
Pro- and antiinflammatory cytokines in threatened miscarriages
9
BASIC SCIENCE: OBSTETRICS Pro- and antiinflammatory cytokines in threatened miscarriages Jean Calleja-Agius, MD; Shanthi Muttukrishna, PhD, DSc; Arnold R. Pizzey; Eric Jauniaux, MD, PhD OBJECTIVE: The purpose of this study was to evaluate circulating and intracellular levels of Th1 and Th2 cytokines in women with threatened miscarriage (TM) and subsequent outcome. STUDY DESIGN: Plasma levels of tumor necrosis factor (TNF)-recep- tors 1 and 2, TNF, interferon gamma (IFN), and interleukins (IL) -6 and -10 were measured by flow cytometric bead assays in 80 women with TM: 53 women with normal outcome and 27 women who miscar- ried. Fluorescent antibody labeling was also performed on whole blood in a subgroup of 27 women of TM: 16 women with normal outcome and 11 women who miscarried. RESULTS: Monocyte expression of TNF and circulating levels of TNF, IFN, IL-10, IL-6, and TNF-R1 were significantly lower, whereas circulating levels of TNF/IL-10, IFN/IL-10, and TNF/IL-6 ratios were significantly higher, in women with TM who subsequently miscar- ried, compared with the women with normal outcome. CONCLUSION: An increased Th1 type of immune response, which was similar to that observed in preterm delivery, was found in TM cases that were complicated by a subsequent miscarriage. Key words: cytokine, interleukin-10, threatened miscarriage, TNF receptor, tumor necrosis factor Cite this article as: Calleja-Agius J, Muttukrishna S, Pizzey AR, et al. Pro- and antiinflammatory cytokines in threatened miscarriages. Am J Obstet Gynecol 2011;205:83.e8-16. T hreatened miscarriage (TM) is de- fined as a history of vaginal bleeding in early pregnancy in the presence of a closed cervix and with ultrasonic evi- dence of an intrauterine gestational sac and a fetal heartbeat. 1 TM is the most common complication of ongoing preg- nancy, which occurs in approximately 30% of pregnant women, and is associ- ated with a 10-14% risk of full miscar- riage. 2,3 Various management protocols have been developed that included con- servative management and hormonal therapy that were based on progester- one 4 and human chorionic gonadotro- pin (hCG). 5 Overall, TM can generate great anxiety in patients, especially be- cause bleeding in early pregnancy can lead to pregnancy loss and other obstet- ric complications. 6 The pathophysiology of TM is linked to bleeding from uteroplacental vessels at the margin of the placenta with blood accumulating between the cho- rionic membrane and uterine wall. 7 The formation of a subchorionic he- matoma may disrupt the placental bed. If the hematoma expands to the rest of the placental mass, it will induce com- plete miscarriage within a week of the first symptoms. 8 If bleeding is limited or happens close to the internal cervi- cal os and is evacuated, the pregnancy may continue; however, this can lead to a chronic inflammatory reaction within the decidua and membranes. 7,8 Within this context, TM is associated with a higher incidence of preterm la- bor, prelabor rupture of membranes, placental abruption, fetal growth re- striction, and low birthweight. 2,9-18 A strong association exists between maternal T helper-1 (Th1)-type immu- nity and pregnancy loss, whereas a shift towards Th2-type cytokine response has been observed in successful pregnancy. 19 Cytokines are known to play an impor- tant role in implantation. An imbalance in cytokine production occurs in early pregnancy loss. 20-22 Cytokine receptors such as tumor necrosis factor-receptor 1 (TNF-R1) have also been associated with miscarriage in their role as apoptosis- mediators through proinflammatory cy- tokines such as tumor necrosis factor al- pha (TNF). 23 Several factors in the maternal his- tory (such as age and smoking, bio- markers that include serum hormones levels, and the presence of a retropla- cental hematoma on ultrasound scan- ning) have been investigated as possi- ble predictors of pregnancy outcome in women with TM. 24-27 It has been shown that after TM, maternal serum inhibin A in combination with other serum markers, such as hCG, are altered in women who subsequently have a first-trimester miscarriage. 28,29 The biomarkers that give the best pre- dictive values are a combination of se- From the Academic Department of Obstetrics and Gynecology, UCL Institute for Women’s Health (Drs Calleja-Agius and Jauniaux) and the Research Department of Haematology, UCL Cancer Institute (Mr Pizzey), University College London, Chenies Mews, London, United Kingdom; and the Anu Research Centre, UCC Department of Obstetrics and Gynaecology, Cork University Maternity Hospital, Wilton, Cork, Republic of Ireland (Dr Muttukrishna). Received Oct. 12, 2010; revised Jan 25, 2011; accepted Feb. 14, 2011. Reprints: Jean Calleja-Agius, MD, Department of Anatomy, Faculty of Medicine and Surgery, University of Malta, Tal-Qroqq, MSD 2080, Malta. [email protected]. Authorship and contribution to the article is limited to the 4 authors indicated. There was no outside funding or technical assistance with the production of this article. 0002-9378/$36.00 © 2011 Published by Mosby, Inc. doi: 10.1016/j.ajog.2011.02.051 Research www. AJOG.org 83.e8 American Journal of Obstetrics & Gynecology JULY 2011
Transcript of Pro- and antiinflammatory cytokines in threatened miscarriages

t
icdac
Research www.AJOG.org
BASIC SCIENCE: OBSTETRICS
Pro- and antiinflammatory cytokinesin threatened miscarriagesJean Calleja-Agius, MD; Shanthi Muttukrishna, PhD, DSc; Arnold R. Pizzey; Eric Jauniaux, MD, PhD
T
wr
OBJECTIVE: The purpose of this study was to evaluate circulating andintracellular levels of Th1 and Th2 cytokines in women with threatenedmiscarriage (TM) and subsequent outcome.
STUDY DESIGN: Plasma levels of tumor necrosis factor (TNF)-recep-ors 1 and 2, TNF�, interferon gamma (IFN�), and interleukins (IL) -6
and -10 were measured by flow cytometric bead assays in 80 womenwith TM: 53 women with normal outcome and 27 women who miscar-ried. Fluorescent antibody labeling was also performed on whole bloodin a subgroup of 27 women of TM: 16 women with normal outcome and
2011;205:83.e8-16.
n3ar
bor, prelabor rupturdoi: 10.1016/j.ajog.2011.02.051
83.e8 American Journal of Obstetrics & Gynecology JULY 2011
RESULTS: Monocyte expression of TNF� and circulating levels ofNF�, IFN�, IL-10, IL-6, and TNF-R1 were significantly lower, whereas
circulating levels of TNF�/IL-10, IFN�/IL-10, and TNF�/IL-6 ratiosere significantly higher, in women with TM who subsequently miscar-
ied, compared with the women with normal outcome.
CONCLUSION: An increased Th1 type of immune response, which wassimilar to that observed in preterm delivery, was found in TM cases thatwere complicated by a subsequent miscarriage.
Key words: cytokine, interleukin-10, threatened miscarriage, TNF
11 women who miscarried. receptor, tumor necrosis factorCite this article as: Calleja-Agius J, Muttukrishna S, Pizzey AR, et al. Pro- and antiinflammatory cytokines in threatened miscarriages. Am J Obstet Gynecol
Threatened miscarriage (TM) is de-fined as a history of vaginal bleeding
n early pregnancy in the presence of alosed cervix and with ultrasonic evi-ence of an intrauterine gestational sacnd a fetal heartbeat.1 TM is the mostommon complication of ongoing preg-
From the Academic Department ofObstetrics and Gynecology, UCL Institutefor Women’s Health (Drs Calleja-Agius andJauniaux) and the Research Department ofHaematology, UCL Cancer Institute (MrPizzey), University College London, CheniesMews, London, United Kingdom; and theAnu Research Centre, UCC Department ofObstetrics and Gynaecology, CorkUniversity Maternity Hospital, Wilton,Cork, Republic of Ireland (DrMuttukrishna).
