The role of epigenetics in personalized medicine: challenges and opportunities
ORIGINAL RESEARCH
Personalized Medicine Through SNP Testing for Breast CancerRisk: Clinical Implementation
Rebecca Howe & Talya Miron-Shatz & Yaniv Hanoch &
Zehra B. Omer & Cristina O’Donoghue &
Elissa M. Ozanne
Received: 21 October 2013 /Accepted: 25 November 2014# National Society of Genetic Counselors, Inc. 2014
Abstract Single nucleotide polymorphisms (SNPs) have thepotential to improve personalized medicine in breast cancercare. As new SNPs are discovered, further enhancing riskclassification, SNP testing may serve to complement familyhistory and phenotypic risk factors when assessed in a clinicalsetting. SNP analysis is particularly relevant to high-riskwomen who may seek out such information to guide theirdecision-making around risk-reduction. However, little isknown about how high-risk women may respond to SNPtesting with regard to clinical decision-making. We examinedhigh-risk women’s interest in SNP testing for breast cancer
risk through an online survey of hypothetical testing scenari-os. Women stated their preferences for sharing test results andselected the most likely follow-up action they would pursue ineach of the test result scenarios (above average and belowaverage risk for breast cancer). Four hundred seventy-eightwomen participated. Most women (89 %) did not knowwhat a SNP was prior to the study. Once SNP testing wasdescribed, 75 % were interested in SNP testing.Participants stated an interest in lifestyle interventions forrisk-reduction and wanted to discuss their testing resultswith their doctor or a genetic counselor. Women areinterested in SNP testing and are prepared to make life-style changes based on testing results. Women’s preferencefor discussing testing results with a healthcare provideraligns with the current trend towards SNP testing in aclinical setting.
Keywords Breast cancer . Risk assessment . SNP testing .
Decisionmaking
Introduction
Personalized medicine in cancer care, such as targetingcare according to an individual’s genetic backgroundand cancer biology, has emerged as a promising optionin the field of breast cancer (Offit 2011; van’t Veer andBernards 2008). Currently best recognized for its use incancer treatment, personalized medicine offers additionalvalue in the areas of cancer risk assessment and pre-vention (Weitzel et al. 2011). Testing for mutations inthe BRCA gene has increased women’s awareness aboutelevated risk for breast cancer and the need for discus-sions with genetic counselors and physicians about risk-reduc ing in te rvent ions (Wei tze l e t a l . 2011) .
R. HoweFrank H. Netter MD School of Medicine, Quinnipiac University,North Haven, CT, USA
T. Miron-ShatzCenter for Medical Decision Making, Ono Academic College,Kiryat Ono, Israel
Y. HanochDepartment of Psychology, Plymouth University, Plymouth, UK
Z. B. OmerSchool of Medicine, University of Massachusetts, Worcester, MA,USA
C. O’DonoghueDepartment of Surgery, University of Illinois at Chicago, Chicago,IL, USA
C. O’Donoghue : E. M. OzanneDepartment of Surgery, University of California at San Francisco,San Francisco, CA, USA
E. M. Ozanne (*)The Dartmouth Institute for Health Policy and Clinical Practice,Lebanon, NH, USAe-mail: [email protected]
J Genet CounselDOI 10.1007/s10897-014-9803-7

Personalized risk communication has been shown toenhance informed decision making and knowledge, withevidence of increasing the accuracy of risk perception(Edwards et al. 2013).
While BRCA testing is already widely established, thispaper examines the newly developed single nucleotide poly-morphism (SNP) testing that provides additional risk stratifi-cation by identifying genetic variants that may be correlatedwith higher or lower risk of various health conditions, includ-ing breast cancer. Studies suggest that in the general popula-tion, certain SNPs may confer between a 0.9 to 1.3 relativerisk of developing breast cancer (Michailidou et al. 2013). Ameta-analysis of the results from 9 genome-wide associationstudies identified 41 new breast cancer susceptibility loci(Michailidou et al. 2013). Along with the previously identifiedloci, these loci account for ~14 % of familial breast cancer risk(Michailidou et al. 2013). This compares to ~20 % of hered-itary breast cancers thought to be due to the BRCA geneticmutations and other high penetrance loci (Michailidou et al.2013).
Several studies have assessed the impact of these newlydiscovered SNPs and found that the inclusion of SNP testingalongside family history and other classic markers of breastcancer risk enhances the accuracy of risk assessment(Brentnall et al. 2014; Campa et al. 2011; Heald et al. 2012;Mealiffe et al. 2010). One study described family history andpersonal genome screening as “complementary tools for can-cer risk assessment” (Heald et al. 2012, p 547), while anotherdiscussed the improvement in classification of breast cancerrisks when SNP risk factors were combined with clinical riskfactors (Mealiffe et al. 2010). This improvement in risk as-sessment has been demonstrated in both high risk women (riskof breast cancer >8 % over 10 years) and moderate risk (5–8 %) (Brentnall et al. 2014).
