CRITICAL CARE AND PERIOPERATIVE MEDICINE
12
PERIOPERATIVE MEDICINE 0889-8537/00 $15.00 + .OO CRITICAL CARE AND PERIOPERATIVE MEDICINE How Goes the Flow? Douglas B. Coursin, MD, Gerald A. Maccioli, MD, FCCM, and Michael J. Murray, MD, PhD, FCCM HISTORICAL PERSPECTIVE Anesthesiologists actively were involved in the development of modern acute and critical care of children and adults. The polio epidem- ics of the early 1950s provided the initial stimulus for anesthesiologists to demonstrate their value and expertise in patient care management outside the operating room. These activities continued their embryogen- esis, ultimately leading to respiratory care units, the forerunners of modern day ICUs. As this care evolved, specialized areas of the hospital for cohorting and continuing care for unstable medical-surgical patients became routine. The need for further subspecialized care units, in which anesthesiology-based intensivists were leaders, occurred because of the growth of cardiology, cardiac surgery, pediatrics, and neuroscience. Anesthesiologists developed innovative technologies for managing patients in the operating room and ICU, including arterial blood gas and noninvasive ventilatory monitoring, unique ventilatory systems, and a broad pharmacopeia. They helped establish leading specialty organizations, such as the Society of Critical Care Medicine (SCCM) and American Society of Critical Care Anesthesiologists (ASCCA). The From the Departments of Anesthesiology and Internal Medicine; and the Trauma and Life Support Center, University of Wisconsin, Madison, Wisconsin (DBC); Critical Health Systems, Raleigh Practice Center, Raleigh, North Carolina (GAM); Department of Anesthesiology, Mayo Medical School; and the Department of Anesthesiology and Critical Care Service, Mayo Clinic, Rochester, Minnesota (MJM) ANESTHESIOLOGY CLINICS OF NORTH AMERICA VOLUME 18 NUMBER 3 - SEPTEMBER 2000 527
Transcript of CRITICAL CARE AND PERIOPERATIVE MEDICINE
PERIOPERATIVE MEDICINE 0889-8537/00 $15.00 + .OO
CRITICAL CARE AND PERIOPERATIVE MEDICINE
How Goes the Flow?
Douglas B. Coursin, MD, Gerald A. Maccioli, MD, FCCM, and Michael J. Murray, MD, PhD, FCCM
HISTORICAL PERSPECTIVE
Anesthesiologists actively were involved in the development of modern acute and critical care of children and adults. The polio epidem- ics of the early 1950s provided the initial stimulus for anesthesiologists to demonstrate their value and expertise in patient care management outside the operating room. These activities continued their embryogen- esis, ultimately leading to respiratory care units, the forerunners of modern day ICUs. As this care evolved, specialized areas of the hospital for cohorting and continuing care for unstable medical-surgical patients became routine. The need for further subspecialized care units, in which anesthesiology-based intensivists were leaders, occurred because of the growth of cardiology, cardiac surgery, pediatrics, and neuroscience.
Anesthesiologists developed innovative technologies for managing patients in the operating room and ICU, including arterial blood gas and noninvasive ventilatory monitoring, unique ventilatory systems, and a broad pharmacopeia. They helped establish leading specialty organizations, such as the Society of Critical Care Medicine (SCCM) and American Society of Critical Care Anesthesiologists (ASCCA). The
From the Departments of Anesthesiology and Internal Medicine; and the Trauma and Life Support Center, University of Wisconsin, Madison, Wisconsin (DBC); Critical Health Systems, Raleigh Practice Center, Raleigh, North Carolina (GAM); Department of Anesthesiology, Mayo Medical School; and the Department of Anesthesiology and Critical Care Service, Mayo Clinic, Rochester, Minnesota (MJM)
ANESTHESIOLOGY CLINICS OF NORTH AMERICA
VOLUME 18 NUMBER 3 - SEPTEMBER 2000 527
528 COURSIN et a1
American Board of Anesthesiologists (ABA) was the first specialty board to sponsor subspecialty certification in critical care medicine.
