Perfluoropropane gas as a Magnetic Resonance Lung Imaging Contrast Agent in Humans
11
1300 CHEST Original Research IMAGING Original Research N onimaging-based techniques used in diagnosing and monitoring pulmonary function (eg, spirom- etry, arterial blood gas analysis) provide information that is averaged over the communicating airways of both lungs. As a consequence, these techniques are relatively insensitive to subtle changes and, in partic- ular, any regional changes. Medical imaging techniques provide a means to address these limitations through volumetric (3-D acquisitions. Stated in imaging terms, the output from global assessments such as spirometry is extracted from a single voxel (or volume element, ie, the entire lung as a single unit), whereas images have thousands of voxel units yielding regional information. Currently available imaging modalities using either ionizing radi- ation or radioactive tracers include CT imaging, 1-3 which offers exquisite anatomic detail but limited func- tional data, and nuclear medicine techniques such as scintigraphy, 4-7 which offer qualitative ventilation and perfusion information with limited spatial resolu- tion (2-D projection images), single photon emission CT imaging 8,9 with limited spatial resolution, or PET scan 10-12 using radioactive nitrogen gas. Developments in the CT imaging arena include dual-energy-based techniques, assessing pulmonary ventilation through the use of gaseous contrast agents such as xenon and krypton. 13-16 CT imaging has also gained prominence by distinguishing airways-predominant vs emphysema- predominant COPD, 17-19 but concern is increasing regarding radiation dose and increased cancer risk. 20 Background: Fluorine-enhanced MRI is a relatively inexpensive and straightforward technique that facilitates regional assessments of pulmonary ventilation. In this report, we assess its suitability through the use of perfluoropropane (PFP) in a cohort of human subjects with normal lungs and subjects with lung disease. Methods: Twenty-eight subjects between the ages of 18 and 71 years were recruited for imaging and were classified based on spirometry findings and medical history. Imaging was carried out on a Siemens TIM Trio 3T MRI scanner using two-dimensional, gradient echo, fast low-angle shot and three-dimensional gradient echo, volumetric, interpolated, breath-hold examination sequences for proton localizers and PFP functional scans, respectively. Respiratory waveforms and physio- logic signals of interest were monitored throughout the imaging sessions. A region-growing algorithm was applied to the proton localizers to define the lung field of view for analysis of the PFP scans. Results: All subjects tolerated the gas mixture well with no adverse side effects. Images of healthy lungs demonstrated a homogeneous distribution of the gas with sufficient signal-to-noise ratios, while lung images from asthmatic and emphysematous lungs demonstrated increased heteroge- neity and ventilation defects. Conclusions: Fluorine-enhanced MRI using a normoxic PFP gas mixture is a well-tolerated, radiation- free technique for regionally assessing pulmonary ventilation. The inherent physical characteristics and applicability of the gaseous agent within a magnetic resonance setting facilitated a clear dif- ferentiation between normal and diseased lungs. CHEST 2013; 144(4):1300–1310 Abbreviations: 1 H 5 proton; 3 He 5 helium 3; 19 F 5 fluorine 19; 129 Xe 5 xenon 129; FOV 5 field of view; hP 5 hyperpolarized; PFP 5 perfluoropropane; PFx 5 perfluorinated gas; SNR 5 signal-to-noise ratio Perfluoropropane Gas as a Magnetic Resonance Lung Imaging Contrast Agent in Humans Ahmed F. Halaweish, PhD; Richard E. Moon, MD, FCCP; W. Michael Foster, PhD; Brian J. Soher, PhD; H. Page McAdams, MD, FCCP; James R. MacFall, PhD; Maureen D. Ainslie, MS; Neil R. MacIntyre, MD, FCCP; and H. Cecil Charles, PhD Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
Transcript of Perfluoropropane gas as a Magnetic Resonance Lung Imaging Contrast Agent in Humans
1300
CHEST Original ResearchIMAGING
Original Research
Nonimaging-based techniques used in diagnosing and monitoring pulmonary function (eg, spirom-
etry, arterial blood gas analysis) provide information that is averaged over the communicating airways of both lungs. As a consequence, these techniques are relatively insensitive to subtle changes and, in partic-ular, any regional changes.
Medical imaging techniques provide a means to address these limitations through volumetric (3-D acquisitions. Stated in imaging terms, the output from global assessments such as spirometry is extracted from a single voxel (or volume element, ie, the entire lung as a single unit), whereas images have thousands of voxel units yielding regional information. Currently available imaging modalities using either ionizing radi-
ation or radioactive tracers include CT imaging, 1-3 which offers exquisite anatomic detail but limited func-tional data, and nuclear medicine techniques such as scintigraphy, 4-7 which offer qualitative ventilation and perfusion information with limited spatial resolu-tion (2-D projection images), single photon emission CT imaging 8,9 with limited spatial resolution, or PET scan 10-12 using radioactive nitrogen gas. Developments in the CT imaging arena include dual-energy-based techniques, assessing pulmonary ventilation through the use of gaseous contrast agents such as xenon and krypton. 13-16 CT imaging has also gained prominence by distinguishing airways-predominant vs emphysema-predominant COPD, 17-19 but concern is increasing regarding radiation dose and increased cancer risk. 20
Background: Fluorine-enhanced MRI is a relatively inexpensive and straightforward technique that facilitates regional assessments of pulmonary ventilation. In this report, we assess its suitability through the use of perfl uoropropane (PFP) in a cohort of human subjects with normal lungs and subjects with lung disease. Methods: Twenty-eight subjects between the ages of 18 and 71 years were recruited for imaging and were classifi ed based on spirometry fi ndings and medical history. Imaging was carried out on a Siemens TIM Trio 3T MRI scanner using two-dimensional, gradient echo, fast low-angle shot and three-dimensional gradient echo, volumetric, interpolated, breath-hold examination sequences for proton localizers and PFP functional scans, respectively. Respiratory waveforms and physio-logic signals of interest were monitored throughout the imaging sessions. A region-growing algorithm was applied to the proton localizers to defi ne the lung fi eld of view for analysis of the PFP scans. Results: All subjects tolerated the gas mixture well with no adverse side effects. Images of healthy lungs demonstrated a homogeneous distribution of the gas with suffi cient signal-to-noise ratios, while lung images from asthmatic and emphysematous lungs demonstrated increased heteroge-neity and ventilation defects. Conclusions: Fluorine-enhanced MRI using a normoxic PFP gas mixture is a well-tolerated, radiation-free technique for regionally assessing pulmonary ventilation. The inherent physical characteristics and applicability of the gaseous agent within a magnetic resonance setting facilitated a clear dif-ferentiation between normal and diseased lungs. CHEST 2013; 144(4):1300–1310
Abbreviations: 1 H 5 proton; 3 He 5 helium 3; 19 F 5 fl uorine 19; 129 Xe 5 xenon 129 ; FOV 5 fi eld of view; hP 5 hyperpolarized; PFP 5 perfl uoropropane; PFx 5 perfl uorinated gas; SNR 5 signal-to-noise ratio
Perfl uoropropane Gas as a Magnetic Resonance Lung Imaging Contrast Agent in Humans Ahmed F. Halaweish , PhD ; Richard E. Moon , MD , FCCP ; W. Michael Foster , PhD ; Brian J. Soher , PhD ; H. Page McAdams , MD , FCCP ; James R. MacFall , PhD ; Maureen D. Ainslie , MS ; Neil R. MacIntyre , MD , FCCP ; and H. Cecil Charles , PhD
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014

journal.publications.chestnet.org CHEST / 144 / 4 / OCTOBER 2013 1301
Kuethe et al 32 demonstrated the use of perfl uoro-ethane mixed with oxygen to image rat lungs using 19 F MRI and respiratory-triggered imaging. Subse-quently, Schreiber et al 34 demonstrated “breath-hold” imaging of the lungs of ventilated pigs using sulfur-hexafl uoride and “ultrafast” MRI and additionally evaluated dynamic imaging including wash-in/wash-out kinetics of pulmonary ventilation, again in venti-lated pigs. 33 Kauczor et al 35 reviewed various strategies for lung ventilation assessment using MRI in 2002 and cited six animal studies using PFx gases for such purposes.
