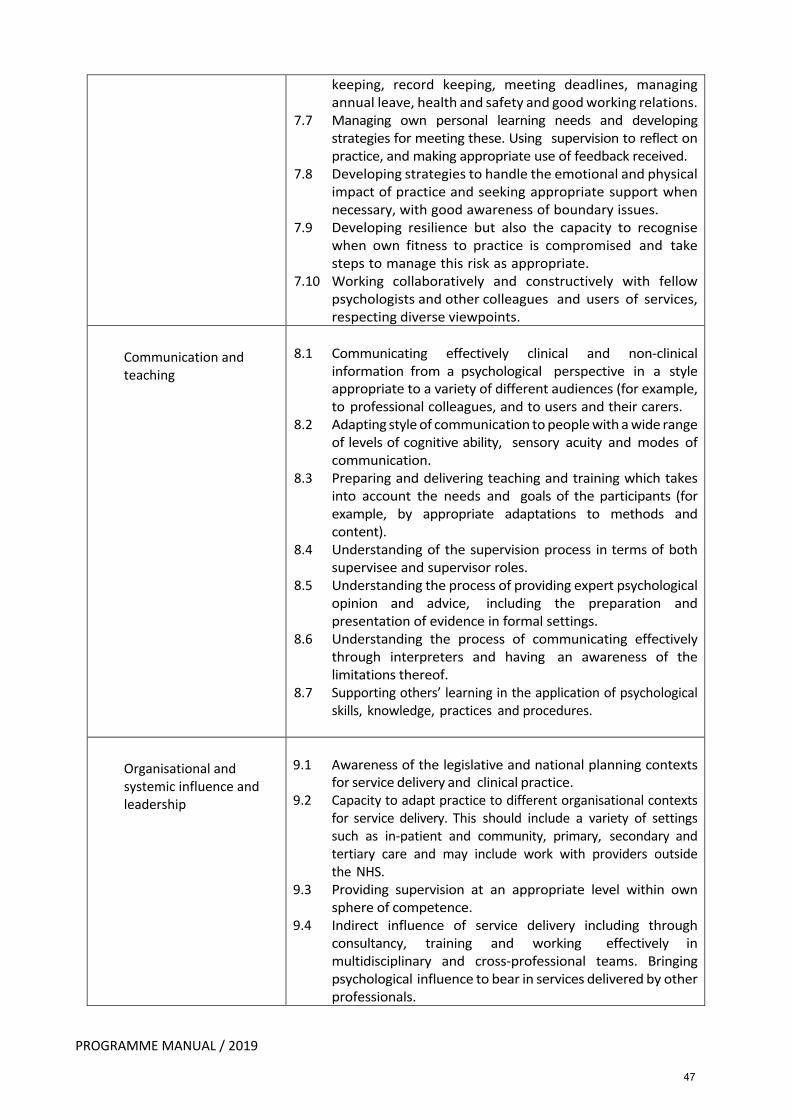
PROGRAMME MANUAL / 2019
keeping, record keeping, meeting deadlines, managing
annual leave, health and safety and good working relations.
7.7 Managing own personal learning needs and developing
strategies for meeting these. Using supervision to reflect on
practice, and making appropriate use of feedback received.
7.8 Developing strategies to handle the emotional and physical
impact of practice and seeking appropriate support when
necessary, with good awareness of boundary issues.
7.9 Developing resilience but also the capacity to recognise
when own fitness to practice is compromised and take
steps to manage this risk as appropriate.
7.10 Working collaboratively and constructively with fellow
psychologists and other colleagues and users of services,
respecting diverse viewpoints.
Communication and
teaching
8.1 Communicating effectively clinical and non-clinical
information from a psychological perspective in a style
appropriate to a variety of different audiences (for example,
to professional colleagues, and to users and their carers.
8.2 Adapting style of communication to people with a wide range
of levels of cognitive ability, sensory acuity and modes of
communication.
8.3 Preparing and delivering teaching and training which takes
into account the needs and goals of the participants (for
example, by appropriate adaptations to methods and
content).
8.4 Understanding of the supervision process in terms of both
supervisee and supervisor roles.
8.5 Understanding the process of providing expert psychological
opinion and advice, including the preparation and
presentation of evidence in formal settings.
8.6 Understanding the process of communicating effectively
through interpreters and having an awareness of the
limitations thereof.
8.7 Supporting others’ learning in the application of psychological
skills, knowledge, practices and procedures.
Organisational and
systemic influence and
leadership
9.1 Awareness of the legislative and national planning contexts
for service delivery and clinical practice.
9.2 Capacity to adapt practice to different organisational contexts
for service delivery. This should include a variety of settings
such as in-patient and community, primary, secondary and
tertiary care and may include work with providers outside
the NHS.
9.3 Providing supervision at an appropriate level within own
sphere of competence.
9.4 Indirect influence of service delivery including through
consultancy, training and working effectively in
multidisciplinary and cross-professional teams. Bringing
psychological influence to bear in services delivered by other
professionals.
47
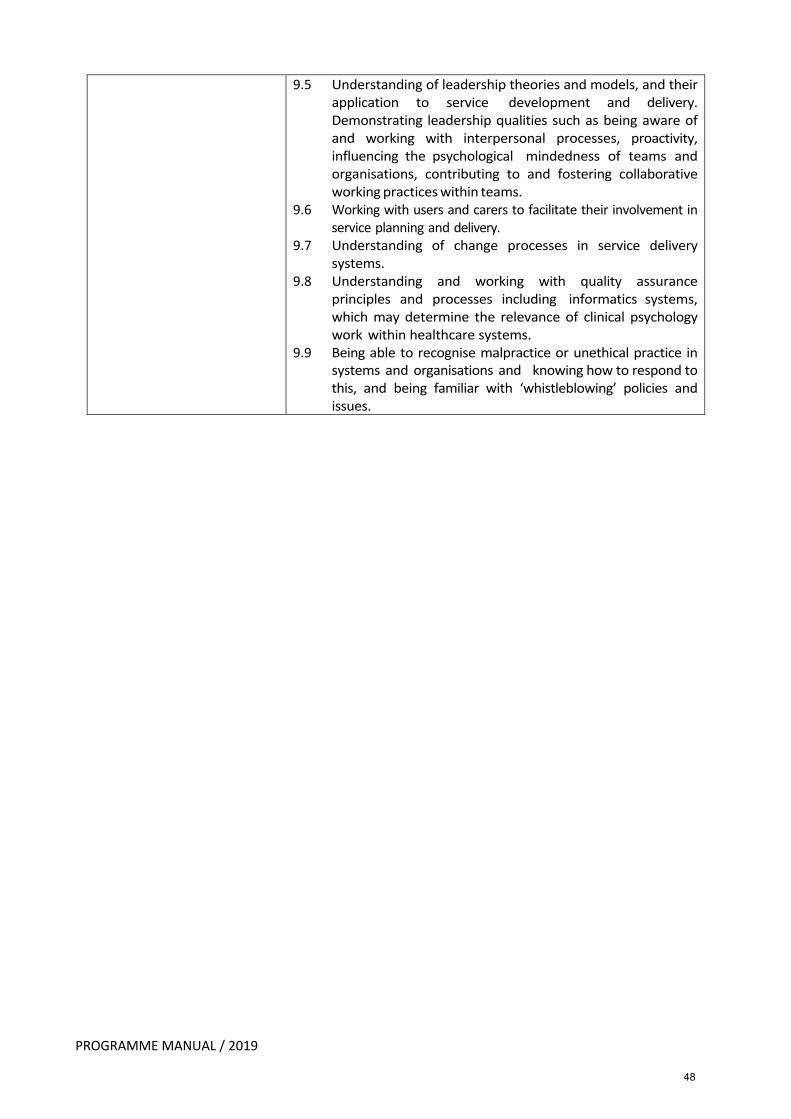
PROGRAMME MANUAL / 2019
9.5 Understanding of leadership theories and models, and their
application to service development and delivery.
Demonstrating leadership qualities such as being aware of
and working with interpersonal processes, proactivity,
influencing the psychological mindedness of teams and
organisations, contributing to and fostering collaborative
working practices within teams.
9.6 Working with users and carers to facilitate their involvement in
service planning and delivery.
9.7 Understanding of change processes in service delivery
systems.
9.8 Understanding and working with quality assurance
principles and processes including informatics systems,
which may determine the relevance of clinical psychology
work within healthcare systems.
9.9 Being able to recognise malpractice or unethical practice in
systems and organisations and knowing how to respond to
this, and being familiar with ‘whistleblowing’ policies and
issues.
48
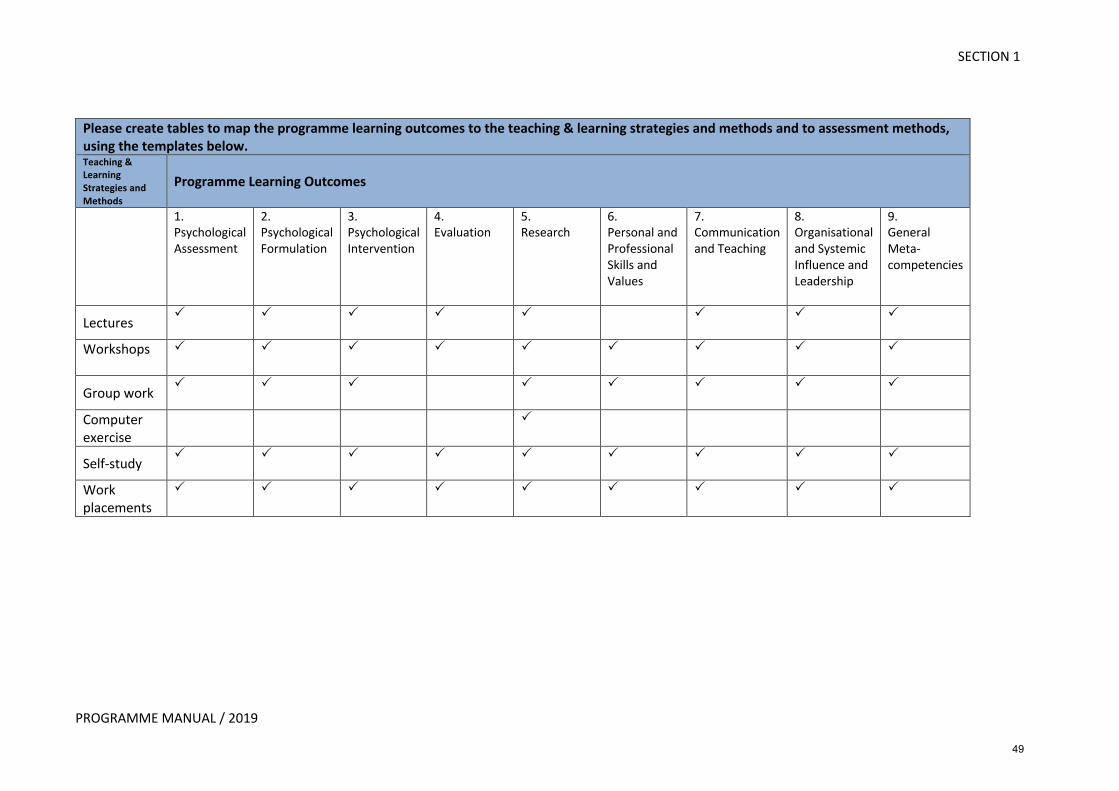
SECTION 1
PROGRAMME MANUAL / 2019
Please create tables to map the programme learning outcomes to the teaching & learning strategies and methods and to assessment methods, using the templates below. Teaching & Learning Strategies and Methods
Programme Learning Outcomes
1. Psychological Assessment
2. Psychological Formulation
3. Psychological Intervention
4. Evaluation
5. Research
6. Personal and Professional Skills and Values
7. Communication and Teaching
8. Organisational and Systemic Influence and Leadership
9. General Meta-competencies
Lectures P
P
P
P P
P
P
P
Workshops
P P P P P P P P P
Group work P
P P P P P P P
Computer exercise
P
Self-study P
P
P
P P
P P
P
P
Work placements
P P P P P P P P P
49
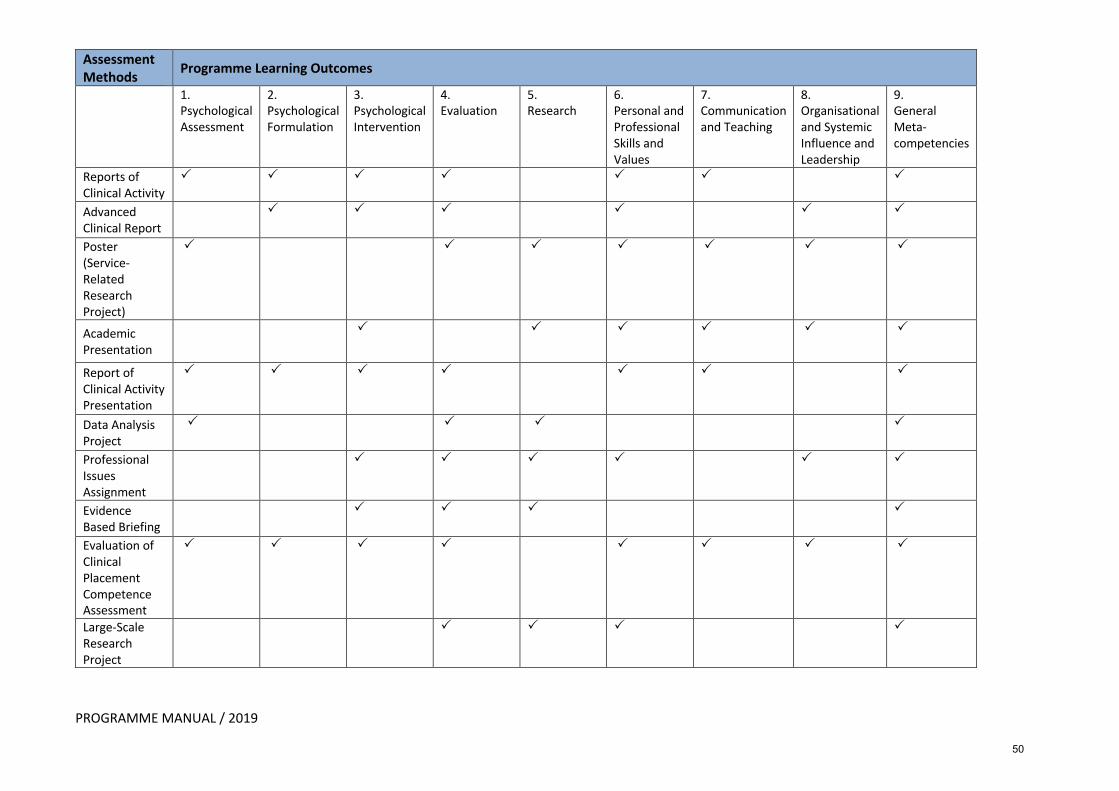
PROGRAMME MANUAL / 2019
Assessment Methods Programme Learning Outcomes
1. Psychological Assessment
2. Psychological Formulation
3. Psychological Intervention
4. Evaluation
5. Research
6. Personal and Professional Skills and Values
7. Communication and Teaching
8. Organisational and Systemic Influence and Leadership
9. General Meta-competencies
Reports of Clinical Activity
P
P
P P P
P
P
Advanced Clinical Report
P
P
P
P
P
P
Poster (Service-Related Research Project)
P
P
P
P
P
P
P
Academic Presentation
P
P
P
P
P P
Report of Clinical Activity Presentation
P
P
P
P
P
P
P
Data Analysis Project
P
P P
P
Professional Issues Assignment
P
P
P
P
P
P
Evidence Based Briefing
P
P
P
P
Evaluation of Clinical Placement Competence Assessment
P
P
P
P
P
P
P
P
Large-Scale Research Project
P P P P
50
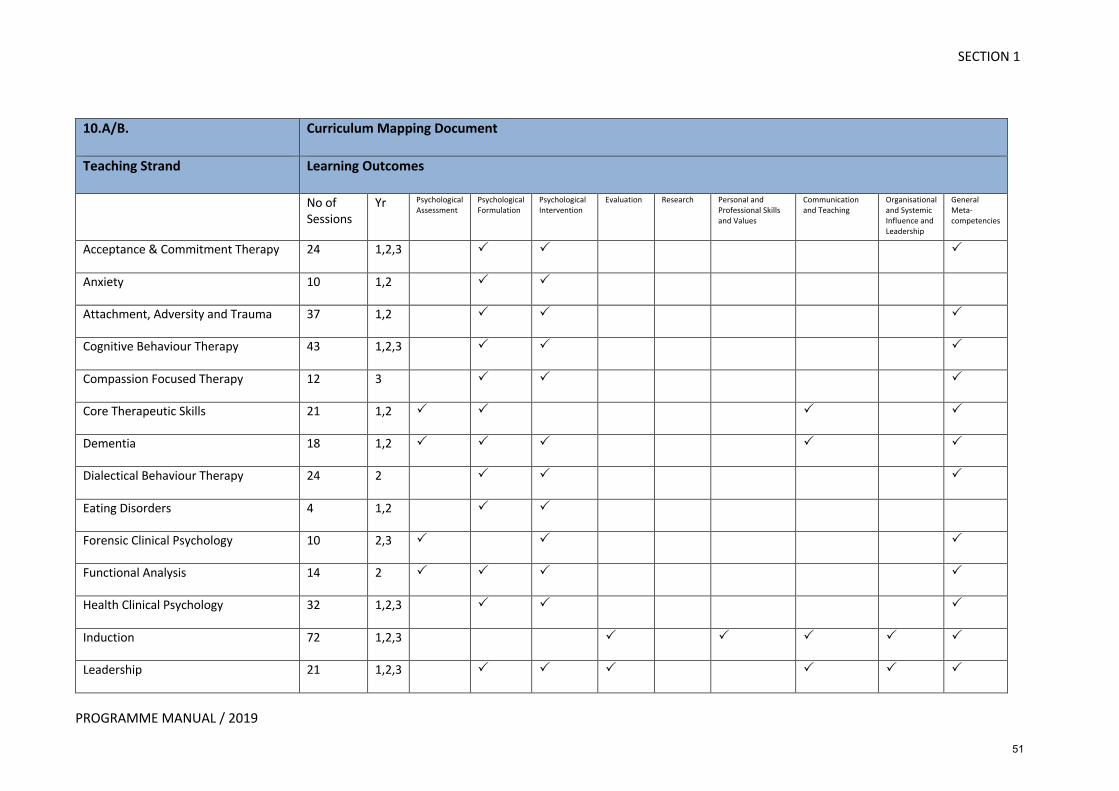
SECTION 1
PROGRAMME MANUAL / 2019
10.A/B. Curriculum Mapping Document
Teaching Strand Learning Outcomes
No of Sessions
Yr Psychological Assessment
Psychological Formulation
Psychological Intervention
Evaluation Research Personal and Professional Skills and Values
Communication and Teaching
Organisational and Systemic Influence and Leadership
General Meta-competencies
Acceptance & Commitment Therapy 24 1,2,3 P
P
P
Anxiety 10 1,2 P
P
Attachment, Adversity and Trauma 37 1,2 P
P
P
Cognitive Behaviour Therapy 43 1,2,3 P
P
P
Compassion Focused Therapy 12 3 P
P
P
Core Therapeutic Skills 21 1,2 P
P
P
P
Dementia 18 1,2 P
P
P
P
P
Dialectical Behaviour Therapy 24 2 P
P
P
Eating Disorders 4 1,2 P
P
Forensic Clinical Psychology 10 2,3 P
P
P
Functional Analysis 14 2 P
P
P
P
Health Clinical Psychology 32 1,2,3 P
P
P
Induction 72 1,2,3 P
P
P
P
P
Leadership 21 1,2,3 P
P
P
P
P
P
51
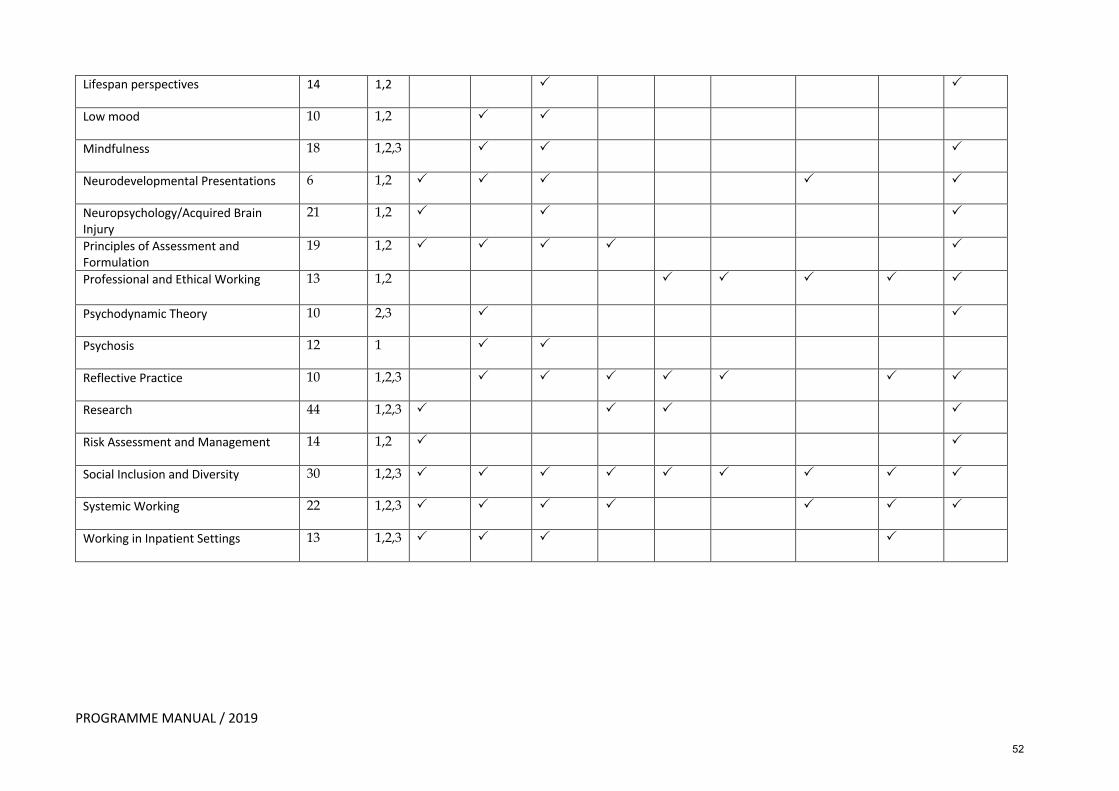
PROGRAMME MANUAL / 2019
Lifespan perspectives 14 1,2 P
P
Low mood 10 1,2 P
P
Mindfulness 18 1,2,3 P
P
P
Neurodevelopmental Presentations 6 1,2 P
P
P
P
P
Neuropsychology/Acquired Brain Injury
21 1,2 P
P
P
Principles of Assessment and Formulation
19 1,2 P
P
P
P
P
Professional and Ethical Working 13 1,2
P
P
P
P
P
Psychodynamic Theory 10 2,3 P
P
Psychosis 12 1 P
P
Reflective Practice 10 1,2,3 P
P
P
P
P
P
P
Research 44 1,2,3 P
P
P
P
Risk Assessment and Management 14 1,2 P
P
Social Inclusion and Diversity 30 1,2,3 P
P
P
P
P
P
P
P
P
Systemic Working 22 1,2,3 P
P
P
P
P
P
P
Working in Inpatient Settings 13 1,2,3 P
P
P
P
52
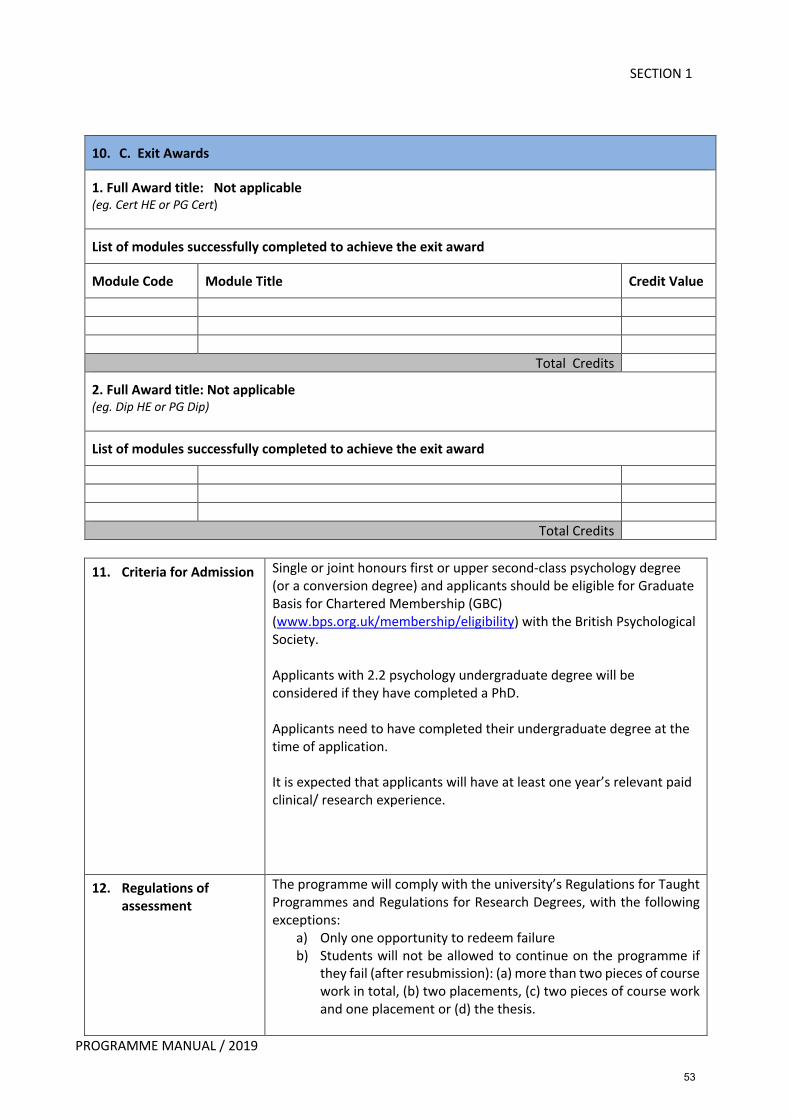
SECTION 1
PROGRAMME MANUAL / 2019
10. C. Exit Awards
1. Full Award title: Not applicable (eg. Cert HE or PG Cert)
List of modules successfully completed to achieve the exit award
Module Code Module Title Credit Value
Total Credits
2. Full Award title: Not applicable (eg. Dip HE or PG Dip)
List of modules successfully completed to achieve the exit award
Total Credits
11. Criteria for Admission Single or joint honours first or upper second-class psychology degree
(or a conversion degree) and applicants should be eligible for Graduate
Basis for Chartered Membership (GBC)
(www.bps.org.uk/membership/eligibility) with the British Psychological
Society.
Applicants with 2.2 psychology undergraduate degree will be
considered if they have completed a PhD.
Applicants need to have completed their undergraduate degree at the
time of application.
It is expected that applicants will have at least one year’s relevant paid
clinical/ research experience.
12. Regulations of assessment
The programme will comply with the university’s Regulations for Taught
Programmes and Regulations for Research Degrees, with the following
exceptions:
a) Only one opportunity to redeem failure
b) Students will not be allowed to continue on the programme if
they fail (after resubmission): (a) more than two pieces of course
work in total, (b) two placements, (c) two pieces of course work
and one placement or (d) the thesis.
53
PROGRAMME MANUAL / 2019
13. Student employability & career opportunities.
Graduates have obtained employment as clinical psychologists after
qualifying from the North Wales Clinical Psychology Programme. A
large group remains in North Wales and work in clinical services. A
smaller group moves away, but often returns when posts become
available in North Wales. Some work in private and third sector or have
taken academic and research positions.
14. Inclusive Provision for Disabled Students (Code 11)
How the needs of all students, including those disabilities and specific
learning difficulties will be addressed.
The programme is an equal opportunities employer and welcomes
candidates from all backgrounds and ages. The programme also
operates the Disability Confident Scheme.
In addition, BCUHB have their own Occupational Health department with
a range of services available to students and the University has a full
range of student support services (including disability support) available
to trainees.
Each person receives a bespoke and confidential provision that is
tailored to their individual needs. There have been many examples in
the past where the Programme has been able to respond flexibly to
students. The process begins with a meeting with the student and the
Programme Manager (and may also include Programme Director and
Training -Co-ordinator if appropriate) where any adaptations or extra
assistance is discussed (e.g. purchase of specialist equipment for
dyslexic students, purchase of special orthopaedic chair for student
with back problems etc). Students with ‘invisible’ disabilities (e.g.
mental health issues) have been successfully trained on the programme
with adaptations that were only known to that student.
54
PROGRAMME MANUAL / 2019
Section C. HEAR Programme Description
Is this degree available as a sandwich degree? N
Is this degree available ‘with International Experience’? N
Single Honours Description (Maximum 550 words)
Major Honours Description (Maximum 400 words)
This description applies to [enter ‘major’ subject] with: [list minor subjects].
Joint Honours Description (Maximum 275 words or 180 for 3 degree programmes)
This description applies to [enter subject] and: [list joint subjects].
Minor Honours Description (Maximum 150 words)
This description applies to another subject with [enter subject] where [enter subject] is the minor
subject with [list major subjects].
Taught Masters Description (Maximum 550 words)
55
SECTION 1
PROGRAMME MANUAL / 2019
Service User and Carer involvement in the North Wales
Clinical Psychology Training Programme
It is recognised that service users have a valuable and meaningful contribution to make in terms of training, service provision and development. The programme team are committed to ensuring that service users and carers are involved with as many aspects of the training programme as possible and that trainees have opportunities to engage in meaningful collaborative dialogue with all members. The group was initially established in 2008 and operates under the title of ‘The People Panel’, which refers to the programme’s Service User and Carers Advisory Group.
The main aims of the People Panel are:
1. To enhance the learning and future practice of clinical psychology trainees by sharing service user and carer experiences which may offer a different perspective to trainees.
2. To ensure that professional and clinical competencies are underpinned by values and practices that acknowledge and respect the goals, needs and strengths of service users, and their carers and families, in a mutual person-centered way.
3. To discuss as a group, action plans, topics of interest, any media coverage relating to service users and service development with the aim of sharing this information with trainees and programme team.
4. To support and encourage creative ideas and innovative ways of working in partnership with Trainee Clinical Psychologists and the programme team.
The People Panel usually meets every two months with representatives currently attending from a number of different specialisms including Adult Mental Health, Intellectual Disability, Health Clinical Psychology, Older Adults and Children’s Services. New members are able to join the People Panel at any time.
People Panel Involvement to date:
Since its inception the People Panel have been actively involved with the following areas:
1. Academic Teaching Service Users, Carers and members of the People Panel contribute on a regular basis to a number of teaching sessions including Adult Mental Health, Intellectual Disability, Child and Adolescent, Health Clinical Psychology and Older Adults. The feedback from trainees remains consistently very positive following these sessions. People Panel members also co-facilitate CBT workshops where feedback is given directly to trainees on their performance from a service user and carers perspective; again, feedback from trainees regarding this experience is very positive and appreciated.
2. Selection Procedure The Programme has had service user representation involved in the selection process since 2008. A member of the People Panel attends the selection committee meetings, where they share the People Panel’s views on the programme’s selection and
56
SECTION 1
PROGRAMME MANUAL / 2019
interviewing process; committee meeting discussions and decisions are feedback to the People Panel by the same representative. In addition, members of the People Panel participate in the programme’s interviewing process, with a member sitting on each interview panel alongside members of the programme team. All members of the interview panels’ marks for candidates have equal weight. People Panel members also take part in interviewing potential members of staff.
3. Clinical Placements The People Panel devised the Service User Feedback form which clients are asked to complete for trainees at the end of their respective placements. The Panel have also been actively involved in designing guidelines regarding the sharing of client information from placements in relation to the role of a clinical psychology trainee and the academic requirements relating to submission of written reports of clinical activity.
4. Research
Trainees regularly ask the People Panel for feedback regarding aspects of projects such as participation information sheets and consent forms, and sometimes present research projects at various stages of development for advice and feedback. Feedback is given to trainees either at the meeting or, later, via e-mail. The lively discussions at People Panel meetings have assisted trainees when they felt they had got ‘stuck’.
People Panel members regularly attend the annual Research Fayre, and contribute by
offering comments and ideas following the research proposals presented.
The People Panel are keen to get more involved in research and this strand of service user and carer involvement is currently being developed to maximise future collaboration and co-production.
5. Programme Committees The People Panel has a representative on each of the following committees: Training Committee, Selection Committee and Supervisors Committee and take forward People Panel ideas to these meetings, and subsequently provide feedback to the People Panel meetings.
In addition, ‘Meet the Trainees’ has become a well-established session where The People Panel meets the new cohort at the beginning of each year, often socialising informally during a buffet lunch before meeting as a group to introduce themselves and share experiences, interests and perspectives. This provides a basis for welcoming the trainees to any People Panel meetings they may wish to attend during their time on the programme, and/or getting in touch at any time. The People Panel is always invited to the Annual Stakeholders’ Day, where qualifying trainees present their research projects, thus following the trainees’ progress from start to finish.
57
SECTION 1
PROGRAMME MANUAL / 2019
People Panel members have enjoyed visits to other programmes during the years, as well as co-hosting an All-Cohort Training Day where renowned Service User and Carer Involvement expert Dr. Barbara Riddell came to visit the programme. The People Panel also has representation on the BPS’ Group of Trainers in Clinical Psychology (GTiCP).
Training and Payment
Members of the People Panel are paid for attending meetings and are also reimbursed for travelling expenses. The programme is fully supportive of members’ health and caring issues if they cannot attend the meetings at any time. Service users and carers involved in teaching are paid in accordance with the payment guidelines for teaching. The University advises service users and carers involved with any work for the University that it is their responsibility to inform the Benefits Agency and /or Inland Revenue about any earnings they receive.
References
Hayward, M & Riddell, B. (2008). Good Practice Guidelines: service user and carer involvement within Clinical Psychology Training, Leicester UK. British Psychological Society.
Cooke, A., & Hayward, M. (2010). Service users and carers as placement advisors: Part 1 Getting started. Clinical Psychology Forum, 209, 21-22
Division of Clinical Psychology (2010). Good Practice Guidelines to support the involvement of Service Users and Carers in Clinical Psychology Services, Leicester: British Psychological Society
Service User Teaching Feedback
Child & Adolescent Service User Workshop
“Excellent session. Both people spoke very openly and honestly – thank you”. “Very relevant to see the other perspective. We could do with more of this to get an idea of the lived experience”. “Really good to hear the perspectives of the service users who gave honest accounts.” “Very valuable and useful to have the service user perspective. Splitting into smaller groups worked as well” “Really helpful to hear from service users” “Would be useful to have more time with the service users”
Health Clinical Psychology Workshop (Renal Service)
“Fantastic to have individual share their experiences”. “Excellent session – really well organised and fantastic variety of speakers”. “Excellent, we need more time on these more specialist areas”. “Excellent teaching session. All presenters were amazing – thank you”. “Excellent session with contributions from so many people”. ‘Fantastic session! Very varied and well planned. Particularly enjoyed input of the service users”.
58
SECTION 1
PROGRAMME MANUAL / 2019
Intellectual Disability Service User Workshop
“Fantastic session. You can’t get this from text books!”. “Excellent session, service users were passionate and many relevant experiences to share”. “I don’t usually find these sessions useful, but the choice of service users, their positive and inspirational, touching stories made it a good, useful session”. “Had an impact on my thinking around opportunities for people with Intellectual disabilities”. “Really insightful session”. “Excellent to have viewpoints from service user, parent and support worker/carer. Really valuable”. “Such an important part of our learning – may it continue!”.
Adult Mental Health Service User Workshop
“Really interesting”. “Very thought provoking”. “Really informative session. Good alternative view on mental health”. “Great to have the opportunity to hear the service users experiences and perspective on psychology and mental health services”. “Very useful, thought provoking and interesting. Useful to have a chance to think about psychology and spirituality”. “Very clear and some interesting ideas!”.
59
SECTION 2
CURRICULUM
60
SECTION 2
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME ACADEMIC SYLLABUS
Within the North Wales Clinical Psychology programme, learning takes place as a result of integrated academic and clinical activity. The teaching syllabus sets the scene for the acquisition of knowledge and skills, which are then observed, applied, reviewed and assessed during clinical placements and in the completion of academic assignments. Teaching sessions also offer further opportunities for trainees’ reflection on their own learning as they progress through the programme. Overarching Aims of the Teaching Syllabus The aim of the syllabus is to teach the academic foundations and professional practice of clinical psychology. By the end of the Programme trainees will be expected to have learned:
1. the features, prevalence and incidence of the major needs and problems of the full range of client groups relevant to clinical psychology, and the influences of life-span development, societal factors and cultural diversity;
2. psychological theories about the aetiology, vulnerability and maintenance of these needs and problems;
3. the results of research investigating the processes underlying such problems; 4. the theory and practice of a range of psychological assessment procedures,
including the interpretation of findings; 5. the theoretical and empirical basis of a range of psychological therapies, and
their application in practice with various client groups; 6. how to evaluate the evidence on the efficacy of treatments; how to inform
clinical decision-making and practice on the basis of evidence synthesis; 7. how to formulate clinical problems and the relationship of the formulation to
assessment, intervention and evaluation; 8. the intervention skills involved in dealing with individual clients, couples,
families, groups, indirect work, and work with health care delivery systems; 9. the professional and organisational framework in which clinical psychology is
practised, including codes of conduct, ethical issues and the relevant legislative framework;
10. to promote non-discriminatory practice and to promote social inclusion; 11. the knowledge and skills necessary to conduct original research in response to
the demands of the workplace and to critically evaluate existing research; 12. the communication and teaching skills required to deliver formal teaching to
other psychologists and non-psychology colleagues, and psychological education to a range of service users.
Each area of knowledge and skill covers a wide range of ages, showing how developmental changes across the lifespan influence psychological processes. By the end of the Programme trainees should have an integrated understanding of a number of ways of working. They will understand psychological theories and interventions that are applied to individual and group work, working with families, indirect and systemic work with carers, teams and broader systems, teaching non-psychologists, service development, consultancy and leadership.
61
SECTION 2
PROGRAMME MANUAL / 2019
Teaching aims to equip trainees with the core theory and skills of clinical psychology, whilst attending to applications, adaptations and limitations of these relevant to distinct client groups. The Programme has a number of strategies to achieve these aims:
• a learning ethos which encourages trainees to engage with the evidence base and to read around psychological models for themselves, and gives regular time for this reading and preparatory work for assignments to be carried out.
• training co-ordinators who are available to read and comment on draft assignments, assisting trainees in integrating and presenting their work coherently;
• extensive use of workshop-based teaching to facilitate learning and skill development, and to encourage the integration of theoretical and clinical aspects.
• a programme structure that ensures that throughout the first two years of the programme, academic teaching is linked to the placement experiences undertaken by trainees during that year.
The focus is on the development of a foundational set of transferable competencies that can be applied broadly across the lifespan and a range of specialisms. This is overlaid by related specialism-specific skills and knowledge to allow trainees to apply these competencies effectively. Teaching Strands In order to combine core competencies with specialism-specific skills and knowledge, our teaching is arranged into ‘strands’ which begin by delivering common components of the topic in question, followed by more specific sessions on their application in different circumstances. For example, teaching on anxiety presentations is one of our strands, which includes theory, assessment, formulation and intervention skills, and a consideration of how these apply across the lifespan. The teaching strands are as follows: Acceptance and Commitment Therapy Anxiety Attachment Adversity and Trauma Cognitive Behavioural Therapy Compassion Focused Therapy Core Therapeutic Skills Dialectical Behaviour Therapy Dementia Eating Disorders Forensic Clinical Psychology Functional Analysis Health Clinical Psychology Induction and NWCPP sessions Leadership Lifespan Perspectives Low Mood Mindfulness
62
SECTION 2
PROGRAMME MANUAL / 2019
Neurodevelopmental Presentations Neuropsychology/ABI Principles of formulation and assessment Professional and ethical working Psychodynamic Theory Psychosis Reflective Practice Research Risk Assessment and Management Social Inclusion and Diversity Systemic Working Working in inpatient settings Overall structure The academic programme in Year 1 includes an Induction Block, providing an introduction to the programme as a whole, and key concepts and theories. Each year an event is scheduled during this time to enable new trainees to meet the other cohorts on the programme. The initial five-week teaching block aims to ensure that trainees are well-prepared academically for their first placement, normally in an Adult Mental Health, or Older Adult context. This block includes a half-day session scheduled for visiting the placement and meeting the clinical supervisor. Teaching continues on regular college days, one day per week, throughout the placement. Between the two first-year placements, another teaching block is scheduled, lasting three weeks. Academic days continue during the second placement, with an August break. Year 2 is structurally similar, with trainees undertaking either Child or Intellectual Disabilities placements, with an integrated academic programme supporting these. An initial 5-week block takes place in October, a further 3-week block in April, and additional weekly teaching days with a break in August. In Year 3, five one-week academic blocks are scheduled, covering a variety of topics, not necessarily linked to particular placements, but supporting the development of advanced knowledge and skills. In the first two years, teaching aims to support the incremental development of knowledge and skills that build core competencies relevant to all CP work. At the same time, the academic syllabus is structured around clients and services in line with clinical placements. Thus, in year one, core psychological theories and skills are introduced, while the bulk of service-specific teaching is designed to be relevant to adult and older adult placements. In year two teaching relevant to child and adolescent and intellectual disability placements is introduced. Towards the end of year one and onwards, teaching sessions relevant to more specialist services such as Health Clinical Psychology and Forensic Clinical Psychology are introduced, so that trainees are aware of the range of Clinical Psychology activities across the Health Service, which may influence their career or specialist placement choices. Therapeutic skills are also introduced incrementally. After an initial introduction to core therapeutic skills, CBT training commences at the start of year one and continues to year
63
SECTION 2
PROGRAMME MANUAL / 2019
three. Other approaches are introduced and developed in stages throughout training, with a particular focus on the development of skills in third wave therapies including Dialectical Behaviour Therapy and Acceptance and Commitment Therapy. The curriculum as a whole is underpinned by the principles of social inclusion and reflective practice, which are woven throughout the teaching. Regular, timetabled specific sessions on reflective practice encourage trainees to consider this across the training programme. Teaching is geared towards the needs of adult learners and includes a range of styles of delivery including lectures, seminars, demonstration and modelling of assessment and intervention strategies and role play and feedback. Strand Descriptors The following sections offer an overview of the content of each of the teaching strands. Whilst the aim is to portion teaching into topics that can be introduced and developed over the course of training by a core set of teachers, it is acknowledged that these topics are not entirely discreet, and there will be overlap in information covered across strands to some degree. Induction and NWCPP sessions This set of teaching sessions supports trainees through the processes and demands associated with their dual role as both a postgraduate student of Bangor University and an employee of the National Health Service. The start of training involves orientation to the academic and clinical processes as well as administrative procedures for completion of the doctoral programme. This includes sessions focused on preparation for supervision, provisions for personal and pastoral care, the role of British Psychological Society and Division of Clinical Psychology, as well attendance at Betsi Cadwaladr University Health Board orientation programme. Further sessions are offered to introduce trainees to their academic assignments, which include supportive information on how to produce work to a high standard as well as how to maximise their own learning through selection of topics. Core Therapeutic Skills The focus on this strand is on developing and maintaining therapeutic communication skills that are required not only to deliver structured therapies effectively but within clinical work more generally. The first two days of this strand are delivered consecutively early in year one by two counselling psychologists, with a focus on one to one clinical conversations. Further sessions across years one and two focus particularly on therapeutic and communication skills required for clinical work with, people with mild, moderate and profound intellectual disabilities multiple disabilities and young children. Attachment Adversity and Trauma At the very start of training, a strong emphasis is placed on understanding our clients in terms of their historical and current context, as well as how the psychological theories that we draw on in clinical work apply to all of us. To this end, an initial four days of teaching follows four life stories of individuals from pre-birth to the present day. Each of these individuals’ stories draw on the clinical experience of the teachers of this strand, who work across adult mental health, child and adolescent mental health, intellectual disability, older adult services and forensic services. There is a strong emphasis on the importance and
64
SECTION 2
PROGRAMME MANUAL / 2019
impact of common factors such as attachment experiences, development (including neurodevelopment), adverse childhood experiences and resilience. This four-day block can be very emotive and time is made for personal reflection and self-care throughout the week. The strand continues into year one and two, with the life-stories being reintroduced as trainees are taught ways of working with people with simple and complex trauma, personality disorders and those who have experienced childhood abuse and neglect. Teaching about CBT for PTSD is also included and thus provides an extension of the core CBT strand. Lifespan Perspectives This strand covers the importance and impact of common life events and issues as relevant to users of clinical psychology services. The teaching is delivered at times that are most appropriate to current placements. For example, in year one and start of year two, following an introduction to lifespan development, there is a focus on adults and older adults’ experiences of aging, grief and loss, sexuality and end of life. In year two, some of these topics are revisited from the perspective of children and young people with an additional focus on adolescence and emotional literacy development in children. Principles of assessment and formulation This strand begins before the start of any clinical placements, and follows on with further sessions throughout the first two years of training, where specialist assessment methods relevant to specific client groups are introduced in line with placement activity. Overall, trainees learn about all assessment methods including clinical interviews, standardised observations, informant interviews, psychometric testing and obtaining information from records. Drawing on psychological models, trainees learn about the principles and purpose of formulation and have the opportunity to practise assembling information from assessments to produce formulations in clinical work. Naturally, formulation teaching and practice also occurs in several other strands, particularly those focused on therapeutic approaches and clinical presentations. Therapies and clinical approaches Each of the strands below offer didactic teaching and skills-based workshops on the relevant therapeutic or clinical approach. Attention is given to the theoretical underpinnings of each, and is followed by opportunities to learn and practice skills within the teaching session. In many of these, teachers will demonstrate skills before asking trainees to try them out for themselves and reflect on their practice. Trainees are then encouraged to apply the models taught within their clinical placements, where they also have the opportunity to practice drawing on more than one model to inform their work with clients. Further detail of each of the strands is given below: Cognitive Behavioural Therapy (CBT) and Schema Therapy (ST) There are five full day CBT workshops during year one which cover the core principles of cognitive and behavioural approaches. Running alongside these workshops we offer additional sessions on the application of CBT with adults with a range of mental health difficulties including low mood and PTSD and the adaptations necessary when undertaking CBT with older people. During year one the trainees also take part in two full-day skills workshops in which they practice and receive feedback on the use of a number of core CBT
65
SECTION 2
PROGRAMME MANUAL / 2019
skills such as Socratic questioning. As part of these workshops, feedback is offered to the trainees by service user consultants. In year two there are workshops on the applications of CBT with children and young people and with people with an intellectual disability. During year three, there is a three-day workshop on Schema Therapy in which trainees have the opportunity to learn more about the theory underpinning Schema Therapy, key principles of the approach, and the opportunity to apply these principles through role-play and experiential exercises. Acceptance and Commitment Therapy (ACT) In year one, trainees are participants in a two-day ACT experiential workshop, where they learn how the principles of the approach apply to their own lives, as well as those of their clients. This is the standard way to start learning how to use ACT clinically. Six follow-on half day sessions take place during the rest of year one and year two, covering the core elements of the ACT ‘hexaflex’ model. In year three, two half-day ACT advanced sessions introduce trainees to different ways to apply the approach, and these sessions in particular are reviewed annually in order to select most recent developments in the field. Dialectical Behaviour Therapy In year two, trainees attend a five-day foundational training in DBT that covers all components of the treatment. This teaching is delivered alongside staff from the local health board who are also learning DBT. Teaching during this week is a mixture of didactic presentations, group discussions, demonstrations and role-play practices. Following this teaching, trainees have the opportunity to join DBT programmes on clinical placement. During years two and three, trainees have the opportunity to attend up to eight additional advanced teaching days on DBT delivered alongside practitioners delivering DBT within the local health board. In year three trainees receive a half-day session on Radically-Open DBT, a more recent evolution of the model. Compassion Focused Therapy The Compassion Focussed Therapy (CFT) strand aims to give trainees a strong grounding in the conceptual and theoretical basis of CFT. This includes formulation drawing on the CFT model, an overview of developments in compassionate care in organisations and the evidence base for the effectiveness of CFT. In addition, experiential training in core CFT strategies and interventions is offered, using practice with group work, and space for trainees to reflect on their own self-compassion. This is delivered as a three-day consecutive programme in the middle of the third year of training. This provides a helpful space to focus on the approach, and to practise in between sessions. Many trainees report that the approach fits well for them at this point in training, in that it integrates concepts and strategies from other approaches around a straightforward but powerful explanatory model. Functional Analysis This strand introduces trainees to the application of behaviour analytic theory and functional analysis to clinical practice. The principles are demonstrated and taught largely from the perspective of intellectual disability services, which allows for a better understanding of challenging behaviours and the importance of values and ethics when working with staff teams. The strand is delivered in year two as a week-long block, to map
66

