PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised...
12
PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised Children Patrice L. (Tamar) Weiss 1 , Carolynn P. Whiteley 2 , Jutta Treviranus 3 and Deborah I. Fels 2 1 Hadassah-Hebrew University, Jerusalem, Israel; 2 Ryerson Polytechnic University, Toronto, Canada; 3 Adaptive Technology Resource Center, University of Toronto, Toronto, Canada Abstract: Wayne Gretzky’s PEBBLES TM (Providing Education By Bringing Learning Environments to Students) is a unique example of a personal technology, one in which PC-based video-conferencing is used to make a real-time link between a hospitalised child and his or her regular classroom. The system provides an opportunity for children who are in isolated situations, such as hospitals, to maintain a meaningful link with their regular educational and social environments, thereby minimising many of the secondary problems that may develop as a result of long-term illness and hospitalisation. The objective of this paper is to illustrate the impact that PEBBLES had on one child who directly benefited from the system and on the people with whom she interacted (classmates, parents, teachers and hospital staff). These results were used to explore how exposure to this personal technology influenced the behaviours and attitudes of those involved in this study. The results indicate that, overall, PEBBLES has a very positive effect on both the young and adult participants; the most dramatic effect of all was on the ill child who used PEBBLES to attend school. Keywords: Hospitalised children; Personal technology; Telepresence; Video-conferencing 1. Introduction When elementary or secondary school students are absent from school for extended periods due to illness they are usually provided with a tutor or access to in-hospital classrooms. Although such instructional techniques help sick students to keep up with some of the missed academic curriculum, they do little to alleviate the stress generated by confinement to and isolation in a hospital setting. The students’ removal from familiar surroundings, such as the home and school environment, and a lack of control over major and even many minor decisions concern- ing themselves, are factors that contribute to this stress [1–4]. Moreover, traditional hospital in- structional techniques do not provide sick children with frequent contact with familiar classmates, a factor that has been reported to be of critical importance for children with cancer [5]. As well as academic gains, contact with peers appears to result in significant non-academic benefits, particularly in social and communica- tion skills and in the development of greater self- confidence and independence [6,7]. Personal technologies typically refer to ubiquitous, pervasive and/or mobile computing in entertainment, business or educational contexts. They can also refer to approaches to computing that demonstrate ways in which advanced technologies can be personalised to meet the unique educational, social and emotional needs of individual users [8]. In this paper we describe users’ experience with a unique PC-based video-conferencing system – Wayne Gretzky’s PEBBLES TM – that has been configured to make a real-time synchronous connection between a hospitalised child and his or her regular classroom [9]. The system provides an opportunity for children who are ill to maintain their link with their regular educational and psychosocial spheres, thereby minimising many of the secondary problems that may develop as a result of long-term illness and hospitalisation. Although PEBBLES (Providing Education By Bringing Learning Environments to Students) is not yet portable or mobile in the sense of wearable computers or personal digital assistants, it shares with 157 # Springer-Verlag London Ltd Personal and Ubiquitous Computing (2001) 5:157–168
Transcript of PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised...

PEBBLES: A Personal Technology for
Meeting Educational, Social and Emotional
Needs of Hospitalised Children
Patrice L. (Tamar) Weiss1, Carolynn P. Whiteley2, Jutta Treviranus3 andDeborah I. Fels2
1Hadassah-Hebrew University, Jerusalem, Israel; 2Ryerson Polytechnic University, Toronto, Canada;3Adaptive Technology Resource Center, University of Toronto, Toronto, Canada
Abstract: Wayne Gretzky’s PEBBLESTM (Providing Education By Bringing Learning Environments to Students) is a unique example of apersonal technology, one in which PC-based video-conferencing is used to make a real-time link between a hospitalised child and his orher regular classroom. The system provides an opportunity for children who are in isolated situations, such as hospitals, to maintain ameaningful link with their regular educational and social environments, thereby minimising many of the secondary problems that maydevelop as a result of long-term illness and hospitalisation. The objective of this paper is to illustrate the impact that PEBBLES had on onechild who directly benefited from the system and on the people with whom she interacted (classmates, parents, teachers and hospital staff).These results were used to explore how exposure to this personal technology influenced the behaviours and attitudes of those involved inthis study. The results indicate that, overall, PEBBLES has a very positive effect on both the young and adult participants; the mostdramatic effect of all was on the ill child who used PEBBLES to attend school.
Keywords: Hospitalised children; Personal technology; Telepresence; Video-conferencing
1. Introduction
When elementary or secondary school studentsare absent from school for extended periods dueto illness they are usually provided with a tutoror access to in-hospital classrooms. Althoughsuch instructional techniques help sick studentsto keep up with some of the missed academiccurriculum, they do little to alleviate the stressgenerated by confinement to and isolation in ahospital setting. The students’ removal fromfamiliar surroundings, such as the home andschool environment, and a lack of control overmajor and even many minor decisions concern-ing themselves, are factors that contribute to thisstress [1–4]. Moreover, traditional hospital in-structional techniques do not provide sickchildren with frequent contact with familiarclassmates, a factor that has been reported to beof critical importance for children with cancer[5]. As well as academic gains, contact with peersappears to result in significant non-academicbenefits, particularly in social and communica-tion skills and in the development of greater self-confidence and independence [6,7].