Though there has been a call for additional research beforeSNP testing can be fully endorsed in the clinical setting(Bellcross et al. 2012; Graves et al. 2011; Hock et al. 2011),the potential for further refinement of risk prediction throughidentification of new SNPs highlights the clinical utility of thistesting (Antoniou et al. 2010; Easton et al. 2007; Ingle et al.2013; Michailidou et al. 2013; Riordan et al. 2012). In partic-ular, the discovery of two SNPs that appear to be associatedwith increased benefit of tamoxifen marks a turning point inthe ability of SNP testing to inform risk counseling discus-sions (Ingle et al. 2013).
The present study was designed to better understandpatient perspectives and the clinical implications of SNPtesting on screening and interventions. Women at increasedrisk of breast cancer are a motivated group with respect toclinical interventions around breast cancer risk and surveil-lance and may be more likely to engage in SNP testing (Hallet al. 2012). Therefore, we were particularly interested inhigh-risk women's response, with emphasis on their interest
in the testing and their potential use of the results fordecision-making.
To date, few studies have examined response to SNPtesting among women at high risk for breast cancer (Graveset al. 2011; Gray et al. 2009), and none have focused onpossible clinical implications in this setting. By understandinghow women might use this information, we aim to inform theimplementation of SNP testing, identifying the needs of wom-en as such testing becomes more prevalent.
Materials and Methods
Study Design
A cross-sectional survey study was conducted among a cohortof women at high risk for breast cancer to understand howthey may approach SNP testing. In an online survey, partici-pants were asked if they were aware of what a SNP is and theirinterest in SNP testing. The survey also included questionsabout direct-to-consumer SNP testing, but these results are notincluded here due to recent changes in the regulation andavailability of direct-to-consumer SNP testing (Annas andElias 2014). Descriptions of SNP testing were provided insimple language (Fig. 1). Interest was assessed through aLikert scale. Two hypothetical scenarios were presented toeach participant based on possible SNP testing results. Thefirst scenario asked participants to imagine that they hadundergone SNP testing and that the results indicated an aboveaverage likelihood of getting breast cancer. The second sce-nario mirrored the first, instead asking participants to imaginea below average likelihood of getting breast cancer.Participants were asked how they would proceed with thisinformation and what interventions they would consider,selecting frommultiple choice answers. The research protocolwas reviewed and approved by the institutional review boardsof the participating institutions.
Study Population
Women were recruited by email invitation from the CancerGenetics Network (CGN), a national network of cancer cen-ters that maintains a database of individuals with cancer andtheir relatives, including both affected individuals and those athigh risk for developing cancer. CGN provides baseline datafor each participant including demographics, family history,and disease history. Women were eligible for our onlinesurvey if they were between 30 and 60 years of age, had noprior history of breast cancer, and were at increased risk ofdeveloping breast cancer defined as: 1) women with at leastone relative diagnosed with breast cancer at age 45 oryounger, 2) women with two or more relatives diagnosed withbreast cancer at age 50 or younger, 3) women with at least one
Howe et al.

relative diagnosed with ovarian cancer, or 4) women with atleast one relative diagnosed with male breast cancer.
Statistical Analysis
Summary statistics were calculated to determine awareness ofSNPs, interest in SNP testing, and the clinical implicationsrelated to follow-up intentions and intervention choices. Forcontinuous variables, mean, median, standard deviation, andrange were calculated; for categorical data, counts and per-centages were used to summarize the variables. Univariatelogistic regressions were performed to determine the predic-tors of interest in SNP testing. Initial predictor variables in-cluded in the univariate regressions included: age, race, eth-nicity, education, marital status, Ashkenazi Jewish heritage,BRCA testing history, perception of breast cancer risk level,subjective and objective numeracy, CGN recruitment site,number of relatives with breast cancer, and trust of direct-to-consumer SNP testing. BRCA testing history included sepa-rate variables for previous personal and family testing historyas well as personal and family BRCA status for BRCA1 andBRCA2. Perception of breast cancer risk level was assessedby asking participants if they perceived themselves to be atlow, medium, or high risk for breast cancer. Subjective nu-meracy, a self-reported preference for numerical instead ofprose information, was calculated according to the questionsand scale developed by Fagerlin et al. (Fagerlin et al. 2007).Objective numeracy, a preference for numerical information,was determined based on the questions and scale developedby Schwartz et al. (1997). Variables that met statistical signif-icance on univariate analysis at p≤ .05 were included in theforward step-wise multivariate logistic regression model.Differences in preferences for post-testing follow-up and in-tervention choices were assessed using McNemar’s tests com-paring the hypothetical above average and below average risk
scenarios. All statistical analyses were completed using Stata/IC statistical software (version 12; Stata Corp., Texas). Allp-values were based on 2-sided tests and considered statisti-cally significant at p≤.05.
