Communicating Coastal and Marine Biodiversity Conservation ...

Physician Frustration in Communicating with PatientsAuthor(s): Wendy Levinson, William B. Stiles, Thomas S. Inui, Robert EngleSource: Medical Care, Vol. 31, No. 4 (Apr., 1993), pp. 285-295Published by: Lippincott Williams & WilkinsStable URL: http://www.jstor.org/stable/3765997Accessed: 26/05/2009 13:39
Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available athttp://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unlessyou have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and youmay use content in the JSTOR archive only for your personal, non-commercial use.
Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained athttp://www.jstor.org/action/showPublisher?publisherCode=lww.
Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printedpage of such transmission.
JSTOR is a not-for-profit organization founded in 1995 to build trusted digital archives for scholarship. We work with thescholarly community to preserve their work and the materials they rely upon, and to build a common research platform thatpromotes the discovery and use of these resources. For more information about JSTOR, please contact [email protected].
Lippincott Williams & Wilkins is collaborating with JSTOR to digitize, preserve and extend access to MedicalCare.
http://www.jstor.org

MEDICAL CARE Volume 31, Number 4, pp 285-295 ( 1993, J. B. Lippincott Company
Physician Frustration in Communicating with Patients
WENDY LEVINSON, MD,* WILLIAM B. STILES, PHD,t THOMAS S. INUI, SCM, MD,: AND ROBERT ENGLE, DBA?
In this study, the nature of practicing physicians' "frustrating" visits was explored and a guide to help physicians identify problems in communicating with patients was developed. The study included 1,076 practicing physicians who attended a voluntary workshop on physician-patient communication. The physicians were from multiple specialties and diverse work settings geographi- cally dispersed throughout the United States. The method included develop- ment of a preliminary item pool (descriptions of frustrating patients and occa- sions) by experienced physicians and teachers of medical communication, addi- tions/deletions/revisions of items within the pool, empirical analyses to reduce redundancy and group-like items, and construct validation of the final 25-item questionnaire. Factor analysis was used to identify subscales. Physi- cians most often attributed communication problems to the patient rather than to their own limitations. Seven types of communication problems (subscales) were identified, including: 1) lack of trust/agreement, 2) too many problems, 3) feeling distressed, 4) lack of understanding, 5) lack of adherence, 6) demanding/ controlling patient, and 7) special problems. Primary care physicians reported greater problems than specialists on four subscales. Physicians practicing in health maintenance organizations reported greater problems than physicians in fee-for-service practice on five subscales. Seven sources of frustration physi- cians experience in their work with patients were identified. Understanding these frustrations will allow physicians to reflect on their own experiences and
potentially improve the quality of their patient visits. Key words: communica- tion; physician frustration. (Med Care 1993; 31:285-295)
*From Good Samaritan Hospital and Medical Center, Portland, Oregon.
t From Miami University, Oxford, Ohio.
: From University of Washington, Seattle, Washing- ton.
? From Quinnipiac College, Hamden, Connecticut.
Supported by a grant from Miles Pharmaceutical In- corporated. The opinions expressed are the authors' and not those of the sponsors.
Address correspondence to: Wendy Levinson, MD, Department of Medicine-R200, Good Samaritan Hospi- tal, 1015 NW 22nd Avenue, Portland, OR 97210.
This article was originally submitted for consider- ation on 6-15-92. It was accepted for publication on 10-21-92 following the completion of all necessary re- views and/or revisions.
It is common for physicians to experience frustration in visits with patients. Despite the frequency of these experiences, we
rarely hear discussions among colleagues about what leads to these frustrations or what specific type of patient visits are most
challenging for a particular physician. Un-
derstanding the nature of these frustrations could reduce the frequency of these occur- rences, improve clinical care, and lead to en- hanced physician satisfaction. This study was designed to identify the specific aspects of patient visits that cause physician frustra-
285

LEVINSON ET AL.
tion and to develop a self-assessment instru- ment for physicians.
The quality of the communication during the interview and the relationship between the doctor and patient are important to both the medical outcome and satisfaction of the doctor and patient.'-14 Although most pa- tient visits go well, occasionally the commu- nication between the doctor and patient is less than optimal, and the visit frustrates the doctor, the patient, or both. Physician frus- tration may interfere in the provision of the
highest quality of care or lead to personal distress for the doctor.
Reasons for physician frustration may in- clude patient nonadherence to recommenda- tions,'5 personality disorders,16-19 and pa- tient characteristics and personality types that pose particular difficulties in the medi- cal encounter. Groves wrote about "hateful
patients," those patients that most physi- cians dread seeing20 and suggested that these patients may receive care that is not best suited to their needs. Physicians may unconsciously or consciously punish, con- front, or try to "get rid of" the patient.21
Characteristics of the physician or the
practice setting can also cause problems in the visit. A particular physician may be up- set or irritated by a patient for reasons re- lated to the physician's own psychological or social situation. Furthermore, in busy practice settings the intense pressure on
physician time may lead to frustration when the patient has more complaints than can be handled in the routine visit.
