
Pre-analysis plan Evaluation of Gram Varta in rural Bihar - 3ie
28
Appendix 7: Pre-analysis plan Evaluation of Gram Varta in rural Bihar – A mixed methods study Analysis plan Christian Bommer 1 , Malavika Subramanyam 2 , Sebastian Vollmer 1,3 October 13, 2015 1 Georg-August University Göttingen 2 IIT Gandhinagar 3 Harvard T.H. Chan School of Public Health
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Pre-analysis plan Evaluation of Gram Varta in rural Bihar - 3ie

Appendix 7: Pre-analysis plan
Evaluation of Gram Varta in rural Bihar – A mixed methods study
Analysis plan
Christian Bommer1, Malavika Subramanyam2, Sebastian Vollmer1,3
October 13, 2015
1Georg-August University Göttingen
2IIT Gandhinagar
3Harvard T.H. Chan School of Public Health
Table of contents
1. Introduction ..................................................................................................................................... 3
2. Description of the Intervention ....................................................................................................... 3
3. Experimental Design ........................................................................................................................ 3
3.1. Sample selection...................................................................................................................... 4
3.2. Treatment assignment ............................................................................................................ 4
4. Data Sources .................................................................................................................................... 5
5. Hypotheses ...................................................................................................................................... 7
6. Methodology ................................................................................................................................. 10
6.1. Estimation of intention-to-treat effects ................................................................................ 11
6.2. Treatment intensity ............................................................................................................... 12
6.3. Subgroup analyses ................................................................................................................. 13
6.4. Spill-over effects .................................................................................................................... 13
6.5. Qualitative analysis................................................................................................................ 13
3
1. Introduction
This pre-analysis plan outlines the main hypotheses about the short-term effects of the Gram Varta
program and specifies the methodologies to be employed in testing them. Gram Varta is a novel
health intervention currently being implemented in rural Bihar, India, building on local women’s Self
Health Groups (SHG) in order to improve health, nutrition, water, sanitation, and hygiene (HNWASH)
knowledge and practices by fostering female empowerment and community solidarity. The impact
evaluation will only deviate from the pre-analysis plan in case of unforeseen events which justify
amendments.
Section 2 of this document describes the intervention in more detail and Section 3 discusses the
study design employed for the evaluation. Section 4 then provides an overview of the different
questionnaires used to obtain the relevant information. Section 5 lists the hypotheses and Section 6
outlines the methodologies used in assessing them.
2. Description of the Intervention
Gram Varta was piloted in 2011 in Bihar and has been gradually expanded within the state since
then. It is implemented through village-based women’s self-help groups (SHG) affiliated with
Women’s Development Corporation, Jeevika and Mahila Samakhya, and relies on a participatory
learning and action (PLA) approach. The evaluation accompanies the program implementation in
Madhepura, Bihar, which was started in August 2015 and is expected to be completed in July 2016.
The core of the intervention is a cycle of 20 pre-structured meetings. A few SHG members are
selected and trained in facilitating these PLA meetings. Each facilitator invites the other SHG
members and the entire village population to participate in the meetings. The facilitator uses games,
stories and activities to bring the women together, enhance women’s sense of agency, and change
their attitude towards working together, service utilization as well as indirectly impact their HNWASH
knowledge and practices. Participants are encouraged to think critically, identify problems in their
households and communities and discuss how HNWASH practices could be improved. Pregnant
women, adolescent girls and children under the age of five are of special interest. This process
includes at least two meetings with the entire community including local authorities and service
providers. The identified problems and solutions are discussed and a community action plan is
formulated. Monitoring progress towards meeting pre-set goals is also a part of Gram Varta.
3. Experimental Design
The impact evaluation of the Gram Varta Program combines a randomized design with a difference-
in-differences approach in order to identify causal effects on maternal and child health, HNWASH
indicators, demand for services as well as female empowerment. It will incorporate both qualitative
and quantitative information, facilitating the understanding of possible channels of change which will
help to explain the presence or absence of certain effects. The following two subsections provide a
short outline of the sampling strategy and the treatment assignment.
4
3.1. Sample selection
As mentioned above, the evaluation of Gram Varta analyzes the program effects in Madhepura. The
district is divided into thirteen blocks comprising a total of 443 gram panchayats. However, given
that Gram Varta is implemented in only six of these thirteen blocks and due to budgetary constraints,
we restricted the sample to 68 gram panchayats, each of which contained about 2.6 villages on
average. This left us with a total of 180 villages. When the enumerators reached the villages, they
talked to local residents as well as the gram panchayat head (Mukhiya) and roughly mapped out the
different hamlets (tolas) in the village which were based on caste in most cases. They also inquired
the number of households in each hamlet. We planned to sample 22 households per village. Based
on the total households in the entire village and the number of households in the different hamlets,
enumerators arrived at the number of households in each hamlet they needed to interview given our
sample size calculations. The number of houses per hamlet was proportional to the total number of
houses each hamlet contained in comparison with the total number of households in the entire
village (probability proportional to size of hamlet).
Once the enumerators calculated how many houses they needed to sample in each hamlet (n), and
the total number of houses in that hamlet (N), they randomly picked the first house (ninth household
from the public facility in the hamlet) and then chose every ninth house. Once they reached the
house, they selected the head of the household for the "main" survey. If the head was not available,
they talked to the adults available at home and picked one adult who seemed to have the
information about the household. After getting information from the head of the household, they
interviewed a woman in the household who is in the 15-49 age group and had the youngest child in
the household, compared to all other women in a similar age group in the household. If no such
woman was available, they interviewed the woman with the next older child and so on. Questions to
adolescent girls (all available adolescent girls in the family) and measurement of height, weight,
hemoglobin as well as stool tests were performed by the female enumerator who visited the same
house the next day. Moreover, pregnant women were oversampled, given that the share of this
group would have been too low in the household sample to achieve sufficient statistical power.
Listing of women who are currently pregnant was done using information obtained from Anganwadi
workers.
3.2. Treatment assignment
To be able to estimate causal effects, we randomly assigned Gram Varta participation. The
randomization process took place on the gram panchayat level and, in order to maximize precision,
we stratified by block. To this end, we first listed all gram panchayat in our study area together with
the block they belonged to. Afterwards, we randomly assigned participation in Gram Varta to gram
panchayats separately by block with a probability of 50%. An alternative strategy involving pair-wise
matching of blocks and treatment assignment on the block level was rejected as census data
revealed a substantial heterogeneity between blocks. Our randomization approach left us with 34
gram panchayats, 90 villages and 1,973 households in the treatment group, while the control group
comprises 34 gram panchayats, 90 villages and 1,980 households. Moreover, the pregnant women
sample contains 1,234 subjects in the treatment group and 766 subjects in the control group.
5
4. Data Sources
We plan to collect data thrice:
Baseline survey prior to Gram Varta implementation.
Small midline survey while the Gram Varta meeting cycle is still ongoing.
End-line after Gram Varta ends.
The differences in changes from baseline to end-line between treatment and control will show us the
causal effects of Gram Varta, while the midline survey will facilitate the monitoring of process
indicators. Given our mixed-method approach, the survey comprises both quantitative and
qualitative elements. For the quantitative part, trained enumerators from the local area will conduct
household and individual interviews guided by pre-coded paper questionnaires developed to
measure process, outcome and impact indicators. Specifically, the following modules will be
administered:
1. Household questionnaire, 1st part (respondent is any adult household member):
For each sampled household a roster to record demographic information and health indicators of
all household members.
2. Household questionnaire, 2nd part (respondents are women and adolescent girls in the
household): This questionnaire will be concerned with women, adolescent girls and child health
and nutrition indicators. We will collect blood and stool samples and anthropometric data from
children.
3. Household questionnaire, 3rd part (respondent is a woman in the household):
This part will contain sections on outcomes (e.g. general HNWASH practices in the household,
related attitudes, beliefs and knowledge, perceived social norms, HNWASH related consumption
behavior) and enabling context (e.g. economic situation of household). Gram Varta participation
and potential obstacles to participation (only treatment group) as well as indicators related to
mediators such as speaking up in groups, a sense of empowerment, critical-thinking, feeling of
community cohesion or even tension, trust in service providers.
4. Pregnant women questionnaire:
A questionnaire for pregnant women will collect data on knowledge, beliefs, social norms and
practices relevant to pregnancy, child birth, and the post-natal period. We will collect blood
samples from these women. In the follow-up we will collect data on the women who were
pregnant at baseline and their newborns as well as newly pregnant women.
5. Facilitator questionnaire:
We will collect data from Gram Varta facilitators on participation of all target groups in meetings
(pregnant women, adolescent girls, marginalized women) and other process indicators (meetings
were implemented as scheduled, any complications, whether frontline workers, men and elderly
participated, which problems were identified and prioritized on the village level, details on the
community action plan, etc.).
6
6. Anganwadi worker questionnaire:
We will collect data from the Anganwadi worker on indicators of service use.
To provide an idea of the impact of Gram Varta in Madhepura as well as other districts of Bihar,
survey information will be further complemented by an analysis of secondary data. We will use
available data from Gram Varta MIS, other sources such as the census, AHS, the concurrent
monitoring survey being conducted by B TAST, and other surveys; routine data collected at
Anganwadi centers; as well as relevant observations from enumerators such as evidence of open
defecation in the village, availability of soaps in households, and method of drinking water storage.
These data will be analyzed quantitatively to investigate differences between treatment and
counterfactual areas, using appropriate statistical techniques for quasi-experimental studies.
For the qualitative part of the analysis we will be guided by the qualitative expert, Dr. Rosa Perez,
and women’s empowerment expert, Dr. Manisha Joshi, and plan to employ researchers experienced
in the use of qualitative inquiry in the Indian context. The underlying goal will continue to be to
inquire what the impact of Gram Varta is and how exactly this impact occurs. However, the
qualitative approach will focus on understanding it in a deeper manner, giving more importance to
understanding what the experience of Gram Varta participation means (to participants/facilitators/
community members/front-line workers), and the various ways it may have affected the lives of
participants as well as community members. The process of change will be of special focus. The
choice of methods will depend on what is appropriate in a given context, but will include participant
observation, key informant interviews, focus groups, in-depth interviews, participatory games, and
others.
