Peer Stressors and Gender Differences in Adolescents' Mental Health: The TRAILS Study
7
Original article Peer Stressors and Gender Differences in Adolescents’ Mental Health: The TRAILS Study Martin P. Bakker, M.Sc. a,b, *, Johan Ormel, Ph.D. a,b,c , Frank C. Verhulst, Ph.D. d , and Albertine J. Oldehinkel, Ph.D. a,b,c,d a Interdisciplinary Center for Psychiatric Epidemiology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands b Graduate School of Health Sciences (SHARE), University Medical Center Groningen, University of Groningen, Groningen, The Netherlands c Graduate School of Behavioral and Cognitive Neurosciences (BCN), University Medical Center Groningen, University of Groningen, Groningen, The Netherlands d Department of Child and Adolescent Psychiatry, Erasmus University Medical Center – Sophia Children’s Hospital Rotterdam, Rotterdam, The Netherlands Manuscript received April 17, 2009; manuscript accepted October 8, 2009 Purpose: This study tested two hypotheses about gender-specific mental health effects of peer stressors during early adolescence: (1) boys and girls are sensitive to different types of peer stressors, and (2) peer stress is associated with different mental health problems in boys and girls. Methods: These two hypotheses were tested in a prospective large population cohort of 2,084 Dutch young adolescents. Internalizing and externalizing problems were measured at baseline and follow-up, whereas stressful life events in the period between baseline and follow-up were measured retrospec- tively at follow-up. We performed the analyses with two types of peer stressors; victimization at school and relationship losses. Results: Relationship losses were more strongly associated with internalizing and externalizing prob- lems in girls than boys, supporting the first hypothesis. Peer victimization at school was also associated with both types of mental health problems, but equally strong in boys and girls. Conclusions: Peer stress is unlikely to be associated with different mental health problems in boys and girls. Instead, boys and girls are more likely to be susceptible to different types of peer stressors. Ó 2010 Society for Adolescent Medicine. All rights reserved. Keywords: Peer stressors; Mental health; Adolescents; Gender During adolescence, the peer group becomes the primary context for socialization and emotional experience [1]. These new bonds not only broaden and enrich the world of adoles- cents but also lead to higher interpersonal demands [2]. Peer group affiliation, social status, and intimate close relation- ships become more important for adolescents [3,4], which in turn increases the risk of loss, rejection, and conflict. Consistent with this increased risk for interpersonal difficul- ties, peer victimization and stressful events involving close friendships and romantic relationships have been found to be major forms of peer stress[1], which are detrimental to adolescents’ mental health [5–7]. For reasons to be explained hereafter, we hypothesized that peer victimization and rela- tionship losses may lead to gender differences in the mental health of adolescents [1,7]. Adolescents’ mental health is likely to be affected by loss of belongingness that occurs when social bonds are threat- ened, broken, or refused [8–10]. Belongingness is a funda- mental human goal, which can be characterized as the need to form and maintain social bonds [8]. Although this goal is assumed to be universally present in human beings, boys and girls might seek belongingness in different social spheres [11]. Specifically, boys are likely to pursue belongingness in the broader peer group by competing for a good social posi- tion within a status hierarchy, whereas girls may pursue belongingness more in dyadic close relationships [1,7,11– 14]. We propose that peer victimization at school is prototyp- ical for a low social position in the peer group [15,16], whereas relationship losses (e.g., loss of friendships, *Address correspondence to: Martin P. Bakker, M.Sc., Interdisciplinary Center for Psychiatric Epidemiology, University Medical Center Groningen, CC72, P.O. Box 30.001, 9700 RB Groningen, The Netherlands. E-mail address: [email protected] 1054-139X/10/$ – see front matter Ó 2010 Society for Adolescent Medicine. All rights reserved. doi:10.1016/j.jadohealth.2009.10.002 Journal of Adolescent Health 46 (2010) 444–450
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Peer Stressors and Gender Differences in Adolescents' Mental Health: The TRAILS Study

Journal of Adolescent Health 46 (2010) 444–450
Original article
Peer Stressors and Gender Differences in Adolescents’ Mental Health:
The TRAILS Study
Martin P. Bakker, M.Sc.a,b,*, Johan Ormel, Ph.D.a,b,c, Frank C. Verhulst, Ph.D.d,and Albertine J. Oldehinkel, Ph.D.a,b,c,d
aInterdisciplinary Center for Psychiatric Epidemiology, University Medical Center Groningen, University of Groningen, Groningen, The NetherlandsbGraduate School of Health Sciences (SHARE), University Medical Center Groningen, University of Groningen, Groningen, The Netherlands
cGraduate School of Behavioral and Cognitive Neurosciences (BCN), University Medical Center Groningen, University of Groningen,Groningen, The Netherlands
dDepartment of Child and Adolescent Psychiatry, Erasmus University Medical Center – Sophia Children’s Hospital Rotterdam, Rotterdam, The Netherlands
Manuscript received April 17, 2009; manuscript accepted October 8, 2009
Purpose: This study tested two hypotheses about gender-specific mental health effects of peer
*Address correspo
Center for Psychiatric
CC72, P.O. Box 30.00
E-mail address: m
1054-139X/10/$ – see
doi:10.1016/j.jadoheal
stressors during early adolescence: (1) boys and girls are sensitive to different types of peer stressors,
and (2) peer stress is associated with different mental health problems in boys and girls.