Advances in the fi eld led to a number of studies in animal models (eg, swine, canine, rodents) 36-39 and excised human lungs, 40,41 demonstrating the suitabil ity of 19 F-enhanced MRI in regional assessments of pul-monary function. The renewable signal characteristics of PFP provide the means for assessing ventilation-defect severity, volume, and gas-trapping severity in patients with COPD and those with asthma, thus, providing a regional insight into the degree of under-lying disease heterogeneity. Here we report, to our knowledge, the fi rst use of PFP-enhanced 3-D MRI in human subjects with normal lung function and var-ious lung disorders as an initial step to elucidate its utility as an imaging tool.
Materials and Methods
This study was approved by the Duke University Medical Cen-ter institutional review board (number PRO-15170) and complied with the Health Insurance Portability Accountability Act; written informed consent was obtained from all subjects prior to partici-pation. The study was accomplished under an investigational new drug designation following US Food and Drug Administration approval. All subjects maintained their dietary routine, normal daily activities, or physical therapy regimens throughout the study to the extent possible. For patients with lung disease, initiation of any new interventions or treatment programs was documented. The inclusion and exclusion criteria for both normal subjects and subjects with lung disease are summarized in Table 1 .
Subject Population
Twenty-eight subjects between the ages of 18 and 71 years were recruited for imaging (clinical referral and/or advertisement). These subjects included nonsmoking normal subjects as well as subjects clinically classifi ed as having COPD, asthma, or under-gone lung transplant. All subjects underwent spirometry in the standard upright position, according to the standards set forth by the American Thoracic Society. Subject demographics, including key spirometric values (FVC, FEV 1 , FEV 1 /FVC ratio, and forced expiratory fl ow) and pre- and postimaging vital signs are summa-rized in Tables 2 and 3 .
Imaging
Imaging was performed on a Siemens TIM Trio 3T MR Scan-ner (Siemens AG) with multinuclear capabilities. Conventional, 1 H localizing scout scans and inspiratory breath-held scans (subject breathing room air) for patient localization and generation of lung masks, respectively, were carried out using the manufacturer’s
In contrast, MRI offers a technique that does not require ionizing radiation or radioactive materials. The general clinical application of MRI uses the intrinsic signals generated from the underlying proton ( 1 H) signal in tissue (eg, water and fat). Due to the low water content in the lung, MRI has seen limited use in the lungs. However, the use of an exogenous contrast agent allows visualization of pulmonary structure and function. For example, hyperpolarized (hP) gas MRI using the stable gaseous isotopes helium 3 ( 3 He) and xenon 129 ( 129 Xe) has offered hope for delivering non-invasive, regional assessment of lung function coupled with conventional MRI to assess structural integrity and variability. 21-26 Unfortunately, the increasing costs and limited supply of 3 He gas 27 limits the feasibility of disseminating the technology within multicenter clinical trials. Thus, attention has turned to 129 Xe hP MRI, 28 facilitating ventilatory, microstructural, and gas-exchange mapping of pulmonary function, with sim-ilar quality to 3 He. 25,26
Perfl uorinated (PFx) gases (eg, perfl uoropropane [PFP]) have been shown to be potentially useful con-trast agents that have the distinct advantages of no anes-thetic effect, high MRI sensitivity (due to molecular symmetry), 29,30 lower cost than hP gases, and availability of multiple liters of gas that enable image acquisition during steady-state breathing. Exploitation of these characteristics, and the lack of a fl ourine 19 ( 19 F) back-ground signal within the body, enables imaging of venti-latory function with a quality similar to that of hP gases.
Several research sites have successfully used PFx gases to image morphology and function in in vivo animal lungs and in ex vivo human lungs. 31-33 In 1998,
Manuscript received October 22, 2012; revision accepted May 1, 2013 . Affi liations: From the Department of Radiology (Drs Halaweish, Soher, MacFall, and Charles and Ms Ainslie); Department of Medicine, Division of Pulmonary Medicine (Drs Moon, Foster, and MacIntyre); Department of Anesthesiology (Dr Moon), GVTU Division; Department of Radiology (Dr McAdams), Division of Chest Radiology; and Department of Radiology (Drs Halaweish and Charles and Ms Ainslie), Duke Image Analysis Laboratory, Duke University School of Medicine, Durham NC. Data from this study have been reported at two conferences (Soher B, Ainslie M, MacFall J, Hashoian R, Charles HC. Lung imaging in humans at 3T using perfl ourinated gases as MR con-trast agents . 2010 Annual Meeting of the International Society of Magnetic Resonance in Medicine, May 2010, Stockholm, Sweden; and Charles HC, MacFall J, Moon R, et al. Initial experience with perfl uorinated gases as lung imaging contrast agents in humans. 2011 American Thoracic Society International Conference, May 2011, Denver, CO). Funding/Support : This study was funded in part by a W. H. Coulter Foundation Translational Partnership Research Award. Correspondence to: H. Cecil Charles, PhD, Duke Image Anal-ysis Laboratory, Duke University School of Medicine–Radiology, DUMC 2702, Durham, NC 27710; e-mail: [email protected] © 2013 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians. See online for more details. DOI: 10.1378/chest.12-2597
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
1302 Original Research
mixtures (79% medical-grade PFP gas and 21% medical-grade oxygen; gas-mixture density: 6.09 g/L). Scanning was initiated after several breaths of PFP-oxygen were taken and contin ued until a steady-state gas concentration in the lung was reached. Each of the acquired breath-holds (about 12-15 s) provided a full 3-D snapshot of the gaseous distribution throughout the airspaces.
Gas Delivery
Using a magnetic resonance compatible pneumotachometer, respiratory waveforms were monitored throughout the duration of the imaging sessions, during both normal room-air breathing and PFP-oxygen gas mixture (Air Liquide SA) breathing. Similarly, oxygen saturation levels and inspiratory and expiratory oxygen and CO 2 levels were monitored throughout with a NONIN 7500FO
body coil. This scan used a 2-D, gradient echo, fast low-angle shot pulse sequence, adjusted for coronal image acquisitions, with the subjects lying feet-fi rst supine (3.125-mm 3 3.125-mm pixels; 15-mm slice thickness; repetition time and echo time : 106 mil-liseconds and 2.72 milliseconds; 128 3 128 acquisition matrix; 40 ° fl ip angle; 400 Hz/pixel bandwidth).