SECTION 2
PROGRAMME MANUAL / 2019
onto intellectual disability placements, but includes reflection on the relevance of behaviour analysis to therapeutic work with adults, older adults and children, with particular emphasis on the behavioural underpinnings of third wave therapies. By the end of the teaching, trainees are able to carry out functional analysis interviews, formulate from a behaviour analytic perspective and begin to develop interventions based on functional analysis. Mindfulness As mindfulness underpins each of the third-wave therapies, trainees are introduced to the subject experientially through an 8-week course delivered by a teacher from the Centre for Mindfulness Research and Practice. Subsequently there are three workshops, one in each of the three years of training covering key topics including theories of mindfulness, the evidence-base underpinning it, learning how to guide mindfulness practices and the clinical applications of these. Reflection on trainees’ experience of their on-going mindfulness practice forms part of each workshop. Psychodynamic Theory This strand provides trainees with an introduction to psychodynamic thinking and therapy. This includes a necessarily very broad overview of the development of psychodynamic thought and practice. This teaching strand also looks in more detail at some core concepts of psychodynamic therapy, such as: the nature of psychological distress; the tripartite psyche; defences – both their nature and function; importance of the relationship and process in psychodynamic therapy; transference and countertransference; and resistance. Time is also given to explore ways to bring psychodynamic thinking into multi-perspective psychological formulation. Finally, this strand of teaching focuses upon the development and practice of short-term dynamic psychotherapies, in particular Intensive Short-Term Dynamic Psychotherapy, including teaching on formulation and techniques.
Clinical Presentations Anxiety Low Mood Eating Disorders Neurodevelopmental Presentations There are four short teaching strands covering some of the most common clinical presentations that trainees will encounter during their placements; anxiety, low mood, eating disorders and neurodevelopmental presentations. Teaching for each of these follows a similar structure, beginning in year one with understanding diagnostic classifications, theoretical models, assessments, formulations and ways of working with adults and older adults presenting with these problems. For anxiety and low mood, these sessions are also an extension of the CBT strand, offering trainees opportunities to learn about and practice disorder- specific models of CBT. In year two each topic is revisited and trainees learn more about differences in presentations and ways of working with children, young people, and people with intellectual disabilities. Psychosis
67
SECTION 2
PROGRAMME MANUAL / 2019
The psychosis strand comprises three consecutive full days of teaching and aims to give trainees a well-grounded, psychologically informed understanding of psychosis and psychotic disorders, some hands-on practice with core therapeutic strategies, and some direct experience of service users with psychosis. As well as informing trainees and offering them some therapeutic tools, the teaching challenges some cultural assumptions about people with psychosis and their suitability for therapy. The first day covers the conceptualisation of psychosis within alternative explanatory frameworks; the epidemiology and outcomes; and the social, cultural and political contexts of psychosis and psychotic disorders. This is followed by a focus on explanatory theories for psychotic disorders, covering a range of biopsychosocial explanations, with an emphasis on broadly cognitive theory. The second day covers CBT for psychosis (CBTp), third wave developments including ACT and CFT, and adventure therapy. This workshop style session gives an experiential grounding in how CBTp develops from more conventional CBT. The third day involves a session of conversations with service users about their experiences of psychosis and mental health services. This can be an intense and moving experience for everyone involved, and it is usually the highlight of the strand for most of the trainees. The final session focusses on early intervention and working with At Risk Mental States, and it provides a reflective space to integrate the different elements of the strand. Dementia Towards the start of year one, as a single block of teaching that takes place during the course of almost a week, trainees are taken through the journey of a person who is being diagnosed with a dementia syndrome. The teaching is delivered by several clinical psychologists working in older adult services, as well as a family member of a person with dementia and a medical colleague. Person-centred care is at the heart of the teaching sessions, which cover: a range of assessment procedures that contribute to the diagnostic process, the sharing of the diagnosis, the psychological support and interventions that can be offered post diagnosis to both the person with dementia as well as their family, and the ways of working with the person as their condition deteriorates, behaviours become more challenging, and where care is transferred into staff in care settings. Further teaching in year one and year two follows on, covering dementia as it presents in younger people and for people with intellectual disabilities. Working in inpatient settings. Sessions take place across all three years of training looking at the different aspects of working psychologically in inpatient settings for young adults, adults, older adults, people with dementia, and people who have had strokes. The teaching is provided by a combination of clinical psychologists who are working across these different services. In year one, the emphasis is on the inpatient journey, including inpatient assessments and interventions. In year two, indirect working through others, and attending to the emotional needs of the team are the main focus. In year three, the emphasis is on leadership and consultation within inpatient settings, including cultural change. An underlying theme used for this teaching strand is the yellow brick road: where trainees need heart, courage, brain and curiosity to undertake this work. Forensic Clinical Psychology
68
SECTION 2
PROGRAMME MANUAL / 2019
This strand is delivered primarily by clinical psychologists working in medium secure hospitals and enables trainees to understand how clinical psychology skills are applied to clients who are involved in the criminal justice system, and to groups of staff working in these areas. As forensic placements are not a part of core training, this teaching starts in year two, as trainees are developing their ability to apply core competencies across a variety of settings. The teaching gives an overview of presenting problems, assessment, formulation and interventions commonly used in forensic services. There are opportunities for case discussions and some of the teaching takes in a medium secure hospital, which enables trainees to better understand the context of the work. Health Clinical Psychology As a growing and important area of practice for clinical psychologists in North Wales, trainees are introduced to ways of working and underpinning competencies of health clinical psychology in year one. Following on from this, further sessions take place across all three years of training covering key clinical areas such as pain management, chronic fatigue, renal failure, psycho-oncology, diabetes, obesity and medically unexplained symptoms. Teaching is planned and delivered by clinical psychologists working in both adult and paediatric settings, other members of multi-disciplinary teams, service users and carers. The focus is on the specialist skills and knowledge required to work in physical health settings in close liaison with medical teams. Neuropsychology/ABI This strand teaches trainees the core skills required to carry out neuropsychological assessments, as well as an introduction to the work of a clinical psychologists in acquired brain injury services. In year one, trainees develop the basic skills necessary to perform a clinical assessment of people with suspected acquired brain injury, which equips them with the ability to identify patients who need formal neuropsychological testing or other neuropsychology/neuroscience input. The teaching covers neuroanatomy, neuropathology, bedside cognitive assessments and mental state examination. In year two further teaching builds on this initial knowledge with a focus on its application to children. As part of this strand, trainees are taught to accurately administer and interpret the Wechsler Adult Intelligence Scale and Wechsler Intelligence Scale for Children. Leadership Trainees are offered the opportunity to complete the Level 5 Award of the Institute of Leadership and Management and all trainees experience teaching to support this qualification, and additional teaching on leadership skills. This includes sessions on theories of leadership, mentoring coaching and supervision, service improvement, working in legal systems and advanced presentation skills. The aim is to support trainees to take up leadership experiences on placement, and more importantly to be ready to be engaged in leadership activities once they are qualified. Professional and ethical working At the start of training this strand begins with the foundations of professional and ethical working, including an overview of HCPC standards of conduct performance and ethics, Guidance on conduct and ethics for students and BPS code of conduct and ethics. These
69
SECTION 2
PROGRAMME MANUAL / 2019
important documents are made real by discussion of clinical scenarios involving ethical dilemmas. The teaching strand continues in a similar vein with the introduction of legal frameworks, local policy and guidelines that inform clinical practice across specialisms. Reflective Practice Set within the teaching timetable, and following an introductory session at the start of year one, each cohort of trainees meets three times a year with two clinical psychologists from the health board, where reflection on their experiences of clinical training is facilitated. Each of these sessions is one and a half hours long and the same facilitators stay with the cohort over the three years of training. The key aim of these sessions is to develop and maintain a safe opportunity for trainees to explore their own strengths and challenges as trainees, and to develop the habit of skilled reflective practice to take forward into their careers once qualified. Research The research strand closely supports the research assignments required during the programme. Delivered by the NWCPP research team, these sessions allow for the acquisition of knowledge and skills regarding research design, a range of methodologies and related analyses, including the theoretical underpinnings, strengths and common criticisms of each. Trainees are given the opportunity to consider the underlying epistemologies of qualitative and quantitative methods, and to consider how these are applicable to their coursework, including their Research Projects. At the start of the programme the teaching focus is on skills required to understand and carry out statistical analyses, which is applied using large data sets for their data analytic project. This focus is intended to be a supportive process to build an early confidence in an area of research practice that some new trainees feel particularly nervous about. As the programme progresses, there is an ongoing focus on specific quantitative and qualitative approaches and their limitations, and the critical evaluation of research findings. Underlying ethical issues, the research permissions process, and good clinical practice in research are covered with colleagues from our Research and Development group. We go on to cover literature search methods, meta-analyses, systematic and narrative literature reviews and research quality assessment. By the end of the programme, each trainee is equipped with the knowledge to critically evaluate, synthesise and disseminate existing research and to understand the importance of these skills as qualified applied scientists. Final year trainees will also have the skills and experience to carry out evaluations and original research in response to the needs of their workplace and to the demands for knowledge advancement in the profession. Risk Assessment and Management The risk assessment and management strand ensures that trainees are proficient at considering, assessing and managing risks that may arise during their clinical work, and to understand how risk issues can be formulated in isolation or embedded within clinical formulations. Teaching includes and extends mandatory risk training required by the health board, covering risk across the lifespan including risk from others, risks posed to the self and to others. Particular focus is given to suicidality as it presents in all specialisms, as this can be one of the most challenging situations for trainees to manage whilst on placements.
70
SECTION 2
PROGRAMME MANUAL / 2019
Social Inclusion and Diversity Within this strand there is the equivalent of nine full days of teaching in which trainees are encouraged to identify key psychological and sociological theories that help us to understand processes such as social exclusion and stigmatisation, and to consider how these processes impact on the individuals and communities that we work with. There is a full day workshop providing an overview of the many ways in which cultural factors may impact on the practice of clinical psychology. Trainees are encouraged to identify and reflect on their own values and biases and to consider how we can work in more culturally responsive ways. Given the geographical location of the programme within North Wales, it is important for trainees to increase their understanding of Welsh language and culture. There are workshops in each year of the programme covering topics relating to working in Wales and trainees are encouraged to reflect on their personal experiences of working in this context. Within the strand there is a strong focus on building relationships with people with lived experience of using human services and understanding more about these experiences and the implications for working effectively as a clinical psychologist There is also an emphasis on the development of strategies to communicate effectively with people from a range of backgrounds through sessions on working with interpreters and working with people who are deaf. Systemic Working There is an increasing need for clinical psychologists to apply their knowledge and skills to working with wider systems that influence the wellbeing and outcomes of service users. This strand includes an introduction to systemic family therapy, along with sessions covering other ways of working effectively with systems. Wider systems include parents, carers, clinical teams and other agencies who hold influence over individual service users. The sessions begin in year one when trainees are introduced to ways of working with systems that influence older adult clients. In year two the focus turns to working with parents, families and other agencies, particularly relevant in child and intellectual disability services. In year three trainees are introduced to more advanced consultation skills including consultancy to organisations.
71
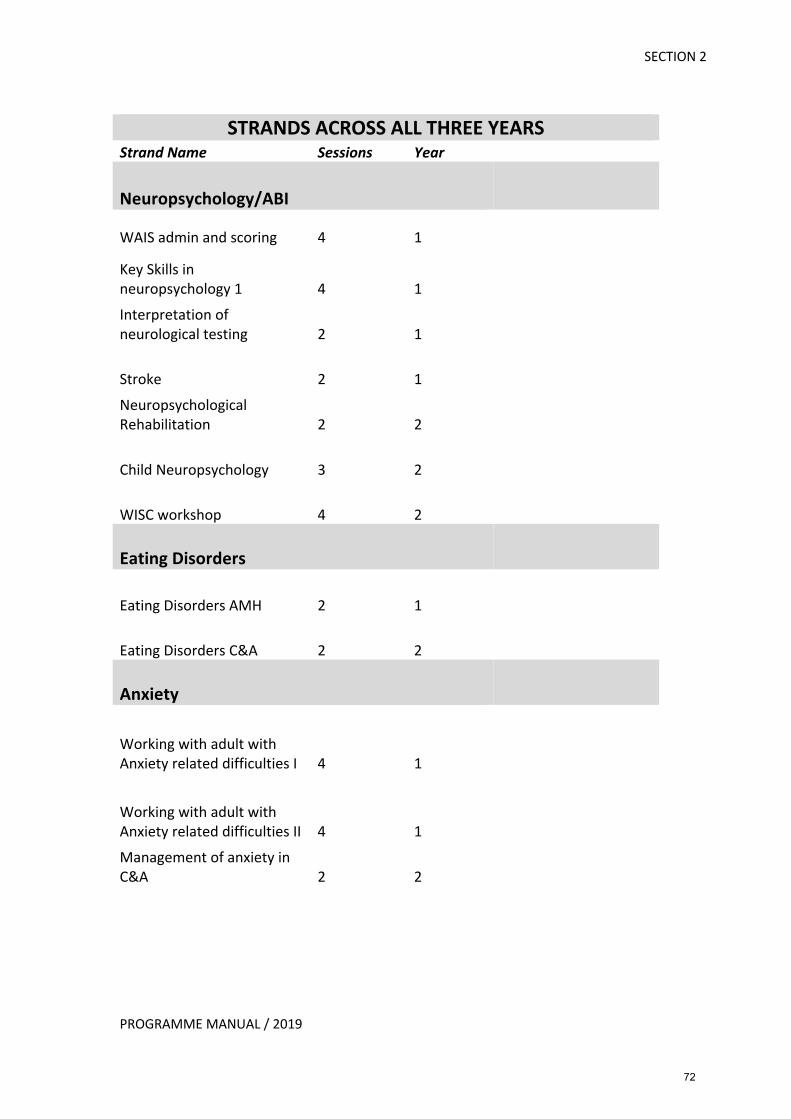
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Neuropsychology/ABI
WAIS admin and scoring 4 1
Key Skills in neuropsychology 1 4 1 Interpretation of neurological testing 2 1
Stroke 2 1 Neuropsychological Rehabilitation 2 2
Child Neuropsychology 3 2
WISC workshop 4 2
Eating Disorders
Eating Disorders AMH 2 1
Eating Disorders C&A 2 2
Anxiety
Working with adult with Anxiety related difficulties I 4 1
Working with adult with Anxiety related difficulties II 4 1 Management of anxiety in C&A 2 2
72
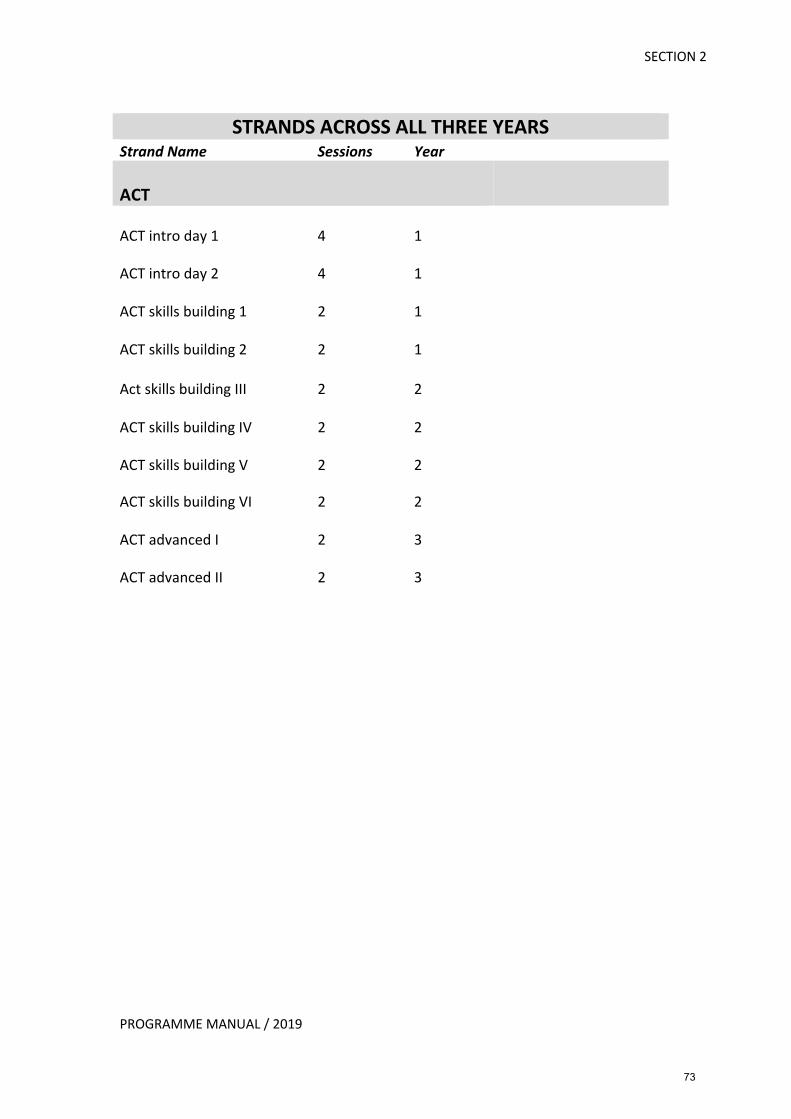
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
ACT
ACT intro day 1 4 1
ACT intro day 2 4 1
ACT skills building 1 2 1
ACT skills building 2 2 1
Act skills building III 2 2
ACT skills building IV 2 2
ACT skills building V 2 2
ACT skills building VI 2 2
ACT advanced I 2 3
ACT advanced II 2 3
73
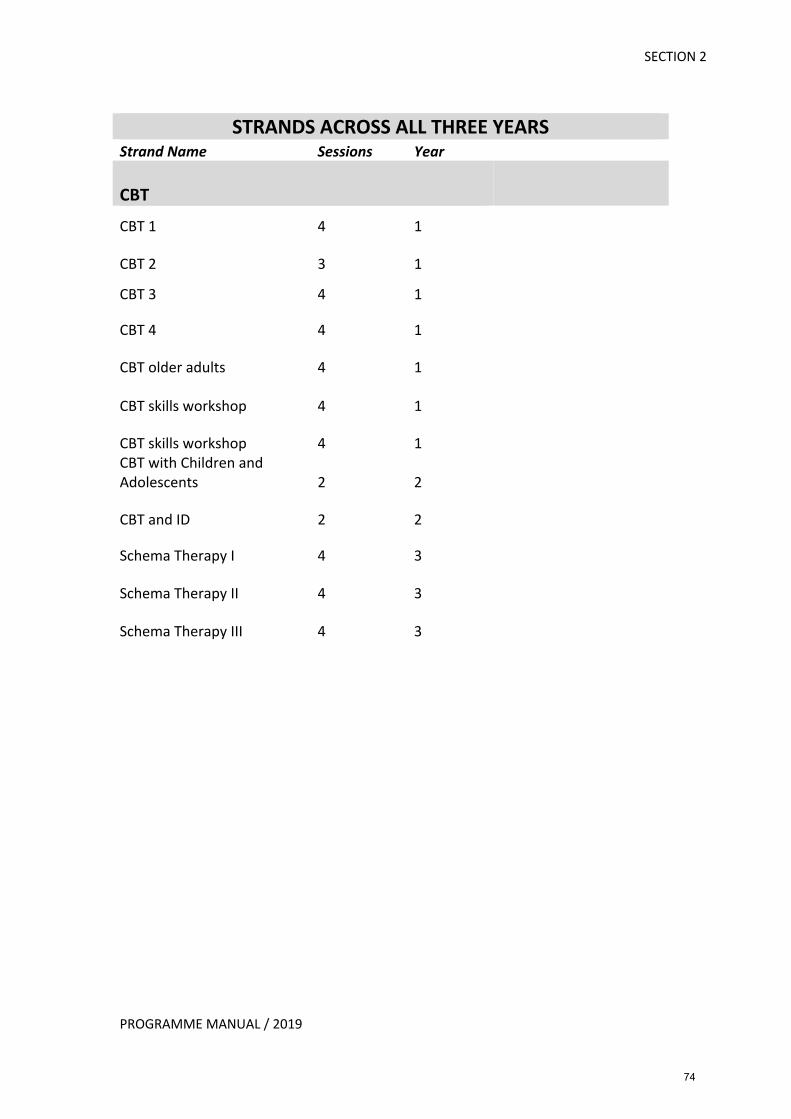
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
CBT CBT 1 4 1
CBT 2 3 1
CBT 3 4 1
CBT 4 4 1
CBT older adults 4 1
CBT skills workshop 4 1
CBT skills workshop 4 1 CBT with Children and Adolescents 2 2
CBT and ID 2 2
Schema Therapy I 4 3
Schema Therapy II 4 3
Schema Therapy III 4 3
74
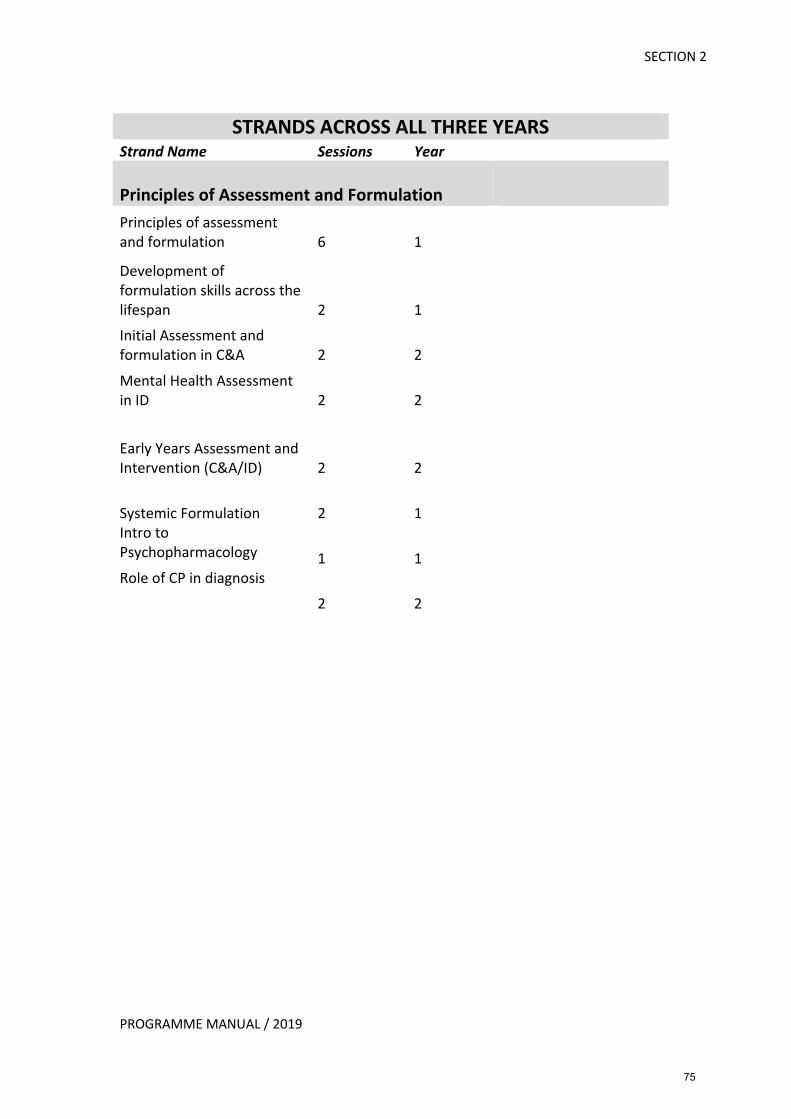
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Principles of Assessment and Formulation Principles of assessment and formulation 6 1 Development of formulation skills across the lifespan 2 1 Initial Assessment and formulation in C&A 2 2 Mental Health Assessment in ID 2 2
Early Years Assessment and Intervention (C&A/ID) 2 2
Systemic Formulation 2 1 Intro to Psychopharmacology 1 1 Role of CP in diagnosis
2 2
75
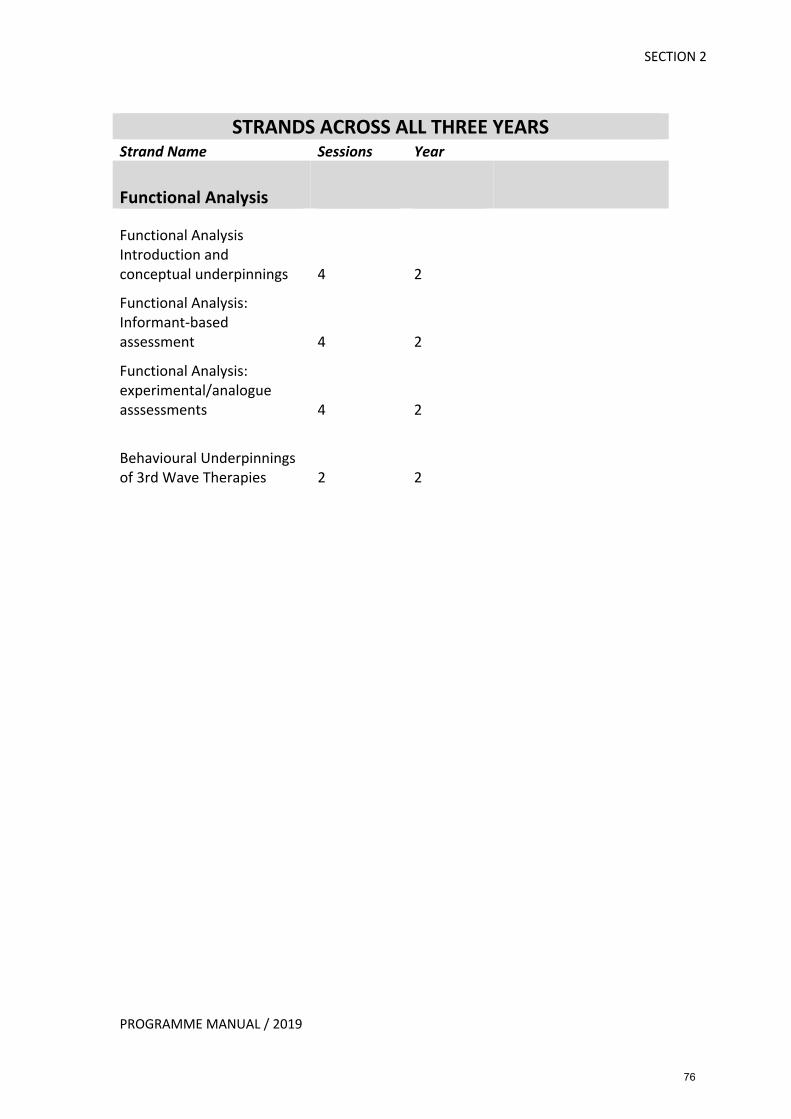
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Functional Analysis
Functional Analysis Introduction and conceptual underpinnings 4 2 Functional Analysis: Informant-based assessment 4 2 Functional Analysis: experimental/analogue asssessments 4 2
Behavioural Underpinnings of 3rd Wave Therapies 2 2
76
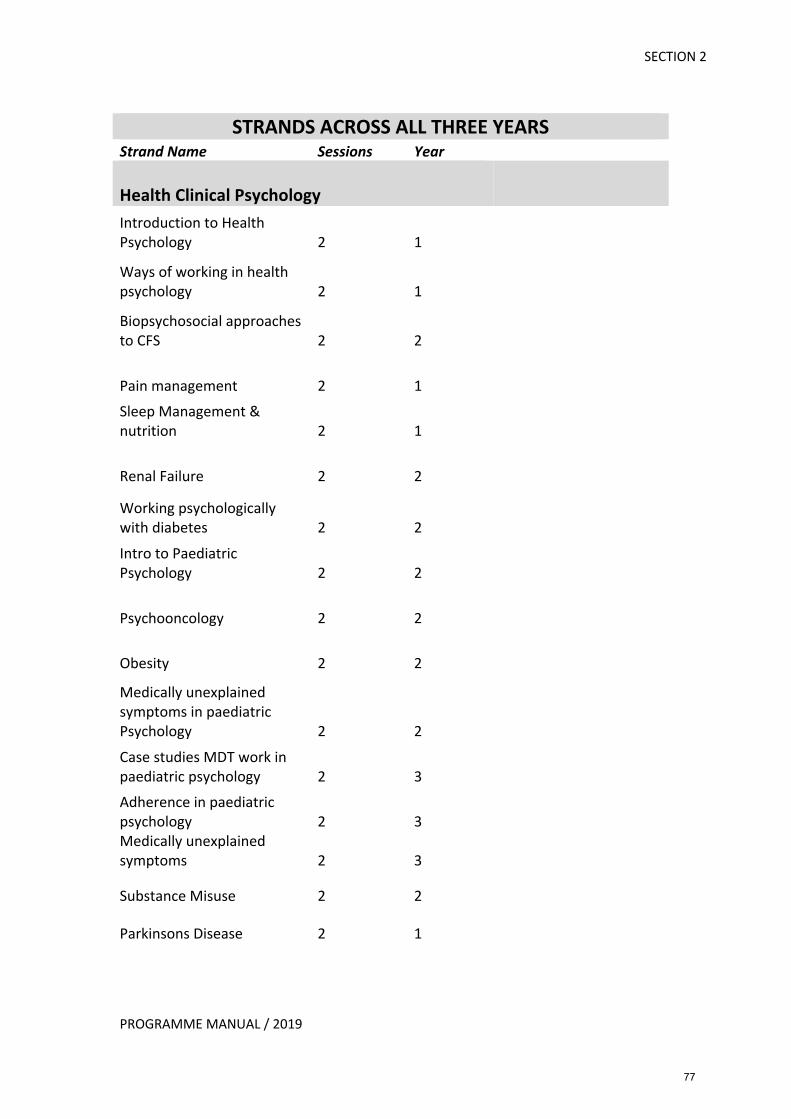
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year Health Clinical Psychology Introduction to Health Psychology 2 1
Ways of working in health psychology 2 1
Biopsychosocial approaches to CFS 2 2
Pain management 2 1 Sleep Management & nutrition 2 1
Renal Failure 2 2
Working psychologically with diabetes 2 2 Intro to Paediatric Psychology 2 2
Psychooncology 2 2
Obesity 2 2 Medically unexplained symptoms in paediatric Psychology 2 2 Case studies MDT work in paediatric psychology 2 3 Adherence in paediatric psychology 2 3 Medically unexplained symptoms 2 3
Substance Misuse 2 2
Parkinsons Disease 2 1
77
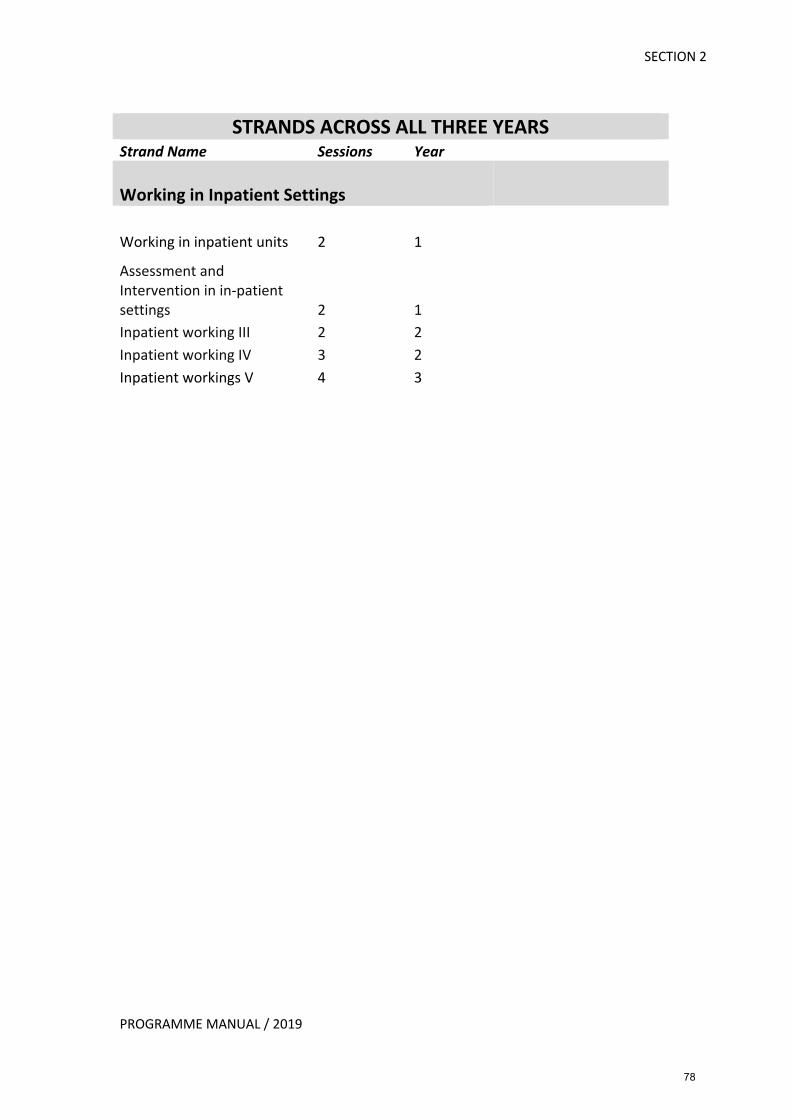
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Working in Inpatient Settings
Working in inpatient units 2 1 Assessment and Intervention in in-patient settings 2 1 Inpatient working III 2 2 Inpatient working IV 3 2 Inpatient workings V 4 3
78
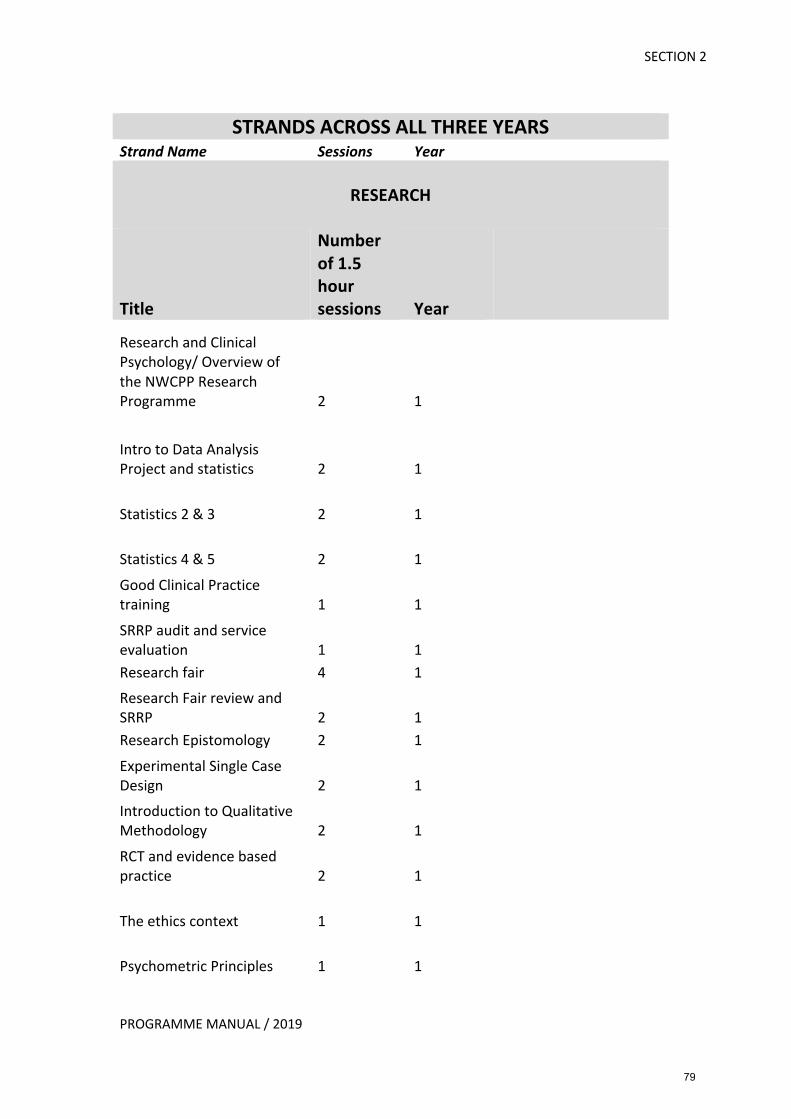
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
RESEARCH
Title
Number of 1.5 hour sessions Year
Research and Clinical Psychology/ Overview of the NWCPP Research Programme 2 1
Intro to Data Analysis Project and statistics 2 1
Statistics 2 & 3 2 1
Statistics 4 & 5 2 1 Good Clinical Practice training 1 1 SRRP audit and service evaluation 1 1 Research fair 4 1 Research Fair review and SRRP 2 1 Research Epistomology 2 1 Experimental Single Case Design 2 1 Introduction to Qualitative Methodology 2 1 RCT and evidence based practice 2 1
The ethics context 1 1
Psychometric Principles 1 1
79
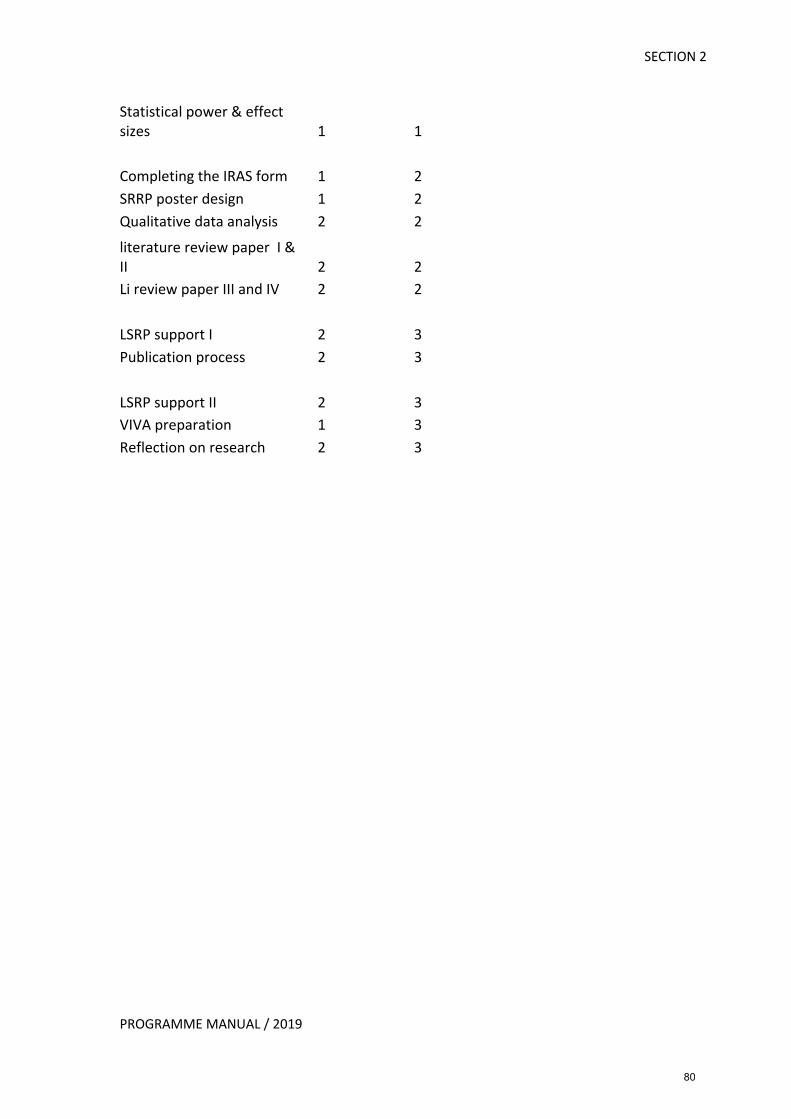
SECTION 2
PROGRAMME MANUAL / 2019
Statistical power & effect sizes 1 1
Completing the IRAS form 1 2 SRRP poster design 1 2 Qualitative data analysis 2 2 literature review paper I & II 2 2 Li review paper III and IV 2 2
LSRP support I 2 3 Publication process 2 3
LSRP support II 2 3 VIVA preparation 1 3 Reflection on research 2 3
80
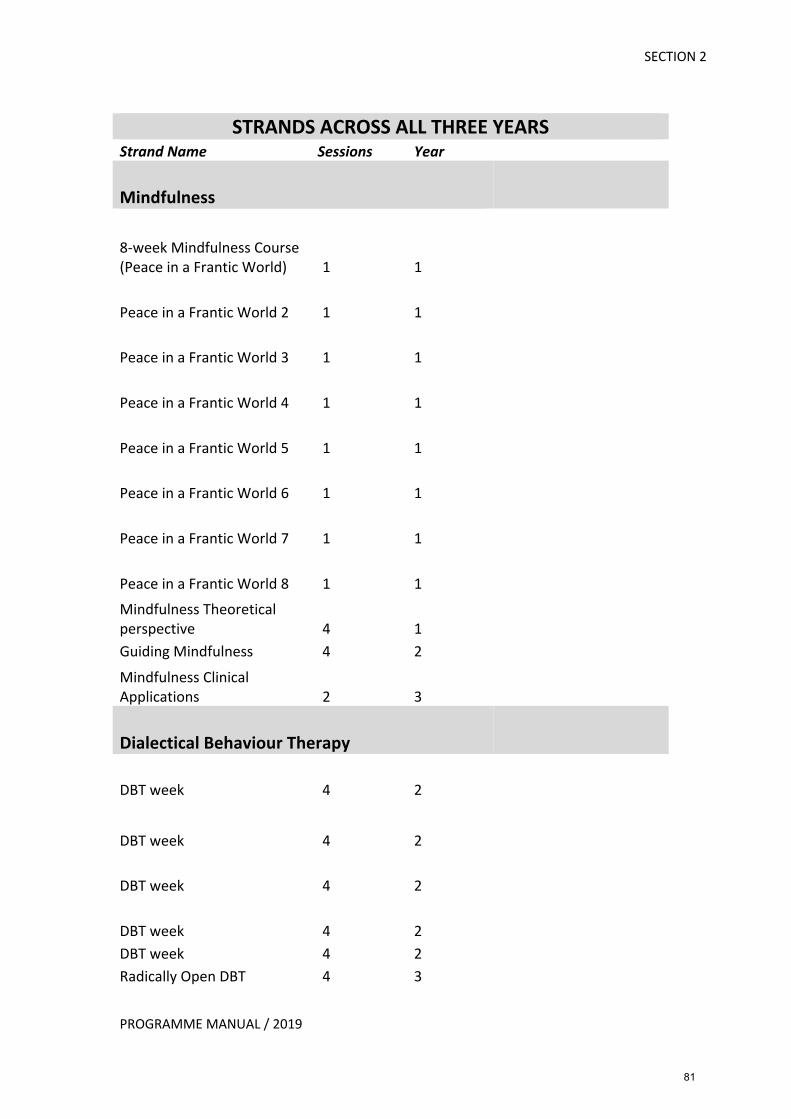
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Mindfulness
8-week Mindfulness Course (Peace in a Frantic World) 1 1
Peace in a Frantic World 2 1 1
Peace in a Frantic World 3 1 1
Peace in a Frantic World 4 1 1
Peace in a Frantic World 5 1 1
Peace in a Frantic World 6 1 1
Peace in a Frantic World 7 1 1
Peace in a Frantic World 8 1 1 Mindfulness Theoretical perspective 4 1 Guiding Mindfulness 4 2 Mindfulness Clinical Applications 2 3
Dialectical Behaviour Therapy
DBT week 4 2
DBT week 4 2
DBT week 4 2
DBT week 4 2 DBT week 4 2 Radically Open DBT 4 3
81
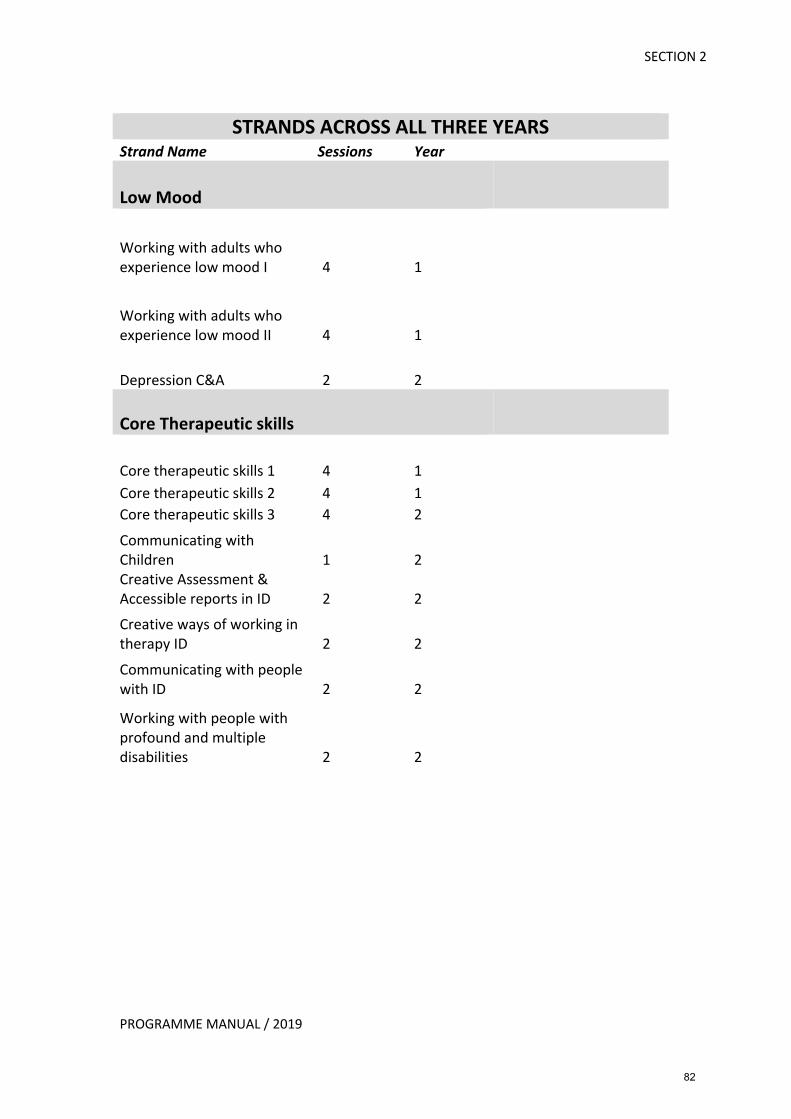
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Low Mood
Working with adults who experience low mood I 4 1
Working with adults who experience low mood II 4 1
Depression C&A 2 2
Core Therapeutic skills
Core therapeutic skills 1 4 1 Core therapeutic skills 2 4 1 Core therapeutic skills 3 4 2 Communicating with Children 1 2 Creative Assessment & Accessible reports in ID 2 2 Creative ways of working in therapy ID 2 2 Communicating with people with ID 2 2 Working with people with profound and multiple disabilities 2 2
82
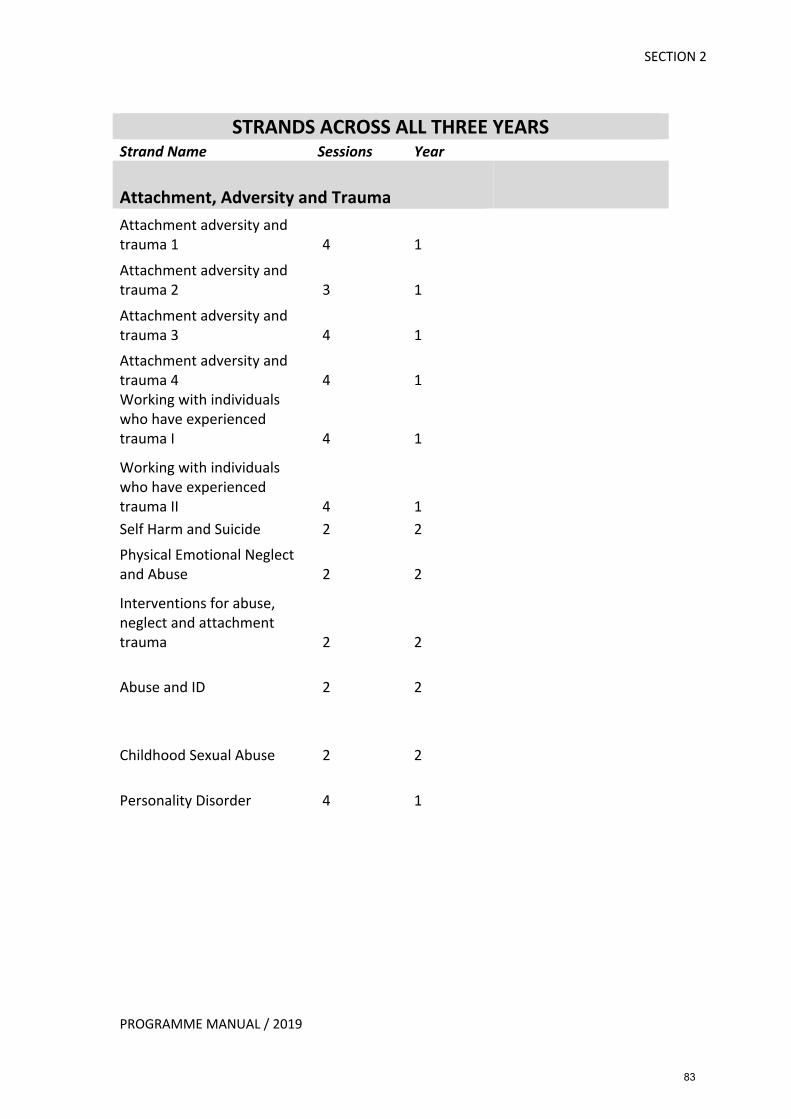
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Attachment, Adversity and Trauma Attachment adversity and trauma 1 4 1 Attachment adversity and trauma 2 3 1 Attachment adversity and trauma 3 4 1 Attachment adversity and trauma 4 4 1 Working with individuals who have experienced trauma I 4 1 Working with individuals who have experienced trauma II 4 1 Self Harm and Suicide 2 2 Physical Emotional Neglect and Abuse 2 2 Interventions for abuse, neglect and attachment trauma 2 2
Abuse and ID 2 2
Childhood Sexual Abuse 2 2
Personality Disorder 4 1
83
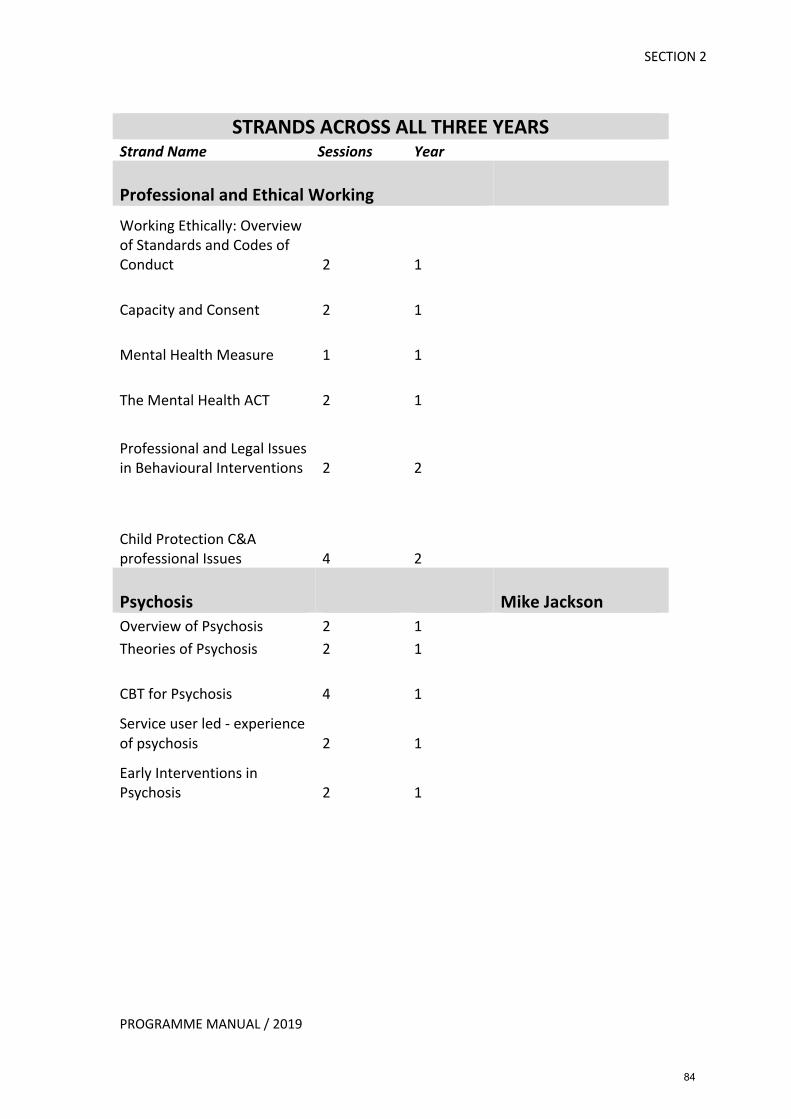
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Professional and Ethical Working Working Ethically: Overview of Standards and Codes of Conduct 2 1
Capacity and Consent 2 1
Mental Health Measure 1 1
The Mental Health ACT 2 1
Professional and Legal Issues in Behavioural Interventions 2 2
Child Protection C&A professional Issues 4 2
Psychosis Mike Jackson Overview of Psychosis 2 1 Theories of Psychosis 2 1
CBT for Psychosis 4 1
Service user led - experience of psychosis 2 1
Early Interventions in Psychosis 2 1
84
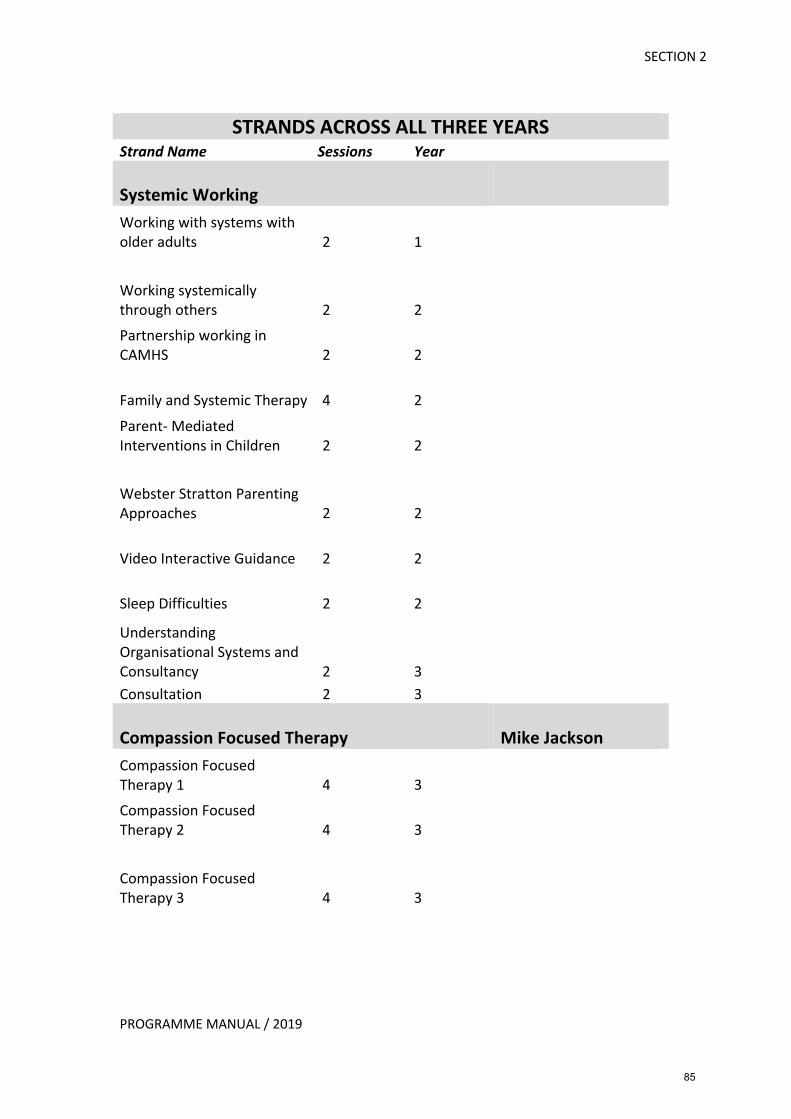
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Systemic Working Working with systems with older adults 2 1
Working systemically through others 2 2 Partnership working in CAMHS 2 2
Family and Systemic Therapy 4 2 Parent- Mediated Interventions in Children 2 2
Webster Stratton Parenting Approaches 2 2
Video Interactive Guidance 2 2
Sleep Difficulties 2 2 Understanding Organisational Systems and Consultancy 2 3 Consultation 2 3 Compassion Focused Therapy Mike Jackson Compassion Focused Therapy 1 4 3 Compassion Focused Therapy 2 4 3
Compassion Focused Therapy 3 4 3
85
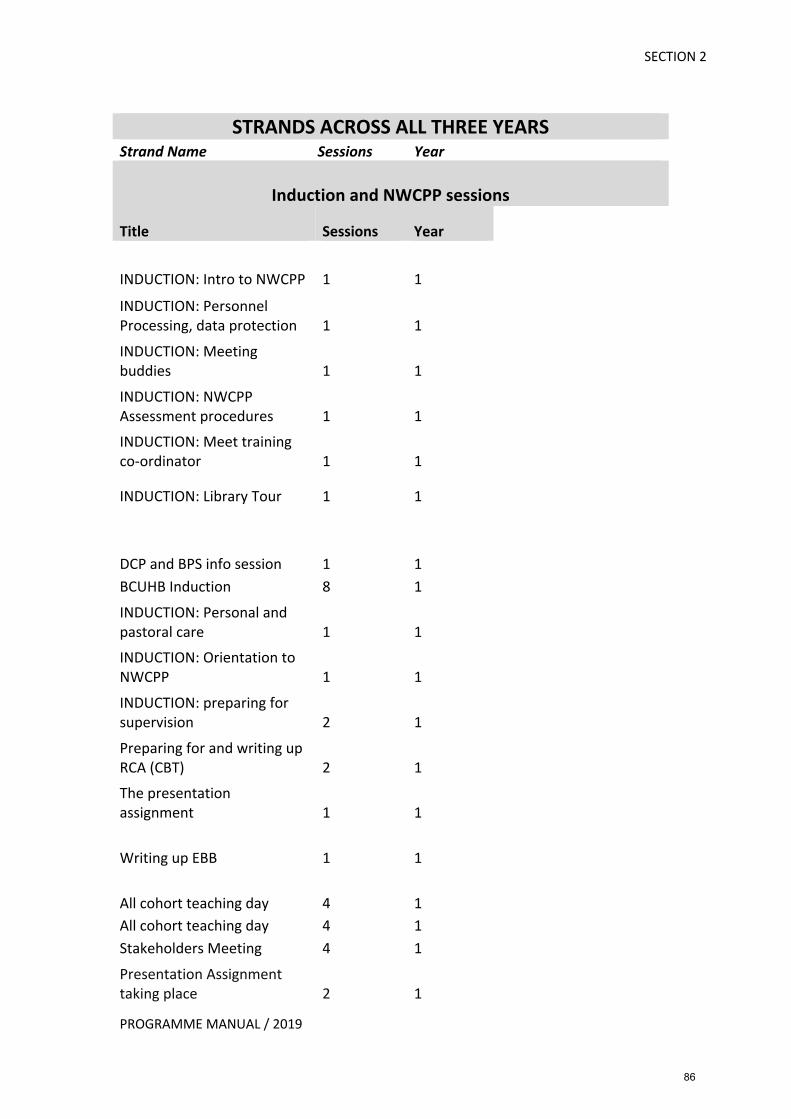
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Induction and NWCPP sessions
Title Sessions Year
INDUCTION: Intro to NWCPP 1 1 INDUCTION: Personnel Processing, data protection 1 1 INDUCTION: Meeting buddies 1 1 INDUCTION: NWCPP Assessment procedures 1 1 INDUCTION: Meet training co-ordinator 1 1
INDUCTION: Library Tour 1 1
DCP and BPS info session 1 1 BCUHB Induction 8 1 INDUCTION: Personal and pastoral care 1 1 INDUCTION: Orientation to NWCPP 1 1 INDUCTION: preparing for supervision 2 1 Preparing for and writing up RCA (CBT) 2 1 The presentation assignment 1 1
Writing up EBB 1 1
All cohort teaching day 4 1 All cohort teaching day 4 1 Stakeholders Meeting 4 1 Presentation Assignment taking place 2 1
86
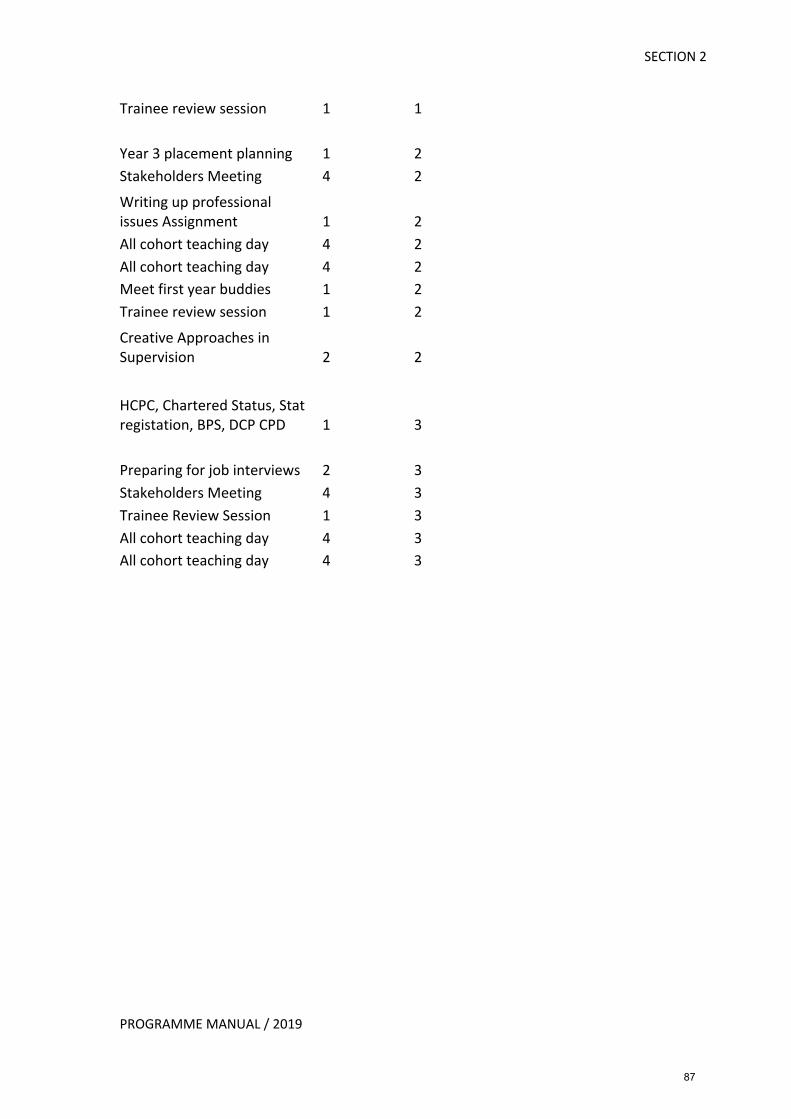
SECTION 2
PROGRAMME MANUAL / 2019
Trainee review session 1 1
Year 3 placement planning 1 2 Stakeholders Meeting 4 2 Writing up professional issues Assignment 1 2 All cohort teaching day 4 2 All cohort teaching day 4 2 Meet first year buddies 1 2 Trainee review session 1 2 Creative Approaches in Supervision 2 2
HCPC, Chartered Status, Stat registation, BPS, DCP CPD 1 3
Preparing for job interviews 2 3 Stakeholders Meeting 4 3 Trainee Review Session 1 3 All cohort teaching day 4 3 All cohort teaching day 4 3
87
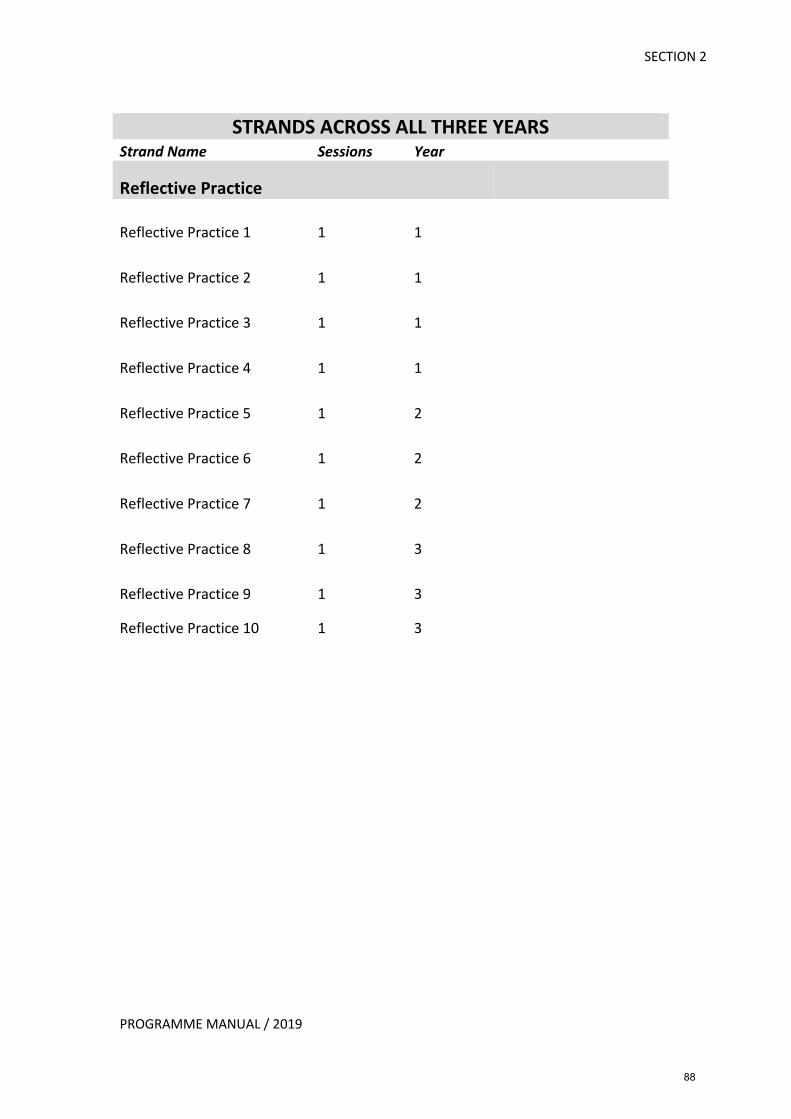
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Reflective Practice
Reflective Practice 1 1 1
Reflective Practice 2 1 1
Reflective Practice 3 1 1
Reflective Practice 4 1 1
Reflective Practice 5 1 2
Reflective Practice 6 1 2
Reflective Practice 7 1 2
Reflective Practice 8 1 3
Reflective Practice 9 1 3
Reflective Practice 10 1 3
88
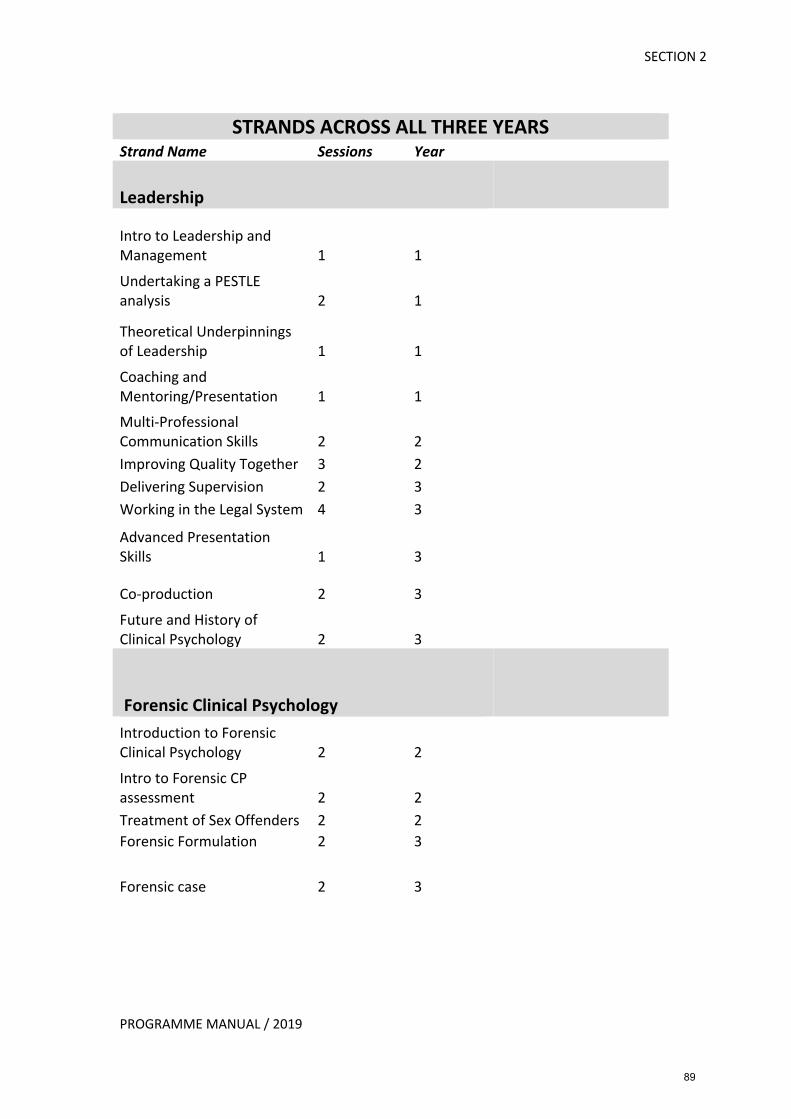
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Leadership
Intro to Leadership and Management 1 1 Undertaking a PESTLE analysis 2 1
Theoretical Underpinnings of Leadership 1 1 Coaching and Mentoring/Presentation 1 1 Multi-Professional Communication Skills 2 2 Improving Quality Together 3 2 Delivering Supervision 2 3 Working in the Legal System 4 3 Advanced Presentation Skills 1 3
Co-production 2 3 Future and History of Clinical Psychology 2 3
Forensic Clinical Psychology Introduction to Forensic Clinical Psychology 2 2 Intro to Forensic CP assessment 2 2 Treatment of Sex Offenders 2 2 Forensic Formulation 2 3
Forensic case 2 3
89
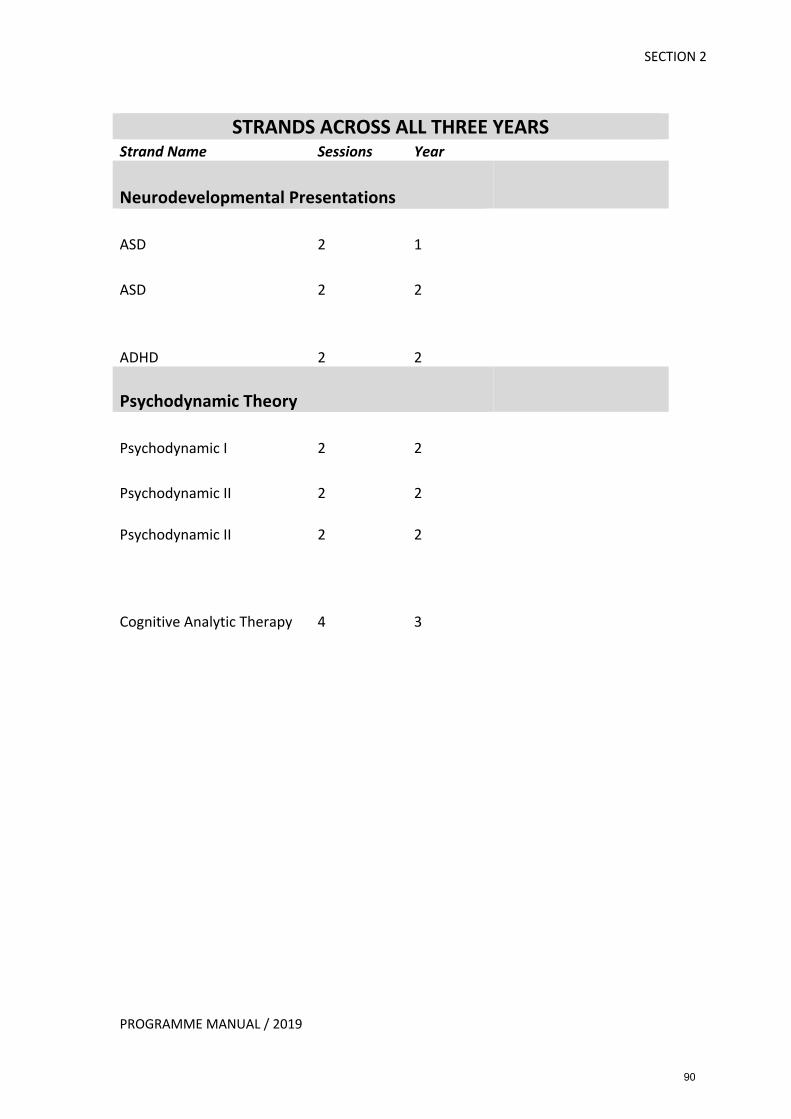
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Neurodevelopmental Presentations
ASD 2 1
ASD 2 2
ADHD 2 2
Psychodynamic Theory
Psychodynamic I 2 2
Psychodynamic II 2 2
Psychodynamic II 2 2
Cognitive Analytic Therapy 4 3
90
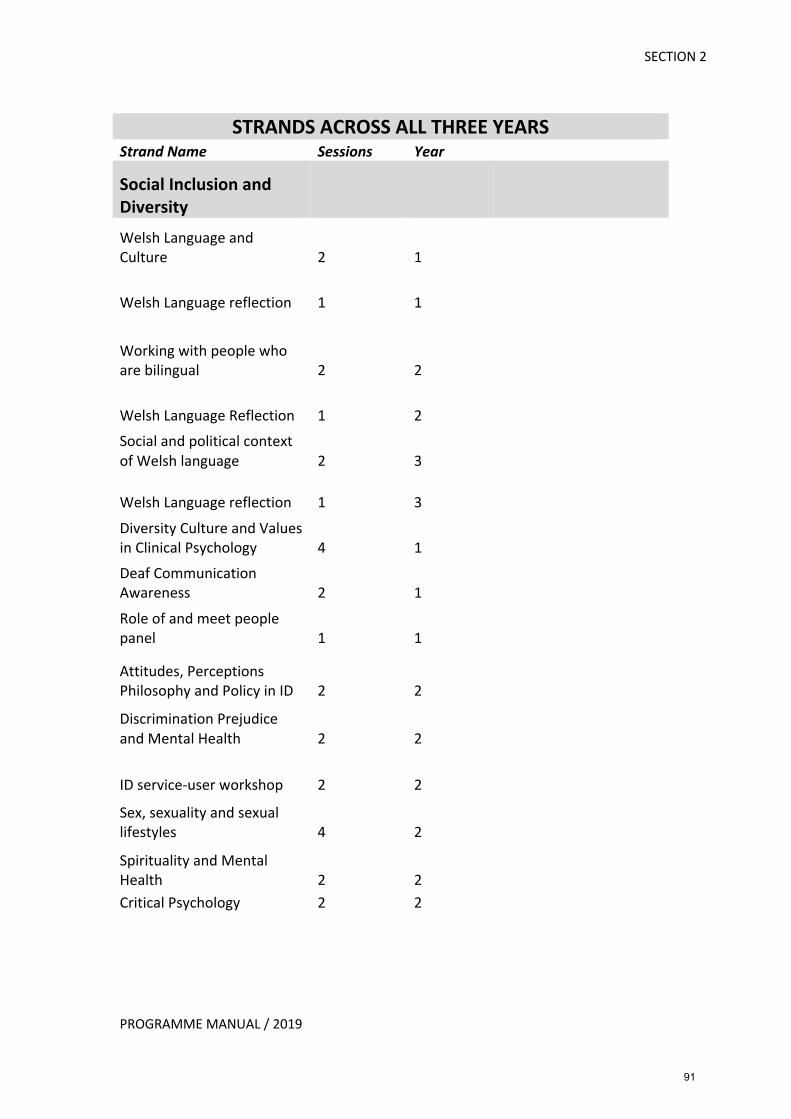
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Social Inclusion and Diversity Welsh Language and Culture 2 1
Welsh Language reflection 1 1
Working with people who are bilingual 2 2
Welsh Language Reflection 1 2 Social and political context of Welsh language 2 3
Welsh Language reflection 1 3 Diversity Culture and Values in Clinical Psychology 4 1 Deaf Communication Awareness 2 1 Role of and meet people panel 1 1
Attitudes, Perceptions Philosophy and Policy in ID 2 2 Discrimination Prejudice and Mental Health 2 2
ID service-user workshop 2 2 Sex, sexuality and sexual lifestyles 4 2 Spirituality and Mental Health 2 2 Critical Psychology 2 2
91
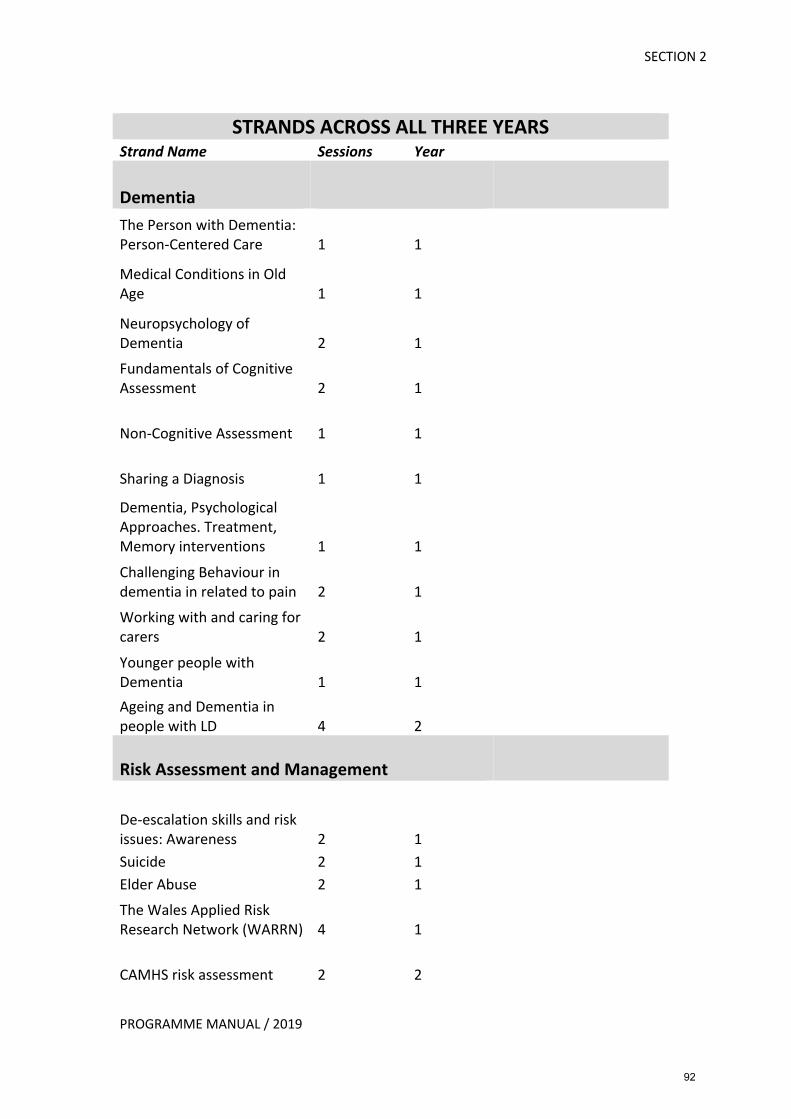
SECTION 2
PROGRAMME MANUAL / 2019
STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Dementia The Person with Dementia: Person-Centered Care 1 1
Medical Conditions in Old Age 1 1
Neuropsychology of Dementia 2 1 Fundamentals of Cognitive Assessment 2 1
Non-Cognitive Assessment 1 1
Sharing a Diagnosis 1 1 Dementia, Psychological Approaches. Treatment, Memory interventions 1 1 Challenging Behaviour in dementia in related to pain 2 1 Working with and caring for carers 2 1 Younger people with Dementia 1 1 Ageing and Dementia in people with LD 4 2
Risk Assessment and Management
De-escalation skills and risk issues: Awareness 2 1 Suicide 2 1 Elder Abuse 2 1 The Wales Applied Risk Research Network (WARRN) 4 1
CAMHS risk assessment 2 2
92
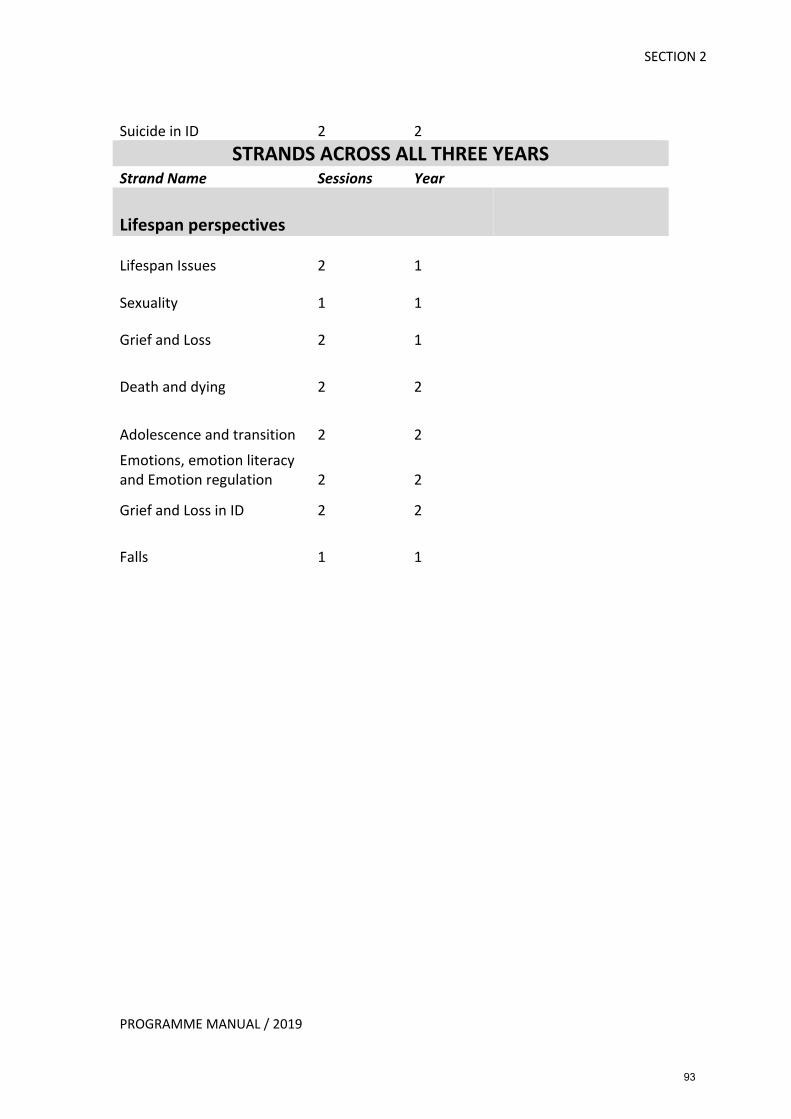
SECTION 2
PROGRAMME MANUAL / 2019
Suicide in ID 2 2 STRANDS ACROSS ALL THREE YEARS
Strand Name Sessions Year
Lifespan perspectives
Lifespan Issues 2 1
Sexuality 1 1
Grief and Loss 2 1
Death and dying 2 2
Adolescence and transition 2 2 Emotions, emotion literacy and Emotion regulation 2 2
Grief and Loss in ID 2 2
Falls 1 1
93
SECTION 2
PROGRAMME MANUAL / 2019
Teaching Strands Reading List
Acceptance and Commitment Therapy Harris, R. (2009). Act Made Simple: An Easy-to-Read Primer on Acceptance and Commitment Therapy. New Harbinger.
Hayes, S., Strosahl, K., & Wilson, K. (2016). Acceptance and Commitment Therapy, Second Edition: The Process and Practice of Mindful Change. New York. Guilford Press. Hayes, L., & Ciarrochi, J. (2015). The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection. Context Press. Luoma, J., Hayes, S., & Walser, R. (2018). Learning ACT, 2nd Edition: An Acceptance and Commitment Therapy Skills-Training Manual for Therapists. Context Press. Polk, K. L., Schoendorff, B., Webster, M., & Olaz, F. (2016). The Essential Guide to the ACT Matrix: A Step-by-Step Approach to Using the ACT Matrix Model in Clinical Practice. Context Press.
Anxiety Beidel, D. C., & Alfano, C. A. (2011). Child Anxiety Disorders A Guide to Research anD Treatment. 2nd Edition, Routledge.
Cartwright-Hatton, S., Laskey, B. Rust, R., & McNally, D. (2010). From Timid To Tiger: A Treatment Manual for Parenting the Anxious Child. Wiley. Clark, D. A., & Beck, A. T. (2010). Cognitive Therapy of Anxiety Disorders. Guilford, New York. Craske, M. G., & Barlow, D. H. (2007). Mastery of your anxiety and panic (Therapist guide- 4th edition). Oxford: Oxford University Press.
Dugas, M. J., & Robichaud, M. (2007). Cognitive - Behavioral Treatment for Generalised Anxiety Disorder. Oxon: Routledge. Ehlers, A., & Clark, D. M. (2000). A Cognitive Model of PTSD. Behaviour Research and Therapy 1-27. Ehlers, A., Clark, D. M., Fennell, M., Herbert, C., & Mayou, R. (2005). Cognitive Therapy for Post-traumatic Stress Disorder. Development and evaluation. Behaviour Research and Therapy 43, 413-431. Foa, E. B., Hembree, E. A., & Rothbaum, B.O. (2007). Prolonged Exposure Therapy for PTSD – Emotional Processing of Traumatic Experiences – Therapist Guide. OUP. New York.
94
SECTION 2
PROGRAMME MANUAL / 2019
Foa, E. B., Yadin, E., & Lichner, T. K. (2012). Exposure and (Ritual). Response Prevention for OCD: Therapist Guide. OUP. USA. Hope, D.A , Heimberg, R.G., & Turk, Cynthia, L. (2006). Managing social anxiety: A cognitive-behavioural approach. Oxford: OUP. James, A. C., James, G., Cowdrey, F. A., Soler, A., & Choke, A. (2015). Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database of Systematic Reviews, Issue 2. Art. No.: CD004690. Mueller, M., & Westbrook, D. Eds. (2004). Oxford guide to behavioural experiments in cognitive therapy. Oxford, OUP. Mayo-Wilson, E., Dias, S., Mazranezouli, I. Kew, K., Clark, D. M., Ades, A. E., & Pilling, S. (2014). Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis. Lancet Psychiatry, 1: 368-376. Steketee, G. S. (2012). The Oxford Handbook of Obsessive Compulsive and Spectrum Disorders. New York. OUP. Tyrer, H. (2013). Tackling Health Anxiety: A CBT Handbook. RCPsych publications. Veale, D. (2009). Cognitive behaviour therapy for a specific phobia of vomiting. The Cognitive Behaviour Therapist, 2, 272-288. Wolitzky-Taylor, K. B., Horowitz., J. D., Powers, M. B., & Telch, M. J. (2008). Psychological approaches in the treatment of specific phobias: a meta-analysis. Clinical Psychology Review 28, 1021–1037. Assessment and Formulation Davey, G. (2014). Psychopathology Research, Assessment and Treatment in Clinical Psychology. BPS. Wiley. Division of Clinical Psychology (2011). Good Practice Guidelines on the Use of Psychological Formulation. BPS Leicester. Johnstone, L., & Dallos, R. (Eds.). (2006). Formulation in psychology and psychotherapy: Making sense of people’s problems. London, New York: Routledge. Kuyken, W., Padesky, C. A., & Dudley, R. (2009). Collaborative case conceptualisation. New York: Guilford Press. Tarrier, N. Ed. (2015). Case formulation in cognitive behaviour therapy: The treatment of
challenging and complex cases. London, New York: Routledge.
95
SECTION 2
PROGRAMME MANUAL / 2019
Attachment Adversity and Trauma Barker-Collo, S., & Read, J. (2003). Models of response to child sexual abuse: Their implication for treatment. Trauma, Violence & Abuse, 4(2), 95-111. Cutajar, M. C, Mullen, P. E., Ogloff, J. R. P., Thomas, S. D., Wells, D. L., & Spataro, J. (2010). Psychopathology in a large cohort of sexually abused children followed up to 43 years. Child Abuse and Neglect, 34, 813–822. Finkelhor, D., & Browne, A., (1985). The Traumatic Impact Model of Child Sexual Abuse: A Conceptualisation. American Journal of Orthopsychiatry, 55(4), 530-541. Pereda, N., Guilera, G.,Forns, M., & Gómez-Benito, J. (2009). The international epidemiology of child sexual abuse: A continuation of Finkelhor (1994). Child Abuse & Neglect, 33, 331–342. Cognitive Behavioural Therapy Beck, J. S. (2011). Cognitive Behaviour Therapy: Basics and Beyond (2nd Ed). Guildford Press: New York. Beck, A. T., Rush, A. J., Shaw, B .F., & Emery, G. (1979). Cognitive therapy of depression. New York: Guilford Press. Bennett-Levy, J., Butler, G., Fennell, M., Hackman, A., Mueller, M., & Westbrook, D. (2004). Oxford Guide to Behavioural Experiments in Cognitive Therapy. Oxford, OUP Craske, M. G., Treanor, M., Conway, C., Zbozinek, T., & Vervliet. B. (2014). Maximizing Exposure Therapy: An Inhibitory Learning Approach. Behaviour research and therapy. 58:10-23. Ekers, D, Webster, L., Van Straten, A., Cuijpers, P., Richards, D., & Gilbody S. (2014). Behavioural Activation for Depression; An Update of Meta-Analysis of Effectiveness and Sub Group Analysis. Aleman A, ed. PLoS ONE. 9(6). Fennell, M. (2000). Depression In: K. Hawton, P.M. Salkovskis, J. Kirk, J & D.M. Clark Eds, Cognitive Behaviour Therapy for Psychiatric Problems (13th Edition). Oxford, OU Press Fredman, G., Anderson, E., & Stott, J. eds (2010). Being with Older People: A systemic Approach. London, Karnac.
Fuggle, P., Dunsmuir, S., & Curry, V. (2013). CBT with children, young people and families. Sage. Grant, A., Townsend, M., Mills, J., & Cockx, A. (2008). Assessment and Case Formulation in Cognitive Behavioural Therapy. Sage. London.
Greenberger, D., & Padesky, C. (2015). Mind Over Mood. Second Edition. Guildford Press: New York.
96
SECTION 2
PROGRAMME MANUAL / 2019
Hackmann, A., Bennett-Levy, J., & Holmes, E.A. (2011). The Oxford Guide to Imagery in Cognitive Therapy. OUP. Hepple, J., Pearce, J., & Wilkinson, P. eds (2002). Psychological Therapies with Older People. Developing Treatments for Effective Practice. Hove: Brunner-Routledge
Holmes, E., Arntz, A., & Smucker, M. R. (2007). Imagery rescripting in cognitive behaviour therapy: Images, treatment techniques and outcomes. Journal of Behaviour Therapy and Experimental Psychiatry, 38, 297-305. Holmes, E.A., Crane, C., Fennell, M. J. V., & Williams, J.M.G. (2007). Imagery about suicide in depression – “Flash-forwards.” Journal of Behaviour Therapy and Experimental Psychiatry, 38, 423-434. Holmes, E.A., Lang, T. J., & Shah, D. M. (2009). Developing interpretation bias modification as a “cognitive vaccine” for depressed mood: Imagining positive events makes you feel better than thinking about them verbally. Journal of Abnormal Psychology, 118, 76-88.
Holmes, E. A., & Mathews, A. (2010). Mental Imagery in emotion and emotional disorders. Clinical Psychology Review, 30, 349-362. Hunt, M., & Fenton, M. (2007). Imagery Rescripting versus in vivo exposure in the treatment of snake fear. Journal of Behaviour Therapy and Experimental Psychiatry, 38, 329-344. Jacobson, N. S., Dobson, K. S., Truax, P. A., Addis, M. E., Koerner, K., Gollan, J. K., Prince, S. E. (1996). A component analysis of cognitive-behavioural treatment for depression. Journal of Consulting and Clinical Psychology, 64(2), 295-304. Kanter, J. W., Busch, A. M & Rusch, L.C. (2009). Behavioral Activation: Distinctive Features Hove, Routledge. Laidlaw, K. (2014). CBT for Older People. Sage.
Laidlaw, K., Kishita, N., & Chellingsworth, M. (2016). A Clinician’s Guide to: CBT with older people. University of East Anglia.
Laidlaw, K., & Pachana, N. (2009). Aging, Mental Health and Demographic Change: Challenges for Psychotherapists. Professional Psychology: Research and Practice, 40, 6, 601-608.
Leahy, R. L. & Holland, S.J. (2000). Treatment Plans and Interventions for Depression & Anxiety New York, The Guilford Press. Lee, S. W., & Kwon, J. H. (2013). The efficacy of imagery rescripting for social phobia: A randomised controlled trial. Journal of Behaviour Therapy and Experimental Psychiatry, 44, 351-360.
97

SECTION 2
PROGRAMME MANUAL / 2019
Martell, C. R., Addis, M. E., & Jacobson, N.S. (2001). Depression in context; strategies for guided action. New York: Norton. Moore, R. G., & Garland, A. (2003). Cognitive Therapy for Chronic & Persistent Depression Chichester, Wiley & Sons. Nilsson, J. E., Lundh, L. G., & Viborg, G. (2012). Imagery rescripting of early memories in social anxiety disorder: An experimental study. Behaviour Research and Therapy, 50, 387-392. Speckens, A.E.M., Kackmann, A., Ehlers, A., & Cuthbert, B. (2007). Intrusive images and memories of earlier adverse events in patients with obsessive compulsive disorder. Journal of Behaviour Therapy and Experimental Psychiatry, 38, 411-422. Stallard, P. (2002). Think good feel good. Wiley. Weslau, C., & Steil, R. (2014). Visual mental imagery in psychopathology – Implications for the maintenance and treatment of depression. Clinical Psychology Review 34, 273-281. Westbrook, D., Kennerley, H., & Kirk, J. (2011). An Introduction to Cognitive Behaviour Therapy: Skills and Applications. Second Edition. Sage, UK.
Wild, J., & Clark, D .M. (2011). Imagery rescripting of early traumatic memories in social phobia. Cognitive and Behavioural Practice, 18, 433-443. Compassion Focused Therapy
Braehler, C., Gumley, A., Harper, J., Wallace, S., Norrie, J., & Gilbert, P. (2013). Exploring change processes in compassion focused therapy in psychosis: Results of a feasibility randomized controlled trial. British Journal of Clinical Psychology, 52, 199-214.
Dutton, J. E., & Workman, K.M. (2014). Compassion at Work. The Annual Review of Organizational Psychology and Organizational Behaviour, 1 :277-304. Gilbert, P. (1993). Defence and safety: Their function in social behaviour and psychopathology. British Journal of Clinical Psychology, 32, 131-153. Gilbert, P. (2005a). Compassion and cruelty: A biopsychosocial approach. In, P. Gilbert (ed). Compassion: Conceptualisations, Research and Use in Psychotherapy (9-74). London: Routledge. Gilbert, P. (2005b). Social Mentalities: A biopsychosocial and evolutionary reflection on social relationships. In, M. W. Baldwin (ed). Interpersonal Cognition. (p. 299-335). New York: Guilford. Gilbert, P., & Choden. (2013). Mindful Compassion. London: Constable.
98
SECTION 2
PROGRAMME MANUAL / 2019
Gilbert, P., & Proctor, S. (2006). Compassionate mind training for people with high shame and self-criticism; Overview and pilot study. Clinical Psychology and Psychotherapy, 13, 353-379). Lee, D (2014). The Compassionate-Mind Guide to Recovering from Trauma and PTSD: Using Compassion-Focused Therapy to Overcome Flashbacks, Shame, Guilt, and Fear (Compassionate-Mind Guides). Oakland CA, New Harbinger. Core Therapeutic Skills Goldbart, J., & Caton, S. 2010 Communication and people with the most complex needs: what works and why this is essential London: Mencap. Kelly, A. 2000 Working with adults with a learning disability Oxon: Winslow. Mansell, J.,2010, Raising our sights: Services for adults with profound intellectual and multiple disabilities Kent: Tizard Centre. Mencap 2007 Death by indifference www.mencap.org.uk. Mencap 2012 Death by indifference: 74 deaths and counting - a progress report 5 years on www.mencap.org.uk. Mencap 2013 Raising our sights guides - 10 how to guides https://www.mencap.org.uk. Ware, J. 2003. Creating a Responsive Environment-For People with Profound and Multiple Learning Difficulties London: David Fulton Publishers. Interviewing People with Intellectual Disabilities Helen Prosser and Jo Bromley. The Handbook of Intellectual Disability and Clinical psychology Practice, Alan Carr Mental Handicap and the Human Condition, Valerie Sinason. Listen to me. Pat Fitton. Books Beyond Words series and issue specific, accessible leaflets from RCPsych Dialectical Behaviour Therapy Dimeff, L., & Koerner, K. (2008). Clinical Applications of Dialectical Behaviour Therapy. New York: Guilford Press. Heard, H., & Swales, M. (2015). Changing Behavior in DBT: Problem-Solving in Action. New York: Guilford Press. Koerner, K. (2012). Doing Dialectical Behavior Therapy. New York: Guilford Press.
99
SECTION 2
PROGRAMME MANUAL / 2019
Linehan, M. M. (1993a). Cognitive Behavioural Treatment of BPD. New York: Guildford. Linehan, M. M. (2015a). Skills Training Manual. Second Edition. New York: Guildford. Linehan, M. M. (2015b). Skills Training Manual: Handouts and Worksheets. Second Edition. New York: Guildford. Swales M. A. (Ed). (2018). Oxford Handbook of Dialectical Behaviour Therapy. Oxford: OUP. Swales, M. A., & Heard, H.L. (2017). Dialectical Behaviour Therapy: The CBT Distinctive Features Series (W. Dryden Ed.). Second Edition. London: Routledge. Linehan, M. M., Armstrong, H. E., Suarez, A., Allman, D., & Heard, H. L. (1991). Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry, 48: 1060–1064.
Linehan, M. M., Comtois, K. A., Murray, A. M., Brown, M .Z., Gallop, R. J., Heard, H. H., Korslund, K. E., Tutek, D. A., Rynolds, S. K. & Lindenboim, N. (2006). Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Archives of General Psychiatry, 63: 757–766.
Lynch T. R., Chapman A. L., Rosenthal M. Z., Kuo, J. R., & Linehan M. (2006). Mechanisms of change in dialectical behavior therapy: theoretical and empirical observations. Journal of Clinical Psychology, 62, 459–80. McMain, S .F., Links, P. S., Gnam, W. H., Guimond, T., Cardish, R. J., Korman, L. & Streiner, D. L. (2009). A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder. American Journal of Psychiatry, 166(12): 1365–1374.
McCauley, E., Berk, M. S., Asarnow, J. R., Adrian, M., Cohen, J., & Linehan, M. M. (2018). Efficacy of Dialectical Behaviour Therapy for adolescents at high-risk of suicide: A randomized clinical trial. JAMA Psychiatry, 1109
Mehlum, L. Ramberg, M., Tørmøen, A .J. et al, (2016). Dialectical behavior therapy compared with enhanced usual care for adolescents with repeated suicidal and self-harming behavior: Outcomes over a one-year follow-up. Journal of the American Academy of Child & Adolescent Psychiatry, 55(4), 295-300.
Dementia Beattie, A. M., Daker-White, G., Gilliard, J., & Means, R. (2002). Younger people in dementia care: A review of service needs, service provision and models of good practice. Aging & Mental Health, 6(3), 205-212.
100

SECTION 2
PROGRAMME MANUAL / 2019
Bentham, P., & La Fontaine, J. (2008), Services for younger people with dementia. Psychiatry, vol.7 (2), 84 87. Freyne, A., Kidd, N., Coen, R., & Lawlor, B.A. (1999). Burden in carers of dementia patients: Higher levels in carers of younger people. International Journal of Geriatric Psychiatry, 14, 784-788. Green, P. (2009). Reviewing diagnostic procedures in a younger people with dementia team. PSIGE Newsletter, No. 107, 23-30. Jefferies, K., Lawrence, R., & Agrawal, N. (2011). Younger People with Dementia. Current Themes in Psychiatry in Theory and Practice, 37. Younger-onset dementia: Understanding your diagnosis. www.alzheimers.org.uk Eating Disorders Waller, G., Cordery, H., Corstorphine, E., Hinrichsen, H., Lawson, R., Mountford, V., & Russell, K. (2007). Cognitive-behavioral therapy for the eating disorders: A comprehensive treatment guide. Cambridge, UK: Cambridge University Press. R. E. McCabe, T., McFarlane, M .P., Olmsted, M. P. (2003). The overcoming bulimia workbook: A comprehensive step-by-step guide to recovery. New Harbinger, California (2003). Cooper. P. (2009). Overcoming bulimia nervosa and binge eating: A self-help guide using cognitive behavioral techniques (2nd ed.), Robinson, London (2009). Fairburn, C. (2008). Cognitive Behaviour Therapy and Eating Disorders. The Guilford Press: Chichester.
Forensic Clinical Psychology
Browne, A., & Finklehor, D. (1986). Impact of child sexual abuse: a review of the research. Psychological Bulletin, 99, 66-77. Hanson, R. K. et al (2002). 1st report of the collaborative outcome data project (etc.). Sexual Abuse: Journal of Research & Treatment, 14, 169-194. Journal of Applied Research in Intellectual Disabilities (Several articles in issue, 15 (2), 2002). Lindsay, W. R. (2002). Research and literature on sex offenders with intellectual and developmental disabilities. Journal of Intellectual Disability Research, 46, 74-85. Marshall, W. L., Laws, D. R., & Barbaree, H. E. (1990). Handbook of Sexual Assault: Issues, Theories & Treatment of the Offender. NY: Plenum Press.
101
SECTION 2
PROGRAMME MANUAL / 2019
Marshall, W. L. et al. (1999). Cognitive Behavioural Treatment of Sexual Offenders. Wiley. Benson, B. A. (1992). Teaching Anger Management to Persons with Mental Retardation. Worthington, OH: International Diagnostic Systems Inc. Eifert, G. H., McKay, M., & Forsyth, J. P. (1996). Act on Life Not on Anger: The New Acceptance & Commitment Therapy Guide to Problem Anger. Oakland, CA: New Harbinger Publications, Inc. Greiger, R. (1982). Anger problems. In R. Grieger & I.Z. Greiger (Eds.). Cognition & Emotional Disturbance. NY: Human Sciences Press. Henderson, M. (1989). Behavioural approaches to violent crimes. In K. Howells & C.R. Hollins (Eds.). Clinical Approaches to Violence. Chichester: John Wiley & Sons. Howells, K. (1998). Cognitive behavioural interventions for anger, aggression and violence. In Tarrier, N., Wells, A., & Haddock, G. (Eds.). Treating Complex Cases. (pp. 295-318). London: Wiley. Michenbaum, D. (1975). Self-Instructional Methods. In F.H. Kanfer & A.P. Goldstein (Eds.). Helping People Change. NY: Pergamum. Monahan, J., & Stephenson, H .J. (Eds.). (1994). Violence & Mental Disorder: Developments in Risk Assessment. Chicago: University of Chicago Press. Novaco, R. W. (1975). Anger Control: the development and evaluation of an experimental treatment. MA, Lexington: D.C. Health. Novaco, R. W. (1985). Anger and its therapeutic regulation. In M.A. Chesney & R. Rosenham (Eds.). Anger & Hostility in Cardiovascular and Behavioural Disorders. NY: Hemisphere. Novaco, R. W. (1994b). Clinical problems of anger and its assessment and regulation through a stress coping skills approach. In W. O’Donohue & L. Kranser (Eds.). Handbook of Psychological Skills Training. Boston: Allyn & Bacon. Novaco, R. W. (1997). Remediating anger and aggression with violent offenders. Legal & Criminological Psychology, 2, 77-78. Novaco, R. W. (1998). Aggression. In Friedman, H. (Ed.), Encyclopaedia of Mental Health. San Diego: Academic Press. O’Neill, H. (1999). Managing Anger. London: Whurr Publications Ltd. Michael Daffern, Lawrence Linda Jones & John Shine. (Eds.). Offence Paralleling Behaviour: A Case Formulation Approach to Offender Assessment and Intervention: Wiley Series in Forensic Clinical Psychology. (2010). Wiley Blackwell Publications.
102
SECTION 2
PROGRAMME MANUAL / 2019
Mary McMurran & Richard Howard (Eds.). Personality, Personality Disorder and Violence: An Evidence-based Approach: Wiley Series in Forensic Clinical Psychology. (2009). Wiley Blackwell Publications. Peter Sturmey & Mary McMurran. (Eds). Forensic Case Formulation: Wiley Series in Forensic Clinical Psychology. (2011). Wiley Blackwell Publications. Raymond Chip Tafrate & Damon Mitchell. (Eds). Forensic CBT: A Handbook for Clinical Practice. (2013). Wiley Blackwell Publications. Functional Analysis Cooper, J. O., Heron, T. E., & Heward, W. L. (2013). Applied Behaviour Analysis. Pearson. Emerson, E. (2011). Challenging Behaviour (3rd ed.). Cambridge University Press. Emerson, E., Dickson, K., Gone, R., Hatton, C., Bromley, J., & Caine, A. (Eds.). (2012). Clinical Psychology and People with Intellectual Disability (2nd ed.). Wiley-Blackwell. Jones, E.W., Hughes, J.C., Williams, B.M., Moseley, Y., Jones, B., Hughes, D.R., Hoerger, M., & Prys, D. (Gol./Eds.). (2011). Geirfa technegol ABA Glossary of ABA technical terms. http://bacb.com/wp-content/uploads/2015/07/welsh-BA-Glossary.pdf. Jones, E.W., Hoerger, M.L., Hughes, J.C., Williams, B.M., Jones, B., Mosley, Y. Hughes, D.R., Prys, D. (2011). ABA and Diverse Cultural and Linguistic Environments: A Welsh Perspective. Journal of Behavioural Education. Newman, B., Reeve, K., Reeve, S., & Ryan, C. (2003). Behaviorspeak: A glossary of terms in Applied Behaviour Analysis. Dove & Orca. NICE Guidance. (2015). Challenging Behaviour and learning disabilities: Prevention and intervention for people with learning disability whose behaviour challenges. nice.org.uk. Repp, A.C., & Horner, R.H. (1999). Functional Analysis of Problem Behaviour: From effective assessment to effective support. Wadsworth Publishing. Challenging behaviour: a unified approach. Clinical and service guidelines for supporting people with learning disabilities who are at risk of receiving abusive or restrictive practices (2007). Royal College of Psychiatrists, British Psychological Society and Royal College of Speech and Language Therapists. College Report CR144. Health Clinical Psychology Brennan, J. (2001). Adjustment to cancer: coping or personal transition? Psych-oncology, 10(1), 1-18.
103
SECTION 2
PROGRAMME MANUAL / 2019
Dunn, J. et al. (2013). Trajectories of psychological distress after colorectal cancer. Psycho-oncology, 22(8), 1759-1765. Wyatt, D., & Hulbert-Williams, N.J. (Eds.). (2015). Cancer and Cancer Care. London: Sage. Das, P., Naylor, C., & Majeed, A. (2016). Bringing together physical and mental health within primary care: a new frontier for integrated care. King’s fund. Kellett, S., Webb, K., Wilkinson, N., Bliss, P., Ayers, T., & Hardy, G. (2016). Developing services for patients with depression or anxiety in the context of long-term physical health conditions and medically unexplained symptoms: Evaluation of an IAPT pathfinder site. Behavioural and cognitive psychotherapy, 44(5), 553-567. Naylor et al (2012). Long term conditions and mental health: The cost of co-morbidities. King’s Fund. Naylor, C., Taggart, H & Charles, A (2017). Mental health models and new models of care: Lessons from the vanguards. King’s Fund. Welsh Government (2018). A Healthier Wales: Our Plan for Health and Social Care. White, P.D. et al. (2013). Recovery from Chronic fatigue syndrome after treatments given in the PACE trial. Psychological Medicine. Burgess, M., & Chalder.C., (2005). Overcoming Chronic Fatigue; a self-help guide using Cognitive Behavioral Techniques. Robinson ISBN 1-84119-942-7. www.bacme.com (website of The British Association for CFS/ME researchers and clinicians). Induction and NWCPP sessions Bamber, M. (2006). CBT for Occupational Stress in Health Professionals. Introducing a schema-focused approach. Routledge. London. Hill, K., Wittkowski, A., Hodgkinson, E., Bell, R., & Hare, D. (2015). Using the Repertory Grid Technique to Examine Trainee Clinical Psychologists’ Construal of their Personal & Professional Development. Clinical Psychology and Psychotherapy. Wileyonlinelibrary.com. DOI: 10.1002/cpp.1961 Pakenham, K.I., & Stafford-Brown, J. (2012). Stress in clinical psychology trainees: A review of current research and future directions. Australian Psychologist,47, 147-155. Kaeding, A., Sougleris, C., Reid, C., Van Vreeswijk, M.F., Hayes, C. et al (2017). Professional burnout, early maladaptive schemas and physical health in clinical and counselling psychology trainees. Journal of Clinical Psychology, 73, 12, 1782-1796.
104
SECTION 2
PROGRAMME MANUAL / 2019
Leadership Care and Treatment Plan Template. Mental Health (Wales). Measure 2010 Section 18 – Care and Treatment Plan. Welsh Government. http://wales.gov.uk/topics/health/publications/health/guidance/careplan/?lang=en Care and Treatment Planning. A step-by-step guide for secondary mental health service users. http://www.hafal.org/pdf/Care_and_Treatment_Planning_1.pdf. The Mental Health (Wales). Measure North Wales Implementation Newsletters 1-4 http://www.wales.nhs.uk/sitesplus/861/page/58653 Hafal (2014). A Working Guide to Mental Health Policy and Legislation in Wales. April. Mental Health (Wales). Measure 2010. National Service Model for Local Primary Mental Health Support Services. Welsh Government August 2011. The Mental Health (Care Coordination and Care and Treatment Planning). (Wales). Regulations 2011 EXPLANATORY NOTE. http://www.legislation.gov.uk/wsi/2011/2942/pdfs/wsi_20112942_mi.pdf The Mental Health (Primary Care Referrals and Eligibility to Conduct Primary Mental Health Assessments). (Wales). Regulations 2012. http://www.legislation.gov.uk/wsi/2012/1305/contents/made The Mental Health (Wales). Measure 2010. Public Summary Leaflet. http://wales.gov.uk/docs/dhss/publications/121017measureency.pdf Wales Mental Health in Primary Care (WaMH in PC). Information Sheet 6. A briefing note for GPs and Primary Care Practitioners. Mental Health (Wales). Measure 2010. www.wamhinpc.org.uk/mental-health-wales-measure-2010 Welsh Government (2011). National Service Model for Local Primary Mental Health Support Services. August. Barnes, M., & Cotterell, P. (2012). “Critical Perspectives on User Involvement.” Bristol. Policy Press. Roberts, A., Greenhill, B., & Talbot, A. (2011). ‘Standing up for my human rights.’ A group’s journey beyond consultation towards co-production. British Journal of Learning Disability, 40, 292-301. British Psychological Society (2015). Psychologists as Expert Witnesses: Guidelines & Procedure for England & Wales. 4th Edition. Carson, D., & Bull, R. (2003). Handbook of Psychology in Legal Contexts. Chichester, Wiley.
105
SECTION 2
PROGRAMME MANUAL / 2019
Gianvanni, E., & Sharma, S.J. (2015). Psychologists as expert witnesses in Australian Courtrooms. Psychiatry, Psychology and Law, 22:6 920-926. Bass, B.M. (1997). Does the Transactional- Transformational Paradigm Transcend. Organizational and National Boundaries? American Psychologist, 52, 130-9. Bresnahan, C.G., & Mitroff, I.I. (2007). Leadership and Attachment Theory. American Psychologist, September, 607-8. Brown, M.E., & Treviño, L.K. (2009). Leader- Follower Values Congruence: Are Socialized Charismatic Leaders Better Able to Achieve it? Journal of Applied Psychology, 94, 478-490. Cardona, P. (2000). Transcendental Leadership. The Leadership and Organization Developmental Journal, 21, 201-6. Chemers, M.M. (2000). Leadership Research and Theory: A Functional Integration. Group Dynamics: Theory, Research and Practice, 4, 27-43. Cohen, B.D., Ettin, M.F., & Fidler, J.W. (1998). Conceptions of Leadership: The “Analytic Stance” of the Group Psychotherapist. Group Dynamics, Theory and Practice, 2, 118-131. Davidovitz, R. Mikulincer, M., Shaver, P.R., Izsak, R., & Popper, M. (2007). Leaders as Attachment Figures: Leaders’ Attachment Orientations Predict Leadership- Related Representations and Followers’ Performance and Mental Health. Journal of Personality and Social Psychology, 93, 632-50. Eagly, A. (2008). Men, women and leadership. The Psychologist, 21, 216-7. Hinkin, T.R., & Schriesheim, C.A. (2008). An Examination of “Non-leadership”: from Laissez-Faire Leadership to Leader Reward Omission and Punishment Omission. Journal of Applied Psychology, 93, 1234-1248. Holmberg, R., Fridell, M., Arnesson, P., & Bäckvall, M. (2008). Leadership and implementation of evidence-based practices. Leadership in Health Services, 21, 168-84. Judge, T.A., & Piccolo, R.F. (2004). Transformational and Transactional Leadership: A Meta- Analytic Test of Their Relative Validity. Journal of Applied Psychology, 89, 755-68. Oberholzer, A. (1996). Psychoanalytic contributions to authority and leadership issues. Leadership & Organisational Development Journal, 17, 53-6. Skogstad, A., Einarsen, S., Torsheim, T., Aasland, M., S., & Hetland, H. (2007). The Destructiveness of Laissez- Faire Leadership Behaviour. Journal of Occupational Health Psychology,12, 80-92. NHS Institute for Innovation and Improvement (2006). NHS Leadership Qualities Framework. www.NHSLeadershipQualtities.org.uk
106
SECTION 2
PROGRAMME MANUAL / 2019
Lifespan Perspectives
Downton. J.H and Andrews, K (1990). postural disturbance and psychological symptoms amongst elderly people living at home. Int J Gerstric Psychiatry. 5; 93 – 98. Lawrence, R.H, Tennstedt, S.L, Kasten, L.E et al. (1998). intensity and correlates of fear of falling and hurting oneself in the next year. journal of aging and health. 10:267 - 286. Arfken C.L, Lach, H.W, et al (1994). the prevalence and correlates of fear of falling in elderly persons living in the community. Am J of Public Health. 84: 565 – 570. Friedman, S.M, Munoz, B et al, (2002). Falls and fear of falling which comes first? Am J Geriatric sociology. 50: 189 – 193. Maki, B.E, Holiday, P.J and Topper, A.K (1991). Fear of Falling and postural performance in the elderly. Journal of Gerontology. 46, 123 – 131. Franzoni, S. Rozzini, R et al, (1994). Fear of Falling in Nursing Home Residents. Gerontology. 40; 38 – 44. Clague, JE, Petrie, PJ and Horan, MA (2000). Hypocapnia and its relation to fear of falling. Arch Phys Med Rehabilitation. 81: 1485 - 1488. Cumming, R.G, Salked, G. et al (2000). prospective study of the impact of fear of falling on activities of daily living. Journal of Gerontology. 5, M229 – 302.
Tennstedt, S., Howland, J., Lachman, M., Peterson, E., Kasten, L., and Jette, A. (1998). A randomised controlled trial of a group intervention to reduce fear of falling and associated activity restriction in older adults. Journal of Gerontology. 53 (6). 384 - 192. Lachman, M.E, Weaver, S.L, Bandura, M., Elliott, E and Lewkowicz, C.J (1992). Improving Memory and Control Beliefs Through Cognitive Restructuring and Self-Generated Strategies. Journal of Gerentology. 47 (5). 293 - 299. Gagnon, N and Flint, A.J (2003). Fear of Falling in the Elderly. Geriatrics and Aging. 6 (7). 15 - 17. Advance Decision to Refuse Treatment: https://thepsychologist.bps.org.uk/volume-28/december-2015/matter-life-and-death. Assisted Dying: https://thepsychologist.bps.org.uk/volume-27/edition-11/assisted-dying-choice-and-recognition. Katz, R. S., & Johnson, T. G. (Eds.). (2013). When professionals weep: Emotional and countertransference responses in end-of-life care. Routledge. NICE - Improving Supportive and Palliative Care for Adults with Cancer. Found here:
107
SECTION 2
PROGRAMME MANUAL / 2019
https://www.nice.org.uk/guidance/csg4/resources/improving-supportive-and-palliative-care-for-adults-with-cancer-773375005. Palliative and End of Life Care Delivery Plan (2017). NHS Wales and Welsh Government. Sandberg, S. F. (2017). Capsule Commentary on Salyers et al., The Relationship Between Professional Burnout and Quality and Safety in Health Care: A Meta-Analysis. Journal of General Internal Medicine, 32(4), 474-474. Sandberg, S. F. (2017). Capsule Commentary on Salyers et al., The Relationship Between Professional Burnout and Quality and Safety in Health Care: A Meta-Analysis. Journal of General Internal Medicine, 32(4), 474-474.
Wren, B. (2012). Schwartz Rounds: Creating new spaces and having new conversations in healthcare organisations. Paper presented at OPUS International Conference, London, November 2012. Bowlby, J. (1980). Loss, sadness and depression. Attachment and Loss Volume 3. New York: Basic Books. Currier, J.M., Irish, J.E.F., Neimeyer, R.A., & Foster, J.D. (2015). Attachment, Continuing Bonds, and Complicated Grief Following Violent Loss: Testing a Moderated Model, Death Studies, 39(4), 201-210, DOI: 10.1080/07481187.2014.975869. Hayes, S.C., Strosahl, K.D., & Wilson, K. G. (2012). Acceptance and Commitment Therapy: The process and practice of mindful change (2nd Eds). London: The Guilford Press. Parkes, C.M. (2014). Diagnostic criteria for complications of bereavement in the DSM-5. Bereavement Care, 33(3), 113-117, DOI:10.1080/02682621.2014.980987. Prigerson H.G., Bierhals A. J, Kasl S.V., Reynolds C.F., Shear M.K., Newsom J.T., et al. (1996). Complicated grief as a disorder distinct from bereavement-related depression and anxiety: a replication study. American Journal of Psychiatry, 153, 1484–1486. Worden, W. (2008). Grief counselling and Grief Therapy: A handbook for the mental health practitioner. New York: Springer Publishing Company.
Archibald C (1994). Sex: is it a problem? Journal of Dementia Care, 2 (4), pp.16-18. Annon J (1976). The PLISSIT Model: a proposed conceptual scheme for the treatment of sexual problems, Journal of Sex Education Therapy, 2, 1976, pp.1-15. Archibald C (1998). Sexuality, dementia and residential care: managers’ report and response, Health and Social Care in the Community, 6 (2), pp.95-101. Archibald C (2001). Resident sexual expression and the key worker relationship: an unspoken stress in residential care work? Practice, 13 (1), pp.5- 12. Bauer M, McAuliffe L, Nay R (2007). Sexuality, health care and the older person: an overview of the literature, International Journal of Older People Nursing, 2 (1), pp.63-68.
108
SECTION 2
PROGRAMME MANUAL / 2019
British Psychological Society (2008). Best interests: guidance on determining the best interests of adults who lack the capacity to make a decision (or decisions). for themselves [England and Wales]. Report by the Professional Practice Board of the British Psychological Society, BPS: Leicester. Cloud GC, Brown R, Salooja N & McLean KA (2003). Newly diagnosed HIV infection in an octogenarian: the elderly are not ‘immune’, Age and Ageing, 32, pp.353- 354. Ferris JA, Smith AM, Pitts MK, Richters J, Shelley JM and Simpson J (2008). Self-reported sexual activity in Australian sexagenarians, British Medical Journal, 337: a239. Goodroad BK (2003). HIV and AIDS in people older than 50: a continuing concern, Journal of Gerontological Nursing, 29 (4), pp.18-24. Gott, M and Hinchliff S (2003a). How important is sex in later life? The views of older people, Social Science & Medicine, 56, pp.1617-1628. Gott, M and Hinchliff S (2003b). Barriers to seeking treatment for sexual problems in primary care: a qualitative study with older people, Family Practice, 20, pp.690-695. Gott, M (2006). Sexual health and the new ageing, Age and Ageing, 35, pp.106-107. Hagus C and Benbow S (2002). Sexuality in older men with mental health problems, Sexual and Relationship Therapy, 17, pp.271-279. Hajjar R and Hosam K (2003). Sexuality in the nursing home Part 1: attitudes and barriers to sexual expression, Journal of the American Medical Directors Association, 4, pp.152-156.
Heath H (2002). Opening doors (Age Concern launches campaign for the rights of gay, lesbian, transsexual and bisexual older adults), Nursing Older People, 14 (4), pp.10-13. Heath, H (2002). Out in the cold (removing barriers in health and social care for lesbian and gay service users), Nursing Standard, 16 (48), pp.18-19. Hill J, Bird H and Thorpe R (2003). Effects of rheumatoid arthritis on sexual activity and relationships, Rheumatology, 42, pp.280-286. McAuliffe L, Bauer, M., & Nay, R (2007). Barriers to the expression of sexuality in the older person: the role of the health professional, International Journal of Older People Nursing, 2 (1), pp.69-75. Panich E, Payne R, South C, Chandler M, Maynard N, Margery M and Newsome M (2004). Sexuality, older people and residential aged care, Geriaction, 22 (4), pp.5-11. Peate, I (2004). Sexuality and sexual health promotion for the older person, British Journal of Nursing, 4, pp.174-180.
109