Where does the future lie for anesthesiologists who expend signifi- cant time and efforts in the critical care arena? Durbin et a17 provided insight into how, why, and how many anesthesiology trainees enter their residency with a significant interest in critical care medicine. They noted, however, that few individuals continue to pursue formal critical care medicine fellowship training and practice, which is disappointing con- sidering the data demonstrating their need and value. The potential benefit of a strong, recognized, and respected presence of anesthesiolo- gists as attending role models in the ICU may help to increase the number of residents who choose to become anesthesiologist-intensivists. Training program directors also must be committed in their programs to the development of intensivists and to the maintenance of a higher profile practice in and out of the operating rooms.7
The separation of anesthesiology and critical care medicine has occurred mainly in the United States. Throughout much of the world, trainees in anesthesiology spend much time on educational and patient care activities in the ICU. In the United Kingdom and Europe, anesthesi- ology explicitly includes critical care, and is perceived as the same field of practice. This perception contradicts that of the United States, where multiple critical care training programs exist as fellowship training in specialties such as anesthesiology, internal medicine, pediatrics, and surgery. Although ASCCA and SCCM promote a multidisciplinary ap- proach to critical care in the United States, much of critical care remains subspecialty-driven. In Europe and the United Kingdom, the full-time intensivist staff is composed of anesthesiologists. In Germany, anesthesi- ologists costaff emergency departments, and are an integral part of the prehospital helicopter rescue and transport service.
Recently, Drs Charles Durbin, William Hanson, and Gerald Maccioli represented ASCCA in exploring avenues of communication and in establishing an ongoing liaison with the leadership of the American Society of Anesthesiologists (ASA) and other subspecialty groups in ASA to address the needs of current and future anesthesiology-inten- sivists (Hanson, CW, MD, 1999, personal communication). Their dialog hopefully will support these organizations on issues regarding training, certification by the resident review committee, ABA, legislative and government affairs, and reimbursement.
Patients and anesthesiology departments need expert anesthesia- intensive care practitioners to allow critically ill patients to continue to benefit from the ongoing presence and influence of members of the specialty. To secure meaningful participation of anesthesiologists as in- tensivists requires an examination of how future practitioners are trained, what types of practice opportunities exist, and acquisition of data regarding how critical care is practiced optimally. Because of in- creasing cost-containment, strained reimbursement, and reallocation of resources, support of the parent specialty is crucial in dealing with managed care organizations, The Health Care Financing Agency, and third-party payers.

CRITICAL CARE AND PERIOPERATIVE MEDICINE 529
DEMOGRAPHIC CHANGES AND PRACTITIONER REQUIREMENTS
Over the past 3 years, a group of physician societies (i.e., SCCM, the American Thoracic Society, and the American College of Chest Physicians) have conducted a broad and far-reaching study called the Committee on Manpower in Pulmonary and Critical Care Services (COMPACCS). They have demonstrated that there is a large vacuum in the number of providers of critical care services, and have identified a growing need for such specialists. According to the COMPACCS study, 49% of critically ill patients receive no input in their care from a specially trained intensivist. Given the overwhelming data establishing the clinical value of intensivists and the improvements in resource use that their presence makes, physicians and leaders in anesthesiology should foster changes that produce more anesthesiology-based intensivists?, lo,
The need for such services is so great and the supply of qualified practitioners so small that Dr. Breslow and Dr. Rosenfield have formed a telemedicine corporation to allow remote delivery of critical care services by off-site intensivists (Michael Breslow, MD, personal commu- nication, 1999). The pilot study of this means of delivery demonstrated improvements in patient outcome, length of time on mechanical ventila- tion, and resource use.*l
CURRENT PERSPECTIVE
To address the issue of critical care practice by anesthesiologists, the authors pose a simple question that they defended in a recent debate? Does anesthesiology encompass the practice of perioperative medicine? Their answer is yes and that it should continue to do so.2, *, l2 Their practice of critical care medicine facilitates the interface with their pri- mary care colleagues, and distinguishes them from hospitalist~.~~ Periop- erutive medicine is defined as ”the care of medical, obstetric, pediatric, and surgical patients who require preoperative assessment; provision of general, regional, or monitored anesthesia care; critical care; or pain evaluation or managerne~~t.”~ Perioperative medicine should be an inclusive-not exclusive-practice that is provided or directed most frequently by an appropriately trained anesthesiologist.