Received Oct. 12, 2010; revised Jan 25, 2011;accepted Feb. 14, 2011.
Reprints: Jean Calleja-Agius, MD, Departmentof Anatomy, Faculty of Medicine and Surgery,University of Malta, Tal-Qroqq, MSD 2080,Malta. [email protected].
Authorship and contribution to the article islimited to the 4 authors indicated. There wasno outside funding or technical assistance withthe production of this article.
0002-9378/$36.00© 2011 Published by Mosby, Inc.
ancy, which occurs in approximately0% of pregnant women, and is associ-ted with a 10-14% risk of full miscar-iage.2,3 Various management protocols
have been developed that included con-servative management and hormonaltherapy that were based on progester-one4 and human chorionic gonadotro-pin (hCG).5 Overall, TM can generategreat anxiety in patients, especially be-cause bleeding in early pregnancy canlead to pregnancy loss and other obstet-ric complications.6
The pathophysiology of TM is linkedto bleeding from uteroplacental vesselsat the margin of the placenta withblood accumulating between the cho-rionic membrane and uterine wall.7
The formation of a subchorionic he-matoma may disrupt the placental bed.If the hematoma expands to the rest ofthe placental mass, it will induce com-plete miscarriage within a week of thefirst symptoms.8 If bleeding is limitedor happens close to the internal cervi-cal os and is evacuated, the pregnancymay continue; however, this can leadto a chronic inflammatory reactionwithin the decidua and membranes.7,8
Within this context, TM is associatedwith a higher incidence of preterm la-
e of membranes,
placental abruption, fetal growth re-striction, and low birthweight.2,9-18
A strong association exists betweenmaternal T helper-1 (Th1)-type immu-nity and pregnancy loss, whereas a shifttowards Th2-type cytokine response hasbeen observed in successful pregnancy.19
Cytokines are known to play an impor-tant role in implantation. An imbalancein cytokine production occurs in earlypregnancy loss.20-22 Cytokine receptorssuch as tumor necrosis factor-receptor 1(TNF-R1) have also been associated withmiscarriage in their role as apoptosis-mediators through proinflammatory cy-tokines such as tumor necrosis factor al-pha (TNF�).23
Several factors in the maternal his-tory (such as age and smoking, bio-markers that include serum hormoneslevels, and the presence of a retropla-cental hematoma on ultrasound scan-ning) have been investigated as possi-ble predictors of pregnancy outcomein women with TM.24-27 It has beenshown that after TM, maternal seruminhibin A in combination with otherserum markers, such as hCG, arealtered in women who subsequentlyhave a first-trimester miscarriage.28,29
The biomarkers that give the best pre-
dictive values are a combination of se-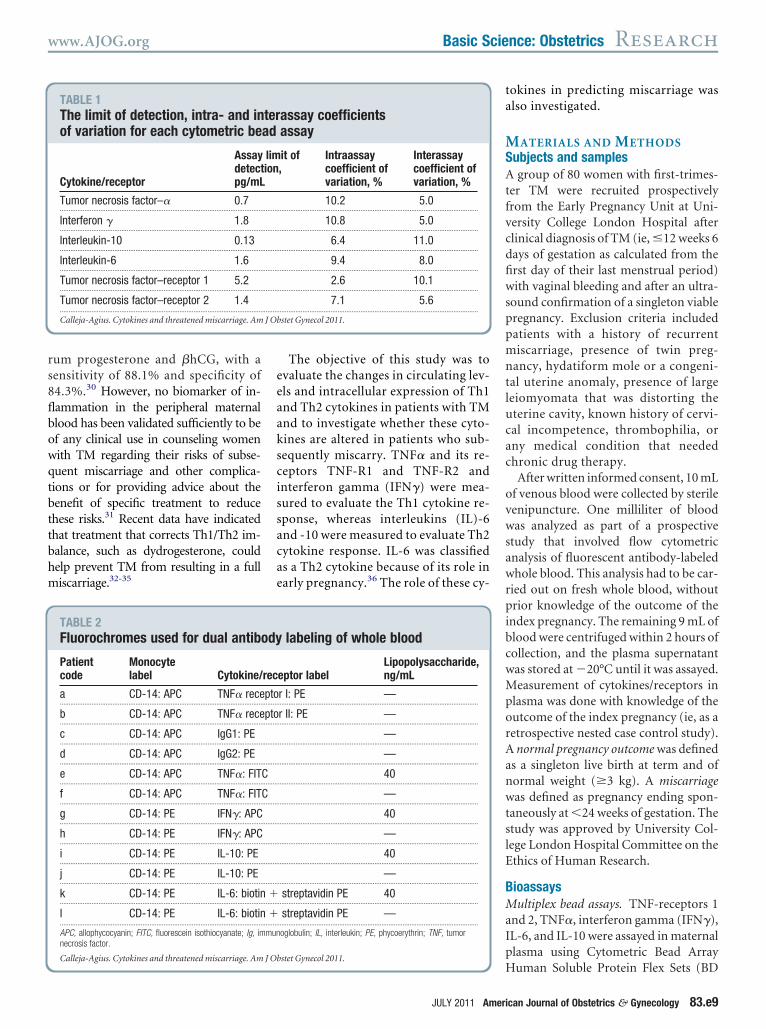
flbowqtbttbhm
ta
J Ob
www.AJOG.org Basic Science: Obstetrics Research
rum progesterone and �hCG, with asensitivity of 88.1% and specificity of84.3%.30 However, no biomarker of in-
ammation in the peripheral maternallood has been validated sufficiently to bef any clinical use in counseling womenith TM regarding their risks of subse-uent miscarriage and other complica-ions or for providing advice about theenefit of specific treatment to reducehese risks.31 Recent data have indicatedhat treatment that corrects Th1/Th2 im-alance, such as dydrogesterone, couldelp prevent TM from resulting in a fulliscarriage.32-35
TABLE 1The limit of detection, intra- and inof variation for each cytometric be
Cytokine/receptor
Assaydetectpg/mL
Tumor necrosis factor–� 0.7...................................................................................................................
Interferon � 1.8...................................................................................................................
Interleukin-10 0.13...................................................................................................................
Interleukin-6 1.6...................................................................................................................
Tumor necrosis factor–receptor 1 5.2...................................................................................................................
Tumor necrosis factor–receptor 2 1.4...................................................................................................................
Calleja-Agius. Cytokines and threatened miscarriage. Am
TABLE 2Fluorochromes used for dual antib
Patientcode
Monocytelabel Cytokine/
a CD-14: APC TNF� rece...................................................................................................................
b CD-14: APC TNF� rece...................................................................................................................
c CD-14: APC IgG1: PE...................................................................................................................
d CD-14: APC IgG2: PE...................................................................................................................
e CD-14: APC TNF�: FIT...................................................................................................................
f CD-14: APC TNF�: FIT...................................................................................................................
g CD-14: PE IFN�: APC...................................................................................................................
h CD-14: PE IFN�: APC...................................................................................................................
i CD-14: PE IL-10: PE...................................................................................................................
j CD-14: PE IL-10: PE...................................................................................................................
k CD-14: PE IL-6: biotin...................................................................................................................
l CD-14: PE IL-6: biotin...................................................................................................................
APC, allophycocyanin; FITC, fluorescein isothiocyanate; Ig, imnecrosis factor.