Methods: These two hypotheses were tested in a prospective large population cohort of 2,084 Dutch
young adolescents. Internalizing and externalizing problems were measured at baseline and follow-up,
whereas stressful life events in the period between baseline and follow-up were measured retrospec-
tively at follow-up. We performed the analyses with two types of peer stressors; victimization at school
and relationship losses.
Results: Relationship losses were more strongly associated with internalizing and externalizing prob-
lems in girls than boys, supporting the first hypothesis. Peer victimization at school was also associated
with both types of mental health problems, but equally strong in boys and girls.
Conclusions: Peer stress is unlikely to be associated with different mental health problems in boys
and girls. Instead, boys and girls are more likely to be susceptible to different types of peer stressors.
� 2010 Society for Adolescent Medicine. All rights reserved.
Keywords: Peer stressors; Mental health; Adolescents; Gender
During adolescence, the peer group becomes the primary
context for socialization and emotional experience [1]. These
new bonds not only broaden and enrich the world of adoles-
cents but also lead to higher interpersonal demands [2]. Peer
group affiliation, social status, and intimate close relation-
ships become more important for adolescents [3,4], which
in turn increases the risk of loss, rejection, and conflict.
Consistent with this increased risk for interpersonal difficul-
ties, peer victimization and stressful events involving close
friendships and romantic relationships have been found to
be major forms of peer stress[1], which are detrimental to
adolescents’ mental health [5–7]. For reasons to be explained
ndence to: Martin P. Bakker, M.Sc., Interdisciplinary
Epidemiology, University Medical Center Groningen,
1, 9700 RB Groningen, The Netherlands.
front matter � 2010 Society for Adolescent Medicine. All
th.2009.10.002
hereafter, we hypothesized that peer victimization and rela-
tionship losses may lead to gender differences in the mental
health of adolescents [1,7].
Adolescents’ mental health is likely to be affected by loss
of belongingness that occurs when social bonds are threat-
ened, broken, or refused [8–10]. Belongingness is a funda-
mental human goal, which can be characterized as the need
to form and maintain social bonds [8]. Although this goal
is assumed to be universally present in human beings, boys
and girls might seek belongingness in different social spheres
[11]. Specifically, boys are likely to pursue belongingness in
the broader peer group by competing for a good social posi-
tion within a status hierarchy, whereas girls may pursue
belongingness more in dyadic close relationships [1,7,11–
14]. We propose that peer victimization at school is prototyp-
ical for a low social position in the peer group [15,16],
whereas relationship losses (e.g., loss of friendships,
rights reserved.

M.P. Bakker et al. / Journal of Adolescent Health 46 (2010) 444–450 445
romantic break ups) are prototypical for stress in dyadic peer
relationships. On the basis of possible gender differences in
pursuit of belongingness, mental health in boys might be
particularly affected by peer victimization at school, while
mental health in girls is more affected by relationship losses.
Gender differences in mental health might also be due to
a differential orientation in the expression of psychological
distress [17–19]. Specifically, sensitivity to peer stress in girls
may be reflected in inward emotional responses, whereas in
boys it may be more reflected in outward-directed behaviors
[7]. In other words, gender differences in internalizing and
externalizing problems could be explained by a gender-
specific sensitivity to particular peer stressors or by gender-
specific expressions of psychological distress [7].
To the best of our knowledge, these two explanations for
gender differences in mental health have never been tested
within a single study. To recapitulate, we expect that peer
victimization is more strongly associated with internalizing
and externalizing problems in boys, and relationship losses
are more strongly associated with both types of mental health
problems in girls. Alternatively, we hypothesize that both
peer victimization and relationship losses are more strongly
associated with internalizing problems in girls and external-
izing problems in boys. This study aims to add to the current
published data by testing both hypotheses in a prospective
large population cohort of Dutch young adolescents.
Methods
Sample
Subjects were participants of the ‘‘TRacking Adolescents’
Individual Lives Survey’’ (TRAILS), a prospective cohort
study of Dutch adolescents, aimed at explaining the develop-
ment of mental health from preadolescence into adulthood.
The TRAILS study was approved by the Central Committee
on Research Involving Human Subjects (Dutch CCMO).
Sample selection involved five municipalities in the North
of the Netherlands, including both urban and rural areas.
The five municipalities were requested to give names and
addresses of all inhabitants born between October 1, 1989,
and September 30, 1990 (first two municipalities: mean
age¼ 11.29 years; SD¼ 0.52; range, 10.0–12.0) or October
1, 1990, and September 30, 1991 (last three municipalities:
mean age¼ 10.72 years; SD¼ 0.37; range, 10.0–11.5).
Two birth cohorts were used to minimize the age range during
the initial assessment. A detailed description of the sampling
procedure and methods is provided by Huisman et al [20].