Results
Four hundred seventy-eight women completed the study(47 % response rate). A large majority of participants werewhite (95 %) and highly educated (72 % college graduate orhigher). Twenty percent of participants had received BRCAtesting, and 7 % of women had previously tested positive for aBRCAmutation. Six women (1 %) had previously undergoneSNP testing. Table 1 lists the characteristics of all studyparticipants.
Awareness of and Interest in SNP Testing
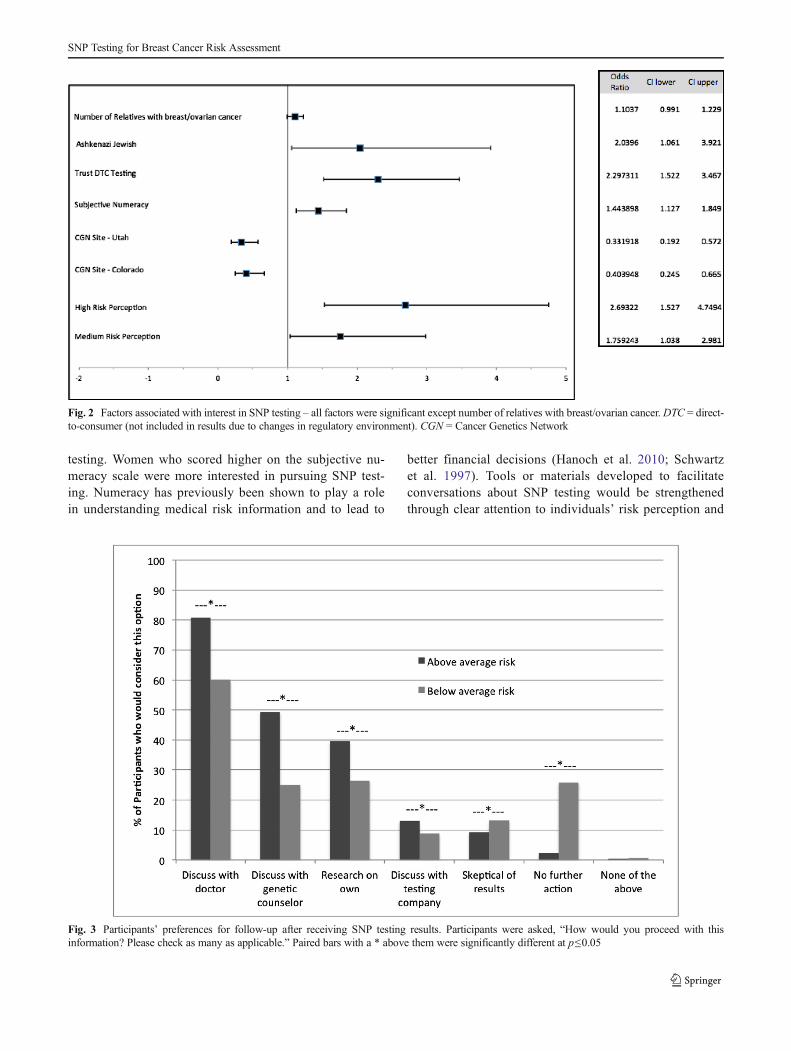
Before being presented with a descriptive paragraph aboutSNP testing, a minority of participants stated that they wereaware of what a SNP is (11 %). After learning about SNPtesting, the majority of participants were interested in SNPtesting (75 %). High perceived risk of breast cancer was moststrongly associated with interest in SNP testing (OR=2.7)(Fig. 2). Participants with Ashkenazi Jewish heritage andhigher subjective numeracy also reported greater interest inSNP testing. Participants from two of the CGN testing sites,Utah and Colorado, were less likely to be interested in SNPtesting (OR=0.3 and OR=0.4, respectively). There was nosignificant difference in the results for participants with aBRCA mutation compared to those without a mutation.
