
Slow force response and auto-regulation of contractility in heterogeneous myocardium
Upload
independentCategory
view
4download
0
Cardiovascular Research 45 (2000) 339–350www.elsevier.com/ locate /cardiores
www.elsevier.nl / locate /cardiores
Preconditioning the human myocardium by simulated ischemia:studies on the early and delayed protection
a b a ,*˜Sudip Ghosh , Nicholas B. Standen , Manuel GalinanesaDivision of Cardiac Surgery, Department of Surgery, University of Leicester, Glenfield Hospital, Leicester LE3 9QP, UK
bDepartment of Cell Physiology and Pharmacology, University of Leicester, Leicester LE1 7RH, UK
Received 1 July 1999; accepted 10 September 1999
Abstract
Background: There are data supporting the existence of ischemic preconditioning in man. This study investigated the most effectivepreconditioning protocol for the human myocardium and whether the second window of ischemic preconditioning (24 h) is as protectiveas the first window (#2 h). Methods and results: Right atrial appendages (n56/group) obtained during coronary bypass surgery wereprepared and superfused with normoxic and normothermic Krebs–Henseleit solution. After 30 min stabilisation, muscles were subjectedto various preconditioning protocols followed by 90 min ischemia and 120 min reperfusion. At the end of each protocol, the leakage ofcreatinine kinase (CK, U/g wet wt) and the reduction of MTT to insoluble formazan dye (OD/mg wet wt), an index of cell viability,were measured. In study 1, preconditioning was induced by 2, 3, 5 and 10 min of ischemia followed by 5 min reperfusion. In study 2, 1–4cycles of 2 or 5 min ischemia–5 min reperfusion were applied. In study 3, preconditioning was induced by 5 min ischemia–5 minreperfusion followed by 1, 2, 3 or 4 h reperfusion before the subsequent 90 min ischemia. In study 4, preconditioning with 5 min ischemiafollowed by 5 min reperfusion either immediately preceded 30 or 90 min ischemia /120 min reperfusion or was applied 24 h before. Instudy 1 and 2, optimal protection was achieved with 5 min or two cycles of 2 min preconditioning ischemia (CK53.0660.31 and2.8960.02; MTT50.5660.05 and 0.4760.09, respectively vs. CK55.5660.52 and MTT50.1860.04 in ischemia alone group; P,0.05).In study 3, protection was observed 2 h after preconditioning (CK53.4360.22 and MTT50.4660.09; P,0.01 vs. ischemia alone group)but it was lost beyond 2 h (CK56.3060.56 and MTT50.1660.02 after 3 h; P5NS vs. ischemia alone group). In study 4, protection wasobserved 24 h following preconditioning when the atrial specimens were exposed to 30 min ischemia (CK52.9660.38 and MTT5
0.6160.01 vs. CK54.5660.26 and MTT50.4360.02 in ischemia alone group, P,0.05); however, when the period of ischemia wasextended to 90 min the beneficial effect of preconditioning was lost (CK510.2860.5 and MTT50.1160.05 vs. CK59.5660.62 andMTT50.10460.05 in ischemia alone group, P5NS). Conclusions: In the isolated human myocardium maximal protection induced bypreconditioning is achieved by a total 4–5 min ischemic stimulus, an effect that is lost beyond 2 h of its application. Two windows ofprotection were identified, the first (#2 h) being more potent than the second (24 h). 2000 Published by Elsevier Science B.V. Allrights reserved.
Keywords: Ischemia; Preconditioning
1. Introduction trabeculae [2], ventricular trabeculae [3] and culturedventricular myocytes [4], studies of patients undergoing
Brief periods of ischemia and reperfusion appear to planned procedures which invariably involve brief periodsprotect the myocardium from a subsequent lethal ischemic of ischemia such as percutaneous transluminal coronaryinjury. This phenomenon of ischemic preconditioning, angioplasty [5] and coronary bypass graft surgery [6].originally described by Murry et al. [1], has been shown to Despite the wealth of information generated by theseexist in all animal species studied to date. There is now human studies, the most effective ischemic preconditioningcompelling evidence that it exists in humans. This evi- protocol in man remains unknown.dence arises from in vitro experiments with human atrial In rats, rabbits, dogs and pigs, separation of the brief
*Corresponding author. Time for primary review 31 days.
0008-6363/00/$ – see front matter 2000 Published by Elsevier Science B.V. All rights reserved.PI I : S0008-6363( 99 )00353-3
by guest on July 30, 2016D
ownloaded from
340 S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350
preconditioning ischemic episodes from the long occlusion an automated blood gas analyser (model 855 Blood Gasby 60 to 120 min results in complete or nearly complete System, Chiron Diagnostics) and the pH was kept betweenloss of protection. However, if the duration of this sepa- 7.36 and 7.45. For the induction of simulated ischemia, theration is extended to 24 to 72 h, the infarct size will be medium was bubbled with 95% N –5% CO (pH 6.80–2 2
reduced again. Hence there appears to be a distinct first 7.00) and D-glucose removed (see below). In this prepara-(early) as well as a second (delayed) phase of protection. tion, tissue injury and viability were assessed (see below)There is no evidence that this biphasic mode of protection but the atrium was not paced and the force developed wasexists in humans. not measured.
Although studies during angioplasty have given evi-dence for ischemic preconditioning in man, clearly there 2.2. Solutionsare practical and ethical limitations on the extent to whichsuch situations can be used to investigate the characteris- The incubation medium was prepared daily with de-tics of preconditioning in the human myocardium. In ionized distilled water and contained (in mmol / l): NaClcontrast, in vitro preparations allow a wide range of (118), KCl (4.8), NaHCO (27.2), KH PO (1), MgCl3 2 4 2
experimental manipulations. The aims of the present study (1.2), CaCl (1.25), D-glucose (10) and HEPES (20).2
were to investigate the most effective preconditioning During simulated ischemia, to maintain a constant osmo-protocol in human myocardium and also the existence and larity, D-glucose was removed and substituted with 2-potency of a second window of protection. To achieve this, deoxy glucose (10 mmol / l). All reagents were obtainedwe subjected to simulated ischemia isolated, sliced and from Sigma.superfused right atrial trabeculae obtained from patientsundergoing elective cardiac surgery. CK leakage and MTT 2.3. Experimental protocolsreduction, an index of cell viability, were measured toassess myocardial injury. After sectioning the atrium, the preparations were
allowed to stabilise for 30 min and then randomly allo-cated to various protocols. In most studies simulatedischemia was induced for a period of 90 min followed by