Of all the children who were approached (N¼ 3,145),
6.7% (n¼ 211) were excluded because of mental or physical
incapability or language problems. Of the remaining 2,934
children, 76.0% (N¼ 2,230; mean age¼ 11.09; SD¼ 0.56;
range, 10.0–12.0; 50.8% girls) were enrolled in the study
(i.e., both child and parent agreed to participate). Of the
2,230 baseline participants, 96.4% (N¼ 2,149) participated
in the first follow-up (mean age, 13.56; SD, 0.53; range,
12.0–15.0; 51.0% girls), held 2–3 years after baseline (T1)
(mean number of months, 29.44; SD, 5.37; range, 16.69–
48.06).
The present study is based on data from both the baseline
(T1) and follow-up (T2) assessment wave. Written informed
consent was obtained from the parents and from the adoles-
cents themselves at both assessment waves. During these
waves, questionnaires were filled out by the adolescents, their
parents, and their teachers. The adolescents filled out their
questionnaires at school, in the classroom, under the supervi-
sion of one or more TRAILS assistants. Both the parent(s)
and adolescents received a small gift after participating in
the study of which they had no prior knowledge (parents
got a pen with the TRAILS logo and the adolescents a gift
certificate of V10 euro). Responders and nonresponders did
not significantly differ in levels of problems behaviors or
on sociodemographic variables [20]. For the present study,
valid data on both stressful life events and internalizing and
externalizing problems were available for 2,084 adolescents
(97.0 % of the follow-up sample).
Measures
Internalizing and externalizing problems. Two broad
domains of mental health problems were included in this
study: internalizing and externalizing problems. These prob-
lems were assessed at baseline (T1) and follow-up (T2) with
the parent-rated Child Behavior Checklist (CBCL) [21], the
Youth Self Report (YSR) [22], and the Teacher Checklist
of Psychopathology (TCP).
The TCP was developed by TRAILS to reduce the respon-
dent burden for teachers, as each had multiple participants to
report on. The TCP is composed of descriptions of problem
behaviors similar to Achenbachs’ Teacher Report Form
(TRF) [23]. The TRF is the teacher-report version of the
CBCL and YSR [23]. The TRF was designed to identify
the same eight syndromes as the CBCL and YSR. The
three syndromes, anxious/depressed, withdrawn/depressed,
and somatic complaints, fall under the larger grouping of
internalizing. The two syndromes, aggressive behavior and
rule-breaking behavior, are grouped under the group of exter-
nalizing. The remaining three syndromes, social problems,
thought problems and attention problems, do not fall under
either of the two mentioned groupings:. Thus, the TCP yields
the same syndrome and domain scales as the TRF, CBCL, and
YSR but based on (sets of) single vignettes rather than sets of
items. For example, the vignette for withdrawn/depressed
syndrome is: ‘‘The adolescent wants to be alone rather than
to have company. He/she is withdrawn and has little contact
with others. The adolescent doesn’t show initiative or shows
a lack of energy’’; the vignette for aggressive behavior is:
‘‘The adolescent is conflictuous and challenges others. He/
she bullies others and physically attacks them. The adolescent
has an explosive and unpredictable nature. He/she gets easily
frustrated by others and frequently uses abusive language.’’
Response options for each description of the TCP ranged
from 0 (not applicable) to 4 (very clearly or frequently

M.P. Bakker et al. / Journal of Adolescent Health 46 (2010) 444–450446
applicable). The TCP vignettes correlated around .60 with the
full TRF syndrome scales filled out by a small sample of
teachers (unpublished internal report, available on request).
We created broadband scales of internalizing (anxious/
depressed, withdrawn/depressed, and somatic complaints)
and externalizing (aggressive behaviors and rule-breaking
behaviors) problems. The validity of these scales has been
documented [21–23] and reiterated in a Dutch sample
[24,25]. In our sample, the reliability statistics for the baseline
sample (T1) were as follows: CBCL-internalizing (32 items,
a¼ .85), CBCL-externalizing (35 items, a¼ .90); YSR-inter-
nalizing (31 items, a¼ .87), YSR-externalizing (32 items,
a¼ .85); TCP-internalizing (3 vignettes, a¼ .71), TCP-
externalizing (2 vignettes, a¼ .78). For the first follow-up
sample (T2), the reliability statistics were as follows:
CBCL-internalizing (31 items, a¼ .86), CBCL-externalizing
(35 items, a¼ .90); YSR-internalizing (31 items, a¼ .88),
YSR-externalizing (32 items, a¼ .86); TCP-Internalizing (3
vignettes, a¼ .71), TCP-externalizing (2 vignettes, a¼ .80).
