Perioperative risk factors affecting hospital stay and hospital costs in open heart surgery for...
10
European Journal of Cardio-thoracic Surgery 11 (1997) 1133 – 1140 Perioperative risk factors affecting hospital stay and hospital costs in open heart surgery for patients ] 65 years old 1 Javier Fernandez a,b, *, Chao Chen a,b , Gail Anolik a , Otto B. Brdlik a,b , Glenn W. Laub a,b , William A. Anderson a,b , Lynn B. McGrath a,b a Di6ision of Cardiothoracic Surgery, Department of Surgery, Deborah Heart and Lung Center, 200 Trenton Road, Browns Mills, New Jersey 08015, USA b Uni6ersity of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School, New Brunswick, New Jersey 08903, USA Received 9 October 1996; received in revised form 10 February 1997; accepted 18 February 1997 Abstract Objective: Demographic changes, associated with increased demands for open heart surgery in the elderly, place increased burden on financial resources. To evaluate perioperative risk factors affecting incidence of hospital events and estimation of hospital charges, 2577 patients ]65 years (range 65–91), operated on from January 1991 to December 1994, were compared with a concurrent cohort of 2642 younger patients. Methods: Statistical analysis, by surgical procedure, focused on hospital mortality, key postoperative complications affecting length of hospital stay and hospital charges. Results: Overall hospital mortality was 4.7%, 3.5% in younger patients versus 6.1% in the older group (P 0.01). Mortality was significantly lower in patients less than 65 years undergoing coronary artery bypass grafting (3% versus 5%, P B0.01) and valve replacement (4% versus 9%, P =0.01). Significant risk factors for hospital death in the elderly: diabetes (P B0.01), hypertension (P B0.01), myocardial infarction (P B0.01) and congestive heart failure (P B0.01). Significant postoperative events, more common in older patients, included prolonged ventilation (P 0.01), congestive heart failure (P 0.01), infection (P 0.01), cerebrovascular accident (P B0.01), and intra aortic balloon pump (P B0.01). Incremental risk factors for morbidity in the elderly were: higher New York Heart Association class, congestive heart failure, emergent operation, and female gender. Mean length of hospital stay for the B65 group was 15.3 versus \19.5 days for the ]65 group (P 0.01). Length of stay over 18 days positively correlated with increased morbidity in both age groups. For patients ]65 years of age, the average hospital charge for open heart surgery was 172% higher for patients with a length of stay greater than 18 days compared with 165% for patients less than 65 years of age. Conclusions: Higher operative mortality and longer length of stay in elderly patients, resulting in increased health care costs, was associated with more co-morbidities. These results suggest interventions designed to reduce congestive heart failure and other co-morbidities may improve patient’s recovery and reduce costs. © 1997 Elsevier Science B.V. Keywords: Risk factors; Hospital stay; Surgery 1. Introduction In recent years we have witnessed increasing numbers of elderly patients referred for cardiac surgery, reflect- ing a general increase in longevity of the population. Increased acceptance of surgical intervention in a popu- lation historically managed by non-surgical methods has contributed heavily to the financial burden of providing open heart surgery (OHS) in an aging popu- lation. Advances in technology contribute to the in- creased acceptance of surgical interventions in the elderly. Important contributions include modern surgi- cal strategies yielding improved results, availability of * Corresponding author. Tel.: +1 609 8936611, ext. 581; fax: +1 609 8930938. 1 Presented at the Tenth Annual Meeting of the European Associa- tion for Cardio-thoracic Surgery, Prague, Czech Republic, 6 – 9 Octo- ber 1996. 1010-7940/97/$17.00 © 1997 Elsevier Science B.V. All rights reserved. PII S1010-7940 97)01216-5
Transcript of Perioperative risk factors affecting hospital stay and hospital costs in open heart surgery for...

