
Prevalence and Persistence of Health Problems After Childbirth: Associations with Parity and Method...
12
Prevalence and Persistence of Health Problems After Childbirth: Associations with Parity and Method of Birth Jane F. Thompson, MSc, PhD, Christine L. Roberts, MBBS, MPH, Marian Currie, BAppSci, RN, RM, and David A. Ellwood, DPhil, FRACGOG ABSTRACT: Background: Awareness about the extent of maternal physical and emotional health problems after childbirth is increasing, but few longitudinal studies examining their duration have been published. The aim of this study was to describe changes in the prevalence of maternal health problems in the 6 months after birth and their association with parity and method of birth. Methods: A population-based, cohort study was conducted in the Australian Capital Territory (ACT), Australia. The study population, comprising women who gave birth to a live baby from March to October 1997, completed 4 questionnaires on the fourth post- partum day, and at 8, 16, and 24 weeks postpartum. Outcome measures were self-reported health problems during each of the three 8-week postpartum periods up to 24 weeks. Results: A total of 1295 women participated, and 1193 (92%) completed the study. Health problems showing resolution between 8 and 24 weeks postpartum were exhaustion/extreme tiredness (60–49%), backache (53–45%), bowel problems (37–17%), lack of sleep/baby crying (30–15%), hemorrhoids (30–13%), perineal pain (22–4%), excessive/prolonged bleeding (20–2%), urinary incontinence (19–11%), mastitis (15–3%), and other urinary problems (5–3%). No significant changes occurred in the prevalence of frequent headaches or migraines, sexual problems, or depression over the 6 months. Adjusting for method of birth, primiparas were more likely than multiparas to report perineal pain and sexual problems. Compared with unassisted vaginal births, women who had cesarean sections reported more exhaustion, lack of sleep, and bowel problems; reported less perineal pain and urinary incontinence in the first 8 weeks; and were more likely to be readmitted to hospital within 8 weeks of the birth. Women with forceps or vacuum extraction reported more perineal pain and sexual problems than those with unassisted vaginal births after adjusting for parity, perineal trauma, and length of labor. Conclusions: Health problems commonly occurred after childbirth with some resolution over the 6 months postpartum. Some important differences in prevalence of health problems were evident when parity and method of birth were considered. (BIRTH 29:2 June 2002) Jane Thompson is a Senior Officer in Women’s and Children’s Health, The Canberra Hospital, Canberra; Christine Roberts is the Research Director at the New South Wales Centre for Perinatal Health Services Research and is a Senior Lecturer in the School of Population Health and Health Services Research at the University of Sydney, Sydney; Marian Currie is a midwife in The Canberra Hospital; and David Ellwood is Professor of Obstetrics and Gynaecology at the University of Sydney Canberra Clinical School, Canberra, Australia. This project was financially supported by a research grant funded by the Salaried Specialists at The Canberra Hospital, Canberra, ACT, Australia, and small grants from The Canberra Hospital Auxiliary, The Nurses’ Board of the ACT, and ACT Department of Health & Community Care, Canberra, Australia. Address correspondence to Dr. Jane F. Thompson, Women’s & Children’s Health, The Canberra Hospital, PO Box 11, Woden, ACT 2606, Australia. Ó 2002 Blackwell Publishing, Inc. BIRTH 29:2 June 2002 83
Transcript of Prevalence and Persistence of Health Problems After Childbirth: Associations with Parity and Method...
Prevalence and Persistence of Health ProblemsAfter Childbirth: Associations with Parity
and Method of Birth
Jane F. Thompson, MSc, PhD, Christine L. Roberts, MBBS, MPH, Marian Currie,BAppSci, RN, RM, and David A. Ellwood, DPhil, FRACGOG
ABSTRACT: Background: Awareness about the extent of maternal physical and emotionalhealth problems after childbirth is increasing, but few longitudinal studies examining theirduration have been published. The aim of this study was to describe changes in the prevalence ofmaternal health problems in the 6 months after birth and their association with parity andmethod of birth. Methods: A population-based, cohort study was conducted in the AustralianCapital Territory (ACT), Australia. The study population, comprising women who gave birthto a live baby from March to October 1997, completed 4 questionnaires on the fourth post-partumday, andat 8, 16, and24weeks postpartum.Outcomemeasureswere self-reportedhealthproblems during each of the three 8-week postpartumperiods up to 24weeks. Results:Atotal of1295 women participated, and 1193 (92%) completed the study. Health problems showingresolution between 8 and 24 weeks postpartum were exhaustion/extreme tiredness (60–49%),backache (53–45%), bowel problems (37–17%), lack of sleep/baby crying (30–15%),hemorrhoids (30–13%), perineal pain (22–4%), excessive/prolonged bleeding (20–2%),urinary incontinence (19–11%), mastitis (15–3%), and other urinary problems(5–3%). No significant changes occurred in the prevalence of frequent headaches or migraines,sexual problems, or depression over the 6 months. Adjusting for method of birth, primiparaswere more likely than multiparas to report perineal pain and sexual problems. Compared withunassisted vaginal births, women who had cesarean sections reported more exhaustion, lack ofsleep, and bowel problems; reported less perineal pain and urinary incontinence in the first 8weeks; andweremore likely to be readmitted to hospital within 8weeks of the birth.Womenwithforceps or vacuum extraction reported more perineal pain and sexual problems than thosewith unassisted vaginal births after adjusting for parity, perineal trauma, and length oflabor. Conclusions:Health problems commonly occurred after childbirth with some resolutionover the 6 months postpartum. Some important differences in prevalence of health problemswere evident when parity and method of birth were considered. (BIRTH 29:2 June 2002)
Jane Thompson is a Senior Officer inWomen’s and Children’s Health,The Canberra Hospital, Canberra; Christine Roberts is the ResearchDirector at the New SouthWales Centre for Perinatal Health ServicesResearch and is a Senior Lecturer in the School of Population Healthand Health Services Research at the University of Sydney, Sydney;Marian Currie is a midwife in The Canberra Hospital; and DavidEllwood is Professor of Obstetrics and Gynaecology at the Universityof Sydney Canberra Clinical School, Canberra, Australia.
This project was financially supported by a research grant funded by theSalaried Specialists at The Canberra Hospital, Canberra, ACT,
Australia, and small grants from The Canberra Hospital Auxiliary,The Nurses’ Board of the ACT, and ACT Department of Health &Community Care, Canberra, Australia.
Address correspondence to Dr. Jane F. Thompson, Women’s &Children’s Health, The Canberra Hospital, PO Box 11, Woden,ACT 2606, Australia.
� 2002 Blackwell Publishing, Inc.
BIRTH 29:2 June 2002 83

The health of women after childbirth is attracting adeserved level of attention (1). Information about theprevalence of a wide range of postpartum healthproblems, and the contribution of birth events, is nowavailable from several cross-sectional studies usingboth large (2–4) and smaller unselected samples (5).Other studies have applied cross-sectional, prospect-ive or retrospective methods to examine specificconditions, such as anal incontinence (6–10); urinaryincontinence (7,8,11–15); perineal pain (16,17); sexualhealth and function (18,19); backache (including apossible association with epidural use) (20–22);headache (23); fatigue (24–29); mastitis (30–32); andpostnatal depression (33–35). Other studies followedup specific subgroups of women for varying frequen-cies and durations, for example, trial participants forspecific outcomes such as perineal pain (36–40) or fora range of outcomes (41), or subgroups experiencingparticular interventions or methods of birth (42–46).
However, few prospective studies have examinedthe extent and duration of a range of morbidities inlarge unselected samples. With the exception of twoBritish studies (47,48) and a recent study conductedin France and Italy (49), previously published pros-pective studies examining women’s general postnatalhealth have had small sample sizes (50–52).
Our study used a large population-based sample todescribe the period prevalence of maternal healthproblems for each 8-week period up to 24 weekspostpartum. It aimed to examine if health problemsshowed significant resolution with time and theeffects of parity and method of birth on health andrecovery after childbirth.
Methods
The study was conducted in the Australian CapitalTerritory (ACT) during 1997 as part of a large projectdesigned to determine risk factors for postnataldepression. The ACT is the district surroundingAustralia’s national capital, Canberra, with an areaof 2400 km2 and a population of 308,000. In 1997, ofthe 4708 women who gave birth in the ACT, 87percent were ACT residents (53). The source popu-lation for the study comprised all women who wereliving in the ACT and planning to live there for atleast 6 months, were aged 16 years or more, and gavebirth to a live baby between March and October 1997in one of the area’s two public hospitals, two privatehospitals, or at home. Exclusions comprised womenwhose babies were admitted to the neonatal intensivecare unit or were adopted, or women who werecritically ill, unable to give informed consent, unableto complete the questionnaires, or participating inany other study. All study women gave their written
informed consent. The study was approved by theACT Department of Health and Community CareResearch Ethics Committee, and the ethics commit-tees of participating hospitals.