SECTION 2
PROGRAMME MANUAL / 2019
Steinke EE (2005). Intimacy needs and chronic illness: strategies for sexual counselling and self-management, Journal of Gerontological Nursing, 31 (5), pp.40-50. Ward R (2000). Waiting to be heard – dementia and the gay community, Journal of Dementia Care, May, pp.24-25. Low Mood Beck, Rush, Shaw & Emery (1979). Cognitive therapy of Depression. Guilford press. Bennett-levy J., Butler, G, et al (2004). Oxford Guide to Behavioural Experiments in Cognitive Therapy. Oxford University Press. Busch, Rudden & Shapiro (2004). Psychodynamic Treatment of Depression. American Psychiatric Publishing. Hawton K, Salkovskis P Kirk J (1989 – 2004). Cognitive behavioural therapy for psychiatric problems a practical guide. Oxford University Press. Klerman, Weissman, Rounsaville & Chevromn (1984). Interpersonal Psychotherapy of Depression. Basic Books. Newman C.F, Leahy L, Beck A (2001). Bipolar disorder a cognitive approach. American Psychological Association. Moorey S. When bad things happen to rational people. In Salkovskis P.M (1996). Frontiers of Cognitive Therapy. Guilford Press. Padesky & Greenberger (1995). Clinicians Guide to Mind over Mood. Guilford press. London. Roth & Pilling (2007). The competences required to deliver effective CBT for people with depression and anxiety disorders. Department of Health. Segal, Williams & Teasdale (2002). Mindfulness Based CBT for depression. A new approach for preventing relapse. The Guilford Press. New York. Zettle (2008). ACT for Depression. A Clinicians Guide for using ACT in treating depression. New Harbinger Publications Mindfulness McCown , D, Reibel, DC & Micozzi, M.S (2011). Teaching Mindfulness: A Practical Guide for Clinicians and Educators. Rimes, K.A., & Wingrove, J. (2011). Pilot Study of Mindfulness-Based Cognitive Therapy for Trainee Clinical Psychologists. Behavioural and Cognitive Psychotherapy, 39, 235-241.
110
SECTION 2
PROGRAMME MANUAL / 2019
Christopher, J.C., & Maris, J.A. (2010). Integrating mindfulness as self-care into counselling and psychotherapy training. Counselling and Psychotherapy Research, 10, 114-125. Germer, C.K., Siegel, R.D., & Fulton, P.R. (2005). Mindfulness and Psychotherapy. Guilford Press. Mardula, J. (2015). from Mindfulness in Therapy, Ch. 15 in Theory and Practice of Counselling and Psychotherapy. Ed. Richard Nelson-Jones. Sage, CA, USA. Segal, Z.V., Williams, J.M.G., & Teasdale, J.D. (2013). Mindfulness-Based Cognitive Therapy for Depression. 2nd Edition. New York: Guilford Press. Shapiro, S.L., Carlson, L.E., Astin, J.A., & Freedman, B. (2006). Mechanisms of Mindfulness. Journal of Clinical Psychology, 62, 373-386. Grabovac, A.D., Lau, M.A., & Willett, B.R. (2011). Mechanisms of Mindfulness: A Buddhist Psychological Model. Mindfulness, 2, 154-166. Bishop, S.R., et al., (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11, 230-241. Hölzel, B. K. et al., (2011). How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspectives on Psychological Science, 6, 537-559. Coffey, K.A., Hartman, M., & Fredrickson, B.L. (2010). Deconstructing mindfulness and constructing mental health: Understanding mindfulness and its mechanisms of action. Mindfulness, 1, 235-253. Keng, S-L, Smoski, M. J., & Robins, C.J. (2011). Effects of Mindfulness on psychological health: A review of empirical studies. Clinical Psychology Review, 31, 1041-1056 Grossman, P. (2010). Mindfulness for psychologists: paying kind attention to the perceptible. Mindfulness, 1, 87-97. Kabat-Zinn, J. (2004 edition), Full catastrophe of living: How to cope with stress, pain and illness using mindfulness meditation. London: Paitkus, p.32. Williams, J. M. G. (2008). Mindfulness, depression and modes of mind. Cogn. Ther. Res. 32, 721–733. doi: 10.1007/s10608-008-9204-z Neurodevelopmental Presentations Professor Elspeth Webb – ADHD, Poverty and Violence Professor Susan Bogels – ADHD and Mindfulness
111
SECTION 2
PROGRAMME MANUAL / 2019
Professor Edmund Sonuga-Barke – Environment vs. genes contribution Professor Anita Thapar and Prof Gordon Harold – pregnancy and ADHD Speed Up and Sit Still by Martin Whitely (www.ADHDisBS.com) BPS/ DCP documents on formulation NICE guidelines DSM-V Attwood, T. (2007). The Complete Guide to Asperger’s Syndrome. Jessica Kingsley Publishing. Attwood, T.( 1998). Asperger’s Syndrome, A guide for parents and professionals. Jessica Kingsley Publishing. Baron-Cohen, Simon. (2008). Autism and Asperger’s Syndrome. Oxford University Press. Frith U. (2008). Autism A Very Short Introduction. Oxford University Press. Wing L. (2002). The Autistic Spectrum. Robinson Neuropsychology/ABI
Lezak, M. D., Howieson, D. B., Bigler, E. D., & Tranel, D. (2012). Neuropsychological Assessment (Fifth Edition). New York, NY 10016, USA: Oxford University Press. Lezak, M. D., Howieson, D. B., Bigler, E. D., & Tranel, D. (2012). Neuropsychological Assessment (Fifth Edition). New York, NY 10016, USA: Oxford University Press. Kipps, C.M., & Hodges, J.R. (2005). Cognitive assessment for clinicians. J Neurol Neurosurg Psychiatry;76(Suppl I): i22–i30. [available for download from journal] Hodges, J.R. (2007). Cognitive assessment for clinicians (2nd Edition). Oxford University Press, UK. Parsons, M. W., & Hammeke, T. A. (2014). Clinical Neuropsychology. A pocket handbook for assessment. Third Edition. American Psychological Association, Washington DC, USA. Coetzer, B.R., Roberts, C.B., Vaughan, F.L., & Rafal, R. (2003). The development of a holistic, community-based neurorehabilitation service in a rural area. Journal of Cognitive Rehabilitation, 21, 4-8. Goldstein, L.H., & McNeil, J.E. (Eds.). (2013). Clinical Neuropsychology: A practical guide to assessment and management for clinicians. Chichester: Wiley-Blackwell.
112
SECTION 2
PROGRAMME MANUAL / 2019
Wilson, B.A., Gracey, F., Evans, J.E., & Bateman, A. (2009). Neuropsychological Rehabilitation: Theory, Models, Therapy and Outcome. Cambridge: Cambridge University Press. Coetzer, R. (2006). Traumatic Brain Injury: A psychotherapeutic approach to loss and grief. New York: Nova Science Publishers. Coetzer, R. (2010). Anxiety and Mood Disorders following Traumatic Brain Injury: Clinical Assessment and Psychotherapy. London: Karnac Books. Wilson, B.A. (2002). Towards a comprehensive model of cognitive rehabilitation. Neuropsychological Rehabilitation, 12, 97-110. Flanahan, D.P., and Kaufman, A.S. (2nd edition). (2009). Essentials of Wisc-IV assessment. Wiley. Principles of formulation and assessment Davey, G. (2014). Psychopathology Research, Assessment and Treatment in Clinical Psychology. BPS.Wiley Division of Clinical Psychology (2011). Good Practice Guidelines on the Use of Psychological Formulation. BPS Leicester. Johnstone, L., & Dallos, R. (Eds.). (2006). Formulation in psychology and psychotherapy: Making sense of people’s problems. London, New York: Routledge. Kuyken, W., Padesky, C.A., & Dudley, R. (2009). Collaborative case conceptualisation. New York: Guilford Press. Tarrier, N. (Ed.), Case formulation in cognitive behaviour therapy: The treatment of challenging and complex cases. London, New York: Routledge. Professional and ethical working BPS. (2009). Code of Ethics and Conduct: Guidance published by the Ethics Committee of the BPS. Health and Care Professions Council. 2016. Standards of conduct, performance and ethics. http://www.hcpc-uk.org/assets/documents/10004EDFStandardsofconduct,performanceandethics.pdf
113
SECTION 2
PROGRAMME MANUAL / 2019
Health and Care Professions Council. 2015. Standards of Proficiency: practitioner psychologists. http://www.hcpc-uk.co.uk/assets/documents/10002963SOP_Practitioner_psychologists.pdf Seedhouse, D. (2009). Ethics the heart of healthcare (3rd Edition.), Chichester, Wiley. Edwards, S.D. (2011). The case of Ashley X. Clinical Ethics, 6, 39-44. Edwards, S.D. (2008). The Ashley Treatment: a step too far, or not far enough? Journal of Medical Ethics. 34, 5, 341-343. Bannerman, D.J., Sheldon, J.B., Sherman, J.A., & Harchick, A.E. (1990). Balancing the right to habilitation with the right to personal liberties; the rights of people developmental disabilities to eat too many doughnuts and take a nap, Journal of Applied Behavior Analysis, 23, 1, 79-89. Goldiamond, I. (2002). Toward a constructional approach to social problems: ethical and constitutional issues raised by applied behavior analysis. Behavior and social issues, 11, 108-197.
Barber, Brown and Martin (2016). Mental Health Law in England and Wales: A Guide for Mental Health Professionals – 3rd Edition. Exeter, Learning Matters. Jones, R. (2015). Mental Health Act Manual – 18th Revised Edition. Sweet and Maxwell. Harbour, A (2008). Mentally Disordered Children and the Law. Jessica Kingsley. Mental Health Act 1983 Code of Practice (2016). Welsh Government. Psychodynamic Theory Bancroft, A., Collins, S., Crowley, V., Harding, C., Kim, Y., Lloyd. J., Murphy (2008). ‘Is CAT an island or a solar system? The dilemmas in the therapeutic frame when working with people with learning disabilities. Summer edition, Reformulation. Carradice, A (2004). Applying cognitive analytic therapy to guide indirect working. Reformulation Conference Paper, 16-23. Clayton, P. (2001). Using cognitive analytic therapy in an institution to understand & help both client & staff. In Landsberg, G & Smiley, A (Ed.). Forensic Mental Health. USA: Civic Research Institute, Inc. Lloyd, J and Clayton, P. (2014). Cognitive Analytic Therapy for people with intellectual disabilities and their careers. London: Jessica Kingsley.
114
SECTION 2
PROGRAMME MANUAL / 2019
Ryle, A. (1975). Self-to-self, self-to-other: The world’s shortest account of object relations theory. New Psychiatry, 12: 53-56. Ryle, A. (1978). A common Language for Psychotherapies? British Journal of Psychiatry, 132: 585-594. Ryle, A and Kerr, I.B. (2002). Introducing Cognitive Analytic Therapy: Principles and Practice. Chichester: John Wiley & Sons. Vygotsky, L.S. (1978). Mind in society; The development of higher psychological processes. Cambridge, MA: Harvard University Press. Psychosis Bentall, R.P. (2003). Madness Explained, London, Allen Lane Birchwood, M., Michail, M. Meaden, S. Tarrier, N. Lewis, S. Wykes, T. Davies, L. Dunn, G. Peters, E. (2014). Cognitive behaviour therapy to prevent harmful compliance with command hallucinations (COMMAND): a randomised controlled trial Lancet Psychiatry; 1: 23–33 Byrne, S; Trower, P; Birchwood, M; Meaden, A; Nelson, A (2003). Command Hallucinations: Cognitive Theory, Therapy, and Research, Journal of Cognitive Psychotherapy, 17, 67-84 Cassie, M. Hazell, C.M. Hayward M. Cavanagh K. Strauss, C. A systematic review and meta-analysis of low intensity CBT for psychosis Clinical Psychology Review 45 (2016). 183–192 Claridge, G.S. (1987). "The schizophrenias as nervous types" revisited. British Journal of Psychiatry, 151, 735-743. Garety, P.A., Bebbington, P. and Fowler, D. et al. (2007). Implications for neurobiological research of cognitive models of psychosis: A theoretical paper. Psychological Medicine, 37, 1377–91. Garety, P. Freeman, D. Jolley, S. Ross, K. Waller, H., & Dunn, G. (2011). Jumping to conclusions: the psychology of delusional reasoning. Advances in psychiatric treatment,, vol. 17, 332–339 Harrop, C and Trower, P. (2003). Why does schizophrenia develop at late adolescence ? Chichester Wiley. McGorry P.D. Hartmann, J.A. Spooner, R. Nelson, B. (2018). Beyond the “at risk mental state” concept: transitioning to transdiagnostic psychiatry World Psychiatry;17:133–14 Morrison, A.P., Barratt, S. (2010). What are the Components of CBT for Psychosis ? A Delphi Study Schizophrenia Bulletin, 36, 136-142
115
SECTION 2
PROGRAMME MANUAL / 2019
Peters E, Ward T, Jackson M, Morgan C, Woodruff P, McGuire, P, Garety P (2018). Clinical Significance of appraisals of persistent psychotic experiences in people with and without a need for care. The Lancet (Psychiatry) Peters E., Ward, T, Jackson, M, Morgan C, Charalambides M, McGuire M, Woodruff P, Jacobsen P, Chadwick P,. Garety P. (2016). Clinical, socio-demographic and psychological characteristics in individuals with persistent psychotic experiences with and without a “need for care” . World Psychiatry. 15, 41-52 van Os, (2009). A Salience Dysregulation syndrome, British Journal of Psychiatry, 194,101–03. van Os, J., Linscott, R.J. Myin-Germeys, I. et al. (2008). A systematic review and meta-analysis of the psychosis continuum: Evidence for a psychosis proneness–persistence–impairment model of psychotic disorder, Psychological Medicine, 8, 1–17. van der Gaag, M. Smit, F. Bechdolf, A. French P. Linszen, D.H. Yung, A.R. McGorry,P. Cuijpers, P. (2013). Preventing a first episode of psychosis: Meta-analysis of randomized controlled prevention trials of 12 month and longer-term follow-ups. Schizophrenia Research, 149, 56–62 British Psychological Society (2014). Understanding Psychosis and Schizophrenia. https://www1.bps.org.uk/networks-and-communities/member-microsite/division-clinical-psychology/understanding-psychosis-and-schizophrenia Schizophrenia Commission (2012). The Abandoned Illness. https://www.rethink.org/media/514093/TSC_main_report_14_nov.pdf Reflective Practice Burnham, J. (2012). Developments in Social GRRRAAACCEEESSS: visible – invisible and voiced – unvoiced. In I.-B. Krause, (ed.). Culture and Reflexivity in Systemic Psychotherapy: Mutual Perspectives (pp. 139–160). London: Karnac. Research BPS - Ethical Principles for Conducting Research with Human Participants, 2009. World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects, 59th WMA General Assembly, Seoul, October 2008. SOMO briefing paper on ethics in clinical trials #1: Examples of unethical trials, 2008. B W Dunlop and J Banja, A renewed, ethical defence of placebo-controlled trials of new treatments for major depression and anxiety disorders, J. Med. Ethics 2009;35;384-389. Beecher, H K., Ethics and clinical research, New England Journal of Medicine, vol 4, no 24
116
SECTION 2
PROGRAMME MANUAL / 2019
M Dixon-Woods and E L Angell, Research involving adults who lack capacity: how have research ethics committees interpreted the requirements? J Med Ethics 2009 35: 377-381 dci: 10.1 136/jme.2008.027094. EJ Robinson, CEP Kerr, AJ Stevens, RJ Lilford, DA Braunholtz, SJ Edwards, SR Beck and MG Rowley - Lay public’s understanding of equipoise and randomisation in randomised controlled trials, Health Technology Assessment, 2005. Cohen, S. (1972). Folk Devils and Moral Panic: The Creation of the Mods and Rockers. New York: St. Martin’s Press. Denscombe, M. (2002). Ground rules of good research. OUP Basingstoke Robson, C. (2011). Real world research: a resource for users of social research methods in applied settings. 3rd ed. Chichester: Wiley. Saks, M., Allsop, J (2010). Researching Health: qualitative, quantitative and mixed methods. Sage, London.
Braun, V. & Clarke, V. (2008) Using thematic analysis in psychology. Qualitative Research in Psychology, 3:2, 77-101
Biggerstaff, D. L. & Thompson, A. R. (2008). Qualitative Research in Psychology 5: 173 – 183
Bishop, D.V. [blog] BishopBlog. Retrieved from http://deevybee.blogspot.co.uk/
Ioannidis, J.P.A. (2005) Why most published research findings are false. PLoS Med 2(8): e124.
Johnsen, T. J., & Friborg, O. (2015). The effects of cognitive behavioral therapy as an anti-depressive treatment is falling: A meta-analysis. Psychological Bulletin, 141(4), 747-768.
Open Science Collaboration (2015) Estimating the reproducibility of psychological science. Science, 349 (6251) aac4716.
Popay, J. Roberts, H., Sowden, A. Petticrew, M., Arai, L., Rodgers, M., Britten, N. Roen, K., & Duffy, S. (2006) ESRC Methods Programme
Silver, N. (2012) The Signal and the Noise. Penguin
Smith, J.A., Jarman, M., & Osborn, M. (1999) Doing interpretive phenomenological analysis. I M.Murray & K. Chamberlain (eds.) Qualitative Health Psychology. Sage.
117
SECTION 2
PROGRAMME MANUAL / 2019
Risk Assessment and Management Deb, S., & Roberts, K. (2003). The evidence base for the management of imminent violence in learning disability settings. Occasional Paper OP57. Royal College of Psychiatrists, London. Inglis, P., & Clifton, A. (2013). De-escalation: the evidence, policy and practice. Journal of Intellectual Disabilities and Offending Behaviour, 4, 3/4, pp.100 – 108. Jambunathan, J., & Bellaire, K. (1996). Evaluating staff use of crisis prevention techniques: a pilot study. Issues in Mental Health Nursing, 17, 6, 541-558. Noll, D. E. (2017). De-Escalate: How to Calm an Angry Person in 90 Seconds or Less. Simon and Schuster. The National Institute of Clinical Excellence. (February 2006). Violence: The short-term management of disturbed/violent behaviour in psychiatric in-patient settings and emergency departments. Clinical Guideline 25. The National Institute of Clinical Excellence. (2015). National Collaborating Centre for Mental Health. Violence and aggression: short-term management in mental-health, health and community settings. NICE Guideline [NG10]. Update. Leicester and London, UK: British Psychological Society & The Royal College of Psychiatrists. Richmond, J.S., Berlin, J.S., Fishkind, A.B., Holloman, G.H., Zeller, S.L., Wilson, M.P., Rifai, M.A., & NG, A.T. (2012). Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. Western Journal of Emergency Medicine, 13(1)17–25. The Royal College of Psychiatrists. (1998). Guidelines for the Management of Imminent Violence. Royal College of Psychiatrists, London. The Royal College of Psychiatrists. (1998). Management of Imminent Violence: Quick Reference Guide. Royal College of Psychiatrists, London. The Royal College of Psychiatrists. (1995). Strategies for the Management of disturbed and violent patients in psychiatric units. Council Report CR41. Royal College of Psychiatrists, London. Spencer S, Johnson P. (2016). De-escalation techniques for managing aggression. Cochrane Database of Systematic Reviews 2016, Issue 1. Art. No.: CD012034. The Cochrane Collaboration. Published by John Wiley & Sons, Ltd. Turnball, J., & Patterson, B. (1999). Managing Aggression & Violence. Pallgrave Macmillan.
118
SECTION 2
PROGRAMME MANUAL / 2019
Social Inclusion and Diversity Beck, A. (2016). Transcultural Cognitive Behaviour Therapy for Anxiety and Depression. Routledge Oxon. Butler, C., O’Donovan, A., & Shaw, E.2010). Sex, Sexuality and Therapeutic Practice Routledge, East Sussex. das Nair, R., & Butler, C. (2012). Intersectionality, Sexuality and Psychological Therapies. Chichester: BPS Blackwell. Ferns, P. (2005). A Holistic Approach to Black and Ethnic Minority Mental Health. Pavilion, Brighton. Hays, P.A., & Iwasama, G. (2006). Culturally Responsive Cognitive-Behavioural Therapy. APA, Washington DC. Hinton, D.E., Rivera, E.I., Hofmann, S.G., Barlow, D.H., & Otto, M.W. (2012). Adapting CBT for traumatized refugees and ethnic minority patients: Examples from culturally adapted CBT (CA-CBT). Transcultural Psychiatry 49, 2 340-365. Meyer, I. (2003). Prejudice, Social Stress and Mental Health in Lesbian, Gay and Bisexual Populations: Conceptual Issues and Research. Psychological Bulletin, 129, 5: 674-697. Sue, D.W. (2008). Counseling the Culturally Diverse, Theory and Practice: 5th Edition. John Wiley & Sons: New Jersey Systemic Working Bruni, O. et al. (1996). The Sleep Disturbance Scale for Children (SDSC). Construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. Sustainable social services for Wales: A framework for action (Welsh Assembly Government, 2011). Bywater, T., Hutchings, J., Daley, D., Whitaker, C., Yeo, S.T., Jones, K., Eames, C., & Edwards, R.T. (2009). Long-term effectiveness of a parenting intervention in Sure Start services in Wales for children at risk of developing conduct disorder. British Journal of Psychiatry, 195, 318-324. Hutchings, J., Bywater, T., & Daley, D. (2007). A pragmatic Randomised Controlled Trial of a Parenting Intervention in Sure Start Services for Pre-School Children at Risk of Developing Conduct Disorder: How and why did it work? Journal of Children’s Services 2,2,4-14. Webster-Stratton, C. (2006). The Incredible Years: A trouble-shooting guide for parents of children aged 2 – 8 years. Incredible Years: USA.
119
SECTION 2
PROGRAMME MANUAL / 2019
Eames, C., Daley, D., Hutchings, J., Whitaker, C. J., Bywater, T., Jones, K., & Hughes, J. C. (2010). The impact of group leader’s behaviour on parent acquisition of key parenting skills during parent training. Behaviour Research and Therapy, 48, 1221-1226. Jones, K., Daley, D., Hutchings, J., Bywater, T., & Eames, C. (2008). Efficacy of the Incredible Years Basic Parent Training Programme as an early intervention for children with Conduct Disorder and ADHD: Long Term Follow-up. Child Care Health and Development, 34, 380-390. Carr, A. (2006). Sleep Problems. In A. Carr (Ed.). The Handbook of Child and Adolescent Clinical Psychology: A Contextual Approach – Second Edition (pp.191-224), London Routledge. Daymond, K (2001). The ParentTalk Guide to Sleep. London: Hodder and Stoughton. http://www.nice.org.uk/nicemedia/pdf/TA102guidance.pdf https://www.nice.org.uk/guidance/cg158 http://www.nice.org.uk/nicemedia/pdf/TA102guidance.pdf https://www.nice.org.uk/guidance/cg158 Hutchings, J., Bywater, T., & Daley, D. (2007). A pragmatic Randomised Controlled Trial of a Parenting Intervention in Sure Start Services for Pre-School Children at Risk of Developing Conduct Disorder: How and why did it work? Journal of Children’s Services 2,2,4-14. Webster-Stratton, C. (2006). The Incredible Years: A trouble-shooting guide for parents of children aged 2 – 8 years. Incredible Years: USA. Working in inpatient settings British Psychological Society (2017). Psychological Best practice in inpatient services for older people. http://www.psige.org/public/files/Psychological%20best%20practice%20in%20inpatient%20services%20for%20older%20people.pdf. Clarke, I., & Wilson, H. (2008). Cognitive Behavioural Therapy for Acute Inpatient Mental Health Units: Working with Clients, Staff and the Milieu. Routledge; Oxon. Clarke, I., & Nicholls, H. (2017). Third Wave CBT Integration for Individuals and Teams: comprehend, Cope & Connect. Routledge; Oxon. New Ways of Working for Applied Psychologists in Health and Social Care: Working Psychologically in teams. http://www.wiltshirepsychology.co.uk/Working%20Psychologically%20in%20Teams.pdf
120
SECTION 2
PROGRAMME MANUAL / 2019
RESEARCH/STUDY TIME During the three years of the Programme trainees are allocated time for research/study. Research/study time is scheduled during academic blocks and allocated during clinical placement. The scheduling of research/study time during clinical placement is flexible however, it must also be arranged to take account of placement requirements. Trainees must therefore consult with their supervisor to agree when would be the most suitable time to schedule research/study time. However, the total allocated time for research/study must remain as specified below: For first and second year trainees:
• During clinical placement trainees are entitled to one day per week for research/study.
• This is in addition to the academic teaching days timetabled when trainees are on placement.
• When no academic teaching days have been scheduled, trainees are expected to be on clinical placement.
For third year trainees:
• In Year 3 when trainees are undertaking final year placements, the usual split of placement and research/study time is two clinical days/three research/study days before Christmas, and three clinical days/two research/study days after Christmas up until thesis submission in June.
• This arrangement is negotiable with the Programme Team and Supervisor depending on the nature of the research project.
• However, if a trainee proposes an alteration to the usual split of clinical and research/study time they must ensure that they complete the same number of clinical and research/study days as the rest of their cohort, as outlined above.
• After thesis submission one day per week is allocated for research/study until submission of the Advanced Clinical Report.
• Subsequently, trainees are on clinical placement for four and a half days per week with half a day allocated for research/study.
121
SECTION 3
CLINICAL EXPERIENCE
122
SECTION 3
PROGRAMME MANUAL / 2019
ALLOCATING CLINICAL PLACEMENTS NWCPP Placement Availability A wide range of clinical placements in various specialisms is available across the NWCPP Programme’s geographical area in North Wales and North Powys. The Programme keeps a directory of local Clinical Psychologists, which outlines the variety of potential placements available. Additionally, local clinicians are asked to complete a placement availability survey, which is updated on an annual basis. The survey gives supervisors the opportunity to outline what kinds of experience trainees can gain on clinical placement as well as options for more specialist clinical experience during the third year of training. Placement Allocation in Years 1 and 2 In Years 1 and 2 of the Programme, the Clinical Director and Clinical Tutor allocate placements to trainees. There are many factors considered in making decisions regarding placement allocation. For example, due to the potential for long travelling distances within North Wales, consideration will be given to where trainees live and the amount of travelling they may have already undertaken on previous placements. Consideration is also given to whether trainees have already worked within any of the services/department in North Wales. Trainees, who have worked as assistants locally, are not usually allocated to a placement in the same service or with the same supervisor. Additionally, for fluent Welsh speakers, we consider placements where trainees will be able to gain the bulk of their placement experience through the medium of Welsh. We would therefore hope to place fluent Welsh speakers with Welsh speaking supervisors, in services where clients would like to receive a service through the medium of Welsh and/or in teams where many colleagues speak Welsh. It is also the case that each trainee’s plan of training is examined as the programme progresses, to ensure sufficient breadth of training, as specified in the standards for accreditation of doctoral programmes in clinical psychology. As a result, sometimes decisions about placements have to be made on the basis of individual training needs. Therefore, although you may wish to express an interest in a particular clinical area or type of therapeutic work and whilst these preferences can be borne in mind, they may not be the primary factor in guiding the allocation process. It is in the 3rd year of training that trainees have the opportunity to specify preferences regarding clinical placements and we do our best to accommodate these requests whilst balancing the needs of all trainees on the Programme
123
SECTION 3
PROGRAMME MANUAL / 2019
Placement Allocation in Year 3 Around January/February each year, the Clinical Director and Clinical Tutor meet with the second-year cohort of trainees to discuss placement opportunities available in the local area. This session enables trainees to begin to consider 3rd year placements and the feasibility of different options. After this session, trainees have until the beginning of March to list 3 placement choices in order of preference, for each 3rd year placement to be undertaken (e.g. two six-month placements or one year long placement either with one supervisor or split between two supervisors). 3rd Year placement preferences should be submitted to the Clinical Director. Trainees who have outstanding learning needs to be met in year 3 or who require further guidance regarding their choice of placements are advised to approach their Training Co-ordinator to discuss their preferences further. The process for arranging 3rd year placements is carefully worked out in conjunction with the arrangement of 1st and 2nd year placements for the forthcoming year. As a result, 3rd year placements are not normally finalised until the placement allocation process is complete for all cohorts. This is not about 1st and 2nd year placements being given priority but rather about making sure that the Programme makes the best use of the placements that are available and that the needs of all trainees are taken into account. The initial approach to potential 3rd year supervisors must come from the Clinical Director and/or Clinical tutor as the potential for inequity is considerable when trainees meet individually with potential supervisors to discuss 3rd year training options. However, trainees may arrange to visit a particular service or team in order to gain a better understanding of the work completed within the specialism. Trainees are therefore free to arrange such a visit with the following two caveats:
• That trainees do not enter into any negotiations regarding 3rd year placements. • That trainees ensure visits are completed on their study day or alternatively, if visits
are arranged within placement time: o that their supervisor is agreeable. o and that they make up the time during a study day at a later date.
Once 3rd year placements have been agreed in principle, trainees will be contacted to suggest that they arrange to meet with prospective 3rd year supervisors to discuss their hopes for the placement in detail.
124
SECTION 3
PROGRAMME MANUAL / 2019
CLINICAL EXPERIENCE IN THE THIRD YEAR Clinical experience in the third year of training aims to help trainees consolidate and further develop the core competencies of a Clinical Psychologist. This can be achieved by working within a clinical area in which the trainee already has some experience, but working at a more advanced level and with a greater focus on leadership and skills of indirect influence; it may involve working in a new clinical area; or it may involve working with a particular therapeutic approach and developing more advanced therapeutic skills. It is hoped that clinical experience in the third year will help trainees further develop generic metacompetencies, as well as their ability to think critically, to reflect on their practice, and to hone their skills in particular areas related to the placements chosen. Placements should enable trainees to generalise and synthesise their prior knowledge and experience and apply this in different settings and novel situations. In addition, the third year is important for trainees who may need to remedy previous gaps in experience, or work more specifically on skills requiring further development. Third year placement options should therefore be discussed with training co-ordinators to ensure that learning needs are met by the end of training. Trainees can take between one and three placements in year three. For trainees opting for two 6-month placements, the first placement begins at the start of the academic year and needs to go on at least until the start of April in order for the supervisor to rate the trainee’s clinical and professional competence. Precise dates for ending the first 6-month placement need to be agreed between the supervisor and the trainee. When trainees are undertaking final year placements, the usual split of placement and research/study time is two clinical days/three research/study days before Christmas, and three clinical days/two research/study days after Christmas up until the thesis hand in date in early June. This arrangement is negotiable with the Programme Team and supervisor depending on the nature of the trainee’s research project. However, if a trainee proposes an alteration to the usual split of clinical and research/study time they must ensure that they complete the same number of clinical and research/study days as the rest of their cohort. After thesis submission there is one day per week study time until the submission of the Advanced Clinical Report. After that, trainees are on clinical placement for four and a half days/week with half a day allocated for study. From each third-year placement, there are four documents that need to be submitted. These are the: Placement Agreement, Evaluation of Clinical and Professional Competence form, Placement Quality Checklist and the updated Clinical Practice Portfolio. These documents should be submitted to the Programme at the end of the placement. Documents for placements due to finish at the end of September when the trainee completes their training, must be submitted to the Programme before the Board of Examiners meet in early September each year. This date will be confirmed once it has been finalised.
125
SECTION 3
PROGRAMME MANUAL / 2019
PREPARING FOR A TRAINEE
• Having agreed to act as a supervisor for a trainee, it is helpful for supervisors to become familiar with the BPS Guidelines on Clinical Supervision (2010) (see Section 3) and the BPS Standards for the Accreditation of Doctoral Programmes in Clinical Psychology (2017). Both are available at www.bps.org.uk/accreditationdownloads .
• Work colleagues should be notified about the trainee’s arrival in advance of the placement.
They will need to know how long the placement is, what sort of work the trainee will be doing and how this will affect the supervisor’s commitments. Supervisors will need to accept a slower pace of working at least initially and arrange to set time aside exclusively for supervision. It is helpful to start the process of creating space for the placement well in advance.
• Although there is variation in how particular services are organised, it is generally helpful for supervisors to look out for suitable cases for the trainee and perhaps even arrange initial appointments soon after the start of placement.
• Prior to the placement, supervisor should prepare information e.g. an induction pack about the Department/Service giving details of administrative support, MDT professionals, psychological tests and equipment, record keeping, management structures, Mental Health Measure documents including risk assessments, and health and safety requirements.
• Supervisors are very busy people and taking on a trainee requires a great commitment of time. It is a good idea to schedule supervision sessions from the start of placement to ensure that sufficient time has been set aside for this purpose.
• It is important to remember that supervisors will need to organise their own workload during the placement such that they can pick up the trainee's clinical work at the end of the placement if necessary.
126
SECTION 3
PROGRAMME MANUAL / 2019
PRE-PLACEMENT VISITS
A 1/2-day pre-placement visit is scheduled in each academic block to allow trainees to visit their forthcoming placement and meet with their supervisor(s) before the start of placement. From Placement 1 onwards, supervisors will have received a copy of the trainee’s ECPC from their most recent placement. This can form the basis of discussions re: strengths and areas for development. The following is a suggested agenda for the visit
• Exchange brief biographies (introductions). • Supervisor provides a general description of the placement and what can be offered. • Trainee describes their hopes and expectations of the placement. • Supervisor provides appropriate information about the placement. This may include
the department or service unit’s expectations of the trainee, including any particular protocols or health and safety requirements.
• Any anxieties the trainee may have about the placement are discussed. • Consider possible goals and placement activities. • Supervisors may wish to provide a reading list and any other introductory material.
127
SECTION 3
PROGRAMME MANUAL / 2019
STARTING OUT ON PLACEMENT Resources & Practice Management In terms of physical placement resources, BPS accreditation criteria in addition to HCPC’s Standards of Education and Training stipulate the following: ‘When trainees are on clinical placements they must have access to (at least) a shared office and telephone. There must be adequate arrangements for secretarial and IT support for their placement work, and trainees must be given guidance on the facilities available.’ Placement Induction It is important for trainees to have a clear and comprehensive induction to the work setting and relevant placement information. Supervisors should introduce the trainee to colleagues and administrative staff and familiarise the trainee with the structure of the Department/Service as follows:
General: • administrative support • hours of work/timekeeping • dress code • psychometric tests and equipment • relevant placement-related documents • library and other facilities
Client-related: • referral routes • decision-making processes • line management of psychology service and other professions • local policies for electronic storage of client related information • clinical notes and note-keeping practices • Mental Health Measure documentation • risk assessment processes and documentation • observational experience of other key services/3rd sector organisations • service user involvement
Clinical Preparation: • review clinical notes • discuss supervisor’s clinical work • review example clinical reports • highlight the assessment/formulation/treatment process
MDT Working & Leadership: • observe/meet with other professionals • attend management/MDT and other meetings • teaching opportunities • observing supervisor’s leadership/consultancy/supervision
128
SECTION 3
PROGRAMME MANUAL / 2019
• possible research opportunities Placement Agreement The Trainee and Supervisor must draw up a Placement Agreement at the start of the placement establishing the general aims of the placement. It is important to select clients who are representative of the typical range of presentations seen by a Clinical Psychologist in the specialism. Additionally, indirect work with carers/staff/teams etc. needs to be representative of the types of work usually carried out by Clinical Psychologists within the service/specialism. Discussion and reference to the following are helpful in drawing up the agreement:
• Guidelines for Clinical Experience in the various specialisms (see relevant pages in Section 3)
• The trainee’s experience prior to training and on previous placements. • From placement 2 onwards, the completed ECPC form from the previous placement
supervisor should be used to identify additional learning needs. • Clinical Practice Portfolio (see relevant pages in Section 3)
The Placement Agreement, signed by the Trainee and the Supervisor, must be completed by the date stipulated on the important dates list and sent to the Administrative Assistant (Curriculum & Clinical). A signed electronic version is acceptable. Any questions or queries regarding the placement agreement can be discussed with the Training Co-ordinator during the first placement review. From year 2 onwards supervisors and trainees are encouraged to contact the relevant Training Co-ordinator with any questions or queries that may arise. Sharing Information and Client Consent The Health and Care Professions Council (HCPC) recommends that ‘wherever possible, service users are aware that students are involved and that appropriate consent has been sought’. The Programme team have devised a formal system to ensure that trainees share information from placements appropriately, that clients are aware of this process and of how and when information may be shared. In particular, clients are informed at the outset that the trainee’s work with them may be written up in the form of an anonymised report of clinical activity and submitted to the University as an academic assignment. Detailed guidelines (including forms) are available for all clinical specialisms (AMH, ID, C&A, OA, Child ID) and these guidelines cover issues relating to training, supervision, confidentiality and submission of reports of clinical activity. Copies of all guidelines (English and Welsh versions) are available on Blackboard. Trainees are required to discuss these guidelines with their clients and where possible obtain signed agreement on the basis of the information provided. If it is not possible for a client to give written consent, verbal consent may be obtained and recorded in the clinical notes. In situations whereby a person lacks capacity, supervisors and trainees are asked to follow the usual guidelines and procedures of the relevant psychology department/service and trainees should record all relevant details in the clinical notes.
129
SECTION 3
PROGRAMME MANUAL / 2019
CLINICAL AND PROFESSIONAL COMPETENCY DEVELOPMENT The new accreditation standards for doctoral programmes in clinical psychology emphasise the following:
• ‘…over-arching competencies to deliver tailored, multi-modal, often complex psychological interventions across a range of ages, presentations and service delivery systems...informed by knowledge and skills from across formal psychological therapies and other evidence bases.’
• ‘…knowledge and skills sets…obtained through transparent benchmarking of work against competence frameworks…’
• ‘Incorporating systematic approaches to in vivo assessment to further quality assure competence development.’
• ‘Deepening collaborative practices with service users and carers…’ • ‘Greater emphasis on skills of indirect influence and leadership in bringing
psychological mindedness to services.’ Core Clinical and Professional Competencies Clinical placements focus on the development of the following core competencies:
• Interviewing and observational skills • Assessment • Formulation and Reformulation • Intervention/Evaluation • Communication • Teaching • Professional and Ethical Behaviour • Organisational, Leadership, and Multi-disciplinary Working • Self-Development
Assessment of Core Competencies In order to ensure that required learning outcomes have been achieved by the end of training, the development, monitoring and evaluation of clinical and professional competence takes place as follows:
• Competency development is monitored through the Clinical Practice Portfolio, which enables trainees to keep a detailed and up to date record of their work across various domains e.g. psychometric assessment, therapeutic competencies, indirect and leadership work with professionals/teams/services.
• Supervisors are asked to formally evaluate trainees’ progress in the development of the above core competencies at the end of each clinical placement using the Evaluation of Clinical and Professional Competence (ECPC) form (see relevant pages in Section 3)
• There is a section in the ECPC form for trainees to comment on the supervisor’s feedback.
• In terms of therapeutic competencies, supervisors are also asked to rate trainees’ competence in CBT, DBT and/or ACT, depending on which models they have used on
130
SECTION 3
PROGRAMME MANUAL / 2019
placement. At the end of the ECPC, supervisors are asked to “RAG” rate (Red/Amber/Green) relevant therapy-specific competencies.
• Once the above RAG ratings have been completed, trainees will transfer them to the Clinical Practice Portfolio so that their developing competence in these therapies can be tracked throughout their training.
• Supervisors are also asked to comment on the feedback received from others regarding the trainee’s work.
• Supervisors are asked to seek feedback from colleagues to contribute to this part of the evaluation.
• Additionally, NWCPPs People Panel devised a feedback/satisfaction questionnaire specifically for the purpose of gaining feedback from service users/carers/families etc.
• Supervisors are asked to provide a rating on the feedback received from others as either exceeded the level, at the level, or below the level expected for the particular stage of training.
• Supervisors are also asked to provide a rating of the trainee’s overall placement performance.
• At the end of Placement 1, the completed ECPC form is forwarded by the Programme to the next placement supervisor(s) so that outstanding learning needs and areas for development can be addressed.
• The Programme forwards ECPC forms routinely to the next placement supervisor from Placement 1 onwards.
Observation & In Vivo Assessment In order to facilitate the development of core clinical and professional competence, trainees must have the opportunity to observe their supervisor(s)’ clinical work. Direct observation of a supervisor’s work is invaluable for trainees throughout training. Supervisors should arrange for the trainee to observe him/her dealing with clinical work that illustrates the beginning, middle and end of psychological intervention/therapy/extended assessment. In this way the trainee can witness the process of specialist assessment and intervention/psychological therapy. When client consent for direct observation is not given, supervisors are encouraged to request consent to audio-record their sessions instead. Supervisors can use the trainee’s recording equipment for this purpose, hence enabling trainees to indirectly observe the supervisor’s clinical work. Additionally, supervisors are encouraged to make use of modelling and role-play during supervision to demonstrate key skills and illustrate their work more directly for the trainee. In line with BPS accreditation standards, supervisors are required to observe a trainee’s clinical work in order to ensure that placement ratings are based on the in-vivo assessment of clinical and professional competencies. Supervisors should therefore make arrangements to observe (live/audio/video) a minimum of 6 clinical sessions. Observations need to be balanced in terms of the clinical/professional activity undertaken on the placement e.g. x3 assessment and x3 intervention/therapy/indirect or leadership work. The exceptions to this are placements focusing on specialist extended assessments e.g. neuropsychology placements or placements based in memory clinics. Additionally, for
131
SECTION 3
PROGRAMME MANUAL / 2019
the purposes of their own learning, trainees are encouraged to record and listen to their clinical work as often as possible - see Guidelines on the Use of Recordings (Section 3). Clinical Practice Portfolio Trainees are required to complete a Clinical Practice Portfolio throughout their training (see Section 3). It is essential that the Clinical Practice Portfolio forms a working document and that trainees update it on an on-going basis as the placement progresses. The Portfolio will be used at mid-placement review and at the trainee’s annual appraisal to ensure that an appropriate breadth of clinical/professional and therapeutic experience is gained. Supervisors validate the portfolio by signing a Supervisor Authentication of Portfolio (SAP) form (see Section 3), which is submitted by the trainee at the end of placement by the deadline given. Reports of Clinical Activity
• In Years 1 and 2, trainees must complete one report of clinical activity per placement to illustrate his/her skill development.
• An RCA may take the form of an extended assessment; however, no more than two extended assessments should be completed.
• One RCA must be a CBT-RCA, which will be submitted together with an audio or video recording of a CBT intervention session (see Section 4)
• Additionally, one of the RCAs in Year 2 will take the form of an RCA-Presentation. (see Section 4).
• Supervisors and trainees need to bear in mind the length of the placement and the need to have collected enough independent clinical information to write/present the report.
132
SECTION 3
PROGRAMME MANUAL / 2019
LONG-TERM THERAPEUTIC WORK During the three years of training, trainees are required to select at least one client to work with on a longer-term basis. It is recognised that the usual 5-month placements undertaken by trainees means that they are only able to do short term pieces of clinical work. Most Clinical Psychologists working in the NHS are dealing routinely with people with more complex problems, which may require longer-term interventions. The opportunity to have experience of this kind of work is seen as an important component of training. It is hoped that longer-term intervention will enable trainees:
• to work with clients in more depth • to work with clients whose problems are more complex • to have experience of dealing with potential obstacles in therapeutic work including
setbacks • to negotiate the ending of therapy in a more natural way.
How long is “long term”? Exact lengths of time are not prescribed, as this will be decided on the basis of clinical need in negotiation with supervisors and clients. However, it is hoped that trainees will have experience of working therapeutically over approximately a 12-month period. This means frequent contact (i.e. weekly, fortnightly or monthly). The client may end up being seen for less than 12 months if the work comes naturally to an end before that time or if the client drops out. It may also extend beyond 12 months if clinically appropriate and if it is feasible for the trainee to continue with the work whilst on subsequent placements. When can the client be selected? A long-term client can be selected from any placement during the first two years or at the beginning of the third year. Trainees on a year-long placement will automatically work for a longer period with clients and are likely to meet this requirement in their routine clinical work. How to select a client Trainees are encouraged to discuss possible clients suitable for longer-term work with their supervisors during the course of placement. They will also need to reach an agreement with the next clinical supervisor about the arrangements (and time) needed to see the client and to receive supervision. If travelling time or other constraints necessitates taking too much time out of the next placement, then a client from a subsequent placement may be selected. The training co-ordinator will ask about suitable clients at mid-placement review. If no client has been selected during the second year, this will need to be prioritised for the third year. Documenting long-term clinical work Contacts with the client are recorded in the Clinical Practice Portfolio for the placement from which the client was selected. Once the therapeutic work has finished, trainees need to complete the Long-Term Therapeutic Work Record Form (see Section 3) and ask the supervisor to complete the relevant section of the form. The completed form should then be submitted to the Programme Office.
133
SECTION 3
PROGRAMME MANUAL / 2019
CLINICAL SUPERVISION
Minimum Supervision Requirements Total ‘contact’ time between supervisors and trainees must be
• at least 3 hours per week. • This must include a formal scheduled supervision meeting each week lasting a
minimum of 1 hour. • The remaining contact can be informal with direct and/or indirect contact. • In some circumstances e.g. when two trainees are being supervised by the same
supervisor or in the same service, group supervision may be appropriate. However, in this instance, individual supervision must also be provided (Min 1 hour).
The Supervisory Relationship It is widely agreed that the development and maintenance of the supervisory relationship (SR) is the most important and central component in effective clinical supervision. This is supported by competency frameworks and a growing body of research, which has identified appropriate measures to monitor and evaluate the supervisory relationship from a trainee and supervisor perspective.
• Supervisors and trainees are encouraged to familiarise themselves with these measures, which include:
o Supervisory Relationship Questionnaire o Supervisory Relationship Measure o Leeds Alliance in Supervision Scale (LASS) - a short 3–item scale designed to
provide session-by-session feedback on the supervisory alliance. o Copies of the above measures are available on Blackboard.
Involving Service Users As a result of increasing collaborative practices with service users and carers several measures are available to seek service user feedback from clients, families and carers:
• Outcome Rating Scale and Session Rating Scale are available for use in therapy/intervention work and trainees are encouraged to use these measures on a session-by-session basis and to present the results regularly in supervision.
• NWCPP’s People Panel devised an End of Assessment/Intervention form as a means of gaining feedback once assessment/therapeutic work is complete.
• Bilingual and placement specific versions of the above form including parent/carer end of intervention feedback forms are included in a folder entitled ‘Service Users’ on Blackboard.
• Trainees are advised to familiarise themselves with the procedure for gaining service user feedback and have the necessary forms available when commencing placements.
• Background information and other procedural details regarding service user feedback are also available in the ‘Service Users’ folder on Blackboard for guidance.
134
SECTION 3
PROGRAMME MANUAL / 2019
Maintaining Placement Quality Accreditation standards state that:
• “Trainees must have the opportunity to provide feedback on the adequacy of placements and supervision and programmes should ensure that it is possible to change important aspects of placements that are found to be unsatisfactory.”
The placement quality checklist (PQC) is the means by which trainees provide feedback to supervisors regarding their placement experience (see Section 3). The PQC focuses on:
• practical aspects of the placement e.g. resources available • placement induction • practical aspects of supervision e.g. that it is private and ring-fenced • more detailed aspects of the supervision provided e.g. provision of clear, open and
timely feedback, reflective practice etc.
The PQC is used at mid-placement review to gain initial trainee feedback on their experience of the placement and supervision. At the end of placement, the PQC is formally completed and submitted to the Programme together with other relevant placement documentation. Providing Successful Supervision
• Early on in placement it is helpful to have a clear structure and agenda for supervision sessions, which takes into account the trainee's needs and stage of development.
• It is important for formal supervision sessions to be ‘ring-fenced’ i.e. to be scheduled in advance, held in a private setting and be free from interruption.
• Supervisors should make it clear to the trainee when and how they are contactable outside formal supervision sessions.
• Trainees will benefit from open/honest, constructive and timely feedback. • It is helpful for supervisors to make their preferred ways of working explicit to the
trainee including theoretical models/interventions. • Supervisors need to be sensitive to the wider issues related to clinical training and
remain aware of and sensitive to the power differential in supervision. • Ensure that supervision is linked to the learning outcomes listed in the Evaluation of
Clinical and Professional Competence form. • Supervisor’s use of modelling and role-play can be invaluable learning tools for
trainees. • Use of the Session Rating Scale and Outcome Rating Scale in supervision provides a
means of systematically exploring both process and outcome in the trainee’s therapeutic work.
• In addition to the required minimum of six observations of the trainee’s clinical work, listening to segments of trainee recordings in supervision is very helpful in providing feedback.
• Supervisors need to be approachable and open to honest feedback from the trainee. • Supervisors are encouraged to demonstrate reflective practice in supervision. It is
important for supervisors to be sensitive to and prepared to discuss personal issues that arise for trainees in the course of their work.
135

SECTION 3
PROGRAMME MANUAL / 2019
• Trainees should be able to discuss any concerns openly without fear of negative appraisal.
• Regular review of supervision in terms of what is working well and not so well, from both perspectives, is a valuable way of developing and maintaining the supervisory relationship.
• It is important for supervisors to be sensitive to diversity and cultural issues in relation to trainee’s personal and professional development.
136
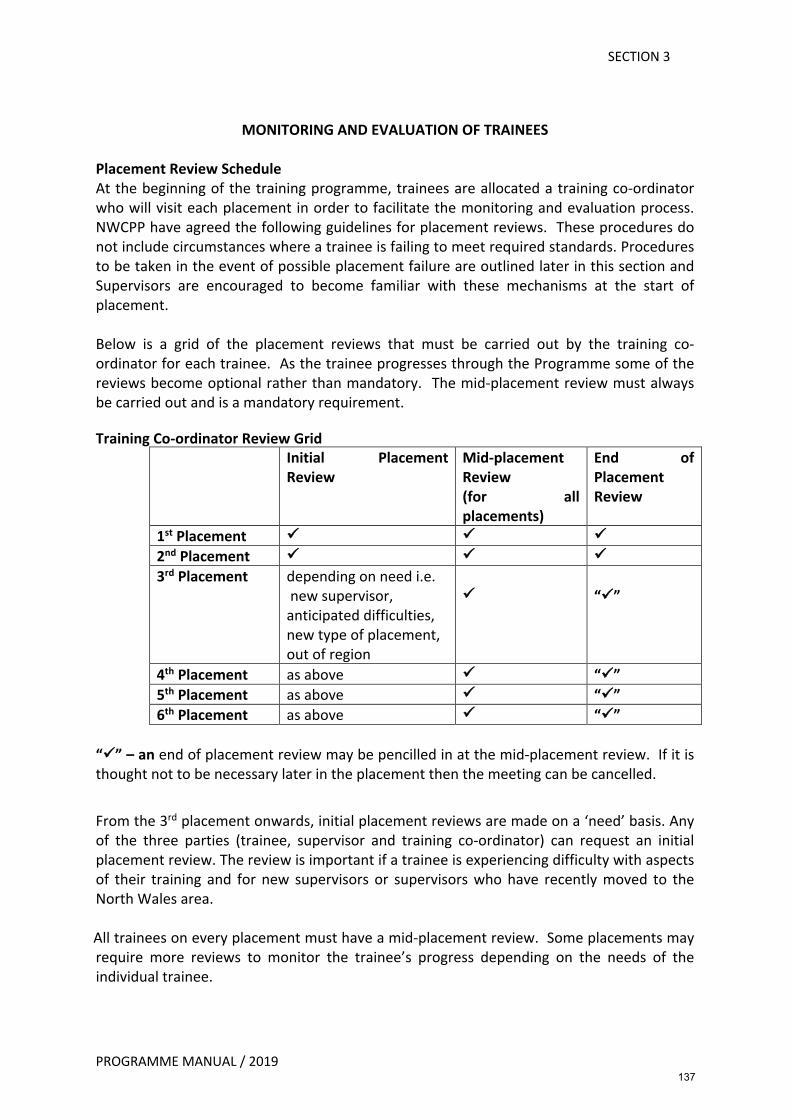
SECTION 3
PROGRAMME MANUAL / 2019
MONITORING AND EVALUATION OF TRAINEES Placement Review Schedule At the beginning of the training programme, trainees are allocated a training co-ordinator who will visit each placement in order to facilitate the monitoring and evaluation process. NWCPP have agreed the following guidelines for placement reviews. These procedures do not include circumstances where a trainee is failing to meet required standards. Procedures to be taken in the event of possible placement failure are outlined later in this section and Supervisors are encouraged to become familiar with these mechanisms at the start of placement. Below is a grid of the placement reviews that must be carried out by the training co-ordinator for each trainee. As the trainee progresses through the Programme some of the reviews become optional rather than mandatory. The mid-placement review must always be carried out and is a mandatory requirement.
Training Co-ordinator Review Grid
Initial Placement Review
Mid-placement Review (for all placements)
End of Placement Review
1st Placement ü ü ü 2nd Placement ü ü ü 3rd Placement depending on need i.e.
new supervisor, anticipated difficulties, new type of placement, out of region
ü
“ü”
4th Placement as above ü “ü” 5th Placement as above ü “ü” 6th Placement as above ü “ü”
“ü” – an end of placement review may be pencilled in at the mid-placement review. If it is thought not to be necessary later in the placement then the meeting can be cancelled.
From the 3rd placement onwards, initial placement reviews are made on a ‘need’ basis. Any of the three parties (trainee, supervisor and training co-ordinator) can request an initial placement review. The review is important if a trainee is experiencing difficulty with aspects of their training and for new supervisors or supervisors who have recently moved to the North Wales area.
All trainees on every placement must have a mid-placement review. Some placements may require more reviews to monitor the trainee’s progress depending on the needs of the individual trainee.
137
SECTION 3
PROGRAMME MANUAL / 2019
Placement Review Schedule for 12-month Placements Involving One Supervisor (Across Two Specialisms) Where one supervisor is providing experience in more than one specialism (e.g. OA and AMH) over a one-year period, two ECPCs are required, one for each speciality at the end of the 12-month period. Supervisor and trainee should discuss which specialism will be designated the lead placement in each half of the year. This will ensure that the balance of clinical time in each specialism mirrors the experience of trainees completing two separate placements. The trainee submits one placement agreement at the start of the placement with separate aims and actions identified for each speciality. At the end of the year, outcome sections of the placement agreement need to be completed for each speciality as well as two PQCs for each placement e.g. AMH and OA. The Clinical Practice Portfolio containing all information relevant to both clinical specialisms must also be submitted at the end of the 12-month period. The trainee produces one RCA at the same time as other trainees submit their first RCA. The second RCA is handed in at the end of the placement at the same time as the rest of the cohort. The trainee, supervisor and training co-ordinator can decide from which specialism the first RCA is written, depending on how the clinical work has progressed. The trainee can consider one client/piece of clinical work commencing early in placement, as fulfilling their requirement for long-term therapeutic work. The following placement reviews are required:
1. First Placement review (NB: First placement reviews are mandatory only if the trainee is in the first year of training).
2. ¼ Placement Telephone Call from training co-ordinator to supervisor and trainee to ensure things are going smoothly. Training co-ordinators will make notes of the telephone conversations and file them in the trainee file.
3. Mid-placement review (to take place at the time Placement 1 or 3 normally finishes). Training co-ordinators will decide whether to complete two separate TC checklists, one for each clinical area or whether to complete one form for both areas. If one form is completed it is essential that the provisional ECPC ratings are clearly recorded for each clinical specialism separately. The PQC needs to contain feedback on the two clinical areas separately. The Clinical Practice Portfolio must be kept up to date with relevant information from both clinical specialisms and be available for the training co-ordinator to view at mid-placement review.
4. ¾ Placement Telephone Call to supervisor and trainee. Again notes will be made of the conversations and filed in the trainee file.
5. End of Placement Review (at the end of the 12 month period) – routine for Year 1 and if required in Year 2.
138
SECTION 3
PROGRAMME MANUAL / 2019
Placement Review Schedule for 12-month Placements Involving Two Supervisors (Across Different Specialisms) Where there are two supervisors providing a yearlong split placement each covering a separate specialism, the same broad principles apply. However, in this instance: • Training co-ordinators review each placement separately as required. • Trainees complete a separate placement agreement for each placement as well as
separate PQCs. • The Clinical Practice Portfolio should be submitted by the deadline given with
information pertaining to both placements. • If the trainee is in year 1 or 2 of the Programme, agreement needs to be reached on
which will be designated as the lead placement in each half of the year. • An RCA from the lead placement in the first half of the year will be submitted by the
deadline for Placement 1 or 3 and from the other placement by the deadline for Placement 2 or 4.
139
SECTION 3
PROGRAMME MANUAL / 2019
Placement Reviews
During all placement reviews at each stage of the placement, training co-ordinators will meet separately with both trainee and supervisor before a joint meeting with all parties takes place. Initial Placement Review In Year one, the training co-ordinator will visit the placement early on and meet with the trainee and supervisor for an initial placement review. The training co-ordinator will complete a checklist designed for initial placement reviews (see Section 3). The review is designed:
• to help finalise the Placement Agreement • to answer any questions or queries that may have arisen • to review additional placement documentation • to identify the trainee’s learning needs on the basis of their experience prior to
training or from placement feedback arising from the previous placement • to discuss requirements for observation (direct of audio/video) of the trainee’s
clinical practice • to discuss forthcoming academic assignments
Mid-Placement Review Mid-way through each placement it is mandatory for the trainee’s progress to be reviewed
as follows: • Separate meetings with the trainee and supervisor enable both parties to discuss, in
confidence, any problems that may have arisen. • Training co-ordinators are there to help trainee and/or supervisor to consider how
best to raise concerns and will support both parties in discussing any difficulties as sensitively as possible in the joint part of the meeting.
• Trainees are asked to complete the Placement Quality Checklist prior to the meeting, as this feedback will form the basis of the separate meeting between trainee and training co-ordinator
• The PQC will also be used by the trainee to provide feedback to the supervisor on their experience of the placement/supervision so far
• The Placement Agreement will be reviewed at this stage to ensure that agreed aims/goals are being achieved.
• Trainees need to ensure that the Clinical Practice Portfolio is available and up-to-date for training co-ordinators to view. This enables the depth and breadth of placement experience to be considered.
• The central part of the mid-placement review is the feedback provided by the supervisor(s) using the Evaluation of Clinical and Professional Competence form as a guide. Supervisors are asked to give a provisional rating for each competency listed on the ECPC form with the intention of noting areas of achievement and areas for further development.
• If any competencies are rated as ‘below the level expected’ at the mid-placement review, an action plan will be put in place to help the trainee address the areas/skills
140
SECTION 3
PROGRAMME MANUAL / 2019
identified for further development. The action plan will be monitored subsequently and Training Co-ordinators will arrange to contact both supervisor(s) and trainee shortly afterward to check on the trainee’s progress.
• If the trainee continues to have difficulty developing the required competencies for their stage of training, the training co-ordinator will liaise with the Programme Director in order to invoke the BCUHB Capabilities Procedure (see Section 3).
• A Training Co-ordinator Checklist is completed at the mid-placement review to summarise the discussions and record the supervisor’s preliminary placement ratings (see Section 3). The checklist covers a range of essential matters such as regular supervision, service user feedback, trainee’s annual leave etc. as well as recording feedback from supervisors on the trainee’s development of core competencies and trainee’s feedback on their experience of the placement so far. The checklist is signed by all parties, copied for both supervisor and trainee and filed subsequently in the trainee’s file.
End of Placement Review This review occurs at the end of placement. The training co-ordinator may also be present
at this meeting. The review covers the following areas: • Placement Agreement is reviewed and any shortfalls noted and recorded in the
ECPC form. • Evaluation of Clinical and Professional Competence form is formally completed and
discussed (see Section 3) • Trainees have the opportunity to comment on the supervisor’s feedback in the
relevant section of the ECPC form. • Strengths as well as areas of development need to be highlighted to help trainees in
their clinical and professional development. • Trainees often express a wish to hear constructive as well as positive feedback from
their supervisors to guide further learning. • After the ECPC feedback has been discussed, trainees are asked to provide feedback
to the supervisor using the Placement Quality Checklist (see Section 3). • Supervisors have the opportunity to comment on the trainee’s feedback in the
relevant section of the PQC form. • The training co-ordinator may be absent from this meeting from year 2 onwards if
the placement is progressing well and all three parties agree that the meeting can proceed with just the supervisor and trainee present.
• In the event of any problems on placement the training co-ordinator’s presence at the end of placement review meeting is mandatory.
• After the ECPC form has been submitted, there is a period of one month at the end of each placement during which supervisors are encouraged to contact the relevant Training Co-ordinator if exceptional information about the trainee arises that would have affected the original evaluation.
• Any additional feedback or alteration to the original feedback will be made available to the trainee for their comment.
141

SECTION 3
PROGRAMME MANUAL / 2019
Ratification of Clinical Placements • It is important for supervisors to be aware that their evaluation of the trainee’s
performance on placement does not solely determine whether or not a trainee passes or fails a placement.
• The decision to pass or fail a clinical placement rests with the Board of Examiners who will consider the supervisor’s evaluation of the trainee together with previous supervisor evaluations and any additional relevant information.
• In situations where any competency is rated as “below the level expected” on the ECPC, the Board of Examiners will discuss the matter further.
• When necessary, the Chair of the Board of Examiners may ask the clinical supervisor to contribute to the Board’s discussions.
• The procedure for Placement Failure is outlined in Section 3
142
SECTION 3
PROGRAMME MANUAL / 2019
PLACEMENT FAILURE 1. Criteria for Passing Placement
The Evaluation of Clinical and Professional Competence form is specific with regard to the range of skills (both clinical and professional) trainees should acquire. The trainee should, by the end of placement, have achieved the Learning Outcomes identified in the Programme Specification (see Section 1). They should be capable of independent working (with the support of consultations with a more senior clinical psychologist) with clinical problems commonly encountered in that setting. The trainee should not be expected to deal with unusual or difficult clinical problems without more active support. They should however be expected to conduct themselves in accordance with Health Board policies, HCPC, the BPS Code of Conduct, Ethical Principles and Guidelines and the DCP Professional Practice Guidelines.
2. Failing a trainee on a placement is one of the most difficult tasks a Clinical
Psychology Programme has to face as well as being a painful and disappointing experience for the trainee. It is of the utmost importance that the criteria for failure and the procedures to be followed in such circumstances are clearly specified. It must be clearly stated here that the supervisor's primary role in these procedures is not to make decisions about whether a trainee has passed or failed, but to supply the Programme Team with relevant information. The Programme Team will then refer appropriate cases to the Board of Examiners who will make the ultimate decision as to whether a trainee has failed a placement or not.
3. Procedures to be Taken in The Event of a Trainee Experiencing Difficulty on a
Placement And For Placement Failure 3.1 If the supervisor notices that the trainee is having an unusual amount of
difficulty for the stage of the placement in acquiring the skills or meeting the requirements specified in the placement agreement, they should inform the trainee of this at the earliest possible stage and attempt to resolve the problems through appropriate supervision. It is important that the supervisor keeps a written record of the difficulties as soon as the situation of unusual difficulty for the stage of placement arises.
3.2 At the mid-placement review, there should be a detailed discussion of the difficulties noted and a clear action plan agreed. If any areas on the draft ECPC form are rated as “Below the Level Expected” then the action plan should specifically address these areas.
3.3 Once such an action plan is agreed, then a period of increased monitoring of the placement ensues. After a period of three weeks the Training Co-ordinator will contact the placement supervisor to enquire if progress is being made towards completion of the action plan. If the supervisor still has concerns about the trainee’s progress, then the BCUHB Capabilities Procedures (WP3a) will be invoked and an initial discussion will occur as soon as possible.
143
SECTION 3
PROGRAMME MANUAL / 2019
Those present at this meeting should include the following: • Programme Director • Programme Manager • Supervisor(s) • Trainee • Personal Tutor or friend of the trainee if they wish
This meeting should follow the initial discussion process outlined in the BCUHB Capabilities Procedure (WP3a).
3.4 At this meeting the supervisor must state clearly and explicitly in what ways difficulties are arising using the Evaluation of Clinical and Professional Competence form, Placement Agreement, Portfolio and the supervisors’ written documentation as an indication of the un-met trainee requirements and skill deficiencies. The trainee is invited to respond to these comments.
3.5 The action plan agreed at the Mid-placement review outlining Areas for Concern and Requiring Attention should be reviewed by all those present and any amendments or additions agreed. Dates for achieving new goals are specified within this. A written copy of this must be provided to each person attending the meeting. A copy must be placed in the trainees’ file along with written information from the supervisor. A review of the trainee’s progress will be formally evaluated by the training co-ordinator at the end of the placement. If there are still areas falling below the level expected on the ECPC form the training coordinator will then refer the case to the Board of Examiners who will make the ultimate decision as to whether a trainee has failed the placement or not.
3.6 Whether or not the trainee passes or fails the placement, the supervisor of the next placement will be made aware of the difficulties on the previous placement and the period of increased placement monitoring by the training co-ordinator will continue into the subsequent placement.
3.7 If the Board of Examiners decides that the initial placement is failed then the second phase of the Capabilities procedure will be instigated. This will be the First Formal interview. Because the interview is of a formal nature, the trainee will be reminded, in advance, of their right to be accompanied by an official of a recognised trade union or staff organisation or by a workplace colleague. In addition to the Programme Director and the Programme Manager a member of HR staff from BCUHB may also be present at the interview.
3.8 At the First Formal interview the level of performance required of the trainee in subsequent placements will be clarified and a revised action plan will be agreed. Following the meeting, this revised action plan will be shared with subsequent placement supervisors. Please see the Capabilities Procedure of BCUHB (WP3a) which is available on the BCUHB intranet for a full outline of this process.
3.9 At the mid-placement review of the next placement, the action plan will be reviewed. If progress is satisfactory, the trainee and training co-ordinator will agree how and when the performance will next be reviewed but it is likely that evidence of sustained progress will be required. This will mean that the
144
SECTION 3
PROGRAMME MANUAL / 2019
monitoring process may extend into subsequent placements. If further issues arise on any subsequent placement during the period of training, then the Capabilities Procedures will move directly to the Second Formal Interview stage.
3.10 If, on the other hand, the mid-placement review is not satisfactory at the next placement, the Second Formal Interview will be held as soon as possible after the date of the mid-placement review. The action plan arising from the mid-placement review will be discussed at this meeting and the trainee will be informed that failure to attain and maintain the improvements required in the action plan (i.e. a second placement failure) will result in termination of employment from BCUHB.
3.11 At the end of the placement the review of the trainee’s progress will again be formally evaluated by the training co-ordinator. If there are still areas falling below the level expected on the ECPC form the training co-ordinator will then refer the case to the Board of Examiners who will make the ultimate decision as to whether a trainee has failed the placement or not.
3.12 In this event, the Chair of the Board of Examiners shall be informed, and an extraordinary Board of Examiners meeting will be arranged. Documents from previous placements should be available at this meeting to provide relevant background information. If this extraordinary meeting concerns the failure of a second placement, the External Examiner must attend as this will normally result in overall programme failure.
4. Criterion for Programme Failure on the basis of Failed Placements Section 5 of the Programme Manual (The DClinPsy assessment procedures) specifies the criteria for programme failure. Trainees should also note carefully paragraph 7.4 of Section 5, which indicates that violations of ethical or other professional codes or guidelines of the University, NHS employer or British Psychological Society will result normally in the Board of Examiners recommending to the University that the candidate be not allowed to continue; this includes any instance where a candidate is dismissed from the NHS employer. The general University rules and regulations governing student conduct also clearly indicate that placement experience is considered an integral part of programmes such as the NWCPP. They unambiguously indicate that violation of professional codes of conduct is unacceptable, and that the University has the right to terminate the student’s training on the basis of placement failure. Extract from University General Regulations for all Students https://www.bangor.ac.uk/ar/main/regulations/BUReg13-v201001b.pdf:
‘Students on courses which involve a placement with an external organisation must comply with the rules and regulations of the placement provider, and with the codes of conduct of any relevant professional body.’
145
SECTION 3
PROGRAMME MANUAL / 2019
MONITORING AND AUDITING PLACEMENT QUALITY BPS Standards for the Accreditation of Doctoral Programmes in Clinical Psychology (2014) and CTCP Guidelines on Clinical Supervision (2010) can be used as a benchmark to ensure that all identified requirements are met on clinical placements. The programme monitors and evaluates the quality of clinical experience gained by trainees on all placements on a regular basis. Monitoring placement quality is a critical function for trainees, supervisors and Programme staff as it: • affords trainees the opportunity to provide open and honest feedback on their
learning experiences on placement • enables the supervisor to maintain and (if required) improve standards of clinical
practice placements • enables the Programme to apply appropriate regulatory and quality control standards
to the range of placements offered.
Gaining Trainee Feedback • Trainees provide detailed feedback on all clinical placements they undertake. • The Placement Quality Checklist (PQC) is used to monitor and evaluate the quality of
placements both during and at the end of placements (see Section 3). • The PQC covers placement resources and clinical practice management issues including,
professional conduct, placement planning and supervision. • Supervisors and trainees are encouraged to raise any anticipated difficulties in meeting
learning outcomes at the mid-placement review so that there is an opportunity to address the concerns during the remainder of the placement.
• Any problems with learning outcomes that are not addressed by the end of placement need to be highlighted in the final PQC.
PQC Feedback at Mid Placement Review • Trainees are asked to informally complete the PQC at mid-placement review and the
feedback is used as a basis for discussion at the review meeting. • It is the trainee’s responsibility to raise concerns regarding any areas of the placement
that they believe is not meeting their learning needs. • Whilst it is appreciated that the power differential in the supervisory relationship means
that raising concerns can be difficult, it is also an important professional skill for trainees to develop in terms of providing constructive feedback and resolving potential conflict.
• The PQC can be used by trainees to highlight areas of concern informally in supervision and/or at mid-placement review.
• If trainees are concerned about how best to give constructive feedback, they are encouraged to discuss the concerns with their Training Co-ordinator in the private meeting held prior to the joint mid-placement review with their supervisor.
• Where required, the Training Co-ordinator will take appropriate action following the mid-placement review to address any concerns raised.
146
SECTION 3
PROGRAMME MANUAL / 2019
PQC Feedback at End of Placement Review • The trainee’s PQC feedback should be shared with the supervisor after the Evaluation of
Clinical and Professional Competence form has been completed and agreed. • Supervisors have the opportunity to comment on the trainee’s feedback in the relevant
section of the PQC form. • Completed PQC forms are submitted by the trainee together with other required
placement documentation by the deadline given.
PQC Feedback and Supervisor PADR In agreement with NWCPP Training Committee and BCUHB Psychology Management Team, the Programme forwards completed PQCs on all placements to relevant Heads of Service to form part of supervisors’ Professional and Development Review (PADR). In this way the excellent placements provided by clinical supervisors can be recognised and acknowledged as well as highlighting any potential problems with placement quality in terms of resources and/or supervisory practice.
Annual Audit of Placement Quality It is necessary for Programmes to establish an audit process for clinical placements and supervision quality in partnership with Heads of Service and clinical supervisors. This should include a mechanism for seeking to overcome problems that are identified. NWCPPs Clinical Team produce an annual audit of all placements, which is presented at the Autumn Training Committee Meeting to all relevant stakeholders. The content of all submitted PQCs across the three trainee cohorts is analysed. Trainee feedback on all aspects of the placement experience (resources, clinical, professional conduct, placement planning and supervision) is reported. Qualitative comments relating to the formative, educative and restorative aspects of supervision are also included.
This audit serves two important functions referred to earlier:
• Firstly, the procedure meets identified BPS accreditation criteria enabling the Programme to maintain standards and enhance placement quality, making appropriate adjustments where required.
• Secondly, it fulfils clinical governance regulatory requirements and is an appropriate mechanism for addressing difficulties identified by trainees.
147
SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR THE USE OF RECORDINGS ON CLINICAL PLACEMENT As specified in earlier sections, the most recent accreditation standards specify that trainees should be observed in vivo and the outcome of that observation should contribute to the overall assessment process. As a result, the Programme requires supervisors to observe (live/audio/video) a minimum of 6 clinical sessions. Observed sessions need to include a range of assessment, therapy, indirect/MDT working as appropriate to the placement. Reasons for Recordings In vivo assessment - Recordings are essential in the evaluation of clinical and professional competence unless supervisors are able to be present to observe the trainee’s work directly. They provide a means of assessing clinical and professional competencies in vivo to ensure adequate standards of performance. Many aspects of clinical work are difficult for trainee’s to accurately report after the event (such as moment-by-moment interactions during critical episodes in therapy). Additionally, trainees like other professionals either qualified or in training, may withhold information about what they perceive as mistakes. They may also be reluctant to share both their positive and negative reactions to clients/carers/families/professionals. As one might expect, the reasons for non-disclosure during supervision may include a difficult supervisory relationship and the wish to avoid being negatively evaluated. CBT-RCA – As outlined earlier, trainees are required to submit an audio or video recording of a CBT intervention session as part of their CBT-RCA. The assignment should be submitted during the first two years of the Programme. As the CBT recording will be rated using the CTS-R, trainees are encouraged to record as many of their clinical sessions as possible. In doing so, they will minimise the difficulty in finding a suitable recording for submission. Trainee Self-Development - Trainees often find it helpful to listen to their own sessions for a variety of reasons including:
• having a choice of recordings for the CBT-RCA • having forgotten or overlooked important information • not understanding everything the client(s) said at the time, • a concern that the intervention was not optimal and wondering how best to proceed • preparation for weekly supervision • for self-assessment and reflection (e.g. using the CTS-R or other therapy equivalent)
In general, listening to recordings of one’s own sessions can help to promote objectivity, an appropriate reflective approach and monitoring of continuing competency development.
148
SECTION 3
PROGRAMME MANUAL / 2019
Informed Consent for Client Recordings Gaining Consent for Assessment/Non-CBT Intervention/Indirect Work A BCUHB standardised consent form for the use of trainee clinical psychologists should be used to gain client consent for the audio/video recording of a clinical session (see Section 3 p126). Copies of this form are also available on Blackboard. Completed consent forms should be stored in client files.
At all times, the interests and well-being of the client must take precedence over other considerations and recordings must be halted at the client’s request or if the trainee believes it is having an adverse effect upon them. Gaining Consent for CBT Intervention Sessions There is a separate client consent form specifically for CBT intervention sessions, which may later be submitted as part of the CBT-RCA (see Section 4). The consent form requires that consent to record the session is gained at the outset. The consent form should be filed in the clinical file. Copies of the above consent form for audio/video recording sessions for the purposes of academic assessment are also available on Blackboard. Additionally, supervisors are required to confirm that client consent was obtained for the submitted recording. The supervisor confirmation form (see Section 4) is also available on Blackboard and trainees must ensure that a signed supervisor confirmation form is submitted together with other relevant documentation for this assignment. Access to Digital Voice and Video Recorders Digital voice and video recorders are available for trainees from the Programme Office. Trainees are also provided with BCUHB encrypted USB sticks for the purposes of submitting a recording for assessment as part of the CBT-RCA. Security of Clinical Recordings It is imperative that digital recorders are stored securely at the placement base and are not removed from the premises until all recordings have been erased. For guidance regarding information governance procedures relating to the submission of recordings for the CBT-RCA (see Section 4). It is the trainee’s responsibility to ensure that recordings are kept securely at all times. Once a recording is no longer required (e.g. when the Supervisor has listened to it and it will not be submitted for the CBT-RCA) the file must be deleted from the recording device or from the computer on which it is stored. Trainees should take care to ensure that the file is completely deleted, i.e. not left in ‘trash’. If recordings are being kept in order to select one for submission of the CBT-RCA then these can be retained until the assignment has been successfully completed. Once the assignment grade has been ratified by the Board of Examiners, it is the trainee’s responsibility to ensure that all video or audio files are deleted.
149

SECTION 3
PROGRAMME MANUAL / 2019
Recordings that do not relate to the CBT-RCA and will not be selected for the purposes of academic assessment should be erased once supervisor and/or trainee have listened to the recording for the purposes of supervision.
150
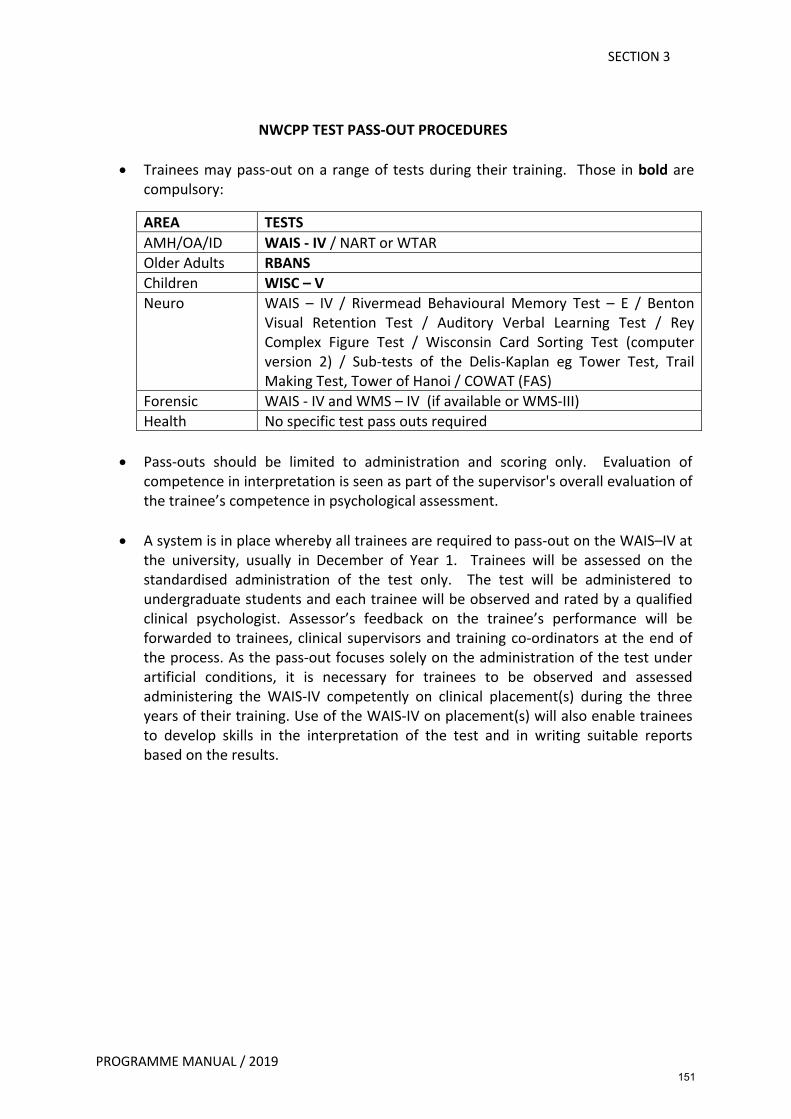
SECTION 3
PROGRAMME MANUAL / 2019
NWCPP TEST PASS-OUT PROCEDURES
• Trainees may pass-out on a range of tests during their training. Those in bold are compulsory:
AREA TESTS AMH/OA/ID WAIS - IV / NART or WTAR Older Adults RBANS Children WISC – V Neuro WAIS – IV / Rivermead Behavioural Memory Test – E / Benton
Visual Retention Test / Auditory Verbal Learning Test / Rey Complex Figure Test / Wisconsin Card Sorting Test (computer version 2) / Sub-tests of the Delis-Kaplan eg Tower Test, Trail Making Test, Tower of Hanoi / COWAT (FAS)
Forensic WAIS - IV and WMS – IV (if available or WMS-III) Health No specific test pass outs required
• Pass-outs should be limited to administration and scoring only. Evaluation of
competence in interpretation is seen as part of the supervisor's overall evaluation of the trainee’s competence in psychological assessment.
• A system is in place whereby all trainees are required to pass-out on the WAIS–IV at the university, usually in December of Year 1. Trainees will be assessed on the standardised administration of the test only. The test will be administered to undergraduate students and each trainee will be observed and rated by a qualified clinical psychologist. Assessor’s feedback on the trainee’s performance will be forwarded to trainees, clinical supervisors and training co-ordinators at the end of the process. As the pass-out focuses solely on the administration of the test under artificial conditions, it is necessary for trainees to be observed and assessed administering the WAIS-IV competently on clinical placement(s) during the three years of their training. Use of the WAIS-IV on placement(s) will also enable trainees to develop skills in the interpretation of the test and in writing suitable reports based on the results.
151
SECTION 3
PROGRAMME MANUAL / 2019
PROGRAMME POLICY REGARDING THE CRITERIA FOR PASS-OUTS ON SELECTED PSYCHOMETRIC TESTS
With the exception of the WAIS-IV, training in psychometric test delivery will normally involve trainees observing their supervisor’s administration of the test and the opportunity for modelling/role play during supervision. The trainee is advised to practise administering and scoring the test until s/he is proficient in its use. Supervisors should then satisfy themselves through direct observation that trainees are competent in each of the following areas:
Administration and Scoring 1. That the test materials have been made ready before the client arrives. 2. That the trainee adequately develops rapport with the client before testing begins. 3. That the various items/components of the test are given in the correct or accepted
order. 4. That responses are recorded accurately, clearly and in sufficient detail for an
independent person who has not witnessed the administration to be able to score the test.
5. That the test is administered smoothly so that the client is not disrupted by the process of its presentation.
6. That responses are scored correctly and in accordance with the instructions in the test manual.
7. That the results are calculated/transformed correctly using appropriate normative tables.
8. The supervisor should not intrude during the administration of the test unless it is considered necessary for clinical reasons, which would then normally negate the session as a successful test pass-out.
Interpretation Whilst the interpretation of psychometric tests is a vital part of the trainee’s development, it does not constitute part of the formal pass-out procedure. Supervisors will work with trainees to develop their understanding and interpretation of relevant psychometric tests throughout the placement and evaluate this as part of the ‘assessment’ ECPC competency at the end of placement. The following points are helpful to be kept in mind by supervisors whilst monitoring trainees' competence in test interpretation:
1. That legitimate conclusions are reached on the basis of the test results obtained. 2. That the trainee abstracts from his/her conclusions. 3. That conclusions from the test are appropriately linked with other information
about the client so that an opinion can be formed. 4. That appropriate action is recommended on the basis of the opinion.
152
SECTION 3
PROGRAMME MANUAL / 2019
SAFETY ISSUES IN CLINICAL TRAINING Introduction Under the Health & Safety at Work Act (2011), employers have a duty to provide a safe working environment for employees. Employees have a responsibility to take reasonable precautions in respect of their own personal safety at work, and to adhere to the policies and procedures of the organisation. Trainees and supervisors should familiarise themselves with BCUHB Health and Safety and Equal Opportunities Policies via the intranet. Safety Issues at the University
• General security arrangements for the university base are clarified in the current version of Bangor University’s General Health and Safety Handbook, which can be found using the following web link: http://www.bangor.ac.uk/studentservices/wellbeing/safety.php.en
• Induction sessions in the first year timetable will also cover safety and security issues related to the use of the Programme office, trainee resource room, keys/codes, photocopying and use of equipment.
• Induction sessions in the first-year timetable include De-escalation and risk issues. The aim of these sessions is to raise awareness of such matters and ensure that appropriate guidelines are adhered to.
• The arrangements for reporting and seeking approval for annual leave, sick leave, compassionate leave and study leave are outlined in the Admin Handbook. All absences from the Programme must be agreed with the trainee’s line manager (Professor Robert Jones, Programme Director). Trainees are also required to inform/seek approval from their supervisor for all absences from placement.
Safety Issues on Placement
• ID Cards – Trainees are provided with a BCUHB identity card, which must be worn whilst on placement.
• Dress Code – Trainees are advised to speak with their supervisor regarding appropriate dress for the placement.
• Working Hours/Working Late. Trainees should consider the following with each placement supervisor:
Ø procedure for safety and security outside routine working hours. Ø access to the building e.g. keys and alarm codes. Ø If there is a panic system in use, how does this work? Ø Security of clinical information – where are the keys for offices/filing cabinets
kept? Ø Are trainees permitted to remove clinical notes from the building? If so, what
are the procedures? Ø Where are clinical psychology session notes recorded? Ø Supervisors and trainees must use the BCUHB Datix system for reporting
untoward incidents.
153
SECTION 3
PROGRAMME MANUAL / 2019
Therapy Issues • It is worth noting that therapy and boundary issues can lead to professional
dilemmas for clinical psychologists at all levels. Trainees are encouraged to raise concerns about these issues should they arise on placement. Such concerns may relate to personal touch, sexual attraction and power imbalances in the therapeutic relationship. Training co-ordinators and supervisors are always available to discuss these issues with trainees.
• Trainees are provided with copies of the BPS Generic Professional Practice Guidelines and Code of Ethics and Conduct when they commence training and are encouraged to refer to these documents for further clarification.
• Seating Arrangements in rooms: Is it possible for the trainee /supervisor to swiftly leave the room if a safety concern arises?
• Home visits: Trainees must be aware of the lone working policy and arrangements in each placement for diary tracking etc.
• Trainees must ensure the information sharing/consent guidelines are used on placement in addition to any service/departmental consent forms.
• Trainee should ensure that all clients have been made aware of the limits to confidentiality.
• Trainees and supervisors need to agree how best to communicate with clients e.g. following non-attendance.
• It is vital that trainees are familiar with the process of password protecting documents when emailing confidential information.
Risk Assessment
• There are a variety of risk issues that trainees may encounter during training. The Wales Applied Risk Research Network (WARRN) training is included as part of the first-year teaching and this will help them negotiate the process of risk assessment and management. Relevant teaching is included regarding other risk issues and trainees have the opportunity to develop their skills in assessing and managing risk during supervised clinical practice.
• Trainees need to discuss the procedure for assessing risk and inform their supervisor if there is cause for concern.
• In the supervisor’s absence, trainees need to be clear what the identified systems are for discussing risk issues within the team/service.
• Dealing with suicide risk is difficult for trainees as well as for qualified clinical psychologists. While trainees gain both teaching and placement experience in assessing and managing suicide risk it is recognised that not all suicides are preventable.
• The death of a client by any means is a difficult experience for a trainee. The Programme will provide support in the event of this happening, primarily through the training co-ordinator. Trainees may also make use of the personal development counselling scheme and personal tutor system to help them in this event.
154
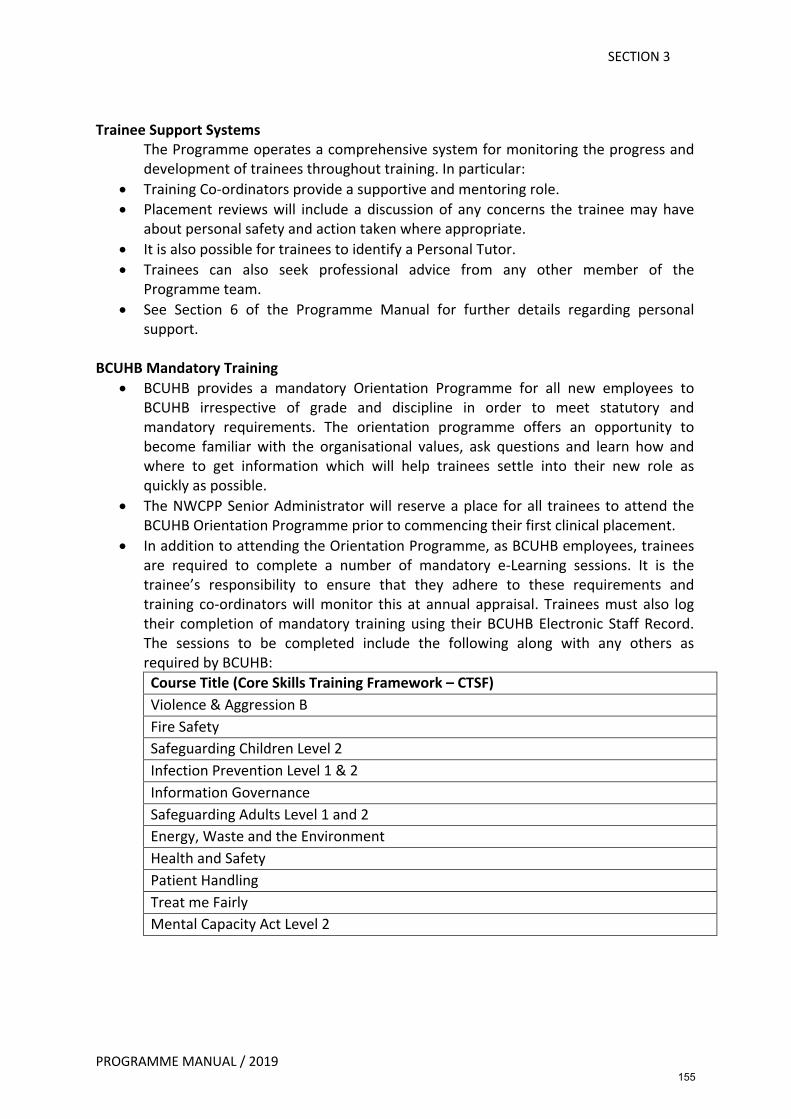
SECTION 3
PROGRAMME MANUAL / 2019
Trainee Support Systems The Programme operates a comprehensive system for monitoring the progress and development of trainees throughout training. In particular:
• Training Co-ordinators provide a supportive and mentoring role. • Placement reviews will include a discussion of any concerns the trainee may have
about personal safety and action taken where appropriate. • It is also possible for trainees to identify a Personal Tutor. • Trainees can also seek professional advice from any other member of the
Programme team. • See Section 6 of the Programme Manual for further details regarding personal
support.
BCUHB Mandatory Training • BCUHB provides a mandatory Orientation Programme for all new employees to
BCUHB irrespective of grade and discipline in order to meet statutory and mandatory requirements. The orientation programme offers an opportunity to become familiar with the organisational values, ask questions and learn how and where to get information which will help trainees settle into their new role as quickly as possible.
• The NWCPP Senior Administrator will reserve a place for all trainees to attend the BCUHB Orientation Programme prior to commencing their first clinical placement.
• In addition to attending the Orientation Programme, as BCUHB employees, trainees are required to complete a number of mandatory e-Learning sessions. It is the trainee’s responsibility to ensure that they adhere to these requirements and training co-ordinators will monitor this at annual appraisal. Trainees must also log their completion of mandatory training using their BCUHB Electronic Staff Record. The sessions to be completed include the following along with any others as required by BCUHB: Course Title (Core Skills Training Framework – CTSF) Violence & Aggression B Fire Safety Safeguarding Children Level 2 Infection Prevention Level 1 & 2 Information Governance Safeguarding Adults Level 1 and 2 Energy, Waste and the Environment Health and Safety Patient Handling Treat me Fairly Mental Capacity Act Level 2
155
SECTION 3
PROGRAMME MANUAL / 2019
SUPPORT FOR SUPERVISORS The clinical supervision of trainees can sometimes be a stressful process, especially if supervisors are new and relatively inexperienced in supervising trainees. However, it is also possible for experienced supervisors to find the process difficult at times. Support for NWCPP supervisors is therefore provided in the following ways:
• The Programme Team are always available to assist Supervisors with any queries or difficulties they man encounter whilst setting up or providing a placement for a trainee. In particular, it is part of the training co-ordinator’s role to help address these problems when they arise.
• The Supervisors Committee of the NWCPP run a series of 3 workshops for new and inexperienced supervisors each year (although more experienced supervisors are also welcome to come along for a refresher). The workshops are timed to coincide with the autumn placements each year. Later in the year there is usually an additional workshop geared more specifically for experienced supervisors (although new supervisors are also welcome to attend). An outside speaker, who is invited by NWCPP, generally delivers this workshop often focusing on a particular aspect of the supervisory process.
• In light of the new BPS accreditation criteria and changes to the Programme as a result, NWCPP will be providing extra workshops/meetings to help supervisors familiarise themselves with these changes.
• In addition, there is a small Supervisor’s library of relevant books available via the Programme Office (see Section 3). Please contact the Admin Assistant (Research & Finance) to arrange to borrow a book.
• There is also a supervisor mentor system, which has the support of local Heads of Service. Supervisors are strongly encouraged to nominate a mentor for support. This person should be another clinical psychologist but need not be in the same specialism as the Supervisor. The purpose of the mentor is to supply support and advice as appropriate. In addition, they may discuss general issues about supervision, which can help the supervisor develop their supervisory skills. The relationship between the supervisor and mentor is confidential and information sharing should be treated with the same degree of confidentiality as client information.
156
SECTION 3
PROGRAMME MANUAL / 2019
Supervisors’ Reading List
1. Bieschke, K. J., & Perez, R. M., & Debord, K.A. (Eds) (2007). Handbook of counselling
and psychotherapy with lesbian, gay, bisexual and transgender clients. (2nd edn). American Psychological Association.
2. Beinart, H., & Clohessy, S. (2017). Effective supervisory relationships best evidence
and practice. Wiley Blackwell.
3. Bradley, L. J. (1989). Counselor Supervision: Principles, Process and Practice. (2nd edn). Accelerated Development Inc.
4. Burck, C., & Daniel, G. (Eds) (2010). Mirrors and reflections, processes of systemic
supervision. Karnac.
5. Carrol, M. (1996). Effective supervision for the helping professions. (2nd edn). SAGE. 6. Dryden, W., & Thorne, B. (Eds) (1991). Training and supervision for counselling in
action. SAGE. 7. Duncan, B. L., & Miller, S.D., & Wampold, B.E., & Hubble, M.A. (Eds) (2010). The
heart and soul of change, delivering what works in therapy. (2nd edn). American Psychological Association.
8. Falander, C. A., & Shafranske, (2008). Clinical Supervision. A Competency Based
Approach. Washington. DC: American Psychological Association 9. Feltham, C., & Dryden, W. (Eds) (1994). Developing counsellor supervision. SAGE.
10. Fleming, I., & Steen, L. (Eds) (2012). Supervision and Clinical Psychology, Theory,
Practice and Perspectives. (2nd edn). Routledge.
11. Hawkins, P., & Shohet, R. (2000). Supervision in the helping professions. (2nd edn). Open University Press.
12. Hawkins, P., & Shohet, R. (2012). Supervision in the helping professions. (4th edn).
Open University Press. 13. Hughes, J., & Youngson, S. (Eds) (2009). Personal development and clinical
psychology. BPS Blackwell.
14. Lahad, M. (2001) Creative Supervision. The use of expressive arts methods in supervision and self-supervision. London: Jessica Kingsley
157
SECTION 3
PROGRAMME MANUAL / 2019
15. Scaife, J. (2001) Supervision in the mental health professions, a practitioner’s guide. Brunner-Routledge.
16. Scaife, J. (2009). Supervision in Clinical Practice: A Practitioner’s Guide. (2nd edn). Hove. Brunner-Rutledge.
17. Schon, D. A. (1983). The reflective practitioner how professionals think in action.
Ashgate. 18. Stedmon, J., & Dallos, R. (Eds) (2009). Reflective practice in psychotherapy and
counselling. Open University Press. 19. Stoltenberg, C.D., & McNeill. B. W. (2010). IDM Supervision: an integrative
developments model for supervising counsellors and therapists. (3rd edn). Routledge. 20. Walker, M., & Jacobs, M. (2004). Supervision questions & answers for counsellors &
therapists. Whurr Publishers. 21. Watkins, Jr. C. E. (Eds) (1997). Handbook for psychotherapy supervision. John Wiley
& Son, Inc. 22. Watkins, Jr. C. E., & Milne, D. L. (Eds) (2014). The Wiley International Handbook of
Clinical Supervision. Wiley Blackwell.
23. Wiener, J., & Mizen, R., & Duckham, J. (Eds) (2013). Supervising and being supervised, a practice in search of a theory. Palgrave MacMillan.
158

SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE IN ADULT MENTAL HEALTH
Introduction In line with the DCP Core Purpose and Philosophy, the placement will focus on reducing psychological distress and enhancing and promoting psychological well-being through the systematic application of knowledge derived from psychological theory and evidence.
Placement Settings and Services Most AMH placements will be based within a local Community Mental Health Team. Other examples may be working within a Psychological Therapies Service or across inpatient and community settings. The trainee will be supervised by a Clinical Psychologist, sometimes with a Counselling Psychologist or Psychological Therapist contributing to the placement.
Placement Induction Trainees will be given the opportunity to become familiar with the organisational structure of the service as well as an awareness of the broader Welsh NHS. This will normally involve shadowing the supervisor, other relevant professionals and becoming familiar with other settings/services e.g. inpatient services, voluntary agencies, primary care services. The supervisor will aid the trainee in organising an induction programme in the first few weeks of placement. A placement agreement will be set up in the early stages of placement and will be reviewed at mid-placement.
Caseload The clinical experience gained on placement should reflect the range of clients (age, gender and presenting problems) typically seen by the supervisor. Some AMH supervisors may also provide experience of Autistic Spectrum Disorder assessments e.g. ADOS. In practice most Clinical Psychologists working in Adult Mental Health see clients with complex and severe problems. Attempts will usually be made by supervisors to select some less complex cases for trainees in view of their stage of training and placement duration. Whilst experience of more complex cases can be gained indirectly through case discussion and observation of the supervisor, trainees are also required to obtain direct experience of complex AMH cases. The actual number of clients seen will vary according to the service setting. Usually by the end of placement the trainee will have had the opportunity to work in some depth with a minimum of six clients. The requirement for long-term client work may come from the AMH placement in negotiation with the supervisor. All referrals will be made through the supervisor.
159
SECTION 3
PROGRAMME MANUAL / 2019
Therapeutic Approaches Most AMH placements will provide a good opportunity to develop and refine skills in specific psychological therapies. Depending on the placement, trainees may gain experience in a range of therapeutic approaches including Cognitive Behaviour Therapy, Dialectical Behaviour Therapy and/or Acceptance and Commitment Therapy. Some AMH supervisors also have experience of approaches such as Compassion Focused Therapy, Schema Focused Therapy and Intensive Short-Term Dynamic Psychotherapy.
Required Learning Outcomes See Programme Specification in Section 1 of the Programme Manual. By the end of placement, trainees should have begun to develop the following core competencies as required by CTCP. Transferable skills in: 1. Generalisable meta-competencies 2. Psychological assessment – in accordance with trainees’ requirement to be assessed
using the WAIS-IV and NART or Wechsler Test of Adult Reading (WTAR) in a clinical setting, this opportunity may be available during some adult mental health placements
3. Psychological formulation 4. Psychological intervention 5. Evaluation 6. Personal and professional skills and values 7. Communication and teaching 8. Organisational and systemic influence and leadership – although AMH placements are
in the first year of training there may be some opportunity for working systemically within teams and for stage-appropriate leadership
9. Research – identifying and critically appraising research evidence relevant to practice 10. Service User involvement (feedback, voluntary organisations, contact with People
Panel) and any other relevant role in service provision.
Supervision The minimum BPS requirement of 1-hour formal supervision per week and three hours contact in total should be adhered to – see Formalities section for Guidelines Clinical Supervision.
160
SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE IN OLDER ADULTS Introduction The minimum requirements and recommended Core Competencies for Trainee Clinical Psychologists working with older people are set out in the Good Practice Guidelines for UK Clinical Psychology Training Providers for the Training and Consolidation of Clinical Practice in Relation to Older People (PSIGE_ Psychology Specialists Working with Older People, 2006). The clinical placements aim to meet these guidelines. Placement Settings and Services The trainee will obtain experience of direct working with clients in a variety of settings, including community, memory clinics, outpatient clinics, day hospitals and day care, hospital wards (mental health and dementia), residential and nursing homes, as well as services run by other agencies e.g. Social Service Day Centres. Where possible, settings will include those allied to physical health e.g. a General Hospital. The trainee will also carry out indirect work with informal (e.g. family and friends) and formal caregivers (care staff, home helps) as indicated. There will be opportunities to work with other professions, such as doctors, psychiatrists, social workers, nurses (including community psychiatric nurses), occupational therapists, physiotherapists and speech and language therapists. The trainee should be aware of non-statutory service provision e.g. Age Concern and Alzheimer Society, Carers Outreach. Caseload Experience with older adults will involve as wide a range of psychological problems presented by older people as possible to include functional, organic and physical health issues. Experience will be obtained in working with psychological therapies used and any adaptations that might be required, when working with this age group. Both men and women should be seen who are over 65 years of age but younger people with difficulties associated with later life may be encountered. Contact with relatives caring for an older person with any of the above problems must be included. Trainees will be required to prepare formulations relating clinical problems with a minimum of seven older people. This experience should encompass the trainee undertaking a minimum of two cognitive assessments. One piece of clinical work will be prepared for Programme requirements. All referrals to the trainee will be made by, or in consultation with the supervisor.
161
SECTION 3
PROGRAMME MANUAL / 2019
Required Learning Outcomes
1. Psychological Assessment, including neuropsychological assessments. The trainee will be expected to develop skills in assessing a range of problems relevant to an older population. The trainee will need to be able to recognise and manage risk in older people. The trainee will need to learn and ‘pass out’ on a cognitive screening test: RBANS.
2. Psychological Formulation. The trainee needs to be able to determine psychological formulations for older people with complex, multiple problems e.g. clients with co-existing dementia, depression, social isolation, substance abuse, and poverty.
3. Psychological Interventions. The trainee needs to be able to effectively intervene, both directly and indirectly, to improve the lives of older people, and their carers, using psychological understanding and techniques based on a scientist-practitioner and reflective-practitioner models. The trainee needs to be able to recognize and manage the effects of differences in age between themselves and older people particularly in the implementation of psychological therapies. They need to be able to encourage and support older people, their carers, and staff to increase autonomy, choice, and psychological well-being and to work effectively in order to increase motivation when it is low.
4. Communication. The trainee needs to be able to effectively communicate with older people, overcome any cognitive and sensory impairments, to enable effective work to take place and provide written information in the right format for the recipient, including an individual older person.
5. Professional and Ethical Issues. The trainee will develop a personal and professional recognition and understanding of how to address age discrimination and minimise psychological barriers to older peoples’ independence. They need to be able to demonstrate cultural sensitivity, and address culture specific expectations of ageing. They will recognise and manage boundary issues when working with older people in different settings, e.g. patients’ homes, medical wards.
6. Organisational working. The trainee will develop a basic knowledge of the range of services and agencies available for older people and how to access them. They will develop an effective working style with other providers of services for older people to address psychological aspects of health and health care. Trainees should begin to develop their thinking about the potential range of leadership roles, including consultancy services, offered by Clinical Psychologists (e.g. service evaluation, health needs, assessment, service design, organisational change, service problem solving).
7. Supervision. The supervisor will be working with the trainee to work towards obtaining the above learning outcomes, while drawing the trainees attention to:
a. the maintenance of a professional relationship with an older person in light of issues pertinent to this age group.
b. The importance of evaluating consent to treatment where an older person is either not capable of giving informed consent or does not share the same view of the problems as carers.
c. The importance of adopting a positive attitude to working with older people, which may challenge their personal assumptions and views about ageing.
162