European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140
Perioperative risk factors affecting hospital stay and hospital costs inopen heart surgery for patients]65 years old1
Javier Fernandez a,b,*, Chao Chen a,b, Gail Anolik a, Otto B. Brdlik a,b, Glenn W. Laub a,b,William A. Anderson a,b, Lynn B. McGrath a,b
a Di6ision of Cardiothoracic Surgery, Department of Surgery, Deborah Heart and Lung Center, 200 Trenton Road, Browns Mills,New Jersey 08015, USA
b Uni6ersity of Medicine and Dentistry of New Jersey, Robert Wood Johnson Medical School, New Brunswick, New Jersey 08903, USA
Received 9 October 1996; received in revised form 10 February 1997; accepted 18 February 1997
Abstract
Objective: Demographic changes, associated with increased demands for open heart surgery in the elderly, place increasedburden on financial resources. To evaluate perioperative risk factors affecting incidence of hospital events and estimation ofhospital charges, 2577 patients]65 years (range 65–91), operated on from January 1991 to December 1994, were compared witha concurrent cohort of 2642 younger patients. Methods: Statistical analysis, by surgical procedure, focused on hospital mortality,key postoperative complications affecting length of hospital stay and hospital charges. Results: Overall hospital mortality was4.7%, 3.5% in younger patients versus 6.1% in the older group (P�0.01). Mortality was significantly lower in patients less than65 years undergoing coronary artery bypass grafting (3% versus 5%, PB0.01) and valve replacement (4% versus 9%, P=0.01).Significant risk factors for hospital death in the elderly: diabetes (PB0.01), hypertension (PB0.01), myocardial infarction(PB0.01) and congestive heart failure (PB0.01). Significant postoperative events, more common in older patients, includedprolonged ventilation (P�0.01), congestive heart failure (P�0.01), infection (P�0.01), cerebrovascular accident (PB0.01), andintra aortic balloon pump (PB0.01). Incremental risk factors for morbidity in the elderly were: higher New York HeartAssociation class, congestive heart failure, emergent operation, and female gender. Mean length of hospital stay for the B65group was 15.3 versus \19.5 days for the ]65 group (P�0.01). Length of stay over 18 days positively correlated with increasedmorbidity in both age groups. For patients ]65 years of age, the average hospital charge for open heart surgery was 172% higherfor patients with a length of stay greater than 18 days compared with 165% for patients less than 65 years of age. Conclusions:Higher operative mortality and longer length of stay in elderly patients, resulting in increased health care costs, was associatedwith more co-morbidities. These results suggest interventions designed to reduce congestive heart failure and other co-morbiditiesmay improve patient’s recovery and reduce costs. © 1997 Elsevier Science B.V.
Keywords: Risk factors; Hospital stay; Surgery
1. Introduction
In recent years we have witnessed increasing numbers
of elderly patients referred for cardiac surgery, reflect-ing a general increase in longevity of the population.Increased acceptance of surgical intervention in a popu-lation historically managed by non-surgical methodshas contributed heavily to the financial burden ofproviding open heart surgery (OHS) in an aging popu-lation. Advances in technology contribute to the in-creased acceptance of surgical interventions in theelderly. Important contributions include modern surgi-cal strategies yielding improved results, availability of
* Corresponding author. Tel.: +1 609 8936611, ext. 581; fax: +1609 8930938.
1 Presented at the Tenth Annual Meeting of the European Associa-tion for Cardio-thoracic Surgery, Prague, Czech Republic, 6–9 Octo-ber 1996.
1010-7940/97/$17.00 © 1997 Elsevier Science B.V. All rights reserved.PII S 1 0 10 -7940 97 )01216 -5

J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–11401134
Table 1Population profile
B65 yearsb ]65 yearsc PTotal patientsa
n (%)d n (%)d
65–91.1/72.921.8–64.99/55.021.8–91.1/63.8Age range/mean1889 (71.5) 1674 (65.0)Males 3563 (68.3) �0.01
NYHA functional class NS54 (2.1) 64 (2.5)118 (2.3)I
587 (23.0)II 1145 (22.1) 558 (21.2)1482 (58.1)1606 (61.1)3088 (59.6)III
334 (12.7) 342 (13.4)IV 676 (13.0)628 (23.8) 718 (28.0)Diabetes 1346 (25.9) �0.01
�0.011533 (59.8)1327 (50.4)2860 (55.0)Hypertension51 (2.0) 43 (1.7)Liver disorder 94 (1.8) NS
�0.01416 (16.3)545 (20.7)961 (18.5)Morbid obesity346 (13.5) �0.01COPD 608 (11.7) 262 (10.0)834 (32.6) �0.01CHF 1547 (29.8) 713 (27.1)
1950 (74.0) 1949 (76.0)Angina 3899 (75.0) NS281 (10.7) �0.01442 (17.2)723 (13.9)Neuro disorder
970 (37.9) 0.01Prior MI 2059 (39.6) 1089 (41.3)
B0.01Operation1808 (68.4) 1645 (63.8)CABG 3453 (66.2)
80 (3.0) 48 (1.9)128 (2.4)Valve repair326 (12.6)Valve replace 748 (14.3) 422 (16.0)316 (12.3)130 (4.9)446 (8.6)CABG+Valve29 (1.1)Repair+Replace 62 (1.2) 33 (1.2)
213 (8.3)Other cardiac 382 (7.3) 169 (6.4)Previous cardiac
976 (38.0)1813 (34.8) �0.01837 (31.7)Surgery
Operation type0.012284 (95.6)2378 (95.2)4662 (95.4)Elective
59 (2.5)Urgent 105 (2.2) 46 (1.8)45 (1.9)Emergency 120 (2.5) 75 (3.0)
NYHA, New York Heart Association; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; MI, myocardial infarction;CABG, coronary artery bypass grafting.a n=5219.b n=2642.c n=2577.d Denominator corresponds to number of patients in each age cohort.
