
Preterm Resuscitation With Low Oxygen Causes Less Oxidative Stress, Inflammation, and Chronic Lung...
13
DOI: 10.1542/peds.2009-0434 2009;124;e439-e449; originally published online Aug 3, 2009; Pediatrics Sastre and Miguel A. Asensi Izquierdo, L. Jackson Roberts, II, Alessandro Arduini, Justo Javier Escobar, Juan Maximo Vento, Manuel Moro, Raquel Escrig, Luis Arruza, Gema Villar, Isabel Inflammation, and Chronic Lung Disease Preterm Resuscitation With Low Oxygen Causes Less Oxidative Stress, http://www.pediatrics.org/cgi/content/full/124/3/e439 located on the World Wide Web at: The online version of this article, along with updated information and services, is rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly . Provided by McMaster University on August 31, 2009 www.pediatrics.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Preterm Resuscitation With Low Oxygen Causes Less Oxidative Stress, Inflammation, and Chronic Lung...

DOI: 10.1542/peds.2009-0434 2009;124;e439-e449; originally published online Aug 3, 2009; Pediatrics
Sastre and Miguel A. Asensi Izquierdo, L. Jackson Roberts, II, Alessandro Arduini, Justo Javier Escobar, Juan Maximo Vento, Manuel Moro, Raquel Escrig, Luis Arruza, Gema Villar, Isabel
Inflammation, and Chronic Lung DiseasePreterm Resuscitation With Low Oxygen Causes Less Oxidative Stress,
http://www.pediatrics.org/cgi/content/full/124/3/e439located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2009 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

Preterm Resuscitation With Low Oxygen Causes LessOxidative Stress, Inflammation, and Chronic Lung Disease
WHAT’S KNOWN ON THIS SUBJECT: In a previous study, thefeasibility of resuscitating ELGANs with an initial FIO2 of 30% andachieving targeted SpO2 values was demonstrated.
WHAT THIS STUDY ADDS: This study confirms the feasibility ofusing lower oxygen concentrations for resuscitating extremelypremature infants, but it also shows that lower FIO2 reduces
oxidative stress, expression of proinflammatory cytokines, and theincidence of BPD.
abstractOBJECTIVE: The goal was to reduce adverse pulmonary adverse out-comes, oxidative stress, and inflammation in neonates of 24 to 28weeks of gestation initially resuscitated with fractions of inspired ox-ygen of 30% or 90%.
METHODS: Randomized assignment to receive 30% (N� 37) or 90%(N� 41) oxygen was performed. Targeted oxygen saturation valueswere 75% at 5 minutes and 85% at 10 minutes. Blood oxidized glu-tathione (GSSG)/reduced glutathione ratio and urinary o-tyrosine,8-oxo-dihydroxyguanosine, and isoprostane levels, isofuran elimi-nation, and plasma interleukin 8 and tumor necrosis factor � levelswere determined.
RESULTS: The low-oxygen group needed fewer days of oxygen supple-mentation (6 vs 22 days; P� .01) and fewer days of mechanical venti-lation (13 vs 27 days; P � .01) and had a lower incidence of broncho-pulmonary dysplasia at discharge (15.4% vs 31.7%; P � .05). GSSG/reduced glutathione � 100 ratios at day 1 and 3 were significantlyhigher in the high-oxygen group (day 1: high-oxygen group: 13.36 �5.25; low-oxygen group: 8.46� 3.87; P� .01; day 3: high-oxygen group:8.87� 4.40; low-oxygen group: 6.97� 3.11; P� .05). Urinary markersof oxidative stress were increased significantly in the high-oxygengroup, compared with the low-oxygen group, in the first week afterbirth. GSSG levels on day 3 and urinary isofuran, o-tyrosine, and8-hydroxy-2�-deoxyguanosine levels on day 7 were correlated signifi-cantly with development of chronic lung disease.
CONCLUSIONS: Resuscitation of preterm neonates with 30% oxygencauses less oxidative stress, inflammation, need for oxygen, and risk ofbronchopulmonary dysplasia. Pediatrics 2009;124:e439–e449
CONTRIBUTORS: Maximo Vento, PhD, MD,a Manuel Moro,MD,b Raquel Escrig, MD,a Luis Arruza, MD,b Gema Villar,MD,b Isabel Izquierdo, MD,a L. Jackson Roberts, II, MD,c
Alessandro Arduini, PhD,d Justo Javier Escobar, PhD,d
Juan Sastre, PhD,d and Miguel A. Asensi, PhDd
aDivision of Neonatology, University Hospital La Fe, Valencia,Spain; bDivision of Neonatology, University Hospital San Carlos,Madrid, Spain; cDepartment of Pharmacology, VanderbiltUniversity, Nashville, Tennessee; dDepartment of Physiology,Faculty of Pharmacy, University of Valencia, Valencia, Spain
KEY WORDSprematurity, resuscitation, oxygen, oxidative stress biomarkers,inflammatory cytokines, bronchopulmonary dysplasia
ABBREVIATIONSELGAN—extremely low gestational age neonateDR—delivery roomBPD—bronchopulmonary dysplasiaROS—reactive oxygen speciesFIO2—fraction of inspired oxygenSpO2—pulse oxygen saturationGSH—reduced glutathioneGSSG—oxidized glutathioneTNF-�—tumor necrosis factor �IL-8—interleukin 8HR—heart rate
This trial has been registered at www.clinicaltrials.gov(identifier NCT00494702).