No studies have systematically explored physicians' feelings of frustration with pa- tient visits. This study identifies specific com-
ponents of frustrating visits and proposed a self-assessment instrument for physicians.
Method
The method included the development of a preliminary "item pool" (descriptions of
frustrating patients and occasions) by ex-
perienced physicians and teachers of medi-
286
cal communication, additions/deletions/re- view of items within the pool by physicians of many specialties, empirical analyses to re- duce redundancy and group like items, and
preliminary construct validation of the final item pool by soliciting responses to it from
physicians who work in diverse settings and
specialties.
Step 1: Generating a Pool of Items
In 1989, a group of 12 nationally recog- nized expertsl in the field of medical inter-
viewing and doctor-patient communication research met to develop a tool to help physi- cians assess and address their educational needs in doctor-patient communication. In unstructured work sessions intended to elicit ideas, they developed lists of the types of frustrations physicians experience in com-
municating with patients. An initial list of 32 common problems were generated and for- matted into statements about patients and occasions ("items") that could be endorsed
by physicians as typical of their experience with frustrating visits. Some items were worded as though the patient was the cause of the difficulties (i.e., "The patient was try- ing to manipulate me."), some emphasized both patient and doctor responsibility (i.e., "We couldn't understand each other."), some took a physician perspective (i.e., "I felt overwhelmed."), and some items em-
phasized the practice setting (i.e., "Problems in my practice setting interfered with the visit.").
Step 2: Pilot Version
An initial questionnaire was developed from this item set which was pilot tested in a
group of 107 practicing physicians. Physi- cians were instructed to "Think back on some patient visits where you left the en- counter feeling that things had not gone as well as you would have liked because you
? See acknowledgement for names of experts.
MEDICAL CARE

PHYSICIAN FRUSTRATION WITH PATIENTS
and the patient didn't communicate effec-
tively." For each of the items, physicians were asked to indicate how typical these were of their experience, using a five-point Likert scale ranging from; 1 "Not at all typi- cal," to 5 "Very typical." This 1-to-5 score was used to analyze responses. In addition, physicians were instructed to add other item statements describing additional situations that they experienced as frustrating. They were asked to indicate the types of problem- atic encounters with which they would like further educational help.
All physicians responding to the self-ad- ministered questionnaire were attending a 4
1/2 hour voluntary workshop on "Physi- cian-Patient Communication." Workshops were hosted by a variety of institutions who invited their physicians to attend. Workshop settings varied, including health mainte- nance organizations (HMOs), community hospitals, large multidisciplinary clinics, and
university settings in geographically dis-
persed settings throughout the United States. Both primary care physicians (family practitioners, general internists, and pediatri- cians) and a broad range of specialists (i.e., obstetrician-gynecologists, surgeons, emer-
gency physicians, psychiatrists) were in- cluded in the study group. All physicians chose to attend one of the 60 workshops for educational reasons, but in some states mal-
practice insurance companies offered a mal-
practice premium reduction as a further in- centive for attendance.
Step 3: Revision and Preliminary Factor Analysis
A revised questionnaire of the 42 items
incorporated new items generated by the pi- lot sample. This second version was distrib- uted to 931 physicians who were also at-
tending the workshops. A factor analysis of this 42-item questionnaire was performed, clustering items into eight clinically mean-
ingful factors: 1) lack of trust/agreement, 2) too many problems, 3) feeling distressed, 4)
lack of understanding, 5) lack of adherence, 6) demanding/controlling patient, 7) inap- propriate visit, and 8) special problems.
Step 4: Refinement and Re-analysis on a New Sample
Based on the analysis of the second ver- sion, the questionnaire was revised again by the authors, deleting items rarely endorsed, rewording items which seemed confus-
ing, and adding new items to help clarify the meaning of a particular factor. The
questionnaire's instructions were modified
slightly for clarification. This third version included 39 items. Data were collected in-
cluding physician sex, race, specialty, prac- tice setting, and years in practice. In addi- tion, the questionnaire included a question about physicians' perceptions of the fre-
quency of frustrating visits, the causes of frustration in the visit (nature of the patient, physician communication skills, practice setting), and their overall satisfaction with their practice.
This 39-item version of the questionnaire was completed by 1,076 physicians who were participating in the workshops as previ- ously described. Their responses were factor
analyzed, and the results were used as a basis for selecting subscales and items for a final version. Their responses are the basis for the results reported in this article.
Step 5: Final Version
On the basis of the results of the analysis of the third (39-item) version, we selected 25 items (Table 1), which included items to rep- resent each of seven subscales. Items less of- ten endorsed or with weaker loadings on factors were deleted. The items included in the "Inappropriate Visit" dimension did not load together consistently and the dimen- sion was deleted.
