PLevin_1.pdf - Sigma Repository
141
PREDICTORS OF GLOVE USE BY HEALTH CARE WORKERS BY PAMELA FOX LEVIN B.S.N., Boston University, 1976 M.S., University of Illinois at Chicago, 1989 THESIS Submitted as partial fulfillment of the requirements for the degree of Doctor of Philosophy in Nursing Sciences in the Graduate College of the University of Illinois at Chicago, 1994 Chicago, Illinois Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of PLevin_1.pdf - Sigma Repository

PREDICTORS OF GLOVE USE BY HEALTH CARE WORKERS
BY
PAM ELA FOX LEVIN B.S.N., Boston University, 1976
M .S., University o f Illinois at Chicago, 1989
THESIS
Submitted as partial fulfillment of the requirements for the degree o f Doctor o f Philosophy in Nursing Sciences
in the Graduate College o f the University of Illinois at Chicago, 1994
Chicago, Illinois
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

THE UNIVERSITY OF ILLINOIS AT CHICAGO G raduate C ollege
CER TIFIC A TE O F APPRO VAL
t, ___
/ hereby recommend that the thesis prepared tinder my supervision by
Pamela Fox Levin
entitled Predictors o f Glove Use By Health Care Workers
be accepted in partial fulfillm ent o f the requirements fo r the degree o fDoctor o f Philosophy
/ concur with this recommendation
Recom m endation concurred in:
UIC The University of Illinois
M e m b e r s o f
T h e s i s o r
D is se r ta t io n
D efen se
C o m m i t t e e
at Chicago
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Copyright by
Pamela Fox Levin
1994
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

ACKNOWLEDGMENTS
I am very grateful for the exceptional support that my thesis committee— Drs. Mary -'Vesta Marston-Scott,
Richard Campbell, Shu-Pi Chen, Julia Cowell, Sally Lusk, Andrew Montgomery, and Thomas Prohaska— provided. I
thank them not only for their expert guidance, but for their encouragement and patience as well.
In addition, I would like to thank Dr. Karen Conrad for her insights along the way of this study, David Child for
his editorial expertise, and Lynn Allison and Dr. Barbara Castleberry from the American Society of Clinical Pathologists
for their support with data collection. This study would not have been possible without the financial support provided by
a National Institute for Occupational Safety and Health traineeship and a predoctoral fellowship from the U.S. Public
Health Service (# F31 NR06654).
Most importantly, immeasurable thanks are extended to my husband, Jonathan. His humor and love smoothed
the rough seas o f graduate study.
PFL
iii
R eproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

TABLE OF CONTENTS
PAGE
INTRODUCTION .............................................................................................................................................................................................1B ack g ro u n d .......................................................................................................................................................................................................... 1Conceptual F ra m e w o rk ....................................................................................................................................................................................2Study P u rp o s e .................................................................................................................................................................................................... 4Hypotheses ..........................................................................................................................................................................................................4Theoretical Definition of T e r m s ....................................................................................................................................................................4S ignificance..........................................................................................................................................................................................................5
REVIEW OF RELATED L IT E R A T U R E ...................................................................................................................................................6Compliance with Universal P re c a u tio n s ......................................................................................................................................................6Theory of Reasoned A c t io n .......................................................................................................................................................................... 15
Constructs and A ssum ptions..........................................................................................................................................................15Empirical Support ........................................................................................................................................................................ 12
M otor vehicle safety devices.......................................................................................................................................... 18Exercise................................................................................................................................................................................ 18
Conceptual and Measurement Issues .........................................................................................................................................18Summary ..........................................................................................................................................................................................22
Extensions of the Theory of Reasoned A c tio n ........................................................................................................................................ 22Theory o f Planned B eh av io r..........................................................................................................................................................................25
Constructs and A ssum ptions.........................................................................................................................................................25Empirical Support ..........................................................................................................................................................................26Measurement Issues .......................................................................................................................................................................27Summary .......................................................................................................................................................................................... 30
Perceived R i s k .................................................................................................................................................................................................. 30Construct .......................................................................................................................................................................................... 30Empirical Support ..........................................................................................................................................................................33Measurement Issues .......................................................................................................................................................................36Summary ..........................................................................................................................................................................................36
Self-Protection M o d e l .................................................................................................................................................................................... 36Summary .......................................................................................................................................................................................................... 37
M E T H O D O L O G Y .......................................................................................................................................................................................... 39Research D e s ig n ................................................................................................................................................................................................39Operationalization o f the Model ................................................................................................................................................................. 39
Attitude .............................................................................................................................................................................................39Perceived C o n tro l............................................................................................................................................................................ 41Perceived R i s k ..................................................................................................................................................................................41In te n tio n .............................................................................................................................................................................................42B e h a v io r .............................................................................................................................................................................................42
S a m p le ................................................................................................................................................................................................................42In stru m en t.......................................................................................................................................................................................................... 43
Content V a lid ity ............................................................................................................................................................................... 43Pilot Study .......................................................................................................................................................................................44
Data Collection Procedures ......................................................................................................................................................................... 44Protection of Human Subjects .................................................................................................................................................................... 44A n a ly s is .............................................................................................................................................................................................................44
iv
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

TABLE OF CONTENTS (continued)
PAGE
R E S U L T S ........................................................................................................................................................................................................... 47Characteristics o f the S a m p le .....................................................................................................................................................................47Descriptive Summary of the V a ria b le s ....................................................................................................................................................47
B e h a v io r ..............................................................................................................................................................................................50In te n tio n ..............................................................................................................................................................................................50Attitude ..............................................................................................................................................................................................50Subjective Norm ..............................................................................................................................................................................50Perceived C o n tro l.......................................................................................................................................................................... 51Perceived R i s k ................................................................................................................................................................................51Additional V aria b le s ........................................................................................................................................................................52
Analysis o f Variance ......................................................................................................................................................................................52Model E stim a tio n ..............................................................................................................................................................................................54
Theory of Reasoned Action— Model I .......................................................................................................................................5oProposed m o d e l ................................................................................................................................................................55Sequence o f models .......................................................................................................................................................55Measurement model .......................................................................................................................................................55Structural m o d e l................................................................................................................................................................56Summary' ...........................................................................................................................................................................60
Theory o f Planned Behavior— Model I I ....................................................................................................................................60Proposed m o d e l ................................................................................................................................................................60Measurement model ....................................................................................................................................................61Structural m o d e l .............................................................................................................................................................61Summary ...........................................................................................................................................................................66
Self-Protection Model— M odel I I I ...............................................................................................................................................66Proposed m o d e l ................................................................................................................................................................66Sequence of models .......................................................................................................................................................66Measurement model .......................................................................................................................................................68Structural m o d e l................................................................................................................................................................68Summary ...........................................................................................................................................................................71
Summary of F in d in g s ......................................................................................................................................................................................73Hypotheses ........................................................................................................................................................................................ 73Comparisons to the L iterature .................................................................................................................................................... 74
Descriptive Summary of Behavioral B e l i e f s ............................................................................................................................................ 77
SUMMARY, CONCLUSIONS, AND IM PLIC A TIO N S.......................................................................................................................81Summary ........................................................................................................................................................................................................... 81C onclusions........................................................................................................................................................................................................ 83Study L im ita tio n s..............................................................................................................................................................................................85Implications of the F ind ings...........................................................................................................................................................................87
Nursing P ra c tice ................................................................................................................................................................................ 87Health Policy and R e g u la tio n s .................................................................................................................................................... 88
Recommendations for Future Research .................................................................................................................................................... 88
A P P E N D IC E S ................................................................................................................................................................................................... 90Appendix A ........................................................................................................................................................................................ 91Appendix B ................................................................................................................................................................................... 109Appendix C ................................................................................................................................................................................... 113Appendix D ................................................................................................................................................................................... 114Appendix E ................................................................................................................................................................................... 115
v
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

TABLE OF CONTENTS (continued)
PAGE
CITED L IT E R A T U R E .............................................................................................................................................................................. 117
V I T A ............................................................................................................................................................................................................... 127
vi
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

LIST OF TABLES
I RESEARCH INDICATING HEALTH CARE WORKERS' FAILURETO WEAR GLOVES WITH POTENTIAL BLOOD C O N T A C T ....................................................................... 7
II FACTORS RELATED TO HEALTH CARE WORKERS' COMPLIANCEWITH UNIVERSAL BARRIER PR EC A U T IO N S...................................................................................................9
III INTERVENTION STUDIES EXAMINING HEALTH CARE WORKERS'COMPLIANCE WITH UNIVERSAL BARRIER PRECAUTIONS ................................................................ 11
IV MOTOR VEHICLE SAFETY AND EXERCISE RESEARCH USING THE THEORY OFREASONED A C T IO N .................................................................................................................................................. 19
V SELECTED HEALTH RELATED RESEARCH USING EXTENSIONS OF THE THEORY OFREASONED A C T IO N ..................................................................................................................................................23
VI SELECTED HEALTH RELATED RESEARCH USING THE THEORY OF PLANNEDBEHAVIOR .....................................................................................................................................................................28
VII HEALTH RELATED RESEARCH USING WEINSTEIN'S MEASURE OF PERCEIVED RISK . . . 34
VIII STUDY VARIABLES ....................................................................................................................................................40
IX HEALTH CARE WORKER SAMPLING PLAN ..................................................................................................42
X DEMOGRAPHIC AND WORK CHARACTERISTICS OF THE SAMPLE (w = 527) .......................... 48
XI MEAN, STANDARD DEVIATION, AND RELIABILITY ESTIMATES FOR V A R IA B L E S 49
XII ANALYSIS OF VARIANCE IN FIELD OF EMPLOYMENT, LOCATION, AND WORKSETTING WITH PAST M ONTH ...............................................................................................................................53
XIII ANALYSIS OF VARIANCE IN FIELD OF EMPLOYMENT, LOCATION, AND WORKSETTING WITH NOT WEAR ....................................................................................................................................53
XIV OVERALL FIT MEASURES FOR THEORY OF REASONED ACTION M ODELS (1.1 -1 .4 ) ................56
XV LISREL ESTIMATES OF REGRESSION OF OBSERVED ON LATENT VARIABLES:THEORY OF REASONED ACTION MODEL 1.3 ..............................................................................................57
XVI LISREL ESTIMATES OF STRUCTURAL COEFFICIENTS FOR THEORY OF REASONEDACTION: MODELS 1.3 AND 1 .4 .............................................................................................................................. 58
XVII DECOMPOSITION OF EFFECTS FOR THEORY OF REASONED ACTION:MODELS 1.3 AND 1.4 ..................................................................................................................................................59
XVIII OVERALL FIT MEASURES FOR THEORY OF PLANNED BEHAVIOR MODELS (II.1-II.3) . . 61
XIX LISREL ESTIMATES OF REGRESSION OF OBSERVED ON LATENT VARIABLES:THEORY OF PLANNED BEHAVIOR M ODEL II.2 ........................................................................................ 62
vii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

LIST OF TABLES
TABLE PAGE
XX LISREL ESTIM ATES OF STRUCTURAL COEFFICIENTS FOR THEORY OF PLANNEDBEHAVIOR MODELS II.2 AND I I . 3 ......................................................................................................................63
XXI DECOM POSITION OF EFFECTS FOR THEORY OF PLANNED BEHAVIOR MODELS II.2AND II.3 ......................................................................................................................................................................... 65
XXII OVERALL FIT MEASURES FOR SELF-PROTECTION MODELS (III. 1—III.5) .....................................67
XXIII LISREL ESTIM ATES OF REGRESSION OF OBSERVED ON LATENT VARIABLES:SELF-PROTECTION MODEL I I I . 4 ........................................................................................................................ 69
XXIV LISREL ESTIM ATES OF STRUCTURAL COEFFICIENTS FOR SELF-PROTECTIONM ODELS III.4 AND I I I . 5 ........................................................................................................................................... 70
XXV DECOM POSITION OF EFFECTS FOR SELF-PROTECTION MODELS III.4 AND I I I . 5 .....................72
XXVI M EAN DIFFERENCES ON STUDY VARIABLES BETW EEN NURSES AND LABORATORYW O R K E R S ...................................................................................................................................................................... 79
XXVII CORRELATIONS OF STUDY VARIABLES .................................................................................................. 114
XXVIII CELL M EANS AND SAMPLE SIZES FOR N O T WEAR AND FOR P A ST M O N T H .......................... 115
viii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

LIST OF FIGURES
FIGURE PAGE
1. The Self-Protection Model..................................................................................................................................................3
2. Theory of Reasoned Action.............................................................................................................................................. 15
3. LISREL Models for the Theory of Reasoned Action, Theory o f Planned Behavior, andSelf-Protection Model....................................................................................................................................................... 46
ix
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

LIST OF ABBREVIATIONS
AGFI Adjusted Goodness-of-Fit Index
CDC Centers for Disease Control (now titled Centers for Disease Control and Prevention)
GFI Goodness-of-Fit Index
HCW s Health care workers
HIV Human immunodeficiency virus
LISREL Linear structural relations model
OSHA Occupational Safety and Health Administration
RMR Root mean-square residual
SPM Self-protection model
TPB Theory of planned behavior
TRA Theory of reasoned action
x
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

SUMMARY
The primary aim of this study was to identify predictors o f health care workers' glove use related to protective
behavior. The self-protection model (SPM) investigated the health care workers' intention to wear gloves and glove use
behavior when there was potential for blood exposure. Additionally, the predictive capability of the SPM was compared
to the theory o f reasoned action (TRA) and the theory of planned behavior (TPB).
A cross-sectional survey approach was used with a stratified-random sample o f nurses and laboratory workers
from Illinois (N = 527). The sample was predominately married, white females, 30 years old, w ith a bachelor's level
education, who worked full-time in a hospital setting and had an average of 14 years' experience. The sample was
surveyed using a 26-itcm questionnaire with acceptable content validity and reliability estimates.
Guided by the SPM, structural equation modeling techniques were used to explore intention and self-reported
glove use behavior. The variables and relationships within the SPM accounted for much of what occurred with glove use;
75% o f the variance in glove use behavior was explained. Intention, attitude, and perceived risk w ere significant
predictors o f behavior. Intention was the best predictor o f glove use. Perceived control and attitude were the significant
determinants o f intention, explaining 74% o f the variance in intention. Perceived control was the variable that contributed
the most to the understanding o f the health care workers' intention towards glove use. Of the three models, the TRA was
the most parsimonious in defining glove use behavior. The TRA, however, did not define what contributed to the health
care workers’ intention to wear gloves as well as the TPB or the SPM did. At least 74% of the variance in glove use
intention and behavior was accounted for by the TPB and the SPM. Overall, the TPB was the most parsimonious model
in explaining why health care workers did or did not intend to wear gloves.
Two departures from the TRA's measurement approach were found. First, contrary to the TRA, intention did not
completely mediate the attitude-behavior relationship. Secondly, multiplying the normative beliefs by motivation to
comply did not add to the predictive capability o f the normative beliefs. These departures from the TRA have been
supported by previous research. An additional methodological concern was the inadequacy of protection effectiveness as
a measure of perceived control.
A secondary aim of this study was to ascertain if glove use varied with the sample's field o f employment, in
addition to the geographical region and type of work setting in which health care workers were employed. Results
indicated that nurses and laboratory workers wore gloves frequently, but only one third to one half o f the sample wore
xi
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

SUMMARY (continued)
gloves every time there was a potential occupational risk. Analysis o f variance procedures revealed that the geographical
region where the nurses and laboratory workers were employed was predictive o f glove use. In addition, the region in
which the HCWs were employed influenced nurses’ and laboratory workers' glove use differently. Suburban laboratory
workers wore gloves m ore frequently than did rural or urban laboratory workers.
Several issues related to glove use continue to be problematic, and occupational health nurses have the
opportunity to take a leadership role in their resolution. These issues include accessibility o f gloves that fit properly,
procedures that facilitate safe work practices, and educational programs that are tailored to meet the special needs of
health care employees. In addition, a national standard on glove quality needs to be established and enforced.
This study concluded that the components of the SPM, as well as field o f employment and geographical region,
are important variables in exploring health care workers' use o f gloves when there is potential exposure to bloodbome
diseases. The results o f this study advanced the work of other researchers in what is known about glove use behavior, as
well as identifying important variables to include in future research. While future research is needed to refine and
validate the relationships within the model, the SPM is a viable approach to study behavior related to injury prevention.
xu
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

INTRODUCTION
Background
The Occupational Safety and Health Administration (OSHA) estimated that the 4.9 m illion health care workers
(HCWs) who frequently handle blood are the most at risk employee group for exposure to bloodbome pathogens such as
human immunodeficiency virus and hepatitis B virus (U.S. Department o f Labor, 1991). To minimize HCWs' exposure
to bloodbome pathogens, the Centers for Disease Control (CDC) in August 1987 issued the universal precautions
mandate. Universal precautions considers all body fluids and materials to be infectious. Universal precautions requires
the use of personal protective equipment, such as gloves, when handling body fluids regardless of the diagnosis or risk of
human immunodeficiency virus (HIV) or hepatitis B (CDC, 1987). Research has demonstrated that a universal
precautions policy is m ore effective than a selective precautions policy (Gordin, Gibert, Hawley, & Willoughby, 1990;
Kelen et al„ 1988).
However, controversy surrounds the universal precautions policy. Experts have debated whether the policy is
cost-effective because it costs so much to stock institutions with necessary supplies and because so few cases of
occupational HIV have been documented (Doebbeling & Wenzel, 1990; Stock, Gafni, & Bloch, 1990). Although
emphasis in the literature has focused on eliminating HIV transmission, many more HCWs die each year from
occupationally transmitted hepatitis B than from HIV (Gerberding, 1990). According to OSHA (U.S. Department of
Labor, 1991) estimates, hepatitis B due to occupational blood exposure infects 8,700 HCWs and kills 200 in the United
States every year. Laboratory workers employed in urban medical centers run a risk of being exposed to hepatitis B
approximately three tim es that o f other hospital employees (Evans, Henderson, & Bennett, 1990).
Other issues relate to the efficiency of universal precautions in the reduction of HCWs' risk for acquiring HIV
and hepatitis B. Concerns have surfaced regarding appropriateness o f the recommendations to prevent percutaneous
transmission (e.g., needlesticks) of bloodbome pathogens (Jagger & Pearson, 1991). However, universal precautions have
been shown to prevent cutaneous (i.e., skin exposure) occupational transmission o f HIV and hepatitis B (Fahey, Koziol,
Banks, & Henderson, 1991; Gonzalez & Naleway, 1988). O f nurses and physicians reporting body fluid exposures,
cutaneous blood exposure was the cause in 68% and 85% o f the cases, respectively (Stotka, Wong, Williams, Stuart, &
Markowitz, 1991).
An additional issue surrounding universal precautions is compliance. Despite the CDC's mandate, research
studies since 1987 indicate that HCWs fail to wear gloves with potential blood contact from 1% to 90% of the time
1
R eproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

2
(Freeman & Chambers, 1992; Loewen, Dhillon, Willy, Wesley, & Henderson, 1989). Results indicate that glove use
varies by work setting, geographical location, and clinical situations. Stotka et al. (1991) reported that 91% o f HCWs'
blood exposures were considered preventable if barrier precautions had been used, and that 98% o f those exposures were
o f the hand. Clearly, clinicians are not always following the CDC universal precaution mandate, and specifically they are
not using gloves when they handle blood.
In an attempt to decrease HCWs' exposure to H IV and hepatitis B, OSHA has enacted a standard governing the
occupational exposure to bloodbome pathogens (U.S. Department of Labor, 1991). The standard includes a combination
o f engineering and work-practice controls, personal protective equipment, training, medical follow-up, and vaccination to
reduce or eliminate the exposure risk. Gloves must be used by HCWs for all types o f blood handling, with the possible
exception o f blood drawing during volunteer blood drives (U.S. Department of Labor, 1991). T his study will focus only
on the use o f gloves as a means to reduce or eliminate the exposure risk.
Conceptual Framework
In the past, health professionals have used a variety o f theoretical approaches to study HCW s' safe behavior
sim ilar to barrier precautions. These theoretical approaches may serve as a springboard for future research. Approaches
used include (a) the health belief model to explain HCW s’ continued recapping of needles (Becker et al., 1990) and
neonatal nurses' use o f universal precautions (Conte, 1992); (b) diffusion o f innovations to predict dentists' use of
infection control procedures (Dorsey et al., 1991); (c) the common sense model to explore nurses' representation of
workplace HIV transmission and risk taking behavior (McNabb & Keller, 1991); (d) social influence to interpret nurses'
handwashing and needle recapping behavior (Seto, Ching, Chu, & Seto, 1991; Seto, Ching, Yuen, Chu, & Seto, 1991;
Seto et al., 1990); (e) performance feedback to increase nurses' use of gloves (DeVries, Burnette, & Redmon, 1991); and
(f) a stress-coping model to explore nccdlesticks in nurses (Sheehy & Trudeau, 1992). Additional theoretical strategies
have been used to foster workers' safe behavior, such as behavior modification techniques (M cAfee & Winn, 1989; Peters,
1991) and the epidemiological model (Suchman, 1967).
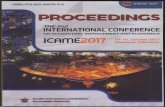
A n additional theoretical approach is the sclf-protection model (SPM), under development by the author, which
seeks to explain IICWs' use of personal protective equipment (sec Figure 1). The SPM is an extension of Ajzen and
Fishbcin's theory of reasoned action (1980) and Ajzen's theory o f planned behavior (1985; 1987; 1991). The concepts
incorporated in the SPM arc belief evaluation, attitude, normative influence, subjective norm, perceived control, and
W einstein's (1980) measure of perceived risk.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

3
Bel efE v a lu a tio n
NormativeInfluence
ControlBeliefs
SubjectiveNorm
Intention
P erceivedRisk
Behavior
PerceivedControl
Figure 1. The Self-Protection Model.
When the theory o f reasoned action (TRA), a value expectancy theory, was applied to such preventive health
behaviors as exercise (Godin, Valois, Shephard, & Deshamais, 1987; Riddle, 1980) and seat belt use (Wittenbraker,
Gibbs, & Kahle, 1983), intention was predictive of behavior. The theory o f planned behavior (TPB) extends the TRA
with perceived control and is more appropriate in situations when individuals do not perceive themselves as having
complete control over their behavior (Ajzen, 1991). The TPB has been used to explain a variety o f preventive health
behaviors, including the use of personal protective measures (Gongaware, 1991). In addition, perceived control was the
best predictor of actual weight loss (Schiftcr & Ajzcn, 1985). W einstein's (1980) measure o f perceived risk has been
employed to explain responses to safety risks such as automobile accidents (Weinstein, Grubb, & Vautier, 1986) as well
as health threats including hepatitis B (Weinstein, 1980, 1982) and HIV (Van Der Velde, Hooykaas, & Van Der Pligt,
1992).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

4
Study Purpose
The study proposed to identify predictors of HCWs' behavior related to injury prevention. Using the SPM, this
study investigated HCW s' intentions and self-reported use o f gloves when there was potential for blood exposure.
Additionally, this study determined which theoretical model (SPM, TRA, or TPB) explained the greatest amount of
variance in HCWs' self-reported use o f gloves. A secondary purpose was to determine if glove use varied with work
setting, location, and field o f employment.
Hypotheses
1. The SPM will fit the data better and explain more o f the variance in HCWs' self-reported use o f gloves
when there is potential blood exposure than the TRA or the TPB.
2. The TPB will f it the data better and explain more o f the variance in HCWs' self-reported use o f gloves
when there is potential blood exposure than the TRA.
3. The HCWs employed in urban hospital settings will differ in frequency of glove use from those
employed in nonhospital rural settings.
a. The HCWs' self-reported use of gloves will vary by the type o f work setting.
b. The HCWs' self-reported use of gloves will vary by the geographical location.
c. Reported use of gloves will vary by the HCWs' field o f employment.
Theoretical Definition o f Terms
Conceptual definitions for the SPM follow:
1. B elief evaluation is the evaluation o f the perceived consequences o f a behavior for a modal set of
behavioral beliefs. Belief evaluation leads to the formation of attitude and is an indicator of attitude.
2. Normative influence is a group of referent others whom the individual perceives as expecting him/her to
perform or not perform the behavior. Normative influence leads to the formation o f and is an indicator of subjective
norm.
3. Control beliefs are a cluster of control factors (internal and external) which are perceived to facilitate or
hinder performing a behavior. Control beliefs lead to the formation o f perceived control and are also an indicator of
perceived control. Control beliefs were not measured in this study.
4. Risk beliefs are a set of beliefs or reasons that the individual perceives to be why he/she is
vulnerable/invulnerable to a hazard. Risk beliefs form the basis of perceived risk but were not measured in this study.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

5
5. Attitude is the personal level determinant o f intention and the individual's evaluation of performing the
behavior (Ajzen & Fishbein, 1980).
6. Subjective norm is the social level determinant of intention; the individual's perception that the people
who are most important think that the individual should or should not perform the behavior and includes the motivation
to comply with them (Ajzen & Fishbein, 1980).
7. Perceived control is the individual's perception as to how easy or difficult it would be to perform the
behavior (Ajzen, 1989).
8. Perceived risk is the individual's evaluation o f the personal degree of risk as compared to others if the
specific precaution or behavior is not performed (Weinstein, 1982).
9. Intention is the individual's perception of whether a specific behavior will be performed. Behavioral
evaluation, normative influence, perceived behavioral control, and perceived risk are postulated to influence intention.
Significance
A National Institutes of Health study indicated that the risks o f occupational cutaneous HIV exposure would be
eliminated if barrier precautions were used; it recommended the development of strategies to increase HCWs' use of
precautions (Henderson et al., 1990). Theory-driven research which examines issues related to HCWs' compliance with
universal precautions is one avenue to provide such strategies. Unfortunately, the current literature contained only a few
theoretically based studies that examined the use o f barrier precautions by HCWs'.
Occupational health nurses are greatly concerned about occupational exposure to bloodbome pathogens because
the 4.9 million HCWs are their clients. One of the major aspects of the occupational health nurse's role is to recognize
worksite hazards and to prevent occupationally-acquired injuries and diseases (Travers, 1987). Furthermore, it is the
occupational health nurse's responsibility to encourage HCWs' compliance with recommended precautions. The American
Association o f Occupational Health Nurses established research priorities which included identifying occupational hazards
of HCW s as well as factors that contribute to behavioral changes among HCWs (Rogers, 1989).
Predictors of intention and use of gloves by HCW s can be identified through the use of the SPM. Future
research using interventions targeted at changing the primary beliefs or perceptions that are negatively correlated with
intention/behavior can then be studied for effectiveness. Results o f future research related to glove use would be
beneficial to occupational health nurses interested in reducing workers' risks.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

REVIEW OF RELATED LITERATURE
T his literature review is divided into two sections: (a) research related to HCWs' com pliance with universal
precautions and (b) literature associated with the constructs used in the SPM (behavioral evaluation, normative influence,
perceived control, and perceived risk) as well as related research. As constructs are presented in relation to the original
models from which the constructs were derived, this part o f the discussion contains four discrete parts: TRA, TPB,
W einstein's (1980) measure o f perceived risk, and the SPM.
Compliance with Universal Precautions
Num erous studies have investigated HCWs' compliance with universal precautions. Results indicated that
compliance varied since universal precautions have been instituted. For example, Table I indicates gloves were not worn
from 1% to 90% o f the tim e when there was potential blood exposure. Studies varied as to whether failure w as of a
single incident (Fox, 1990, unpublished data) or as a percentage o f always wearing (Smyser, Bryce, & Joseph, 1990).
Glove use also varied across studies whether a self-report or observational measure was used. No difference w as found in
the frequency of glove use when self-reported use was compared to observed use (Henry, Campbell, & Maki, 1992).
Table I indicates that glove use varied by clinical situation. In emergency situations, HCW s' use of gloves
differed according to the extensiveness of the HCWs' interventions (Baraff & Talan, 1989; Kclen et al., 1989; Kelen et
al., 1991; Talan & Baraff, 1990). In nonemergency situations, failure to wear gloves was highest when the HCW
perceived the patient to be low risk (Lusk, 1989, unpublished data; Stevens, Mentis, & Downs, 1991).
In the Fox (1990, unpublished data) study, glove use was significantly associated with type of setting. More
often H CW s failed to wear gloves when drawing blood in perceived low risk areas such as physician offices and suburban
hospitals. Additional studies also indicated that gloves were not frequently worn in physician offices (Freeman &
Chambers, 1992; M iller, Krol, & Losh, 1992; U.S. Department o f Labor, 1989).
In addition to the type of setting, setting location was associated w ith glove use in one study. In a national study
of certified nurse midwivcs, Willy, Dhillon, Loewen, Wesley, and Henderson (1990) found that universal barrier
precautions varied significantly with size of the city o f residence.
In a search for reasons for noncompliance, researchers have indicated several factors associated with nonuse (see
Table II). These factors are related to (a) perceived control (time, availability, habit); (b) risk (perceived risk, type o f
patient contact); (c) behavioral beliefs (inconvenience, discomfort, relationship with patient); (d) awareness of universal
precautions; and (e) protection effectiveness (effectiveness, necessity).
6
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