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0434
doi:10.1542/peds.2009-0434
Accepted for publication Apr 14, 2009
Address correspondence to Maximo Vento, PhD, MD, Departmentof Pediatrics, Neonatal Research Unit, Division of Neonatology,University Hospital La Fe, Avenida de Campanar, 21, E46009Valencia, Spain. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
ARTICLES
PEDIATRICS Volume 124, Number 3, September 2009 e439. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from
Rates of survival of extremely low ges-tational age neonates (ELGANs) (�28weeks of gestation) have increasedsteadily since the late 1990s.1–3 How-ever, death in the delivery room (DR)still represents 32% of total ELGANdeaths at discharge, and morbidityrates are especially high at 23 to 25weeks of gestation.4,5 Of note, the use ofpositive pressure ventilation with ahigh oxygen concentration has been as-sociated with development of chroniclung disease.6,7 Lung-stretching and hy-peroxia may act synergistically on pre-natally inflamed fetal membranes andmay elicit a systemic inflammatory re-sponse that contributes to the develop-ment of bronchopulmonary dysplasia(BPD).8 In fact, in experimental andclinical settings, hyperoxia has beenassociated with serious injury to thedeveloping brain, lung, myocardium,and kidney.9 Therefore, excessive oxy-genation contributes to the formationof reactive oxygen species (ROS).10
These highly reactive compounds re-act with nearbymolecules (eg, protein,lipids, DNA, and RNA), modifying theirstructure and function.11 In addition, itwas shown experimentally that ROSmay act in the lung as upstream signal-ingmolecules favoring alveolar epithe-lial cell apoptosis.12
To prevent adverse effects of oxygenduring resuscitation, room air insteadof 100% oxygen was used in random-ized, clinical trials.13 In those studies,room air reduced significantly thetime of resuscitation,14,15 biomarkersof heart (troponin C) and kidney(N-acetyl-glucosaminidase) damage,16
and oxidative stress17; moreover, roomair reduced mortality rates13 withoutincreasing long-term neurologic mor-bidity rates for survivors.18
The antioxidant defense system de-velops late in gestation.19,20 There-fore, premature neonates are highlysusceptible to the negative side ef-fects of excess oxygen.21 Conse-
quently, it would be especially advis-able to avoid hyperoxia duringneonatal resuscitation of pretermneonates.22 However, few studiesmonitored oxygen supplementationduring resuscitation of ELGANs.23–26
Wang et al24 failed to achieve clinicalstabilization of ELGANs by using roomair. Dawson et al25 compared 2 co-horts of ELGANs, before and after es-tablishment of room air as the initialstandard of care in the DR, and re-ported similar results. Harling et al23
did not find differences in clinical re-covery of premature neonates withthe use of 50% instead of 100%oxygen during resuscitation. Con-versely, in a previous trial in ourgroup, Escrig et al,26 using initial FIO2of 30%, showed the feasibility ofELGANs achieving targeted pulse oxy-gen saturation (SpO2) values of 85%at 10 minutes after birth. Further-more, neonates in the lower-oxygengroup received significantly smalleroxygen loads during resuscitation.26
The only medical intervention that dif-ferentiated the 2 groups in our studywas oxygen concentration during re-suscitation. The remaining interven-tions followed established standardsof care. We hypothesized that lower ox-ygen levels during resuscitation wouldcause less oxidative stress and inflam-mation and would reduce the need foroxygen supplementation and mechan-ical ventilation and/or the incidence ofBPD. To validate our hypothesis, welaunched a new trial enrolling ELGANsassigned randomly to an initial FIO2 of30% or 90%. Targeted SpO2 valueswere75% at 5 minutes and 85% at 10 min-utes after birth. For evaluation of oxi-dative stress and redox status, thereduced glutathione (GSH)/oxidizedglutathione (GSSG) ratio was deter-mined.14,15,17,18 In addition, we evaluatedoxidation of proteins (o-tyrosine/phe-nylalanine ratio), DNA (8-hydroxy-2�-deoxyguanosine/2-deoxyguanosine ra-
tio),27 and lipids (isoprostanes andisofurans).28 Furthermore, for assess-ment of inflammation, plasma inter-leukin 8 (IL-8) and tumor necrosisfactor � (TNF-�) levels were deter-mined.29 We correlated oxygen levels atresuscitation with biomarkers of oxi-dative stress and inflammation andclinical outcomes.
METHODS
Design
A prospective clinical trial enrolledELGANs (�28 weeks of gestation, asdetermined with fetal ultrasonogra-phy) in 2 tertiary referral centers inSpain during a 30-month period(September 2005 through March2008). Eligible patients were as-signed randomly to be resuscitatedwith a lower (30%) or higher (90%)fraction of inspired oxygen (FIO2). Thehigher FIO2 was chosen because a re-cent meta-analysis showed highermortality rates among neonates re-suscitated with pure oxygen.13 Thestudy was not blinded with respect tothe neonatologist in charge of the re-spiratory airway but it was with re-spect to the rest of the caregiversin the DR. The institutional reviewboard of our hospital counseledagainst complete blinding, citing alack of published experience with theresuscitation and follow-up care ofELGANs with lower oxygen concentra-tions. Interventions in the DR wererecorded scrupulously and were an-alyzed to evaluate possible bias. Thestudy protocol was approved by theethics and scientific research com-mittees of both participating hospi-tals. Parents’ informed consent wasobtained for all enrolled infants.
The main clinical outcome was neo-natal death (death at�28 days) plusthe incidence of BPD, defined as theneed for oxygen supplementation atpostconceptional age of 36 weeks.30
Secondary outcomes were durations
e440 VENTO et al. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

of supplementary oxygen treatmentand mechanical ventilation and useof surfactant. Biochemical outcomeswere biomarkers of oxidative stressand proinflammatory cytokines andtheir correlation with BPD.
Women who were admitted at gesta-tional ages of�28 weeks were askedto sign informed consent forms andwere assigned to the high-oxygenor low-oxygen group, according tocomputer-generated random num-bers in sealed envelopes. In cases ofrefusal, the patients were not as-signed. Moreover, if an infant was as-signed randomly but was not resus-citated, then the data were notincluded in the study. Twin gesta-tions were considered as a unit forthe purpose of randomization. Tar-geted objectives were preductal SpO2values of 75% at 5 minutes and 85%at 10 minutes after birth. The samplesize was calculated to reduce the in-cidence of BPD from 30% to 20%(minimum of 35 patients per group).Moreover, patients were stratified ingroups of 27 to 28 weeks and �26weeks of gestation, to ensure a ho-mogeneous representation of allgestational ages.