Fig. 1 Explanation of SNPtesting and question about interestin testing from online survey
SNP Testing for Breast Cancer Risk Assessment

Participant Follow-up and Decision Making Based on SNPTesting Results
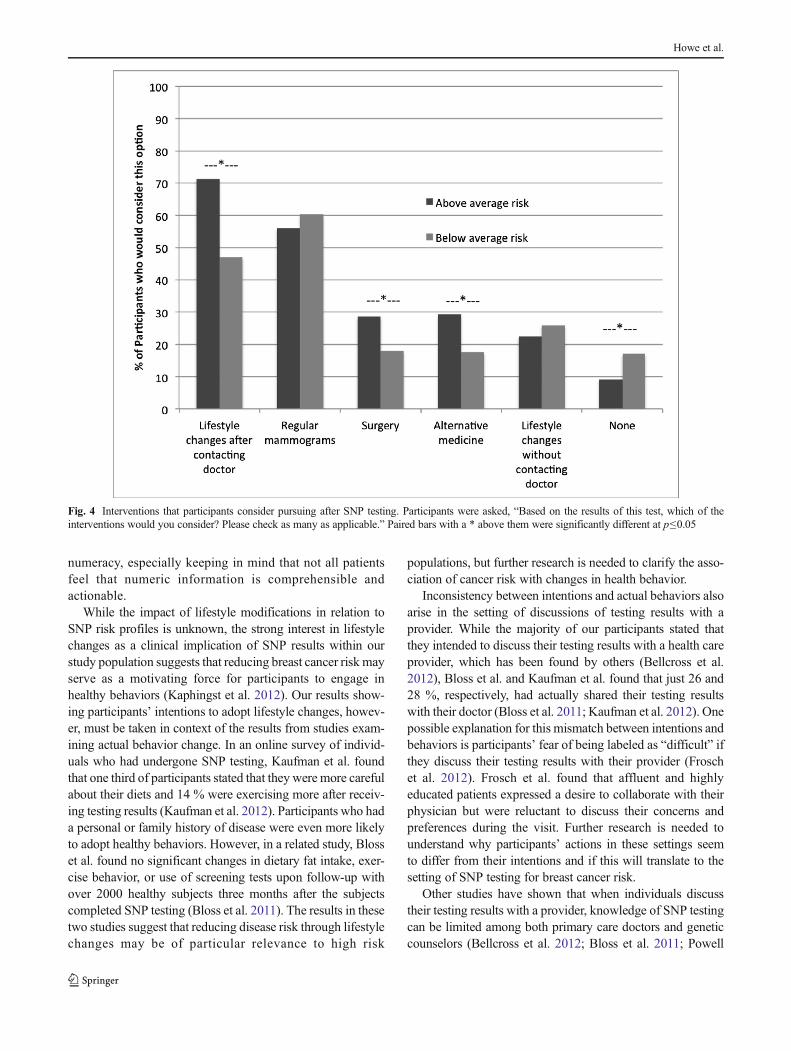
When asked how they would proceed with SNP testing resultsthat identified them as either below average or above averagerisk for breast cancer, participants preferred to discuss thetesting results with a doctor (60 % if below average risk,81 % if above average risk) or a genetic counselor (25 % ifbelow average risk, 49 % if above average risk) (Fig. 3).Participants in both the below average and above averagesettings were most likely to consider lifestyle changes (e.g.diet, exercise, etc.) and screening mammograms as interven-tions (Fig. 4). When identified as above average risk for breastcancer, participants were more likely to consider surgery as anintervention choice than when they were identified as being atbelow average risk. Differences in preference for each of theintervention choices between the below average and aboveaverage risk settings were significant for all intervention
options except regular mammograms and interest in makinglifestyle changes without contacting a provider first.
Discussion
Our study found that a large majority of women at increasedrisk of breast cancer are interested in SNP testing and that theresults of such a test are likely to influence their health caredecision-making. As we move into an age of personalizedmedicine and increased genetic testing, these data will becritical to understanding the implications for women’sfollow-up choices. While the research on SNP testing forbreast cancer risk stratification is still in the early stages,genetic counselors and physicians may soon be asked tointerpret SNP testing results alongside family history andother established risk factors. The results from this study helpto anticipate these changes in risk assessment by presentingresponses from high risk women.
The rates of awareness and interest in SNP testingamong our participant population are similar to ratesfound in similar studies. In a review, Bellcross et al. foundthat awareness of SNP testing ranged from 13-29 %(Bellcross et al. 2012). Graves et al. surveyed women atincreased risk for breast or ovarian cancer and found that77 % reported ‘definite’ interest in SNP testing (Graveset al. 2011). Interest was associated with the cost of thetesting and the amount of risk conveyed through thetesting. In another study, by Hall et al., 19 % of partici-pants drawn from the Northwest Cancer GeneticsNetwork were interested in SNP testing (Hall et al.2012). Two factors could explain the divergent resultsbetween our and Hall et al.’s results. First, in Hallet al.'s examination, women were eligible for the studyif they were at increased risk for cancer, but not exclu-sively breast or ovarian cancer. In addition, the greaterinterest in SNP testing found in our study, conducted afterHall’s, could be a sign of increased awareness and com-fort with these types of tests over time.