Results
Demographic and professional character- istics of the 1,076 physicians are shown in
287
Vol. 31, No. 4

LEVINSON ET AL.
TABLE 1. Item Means and Standard Deviations
Mean
Lack of trust or agreement 1. There was a lack of trust between us. 2. The patient was unwilling to accept the diagnosis. 3. The patient and I could not see eye to eye on the goal of the visit. 4. I felt that the patient didn't believe me.
Too many problems 5. The patient had a million complaints. 6. There were too many problems. 7. I spent more time in the visit than I wanted to. 8. On the way out the door, the patient said, "Oh, by the way ..."
Feeling distressed 9. I felt depressed after seeing the patient.
10. There were times when I didn't know what to do next. 11. I felt angry after seeing the patient. 12. I felt overwhelmed.
Lack of adherence 13. The patient didn't follow my instructions. 14. The patient had not complied with the therapy I prescribed. 15. The patient did not accept responsibility for his/her own health care.
Lack of understanding 16. The patient couldn't give me a clear history. 17. We couldn't understand each other. 18. I couldn't understand what the patient wanted to tell me.
Demanding/controlling patient 19. The patient was trying to manipulate me. 20. The patient was too controlling. 21. The patient was telling me what to do to diagnose or treat the problem. 22. The family was demanding and complaining.
Special problems (alcohol, drugs, chronic pain) 23. Working with this drug abusing patient was difficult for me. 24. Working with this alcoholic patient was difficult for me. 25. This patient with chronic pain gave me trouble.
2.72 2.84 2.73 2.81
3.55 3.06 3.40 3.15
2.60 2.60 2.90 2.65
3.20 3.32 3.68
3.38 2.80 2.63
3.23 2.84 3.10 3.39
3.12 2.65 3.26
SD
1.28 1.15 1.17 1.21
1.21 1.19 1.27 1.27
1.28 1.16 1.35 1.31
1.14 1.12 1.11
1.12 1.16 1.16
1.22 1.15 1.15 1.18
1.43 1.32 1.21
Note: Based on 1,076 returned questionnaires. Because some physicians skipped some items, the means were based on 1,058 to 1,073 responses, except that somewhat fewer responded to item 23, which concerned drug-abus- ing patients (N = 1,044), and item 26, which concerned alcohol-abusing patients (N = 1,035).
Table 2. Approximately half of the physi- cians were practicing in primary care disci-
plines-family medicine (N = 201), general internal medicine (N = 192), and pediatrics (N = 69). The others were in more than 40
specialties, of which the most common were obstetrics (N = 108), surgery (N = 70), ortho-
pedics (N = 48), psychiatry (N = 32), and
emergency medicine (N = 31). Physicians' overall satisfaction with prac-
tice was evaluated by responses to the ques- tion, "All in all on a daily basis, how satis- fied are you with your practice in general?"
Of those who responded to this item (N = 1,014), 49% reported they were very satis- fied, 44% somewhat satisfied, 6% some- what dissatisfied, and 1% very dissatisfied. In response to the question, "What percent- age of your patient visits are frustrating in one way or another?" (N = 1,027), 54% said this occurred in less than 10% of visits; 36%
reported frustration in 11% to 25% of visits; 8% reported frustration in 26% to 50% of visits; and 2% reported frustration in greater than 51% of visits. The cause of the frustrat-
ing visits was most frequently attributed to
288
MEDICAL CARE
PHYSICIAN FRUSTRATION WITH PATIENTS
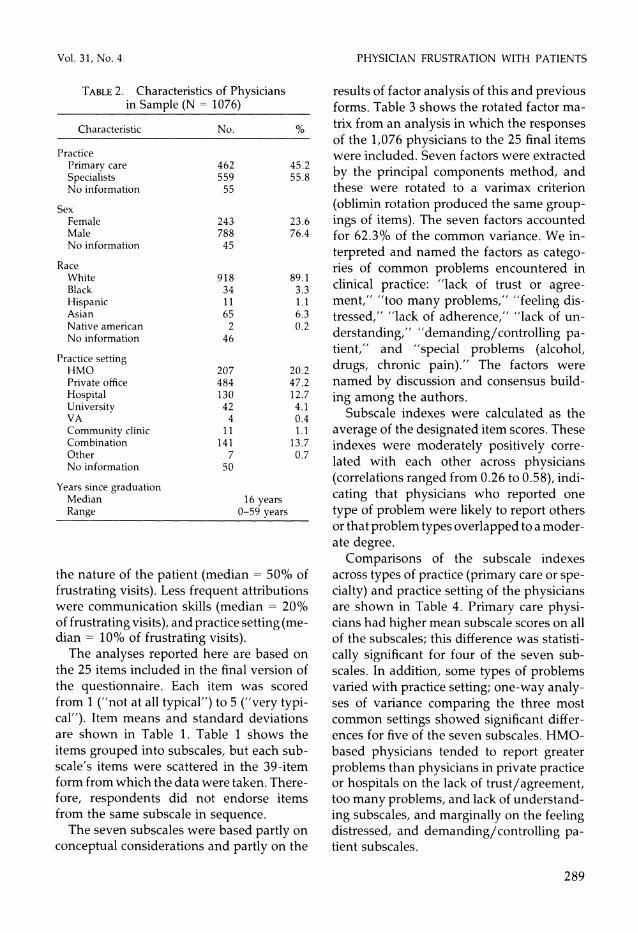
TABLE 2. Characteristics of Physicians in Sample (N = 1076)
Characteristic No. %
Practice Primary care 462 45.2 Specialists 559 55.8 No information 55
Sex Female 243 23.6 Male 788 76.4 No information 45
Race White 918 89.1 Black 34 3.3 Hispanic 11 1.1 Asian 65 6.3 Native american 2 0.2 No information 46
Practice setting HMO 207 20.2 Private office 484 47.2 Hospital 130 12.7 University 42 4.1 VA 4 0.4 Community clinic 11 1.1 Combination 141 13.7 Other 7 0.7 No information 50
Years since graduation Median 16 years Range 0-59 years
the nature of the patient (median = 50% of frustrating visits). Less frequent attributions were communication skills (median = 20% of frustrating visits), and practice setting (me- dian = 10% of frustrating visits).