Reports from different sources are needed to reduce rater
bias in the prediction of mental health problems and provide
better estimates of diagnosis than those based on a single
source [26,27]. For this reason, we computed a combined
measure of mental health problems, using the scores given
by the adolescents, parents, and teachers. To place the
same weight on information from different informants, the
scores on CBCL, YSR, and TCP were first standardized to
mean zero and standard deviation one (z-scores) before aver-
aging over informants. When data of one informant were
missing or unreliable (for internalizing: CBCL: T1 n¼ 157;
T2 n¼ 225; YSR: T1 n¼ 41; T2 n¼ 17; TCP: T1 n¼ 281;
T2 n¼ 601. For externalizing: CBCL: T1 n¼ 148; T2
n¼ 203; YSR: T1 n¼ 32; T2 n¼ 2; TCP: T1 n¼ 279;
T2 n¼ 590), the composite score was based on the other
informants. The composite scores of internalizing problems
and externalizing problems were subsequently standardized
to mean zero and standard deviation one (z-scores).
Stressful life events. Stressful life events were assessed retro-
spectively with a self-report questionnaire at follow-up (T2),
including 20 stressful life events. The items had a yes/no
Table 1
Prevalence rates of the specific peer stressors during early adolescence, by gender
Girls (n¼ 1,069)
N (experienced event)
Loss of close frienda 160
Romantic breakupa 228
Victim of physical violencea,b 22
Victim of negative gossipa,b 256
Victim of bullyinga,b 219
Victim of sexual harrassmenta,b,c 46
a Stressful life events are dummy variables (0, not experienced; 1, experienced)b Victimization experienced at school.c Includes both verbal and physical forms of harassment.
* p < .05.
format to indicate whether the event had occurred in the
last 2 years (between baseline [T1] and follow-up [T2]).
For each stressful event, the level of experienced severity
was also asked, which the adolescents could rate as 0, not
unpleasant; 1, somewhat unpleasant; 2, rather unpleasant;
or 3, very unpleasant. We used this measure to exclude events
that were not experienced as unpleasant.
Of the list of 20 stressful life events, we selected those
peer-related events that were prototypical for either peer
victimization at school or relationship losses. Peer victimiza-
tion at school includes physical, verbal, and psychological
forms of degrading actions by peers [5,28]. We selected
the following prototypical events for this category: victim
of physical violence at school, victim of sexual harassment
at school (both verbal and physical), victim of bullying
at school, and victim of negative gossip at school. The cate-
gory of relationship losses included the loss of a close friend-
and romantic breakup. The prevalence of the specific stressful
life events within each category is given separately for boys
and girls in Table 1. Numbers of stressful events within these
two categories were used as variables in the analyses.
Statistical analyses
Gender differences in peer stressors and mental health
problems were examined using t-tests. Associations between
the variables were tested for boys and girls separately by
Pearson correlations. Multiple linear regression analyses
were used to test gender differences in the effects of peer
victimization and relationship losses on internalizing and
externalizing problems. All continuous variables were stan-
dardized to M¼ 0 and SD¼ 1, and gender was dummy
coded (0¼ girls, 1¼ boys), so as to ease the interpretation
of the interaction effects. For each mental health outcome,
we tested the main and interaction effects of peer victimiza-
tion at school and gender, as well as the main and interaction
effects of relationship losses and gender. The interaction
effects were only maintained in the model if significant.
We adjusted for pre-event mental health problems because
some events might in part reflect prior manifestations of
psychiatric symptoms [29].
Boys (n¼ 1,015) c2 test
N (experienced event)
40 c2 ¼ 72.723, p < .001*
152 c2 ¼ 14.171, p < .001*
39 c2 ¼ 5.974, p < .01*
129 c2 ¼ 43.534, p < .001*
176 c2¼ 3.236, p¼ .072
37 c2¼ 1.301, p¼ .254
.
M.P. Bakker et al. / Journal of Adolescent Health 46 (2010) 444–450 447
To provide an impression of the effect size and facilitate
the interpretation of the interaction effect, we wrote out
multiple equations using simple slope analysis [30]. In these
analyses, low and high levels of the predictor indicate one
standard deviation below and above the mean, respectively,
while holding all other variables to their sample means.
Results
Descriptive statistics
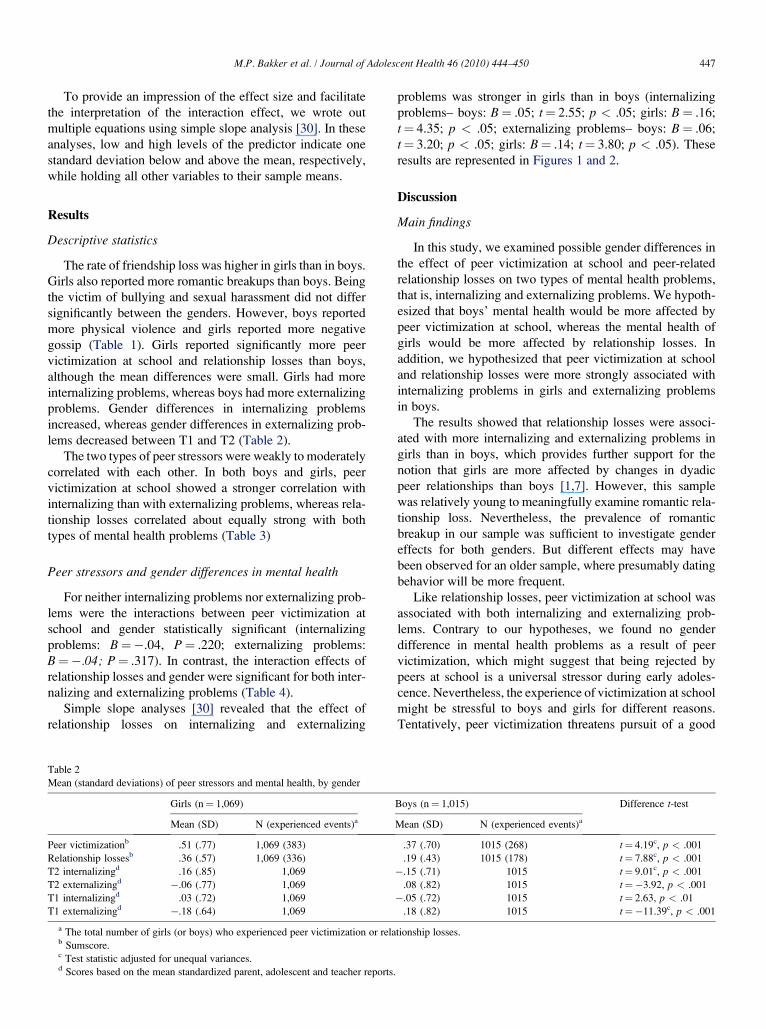
The rate of friendship loss was higher in girls than in boys.