Patients
Eligible neonates were inborn pa-tients with 1 of the following resusci-tation criteria: (1) absence of spon-taneous respiration at �1 minute;(2) bradycardia (�60 beats perminute) for �2 minutes, hypoactiv-ity, and/or hypotonia; or (3) inef-fective ventilation, as determinedthrough auscultation and/or lack ofthoracic expansion. Exclusion crite-ria were (1) uncertain gestationalage or (2) severe congenital malfor-mations or chromosomal abnormal-ities. Of a total of 106 eligible neo-nates, 9 in the low-oxygen group and10 in the high-oxygen group were lost
to randomization because parentsdeclined to participate. Of the re-maining subjects, 4 in the low-oxygengroup and 3 in the high-oxygen groupdied and did not complete the study.
Resuscitation Procedure
The resuscitation procedure was de-scribed previously.26,31 Neonates withheart rate (HR) of �80 to 100 beatsper minute and increased work ofbreathing in the first 2 minutes of lifeinitially underwent ventilation with aface mask (5– 8 cm H2O), with aT-piece resuscitator (Neopuff; Fisher& Paykel Healthcare, Penmure, NewZealand); if clinical responses (HRand/or SpO2) were insufficient, thenthe neonates were switched to inter-mittent positive pressure ventilation.For infants with gestational ages of�27 weeks, endotracheal intubationwas performed; however, for infantswith gestational ages of 27 or 28weeks, noninvasive ventilation waspursued for several minutes and in-tubation was performed only if thepatient’s condition did not improve.Initial parameters for intermittentpositive pressure ventilation were
positive inspiratory pressure of 20cm H2O and positive end expiratorypressure of 5 cm H2O. If no improve-ment was detected after 2 minutes,then respirator parameters weremodified to achieve the targeted ob-jectives. Immediately after birth, anoximeter probe with sensors with2-second averaging (Radical 7;Masimo, Irvine, CA) was set on theright wrist for preductal SpO2 moni-toring.32 FIO2 was titrated to attaintargeted SpO2 values, and 60 to 90seconds were allowed for responsesafter each change. Abrupt FIO2changes (�10% every 30 seconds)were avoided, to prevent pulmonaryvessel constriction.33 HR indicatedthe effectiveness of resuscitation; ifbradycardia (HR of �60 beats perminute) lasted �30 seconds, thenthe FIO2 was switched to 100%. SpO2was recorded continuously, and theinformation was downloaded and an-alyzed once oxygen treatment wasdiscontinued.
Analytical Determinations
Cord blood (3 mL) was collected inthe DR before clamping, and blood
TABLE 1 Characteristics of ELGANs Resuscitated With Lower (30%) or Higher (90%) OxygenConcentrations at Birth and Management in DR
Low Oxygen(N� 37)
High Oxygen(N� 41)
Gestational age, mean� SD, wk 26.0� 1.5 26.3� 1.3Birth weight, mean� SD, g 854.7� 170.1 901.7� 195.4Gender, nMale 14 18Female 23 23Multiple birth, n 11 9Small for gestational age, n 13 12Prenatal corticosteroid therapy (full schedule), n (%) 36 (97.2) 38 (92.7)Type of delivery, n (%)Vaginal 18 (48.6) 17 (41.4)Cesarean section 19 (51.4) 24 (58.6)Cord blood pH at birth, mean� SD 7.05� 0.9 7.09� 1.1Apgar score, median (interquartile range)1 min 5 (2–7) 6 (2–8)5 min 8 (5–9) 8 (5–9)Received supplementary oxygen during resuscitation, n (%) 32 (86.5) 34 (82.9)Tracheal intubation in DR, n (%) 21 (56.7) 25 (60.9)Breathing 21% oxygen at arrival at NICU, n (%) 28 (75.6) 23 (56.0)a
a Statistical comparison between groups (�2 test), P� .05, compared with low-oxygen group.
ARTICLES
PEDIATRICS Volume 124, Number 3, September 2009 e441. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from
was collected from a peripheral veinat days 1 and 7. One milliliter of totalblood was used for GSH and GSSG as-says. Two milliliters were centri-fuged (2000 rpm for 20 minutes), andthe supernatant was divided into0.5-mL aliquots and deep-frozen(�80°C). One 0.5-mL aliquot wasused for TNF-� and IL-8 determina-tions, and the rest was kept deep-frozen. Urine samples were deep-frozen (�80°C). GSH and GSSG levelswere determined through high-performance liquid chromatogra-phy,34 IL-8 and TNF-� levels throughflow cytometry (CBA Flex Set System;Becton-Dickinson, Franklin Lakes,NJ), o-tyrosine, phenylalanine, 8-hydroxy-2�-deoxyguanosine, and 2�-deoxyguanosine levels through high-performance liquid chromatography/mass spectrometry,27 and levels of iso-prostane metabolites and isofuransthrough gas chromatography/massspectrometry.28
Statistical Analyses
Baseline characteristics were deter-mined by using SPSS 13 (SPSS Inc,Chicago, IL). For parameters withnormal distribution (as assessedwith the Kolmogorov-Smirnov test),1-way analysis of variance was per-formed and differences betweengroups were calculated with Tukey’smethod. The level of significance was.05. The Mann-Whitney U test wasused for comparison of nonpairedsamples and the Kruskal-Wallis testfor �2 nonpaired (independent)samples for nonnormally distributedvalues.35
RESULTS
General Characteristics of thePopulation and Management in theDR and NICU
Table 1 shows no differences in thegeneral characteristics of the popula-tion or management in the DR. The
number of neonates breathing roomair on arrival in the NICU was signifi-cantly higher in the low-oxygen group(P� .05).