2. Methods 120 min of reperfusion.
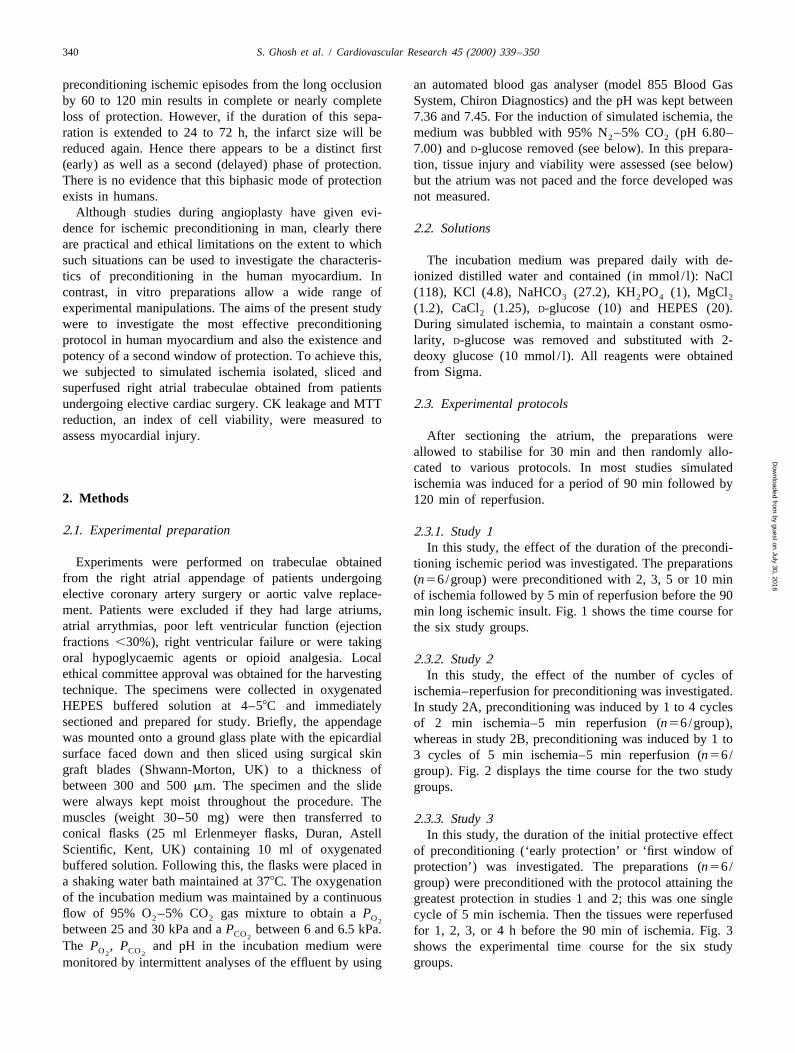
2.1. Experimental preparation 2.3.1. Study 1In this study, the effect of the duration of the precondi-
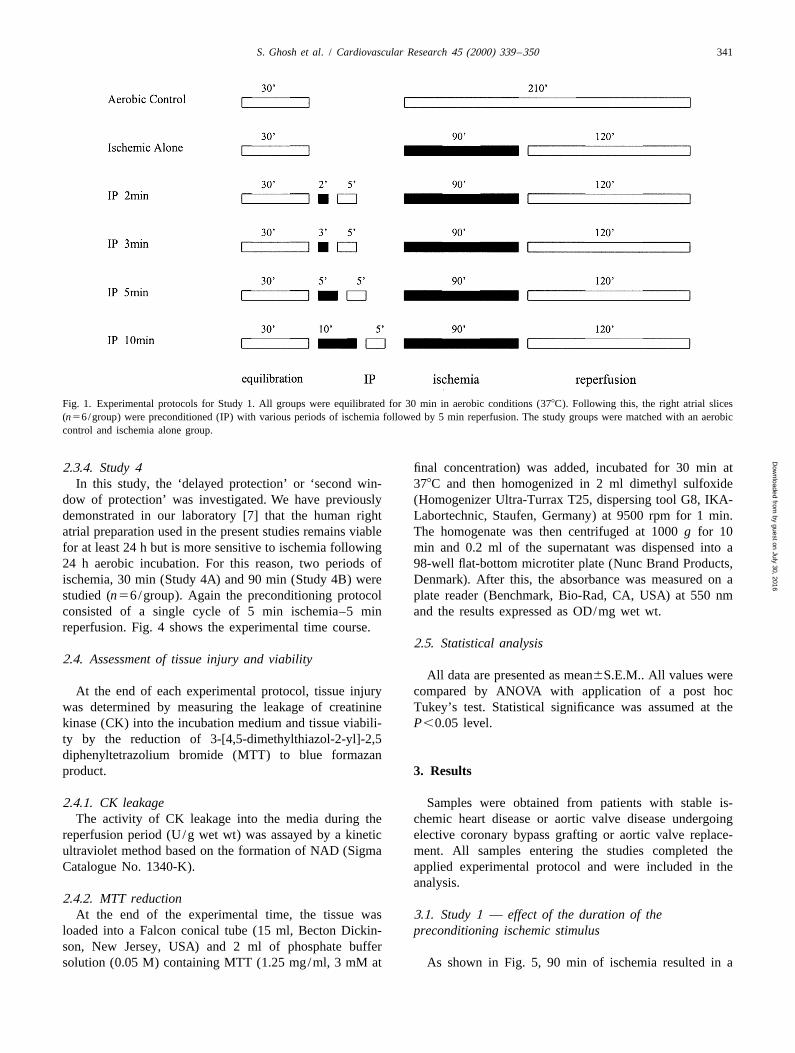
Experiments were performed on trabeculae obtained tioning ischemic period was investigated. The preparationsfrom the right atrial appendage of patients undergoing (n56/group) were preconditioned with 2, 3, 5 or 10 minelective coronary artery surgery or aortic valve replace- of ischemia followed by 5 min of reperfusion before the 90ment. Patients were excluded if they had large atriums, min long ischemic insult. Fig. 1 shows the time course foratrial arrythmias, poor left ventricular function (ejection the six study groups.fractions ,30%), right ventricular failure or were takingoral hypoglycaemic agents or opioid analgesia. Local 2.3.2. Study 2ethical committee approval was obtained for the harvesting In this study, the effect of the number of cycles oftechnique. The specimens were collected in oxygenated ischemia–reperfusion for preconditioning was investigated.HEPES buffered solution at 4–58C and immediately In study 2A, preconditioning was induced by 1 to 4 cyclessectioned and prepared for study. Briefly, the appendage of 2 min ischemia–5 min reperfusion (n56/group),was mounted onto a ground glass plate with the epicardial whereas in study 2B, preconditioning was induced by 1 tosurface faced down and then sliced using surgical skin 3 cycles of 5 min ischemia–5 min reperfusion (n56/graft blades (Shwann-Morton, UK) to a thickness of group). Fig. 2 displays the time course for the two studybetween 300 and 500 mm. The specimen and the slide groups.were always kept moist throughout the procedure. Themuscles (weight 30–50 mg) were then transferred to 2.3.3. Study 3conical flasks (25 ml Erlenmeyer flasks, Duran, Astell In this study, the duration of the initial protective effectScientific, Kent, UK) containing 10 ml of oxygenated of preconditioning (‘early protection’ or ‘first window ofbuffered solution. Following this, the flasks were placed in protection’) was investigated. The preparations (n56/a shaking water bath maintained at 378C. The oxygenation group) were preconditioned with the protocol attaining theof the incubation medium was maintained by a continuous greatest protection in studies 1 and 2; this was one singleflow of 95% O –5% CO gas mixture to obtain a P cycle of 5 min ischemia. Then the tissues were reperfused2 2 O2
between 25 and 30 kPa and a P between 6 and 6.5 kPa. for 1, 2, 3, or 4 h before the 90 min of ischemia. Fig. 3CO2
The P , P and pH in the incubation medium were shows the experimental time course for the six studyO CO2 2
monitored by intermittent analyses of the effluent by using groups.
by guest on July 30, 2016D
ownloaded from
S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350 341
Fig. 1. Experimental protocols for Study 1. All groups were equilibrated for 30 min in aerobic conditions (378C). Following this, the right atrial slices(n56/group) were preconditioned (IP) with various periods of ischemia followed by 5 min reperfusion. The study groups were matched with an aerobiccontrol and ischemia alone group.