7
TABLE I
RESEARCH INDICATING HEALTH CARE WORKERS' FAILURE TO WEAR GLOVES WITH POTENTIAL BLOOD CONTACT
Researchers Sample Measure Failure to Wear
Freeman & Chambers, 1992 34 physician office staff Self-reported and observed glove use
Self-reported: 1-39% Observed: 56%
Friedland, Joffe, Wiley, Schapire, & M oore, 1992
23 pediatric emergency room nurses
Observed glove use 3-50%
Henry, Campbell, & Maki, 1992
1,018 emergency room observations
Self-reported and observed glove use
Self-reported: 23% Observed: 26%
Jagger, Detmer, Cohen, Scarr, & Pearson, 1992
276 hospital laboratory workers Self-reported glove use 45%
McKay, 1992 60 anesthesia providers Observed glove use 45%
Miller, Krol, & Losh, 1992 1,409 family practice physicians Self-reported glove use 68%
Bauer, 1991 25 circulating operating room nurses
Self-reported glove use 20-32%
Kaczmarek et al., 1991 405 HCW a-patient observations Observed glove use 8-29%
Kclen et al., 1991 127 emergency room FICW Observed glove use Intervention Minor: 9-11% Examination: 19%
Panlilio et at., 1991 146 operating room personnel Observed glove use 14%
Schwartz, Jacobs, & Juda, 1991 86 I-ICW-patient interactions Observed glove use 31-44%
Stevens, Mentis, & Downs, 1991
24 anesthetists Self-reported and observed glove use
Observed: 22-58% Self-reported:High risk: 4% Routine care: 50%
W ilkinson, 1992 574 HCW -patient interactions Observed glove use 22%
Bowman & Nicholas, 1990 Nursing personnel (size not reported)
Observed glove use 11-23%
Doebbeling & Wenzel, 1990 154 intensive care unit HCW Self-reported glove use 28%
Fox, 1990, unpublished data 181 college faculty/staff reporting on HCW
Recall o f observed glove use
35%City hospital: 23% Suburban hospital: 4" Physician office: 54°/
Gauch, Feeney, & Brown, 1990 212 hospital laboratory workers Self-reported glove use 54%
Smyser, Bryce, & Joseph, 1990 877 emergency medical technicians
Self-reported glove use 63%
Talan & Baraff, 1990 24 emergency room nursing personnel
Observed glove use Interventions Major: 12% Minor: 35%
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

TABLE I (continued)
RESEARCH INDICATING HEALTH CARE WORKERS' FAILURE TO WEAR GLOVES WITH POTENTIAL BLOOD CONTACT
Researchers Sample Measure Failure to Wear
Albrecht & Miller, 1989 307 hospital laboratory workers Self-reported glove use 34%
Baraff & Talan, 1989 Emergency room HCW (size not reported)
Observed glove use Interventions Major: 35% Minor: 48%
Kelen et al., 1989 129 emergency room HCW Observed glove use Interventions Major: 83% Minor: 44%
Loewen, Dhillon, Willy, Wesley, & Henderson, 1989
1,562 nurse midwives Self-reported glove use 90%
Lusk, 1989, unpublished data 35 hospital laboratory workers Self-reported glove use Low risk: 34-36% High risk: 4-5%
aITCW = Health care worker.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

9
TABLE II
FACTORS RELATED TO HEALTH CARE WORKERS' COMPLIANCE W ITH UNIVERSAL BARRIER PRECAUTIONS
Factors Researchers
Time Courington, Patterson, & Howard, 1991; Hammond, Eckes, Gomez, & Cunningham, 1990; Henry, Campbell, & Maki, 1992; Hoffman-Terry, Rhodes, & Reed, 1992; Kelen et al., 1990; McNabb & Keller, 1991
Interference or Conte, 1992; Courington et al., 1991; Henry et al., 1992; Kelen et al., 1990; Linn, Kahn, &inconvenience Leake, 1990; McNabb & Keller, 1991; Ros & Cabrera-Ros, 1990; Willy, Dhillon, Loewen,
Wesley, & Henderson, 1990
Discomfort Baraff & Talan, 1989; Bauer, 1991; Kelen et al., 1990; McNabb & Keller, 1991
Effectiveness of protection
Baraff & Talan, 1989; Conte, 1992; Hoffman-Terry et al., 1992; Kelen et al., 1990
Supply availability Baraff & Talan, 1989; Courington et al., 1991; Gruber et al., 1989; Henry et al., 1992; Hoffman-Terry et al., 1992; Kelen et al., 1990; McNabb & Keller, 1991; Willy et al., 1990
Perceived risk Conte, 1992; Hammond et al., 1990; Henry et al., 1992; Hoffman-Terry et al., 1992; Kelen et al., 1990; McNabb & Keller, 1991; Talan & Baraff, 1990; R os & Cabrera-Ros, 1990; Willy et al., 1990
Awareness o f universal Baraff & Talan, 1989; Conte, 1992; Courington ct al., 1991; Hamm ond et al., 1990; Henryprecautions et al., 1992; Kelen et al., 1990; Talan & Baraff, 1990; Willy et al., 1990
Habit or remembrance Gruber et al., 1989; Hammond et al., 1990; Henry et al., 1992; McNabb & Keller, 1991
Necessity Courington et al., 1991; Hammond et al., 1990; Hoffman-Terry et al., 1992; Linn ct al., 1990; Willy et al., 1990
Relationships Linn et al., 1990; McNabb & Keller, 1991; Willy et al., 1990
Type o f contact Baraff & Talan, 1989; Bauer, 1991; Bowman & Nicholas, 1990; Henry et al., 1992; Kelen et al., 1990; McNabb & Keller, 1991; Smyser, Bryce, & Joseph, 1990; Talan & Baraff, 1990; Willy et al., 1990; Wong et al., 1991
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

10
Calls for strategies to change HCW s' attitudes and behavior have been answered by additional as well as more
intensive educational programs (Becker, Cone, & Gcrberding, 1989; Klein, 1991). Several studies have investigated the
effects o f interventions, including education, to increase HCWs' compliance with universal barrier precautions (see Table
III). Fourteen studies were located that investigated the impact o f interventions on hospital-based HCWs' compliance
with universal barrier precautions since the CDC issued the universal precautions mandate in August 1987 and through
June 1993. Of note, one study was a follow-up to an earlier one (Kelen et al., 1990; Kelen et al., 1991). These studies
were mainly atheoretical in nature; o f the studies presented in Table HI, only one study reported any form o f conceptual
framework guiding the research (DeVries et al., 1991).
Nonexperimental designs w ere used exclusively, w ith a pretest/posttest design being used by 85% o f the studies.
Samples were predominately convenient and the emergency room was the most frequent setting. Sample size of
individuals ranged from 4 to 283. However, the unit o f analysis w as frequently the HCW -patient contact; sample size
ranged from 40 to 1,861 contacts or events. M ost studies included a variety of HCW personnel including nurses,
physicians, and emergency medical technicians. Several studies classified HCW -patient contacts according to blood and
body fluid exposure risk or type o f barrier needed. Contacts were classified as critical or major contacts when multiple
barriers were required. Noncritical or m inor contacts required only the use of gloves for protection.
All of the studies lacked any analysis o f power. A power analysis determines if the sample size was large
enough to eliminate the chance of a Type II error, given treatment (intervention) effects. W ithout power calculations,
conclusions about possible treatment effects are difficult to make (Polit & Sherman, 1990). Six studies provided enough
information to perform a post hoc pow er analysis. Cohen's (1988) tables and an alpha error o f .05 w ere used. Overall,
there was little likelihood of detecting small treatment effects in these studies. Being able to detect small effects is
important as research in new areas usually generates small treatment effects (Cohen, 1988).
Education, as an intervention, was used in all but one study. Other interventions included performance feedback,
reminder posters, and equipment purchases. Although studies frequently supplied multiple interventions, only three
reported any standardization o f procedures (DeVries et al., 1991; Talan & Baraff, 1990; Wong et al., 1991).
The definition o f compliance was not consistent across the studies. For example, use o f any of the required
barriers was considered compliance in the Courington, Patterson, and Howard (1991) study, as well as in W ong ct al.
(1991). Conversely, compliance in the Kelen et al. (1991) study occurred only if all of the required barriers were used.
All of the studies measured glove use and additional barriers (e.g., masks, gowns, eyewear) were assessed in 62% of the
studies. Three studies used a self-report measure; the remaining studies used observational measures. As instrument
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

11
TABLE III
INTERVENTION STUDIES EXAMINING HEALTH CARE W ORKERS’COMPLIANCE WITH UNIVERSAL BARRIER PRECAUTIONS
ResearchersD esign and Intervention Sample Measures Significant Findings
Albrecht & M iller, 1989
B araff & Talan, 1989
Talan & Baraff, 1990
Bowman & Nicholas, 1990
Hammond, Eckes, Gomez, & Cunningham, 1990
NonexperimentalCross-sectionalEducation
NonexperimentalCross-sectionalEducation
Nonexperimental Pretest/posttest Education, feedback
Nonexperimental Pretest/posttest Education, feedback
Nonexperimental Pretest/posttest Education, feedback, equipment purchases
283 medical laboratory workers from 8 hospitals (convenience)
169 HCW*5-Emergency Room patient contacts (convenience)
24 Emergency Room nursing personnel (convenience)
Nursing-patientcontactsPretest: 112 contacts Posttest: 121 contacts (random)
Emergency Room resuscitation contacts Pretest: 81 Emergency Room patients Post test: 84 Emergency Room patients(stratified random)
Self-reported glove use with all specimens
Observation critical: gloves, masks, eyewear, gownnoncritical: gloves
Observation cn7;'ca/:gloves, masks, eyewear, gownnoncritical: gloves
Observation glove use
Observation gloves, mask, eyewear,apron/gown, ankle protectionInvasive procedures (all barriers required)
Type of Barrier8 glove use increased with the number o f educational programs attended p < .005
Type of Contactc critical: gloves = 73% gown = 26% mask = 2% eyewear = 18% noncritical: gloves = 52%
Type of HCW d Glove use nurse = 51% EM Te = 71% physician = 50%
Type of Contact critical: gloves = p < .025 eyewear = p < .05
Type of Barrier Pretest = 66 - 79% Posttest = 11 - 89%
Type of Barrier Pretestapron/gown = 82% gloves = "nearly universal" mask = 63% ankle = 67%
Type of Contact Invasive procedures Pretest = 37%Posttest = 61%
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

12
TABLE III (continued)
INTERVENTION STUDIES EXAMINING HEALTH CARE WORKERS'COMPLIANCE WITH UNIVERSAL BARRIER PRECAUTIONS
Design andResearchers Intervention Sample Measures Significant Findings
Courington, Nonexperimental HCW-patient contacts Observation Tvdc o f BarrierPatterson, & Pretest/posttest Operating room'. Operating room: Surgical care:Howard, 1991 Education, feedback Pretest: 266
Posttest: 310 Surgical ward: Pretest: 243 Posttest: 253 Intensive care: Pretest: 40 Posttest: 53 (convenience)
eyewearSurgical w ard & intensive care: mask, gloves
eyewear p < .05 gloves p < .05
TvDe o f Contact Surgical ward: minor p < .05
Tvne o f HCW Operating room: surgeon & nursing p_< .05 Surgical ward: physician p < .05
DeVries, Nonexperimental 4 Emergency Room Observation Tvoe o f BarrierBurnette, & Pretcst/posttest nurses glove use Pretest = 41%Redmon, 1991 Feedback (convenience) Posttest = 73%
Kelen et al., Nonexperimental Emergency Room Observation Tvne o f Contact1991 Pretcst/posttest personnel M inor & Posttest Exam = 71%
Education, feedback, Pretest: 129 HCWs examination: M inor = 82% Major =reminder posters 1,274 patient contacts
Posttest: 127 HCWs 1,861 patient contacts (convenience)
glovesMajor: gloves, gown, mask, and eyewear (all required)
55%p < .01
Tvne o f HCW Pretestphysicians, nurses, X-ray personnel, EMT, housekeeping, p < .01
Stevens, Mentis, Nonexperimental Anesthetists Self-report Tvne o f Barrier& Downs, 1991 Pretest/posttest Pretest: 46 gloves, masks, Glove use increased in 3
Education Posttest: 24 (convenience)
eyewear, gown in 5 clinical situations
out of 5 situations, eyewear in 1 situation p < .05
W ong ct al., Nonexperimental 277 physicians, 1,553 Self-report Tvne o f Barrier1991 Prctest/posttest
Education, feedback, equipment
exposure incidence (convenience)
gloves, gown, mask, eyewear
Odds Ratio= 3.3 p < .001
Tvne o f Contact emergency status Odds Ratio = .61 p < .01
Freeman & Nonexperimental Physician office HCWs Observation Tvne o f BarrierChambers, Prctest/posttest Pretest: 97 blood gloves Pretest: 44%1992 Education exposures
Posttest: 98 bloodPosttest: 49%p > .2
exposures(convenience)
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

13
TABLE III (continued)
INTERVENTION STUDIES EXAMINING HEALTH CARE WORKERS'COMPLIANCE WITH UNIVERSAL BARRIER PRECAUTIONS
ResearchersDesign and Intervention Sample Measures Significant Findings
Friedland, Joffe, Wiley, Schapire, & Moore, 1992
Nonexperimental Pretest/posttest Education, reminder posters
23 Emergency Room pediatric nurses Experienced'. 16 N ot experienced: 1 (convenience)
Observation glove use
TvDe o f Barrier Experienced: Pretest = 15% Posttest 3 = 50%
Not Experienced: Pretest = 70% Posttest 3 = 97%
Schwartz, Jacobs, & Juda, 1992
NonexperimentalPretest/posttestEducation
Acromedical HCWs Pretest: 162 flights Posttest: 86 flights (convenience)
Observation gloves, goggles
Tvne o f Barrier Posttest: no change Goggles = 0% Gloves:
Nurses = 56% Physicians = 69% p > .05
aTypc o f Barrier = Findings placed in this category if study analyzed compliance by type o f barrier used.
^HCW = health care worker.
cType o f Contact = Findings placed in this category if study analyzed compliance by the extensiveness of HCW-patient contact.
‘'Type o f HCW = Findings placed in this category if study analyzed compliance according to the H C W s job classification.
CEMT = emergency medical technician or paramedic.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

14
reliability or observer training procedures were rarely reported, it is not clear how consistently compliance was measured.
An exception was the DeVries et al. (1991) study which reported inter-rater agreement o f 93% to 100%.
Frequency distribution was the sole method of analysis in 38% o f the studies. O f the studies which tested for
significance, 75% used chi-square or Fisher's exact test fo r analysis.
Findings were categorized in relation to compliance with universal barrier precautions by (a) type o f barrier such
as gloves or gowns; (b) type of HCW including nursing, physicians, and paramedics; and (c) type of patient contact such
as critical or noncritical, major or examination. Related to the type of barrier used, the greatest compliance was with
glove use. Glove use varied from 15% to "nearly universal" before the intervention to 49% to 97% post intervention.
Two studies indicated a trend that barrier compliance was significantly associated with type o f contact; the more emergent
or extensive the contact, the less likely the HCW was to use the barriers (Kelen et al., 1991; Wong et al., 1991). In
addition, Kelen et al. (1991) found that compliance varied between HCW groups.
Two studies reported no change in compliance after the intervention. Determining the effects o f treatment is
hampered by the small number of studies with similar methods of reporting significant results. For example, four studies
reported results in relation to the effects o f the intervention on barrier compliance. No conclusions can be drawn from
the four studies. Wong et al. (1991) reported a positive significant effect for all barriers combined. Albrecht and Miller
(1989) reported a positive significant effect for glove use. And finally, the Courington et al. (1991) and Stevens et al.
(1991) studies described both significant and nonsignificant (positive or negative) results for the use of gloves or eyewear.
Although inconclusive, results o f these 13 intervention studies indicate that HCW s' compliance may vary with
type of barrier used, type o f patient contact, and type of HCW. No conclusions, however, can be made regarding the
effect o f the interventions due to the small number of articles reporting significant results, lack of power, and the
weakness of the study designs.
In summary, several variables were identified which may be associated with HCW s' compliance with universal
barrier precautions. These variables included type o f setting and location, type of patient contact/HCW /barrier, perceived
control, perceived risk, behavioral beliefs, awareness of universal precautions, and protection effectiveness. Variables
identified through research focusing on universal precaution compliance could be used as a basis for new model
development or to extend an existing framework.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

15
Theory of Reasoned Action
Constructs and Assumptions
As the TRA (Ajzen & Fishbein, 1980) was influenced by Lewin's (1951) field theory, several of Lewin's
assumptions apply to the TRA as well. These assumptions include (a) behavior is a function people’s interaction with
their meaningful environment; (b) people's behavior is determined by their perception o f the situation in which they find
themselves; and (c) the present, and not the past, primarily determines people's behavior. An additional assumption of the
TRA is that people usually behave in a rational manner, giving consideration to the consequences of their actions.
According to the TRA, this process is mostly automatic. Many routine behaviors o f social relevance are under the
individual's volitional control. These behaviors are ones that do not require skills or cooperation of others. The person
can chose to act or not. Therefore, the person's intention is the deciding factor o f whether the behavior is performed.
Behavior is a function of intention (see Figure 2).
Factors associated with intention need to be assessed in order to understand and predict behavior. There are two
determinants o f behavioral intention. One is that the beliefs about consequences of the behavior and the evaluation of
consequences lead to attitude toward the behavior. In addition, perceptions of significant others regarding the behavior
and the motivation to comply determine subjective norm. Both subjective norm and attitude toward the behavior may
lead to intention. Action is likely to occur when the person positively views the outcome of the behavior, assumes that
Attitudetow ard
behavior
BehaviorIntention
SubjectiveNormMotivation to com ply
Normative beliefs
Behavioral beliefs
Belief evaluation
Figure 2. Theory o f Reasoned Action.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

16
significant others want the individual to perform the behavior, and the individual is motivated to comply with these.
Contributions that attitude and subjective norm make to the prediction of intention vary with the behavior. The theory is
represented symbolically as B ~ I = [Abwj + SNw2]. Intention (I) is predictive of behavior (B) and intention is a
function o f the weighted (Wj, w2) sum of attitude toward the behavior (Ab) and subjective norm (SN).
The TRA states that a person's behavioral beliefs determine the attitude toward the behavior. Individuals
acknowledge there are possible outcomes or consequences to their actions and rate these outcomes as good or bad.
Symbolically, Ab = attitude toward the behavior is determined by summing the products o f specific beliefs (b)
that performing the behavior w ill lead to an outcome (i) and the evaluation (e) o f that outcome (i).
Similarly, the individual's normative beliefs determine subjective norm. In the individual's perception, important
or referent others have expectations regarding the behavior and the person decides how motivated he/she is to comply
with those expectations. This relationship is represented symbolically as, SN s 2,bjmj. Subjective norm (SN) is the sum
of the products of the normative beliefs (b) regarding referent others (j) and the person's motivation to comply (m) with
each.
There are several conditions that may affect the relationship between intention and behavior. Jaccard (1975)
identified seven such conditions: (a) time interval between measurement o f intention and the measurement o f behavior;
(b) exposure o f new information between the measurement of intention and behavior; (c) number of steps that must be
taken before the behavior can be performed; (d) lack of abilities; (e) force of habit; (0 effect of memory ; and (g)
specificity of the measure of intention and behavior.
Ajzen and Fishbein (1980) emphasized the importance o f specificity or correspondence between the measures of
prediction of behavior. The measures of attitude, intention, and behavior must be at the same level of generality and
correspond. Correspondence between measures is critical in regard to action, target o f the action, context that the action
is performed within, and the tim e the action was performed. These four elements o f action, target, context, and time
should be defined prior to instrument development.
In order to assess the individual's intentions, beliefs about attitude and the subjective norm must first be
determined. Beliefs associated with a specific behavior and the related referents are usually elicited by interview. The
purpose o f the elicitation study is to identify the salient beliefs and referents o f the sample. These salient beliefs and
referents arc then used to develop an instrument to measure attitude and subjective norm.
Ajzen and Fishbein (1980) recommend eliciting beliefs in a free response format from a sample sim ilar to the
intended study sample. The subjects are asked to identify the advantages and disadvantages of performing the behavior.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

17
In addition, subjects identify the people who think the subject should or should not perform the behavior. As a rule of
thumb, individuals hold five to nine salient beliefs at a time; those beliefs that are elicited first are the ones most
important to them.
Comparable responses are grouped together and the most frequent form what is term ed the "modal set." The
modal set is used in developing the questionnaire. The subject rates the strength, on a bipolar Likert-type scale, of the
belief that the performance of the behavior will lead to that outcome and similarly ranks the value of the outcome. The
individual also indicates how likely or unlikely it is that the referents expect the person to perform the behavior. The
motivation to comply with these referents is measured on a unipolar scale, strongly to not at all strongly.
The use o f the modal set of beliefs and referents provides indirect measures o f attitude and subjective norm.
Direct measures of subjective norm and attitude can also be obtained. Subjective norm is directly measured by asking
how likely it is that most people important to them would approve o f their performing the behavior. A direct measure of
attitude is obtained by using several bipolar evaluative adjectives to judge behavior performance. Ajzen and Fishbein
(1980) report good correlations between direct and indirect measures (/■ = .60-.80) and both measurement approaches are
predictive o f intention. A determination of beliefs associated with nonintention which is important for intervention
purposes can, however, only be obtained from indirect measures.
Using equations previously mentioned, attitude and subjective norm are defined. Regression analysis determines
the weights o f the behavioral and normative components. Identifying which component contributes more to intention is
important for intervention purposes. Interventions are targeted at changing the primary beliefs that correlate highest with
nonintention. Changing beliefs, however, does not always result in a change in intention as the new belief may carry the
same strength and evaluation.
Additional or external variables are not directly included in the TRA (e.g., demographics, self-efficacy, perceived
risk). The TRA assumes that these external variables influence intentions and/or behavior indirectly through the
formation o f attitude and subjective norm (Fishbein & Middlcstadt, 1989).
Empirical Support
The ability of attitude and subjective norm to be predictive o f intention, as well as intention predictive o f
behavior, has been demonstrated in a variety of studies. Several of these studies are in the area of preventive health.
According to the TRA, intention must be related to the specific behavior. Therefore, caution should be taken in
interpreting related but unlike behaviors. The studies that follow deal with protective behaviors. Research that
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

18
investigates protective behavior of the chronically ill is not included because perceptions of this population may be
significantly different from a healthy population.
M otor vehicle safety devices. The TRA has been tested in the area of safety behavior related to the use o f seat
belts, child car restraints, and helmet use (see Table IV). Nonexperimental, with a cross-sectional approach, was the
predom inant design used in the research. A ll of the studies developed instruments based on elicited beliefs. However,
only two reported acceptable measures o f internal consistency for the attitude scale and none reported inter-item
correlations (Gielen, Ericksen, Daltroy, & Rost, 1984; Jonah & Dawson, 1982). According to Nunnally (1978), .70 is an
acceptable level of internal consistency for a new instrument. Inter-item correlations should also be reviewed to
determine if coefficient alpha is inflated due to redundancy and not because of consistency of the items. Inter-item
correlations in the range o f .30 to .70 indicate content similarity without redundancy (Kerlinger, 1986). As elicited
beliefs are often close semantically (Fox, 1989), a determination o f inter-item correlations is important to assure that item
redundancy is not an issue. Allegrante, Mortimer, and O'Rourke (1980) measured only the stability o f the instrument.
No reliability information was reported on the subjective norm scales. Additionally, none o f the studies discussed
whether validity had been established for the instrument.
The studies used both direct and indirect measures of attitude and subjective norm. Attitude contributed more
than subjective norm to motorcycle helmet use, seat belt use, and the intended parental use of a child car restraint.
Exercise. Exercise can be viewed as a protective behavior used to prevent weight gain and promote
cardiovascular fitness. O f the studies testing the TRA in relation to exercise, all were nonexperimental in design and
three out o f five used a random sample (see Table IV). Three used a longitudinal approach to measure behavior.
Instrum ents were based on elicited beliefs in all o f the studies and there was no report o f validity. Acceptable measures
o f internal consistency were reported in two studies. Three studies measured stability o f the scales, which ranged from
r = .72 to .87.
Both direct and indirect measures were used, and Table IV indicates that attitude was m ore predictive than
subjective norm of intention to exercise in four out o f five studies. However, Pender and Pender (1986) concluded that
subjective norm contributed more to the prediction o f intention to exercise than did attitude. In the four studies
m easuring exercise behavior, intention correlated significantly with behavior.
Conceptual and Measurement Issues
Over the years, several concerns have surfaced regarding the TRA's structure. The following w ill discuss two of
the m ajor concerns related to the internal structure of the TRA which have emerged from the literature: (a) whether
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

19
TABLE IV
M OTOR VEHICLE SAFETY AND EXERCISE RESEARCH USING THE THEORY OF REASONED ACTION
Researchers and Topic
Design Sample Measures Significant Findings
Allegrante, M ortimer, & O 'Rourke, 1980 M otorcycle helmet
Gielen, Eriksen, Daltroy, & Rost, 1984 Child car restraints
Jonah & Dawson, 1982 Seat belts
M artin & Newman, Seat belt
1990
Pieterse, Kok, & Verbeek, 1992 Child car restraints
Godin & Shephard, 1986 Exercise
Dzewaltowski,1989Active sports orphysicalactivities
Nonexperimental Longitudinal (6 weeks)
NonexperimentalCross-sectional
NonexperimentalCross-sectional
NonexperimentalCross-sectional
NonexperimentalCross-sectional
NonexperimentalCross-sectional
Nonexperimental Longitudinal (7 weeks)
235 motorcyclists (random)
339 parents with children under 5 years (random)
445 Canadiandrivers(random)
200 female drivers(convenience)
419 parents with children under 5 years in the Netherlands (convenience)
90 universityemployees(random)
328 undergraduatestudents(convenience)
Aba (INb & Dc) 16 beliefs Behavior 4 items Test retest: r = .80
Ab (IN) 6 beliefs (a = .76)
Ab (IN) 6 beliefs ( a = .82) Ab (D) 1 item SN (D) 2 items
Ab (IN) 8 beliefs SN (IN) 4 referents I 1 item
Ab (D) 2 items Ab (IN) 18 beliefs SN (D) 1 item SN (IN) 6 referents
Ab (IN) 5 beliefs Ab (D) 1 item SN (D) 1 item
Ab (IN) 13 beliefs Ab (D) 6 items SN (D) 1 item I 4 items a = .80-.97
IntentionAb + SN*1: R2 = .53 Ab: /3e = .64 SN: 0 = .15 Behavior I1: r = .66:96
Intention Ab: r = .40 SN: r = .26
BehaviorAb + SN: R2 = .48
Intention AbAb: r = .37
SN: R2 = .61
IntentionAb + SN: R2 = .50 Ab: r = .47 SN: r = .33 Behavior I: r = .50
IntentionAb + SN: R2 = .31 Ab: /3 = .45 Behavior I: r = .41
IntentionAb + SN: R2 = .20 Ab: r = .49 Behavior I: r = .22
Pender & Pender, 1986 Exercise
NonexperimentalCross-sectional
337 adults (random)
Ab (IN) 6 beliefs(a = .87 Test retest: r = .78)SN (IN) 6 referents(a = .90 Test retest: r.82)I 1 item (Test retest: r = .78)
IntentionA b + SN: R2 = .06 Ab: r = .18 SN: r = .26
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

20
TABLE IV (continued)
MOTOR VEHICLE SAFETY AND EXERCISE RESEARCH USING THE THEORY OF REASONED ACTION
Researchers and Topic
Design Sample Measures8 Significant Findings*3
Riddle, 1980 Jog regularly
Nonexperimental Longitudinal (2 weeks)
296 joggers andnonexercisers(convenience)
Ab (IN) 19 beliefs (Test retest: r = .87) Ab (D) 14 items (Test retest: r = .72) SN (IN) 7 referents (Test retest: r = .78) SN (D) 1 item I 1 item
IntentionAb + SN: R2 = .55 Ab: /3 = .64 SN: j3 = .16 Behavior I: r = .82
Schmelling,1985Exercise
Nonexperimental Longitudinal (1 month)
135 universityemployees(random)
Ab (IN) 5 beliefs Ab (D) 1 item SN (D) 1 item
IntentionAb + SN: R2 = .77 Ab: (3 = .76 Behavior I: r = .65
aAb = Attitude toward behavior.
^IN = Indirect measure.
CD = Direct measure.
^SN = Subjective norm.
c ft = Standardized regression coefficient.
rI = Intention.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

21
attitude affects behavior independent o f intention and (b) whether the TRA is an additive or multiplicative model.
Additionally, issues associated with item development w ill be discussed.
Ajzen and Fishbein (1980) argued that when attitude, intention, and behavior are measured with attention to
correspondence, intention fully mediates the attitude-behavior relationship. Intention has been supported as a mediating
variable in laboratory studies, but not consistently in field studies (Bentler & Speckart, 1979, 1981; Liska, 1984).
However, Bagozzi, Baumgartner, and Y i's (1989) re-analysis o f 11 studies indicated that intention did fully mediate the
attitude-behavior relationship only when a study had (a) reliable intention measures, (b) correspondence between the
intention and behavior measures, and (c) sufficient power.
Secondly, although Fishbein and Ajzen (1975, 1980) provided no empirical support for the additive model, an
interactive effect between attitude and subjective norm has not been found (Andrews & Kandel, 1979; Liska, 1984). A
related issue is whether the belief scores should be added to or multiplied with the evaluative/motivation-to-comply items.
Fishbein and Ajzen (1975) provided limited theoretical or empirical support for the use of multiplicative composites.
There was no discussion o f the additive approach. Hewstone and Young (1988) found the additive approach more stable
in their study on the European economic community. Four studies found that motivation to comply did not significantly
contribute to normative beliefs' prediction of intention (Ajzen & Driver, 1992; Budd, North, & Spencer, 1984; Saltzer,
1981; Vallerand, Deshaics, Cuerrier, Pellerier, & Mongeau, 1992). In addition, the issue of using multiplicative
composites in correlational analysis has been raised (Evans, 1991; Lauver & Knapp, 1993; Schmidt, 1973).
Finally, issues related to the item clarity have recently surfaced in the nursing literature (Young, Lierman,
Powcll-Cope, Kasprzyk, & Benoliel, 1991). Ajzen and Fishbein (1980) provided a structured process to develop
questionnaire items from the elicitation interviews. Although this item development process may accurately reflect the
beliefs o f the population of interest, the TRA docs not address issues related to item clarity. Clarity deals not only with
readability of the item but also with whether a single message is being conveyed. Ajzen and Fishbein (1980)
recommended retaining as much o f the elicited response as possible when constructing items. However, evaluation of a
negative outcome on a good/bad scale is awkward and confusing. The effect of rewording a negative outcome was not
discussed.
Unclear items may introduce systematic error. Both Mullen, Hcrsey, and Iverson (1987) and Young et al. (1991)
identified some respondent difficulty in answering the evaluative items. Respondents were confused when asked to
evaluate an outcome if they themselves did not hold the belief. If a person does not agree that a possible outcome is, for
example, uncomfortable then how docs that person rate how good or bad being uncomfortable will be for him or herself?
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

