
Predictors of cognitive and functional improvement and normalization after cognitive remediation in...
7
Predictors of cognitive and functional improvement and normalization after cognitive remediation in patients with schizophrenia Antonio Vita a,b, ⁎, Giacomo Deste b , Luca De Peri a , Stefano Barlati b , Roberto Poli c , Bruno M. Cesana d , Emilio Sacchetti a,b a Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy b Department of Psychiatry, Spedali Civili Hospital, Brescia, Italy c Hospital Istituti Ospitalieri of Cremona, Cremona, Italy d Department of Molecular and Translational Sciences, University of Brescia, Brescia, Italy abstract article info Article history: Received 5 May 2013 Received in revised form 24 July 2013 Accepted 10 August 2013 Available online 30 August 2013 Keywords: Cognitive remediation Schizophrenia Cognitive improvement Cognitive normalization Functional improvement Functional normalization Objective: Although the efficacy of cognitive remediation interventions has been demonstrated in several experi- mental studies on schizophrenia, few studies have investigated the predictors of response to such interventions. We were interested in determining what factors contribute to a positive outcome after cognitive rehabilitation and whether different factors are associated with different degrees of improvement in cognitive and real-world functioning in individual patients after cognitive remediation. Methods: The study sample consisted of 56 patients with schizophrenia who had completed a 6-month cognitive remediation intervention and showed different cognitive and functional outcomes. Measures of cognitive and functional amelioration after cognitive remediation were analyzed in relation to patients' clinical, neuropsycholog- ical and functional variables at baseline using logistic regression analysis. Results: Lower antipsychotic intake at baseline predicted cognitive improvement, whereas lower antipsychotic in- take, severity of specific symptoms, and higher neurocognitive functioning (particularly executive functions and verbal memory) at baseline were associated with cognitive normalization after remediation treatment. Functional improvement was predicted by lower patient age and type of cognitive remediation intervention, whereas func- tional normalization was related to lower baseline antipsychotic intake and, at a trend level, to higher executive functioning and type of cognitive remediation intervention. Conclusion: Cognitive remediation could be more effective in younger, less disorganized, and cognitively less im- paired patients, who take a smaller amount of antipsychotics. The predictive role of lower antipsychotic dosage on cognitive and functional outcome after remediation suggests either that patients with less severe illness could gain better advantage from cognitive remediation interventions or that high dose or complex antipsychotic therapy may limit the effectiveness of such interventions. © 2013 Elsevier B.V. All rights reserved. 1. Introduction Cognitive dysfunctions are a core feature of schizophrenia (Green et al., 2004; Keefe et al., 2006) and have been shown to play a major role in the functional outcome of the disorder (Bowie et al., 2006, 2008). Various cognitive remediation interventions for schizophrenia have been developed in recent years and adopted in the multimodal treatment approaches to schizophrenia. The efficacy of such interven- tions in ameliorating cognitive performance and psychosocial function- ing is now well recognized (McGurk et al., 2007; Grynszpan et al., 2010; Wykes et al., 2011; Medalia and Saperstein, 2013). Despite the amount of data supporting the benefits of cognitive remediation interventions in schizophrenia, a number of questions remain to be answered. Identifi- cation of potential predictors of effectiveness of cognitive rehabilitation is of primary interest to researchers and clinicians, because the efficacy of treatments largely depends on the appropriate selection of individ- uals and treatment methodologies (Medalia and Richardson, 2005; Bowie et al., 2013; Kontis et al., 2013; Medalia and Saperstein, 2013). Few studies have investigated the relationship between baseline char- acteristics and the response to cognitive remediation interventions in patients with schizophrenia. A study by Medalia and Richardson (2005) found that baseline cognitive performance, intrinsic motivation and greater clinician experience predicted improvement in cognitive performance in patients with schizophrenia who participated in the Neuropsychological Educational Approach to Remediation (NEAR) pro- gram. Another study by Fiszdon et al. (2005) showed that better vigi- lance, better immediate verbal memory and less hostility predicted remediation success and accounted for 70% of the chance of ameliora- tion in a selected memory task (Wechsler Adult Intelligence Scale Schizophrenia Research 150 (2013) 51–57 ⁎ Corresponding author at: Dept of Clinical and Experimental Sciences, University of Brescia, via Europa 11, 25123 Brescia, Italy. Tel.: +39 030 2184856; fax: +39 030 2184871. E-mail address: [email protected] (A. Vita). 0920-9964/$ – see front matter © 2013 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.schres.2013.08.011 Contents lists available at ScienceDirect Schizophrenia Research journal homepage: www.elsevier.com/locate/schres
Transcript of Predictors of cognitive and functional improvement and normalization after cognitive remediation in...

Schizophrenia Research 150 (2013) 51–57
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r .com/ locate /schres
Predictors of cognitive and functional improvement and normalizationafter cognitive remediation in patients with schizophrenia
Antonio Vita a,b,⁎, Giacomo Deste b, Luca De Peri a, Stefano Barlati b, Roberto Poli c,Bruno M. Cesana d, Emilio Sacchetti a,b
a Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italyb Department of Psychiatry, Spedali Civili Hospital, Brescia, Italyc Hospital Istituti Ospitalieri of Cremona, Cremona, Italyd Department of Molecular and Translational Sciences, University of Brescia, Brescia, Italy
⁎ Corresponding author at: Dept of Clinical and ExperBrescia, via Europa 11, 25123 Brescia, Italy. Tel.: +392184871.
E-mail address: [email protected] (A. Vita).
0920-9964/$ – see front matter © 2013 Elsevier B.V. All rihttp://dx.doi.org/10.1016/j.schres.2013.08.011
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 5 May 2013Received in revised form 24 July 2013Accepted 10 August 2013Available online 30 August 2013Keywords:Cognitive remediationSchizophreniaCognitive improvementCognitive normalizationFunctional improvementFunctional normalization
Objective: Although the efficacy of cognitive remediation interventions has been demonstrated in several experi-mental studies on schizophrenia, few studies have investigated the predictors of response to such interventions.We were interested in determining what factors contribute to a positive outcome after cognitive rehabilitationand whether different factors are associated with different degrees of improvement in cognitive and real-worldfunctioning in individual patients after cognitive remediation.Methods: The study sample consisted of 56 patients with schizophrenia who had completed a 6-month cognitiveremediation intervention and showed different cognitive and functional outcomes. Measures of cognitive andfunctional amelioration after cognitive remediationwere analyzed in relation to patients' clinical, neuropsycholog-ical and functional variables at baseline using logistic regression analysis.Results: Lower antipsychotic intake at baseline predicted cognitive improvement, whereas lower antipsychotic in-take, severity of specific symptoms, and higher neurocognitive functioning (particularly executive functions andverbal memory) at baselinewere associatedwith cognitive normalization after remediation treatment. Functional
improvement was predicted by lower patient age and type of cognitive remediation intervention, whereas func-tional normalization was related to lower baseline antipsychotic intake and, at a trend level, to higher executivefunctioning and type of cognitive remediation intervention.Conclusion: Cognitive remediation could be more effective in younger, less disorganized, and cognitively less im-paired patients, who take a smaller amount of antipsychotics. The predictive role of lower antipsychotic dosageon cognitive and functional outcome after remediation suggests either that patients with less severe illnesscould gain better advantage from cognitive remediation interventions or that high dose or complex antipsychotictherapy may limit the effectiveness of such interventions.© 2013 Elsevier B.V. All rights reserved.