We found that among our study population, certaingroups are more interested in SNP testing and may benefitf rom more targeted informat ion about tes t ing.Specifically, women who perceived themselves to be athigh risk for breast cancer expressed more interest in SNPtesting. Since research has shown that women tend tomisunderstand their breast cancer risk (Bowen et al.1997; Cyrus-David 2010; Daly et al. 1996; Gurmankinet al. 2005; Senay and Kaphingst 2009; Vernon 1999),providing women with information and tools to accuratelyinterpret their risk is a critical component of counselingrelated to SNP testing. A second factor, subjective numer-acy, was also found to be associated with interest in SNP
Table 1 Demographic characteristics of the sample (N=478)
Characteristics N (%)
Age (years) Mean: 50 Range: 30–61
Race
White 455 (95)
Other 22 (5)
Ashkenazi Jewish heritage 46 (10)
Education
Some college or less 135 (28)
College graduate or more 342 (72)
Marital status
Married 370 (78)
Unmarried 107 (22)
BRCA testing (proportions are of full sample)
Previously tested 93 (20)
Tested positive 31 (7)
Family member positive 39 (8)
Previous SNP testing 6 (1)
Number of relatives with breast cancer Median:2
Range: 0–13
Number of relatives with ovarian cancer Median:0
Range: 0–7
Cancer Genetics Network site
Duke (Durham, NC) 40 (8)
MD Anderson (Houston, TX) 25 (5)
University of North Carolina (Chapel Hill,NC)
26 (5)
Emory (Atlanta, GA) 25 (5)
Johns Hopkins (Baltimore, MD) 75 (16)
Utah (Salt Lake City, UT) 129 (27)
Colorado (Aurora, CO) 157 (33)
Howe et al.
testing. Women who scored higher on the subjective nu-meracy scale were more interested in pursuing SNP test-ing. Numeracy has previously been shown to play a rolein understanding medical risk information and to lead to
better financial decisions (Hanoch et al. 2010; Schwartzet al. 1997). Tools or materials developed to facilitateconversations about SNP testing would be strengthenedthrough clear attention to individuals’ risk perception and
Fig. 2 Factors associated with interest in SNP testing – all factors were significant except number of relatives with breast/ovarian cancer.DTC = direct-to-consumer (not included in results due to changes in regulatory environment). CGN = Cancer Genetics Network
Fig. 3 Participants’ preferences for follow-up after receiving SNP testing results. Participants were asked, “How would you proceed with thisinformation? Please check as many as applicable.” Paired bars with a * above them were significantly different at p≤0.05
SNP Testing for Breast Cancer Risk Assessment
numeracy, especially keeping in mind that not all patientsfeel that numeric information is comprehensible andactionable.
While the impact of lifestyle modifications in relation toSNP risk profiles is unknown, the strong interest in lifestylechanges as a clinical implication of SNP results within ourstudy population suggests that reducing breast cancer risk mayserve as a motivating force for participants to engage inhealthy behaviors (Kaphingst et al. 2012). Our results show-ing participants’ intentions to adopt lifestyle changes, howev-er, must be taken in context of the results from studies exam-ining actual behavior change. In an online survey of individ-uals who had undergone SNP testing, Kaufman et al. foundthat one third of participants stated that they were more carefulabout their diets and 14 % were exercising more after receiv-ing testing results (Kaufman et al. 2012). Participants who hada personal or family history of disease were even more likelyto adopt healthy behaviors. However, in a related study, Blosset al. found no significant changes in dietary fat intake, exer-cise behavior, or use of screening tests upon follow-up withover 2000 healthy subjects three months after the subjectscompleted SNP testing (Bloss et al. 2011). The results in thesetwo studies suggest that reducing disease risk through lifestylechanges may be of particular relevance to high risk
populations, but further research is needed to clarify the asso-ciation of cancer risk with changes in health behavior.
Inconsistency between intentions and actual behaviors alsoarise in the setting of discussions of testing results with aprovider. While the majority of our participants stated thatthey intended to discuss their testing results with a health careprovider, which has been found by others (Bellcross et al.2012), Bloss et al. and Kaufman et al. found that just 26 and28 %, respectively, had actually shared their testing resultswith their doctor (Bloss et al. 2011; Kaufman et al. 2012). Onepossible explanation for this mismatch between intentions andbehaviors is participants’ fear of being labeled as “difficult” ifthey discuss their testing results with their provider (Froschet al. 2012). Frosch et al. found that affluent and highlyeducated patients expressed a desire to collaborate with theirphysician but were reluctant to discuss their concerns andpreferences during the visit. Further research is needed tounderstand why participants’ actions in these settings seemto differ from their intentions and if this will translate to thesetting of SNP testing for breast cancer risk.