2.3.4. Study 4 final concentration) was added, incubated for 30 min atIn this study, the ‘delayed protection’ or ‘second win- 378C and then homogenized in 2 ml dimethyl sulfoxide
dow of protection’ was investigated. We have previously (Homogenizer Ultra-Turrax T25, dispersing tool G8, IKA-demonstrated in our laboratory [7] that the human right Labortechnic, Staufen, Germany) at 9500 rpm for 1 min.atrial preparation used in the present studies remains viable The homogenate was then centrifuged at 1000 g for 10for at least 24 h but is more sensitive to ischemia following min and 0.2 ml of the supernatant was dispensed into a24 h aerobic incubation. For this reason, two periods of 98-well flat-bottom microtiter plate (Nunc Brand Products,ischemia, 30 min (Study 4A) and 90 min (Study 4B) were Denmark). After this, the absorbance was measured on astudied (n56/group). Again the preconditioning protocol plate reader (Benchmark, Bio-Rad, CA, USA) at 550 nmconsisted of a single cycle of 5 min ischemia–5 min and the results expressed as OD/mg wet wt.reperfusion. Fig. 4 shows the experimental time course.
2.5. Statistical analysis2.4. Assessment of tissue injury and viability
All data are presented as mean6S.E.M.. All values wereAt the end of each experimental protocol, tissue injury compared by ANOVA with application of a post hoc
was determined by measuring the leakage of creatinine Tukey’s test. Statistical significance was assumed at thekinase (CK) into the incubation medium and tissue viabili- P,0.05 level.ty by the reduction of 3-[4,5-dimethylthiazol-2-yl]-2,5diphenyltetrazolium bromide (MTT) to blue formazanproduct. 3. Results
2.4.1. CK leakage Samples were obtained from patients with stable is-The activity of CK leakage into the media during the chemic heart disease or aortic valve disease undergoing
reperfusion period (U/g wet wt) was assayed by a kinetic elective coronary bypass grafting or aortic valve replace-ultraviolet method based on the formation of NAD (Sigma ment. All samples entering the studies completed theCatalogue No. 1340-K). applied experimental protocol and were included in the
analysis.2.4.2. MTT reduction
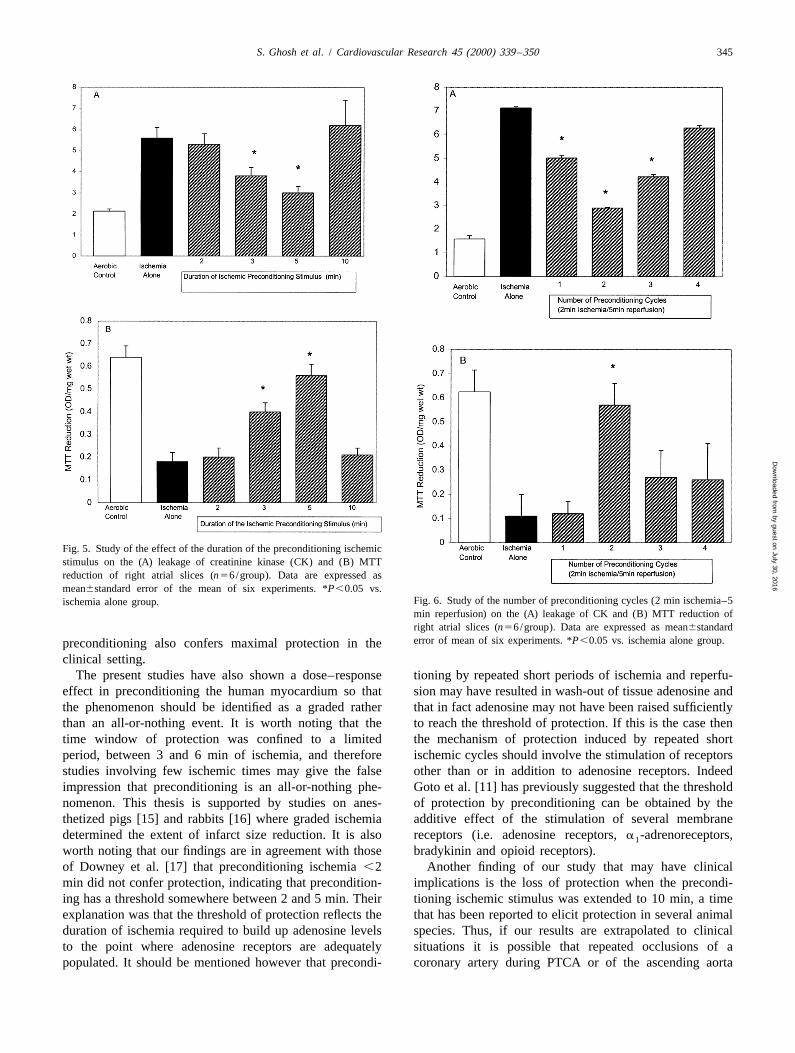
At the end of the experimental time, the tissue was 3.1. Study 1 — effect of the duration of theloaded into a Falcon conical tube (15 ml, Becton Dickin- preconditioning ischemic stimulusson, New Jersey, USA) and 2 ml of phosphate buffersolution (0.05 M) containing MTT (1.25 mg/ml, 3 mM at As shown in Fig. 5, 90 min of ischemia resulted in a
by guest on July 30, 2016D
ownloaded from
342 S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350
Fig. 2. Experimental protocols for Study 2A and 2B. Right atrial slices in all groups (n56/group) were equilibrated for 30 min. In Study 2A, the sliceswere then preconditioned(IP) with 1–4 cycles of 2 min ischemia–5 min reperfusion before being subjected to 90 min of ischemia–120 min reperfusion. InStudy 2B, after equilibration, the slices were subjected to 1–3 cycles of 5 min ischemia–5 min reperfusion preconditioning before the 90-min ischemicperiod.