22
Although the research reviewed here used this approach to evaluate outcomes, Fishbein recently (personal communication,
May 27, 1993) acknowledged the difficulty in evaluating health outcomes.
Summary
The accumulated studies supported the use o f the TRA in relation to protective behavior. Attitude and subjective
norm were predictive of intention to use selected protective behaviors, though their individual contributions varied with
the specific behavior. Future research should consider the impact o f item clarity as well as the effects of combination
practices on findings. Although criticism of the TRA exists, researchers continue to find the theory useful in explaining
and predicting health related behaviors. Researchers examining protective health behaviors have extended the TRA in an
attempt to increase the theory's predictive capabilities.
Extensions of the Theory o f Reasoned Action
Constructs such as self-efficacy, habit or past behavior, and facilitating factors have been added by researchers to
the TRA (see Table V). These additional constructs usually contributed significantly to intention or behavior. Self-
efficacy made a significant contribution to intention to brush and floss teeth (McCaul, O'Neill, & Glascow, 1988).
Factors that facilitated or hindered the performance o f behavior were measured with breast self-examination, obtaining a
Pap test, industrial respirator use, and exercise. Facilitating factors or barriers correlated significantly with intention and
behavior related to breast self-examination and respirator use (Hill, Gardner, & Rassaby, 1985; Lierman, Young,
Kasprzyk, & Benoliel, 1990; White, Baker, Larson, & Wolford, 1988). Additionally, facilitating factors contributed
significantly to the prediction o f breast self-examination and Pap test intentions, as well as exercise behavior (Hill et al.,
1985; Lierman et al., 1990; Valois, Deshamais, & Godin, 1988). A number of researchers have extended the TRA with
habit, as suggested by Triandis (1977). Past behavior or habit consistently contributed to the prediction of intention or
current behavior. With exercise, habit contributed more than any other variable to intention. Habit was the best predictor
o f seat belt use in only one study (Wittenbraker et al., 1983) and habit had a small effect on seat belt behavior
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

23
TABLE V
SELECTED HEALTH RELATED RESEARCH USING EXTENSIONS OF THE THEORY OF REASONED ACTION
Researchers Behavior Extension Variable Significant Finding
McCaul, O'Neill, & Glasgow, 1988
Hill, Gardner, & Rassaby, 1985
Lierman, Young, Kasprzyk, & Benoliel, 1990
White, Baker, Larson, & Wolford, 1988
Valois, Deshamais, & Godin, 1988
Godin, Valois, Shephard, & Deshamais, 1987
Godin, Cox, & Shephard, 1983
Wittenbraker, Gibbs, & Kahle, 1983
Budd, North, & Spencer, 1984
Mittal, 1988
Stasson & Fishbein, 1990
Brushing and flossing teeth
Breast self-examination, Pap test
Breast self-examination
Respirator use by painters
Employee exercise
Employee exercise
Employee exercise
Seat belt use
Seat belt use
Seat belt use
Seat belt use
Self-efficacy (SE)
Benefit/barrier factors (F)
Facilitating factors (F)
Availability factors (F)
Facilitating factors (F) Habit (H)
Habit (H)
Habit (FI)
Habit (H)
Past behavior (H)
Habit (H)
Perceived risk (PR)
IntentionSEa: R2 = .08-. 19
Intention F b: R2 = .20-.57
Behavior F :r = -.30- -.52
Behavior F: p = .46
BehaviorH c + F + Id: R 2 = .39 H: f3c = .37 I: /3 = .31
Proximal Behavior H: y = -82
IntentionH + Ab1 + SN8: R2 = .59 H: P = .30
Behavior H + I: R2 = .50 H: /J = .4 I: /3 = .30
IntentionH + Ab + SN: R2 = .80-.88 H: (3 = .38 Ab: /? = .42
BehaviorH + I: R2 = .82H: p = .20 I: (3 = .71
IntentionAb: /? = .57 SN: f3 = .3
R eproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

24
TABLE V (continued)
SELECTED HEALTH RELATED RESEARCH USING EXTENSIONS OF THE THEORY OF REASONED ACTION
Researchers Behavior Extension Variable Significant Finding
Radius, McDonald, & Bemstein, 1991
Child car-safety seat Perceived risk (PR) BehaviorPRh: r = .2 Ab: r = .15
aSE = Self-efficacy.
bF = Benefit/barrier factors.
°H = Habit.
^1 = Intention.
e/3= Standardized regression coefficient.
*Ab = Attitude.
gSN = Subjective norm.
L
PR = Perceived risk.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

25
independent o f intention in the Mittal (1988) study. Although perceived risk correlated significantly with intention in one
study (Radius, McDonald, & Bernstein, 1991), perceived risk was not predictive o f intention in the Stasson and Fishbein
study (1990).
Perceived risk, facilitating factors, habit, and self-efficacy are elements that indicate that the behavior is not
completely under the person's volitional control. Additional responses indicating elements not under the person's
volitional control have been identified in several studies. One such study is the Fox (1989) analysis o f the behavioral and
normative beliefs o f medical laboratory workers about glove use when handling blood. Responses from the Fox (1989)
and White et al. (1988) studies, and other research on HCWs' use o f gloves (not guided by the TRA), are not adequately
defined by the concept o f behavioral beliefs (see Table II). These responses include (a) equipment availability, (b) lack
of time, (c) interference with job performance, and (d) protection effectiveness.
Theory of Planned Behavior
Constructs and Assumptions
In contrast to the TRA, Ajzen's (1985, 1991) TPB assumes that many behaviors are not within the person's
volitional control and that many behaviors depend on non-motivational factors. The TPB has modified the TRA by
adding the variable perceived control to address the issue of incomplete volitional control. Perceived control deals with
the ease or difficulty of performing the behavior and relates to the past experiences, resources, opportunities, and barriers
to performing the behavior. The TPB is applicable to behaviors which are not totally within the individual's volitional
control, such as smoking cessation and the use of personal protective equipment. Perceived control is comprised of
internal factors, such as lack of skills, ability, information, emotions, and prior behavior. External factors also comprise
perceived control (e.g., time, opportunity, cooperation of others).
Ajzen (1991) considered perceived control to be related to Bandura's (1986) concept of self-efficacy. According
to Bandura's (1986) social learning theory, both perceived self-efficacy and outcome expectations are mediators of
treatment outcome. Self-efficacy refers to individuals' judgments about their ability to monitor, plan, and carry out a
behavior. Outcom e expectations is the belief that the behavior will lead to a specific outcome. Self-efficacy has been a
strong predictor o f a variety of health behaviors, including smoking cessation, pain experiences, weight control, cardiac
rehabilitation, and adherence to medical regimens (O'Leary, 1985; Strecher, DeVellis, Becker, & Rosenstock, 1986).
Taylor (1990) identified sclf-efficacy as one of four variables which consistently explained health practices. As
previously discussed, studies used self-efficacy to extend the TRA (see Table V). Ajzen, however, placed sclf-efficacy
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

26
(i.e., perceived control) within "a more general framework o f the relations among beliefs, attitudes, intention, and
behavior" (Ajzen, 1991, p. 184).
As with attitude and subjective norm, the contribution that perceived control makes to the prediction o f intention
varies with the behavior. Ajzen (1989) identified three conditions when perceived control may not contribute to the
prediction o f intention. These conditions occured when there w as (a) a lack of information, (b) a change in requirements
or resources, o r (c) a new situation.
Ajzen (1985, 1991) represented the relationship between perceived control and behavior as a broken arrow.
Perceived control has a direct effect on behavior when perceived control reflects actual control. Consequently, a direct
effect is seen when the person is realistic about what is needed to successfully perform the behavior. The direct effect on
behavior should be significant when behavior is not completely under the person's control and the person's perception of
control is accurate. The TPB is a special case o f the TRA. In behaviors where the person has close to complete control
(e.g., voting), only subjective norm and attitude are of interest. Madden, Ellen, and Ajzen (1992) found that perceived
control was not predictive of behaviors thought to be high in volitional control. In turn, when controlling for intention,
perceived control was most predictive of behavior when volitional control was low.
The theory is represented symbolically in the same manner as the TRA with the addition of PCWj. This addition
reflects that intention (I) is a function of the weighted (w j, w2, w-j) sum of attitude, subjective norm, and perceived
control.
As with behavioral and normative beliefs, the individual's control beliefs determine perception o f behavioral
control. Factors which help or hinder performing the behavior are elicited by interview. The modal set o f control beliefs
is used to measure the likelihood that the control factors would occur. An indirect measure of perceived control is the
sum of the products of control beliefs and the perceived power of the control beliefs to help or hinder performing the
behavior (Ajzen, 1989). The direct measure of perceived control is obtained using the sum o f responses from three
questions: (a) how much control one has to perform the behavior, (b) the ease or difficulty in performing the behavior;
and (c) if one wanted to, how easily could one perform the behavior. Moderate correlations between the direct and
indirect measures o f perceived control have been reported (Ajzen, 1991; Ajzen & Driver, 1991; Ajzen & Madden, 1986).
Empirical Support
The TPB has been tested with a variety o f health behaviors such as smoking cessation, condom use, and
automobile safety (Babrow, Black, & Tiffany, 1990; Lavoie & Godin, 1991; Parker, Manstead, Stradling, Reason, &
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

27
Baxter, 1992). The following is a discussion o f studies testing the TPB with exercise, weight loss, and the use of
protective equipment (sec Table VI).
As with the protective behavior research using the TRA, nonexperimental designs were used exclusively. Of the
studies employing a longitudinal approach, time ranged from four weeks to one year. Samples were all convenient. Only
two studies based instruments on data gathered from an elicitation study (Gongaware, 1991; Kimiecik, 1992). Only the
Kimiecik (1992) study used an indirect measure o f perceived control, as well as a direct measure.
Reliability of the direct perceived control measure w as generally adequate in the six studies reporting reliability
information. Kimiecik (1992) reported a high internal consistency level (a = .92) for the indirect measure o f perceived
control which was based on seven exercise barriers.
Regression analysis was the statistical method used in all o f the studies. Findings indicate that perceived control
exerted an independent and significant effect on intentions in all but the Gongaware (1991) study. However, the
Gongaware (1991) study was with a small sample and used a two-item perceived control scale. In addition, perceived
control contributed to the prediction of behavior, independent o f intentions, in all but one study (Dzewaltowski, Noble, &
Shaw, 1990). In Schifter and Ajzen's (1985) study of college women's weight loss, perceived control was the best
predictor of actual weight loss. Interestingly, one study compared the predictive capabilities of self-efficacy and
perceived control (Dzewaltowski et al., 1990). This study found that both variables were predictive of behavior, but the
correlation between perceived control and self-efficacy was low (r = .38). If perceived control is considered to be a
construct similar to self-efficacy, a higher correlation would be expected.
Measurement Issues
Although Ajzen and Madden (1986) proposed both a direct and indirect measure of perceived control, few
studies have used an indirect measure (Babrow et al., 1990; Kimiecik, 1992; Lavoie & Godin, 1991). Ajzen (1989)
recommended the use of three questions to measure perceived control directly. Little data was available regarding the
validity o f the direct measure. Ajzen and Madden (1986) reported that confirmatory factor analysis indicated that both a
3- and 5-item direct measure were unidimensional. Although no data were given, results of the factor analysis provide
some indication o f construct validity. An opinion of this writer is that the questions recommended by Ajzen do not fit
with the conceptual definition o f perceived control. As it is not clear whether these items are measuring what is intended,
a measure of content validity is needed.
Although it is questionable how well the direct method measures perceived control, Ajzen's (1989) recently
proposed indirect method appeared to capture the construct as defined. Identifying how much resources help or hinder
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

28
TABLE VI
SELECTED HEALTH RELATED RESEARCH USING THE THEORY OF PLANNED BEHAVIOR
Researchers Design Sample Measures Significant Findings
Schifter & Ajzen, 1985Weight loss
Gongaware, 1991 Personal protective equipment use
Ajzen & Driver, 1992Leisure activities
Dzewaltowski, Noble, & Shaw, 1990 Exercise
Gatch &Kendzierski, 1990 Aerobic exercise
Godin & Gionet,1991Exercise
Nonexperimental Longitudinal (6 weeks)
Nonexperimental Longitudinal (8 weeks)
Nonexperimental Longitudinal (1 year)
Nonexperimental Longitudinal (4 weeks)
NonexperimentalCross-sectional
NonexperimentalCross-scctional
76 female collegestudents(convenience)
28 oncology nurses(convenience)
143 undergraduatestudents(convenience)
254 undergraduatestudents(convenience)
100 female college students (convenience)
444 power plantemployees(convenience)
Aba (T)k) 6 items a = .82 SN® (D) 4 item s a = .88 PC^ (D) 2 item s r = .68 Ie 4 items a = .88
Ab (IN8) 8 items a = .75 SN (IN) 7 items a = .90 PC (D) 2 item s a = .78 I 3 items a = .61
Ab (D) 12 items a = .89 SN (D) 2 item s a = .77 PC (D) 2 item s a = .70 I 2 items a = .93
Ab (D) 6 item s a = .83 SN (D) 1 item PC (D) 3 items a = .87 I 4 items a = .96
Ab (D) 7 items a = .79 SN (D) 2 items PC (D) 5 item s a = .81 I 5 items a = .93
Ab (D) 6 items a = .87 SN (D) 1 items PC (D) 1 item I 1 item
IntentionAb + SN + PC : R = .74 Ab: /3f = .79 SN: /3 = .17 PC: (i = .30
IntentionAB + SN +PC : R 2 = .35 SN: P = .50
IntentionAb + SN + PC : R2 = .86 Ab: p = .26 PC: P = .69 Behavior I + PC: R2 = .78 I: P = .46 PC: P = .37
IntentionAb + SN + PC: R2 = .52 Ab: p = .33 PC: P = .30 Behavior I + PC: R = .32 I: p = .32
IntentionAb + SN + PC: R2 = .55 Ab: P = .30 SN: p = .23 PC: p = .25
IntentionAb + SN + PC : R2 = .26 Ab: P = .39 PC: P = .35
Godin, Vezina, & Leclcrc, 1989 Exercise
NonexperimentalCross-sectional
98 pregnantwomen(convenience)
AB (D) 6 items a = .82 SN (D) 1 item PC (D) 1 item
IntentionAb + SN + PC: R2 = .47 Ab: P = .36 PC: p = -.50
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

29
TABLE VI (continued)
SELECTED HEALTH RELATED RESEARCH USING THE THEORY OF PLANNED BEHAVIOR
Researchers Design Sample Measures Significant Findings
Kimiecik, 1992 Physical activity
Nonexperimental Longitudinal (4 weeks)
332 corporateemployees(convenience)
Ab (D) 1 item Ab (IN) 6 items a — .86 SN (D) 1 item SN (IN) 3 items a = .85 PC (D) 3 items a = .83 PC (IN) 7 items a . 92 I 1 item
IntentionAb + SN + PC: R2 = .66 Ab: (} = .53 PC: P = .35 Behavior I + PC: R2 = .49 I: 0 = .52 PC: p = .23
aAb = A ttitude toward behavior.
^D = Direct measure.
CSN = Subjective norm.
^PC = Perceived control.
CI = Intention.
r/3 = Standardized regreession coefficient.
gIN = Indirect measure.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

30
the performance o f the behavior should tap into both internal and external control factors. To date, there has been no
report o f a study measuring perceived control as the product sum o f the likelihood of the control beliefs occurring and
perceived strength o f the facilitator. Usually, studies which used an indirect measure had summed the beliefs regarding
barriers to the behavior. One study summed the perceived strength o f the facilitator or inhibitor (Babrow et al., 1990).
As with the TRA, there was no empirical rationale given for m ultiplying the control beliefs by strength. In one study, the
prediction of intention was not significantly different whether the direct or the partial indirect (control beliefs only)
measure was used (Ajzen & Madden, 1986).
Unlike the additive model approach with the TRA, Ajzen initially proposed that perceived control would
statistically interact with attitude when predicting intention and with intention when predicting behavior. However,
studies which have included these interaction terms have found the term s nonsignificant (Ajzen, 1991; Ajzen & Driver,
1992; Ajzen & Madden, 1986; DeVellis, Blalock, & Sandler, 1990; Dzewaltowski et al., 1990). Ajzen (1989) currently
presents the TPB as an additive model.
Summary
Under what circumstances perceived control exerts an effect on behavior independent o f intention has yet to be
determined. Perceived control was the best predictor o f actual behavior in one study and was a significant predictor of
behavior in three additional studies. In addition, habit and past behavior are considered control factors. Habit or past
behavior, when measured in addition to attitude and subjective norm, contributed to the prediction o f behavior
independent o f intention (Fredricks & Dossett, 1983; Mittal, 1988; W ittenbraker et al., 1983).
The findings presented here as well as from studies extending the TRA with self-efficacy supported the use of
the TPB in explaining health behaviors. Perceived control was predictive of intention and behavior. Although the
empirical support to date was limited, perceived control is a worthwhile addition to the TRA.
Perceived Risk
Construct
Findings from research on HCWs' use of protective equipment were not adequately defined by the concepts
within the TPB. Responses related to perceived risk were identified in the Fox (1989) study as well as other research on
ITCWs' use of protective equipment (see Table II).
As a component of the health belief model, perceived vulnerability or risk predicted a variety of preventative
health behaviors (Janz & Becker, 1984). However, according to W einstein (1980), perception o f vulnerability or
perceived risk, is inaccurate. Individuals often and nonrandomly exhibit unrealistic optimism about their risk. Unrealistic
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

31
optimism is the erroneous belief that one's risk is less than that o f your peers or is less than the actual risk. People
consistently believe that good things will happen to them and bad things w ill not. Unrealistic optim ism is related to the
theory o f downward comparison, an extension o f social comparison theory (Festinger, 1954; Wills, 1991). When
appraising their risk for a hazard, people compare themselves downwards to someone more at risk than themselves. As
people attempt to be less at risk than their peers, a uniqueness or optim istic bias occurs (Gibbons & Gerrad, 1991;
Goethals, M essick, & Allison, 1991). Studies indicated that individuals perceive themselves to be at a lesser risk than
their peers fo r a variety of health threats. These health threats include HIV, hepatitis B, lung cancer, as well as safety
risks such as radon exposure and automobile accidents (Bauman & Siegel, 1987; Emmons et al., 1986; Joseph et al.,
1987; W einstein, 1980, 1982; Weinstein et al., 1986; Weinstein, Klotz, & Sandman, 1988; W einstein, Sandman, &
Roberts, 1991).
W hether optimistic bias is evoked may be related to characteristics of the specific hazard, such as the frequency
of exposure and personal experience with the hazard. As many hazards are infrequent, individuals forget that others may
have as m uch interest and ability to cope with the hazard as they do. Weinstein and Lachendro (1982) referred to this
failure to consider other people's risks carefully as egocentrism.
Individuals also use experience to rationalize their personal vulnerability. College students who had not
experienced m ajor life threatening events perceived themselves to be invulnerable (Pcrloff & Fetzer, 1986). In
W einstein's (1987) report o f a combined data set from three community studies, infrequent hazards and the lack of
experience w ith a hazard were highly correlated (r = .90), as well as predictive of optimistic bias.
The drive to maintain a level o f self-esteem appeared to be related to unrealistic optimism. In protecting their
self-esteem, people make downward comparisons, exaggerating the risk to others (Kunda, 1987; W ills, 1991). This
downward comparison was exhibited in college students who consistently chose high risk friends for comparison (Perloff
& Fetzer, 1986). Perloff and Fetzer (1986) also found that the less fam iliar the comparison person was, the more biased
the student became. Additional research indicated that when confronted with an actual threat/hazard such as cancer,
individuals made downward comparisons to a less fortunate peer (Gibbons & Gerrad, 1991; Hakmiller, 1966; Taylor &
Lobel, 1989).
Downward comparisons should produce optimism only when the threat is perceived to be controllable. Self
esteem is not maintained if the downward target cannot prevent the threat (Weinstein, 1984; Wills, 1991). Preventability
was predictive o f optimistic bias in Weinstein's (1987) combined data set o f health problems and hazards.
R eproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

32
In general, optim istic bias is generated when (a) the person views the hazard as preventable and infrequent, (b)
when there is a lack o f personal experience with the hazard, or (c) when the person does not share similar characteristics
with those who are at higher risk. An exception, unrealistic pessimism, w as found by Dolinski, Gromski, and Zawisza
(1987) in a study o f women who had been exposed to radiation during the Chernobyl nuclear accident. In this group of
women, optimistic bias was evoked for m ore remote hazards such as heart attacks and vehicular accidents. However,
these women perceived their risk to be greater than their radiation-exposed peers (e.g., unrealistic pessimism) for
consequences of radiation exposure (Dolinski et al., 1987).
Although optim istic bias may be a barrier to the adoption of protective health behaviors, little is known about
altering biases (Weinstein et al., 1991). A message campaign targeted at changing perception of automobile injury risk
significantly increased seat belt use by 31% in a group of workers (Weinstein et al., 1986). Additionally, the correlation
between perceived risk and self-reported seat belt use changed significantly. However, it is unclear if altered risk
perceptions were the cause o f the behavior change as there was little acknowledged link between not wearing a seat belt
and risk of injury (W einstein et al., 1986). Another message campaign did significantly decrease optimistic bias related
to risk o f radon (Weinstein et al., 1991). However, there was no difference between the treatment groups in the actual
purchasing of radon test kits. Out o f 13 reasons given by the sample for no t testing their home for radon, only 2 changed
significantly after treatment. Weinstein et al. (1991) acknowledged in order to alter optimistic biases, researchers may
need to target interventions specifically at the reasons or beliefs given for not being at risk for the hazard.
The extent o f optim istic bias is determined on a group level using a comparative risk assessment. Comparisons
to a peer arc generated (e.g., average man/woman my age) for the hazard. Weinstein (1989a) recommended that
optimistic bias be measured using the mean response on an ordinal scale (-3, much below average, to +3, much above
average) with a randomly selected sample. A mean of zero would indicate that no systematic bias occurred. Optimistic
bias occurs when the mean falls significantly below zero; the group estimates the risk to be less than their peers.
Similarly, a pessimistic bias would result if the mean were greater than zero.
A second measure o f risk is obtained from the difference of two absolute risk scales, absolute-own and absolute-
other. Individuals rate (-3, no chance, to +3, certain chance) the likelihood of their own risk for the hazard (absolute-
own) and the likelihood for an average other (absolute-other). A mean significantly different from zero for the difference
of absolute-other from absolute-own, would indicate optimistic bias (W einstein, 1989b).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

33
Empirical Support
Initial studies investigated unrealistic optimism involving multiple health problems or safety hazards in college
students (Dolinski et al., 1987; Kulik & Mahler, 1987; Perloff & Fetzer, 1986; Weinstein, 1980, 1982, 1983, 1984). The
following is a review of optim istic bias studies related to a specific preventive health risk such as HIV, automobile injury,
and home radon exposure (see Table VII).
Nonexperimental designs were used in over half o f the studies in Table VII, with the Joseph et al. (1987) study
using a prospective approach over 6 months. The quasi-experimental design studies used nonequivalent groups. With the
exception of the Weinstein et al. (1986) automobile injury study, all samples were obtained from a high risk population.
The three studies that investigated perceived risk for HIV used convenience samples, the remaining samples were random.
Measures of perceived risk varied. All but one study measured com parative risk to a peer with one item
(Weinstein et al., 1991). M ost o f the researchers used some measure of personal risk likelihood (absolute-own), with two
exceptions (Bauman & Siegel, 1987; Weinstein et al., 1986). Two studies com bined the absolute-own and comparative
risk scales (Emmons et al., 1986; Joseph ct al., 1987). Absolute risk was also measured as the difference between the
likelihood of risk for others and own risk likelihood (Weinstein et al., 1988, 1990). None o f the studies reported any
reliability or validity for the measures.
Findings indicated that optimistic bias was operating. In the radon studies, respondents displayed significant
optimistic bias without prior knowledge of personal home radon levels on both comparative and absolute risk scales.
However, optimistic bias disappeared with experience; 75% of the respondents w ith confirmed high radon levels rated
themselves at equal risk to the average home in the community for home radon exposure (Weinstein ct al., 1988).
Self-serving bias was also present in the three HIV studies. From 40% to 54% of the respondents felt they were
at less risk for HIV than other gay men. Bauman and Siegel (1987) reported that this bias was significant (mean =
-0.35).
Several studies investigated the relationship of perceived risk with behavior or intention. Comparative and
absolute risk correlated significantly with intention to test for radon, seat belt use, and completed radon testing (Weinstein
et al., 1986, 1990, 1991). In a cross-sectional study, comparative risk was predictive of three outcome measures related
to changes in risky sexual behavior (Emmons ct al., 1986). However, in the Joseph ct al. (1987) prospective study, risk
was not predictive of a change in risky sexual behavior when initial behavior and sociodemographic factors were
controlled. With radon testing and seat belt use, perceived risk was also not predictive of behavior change (Weinstein et
al., 1986, 1990, 1991). Personal risk likelihood (absolute-own) was predictive o f ordering test kits where likelihood of
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

34
TABLE VII
HEALTH RELATED RESEARCH USING WEINSTEIN'S MEASURE OF PERCEIVED RISK
Researchers Design Sample Measures Significant Findings
Weinstein, Klotz, & Sandman,1988Risk o f home radon
NonexperimentalCross-sectional
Study 1657 home owners in high radon area (random)
Study 1 CRa: 1 itemARb: 1 item own, 1 item
community (AR = ARq - ARC)
Study 1CR: lessc = 51%, equald = 44%, greatere = 6% AR: less = 52%, equal = 45%, greater = 3%
Weinstein, Sandman, & Roberts, 1990 Risk of home radon
Quasi-experimentalNonequivalentgroups
Study 2141 home owners with confirmed high radon level (convenience)
271 home owners in high radon area (random)
Study 2 CR: 1 item
CR: 1 itemAR: 1 item own, 1 itemcommunity(AR = ARC - ARC)
Study 2CR: less = 16%, equal = 75%, less = 10
CR: less = 36%, equal = 51%, less = 13%, m ean = -0.32 AR: mean = -0.57
Weinstein, Sandman, & Roberts, 1991 Risk of home radon
Weinstein, Grubb, & Vautier, 1986 Risk o f auto injury
Emmons et al. 1986Risk of HIV
Bauman & Siegel, 1987 Risk o f HIV
Quasi-experimentalNonequivalentgroups
Quasi-experimental
NonexperimentalCross-sectional
NonexperimentalCross-sectional
300 (group 1) 347 (group 2) Home owners in high radon area (random)
50 corporateemployees(random)
907 homosexual men, HIV negative (convenience)
160 homosexual men, HIV negative (convenience)
AR: 1 item own, 1 item community
CR: 1 item
CRAR:
1 item 1 item
PRf: AR + CR
CR: 1 item
Intention (to test)CR: r = .29,A R 0:r = .50,A RC: r = .41
Behavior (order tests) A R0: F (l, 257) = 6.2
Intention (to test) A R0:r = .49 A RC: r = .38
Behavior (order tests) .25 .11
AR0: r = ARC: r =
Behavior (seat belt use) CR pretest: r = -.5
CR: greater = 15% AR: less = 40%, equal = 50%, greater = 10%
CR: less = 51% mean = -0.35
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

35
TABLE VII (continued)
HEALTH RELATED RESEARCH USING WEINSTEIN'S MEASURE OF PERCEIVED RISK
Researchers Design Sample Measures Significant Findings
Joseph et al., 1987Risk of HIV
Nonexperimental Longitudinal (6 months)
637 homosexual men, HIV negative (convenience)
CR: 1 item AR: 1 item CombR8: Ar + CR
CR: less = 54%, equal = 33%, greater = 14%AR: less = 43%, equal = 47%, greater = 7% CombR: less = 40%, equal = 54%, greater = 6%
aCR = Comparative risk.
bAR = Absolute risk; ARQ = Absolute-own risk; ARC = Absolute-other risk.
cLess = Less than average risk.
dEqual = About average risk.
eGreater = Greater than average risk.
*PR = Perceived risk.
8CombR = Combined risk.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

36
risk for others (absolute-other) was not (Weinstein et al., 1990). Whether comparative or absolute risk contributes more
to the prediction of behavior cannot be determined from the studies in Table VII due to differences in measurement
approaches and reporting o f results.
Measurement Issues
W einstein provided limited empirical support for measures o f perceived risk. And it is not clear whether a single
measure o f comparative risk or in combination with absolute risk sufficiently taps the domain o f perceived risk.
Although not a measure of content validity, inter-item correlations for comparative risk and absolute risk measures
provide som e indication that the items may represent the same domain. Comparative and absolute risks were highly
correlated ( r = .84) in one group o f college students (Weinstein, 1989b). However, in another sample of college students
who rated 10 hazards, it was unclear from the correlations if comparative and absolute risk tap into the same domain (r =
.22-.75, m edian r = .64) (Weinstein, 1989b). From these two studies, comparative and absolute risk may both be
necessary measures for perceived risk, but it is not clear if the usual single item measure is sufficient to represent the
domain. A lthough further research is needed to develop these measures, Weinstein provides a useful approach to
understanding adoption of protective health behaviors.
Summary
In summary, these studies indicated that individuals with actual risks for a specific hazard perceived themselves
to be invulnerable. Comparative and absolute risk correlated with intention and behavior. Underestimating risk may
inhibit behavior change. However, no conclusions could be drawn whether underestimating risk (unrealistic optimistic
bias) is predictive o f behavior change.
Self-Protection Model
The SPM is an extension of the TRA and TPB and incorporates perceived risk as an additional variable that
directly influences intention (see Figure 1). The SPM proposes that belief evaluation alone contributes significantly to the
formation o f attitude. Similarly, normative influence is not multiplied by motivation to comply as in the TRA and TPB.
The model was developed from responses obtained during an elicitation study o f HCWs' behavioral and normative beliefs
regarding glove use when handling blood (Fox, 1989). As previously discussed, responses from the Fox (1989) study and
other research on HCWs indicated that the use o f protective equipment was not totally under the person’s volitional
control. Responses such as equipment availability, lack of time, interference w ith job performance, effectiveness o f the
protection, and habit are control beliefs. Control beliefs in the SPM are the summation of internal factors such as self-
efficacy and external factors (e.g., response efficacy, protection effectiveness, availability).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