19 F-enhanced acquisitions were performed using a fl exible vest-like coil (Clinical MR Solutions LLC) specifi cally tuned to the frequency of 19 F. These scans were acquired using a 3-D gradient echo volumetric interpolated breath-hold examination similarly adjusted for coronal image acquisitions in the feet-fi rst supine posi-tion (6.25-mm 3 6.25-mm pixels; 15-mm slice thickness, repetition time to echo time : 13 milliseconds/1.62 milliseconds; 64 3 64 acquisi-tion matrix; 70 ° fl ip angle; 130 Hz/pixel bandwidth). End-inspiration, 19 F-enhanced acquisitions were carried out follow ing inspiration of normoxic PFP (molar mass: 188 g/mol; density: 8.17 g/L) gas
Table 1— Study Inclusion and Exclusion Criteria
Inclusion Criteria a Exclusion Criteria b,c
Must be aged � 18 y Unable to undergo 3 T MRI due to contraindications (ie, metal, claustrophobia)Willing and able to comply with procedures Unable to receive gas mixture due to contraindications… Participation in a clinical trial affecting lung function 14 d prior to imaging… Severe, acute, or chronic medical or psychiatric conditions that may increase the
associated risk or interfere with interpretation of results… Women of childbearing potential must have confi rmed negative urine pregnancy
test results on the day of the MR scan
MR 5 magnetic resonance. a Subjects had to have met all inclusion criteria. b Subjects presenting with any of the exclusion criteria were not included. c Imaging was terminated if oxygen saturation levels dropped , 90% at any time during the sessions.
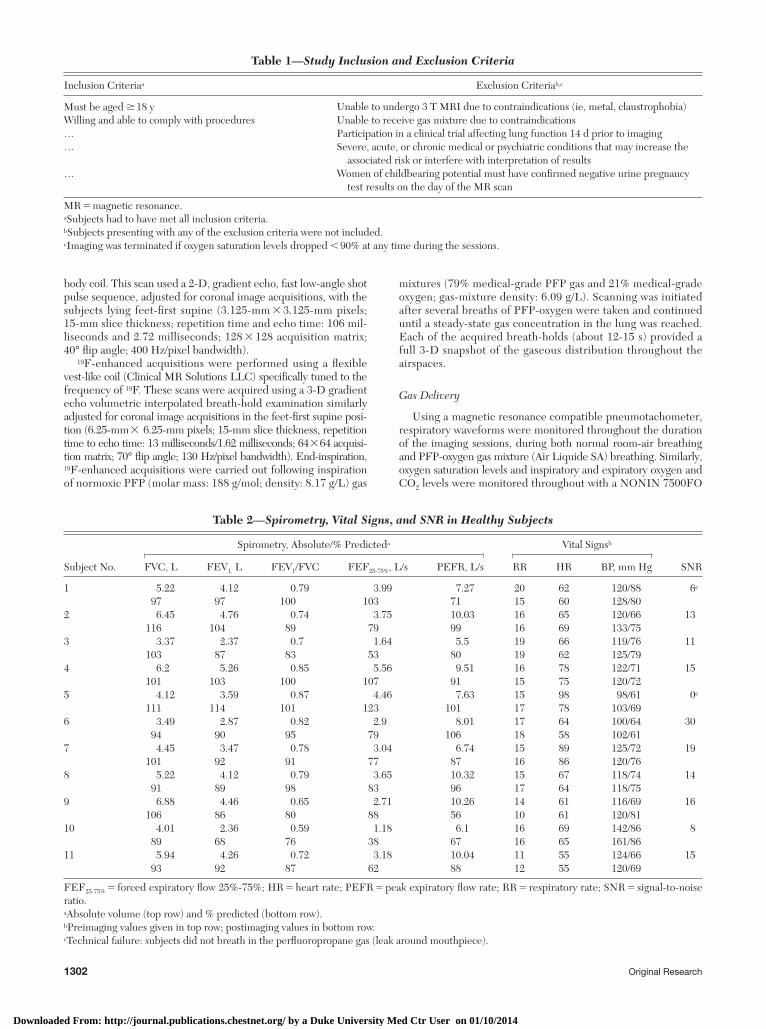
Table 2— Spirometry, Vital Signs, and SNR in Healthy Subjects
Subject No.
Spirometry, Absolute /% Predicted a Vital Signs b
SNRFVC, L FEV 1, L FEV 1 /FVC FEF 25-75% , L/s PEFR, L/s RR HR BP, mm Hg
1 5.22 4.12 0.79 3.99 7.27 20 62 120/88 6 c 97 97 100 103 71 15 60 128/80
2 6.45 4.76 0.74 3.75 10.03 16 65 120/66 13116 104 89 79 99 16 69 133/75
3 3.37 2.37 0.7 1.64 5.5 19 66 119/76 11103 87 83 53 80 19 62 125/79
4 6.2 5.26 0.85 5.56 9.51 16 78 122/71 15101 103 100 107 91 15 75 120/72
5 4.12 3.59 0.87 4.46 7.63 15 98 98/61 0 c 111 114 101 123 101 17 78 103/69
6 3.49 2.87 0.82 2.9 8.01 17 64 100/64 3094 90 95 79 106 18 58 102/61
7 4.45 3.47 0.78 3.04 6.74 15 89 125/72 19101 92 91 77 87 16 86 120/76
8 5.22 4.12 0.79 3.65 10.32 15 67 118/74 1491 89 98 83 96 17 64 118/75
9 6.88 4.46 0.65 2.71 10.26 14 61 116/69 16106 86 80 88 56 10 61 120/81
10 4.01 2.36 0.59 1.18 6.1 16 69 142/86 889 68 76 38 67 16 65 161/86
11 5.94 4.26 0.72 3.18 10.04 11 55 124/66 1593 92 87 62 88 12 55 120/69
FEF 25-75% 5 forced expiratory fl ow 25%-75%; HR 5 heart rate; PEFR 5 peak expiratory fl ow rate; RR 5 respiratory rate; SNR 5 signal-to-noise ratio. a Absolute volume (top row) and % predicted (bottom row). b Preimaging values given in top row; postimaging values in bottom row. c Technical failure: subjects did not breath in the perfl uoropropane gas (leak around mouthpiece).
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
journal.publications.chestnet.org CHEST / 144 / 4 / OCTOBER 2013 1303
(Vacumetrics Inc) was placed inline with the breathing circuit to isolate the subject from the delivery system.