Girls also reported more romantic breakups than boys. Being
the victim of bullying and sexual harassment did not differ
significantly between the genders. However, boys reported
more physical violence and girls reported more negative
gossip (Table 1). Girls reported significantly more peer
victimization at school and relationship losses than boys,
although the mean differences were small. Girls had more
internalizing problems, whereas boys had more externalizing
problems. Gender differences in internalizing problems
increased, whereas gender differences in externalizing prob-
lems decreased between T1 and T2 (Table 2).
The two types of peer stressors were weakly to moderately
correlated with each other. In both boys and girls, peer
victimization at school showed a stronger correlation with
internalizing than with externalizing problems, whereas rela-
tionship losses correlated about equally strong with both
types of mental health problems (Table 3)
Peer stressors and gender differences in mental health
For neither internalizing problems nor externalizing prob-
lems were the interactions between peer victimization at
school and gender statistically significant (internalizing
problems: B¼�.04, P¼ .220; externalizing problems:
B¼�.04; P¼ .317). In contrast, the interaction effects of
relationship losses and gender were significant for both inter-
nalizing and externalizing problems (Table 4).
Simple slope analyses [30] revealed that the effect of
relationship losses on internalizing and externalizing
Table 2
Mean (standard deviations) of peer stressors and mental health, by gender
Girls (n¼ 1,069)
Mean (SD) N (experienced events)a
Peer victimizationb .51 (.77) 1,069 (383)
Relationship lossesb .36 (.57) 1,069 (336)
T2 internalizingd .16 (.85) 1,069
T2 externalizingd �.06 (.77) 1,069
T1 internalizingd .03 (.72) 1,069
T1 externalizingd �.18 (.64) 1,069
a The total number of girls (or boys) who experienced peer victimization or relab Sumscore.c Test statistic adjusted for unequal variances.d Scores based on the mean standardized parent, adolescent and teacher reports.
problems was stronger in girls than in boys (internalizing
problems– boys: B¼ .05; t¼ 2.55; p < .05; girls: B¼ .16;
t¼ 4.35; p < .05; externalizing problems– boys: B¼ .06;
t¼ 3.20; p < .05; girls: B¼ .14; t¼ 3.80; p < .05). These
results are represented in Figures 1 and 2.
Discussion
Main findings
In this study, we examined possible gender differences in
the effect of peer victimization at school and peer-related
relationship losses on two types of mental health problems,
that is, internalizing and externalizing problems. We hypoth-
esized that boys’ mental health would be more affected by
peer victimization at school, whereas the mental health of
girls would be more affected by relationship losses. In
addition, we hypothesized that peer victimization at school
and relationship losses were more strongly associated with
internalizing problems in girls and externalizing problems
in boys.
The results showed that relationship losses were associ-
ated with more internalizing and externalizing problems in
girls than in boys, which provides further support for the
notion that girls are more affected by changes in dyadic
peer relationships than boys [1,7]. However, this sample
was relatively young to meaningfully examine romantic rela-
tionship loss. Nevertheless, the prevalence of romantic
breakup in our sample was sufficient to investigate gender
effects for both genders. But different effects may have
been observed for an older sample, where presumably dating
behavior will be more frequent.
Like relationship losses, peer victimization at school was
associated with both internalizing and externalizing prob-
lems. Contrary to our hypotheses, we found no gender
difference in mental health problems as a result of peer
victimization, which might suggest that being rejected by
peers at school is a universal stressor during early adoles-
cence. Nevertheless, the experience of victimization at school
might be stressful to boys and girls for different reasons.