Other studies have shown that when individuals discusstheir testing results with a provider, knowledge of SNP testingcan be limited among both primary care doctors and geneticcounselors (Bellcross et al. 2012; Bloss et al. 2011; Powell
Fig. 4 Interventions that participants consider pursuing after SNP testing. Participants were asked, “Based on the results of this test, which of theinterventions would you consider? Please check as many as applicable.” Paired bars with a * above them were significantly different at p≤0.05
Howe et al.

et al. 2012). Our results, taken in the context of thesesupporting studies, call for awareness and education amongproviders about how to discuss SNP testing and engage pa-tients in such conversations. Given that both below averageand above average risk individuals may have questions orconcerns about SNP testing, developing an infrastructure tobest support these discussions is imperative.
There are a few limitations to our study that need to beconsidered in light of these results. Since we presented partic-ipants with hypothetical results based on SNP testing, wecannot be sure whether participants’ responses to actual test-ing would differ from their intentions based on these hypo-thetical scenarios. We also were not able to conduct follow-upsurveys with participants, as intentions to discuss the resultswith a provider or adopt other interventions may change overtime. While the selection of a high-risk population for studywas appropriate given the potential clinical utility of SNPtesting to further refine risk among women at increased risk(Ingham et al. 2012), high-risk participants may have strug-gled to imagine how they would respond to testing resultsidentifying them as below average risk for breast cancer. Wewere also unable to control for the lack of independence in agiven woman’s responses to the two different risk scenarios.Finally, our participant population included predominantlywhite, highly educated women. Though reflective of the pop-ulation most likely to undergo genetic testing for cancer risk,these participants’ responses may not be representative of amore diverse population.
SNP testing has the potential to serve as a novel riskstratifying technique for cancer and as a motivator for healthylifestyle changes and other breast cancer prevention options.Further research concerning women’s response to alternativemeans of conducting SNP testing, such as testing within ahealth care setting administered by a clinician and accompa-nied by genetic counseling, may offer additional clarity on thistopic. Even as studies presenting the clinical validity of SNPtesting continue to emerge, a shared understanding of not justgenetics, but also an individual’s family history and otherestablished risk factors will ensure a thorough assessment ofcancer risk.
Acknowledgments This work was supported in part by grant numberMRSG112037 from the American Cancer Society. Additional resourcesfor this study were obtained from the Cancer Genetics Network (RFACA-97-004, RFA CA-97-019, RFP No. N01-PC-55049-40), a Universityof Plymouth award, and a European Research Council Marie CurieReintegration Grant [No. PIRG7-GA-2010-268224]. These fundingsources ensured the authors’ independence in designing the study,interpreting the data, writing, and publishing the report. We would alsolike to thank Elaine Allen for her guidance with the statistical analysis forthis study.
Human Studies and InformedConsent All procedures followed werein accordance with the ethical standards of the responsible committee onhuman experimentation (institutional and national) and with the Helsinki
Declaration of 1975, as revised in 2000. Informed consent was obtainedfrom all patients for being included in the study.
Conflicts of Interest Rebecca Howe, Talya Miron-Shatz, YanivHanoch, Zehra B. Omer, Cristina O’Donoghue, and Elissa M. Ozannedeclare that they have no conflict of interest.
References
Annas, G. J., & Elias, S. (2014). 23andMe and the FDA. The NewEngland Journal of Medicine, 370(11), 985–988.
Antoniou, A. C., Beesley, J., McGuffog, L., Sinilnikova, O. M., Healey,S., Neuhausen, S. L., & Easton, D. F. (2010). Common breast cancersusceptibility alleles and the risk of breast cancer for BRCA1 andBRCA2 mutation carriers: implications for risk prediction. CancerResearch, 70(23), 9742–9754.
Bellcross, C. A., Page, P. Z., & Meaney-Delman, D. (2012). Direct-to-consumer personal genome testing and cancer risk prediction.Cancer Journal (Sudbury, Mass.), 18(4), 293–302. Retrieved fromhttp://www.ncbi.nlm.nih.gov/pubmed/22846729.
Bloss, C. S., Schork, N. J., & Topol, E. J. (2011). Effect of direct-to-consumer genomewide profiling to assess disease risk. The NewEngland Journal of Medicine, 364(6), 524–534.
