Preparing the community health nursing workforce: Internal and external enablers and challenges...
23
International Journal of Nursing Education Scholarship Volume 5, Issue 1 2008 Article 22 Preparing the Community Health Nursing Workforce: Internal and External Enablers and Challenges Influencing Undergraduate Nursing Programs in Canada Ruta K. Valaitis * Christina J. Rajsic † Benita Cohen ‡ Lynnette Leeseberg Stamler ** Donna Meagher-Stewart †† Susan A. Froude ‡‡ * McMaster University, [email protected] † University of Toronto, [email protected] ‡ University of Manitoba, benita [email protected] ** University of Saskatchewan, [email protected] †† Dalhousie University, [email protected] ‡‡ Western Regional School of Nursing, [email protected] Copyright c 2008 The Berkeley Electronic Press. All rights reserved.
Transcript of Preparing the community health nursing workforce: Internal and external enablers and challenges...

International Journal of NursingEducation Scholarship
Volume 5, Issue 1 2008 Article 22
Preparing the Community Health NursingWorkforce: Internal and External Enablers and
Challenges Influencing UndergraduateNursing Programs in Canada
Ruta K. Valaitis∗ Christina J. Rajsic† Benita Cohen‡
Lynnette Leeseberg Stamler∗∗ Donna Meagher-Stewart†† Susan A. Froude‡‡
∗McMaster University, [email protected]†University of Toronto, [email protected]‡University of Manitoba, benita [email protected]
∗∗University of Saskatchewan, [email protected]††Dalhousie University, [email protected]‡‡Western Regional School of Nursing, [email protected]
Copyright c©2008 The Berkeley Electronic Press. All rights reserved.

Preparing the Community Health NursingWorkforce: Internal and External Enablers and
Challenges Influencing UndergraduateNursing Programs in Canada∗
Ruta K. Valaitis, Christina J. Rajsic, Benita Cohen, Lynnette Leeseberg Stamler,Donna Meagher-Stewart, and Susan A. Froude
Abstract
The Canadian Schools of Nursing (CASN) task force on public health was mandated to fa-cilitate Schools of Nursing to provide students with the foundation required to meet the CanadianCommunity Health Nursing Standards of Practice. This paper reports on an environmental scanthat explored barriers and enablers influencing the integration of community health nursing con-tent in baccalaureate education in Canada. Data was collected over three phases including: 1)a pan-Canadian survey of nursing schools, 2) completion of open-ended workbook questions byeducators, policy makers, administrators, and community health nursing managers attending apan-Canadian symposium on community health nursing, and 3) recorded notes from the sym-posium. The response rate for the survey was 72.5% (n = 61 schools) and approximately 125stakeholders participated in symposium activities. Internal and external enablers and challengesas well as recommendations for practice and education are presented.
KEYWORDS: nursing education, community health nursing, standards, baccalaureate
∗We would like to acknowledge the contributions of all members of the Canadian Association ofSchools of Nursing’s (CASN) Subcommittee on Public Health in the design of the methods anddata collection in this work. Members include: Margaret Antolovich, Pat Gibson, Pat Griffin,Omaima Mansi, Heather Pattulo, Pat Seaman, Jo Ann Tober, and all authors on this paper. Wewould also like to sincerely thank and acknowledge the Public Health Agency of Canada, JaneUnderwood and Joan Reiter for their support that enabled this work to be completed and DinaIdriss for her expert assistance with recruitment, data gathering and cleaning.

Canadian Schools of Nursing that deliver all or part of nursing
baccalaureate education are invited to become members of the Canadian
Association of Schools of Nursing (CASN), the Canadian nursing education
accreditation body. In response to a growing awareness and interest in community
health issues across the country, CASN created a taskforce in 2004 to examine
community health nursing undergraduate education. The mandate of the task
force was to assist CASN members in ensuring that all baccalaureate graduates of
Canadian schools of nursing obtain a foundation towards meeting the expected
entry-level competencies based on the Canadian Community Health Nursing
Standards of Practice (CCHNSoP), which were released in 2003 (Community
Health Nurses Association of Canada). In the CCHNSoP, outlined are
expectations for a community nurse after two years of practice. Membership in
the taskforce included educators from CASN member schools and representatives
from practice.
A mandate of the Public Health Agency of Canada is to build human
resource capacity in public health, including nursing. In collaboration with the
Public Health Agency of Canada and CASN, the taskforce conducted an
environmental scan. The purpose was to identify strengths and gaps within current
undergraduate nursing curricula (structures/content), and identify enablers and
challenges in delivering community health nursing education (processes) in
CASN member undergraduate nursing schools. A guiding framework was the
CCHNSoP. Process issues (enablers and challenges) were largely explored
through qualitative data collection strategies and are reported in this article.
LITERATURE REVIEW
The majority of literature on integration of community health concepts in
undergraduate nursing education comes from the United States (U.S.), where a
curriculum revolution initiated at the federal level led to major changes in
professional nursing. The Pew Health Professions Commission (O’Neil, 1993)
recommended that U.S. nursing programs reorient curricula to provide greater
emphasis on health promotion and population-based care. The rationale for the
shift from acute, hospital-based care to community-based care was part of a broad
policy change, which would see a care location shift resulting in cost savings
related to lowered hospitalizations. The community nursing role was considered
to be integral for ongoing health education and disease monitoring in the
community. The role was also viewed in the context of working with populations
in partnership with communities rather than individuals, and required
“fundamental realignments of nursing education program[s], not merely add-on
courses or educational experiences to the existing curricula” (O’Neil, p. 89). The
1
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