significant increase in CK leakage and a decrease in MTT the duration of ischemia was less than 3 min or increasedreduction. An inverted bell shape curve was observed for to 10 min.CK leakage when various periods of ischemic precondi-tioning were applied. 2 min of ischemia was not protective; 3.2. Study 2 — effect of the number of cycles of3 min of ischemia was the minimum period required to preconditioningachieve a significant reduction in CK leakage but maximalprotection was obtained with 5 min ischemic precondition- Fig. 6 shows the results of preconditioning with increas-ing with mean CK leakage values not significantly differ- ing cycles of 2 min ischemia–5 min reperfusion. Theent from those in the aerobic control group. Surprisingly, results from CK leakage and MTT reduction show thatprotection was lost when ischemic preconditioning was maximal protection was obtained with two cycles of 2 minextended to 10 min. ischemia. Interestingly, in this study preconditioning with
A mirror image to that seen for CK leakage was one cycle of 2 min ischemia resulted in a small butobserved for MTT reduction. Thus, 5 min of ischemic statistically significant decrease in CK leakage. This resultpreconditioning afforded maximal protection such that contrasts with that observed in study 1 where the enzymeMTT reduction values were similar to those seen in the leakage resulting from preconditioning with 2 min is-aerobic control group, and again, protection was lost when chemia was similar to the mean values of the ischemia
by guest on July 30, 2016D
ownloaded from
S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350 343
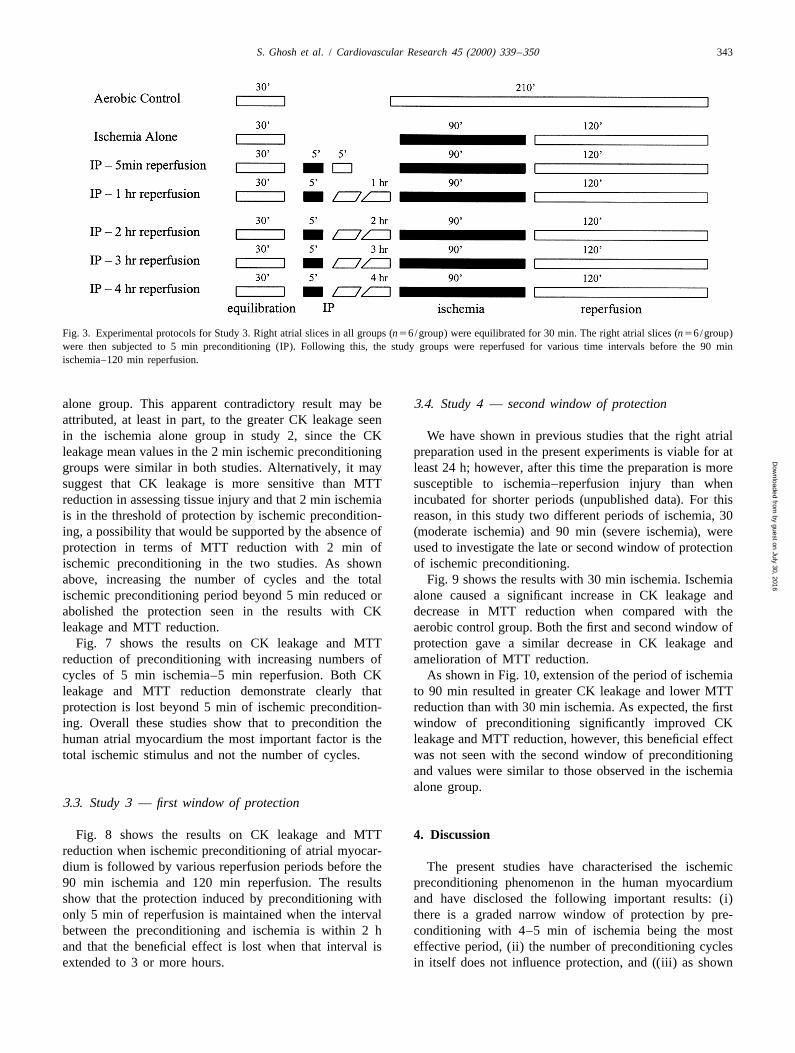
Fig. 3. Experimental protocols for Study 3. Right atrial slices in all groups (n56/group) were equilibrated for 30 min. The right atrial slices (n56/group)were then subjected to 5 min preconditioning (IP). Following this, the study groups were reperfused for various time intervals before the 90 minischemia–120 min reperfusion.
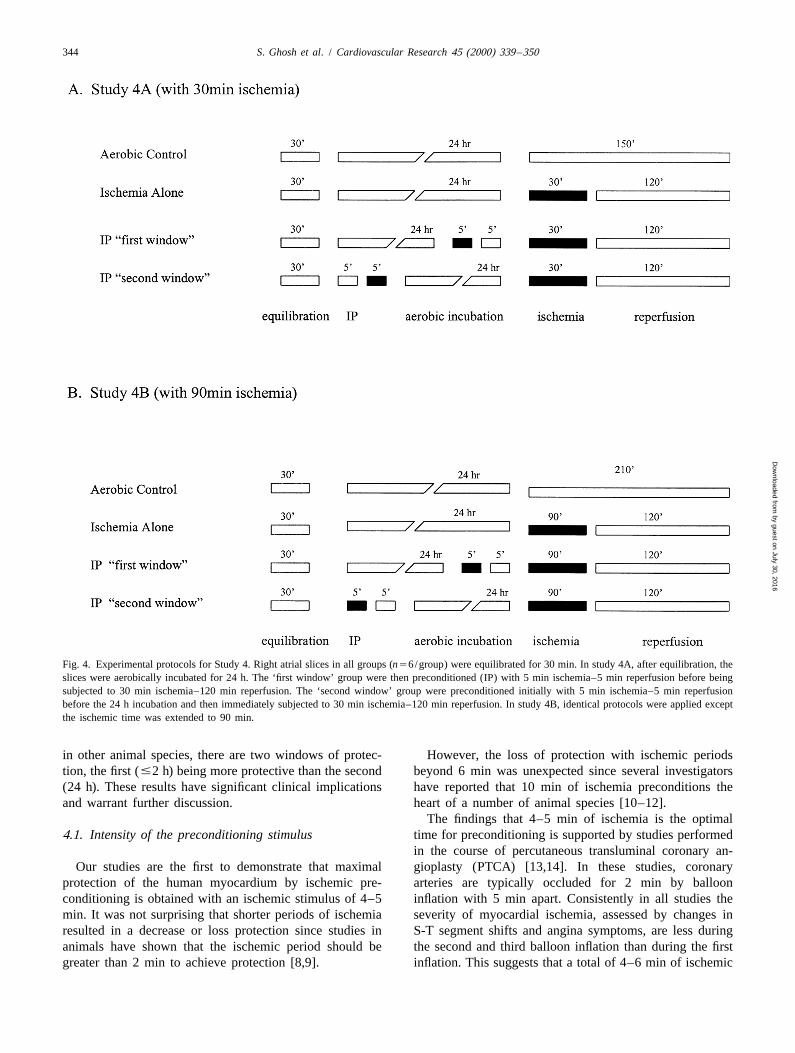
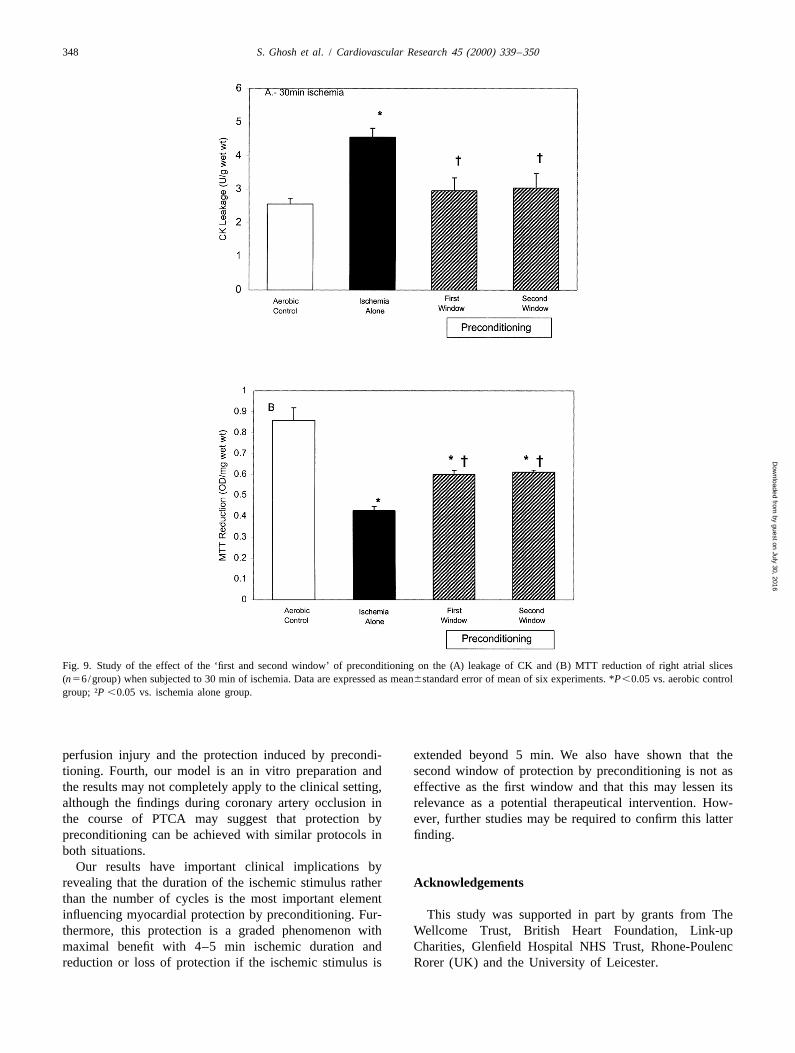