1. Introduction
Cognitive dysfunctions are a core feature of schizophrenia (Greenet al., 2004; Keefe et al., 2006) and have been shown to play a majorrole in the functional outcome of the disorder (Bowie et al., 2006,2008). Various cognitive remediation interventions for schizophreniahave been developed in recent years and adopted in the multimodaltreatment approaches to schizophrenia. The efficacy of such interven-tions in ameliorating cognitive performance and psychosocial function-ing is nowwell recognized (McGurk et al., 2007; Grynszpan et al., 2010;Wykes et al., 2011; Medalia and Saperstein, 2013). Despite the amountof data supporting the benefits of cognitive remediation interventions in
imental Sciences, University of030 2184856; fax: +39 030
ghts reserved.
schizophrenia, a number of questions remain to be answered. Identifi-cation of potential predictors of effectiveness of cognitive rehabilitationis of primary interest to researchers and clinicians, because the efficacyof treatments largely depends on the appropriate selection of individ-uals and treatment methodologies (Medalia and Richardson, 2005;Bowie et al., 2013; Kontis et al., 2013; Medalia and Saperstein, 2013).Few studies have investigated the relationship between baseline char-acteristics and the response to cognitive remediation interventions inpatients with schizophrenia. A study by Medalia and Richardson(2005) found that baseline cognitive performance, intrinsic motivationand greater clinician experience predicted improvement in cognitiveperformance in patients with schizophrenia who participated in theNeuropsychological Educational Approach to Remediation (NEAR) pro-gram. Another study by Fiszdon et al. (2005) showed that better vigi-lance, better immediate verbal memory and less hostility predictedremediation success and accounted for 70% of the chance of ameliora-tion in a selected memory task (Wechsler Adult Intelligence Scale

Table 1Demographic characteristics of the study sample at baseline.
Variable Sample at baseline
Number 56Sex (M:F) 40:16Age (years) 37.00 ± 10.30Age at onset (years) 22.43 ± 5.72Duration of illness (years) 14.87 ± 9.68Education (years) 10.45 ± 2.91WAIS-R full scale IQ 86.30 ± 12.71Dose of antipsychotics at baseline (CPZ-eq) 634.48 ± 387.44
52 A. Vita et al. / Schizophrenia Research 150 (2013) 51–57
[WAIS] digit span) after Neurocognitive Enhancement Therapy (NET).Eack et al. (2011) showed that greater neurobiological reserve (pretreat-ment cortical surface area and gray matter volume) predicted a rapidsocial-cognitive response to cognitive enhancement therapy (CET) inthe first year of treatment. Kontis et al. (2013) showed that younger,but not older patientswith schizophrenia, improved inworkingmemoryperformance after cognitive remediation. This result is complemented bythe one of Bowie et al. (2013) that evidenced that early course patientshad lager improvements in cognitive measures such as processingspeed and executive functions than patients in the chronic course ofschizophrenia. Research on the potential predictors of psychosocial im-provement after remediation interventions is sparse. Kurtz et al. (2009)demonstrated that after 1 year of Computer-Assisted Cognitive Re-mediation (CACR), a measure of everyday life skills, assessed withthe University of California Performance-based Skills Assessment(UPSA), was predicted by baseline verbal learning performance.Moreover, in a controlled study by Bosia et al. (2007), it was demon-strated that catechol-O-methyltransferase polymorphismmay affectindividual capacity to recover from cognitive deficits after 3 monthsof CACR intervention, with a significantly greater improvement inthe Quality of Life Scale total score in Met carriers on active treat-ment compared with Val/Val carriers on placebo. More recently,Bowie et al. (2013) demonstrated larger improvement in adaptativecompetence and real-world work skills in patients with early- vslong-term course schizophrenic illness.
In a previous prospective controlled study performed by our group,we demonstrated the effectiveness of different modalities of cognitiveremediation in schizophrenia, i.e. the cognitive subprograms of the Inte-grated Psychological Therapy (IPT-cog), and CACR (Cogpack), comparedwith usual rehabilitative interventions in a group of patients withschizophrenia treated in a naturalistic setting of care (Vita et al., 2011a).
In this study, we examined whether specific factors differentiatedthose individuals who showed a positive response to cognitive remedi-ation and those who did not in cognitive and psychosocial functioningdomains to possibly identify the characteristics that predict outcomein individual patients. We were also interested in analyzing whetherdifferent factors were associated with different degrees of ameliorationin both cognitive and real-world functioning in individual patients aftercognitive remediation.
2. Materials and methods
2.1. Participants
Participants were patients who had taken part in a previous studyperformed by our group (Vita et al., 2011a) in which 84 patients fulfill-ing the diagnostic criteria for schizophrenia according to the DSM-IV-TR(American Psychiatric Association, 2000), have been followed up natu-ralistically in three rehabilitative centers at the department of MentalHealth of the Spedali Civili Hospital in Brescia (Italy) and Cremona Hos-pital, for a period of 6 months. Exclusion criteria were: (a) a concomi-tant diagnosis of mental retardation (as revealed by a Wechsler AdultIntelligence Scale—Revised (WAIS-R) (Wechsler, 1981) full scale IQless than 70) or substance use disorder; (b) severe positive symptomsor impulsive behavior requiring a higher security setting; (c) significantchanges in psychopathologic status (requiring hospitalization or majorchange in pharmacologic treatment) in the last 3 months; (d) age lessthan 18 ormore than 50 years. These are the same criteria for exclusionof patients to the rehabilitative centers where the studywas conducted,according to the admission/discharge criteria for day centers and reha-bilitation centers in the Lombardia Region, Italy, so that no further selec-tion of patients among those treated in these centers was done.
Fifty-six patients received a cognitive remediation intervention inaddition to usual rehabilitation intervention. In particular, twenty-sixpatients received the first 2 subprograms (cognitive differentiationand social perception) of the Integrated Psychological Treatment (IPT-
cog), and 30 patients received a CACR intervention (for details see Vitaet al., 2011a). The IPT is a group-based structured cognitive behavioralprogram for schizophrenia in which neurocognitive remediation andsocial cognitive remediation are integrated with psychosocial rehabili-tation (Brenner et al., 1994). The IPT-cog groups, composed of 8–10 pa-tients, attended therapy sessions twice a week, 45 min each session, for24 weeks. They were conducted by one trained psychiatrist or psychol-ogist and another professional who administered the 2 cognitive sub-programs following the IPT manual (Brenner et al., 1997). The CACRused the Cogpack (Marker Software®) program. The Cogpack includesdifferent neurocognitive exercises that can be divided into domain-specific exercises, aimed at training specific cognitive areas amongthose known to be impaired in schizophrenia (verbalmemory, verbalflu-ency, psychomotor speed and coordination, executive function, workingmemory, attention) and non-domain-specific exercises that require theuse of various functions at the same time and engage culture, languageand calculation skills. The CACR was administered individually twice aweek, in 45-min sessions, for 24 weeks. Another group of patients(N = 28) had been followed up with the usual rehabilitation interven-tions and, for the same period of time, received non-cognitive specific re-habilitation interventions (such as expressive groups as art therapies,physical training, or occupational therapies), with the same frequencyand duration of cognitive remediation interventions (Rehabilitation(REHAB) program). In addition to participating in the IPT-cog, CACR orREHAB programs, the patients continued with standard psychiatric careprovided by a multidisciplinary mental health team, including othernon-cognitive-oriented rehabilitative interventions aimed at improvingpatients' skills, social relationships or work abilities, individually tailoredin relation to clinical needs and personal preferences and delivered in abalanced way between groups (Vita et al., 2011a).