37
Several responses from the Fox (1989) study also were related to perceived risk. Weinstein's approach to
perceived risk w as used. W ithin the SPM, perceived risk is a function o f risk beliefs. Risk beliefs determine the
individual's sense of personal vulnerability. Risk beliefs are elicited in a sim ilar manner as behavioral, normative, and
control beliefs. For intervention purposes, risk beliefs associated with intention and behavior need to be identified.
However, it is not clear what the relationship between perceived risk and risk beliefs is and whether risk beliefs
contribute to the prediction of intention. It is assumed that intention mediates the perceived risk-behavior relationship.
Comprehensive reviews o f the health psychology literature have identified variables that are components o f the
SPM which are important for studying health behaviors. Taylor (1990) identified four variables which consistently
explained health behaviors: (a) the perceived threat to health is severe (i.e., behavioral belief); (b) perceived
vulnerability (i.e., perceived risk); (c) person's beliefs that he/she is able to perform the response to reduce a threat (i.e.,
self-efficacy or control belief-internal factor); and (d) effectiveness o f the response to overcome the threat (i.e., protection
effectiveness o r control belief-external factor). In an analysis o f 99 health behavior variables, Cummings, Becker, and
Maile (1980) found six clusters: (a) accessibility and availability o f health services; (b) attitudes toward health care (i.e.,
attitude); (c) perception o f susceptibility, threat of illness (i.e., perceived risk); (d) social norms, social structure (i.e.,
subjective norm); (e) knowledge of disease; and (f) demographic characteristics.
W einstein (1989a), in reviewing research on self-protective behaviors, recognized that personal experience and
the perceived efficacy of the preventive measure were important for the individual to adopt the protective behavior. Both
Weinstein (1989a) and Taylor (1990) identified the significance of perceived effectiveness of the protective measure, or
response efficacy. Response efficacy, as part of Roger's (1983) protection motivation theory, has been predictive of
intention and behavior. Response efficacy or protection effectiveness is incorporated within the SPM. Protection
effectiveness is considered a component o f perceived control as an external control factor.
Summary
This discussion has focused on the research and theoretical literature related to HCWs' compliance with universal
barrier precautions and the constructs used in the SPM. Variables identified from this literature review which may be
associated with use o f universal barrier precautions included behavioral and normative beliefs, perceived control,
perceived risk, type o f setting and location, type of patient contact, and type o f HCW. Guided by the SPM, these
variables can contribute to the understanding of HCWs' use of universal barrier precautions. In addition, the accumulated
studies support the use o f the TRA, TPB, and Weinstein's measure of perceived risk. Future research, however, should
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

38
consider the impact o f measurement issues related to these variables, such as the definition of compliance, item clarity,
and reliability of measures.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

METHODOLOGY
This section will provide a description o f the study design, operationalization of the model, sample, and
instruments used, as well as data collection and analysis procedures. In addition, procedures to protect human subjects are
discussed.
Research Design
The design o f this study was nonexperimental. The study used a cross-sectional survey approach to describe the
use of gloves by HCW s, as well as to describe the relationships among the variables w ithin the theoretical models. The
study used a self-report, self-administered questionnaire.
Operationalization o f the Model
Variables w ere measured within the context o f the various models from which the concepts were originally
derived. Using Ajzen and Fishbein's (1980) guidelines, the first step in determining the predictors of glove use was an
elicitation o f medical laboratory workers' behavioral and normative beliefs about wearing gloves when handling blood
(Fox, 1989). The m ost frequently reported beliefs, described as the modal set, were used to develop an instrument that
measured behavioral beliefs, normative beliefs, attitude, and subjective norm (see Appendix A). As the concepts of
perceived risk and perceived control were added after the elicitation study was completed, control beliefs and risk beliefs
were not determined. The following is a discussion of the operational variables in this study (see Table VIII).
A ttitude
Initially, attitude was to be measured by three variables: attitude-direct, attitude-indirect, and belief evaluation.
Attitude-direct followed the direct measurement approach o f the TRA, using the sum o f three bipolar semantic evaluation
scales (foolish/wise, valuable/worthless, useless/useful). The modal set o f behavioral beliefs was used to develop the
5-point Likert-type scales which comprised the behavioral belief and belief evaluation items. The modal set included
m ore awkward, uncomfortable, less handwashing, protects the patient, hard to draw blood, protection from bloodbome
disease, doesn't provide as much protection as needed, cross-contamination to surfaces, inconvenient to take on and off,
and makes you feel partially safe. Attitude-indirect was to be the sum o f the products o f behavioral beliefs and belief
evaluation items. A lthough belief evaluation items were included in the instrument (see Appendix A), these items could
not be used to form the attitude-indirect measure. The anchors used w ith the belief evaluation items (important/not
important) resulted in these items being useless as the evaluative component o f the attitude-indirect measure. In research
using the semantic differential scale, importance loads on both the evaluation and activity dimension (Osgood, Suci, &
39
R eproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

40
TABLE VIII
STUDY VARIABLES
Theoretical Constructs Operational Variables Questionnaire Item Number
Attitude Altitude-direct (TRAa, TPBb, SPMC)
4 a,c,d,e
Attitude-indirect (TRA, TPB, SPM)
2, 4 b
Subjective norm Norm-direct (TRA, TPB, SPM)
6
Norm-indirect (TRA, TPB)
5,7
Normative influence (SPM)
5
Perceived control Control-direct (TPB, SPM)
8 a-e
Self-efficacy (TPB, SPM)
8 f, g
Protection effectiveness (SPM)
15
Perceived risk Comparative risk (SPM)
13, 14
Intention Intend(TRA, TPB, SPM)
9
Next month (TRA, TPB, SPM)
10
Behavior Not wear (TRA, TPB, SPM)
12
Past month (TRA, TPB, SPM)
11
aTRA = Theory of reasoned action.
'’TPB = Theory of planned behavior.
CSPM = Self-protection model.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

41
Tannenbaum, 1967). After consultation with Fishbein (personal communication, May 27, 1993), the evaluative items
were dropped. As there was no longer a set o f evaluative items to use, attitude-direct became the only measure of
attitude.
Subjective Norm
Three variables (norm-direct, norm-indirect, and normative influence') measured subjective norm. The direct
measure, norm-direct, used a 5-point scale to determine whether most people important to the HCW think the HCW
should or should not wear gloves. The modal set o f normative beliefs was used to develop the norm-indirect variable:
supervisors, co-workers, outside regulators, patients, family, and other health professionals. These normative beliefs were
measured on 5-point Likert-type scales to determine whether people who are important to the HCW think they
should/should not wear gloves when there is potential blood contact over the next week. And, in addition, whether the
HCW is motivated to comply with these people. Norm-indirect was the sum of the products of these two scales
(normative beliefs, motivation to comply). To comply with TRA measurement practices, the normative belief items were
converted to bipolar scales. In the SPM, the six normative belief items were summed, without multiplying the beliefs
with the motivation to comply items (normative influence).
Perceived Control
Perceived control was measured by three scales (control-direct, self-efficacy, protection effectiveness). Control-
direct was the sum of five 5-point Likert-type scales adapted from the Gatch and Kendzierski (1990) perceived control
scale. The 5-item Gatch and Kendzierski scale was reliable with an alpha coefficient of .81. The items used in the
control-direct scale measured how easy, how likely, how much control, whether mostly up to you, and very little that you
can do to wear gloves every time there is a potential for blood contact. Self-efficacy was a measure of internal control
factors and summed two items which measured the HCWs' confidence level in the ability to wear gloves. The HCWs'
perception of the ability of gloves to protect against HIV and hepatitis B comprised the measure o f external control
factors {protection effectiveness).
Perceived Risk
As compared to other HCWs who do similar work, comparative risk was the sum o f two items assessing the
I-ICWs' perception of the chances o f acquiring HIV or hepatitis B, measured as much below average to much above
average, on a 5-point scale.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

42
Intention
The variable next month measured the HCW s' indication of what will be the frequency o f glove use with
potential blood exposure over the next month. Intend measured the level of determination to wear gloves.
Behavior
Past month was the HCWs' self-reported frequency o f glove use measured on a range from 0 to 100. An
additional measure of behavior was not wear, which indicated the number of times that gloves were not worn when there
was actual blood contact.
Other variables of interest to this study were (a) health care worker (medical laboratory worker o r registered
nurse who came in contact with human blood either through direct care, specimen collection, or specimen processing) and
(b) professional and personal characteristics (work setting/location, work experience, hepatitis B vaccination, and
demographic information).
Sample
A disproportionate-stratified-random sample was drawn (see Table IX). The sample was randomly selected by
telephone area codes for a major midwestem city, its suburbs, and the rural area of the state. Target populations were
chosen to assure representation from all areas of the state. A listing of all registered nurses with active registration status
through the state department o f professional registration constituted the target nurse population (N = 104,499). As
medical laboratory professionals were not licensed, a comparable sample to the nurses was medical laboratory workers
who had received certification through the American Society of Clinical Pathologists' Board o f Registry (B. Castleberry,
personal communication, November, 1990). The American Society o f Clinical Pathologists' Board o f Registry
TABLE IX
HEALTH CARE WORKER SAMPLING PLAN
Regional Location
Nurses Laboratory Workers
Number Proportion8 Number Proportion
Urban 151 (.009) 158 (.200)
Suburban 149 (.003) 152 (.031)
Rural 148 (.004) 151 (.053)
TOTAL 448 461
P roportion of total population.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

43
certification mailing list contained 8,499 medical laboratory technologists, medical technicians, and phlebotomists living
within the state.
The proposed sample size needed to compare the three theoretical models was 450. This sample size was
considered adequate for the 13 independent variables in the study. In order to obtain the estim ated sample, oversampling
by 100% (n = 909) was done to account for respondents who had no potential blood contact, as well as for nonresponse.
O f the respondents, 527 (83%) were employed in positions with potential blood contact.
Instrument
The Protection from Blood Contact: Opinions o f TState Name! Health Care W orkers questionnaire is a self
administered instrument containing 26 closed-ended questions (see Appendix A). Dillman's (1978) total design method
for mailed surveys was used to develop the instrument. Results from the elicitation study were used as a basis for
measuring the norm-indirect and normative influence variables.
Content Validity
An initial draft o f the instrument which contained study variables underwent an assessment for clarity and
content validity. First, a clarity assessment was done on 69 items to determine readability and whether a single message
was being conveyed. An a priori-criterion of 80% was set for rater agreement on clarity for each item and for overall
agreement. Item clarity was acceptable if there was greater than 80% agreement, questionable if agreement was between
60% and 79%, and unacceptable if less than 60%. Judges were selected based on theory or practice expertise. Seven of
the eight judges responded and rated 33 items with acceptable clarity (47.8%), 11 items questionable (15.9%), and 25
unacceptable (36.2%). The 33 items with acceptable clarity were retained and the 11 questionable items were modified
using the judges' comments. Eight of the unacceptable item s were revised and the remaining 17 were deleted. An
additional seven item s were written from the judges' comments. The revised item list resulted in an overall clarity pair-
agreement o f 82% among a second panel o f judges.
A sim ilar panel of eight judges rated the relevance o f each item to the concept label and definition. Agreement
for relevancy was 100% for 48 items, 86-88% for 10 items, and 71% for the remaining item. The content validity index
was .97 for the 59 items (Lynn, 1986). These judges also rated whether item s grouped into theoretical categories
belonged together; there was universal agreement regarding these groupings.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

44
Pilot Study
A convenience sample o f 16 nurses participated in a pilot study of the instrument. The purpose o f this pilot
study was to identify any items that m ight be unclear to the final sample. Only one of the pilot sample respondents rated
any o f the items unclear. Unclear item s were revised as needed.
Data Collection Procedures
Each member of the sample received a questionnaire, a postage-free return envelope, and a cover letter that
explained the study. The laboratory worker sample also received a letter from the American Society of Clinical
Pathologists' Board o f Registry that encouraged participation in the study (see Appendix B). To increase response rate, a
follow-up postcard was sent one week after the first mailing. A second questionnaire was mailed to nonrespondents three
weeks later (see Appendix B).
The overall response rate was 69.7%. Out of the 634 returns, 13 were not used because respondents had either
moved out o f the state or had returned a totally blank questionnaire. An additional 94 questionnaires were not included
in the final sample as these respondents had no potential contact with blood during their work-day. There was no
significant difference between the nurse response rate (66.8%) and the laboratory worker response rate (69.7%).
However, response rate did vary significantly by location, x (2, N = 634) = 47.5, p < .00. This difference in response
rate was primarily due to the lower number o f returns from the nurses in the city (58%).
Protection of Human Subjects
The University o f Illinois at Chicago's Institutional Review Board approved this research (see Appendix C). In
addition, the study was reviewed and approved by the American Society of Clinical Pathologists' Board o f Registry
Executive Committee. A cover letter which explained the study to the HCWs w as sent along with the questionnaire (see
Appendix B). Respondents were informed that (a) participation was voluntary, (b) confidentiality would be assured, and
(c) consent was implied by return o f the questionnaire. Risks and benefits were also explained. In addition, if the
respondents wanted more information, the investigator's address and phone number were included in the cover letter as
well as in the questionnaire.
Analysis
Descriptive statistics were used to describe the HCW sample. Analysis o f variance procedures were performed to
determine if there were significant effects for field of employment, location, and work setting on ITCWs' use of gloves.
The linear structural relations model (LISREL) was used to determine which model was the best fit for the data
as other researchers had done with modifications of the TRA (Godin et al., 1987; Rcnfroc, O’Sullivan, & McGee, 1990).
R eproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

45
The LISREL model is an approach used to estimate unknown parameters within a set of structural equations that are
theorized to be related to observed variables. A causal structure is assumed among a set o f latent variables (theoretical
constructs). These latent constructs emerge as underlying causes of the observed variables. The LISREL procedure
allows for the inclusion of m ultiple measures of the latent constructs and adjusts for measurement error (Long, 1983).
There are two models in LISREL: measurement and structural. The measurement model describes the adequacy
or accuracy of the observed variables as indicators o f the latent constructs. The structural model provides estimates of the
hypothesized interrelationships among the variables for the TRA, TPB, and SPM. Figure 3 identifies the latent and
observed variables for each theoretical model. Initially, models were tested as proposed and then additional possible
causal relationships were tested for the models. Models were modified according to the information provided by the
analysis (e.g., parameter estimates, normalized residual plots, modification indices).
Three measures of overall goodness o f fit were used to determine how well the theoretical models fit the data
including chi-square, Adjusted Goodness-of-Fit Index (AGFI), and root mean-square residuals (RMR). The critical value
of the chi-square statistic (x2) is a function o f the number of the degrees o f freedom and the sample size. The AGFI
provides a measure of goodness o f fit that corrects for degrees of freedom as well as sample size. The closer the AGFI is
to one, the better the fit of the model to the data (Long, 1983).
The RMR is a measure o f the average of the residual variances and covariances. The closer the RMR is to zero,
the belter the fit. Q-plots of normalized residuals were inspected for outliers which w ould indicate possible model
-•)misspecification (JOreskog & SOrbom, 1989). Finally, the squared m ultiple correlation coefficients (R ) were compared
for the models to determine which of the theoretical models explained the greatest am ount of variance in glove use
intentions and behavior.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

46
Theory of Reasoned Action
A ttitu d eD ire c t
x,
N o rmD irec t
* 2
N o rmIn d ire c t
In ten d N e x t M on thyi y 2
A ttitu d e
In te n tio n
P a s t M o n thS u b je c tiv e
N o rm B e h a v io rn3
N o t W e a r
Theory of Planned BehaviorA t t i t u d e
D i r e c tx,
N ormD irect
__N orm
In d irec t*3
C o n tro lD irec t
X«
Self-E fficacy
* 5
In te n d N ex t M o n thy, Vi
S u b je c tiv e N orm
IIn ten tio n
1
P a s t M o n thy3P e rc e iv e d
C o n tro l5
B e h a v io rn2
N o t W e a r
Self-Protection M odelA tt i tu d e
D i r e c tx,
NormD irect
*2
N orm ativeInfluence
C om parativeRiskx4
C ontrolD irect
*5
Self-Efficacy
*0P rotectionEffective
x7
Attitude
In tend N ext M onth
SubjectiveNorm
IntentionP erce iv edRisk
P a s t M onth
B ehavior
P erceivedC ontrol N ot W ear
Figure 3. LISREL Models for the Theory of Reasoned Action, Theory of Planned Behavior, and Self-ProtectionModel.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

RESULTS
This section consists o f the results o f the data analysis and includes descriptive statistics, reliability estimates,
analysis o f variance procedures, and tests for estimating the three theoretical models. The study's hypotheses are used as
a framework for discussing and summarizing the findings. In addition, comparisons are m ade to previous research.
Characteristics o f the Sample
The sample included 527 nurses and laboratory workers who had potential contact w ith a patient's blood. The
sample was predominately white, married females who worked full-time in a hospital setting (see Table X). Laboratory
workers comprised 53% (280) o f the sample. Over half o f the sample had a bachelor's degree. The mean age for the
group was 38.7 ± 9.8 years, w ith a range o f 20 to 68 years. Average length o f employment in the health care area was
14.3 ± 8.9 years, ranging from 1 to 45 years. M ost of the sample (76.5%) had at least begun the series o f injections for
the hepatitis B vaccine. Additional demographic and work characteristics are summarized in Table X.
The data were examined for any significant differences between the nurses and laboratory workers on
demographic or work characteristics. Significant differences between these two groups were found only for education,
X2(2, N - 523) = 57.0, p = .00; gender, x2(L N ~ 523) = 18.7, p - .00; and age, r(486) = 2.03, p = .04. In general, the
nurses were more likely to be female, older, and less likely to have a bachelor's degree than the laboratory workers.
Nurses and laboratory workers did not differ on years of experience or status o f hepatitis B vaccination. Previous
research has reported a difference in glove use between more experienced HCW s and those with less experience (Freeman
et al., 1992; Fricdland et al., 1992; Kclen et al., 1990). In addition, differences between the nurses and laboratory
workers as to whether they had been vaccinated for hepatitis B may have influenced the HCW s' sense of risk towards
hepatitis B. Earlier studies have not investigated the effect o f demographic characteristics on glove use; it is doubtful that
these differences would have much o f an impact.
Descriptive Summary o f the Variables
The following is a descriptive summary o f the variables used in this study and includes reliability estimates. The
dependent variables are listed first. A description of all o f the variables is contained in Table XI. In addition, Table VIII
identified study variables according to the theoretical models in which they were used.
47
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

48
TABLE X
DEMOGRAPHIC AND WORK CHARACTERISTICS OF THE SAMPLE(n = 527)
Laboratory Workers Nurses Total
Characteristic Frequency Percent Frequency Percent Frequency Percent
GenderFemale 240 86 239 97 479 91M ale 37 13 7 3 44 8Missing 3 1 1 <1 4 1
EducationDiploma/Certificate 15 5 57 23 72 14Associate Degree 48 17 71 29 119 23Bachelor's Degree 194 69 92 37 286 54Post Bachelor's Degree 21 6 25 10 46 9Missing 2 1 2 1 4 1
EthnicityWhite/Caucasian 215 77 196 79 411 78African American/Black 23 8 16 17 39 7Asian/Oriental 39 11 25 10 55 10Hispanic 8 3 4 2 12 2Other 1 <1 2 1 3 1Missing 3 1 4 2 7 1
Marital StatusMarried 191 68 166 67 357 68Single 59 21 42 17 101 19Divorced/Separated/Widowcd 28 10 36 15 64 12Missing 2 1 3 1 5 1
Employm ent StatusEmployed Full-time 211 75 173 70 384 73Employed Part-time 68 24 69 28 137 26Missing 1 <1 5 2 6 1
Work SettingHospital 221 79 171 69 392 74Nonhospital 59 21 71 29 130 25Missing 0 - 5 2 5 1
W ork LocationUrban 92 33 69 28 161 31Suburbs 87 31 87 35 174 33Rural 101 36 86 35 187 36Missing 0 - 5 2 5 1
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

49
TABLE XI
M EAN, STANDARD DEVIATION, AND RELIABILITY ESTIMATES FOR VARIABLES
Variable Number of Items Scale Mean Scale Standard Deviation Measures o f Reliability
A tlilude-direct 2 9.54 1.09 .63e
N orm -ind irect 6 43.04 13.48 ,80fN orm -direct 1 4.81 0.49 -
Normative influencea 6 9.33 2.68 ,78f
C ontrol-d irect 3 12.80 2.30 .67fSelf-efficacya 2 8.03 2.19 ,55eProtection effectivenessa 2 7.72 1.52 .80e
Comparative r is l t 2 4.91 1.99 .74°
In tenc t 1 4.13 1.18 _
Next montha 1 6.46 0.89 -
Not weara 1 2.05 1.09 _
Past montha 1 6.25 1.06 -
F ie ltft 1 1.53 0.50 -
Location0 1 2.05 0.82 -
W ork setting^ 1 1.24 0.43 -
aMeasured using an ordinal scale.
^Measured using a dichotomous scale.
cMeasured using 7 categories, recoded into 3 categories.
^Measured using 11 categories, recoded into 2 categories.
“Spearman correlation coefficient.
rStandardized alpha coefficient.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

50
Behavior
Glove use behavior was measured by two variables in the questionnaire. The variable past month measured the
frequency o f wearing gloves when there was potential blood contact. This measure used a 7-point scale with responses
that ranged from 0% to 96%-100%. Past month had a median o f 7.00, which is equivalent to wearing gloves all o f the
time (96%-100%). This item was negatively skewed (-2.09). O f all the respondents, 52% reported wearing gloves all of
the tim e and 32% reported wearing gloves m ost o f the tim e (76%-95%) when there was potential blood contact. Not
wear measured the frequency of actual blood contact when gloves were not worn, over the last month. N ot wear used a
5-point scale with responses that ranged from 0 to 10 o r more times. The median response for this item was 2.00; this
meant that 47% of the sample had blood contact 1 to 3 times during the last month when gloves were not worn. Another
33% of the respondents reported always wearing gloves when there had been actual blood contact, a response o f (0) blood
contact. The correlation between past month and not wear was .47 (see Table XXVII, Appendix D).
Intention
Two variables (next month, intend) measured intention. Next month is similar to past month with the exception
that next month rated the intended glove use over the coming month. This variable was also negatively skewed (-2.39)
and had a median of 7.00 on a 7-point scale. Of those responding, 63% intended to wear gloves all of tim e (96%-100%)
during the coming month.
The other variable, intend, was measured on a 5-point scale. Negatively skewed (-1.40), intend's median was
5.00; 53% of the sample was determined to wear gloves every time there was potential blood contact. Correlation
between intend and next month was .55 (sec Table XXVII, Appendix D).
Attitude
Corrected item-total correlations ranged from .69 to .88 for the four items measuring attitude-direct. The two
items with corrected item-total correlations greater than .80 were dropped. Item-total correlations greater than .70
indicate that the item is redundant and may cause an inflated alpha because o f increasing the number of items (Kcrlinger,
1986). This left the two items wise and useful. The correlation coefficient for these two items was high (.63).
Responses for the sum of these two items ranged from 2 to 10. This variable had a median of 10.00 and was negatively
skewed (-3.27). Seventy-eight percent of the sample thought that it was wise and useful to wear gloves.
Subjective Norm
Three variables were used as measures o f subjective norm: norm-direct, norm-indirect, and normative influence.
Norm-direct used a 5-point scale and responses ranged from 2 to 5. This variable was also negatively skewed (-2.70),
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

51
with 84% o f the sample responding that m ost people think they should wear gloves; the median was 5.00. Correlations
with norm-indirect and normative influence were .53 and .54, respectively (see Table XXVII, Appendix D).
Norm-indirect was the sum of the products o f normative beliefs and motivation to comply. The range of
responses fo r this variable w as -13 to 60 and the mean was 43.04. Finally, normative influence was the sum of the six
normative beliefs; responses ranged from -6 to 12. With a mean o f 9.33, 30% o f the sample thought that all six referents
would strongly agree that the respondents should wear gloves. Standardized alpha coefficients for normative influence
and norm-indirect were .78 and .80, respectively.
Perceived Control
Control-direct, self-efficacy, and protection effectiveness were the three variables used to measure perceived
control. O f the five original items in the control-direct scale, two were dropped because of very low (.17 - .23) item to
total correlations. The two items which were dropped were (a) mostly up to you, and there is (b) very little you can do to
wear gloves every time. The remaining three items achieved an alpha reliability of only .67. The sum o f these three
items had a mean of 12.80, w ith a range o f responses from 3 to 15. In addition, 30% of the sample indicated that they
thought wearing gloves was completely under their control as well as being likely and easy to wear every tim e there was
potential blood contact.
Both self-efficacy and protection effectiveness were the sum of two items that were measured on 5-point scales.
Items were recoded so that a response of (1) was equivalent to disagree or not all effective. Responses for both scales
ranged from 2 to 10. With self-efficacy, 42% of the sample felt confident and sure that they could wear gloves every
time. Only 17% thought that gloves were very effective against both HIV and hepatitis B (protection effectiveness). The
means and reliability estimates are reported in Table XI.
Protection effectiveness correlated only moderately with control-direct (.31) and self-efficacy (.28). However,
there was a stronger correlation between control-direct and self-efficacy (.59) (see Tabic XXVII, Appendix D).
Perceived Risk
The sum of two item s comprised the comparative risk variable. Both items were measured on a 5-point scale,
with responses ranging from 2 to 10. The mean was 4.91, indicating that over half (54%) o f the sample rated themselves
at below average risk for H IV and hepatitis B when compared to similar HCWs. Another 30% rated their risk to be
average. The correlation coefficient between these two items was high (.74) (see Table XXVII, Appendix D).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

52
Additional Variables
Field, location, and w ork setting were variables used to explain how glove use varied. The response as to
whether the HCW was employed in the nursing profession (47%) or the medical laboratory area (53%) comprised the
measure of fie ld . Location consisted of the seven area codes for the midwestem state which were recoded into urban
(31%), suburban (33%), and rural (36%). The measure of w ork setting consisted o f the types o f facilities the HCWs were
employed in ; the 11 types o f facilities were recoded into the two categories of hospital (74%) and nonhospital (25%).
Scale means are reported in Table XI.
Analysis o f Variance
The data were examined as to whether glove use varied by (a) the field o f employment, (b) the type o f work
setting, and (c) location within the state where the HCW was employed. A s field , location, and work setting arc
variables which are not included in the theoretical models, analysis o f variance procedures were used to determine if these
variables had an affect on HCW s' glove use. Analysis of variance procedures were performed using the two dependent
variables, not wear and past month.
As Table XII indicates, field of employment, geographical location, and type o f work setting were not predictive
o f the frequency of glove use over the last month (past month). These variables were predictive of blood contact (not
wear) (see Table XIII). Specifically geographical location was predictive o f blood contact (not wear) when type of work
setting and field of employment were controlled. Since HCW s that had more contact with blood would mean that they
were less likely to always wear gloves, then HCWs' glove use varied between urban, rural, and suburban areas.
A significant effect was found for the interaction o f field of employment with location on the frequency o f blood
contact. The cell means revealed that laboratory workers in suburban areas came in less contact with blood than did
those working in urban or rural areas (see Appendix E). In other words, suburban laboratory workers wore gloves more
often then others did, since they reported less frequent contact with blood. The nurses did not differ in their frequency o f
blood contact by location, meaning that urban, suburban, and rural nurses were consistent in their glove use.
There are possible reasons why glove use varied. First, nurses and laboratory workers differ in the type o f work
activities they perform in relation to blood products. In general, laboratory workers more frequently draw blood from a
patient's vein and process blood samples. Nurses tend to administer blood products, draw blood from established access
lines, or care for patients with bleeding wounds. The work activities of suburban laboratory workers may be different
from urban and rural laboratory workers. Perhaps suburban laboratory workers draw less blood than the other laboratory
workers. Differences in the frequency of drawing blood could affect glove use as laboratory workers have been observed
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

53
TABLE XII
ANALYSIS OF VARIANCE IN FIELD OF EMPLOYMENT, LOCATION, AND WORK SETTINGWITH PAST MONTH*
Source of VariationSum of Squares
Degrees of Freedom Mean Square F Statistic F Probability
Main Effects 5.81 4 1.45 1.29 .27Field 0.00 1 0.00 0.00 .99Work setting 3.79 2 3.77 3.37 .07Location 2.79 1 1.40 1.24 .29
2-Way Interactions 6.04 5 1.21 1.07 .37Field x work setting 0.20 2 0.20 0.17 .68Field x location 0.52 1 0.26 0.23 .79Work setting x location 4.73 2 2.36 2.10 .12
3-Way Interaction 2.88 2 1.44 1.28 .28Field x work setting x location
Explained 13.81 11 1.26 1.12 .35Residual 572.75 509 1.13Total 586.56 520 1.13
aModcl estimated using a regression approach.
TABLE XIII
ANALYSIS OF VARIANCE IN FIELD OF EMPLOYMENT, LOCATION, AND WORK SETTINGWITH NOT WEARa
Sum of Degrees ofSource of Variation Squares Freedom Mean Square F Statistic F Probability
Main Effects 15.16 4 3.79 3.26 .01Field 3.65 1 3.65 3.14 .08Work setting 0.13 2 0.13 0.11 .74Location 11.04 1 5.52 4.74 .01
2-Way Interactions 11.29 5 2.26 1.94 .09Field x work setting 0.02 2 0.02 0.02 .90Field x location 9.58 1 4.79 4.12 .02Work setting x location 1.61 2 0.81 0.69 .50
3-Way Interaction 2.78 2 1.39 1.20 .30Field x work setting x location
ExplainedResidual 29.62 11 2.69 2.31 .01Total 586.64 504 1.16
616.26 515 1.20
aModel estimated using a regression approach.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