alone group. This apparent contradictory result may be 3.4. Study 4 — second window of protectionattributed, at least in part, to the greater CK leakage seenin the ischemia alone group in study 2, since the CK We have shown in previous studies that the right atrialleakage mean values in the 2 min ischemic preconditioning preparation used in the present experiments is viable for atgroups were similar in both studies. Alternatively, it may least 24 h; however, after this time the preparation is moresuggest that CK leakage is more sensitive than MTT susceptible to ischemia–reperfusion injury than whenreduction in assessing tissue injury and that 2 min ischemia incubated for shorter periods (unpublished data). For thisis in the threshold of protection by ischemic precondition- reason, in this study two different periods of ischemia, 30ing, a possibility that would be supported by the absence of (moderate ischemia) and 90 min (severe ischemia), wereprotection in terms of MTT reduction with 2 min of used to investigate the late or second window of protectionischemic preconditioning in the two studies. As shown of ischemic preconditioning.above, increasing the number of cycles and the total Fig. 9 shows the results with 30 min ischemia. Ischemiaischemic preconditioning period beyond 5 min reduced or alone caused a significant increase in CK leakage andabolished the protection seen in the results with CK decrease in MTT reduction when compared with theleakage and MTT reduction. aerobic control group. Both the first and second window of
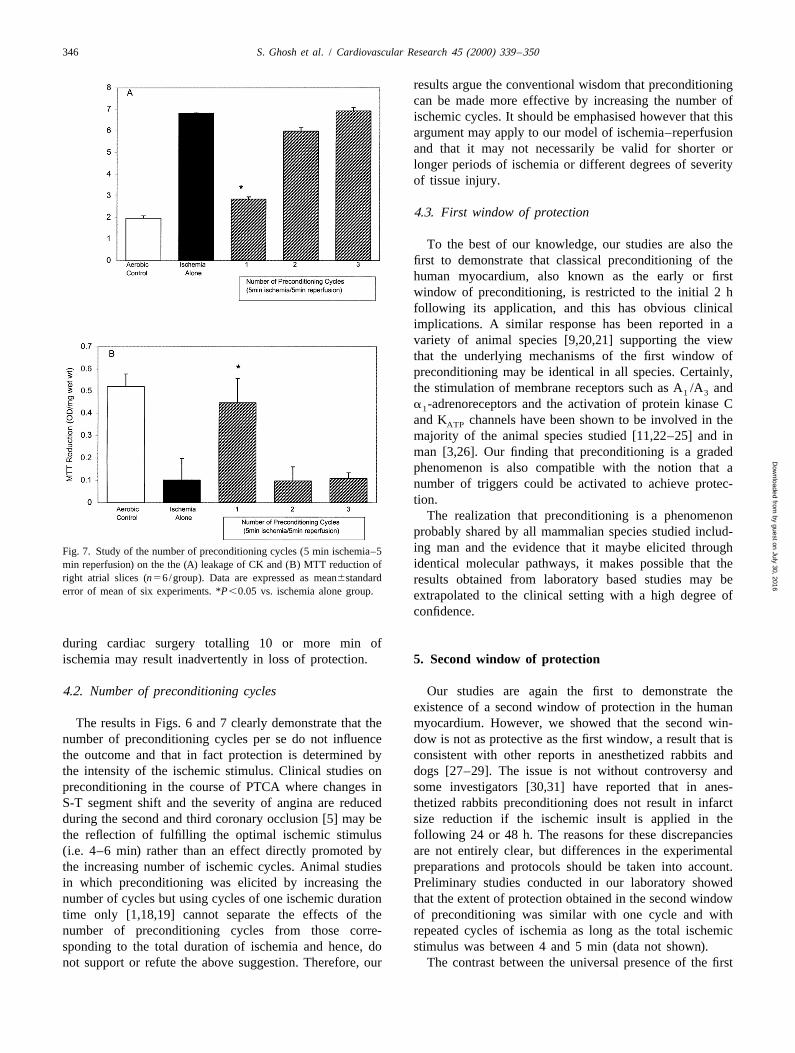
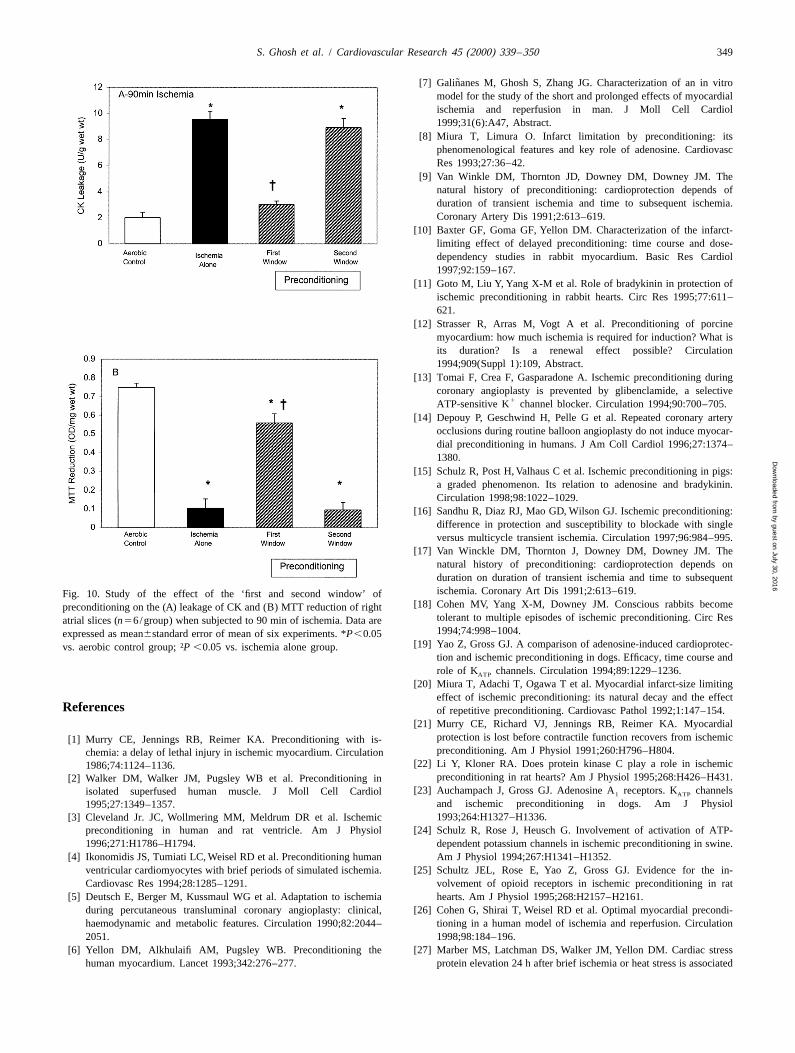
Fig. 7 shows the results on CK leakage and MTT protection gave a similar decrease in CK leakage andreduction of preconditioning with increasing numbers of amelioration of MTT reduction.cycles of 5 min ischemia–5 min reperfusion. Both CK As shown in Fig. 10, extension of the period of ischemialeakage and MTT reduction demonstrate clearly that to 90 min resulted in greater CK leakage and lower MTTprotection is lost beyond 5 min of ischemic precondition- reduction than with 30 min ischemia. As expected, the firsting. Overall these studies show that to precondition the window of preconditioning significantly improved CKhuman atrial myocardium the most important factor is the leakage and MTT reduction, however, this beneficial effecttotal ischemic stimulus and not the number of cycles. was not seen with the second window of preconditioning
and values were similar to those observed in the ischemiaalone group.