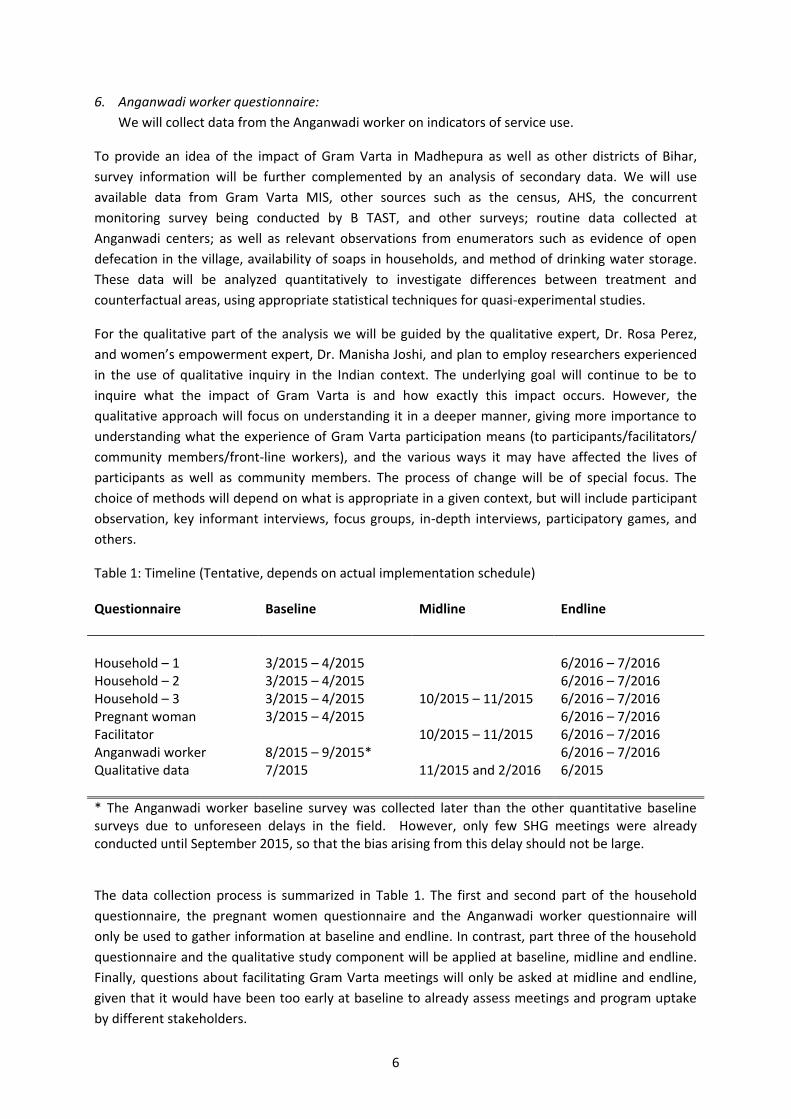
Table 1: Timeline (Tentative, depends on actual implementation schedule) Questionnaire Baseline Midline Endline
Household – 1 3/2015 – 4/2015 6/2016 – 7/2016 Household – 2 3/2015 – 4/2015 6/2016 – 7/2016 Household – 3 3/2015 – 4/2015 10/2015 – 11/2015 6/2016 – 7/2016 Pregnant woman 3/2015 – 4/2015 6/2016 – 7/2016 Facilitator 10/2015 – 11/2015 6/2016 – 7/2016 Anganwadi worker 8/2015 – 9/2015* 6/2016 – 7/2016 Qualitative data 7/2015 11/2015 and 2/2016 6/2015
* The Anganwadi worker baseline survey was collected later than the other quantitative baseline surveys due to unforeseen delays in the field. However, only few SHG meetings were already conducted until September 2015, so that the bias arising from this delay should not be large.
The data collection process is summarized in Table 1. The first and second part of the household
questionnaire, the pregnant women questionnaire and the Anganwadi worker questionnaire will
only be used to gather information at baseline and endline. In contrast, part three of the household
questionnaire and the qualitative study component will be applied at baseline, midline and endline.
Finally, questions about facilitating Gram Varta meetings will only be asked at midline and endline,
given that it would have been too early at baseline to already assess meetings and program uptake
by different stakeholders.

7
5. Hypotheses
Group 1: Women’s self-help groups
Women’s self-help groups (SHG) are at the center of the Gram Varta program. One part of our
analysis will therefore focus on the processes happening within SHG groups and look at the
interaction of SHG members with the community. To this end, we will use indicators acquired from
the facilitator surveys at midline and endline. Specifically, we will test the following eight hypotheses:
H1: Gram Varta improves participation in SHG meetings.
H2: Gram Varta increases SHG acceptance in and cooperation with community.
H3: Gram Varta improves provision of information on health practices within SHG.
H4: Gram Varta improves provision of health finance information and practices within SHG.
H5: Gram Varta improves awareness and usage of government health services by SHG members.
H6: Gram Varta improves frequency of promoting enrolment to VO nutrition center
H7: Gram Varta improves awareness and usage of VO nutrition centers by SHG members.
H8: Gram Varta improves facilitators' health knowledge.
H9: Gram Varta improves facilitators' opinion on their work.
Group 2: Women's agency and empowerment
Next, we will look at Gram Varta's effect on women's agency and empowerment. The ways in which
the program may impact women's standing in the family and community are manifold. First, we
anticipate that the participatory learning approach will encourage self-help group members to think
more critically and to question societal standards as well as make them more comfortable at voicing
their opinion in public. Second, adolescent girls will indirectly benefit from their mothers'
involvement and develop a stronger self-esteem and a more positive outlook on their future. Lastly,
we expect that the involvement of men in some SHG sessions will also increase the willingness of
husbands to support their wives and to rethink cultural standards. The indicators which will be used
to test the following hypotheses are taken from the household surveys and pregnant women
surveys.
H10: Gram Varta encourages women to acquire paid work and to become economically more
independent.
H11: Gram Varta increases women's bargaining power within the household.
H12: Gram Varta enables women to become more independent of their husbands.
H13: Gram Varta enables women to develop an identity of their own.
H14: Gram Varta increases women's involvement in the community.
8
H15: Gram Varta makes women become more comfortable at speaking out in public.
H16: Gram Varta makes self-confident when it comes to refusing sexual intercourse with husband or
demanding him to use a condom.
H17: Gram Varta reduces women's acceptance of domestic violence.
H18: Gram Varta reduces the practice of domestic violence and oppression.
H19: Gram Varta gives adolescent girls a more positive outlook on their future.
H20: Gram Varta reduces adolescent girls' preferred number of children.
H21: Gram Varta decreases women's preference for sons.
H22: Gram Varta makes it more likely that women desire a higher age at marriage for themselves or
their daughters.
H23: Gram Varta reduces the likelihood of early pregnancies.
H24: Gram Varta improves attitudes towards and practices of care for daughters.
H25: Gram Varta makes adolescent girls more confident to cook for themselves in order to take care
of their own nutrition.
H26: Gram Varta increases husbands' support for their wives' SHG membership.
Group 3: HNWASH knowledge and practices
The key element of Gram Varta is the uptake of health knowledge among SHG members through the
use of participatory learning methods. In order to evaluate the program's success, it is hence crucial
to look at the development of HNWASH knowledge and practices in SHG and the community. We
expect households and pregnant women in treatment areas to exhibit a better understanding of
basic issues in health, hygiene and nutrition as well as to implement their knowledge through the use
of proper practices. The indicators we will use to test our hypotheses in this section will be taken
from the household and pregnant women surveys.
H27: Gram Varta increases the intake of micronutrients.
H28: Gram Varta raises awareness of importance of balanced diet for family.
H29: Gram Varta improves knowledge and attitudes toward proper feeding of newborns.
H30: Gram Varta encourages parents to prevent diseases in children, e.g. through vaccinations and
bednets.
H31: Gram Varta reduces risky consumption behavior (tobacco/alcohol).
H32: Gram Varta improves domestic storage and treatment of water.
H33: Gram Varta improves domestic hygiene (hand-washing/use of toilets).

9
H34: Gram Varta increases women's awareness about infectious diseases such as malaria.
H35: Gram Varta improves adolescent girls' and women's knowledge about sexuality and
contraception.
Group 4: Pregnancy
An important group of beneficiaries of Gram Varta are pregnant women, given that their health
knowledge and practices do not only affect themselves but also the health of their unborn children.
This group of hypotheses will therefore in particular look at pregnant women's behavior during
pregnancy as well as antenatal care.
H36: Gram Varta encourages pregnant women to be mindful of their health, to take healthy and
sufficient diet, to avoid stress and to avoid health risks.
H37: Gram Varta increases the frequency of antenatal care visits as well as their quality.
H38: Gram Varta increases support to pregnant women for obtaining antenatal care.
H39: Gram Varta increases pregnant women's satisfaction with antenatal care.
H40: Gram Varta encourages women to accept their pregnancy, making them more optimistic about
their situation.
H41: Gram Varta raises awareness and understanding of abortions among pregnant women.
Group 5: Anganwadi centers
An important part of the intervention is the participation of local service providers in selected SHG
meetings. We expect that these meetings will improve the health knowledge of Anganwadi workers
and increase the quality of offered services. To assess the following hypotheses, we will make mainly
use of data collected directly from local Anganwadi workers.
H42: Gram Varta increases use of Anganwadi health centers.
H43: Gram Varta improves malnutrition treatment and prevention.
H44: Gram Varta improves the quality of child weighing practices.
H45: Gram Varta improves the cleanliness of and hygiene practices at the Anganwadi center.
H46: Gram Varta improves quality of work and activities related to preschool children.
H47: Gram Varta improves counseling for pregnant and lactating women.
H48: Gram Varta improves postnatal care.
H49: Gram Varta improves Anganwadi workers' health knowledge.
H50: Gram Varta improves immunization practices.
10
H51: Gram Varta improves facilitation of routine check-ups.
H52: Gram Varta increases job satisfaction of Anganwadi workers.
H53: Gram Varta improves participation of Anganwadi workers in community health events.
H54: Gram Varta improves perception of and respect for Anganwadi workers by community.
Group 6: Health outcomes
Provided that Gram Varta is successful in improving health knowledge and services as well as in
altering health-related behavior, we expect to see some mild improvements in the health status of
women, men and children at endline. For instance, improved iron intake due to nutritional training is
expected to improve hemoglobin levels in subjects, provided that they are anemic. To assess
whether this is true, we will use a mix of verbal autopsy data and anthropometric measures from the
household and pregnant women surveys.
H55: Gram Varta improves women's health.
H56: Gram Varta improves husbands' health.
H57: Gram Varta improves child health.
Group 7: Social cohesion
Lastly, we expect Gram Varta to strengthen the general social relationships within the community. To
test our related hypotheses, we will make use of indicators collected in the household surveys.
H58: Gram Varta increase mutual trust within the community.
H59: Gram Varta reduces tensions in the neighbourhood.
A detailed overview of all hypotheses and indicators is given in Appendix Table A1. For each
indicator, we provide the data source, the format of the data and the anticipated direction of the
effect.
6. Methodology
The estimation methods we plan to use depend on the format of the indicators which form the basis
for the hypotheses tests. Integer and real variables will be analyzed using ordinary least squares.
However, the majority of indicators is based on binary data and requires the use of more
sophisticated methods, as linear probability models are inefficient and may lead to unrealistic
predictions. We therefore plan to model the probability that a binary indicator equals one as a
logistic function which will guarantee predictions within the [0,1] interval. Moreover, in some cases,
indicators are coded on an ordinal scale, requiring the use ordered logit models since linear models

11
would implicitly assume that the data are defined on a cardinal rather than ordinal scale. Standard
errors will be clustered on the ID-level (i.e. household head, pregnant woman, Anganwadi worker
etc., depending on the context) in order to account for serial correlation and heteroscedasticity, and
on the village-level to reflect the multi-level sampling design.1,2
Given that not all self-help group members necessarily attend and participate in every meeting,
comparing treated and not treated gram panchayats will provide an estimate for the effect of the
intention to treat rather than the treatment itself. In other words, we would not measure the effect
of participatory learning in self-help groups, but rather the effect of offering it. Since voluntary
participation is a key element of these groups, we believe that the intention-to-treat effect will be
more interesting to policy makers than the treatment effect on the treated and the main emphasis of
our analysis will hence be on the effect of program assignment. Nevertheless, it will be useful to take
a closer look at the extent to which the treatment effects vary depending on the number of meetings
SHG group members have attended, as this will provide us with information on the effect of
treatment intensity and allow us to assess whether there are decreasing marginal returns to holding
additional meetings. Additionally, we plan to investigate spill-over effects of Gram Varta membership
on non-participating households in treatment areas and heterogeneous intention-to-treat effects
depending on a range of individual and household characteristics, such as caste, age and poverty.
By virtue of random assignment of the intervention, a simple comparison of post-intervention
outcomes between treated and non-treated gram panchayats will on average provide us with the
correct intention-to-treat effect. Nevertheless, it is possible that imbalances between the treatment
and control group in our experiment regarding observable or unobservable characteristics occur by
chance, leading to selection bias. We will thus exploit the panel-structure of our study and employ a
difference-in-differences approach in order to control for baseline differences and a common time
trend. In order to further reduce potential bias, we also control for a range of observable individual
and household characteristics, such as socioeconomic status. This will also have the side effect of
increasing the precision of our estimate even if our controls are uncorrelated to treatment
assignment but correlated to the outcome since the share of unexplained variation in the outcome
will decline. The following subsections provide a description of the main elements of our analysis.