54
to wear only one glove or to cut off a fingertip in order to feel a vein more easily. Given this perceived difficulty with
wearing gloves while drawing blood, it is logical that laboratory workers who draw blood more often may not wear
gloves as frequently as others. Another explanation is that rural HCW s may not perceive themselves to be at risk for
HIV or hepatitis B as these disease are considered to be an inner city problem. However, this does not explain why
urban laboratory workers do not wear gloves the m ost frequently. And finally, urban and rural laboratory workers may
be involved with m ore emergent situations than suburban laboratory workers. Studies have indicated that barriers, such as
gloves, were less likely to be worn during emergent contacts (Kelen et al., 1991; Wong et al., 1991).
A post hoc power analysis was performed to determine if the sample size were large enough to eliminate the
chance of a Type II error, given the effect sizes found. Cohen's (1988) tables and an alpha error of .05 wrere used. For
the dependent variable not wear (n = 516), power w as adequate to detect differences between the groups on field of
employment and location. However, as there were only small differences found between the hospital and nonhospital
settings (effect size = .044, power = .30), the chance of a difference existing between these types of work settings cannot
be eliminated. Similarly, with past month (n = 521) there was insufficient power (.11-.53) to detect the small differences
(effect size = .016-.069) associated with field o f employment, location, and work setting. Very large sample sizes of
approximately 800 to 1,570 would be needed to elim inate the chance of a Type II error given the effects found with past
month.
Model Estimation
A structural equation modeling technique, LISREL, was used to test how well the three theoretical models (TRA,
TPB, SPM) fit the data. A covariance matrix was used for this phase of the analysis and analysis was based on 527
respondents. The theoretical models were tested as originally proposed and then modified when indicated. Each of the
theoretical models w ill be discussed separately. In order to clarify the discussion, as well as the tabular entries, the
theoretical models have been classified as Model I (TRA), Model II (TPB), and Model III (SPM).
For each of the three theoretical models, a series o f models was estimated. The first model that was estimated
was the baseline m odel; the baseline model tested the theoretical model as originally proposed with no added correlated
measurement errors or additional structural paths. The baseline model was examined for indications o f how well the
model fit the data, as well as for indications of w here the model fit was not perfect. Overall goodness of fit measures
that were reviewed included x“, Adjusted Goodness-of-Fit Index (AGFI), and root mean-square residual (RMR) (see
Methodology section). In addition, standardized residuals and modification indices were examined for indications of
where the model did not fit the data perfectly.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

55
At first, additional models were tested that allowed measurement errors to correlate. To determine if these
subsequent models were a significant improvement in fit over the baseline model, a x difference test was performed.
The structural components o f the model were examined after each correlated error was added. Structural order should not
change if the measurement model is adjusted by correlating measurement errors. Changes in the structural order when a
correlated error is introduced would indicate that the relationship between the latent variables is influenced by the
measurement approach taken.
The second phase o f model estimation added structural paths if the analysis revealed a possible improvement in
fit. An example o f an added structural path would be the path from attitude to behavior that has been found in prior
research. A x difference test was then done to see if there was any improvement in fit over prior models.
Theory of Reasoned Action— Model I
Proposed model. The model, as proposed, is illustrated in Figure 3. Four observed variables (yj to y^) served
as measures of intention and behavior. The y-variables included two measures o f intention {intend, next month) and two
measures o f behavior {past month, not wear). In addition, there were three observed variables (Xj to x3) which served as
measures o f attitude and subjective norm: attitude-direct measured attitude and subjeative norm was measured by norm-
direct and norm-indirect. In LISREL if a latent variable has more than one observed or indicator variable, LISREL is
able to estimate the error terms. As attitude was measured by only one variable, an assumption was made that attitude-
direct was perfectly measured. This would mean that there was no measurement error in attitude-direct (JOreskog &
SOrbom, 1989).
Sequence of m odels. The baseline model (Model 1.1) is shown in Table XIV. Measurement error terms were
allowed to correlate (M odels 1.2, 1.3). As Table XIV shows, the differences in the x" statistics indicate a significant
improvement in fit of Model 1.3 over Models 1.1 and 1.2. With 9 degrees of freedom, the x~ statistic for Model 1.3 was
20.9. The probability value of .01 indicates that this model did not fit the data perfectly. The AGFI and the RMR
indicate a good fit for the model. A lthough the RM R is not close to zero, the standardized residuals behaved normally;
residuals were symmetrically distributed, the average residual was zero, and there were no large residuals. The structural
component of the model was stable with each addition o f a correlated error.
M easurement m odel. The measurement model provided information related to how adequately the observed
variables measured the four latent variables (see Table XV). Where / values could be estimated, values were significant
for the x and y variables. The measurement model for the x variables included the single measure of attitude and the two
measures o f subjective norm. W ithin the measurement model, R~ is an estimate of the measure's reliability or how much
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

56
TABLE XIV
OVERALL FIT MEASURES FOR THEORY OF REASONED ACTION MODELS (1.1-1.4)
Model
Degreesof
Freedom X2
Goodness-of-FitIndex
AdjustedGoodness-
of-FitIndex
RootMean-Square
Residualx2
p value
0X”
difference p value8
Model 1.1(Baseline model: no correlated errors)
11 41.1 .98 .95 .52 .00 -
M odel 1.2(Model 1.1 and correlated error between past month and next month)
10 25.2 .99 .96 .34 .01 < .00
M odel 1.3(Final model: Model 1.2 and correlated error between not wear and next month)
9 20.9 .99 .96 .32 .01 < .05
M odel 1.4(Model 1.3 and direct path from attitude to behavior)
8 16.7 .99 .97 .32 .03 < .05
ap value for the difference in chi-square statistic from previous model.
o f the variance m the latent variable is accounted for by that measure. For subjective norm, nonn-direct (R = .62) was a
9 9better measure of subjective norm than w as norm-indirect (R = .46). The closer R is to one, the better the measure is a
9 9good indicator for that latent variable or construct. In turn, a low R indicates more measurement error. The R values
associated w ith norm-direct and norm-indirect show that there was more measurement error associated with the indirect
measure than with the direct measure of subjective norm.
The measurement model for the y variables included the two measures of intention and the two measures of
behavior. Both intend and next month were acceptable measures of intention (R = .52 and .61, respectively). Although
9 2not wear (R = .30) would be considered a poor indicator of behavior, past month (R = .74) was an acceptable measure.
Structural model. The LISREL estimates o f structural coefficients and t values for the structural paths are shown
in Table XVI. The R for the structural equations was .41 for intention and .70 for behavior. This means that 41% of
the HCWs' intention to wear gloves was a function o f their attitude and the influence of important others. In turn, 70%
o f glove use was a function of the HCW s' intention to wear them. Attitude and subjective norm were moderate, but
significant, predictors of intention, and intention was a strong predictor o f behavior.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

57
TABLE XV
LISREL ESTIMATES OF REGRESSION OF OBSERVED ON LATENT VARIABLES: THEORY OF REASONED ACTION MODEL I.3a
Latent Variables
ObservedVariables
Attitude Subjective Norm Intention Behavior
R2 U b Sc td U S t U S t U S t
Attitude-direct 1.00 1.0C 1.0 0C _f - - - - - - -
Norm-indirect .46 1.0e .68 0C - - - - -
Norm-direct .62 0.04 .78 11.9 - - - - -
Intend .52 1.0e .72 0C - -
Next month .61 0.82 .78 11.4 - -
Past month .74 1.0e .86 0 c
Not wear .30 0.66 .55 9.3
aFit measures are reported in Table XIV.
'’Unstandardized LISREL lambda coefficients.
cStandardized LISREL lambda coefficients.
dCritical value for / approximately ± 1.96.
cFixed parameter value.
fAccording to the theory of reasoned action, theoretically implausible path, which was fixed to zero in analysis.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

58
TABLE XVI
LISREL ESTIM ATES OF STRUCTURAL COEFFICIENTS FOR THEORY OF REASONED ACTION:MODELS 1.3 AND I.4a
Independent Variables
Dependent Variables
Intention Behavior
Ub Sc /d U S /
Model 1.3
Attitude 0.28 .36 5.0 _c - -
Subjective norm 0.03 .34 4.1 - - -
Intention 0.90 .84 10.8
R2 .41 .70
Model 1.4
Attitude 0.29 .38 5.3 -0.08 -.10 -2.0
Subjective norm 0.03 .33 4.2
Intention 1.02 .93 9.2
R2 .42 .77
aFit measures are reported in Table XIV.
'’Unstandardized LISREL gamma and beta coefficients.
cStandardized LISREL gamma and beta coefficients.
‘'Critical value for t is approximately ± 1.96.
eAccording to the theory of reasoned action, a theoretically implausible path, which was fixed to zero in analysis.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

59
As the standardized coefficients in Table XVI indicate, attitude and subjective norm were equally strong as
predictors o f intention. The HCWs' attitude and the influence o f important others contributed equally to any change in
their intention to wear gloves. However, Table XVII shows that for this model (1.3) most o f subjective norm's effect on
intention was a result o f subjective norm's correlation with attitude. Attitude's effect on intention (.28) is about 10 times
that of subjective norm (.03). Intention strongly impacted behavior (.90). In addition, attitude indirectly influenced
behavior by increasing HCW s’ intention to wear gloves; this indirect influence (.25) was also 10 tim es more than
subjective norm 's influence (.03). The relationship between attitude, subjective norm, and intention may have been
affected by the passage o f time. Initially, when universal precautions were first introduced, im portant others may have
more directly influenced the HCWs' level o f determination to wear gloves. With the passage o f tim e, the necessity for
others to monitor glove use lessens as HCWs' adopt the regulations into their behavioral belief system.
The data were further examined to determine if the path from attitude to behavior would improve the fit of the
model. The modification index for this path revealed a possible improvement in fit. Model 1.4 represents this addition
TABLE XVII
DECOMPOSITION OF EFFECTS FOR THEORY OF REASONED ACTION:MODELS 1.3 AND 1.4
IndependentVariables
Dependent Variables
Intention Behavior
TotalEffect
StandardError
DirectEffect
StandardError
TotalEffect
StandardError
DirectEffect
StandardError
IndirectEffect
StandardError
Model 1.3
Attitude .28 .06 .28 .06 .25 .05 a - .253 .050
Subjective norm .03 .01 .03 .01 .03 .01 - - .027 .007
Intention .90 .08 .90 .08
Model 1.4
Attitude .29 .06 .29 .06 .21 .06 -.08 .04 .294 .059
Subjective norm .03 .01 .03 .01 .03 .01 0 0 .030 .007
Intention 1.0 .11 1.0 .11
“According to the theory of reasoned action, theoretically implausible path, which was fixed to zero in analysis.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

60
(see Table XIV). The difference in the x statistic indicates a significant improvement over Model 1.3. The / value for
the added path was significant (-1.99) (see Table XVI). Table XVII shows that attitude not only affected behavior in part
through its effect on intention, but also directly influenced behavior independently o f intention. However, this direct
influence o f attitude was a small and negative one. When HCWs' thought about whether they intended to wear gloves,
their attitude about gloves positively influenced their decision. A lthough those who were determined to wear gloves were
the most likely to do so, HCW s were also likely to wear gloves if they held a negative attitude about gloves. As glove
use is a mandatory behavior, HCWs’ may still wear gloves even though gloves are not well liked.
Table XVII indicated that attitude continued to influence intention more so than subjective norm and that attitude
influenced behavior independently o f intention. The R for behavior increased modestly; 77% o f glove use was a
function o f the HCW s' determination to wear gloves and their attitude toward glove use (see Table XVI).
Sum m ary. The I-ICWs' attitude toward glove use was predictive of their intention to wear gloves, as well as
their glove use behavior. Subjective norm had a minimal effect on HCW s' intention to wear gloves. Together, HCWs'
positive attitude about glove use and important others explained 41% o f the variance in intention. Those HCWs who
intended to wear gloves and held a negative attitude about glove use w ere more apt to wear gloves; 77% of glove use was
a function of the HCW s’ attitude and their determination to wear gloves. In addition, intention did not fully mediate the
attitude-behavior relationship; when intention was not an intervening variable, attitude had a negative relationship to
behavior. HCW s who held a negative attitude toward glove use would still wear gloves. Overall, Model 1.4 explained a
large amount o f the variance in glove use behavior and the model was a good fit to the data.
Theory o f Planned Behavior— Model II
Proposed m odel. Figure 3 displays the model as proposed. M odel II varies from Model I with the addition of
perceived control as discussed in the Review of the Literature section. Control-direct and self-efficacy were the two
observed variables (x4 , x5) which measured perceived control. Other variables were measured as in Model I.
Sequence of m odels. Table XVIII displays the baseline model (Model II. 1). Results were reviewed for model
misspecifications and correlated measurement errors as was done with Model I. The results of the final model, Model
yII.2, are reported in Table XVIII. Differences in the x statistics between the baseline and final model indicated a
significant improvement in fit. All o f the goodness of fit indicators showed that this model was a good fit with the data.
yWith 18 degrees o f freedom, the x statistic for Model II.2 was 35.7 and the probability value was .01. Although the
RM R value was high (.46), the standardized residuals behaved normally; residuals were symmetrically distributed, the
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

61
TABLE XVIII
OVERALL FIT MEASURES FOR THEORY OF PLANNED BEHAVIOR MODELS (II. I-II.3)
Model
Degreesof
Freedom X2
Goodness-of-FitIndex
AdjustedGocdness-
of-FitIndex
RootMean-Square
Residualx2
p value
X“difference p value8
Model II. 1(Baseline model: no correlated errors)
20 71.8 .97 .93 .54 .00 -
Model II.2(Final model: Model II. 1 and correlated errors between past month and next month and not wear and next month)
18 35.7 .99 .96 .46 .01 < .00
Model II.3(Model II.2 and direct path from attitude to behavior)
17 31.4 .99 .97 .46 .02 < .05
ap value for the difference in chi-square statistic from previous model.
average residual was zero, and there were no large residuals. The structural component of the model remained stable
with the addition of the correlated errors.
In comparing the TPB Model II.2 (see Table XVIII) to the TRA Model 1.3 (see Table XIV), the difference
9 9between their respective x“ statistics was not significant (x“ difference = 14.8, 9 degrees o f freedom). Though the
previous TRA Model 1.3 did not fit the data perfectly, this TPB model did not significantly improve the fit.
Measurement m odel. As the measurement model for Model II.2 is an extension o f Model I, values were the
same for repeated variables (see Table XIX). This would mean the measurement model for the y variables, as well as for
the variables that measured attitude and subjective norm should remain the same, which was the case. The measurement
model for the x vanablcs included the two new measures of perceived control. For perceived control, control-direct
9 9(R~ = .78) was a very good measure of perceived control. Self-efficacy had an R o f only .44, meaning it was not a good
indicator of perceived control and that there was significant measurement error associated with self-efficacy.
Structural model. With the introduction o f perceived control, the role of subjective norm and attitude in the
prediction of intention declined (see Table XX). The amount of variance explained in intention increased to 74%.
Subjective norm was no longer a significant predictor o f intention (/ = 1.27). In regard to their intention to wear gloves,
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Reproduced
with perm
ission of the
copyright ow
ner. Further
reproduction prohibited
without
permission.
TABLE XIX
LISREL ESTIMATES OF REGRESSION OF OBSERVED ON LATENT VARIABLES: THEORY OF PLANNED BEHAVIOR MODEL II.2
ObservedVariables R2
Latent Variables
Attitude Subjective Norm Perceived Control Intention Behavior
Ua Sb /c U S t U S t U S t U S I
Attitude-direct 1.0 1.0d 1.0 0d e - - - - - - - - - - -
Norm-indirect .47 1.0d .69 0d - - - - - - - - -
Norm-direct .60 0.04 .75 12.2 - - - - - - - - -
Control-direct .78 1.0d .85 0d - - - - - -
Self-efficacy .44 0.72 .67 13.9 - - - - - -
Intend .52 I.0d .72 0d - - -
Next month .61 0.82 .78 14.7 - - -
Past month .80 1.0d .83 0d
Not wear .28 0.61 .53 9.7
aUnstandardized LISREL lambda coefficients.
^Standardized LISREL lambda coefficients.
cCritical value for t approximately ± 1.96.
dFixed parameter value.
eAccording to the theory of planned behavior, theoretically implausible path, which was fixed to zero in analysis.ONto

63
TABLE XX
LISREL ESTIMATES OF STRUCTURAL COEFFICIENTS FOR THEORY OF PLANNED BEHAVIOR MODELS II.2 AND II.3a
Independent Variables
Dependent Variables
Intention Behavior
U b Sc ,d U S t
Model II.2
Attitude 0.14 .18 2.9 _c - -
Subjective norm 0.01 .10 1.3 - - -
Perceived control 0.29 .69 9.0 0.01 .17 1.2
Intention 0.80 .71 6.5
R 2 .74 .66
Model II.3
Attitude 0.14 .19 3.09 -0.08 -.09 -2.0
Subjective norm 0.01 .10 1.34
Perceived control 0.29 .69 8.99 0.02 .04 0.3
Intention 0.97 .86 6.0
R 2 .74 .71
aFit measures are reported in Table XVIII.
'’Unstandardized LISREL gamma and beta coefficients.
cStandardized LISREL gam m a and beta coefficients.
‘'critical value for / is approximately ± 1.96.
cAccording to the theory o f planned behavior, a theoretically implausible path, which was fixed to zero in analysis.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

64
74% of HCWs1 intentions were accounted for by their attitude about gloves and their perception of how easy gloves are to
wear.
The standardized regression coefficients in Table XX describe the relationship between attitude, subjective norm,
and perceived control in their ability to predict intention. The HCWs who differed in their intention to wear gloves,
differed by about 69% in their perception o f how easy gloves are to wear, about 18% in their attitudes about gloves, and
about 10% on how much influence important others have on their glove use.
Although perceived control was very important in predicting HCWs' intention, this variable was not an important
predictor o f glove use (/ = 1.23) independent o f intention. The amount o f variance in glove use behavior did not change
over what was accounted for by the TRA models; 66% of glove use was a function o f the HCWs' intent to wear them.
With the addition of perceived control, perceived control's affect on intention (.29) was twice that o f attitude's
(.14), with subjective norm 's impact being negligible (.01) (see Table XXI). A possible reason for the decline in attitude's
impact on intention is that part o f the HCWs' opinion about wearing gloves is related to how easy or difficult gloves are
to wear. In addition, intention continued to strongly impact behavior (.80). Perceived control and attitude indirectly
influenced behavior through their affect on HCWs' intention. Perceived control's indirect influence (.23) on behavior was
twice that o f attitude's (.11).
According to the TPB, perceived control influences behavior directly when behavior is not completely under the
person's control and when the person's perception of control is accurate. Given the results, this would suggest that glove
use is completely under the HCW s' control or that their perception of control is not accurate. Only 30% of HCWs
thought that wearing gloves was completely under their control; additional concerns may impact on whether gloves are
worn. Other studies have reported that gloves were not always worn during emergent contacts (Kelen et al., 1991; Wong
ct al., 1991); emergent situations are when HCW s are least likely to be in control o f events. When confronted with an
emergency situation, HCW s may chose to protect the patient's safety before their own. Another issue that may also
contribute to the degree o f control HCWs have over glove use is whether gloves are easily accessible at all limes.
Perceived control did not directly influence glove use and perhaps this may be the reality of working in a health care
environment. In health care, there will always be unexpected and emergent situations and these emergent situations do
not always occur where supplies are immediately accessible.
As with the TRA models, the modification index for the path from attitude to behavior revealed that adding this
'ypath may im prove the fit o f the model. M odel II.3 represents this addition (see Table XVIII). The difference in the x~
statistics indicated an improvement in fit over Model II.2 The / value for the path from attitude to behavior was
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

65
TABLE XXI
DECOMPOSITION OF EFFECTS FOR THEORY OF PLANNED BEHAVIOR MODELS II.2 AND II.3
IndependentVariables
Dependent Variables
Intention Behavior
TotalEffect
StandardError
DirectEffect
StandardError
TotalEffect
StandardError
DirectEffect
StandardError
IndirectEffect
StandardError
Model II.2
Attitude .14 .05 .14 .05 .11 .04 a - .11 .04
Subjective norm .01 .01 .01 .01 .01 .01 - - .01 .01
Perceived control .29 .03 .29 .03 .29 .03 .06 .04 .23 .04
Intention .80 .12 .80 .12
Model II.3
Attitude .14 .05 .14 .05 .06 .05 -.08 .04 .14 .05
Subjective norm .01 .01 .01 .01 .01 .01 0 0 .01 .01
Perceived control .29 .03 .29 .03 .29 .03 .02 .05 .28 .05
Intention .97 .16 .97 .16
aAccording to the theory of planned behavior, theoretically implausible path, which was fixed to zero in analysis.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

66
significant. Table XXI shows that attitude affected behavior in part through its effect on intention and that attitude also
directly influenced behavior independently o f intention. As before in the TRA Model 1.4, this direct influence of attitude
w as a small and negative one. Perceived control continued to influence intention more so than did attitude or subjective
norm. In Model II.3, 71% of glove use behavior was accounted for by the HCWs' determination to wear gloves and their
opinions about gloves. In turn, 74% of the HCWs' intention to wear gloves was accounted for by their opinions about
gloves and their perceptions of how easy gloves are to wear.
Summary. The HCWs' attitude about gloves and their perception of how easy gloves are to wear were predictive
o f their intention to wear gloves. Also, how determined HCW s were to wear gloves and their attitude about gloves were
predictive o f their glove use. The HCWs' perception about how much control they had over their glove use and their
positive attitude about gloves accounted for 74% o f their intentions to wear gloves. The HCWs w ho intended to wear
gloves but who also held a negative attitude about gloves, were more likely to wear them. Intention was an important
intervening variable for behavior with perceived control and attitude. Only the HCWs' attitude about gloves influenced
their glove use separately from their intentions to wear gloves.
Model II.3 was a good fit to the data. Compared to the TRA Model 1.4, the TPB models explained more about
HCW s' intention to wear gloves but did not add anything to the explanation of glove use behavior.
Self-Protection M odel—Model III
Proposed m odel. The LISREL model is illustrated in Figure 3. Model III varies from M odel II with the
addition o f the construct perceived risk, as well as changes in the observed variables that measured subjective norm and
perceived control. Referring to Figure 3, perceived risk was measured by the observed variable comparative risk (xf).
Norm-direct (x2) and normative influence (x^) served as the observed measures of subjective norm. The observed
variable protection effectiveness (x-y) measured perceived control along with control-direct (x fi and self-efficacy (\g).
Other variables were measured as in Models I and II.
Sequence o f models. Table XXII shows the fit statistics for the baseline model (III. 1). Protection effectiveness
was eliminated from the model. This variable was eliminated after examination of the data revealed that protection
effectiveness was a poor indicator of perceived control (R = .1 8 ) and contained a great deal of measurement error.
Control-direct and self-efficacy remained as the only measures o f perceived control.
After eliminating protection effectiveness from the model (Model III.2), measurement errors were allowed to
correlate (M odels III.3, III.4). As with attitude-direct, comparative risk was assumed to be perfectly measured and
therefore, other error parameters were not allowed to correlate with comparative risk.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

67
TABLE XXII
OVERALL FIT M EASURES FOR SELF-PROTECTION M ODELS (III.1-III.5)
M odel
Degreesof
Freedom X2
Goodness-of-FitIndex
AdjustedGoodness-
of-FitIndex
RootMean-Square
Residualx2
p value
X" difference p valuea
M odel III. 1 34 105.1 .97 .93 .11 .00 _
(Model III. 1 = baseline model: no correlated errors) 25 75.2 .97 .94 .11 .00 < .00
M odel III.2 24 51.9 .98 .96 .10 .00 < .00(Model III.2 = M odel III. 1 and elim inating protection effectiveness) 22 39.7 .97 .96 .08 .01 < .01
M odel III. 3 20 29.0 .99 .97 .07 .09 < .01(M odel III.3 = M odel III.2 and correlated error between past month and next month)
M odel III.4(Model III.4 = Model III.3 and correlated errors between not wear and next month and self-efficacy and normative influence)
M odel III.5(Model III.5 = Model III.4 and direct path from attitude to behavior and from perceived risk to behavior)
a/7 value for the difference in chi square statistic from previous model.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

68
Results o f the final model (Model III.4) are reported in Table XXII. The differences in the x“ statistics
indicated a significant improvement in fit o f Model III.4 over the previous models (III. 1 to III.3). With 22 degrees of
freedom, the x" statistic for Model III.4 was 39.7. With a probability value o f .012, this model and the data were not a
perfect fit. The RM R o f .077 indicates that more o f the residual variances was accounted for by Model III.4 than in the
other models. W ith the addition o f the correlated errors, the structural model remained stable. Overall, this model was a
good fit.
Measurement m odel. The measurement model for the y variables, perceived control, and attitude remained the
same as in Model II (see Table XXIII). The measurement m odel for the remaining x variables included the new measure
o f subjective norm (nonnative influence) and the comparative risk measure. For subjective norm the two observed
variables, norm-direct and normative influence, were acceptable measures. Norm-direct (R~ = .64) was a better indicator
o f subjective norm then was nonnative influence (R^ = .46). The t value for normative influence was significant. Of
note, the A2 value for nonnative influence was approximately the same as for norm-indirect which was used in the
previous TRA and TPB models. This would be expected as the items used in normative influence were also used in the
norm-indirect scale. However, the similarity in results would indicate that the motivation-to-comply items used within
the nonn-indirect scale do not improve the reliability o f the measure and that nonnative influence is as good a measure of
subjective norm as is norm-indirect.
Structural m odel. As Table XXIV indicates, perceived risk was a significant but minimal predictor of intention
(t = 2.08). The amount o f variance explained in intention remained the same as with the TPB models. Among HCWs
who differ in their intention to wear gloves, they differed by 69% in their perception o f how easy gloves were to wear,
by 18% in their attitudes about gloves, and by 8% by whether they perceived themselves to be at risk for HIV or hepatitis
B, as well as how much influence important others had on their glove use.
Although perceived risk w as a significant predictor o f intention, perceived risk minimally influenced (.03)
HCW s1 intention to wear gloves. How easy or difficult HCW s' perceived gloves are to wear continued to be the most
influential in deciding HCWs' intention towards glove use. W ith the addition of perceived risk, subjective norm's affect
on intention (.07) was twice that o f perceived risk (.03). Perceived risk, perceived control, attitude, and subjective norm
indirectly influenced behavior through their affect on HCW s' intention. Important others impacted glove use behavior by
influencing HCW s’ intention (.15) m ore so than did the HCWs' perception o f risk (.03) or their attitudes about glove use
(.12). The influence o f important others may be related to supervisors and regulatory bodies who have been informing
HCWs they are at risk for HIV and hepatitis B. In this study, the HCW s perceived themselves to be at less risk than
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Reproduced
with perm
ission of the
copyright ow
ner. Further
reproduction prohibited
without
permission.
TABLE XXIII
LISREL ESTIMATES OF REGRESSION OF OBSERVED ON LATENT VARIABLES: SELF-PROTECTION MODEL III.4
Observed Variables R2
Latent Variables
Attitude Subjective Norm Perceived Control Perceived Risk Intention Behavior
Ua Sb t° U S t U S t U S / U S t U S t
A ttitude-direct 1.0 1.0d 1.0 0d - - - - - - - - - - - - -
Nonn-direct .64 1.0d .80 0d - - - - - - - - - - -
Nonnative influence .46 4.83 .68 12.0 - - - - - - - - - - -
Control-direct .79 1.0d .89 0d - - - - - - - -
Self-efficacy .44 0.71 .66 13.7 - - - - - - - -
Comparative risk 1.0 1 00d 1.00 od - - - - - -
Intend .51 1.0d .71 0d - - -
Next month .62 0.83 .79 14.7 - - -
Past month .79 l.Od .89 0d
Not wear .28 0.61 .53 9.9
aUnstandardized LISREL lambda coefficients.
^Standardized LISREL lambda coefficients.
°Critical value for t approximately ± 1.96.
dFixed parameter value.
cAccording to the self-protection model, theoretically implausible path, which was fixed to zero in analysis.OsVO

70
TABLE XXIV
LISREL ESTIMATES OF STRUCTURAL COEFFICIENTS FOR SELF-PROTECTION MODELS III.4 AND III.5a
Independent Variables
Dependent Variables
Intention Behavior
Ub Sc rd U S I
Model III.4
Attitude 0.14 .18 3.0 _c - -
Subjective norm 0.17 .08 1.1 - - -
Perceived control 0.29 .69 9.2 0.03 .07 0.7
Perceived risk 0.03 .08 2.1 - - -
Intention 0.87 .77 7.0
R2 .73 .69
Model III.5
Attitude 0.15 .20 3.3 -0.08 -.09 -2.0
Subjective norm 0.17 .08 1.2
Perceived control 0.28 .68 9.1 0.01 .03 0.2
Perceived risk 0.03 .07 1.7 0.03 .07 2.1
Intention 0.99 .88 6.0
R2 .74 .75
aFit measures are reported in Table XXII.
LUnstandardized LISREL gamma and beta coefficients.
S tandardized LISREL gamma and beta coefficients.
clCritical value for t is approximately ± 1.96.
eAccording to the self-protection model, a theoretically implausible path, which was fixed to zero in analysis.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

71
their peers for these diseases. Regardless o f whether HCWs themselves think they are at risk, HCW s are being told they
are at risk. In addition, w ith the passage o f time, the influence o f perceived risk may have been incorporated into the
HCWs' belief systems. Initially, when gloves were first required, risk may have influenced HCW s' intention to wear
gloves m ore significantly. But with time, the influence o f risk may be incorporated into their perceptions that important
others want them to wear gloves because o f potential risk, as well as incorporated into their attitude about gloves which
are worn to protect them from risk.
The results indicated a possible improvement in fit if there were paths from attitude and perceived risk to
behavior. Model III. 5 in Table XXII represents these additions. All o f the goodness o f fit m easures revealed that this
model is a good fit to the data. With 20 degrees o f freedom, the x2 statistic for M odel III.5 was 29.0; with a probability
value of .087, this model fit the data. The / values associated with the direct paths o f attitude and perceived risk to
behavior were significant (see Table XXIV). However, these added paths did not significantly add to the prediction of
glove use; Model III.5 explained 75% of the variance in glove use behavior.
Table XXV shows that perceived risk and attitude influenced glove use partially through their affect on intention
and that these variables also directly influenced HCWs' behavior independently o f intention. The impact of perceived risk
was small and perceived risk had about the same impact on glove use as did the HCW s' attitude. Subjective norm and
perceived control indirectly affected behavior by increasing HCWs' intention; these variables direct influence on behavior
were minimal. Overall, intention was an important intervening variable for perceived control, perceived risk, subjective
norm, and attitude. The majority of the influence o f these variables on behavior was moderated through intention.
y y 2The x statistics and R~ values for the SPM models cannot be strictly com pared to the x statistics in the TRA
models o r TPB models. This comparison should not be made because the SPM m odels differ from the other models in
terms of the measurement o f subjective norm. In general, however, Model III.5 did not explain any more o f the variance
in glove use over the TPB (Model II.3). The SPM model explained 74% of the variance in intention and 75% of the
variance in behavior.
Summary. In Model III.5, attitude and perceived control were predictive of intention. HCW s who held a
positive evaluation of wearing gloves and w ho also perceived that wearing gloves was easy, were more likely to intend to
wear gloves. Those who were confident in their ability to wear gloves and found it easy to do so were the most likely to
intend to wear gloves when there was potential for blood contact.
Attitude, perceived risk, and intention were significant predictors of behavior; those who intended to wear gloves
were the most likely to report wearing gloves. In addition, HCWs were likely to report wearing gloves if they held a
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Reproduced
with perm
ission of the
copyright ow
ner. Further
reproduction prohibited
without
permission.
TABLE XXV
DECOMPOSITION OF EFFECTS FOR SELF-PROTECTION MODELS III.4 AND III.5
Independent Variables
Dependent Variables
Intention Behavior
TotalEffect
StandardError
DirectEffect
StandardError
TotalEffect
StandardError
DirectEffect
StandardError
IndirectEffect
StandardError
Model III.4
Attitude .14 .05 .14 .05 .12 .04 a - .12 .04
Subjective norm .07 .15 .07 .15 .15 .13 - - .15 .13
Perceived control .29 .03 .29 .03 .28 .03 .03 .04 .25 .04
Perceived risk .03 .02 .03 .02 .03 .01 a .03 .01
Intention .87 .12 .87 .13
Model III.5
Attitude .15 .05 .15 .05 .07 .05 -.08 .04 .15 .05
Subjective norm .17 .14 .17 .14 .17 .14 0 0 .17 .14
Perceived control .28 .03 .28 .03 .29 .03 .01 .05 .28 .05
Perceived risk .03 .02 .03 .02 .06 .02 .03 .01 .03 .02
Intention .99 .17 .99 .17
“According to the self-protection model, theoretically implausible path, which was fixed to zero in analysis.