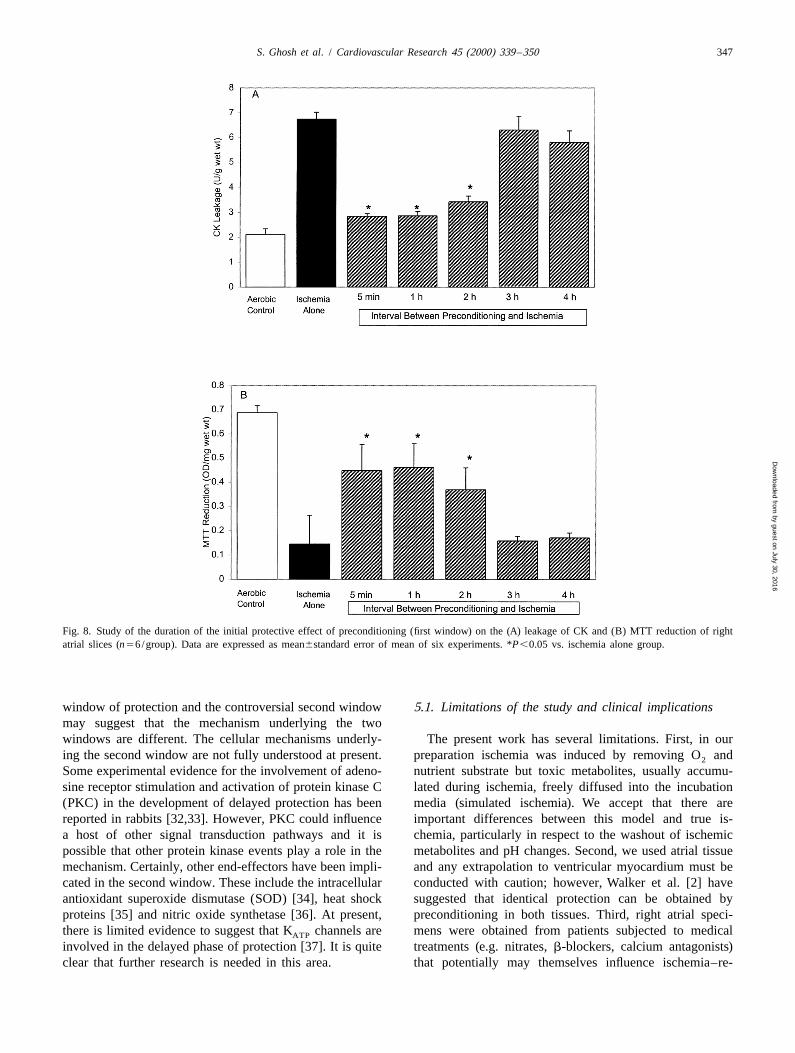
3.3. Study 3 — first window of protection
Fig. 8 shows the results on CK leakage and MTT 4. Discussionreduction when ischemic preconditioning of atrial myocar-dium is followed by various reperfusion periods before the The present studies have characterised the ischemic90 min ischemia and 120 min reperfusion. The results preconditioning phenomenon in the human myocardiumshow that the protection induced by preconditioning with and have disclosed the following important results: (i)only 5 min of reperfusion is maintained when the interval there is a graded narrow window of protection by pre-between the preconditioning and ischemia is within 2 h conditioning with 4–5 min of ischemia being the mostand that the beneficial effect is lost when that interval is effective period, (ii) the number of preconditioning cyclesextended to 3 or more hours. in itself does not influence protection, and ((iii) as shown
by guest on July 30, 2016D
ownloaded from
344 S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350
Fig. 4. Experimental protocols for Study 4. Right atrial slices in all groups (n56/group) were equilibrated for 30 min. In study 4A, after equilibration, theslices were aerobically incubated for 24 h. The ‘first window’ group were then preconditioned (IP) with 5 min ischemia–5 min reperfusion before beingsubjected to 30 min ischemia–120 min reperfusion. The ‘second window’ group were preconditioned initially with 5 min ischemia–5 min reperfusionbefore the 24 h incubation and then immediately subjected to 30 min ischemia–120 min reperfusion. In study 4B, identical protocols were applied exceptthe ischemic time was extended to 90 min.
in other animal species, there are two windows of protec- However, the loss of protection with ischemic periodstion, the first (#2 h) being more protective than the second beyond 6 min was unexpected since several investigators(24 h). These results have significant clinical implications have reported that 10 min of ischemia preconditions theand warrant further discussion. heart of a number of animal species [10–12].
The findings that 4–5 min of ischemia is the optimal4.1. Intensity of the preconditioning stimulus time for preconditioning is supported by studies performed
in the course of percutaneous transluminal coronary an-Our studies are the first to demonstrate that maximal gioplasty (PTCA) [13,14]. In these studies, coronary
protection of the human myocardium by ischemic pre- arteries are typically occluded for 2 min by balloonconditioning is obtained with an ischemic stimulus of 4–5 inflation with 5 min apart. Consistently in all studies themin. It was not surprising that shorter periods of ischemia severity of myocardial ischemia, assessed by changes inresulted in a decrease or loss protection since studies in S-T segment shifts and angina symptoms, are less duringanimals have shown that the ischemic period should be the second and third balloon inflation than during the firstgreater than 2 min to achieve protection [8,9]. inflation. This suggests that a total of 4–6 min of ischemic
by guest on July 30, 2016D
ownloaded from
S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350 345
Fig. 5. Study of the effect of the duration of the preconditioning ischemicstimulus on the (A) leakage of creatinine kinase (CK) and (B) MTTreduction of right atrial slices (n56/group). Data are expressed asmean6standard error of the mean of six experiments. *P,0.05 vs.
Fig. 6. Study of the number of preconditioning cycles (2 min ischemia–5ischemia alone group.min reperfusion) on the (A) leakage of CK and (B) MTT reduction ofright atrial slices (n56/group). Data are expressed as mean6standarderror of mean of six experiments. *P,0.05 vs. ischemia alone group.preconditioning also confers maximal protection in the
clinical setting.The present studies have also shown a dose–response tioning by repeated short periods of ischemia and reperfu-
effect in preconditioning the human myocardium so that sion may have resulted in wash-out of tissue adenosine andthe phenomenon should be identified as a graded rather that in fact adenosine may not have been raised sufficientlythan an all-or-nothing event. It is worth noting that the to reach the threshold of protection. If this is the case thentime window of protection was confined to a limited the mechanism of protection induced by repeated shortperiod, between 3 and 6 min of ischemia, and therefore ischemic cycles should involve the stimulation of receptorsstudies involving few ischemic times may give the false other than or in addition to adenosine receptors. Indeedimpression that preconditioning is an all-or-nothing phe- Goto et al. [11] has previously suggested that the thresholdnomenon. This thesis is supported by studies on anes- of protection by preconditioning can be obtained by thethetized pigs [15] and rabbits [16] where graded ischemia additive effect of the stimulation of several membranedetermined the extent of infarct size reduction. It is also receptors (i.e. adenosine receptors, a -adrenoreceptors,1
worth noting that our findings are in agreement with those bradykinin and opioid receptors).of Downey et al. [17] that preconditioning ischemia ,2 Another finding of our study that may have clinicalmin did not confer protection, indicating that precondition- implications is the loss of protection when the precondi-ing has a threshold somewhere between 2 and 5 min. Their tioning ischemic stimulus was extended to 10 min, a timeexplanation was that the threshold of protection reflects the that has been reported to elicit protection in several animalduration of ischemia required to build up adenosine levels species. Thus, if our results are extrapolated to clinicalto the point where adenosine receptors are adequately situations it is possible that repeated occlusions of apopulated. It should be mentioned however that precondi- coronary artery during PTCA or of the ascending aorta
by guest on July 30, 2016D
ownloaded from
346 S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350
results argue the conventional wisdom that preconditioningcan be made more effective by increasing the number ofischemic cycles. It should be emphasised however that thisargument may apply to our model of ischemia–reperfusionand that it may not necessarily be valid for shorter orlonger periods of ischemia or different degrees of severityof tissue injury.