additional devices such as implantable defibrillators,and newer cardiac valves offering improved hemody-namics and enhanced durability. Our recent experiencewith octogenarians [2] demonstrated acceptable earlyand late results. Other authors have reported similarseries [3,6,13].
The purpose of this research was to investigate age-related differences between preoperative risk factors,hospital events, length of stay (LOS) and hospitalcharges. It was theorized that for older patients, themanagement of and recuperation associated with post-operative complications would result in higher chargesthan for younger patients. It is proposed that betterunderstanding the relationship between age and periop-erative factors, and their impact on how resources areutilized, may lead to an improved model to reducepostoperative morbidity and subsequent cost.
2. Materials and methods
The study population was comprised of 5219 consec-utive patients undergoing open heart surgery at Debo-rah Heart and Lung Center between January 1991 andDecember 1994. This population was divided into twoage cohorts for comparison: patients ]65 years of age(n=2577) and patients B65 years of age (n=2642);ranging in age from 21 to 91 years. The clinical profile,including preoperative risk factors and types of opera-tive procedures performed, is shown in Table 1. Therewere proportionately more males (P�0.01). Co-mor-bidity in patients ]65 years of age was more likely toinclude diabetes, hypertension, chronic obstructive pul-monary disease (COPD), congestive heart failure(CHF), and history of neurological The ma-jority of operations were coronary artery bypass graft

J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140 1135
(CABG) procedures for both age groups. Mean bypassand cross-clamp times were 74.3937.3 min and 38.4921.3 min, respectively. The bypass time (min) was sig-nificantly longer in the ]65 year old (78.4 versus 70.4,P�0.01) as was the crossclamp time (min) (40.6 versus36.3, P�0.01). The mean ejection fraction, similar inboth age groups, as determined by surgical assessmentof cineangiography, was 46.6913.4%. Due to missingvalues, New York Heart Association (NYHA) func-tional status and urgency of operation do not equal thepopulation total.
2.1. Statistical analysis
Hospital charges were retrieved from our accountingsystem. All other clinical information, including demo-graphic variables, medical history, admission and dis-charge dates, operative data and presence ofpostoperative complications were retrieved from thesurgical department’s database.
Initial analysis revealed the distribution of most vari-ables were highly skewed. The skewness was particu-larly obvious in hospital charge and length of hospitalstay. This digression from the normal distribution as-sumed with parametric approach necessitated the use ofnonparametric methods. For comparison of continuousvariables, Kruskal–Wallis test was used. The associa-tion between hospital LOS and hospital charge wasanalyzed by Spearman’s correlation coefficient. Discretevariables having two levels were analyzed by the Fish-er’s exact test. Discrete variables with more than twolevels were analyzed by the x2 method.
Hospital death was analyzed using two different ap-proaches. The first approach assessed whether the pres-ence of risk factors affected hospital mortality. Thisapproach compared the mortality rate for all patientswith and without perioperative risk factors present. Thesecond approach assessed the effect of age on mortalityby comparing mortality rates in the younger and oldergroups for patients having selected risk factors.
Analysis was guided by the assumption that compli-cations affected hospital charge in two interdependentways. First, complications necessitate costly therapeuticinterventions and secondly, complications necessitateadditional hospital days. Complications were comparedfor patients with and without selected preoperative riskfactors to identify those increasing the probability of ahigher hospital charge. Postoperative complicationsthat were similarly managed and of comparable clinicalrelevance were grouped together for the purpose ofstatistical analysis. The composition of groupings aredetailed in the morbidity section. The effect of compli-cations on hospital charge was assessed by comparingmean charges incurred by patients with LOS (admissionto discharge) 518 days with that of LOS\18 days forthe two age cohorts and by recording the mean charges
with the type of surgery. For this series, the 18 daycriteria was based on an institutional mean admissionto operation interval of 4 days and a mean operation todischarge interval of 14 days.
