
Patients' Self-Report and Handwriting Performance Features ...
11
Citation: Rosenblum, S.; Meyer, S.; Richardson, A.; Hassin-Baer, S. Patients’ Self-Report and Handwriting Performance Features as Indicators for Suspected Mild Cognitive Impairment in Parkinson’s Disease. Sensors 2022, 22, 569. https://doi.org/10.3390/s22020569 Academic Editor: Loris Nanni Received: 19 December 2021 Accepted: 10 January 2022 Published: 12 January 2022 Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affil- iations. Copyright: © 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https:// creativecommons.org/licenses/by/ 4.0/). sensors Article Patients’ Self-Report and Handwriting Performance Features as Indicators for Suspected Mild Cognitive Impairment in Parkinson’s Disease Sara Rosenblum 1, * , Sonya Meyer 2 , Ariella Richardson 3 and Sharon Hassin-Baer 4,5,6 1 The Laboratory of Complex Human Activity and Participation (CHAP), Department of Occupational Therapy, Faculty of Social Welfare & Health Sciences, University of Haifa, Haifa 3498838, Israel 2 Department of Occupational Therapy, Ariel University, Ariel 4077603, Israel; [email protected] 3 Department of Industrial Engineering, Jerusalem College of Technology, Jerusalem 9372115, Israel; [email protected] 4 Movement Disorders Institute, Sheba Medical Center, Ramat Gan 5262000, Israel; [email protected] 5 Department of Neurology, Sheba Medical Center, Ramat Gan 5262000, Israel 6 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv 6997801, Israel * Correspondence: [email protected]; Tel.: +972-4-824-0474 Abstract: Early identification of mild cognitive impairment (MCI) in Parkinson’s disease (PD) patients can lessen emotional and physical complications. In this study, a cognitive functional (CF) feature using cognitive and daily living items of the Unified Parkinson’s Disease Rating Scale served to define PD patients as suspected or not for MCI. The study aimed to compare objective handwriting performance measures with the perceived general functional abilities (PGF) of both groups, analyze correlations between handwriting performance measures and PGF for each group, and find out whether participants’ general functional abilities, depression levels, and digitized handwriting measures predicted this CF feature. Seventy-eight participants diagnosed with PD by a neurologist (25 suspected for MCI based on the CF feature) completed the PGF as part of the Daily Living Questionnaire and wrote on a digitizer-affixed paper in the Computerized Penmanship Handwriting Evaluation Test. Results indicated significant group differences in PGF scores and handwriting stroke width, and significant medium correlations between PGF score, pen-stroke width, and the CF feature. Regression analyses indicated that PGF scores and mean stroke width accounted for 28% of the CF feature variance above age. Nuances of perceived daily functional abilities validated by objective measures may contribute to the early identification of suspected PD-MCI. Keywords: assessment; activities of daily living; functional cognition; Parkinson’s disease 1. Introduction The reported frequency rate of mild cognitive impairment (MCI) among patients with Parkinson’s disease (PD), ranging from 20% to 50% [1,2], reflects the difficulty in defining and identifying PD-MCI. Early recognition of MCI is vital for both patients and their caregivers, enabling prompt intervention to lessen further emotional and physical health complications and improve patients’ life quality [3,4]. A central challenge lies in how to capture “the gradual cognitive decline, which does not significantly interfere with patients’ functional independence as subjectively reported by the patient and/or informant”, as determined by PD Brain Bank criteria [5]. These criteria lead to the need to assess functional cognitive decline and its possible consequences as reported by the patient. Functional cognition means the cognitive ability to perform daily tasks while incorporating varied cognitive domains. These motor/sensory skill domains support action and performance patterns, such as habits, routines, and roles, rather than specific cognitive skills, such as inhibition, attention, or memory, in isolation [6]. Sensors 2022, 22, 569. https://doi.org/10.3390/s22020569 https://www.mdpi.com/journal/sensors
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Patients' Self-Report and Handwriting Performance Features ...
�����������������
Citation: Rosenblum, S.; Meyer, S.;
Richardson, A.; Hassin-Baer, S.
Patients’ Self-Report and
Handwriting Performance Features
as Indicators for Suspected Mild
Cognitive Impairment in Parkinson’s
Disease. Sensors 2022, 22, 569.
https://doi.org/10.3390/s22020569
Academic Editor: Loris Nanni
Received: 19 December 2021
Accepted: 10 January 2022
Published: 12 January 2022
Publisher’s Note: MDPI stays neutral
with regard to jurisdictional claims in
published maps and institutional affil-
iations.
Copyright: © 2022 by the authors.
Licensee MDPI, Basel, Switzerland.
This article is an open access article
distributed under the terms and
conditions of the Creative Commons
Attribution (CC BY) license (https://
creativecommons.org/licenses/by/
4.0/).
sensors
Article
Patients’ Self-Report and Handwriting Performance Features asIndicators for Suspected Mild Cognitive Impairment inParkinson’s DiseaseSara Rosenblum 1,* , Sonya Meyer 2 , Ariella Richardson 3 and Sharon Hassin-Baer 4,5,6
1 The Laboratory of Complex Human Activity and Participation (CHAP), Department of Occupational Therapy,Faculty of Social Welfare & Health Sciences, University of Haifa, Haifa 3498838, Israel
2 Department of Occupational Therapy, Ariel University, Ariel 4077603, Israel; [email protected] Department of Industrial Engineering, Jerusalem College of Technology, Jerusalem 9372115, Israel;
[email protected] Movement Disorders Institute, Sheba Medical Center, Ramat Gan 5262000, Israel;
[email protected] Department of Neurology, Sheba Medical Center, Ramat Gan 5262000, Israel6 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv 6997801, Israel* Correspondence: [email protected]; Tel.: +972-4-824-0474
Abstract: Early identification of mild cognitive impairment (MCI) in Parkinson’s disease (PD) patientscan lessen emotional and physical complications. In this study, a cognitive functional (CF) featureusing cognitive and daily living items of the Unified Parkinson’s Disease Rating Scale served todefine PD patients as suspected or not for MCI. The study aimed to compare objective handwritingperformance measures with the perceived general functional abilities (PGF) of both groups, analyzecorrelations between handwriting performance measures and PGF for each group, and find outwhether participants’ general functional abilities, depression levels, and digitized handwritingmeasures predicted this CF feature. Seventy-eight participants diagnosed with PD by a neurologist(25 suspected for MCI based on the CF feature) completed the PGF as part of the Daily LivingQuestionnaire and wrote on a digitizer-affixed paper in the Computerized Penmanship HandwritingEvaluation Test. Results indicated significant group differences in PGF scores and handwriting strokewidth, and significant medium correlations between PGF score, pen-stroke width, and the CF feature.Regression analyses indicated that PGF scores and mean stroke width accounted for 28% of the CFfeature variance above age. Nuances of perceived daily functional abilities validated by objectivemeasures may contribute to the early identification of suspected PD-MCI.
Keywords: assessment; activities of daily living; functional cognition; Parkinson’s disease
1. Introduction
The reported frequency rate of mild cognitive impairment (MCI) among patientswith Parkinson’s disease (PD), ranging from 20% to 50% [1,2], reflects the difficulty indefining and identifying PD-MCI. Early recognition of MCI is vital for both patients andtheir caregivers, enabling prompt intervention to lessen further emotional and physicalhealth complications and improve patients’ life quality [3,4].
A central challenge lies in how to capture “the gradual cognitive decline, which doesnot significantly interfere with patients’ functional independence as subjectively reportedby the patient and/or informant”, as determined by PD Brain Bank criteria [5]. Thesecriteria lead to the need to assess functional cognitive decline and its possible consequencesas reported by the patient. Functional cognition means the cognitive ability to performdaily tasks while incorporating varied cognitive domains. These motor/sensory skilldomains support action and performance patterns, such as habits, routines, and roles,rather than specific cognitive skills, such as inhibition, attention, or memory, in isolation [6].
Sensors 2022, 22, 569. https://doi.org/10.3390/s22020569 https://www.mdpi.com/journal/sensors
Sensors 2022, 22, 569 2 of 11
Functional cognition decline may be tied to negative emotional response, less efficiencyand participation in activities of daily living (ADL) and life domains, and diminishedlife quality and depression [7,8]. Thus, we measured depression by the Beck DepressionInventory (BDI) test [9].