Bowen, D., Hickman, K. M., & Powers, D. (1997). Importance ofpsychological variables in understanding risk perceptions and breastcancer screening of African American women. Women’s Health(Hillsdale, N.J.), 3(3–4), 227–242. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9426495.
Brentnall, A. R., Evans, D. G., & Cuzick, J. (2014). Distribution of breastcancer risk from SNPs and classical risk factors in women of routinescreening age in the UK. British Journal of Cancer, 110(3), 827–828.
Campa, D., Kaaks, R., Le Marchand, L., Haiman, C. A., Travis, R. C.,Berg, C. D., & Canzian, F. (2011). Interactions between geneticvariants and breast cancer risk factors in the breast and prostatecancer cohort consortium. Journal of the National CancerInstitute, 103(16), 1252–1263.
Cyrus-David, M. S. (2010). Knowledge and accuracy of perceived per-sonal risk in underserved women who are at increased risk of breastcancer. Journal of Cancer Education : The Official Journal of theAmerican Association for Cancer Education, 25(4), 617–623.
Daly, M. B., Lerman, C. L., Ross, E., Schwartz, M. D., Sands, C. B., &Masny, A. (1996). Gail model breast cancer risk components arepoor predictors of risk perception and screening behavior. BreastCancer Research and Treatment, 41(1), 59–70.
Easton, D. F., Pooley, K. A., Dunning, A. M., Pharoah, P. D. P.,Thompson, D., Ballinger, D. G., & Ponder, B. A. J. (2007).Genome-wide association study identifies novel breast cancer sus-ceptibility loci. Nature, 447(7148), 1087–1093.
Edwards, A. G., Naik, G., Ahmed, H., Elwyn, G. J., Pickles, T., Hood, K.,& Playle, R. (2013). Personalised risk communication for informeddecision making about taking screening tests. Cochrane Databaseof Systematic Reviews (Online), 2, CD001865.
Fagerlin, A., Zikmund-Fisher, B. J., Ubel, P. A., Jankovic, A., Derry, H.A., & Smith, D. M. (2007). Measuring numeracy without a mathtest: development of the Subjective Numeracy Scale. MedicalDecision Making : An International Journal of the Society forMedical Decision Making, 27(5), 672–680. doi:10.1177/0272989X07304449.
Frosch, D. L., May, S. G., Rendle, K. A. S., Tietbohl, C., & Elwyn, G.(2012). Authoritarian physicians and patients’ fear of being labeled“difficult” among key obstacles to shared decision making. Health
SNP Testing for Breast Cancer Risk Assessment

Affairs (Project Hope), 31(5), 1030–1038. doi:10.1377/hlthaff.2011.0576.
Graves, K. D., Peshkin, B. N., Luta, G., Tuong, W., & Schwartz, M. D.(2011). Interest in genetic testing for modest changes in breastcancer risk: implications for SNP testing. Public Health Genomics,14(3), 178–189.
Gray, S. W., O’Grady, C., Karp, L., Smith, D., Schwartz, J. S., Hornik, R.C., & Armstrong, K. (2009). Risk information exposure and direct-to-consumer genetic testing for BRCA mutations among womenwith a personal or family history of breast or ovarian cancer. CancerEpidemiology, Biomarkers & Prevention : A Publication of theAmerican Association for Cancer Research, Cosponsored by theAmerican Society of Preventive Oncology, 18(4), 1303–1311.
Gurmankin, A., Domchek, S., Stopfer, J., Fels, C., &Armstrong, K. (2005).Patients’ resistance to risk information in genetic counseling forBRCA1/2. Archives of Internal Medicine, 14(165), 523–529.Retrieved from https://vpn.ucsf.edu/pubmed/,DanaInfo=www.ncbi.nlm.nih.gov+?term=gurmankin+2005+patients’+resistance+to+risk.
Hall, T. O., Renz, A. D., Snapinn, K.W., Bowen, D. J., & Edwards, K. L.(2012). Awareness and uptake of direct-to-consumer genetic testingamong cancer cases, their relatives, and controls: the NorthwestCancer Genetics Network. Genetic Testing and MolecularBiomarkers, 16(7), 744–748.
Hanoch, Y., Miron-Shatz, T., Cole, H., Himmelstein,M., & Federman, A.(2010). Choice, numeracy, and physicians-in-training performance:the case of Medicare Part D. Retrieved from https://vpn.ucsf.edu/pubmed/,DanaInfo=www.ncbi.nlm.nih.gov+?term=Hanoch,+Y.,+Miron-Shatz,+T,+Cole,+H.,+Himmelstein,+M.,+&+Federman,+A.+D.+(2010).+Choice,+numeracy++and+physicians-in-training+performance:+the+case+of+Medicare+Part+D.+Health+Psychology,+29(4),+454-459.