Image Processing
Analysis of the images was performed via semiautomated in-house scripts using the Insight Toolkit library of image process-ing functions (National Library of Medicine) and 3D Slicer ( http://www.slicer.org ) 42-44 for visualization. Lung masks were generated via a semiautomated segmentation of the 1 H lung-cavity images, using a simple region-growing algorithm and three user-placed threshold (image intensity) markers as the threshold criterion. Following generation of the lung masks, the 1 H images were registered to their PFP equivalents through the use of a rigid reg-istration transform, allowing for matching of anatomic and func-tional coverage, and, thus, placing the aforementioned lung masks in the same image space as the PFP datasets. Lung masks were then used to eliminate noise regions outside of the lung fi eld of view (FOV) and allow for proper overlay of the functional maps on top of their anatomic equivalents. Signal-to-noise ratios (SNRs)
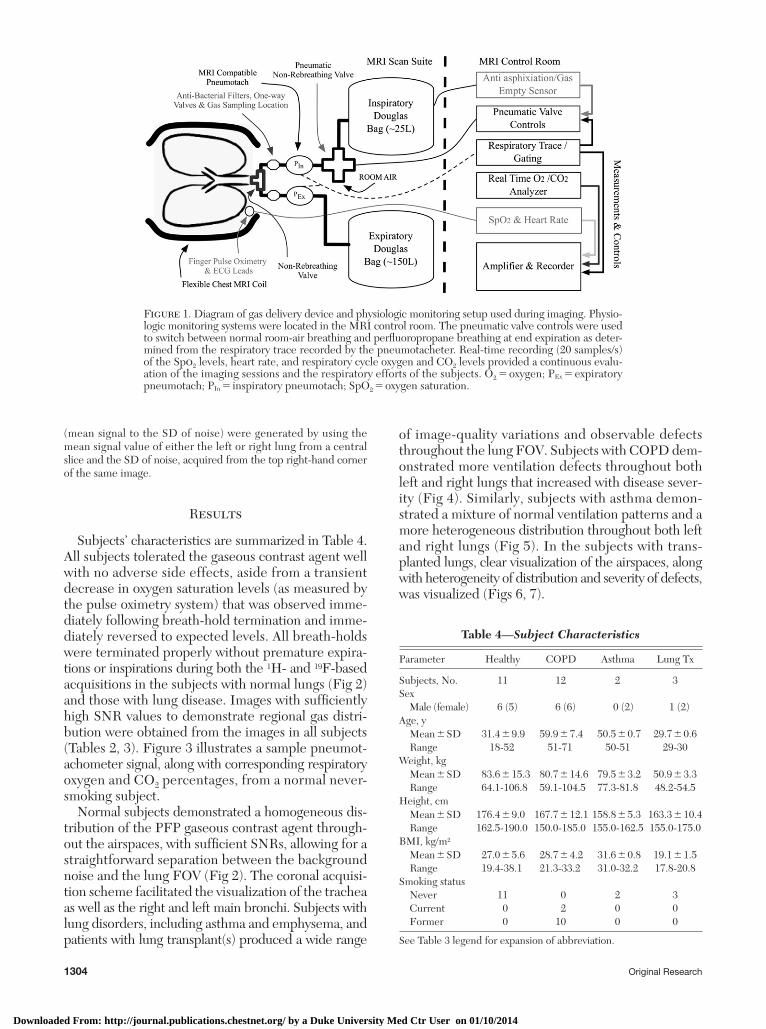
fi nger pulse-oximetry system (Nonin Medical Inc) and an Oxigraf gas analyzer (Oxigraf Inc), respectively ( Fig 1 ).
Gas delivery was accomplished through the use of a magnetic resonance compatible pneumotachometer (Biopac TSD 117 MRI transducer; Biopac Systems Inc), providing calibrated respiratory-cycle data and a robust respiratory gating mechanism, in conjunc-tion with a three-way pneumatically controlled Hans Rudolph Valve (Hans Rudolph Inc) connected to a 25-L Douglas bag containing the PFP-oxygen gas mixture. This setup facilitated remote switch-ing between normal room air and the PFP gas mixture. Subjects were fi tted with either a mouthpiece or an oronasal Hans Rudolph disposable mask and instructed to perform normal respiratory efforts throughout the duration of the imaging, during which several 12-15 s breath-holds at end inspiration were performed. Choice of mask or mouthpiece was assessed prior to imaging based on comfort levels and ability to perform the desired breathing maneu-vers. A nose clip was used in conjunction with the mouthpieces only. Gas samples for monitoring oxygen and CO 2 levels were acquired directly at the mouthpiece/mask for continuous moni-toring throughout the imaging sessions ( Fig 1 ). A Vacumed fi lter
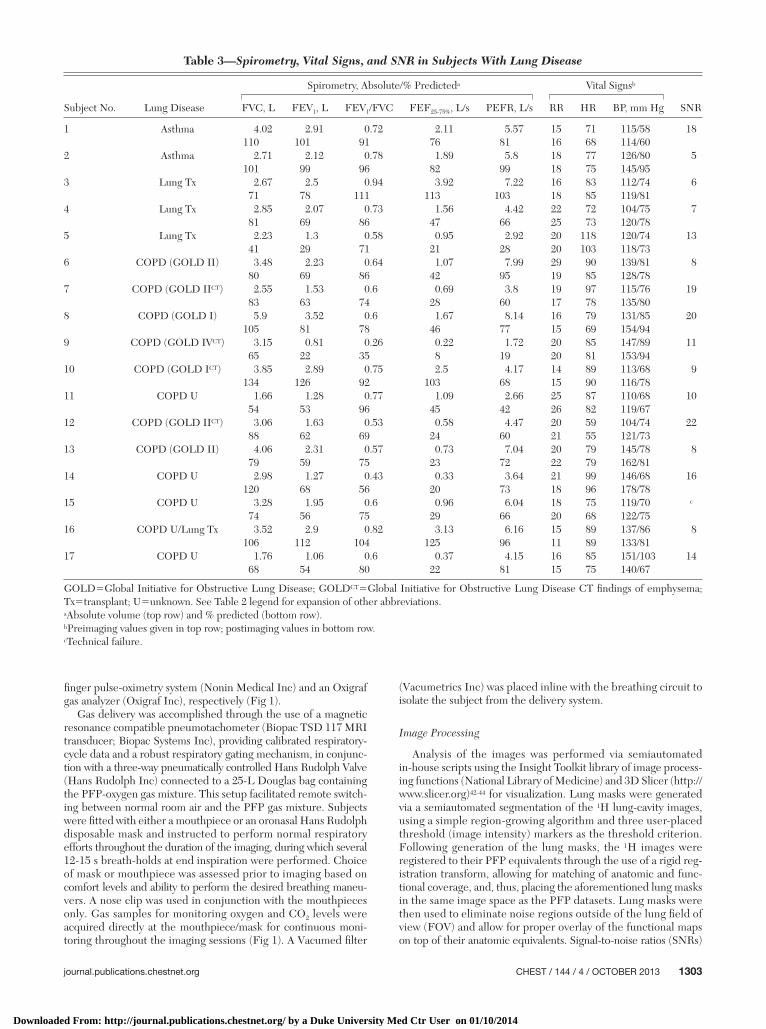
Table 3— Spirometry, Vital Signs, and SNR in Subjects With Lung Disease
Subject No. Lung Disease
Spirometry, Absolute/% Predicted a Vital Signs b
SNRFVC, L FEV 1 , L FEV 1 /FVC FEF 25-75% , L/s PEFR, L/s RR HR BP, mm Hg
1 Asthma 4.02 2.91 0.72 2.11 5.57 15 71 115/58 18110 101 91 76 81 16 68 114/60
2 Asthma 2.71 2.12 0.78 1.89 5.8 18 77 126/80 5101 99 96 82 99 18 75 145/95
3 Lung Tx 2.67 2.5 0.94 3.92 7.22 16 83 112/74 671 78 111 113 103 18 85 119/81
4 Lung Tx 2.85 2.07 0.73 1.56 4.42 22 72 104/75 781 69 86 47 66 25 73 120/78
5 Lung Tx 2.23 1.3 0.58 0.95 2.92 20 118 120/74 1341 29 71 21 28 20 103 118/73
6 COPD (GOLD II) 3.48 2.23 0.64 1.07 7.99 29 90 139/81 880 69 86 42 95 19 85 128/78
7 COPD (GOLD II CT ) 2.55 1.53 0.6 0.69 3.8 19 97 115/76 1983 63 74 28 60 17 78 135/80
8 COPD (GOLD I) 5.9 3.52 0.6 1.67 8.14 16 79 131/85 20105 81 78 46 77 15 69 154/94
9 COPD (GOLD IV CT ) 3.15 0.81 0.26 0.22 1.72 20 85 147/89 1165 22 35 8 19 20 81 153/94
10 COPD (GOLD I CT ) 3.85 2.89 0.75 2.5 4.17 14 89 113/68 9134 126 92 103 68 15 90 116/78
11 COPD U 1.66 1.28 0.77 1.09 2.66 25 87 110/68 1054 53 96 45 42 26 82 119/67
12 COPD (GOLD II CT ) 3.06 1.63 0.53 0.58 4.47 20 59 104/74 2288 62 69 24 60 21 55 121/73
13 COPD (GOLD II) 4.06 2.31 0.57 0.73 7.04 20 79 145/78 879 59 75 23 72 22 79 162/81
14 COPD U 2.98 1.27 0.43 0.33 3.64 21 99 146/68 16120 68 56 20 73 18 96 178/78
15 COPD U 3.28 1.95 0.6 0.96 6.04 18 75 119/70 c
74 56 75 29 66 20 68 122/7516 COPD U/Lung Tx 3.52 2.9 0.82 3.13 6.16 15 89 137/86 8
106 112 104 125 96 11 89 133/8117 COPD U 1.76 1.06 0.6 0.37 4.15 16 85 151/103 14
68 54 80 22 81 15 75 140/67
GOLD 5 Global Initiative for Obstructive Lung Disease; GOLD CT 5 Global Initiative for Obstructive Lung Disease CT fi ndings of emphysema; Tx 5 transplant; U 5 unknown. See Table 2 legend for expansion of other abbreviations. a Absolute volume (top row) and % predicted (bottom row). b Preimaging values given in top row; postimaging values in bottom row. c Technical failure.