All patients received an antipsychotic treatment at baseline andwere then maintained on pharmacologic treatment during the studyperiod but the drug dose or regimen could be modified as needed. Inparticular, 15 patients received a first generation antipsychotic therapy,either as amonotherapy or as an add-on to a second generation therapy,and 41 patients were treated with second generation antipsychotics.Use of benzodiazepines and anticholinergics was allowed, based ontreating psychiatrist's clinical judgment. Doses of antipsychotics takenwere calculated as chlorpromazine equivalents (CPZ-eq) using the con-version proposed byWoods (2003) both at baseline and throughout thetreatment period. Patients were assessed at baseline and after a six-month follow-up with clinical, functional, and neurocognitive mea-sures. In this study, we considered the 56 patients who received a cog-nitive remediation intervention (IPT-cog or CACR). Demographic datafor this group are shown in Table 1.
2.2. Assessment
The participants were clinically assessed using the Positive and Neg-ative Syndrome Scale (PANSS) (Kay et al., 1987), and the Clinical GlobalImpression-Severity (CGI-S) scale (Guy, 1976) at baseline and, at theend point of the study, by the psychiatrists who followed up each pa-tient in the psychiatric outpatient units and who were not directly

53A. Vita et al. / Schizophrenia Research 150 (2013) 51–57
involved in the study or aware of the rehabilitative treatments followedby their patients.
The neuropsychological battery administered to patients comprisedthe WAIS-R, adopted only at study entry as an inclusion criterion mea-sure, and the following neuropsychological tests administered: the TrailMaking Test A (TMT-A), Trail Making Test B (TMT-B) (Reitan, 1979);the Wisconsin Card Sorting Test (WCST) (Heaton, 1981); the Self-Ordered Pointing Task (SOPT) (Petrides and Milner, 1982); and theCalifornia Verbal Learning Test (CVLT) (Benton and Hamsher, 1989).These testswere chosen among those frequently used inneuropsycholog-ical studies of schizophrenia, as being an acceptable compromise betweencompleteness in relation to cognitive domains found to be affected inschizophrenia and their ease of use, or because theywere already usuallyapplied in our centers (Sacchetti et al., 2008; Vita et al., 2011a,b).
Four cognitive constructs were used to represent specific domainsof cognitive functioning: processing speed, working memory, verbalmemory, and executive functions. A global cognitive composite scorewas calculated by averaging the other cognitive indexes. When aneurocognitive test was missing, the relative composite score, andglobal cognitive score were not calculated, and considered as missingvalues (see below, Statistical analyses). Z scores for each neuropsycho-logical test were obtained using Italian normative data for TMT andWCST (Giovagnoli et al., 1996) or using control data published in pre-vious studies for SOPT (Sacchetti et al., 2008) or obtained in healthysubjects (N = 109) recruited by our group for CVLT.
The Z score for each cognitive construct was calculated by averagingthe Z scores of the different tests for evaluating the specific construct asfollows (see Vita et al., 2011a): (1) processing speed, TMT-A; (2) verbalmemory, mean number of correct responses at immediate free recall,short- and long-delay free recall and short- and long-delay cued recall,CVLT; (3) executive functions, TMT-Bminus TMT-A (used as a flexibilityindex; Reitan and Wolfson, 1993), and mean percentage of persevera-tive and total errors, WCST; and (4) working memory, TMT-B andSOPT, number of errors. The pre-treatment score was then subtractedfrom the post-treatment score for each of the 5 variables (4 cognitivedimensions and global cognitive score).
Psychosocial functioning measures were the Global Assessment ofFunctioning (GAF) scale (American Psychiatric Association, 2000) andthe Health of the Nation Outcome Scale (HoNOS) (Wing et al., 1998;Lora et al., 2001).
All scales and testswere administered at baseline and after 24 weeks.Neuropsychological testswere administered by trained personnel, exter-nal to the treatment teams, who did not know individual patients andtheir treatment allocation. On the other hand, the functional outcomemeasures were completed by the multiprofessional team taking care ofthe patients in the rehabilitative centers, who were trained in the useof these instruments and used them routinely. This team, which didnot include any personnel involved in the experimental treatment forthe individual patients, completed the evaluations with team consensus.
2.3. Definition of outcome variables: cognitive improvement andnormalization and psychosocial functioning improvementand normalization
All patients were characterized as to whether theymanifested cogni-tive improvement or normalization for each cognitive domain after theremediation intervention. In this study, we defined as cognitively im-proved patients whose change in global cognitive performance frombaseline to end pointwas greater than or equal to Z = 0.5, reflecting po-tentially meaningful change (Norman et al., 2003); patients whosechange in global cognitive performance did not reach Z = 0.5 were de-fined as not improved. This definition is the same as that proposed byHarvey et al. (2006).
On the other hand, we defined patients as normalized if theirglobal cognitive performance changed from Z b −0.5 at baseline toZ ≥ −0.5 at end point, and not normalized if their performance at the
end point was below Z = −0.5. This definition is similar to, but morerestrictive than that proposed by Harvey et al. (2006).
As for psychosocial functioning, we adopted HoNOS cut-off thresh-olds proposed by the authors who validated the Italian version of thescale (Parabiaghi et al., 2005) to identify meaningful functional change,defining patients as improved if their HoNOS total score decreased atleast by 8 points after treatment and functionally normalized if theirHoNOS total score at the end point was ≤5, starting from a baselinescore N5.
2.4. Statistical analyses
To explore the presence of potential predictors of meaningfulchange in the outcome measures, univariate differences in baselinesociodemographic variables (age, sex, and educational level), clinicalvariables (age at onset, duration of illness and antipsychotic daily doseexpressed as CPZ equivalents, all PANSS items and CGI-S score, durationand type of previous rehabilitative interventions), neurocognitive vari-ables (WAIS-R full scale IQ and scores for the cognitive domains of pro-cessing speed, working memory, verbal memory, executive functions)and functional variables (all HoNOS items and GAF scores), as well asthe type of cognitive remediation treatment received (CACR or IPT-cog) between cognitively and functionally improved/not improved andnormalized/not normalized patients after treatment were evaluatedusing t tests for continuous variables and the chi-square test (or Fisherexact test, when appropriate) for categorical variables. Subsequently, alogistic regression analysis according to a backward procedure wasadopted to identify independent baseline predictors of improvementand normalization. The backward procedure involves starting with allcandidate variables and deleting (one at the time) those that are not sta-tistically significantly in relation to the dependent variables until theremaining variables represent the independent (predictor) variablesthat may influence the outcome. We decided to use a backward logisticregression procedure since it was our intention to explore the presenceof individual predictors of amelioration following cognitive remediation.For this reason we decided not to force a-priori or hypothesis-selectedspecific variables into the logistic regression models.