Given the large number of tests performed, the con-ventional criterion for statistical significance (P=0.05)needs to be adjusted by Bonferroni’s inequality, to asmaller P-value. P-values between 0.001–0.01 are pre-sented as PB0.01. P-values B0.001 are presented asP�0.01 and considered strong evidence to supportstatistical significance.
3. Results
The overall hospital mortality was 4.7%. Youngerpatients experienced 93 (3.5%) hospital deaths while inthe older group there were 156 (6.1%) deaths, a highlysignificant difference (P�0.01). Mortality rate washigher in the elderly for most surgical procedures butdifferences were statistically significant only in patientsundergoing isolated coronary bypass (3.1% versus 5%,PB0.01) and isolated valve replacement (4.3% versus8.9%, P=0.01). Cardiac causes of death accounted for74% (n=69) of deaths in the younger group and 53%(n=83) in the elderly. Acute cardiac failure was themost frequent cause of death for both age groups.Non-cardiac causes of death accounted for 26% (n=24) of deaths in the younger group and 47% (n=73) inthe elderly.
Preoperative risk factors for hospital death werecompared by univariate analysis between patients withand without these risk factors in each age group. Fac-tors significant for hospital death in the elderly and inthe young included female gender (PB0.01), higherNYHA functional class (PB0.01), COPD (P=0.02),and CHF (PB0.01). Risk factors which were signifi-cant for hospital death and exclusive to the elderlygroup were diabetes (P=0.03) and type of operation(PB0.01): (in descending order) CABG+valve, valvereplacement, valve repair, CABG, and valve repair+replacement. Surprisingly, morbid obesity reached sig-nificance only in the young (P�0.01). Left ventricularejection fraction was lower in non-survivors in compari-son to survivors in both age groups but the differencedid not reach statistical significance.
Mortality was also compared for patients with selectperioperative risk factors. This analysis identified pa-tients with diabetes (PB0.01), hypertension (P�0.01),CHF (PB0.01) and prior myocardial infarction (PB0.01) as having higher mortality rates in the ]65 yearold group. However, previous cardiac surgery andCOPD at the time of operation did not affect hospitalmortality.

J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–11401136
Table 2Hospital morbidity
B65 years P]65 yearsPost-op complications
n (%)n (%)
106 (4.0) 120 (4.6) NSVentricular arrhythmia27 (1.0) NSHeart block (requiring permanent pacemaker) 42 (1.6)
59 (2.3) NSPeriop myocardial infarction 66 (2.5)63 (2.4) NSCardiac arrest 62 (2.4)
102 (3.9) 140 (5.4)Postop intra aortic balloon pump B0.01127 (4.8) 206 (8.0)Congestive heart failure (inotropes\24 h) �0.01
29 (1.1) NSAcute cardiac failure w/assist device 46 (1.7)NS78 (3.0)Hemodynamic instability (chest closure delay) 77 (2.9)
76 (2.9) �0.01Cerebrovascular accident 41 (1.6)17 (.7) 0.04Neuropsychiatric 7 (.3)
303 (11.5) 324 (12.6)General pulmonarya NS�0.01135 (5.1)Prolonged ventilation (\48 h) 228 (8.8)
14 (.5) 22 (.8) NSRenal dialysisb
137 (5.3) NSBleedingc 111 (4.2)134 (5.1) 223 (8.6)Infectiond �0.01
41 (1.6) 31 (1.2)Vasculare NS
a Bronch+re-intubation, bronchopleural fistula, diaphragmatic paralysis, pneumothorax, pulmonary emboli, pleural effusion+tap, pneumonia,hemothorax, chylothorax, upper respiratory infection (treated).b Peritoneal dialysis, hemodialysis, continuous arterio-venous hemodialysis, ultrafiltration.c Coagulopathy, cardiac tamponade, bleeding, severe (requiring re-entry).d Genitourinary, leg wound, mediastinitis, native valvular, prosthetic valvular, sepsis, sterile sternal dehiscence, superficial sternal wound, intraaortic balloon pump site, other incision a infection, non-incisional (ulcer, wound).e Dissection, embolism, pseudoaneurysm, thrombosis, deep vein thrombosis, amputation, occlusion of graft or artery.