Personal technologies typically refer toubiquitous, pervasive and/or mobile computingin entertainment, business or educationalcontexts. They can also refer to approachesto computing that demonstrate ways in whichadvanced technologies can be personalised tomeet the unique educational, social andemotional needs of individual users [8]. Inthis paper we describe users’ experience with aunique PC-based video-conferencing system –Wayne Gretzky’s PEBBLESTM – that has beenconfigured to make a real-time synchronousconnection between a hospitalised child andhis or her regular classroom [9]. The systemprovides an opportunity for children who areill to maintain their link with their regulareducational and psychosocial spheres, therebyminimising many of the secondary problemsthat may develop as a result of long-termillness and hospitalisation. Although PEBBLES(Providing Education By Bringing LearningEnvironments to Students) is not yet portableor mobile in the sense of wearable computersor personal digital assistants, it shares with
157
# Springer-Verlag London LtdPersonal and Ubiquitous Computing (2001) 5:157–168

such devices a common vision of the impor-tance of fostering a close link between the userand the technology [8].
PEBBLES has been designed to promote apersonal aura of ‘‘telepresence’’ for its partici-pants, a crucial element in Buxton’s [10] viewtowards successful video-conferencing. Telepre-sence may be defined as the extent to whichpeople feel immersed within a real or virtualsituation even though they are not physicallyconnected to it. There has been some consensusthat telepresence is related to the way in which auser experiences the events and interpersonalinteractions which take place in a given remotelocation [11]. Over the past decade, the conceptof telepresence has been accorded a central rolein a variety of educational and vocationalsettings, with each application refining theterm to satisfy its particular application. In thePEBBLES project we endeavour to provide bothphysical and virtual elements of telepresence inorder to improve the users’ sense of jointparticipation in a shared experience.
With PEBBLES, virtual telepresence is facili-tated by a video-conferencing system thatprovides a two-way audio and video link viaISDN (Integrated Services Digital Network), ahigh speed, broadband digital public commu-nications network. The system consists of twodesktop computers, each equipped with video-conferencing hardware and software. Both theremote and classroom units have been designedto provide video-conferencing capability in asafe, accessible and easy-to-use and maintainconfiguration.
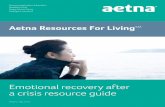
The child is also represented by a physicalpresence in the form of a robot-like unit in theclassroom, providing a form of social telepre-sence that is emphasised by Buxton [10]. Thisunit, shown in Fig. 1, is mobile, and is housed ina unique, ‘‘child-friendly’’, custom-designedshell. The head is egg-shaped with smooth,‘‘huggable’’ contours. The base is rounded andhouses all of the hardware components. The‘‘neck’’ is a rotating structure that contains theservo-motor and electronic control box. Thehead structure covers most of the neck so thatthe rotating and power mechanisms cannot beaccessed by children’s hands. It has a turquoise/yellow colour scheme that was selected to rendera pleasing and friendly appearance. The atten-tion control signal activates an animated handprotruding from the side of the head and is used
to gain the attention of the teacher andclassmates. The unit at the remote setting (i.e.in the hospital), shown in Fig. 2, can be easilyused by the child, maintained by support staffand stored safely away after use.
The system works in the following manner.The remote user’s image (head and shoulders)and voice are captured by a tracking videocamera and hands-free microphone respectively.The video and audio signals are transmitted tothe classroom site and output to a computer
158
Fig. 1. Wayne Gretzky’s PEBBLES in the classroom. This endof the system is used to display the sick child’s video andaudio transmission from the hospital.
Fig. 2. The hospital end of PEBBLES. The sick child controlsthe classroom unit from this device which also displays videoand audio transmission from his/her classmates.
P. L. (Tamar) Weiss, C. P. Whiteley, J. Treviranus and D. I. Fels

monitor and speakers. In the classroom, imagesand sounds are gathered using a video camera,room microphones and a wireless microphoneworn by the teacher. The classroom video andaudio signals are transmitted to the remote siteand output on the computer screen and speakers.At both sites, the video-conferencing systemprovides local video feedback to enable the userto see him/herself on the computer screen and/orseparate LCD panel. A game-pad controller isused by the remote student as the interface to thevideo-conferencing system to manipulate thesystem including the camera (tilt it up and down,zoom it in and out), the PEBBLES head (turn itleft and right), and the attention getting device(wave the hand).
By providing only the necessary functionalityand feedback, the software interface is designedto be both child-friendly and robust. Due to thecomplexity of PictureTel’s LIVE200TM video-conferencing software interface, the standardcontrol panel is not accessible to the user.Instead, all required commands are performedvia a game-pad control device. Icons represent-ing each command are also displayed on thescreen to provide feedback to the user. Forexample, pan left and pan right are indicatedwith a yellow bar on the corresponding side of aframe surrounding the video-conferencingwindow. The child activates a ‘‘go to school’’icon to connect to the classroom unit. All callmanagement functions such as dialling andhanging up are performed in the background ofthe customised interface.
While there are many aspects of this projectto report, this paper will focus on data that showthe impact that PEBBLES had on one child whodirectly benefited from the system, and on thepeople with whom she interacted (classmates,parents, teachers and hospital staff). Theseresults will be used to explore how exposure tothis personal technology influenced the beha-viours and attitudes of the study participants.
2. Methods
2.1. Subjects
The subjects in this study consisted of:
. Naama (not her real name), a 12-year-old girlsuffering from acute renal failure as a result ofchronic kidney disease
. her father
. regular grade 7 classroom teacher
. one hospital teacher who provided one-on-one teaching for one hour per day to Naama
. primary medical caregiver (the dialysis nurse)
. 26 11–13 year old male and female studentswho attended grade 7 in the senior publicschool in which Naama was enrolled.