Calleja-Agius. Cytokines and threatened miscarriage. Am J Ob
The objective of this study was toevaluate the changes in circulating lev-els and intracellular expression of Th1and Th2 cytokines in patients with TMand to investigate whether these cyto-kines are altered in patients who sub-sequently miscarry. TNF� and its re-ceptors TNF-R1 and TNF-R2 andinterferon gamma (IFN�) were mea-sured to evaluate the Th1 cytokine re-sponse, whereas interleukins (IL)-6and -10 were measured to evaluate Th2cytokine response. IL-6 was classifiedas a Th2 cytokine because of its role inearly pregnancy.36 The role of these cy-
assay coefficientsassay
it of,
Intraassaycoefficient ofvariation, %
Interassaycoefficient ofvariation, %
10.2 5.0..................................................................................................................
10.8 5.0..................................................................................................................
6.4 11.0..................................................................................................................
9.4 8.0..................................................................................................................
2.6 10.1..................................................................................................................
7.1 5.6..................................................................................................................
stet Gynecol 2011.
labeling of whole blood
eptor labelLipopolysaccharide,ng/mL
r I: PE —..................................................................................................................
r II: PE —..................................................................................................................
—..................................................................................................................
—..................................................................................................................
40..................................................................................................................
—..................................................................................................................
40..................................................................................................................
—..................................................................................................................
40..................................................................................................................
—..................................................................................................................
streptavidin PE 40..................................................................................................................
streptavidin PE —..................................................................................................................
oglobulin; IL, interleukin; PE, phycoerythrin; TNF, tumor
stet Gynecol 2011.
JULY 2011 Ameri
okines in predicting miscarriage waslso investigated.
MATERIALS AND METHODSSubjects and samplesA group of 80 women with first-trimes-ter TM were recruited prospectivelyfrom the Early Pregnancy Unit at Uni-versity College London Hospital afterclinical diagnosis of TM (ie, �12 weeks 6days of gestation as calculated from thefirst day of their last menstrual period)with vaginal bleeding and after an ultra-sound confirmation of a singleton viablepregnancy. Exclusion criteria includedpatients with a history of recurrentmiscarriage, presence of twin preg-nancy, hydatiform mole or a congeni-tal uterine anomaly, presence of largeleiomyomata that was distorting theuterine cavity, known history of cervi-cal incompetence, thrombophilia, orany medical condition that neededchronic drug therapy.
After written informed consent, 10 mLof venous blood were collected by sterilevenipuncture. One milliliter of bloodwas analyzed as part of a prospectivestudy that involved flow cytometricanalysis of fluorescent antibody-labeledwhole blood. This analysis had to be car-ried out on fresh whole blood, withoutprior knowledge of the outcome of theindex pregnancy. The remaining 9 mL ofblood were centrifuged within 2 hours ofcollection, and the plasma supernatantwas stored at �20°C until it was assayed.Measurement of cytokines/receptors inplasma was done with knowledge of theoutcome of the index pregnancy (ie, as aretrospective nested case control study).A normal pregnancy outcome was definedas a singleton live birth at term and ofnormal weight (�3 kg). A miscarriagewas defined as pregnancy ending spon-taneously at �24 weeks of gestation. Thestudy was approved by University Col-lege London Hospital Committee on theEthics of Human Research.
BioassaysMultiplex bead assays. TNF-receptors 1and 2, TNF�, interferon gamma (IFN�),IL-6, and IL-10 were assayed in maternalplasma using Cytometric Bead Array
terad
limion
.........
.........
.........
.........
.........
.........
ody
rec
pto.........
pto.........
.........
.........
C.........
C.........
.........
.........
.........
.........
�.........
�.........
mun
Human Soluble Protein Flex Sets (BD
can Journal of Obstetrics & Gynecology 83.e9

wcegFTto
FawtLglsrDwjcAafcatt
1vosmpw
sw
a3mu
qtptaCpmP(Uu
1ticiwpCGt
Tfto
T
CO
J Ob
Research Basic Science: Obstetrics www.AJOG.org
Biosciences, San Jose, CA). The scope ofthis cytometric bead array was to allowfor multiplexed analysis of different cy-tokines and receptors on smaller quanti-ties of plasma, when compared with theuse of conventional enzyme-linked im-munosorbent assay. The experiment wascarried out according to the manufactur-er’s instructions and as previously pub-lished.37 Acquisition of the sample data
as performed with a bioanalyzer flowytometer (BD FACSArray; BD Biosci-nces). The data were presented inraphic and tabular formats with theCAP Array software (BD Biosciences).he limit of detection for each assay and
he intraassay and interassay coefficientsf variation are shown in Table 1.
low cytometric analysis of fluorescentntibody-labeled whole blood. Initialhole blood validation experiments showed
hat 40 ng/mL of lipopolysaccharide (40PS) and an incubation period of 12 hoursave the highest increment above basalevel (0 LPS) in terms of cytokine expres-ion by the activated monocytes, whileetaining a high monocyte population.ual antibody labeling was carried outith specific antibodies that were con-
ugated to spectrally distinct fluoro-hromes to enable easy discrimination.ll samples were labeled with mousenti-human antibody (AbD Serotec, Ox-ord, UK) that was specific for mono-ytes (CD 14). Different aliquots werelso labeled with antihuman antibodieshat were specific to the cytokine/recep-or of interest (Table 2).
With the use of aseptic techniques,.5 mL of whole blood from each indi-idual patient was mixed with 1.5 mLf Dulbecco phosphate-buffered salineolution without Ca��, Mg��. One
illiliter of this whole blood/Dulbeccohosphate-buffered saline solutionas placed into 4 200-�L aliquots (Ta-
ble 2). The other 2 mL aliquots wereseparated into 2 separate 1-mL ali-quots. Ten microliters of monensinsodium solution (Sigma-Aldrich, St.Louis, MO) and 10 �L of 40 LPS solu-tion were added to 1 aliquot (stimu-lated); only 10 �L of monensin sodiumolution (Sigma-Aldrich) without LPS
as added to the other aliquot. Both 483.e10 American Journal of Obstetrics & Gynecolo
liquots were placed in a water bath at7°C and shaken at 20 rev/min. Nor-al atmospheric composition was
sed instead of a CO2 system to ensurethat the samples were kept as close tothe physiologic state as possible. After12 hours incubation, the samples ineach tube were further divided into 4200-�L aliquots, to a total of 8 ali-
uots, each of which was labeled withhe patient’s code and lettered e-l, de-ending on the antibody combinationo be added and whether LPS wasdded (Table 2). Ten microliters ofD14 antibody were added to the sam-le and incubated in the dark for 15inutes at room temperature. Fix and
erm Cell Permeabilization ReagentsCaltag; Invitrogen, Paisley, Scotland,K) were added according to the man-facturer’s instructions, followed by 5
�L of the second antibody (TNF�, IL-0, TNF� receptor, or negative con-rol). The sample was again incubatedn the dark for 20 minutes, washed, andentrifuged. The pellet was resuspendedn 200 �L of wash buffer. Each cryovialas kept at 4°C in the dark until the sam-le was read by the flow cytometer (DakoyAn ADP; Advanced Digital Processing,lostrup, Denmark), which was operated
hrough the Summit software (version
TABLE 3Patient demographics
Parameter Outcome
Body mass index, kg/m2 Normal outco................................
Miscarriage...................................................................................................................
Gestation, wk Normal outco................................
Miscarriage...................................................................................................................
Parity, births Normal outco................................
Miscarriage...................................................................................................................
Age, y Normal outco................................
Miscarriage...................................................................................................................
White ethnicity, % Normal outco................................
Miscarriage...................................................................................................................
Patient demographics of all the patients with threatened mipregnancy outcome, 53 women; TM with subsequent miscarri2 groups in terms of body mass index, gestation, parity, age,a Considered to be not significant.
Calleja-Agius. Cytokines and threatened miscarriage. Am
.31; Summit Software, Little Rock, AR).
gy JULY 2011
he results were then saved in file formator post-acquisition spectral compensa-ion and data analysis (FCS 2.0; Dako Col-rado Inc, Fort Collins, CO).