3.1. Morbidity
The prevalence and proportion of postoperativemorbidities, grouped together by clinical relevanceand management, are depicted in Table 2. Significantevents, more common in the older patient group, in-cluded postoperative intra aortic balloon pump(IABP) for low cardiac output (PB0.01), CHFtreated only with inotropes greater than 24 h. (P�0.01), cerebrovascular accident (P�0.01), neuropsy-chiatric symptoms (P=0.04), prolonged ventilationgreater than 48 h (P�0.01) and infection (P�0.01).Acute cardiac failure treated with an assist device oc-curred in both age groups but the difference was notsignificant.
Although univariate analysis did not identify adefinite correlation between preoperative risk factorsand postoperative morbidity, higher NYHA func-tional class and CHF showed a strong correlationwith postoperative complications in the ]65 yearold. In contrast, female gender, diabetes mellitus, andurgency of operation correlated with a smaller num-ber of postoperative events in both age groups. Post-operative infection and prolonged ventilationappeared more commonly in: females, diabetics,higher NYHA functional class III/IV, CHF, patientswith previous cardiac surgery, and in emergent opera-tions (Appendix A).
3.2. Length of stay and charges
In this series, the average interval from admission tooperation was 3.98 days in the B65 year old group and4.33 days in the ]65 year old group (P�0.01). Thisdifference was statistically significant but not relevanteconomically. During this preoperative time interval,catheterization and a variety of medical tests were oftenperformed. The overall LOS was significantly longer inthe ]65 year old: 19.5 versus 15.3 days in the youngergroup (P�0.01). According to operative procedure,longer LOS in the elderly was significant in isolatedCABG (P�0.01), CABG+valve replacement (P�0.01), and valve repair+replacement (P�0.01).
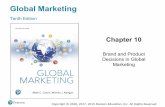
Subtracting the interval between admission and oper-ation, the mean postoperative length of stay was 11.3days for the younger patients and 15.2 days in the oldergroup. Our institutional standard LOS for open heartprocedures is approximately 10–14 days. Reimburse-ment for length of stay varies depending on the con-tract negotiated between the provider and the thirdparty payer. Most patients were discharged from thehospital by the 18th day after admission leaving 461(17.5%) of patients B65 years and 761 (29.6%) ofpatients ]65 years old remaining in the hospital pastthis time. Fig. 1 depicts the length of hospital staydistribution for non-survivors and in each agecohort, represented by coded bars. For non-survivors,

J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140 1137
Fig. 1. Hospital length of stay following open heart procedures. Redand purple bars represent percent of non-surviving patients at eachinterval (total deaths=250: ]65=156, B65=94). Yellow and bluebars indicate percent of patients discharged alive from the hospital atthe indicated intervals (total survivors entered in this calculation=4964: ]65=2416, B65=2548). Percentages indicated at top ofeach bar.
The economic impact on a longer LOS for both agegroups is seen in Table 3 where operative proceduresare listed in ascending order of clinical, operative, andmedical management resource consumption. The morecomplex the surgical procedure, the longer the length ofhospital stay. This finding correlated with a progressiveincrease in hospital charges (r=0.7; P�0.01). Whilethe strength of this correlation is similar overall, theactual charges are higher in the ]65 year old.
For both age groups, length of hospital stay greaterthan 18 days resulted in dramatically higher hospitalcharges. When LOS was 518 days in patients less than65 years of age, mean hospital charge was $39,404. Incontrast, the mean hospital charge was $104,462 for ahospital stay more than 18 days (P�0.01) for the sameage group. This difference was also observed in theolder cohort when, for a LOS518 days, mean hospitalcharge was $42,636 and $116,154 for hospital staysgreater than 18 days (P�0.01).
Table 4 shows a pattern of significantly highercharges overall for hospital deaths compared with hos-pital survivors (PB0.01). It is noteworthy that therewas a dramatic three-fold increase in overall charges fornon-survivors.
4. Discussion
This investigation disclosed a relationship betweenselected perioperative risk factors and hospital death,hospital morbidity and hospital length of stay, andtheir financial impact as reflected in the hospital charge.Several reports have correlated preoperative risk factorswith early operative mortality [5], or morbidity withhospitalization, particularly in the elderly since it ap-pears the cost of open heart surgery for this segment ofthe population is significantly higher than in the young[7–12].