Naama required hospitalisation as a day patientthree times a week (Mondays, Wednesdays andFridays) in order to receive haemodialysis.Owing to her chronic kidney disease as well asother systemic disorders (Schmeinkes Syndromeand Moyamoya, a blood vessel condition thatcan affect memory), Naama is small for her age,and had only little prior or current contact withher classmates. She has a gastrostomy for feedingand a central line for haemodialysis. Her bloodpressure must be checked regularly as she hashypertension and is prone to cerebral haemor-rhage. During dialysis, Naama sometimes experi-enced nausea, cramping in her legs and feet anda tugging sensation at the dialysis ports but shewas not in physical pain. Naama is a very quietstudent who is reluctant to communicate;indeed, in the several years prior to this studyshe had been classified as a selective mute,interacting freely with family members and closefriends only. On alternate days when notrequired to undergo haemodialysis, Naama waspermitted to attend school but was often too sickto do so.
2.2. PEBBLES
In the present study, the classroom end ofPEBBLES was located in Naama’s regularschool classroom. The hospital end was locatedin the dialysis unit of a major children’s hospitalin the same city as Naama’s regular school.Although the unit was used in this classroom for11 weeks, the results reported in this paper arebased on usage during the first six weeks of thePEBBLES experience. PEBBLES was used threetimes weekly in the mornings while Naama wasreceiving haemodialysis. She would be ready tostart ‘‘attending’’ class together with her class-mates at 9:00am (or shortly thereafter), havingbeen already prepared for and attached to thehaemodialysis unit. Naama would often connectto the school prior to the arrival of the hospitalteacher, and would take part in whicheverclassroom activity was in progress. Once the
159
PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised ChildrenPEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised Children

hospital teacher arrived, she would help Naamawith any difficulties she had in carrying outassigned tasks. Naama would normally be linkedto the school classroom for 11.5 hours. Theclassroom activities in which Naama partici-pated were related to homeroom-based topicssuch as English, maths and social studies. (Othersubjects, such as science and music, were taughtin classrooms which did not support the requisiteISDN connections.) Activities varied from silentreading and journal entry to class presentationsand discussions. At least one new topic wasintroduced to the class each day.
2.3. Outcome measures
A wide variety of different outcome measures,obtained from data from the remote student(Naama), her classmates, and the adult partici-pants, were used to evaluate the effectiveness ofthis personal video-conferencing system.
Data from remote student: Eleven video record-ings of one-hour PEBBLES sessions were col-lected during the six-week study via a videocamera that was located in the haemodialysisunit behind Naama’s chair. The recordings weremade during each of the first eight sessions, onone session midway through the study, andduring the last two sessions. The camera wasadjusted to focus on the computer screencapturing the computer screen images (bothlocal and remote video windows) and the audio(again both local and remote). Taping began assoon as Naama established the video-conferen-cing link to the classroom and continued untilthe conclusion of the day’s session. In addition,two members of the research team, one at thehospital and one in the classroom, made writtenrecords of any noteworthy incidents which tookplace during the sessions.
The videotape records were examined withthe objective of tracking changes that occurredto the following factors:
(1) ability to operate PEBBLES;
(2) communication interactions;
(3) attitudes and behaviours (e.g. concentration,motivation, initiative); and
(4) academic progress.
Data from classmates:Drawings of PEBBLES: Each classmate was askedto make a drawing of PEBBLES after the system
and its function had been described to them butbefore it was actually installed in the classroom.They were also asked to draw it at the end oftheir PEBBLES experience.
Classmates’ responses to discussion/questionnaire: Agroup discussion was conducted with the class-mates prior to and following the PEBBLESexperience. A facilitator asked the group eightquestions and the responses were recorded onaudiotape. The questions were formulated toobtain information about how the childrenviewed:
. hospitals (e.g. What kind of people work inhospitals? Who has been in a hospital? Didyou like it or dislike it? Why or why not?);
. their sick classmate (e.g. What do you thinkyour classmate will miss while he or she is inthe hospital? What will (did) you miss aboutyour classmate not being here?); and
. PEBBLES (e.g. What do you think the systemwill be able to do? What are the good (bad)things about the system?)
Upon completion of the questionnaire, a paperwas handed out to the students on which wastyped the following question: ‘‘When you thinkabout [remote student’s name] in the hospitaland using PEBBLES to connect to the classroom,how much has it helped you understand what shehas gone through while in the hospital?’’ Eachstudent was asked to mark his or her response ona 10 cm visual analog scale where the left end ofthe line was anchored with the label ‘‘no help’’,and the right end of the line was anchored withthe label ‘‘best possible help’’. At equal intervalsalong this line between the two anchors thelabels ‘‘little help’’, ‘‘medium help’’ and ‘‘largehelp’’ were placed.
Drawings of a sick person: The classmates werealso asked to make two drawings illustrating theirview of a sick person in the hospital. Onedrawing was made immediately prior to thecommencement of the PEBBLES’ experiencewhile the second drawing was made shortly afterits completion. The purpose of these drawingswas to determine whether PEBBLES had apositive or negative influence on children’sperceptions of hospitals and individuals whostay in hospitals. These drawings were reviewedby two members of the research team and ratedon four seven-point scales (see Fig. 3). The first
160
P. L. (Tamar) Weiss, C. P. Whiteley, J. Treviranus and D. I. Fels

scale was ‘‘health’’, i.e. was a person in hospitalperceived as being very sick (a rating of ‘‘1’’) allthe way to being very healthy (‘‘7’’). The secondscale was ‘‘attitude’’, i.e. was a person in hospitalperceived as being very negative (unhappy)(‘‘1’’) all the way to being very positive(happy) (‘‘7’’). The third scale was ‘‘individual-ity’’, i.e. was the person in hospital perceived asbeing essentially generic of all sick or hospita-lised people (‘‘1’’) all the way to being acompletely unique individual (‘‘7’’). The forthscale was ‘‘vitality’’, i.e. was the person inhospital perceived as being very passive (‘‘1’’)all the way to being very active (‘‘7’’).