In a previous study, we presented the inadequate PD-MCI identification achievedby cognitive and neuropsychological tests due to the discorrelation found between testscores and individuals’ reports about their daily functional cognitive abilities [3]. Wehad emphasized the discrepancy between the results of the cognitive battery offeredby the Movement Disorder Society (MDS) and the individuals’ self-reports of changesin their daily functioning related to cognitive decline. That study supported previousliterature addressing the problem of making conclusions about human functional cognitiveabilities from neuropsychological tests that evaluate each cognitive domain separately.Instead, this literature suggested the need for questionnaires/tests that relate to real-lifefunctional scenarios that require integrating varied cognitive domains for efficient dailyfunction [10,11].
We next presented the cognitive functional (CF) feature, which we created based onpatients’ reports of certain items in the MDS Unified Parkinson’s Disease Rating Scale(UPDRS) [3,12]. The CF feature is calculated as the mean score of seven MDS-UPDRS-derived items: the cognitive impairment Item 1.1 from the UPDRS nonmotor experienceof the daily living subscale and Items 2.1 speech, 2.4 eating, 2.5 dressing, 2.6 hygiene,2.7 handwriting, and 2.8 doing hobbies from the UPDRS motor experience of the dailyliving subscale. As the CF feature has not been approved yet, we suggest the term suspectedof PD-MCI based on results of these two prior studies (one in publication [3] and one indraft [4]) and participants’ reports of their real-life confrontations that are herein validatedby objective measures. We assume the changes participants feel in their daily functioningare still too subtle for instruments such as the Montreal Cognitive Assessment (MoCA) todetect but significant enough to affect their functional capabilities.
In the second study, we found that PD patients defined as having suspected PD-MCIbased on their self-reported CF feature exhibited significantly lower CF abilities than didPD patients without suspected MCI [4]. Furthermore, specific items of the self-reportedDaily Living Questionnaire (DLQ) [13] and Time Organization and Participation Scale(TOPS) [14] accounted for up to 35% of the variance in the CF feature [4].
The results indicated that PD patients with suspected MCI feel something has changedin their CF abilities, as reflected in the amount of cognitive effort they need to invest intheir daily activities and in their ability to organize time [4]. Their CF decline, emotionalstatus, activity performance features, and motivation were related [15]. These relationshipsraise the question of how PD patients with suspected MCI would report on their generalfunctional ability, satisfaction from their daily activities, and the changes in their rolescompared to patients not suspected for MCI. It is further intriguing to consider whether thedeclined functional ability of patients suspected for MCI would manifest through objectivemeasures of their actual activity performance, such as in their handwriting.
Handwriting is a complex human activity taught in childhood and a daily activitythat adults perform in various settings. In a handwriting task, people operate and inte-grate lower-level perceptual–motor and higher-level cognitive processes [16]. Abnormalhandwriting changes and specifically micrographia (abnormally small letter size) havebeen reported among PD patients [17]. Previous findings also indicated that handwritingmeasures potentially differentiate between PD and healthy subjects [18–21], and identifyvarious stages of PD and both medication and intervention effects [22,23]. Thus, measuresof handwriting also may support PD-MCI identification.
Past studies have indicated that using a computerized handwriting evaluation sys-tem, such as ComPET [24], to collect handwriting data enables an efficient and objectivemethod to evaluate functional handwriting performance. Applying dynamic handwritinganalysis in neurodegenerative disease assessment focused on PD also has been reviewedin the literature [25]. Specifically, digitized spiral drawing has been used to differentiate
Sensors 2022, 22, 569 3 of 11
between PD and healthy controls [26,27]. Tasks in which sensing user handwriting with adigitized tablet was used include demonstrating performance change in patients with mildmajor depressive disorder (MDD) [28], differentiating between PD patients and healthycontrols [17,29,30], and reflecting executive functions among patients with developmen-tal coordination disorders [31,32]. In a previous PD study [17], 20 people with PD and20 healthy people wrote their full names and copied an address. The variables that madethe greatest contribution to group membership in that study—and thus were implanted inthe current study—were mean width, duration, and height in both tasks. Based on thesefunctions, we were able to classify 97.5% of participants as with or without PD. However,the distinction between PD with and without PD-MCI is not trivial. Therefore, in the cur-rent study, we used a handwriting task that requires integrating cognitive domains founddeficient among people with PD-MCI. Based on evidence of visuospatial, working memory,organization, and psychomotor speed deficits among people with PD-MCI (e.g., [33–35]),we requested participants to fill in a check-formatted paper.
This study aims to further analyze the impact of the self-reported CF feature onsuspected PD-MCI identification. We compare perceived general functional ability (PGF)and digitized handwriting performance measures of PD participants with and withoutsuspected MCI based on their CF features. Furthermore, correlations between participants’PGF, BDI scores, and digitized handwriting measures are analyzed. Finally, we addressthe question of whether participants’ global functional abilities, BDI scores, and digitizedhandwriting measures may predict the CF feature.
2. Materials and Methods2.1. Participants
The study included 78 participants recruited at the Sheba Movement Disorders Insti-tute in Israel and diagnosed with PD by expert neurologists. Inclusion criteria were an ageof 40 years or older, living in Israel for at least 10 years, being functionally independent,with ability to read and speak Hebrew, normal or corrected hearing, and vision abilities.Furthermore, participants had to score 18 or less on the BDI [9] and 23 or more on theMoCA [36–38].
Exclusion criteria for all participants were significant systemic diseases, such as can-cer or congestive heart failure; any neurological or psychiatric condition or damage; ortreatment with antipsychotic or anticholinergic medications.
The 78 patients in the sample met the MDS clinical diagnostic criteria for probableor possible PD [39], and were Hoehn and Yahr Stage 1 or 2 [40]. The disease durationat inclusion was up to 10 years. A movement disorders neurologist assessed PD-relatedsymptoms and signs using the MDS-UPDRS [12].
The PD patients were divided into two groups based on their CF features. Group A(1 point or more) were PD patients with CF difficulties (n = 25) suspected for PD-MCI (s.PD-MCI). Group B (less than 1 point) were PD patients without CF difficulties (n = 53). Fordetailed descriptions of both groups’ demographic characteristics, see [4] and Section 3.1.
2.2. Measures
A medical evaluation was conducted and self-report questionnaires that focused onfunctional cognition were administered to all participants.Daily Living Questionnaire (DLQ) [13]
Our previous study implemented Parts A and B of the DLQ [13], which evaluatesfunctional cognition through 52 items scored on a 5-point Likert scale. In the current study,we used Part C, which captures the individual’s PGF. The Part C score is comprised ofseven items that ask the respondents about their overall ability to function, perceivedchanges in roles and responsibilities, and the degree of satisfaction with what they needand want to do in their daily lives [41]. The scores range from 1 (excellent/satisfied/nochange) to 5 (weak/disappointing/completely changed). Thus, higher scores indicate agreater decline. For each group, we calculated a mean score for each item and a total mean
Sensors 2022, 22, 569 4 of 11
score for all seven items. Cronbach’s alpha for the DLQ Part C general score was 90 in thecurrent study.Computerized Penmanship Evaluation Tool [24]
The ComPET, an online computerized handwriting evaluation system, was used inthis study to collect and analyze handwriting data. The ComPET contains two main parts:data collection, which is not language-dependent, and data analysis, programmed usingMATLAB software. Participants performed the writing task on A4-size lined paper affixedto the surface of a WACOM Intuos 4 digitizing tablet using a wireless electronic inking pen(Model GP-110). The displacement, pressure, and pen-tip angle were sampled at 100 Hzvia a 1300 MHz Pentium (R) M laptop computer. The computerized system enables thecollection of spatial, temporal, and pressure data while the subject is writing. Pen strokeon paper was measured each time the pen contacted the writing surface with an appliedpressure above 50 non-scaled units. The ComPET also enables detecting pen motion in theair when the pen is up to 6 mm and pen-stroke time continues when the pen again contactsthe paper. Pen-stroke height and width also are computed when the pen is on the paper.Notably, these measures relate to pen strokes and not letters because forming a letter mayrequire combining two or more pen strokes.