73
negative attitude toward glove use or if they perceived themselves to be at less risk for HIV or hepatitis B than their
peers. The HCW s were unrealistically optimistic about their risk o f HIV and hepatitis B and this influenced their use of
gloves. When asked what their intention toward glove use was, HCWs had a positive attitude toward gloves. Asking
about their intentions required the HCWs to think and rationalize their glove use. However, HCWs do not like to wear
gloves. They know that gloves are required, but gloves are uncomfortable, inconvenient, and interfere with their work.
Understandably, HCW s have a negative attitude toward wearing gloves. But since gloves are required, HCW s still wear
them. Deciding what they intend to do about gloves seems to in some way moderate their negative opinion toward
gloves.
Overall, perceived control was the strongest predictor of intention to wear gloves and in turn, intention was the
strongest predictor o f glove use. Attitude and perceived risk contributed trivial but statistically significant amounts to the
prediction o f glove use. The HCWs' intention to wear gloves or their actual glove use was not influenced by important
others. It is at first surprising that important others, such as OSHA and supervisors, did not influence HCWs. However,
the passage o f tim e may have impacted the influence o f important others on intention. The direct effect of policy
changes would probably decrease with time as HCW s incorporate the need to wear gloves into their other belief systems.
The model is a good fit to the data. Overall, attitude, perceived control, perceived risk, and intention are
important variables in predicting glove use behavior. This model accounted for a large amount of the variance in glove
use behavior.
Summary of Findings
The study's hypotheses are used as an organizing framework to discuss and summarize the findings. In addition,
comparisons to previous research are made. This section also contains a descriptive summary o f the behavioral belief
items.
Hypotheses
The first hypothesis was, The SPM will fit the data better and explain m ore of the variance in HCWs' self-
reported use of gloves when there is potential blood exposure than the TRA or the TPB. The variables and their
relationships within the SPM explained 74% o f the variance in self-reported glove use. The final SPM was, overall, the
best fit of the theoretical models to the data. The SPM accounted for the same amount o f variance in intention as did the
TPB; neither the SPM nor the TPB explained any more about glove use behavior than did the TRA model. Therefore,
this hypothesis was not supported.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

74
The second hypothesis was, The TPB will fit the data better and explain more o f the variance in HCWs' self-
reported use of gloves when there is potential blood exposure than the TRA. The addition o f perceived control
significantly increased w hat was known about HCWs' intention to wear gloves but did not add to what the TRA had
already explained about H CW s1 glove use. Overall, the TPB Model II.3 explained 71% o f the variance in self-reported
glove use. Therefore, the second hypothesis was not supported. There was not a statistically significant improvement in
fit o f the TPB over the TRA, and the TPB did not explain any more o f the variance in glove use behavior.
The third hypothesis was, HCWs employed in urban hospital settings will differ in frequency of glove use from
those employed in nonhospital rural settings. Subhypotheses included (a) HCWs' self-reported use o f gloves will vary by
the type of work setting, (b) HCWs' self-reported use of gloves will vary by the geographical location, and (c) reported
use of gloves will vary by the HCWs' field of employment. Both nurses and laboratory workers reported frequent glove
use. However, only one-half of the sample (52%) reported wearing gloves every time there was potential blood contact.
In addition, only 33% reported that they always had gloves on when there had been actual blood contact. The general
hypothesis that glove use would vary between urban hospital settings and nonhospital rural settings was not supported.
There was no significant difference in glove use between hospital and nonhospital settings. The HCW s employed in
suburban areas were m ore likely to wear gloves than those working in urban and rural areas. Suburban laboratory
workers were more likely to wear gloves than were urban or rural laboratory workers. Therefore, two out of the three
subhypotheses were supported. Glove use did vary by geographical location and there was an interaction with field of
employment. Glove use did not vary by type o f work setting. This lack of association may be a result of insufficient
sample size to detect any difference in glove use between hospitals and nonhospitals.
Comparisons to the Literature
Comparisons can be made to this study's findings from previous research. There were several similarities with
findings of this research and other research that investigated HCWs' use of gloves. In the present study, nurses and
laboratory workers failed to always wear gloves 48% of the time; 67% reported having some contact with blood during
the last month. This level of noncompliance falls within the range of glove use previously reported in the literature (see
Table I). A recent study reported that 29% of Michigan nurses failed to almost always wear gloves (Schillo & Reischl,
1993). This is a higher compliance rate than was reported by the nurses in the present study— 50% failed to always wear
gloves. The difference in magnitude between the two studies is probably related to the measurement approach taken.
The Schillo and Reischl (1993) measure contained only three response categories for frequency of glove use whereas this
study included seven categories.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

75
Although few studies examined differences in glove use by field o f employment, geographical location, or work
setting, results are supportive. Studies that examined various HCW s' compliance with universal barrier precautions found
that the frequency o f barrier use varied between various professional and nonprofessional employment groups (Baraff &
Talan, 1990; Henry et al., 1992; Kelen et al., 1991). None o f these studies, however, compared glove use between nurses
and laboratory workers. Similarly, few studies have examined glove use by geographical location. Findings from the
Willy et al. (1990) and Fox (1990, unpublished data) studies also found differences in glove use by geographical location.
However, contrary to the last two studies, Schillo and Reischl (1993) did not find any geographical differences; the
comparison between the Detroit area and the remainder o f the state may have masked any possible affect by the suburbs.
No studies were found that reported or investigated whether geographical location impacted the use o f gloves within
various employment groups.
Finally, the present study did not find that glove use varied by type of work setting. Nevertheless, other studies
have reported such differences. The Schillo and Reischl (1993) study reported differences in glove use between nurses
working in acute care, nonacute care, administrative, and educational settings. Whether Schillo and Reischl's findings are
contradictory is difficult to assess; the present study classified settings in such a manner that nonacute, administrative, and
educational settings would be included in both hospital and nonhospital settings. However, the Fox (1990, unpublished
data) study did find that glove use varied between hospital and nonhospital settings.
Overall, previous research is supportive of findings reported here in relation to glove use. Frequency of glove
use and variations in glove use by field o f employment and geographical location were supported. Although the present
study contradicts previous studies in relation to glove use in various type o f work settings, different measurement
approaches confounded direct comparisons.
There are also similarities between the present study and other studies which used the TRA, TPB, and elements
of the SPM. As with the TRA research reported in Table IV, subjective norm and attitude were predictive of intention in
the present study. In addition, intention was a strong predictor o f behavior. The amount of variance explained in
intention, and in turn, behavior, was within the range o f what was reported in Table IV. Consistent with the TRA, the
direct measure of subjective norm was a better gauge o f subjective norm than was the indirect measure. However, the
motivation-to-comply items contained within the indirect measure did not add to the predictive capabilities of the
normative belief items. This was seen when the normative influence measure explained about the same amount of the
variance in intention as did norm-indirect. Although this finding is contrary to what the TRA postulates, other studies
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

76
have found that motivation to comply did not significantly contribute to normative beliefs' prediction o f intention (Ajzen
& Driver, 1992; Budd et al., 1984; Saltzer, 1981; Vallerand et al., 1992).
Other studies have also reported a direct path from attitude to behavior, suggesting that intention did not fully
m ediate the attitude-behavior relationship (Bentler & Speckart, 1979, 1981; Liska, 1984). However, Bagozzi et al. (1989)
reported that a direct path occurred only when there was insufficient power, the intention measures were unreliable, or
w hen the intention-behavior measures did not correspond. Given Bagozzi's et al. (1989) findings, it is possible that the
direct path found in this study w as due to a lack of correspondence. According to the TRA, the intention and behavior
measures must correspond in relation to action, target o f action, the tim e the action was performed, and context that the
action is performed within. One could argue that one o f the measures o f behavior (i.e., not wear) did not correspond
with intention in relation to context; not wear measured actual blood contact where the measures o f intention dealt with
potential blood contact. Regardless o f the correspondence issue, the direct path of attitude to behavior contributed only
trivially to the prediction of behavior. In other words, intention significantly mediated the attitude-behavior relationship.
The present study supported the TPB in that perceived control was an important addition to the understanding of
intention. In this study, perceived control was the strongest predictor o f HCW s' determination to wear gloves. In two out
o f the seven studies presented in Table VI, perceived control was the best predictor of intention. However, as the studies
in Table IV showed, perceived control did not always influence behavior independently of intention. The addition of
perceived control in this study did not improve the overall prediction o f glove use.
An additional question arises regarding the relationships between self-efficacy, protection effectiveness, and
perceived control. The TPB states that perceived control is a construct sim ilar to self-efficacy. In that case, there should
be good correlations between self-efficacy and perceived control. This study did find a good correlation; however, a
previous study did not (Dzewaltowski et al., 1990). Dzewaltowski et al. (1990) used a self-efficacy scale that combined
perceived strength of ability to participate in physical activities along w ith confidence in participating despite the presence
of barriers. Although the present study and the Dzewaltowski et al. (1990) study used sim ilar measures o f perceived
control, the differences in measurement approach with self-efficacy may account for the dissimilarity in correlations.
Previous researchers (Rogers, 1983; Taylor, 1990; Weinstein, 1989a) have recognized the importance of
protection effectiveness in predicting protective behaviors. The SPM incorporated protection effectiveness into perceived
control as an external control factor. However, protection effectiveness, as measured in this study, failed as an adequate
measure of perceived control. There is little discussion within the TPB about external control factors and this is an area
that warrants further study.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

77
In this study, perceived control was a strong predictor of intention and this may partially have been due to the
measure o f control-direct. The control-direct scale was based on items previously used w ith the TPB (Ajzen, 1991;
Ajzen & Madden, 1986) as well as items taken from a scale which was reliable in measuring perceived control (Gatch &
Kendzierski, 1990). During the content validity process, one o f the items was changed from how likely is it that you
could wear gloves to how likely is it that you would wear gloves. This item seems to tap m ore into the construct o f
intention than that o f perceived control. However, the perceived control scale was more highly correlated with self-
efficacy than with either o f the intention measures.
Within the SPM, perceived risk was a statistically significant, although trivial, predictor o f behavior. However,
the HCW s in this study did exhibit unrealistic optimism; over half rated themselves at below average risk for HIV and
hepatitis B when compared to their peers. This is consistent with previous research dealing with preventive health risks.
In extensions o f the TRA, two out o f three studies reported significant correlations with intention (Godin, Valois, Jobin,
& Ross, 1991; Radius et al., 1991; Stasson & Fishbein, 1990). In addition, Weinstein et al. (1986, 1990, 1991) reported
significant correlations between comparative risk and intention. Perceived risk was also predictive of behavior in this
study; in previous research there w as no consistent pattern as to whether perceived risk w as predictive of health related
behavior (see Table VII). In a recent paper, Weinstein and Nicolich (1993) stated that the correlation between perceived
risk and behavior should decrease over time. As there is more experience with the risk or hazard, perceived risk may no
longer influence behavior change. However, a small correlation in the present study docs not mean that perceived risk
was not initially im portant in influencing the decision to wear gloves (Weinstein & Nicolich, 1993). Data for the present
study were collected at least 5 years after the CDC first issued the universal precautions mandate, which required the use
of gloves with potential blood contact. The passage o f time may have had an effect on the magnitude o f the perceived
risk's correlation w ith behavior.
In summary, previous research is supportive of this study's findings. Overall, this study helps to demonstrate the
usefulness of these theoretical m odels in examining HCWs' use of gloves.
Descriptive Summary of Behavioral Beliefs
As previously discussed, the behavioral belief and belief evaluation items were eliminated from further analysis
as a result of a measurement error w ith the belief evaluation items. Although the behavioral belief items could not be
used in estimating the models, a descriptive summary of the items may be useful for future research.
Ten items comprised the behavioral belief scale. Using a 5-point scale, the sum of the responses ranged from 11
to 47. The 10-item scale mean was 33.93, with a standardized alpha coefficient of .55. As the corrected item-total
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

78
correlations ranged from .07 to .57, the correlations that were less than .40 were dropped. T his left five items with a
standardized alpha of .81 and item-total correlations ranging from .38 to .68. The items that remained were
uncomfortable, awkward, inconvenient, cause cross-contamination, and hard to draw blood. M ore than half of the sample
reported that wearing gloves was likely to be uncomfortable (53%), awkward (59%), inconvenient (52%), and make it
harder to draw blood (61%). An additional 47% reported that wearing gloves would likely cause cross-contamination.
A question arose as to why half o f the items needed to be dropped to create a reliable scale. The items were
based on an elicitation study performed in 1988 on laboratory workers. The passage o f time may have affected the
saliency of these beliefs as OSHA had released regulations regarding bloodbome pathogens since the elicitation study was
performed. When gloves were first required, many HCWs were reluctant to change their work practices. Most o f the
beliefs that were elicited were disadvantages; all o f the items which comprised the scale were disadvantages of wearing
gloves. With time, the use of gloves may have become more acceptable to HCWs and more advantages o f wearing
gloves would be elicited. In addition, there may have been a difference in belief saliency between nurses and laboratory
workers; there were no nurses in the elicitation study.
To determine if there was a difference in belief saliency, the behavioral beliefs of the nurses were compared to
those o f the laboratory workers. First, the results indicated that the nursing and laboratory' w orker population variances
were equal. Results were the same whether all 10 behavioral belief items were used, Levene statistic(l, 5160 = .02, p =
.90, or the 5-item reliable scale was used, Levene statistic(l, 511) = .61, p = .44. However, t test results revealed that
there were significant differences in the belief means between the nursing and laboratory w orker groups (see Table
XXVI). Specifically, for half of the beliefs items, there was a significant difference in the nurses' and laboratory workers'
responses. Nurses and laboratory workers differed on all the beliefs except that gloves were awkward. Laboratory
workers were more likely to report that gloves were uncomfortable, /(522) = -2.1, p = .04; inconvenient, /(522) = -2.2, p
= .03; and would cause cross-contamination, /(522) = -7.8, p = .00; as well as make it harder to draw blood, /(519) =
-6.9, p = .00.
As there were differences between the nurses' and laboratory workers' responses on the behavioral belief scale, t
tests were done for the other study variables. As Table XXVI indicates, nurses and laboratory workers responded
differently on the variables developed from the elicitation study (e.g., norm-indirect, normative influence) as well as on
nonclicited variables (e.g., attitude-direct, self-efficacy, not wear). One of the study hypotheses was, however, that glove
use would vary between employment groups.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

79
TABLE XXVI
M EAN DIFFERENCES ON STUDY VARIABLES BETW EEN NURSES AND LABORATORY WORKERS
Variable t valueDegrees of Freedom
Probabilityvalue
Behavioral beliefs 10 items -3.4 511 .005 items -4.9 516 .00
Attitude-direct 2.6 509 .01
Norm-direct 1.6 510 .11
Norm-indirect 3.8 506 .00
Normative influence 3.6 508 .00
Control-direct 0.4 523 .69
Self-efficacy -2.5 522 .01
Comparative risk 0.5 519 .61
Intend 1.6 501 .10
Next month 0.3 525 .80
Past month -0.4 525 .69
Not wear 2.5 520 .01
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

80
Beliefs about glove use found in this study were supported by those reported in Table II. However, no study
could be found that compared beliefs about glove use among different employment groups.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

SUMMARY, CONCLUSIONS, AND IMPLICATIONS
A summary o f the study as well as conclusions drawn from the findings are presented. This section closes with
the limitations of the study and the im plications for the study findings.
Summary
The purpose o f this study was to identify predictors o f HCWs' behavior related to injury prevention. Using the
SPM, this study investigated HCWs' intentions towards glove use as well as glove use when there was potential for blood
exposure. Additionally, this study determined which of the three theoretical models (SPM, TPB, TRA) was the best at
explaining glove use behavior. A secondary aim of this study was to ascertain if glove use varied with the field o f
employment o f the HCW in addition to the geographical location and type o f work setting.
To meet the stated purposes, a cross-sectional approach was used to survey a stratified-random sample of 909
nurses and laboratory workers from w ithin a midwestem state. The survey response rate was good (70%), resulting in a
sample o f 527 HCWs who had potential contact with blood. The sample was predominantly white, married females, who
were 30 years old. The sample typically held a bachelor's degree, had worked in their field for 14 years, and worked
full-time in a hospital setting. Most o f the sample were in the process of being vaccinated for hepatitis B. Although the
nurses were more likely to be female, older, and less likely to hold a bachelor's degree than the laboratory workers, these
differences were not considered to have affected the results.
The sample was surveyed using a 26-item questionnaire with acceptable content validity and reliability estimates.
The questionnaire was based on items derived from an elicitation study and followed the TRA approach for item
generation.
Guided by the SPM, structural equation modeling techniques were used to explore HCWs' intentions and glove
use behavior. The variables and relationships within the SPM accounted for much o f what occurred with glove use; 75%
o f the variance in glove use behavior was explained. Intention, attitude, and perceived risk were significant predictors of
behavior; those who were determined to wear gloves were the most likely to report wearing them. In addition, HCWs
were likely to report wearing gloves if they held a negative attitude about glove use o r if they perceived themselves to be
at less risk for bloodbome diseases than their peers. Intention was the best predictor o f glove use. Perceived control and
attitude were the significant determinants o f intention, explaining 74% of the variance in intention. Perceived control was
the variable that contributed the most to the understanding of HCWs' intentions towards glove use. HCWs who felt that
they could control whether they wore gloves had a positive evaluation about gloves, and who also were confident in their
81
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

82
ability to wear gloves, were determined to wear them. HCW s' intention to wear gloves was not influenced by important
others, such as supervisors and OSHA. Overall, the SPM w as very useful in identifying the predictors of HCWs' glove
use.
An additional purpose of this study was to determine if the SPM explained any more of the variance in glove use
than the TRA o r the TPB. The SPM accounted for the sam e amount o f variance in intentions as did the TPB and neither
the SPM nor the TPB explained any additional variance than what was accounted for by the TRA with glove use.
Although the variables which extended the TRA (e.g., perceived control, perceived risk) contributed to the understanding
o f HCWs' intentions, these variables did not improve the TRA's predictive capabilities in terms o f glove use behavior.
However, perceived control and perceived risk enhanced the understanding o f HCWs' glove use intentions. Knowing the
determinants o f intention can guide the development o f interventions aimed at increasing glove use.
The findings from this study were generally supportive o f previous research using the TRA, TPB, and the
elements o f the SPM. Intention was the best predictor o f behavior and perceived control was the best predictor o f
intention. Contrary to the TRA, a direct path from attitude to behavior was found. However, the impact o f attitude on
behavior was minimal. In general, intention was an important intervening variable for behavior for perceived control,
subjective norm, perceived risk, and attitude. Contrary to the TRA, motivation to comply did not significantly increase
the predictive pow er of the normative beliefs. These findings have been supported by other research as well.
Previous research has indicated the importance of the protection effectiveness concept in relation to protective
behaviors. The SPM proposed that protection effectiveness was a measure o f the external control factors within perceived
control. However, protection effectiveness was not a successful indicator of the external control factors. This finding
does not clarify the relationship between protection effectiveness and perceived control.
This study's findings are supportive of the TRA in relation to the saliency of beliefs. According to the TRA,
items should be developed from beliefs based on an elicitation study performed on a group as sim ilar as possible to the
sample of interest. The items used in this study were based on an elicitation study performed on a group of laboratory
workers four years prior to the present study's data collection. Differences in the present study were found between
nurses and laboratory workers on their behavioral and normative beliefs. This difference in the saliency o f beliefs may be
due in part to the dissimilar jo b functions o f the nurses and laboratory workers. An additional factor which may have
impacted the saliency o f the beliefs, was time. As time passed between the elicitation study and the present study, new
regulations were enacted to prevent occupational transmission of bloodbome diseases. In addition, HCWs attended
mandatory educational sessions and were bombarded with professional and lay material on bloodbome diseases and the
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

83
HIV epidemic. W ith such frequent exposure to information concerning HIV and hepatitis B, the passage o f time is apt to
have played an influential role in affecting the beliefs of the nurses and laboratory workers.
This passage of tim e may have also impacted the role that subjective norm and perceived risk played in th"
prediction of intention and behavior. Earlier on, important others may have influenced the HCW s' use of gloves through
policy enforcement and educational sessions where HCWs were informed o f their potential occupational risks. As time
passed and HCW s became m ore experienced with using gloves to protect themselves, the influence of risk and important
others may have been incorporated into the HCWs' behavioral belief system.
The final purpose o f this study was to determine if glove use varied with the type o f work setting, field of
employment, and geographical location in which the HCWs were employed. Results indicated that although HCWs wore
gloves frequently, only one-third to one-half o f the sample wore gloves every time there was a potential occupational risk.
Analysis o f variance procedures revealed that the geographical region where the HCW s w ere employed was predictive of
glove use. In addition, the region in which the HCWs were employed influenced nurses' and laboratory workers' glove
use differently. Specifically, nurses were found to wear gloves consistently regardless o f the region where they worked.
But suburban laboratory workers wore gloves more often than did rural or urban laboratory workers. This dissimilarity in
glove use may be due in part to regional differences in job responsibilities o r regional differences in the frequency of
emergent clinical situations. For laboratory workers, the work environment, work practices, and staffing patterns may be
different across the various regions.
Although the study did not find the proposed association between glove use and work setting, other studies have
indicated that glove use is m ore frequent in acute or hospital settings. This lack of support for previous studies may be a
result of the sampling design. The sample used in the present study was not initially stratified on the type of work setting
and as a result, the majority o f respondents were employed in hospital settings. A larger and more evenly distributed
sample would be needed to detect any differences in glove use between types of work settings.
The results of this study advance the work of other researchers in what is known about glove use behavior as
well as identifying important variables to include in future research. Furthermore, this study found that the SPM was a
viable model to study behavior related to injury prevention.
Conclusions
There are several conclusions that can be drawn from this study. First, the three theoretical models provided a
sound framework for investigating the predictors of glove use intentions and behavior. A great deal was achieved in
learning what contributes to HCWs' decisions regarding glove use. In all o f the models, the HCWs' level o f
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

84
determination (i.e., intention) was the best predictor of their behavior. Of the three models, the TRA was the most
parsimonious in defining glove use behavior. The TRA, however, did not define what contributed to the HCWs'
determination as well as did the TPB or the SPM. At least 74% of glove use intention and behavior was accounted for
by the TPB and the SPM. Overall, the TPB was the most parsimonious m odel in explaining why HCWs were or were
not determined to wear gloves.
The use of the SPM provided a framework to explore the relationships of perceived control, attitude, subjective
norm, and perceived risk to intention and behavior. Perceived control was the best predictor of intention; attitude
contributed only trivially to the prediction of intention. Important others, such as supervisors, OSHA, and co-workers,
did not influence HCWS' determination to wear gloves, but the cooperation o f others may have impacted glove use.
Attitude, perceived risk, and intention were predictive o f behavior.
The SPM provided a framework to explore several methodological concerns o f interest to future research. Two
departures from the TRA’s measurement approach were found. First, intention was found to be an important intervening
variable for behavior between attitude, subjective norm, perceived control, and perceived risk. However, contrary to the
TRA, intention did not completely mediate the attitude-behavior relationship. Secondly, multiplying the normative beliefs
by motivation to comply did not add to the predictive capabilities of the norm ative beliefs. These departures from the
TRA have been supported by previous research.
An additional methodological concern was the inadequacy o f protection effectiveness as a measure o f the
external control factors w ith perceived control. As previous protective behavior research had found protective
effectiveness an important variable, the relationship between this variable and perceived control needs to be explored.
The final methodological concern deals with the impact of time. T im e is a factor with any study that involves a
rapidly changing issue, such as H IV or the occupational exposure to bloodbom e diseases. The passage of time may have
impacted the results o f this study. Since the beliefs used in this study were first elicited, health care settings as well as
the media have emphasized compliance with OSFIA's bloodbom e disease regulations. W ith time, this emphasis may have
impacted the relationships between the variables and the saliency of the beliefs.
Despite the em phasis on regulatory compliance, this study concluded that glove use was not optimal when there
is potential for blood exposure. Several workplace factors may be associated with glove use. First, geographical location
influenced the frequency o f glove use. As suburban HCWs came in less contact with blood then did HCWs in other
regions, more emphasis needs to be placed on glove use in urban and rural areas. Suburban laboratory workers came in
less contact with blood and were the most likely to wear gloves. Differences in job functions, type o f patient contacts,
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

85
work environment, and work practices between the different fields may be reasons for variations in glove use. The
potential effect of differences in job functions (e.g., field o f employment) on glove use was also supported by the
dissimilarities between nurses and laboratory workers in their behavioral and normative beliefs. Although this study
cannot conclude that work setting affected glove use, type of work setting has been found by other researchers to affect
glove use.
In summary, this study concludes that the components o f the SPM, as well as field of employment and
geographical location, are important variables in exploring HCWs' use of gloves. Though this study cannot conclude that
type of work setting affects glove use, work setting is another variable which may add to the understanding o f HCWs' use
o f gloves.
Study Limitations
There are several limitations on the generalization of this study's findings. Limitations related to the theoretical
models and methodological approaches that were used are discussed.
The TRA specifics a methodological approach which requires the use of a single behavior and this model is not
recommended to be used with multiple behaviors. Although this approach strengthens the model's predictive powers, the
approach limits the gcneralizability of this study's findings. First, this study only addressed the single protective measure
o f glove use. Other protective measures prevent the transmission of bloodbome disease; these measures include barriers,
such as masks, goggles, and gowns, as well as procedures that prevent needlesticks. Secondly, this study only
investigated potential blood contact. The HCWs are potentially exposed to all body fluids that have been documented to
transmit bloodbome disease. This study's findings are not expected to generalize to other preventive approaches or other
body fluids.
An additional constraint that the TRA imposes is the use of an elicitation study to identify beliefs that are used
in developing items. Belief-based items assist in identifying the beliefs that are negatively associated with intention and
upon which interventions may be based. Regardless of the benefit of belief-based items, elicitation studies take time.
The extra time involved with an elicitation study may impact results when investigating a behavior that involves an
emerging and highly charged issue, such as HIV. As was suggested by this study, passage of time may have affected the
HCW s’ beliefs.
Another limitation which is associated with the TRA's approach and the passage o f time, is the limitation related
to the research design. As this was a cross-sectional study, the predictors of intention and glove use behavior were
measured at a single point in time. Ideally, to determine more assuredly the causal order o f the variables, studies should
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

86
use a prospective design; measures then could be taken at several points in time. However, the TRA is based on Lewin's
(1951) field theory which assumes that the person's perceptions at a single point in tim e primarily determine a person's
behavior at that moment. Thus, the predictive capabilities o f the TRA would diminish with designs that use multiple
measures over time. Models based on the TRA are predictive of behavior when short periods o f time are allowed to pass
between the measures of intention and behavior. Designs that advocate long time periods between measures or multiple
measures over time may benefit from a different theoretical approach.
A final theoretical limitation is that this study was not a full test of the TRA, TPB, or the SPM. Control and
risk beliefs were not elicited. Behavioral beliefs were available but data based on these beliefs could not be used due to
instrument error. Developing the proposed indirect measures based on elicited beliefs would contribute to the
understanding of the relationships between the beliefs and the other constructs in the models.
There are several limitations which are not related to the theoretical models. The first is the measure o f the
dependent variable, glove use behavior. Although other studies have reported no differences between observed and self-
reported glove use, this study relied on a retrospective self-report measure. The estimates of how often gloves were worn
could not be verified. Therefore, glove use estimates could be influenced by this sample's poor recall or social
desirability factors associated with a mandated behavior.
Second, participation in this study was voluntaiy, so self-selection bias may be a threat. Although there was a
range of responses for glove use, nonrespondents may wear gloves more or less frequently than did the sample.
Nonrespondents may have different perceptions about glove use. As this sample of nurses and laboratory workers may
not be representative of all HCWs who are at risk for occupational exposure to bloodbome diseases, generalization o f the
findings is limited to the study population. Strictly speaking, the results cannot be generalized to other HCW s employed
in fields other than nursing or medical laboratory.
This study did not include variables which measured situational or environmental factors that may influence
glove use. Flay and Petraitis (1993, unpublished manuscript) in their new macro-level model, discussed the importance of
including situational factors along with personal factors when studying health-related behaviors. Examples o f situational
factors which may impinge upon glove use are whether glove boxes are located conveniently for each work station or
whether vinyl gloves arc available for latex-sensitive employees.
The last limitation is that the stratified-random sampling approach used in this study did not generate an adequate
sample of nonhospital settings. Without an adequate sample, no conclusions could be reasonably drawn regarding the
affect of work setting on glove use. In the future, an approach that assures equal representation of hospital and
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