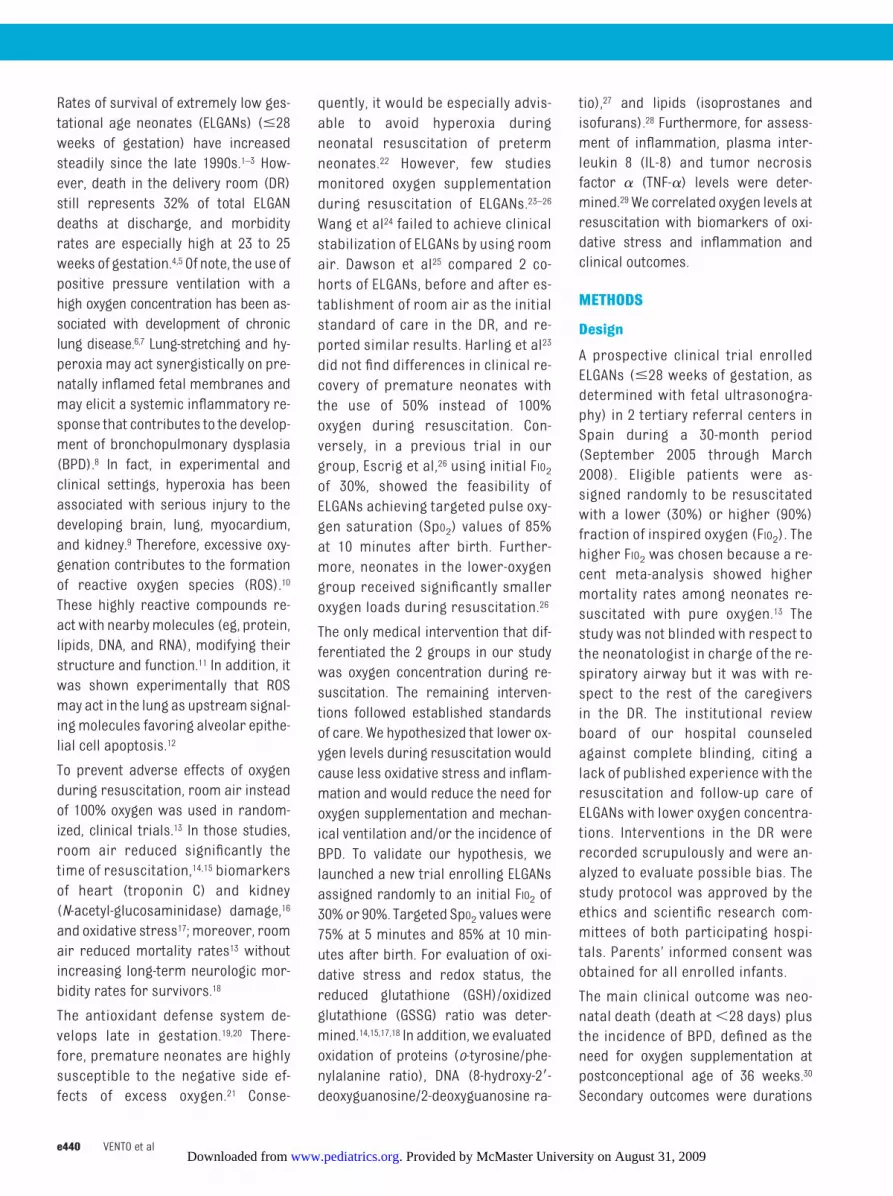
FIO2, HR, and SpO2 in the DR
Reliable SpO2 readings were achievedat 76 � 13 seconds. Figure 1 depictsboth FIO2 and HR at 60-second intervalsfrom the first reliable reading to 30minutes after birth. The initial FIO2 in
the low-oxygen group was increased ina stepwise manner to 55% at 5 min-utes; conversely, the initial FIO2 in thehigh-oxygen group was reduced in astepwise manner, reaching 55% at 5minutes. Significant differences in FIO2values used in the first 4minutes of lifewere found (P � .01), whereas no dif-ferences were found thereafter. No dif-ferences in HR between groups werefound.
FIGURE 1A, FIO2 received by ELGANs in the low-oxygen group (initial FIO2 of 30%) and in the high-oxygen group(initial FIO2 of 90%) in the first 30 minutes after birth. Student’s t test comparisons (minute to minute)found significant differences between groups at minutes 2, 3, 4, and 6 after birth (aP � .01). B, HR,expressed in beats perminute (bpm), in the low-oxygen (Lox) and high-oxygen (Hox) groups in the first30 minutes after birth.
e442 VENTO et al. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

SpO2 in the Low-Oxygen andHigh-Oxygen Groups
Figure 2 shows no significant differ-ences in SpO2 values between the low-oxygen group and the high-oxygengroup at any time point in the first 30minutes after birth. Both groupsreached targeted SpO2 values at 5 and10 minutes.
Clinical Outcomes
Table 2 shows outcomes for relevantitems related to management andconditions. Patients in the low-oxygen group received significantlyfewer days of oxygen supplementa-tion (P � .01), mechanical ventila-tion (P � .01), and continuous posi-
tive airway pressure treatment (P�.05) and developed less BPD (P �.05), compared with infants in thehigh-oxygen group. No differencesregarding rates of neonatal death,nosocomial infections, patent ductusarteriosus, grade III/IV intraventricu-lar/periventricular hemorrhage, orretinopathy of prematurity werefound (Table 2).
Analytical Results
Blood GSSG/GSH Ratio
Figure 3 shows no significant differ-ences in GSSG/GSH ratios at birth (um-bilical cord) between the high-oxygengroup and the low-oxygen group. On
day 1 (high-oxygen group: 13.36� 5.25;low-oxygen group: 8.46� 3.87; P� .01)and day 3 (high-oxygen group: 8.87 �4.40; low-oxygen group: 6.97 � 3.11;P � .05), however, the high-oxygengroup had significantly greater GSSG/GSH ratios than did the low-oxygengroup.
Urinary Isoprostane Metabolites andIsofurans
Figure 4A shows no differences inurinary isoprostane metabolite lev-els between the groups at either day1 or day 7. Figure 4B shows signifi-cantly greater elimination of iso-furans in the high-oxygen group onday 1 (P� .01) but no significant dif-ferences on day 7.
Urinary o-Tyrosine/PhenylalanineRatio
Figure 5A shows increased urinaryelimination of o-tyrosine in the high-oxygen group, compared with the low-oxygen group, on day 1 (P � .05) andday 7 (P� .05).
8-Hydroxy-2�-deoxyguanosine/2�-Deoxyguanosine Ratio in Urine
Figure 5B depicts significantly in-creased urinary elimination of oxi-dized guanosine in the high-oxygengroup on both day 1 (P� .01) and day7 (P� .01).
Plasma TNF-� Levels
Figure 6A shows serial determinationsof plasma TNF-� levels in weeks 1, 2, 3,
FIGURE 2SpO2 values in the first 30minutes after birth for the low-oxygen (Lox) group (initially resuscitatedwithFIO2 of 30%) and the high-oxygen (Hox) group (initially resuscitated with FIO2 of 90%). No significantdifferences between groups were found.