6.1. Estimation of intention-to-treat effects
The main analysis of our evaluation will test the hypotheses outlined in Section 5 by an intention-to-
treat analysis. As illustrated in Table 1, some surveys are collected at baseline, midline and endline,
while other surveys are either only collected at baseline and endline or at midline and endline. In
case the data is collected thrice and assuming that the outcome variable is cardinal, the analysis will
have the following form:
𝑌𝑖𝑔𝑡 = 𝛾𝑖 + 𝜆𝑡 + 𝛽1𝐷𝑔1 + 𝛽2𝐷𝑔2 + 𝑋𝑖𝑔𝑡𝛿 + 휀𝑖𝑔𝑡 (1)
1 While efficiency gains might be realized by using a random effects (RE) model instead, the underlying assumptions about RE are very restrictive and unlikely to be fulfilled in the setting of our study. 2 As the number of hypotheses we intend to test is high, we will investigate the robustness of our inference by applying the Benjamini-Hochberg correction for multiple hypotheses tests.

12
where 𝑌𝑖𝑔𝑡 is the outcome for unit i (e.g. pregnant woman/household head/Anganwadi) in gram
panchayat g at time t, with 𝑡 = 0 at baseline, 𝑡 = 1 at midline and 𝑡 = 2 at endline. 𝛾𝑖 and 𝜆𝑡 are
unit-level and time fixed effects, respectively, where 𝜆0 = 0. 𝐷𝑔1 and 𝐷𝑔2 are dummy variables that
equal 1 if the data comes from midline or endline, respectively, and gram panchayat g was assigned
to the treatment group. The corresponding coefficients 𝛽1 and 𝛽2 will therefore estimate the
intention-to-treat effects at midline and endline, taking the outcomes at baseline as reference
values. Moreover, 𝛿 is a vector of coefficients, capturing the contribution of a range of control
variables.
If only two time periods are available, equation 1 simplifies to:
𝑌𝑖𝑔𝑡 = 𝛾𝑖 + 𝜆𝑡 + 𝛽1𝐷𝑔1 + 𝑋𝑖𝑔𝑡𝛿 + 휀𝑖𝑔𝑡 (2)
with 𝑡 = 0 at baseline or midline, depending on when the first survey is conducted, and 𝑡 = 1 at
endline. The treatment effect at endline will now be given by 𝛽1 rather than 𝛽2, but the underlying
concept remains identical. Note, that in case of binary or ordinal outcomes, 𝑌𝑖𝑔𝑡 in the above
equations does not denote the outcome itself but rather the propensity of unit i to achieve a certain
outcome. While the logic of the difference-in-differences approach still applies, the consequence of
this more complicated setup is that 𝛽1 and 𝛽2 are not interpretable as marginal effects on the
probability of a certain outcome, as we model this probability as a logistic (i.e. non-linear) function of
the right-hand side variables. Therefore, we plan to express effect sizes as odds ratios, which are
simply the antilog of the respective coefficients and a widely applied metric in health economics.
To put the estimated effect sizes into perspective, we plan to conduct a cost-benefit analysis. For
health indicators there is a standard procedure which we will follow. We will express effects on all
health indicators in terms of Disability-adjusted life years (DALYs) averted. DALYs are a metric that is
officially adopted by the World Health Organization and constructed by a group of researchers
including the Institute for Health Metrics and Evaluation at the University of Washington and the
Harvard T.H. Chan School of Public Health. DALYs are a tool to quantitatively compare the burden
from different diseases. After converting the effects of Gram Varta into DALYs averted for all
indicators, we will sum up the total number of DALYs averted through Gram Varta. These will then be
compared to the program's costs, allowing us to obtain the number of DALYs prevented per $1.
Moreover, Gram Varta also aims at improving non-health indicators such as female empowerment.
Here we will express the improvement in the indicators in terms of $1 invested in Gram Varta. These
effects would be in addition to the health effects of Gram Varta. There is no standard metric for
quantitatively comparing DALYs with non-health indicators, thus we will present these indicators side
by side.
6.2. Treatment intensity
The fact that participation in SHG meetings is voluntary makes it likely that there will be differences
in the treatment intensity for different women. We plan to exploit this design feature in order to
estimate the marginal effect of an additional SHG meeting. The analysis will focus on data acquired
from the household surveys and the pregnant women surveys as we do not expect much variation in
the treatment intensity for Anganwadi workers. We plan to use an approach similar to those outlined
in equation 1 and 2 with the difference that 𝐷𝑔1 and 𝐷𝑔2 are now not simple dummies but rather
13
integer variables counting the number of times a women from a treated gram panchayat has
participated in SHG meetings in case the outcome is measured at endline.
6.3. Subgroup analyses
We plan to augment our study by estimating separate intention-to-treat effects by subgroups. To this
end, we will stratify our sample by caste, age and poverty and run separate regressions of the types
depicted in equation 1 and 2. We expect that intention-to-treat effects on HNWASH knowledge and
practices as well as health outcomes and female empowerment will be smaller for scheduled castes
and the poor, as SHG meetings may not be completely inclusive for members of these groups who
may consequently not feel a strong sense of ownership of the program.
In addition, we will analyze, whether the intention-to-treat effects vary with the length of time the
SHGs have been operational (this may just be applicable in non-Jeevika areas, since Jeevika employs
a model where SHG activities are initiated only when the SHG attains a certain level of maturity in
functioning, but there might still be differences in the length of time since the SHGs were
operational). Gram Varta relies on the functionality of SHGs and might be less influential if a SHG is
not already well established. Moreover, we plan to stratify on infrastructural indicators, as some of
Gram Varta's possible behavioral effects will potentially depend on infrastructural prerequisites. For
instance, we will try to answer questions like `Do individuals not use toilets because they are not
aware that open defecation is harmful for good health in their community or is the necessary
infrastructure just lacking?´
6.4. Spill-over effects
A further aim of the study will be to measure spill-over effects of Gram Varta on non-participating
households in the same gram panchayat. We expect that the non-SHG members in treatment
communities will self-select into participating in Gram Varta meetings. We will not be able to obtain
credible information from non-SHG-individuals in the counterfactual communities on their potential
for self-selection into participation (had they gotten an opportunity to do so). Therefore, a simple
comparison of the non-SHG-individuals in the counterfactual communities with the non-participants
in the treatment communities might suffer from selection bias. To deal with this, we will draw
random samples of non-SHG-households in the counterfactual and treatment communities
independent of their participation status. We will then match the treatment group in non-
participating households with comparable households in the counterfactual group using propensity
scores. The propensity score will be based on a wide range of socio-economic characteristics with a
special focus on indicators which are hypothesized to determine self-selection into participation such
as sense of empowerment, child care obligations, distance to venue, economic situation, etc.
6.5. Qualitative analysis
In addition to the quantitative part of the evaluation, we will make use of qualitative information in
order to understand what experiencing Gram Varta means to participants. This will allow us to better
understand the process of change, enable us to draw conclusions about the causal pathways driving
our results and enhance our ability to assess the external validity of our results. As mentioned above,

14
we will make use of a broad range of methods, including participant observation, key informant
interviews, focus groups, in-depth interviews as well as participatory games.
The qualitative component of the study will be leveraged to provide insights into the transferability
of findings by delving deeper into the context of program implementation and asking questions such
as: how much of the program is driven by the particular personalities involved and how much of it is
due to the design of the program itself; what aspects of context matter when it comes to
acceptability and sustained interest in program participation; how do the experiences of participants
and facilitators in other districts differ from those in Madhepura district; and, which aspects of the