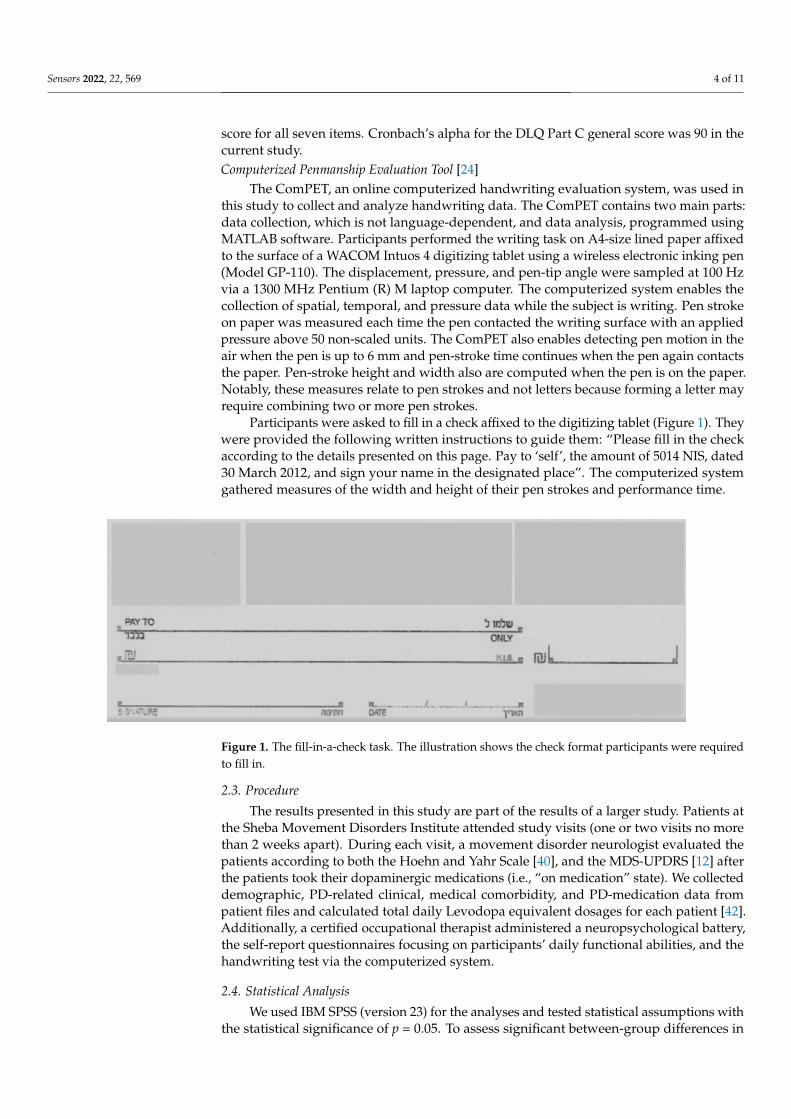
Participants were asked to fill in a check affixed to the digitizing tablet (Figure 1). Theywere provided the following written instructions to guide them: “Please fill in the checkaccording to the details presented on this page. Pay to ‘self’, the amount of 5014 NIS, dated30 March 2012, and sign your name in the designated place”. The computerized systemgathered measures of the width and height of their pen strokes and performance time.
Sensors 2022, 22, x FOR PEER REVIEW 4 of 11
changes in roles and responsibilities, and the degree of satisfaction with what they need and want to do in their daily lives [41]. The scores range from 1 (excellent/satisfied/no change) to 5 (weak/disappointing/completely changed). Thus, higher scores indicate a greater decline. For each group, we calculated a mean score for each item and a total mean score for all seven items. Cronbach’s alpha for the DLQ Part C general score was 90 in the current study. Computerized Penmanship Evaluation Tool [24]
The ComPET, an online computerized handwriting evaluation system, was used in this study to collect and analyze handwriting data. The ComPET contains two main parts: data collection, which is not language-dependent, and data analysis, programmed using MATLAB software. Participants performed the writing task on A4-size lined paper affixed to the surface of a WACOM Intuos 4 digitizing tablet using a wireless electronic inking pen (Model GP-110). The displacement, pressure, and pen-tip angle were sampled at 100 Hz via a 1300 MHz Pentium (R) M laptop computer. The computerized system enables the collection of spatial, temporal, and pressure data while the subject is writing. Pen stroke on paper was measured each time the pen contacted the writing surface with an applied pressure above 50 non-scaled units. The ComPET also enables detecting pen mo-tion in the air when the pen is up to 6 mm and pen-stroke time continues when the pen again contacts the paper. Pen-stroke height and width also are computed when the pen is on the paper. Notably, these measures relate to pen strokes and not letters because form-ing a letter may require combining two or more pen strokes.
Participants were asked to fill in a check affixed to the digitizing tablet (Figure 1). They were provided the following written instructions to guide them: “Please fill in the check according to the details presented on this page. Pay to ‘self’, the amount of 5014 NIS, dated 30 March 2012, and sign your name in the designated place.” The computer-ized system gathered measures of the width and height of their pen strokes and perfor-mance time.
Figure 1. The fill-in-a-check task. The illustration shows the check format participants were required to fill in.
2.3. Procedure The results presented in this study are part of the results of a larger study. Patients at
the Sheba Movement Disorders Institute attended study visits (one or two visits no more than 2 weeks apart). During each visit, a movement disorder neurologist evaluated the patients according to both the Hoehn and Yahr Scale [40], and the MDS-UPDRS [12] after the patients took their dopaminergic medications (i.e., “on medication” state). We col-lected demographic, PD-related clinical, medical comorbidity, and PD-medication data from patient files and calculated total daily Levodopa equivalent dosages for each patient [42]. Additionally, a certified occupational therapist administered a neuropsychological
Figure 1. The fill-in-a-check task. The illustration shows the check format participants were requiredto fill in.
2.3. Procedure
The results presented in this study are part of the results of a larger study. Patients atthe Sheba Movement Disorders Institute attended study visits (one or two visits no morethan 2 weeks apart). During each visit, a movement disorder neurologist evaluated thepatients according to both the Hoehn and Yahr Scale [40], and the MDS-UPDRS [12] afterthe patients took their dopaminergic medications (i.e., “on medication” state). We collecteddemographic, PD-related clinical, medical comorbidity, and PD-medication data frompatient files and calculated total daily Levodopa equivalent dosages for each patient [42].Additionally, a certified occupational therapist administered a neuropsychological battery,the self-report questionnaires focusing on participants’ daily functional abilities, and thehandwriting test via the computerized system.
2.4. Statistical Analysis
We used IBM SPSS (version 23) for the analyses and tested statistical assumptions withthe statistical significance of p = 0.05. To assess significant between-group differences in

Sensors 2022, 22, 569 5 of 11
medical status and demographics, we used t-tests for continuous variables and Chi-squaredtests for categorical variables. Given the significant between-group age difference and thecorrelations between the main study variables and age that indicated no significant corre-lation, we did not include age as a covariate variable in comparisons of the study’s mainvariables (PGF and handwriting measures). A Cronbach’s alpha analysis was implementedto check the internal variability of the PGF self-report (Part C of the DLQ). Tests of normalityfor each main study variable indicated normal distribution. Further comparison analysisat the mean-score and item levels of the PGF provided insight about which functionalitems best differentiated between the PD patients with and without suspected PD-MCI. Weconducted additional t-tests to compare the handwriting process measures of both groups.Pearson correlations were conducted on the entire sample of PD patients (N = 78) betweenthe handwriting process measure that differentiated the groups, the BDI score, the PGFscore, and the CF feature. Finally, stepwise regression was conducted to examine whetherthe handwriting process measure that differentiated between the groups, the BDI score,and/or the PGF score may predict the CF feature above age.
3. Results3.1. Participants’ Demographic and Medical Status
There were no significant differences between PD participants without CF difficulties(PD-n.MCI) and those suspected for MCI (s.PD-MCI) based on their CF feature in genderfrequency (68% and 69.80% male) or in years of education (M = 16.4 years and SD = 3.68;M = 15.64 and SD = 3.67). No significant group differences were found for the percentile ofparticipants treated with Levodopa (49.10% and 48%) or for PD duration since diagnosis inyears (M = 4.21 and SD = 3.42, and M = 4.09 and SD = 2.88). The Hoehn and Yahr stageof the participants in the PD group ranged from 1.0 to 3.0, with the same median of 2.0 s,and of the participants in the PD-MCI group ranged from 1.0 to 2.5, with a median of 2.0.However, significant group differences were found for age ((M = 60.24 years and SD = 8.36;M = 66.26 and SD = 7.24), t(76) = −3.46, p = 0.004)); MoCA scores ((M = 26 and SD = 2.00;M = 24.98 and SD = 2.00), t(76) = 2.05, p = 0.043)); and BDI scores ((M = 7.79 and SD = 4.92;M = 5.43 and SD = 4.43), t(76) = 2.64, p = 0.010)).