Pew Commission encouraged university-community partnerships, leading to an
increase in ‘service-learning’ opportunities for health professional students to fill
the health care gap in under-serviced populations. While models of ‘service
learning’ vary, Redman and Clark (2002) suggest that the essential component is
a partnership between the campus and a community, with community agencies
defining their needs for service and educators providing structured learning
experiences for students to meet those needs. They also noted that students’
critical reflections on the social forces that led to the community need and the
student-as-citizen’s civic responsibility in addressing that need, are characteristics
of service-learning models.
The National League for Nursing’s (1993) position statement pointed to
the importance of moving the focus of a large part of content and clinical nursing
education from acute care to community-based settings. These developments
spawned widespread curriculum revision across the U.S. to the end of the decade.
Since the mid-1990s, most American literature on the integration of community
health content into undergraduate curricula, describes experiences of various
nursing programs as they shifted from a traditional medical model to a
community-based care model (Conger, Baldwin, Agegglen, & Callister, 1999;
Edwards & Alley, 2002; Reece, Mawn, & Scollin, 2003; Speck, 2003; Staats,
2003; Thomas & Carroll, 2006).
In Europe, the World Health Organization (2000) called for the inclusion
of health promotion in all nursing curricula. Results from a literature review
conducted by Whitehead (2006), showed that health promotion has been
inadequately incorporated into nursing education programs. Students have had
little opportunity to apply health promotion theory in their practice. And when
they have, the focus has been primarily on health education in disease and life-
style oriented contexts as opposed to a broader ‘determinants of health’ approach
to health promotion. A stronger curriculum focused on health promotion and
education has been placed on pre- and post-registration nursing programs in the
U.K. (Holt & Warne, 2007). This is believed to be related to U.K. policies that
have emphasized health promotion and prevention within nursing activities, in all
nursing settings beyond primary care, school health and health visiting. Holt and
Warne found a perceived lack of health promotion and education practice
opportunities in student clinical placements which has resulted in devaluing of
this role. Results from a literature review and key informant interviews in the
U.K. conducted by Latter, Speller, Westwood, and Latchem (2003) indicated that
exposure to public health practice placements for pre-registration students “is
limited at present, due to the demands on placement availability created by large
2
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

student cohorts, the requirement for longer placement experiences and the
comparative lack of development of public health nursing roles to date" (p.215).
In Canada, there have been no policy statements leading to radical reform
of community health nursing education. Furthermore, the literature on integration
of community health content into Canadian undergraduate curricula is sparse.
However, there is evidence of nursing’s widespread adoption in Canada of the
concept of Primary Health Care (PHC), which emphasizes community
participation and empowerment, health promotion and disease prevention, inter-
disciplinary and inter-sectoral partnerships for health and social development, and
appropriate use of technology (Smith, 2004). The application of the principles of
PHC has had a major influence on Canadian undergraduate nursing education. A
2005 survey of Canadian nursing programs conducted by the CASN Task Force
on Public Health Education (CASN, 2007) found that most undergraduate
programs in Canada report covering the topic of PHC in some way. A review of
approaches to community health clinical education in Canadian baccalaureate
nursing programs (Cohen & Gregory, 2007), indicated that about 20 percent of
programs used PHC as a conceptual framework for community health clinical
education; however, the understanding and/or application of PHC principles to
community health nursing practice was a common expectation in clinical course
objectives. They found that, unlike the U.S., where the emphasis in baccalaureate
education has been on a shift toward community-based nursing (i.e., providing
nursing care to clients in community settings), Canadian programs stress
community health nursing, emphasizing health promotion and disease prevention.
However, there was significant variation in community health clinical courses
(content, process, outcomes) across the country, which suggests a need for
national dialogue/consensus regarding standard curriculum content for
community health nursing education in Canada.
PURPOSE AND OBJECTIVES
The purpose of this environmental scan was to explore internal and
external enablers and challenges influencing the integration of community health
content in baccalaureate nursing education in Canada. The objectives of the paper
are to: 1. describe enablers and challenges with respect to intra-organizational
factors in community health settings (external) that influence the teaching
learning process; 2. explore enablers and challenges with respect to intra-
organizational factors in academe (internal) that influence the teaching-learning
process; 3. investigate the enablers and challenges with respect to partnerships
between community health settings and academe that influence the teaching-
3
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

learning process, and; 4. identify recommendations to guide further enhancement
of community health content in baccalaureate curricula in Canada.
METHODS
To obtain a comprehensive understanding of the enablers and challenges,
three phases of data collection were conducted involving different sources and
methods, each phase building on the next. In Phase 1, an online survey was
conducted with CASN member schools; in Phase 2, key stakeholders answered
broad open-ended questions in a workbook prior to attending a Pan-Canadian
symposium on community health nursing education; in Phase 3, recorded notes
were collected from all symposium discussions to include in the analysis (Table
1). Although the authors did not obtain ethics clearance for this environmental
scan, permission was obtained from participants for all quotes used in this
manuscript.
Table 1
Summary of Data Collection
Phase Strategy Participant response
1 – Pan-Canadian
Survey
Survey sent to all 91
CASN member Schools
of Nursing
66 member schools
responded
(72.5% response rate)
2 – Pre-symposium
Workbooks
Workbook questions pre-
circulated by email to all
registered participants
65 workbooks completed
by nurse educators and
nurse leaders
3 – Symposium Invitations emailed to
CASN member schools
and key nursing leaders
125 community health
nursing educators and
leaders attended
In Phase 1, the CASN taskforce developed a web-based survey to examine
the current status of Canadian undergraduate public health nursing education.
Questions pertained to internal and external enabling and challenging influences
that impacted community health nursing curriculum content and delivery as well
as participant’s interest in participating in a pan-Canadian follow up symposium.
The survey was pilot-tested with 5 member schools, suggested areas for
improvements were identified, and edits were made accordingly. Based on pilot-
test results, respondents needed to consult with colleagues to complete the survey.
4
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