Statistical analysisThe results generated by the FCAPArray software and Summit softwarewere entered in Microsoft Excel (ver-sion 2003; Microsoft Corporation,
FIGURE 1Comparison of cytokinelevels in plasma
TNF IFN IL-10 IL-60
2
4
6
8
10
TM - Normal Pregnancy OutcomeTM - Miscarriage
Cyt
oki
ne
in p
g/m
L
Graph shows significantly higher cytokine levelsin patients with threatened miscarriage (TM )with normal outcome. See Table 4 for probabilityvalues.IL, interleukin; IFN, interferon; pg/mL, picograms per milliliter;NF, tumor necrosis factor.
alleja-Agius. Cytokines and threatened miscarriage. Am Jbstet Gynecol 2011.
Mean SEM P valuea
23.63 .47 .63.................................................................................................................
24.18 1.05..................................................................................................................
8.10 .40 .24.................................................................................................................
7.45 .37..................................................................................................................
.43 .10 .61.................................................................................................................
.52 .14..................................................................................................................
30.57 .74 .07.................................................................................................................
32.41 .68..................................................................................................................
77 .59.................................................................................................................
70..................................................................................................................
iage (TM) who were recruited in this study (TM normal27 women) showed no significant difference between thethnicity.
stet Gynecol 2011.
me.........
.........
me.........
.........
me.........
.........
me.........
.........
me.........
.........
scarrage,and e

geenrfpscw
.Iisw.u
dt9bptaatT
www.AJOG.org Basic Science: Obstetrics Research
Redmond, WA). For the purpose ofanalysis, patients were matched for eth-nicity, gestation, body mass index, age,and parity. Data were normalized by log
FIGURE 2Comparison of tumor necrosis fact
TNF-R1 in pg/mL
TM -
Liveb
irths
TM -
Mis
carri
age
0
50
100
150
200
TM - Normal Pregnancy OutcomeTM - Miscarriage
There is a significantly higher level of TNF-R1normal pregnancy outcome (P � .05).Calleja-Agius. Cytokines and threatened miscarriage. Am J O
FIGURE 3Comparison of Th1/Th2 cytokineratios in plasma
There are significantly higher tumor necrosis factor(TNF )-�/IL-10, TNF-�/interleukin (IL)-6, and inter-feron (IFN )�/IL-10 ratios in patients with threatenedmiscarriage (TM ) who subsequently miscarried thanin women with a normal pregnancy outcome (P �.001, P � .049, P � .001, respectively).Calleja-Agius. Cytokines and threatened miscarriage. Am JObstet Gynecol 2011.
transformation, and unpaired t test wascarried out for the plasma and intracel-lular cytokine and receptor levels. Themean and SEM of the actual values wereentered in GraphPad Prism 5 (GraphPadSoftware Inc, La Jolla, CA) to generategraphs. Analysis was carried out withSPSS software (version 12 for Windows;SPSS Inc, Chicago, IL) for significancetesting. A probability value of � .05 wasconsidered statistically significant.
Intercooled STATA 9.1 (StataCorp,College Station, TX) was used to gener-ate nonparametric receiver operatorcharacteristics curves for each cytokine/receptor. Each biomarker was ranked ac-cording to the area under the graph, andconfidence intervals were calculated. Toidentify the best biomarker combinationfor the prediction of miscarriage, step-wise logistic regression was carried out,followed by discriminant analysis on theresulting combination to quantify thespecificity, sensitivity, and positive pre-dictive value.38
RESULTSOf the 80 patients with TM who were re-cruited in the retrospective nested casecontrol study, 53 patients had normalpregnancy outcome that resulted in a
(TNF ) receptors in plasma
TNF-R2 in pg/mL
TM- Liv
ebirt
hs
TM- M
isca
rriag
e
0
000
000
000
000
TM - Normal Pregnancy Outcome
TM - Miscarriage
atients with threatened miscarriage (TM ) with
t Gynecol 2011.
singleton live birth at term and of normal
JULY 2011 Americ
weight (10-90th percentile); 27 patientssubsequently miscarried at �24 weeks ofestation. There was no statistical differ-nce in body mass index, parity, age, andthnicity between patients with TM withormal outcome and those who miscar-ied (Table 3). The mean gestational ageor patients with TM who had normalregnancy outcome and those who sub-equently miscarried was not signifi-antly different (9 weeks 6 days and 8eeks 3 days, respectively; P � .73). Flow
cytometric analysis of fluorescent anti-body-labeled whole blood was carriedout on a subgroup of 27 patients: 16 pa-tients had normal outcome, and 11 pa-tients subsequently miscarried.
Circulating cytokine and receptorlevels in the plasmaCirculating levels of TNF�, IFN�, IL-10,IL-6, and TNF-R1 in plasma were signif-icantly higher in patients with TM whohad normal pregnancy outcome than inpatients who subsequently miscarried(P � .001, � .05, � .001, � .005, and �05, respectively). TNF�/IL-10, TNF�/L-6, and IFN�/IL-10 ratios were signif-cantly higher in patients with TM whoubsequently miscarried than in thoseith normal pregnancy outcome (P �
001, � .05, and � .001, respectively; Fig-res 1-3; Table 4).The biomarker that was the best pre-
ictor of miscarriage was TNF-R2, withhe highest area under the curve (0.65;5% confidence interval, 0.47– 0.75; Ta-le 5; Figure 4). At a cutoff value of 2202g/mL, TNF-R2 gave a positive predic-ive value of 44%, a sensitivity of 63%,nd a specificity of 62%. Discriminantnalysis showed that the best combina-ion of biomarkers was TNF-R2 andNF�, which gave a positive predictive
value of 66%, a sensitivity of 54%, and aspecificity of 92%.
Intracellular cytokine and receptorlevels in whole bloodIn whole blood, the number of CD-14cells that were positive for each indi-vidual cytokine was measured both atunstimulated basal level (0 LPS) andafter LPS stimulation (40 LPS; Figure4). In monocytes, there was a signifi-
or
1
2
3
4
in p
bste
cantly higher level of stimulated TNF�
an Journal of Obstetrics & Gynecology 83.e11

aiopuwr
nw
mit
stirasbp
iTcatrsacsimipc
pvi
Research Basic Science: Obstetrics www.AJOG.org
levels (TNF 40 LPS/TNF 0 LPS; P �.05) in women with TM who had nor-mal pregnancy outcome comparedwith those who miscarried. The me-dian number of CD-14 cells that werepositive for TNF-Rs were measured atunstimulated basal levels only, andthere was no significant difference be-tween women with TM who had nor-mal pregnancy outcome and those whomiscarried (Figure 5).
The ratio of Th1/Th2 cytokines wascalculated both at unstimulated basallevel and as a ratio of percentage fold in-crease in cytokine expression. At basallevel, Th1/Th2 ratio was measured inwhole blood without LPS stimulation asTNF�/IL-10, TNF�/IL-6, IFN�/IL-10,nd IFN�/IL-6. Also, the percentage foldncrease with LPS stimulation (40/0 LPS)f each individual Th1 cytokine overercentage fold increase of each individ-al Th2 cytokine was calculated. Thereas no significant difference in any of the
TABLE 4Comparison of circulatingcytokine and receptor levelsin the plasma in threatenedmiscarriage with normalpregnancy outcome andwith subsequent miscarriage
Cytokine/receptor P value
TNF� � .001a
...........................................................................................................
IFN� � .05a
...........................................................................................................
IL-10 � .001a
...........................................................................................................
IL-6 � .005a
...........................................................................................................
TNF-R1 � .05a
...........................................................................................................
TNF-R2 Not significant...........................................................................................................
TNF�/IL-10 � .001a
...........................................................................................................
TNF�/IL-6 � .05a
...........................................................................................................
IFN�/IL-10 � .001a
...........................................................................................................