At its 1998 interim meeting, the American Medical Association endorsed the obvious: anesthesiology is the practice of medicine; and because preoperative evaluation, intraoperative management, critical care medicine, and alleviation of acute and chronic pain are integral activities of physicians, many anesthesiologists currently practice periop- erative medicine (see box on page 530). This comment does not imply that every practitioner should focus his or her energies on all areas in the domain of perioperative medicine. Presently, many anesthesiologists limit much of their time and energy to preoperative assessment and intraoperative care, whereas others exclusively care for the critically ill or patients with acute and chronic pain.
The specialty of anesthesiology is at a defining crossroad. How anesthesiologists choose to proceed determines their future. This article
530 COURSIN et a1
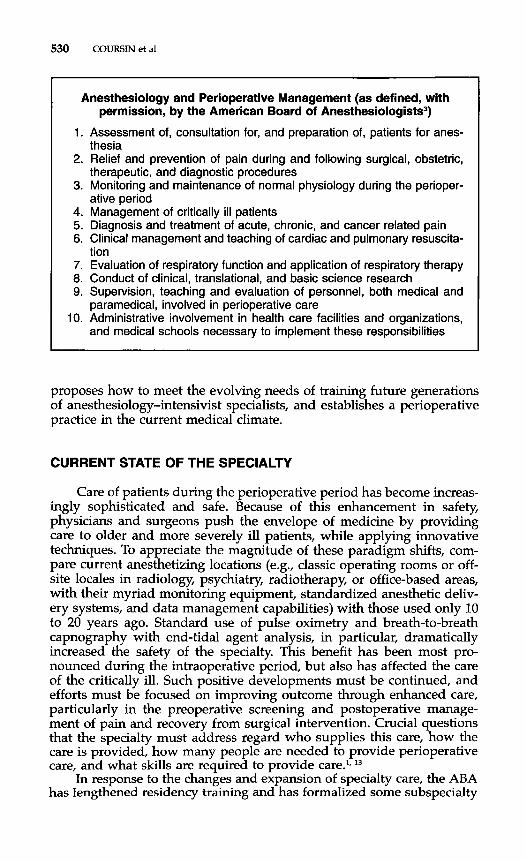
I Anesthesiology and Perioperative Management (as defined, with
permission, by the American Board of Anesthesiologists3)
1. Assessment of, consultation for, and preparation of, patients for anes-
2. Relief and prevention of pain during and following surgical, obstetric,
3. Monitoring and maintenance of normal physiology during the perioper-
4. Management of critically ill patients 5. Diagnosis and treatment of acute, chronic, and cancer related pain 6. Clinical management and teaching of cardiac and pulmonary resuscita-
tion 7. Evaluation of respiratory function and application of respiratory therapy 8. Conduct of clinical, translational, and basic science research 9. Supervision, teaching and evaluation of personnel, both medical and
paramedical, involved in perioperative care 10. Administrative involvement in health care facilities and organizations,
and medical schools necessary to implement these responsibilities
thesia
therapeutic, and diagnostic procedures
ative period
proposes how to meet the evolving needs of training future generations of anesthesiology-intensivist specialists, and establishes a perioperative practice in the current medical climate.