In addition, Pearson correlations indicated no significant correlations between ageand the main study variables (i.e., general functional DLQ score or handwriting measures).Thus, age was not held as a covariate in the between-group comparison.
3.2. Comparison of PGF Ability
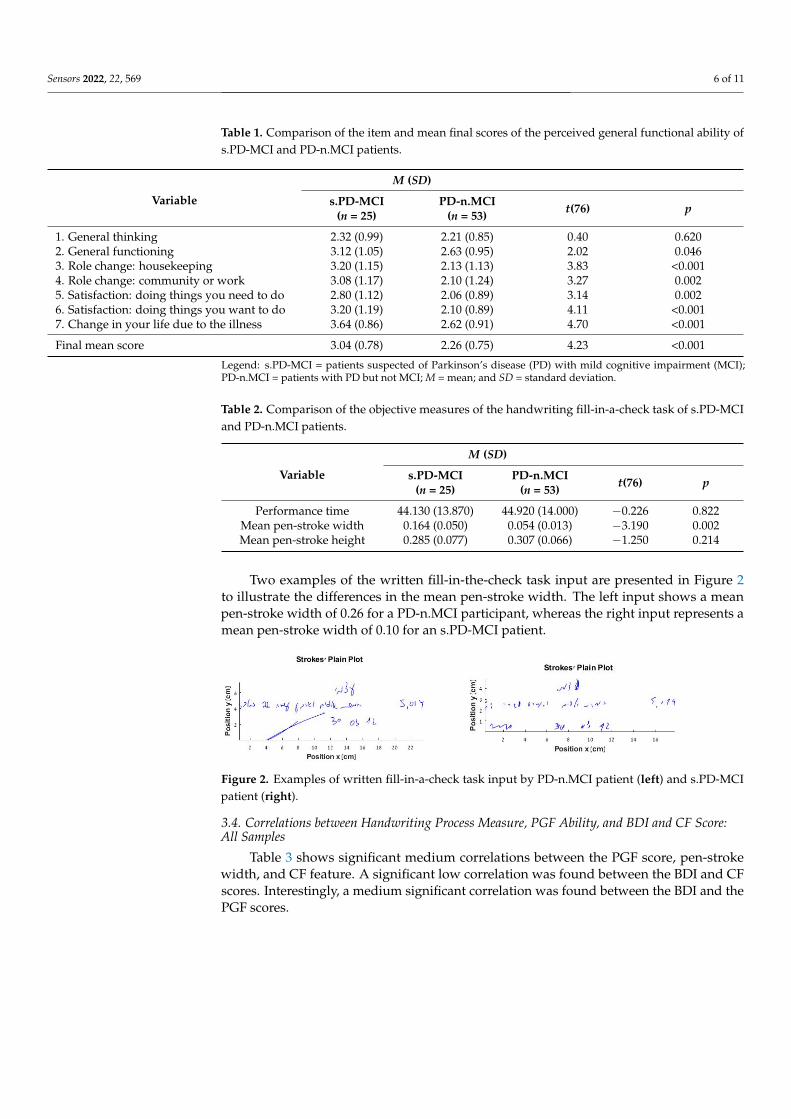
Table 1 shows the significant group differences found for the participants’ PGF abilitymean scores. The mean scores for each questionnaire also are presented to indicate thesources of the differences; high scores indicate more difficulties, less satisfaction, or greaterchange due to the disease. Although there were no significant differences for generalthinking, we found significant differences for all other items capturing general functioning,roles changes, satisfaction level, and life change due to the disease.
3.3. Comparison of Objective Handwriting Measure (Fill in a Check)
As presented in Table 2, only the mean pen-stroke width significantly differentiatedthe groups, with the mean significantly smaller among participants with s.PD-MCI.
Sensors 2022, 22, 569 6 of 11
Table 1. Comparison of the item and mean final scores of the perceived general functional ability ofs.PD-MCI and PD-n.MCI patients.
Variable
M (SD)
s.PD-MCI(n = 25)
PD-n.MCI(n = 53) t(76) p
1. General thinking 2.32 (0.99) 2.21 (0.85) 0.40 0.6202. General functioning 3.12 (1.05) 2.63 (0.95) 2.02 0.0463. Role change: housekeeping 3.20 (1.15) 2.13 (1.13) 3.83 <0.0014. Role change: community or work 3.08 (1.17) 2.10 (1.24) 3.27 0.0025. Satisfaction: doing things you need to do 2.80 (1.12) 2.06 (0.89) 3.14 0.0026. Satisfaction: doing things you want to do 3.20 (1.19) 2.10 (0.89) 4.11 <0.0017. Change in your life due to the illness 3.64 (0.86) 2.62 (0.91) 4.70 <0.001
Final mean score 3.04 (0.78) 2.26 (0.75) 4.23 <0.001
Legend: s.PD-MCI = patients suspected of Parkinson’s disease (PD) with mild cognitive impairment (MCI);PD-n.MCI = patients with PD but not MCI; M = mean; and SD = standard deviation.
Table 2. Comparison of the objective measures of the handwriting fill-in-a-check task of s.PD-MCIand PD-n.MCI patients.
Variable
M (SD)
s.PD-MCI(n = 25)
PD-n.MCI(n = 53) t(76) p
Performance time 44.130 (13.870) 44.920 (14.000) −0.226 0.822Mean pen-stroke width 0.164 (0.050) 0.054 (0.013) −3.190 0.002Mean pen-stroke height 0.285 (0.077) 0.307 (0.066) −1.250 0.214
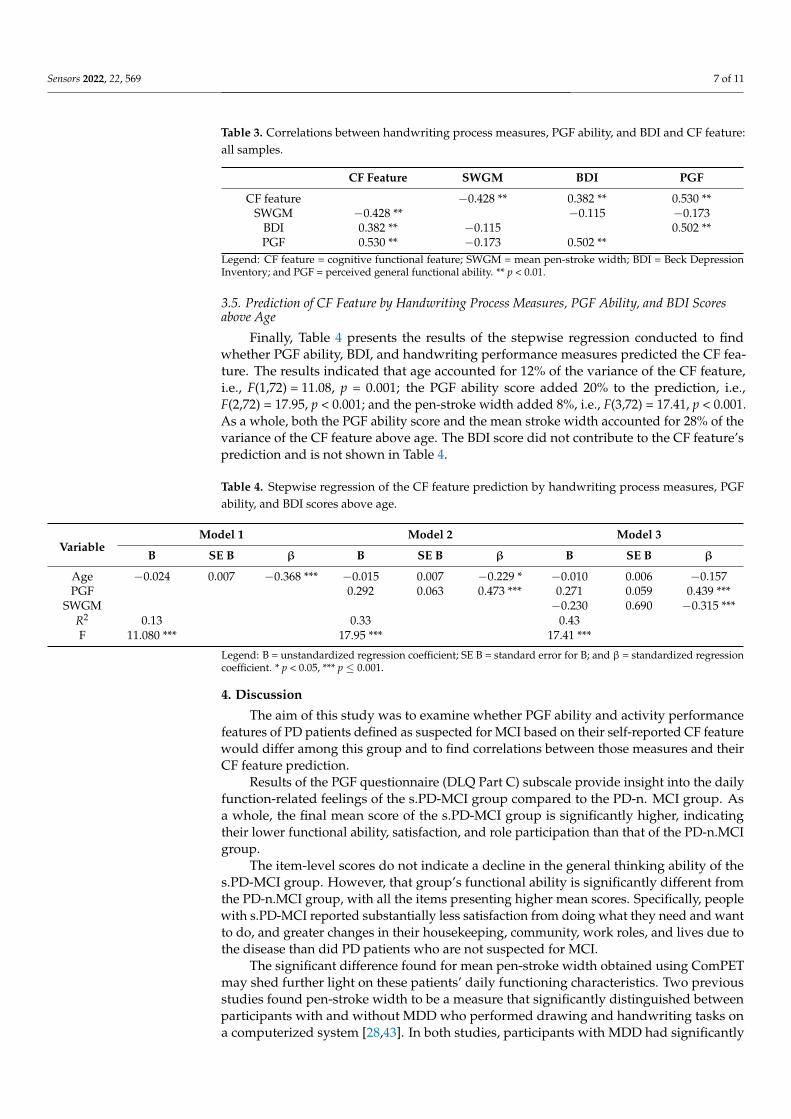
Two examples of the written fill-in-the-check task input are presented in Figure 2to illustrate the differences in the mean pen-stroke width. The left input shows a meanpen-stroke width of 0.26 for a PD-n.MCI participant, whereas the right input represents amean pen-stroke width of 0.10 for an s.PD-MCI patient.