Postnatal ward or domiciliary midwives gaveinformation sheets to women in the first few daysafter birth. The first questionnaire was completed asclose to the fourth postpartum day as possible; womenwere then mailed questionnaires at 8, 16, and 24 weeksafter birth. To minimize loss to follow-up, remindercards were sent if questionnaires were not returnedwithin 2 weeks of mailing, and reminder telephonecalls were made at 3 and 4 weeks if necessary.
Questionnaire 1 covered sociodemographic char-acteristics of mother and partner, and obstetricdetails of the index and past pregnancies. Subsequentquestionnaires included the following question which,for comparability, was similar to that used in aprevious cross-sectional study in another Australianpopulation (4): Thinking about your health and howyou have been feeling over the past 8 weeks, have anyof the following been a problem for you? A list of12 common health problems followed: exhaustion/extreme tiredness; lack of sleep through baby crying;excessive or prolonged bleeding; backache; frequentheadaches or migraines; sexual problems; hemor-rhoids (piles); sore perineum; mastitis; bowel prob-lems (e.g., constipation or diarrhea); and urinaryincontinence (e.g., hard to hold urine when coughing,sneezing, or exercising) or other urinary problems(e.g., passing urine frequently or trouble passingurine). A ‘‘yes’’ or ‘‘no’’ answer was requested. Anopen-ended question asked women to list any otherhealth problems. The option ‘‘lack of sleep throughbaby crying’’ was included to distinguish the itemfrom sleeping difficulties due to maternal anxiety,depression, or other causes.
Depressive symptoms were assessed at 8, 16, and24 weeks using the 10-item Edinburgh PostnatalDepression Scale (EPDS), a self-report measure ofdepression developed for use in the postpartumperiod (54–56). Women who score above 12 arelikely to be suffering from a depressive illness. Thiscutoff is widely used in research and clinical practiceto differentiate between depressed and nondepressedwomen. Questions were also included about the useof health services in the 6 months postpartum,including readmission to hospital for either maternalor infant problems, and need for help and advice.
Data Analysis
The sample size estimate was based on assumptionsrelevant to the primary study hypothesis and isdescribed elsewhere (57). Statistical analyses were
84 BIRTH 29:2 June 2002
carried out usingSPSS forWindows, version 6.1.3. Theperiod prevalence of each health problem was deter-mined for each 8-week period. The CochranQ test wasused for more than two related proportions to assessdifferences over time. Differences between unrelatedproportions were tested using v2 tests. Unconditionallogistic regression was applied to determine adjustedodds ratios (AOR) with 95% confidence intervals.Variables to be included in logistic regression analyseswere selected after examining potential confoundingvariables (e.g., parity, perineal trauma, length oflabor, depression, breastfeeding status) and excludingthose not associated with both the exposure (e.g.,type of delivery) and outcome. Variables were notsimultaneously included in logistic regression analy-ses if they were likely to be intervening variables inthe exposure and outcome relationship (e.g., length oflabor, perineal trauma, perineal pain).
Women who had vaginal births assisted by eithervacuum extraction or forceps were grouped for theanalyses to increase the sample size. No statisticallysignificant differences occurred for any outcomesbetween women who had cesarean section with laborand without labor, so these two groups were alsopooled for analysis.
The significance level for statistical testing was setat p < 0:01 because of the number of tests beingconducted and the possibility of chance effects.
Results
Of the women eligible and approached, 1295 (70%)agreed to participate in the study, and of these, 1193(92%) were retained in the cohort to 6 monthspostpartum. The characteristics of the sample areshown in Table 1. The characteristics of those lost tofollow-up and a comparison of participants with allwomen who gave birth in 1997 are given elsewhere(57). Overall, participants were slightly older, morelikely to be in married or de facto relationships, tohave given birth in private hospitals, to be privatepatients, and to be of English-speaking backgroundthan all women who gave birth in the ACT in 1997.
Self-reported Health Problems
Complete data on the physical health problems ofinterest were available for all participants whoreturned questionnaires 2 (n ¼ 1254) and 3(n ¼ 1221). Of the 1193 participants who returnedquestionnaire 4, all but 4 women answered all partsof the question and 1 woman gave an ambiguousresponse (exhaustion/extreme tiredness). Two womendid not complete the EPDS at 8 weeks, 2 at 16 weeks,and 6 at 24 weeks.
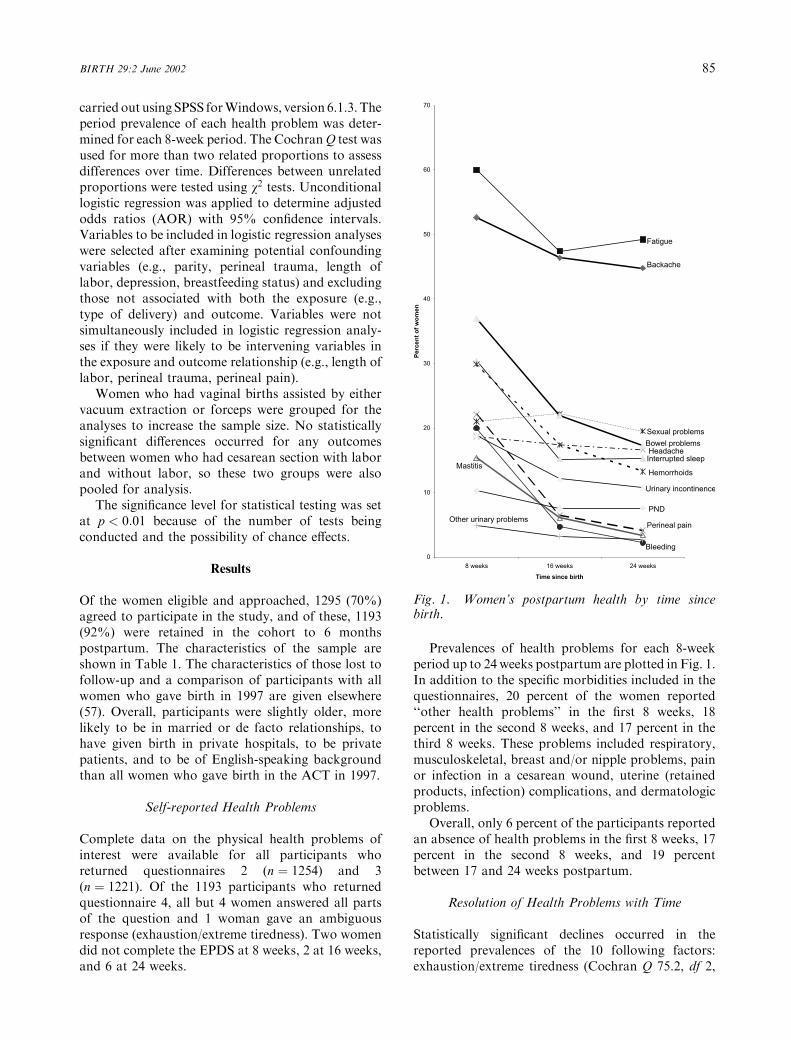
Prevalences of health problems for each 8-weekperiod up to 24 weeks postpartum are plotted in Fig. 1.In addition to the specific morbidities included in thequestionnaires, 20 percent of the women reported‘‘other health problems’’ in the first 8 weeks, 18percent in the second 8 weeks, and 17 percent in thethird 8 weeks. These problems included respiratory,musculoskeletal, breast and/or nipple problems, painor infection in a cesarean wound, uterine (retainedproducts, infection) complications, and dermatologicproblems.
Overall, only 6 percent of the participants reportedan absence of health problems in the first 8 weeks, 17percent in the second 8 weeks, and 19 percentbetween 17 and 24 weeks postpartum.
Resolution of Health Problems with Time
Statistically significant declines occurred in thereported prevalences of the 10 following factors:exhaustion/extreme tiredness (Cochran Q 75.2, df 2,
Fig. 1. Women’s postpartum health by time sincebirth.