CURRENT STATE OF THE SPECIALTY
Care of patients during the perioperative period has become increas- ingly sophisticated and safe. Because of this enhancement in safety, physicians and surgeons push the envelope of medicine by providing care to older and more severely ill patients, while applying innovative techniques. To appreciate the magnitude of these paradigm shifts, com- pare current anesthetizing locations (e.g., classic operating rooms or off- site locales in radiology, psychiatry, radiotherapy, or office-based areas, with their myriad monitoring equipment, standardized anesthetic deliv- ery systems, and data management capabilities) with those used only 10 to 20 years ago. Standard use of pulse oximetry and breath-to-breath capnography with end-tidal agent analysis, in particular, dramatically increased the safety of the specialty. This benefit has been most pro- nounced during the intraoperative period, but also has affected the care of the critically ill. Such positive developments must be continued, and efforts must be focused on improving outcome through enhanced care, particularly in the preoperative screening and postoperative manage- ment of pain and recovery from surgical intervention. Crucial questions that the specialty must address regard who supplies this care, how the care is provided, how many people are needed to provide perioperative care, and what skills are required to provide
In response to the changes and expansion of specialty care, the ABA has lengthened residency training and has formalized some subspecialty

CRITICAL CARE AND PENOPERATIVE MEDICINE 531
fellowship training3 Along with such changes, the Accreditation Council of Graduate Medical Education (ACGME) has established more struc- tured guidelines to ensure standardization of training. Despite the dra- matic growth in the number and quality of trainees in the late 1980s and early 1990s, the number of American medical graduates pursuing graduate education in anesthesiology has dropped.* This decrease is partly related to economic issues, perceived changes in quality of life, the nationwide push for entry of graduates into primary care specialties, and misperceptions about the specialty. This downward trend may have flattened or reversed. To sustain this favorable reversal, anesthesiologists must be proactive and anticipate future needs and niches. Critical care has strong roots in anesthesiology; ICU heritage must be revisited, and these skills must be applied to innovative, broad-based care of the perioperative patient.
The ASA, ABA, and ACGME, in conjunction with anesthesiology medical educators, investigators, and program directors, must change course to preserve and strengthen the specialty and continue to respond to ongoing changes in health care delivery as a means to improve patient care. As LongneckerI2 warned in his insightful lecture, "Far too often, we have limited our activities to intraoperative care only, and thus have been invisible to our patients [in the preoperative and postoperative periods] ." Critical care remains a natural complementary role to the intraoperative expertise of anesthesiologists; it heightens visibility to patients, other physician groups, and administrators, and is a natural means of interfacing with hospitalists and primary care physicians. The practice of critical care may provide economic avenues worth pursuing and add value to patient care.
The formal program of physicians-in-training must be addressed to prepare these physicians for the rapidly changing landscape of medicine. This review must address how they should be trained, what they need to know, and whether there are a job market and practice opportunities. The specialty of anesthesiology and subspecialty of critical care must anticipate the needs of trainees and their patients and internal consumers (e.g., society, administrators, other physicians, and medical organiza- tions) to ensure participation of competent physicians in a comprehen- sive practice.
TRAINING PARADIGM
Tremendous economic and service pressures have been applied to training directors and programs, which are exacerbated by the decrease in numbers of trainees, growth in service demands, increasingly struc- tured training, limits in patient availability, cost-containment, fiscal and time restrictions on graduate medical education, and a rapidly growing body of information. The current dynamic developments in the fields of molecular biology, human genomics, computer science, and informatics continue to challenge the ability to absorb information and efforts to keep abreast of innovations. As Silverstein" states in a recent commen- tary on medicine in the 21st century, medical schools and centers that catch the wave of informatics, genomics, and electronic medical data bases

532 COURSIN et a1
survive and are positioned to flourish. The same paradigm can be extrapolated to anesthesiology and critical care. The challenge for the specialty is to adapt to and anticipate such changes and develop and apply innovative approaches. Developments to improve patient preoper- ative screening, intraoperative monitoring, drug selection, pain manage- ment, and critical care should be participated in and anticipated.
An outline of a proposed 5-year training continuum is provided.