The analyses reported here are based on the 25 items included in the final version of the questionnaire. Each item was scored from 1 ("not at all typical") to 5 ("very typi- cal"). Item means and standard deviations are shown in Table 1. Table 1 shows the items grouped into subscales, but each sub- scale's items were scattered in the 39-item form from which the data were taken. There- fore, respondents did not endorse items from the same subscale in sequence.
The seven subscales were based partly on conceptual considerations and partly on the
results of factor analysis of this and previous forms. Table 3 shows the rotated factor ma- trix from an analysis in which the responses of the 1,076 physicians to the 25 final items were included. Seven factors were extracted
by the principal components method, and these were rotated to a varimax criterion (oblimin rotation produced the same group- ings of items). The seven factors accounted for 62.3% of the common variance. We in-
terpreted and named the factors as catego- ries of common problems encountered in clinical practice: "lack of trust or agree- ment," "too many problems," "feeling dis- tressed," "lack of adherence," "lack of un-
derstanding," "demanding/controlling pa- tient," and "special problems (alcohol, drugs, chronic pain)." The factors were named by discussion and consensus build-
ing among the authors. Subscale indexes were calculated as the
average of the designated item scores. These indexes were moderately positively corre- lated with each other across physicians (correlations ranged from 0.26 to 0.58), indi-
cating that physicians who reported one
type of problem were likely to report others or that problem types overlapped to a moder- ate degree.
Comparisons of the subscale indexes across types of practice (primary care or spe- cialty) and practice setting of the physicians are shown in Table 4. Primary care physi- cians had higher mean subscale scores on all of the subscales; this difference was statisti- cally significant for four of the seven sub- scales. In addition, some types of problems varied with practice setting; one-way analy- ses of variance comparing the three most common settings showed significant differ- ences for five of the seven subscales. HMO- based physicians tended to report greater problems than physicians in private practice or hospitals on the lack of trust/agreement, too many problems, and lack of understand- ing subscales, and marginally on the feeling distressed, and demanding/controlling pa- tient subscales.
289
Vol. 31, No. 4

LEVINSON ET AL.
TABLE 3. Varimax Rotated Factor Matrix
Factor Number
Item 1 2 3 4 5 6 7
Lack of trust/agreement Q1 Q2 Q3 Q4
Too many problems Q5 Q6 Q7 Q8
Feeling distressed Q9 Q10 Qll Q12
Lack of adherence Q13 Q14 Q15
Lack of understanding Q16 Q17 Q18
Demanding/controlling patient Q19 Q20 Q21 Q22
Special problems (alcohol, drugs, chronic pain) Q23 Q24 Q25
0.67 0.66 0.65 0.63
0.75 0.73 0.71 0.56
0.73 0.59 0.57 0.54
0.83 0.82 0.68
0.72 0.70 0.66
0.75 0.63 0.58 0.55
0.87 0.84 0.47
Note: Based on N = 1076 questionnaires. See Table 1 for item content. The factor analysis used principal compo- nents extraction with varimax rotation; item means were substituted for missing data. Loadings of absolute value less than 0.40 were omitted (none of the items had loadings this high on more than one factor).
Correlations of subscale indexes with
physicians' characteristics and attitudes (Ta- ble 5) showed the following:
1) More recent graduates tended to have slightly-but significantly higher scores on all of the subscales, most strongly for the feel- ing distressed subscale, shown by negative correlations of physician years since gradua- tion with subscale scores. One interpretation of this finding is that physicians learn to cope as they gain experience;
2) Greater time spent in primary care was associated with higher scores on several of
the subscales, most strongly on too many problems, feeling distressed, and demand- ing/controlling patient. This echoes the pat- tern of differences between primary care physicians and specialists (Table 4);
3) Physicians' general level of satisfaction and the percentage of visits they reported as frustrating were correlated with most of the subscale scores, negatively and positively, re- spectively. This pattern supports the conver- gent validity of the scales.