entire program are reported as important/helpful by facilitators and participants in Madhepura
versus other districts.
Appendix
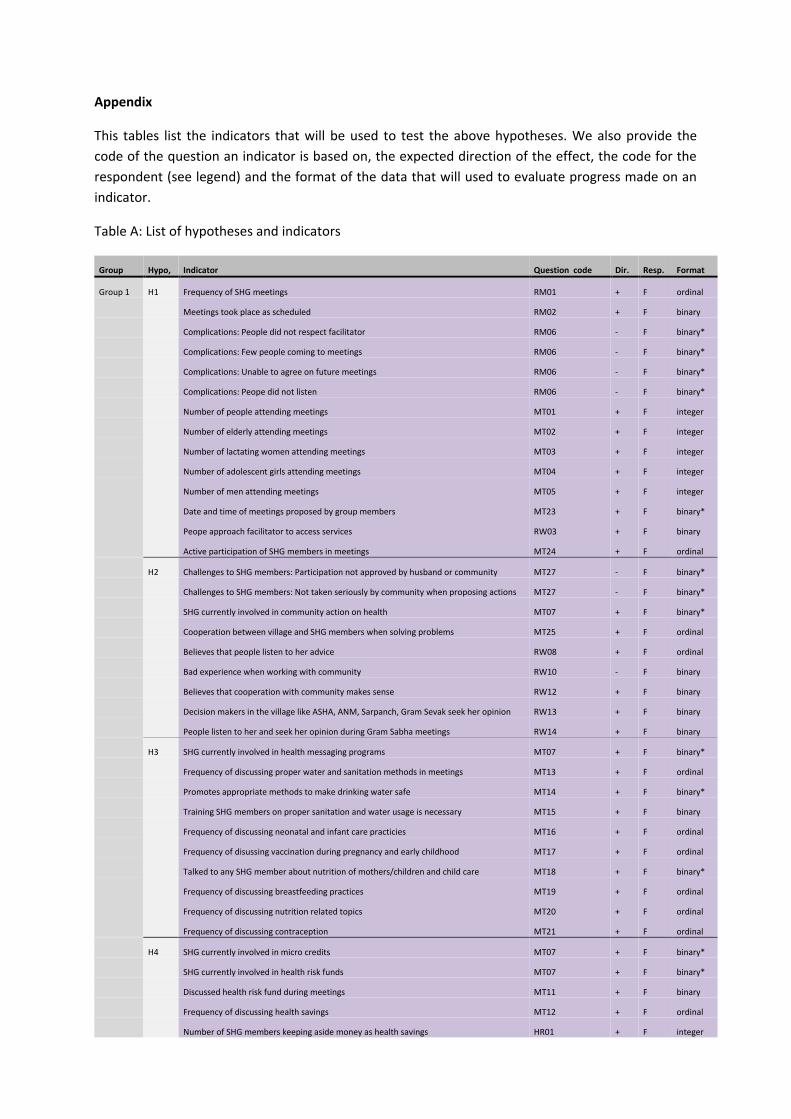
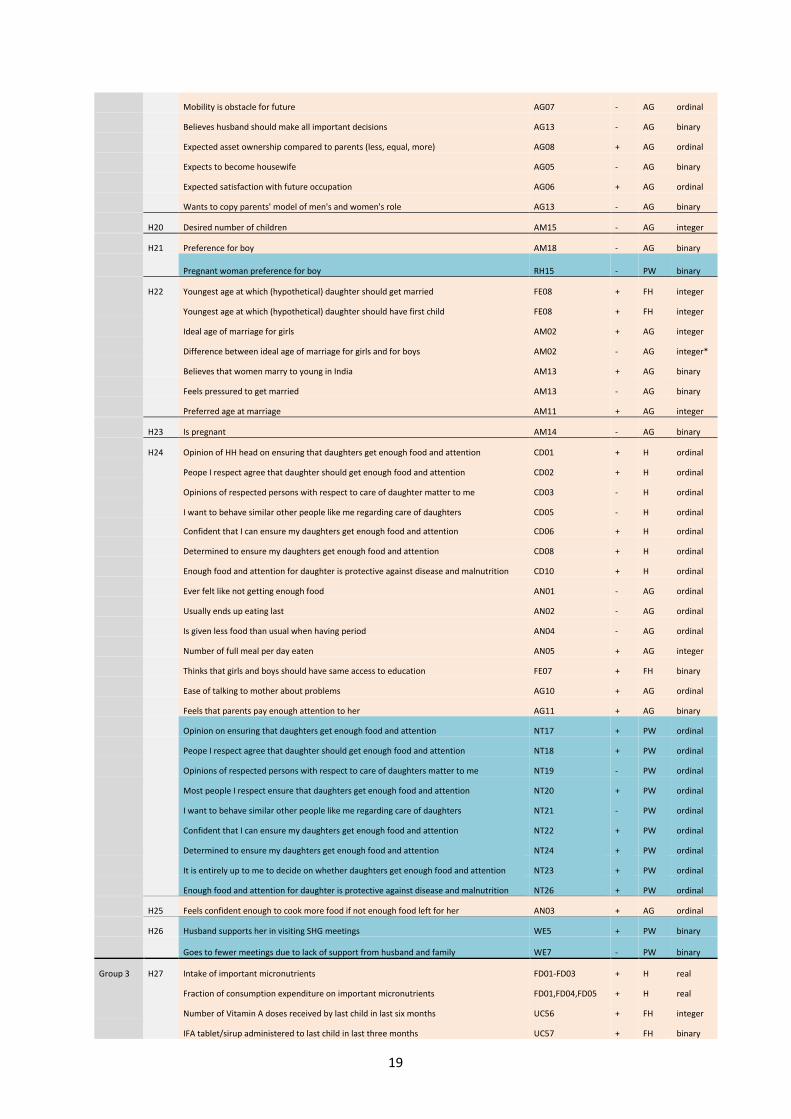
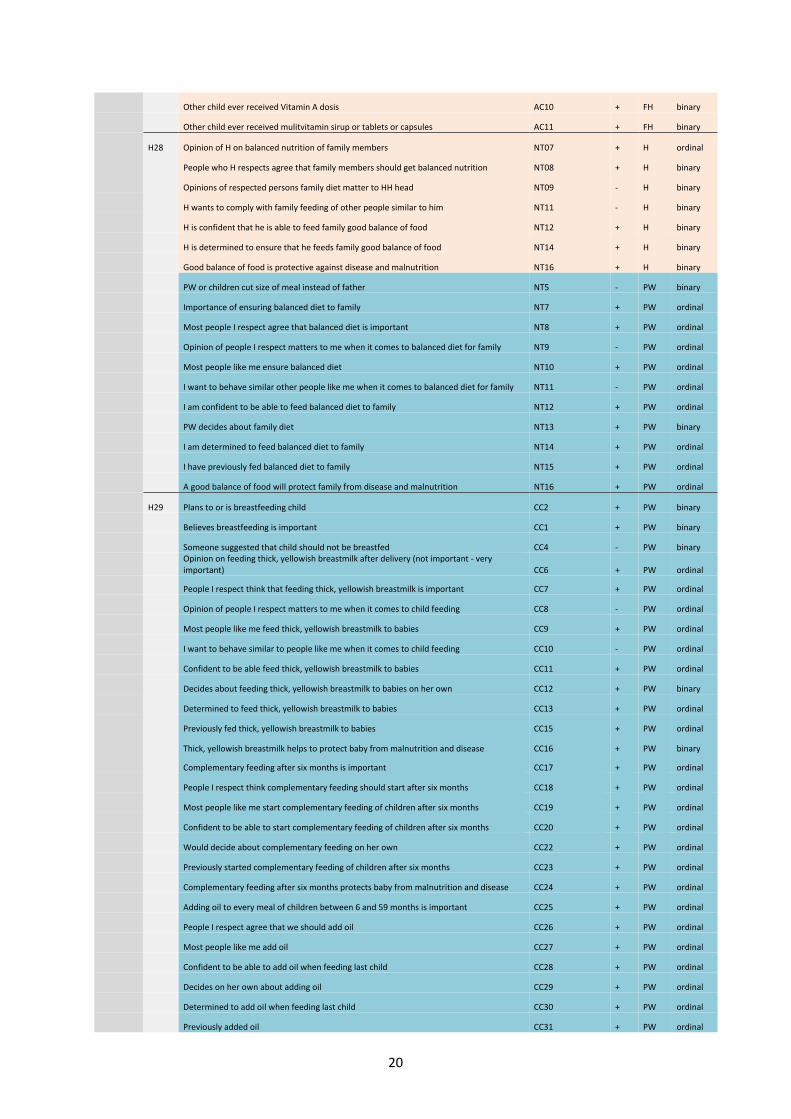
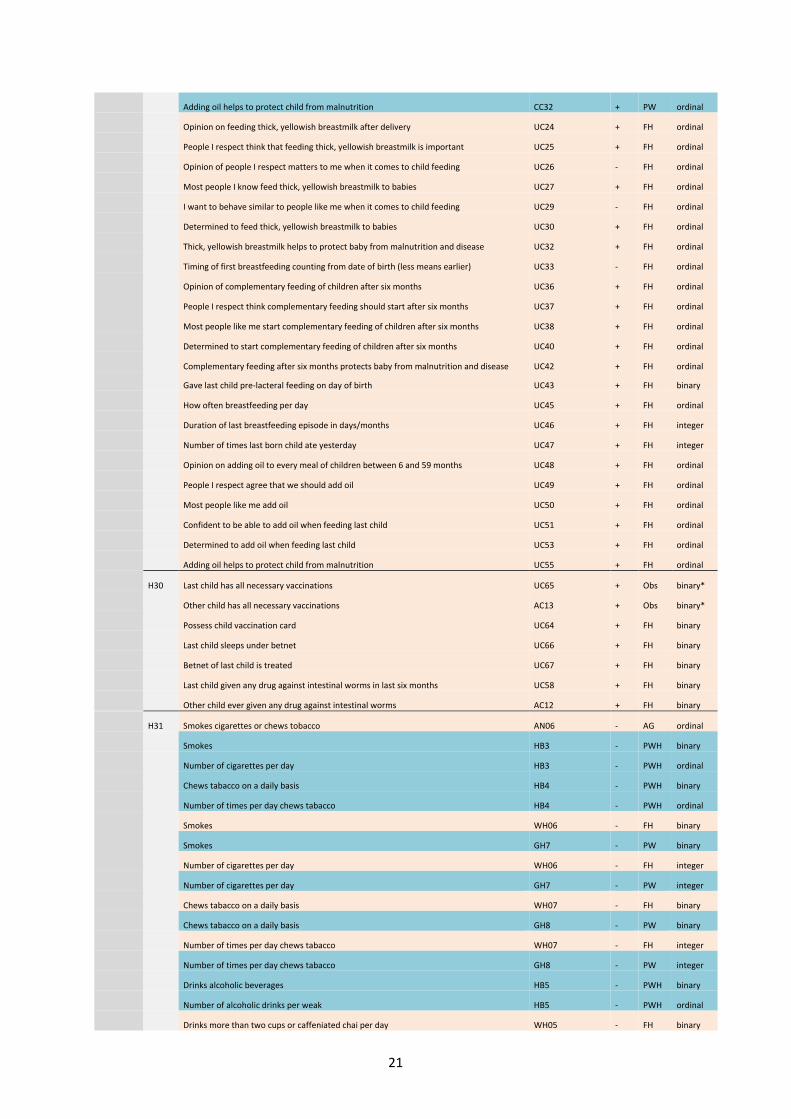
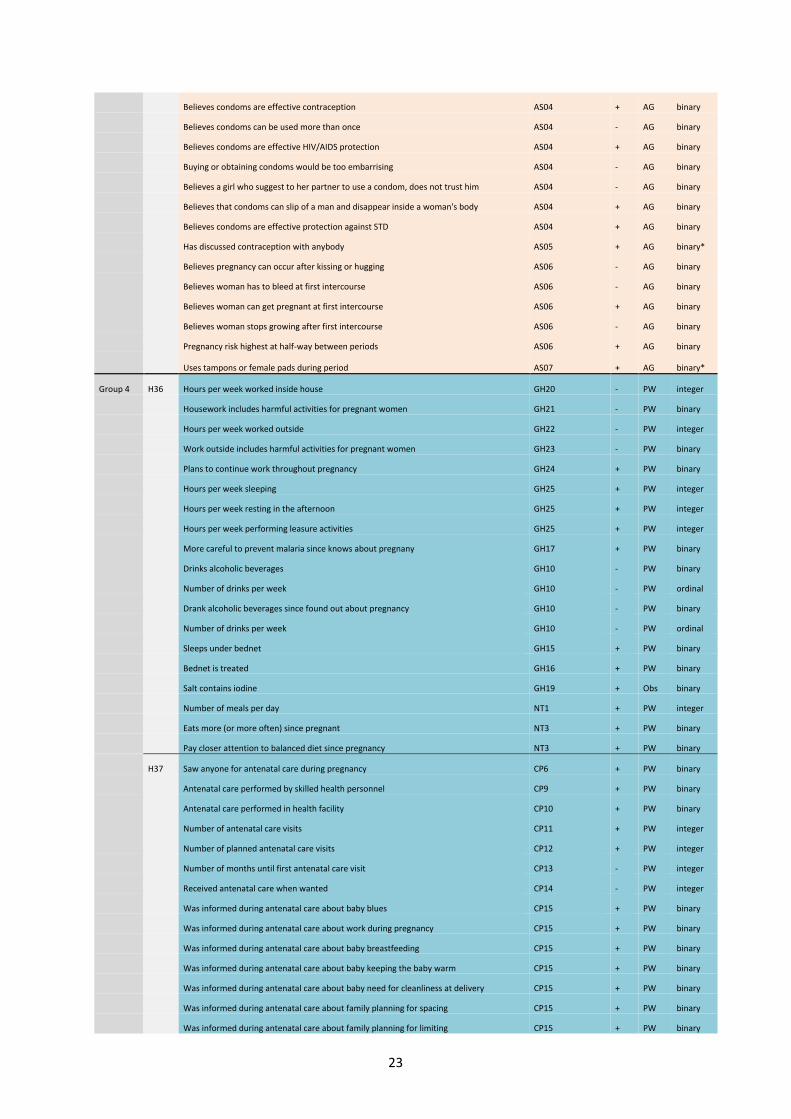
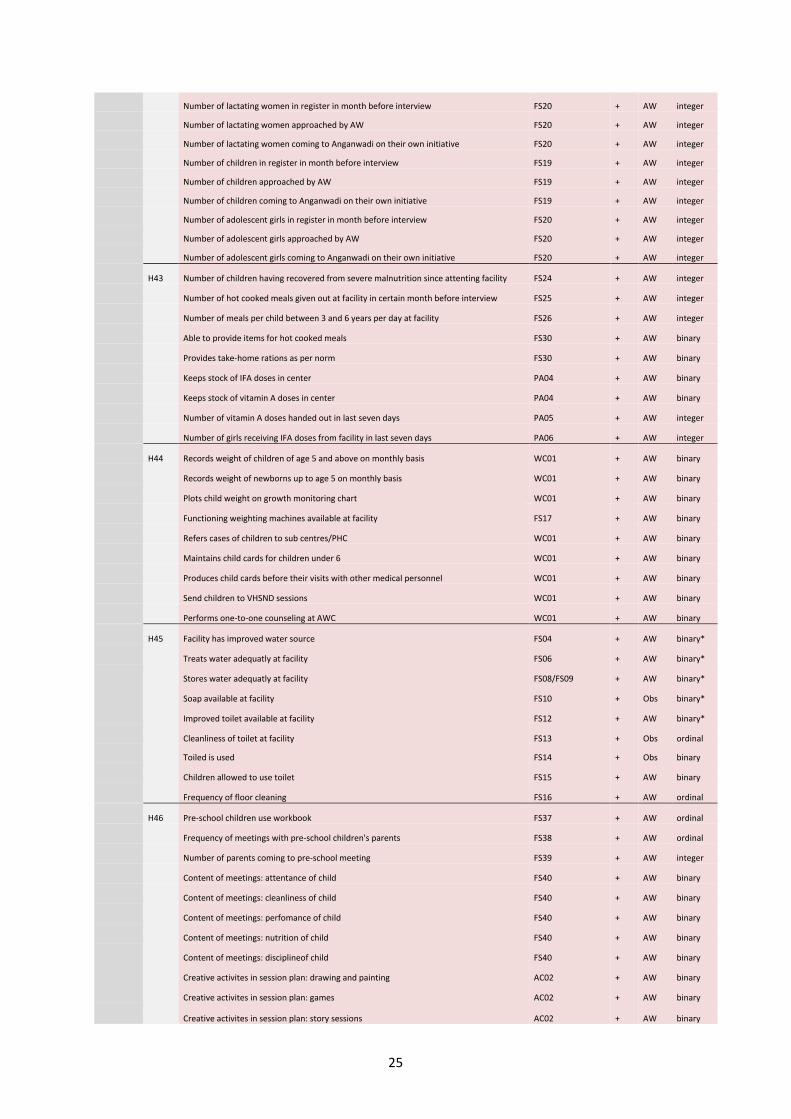
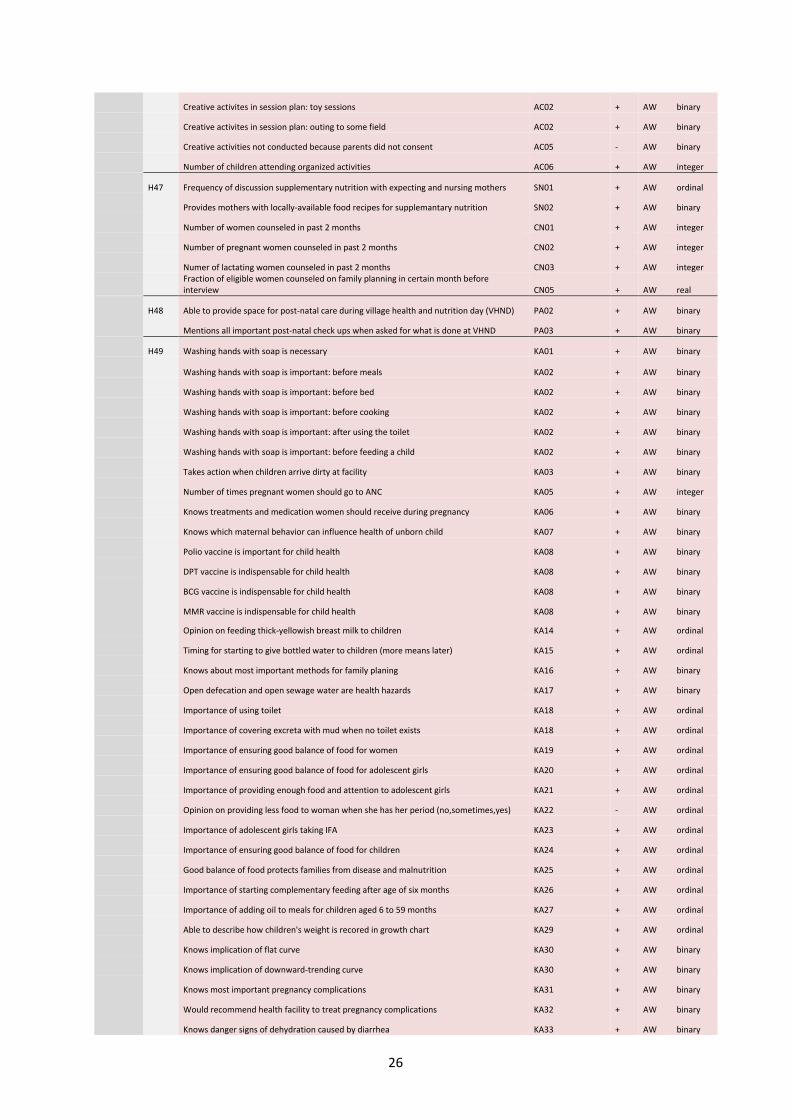
This tables list the indicators that will be used to test the above hypotheses. We also provide the
code of the question an indicator is based on, the expected direction of the effect, the code for the
respondent (see legend) and the format of the data that will used to evaluate progress made on an
indicator.
Table A: List of hypotheses and indicators
Group Hypo, Indicator Question code Dir. Resp. Format
Group 1 H1 Frequency of SHG meetings RM01 + F ordinal
Meetings took place as scheduled RM02 + F binary
Complications: People did not respect facilitator RM06 - F binary*
Complications: Few people coming to meetings RM06 - F binary*
Complications: Unable to agree on future meetings RM06 - F binary*
Complications: Peope did not listen RM06 - F binary*
Number of people attending meetings MT01 + F integer
Number of elderly attending meetings MT02 + F integer
Number of lactating women attending meetings MT03 + F integer
Number of adolescent girls attending meetings MT04 + F integer
Number of men attending meetings MT05 + F integer
Date and time of meetings proposed by group members MT23 + F binary*
Peope approach facilitator to access services RW03 + F binary
Active participation of SHG members in meetings MT24 + F ordinal
H2 Challenges to SHG members: Participation not approved by husband or community MT27 - F binary*
Challenges to SHG members: Not taken seriously by community when proposing actions MT27 - F binary*
SHG currently involved in community action on health MT07 + F binary*
Cooperation between village and SHG members when solving problems MT25 + F ordinal
Believes that people listen to her advice RW08 + F ordinal
Bad experience when working with community RW10 - F binary
Believes that cooperation with community makes sense RW12 + F binary
Decision makers in the village like ASHA, ANM, Sarpanch, Gram Sevak seek her opinion RW13 + F binary
People listen to her and seek her opinion during Gram Sabha meetings RW14 + F binary
H3 SHG currently involved in health messaging programs MT07 + F binary*
Frequency of discussing proper water and sanitation methods in meetings MT13 + F ordinal
Promotes appropriate methods to make drinking water safe MT14 + F binary*
Training SHG members on proper sanitation and water usage is necessary MT15 + F binary
Frequency of discussing neonatal and infant care practicies MT16 + F ordinal
Frequency of disussing vaccination during pregnancy and early childhood MT17 + F ordinal
Talked to any SHG member about nutrition of mothers/children and child care MT18 + F binary*
Frequency of discussing breastfeeding practices MT19 + F ordinal
Frequency of discussing nutrition related topics MT20 + F ordinal
Frequency of discussing contraception MT21 + F ordinal
H4 SHG currently involved in micro credits MT07 + F binary*
SHG currently involved in health risk funds MT07 + F binary*
Discussed health risk fund during meetings MT11 + F binary
Frequency of discussing health savings MT12 + F ordinal
Number of SHG members keeping aside money as health savings HR01 + F integer

16
Discussed health risk fund with SHG members during training HR02 + F binary
Number of people in community currently enrolled HR03 + F integer
Number of deposits made last month HR04 + F integer
H5 Informs SHG households about benefits from government health facilities PH01 + F binary
Number of SHG women using government health facilities in last months PH02 + F integer
Discusses problems faced by SHG households when using health facilities PH15 + F binary
H6 Frequency of promoting enrolment to VO nutrition center VO02 + F ordinal
H7 Number of SHG members succesfully enrolled to VO nutrition center in last 2 months VO03 + F integer
Number of women enrolled in VO nutrition center in total at the moment VO04 + F integer
Amount of time spend in VO centers per week by facilitator VO05 + F real
Number of training programs conducted at VO centers per months VO06 + F integer
Number of women participating in training programs VO07 + F integer
Number of households the facilitator provided counseling to during last month VO09 + F integer
H8 Believes that hands need to be washed frequently KA01 + F binary
Believes that soap should be used when washing hands KA01 + F binary*
Using soap after toilet is important KA02 + F binary*
Using soap before eating is important KA02 + F binary*
Using soap before cooking is important KA02 + F binary*
Using soap before feeding children is important KA02 + F binary*
Using soap before going to bed is important KA02 + F binary*
Knows required frequency of ANC KA03 + F binary*
Believes women should take IFA tablets during pregnancy KA04 + F binary
Importance of tetanus injection before giving birth KA05 + F ordinal
Important that pregnant women get enough food KA06 + F binary*
Important that pregnant women get balanced diet KA06 + F binary*
Knows health effects of polio vaccine KA07 + F binary*
Knows health effects of MMR vaccine KA07 + F binary*
Importance of feeding thick yellowish breast milk KA08 + F ordinal
Breastfeeding instead of giving water to drink can protect babies from diseases KA09 + F ordinal
Timing of starting to giving bottled water to a child KA10 + F ordinal
Knows most important methods of family planning KA11 + F binary*
Condoms are effective in preventing STDs like HIV/Aids KA13 + F binary
Wife justified in asking husband to use condom if he has STD KA14 + F binary
Open defecation and open sewage water are health hazards KA15 + F binary
Importance of using toilet KA16 + F ordinal
Importance of covering excreta with mud when no toilet exists KA16 + F ordinal
Importance of ensuring that women get a good balance of food KA17 + F ordinal
Importance of ensuring that adolescent girls get a good balance of food KA18 + F ordinal
Importance of ensuring that adolescent girls get enough food and attention KA19 + F ordinal
Amount of food women should be given during period KA20 + F ordinal
Importance of IFA tablets for adolescent girls KA21 + F ordinal
Importance of ensuring that children get good balance of food KA22 + F ordinal
Good balance of food protects families from disease and malnutrition KA23 + F binary
Importance of starting complementary feeding after age of six months KA24 + F ordinal
Importance of adding oil to meals for children aged 6 to 59 months KA25 + F ordinal
Importance of cutting children's hair short KA26 + F ordinal
Knows appropriate ways to make water safe to drink KA27 + F binary*

17
Knows danger signs of malaria KA28 + F binary*
Knows danger signs of acute respiratory infection KA29 + F binary*
Knows what to do when child suffers from diarrhea KA30 + F binary*
Knows danger signs of dehydration caused by diarrhea KA31 + F binary*
Holding babies in contact with mother's warm skin is good practice KA32 + F binary
Knows information on DIDI sheet KA33 + F ordinal
Knows 5 Panchsutras KA34 + F binary
H9 Satisfied with work as community mobilizer RW01 + F binary
Feels respected by SHG members and community RW05 + F binary
Feels that her work is appreciated by SHG members RW06 + F binary
Believes that SHG members are happy with her services RW07 + F binary
Group 2 H10 Women earns any income JB02a, JB03a + H binary
Woman has any savings SV02 + H binary
Level of women's savings SV04 + H real
Hours spent on unpaid household work in last seven days AG03 - AG integer
Woman has ever taken loan to start business FE03 + FH binary
Husband does/did not trust woman with money HR05 - FH binary
H11 Woman has say in use of income JB02e, JB03e + H binary
Woman can decide on her own how savings are spent SV06, SV07 + H binary
Participates in health care decisions FE01 + FH binary*
Participates in major household purchase decisions FE01 + FH binary*
Participates in decisions on visits to family and relatives FE01 + FH binary*
Participates in major farm decisions FE01 + FH binary*
Participates in decisions on use of own earnings FE01 + FH binary*
Woman participates in decisions on use of husbands earnings FE01 + FH binary*
Woman participates in decisions on land/house purchase and use FE01 + FH binary*
Makes decision about health care alone or jointly with husband WE3 + PW binary*
Makes decision about major household purchases alone or jointly with husband WE3 + PW binary*