BIRTH 29:2 June 2002 85
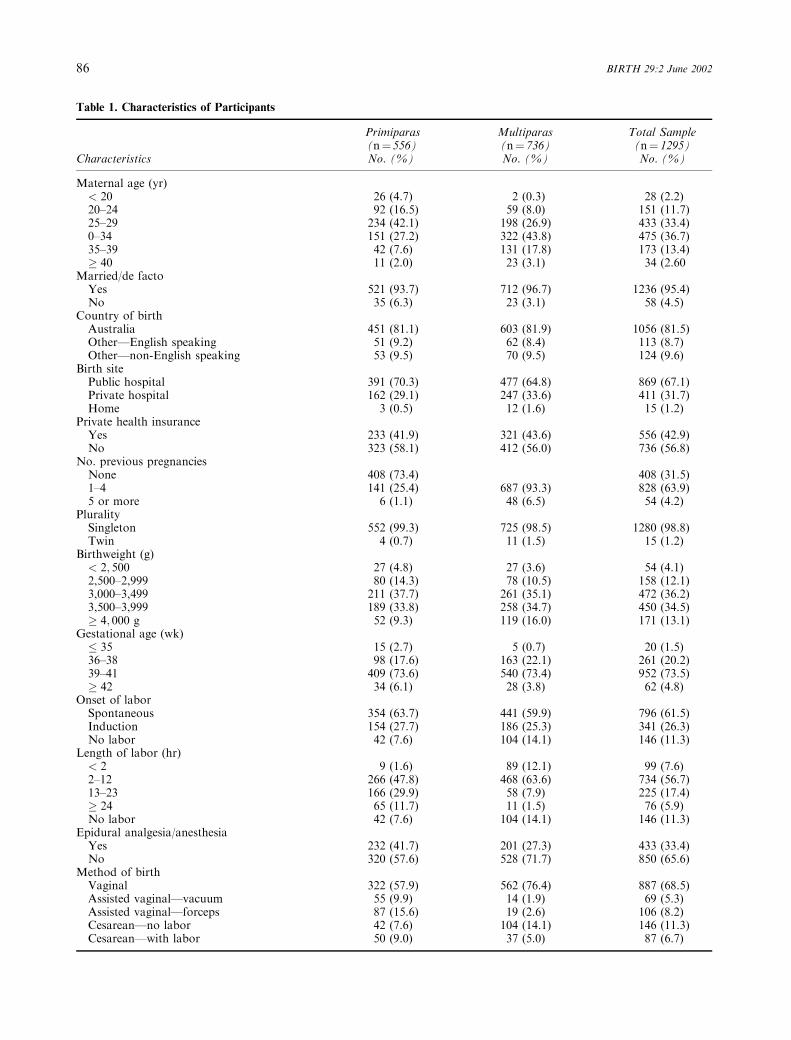
Table 1. Characteristics of Participants
Primiparas Multiparas Total Sample(n¼ 556) (n¼ 736) (n¼ 1295)
Characteristics No. (%) No. (%) No. (%)
Maternal age (yr)< 20 26 (4.7) 2 (0.3) 28 (2.2)20–24 92 (16.5) 59 (8.0) 151 (11.7)25–29 234 (42.1) 198 (26.9) 433 (33.4)0–34 151 (27.2) 322 (43.8) 475 (36.7)35–39 42 (7.6) 131 (17.8) 173 (13.4)� 40 11 (2.0) 23 (3.1) 34 (2.60
Married/de factoYes 521 (93.7) 712 (96.7) 1236 (95.4)No 35 (6.3) 23 (3.1) 58 (4.5)
Country of birthAustralia 451 (81.1) 603 (81.9) 1056 (81.5)Other—English speaking 51 (9.2) 62 (8.4) 113 (8.7)Other—non-English speaking 53 (9.5) 70 (9.5) 124 (9.6)
Birth sitePublic hospital 391 (70.3) 477 (64.8) 869 (67.1)Private hospital 162 (29.1) 247 (33.6) 411 (31.7)Home 3 (0.5) 12 (1.6) 15 (1.2)
Private health insuranceYes 233 (41.9) 321 (43.6) 556 (42.9)No 323 (58.1) 412 (56.0) 736 (56.8)
No. previous pregnanciesNone 408 (73.4) 408 (31.5)1–4 141 (25.4) 687 (93.3) 828 (63.9)5 or more 6 (1.1) 48 (6.5) 54 (4.2)
PluralitySingleton 552 (99.3) 725 (98.5) 1280 (98.8)Twin 4 (0.7) 11 (1.5) 15 (1.2)
Birthweight (g)< 2; 500 27 (4.8) 27 (3.6) 54 (4.1)2,500–2,999 80 (14.3) 78 (10.5) 158 (12.1)3,000–3,499 211 (37.7) 261 (35.1) 472 (36.2)3,500–3,999 189 (33.8) 258 (34.7) 450 (34.5)� 4; 000 g 52 (9.3) 119 (16.0) 171 (13.1)
Gestational age (wk)� 35 15 (2.7) 5 (0.7) 20 (1.5)36–38 98 (17.6) 163 (22.1) 261 (20.2)39–41 409 (73.6) 540 (73.4) 952 (73.5)� 42 34 (6.1) 28 (3.8) 62 (4.8)
Onset of laborSpontaneous 354 (63.7) 441 (59.9) 796 (61.5)Induction 154 (27.7) 186 (25.3) 341 (26.3)No labor 42 (7.6) 104 (14.1) 146 (11.3)
Length of labor (hr)< 2 9 (1.6) 89 (12.1) 99 (7.6)2–12 266 (47.8) 468 (63.6) 734 (56.7)13–23 166 (29.9) 58 (7.9) 225 (17.4)� 24 65 (11.7) 11 (1.5) 76 (5.9)No labor 42 (7.6) 104 (14.1) 146 (11.3)
Epidural analgesia/anesthesiaYes 232 (41.7) 201 (27.3) 433 (33.4)No 320 (57.6) 528 (71.7) 850 (65.6)
Method of birthVaginal 322 (57.9) 562 (76.4) 887 (68.5)Assisted vaginal—vacuum 55 (9.9) 14 (1.9) 69 (5.3)Assisted vaginal—forceps 87 (15.6) 19 (2.6) 106 (8.2)Cesarean—no labor 42 (7.6) 104 (14.1) 146 (11.3)Cesarean—with labor 50 (9.0) 37 (5.0) 87 (6.7)
86 BIRTH 29:2 June 2002

p < 0:001); lack of sleep through baby crying (Coch-ran Q 154.9, df 2, p < 0:001); excessive or prolongedbleeding (Cochran Q 308.6, df 2, p < 0:001); back-ache (Cochran Q 26.2, df 2, p < 0:001); hemorrhoids(Cochran Q 190.5, df 2, p < 0:001); perineal pain(Cochran Q 308.0, df 2, p < 0:001); mastitis (CochranQ 134.1, df 2, p < 0:001); bowel problems (CochranQ 190.6, df 2, p < 0:001); urinary incontinence(Cochran Q 71.4, df 2, p < 0:001); other urinaryproblems (Cochran Q 9.3, df 2, p < 0:01).
No statistically significant changes were detectedin the proportions of women reporting frequentheadaches or migraines, sexual problems, depressionand ‘‘other’’ health problems over the 6-monthfollow-up period.
Epidural Use
Of the participants with complete data, 433/1283(33%) reported use of epidural analgesia or anesthe-sia during delivery. No statistically significant associ-ation occurred between epidural use and backache atany time (8 wk: OR 1.04 [95% CI 0.83–1.33]; 16 wk:OR 1.29 [95% CI 1.02–1.64]; 24 wk: OR 1.15 [95%CI 0.90–1.46]). Similarly, women who had epiduralswere not significantly more likely to report headachesat any time (8 wk: OR 1.34 [95% CI 0.99–1.79]; 16wk: OR 1.28 [95% CI 0.94–1.73]; 24 wk: OR 1.36[95% CI 0.99–1.86]).
Differences by Parity
Data on parity were available for 1292 women, 556(43%) of whom were primiparas and 736 (57%)multiparas. Table 1 shows participants’ demographicand obstetric data. Among those who had a vaginaldelivery, primiparas were significantly more likely tohave vacuum or forceps assistance than multiparas(31% vs 6%, p < 0:001; (OR 7.51 [95% CI 4.94–11.47]) and to experience perineal trauma (episio-tomy, tear requiring stitches, or both) (71% vs 50%,p < 0:001 (OR 2.54 [95% CI 1.96–3.29]).