Female physicians averaged slightly higher scores than male physicians on the
290
MEDICAL CARE

PHYSICIAN FRUSTRATION WITH PATIENTS
TABLE 4. Communication Problem Subscale Means: Comparisons of Primary Care Physicians Versus
Specialists and Comparisons Across Practice Settings
Lack of Lack of Demanding Trust or Too Many Feeling Lack of Under- Contrig. Special
Comparison Agreement Problems Distressed Adherence standing Patient Problems
Type of practice Primary care 2.83 3.52 2.83 3.46 2.98 3.27 3.12 Specialty 2.72 3.11a 2.56' 3.35 2.90 3.04 2.93
t-statistic 1.94 7.04a 4.46a 1.81 1.34 4.33a 2.70b
Practice setting HMO 2.99 3.45 2.81 3.45 3.16 3.28 2.88 Private office 2.72 3.31 2.60 3.32 2.84 3.10 2.98 Hospital 2.67 3.01 2.65 3.40 2.88 3.16 3.13
F value 7.20" 8.87a 3.62c 1.46 8.89a 3.03c 2.14
Note: N varied from 978 to 1,011 for type of practice comparisons and from 783 to 813 for the practice setting comparisons because of missing data on some measures. Comparisons used t-tests (for type of practice) or one-way analyses of variance (for practice setting).
aP < 0.001. P < 0.01.
c P < 0.05.
too many problems subscale (3.50 versus 3.24, t = 3.85, df = 1014, P < 0.001), the feeling distressed subscale, (2.82 versus 2.64; t = 2.46, df = 1016, P < 0.05), and the lack of adherence subscale (3.54 versus 3.35, t = 2.62, df = 1012, P < 0.01). Comparisons of white physicians with nonwhite physi- cians showed no significant differences in subscale scores.
Discussion
It is indeed common for physicians to ex- perience frustration in visits with patients. In this study, more than one third of physi- cians reported experiencing frustration in up to 25% of patient visits and 8% of physi- cians felt frustrated in up to half of their pa- tient encounters. The types of frustrations
TABLE 5. Correlates of Communication Problem Subscale Scores
Lack of Lack of Demanding Trust or Too Many Feeling Lack of Under- Contrig. Special
Comparison Agreement Problems Distressed Adherence standing Patient Problems
Years since graduation -0.13 -0.17a -0.24a -0.16a -0.16a -0.16" -0.09b
Time spent in primary care 0.06 0.22a 0.15a 0.08c 0.05 0.13a 0.10b
General satisfaction -0.13a -0.17a -0.16a -0.10b -0.13a -0.14a -0.08c
Percent of visits experienced as frustrating 0.11b 0.22a 0.24a 0.15a 0.19a 0.11b 0.19a
Note: N varied from 957 to 1,017 because of missing data on some measures. 'P < 0.001.
p < 0.01. P < 0.05.
291
Vol. 31, No. 4

LEVINSON ET AL.
distinguished empirically in our factor analy- sis reflect frequently occurring problems in the physician-patient relationship. Identify- ing specific types of frustrations may facili- tate better targeted efforts at amelioration. Below we discuss each of the seven types of frustrations identified in the study. Table 6
suggests additional literature pertinent to each of these areas.
Lack of Trust or Agreement
Lack of trust or agreement may result from differences between the beliefs of pa- tients and physicians about the medical
problem. Patients may have beliefs about the etiology of the problem or appropriate treatment that conflict with the model of the
physician.2223 Often unspoken differences lead the patient to feel that the physician does not understand them and leave the
physician frustrated that they aren't "get- ting through" to the patient. Both parties can feel unhappy with the experience. Specific communication skills may be helpful in
building a trusting rapport between physi- cians and patient. Trust and agreement can be enhanced with the use of open-ended questions, active listening to the patient's concerns, repeating and summarizing the
patient's problem, and involving the patient in decisionmaking about treatment op- tions.24'25 Skills in negotiation may help clar-
ify a plan of action acceptable to both the
physician and the patient.26'27
Lack of Adherence
Extensive literature has demonstrated that a significant percentage of patients do not follow through with instructions or medica- tions recommended by their doctors.11'28'29
Specific communication strategies can signif- icantly improve patient adherence. These
strategies include checking patient's opinion of treatments prescribed, written instruc- tions, and asking the patient to repeat the treatment plan. In practice, physicians spend a relatively short period explaining
292
TABLE 6. Selected Literature Relevant to Each of the Frustrations
Communication Problem References
1. Lack of trust/agreement 6,38-40 2. Lack of understanding 34,41-44 3. Feeling distressed 20,45-48 4. Too many problems 49 5. Lack of adherence 7,23,39,50,51 6. Demanding/controlling 20,38,45 7. Special problems 52-62
the diagnosis and giving treatment instruc- tions to patients.4 Patients are frequently dis- satisfied by the lack of instruction they re- ceive.30 Strategies to improve communica- tion in the area of giving instructions may result in improved patient satisfaction and better patient outcomes.