Data from adult participants: Subjective atti-tudes and opinions regarding the impact ofPEBBLES on the remote student and on thestudents in the classroom were gathered from theadult participants in the study (the hospitalteacher, the homeroom teacher at the school,Naama’s father and the primary dialysis nurse).The adult participants also answered questionsabout their own attitudes towards and opinionsof the PEBBLES system. The objective in usingthis outcome measure was to track changes inthe subjective opinions (both positive andnegative) of the major adult participants regard-ing Naama’s participation in school, effective-ness of communication strategies, motivation,emotional state and coping abilities. The ques-tionnaire was composed of three sections includ-ing:
. demographic information about the respon-dent;
. his or her evaluation of PEBBLES’ effective-ness; and
. his or her assessment of the positive andnegative aspects of the project.
To assess PEBBLES’ effectiveness, the adultparticipants were asked to rate the changes thatoccurred as Naama used PEBBLES throughoutthe six-week study. A five-point scale, rangingfrom ‘‘1’’ denoting a significant negative changeto ‘‘5’’ denoting a significant positive change, wasused to rate the effect that using PEBBLES hadon Naama’s level of participation, communica-tion, emotional state, and motivation. Thedialysis nurse was also asked to rate any changethat occurred in Naama’s ability to cope. Thepositive and negative aspects of the project wereassessed using open-ended questions whererespondents were permitted to make free-formcomments that were not addressed in previoussections in the questionnaire. Each adult parti-cipant completed the full questionnaire on thefirst day of the study. They then completed thelatter two sections a further five times atapproximately one-week intervals, with theexception of the dialysis nurse who onlycompleted it four additional times.
2.4. Statistical analysis
Wherever the sample size permitted (e.g. theresponses of Naama’s classmates), non-para-
161
Fig. 3. Scales used to rate classmates’ view of a person in the hospital.
PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised ChildrenPEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised Children

metric or parametric statistical analyses proce-dures were used. Thus, the Intraclass correlationcoefficient (ICC) and the Pearson CorrelationCoefficient were used to test the reliability forthe ratings of the drawings of a sick person. TheWilcoxon Signed Ranks test for related sampleswas then used to determine whether there weresignificant differences between pre- and post-ratings of the drawings. In other cases (e.g. inevaluating the responses of Naama and the adultparticipants), qualitative descriptions of pre- andpost-assessments have been provided.
3. Results
3.1. Data from remote student
Throughout the study, Naama continued to be aquiet student who was reluctant to communi-cate. However, remarkable changes occurredduring her participation in the study. Sheagreed to every request and suggestion (e.g.wanting to use PEBBLES, having her picturetaken or writing a story about PEBBLES).Noticeable improvements in Naama’s behaviourand performance were observed in her ability tooperate the system, her communication withteachers and classmates, her behaviour and heracademic progress.
Ability to operate PEBBLES: Naama learned touse the game-pad to control the various PEB-BLES’ functions with ease. For example, Naamawas quite adept at manipulating the variouscamera functions, such as zooming in to get acloser look at the blackboard or at a map. Shedid not, however, take advantage of some of theextra features (e.g. switching from one camera toanother) that would have made it easier toalternate between different views of the class-room. Whenever Naama was reminded of thesefeatures she was able to operate them; she justdid not initiate their use, an omission that maybe due to unclear labelling of the game-padcontroller
Communication interactions: Naama frequentlypressed the hand button to wave ‘‘hello’’ to herclassmates and to answer a question from theteacher. Initially she appeared to use the hand asa way of avoiding a verbal answer, a responsethat was typical of her discomfort with speaking.However, as the study progressed, and she
became more comfortable using PEBBLES,Naama relied more on brief spoken responses,especially when a question was specificallydirected at her. The school teacher quicklydiscovered that the best way to encourageNaama to respond was to warn her that shewould be asked a question on a particular topicin a few minutes’ time. She would then prepareher response, often discussing possible answerswith the hospital teacher. Towards the end ofthe six-week study, Naama demonstrated greaterreadiness to respond verbally, to the point ofanswering a multiplication drill question withoutany prior notice.
The topic of PEBBLES itself proved to be aneffective way of starting a conversation betweenNaama and her friends. Naama was pleased toshow the game-pad and demonstrate what thevarious buttons and triggers would do. Herclassmates were quite intrigued with this andseemed to gain a clearer understanding of howthe system worked. They were keen to ask her to‘‘wave the hand’’ and ‘‘turn to look at me’’.
Attitudes and behaviours: Naama’s ability toconcentrate was excellent, even under thedifficult conditions of a busy and noisy haemo-dialysis ward. She was able to read and completeher schoolwork regardless of external distractionseven when visitors arrived to see PEBBLES inaction.
There were times, however, when PEBBLESmay have been misused. For example, one of thestanding rules of system usage was that, exceptfor urgent needs, the student had to requestpermission to take a break if she felt greatfatigue, discomfort or illness. At times thehospital teacher had difficulty in distinguishingbetween such justifiable reasons for discontinu-ing class and other less legitimate reasons (suchas the wish to avoid a challenging maths lesson).
As the study progressed, Naama became moreassertive in her use of the mechanical hand togain the attention of the teacher. Toward theend of the six-week period, she was using thehand on her own initiative at appropriate timeswithout any prompting from either teacher.