SECTION 3
PROGRAMME MANUAL / 2019
d. Awareness of the clients’ position in history and the fact that older people have a history that is not necessarily shared by the trainee.
8. Service User involvement (feedback, voluntary organisations, contact with People Panel) and any other relevant role in service provision.
163
SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE IN NEUROPSYCHOLOGY Introduction The Division of Neuropsychology (BPS) provides guidelines for professional practice. Clinical activity during the placement will cover the assessment and management of neuropsychological impairments following acquired brain injury, based on current evidence of best practise. Placement Settings and Services Trainees are based at the North Wales Brain Injury Service, Colwyn Bay Hospital for the duration of their placements. The service covers North Wales and can include a significant amount of travel. More detailed information about the service is available in:
Coetzer, B.R., Vaughan, F.L., Roberts, C.B. & Rafal, R. (2003). The development of a holistic, community-based neurorehabilitation service in a rural area. The Journal of Cognitive Rehabilitation, 21 (2): 4-8.
Trainees will be given the opportunity to become familiar with the organisational structure of the service as well as an awareness of the broader NHS and National Service Frameworks. A key policy document the trainees are expected to read is the Division of Neuropsychology (BPS) document providing guidance to commissioners (2015). Trainees will normally initially shadow the supervisor, other relevant professionals and become familiar with other settings/services e.g. inpatient services, voluntary agencies, and primary care services. The trainee is usually provided with relevant papers etc. to read. The supervisor will aid the trainee in organising an induction programme in the first few weeks of placement. A placement agreement should be set up in the early stages of placement and should be reviewed at mid-placement. The Training Co-ordinator will visit the placement at the beginning and can help to set up the Placement Agreement. Caseload The clinical experience gained on placement should reflect the range of patients (age, gender and presenting problems) typically seen in the service. It is expected that the trainee will identify an initial caseload with the supervisor as soon as possible after starting the placement. In practise most Clinical Neuropsychologists working in community neuro-rehabilitation services see patients with moderate to severe acquired brain injury that have led to complex disability. Attempts will usually be made by supervisors to select less complex cases for trainees in view of their stage of training and placement duration. However ideally some experience of more complex cases can be gained indirectly through case discussion, observation of the supervisor and sometimes through co-working within the multi-disciplinary team. The actual number of patients seen will vary depending on the needs identified during assessment. Usually by the end of placement the trainee will have had the opportunity to work in some depth with between six patients (six-month placement) and ten patients (1-year placement). The requirement for a long-term case may come from the neuropsychology placement in negotiation with the supervisor.
164
SECTION 3
PROGRAMME MANUAL / 2019
All referrals will be made through the supervisor, following the multi-disciplinary referral meeting. Required Learning Outcomes See Programme Specification in Section 1 of the Programme Manual. By the end of placement, trainees should have begun to develop the following core competencies as required by the British Psychological Society. Transferable skills in: 1. Clinical assessment in neuropsychology (including presenting problems, history,
clinical picture, diagnosis, interviewing carers, interpretation of findings and case formulation).
2. Psychometric assessment in neuropsychology (including measures of general ability, attention, language, memory, and executive control function among others).
3. Writing clinical neuropsychology reports. 4. Neuropsychological rehabilitation (individuals and groups) within a multi-disciplinary
setting (including cognitive rehabilitation, psycho-education, work with carers, among others)
5. Gaining a thorough understanding of what other professionals contribute to Neuro-rehabilitation.
6. Personal and Professional skills 7. Communication and Teaching 8. Service Delivery 9. Research – identifying and critically appraising research evidence relevant to practice. 10. Service User involvement (feedback, voluntary organisations) and any other relevant
role in service provision. Supervision The minimum BPS requirement of 1-hour formal supervision per week and three hours contact in total should be adhered to – see Formalities section for Guidelines Clinical Supervision.
165
SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE IN CHILD AND ADOLESCENT PSYCHOLOGY Introduction This document provides an outline of the minimum requirements and recommended Core Competencies for Trainee Clinical Psychologists working with Children, Young People and their families. Included here are guidelines indicating the minimum experience a Trainee Clinical Psychologist should have achieved at the conclusion of placement.
Placement settings and services Child and Adolescent placements will be based within local Specialist Child and Adolescent Mental Health teams, North Wales Adolescent service, and hospital based Paediatric Psychology departments. Placement Induction The supervisor will help the trainee to organise an induction programme in the early part of the placement where an understanding of multi-disciplinary and inter-agency work is gained. The trainee will be expected to familiarise themselves with and work within the All Wales Child Protection Procedures, with the support of and in consultation with their supervisors. The trainee will become familiar with how the teams are organised, how referrals are prioritised, and issues around the source and allocation of referrals to be described by the supervisor. Clinical Activity Over the course of the placement, the trainee will have taken the lead in clinical work with at least 6 clients, although the number of individual clients may be lower if the trainee is involved in delivering group work. Individual interventions will include work with children, adolescents, and their families with some boys and girls. By the end of their training the trainee’s child and adolescent clients will be across the age-range but reflecting those typically referred to the service where the placement is set. On completion of the Child and Adolescent placement the trainee will have had some experience of working in partnership with families, educational services, social services, health services and voluntary agencies (where appropriate). At least some of the work that the trainee is involved with will have taken place in a setting other than the placement base, for example home or school, and involved working collaboratively with colleagues in other agencies. The trainee will have the opportunity for direct observation of the clinical work of the supervisor throughout the placement, this will include work at different stages in the course of treatment and in different contexts, for example both direct and consultation work. In
166
SECTION 3
PROGRAMME MANUAL / 2019
addition, observation of the trainee will be organised at different stages of clinical intervention. There will be an opportunity for the trainee to deliver information/training to other professional groups, either in the form of a lecture of seminar, or a structured workshop. Required Learning Outcomes 1. Psychological Assessment. During the placement the trainee will be required to
develop competence in the assessment of children, adolescents and their families incorporating a developmental perspective. Awareness of attachment theory and biological/ psycho-social models of child development will also be considered in terms of presenting difficulties.
2. Psychometric Assessment. The trainee will demonstrate an understanding of
psychometric assessment and measures for use with children and adolescents, and to be able to select, administer and interpret first stage psychometric assessments with children and adolescents, for example the WISC-IV–UK. Other child neuro-psychological assessments can be used where appropriate.
3. Psychological Formulation. The trainee needs to demonstrate an ability to identify the
maintaining, predisposing, protective and precipitating factors and identify the most appropriate therapeutic intervention (for example, CBT, behavioural, systemic and psychodynamic).
4. Psychological Intervention. The trainee will be able to utilise the main theoretical
models, which underpin therapeutic interventions in accordance with the current evidence base and approaches adopted on the placement.
5. Professional /Clinical Skills. The trainee will be able to build a rapport and work in
partnership with children, adolescents and their families/carers. There will also be an emphasis on promoting leadership skills during placements.
6. Evaluation. Over the course of the placement the trainee will be encouraged to use a
range of psychological questionnaires to assess the severity of the presenting concerns and evaluate the effectiveness of the intervention.
7. Supervision. The trainee will bring to supervision an awareness of the clinical material
and an ability to reflect on their clinical practice. There will also be an expectation that the trainee shows an awareness of the impact of working with children at risk, (e.g. deliberate self-harm, child protection, and the need for support and supervision).
8. Service User Involvement. Feedback, voluntary organisations, contact with People
Panel and any other relevant role in service provision.
167
SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE WHEN WORKING WITH INDIVIDUALS WITH AN
INTELLECTUAL DISABILTY Introduction The aim of the placement is to teach skills that will help improve the psychological well-being of the person with intellectual disability, and their families and carers in accordance with the Division of Clinical Psychology statement of core purpose and philosophy. This will be achieved through systematic application of knowledge derived from psychological theory and evidence and will be based upon the premise that all people have the same human value and the right to be treated as unique individuals. Placement Settings and Services Most intellectual disability placements will be based within a local multidisciplinary team serving the community. The trainee will be placed with a team primarily working with adults but might also have the opportunity to gain relevant experience of working in children’s services as well, if available. Assessment and working with individuals with an intellectual disability forms part of the service provided by Intellectual Disability Services. Liaison and co-operation with other professionals is an important part of the work, which may be carried out in a variety of settings. Liaison with other services will also be an aspect of working in Intellectual Disability Services. Placement Induction Trainees will be given the opportunity to become familiar with the organisational structure of the service as well as NHS and National Service frameworks. This will involve reading relevant documentation, talking to key members of the organisation and shadowing the supervisor and other relevant professionals to various settings such as day services, work placements, colleges and schools for individuals with ID. The trainee and supervisor will set up an induction programme at the start of the placement. A placement agreement should be set up at an early stage of the placement and reviewed mid-placement. Caseload The trainee will be given the opportunity to work with as wide a range of clients as possible. This will involve clients varying in their degree and type of disability, their presenting problem and who are at different life stages. Part of the intervention work is often carried out through and/or with the help of carers and family members. Trainees may be given the opportunity to be involved in group work, and assessments of eligibility for the service, along with assessing individuals in the later stage of life for cognitive decline that may be associated with dementia. Each trainee will work with approximately six clients individually.
168
SECTION 3
PROGRAMME MANUAL / 2019
Required Learning Outcomes 1. To gain an understanding of current policies and contexts of services for people with
an intellectual disability. 2. To gain an appreciation of the heterogeneity of people classified as having an
intellectual disability and of relevant biological and neurological issues. 3. To gain an understanding of the various contexts in which people with an intellectual
disability function and live and of life span issues which they face. 4. To gain an ability to communicate with people with an intellectual disability with
various levels of communicative skills. 5. To gain experience of conducting a capacity assessment with an individual with an
intellectual disability 6. To gain an understanding of consent issues between professionals and people with an
intellectual disability and the potential vulnerability of this client group. 7. To gain an ability to adapt psychological assessments and interventions to the
cognitive, communication, sensory, social and physical needs of people with an intellectual disability.
8. To gain an ability to complete a detailed functional analysis and translate the results into appropriate guidelines which are sensitive to the needs of those implementing them, as well as recognising common barriers to successful implementation.
9. To gain an ability to develop multi-faceted formulations and interventions that take into account individual, systemic and organisational factors.
10. To gain an ability to work with a range of service providers including health, social services, voluntary and private sectors.
11. To have an opportunity to work either directly or indirectly with someone who has profound and multiple disabilities.
12. To gain experience of providing consultancy and a greater understanding of the contribution of consultancy to practice.
13. To gain experience of quality improvement work, such as involvement in service development.
14. To gain an understanding of diversity issues, including cultural and linguistic factors as they impact on this client group, within the bilingual context of Wales.
15. Service User involvement (feedback, voluntary organisations, contact with People Panel) and any other relevant role in service provision.
Supervision The minimum BPS requirement of 1-hour formal supervision per week and three hours overall contact with the supervisor in total will be provided. Professional Issues Written records must be legible, signed and kept secure at all times in a manner agreed by the supervisor. The trainee must be aware of the local Health and Safety measures in place and should attend referral meetings, sufficient to understand the referral process between the various involved professionals. In addition, he or she should attend the meetings of the Psychology Services.
169

SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE IN HEALTH CLINICAL PSYCHOLOGY Introduction Health Clinical Psychology placements are generally only available as third year specialist placements and usually occur in adult or child and family services. However, some second year Child and Adolescent Placements may include paediatric casework, where the supervisor has a split CAMHS – Paediatric post. In line with the DCP core purpose and philosophy, the placement will focus on reducing psychological distress and enhancing and promoting psychological well-being associated with clients with chronic medical and physical health problems. It may also involve working psychologically with patients to help improve adherence with necessary medical treatment where this has been compromised by psychological factors. This will be carried out through the systematic application of knowledge derived from psychological theory and evidence. Placement Settings and Services Health Clinical Psychology placements will be based within community and/or general hospital settings, under the supervision of a Clinical Psychologist and/or Psychological Therapist in one or more of the following services: pain management; chronic fatigue; renal; cancer; paediatrics; diabetes and other. Most of the work will occur in out-patient settings, with some inpatient and home visits a possibility. Placement Induction Trainees will be given the opportunity to become familiar with the organisational structure of the service(s) as well as an awareness of the broader NHS and relevant National Service Frameworks. This will normally involve shadowing the supervisor and other relevant professionals in hospital settings. The supervisor will aid the trainee in organising an induction programme in the first few weeks of placement. A placement agreement should be set up in the early stages of placement and should be reviewed at mid-placement. Caseload The clinical experience gained on placement should reflect the range of clients (age, gender and presenting problems) typically seen by the supervisor. In some services (e.g. pain management, chronic fatigue), Clinical Psychologists typically see clients with chronic health problems for whom medical and physical treatments and interventions have led to an unsatisfactory outcome. As a result these clients are likely to have moderate mental health problems and/or significant cognitive and behavioural obstacles to successful self-management of their enduring chronic health problem. In other services (e.g. renal, cancer), Clinical Psychologists typically see patients whose sense of self, emotional well being and quality of life is affected by the relentless, intrusive nature of treatments and end of life issues. Working systemically is as important as working with individuals and groups in all areas of Health Clinical Psychology. In Paediatric settings work will often be with parents and/or siblings, as well as the child patient. In adult settings, family members/carers are seen as patients in their own right as the burden on them of having a loved one with a chronic
170
SECTION 3
PROGRAMME MANUAL / 2019
health condition can be considerable. Whilst working systemically with MDT staff for the benefit of specific patients is common practice, providing teaching to staff can also occur on a placement and can help staff to not only better understand how to undertake psychological care but also how to help support their own psychological wellbeing. Cases range in level of complexity. Supervisors will select cases for trainees dependent on stage of training, placement duration, specific interests/requirements of trainees (e.g. involvement in group work) and level of complexity of individual cases. If direct experience of highly complex cases is not possible, some experience of such cases can be gained indirectly through case discussion and observation of the supervisor. The actual number of clients seen will vary according to the service setting and type of placement required. Usually by the end of placement the trainee will have had the opportunity to work in some depth with a minimum of six clients. All referrals will be made through the supervisor.
Required Learning Outcomes See CTCP Document – B: The required learning outcomes and the structure of training – Section 1 of the Programme Manual. By the end of placement, trainees should have built upon the following core competencies as required by CTCP. Transferable skills in: 1. Psychological Assessment – in accordance with trainees’ requirement to pass-out on
the WAIS-III and NART/WTAR this opportunity may be available during some Health Clinical Psychology placements. However, it is not common for neuro-psychological assessment to be undertaken in adult settings. In the main, psychological assessment is likely to involve the following methods: interview, psychometric measures, observation, review of medical notes, and consulting with MDT colleagues and other services.
2. Psychological Formulation 3. Psychological Intervention 4. Evaluation 5. Personal and Professional Skills 6. Communication and Teaching 7. Service Delivery 8. Research – identifying and critically appraising research evidence relevant to practice 9. Service User involvement (feedback, voluntary organisations, contact with People
Panel) and any other relevant role in service provision
Supervision The minimum BPS requirement of 1-hour formal supervision per week and three hours contact in total should be adhered to – see Formalities section for Guidelines Clinical Supervision.
171
SECTION 3
PROGRAMME MANUAL / 2019
GUIDELINES FOR CLINICAL EXPERIENCE IN FORENSIC CLINICAL PSYCHOLOGY
Introduction At the North Wales Forensic Psychiatric Service, trainees work with inpatient and outpatient adult clients who have a forensic history. Many of them have also had a history of previous involvement with other Mental Health and / or Substance Misuse Services. The placement will focus on assessment of psychological skills and of risk for violence and further offending. If the placement is of sufficient duration, it will also provide an opportunity for trainees to implement psychological therapies, delivered in an individual or group setting, and other interventions appropriate to the presenting problem, to assist the client to reduce their psychological distress and enhance their sense of well-being. This is accomplished through the systematic application of knowledge derived from psychological theory and evidence. Placement Settings and Services The base for the Forensic Placement is the North Wales Forensic Psychiatric Service at Ty Llywelyn Medium Secure Unit, Bryn y Neuadd Hospital, Llanfairfechan. This is a 25 bed Medium Secure inpatient unit, with facilities for outpatient services on site. The trainee will work alongside a Clinical Psychologist with Forensic Clinical Psychology training and experience. Duration of the Placement The length of the Forensic Placement should be between 6 and 12 months, depending on the specific goals for the placement. Six months is considered the minimum time to ensure that the relevant experience is gained. The goals are agreed in advanced between trainee, placement supervisor and training coordinator. Placement Induction Trainees will be given the opportunity to become familiar with the broad structure of the North Wales Forensic Psychiatric Service, the broader NHS framework and the relationship of forensic services with North Wales residential facilities, the Courts, Probation Services, The Ministry of Justice and the Prison Services. This will involve observing the supervisor and other relevant professions both within the inpatient unit and out in the community. A placement agreement will be set up in the early stages of the placement and will be reviewed at mid-placement. Caseload The clinical experience gained on this placement will reflect a range of clients over 18 years of age, with a wide range of identified moderate to severe psychological problems. All clients within the inpatient setting are male, but some assessments may be conducted with female clients in other settings. Many of the clients will have both complex psychiatric or psychological histories, and all will have forensic involvement. Some may have borderline intellectual disability, and many will have a history of violence. The actual numbers of clients seen will vary according to the length of time of the placement and the complexity of the clients’ presenting problems.
172
SECTION 3
PROGRAMME MANUAL / 2019
The trainee will have the opportunity to observe the supervisor on some of the more complex cases presented to the service, either in individual sessions or within group therapy settings. However, usually by the end of a six-month placement, the trainees will have the opportunity to become involved in some in-depth work with a minimum of four clients. There may be an opportunity for work on a long-term case, in negotiation with the supervisor. All referrals will be made through the supervisor. Required Learning Outcomes By the end of the Forensic Placement, trainees should have demonstrated progress in further developing core competencies gained on other Adult Placements. In particular: 1. Deciding, using a broad evidence and knowledge base, how to assess, formulate
psychologically and suggest possible psychological interventions, with clients from a forensic setting
2. In the areas of assessment, formulation and suggested interventions, demonstrate in both individual supervision and in multi-disciplinary meetings, self-awareness and ability to work as a reflective practitioner with clients in a forensic setting
3. In assessment, demonstrate an ability to choose appropriate assessment tools, relevant to the forensic setting and to the client’s needs. Assessment tools that may be utilised on placement will include standardised instruments (e.g., WAIS-IV, WTAR, WASI, WMS-III), risk assessment (e.g., HCR-20), systematic interviewing procedures and observation or gathering information from others.
4. In psychological formulation, integrate data from assessments, forensic and other background history, within a coherent framework that incorporates interpersonal, cultural, social and biological factors
5. In psychological formulation, demonstrate that they can then assist the multi-disciplinary team members and / or the Courts or Probation Services in better understanding the forensic client and their care
6. If new information or assessment is obtained, demonstrate their ability to re-formulate the problem and then assist the multi-disciplinary team in understanding the re-formulation.
7. If the placement is 6-9 months long and the trainee is helping clients to implement psychological interventions, then they would be expected to demonstrate that they can do so in a collaborative manner with both the individual client and the North Wales Forensic Psychiatric Service multidisciplinary team.
8. Understanding the ethical issues in this complex clinical context, including informed consent and the relationship of forensic services to other legal services and the Ministry of Justice.
9. Appreciating the inherent power imbalance between clinicians and clients, particularly those in an inpatient setting against their will, and appreciate how abuse of this can be minimised.
10. Learning when to work with relative autonomy and when to involve other members of the multidisciplinary team in decision making and the formulation of recommendations.
173
SECTION 3
PROGRAMME MANUAL / 2019
11. Accepting the accountability of clinicians within forensic services, to managers, and to the courts and the Ministry of Justice.
12. Using supervision to reflect on clinical practice and making use of feedback received. 13. Working collaboratively and constructively with clinical psychologists and assistant
psychologists working in Forensic Clinical Psychology Services, as well as other members of the multidisciplinary team, including psychiatrists, other medical doctors, social workers, arts therapists, occupational therapists, nurses and health-care assistants.
14. Communicating the information contained in psychological assessments, case formulations and therapy progress accounts to a variety of audiences, including clients, carers and professional colleagues, in a manner that can be easily understood. This would involve taking into account the abilities, needs and goals of the participant, and adapting accordingly.
15. Understanding the role and value of consulting with other North Wales Forensic Psychiatric Service professionals in the multi-disciplinary team and of working with them effectively.
16. Service User involvement (feedback, voluntary organisations) and any other relevant role in service provision.
Supervision A minimum of one-hour formal supervision per week is provided. However, there are always opportunities available for more informal discussions with other members of the Forensic Clinical Psychology team and the North Wales Forensic Psychiatric Service Multidisciplinary Team, in weekly clinical team meetings and case conferences. N.B. Before commencing this placement, trainees must have undergone Betsi Cadwaladr
University Health Board De-escalation and Breakaway Training.
Trainees wishing to undertake a forensic placement whilst pregnant will require an on-going risk assessment and should, therefore, approach the Clinical Director or Clinical Tutor for further details.
174
ACCREDITATION THROUGH PARTNERSHIP
175
176
177
178
179
180
181
SECTION 3
PROGRAMME MANUAL / 2019
Fair Processing Information As part of the regular training and development process, it is a requirement for the trainee clinical psychologist you are seeing to use audio or video recordings of their work in clinical supervision sessions with their supervisor. He/she will also be required to submit one of these sessions as part of the assessment process for their Doctorate in Clinical Psychology to demonstrate their clinical skills. Your written consent is required before any recording of sessions takes place. You must give your consent freely and understand what we are going to do with the recording. Your written consent is required before any recording of sessions can take place. The consent you are giving is only for us to use the recording in this way and not for anything else. Once you have consented for recording of sessions in writing the trainee will check with you at each session verbally if you are happy for the recording to take place. At a later date, the trainee will ask you separately for explicit consent to submit one of the recorded sessions for assessment. Please initial
I understand that each recording may be used for supervision where the Clinical Psychologist in Training and his/her supervisor need to listen to / view the recording.
I understand that the recordings will be stored securely at all times until it is confidentially destroyed (which will be no longer than the end of the trainee’s placement).
I understand that written notes on the sessions will be made as a matter of routine. Recordings are additional to, not in place of, case-notes.
I understand that I can ask for the recording to be stopped at any time and this will not affect my care in any way.
I understand that at the end of each session the recording can be erased immediately if I am unhappy.
I have read the information above and am happy to agree to my sessions being recorded. Patient: Print Name: ______________________________________________________ Signature: ______________________________ Date: _________________ Psychologist: Print Name: ______________________________________________________ Signature: ______________________________ Date: _________________
CLIENT CONSENT FORM FOR AUDIO/VIDEO RECORDING OF PSYCHOLOGY SESSION FOR
ACADEMIC ASSESSMENT
182
SECTION 3
PROGRAMME MANUAL / 2019
LONG TERM CLINICAL WORK RECORD FORM
Trainee: Placement: Supervisor: Training Co-ordinator:
It is a requirement of the North Wales Clinical Psychology Programme that trainees have experience of long-term therapeutic work with at least one client/family/system during the three years of their training. Please give a short summary and outcome of the work you have undertaken and the dates of the therapeutic work. Trainee to complete:
Frequency of contact during placement: Frequency of contact after end of placement: Frequency of supervision:
Summary of work including therapeutic model/specific competencies used
Outcome
Reflection: (what have you learned from this piece of work)
183
SECTION 3
PROGRAMME MANUAL / 2019
Supervisor to complete: Evaluation of long-term clinical work: (strengths, weaknesses, areas for development, use of supervision)
Any additional comments: Supervisor’s signature:
Date:
Trainee’s signature: Date:
184
SECTION 3
PROGRAMME MANUAL / 2019
SAMPLE PLACEMENT AGREEMENT
Trainee: Supervisor: Specialism: Placement Dates: Back-up Supervisor:
AIMS:
• To provide the trainee with clinical and professional practice experience as outlined in Section 3 of the programme manual.
• The aim will be to provide the trainee with suitable experience to develop the range of clinical and professional competencies outlined in the Evaluation of Clinical and Professional Competence form, as applied to the above-named specialism.
PLACEMENT REQUIREMENTS Induction • The placement will commence with a suitable induction. • The supervisor will facilitate observation of his/her work either directly or indirectly
(live/audio/video). • Observation of assessment, intervention and/or leadership/consultancy work will be
facilitated. Placement Agreement • From Placement 2 onwards, the completed ECPC feedback from the previous
placement should be used to inform this agreement. Supervision • Supervision will be tailored to the development of the clinical and professional
competencies required. • The supervisor will provide 1-hour minimum formal supervision/week plus informal
supervision - total contact time 3-hours/week (core placements). • Supervision will be scheduled in advance and the Placement Quality Checklist used
as a guide to providing helpful/reflective supervision. • The supervisor will observe the trainee (live/audio/video) in a minimum of six
sessions across a range of assessment, intervention, indirect/MDT work as appropriate to the placement.
• The trainee will accept referrals only from the supervisor. • The trainee will keep an up-to-date clinical practice portfolio, which should be
available for the supervisor to view when requested. • As outlined in the BPS Generic Professional Practice Guidelines (2008), trainees are
informed that “…they are individually responsible for their conduct with clients and the extent to which responsibility for the work is shared with the supervisor.”
• Trainees will complete a Report of Clinical Activity (RCA/CBT-RCA or RCA-Presentation) by the deadline set as part of the assessment for the DClinPsy.
185
SECTION 3
PROGRAMME MANUAL / 2019
• The trainee will provide the supervisor with a copy of the RCA and the feedback provided by the assessors.
Annual Leave • The trainee will take no more than 11 days annual leave [22 days per year] from
clinical placement time. Research/Study Time • Year 1 & 2 trainees are allocated one day/week for study/research. The trainee
should agree with their supervisor which weekday is to be taken. General Points • The Programme is not at leave to provide trainee telephone contact details. Trainee
and supervisor(s) need to exchange relevant numbers and agree the best mechanism for leaving messages.
• The trainee must inform NWCPP if their supervisor is on sick leave for more than one week.
• In the event of long-term sick leave, NWCPPs clinical team will negotiate a new placement arrangement with the relevant Head of Service.
• The trainee will abide by NWCPP and BCUHB guidance in relation to: information sharing/client consent; service user feedback; client consent for audio/video recording; storage of clinical information and note-keeping.
• The trainee should familiarise themselves with Health & Safety & Equal Opportunities Policies via the BCUHB intranet.
186
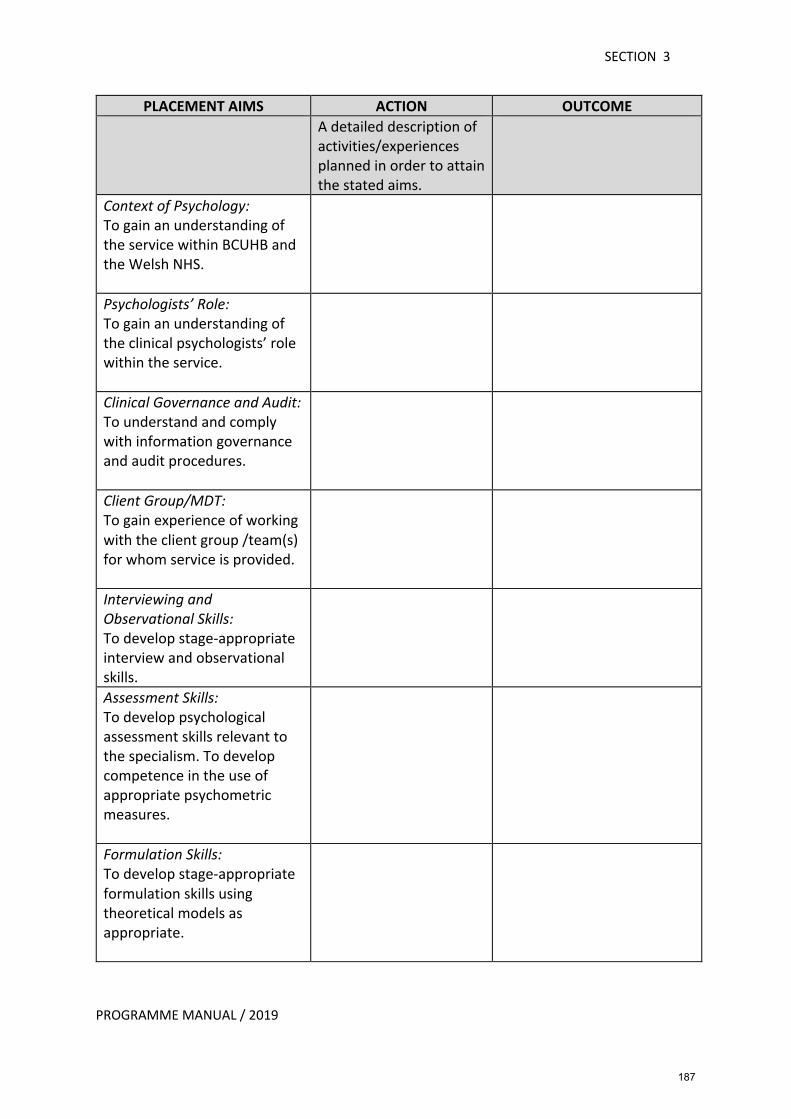
SECTION 3
PROGRAMME MANUAL / 2019
PLACEMENT AIMS ACTION OUTCOME A detailed description of
activities/experiences planned in order to attain the stated aims.
Context of Psychology: To gain an understanding of the service within BCUHB and the Welsh NHS.
Psychologists’ Role: To gain an understanding of the clinical psychologists’ role within the service.
Clinical Governance and Audit: To understand and comply with information governance and audit procedures.
Client Group/MDT: To gain experience of working with the client group /team(s) for whom service is provided.
Interviewing and Observational Skills: To develop stage-appropriate interview and observational skills.
Assessment Skills: To develop psychological assessment skills relevant to the specialism. To develop competence in the use of appropriate psychometric measures.
Formulation Skills: To develop stage-appropriate formulation skills using theoretical models as appropriate.
187
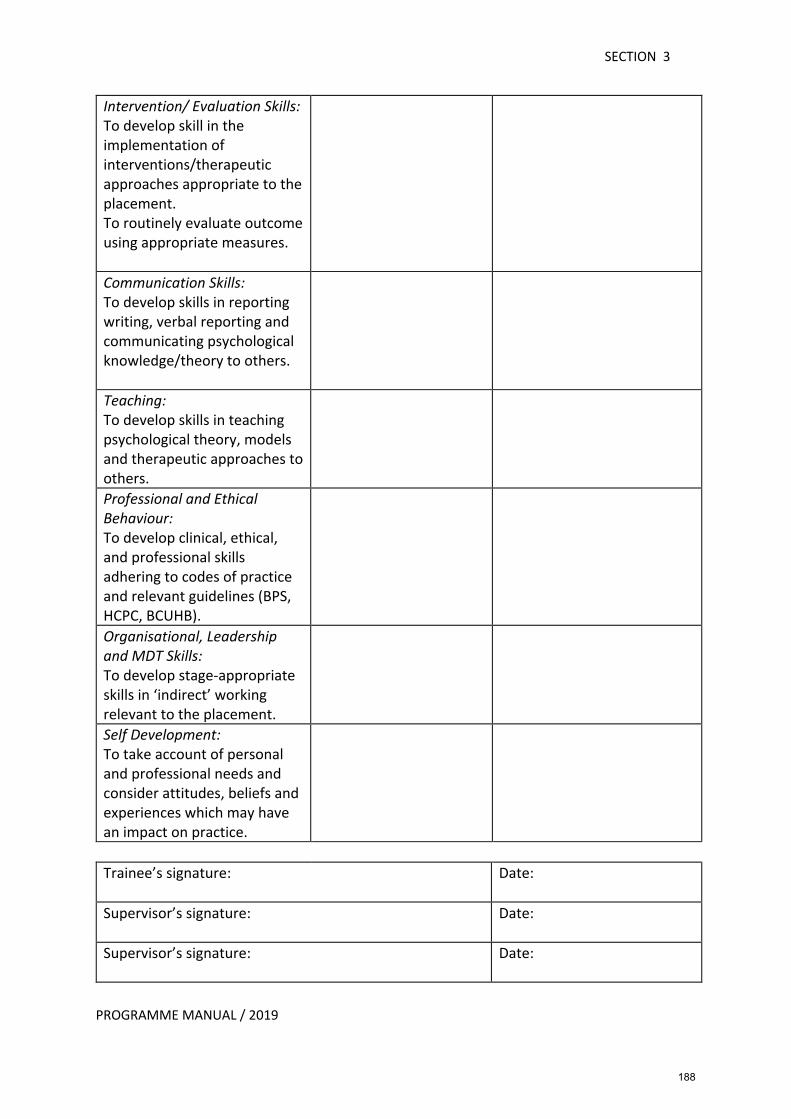
SECTION 3
PROGRAMME MANUAL / 2019
Intervention/ Evaluation Skills: To develop skill in the implementation of interventions/therapeutic approaches appropriate to the placement. To routinely evaluate outcome using appropriate measures.
Communication Skills: To develop skills in reporting writing, verbal reporting and communicating psychological knowledge/theory to others.
Teaching: To develop skills in teaching psychological theory, models and therapeutic approaches to others.
Professional and Ethical Behaviour: To develop clinical, ethical, and professional skills adhering to codes of practice and relevant guidelines (BPS, HCPC, BCUHB).
Organisational, Leadership and MDT Skills: To develop stage-appropriate skills in ‘indirect’ working relevant to the placement.
Self Development: To take account of personal and professional needs and consider attitudes, beliefs and experiences which may have an impact on practice.
Trainee’s signature: Date:
Supervisor’s signature: Date:
Supervisor’s signature: Date:
188
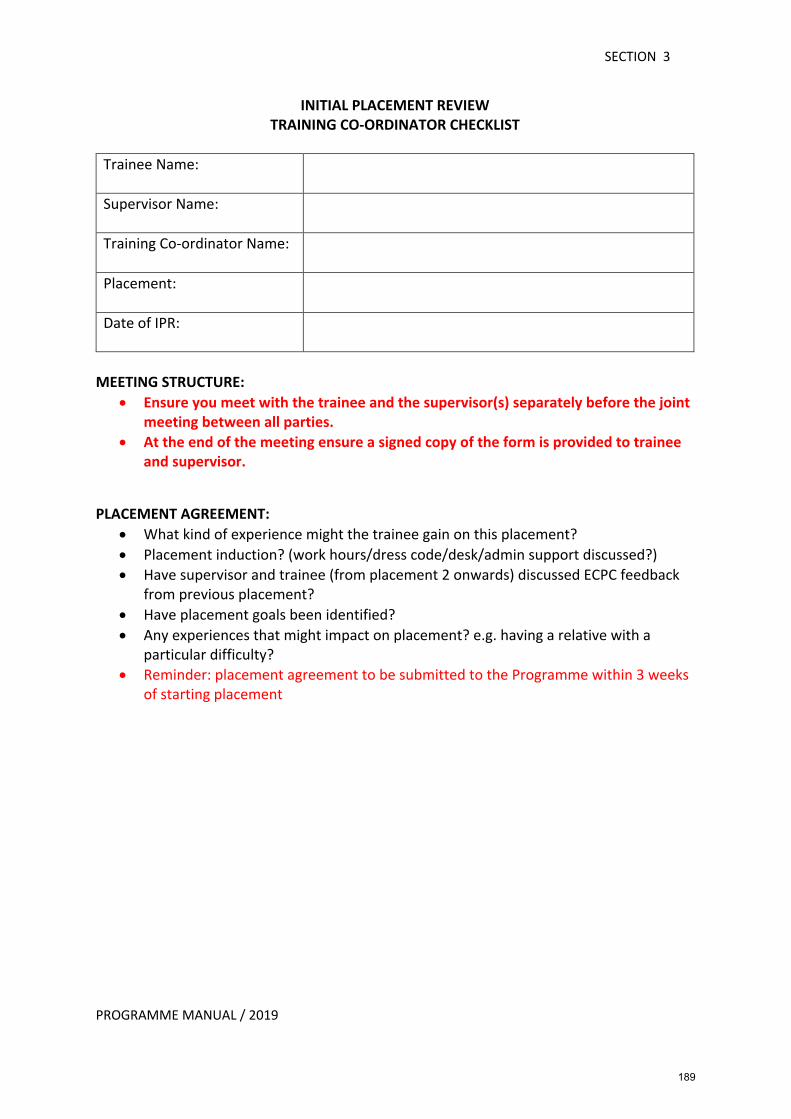
SECTION 3
PROGRAMME MANUAL / 2019
INITIAL PLACEMENT REVIEW TRAINING CO-ORDINATOR CHECKLIST
Trainee Name:
Supervisor Name:
Training Co-ordinator Name:
Placement:
Date of IPR:
MEETING STRUCTURE: • Ensure you meet with the trainee and the supervisor(s) separately before the joint
meeting between all parties. • At the end of the meeting ensure a signed copy of the form is provided to trainee
and supervisor.
PLACEMENT AGREEMENT:
• What kind of experience might the trainee gain on this placement? • Placement induction? (work hours/dress code/desk/admin support discussed?) • Have supervisor and trainee (from placement 2 onwards) discussed ECPC feedback
from previous placement? • Have placement goals been identified? • Any experiences that might impact on placement? e.g. having a relative with a
particular difficulty? • Reminder: placement agreement to be submitted to the Programme within 3 weeks
of starting placement
189
SECTION 3
PROGRAMME MANUAL / 2019
SUPERVISION:
• Plans for supervision? • Reminder: BPS requirement Min 1-hour formal supervision plus informal supervision
– total contact time at least 3 hours/week BACK-UP SUPERVISOR: _______________________________________________________ OBSERVATION - of Supervisor:
• Opportunities for trainee to observe supervisor – in assessment/therapy/intervention/indirect working?
• Reminder: Supervisors encouraged to facilitate trainee observation as much as possible
OBSERVATION - of Trainee:
• Plans for observation? • Live or audio/video recording preferred by supervisor? • Reminder: Trainees to be observed across range assessment/therapy/indirect
working min 6 times per 5/6-month placement CBT-RCA:
• Trainees are required to submit a CBT-RCA during Year 1 or 2, ideally in Year 1. This will involve submitting a 60-minute (or 90-minute if appropriate e.g. trauma-focused CBT) recording of a CBT intervention session.
• Reminder: Trainees are encouraged to audio record as many of their sessions as possible to be used in supervision and for self-assessment/reflection.
190
SECTION 3
PROGRAMME MANUAL / 2019
USE OF THE COGNITIVE THERAPY SCALE – REVISED (CTS-R):
• CTS-R to be used by assessors to rate CBT-RCA recording. CTS-R score of 36 required to pass this part of the assignment.
• Reminder: Supervisors encouraged to use CTS-R (or equivalent for DBT or ACT) when observing trainees (live/audio/video) to structure feedback. Trainees encouraged to use CTS-R or equivalent for self-assessment and reflection.
CLINICAL PRACTICE PORTFOLIO:
• Any questions about the portfolio? The content can be shared at intervals with supervisor to discuss therapeutic competency development (CBT/DBT/ACT).
• Reminder: Trainees must keep the clinical practice portfolio updated on a regular basis.
SUPERVISOR AUTHENTICATION OF PORTFOLIO FORM:
• Supervisors ‘sign-off’ the portfolio with this form confirming that the content reflects the clinical work completed.
• Trainees submit a hard copy of this form to the Programme, which will be scanned into the clinical practice portfolio.
SERVICE USER INFORMATION:
• Are both Trainee and Supervisor aware of the relevant service user documentation? (e.g. consent/sharing information forms, end of intervention/assessment forms and service-user outcome measurement)
TRAINEE CASELOAD:
• Minimum x 6 on-going pieces of direct/indirect clinical work throughout placement. • Any queries re: caseload? • Any group work planned that may affect caseload size?
191
SECTION 3
PROGRAMME MANUAL / 2019
TEACHING: • Trainees must complete a teaching session on each placement. What teaching
opportunities might be available on this placement? ANNUAL LEAVE:
• Trainees required to complete 50% of their training excluding annual leave in clinical practice. Annual leave must not therefore be taken solely from placement.
• Reminder: Core placements - no more than 11 days annual leave [22 days per year] can be taken from clinical placement. Although structure may alter, same principles apply in Year 3.
Signed by Trainee:
Date:
Signed by Supervisor(s): Date:
Signed by Supervisor(s):
Date:
Signed by Training Co-ordinator: Date:
COPY OF CHECKLIST MUST BE GIVEN TO SUPERVISOR & TRAINEE
192
SECTION 3
PROGRAMME MANUAL / 2019
MID-PLACEMENT REVIEW TRAINING CO-ORDINATOR CHECKLIST
Trainee Name:
Supervisor(s) Name(s):
Training Co-ordinator Name:
Placement:
Date of MPR:
MEETING STRUCTURE:
• Individual meeting with trainee – review completed PQC ☐ YES • Individual meeting with supervisor – general review ☐ YES • Joint Meeting – complete/check the following paperwork:
Training Co-ordinator Checklist Portfolio (2016 Intake) or Logbook & Placement Agreement ECPC Feedback from supervisor PQC Feedback from trainee
SUPERVISION: Minimum 1-hour formal supervision plus informal supervision – at least 3 hours per week in total?
☐YES ☐NO ☐MORE NEEDED
Number of sessions
Minimum x 6 / core placement
Observation (Direct/Audio/Video)
Assessment Intervention/ Indirect work
More needed
Trainee observing Supervisor
Supervisor observing Trainee
NAMED BACK UP SUPERVISOR: _____________________________________________
193
SECTION 3
PROGRAMME MANUAL / 2019
PLACEMENT AGREEMENT: Are goals being reached? TRAINEE CASELOAD: Number/range of clients & portfolio or logbook review THERAPEUTIC APPROACHES: Approaches being used/developed? REPORT OF CLINICAL ACTIVITY: Including CBT-RCA 2016 Intake:
Is it appropriate? Is it on schedule? ☐YES ☐NO ☐YES ☐NO Will the CBT-RCA be submitted from this placement? If yes, any queries?
Reminder: Trainee must use specific CBT-RCA consent form for recording all CBT intervention sessions and Supervisor Confirmation form must be signed to confirm consent was gained for submitted recording.
• Has trainee given a copy of previous RCA/SRRP to relevant Supervisor? ☐YES ☐NO
• Long term clinical work: Possible client identified?
☐YES ☐NO
194
SECTION 3
PROGRAMME MANUAL / 2019
If yes, include in logbook or portfolio and complete long-term record form PASS OUTS: Have any required pass outs been completed?
☐YES ☐NO ☐To be arranged
TEACHING: Has a teaching/training opportunity been identified?
☐YES ☐NO ☐To be arranged SERVICE USER INFORMATION:
• Has the trainee discussed the guidelines re: confidentiality/sharing client information with clients?
☐YES ☐NO
• Any queries re: End of Intervention/Assessment forms?
☐YES ☐NO ☐N/A
• Opportunity to liaise with voluntary/3rd sector organisations? ☐YES ☐NO ☐MORE NEEDED
OUTCOME MEASUREMENT/EVALUATION: What outcome measures will be used to evaluate intervention and/or to track service-user response during therapy/intervention? ANNUAL LEAVE: Has leave been agreed with Supervisor & Programme Director? No more than 11 clinical placement days to be taken per placement [except 12-month placements - max 22 days per year]
☐YES ☐NO ☐To be arranged
ANNUAL LEAVE
Clinical Placement Study/Research Academic Teaching
195

SECTION 3
PROGRAMME MANUAL / 2019
Number of days taken/scheduled
196
SECTION 3
PROGRAMME MANUAL / 2019
TRAINING CO-ORDINATOR CHECKLIST ECPC FEEDBACK FROM SUPERVISOR ISSUES: ACTION: Are there any concerns that might require further review between now and the end of the placement? ☐YES ☐NO If Yes, please provide details: PQC FEEDBACK FROM TRAINEE ISSUES: ACTION: COMMENTS/AREAS FOR FURTHER DEVELOPMENT
197
SECTION 3
PROGRAMME MANUAL / 2019
Preliminary Summary of Ratings at Mid Placement
Exceeded the level at this stage
At the level expected at this stage
Below the level expected at this stage
Interviewing and observational skills
Assessment
Formulation and reformulation
Intervention/Evaluation
Communication
Teaching
Professional and Ethical Behaviour
Organisational, Leadership, and Multi-disciplinary Working
Self-development
Feedback from others
Overall
Signed by Trainee:
Date:
Signed by Supervisor: Date:
Signed by Training Co-ordinator’s: Date:
COPY OF CHECKLIST MUST BE GIVEN TO SUPERVISOR & TRAINEE
198
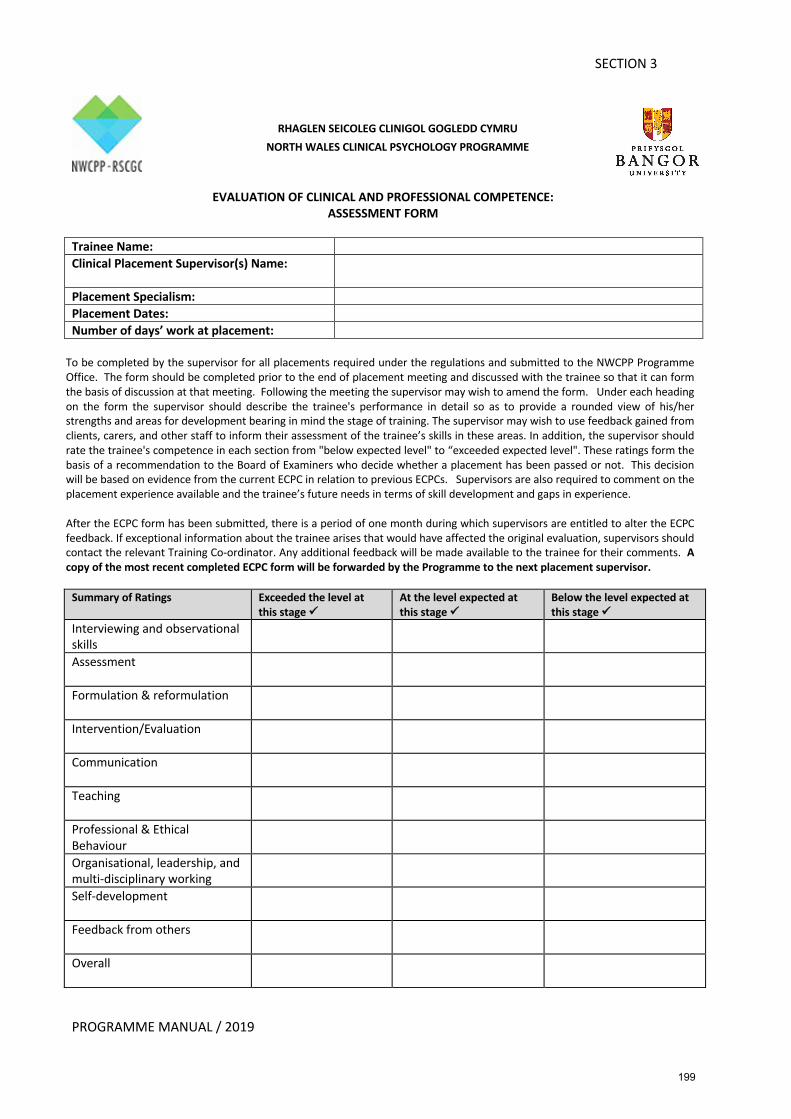
PROGRAMME MANUAL / 2019
SECTION 3
EVALUATION OF CLINICAL AND PROFESSIONAL COMPETENCE: ASSESSMENT FORM
Trainee Name: Clinical Placement Supervisor(s) Name:
Placement Specialism: Placement Dates: Number of days’ work at placement:
To be completed by the supervisor for all placements required under the regulations and submitted to the NWCPP Programme Office. The form should be completed prior to the end of placement meeting and discussed with the trainee so that it can form the basis of discussion at that meeting. Following the meeting the supervisor may wish to amend the form. Under each heading on the form the supervisor should describe the trainee's performance in detail so as to provide a rounded view of his/her strengths and areas for development bearing in mind the stage of training. The supervisor may wish to use feedback gained from clients, carers, and other staff to inform their assessment of the trainee’s skills in these areas. In addition, the supervisor should rate the trainee's competence in each section from "below expected level" to “exceeded expected level". These ratings form the basis of a recommendation to the Board of Examiners who decide whether a placement has been passed or not. This decision will be based on evidence from the current ECPC in relation to previous ECPCs. Supervisors are also required to comment on the placement experience available and the trainee’s future needs in terms of skill development and gaps in experience. After the ECPC form has been submitted, there is a period of one month during which supervisors are entitled to alter the ECPC feedback. If exceptional information about the trainee arises that would have affected the original evaluation, supervisors should contact the relevant Training Co-ordinator. Any additional feedback will be made available to the trainee for their comments. A copy of the most recent completed ECPC form will be forwarded by the Programme to the next placement supervisor.
Summary of Ratings Exceeded the level at
this stage ü At the level expected at this stage ü
Below the level expected at this stage ü
Interviewing and observational skills
Assessment
Formulation & reformulation
Intervention/Evaluation
Communication
Teaching
Professional & Ethical Behaviour
Organisational, leadership, and multi-disciplinary working
Self-development
Feedback from others
Overall
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
199
PROGRAMME MANUAL / 2019
SECTION 3
GENERAL COMMENTS AND SUMMARY (to be completed last) General Comments by the supervisor: Specific trainee strengths SPECIFY TRAINEE NEEDS /AREAS FOR DEVELOPMENT RE: a. Experience b. Skills TRAINEE’S COMMENTS ON ACCURACY OF FEEDBACK: Clinical Placement Supervisor(s) Signature:
Date:
Trainee Signature: Date:
200
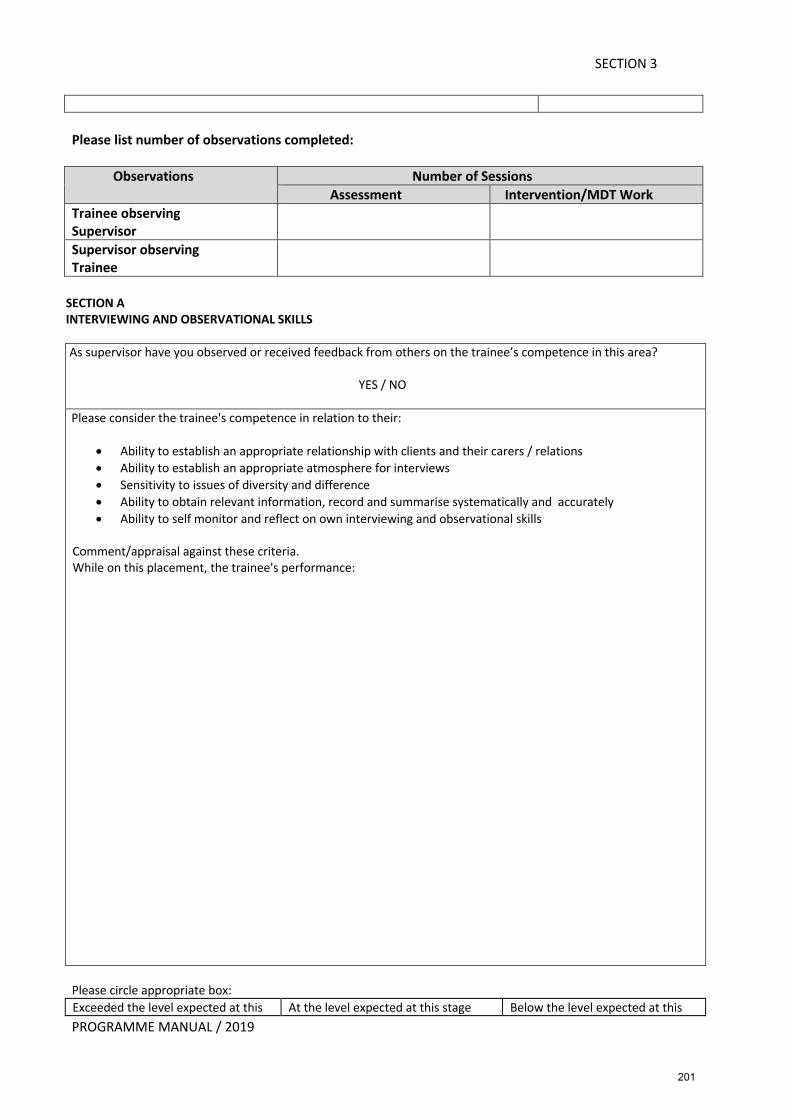
PROGRAMME MANUAL / 2019
SECTION 3
Please list number of observations completed:
Observations Number of Sessions Assessment Intervention/MDT Work
Trainee observing Supervisor
Supervisor observing Trainee
SECTION A INTERVIEWING AND OBSERVATIONAL SKILLS As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO Please consider the trainee's competence in relation to their:
• Ability to establish an appropriate relationship with clients and their carers / relations • Ability to establish an appropriate atmosphere for interviews • Sensitivity to issues of diversity and difference • Ability to obtain relevant information, record and summarise systematically and accurately • Ability to self monitor and reflect on own interviewing and observational skills
Comment/appraisal against these criteria. While on this placement, the trainee's performance:
Please circle appropriate box: Exceeded the level expected at this At the level expected at this stage Below the level expected at this
201

PROGRAMME MANUAL / 2019
SECTION 3
stage stage SECTION B ASSESSMENT As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO
Please consider the trainee's competence in relation to:
• Ability to choose, administer and interpret a broad range of appropriate assessment methods appropriate to the client and service in which the assessment takes place
• Competence demonstrated in both performance-based psychometric measures (e.g. cognitive function and developmental measures and self/other reported psychometric measures (mood, feelings behaviours etc.)
• Understanding demonstrated in relation to the key elements of psychometric theory, which have relevance for psychological assessment (e.g. sources of error/bias, language used/ effect sizes etc.)
• Using the above information to aid interpretation and final analysis • Where appropriate information/observation is sought, and obtained from other sources acknowledging
the social context and other organisational involvement. • Evidence that appropriate risk assessments have been conducted and where appropriate other
service/organisation-related documentation such as the Mental Health Measure under designated supervisory conditions
• Communication of results, written and verbal reporting in a style appropriate for the intended audience Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
202

PROGRAMME MANUAL / 2019
SECTION 3
SECTION C FORMULATION AND REFORMULATION As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO Please consider the trainees competence in relation to:
• Using assessment information to develop formulations which are informed by theory and practice and relevant individual, systemic, cultural and biological factors
• Developing a collaborative formulation through a shared understanding of it’/s personal meaning for the client
• Demonstrating the ability to share a formulation collaboratively with service users, carers teams and services
• Ensuring that formulations are shared in accessible language or pictorial form and are culturally sensitive and non-discriminatory in terms of issues of difference and diversity
• Ability to evaluate and review formulation in the light of subsequent evidence and re-formulate accordingly.
Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
203
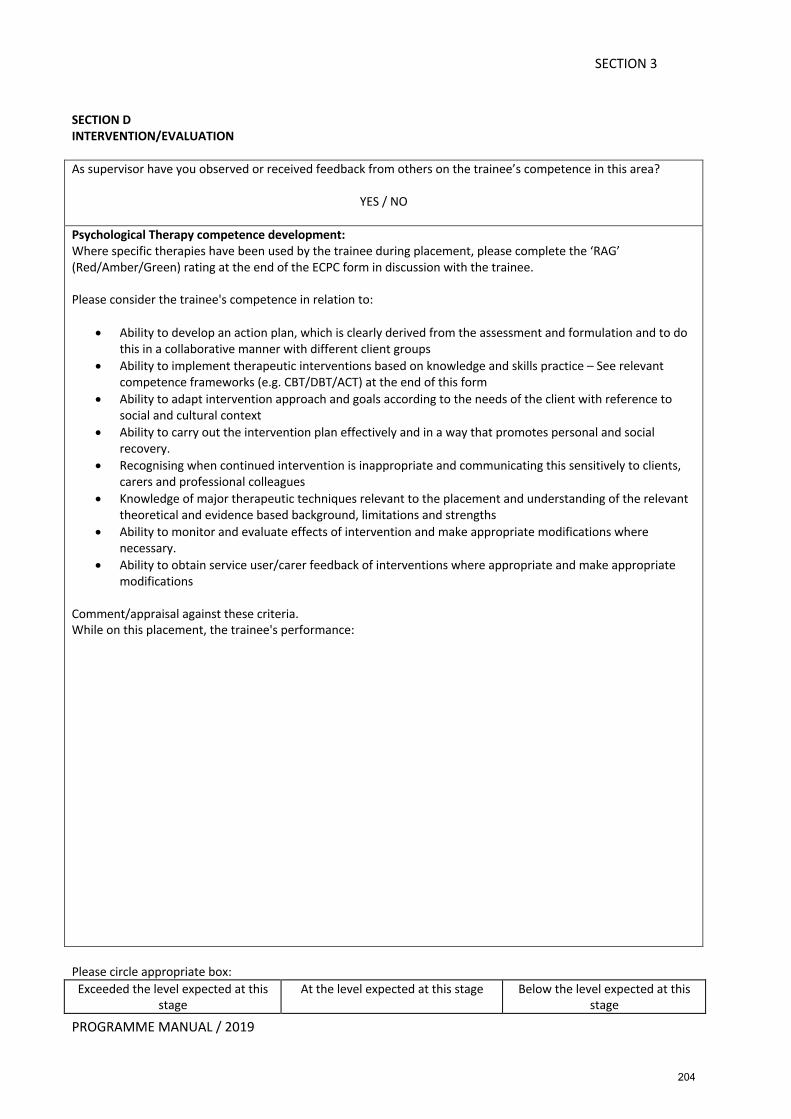
PROGRAMME MANUAL / 2019
SECTION 3
SECTION D INTERVENTION/EVALUATION As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO
Psychological Therapy competence development: Where specific therapies have been used by the trainee during placement, please complete the ‘RAG’ (Red/Amber/Green) rating at the end of the ECPC form in discussion with the trainee. Please consider the trainee's competence in relation to:
• Ability to develop an action plan, which is clearly derived from the assessment and formulation and to do this in a collaborative manner with different client groups
• Ability to implement therapeutic interventions based on knowledge and skills practice – See relevant competence frameworks (e.g. CBT/DBT/ACT) at the end of this form
• Ability to adapt intervention approach and goals according to the needs of the client with reference to social and cultural context
• Ability to carry out the intervention plan effectively and in a way that promotes personal and social recovery.
• Recognising when continued intervention is inappropriate and communicating this sensitively to clients, carers and professional colleagues
• Knowledge of major therapeutic techniques relevant to the placement and understanding of the relevant theoretical and evidence based background, limitations and strengths
• Ability to monitor and evaluate effects of intervention and make appropriate modifications where necessary.
• Ability to obtain service user/carer feedback of interventions where appropriate and make appropriate modifications
Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
204

PROGRAMME MANUAL / 2019
SECTION 3
SECTION E COMMUNICATION As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO
Please consider the trainee's competence in relation to:
• Ability to give clear, comprehensive and relevant verbal reports • Ability to give clear, comprehensive, accurate and relevant written reports devoid of careless mistakes and
the need for correction • Effectively communicating information from a psychological perspective in a style appropriate to a variety
of different audiences (clients, carers, staff, professional colleagues) • Ability to adapt style of communication to people with a wide range of cognitive ability and other physical
difficulties • Understand the process of supervision and trainees’ role in contributing to good supervisory relationships •
Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
205