Primiparas were more likely than multiparas toreport lack of sleep through baby crying (OR 1.44[95% CI 1.13–1.84]) and backache (OR 1.27 [95%CI 1.01–1.58]) as problems for them in the first 8weeks postpartum; to report perineal pain at 8 (OR2.90 [95% CI 2.19–3.82]), 16 (OR 3.70 [95% CI2.23–6.14]), and 24 weeks (OR 4.28 [95% CI 2.21–8.30]); and to report sexual problems at 8 (OR 1.81[95% CI 1.38–2.38]), 16 (OR 1.58 [95% CI 1.21–2.08]), and 24 weeks (OR 1.40 [95% CI 1.05–1.87]).After adjustment for method of birth, a significantassociation remained between parity and perinealpain at 8 weeks postpartum (AOR 2.31 [95% CI1.71–3.14]), 16 weeks (AOR 3.15 [95% CI 1.85–5.36]), and 24 weeks (AOR 3.15 [95% CI 1.56–6.35]); and similarly, between parity and sexualproblems at 8 weeks postpartum (AOR 1.65 [95%CI 1.24–2.21]) and 16 weeks (AOR 1.42 [95% CI1.07–1.89]), but not at 24 weeks (AOR 1.26 [95% CI0.93–1.71], p ¼ 0:14). No statistically significantdifferences occurred between women having theirfirst or subsequent births in any of the otheroutcomes assessed.
Although both primiparas and multiparas showedsimilar trends in resolution of health problems overtime, exceptions occurred. Multiparas did not reportstatistically significant declines in either backache(Cochran Q 7.8, df 2, p ¼ 0:02) or other urinaryproblems (Cochran Q 1.8, df 2, p ¼ 0:41), whereasprimiparas did report declines: (Cochran Q 20.1, df 2,p < 0:001) and (Cochran Q 9.3, df 2, p < 0:01),respectively. In addition, whereas multiparas showeda trend toward resolution of symptoms of depressionover the 6-month follow-up period (Cochran Q 17.6,df 2, p ¼ 0:02), primiparas did not (Cochran Q 1.8,df 2, p ¼ 0:4).
Differences by Method of Birth
Data on method of birth were available for all 1295study participants (Table 1). Table 2 shows mater-nal health problems for all women by method of
Table 1. Continued
Primiparas Multiparas Total Sample(n¼ 556) (n¼ 736) (n¼ 1295)
Characteristics No. (%) No. (%) No. (%)
Perineal traumaTear requiring stitches 195 (35.1) 216 (29.3) 412 (31.8)Episiotomy 107 (19.2) 64 (8.7) 171 (13.2)Tear requiring stitches plus episiotomy 28 (5.0) 15 (2.0) 43 (3.3)Intact perineum 224 (40.3) 439 (59.6) 664 (51.3)
*Percentages may not add to 100 because of missing values.
BIRTH 29:2 June 2002 87

birth grouped for analysis as described above (seeMethods).
Cesarean Section Versus Unassisted Vaginal Delivery
Overall, compared with women having unassistedvaginal births, women who had cesarean sectionswere significantly more likely to report exhaustion/extreme tiredness (OR 1.45 [95% CI 1.07–1.98]); tobe troubled by lack of sleep through their baby crying(OR 1.56 [95% CI 1.15–2.12]) in the first 8 weeks; andto report bowel problems at 8 weeks (OR 1.57 [95%CI 1.16–2.11]) and 24 weeks (OR 1.61 [95% CI 1.11–2.34]), but this association was not significant at 16weeks (OR 1.39 [95% CI 0.99–1.96]).
Compared with women having unassisted vaginaldeliveries, women with cesarean sections were signi-ficantly (p< 0.001) less likely to report perineal painat 8 weeks (1.8% vs 21.8%), 16 weeks (0.9% vs6.2%), and 24 weeks (0.9% vs 3.3%); and to reporturinary incontinence at 8 weeks (OR 0.25 [95% CI0.14–0.44]), but this difference was not statisticallysignificant at 16 weeks (OR 0.59 [95% CI 0.35–0.99],p ¼ 0.05) and 24 weeks (OR 0.55 [95% CI 0.31–0.98], p ¼ 0.04). At 24 weeks postpartum, cesareandelivery women were more likely to report otherurinary problems than women having unassistedvaginal deliveries (OR 3.63 [95% CI 1.68–7.85]).
Cesarean Section Versus Assisted Vaginal Delivery
Compared with women having assisted vaginaldeliveries, women having cesarean sections weresignificantly less likely to report hemorrhoids at 8weeks (OR 0.56 [95% CI 0.36–0.86]); perineal pain at8 weeks (OR 0.02 [95% CI 0.01–0.05]), 16 weeks (OR0.05 [95% CI 0.01–0.22]), and 24 weeks (OR 0.07[95% CI 0.02–0.29]); and urinary incontinence at 8weeks (OR 0.18 [95% CI 0.10–0.35]), but not at16 weeks (OR 0.58 [95% CI 0.30–1.12], p ¼ 0:10) or24 weeks (OR 0.61 [95% CI 0.30–1.25], p ¼ 0:18).Cesarean delivery women were slightly more likely toreport other urinary problems at 24 weeks than thosehaving assisted vaginal deliveries, but this did notreach statistical significance (6.0% vs 3.6%,p ¼ 0:30).
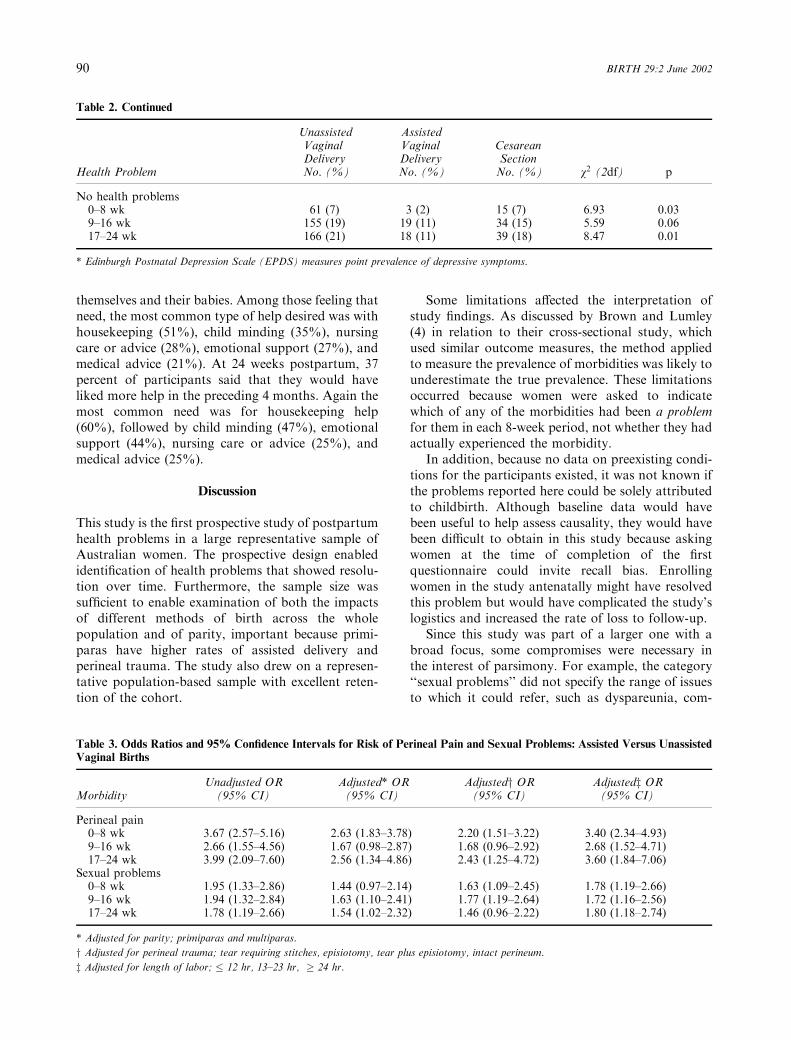
Assisted Vaginal Versus Unassisted Vaginal Delivery
The 175 women who had assisted vaginal deliverieswere more likely to report sexual problems andperineal pain at all three time periods than those whohad unassisted vaginal deliveries (Table 3). To assesswhether the associations between assisted vaginalbirth and higher rates of perineal pain and sexual
problems could be accounted for by differences inparity, length of labor, or perineal trauma, logisticregression models examined each of these factorsseparately. The associations of assisted vaginal birthwith sexual problems and perineal pain remainedsignificant even after separate adjustments for thesevariables (Table 3).