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
1304 Original Research
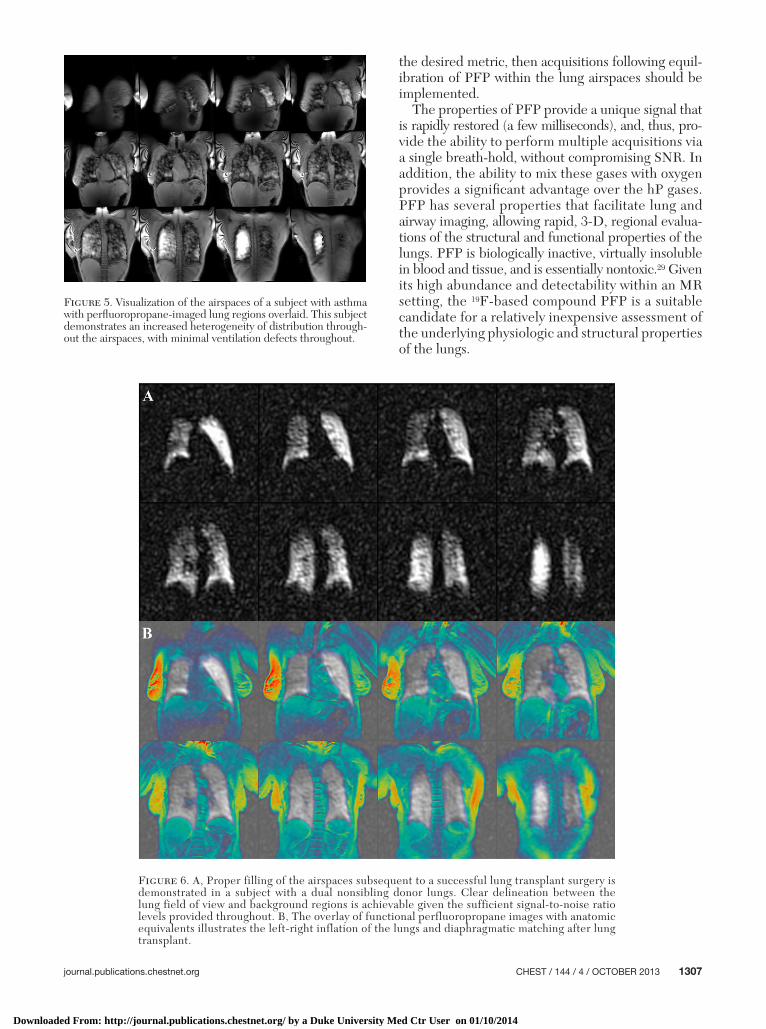
of image-quality variations and observable defects throughout the lung FOV. Subjects with COPD dem-onstrated more ventilation defects throughout both left and right lungs that increased with disease sever-ity ( Fig 4 ). Similarly, subjects with asthma demon-strated a mixture of normal ventilation patterns and a more heterogeneous distribution throughout both left and right lungs ( Fig 5 ). In the subjects with trans-planted lungs, clear visualization of the airspaces, along with heterogeneity of distribution and severity of defects, was visualized ( Figs 6, 7 ).
(mean signal to the SD of noise) were generated by using the mean signal value of either the left or right lung from a central slice and the SD of noise, acquired from the top right-hand corner of the same image.
Results
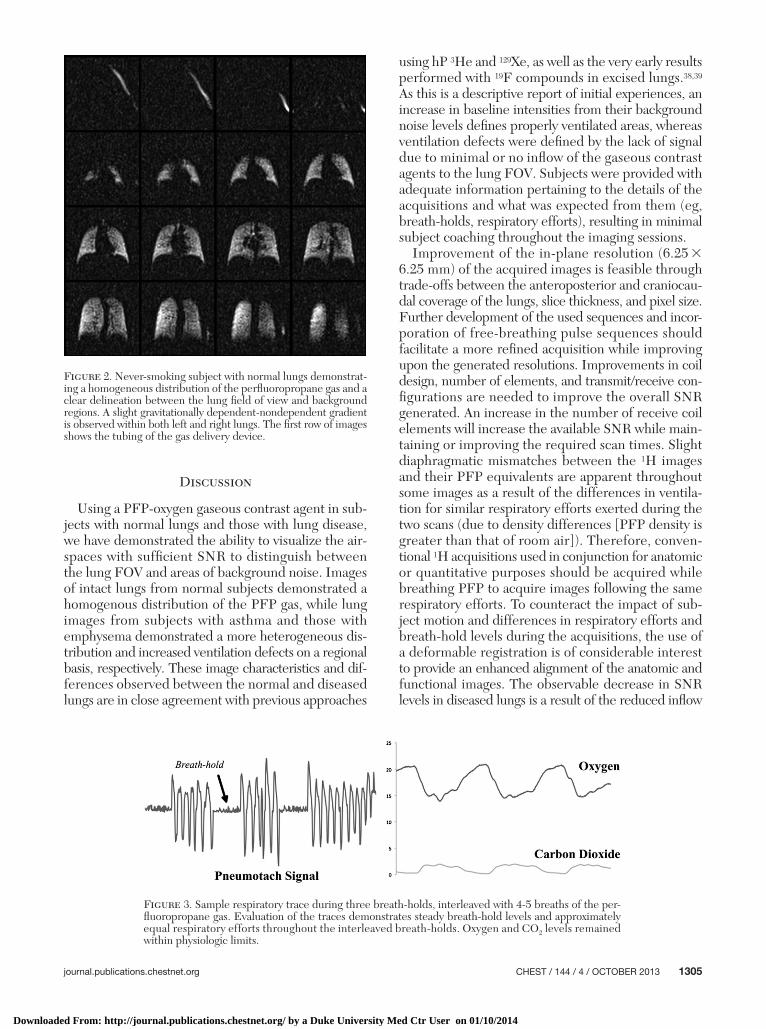
Subjects’ characteristics are summarized in Table 4 . All subjects tolerated the gaseous contrast agent well with no adverse side effects, aside from a transient decrease in oxygen saturation levels (as measured by the pulse oximetry system) that was observed imme-diately following breath-hold termination and imme-diately reversed to expected levels. All breath-holds were terminated properly without premature expira-tions or inspirations during both the 1 H- and 19 F-based acquisitions in the subjects with normal lungs ( Fig 2 ) and those with lung disease. Images with suffi ciently high SNR values to demonstrate regional gas distri-bution were obtained from the images in all subjects ( Tables 2, 3 ). Figure 3 illustrates a sample pneumot-achometer signal, along with corresponding respiratory oxygen and CO 2 percentages, from a normal never-smoking subject.