Academic progress: There were a number ofindicators that demonstrated PEBBLES’ abilityto facilitate Naama’s academic progress. When-ever the school teacher used the blackboardduring a lesson, Naama would use the camera’szoom-in feature to focus on the blackboard or to
162
P. L. (Tamar) Weiss, C. P. Whiteley, J. Treviranus and D. I. Fels

track his hand as he pointed at various locationson the TV monitor when a video was shown.Moreover, the hospital teacher’s immediateawareness of a given lesson’s content and paceenabled her to adjust it to better suit Naamawhile preserving the essence of the class’s work.The school teacher was able to incorporateNaama’s responses to questions into class discus-sions which, in turn, served to encourage Naamato respond with greater frequency.
3.2. Classmates’ drawings of PEBBLES
The pre- and post-drawings of PEBBLES did notprovide much insight into class attitudes aboutPEBBLES. For example, as expected, the shapeof the unit varied considerably in the pre-drawings (from a drawing of a tank to a drawingthat had a similar shape to PEBBLES), while thepost-drawings all resembled the actual unit inshape and size. Many of the students had seenPEBBLES prior to the study because there hadbeen much media attention as well as manypublic exhibitions. One interesting observationfrom these drawings is that the majority (11/18)of pre-study drawings included a face whereas themajority (15/18) of post-study drawings did not.In previous studies [9], we observed the opposite(i.e. the students added personality to the robotunit in the post-study drawings and not the pre-study drawings).
3.3. Classmates’ responses todiscussion/questionnaire
During the group discussion that took place priorto the PEBBLES experience, the studentsappeared to have a fairly typical view of whattakes place in hospital environments. Forexample, statements such as ‘‘I don’t like it [ahospital], but they are good it helps people’’ and‘‘doctors, nurses, surgeons, secretaries, pediatri-cians work there’’. The number and length ofresponses were sparse. In contrast, the discussionfollowing the six-week PEBBLES experience wasmuch richer in both quantity and quality. Thestudents now included ‘‘teachers of little kids’’ aspeople who work at a hospital. They also mademany more references to the remote student;statements such as ‘‘PEBBLES is helping [stu-dent’s name] learn at home’’, ‘‘it’s kind of coolhaving a robot sit next to [her]’’, ‘‘it lets her bewith her friends’’, and ‘‘it allows her to keep upwith her school work’’ were common. Although
the mean score of the students’ response (on themarked scale) to whether PEBBLES had helpedthe remote student was higher after six weeks(4.1 ± 0.5) than it had been before they startedusing the system (3.8 ± 0.6), the difference wasnot statistically significant.
3.4. Drawings of a sick person
The inter-rater reliability of the four scales usedto evaluate the students’ perception of a sickperson was generally good with pre-scale coeffi-cients for health (ICC=0.61, p=0.001), attitude(ICC=0.87, p=0.000), individuality (0.75,p=0.000), and vitality (ICC=0.54, p=0.005).The post-scale inter-rater reliability was alsogood for the attitude (ICC=0.84, p=.000) andvitality (ICC=0.72, p=0.000) scales, weaker forthe individuality scale (ICC=0.55, p=0.003) andquite low for the health scale (ICC=0.38,p=0.04). The results of the Wilcoxon signedranks test for related samples showed that therewas a significant difference between the pre- andpost-attitude scales (p=0.01). Although thereappeared to be a trend for the other three scales,with the post-scores being higher than the pre-scores in all cases, these results were notsignificant. These results suggest that interactingwith PEBBLES does affect students’ impressionsof hospitals (and of people’s experience inhospitals).
3.5. Data from adult participants
Overall, three of the adult participants (thehospital teacher, the classroom teacher and theparent) rated the PEBBLES experience as beinga positive one for Naama. At the start of thestudy, their ratings were neutral, positive or verypositive (scores of 3, 4 or 5 on the five-pointscale) on participation in school, effectiveness ofcommunication strategies, motivation and emo-tional state. At the end of six weeks, the hospitalteacher increased her scores, rating PEBBLES tohave had a positive effect in all four categories.She noted that she was ‘‘thrilled with the remotestudent’s delight in joining her class’’ and thatshe ‘‘noticed great changes with her [Naama’s]school work’’. The school teacher rated themotivation and emotion categories as being verypositive but decreased his rating of participationand communication as the study progressed.Naama’s father gave high scores throughout thesix weeks and verbally supported his scores with
163
PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised ChildrenPEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised Children

comments such as ‘‘with the help of PEBBLES Ihave noticed great changes with her schoolwork. She seems to be enjoying the day withschoolwork. She seems to be catching up fasternow, making up the lost time. PEBBLES is thekey to lost education’’.
In contrast to these overall positive scores,the dialysis nurse indicated that she observed noor a very small change for the four categories.This result was not surprising in this case sincethe nurse’s role related primarily to the provisionof the medical care required by the haemodialysisprocedure. The other adult participants, as wellas members of the PEBBLES research team,supervised and guided all interactions withPEBBLES. Given the space limitations in thehaemodialysis treatment room and the heavycase load of other patients, it was neithernecessary nor feasible for the dialysis nurse toplay a role in Naama’s classroom interactions.
It is important to note that the school teacherconsistently rated his workload as increased as aresult of PEBBLES being used in the classroom.The hospital teacher rated her workload asunchanged throughout the study. All partici-pants expressed some concern related to techni-cal difficulties with the system, especially relatedto the audio levels.
4. Discussion
4.1. Effect on remote student
The objective and subjective data clearlyindicate that PEBBLES had an overall positiveimpact on the majority of the people whoparticipated in this study. As expected, theperson most positively affected was the remotestudent herself. Prior to the commencement ofthis project, Naama was identified as a very quietand shy individual who had extremely weakcommunication skills; she was recommended as acandidate for PEBBLES by the hospital teachersbecause she had missed so much school andmight benefit from contact with her regular class.In fact, over the past several years there has beenmuch concern about Naama’s chronic truancy.Although children undergoing haemodialysisoften experience fatigue by the end of thesession, and may not be well enough to attendschool in the afternoon, they are usually able toattend on the alternate days. In Naama’s case,before this study commenced, she had been
attending school very infrequently (she had goneto school for several days at the beginning of theschool year but rarely since) and contactbetween the school and hospital teachers hadbeen minimal. Prior to PEBBLES there did notappear to be any practical mechanism forresolving the problem.