A Proposed Training Program for Anesthesiologist-Perioperative Physicians
I. Basic-five-year continuum of training* A. Incorporate classic operating room specialty and subspecialty rota-
B. Additional training (2.0 years and 0.5 year elective) tions, pain clinic, and ICU training (2.5 years)
1. Internal Medicine a. outpatient electives in primary care cardiology, preventive
and general medicine, and pediatrics. b. hospitalist training rotation (coordinated with medicine and
surgery). c. greater experience with in-house management of complex
medical and surgical patients (focus on infectious disease, nephrology, pulmonary medicine and specific populations such as the diabetic and patients with ischemia be it CNS, cardiac, or peripheral vascular).
2. Business curriculum (3-6 month section focusing on periopera- tive business issues) a. personnel and time management, b. organizational hierarchy and conflict resolution, c. cost containment, d. negotiating/ bargaining
3. Informatics / statistics-to facilitate data acquisition, data manage- ment, communications, and scientific evaluation of new data and evidence-based medicine
11. Advanced training (optional and individualized) A. Classical subspecialty tract-Critical Care, Pain, Obstetrics, Pediat-
B. Basic scientist tract-GCRC or NIH training center directed, or
C. Management / informatics tract-MBA, MHA, MPH, epidemiol-
This paradigm provides standard clinical training that focuses on op- erating room management, critical care, and pain therapies, supple- mented by expanded modules in business, informatics, computer sci- ence, and statistics. The acquisition of such expertise strengthens the
rics, CV, Neurology, etc.
formal PhD program
ogy tract
*At the end of the basic residency, the trainee would be able to assess perioperative patient risk, be skilled in techniques of intraoperative management and postoperative care including hospital-based care, and be well grounded in business skills including personnel and time management, organizational hierarchy, cost containment, conflict resolution, and informatics.
CRITICAL CARE AND PEIUOPERATIVE MEDICINE 533
scientific basis of the specialty, facilitates application of evidence-based medicine and outcomes research, and enhances business strategies and negotiations. Current Medicare A regulations pay for only up to a maximum of 5 years for primary certification. After 5 years, Medicare provides 50% support for additional training. Any change in the overall training paradigm that increases the duration of training must factor the training costs into physician reimbursement. Specialist intensivists, however, have been shown not only to improve care but enhance re- source use, decreasing overall costs.19 The additional money spent to train such specialists definitely improves patient care, and clinical train- ing programs potentially can recoup more than their direct cost.
Formal training in cardiology, risk stratification, and preventive medicine and broader experience in caring for hospitalized patients with common pathologies can complement the previous base year of the clinical curriculum, and can enhance preoperative assessment and risk stratification. Standard hands-on hospital and clinical patient care, com- bined with didactic sessions and simulated care, would be used.
The approach to research must be redefined to ensure that anesthesi- ologist-perioperative physicians engage in clinical or translational re- search efforts that benefit patient care. The chance of having anesthesiol- ogist-perioperative physicians funded by the National Institutes of Health (NIH) is increasingly remote unless changes in training proac- tively are made. A motivated physician-in-training must be identified and aligned with a mentor, who does not use him or her as a workhorse to finish projects but serves as a guide to ensure that the trainee matures into an independent investigator. Identifying a mentor with current NIH support, preferably one with clinical projects in a general clinical re- search center or with translational bench research complemented by an understanding of clinical priorities and practices, facilitates such efforts.
Fifty percent of physicians who participate in the Clinical Associate Physician program are successful in securing NIH funding at the com- pletion of their program (Judith Vaitukaitis, MD, personal communica- tion, 1999). The National Center for Research Resources oversees general clinical research center programs, and has a projected 22% increase in its funding for the year 2000. This increase in congressionally funded clinical research presents an opportunity for the specialty to ensure that there are enough well-trained anesthesiologist-perioperative physicians available to secure this funding.