Makes decision about visits to family alone or jointly with husband WE3 + PW binary*
Makes decision about farm matters alone or jointly with husband WE3 + PW binary*
Makes decision about number and timing of children alone or jointly with husband WE4 + PW binary*
H12 Allowed to go to market alone FE05 + FH binary
Allowed to go to health facility alone FE05 + FH binary
Allowed to go to neighbour's home alone FE05 + FH binary
Allowed to go to friends/relatives outside the village alone FE05 + FH binary
Allowed to go to places of worship alone FE05 + FH binary
Allowed to go to market alone FE05 + FH binary
Feels recognized in community as herself rather than mother/wife WE1 + PW binary*
Allowed to go alone to market WE2 + PW binary
Allowed to go alone to health facility WE2 + PW binary
Allowed to go alone to neighbor's home WE2 + PW binary
Allowed to go alone to friends/relatives outside the village WE2 + PW binary
Allowed to go alone to place of worship WE2 + PW binary
H13 Mostly known as husband's wife in village FE04 - FH binary*
H14 Acquainted with health staff SC01 + FH binary
Acquainted with government officials SC01 + FH binary
Acquainted with school officials SC01 + FH binary

18
Acquainted with official from village panchayat / nagarpalika / ward committee SC01 + FH binary
Not allowed to participate in community activities SC03 - FH binary
Not allowed to participate in community activities because of gender SC04 - FH binary*
Voted in most recent national election SC05 + FH binary
Attended public meeting of village Panchayat / Nagarpalika / ward committee last year SC06 + FH binary
H15 How often states own opinion in public FE06 + FH ordinal
H16 Wife can refuse intercourse if husband has STD RH23 + FH binary*
Wife can refuse intercourse if husband has sex with other women RH23 + FH binary*
Wife can refuse intercourse if she is tired/not in mood RH23 + FH binary*
Wife can demand husband to use condom if he has STD RH24 + FH binary
Women can decide on her own about family planning KA12 + F binary*
H17 Husband justified in hitting wife if she goes out without telling him HR04 - FH binary
… if she neglects children HR04 - FH binary
… if she argues with him HR04 - FH binary
… if she refuses to have sex with him HR04 - FH binary
… if she burns the food HR04 - FH binary
Believes husband is justified in beating wife is she goes out without telling him AG12 - AG binary
Believes husband is justified in beating wife is she neglects children AG12 - AG binary
Believes husband is justified in beating wife is she argues with him AG12 - AG binary
Believes husband is justified in beating wife is she refuses to have sex with him AG12 - AG binary
Believes husband is justified in beating wife is she burns the food AG12 - AG binary
H18 Afraid of husband HR03 - FH ordinal
Husband jealous or angry if woman talks/talked to other men HR05 - FH binary
Husband frequently accuses/accused woman of being unfaithful HR05 - FH binary
Husband does/did not allow woman to meet her female friends HR05 - FH binary
Husband tries/tried to limit woman's contact with her family HR05 - FH binary
Husband insists/insisted on knowing where woman is HR05 - FH binary
Husband pushed/shaked woman or threw something at her in last 12 months HR06 - FH binary
Number of times pushed/shaked or being thrown at by husband in last 12 months HR06 - FH integer
Husband kicked/dragged/beat up woman in last 12 months HR06 - FH binary
Number of times kicked/dragged/beaten up by husband in last 12 months HR06 - FH integer
Husband tried to choke woman or burn her on purpose in last 12 months HR06 - FH binary
Number of times choked or burned on purpose by husband in last 12 months HR06 - FH integer
Husband forced women to perform non-consensual sexual activity in last 12 months HR06 - FH binary
Number of times forced to perform non-consensual sexual activity in last 12 months HR06 - FH integer
Pushed/shaked/having things thrown at by husband during pregnancy WE8 - PW binary
How often? WE8 - PW integer
Kicked/dragged/beaten up by husband during pregnancy WE8 - PW binary
How often? WE8 - PW integer
Choked/burned on purpose by husband during pregnancy WE8 - PW binary
How often? WE8 - PW integer
Forced to do perform non-consensual sexuality activites by husband during pregnancy WE8 - PW binary
How often? WE8 - PW integer
H19 Lack of self-confidence is obstacle for future AG07 - AG ordinal
Lack of family support is obstacle for future AG07 - AG ordinal
Marriage is obstacle for future AG07 - AG ordinal
Domestic responsibility is obstacle for future AG07 - AG ordinal
19
Mobility is obstacle for future AG07 - AG ordinal
Believes husband should make all important decisions AG13 - AG binary
Expected asset ownership compared to parents (less, equal, more) AG08 + AG ordinal
Expects to become housewife AG05 - AG binary
Expected satisfaction with future occupation AG06 + AG ordinal
Wants to copy parents' model of men's and women's role AG13 - AG binary
H20 Desired number of children AM15 - AG integer
H21 Preference for boy AM18 - AG binary
Pregnant woman preference for boy RH15 - PW binary
H22 Youngest age at which (hypothetical) daughter should get married FE08 + FH integer
Youngest age at which (hypothetical) daughter should have first child FE08 + FH integer
Ideal age of marriage for girls AM02 + AG integer
Difference between ideal age of marriage for girls and for boys AM02 - AG integer*
Believes that women marry to young in India AM13 + AG binary
Feels pressured to get married AM13 - AG binary
Preferred age at marriage AM11 + AG integer
H23 Is pregnant AM14 - AG binary
H24 Opinion of HH head on ensuring that daughters get enough food and attention CD01 + H ordinal
Peope I respect agree that daughter should get enough food and attention CD02 + H ordinal
Opinions of respected persons with respect to care of daughter matter to me CD03 - H ordinal
I want to behave similar other people like me regarding care of daughters CD05 - H ordinal
Confident that I can ensure my daughters get enough food and attention CD06 + H ordinal
Determined to ensure my daughters get enough food and attention CD08 + H ordinal
Enough food and attention for daughter is protective against disease and malnutrition CD10 + H ordinal
Ever felt like not getting enough food AN01 - AG ordinal
Usually ends up eating last AN02 - AG ordinal
Is given less food than usual when having period AN04 - AG ordinal
Number of full meal per day eaten AN05 + AG integer
Thinks that girls and boys should have same access to education FE07 + FH binary
Ease of talking to mother about problems AG10 + AG ordinal
Feels that parents pay enough attention to her AG11 + AG binary
Opinion on ensuring that daughters get enough food and attention NT17 + PW ordinal
Peope I respect agree that daughter should get enough food and attention NT18 + PW ordinal
Opinions of respected persons with respect to care of daughters matter to me NT19 - PW ordinal
Most people I respect ensure that daughters get enough food and attention NT20 + PW ordinal
I want to behave similar other people like me regarding care of daughters NT21 - PW ordinal
Confident that I can ensure my daughters get enough food and attention NT22 + PW ordinal
Determined to ensure my daughters get enough food and attention NT24 + PW ordinal
It is entirely up to me to decide on whether daughters get enough food and attention NT23 + PW ordinal
Enough food and attention for daughter is protective against disease and malnutrition NT26 + PW ordinal
H25 Feels confident enough to cook more food if not enough food left for her AN03 + AG ordinal
H26 Husband supports her in visiting SHG meetings WE5 + PW binary
Goes to fewer meetings due to lack of support from husband and family WE7 - PW binary
Group 3 H27 Intake of important micronutrients FD01-FD03 + H real
Fraction of consumption expenditure on important micronutrients FD01,FD04,FD05 + H real
Number of Vitamin A doses received by last child in last six months UC56 + FH integer
IFA tablet/sirup administered to last child in last three months UC57 + FH binary
20
Other child ever received Vitamin A dosis AC10 + FH binary
Other child ever received mulitvitamin sirup or tablets or capsules AC11 + FH binary
H28 Opinion of H on balanced nutrition of family members NT07 + H ordinal
People who H respects agree that family members should get balanced nutrition NT08 + H binary
Opinions of respected persons family diet matter to HH head NT09 - H binary
H wants to comply with family feeding of other people similar to him NT11 - H binary
H is confident that he is able to feed family good balance of food NT12 + H binary
H is determined to ensure that he feeds family good balance of food NT14 + H binary