Variables that differentiated improved from not improved andnormalized from not normalized groups in univariate comparisons(P b 0.10 at least) were considered eligible for entry into the multiplevariable logistic regression model. However, only the most statisticallysignificant variables from the univariate analysis were included in thelogistic regression as covariates, if their number exceeded 1/10 of theanalyzed sample. In the case of functional normalization only, we in-cluded one variable more than those allowed (1/10 of the sample),since the 2 last variables included had similar level of significance andwere both of particular interest for the model.
To avoid multicollinearity, PANSS total or global scores were not in-cluded as covariates because of the inclusion of PANSS single items. Forthe same reason, only HoNOS single items and not the HoNOS totalscore were included as covariates in the logistic regressions. Further-more, cognitive composites were not used in the logistic regressionsof cognitive improvement and normalization, and HoNOS items werenot used as covariates in the logistic regressions in which HoNOS im-provement and remission were the dependent variables.
For cognitive improvement and normalization, however, we con-sidered it worthwhile to perform an independent, logistic regressionanalysis including as covariates only the cognitive variables that weresignificant in the univariate analysis. In this case, the single cognitivecomposites, but not the global cognitive composite score,were includedin the analysis.
The analyseswere performed on available data, i.e. for patients com-pleting assessments and treatment; missing values, previously treatedwith an intention-to-treat methodology (Vita et al., 2011a), could notcontribute to the present analyses. Patients whose cognitive or psycho-social functioning score fell within the range of normality (as defined

Table 3Predictors of cognitive improvement and normalization after cognitive remediation inpatients with schizophrenia (backward logistic regression).
Degrees of freedom Exp(B)a P
Predictors of cognitive improvementAntipsychotic dose (CPZ-eq) 1 0.997 0.017Model 0.006
Predictors of cognitive normalizationAntipsychotic dose (CPZ-eq) 1 0.993 0.040Conceptual disorganization (PANSS) 1 0.202 0.016Preoccupation (PANSS) 1 7.497 0.012Model b0.001
Predictors of cognitive normalizationVerbal memory 1 2.140 0.074Executive functions 1 6.393 0.015Model b0.001
a Exp(B) describesmodification of the odds ratio of achieving the specific outcomewitha 1-point change in the predictor variable.
54 A. Vita et al. / Schizophrenia Research 150 (2013) 51–57
above) at baselinewere not considered in the analyses of normalizationof the relative score after treatment.
P values b0.05 were considered statistically significant. All P valueswere two-tailed. Data were analyzed using SPSS 14.0 software.
3. Results
All but 2 of the treated patients completed the study according to thecriterion of at least 70% attendance at treatment sessions. A mean of 42(range = 37–48) sessions were completed, with no differences be-tween treatment conditions (P N 0.8). Data for the cognitive outcomevariable were available for 52 patients since 2 patients in the IPT-coggroup left the study, and 2 patients in the CACR group missed a singlecognitive test. Moreover, 15 patients were classified as already normalat baseline, thus they were not considered in the analyses of cognitivenormalization. Statistical analyses were performed on 55 patients forthe functional outcome variable, since for one patient that left thestudy it was not possible to assess functioning at follow-up. None ofthese patients were within the range of normality at baseline. Demo-graphic and baseline clinical and cognitive characteristics of the fewdropout patients were not any different from those of patients includedin the analyses.
A substantial number of the patients in the study experienced an im-provement (46.2%) or normalization (32.4%) of their cognitive perfor-mance according to the criteria described above (Table 2).
For the cognitive outcome, variables at baseline that differentiatedbetween improved and not improved patients in the univariate com-parisons were a lower antipsychotic intake at baseline (CPZ-eq) (t testP = 0.001), a higher GAF score (t test P = 0.030), a lower score forthe PANSS item delusions (t test P = 0.024), poor attention (t testP = 0.027), disturbance of volition (t test P = 0.039) and lower sever-ity of the HoNOS item problems with occupation and activities (t testP = 0.026). Backward logistic regression analysis identified lower anti-psychotic drug intake (CPZ-eq) at baseline as the most significant indi-vidual predictor of patient's global cognitive improvement. This modelwas highly statistically significant (P = 0.006), with a predictive valueof 67.4% (Table 3). No cognitive variable at baseline differentiated cogni-tively improved vs not improved patients in the univariate analysis,therefore no separate regression analysis was performed for cognitivepredictors of cognitive improvement.
Univariate comparisons at baseline that differentiated normalized vsnot normalized patients for cognitive performance were younger age(t test P = 0.050), shorter duration of illness (t test P = 0.022), lowerantipsychotic intake at baseline (CPZ-eq) (t test P = 0.001), lowerscores for the PANSS item conceptual disorganization (t test P =0.001), excitement (t test P = 0.027) and poor attention (t test P =0.033) and higher score for the item preoccupation (t test P = 0.017).Higher score for the HoNOS item problem with depressed mood(t test P =0.025) also discriminated normalized and not normalized pa-tients as well as better cognitive performance at baseline for the cogni-tive domains of working memory (t test P = 0.008), verbal memory(t test P = 0.006), and executive functions (t test P = 0.001). In the lo-gistic regression analysis, lower antipsychotic intake (CPZ-eq), less
Table 2Frequency of cognitive improvement and normalization after cognitive remediation inpatients with schizophrenia.
Frequency Percent
Global cognitive improvementImproved 24 46.2Not improved 28 53.8
Global cognitive normalizationNormalized 12 32.4Not normalized 25 67.6Normal at baseline 15
severe conceptual disorganization and more severe preoccupation atbaseline, asmeasuredwith the PANSS, emerged as significant individualpredictors of patient's global cognitive normalization. This model wasstatistically highly significant (P b 0.001) and had a predictive value of88.9%. In a separate logistic regression analysis, a better performancefor executive functions and, at a trend level, of verbal memory at base-line were significant cognitive predictors of patient's cognitive normal-ization (model P b 0.001), with a predictive value of 81.1% (Table 3).
For the psychosocial outcome, the percentages of patients showingfunctional improvement and normalization after the cognitive rehabili-tative interventions were 41.8% and 23.6%, respectively (Table 4).