TABLE 2 Variables Recorded During Hospitalization and Long-Term Outcomes of ELGANs Resuscitated With Lower (30%) or Higher (90%) OxygenConcentrations
Group Duration of OxygenTreatment, Median
(IQR), d
Duration ofMechanicalVentilationMedian(IQR), d
Duration of CPAPTherapy, Median(IQR), d
SurfactantTreatment,n (%)
BPD, n(%)
ROP, n(%)
NosocomialSepticemia,n (%)
PDA, n(%)
IPVH (GradeIII/IV), n (%)
Neonatal Death(�28 d), n (%)
Low-oxygen (N� 37) 6 (1–67) 13 (6–57) 4 (1–38) 13 (36) 6 (15.4) 4 (10.8) 10 (27.0) 19 (51.3) 7 (18.9) 4 (10.8)High-oxygen (N� 41) 22 (7–132)a 27 (10–98)a 12 (6–45)b 13 (33) 13 (31.7)b 6 (14.6) 9 (23.5) 27 (65.8) 5 (12.2) 3 (7.3)
IQR indicates interquartile range; CPAP, continuous positive airway pressure; ROP, retinopathy of prematurity (stage 2, stage 3, or plus disease)52; PDA, patent ductus arteriosus; IPVH,intraventricular/periventricular hemorrhage.53 BPD was defined as described.54a P� .01, versus low-oxygen group.b P� .05, versus low-oxygen group.
ARTICLES
PEDIATRICS Volume 124, Number 3, September 2009 e443. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

and 5 after birth. TNF-� levels weresignificantly lower in the low-oxygengroup than in the high-oxygen group atthe end of the first week of life (high-
oxygen group: 3.47� 1.12 pg/mL; low-oxygen group: 2.64� 0.94 pg/mL; P�.05), but no differences were foundthereafter.
Plasma IL-8 Levels
Figure 6B shows IL-8 levels in the first 5weeks after birth. IL-8 levels were sig-nificantly higher in the high-oxygengroup in the first 3 weeks after birth(P� .01) but not thereafter.
Association of Oxidative StressMarkers With BPD
Figure 7A shows blood GSSG and uri-nary isofuran levels for neonates wholater developed BPD (n� 19) or did notdevelop BPD (n� 59). Blood GSSG lev-els on day 3 and urinary isofuran levelsat the end of the first week were cor-related significantly (P� .01) with thedevelopment of BPD. Moreover, the o-tyrosine/phenylalanine and 8-hydroxy-2�-deoxyguanosine/2-deoxyguanosineratios also were correlated signifi-cantly with later development of BPD(Fig 7B).
DISCUSSION
The fetal to neonatal transition is char-acterized by initiation of breathing andchanges in the cardiopulmonarycirculation, which increases tissue ox-ygenation abruptly.33 For adequatepostnatal adaptation, both effectiveventilation and establishment of func-tional residual capacity are essential.Frequently, ELGANs are incapable of es-tablishing effective respiration andtherefore require positive pressureventilation and oxygen treatment inthe DR.7 Of note is that high oxygen andlung-stretching lead to increased ROSproduction and expression of proin-flammatory cytokines.8 In addition,prenatal fetal lung colonization withvaginal flora and/or commensal or-ganisms in ELGANs predisposes themto lung inflammation.36 We hypothe-sized that use of a high oxygen concen-tration in the DR would constitute a su-perimposed factor contributing tolung inflammation and architecturalremodeling and leading to chroniclung disease. To validate this hypothe-sis, we launched a clinical trial to com-
FIGURE 3GSSG/GSH ratio� 100 in cord blood on days 1 and day 3 in ELGANs resuscitated with initial FIO2 of 90%(high-oxygen [Hox] group) or 30% (low-oxygen [Lox] group). Mann-Whitney comparisons betweengroups were as follows: aP� .01, versus low-oxygen group; bP� .05, versus low-oxygen group.
FIGURE 4Urinary levels of isoprostane metabolites (A) and urinary isofurans (B), determined through gaschromatography/mass spectrometry, in ELGANs resuscitated with an initial FIO2 of 90% (high-oxygen[Hox] group) or 30% (low-oxygen [Lox] group) at days 1 and 7 after birth. Mann-Whitney comparisonsbetween groups were as follow: aP� .01, versus low-oxygen group.
e444 VENTO et al. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

pare the clinical and biochemical con-sequences of using 2 different oxygenloads during resuscitation. Further-more, to attenuate the influence oflung-stretch damage, we used gentleventilation for both groups.31 To date,only 2 randomized studies have com-pared different FIO2 values for the re-suscitation of ELGANs.24,26 Those stud-ies confirmed that room air wasinsufficient for ELGANs to achieve tar-geted SpO2 values in the DR, whereasuse of FIO2 of 30% was effective, thus
avoiding the need for rescue therapywith pure oxygen. Our study confirmsthe suitability of an initial FIO2 of 30%and titration of oxygen supplementa-tion according to SpO2 values. Oxygen-ation of patients with impaired lungfunction is an important and life-saving measure. Although oxygen-ation relieves the immediate life-threatening consequences transiently,it also may exacerbate lung injury.37
Hyperoxia leads to increased produc-tion of oxygen free radicals, which di-
rectly cause damage and induce im-paired remodeling of the lungstructure through activation of proin-flammatory cytokines.38,39 Oxygen freeradical-induced TNF receptor activa-tion of pulmonary cells upregulatesinflammatory effector gene expres-sion.39 In addition, oxygenation mayweaken or even suppress the adeno-sine A2A receptor-mediated antiinflam-matory mechanism and thereby exac-erbate lung injury.40 In our study, theGSSG/GSH ratio, a reliable marker ofintracellular oxidative stress and re-dox status,41,42 was increased signifi-cantly in the group receiving higher ox-ygen levels, which confirmed previousfindings that indicated that high oxy-gen exposure on reoxygenation in-creases oxidative stress and prolongsprooxidant status.14,15,17,18 Moreover,correlation between oxidative stressand later development of BPD wasestablished in this study. Increased o-tyrosine/phenylalanine and 8-hydroxy-2�-deoxyguanosine/2-deoxyguanosineratios both indicated that neonates re-ceiving high oxygen levels generatedmore ROS, especially hydroxyl radicals,which have been associated with thepathophysiologic processes of hypoxic-ischemic encephalopathy.43 Interest-ingly, in a piglet model of asphyxia, therates of urinary elimination of o-tyrosine/phenylalanine and 8-hydroxy-2�-deoxyguanosine/2-deoxyguanosinewere correlated significantly withthe amount of oxygen administeredduring resuscitation.27 Increased lev-els of markers of protein and DNAoxidation also were correlated withlater development of BPD. We alsomeasured prostaglandin F2-like com-pounds, which are considered themost-reliable markers of lipid per-oxidation. Under hyperoxic condi-tions, these compounds incorporatean oxygen molecule into their innerstructure, leading to the formation ofisofurans. Isofurans are excellentmarkers of hyperoxia-derived lipid
FIGURE 5Urinary o-tyrosine/phenylalanine (o-Tyr/Phenyl) � 1000 ratio (A) and urinary 8-hydroxy-2�-deoxyguanosine/2�-deoxyguanosine � 100 ratio (8oxodG/2dG � 100) (B), both determined throughhigh-performance liquid chromatography/tandem mass spectrometry, on days 1 and 7 after birth inELGANs resuscitated with an initial FIO2 of 90% (high-oxygen [Hox] group) or 30% (low-oxygen [Lox]group). Mann-Whitney comparisons between groups were as follows: aP � .05, bP � .01, versuslow-oxygen group.