Therefore, participants were provided with a printer-friendly survey to enable
easier survey completion. The survey was distributed in web-based and paper
formats to 91 CASN member schools in May 2005. Deans or Program Directors
were sent a letter of invitation to participate, survey instructions, a glossary of
terms, a survey formatted for printing, and a link to the online version. They were
asked to forward the survey to faculty most knowledgeable about the curriculum.
Respondents were asked to enter their responses online, by mail or fax, and phone
reminders were made to increase response rates.
A full day, pan-Canadian symposium on public heath nursing education
was held in May, 2006 to gain further understanding of enablers and challenges
for integrating community health nursing in the curricula. In Phase 2, participants
were asked to complete workbook questions prior to attending the symposium.
The objectives were to present, validate and expand on Phase 1 findings and assist
in the development of key community health nursing education recommendations
for CASN. Symposium participants included representatives from more than 60
of the 91 CASN member schools, with some schools supporting more than one
participant. Other attendees included staff from the Public Health Agency of
Canada, the Canadian Nurses Association, provincial nursing associations, and
nursing policy officers from various provinces. More than 20 public health
nursing directors and managers, who were attending a concurrent meeting, joined
the symposium for parts of the day. Thus, the symposium was represented by
approximately 125 key stakeholders including educators, policy makers and
decision-makers in community health nursing. Workbook questions explored
student placements in community, enablers and barriers in supporting students’
move to meeting the CCHNSoP, and the nature of internal and external
relationships required for successful partnerships between academia and
community agencies.
In Phase 3, results from Phase 1 and 2 were shared at the symposium,
followed by small and large group discussions to help interpret results and begin
formulating recommendations. Notes recorded from the day were collected. In
addition, approximately 100 public health nurse managers met in British
Columbia to discuss the workbook questions and submitted a joint response to the
taskforce for inclusion.
ANALYSIS
NVivo2 qualitative analysis software was used to code the open-ended
questions in the Phase 1 survey. The lead author coded responses and reviewed
coding with a sub-group of the taskforce in a face-to-face meeting. Consensus
5
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

was reached on all coding, thereby strengthening research rigor. Minor codes
were grouped into larger themes by the sub-group. All data collected from Phase
1 and 2 were reviewed in a face-to-face meeting prior to the symposium. The
major findings were shared with symposium participants in order to validate
results, expand upon interpretations, and serve as a member check. This was
followed by the second author who conducted more detailed analysis of data from
Phase 2 and 3, building and expanding on the themes from Phase I using
HyperRESEARCH software; and the coding structure, which was reviewed by the
first author. Codes mapped onto the initial Phase I coding structure went well. All
French language responses (online, handwritten and verbal responses) were
translated and coded. The final analysis was reviewed in depth by taskforce
members as a peer-review.
RESULTS
Sixty-six surveys were received from the 91 CASN member schools of
nursing (72.5% response rate), which offer generic, collaborative integrated
‘DEC-BAC’ programs (College Diploma to Degree programs in the Province of
Quebec), and/or post-RN programs with degree designations of BScN or BN. Of
these, 86.4% of programs were offered in English, 9.1% in French and 4.5% were
bilingual. The highest response rates were from Atlantic and Prairie Provinces and
the Territories. Although the lowest percentage response rates were from British
Columbia, Quebec, and Ontario, these provinces had a greater number of
responses than others, since they have more schools.
6
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