Variables at baseline that differentiated between improved and notimproved patients for functional outcome in the univariate comparisonswere type of cognitive remediation intervention (CACR vs IPT-cog, chi-square test P = 0.001), lower age (t test P = 0.002), shorter duration ofillness (t test P = 0.008), lower antipsychotic intake at baselineexpressed as CPZ-eq (t test P = 0.030), as well as lower PANSS scorefor severity of uncooperativeness (t test P = 0.046) and higher scoresfor severity of somatic concern (t test P = 0.034), depression (t testP = 0.001), motor retardation (t test P = 0.037), and disorientation(t test P = 0.040). Higher baseline scores for the cognitive domains ofprocessing speed (t test P = 0.038) and working memory (t test P =0.044) also distinguished between patients who improved and thosewho did not. In the logistic regression analysis, lower patient age andtype of cognitive remediation intervention received (CACR vs IPT-cog) were significant individual predictors of functional improve-ment (model P b 0.001), with a predictive value of 75.5% (Table 5).
In univariate comparisons, the characteristics that differentiatedfunctionally normalized patients from those who did not show normal-ization after treatment using the HoNOS were lower antipsychotic in-take at baseline (CPZ-eq) (t test P = 0.002), shorter duration of illness(t test P = 0.017), younger age (t test P = 0.044) and type of cognitiveremediation intervention (CACR vs IPT-cog, chi-square test P = 0.046).A lower score of the PANSS item cognitive problems (t test P = 0.014)
Table 4Frequency of functional improvement and normalization after cognitive remediation inpatients with schizophrenia.
Frequency Percent
Functional improvementImproved 23 41.8Not improved 32 58.2
Functional normalizationNormalized 13 23.6Not normalized 42 76.4Normal at baseline 0 0
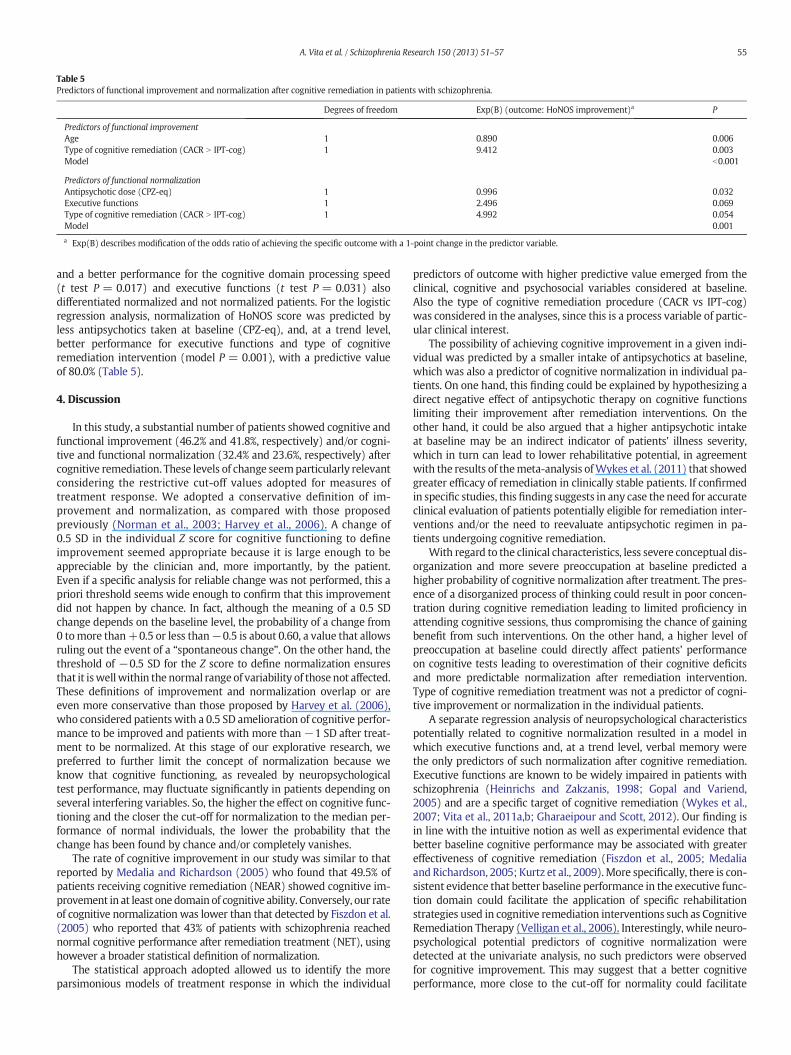
Table 5Predictors of functional improvement and normalization after cognitive remediation in patients with schizophrenia.
Degrees of freedom Exp(B) (outcome: HoNOS improvement)a P
Predictors of functional improvementAge 1 0.890 0.006Type of cognitive remediation (CACR N IPT-cog) 1 9.412 0.003Model b0.001
Predictors of functional normalizationAntipsychotic dose (CPZ-eq) 1 0.996 0.032Executive functions 1 2.496 0.069Type of cognitive remediation (CACR N IPT-cog) 1 4.992 0.054Model 0.001
a Exp(B) describes modification of the odds ratio of achieving the specific outcome with a 1-point change in the predictor variable.
55A. Vita et al. / Schizophrenia Research 150 (2013) 51–57
and a better performance for the cognitive domain processing speed(t test P = 0.017) and executive functions (t test P = 0.031) alsodifferentiated normalized and not normalized patients. For the logisticregression analysis, normalization of HoNOS score was predicted byless antipsychotics taken at baseline (CPZ-eq), and, at a trend level,better performance for executive functions and type of cognitiveremediation intervention (model P = 0.001), with a predictive valueof 80.0% (Table 5).
4. Discussion
In this study, a substantial number of patients showed cognitive andfunctional improvement (46.2% and 41.8%, respectively) and/or cogni-tive and functional normalization (32.4% and 23.6%, respectively) aftercognitive remediation. These levels of change seemparticularly relevantconsidering the restrictive cut-off values adopted for measures oftreatment response. We adopted a conservative definition of im-provement and normalization, as compared with those proposedpreviously (Norman et al., 2003; Harvey et al., 2006). A change of0.5 SD in the individual Z score for cognitive functioning to defineimprovement seemed appropriate because it is large enough to beappreciable by the clinician and, more importantly, by the patient.Even if a specific analysis for reliable change was not performed, this apriori threshold seems wide enough to confirm that this improvementdid not happen by chance. In fact, although the meaning of a 0.5 SDchange depends on the baseline level, the probability of a change from0 tomore than+0.5 or less than−0.5 is about 0.60, a value that allowsruling out the event of a “spontaneous change”. On the other hand, thethreshold of −0.5 SD for the Z score to define normalization ensuresthat it iswellwithin the normal range of variability of those not affected.These definitions of improvement and normalization overlap or areeven more conservative than those proposed by Harvey et al. (2006),who considered patients with a 0.5 SD amelioration of cognitive perfor-mance to be improved and patients with more than −1 SD after treat-ment to be normalized. At this stage of our explorative research, wepreferred to further limit the concept of normalization because weknow that cognitive functioning, as revealed by neuropsychologicaltest performance, may fluctuate significantly in patients depending onseveral interfering variables. So, the higher the effect on cognitive func-tioning and the closer the cut-off for normalization to the median per-formance of normal individuals, the lower the probability that thechange has been found by chance and/or completely vanishes.