Normal subjects demonstrated a homogeneous dis-tribution of the PFP gaseous contrast agent through-out the airspaces, with suffi cient SNRs, allowing for a straightforward separation between the background noise and the lung FOV ( Fig 2 ). The coronal acquisi-tion scheme facilitated the visualization of the trachea as well as the right and left main bronchi. Subjects with lung disorders, including asthma and emphysema, and patients with lung transplant(s) produced a wide range
Figure 1. Diagram of gas delivery device and physiologic monitoring setup used during imaging. Physio-logic monitoring systems were located in the MRI control room. The pneumatic valve controls were used to switch between normal room-air breathing and perfl uoropropane breathing at end expiration as deter-mined from the respiratory trace recorded by the pneumotacheter. Real-time recording (20 samples/s) of the Sp o 2 levels, heart rate, and respiratory cycle oxygen and CO 2 levels provided a continuous evalu-ation of the imaging sessions and the respiratory efforts of the subjects. O 2 5 oxygen; P Ex 5 expiratory pneumotach; P In 5 inspiratory pneumotach; SpO 2 5 oxygen saturation.
Table 4— Subject Characteristics
Parameter Healthy COPD Asthma Lung Tx
Subjects, No. 11 12 2 3Sex Male (female) 6 (5) 6 (6) 0 (2) 1 (2)Age, y Mean � SD 31.4 � 9.9 59.9 � 7.4 50.5 � 0.7 29.7 � 0.6 Range 18-52 51-71 50-51 29-30Weight, kg Mean � SD 83.6 � 15.3 80.7 � 14.6 79.5 � 3.2 50.9 � 3.3 Range 64.1-106.8 59.1-104.5 77.3-81.8 48.2-54.5Height, cm Mean � SD 176.4 � 9.0 167.7 � 12.1 158.8 � 5.3 163.3 � 10.4 Range 162.5-190.0 150.0-185.0 155.0-162.5 155.0-175.0BMI, kg/m 2 Mean � SD 27.0 � 5.6 28.7 � 4.2 31.6 � 0.8 19.1 � 1.5 Range 19.4-38.1 21.3-33.2 31.0-32.2 17.8-20.8Smoking status Never 11 0 2 3 Current 0 2 0 0 Former 0 10 0 0
See Table 3 legend for expansion of abbreviation.
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
journal.publications.chestnet.org CHEST / 144 / 4 / OCTOBER 2013 1305
using hP 3 He and 129 Xe, as well as the very early results performed with 19 F compounds in excised lungs. 38,39 As this is a descriptive report of initial experiences, an increase in baseline intensities from their background noise levels defi nes properly ventilated areas, whereas ventilation defects were defi ned by the lack of signal due to minimal or no infl ow of the gaseous contrast agents to the lung FOV. Subjects were provided with adequate information pertaining to the details of the acquisitions and what was expected from them (eg, breath-holds, respiratory efforts), resulting in minimal subject coaching throughout the imaging sessions.
Improvement of the in-plane resolution (6.25 3 6.25 mm) of the acquired images is feasible through trade-offs between the anteroposterior and craniocau-dal coverage of the lungs, slice thickness, and pixel size. Further development of the used sequences and incor-poration of free-breathing pulse sequences should facilitate a more refi ned acquisition while improving upon the generated resolutions. Improvements in coil design, number of elements, and transmit/receive con-fi gurations are needed to improve the overall SNR generated. An increase in the number of receive coil elements will increase the available SNR while main-taining or improving the required scan times. Slight diaphragmatic mismatches between the 1 H images and their PFP equivalents are apparent throughout some images as a result of the differences in ventila-tion for similar respiratory efforts exerted during the two scans (due to density differences [PFP density is greater than that of room air]). Therefore, conven-tional 1 H acquisitions used in conjunction for anatomic or quantitative purposes should be acquired while breathing PFP to acquire images following the same respiratory efforts. To counteract the impact of sub-ject motion and differences in respiratory efforts and breath-hold levels during the acquisitions, the use of a deformable registration is of considerable interest to provide an enhanced alignment of the anatomic and functional images. The observable decrease in SNR levels in diseased lungs is a result of the reduced infl ow
Discussion
Using a PFP-oxygen gaseous contrast agent in sub-jects with normal lungs and those with lung disease, we have demonstrated the ability to visualize the air-spaces with suffi cient SNR to distinguish between the lung FOV and areas of background noise. Images of intact lungs from normal subjects demonstrated a homogenous distribution of the PFP gas, while lung images from subjects with asthma and those with emphysema demonstrated a more heterogeneous dis-tribution and increased ventilation defects on a regional basis, respectively. These image characteristics and dif-ferences observed between the normal and diseased lungs are in close agreement with previous approaches
Figure 2. Never-smoking subject with normal lungs demonstrat-ing a homogeneous distribution of the perfl uoropropane gas and a clear delineation between the lung fi eld of view and background regions. A slight gravitationally dependent-nondependent gradient is observed within both left and right lungs. The fi rst row of images shows the tubing of the gas delivery device.
Figure 3. Sample respiratory trace during three breath-holds, interleaved with 4-5 breaths of the per-fl uoropropane gas. Evaluation of the traces demonstrates steady breath-hold levels and approximately equal respiratory efforts throughout the interleaved breath-holds. Oxygen and CO 2 levels remained within physiologic limits.
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014

1306 Original Research
Figure 4. A, Visualization of the airspaces of a subject with COPD with emphysema. Increased hetero-geneity and ventilation defects are seen in both lungs, with lower signal-to-noise ratio values throughout. A clear difference between the airspaces of the subject with normal lungs and the subject with lung disease can be seen compared to Figure 2 . B, Matching of the functional perfl uoropropane (PFP) maps to their proton-based anatomic equivalents is demonstrated in the lower portion of the image following generation of the lung masks and a simple nonrigid registration of the image spaces. A misalignment in the diaphragmatic region of the images is a result of differences in exerted respiratory efforts between the proton and PFP scans (PFP gas is denser).
of PFP throughout the lung and the regional hetero-geneity of pulmonary ventilation, similar to fi ndings within the hP MRI arena. 45 If the desired quantitative
end point is ventilation-defect volume and severity, acquisitions following a couple of PFP breaths are desired. On the other hand, if ventilation effi ciency is
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
journal.publications.chestnet.org CHEST / 144 / 4 / OCTOBER 2013 1307
the desired metric, then acquisitions following equil-ibration of PFP within the lung airspaces should be implemented.
The properties of PFP provide a unique signal that is rapidly restored (a few milliseconds), and, thus, pro-vide the ability to perform multiple acquisitions via a single breath-hold, without compromising SNR. In addition, the ability to mix these gases with oxygen provides a signifi cant advantage over the hP gases. PFP has several properties that facilitate lung and airway imaging, allowing rapid, 3-D, regional evalua-tions of the structural and functional properties of the lungs. PFP is biologically inactive, virtually insoluble in blood and tissue, and is essentially nontoxic. 29 Given its high abundance and detectability within an MR setting, the 19 F-based compound PFP is a suitable candidate for a relatively inexpensive assessment of the underlying physiologic and structural properties of the lungs.