ARTICLES
PEDIATRICS Volume 124, Number 3, September 2009 e445. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

peroxidation, whereas isoprostanemetabolites reflect oxidative stressunder normoxic conditions.44,45 Inter-estingly, although isoprostane me-tabolite levels were no different inthe 2 groups, isofuran levels weresignificantly higher in the high-oxygen group, evidencing hyperoxia-derived oxidative stress duringreoxygenation. It is noteworthy that asignificant number of patients withincreased levels of isofurans laterdeveloped BPD. Previous studies cor-related oxidative stress and develop-ment of BPD.46,47 In addition, Ahola et
al48 found that, among ELGANs need-ing ventilatory assistance, those wholater developed BPD had significantlyhigher plasma free 8-epi-prostaglandinF2� levels on days 3 and 7, comparedwith survivorswithout BPD. Reuter et al49
did not find such correlation betweenBPD and urinary elimination of 8-iso-prostaglandin F2� in preterm neo-nates. Apparently not all isoprostanemetabolites have similar predictivevalue regarding the development ofBPD, and we did not find a correlationbetween isoprostane metaboliteelimination and BPD, although there
was a positive correlation with isofu-ran levels.
The present study has several limita-tions that need to be addressed.First, this was not a blinded study.Our group previously studied the po-tentially harmful effects of pure oxy-gen resuscitation in term infants andmight have been influenced in subse-quent care by the initial patient as-signment. We recorded and analyzedscrupulously all data and decisionsmade in the DR and NICU, and care-givers who were able to observe theoxygen blender did not make deci-sions that might have put the pa-tients at risk of hypoxia or hyperoxiato influence the randomization as-signment. Moreover, caregivers inthe DR did not care for the neonatesduring their hospitalizations. An-other limitation is the number of pa-tients studied, which might have pre-cluded obtaining more-definitivedata regarding the correlation be-tween initial management in the DRand subsequent development of BPD.Although the sample size was pow-ered for 10% reduction of BPD, thenumber of patients in the lower ges-tational age range (�26 weeks ofgestation), who more frequently de-velop BPD, should be increased in fu-ture studies. Despite these limita-tions, our study showed that anincreased oxygen load in the first fewminutes of life caused oxidativestress and inflammation, which wascorrelated with later development ofBPD. Only a few minutes of oxygen ex-cess have been shown to cause long-term oxidative stress in term infantswith mature antioxidant defense sys-tems,14 and even serious conditionssuch as cancer.50 It was proposed re-cently that oxygen serves as amorpho-gen to promote development by influ-encing the production of metabolicoxidants such as ROS. Therefore, an ex-cess of oxygen for even a short period
FIGURE 6TNF-� (A) and IL-8 (B) levels in plasma, as determined through flow cytometry, duringweeks 1, 2, 3, and5 after birth in ELGANs initially resuscitated with FIO2 of 90% (high-oxygen [Hox] group) or 30%(low-oxygen [Lox] group). Mann-Whitney comparisons between groupswere as follows: aP� .05, bP�.01, versus low-oxygen group.
e446 VENTO et al. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

could trigger structural changes in theimmature lung.51
We conclude that ELGAN resuscitationshould be initiated with lower FIO2(�30%) and titrated according to SpO2values, to avoid oxidative damage andinflammation. However, there is a needfor randomized, blinded studies thatare powered adequately for evaluationof the correlation between oxygen lev-els during resuscitation and develop-ment of BPD.
ACKNOWLEDGMENTS
This study was funded by a grant fromthe Spanish Ministry of Health (Insti-tuto Carlos III) (grant FIS PI05/1505) toDr Vento, a research fellowship fromthe Research Foundation Hospital LaFe to Dr Escrig, a research grant fromMutua Madrilena to Dr Moro, Consol-ider grant CSD-2007-00020 to Mr Ar-duini and Dr Sastre, and National Insti-tutes of Health Grant GM42056 to DrRoberts.
We express our gratitude to Drs Neil N.Finer and Tina A. Leone (University ofCalifornia, San Diego, CA) for their in-estimable help in reviewing and edit-ing this manuscript.