Too Many Problems
Often, a patient comes to the office visit with a list of complaints. The physician may have less than 10 minutes scheduled for the visit and cannot adequately address each
complaint. Sometimes when the allotted time is almost over, the patient reveals the real reason for the visit, saying "Oh, by the
way doctor. . .". Presentation of new prob- lems at this late stage can be avoided by use of open-ended questions and allowing the
patient to talk uninterrupted at the begin- ning of the interview.31 Identifying all the
patient's concerns early in the interview al- lows the physician and patient to negotiate what problems will be covered in this or
subsequent visits.
Feeling Distressed
Physicians can "feel distressed" during or after a visit with a patient. These feelings can include sadness, being overwhelmed, anger, and rejection. Sometimes physicians may feel more comfortable by recognizing their
feelings and reflecting about the cause. Dis- cussion groups, like Balint groups, are de-
signed for physicians to talk together about
MEDICAL CARE

PHYSICIAN FRUSTRATION WITH PATIENTS
the negative and positive feelings they expe- rience working with patients.32
Demanding or Controlling Patient
Physicians are used to being in charge of the medical situation and can feel uncom- fortable with the patients or families exert- ing too much control in the medical en- counter. These "demanding" patients may pressure doctors to order specific tests or in- sist on referrals to various specialists. In some cases strategies to shift the interview to a more "patient-centered model" can help avoid these frustrations. It is important for physicians to learn to set limits in a firm but supportive fashion to decrease the frustra- tions associated with feeling "manipu- lated." Skilled-based continuing medical ed- ucation programs may be particularly help- ful in this area to explore ways to manage the power and control in the interview.33
Lack of Understanding
Physicians and patients express them- selves using a different language from one another.34 The physicians' medical language and the patients' difficulty in describing their problem in medically understandable terms can lead to frustration for both parties. Attention to avoiding the use of medical jar- gon and understanding some of the com- mon breakdowns in communication from a linguistic viewpoint can be helpful to physi- cians in this area.
Special Problems
Finally, some physicians experience frus- tration in specific problem areas including alcohol, drugs, chronic pain, or somatiza- tion. Specific medical literature focused on those topics may help physicians develop specific knowledge useful for working with these patient problems (Table 6).
In addition to the specific nature of physi- cian frustrations, this study found differ- ences in the experiences of groups of physi- cians. Primary care physicians reported
higher frustrations on all factors. This find-
ing seems particularly relevant in these days of declining interest in graduating medical students in selecting residencies in primary care disciplines.35 Do students perceive the nature of visits to primary care physicians as more "unpleasant" for the doctor than visits to subspecialists? Is this a significant source of "burn out" for doctors? Would particular skills introduced in medical education help primary care physicians be happier in prac- tice? Is clinical practice bound to be more frustrating to primary care providers than subspecialists because of the nature of the work? While we do not have answers for these questions, this study suggests that dis- cussion and education in the field of commu- nication is particularly important to physi- cians practicing in primary care disciplines.
Physicians practicing in HMOs reported greater frustration with "lack of trust," "lack of understanding," and "too many prob- lems," compared with physicians in private practice or hospital-based settings. Perhaps physicians and patients in HMO settings are more likely to have differing expectations or less time to build relationships than those in private practice. For these physicians, skills in negotiating an agenda for the visit may be
particularly important to deal with "too
many problems" for the length of time avail- able. Educational programs geared to help HMO physicians improve their communica- tion skills are provided in some large HMO settings and may address the challenges ex- perienced based by this particular group of doctors.36,37
Finally, physicians in this study perceived the source of frustration as resulting from the characteristics of the patient in more than 50% of frustrating visits. A smaller fraction of the time they assumed responsi- bility themselves, shared it with patients, or blamed the organization for their frustra- tion. Many of the original items that were worded to emphasize either physician re- sponsibility for communication problems or shared responsibility with the patients were
293
Vol. 31, No. 4

LEVINSON ET AL.
not endorsed by the physicians and hence, were deleted in revisions of the question- naire. This tendency to blame the patient is a
dangerous position for physicians, and one which patients should find worrisome as well. Attributing our frustration to patients' characteristics alone may interfere in build-
ing a trusting relationship necessary for op- timal patient care. It is preferable for physi- cians to be able to analyze the source of their frustration and seek ways to modify the ex-
perience. In conclusion, this instrument may assist
physicians in identifying areas that they ex-
perience as particularly frustrating in work-
ing with patients. Through identification, ed- ucation, and reflection, patient care can be
improved while making the experience of
day-to-day practice more rewarding. The last person an ill patient wants to see is a frustrated doctor. As the saying goes, "Phy- sician heal thyself."