Good balance of food is protective against disease and malnutrition NT16 + H binary
PW or children cut size of meal instead of father NT5 - PW binary
Importance of ensuring balanced diet to family NT7 + PW ordinal
Most people I respect agree that balanced diet is important NT8 + PW ordinal
Opinion of people I respect matters to me when it comes to balanced diet for family NT9 - PW ordinal
Most people like me ensure balanced diet NT10 + PW ordinal
I want to behave similar other people like me when it comes to balanced diet for family NT11 - PW ordinal
I am confident to be able to feed balanced diet to family NT12 + PW ordinal
PW decides about family diet NT13 + PW binary
I am determined to feed balanced diet to family NT14 + PW ordinal
I have previously fed balanced diet to family NT15 + PW ordinal
A good balance of food will protect family from disease and malnutrition NT16 + PW ordinal
H29 Plans to or is breastfeeding child CC2 + PW binary
Believes breastfeeding is important CC1 + PW binary
Someone suggested that child should not be breastfed CC4 - PW binary
Opinion on feeding thick, yellowish breastmilk after delivery (not important - very important) CC6 + PW ordinal
People I respect think that feeding thick, yellowish breastmilk is important CC7 + PW ordinal
Opinion of people I respect matters to me when it comes to child feeding CC8 - PW ordinal
Most people like me feed thick, yellowish breastmilk to babies CC9 + PW ordinal
I want to behave similar to people like me when it comes to child feeding CC10 - PW ordinal
Confident to be able feed thick, yellowish breastmilk to babies CC11 + PW ordinal
Decides about feeding thick, yellowish breastmilk to babies on her own CC12 + PW binary
Determined to feed thick, yellowish breastmilk to babies CC13 + PW ordinal
Previously fed thick, yellowish breastmilk to babies CC15 + PW ordinal
Thick, yellowish breastmilk helps to protect baby from malnutrition and disease CC16 + PW binary
Complementary feeding after six months is important CC17 + PW ordinal
People I respect think complementary feeding should start after six months CC18 + PW ordinal
Most people like me start complementary feeding of children after six months CC19 + PW ordinal
Confident to be able to start complementary feeding of children after six months CC20 + PW ordinal
Would decide about complementary feeding on her own CC22 + PW ordinal
Previously started complementary feeding of children after six months CC23 + PW ordinal
Complementary feeding after six months protects baby from malnutrition and disease CC24 + PW ordinal
Adding oil to every meal of children between 6 and 59 months is important CC25 + PW ordinal
People I respect agree that we should add oil CC26 + PW ordinal
Most people like me add oil CC27 + PW ordinal
Confident to be able to add oil when feeding last child CC28 + PW ordinal
Decides on her own about adding oil CC29 + PW ordinal
Determined to add oil when feeding last child CC30 + PW ordinal
Previously added oil CC31 + PW ordinal
21
Adding oil helps to protect child from malnutrition CC32 + PW ordinal
Opinion on feeding thick, yellowish breastmilk after delivery UC24 + FH ordinal
People I respect think that feeding thick, yellowish breastmilk is important UC25 + FH ordinal
Opinion of people I respect matters to me when it comes to child feeding UC26 - FH ordinal
Most people I know feed thick, yellowish breastmilk to babies UC27 + FH ordinal
I want to behave similar to people like me when it comes to child feeding UC29 - FH ordinal
Determined to feed thick, yellowish breastmilk to babies UC30 + FH ordinal
Thick, yellowish breastmilk helps to protect baby from malnutrition and disease UC32 + FH ordinal
Timing of first breastfeeding counting from date of birth (less means earlier) UC33 - FH ordinal
Opinion of complementary feeding of children after six months UC36 + FH ordinal
People I respect think complementary feeding should start after six months UC37 + FH ordinal
Most people like me start complementary feeding of children after six months UC38 + FH ordinal
Determined to start complementary feeding of children after six months UC40 + FH ordinal
Complementary feeding after six months protects baby from malnutrition and disease UC42 + FH ordinal
Gave last child pre-lacteral feeding on day of birth UC43 + FH binary
How often breastfeeding per day UC45 + FH ordinal
Duration of last breastfeeding episode in days/months UC46 + FH integer
Number of times last born child ate yesterday UC47 + FH integer
Opinion on adding oil to every meal of children between 6 and 59 months UC48 + FH ordinal
People I respect agree that we should add oil UC49 + FH ordinal
Most people like me add oil UC50 + FH ordinal
Confident to be able to add oil when feeding last child UC51 + FH ordinal
Determined to add oil when feeding last child UC53 + FH ordinal
Adding oil helps to protect child from malnutrition UC55 + FH ordinal
H30 Last child has all necessary vaccinations UC65 + Obs binary*
Other child has all necessary vaccinations AC13 + Obs binary*
Possess child vaccination card UC64 + FH binary
Last child sleeps under betnet UC66 + FH binary
Betnet of last child is treated UC67 + FH binary
Last child given any drug against intestinal worms in last six months UC58 + FH binary
Other child ever given any drug against intestinal worms AC12 + FH binary
H31 Smokes cigarettes or chews tobacco AN06 - AG ordinal
Smokes HB3 - PWH binary
Number of cigarettes per day HB3 - PWH ordinal
Chews tabacco on a daily basis HB4 - PWH binary
Number of times per day chews tabacco HB4 - PWH ordinal
Smokes WH06 - FH binary
Smokes GH7 - PW binary
Number of cigarettes per day WH06 - FH integer
Number of cigarettes per day GH7 - PW integer
Chews tabacco on a daily basis WH07 - FH binary
Chews tabacco on a daily basis GH8 - PW binary
Number of times per day chews tabacco WH07 - FH integer
Number of times per day chews tabacco GH8 - PW integer
Drinks alcoholic beverages HB5 - PWH binary
Number of alcoholic drinks per weak HB5 - PWH ordinal
Drinks more than two cups or caffeniated chai per day WH05 - FH binary

22
Drinks more than two cups or caffeniated chai per day GH5 - PW binary
H32 Household treats water adequatly HV07, HV08 + H binary*
Household of pregnant woman treats water adequatly HV7,HV8 + PW binary
Stored water contaminated with e.coli HV13 - Obs binary
H33 Frequency of buying soap HV14 + H ordinal
Improved toiled in HH HV15 + Obs binary*
Cleanliness of toilet HV17 + Obs binary
Stool piles or sewage water nearby HV18 - Obs binary*
Adequate stool disposal of infant HV19 + H binary*
Open defecation despite toilet by any HH member HV20 - H binary
H ever reprehended open defecation by others near own house HV22 + H binary
H believes open defecation is health hazard HV23 + H binary
H opinion of using toilets or covering excreta with mud HV24 + H ordinal
People who HH head respects agree that one should use toilet or cover excreta with mud HV25 + H ordinal
Opinions of respected persons on toiled use matter to HH head HV26 - H ordinal
H wants to comply with toilet behavior of other people similar to him HV28 - H ordinal
H is confident that he is able to use toilet/cover extreta with mud HV29 + H ordinal
H is determined to ensure that he uses toilet/cover extreta with mud HV31 + H ordinal
H uses soap after toilet HV34 + H binary*
H uses soap before meals HV34 + H binary*
Frequency of soap usage by HH head HV35 + H ordinal
Frequency of baths by HH members HV36 + H ordinal
Importante of using toilets or covering excreta with mud SB1 + PW ordinal
People who I respect agree that one should use toilet or cover excreta with mud SB2 + PW binary
Opinions of respected persons on toiled use matter to me SB3 - PW binary
Most people like me use toilet or cover excreta with mud SB4 + PW binary
PW wants to comply with toilet behavior of other people similar to her SB5 - PW ordinal
PW is confident that he is able to use toilet/cover extreta with mud SB6 + PW ordinal
PW is determined to ensure that he uses toilet/cover extreta with mud SB8 + PW ordinal
PW decides about toilet use SB7 + PW binary
PW has previously used toilet or covered excreta with mud SB9 + PW binary
Using toiled or covering excreta with mud protects me and everyone in village from disease SB10 + PW binary
H34 Seen/heard/read messages about malaria/dengue programme WH10 + FH binary*
Seen/heard/read messages about diarrhea WH10 + FH binary*
Seen/heard/read messages about acute respiratory infection WH10 + FH binary*
Seen/heard/read messages about STI WH10 + FH binary*
Knows danger signs of malaria WH11 + FH binary*
Knows danger signs of acute respiratory infection WH12 + FH binary*
