Présentation PowerPoint - AIOM
36
The evolving landscape of biomarkers for immune checkpoint inhibitors in thoracic oncology Paul Hofman Laboratory of Clinical and Experimental Pathology FHU OncoAge, Inserm U1081/CNRS 7284 Côte d’Azur University, Nice, France
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Présentation PowerPoint - AIOM

The evolving landscape of biomarkers for immune checkpoint inhibitors
in thoracic oncology
Paul Hofman
Laboratory of Clinical and Experimental PathologyFHU OncoAge, Inserm U1081/CNRS 7284
Côte d’Azur University, Nice, France

Biomarkers
Response Resistance Toxicity Hyperprogression

Biomarkers
Response

Two independent predictive biomarkers
IHC PD-L1 Tumor mutational burden
+ EGFR, ALK, ROS1 & BRAF
ValidatedDaily practice
Not ValidatedClinical trials

PD-L1 has limitations
– Patient with 0% of PD-L1 IHC positivity can be good responder– Patient with > 50% of PD-L1 IHC positivity can be non responder–Heterogeneity of PD-L1 IHC staining limits the assessment in small biopsies – Inter & intra oberver variability– PD-L1 IHC is not well-validated to date –Many PD-L1 clones, many devices, different performances–Many cut off (>1%, > 25%, > 50%)– Clinical value of positive immune cells for PD-L1 is controversial

PD-L1 IHC
<1%
>50%
Prembrolizumabfirst line
Chemotherapyfirst line
…..or…..!

Matched specimens in NSCLC patientsIlie et al, Ann Oncol 2016

> 50% TC ?
First line I-O according to the PD-L1 expression on TC (May 2018)
> 25% TC ? > 1% TC ? …All comers ?

Controversies about EMA decision
EMA excluded patients with PD-L1 <1%from access to durvalumab
Expands pembrolizumab indication for first-line treatment of NSCLC (TPS ≥1%). Accessed April 11, 2019. https://www.fda.gov/Drugs/InformationOnDrugs/ ApprovedDrugs/ucm635857.htm.FDA
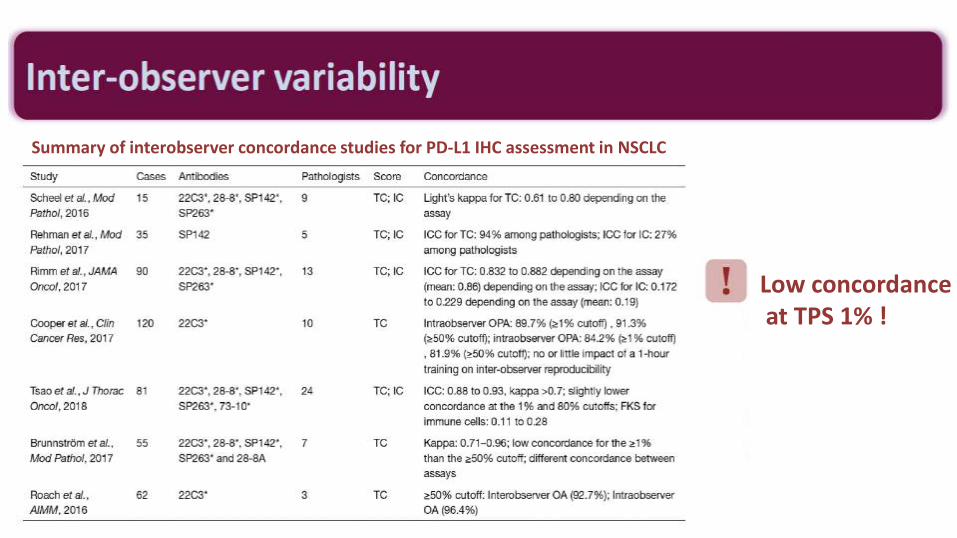
Summary of interobserver concordance studies for PD-L1 IHC assessment in NSCLC
Low concordanceat TPS 1% !

Tumor mutational burden
What’s next ?


CheckMate 026: Nivolumab in first-line in stage IV NSCLCPFS by TMB subgroup
Nivolumab Chemotherapy

CheckMate 227: PFS in Patients With High TMB (≥10 mut/Mb) by Tumor PD-L1 Expression
≥1% PD-L1 expression <1% PD-L1 expression
Nivo + ipi(n = 38)
Chemo(n = 48)
Median PFS, mob 7.7 5.3
HR95% CI
0.480.27, 0.85
Chemotherapy
Nivolumab +ipilimumab
Months
0
20
40
60
80
100
0 6 12 183 9 15 21 24
1-y PFS = 45%
1-y PFS = 8%
1-y PFS = 42%
1-y PFS = 16%
PF
S (
%)
Chemotherapy
Nivolumab +ipilimumab
Months
0
20
40
60
80
100
0 6 12 183 9 15 21 24
Nivo + ipi(n = 101)
Chemo(n = 112)
Median PFS, moa 7.1 5.5
HR95% CI
0.620.44, 0.88
2018