Acknowledgments The authors thank the following individuals for their
help in the development of the initial items used in the instrument: Paul Arntson, Howard Beckman, Richard Frankel, Craig Kaplan, Suzanne Kurtz, Vaughn Keller, Mack Lipkin, Jr., Sam Putnam, and Debra Roter.
We also thank Barbara Olsen and Dr. James Shaw for their help in manuscript preparation.
References
1. Roter D, Hall J, Katz N. Patient-physician commu- nication: a description summary of the literature. Pa- tient Education and Counseling 1988; 12:99.
2. Hall JA, Roter DL, Katz NR. Meta-analysis of cor- relates of provider behavior in medical encounters. Med Care 1988;26:657.
3. Hall JA, Dornan MC. Meta-analysis of satisfaction with medical care: description of research design and analysis of overall satisfaction levels. Soc Sci Med 1988; 27:637.
4. Waitzkin H. Doctor-patient communication: Clin- ical implications of social scientific research. JAMA 1984; 252(17):2441.
5. Woolley FR, Kane RL, Hughes CC, Wright DD. The effects of doctor-patient communication on satis- faction and outcome of care. Soc Sci Med (12):123-8.
6. Starfield B, Wray C, Hess K, et al. The influence of patient-practitioner agreement on outcome of care. Am J Public Health 1981;71:127.
7. DiMatteo MR, DiNicola DD. Achieving patient compliance. New York, NY: Pergamon Press, 1982:35.
8. Reading AE. The short term effects of psychologi- cal preparation for surgery. Soc Sci Med 1979; 13:641.
9. Mumford E, Schlesinger HJ, Glass VG. The effects of psychological intervention on recovery from surgery and heart attacks: An analysis of the literature. Am J Public Health 1982; 72:141.
10. Greenfield S, Kaplan S, Ware JE. Expanding pa- tient involvement in care. Ann Intern Med 1985; 102:520.
11. Mushlin AI, Appal FA. Diagnosing patient non- compliance. Arch Intern Med 1977; 137:318.
12. Svarstad B. Physician-patient communication and patient conformity with medical advice. In: Me- chanic D. The Growth of Bureaucratic Medicine. New York, NY: Wiley, 1976.
13. Eraker SA, Kirscht JP, Becker MH. Understand- ing and improving patient compliance. Ann Intern Med 1984; 100:258.
14. Korsch BM, Gozzi EK, Francis V. Gaps in doctor patient communication. I. Doctor-patient interaction and patient satisfaction. Pediatrics 1968;42:855.
15. Heszen, Klemens I. Patients' noncompliance and how doctors manage this. Soc Sci Med 1987;24:409.
16. Nowlis DP. Borderline personality disorder in primary care. J Fam Pract 1990;30:329.
17. Levinson W. Frustrating patients: using our feel- ings as diagnostic clues. J Gen Intern Med 1990;6:259.
18. Lin EHB, Katon W, Von Korff M, et al. Frustrat- ing patients: physician and patient perspectives among distressed high users of medical services. J Gen Intern Med 1991;6:241.
19. Putnam SM, Lazare A, Lipkin M. Personality disorders and patients whom the physician find diffi- cult. In: Lipkin M. Putnam SM, Lazare A, eds. The Medi- cal Interview. New York, NY: Springer-Verlag, 1990.
20. Groves JE. Taking care of the hateful patient. N Engl J Med 1978; 298:883.
21. Mizrahi T. Getting rid of patients: contradictions in the socialization of physicians. New Brunswick, NJ: Rutgers University Press, 1986.
22. Becker MH. The health belief model and sick role behavior. Health Education Monograph 1974; 2:409.
23. Helman CG. Communication in primary care: the role of patient and practitioner explanatory models. Soc Sci Med 1985;20:923.
24. Lipkin M. The medical interview and related skills. In: Branch WT, (Ed). The Office Practice of Medi- cine. Philadelphia, Pa: W.B. Saunders Co, 1987:1287.
25. Cohen-Cole SA. Kist K, Rudolph P (Eds). The Medical Interview: The Three-Function Approach. St. Louis, Mo: Mosby-Year Book, Inc., 1991.
26. Meichenbaum D, Turk D. Facilitating treatment adherence, 1990. New York, NY: Plenum Press.
27. Becker MH. Patient adherence to prescribed therapies. Med Care 1985;23:539.
294
MEDICAL CARE

PHYSICIAN FRUSTRATION WITH PATIENTS
28. Stimson GV. Obeying doctor's orders: a view from the other side. Soc Sci Med 1974; 8:97.
29. Podell RN, Gary LR. Compliance: a problem in medical management. Am Fam Physician 1976; 13:74.
30. Tuckett D, Boulton M, Olson C, Williams A. Meetings between experts. New York, NY: Tavistock Publications, 1985.
31. Beckman H, Frankel R. The impact of physician behavior on the collection of data. Ann Intern Med 1984; 101:692.
32. Frenette J, Blondeau F. Balint groups in clinical training. In: Stewart M, Roter D, (Eds). Communicating with Medical Patients. Newbury Park, Calif: Sage, 1989:58.