4.3. First window of protection
To the best of our knowledge, our studies are also thefirst to demonstrate that classical preconditioning of thehuman myocardium, also known as the early or firstwindow of preconditioning, is restricted to the initial 2 hfollowing its application, and this has obvious clinicalimplications. A similar response has been reported in avariety of animal species [9,20,21] supporting the viewthat the underlying mechanisms of the first window ofpreconditioning may be identical in all species. Certainly,the stimulation of membrane receptors such as A /A and1 3
a -adrenoreceptors and the activation of protein kinase C1
and K channels have been shown to be involved in theATP
majority of the animal species studied [11,22–25] and inman [3,26]. Our finding that preconditioning is a gradedphenomenon is also compatible with the notion that anumber of triggers could be activated to achieve protec-tion.
The realization that preconditioning is a phenomenonprobably shared by all mammalian species studied includ-ing man and the evidence that it maybe elicited throughFig. 7. Study of the number of preconditioning cycles (5 min ischemia–5identical molecular pathways, it makes possible that themin reperfusion) on the the (A) leakage of CK and (B) MTT reduction of
right atrial slices (n56/group). Data are expressed as mean6standard results obtained from laboratory based studies may beerror of mean of six experiments. *P,0.05 vs. ischemia alone group. extrapolated to the clinical setting with a high degree of
confidence.
during cardiac surgery totalling 10 or more min ofischemia may result inadvertently in loss of protection. 5. Second window of protection
4.2. Number of preconditioning cycles Our studies are again the first to demonstrate theexistence of a second window of protection in the human
The results in Figs. 6 and 7 clearly demonstrate that the myocardium. However, we showed that the second win-number of preconditioning cycles per se do not influence dow is not as protective as the first window, a result that isthe outcome and that in fact protection is determined by consistent with other reports in anesthetized rabbits andthe intensity of the ischemic stimulus. Clinical studies on dogs [27–29]. The issue is not without controversy andpreconditioning in the course of PTCA where changes in some investigators [30,31] have reported that in anes-S-T segment shift and the severity of angina are reduced thetized rabbits preconditioning does not result in infarctduring the second and third coronary occlusion [5] may be size reduction if the ischemic insult is applied in thethe reflection of fulfilling the optimal ischemic stimulus following 24 or 48 h. The reasons for these discrepancies(i.e. 4–6 min) rather than an effect directly promoted by are not entirely clear, but differences in the experimentalthe increasing number of ischemic cycles. Animal studies preparations and protocols should be taken into account.in which preconditioning was elicited by increasing the Preliminary studies conducted in our laboratory showednumber of cycles but using cycles of one ischemic duration that the extent of protection obtained in the second windowtime only [1,18,19] cannot separate the effects of the of preconditioning was similar with one cycle and withnumber of preconditioning cycles from those corre- repeated cycles of ischemia as long as the total ischemicsponding to the total duration of ischemia and hence, do stimulus was between 4 and 5 min (data not shown).not support or refute the above suggestion. Therefore, our The contrast between the universal presence of the first
by guest on July 30, 2016D
ownloaded from
S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350 347
Fig. 8. Study of the duration of the initial protective effect of preconditioning (first window) on the (A) leakage of CK and (B) MTT reduction of rightatrial slices (n56/group). Data are expressed as mean6standard error of mean of six experiments. *P,0.05 vs. ischemia alone group.
window of protection and the controversial second window 5.1. Limitations of the study and clinical implicationsmay suggest that the mechanism underlying the twowindows are different. The cellular mechanisms underly- The present work has several limitations. First, in ouring the second window are not fully understood at present. preparation ischemia was induced by removing O and2
Some experimental evidence for the involvement of adeno- nutrient substrate but toxic metabolites, usually accumu-sine receptor stimulation and activation of protein kinase C lated during ischemia, freely diffused into the incubation(PKC) in the development of delayed protection has been media (simulated ischemia). We accept that there arereported in rabbits [32,33]. However, PKC could influence important differences between this model and true is-a host of other signal transduction pathways and it is chemia, particularly in respect to the washout of ischemicpossible that other protein kinase events play a role in the metabolites and pH changes. Second, we used atrial tissuemechanism. Certainly, other end-effectors have been impli- and any extrapolation to ventricular myocardium must becated in the second window. These include the intracellular conducted with caution; however, Walker et al. [2] haveantioxidant superoxide dismutase (SOD) [34], heat shock suggested that identical protection can be obtained byproteins [35] and nitric oxide synthetase [36]. At present, preconditioning in both tissues. Third, right atrial speci-there is limited evidence to suggest that K channels are mens were obtained from patients subjected to medicalATP
involved in the delayed phase of protection [37]. It is quite treatments (e.g. nitrates, b-blockers, calcium antagonists)clear that further research is needed in this area. that potentially may themselves influence ischemia–re-
by guest on July 30, 2016D
ownloaded from
348 S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350
Fig. 9. Study of the effect of the ‘first and second window’ of preconditioning on the (A) leakage of CK and (B) MTT reduction of right atrial slices(n56/group) when subjected to 30 min of ischemia. Data are expressed as mean6standard error of mean of six experiments. *P,0.05 vs. aerobic controlgroup; †P,0.05 vs. ischemia alone group.
perfusion injury and the protection induced by precondi- extended beyond 5 min. We also have shown that thetioning. Fourth, our model is an in vitro preparation and second window of protection by preconditioning is not asthe results may not completely apply to the clinical setting, effective as the first window and that this may lessen itsalthough the findings during coronary artery occlusion in relevance as a potential therapeutical intervention. How-the course of PTCA may suggest that protection by ever, further studies may be required to confirm this latterpreconditioning can be achieved with similar protocols in finding.both situations.
Our results have important clinical implications byrevealing that the duration of the ischemic stimulus rather Acknowledgementsthan the number of cycles is the most important elementinfluencing myocardial protection by preconditioning. Fur- This study was supported in part by grants from Thethermore, this protection is a graded phenomenon with Wellcome Trust, British Heart Foundation, Link-upmaximal benefit with 4–5 min ischemic duration and Charities, Glenfield Hospital NHS Trust, Rhone-Poulencreduction or loss of protection if the ischemic stimulus is Rorer (UK) and the University of Leicester.
by guest on July 30, 2016D
ownloaded from
S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350 349
˜[7] Galinanes M, Ghosh S, Zhang JG. Characterization of an in vitromodel for the study of the short and prolonged effects of myocardialischemia and reperfusion in man. J Moll Cell Cardiol1999;31(6):A47, Abstract.
[8] Miura T, Limura O. Infarct limitation by preconditioning: itsphenomenological features and key role of adenosine. CardiovascRes 1993;27:36–42.