PRACTICE MODELS
Various models exist for anesthesiology and critical care medicine practices, and they range from residency-driven academic university centers and nonuniversity programs to private practitioners, single-spe- cialty practices, or those in integrated multidisciplinary group practices without residents. There is marked regional variability in modes of delivery of care (i.e., with or without the anesthesia care team, subspeci- alty practice in groups) and scope (i.e., highly subspecialized, trauma, transplant, pediatric, and so forth) of practice. This pattern of care

Practice Center
Practice Center
Coord inator
Hospital Chairman
Dept of Aries & CCM
Director of Critical Care Medicine
Dept Vice-chairman 1 Director of Pain Management
Medical Director
I
Hospital Committees or Service Line Teams
\ Examples -Critical Care Committee, Blood Utilization Committee, Code Blue Committee, i Information Mangement Committee
534
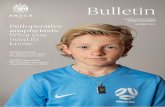
Figure 1. See legend on opposite page
CRITICAL CARE AND PERIOPERATIVJ? MEDICINE 535
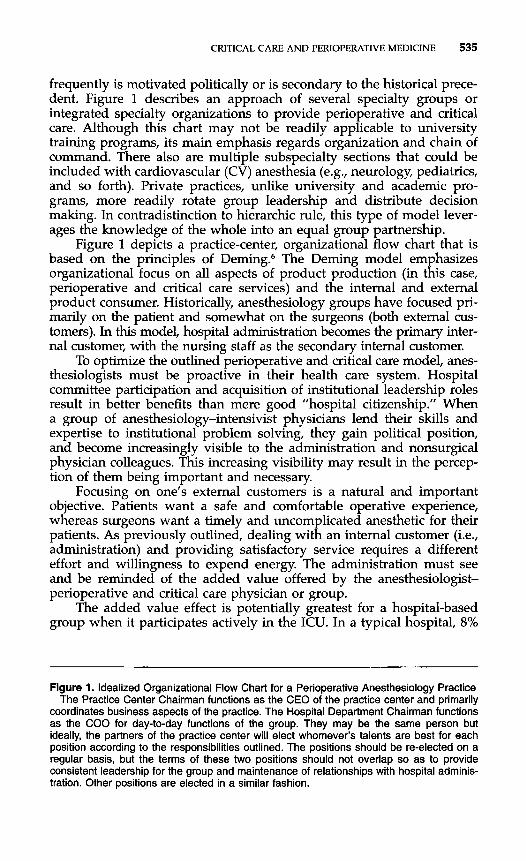
frequently is motivated politically or is secondary to the historical prece- dent. Figure 1 describes an approach of several specialty groups or integrated specialty organizations to provide perioperative and critical care. Although this chart may not be readily applicable to university training programs, its main emphasis regards organization and chain of command. There also are multiple subspecialty sections that could be included with cardiovascular (CV) anesthesia (e.g., neurology, pediatrics, and so forth). Private practices, unlike university and academic pro- grams, more readily rotate group leadership and distribute decision making. In contradistinction to hierarchic rule, this type of model lever- ages the knowledge of the whole into an equal group partnership.
Figure 1 depicts a practice-center, organizational flow chart that is based on the principles of Deming.6 The Deming model emphasizes organizational focus on all aspects of product production (in this case, perioperative and critical care services) and the internal and external product consumer. Historically, anesthesiology groups have focused pri- marily on the patient and somewhat on the surgeons (both external cus- tomers). In this model, hospital administration becomes the primary inter- nal customer, with the nursing staff as the secondary internal customer.
To optimize the outlined perioperative and critical care model, anes- thesiologists must be proactive in their health care system. Hospital committee participation and acquisition of institutional leadership roles result in better benefits than mere good ”hospital citizenship.” When a group of anesthesiology-intensivist physicians lend their skills and expertise to institutional problem solving, they gain political position, and become increasingly visible to the administration and nonsurgical physician colleagues. This increasing visibility may result in the percep- tion of them being important and necessary.
Focusing on one’s external customers is a natural and important objective. Patients want a safe and comfortable operative experience, whereas surgeons want a timely and uncomplicated anesthetic for their patients. As previously outlined, dealing with an internal customer (i.e., administration) and providing satisfactory service requires a different effort and willingness to expend energy. The administration must see and be reminded of the added value offered by the anesthesiologist- perioperative and critical care physician or group.