Sensors 2022, 22, x FOR PEER REVIEW 6 of 11
Table 1. Comparison of the item and mean final scores of the perceived general functional ability of s.PD-MCI and PD-n.MCI patients.
Variable M (SD)
s.PD-MCI (n = 25)
PD-n.MCI (n = 53) t(76) p
1. General thinking 2.32 (0.99) 2.21 (0.85) 0.40 0.620 2. General functioning 3.12 (1.05) 2.63 (0.95) 2.02 0.046 3. Role change: housekeeping 3.20 (1.15) 2.13 (1.13) 3.83 <0.001 4. Role change: community or work 3.08 (1.17) 2.10 (1.24) 3.27 0.002 5. Satisfaction: doing things you need to do 2.80 (1.12) 2.06 (0.89) 3.14 0.002 6. Satisfaction: doing things you want to do 3.20 (1.19) 2.10 (0.89) 4.11 <0.001 7. Change in your life due to the illness 3.64 (0.86) 2.62 (0.91) 4.70 <0.001 Final mean score 3.04 (0.78) 2.26 (0.75) 4.23 <0.001
Legend: s.PD-MCI = patients suspected of Parkinson’s disease (PD) with mild cognitive impairment (MCI); PD-n.MCI = patients with PD but not MCI; M = mean; and SD = standard deviation.
3.3. Comparison of Objective Handwriting Measure (Fill in a Check) As presented in Table 2, only the mean pen-stroke width significantly differentiated
the groups, with the mean significantly smaller among participants with s.PD-MCI.
Table 2. Comparison of the objective measures of the handwriting fill-in-a-check task of s.PD-MCI and PD-n.MCI patients.
Variable M (SD)
s.PD-MCI (n = 25)
PD-n.MCI (n = 53) t(76) p
Performance time 44.130 (13.870) 44.920 (14.000) −0.226 0.822 Mean pen-stroke width 0.164 (0.050) 0.054 (0.013) −3.190 0.002 Mean pen-stroke height 0.285 (0.077) 0.307 (0.066) −1.250 0.214
Two examples of the written fill-in-the-check task input are presented in Figure 2 to illustrate the differences in the mean pen-stroke width. The left input shows a mean pen-stroke width of 0.26 for a PD-n.MCI participant, whereas the right input represents a mean pen-stroke width of 0.10 for an s.PD-MCI patient.
Figure 2. Examples of written fill-in-a-check task input by PD-n.MCI patient (left) and s.PD-MCI patient (right).
3.4. Correlations between Handwriting Process Measure, PGF Ability, and BDI and CF Score: All Samples
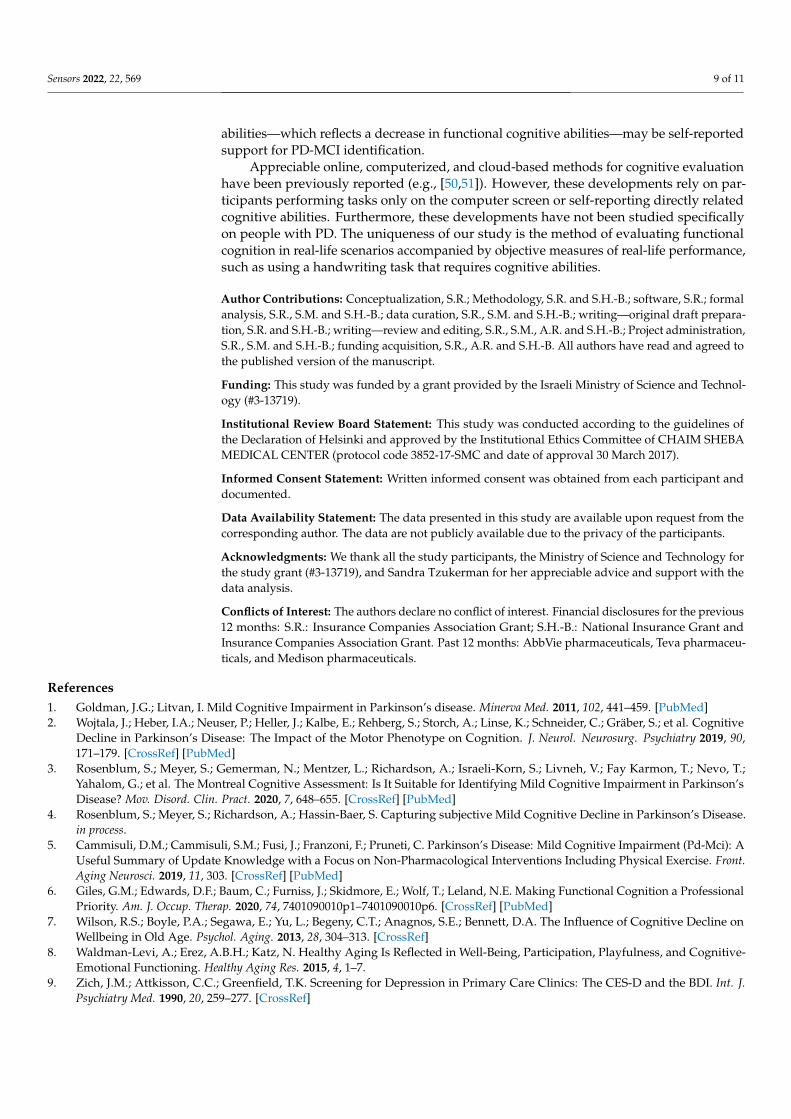
Table 3 shows significant medium correlations between the PGF score, pen-stroke width, and CF feature. A significant low correlation was found between the BDI and CF scores. Interestingly, a medium significant correlation was found between the BDI and the PGF scores.
Figure 2. Examples of written fill-in-a-check task input by PD-n.MCI patient (left) and s.PD-MCIpatient (right).
3.4. Correlations between Handwriting Process Measure, PGF Ability, and BDI and CF Score:All Samples
Table 3 shows significant medium correlations between the PGF score, pen-strokewidth, and CF feature. A significant low correlation was found between the BDI and CFscores. Interestingly, a medium significant correlation was found between the BDI and thePGF scores.
Sensors 2022, 22, 569 7 of 11
Table 3. Correlations between handwriting process measures, PGF ability, and BDI and CF feature:all samples.
CF Feature SWGM BDI PGF
CF feature −0.428 ** 0.382 ** 0.530 **SWGM −0.428 ** −0.115 −0.173
BDI 0.382 ** −0.115 0.502 **PGF 0.530 ** −0.173 0.502 **
Legend: CF feature = cognitive functional feature; SWGM = mean pen-stroke width; BDI = Beck DepressionInventory; and PGF = perceived general functional ability. ** p < 0.01.