Our study showed that, at the time of surgery, theelderly group was in worse clinical condition whencompared with the younger cohort. The elderly popula-
most deaths occurred early or very late in hospitaliza-tion. In contrast, survivor discharge followed a smoothdescent after the 19th post admission day. The longesthospital stay recorded for non-survivors was 330 daysand for survivors was 219 days.
Univariate analysis identified 15 of the 16 postopera-tive complications reviewed as significant for increasingLOS in the elderly group beyond the 18th day afteradmission (Appendix B). Specifically, heart block, pro-longed ventilation, and CVA had the greatest impacton LOS\18 days. This data also demonstrated olderpatients without these complications had a higher per-centage of hospitalization greater than 18 days thantheir younger counterparts. With the exception of peri-operative MI, cardiac failure, and hemodynamic insta-bility treated by an assist device, the same morbidevents also significantly prolonged hospitalization in theless than 65 year old group but to a lesser degree thanin the ]65 year old. In the younger age group, cere-brovascular accident had the highest impact on LOS\18 days.
Table 3Correlation between length of stay and hospital charges by age group and procedure
B65 years ]65 Years
r*Mean charge $Pr* LOSLOSMean charge $ P
44,122 0.755,852�0.01CABG 0.514.0 18.3 �0.01Valve repair 0.750,725 �0.0116.9 0.7 �0.01 64,557 22.6
81,005 22.8 0.7 �0.01Valve replace 18.160,978 0.5 �0.010.7 �0.01CABG+valve 71,641 19.9 0.7 �0.01 84,655 24.2
0.881,370 23.6Repair+replace �0.010.828.395,832�0.01
Overall, mean charge=$56 663, LOS=17.4 days.LOS, length of stay; CABG, coronary artery bypass grafting.r*=Spearman’s rank correlation coefficient.

J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–11401138
Table 4Comparison of mean hospital charges between hospital survivors and hospital deaths by procedure and age group
B65 years ]65 years
Hospital deaths Hospital survivorsHospital deaths Hospital survivors P* P*
$154,045 $50,554 �0.01CABG �0.01$102 890 $42,195�0.01 $160,914 $55,797Valve repair B0.01$246 131 $42,909
�0.01$71,325$156,462Valve replace �0.01$133 702 $58,145�0.01$76,234CABG+valve $124 709 $68,520 NS $150,822NS$83,340Repair+replace $132 781 $76,229 NS $445,606
Overall: hospital deaths=$141 770, hospital survivors=$52 068; PB0.01.CABG: coronary artery bypass grafting.* Kruskal–Wallis.
tion had a higher incidence of co-morbid conditions,particularly CHF, diabetes, hypertension, COPD, andprevious cardiac surgery, and were more likely to re-quire emergent surgery. New York Heart Associationfunctional class was similar in both groups. Thesebaseline clinical characteristics clearly impacted on hos-pital mortality and was significantly higher in the oldercohort. Overall mortality was, nevertheless, well withinthe ranges reported for OHS in elderly populations[1–3,6,7,13].
The only preoperative risk factors showing a strongcorrelation with postoperative morbidity were increasedNYHA functional class and congestive heart failure. Ingeneral, preoperative risk factors diversely affectedpostoperative events, in varying degrees (as expressedby the magnitudes of individual P values), for both agegroups.
It appeared, from our findings, that younger as wellas older patients affected by morbidity had a commondenominator -a significant increase in length of hospi-talization, an occurrence which has been pointed out byothers [8,9,11]. This finding, in our series, was consis-tently associated with increased hospital charges, as hasbeen previously described. [12] Although the mean hos-pital stay of 17.4 days characterized the average popu-lation, a smaller portion of patients remainedhospitalized beyond this time, an aspect particularlynoted in the older population. Presumably this phe-nomenon in the older population was related to delayedwound healing and prolonged recovery following post-operative complications when compared with theyounger cohort which can ambulate and recuperatemore readily. This series established a clear relationshipbetween increased hospital LOS, charges, and complex-ity of operative procedures performed (r=0.7). Lengthof stay was extended in complex cases such asCABG+valve replacement, or valve repair+replace-ment, as were the charges. Hospital charges were pro-gressively higher with more resource consumption. Thisimpacted most dramatically on elderly non-survivors.Based on these findings, one can surmise that imple-
mentation of measures to decrease postoperative mor-bidity in both age populations (with emphasis on theolder group) would decrease the duration of hospital-ization thereby reducing costs incurred in caring forcardiac surgery patients.