The added value effect is potentially greatest for a hospital-based group when it participates actively in the ICU. In a typical hospital, 8%
Figure 1. Idealized Organizational Flow Chart for a Perioperative Anesthesiology Practice The Practice Center Chairman functions as the CEO of the practice center and primarily
coordinates business aspects of the practice. The Hospital Department Chairman functions as the COO for day-to-day functions of the group. They may be the same person but ideally, the partners of the practice center will elect whomever’s talents are best for each position according to the responsibilities outlined. The positions should be re-elected on a regular basis, but the terms of these two positions should not overlap so as to provide consistent leadership for the group and maintenance of relationships with hospital adminis- tration. Other positions are elected in a similar fashion.
536 COURSIN et a1
to 10% of in-patient beds are designated as ICU beds. In some centers, an additional 10% to 15% of hospital beds are designated as ICU step- down or intermediate care beds. Critically ill patients typically consume 33% of the resources of an institution, which translates to approximately 1% to 1.5% of the gross national product. Naturally, this expense repre- sents an area of ongoing concern to hospital and governmental adminis- trators.
How can an anesthesiology group address this concern and still maintain excellent patient care and cost-containment? Numerous studies in the past 1 to 10 years have shown that appropriately trained intensiv- ists (see page 532) have profound effects on patient care and resource use in the ICU. Reported benefits include, but are not limited to, reduc- tions in predicted mortality, ICU and hospital length of stay, duration of mechanical ventilation, and resource use.4, 11, 2o Anesthesiologist- perioperative and critical care practitioners can help address a primary focus and concern of the internal customer positively and proactively. The reported reduction in iatrogenic complications; nosocomial infec- tions, such as bacteremia and ventilator-associated pneumonia; acute renal failure, blood product use, and Medicare charges is a positive benefit for the internal and external customer base?, lo, lPl6, 2o Informing administrators and group practice leaders of the added value effect of such a practice is a priority. To provide optimal and cost-effective critical care, these organizations must be provided with fiscal and logistic sup- port or cross-subsidization of such activities.
The skills of anesthesiologists-intensivists who function as intensiv- ists are contradistinct to those of hospitalists, whose primary focus is on in-patient, nonoperative, or out-of-operating-room non-ICU care. By training, hospitalists are not critical care physicians,17 but are partners to the perioperative physician when patients leave the operating room, step-down unit, or ICU venue and are transitioned to general ward care.
The common goal of these approaches is integration between the critical care physician, hospitalist, and primary care physician to provide cost-efficient, state-of-the-art care. This successful integration makes the anesthesiologist-critical care physician increasingly valuable for improv- ing outcome in his or her health care system, and should be a prime goal for the training of the next generation of practitioners.
SUMMARY
The specialty of anesthesiology is at a crossroad. Do anesthesiolo- gists stay in the illusionary safe harbor of the operating room and allow critical care anesthesiologists to float alone? How can in-fighting with other medical and nonmedical providers be avoided, while maintaining or expanding the historic and hopefully future roles of anesthesiologists as hospital-based physicians? A different tact is required to redefine the scope of the practice with broadened training to provide increased expertise in the evolving medical marketplace. This approach would include solid training in business, informatics, data management, and critical thinking on outcomes.

ClUTICAL CARE AND PERIOPERATIVE MEDICINE 537
This paradigm shift may be challenging, and requires redirection, reallocation of assets, re-education, and a new mindset. If successfully applied, however, it presents a means to strengthen the respected position of the specialty and to promote the medical care and practice of periopera- tive specialists in the rapidly changing landscape of modern medicine.
Regarding the question of turf and ownership of the ICU, the authors suggest pursuing the higher ground of an excellent scope of practice, which facilitates the care and activities of surgical and primary care colleagues. These colleagues, administrators, and governmental agencies will have to be re-educated to support training and provide equitable remuneration. Appropriately trained anesthesiologist-intensiv- ists can complement many other care providers, while providing a wide range of services with an economy of care, whether in a semiclosed or closed ICU setting.