IFN�/IL-6 Not significant...........................................................................................................
t test showed that there were statistically significantelevated levels of TNF�, IFN�, IL-10, IL-6, and TNF-R1in threatened miscarriage in women who proceeded tolive birth; the women with threatened miscarriage whomiscarried had statistically higher ratios of TNF�/IL-10, TNF�/IL-6, and IFN�/IL-10.IFN, interferon; IL, interleukin; TNF, tumor necrosis fac-tor.a Considered to be statistically significant.
Calleja-Agius. Cytokines and threatened miscarriage.Am J Obstet Gynecol 2011.
atios between patients with TM with
83.e12 American Journal of Obstetrics & Gynecolo
ormal pregnancy outcome and thoseho miscarried (Figure 6).
COMMENTThe results of this study indicated thatwomen with TM during the first trimes-ter who subsequently miscarried had animbalance in the circulatory Th1/Th2cytokine levels, with a shift towards aTh1 type of immune response. Similarfindings have been found previously inwomen with recurrent or complete mis-carriage,21,22 whereas women with a nor-
al pregnancy outcome do not have anmbalance in their plasma Th1/Th2 cy-okine ratio.19,39,40 These findings sug-
gest that changes in levels of cytokinescould play a role in the determination ofthe risk of miscarriage in women withfirst trimester TM.
The mechanism by which intrauterinebleeding alters maternal circulating hor-mone and cytokine levels is not well-de-fined. Up to week 9-10 of gestation, pla-cental villi cover the entire surface of thechorionic sac. As the gestational sacgrows during fetal life, the villi that areassociated with the decidua capsularissurrounding the amniotic sac degenerateand form the chorion leave, whereas villithat are associated with the deciduabasalis proliferate and form the defini-tive placenta.7 We previously havehown that the underlying uteroplacen-al circulation in the center of the prim-tive placenta is plugged, whereas in pe-iphery the mouth of the spiral arteriesre never plugged by the trophoblastichell, which allows limited maternallood flow to enter the marginal zone oflacenta from 8-9 weeks of gestation.8
This leads to higher local O2 concentra-tion at a stage of pregnancy when the tro-phoblast possesses low concentrations ofthe main antioxidant enzymes superox-ide dismutase, catalase, and glutathioneperoxidase.7 Focal trophoblastic oxi-dative damage and progressive villousdegeneration trigger the formation of fe-tal membranes, which remodels theuteroplacental interface. First-trimestervaginal bleeding has been associatedwith increased maternal levels of free se-rum �-hCG,41 possibly because of a rise
in hCG transfer into the maternal circu-gy JULY 2011
lation because of the disruption of thematernofetal interface. Bleeding in thesubchorionic space can result in elevatedbioavailability of free iron, catalyzing thegeneration of hydroxyl radicals and sub-sequent free-radical damage to the sur-rounding tissues. The oxidative stressand focal rise in oxygenation may alsostimulate the synthesis of various tro-phoblastic proteins such as hCG andestrogens.
We found that all cytokines that wereinvestigated in our study, both proin-flammatory (TNF� and IFN�) and anti-nflammatory (IL-10 and IL-6) andNF-R1, were significantly higher in theirculation of women with TM who had
normal pregnancy outcome than inhose women who subsequently miscar-ied. Intracellular TNF� levels after LPStimulation were also higher in TM with
normal pregnancy outcome. This isomparable with the findings of anothertudy that shows that TNF� productionn women with a history of recurrent
iscarriage who subsequently miscarrys significantly lower than in normalregnant women with successful out-ome.42 It has been proposed that TNF�
is essential in preventing the birth of off-spring with structural anomalies43 and
rotects embryos who are exposed to de-elopmental toxins.44 Therefore, the risen TNF� and other cytokines could be
TABLE 5Values of AUC of the ROCcurves and CIs for eachcytokine and receptor
BiomarkerArea underthe curve 95% CI
TNF-R2 0.65 0.47–0.75...........................................................................................................
TNF-R1 0.36 0.22–0.50...........................................................................................................
IFN� 0.36 0.22–0.49...........................................................................................................
IL-6 0.31 0.18–0.43...........................................................................................................
TNF� 0.29 0.19–0.39...........................................................................................................
IL-10 0.12 0.01–0.23...........................................................................................................
TNF-R2 is the best single predictor of miscarriage, withan area under the curve of 0.65.AUC, area under the curve; CI, confidence interval; IFN,interferon; IL, interleukin; ROC, receiver operator char-acteristic; TNF, tumor necrosis factor.
Calleja-Agius. Cytokines and threatened miscarriage.Am J Obstet Gynecol 2011.
secondary to the insult caused by the pre-

slc
T
tw
I
p
it
C
www.AJOG.org Basic Science: Obstetrics Research
mature entry of oxygenated maternalblood in the developing placenta in TM.If the offspring is otherwise normal, ele-vated TNF� levels, in fact, might have aprotective effect to dampen the harmthat is caused by oxidative stress, thus al-lowing the TM to proceed to a normaloutcome. IFN� production by periph-eral lymphocytes in very early pregnancyis higher in normal women comparedwith women with recurrent miscar-riage.42 By contrast, IL-10 is known to bean antiinflammatory cytokine,45 and ashown in our study and others,46,47 highevels of IL-10 are associated with suc-essful outcome.
We also found that, when the ratios of
FIGURE 4Receiver operator characteristics (
Tumor necrosis factor (TNF )-R2 was shown to bnterval, 0.47-0.75). A cutoff level of 2202 pg/mhe prediction of miscarriage.
IFN, interferon; IL, interleukin.
alleja-Agius. Cytokines and threatened miscarriage. Am J O
h1/Th2 cytokines were calculated,
here was a shift towards Th1 cytokinesith elevated TNF�/IL-10 and IFN�/
IL-10 ratios in patients with TM whosubsequently miscarried. This suggeststhat, if there is a rise in proinflammatorycytokines in women with TM, there is aneven bigger rise in the antiinflammatorycytokines to counteract the harmful ef-fect of proinflammatory cytokines suchas TNF� and IFN�. TNF�/IL-10 andFN�/IL-10 ratios are more representa-
tive of the Th1/Th2 balance, rather thanthe absolute individual cytokine levels. Ifthere is an overall imbalance with a pre-dominance of Th1 cytokines, then TMends up in miscarriage. This pattern iscomparable with that found in women
C ) curves for each cytokine and rece
e biomarker that best predicts miscarriage, withf TNF-R2 gave a sensitivity of 63%, a specificity
t Gynecol 2011.
with recurrent miscarriages; the Th1/
JULY 2011 Americ
Th2 cytokine balance of women with TMwho proceed to normal pregnancy out-come is similar to women with successfulpregnancy outcome.48-55
Our data also show that the TNF�/IL-6 ratio, but not the IFN�/IL-6 ratio,was also significantly higher in womenwith subsequent miscarriage. This couldbe explained by the fact that IL-6 hasboth pro- and antiinflammatory proper-ties. The classification of IL-6 as a Th1-type cytokine in studies on preterm la-bor56,57 or as a Th2 type cytokine in early
regnancy58-61 remains controversial.Recently, it has been demonstrated thatIL-6 is involved in the promotion of Th2differentiation and the inhibition of Th1
or
area under the curve of 0.65 (95% confidence62%, and a positive predictive value of 44% for
RO pt
e th anL o of
bste
polarization.62 During the first trimes-
an Journal of Obstetrics & Gynecology 83.e13

tTolai
c
e
mflwbhg
tocmmctkiko
C
Research Basic Science: Obstetrics www.AJOG.org
ter, IL-6 contributes to tissue remodelingthat is associated with placentation, thehematopoiesis function of the secondaryyolk sac, and the generation of newvessels in placental villi.36 One possiblemechanism of IL-6 in preventing mis-carriage is modulation of the quality ofthe Th2 response by increasing the pro-portion of blocking asymmetric anti-bodies during implantation and placen-tal vascularization.62
Although the sensitivity and specificityof the cytokines/receptors in our studyare not accurate enough for treatmentdecisions, a combination of cytokines to-gether with other biomarkers in the fu-ture may prove to be useful clinically.Previous studies have shown that TNF-receptors are useful in first-trimesterscreening of women who are at subse-quent risk of preeclampsia.63,64 By con-rast, elevated levels of TNF-R1 andNF-R2 have been described as markersf normal human pregnancy, although a
ack of soluble TNF-receptors have beenssociated with spontaneous miscarriage
FIGURE 5Cytokines in monocytes in whole b
TNFalpha
TM-N
ormal
TM-M
isca
rriag
e
0
2
4
6
8
100 LPS40 LPS
TN
Fal
ph
a /
pg
/mL
IL10
TM-N
ormal
TM-M
isca
rriag
e
0
5
10
150 LPS40 LPS
IL1
0 /
pg
/mL
There is a significantly higher tumor necrosis facstimulation in patients with threatened miscarriagIFN, interferon; IL, interleukin; pg/mL, picograms per milliliter.
