
Paclitaxel plus high-dose cyclosphosphamide with G-CSF support in patients with relapsed and...
6
Paclitaxel plus high-dose cyclosphosphamide with G-CSF support in patients with relapsed and refractory aggressive non-Hodgkin’s lymphoma A NAS YOUNES ,J ORGE ROMAGUERA ,O FELIA MESINA,F REDERICK H AGEMEISTER ,A NDREAS H. S ARRIS , MARIA A. RODRIGUEZ ,P ETER MC L AUGHLIN,H ECTOR A. P RETI ,C ARLOS B ACHIER AND F ERNANDO C ABANILLAS Department of Lymphoma, University of Texas M. D. Anderson Cancer Center, Houston, Texas, U.S.A. Received 18 May 1998; accepted for publication 21 August 1998 Summary. Based on the single-agent activity of both paclitaxel and cyclophosphamide in the treatment of non- Hodgkin’s lymphoma (NHL), we conducted a phase II study to evaluate the efficacy of the combination of the two drugs in patients with refractory and relapsed aggressive NHL. All patients received 900 mg/m 2 bolus of cyclophosphamide intravenously daily for 3 consecutive days with a concurrent infusion of 150 mg/m 2 of paclitaxel over 72 h (50 mg/m 2 /d). 24h after the completion of chemotherapy, patients received subcutaneous injections of 5 mg/kg of granulocyte-colony stimulating factor (G-CSF) daily until white cell count recovery. Treatment was repeated every 3 weeks. Patients who had at least a partial response (PR) after two courses continued to receive a maximum of four courses. Patients with responding disease were allowed to undergo high-dose chemotherapy followed by stem-cell/bone marrow transplantation if they were eligible. Of the 77 patients who were eligible for the study, 74 (96%) were evaluable for toxicity and treatment response. The overall response rate was 45% (95% CI 33–57%). Patients who received treatment after their disease relapsed from a complete response (CR) had an 81% response rate (38% CRs), whereas those with primary refractory disease had a 22% response rate. Toxicities of >grade 2 included alopecia (100%) and stomatitis (25%). Neutropenic fever of grade >2 occurred after 18% of the courses, and platelet count of <20 × 10 9 /l developed after 20% of the courses. Thus, the combination of paclitaxel plus high-dose cyclophosphamide is an effective new regimen in the treatment of refractory and relapsed NHL. Keywords: paclitaxel, cyclophosphamide, lymphoma. Although aggressive non-Hodgkin’s lymphoma (NHL) was among the first human cancers to be cured with combina- tion chemotherapy, the cure rate of this disease remains about 50%, which has not changed since the introduction of CHOP (cyclophosphamide, hydroxydoxorubicin, vincristine, prednisolone) combination chemotherapy in the 1970s (Armitage, 1993). Later combination programmes failed to improve survival and were more toxic than CHOP (Armitage, 1992; Fisher et al, 1993; Hryniuk, 1993). For patients whose disease fails to respond to primary therapy or relapses from a complete remission (CR), the prognosis remains poor. Various salvage programmes can achieve high response rates, but the responses achieved are rarely durable (Rodriguez, 1995; Velasquez et al, 1994; Wilson et al, 1993), leaving high-dose chemotherapy and stem-cell transplantation as the only potentially curative treatment (Armitage, 1993). The success of stem cell and bone marrow transplantation in the treatment of relapsed lymphoma increased the demand for more effective salvage therapy that could reduce the tumour load and mobilize stem cells into peripheral blood prior to their collection. Although several salvage programmes have been reported to induce high response rates in patients with relapsed and refractory aggressive NHL, they predominantly targeted patients who had previously failed CHOP or CHOP-like therapy. Thus, new effective treatment programmes are needed for those who do not respond to or relapse after salvage therapy. Paclitaxel (Taxol; Bristol-Myers Squibb, Princeton, N.J.) has been recently tested for the treatment of NHL (Younes et al, 1997b). In our experience with 44 previously treated patients with aggressive NHL, paclitaxel alone induced an British Journal of Haematology , 1998, 103, 678–683 678 q 1998 Blackwell Science Ltd Correspondence: Dr Anas Younes, Department of Hematology, Section of Lymphoma, Box 68, University of Texas M. D. Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030, U.S.A.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Paclitaxel plus high-dose cyclosphosphamide with G-CSF support in patients with relapsed and...