Tentatively, peer victimization threatens pursuit of a good
Boys (n¼ 1,015) Difference t-test
Mean (SD) N (experienced events)a
.37 (.70) 1015 (268) t¼ 4.19c, p < .001
.19 (.43) 1015 (178) t¼ 7.88c, p < .001
�.15 (.71) 1015 t¼ 9.01c, p < .001
.08 (.82) 1015 t¼�3.92, p < .001
�.05 (.72) 1015 t¼ 2.63, p < .01
.18 (.82) 1015 t¼�11.39c, p < .001
tionship losses.

Table 3
Correlations between peer stressors and mental health, in girls (above the diagonal) and boys (below the diagonal)
Peer victimization Relationship losses T2 internalizing T2 externalizing T1 internalizing T1 externalizing
Peer victimizationa .27 (<.001) .31 (<.001) .18 (<.001) .20 (<.001) .17 (<.001)
Relationship lossesa .26 (<.001) .20 (<.001) .21 (<.001) .05 (0.10) .09 (<.01)
T2 internalizingb .33 (<.001) .12 (<.001) .45 (<.001) .50 (<.001) .26 (<.001)
T2 externalizingb .12 (<.001) .10 (<.01) .37 (<.001) .30 (<.001) .57 (<.001)
T1 internalizingb .27 (<.001) .12 (<.001) .55 (<.001) .23 (<.001) .49 (<.001)
T1 externalizingb .13 (<.001) .08 (<.01) .21 (<.001) .57 (<.001) .43 (<.001)
a Sumscore.b Scores based on the mean standardized parent, adolescent and teacher reports.
M.P. Bakker et al. / Journal of Adolescent Health 46 (2010) 444–450448
status position by boys within the peer group, whereas for
girls peer victimization poses constraints to establish affilia-
tive ties at school.
Previous research provides mixed support for gender
differences in mental health because of peer victimiza-
tion[1,31], which could be due to heterogeneity within this
category of events. Boys are assumed to be more affected
by overt victimization, whereas girls experience more mental
health problems caused by relational victimization [1,31].
We performed post hoc analyses to examine this possibility.
Gender differences in mental health were tested separately
for being a victim of physical violence (overt victimization)
and negative gossip (relational victimization) at school.
The interaction with gender was not significant (results are
available on request) in either of the regression models, sug-
gesting that our combined measure of peer victimization did
not obscure gender-specific pathways toward mental health
problems.
The results for both relationship losses and peer victimiza-
tion at school did not support the hypothesis that peer stress is
associated with different mental health problems in boys and
girls. Hence, our findings suggest that gender per se is
unlikely to result in different reactions to the same peer
Table 4
Main and interaction effects of peer stressors and gender on mental health
problems
T2 internalizing
problemsa
T2 externalizing
problemsa
Bb (p) Bb (p)
Model 1c,d
Peer victimizatione .20 (<.001) .07 (<.001)
Gender (1¼ boys)f �.29 (<.001) �.10 (<.01)
Model 2d
Relationship lossese .16 (<.001) .14 (<.001)
Gender (1¼ boys)f �.29 (<.001) �.08(<.05)
Relationship losses 3 gender �.11 (<.01) �.08(<.05)
a Regression analyses for T2 internalizing problems are adjusted for T1
internalizing problems; Regression analyses for T2 externalizing problems
are adjusted for T1 externalizing problems.b Unstandardized regression coefficients.c Main effects are presented because interaction effects between peer
victimization at school and gender were not significant.d All continuous variables in the model were standardized to M¼ 0;
SD¼ 1.e Sumscore.f Dummy coded variable (0¼ girls, 1¼ boys).
stressor; rather boys and girls are more likely to react to
different peer stressors.
In additional, girls reported more peer victimization at
school than boys. One well-documented explanation is that,
in general, girls are more likely to report interpersonal stress
and conflicts than boys [32,33]. It is therefore possible that
girls are more willing to admit peer victimization than boys
[33]. Another explanation for this result could relate to
gender differences in the onset of puberty during early
adolescence. According to the social misfit hypothesis, early
maturers are perceived as social deviants by same-age peers
[34]. As a result, early maturers are more likely to be targeted
for victimization by peers [34]. In general, girls tend to expe-
rience puberty at an earlier age than boys [35]. Thus, more
girls than boys were likely to have been early maturers in
our relatively young sample. This might also possibly explain
why we found that girls reported more peer victimization at
school than boys during early adolescence.
Limitations and strengths
A limitation of this study is that the life events were
measured retrospectively, without regard to contextual infor-
mation, and were based on self-reports [36]. Retrospective
self-reports are likely to be susceptible to recall bias. For
example, people with mental health problems have been sug-
gested to over-report the severity as well as the number of
Figure 1. Interaction between relationship losses and gender on internalizing
problems.

Figure 2. Interaction between relationship losses and gender on external-
izing problems.
M.P. Bakker et al. / Journal of Adolescent Health 46 (2010) 444–450 449
stressful life events [36,37]. Tentatively, recall bias in self-
reports about peer victimization at school and relationship
losses might be more pronounced in severity ratings than in
occurrence ratings of these stressful life events [38]. To
reduce possible state-related biases, we only used the number
of stressful life events in the analyses, not their reported
severity. Important assets of this study are the size and repre-
sentativeness of our sample, the use of multiple informants,
and multiple outcome measures. The longitudinal nature of
our study made it possible to adjust for pre-event mental
health problems as well.