Naama’s response to and performance withPEBBLES was extremely positive. Naama reg-ularly attended school via PEBBLES throughoutthe study and did experience some very dramaticchanges in attitudes and behaviours. After onlyfive sessions with PEBBLES, Naama informedher father that she wanted to return to class,which she did. Unfortunately, shortly after shebegan going to school, a number of eventsoccurred which prevented her from attending fora two-week period (she became ill, the schoolwas closed due to a maintenance workers’ strikeand a school holiday intervened). She did,however, resume her attendance after theseoccurrences. The PEBBLES experience appearedto help Naama demonstrate a positive interest inbecoming a part of her class and an ability tomake this desire known. She also became moreassertive. This was nicely illustrated by herincreasingly frequent use of the mechanicalhand to gain the attention of the teacher.Toward the end of the study, she was using thehand on her own initiative without any prompt-ing. The above examples illustrate the variety ofways in which PEBBLES helped to nurtureNaama’s latent abilities that had been concealedby her reserved and timid nature.
Naama’s use of PEBBLES was reminiscent ofyoung or very shy children who often find iteasier to communicate with the aid of a puppet.A puppet is an inanimate object that is used as avisual metaphor to depict real life but is not quitepart of the real world [13]. Puppetry has beenused in educational settings with children ofdifferent ages and has been shown to be effectivein helping children communicate sensitive issuesbecause it can provide a safe way for children toexpress themselves [14]. We suggest that Naamafound comfort in being represented by the warmand friendly PEBBLES who, much as a puppetwould, acted as a congenial intermediary ininteractions with the school teacher and class-mates. The ability of PEBBLES to establish anaura of telepresence removed the stigma that theclassroom participants may otherwise haveassociated with Naama’s reliance on an inter-
164
P. L. (Tamar) Weiss, C. P. Whiteley, J. Treviranus and D. I. Fels

mediary. Fortunately, Naama’s need to usePEBBLES as an ‘‘arm’s length’’ representativeabated with time, as she improved her commu-nication skills and gained confidence. PEBBLESthen assumed its traditional role of being aphysical and social representative of the absentstudent.
It is important to note that there seems to bea great flexibility in the way that a given student,her classmates and the adult participants takeadvantage of the many ways that PEBBLES canenhance the learning environment. For a quietand withdrawn child such as Naama, PEBBLESserved as the intermediary through which shecould reconnect to her educational setting andinteract more freely with her classmates andteachers. Naama’s needs and responses presenteda startling contrast to a previous PEBBLES user,a very precocious, articulate grade 3 student whohad a tendency to overreact and behave in a sillymanner. In this latter case the PEBBLESexperience appeared help him calm down andfocus on his studies while he was in the hospital.In all cases to date, including students with largedifferences in age, illness, intelligence andpersonality, we can confidently report thatthere was a positive behavioural change in thestudent as a result of using PEBBLES.
4.2. Effect on classmates
The remote student was by no means the onlyone to benefit from the PEBBLES experience.
Naama’s classmates welcomed her use ofPEBBLES with great enthusiasm. They weregreatly intrigued by this application of computersand were impressed by the association of acelebrity figure with the project. PEBBLES had asignificant impact on their awareness of andattention to their shy classmate and seemed tohelp them become more sensitive to people indifficult situations. As noted previously, Naamawas very soft spoken and it was often difficult tohear her during face-to-face conversations. Fromthe start, the fact that Naama’s voice could beheard much more easily (since it was projectedvia a high-quality wireless lavaliere micro-phone), greatly facilitated communication be-tween Naama and her classmates.
The early excitement generated by PEBBLES’presence in the classroom was followed by amodest, and not unexpected, decrease in en-thusiasm. Nevertheless, the classmates main-tained their interest in the system throughout
the study and readily agreed to use the teacher’slavaliere microphone during class presentations(to improve the quality of their audio transmis-sion for Naama’s benefit). They approached theclassroom unit to chat with Naama and made anumber of suggestions for improving PEBBLES’effectiveness.
4.3. Effect on adult participants
Overall, the adult participants were positiveabout the PEBBLES experience and the effect ithad on Naama. Nevertheless, several issues ofconcern were expressed. The school teacherreported that his workload increased whilePEBBLES was in used in the classroom as hehad to prepare extra teaching materials forNaama prior to each session. Moreover, incontrast to his behaviour with the rest of theclass, the school teacher tended to interact withNaama individually when using PEBBLES,instructing her separately from the class anddirecting questions personally to her. From thevideotaped records it is not clear how much ofthe extra attention paid to Naama was actuallyrequired versus how much was due to the schoolteacher’s uncertainty whether PEBBLES wouldreally enable Naama to perform like any otherstudent.
In his written comments, the teacher alsoexpressed an initial apprehension regarding thetechnology and also regarding his perceived needto alter his teaching style. In later comments, hestated that these impressions were unfoundedand that he did not really need to alter histeaching style to suit PEBBLES. He also statedthat he recognised the significant benefits to theremote student in maintaining a connection toher peers, and the very positive benefits to theclassroom students as result of interaction withthe remote student (e.g. gaining sensitivity toothers in difficult situations).
The remote student’s father was the mostpositive of all of the adult participants in hisreactions to PEBBLES, often remarking thatthere were impressive changes in his daughter’sbehaviour and school work. He expressed greatpleasure with this experience.