87
nonhospital work settings would be necessary if work setting is investigated. To obtain an adequate sample from
nonhospital settings could be accomplished by randomly selecting work settings within each region and then sampling the
employee groups.
Im plications o f the Findings
Nursing Practice
The National Institute for Occupational Health and Safety, the American Association o f Occupational Health
Nurses, and OSHA have all taken measures to support safe work practices within health care settings (U.S. Department o f
Labor, 1991). These measures include guidelines and regulations concerning work practice controls, mandated
educational sessions, hepatitis B vaccination programs, and the use of protective equipment such as gloves. Despite some
improvements in practice that have occurred, such as the advent o f retractable needles, considerable improvement is still
needed.
Several issues continue to be problematic, and occupational health nurses have the opportunity to take a
leadership role in their resolution. These issues include accessibility of proper fitting gloves, practices that facilitate safe
work practices, and educational programs tailored to meet the special needs o f health care employees. First, gloves must
be accessible for all HCWs at all times. As gloves are probably least likely to be wom during unexpected or emergent
situations, equipment used in health care settings requires designs that accommodate this need. Innovative design
approaches, such as small glove packs which attach to the HCWs' uniform or to the patient's cart, need to be devised and
tested. Second, gloves that do not fit properly may result in accidents, and in turn not be wom. The OSHA regulations
stipulate that an adequate supply of appropriately sized gloves be available for employees (U.S. Department o f Labor,
1991). However, many health care settings may resist keeping multiple sizes in stock due to the perceived burden o f
cost. And third, job responsibilities need to be evaluated in light o f the additional time that donning gloves requires. In
the laboratory area, preventing glove tears necessitates extra care with specimen labeling. Adequate time is usually not
available to take this extra care.
The occupational health nurse, along with management, can be instrumental in developing cost-effective
strategies to assure accessibility o f adequately sized gloves and to encourage safe work practices. With the understanding
that the traditional emphasis on regulatory compliance is not sufficient to motivate employees to wear gloves,
occupational health nurses can recommend alternative approaches to management. Decreasing barriers to glove use is one
approach which may be more practical and successful. Techniques, such as focus groups, may help to elicit the perceived
barriers to glove use and this information would provide a foundation for developing cost-effective strategies.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

88
Finally, educational programs tailored to meet regional concerns regarding glove use, as well as to m eet the
special needs of each type o f health care worker, should be more successful then a single generic approach which is often
used. Program planners may not be able to develop such specialized programs but in developing any program , planners
should incorporate the awareness that location and type of worker are significant and interact in various ways to influence
glove use.
Health Policy and Regulations
Under the existing OSHA regulations, employers are responsible for providing appropriate sized gloves and other
protective supplies (U.S. Department of Labor, 1991). Quality should be a major consideration when worker protection is
the concern. However, there are no quality standards established for the glove industry. Glove integrity studies reported
a broad spectrum of performance in relation to permeability and intactness (Komiewicz, Laughon, Butz, & Larson, 1989).
In an era o f cost-containment, price has often been an overriding consideration when gloves are purchased. Perhaps,
glove compliance is related to glove quality: Why wear gloves which are awkward, when the gloves are defective
anyway? Thus, a national standard on glove quality must be established and enforced. This standard would come under
the jurisdiction of the Food and Drug Administration, which currently regulates other medical devices.
Recommendations for Future Research
Future research could investigate the predictive capabilities of these theoretical models using other protective
measures, other types of HCWs, and other body fluids. A possible extension of the present study would be to separate
the nurse and laboratory worker sample and estimate the theoretical models to determine if there is an improvement in fit.
The salient beliefs o f nurses and laboratory workers would need to be identified and compared to those beliefs used in
this study. Results o f these future studies may indicate a range of beliefs that could be generalized to all workers who
use protective equipment. Flowever, if multiple behaviors are studied at one time, the approach used w ith the SPM may
be burdensome.
Secondly, future research needs to confirm the theoretical relationships found in this and other studies.
Researchers may be interested in exploring under what circumstances intention does not fully mediate the attitude-
behavior relationship, as well as investigate the predictive capabilities o f motivation to comply. In addition, the
relationship among self-efficacy, protection effectiveness, and perceived control needs to be explored. The dimensionality
o f the perceived control construct should be examined to determine the role o f internal and external factors. And finally,
the function of perceived risk needs to be explored with a newer hazard. A longitudinal approach could determine
perceived risk's contribution to the decision to use protective equipment; this approach would dictate a theoretical model
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

89
other than the SPM. Possible alternative models include Weinstein's (1988) precaution adoption model and Rogers'
(1983) protection motivation theory.
Future research may also expand the present study in order to test all of the proposed relationships within the
SPM. Further testing is necessary to determine if the model is viable for studying protective behaviors. Basing measures
on behavioral, normative, control, and risk beliefs would be beneficial to identify the beliefs which contribute to glove
use. Using these beliefs in a refined instrument would more fully test the SPM, as well as the TRA, and TPB and would
also determine the contribution of the beliefs in predicting intention and glove use behavior. Interventions targeted at
changing the primary beliefs that are negatively associated with intention/behavior could then be studied for effectiveness.
Lastly, consistency is needed across studies which investigate glove use. When consistent definitions o f
compliance, work setting, geographical location, and type of HCW are used, conclusions based on comparisons across
studies can be made more confidently. Results of this future research related to glove use would be beneficial to
occupational health nurses and all health care professionals interested in increasing glove use and reducing workers' risks
to bloodbome diseases.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

APPENDICES
90
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

91
Appendix A
SURVEY
Questionnaire.
P ro tectio n from B lo o d C ontact:
Opinions o f Illinois Health Care Workers
Department of Public Health Nursing • College of Nursing (m/c 802) University of Illinois at Chicago • Box 6998 • Chicago, Illinois 60680
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
page I
Objective
' Qpiniori Siirvey
The purpose of this survey is to determine what health care workers believe is important to protect themselves against bloodbome pathogen exposure. For each question, check the number which best represents your response. Please answer all of the questions. If you want to comment on any of the questions, or qualify your answer, please feel free to use the space in the margins. Your comments will be read and considered.
Thank you for your help.
Department of Public Health Nursing College of Nursing (m/c 802)
University of Illinois at Chicago Box 6998
Chicago, Illinois 60680
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

93
Appendix A (continued)
SURVEY (continued)
page 2
Question One
In your present position, is there a possibility that you will come in contact with a patient’s blood? Contact with a patient’s blood could occur when drawing blood, handling or processing a blood sample, starting or discontinuing an IV, performing a finger or heel stick, performing a non-sterile dressing change on a draining wound, or when assisting a patient who is actively bleeding. (Check one)
YES [ J j
NO □ (If NO)Because the purpose of this survey is to learn more about what health care workers think is important to protect themselves against bloodbome pathogen exposure, please skip to Question Sixteen on page 14.1 appreciate any comments you would like to make. Please continue with Question Sixteen and return the questionnaire, so I will know that you work in an area without potential contact with patient’s blood.
Opinion Survey .
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

94
Appendix A (continued)
SURVEY (continued)
page 3
Health care professionals have recommended wearing gloves to protect against blood contact. The following is a list of statements of what you may believe about wearing gloves. There are no right or wrong answers. It is important that you answer the statements according to your beliefs and not what you think others may want you to believe.
Question TwoHow likely is it that wearing gloves when there is a potential for blood contact will:
VeryUnlikely Unlikely Uncertain Likely
VeryLikely
a) Protect you from bloodbome disease
□ □ a a ab) Be uncomfortable □ a a a ac) Be awkward □ a a a ad) Make it harder to
draw blood□ a a a a
e) Cause cross contamination to work surfaces
□ a a a a
f) Encourage less handwashing
□ a a a ag) Be inconvenient □ a a a a
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
: Opiriion Survey

95
Appendix A (continued)
SURVEY (continued)
page 4
Question Two • Continued
How likely is it that wearing gloves when there is a potential for blood contact will:
Very VeryUnlikely Unlikely Uncertain Likely Likely
h) Make you feel safe □ a a a aI) Not provide □ 0 0 0 0
complete protection
j) Protect your patient’ CD 0 HI ID H)from bloodbome disease
The next statements are very similar to those in Question Two, but the statements in Question Three are about the effects or outcomes of wearing gloves.
Question Three
How important to you is each of the following effects of wearing gloves:
Very VeryUnimportant Unimportant Uncertain Important Important
a) Protecting you from □ □ D D Dbloodbome disease
b) Being uncomfortable □ a D D Dc) Being awkward (T^ [^ j [sjj
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
page 5
Question Three • continuedHow important to you is each of the following effects of wearing gloves:
Very VeryUnimportant Unimportant Uncertain Important Important
d) Making it harder to draw blood
HI HI a a ae) Causing cross
contamination to work surfaces
HI a a a a
f) Encouraging less handwashing
HI a a a ag) Being inconvenient HI a a a ah) Making you feel safe HI a a a ai) Not providing complete □ a a a a
protection
j) Protecting your patient HI HI El □ 0from bloodbome disease
Opinion Survey
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

97
Appendix A (continued)
SURVEY (continued)
Op.inion Survey
Question Four
In general, do you think that wearing gloves when there is a potential for blood contact is:
a) Foolish □ a a a a Wise
b) Harmful □ a a a a Beneficial
c) Worthless □ a a a a Valuable
d) Useless □ a a a a Useful
Another important part of this survey is to learn more about what other people think of health care workers wearing gloves.
Question FiveDo you agree or disagree that the following people want you to wear gloves when there is a potential for blood contact?
a) Your supervisors
b) Your co-workers
c) Officials from regulatory agencies such as CDC, OS o r the health department
StronglyDisagree Disagree Uncertain Agree
StronglyAgree
a a a a aa a a a aa a a a a
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
98
page 7
Question Five • continued
Do you agree or disagree that the following people want you to wear gloves when there is a potential for blood contact?
StronglyDisagree Disagree Uncertain Agree
StronglyAgree
d) Your patients □ CD a a ae) Other health professionals □ a a a af) Your family or friends CD a a a aQuestion Six
In general, do most of the people or groups that are important to you think you should wear gloves when there is potential for blood contact?
Should not (D a ID a IU Should
' Opinibn Survey•,■
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
99
page 8
Q uestion Seven
Generally speaking, how much do you want to do what the following people think you should do?
Not Not VeryAt All Much Uncertain Somewhat Much
a) Your supervisors □ a a a ab) Your co-workers CD a a a ac) Officials from regulatory
agencies such as CDC, OSHA, or the health department
□ a a a a
d) Your patients □ a a a ae) Other health professionals CD a a a af) Your family or friends ID a a a a
Q uestion Eight
Now, would you please indicate how easy it is for you to wear gloves.
Difficult Easya) How easy is it for you to □ a a a a
wear gloves every time there is potential for blood contact is?
O p i n i o h Survey
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

100
Appendix A (continued)
SURVEY (continued)
page 9 “ O pi n j o n S u rv ey
Question Eight * continuedNow, would you please indicate how easy it is for you to wear gloves.
b) How much control do you have Little Completeover whether you wear gloves every Control — — — Control
time there is potential for blood contact? LU ILI Ijj Lii IJLl
c) How likely is it that you would wear Unlikely ______ ___ ___ Likelygloves every time there is potential I j J I^J i^ J I^J IJLjfor blood contact?
d) It is mostly up to you whether or Disagree Agreenot you wear gloves every time □ a a □ u sthere is potential for blood contact:
e) There is very little that you can do Disagree Agreeto make sure you wear gloves every [ o □ m □ [ ntime there is potential for blood contact:
f) You are confident in your ability to Disagree Agreewear gloves every time there is q i n a a apotential for blood contact:
g) You are not sure that you can wear Disagree Agreegloves every time there is potential [J J [^J [jjjj I"*! l~S~|for blood contact:
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

101
Appendix A (continued)
SURVEY (continued)
page 10
Could you please tell me how you feel about wearing gloves.
Question NineOver the next month, which statement best describes what you will do about wearing gloves when there is potential for blood contact?
I am determined to wear gloves every time □there is potential for blood contact over the next month
I want to wear gloves every time there is potential for blood contact over the next month
I don’t intend to wear gloves every time there is potential for blood contact over the next month
1 will try to wear gloves every time there is potential for blood contact over the next month
It is possible that 1 will not wear gloves every \1time there is potential for blood contact over the next month
HI
□
H I
Opinion Survey
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
102
page 11
Question TenOver the next month, what percentage of time do you think you will wear gloves when there is a potential for blood contact?
0% □
I to 5% Q 51 to 75% □
6 to 25% □ 76 to 95% □
26 to 50% 96 to 100% □
Opinieti Survey
Question ElevenOver the past month, generally what percentage of time did you wear gloves when there was potential for blood contact?
0% □
1 to 5% □ 51 to 75% a6 to 25% a 76 to 95% a
26 to 50% a 96 to 100% a
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
page 12
Question Twelve
Over the past month, how many times were you not wearing gloves and you came in contact with a patient’s blood?
0 □1 to 3 a4 to 6 a
7 to 10 a10 or more a
The next questions are about the AIDS virus and Hepatitis B.
Question ThirteenHow b'Vr.’y is it that you will get the AIDS virus as compared to other health care workers who do a similar job as you do where you work?
Much below average aBelow average a
Average for your group aAbove average a
Much above average a
Opinion Survey '
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

104
Appendix A (continued)
SURVEY (continued)
page 13
Question Fourteen
How likely is it that you will get Hepatitis B as compared to other health care workers who do a similar job as you do where you work?
Much below average □Below average a
Average for your group aAbove average a
Much above average a
Op ini on.S u r v ey
Question FifteenDo you think gloves are effective in protecting you against
Not at all VeryEffective Uneffective Uncertain Effective Effective
a) AIDS) □ (3 ID □ H)
b) Hepatitis B! □ □ □ □ ( D
Finally, I would like to ask a few questions about yourself and where you work for statistical purposes.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix A (continued)
SURVEY (continued)
105
Opinion Survey page 14
Question Sixteen
Are you presently:
Employed Full-time □Employed Part-time □
Seeking Employment □ [S kip to
Not Employed □ [S kip to
Retired a [S kip to
Question Seventeen
Which of the following best describes your primary work setting?
Hospital □ Community/Public Health Agency aHospital Clinic a Medical Office a
Clinic a Home Care Agency aLong Term Care Facility a Student Health a
HMO a Occupational Health
Other(Pleue Specify)
aa
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

106
Appendix A (continued)
SURVEY (continued)
page 15
Question Eighteen
Where is your primary place of work located by telephone area code?
312 □ 309 □708 □ 618 □217 □ 815 □
Other □
Question NineteenPlease indicate how many years you have worked in the health care field:
_________ YEARS
Question TwentyWhich health care field do you work in?
Nursing [T) Medical Laboratory [Tj|
Question Twenty OneHave you either begun or completed a series of vaccination injections for Hepatitis B?
YES |7 ] NO [T)
Opinion Survey
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

107
Appendix A (continued)
SURVEY (continued)
' Opinidn. Survey
Question Twenty Two
Which is the highest level of education that you have completed?
Diploma/Certificate CD Associate Degree □
Baccalaureate □
Question Twenty ThreeYour gender.
Female CDQuestion Twenty FourYour ethnic group.
African American/Black CD Asian/Oriental CD
Other______________(Please Specify)
Question Twenty Five
Your present marital status.
Single CD Married [~2~|
Master’s □
Doctorate a
Male [TJ
White/Caucasian H I
Hispanic a
a
Divorced/Separated/Widowed
page 16
a
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

108
Appendix A (continued)
SURVEY (continued)
Question Twenty Six
Your age at last birthday:_______ YEARS
Is there anything else you would like to add? Please use this space for your comments.
Your tim e and effort is greatly appreciated. Please check that you have answered all the questions. If you would like a summ ary of resul ts, please call m e a t _'or'write “results” and your address on the enclosed env'elope: I v/ill see that you receive a copy of the results.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

109
Appendix B
CORRESPONDENCE TO THE SAMPLE
September 8, 1992
Dear :
As you know, regulations now protect health-care workers against bloodbome diseases such as HIV and Hepatitis B. However, this is a subject on which you, as a nurse, may have your own views.
I am asking you to take part in a study o f what you think is important about protecting yourself against bloodbome diseases.
So that results will truly represent nurses in Illinois, I have selected a special sample, which includes yourself. Thus it is very important that you respond.
I ask only 20 minutes o f your time. Most o f the enclosed questionnaire asks that you simply check a number that best represents your opinion. Then return the completed questionnaire in the enclosed pre-addressed stamped envelope by September 29th.
Your responses are completely confidential. Please do not put your name anywhere on the questionnaire. I will report the results as grouped data only; no individual results will be reported.
Your participation in this study is entirely voluntary, and that participation implies consent. There is no compensation for participation, and there are no known risks or benefits.
The results o f this study will be made available to employee-health providers and interested researchers. You may receive a summary o f the results: simply write "results" and your address on the return envelope. (Please do not put "results" or your name on the questionnaire).
I would be happy to answer any questions; you may reach me at Thank you very much for your cooperation and help.
Sincerely,
Pamela Fox Levin, MS, RN
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix B (continued)
CORRESPONDENCE TO THE SAMPLE (continued)
110
Dear Colleague:
Last week, a questionnaire was mailed to you asking your opinion about protecting yourself against bloodbome disease exposure at work. Your name was chosen as a representative o f Illinois health care workers.
If you have already completed and returned the questionnaire to me, please accept my sincere thanks. If not, please do so today. As only a small sample o f Illinois health professionals were sent the questionnaire, it is extremely important that yours also be included i f the results are to accurately represent the opinions o f Illinois health care workers.
If by some chance you did not receive the questionnaire or it got misplaced, please call me at and another will be mailed to you.
Sincerely,Pamela Fox Levin, MS, RN
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

I l l
Appendix B (continued)
CORRESPONDENCE TO THE SAMPLE (continued)
October 19, 1992
Dear Colleague:
About a month ago, I asked that you take part in a study of what you think is important about protecting yourself against bloodbome diseases.
Unfortunately, I have not received your completed questionnaire. So that results will truly represent medical-laboratory professionals in Illinois, I have selected a special sample, which includes yourself. Thus it is very important that you respond.
I ask only 20 minutes o f your time. Most o f the enclosed questionnaire asks ch«i you simply check a number that best represents your opinion. Then return the completed questionnaire in the enclosed pre-addressed stamped envelope.
I would be happy to answer any questions; you may reach me at . Thank you very much for your cooperation and help.
Sincerely,
Pamela Fox Levin, MS, RN
P.S. Even if you are no longer working in the health-care field, it is still very important foryou to respond.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

112
Appendix B (continued)
CORRESPONDENCE TO THE SAMPLE (continued)
m53BOARD OF REGISTRY Steven D. Wright. MT(ASCP)
Chairman
P.O. Box 12270. Chicago. It 60612-0270 (312) 736-1336 (312) 738-1619 FAX
September 8,1992
Dear Registrant:
Enclosed with this letter is a survey which is being conducted by Pamela Fox Levin as part of a research project. In order to assist this individual, the Board of Registry is distributing this material to a randomly selected audience of Medical Laboratory Technicians, Medical Technologists and Phlebotomists within the state of Illinois.
We believe research is important and encourage you to participate; however, the study is in no way endorsed or supported by the Board of Registry.
Sincerely,
Chairman
SDW:lcaEnc.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Appendix C
INSTITUTIONAL REVIEW BOARD APPROVAL
I I B 4 1* University °f Illinois H at Chicago
O ffice o f the V ice C h a n c e llo r for R e s e a rc h (W C 672)3 1 0 A d m in is tra tiv e O ffice Building1 7 3 7 W e s t P o lk S tre e tC h ic a g o . Illinois 6 0 6 1 2(3 1 2 ) 9 9 6 -4 9 9 5
NO TIC E OF RECEIPT OF H UM AN SU B JE C T RESEARC H PROTOCOL NOT REQUIRING IRB REVIEW
P roject T itle: Predictors o f G love U se by Health Care Workers
P rincipal Investigator. Pamela Fox Levin ,
Your hum an su b ject research protocol has been received. The inform ation w hich you have provided indicates that this protocol does not require IRB review . As long as you fo iiow the study m ethod described you are in full com pliance w ith U n iversity o f Illinois at Chicago human research policy .
If you alter your study plan in anyway, it is your responsib ility to report these changes to the O ffice for P rotection from Research Risks.
IRB NO: H -9 2 -2 8 1 P roject Period: 0 7 /9 2 -0 7 /9 3
Departm ent: N ursing Sciences
Your study meets criterion # # 3 in 45 CFR 46.
Lynda Brodsky Director 0 7 /1 6 /9 2O ffice for Protection from Research Risks
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Reproduced
with perm
ission of the
copyright ow
ner. Further
reproduction prohibited
without
permission.
TABLE XXVII
CORRELATIONS OF STUDY VARIABLES
Attitude-direct
Norm-indirect
Norm-direct
Normativeinfluence
Control-direct
Self-efficacy
Protectioneffective
Comparerisk Intend
Nextmonth
Pastmonth
Norm-indirect
.43**
Norm-direct .54** .53**
Normativeinfluence .43** .95** .54**
Control-direct .46** .38** .34** .35**
Self-efficacy .32** .31** .23** .30** .59**
Protectioneffective .38** .22** .20** .21** .31** .28**
Comparerisk .04 .08 .05 .07 .07 .11* .05
Intend .42** .36** .28** .32** .52** .43** .26** .07
Next month .47** .35** .34** .32** .57** .44** .32** .13** .55**
Past month .40** .33** .29** .31** .57** .40** .27** .17** .53** .80**
Not wear .24** .23** .19** .19** .30** .23** .16** .17** .35** .44** .47**
*p < .05.
**p < .01.
CO
RR
ELATIO
N
MA
TR
IX

115
Appendix E
TABLE XXVIII
CELL M EANS AND SAMPLE SIZES FOR NO T WEAR AND FOR PAST M ONTH
Not Wear Past Month
Sample SampleCell Mean Size Mean Size
One-Way GroupingsTotal Population 2.06 (516) 6.25 (521)
Total FieldNurse 1.94 (240) 6.24 (241)Laboratory W orker 2.16 (276) 6.27 (280)
Total SettingHospital 2.08 (388) 6.29 (391)Nonhospital 1.98 (128) 6.13 (130)
Total LocationUrban 2.08 (158) 6.24 (161)Suburb 1.86 (172) 6.34 (173)Rural 2.22 (186) 6.18 (187)
Two-Way GroupingsWork Setting x Field
HospitalNurse 1.95 (170) 6.27 (170)Laboratory Worker 2.18 (218) 6.31 (221)
NonhospitalNurse 1.90 (70) 6.15 (71)Laboratory Worker 2.09 (58) 6.10 (59)
Location x FieldUrban
Nurse 1.97 (68) 6.17 (69)Laboratory W orker 2.17 (90) 6.29 (92)
SuburbanNurse 1.90 (86) 6.33 (86)Laboratory W orker 1.83 (86) 6.36 (87)
RuralNurse 1.90 (86) 6.20 (86)Laboratory Worker 2.45 (100) 6.17 (101)
Location x Work SettingUrban
Hospital 2.06 (128) 6.35 (130)Nonhospital 2.17 (30) 5.81 (31)
SuburbanHospital 1.92 (122) 6.38 (123)Nonhospital 1.72 (50) 6.24 (50)
RuralHospital 2.25 (138) 6.17 (138)Nonhospital 2.15 (48) 6.22 (49)
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

116
Appendix E (continued)
TABLE XXVIII (continued)
CELL MEANS AND SAMPLE SIZES FOR N OT WEAR AND FOR PAST MONTH
Not W ear Past Month
Sample SampleCell Mean Size Mean Size
Location x Setting x Field Urban
HospitalNurse
Three-Way Grouping
1.90 (50) 6.34 (60)Laboratory Worker 2.17 (78) 6.35 (80)
NonhospitalNurse 2.17 (18) 5.74 (19)Laboratory Worker 2.17 (12) 5.92 (12)
SuburbanHospital
Nurse 1.92 (60) 6.28 (60)Laboratory W orker 1.92 (62) 6.48 (63)
NonhospitalNurse 1.85 (26) 6.42 (26)Laboratory W orker 1.58 (24) 6.04 (24)
RuralHospital
Nurse 2.03 (60) 6.20 (60)Laboratory Worker 2.41 (78) 6.14 (78)
NonhospitalNurse 1.77 (26) 6.19 (26)Laboratory Worker 2.59 (22) 6.29 (23)
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

CITED LITERATURE
Ajzen, I. (1985). From intentions to actions: A theory o f planned behavior. In J. Kuhl & J. Beckman (Eds.), Action control: From cognition to behavior (pp. 11-39). New York: Springer.
Ajzen, I. (1987). A ttitudes, traits and actions: Dispositional prediction o f behavior in personality and social psychology. Advances in Experimental Social Psychology, 20, 1-63.
Ajzen, I. (1988). Attitudes, personality, and behavior. Chicago: Dorsey Press.
Ajzen, I. (1989). A ttitude structure and behavior. In A. R. Pratkinis, S. J. Breckler, & A. G. Greenwald (Eds.),Attitude, structure and function (pp. 241-274). Hillsdale, NJ: Lawrence Erlbaum Associates.
Ajzen, I. (1991). The theory o f planned behavior. Organizational Behavior and Human Decision Processes, 50, 179- 2 11 .
Ajzen, I., & Driver, B. L. (1991). Prediction of leisure participation from behavioral, normative, and control beliefs: An application of the theory of planned behavior. Leisure Sciences, 13, 185-204.
Ajzen, I., & Driver, B. L. (1992). Application o f the theory o f planned behavior to leisure choice. Journal o f Leisure Research, 24, 207-224.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood, NJ: Prentice Hall.
Ajzen, I., & Madden, T. J. (1986). Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal o f Experimental Social Psychology, 22, 453-474.
Albrecht, C. M., & Miller, L. E. (1989). Impact of AIDS on clinical laboratorians. Laboratory Medicine, 20, 187-191.
Allegrante, J. P., M ortimer, R. G., & O'Rourke, T. W. (1980). Social-psychological factors in motorcycle safety helmet use: Implications for public policy. Journal o f Safety Research, 12, 115-126.
Andrews, P., & Kandel, D. B. (1979). Attitude and behavior: A specification o f the contingency consistency hypothesis. American Sociological Review, 44, 280-297.
Babrow, A. S., Black, D. R., & Tiffany, S. T. (1990). Beliefs, attitudes, intentions, and a smoking-cessation program: A planned behavior analysis o f communication campaign development. Health Communication, 2, 145-163.
Bagozzi, R. P., Baumgartner, J., & Yi, Y. (1989). An investigation into the role o f intentions as mediators of the attitude-behavior relationship. Journal o f Economic Psychology, 10, 35-62.
Bandura, A. (1986). Social foundations o f thought and action: A social cognitive theory. New York: Prentice Hall.
Baraff, L. J., & Talan, D. A. (1989). Compliance with universal precautions in a university hospital emergency department. Annals o f Emergency Medicine, 18, 89-92.
Bauer, P. (1991). Universal precautions in OR practice, part III: Compliance and knowledge. Nursing Management, 22 (8), 48Q-48S, 48V-48X.
Bauman, L. J., & Siegel, K. (1987), Misperceptions among gay men of the risk for AIDS associated with their sexual behavior. Journal o f Applied Social Psychology, 17, 329-350.
117
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

118
Becker, C. E., Cone, J. E., & Gerberding, J. (1989). Occupational infection with human immunodeficiency virus (HIV). Annals o f Internal M edicine, 110, 653-656.
Becker, M. H., Janz, N. K., Band, J., Bartley, J., Snyder, M. B., & Gaynes, R. P. (1990). Noncompliance with universal precautions policy: Why do physicians and nurses recap needles? American Journal o f Infection Control, 18, 232-239.
Bentler, P. M ., & Speckart, G. (1979). Models o f attitude-behavior relations. Psychological Review, 86, 452-664.
Bentler, P. M ., & Speckart, G. (1981). Attitudes "cause" behaviors: A structural equation analysis. Journal o f Personality and Social Psychology, 40, 226-238.
Bowman, A. M., & Nicholas, T. J. (1990). Improving compliance with universal blood and body fluid precautions in a rural medical center. Journal o f Nursing Quality Assurance, 5, 73-81.
Budd, R. J., North, D., & Spencer, C. (1984). Understanding seat-belt use: A test o f Bentler and Speckart's extension of the 'theory o f reasoned action.' European Journal o f Social Psychology, 14, 69-78.
Centers for Disease Control (1987). Recommendations for prevention o f HIV transmission in health care settings. M orbidity and M ortality Weekly Report: M MWR, 36 (suppl. 2S), 3S-18S.
Cohen, J. (1988). Statistical power analysis fo r the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum Associates.
Conte, L. (1992). Factors that influence the use of universal precautions by neonatal nurses. Neonatal Network, 11, 27-31.
Courington, K. R., Patterson, S. L., & Howard, R. J. (1991). Universal precautions are not universally followed. Archives o f Surgery, 126, 93-96.
Cummings, K. M., Becker, M. H., & Maile, M. C. (1980). Bringing the models together: An empirical approach to combining variables used to explain health actions. Journal o f Behavioral Medicine, 3, 123-145.
DeVellis, B. M., Blalock, S. J., & Sandler, R. S. (1990). Predicting participation in cancer screening: The role of perceived behavioral control. Journal o f Applied Social Psychology, 20, 639-660.
DeVries, J. E., Burnette, M. M., & Redmon, W. K. (1991). AIDS prevention: Improving nurses' compliance with glove wearing through performance feedback. Journal o f Applied Behavior Analysis, 24, 705-711.
Dillman, D. A. (1978). M ail and telephone surveys: The total design method. New York: Wiley & Sons.
Doebbeling, B. N., & Wenzel, R. P. (1990). The direct costs of universal precautions in a teaching hospital. Journal o f the American M edical Association, 264, 2083-2087.
Dolinski, D., Gromski, W., & Zawiska, E. (1987). Unrealistic pessimism. Journal o f Social Psychology, 127, 511-516.
Dorsey, M., Overman, P., Hayden, W. J., Mayberry, W., Requa-Clark, B., & Krust, K. (1991). Relationships among and demographic predictors o f dentists' self-reported adherence to national guidelines. Social Science and Medicine,32, 1263-1268.
Dzewaltowski, D. A. (1989). Toward a model o f exercise motivation. Journal o f Sport & Exercise Psychology, 11, 251-269.
Dzewaltowski, D. A., Noble, J. M., & Shaw, J. M. (1990). Physical activity participation: Social cognitive theory versus the theories of reasoned action and planned behavior. Journal o f Sport & Exercise Psychology, 12, 388-405.
Reproduced with perm ission o f the copyright owner. Further reproduction prohibited without perm ission.