0 10 20 30 40 50 60 70
Number of faculty teaching CHN
Faculty preparation for CHN
Understanding community as partner
Faculty commitment to CHN
Curriculum renewal
Culture of collaborative program
Accelerated Program
Funding
Space
Time
Percentage
Enabling Neutral Challenging Not Applicable
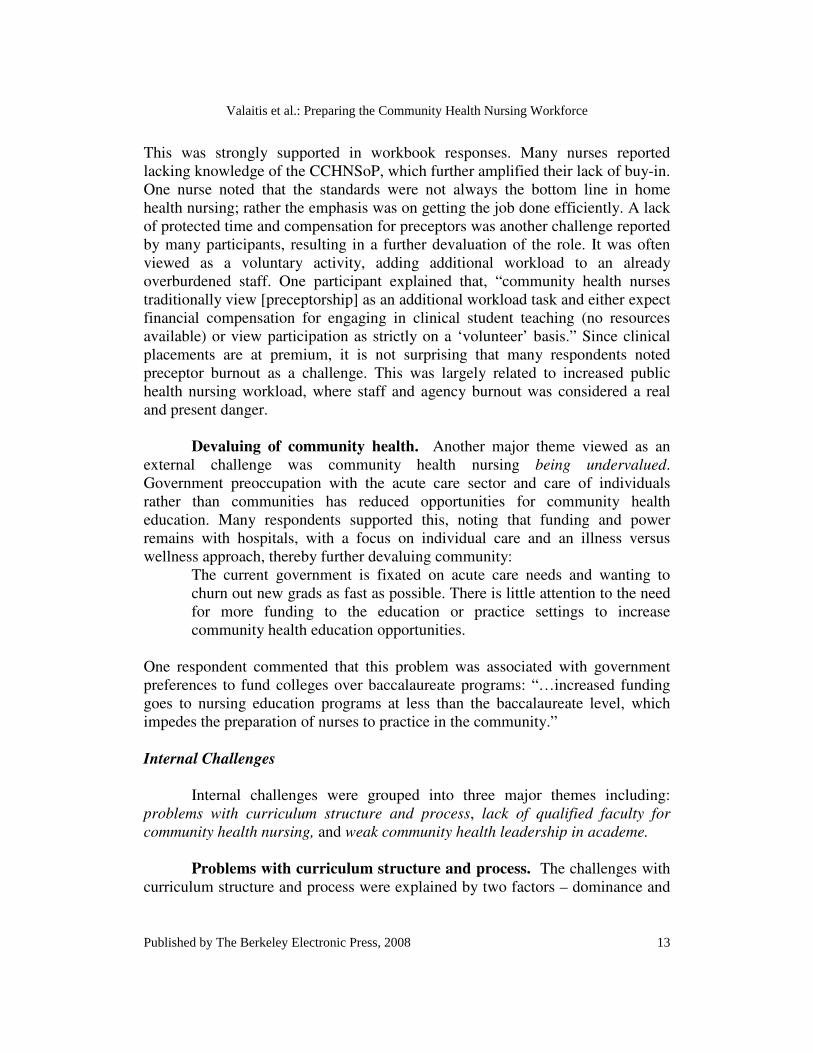
Figure 1 Internal influences on community health nursing curriculum (n=61).
Respondents rated a list of internal and external influences with respect to
their impact on community health content in their program (1 to 5 scale, and not
applicable) (Figures 1 and 2). Enablers referred to influences enabling the
delivery of community health nursing content in program(s). Internal enabling
influences (scored 1 or 2) were curriculum revision/renewal (65.6%);
understanding of the concept of community as partner versus community as
context (63.9%); faculty preparation for teaching community health nursing
(63.9%); number of faculty teaching community health nursing content (63.9%);
and faculty commitment to community health nursing (62.3%). Issues rated as the
greatest internal challenges (scored 4 or 5) were space (60.7%) and funding
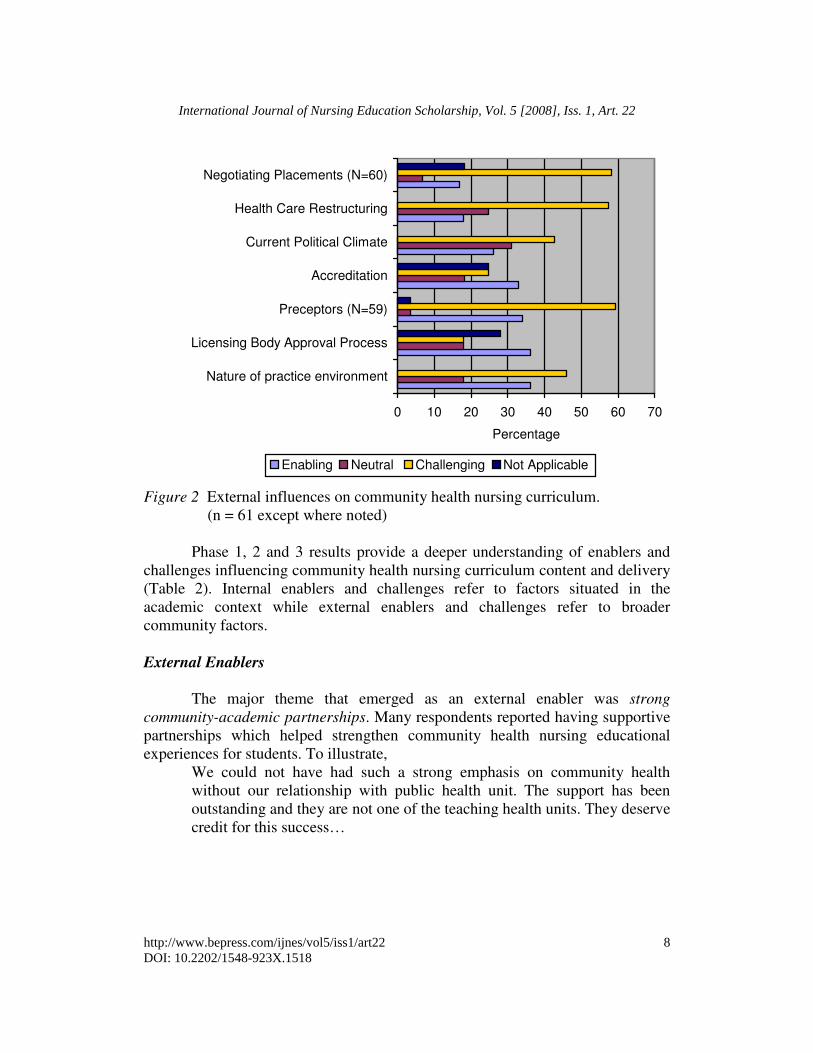
(39.3%). External challenges were preceptors (59.3%); negotiating placements
with others (e.g., LPNs, NPs, MDs, Midwifery, geography, social science, and
kinesiology) (58.3%); health care restructuring (57.4%); the nature of the practice
environment (45.9%); and the current political climate (42.6%). A smaller
percentage of respondents identified external enabling influences as, the nature of
the practice environment (36.1%); the licensing body approval process (36.1%);
preceptors (33.9%); accreditation (32.8%); and current political climate (26.2%).
7
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008
0 10 20 30 40 50 60 70
Nature of practice environment
Licensing Body Approval Process
Preceptors (N=59)
Accreditation
Current Political Climate
Health Care Restructuring
Negotiating Placements (N=60)
Percentage
Enabling Neutral Challenging Not Applicable
Figure 2 External influences on community health nursing curriculum.
(n = 61 except where noted)
Phase 1, 2 and 3 results provide a deeper understanding of enablers and
challenges influencing community health nursing curriculum content and delivery
(Table 2). Internal enablers and challenges refer to factors situated in the
academic context while external enablers and challenges refer to broader
community factors.
External Enablers
The major theme that emerged as an external enabler was strong
community-academic partnerships. Many respondents reported having supportive
partnerships which helped strengthen community health nursing educational
experiences for students. To illustrate,
We could not have had such a strong emphasis on community health
without our relationship with public health unit. The support has been
outstanding and they are not one of the teaching health units. They deserve
credit for this success…
8
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

Table 2
Summary of Major Themes Influencing Community Health Content in Schools of
Nursing in Canada
Enablers Challenges
External:
• Strong community-
academic partnerships
• Placement: increased demand /
reduced supply, limited exposure to
varieties of community nursing
placements and activities within
placements (resulting in fewer
nursing role models), as well as
limited clinical space for students
• Preceptor: lack of valuing of the
preceptor role, lack of skilled
preceptors, lack of protected time and
compensation for preceptors, and
burnout.
• Community health devalued versus
acute care sector
Internal:
• Supportive curriculum
structure and process
• Faculty champions
• Problems with curriculum structure
and process: dominance and valuing
of illness / acute care in academe and
difficulties integrating community
health nursing components
throughout the curriculum.
• Lack of qualified faculty to teach
community health: shortage of faculty
prepared to teach community health,
with an understanding community
health concepts.
• Weak community health leadership in
academe: negatively impacting
integration of community health
curriculum content, and budget
implications for community health
nursing educational resources.
9
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