Our results do not extend to answer the question‘‘which patients should be excluded from operation dueto higher risk?’’ but does emphasizes that the therapeu-tic approach in patients with the specific risk factorsmentioned should be planned and managed with ex-treme care preoperatively. As Engelman et al. [4] sug-gests, newer strategies to hasten patient recovery in theimmediate postoperative period, for the young and old,may be promising. At this institution, implementationof strategies to decrease length of stay, including ‘fasttrack’ protocols, same day surgery, and early extuba-tion are underway. Furthermore, advances in linkingfinancial and clinical databases promise to affordgreater ability for building prediction models to identifythe effect of specific co-morbidities on hospital eventsand charges.
In conclusion, the operative mortality in patients]65 years old was significantly higher than in theyounger cohort and was consistent with other publishedreports. Increased length of stay and hospital charges inthe elderly population, strongly related to postoperativecomplications, could be theoretically (and practically)reduced by judicious patient selection and careful plan-ning of operative procedures.
Acknowledgements
The authors wish to thank Marcia Graybeal for thetyping and meticulous revision of the manuscript, RayEllis for figure preparation, William Perkins for exten-sive literature review, Lynn Wang for database organi-zation, Kimberly Dillon for data entry, Gabriela Lanefor programming assistance, and Catherine Stemmerfor assisting table preparation. Special thanks toDr. Frank Lumia for his valuable assistance in review-ing the manuscript.

J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140 1139
Appendix A. Perioperative factors and postoperative morbidity*
Renal dialysis PBleeding P Cardiac IABPInfection P Neuro CVAProlonged ventilationPPP
NS NSNSNYHA class NSB65 NS NSB0.01 B0.01 B0.01(III/IV) ]65 0.04 B0.01B0.01
0.030.02NSCongestive NSB65 0.01 �0.01�0.01 0.02Heart failure ]65 0.03 �0.01 B0.01 NSNS NSUrgency of B65 NS B0.01 B0.01 NS
NSNS NSOperation B0.01]65 B0.01 B0.01NS B0.01 �0.01Female B65 �0.01 NSB0.01
NSNSNSNS]65 B0.01 �0.01NS NSDiabetes B65 0.03 NS NS NSNS NS]65 �0.01 B0.01 NS �0.01
0.02B0.01 NSPrior open B0.01B65 0.02 B0.010.01 NS NS NSHeart surgery ]65 NS NS
NSNSB0.01Hypertension NSB65 0.03 B0.01NS NS]65 B0.01 NS NS NSNS NSPrior MI B65 NS NS NS NS
NSNS NSB0.01]65 NS NS
NYHA, New York Heart Association; MI, myocardial infarction.NS, P]0.05.* For explanation of morbidity, see Section 2.
Appendix B. Effect of morbidity on hospital LOS\18 days
B65 years ]65 years
Complication P valueP value ComplicationComplication ab- Complication ab-present %sent %present %sent %
50.0 �0.01Ventricular arrhythmia 16.6 26.4 0.01 27.9�0.0176.228.2Heart block �0.0116.6 55.6
28.6 45.8 B0.01Perioperative myocardial16.8 25.8 NSinfarction
39.7 NSCardiac arrest 16.7 29.0 0.02 28.727.9 47.9Postop IABP 16.5 30.4 �0.01 �0.0126.8 53.4 �0.01Congestive heart failurea �0.0115.7 44.129.2 10.3Acute cardiac failureb 17.1 15.2 NS 0.02
0.0142.328.5Hemodynamic instability NS16.8 24.7�0.01 27.6Cerebrovascular acci- 72.416.3 63.4 �0.01
dent28.7 58.8Neuropsychiatric 16.9 57.1 0.010.02
48.226.2 �0.01Pulmonary, general �0.0115.3 30.772.8 �0.01Prolonged ventilation 14.8 58.5 �0.01 24.7
28.7 54.6Renal dialysis 16.9 50.0 B0.01 0.0254.027.5 �0.01Bleeding �0.0116.3 33.3
�0.01 25.3 67.7Infection 14.9 �0.0157.567.7 �0.01Vascular 16.5 51.2 �0.01 28.5
a Inotropes greater than 24 h.b With assist device.


J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–1140J. Fernandez et al. / European Journal of Cardio-thoracic Surgery 11 (1997) 1133–11401140
References
[1] Antunes MJ. Valve replacement in the elderly: Is the mechanicalvalve a good alternative? J Thorac Cardiovasc Surg1989;98:485–491.