alleja-Agius. Cytokines and threatened miscarriage. Am J O
n women who undergo recurrent mis-
83.e14 American Journal of Obstetrics & Gynecolo
arriage.65 In our study, there was signif-icantly higher TNF-R1 levels in theplasma of patients with TM who had anormal pregnancy. Circulating TNF-re-ceptor levels reflect TNF� activity; thus,levated plasma levels of TNF� can be
explained by increased levels of TNF-receptors.
The novelty of this study is that bloodsampling has been carried out in patientswith TM at the time of presentation witha viable fetus who then were followedprospectively. Most other studies in-clude women who had already miscar-ried.66-68 In contrast to what previousinvestigators have carried out, whereexperiments were done on cultured pe-ripheral blood mononuclear cells,69,70
fluorescent antibody-labeled whole bloodwas analyzed by flow cytometry in thiscase. In view of the patient groups thatwere recruited (pregnant women whowere experiencing vaginal bleeding inthe first trimester), we aimed to samplesmaller volumes of blood (1 mL) for theentire experiment (100 �L/cytokine or
dIFN gamma
TM-N
ormal
TM-M
isca
rriag
e
0
20
40
60
80
1000 LPS40 LPS
IFN
gam
ma
/ p
g/m
L
IL6
TM-N
ormal
TM-M
isca
rriag
e
0
20
40
600 LPS40 LPS
IL6
/ p
g/m
L
(TNF )-� elevation on lipopolysaccharide (LPS )TM ) with normal pregnancy outcome (P � .05).
t Gynecol 2011.
receptor), compared with a minimum of m
gy JULY 2011
50 mL in the peripheral blood mononu-clear cell culture experiments. Also,whole blood analysis with incubation, ascarried out in our study, with the use of awater bath at 37°C in atmospheric con-ditions, rather than in a CO2 incubator,
imics physiologic conditions and re-ects the in vivo scenario, comparedith experiments on isolated peripherallood mononuclear cells. This methodas been used successfully by otherroups as well.71-73
The limitation of this study was thatinevitably there were fewer women whowere recruited whose threatened preg-nancy ended up in miscarriage, espe-cially in the flow cytometry subgroup.Epidemiologic studies have shown thatthe miscarriage rate in women with TMis up to 14%.74 The other drawback ofhis study was that we did not have datan the karyotype of the products of con-eption of the patients who eventuallyiscarried. The reason for this is thatost patients either had a complete mis-
arriage or were treated expectantly;herefore, it was not possible to carry outaryotyping. The reason that karyotyp-ng would have been useful is that it isnown that up to 50% of miscarriagesccur because of a chromosomal abnor-
FIGURE 6Median levels of TNF receptorsin monocytes at basal(unstimulated) levels
TNFR1 TNFR20
10
20
30
40
TM - Normal Pregnancy OutcomeTM - Miscarriage
Type of TNF receptors
Rec
epto
rs in
pg
/mL
There were no significant differences betweenthreatened miscarriage (TM ) with normal preg-nancy outcome and miscarriage.pg/mL, picograms per milliliter; TNF, tumor necrosis factor.
Calleja-Agius. Cytokines and threatened miscarriage. Am JObstet Gynecol 2011.
loo
tore (
bste
ality.75,76 Also, it has been shown that

tds
m
www.AJOG.org Basic Science: Obstetrics Research
patients with a history of miscarriage anddecreased circulating levels of TNF� hada significantly higher chance of having asubsequent miscarriage with normalkaryotype.77
The immune response towards ele-vated Th1 cytokines that has been dem-onstrated in our study in patients withTM who subsequently miscarry is simi-lar to that described in preterm delivery.The onset of preterm labor is associatedwith increased proinflammatory cyto-kines such as TNF�.78 Progesteronereatment reduces the rates of pretermelivery in singleton pregnancies withhort cervical length79 and in women
with a history of preterm birth80 by pre-venting TNF�-induced apoptosis of fetal
embranes.81,82 Future clinical trialsand in vitro studies should be carried outto confirm the effect of progesterone inreversing the imbalance of Th1/Th2 inwomen with TM. f
REFERENCES1. Cunningham FG, Leveno KJ, Bloom S,Hauth J, Rouse D, Spong C. William’s Obstet-rics. New York: McGraw-Hill, 2010.2. Basama FM, Crosfill F. The outcome of preg-nancies in 182 women with threatened miscar-riage. Arch Gynecol Obstet 2004;270:86-90.3. Hill LM, Guzick D, Fries J, Hixson J. Fetal lossrate after ultrasonically documented cardiac ac-tivity between 6 and 14 weeks, menstrual age.J Clin Ultrasound 1991;19:221-3.4. Wahabi HA, Abed Althagafi NF, Elawad M.Progestogen for treating threatened miscar-riage. Cochrane Database Syst Rev 2007;3:CD005943.5. Devaseelan P, Fogarty PP, Regan L. Humanchorionic gonadotropin for threatened miscar-riage. Cochrane Database Syst Rev 2010;5:CD007422.6. Saraswat L, Bhattacharya S, Maheshwari A,Bhattacharya S. Maternal and perinatal out-come in women with threatened miscarriage inthe first trimester: a systematic review. BJOG2010;117:245-57.7. Jauniaux E, Hempstock J, Greenwold N,Burton GJ. Trophoblastic oxidative stress in re-lation to temporal and regional differences inmaternal placental blood flow in normal and ab-normal early pregnancies. Am J Pathol 2003;162:115-25.8. Jauniaux E, Watson AL, Hempstock J, BaoYP, Skepper JN, Burton GJ. Onset of maternalarterial blood flow and placental oxidativestress: a possible factor in human early preg-nancy failure. Am J Pathol 2000;157:2111-22.9. Johns J, Jauniaux E. Threatened miscarriageas a predictor of obstetric outcome. Obstet Gy-