Respondents described formal and informal community-academic partnerships.
One supportive formal partnership model was the teaching health unit.
The Ontario PHRED (Public Health Research Education and Development
Program) model has strengthened public health nursing education,
research and practice through increased opportunities provided to our
students by the partnerships and experience that faculty have brought from
their PHRED joint appointments.
Another example was provincial legislation that supported collaboration
between education and the health sector to facilitate student learning. In this
structure, faculty maintained ongoing consultations with inter-professional
clinical coordinators and nurse leaders. They created a new nurse educator faculty
position to assist preceptors (the position is dependent upon agency accepting a
significant cohort of students). Marketing strategies were designed to help
agencies value student contributions, particularly through community health
promotion projects. Faculty visited clinical sites to collaborate with preceptors
and monitor student learning. Nurse preceptors were offered 3 year positions as
clinical instructors where they were offered privileges within the university,
thereby encouraging sustained involvement.
Internal Enablers
Two major themes denoted internal enablers that influenced community
health content in nursing schools - curriculum structure and process, and faculty
champions. Curriculum structures and processes referred to establishing a
curriculum rooted in the CCHNSoP, sequencing the curriculum to support
community health nursing throughout the program, and teaching foundational
concepts and supporting a PHC-based curriculum. One school reported having a
course including a learning plan and evaluation template rooted in the CCHNSoP.
Many schools sequenced community health nursing throughout the program
rather than as a stand-alone course, and health promotion was emphasized in the
first year. Some schools reported that their programs were strengthened by the
inclusion of foundational concepts, such as health promotion, caring, PHC,
determinants of health, and critical social theory. Others developed their curricula
based on PHC, which positively impacted community content in the program. As
described by one respondent,
…due to new program development, faculty have embraced the primary
health care approach to professional nursing practice and delivery of
health care. We aim to work at embedding the principles of PHC and
community health into the integrated program.
10
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518
Having faculty champions in community health nursing was found to be
an important enabler in Canadian nursing schools. Many, but not all, respondents
reported that their faculty had good preparation, passion and commitment for
community health, which resulted in students having excellent supervision in
community. Respondents often commented on the quality and quantity of faculty
preparation in community health as an enabler:
…[ an enabler is] the number of faculty members in our department with
advanced practice and education in the area of community health nursing.
Additionally, faculty members who do not have this background are very
receptive to learning more about community health concepts and
incorporating these into their classes.
External Challenges
Three external challenges emerged including: placement challenges,
preceptor challenges, and devaluing of community health (versus acute care).
Placement challenges. These were related to: a) increased demand /
reduced supply of placements, b) limited exposure to varieties of community
nursing placements and few activities within placements (resulting in fewer
nursing role models), and c) limited clinical office space for students. Increased
demand / reduced supply of student placements was related to two factors –
increased competition for placements and health care restructuring. Increased
competition for placements was described as being the result of higher student
numbers related to the growth of college programs, as well as a general lack of
community resources. Many comments addressed challenges related to a lack of
available traditional community placements. Restructuring of health care
environments also had an impact on the supply of community placements. One
respondent wrote that:
The government of this province is restructuring public health into the
hospital corporation with no protected budget. The future role of public
health is of major concern. Because of this restructuring, there is no
opportunity at this time, for our students to have placement with public
health.
The second placement challenge was related to limited exposure to
varieties of community nursing placements and activities within them. Placement
activities were often restricted (such as, lack of permission to administer
immunizations, limited access to vulnerable populations, and observation-only
placements). For example, agency staff working with vulnerable populations can
overprotect their population. Limited role modeling by nurses was also reported
11
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008
as a challenge; students had minimal contact with community health nurses and
thus limited exposure to their roles and activities. The use of non-traditional
placements and non-nursing teachers has, therefore, created complex challenges
for educators:
Community settings can usually accommodate small groups of students,
usually one at a time. With increases in enrolment, this presents a
challenge to find meaningful community health placements where
community health nurses are there to model their role.
A third placement challenge was limitation in clinical space for students,
which potentially made students feel unwelcome in their placements. The above
challenges represented a general apathy in community agencies towards students,
which transferred to clinical preceptors.
Preceptor challenges. These were related to four factors including: a)
lack of valuing of the preceptor role, b) lack of skilled preceptors, c) lack of
protected time and compensation for preceptors, and d) preceptor burnout. Lack
of valuing of the preceptor role by agencies was reported repeatedly. This was
linked to the lack of skilled preceptors and protected time for preceptorship. The
following comment describes preceptor challenges exacerbated by the focus on
illness care:
The focus in nursing remains on illness care and therefore community is
devalued at times. We are in CONSTANT competition for placements
and we have to beg for preceptors and sites. We believe that in order for
facilities that employ nurses to receive accreditation, they have to take a
certain percentage of students annually (some sort of a ratio system) or
they do not get accredited. Further, that those that precept, have this
valued and affirmed and that a part of their work is taken away so they
have the time to do this. It is such a stretch for them and we find it is rare
that agencies value preceptorship as much as universities invite them to.
A challenge for preceptors was the need to increase their knowledge and skills,
including PHC principles and the CCHNSoP:
…additional challenges include [the] community health nursing
professional population that does not necessarily have the educational
preparation to engage in co-teaching community health nursing concepts:
local community health nurses are largely unaware of Primary Health Care
principles; Population Health Promotion; may not value participating in
student teaching.
12
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518
This was strongly supported in workbook responses. Many nurses reported
lacking knowledge of the CCHNSoP, which further amplified their lack of buy-in.
One nurse noted that the standards were not always the bottom line in home
health nursing; rather the emphasis was on getting the job done efficiently. A lack
of protected time and compensation for preceptors was another challenge reported
by many participants, resulting in a further devaluation of the role. It was often
viewed as a voluntary activity, adding additional workload to an already
overburdened staff. One participant explained that, “community health nurses
traditionally view [preceptorship] as an additional workload task and either expect
financial compensation for engaging in clinical student teaching (no resources
available) or view participation as strictly on a ‘volunteer’ basis.” Since clinical
placements are at premium, it is not surprising that many respondents noted
preceptor burnout as a challenge. This was largely related to increased public
health nursing workload, where staff and agency burnout was considered a real
and present danger.
Devaluing of community health. Another major theme viewed as an
external challenge was community health nursing being undervalued.
Government preoccupation with the acute care sector and care of individuals
rather than communities has reduced opportunities for community health
education. Many respondents supported this, noting that funding and power
remains with hospitals, with a focus on individual care and an illness versus
wellness approach, thereby further devaluing community:
The current government is fixated on acute care needs and wanting to
churn out new grads as fast as possible. There is little attention to the need
for more funding to the education or practice settings to increase
community health education opportunities.
One respondent commented that this problem was associated with government
preferences to fund colleges over baccalaureate programs: “…increased funding
goes to nursing education programs at less than the baccalaureate level, which
impedes the preparation of nurses to practice in the community.”
Internal Challenges
Internal challenges were grouped into three major themes including:
problems with curriculum structure and process, lack of qualified faculty for
community health nursing, and weak community health leadership in academe.
Problems with curriculum structure and process. The challenges with
curriculum structure and process were explained by two factors – dominance and
13
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