[2] Cane ME, Chen C, Bailey BM, Fernandez J, Laub GW, Ander-son WA, McGrath LB. CABG in Octogenarians: early and lateevents and actuarial survival in comparison with a matchedpopulation. Ann Thorac Surg 1995;60:1033–1037.
[3] Deviri E, Merin G, Medalion B, Borman JB. Open heart surgeryin Octogenarians: A review. Am J Geriatric Cardiol 1995;4:8,14–16, 41.
[4] Engleman RM. Mechanisms to reduce hospital stays. Ann Tho-rac Surg 1996;61:S26–29.
[5] Holmes L, Loughead K, Treasure T, Gallivan S. Which patientswill not benefit from further intensive care after cardiac surgery?Lancet 1994;344:1200–1202.
[6] Horvath KA, DiSesa VJ, Peigh PS, Couper GS, Collins JJ, CohnLH. Favorable results of coronary artery bypass grafting inpatients older than 75 years. J Thorac Cardiovasc Surg1990;99:92–96.
[7] Katz NM, Ahmed SW, Clark BK, Wallace RB. Predictors oflength of hospitalization after cardiac surgery. Ann Thorac Surg1988;45:656–660.
[8] Katz NM, Hannan RL, Hopkins RA, Wallace RB. Cardiacoperations in patients aged 70 years and over: mortality, lengthof stay and hospital charge. Ann Thorac Surg 1995;60:96–101.
[9] Lahey SJ, Borlase BC, Lavin PT, Levitsky S. Preoperative riskfactors that predict hospital length of stay in coronary arterybypass patients \60 years old. Circulation 1992;86(suppl II):II-181–185.
[10] Mark DB. Implications of cost in treatment selection for patientswith coronary heart disease. Ann Thorac Surg 1996;61:S12–15.
[11] Peigh PS, Swartz MT, Vaca KJ, Lohmann DP, Naumheim KS.Effect of advancing age on cost and outcome of coronary arterybypass grafting. Ann Thorac Surg 1994;58:1362–1367.
[12] Taylor GJ, Mikell FL, Moses W, Dove JT, Katholi RE, MalikSA, Markwell SJ, Korsmeyer C, Schneider JA, Wellons HA.Determinants of hospital charges for coronary artery bypasssurgery: The economic consequences of postoperative complica-tions. Am J Cardiol 1990;65:309–313.
[13] Tsai T-P, Nessim S, Kass RM, Chaux A, Gray RJ, Khan SS,
Blanche C, Utley C, Matloff JM. Morbidity and mortality aftercoronary artery bypass in Octogenarians. Ann Thorac Surg1991;51:983–986.
Appendix C. Conference discussion
Dr W. Mohl (Vienna, Austria): Do you think, that the age is theultimate cause of this length of stay or did you do a stepwise logisticregression, finding out whether co-morbidity would be the mostimport ant factor in older patients because they are more ill, moresick than the others?
Dr J. Fernandez: We did not do the regression equation. We didunivariate and multivariate analysis, and the strongest correlationwas the morbidity with the length of stay. The more morbidity, thegreater the number of postoperative complications and correlatedincrease in length of stay. After 18 days post admission, defined aslength of stay, the cost skyrocketed. Practically, the longer the patientstayed the more the cost.
Dr S. Schueler (Dresden, Germany): Do these data affect yourreimbursement system? The reason I am asking is, that in Germany,we have kind of a fixed rate system where we get reimbursed by fixedrates for each individual procedure regardless of the risk factors ofthe patient. So could you tell me if there is a different negotiationpractice to the health insurance companies in your country?
Dr J. Fernandez: Definitely. Patients over 65 years old are reim-bursed by the government, and you can see that half of the patientsare over 65 years of age. Those that are under 65 years of age arereimbursed by the insurance companies. These companies are puttingpressure on the institutions to decrease costs. There is a widespreadsense at the present time in the US to achieve cost containment. Therestrictions are coming from the third party payers, particularly theinsurance companies but also the government. Does that answer yourquestion?
Dr S. Schueler: But how can you get along with a reimbursementfor these patients?
Dr J. Fernandez: In our institution, as opposed to other institutionsin the United States, traditionally it is subsidized by contributions;20% of the cost is carried out by donations. In a way it is a charityhospital that does not bill the patients. But in general I would saythat many of the institutions do have a big problem in this respect.
.

.