Figure 5. Visualization of the airspaces of a subject with asthma with perfl uoropropane-imaged lung regions overlaid. This subject demonstrates an increased heterogeneity of distribution through-out the airspaces, with minimal ventilation defects throughout.
Figure 6. A, Proper filling of the airspaces subsequent to a successful lung transplant surgery is demonstrated in a subject with a dual nonsibling donor lungs. Clear delineation between the lung field of view and background regions is achievable given the sufficient signal-to-noise ratio levels provided throughout. B, The overlay of functional perfluoropropane images with anatomic equivalents illustrates the left-right inflation of the lungs and diaphragmatic matching after lung transplant.
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014

1308 Original Research
Ms Ainslie: contributed to concept and design of the study and writing and revising of the manuscript and provided managerial support through subject recruitment and scheduling. Dr MacIntyre: contributed to concept and design of the study and writing and revising of the manuscript and provided clinical and patient selection support. Dr Charles: contributed to concept and design of the study and writing and revising of the manuscript, was involved in all critical aspects of the study design and implementation, and served as the guarantor of the manuscript and senior author overseeing the study from concept to completion. Financial/nonfi nancial disclosures: The authors have reported to CHEST the following confl icts of interest: Drs Charles and Soher are listed as inventors on patent application serial number 61/305,025, fi led February 16, 2010, and titled “Systems, methods, compositions and devices for in vivo magnetic resonance imaging of lungs using perfl uorinated gas mixtures.” Dr Charles has received funding or will receive funding related to this general area of research from the National Institutes of Health and Merck & Co Inc. He is an inventor on the patent related to this research that is assigned to Duke University. The other authors have reported that no potential confl icts of interest exist with any companies/organi-zations whose products or services may be discussed in this article .
Acknowledgments Author contributions: Dr Halaweish had full access to all the data in the study and takes responsibility for the integrity and the accuracy of the data analysis. Dr Halaweish: contributed to the overall concept and design of the study, implementation of the data analysis, and writing and editing of the manuscript; and served as principle author. Dr Moon: contributed to the overall concept and design of the study and the writing and revising of the manuscript and provided mixed-gas expertise throughout. Dr Foster: contributed to concept and design of the study and the writing and revising of the manuscript and provided pulmonary function testing support and a physiologic perspective of the probed structure and function. Dr Soher: contributed to the concept and design of the study, modifi cation of the MRI pulse sequences, and writing and revis-ing of the manuscript. Dr McAdams: contributed to concept and design of the study and writing and revising of the manuscript and provided a radiologic perspective toward the acquired images. Dr MacFall: contributed to concept and design of the study and writing and revising of the manuscript.
Figure 7. A, Airspaces of a lung transplant recipient, following a single sibling-lung transplant (right lung). Both left and right lungs had developed bronchiolitis obliterans (BOS) following an earlier, dual, nonsi-bling transplant. Visualization via perfl uoropropane provides a regional evaluation of the distribution throughout and function of the lungs. It can be clearly seen that the BOS lung (left lung) has severe ventilation defects with minimal function, while the newly transplanted lung (right lung) shows signifi cantly improved distribution and minimal ventilation defects. B, Matching CT slices demonstrate the structural integrity of the lungs after lung transplant.
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014
journal.publications.chestnet.org CHEST / 144 / 4 / OCTOBER 2013 1309
Correlation with lung function . Am J Respir Crit Care Med . 2000 ; 162 ( 3 pt 1 ): 1102 - 1108 .
18 . Han MK , Agusti A , Calverley PM , et al . Chronic obstructive pulmonary disease phenotypes: the future of COPD . Am J Respir Crit Care Med . 2010 ; 182 ( 5 ): 598 - 604 .
19 . Han MK , Kazerooni EA , Lynch DA , et al ; COPDGene Inves-tigators . Chronic obstructive pulmonary disease exacerbations in the COPDGene study: associated radiologic phenotypes . Radiology . 2011 ; 261 ( 1 ): 274 - 282 .
20 . Redberg RF . Cancer risks and radiation exposure from com-puted tomographic scans: how can we be sure that the ben-efits outweigh the risks? Arch Intern Med . 2009 ; 169 ( 22 ): 2049 - 2050 .
21 . MacFall JR , Charles HC , Black RD , et al . Human lung air spaces: potential for MR imaging with hyperpolarized He-3 . Radiology . 1996 ; 200 ( 2 ): 553 - 558 .
22 . Conradi MS , Yablonskiy DA , Woods JC , et al . 3He diffusion MRI of the lung . Acad Radiol . 2005 ; 12 ( 11 ): 1406 - 1413 .
23 . Woods JC , Choong CK , Yablonskiy DA , et al . Hyperpolarized 3He diffusion MRI and histology in pulmonary emphysema . Magn Reson Med . 2006 ; 56 ( 6 ): 1293 - 1300 .
24 . Zheng J , Leawoods JC , Nolte M , et al . Combined MR proton lung perfusion/angiography and helium ventilation: poten-tial for detecting pulmonary emboli and ventilation defects . Magn Reson Med . 2002 ; 47 ( 3 ): 433 - 438 .
25 . Driehuys B , Martinez-Jimenez S , Cleveland ZI , et al . Chronic obstructive pulmonary disease: safety and tolerability of hyper-polarized 129Xe MR imaging in healthy volunteers and patients . Radiology . 2012 ; 262 ( 1 ): 279 - 289 .
26 . Kaushik SS , Cleveland ZI , Cofer GP , et al . Diffusion-weighted hyperpolarized (129)Xe MRI in healthy volunteers and sub-jects with chronic obstructive pulmonary disease . Magn Reson Med . 2011 ;65( 4 ): 1154 - 1165 .
27 . Wittenberg LJ , Cameron EN , Kulcinski GL , et al . A review of He-3 resources and acquisition for use as fusion fuel . Fusion Technol. 1992 ; 21 ( 4 ): 2230 - 2253 .
28 . Patz S , Muradian I , Hrovat MI , et al . Human pulmonary imag ing and spectroscopy with hyperpolarized 129Xe at 0.2T . Acad Radiol . 2008 ; 15 ( 6 ): 713 - 727 .
29 . Ruiz-Cabello J , Barnett BP , Bottomley PA , Bulte JW . Fluorine ( 19 F) MRS and MRI in biomedicine . NMR Biomed . 2011 ; 24 ( 2 ): 114 - 129 .
30 . Willock DJ . Molecular Symmetry . Vol 1 . Hoboken, NJ : John Wiley & Sons Inc ; 2009 .
31 . Rinck PA , Petersen SB , Lauterbur PC . NMR imaging of fl u-orine-containing substances. 19-Fluorine ventilation and per-fusion studies [in German] . ROFO Fortschr Geb Rontgenstr Nuklearmed . 1984 ; 140 ( 3 ): 239 - 243 .
32 . Kuethe DO , Caprihan A , Fukushima E , Waggoner RA . Imag-ing lungs using inert fl uorinated gases . Magn Reson Med . 1998 ; 39 ( 1 ): 85 - 88 .
33 . Schreiber WG , Eberle B , Laukemper-Ostendorf S , et al . Dynamic (19)F-MRI of pulmonary ventilation using sulfur hexafl uoride (SF(6)) gas . Magn Reson Med . 2001 ; 45 ( 4 ): 605 - 613 .