Knows what to do when child has diarrhea WH13 + FH binary*
Seen/heard/read messages about malaria/dengue/chikungunya programme GH13 + PW binary
Knows danger signs of malaria GH14 + PW binary
H35 Number of known family planning methods RH06 + FH integer
Contraception currently used by FH or partner RH07 + FH binary
Knows were to get the pill AS03 + AG binary
Knows were to get emergency contraception AS03 + AG binary
Knows were to get condom or nirodh AS03 + AG binary
Knows were to get female condom AS03 + AG binary
23
Believes condoms are effective contraception AS04 + AG binary
Believes condoms can be used more than once AS04 - AG binary
Believes condoms are effective HIV/AIDS protection AS04 + AG binary
Buying or obtaining condoms would be too embarrising AS04 - AG binary
Believes a girl who suggest to her partner to use a condom, does not trust him AS04 - AG binary
Believes that condoms can slip of a man and disappear inside a woman's body AS04 + AG binary
Believes condoms are effective protection against STD AS04 + AG binary
Has discussed contraception with anybody AS05 + AG binary*
Believes pregnancy can occur after kissing or hugging AS06 - AG binary
Believes woman has to bleed at first intercourse AS06 - AG binary
Believes woman can get pregnant at first intercourse AS06 + AG binary
Believes woman stops growing after first intercourse AS06 - AG binary
Pregnancy risk highest at half-way between periods AS06 + AG binary
Uses tampons or female pads during period AS07 + AG binary*
Group 4 H36 Hours per week worked inside house GH20 - PW integer
Housework includes harmful activities for pregnant women GH21 - PW binary
Hours per week worked outside GH22 - PW integer
Work outside includes harmful activities for pregnant women GH23 - PW binary
Plans to continue work throughout pregnancy GH24 + PW binary
Hours per week sleeping GH25 + PW integer
Hours per week resting in the afternoon GH25 + PW integer
Hours per week performing leasure activities GH25 + PW integer
More careful to prevent malaria since knows about pregnany GH17 + PW binary
Drinks alcoholic beverages GH10 - PW binary
Number of drinks per week GH10 - PW ordinal
Drank alcoholic beverages since found out about pregnancy GH10 - PW binary
Number of drinks per week GH10 - PW ordinal
Sleeps under bednet GH15 + PW binary
Bednet is treated GH16 + PW binary
Salt contains iodine GH19 + Obs binary
Number of meals per day NT1 + PW integer
Eats more (or more often) since pregnant NT3 + PW binary
Pay closer attention to balanced diet since pregnancy NT3 + PW binary
H37 Saw anyone for antenatal care during pregnancy CP6 + PW binary
Antenatal care performed by skilled health personnel CP9 + PW binary
Antenatal care performed in health facility CP10 + PW binary
Number of antenatal care visits CP11 + PW integer
Number of planned antenatal care visits CP12 + PW integer
Number of months until first antenatal care visit CP13 - PW integer
Received antenatal care when wanted CP14 - PW integer
Was informed during antenatal care about baby blues CP15 + PW binary
Was informed during antenatal care about work during pregnancy CP15 + PW binary
Was informed during antenatal care about baby breastfeeding CP15 + PW binary
Was informed during antenatal care about baby keeping the baby warm CP15 + PW binary
Was informed during antenatal care about baby need for cleanliness at delivery CP15 + PW binary
Was informed during antenatal care about family planning for spacing CP15 + PW binary
Was informed during antenatal care about family planning for limiting CP15 + PW binary

24
Was informed during antenatal care about maternal nutrition CP15 + PW binary
Was informed during antenatal care about child nutrition CP15 + PW binary
Was informed during antenatal care about need for institutional delivery CP15 + PW binary
Was informed during antenatal care about danger of malaria infection CP15 + PW binary
Was informed during antenatal care about danger signs to look out for CP16 + PW binary
Was informed during antenatal care about bleeding CP17 + PW binary
Was informed during antenatal care about convulsions CP17 + PW binary
Was informed during antenatal care about prolonged labor CP17 + PW binary
Was informed during antenatal care about preterm labor CP17 + PW binary
Was told were to go in case of complications CP18 + PW binary
Blood pressure measured during antenatal care CP19 + PW binary
Weight measured during antenatal care CP20 + PW binary
Urine sample taken during antenatal care CP21 + PW binary
Blood sample taken during antenatal care CP22 + PW binary
Ultrasound test during pregnancy CP29 + PW binary
Received tetanus injection during pregnancy CP30 + PW binary
Number of tetanus injections during pregnancy CP31 + PW integer
Number of iron & folic acid tablets/bottles during pregnancy CP34 + PW integer
Duration of iron & folic acid intake in days CP35 + PW integer
Other nutritional supplements during pregnancy CP36 + PW binary
H38 Was accompanied by anyone to antenatal care CP23 + PW binary
Was accompanied by husband to antenatal care CP24 + PW binary
H39 Satisfaction of antenatal care CP25 + PW ordinal
Satisfied with waiting time CP26 + PW binary
Satisfied with number of visits CP26 + PW binary
Satisfied withamount of time with health staff CP26 + PW binary
Satisfied with advice and information CP26 + PW binary
Satisfied with understanding and respect CP26 + PW binary
H40 Happiness with pregnancy CP3 + PW ordinal
How often stressed or strongly worried in last 12 months GH26 + PW ordinal
Worried about not knowing how to care for baby CP4 - PW binary
Thinks baby will keep her from things she is used to CP4 - PW binary
Looks forward to teaching and caring for baby CP4 + PW binary
Looks forward to new experience that baby brings CP4 + PW binary
Looks forward to telling friends and family about pregnancy CP4 + PW binary
Worried about money CP4 - PW binary
Does not look forward to telling friends and family about pregnancy CP4 - PW binary
Has possibility in household to adapt to challenges of pregnancy CP5 + PW binary
Feeling when got to know about pregnancy (very unhappy to very happy) RH13 + PW ordinal
Partner's feeling when got to know about pregnancy (very unhappy to very happy) RH14 + PW ordinal
H41 Knows about abortion RH7 + PW binary
Knows were to get safe abortion RH8 + PW binary
Would discuss abortion jointly with partner RH9 + PW binary
Group 5 H42 Number of times visited nearest Anganwadi health center in last 3 months WH09 + FH integer
Number of pregnant women in register in month before interview FS19 + AW integer
Number of pregnant women approached by AW FS19 + AW integer
Number of pregnant women coming to Anganwadi on their own initiative FS19 + AW integer
25
Number of lactating women in register in month before interview FS20 + AW integer
Number of lactating women approached by AW FS20 + AW integer
Number of lactating women coming to Anganwadi on their own initiative FS20 + AW integer
Number of children in register in month before interview FS19 + AW integer
Number of children approached by AW FS19 + AW integer
Number of children coming to Anganwadi on their own initiative FS19 + AW integer
Number of adolescent girls in register in month before interview FS20 + AW integer
Number of adolescent girls approached by AW FS20 + AW integer
Number of adolescent girls coming to Anganwadi on their own initiative FS20 + AW integer
H43 Number of children having recovered from severe malnutrition since attenting facility FS24 + AW integer
Number of hot cooked meals given out at facility in certain month before interview FS25 + AW integer
Number of meals per child between 3 and 6 years per day at facility FS26 + AW integer
Able to provide items for hot cooked meals FS30 + AW binary
Provides take-home rations as per norm FS30 + AW binary
Keeps stock of IFA doses in center PA04 + AW binary
Keeps stock of vitamin A doses in center PA04 + AW binary
Number of vitamin A doses handed out in last seven days PA05 + AW integer
Number of girls receiving IFA doses from facility in last seven days PA06 + AW integer
H44 Records weight of children of age 5 and above on monthly basis WC01 + AW binary
Records weight of newborns up to age 5 on monthly basis WC01 + AW binary
Plots child weight on growth monitoring chart WC01 + AW binary
Functioning weighting machines available at facility FS17 + AW binary
Refers cases of children to sub centres/PHC WC01 + AW binary
Maintains child cards for children under 6 WC01 + AW binary
Produces child cards before their visits with other medical personnel WC01 + AW binary
Send children to VHSND sessions WC01 + AW binary
Performs one-to-one counseling at AWC WC01 + AW binary