valuing of illness/acute care in academe, and difficulties integrating community
health nursing components throughout the curriculum. Coinciding with the
external challenge of community health devalued, numerous respondents felt that
dominance of acute care also exists in academic settings. Some respondents
voiced this as a constant threat to community health: “what challenges us is the
power of the dominant voice that insists that nursing students must have more
thorough and senior preparation (theory and especially clinical practice) in acute
care/institutional nursing, rather than community practice.” “Community health
content never seems to be given as much recognition as content such as med-surg
which seems to receive more monetary / staff resources for ensuring
comprehensive clinical education etc..” Faculty felt that students also devalued
community health nursing. A number of respondents commented on students’
preferences for hospital placements: “the majority of jobs for new graduates are
hospital based. As the students plan their final practice placements, they often
choose acute care.”
Lack of qualified faculty for community health nursing. The second
challenge was related to problems with integration of community health into the
curriculum. This theme took into account philosophies and approaches to teaching
community health. For example, one respondent felt it was challenging to assist
placement staff to understand the philosophy of the curriculum and course
expectations of students. Another explained that philosophical conflicts exist
when delivery programs are based on a behavioural orientation rather than
determinants of health, and social environmental approaches which are more
consistent with CCHNSoP. A manager noted that there were unrealistic course
goals in education that must be made more compatible with public health agency
goals and objectives. A few comments were also made indicating the importance
of teaching community health nursing as a process integrated into the curriculum,
rather than as a series of topics.
In contrast to the internal enabler,-faculty champions, the second theme
that was a challenge for many schools was lack of qualified faculty to teach
community health. Shortages of faculty prepared to teach community health
nursing were explained by faculty retirements and moves, few graduate-degree
prepared community health nursing faculty, and few faculty members with
practical community health experience. The shortage was exacerbated by faculty
members’ lack of knowledge of current community health issues and concepts. As
noted by one participant, “adding to this challenge [are] instructors who have
never worked in the community or having very little practice experience in the
community, have poor understanding of key community concepts and then being
thrust into this clinical practice setting.” A participant also commented that
14
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

community college collaborative program faculty members do not have expertise
in community health nursing.
Weak community health leadership in academe. Weak community
health nursing leadership in educational nursing organizations impacted
negatively on integration of community health curriculum content and educational
resources. Several respondents lamented that few nursing program leaders have
community health backgrounds. Some participants noted that it was essential for
top administration to buy-in to community health nursing and the CCHNSoP. One
participant shared some of these challenges:
Community health nursing faculty are not represented within the Program
Director positions. Program decision makers are unaware of the impact of
the province’s community health nursing population profile on our
community health nursing program, therefore are unaware of the unique
challenges faculty experience recruiting community partners (nurse
preceptors at community sites), collaborating with these partners, and
developing the necessary supports for student learning (student health
promotion projects; focus on family, aggregates; health promotion rather
than medical care; need for bilingual teaching materials).
A lack of valuing of community health by academic administrators led to budget
allocation problems that impacted negatively on community health nursing
education including: high faculty-student ratios, administrative complexity from
offering multiple programs (Post RN/BN, accelerated, collaborative), and space
problems. The variety of program options offered by many schools was reported
to overburden clinical resources. In addition, participants also reported higher
student/faculty ratios in community (1:12) compared to hospitals settings (1:8).
Community health nursing faculty resources were further stretched by requiring
faculty to monitor students in up to 10 to12 rural and urban communities, which
imposed additional travel time. The result: reduced faculty time spent with each
student in community.
Strategies to Overcome Challenges
Respondents identified a number of strategies to overcome these
challenges. To promote preceptor availability within programs, respondents
suggested: a) permitting nurses to have a choice to be preceptors rather than
being forced by management; b) increasing incentives through access to library
resources and other recognition strategies; and c) providing nurses with lighter
workloads to accommodate students. Despite the problems associated with non-
traditional placements, a number of respondents identified unique non-traditional
15
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