119
Emmons, C. A., Joseph, J. G., Kessler, R. C., Wortman, C. B., Montgomery, S. B., & Ostrow, D. G. (1986).Psychological predictors of reported behavior change in homosexual men at risk for AIDS. Health Education Quarterly, 13, 331-345.
Evans, M. G. (1991). The problem of analyzing multiplicative composites. American Psychologist, 46, 6-15.
Evans, M. R., Henderson, D. K., & Bennett, J. E. (1990). Potential for laboratory exposures to bloodbome biohazardous agents found in blood. American Journal o f Public Health, 80, 423-427.
Fahey, B. J., Koziol, D. E., Banks, S. M., & Henderson, D. K. (1991). Frequency of nonparenteral occupational exposures to blood and body fluids before and after universal precautions training. American Journal o f Medicine, 90, 145-153.
Festinger, L. (1954). A theory o f social comparison processes. Human Relations, 7, 117-140.
Fishbein, M., & Ajzen, I. (1975). B elief attitude, intention, and behavior. Reading, MA: Addison-Wesley.
Fishbein, M., & Middlestadt, S. E. (1989). Using the theory of reasoned action as framework for understanding andchanging AIDS-related behaviors. In V. Mays, G. Albee, & S. Schneider (Eds.), Primaty prevention o f AIDS: Psychological approaches (pp 93-110). Newbury Park, CA: Sage.
Flay, B. R., & Petraitis, J. (in press). The theory of triadic influence: A new theory of health behavior with implications for preventive interventions. In G. L. Albrecht (Ed.), Advances in medical sociology, Vol. IV: A reconsideration o f models o f health behavior change. Greenwich, CT: JAI Press.
Fox, P. J. (1989). Beliefs o f medical laboratory workers concerning glove use. Unpublished master's thesis, University o f Illinois at Chicago, Chicago.
Fredricks, A. J., & Dossctt, D. L. (1983). Attitudc-behavior relations: A comparison of the Fishbcin-Ajzcn and the Bentler-Speckart models. Journal o f Personality and Social Psychology, 45, 501-512.
Freeman, S. W., & Chambers, C. V. (1992). Compliance with universal precautions in a medical practice with a highrate of HIV infection. Journal o f the American Board o f Family Practice, 5, 313-318.
Friealand, L. R., Joffe, M., Wiley, J. F., Schapirc, A., & Moore, D. F. (1992). Effect o f educational program oncompliance with glove use in a pediatric emergency department. American Journal o f Diseases o f Children, 146, 1355-1358.
Gatch, C. L., & Kcndzierski, D. (1990). Predicting exercise intentions: The theory of planned behavior. Research Quarterly fo r Exercise and Sport, 61, 100-102.
Gauch, R. R., Feeney, K. B., & Brown, J. W. (1990). Fear o f AIDS and attrition among medical technologists.American Journal o f Public Health, 80, 1264-1265.
Gerberding, J. L. (1990). Current epidemiologic evidence and case reports of occupationally acquired HIV and other bloodbome diseases. Infection Control and H ospital Epidemiology, I I (suppl), 558-560.
Gibbons, F. X., & Gcrrad, M. (1991). Downward comparison and coping with threat. In J. Suls & T. A. Wills (Eds.),Social comparison: Contemporaiy theoty and research (pp. 317-345). Hillsdale, NJ: Lawrence Erlbaum Associates.
Gielen, A. C., Eriksen, M. P., Daltroy, L. H., & Rost, K. (1984). Factors associated with the use o f child restraint devices. Health Education Quarterly, I I , 195-206.
Godin, G., Cox, M. II., & Shephard, R. J. (1983). The impact o f physical fitness evaluation on behavioral intentionstowards regular exercise. Canadian Journal o f Applied Sport Sciences, 8, 240-245.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

120
Godin, G., & Gionet, N. J. (1991). Determinants of an intention to exercise o f an electric power commission's employees. Ergonomics, 34, 1221-1230.
Godin, G., & Shephard, R. J. (1986). Importance of type o f attitude to the study o f exercise-behavior. Psychological Reports, 58, 991-1000.
Godin, G., Valois, P ., Shephard, R. J., & Deshamais, R. (1987). Prediction o f leisure-time exercise behavior: A path analysis (Lisrel V) model. Journal o f Behavioral M edicine, 10, 145-158.
Godin, G., Vezina, L ., & Leclerc, O. (1989). Factors influencing intentions o f pregnant women to exercise after giving birth. Public Health Reports, 104, 188-195.
Goethals, G. R., Messick, D. M., & Allison, S. T. (1991). The uniqueness bias: Studies of constructive socialcomparison. In J. Suls & T. A. Wills (Eds.), Social comparison: Contemporary theory and research, (pp. 149- 176). Hillsdale, NJ: Lawrence Erlbaum Associates.
Gongaware, V. E. (1991). Nurses' beliefs about the use o f personal protective measures when handling antineoplastic agents. Unpublished master's thesis, University o f Illinois at Chicago, Chicago.
Gonzalez, E ., & Naleway, C. (1988). Assessment of the effectiveness of glove use as a barrier technique in the dental operatory. Journal o f the American Dental Association, 117, 467-469.
Gordin, F. M ., Gibert, C., Hawley, H. P., & Willoughby, A. (1990). Prevalence o f human immunodeficiency virus and hepatitis B virus in unselected hospital admissions: Implications fo r mandatory testing and universal precautions. Journal o f Infectious Diseases, 161, 14-17.
Gruber, M., Beavers, F. E., Johnson, B., Brackett, M., Lopez, T ., Feldman, M. J., & Ventura, M. (1989). Therelationship between knowledge about acquired immunodeficiency syndrome and the implementation o f universal precautions by registered nurses. Clinical Nurse Specialist, 3, 182-185.
Hakmiller, K. L. (1966). Threat as a determinant of downward comparison. Journal o f Experimental Social Psychology, 2 (suppl. 1), 32-39.
Hammond, J. S., Eckes, J. M ., Gomez, G. A., & Cunningham, D. N. (1990). HIV, trauma, and infection control: Universal precautions are universally ignored. Journal o f Trauma, 30, 555-561
Henderson, D. K., Fahey, B. J., Willy, M., Schmitt, J. M., Carey, K., Koziol, D. E., Lane, H. C., Fedio, J., & Saah, A. J. (1990). R isk o f occupational transmission of human immunodeficiency virus type 1 (HIV-1) associated with clinical exposures. Annals o f Internal Medicine, 113, 740-746.
Henry, K., Campbell, S., & Maki, M. (1992). A comparison o f observed and self-reported compliance w ith universal precautions among emergency department personnel at a Minnesota public teaching hospital: Implications for assessing infection control programs. Annals o f Emergency M edicine, 21, 940-946.
Hewstonc, M., & Young, L. (1988). Expectancy-value m odels of attitude: M easurement and combination of evaluations and beliefs. Journal o f Applied Social Psychology, 18, 958-971.
Hill, D ., Gardner, G., & Rassaby, J. (1985). Factors predisposing women to take precautions against breast and cervix cancer. Journal o f Applied Social Psychology, 15, 59-79.
FIoffman-Terry, M., Rhodes, L. V., & Reed, J. F. (1992). Impact o f human immunodeficiency virus on medical and surgical residents. Archives o f Internal Medicine, 152, 1788-1796.
Jaccard, J. (1975). A theoretical analysis o f selected factors important to health education strategies. Health Education Monographs, 3, 152-167.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

121
Jagger, J., Detmer, D. E., Cohen, M. L., Scarr, P. R., & Pearson, R. D. (1992). Reducing blood and body flu idexposures among clinical laboratory workers: M eeting the OSHA standard (Report No. KL-1205). Roswell, GA: Kim berly-Clark Corporation.
Jagger, J. & Pearson, R. D. (1991). Universal precautions: Still missing the point on needlesticks. Infection Control and H ospital Epidemiology, 12, 211-213.
Janz, N., & Becker, M. (1984). The health belief model: A decade later. Health Education Quarterly, 11, 1-47.
Jonah, B. A ., & Dawson, N. E. (1982). Predicting reported seat belt use from attitudinal and normative factors.Accident Analysis and Prevention, 14, 305-310.
Jdreskog, K. G., & SOrbom, D. (1989). LISREL 7: A guide to the program and applications (2nd ed). Chicago: SPSS.
Joseph, J. G., M ontgomery, S. B., Emmons, C. A., Kirscht, J. P ., Kessler, R. C., Ostrow, D. G., W ortman, C. B., & O 'Brien, K. (1987). Perceived risk o f AIDS: Assessing the behavioral and psychological consequences in a cohort o f gay men. Journal o f Applied Social Psychology, 17, 231-250.
Kaczmarek, R. G., Moore, R. M., McCrohan, J., Arrowsmith-Lowe, J. T., Caquelin, C., Reynolds, C., Israel, E. (1991).G love use by health care workers: Results of a tristate investigation. American Journal o f Infection Control, 19, 228-232.
Kelen, G. D ., DiGiovanna, T., Bisson, L., Kalainov, D., Sivertson, K. T., & Quinn, T. C. (1989). Humanimmunodeficiency virus infection in emergency department patients. Journal o f the American M edicalAssociation, 262, 516-522.
Kelen, G. D ., DiGiovanna, T. A., Celcntano, D. D ., Kalainov, D., Bisson, L., Junkins, E., Stein, A., Lofy, L., Scott, C. R.J., Sivertson, K. T., & Quinn, T. C. (1990). Adherence to universal (barrier) precautions during interventionson critically ill and injured emergency department patients. Journal o f Acquired Immune Deficiency Syndromes,3, 987-994.
Kelen, G. D ., Fritz, S., Qaqish, B., Brookmeycr, R ., Baker, J. L ., Kline, R. L., Cuddy, R. M., Goessel, T. K., Floccare,D ., W illiams, K. A., Sivertson, K. T., Altman, S., & Quinn, T. C. (1988). Unrecognized human immunodeficiency virus infection in emergency department patients. New England Journal o f Medicine, 318, 1645-1650.
Kelen, G., Green, G. B., Hexter, D. A., Fortenberry, D. C., Taylor, E., Fleetwood, D. IT., & Sivertson, K. T. (1991). Substantial improvement in compliance with universal precautions in an emergency department following institution o f policy. Archives o f Internal Medicine, 151, 2051-2056.
Kerlinger, F. N. (1986). Foundations o f behavioral research (3rd cd.). New York: Holt, Rinehart, & Winston.
Kimiccik, J. (1992). Predicting vigorous physical activity of corporate employees: Comparing the theories of reasoned action and planned behavior. Journal o f Sport & Exercise Psychology, 14, 192-206.
Klein, R. S. (1991). Universal precautions for preventing occupational exposures to human immunodeficiency vims type 1. American Journal o f Medicine, 90, 141-144.
Komiewicz, D. M., Laughon, B. E., Butz, A., & Larson, E. (1989). Integrity of vinyl and latex procedure gloves. Nursing Research, 38, 144-146.
Kulik, J. A ., & M ahler, H. I. (1987). Health status, perceptions of risk, and prevention interest for health and nonhcalth problems. Health Psychology, 6, 15-27.
Kunda, Z. (1987). Motivated inference: Self-serving generation and evaluation of causal theories. Journal o f Personality and Social Psychology, 53, 636-647.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

122
Lauver, D., & Knapp, T. R. (1993). Sum-of-products variables: A methodological critique. Research > .lursing & Health, 16, 385-391.
Lavoie, M., & Godin, G. (1991). Correlates o f intention to use condoms among auto mechanic students. Health Education Research, 6, 313-316.
Lewin, K. (1951). F ield theory in social science: Selected theoretical papers. Chicago: The University of Chicago Press.
Lierman, L. M., Young, H. M., Kasprzyk, D., & Benoliel, J. Q. (1990). Predicting breast self-examination using the theory of reasoned action. Nursing Research, 39, 97-101.
Linn, L. S., Kahn, K. L., & Leake, B. (1990). Physicians' perceptions about increased glove wearing in response to risk of HIV infection. Infection Control and Hospital Epidemiology, 11, 248-254.
Liska, A. E. (1984). A critical examination of the causal structure o f the Fishbein/Ajzen attitude-behavior model. Social Psychology Quarterly, 47, 61-74.
Loewen, N. L., Dhillon, G. L., Willy, M. E., Wesley, R. A., & Henderson, D. K. (1989). Use of precautions by nurse- midwives to prevent occupational infections with HIV and other blood-bome diseases. Journal o f Nurse- Midwifery, 34, 309-317.
Long, J. S. (1983). Confirmatory fac tor analysis. Newbury Park, CA: Sage.
Lynn, M. R. (1986). Determination and quantification of content validity. Nursing Research, 35, 382-385.
Madden, T. J., Ellen, P. S., & Ajzen, I. (1992). A comparison o f the theory of planned behavior and the theory o f reasoned action. Personality and Social Psychology Bulletin, 18, 3-9.
Martin, G. L., & Newman, I. M. (1990). Women as motivators in the use of seat belts. Health Values, 14, 37-47.
McAfee, R. B., & Winn, A. R. (1989). The use of incentives/feedback to enhance work place safety: A critique o f the literature. Journal o f Safety Research, 20, 7-19.
McCaul, K. D., O'Neill, H. K., & Glasgow, R. E. (1988). Predicting the performance of dental hygiene behaviors: An examination of the Fishbein and Ajzen model and self-efficacy expectations. Journal o f Applied Social Psychology, 18, 114-128.
McKay, G. (1992). Comparing perceived and observed infection control practices among anesthesia providers. Journal o f the American Association o f Nurse Anesthetists, 60, 360.
McNabb, K., & Keller, M. L. (1991). Nurses' risk taking regarding HIV transmission in the workplace. Western Journal o f Nursing Research, 13, 732-745.
Miller, K. E., Krol, R. A., & Losh, D. P. (1992). Universal precautions in the family physician's office. Journal o fFamily Practice, 35, 163-168.
Mittal, B. (1988). Achieving higher seat belt useage: The role of habit in bridging the attitude-behavior gap. Journal o f Applied Social Psychology, 18, 993-1016.
Mullen, P. D., Hersey, J. C., & Iverson, D. C. (1987). Health behavior models compared. Social Science and Medicine, 24, 973-981.
Nunnally, J. C. (1978). Psychometric theory. New York: McGraw Hill.
O’Leary, A. (1985). Self-cfficacy and health. Behavioral Research and Theory, 23, 437-451.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

123
Osgood, C. E., Suci, G. J., & Tanncbaum, P. H. (1967). The measurement o f meaning. Urbana: University of Illinois Press.
Panlilio, A., Foy, D. R., Edwards, J. R., Bell, D. M., Welch, B. A., Parrish, C. M., Culver, D. H., Lowry, P. W., Jarvis, W. R., & Perlino, C. A. (1991). Blood contacts during surgical procedures. Journal o f the American M edical Association, 265, 1533-1537.
Parker, D., Manstead, A. S., Stradling, S. G ., Reason, J. T., & Baxter, J. S. (1992). Intention to commit driving violations: An application of the theory o f planned behavior. Journal o f Applied Psychology, 77, 94-101.
Pender, N. J., & Pender, A. R. (1986). Attitudes, subjective norms, and intentions to engage in health behavior.Nursing Research, 35, 15-18.
Pieterse, M. E., Kok, G., & Verbeek, J. (1992). Determinants of the acquisition and utilization of automobile child restraint devices: A survey among Dutch parents. Health Education Research, 7, 349-358.
Perloff, L. S., & Fetzer, B. K. (1986). Self-other judgm ents and perceived vulnerability to victimization. Journal o f Personality and Social Psychology, 50, 502-510.
Peters, R. H. (1991). Strategies for encouraging self-protective employee behavior. Journal o f Safety Research, 22, 53- 70.
Polit, D. F., & Sherman, R. E. (1990). Statistical power in nursing research. Nursing Research, 39, 365-369.
Radius, S. M., McDonald, E. M., & Bernstein, L. (1991). Influencing car safely scat use: Prenatal and postnatal predictors. Health Values, 15(A), 29-38.
Renfroe, D. H., O'Sullivan, P. S., & McGee, G. W. (1990). The relationship of attitude, subjective norm, and behavioral intent to the documentation behavior o f nurses. Scholarly Inquiry fo r Nursing Practice: An International Journal, 4, 47-60.
Riddle, P. K. (1980). Attitudes, beliefs, behavioral intentions, and behaviors of women and men toward regular jogging. Research Quarterly fo r Exercise and Sport, 51, 663-674.
Rogers, B. (1989). Establishing research priorities in occupational health nursing. AAOH N Journal, 37, 493-500.
Rogers, R. W. (1983). Cognitive and physiological processes in fear appeals and attitude change: A revised theory o fprotection motivation. In R. Cacioppo & R. Petty (Eds.), Social psychophysiology: A sourcebook (pp. 153-176). New York: Guilford Press.
Ros, S. P., & Cabrera-Ros, B. L. (1990). Poor compliance with universal precautions: A universal phenomenon? Pediatric Emergency Care, 6, 183-185.
Saltzer, E. B. (1981). Cognitive moderators of the relationship between behavioral intentions and behavior. Journal o f Personality and Social Psychology, 41, 260-271.
Schifter, D. E., & Ajzen, I. (1985). Intention, perceived control, and weight loss: An application of the theory of planned behavior. Journal o f Personality and Social Psychology, 49, 843-851.
Schillo, M. A., & Reischl, T. M. (1993). I-IIV-relatcd knowledge and precautions among Michigan nurses. American Journal o f Public Health, 83, 1438-1442.
Schmelling, E. C. (1985). Identifying the salient outcomes o f exercise: Application of marketing principles to preventive health behavior. Public Health Nursing, 2, 93-103.
Schmidt, F. L. (1973). Implications of a measurement problem for expectancy theory research. Organizational Behavior and Human Performance, 10, 243-251.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

124
Schwartz, R. J., Jacobs, L. M., & Juda, R. J. (1992). Evaluating the compliance o f universal precautions by aeromedical personnel before and after an educational seminar on infectious diseases. Connecticut M edicine, 56, 3-5.
Seto, W. H., Ching, T. Y., Chu, Y. B., & Seto, W. L. (1991). Social power and motivation for the compliance of nurses and housekeeping staff with infection control policies. American Journal o f Infection Control, 19, 42-44.
Seto, W. H., Ching, T. Y., Yuen, K. Y., Chu, Y. B., & Seto, W. L. (1991). The enhancement of infection control in- service education by ward opinion leaders. American Journal o f Infection Control, 19, 86-90.
Seto, W. H., Ong, S. G„ Ching, T. Y„ Ng, S. H., Chu, Y. B., Yung, W. H „ & Ho, L. M. (1990). B rief report: The utilization o f influencing tactics for the implementation o f infection control policies. Infection Control and H ospita l Epidemiology, 11, 144-150.
Sheehy, C., & Trudeau, V. (1992). AIDS education strategies: Evaluating the fear response. AAO H N Journal, 40, 271 - 278.
Smyser, M. S., Bryce, J., & Joseph, J. G. (1990). AIDS-related knowledge, attitudes, and precautionary behaviors among emergency medical professionals. Public H ealth Reports, 105, 496-505.
Stasson, M ., & Fishbein, M. (1990). The relation between perceived risk and preventive action: A within-subjectanalysis of perceived driving risk and intentions to wear seatbelts. Journal o f Applied Social Psychology, 20, 1541-1557.
Stevens, C. K., Mentis, S. W., & Downs, J. B. (1991). The human immunodeficiency virus: Knowledge and precautions among anesthesiology personnel. Journal o f C linical Anesthesiology, 3, 266-275.
Stock, S. R., Gafni, A., & Bloch, R. F. (1990). Universal precautions to prevent HIV transmission to health care workers: An economic analysis. Canadian M edical Association Journal, 142, 937-946.
Stotka, J. L., Wong, E. S., W illiams, D. S., Stuart, C. G., & Markowtitz, S. M. (1991). An analysis o f blood and bodyfluids exposures sustained by house officers, medical students, and nursing personnel on acute-care general medical wards: A prospective study. Infection Control and Hospital Epidemiology, 12, 583-590.
Strecher, V. J., DeVellis, B. M., Becker, M. H., & Rosenstock, I. M. (1986). The role o f self-efficacy in achievinghealth behavior change. Health Education Quarterly, 13, 73-92.
Suchman, E. A. (1967). Preventive health behavior: A model for research on community health campaigns. Journal o f H ealth and Social Behavior, 8, 197-209.
Talan, D. A., & Baraff, L. J. (1990). Effect of education on the use of universal precautions in a university hospital emergency department. Annals o f Emergency M edicine, 19, 1322-1326.
Taylor, S. E. (1990). Health psychology: The science and the field. American Psychologist, 45, 40-50.
Taylor, S. E., & Lobel, M. (1989). Social comparison activity under threat: Downward evaluation and upward contacts. Psychological Review, 96, 569-575.
Travers, P. (1987). A comprehensive guide fo r establishing an occupational health seivice. Atlanta: American Association of Occupational Health Nurses.
Triandis, H. C. (1977). Interpersonal behavior. Monterey, CA: Brooks/Cole.
U.S. Department of Labor. (1989). Proposed OS1IA rule governing occupational exposure to bloodbom e pathogens. Washington, DC: Bureau o f National Affairs.
U.S. Department of Labor. (1991). Occupational exposure to bloodbome pathogens: Final Rule. Federal Register, 56 (235), 64004-64182.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

125
Vallerand, R, J., Deshaies, P., Cucrrier, J. P., Pellerier, L. G., & Mongeau, C. (1992). Ajzen and Fishbein's theory of reasoned action as applied to moral behavior: A confirmatory analysis. Journal o f Personality and Social Psychology, 62, 98-109.
Valois, P., Deshamais, R., & Godin, G. (1988). A comparison o f the Fishbein and Ajzen and Triandis attitudinal models for the prediction o f exercise intention and behavior. Journal o f Behavioral Medicine, 11, 459-472.
Van Der Velde, F. W., Hooykaas, C., & Van D er Pligt, J. (1992). Risk perception and behavior: Pessimism, realism, and optimism about AIDS-related health behavior. Psychology and Health, 6, 23-38.
Weinstein, N. D. (1980). Unrealistic optimism about future life events. Journal o f Personality and Social Psychology, 39, 806-820.
Weinstein, N. D. (1982). Unrealistic optimism about susceptibility to health problems. Journal o f Behavioral Medicine, 5, 441-460.
Weinstein, N. D. (1983). Reducing unrealistic optim ism about illness susceptibility. Health Psychology, 2, 11-20.
Weinstein, N. D. (1984). Why it won't happen to me: Perceptions o f risk factors and susceptibility. Health Psychology, 3, 431-457.
Weinstein, N. D. (1987). Unrealistic optimism about susceptibility to health problems: Conclusions from a community- wide sample. Journal o f Behavioral M edicine, 10, 481-500.
Weinstein, N. D. (1988). The precaution adoption process. Health Psychology, 7, 355-386.
Weinstein, N. D. (1989a). Effects of personal experience on self-protective behavior. Psychological Bulletin, 105, 31- 50.
Weinstein, N. D. (1989b). Perceptions of personal susceptibility to harm. In V. M. Mays, G. W. Albee, & S. F. Schneider (Eds.), Primary prevention o f A ID S (pp. 142-167). Newbury Park, CA: Sage.
Weinstein, N. D., Grubb, P. D., & Vautier, J. S. (1986). Increasing automobile seat belt use: An intervention emphasizing risk susceptibility. Journal o f Applied Psychology, 71, 285-290.
Weinstein, N. D., Klotz, M. L., & Sandman, P. M. (1988). Optimistic biases in public perceptions o f the risk from radon. American Journal o f Public Health, 78, 796-800.
Weinstein, N. D., & Lachendro, E. (1982). Egocentrism as a source of unrealistic optimism. Personality and Social Psychology Bulletin, 8, 195-200.
Weinstein, N. D., & Nicolich, M. (1993). Correct and incorrect interpretations between risk perceptions and risk behavior. Health Psychology, 12, 235-245.
Weinstein, N. D., Sandman, P. M ., & Roberts, N. E. (1990). Determinants of self-protective behavior: Hom e radon testing. Journal o f Applied Social Psychology, 20, 783-801.
Weinstein, N. D., Sandman, P. M., & Roberts, N. E. (1991). Perceived susceptibility and self-protective behavior: A field experiment to encourage home radon testing. Health Psychology, 10, 25-33.
White, M. C., Baker, E. L ., Larson, M. B., & W olford, R. (1988). The role of personal beliefs and social influences as determinants of respirator use among construction painters. Scandinavian Journal o f Work and Environmental Health, 14, 239-245.
Wilkinson, W. E. (1992). Medical center studies how consistently workers use gloves to prevent infection. Occupational Health & Safety, 61 ( 11), 35, 36, 38, 39, 43.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

126
Wills, T. A. (1991). Similarity and self-esteem in downward comparison. In J. Suls & T. A. Wilis (Eds.), Social comparison: Contemporary theory and research (pp. 51-78). Hillsdale, NJ: Lawrence Erlbaum Associates.
Willy, M. E ., Dhillon, G. L., Loewen, N. L., Wesley R. A., & Henderson, D. K. (1990). Adverse exposures anduniversal precautions practices among a group of highly exposed health professionals. Infection Control and Hospital Epidemiology, 11, 351-356.
Wittenbraker, J., Gibbs, B. L., & Kahle, L. R. (1983). Seat belt attitudes, habits, and behaviors: An adaptive amendment to the Fishbein model. Journal o f A pplied Social Psychology, 13, 406-421.
Wong, E. S., Stotka, J. L ., Chinchilli, V. M., W illiams, D. S., Stuart, C. G., & Markowitz, S. M. (1991). Are universal precautions effective in reducing the num ber of occupational exposures among health care workers? Journal o f the American M edical Association, 265, 1123-1128.
Young, H. M ., Lierman, L., Powell-Cope, G., Kasprzyk, D., & Benoliel, J. Q. (1991). Operationalizing the theory of planned behavior. Research in Nursing & Health, 14, 137-144.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

VITA
NAME:
EDUCATION:
PROFESSIONALEXPERIENCE:
HONORS:
PUBLICATIONS:
Pamela Fox Levin
B.S.N., Nursing, Boston University, Boston, Massachusetts, 1976
M.S., Nursing Sciences, University o f Illinois at Chicago, Chicago, Illinois, 1989
Ph.D., Nursing Sciences, University o f Illinois at Chicago, Chicago, Illinois, 1994
Instructor, Community Health Nursing, St. Xavier University, Chicago, Illinois, 1993
Teaching Assistant, Department of Public Health Nursing, University o f Illinois at Chicago, Chicago, Illinois, 1990 to present
Project Coordinator, Department of Public Health Nursing, University o f Illinois at Chicago, Chicago, Illinois, 1989-1990
Research Assistant, Department of Public Health Nursing, University o f Illinois at Chicago, 1988-1990
Special Projects Coordinator, Division of Nursing, Lake Forest Hospital, Lake Forest, Illinois, 1987-1988
Coordinator, Nursing Education Department, Lake Forest Hospital, Lake Forest, Illinois, 1982-1987
Quality Assurance Coordinator, Nursing Quality Assurance Program, Rush-Presbyterian-St. Luke’s Medical Center, Chicago, Illinois, 1979-1987
Staff Nurse, Medical Nursing, Rush-Presbyterian-St. Luke's Medical Center, Chicago, Illinois, 1976-1979
University of Illinois at Chicago Chancellor's Student Service Award, 1993 University of Illinois Alumni Association Student Leadership Award, 1993 Predoctoral Fellow, Public Health Service, National Research Service Award, 1991-1993 National Institute of Occupational Safety and Health Trainecship, 1990-1991 Sigma Theta Tau International Nursing Honor Society, 1989
Fox, P. J. (1991). H ow to comply with the OSHA hazard communication standard, [book review], AAO H N Journal, 39, 447.
Fox, P. J., & Kulbok, P. P. (1989). Preparing tomorrow's leaders in home health care. The Nursing Spectrum, Illinois Edition, 2 (9), 18.
Hewitt, J. B., Misncr, S. T., & Levin, P. F. (1993). Health hazards o f nurses: Identifying workplace hazards and reducing risks. AW HONN Clinical Issues in Perinatal and Women's H ealth Nursing, 4(2), 320-327.
127
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

128
PROFESSIONALMEMBERSHIP:
VITA (continued)
Hewitt, J. B., Misner, S. T., & Levin, P. F. (1991). Nurse's health in the workplace. The Nursing Spectrum, Illinois Edition, 4 (9), 23-24.
Levin, P. F. (in press). Effectiveness o f methods to increase health care workers' compliance w ith universal precautions. A A O H N Journal.
Levin, P. F., Hewitt, J. B., & Misner, S. T. (1992). Female workplace homicide: An integrative research review. A A O H N Journal, 40, 229-236.
Misner, S. T., & Levin, P. F. (1993). M urder on the job: How to protect yourself. Well- Woman Journal, 4(2), 14.
Misner, S. T., Levin, P. F., & Hewitt, J. B. (1993). Occupational issues in w om en's health. Annual Review o f Women's Health, 1, 29-66.
American Association o f Occupational Health Nurses American Nurses' Association American Public Health AssociationAssociation of Hospital and Employee Health Professionals Chicago Area Committee for Occupational Safety and Health Illinois Public Health Association Midwest Nursing Research Society Sigma Theta Tau International
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.