Bowel problems were more common amongwomen who had assisted vaginal deliveries thanthose with unassisted vaginal deliveries at all threetime periods (Table 2), but this trend did not reachstatistical significance at p < 0:01 : 8 weeks (OR 1.47[95% CI 1.05–2.06], p ¼ 0:03), 16 weeks (OR 1.30[95% CI 0.88–1.57], p ¼ 0:18), and 24 weeks (OR1.63 [95% CI 1.07–2.46], p ¼ 0:02). Among womenwith vaginal deliveries, those assisted by forceps orvacuum were not significantly more likely to reporturinary incontinence than those having unassisteddeliveries at any time (Table 2).
Hospital Readmissions by Method of Birth
Of the 1246 women with complete data, 90 (7.2%)reported readmission to hospital within 8 weeks ofthe birth for reasons related to either their baby’s(4.1%) or their own (2.9%) health, or both (0.2%).Overall, 120/1224 (9.8%) women with complete datareported admission to either secondary or tertiarymother and baby units for outreach, day stay, and/orresidential services. This group included 13 womenwho had also reported a readmission to hospital.
The primary reason for admission to hospital wasrelated the woman’s own health for 36/90 (40%), 51/90 (57%) for their baby’s health, and 3/90 (3%) forboth. Seventy-one women (78.9%) spent at least onenight in hospital; primiparas and multiparas wereequally likely to be readmitted (6.9% vs 7.3%,respectively).
Compared with women having unassisted vaginalbirths, cesarean delivery women were significantlymore likely to report readmission to hospital formaternal reasons (5.3% vs 2.2%; OR 2.46 [95% CI1.11–5.43]), as were women who had assisted vaginalbirths (4.8% vs 2.2%; OR 2.23 [95% CI 0.88–5.48],p ¼ 0:06), although this did not reach statisticalsignificance (p ¼ 0:01). No association was foundbetween method of birth and readmission to hospitalfor baby’s health (cesarean birth 5.8%, assistedvaginal birth 4.2%, unassisted vaginal birth 4.0%).
New Mothers’ Needs for Help and Advice
Overall, 40 percent of participants reported that theywould have liked more help and advice in the first 8weeks postpartum to assist them in looking after
88 BIRTH 29:2 June 2002
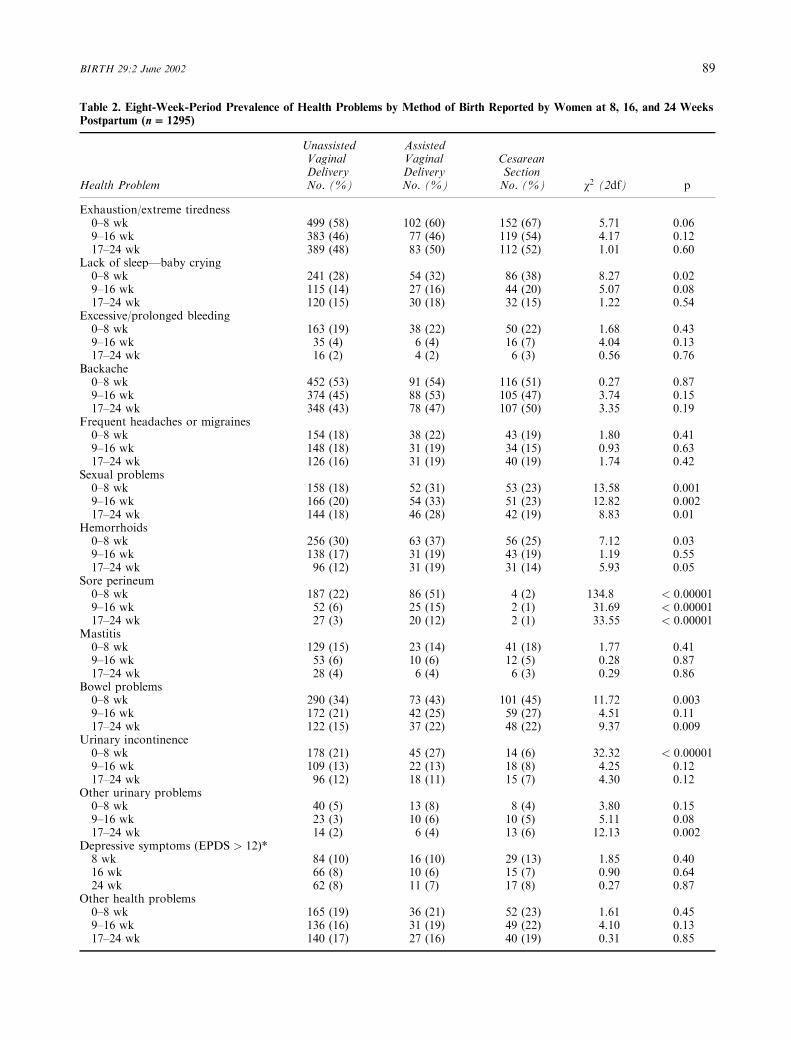
Table 2. Eight-Week-Period Prevalence of Health Problems by Method of Birth Reported by Women at 8, 16, and 24 Weeks
Postpartum (n = 1295)
Unassisted AssistedVaginal Vaginal CesareanDelivery Delivery Section
Health Problem No. (%) No. (%) No. (%) v2 (2df) p
Exhaustion/extreme tiredness0–8 wk 499 (58) 102 (60) 152 (67) 5.71 0.069–16 wk 383 (46) 77 (46) 119 (54) 4.17 0.1217–24 wk 389 (48) 83 (50) 112 (52) 1.01 0.60
Lack of sleep—baby crying0–8 wk 241 (28) 54 (32) 86 (38) 8.27 0.029–16 wk 115 (14) 27 (16) 44 (20) 5.07 0.0817–24 wk 120 (15) 30 (18) 32 (15) 1.22 0.54
Excessive/prolonged bleeding0–8 wk 163 (19) 38 (22) 50 (22) 1.68 0.439–16 wk 35 (4) 6 (4) 16 (7) 4.04 0.1317–24 wk 16 (2) 4 (2) 6 (3) 0.56 0.76
Backache0–8 wk 452 (53) 91 (54) 116 (51) 0.27 0.879–16 wk 374 (45) 88 (53) 105 (47) 3.74 0.1517–24 wk 348 (43) 78 (47) 107 (50) 3.35 0.19
Frequent headaches or migraines0–8 wk 154 (18) 38 (22) 43 (19) 1.80 0.419–16 wk 148 (18) 31 (19) 34 (15) 0.93 0.6317–24 wk 126 (16) 31 (19) 40 (19) 1.74 0.42
Sexual problems0–8 wk 158 (18) 52 (31) 53 (23) 13.58 0.0019–16 wk 166 (20) 54 (33) 51 (23) 12.82 0.00217–24 wk 144 (18) 46 (28) 42 (19) 8.83 0.01
Hemorrhoids0–8 wk 256 (30) 63 (37) 56 (25) 7.12 0.039–16 wk 138 (17) 31 (19) 43 (19) 1.19 0.5517–24 wk 96 (12) 31 (19) 31 (14) 5.93 0.05
Sore perineum0–8 wk 187 (22) 86 (51) 4 (2) 134.8 < 0:000019–16 wk 52 (6) 25 (15) 2 (1) 31.69 < 0:0000117–24 wk 27 (3) 20 (12) 2 (1) 33.55 < 0:00001
Mastitis0–8 wk 129 (15) 23 (14) 41 (18) 1.77 0.419–16 wk 53 (6) 10 (6) 12 (5) 0.28 0.8717–24 wk 28 (4) 6 (4) 6 (3) 0.29 0.86
Bowel problems0–8 wk 290 (34) 73 (43) 101 (45) 11.72 0.0039–16 wk 172 (21) 42 (25) 59 (27) 4.51 0.1117–24 wk 122 (15) 37 (22) 48 (22) 9.37 0.009
Urinary incontinence0–8 wk 178 (21) 45 (27) 14 (6) 32.32 < 0:000019–16 wk 109 (13) 22 (13) 18 (8) 4.25 0.1217–24 wk 96 (12) 18 (11) 15 (7) 4.30 0.12
Other urinary problems0–8 wk 40 (5) 13 (8) 8 (4) 3.80 0.159–16 wk 23 (3) 10 (6) 10 (5) 5.11 0.0817–24 wk 14 (2) 6 (4) 13 (6) 12.13 0.002
Depressive symptoms (EPDS > 12)*8 wk 84 (10) 16 (10) 29 (13) 1.85 0.4016 wk 66 (8) 10 (6) 15 (7) 0.90 0.6424 wk 62 (8) 11 (7) 17 (8) 0.27 0.87
Other health problems0–8 wk 165 (19) 36 (21) 52 (23) 1.61 0.459–16 wk 136 (16) 31 (19) 49 (22) 4.10 0.1317–24 wk 140 (17) 27 (16) 40 (19) 0.31 0.85
BIRTH 29:2 June 2002 89
themselves and their babies. Among those feeling thatneed, the most common type of help desired was withhousekeeping (51%), child minding (35%), nursingcare or advice (28%), emotional support (27%), andmedical advice (21%). At 24 weeks postpartum, 37percent of participants said that they would haveliked more help in the preceding 4 months. Again themost common need was for housekeeping help(60%), followed by child minding (47%), emotionalsupport (44%), nursing care or advice (25%), andmedical advice (25%).