necol 2006;107:845-50.10. Mulik V, Bethel J, Bhal K. A retrospectivepopulation-based study of primigravid womenon the potential effect of threatened miscarriageon obstetric outcome. J Obstet Gynaecol2004;24:249-53.11. Wijesiriwardana A, Bhattacharya S, ShettyA, Smith N, Bhattacharya S. Obstetric outcomein women with threatened miscarriage in thefirst trimester. Obstet Gynecol 2006;107:557-62.12. Verma SK, Premi HK, Gupta TV, Thakur S,Gupta KB, Randhawa I. Perinatal outcome ofpregnancies complicated by threatened abor-tion. J Indian Med Assoc 1994;92:364-5.13. Ananth CV, Savitz DA. Vaginal bleeding andadverse reproductive outcomes: a meta-analy-sis. Paediatr Perinat Epidemiol 1994;8:62-78.14. Weiss JL, Malone FD, Vidaver J, et al.Threatened abortion: a risk factor for poor preg-nancy outcome, a population-based screeningstudy. Am J Obstet Gynecol 2004;190:745-50.15. van Oppenraaij RHF, Jauniaux E, Christian-sen OB, Horcajadas JA, Farquharson RG, Ex-alto N. Predicting adverse obstetric outcomeafter early pregnancy events and complications:a review. Hum Reprod Update 2009;15:409-21.16. Tongsong T, Srisomboon J, Wanapirak C,Sirichotiyakul S, Pongsatha S, Polsrisuthikul T.Pregnancy outcome of threatened abortionwith demonstrable fetal cardiac activity: a co-hort study. J Obstet Gynaecol 1995;21:331-5.17. Saraswat L, Bhattacharya S, MaheshwariA, Bhattacharya S. Maternal and perinatal out-come in women with threatened miscarriage inthe first trimester: a systematic review. BJOG2010;117:245-57.18. Johns J, Hyett J, Jauniaux E. Obstetric out-come after threatened miscarriage with andwithout a hematoma on ultrasound. Obstet Gy-necol 2003;102:483-7.19. Wegmann TG, Lin H, Guilbert L, MosmannTR. Bidirectional cytokine interactions in thematernal-fetal relationship: is successful preg-nancy a TH-2 phenomenon? Immunol Today1993;14:353-6.20. Chaouat G, Dubanchet S, Ledee N. Cyto-kines: important for implantation? J Assist Re-prod Genet 2007;24:491-505.21. Niederkorn JY. See no evil, hear no evil, dono evil: the lessons of immune privilege. NatImmunol 2006;7:354-9.22. Haider S, Knofler M. Human tumour necro-sis factor: physiological and pathological rolesin placenta and endometrium. Placenta 2009;30:111-23.23. Yu XW, Yan CF, Jin H, Li X. Tumor necrosisfactor receptor 1 expression and early sponta-neous abortion. Int J Gynaecol Obstet 2005;88:44-8.24. Choong S, Rombauts L, Ugoni A, MeagherS. Ultrasound prediction of risk of spontaneousmiscarriage in live embryos from assisted con-ceptions. Ultrasound Obstet Gynecol 2003;22:571-7.25. Makrydimas G, Sebire NJ, Lolis D, Vlassis
N, Nicolaides KH. Fetal loss following ultra-JULY 2011 Americ
sound diagnosis of a live fetus at 6-10 weeks ofgestation. Ultrasound Obstet Gynecol 2003;22:368-72.26. Dumps P, Meisser A, Pons D, et al. Accu-racy of single measurements of pregnancy-as-sociated plasma protein-A, human chorionicgonadotropin and progesterone in the diagno-sis of early pregnancy failure. Eur J Obstet Gy-necol Reprod Biol 2002;100:174-80.27. Johns J, Muttukrishna S, Lygnos M,Groome N, Jauniaux E. Maternal serum hor-mone concentrations for prediction of adverseoutcome in threatened miscarriage. ReprodBiomed Online 2007;15:413-21.28. Florio P, Luisi S, D’Antona D, Severi FM,Rago G, Petraglia F. Maternal serum inhibin Alevels may predict pregnancy outcome inwomen with threatened abortion. Fertil Steril2004;81:468-70.29. Treetampinich C, O’Connor AE, MacLachlanV, Groome NP, de Kretser DM. Maternal seruminhibin A concentrations in early pregnancy afterIVF and embryo transfer reflect the corpus luteumcontribution and pregnancy outcome. Hum Re-prod 2000;15:2028-32.30. Duan L, Yan D, Zeng W, Yang X, Wei Q.Predictive power progesterone combined withbeta human chorionic gonadotropin measure-ments in the outcome of threatened miscar-riage. Arch Gynecol Obstet 2011;283:431-5.31. Christiansen OB, Nielsen HS, Kolte AM. In-flammation and miscarriage. Semin Fetal Neo-natal Med 2006;11:302-8.32. Liu F, Luo SP. Effect of Chinese herbaltreatment on Th1- and Th2-type cytokines, pro-gesterone and beta-human chorionic gonado-tropin in early pregnant women of threatenedabortion. Chin J Integr Med 2009;15:353-8.33. Clark DA. Should anti-TNF-alpha therapybe offered to patients with infertility and recur-rent spontaneous abortion? Am J Reprod Im-munol 2009;61:107-12.34. Ali YM, Kuriya B, Orozco C, Cush JJ, Key-stone EC. Can tumor necrosis factor inhibitorsbe safely used in pregnancy? J Rheumatol2010;37:9-17.35. Raghupathy R, Kalinka J. Cytokine imbal-ance in pregnancy complications and its mod-ulation. Front Biosci 2008;13:985-94.36. Jauniaux E, Gulbis B, Schandene L, Col-lette J, Hustin J. Distribution of interleukin-6 inmaternal and embryonic tissues during the firsttrimester. Mol Hum Reprod 1996;2:239-43.37. Chen R, Lowe L, Wilson JD, et al. Simulta-neous quantification of six human cytokines in asingle sample using microparticle-based flowcytometric technology. Clin Chem 1999;45:1693-4.38. Mamtani MR, Thakre TP, Kalkonde MY, etal. A simple method to combine multiple molec-ular biomarkers for dichotomous diagnosticclassification. BMC Bioinformatics 2006;7:442.39. Sacks GP, Clover LM, Bainbridge DR, Red-man CW, Sargent IL. Flow cytometric measure-ment of intracellular Th1 and Th2 cytokine pro-duction by human villous and extravillous
cytotrophoblast. Placenta 2001;22:550-9.an Journal of Obstetrics & Gynecology 83.e15

Research Basic Science: Obstetrics www.AJOG.org
40. Sacks GP, Redman C, Sargent I. The im-munology of human pregnancy. In: Studd J, ed.Progress in obstetrics and gynaecology. Kid-lington, UK: Elsevier Science Limited; 2003:17-32.41. De Biasio P, Canini S, Crovo A, Prefumo F,Venturini PL. Early vaginal bleeding and first-trimester markers for Down syndrome. PrenatDiagn 2003;23:470-3.42. Bates MD, Quenby S, Takakuwa K, John-son PM, Vince GS. Aberrant cytokine produc-tion by peripheral blood mononuclear cells inrecurrent pregnancy loss? Hum Reprod 2002;17:2439-44.43. Toder V, Fein A, Carp H, Torchinsky A. TNF-alpha in pregnancy loss and embryo maldevel-opment: a mediator of detrimental stimuli or aprotector of the fetoplacental unit? J Assist Re-prod Genet 2003;20:73-81.44. Torchinsky A, Shepshelovich J, OrensteinH, et al. TNF-alpha protects embryos exposedto developmental toxicants. Am J Reprod Im-munol 2003;49:159-68.45. Blanco O, Tirado I, Munoz-Fernandez R, etal. Human decidual stromal cells expressHLA-G: Effects of cytokines and decidualiza-tion. Hum Reprod 2008;23:144-52.46. Marzi M, Vigano A, Trabattoni D, et al. Char-acterization of type 1 and type 2 cytokine pro-duction profile in physiologic and pathologic hu-man pregnancy. Clin Exp Immunol 1996;106:127-33.47. Koch CA, Platt JL. T cell recognition andimmunity in the fetus and mother. Cell Immunol2007;248:12-7.48. Rezaei A, Dabbagh A. T-helper (1) cyto-kines increase during early pregnancy inwomen with a history of recurrent spontaneousabortion. Med Sci Monit 2002;8:CR607-10.49. Raghupathy R. Pregnancy: success andfailure within the Th1/Th2/Th3 paradigm. SeminImmunol 2001;13:219-27.50. Raghupathy R, Makhseed M, Azizieh F,Omu A, Gupta M, Farhat R. Cytokine produc-tion by maternal lymphocytes during normal hu-man pregnancy and in unexplained recurrentspontaneous abortion. Hum Reprod 2000;15:713-8.51. Lim KJ, Odukoya OA, Ajjan RA, Li TC,Weetman AP, Cooke ID. The role of T-helpercytokines in human reproduction. Fertil Steril2000;73:136-42.52. Kwak-Kim JY, Chung-Bang HS, Ng SC, etal. Increased T helper 1 cytokine responses bycirculating T cells are present in women withrecurrent pregnancy losses and in infertilewomen with multiple implantation failures afterIVF. Hum Reprod 2003;18:767-73.53. Yamada H, Morikawa M, Furuta I, et al. Cir-culating cytokines during early pregnancy inwomen with recurrent spontaneous abortion:decreased TNF-á levels in abortion with normalchromosome karyotype. Hokkaido J Med Sci2004;79:237-41.54. Yamada H, Morikawa M, Furuta I, et al. In-travenous immunoglobulin treatment in women