Paclitaxel plus high-dose cyclosphosphamide with G-CSFsupport in patients with relapsed and refractoryaggressive non-Hodgkin’s lymphoma
ANAS YOUNES, JORGE ROMAGUERA, OFELIA MESINA, FREDERICK HAGEMEISTE R, ANDREAS H. SARRIS,MARIA A. RODRIGUEZ, PE TER MCLAUGHLIN, HECTO R A. PRETI, CARL OS BACHIER AND FE RNANDO CABANIL LAS
Department of Lymphoma, University of Texas M. D. Anderson Cancer Center, Houston, Texas, U.S.A.
Received 18 May 1998; accepted for publication 21 August 1998
Summary. Based on the single-agent activity of bothpaclitaxel and cyclophosphamide in the treatment of non-Hodgkin’s lymphoma (NHL), we conducted a phase II studyto evaluate the efficacy of the combination of the two drugsin patients with refractory and relapsed aggressive NHL. Allpatients received 900 mg/m2 bolus of cyclophosphamideintravenously daily for 3 consecutive days with a concurrentinfusion of 150 mg/m2 of paclitaxel over 72 h (50 mg/m2/d).24 h after the completion of chemotherapy, patients receivedsubcutaneous injections of 5 mg/kg of granulocyte-colonystimulating factor (G-CSF) daily until white cellcount recovery. Treatment was repeated every 3 weeks.Patients who had at least a partial response (PR) after twocourses continued to receive a maximum of four courses.Patients with responding disease were allowed to undergohigh-dose chemotherapy followed by stem-cell/bone marrow
transplantation if they were eligible. Of the 77 patients whowere eligible for the study, 74 (96%) were evaluable fortoxicity and treatment response. The overall response ratewas 45% (95% CI 33–57%). Patients who receivedtreatment after their disease relapsed from a completeresponse (CR) had an 81% response rate (38% CRs), whereasthose with primary refractory disease had a 22% responserate. Toxicities of >grade 2 included alopecia (100%) andstomatitis (25%). Neutropenic fever of grade >2 occurredafter 18% of the courses, and platelet count of <20 × 109/ldeveloped after 20% of the courses. Thus, the combination ofpaclitaxel plus high-dose cyclophosphamide is an effectivenew regimen in the treatment of refractory and relapsedNHL.
Keywords: paclitaxel, cyclophosphamide, lymphoma.
Although aggressive non-Hodgkin’s lymphoma (NHL) wasamong the first human cancers to be cured with combina-tion chemotherapy, the cure rate of this disease remainsabout 50%, which has not changed since the introduction ofCHOP (cyclophosphamide, hydroxydoxorubicin, vincristine,prednisolone) combination chemotherapy in the 1970s(Armitage, 1993). Later combination programmes failedto improve survival and were more toxic than CHOP(Armitage, 1992; Fisher et al, 1993; Hryniuk, 1993). Forpatients whose disease fails to respond to primary therapy orrelapses from a complete remission (CR), the prognosisremains poor. Various salvage programmes can achieve highresponse rates, but the responses achieved are rarelydurable (Rodriguez, 1995; Velasquez et al, 1994; Wilson
et al, 1993), leaving high-dose chemotherapy and stem-celltransplantation as the only potentially curative treatment(Armitage, 1993).
The success of stem cell and bone marrow transplantationin the treatment of relapsed lymphoma increased thedemand for more effective salvage therapy that couldreduce the tumour load and mobilize stem cells intoperipheral blood prior to their collection. Although severalsalvage programmes have been reported to induce highresponse rates in patients with relapsed and refractoryaggressive NHL, they predominantly targeted patients whohad previously failed CHOP or CHOP-like therapy. Thus, neweffective treatment programmes are needed for those who donot respond to or relapse after salvage therapy.
Paclitaxel (Taxol; Bristol-Myers Squibb, Princeton, N.J.)has been recently tested for the treatment of NHL (Youneset al, 1997b). In our experience with 44 previously treatedpatients with aggressive NHL, paclitaxel alone induced an
British Journal of Haematology, 1998, 103, 678–683
678 q 1998 Blackwell Science Ltd
Correspondence: Dr Anas Younes, Department of Hematology,Section of Lymphoma, Box 68, University of Texas M. D. AndersonCancer Center, 1515 Holcombe Blvd, Houston, TX 77030, U.S.A.