The rate of cognitive improvement in our study was similar to thatreported by Medalia and Richardson (2005) who found that 49.5% ofpatients receiving cognitive remediation (NEAR) showed cognitive im-provement in at least one domain of cognitive ability. Conversely, our rateof cognitive normalization was lower than that detected by Fiszdon et al.(2005) who reported that 43% of patients with schizophrenia reachednormal cognitive performance after remediation treatment (NET), usinghowever a broader statistical definition of normalization.
The statistical approach adopted allowed us to identify the moreparsimonious models of treatment response in which the individual
predictors of outcome with higher predictive value emerged from theclinical, cognitive and psychosocial variables considered at baseline.Also the type of cognitive remediation procedure (CACR vs IPT-cog)was considered in the analyses, since this is a process variable of partic-ular clinical interest.
The possibility of achieving cognitive improvement in a given indi-vidual was predicted by a smaller intake of antipsychotics at baseline,which was also a predictor of cognitive normalization in individual pa-tients. On one hand, this finding could be explained by hypothesizing adirect negative effect of antipsychotic therapy on cognitive functionslimiting their improvement after remediation interventions. On theother hand, it could be also argued that a higher antipsychotic intakeat baseline may be an indirect indicator of patients' illness severity,which in turn can lead to lower rehabilitative potential, in agreementwith the results of themeta-analysis ofWykes et al. (2011) that showedgreater efficacy of remediation in clinically stable patients. If confirmedin specific studies, this finding suggests in any case the need for accurateclinical evaluation of patients potentially eligible for remediation inter-ventions and/or the need to reevaluate antipsychotic regimen in pa-tients undergoing cognitive remediation.
With regard to the clinical characteristics, less severe conceptual dis-organization and more severe preoccupation at baseline predicted ahigher probability of cognitive normalization after treatment. The pres-ence of a disorganized process of thinking could result in poor concen-tration during cognitive remediation leading to limited proficiency inattending cognitive sessions, thus compromising the chance of gainingbenefit from such interventions. On the other hand, a higher level ofpreoccupation at baseline could directly affect patients' performanceon cognitive tests leading to overestimation of their cognitive deficitsand more predictable normalization after remediation intervention.Type of cognitive remediation treatment was not a predictor of cogni-tive improvement or normalization in the individual patients.
A separate regression analysis of neuropsychological characteristicspotentially related to cognitive normalization resulted in a model inwhich executive functions and, at a trend level, verbal memory werethe only predictors of such normalization after cognitive remediation.Executive functions are known to be widely impaired in patients withschizophrenia (Heinrichs and Zakzanis, 1998; Gopal and Variend,2005) and are a specific target of cognitive remediation (Wykes et al.,2007; Vita et al., 2011a,b; Gharaeipour and Scott, 2012). Our finding isin line with the intuitive notion as well as experimental evidence thatbetter baseline cognitive performance may be associated with greatereffectiveness of cognitive remediation (Fiszdon et al., 2005; Medaliaand Richardson, 2005; Kurtz et al., 2009).More specifically, there is con-sistent evidence that better baseline performance in the executive func-tion domain could facilitate the application of specific rehabilitationstrategies used in cognitive remediation interventions such as CognitiveRemediation Therapy (Velligan et al., 2006). Interestingly, while neuro-psychological potential predictors of cognitive normalization weredetected at the univariate analysis, no such predictors were observedfor cognitive improvement. This may suggest that a better cognitiveperformance, more close to the cut-off for normality could facilitate

56 A. Vita et al. / Schizophrenia Research 150 (2013) 51–57
normalization, while a clinically relevant cognitive improvement ispossible regardless of the subject's baseline neuropsychological perfor-mance. Moreover, more variables explained cognitive normalization,compared to those explaining improvement. It may be speculated thatthe narrow definition of cognitive normalization used in this studymay have defined a more homogeneous group of patients, facilitatingthe detection of specific predictive variables on this outcome. On theother hand, the broader concept of improvement probably is applicableto a more heterogeneous group of patients, and this could diminish thepossibility to detect specific predictors of improvement.
Functional improvement was predicted by the younger age of thepatient and type of cognitive remediation intervention (CACR N IPT-cog) received. The efficacy of remediation interventions on cognitionin patients in the early phases of schizophrenia has already been docu-mented (Wykes et al., 2007; Eack et al., 2009; and, for a review, Barlatiet al., 2012). Our results indicate that younger patients may also havea higher chance of a relevant beneficial effect on psychosocial function-ing after cognitive remediation, consistent with previous preliminaryfindings (Medalia and Richardson, 2005; McGurk et al., 2007; Wykeset al., 2009). If this result is confirmed by further investigations, itcould represent a clinical guideline for cognitive remediation interven-tions and support the recommendation to begin treatment as soon aspossible in the earliest phases of the illness. The different probabilityto attain improvement for patients treated with different remediationmodalities is consistent with the larger effect on functioning found inthe CACR vs IPT-cog group in the study from which this analysis is de-rived (Vita et al., 2011a) and may be due to the fact that compensatorystrategies, although present in bothmodalities, aremore openly includ-ed in the learning process of the CACR method. It is also possible to hy-pothesize that the differential effects on functional outcome found inour study may have been influenced by the prevailing role of concomi-tant factors related to the naturalistic setting in which the cognitive re-mediation interventions were offered. Functional normalization refersto a psychosocial performance that is indistinguishable from that ofhealthy people, a goal now considered appropriate for patients withschizophrenia (Frese et al., 2009). In this case, smaller intake of antipsy-chotics at baseline and, at a nonsignificant level, type of cognitive reme-diation intervention (CACR N IPT-cog) received and better performancein executive functions at baseline predicted functional normalizationafter cognitive remediation. This emphasizes the role of the amount ofantipsychotic therapy taken also on patient's functional outcome aftercognitive remediation, and of skills such asmentalflexibility in allowingchange in psychosocial functioning, which may have been more effec-tively trained by CACR method in this sample.
This study has a number of limitations. The most relevant is its rela-tively small sample size. This limited the number of potential predictorsthat could be explored and possibly included as covariates in the logisticregressions.Moreover, it was not possible to analyze the specific predic-tors of cognitive and functional response to each of the two cognitive re-mediation interventions applied in the study, i.e. IPT-cog and CACR. Forthe same reason, the role of the use of specific antipsychotics as poten-tial predictors of cognitive and functional improvement and normaliza-tion after cognitive remediation could not be analyzed. The absence ofadditional specific tests in our neuropsychological battery, for instancethose for visual and spatial memory, could have limited the possibilityto detect positive effects of cognitive remediation interventions and/orputative predictors of their effectiveness in the present study. Finally,we did not calculate any specific index to account for practice effectsof neuropsychological tests. However, the conservative definitions ofimprovement and normalization, consistent with, and evenmore rigor-ous than those used by other authors, allow excluding that such effectsmay have played a major role on our results.