3.5. Prediction of CF Feature by Handwriting Process Measures, PGF Ability, and BDI Scoresabove Age
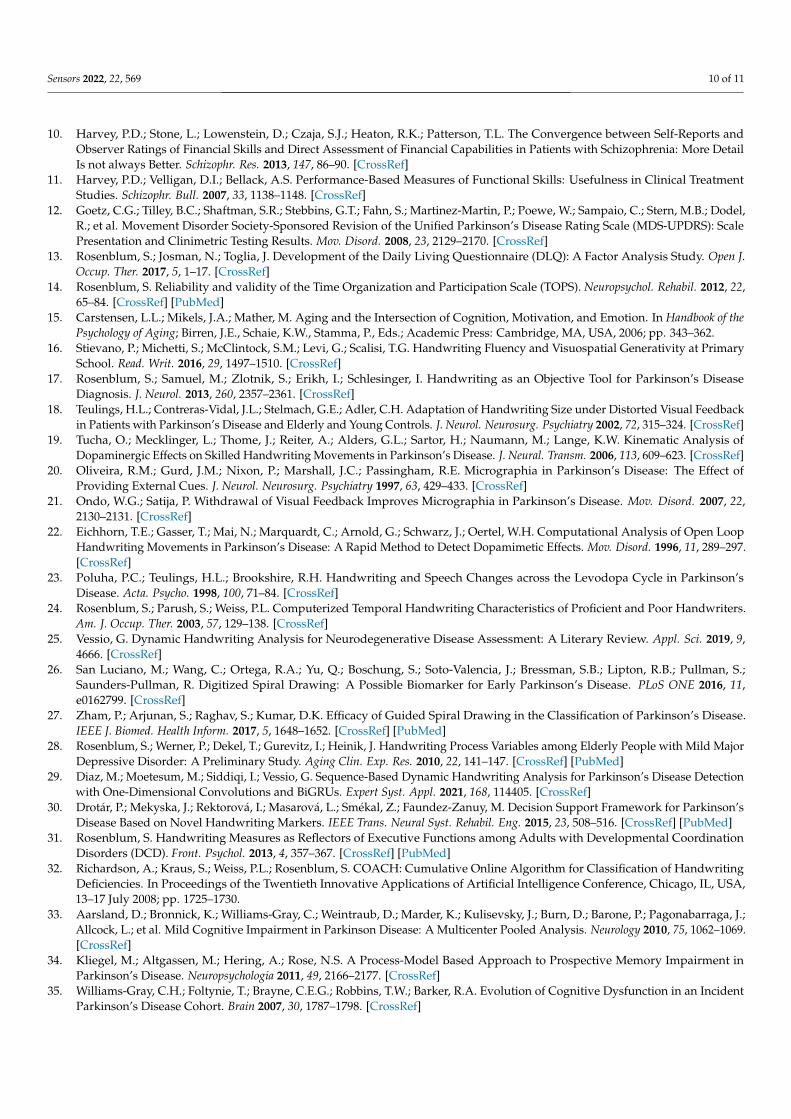
Finally, Table 4 presents the results of the stepwise regression conducted to findwhether PGF ability, BDI, and handwriting performance measures predicted the CF fea-ture. The results indicated that age accounted for 12% of the variance of the CF feature,i.e., F(1,72) = 11.08, p = 0.001; the PGF ability score added 20% to the prediction, i.e.,F(2,72) = 17.95, p < 0.001; and the pen-stroke width added 8%, i.e., F(3,72) = 17.41, p < 0.001.As a whole, both the PGF ability score and the mean stroke width accounted for 28% of thevariance of the CF feature above age. The BDI score did not contribute to the CF feature’sprediction and is not shown in Table 4.
Table 4. Stepwise regression of the CF feature prediction by handwriting process measures, PGFability, and BDI scores above age.
VariableModel 1 Model 2 Model 3
B SE B β B SE B β B SE B β
Age −0.024 0.007 −0.368 *** −0.015 0.007 −0.229 * −0.010 0.006 −0.157PGF 0.292 0.063 0.473 *** 0.271 0.059 0.439 ***
SWGM −0.230 0.690 −0.315 ***R2 0.13 0.33 0.43F 11.080 *** 17.95 *** 17.41 ***
Legend: B = unstandardized regression coefficient; SE B = standard error for B; and β = standardized regressioncoefficient. * p < 0.05, *** p ≤ 0.001.
4. Discussion
The aim of this study was to examine whether PGF ability and activity performancefeatures of PD patients defined as suspected for MCI based on their self-reported CF featurewould differ among this group and to find correlations between those measures and theirCF feature prediction.
Results of the PGF questionnaire (DLQ Part C) subscale provide insight into the dailyfunction-related feelings of the s.PD-MCI group compared to the PD-n. MCI group. Asa whole, the final mean score of the s.PD-MCI group is significantly higher, indicatingtheir lower functional ability, satisfaction, and role participation than that of the PD-n.MCIgroup.
The item-level scores do not indicate a decline in the general thinking ability of thes.PD-MCI group. However, that group’s functional ability is significantly different fromthe PD-n.MCI group, with all the items presenting higher mean scores. Specifically, peoplewith s.PD-MCI reported substantially less satisfaction from doing what they need and wantto do, and greater changes in their housekeeping, community, work roles, and lives due tothe disease than did PD patients who are not suspected for MCI.
The significant difference found for mean pen-stroke width obtained using ComPETmay shed further light on these patients’ daily functioning characteristics. Two previousstudies found pen-stroke width to be a measure that significantly distinguished betweenparticipants with and without MDD who performed drawing and handwriting tasks ona computerized system [28,43]. In both studies, participants with MDD had significantly

Sensors 2022, 22, 569 8 of 11
smaller pen-stroke width in the clock-drawing task [43] and in writing their names andsurnames [28] than did those of the control group. The pen-stroke width alongside otherdigitized spatial measures, such as pen-stroke height and length, pen azimuth, and pressuremeasures, distinguished 89% of the MDD group in each study and more than 80% of allsamples collectively.
The findings of the significantly smaller pen-stroke width among participants withcertain emotional decline (MDD) were similar to the current results. Thus, it seems that thesmaller mean pen-stroke width in the current study may reflect declining emotional health.
When considering the PGF questionnaire results and the decreased mean stroke widthtogether, an interesting point arises. Previous studies reported correlations between hand-writing measures and patients’ status/report among participants with varied pathologies(e.g., depression [28], Alzheimer’s disease [44], and developmental coordination disor-ders [31]). Given those results, we assume that an individual’s pen motions on the papermay reflect their motions in their real-life space. It seems that due to the cognitive decline(exhibited by their CF report) and accompanying emotional consequences, their space isdecreasing. They do less and both their role and life space are diminished. The significantmedium correlations found between the CF feature, PGF score, mean pen-stroke width, andBDI score enhance the message of this study’s results regarding the relationships betweencognitive and emotional components. Such functional cognitive–emotional decline seemsto lead people with suspected MCI to decrease their activities and participation, and thustheir emotional and perhaps physical health and well-being, and vice versa.
As for the regression results, it is interesting to note that in a previous study, the DLQand TOPS accounted for up to 35% of the variance. In contrast, the PGF and pen-strokewidth predicted only 28% of the variance of the CF feature in this study. Such results supportthe need to enable participants to provide a detailed description of their daily functioncapabilities in the real world through appropriate questions based on theoretical and clinicalknowledge. These descriptions may assist in capturing this hidden phenomenon of being atrisk for MCI because referring to patients’ general functional abilities may not be accurateenough to provide a complete picture.
The regression results indicating that both the PGF ability feature and the mean strokewidth accounted for 28% of the variance of the CF feature above age enhance support forthe relationships found between pen-stroke width and the individual’s general functioning.It further supports the CF benefit as a possible assistance marker for suspected PD-MCIidentification.
The study had some limitations. The sample was a small convenience sample thatdid not necessarily represent the typical population with PD. Further studies about thereliability and validity of the scale used in the current study to measure PGF abilities (i.e.,DLQ Part C) are still needed despite the high reliability found in this study.
5. Conclusions
Future integration of varied analysis methods for the handwriting data taken fromhandwriting recognition methods [45], machine learning algorithms [46], and combingintelligent pen devices [47] may support the PD-MCI early detection process.
Thus, it appears that the self-reported CF feature might enable people to reflect theirCF decline through this simple measure, which combines one cognitive item and sixitems related to ADL performance. Those items currently appear under the UPDRS motorexperiences of the daily living subscale. However, participating in ADL also requirescognitive components such as inhibition (ignoring irrelevant stimuli not appropriate to thepurpose), attention, working memory (action sequence), organization (what first, whatnext), spatial orientation (from which direction to begin dressing), visuospatial abilities(such as finding a car in a parking lot), and additional executive functions [48,49].
Given the associations between specific cognitive abilities and deficient ADL abil-ities [48], reporting through the CF feature even a slight decline in cognitive and ADL
Sensors 2022, 22, 569 9 of 11
abilities—which reflects a decrease in functional cognitive abilities—may be self-reportedsupport for PD-MCI identification.