Implications and Conclusion
To the best of our knowledge, this study was the first to
examine two plausible explanations for gender differences
in mental health because of peer stressors in a large prospec-
tive population cohort of Dutch young adolescents.
An important result of this study is that gender per se does
not predispose adolescents to either internalizing or external-
izing problems in response to peer stress. Whether adoles-
cents react to stressful events by developing internalizing
or externalizing problems does not seem to be strongly
related to gender. Previous research suggests that differences
in temperamental traits partly explain the risk for either inter-
nalizing or externalizing problems in adolescents [39]. For
example, adolescents with low effortful control are more at
risk to experience externalizing problems than internalizing
problems, whereas this pattern is reversed for fearful adoles-
cents [39]. Thus, low effortful control and fearfulness, rather
than gender, might in part account for a possible differential
expression of mental health problems in response to peer
stress. However, this conjecture awaits future research.
Another noteworthy result of this study is that rejection by
peers at school is an important stressor for both genders
during early adolescence. Furthermore, girls reported more
peer victimization than boys. Taken together, girls might
be particularly at risk for peer victimization during this devel-
opmental period. Our results therefore provide additional
support to the emerging view that girls’ experience with
victimization at school deserves much closer scrutiny from
researchers, parents, and teachers [40].
Acknowledgments
This research is part of the TRacking Adolescents’ Indi-
vidual Lives Survey (TRAILS). Participating centers of
TRAILS include various departments of the University
Medical Center and University of Groningen, the Erasmus
University Medical Center Rotterdam, the University of
Utrecht, the Radboud Medical Center Nijmegen, and the
Trimbos Institute, all in the Netherlands. Principal investiga-
tors are Professor Dr. J. Ormel (University Medical Center
Groningen) and Professor Dr. F.C. Verhulst (Erasmus
University Medical Center). TRAILS has been financially
supported by various grants from the Netherlands Organiza-
tion for Scientific Research NWO (Medical Research Council
program grant GB-MW 940-38-011; ZonMW Brainpower
grant 100-001-004; ZonMw Risk Behavior and Dependence
grants 60-60600-98-018 and 60-60600-97-118; ZonMw
Culture and Health grant 261-98-710; Social Sciences
Council medium-sized investment grants GB-MaGW 480-
01-006 and GB-MaGW 480-07-001; Social Sciences Council
project grants GB-MaGW 457-03-018, GB-MaGW 452-04-
314, and GB-MaGW 452-06-004; NWO large-sized invest-
ment grant 175.010.2003.005); the Sophia Foundation for
Medical Research (projects 301 and 393), the Dutch Ministry
of Justice (WODC), and the participating universities. We are
grateful to all adolescents, their parents, and their teachers
who participated in this research, and to everyone who
worked on this project and made it possible.
References
[1] Rose AJ, Rudolph KD. A review of sex differences in peer relationship
processes: Potential trade-offs for the emotional and behavioral devel-
opment of girls and boys. Psychol Bull 2006;132:98–131.
[2] Compas BE, Wagner BM. Psychosocial stress during adolescence:
Intrapersonal and interpersonal processes. In: Colten ME, Gore S,
eds. Adolescent Stress: Causes and Consequences. New York, NY:
Walter de Gruyter Inc, 1991:67–85.
[3] La Greca AM, Harrison M. Adolescent peer relations, friendships, and
romantic relationships: Do they predict social anxiety and depression?
J Clin Child Adolesc Psychol 2005;34:49–61.
[4] Pellegrini AD, Long JD. A longitudinal study of bullying, dominance,
and victimization during the transition from primary school through
secondary school. Br J Dev Psychol 2002;20:259–80.
[5] Graham S, Bellmore AD. Peer victimization and mental health during
early adolescence. Theory Pract 2007;46:138–46.
[6] Monroe SM, Rohde P, Seeley JR, Lewinsohn PM. Life events and
depression in adolescence: Relationship loss as a prospective risk factor
for first onset of major depressive disorder. J Abnorm Psychol 1999;
108:606–14.
[7] Rudolph KD. Gender differences in emotional responses to interper-
sonal stress during adolescence. J Adolesc Health 2002;30S:3–13.

M.P. Bakker et al. / Journal of Adolescent Health 46 (2010) 444–450450
[8] Baumeister RF, Leary MR. The need to belong: Desire for interpersonal
attachments as a fundamental human motivation. Psychol Bull 1995;
117:497–529.
[9] Bowlby J. Attachment. Attachment and Loss, Volume 1. New York,
NY: Basic Books, 1969.
[10] Bowlby J. Separation Anxiety and Anger. Attachment and Loss,
Volume 2. New York, NY: Basic Books, 1973.
[11] Baumeister RF, Sommer KL. What do men want? Gender differences
and two spheres of belongingness: Comments on Cross and Madson.
Psychol Bull 1997;1997(122):38–44.
[12] Cyranowski JM, Frank E, Young E, Shear K. Adolescent onset of the
gender difference in lifetime rates of major depression: A theoretical
model. Arch Gen Psychiatry 2000;57:21–7.