placements as a solution for placement shortages. School administrators were
urged to construct learning opportunities that develop competencies outside of
formal practice settings through non-traditional placements, such as correctional
facilities, seniors and drop-in centres. For example, one respondent described a
provincially-funded rural incentive program, which enabled students to complete
practicum experiences in remote and rural settings. Solutions to overcome
practice environment challenges focused on improving communication between
academic and practice settings. For example, preceptors and managers were
encouraged to discuss the amount of guidance and supervision to expect from
faculty, and community program managers could meet with faculty as a group to
discuss student placement opportunities.
DISCUSSION AND RECOMMENDATIONS
It is generally accepted that teaching community health nursing requires a
strong practice component. Nursing is an applied science that requires theory and
practice to adequately prepare individuals to meet expected entry-level
competencies for community health nursing. Supported by the findings, there are
decreasing supplies of clinical placements to support community nursing
education (Latter et al., 2003; UKCC, 1999). Although there are a number of
valid and significant reasons for this, three major themes were identified that
contributed most significantly to the success or ‘failure’ of integrating community
health content into undergraduate nursing programs. Overall, placement
challenges, preceptor challenges and devaluing of community health nursing as
compared to acute care, were the major overarching themes. These factors are
well supported in the literature. Research has also shown that there are
insufficient community health clinical sites to accommodate students (Sweeney &
de Peyster, 2005). In the U.S., funding for illness prevention and health promotion
activities was cut dramatically, and there have been serious shortages of public
health nurses. At the same time, schools have been encouraged to increase
community-based curriculum content (Quad Council of Public Health Nursing
Organizations, 2007). In addition, students have preconceived ideas that ‘real’
nursing involves taking care of sick patients in the hospital (Ervin, Bickes, &
Myers Schim, 2006; Speck, 2003). There is pressure for students to master acute
care content to pass licensing examinations and manage “high-tech” care in
community-based settings (Ervin et al.). Other challenges include the mismatch of
didactic content delivered in courses, such as the care of adults in acute care and
the community as the care setting (Ervin et al.). The present environmental scan
results corroborated the findings of Edwards and Alley (2002), who found
resistance from faculty members regarding the balance of community-based
versus acute care curriculum content. The results also supported Ervin et al., as
16
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

well as Speck’s (2003) work, who found that there are few faculty members with
community health clinical experience, which leads to work overload for
experienced faculty.
To address these challenges, respondents identified value in a curriculum
that supports community health nursing content. It has been suggested by others
(Irvine, 2007; Nehls & Vandermause, 2004; Thomas & Carroll, 2006) that a
supportive academic environment which ensures faculty knowledge of
community health content and principles is essential to ensure community nursing
practice is addressed adequately in undergraduate education. When nursing
schools have a strong community health curriculum, improved relationships
between clinical agencies and academe can and should be built. These
relationships are essential to ensure enough community placements and
opportunities exist for students. Nehls and Vandermause, discussed the need to
have community-focused nursing education to support students, faculty and
agencies. Although having strong community relationships were found to be an
enabler in the present study, others have identified that it has been a challenge to
establish long-term relationships with community agencies and groups (Edwards
& Alley, 2002).
The findings of this investigation highlight examples of successful
relationships between academe and clinical agencies, which are shown to provide
mutual benefits to all partners involved. Although community-academic
partnerships can be formal or informal, the teaching health unit model (Black,
Edwards, McKnight, Valaitis, & Van Dover, 1989) and the Community Academic
Practice Alliance (Ganley et al. 2004), which represent formal partnerships, have
been found to support community health nursing education. The models described
in the current findings required local government support. With such dedicated
resources, programs can provide appropriate community faculty and funding for
placements to integrate all program components required for beginning entry level
community health nursing standards. Although having strong community
relationships were found to be an enabler in this study, others have identified that
it has been challenging to establish long-term relationships with community
agencies and groups (Edwards & Alley, 2002). Latter et al., (2003), and Thomas
and Carroll (2006) support the notion that legislative policy helped the transition
from acute care focused health education to community health education. As
governments and administration provide more financial and personnel resources,
the opportunity to shift curriculum and create stronger partnerships increases.
This foundation is the basis of the key recommendations taken forward to CASN.
17
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

As problems contributing to limitations with preceptors and practice
environments become more complicated, so do the strategies required to
overcome them. The present scan identified a variety of strategies to manage
preceptor stressors: providing nurses a choice whether or not to be preceptors,
increasing incentives and recognition for the role, and reducing workload to
accommodate students. Providing nurses a choice of whether or not to be
preceptors has been supported in the literature. If qualified and valued staff
members are asked repeatedly to be preceptors and do not receive rewards or
support, burnout can occur (Dibert & Goldenberg, 1995; Usher, Nolan, Reser,
Owens, & Tollefson, 1999). With respect to workload, research supports the need
for preceptors to have release time from normal duties to orient students, review
and revise goals and objectives throughout the experience, as well as conduct
evaluations (Ohrling & Hallberg, 2001; Usher et al.). This scan also addressed
solutions to placement stressors, namely the use of non-traditional placements.
Also urged in the literature is that innovative community placements such as
parish, corrections, aboriginal, rural and international placement settings, can be
transformative for gaining witness to poverty, inequities and marginalization, as
well as increasing critical engagement and commitment to social change (Reimer-
Kirkham, VanHofwegen & Hoe Harwood, 2005). In addition, innovative
partnerships with housing authorities for the elderly and disabled have been found
to be valuable for student placements (Ellenbecker, O’Brien, & Byrne, 2002).
Educators in the U.K. have delineated criteria for non-traditional nursing
community experiences, including placements which can provide: a) variety of
health and social care resources over 14 weeks: and b) qualified and enthusiastic
nurse mentors who have the knowledge to facilitate a broad community
experience, and can offer weekly contact for a minimum of 2 shifts weekly.
CONCLUSION
This environmental scan illustrates the need for stronger partnerships
between academe and community clinical agencies. Allocation of resources for
education in community nursing is as important as that for acute care, if we wish
to have a nursing workforce prepared to meet future health care demands.
Recommendations encouraging this balance have been forwarded to the CASN
Board of Directors and the Public Health Agency of Canada. This scan has
highlighted the need to send a strong message to governments, educators and
administrators to ensure that there are adequate and appropriate resources, in
funding, and human and technical resources, to guarantee deserved recognition
for undergraduate community nursing preparation in Canadian nursing schools.
Through the efforts of CASN and the Public Health Agency of Canada, it is
hoped that faculty will champion and be supported in their efforts to prepare new
18
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