with recurrent abortions: increased cytokine83.e16 American Journal of Obstetrics & Gynecolo
levels and reduced Th1/Th2 lymphocyte ratio inperipheral blood. Am J Reprod Immunol 2003;49:84-9.55. Zammiti W, Mtiraoui N, Finan RR, AlmawiWY, Mahjoub T. Tumor necrosis factor alphaand lymphotoxin alpha haplotypes in idiopathicrecurrent pregnancy loss. Fertil Steril 2009;91:1903-8.56. Challis JR, Lockwood CJ, Myatt L, NormanJE, Strauss JF III, Petraglia F. Inflammation andpregnancy. Reprod Sci 2009;16:206-15.57. Greig PC, Murtha AP, Jimmerson CJ, Her-bert WN, Roitman-Johnson B, Allen J. Maternalserum interleukin-6 during pregnancy and dur-ing term and preterm labor. Obstet Gynecol1997;90:465-9.58. Orsi NM, Tribe RM. Cytokine networks andthe regulation of uterine function in pregnancyand parturition. J Neuroendocrinol 2008;20:462-9.59. Coffman RL, Romagnani S. Redirection ofTh1 and Th2 responses. Berlin: Springer-Ver-lag; 1999.60. Mosmann TR, Sad S. The expanding uni-verse of T-cell subsets: Th1, Th2 and more.Immunol Today 1996;17:138-46.61. Dubinsky V, Junovich G, Gentile T, Gutier-rez G. IL-6 as a regulatory factor of the humoralresponse during pregnancy. Am J Reprod Im-munol 2008;60:197-203.62. Snyder SK, Wessner DH, Wessells JL, et al.Pregnancy-specific glycoproteins function asimmunomodulators by inducing secretion of IL-10, IL-6 and TGF-beta1 by human monocytes.Am J Reprod Immunol 2001;45:205-16.63. Leal AM, Poon LC, Frisova V, Veduta A,Nicolaides KH. First-trimester maternal serumtumor necrosis factor receptor-1 and pre-ec-lampsia. Ultrasound Obstet Gynecol 2009;33:135-41.64. Visser W, Beckmann I, Knook MA, Wallen-burg HC. Soluble tumor necrosis factor recep-tor II and soluble cell adhesion molecule 1 asmarkers of tumor necrosis factor-alpha releasein preeclampsia. Acta Obstet Gynecol Scand2002;81:713-9.65. Chernyshov VP, Vodyanik MA, Pisareva SP.Lack of soluble TNF-receptors in women withrecurrent spontaneous abortion and possibilityfor its correction. Am J Reprod Immunol 2005;54:284-91.66. Christiaens I, Zaragoza DB, Guilbert L, Rob-ertson SA, Mitchell BF, Olson DM. Inflammatoryprocesses in preterm and term parturition. J Re-prod Immunol 2008;79:50-7.67. Dumps P, Meisser A, Pons D, et al. Accu-racy of single measurements of pregnancy-as-sociated plasma protein-A, human chorionicgonadotropin and progesterone in the diagno-sis of early pregnancy failure. Eur J Obstet Gy-necol Reprod Biol 2002;100:174-80.68. Johnson MR, Riddle AF, Grudzinskas JG,Sharma V, Collins WP, Nicolaides KH. Reducedcirculating placental protein concentrationsduring the first trimester are associated withpreterm labour and low birth weight. Hum Re-
prod 1993;8:1942-7.gy JULY 2011
69. Raghupathy R, Kalinka J. Cytokine imbal-ance in pregnancy complications and its mod-ulation. Front Biosci 2008;13:985-94.70. Sacks GP, Redman CW, Sargent IL. Mono-cytes are primed to produce the Th1 type cyto-kine IL-12 in normal human pregnancy: an in-tracellular flow cytometric analysis of peripheralblood mononuclear cells. Clin Exp Immunol2003;131:490-7.71. Bates MD, Quenby S, Takakuwa K, John-son PM, Vince GS. Aberrant cytokine produc-tion by peripheral blood mononuclear cells inrecurrent pregnancy loss? Hum Reprod 2002;17:2439-44.72. van Nieuwenhoven AL, Moes H, HeinemanMJ, Santema J, Faas MM. Cytokine productionby monocytes, NK cells, and lymphocytes isdifferent in preeclamptic patients as comparedwith normal pregnant women. Hypertens Preg-nancy 2008;27:207-24.73. Zahran WA, Ghonaim MM, Koura BA, El-Banna H, Ali SM, El-Sheikh N. A study of therole of IL-12 in pulmonary tuberculosis using thewhole blood flow cytometry technique. EgyptJ Immunol 2006;13:53-65.74. Colin IM, Isaac J, Dupret P, Ledant T,D’Hautcourt JL. Functional lymphocyte subsetassessment of the Th1/Th2 profile in patientswith autoimmune thyroiditis by flow cytometricanalysis of peripheral lymphocytes. J Biol RegulHomeost Agents 2004;18:72-6.75. Basama FM, Crosfill F. The outcome ofpregnancies in 182 women with threatenedmiscarriage. Arch Gynecol Obstet 2004;270:86-90.76. Lathi RB, Milki AA. Rate of aneuploidy inmiscarriages following in vitro fertilization andintracytoplasmic sperm injection. Fertil Steril2004;81:1270-2.77. Ljunger E, Cnattingius S, Lundin C, AnnerenG. Chromosomal anomalies in first-trimestermiscarriages. Acta Obstet Gynecol Scand2005;84:1103-7.78. Yamada H, Morikawa M, Furuta I, et al. Cir-culating cytokines during early pregnancy inwomen with recurrent spontaneous abortion:decreased TNF-� levels in abortion with normalchromosome karyotype. Hokkaido J Med Sci2004;79:237-41.79. Fonseca EB, Celik E, Parra M, Singh M,Nicolaides KH. Progesterone and the risk ofpreterm birth among women with a short cervix.N Engl J Med 2007;357:462-9.80. Meis PJ. Prevention of recurrent pretermdelivery by 17 alpha-hydroxyprogesteronecaproate. N Engl J Med 2003;348:2379-85.81. Luo G, Abrahams VM, Tadesse S, et al.Progesterone inhibits basal and TNF-alpha-in-duced apoptosis in fetal membranes: a novelmechanism to explain progesterone-mediatedprevention of preterm birth. Reprod Sci 2010;17:532-9.82. Kuon RJ, Shi SQ, Maul H, et al. Pharmaco-logic actions of progestins to inhibit cervical rip-ening and prevent delivery depend on theirproperties, the route of administration, and the
vehicle. Am J Obstet Gynecol 2010;202:455-9.



