[9] Van Winkle DM, Thornton JD, Downey DM, Downey JM. Thenatural history of preconditioning: cardioprotection depends ofduration of transient ischemia and time to subsequent ischemia.Coronary Artery Dis 1991;2:613–619.
[10] Baxter GF, Goma GF, Yellon DM. Characterization of the infarct-limiting effect of delayed preconditioning: time course and dose-dependency studies in rabbit myocardium. Basic Res Cardiol1997;92:159–167.
[11] Goto M, Liu Y, Yang X-M et al. Role of bradykinin in protection ofischemic preconditioning in rabbit hearts. Circ Res 1995;77:611–621.
[12] Strasser R, Arras M, Vogt A et al. Preconditioning of porcinemyocardium: how much ischemia is required for induction? What isits duration? Is a renewal effect possible? Circulation1994;909(Suppl 1):109, Abstract.
[13] Tomai F, Crea F, Gasparadone A. Ischemic preconditioning duringcoronary angioplasty is prevented by glibenclamide, a selective
1ATP-sensitive K channel blocker. Circulation 1994;90:700–705.[14] Depouy P, Geschwind H, Pelle G et al. Repeated coronary artery
occlusions during routine balloon angioplasty do not induce myocar-dial preconditioning in humans. J Am Coll Cardiol 1996;27:1374–1380.
[15] Schulz R, Post H, Valhaus C et al. Ischemic preconditioning in pigs:a graded phenomenon. Its relation to adenosine and bradykinin.Circulation 1998;98:1022–1029.
[16] Sandhu R, Diaz RJ, Mao GD, Wilson GJ. Ischemic preconditioning:difference in protection and susceptibility to blockade with singleversus multicycle transient ischemia. Circulation 1997;96:984–995.
[17] Van Winckle DM, Thornton J, Downey DM, Downey JM. Thenatural history of preconditioning: cardioprotection depends onduration on duration of transient ischemia and time to subsequentischemia. Coronary Art Dis 1991;2:613–619.Fig. 10. Study of the effect of the ‘first and second window’ of
[18] Cohen MV, Yang X-M, Downey JM. Conscious rabbits becomepreconditioning on the (A) leakage of CK and (B) MTT reduction of righttolerant to multiple episodes of ischemic preconditioning. Circ Resatrial slices (n56/group) when subjected to 90 min of ischemia. Data are1994;74:998–1004.expressed as mean6standard error of mean of six experiments. *P,0.05
[19] Yao Z, Gross GJ. A comparison of adenosine-induced cardioprotec-vs. aerobic control group; †P,0.05 vs. ischemia alone group.tion and ischemic preconditioning in dogs. Efficacy, time course androle of K channels. Circulation 1994;89:1229–1236.ATP
[20] Miura T, Adachi T, Ogawa T et al. Myocardial infarct-size limitingeffect of ischemic preconditioning: its natural decay and the effect
References of repetitive preconditioning. Cardiovasc Pathol 1992;1:147–154.[21] Murry CE, Richard VJ, Jennings RB, Reimer KA. Myocardial
protection is lost before contractile function recovers from ischemic[1] Murry CE, Jennings RB, Reimer KA. Preconditioning with is-preconditioning. Am J Physiol 1991;260:H796–H804.chemia: a delay of lethal injury in ischemic myocardium. Circulation
[22] Li Y, Kloner RA. Does protein kinase C play a role in ischemic1986;74:1124–1136.preconditioning in rat hearts? Am J Physiol 1995;268:H426–H431.[2] Walker DM, Walker JM, Pugsley WB et al. Preconditioning in
[23] Auchampach J, Gross GJ. Adenosine A receptors. K channelsisolated superfused human muscle. J Moll Cell Cardiol 1 ATP
and ischemic preconditioning in dogs. Am J Physiol1995;27:1349–1357.1993;264:H1327–H1336.[3] Cleveland Jr. JC, Wollmering MM, Meldrum DR et al. Ischemic
preconditioning in human and rat ventricle. Am J Physiol [24] Schulz R, Rose J, Heusch G. Involvement of activation of ATP-1996;271:H1786–H1794. dependent potassium channels in ischemic preconditioning in swine.
[4] Ikonomidis JS, Tumiati LC, Weisel RD et al. Preconditioning human Am J Physiol 1994;267:H1341–H1352.ventricular cardiomyocytes with brief periods of simulated ischemia. [25] Schultz JEL, Rose E, Yao Z, Gross GJ. Evidence for the in-Cardiovasc Res 1994;28:1285–1291. volvement of opioid receptors in ischemic preconditioning in rat
[5] Deutsch E, Berger M, Kussmaul WG et al. Adaptation to ischemia hearts. Am J Physiol 1995;268:H2157–H2161.during percutaneous transluminal coronary angioplasty: clinical, [26] Cohen G, Shirai T, Weisel RD et al. Optimal myocardial precondi-haemodynamic and metabolic features. Circulation 1990;82:2044– tioning in a human model of ischemia and reperfusion. Circulation2051. 1998;98:184–196.
[6] Yellon DM, Alkhulaifi AM, Pugsley WB. Preconditioning the [27] Marber MS, Latchman DS, Walker JM, Yellon DM. Cardiac stresshuman myocardium. Lancet 1993;342:276–277. protein elevation 24 h after brief ischemia or heat stress is associated
by guest on July 30, 2016D
ownloaded from

350 S. Ghosh et al. / Cardiovascular Research 45 (2000) 339 –350
with resistance to myocardial infarction. Circulation 1993;88:1264– [33] Baxter GF, Mocanu M, Yellon DM. Diacylglycerol treatment in vivo1272. increases ischemic tolerance 24 h later in a rabbit model of
[28] Kuzuya T, Hoshida S, Yamashita N et al. Delayed effects of myocardial infarction. J Moll Cell Cardiol 1996;28:A19.sublethal ischemia on the acquisition of tolerance to ischemia. Circ [34] Yamashita N, Nishida M, Hoshida S. Induction of manganeseRes 1993;72:1293–1299. superoxide dismutase in rat cardiac myocytes increases tolerance to
[29] Yang X-M, Baxter GF, Heads RJ et al. Infarct limitation in the hypoxia 24 h after preconditioning. J Clin Invest 1994;94:2193–second window of protection in a conscious rabbit model. Cardivasc 2199.Res 1996;31:777–783. [35] Yellon DM, Marber MS. Hsp 70 in myocardial ischemia. Ex-
[30] Tanaka M, Fujiwara H, Yamasaki K et al. Ischemic preconditioning perimentia 1994;50:1075–1084.elevates cardiac stress protein but does not limit infarct size 24 h or [36] Parratt JR, Szekeres L. Delayed protection of the heart against48 h later in rabbit hearts. Am J Physiol 1994;267:H1476–H1482. ischemia. Trends Pharmacol Sci 1995;16:351–355.
[31] Qian YZ, Bernado NL, Nayeem MA et al. Induction of 72-kDa heat [37] Fryer RM, Hsu AK, Eells JT et al. Opioid-induced second windowshock protein does not produce a second window of ischemic of cardioprotection. Potential role of mitochondrial K channels.ATP
preconditioning in rat heart. Am J Physiol 1999;276:H224–H234. Circ Res 1999;84:846–851.[32] Baxter GF, Goma FM, Yellon DM. Involvement of protein kinase C
in the delayed cytoprotection following sublethal ischemia in rabbitmyocardium. Br J Pharmacol 1995;115:222–224.
by guest on July 30, 2016D
ownloaded from
Copyright © 2022 FDOKUMEN




