References
1. Abt Associates: Estimation of the physician work force requirements in anesthesiology. Park Ridge, IL, American Society of Anesthesiologists, 1994, 1-53
2. Alpert CC, Conroy JM, Roy RC: Anesthesia and perioperative medicine: A department of anesthesiology changes its name. Anesthesiology 84:712-715, 1996
3. American Board of Anesthesiology: Booklet of Information. Raleigh, NC, American Board of Anesthesiology, 1999, pp 1-39
4. Brown JJ, Sullivan G: Effect on ICU mortality of a full-time critical care specialist. Chest 96:127-129, 1989
5. Coursin DB, Maccioli G, Murray MJ: The anesthesiologist as perioperative physician: Three views-pro. Prob Anesth, in press
6. Dobyns L, Crawford-Mason C Thinking About Quality: Progress, Wisdom, and the Deming Philosophy. Times Books, New York, 1994, pp 1-280
7. Durbin CG Jr, McLafferty CL Jr: Attitudes of anesthesiology residents toward critical care medicine. Anesth Analg 77418426, 1993
8. Feeley TW The anesthesiologist as perioperative physician, new challenges, new roles. American Society of Anesthesiologists Refresher Course Lectures. Lecture 2241-7,1998
9. Ghorra S, Reinert SE, Cioffi W, et al: Analysis of the effect of conversion from open to closed surgical intensive care unit. Ann Surg 229:163-171, 1999
10. Hanson CW, Deutschman CS, Anderson HL, et al: The effect of an organized critical care service on outcomes and resource utilization: A prospective cohort study. Crit Care Med 27270-274, 1999
11. Li TC, Phillips MC, Shaw L, et al: On-site physician staffing in a community hospital intensive care unit: Impact on test and procedure use and on patient outcome. JAMA 252:2023, 1984
12. Longnecker DE: Navigation in uncharted waters: Is anesthesiology on course for the 21st century? Anesthesiology 86:736-742, 1997
13. Longnecker DE: Planning the future of anesthesiology. Anesthesiology 84.495-497,1996 14. Manthous CA, Amoateng-Adjepong Y, Al-Kharrat T, et al: Effects of a medical intensiv-
ist on patient care in a community teaching hospital. Mayo Clin Proc 72391-399, 1997 15. Multz AS, Chalfin DB, Samson IM, et al: A closed medical intensive care unit (MICU)
improves resource utilization when compared with an open MICU. Am J Respir Crit Care Med 1571468-1473, 1998
16. Multz AS, Samson I, Scharf S M A closed ICU is more efficient compared to an open ICU. Crit Care Med 25(suppl):A106, 1997
17. Nelson JR, Winthrop FW The hospitalist How we’ve grown, where we’re going. Today’s Internist September/ October: 10-13, 1998
538 COURSIN et a1
18. Pollack MM, Katz RW, Ruttimann UE, et al: Improving the outcome and efficiency of intensive care: The impact of an intensivist. Crit Care Med 16:ll-17, 1988
19. Pronovost P, Jenckes M, Dorman T, et al: Organizational characteristics of intensive care units related to outcomes of abdominal aortic surgery. JAMA 281:1310-1317, 1999
20. Reynolds HN, Haupt MT, Thill-Baharozian MC, et al: Impact of critical care physician staffing on patients with septic shock in a university hospital medical intensive care unit. JAMA 260:344&3450, 1988
21. Rosenfield 8, Dorman T, Pronovost P, et al: Remote management improves ICU outcomes. Crit Care Med 27A153, 1999
22. Silverstein SC. Medicine in the 21st century: Preparing for a paradigm shift. J Investig Med 46342-347, 1998
23. Wachter RM, Goldman L The emerging role of hospitalists in the American health care system. N Engl J Med 335514-517, 1996
Address reprint requests to Douglas B. Coursin, MD
Professor of Anesthesiology and Internal Medicine B6/319 UW CSC
Madison, WI 53792-3272
e-mail: [email protected]