REFERENCES
1. Markestad T, Kaaresen P, Ronnestad A. Early death, morbidity and need of treatment amongextremely premature infants. Pediatrics. 2005;115(5):1289–1298
2. Fanaroff AA, Stoll BJ, Wright LL, et al. Trends in neonatal morbidity andmortality for very low birthweight infants. Am J Obstet Gynecol. 2007;196(2):147.e1–147.e8
3. Branco de Almeida MF, Guinsburg R, Martinez FE, et al. Perinatal factors associated with earlydeaths of preterm infants born in Brazilian Network on Neonatal Research centers[inPortuguese]. J Pediatr (Rio J). 2008;84(4):300 –307
4. Field DJ, Dorling JS, Manktelow BN, Draper ES. Survival of extremely premature babies in ageographically defined population: prospective cohort study of 1994–9 compared with 2000–5.BMJ. 2008;336(7655):1221–1223
5. Landmann E, Misselwitz B, Steiss JO, Gortner L. Mortality and morbidity of neonates born at�26weeks gestation (1998–2003): a population-based study. J Perinat Med. 2008;36(2):168–174
6. Baraldi E, Filippone M. Chronic lung disease after premature birth. N Engl J Med. 2007;357(19):1946–1955
7. Leone TA, Rich W, Finer NN. A survey of delivery room resuscitation practices in the United States.Pediatrics. 2006;117(2). Available at: www.pediatrics.org/cgi/content/full/117/2/e164
8. Jobe AH, Hillman N, Polglase G, Kramer BW, Kallapur SH, Pillow J. Injury and inflammation fromresuscitation of the preterm infant. Neonatology. 2008;94(3):190–196
FIGURE 7A, Blood GSSG levels at day 3 after birth and urinary isofuran (Iso F) levels at day 7 after birth in ELGANswho were resuscitated with an initial FIO2 of either 90% or 30% and later developed BPD or not. B,Urinary o-tyrosine/phenylalanine � 1000 ratio (o-tyr/Phenyl ratio) and urinary 8-hydroxy-2�-deoxyguanosine/2�-deoxyguanosine� 100 ratio (8-oxodG/2dG ratio) in ELGANswhowere resuscitatedwith an initial FIO2 of either 90% or 30% and later developed BPD or not. a P� .01.
ARTICLES
PEDIATRICS Volume 124, Number 3, September 2009 e447. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

9. Saugstad OD. Optimal oxygenation at birth and in the neonatal period. Neonatology. 2007;91(4):319–322
10. Maltepe E, Saugstad OD. Oxygen in health and disease: regulation of oxygen homeostasis: clinicalimplications. Pediatr Res. 2009;65(3):261–268
11. Bhandari V. Molecular mechanisms of hyperoxia-induced acute lung injury. Front Biosci. 2008;13:6653–6661
12. Buccellato LJ, TsoM, Akinci OI, Chandel NS, Budinger GRS. Reactive oxygen species are required forhyperoxia-induced Bax activation and cell death in alveolar epithelial cells. J Biol Chem. 2004;279(8):6753–6760
13. Saugstad OD, Ramji S, Soll RF, VentoM. Resuscitation of newborn infants with 21% or 100% oxygen:an updated systematic review and meta-analysis. Neonatology. 2008;94(3):174–182
14. Vento M, Asensi M, Sastre J, García-Sala F, Pallardo FV, Vina J. Resuscitation with room air insteadof 100% oxygen prevents oxidative stress in moderately asphyxiated term neonates. Pediatrics.2001;107(4):642–647
15. Vento M, Sastre J, Asensi MA, Vina J. Room-air resuscitation causes less damage to heart andkidney than 100% oxygen. Am J Respir Crit Care Med. 2005;172(11):1393–1398
16. Saugstad OD, Ramji S, Irani SF, et al. Resuscitation of newborn infants with 21% or 100% oxygen:follow-up at 18 to 24 months. Pediatrics. 2003;112(2):296–300
17. Vento M, Asensi M, Sastre J, et al. Hyperoxemia caused by resuscitation with pure oxygen mayalter intracellular redox status by increasing oxidized glutathione in asphyxiated newly borninfants. Semin Perinatol. 2002;26(6):406–410
18. Vento M, Asensi M, Sastre J, Lloret A, García-Sala F, Vina J. Oxidative stress in asphyxiated terminfants resuscitated with 100% oxygen [published correction appears in J Pediatr. 2003;142(6):616]. J Pediatr. 2003;142(3):240–246
19. Vina J, Vento M, García-Sala F, et al. L-Cysteine and glutathione metabolism are impaired inpremature infants due to cystathionase deficiency. Am J Clin Nutr. 1995;61(5):1067–1069
20. Ledo A, Arduini A, Asensi MA, et al. Human milk enhances antioxidant defenses against hydroxylradical aggression in preterm infants. Am J Clin Nutr. 2009;89(1):210–215
21. Asikainen TM, White CW. Antioxidant defenses in the preterm lung: role for hypoxia-induciblefactors in BPD? Toxicol Appl Pharmacol. 2005;203(2):177–188
22. Ballard PL, Truog WE, Merrill JD, et al. Plasma biomarkers of oxidative stress: relationship to lungdisease and inhaled nitric oxide therapy in premature infants. Pediatrics. 2008;121(3):555–561
23. Harling AE, BeresfordMW, Vince GS, BatesM, Yoxall CW. Does use of 50% oxygen at birth in preterminfants reduce lung injury? Arch Dis Child Fetal Neonatal Ed. 2005;90(5):F401–F405
24. Wang CL, Anderson C, Leone TA, Rich W, Govindaswami B, Finer NN. Resuscitation of pretermneonates by using room air or 100% oxygen. Pediatrics. 2008;121(6):1083–1089
25. Dawson JA, Kamlin CO, Wong C, et al. Oxygen saturation and heart rate during delivery roomresuscitation of infants �30 weeks’ gestation with air or 100% oxygen. Arch Dis Child FetalNeonatal Ed. 2009;94(2):F87–F91
26. Escrig R, Arruza L, Izquierdo I, et al. Achievement of targeted saturation values in extremely lowgestational age neonates resuscitated with low or high oxygen concentrations: a prospective,randomized trial. Pediatrics. 2008;121(5):875–881
27. Solberg R, Andresen JH, Escrig R, Vento M, Saugstad OD. Resuscitation of hypoxic newborn pigletswith oxygen induces a dose-dependent increase in markers of oxidation. Pediatr Res. 2007;62(5):559–563