PROGRAMME MANUAL / 2019
SECTION 3
SECTION F TEACHING As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO
Please consider the trainee's competence in relation to:
• Preparing and delivering teaching and training, which takes into account the needs and goals of the participants
• Can present material in a clear and interesting way avoiding jargon and with appropriate use of handouts and A/V aids
• Ability to support others’ learning in the application of psychological skills, knowledge practices and procedures
• Deal appropriately with questions and feedback Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
206
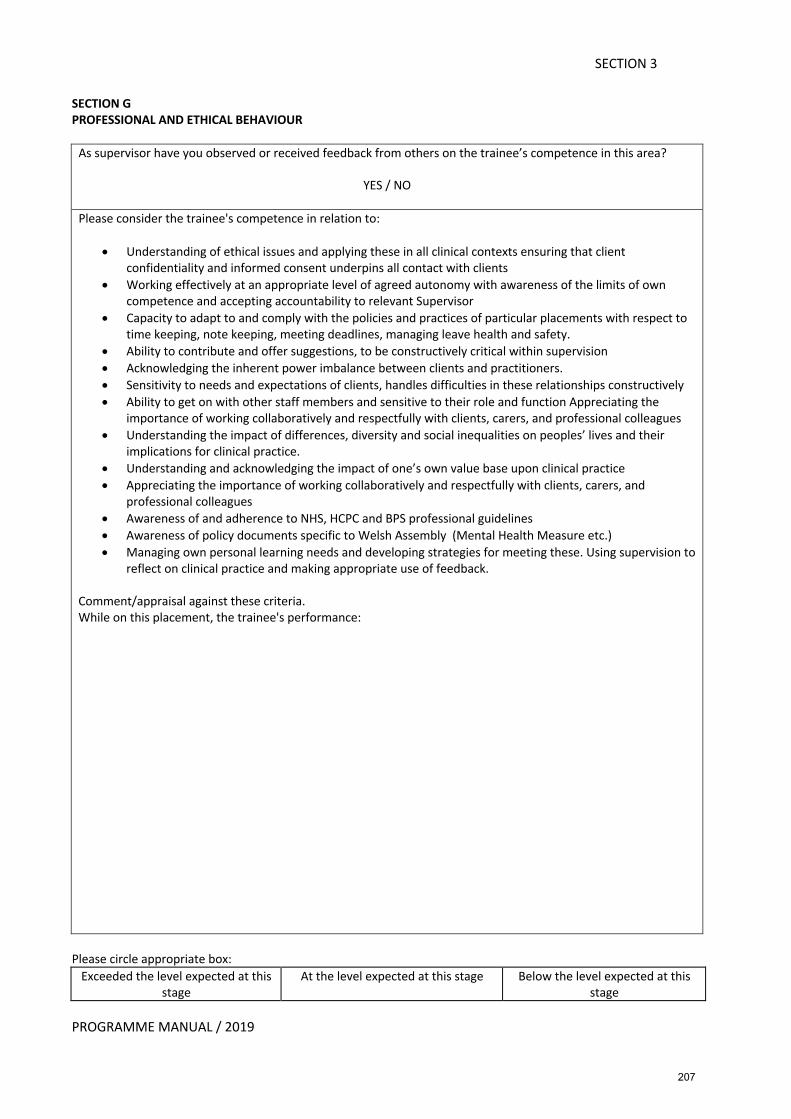
PROGRAMME MANUAL / 2019
SECTION 3
SECTION G PROFESSIONAL AND ETHICAL BEHAVIOUR
As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO Please consider the trainee's competence in relation to:
• Understanding of ethical issues and applying these in all clinical contexts ensuring that client confidentiality and informed consent underpins all contact with clients
• Working effectively at an appropriate level of agreed autonomy with awareness of the limits of own competence and accepting accountability to relevant Supervisor
• Capacity to adapt to and comply with the policies and practices of particular placements with respect to time keeping, note keeping, meeting deadlines, managing leave health and safety.
• Ability to contribute and offer suggestions, to be constructively critical within supervision • Acknowledging the inherent power imbalance between clients and practitioners. • Sensitivity to needs and expectations of clients, handles difficulties in these relationships constructively • Ability to get on with other staff members and sensitive to their role and function Appreciating the
importance of working collaboratively and respectfully with clients, carers, and professional colleagues • Understanding the impact of differences, diversity and social inequalities on peoples’ lives and their
implications for clinical practice. • Understanding and acknowledging the impact of one’s own value base upon clinical practice • Appreciating the importance of working collaboratively and respectfully with clients, carers, and
professional colleagues • Awareness of and adherence to NHS, HCPC and BPS professional guidelines • Awareness of policy documents specific to Welsh Assembly (Mental Health Measure etc.) • Managing own personal learning needs and developing strategies for meeting these. Using supervision to
reflect on clinical practice and making appropriate use of feedback.
Comment/appraisal against these criteria. While on this placement, the trainee's performance:
Please circle appropriate box:
Exceeded the level expected at this stage
At the level expected at this stage Below the level expected at this stage
207
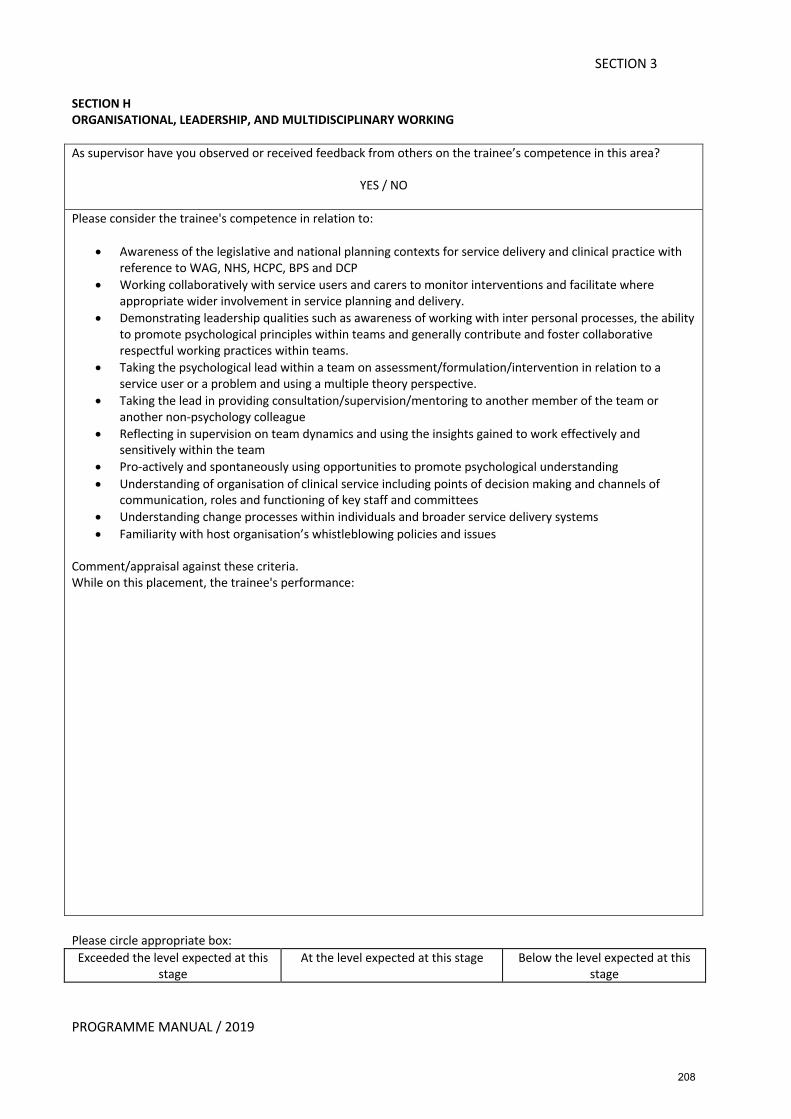
PROGRAMME MANUAL / 2019
SECTION 3
SECTION H ORGANISATIONAL, LEADERSHIP, AND MULTIDISCIPLINARY WORKING As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO
Please consider the trainee's competence in relation to:
• Awareness of the legislative and national planning contexts for service delivery and clinical practice with reference to WAG, NHS, HCPC, BPS and DCP
• Working collaboratively with service users and carers to monitor interventions and facilitate where appropriate wider involvement in service planning and delivery.
• Demonstrating leadership qualities such as awareness of working with inter personal processes, the ability to promote psychological principles within teams and generally contribute and foster collaborative respectful working practices within teams.
• Taking the psychological lead within a team on assessment/formulation/intervention in relation to a service user or a problem and using a multiple theory perspective.
• Taking the lead in providing consultation/supervision/mentoring to another member of the team or another non-psychology colleague
• Reflecting in supervision on team dynamics and using the insights gained to work effectively and sensitively within the team
• Pro-actively and spontaneously using opportunities to promote psychological understanding • Understanding of organisation of clinical service including points of decision making and channels of
communication, roles and functioning of key staff and committees • Understanding change processes within individuals and broader service delivery systems • Familiarity with host organisation’s whistleblowing policies and issues
Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
208
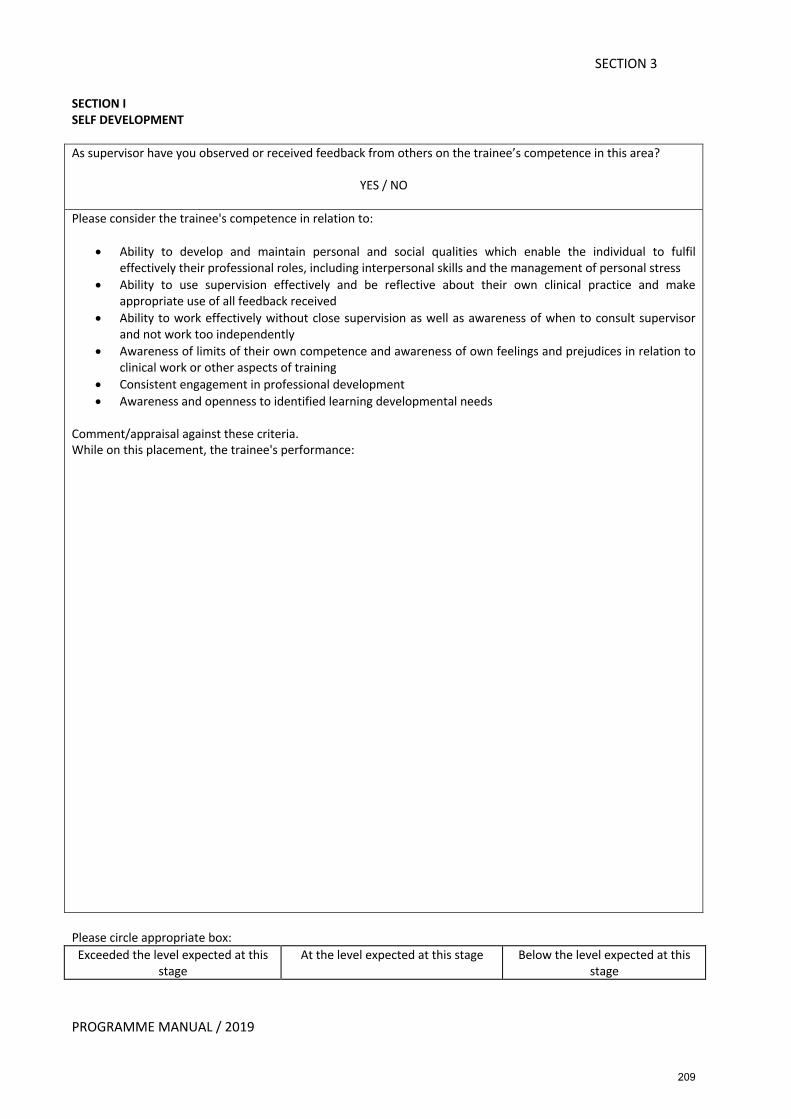
PROGRAMME MANUAL / 2019
SECTION 3
SECTION I SELF DEVELOPMENT As supervisor have you observed or received feedback from others on the trainee’s competence in this area?
YES / NO
Please consider the trainee's competence in relation to:
• Ability to develop and maintain personal and social qualities which enable the individual to fulfil effectively their professional roles, including interpersonal skills and the management of personal stress
• Ability to use supervision effectively and be reflective about their own clinical practice and make appropriate use of all feedback received
• Ability to work effectively without close supervision as well as awareness of when to consult supervisor and not work too independently
• Awareness of limits of their own competence and awareness of own feelings and prejudices in relation to clinical work or other aspects of training
• Consistent engagement in professional development • Awareness and openness to identified learning developmental needs
Comment/appraisal against these criteria. While on this placement, the trainee's performance: Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
209
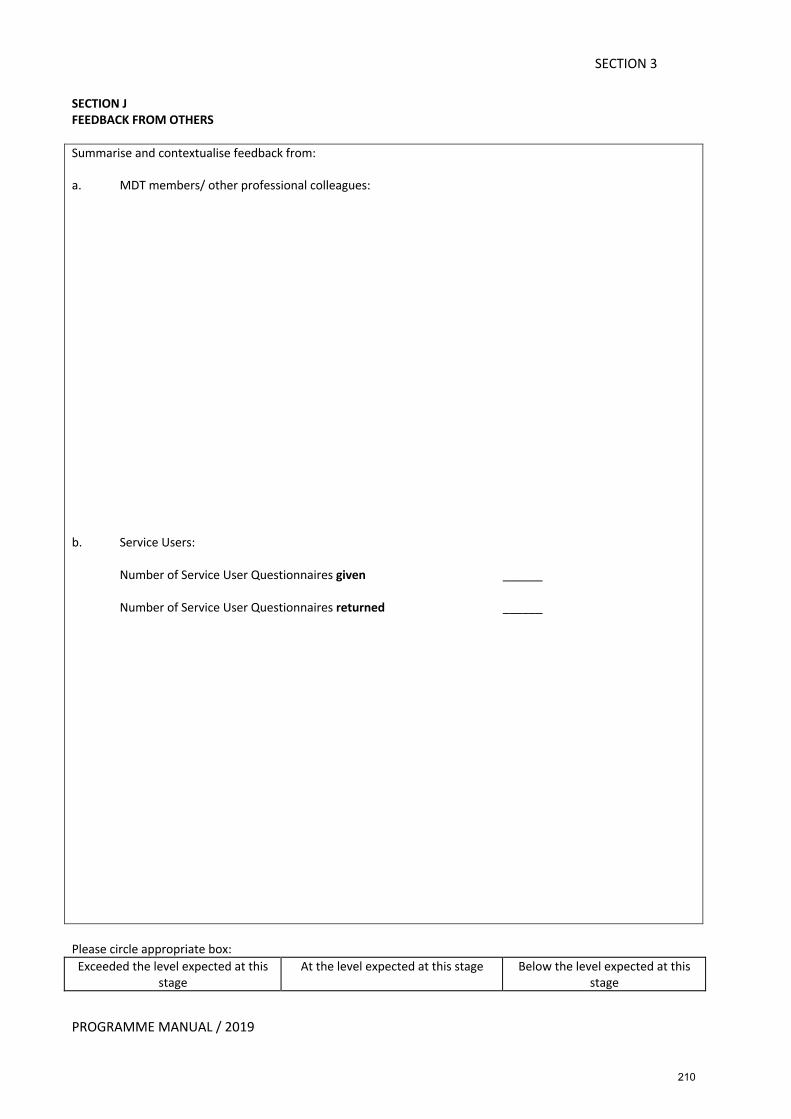
PROGRAMME MANUAL / 2019
SECTION 3
SECTION J FEEDBACK FROM OTHERS Summarise and contextualise feedback from: a. MDT members/ other professional colleagues: b. Service Users:
Number of Service User Questionnaires given ______ Number of Service User Questionnaires returned ______
Please circle appropriate box: Exceeded the level expected at this
stage At the level expected at this stage Below the level expected at this
stage
210
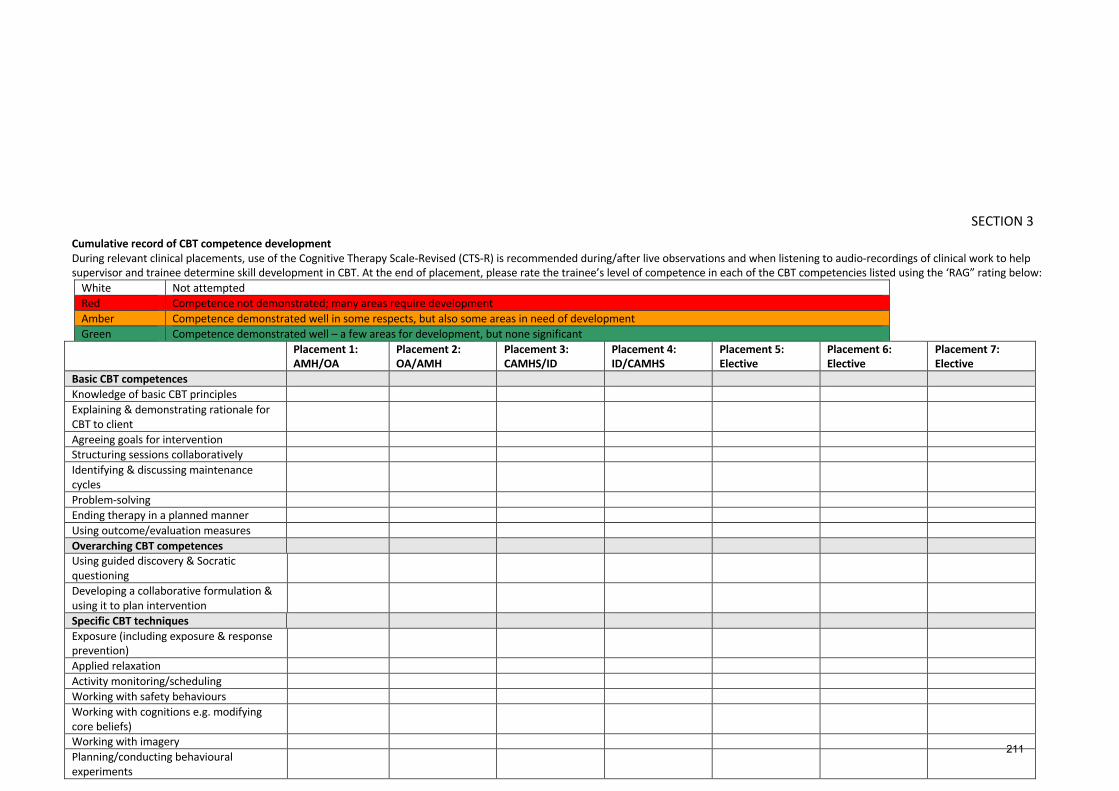
PROGRAMME MANUAL / 2019
SECTION 3 Cumulative record of CBT competence development
During relevant clinical placements, use of the Cognitive Therapy Scale-Revised (CTS-R) is recommended during/after live observations and when listening to audio-recordings of clinical work to help supervisor and trainee determine skill development in CBT. At the end of placement, please rate the trainee’s level of competence in each of the CBT competencies listed using the ‘RAG” rating below:
White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need of development Green Competence demonstrated well – a few areas for development, but none significant
Placement 1: AMH/OA
Placement 2: OA/AMH
Placement 3: CAMHS/ID
Placement 4: ID/CAMHS
Placement 5: Elective
Placement 6: Elective
Placement 7: Elective
Basic CBT competences Knowledge of basic CBT principles Explaining & demonstrating rationale for CBT to client
Agreeing goals for intervention Structuring sessions collaboratively Identifying & discussing maintenance cycles
Problem-solving Ending therapy in a planned manner Using outcome/evaluation measures Overarching CBT competences Using guided discovery & Socratic questioning
Developing a collaborative formulation & using it to plan intervention
Specific CBT techniques Exposure (including exposure & response prevention)
Applied relaxation Activity monitoring/scheduling Working with safety behaviours Working with cognitions e.g. modifying core beliefs)
Working with imagery Planning/conducting behavioural experiments
211
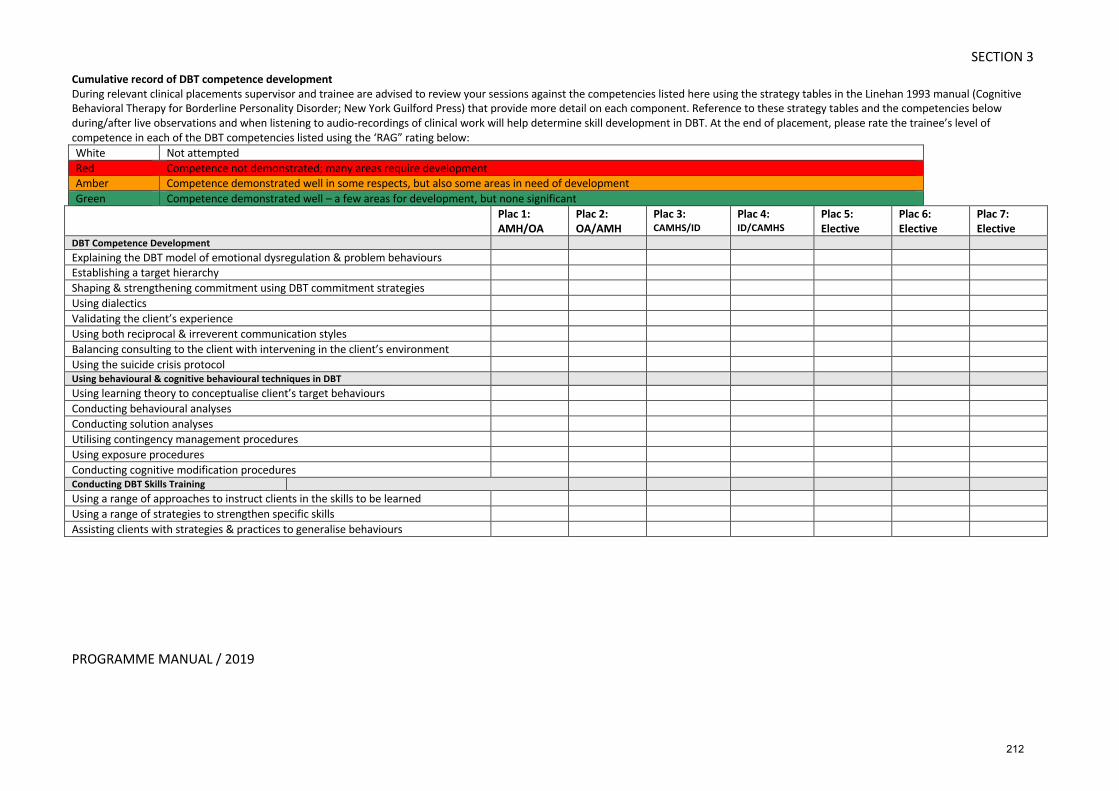
PROGRAMME MANUAL / 2019
SECTION 3 Cumulative record of DBT competence development
During relevant clinical placements supervisor and trainee are advised to review your sessions against the competencies listed here using the strategy tables in the Linehan 1993 manual (Cognitive Behavioral Therapy for Borderline Personality Disorder; New York Guilford Press) that provide more detail on each component. Reference to these strategy tables and the competencies below during/after live observations and when listening to audio-recordings of clinical work will help determine skill development in DBT. At the end of placement, please rate the trainee’s level of competence in each of the DBT competencies listed using the ‘RAG” rating below: White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need of development Green Competence demonstrated well – a few areas for development, but none significant
Plac 1:
AMH/OA
Plac 2:
OA/AMH
Plac 3: CAMHS/ID
Plac 4: ID/CAMHS
Plac 5:
Elective
Plac 6:
Elective
Plac 7:
Elective DBT Competence Development Explaining the DBT model of emotional dysregulation & problem behaviours Establishing a target hierarchy Shaping & strengthening commitment using DBT commitment strategies Using dialectics Validating the client’s experience Using both reciprocal & irreverent communication styles Balancing consulting to the client with intervening in the client’s environment Using the suicide crisis protocol Using behavioural & cognitive behavioural techniques in DBT Using learning theory to conceptualise client’s target behaviours Conducting behavioural analyses Conducting solution analyses Utilising contingency management procedures Using exposure procedures Conducting cognitive modification procedures Conducting DBT Skills Training Using a range of approaches to instruct clients in the skills to be learned Using a range of strategies to strengthen specific skills Assisting clients with strategies & practices to generalise behaviours
212
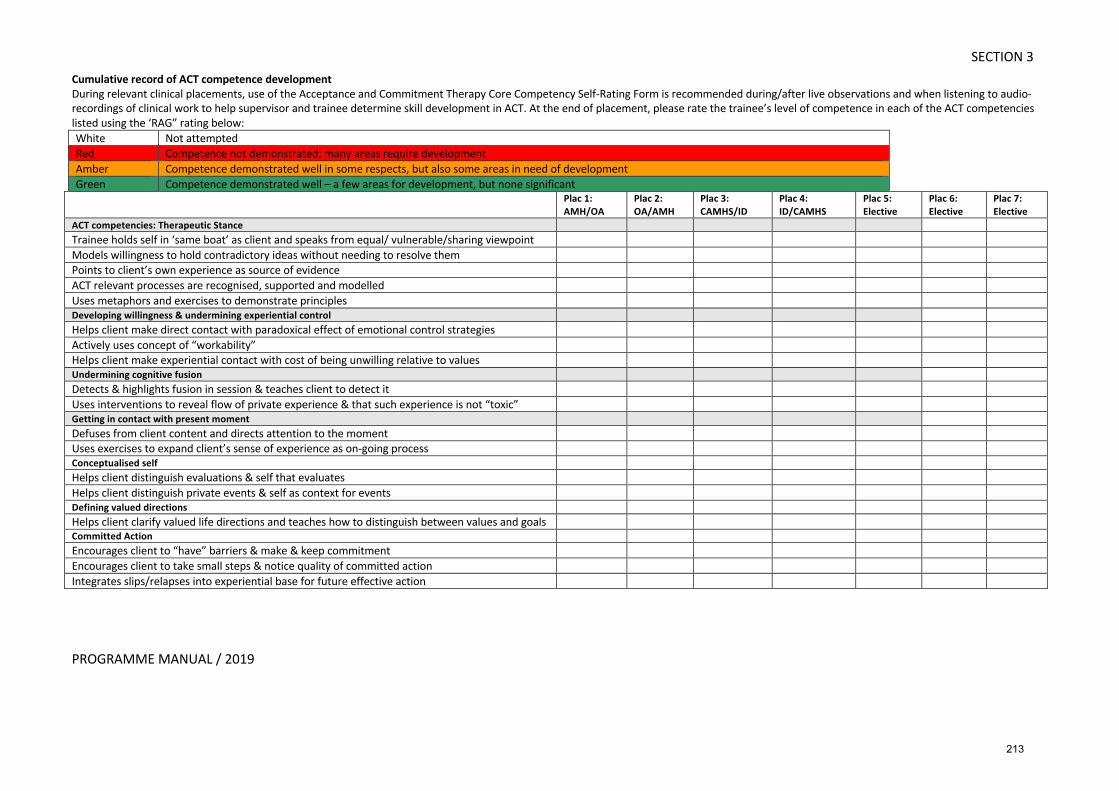
PROGRAMME MANUAL / 2019
SECTION 3 Cumulative record of ACT competence development
During relevant clinical placements, use of the Acceptance and Commitment Therapy Core Competency Self-Rating Form is recommended during/after live observations and when listening to audio-recordings of clinical work to help supervisor and trainee determine skill development in ACT. At the end of placement, please rate the trainee’s level of competence in each of the ACT competencies listed using the ‘RAG” rating below: White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need of development Green Competence demonstrated well – a few areas for development, but none significant
Plac 1:
AMH/OA
Plac 2:
OA/AMH
Plac 3:
CAMHS/ID
Plac 4:
ID/CAMHS
Plac 5:
Elective
Plac 6:
Elective
Plac 7:
Elective
ACT competencies: Therapeutic Stance Trainee holds self in ‘same boat’ as client and speaks from equal/ vulnerable/sharing viewpoint Models willingness to hold contradictory ideas without needing to resolve them Points to client’s own experience as source of evidence ACT relevant processes are recognised, supported and modelled Uses metaphors and exercises to demonstrate principles Developing willingness & undermining experiential control Helps client make direct contact with paradoxical effect of emotional control strategies Actively uses concept of “workability” Helps client make experiential contact with cost of being unwilling relative to values Undermining cognitive fusion Detects & highlights fusion in session & teaches client to detect it Uses interventions to reveal flow of private experience & that such experience is not “toxic” Getting in contact with present moment Defuses from client content and directs attention to the moment Uses exercises to expand client’s sense of experience as on-going process Conceptualised self Helps client distinguish evaluations & self that evaluates Helps client distinguish private events & self as context for events Defining valued directions Helps client clarify valued life directions and teaches how to distinguish between values and goals Committed Action Encourages client to “have” barriers & make & keep commitment Encourages client to take small steps & notice quality of committed action Integrates slips/relapses into experiential base for future effective action
213
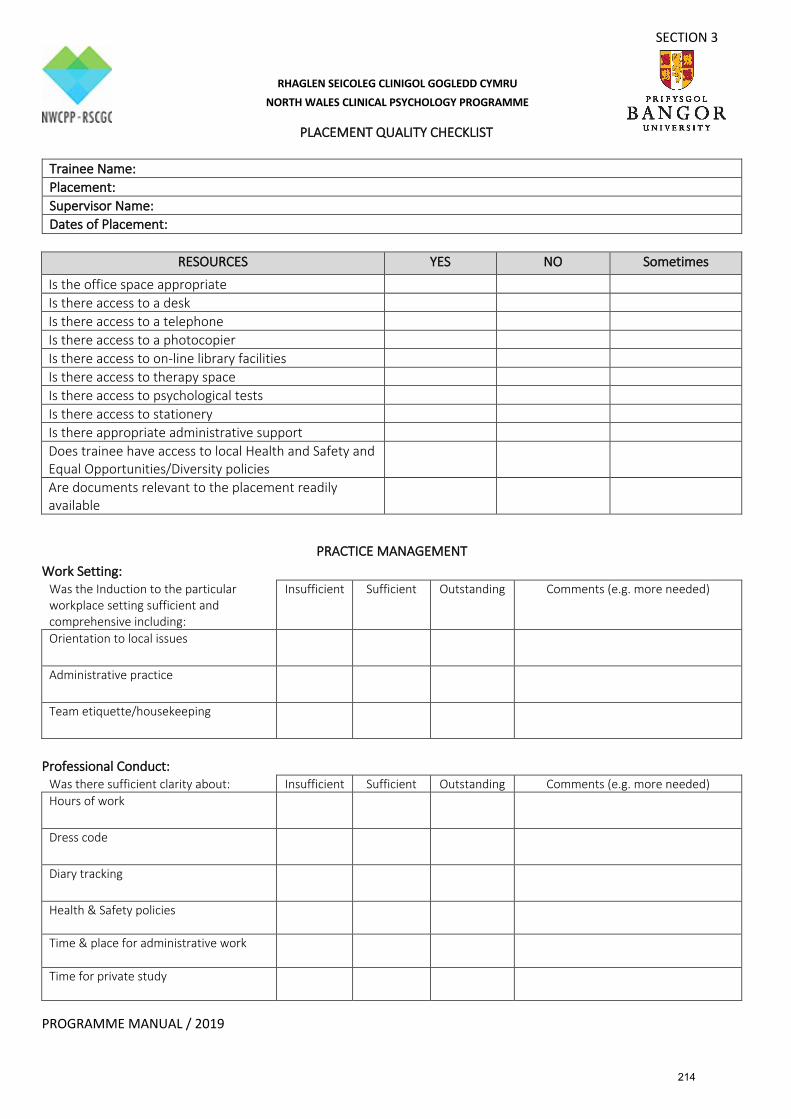
SECTION 3
PROGRAMME MANUAL / 2019
PLACEMENT QUALITY CHECKLIST
Trainee Name: Placement: Supervisor Name: Dates of Placement:
RESOURCES YES NO Sometimes
Is the office space appropriate Is there access to a desk Is there access to a telephone Is there access to a photocopier Is there access to on-line library facilities Is there access to therapy space Is there access to psychological tests Is there access to stationery Is there appropriate administrative support Does trainee have access to local Health and Safety and Equal Opportunities/Diversity policies
Are documents relevant to the placement readily available
PRACTICE MANAGEMENT Work Setting:
Was the Induction to the particular workplace setting sufficient and comprehensive including:
Insufficient Sufficient Outstanding Comments (e.g. more needed)
Orientation to local issues
Administrative practice
Team etiquette/housekeeping
Professional Conduct:
Was there sufficient clarity about: Insufficient Sufficient Outstanding Comments (e.g. more needed) Hours of work
Dress code
Diary tracking
Health & Safety policies
Time & place for administrative work
Time for private study
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
214
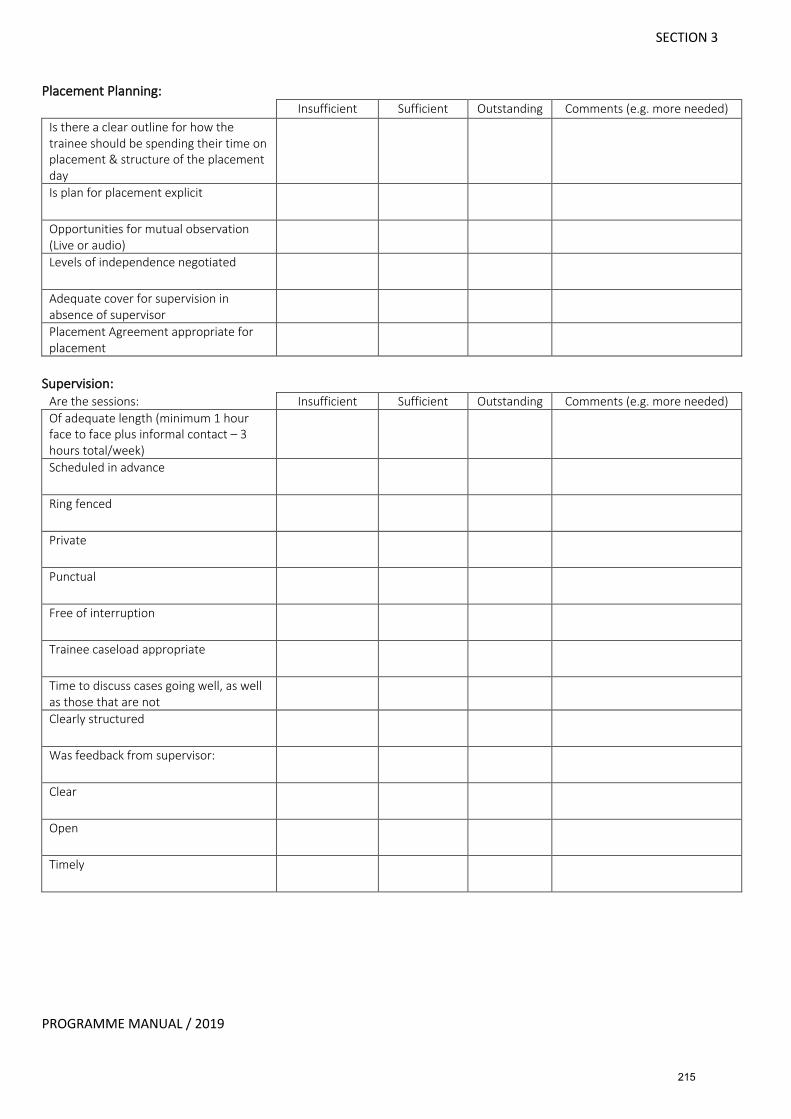
SECTION 3
PROGRAMME MANUAL / 2019
Placement Planning:
Insufficient Sufficient Outstanding Comments (e.g. more needed) Is there a clear outline for how the trainee should be spending their time on placement & structure of the placement day
Is plan for placement explicit
Opportunities for mutual observation (Live or audio)
Levels of independence negotiated
Adequate cover for supervision in absence of supervisor
Placement Agreement appropriate for placement
Supervision:
Are the sessions: Insufficient Sufficient Outstanding Comments (e.g. more needed) Of adequate length (minimum 1 hour face to face plus informal contact – 3 hours total/week)
Scheduled in advance
Ring fenced
Private
Punctual
Free of interruption
Trainee caseload appropriate
Time to discuss cases going well, as well as those that are not
Clearly structured
Was feedback from supervisor:
Clear
Open
Timely
215
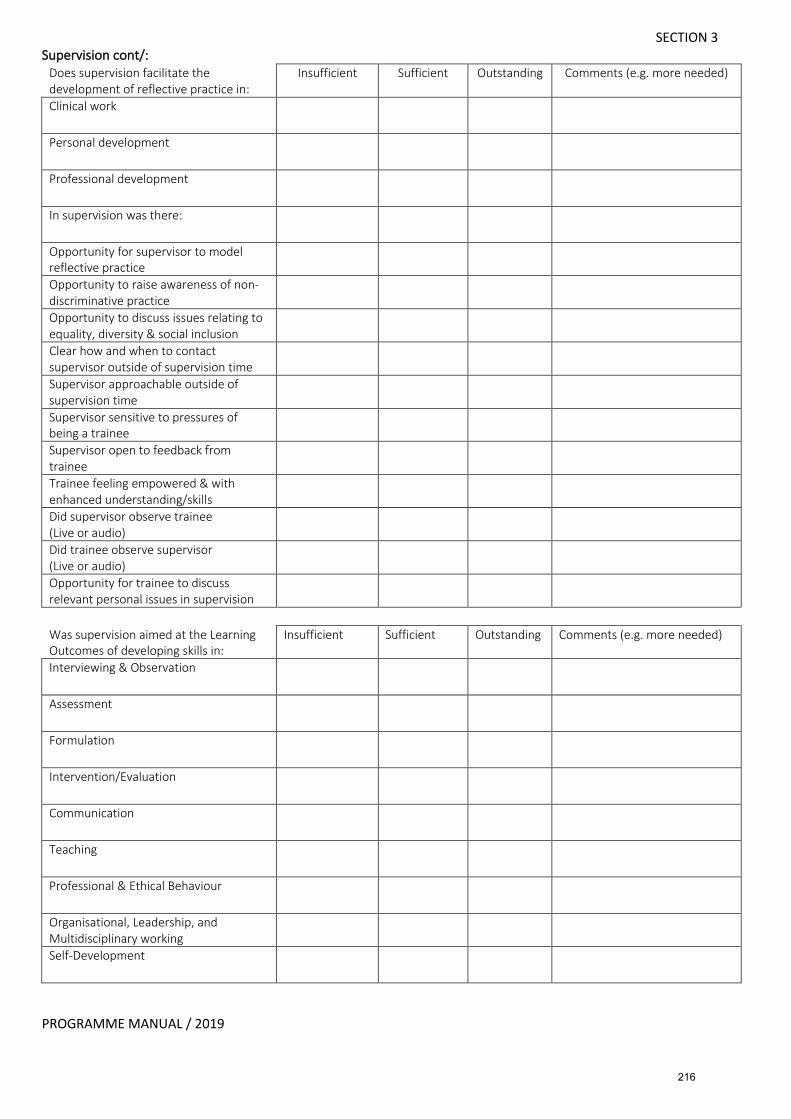
SECTION 3
PROGRAMME MANUAL / 2019
Supervision cont/: Does supervision facilitate the development of reflective practice in:
Insufficient Sufficient Outstanding Comments (e.g. more needed)
Clinical work
Personal development
Professional development
In supervision was there:
Opportunity for supervisor to model reflective practice
Opportunity to raise awareness of non-discriminative practice
Opportunity to discuss issues relating to equality, diversity & social inclusion
Clear how and when to contact supervisor outside of supervision time
Supervisor approachable outside of supervision time
Supervisor sensitive to pressures of being a trainee
Supervisor open to feedback from trainee
Trainee feeling empowered & with enhanced understanding/skills
Did supervisor observe trainee (Live or audio)
Did trainee observe supervisor (Live or audio)
Opportunity for trainee to discuss relevant personal issues in supervision
Was supervision aimed at the Learning Outcomes of developing skills in:
Insufficient Sufficient Outstanding Comments (e.g. more needed)
Interviewing & Observation
Assessment
Formulation
Intervention/Evaluation
Communication
Teaching
Professional & Ethical Behaviour
Organisational, Leadership, and Multidisciplinary working
Self-Development
216
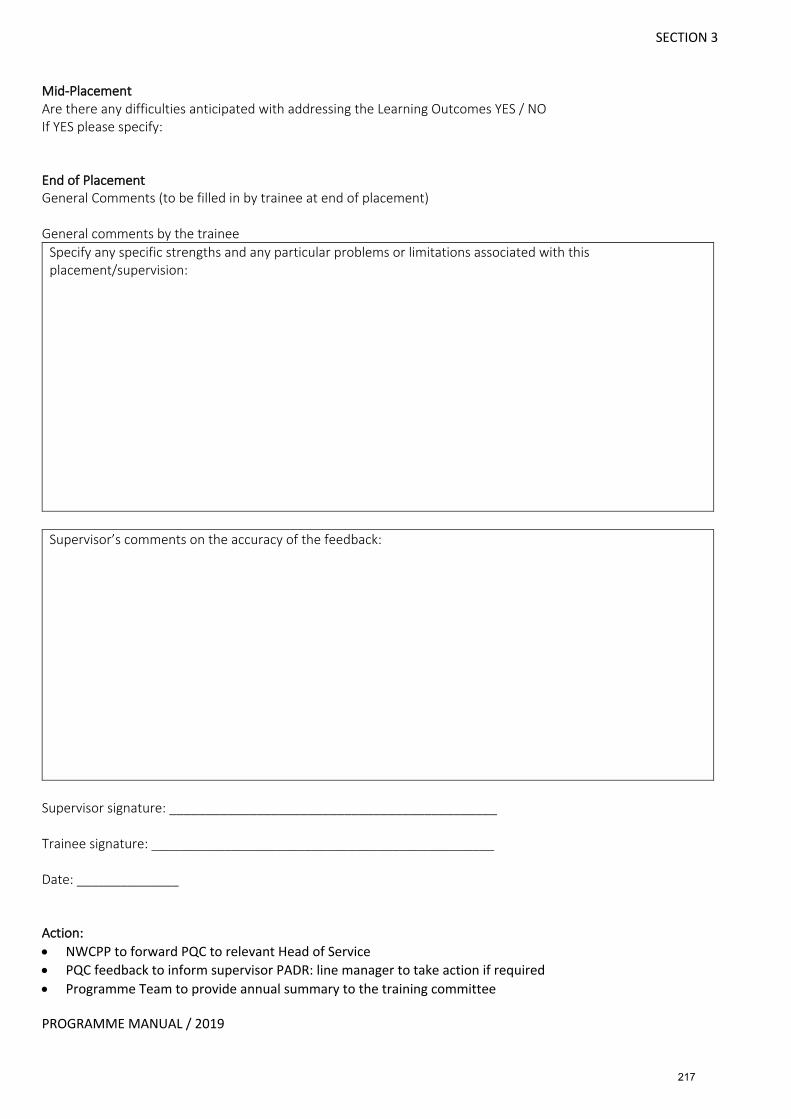
SECTION 3
PROGRAMME MANUAL / 2019
Mid-Placement Are there any difficulties anticipated with addressing the Learning Outcomes YES / NO If YES please specify: End of Placement General Comments (to be filled in by trainee at end of placement) General comments by the trainee
Specify any specific strengths and any particular problems or limitations associated with this placement/supervision:
Supervisor’s comments on the accuracy of the feedback:
Supervisor signature: _____________________________________________ Trainee signature: _______________________________________________ Date: ______________ Action: • NWCPP to forward PQC to relevant Head of Service • PQC feedback to inform supervisor PADR: line manager to take action if required • Programme Team to provide annual summary to the training committee
217
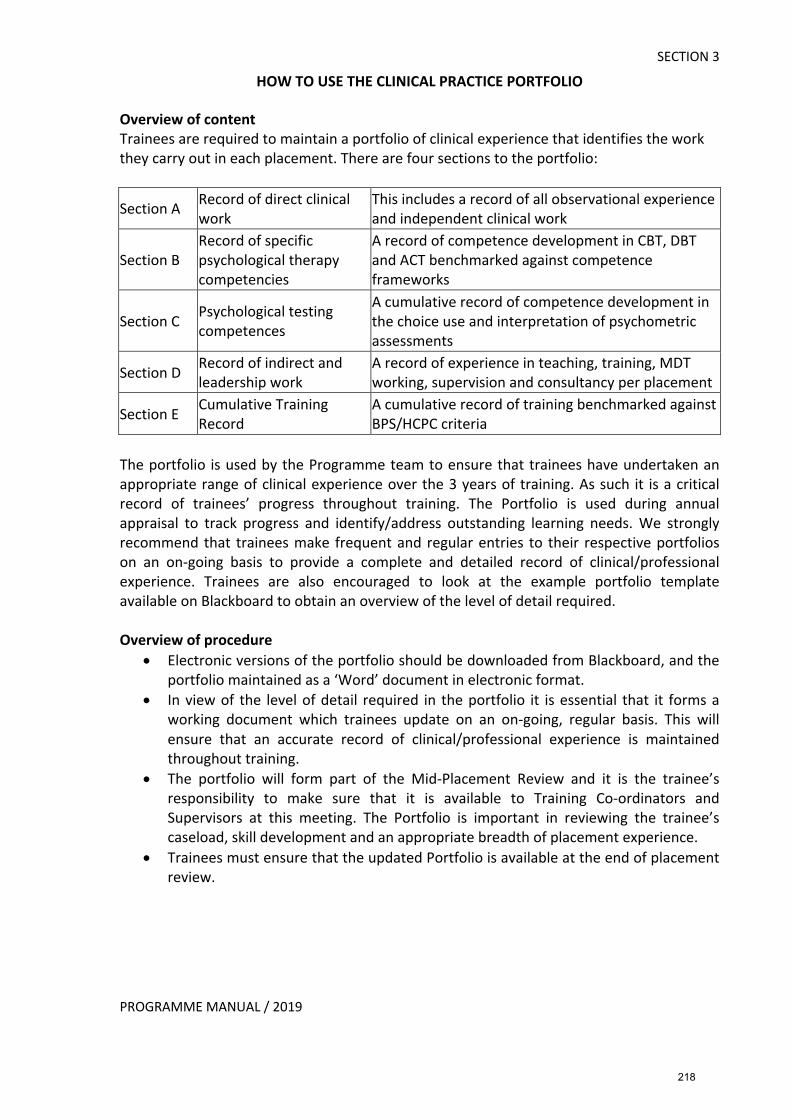
PROGRAMME MANUAL / 2019
SECTION 3 HOW TO USE THE CLINICAL PRACTICE PORTFOLIO
Overview of content Trainees are required to maintain a portfolio of clinical experience that identifies the work they carry out in each placement. There are four sections to the portfolio:
Section A Record of direct clinical work
This includes a record of all observational experience and independent clinical work
Section B Record of specific psychological therapy competencies
A record of competence development in CBT, DBT and ACT benchmarked against competence frameworks
Section C Psychological testing competences
A cumulative record of competence development in the choice use and interpretation of psychometric assessments
Section D Record of indirect and leadership work
A record of experience in teaching, training, MDT working, supervision and consultancy per placement
Section E Cumulative Training Record
A cumulative record of training benchmarked against BPS/HCPC criteria
The portfolio is used by the Programme team to ensure that trainees have undertaken an appropriate range of clinical experience over the 3 years of training. As such it is a critical record of trainees’ progress throughout training. The Portfolio is used during annual appraisal to track progress and identify/address outstanding learning needs. We strongly recommend that trainees make frequent and regular entries to their respective portfolios on an on-going basis to provide a complete and detailed record of clinical/professional experience. Trainees are also encouraged to look at the example portfolio template available on Blackboard to obtain an overview of the level of detail required. Overview of procedure
• Electronic versions of the portfolio should be downloaded from Blackboard, and the portfolio maintained as a ‘Word’ document in electronic format.
• In view of the level of detail required in the portfolio it is essential that it forms a working document which trainees update on an on-going, regular basis. This will ensure that an accurate record of clinical/professional experience is maintained throughout training.
• The portfolio will form part of the Mid-Placement Review and it is the trainee’s responsibility to make sure that it is available to Training Co-ordinators and Supervisors at this meeting. The Portfolio is important in reviewing the trainee’s caseload, skill development and an appropriate breadth of placement experience.
• Trainees must ensure that the updated Portfolio is available at the end of placement review.
218
PROGRAMME MANUAL / 2019
SECTION 3 End of placement Portfolio submission
• Once supervisors have completed the Evaluation of Clinical and Professional Competence form, trainees should transfer the therapeutic competency ‘RAG’ (Red/Amber/Green) ratings to the portfolio for the approaches used on placement – CBT/DBT/ACT.
• Supervisors are required to validate the trainee’s Portfolio by signing a ‘Supervisor Authentication of Portfolio’ form (see Section 3 p113).
• The Supervisor Authentication of Portfolio form is available on Blackboard and trainees should ensure that a signed, paper copy of this form is submitted to the Programme Office together with other relevant placement documentation.
• Trainees should submit an electronic copy of the approved portfolio to the programme office by the deadline specified.
• After submission, programme administrative staff will scan the ‘Supervisor Authentication of Portfolio’ form, adding it to the end of the trainee’s Clinical Practice Portfolio. Subsequently, the complete document will be saved in PDF format.
Maintaining a cumulative Clinical Practice Portfolio Trainees must always keep an electronic copy of the most up-to-date ‘Word’ version of the portfolio. The portfolio forms a cumulative record across placements culminating in a complete record of clinical/professional experience and skill development by the end of training. As such, trainees also need to ensure that the portfolio is kept after training as evidence of clinical/professional experience and competence development. The Portfolio will be essential if applying for further training, post-qualification accreditation in psychological therapy and/or applying to work in another country. SECTION A: RECORD OF DIRECT CLINICAL WORK The record of direct clinical work serves several functions:
•� It creates and maintains an accurate and detailed record of the observational, joint and/or independent work trainees have undertaken and the supervision they have received.
•� It identifies gaps in experience or areas for further development, which need to be addressed
•� It aids placement planning (for example, when reviewing progress in a current placement or thinking about the content of future placements)
•� It may be used as evidence of clinical activity and hours of supervised clinical practice when seeking accreditation with external bodies (e.g. BABCP)
As can be seen from the example Clinical Practice Portfolio on Blackboard, Section A provides a summary of clients seen, presenting problems, work undertaken, supervision received including the amount of in vivo observation. The examples in the CPP on Blackboard are intended as a guide to the level of detail required.
219
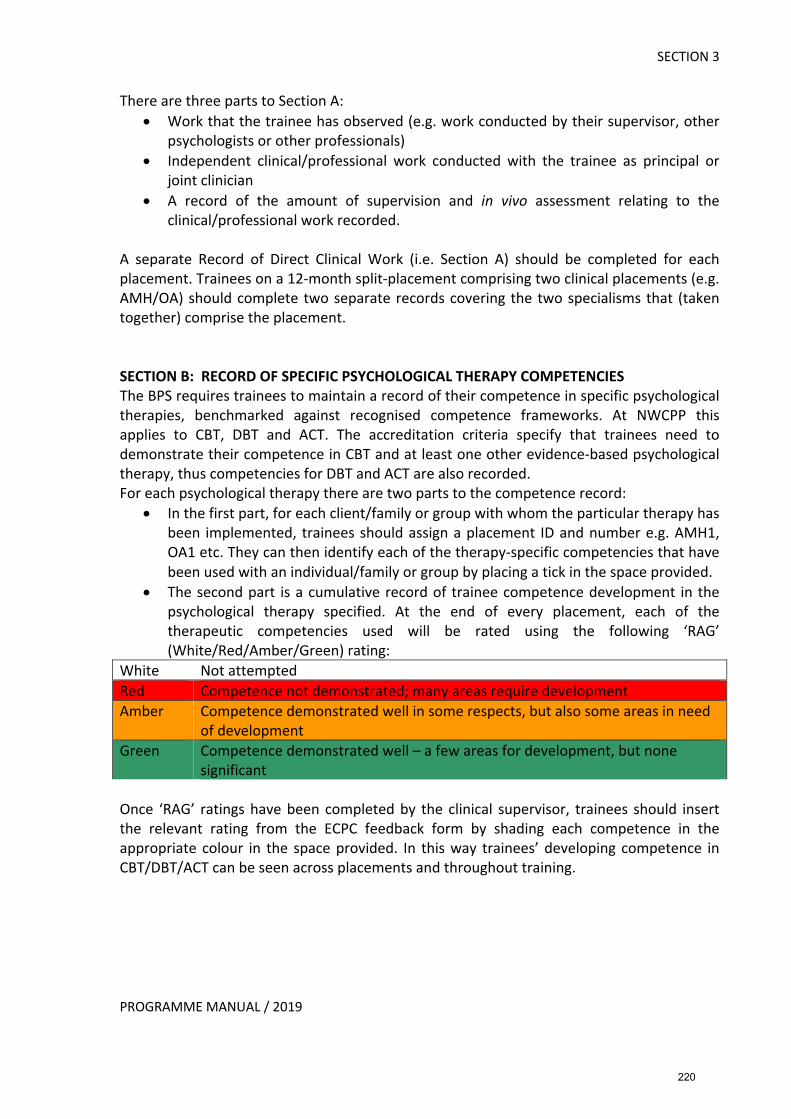
PROGRAMME MANUAL / 2019
SECTION 3 There are three parts to Section A:
• Work that the trainee has observed (e.g. work conducted by their supervisor, other psychologists or other professionals)
• Independent clinical/professional work conducted with the trainee as principal or joint clinician
• A record of the amount of supervision and in vivo assessment relating to the clinical/professional work recorded.
A separate Record of Direct Clinical Work (i.e. Section A) should be completed for each placement. Trainees on a 12-month split-placement comprising two clinical placements (e.g. AMH/OA) should complete two separate records covering the two specialisms that (taken together) comprise the placement. SECTION B: RECORD OF SPECIFIC PSYCHOLOGICAL THERAPY COMPETENCIES The BPS requires trainees to maintain a record of their competence in specific psychological therapies, benchmarked against recognised competence frameworks. At NWCPP this applies to CBT, DBT and ACT. The accreditation criteria specify that trainees need to demonstrate their competence in CBT and at least one other evidence-based psychological therapy, thus competencies for DBT and ACT are also recorded. For each psychological therapy there are two parts to the competence record:
• In the first part, for each client/family or group with whom the particular therapy has been implemented, trainees should assign a placement ID and number e.g. AMH1, OA1 etc. They can then identify each of the therapy-specific competencies that have been used with an individual/family or group by placing a tick in the space provided.
• The second part is a cumulative record of trainee competence development in the psychological therapy specified. At the end of every placement, each of the therapeutic competencies used will be rated using the following ‘RAG’ (White/Red/Amber/Green) rating:
White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need
of development Green Competence demonstrated well – a few areas for development, but none
significant Once ‘RAG’ ratings have been completed by the clinical supervisor, trainees should insert the relevant rating from the ECPC feedback form by shading each competence in the appropriate colour in the space provided. In this way trainees’ developing competence in CBT/DBT/ACT can be seen across placements and throughout training.
220
PROGRAMME MANUAL / 2019
SECTION 3 SECTION C: PSYCHOLOGICAL TESTING COMPETENCIES
• This is a record of trainees’ experience and skill development in psychological testing.
• Trainees maintain a summary record of client self-report and performance-based measures with reference to choice, use and interpretation.
• The example on Blackboard illustrates the level of detail required. SECTION D: RECORD OF INDIRECT AND LEADERSHIP WORK WITH PROFESSIONALS/TEAMS/SERVICES
• This section provides a summary record of all ‘indirect’ clinical work including organisational, leadership, and MDT working. Examples of such activities include teaching, training, inter-professional liaison, supervision, service development, organisational initiatives and consultancy work.
• A separate record should be completed for each clinical placement undertaken during the three years of training outlining a brief summary of the work completed.
SECTION E: CUMULATIVE TRAINING RECORD
• The cumulative training record summarises clinical activity as benchmarked across the BPS accreditation criteria for clinical presentations, service settings, age ranges, modes of work etc. (Please refer to the BPS standards for the accreditation of Doctoral programmes in clinical psychology, October 2014 and the HCPC Standards of education and training for clinical psychologists for more information).
• The summary record should be completed for each placement by counting the number of clients and/or pieces of indirect clinical work matching the relevant clinical presentations, age ranges, services, modes of work etc. across placements.
• The various categories are not mutually exclusive and each client /carer/family/group may undoubtedly have relevance to multiple domains.
• The cumulative training record and Clinical Practice Portfolio more generally, are used during annual appraisal to consider trainees’ learning needs and to plan future training experience.
• The cumulative training record ensures that by the end of training, trainees have attained a satisfactory range of experience upon which competencies have been evidenced.
• The cumulative record encourages trainees to reflect on their overall development and in so doing can contribute to their development as reflective practitioners.
221
SECTION 3
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
CLINICAL PRACTICE PORTFOLIO
NAME OF CANDIDATE: _____________________________________________ [Please use block capitals]
START AND END DATES ON NWCPP PROGRAMME:
START DATE : ______________________________________________________
END DATE: __________________________________________________________
222
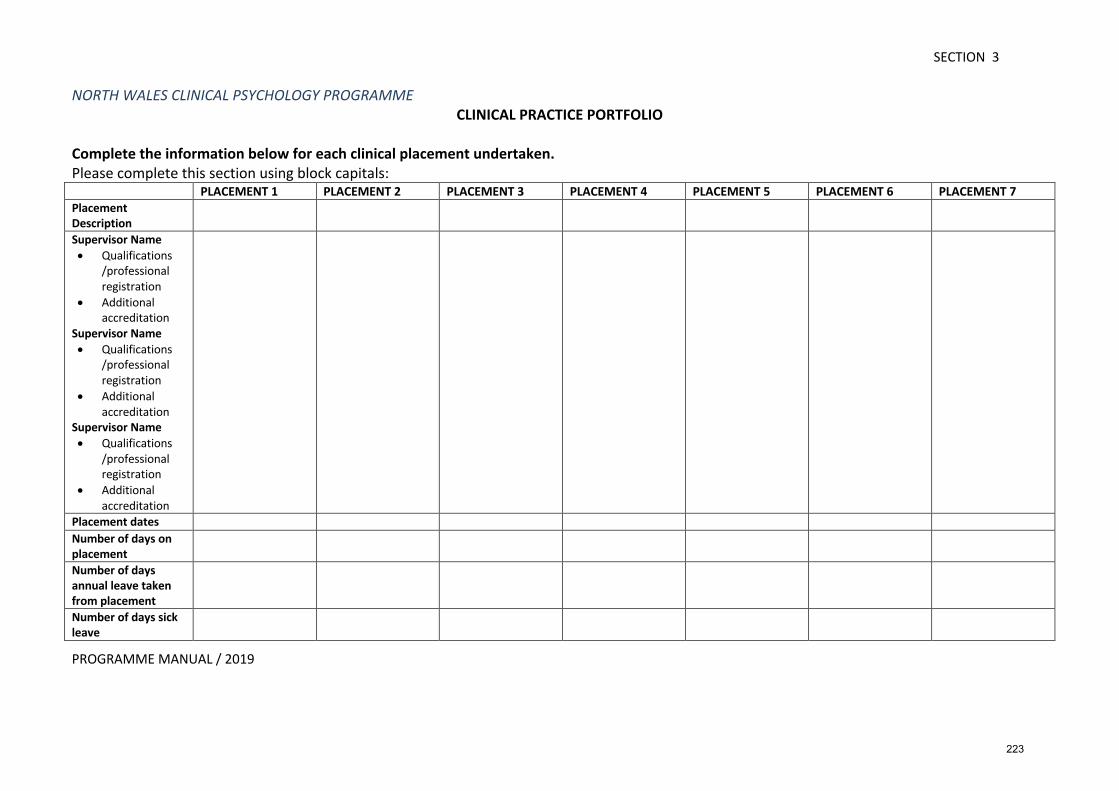
SECTION 3
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME CLINICAL PRACTICE PORTFOLIO
Complete the information below for each clinical placement undertaken. Please complete this section using block capitals: PLACEMENT 1 PLACEMENT 2 PLACEMENT 3 PLACEMENT 4 PLACEMENT 5 PLACEMENT 6 PLACEMENT 7 Placement Description
Supervisor Name • Qualifications
/professional registration
• Additional accreditation
Supervisor Name • Qualifications
/professional registration
• Additional accreditation
Supervisor Name • Qualifications
/professional registration
• Additional accreditation
Placement dates Number of days on placement
Number of days annual leave taken from placement
Number of days sick leave
223
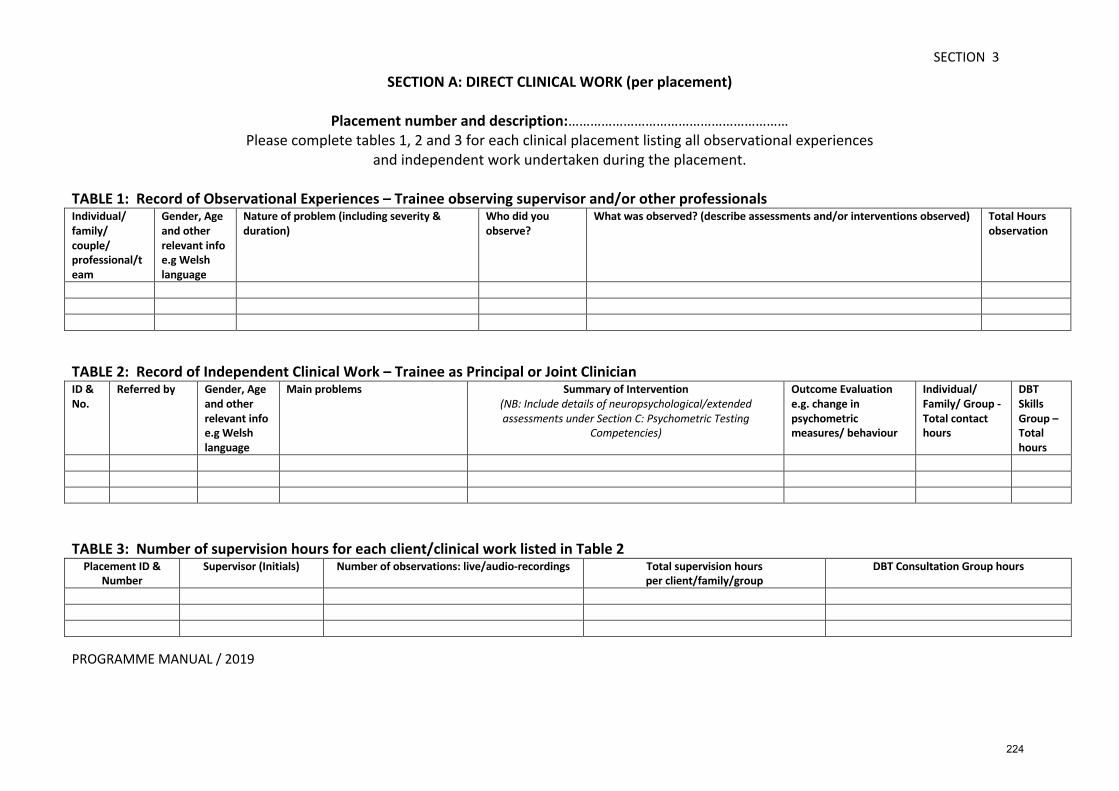
SECTION 3
PROGRAMME MANUAL / 2019
SECTION A: DIRECT CLINICAL WORK (per placement)
Placement number and description:……………………………………………………
Please complete tables 1, 2 and 3 for each clinical placement listing all observational experiences and independent work undertaken during the placement.
TABLE 1: Record of Observational Experiences – Trainee observing supervisor and/or other professionals Individual/ family/ couple/ professional/team
Gender, Age and other relevant info e.g Welsh language
Nature of problem (including severity & duration)
Who did you observe?
What was observed? (describe assessments and/or interventions observed) Total Hours observation
TABLE 2: Record of Independent Clinical Work – Trainee as Principal or Joint Clinician ID & No.
Referred by Gender, Age and other relevant info e.g Welsh language
Main problems Summary of Intervention (NB: Include details of neuropsychological/extended assessments under Section C: Psychometric Testing
Competencies)
Outcome Evaluation e.g. change in psychometric measures/ behaviour
Individual/ Family/ Group - Total contact hours
DBT Skills Group – Total hours
TABLE 3: Number of supervision hours for each client/clinical work listed in Table 2
Placement ID & Number
Supervisor (Initials) Number of observations: live/audio-recordings Total supervision hours per client/family/group
DBT Consultation Group hours
224
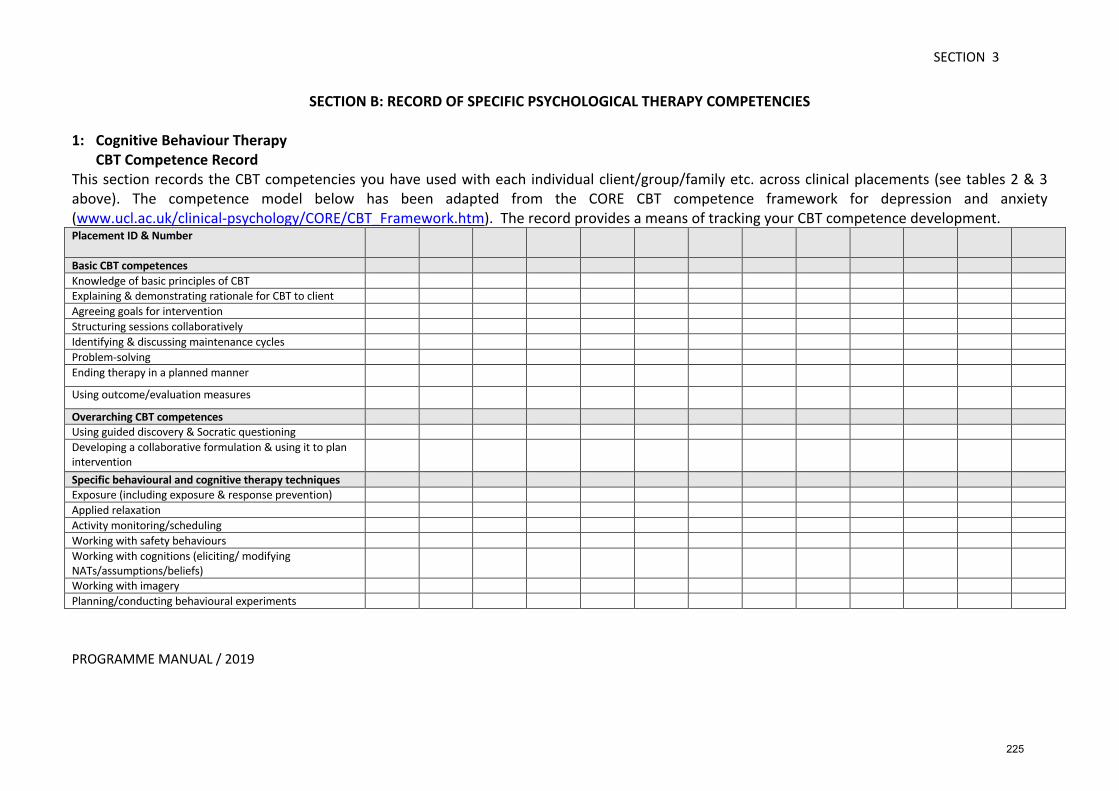
SECTION 3
PROGRAMME MANUAL / 2019
SECTION B: RECORD OF SPECIFIC PSYCHOLOGICAL THERAPY COMPETENCIES
1: Cognitive Behaviour Therapy CBT Competence Record This section records the CBT competencies you have used with each individual client/group/family etc. across clinical placements (see tables 2 & 3 above). The competence model below has been adapted from the CORE CBT competence framework for depression and anxiety (www.ucl.ac.uk/clinical-psychology/CORE/CBT_Framework.htm). The record provides a means of tracking your CBT competence development. Placement ID & Number
Basic CBT competences Knowledge of basic principles of CBT Explaining & demonstrating rationale for CBT to client Agreeing goals for intervention Structuring sessions collaboratively Identifying & discussing maintenance cycles Problem-solving Ending therapy in a planned manner
Using outcome/evaluation measures
Overarching CBT competences Using guided discovery & Socratic questioning Developing a collaborative formulation & using it to plan intervention
Specific behavioural and cognitive therapy techniques Exposure (including exposure & response prevention) Applied relaxation Activity monitoring/scheduling Working with safety behaviours Working with cognitions (eliciting/ modifying NATs/assumptions/beliefs)
Working with imagery Planning/conducting behavioural experiments
225
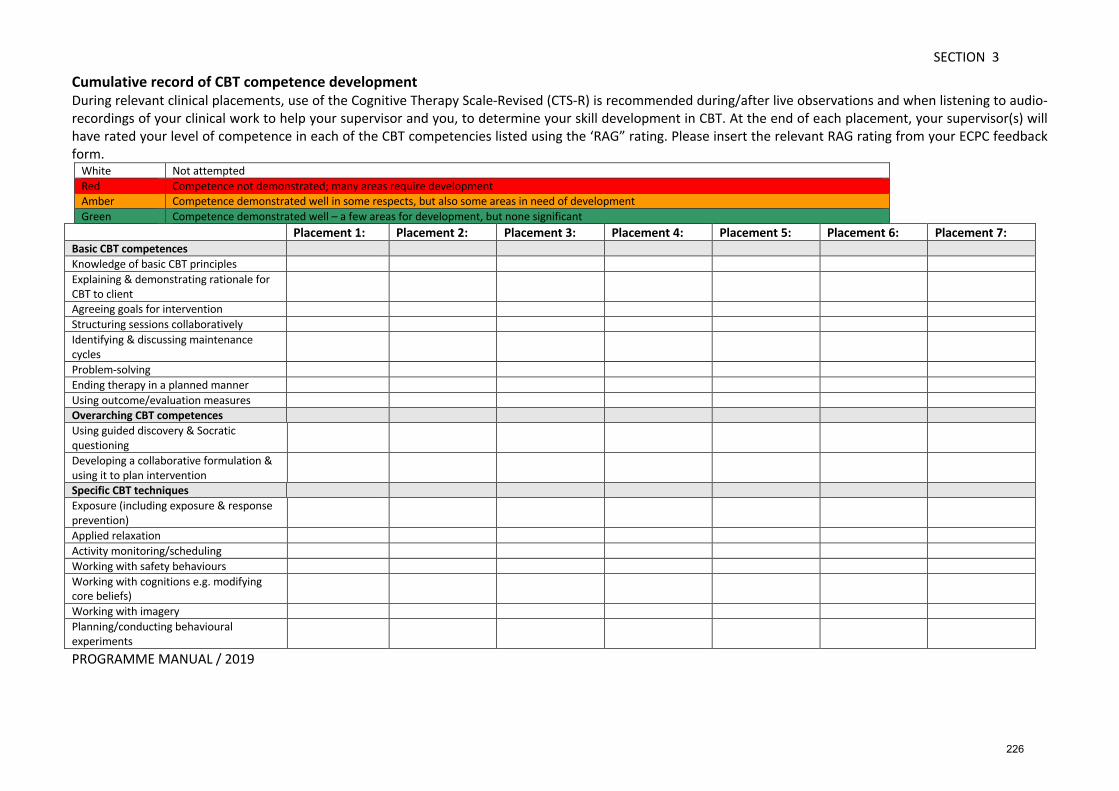
SECTION 3
PROGRAMME MANUAL / 2019
Cumulative record of CBT competence development During relevant clinical placements, use of the Cognitive Therapy Scale-Revised (CTS-R) is recommended during/after live observations and when listening to audio-recordings of your clinical work to help your supervisor and you, to determine your skill development in CBT. At the end of each placement, your supervisor(s) will have rated your level of competence in each of the CBT competencies listed using the ‘RAG” rating. Please insert the relevant RAG rating from your ECPC feedback form.
White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need of development Green Competence demonstrated well – a few areas for development, but none significant
Placement 1: Placement 2: Placement 3: Placement 4: Placement 5: Placement 6: Placement 7: Basic CBT competences Knowledge of basic CBT principles Explaining & demonstrating rationale for CBT to client
Agreeing goals for intervention Structuring sessions collaboratively Identifying & discussing maintenance cycles
Problem-solving Ending therapy in a planned manner Using outcome/evaluation measures Overarching CBT competences Using guided discovery & Socratic questioning
Developing a collaborative formulation & using it to plan intervention
Specific CBT techniques Exposure (including exposure & response prevention)
Applied relaxation Activity monitoring/scheduling Working with safety behaviours Working with cognitions e.g. modifying core beliefs)
Working with imagery Planning/conducting behavioural experiments
226
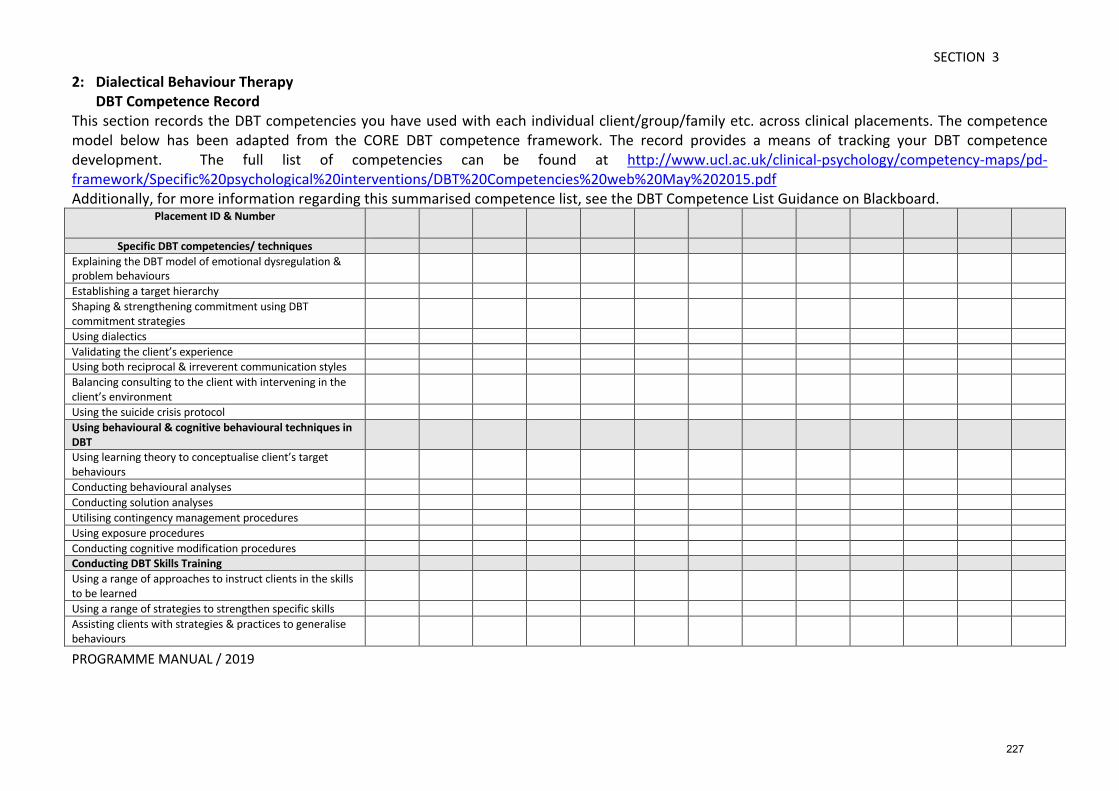
SECTION 3
PROGRAMME MANUAL / 2019
2: Dialectical Behaviour Therapy DBT Competence Record This section records the DBT competencies you have used with each individual client/group/family etc. across clinical placements. The competence model below has been adapted from the CORE DBT competence framework. The record provides a means of tracking your DBT competence development. The full list of competencies can be found at http://www.ucl.ac.uk/clinical-psychology/competency-maps/pd-framework/Specific%20psychological%20interventions/DBT%20Competencies%20web%20May%202015.pdf Additionally, for more information regarding this summarised competence list, see the DBT Competence List Guidance on Blackboard.
Placement ID & Number
Specific DBT competencies/ techniques Explaining the DBT model of emotional dysregulation & problem behaviours
Establishing a target hierarchy Shaping & strengthening commitment using DBT commitment strategies
Using dialectics Validating the client’s experience Using both reciprocal & irreverent communication styles Balancing consulting to the client with intervening in the client’s environment
Using the suicide crisis protocol Using behavioural & cognitive behavioural techniques in DBT
Using learning theory to conceptualise client’s target behaviours
Conducting behavioural analyses Conducting solution analyses Utilising contingency management procedures Using exposure procedures Conducting cognitive modification procedures Conducting DBT Skills Training Using a range of approaches to instruct clients in the skills to be learned
Using a range of strategies to strengthen specific skills Assisting clients with strategies & practices to generalise behaviours
227
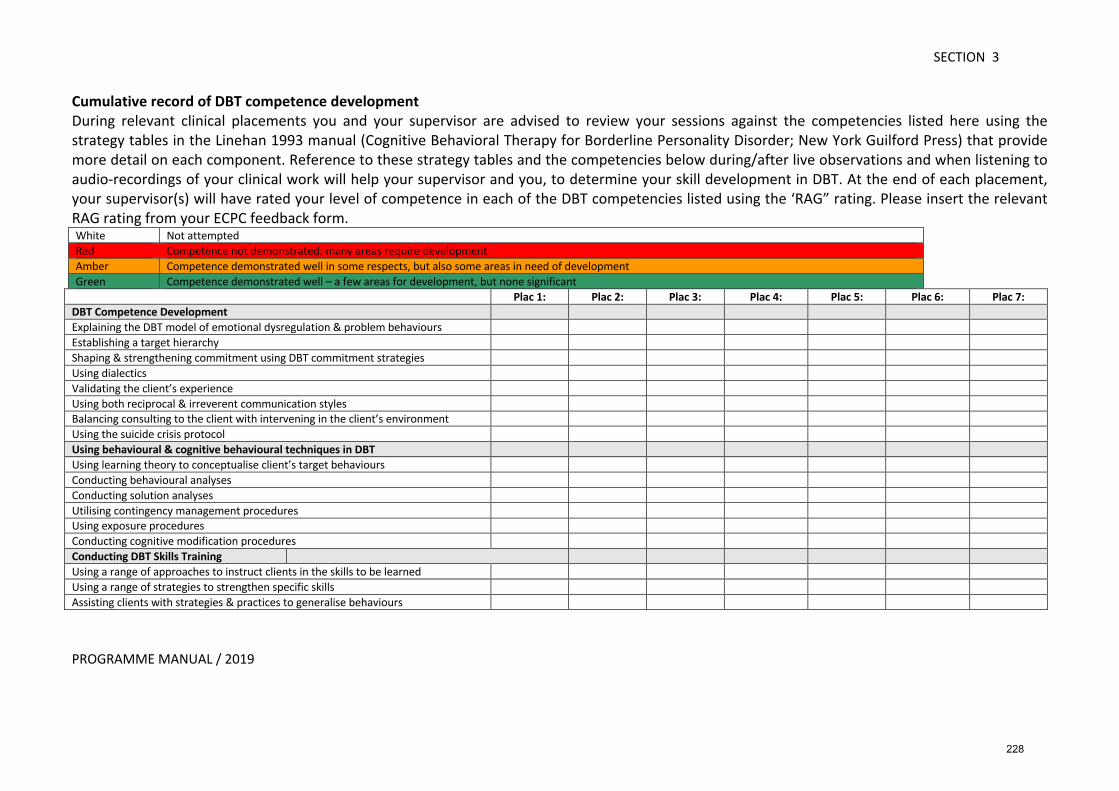
SECTION 3
PROGRAMME MANUAL / 2019
Cumulative record of DBT competence development During relevant clinical placements you and your supervisor are advised to review your sessions against the competencies listed here using the strategy tables in the Linehan 1993 manual (Cognitive Behavioral Therapy for Borderline Personality Disorder; New York Guilford Press) that provide more detail on each component. Reference to these strategy tables and the competencies below during/after live observations and when listening to audio-recordings of your clinical work will help your supervisor and you, to determine your skill development in DBT. At the end of each placement, your supervisor(s) will have rated your level of competence in each of the DBT competencies listed using the ‘RAG” rating. Please insert the relevant RAG rating from your ECPC feedback form. White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need of development Green Competence demonstrated well – a few areas for development, but none significant
Plac 1: Plac 2: Plac 3: Plac 4: Plac 5: Plac 6: Plac 7: DBT Competence Development Explaining the DBT model of emotional dysregulation & problem behaviours Establishing a target hierarchy Shaping & strengthening commitment using DBT commitment strategies Using dialectics Validating the client’s experience Using both reciprocal & irreverent communication styles Balancing consulting to the client with intervening in the client’s environment Using the suicide crisis protocol Using behavioural & cognitive behavioural techniques in DBT Using learning theory to conceptualise client’s target behaviours Conducting behavioural analyses Conducting solution analyses Utilising contingency management procedures Using exposure procedures Conducting cognitive modification procedures Conducting DBT Skills Training Using a range of approaches to instruct clients in the skills to be learned Using a range of strategies to strengthen specific skills Assisting clients with strategies & practices to generalise behaviours
228
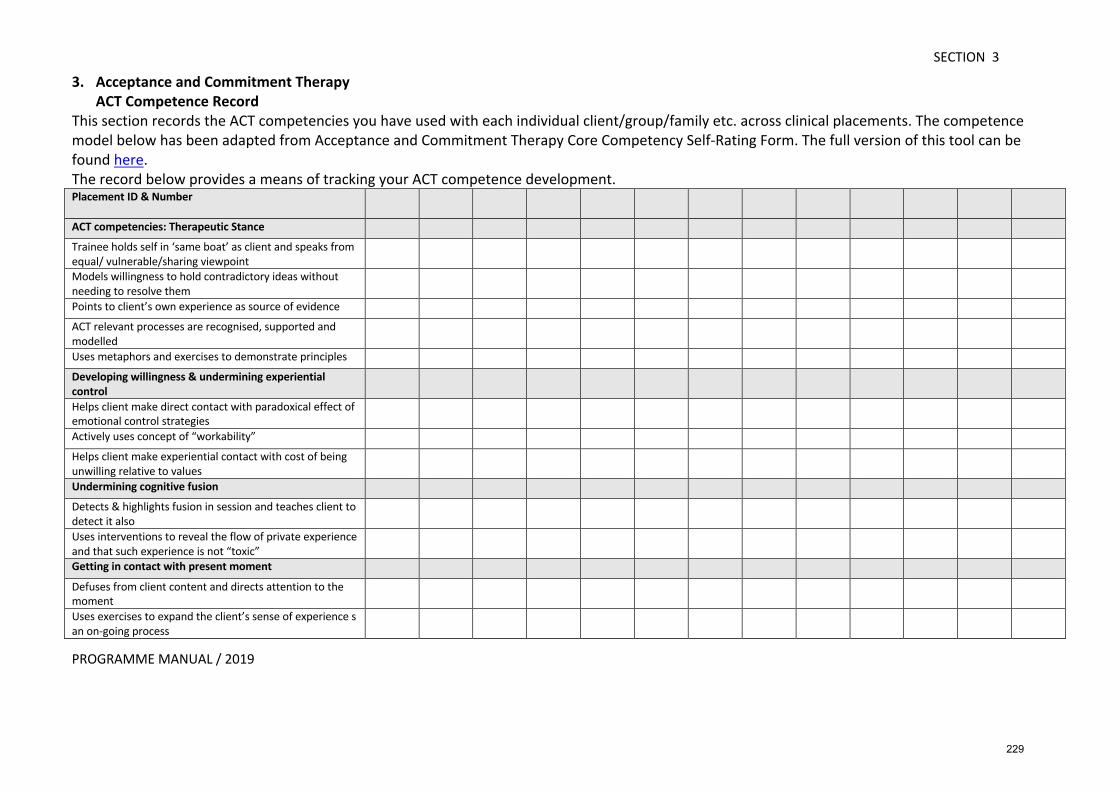
SECTION 3
PROGRAMME MANUAL / 2019
3. Acceptance and Commitment Therapy ACT Competence Record This section records the ACT competencies you have used with each individual client/group/family etc. across clinical placements. The competence model below has been adapted from Acceptance and Commitment Therapy Core Competency Self-Rating Form. The full version of this tool can be found here. The record below provides a means of tracking your ACT competence development. Placement ID & Number
ACT competencies: Therapeutic Stance Trainee holds self in ‘same boat’ as client and speaks from equal/ vulnerable/sharing viewpoint
Models willingness to hold contradictory ideas without needing to resolve them
Points to client’s own experience as source of evidence ACT relevant processes are recognised, supported and modelled
Uses metaphors and exercises to demonstrate principles Developing willingness & undermining experiential control
Helps client make direct contact with paradoxical effect of emotional control strategies
Actively uses concept of “workability” Helps client make experiential contact with cost of being unwilling relative to values
Undermining cognitive fusion Detects & highlights fusion in session and teaches client to detect it also
Uses interventions to reveal the flow of private experience and that such experience is not “toxic”
Getting in contact with present moment Defuses from client content and directs attention to the moment
Uses exercises to expand the client’s sense of experience s an on-going process
229
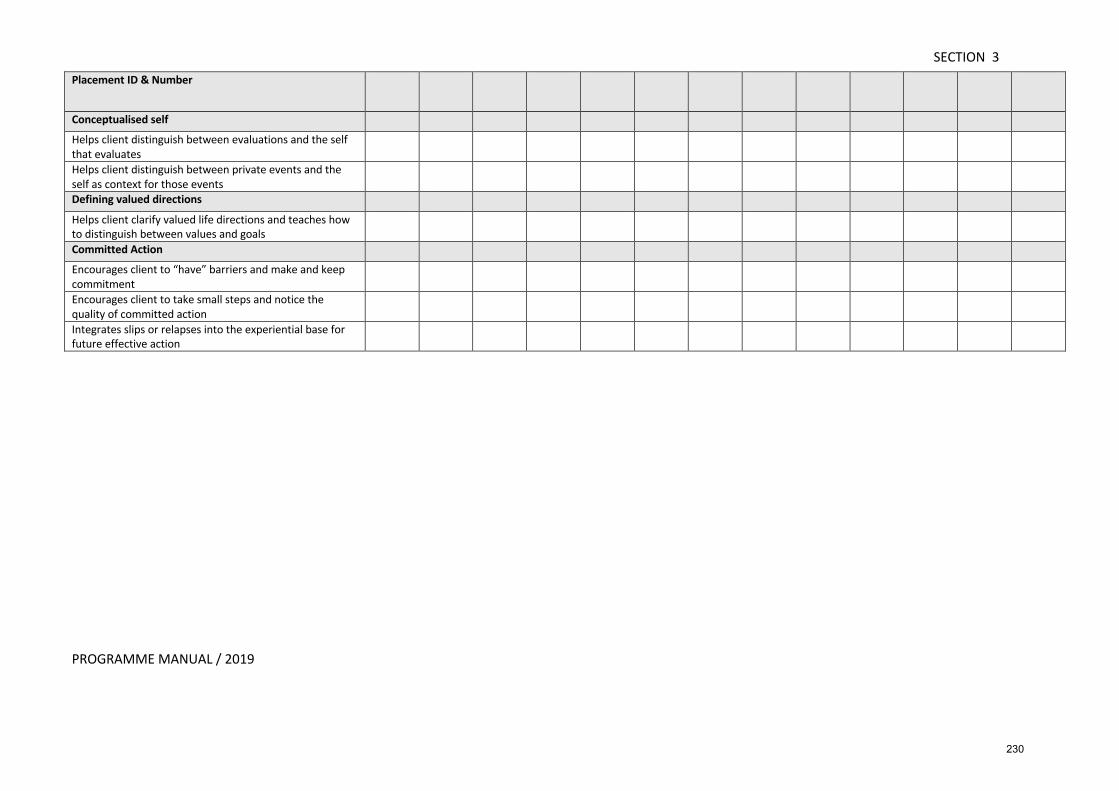
SECTION 3
PROGRAMME MANUAL / 2019
Placement ID & Number
Conceptualised self Helps client distinguish between evaluations and the self that evaluates
Helps client distinguish between private events and the self as context for those events
Defining valued directions Helps client clarify valued life directions and teaches how to distinguish between values and goals
Committed Action Encourages client to “have” barriers and make and keep commitment
Encourages client to take small steps and notice the quality of committed action
Integrates slips or relapses into the experiential base for future effective action
230
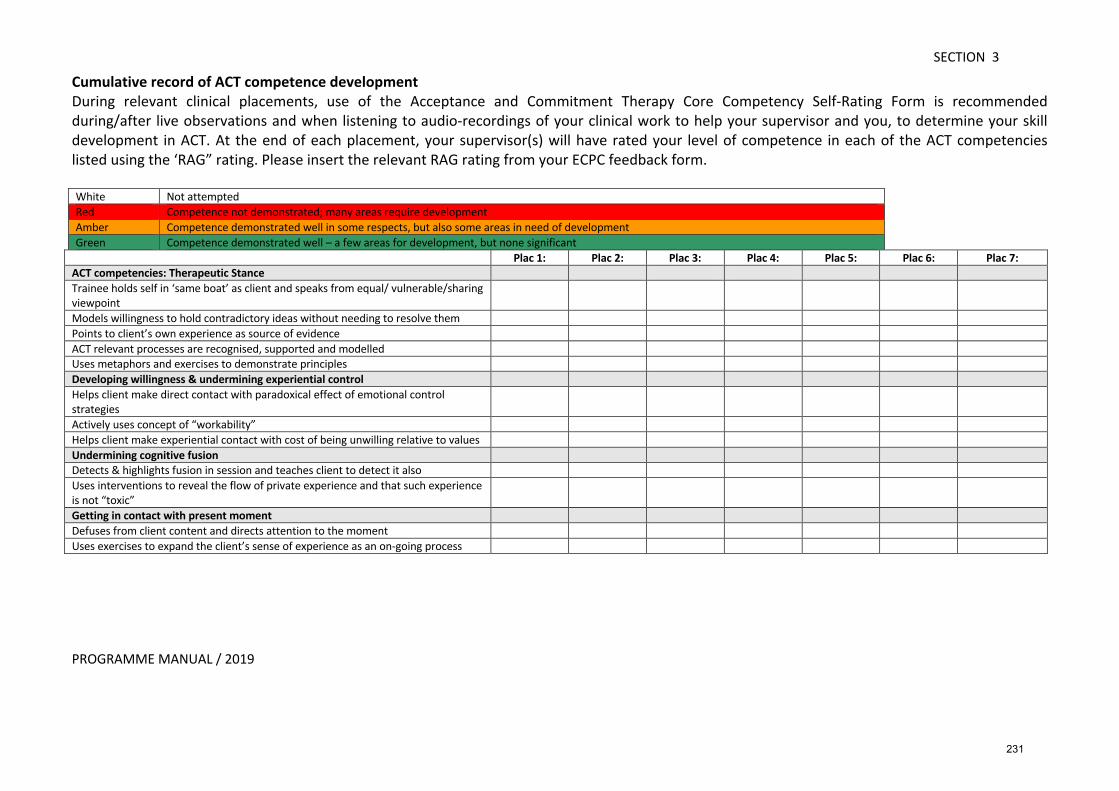
SECTION 3
PROGRAMME MANUAL / 2019
Cumulative record of ACT competence development During relevant clinical placements, use of the Acceptance and Commitment Therapy Core Competency Self-Rating Form is recommended during/after live observations and when listening to audio-recordings of your clinical work to help your supervisor and you, to determine your skill development in ACT. At the end of each placement, your supervisor(s) will have rated your level of competence in each of the ACT competencies listed using the ‘RAG” rating. Please insert the relevant RAG rating from your ECPC feedback form. White Not attempted Red Competence not demonstrated; many areas require development Amber Competence demonstrated well in some respects, but also some areas in need of development Green Competence demonstrated well – a few areas for development, but none significant
Plac 1: Plac 2: Plac 3: Plac 4: Plac 5: Plac 6: Plac 7: ACT competencies: Therapeutic Stance Trainee holds self in ‘same boat’ as client and speaks from equal/ vulnerable/sharing viewpoint
Models willingness to hold contradictory ideas without needing to resolve them Points to client’s own experience as source of evidence ACT relevant processes are recognised, supported and modelled Uses metaphors and exercises to demonstrate principles Developing willingness & undermining experiential control Helps client make direct contact with paradoxical effect of emotional control strategies
Actively uses concept of “workability” Helps client make experiential contact with cost of being unwilling relative to values Undermining cognitive fusion Detects & highlights fusion in session and teaches client to detect it also Uses interventions to reveal the flow of private experience and that such experience is not “toxic”
Getting in contact with present moment Defuses from client content and directs attention to the moment Uses exercises to expand the client’s sense of experience as an on-going process
231
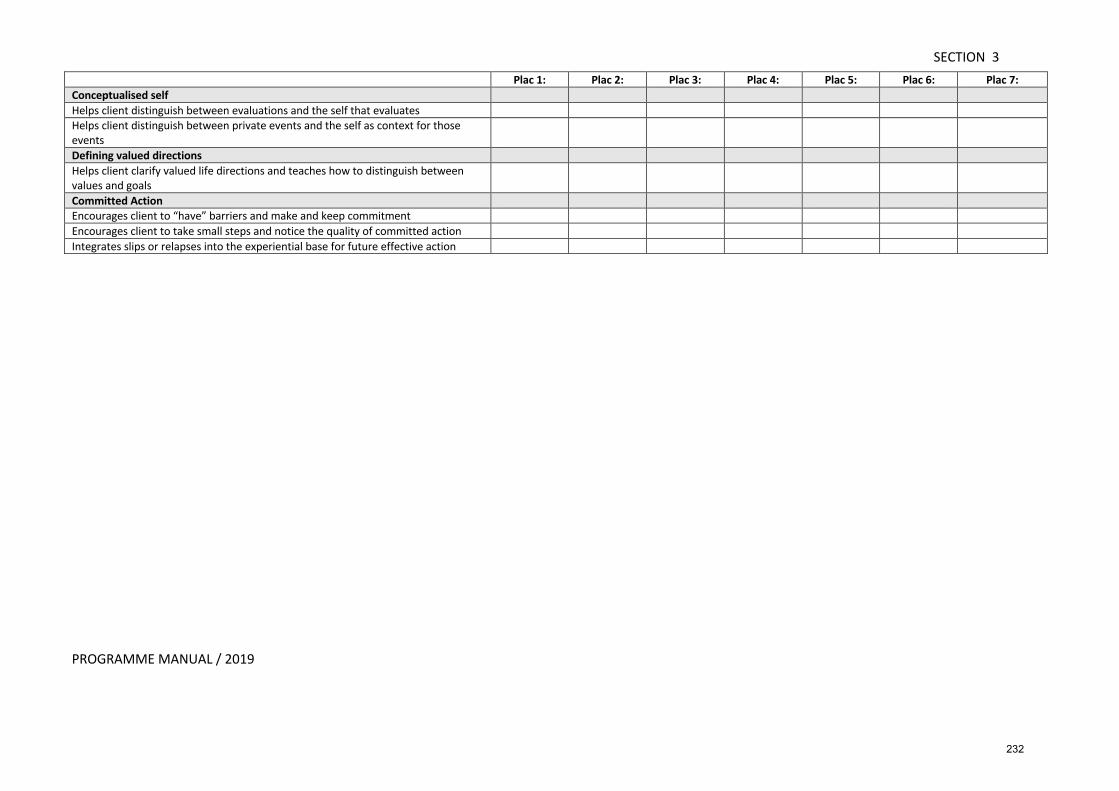
SECTION 3
PROGRAMME MANUAL / 2019
Plac 1: Plac 2: Plac 3: Plac 4: Plac 5: Plac 6: Plac 7: Conceptualised self Helps client distinguish between evaluations and the self that evaluates Helps client distinguish between private events and the self as context for those events
Defining valued directions Helps client clarify valued life directions and teaches how to distinguish between values and goals
Committed Action Encourages client to “have” barriers and make and keep commitment Encourages client to take small steps and notice the quality of committed action Integrates slips or relapses into the experiential base for future effective action
232
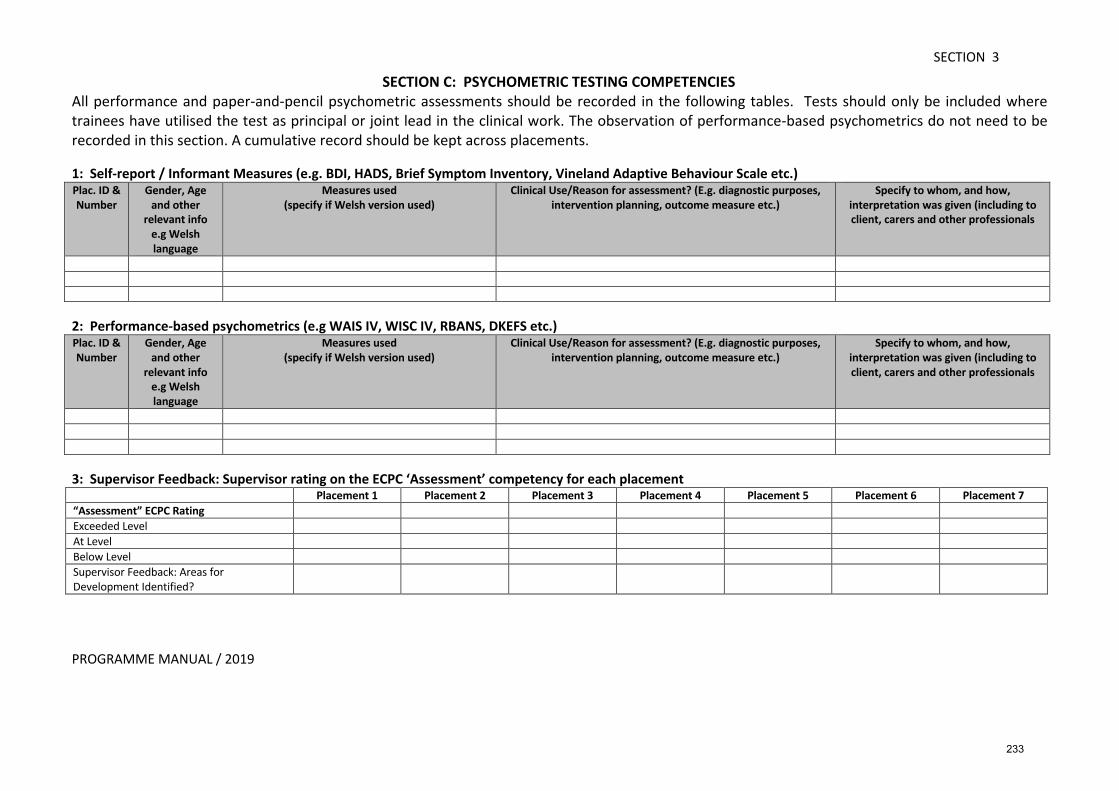
SECTION 3
PROGRAMME MANUAL / 2019
SECTION C: PSYCHOMETRIC TESTING COMPETENCIES
All performance and paper-and-pencil psychometric assessments should be recorded in the following tables. Tests should only be included where trainees have utilised the test as principal or joint lead in the clinical work. The observation of performance-based psychometrics do not need to be recorded in this section. A cumulative record should be kept across placements. 1: Self-report / Informant Measures (e.g. BDI, HADS, Brief Symptom Inventory, Vineland Adaptive Behaviour Scale etc.) Plac. ID & Number
Gender, Age and other
relevant info e.g Welsh language
Measures used (specify if Welsh version used)
Clinical Use/Reason for assessment? (E.g. diagnostic purposes, intervention planning, outcome measure etc.)
Specify to whom, and how, interpretation was given (including to client, carers and other professionals
2: Performance-based psychometrics (e.g WAIS IV, WISC IV, RBANS, DKEFS etc.) Plac. ID & Number
Gender, Age and other
relevant info e.g Welsh language
Measures used (specify if Welsh version used)
Clinical Use/Reason for assessment? (E.g. diagnostic purposes, intervention planning, outcome measure etc.)
Specify to whom, and how, interpretation was given (including to client, carers and other professionals
3: Supervisor Feedback: Supervisor rating on the ECPC ‘Assessment’ competency for each placement Placement 1 Placement 2 Placement 3 Placement 4 Placement 5 Placement 6 Placement 7 “Assessment” ECPC Rating Exceeded Level At Level Below Level Supervisor Feedback: Areas for Development Identified?
233
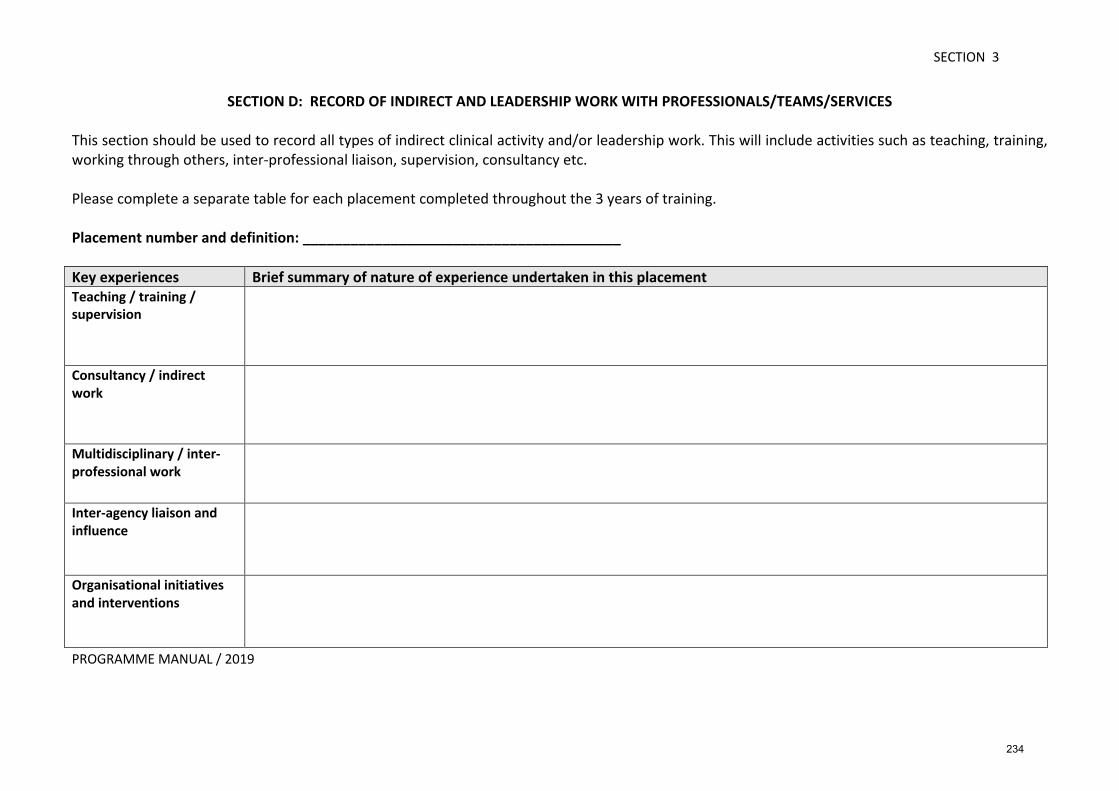
SECTION 3
PROGRAMME MANUAL / 2019
SECTION D: RECORD OF INDIRECT AND LEADERSHIP WORK WITH PROFESSIONALS/TEAMS/SERVICES
This section should be used to record all types of indirect clinical activity and/or leadership work. This will include activities such as teaching, training, working through others, inter-professional liaison, supervision, consultancy etc. Please complete a separate table for each placement completed throughout the 3 years of training. Placement number and definition: ________________________________________ Key experiences Brief summary of nature of experience undertaken in this placement Teaching / training / supervision
Consultancy / indirect work
Multidisciplinary / inter-professional work
Inter-agency liaison and influence
Organisational initiatives and interventions
234
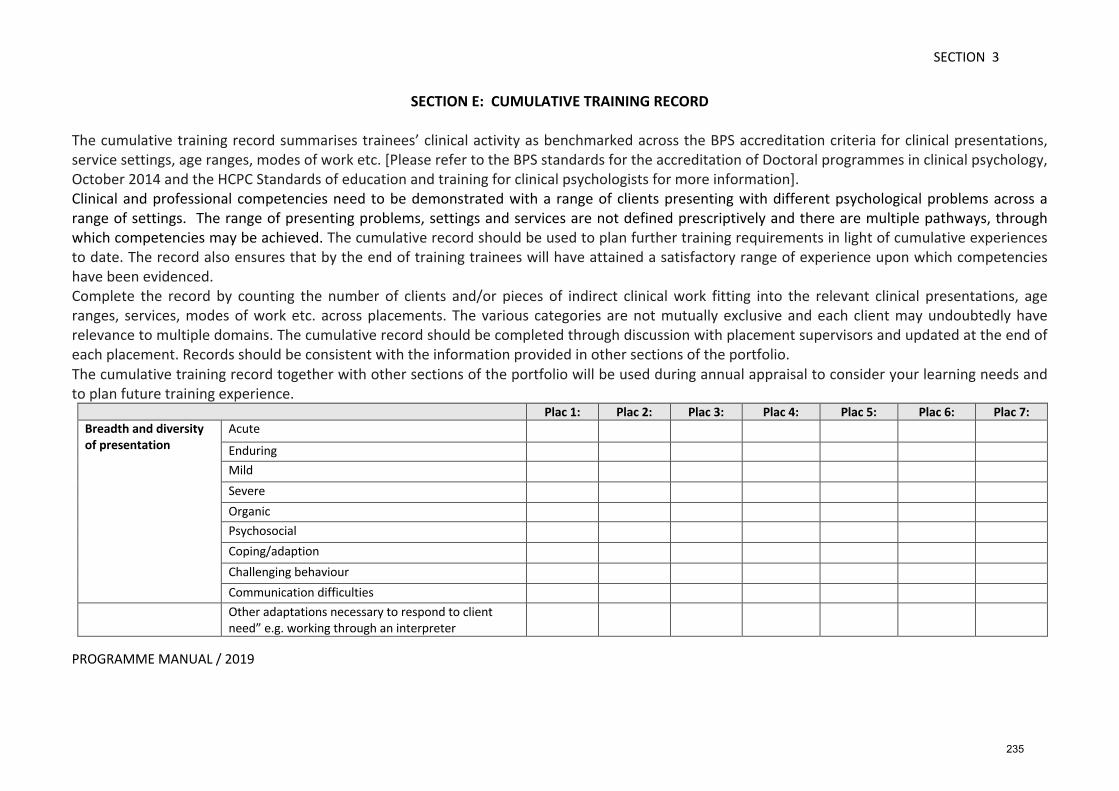
SECTION 3
PROGRAMME MANUAL / 2019
SECTION E: CUMULATIVE TRAINING RECORD
The cumulative training record summarises trainees’ clinical activity as benchmarked across the BPS accreditation criteria for clinical presentations, service settings, age ranges, modes of work etc. [Please refer to the BPS standards for the accreditation of Doctoral programmes in clinical psychology, October 2014 and the HCPC Standards of education and training for clinical psychologists for more information]. Clinical and professional competencies need to be demonstrated with a range of clients presenting with different psychological problems across a range of settings. The range of presenting problems, settings and services are not defined prescriptively and there are multiple pathways, through which competencies may be achieved. The cumulative record should be used to plan further training requirements in light of cumulative experiences to date. The record also ensures that by the end of training trainees will have attained a satisfactory range of experience upon which competencies have been evidenced. Complete the record by counting the number of clients and/or pieces of indirect clinical work fitting into the relevant clinical presentations, age ranges, services, modes of work etc. across placements. The various categories are not mutually exclusive and each client may undoubtedly have relevance to multiple domains. The cumulative record should be completed through discussion with placement supervisors and updated at the end of each placement. Records should be consistent with the information provided in other sections of the portfolio. The cumulative training record together with other sections of the portfolio will be used during annual appraisal to consider your learning needs and to plan future training experience.
Plac 1: Plac 2: Plac 3: Plac 4: Plac 5: Plac 6: Plac 7: Breadth and diversity of presentation
Acute
Enduring
Mild
Severe
Organic
Psychosocial
Coping/adaption
Challenging behaviour
Communication difficulties
Other adaptations necessary to respond to client need” e.g. working through an interpreter
235
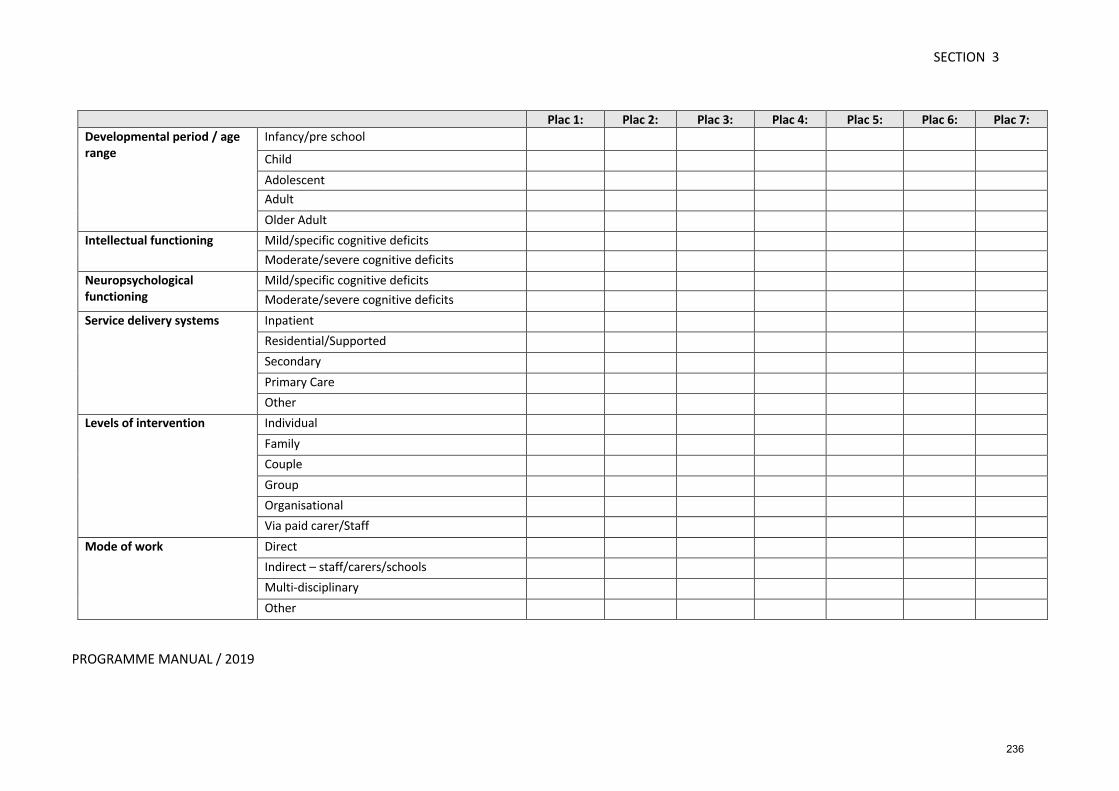
SECTION 3
PROGRAMME MANUAL / 2019
Plac 1: Plac 2: Plac 3: Plac 4: Plac 5: Plac 6: Plac 7: Developmental period / age range
Infancy/pre school
Child
Adolescent Adult
Older Adult
Intellectual functioning Mild/specific cognitive deficits
Moderate/severe cognitive deficits
Neuropsychological functioning
Mild/specific cognitive deficits
Moderate/severe cognitive deficits
Service delivery systems Inpatient
Residential/Supported
Secondary
Primary Care
Other
Levels of intervention Individual
Family
Couple
Group
Organisational
Via paid carer/Staff
Mode of work Direct
Indirect – staff/carers/schools
Multi-disciplinary
Other
236
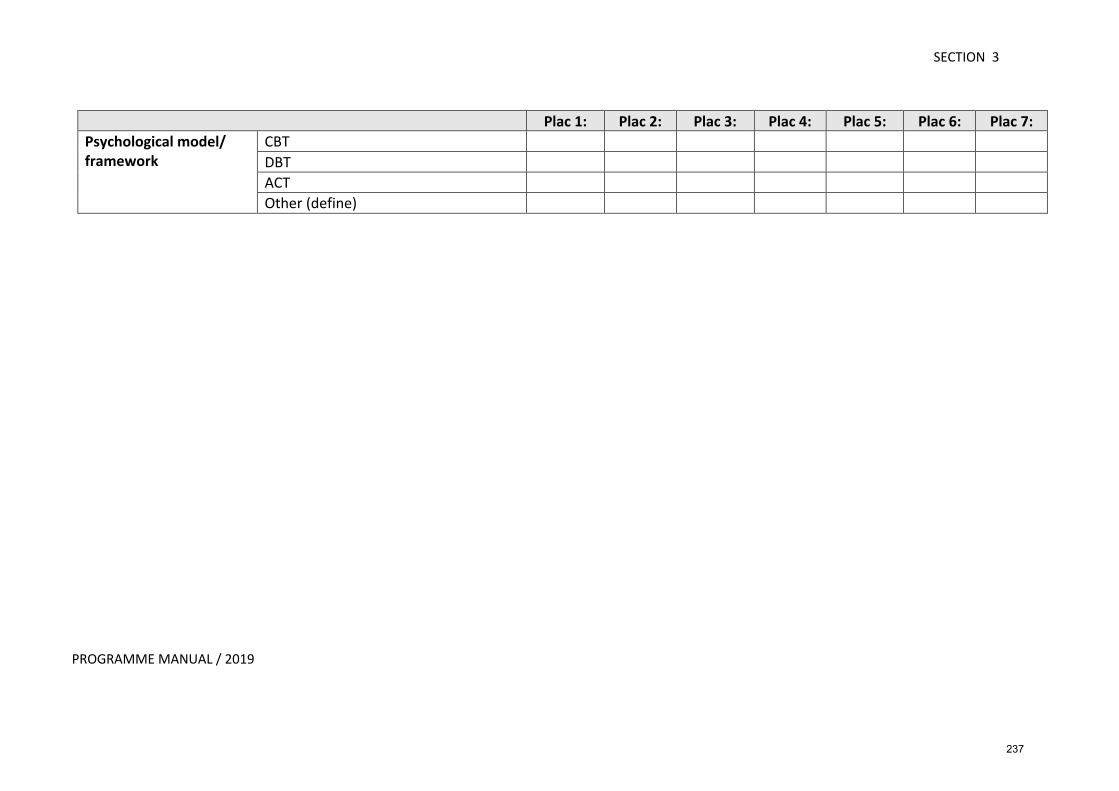
SECTION 3
PROGRAMME MANUAL / 2019
Plac 1: Plac 2: Plac 3: Plac 4: Plac 5: Plac 6: Plac 7: Psychological model/ framework
CBT DBT ACT Other (define)
237

SECTION 3
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME SUPERVISOR AUTHENTICATION OF PORTFOLIO FORM
At the end of all placements, trainees must submit a hard copy of the following form. This form will be subsequently scanned as an attachment with the trainees e-portfolio and be included with their respective records) Trainee: ______________________________________________________ Specialism: ______________________________________________________ I hereby confirm that the clinical work described in the clinical practice portfolio was carried out on this placement and accurately reflects the clinical work undertaken by the trainee under my supervision. I also confirm that areas for further development in terms of therapeutic competencies have been jointly discussed and agreed with the trainee. Signed: ________________________________________________________ Supervisor Signed: ________________________________________________________ Trainee Date: __________________________________
238
SECTION 4
GUIDELINES FOR ASSIGNMENTS
239
PROGRAMME MANUAL / 2019
SECTION 4 IMPORTANT DATES
Deadlines and Academic Days The following pages are provisional dates for all deadlines and academic days. Please contact the Admin’ Office [email protected] 01248 382205 if you have any queries.
240
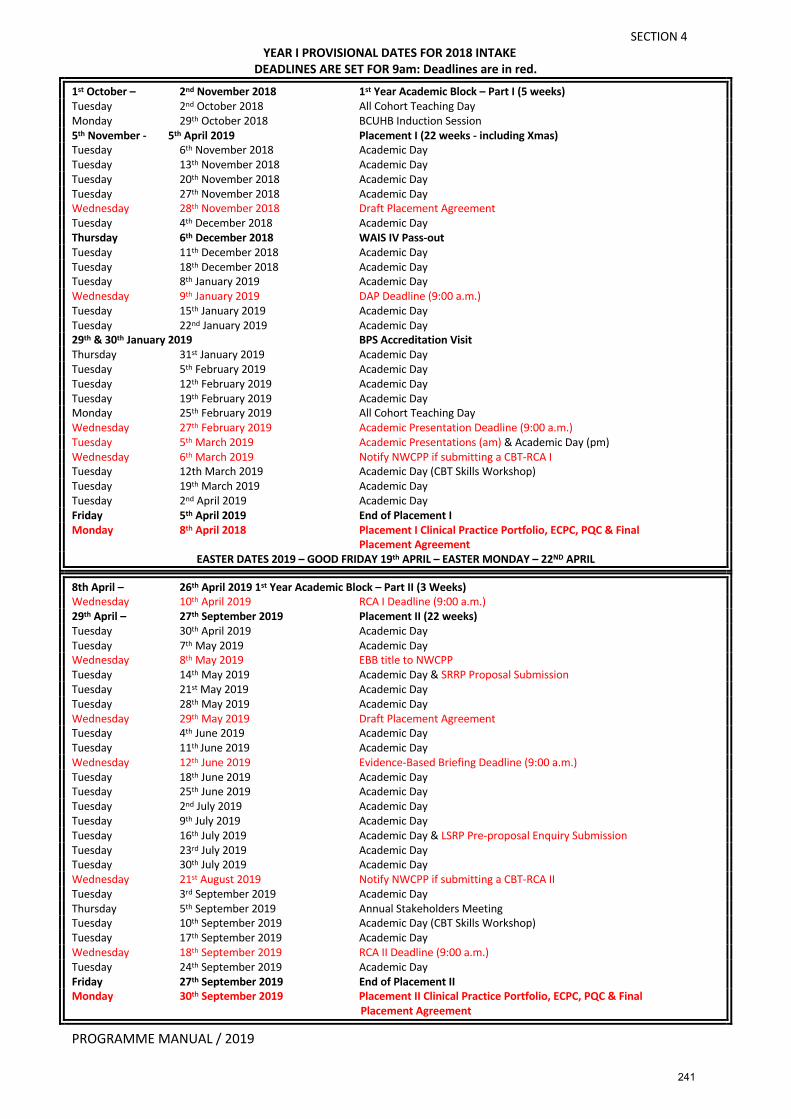
SECTION 4
PROGRAMME MANUAL / 2019
YEAR I PROVISIONAL DATES FOR 2018 INTAKE DEADLINES ARE SET FOR 9am: Deadlines are in red.
1st October – 2nd November 2018 1st Year Academic Block – Part I (5 weeks) Tuesday 2nd October 2018 All Cohort Teaching Day Monday 29th October 2018 BCUHB Induction Session 5th November - 5th April 2019 Placement I (22 weeks - including Xmas) Tuesday 6th November 2018 Academic Day Tuesday 13th November 2018 Academic Day Tuesday 20th November 2018 Academic Day Tuesday 27th November 2018 Academic Day Wednesday 28th November 2018 Draft Placement Agreement Tuesday 4th December 2018 Academic Day Thursday 6th December 2018 WAIS IV Pass-out Tuesday 11th December 2018 Academic Day Tuesday 18th December 2018 Academic Day Tuesday 8th January 2019 Academic Day Wednesday 9th January 2019 DAP Deadline (9:00 a.m.) Tuesday 15th January 2019 Academic Day Tuesday 22nd January 2019 Academic Day 29th & 30th January 2019 BPS Accreditation Visit Thursday 31st January 2019 Academic Day Tuesday 5th February 2019 Academic Day Tuesday 12th February 2019 Academic Day Tuesday 19th February 2019 Academic Day Monday 25th February 2019 All Cohort Teaching Day Wednesday 27th February 2019 Academic Presentation Deadline (9:00 a.m.) Tuesday 5th March 2019 Academic Presentations (am) & Academic Day (pm) Wednesday 6th March 2019 Notify NWCPP if submitting a CBT-RCA I Tuesday 12th March 2019 Academic Day (CBT Skills Workshop) Tuesday 19th March 2019 Academic Day Tuesday 2nd April 2019 Academic Day Friday 5th April 2019 End of Placement I Monday 8th April 2018 Placement I Clinical Practice Portfolio, ECPC, PQC & Final Placement Agreement
EASTER DATES 2019 – GOOD FRIDAY 19th APRIL – EASTER MONDAY – 22ND APRIL
8th April – 26th April 2019 1st Year Academic Block – Part II (3 Weeks) Wednesday 10th April 2019 RCA I Deadline (9:00 a.m.) 29th April – 27th September 2019 Placement II (22 weeks) Tuesday 30th April 2019 Academic Day Tuesday 7th May 2019 Academic Day Wednesday 8th May 2019 EBB title to NWCPP Tuesday 14th May 2019 Academic Day & SRRP Proposal Submission Tuesday 21st May 2019 Academic Day Tuesday 28th May 2019 Academic Day Wednesday 29th May 2019 Draft Placement Agreement Tuesday 4th June 2019 Academic Day Tuesday 11th June 2019 Academic Day Wednesday 12th June 2019 Evidence-Based Briefing Deadline (9:00 a.m.) Tuesday 18th June 2019 Academic Day Tuesday 25th June 2019 Academic Day Tuesday 2nd July 2019 Academic Day Tuesday 9th July 2019 Academic Day Tuesday 16th July 2019 Academic Day & LSRP Pre-proposal Enquiry Submission Tuesday 23rd July 2019 Academic Day Tuesday 30th July 2019 Academic Day Wednesday 21st August 2019 Notify NWCPP if submitting a CBT-RCA II Tuesday 3rd September 2019 Academic Day Thursday 5th September 2019 Annual Stakeholders Meeting Tuesday 10th September 2019 Academic Day (CBT Skills Workshop) Tuesday 17th September 2019 Academic Day Wednesday 18th September 2019 RCA II Deadline (9:00 a.m.) Tuesday 24th September 2019 Academic Day Friday 27th September 2019 End of Placement II Monday 30th September 2019 Placement II Clinical Practice Portfolio, ECPC, PQC & Final Placement Agreement
241
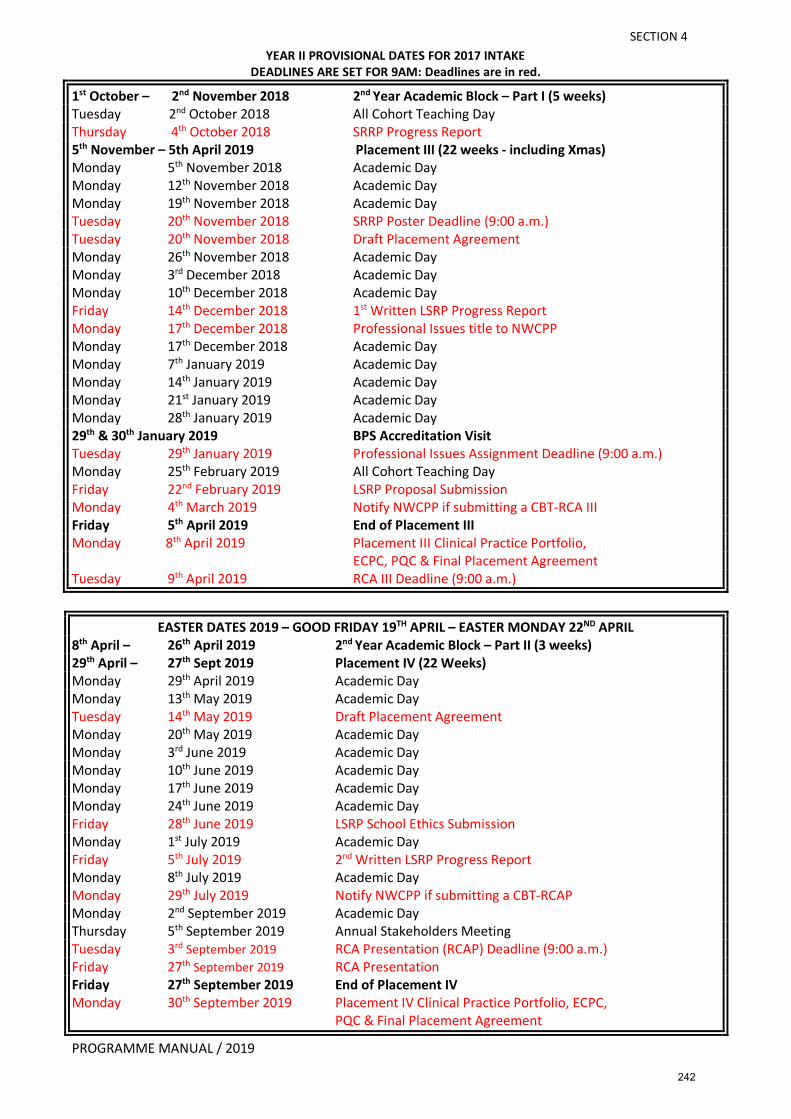
SECTION 4
PROGRAMME MANUAL / 2019
YEAR II PROVISIONAL DATES FOR 2017 INTAKE DEADLINES ARE SET FOR 9AM: Deadlines are in red.
1st October – 2nd November 2018 2nd Year Academic Block – Part I (5 weeks) Tuesday 2nd October 2018 All Cohort Teaching Day Thursday 4th October 2018 SRRP Progress Report 5th November – 5th April 2019 Placement III (22 weeks - including Xmas) Monday 5th November 2018 Academic Day Monday 12th November 2018 Academic Day Monday 19th November 2018 Academic Day Tuesday 20th November 2018 SRRP Poster Deadline (9:00 a.m.) Tuesday 20th November 2018 Draft Placement Agreement Monday 26th November 2018 Academic Day Monday 3rd December 2018 Academic Day Monday 10th December 2018 Academic Day Friday 14th December 2018 1st Written LSRP Progress Report Monday 17th December 2018 Professional Issues title to NWCPP Monday 17th December 2018 Academic Day Monday 7th January 2019 Academic Day Monday 14th January 2019 Academic Day Monday 21st January 2019 Academic Day Monday 28th January 2019 Academic Day 29th & 30th January 2019 BPS Accreditation Visit Tuesday 29th January 2019 Professional Issues Assignment Deadline (9:00 a.m.) Monday 25th February 2019 All Cohort Teaching Day Friday 22nd February 2019 LSRP Proposal Submission Monday 4th March 2019 Notify NWCPP if submitting a CBT-RCA III Friday 5th April 2019 End of Placement III Monday 8th April 2019 Placement III Clinical Practice Portfolio, ECPC, PQC & Final Placement Agreement Tuesday 9th April 2019 RCA III Deadline (9:00 a.m.)
EASTER DATES 2019 – GOOD FRIDAY 19TH APRIL – EASTER MONDAY 22ND APRIL 8th April – 26th April 2019 2nd Year Academic Block – Part II (3 weeks) 29th April – 27th Sept 2019 Placement IV (22 Weeks) Monday 29th April 2019 Academic Day Monday 13th May 2019 Academic Day Tuesday 14th May 2019 Draft Placement Agreement Monday 20th May 2019 Academic Day Monday 3rd June 2019 Academic Day Monday 10th June 2019 Academic Day Monday 17th June 2019 Academic Day Monday 24th June 2019 Academic Day Friday 28th June 2019 LSRP School Ethics Submission Monday 1st July 2019 Academic Day Friday 5th July 2019 2nd Written LSRP Progress Report Monday 8th July 2019 Academic Day Monday 29th July 2019 Notify NWCPP if submitting a CBT-RCAP Monday 2nd September 2019 Academic Day Thursday 5th September 2019 Annual Stakeholders Meeting Tuesday 3rd September 2019 RCA Presentation (RCAP) Deadline (9:00 a.m.) Friday 27th September 2019 RCA Presentation Friday 27th September 2019 End of Placement IV Monday 30th September 2019 Placement IV Clinical Practice Portfolio, ECPC, PQC & Final Placement Agreement
242
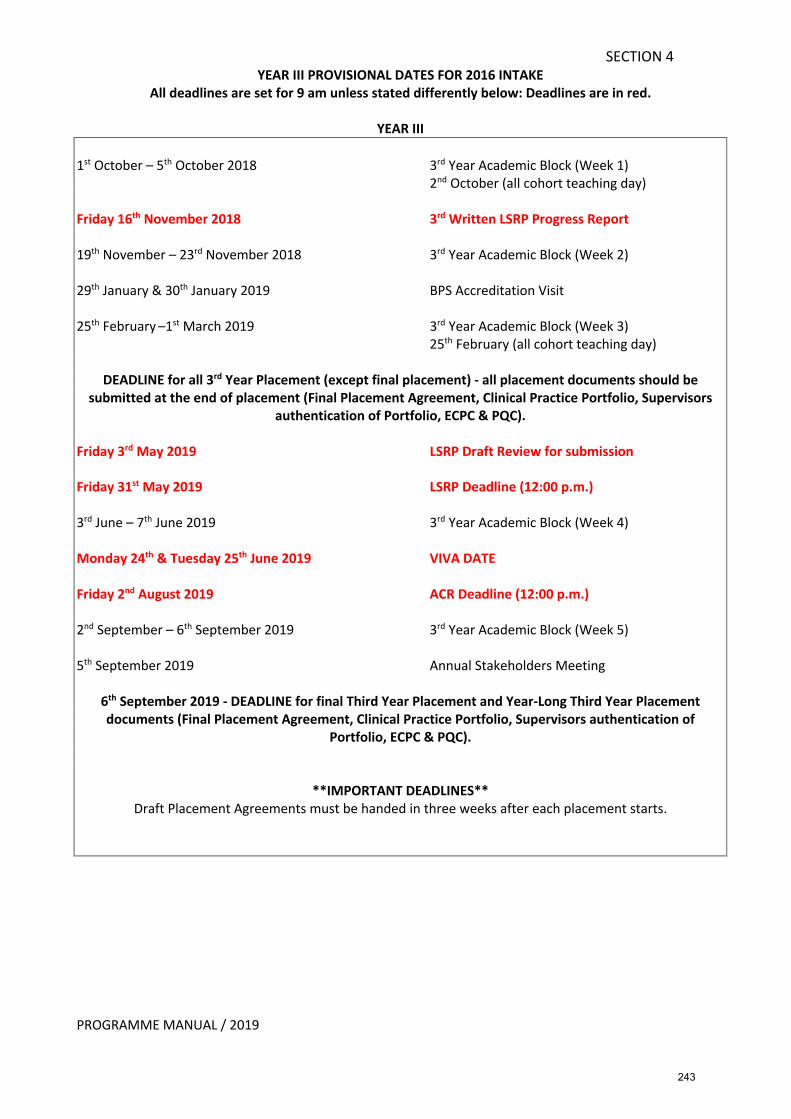
SECTION 4
PROGRAMME MANUAL / 2019
YEAR III PROVISIONAL DATES FOR 2016 INTAKE All deadlines are set for 9 am unless stated differently below: Deadlines are in red.
YEAR III
1st October – 5th October 2018 3rd Year Academic Block (Week 1) 2nd October (all cohort teaching day) Friday 16th November 2018 3rd Written LSRP Progress Report 19th November – 23rd November 2018 3rd Year Academic Block (Week 2) 29th January & 30th January 2019 BPS Accreditation Visit 25th February –1st March 2019 3rd Year Academic Block (Week 3) 25th February (all cohort teaching day)
DEADLINE for all 3rd Year Placement (except final placement) - all placement documents should be submitted at the end of placement (Final Placement Agreement, Clinical Practice Portfolio, Supervisors
authentication of Portfolio, ECPC & PQC). Friday 3rd May 2019 LSRP Draft Review for submission Friday 31st May 2019 LSRP Deadline (12:00 p.m.) 3rd June – 7th June 2019 3rd Year Academic Block (Week 4) Monday 24th & Tuesday 25th June 2019 VIVA DATE Friday 2nd August 2019 ACR Deadline (12:00 p.m.) 2nd September – 6th September 2019 3rd Year Academic Block (Week 5) 5th September 2019 Annual Stakeholders Meeting
6th September 2019 - DEADLINE for final Third Year Placement and Year-Long Third Year Placement documents (Final Placement Agreement, Clinical Practice Portfolio, Supervisors authentication of
Portfolio, ECPC & PQC).
**IMPORTANT DEADLINES** Draft Placement Agreements must be handed in three weeks after each placement starts.
243
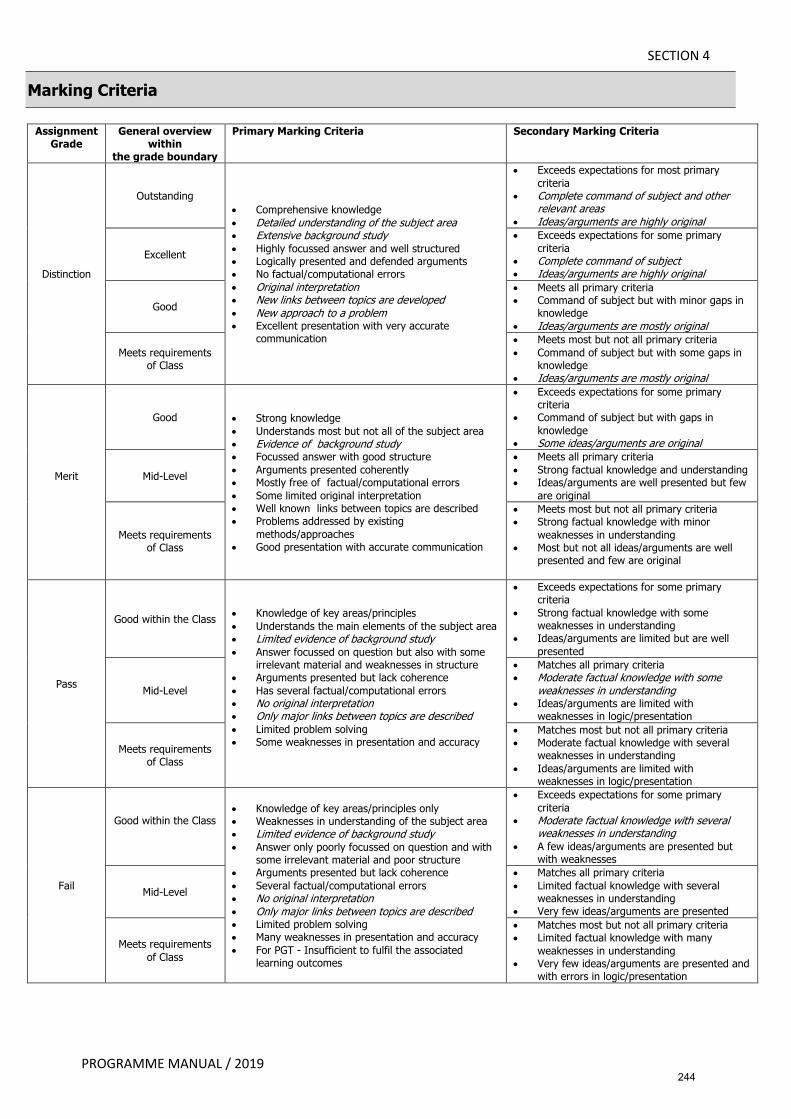
SECTION 4
PROGRAMME MANUAL / 2019
Marking Criteria
Assignment Grade
General overview within
the grade boundary
Primary Marking Criteria Secondary Marking Criteria
Distinction
Outstanding • Comprehensive knowledge • Detailed understanding of the subject area • Extensive background study • Highly focussed answer and well structured • Logically presented and defended arguments • No factual/computational errors • Original interpretation • New links between topics are developed • New approach to a problem • Excellent presentation with very accurate
communication
• Exceeds expectations for most primary criteria
• Complete command of subject and other relevant areas
• Ideas/arguments are highly original
Excellent
• Exceeds expectations for some primary criteria
• Complete command of subject • Ideas/arguments are highly original
Good
• Meets all primary criteria • Command of subject but with minor gaps in
knowledge • Ideas/arguments are mostly original
Meets requirements of Class
• Meets most but not all primary criteria • Command of subject but with some gaps in
knowledge • Ideas/arguments are mostly original
Merit
Good • Strong knowledge • Understands most but not all of the subject area • Evidence of background study • Focussed answer with good structure • Arguments presented coherently • Mostly free of factual/computational errors • Some limited original interpretation • Well known links between topics are described • Problems addressed by existing
methods/approaches • Good presentation with accurate communication
• Exceeds expectations for some primary criteria
• Command of subject but with gaps in knowledge
• Some ideas/arguments are original
Mid-Level
• Meets all primary criteria • Strong factual knowledge and understanding • Ideas/arguments are well presented but few
are original
Meets requirements of Class
• Meets most but not all primary criteria • Strong factual knowledge with minor
weaknesses in understanding • Most but not all ideas/arguments are well
presented and few are original
Pass
Good within the Class • Knowledge of key areas/principles • Understands the main elements of the subject area • Limited evidence of background study • Answer focussed on question but also with some
irrelevant material and weaknesses in structure • Arguments presented but lack coherence • Has several factual/computational errors • No original interpretation • Only major links between topics are described • Limited problem solving • Some weaknesses in presentation and accuracy
• Exceeds expectations for some primary criteria
• Strong factual knowledge with some weaknesses in understanding
• Ideas/arguments are limited but are well presented
Mid-Level
• Matches all primary criteria • Moderate factual knowledge with some
weaknesses in understanding • Ideas/arguments are limited with
weaknesses in logic/presentation
Meets requirements of Class
• Matches most but not all primary criteria • Moderate factual knowledge with several
weaknesses in understanding • Ideas/arguments are limited with
weaknesses in logic/presentation
Fail
Good within the Class
• Knowledge of key areas/principles only • Weaknesses in understanding of the subject area • Limited evidence of background study • Answer only poorly focussed on question and with
some irrelevant material and poor structure • Arguments presented but lack coherence • Several factual/computational errors • No original interpretation • Only major links between topics are described • Limited problem solving • Many weaknesses in presentation and accuracy • For PGT - Insufficient to fulfil the associated
learning outcomes
• Exceeds expectations for some primary criteria
• Moderate factual knowledge with several weaknesses in understanding
• A few ideas/arguments are presented but with weaknesses
Mid-Level
• Matches all primary criteria • Limited factual knowledge with several
weaknesses in understanding • Very few ideas/arguments are presented
Meets requirements of Class
• Matches most but not all primary criteria • Limited factual knowledge with many
weaknesses in understanding • Very few ideas/arguments are presented and
with errors in logic/presentation
244
SECTION 4
PROGRAMME MANUAL / 2019
GRADE CATEGORIES FOR ACADEMIC ASSIGNMENTS ON THE DCLINPSY
The marking criteria and grade categories for assignments on the DClinPsy follow Bangor University guidelines with a pass mark of 50%. Assignments may be awarded a Merit (equivalent of 60-69%) or a Distinction (70% and above). The BU marking criteria are displayed in tabular form on Page 5. Below is a narrative description of these categories to aid markers in making a determination of the grade. Narrative descriptions of the grade categories for RCAs can be found on Page 69 DISTINCTION 70%+ (Excellent) Learning objectives have been met to a high standard. The submitted work (either written or as a presentation) demonstrates a very high standard of critical appraisal. There is a concise but thorough description of the appropriate clinical, research and service context as they apply to the assignment. The appraisal of the work conducted demonstrates an excellent and detailed grasp of clinical and academic issues as they relate to the question posed. The trainee also demonstrates a solid grasp of the limitations of the work that they have completed. The trainee’s work demonstrates (if appropriate to the assignment) a sound understanding of measurement issues and a good grasp of psychometrics. In addition, the trainee demonstrates careful consideration of relevant ethical issues including, where relevant, careful extrapolation of research findings to their clinical and service implications. The report has a strong and coherent structure with lucid and succinct writing. There is a high standard of presentation with few errors of grammar, typography and style. In written assignments there is a high standard of referencing throughout conforming to APA, or BPS guidelines. In presented assignments, the trainee presents in a coherent and engaging manner making excellent use of audio-visuals. The trainee is skilled in providing thoughtful and nuanced answers to questions. MERIT 60-69% (Good to Very Good) Learning objectives have been met to a good standard. A meritorious academic assignment shares many of the features of work at a distinction level with a strong emphasis on critical analyses however, application of clinical, research and academic knowledge and depth of analysis is weaker in some domains. The submission (either written or as a presentation) clearly shows the trainee understands the wider service, research and clinical context. The trainee demonstrates a good grasp of measurement issues with psychometric data and a good grasp of potential limitations although some gaps in understanding may be evident. The trainee extrapolates from appropriate research literature to draw valid clinical and service implications relevant to the context of the assignment. There is evidence that the trainee has carefully considered any ethical issues (where appropriate) and their implications. The report demonstrates a good standard of presentation with a systematic and logical structure but may contain minor errors of grammar, typography and style. In written assignments there is a good standard of referencing throughout conforming to APA, or BPS guidelines, with only minor errors. In presented assignments, the trainee presents well making good use of the audio-visuals and responding accurately to questions.
PASS 50-59% (Satisfactory) Learning objectives have been met to satisfactory standard. The submission may be good or very good in places but with some areas of weakness. The submission style (either written or as a presentation) tends towards the descriptive level of analysis with a superficial understanding of the wider clinical, research or service context. The range and breadth of literature used to support
245