Even with these limitations, our findings extend existing knowledgeon the predictors of response to cognitive remediation treatment inschizophrenia. Furthermore, the naturalistic approach adopted allowsus to draw some clinically relevant conclusions on the application of
cognitive remediation in the “real world”. In fact, particular attentionwas given to maintaining a naturalistic setting of care, close to theusual delivery of treatment in Italian psychiatric services. This increasedthe study's external validity and the likelihood of having detected reli-able predictors of treatment response that could be useful in routineclinical practice. Improvement and normalization of cognitive and func-tional performancemay be obtained in a substantial number of patientswith schizophrenia undergoing cognitive remediation treatments. Cog-nitive remediation may be more effective in younger, less disorganized,and less cognitively impaired patients, who are taking smaller amountsof antipsychotics. The predictive role of a smaller antipsychotic dose forbetter cognitive and functional outcome after remediation suggestseither that patients with less severe illness, i.e. patients who do notneed high doses of antipsychotics or complex polypharmacotherapies,could gain more benefit from cognitive remediation, or that high dosesor complex antipsychotic therapies may limit the effectiveness of suchinterventions.
Role of funding sourceFunding for this studywas partially provided by theHealth Authority of the Lombardia
Region (project TR11).
ContributorsAV designed the project, reviewed and discussed the data and statistical analyses, and
the final version of the paper; LDP participated in the design of the study, in the choice ofassessment scales and tests, reviewed the methodology of remediation interventions andof scale completion by the centers and contributed to write the first draft of the paper; GDadministered and scored neuropsychological tests, prepared the database, participated inthe analyses and contributed to write the first draft of the paper; SB and RP followed uppatients in the rehabilitative interventions and discussed the design of the study andstudy results; BMC designed and undertook the statistical analyses; ES participated inthe design of the project, and discussion of the data andmanuscript. All authors contribut-ed to and approved the final manuscript.
Conflict of interestIn the past 3 years, Professor Vita has received funding for research, advisory board
membership and sponsored lectures from: Astra Zeneca Pharmaceuticals, Eli Lilly,Janssen-Cilag, Lundbeck, Pfizer, Sanofi, Servier, and Stroder. He is not a shareholder inany of these corporations.
Professor Sacchetti has received funding for research, advisory board membershipand sponsored lectures from: Angelini, AstraZeneca Pharmaceuticals, Bristol-MyersSquibb, Dainippon Sumitomo Pharma, Eli Lilly, Glaxo SmithKline, Janssen-Cilag, Lundbeck,Pfizer, Rottapharm, Servier, and Stroder. He is not a shareholder in any of thesecorporations.
No declaration of interest by the other authors.
AcknowledgmentsThe studywas presented in part at the 3rd Congress of the Schizophrenia Internation-
al Research Society, Florence, 14–18 April 2012. The authors wish to thank Paolo Cacciani,MD, for participating in patient recruitment, and Lorna O'Brian for the revision of theEnglish language.
References
American Psychiatric Association, 2000. Diagnostic and Statistical Manual of Mental Dis-orders, 4th ed. Text Revision. American Psychiatric Association, Washington, DC.
Barlati, S., De Peri, L., Deste, G., Fusar-Poli, P., Vita, A., 2012. Cognitive remediation in theearly course of schizophrenia: a critical review. Curr. Pharm. Des. 18 (4), 534–541.
Benton, A.L., Hamsher, K.D., 1989. Multilingual Aphasia Examination. AJA Associates, IowaCity, IA.
Bosia, M., Bechi, M., Marino, E., Anselmetti, S., Poletti, S., Cocchi, F., Smeraldi, E., Cavallaro,R., 2007. Influence of catechol-O-methyltransferase Val158Met polymorphism onneuropsychological and functional outcomes of classical rehabilitation and cognitiveremediation in schizophrenia. Neurosci. Lett. 417 (3), 271–274.
Bowie, C.R., Reichenberg, A., Patterson, T.L., Heaton, R.K., Harvey, P.D., 2006. Determinantsof real-world functional performance in schizophrenia subjects: correlations withcognition, functional capacity, and symptoms. Am. J. Psychiatry 163 (3), 418–425.
Bowie, C.R., Leung, W.W., Reichenberg, A., McClure, M.M., Patterson, T.L., Heaton, R.K.,Harvey, P.D., 2008. Predicting schizophrenia patients' real-world behavior with spe-cific neuropsychological and functional capacity measures. Biol. Psychiatry 63 (5),505–511.
Bowie, C.R., Grossman, M., Gupta, M., Oyewumi, L.K., Harvey, P.D., 2013. Cognitive remedia-tion in schizophrenia: efficacy and effectiveness in patients with early versus long-termcourse of illness. Early Interv. Psychiatry. http://dx.doi.org/10.1111/eip.12029 ([Epubahead of print]).
Brenner, H., Roder, V., Hodel, B., Kienzie, N., Reed, D., Liberman, R., 1994. Integrated Psy-chological Therapy for Schizophrenic Patients. Hogrefe & Huber, Seattle, WA.

57A. Vita et al. / Schizophrenia Research 150 (2013) 51–57
Brenner, V., Roder, V., Hodel, B., Kienzle, N., Invernizzi, G., Vita, A., 1997. Terapia PsicologicaIntegrata (ITP). In: Vita, A., Invernizzi, G. (Eds.), Programma per la Riabilitazione delPaziente Schizofrenico. Milan, McGraw-Hill (Italian edition).
Eack, S.M., Greenwald, D.P., Hogarty, S.S., Cooley, S.J., DiBarry, A.L., Montrose, D.M.,Keshavan, M.S., 2009. Cognitive enhancement therapy for early-course schizophrenia:effects of a two-year randomized controlled trial. Psychiatr. Serv. 60 (11), 1468–1476.
Eack, S.M., Pogue-Geile, M.F., Greenwald, D.P., Hogarty, S.S., Keshavan, M.S., 2011. Mech-anisms of functional improvement in a 2-year trial of cognitive enhancement therapyfor early schizophrenia. Psychol. Med. 41 (6), 1253–1261.
Fiszdon, J.M., Cardenas, A.S., Brysonm, G.J., Bell, M.D., 2005. Predictors of remediation suc-cess on a trained memory task. J. Nerv. Ment. Dis. 193 (9), 602–608.
Frese 3rd, F.J., Knight, E.L., Saks, E., 2009. Recovery from schizophrenia: with views of psy-chiatrists, psychologists, and others diagnosed with this disorder. Schizophr. Bull. 35(2), 370–380.
Gharaeipour, M., Scott, B.J., 2012. Effects of cognitive remediation on neurocognitive func-tions and psychiatric symptoms in schizophrenia inpatients. Schizophr. Res. 142(1–3), 165–170.
Giovagnoli, A.R., Del Pesce, M., Mascheroni, S., Simoncelli, M., Laiacona, M., Capitani, E.,1996. Trail making test: normative values from 287 normal adult controls. Ital.J. Neurol. Sci. 17, 305–309.
Gopal, Y., Variend, H., 2005. First-episode schizophrenia: review of cognitive deficits andcognitive remediation. Adv. Psychiatr. Treat. 11, 38–44.