33. Levinson W, Roter D. Can educational programs change the actual communication skills of practicing primary care physicians?-the results of two types of
continuing medical education programs. Clin Research 1992;40(2):615A.
34. Mishler EG. The discourse of medicine: dialectics of medical interviews. Norwood, NJ: Ablex Publishing Corp., 1984:211.
35. Lipkin M, Levinson W, Barker R, et. al. Primary care internal medicine: a challenging career choice for the 1990s. Ann Intern Med 1990;112:371.
36. Levinson W. Physician-patient communication in the managed care environment. Medical Interface, May 1991.
37. Carroll JG, Engle RL. Communication tech- niques for HMO physicians. HMO Practice (In press).
38. Quill TE. Partnerships in patient care: a contrac- tual approach. Ann Intern Med 1983;98:228.
39. Lazare A, Eisenthal S, Wasserman L. The cus- tomer approach to patienthood. Arch Gen Psych 1975; 32:553.
40. Rogers CR. The characteristics of a helping rela- tionship. In: On Becoming a Person: A Therapist's View of Psychotherapy. Boston, Mass: Houghton Mifflin, 1961:39.
41. Kleinman A, Eisenberg L, Good B. Culture, ill- ness, and care: Clinical lessons from anthropologic and cross-cultural research. Ann Intern Med 1978;88:251.
42. Smith RC, Hoppe RB. The patient's story: inte- grating the patient-and physician-centered approaches to interviewing. Ann Intern Med 1991;115:470.
43. Roter DL. Patient participation in patient-pro- vider interaction: Effects of patient question-asking on the quality of interaction, satisfaction, and compliance. Health Education Monograph 1977;5:281.
44. Starfield B, Steinwachs D, Morris I, et al. Patient-
doctor agreement about problems needing follow-up visit. JAMA 1979; 242:344.
45. Drossman DA. The problem patient: evaluation and medical care of patients with psychosocial distur- bances. Ann Intern Med 1978;88:366.
46. Sansone RA. Borderline personality disorder: of- fice diagnosis and management. Am Fam Physician 1991;44:194.
47. Smith RC, Zimny GH. Physicians' emotional re- actions to patients. Psychosomatics 1988;29:392.
48. Gorlin R, Zucker HD. Physicians' reactions to pa- tients: A key to teaching humanistic medicine. N Engl J Med 1983;308:1059.
49. Cohen-Cole SA. Interviewing the cardiac pa- tient: I. A practical guide for assessing quality of life. Quality of Life and Cardiovascular Care 1985;2:7.
50. Brody DS. The patient's role in clinical decision- making. Ann Intern Med 1980;93:718.
51. Barsky AJ. Patient heal thyself: activating the ambulatory medical patient. J Chron Dis 1976;29:585.
52. Johnson B, Clark W. Alcoholism: a challenging physician-patient encounter. J Gen Intern Med 1989;4:445.
53. Barnes HN, Aronson M, Delbanco TL. Alcohol- ism: a guide for the primary care physician. New York, NY: Springer-Verlag, 1988:231.
54. Clark WD. The generalist and alcoholism: dilem- mas and Progress. In: Noble J, ed. Textbook of General Medicine and Primary Care. Boston, Mass: Little Brown & Co, 1987:1619.
55. Shine DD. Approach to the drug abusing pa- tient. In: Noble J, ed. Textbook of General Medicine and Primary Care. Boston, Mass: Little Brown & Co, 1987:1645.
56. Shine DD. Management of drug abusers. In: No- ble J, ed. Textbook of General Medicine and Primary Care. Boston, Mass: Little Brown & Co;1987:1675.
57. Engle GL. 'Psychogenic' pain and the pain- prone patient. Am J Med 1959;26:899.
58. Reuler JB, Girard DE, Nardone DA. The chronic pain syndrome: misconceptions and management. Ann Intern Med 1980;93:588.
59. Melzack R, Wall PD. The challenge of pain. New York, NY: Basic Books, Inc., 1983.
60. Kaplan C, Lipkin M, Gordon GH. Somatization in primary care: patients with unexplained and vexing medical complaints. J Gen Int Med 1988;3:177.
61. Smith RC. Somatization disorder: defining its role in clinical medicine. J Gen Int Med 1991;6:168.
62. Barksy AJ. Patients who amplify bodily sensa- tions. Ann Intern Med 1979;91:63.
295
Vol. 31, No. 4
Copyright © 2022 FDOKUMEN