SECTION 4
PROGRAMME MANUAL / 2019
assertions are narrower, restricted and less contemporary. Changes to services or clinical practice may be described but without a clear or only a superficial rationale for them being provided. There is a more limited and uncertain grasp of measurement issues and the use of psychometrics. The content is noticeably weak in parts with omissions and gaps in how relevant literature is used to support the arguments being made. The content overall is less lucid and there is less coherence in the presentation of information overall. There are a few errors of grammar, typography and style. In written assignments there is a competent standard of referencing throughout the text and bibliography with some violations of consensus guidelines. Overall the work demonstrates sufficient competence, understanding and standards of scholarship to merit a pass at doctoral level. In presented assignments, the trainee gives an adequate presentation. There may be some hesitancy and inaccuracies. Audio-visuals may simply provide the written information that is delivered orally by the trainee or do not provide greatly augment the oral narrative. Answers to questions will be adequate but may not provide a great deal of depth. FAIL <50% (Fail) Learning outcomes are not met to a satisfactory standard. Relevant clinical and academic issues have been missed or core concepts have been misunderstood in their application to answering the question posed. There is an inadequate application of psychological theory to clinical practice or service change. Recommendations for changes in services or clinical practice are not justified by theoretical knowledge. Psychometric data may be misunderstood or misinterpreted. The appraisal is not concise, and irrelevant material is included at the cost of more relevant material. The argument is not clearly presented or articulated and some of the conclusions drawn may not be valid. The report may be poorly structured. The trainee fails to discuss limitations of their work in a way that convinces that they understand them. There is little or no consideration of any ethical issues that may be relevant to the assignment (where relevant). Consideration of relevant research and clinical context is missing. Writing may be of an unsatisfactory standard with errors and inaccuracies. There may be a poor standard of referencing throughout the text and bibliography. In presented assignments, the trainee presents poorly. They may be chaotic and disorganized, lacking in coherence or provide only minimal information to answer the question posed. Answers to questions may be inaccurate or very minimal.
246
PROGRAMME MANUAL / 2019
SECTION 4 SUBMISSION OF ASSIGNMENTS
Deadlines and Guidance • Deadlines are normally set for 9am on the day following a teaching day except where an
assignment submission deadline falls during a period where there is no teaching, please see the Important Dates section of this manual for the assignment submission dates and times. We have deliberately chosen this day and time to allow for submission on a day when trainees are typically in the University to prevent having to make an extra trip. We expect most trainees will submit on the teaching day itself but as trainees are not allowed to miss teaching in order to submit the office may be closed when they are ready to hand-in. Thus, we have set the deadline as 9am the following morning so that assignments can be handed in even after the office is closed. If you will be handing in your assignment outside office hours, you should leave the assignment in an envelope FAO Debbie/Anna in the pigeon hole labelled ‘Assignment Submissions’ in the Staff Resource Room, Brigantia.
• NB - If you are submitting a CBT – RCA, the encrypted safe stick MUST be handed to a member of the Admin Team in person; DO NOT leave encrypted safe-sticks in pigeon-holes.
• The only exception to the above is the LSRP Thesis hand-in, the ACR hand-in and any re-
submitted assignments (first fail) or second submissions (i.e. assignments which were found to contain identifiers) which will be at 12 noon on the assigned day.
• Trainees may submit their assignments in Welsh or English. Assignments submitted in
Welsh will need to be translated by the University translation service. The Programme will arrange for the translation, but the trainee needs to check the translation is adequate before it can be marked.
• Three hard copies of all assignments must be submitted to the Admin’ Assistant (Curriculum & Clinical), plus an exact electronic version submitted on 'Turnitin’ via Blackboard https://blackboard.bangor.ac.uk/ https://www.bangor.ac.uk/itservices/lt/helpsheets/turnitin/turnitin_guide_students.pdf The deadline for both the hard copies and the electronic copy are the same.
• You MUST ensure that electronic versions are clearly labelled as follows:
Trainee No-Type of assignment-Specialism.doc (e.g. 123-RCAI-AMH.doc or 123-LSRP Presentation.ppt etc.). Wrongly labelled electronic versions will be returned for re-labelling. This could mean that you miss the required deadline.
• The hard copies must have the Assignment Cover Sheet completed and attached (available
on Blackboard and template available from the Admin Office). Please ensure that assignments are firmly held together (not paper clipped). It is essential to indicate the specialism of the assignment where appropriate on the front sheet. Apart from the Assignment Cover Sheet, no other declaration forms (see list below) should be attached to or included in the assignment, all other declaration forms should be handed in separately at the same time as the assignment.
247
PROGRAMME MANUAL / 2019
SECTION 4 • If sending hard copies by post, all envelopes must be addressed to the Programme Manager
and a dated postage receipt must be retained as proof of postage. Packages MUST BE received in the office on the deadline date not simply mailed on the deadline date.
• Please note that the above guidelines also apply to the submission of the two presentation assignments (Academic presentation, Year 1 and the Report of Clinical Activity Presentation in Year 2). In practice, as the submission date for both of these assignments is before the actual presentation date to allow for marking and administrative preparation, modifications to these assignments can not be made after submission. Requests to change the electronic version to present will be declined. Any desired changes can only be made verbally during the presentation itself.
• If you have to re-submit an assignment ensure that this is clearly indicated on the
Assignment Cover Sheet and submit three copies in the usual way. An electronic version is also required via ‘Turnitin’ and ensure that it is clearly labelled as a re-submission.
• Please make sure you do not add your name to any running header as all assignments are
marked anonymously and do not include any declaration forms in the assignment/attached to the assignment as these will have your name on them.
• A supply of Assignment Cover Sheets is included in your starter box. If you require more,
there is a template for you to use in the NWCPP Admin Office, Room 246, Brigantia. • Plagiarism and word count checks will be carried out on submitted assignments. • Once the assignment has been assessed you will receive a letter notifying you of your
provisional grade and feedback from the assessors. All marks are provisional until they have been moderated by an External Examiner and ratified by the Board of Examiners.
• For LSRP submissions, see also LSRP Section in this manual for more detailed information.
Forms to be Submitted with each Assignment (do NOT include declaration forms in your academic assignments as these will have your name on them. The only form which should be attached to the academic assignment is the Assignment Cover Sheet, the others should be handed in separately). Separate guidance is provided below for the LSRP. All forms are available on Blackboard or can be photocopied from this Programme Manual and should be handed in with the assignment as specified below: Assignment Form(s) Data Analysis Project (DAP) Assignment Front Sheet
Academic Presentation (AP) Assignment Front Sheet
Report of Clinical Activity (RCA) Assignment Front Sheet
RCA Trainee Declaration Form
Report of Clinical Activity-CBT (RCA-CBT) Assignment Front Sheet RCA Trainee Declaration Form Confirmation of Receipt of Client Consent for
248
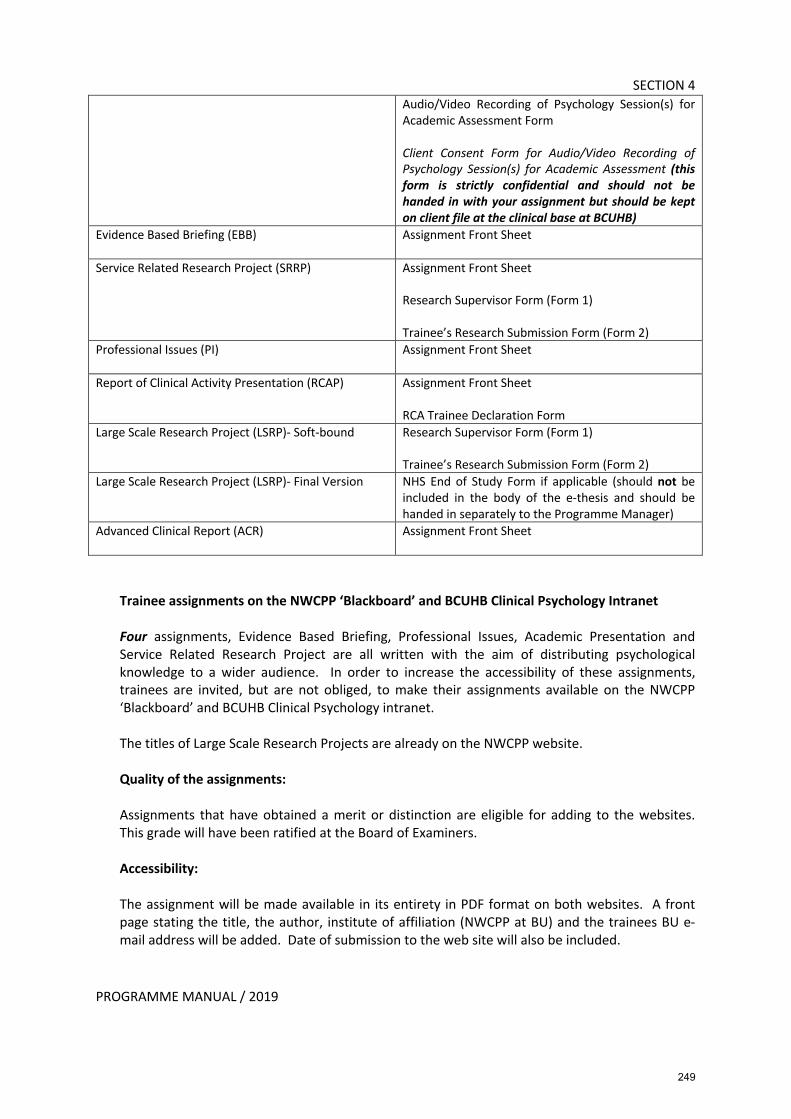
PROGRAMME MANUAL / 2019
SECTION 4 Audio/Video Recording of Psychology Session(s) for Academic Assessment Form Client Consent Form for Audio/Video Recording of Psychology Session(s) for Academic Assessment (this form is strictly confidential and should not be handed in with your assignment but should be kept on client file at the clinical base at BCUHB)
Evidence Based Briefing (EBB) Assignment Front Sheet
Service Related Research Project (SRRP) Assignment Front Sheet Research Supervisor Form (Form 1) Trainee’s Research Submission Form (Form 2)
Professional Issues (PI) Assignment Front Sheet
Report of Clinical Activity Presentation (RCAP) Assignment Front Sheet RCA Trainee Declaration Form
Large Scale Research Project (LSRP)- Soft-bound Research Supervisor Form (Form 1) Trainee’s Research Submission Form (Form 2)
Large Scale Research Project (LSRP)- Final Version NHS End of Study Form if applicable (should not be included in the body of the e-thesis and should be handed in separately to the Programme Manager)
Advanced Clinical Report (ACR) Assignment Front Sheet
Trainee assignments on the NWCPP ‘Blackboard’ and BCUHB Clinical Psychology Intranet Four assignments, Evidence Based Briefing, Professional Issues, Academic Presentation and Service Related Research Project are all written with the aim of distributing psychological knowledge to a wider audience. In order to increase the accessibility of these assignments, trainees are invited, but are not obliged, to make their assignments available on the NWCPP ‘Blackboard’ and BCUHB Clinical Psychology intranet. The titles of Large Scale Research Projects are already on the NWCPP website. Quality of the assignments: Assignments that have obtained a merit or distinction are eligible for adding to the websites. This grade will have been ratified at the Board of Examiners. Accessibility: The assignment will be made available in its entirety in PDF format on both websites. A front page stating the title, the author, institute of affiliation (NWCPP at BU) and the trainees BU e-mail address will be added. Date of submission to the web site will also be included.
249
PROGRAMME MANUAL / 2019
SECTION 4 Consent from Trainees: Trainees are asked to complete and return a ‘Trainee Publication Consent Form’ when they commence their studies (the form will be included in the trainee’s starter box). Trainees will indicate whether or not they agree to have their assignment added to both websites if the above criteria are met.
The trainee has the right to ask for the assignment to be removed from either or both websites at any time. The request needs to be made in writing to the NWCPP Programme Manager. Manager.
250
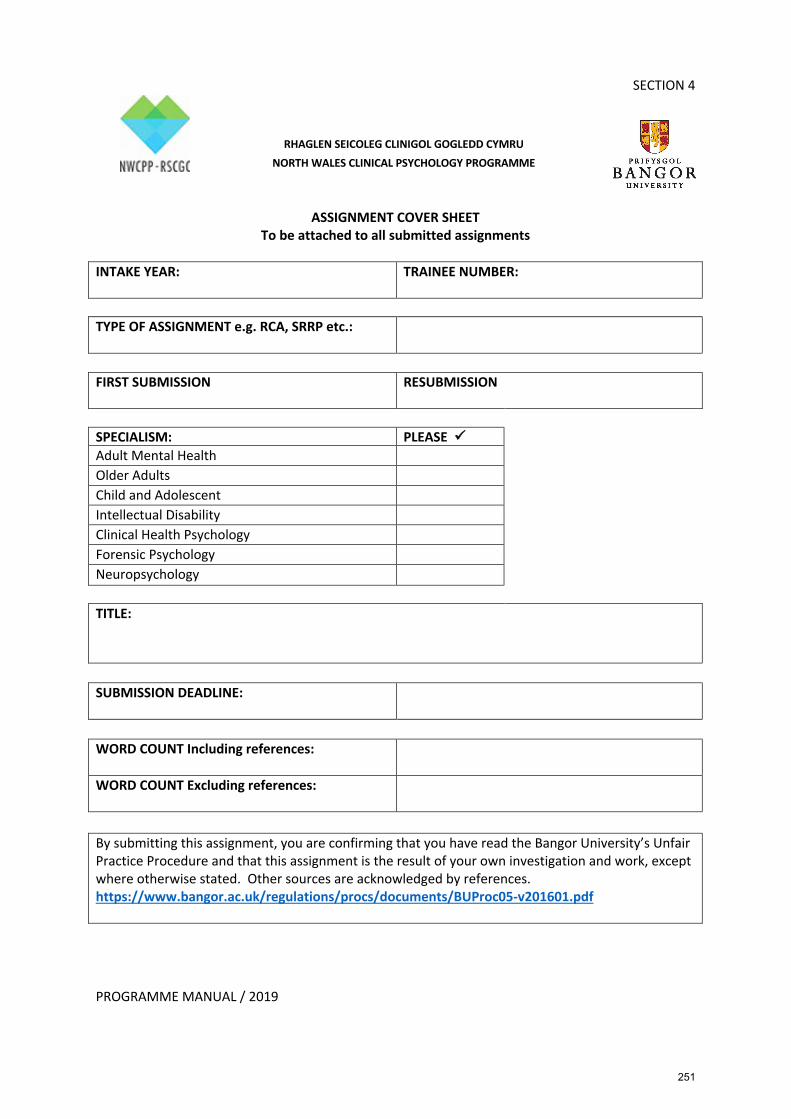
PROGRAMME MANUAL / 2019
SECTION 4
ASSIGNMENT COVER SHEET To be attached to all submitted assignments
INTAKE YEAR:
TRAINEE NUMBER:
TYPE OF ASSIGNMENT e.g. RCA, SRRP etc.:
FIRST SUBMISSION RESUBMISSION
SPECIALISM: PLEASE ü Adult Mental Health Older Adults Child and Adolescent Intellectual Disability Clinical Health Psychology Forensic Psychology Neuropsychology TITLE:
SUBMISSION DEADLINE:
WORD COUNT Including references:
WORD COUNT Excluding references:
By submitting this assignment, you are confirming that you have read the Bangor University’s Unfair Practice Procedure and that this assignment is the result of your own investigation and work, except where otherwise stated. Other sources are acknowledged by references. https://www.bangor.ac.uk/regulations/procs/documents/BUProc05-v201601.pdf
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
251
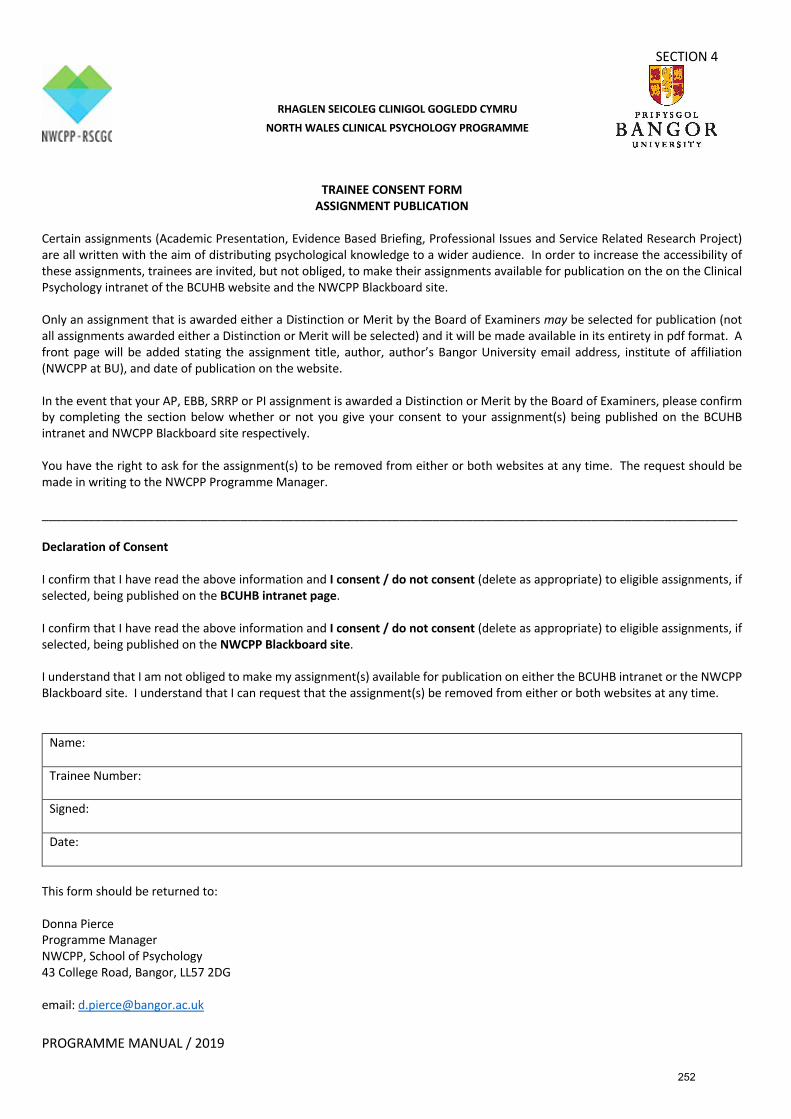
SECTION 4
PROGRAMME MANUAL / 2019
TRAINEE CONSENT FORM
ASSIGNMENT PUBLICATION Certain assignments (Academic Presentation, Evidence Based Briefing, Professional Issues and Service Related Research Project) are all written with the aim of distributing psychological knowledge to a wider audience. In order to increase the accessibility of these assignments, trainees are invited, but not obliged, to make their assignments available for publication on the on the Clinical Psychology intranet of the BCUHB website and the NWCPP Blackboard site. Only an assignment that is awarded either a Distinction or Merit by the Board of Examiners may be selected for publication (not all assignments awarded either a Distinction or Merit will be selected) and it will be made available in its entirety in pdf format. A front page will be added stating the assignment title, author, author’s Bangor University email address, institute of affiliation (NWCPP at BU), and date of publication on the website. In the event that your AP, EBB, SRRP or PI assignment is awarded a Distinction or Merit by the Board of Examiners, please confirm by completing the section below whether or not you give your consent to your assignment(s) being published on the BCUHB intranet and NWCPP Blackboard site respectively. You have the right to ask for the assignment(s) to be removed from either or both websites at any time. The request should be made in writing to the NWCPP Programme Manager. _________________________________________________________________________________________________________ Declaration of Consent I confirm that I have read the above information and I consent / do not consent (delete as appropriate) to eligible assignments, if selected, being published on the BCUHB intranet page. I confirm that I have read the above information and I consent / do not consent (delete as appropriate) to eligible assignments, if selected, being published on the NWCPP Blackboard site. I understand that I am not obliged to make my assignment(s) available for publication on either the BCUHB intranet or the NWCPP Blackboard site. I understand that I can request that the assignment(s) be removed from either or both websites at any time.
Name: Trainee Number: Signed: Date:
This form should be returned to: Donna Pierce Programme Manager NWCPP, School of Psychology 43 College Road, Bangor, LL57 2DG email: [email protected]
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
252
SECTION 4
PROGRAMME MANUAL / 2019
POLICY ON EXTENSIONS FOR ASSIGNMENTS 1. As part of the evaluation of the acquisition and development of trainees’ knowledge,
skills and competencies, a number of assignments must be satisfactorily completed during the training period. Deadlines for each assignment are communicated well in advance to enable trainees to plan and manage their work-load, demonstrate their organisational skills and to ensure that foreseeable difficulties (such as computer and photocopier failure) do not prevent deadlines being met.
2. Deadlines are typically set for 9 a.m. on the day following a teaching day (see also the
guidance on Submission of Assignments earlier in this section for detailed information and exceptions). This is to enable assignments to be forwarded to markers that day.
3. It is recognised that from time to time trainees may have extended periods of ill health
or unusually difficult personal circumstances that interfere with the completion of an assignment. In such cases, the trainee may contact the Chair of the Board of Examiners (Dr Michaela Swales) or in her absence the Programme Director (Professor Robert Jones), as soon as possible before the deadline to request an extension, forwarding a medical certificate in the case of health problems. In the case of personal difficulties, these should be set out in writing. A revised deadline will then be set for the assignment in question.
4. Extensions granted will be routinely reported to the Board of Examiners. Where trainees
wish any personal difficulties to remain confidential, this will of course be respected and they will be reported only in general terms.
5. Where trainees hand in assignments after the deadline, without an extension, this will
normally result in a reduced grade, at the discretion of the Board of Examiners, as indicated in the Doctor of Clinical Psychology Assessment Procedures. Trainees should ensure that they apprise the Board (via the Chair) of any extenuating circumstances, which they wish to be taken into account.
6. Where a piece of work (a research project or a case for a RCA) is not proceeding to plan,
and the trainee has doubts regarding completing it on time (e.g. through delays in data collection or a patient not attending), the trainee should discuss the matter as soon as possible with the Research Director (for research projects) or Training Coordinator (for clinical assignments). They will advise on strategies for completing the assignment in a timely manner, or completing it as far as is possible, without the need for an extension.
Please copy any e-mails regarding extensions to the Programme Manager.
253
PROGRAMME MANUAL / 2019
SECTION 4
POLICY ON BREADTH OF EXPERIENCE REFLECTED IN ASSIGNMENTS Paragraph 1.2 of the Doctor of Clinical Psychology Assessment Procedures, encourages trainees to choose assignment topics covering a range of types of problems or procedures. However, on occasion, trainees wish to carry out a Large-Scale Research Project in an area where they have previously completed one or more assignments. For example, the trainee may wish to carry out a study on cognitive function in people with Parkinson’s disease, having previously written an Evidence Based Briefing on depression and Parkinson’s, and completed an RCA on CBT with a person with Parkinson’s. The over-riding principles that operate in this area are: 1. The same piece of work cannot be presented for more than one assignment (or for
that matter, work presented for a previous degree). Thus a trainee may not use an Evidence Based Briefing as the basis for the literature review for their LSRP. In their LSRP proposal, trainees should make clear any potential overlap with any previous work, so that this can be considered in approving the proposal.
2. Each trainee must fulfil the Programme’s core competencies, as laid out in the
Programme Specification. Within this overall framework, trainees may, if they wish, develop areas of specialist interest. Trainees submit all assignment titles to the Chair of the Board of Examiners in advance of submission to allow the Chair to monitor extensive overlap among a trainee’s assignments. Trainees are encouraged to contact the Chair for advice to request clarification on the degree of overlap allowed between their assignments.
254

SECTION 4
PROGRAMME MANUAL / 2019
POLICY ON SUPPORT FOR TRAINEES WITH ACADEMIC ASSIGNMENTS
The Programme aims to provide tuition and support that is individually tailored to ensure all trainees have the opportunity to reach the required standard in clinical, academic and research domains. One element of this is feedback on draft assignments from Training Co-ordinators, Research Tutors and Supervisors and (where appropriate) Clinical Supervisors. The aim of such feedback is to help to improve the assignment, and as such they are formative comments and not an assessment procedure. The process of assessing trainees’ work is independent from the process of assisting its development. Trainees wishing to benefit from such feedback should provide drafts in accordance with an agreed timescale.
255
SECTION 4
PROGRAMME MANUAL / 2019
WORD LIMITS AND PRESENTATION GUIDELINES The format of all assignments should follow the presentation style of the latest edition of the American Psychological Association (APA) Publication Manual. Assignments should be printed on both sides of the paper. Word limits for assignments are as follows:
• RCAs: 5,500 words, excluding the abstract (not more than 200 words including titles), appendices and reference list, but including all words in Figures, Titles, Tables and text boxes.
• RCA (CBT): 5,500 words, excluding the abstract (not more than 200 words including titles), appendices and reference list, but including all words in Figures, Titles, Tables and text boxes.
• ACRs: Between 3,000 and 5,000 words, excluding the abstract (not more than 200 words including titles), appendices and reference list, but including all words in Figures, Titles, Tables and text boxes. Further, the report should be able to be read without excessive reference to appendices.
• DAP: The total word count, including titles but not including tables or references, must not exceed 4,000 words
• SRRP: See format requirements for this poster presentation. • All other assignments: see documentation for each of the assignments, as they have
a different word limit and format requirement. Abstracts:
• RCAs: The RCA must be preceded by an abstract of not more than 200 words, which must include the type of report, (e.g. individual or group therapy, assessment, indirect work with carers) and client group (e.g. adult, child). Each RCA must include in an appendix copies of any letters or official reports written by the candidate. It must be noted that report writing, as a professional communication skill, will also be assessed. Information identifying clients, other professionals and institutions must be removed. The RCA must be able to be read without frequent reference to the appendices.
• RCA (CBT): The RCA must be preceded by an abstract of not more than 200 words, summarising key elements of the work detailed in the report. Copies of relevant therapy materials such as thought records and behavioural experiment recording sheets should be included within the appendices. Information identifying clients, other professionals and institutions must be removed from these therapy materials. The RCA must be able to be read without frequent reference to the appendices.
• Portfolio of RCA Presentation: All candidates are requested to submit a Portfolio with their RCAP. The Portfolio should contain the following documents; 1. Abstract. The Abstract should not exceed 1000 words and should include a summary
of the identified key areas in the general guidelines for RCA presentation
256

SECTION 4
PROGRAMME MANUAL / 2019
2. Copies of letters or official reports written by the candidate to the referrer/team/ other agencies (Trainees are reminded that reports/referral letters etc. by other professionals should not be included.)
3. A summary/graph of Service User Feedback if available. 4. Print out of Power Point Slides 5. Trainee Declaration Form (not to be included in the body of the assignment) 6. If you are submitting a CBT-RCA for this assignment you must also submit your
session recording, including the guidance on consent documentation, following the guidance later in Section 4 ‘Guidelines on Submission of Recordings for the CBT-RCA’.
Please note that all word limits are absolute, and there is NO provision for, say, a 10% margin of error. Exceeding the word limit for an assignment or failing to follow the prescribed presentation style may result, at the discretion of the Board of Examiners in a reduced grade, proportionate to the extent of deviation from the required standard, as indicated in the Doctor of Clinical Psychology Assessment Procedures. Where word counts for assignments include all text within Tables and Figures, trainees are advised to check their word counts very carefully indeed, as some word-processing packages exclude certain types of text boxes from the word count. In all assignments, any footnotes are included in the word count. A word count for each assignment must be included on the cover of the assignment. Titles (except where on cover page) are necessary for assignment identification and are included in the word count.
257
PROGRAMME MANUAL / 2019
SECTION 4
PLAGIARISM Trainees must be aware of the University’s Unfair Practice Procedure. The most recent version is can be found at: https://www.bangor.ac.uk/regulations/codes/code13.php.en See also the University’s guidelines on avoiding plagiarism: https://www.bangor.ac.uk/studyskills/study%20guides/avoiding_plagiarism.php.en
258

SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR ENSURING CONFIDENTIALITY IN REPORTS OF CLINICAL ACTIVITY & ADVANCED CLINICAL REPORTS
Nothing, which would allow the identification of the persons concerned, may appear in any case records or other material submitted as part of the assessment for Bangor University DClinPsy. In addition to the obliteration of names and addresses of clients (and the trainee’s own name), names of hospitals, clinics, and staff must also be obliterated. It may be helpful though to the examiners to retain a statement of the type of institution involved and the status of collaborating professionals. In addition, background information about clients can be potentially identifying. This is especially the case when various pieces of information are presented for example, education, occupation and family composition. Where possible, information provided should be general rather than specific. Trainees should consider whether information presented is specifically related to the formulation. Where the information is not germane to the assessment/formulation, trainees are advised to consider whether it can be omitted or alternatively, it should be presented in general terms. For example, if the client’s birth order in their family of origin is not directly relevant to the psychological understanding of their problems, it would be better to say that he/she came from a small or a large family or grew up locally with his/her siblings, rather than that he/she had two brothers three and five years his/her senior and a sister two years younger. Similarly, if the client’s relationship history is considered relevant, it would be preferable to say that she/he married several times with each marriage lasting for a short period of time rather than; he met his first wife in September 2000 and divorced in April 2003, his second wife in May 2005 and separated in July 2008 and married again in 2009, separating from his third wife in 2011. In summary, you are advised to avoid unnecessary detail and if in doubt consult your Training Co-ordinator. Reports from other people (e.g. referral letters) should not be included without first gaining the author's permission. Confirmation that consent was sought and obtained should be included. Normally a brief précis of relevant reports/letters within the text of the Report of Clinical Activity is sufficient. In the appendices, particular care should be taken that where information has been obliterated it is not possible to read the information either through the obliteration or by looking at the reverse side of the document. To ensure against this happening, a photocopy of the sheet with obliterations should be submitted, not the originals. Trainees are advised to check their reports with the utmost care, particularly all information contained in the appendices, to ensure that no identifiers are present.
• All submitted assignments that contain identifiers are returned to the candidate for removal of the identifiers.
• The assignment will not be assessed until all identifiers are removed.
259

SECTION 4
PROGRAMME MANUAL / 2019
• Inclusion of identifiers in a piece of work counts as a serious breach of confidentiality.
• All such breaches will be discussed at the Board of Examiners. The Board will reach a view on how to proceed following a discussion of the nature and seriousness of the breach.
• Typically for more ‘minor’ breaches e.g. leaving a standard health board header on a copy of the letter in the appendices, trainees will receive a written reprimand.
• The Board of Examiners reserves the right to reduce the grade of an assignment where identifiers may be ‘minor’ but in circumstances where there is more than one breach within the assignment or where the trainee has demonstrated a pattern of minor breaches across assignments, the Board may take a view in these circumstances that the trainee is paying insufficient attention to protecting the anonymity of their clients.
• Typically for more major breaches such as, for example, leaving in the name of a client, the Board will recommend a reduction in grade. Trainees should bear in mind that this could lead to the substantive failure of an assignment if the assignment has received a pass grade. The Board reserves the right to substantively fail any assignment regardless of grade in the case of a significant breach of confidentiality. In cases where an assignment is substantively failed because of the presence of identifiers, the candidate will not be offered an opportunity to resubmit the assignment. Inclusion of a client’s name in an assignment is also a matter of professional conduct and, as with any other substantive failure of an assignment, will result in the invocation of the BCUHB capabilities procedures.
Breaching confidentiality is potentially a serious disciplinary offence. Please make yourself familiar with the relevant sections of the latest HCPC & DCP Professional Practice Guidelines, which is included in your starter box. Examples Unnecessary Detail Suggested Alternative Aged 47 yrs In his/her forties Birmingham A city elsewhere in the UK Ward Clerk Works in administration Chief Executive of a large food business A senior manager in private industry Geography teacher in a Comprehensive school Works in education in Denbighshire
260
SECTION 4
PROGRAMME MANUAL / 2019
Guidelines on non-client identifiers in academic and research assignments Some assignments on the programme may involve reporting or describing typical service delivery patterns or outcomes. Occasionally these reports may involve information that BCUHB may consider sensitive or confidential e.g. data on waiting times or differential performance of services. To guard against breaching BCUHB policies ensure that in assignments submitted for marking that descriptions of services only refer to a type of service rather than a specific location e.g. Waiting Times in a Community CAMHS team rather than Waiting Times in Denbighshire CAMHS.
261
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR THE PREPARATION OF RESEARCH ASSESSMENTS These guidelines should be read in conjunction with the DClinPsy Regulations and the general Bangor University Regulations. General Issues The DAP is based on an analysis of publically available or anonymised local data. SRRPs usually involve the analysis of existing data, but may also involve data collection by the trainee. In either case, trainees must be actively involved in collating and analysing the data. The LSRP can draw on primary analysis of new data, or an advanced secondary analyses of an existing research data set. In projects where trainees are using secondary data, rather than collecting data themselves, trainees and supervisors should take care to ensure that the project is sufficiently substantial to qualify as a doctoral thesis. Trainees may work with other students or researchers to carry out any of the research assessments, except the DAP. SRRPs may be carried out with the involvement of other people who are not supervising the project (e.g., a non-psychologist in a clinical service, a student from another profession). However, the trainee would work independently to present the study results in their submitted assignment. Collaborations between trainees, their supervisors and other researchers is positively encouraged for LSRP projects. In the context of collaborative projects, the trainee’s unique contribution to the design, implementation and interpretation of the research must be clear from the outset (and in the finished thesis). These issues are clarified during the LSRP proposal process. The focus of research assessments reflects the learning outcomes of the clinical psychology programme and therefore will be monitored by the research team and training co-ordinators. The general principle is that each trainee should avoid duplication of topic or method across projects; advice will be given on a case-by-case basis to trainees on this issue. Trainees must submit formal proposals for SRRPs and LSRPs to the Administrative Assistant (Research & Clinical) for approval by the research team, by the specified deadline. After submission, there is likely to be a short period of clarification with the research team before projects are formally approved. Trainees may not begin a research project without having gained formal approval from the Programme team for the planned project. Any changes to the project must also be approved by the Research Team. Projects which have not received such approval will receive an automatic Fail grade.
262

SECTION 4
PROGRAMME MANUAL / 2019
Any research project that requires research ethics approval or other permissions (see guidance on ethical approval) must be approved by the relevant committee(s) in advance of any data collection and in advance of submission of the assessment. Any assessment requiring ethical approval which is submitted before this approval has been granted will receive an automatic Fail grade. Note that all of the above points apply to the research thesis that is based on the LSRP as well as SRRPs. All projects that involve data collection from participants or from a service (SRRPs, LSRPs) must be conducted in an ethical and professional manner with special reference to the most recent guidelines available from the British Psychological Society. If this is found not to be the case, the assessment will normally receive a Fail grade.
263
SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH TRAINING – RESEARCH ASSESSMENTS
The central vehicle for research training on the Programme is the completion of clinically relevant research studies. One Service-Related Research Project (SRRP) and one Database Analysis Project (DAP) are completed during the first two years of training and the Large-Scale Research Project (LSRP) is planned and conducted throughout the three years of training. For the SRRP and LSRP, trainees collaborate with one or more research supervisor(s) who assist(s) with all stages of the research process. Supervisors can be clinicians, academics, service users, or other relevant people, and for the LSRP, at least one supervisor must be a staff member of the School of Psychology. Additional support, where required, is also available from members of the programme’s research team. Training Co-ordinators may also provide some input to the process of conducting SRRPs during clinical placements. Database Analysis Project (DAP) Trainees work on conducting an original analysis on an existing anonymous database containing real data. This work will be completed alongside teaching sessions detailing approaches to statistical analysis. Some of these skills will be used in the SRRP and LSRP project in Years 2 and 3. The final report is an individual piece of work, roughly corresponding to the methods and results sections of an academic journal article. Service-Related Research Project Trainees produce a written proposal detailing their plans for their SRRP. Trainees are encouraged to select service audits or service evaluation projects as their SRRP, or, alternatively, any other small-scale project with a direct relevance to clinical psychology services. The SRRP proposal describes the design and methods, plans for data analysis, supervision and support required to complete the work, and a clear timetable identifying appropriate milestones. These proposals are reviewed by a member of the Programme team, usually one or more of the Research Team, and the timetables are used by Programme staff in order to monitor SRRP progress and identify potential difficulties as early as possible. As a part of the agreed timetable, written progress reports are also required for SRRPs at various points. In addition to formal assessment by the Programme, SRRP supervisors complete a formative feedback form (copy submitted by the trainee with the SRRP report). This feedback can be used by trainees in collaboration with their Training Co-ordinator to plan future learning. The final report is submitted in the form of a conference poster, with an accompanying letter explaining who the target audience is, and how the poster will be disseminated. Large-Scale Research Project The planning procedure for the LSRP begins in the first year with an outline of the Programme requirements and timetable being presented to the trainees in their first Induction block. Trainees begin to formulate ideas for the large-scale research thesis throughout the first year. After the Christmas break in the first year, trainees will receive information about potential research supervisors who may be willing to be contacted to develop research proposals. Following this, trainees will be supported by the Programme team to develop their LSRP ideas and write a pre-proposal enquiry (PPE).
264

SECTION 4
PROGRAMME MANUAL / 2019
Using this initial feedback, trainees then complete a detailed LSRP proposal including background information, design and samples, ethical approval and risks, data analysis, budget, supervision arrangements, and a detailed initial timetable. This proposal is reviewed by one or more members of the Research Team. Amendments may be required, or trainees may be advised to develop a new proposal. This process is designed to ensure that trainees and supervisors select realistic research projects, which are appropriate for a DClinPsy thesis. Once Programme approval has been granted, trainees need to obtain permission from the relevant ethics committees. Trainees are encouraged to obtain ethical permission as soon as possible, but should have submitted their application to the School of Psychology ethics committee no later than June of their second year. Failure to do so will be addressed during their PADR meetings. Data collection should normally be completed by the end of February of the third year leaving sufficient time for analysis and writing up. Final drafts are to be submitted to supervisors for feedback in early May of the third year. These will be reviewed for suitability for final submission in early June, or for postponed submission if significant issues are identified. Vivas will be completed in late June or July, leaving time to complete revisions before the end of the Programme in September.
265
SECTION 4
PROGRAMME MANUAL / 2019
GUIDANCE ON THE RECEIPT OF FEEDBACK ON RESEARCH ASSIGNMENTS During your clinical psychology training, you will submit three research assignments. The process of gaining feedback on drafts of research assignments is different than for other assignments (normally read by your Training Co-ordinator). Because more people are potentially involved in research projects, it is useful to plan the feedback process, and to avoid simultaneous review by different people, which can waste time and effort, and generate confusion. Database Analysis Project (DAP)
You will receive on-going supervision during the completion of the task. If you would like to receive feedback on a draft of this assessment, arrangements should be made with a research team member. A deadline for the receipt of draft DAPs for feedback is likely to be identified in advance of the main submission deadline.
Service-Related Research Projects (SRRP)
The general expectation here is that your project supervisor should provide you with feedback on a draft. The research team are also available to review drafts, by arrangement. A deadline for the receipt of draft reports for feedback is likely to be identified in advance of the main submission deadline.
Large Scale Research Projects (LSRP)
The expectation is that your supervisory team should provide feedback on drafts of the various sections of the thesis (and this is stated clearly in the Research Contract). The research team are also available to review drafts (within reason), by arrangement. Before final submission, the research team must review trainees’ progress to decide whether their work is likely to reach the required standard, or whether to recommend that submission is postponed. Trainees are expected to submit their current draft of the thesis four weeks before the final submission date to supervisors and the Research Team for this review. It is also helpful to find a colleague who is not involved in your research to review a draft during the writing process. We recommend that you recruit an additional thesis reader as early as possible, but certainly no later than March in your final year (to give readers the chance to plan time in the diaries to help you). The purpose of this additional feedback is not to tell you whether the project will pass or not, but to read for structure, errors, and the general style and flow. An additional reader should ideally be someone who has not been involved in your research but can read it as an informed person (much like an external examiner might be).
266

PROGRAMME MANUAL / 2019
SECTION 4
GUIDELINES ON ETHICS APPROVAL AND RESEARCH GOVERNANCE FOR NWCPP PROJECTS
The requirement to seek ethics and other approval for the NWCPP research assignments depends on the exact nature of the project. The following guidance is designed to help you think through the implications for your own project. In general, the expectation is that SRRPs will be registered as Audits or Service Evaluations with the Audit Department of BCUHB; while LSRPs will normally require Ethics approval first from the university and then from an NHS REC. There may be exceptions depending on the constraints of the specific project. It can be difficult to work out exactly where to draw the line between research and service evaluation/ audit. The research team can advise on specifics, and for guidance the following table is used by the R+D department in making this distinction. See also http://www.hra-decisiontools.org.uk/research/
267
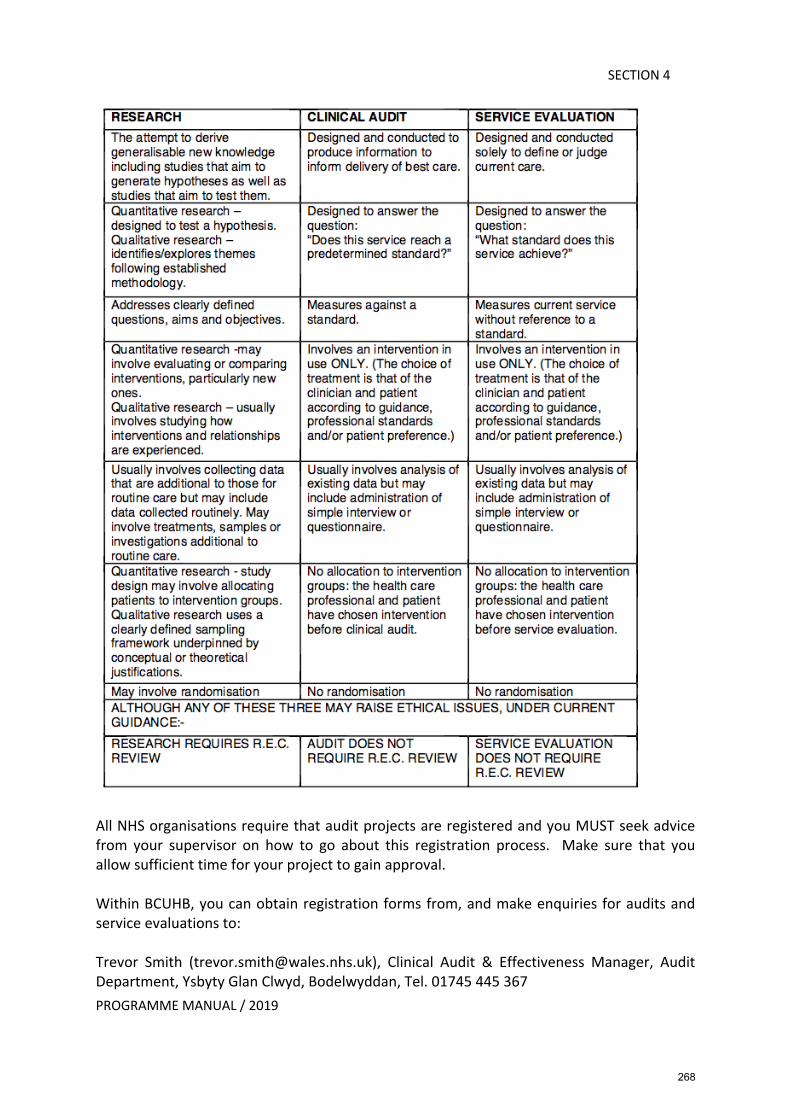
PROGRAMME MANUAL / 2019
SECTION 4
All NHS organisations require that audit projects are registered and you MUST seek advice from your supervisor on how to go about this registration process. Make sure that you allow sufficient time for your project to gain approval. Within BCUHB, you can obtain registration forms from, and make enquiries for audits and service evaluations to: Trevor Smith ([email protected]), Clinical Audit & Effectiveness Manager, Audit Department, Ysbyty Glan Clwyd, Bodelwyddan, Tel. 01745 445 367
268
PROGRAMME MANUAL / 2019
SECTION 4
Any project meeting the definition of research MUST be submitted for ethics approval and research governance review. For advice regarding the R&D and ethics procedure please contact: Dr Rossela Roberts, R+D Manager, Ysbyty Gwynedd, Bangor, email: [email protected], Tel. 01248 384 877 For advice regarding submission of the ethics application please contact: Dr Rossela Roberts, R+D Manager, Ysbyty Gwynedd, Bangor, email: [email protected], Tel. 01248 384 877 As of July 2016, all applications for R&D permissions across Wales are managed by the HCRW Permissions Coordinating Unit (PCU). The HCRW Permissions Co-ordinating Process (PCP) provides a single point of contact for all R&D registrations across NHS Wales. After the Programme has formally approved your project proposal, the basic process for approval of research is as follows:
1. Submit your research to the School of Psychology Ethics Committee. Allow at least three weeks for this review process and to complete any required amendments to your proposal.
2. Ensure that your proposal is submitted through the relevant research governance process. This may need to happen before your proposal goes to an Ethics Committee. To do this, you initialise your IRAS application (www.myresearchproject.org.uk), and you fill in the relevant sections required for the R&D registration. All required documents and the xml file generated in IRAS are emailed to: [email protected] who examine the validity of the application and guide you though the remaining stages for finalising the R&D registration of your project. Make sure you find out how long this process will take well in advance so that you can be ready to meet the appropriate NHS Ethics Committee deadline.
3. If you are conducting research in more than one NHS organisation area, it should not be necessary to go to more than one Ethics Committee but a separate R&D registration is required for each participating NHS organisation. However, applications for multi-site registrations are now managed in the context of a single application to the HCRW PCU where site-specific information (SSI) is provided for each participating NHS organisation.
269
PROGRAMME MANUAL / 2019
SECTION 4
Database Analysis Project (DAP) This should involve the original analysis of anonymous data already collected in an ethically approved research project. As these databases will not contain any identifiable personal data you should not need any ethics approval to conduct this project, nor will you need to register the project with any NHS organisation. Service Related Research Project (SRRP) The intention of these projects is that they are based on data already being collected in services or projects that arise during clinical practice. Thus, the projects are likely to be audits of practice or evaluations of interventions carried out within a service. For the purposes of the SRRP, it would not generally be appropriate to conduct a project that is driven by theory or designed to uncover new knowledge. Of course, presentation of the SRRP findings (in a poster) will refer to theory and any new findings from the project but this is not the general purpose of the project. You will usually be required to register a SRRP project within the host organisation. Your NHS SRRP supervisor should help you with this process. You can also seek advice from the Audit department of BCUHB. Research ethics approval would not normally be required for SRRPs. However, you must still adhere to appropriate ethical standards in the conduct of your project. For example, you would need to establish that patients had given their consent for evaluation questionnaires to be used as a part of the process of monitoring and improvement within the service. Large Scale Research Project (LSRP) These projects will always count as research as they are designed to be based on a protocol, theory-driven, and expected to identify new knowledge. As students of the University, all LSRPs must receive ethics approval from the School of Psychology’s Committee : https://legacy.apps.bangor.ac.uk/ethics/ If a project already has NHS ethics approval and has passed through the appropriate research governance process (e.g., your supervisor has already applied):
1. Apply to the committee to add you as a named researcher. 2. Check to see if you will need an Honorary Contract in order to carry out the research. 3. Submit a full application to the School of Psychology Ethics Committee.
If a programme of research or larger project already has ethics approval and has passed through the appropriate research governance process:
1. You may be able to add a sub-project to an existing one, perhaps using a fast-track procedure. Such an addition might also need to pass through the research governance review process.
2. Check to see if you will need an honorary contract in order to carry out the research. 3. Submit a full application to the School of Psychology Ethics Committee.
270
PROGRAMME MANUAL / 2019
SECTION 4
If no prior approval exists:
Follow the full ethics and research governance procedure outlined above. Under some circumstances, you might carry out research that does not use NHS clinics, staff, or other resources to recruit participants (e.g., recruiting children via schools). You must still submit a full ethics application to the School of Psychology. For these projects not making use of NHS resources or “patients”, you may not be required to go to another local Ethics Committee. However, some researchers still use the committee review process to ensure that the project has been through rigorous ethical review. There are also likely to be some grey areas. So, you should discuss the situation with your supervisor and seek advice from the BCUHB R+D Manager (currently Dr Rossela Roberts). Please remember that failure to obtain appropriate ethical approval before conducting any research project, or unethical behaviour on your part during the conduct of any research project, will normally result in a Fail grade for the assessment concerned. Additional Advice on Ethics Applications You should read the IRAS (Integrated Research Application System) notes for completing the form, which are generally very helpful. On the website, there are FAQs and information about preparing information sheets and consent forms. See: http://www.myresearchproject.org.uk SRRPs are audit-type projects only. The projects will probably still need to be registered as audit projects with the NHS organisation in which they are to be carried out. When you submit your proposals to NWCPP, you are asked to clarify the registrations that will be required. Your supervisor should be able to help and/or direct you to the clinical audit registration manager in the relevant NHS organisation. If the project comes under a definition of research (probably varies throughout NHS organisations and has never been crystal clear), then your supervisor should probably be the Chief Investigator. You will probably be carrying out a project that they want done, so this makes sense. It also means that it is then clear who should fund the research (i.e., this will be NHS “own account” research that they fund internally), and who is Sponsor for the research (the NHS organisation concerned) and so responsible for insurance. Do You Need IRAS Approval? You only need to go to IRAS if your study involves NHS patients/staff, or if your study is intending to use diagnostic measures on general population samples. If you recruit through schools, Social Services, University participant panel etc., you may not need to go to IRAS. You can submit an application so that they can give you a view on your research if that would be helpful, for example, in securing agreement from an organisation to help with your recruitment. However, you MUST ALWAYS submit any research study to the School of Psychology Ethics Committee.
271
PROGRAMME MANUAL / 2019
SECTION 4
R&D Registration Process The Ethics Committee can come to a decision that a research study is ethical but they cannot also give you permission to carry out a study within the NHS. You need to go through a separate R&D registration process with ALL of the NHS organisations within which you will collect data. The R&D registration form is also created within the IRAS system when you select the R&D registration option. BCUHB is at present insisting that every single person has an Honorary Contract with them no matter if they already hold a NHS Employment Contract or an Honorary Contract with a local NHS organisation. If you are collecting data in BCUHB, you cannot avoid getting their approval to carry out the research. Make sure you check out the R&D registration process with the NHS organisation concerned early on in your project planning. R&D registration applications are co-ordinated by HCRW Permissions Co-ordinating Process (HCRW PCP). Research Protocol Most committees expect to see a separate research protocol with the ethics application. You can submit an edited version of your LSRP proposal (i.e., full background, methods/measures sections with references) with your ethics application. Make sure that you answer all the IRAS form sections in as much detail as you can even if it seems to repeat information in your “Protocol”. You could also attach a copy of a grant application if your study is a part of a larger externally funded research grant held by your supervisor. Who Signs the IRAS Forms? For LSRP studies, you will probably need your supervisors and appropriate people in the relevant NHS organisation (e.g., manager of the service where you want to collect data) to sign the form electronically. No-one will sign a form unless they are happy with its content, so make sure that you allow time to get these signatures and send them a brief summary of your study in addition to the rest of the documentation.
272
PROGRAMME MANUAL / 2019
SECTION 4
Advice on completing your IRAS form Once you access the IRAS system at www.myresearchproject.org.uk the system will ask you to complete a screening questionnaire about your study, you can also state whether you just need NHS ethics approval or ethics and R&D approval. The system then generates a bespoke application form for your study. If you are unsure about the meaning of any question then click on the green tab beside the question to get an explanation of the question and the possible range of answers. Some of the answers
1. Trainees are the Principal Investigators for their study. 2. You can detail on your IRAS form that your protocol has been reviewed by your
educational supervisor, and dual reviewed and approved by the School of Psychology Ethics Committee.
3. You can say that the statistical components of your study, have been reviewed by your Supervisor, and the Research Director from the Programme.
4. The University has the appropriate level of insurance cover for research projects, and non-negligent harm cover is normally the one which should be selected.
5. The sponsor for the research is the University, and the lead representative for the sponsor is the School of Psychology manager, (currently Huw Ellis)
Language Awareness in Health & Social Care Research As part of conducting research it is important to consider issues of language. This becomes even more pertinent for studies conducted in Wales. It is very important when conducting research in health and social care to take full account of the bilingual nature of Wales and its speakers. LLAIS (Language Awareness Infrastructure Support Service) have produced a useful report on this topic, which we have placed on Blackboard for you and encourage you to read.
273
SECTION 4
PROGRAMMRE MANUAL / 2019
GUIDELINES ON WRITING-UP DATA ANALYSIS PROJECT Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. The data analysis project (DAP) is designed to teach and assess statistical analysis skills. Trainees will be given a set of clinically-relevant quantitative data and a series of questions about the data. Trainees should then answer these questions using appropriate statistical techniques, and write up a report of these analyses. Assignment Structure The DAP should begin with a short general description of the database and a description of the pre-processing steps used to 'clean' the data, including procedures for missing data and exclusion of participants etc. Then each question should be answered in turn. These sections should include:
• Methods: A description of the analyses used to answer the question. • Results: A report of the results, including appropriate statistical information
(test statistics, p-values etc.). Where possible, illustrative figures. • Discussion: A brief section critically evaluating your analyses, and how well
they answered the question. The entire report, not including references, tables, or figures, should not exceed 4000 words, and may be shorter. Further guidance is provided below. Methods A key part of the assignment is to assess whether trainees are able to identify appropriate analyses to answer a question. Trainees should think carefully about how they turn a research question into a statistical analysis, making sure that the analysis they choose answers the question. Note that it may be possible to answer the same question in many different ways, and trainees should be looking for a correct answer, rather than the correct answer. It may also be possible to use a set of complementary analyses, rather than a single one, so long as this does not violate word counts and so long as these multiple analyses are not redundant. You should also show that you understand the assumptions that these analyses make, outline how you assessed whether these assumptions were met, and any changes you made to your analysis as a result. Finally, make sure that your analyses are described in sufficient detail that it would be possible to replicate your analyses by following the description. You are encouraged to consult the research team for feedback on your ideas.
274
SECTION 4
PROGRAMMRE MANUAL / 2019
Results Report the outcome of your analyses in a concise and coherent manner in the style of an empirical paper. Your description of the results should be supported by appropriate tables and/or figures. Make sure you provide an appropriate amount of information on your analyses. All important information should be included, but unnecessary information should not. Use your editorial judgement, rather than pasting entire SPSS outputs into the document. You are strongly encouraged to illustrate your results using figures. Try to choose figures which are most helpful for understanding the data. Discussion You should evaluate how well your chosen analyses answered the research question. You should identify any shortcomings, ambiguities, or trade-offs in your analyses, and, if appropriate, suggest how your analysis could be improved. References Any references cited in must be listed. As this assignment does not require you to integrate your findings with the literature, this is likely to be very short. CHECKLIST A checklist of issues to address when writing a DAP follows. Make sure that you think carefully about them before submitting a report.
General Issues • Check that the assignment meets the overall expectations for the nature
of a DAP as outlined above. • Make sure that you pay attention to the clarity of the report and
communicate the results effectively. • Make sure that the DAP is appropriately structured (see general
guidance). • Maintain a critical stance to your data and analyses throughout. • Where relevant, be sensitive to issues such as ethics and the impact of
diversity – including gender, culture, religion, and language. • Remember that there are often many reasonable ways to answer the
same question. Data Pre-processing
• Check that you have explained why you excluded any participants. • If different pre-processing steps were used for different questions, detail
the steps that varied in the sections they are associated with. Methods
• Clearly show how you have operationalised your chosen research question into a testable hypothesis or a similarly narrow question.
• Make sure your method contains sufficient detail so that the procedure could be replicated.
• Make sure your chosen analysis method is an appropriate way to address your research question.
• Make sure your chosen analysis method is appropriate for the
275

SECTION 4
PROGRAMMRE MANUAL / 2019
type/distribution of data. Results
• You should include tables and, where possible, figures that effectively summarise the results.
• Format the reporting of statistical tests appropriately • Clearly report the results of your analysis. • Exercise editorial judgement in what you report.
Discussion • Offer interpretations of your findings making sure you demonstrate an
understanding of the meaning of statistical methods used. • Be careful to show that you understand the limitations of the data and
methods.
276
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR ASSESSORS MARKING DATA ANALYSIS PROJECTS
These guidelines incorporate the essential learning outcomes agreed by the Board of Examiners. For the DAP, the relevant Learning Objectives are as follows: Generalisable Meta-Competencies
• Making informed judgements on complex issues in specialist fields, often in the absence of complete information
Psychological assessment
• Understanding of key elements of psychometric theory, which have relevance to psychological assessment (e.g. effect sizes, reliable change scores, sources of error and bias, base rates, limitations etc.) and utilising this knowledge to aid assessment practices and interpretations thereof
Evaluation
• Appreciating outcomes frameworks in wider use within national healthcare systems, the evidence base and theories of outcomes monitoring (e.g. as related to dimensions of accessibility, acceptability, clinical effectiveness and efficacy) and creating synergy with personal evaluative strategies
Research
• Conceptualising, designing and conducting independent, original and translational research of a quality to satisfy peer review, contribute to the knowledge base of the discipline, and merit publication including: identifying research questions, demonstrating an understanding of ethical issues, choosing appropriate research methods and analysis (both quantitative and qualitative), reporting outcomes and identifying appropriate pathways for dissemination
The grade awarded and feedback comments should reflect these ratings as well as appropriateness of presentation and style. Please refer to guidance on Grade Categories on p187-188. Please consider the following when marking: General Issues
1. Is the report clear? Does it communicate the methods and results effectively?
2. Is information divided appropriately into Pre-Processing (if appropriate), Methods, Results, and Discussion sections?
3. Does the trainee demonstrate a critical stance to data throughout? 4. Is the trainee, where relevant, sensitive to issues such as ethics and the
impact of diversity – including gender, culture, religion, and language?
277
SECTION 4
PROGRAMME MANUAL / 2019
Pre-processing
1. Is the sample described in an appropriate level of detail? 2. If appropriate, are procedures for treatment missing data and other ‘pre-
processing’ steps well-described, well-justified, and reasonable? Methods
1. Has the trainee operationalised the research question into a testable hypothesis, or similar?
2. Would it be possible to replicate the trainee’s procedure on the reported methods?
3. Are the statistical methods appropriate for the characteristics of the data? Are the important assumptions of the methods met? Are the analyses appropriate for addressing the research question?
Results
1. Are results reported clearly and using appropriate formatting? 2. Does the trainee balance comprehensiveness with brevity appropriately
when reporting results? 3. Is the trainees use of tables and figures effective in communicating the
results of the analysis? Discussion
1. Does the trainee show that they understand the limitations of the data and their analyses?
278
PROGRAMME MANUAL / 2019
SECTION 4
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: Data Analysis Project - DAP Specialism:
General Presentation / Overall Comments: Method: Results: Discussion: Additional Comments (optional):
Assignment strengths:
Areas for improvement:
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
279
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON WRITING-UP ACADEMIC PRESENTATION Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. Format: 20-minute presentation, plus 10 minutes question / discussion time. The presentation, response to questions and accompanying handout (which would usually comprise the PowerPoint presentation plus a reference list in APA format) will form the basis of the assessment. The presentation will be made to a small group of trainees and two assessors. For trainees who wish to present in Welsh, the programme will provide simultaneous translation in English using the University Translation Unit (Canolfan Bedwyr). Please be aware that although the translators will have been given a copy of the written version of the assignment in advance of your presentation, they will not be able to prepare in advance for the 10 - minute question/discussion time that follows from the 20-minute presentation. As some of these discussions may contain psychological terms and phrases that may be unfamiliar to the translators, please be sensitive to the difficulties of simultaneous translation in such circumstances. You may wish to slow down the discussion and/or use less technical terms for this part of the presentation. Content: Trainees should agree a topic with their Training Coordinator by their mid-placement review of Placement 1, and notify the Chair of the Board of Examiners. The topic should arise from the trainee’s current placement, and demonstrate critical thinking and appraisal of relevant literature, theories, debates and models around the topic. The presentation might begin with a very brief explanation of how the topic arose from a clinical context, but the presentation is not expected to focus on the trainee’s clinical work or clinical experience. Example topics: could include: How useful is a diagnosis of Mild Cognitive Impairment to an older person with memory difficulties? Eating disorders experienced by older people – what factors contribute to their development and maintenance? Family care giving in dementia – the effects of role reversal. Does CBT help people with common mental health problems return to work? Co-morbidity of substance abuse and mental health problems – how to assess? Suicide in young men – how can mental health services respond? Timing: A presentation session will be timetabled in late February / early March of Year 1, and will take place at the University. Assessment:
280
SECTION 4
PROGRAMME MANUAL / 2019
Internal: Two assessors appointed by the Board of Examiners will attend and assess each presentation, using the appropriate evaluation and feedback form, which specifies the range of learning outcomes to be achieved. Both the content and the presentation will be evaluated. Assessors are in charge of the delivery of the presentation and will indicate when the presentation is to begin and end. Internal assessors will be the first to ask questions after the presentation has concluded. Effectively answering questions posed by the internal examiners is a central part of the assessment which is why their questions must be asked first. Other cohort members will be invited to ask questions AFTER the assessors if there is time available.
External: Handouts from each presentation will be made available for External moderation. Presentations will be recorded on DVD for later moderation, if required. Resubmissions: A presentation that has received a ‘Fail’ grade will require the trainee, at the discretion of the assessors, to either redo the presentation or make a further presentation, on another topic, later in Year 1, to the assessors only. Extensions: If an extension is granted for this assignment, this will typically require the trainee to present later in Year 1, at the same time as any resubmissions. As the submission date for both of this assignment is before the actual presentation date to allow for marking and administrative preparation, modifications to this assignment cannot be made after submission. Requests to change the electronic version to present will be declined. Any desired changes can only be made verbally during the presentation itself.
281
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR ASSESSORS MARKING ACADEMIC PRESENTATIONS Conduct of the Presentation Assessment Assessors are in charge of the presentation session and will indicate when each presentation is to begin and end. Sticking to the times allocated for the presentations is essential to ensure equity in the assessment for all trainees. We provide a schedule, however, if you need a little more time to consider your marks, please feel free to take a few more minutes than scheduled if necessary. Significant discussions about an individual presentation are perhaps best left until the session is over. Internal assessors will be the first to ask questions after the presentation has concluded. Effectively answering questions posed by you is a central part of the assessment and you may use your questions to clarify anything that was unclear. You may also use questions to test the trainee’s depth of understanding of the topic. You can invite other members of the trainee’s cohort to ask questions AFTER yourselves if there is time available. For trainees who wish to present in Welsh, the programme will provide simultaneous translation in English using the University Translation Unit (Canolfan Bedwyr). Markers who are not Welsh speakers themselves will be provided with headphones and hear the presentation in English. Our experience is that this can sometimes be challenging, especially if the trainee presents information very quickly. Under these circumstances, it is appropriate to ask a trainee to slow the pace of their delivery to allow for full appreciation of the content. Trainees will have been reminded that although the translators will have been given a copy of the written version of the assignment in advance of their presentation, they will not be able to prepare in advance for the 10 - minute question/discussion time that follows from the 20-minute presentation. As some of these discussions may contain psychological terms and phrases that may be unfamiliar to the translators, the trainees have been asked to be sensitive to the difficulties of simultaneous translation in such circumstances. (e.g. to slow down the discussion and/or use less technical terms for this part of the presentation). In terms of marking, however, it is important to ensure that no extra requirements are made of trainees who do wish to avail of translation services. For this reason, although trainees are asked to be sensitive to the needs of the translators, they should not be marked down if they do not comply with this request. Learning Outcomes assessed As trainees choose their own titles for assignments not all of the learning objectives below may be relevant to any particular assignment. Markers are encouraged to use their judgement and only assess those learning outcomes relevant to the assignment presented. All Part I assignments are marked in accordance with Bangor University’s Assessment and Marking Guidance for Taught Post-Graduate Programmes. Please refer to guidance on Grade Categories on pages 187-188.
282
SECTION 4
PROGRAMME MANUAL / 2019
Generalisable Meta-Competencies Capacity to: • Generalise and synthesise prior knowledge and experience in order to apply them
critically and creatively in different settings and novel situations
Psychological Intervention Knowledge & capacity to: • Conduct interventions related to, secondary prevention and the promotion of health
and well-being
Research Capacity to: • Be a critical and effective consumer, interpreter and disseminator of the research
evidence base relevant to clinical psychology practice and that of psychological services and interventions more widely. Utilising such research to influence and inform the practice of self and others
Personal and Professional Skills and Values Capacity to: • Understand relevant ethical issues and apply these in complex clinical contexts,
ensuring that informed consent underpins all contact with clients and research participants
Communication and Teaching Capacity to: • Communicate effectively clinical and non-clinical information from a psychological
perspective in a style appropriate to a variety of different audiences (for example, to professional colleagues, and to users and their carers).
• Prepare and deliver teaching and training, which takes into account the needs and goals of the participants (for example, by appropriate adaptations to methods and content).
Writing and Presentation style • Does the assignment demonstrate a clear structure? • Does the assignment present a coherent argument? • Does the assignment demonstrate the writer’s ability to use a clear, concise writing
style, avoiding grammatical and presentational errors? • Does the assignment demonstrate the ability to interpret, where relevant, statistical
information? • Does the assignment make good use of presentation aids?
283
SECTION 4
PROGRAMME MANUAL / 2019
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: Academic Presentation Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional): Any problems with timing?
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
284
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR REPORTS OF CLINICAL ACTIVITY (RCA) ASSESSMENT The learning objectives should be used as a guide in preparing, writing (and if relevant presenting) of the clinical work and can be found along with the marking guidance for the assignment at the end of the section on structuring the report. This guidance is for all Reports of Clinical Activity including the CBT RCA and the RCAP. Additional guidance on the RCAP is provided in the additional guidance for that assignment. Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. STRUCTURING THE RCA The purpose of a Report of Clinical Activity is for trainees to demonstrate that they can apply psychological thinking and clinical skills to clinical problems as reflective scientist practitioners. As well as showing evidence of general therapeutic skills such as reflectiveness, empathy and sensitivity, a respectful and non-judgmental attitude towards culture, ethnicity and gender should be evident in the work. In addition, trainees need to show an awareness of how presenting problems are influenced by age, developmental stage, context, health and cognitive status. There is an expectation that all clinical assignments will describe evidence based practice and / or psychological theories or models and as such referencing to relevant evidence / guidelines when writing reports is expected.
Do not avoid writing about clinical work that does not turn out as expected. Such circumstances often provide more scope to demonstrate critical thinking and an ability to flexibly review and reformulate the client’s presentation or particular clinical activity. The topic chosen for a Report of Clinical Activity should be representative of the type of work on that placement and of clinical relevance. Reports should be clear and succinct.
The report should follow a logical structure and will contain a number of sections. The structure outlined below may fit best with a clinical report focusing on work with an individual client. Additional guidance for writing a report focusing on group work, extended assessment and/or indirect work can be found at the end of this section on structuring the report. No more than two RCAs should be extended assessments only. Normally an RCA structure would include the following:
285
SECTION 4
PROGRAMME MANUAL / 2019
Abstract The RCA must be preceded by an abstract of no more than 200 words which must include the type of report (e.g. individual, group work, extended assessment, indirect work with carers) and client group (e.g. adult, child). Reason for Referral A concise summary of how and why the client came to be seen. This is a very short section and need not be more than two or three sentences and should be limited to information such as who is being referred, who made the referral and why, and to whom the referral was made. Assessment An account of the information collected in a logical sequence. The section will include any hypotheses that were made during the assessment and how these hypotheses were evaluated. The information in this section should relate to evidence based practice and / or relevant psychological theory. You should evidence how the assessment provides the basis for the formulation. Formulation
This is your psychological understanding of your client’s problems after the initial assessment phase; integrating the assessment information and giving the basis for your action plan and interventions. In your formulation you must use psychological theory and evidence explicitly to explain the development and maintenance of your client’s problems. Your formulation will lead into the action plan, intervention and outcome evaluation. If you are planning to work within a particular therapeutic model, your formulation will be based upon the underpinning psychological theory inherent to that model e.g. CBT, DBT, ACT.
Your formulation would be an appropriate place to include evidence of knowledge of more than one psychological model by considering the problems from a variety of perspectives before settling on the one (s), if you are using more than one model, that you are going to follow for the intervention. However, it is not essential to do this in every report or oral presentation of clinical activity.
An integrated, narrative account that describes how the various factors operate and psychological processes that underlie the problems is required. Formulations presented as lists of important factors or solely diagrammatic formulations are insufficient on their own.
A formulation is not expected to be static. It is in essence a Working Hypothesis. It may well
286
SECTION 4
PROGRAMME MANUAL / 2019
be wrong or incomplete and change in the light of new information. It must however have been derived coherently, with reference to current theory and knowledge and from specific information and observations you have made about the client(s). It must also be capable of being shared with the client(s) and relevant others in a comprehensible way. For the purpose of the RCA, you must be able to demonstrate why the formulation needed to change and develop and that you are able to revise and reformulate it appropriately.
It is helpful at this stage to outline the aims/goals that have been agreed between the client(s) and yourself with some information about how these were agreed. For example, how realistic were the client(s) original aims or were the client’s aims different to those of other interested parties. Sometimes clients may not have capacity to set out their aims, or the referred client is not the person that you will be working with. In these circumstances, you will need to describe how you handled these issues and how you chose the focus of your intervention. Action plan This should follow logically from your assessment and formulation. Reasons for choosing an approach or model rather than another should be described and justified with reference to available evidence. The order and timing in which you plan to introduce different components across the intervention will be set out here. If not already addressed earlier in the report, it may also be relevant to refer to professional and ethical issues, e.g. informed consent, capacity, risk assessment, multidisciplinary working. Intervention: Implementation of the action plan This is not a detailed chronological account of what happened, however, it should present a clear picture of:
• The approach and procedures adopted. • The general structure of the sessions (if they share a similar format). It may be helpful
to give a more detailed account of one session or part of a session as an example of the way you are working and what the session was like.
• A brief description of the techniques used. • How the client responded, including at least, the minimum dataset used in practice
with the service that the client is attending. Valid and reliable measures of outcome are expected alongside other relevant indicators of change for example, returning to work, frequency of social contacts, reductions in crisis calls to CMHT etc.
• Key issues, problems, and/or themes. • Any requirements to reformulate, what these changes were and how these impacted
upon the intervention
287
SECTION 4
PROGRAMME MANUAL / 2019
• A brief critical appraisal of relevant theory-practice links. For the CBT RCA you are required to submit a recording of a session and it is in this section that you will briefly outline this session. Details about the format for submission of the audio or video recording are given in the section on guidelines for submission at the end of this section. Trainees must also indicate how the session submitted by means of audio or video recording fits into the intervention as a whole. For example: - “…The recording submitted is the tenth session, and the fifth involving active CBT interventions. Having undertaken work to increase the range of activities engaged in by the client, in this session I was helping the client to identify and challenge negative automatic thoughts …” Word limits do not allow for either verbatim accounts or session-by-session descriptions to be included here. Rather an account of the therapeutic strategies adopted and information gathered to evaluate their impact (e.g. client(s) self report, rating scales, records, psychological tests, behavioural evidence, homework diaries etc.) should be included. Quotes taken from session notes/recordings may be included when relevant to illustrate the use of particular therapeutic strategies e.g. guided discovery, cognitive defusion. Samples of relevant therapeutic materials such as thought records and behavioural experiment recording sheets can be included in the appendices. Take especial care to ensure the removal of all identifiers. The work within the submitted session is evaluated using a relevant rating scale such as the Revised Cognitive Therapy Rating Scale (Blackburn, James, Milne and Reichelt, 2001). In order to pass this component of the assignment a score of at least 50% should be achieved with no score on any of the individual items falling below a 2. Outcome In this section, you need to present and discuss your client’s outcomes presenting information that demonstrates what change was achieved, if any. Ideally multiple sources of information, for example, psychometrics, ratings, observations, self-report etc. will be available. All RCAs must use at least one psychometrically valid assessment measure reporting on pre-post outcome as a minimum unless in circumstances where there are no recognized reliable and valid measures available – in such circumstances bespoke measures may be used and their use explained. The measures chosen should relate to the therapeutic aims or goals of the intervention and ideally each goal or aim should have a measure(s) of change. Sometimes, multiple sources of information cannot be achieved in practice. If this is the case, report at least one and explain the reasons for limited information. Ideas on how these problems could be overcome would be a good item for the next section. Follow-up information should be given where possible.
288
SECTION 4
PROGRAMME MANUAL / 2019
Critical review and self-reflection This section is a critical appraisal of your work and what you have learned. Things that are useful to cover are a review of the formulation, review of strengths and weaknesses of the clinical work, a reflection on what you have learned, the personal impact of work, and/or any unresolved issues that might have been dealt with more effectively.
Appendices
Trainees need to include all letters or reports they have written about the work. In circumstances where the placement does not expect written reports or letters, the trainee is expected to write a formal report to include in the RCA that must be signed off by the supervisor. Failure to include appropriate report(s) may lead to a fail grade being awarded to the RCA. Copies of risk assessments, mental health measure documentation or psychometric measures, are NOT required for submission, however, outcomes and conclusions from these assessments must be reported within the main body of the report, typically in the assessment and outcome sections. Copies of letters/reports that have been written by other professionals must NOT be included. Information that can identify clients, professionals (including the trainee) or institutions must be removed from any letters or reports. RCAs that contain identifying material, will be returned to the candidate and cannot be formally assessed until such information is removed. RCAs that include identifiers will be discussed at the Board of Examiners and may be subject to a grade penalty which may include an automatic FAIL grade. Please see the Guidelines for ensuring confidentiality in RCAs and ACRs earlier in this section of the manual.
The report should also contain a Reference List.
Extended Assessment RCAs
Sometimes a piece of work focuses on undertaking a thorough assessment. This can still be written up in a similar format as the above RCA. It needs to consider the same issues; referral, initial assessment, formulation. The assessment part is likely to be the most extensive part of the RCA, where specific hypotheses guide the nature and type of assessments that will need to be undertaken. Sometimes the findings of testing out one hypothesis, leads to the formulation of the next hypothesis. This process can be stepwise and iterative and might resemble an ongoing reformulation. The choices of assessment tools need to be made explicit: why was the assessment needed and how can it affect the outcome for the client? Issues of capacity and consent to the assessment are addressed here. The outcomes of the different assessments are then interpreted and summarized and form the basis for the formulation. Here again, theoretical models and theories (and
289