Discussion
This study is the first prospective study of postpartumhealth problems in a large representative sample ofAustralian women. The prospective design enabledidentification of health problems that showed resolu-tion over time. Furthermore, the sample size wassufficient to enable examination of both the impactsof different methods of birth across the wholepopulation and of parity, important because primi-paras have higher rates of assisted delivery andperineal trauma. The study also drew on a represen-tative population-based sample with excellent reten-tion of the cohort.
Some limitations affected the interpretation ofstudy findings. As discussed by Brown and Lumley(4) in relation to their cross-sectional study, whichused similar outcome measures, the method appliedto measure the prevalence of morbidities was likely tounderestimate the true prevalence. These limitationsoccurred because women were asked to indicatewhich of any of the morbidities had been a problemfor them in each 8-week period, not whether they hadactually experienced the morbidity.
In addition, because no data on preexisting condi-tions for the participants existed, it was not known ifthe problems reported here could be solely attributedto childbirth. Although baseline data would havebeen useful to help assess causality, they would havebeen difficult to obtain in this study because askingwomen at the time of completion of the firstquestionnaire could invite recall bias. Enrollingwomen in the study antenatally might have resolvedthis problem but would have complicated the study’slogistics and increased the rate of loss to follow-up.
Since this study was part of a larger one with abroad focus, some compromises were necessary inthe interest of parsimony. For example, the category‘‘sexual problems’’ did not specify the range of issuesto which it could refer, such as dyspareunia, com-
Table 3. Odds Ratios and 95% Confidence Intervals for Risk of Perineal Pain and Sexual Problems: Assisted Versus Unassisted
Vaginal Births
Unadjusted OR Adjusted* OR Adjustedy OR Adjustedz ORMorbidity (95% CI) (95% CI) (95% CI) (95% CI)
Perineal pain0–8 wk 3.67 (2.57–5.16) 2.63 (1.83–3.78) 2.20 (1.51–3.22) 3.40 (2.34–4.93)9–16 wk 2.66 (1.55–4.56) 1.67 (0.98–2.87) 1.68 (0.96–2.92) 2.68 (1.52–4.71)17–24 wk 3.99 (2.09–7.60) 2.56 (1.34–4.86) 2.43 (1.25–4.72) 3.60 (1.84–7.06)
Sexual problems0–8 wk 1.95 (1.33–2.86) 1.44 (0.97–2.14) 1.63 (1.09–2.45) 1.78 (1.19–2.66)9–16 wk 1.94 (1.32–2.84) 1.63 (1.10–2.41) 1.77 (1.19–2.64) 1.72 (1.16–2.56)17–24 wk 1.78 (1.19–2.66) 1.54 (1.02–2.32) 1.46 (0.96–2.22) 1.80 (1.18–2.74)
* Adjusted for parity; primiparas and multiparas.
y Adjusted for perineal trauma; tear requiring stitches, episiotomy, tear plus episiotomy, intact perineum.z Adjusted for length of labor; � 12 hr, 13–23 hr, � 24 hr.
Table 2. Continued
Unassisted AssistedVaginal Vaginal CesareanDelivery Delivery Section
Health Problem No. (%) No. (%) No. (%) v2 (2df) p
No health problems0–8 wk 61 (7) 3 (2) 15 (7) 6.93 0.039–16 wk 155 (19) 19 (11) 34 (15) 5.59 0.0617–24 wk 166 (21) 18 (11) 39 (18) 8.47 0.01
* Edinburgh Postnatal Depression Scale (EPDS) measures point prevalence of depressive symptoms.
90 BIRTH 29:2 June 2002

munication difficulties with partner, lack of desire, orresumption of sexual intercourse. Studies have indi-cated that 76 percent of women with partners willresume or attempt intercourse by 8 weeks (18) and89 percent by 6 months postpartum (19). Constipa-tion or diarrhea were given as examples of bowelproblems, but women may not have reported prob-lems such as incontinence of flatus or feces or analfissures under this heading, resulting in some under-reporting.
Someomissions occurred in the study. For example,pain or infection of woundsmay affect up to 60 percentof women who underwent a cesarean sections (4). Thisspecific option was not included, although somewomen volunteered information about cesareanwound problems under the category ‘‘other.’’ Anemia,high blood pressure, and other medical conditions alsowere not included.
We reported only changes in prevalence of healthproblems in the first 6 postpartum months. Saurel-Cubizolles et al (49) reported an increase in theprevalence of some problems between 5 and 12months postpartum. A 2-year follow-up of ourAustralian cohort was conducted, and the 6-monthand 2-year postpartum prevalences will be comparedand reported in the future, adjusting for any inter-vening pregnancies or births.
Comparison with Previous Studies
Overall, in our study the prevalences of specific healthproblems in the first 8 weeks postpartum were similarto those reported as occurring in the first 7 postpar-tum months by Brown and Lumley (4). Since in ourstudy all health problems were most likely to occur inthe early postpartum period, we would expect periodprevalences over 7 months to be similar to those overthe first 8 weeks.
Our findings of a high level of exhaustion orextreme tiredness were consistent with other reports(4,48,49). In keeping with the findings of Glazeneret al (48) and Brown and Lumley (4), tiredness wasunrelated to parity. In contrast to those authors,however, we reported a significantly higher preval-ence of tiredness in the first 8 weeks postpartumamong women who had cesarean sections. Althoughtiredness declined significantly over the first 6 post-partum months, the prevalence still remained highbetween 17 and 24 weeks postpartum, when 49percent of the women still reported exhaustion orextreme tiredness.
Backache was also commonly reported and affec-ted more than half of the sample in the first 8 weekswith a small decline over 6 months. Multiparas didnot report statistically significant declines in back-
ache over the 6 postpartum months as reported byprimiparas. Backache was not associated with epi-dural use during birth, in contrast to previous reports(2,4,58).
The percentage of women reporting frequentheadaches or migraines was similar over all threetime periods (17%–19%). This finding was similar tothose of Glazener et al (48), who reported prevalencesof 15 percent, and Saurel-Cubizolles et al (49), 22.5percent at 5 months postpartum. MacArthur et al (2)reported an incidence of headache of 4 percent butprevalence was not reported. Headache was unrelatedto parity or method of birth in our study and that ofGlazener et al (48). Estrogen may play an importantrole in the etiology of headache in women. Previousstudies have shown a decrease in headache duringpregnancy with rising estrogen levels and a worseningof headache during times of estrogen withdrawal, asoccurs after birth (23,59,60). Data on headache ormigraines either before or during pregnancy were notcollected for our study but should be collected infuture research.
The percentage of women with EPDS scoresgreater than 12 is lower than that reported by Brownand Lumley (4), which may reflect differences inpopulation characteristics but the possibility of atherapeutic effect of participating in the study mustalso be considered. Many women volunteered thatthey found participation in the study to be a positiveexperience. Simply providing women with the oppor-tunity to express how they feel, as well as showing aninterest in them, may in itself be therapeutic. Inaddition, an ethical requirement bound us to contactwomen whose scores on the EPDS were greater than12 at any time, and to offer help if appropriate ordesired. This intervention may have been effective initself, or led to an effective form of therapy ortreatment, thus reducing the prevalence of depressivesymptoms at subsequent time points.