graduates for community health nursing positions, and thereby meet the health
care needs of the 21st century.
REFERENCES
Black, M., Edwards, N., McKnight, J., Valaitis, R., Van Dover, L. (1989). The
McMaster University: Hamilton-Wentworth Teaching Health Unit Project.
Experiences of the Nursing Joint Appointees. Public Health Nursing, 6,
135-140.
Canadian Association of Schools of Nursing Task Force on Public Health
Education (2007). Final report: Public health nursing education at the
baccalaureate level in Canada today. Retrieved March 20, 2008, from
http://www.casn.ca/media.php?mid=650&xwm=true
Community Health Nurses Association of Canada (2003). Canadian community
health nursing standards of practice. Ottawa: Canadian Community
Health Nurses Association. Retrieved October 9, 2007, from
http://www.chnac.ca/images/downloads/standards/chn_standards_of_pract
ice_jun04_english.pdf
Cohen, B., & Gregory, D. (2007). Toward an evidence-based approach to
curriculum revision: Clinical education for community health nursing
practice in Canada. A report submitted to the Faculty of Nursing,
University of Manitoba, Winnipeg, Canada.
Conger, C. O., Baldwin, J. H., Abegglen, J., & Callister, L. C. (1999). The
shifting sands of health care delivery: Curriculum revision and integration
of community health nursing. Journal of Nursing Education, 38, 304-311.
Dibert, C. & Goldenberg, D. (1995). Preceptors' perceptions of benefits, rewards,
supports and commitment to the preceptor role. Journal of Advanced
Nursing, 21, 1144-1151.
Edwards, J. B., & Alley, N. M. (2002). Transition to community-based nursing
curriculum processes and outcomes. Journal of Professional Nursing, 18,
78-84.
Ellenbecker, C. H., O'Brien, E., & Byrne, K. (2002). Establishing partnerships
with social services agencies for community health education. Journal of
Community Health Nursing, 19, 1-6.
Ervin, N., Bickes, J., & Myers Schim, S. (2006). Environments of care: A
curriculum model for preparing a new generation of nurses. Journal of
Nursing Education, 45, 75-80.
Ganley, B., Sheets, I., Buccheri, R., Thomas, S. A., Doerr-Kashani, P.,
Widergren, R., Bolla, A., Stoker, D. & West, D. (2004). Collaboration
versus competition: Results of an academic practice alliance. Journal of
Community Health Nursing, 21, 153-165.
19
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008

Holt, M. & Warne, T. (2007). The educational and practice tensions in preparing
pre-registration nurses to become future health promoters: A small scale
explorative study. Nurse Education in Practice, 7, 373-380.
Irvine, F. (2007). Examining the correspondence of theoretical and real
interpretations of health promotion. Journal of Clinical Nursing, 16, 593-
602.
Latter, S., Speller, V., Westwood, G., & Latchem, S. (2003). Education for
public health capacity in the nursing workforce: findings from a review of
education and practice issues. Nurse Education Today, 23, 211-218.
National League for Nursing. (1993). A Vision for Nursing Education. New
York: National League for Nursing.
Nehls, N., & Vandermause, R. (2004). Community-driven nursing: Transforming
nursing curricula and instruction Nursing Education Perspectives, 25, 81–
85.
O'Neil, E. H. (1993). Health Professions Education for the Future: Schools in
Service to the Nation (Report of the Pew Health Professions Commission).
San Francisco, CA: Pew Health Professions Commission.
Ohrling, K. & Hallberg, I. R. (2001). The meaning of preceptorship: nurses' lived
experience of being a preceptor. Journal of Advanced Nursing, 33, 530-
540.
Quad Council of Public Health Nursing Organizations (Feb. 2007). The public
health nursing shortage: A threat to the public’s health. Retrieved October
9, 2007, from
http://www.astdn.org/downloadablefiles/Final%20Nursing%20Shortage%
20Paper.pdf
Redman, R., & Clark, L. (2002). Service learning as a model for integrating
social justice in the nursing curriculum. Journal of Nursing Education,
41, 446-449.
Reece, S. M., Mawn, B., & Scollin, P. (2003). Evaluation of faculty transition
into a community-based curriculum. Journal of Nursing Education, 42,
43-47.
Reimer-Kirkham, S., Van Hofwegen, L., & Hoe Harwood. C. (2005). Narratives
of social justice: Learning in innovative clinical settings. International
Journal of Nursing Education Scholarship, 2, Article 28.
Smith, D. (2004). Primary health care. In Stamler, L., & Yiu, L. (Eds.).
Community health nursing: A Canadian perspective. Toronto: Pearson
Prentice Hall.
Speck, B. J. (2003). Educational innovations. Undergraduate community health
in the first semester: opportunities and challenges. Journal of Nursing
Education, 42, 329-332.
20
International Journal of Nursing Education Scholarship, Vol. 5 [2008], Iss. 1, Art. 22
http://www.bepress.com/ijnes/vol5/iss1/art22DOI: 10.2202/1548-923X.1518

Staats, C. R. (2003). The development of a community-based baccalaureate
curriculum model in a culturally diverse health care delivery area.
Nursing Education Perspectives, 24, 94-97.
Sweeney, N., & de Peyster, A. (2005). Integrating environmental health into an
undergraduate community health nursing course. Public Health Nursing,
22, 439-444.
Thomas, G., & Carroll, S. (2006). Curriculum revision: Product innovation for
quality outcomes. Quality Management in Health Care, 15, 285-290.
United Kingdom Central Council [UKCC] for Nursing, Midwifery and Health
Visiting. (1999). Fitness for Practice: The UKCC Commission on Nursing
and Midwifery Practice London: United Kingdom Central Council for
Nursing, Midwifery and Health Visiting.
Usher, K., Nolan, C., Reser, P., Owens, J., & Tollefson, J. (1999). An exploration
of the preceptor role: preceptors' perceptions of benefits, rewards, supports
and commitment to the preceptor role. Journal of Advanced Nursing, 29,
506-514.
Whitehead, D. (2007). Reviewing health promotion in nursing education. Nurse
Education Today, 27, 225-237.
World Health Organization (2000). Nurses and midwives for health. Copenhagen:
WHO Regional Office for Europe.
21
Valaitis et al.: Preparing the Community Health Nursing Workforce
Published by The Berkeley Electronic Press, 2008