The positive subjective results from all of theadults are encouraging and seem to indicate thatthere is consistent and noticeable change insalient behaviours of the remote student includ-ing communication, motivation and participa-tion.
165
PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised ChildrenPEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised Children

4.4. Effect on teaching
Hospitalised students are prone to regressingacademically. One of the primary roles of thehospital teacher is to retard that regression bycustomising the curriculum (that has beenprovided by the school teacher) to suit the sickstudent’s abilities. PEBBLES was invaluable infacilitating team teaching between school andhospital teachers, helping them to appreciateeach other’s role, and actualising the curriculumin the best way possible. Despite the reportedincrease in workload, both the school andhospital teachers agreed that PEBBLES had agenerally positive effect on teaching practices,procedures and logistics.
The hospital teacher commented that shegreatly benefited from hearing the way in whichthe school teacher interacted with his otherstudents; it helped her understand his teachingmethods and to gain a clearer idea of the overallacademic goal in each subject area. The hospitalteacher was thereby able to tailor her teaching tomeet Naama’s needs in a way that would satisfythe school teacher’s objectives. This unantici-pated use of PEBBLES raised a potentially seriousmoral dilemma in that ‘‘private’’ conversationsbetween the school teacher and another studentwere ‘‘overheard’’ by Naama and the hospitalteacher. All classroom participants had agreed totake part in the study, and had been informedthat all conversations were transmitted to thehospital. However, the natural acceptance ofPEBBLES as a normal and regular presence inthe classroom may have lulled the teacher andstudents into forgetting that many of theirindividual conversations were being shared.
One aspect of team teaching that can imposea serious challenge is coordinating the timetablesof the school and hospital teachers, especiallywhen the time allotted for the hospital teacher isonly one half hour per day per student. Thetimetables generally matched very well inNaama’s case, but there were some less appro-priate uses of PEBBLES, mostly arising from theschool teacher’s preference for starting class eachday with 15 minutes of individual reading from anovel. Although the hospital teacher was able touse this time to explore difficulties that Naamahad with the reading material, PEBBLES wasclearly put to better use for more dynamicactivities. An example from a maths class on
learning how to determine surface area illustratesthis point.
Naama’s classmates were asked to calculatethe surface area of regular-sized cereal boxeswhich had been brought to class for that purpose.Naama carried out the same task using a single-serving size cereal box from her breakfast tray.This size was easier for her small hands tomanipulate on a bedside table. After observingthe other students present their results to the restof the class, Naama felt more comfortable withthe assignment and was able to take hers toschool. On another occasion, when the schoolteacher began a discussion of recent events inKosovo, the hospital teacher used an atlas toensure that Naama had immediate access toinformation about its location.
One final issue that arose was the exchange ofpaper-based materials between the school andhospital. The installation of a printer/scanner atboth the classroom and hospital ends of PEB-BLES is now available but was not fullyimplemented at the time of this study. A faxsystem was available at the school and at thehospital but it was not located close to either theclassroom or to Naama’s area, making it incon-venient for the teachers to use. In any case, bothof these solutions only support single pages andnot books or other bulky materials such as specialart supplies. A related problem was that therewere insufficient numbers of textbooks inNaama’s school to provide her with her owncopy of them. Again, the hospital school hadtextbooks to use but none were ones used byNaama’s school. It is recommended that aninitial preparation session is required for studentsusing PEBBLES to ensure that textbooks andother materials that cannot be sent by fax aremade available prior to using PEBBLES.
4.5. Technical aspects
The major technical problem continues to be thequality of the audio system. The difficulties withthe sound were often due to:
(1) the hospital noises being picked up andtransmitted to the classroom by Naama’smicrophone; and
(2) the dynamics of the classroom acoustics. Asystem is required that can automaticallydetect and adjust the level of desired soundsand filter out undesirable noise.
The sound landscape for PEBBLES is very
166
P. L. (Tamar) Weiss, C. P. Whiteley, J. Treviranus and D. I. Fels

complex and dynamic. For instance, the class-room contains many potential sound sources,including students, teachers, visitors, the publicaddress system and general noise. All of thesesounds can originate from any physical locationin the room. There is also a very large volumerange to capture, regulate and transmit, fromvery soft-spoken individuals to the loud sound ofa fire alarm. Compounding the difficulty is thefact that PEBBLES is equipped with only twomicrophones, one for the teacher and one roommicrophone fixed in one location; an automaticmixer switches between the two microphonesdepending on which one is receiving the bestinput. Currently, gain levels are established onlyduring PEBBLES’ set-up and cannot be altereddynamically. We would like to implement a typeof automatic speaker location system with multi-ple microphones that would detect and amplifythe sound of the person speaking. Speakerlocation systems have been developed [12] butthey are usually designed for quiet and acousti-cally managed environments. One temporarysolution has been to share the teacher’s lavalieremicrophone when students wished or wererequired to speak individually. However, thisoften created logistical problems for the teacher.
Naama was able to adjust the volume of theclassroom speaker via a thumbwheel controlplaced on her work surface. This allowed her toreduce audio distractions but still be aware ofwhat was taking place in the classroom. Volumecontrol was preferable to pausing the system as itenabled Naama and her teacher to be aware ofwhen the next lesson was about to begin.
At the hospital, the sound landscape is not asdynamic as that of the classroom, primarilybecause there is only one main speaker, butdifficulties were nevertheless present. For in-stance, when Naama had a cold, her classmatescould clearly hear her blowing her nose. More-over, noise in the dialysis unit, especially fromsome of the other patients, frequently disturbedstudents in the classroom, especially during silentreading times. Naama’s microphone wasequipped with a user-controlled mute switchbut she did not always remember to turn it on oroff as needed. A voice-activated microphonesystem may be the solution to this problem (butit would have to be calibrated to the user’svoice).