Some differences between primiparas and multi-paras reported in this study may be amenable tointervention. Even after adjustment for method ofbirth, primiparas were more likely to report sexualproblems and perineal pain, which may be due tounrealistic expectations for postpartum recovery, toadjustment difficulties in this subgroup, or both. Thisissue should be explored further. In addition, primi-paras were less likely than multiparas to haveresolution of depression symptoms over the 6-monthpostpartum period. This finding could be attributedto their lack of knowledge about postpartum depres-sion, inability to recognize early signs of depression,and perhaps reluctance to seek help.
After cesarean delivery women can suffer seriousmorbidity compared with vaginal delivery (61). The
BIRTH 29:2 June 2002 91

effects of assisted vaginal deliveries may be equally ormore debilitating (62), a finding of increasing recog-nition and concern. As an indicator of excessmorbidity, we reported a higher rate of hospitalreadmission within 2 months of the birth amongwomen who had a cesarean section, and possiblyassisted vaginal births, a finding also reported in arecent United States study (63). The specific reasonsfor readmissions could not be ascertained from ourstudy, and further research is underway to examinethis factor.
Instrumental delivery is associated with anincreased risk of vaginal or perineal trauma anddamage to the anal sphincter, leading to urinaryincontinence and bowel and sexual problems (9). Ourstudy lacked the power to distinguish between forcepsand vacuum extraction; other studies have suggestedthe former may be more damaging (64). Our findingof an increased risk of perineal pain and sexualproblems after vaginal birth assisted by eithervacuum or forceps concurs with that of previousstudies (4). An increased risk of urinary incontinencewas not found in the study group compared withwomen who had unassisted vaginal births, as wasreported by others (4). Our study observed a trendtoward an increased risk of bowel problems amongwomen who had assisted vaginal deliveries. Incon-tinence of flatus and/or feces, associated with instru-mental births in previous studies, may have beenunderreported because of the limitations in ourmethod. Studies with longer follow-up and moreprecise assessments are needed to evaluate theassociation between instrumental deliveries and pel-vic floor problems accurately.
Our data suggest that, in the short term, womenwho have cesarean sections are at a reduced risk ofurinary stress incontinence compared with those whohave vaginal births. A similar finding was alsoreported by Wilson et al (13), but with higherabsolute prevalences. However, by 24 weeks postpar-tum the reduction in risk was not statisticallysignificant. This is important information. Changingattitudes toward cesarean delivery (65) have resultedin an increasing acceptance of prophylactic cesareansection (66) for prevention of problems such asurinary incontinence. In the United Kingdom asurvey of female obstetricians reported that 31percent would choose an elective cesarean in anuncomplicated pregnancy to avoid future pelvic floorproblems (67). In a similar survey among midwives,only 4 percent said they would choose an electivecesarean (68). Since incontinence may not increasesubstantially until many years after childbirth (69),studies with long follow-up are needed to properlyevaluate the association between cesarean delivery
and preservation of urinary continence and otherproblems associated with pelvic floor integrity. In theabsence of such studies, recent findings from apopulation survey in South Australia indicate thatcesarean section may not, in fact, be associated with asignificant reduction in long-term pelvic floor mor-bidity compared with spontaneous vaginal delivery(70).
Forty percent of the women in our study wouldhave liked more help and advice to assist them inlooking after themselves and their baby. This findingrepresents a high level of unmet need in thecommunity, and strategies to assist women in thedemanding task of child care after the physical andemotional demands of childbirth with its sequelaeare clearly indicated. Knowledge of normal bodychanges and the time taken to recover from preg-nancy and childbirth is important so that womenhave realistic expectations of the postpartum period.Furthermore, the possible association between phys-ical health and recovery in the postpartum periodand maternal emotional well-being or depressiondeserves further exploration (71) as do their tem-poral relationships. This will be the subject of futureresearch.
Conclusions
This population-based study confirmed that a highprevalence of morbidity occurs in women afterchildbirth. In addition, the study indicated evidenceof some resolution of certain complications within 6months of the birth, such as bowel problems, urinaryincontinence, and perineal pain. Problems such asexhaustion/extreme tiredness and backache, althoughdeclining in prevalence, are still common after 6months, perhaps reflecting the exigencies of parentingas well as the physical impact of pregnancy andchildbirth itself. The importance of recognizinghealth problems after childbirth, as well as theirassociations, is that measures to reduce and alleviatethem can be sought and implemented. In addition,realistic expectations can be given to women aboutthe expected time taken to recover from childbirthand the physical and emotional demands of earlyparenting.
Acknowledgments
The assistance of the midwives in recruiting womento participate in this study is gratefully acknow-ledged. Robyn Attewell provided statistical advice.We are especially grateful to the women of the ACTwho so generously gave their time to complete thisstudy.
92 BIRTH 29:2 June 2002
References
1. MacArthur C, Lewis M, Knox EG. Commentaries. Health
after childbirth. Br J Obstet Gynaecol 1991;98:1193–1204.
2. MacArthur C, Lewis M, Knox E. Health after Childbirth,
London, Her Majesty’s Stationery Office, 1991:1.
3. Bick D, MacArthur C. The extent, severity and effect of
health problems after childbirth. Br J Midwifery 1995;3:27–
31.
4. Brown S, Lumley J. Maternal health after childbirth: Results
of an Australian population based survey. Br J Obstet
Gynaecol 1998;105:156–161.
5. Blomquist HK, Soderman P. The occurrence of symptoms
and the proportion treated in Swedish infants and their
mothers. Scand J Primary Health Care 1991;9:217–223.
6. MacArthur C, Bick DE, Keighley MR. Faecal incontinence
after childbirth. Br J Obstet Gynaecol 1997;104:46–50.
7. Meyer S, Schreyer A, De Grandi P, Hohlfeld P. The effects of
birth on urinary continence mechanisms and other pelvic-
floor characteristics. Obstet Gynecol 1998;92:613–618.
8. Ryhammer AM, Bek KM, Laurberg S. Multiple vaginal
deliveries increase the risk of permanent incontinence of flatus
and urine in normal premenopausal women. Dis Colon
Rectum 1995;38:1206–1209.
9. Sultan AH, Kamm MA, Hudson CN, et al. Anal-sphincter
disruption during vaginal delivery. N Engl J Med
1993;329:1905–1911.
10. Zetterstrom JP, Lopez A, Anzen B, et al. Anal incontinence
after vaginal delivery: A prospective study in primiparous
women. Br J Obstet Gynaecol 1999;106:324–330.
11. Viktrup L, Lose G, Rolff M, Barfoed K. The symptoms of
stress incontinence caused by pregnancy or delivery in
primiparas. Obstet Gynecol 1992;79:945–949.
12. MacArthur C, Lewis M, Bick DE. Stress incontinence after
childbirth. Br J Midwifery 1993;1:207–215.
13. Wilson PD, Herbison RM, Herbison GP. Obstetric practice
and the prevalence of urinary incontinence three months after
delivery. Br J Obstet Gynaecol 1996;103:154–161.
14. Mason L, Glenn S, Walton I, Appleton C. The prevalence of
stress incontinence during pregnancy and following delivery.
Midwifery 1999;15:120–128.
15. Foldspang A, Mommsen S, Djurhuus JC. Prevalent urinary
incontinence as a correlate of pregnancy, vaginal childbirth,
and obstetric techniques. Am J Public Health 1999;89:209–
212.
16. Abraham S, Child A, Ferry J, et al. Recovery after
childbirth: A preliminary prospective study. Med J Aust
1990;152:9–12.
17. Stainton MC, Edwards S, Jones B, Switonski C. The nature
of maternal postnatal pain. J Perinat Educ 1999;8:1–10.
18. Glazener CM. Sexual function after childbirth: Women’s
experiences, persistent morbidity and lack of professional
recognition. Br J Obstet Gynaecol 1997;104:330–335.
19. Barrett G, Pendry E, Peacock J, et al. Women’s sexual health
after childbirth. Br J Obstet Gynaecol 2000;107:186–195.
20. Ostgaard HC, Andersson GB. Postpartum low-back pain.
Spine 1992;17:53–55.
21. Russell R, Dundas R, Reynolds F. Long term backache after
childbirth: Prospective search for causative factors. BMJ
1996;312:1384–1388.
22. Russell R, Groves P, Taub N, et al. Assessing long term
backache after childbirth. BMJ 1993;306:1299–1303.
23. Scharff L, Marcus DA, Turk DC. Headache during
pregnancy and in the postpartum: A prospective study.
Headache 1997;37:203–210.
24. Gardner DL. Fatigue in postpartum women. Appl Nurs Res
1991;4:57–62.