[13] Geary DC, Byrd-Graven J, Hoard MK, et al. Evolution and develop-
ment of boys’ social behavior. Dev Rev 2003;23:444–70.
[14] Troisi A. Gender differences in vulnerability to social stress: A
Darwinian perspective. Physiol Behav 2001;73:443–9.
[15] Salmivalli C, Huttunen A, Lagerspetz KMJ. Peer networks and
bullying in school. Scand J Psychol 1997;38:305–12.
[16] Veenstra R, Lindenberg SM, Zijlstra BJH, et al. The dyadic nature of
bullying and victimization: Testing a dual-perspective theory. Child
Dev 2007;78:1843–54.
[17] Gjerde PF, Block J, Block JH. Depressive symptoms and personality
during late adolescence: Gender differences in the externalization-inter-
nalization of symptom expression. J Abnorm Psychol 1988;97:475–86.
[18] Gjerde PF. Alternative pathways to chronic depressive symptoms in
young adults: Gender differences in developmental trajectories. Child
Dev 1995;66:1277–300.
[19] Leadbeater BJ, Blatt SJ, Quinlan DM. Gender-linked vulnerabilities
to depressive symptoms, stress and problem behaviors in adolescents.
J Res Adolesc 1995;5:1–29.
[20] Huisman M, Oldehinkel AJ, de Winter A, et al. Cohort profile: The
Dutch "Tracking Adolescents’ Individual Lives’ Survey"; TRAILS.
Int J Epidemiol 2008;37:1227–35.
[21] Achenbach TM. Manual for the Child Behavior Checklist/4-18 and
1991 Profile. Burlington, VT: University of Vermont, 1991.
[22] Achenbach TM. Manual for the Youth Self-Report and 1991 Profile.
Burlington, VT: University of Vermont, 1991.
[23] Achenbach TM. Manual for the Teachers’ Report Form and 1991
Profile. Burlington, VT: University of Vermont, 1991.
[24] Verhulst FC, Van der Ende J, Koot HK. Handleiding voor de Youth
Self-Report (YSR). Rotterdam, The Netherlands: Sophia Children’s
Hospital Rotterdam, 1997.
[25] Verhulst FC, Van der Ende J, Koot HK. Handleiding voor de CBCL/
4-18. Rotterdam, The Netherlands: Sophia Children’s Hospital
Rotterdam, 1996.
[26] Noordhof A, Oldehinkel AJ, Verhulst FC, Ormel J. Optimal use of
multi-informant data on co-occurrence of internalizing and external-
izing problems. Int J Methods Psychiatr Res 2008;17:174–83.
[27] Verhulst FC, Koot HM, Van der Ende J. Differential predictive value of
parents’ and teachers’ reports of childrens’ problem behaviors: A longi-
tudinal study. J Abnorm Child Psychol 1994;22:531–46.
[28] Olweus D. Bullying at School. Malden, MA: Blackwell Publishers,
1993. Inc.
[29] Hammen C. Stress generation in depression: Reflections on origins,
research, and future directions. J Clin Psychol 2006;62:1065–82.
[30] Aiken LS, West SG. Multiple Regression: Testing and Interpreting
Interactions. Newbury Park, CA: Sage, 1991.
[31] Gershon A, Minor K, Hayward C. Gender, victimization, and psychi-
atric outcomes. Psychol Med 2008;38:1377–91.
[32] Rudolph KD, Hammen C. Age and gender as determinants of stress
exposure, generation and reactions in youngsters: A transactional
perspective. Child Dev 1999;70:660–77.
[33] Wagner BM, Compas BE. Gender, instrumentality, and expressivity:
Moderators of the relation between stress and psychological symptoms
during adolescence. Am J Community Psychol 1990;18:383–406.
[34] Nadeem E, Graham S. Early puberty, peer victimization and internal-
izing symptoms in ethnic minority adolescents. J Early Adolesc
2005;25:197–222.
[35] Waylen A, Wolke D. Sex ‘n’ drugs ‘n’ rock ‘n’ roll: The meaning and
social consequences of pubertal timing. Eur J Endocrinol 2004;151:
U151–9.
[36] Dohrenwend BP. Inventorying stressful life events as risk factors for
psychopathology: Toward resolution of the problem of intracategory
variability. Psychol Bull 2006;132:477–95.
[37] Monroe SM. Modern approaches to conceptualizing and measuring
human life stress. Annu Rev Clin Psychol 2008;4:33–52.
[38] Wagner C, Abela JRZ, Brozina K. A comparison of stress measure in
children and adolescents: A self-report checklist versus an objectively
rated interview. J Psychopathol Behav Assess 2006;28:251–61.
[39] Oldehinkel AJ, Hartman CA, De Winter AF, et al. Temperament
profiles associated with internalizing and externalizing problems in
preadolescence. Dev Psychopathol 2004;16:421–40.
[40] Berger C, Rodkin PC. Male and female victims of male bullies: Social
status differences by gender and informant source. Sex Roles 2009;61:
72–84.