34 . Schreiber WG , Weiler N , Kauczor HU , et al . Ultrafast MRI of lung ventilation using hyperpolarized helium-3 [in German] . ROFO Fortschr Geb Rontgenstr Nuklearmed . 2000 ; 172 ( 2 ): 129 - 133 .
35 . Kauczor HU , Hanke A , Van Beek EJ . Assessment of lung ventilation by MR imaging: current status and future per-spectives . Eur Radiol . 2002 ; 12 ( 8 ): 1962 - 1970 .
36 . Pérez-Sánchez JM , Pérez de Alejo R , Rodríguez I , Cortijo M , Peces-Barba G , Ruiz-Cabello J . In vivo diffusion weighted 19 F MRI using SF6 . Magn Reson Med . 2005 ; 54 ( 2 ): 460 - 463 .
37 . Ruiz-Cabello J , Pérez-Sánchez JM , Pérez de Alejo R , et al . Diffusion-weighted 19 F-MRI of lung periphery: Influence
Role of sponsors: The sponsor had no role in the design of the study, the collection and analysis of the data, or the preparation of the manuscript. Other contributions : The authors thank Ralph S. Hashoian (Clinical MR Solutions LLC) for his efforts in RF coil development; Samantha Womack, BS, for her efforts in subject recruitment, spi-rometry, and screening; and Wandra Davis, RT(R)(MR), for oper-ation of the MRI scanner and experimental setup. We would also like to thank Siemens Healthcare (Siemens Corp) for their con-tinuous MRI support, and Air Liquide SA (formerly Scott Specialty Gases) for the gas supply.
References 1 . van Beek EJR , Hoffman EA . Functional imaging: CT and
MRI . Clin Chest Med . 2008 ; 29 ( 1 ): 195 - 216 . 2 . Chon D , Simon BA , Beck KC , et al . Differences in regional
wash-in and wash-out time constants for xenon-CT ventila-tion studies . Respir Physiol Neurobiol . 2005 ; 148 ( 1-2 ): 65 - 83 .
3 . Hoffman EA , Tajik JK , Kugelmass SD . Matching pulmonary structure and perfusion via combined dynamic multislice CT and thin-slice high-resolution CT . Comput Med Imaging Graph . 1995 ; 19 ( 1 ): 101 - 112 .
4 . Milic-Emili J . Regional distribution of pulmonary ventilation [in French] . Poumon Coeur . 1968 ; 24 ( 9 ): 1007 - 1018 .
5 . Milic-Emili J. Regional distribution of gas in the lung . Can Resp J . 2000 ; 7 ( 1 ): 71 - 76 .
6 . Milic-Emili J , Henderson JA , Dolovich MB , Trop D , Kaneko K . Regional distribution of inspired gas in the lung . J Appl Physiol . 1966 ; 21 ( 3 ): 749 - 759 .
7 . Nyrén S , Mure M , Jacobsson H , Larsson SA , Lindahl SG . Pulmonary perfusion is more uniform in the prone than in the supine position: scintigraphy in healthy humans . J Appl Physiol . 1999 ; 86 ( 4 ): 1135 - 1141 .
8 . Meignan MA . Lung ventilation/perfusion SPECT: the right technique for hard times . J Nucl Med . 2002 ; 43 ( 5 ): 648 - 651 .
9 . Suga K . Technical and analytical advances in pulmonary ven-tilation SPECT with xenon-133 gas and Tc-99m-Technegas . Ann Nucl Med . 2002 ; 16 ( 5 ): 303 - 310 .
10 . Musch G , Layfi eld JD , Harris RS , et al . Topographical dis-tribution of pulmonary perfusion and ventilation, assessed by PET in supine and prone humans . J Appl Physiol . 2002 ; 93 ( 5 ): 1841 - 1851 .
11 . Vidal Melo MF , Layfi eld D , Harris RS , et al. Quantifi cation of regional ventilation-perfusion ratios with PET . J Nucl Med . 2003 ; 44 ( 12 ): 1982 - 1991 .
12 . Wellman TJ , Winkler T , Costa EL , et al. Measurement of regional specific lung volume change using respiratory-gated PET of inhaled 13N-nitrogen . J Nucl Med . 2010 ; 51 ( 4 ): 646 - 653 .
13 . Chae EJ , Seo JB , Goo HW , et al . Xenon ventilation CT with a dual-energy technique of dual-source CT: initial experience . Radiology . 2008 ; 248 ( 2 ): 615 - 624 .
14 . Chae EJ , Seo JB , Lee J , et al . Xenon ventilation imaging using dual-energy computed tomography in asthmatics: initial experience . Invest Radiol . 2010 ; 45 ( 6 ): 354 - 361 .
15 . Ferda J , Ferdová E , Mírka H , et al . Pulmonary imaging using dual-energy CT, a role of the assessment of iodine and air distribution . Eur J Radiol . 2011 ; 77 ( 2 ): 287 - 293 .
16 . Hachulla AL , Pontana F , Wemeau-Stervinou L , et al . Krypton ventilation imaging using dual-energy CT in chronic obstruc-tive pulmonary disease patients: initial experience . Radiology . 2012 ; 263 ( 1 ): 253 - 259 .
17 . Nakano Y , Muro S , Sakai H , et al . Computed tomographic mea-surements of airway dimensions and emphysema in smokers.
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014

1310 Original Research
42 . The Insight Segmentation and Registration Toolkit. National Library of Medicine/ITK website. http://www.itk.org .
43 . 3D Slicer: A multi-platform, free and open-source software package for visualization and medical image computing. 3D Slicer website . http://www.slicer.org . Accessed August 1, 2013.
44 . Pieper SLB , Schroeder W , Kikinis R . The NA-MIC Kit: ITK, VTK, pipelines, grids and 3D slicer as an open platform for the medical image computing community . Proceedings of the 3rd IEEE International Symposium on Biomedical Imaging: From Nano to Macro . 2006 ; 698 - 701 .
45 . Fain S , Schiebler ML , McCormack DG , Parraga G . Imaging of lung function using hyperpolarized helium-3 magnetic resonance imaging: review of current and emerging trans-lational methods and applications . J Magn Reson Imaging . 2010 ; 32 ( 6 ): 1398 - 1408 .
of pressure and air-SF6 composition on apparent diffu-sion coeffi cients . Respir Physiol Neurobiol . 2005 ; 148 ( 1-2 ): 43 - 56 .
38 . Jacob RE , Chang YV , Choong CK , et al . 19 F MR imaging of ventilation and diffusion in excised lungs . Magn Reson Med . 2005 ; 54 ( 3 ): 577 - 585 .
39 . Wolf U , Scholz A , Heussel CP , Markstaller K , Schreiber WG . Subsecond fl uorine-19 MRI of the lung . Magn Reson Med . 2006 ; 55 ( 4 ): 948 - 951 .
40 . Scholz AW , Wolf U , Fabel M , et al . Comparison of magnetic resonance imaging of inhaled SF(6) with respiratory gas analysis . Magn Reson Imaging . 2009 ; 27 ( 4 ): 549 - 556 ..
41 . Conradi MS , Saam BT , Yablonskiy DA , Woods JC . Hyperpo-larized 3He and perfl uorocarbon gas diffusion MRI of lungs . Prog Nucl Magn Reson Spectrosc . 2006 ; 48 ( 1 ): 63 - 83 .
Downloaded From: http://journal.publications.chestnet.org/ by a Duke University Med Ctr User on 01/10/2014