25. Lee KA, Zaffke ME. Longitudinal changes in fatigue and
energy during pregnancy and the postpartum period. J Obstet
Gynecol Neonatal Nurs 1999;28:183–191.
26. Parks PL, Lenz ER, Milligan RA, Han HR. What happens
when fatigue lingers for 18 months after delivery? J Obstet
Gynecol Neonatal Nurs 1999;28:87–93.
27. Carty EM, Bradley C, Winslow W. Women’s perceptions of
fatigue during pregnancy and postpartum: The impact of
length of hospital stay. Clin Nurs Res 1996;5:67–80.
28. Waters MA, Lee KA. Differences between primigravidae and
multigravidae mothers in sleep disturbances, fatigue, and
functional status. J Nurse Midwifery 1996;41:364–367.
29. Troy NW, Dalgas-Pelish P. The natural evolution of
postpartum fatigue among a group of primiparous women.
Clin Nurs Res 1997;6:126–141.
30. Fetherston C. Characteristics of lactation mastitis in a
Western Australian cohort. Breastfeeding Rev 1997;5:5–11.
31. Kinlay JR, O’Connell DL, Kinlay S. Incidence of mastitis in
breastfeeding women during the six months after delivery:
A prospective cohort study. Med J Aust 1998;169:310–312.
32. Vogel A, Hutchison BL, Mitchell EA. Mastitis in the first year
postpartum. Birth 1999;26:218–225.
33. Cooper PJ, Campbell EA, Day A, et al. Non-psychotic
psychiatric disorder after childbirth: A prospective study of
prevalence, incidence, course and nature. Br J Psychiatry
1988;152:799–806.
34. Cox JL, Murray D, Chapman G. A controlled study of the
onset, duration and prevalence of postnatal depression. Br J
Psychiatry 1993;163:27–31.
35. O’Hara MW. Postpartum Depression. Causes and Conse-
quences, New York, Springer–Verlag, 1995:1.
36. Sleep J, Grant A. West Berkshire perineal management trial:
Three year follow up. Br Med J 1987;295:749–751.
37. Johanson RB, Wilkinson P, Bastible A, et al. Health after
assisted vaginal delivery: Follow up of a random controlled
study. J Obstet Gynaecol 1993;13:242–246.
38. Johanson RB, Heycock E, Carter J, et al. Maternal and child
health after assisted vaginal delivery: Five-year follow up of a
randomised controlled study comparing forceps and
ventouse. Br J Obstet Gynaecol 1999;106:544–549.
39. McCandlish R, Bowler U, van Asten H, et al. A randomised
controlled trial of care of the perineum during second stage of
normal labour. Br J Obstet Gynaecol 1998;105:1262–1272.
40. Gordon B, Mackrodt C, Fern E, et al. The Ipswich Childbirth
Study: 1. A randomised evaluation of two stage postpartum
perineal repair leaving the skin unsutured. Br J Obstet
Gynaecol 1998;105:435–440.
41. Gunn J, Lumley J, Chondros P, Young D. Does an early
postnatal check-up improve maternal health: Results from a
randomised trial in Australian general practice. Br J Obstet
Gynaecol 1998;105:991–997.
42. Fynes M, Donnelly V, Behan M, et al. Effect of second
vaginal delivery on anorectal physiology and faecal
continence: A prospective study [see comments]. Lancet
1999;354:983–986.
43. Hillan EM. Short-term morbidity associated with cesarean
delivery. Birth 1992;19:190–194.
44. Malouf AJ, Norton CS, Engel AF, et al. Long-term results of
overlapping anterior anal-sphincter repair for obstetric
trauma. Lancet 2000;355:260–265.
45. Snooks SJ, Swash M, Mathers SE, Henry MM. Effect of
vaginal delivery on the pelvic floor: A 5-year follow-up. Br J
Surg 1990;77:1358–1360.
BIRTH 29:2 June 2002 93

46. Sultan AH, Kamm MA, Hudson CN, Bartram CI. Third
degree obstetric anal sphincter tears: Risk factors and
outcome of primary repair. BMJ 1994;308:887–891.
47. Baker D, Taylor H. Inequality in health and health service use
for mothers of young children in south west England. Survey
Team of the Avon Longitudinal Study of Pregnancy and
Childhood Team. J Epidemiol Commun Health 1997;51:74–79.
48. Glazener CM, Abdalla M, Stroud P, et al. Postnatal maternal
morbidity: Extent, causes, prevention and treatment. Br J
Obstet Gynaecol 1995;102:282–287.
49. Saurel-Cubizolles MJ, Romito P, Lelong N, Ancel PY.
Women’s health after childbirth: A longitudinal study in
France and Italy. BJOG 2000;107:1202–1209.
50. Field S, Draper J, Kerr M, Hare MJ. Women’s illness in the
postnatal period. Mat Child Health 1983;8:302–304.
51. Gjerdingen DK, Froberg DG, Kochevar L. Changes in
women’s mental and physical health from pregnancy through
six months postpartum. J Fam Pract 1991;32:161–166.
52. Tulman L, Fawcett J, Groblewski L, Silverman L. Changes in
functional status after childbirth. Nurs Res 1990;39:70–75.
53. Bourne M.Maternal and Perinatal Status, ACT, 1997 Tables.
Health Series No 25, Canberra, ACT: Clinical Epidemiology
and Health Outcomes Centre, ACT Department of Health &
Community Care, 2000.
54. Boyce P, Stubbs J, Todd A. The Edinburgh postnatal
depression scale: Validation for an Australian sample. Aust
NZ J Psychiatry 1993;27:472–476.
55. Cox JL, Holden JM, Sagovsky R. Detection of postnatal
depression: Development of the 10-item Edinburgh Postnatal
Depression Scale. Br J Psychiatry 1987;150:782–786.
56. Murray L, Carothers AD. The validation of the Edinburgh
Post-natal Depression Scale on a community sample. Br J
Psychiatry 1990;157:288–290.
57. Thompson JF, Roberts CL, Currie MJ, Ellwood DA. Early
discharge and postnatal depression: A prospective cohort
study. Med J Aust 2000;172:532–536.
58. MacArthur C, Lewis M, Knox EG. Investigation of long term
problems after obstetric epidural anaesthesia. BMJ
1992;304:1279–1282.
59. Stein G, Morton J, Marsh A, et al. Headaches after
childbirth. Acta Neurol Scand 1984;69:74–79.
60. Zib M, Lim L, Walters WA. Symptoms during normal
pregnancy: A prospective controlled study. Aust NZ J Obstet
Gynaecol 1999;39:401–410.
61. Sultan AH, Stanton SL. Preserving the pelvic floor and
perineum during childbirth-elective caesarean section? Br J
Obstet Gynaecol 1996;103:731–734.
62. Roberts CL, Tracy S, Peat B. Rates for obstetric intervention
among private and public patients in Australia: Population
based descriptive study. BMJ 2000;321:137–141.
63. Lydon-Rochelle M, Holt VL, Martin DP, Easterling TR.
Association between method of delivery and maternal
rehospitalization. JAMA 2000;283:2411–2416.
64. Johanson RB, Menon BKV. Vacuum extraction versus
forceps for assisted vaginal delivery (Cochrane Review). In:
The Cochrane Library. Issue 3. Oxford: Update Software,
2000.
65. Roberts JM. Recent advances: Obstetrics. BMJ 2000;321:33–
35.
66. Paterson-Brown S. Should doctors perform an elective
caesarean section on request? Yes, as long as the woman is
fully informed. BMJ 1998;317:462–463.
67. Al-Mufti R, McCarthy A, Fisk NM. Survey of obstetricians’
personal preference and discretionary practice. Eur J Obstet
Gynecol Reprod Biol 1997;73:1–4.
68. Dickson MJ, Willett M. Midwives would prefer a vaginal
delivery. BMJ 1999;319:1008.
69. Thom DH, van den Eeden SK, Brown JS. Evaluation of
parturition and other reproductive variables as risk factors for
urinary incontinence in later life. Obstet Gynecol 1997;90:983–
989.
70. MacLennan AH, Taylor AW, Wilson DH, Wilson D. The
prevalence of pelvic floor disorders and their relationship to
gender, age, parity and mode of delivery. BJOG 2000;
107:1460–1470.
71. Brown S, Lumley J. Physical health problems after childbirth
and maternal depression at six to seven months postpartum.
BJOG 2000;107:1194–1201.
94 BIRTH 29:2 June 2002




