Heald, B., Edelman, E., & Eng, C. (2012). Prospective comparison offamily medical history with personal genome screening for riskassessment of common cancers. European Journal of HumanGenetics : EJHG, 20(5), 547–551.
Hock, K. T., Christensen, K. D., Yashar, B. M., Roberts, J. S., Gollust, S.E., & Uhlmann, W. R. (2011). Direct-to-consumer genetic testing:an assessment of genetic counselors’ knowledge and beliefs.Genetics in Medicine : Official Journal of the American College ofMedical Genetics, 13(4), 325–332. doi:10.1097/GIM.0b013e3182011636.
Ingham, S. L., Warwick, J., Byers, H., Lalloo, F., Newman, W. G., &Evans, D. G. R. (2012). Is multiple SNP testing in BRCA2 andBRCA1 female carriers ready for use in clinical practice? Resultsfrom a large Genetic Centre in the UK. Clinical Genetics. Retrievedfrom http://www.ncbi.nlm.nih.gov/pubmed/23050611
Ingle, J. N., Liu, M., Wickerham, D. L., Schaid, D. J., Wang, L.,Mushiroda, T., & Weinshilboum, R. M. (2013). Selective EstrogenReceptor Modulators and Pharmacogenomic Variation in ZNF423
Regulation of BRCA1 Expression: Individualized Breast CancerPrevention. Cancer Discovery, 3(7), 812–825.
Kaphingst, K. A., McBride, C. M., Wade, C., Alford, S. H., Reid, R.,Larson, E., … Brody, L. C. (2012). Patients’ understanding of andresponses to multiplex genetic susceptibility test results.Genetics inMedicine : Official Journal of the American College of MedicalGenetics. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22481132
Kaufman, D. J., Bollinger, J. M., Dvoskin, R. L., & Scott, J. A. (2012).Risky business: risk perception and the use of medical servicesamong customers of DTC personal genetic testing. Journal ofGenetic Counseling, 21(3), 413–422.
Mealiffe, M. E., Stokowski, R. P., Rhees, B. K., Prentice, R. L., Pettinger,M., & Hinds, D. A. (2010). Assessment of clinical validity of abreast cancer risk model combining genetic and clinical information.Journal of the National Cancer Institute, 102(21), 1618–1627.
Michailidou, K., Hall, P., Gonzalez-Neira, A., Ghoussaini, M., Dennis, J.,Milne, R. L., & Easton, D. F. (2013). Large-scale genotypingidentifies 41 new loci associated with breast cancer risk. NatureGenetics, 45(4), 353–361. doi:10.1038/ng.2563.
Offit, K. (2011). Personalized medicine: new genomics, old lessons.Human Genetics, 130(1), 3–14. doi:10.1007/s00439-011-1028-3.
Powell, K. P., Cogswell, W. A., Christianson, C. A., Dave, G., Verma, A.,Eubanks, S., & Henrich, V. C. (2012). Primary care physicians’awareness, experience and opinions of direct-to-consumer genetictesting. Journal of Genetic Counseling, 21(1), 113–126. doi:10.1007/s10897-011-9390-9.
Riordan, S., Rodriguez, D. F., & Kieran, S. (2012). Personal genomictesting as part of the complete breast cancer risk assessment: a casereport. Journal of Genetic Counseling, 21(5), 638–644.
Schwartz, L. M., Woloshin, S., Black, W. C., &Welch, H. G. (1997). Therole of numeracy in understanding the benefit of screening mam-mography. Annals of Internal Medicine, 127(11), 966–972.
Senay, I., & Kaphingst, K. A. (2009). Anchoring-and-adjustment bias incommunication of disease risk. Medical Decision Making : AnInternational Journal of the Society for Medical Decision Making,29(2), 193–201.
van’t Veer, L. J., & Bernards, R. (2008). Enabling personalized cancermedicine through analysis of gene-expression patterns. Nature,452(7187), 564–570. doi:10.1038/nature06915.
Vernon, S.W. (1999). Risk perception and risk communication for cancerscreening behaviors: a review. Journal of the National CancerInstitute Monographs, 25, 101–119. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10854465.
Weitzel, J. N., Blazer, K. R., & Macdonald, D. J. (2011). Genetics,Genomics, and Cancer Risk Assessment State of the Art andFuture Directions in the Era of Personalized Medicine. CA:Cancer Journal for Clinicians, 61(5), 327–359. doi:10.3322/caac.20128.Available.
Howe et al.
Copyright © 2022 FDOKUMEN