H45 Facility has improved water source FS04 + AW binary*
Treats water adequatly at facility FS06 + AW binary*
Stores water adequatly at facility FS08/FS09 + AW binary*
Soap available at facility FS10 + Obs binary*
Improved toilet available at facility FS12 + AW binary*
Cleanliness of toilet at facility FS13 + Obs ordinal
Toiled is used FS14 + Obs binary
Children allowed to use toilet FS15 + AW binary
Frequency of floor cleaning FS16 + AW ordinal
H46 Pre-school children use workbook FS37 + AW ordinal
Frequency of meetings with pre-school children's parents FS38 + AW ordinal
Number of parents coming to pre-school meeting FS39 + AW integer
Content of meetings: attentance of child FS40 + AW binary
Content of meetings: cleanliness of child FS40 + AW binary
Content of meetings: perfomance of child FS40 + AW binary
Content of meetings: nutrition of child FS40 + AW binary
Content of meetings: disciplineof child FS40 + AW binary
Creative activites in session plan: drawing and painting AC02 + AW binary
Creative activites in session plan: games AC02 + AW binary
Creative activites in session plan: story sessions AC02 + AW binary
26
Creative activites in session plan: toy sessions AC02 + AW binary
Creative activites in session plan: outing to some field AC02 + AW binary
Creative activities not conducted because parents did not consent AC05 - AW binary
Number of children attending organized activities AC06 + AW integer
H47 Frequency of discussion supplementary nutrition with expecting and nursing mothers SN01 + AW ordinal
Provides mothers with locally-available food recipes for supplemantary nutrition SN02 + AW binary
Number of women counseled in past 2 months CN01 + AW integer
Number of pregnant women counseled in past 2 months CN02 + AW integer
Numer of lactating women counseled in past 2 months CN03 + AW integer
Fraction of eligible women counseled on family planning in certain month before interview CN05 + AW real
H48 Able to provide space for post-natal care during village health and nutrition day (VHND) PA02 + AW binary
Mentions all important post-natal check ups when asked for what is done at VHND PA03 + AW binary
H49 Washing hands with soap is necessary KA01 + AW binary
Washing hands with soap is important: before meals KA02 + AW binary
Washing hands with soap is important: before bed KA02 + AW binary
Washing hands with soap is important: before cooking KA02 + AW binary
Washing hands with soap is important: after using the toilet KA02 + AW binary
Washing hands with soap is important: before feeding a child KA02 + AW binary
Takes action when children arrive dirty at facility KA03 + AW binary
Number of times pregnant women should go to ANC KA05 + AW integer
Knows treatments and medication women should receive during pregnancy KA06 + AW binary
Knows which maternal behavior can influence health of unborn child KA07 + AW binary
Polio vaccine is important for child health KA08 + AW binary
DPT vaccine is indispensable for child health KA08 + AW binary
BCG vaccine is indispensable for child health KA08 + AW binary
MMR vaccine is indispensable for child health KA08 + AW binary
Opinion on feeding thick-yellowish breast milk to children KA14 + AW ordinal
Timing for starting to give bottled water to children (more means later) KA15 + AW ordinal
Knows about most important methods for family planing KA16 + AW binary
Open defecation and open sewage water are health hazards KA17 + AW binary
Importance of using toilet KA18 + AW ordinal
Importance of covering excreta with mud when no toilet exists KA18 + AW ordinal
Importance of ensuring good balance of food for women KA19 + AW ordinal
Importance of ensuring good balance of food for adolescent girls KA20 + AW ordinal
Importance of providing enough food and attention to adolescent girls KA21 + AW ordinal
Opinion on providing less food to woman when she has her period (no,sometimes,yes) KA22 - AW ordinal
Importance of adolescent girls taking IFA KA23 + AW ordinal
Importance of ensuring good balance of food for children KA24 + AW ordinal
Good balance of food protects families from disease and malnutrition KA25 + AW ordinal
Importance of starting complementary feeding after age of six months KA26 + AW ordinal
Importance of adding oil to meals for children aged 6 to 59 months KA27 + AW ordinal
Able to describe how children's weight is recored in growth chart KA29 + AW ordinal
Knows implication of flat curve KA30 + AW binary
Knows implication of downward-trending curve KA30 + AW binary
Knows most important pregnancy complications KA31 + AW binary
Would recommend health facility to treat pregnancy complications KA32 + AW binary
Knows danger signs of dehydration caused by diarrhea KA33 + AW binary
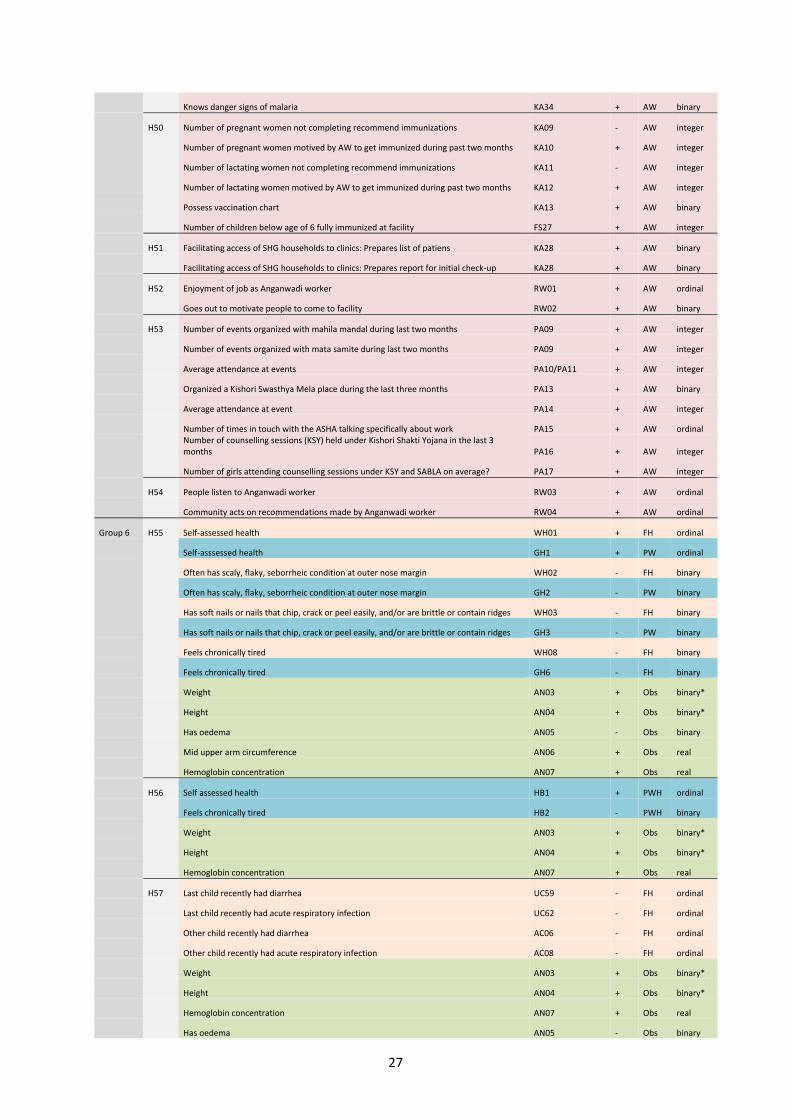
27
Knows danger signs of malaria KA34 + AW binary
H50 Number of pregnant women not completing recommend immunizations KA09 - AW integer
Number of pregnant women motived by AW to get immunized during past two months KA10 + AW integer
Number of lactating women not completing recommend immunizations KA11 - AW integer
Number of lactating women motived by AW to get immunized during past two months KA12 + AW integer
Possess vaccination chart KA13 + AW binary
Number of children below age of 6 fully immunized at facility FS27 + AW integer
H51 Facilitating access of SHG households to clinics: Prepares list of patiens KA28 + AW binary
Facilitating access of SHG households to clinics: Prepares report for initial check-up KA28 + AW binary
H52 Enjoyment of job as Anganwadi worker RW01 + AW ordinal
Goes out to motivate people to come to facility RW02 + AW binary
H53 Number of events organized with mahila mandal during last two months PA09 + AW integer
Number of events organized with mata samite during last two months PA09 + AW integer
Average attendance at events PA10/PA11 + AW integer
Organized a Kishori Swasthya Mela place during the last three months PA13 + AW binary
Average attendance at event PA14 + AW integer
Number of times in touch with the ASHA talking specifically about work PA15 + AW ordinal
Number of counselling sessions (KSY) held under Kishori Shakti Yojana in the last 3 months PA16 + AW integer
Number of girls attending counselling sessions under KSY and SABLA on average? PA17 + AW integer
H54 People listen to Anganwadi worker RW03 + AW ordinal
Community acts on recommendations made by Anganwadi worker RW04 + AW ordinal
Group 6 H55 Self-assessed health WH01 + FH ordinal
Self-asssessed health GH1 + PW ordinal
Often has scaly, flaky, seborrheic condition at outer nose margin WH02 - FH binary
Often has scaly, flaky, seborrheic condition at outer nose margin GH2 - PW binary
Has soft nails or nails that chip, crack or peel easily, and/or are brittle or contain ridges WH03 - FH binary
Has soft nails or nails that chip, crack or peel easily, and/or are brittle or contain ridges GH3 - PW binary
Feels chronically tired WH08 - FH binary
Feels chronically tired GH6 - FH binary
Weight AN03 + Obs binary*
Height AN04 + Obs binary*
Has oedema AN05 - Obs binary
Mid upper arm circumference AN06 + Obs real
Hemoglobin concentration AN07 + Obs real
H56 Self assessed health HB1 + PWH ordinal
Feels chronically tired HB2 - PWH binary
Weight AN03 + Obs binary*
Height AN04 + Obs binary*
Hemoglobin concentration AN07 + Obs real
H57 Last child recently had diarrhea UC59 - FH ordinal
Last child recently had acute respiratory infection UC62 - FH ordinal
Other child recently had diarrhea AC06 - FH ordinal
Other child recently had acute respiratory infection AC08 - FH ordinal
Weight AN03 + Obs binary*
Height AN04 + Obs binary*
Hemoglobin concentration AN07 + Obs real
Has oedema AN05 - Obs binary
28
Mid upper arm circumference AN06 + Obs real
Group 7 H58 Believes most people in neighbourhood can be trusted SC07 + FH ordinal
Believes in neighbourhood/village someone is likely to take advantage of you SC07 - FH ordinal
People in village do not trust each other in matters of borrowing/lending money SC07 - FH ordinal
H59 Differences in caste/race/religion/sex/etc. cause problems in neighbourhood SC08 - FH binary
A star (see column format) indicates that the indicated format is obtained after recoding a variable (e.g. by collapsing different categories)
Legend
F=Facilitator
H=Household head
FH=Female household head
Obs=Observed by fieldworker
AG=Adolescent girl
PW=Pregnant woman
PWH=Husband of pregnant woman
AW=Anganwadi worker
Information taken from household surveys
Information taken from facilitator survey
Information taken from pregnant women survey
Information taken from Anganwadi worker survey
Information taken from antropometic measurement




