Appreciable online, computerized, and cloud-based methods for cognitive evaluationhave been previously reported (e.g., [50,51]). However, these developments rely on par-ticipants performing tasks only on the computer screen or self-reporting directly relatedcognitive abilities. Furthermore, these developments have not been studied specificallyon people with PD. The uniqueness of our study is the method of evaluating functionalcognition in real-life scenarios accompanied by objective measures of real-life performance,such as using a handwriting task that requires cognitive abilities.
Author Contributions: Conceptualization, S.R.; Methodology, S.R. and S.H.-B.; software, S.R.; formalanalysis, S.R., S.M. and S.H.-B.; data curation, S.R., S.M. and S.H.-B.; writing—original draft prepara-tion, S.R. and S.H.-B.; writing—review and editing, S.R., S.M., A.R. and S.H.-B.; Project administration,S.R., S.M. and S.H.-B.; funding acquisition, S.R., A.R. and S.H.-B. All authors have read and agreed tothe published version of the manuscript.
Funding: This study was funded by a grant provided by the Israeli Ministry of Science and Technol-ogy (#3-13719).
Institutional Review Board Statement: This study was conducted according to the guidelines ofthe Declaration of Helsinki and approved by the Institutional Ethics Committee of CHAIM SHEBAMEDICAL CENTER (protocol code 3852-17-SMC and date of approval 30 March 2017).
Informed Consent Statement: Written informed consent was obtained from each participant anddocumented.
Data Availability Statement: The data presented in this study are available upon request from thecorresponding author. The data are not publicly available due to the privacy of the participants.
Acknowledgments: We thank all the study participants, the Ministry of Science and Technology forthe study grant (#3-13719), and Sandra Tzukerman for her appreciable advice and support with thedata analysis.
Conflicts of Interest: The authors declare no conflict of interest. Financial disclosures for the previous12 months: S.R.: Insurance Companies Association Grant; S.H.-B.: National Insurance Grant andInsurance Companies Association Grant. Past 12 months: AbbVie pharmaceuticals, Teva pharmaceu-ticals, and Medison pharmaceuticals.
References1. Goldman, J.G.; Litvan, I. Mild Cognitive Impairment in Parkinson’s disease. Minerva Med. 2011, 102, 441–459. [PubMed]2. Wojtala, J.; Heber, I.A.; Neuser, P.; Heller, J.; Kalbe, E.; Rehberg, S.; Storch, A.; Linse, K.; Schneider, C.; Gräber, S.; et al. Cognitive
Decline in Parkinson’s Disease: The Impact of the Motor Phenotype on Cognition. J. Neurol. Neurosurg. Psychiatry 2019, 90,171–179. [CrossRef] [PubMed]
3. Rosenblum, S.; Meyer, S.; Gemerman, N.; Mentzer, L.; Richardson, A.; Israeli-Korn, S.; Livneh, V.; Fay Karmon, T.; Nevo, T.;Yahalom, G.; et al. The Montreal Cognitive Assessment: Is It Suitable for Identifying Mild Cognitive Impairment in Parkinson’sDisease? Mov. Disord. Clin. Pract. 2020, 7, 648–655. [CrossRef] [PubMed]
4. Rosenblum, S.; Meyer, S.; Richardson, A.; Hassin-Baer, S. Capturing subjective Mild Cognitive Decline in Parkinson’s Disease.in process.
5. Cammisuli, D.M.; Cammisuli, S.M.; Fusi, J.; Franzoni, F.; Pruneti, C. Parkinson’s Disease: Mild Cognitive Impairment (Pd-Mci): AUseful Summary of Update Knowledge with a Focus on Non-Pharmacological Interventions Including Physical Exercise. Front.Aging Neurosci. 2019, 11, 303. [CrossRef] [PubMed]
6. Giles, G.M.; Edwards, D.F.; Baum, C.; Furniss, J.; Skidmore, E.; Wolf, T.; Leland, N.E. Making Functional Cognition a ProfessionalPriority. Am. J. Occup. Therap. 2020, 74, 7401090010p1–7401090010p6. [CrossRef] [PubMed]
7. Wilson, R.S.; Boyle, P.A.; Segawa, E.; Yu, L.; Begeny, C.T.; Anagnos, S.E.; Bennett, D.A. The Influence of Cognitive Decline onWellbeing in Old Age. Psychol. Aging. 2013, 28, 304–313. [CrossRef]
8. Waldman-Levi, A.; Erez, A.B.H.; Katz, N. Healthy Aging Is Reflected in Well-Being, Participation, Playfulness, and Cognitive-Emotional Functioning. Healthy Aging Res. 2015, 4, 1–7.
9. Zich, J.M.; Attkisson, C.C.; Greenfield, T.K. Screening for Depression in Primary Care Clinics: The CES-D and the BDI. Int. J.Psychiatry Med. 1990, 20, 259–277. [CrossRef]
Sensors 2022, 22, 569 10 of 11
10. Harvey, P.D.; Stone, L.; Lowenstein, D.; Czaja, S.J.; Heaton, R.K.; Patterson, T.L. The Convergence between Self-Reports andObserver Ratings of Financial Skills and Direct Assessment of Financial Capabilities in Patients with Schizophrenia: More DetailIs not always Better. Schizophr. Res. 2013, 147, 86–90. [CrossRef]
11. Harvey, P.D.; Velligan, D.I.; Bellack, A.S. Performance-Based Measures of Functional Skills: Usefulness in Clinical TreatmentStudies. Schizophr. Bull. 2007, 33, 1138–1148. [CrossRef]
12. Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel,R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): ScalePresentation and Clinimetric Testing Results. Mov. Disord. 2008, 23, 2129–2170. [CrossRef]
13. Rosenblum, S.; Josman, N.; Toglia, J. Development of the Daily Living Questionnaire (DLQ): A Factor Analysis Study. Open J.Occup. Ther. 2017, 5, 1–17. [CrossRef]
14. Rosenblum, S. Reliability and validity of the Time Organization and Participation Scale (TOPS). Neuropsychol. Rehabil. 2012, 22,65–84. [CrossRef] [PubMed]
15. Carstensen, L.L.; Mikels, J.A.; Mather, M. Aging and the Intersection of Cognition, Motivation, and Emotion. In Handbook of thePsychology of Aging; Birren, J.E., Schaie, K.W., Stamma, P., Eds.; Academic Press: Cambridge, MA, USA, 2006; pp. 343–362.