28. Davies SS, Zackert W, Luo Y, Cunningham CC, Frisard M, Roberts LJ II. Quantification of dinor,dihy-dro metabolites of F2-isoprostanes in urine by liquid chromatography/tandem mass spectrome-try. Anal Biochem. 2006;348(2):185–191
29. Naik AS, Kallapur SG, Bachurski CJ, et al. Effects of ventilation with different positive end-expiratory pressures on cytokine expression in the preterm lamb lung. Am J Respir Crit CareMed.2001;164(3):494–498
30. Ehrenkranz RA, Walsh MC, Vohr BR, et al. Validation of National Institutes of Health consensusdefinition of bronchopulmonary dysplasia. Pediatrics. 2005;116(6):1353–1360
31. Spanish Society for Neonatology, Neonatal Resuscitation Group.Manual de Reanimacion Neonatal[Manual of Neonatal Resuscitation; in Spanish]. Madrid, Spain: Ergon Editores; 2006
32. O’Donnell CP, Kamlin CO, Davis PG, Morley CJ. Feasibility of and delay in obtaining pulse oximetryduring neonatal resuscitation. J Pediatr. 2005;147(5):698–699
33. Fineman JR, Soifer SJ, Heymann MA. Regulation of pulmonary vascular tone in the perinatalperiod. Annu Rev Physiol. 1995;57:115–134
34. Asensi M, Sastre J, Pallardo FV, Garcia de la Asuncion J, Estrela JM, Vina J. A high-performance
e448 VENTO et al. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

liquid chromatography method for measurement of oxidized glutathione in biological samples.Anal Biochem. 1994;217(2):323–328
35. Riffenburgh RH. Statistics in Medicine. 2nd ed. New York, NY: Academic Press; 2005
36. Hansen-Pupp I, Hallin AL, Hellstrom-Westas L, et al. Inflammation at birth is associated withsubnormal development in very preterm infants. Pediatr Res. 2008;64(2):183–188
37. Thiel M, Chouker A, Ohta A, et al. Oxygenation inhibits the physiological tissue-protecting mecha-nism and thereby exacerbates acute inflammatory lung injury. PLoS Biol. 2005;3(6):e174
38. Deng H, Mason SN, Auten RL Jr. Lung inflammation in hyperoxia can be prevented by antichemo-kine treatment in newborn rats. Am J Respir Crit Care Med. 2000;162(6):2316–2323
39. Cho H-Y, Morgan DL, Bauer AK, Kleeberger SR. Signal transduction pathways of tumor necrosisfactor-mediated lung injury induced by ozone in mice. Am J Respir Crit Care Med. 2007;175(8):829–839
40. Fredholm BB, Chern Y, Franco R, Sitkovsky M. Aspects of the general biology of adenosine A2Asignaling. Prog Neurobiol. 2007;83(5):263–276
41. Borras C, Esteve JM, Vina JR, Sastre J, Vina J, Pallardo FV. Gutathione regulates telomerase activityin 3T3 fibroblasts. J Biol Chem. 2004;279(33):34332–34335
42. Markovic J, Borras C, Ortega A, Sastre J, Vina J, Pallardo FV. Glutathione is recruited into thenucleus in early phases of cell proliferation. J Biol Chem. 2007;282(28):20416–20424
43. Ogihara T, Hirano K, Ogihara H, et al. Non-protein transition metals and hydroxyl radical genera-tion in cerebrospinal fluid of newborn infants with hypoxic-ischemic encephalopathy. Pediatr Res.2003;53(4):594–599
44. Montuschi P, Barnes PJ, Roberts LJ. Isoprostanes: markers and mediators of oxidative stress.FASEB J. 2004;18(15):1791–1800
45. Patel M, Liang LP, Hou H, et al. Seizure-induced formation of isofurans: novel products of lipidperoxidation whose formation is positively modulated by oxygen tension. J Neurochem. 2008;104(1):264–270
46. Banks BA, Ischiropoulos H, McClellandM, Ballard PL, Ballard RA. Plasma 3-nitrotyrosine is elevatedin premature infants who develop bronchopulmonary dysplasia. Pediatrics. 1998;101(5):870–874
47. Saugstad OD. Chronic lung disease: the role of oxidative stress. Biol Neonate. 1998;74(suppl1):21–28
48. Ahola T, Fellman V, Kjellmer I, Raivio KO, Lapatto R. Plasma 8-isoprostane is increased in preterminfants who develop bronchopulmonary dysplasia or periventricular leukomalacia. Pediatr Res.2004;56(1):88–93
49. Reuter SD, O’Donovan DJ, Hegemier SE, Smith EO, Heird WC, Fernandes CJ. Urinary F2-isoprostanesare poor prognostic indicators for the development of bronchopulmonary dysplasia. J Perinatol.2007;27(5):303–306
50. Spector LG, Klebanoff MA, Feusner JH, Georgieff MK, Ross JA. Childhood cancer following neonataloxygen supplementation. J Pediatr. 2005;147(1):27–31
51. Hitchler MJ, Domann FE. An epigenetic perspective on the free radical theory of development. FreeRadic Biol Med. 2007;43(7):1023–1036
52. International Committee for the Classification of Retinopathy of Prematurity. The InternationalClassification of Retinopathy of Prematurity revisited. Arch Ophthalmol. 2005;123(7):991–999
53. Papile LA, Munsick-Bruno G, Schaefer A. Relationship of cerebral intraventricular hemorrhageand early childhood neurologic handicaps. J Pediatr. 1983;103(2):273–277
54. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163(7):1723–1729
ARTICLES
PEDIATRICS Volume 124, Number 3, September 2009 e449. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.2009-0434 2009;124;e439-e449; originally published online Aug 3, 2009; Pediatrics
Sastre and Miguel A. Asensi Izquierdo, L. Jackson Roberts, II, Alessandro Arduini, Justo Javier Escobar, Juan Maximo Vento, Manuel Moro, Raquel Escrig, Luis Arruza, Gema Villar, Isabel
Inflammation, and Chronic Lung DiseasePreterm Resuscitation With Low Oxygen Causes Less Oxidative Stress,
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/124/3/e439including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/124/3/e439#BIBLat: This article cites 51 articles, 24 of which you can access for free
Subspecialty Collections
nhttp://www.pediatrics.org/cgi/collection/premature_and_newbor
Premature & Newbornfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by McMaster University on August 31, 2009 www.pediatrics.orgDownloaded from




