CheckMate 227: PFS in Patients With High TMB (≥10 mut/Mb) by Tumor PD-L1 Expression
≥1% PD-L1 expression <1% PD-L1 expression
Nivo + ipi(n = 38)
Chemo(n = 48)
Median PFS, mob 7.7 5.3
HR95% CI
0.480.27, 0.85
Chemotherapy
Nivolumab +ipilimumab
Months
0
20
40
60
80
100
0 6 12 183 9 15 21 24
1-y PFS = 45%
1-y PFS = 8%
1-y PFS = 42%
1-y PFS = 16%
PF
S (
%)
Chemotherapy
Nivolumab +ipilimumab
Months
0
20
40
60
80
100
0 6 12 183 9 15 21 24
Nivo + ipi(n = 101)
Chemo(n = 112)
Median PFS, moa 7.1 5.5
HR95% CI
0.620.44, 0.88

The pros
The cons
1. Alternative / complementary biomarker to PD-L1 2. Compatible with targeted panel NGS tests
3. Less heterogeneity than PD-L1 (?)
1. Turnaround times for getting the results2. Sensitivity links to DNA quantity/quality
3. Proposed cutpoints for TMB High4. Reproducibility across sequencing platforms
5. Cost effectivness6. Accreditation is mandatory
TMB

Lung Cancer with a High Tumor Mutational BurdenVanderLaan PA, et al. N Engl J Med 2018
VanderLaan PA. N Engl J Med 2018; 379: 11.
In-House Testingversus
External to Referral Center?

TMBTMBMain challenge
in thoracic oncology

Samstein et al, Nat Genet. 2019 Feb;51(2):202-206.
Which cutoff?

Estimated number of patients over 100 cases who will benefit to ICIs according to a high TMB
WithoutWithout TAT consideration
(>10 mut/Mb)
(<10 mut/Mb)
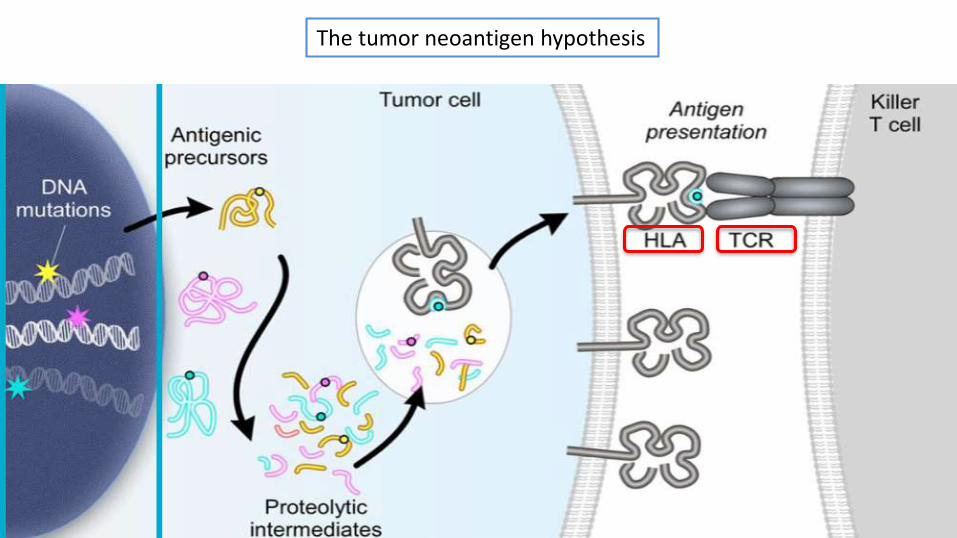
The tumor neoantigen hypothesis

TCR repertoire variability may serve as a predictivebiomarker for immunotherapy in solid tumors,including those where TMB is not predictive of response

Biomarkers
Resistance

Skoulidis et al, Cancer Discovery May 2018
Patients treated by PD1/PD-L1 inhibitors
STK11 mutation
Biomarkers
Toxicity
TCR repertoire ?

Biomarkers
Hyperprogression
MDM2 amplification?EGFR amplification?

More and more biomarkersin I-O pipeline
PD-L1
TMB
TCR
GEP
?

Tumor mutational burden &genomic alterations
PD1/PD-L1 and other ICIs
Adaptative immunity TCR repertoire
SNPs (germline DNA)
Microbiome
Innate immunity

Combination oftherapies
Combination ofbiomarkers

J Clin Oncol. 2019 Feb 1;37(4):318-327

Which targets?Which methods?How many fields to assess per tumor?Primary and/or metastatic site (s)?How to quantify the different signals?How to assess the different cut off?
&How to integrate genomic associated data ?

Comment optimiser?How to optimize?
The evolving landscape of biomarkers for immune checkpoint inhibitors

How to integrate?

The evolving landscape of biomarkers for immune checkpoint inhibitors
in thoracic oncology
Paul Hofman
Laboratory of Clinical and Experimental PathologyFHU OncoAge, Inserm U1081/CNRS 7284
Côte d’Azur University, Nice, France