SECTION 4
PROGRAMME MANUAL / 2019
sometimes diagnostic criteria) underpin the formulation. The action plan will set out how the formulation (or diagnosis) obtained will be used in further work with the client, their caregiver or wider MDT systems. Implications of the formulations obtained and possible related actions will also be presented and discussed. The implementation of the action plan and the outcomes section can be limited, as the RCA is primarily focused on an extended assessment. RCAs of this type still require evidence of critical review as described above. Groups
In writing up a group full account of what happens to every client is not possible within the word limit. One way to deal with this is to write mainly about the group’s aims; rationale and theoretical basis; structure; methods; content; assessment measures; systems issues; brief summary of individuals' problems and progress and group dynamics. This can be supplemented with detail about one individual, for example, their initial problems, how they fit the formulation being applied to the group generally, their progress in the group and how they responded to the group. This approach enables the group as a whole to form the focus of the report but also for the examiner to obtain a clear idea of the experience of individuals within it. The mention of 'systems issues' above refers to factors such as efficiency in dealing with waiting lists or training co-facilitators. It helps to make these factors explicit at all stages of the report because they may well be part of the rationale for the group and thus need to be addressed and discussed in the various sections of the report.
Other types of RCAs Reports of clinical activity may also be submitted that involve other aspects of the work of the clinical psychologist. For example, systemic intervention with a clinical team, development, delivery and evaluation of a training programme, implementation of an evidence-based approach to treatment with an entire clinical team. In selecting to write up this type of clinical work for an RCA it is important to discuss with your TC and supervisor at the earliest opportunity and review the learning objectives for the assignment to ensure that your RCA clearly meets them. The RCA will need to clearly define the problem that your intervention was endeavoring to solve, how you assessed and formulated the problem using psychological theories and principles and how your action and intervention plan clearly flowed from the formulation. You will need to include and discuss the outcomes of your intervention. You must also include a report that was prepared for the service in which the intervention was delivered signed by your supervisor and that meets the learning objectives of an RCA in relation to the communication of information.
290
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON WRITING-UP REPORT CLINICAL ACTIVITY PRESENTATION
Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. Format:
20-minute presentation, plus 15-20 minutes’ question / discussion time. Trainees are also required to complete and submit a portfolio containing key supporting documentation, (see Portfolio section below for details of what to include). The oral presentation, response to questions, general discussion and accompanying portfolio will form the basis of the assessment. Guidance on preparing and delivering a presentation can be found on Blackboard under ‘General Teaching Information’ (Tips on using Powerpoint). Trainees are also reminded that information identifying client(s), other professionals and institutions must be removed and RCAs, which do contain identifying material, will be returned to the candidate and the oral RCA will not formally be assessed until such information is removed. The presentation will be made to two assessors appointed by the Board of Examiners.
Timing:
A presentation session will be timetabled in September toward the end of placement IV (Year Two), and will take place at the University.
Content:
While the presentation assesses the same core competencies as a written RCA or the written component of a CBT-RCA (for further guidance on content refer to the section on Structure for Reports of Clinical Activity) it also assesses the trainee’s ability to summarise and present clinical work concisely and succinctly. This is a key skill for future clinical and professional practice. Equally, the assessment will enable the trainee to respond to examiners’ queries, facilitating a broader discussion of their work beyond the actual presentation. The presentation also provides the trainee with an opportunity to present and discuss their clinical work in a more creative and flexible manner. For example, a trainee may choose to structure their slides around a formulation whilst verbally referring to other relevant information e.g. background/assessment/intervention. It is therefore not essential for slides to follow a sequential order in presenting the key areas identified below:
Reasons for Referral: “A brief statement of how and/or why the problem came to the candidate or their supervisor”
291
SECTION 4
PROGRAMME MANUAL / 2019
Assessment: An initial assessment which might include information from interviews, case notes, meetings, telephone calls, psychometric measures, observation or daily diaries. Such assessment should form the basis for subsequent action including assessment of outcome
Formulation: A formulation, which consists of a brief statement about how the problem was understood after the assessment phase or during the early stages of assessment if the whole intervention was an extended assessment. Such an initial formulation may require modification but should lead coherently to the initial intervention. If you are presenting a CBT case, you will need to present your CBT formulation diagram
Intervention: An action plan following logically from the initial assessment and formulation of the problem. This action plan might involve further detailed assessment, and/or outline of therapeutic intervention and/or proposals for service development, and/or outline of teaching programme. Where relevant it should refer to the professional and ethical issues raised
Implementation and Outcome: A description of what was implemented and achieved. This might include accounts and/or measures of change in psychological functioning, skills, settings, management practice, effectiveness of teaching programmes. In a CBT-RCA this will include discussion of the different CBT procedures used and their outcomes.
Discussion/Reflection: A review of the clinical work (including possible ethical implications), from the perspective of the trainee’s personal and professional development.
Assessment:
Internal: Two assessors appointed by the Board of Examiners will attend and assess each presentation, using the appropriate evaluation and feedback form, which specifies the range of learning outcomes to be achieved. Both the content and the presentation will be evaluated. Assessors are in charge of the delivery of the presentation and will indicate when the presentation is to begin and end. Internal assessors will be the first to ask questions after the presentation has concluded. Effectively answering questions posed by the internal examiners is a central part of the assessment which is why their questions must be asked first. Other cohort members will be invited to ask questions AFTER the assessors if there is time available.
External: Portfolios from each presentation will be made available for External moderation. Presentations will be recorded on DVD for later moderation, if required.
292
SECTION 4
PROGRAMME MANUAL / 2019
Resubmissions: An RCAP, which has received a ‘Fail’ grade, will either require the trainee to make an amended presentation of the original submission or present a new RCAP later in Year Three. The Board of Examiners will advise accordingly.
Extensions:
If an extension is granted for this assignment, this will typically require the trainee to present in Year Three, at the same time as any resubmissions.
Portfolio: All candidates are requested to submit a Portfolio with their RCAP. The Portfolio should contain the following documents; 1. Abstract. The Abstract should not exceed 1000 words and should include a
summary of the identified key areas in the general guidelines for RCA presentation 2. Copies of letters or official reports written by the candidate to the referrer/team/
other agencies (Trainees are reminded that reports/referral letters etc. by other professionals should not be included.)
3. A summary/graph of Service User Feedback if available. 4. Print out of Power Point Slides 5. Trainee Declaration Form (not to be included in the body of the assignment) 6. If you are submitting a CBT-RCA for this assignment you must also submit your
session recording, including the guidance on consent documentation, following the guidance in Section 4 p242-243.
293
PROGRAMME MANUAL / 2019
SECTION 4
REPORT OF CLINICAL ACTIVITY TRAINEE DECLARATION FORM
To be completed and submitted with every RCA assignment Please note that this form should not be included in the body of your assignment and should be handed
in separately with your assignment
Trainee Name: Type of Assignment: REPORT OF CLINICAL ACTIVITY Specialism: Declaration
Yes ü
No ü
I was the main professional working with the client
The background information provided is an accurate account
The assessment was carried out as stated
The formulation reflects the discussions held in supervision
The intervention accurately reflects the work undertaken
I have given a final copy of the RCA to the Clinical Supervisor(s)
I confirm that I will forward a copy of the Assignment Feedback Form pertaining to this RCA to the Clinical Supervisor(s)
I discussed the Information Sharing Guidelines with the client and gained consent from the client to use our work as part of an academic assignment
Signed: Date
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
294
PROGRAMME MANUAL / 2019
SECTION 4
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: RCA Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
295
SECTION 4
PROGRAMME MANUAL / 2019
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee
Trainee Number: Type of Assignment: RCA - CBT Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
296
SECTION 4
PROGRAMME MANUAL / 2019
COGNITIVE THERAPY RATING SCALE – REVISED (CTS-R)
Trainee Number: Date Submitted: Assessor: Date Marked:
CTS-R ITEMS
SCORE
1. Agenda Setting and Adherence Did the therapist set a good agenda and adhere to it?
2. Feedback Did the therapist regularly provide and elicit feedback and summaries?
3. Collaboration Was good teamwork evident? Were there statements and/or actions encouraging the client to participate appropriately and preventing an unequal power relationship developing?
4. Pacing and Efficient Use of Time Was the session well-paced and time used efficiently?
5. Interpersonal Effectiveness Was a good therapeutic alliance evident (trust, warmth, humor etc.)?
6. Eliciting Appropriate Emotional Expression Did the therapist elicit relevant emotions? For example, were there good questions and / or actions designed to elicit relevant emotions and promote a good emotional ambience?
7. Elicit Key Cognitions Did the therapist elicit relevant cognitions? For example, were there questions and/or actions designed to elicit relevant cognitions (thoughts, beliefs etc.)?
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
297
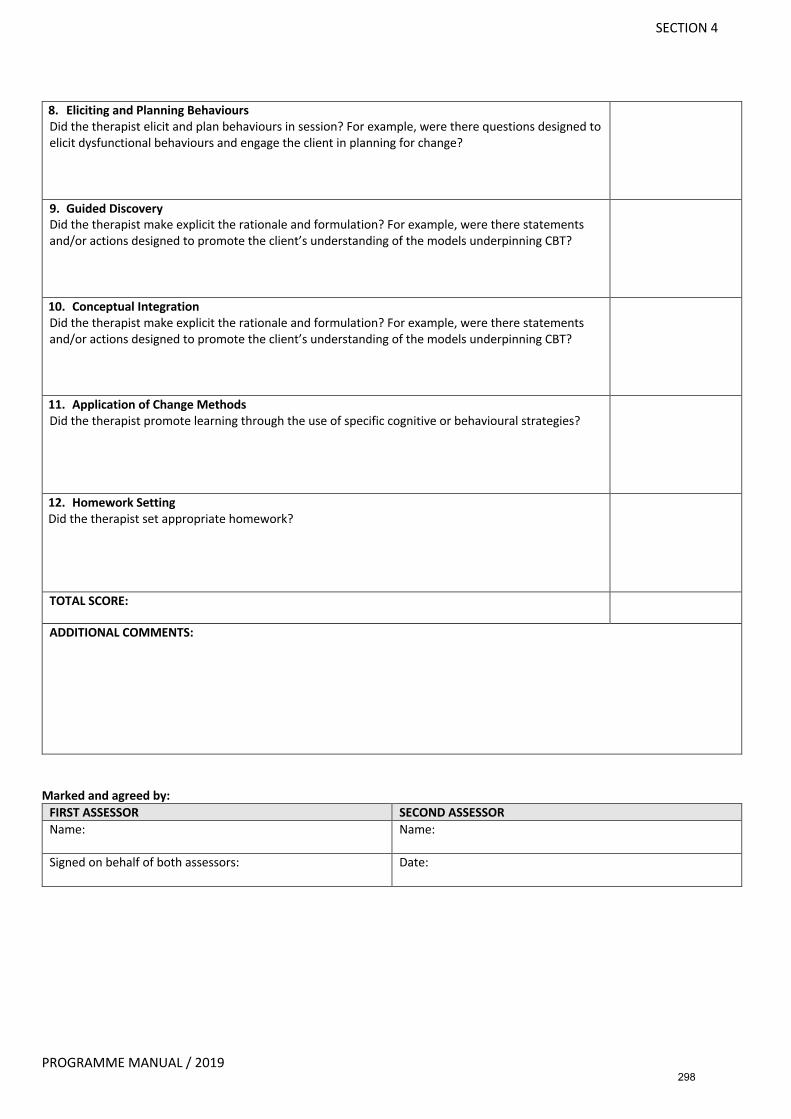
SECTION 4
PROGRAMME MANUAL / 2019
8. Eliciting and Planning Behaviours Did the therapist elicit and plan behaviours in session? For example, were there questions designed to elicit dysfunctional behaviours and engage the client in planning for change?
9. Guided Discovery Did the therapist make explicit the rationale and formulation? For example, were there statements and/or actions designed to promote the client’s understanding of the models underpinning CBT?
10. Conceptual Integration Did the therapist make explicit the rationale and formulation? For example, were there statements and/or actions designed to promote the client’s understanding of the models underpinning CBT?
11. Application of Change Methods Did the therapist promote learning through the use of specific cognitive or behavioural strategies?
12. Homework Setting Did the therapist set appropriate homework?
TOTAL SCORE:
ADDITIONAL COMMENTS:
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Signed on behalf of both assessors: Date:
298
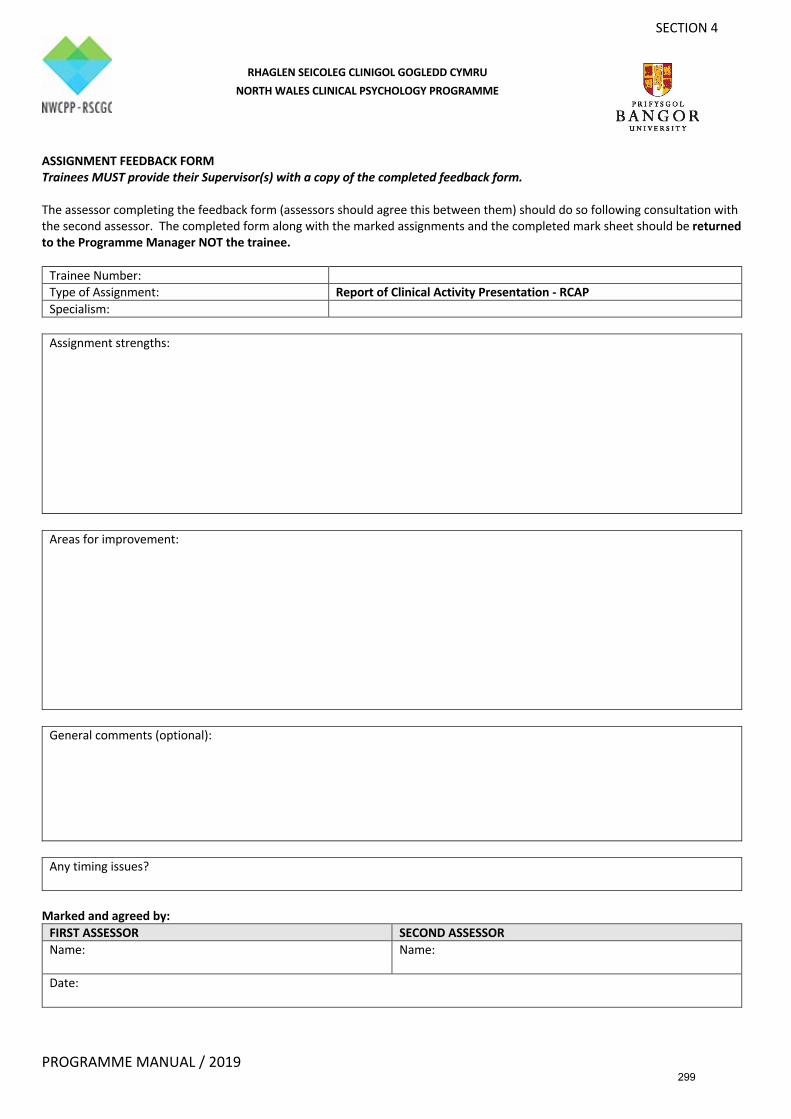
SECTION 4
PROGRAMME MANUAL / 2019
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: Report of Clinical Activity Presentation - RCAP Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Any timing issues?
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
299
SECTION 4
PROGRAMME MANUAL / 2019
SEEKING ADVICE ON REPORTS OF CLINICAL ACTIVITY AND THE STATUS OF ADVICE Discuss your choice of case for the Report of Clinical Activity with your Supervisor and Training Co-ordinator early on in the placement. It is often a good idea to write up several cases as if they were Reports of Clinical Activity to maximise your choices. In principle any case you see should be capable of being written up as a Report of Clinical Activity. Prior to submitting your Report of Clinical Activity by the relevant deadline you are strongly advised to ask your Supervisor and Training Co-ordinator to read it through and comment. It is best for your Supervisor to read it first and then to show it to your Training Co-ordinator after incorporating your Supervisor's comments. Make sure the draft is as complete as possible before asking for feedback. There is little point in Supervisors and Training Co-ordinators reading through unfinished work with sections and appendices missing, or work that you have already substantially changed before they have given feedback. In the early stages of the clinical training Programme you may find your Training Co-ordinator making substantial suggestions for change. You need therefore to allow sufficient time before the deadline to incorporate the relevant changes. It is usually the case that Supervisors and Training Co-ordinators focus on different aspects of your drafts. As a rule your Supervisor will concentrate primarily on the clinical competence aspect of your Report e.g. is this an accurate description of the clinical work, is it an appropriate intervention etc. Your Training Co-ordinator, on the other hand, will primarily focus on the extent to which your Report adheres to the guidelines in the Assessment procedures e.g. are the provisional hypotheses clear, is the formulation adequate and appropriately based in theory etc. However, incorporating the advice of your Supervisors and Training Co-ordinator will not guarantee that the assignment will be passed by the assessors. The aim of their advice is to help you improve the Report and as such they are formative comments and not an assessment procedure. The process of assessing your work is independent from the process of helping you develop it. Please note that Supervisors and Training Co-ordinators are not expected to proof read your work.
300
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON SUBMISSION OF RECORDINGS FOR THE CBT RCA Alongside your written CBT case report you need to submit an audio or video recording of a clinical session. Voice recorders and camcorders can be requested from the NWCPP Admin Office. The session needs to be between 50-60 minutes long during which you need to demonstrate competence in CBT to a level of 36 or above on the CTS-R rating scale. In order to use a recording of a clinical session for this assignment you MUST have freely given, specified, informed and unambiguous consent from your client for this specific use of the recording. Please use the consent form for the submission of audio/video recording for academic assessment later in this section for this purpose. This consent form must be retained in the client’s clinical file. You must show the client consent form to your supervisor who can then sign and confirm that you had consent to record and submit the recording to the clinical programme (see Confirmation of Receipt of Client Consent Form). You must submit the Confirmation of Receipt of Client Consent Form with your CBT RCA (but not included in the body of the assignment, it should be handed in separately). DO NOT SUBMIT the actual Client Consent Form from your client as this will breach confidentially and data protection. Once you have consent from your client you can then proceed to record sessions with him or her. When you have a session that you wish to submit with your case study you need to connect your audio device or SD card to a BCUHB computer and copy the audio or video file from the audio recorder or SD card to a BCUHB encrypted USB stick with which you were provided at the start of your training. When you insert your digital audio recorder into the BCUHB computer that you are using the computer may activate WAVE software that asks you if you wish to encrypt your device. YOU MUST DECLINE TO DO THIS. If you do not the device will be unusable. In some cases you will not be able to copy the file off your audio device onto the computer without going through a process called Whitelisting. If you cannot copy the file from the audio device call IT and explain that you need to have a device/SD card whitelisted. They will then require you to either connect your audio recording device to a BCUHB computer or insert the SD card from the video camera into a BCUHB computer. They will then Whitelist the device allowing you to copy the file onto the computer. You need to hand in the USB device/safe stick in person. Do not at any time have the password or decryption information in the same location as the USB device. Please note that it is your responsibility to ensure that recordings are kept securely at all times. Once a recording is no longer required (e.g. when the Supervisor has listened to it and you are not intending to submit it for your CBT-RCA) the file must be deleted from the recording device or from the computer on which it is stored. Take care to ensure that the file is completely deleted, i.e. not left in ‘trash’. If you are keeping recordings in order to select one for submission then you can retain these until the assignment has been successfully completed. Once the assignment grade has been ratified by the Board of Examiners, it is your responsibility to ensure that all video or audio files are deleted.
301
SECTION 4
PROGRAMME MANUAL / 2019
Recordings that do not relate to the CBT-RCA and will not be selected for the purposes of academic assessment should be erased once supervisor and/or trainee have listened to the recording for the purposes of supervision. Guidance for RCA – CBT recordings using the Integral Crypto USB Flash Drive The safe stick provided to you has already been encrypted and you have been allocated a password therefore you are not required to do this again. Please note that these safe sticks only work on newer BCUHB computers. Let the voice recorder / camcorder run for about 5-10 seconds before you start speaking/recording the session. When you are ready to transfer the recording onto the safe stick do as follows: Copy the voice / video recording onto the BCUHB computer desktop or alternatively, if there are multiple USB ports available you can insert both the voice recorder and the safe stick at the same time. Insert Safe Stick into BCUHB computer Click on Windows Explorer or MyComputer Double-click on F: Total Lock Double-click on TotalLock.exe You will then be prompted to log in using the password allocated to you. Once you have logged in you will see that the G: drive will become visible on MyComputer/Windows Explorer You can then copy your voice recording onto G: Once you are satisfied that the recording has copied successfully onto G: remember to delete the recording from the BCUHB computer and from Recycle Bin/Trash. To log out safely click on the padlock icon and eject the safe stick correctly using the eject function.
302
PROGRAMME MANUAL / 2019
SECTION 4
CONFIRMATION OF RECEIPT OF CLIENT CONSENT FOR AUDIO / VIDEO RECORDING OF PSYCHOLOGY SESSION(S) FOR ACADEMIC ASSESSMENT
Fair Processing Information As part of the regular training and development process, it is a requirement for the trainee clinical psychologist you are supervising to use audio or video recordings of their work in clinical sessions. They are also required to submit one of these sessions as part of the assessment process for their Doctorate in Clinical Psychology. Clinical Psychology Trainees are required to gain consent for recording and for submission of recordings from their clients. The clients must give their consent freely and understand what we are going to do with the recording. To protect client confidentiality the NWCPP does not wish to receive the client consent form, however, we do need formal confirmation that the trainee requested and obtained consent from the client. Supervisor Declaration
Please Initial
I confirm that written consent was obtained from the client for the purposes specified below. I confirm that the client gave their consent freely and understands what the recording will be used for.
• Recording of clinical sessions • Submission of the recordings to NWCPP
I confirm that I have seen the signed Client Consent Form
Name - Clinical Psychologist in Training: Signed:
Date:
Name - Supervising Clinical Psychologist: Signed:
Date:
303
SECTION 4
PROGRAMME MANUAL / 2019
Fair Processing Information As part of the regular training and development process, it is a requirement for the trainee clinical psychologist you are seeing to use audio or video recordings of their work in clinical supervision sessions with their supervisor. He/she will also be required to submit one of these sessions as part of the assessment process for their Doctorate in Clinical Psychology to demonstrate their clinical skills. Your written consent is required before any recording is submitted for assessment. You must give your consent freely and understand what we are going to do with the recording (see the boxes below for a list). The consent you are giving is only for us to use the recording in this way and not for anything else. Date and Time of session to be submitted: Please initial
• I agree that the Clinical Psychologist in Training can submit this recording for academic assessment.
• I understand that the recording will be encrypted and transferred securely.
• I understand that sometimes a qualified assessor outside of BCUHB may need to listen to the recording to assess the Clinical Psychologist in Training’s skills. This person will always be an appropriately qualified Clinical Psychologist adhering to confidentiality guidelines and professional codes of conduct.
• I understand that the recording will be kept securely until the assessment process is complete. Once the assessment has been completed the recording will be
confidentially destroyed.
Patient: Print Name: ______________________________________________________ Signature: ______________________________ Date: _________________ Psychologist: Print Name: ______________________________________________________ Signature: ______________________________ Date: _________________
CLIENT CONSENT FORM FOR AUDIO/VIDEO RECORDING OF PSYCHOLOGY SESSION(S) FOR
ACADEMIC ASSESSMENT
304
SECTION 4
PROGRAMME MANUAL / 2019
ASSESSMENT AND MARKING GUIDANCE FOR REPORTS OF CLINICAL ACTIVITY Assessment All written assignments will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Recordings submitted as part of the RCA-CBT recordings will be marked by an accredited CBT practitioner and a sample will be moderated by another suitably qualified internal assessor. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. Learning Outcomes Assessed Trainees submit four reports of clinical activity during their training programme. Not all of the following competencies may be relevant in every one of these. Markers are encouraged to use their judgement and only assess those competencies relevant to the particular case presented. All Part I assignments are marked in accordance with Bangor University’s Assessment and Marking Guidance for Taught Post-Graduate Programmes. Guidance on grade boundaries and aspects of the assignment to consider follow the learning outcomes. Generalisable Meta-Competencies Capacity to:
• Draw on psychological knowledge of developmental, social and neuropsychological processes across the lifespan to facilitate adaptability and change in individuals, groups, families, organisations and communities.
• Decide, using a broad evidence and knowledge base, how to assess, formulate and intervene psychologically, from a range of possible models and modes of intervention with clients, carers and service systems. Ability to work effectively whilst holding in mind alternative, competing explanations
• Generalise and synthesise prior knowledge and experience in order to apply them critically and creatively in different settings and novel situations
• Demonstrate familiarity with theoretical frameworks, the evidence base and practice guidance frameworks such as NICE and SIGN, and to critically utilise these in complex clinical decision making without being formulaic in application
• Make informed judgments on complex issues in specialist fields, often in the absence of complete information
• Demonstrate self-awareness and sensitivity, and working as a reflective practitioner within ethical and professional practice frameworks.
Psychological Assessment Capacity to:
• Choose, use and interpret a broad range of assessment methods appropriate: to the client and service delivery system in which the assessment takes place; and to the type of intervention which is likely to be required
• For the CBT RCA – plan and conduct an appropriate CBT assessment and demonstrate sound clinical judgement in deciding how to proceed on the basis of the assessment
305
SECTION 4
PROGRAMME MANUAL / 2019
• Conduct appropriate risk assessment and using this to guide practice. Psychological Formulation Capacity to:
• Develop formulations, which are informed by theory and evidence about relevant individual, systemic, cultural and biological factors
• Construct formulations of presentations which may be informed by, but which are not premised on, formal diagnostic classification systems; developing formulation in an emergent trans diagnostic context.
• For the CBT RCA: Ø Construct a relevant CBT formulation drawing upon psychological therapy and
contextual information and providing a clear explanation as the how the formulation accounts for the development and maintenance of the identified difficulties
• Develop a formulation through a shared understanding of its personal meaning with the client(s) and / or team in a way which helps the client better understand their experience
• Make justifiable choices about the format and complexity of the formulation that is presented or utilised as appropriate to a given situation
• Ensure that formulations are expressed in accessible language, culturally sensitive, and non-discriminatory in terms of, for example, age, gender, disability and sexuality.
• Use formulations to guide appropriate interventions • Reflect on and revise formulations in the light of on-going feedback and intervention.
Psychological Intervention Capacity to:
• Implement psychological therapy or other interventions appropriate to the presenting problem and to the psychological and social circumstances of the client(s), based on the formulation and in collaboration with service users and clinical teams
• Understand therapeutic techniques and processes as applied when working with a range of different individuals and presenting problems.
• Conduct interventions in a way, which promotes recovery of personal and social functioning as informed by service user values and goals
• Consider the impact and relevance of psychopharmacological and other multidisciplinary interventions
• When appropriate, implement interventions and care plans through, and with, other professions and/or with individuals who are formal (professional) carers for a client, or who care for a client by virtue of family or partnership arrangements.
306
SECTION 4
PROGRAMME MANUAL / 2019
Evaluation Capacity to:
• Evaluate practice through the monitoring of processes and outcomes, across multiple dimensions of functioning, in relation to recovery, values and goals and as informed by service user experiences as well as clinical indicators
• Devise innovate evaluative procedures where appropriate. For the CBT RCA Audio or video recording of a client session
• Achieve a score of at least 50% (with no individual score falling below 2) on the CTS-R or other appropriate measure
• Reflect in the written report on the strengths and areas for improvement within the clinical session that has been submitted.
Personal and Professional Skills and Values Capacity to:
• Understand ethical issues and apply these in complex clinical contexts, ensuring that informed consent underpins all contact with clients
• Understanding the impact of differences, diversity and social inequalities on people’s lives, and their implications for working practices.
Communication and Teaching Capacity to:
• Communicate effectively clinical and non-clinical information from a psychological perspective in a style appropriate to a variety of different audiences (for example, to professional colleagues, and to users and their carers)
• Adapt style of communication to people with a wide range of levels of cognitive ability, sensory acuity and modes of communication.
307
SECTION 4
PROGRAMME MANUAL / 2019
MARKING GUIDANCE FOR REPORTS OF CLINICAL ACTIVITY – WRITTEN AND CBT RCA
The following general marking criteria provides guidance on the allocation of marks, and how each grade is achieved. In the main, more successful answers have more evidence of critical evaluation within a context of consideration of wider issues, most often evidenced by wider reading concerning the topic and the task being addressed. Please consider the following when marking: General Presentation:
• Does the report have a clear and logical structure? • Is the writing style accurate i.e. free of grammatical and presentational errors and
appropriate to the nature of the report? Background Information:
• Does the report clarify how consent was sought/obtained? • Does the report provide sufficient information about the service context and the
referral route? Assessment:
• Does the report clearly describe the assessment process and outcome including choice of methods; psychometric measures used and with links to theory as appropriate?
• Where applicable, does the report clearly set out the decision-making steps for carrying out an extended assessment?
• Does the report indicate what steps were taken to develop and maintain an effective working alliance with the client?
• Does the report demonstrate competence in conducting appropriate risk assessments and use these to guide practice?
• Does the report show evidence of sound clinical judgement in deciding how to proceed on the basis of the assessment?
Formulation/Reformulation:
• Does the report include a relevant formulation(s) drawing upon psychological theory/evidence and incorporating contextual factors?
• Is the formulation expressed in accessible language and is it culturally sensitive and non-discriminatory in terms of factors such as age, gender, disability and sexuality?
• Does the report include a clear explanation as to how the formulation accounts for the development and maintenance of the client’s difficulties?
• Does the report clarify how the formulation was shared/used with clients/families/group/team to promote psychological thinking?
• Where reformulation has been necessary, does the report describe this and provide a rationale for why reformulation was undertaken?
Intervention
• Does the report demonstrate the ability to plan and implement an appropriate intervention(s) which is consistent with the formulation and the evidence base?
308
SECTION 4
PROGRAMME MANUAL / 2019
• Has the intervention been conducted so as to promote the recovery of personal and social functioning?
• In the case of the CBT RCA, does the report indicate how work undertaken within the audio or videotaped session that has been submitted fits with the intervention as a whole?
• Does the report indicate how the ending of therapy was or is planned to be managed? Outcome:
• Does the report include an evaluation of the process and outcomes of the intervention and how this was obtained/measured?
• Does the report include feedback from the relevant service user/family/team/professional?
Professional Issues:
• Does the report demonstrate knowledge and understanding of relevant professional and ethical issues?
• Does the report demonstrate sensitivity to issues of difference, diversity and social inequality?
• Does the report take account of the inherent power balance between practitioners and clients?
Reflective Practice:
• Does the candidate reflect on the clinical work undertaken in terms of their own personal and professional development and recognition of the impact of their own value base on the work undertaken?
• Has the candidate provided specific examples of how supervision shaped their own practice and the development of this work?
• Does the report demonstrate self-awareness and working as a reflective practitioner? • Has the candidate accurately reflected on the strengths and areas for improvement
within the sample of clinical work submitted in the form of an audio or video recording?
Appendices:
• Was all relevant documentation included in the Appendices? • Were the abstract /letters/reports /measures completed to a satisfactory professional
standard? Audio or video recording of a client session (CBT RCA only)
• Does the work undertaken in the session achieve a score of at least 50% (with no individual score falling below 2) on the CTS-R or other appropriate measure?
309
SECTION 4
PROGRAMME MANUAL / 2019
MARKING GUIDANCE FOR REPORTS OF CLINICAL ACTIVITY PRESENTATIONS (RCAP)
Conduct of the RCAP Assessment Assessors are in charge of the presentation session and will indicate when each presentation is to begin and end. Sticking to the times allocated for the presentations is essential to ensure equity in the assessment for all trainees. We provide a schedule, however, if you need a little more time to consider your marks, please feel free to take a few more minutes than scheduled if necessary. Significant discussions about an individual presentation are perhaps best left until the session is over. Internal assessors will be the first to ask questions after the presentation has concluded. Effectively answering questions posed by you is a central part of the assessment and you may use your questions to clarify anything that was unclear. You may also use questions to test the trainee’s depth of understanding of the topic. You can invite other members of the trainee’s cohort to ask questions AFTER yourselves if there is time available. These guidelines incorporate the essential learning outcomes agreed by the Board of Examiners. The grade awarded and feedback comments should reflect these ratings as well as appropriateness of presentation and style. Please consider the following when marking: General Presentation: 1a) Does the presentation demonstrate a clear logical structure? 1b) Is the material presented fluently with appropriate use of presentation aids? 1c) Is the trainee able to expand on their work in response to questions from the
assessors? 1d) Does the presentation keep within time boundaries? Background Information: 2a) Does the presentation clarify how consent was sought/obtained? 2b) Does the presentation provide sufficient information regarding the nature of the
clinical work undertaken (individual/group/systemic); reasons for referral/consultation; relevant history; presenting problems; service context and any relevant issues re: MDT working?
Assessment: 3a) Does the presentation clearly describe the assessment process and outcome including
choice of methods; psychometric measures used and with links to theory as appropriate?
3b) Does the presentation demonstrate competence in conducting appropriate risk assessments and use these to guide practice?
Formulation/Reformulation: 4a) Does the presentation illustrate a formulation(s) drawing upon psychological
theory/evidence and incorporating contextual factors? 4b) Does the presentation clarify how the formulation was shared/used with
310
SECTION 4
PROGRAMME MANUAL / 2019
clients/families/group/team to promote psychological thinking. 4c) Where reformulation has been necessary, does the presentation illustrate this? Intervention 5) Does the presentation demonstrate the ability to plan/implement an appropriate
intervention(s) based on the formulation presented with reference to relevant theory and evidence-based.
Outcome: 6a) Does the presentation include an evaluation of the intervention and how this was
obtained/measured? 6b) Does the presentation include feedback from the relevant service
user/family/team/professional? Professional Issues: 7a) Does the presentation demonstrate knowledge and understanding of relevant
professional and ethical issues? 7b) Does the presentation demonstrate sensitivity to issues of difference and diversity? Reflective Practice: 8a) Does the presenter reflect on the clinical work discussed in terms of their own
personal and professional development? 8b) Does the presentation demonstrate self-awareness and working as a reflective
practitioner? Portfolio: 9a) All relevant documentation included in portfolio. 9b) Were the abstract /letters/reports /measures completed to a satisfactory professional
standard?
311
SECTION 4
PROGRAMME MANUAL / 2019
GRADE CATEGORIES FOR RCAs, CBT-RCA & RCAP DISTINCTION 70%+ (Excellent) Learning objectives have been met to a high standard. The submitted work (either written or as a presentation) demonstrates a very high standard of critical appraisal. There is a concise but thorough description of the appropriate clinical and research context as it applies to the clinical work presented. The appraisal of the work conducted demonstrates an excellent and detailed grasp of clinical and academic issues as they relate to the assessment, formulation and intervention with the client or the group or system within which the work was conducted. The trainee also demonstrates a solid grasp of the limitations of the work that they have completed. The trainee’s work demonstrates a sound understanding of measurement issues and a good grasp of psychometrics. In addition, the trainee demonstrates careful consideration of relevant ethical issues including, where relevant, careful extrapolation of research findings to their clinical implications. The report has a strong and coherent structure with lucid and succinct writing. There is a high standard of presentation with few errors of grammar, typography and style. In written RCAs there is a high standard of referencing throughout conforming to APA, or BPS guidelines. MERIT 60-69% (Good to Very Good) Learning objectives have been met to a good standard. A meritorious report of clinical activity shares many of the features of work at a distinction level with a strong emphasis on critical analyses however, application of clinical and academic knowledge and depth of analysis is weaker in some domains. The submission (either written or as a presentation) clearly shows the trainee understands the wider research and clinical context with which the work is embedded. The trainee demonstrates a good grasp of measurement issues with psychometric data and a good grasp of potential limitations although some gaps in understanding may be evident. The trainee extrapolates from appropriate research literature to draw valid clinical implications relevant to the clinical, group or system’s presentation. There is evidence that the trainee has carefully considered any ethical issues (where appropriate) and the implications for the assessment, formulation and intervention that they provided. The report demonstrates a good standard of presentation with a systematic and logical structure but may contain minor errors of grammar, typography and style. In written RCAs there is a good standard of referencing throughout conforming to APA, or BPS guidelines, with only minor errors.
PASS 50-59% (Satisfactory) Learning objectives have been met to satisfactory standard. The submission may be good or very good in places but with some areas of weakness. The submission style tends towards the descriptive level of analysis with a superficial understanding of the wider clinical or academic context. The range and breadth of literature used to support assessment and
312
SECTION 4
PROGRAMME MANUAL / 2019
interventions are narrower, restricted and less contemporary. Clinical interventions may be described but without a clear or only a superficial rationale for them being provided. There is a more limited and uncertain grasp of measurement issues and the use of psychometrics. The content is noticeably weak in parts with omissions and gaps in how relevant literature is used to support the clinical work. The content overall is less lucid and there is less coherence in the presentation of information overall. There are a few errors of grammar, typography and style. In written RCAs there is a competent standard of referencing throughout the text and bibliography with some violations of consensus guidelines. Overall the work demonstrates sufficient competence, understanding and standards of scholarship to merit a pass at doctoral level. FAIL <50% (Fail) Learning outcomes are not met to a satisfactory standard. Relevant clinical and academic issues have been missed or core concepts have been misunderstood in the application to the clinical work. There is an inadequate application of psychological theory to clinical practice. Application of clinical actions is not justified by theoretical knowledge. Psychometric data may be misunderstood or misinterpreted. The appraisal is not concise, and irrelevant material is included at the cost of more relevant material. The argument is not clearly presented or articulated and some of the conclusions drawn may not be valid. The report may be poorly structured. The trainee fails to discuss limitations of their work in a way that convinces that they understand them. There is little or no consideration of any ethical issues that may be relevant to the work or presentation. Indeed, unethical practice alone may merit a fail grade even in the face of other areas of skill. Consideration of relevant research and clinical context is missing. Writing may be of an unsatisfactory standard with errors and inaccuracies. There may be a poor standard of referencing throughout the text and bibliography. Non-submission of a clinical report about the work is also justification for failing the report of clinical activity. For the CBT Report of Clinical Activity, a score of less than 36 on the CTSR for the submitted session will result in the failure of that component of the assignment. Procedures for Resubmission of Reports of Clinical Activity given a Fail Grade • If a fail grade is obtained for an RCA or on the written component of the CBT RCA the
trainee will usually be required to revise and resubmit the RCA or the written component only in the case of the CBT RCA.
• If an RCAP fails the trainee may be required to resubmit the portfolio and presentation
slides only or present again, or both. • In the event of a fail being obtained on the audio or video recording component of the
CBT RCA the Board of Examiners will specify how the work should be resubmitted. There are a number of possible options as to how an alternative piece of work for resubmission can be identified:
o Submit an audio or video recording of another CBT session with the same client
313
SECTION 4
PROGRAMME MANUAL / 2019
o Submit an audio or video recording of a CBT session with a different client. If this option is chosen the trainee will be required to submit a written report of no more than 1500 words detailing:
• The presenting problem for the client • A summary of the outcomes of the assessment and the formulation • Details of work being undertaken in the session and how this fits
into the overall intervention • A reflection on the strengths of the work undertaken in the session
and areas for improvement
• If a fail grade is obtained on both the written component and work undertaken in the audio or video recording the Board of Examiners will specify arrangements for the resubmission of both pieces of work.
• If a fail grade is given on the second submission of the audio or video recording of the CBT
session then the trainee will be required by the Board of Examiners to submit a further recording for assessment on a subsequent placement.
314
SECTION 4
PROGRAMME MANUAL / 2019
NWCPP POLICY FOR RECEIPT OF VIDEO/AUDIO RECORDINGS FOR ASSESSMENT
1. The NWCPP will provide trainees with BCUHB white listed encrypted USB safe sticks to be used for storing and submitting their video/audio recordings. Each trainee will be required to collect the USB Safe Stick in person and will be allocated their unique password. Trainees must keep their password secure and separately from the USB safe stick. Trainees must not to change the password unless the original password security has been compromised in which case they should contact the Programme Manager immediately.
2. USB Safe Sticks are numbered and logged out to each individual trainee. This information
is stored on a password protected document on the University’s secure NWCPP network drive.
3. The NWCPP will provide trainees with ‘Guidance for RCA – CBT recordings using the
Integral Crypto USB Flash Drive’. 4. Trainees are also referred to additional ‘Guidelines on Submission of Recordings for the
CBT RCA’ included in the Programme Manual (Section 4).
5. Trainees must submit their USB safe stick in person to the Administrative Assistant (Curriculum and Clinical).
6. When recordings are submitted, they will be placed in individual envelopes marked with
the trainee ID number and then placed in the securely locked safe until they are requested by the Assessors.
7. USB Safe Sticks will be placed back in the securely locked safe once the Assessor has
completed their assessment. 8. Assignments plus recordings will be listened to by a suitably qualified member of the
Programme Team.
9. Recordings will be transferred onto one USB encrypted safe stick to be sent to the External Examiner.
10. Assignments and USB safe sticks sent to External Examiners must be sent and returned by
registered delivery.
11. The External Examiner will be advised to contact the NWCPP Admin Office by telephone upon receipt of the USB safe stick in order to obtain the password to access the data.
12. Once the assignments have been moderated and marks confirmed by the Board of
Examiners the recordings will be destroyed. Paperwork describing the marks will be retained in accordance with University regulations.
315

SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON WRITING-UP EVIDENCE-BASED BRIEFING Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. Format The focus of the assignment is a concise, jargon-free report, targeted at service planners, managers or practitioners, with varying degrees of psychological knowledge and awareness. This brief report must be no more than 1000 words in length. In addition, an appendix of up to 4500 words (not including a reference list) is required, to provide contextual and supporting information demonstrating explicitly the critical appraisal that has led to the production of the briefing. Tables included in an appendix must be accompanied by a contextual narrative (critical appraisal and synthesis of studies). Content Evidence-based practice requires the weighing up of a variety of sources of evidence and placing them within a context of values and principles. However, the assignment differs from the Data-Analytic Project, in that the trainee will access a wide range of evidence on a topic, including systematic reviews of randomised controlled trials, where relevant, but will also be expected to have critically reviewed evidence from qualitative studies, expert opinion (including views from service users and carers), consensus statements and guidelines. It is important that the evidence-base regarding psychological interventions is accurately and fully represented in the appendix and summarised in the brief report, to help inform service planning, development and practice. Therefore, the trainee will make clear recommendations, making explicit the level of evidential support for these, and highlight areas of certainty and uncertainty, including areas for further investigation and consideration. The topic for this assignment should be agreed with the trainee’s Training Coordinator, and is subject to approval by the Chair of the Board of Examiners. Example Topics CBT-based anger management interventions for adults with learning disabilities. Mindfulness training for children and adolescent mental health services. The suitability of Dialectical Behaviour Therapy for individuals with learning disabilities. * Addressing deliberate self-harm in young people: A psychologically informed approach* Cognitive rehabilitation for executive functioning difficulties following traumatic brain injury. *Copies of these assignments are available on Blackboard
316
SECTION 4
PROGRAMME MANUAL / 2019
Timing The submission date for this assignment will be in June of Year 1. You will be required to submit the title of your EBB to the Chair of the Board of examiners in advance to ensure that there is no substantial overlap with previous assignments and to allow sufficient time for appropriate assessors to be identified.
317
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR ASSESSORS MARKING EVIDENCE BASED BRIEFINGS Learning Outcomes assessed As trainees choose their own titles for assignments not all of the learning objectives below may be relevant to any particular assignment. Markers are encouraged to use their judgement and only assess those learning outcomes relevant to the submitted assignment. All Part I assignments are marked in accordance with Bangor University’s Assessment and Marking Guidance for Taught Post-Graduate Programmes. Please refer to guidance on Grade Categories on pages 187-188.
Generalisable Meta-Competencies Capacity to: • Complement evidence-based practice with an ethos of practice-based evidence
where processes, outcomes, progress and needs are critically and reflectively evaluated.
• Make informed judgments on complex issues in specialist fields, often in the absence of complete information.
Psychological Intervention Knowledge of: • Interventions related to, secondary prevention and the promotion of health and
well-being
Evaluation Capacity to: • Appreciate outcomes frameworks in wider use within national healthcare systems,
the evidence base and theories of outcomes monitoring (e.g. as related to dimensions of accessibility, acceptability, clinical effectiveness and efficacy) and creating synergy with personal evaluative strategies
Research Capacity to: • Be a critical and effective consumer, interpreter and disseminator of the research
evidence base relevant to clinical psychology practice and that of psychological services and interventions more widely. Utilising such research to influence and inform the practice of self and others
• Conceptualise, design and conduct independent, original and translational research of a quality to satisfy peer review, contribute to the knowledge base of the discipline, and merit publication including: identifying research questions, demonstrating an understanding of ethical issues, choosing appropriate research methods and analysis (both quantitative and qualitative), reporting outcomes and identifying appropriate pathways for dissemination
• Understand the need and value of undertaking translational (applied and applicable) clinical research post-qualification, contributing substantially to the development of theory and practice in clinical psychology
318
SECTION 4
PROGRAMME MANUAL / 2019
Personal & Professional Skills & Values Capacity to:
• Understand the impact of differences, diversity and social inequalities on people’s lives, and their implications for working practices.
In addition, please consider the following when marking: Writing & Presentation style
• Does the assignment demonstrate a clear structure? • Does the assignment present a coherent argument? • Does the assignment demonstrate the writer’s ability to use a clear, concise writing
style, avoiding grammatical and presentational errors? • Does the assignment demonstrate the ability to write reports that are clear and
concise for a range of readerships? • Does the assignment demonstrate the ability to interpret statistical information? • Does the trainee make clear recommendations (summarised in the briefing paper
and elaborate more fully in the appendix)?
319
SECTION 4
PROGRAMME MANUAL / 2019
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: EBB Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
320
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON WRITING-UP SERVICE RELATED RESEARCH PROJECTS Service Related Research Projects (SRRPs) are projects that inform a service, usually using data already collected or collected during normal clinical practice. A good SRRP will address an identified problem, impact on service provision, and help the service to improve. Thus, typical project topics include an audit of whether a service is meeting a specified standard, with recommendations and action plan; an analysis of referral patterns; a pre-post evaluation of a group intervention; or a survey of service user or staff perceptions of a service. The SRRP is submitted and presented as a poster with an accompanying letter which explains who the poster is targeted at, and what the plan for dissemination will be. The style and content of the poster must reflect the purpose of the project and the intended “audience”. For example, a report of a service evaluation should be in a form suitable to communicate the findings to a multi-disciplinary group of colleagues with limited research expertise. The poster should normally include the following elements:
• A short introduction to the problem with reference to relevant literature and clear statement of specific questions being addressed.
• An account of the sample and methods used in the study and of the practical work undertaken.
• A clear presentation of the results of the study. The emphasis in the SRRP is to be placed on the clear presentation of findings.
• A short discussion/conclusion relating to the research findings in the context of the specific problem addressed, together with recommendations for service provision and future research.
SRRP posters should be prepared in PowerPoint and submitted in A3 size for marking. The version of the poster submitted for marking must be anonymised, as for any assignment. Trainee/supervisor names and affiliations, including identifying logos must be removed before submission. Once the assessors have given you feedback on the poster, and you have made any relevant revisions, an A1 size poster in colour should be printed for presentation at the Programme’s Annual Research Conference. When the poster is presented at the conference, author names and relevant logos should be re-inserted. Three A3 copies of each poster must be handed in by the dates set by the Examining Board. A signed copy of the Research Supervisor’s Form and the Research Submission Form must also be included (copied below). IN addition, a brief letter to the markers, explaining i) who the intended audience for the SRRP is and ii) the plan for disseminating the findings should be included. In addition to the creation of a poster, candidates may be required to provide a short report for the relevant service. This short report should cover in greater detail the methods used and results found. Candidates will be required to provide this additional report for their SRRP supervisor if this has been requested on their SRRP research supervision agreement form.
321
SECTION 4
PROGRAMME MANUAL / 2019
The following is general advice about the content of a good SRRP:
• Choose a title that will appeal to your prospective audience as they walk by. • Consider design issues like colour and font carefully (a point 28 font is a good
approximate size for text). • State clearly the problem being addressed. • Ensure that your poster has a clear structure. • Cite appropriate empirical literature sparingly. • Always bear in mind who your audience is and present information in the best
way for this group. For example, if the poster is for an audience with limited technical knowledge, then technical details about the methodology should be visually separated from the main content of the poster – for example a method section could be in a different colour, or a smaller font, on one side.
• Maintain a critical view of empirical literature, other evidence, and/or theory. • Describe the data collection and analysis methods in appropriate detail. • Less is more – try to use the minimum amount of text to convey the information
your audience needs. • Where possible, use figures to present data rather than text. • Consider any copyright issues with images. • State clearly the main finding(s). Try to stick to one or two clear messages. • Consider the clinical implications of the results. • Show awareness of the limitations of the data and methods, and be cautious
about interpreting the data in the light of these limitations. • Don’t forget to include references, but these can be presented in a smaller font.
Sample posters will be available to inform the development of SRRP posters. Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. It is the trainee’s responsibility to inform the Supervisor that the relevant assignment has been passed before it can be publicly disseminated. Preparing your poster for the Annual Conference Put your name and contact details on your poster and make any appropriate changes suggested by the Programme assessors.
• E-mail the final version of the poster in pdf or ppt file format to [email protected]. (You must cc. the research secretary into your e-mail as your poster will not be created without their authorisation).
• Explain to the print unit that the poster must be size A1, and in colour. Ask if you can have a poster tube to keep it safe.
• Deliver the poster to the Programme office at last 3 working days before the conference.
Presenting your poster at the Annual Conference Your A1 colour poster will be fixed to a poster board or a wall. You will need to stand by
322
SECTION 4
PROGRAMME MANUAL / 2019
your poster during some specified times. Your job is to help people understand the study presented on the poster. Thus, you should be prepared to:
• Give a short verbal ‘walk through’ the rationale, methods, findings, and your main conclusion. Always offer to do this when someone first comes up to your poster.
• Be generally engaging and sociable – acknowledge the arrival of a new person even if you are already engaged with someone else.
• Answer questions that anyone looking at your poster may have. • Offer an A4 black and white copy of your poster to anyone who is interested.
323
PROGRAMME MANUAL / 2019
SECTION 4
SERVICE RELATED RESEARCH PROJECTS PROPOSALS See the Important Dates section for exact deadlines Proposals should be discussed with your proposed supervisor(s) and approved by them. Proposals should address each of the numbered points below, and typically will be between 4-6 pages in length: 1. Project title 2. Supervision (who will supervise, and will they be able to provide supervision for
all aspects of the project including data analysis. If not, what additional supervision support would you need)
3. Background (gives a summary of the literature which supports the need for the study)
4. Clinical question/service need identified 5. Proposed design and methods (where will the data come from, how many
people involved, availability of sample, what measures will you use, what is the overall design?)
6. Access (state from whom you need permission to access participants or data and indicate whether their co-operation has been assured)
7. Data analysis (what techniques will you use?) 8. Ethical/Registration issues (describe as relevant and indicate whether an ethics
application will be needed. Specify the procedure required to register your project with the Health Board)
9. Data storage (what happens to the data at the end of the project?) 10. Financial information (NB. Normally, clinical services would be expected to cover
any SRRP costs as the projects are intended to be of benefit to the service directly. Please detail any additional costs to the Programme that we should be aware of – e.g., requirements for copies of copyright measures. Please detail amounts. Bear in mind that if you require additional measures, you are likely to be straying into the territory of a project defined as research and requiring ethics approval)
11. Timetable (a detailed timetable from the present date to submission – include all relevant milestones)
12. References (any key references cited should be listed) Throughout the proposal, trainees should consider any relevant diversity issues (e.g., in relation to questions asked, samples to be recruited, exclusion as a result of the methods to be adopted).
Submission of the SRRP proposal 1. Supervision Agreement:
Both the trainee and supervisor must sign and date a hard copy of the Supervision Agreement. This document must be attached to the SRRP
2. SRRP Proposal: A signed, hard copy of the SRRP proposal containing the Supervision Agreement must be submitted by the deadline date to the Admin Assistant (Research &
324
PROGRAMME MANUAL / 2019
SECTION 4
Finance). Both the trainee and supervisor must sign and date the document. E-mail submission of a scanned copy of the signed and dated proposal is acceptable.
SRRP Progress Report By the dates indicated in the trainee’s individual SRRP timetable, trainees must submit a SRRP progress report to the Programme. This does not need to be overly long, but should address the following numbered headings: 1. Progress (have you managed to adhere to your timetable milestones. If not,
please explain why and also provide a revised timetable showing new milestones up to completion)
2. Problems/Changes to Project (describe problems/difficulties that have arisen and indicate how you have resolved them or plan to resolve them. Any major changes to the project should already have been approved by the Programme team, but please also include reference to them in this section).
3. Supervisors’ comments (please ask your supervisor to write any comments that they feel are useful. If no additional comments are necessary, please state “none”)
4. A signed, hard copy of the progress report must be submitted to the Admin Assistant (Research & Finance). Both the trainee and supervisor MUST sign and date the document. E-mail submission of a scanned copy of the signed and dated progress report is acceptable.
325
SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH SUPERVISION AGREEMENT: SRRP This agreement MUST be attached to the SRRP proposal when submitted NOTE – THIS IS A SAMPLE FRAMEWORK ONLY. YOU SHOULD OBTAIN AN ELECTRONIC VERSION OF THIS DOCUMENT AND ADAPT IT FOR YOUR SPECIFIC NEEDS. THE SUPERVISION CONTRACT STATED HERE IS THE RECOMMENDED MINIMUM ONLY AND YOU SHOULD CLARIFY THIS WITH YOUR SUPERVISORS. YOU SHOULD ALSO SPECIFY AUTHORSHIP ORDER AT THIS POINT. TRAINEE AND SUPERVISORS’ NAMES SHOULD BE INSERTED IN THE SPACES INDICATED BY SQUARE BRACKETS. DELETE THIS INSTRUCTION PARAGRAPH FROM YOUR PERSONALISED AGREEMENT. Research Supervisor: ________________________________ Trainee: ________________________________ This agreement is between:
SUPERVISOR(S): ________________________________ JOB TITLE(S): ________________________________ PLACE(S) OF WORK: ________________________________ TRAINEE: ________________________________
The purpose of the agreement is to ensure co-operation from all parties toward the completion of the trainee’s Service Related Research Project. It is accepted that the primary responsibility for completion of the project lies with the trainee. The research supervisor and the trainee agree to meet at least fortnightly or monthly in the initial stages of the research. However, during the period of data collection, it is accepted that meetings may be less frequent. Contact during this period will be maintained by e-mail or phone, but there should be no more than four weeks without a joint meeting. During the period of supervision, the research supervisor will attend any research supervisor meetings that are held. These meetings are chaired by the research director or other member of the Programme team. It is expected that the trainee will endeavour to meet the tasks and deadlines as agreed together with the supervisor and the Programme. In particular the trainee will submit to the supervisor(s), a near-final draft of the poster by DATE - actual date to be agreed under negotiation with supervisor(s). The supervisor(s) will endeavour to read and comment on draft poster and other contributions without undue delay. In the event of a delay of more than 3 weeks, the supervisor will contact the trainee and agree a date by which feedback will be provided. Trainees may also submit a near final draft of the poster to a Programme staff member for feedback, for example their training coordinator or research tutor.
326
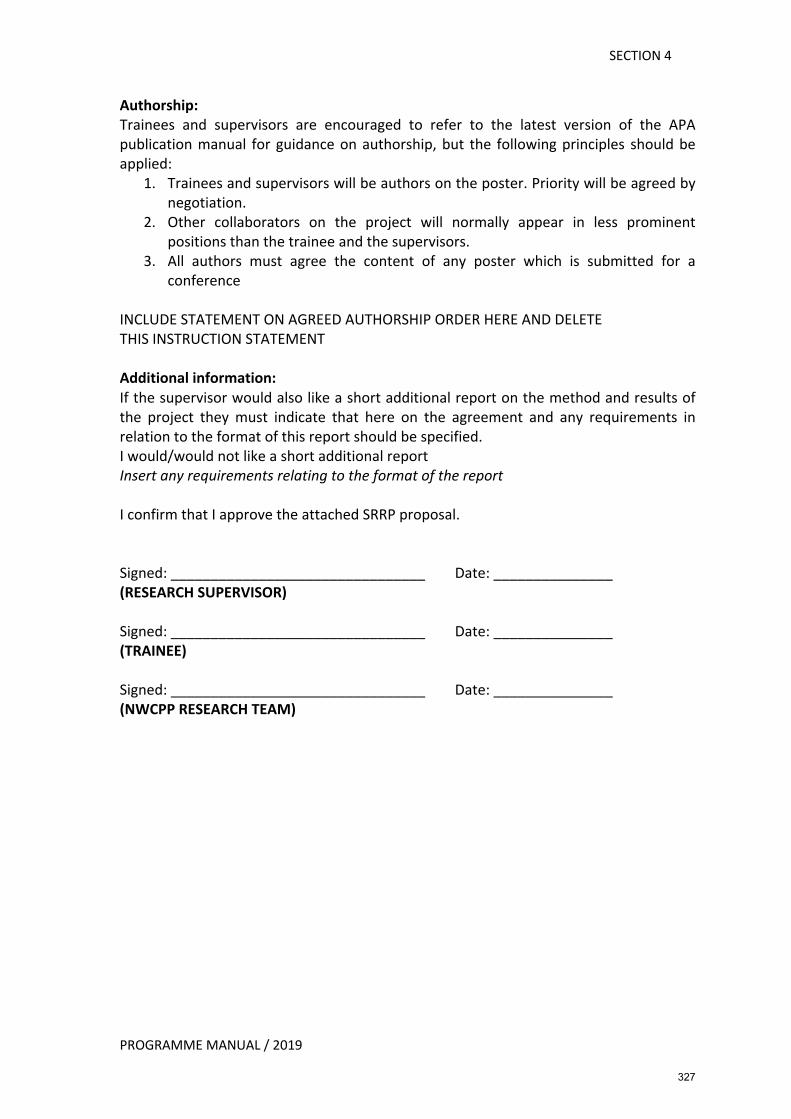
SECTION 4
PROGRAMME MANUAL / 2019
Authorship: Trainees and supervisors are encouraged to refer to the latest version of the APA publication manual for guidance on authorship, but the following principles should be applied:
1. Trainees and supervisors will be authors on the poster. Priority will be agreed by negotiation.
2. Other collaborators on the project will normally appear in less prominent positions than the trainee and the supervisors.
3. All authors must agree the content of any poster which is submitted for a conference
INCLUDE STATEMENT ON AGREED AUTHORSHIP ORDER HERE AND DELETE THIS INSTRUCTION STATEMENT Additional information: If the supervisor would also like a short additional report on the method and results of the project they must indicate that here on the agreement and any requirements in relation to the format of this report should be specified. I would/would not like a short additional report Insert any requirements relating to the format of the report I confirm that I approve the attached SRRP proposal. Signed: ________________________________ Date: _______________ (RESEARCH SUPERVISOR) Signed: ________________________________ Date: _______________ (TRAINEE) Signed: ________________________________ Date: _______________ (NWCPP RESEARCH TEAM)
327
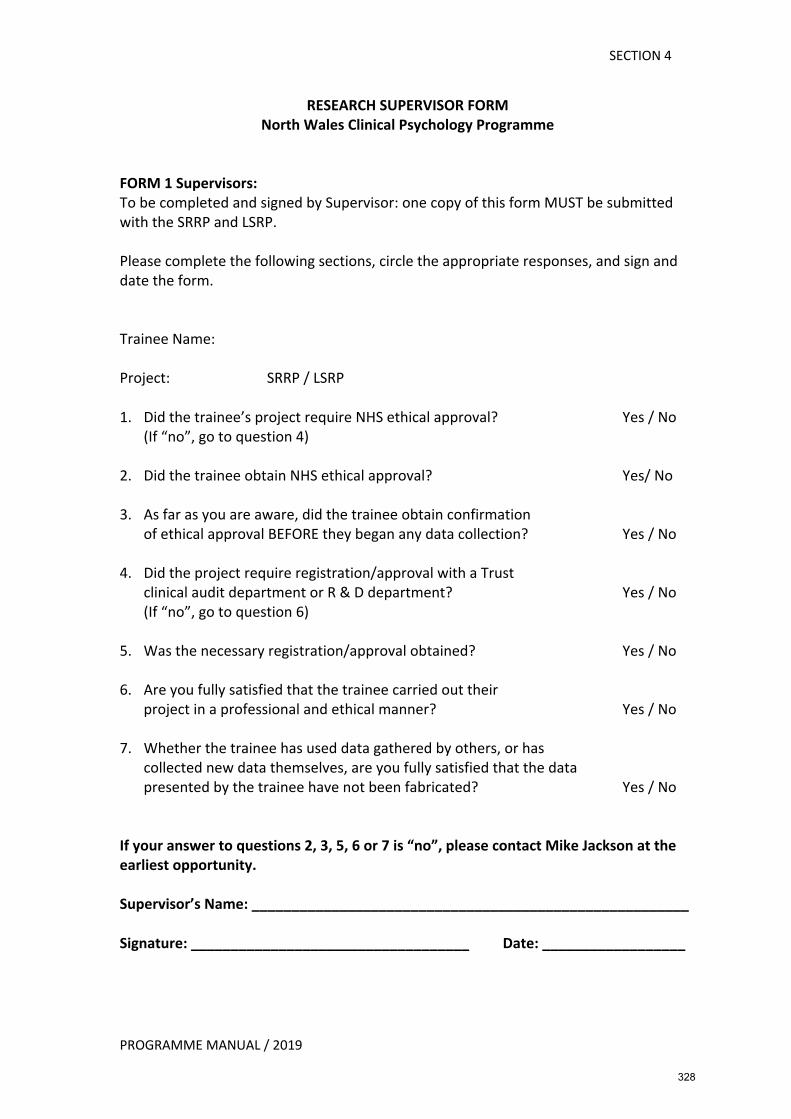
SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH SUPERVISOR FORM North Wales Clinical Psychology Programme
FORM 1 Supervisors: To be completed and signed by Supervisor: one copy of this form MUST be submitted with the SRRP and LSRP. Please complete the following sections, circle the appropriate responses, and sign and date the form. Trainee Name: Project: SRRP / LSRP 1. Did the trainee’s project require NHS ethical approval? Yes / No
(If “no”, go to question 4) 2. Did the trainee obtain NHS ethical approval? Yes/ No 3. As far as you are aware, did the trainee obtain confirmation
of ethical approval BEFORE they began any data collection? Yes / No 4. Did the project require registration/approval with a Trust
clinical audit department or R & D department? Yes / No (If “no”, go to question 6)
5. Was the necessary registration/approval obtained? Yes / No 6. Are you fully satisfied that the trainee carried out their
project in a professional and ethical manner? Yes / No 7. Whether the trainee has used data gathered by others, or has
collected new data themselves, are you fully satisfied that the data presented by the trainee have not been fabricated? Yes / No
If your answer to questions 2, 3, 5, 6 or 7 is “no”, please contact Mike Jackson at the earliest opportunity. Supervisor’s Name: _______________________________________________________ Signature: ___________________________________ Date: __________________
328
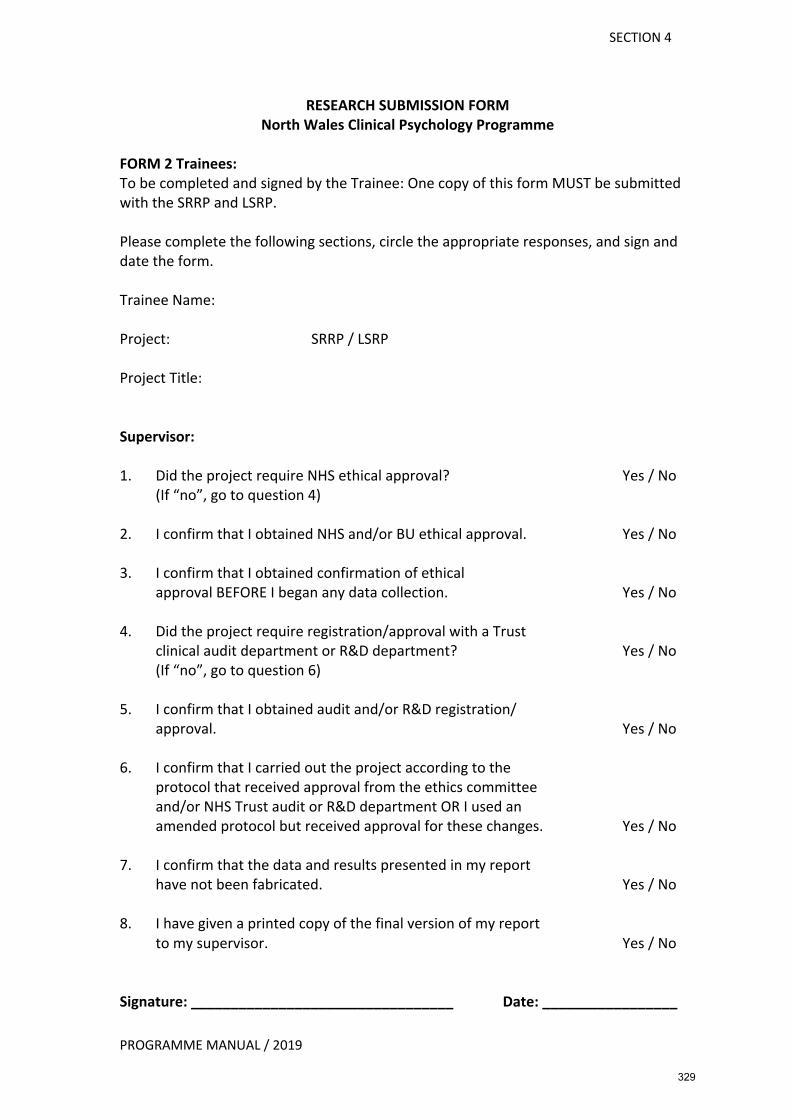
SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH SUBMISSION FORM North Wales Clinical Psychology Programme
FORM 2 Trainees: To be completed and signed by the Trainee: One copy of this form MUST be submitted with the SRRP and LSRP. Please complete the following sections, circle the appropriate responses, and sign and date the form. Trainee Name: Project: SRRP / LSRP Project Title: Supervisor: 1. Did the project require NHS ethical approval? Yes / No
(If “no”, go to question 4) 2. I confirm that I obtained NHS and/or BU ethical approval. Yes / No 3. I confirm that I obtained confirmation of ethical
approval BEFORE I began any data collection. Yes / No 4. Did the project require registration/approval with a Trust
clinical audit department or R&D department? Yes / No (If “no”, go to question 6)
5. I confirm that I obtained audit and/or R&D registration/
approval. Yes / No 6. I confirm that I carried out the project according to the
protocol that received approval from the ethics committee and/or NHS Trust audit or R&D department OR I used an amended protocol but received approval for these changes. Yes / No
7. I confirm that the data and results presented in my report
have not been fabricated. Yes / No 8. I have given a printed copy of the final version of my report
to my supervisor. Yes / No Signature: _________________________________ Date: _________________
329

PROGRAMME MANUAL / 2019
SECTION 4
RESEARCH TIMETABLE FOR SERVICE RELATED RESEARCH PROJECTS SRRP ideas can be developed during the first year of training. Trainees will be provided with information on potential SRRP supervisors after the Christmas break of the first year, and contact with potential supervisors will be facilitated. SRRP proposals are then developed and submitted to NWCPP by mid-May of the first year. The deadline for submission of the final SRRP project (in the form of a poster) will be in November of your second year. Exact deadlines for proposal and SRRP submissions are available in the Important Dates document for your cohort. SRRP ideas may emerge in at least three ways. First, the programme will provide initial information on potential supervisors’ interests and projects during the first year. The programme will facilitate contact with supervisors. You can approach supervisors and services at any time. Second, you and/or your supervisor might identify ideas whilst you are on placement or during the planning process for a future placement. You will not be required to design and complete a SRRP within the timeline of a placement. You are welcome to do so, but more likely the process will take longer. There may be some advantages to being in a service on placement when you are trying to collate or collect data for a SRRP. Placement supervisors are under no obligation to develop SRRP ideas with you and under no obligation to supervise you. The intention is to create some flexibility for SRRP ideas to emerge from placement experiences and to then be supported by NWCPP. Thus, supervision support for the research aspects of any SRRP can be provided by a Research Team member. A clinical supervisor may need to help design a project and facilitate the practical aspects, but they may not need to get involved with the research supervision. Supervision arrangements would be negotiated and specified in the SRRP proposal (the supervision agreement section). A third option for the development of a SRRP would be an idea that you have yourself for a suitable piece of work. If you have ideas and want to discuss how they might be developed and who could potentially supervise the project, please discuss with the research team member responsible for SRRPs.
330
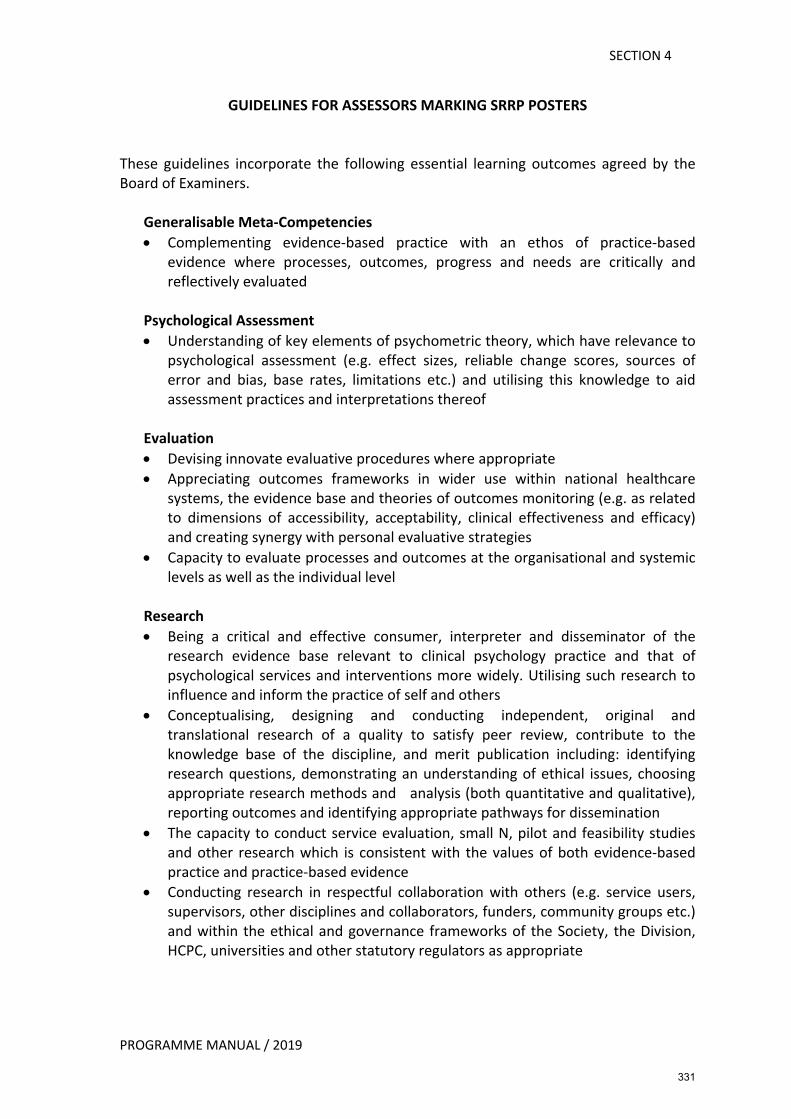
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR ASSESSORS MARKING SRRP POSTERS These guidelines incorporate the following essential learning outcomes agreed by the Board of Examiners.
Generalisable Meta-Competencies • Complementing evidence-based practice with an ethos of practice-based
evidence where processes, outcomes, progress and needs are critically and reflectively evaluated
Psychological Assessment • Understanding of key elements of psychometric theory, which have relevance to
psychological assessment (e.g. effect sizes, reliable change scores, sources of error and bias, base rates, limitations etc.) and utilising this knowledge to aid assessment practices and interpretations thereof
Evaluation • Devising innovate evaluative procedures where appropriate • Appreciating outcomes frameworks in wider use within national healthcare
systems, the evidence base and theories of outcomes monitoring (e.g. as related to dimensions of accessibility, acceptability, clinical effectiveness and efficacy) and creating synergy with personal evaluative strategies
• Capacity to evaluate processes and outcomes at the organisational and systemic levels as well as the individual level
Research • Being a critical and effective consumer, interpreter and disseminator of the
research evidence base relevant to clinical psychology practice and that of psychological services and interventions more widely. Utilising such research to influence and inform the practice of self and others
• Conceptualising, designing and conducting independent, original and translational research of a quality to satisfy peer review, contribute to the knowledge base of the discipline, and merit publication including: identifying research questions, demonstrating an understanding of ethical issues, choosing appropriate research methods and analysis (both quantitative and qualitative), reporting outcomes and identifying appropriate pathways for dissemination
• The capacity to conduct service evaluation, small N, pilot and feasibility studies and other research which is consistent with the values of both evidence-based practice and practice-based evidence
• Conducting research in respectful collaboration with others (e.g. service users, supervisors, other disciplines and collaborators, funders, community groups etc.) and within the ethical and governance frameworks of the Society, the Division, HCPC, universities and other statutory regulators as appropriate
331
SECTION 4
PROGRAMME MANUAL / 2019
Personal and Professional Skills and Values • Capacity to adapt to, and comply with, the policies and practices of a host
organisation with respect to time-keeping, record keeping, meeting deadlines, managing leave, health and safety and good working relations
• Working collaboratively and constructively with fellow psychologists and other colleagues and users of services, respecting diverse viewpoints
Communication and Teaching • Communicating effectively clinical and non-clinical information from a
psychological perspective in a style appropriate to a variety of different audiences (for example, to professional colleagues, and to users and their carers).
Organisational and Systemic Influence and Leadership • Understanding and working with quality assurance principles and processes
including informatics systems, which may determine the relevance of clinical psychology work within healthcare systems.
The grade awarded and feedback comments should reflect these ratings as well as appropriateness of presentation and style. Please refer to guidance on Grade Categories on pages 187-188. Please consider the following when marking: General presentation Is the poster well presented, with a consistent style, clear headings, and consideration of the needs of the intended audience? Poster content 1. Is there a cohesive flow from the Introduction through to final Conclusion,
centered around a succinctly stated research question or aim? 2. Is the clinical service context and relevance of the project clear? 3. Is the relevant research, policy or theory literature clearly summarised? (with
references for core papers only provided) 4. Is the study design and sampling approach appropriate and clear? 5. Is the methodology clearly described and replicable (within constraints of space) 6. Are ethical issues discussed and addressed appropriately? 7. Is the study correctly registered? 8. Are the statistical analyses or qualitative methods appropriate? 9. Are the results described clearly and with awareness of limitations? 10. Are the implications of the results for the service/for clinical practice discussed? 11. Are the main methodological problems/limitations noted appropriately? 12. Is there an appropriate level of critical reflection throughout the poster? 13. Does the trainee show awareness of diversity and social inclusion issues where
relevant?
332
PROGRAMME MANUAL / 2019
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee. Please see overleaf for guidelines for assessors marking SRRP posters.
Trainee Number: Type of Assignment: SRRP POSTER Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
333
PROGRAMME MANUAL / 2019
GUIDELINES FOR ASSESSORS MARKING SRRP POSTER See also Programme Manual for additional information General presentation Is the poster well presented, with a consistent style, clear headings, and consideration of the needs of the intended audience? Poster content 1. Is there a cohesive flow from the Introduction through to final Conclusion, centred around a
succinctly stated research question or aim? 2. Is the clinical service context and relevance of the project clear? 3. Is the relevant research, policy or theory literature clearly summarised? (with references for core
papers only provided) 4. Is the study design and sampling approach appropriate and clear? 5. Is the methodology clearly described and replicable (within constraints of space) 6. Are ethical issues discussed and addressed appropriately? 7. Is the study correctly registered? 8. Are the statistical analyses or qualitative methods appropriate? 9. Are the results described clearly and with awareness of limitations? 10. Are the implications of the results for the service/for clinical practice discussed? 11. Are the main methodological problems/limitations noted appropriately? 12. Is there an appropriate level of critical reflection throughout the poster? 13. Does the trainee show awareness of diversity and social inclusion issues where relevant?
334

SECTION 4
PROGRAMME MANUAL / 2019
NWCPP – FINANCIAL RESOURCES FOR SRRPs The NWCPP team is well aware of the difficulties that the funding of research projects can precipitate in today's NHS, and the following guidelines are intended to make clear to trainees and supervisors how the programme can help with the financial support for research projects. Service Related Research Projects are intended to be projects that involve the evaluation of services, examination of the effectiveness of standard clinical interventions, and audits or surveys relating to various service questions. Thus, the intention is that trainees are helping local services and clinicians by carrying out a project of practical importance to the service. It is expected that services would offer ideas to trainees rather than vice versa. Under these circumstances, services receive the time of the trainee for free and also receive copies of any reports produced for their own use. Any travel expenses incurred by the trainee would also be claimed by the trainee through the normal procedures and so do not need to be covered by the service. However, photocopying, stationary, postage, any administrative support required to help access data, the costs of purchasing copies of copyright measures, and any other procedural costs would be expected to be covered by the service(s) in question. Where SRRPs require the use of an expense that is clearly out of the ordinary and that would be very difficult to absorb within a service, trainees may make a case to NWCPP to cover all or a part of the cost for these extraordinary items. Trainees must accurately cost such items and make a detailed case why the service cannot cover all or part of the expense and include this in their SRRP written proposal. NWCPP will not normally honour such requests, but will consider any requests on a case-by-case basis Any trainee who anticipates making such a request is encouraged to discuss the issue early in the SRRP planning process with the research team member responsible for SRRPs.
335
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON WRITING-UP PROFESSIONAL ISSUES ASSIGNMENT Trainees choose their own titles for assignments and are encouraged to consult with Clinical Psychologists working in the specific clinical area specialism before finalising. Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. Format A document suitable for professional use, of no more than 5500 words (not including reference list, but including words in Figures, Tables, text boxes and Appendices). Content The document will apply knowledge, theory and models in clinical psychology to an area of professional or service development. The topic will be agreed with the trainee’s Training Coordinator, and subject to approval by the Chair of the Board of Examiners. The content must address the learning outcomes specified in the appropriate evaluation and feedback form. Where the form of the document is constrained e.g. by consultation questions or is adapted to a particular audience, additional supporting material and argument may be provided in an appendix to demonstrate critical evaluation and appraisal skills. Example topics
Responses to a current (or recent) consultation by government or relevant professional bodies or a review of such a document e.g.:
• Response to the draft National Dementia Plan for Wales (WAG - June 2009). • Response to draft Intelligent Targets for first episode psychosis (NHS Wales, April
2009). • Response to consultation on a relevant NICE guideline. • A Critical Psychological Response to the UK Government (2012) Consultation:
“Improving Permanence for Looked after Children. • Are people with learning disabilities rights to be part of a community, and live in
a home of their choice being address? A response to the Department of Health (2015) Consultations: No voice unheard, no right ignored
Service development proposals e.g.: • A proposal for the involvement of service users and carers in a service
development. • A proposal for the management of change in the context of a service
development. • A proposal for ensuring access to psychological services for people of diverse
cultural backgrounds. • A proposal for the involvement of clinical psychology in developing service
provision for refugees and asylum seekers.
336
SECTION 4
PROGRAMME MANUAL / 2019
Topics of relevance to clinical psychology e.g.: • Occupational stress and burnout in trainees and qualified clinical psychologists
in North Wales; recommendations for minimisation and managements through the promotions of resilience.
• The Clostridium Difficile Infection at Ysbyty Glan Clwyd: A Psychological Analysis of Factors that Contributed to the Outbreak.
• Compassionately Responding to the Francis Report – A Psychological Analysis of the Inhibitors and Facilitators of Compassionate Healthcare.
• Time to think differently? Applying Psychological Understanding to Prevent Radicalisation
• Clinical Psychologists role in widening access to mental health services for people from social- economically deprived backgrounds
Timing The submission date for this assignment will be set in January of Year 2. You will be required to submit the title of your PI assignment to the Chair of the Board of examiners in advance to ensure that there is no substantial overlap with previous assignments and to allow sufficient time for appropriate assessors to be identified.
337
SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES FOR ASSESSORS MARKING PROFESSIONAL ISSUES ASSIGNMENTS Learning Outcomes assessed As trainees choose their own titles for assignments not all of the learning objectives below may be relevant to any particular assignment. Markers are encouraged to use their judgement and only assess those learning outcomes relevant to the submitted assignment. All Part I assignments are marked in accordance with Bangor University’s Assessment and Marking Guidance for Taught Post-Graduate Programmes. Please refer to guidance on Grade Categories on pages 187-188.
Generalisable Meta-Competencies Capacity to: • Make informed judgments on complex issues in specialist fields, often in the absence
of complete information. • Reflectively apply ethical and professional practice frameworks
And if appropriate to the trainees chosen title: • Collaborate with service users and carers, and other relevant stakeholders, in
advancing psychological initiatives such as interventions and research
Organisational and Systemic Influence and Leadership Capacity to: • Demonstrate awareness of the legislative and national planning contexts for service
delivery and clinical practice • Adapt practice to different organisational contexts for service delivery. This should
include a variety of settings such as in-patient and community, primary, secondary and tertiary care and may include work with providers outside of the NHS
• Understand leadership theories and models, and their application to service development and delivery. Demonstrating leadership qualities such as being aware of and working with interpersonal processes, proactivity, influencing the psychological mindedness of teams and organisations, contributing to and fostering collaborative working practices within teams
• Understand change processes in service delivery systems
Evaluation Capacity to: • Appreciate outcomes frameworks in wider use within national healthcare systems,
the evidence base and theories of outcomes monitoring (e.g. as related to dimensions of accessibility, acceptability, clinical effectiveness and efficacy) and creating synergy with personal evaluative strategies
• Evaluate processes and outcomes at the organisational and systemic levels as well as the individual level
338
SECTION 4
PROGRAMME MANUAL / 2019
Research Capacity to: • Be a critical and effective consumer, interpreter and disseminator of the research
evidence base relevant to clinical psychology practice and that of psychological services and interventions more widely. Utilising such research to influence and inform the practice of self and others.
Personal and Professional Skills and Values Capacity to: • Understand the impact of differences, diversity and social inequalities on people’s
lives, and their implications for working practices Psychological Intervention (if appropriate to the assignment title selected by the trainee) Capacity to: • Understand social approaches to intervention; for example, those informed by
community, critical, and social constructionist perspectives
Writing and Presentation style • Does the assignment demonstrate a clear structure? • Does the assignment present a coherent argument? • Does the assignment demonstrate the writer’s ability to use a clear, concise writing
style, avoiding grammatical and presentational errors? • Does the assignment demonstrate the ability to write reports that are clear and
concise for a range of readerships? • Does the assignment demonstrate the ability to interpret statistical information (if
appropriate to the assignment title)?
339
PROGRAMME MANUAL / 2019
SECTION 4
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: Professional Issues Assignment - PI Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
340
SECTION 4
PROGRAMME MANUAL / 2019
GUIDANCE ON LARGE SCALE RESEARCH PROJECTS
1. The large-scale research project will be presented in two formats: a research thesis, and a presentation at the annual Stakeholder conference in September. The conference presentation is a formative assessment exercise. Comments and feedback will be provided by the delegates/audience, but there is no formal assessment conducted during the conference presentation. The thesis is the summative (i.e., formally assessed) assessment for the LSRP. The thesis should report investigative work, the results of which can be judged to constitute substantial contribution to knowledge, and should show evidence of originality by the discovery of new findings and by the exercise of independent critical power. The candidate should be able to demonstrate in what respect her or his work appears to advance knowledge or practice in clinical psychology. The main substance of the report of the large-scale research should not exceed: • 20,000 words excluding tables, figures, reference lists and appendices; • 40,000 words including tables, figures, references and appendices.
Trainees submitting qualitative research studies must also adhere to these requirements. Extensive presentation of quoted/sample material can be presented in a suitable tabular form in order to comply with the above word count.
All LSRPs require a supervisor who is a staff member of the University School of Psychology. Usually this will be a member of the Programme Team. Most projects will also have a clinical Research Supervisor. Whether your project is qualitative or quantitative, your supervision team needs to be competent and confident with the methodology you are using. The research team can offer additional support 2. The thesis shall constitute the following components: 2.1 A thesis abstract of not more than 300 words, outlining the major issues,
methods and findings of the large-scale research project (covering all aspects of the thesis – this is an overall summary, not an abstract simply for the empirical study paper). The abstract of the thesis should contain: (a) A title for the thesis (most likely different to the titles of the papers within the thesis) of not more than 15 words, and (b) The abstract itself, presented in 12- point font, double-spaced, with page margins not less than one inch.
2.2 A literature review, written in the format of a specified peer reviewed
academic journal but using the following format: (a) a title page, (b) an abstract in the appropriate format for the journal, and (c) other sections as specified by the journal requirements. The title page should provide a web address where the journal author guidelines can be found. The text of this literature review (excluding tables, figures, captions, and reference lists) will normally be not less than 3,000 words and not more than 6,000 words, according to the submission guidelines for the chosen journal. If your word count does not fall into this range, consult with the research team. Remember to comply with the
341
SECTION 4
PROGRAMME MANUAL / 2019
overall thesis word count. The literature review may be a systematic review, as defined by PRISMA guidelines or similar, a meta-analysis or meta-synthesis, or a narrative review. The format of the review should, however, be appropriate for its topic. Both the literature review and the empirical paper should conform to the author guidelines, with one exception: Where tables and figures would normally be placed at the end of a paper, with an indication of their approximate location in the main text, it is preferable to include them in the main body of the text. The selected journal should be approved by the programme team as a part of the LSRP proposal process. The candidate should be the first author of the literature review, with research supervisor(s) as subsequent author(s). Normally this should be according to the signed supervision and authorship agreement submitted with the LSRP proposal, but this can be changed with the agreement of all authors if the degree of contribution from different authors differs from what was anticipated. It is important to note that the literature review bound into the thesis is presented in the format for a specified peer-reviewed academic journal. There is an expectation that the literature review is actually submitted to the journal in question. However, there is no requirement that the literature review be accepted by the journal.
2.3 A research paper describing the major findings of the large-scale research project, written in the format of a specified peer-reviewed academic journal but using the following format:
(a) a title page (b) an abstract in the appropriate format for the journal (c) other sections as specified by the journal requirements The text of this research paper (excluding tables, figures and reference lists) will normally be not less than 2,500 words and not more than 6,000 words, according to submission guidelines for the chosen journal. If your word count does not fall into this range, consult with the research team. Remember to comply with the overall thesis word count. As with the literature review, the research paper should conform to the style laid out in the notes to contributors, again except that figures and tables should be placed in the intended location in the text, rather than at the end of the manuscript. The purpose of the research paper is to summarise the findings from the empirical study carried out for the large-scale research project. The candidate should be the first author of theresearch paper, with research supervisor(s)
342
SECTION 4
PROGRAMME MANUAL / 2019
and any other research team members as subsequent author(s). Again, normally this should be as agreed in the signed supervision and authorship agreement, but this can be changed with the agreement of all authors if the degree of contribution from different authors differs from what was anticipated. As with the literature review, there is an expectation that the research paper is actually sent to the journal in question. However, there is no requirement that the research paper is accepted by the journal. Please note that in the case of the review and empirical paper, you will not be examined on the precise suitability of the paper for the selected journal. However, you are expected to conform to the journal’s style guidelines, and broad scope.
2.4 A final discussion paper entitled “Contributions to Theory and Clinical
Practice”. This paper should focus on these issues and should be organised using a minimum of these two subheadings but probably more):
(a) Implications for future research and theory development (b) Implications for clinical practice This paper should not simply be a review of the issues already addressed in the discussions of the review or empirical papers but should focus more broadly on the whole of the LSRP. Implications for clinical practice should be as detailed and specific as possible. Very little space is likely to be devoted to clinical implications in the discussion to a research paper, and so the final paper is an opportunity to think clearly about how your research might be applied. This paper will normally be around 3,000 words in length but must not exceed 5,000 words. Where relevant, trainees can include a short reflective commentary in this paper, covering process/personal issues arising from the conduct of the research. An abstract may be included where this would be helpful, but this is not a requirement.
2.5 Optional appendices. These appendices, together with the figures, tables and
reference lists of the earlier parts of the thesis, shall not be more than 20,000 words. The contents of these will vary from project to project, but we suggest that you consider including: • Copies of measures and materials used in the research project (although
be sure to consider any copyright issues). • Blank copies of information sheets and consent forms used in the project. • A copy of the research protocol reviewed by the Research Ethics
Committee (the protocol, not the entire form). • For qualitative research projects either a full example transcript, or a
343
SECTION 4
PROGRAMME MANUAL / 2019
section of transcript, annotated to illustrate the process of analysis should be included. This appendix might also include further descriptive detail about the analysis process that would typically be excluded from a research paper but might be needed to inform an examiner or other reader of the thesis.
2.6 A statement for the word count for each component of the thesis. Word
counts for the thesis abstract, literature review, research paper and final discussion paper should not include tables, figures and reference lists, and in total should not exceed 20,000 words. Word counts for tables, figures and reference lists should be calculated separately, and counted towards the appendix word count, which in total should also not exceed 20,000 words.
When the soft-bound LSRP is submitted, you must also submit a signed copy of the Research Supervisor’s Form and the Research Submission Form. These forms must not be bound into the thesis.
344
PROGRAMME MANUAL / 2019
SECTION 4
LARGE SCALE RESEARCH PROJECTS PROPOSALS Pre-proposal enquiry By the date indicated in the LSRP timetable, trainees must submit a pre-proposal enquiry to the Research Team. This is a short outline of their LSRP topic, possible questions, and possible supervisors. We would generally expect this document to be roughly 500 words, but trainees are free to write more or less, depending on how detailed their plans are at that stage. The research team will give formative feedback on these documents to help trainees to develop their ideas. Research ‘placement visit’ After the pre-proposal enquiry submission, but before the proposal deadline, trainees are responsible for convening a meeting between themselves, their proposed supervisors, and the Research Team. This meeting will be an opportunity to develop the ideas outlined in the pre-proposal enquiry and to negotiate the terms of the Supervision and Authorship Contract. The proposal By the date indicated in the LSRP timetable, trainees must submit a LSRP proposal to the Programme for consideration to ensure that the proposed project will meet the criteria for a LSRP (See Guidance on Large Scale Research Projects Section). Proposals should be discussed with your proposed supervisor(s) and approved by them. Proposals should be no longer than approximately 3,000 words (this is a guide only, you may need fewer or more) and should address each of the numbered points below. The important thing is that you communicate clearly the nature of your proposed project so that it can be fully assessed. These proposals MUST be completed and approved before any application for ethical approval is made. The material prepared for the LSRP proposal will provide a useful starting point for any ethics application, so it is not a wasted effort. As a result of this approval process, you may be asked to make amendments or to devise a new project proposal. On rare occasions, the Programme team may also seek a view from an external examiner. Once the details of the empirical research proposal are approved, any changes made will require checking with the research team. Changes to the focus of the literature review are more typical throughout an LSRP study, but again changes will need to be checked with the research team. The main reason for these checks is to ensure that the research and literature review will be relevant for a doctoral degree in clinical psychology. Trainees are encouraged to discuss ideas for LSRPs with the research team at an early stage, rather than just submitting a proposal. This helps to ensure that time is not wasted on unfeasible ideas and that the research team’s suggestions can be integrated at an early stage.
345
PROGRAMME MANUAL / 2019
SECTION 4
Please include your name at the beginning of the LSRP proposal. 1. Project title 2. Supervision (who will be a part of the supervision team, what roles will each
supervisor take on, and who will be nominated as the lead supervisor. The proposal needs to make it clear that you have sorted out all aspects of supervision needed to complete the proposed research). A copy of the signed LSRP Supervision and Authorship Contract should also be attached. NB Bangor University now requires all doctoral research to have a university member of staff on the supervision team. This would normally be one of the research team, or if more appropriate another programme team member, acting as ‘academic supervisor’
3. Background (a literature review outlining the key theoretical, methodological and clinical issues. No more than 1,500 words. Cite appropriate literature and include full references at the end of the proposal. End this section with a brief summary of how your proposed project builds on/extends existing research)
4. Research question (question(s) addressed, hypotheses if relevant, expected findings)
5. Overlap with previous assessments (state clearly the topics of your SRRP, DAP, and essays to show that there is no major overlap with these previous assessments)
6. Participant recruitment (who are they, numbers, sources, procedure for recruitment, have you got initial approval to access participants from relevant people?)
7. Design and Procedures (what is the overall design – linked to your research questions – and what essentially will participants be asked to do? Where will the research take place?)
8. Measures (include information about all data to be collected – including a brief list of demographic information to be gathered. Name each measure, include a source reference, and state in a single paragraph information about the previous use of the scale and its psychometric properties. If you have developed your own measure, describe in more detail how you have done this and include a full copy. For all non-standard measures, please include a copy in the Appendices)
9. Data management and analysis (how do you propose to store your data? what data analysis techniques will you use? How do you know that your proposed sample size is adequate)?
10. Diversity (explicitly discuss how you have addressed salient diversity issues in your choice of research question, methods and analysis approaches. Ideally, you will already have done all possible to address these issues in earlier proposal sections. This section is designed to make sure that you have done this and also to provide an opportunity for you to discuss relevant issues of which you are aware and that you feel cannot be adequately addressed within your study)
11. Proposed journals (specify the titles of the journals that you propose to use as the publication targets for your review and your research paper in the final thesis. A different journal is likely to be chosen for each paper to ensure a good match)
12. Ethical/Registration issues (what are the likely “problematic” aspects of the
346
PROGRAMME MANUAL / 2019
SECTION 4
proposal as far as ethical practices are concerned? How do you propose to deal with each of these? Which ethics committees will you need to make applications to? Which research governance procedures will you need to go through – with which NHS organisations?)
13. Feedback (how do you plan to feedback information about your study results to participants?)
14. Risk Assessment (briefly identify the potential risks to participants and to you as the researcher. Evaluate each risk and indicate how you will deal with each potentially significant risk. Common risks ought to be able to be dealt with using NHS policies – e.g., a lone worker policy. Please be explicit about the issues raised in this section. It is very important that you carefully consider all potential risks to yourself as researcher as well as to participants)
15. Data storage (Explain briefly how you will store the data during the course of the study to comply with Data Protection legislation. Also specify what happens to the data at the end of the project)
16. Financial information On the LSRP expenses form (Section 4 Page 126) provide a full budget of the costs associated with your proposal – include costs of measures/questionnaires, equipment required for purchase, participant payments, photocopying costs, postage costs, stationery costs etc. Additional guidance is included in the Programme Manual – Financial Resources for trainee – Research Projects – Section 4.
17. Literature Review: briefly describe the focus/question that you plan to address in the literature review paper. A literature review should focus in the same general area as the empirical paper, but the literature review does not serve as an introduction to your empirical paper. A literature review is a stand-alone piece of work. At this stage, there only needs to be one paragraph initial description and may change during your LSRP work
18. Timetable (a detailed – at least month by month - timetable from the present date to submission – include all relevant milestones e.g., research governance registration and review, ethical submission, pilot work, data collection, data analysis, writing up, literature review. Remember to allow for your holidays and potentially for periods when participants are also likely to be difficult to get hold of – such as during the Christmas and summer periods)
19. References (any key references cited should be listed) 20. Appendices (include copies of measures or any other supporting documentation
that you feel is useful in assessing your proposal)
A copy of your proposal must be emailed to the Admin Assistant (Research, Finance & Selection), copying in your supervisor, by the deadline date. The Research Team will then review your proposal and request amendments or further information where appropriate. Once the Research Team are happy with your proposal, to finalise approval, a copy of the LSRP proposal containing the ‘Research Supervision Agreement’ must be submitted to the Admin Assistant (Research & Finance). Both the trainee and supervisor MUST sign and date the document (including authorship). E-mail submission of a scanned copy of the signed and dated proposal is acceptable.
347
SECTION 4
PROGRAMME MANUAL / 2019
LARGE SCALE RESEARCH PROJECTS PROGRESS REPORTS By the dates indicated in the key dates document, trainees must submit an LSRP progress report to the Programme. This does not need to be overly long, but should address the following numbered headings: 1. Progress (have you managed to adhere to your timetable milestones? If not, please
explain why and also provide a revised timetable showing new milestones up to completion)
2. Problems/Changes to Project (describe problems/difficulties that have arisen and
indicate how you have resolved them or plan to resolve them. Any major changes to the project should already have been approved by the research team, but please also include reference to them in this section)
3. Supervisors’ comments (please ask your supervisor to write any comments that they
feel are useful. If no additional comments are necessary, please state “none”) Trainees must include the following at the beginning of the Report:
• Correct version of Report (e.g. 1st Draft, 2nd Draft etc.) • Submission date • Project title • Full name of Supervisor/s
An emailed progress report, copied to all supervisors must be submitted to the Administrative Assistant (Research, Finance & Selection) by the specified date.
348

SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH PROJECTS USING QUALITATIVE RESEARCH METHODOLOGY: ASSESSMENT ISSUES
Introduction The aim of qualitative research is to analyse the experiences, perceptions, interpretations and actions of people; in other words, to capture their ‘lived experiences’. Qualitative methods describe and analyse their subject matter using ordinary language. Traditionally there has been a debate between proponents of qualitative methods and quantitative methods as to the value of each approach. This distinction sometimes obscures a more central distinction between two different epistemologies or approaches to knowledge. These are essentially at one extreme an epistemology which embraces the scientific method and the notion of an ‘objective truth’ that can be measured and analysed, and at the other extreme, an epistemology that calls into question the basic tenets of science, the concept of objective truth, and emphasises the social constructional nature of much that is currently regarded by the scientific community as factual (the 'social constructionist' approach). In keeping with the overall Programme Aims and Objectives, qualitative methods are appropriate for clinical psychology trainee projects in the same way as quantitative methods. When selecting which method to use, the important question is the match between the research goal and the analytic approach. In other words, the choice of methodology needs to be able to answer the research question in the best possible way. Furthermore, the same high standards that apply to the evaluation of quantitative projects will be applied to qualitative research. In the absence of the availability of appropriate supervision for any piece of research, including qualitative studies, trainees will be asked to develop amended research proposals. In terms of basic guidance about quality standards for research projects using qualitative methods, the following guidelines apply: Setting the Scene The research project should specify where the study fits within relevant literature and state the intended purposes or questions of the study. In particular the trainee should outline why the particular qualitative methodology used in the research project is felt to be appropriate or responsive to the intended purposes or questions of the study. Could another methodology have addressed the issue better? Trainees need to consider their own perspective and where they feel they and their question fit within the objectivist-constructivist continuum. Specify the methods used Methods and procedures should be specified clearly so that readers may see how to conduct a similar study themselves, and may judge for themselves how well the reported study was carried out. It is not sufficient to simply state for example that “grounded theory was used to analyse the transcripts”. Trainees should report all procedures for gathering data, including specific questions posed to participants.
349
SECTION 4
PROGRAMME MANUAL / 2019
Ways of organising the data and methods of analysis should be specified in sufficient detail to assist readers in understanding and appraising the researchers' descriptive reports about the form of experience or action under study. Situating the sample Trainees should describe the research participants and their circumstances to aid readers in judging how typical the data and findings might be. In particular, consideration should be given to whether the participants chosen were unusual in some important way. Owning one's perspective When using qualitative methods, trainees need to specify their theoretical and personal anticipations, both as known in advance and as they become apparent during the research. Trainees should attempt to recognise their values, interests and assumptions and to explicitly discuss their relation to the study’s findings. This disclosure of values and assumptions helps readers to interpret the researcher's data and findings, and to consider possible alternatives. In particular, any speculation on the part of the trainee should be clearly identified as speculation. Grounding in examples Trainees should illustrate analytic procedures, data and findings with examples. The examples allow appraisal of the fit between data and findings and allow readers to perceive possible alternative meanings and understandings. Are quotations, field notes, etc. identified in a way that enables thereafter to judge the range of evidence being used? Providing credibility checks In the field of qualitative research, investigators may use any of a number of methods for checking the credibility of their categories, themes or accounts as descriptions of the phenomenon. Where relevant, these may include (1) checking these findings with the original informants or others similar to them; (2) using multiple qualitative analysts, an additional analytic ‘auditor’, or the original analyst for a ‘verification step’ of reviewing the data for discrepancies, overstatements, or errors; (3) comparing multiple, varied qualitative perspectives, or (4) where appropriate, comparison or contrast with quantitative data (e.g., in a mixed methods approach). Awareness of the research focus It is important that the trainee shows an understanding of the focus of the research. In particular the trainee should be aware of limitations to generalisability in terms of context and information available. Where a general understanding of a phenomenon is intended, data and findings are based on an appropriate range of instances (informants or situations) should be included. Where understanding one instance or case is the goal, this should be clearly stated and the trainee should strive to describe the single instance systematically and comprehensively enough to provide the reader with a basis for attaining that understanding.
350
SECTION 4
PROGRAMME MANUAL / 2019
Are the results credible and appropriate? Do the results address the research question(s)? Are they plausible and coherent? Are they important, either theoretically or practically, or trivial?
351
SECTION 4
PROGRAMME MANUAL / 2019
SAMPLE RESEARCH SUPERVISION AGREEMENT: LSRP This agreement MUST be attached to the LSRP proposal when submitted NOTE – THIS IS A SAMPLE FRAMEWORK ONLY. YOU SHOULD OBTAIN AN ELECTRONIC VERSION OF THIS DOCUMENT AND ADAPT IT FOR YOUR SPECIFIC NEEDS. THE SUPERVISION CONTRACT STATED HERE IS THE RECOMMENDED MINIMUM ONLY AND YOU SHOULD CLARIFY THIS WITH YOUR SUPERVISORS. YOU SHOULD ALSO SPECIFY AUTHORSHIP ORDER AT THIS POINT. TRAINEE AND SUPERVISORS’ NAMES SHOULD BE INSERTED IN THE SPACES INDICATED BY SQUARE BRACKETS. DELETE THIS INSTRUCTION PARAGRAPH FROM YOUR PERSONALISED AGREEMENT. Research Supervisor: ________________________________ Trainee: ________________________________ This agreement is between:
SUPERVISOR(S): ________________________________ JOB TITLE(S): ________________________________ PLACE(S) OF WORK: ________________________________ TRAINEE: ________________________________
The purpose of the agreement is to ensure co-operation from both parties toward the completion of [the trainee’s] large-scale research project. It is accepted that the primary responsibility for completion of the project lies with [the trainee]. [The research supervisor] and [the trainee] agree to meet at least fortnightly or monthly in the initial stages of the research. However, during the period of data collection, it is accepted that meetings may be less frequent. Contact during this period will be maintained by e-mail or phone, but there should be no more than four weeks without a joint meeting. Summaries of these meetings will be circulated by email by the trainee. It is expected that [the trainee] will endeavour to meet the tasks and deadlines as agreed together with [the supervisor] and the Programme. In particular [the trainee] will submit to the supervisor(s), a near-final draft of the thesis by early May of the third year [actual date to be agreed and entered here]. [The supervisor(s)] will endeavour to read and comment on drafts and other contributions without undue delay. In the event of a delay of more than 3 weeks, [the supervisor] will contact [the trainee] and agree a date by which feedback will be provided.
352
SECTION 4
PROGRAMME MANUAL / 2019
Authorship: Trainees and supervisors are encouraged to refer to the latest version of the APA publication manual for guidance on authorship, but the following principles should be applied:
1. Trainees and supervisors will be authors on the paper. Priority will be agreed by negotiation.
2. Other collaborators on the project will normally appear after the trainee and the supervisors.
3. Trainees and supervisors and other authors must agree the content of any paper which is submitted for publication.
I confirm that I approve the attached LSRP proposal. Signed: ________________________________ Date: ___________________ (RESEARCH SUPERVISOR) Signed: ________________________________ Date: ___________________ (TRAINEE) Signed: ________________________________ Date:___________________ (NWCPP RESEARCH TEAM)
353
SECTION 4
PROGRAMME MANUAL / 2019
FINANCIAL RESOURCES FOR LARGE SCALE RESEARCH PROJECTS The NWCPP team is well aware of the difficulties that the funding of research projects can precipitate in today's NHS, and the following guidelines are intended to make clear to trainees and supervisors how the programme can help with the financial support for research projects. The costs of running LSRPs are normally fully covered by NWCPP, subject to approval by the Programme Team. All trainees must provide a full and detailed set of costs in their written LSRP proposals on the form provided. Day-to-day running expenses would be met through the use of the normal mechanisms supporting trainees' studies. For example, photocopying should be completed using the NWCPP copier, stationary should be ordered from the programme office, postage should go through the normal School of Psychology system (note that return postage costs would normally be organised through the Programme's business reply service), and travel expenses can be claimed in the usual way. The preceding items should be included in LSRP proposal Finance Sections, but all other items must be justified clearly in the LSRP research proposal. Reasonable requests to cover purchase of essential copyright measures and other small items of equipment not already possessed by the programme will normally be met. The research team, as a part of the LSRP approval process, will approve day-to-day running expenses and other typical expenses. Trainees may also make a request to use items of equipment already possessed by NWCPP and approval for this will normally be granted. Any unusual or expensive items or services required to support a LSRP study may also be requested by trainees and must be justified in detail in LSRP proposals. All such requests will be considered by the NWCPP Programme Team at their monthly meeting. Decisions will be taken on a case-by-case basis but the general principle adopted by the programme is that we will do our best to meet the costs of all reasonable requests essential to an LSRP, or to come to a compromise position. Trainees are encouraged to discuss such requests with the Research Team early in the LSRP process. NWCPP does not pay for research supervisors' time. Where a trainee requires expert supervision for a part of their LSRP, and such support cannot be provided locally, trainees may request these costs from the programme using the mechanism described above. There is no guarantee that such a request would be granted and it would be very unusual for requests for external supervision to be supported. Training in the use of measures/techniques (e.g., a specialist data analysis technique, training in a specialised measure) would normally be viewed more positively but trainees would be expected to propose using their Study Leave budget (see Programme Administration Manual) for such training.
354
SECTION 4
PROGRAMME MANUAL / 2019
Participant Expenses • Participant payments should be incorporated into your LSRP proposal as part of
your costing. • The preferred method for paying participants is through the form of vouchers
that can be purchased online (e.g. Amazon, Love to Shop). • Contact the Admin Assistant (Research & Finance) to make any purchases for
vouchers, which will be checked against your financial costings from your LSRP proposal.
Ordering Equipment, Test Materials and Consumables When ordering equipment, test materials or consumables in relation to your LSRP, all requests must be sent by email to the Admin Assistant (Research & Finance) to provide sufficient notice. This will be checked against your financial costings from your LSRP proposal. Furthermore:
• When ordering test materials, it is your responsibility to contact the relevant test company to establish the correct costs and ISBN numbers of the test materials you would like to purchase, and then forward these to the Admin Assistant (Research & Finance) with a request to order them.
• A freepost address for research purposes is available from the Admin Assistant (Research & Finance) at the admin office.
• An electronic letterhead is available upon request to the Admin Assistant (Research & Finance)
• Any purchases required for your LSRP project must be made through the Admin Assistant (Research & Finance). Do not make purchases yourself, as the Finance Office will not reimburse you. Purchases will only be processed once they have been checked against your financial costings in your LSRP proposal.
355
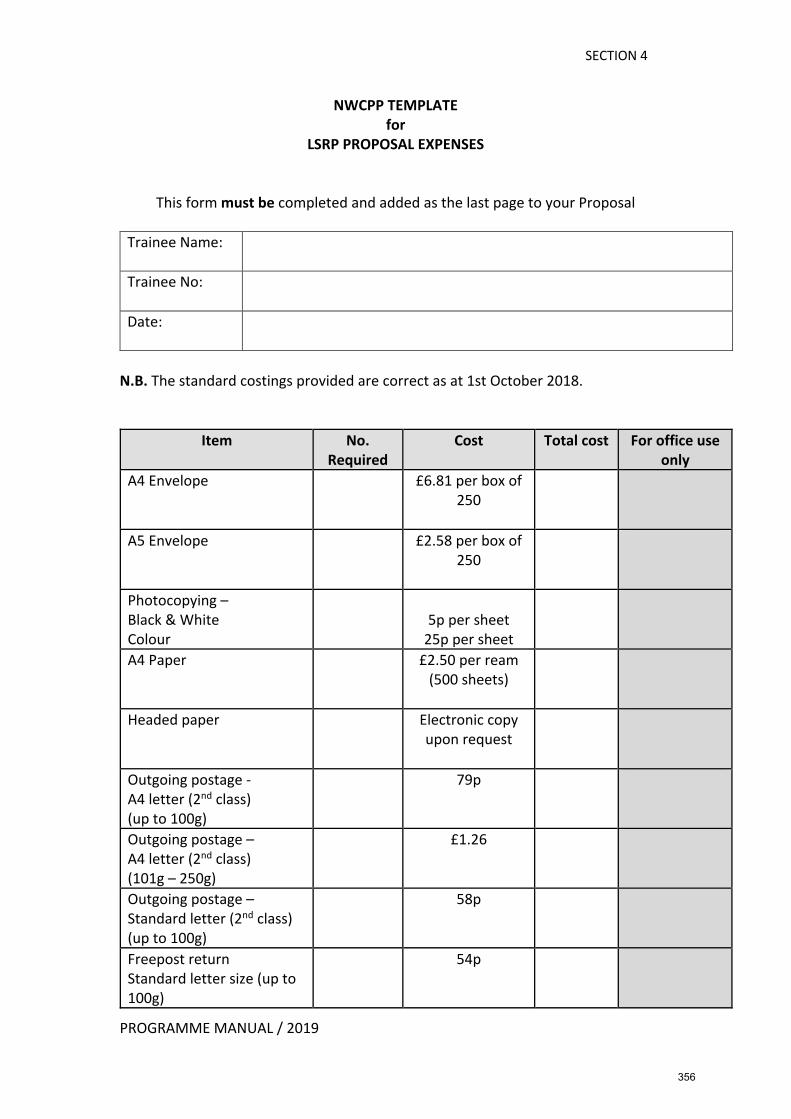
SECTION 4
PROGRAMME MANUAL / 2019
NWCPP TEMPLATE for
LSRP PROPOSAL EXPENSES
This form must be completed and added as the last page to your Proposal
Trainee Name:
Trainee No:
Date:
N.B. The standard costings provided are correct as at 1st October 2018.
Item No. Required
Cost Total cost For office use only
A4 Envelope £6.81 per box of 250
A5 Envelope £2.58 per box of 250
Photocopying – Black & White Colour
5p per sheet
25p per sheet
A4 Paper £2.50 per ream (500 sheets)
Headed paper Electronic copy upon request
Outgoing postage - A4 letter (2nd class) (up to 100g)
79p
Outgoing postage – A4 letter (2nd class) (101g – 250g)
£1.26
Outgoing postage – Standard letter (2nd class) (up to 100g)
58p
Freepost return Standard letter size (up to 100g)
54p
356
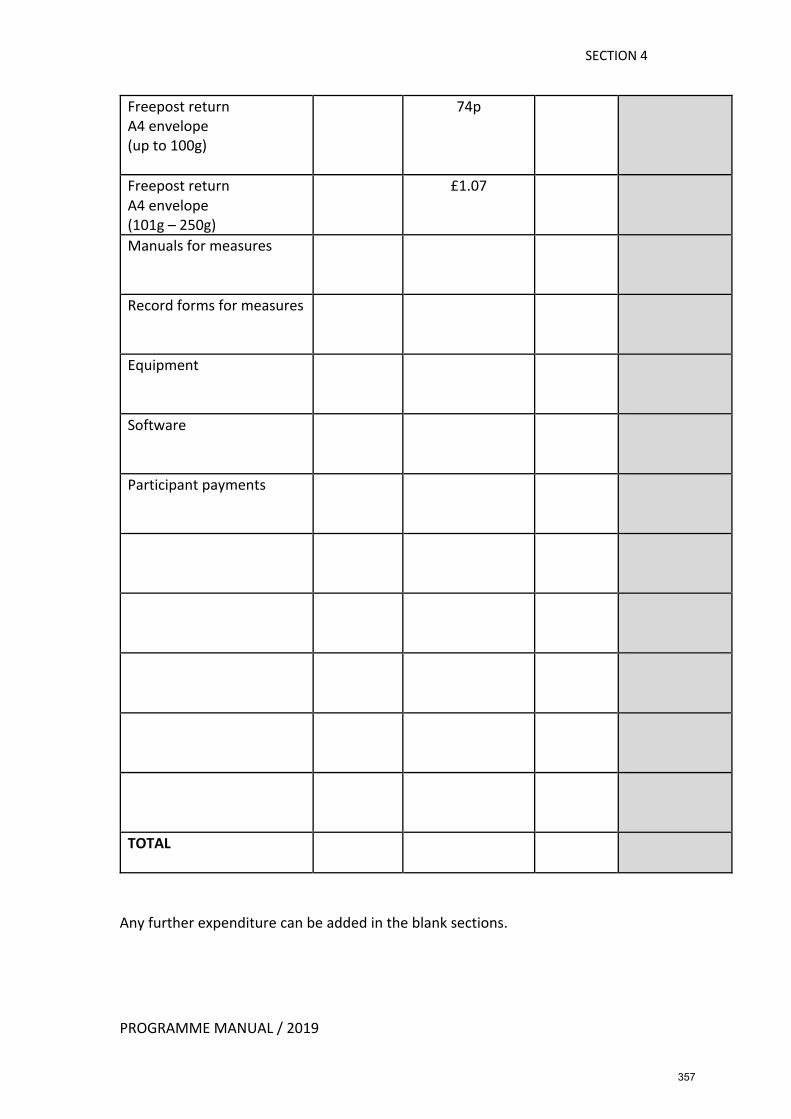
SECTION 4
PROGRAMME MANUAL / 2019
Freepost return A4 envelope (up to 100g)
74p
Freepost return A4 envelope (101g – 250g)
£1.07
Manuals for measures
Record forms for measures
Equipment
Software
Participant payments
TOTAL
Any further expenditure can be added in the blank sections.
357
SECTION 4
PROGRAMME MANUAL / 2019
DATA STORAGE POLICY During and after all research studies, trainees have an individual responsibility to adhere to the latest Data Protection legislation. Data (including hard copies and electronic files) collected for the SRRP should normally be stored after the study is completed at a clinical base associated with the project. Data from LSRPs would also normally be stored at a clinical base after completion of the project when the main supervisor is a local NHS employee and data were gathered using NHS resources. Where the main supervisor is University based, data would normally be stored at the University by the supervisor after the project is completed. Where neither an NHS or University supervisor has a suitable storage facility, data must be prepared for storage in the Programme archive and clearly marked with a date for destruction. Data storage must conform to ethical procedures, particularly any statement about data storage included in an ethics application or information given to research participants. Thus, where it has been stated that data are to be destroyed at a certain point, trainees must ensure that this is carried out. Where data are to be stored without identifying information, this must be achieved with appropriate care. Research Supervisors should be named as custodians of data. A normal expectation is that data used in published research, where this does not infringe participants’ rights, should be available for scrutiny up to five years after a paper is published. Where trainees do not have an appropriate clinical base at which to store research data, on no account should they store data at their home. Appropriate arrangements should be made to store data either at a supervisor’s University base or in the Programme archive. Note that for many projects where data has been fully entered into an electronic anonymised file, it may be possible to destroy raw data (copies of completed questionnaires or audio recordings of interviews, for example) as soon as trainees have been awarded their DClinPsy.
358
PROGRAMME MANUAL / 2019
SECTION 4
SUBMITTING YOUR THESIS As part of the submission process for your thesis, you are required to complete a ‘Final Award Check’ available here https://apps.bangor.ac.uk/student/sd1/. Once you have successfully completed the award checks you will be able to submit your document. If you are unable to complete any section of the form and/or have any queries about the checks, please email [email protected]. The on-line form must be submitted at least 10 days but no more than 28 days before your thesis submission deadline. The thesis title is required on the ‘Final Award Check’ form and cannot be amended once the form has been submitted. The ‘Final Award Check’ is where the University’s central Student Administration Office check the following before confirming that students are eligible to submit their thesis: • All library books have been returned • All matriculation requirements have been met (you will have met this requirement) • All financial accounts have been paid (you do not pay tuition fees) • Any additional submission fees are paid (this only applies when a student is re-
submitting the thesis) • Establish if a student upon successful completion of their course wishes to attend a
graduation ceremony or graduate ‘in absentia’. Graduation ceremonies now take place twice a year, in December and July. You will be invited to attend the ceremony closest in date to when your award is finalised.
If you have failed to comply with any of the above requirements the Student Administration Office will be in touch to advise you what is required. The University’s Awards Office will not issue your final award until all the requirements have been met. Detailed guidance on how the thesis should be submitted, including the declaration that should be included in your thesis, is available on the Doctoral School website: https://www.bangor.ac.uk/library/copyright/esubmission.php.en For the purpose of examination, a candidate shall submit the following to the Programme Manager on or before your deadline date:
Two soft bound copies of the thesis containing; • a summary of up to 300 words • a signed declaration as specified in the guidance on the Doctoral School website • an electronic copy (to [email protected]) of the thesis, in a
structure and format that is exactly the same as the printed version. Two other forms, the Research Submission Form and the Research Supervisors Form (one to be completed and signed by the trainee, the other for the supervisor to complete and sign) are also handed in with the thesis (not to be included in the body of the soft-bound thesis).
359
PROGRAMME MANUAL / 2019
SECTION 4
Except with the permission of the Examining Board a candidate may not amend, add to or delete from the thesis after it has been submitted. For details of where LSRPs are bound, these are: https://www.bangor.ac.uk/itservices/thesis-printing-binding.php.en Printing and Binding Unit Bangor University Nantlle, Normal Site Bangor Gwynedd, LL57 2PZ Email: [email protected] Tel: 01248 383997
360
SECTION 4
PROGRAMME MANUAL / 2019
AFTER SUBMISSION
Electronic Copies of LSRP Documents After submitting your soft-bound paper copies of your LSRP, please email the Admin Assistant (Curriculum & Clinical) [email protected] with copies of your Empirical Paper, Review Paper, Paper 3, and appendices.
The Viva Voce After submission, two soft-bound theses are forwarded to the Internal and External examiners for them to review in time for the trainee’s viva. The vivas are attended by an External Examiner, Internal Examiner and a Chair. The Chair is there to oversee the procedure and will not usually ask any questions. During the viva, the trainee is asked to comment on various aspects of their thesis concerning points of interest to the examiners. Vivas usually take approximately 45 minutes. You will then be asked to leave the room for a few minutes while the Examiners decide on the outcome. There are several recommendations that the Examiners can make from simply being approved for the degree to having to resubmit. The recommendation given will be fully explained to you. If there are any amendments, a list will be supplied by the Examiners.
E- thesis final submission to the Library (PURE) Upon successful completion of the viva and once any amendments to the thesis that were required have been accepted and approved by the Internal Examiner, a final version of the thesis should be submitted to the Library in e-version only.
Please see here for detailed information on guidance on how to submit your e-thesis:
https://www.bangor.ac.uk/research-innovation-and-impact- office/pure.php.en#gettinghelp
https://www.bangor.ac.uk/doctoral-school/
Further details on this system will also be provided by the Research Team.
A hard-bound copy of the thesis is not required for University purposes; however, you may wish to purchase a hard-bound copy for yourself:
For details of where LSRPs are bound, these are: https://www.bangor.ac.uk/itservices/thesis-printing-binding.php.en
Printing and Binding Unit Bangor University Nantlle, Normal Site Bangor Gwynedd, LL57 2PZ Email: [email protected] Tel: 01248 383997
361
SECTION 4
PROGRAMME MANUAL / 2019
In addition to submitting your e-thesis to the Library, you are also required to do the following:
• If you were issued with a Safestick by the Programme for your thesis data, then this
must be returned to the Programme Manager. • If your thesis data is not being stored on the Safestick, then you must email the
Programme Manager to confirm where your thesis data will be stored (normally at the clinical base with your Supervisor).
• NHS Ethics End of Study confirmation must be submitted to the Programme Manager (where applicable)
• Return any trainee equipment to the Admin’ Office
Only once all the above have been completed will we be able to confirm the successful completion of the DClinPsy programme with the University and the HCPC. Report Forms (completed by the examiners during the viva and copied to you) are sent to the University’s Awards Office following the September Board of Examiners meeting in order to register the trainee’s successful completion of the Programme. The HCPC are also notified of trainees’ successful completion following the September Board of Examiners meeting. The HCPC can take up to 10 working days to update their records. Only when the HCPC have updated their records should trainees apply for HCPC registration. The University’s Awards Office will issue your final DClinPsy certificate and you will be contacted regarding the Graduation Ceremony in due course.
Presentation of LSRP Findings at NWCPP Annual Stakeholders Meeting It is a Programme requirement that trainees present their LSRP findings at this meeting. You will need to prepare a 10-15-minute PowerPoint presentation of your empirical paper, in a format accessible to a ‘general’ clinical audience. Trainees are provided with a conference/meeting dates list at the beginning of the academic year.
362
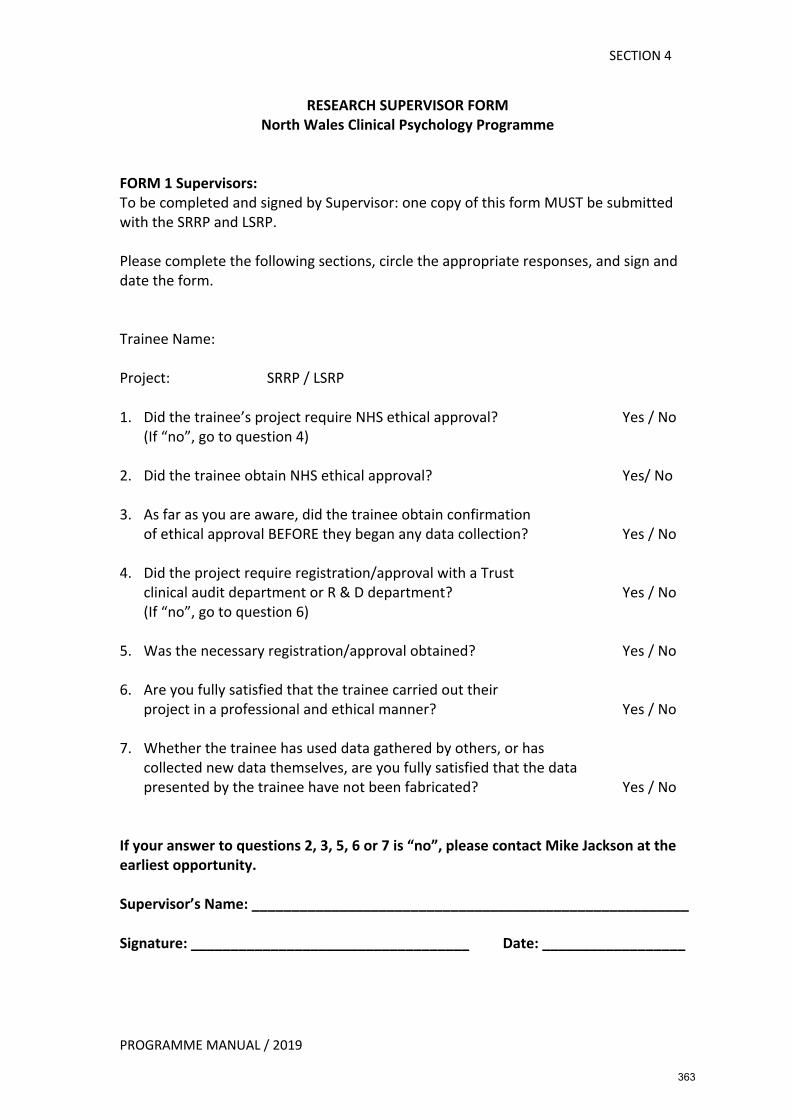
SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH SUPERVISOR FORM North Wales Clinical Psychology Programme
FORM 1 Supervisors: To be completed and signed by Supervisor: one copy of this form MUST be submitted with the SRRP and LSRP. Please complete the following sections, circle the appropriate responses, and sign and date the form. Trainee Name: Project: SRRP / LSRP 1. Did the trainee’s project require NHS ethical approval? Yes / No
(If “no”, go to question 4) 2. Did the trainee obtain NHS ethical approval? Yes/ No 3. As far as you are aware, did the trainee obtain confirmation
of ethical approval BEFORE they began any data collection? Yes / No 4. Did the project require registration/approval with a Trust
clinical audit department or R & D department? Yes / No (If “no”, go to question 6)
5. Was the necessary registration/approval obtained? Yes / No 6. Are you fully satisfied that the trainee carried out their
project in a professional and ethical manner? Yes / No 7. Whether the trainee has used data gathered by others, or has
collected new data themselves, are you fully satisfied that the data presented by the trainee have not been fabricated? Yes / No
If your answer to questions 2, 3, 5, 6 or 7 is “no”, please contact Mike Jackson at the earliest opportunity. Supervisor’s Name: _______________________________________________________ Signature: ___________________________________ Date: __________________
363
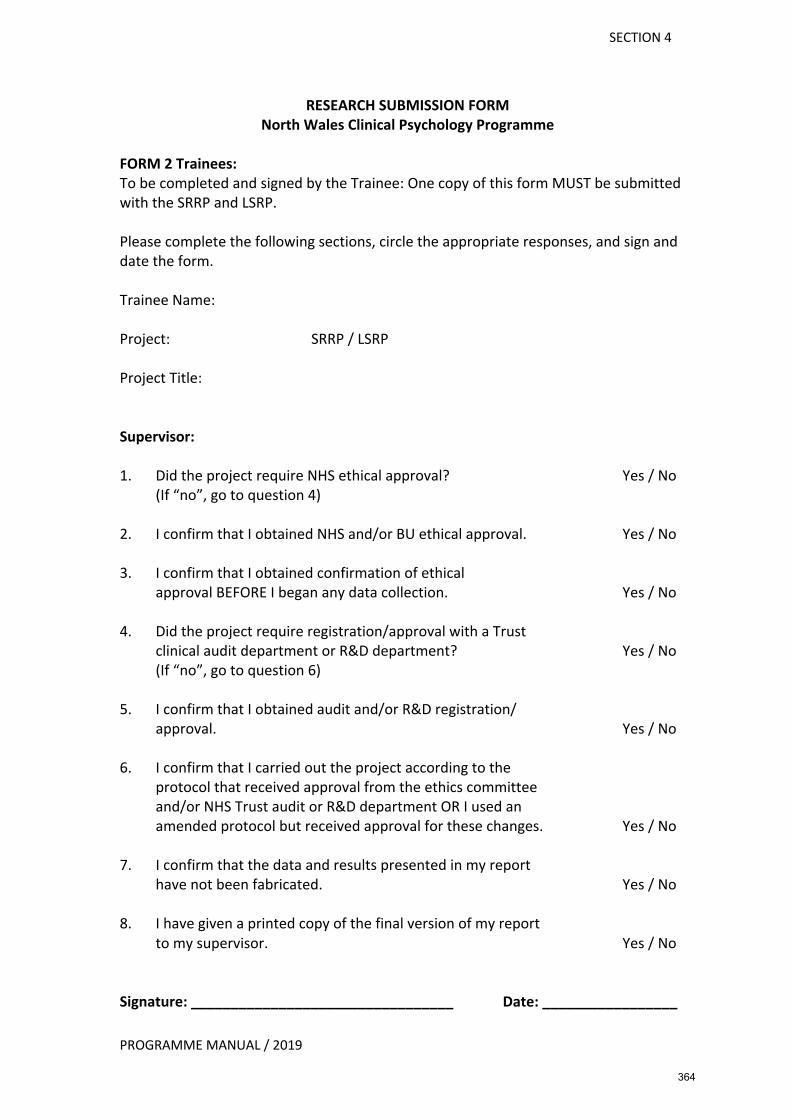
SECTION 4
PROGRAMME MANUAL / 2019
RESEARCH SUBMISSION FORM North Wales Clinical Psychology Programme
FORM 2 Trainees: To be completed and signed by the Trainee: One copy of this form MUST be submitted with the SRRP and LSRP. Please complete the following sections, circle the appropriate responses, and sign and date the form. Trainee Name: Project: SRRP / LSRP Project Title: Supervisor: 1. Did the project require NHS ethical approval? Yes / No
(If “no”, go to question 4) 2. I confirm that I obtained NHS and/or BU ethical approval. Yes / No 3. I confirm that I obtained confirmation of ethical
approval BEFORE I began any data collection. Yes / No 4. Did the project require registration/approval with a Trust
clinical audit department or R&D department? Yes / No (If “no”, go to question 6)
5. I confirm that I obtained audit and/or R&D registration/
approval. Yes / No 6. I confirm that I carried out the project according to the
protocol that received approval from the ethics committee and/or NHS Trust audit or R&D department OR I used an amended protocol but received approval for these changes. Yes / No
7. I confirm that the data and results presented in my report
have not been fabricated. Yes / No 8. I have given a printed copy of the final version of my report
to my supervisor. Yes / No Signature: _________________________________ Date: _________________
364

SECTION 4
PROGRAMME MANUAL / 2019
GUIDELINES ON WRITING-UP ADVANCED CLINICAL REPORT Assessment Each assignment will be marked independently by two internal assessors, appointed by the Board of Examiners, and be subject to moderation by an External Examiner. Marking guidelines follow that highlight the learning outcomes assessed for this assignment. Introduction The ACR is a Part II coursework requirement and is designed to reflect developments within the Bangor Clinical Psychology Programme, and more widely within the field of Clinical Psychology, focusing in particular on Reflective Practice. Consequently, it will provide Trainees an opportunity, immediately prior to qualification, to demonstrate mature, reflective ‘high level’ clinical thinking in at least one of the following areas.
• Reflective practice • Process issues • Personal and professional development • Systemic thinking
There is considerable overlap in these areas and it is proposed that Trainees, irrespective of the area discussed, will be required to demonstrate knowledge of reflective practice. In particular candidates will be encouraged to consider how personal issues may impact on clinical practice. Assignment Questions Trainees are required to answer one of the following questions: 1. Consider one or more of the cases you have been involved with during your clinical
training. Critically reflect on this work with reference to at least two of the following: (i) process issues; (ii) systemic influences; (iii) you as a Reflective Practitioner, and, (iv) your development as a clinician at the time. With the benefit of reflection consider things you did well and things you would change?
2. You are soon to embark on a career as a Qualified Clinical Psychologist. Using examples from throughout your training, outline what you consider to be your strengths and weaknesses as a clinician. How have these developed during training, and what do you think your CPD needs are for the first two years post qualification?
3. What have you found to be the more and less challenging aspects of clinical practice, focusing particularly on direct work with clients? Consider these experiences in light of your development as a Reflective Practitioner.
4. Choose a clinical model that you are particularly interested in. Implement this model in one or more areas of your life for a minimum of four weeks. Outline why you have chosen the particular model, and reflect on your experiences both from a practical and a personal perspective. What impact will this exercise have on your clinical practice in the future?
5. Do you know someone in your personal life that has experienced similar difficulties to that of one (or more) of your clients? Consider how the experiences gained through your relationship with that individual have impacted on your work with relevant clients. If applicable, also consider how your clinical training has impacted on this area of your personal life. (Examples suitable for this assignment would include: a sibling
365
SECTION 4
PROGRAMME MANUAL / 2019
with a learning disability; a family member with a significant mental health difficulty or dementia; a sibling/child with a developmental disorder.)
6. Complete a confidential clinical log for at least six months. Discuss the following: (i) advantages and disadvantages of this exercise, (ii) benefits to your clinical practice, and, (iii) how this has helped/hindered your development as a Reflective Practitioner.
Please note: Although personal reflection is required during the ACR, it is neither necessary nor expected that Trainees share information of a very personal, sensitive or confidential nature. In terms of confidentiality the ACR will be treated in the same way as other course work/presentations undertaken during training. Format In line with other coursework requirements the ACR is a written assignment, between 3,000 and 5,000 words, excluding the abstract (not more than 200 words), appendices and reference list, but including all words in Figures, Tables and text boxes. Further, the report should be able to be read without excessive reference to appendices. Advice on Structure Trainees will not be provided a predetermined structure for the ACR, as is the case with the Report of Clinical Activity. Instead there will be an expectation that the candidate devise a structure that allows the chosen assignment to be appropriately addressed. Trainees will be encouraged to discuss all aspects of the ACR (e.g., structure, content, issues relating to confidentiality) with their Training Coordinator well in advance of the deadline. Given sufficient notice the Training Coordinator will also provide feedback on a written draft. The guidelines concerning confidentiality in Reports of Clinical Activity will also apply to the ACR. Given that this assignment is not designed to examine the candidate’s professional communication skills, inclusion of reports and letters is not mandatory. However, such material can be included if the candidate believes this to be appropriate to answering the chosen assignment. Assignment Failure At present a failed assignment will likely fall into one of the following categories:
1. An assignment that violates the word limit. 2. An assignment which fails to address the chosen assignment 3. Work of insufficient quality, i.e., that which contains superficial consideration of
topics, or which does not provide evidence of a sufficient level of critical thinking. Work with excessive typographical errors, errors in referencing, a small number of under developed points/issues may be required to be corrected. Failed assignments will need to be resubmitted and awarded a pass grade prior to graduation. Where necessary a resubmission date will be negotiated with the Trainee. A fail grade on the ACR will be treated as any other course work failure (including substantive failure as the result of identifiers), and consequently may contribute to a Trainee’s overall failure (as outlined in the Programme Manual).
366
PROGRAMME MANUAL / 2019
SECTION 4
GUIDELINES FOR ASSESSORS MARKING ADVANCED CLINICAL REPORTS Learning Outcomes assessed As trainees choose their own titles for assignments not all of the learning objectives below may be relevant to any particular assignment. Markers are encouraged to use their judgement and only assess those learning outcomes relevant to the submitted assignment.
Generalisable Meta-Competencies • Being familiar with theoretical frameworks, the evidence base and practice
guidance frameworks such as NICE and SIGN, and having the capacity to critically utilise these in complex clinical decision making without being formulaic in application
• Exercising personal responsibility and largely autonomous initiative in complex and unpredictable situations in professional practice
• Demonstrating self-awareness and sensitivity, and working as a reflective practitioner within ethical and professional practice frameworks
Psychological Formulation • Using assessment to develop formulations, which are informed by theory and
evidence about relevant individual, systemic, cultural and biological factors
Psychological Intervention • Conducting interventions in a way, which promotes recovery of personal and
social functioning as informed by service user values and goals
Evaluation • Capacity to evaluate processes and outcomes at the organisational and
systemic levels as well as the individual level
Personal and Professional Skills and Values • Understanding the impact of differences, diversity and social inequalities on
people’s lives, and their implications for working practices • Understanding the impact of one’s own value base upon clinical practice • Managing own personal learning needs and developing strategies for
meeting these. Using supervision to reflect on practice, and making appropriate use of feedback received
Organisational and Systemic Influence and Leadership • Capacity to adapt practice to different organisational contexts for service
delivery. This should include a variety of settings such as in-patient and community, primary, secondary and tertiary care and may include work with providers outside of the NHS
• Understanding of leadership theories and models, and their application to service development and delivery. Demonstrating leadership qualities such as being aware of and working with interpersonal processes, proactivity,
367

PROGRAMME MANUAL / 2019
SECTION 4
influencing the psychological mindedness of teams and organisations, contributing to and fostering collaborative working practices within teams
• Understanding of change processes in service delivery systems
368
SECTION 4
PROGRAMME MANUAL / 2019
SEEKING ADVICE ON THE ADVANCED CLINICAL REPORT AND THE STATUS OF ADVICE Trainees are advised to begin thinking about the ACR as early as possible, and are strongly advised not to leave preparation until after the thesis is completed. The scope of this report is potentially very broad, drawing on experiences from all placements, and focusing on Reflective Practice. At the outset trainees should also familiarise themselves with the marking guidelines. It is suggested that an initial meeting with the Training Coordinator is arranged to discuss choice of question and consider initial ideas about content. Trainees may then wish to formulate their ideas more clearly and discuss these again with the Training Coordinator to get feedback on the general direction and content of the report. Throughout this process Trainees may be advised to discuss their ideas with other members of the Programme Team. Trainees are clearly at liberty to discuss the ACR with past or present placement Supervisors. However, depending on the scope and breadth of the proposed content, any Supervisor may be more or less familiar with certain client related issues in the report. Given sufficient time, Training Coordinators will provide feedback on a draft manuscript of the ACR. As with other assignments, there is little point in handing in an incomplete draft. Trainees should allow sufficient time before the deadline to incorporate any feedback. As with other pieces of course work, advice incorporated from Training Coordinators will not guarantee that the assessors will pass the ACR. The aim of their advice is to help you improve the Report and as such they are formative comments and not an assessment procedure. The process of assessing your work is independent from the process of helping you develop it.
369
SECTION 4
PROGRAMME MANUAL / 2019
ASSIGNMENT FEEDBACK FORM Trainees MUST provide their Supervisor(s) with a copy of the completed feedback form. The assessor completing the feedback form (assessors should agree this between them) should do so following consultation with the second assessor. The completed form along with the marked assignments and the completed mark sheet should be returned to the Programme Manager NOT the trainee.
Trainee Number: Type of Assignment: Advanced Clinical Report - ACR Specialism:
Assignment strengths:
Areas for improvement:
General comments (optional):
Marked and agreed by:
FIRST ASSESSOR SECOND ASSESSOR Name:
Name:
Date:
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
370
SECTION 5
ASSESSMENT PROCEDURES AND
UNIVERSITY REGULATIONS
371
SECTION 5
PROGRAMME MANUAL / 2019
BANGOR UNIVERSITY THE DOCTOR OF CLINICAL PSYCHOLOGY
ASSESSMENT PROCEDURES 1. Overview 1.1 The aim of these Procedures is to describe the evaluation of academic, research and
clinical competence on the Doctor of Clinical Psychology Programme. Unless exempted from any assessment under appropriate sections of the Regulations for Postgraduate Research Programmes, candidates will be required to demonstrate their competence in academic, research and clinical work by completing eleven assignments during the course of the three years. These will consist of: • Three academic assignments (spread over the first two years, as described in the
latest Programme Manual). • Four Reports of Clinical Activity (RCA) (one from each of four areas of clinical
experience, usually undertaken in years 1 and 2). • One Service Related Research Project (SRRP). • One Database Analysis Project (DAP). • One Advanced Clinical Report (ACR). • One Report of a Large-Scale Research Project (LSRP).
1.2 Candidates will be required to choose topics for academic assignments, research
assignments and RCAs, which, between them, cover a range of types of problem or procedures, in accord with the Programme’s policy on Breadth of Experience Reflected in Assignments. Across all types of work, the trainees must demonstrate awareness of and competence in professional and ethical issues and practice. Clinical competence will additionally be assessed using the Evaluation of Clinical and Professional Competence Forms.
2. Part I 2.1 Academic
• This will be assessed by the submission of three pieces of assessed course work in three different areas of clinical psychology.
• Each assignment must be prepared and submitted in accordance with the latest guidelines contained within the Programme Manual.
• The topic for each assignment must be approved by the Chair of the Examining Board.
• All candidates shall be informed in writing by the Programme, at the beginning of the relevant session, of the deadlines for the submission of all assignments.
• Assignments, which exceed the word limit, or do not follow the prescribed presentation style, may result, at the discretion of the Board of Examiners, in a reduced grade, proportionate to the extent of deviation from the required standard. In circumstances where the reduction in grade is the result of a significant breach of confidentiality the candidate will not be allowed to resubmit the assignment.
372
SECTION 5
PROGRAMME MANUAL / 2019
2.2. Clinical This will be assessed in the following ways: • The submission of four RCAs. Normally, this will be one from each area of clinical
work undertaken in years 1 and 2. • Four Evaluations of Clinical and Professional Competence by the candidate’s
clinical supervisors for placements in the first two years of the Programme, using the form prescribed for this purpose. Supervisors will report to the Examining Board whether a candidate’s placement performance is satisfactory. The Examining Board will consider these evaluations alongside the Clinical Practice Portfolio (for recording clinical experience) to ensure that an appropriate range of clinical experience has been gained.
Reports of Clinical Activity • Four RCAs are required. These must be selected to demonstrate the candidate's
clinical competence. They must cover a wide age range, types of problem and clinical procedures and must include some cases involving direct work with individual clients or groups of clients. Evidence of knowledge of more than one psychological model is required. The structure will vary with the type of report, (e.g. detailed assessment only; group work; individual therapy; family work; indirect work with carers; service development; consultancy). One RCA must be presented from four areas of supervised clinical experience. These will normally be those undertaken in years 1 and 2.
• It is not appropriate to include material in the RCA that has been submitted for another examination. Published work may be included when the candidate is sole author or, in the case of multiple authorship, when the candidate's responsibility can be, and is, clearly specified. In such cases the candidate must have taken the primary responsibility. Work undertaken jointly with another trainee clinical psychologist or in which the candidate took a subsidiary role must not be submitted. In all cases it must be made absolutely clear which procedures were carried out by the candidate and which by the collaborator, although candidates will be expected to take responsibility for the whole of what is submitted.
• RCAs must be prepared and submitted in accordance with the latest guidance provided by the Programme and contained in the Programme Manual.
• RCAs, which exceed the word limit, breach confidentiality, or do not follow the prescribed presentation style may, at the discretion of the Board of Examiners, result in a reduced grade, proportionate to the extent of deviation from the required standard. In circumstances where the reduction in grade is the result of a significant breach of confidentiality the candidate will not be allowed to resubmit the assignment.
373
SECTION 5
PROGRAMME MANUAL / 2019
Evaluation of Clinical and Professional Competence Form • The Evaluation of Clinical and Professional Competence Form(s) must be
completed by the supervisor at the specified point(s) for each placement. Completion and submission of these forms must comply with the latest guidelines described in the Programme Manual.
Clinical Practice Portfolio • The Clinical Practice Portfolio must be kept up-to-date throughout each
placement. At the end of the placement, the completed Portfolio must be signed by the supervisor and candidate and agreed as a correct record of the experience on placement.
• The Portfolio must be submitted to the Programme at the end of the placement as specified in the Programme Manual.
2.3 Research
Service Related Research Project One SRRP is required. This can be linked to any approved area of clinical experience. Proposed projects should be approved by the Research Team. The aims of the SRRP are two-fold: • To provide candidates with experience of completing pieces of service-related
research within a clinical context (typically audit or service development) and • To foster the development of research awareness and skills.
In contrast to the LSRP, the SRRPs need not be of an explicitly psychological nature, i.e. they do not need to be investigations of psychological phenomena. They must, however, address problems of relevance to the practice of clinical psychology.
The projects are intended to be small in scale. It is envisaged that the SRRPs will demonstrate competence in the application of research skills to the evaluation or audit of aspects of the practice of clinical psychology. Examples of potential projects include the following: • A single case experiment evaluating an intervention • A small-scale survey, e.g. consumer satisfaction survey • An analysis of data routinely collected by a service • A small piece of service related qualitative research.
The format, style of presentation, and submission of the SRRPs should conform with the latest guidance provided in the Programme Manual. • SRRPs may not meet the definition of ‘research’ for the purposes of applying for
ethical approval and guidance on this topic is provided to trainees in the latest version of the Programme Manual. However, in all projects, candidates must carefully consider ethical issues raised by the project, which they undertake and
374
SECTION 5
PROGRAMME MANUAL / 2019
must adhere to the “Code of Human Research Ethics”, published by the British Psychological Society.
• SRRPs, which exceed the word limit or do not follow the prescribed presentation style may result, at the discretion of the Board of Examiners, in a reduced grade, proportionate to the extent of deviation from the required standard. In circumstances where the reduction in grade is the result of a significant breach of confidentiality the candidate will not be allowed to resubmit the assignment.
Data Analysis Project • One DAP is required. The research team will provide a dataset and questions to
trainees. • The aims of the DAP are:
• To provide the opportunity for candidates to apply quantitative data analysis techniques to the evaluation of research databases, and
• To provide an opportunity for future clinical psychologists to engage with the process of exploring research questions using a statistical approach
• The format, style of presentation, and submission of the DAP should conform with the latest guidance provided in the Programme Manual.
• DAPs which exceed the word limit or do not follow the prescribed presentation style may result, at the discretion of the Board of Examiners, in a reduced grade, proportionate to the extent of deviation from the required standard.
2.4 Assessment of Part I
All assignments will be marked, in line with Bangor University marking guidelines (as specified in Section 4 of the NWCPP programme manual) independently by two internal assessors appointed by the Examining Board. Recordings submitted as part of the RCA-CBT assignment will be marked by an accredited CBT practitioner and a sample will be moderated by another suitably qualified internal assessor. • An External Examiner(s) will moderate the internal marking of these. The guiding
principle is that an External Examiner must have enough evidence to determine that the internal marking is of an appropriate standard and is consistent. An External Examiner will normally see any work that has failed, and a sample of other assignments.
• External Examiners are normally expected to participate in the decisions made by an Examining Board meeting when the results of Part I examinations are determined.
375
SECTION 5
PROGRAMME MANUAL / 2019
3. PART II 3.1 Academic
This will be assessed with a written clinical report of an advanced nature (ACR). This must be prepared and submitted in accordance with the latest guidelines contained within the Programme Manual.
3.2 Clinical This will be assessed in the following way: • An Evaluation of Clinical and Professional Competence by the candidate’s clinical
supervisor for the main third year placement using the form prescribed for this purpose. The supervisor will report to the Examining Board whether a candidate’s placement performance is satisfactory. The Evaluation of Clinical and Professional Competence Form must be completed by the supervisor at the specified point for the placement. Completion and submission of this form must comply with the latest guidelines described in the Programme Manual.
• The Clinical Practice Portfolio must be kept up-to-date throughout. At the end of the placement, the completed portfolio must be signed by the supervisor and candidate and agreed as a correct record of the experience on placement.
• The Examining Board will consider the Evaluation of Clinical and Professional Competence alongside the Clinical Portfolio (for recording clinical experience) to ensure that an appropriate range of clinical experience has been gained.
3.3 Large Scale Research Project (LSRP)
• This Research project must consist of an investigation with human participants and be of clinical relevance. It represents a more substantial piece of work than the SRRP. The LSRP must not exceed 20,000 words excluding the reference list and appendices, 40,000 words including the reference list and appendices.
• Candidates must carefully consider ethical issues raised by the research which they undertake and must adhere to the “Code of Human Research Ethics”, published by the British Psychological Society.
• Research design, execution, analysis and interpretation must be of a high standard and appropriate to the research problem. Candidates must be able to justify them at the oral examination.
3.4 Presentation of Thesis
• Candidates will present a thesis, which reports the results of the LSRP undertaken during the scheme of study and research. The report must include new investigative work, the results of which can be judged to constitute substantial contribution to knowledge, and should afford evidence of originality either by the discovery of new facts or by the exercise of independent critical power. The candidate must be able to demonstrate in what respect his or her work appears to him or her to advance knowledge or practice in clinical psychology.
• The thesis must consist of three parts: a literature review, a report of an empirical study, and a general discussion of the research. The former two parts must be presented in a format suitable for submission to an appropriate peer-review journal.
376
SECTION 5
PROGRAMME MANUAL / 2019
• The work must not have been submitted in fulfilment of the requirements of any other examination.
• Candidates will normally be required to submit their theses approximately three months before the end of their final year by a date determined by the Examining Board.
• The thesis must be submitted in accordance with the current Bangor University Regulations for Postgraduate Research Programmes.
3.5 Examination of Thesis
• The thesis must be examined in accordance with the current Regulations for Postgraduate Research Programmes.
• The internal examiner must not be the candidate’s research supervisor. 4. Course work Marking - Scales and Procedures 4.1 Scales
• Each Academic Assignment, RCA, SRRP, DAP and ACR will be assigned a category. The following structure, following the marking guidance in the Bangor University’s Regulations for Taught Programmes and described in Section 4 page 186-187, will be adopted:
GRADE CATEGORY PASS Distinction
Merit Pass
FAIL Fail
Whilst the award itself is unclassified, assignments are assigned a pass, merit or distinction to assist students in gauging the standard of their work.
• Distinction: All of the key issues in the Guidelines for Assessors for the piece of assessed work concerned have been addressed appropriately, and there is evidence of excellence in most of the main areas of the work as appropriate to the assignment.
• Merit: All of the issues outlined in the Guidelines for Assessors for the piece of assessed work concerned have been addressed appropriately and there is evidence of excellence in some areas of the work.
• Pass: This grade is applied to a piece of assessed work under three general circumstances:
• The candidate has dealt with all the main issues listed in the Guidelines for Assessors for the piece of assessed work concerned to an acceptable standard.
377
SECTION 5
PROGRAMME MANUAL / 2019
• The trainee has failed to deal adequately with one or more issues of lower importance, but these are not sufficient to warrant a fail grade.
• There are a small number of slightly weaker areas of the work compensated for by some strong aspects. However, the weaker aspects are not sufficient to warrant a fail grade.
• Fail: Work in this category will typically have one or more substantial deficits or the accumulation of minor defects is such that it does not meet the standard for a Pass. In these circumstances, the Board of Examiners will require candidates either to substantially revise the work or prepare a new piece of work for submission. The candidate will be informed by the Board whether revision or a new piece of work is required. If on resubmission the work is of a Pass standard the work will Pass (with a grade cap of a Pass) and the ‘fail’ will be expunged from the candidate’s record. If a resubmission fails no further resubmission is permitted and the fail remains on the candidate’s record.
4.2 Procedures
• All pieces of work are initially marked by two assessors, appointed by the Examining Board. This follows the procedures for Blind Double Marking as outlined in Bangor University’s Regulations for Taught Programmes (section 7.4). Assessors will reach an agreed mark. Recordings submitted as part of the RCA-CBT assignment will be marked by an accredited CBT practitioner and a sample will be moderated by another suitably qualified internal assessor. The Chair of the Board of Examiners may arbitrate on marks for an assignment where the two markers cannot reach a consensus about the final grade. Assessors will not assess assignments where they have acted in a supervisory capacity (RCAs, SRRPs).
• Material to illustrate the bottom, middle and top of the ranges of marks, including any failed assignments, will normally be forwarded for moderation to the External Examiner. The External Examiner may request to see any material that any candidate has presented.
5. Submission Deadlines
The Examining Board, at the start of each academic year, will publish deadlines for submission of all material, which includes all placement paperwork as well as academic assignments. Failure to submit course work by the deadline required without good prior reason having been given will normally result in a Fail grade for that piece of work.
6. Failure
6.1 In the event that a failure rating is given to an assignment the following procedure for re-submission will be followed:
• The Chair of the Board of Examiners will require the candidate either to rewrite the assignment or to present new material for assessment. Such new
378
SECTION 5
PROGRAMME MANUAL / 2019
material will normally be on a topic from the same clinical, academic or research area. Only one re-submission is permitted per assignment.
• The deadline for submission of this further work will be specified by the Examining Board in consultation with the candidate and their Training Co-ordinator, and formally communicated to the candidate.
6.2 Resubmitted assignments will first be marked internally by one of the original assessors, and one new assessor. Assignments that Pass on a resubmission will be capped at a Pass grade regardless of their quality. If an assignment passes on a resubmission then the ‘fail’ is expunged from the candidates record. If the assignment fails on a resubmission then the fail grade stands.
6.3 The Examining Board will normally recommend to the University that the candidate
be not allowed to continue with the Scheme of Study if he or she fails (after resubmission): (a) more than two pieces of course work in total, (b) two placements, (c) two pieces of course work and one placement or (d) the thesis. As there is no exit award, candidates receiving a C2 rating by the Exam Board following the Oral Examination of their thesis will no longer be able to continue with the Scheme of Study. An External Examiner will be required to be present at the meeting of the Examining Board at which any such recommendation is made.
6.4 The Examining Board will normally recommend to the University that the candidate
be not allowed to continue with the Scheme of Study if he or she is found to have violated ethical or other professional codes or guidelines of the University, NHS employer, Health & Care Professions Council or British Psychological Society. Where a candidate is dismissed from the National Health Service employer, the Examining Board will normally recommend to the University that the candidate be not allowed to continue with the Scheme of Study.
6.5 The Chair of the Examining Board shall be responsible for ensuring that the
communications to the candidate notifying him or her of the possibility of failure are consistent with the Disciplinary and Appeals Procedures of the Health Board with which the candidate holds his or her Contract of Employment.
6.6 A candidate may appeal against the decision of the Examining Board using the
Academic Appeals Procedure of Bangor University. https://www.bangor.ac.uk/regulations/procs/documents/BUProc02-v201801-1.pdf
379

SECTION 5
PROGRAMME MANUAL / 2019
NWCPP BOARD OF EXAMINERS The Board of Examiners oversees the implementation of the assessment procedures of the NWCPP in line with University regulations, HCPC and BPS standards. Membership of the Board of Examiners
The Board of Examiners comprises the following members: • Director of the NWCPP Programme • All members of the NWCPP team who mark assignments • The Head of School for the School of Psychology • The External Examiners • An assessor from each specialism who is not a member of the Programme
team • The Professional Lead for Clinical Psychology within the local Health Board.
A senior member of the Programme Team, nominated by the Programme Director, Chairs the Board.
Terms of Reference
The Board of Examiners is responsible for: • Equitable implementation of the assessment procedures of the programme • Reviewing, ratifying and modifying the marks for academic and research
assignments as appropriate in line with NWCPP and BU guidance • Reviewing, ratifying and modifying the placement decisions
as appropriate in line with NWCPP and BU guidance • Confirmation of progression from Part I to Part II of the programme • Consideration of extenuating circumstances for trainees failing assignments
and / or placements • Deciding whether trainees are eligible for re-assessment if an assignment or
undertaking a further placement if this has been failed • Making recommendations to the Academic Registry in relation to passing or
failing parts or the entire programme. • Recruiting internal and external examiners?
The Programme Manager acts as Secretary to the Board of Examiners. The Secretary to the Board is responsible for:
• Coordinating the distribution of assignments for marking • Maintaining comprehensive records of assignment marks • Informing Trainees of their provisional marks before the Board and confirming
final marks after the Board has ratified them • Drawing any matters of concern in relation to marking or its execution to the
Chair of the Board.
380
SECTION 5
PROGRAMME MANUAL / 2019
Boards of Examiners Meetings Meetings occur four times a year. Once in June where results for Part II of the DClinPsy award are considered and once in September when transition from Part I to Part II of the award are reviewed. Meetings are also held in March and November to discuss and ratify academic assignments and clinical placements.
Recording the activity of the Board
Agenda and Minutes • The Secretary of the Board in consultation with the Chair will prepare an
agenda for Board of Examiners meetings • Boards of Examiners minutes will be written by the Secretary’s nominee and
signed by the Chair • The minutes will be kept in accordance with the University’s record retention
schedule. Minutes should be taken at each Board of Examiners to:
• Record relevant discussion and decisions • Record the reasons for special recommendations/decisions for students, e.g.
special examination arrangements, medical issues, plagiarism • Provide examples for future Board of Examiners to ensure consistency • Record comments of External Examiners
The agenda should follow a basic outline as follows: 1. Date of the meeting 2. Declarations of conflicts of interest 3. Members present and apologies 4. Minutes of the previous meeting and any matters arising 5. Any actions by the Chair since the most recent meeting 6. Confirmation of assignment marks: to confirm that the Board agrees with the
marks as listed in an attached appendix. This section must include generic information on the reasons for any changes to marks (the reasons can be categorised and specific details of a medical/personal nature should not be included)
7. Confirmation of clinical placement evaluations 8. Confirmation of transitioning to Part II of the award and of successful
completion of the award 9. External Examiners’ comments
Conflicts of interest Members of staff must inform the Chair of the Board of Examiners of any personal interests, involvement or relationship with any students. The Chair must decide whether the circumstances have to be declared at the meeting. The member of staff must withdraw from the meeting when the student’s case is being discussed. Any declaration of interest and/or withdrawal of a member of staff must be recorded in the minutes of the Board.
Notification of results Notification of Results Form (NORF): The NORF form records the Viva results for individual students. The Chair and members of the Board present at the relevant meeting will sign this form, usually at the end of the Board of Examiners meeting.
381
SECTION 5
PROGRAMME MANUAL / 2019
BANGOR UNIVERSITY REGULATIONS AND PROCEDURES The University Registry recommend that links are provided rather than hard copies as Regulations and Procedures may change within the year. All Bangor University Regulations, Procedures and Codes of Practice can be found here: https://www.bangor.ac.uk/ar/main/regulations/home.htm For example: • General Regulations for all Students
• Regulations for Postgraduate Research Programmes
• Academic Appeals Procedure
382
SECTION 6
PERSONAL SUPPORT
383
SECTION 6
PROGRAMME MANUAL / 2019
PERSONAL SUPPORT There are a variety of sources of personal support available to trainees on the NWCPP. These are outlined below: 1. Shortly after appointment trainees attend the Occupational Health Department of
their local District General Hospital and are advised that they may seek help from that Department. They are informed that staff members of all disciplines in the Health Authority have access to specialist services through the Occupational Health Department.
2. Trainees have a Training Co-ordinator (details explained later in this Section).
3. Trainees have a Personal Tutor (details explained later in this Section). 4. Trainees have access to the Personal & Professional Development Scheme (details
explained later in this Section). 5. Trainees have an appraisal (PADR) once a year with their Training Co-ordinator. This
gives an opportunity for their whole progress and development to be reviewed. Appraisals are partly based on information from clinical practice portfolio and summaries of academic marks. In addition, the Programme needs to monitor trainee attendance at BCUHB mandatory training events. This is also a good opportunity for trainees to discuss their individual training plans in terms of clinical experience and research. Trainees need to consider any other issues they would like to raise for discussion, as well as feedback they wish to give about aspects of the training. Please remember that this is not part of the Programme assessments and the aim of such meetings is to facilitate progress and development, and try and ensure that the Programme is meeting individual trainee needs and the needs of others in the future. Trainees need to complete the Appraisal Form and send a copy to the Programme Director within one week of the appraisal meeting.
6. Trainees may approach the HR Department of BCUHB who may be able to provide
help or refer them appropriately to a range of support services available e.g. Celtic Pride and information on a range of other organisations.
7. On their appointment, trainees are advised to register with a local General
Practitioner. 8. Trainees also have access as Bangor University students to all the support services
provided by the University’s Student Services Department including, disability support, dyslexia support, counselling services etc.
https://www.bangor.ac.uk/studentservices/index.php.en
384
SECTION 6
PROGRAMME MANUAL / 2019
9. While Programme staff recognise that trainees might not necessarily want to approach them with problems, they are advised that if these are likely to affect their academic and clinical work, they should contact their Training co-ordinator to discuss the situation. Programme staff are aware of the pressures of being a trainee and of their need to remain approachable. It is the aim of the Programme team to help trainees through the Programme, and alerting Programme staff to any problems at an early stage will assist them with this aim.
385
SECTION 6
PROGRAMME MANUAL / 2019
TRAINING CO-ORDINATOR ROLE
For the three years of the Programme each Trainee has a Training Co-ordinator allocated who will oversee their development. Trainees usually have the same Training Co-ordinator for the duration of the Programme, but this cannot be guaranteed. The main duties of Training Co-ordinators are listed below: Co-ordination of training programmes for individual trainees throughout the Programme and monitoring development of clinical and professional skills.
1. Supporting and mentoring trainees throughout their training. 2. Placement Visits
2.1 Monitoring and evaluation of the clinical experience provided and the
individual trainee’s progress and development whilst on placement. Using the Placement Agreement, Placement Quality Checklist and Evaluation of Clinical and Professional Competence to guide discussion and provide formal documentation.
2.2 Monitoring progress and advising supervisor and trainee regarding essays and Reports of Clinical Activity. Liaising as appropriate with the research team regarding the trainee’s progress.
2.3 Facilitation of the relationship between supervisor and trainee, troubleshooting difficulties and advocating on the trainee’s behalf as necessary.
2.4 Ensuring Placement Agreements adequately address the needs of individual trainees, for example with reference to skills deficits/experience deficits. Special requirements for clinical or professional development on placement should be discussed with the Clinical Director and/or Clinical Tutor.
3. Reading drafts of essays and RCAs and advising trainees on any changes that would
improve overall quality. The Training Co-ordinator will not usually read research assignments but this can be negotiated if appropriate.
4. Attendance at monthly Team Meetings to provide regular feedback to the
Programme Team regarding individual trainees’ progress.
5. Reviewing the trainees overall progress at annual appraisal meetings.
386
SECTION 6
PROGRAMME MANUAL / 2019
THE PERSONAL TUTOR SCHEME
1. The North Wales Clinical Psychology Programme has a system whereby each trainee selects a Personal Tutor who is a local Clinical Psychologist and not a member of the Programme Team.
2. The Personal Tutor’s role is to counsel trainees on matters to do with their training and to advise and help them in seeking suitable advice/support etc., with regard to any specific issues connected with the Programme.
3. A trainee’s Personal Tutor cannot at the same time act as their placement supervisor. In the event of a trainee’s Personal Tutor becoming their placement supervisor, then an alternative Personal Tutor must be sought.
4. It is suggested that there be no maximum level of contact between each trainee and his/her Personal Tutor, only a minimum level of at least once every six months.
5. The relationship between the trainee and his/her tutor would be confidential at all times unless mutually agreed.
6. In the event of the trainee bringing a problem to the Personal Tutor that they are unable to resolve between them and which the trainee does not wish to be raised with the Programme Team, the Personal Tutor may, on behalf of the trainee with their consent, raise the issue with either the Lead Clinical Psychologist with the North Wales NHS Trust or the Head of the School of Psychology, BU as appropriate.
7. The Programme Director invites people to submit themselves as Personal Tutors and circulates the list to trainees.
8. The trainee/tutor have an option for either party concerned to opt out of the arrangement. Under such circumstances the trainee should seek a "new" Personal Tutor.
387
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
PERSONAL TUTORS
Alan Dowey Alison Firth Angela Brennan Beth Parry-Jones Cara Rogowski Carmel Harrison Caroline Jones Eleri Jones Elin Walker Jones Esme Paynter Fiona Sanders Freya Spicer-White Gwenllian Parry Jody Etheridge Jonathan Williams Julia Wane Kate Dickson Katie Elliott Kristina Cole Laura Spencer Leah Jones Lesley Leeds Lisa Train Liz Whitehead Louise Cunliffe Lucy Piggin Megan Marks Nick Horn Nicola Weatherall Rose Stewart Samantha Owen Sarah Bailey-Rogers Simon Moseley Siwan Roberts Trish Girling
388
SECTION 6
PROGRAMME MANUAL / 2019
THE PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
(PPD Scheme)
This scheme commenced in 1989 as a new initiative on the NWCPP and has undergone two positive evaluation exercises (Ref. Eayrs, Appleton and Lewis 1992). The scheme is optional and is independent from the Programme. It was devised to provide confidential individual attention to the overlap between a trainee's professional and personal development during clinical training. Awareness of these processes by the trainee may be of considerable advantage in their continued self-monitoring and self-development. The Scheme is reviewed annually and a report submitted to the Training Committee. Some of the issues that may arise for trainees will be very highly personal and trainees may find it difficult to talk about such issues except to someone with whom they have a trusting relationship and who is also completely separate from the assessment process. The responsibilities of individual Clinical Psychologists both in relation to the self and to others are outlined in:
• HCPC – Standards of conduct, performance and ethics http://www.HCPC-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
• HCPC - Guidance on conduct and ethics for students http://www.hcpc-uk.org/assets/documents/10002C16Guidanceonconductandethicsforstudents.pdf http://www.hcpc-uk.org/publications/brochures/index.asp?id=219
• BPS Code of Ethics and Conduct
https://www.bps.org.uk/news-and-policy/bps-code-ethics-and-conduct • Generic Professional Practice Guidelines • BPS Code of Human Research Ethics
https://www.bps.org.uk/news-and-policy/bps-code-human-research-ethics-2nd-edition-2014
Self-monitoring of stress levels may be better facilitated when this is done as part of a proactive and reflective personal development counselling relationship (rather than as a reactive approach which can occur in clinical supervision arrangements). The individual trainee can then begin to identify the particular situations which cause stress, their own individual patterns of reactivity, and develop more appropriate coping mechanisms. Of course, stress can simply occur through the enormous pressure of different types of work which are involved in the post-graduate Programme. Personal and professional development sessions can help trainees monitor this and take appropriate action.
389
SECTION 6
PROGRAMME MANUAL / 2019
Personal and professional development should allow the trainee to gradually work through a range of personal issues in the overlap between personal and professional life. Potentially it should not be 'reactive' to individual occurrences of stress but should handle stress within the wider brief of the work undertaken. Being in the personal & professional development scheme can be stressful in itself. It can lead to personal change and development and might entail having to deal with painful issues. Trainees need to be aware of this before embarking on the scheme. The PPD Scheme is not intended to provide psychological therapy to trainees and should not be seen as a resource for personal crisis. The University offers a counselling service for students and further information can be found here: https://www.bangor.ac.uk/studentservices/counselling/index.php.en The scheme is available as a means of enhancing the exploration of trainees’ own development as clinical psychologists. New trainees who are already receiving counselling prior to joining the programme are not encouraged to transfer their counsellors or therapists to the scheme as this perpetuates the impression that the scheme exists for personal therapy rather than professional development. Such trainees might wish to continue their own counselling while on the Programme, but such counselling would be in addition to the PPD scheme and would need to continue to be funded by the trainee. The Psychological Therapists are trained and experienced in counselling and/or psychotherapy and are all individuals who are not providing placement supervision or academic supervision on the Clinical Programme and as such are not in the position of evaluating the trainees. All Psychological Therapists are approved by the Programme on the basis of a CV and interview. Subsequent approval is on an annual basis. Psychological Therapists complete an annual personal information sheet, which is included in the Programme Manual. All contact made by the trainees is at their own discretion and is confidential. Programme staff will be unaware of any trainee’s contact with a Psychological Therapist unless the trainee chooses to disclose it in their own time/study time. Desired Benefits
• Increased appropriate self-awareness and reflectiveness by trainees of areas of overlap between personal and professional development.
• Increase in coping skills in relation to stress. • Increase in personal confidence in therapeutic and professional work.
Accessing the Personal & Professional Development Scheme
Trainees are funded for 24 sessions for the duration of the Programme and are issued with 24 vouchers at the start of their training. One voucher must be handed to the Psychological Therapist during each session to enable the appropriate fee to be claimed. Any further sessions (than the 24) must be self-funded. Trainees may wish to bear in mind that it is often useful to receive personal & professional development while they are on specialist placements in their third year. Trainees are free to contact one of the
390
SECTION 6
PROGRAMME MANUAL / 2019
listed Psychological Therapists to arrange to meet with them. The Psychological Therapists invoice NWCPP directly (using the vouchers) for sessions and so trainees need not be further concerned with this aspect of the Scheme.
Feedback from trainees
Trainees are encouraged to provide general, anonymous feedback on the scheme on an annual basis to the Training Committee. This feedback should be provided on the attached form and submitted in May of each year. Trainees should ensure any concerns about the scheme are passed on to the Programme Team, either directly or via their Personal Tutor/Training Co-ordinator. Significant concerns about the behaviour/competence of any individual counsellor should be directed to that counsellor’s professional body.
391
SECTION 6
PROGRAMME MANUAL / 2019
PERSONAL AND PROFESSIONAL DEVELOPMENT SCHEME TRAINEE FEEDBACK FORM
This Feedback Form is part of the PPD Scheme monitoring process. Feedback is voluntary and anonymous and you are not required to provide the name of your counsellor(s). The feedback received from all trainees will be summarised and presented to the Training Committee annually. 1. Have you used the PPD Scheme? (if YES proceed to question 3, if NO proceed to question 2 only) 2. Are you planning to use the PPD Scheme during your time on the programme (please give details)? 3. How many sessions have you had to date? 4. What is your opinion of the PPD Scheme and what has influenced your decision about whether to participate at this stage?
RHAGLEN SEICOLEG CLINIGOL GOGLEDD CYMRU NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
392
SECTION 6
PROGRAMME MANUAL / 2019
5. How has the PPD Scheme been helpful to you? 6. Is there anything about the PPD Scheme that you have found unhelpful? 7. Do you have any positive comments or any concerns about the content of your PPD sessions? (e.g. issues covered, advice given) 8. Do you have any positive comments or concerns about the process of your PPD sessions? (e.g. availability, punctuality, professional boundaries)
393
SECTION 6
PROGRAMME MANUAL / 2019
9. As you know we review the PPD Scheme on annual basis. If you have anything specific you would like to report please indicate below: 10. Form completed date:
394
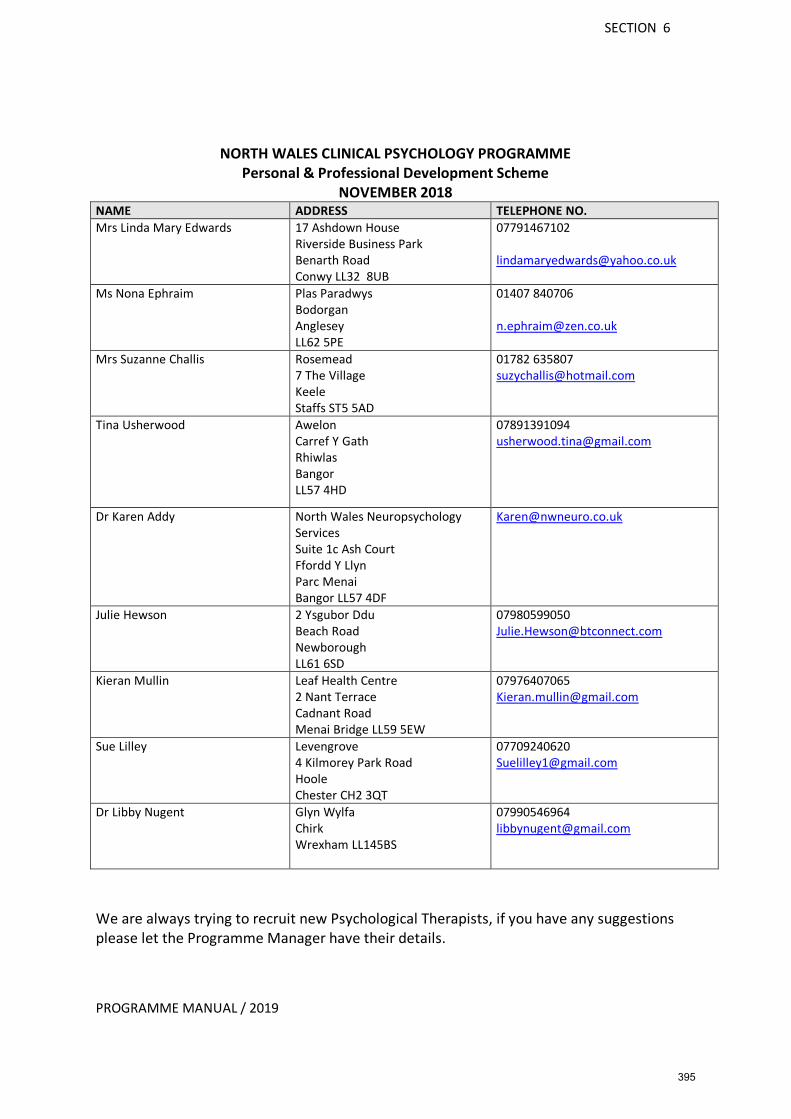
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME Personal & Professional Development Scheme
NOVEMBER 2018 NAME ADDRESS TELEPHONE NO. Mrs Linda Mary Edwards
17 Ashdown House Riverside Business Park Benarth Road Conwy LL32 8UB
07791467102 [email protected]
Ms Nona Ephraim
Plas Paradwys Bodorgan Anglesey LL62 5PE
01407 840706 [email protected]
Mrs Suzanne Challis Rosemead 7 The Village Keele Staffs ST5 5AD
01782 635807 [email protected]
Tina Usherwood Awelon Carref Y Gath Rhiwlas Bangor LL57 4HD
07891391094 [email protected]
Dr Karen Addy North Wales Neuropsychology Services Suite 1c Ash Court Ffordd Y Llyn Parc Menai Bangor LL57 4DF
Julie Hewson 2 Ysgubor Ddu Beach Road Newborough LL61 6SD
07980599050 [email protected]
Kieran Mullin Leaf Health Centre 2 Nant Terrace Cadnant Road Menai Bridge LL59 5EW
07976407065 [email protected]
Sue Lilley Levengrove 4 Kilmorey Park Road Hoole Chester CH2 3QT
07709240620 [email protected]
Dr Libby Nugent Glyn Wylfa Chirk Wrexham LL145BS
07990546964 [email protected]
We are always trying to recruit new Psychological Therapists, if you have any suggestions please let the Programme Manager have their details.
395
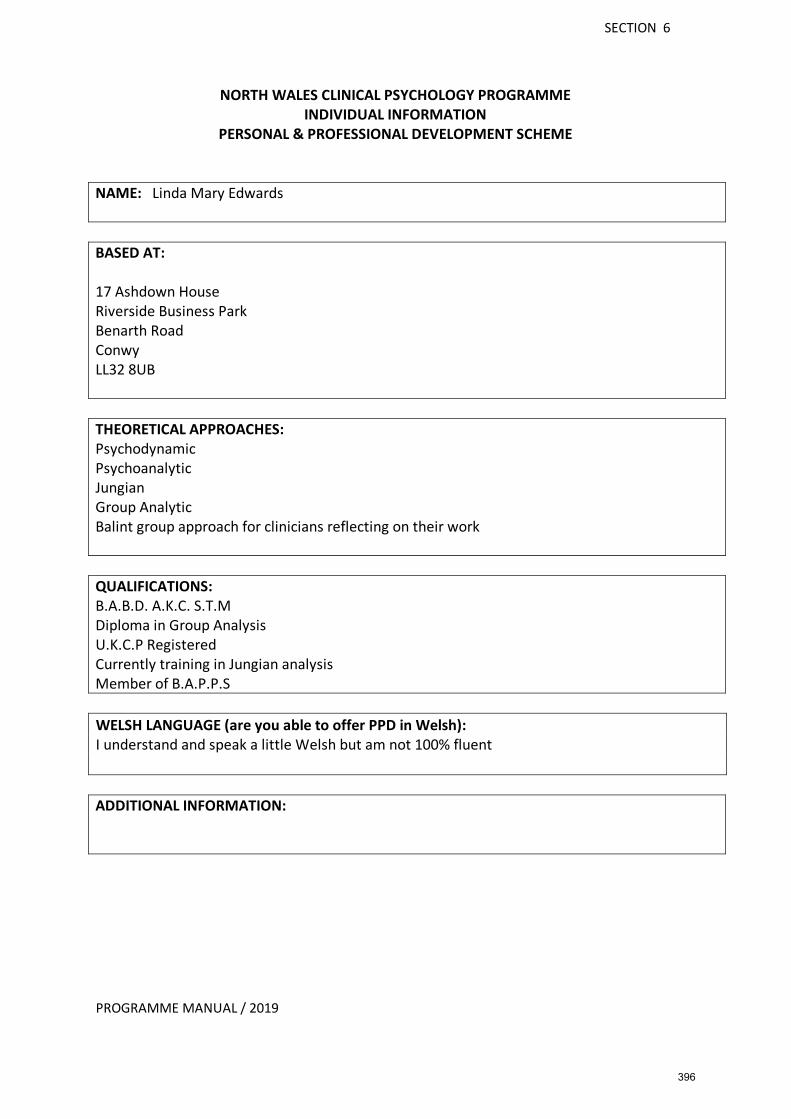
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME INDIVIDUAL INFORMATION
PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Linda Mary Edwards BASED AT: 17 Ashdown House Riverside Business Park Benarth Road Conwy LL32 8UB THEORETICAL APPROACHES: Psychodynamic Psychoanalytic Jungian Group Analytic Balint group approach for clinicians reflecting on their work QUALIFICATIONS: B.A.B.D. A.K.C. S.T.M Diploma in Group Analysis U.K.C.P Registered Currently training in Jungian analysis Member of B.A.P.P.S WELSH LANGUAGE (are you able to offer PPD in Welsh): I understand and speak a little Welsh but am not 100% fluent ADDITIONAL INFORMATION:
396

SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME INDIVIDUAL INFORMATION
PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Nona Ephraim BASED AT: Independent Practice based at: Plas Paradwys Bodorgan Ynys Môn LL62 5PE (20 minutes approx. from Bangor) THEORETICAL APPROACHES: Psychodynamic psychotherapy with a strong attachment theory base QUALIFICATIONS: MA Counselling Post Grad Diploma Psychodynamic Psychotherapy
WELSH LANGUAGE (are you able to offer PPD in Welsh): Yes ADDITIONAL INFORMATION: I started my psychotherapy training at the Institute of Psychotherapy & Social Studies which included Ronnie Lang and John Southgate on the staff. John Southgate was at one time supervised by John Bowlby. I continue to have attachment based psychodynamic supervision.
397

SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME INDIVIDUAL INFORMATION
PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME NAME: Tina Usherwood BASED AT: Rhiwlas
THEORETICAL APPROACHES: I am a Psychodynamic Psychotherapist with a particular interest in Attachment Theory and Mentalization Based Therapy (MBT)
QUALIFICATIONS: In 2005, I completed my Postgraduate Diploma in Psychodynamic Psychotherapy through the Merseyside Psychotherapy Institute. In 2011, I completed my Diploma in Psychoanalytic Supervision with the Guild of Psychotherapists, London. In 2015 & 2016 I completed training in Mentalization-Based Treatment for Adults and Adolescents with the Anna Freud Centre, London. WELSH LANGUAGE (are you able to offer PPD in Welsh): No ADDITIONAL INFORMATION: I have experience of working in a variety of settings including the NHS, the voluntary sector for Relate and Stepping Stones, a sexual abuse service, in private practice and for University Counselling Services here in Bangor and Liverpool. Additionally, I founded and run a Peer Support Service for Liverpool Veterinary School. I am a UKCP (United Kingdom Council for Psychotherapy) registered Psychoanalytic Psychotherapist and Supervisor, Member of Council for Psychoanalysis and Jungian Analysis College, Member of the Merseyside Psychotherapy Network, BAPPS (British Association for Psychoanalytic and Psychodynamic Supervision) registered member.
398
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
INDIVIDUAL INFORMATION PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Karen Addy BASED AT: North Wales Neuropsychology Services Suite 1c Ash Court, Ffordd Y Llyn Park Menai, Bangor LL57 4DF [email protected] / [email protected]
THEORETICAL APPROACHES: CAT CBT Neuropsychology - Cognitive Rehabilitation
QUALIFICATIONS: 1997–2000 - Liverpool John Moores University BSc Hons Psychology and Biology 1997-2002 - The Open University MSc Psychology 2002-2005 - The University of Manchester Doctorate in Clinical Psychology 2008 – 2012 - The British Psychological Society Qualification in Clinical Neuropsychology 2015 – 2017 - Catalyse ACAT North Cognitive Analytic Therapy Practitioner (pending in training)
WELSH LANGUAGE (are you able to offer PPD in Welsh): No ADDITIONAL INFORMATION: I am currently training in Cognitive Analytic therapy and will be able to provide CAT as the main therapy approach. I also have extensive experience in CBT having trained at the University of Manchester DClinPsych programme, which has a strong CBT framework base for the training in years 1 and 2. In addition, I am a fully qualified Neuropsychologist and as such have wide experience of working with disabilities and dyslexia. I have experience of stress management, pacing and study approaches to overcoming cognitive impairment.
399
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME INDIVIDUAL INFORMATION
PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Suzy Challis BASED AT: Rosemead 7 The Village Keele Staffs ST5 5AD Consultation venue may be different Tel: 01782 635 807 Email: [email protected] THEORETICAL APPROACHES:
Psychoanalytic Psychotherapy QUALIFICATIONS:
MSc Clinical Psychology Diploma in Psychoanalytic Psychotherapy WELSH LANGUAGE (are you able to offer PPD in Welsh): No ADDITIONAL INFORMATION:
400
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
INDIVIDUAL INFORMATION PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Kieran Mullin BASED AT:
Leaf Health Centre 2 Nant Terrace Cadnant Road Menai Bridge Anglesey LL59 5EW
THEORETICAL APPROACHES:
Cognitive Behavioural Therapy
QUALIFICATIONS:
PGDip Cognitive Behavioural Psychotherapies
WELSH LANGUAGE (are you able to offer PPD in Welsh): No ADDITIONAL INFORMATION: I am slightly limited in times of appointments due to the opening times of the Leaf Health Centre, however if there is a problem I can source another clinic to hire a room at that time.
401
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME INDIVIDUAL INFORMATION
PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Sue Lilley BASED AT: Hoole in Chester THEORETICAL APPROACHES:
Person Centred Approach Cognitive Behavioural Therapy
QUALIFICATIONS:
BACP Accreditation Diploma in Counselling (Integrative) Diploma in CBT Certificate in Couple and Family Counselling Certificate in Coaching Certificate in Supervision MSc in Financial Management PGCE
WELSH LANGUAGE (are you able to offer PPD in Welsh): No ADDITIONAL INFORMATION: I am an experienced and BACP accredited counsellor and am able to offer a very supportive and positive learning environment. I work with individuals, couples and families in my private practice and having been trained integratively, I am able to use a variety of approaches to suit the needs of the individual client. I have 5 years experience as a counselling supervisor, 16 years experience as a lecturer and 6 years experience of mentoring students at The University of Chester so I have a long history of working with individuals to achieve their potential.
402
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME
INDIVIDUAL INFORMATION PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Julie Anne Hewson BASED AT:
Menai Bridge Tel: 07980599050 Llandudno Email: [email protected] Newborough
THEORETICAL APPROACHES:
Integrative (not eclectic) Transactional Analytic Gestalt Psychoanalytic/object relations. Jungian Analytic concepts A range of interventions for PTSD Art therapeutic approaches
QUALIFICATIONS: M.A. B.A. Hons Dip SW. CQSW. Dip Supervision. Training and Supervising Transactional Analyst. Diploma in Integrative Psychotherapy, Clinical Transactional Analyst, UKCP accredited, BACP Snr Accredited. Trained mediator, European Qualified Supervisor, Coach and Trainer. Undergone 4 5 years Jungian Analysis. Founded and set up the Iron Mill in Exeter, sold on as a going concern 6 years ago. Professional artist and writer. WELSH LANGUAGE (are you able to offer PPD in Welsh): No ADDITIONAL INFORMATION: I am kind, interested, continue to learn and grow. I am 71 this coming birthday so a wise but juicy crone! I have worked all over Europe and taught post graduate trainees for over 30 years.
403
SECTION 6
PROGRAMME MANUAL / 2019
NORTH WALES CLINICAL PSYCHOLOGY PROGRAMME INDIVIDUAL INFORMATION
PERSONAL & PROFESSIONAL DEVELOPMENT SCHEME
NAME: Dr Libby Nugent
BASED AT: Glyn Wylfa, Chirk, Wrexham, LL145BS
THEORETICAL APPROACHES:
Individual work: systemic and narrative therapies. Group work: group analytic.
QUALIFICATIONS:
Doctorate in Clinical Psychology EMDR practitioner Currently training for diploma as as group work practitioner in group analysis.
WELSH LANGUAGE (are you able to offer PPD in Welsh): No
ADDITIONAL INFORMATION:
Should wheelchair/ supported access be needed please let me know on contact, as my room is on the first floor. I can then make arrangements for a more appropriate space.
404
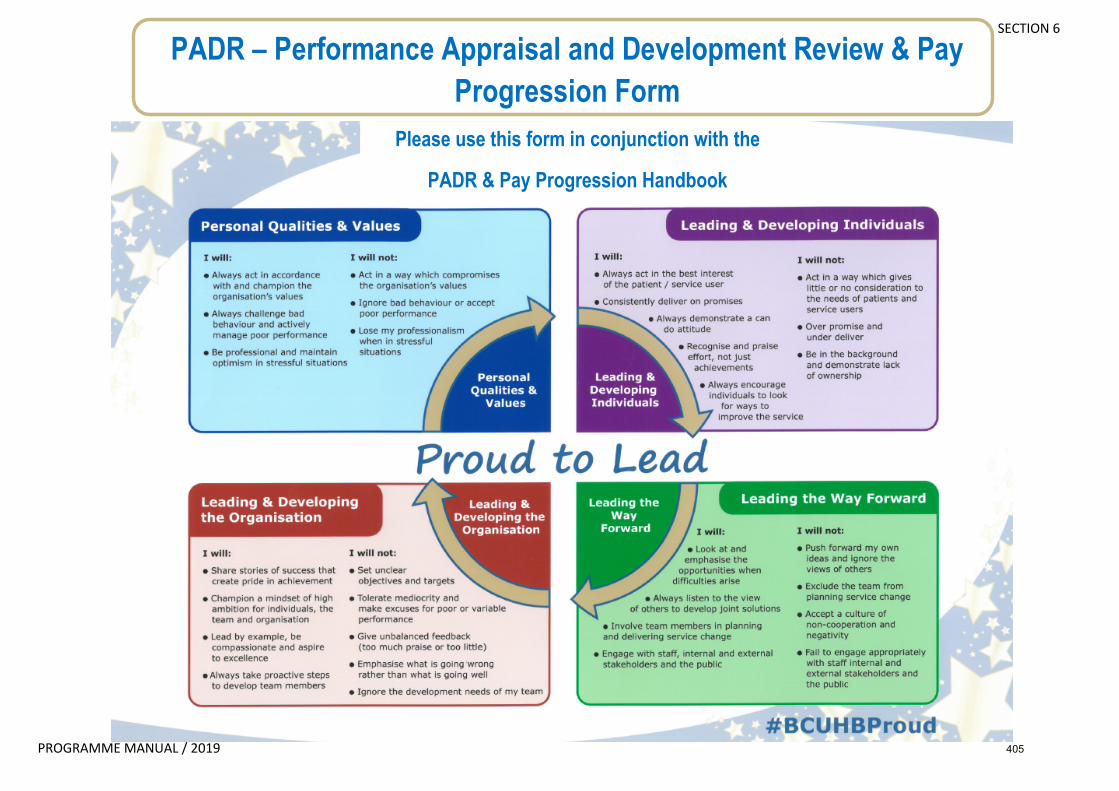
SECTION 6
PROGRAMME MANUAL / 2019
PADR – Performance Appraisal and Development Review & Pay Progression Form
Please use this form in conjunction with the
PADR & Pay Progression Handbook
405
SECTION 6
PROGRAMME MANUAL / 2019
Name & Employee Number:
Today’s date:
Job title:
Manager & Team:
Our Values
Please note all appraisees should aim to complete section 1-4 prior to the PADR and can discuss this with the appraiser during the PADR
406
SECTION 6
PROGRAMME MANUAL / 2019
1. Looking back over the past 12 months, what have I done really well in terms of demonstrating our values? (For further information please see relevant section in PADR & Pay Progression handbook)
• Review of clinical and professional competence development so far, including range of placements, assessments, therapeutic interventions
• Review of academic progress so far, including range of topics/methodologies
• Review of research plans/progress (SRRP/LSRP)
407
SECTION 6
PROGRAMME MANUAL / 2019
2. Looking back over the past 12 months, what could I have done better / differently in terms of our values? (For further information please see relevant section in PADR & Pay Progression handbook)
• Any development needs arising from clinical placement feedback and/or reflective practice?
• Any development needs in relation research activity?
• Any development needs in relation to academic assignments?
408
SECTION 6
PROGRAMME MANUAL / 2019
3. In what way has feedback from others contributed towards my development? (For further information please see relevant section in PADR & Pay Progression handbook)
4. How am I meeting my KSF outline and what examples can I give to show progress in my skills and development? (For further information please see relevant section in PADR & Pay Progression handbook)
Comments
Core 1. Communication
Develop and maintain communication with people about difficult matters and / or in difficult situations
Core 2. Personal and People Development
Develop own skills and knowledge and provide information to others to help their
409
SECTION 6
PROGRAMME MANUAL / 2019
development
Core 3. Health , Safety and Security
Monitor and maintain health, safety and security of self and others
Core 4. Service Improvement
Make changes in own practice and offer suggestions for improving services
Core 5. Quality
Maintain quality in own work and encourage others to do so
Core 6. Equality and Diversity
Support equality and value diversity
Health and wellbeing: Assessment and treatment planning
Assess psychological functioning and develop, monitor and review related treatment plans
410
SECTION 6
PROGRAMME MANUAL / 2019
Health and wellbeing: Interventions and treatments
Contribute to planning, delivering and monitoring interventions and/or treatments
Information and Knowledge. Information collection and analysis
Gather, analyse, interpret and present extensive and/or complex data and information
General Development and innovation
Test and review new concepts, models, methods, practices, products and equipment
411
SECTION 6
PROGRAMME MANUAL / 2019
5. Core Objectives Core objectives must be relevant to job role and linked to service & organisational goals and/or Proud to Lead. Performance is measured against core objectives. Must include the following objectives as a minimum:-
• Demonstrate Statutory & Mandatory Training compliance • Demonstrate meeting KSF post outline • Demonstrate you are meeting BCUHB values
Review of last year’s objectives (For further information please see relevant section in PADR & Pay Progression handbook) What is your current compliance score on Mandatory Training?
Date this score was
Outstanding training already booked
Date Training is booked for
Training not yet booked
412
SECTION 6
PROGRAMME MANUAL / 2019
checked % / / / /
This year’s objectives with dates (For further information please see relevant section in PADR & Pay Progression handbook)
6. Development Objectives Development objectives are ambitious and aspirational taking the individual beyond current required competence. Development objectives are reviewed but will not be taken into account in determining unsatisfactory performance. Review of last year’s objectives (For further information please see relevant section in PADR & Pay Progression handbook)
• What areas do you need to target for further development over the next year?
413
SECTION 6
PROGRAMME MANUAL / 2019
This year’s objectives with dates (For further information please see relevant section in PADR & Pay Progression handbook)
• Plan for future training needs on the basis of sections 1-4 above?
7. Looking ahead, what am I going to do now? (My Development Plan) (For further information please see relevant section in PADR & Pay Progression handbook)
• Areas of interest for 3rd year placement and/or future employment post-qualification – implications for training?
414
SECTION 6
PROGRAMME MANUAL / 2019
8. What support will I need to get there? (For further information please see relevant section in PADR & Pay Progression handbook)
• Feedback to the Programme?
415
SECTION 6
PROGRAMME MANUAL / 2019
9. A few words that sum up the last year for me (For further information please see relevant section in PADR & Pay Progression handbook)
Will the increment be rewarded? Yes / No / N/A
If ‘No’ detail reasons why and ensure development plan above is completed with a review date.
(If no it is crucial that you see relevant section in PADR & Pay Progression handbook)
My signature and date
My managers signature and date
REMEMBER!!!! You should record the PADR date on ESR as a minimum
416
Copyright © 2022 FDOKUMEN