16. Stievano, P.; Michetti, S.; McClintock, S.M.; Levi, G.; Scalisi, T.G. Handwriting Fluency and Visuospatial Generativity at PrimarySchool. Read. Writ. 2016, 29, 1497–1510. [CrossRef]
17. Rosenblum, S.; Samuel, M.; Zlotnik, S.; Erikh, I.; Schlesinger, I. Handwriting as an Objective Tool for Parkinson’s DiseaseDiagnosis. J. Neurol. 2013, 260, 2357–2361. [CrossRef]
18. Teulings, H.L.; Contreras-Vidal, J.L.; Stelmach, G.E.; Adler, C.H. Adaptation of Handwriting Size under Distorted Visual Feedbackin Patients with Parkinson’s Disease and Elderly and Young Controls. J. Neurol. Neurosurg. Psychiatry 2002, 72, 315–324. [CrossRef]
19. Tucha, O.; Mecklinger, L.; Thome, J.; Reiter, A.; Alders, G.L.; Sartor, H.; Naumann, M.; Lange, K.W. Kinematic Analysis ofDopaminergic Effects on Skilled Handwriting Movements in Parkinson’s Disease. J. Neural. Transm. 2006, 113, 609–623. [CrossRef]
20. Oliveira, R.M.; Gurd, J.M.; Nixon, P.; Marshall, J.C.; Passingham, R.E. Micrographia in Parkinson’s Disease: The Effect ofProviding External Cues. J. Neurol. Neurosurg. Psychiatry 1997, 63, 429–433. [CrossRef]
21. Ondo, W.G.; Satija, P. Withdrawal of Visual Feedback Improves Micrographia in Parkinson’s Disease. Mov. Disord. 2007, 22,2130–2131. [CrossRef]
22. Eichhorn, T.E.; Gasser, T.; Mai, N.; Marquardt, C.; Arnold, G.; Schwarz, J.; Oertel, W.H. Computational Analysis of Open LoopHandwriting Movements in Parkinson’s Disease: A Rapid Method to Detect Dopamimetic Effects. Mov. Disord. 1996, 11, 289–297.[CrossRef]
23. Poluha, P.C.; Teulings, H.L.; Brookshire, R.H. Handwriting and Speech Changes across the Levodopa Cycle in Parkinson’sDisease. Acta. Psycho. 1998, 100, 71–84. [CrossRef]
24. Rosenblum, S.; Parush, S.; Weiss, P.L. Computerized Temporal Handwriting Characteristics of Proficient and Poor Handwriters.Am. J. Occup. Ther. 2003, 57, 129–138. [CrossRef]
25. Vessio, G. Dynamic Handwriting Analysis for Neurodegenerative Disease Assessment: A Literary Review. Appl. Sci. 2019, 9,4666. [CrossRef]
26. San Luciano, M.; Wang, C.; Ortega, R.A.; Yu, Q.; Boschung, S.; Soto-Valencia, J.; Bressman, S.B.; Lipton, R.B.; Pullman, S.;Saunders-Pullman, R. Digitized Spiral Drawing: A Possible Biomarker for Early Parkinson’s Disease. PLoS ONE 2016, 11,e0162799. [CrossRef]
27. Zham, P.; Arjunan, S.; Raghav, S.; Kumar, D.K. Efficacy of Guided Spiral Drawing in the Classification of Parkinson’s Disease.IEEE J. Biomed. Health Inform. 2017, 5, 1648–1652. [CrossRef] [PubMed]
28. Rosenblum, S.; Werner, P.; Dekel, T.; Gurevitz, I.; Heinik, J. Handwriting Process Variables among Elderly People with Mild MajorDepressive Disorder: A Preliminary Study. Aging Clin. Exp. Res. 2010, 22, 141–147. [CrossRef] [PubMed]
29. Diaz, M.; Moetesum, M.; Siddiqi, I.; Vessio, G. Sequence-Based Dynamic Handwriting Analysis for Parkinson’s Disease Detectionwith One-Dimensional Convolutions and BiGRUs. Expert Syst. Appl. 2021, 168, 114405. [CrossRef]
30. Drotár, P.; Mekyska, J.; Rektorová, I.; Masarová, L.; Smékal, Z.; Faundez-Zanuy, M. Decision Support Framework for Parkinson’sDisease Based on Novel Handwriting Markers. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 508–516. [CrossRef] [PubMed]
31. Rosenblum, S. Handwriting Measures as Reflectors of Executive Functions among Adults with Developmental CoordinationDisorders (DCD). Front. Psychol. 2013, 4, 357–367. [CrossRef] [PubMed]
32. Richardson, A.; Kraus, S.; Weiss, P.L.; Rosenblum, S. COACH: Cumulative Online Algorithm for Classification of HandwritingDeficiencies. In Proceedings of the Twentieth Innovative Applications of Artificial Intelligence Conference, Chicago, IL, USA,13–17 July 2008; pp. 1725–1730.
33. Aarsland, D.; Bronnick, K.; Williams-Gray, C.; Weintraub, D.; Marder, K.; Kulisevsky, J.; Burn, D.; Barone, P.; Pagonabarraga, J.;Allcock, L.; et al. Mild Cognitive Impairment in Parkinson Disease: A Multicenter Pooled Analysis. Neurology 2010, 75, 1062–1069.[CrossRef]
34. Kliegel, M.; Altgassen, M.; Hering, A.; Rose, N.S. A Process-Model Based Approach to Prospective Memory Impairment inParkinson’s Disease. Neuropsychologia 2011, 49, 2166–2177. [CrossRef]
35. Williams-Gray, C.H.; Foltynie, T.; Brayne, C.E.G.; Robbins, T.W.; Barker, R.A. Evolution of Cognitive Dysfunction in an IncidentParkinson’s Disease Cohort. Brain 2007, 30, 1787–1798. [CrossRef]
Sensors 2022, 22, 569 11 of 11
36. Dalrymple-Alford, J.C.; MacAskill, M.R.; Nakas, C.T.; Livingston, L.; Graham, C.; Crucian, G.P.; Melzer, T.R.; Kirwan, J.; Keenan,R.; Wells, S.; et al. The MoCA Well-Suited Screen for Cognitive Impairment in Parkinson Disease. Neurology 2010, 75, 1717–1725.[CrossRef]
37. Hoops, S.; Nazem, S.; Siderowf, A.D.; Duda, J.E.; Xie, S.X.; Stern, M.B.; Weintraub, D. Validity of the MoCA and MMSE in theDetection of MCI and Dementia in Parkinson Disease. Neurology 2009, 73, 1738–1745. [CrossRef]
38. Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. TheMontreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53,695–699. [CrossRef]
39. Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDSClinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [CrossRef]
40. Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, Progression and Mortality. Neurology 1967, 17, 427–442. [CrossRef] [PubMed]41. Toglia, J.; Foster, E. The Multicontext Approach: A Metacognitive Strategy Based Intervention to Optimize Functional Cognition;
Gatekeeper Press: Grove City, OH, USA, 2022; in press.42. Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic Review of Levodopa dose Equivalency Reporting
in Parkinson’s Disease. Mov. Disord. 2010, 25, 2649–2653. [CrossRef] [PubMed]43. Heinik, J.; Wenre, P.; Dekel, T.; Gurevitz, I.; Rosenblum, S. Computerized Kinematic Analysis of the Clock Drawing Task in Elderly
People with Mild Major Depressive-Disorder: An Exploratory Study. Int. Psychogeriatr. 2010, 22, 479–488. [CrossRef] [PubMed]44. Werner, P.; Rosenblum, S.; Bar-On, G.; Heinik, J.; Korczyn, A. Handwriting Process Variables Discriminating Mild Alzheimer’s
Disease and Mild Cognitive Impairment. J. Gerontol. B Psychol. Sci. Soc. Sci. 2006, 61B, 228–236. [CrossRef] [PubMed]45. Al-Saffar, A.; Awang, S.; Al-Saiagh, W.; Al-Khaleefa, A.S.; Abed, S.A. A Sequential Handwriting Recognition Model Based on a
Dynamically Configurable CRNN. Sensors 2021, 21, 7306. [CrossRef] [PubMed]46. Devillaine, L.; Lambert, R.; Boutet, J.; Aloui, S.; Brault, V.; Jolly, C.; Labyt, E. Analysis of Graphomotor Tests with Machine
Learning Algorithms for an Early and Universal Pre-Diagnosis of Dysgraphia. Sensors 2021, 21, 7026. [CrossRef]47. Júnior, E.P.; Delmiro, I.L.D.; Magaia, N.; Maia, F.M.; Hassan, M.M.; Albuquerque, V.H.; Fortino, G. Intelligent Sensory Pen for
Aiding in the Diagnosis of Parkinson’s Disease from Dynamic Handwriting Analysis. Sensors 2020, 20, 5840. [CrossRef] [PubMed]48. Kalbe, E.; Folkerts, A.-K.; Ophey, A.; Eggers, C.; Elben, S.; Dimenshteyn, K.; Sulzer, P.; Schulte, C.; Schmidt, N.; Schlenstedt,
C.; et al. Enhancement of Executive Functions but Not Memory by Multidomain Group Cognitive Training in Patients withParkinson’s Disease and Mild Cognitive Impairment: A Multicenter Randomized Controlled Trial. Parkinsons Dis. 2020, 2020,4068706. [CrossRef] [PubMed]
49. Lau, K.M.; Parikh, M.; Harvey, D.J.; Huang, C.J.; Farias, S.T. Early Cognitively Based Functional Limitations Predict Loss ofIndependence in Instrumental Activities of Daily Living in Older Adults. J. Int. Neuropsychol. Soc. 2015, 21, 688–698. [CrossRef][PubMed]
50. Feenstra, H.E.; Vermeulen, I.E.; Murre, J.M.; Schagen, S.B. Online Self-Administered Cognitive Testing Using the AmsterdamCognition Scan: Establishing Psychometric Properties and Normative Data. J. Med. Internet Res. 2018, 20, e9298. [CrossRef]
51. Sciuto, G.L.; Russo, S.; Napoli, C. A Cloud-Based Flexible Solution for Psychometric Tests Validation, Administration andEvaluation. Proc. SYSTEM 2019, 2468, 16–21.




