Green, M.F., Kern, R.S., Heaton, R.K., 2004. Longitudinal studies of cognition and functionaloutcome in schizophrenia: implications for MATRICS. Schizophr. Res. 72 (1), 41–51.
Grynszpan, O., Perbal, S., Pelissolo, A., Fossati, P., Jouvent, R., Dubal, S., Perez-Diaz, F., 2010.Efficacy and specificity of computer-assisted cognitive remediation in schizophrenia:a meta-analytical study. Psychol. Med. 41 (1), 163–173.
Guy, W., 1976. ECDEU Assessment Manual for Psychopharmacology. US Department ofHealth, Education and Welfare, National Institute of Mental Health, Washington, DC76–338.
Harvey, P.D., Bowie, C.R., Loebel, A., 2006. Neuropsychological normalizationwith long-termatypical antipsychotic treatment: results of a six-month randomized, double-blind com-parison of ziprasidone vs. olanzapine. J. Neuropsychiatry Clin. Neurosci. 18 (1), 54–63.
Heaton, R.K., 1981. The Wisconsin Card Sorting Test Manual. Psychological Assessment Re-sources, Odessa (FL (Italian translation and validation edited by Giunti OrganizzazioniSpeciali, Florence, 2000)).
Heinrichs, R.W., Zakzanis, K.K., 1998. Neurocognitive deficit in schizophrenia: a quantita-tive review of the evidence. Neuropsychology 12 (3), 426–445.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The Positive and Negative Syndrome Scale(PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276.
Keefe, R.S., Bilder, R.M., Harvey, P.D., Davis, S.M., Palmer, B.W., Gold, J.M.,Meltzer, H.Y., Green,M.F., Miller, D.D., Canive, J.M., Adler, L.W., Manschreck, T.C., Swartz, M., Rosenheck, R.,Perkins, D.O., Walker, T.M., Stroup, T.S., McEvoy, J.P., Lieberman, J.A., 2006. Baselineneurocognitive deficits in the CATIE schizophrenia trial. Neuropsychopharmacology 31(9), 2033–2046.
Kontis, D., Huddy, V., Reeder, C., Landau, S., Wykes, T., 2013. Effects of age and cognitivereserve on cognitive remediation therapy outcome in patients with schizophrenia.Am. J. Geriatr. Psychiatry 21 (3), 218–230.
Kurtz, M.M., Seltzer, J.C., Fujimoto, M., Shagan, D.S., Wexler, B.E., 2009. Predictors ofchange in life skills in schizophrenia after cognitive remediation. Schizophr. Res.107 (2–3), 267–274.
Lora, A., Bai, G., Bianchi, S., Bolongaro, G., Civenti, G., Erlicher, A., 2001. La versione italianadella HoNOS (Health of the Nation Outcome Scales), una scala per la valutazione dellagravità e dell'esito nei servizi di salute mentale. Epidemiol. Psichiatr. Soc. 10, 198–212.
McGurk, S.R., Twamley, E.W., Sitzer, D.I., McHugo, G.J., Mueser, K.T., 2007. A meta-analysisof cognitive remediation in schizophrenia. Am. J. Psychiatry 164 (12), 1791–1802.
Medalia, A., Richardson, R., 2005.What predicts a good response to cognitive remediationinterventions? Schizophr. Bull. 31 (4), 942–953.
Medalia, A., Saperstein, A.M., 2013. Does cognitive remediation for schizophrenia improvefunctional outcomes? Curr. Opin. Psychiatry 26 (2), 151–157.
Norman, G.R., Sloan, J.A., Wyrwich, K.W., 2003. Interpretation of changes in health-relatedquality of life: the remarkable universality of half a standard deviation. Med. Care 41,582–592.
Parabiaghi, A., Barbato, A., D'Avanzo, B., Erlicher, A., Lora, A., 2005. Assessing reliable andclinically significant change on Health of the Nation Outcome Scales: method fordisplaying longitudinal data. Aust. N.Z. J. Psychiatry 39 (8), 719–725.
Petrides, M., Milner, B., 1982. Deficits on subject-ordered tasks after frontal- andtemporal-lobe lesions in man. Neuropsychologia 20, 249–262.
Reitan, R.M., 1979. Trail Making Test: Manual for Administration and Scoring. Reitan Neu-ropsychology Laboratory, South Tucson, AZ.
Reitan, R.M., Wolfson, D., 1993. The Halstead–Reitan Neuropsychological Test Battery:Theory and Clinical Interpretation, 2nd ed. Neuropsychology Press, Tucson, AZ.
Sacchetti, E., Galluzzo, A., Panariello, A., Parrinello, G., Cappa, S.F., 2008. Self-orderedpointing and visual conditional associative learning tasks in drug-free schizophreniaspectrum disorder patients. BMC Psychiatry 8, 6.
Velligan, D.I., Kern, R.S., Gold, J.M., 2006. Cognitive rehabilitation for schizophrenia andthe putative role of motivation and expectancies. Schizophr. Bull. 32 (3), 474–485.
Vita, A., De Peri, L., Barlati, S., Cacciani, P., Deste, G., Poli, R., Agrimi, E., Cesana, B.M.,Sacchetti, E., 2011a. Effectiveness of different modalities of cognitive remediationon symptomatological, neuropsychological, and functional outcome domains inschizophrenia: a prospective study in a real-world setting. Schizophr. Res. 133(1–3), 223–231.
Vita, A., De Peri, L., Barlati, S., Cacciani, P., Cisima, M., Deste, G., Cesana, B.M., Sacchetti, E.,2011b. Psychopathologic, neuropsychological and functional outcome measures dur-ing cognitive rehabilitation in schizophrenia: a prospective controlled study in a real-world setting. Eur. Psychiatry 26 (5), 276–283.
Wechsler, D., 1981. Wechsler Adult Intelligence Scale—Revised. Harcourt, Brace,Jovanovich, New York.
Wing, J.K., Beevor, A.S., Curtis, R.H., Park, S.B., Hadden, S., Burns, A., 1998. Health of theNation Outcome Scales (HoNOS). Research and development. Br. J. Psychiatry 172,11–18.
Woods, S.W., 2003. Chlorpromazine equivalent doses for the newer atypical antipsy-chotics. J. Clin. Psychiatry 64, 663–667.
Wykes, T., Reeder, C., Landau, S., Everitt, B., Knapp, M., Patel, A., Romeo, R., 2007. Cognitiveremediation therapy in schizophrenia: randomised controlled trial. Br. J. Psychiatry190, 421–427.
Wykes, T., Reeder, C., Landau, S., Matthiasson, P., Haworth, E., Hutchinson, C., 2009. Doesagematter? Effects of cognitive rehabilitation across the age span. Schizophr. Res. 113(2–3), 252–258.
Wykes, T., Huddy, V., Cellard, C., McGurk, S.R., Czobor, P., 2011. A meta-analysis of cogni-tive remediation for schizophrenia: methodology and effect sizes. Am. J. Psychiatry168 (5), 472–485.




