One additional technical concern wasNaama’s difficulty in grasping the importance
of switching between the two cameras. It wouldappear that improvements in labelling of the twocameras as well as better training would help.However, new technical solutions may also berequired. The purpose of the secondary (extra)camera is to provide a global view of theclassroom so that the view from the primarycamera (if the primary camera is zoomed-inclose) can be maintained simultaneously. Thismay be useful for the remote student to captureperipheral information, such as someone enter-ing the room, with one simple control action toswitch cameras. The user would not be requiredto divert attention from his/her main activitysuch as looking at the blackboard due to thecontrol actions required to change the focus ofthe primary camera to perform another task.
5. Conclusion
The ultimate goal of the PEBBLES interactivetelepresence system is to become a truly mobileand portable system, one which would fulfil thedefinition of a personal technology in every senseof the phrase. Notwithstanding the manytechnical difficulties still to resolve (e.g. accessto a fast, reliable communication link), theongoing, highly-successful efforts towards minia-turisation of related mobile devices (e.g. wrist-phones) [15] appear to indicate that such a goalis feasible within the next few years. Theachievement of mobility and portability willcertainly enhance PEBBLES users’ sense of jointparticipation in a shared experience, and makepossible a number of other important applica-tions. We are currently developing strategies forusing video-conferencing interactivity via PEB-BLES-like devices for helping teleworkers (par-ticularly, but not only, for those with disabilities)achieve a more effective link between the worksite and their remote work location [16]. We arealso involved in the development of synchronoustools for the support of distance education forstudents with disabilities. These and otherdevelopments should help make PEBBLES aneffective personal technology for a large varietyof users.
Acknowledgements
The authors would like to thank The Bay andWayne Gretzky, CANARIE, The OntarioMinistry of Education and Training (TIPPS II),
167
PEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised ChildrenPEBBLES: A Personal Technology for Meeting Educational, Social and Emotional Needs of Hospitalised Children

The Royal Bank of Canada, NSERC grant# OGP0184220, the Ontario Provincial andDemonstration Schools, Human Resources De-velopment Canada, Ryerson Polytechnic Uni-versity, Telbotics Inc. and The University ofToronto. We also would like to acknowledge theMcCaul Street School, The Toronto Hospital forSick Children and J.S. Woodsworth SeniorPublic School (grade 7 class) for their participa-tion in the PEBBLES project. Partial results ofthis study were presented at the CybErg 1999 on-line conference (August 1999) and are availableon their website (cyberg.curtin.edu.au).
References
1. Bossert E. Stress appraisals of hospitalized school-agechildren. Children’s Health Care 1994; 23(1): 33–49
2. Ellerton ML, Ritchie JA, Caty S. Factors influencingyoung children’s coping behaviours during stressfulhealthcare encounters. Maternal-Child Nursing Journal1994; 22(3): 74–82
3. Lambert SA. Variables that affect the school-age child’sreaction to hospitalization and surgery: a review of theliterature. Maternal-Child Nursing Journal 1984; 13: 1–18
4. Thompson ML. Information-seeking, coping and anxietyin school-age children anticipating surgery. Children’sHealth Care 1994; 23(2): 87–97
5. Katz E, Varni J, Rubenstein C, Blew A, Hubert N.Teacher, parent, and child evaluation ratings of a schoolre-integration intervention for children with newlydiagnosed cancer. Children’s Health Care 1992; 21(2):69–75
6. Calculator S, Jorgensen C. Including students withsevere disabilities in schools: fostering communication,
interaction and participation. Singular Publishing, SanDiego, CA, 1994
7. Lipsky D. National study on inclusion: overview andsummary report. Bulletin of the NCERI 1995; 2(2): 6–7
8. Frolich D, Thomas P, Hawley M, Hirade K. Inauguralissue editorial: future personal computing. PersonalTechnologies 1997; 1:1–5
9. Fels DI, Williams LA, Smith G, Treviranus J, EaglesonR. Developing a video-mediated communication systemfor hospitalized children. Telemedicine 1999; 5(2): 193–207
10. Buxton W. Telepresence: integrating shared task andperson spaces. In: Proceedings of Graphics Interface ’92,1992; 23–29
11. Draper D, Kaber DB, Usher JM. Telepresence. HumanFactors 1998; 40(3): 354–375
12. Brandstein MS, Silverman HF. A practical methodologyfor speech source localization with microphone arrays.Computer Speech and Language 1997; 11: 91–126
13. Retrieved from the world wide web on 9 August 1999.http://www.abel.co.uk/~dianalan/Classroom.html
14. Kelton SC, Hamilton AC. Using puppets with youngchildren. Proceedings of the Annual Conference of theAlabama Association for Young Children (Mobile, AL),16 February 1990: 1–12
15. Cochrane P, Payne R, MacDonald B. From Kirk to Picard(a vision of mobility). Personal Technologies 1997; 1: 6–10
16. Weiss PL, Fels D, Treviranus J. Telework enhanced byvideo-conferencing: importance of real-time, interactivecommunication for workers with disabilities. 14thAnnual Meeting of the CSUN Center for Disabilities,Los Angeles, CA, 1999: on-line proceedings http://www.dinf.org/csun_99/session0238.html
Correspondence to: Dr Deborah Fels, Ryerson PolytechnicUniversity, 350 Victoria St., Toronto, Canada M5B 2K3.Email: [email protected]
168
P. L. (Tamar) Weiss, C. P. Whiteley, J. Treviranus and D. I. Fels