679Paclitaxel plus Cyclophosphamide in NHL
q 1998 Blackwell Science Ltd, British Journal of Haematology 103: 678–683
overall response rate of 30% (16% CRs). The most favourableactivity of paclitaxel was observed in patients with relapsedaggressive NHL who did not have a primary refractorydisease as it induced a 50% response rate (Younes et al,1997a), Based on this favourable single-agent activity, webecame interested in evaluating paclitaxel-based new treat-ment programmes that can be tested in patients withrelapsed and refractory aggressive NHL. Active regimenscan then be tested in untreated patients with poor prognosticfeatures (Shipp et al, 1993). In this study we reportour experience with paclitaxel combined with high-dosecyclophosphamide. The dose and schedule of this combina-tion were adopted from a recently published phase I trialin patients with breast carcinoma (Tolcher et al, 1996).The addition of high-dose cyclophosphamide with growthfactor support to paclitaxel was appealing because itenhanced peripheral blood stem cell collection in respondingpatients prior to stem-cell transplantation.
PATIENTS AND METHODS
Patients. Patients were eligible for this phase II clinical trialif they had histologically documented refractory or relapsedaggressive NHL, which included the following histologiesaccording to the REAL classification: diffuse large B-cell,follicular centre-cell (follicular, grade III), peripheral T-cell,and anaplastic large-cell lymphoma (Harris et al, 1994).All patients were required to have bidimensionally measur-able disease, a bilirubin level <25 mmol/l, SGPT level <twicethe upper normal value, a platelet count >100 × 109/lunless caused by marrow infiltration of NHL, and anabsolute neutrophil count (ANC) >1 × 109/l. Patients wereexcluded if they had HIV infection, central nervous systemlymphoma, prior treatment with paclitaxel or high dosesof cyclophosphamide or ifosfamide, a life expectancy<12 weeks, or serious cardiac disease. Patients wereregistered after signing a consent form according toinstitutional guidelines.
Staging. Before starting therapy all patients had acomplete physical examination, a chest X-ray, a CT scan ofthe chest, abdomen and pelvis, a gallium scan, and bilateralbone marrow biopsies. These tests were repeated after twocourses and after the completion of therapy.
Chemotherapy. The dose and schedule of drugs used in thisstudy were adopted from a recently published phase I trial inbreast carcinoma patients (Tolcher et al, 1996). Patientsreceived 20 mg of dexamethasone orally 4 h before thechemotherapy infusion. 30 min before the infusion ofpaclitaxel, patients received premedication with intravenousinjections of dexamethasone (20 mg), cimetidine (300 mg)and diphenhydramine (50 mg). Cyclophosphamide wasgiven intravenously at a dose of 900 mg/m2/d on days 1, 2and 3 (total dose 2700 mg/m2) with mesna given intrave-nously at a dose of 900 mg/m2/d by continuous infusion for72 h. Paclitaxel was given intravenously at a dose of 50 mg/m2/d by continuous infusion for 72 h (total dose 150 mg/m2). 24 h after completion of the paclitaxel infusion, G-CSF(filgrastim, Amgen, Thousand Oaks, Calif.) was administeredsubcutaneously at a dose of 5 mg/kg/d for 14 d or until an
ANC >10 × 109/l was achieved. Courses were repeated every3 weeks.
Responding patients were allowed to receive consolidationwith high-dose chemotherapy and bone marrow or stem celltransplantation after at least two courses of paclitaxel andcyclophosphamide. Patients who were not eligible for orrefused bone marrow transplantation continued to receive amaximum of four courses. Patients whose disease progressedafter any course were removed from the study.
Dose modification. Dose reduction was allowed if the ANCcount on day 21 was <0·75 × 109/l or the platelet count was<100 × 109/l, and for patients who had grade III non-haematological toxicities other than nausea. The reduced
Table I. Characteristics of 74 evaluable patients.
No. %
Age (years)Median 59Range 24–76
Male/female 42/32 57%, 43%
HistologyDiffuse large B-cell 53 72%Peripheral T-cell 6 8%Anaplastic Ki-1þ 3 4%Transformed lymphoma 12 16%
Performance status (ECOG)0 12 16%1 48 65%
>2 14 19%
Prior chemotherapy regimens1* 37 50%2 19 26%
>3 18 24%
No. of prior chemotherapy drugs4 13 18%
>4 61 82%
LDH (upper normal value 618 IU/l)Mean 2085Median 928Range 213–4111Elevated (>618 IU/l) 56 76%>1000 IU/l 33 45%
Response to prior therapyNo prior CR 41 55%Resistant relapse 12 16%Relapse from CR 21 28%
Prior induction regimensASHAP/MBACOS/MINE 20 27%CHOP or equivalent 54 73%
Prior ara-C/platinum 38 51%
ASHAP: adriamycin, solumedrol, high-dose ara-C, platinum;MBACOS: methotrexate, bleomycin, adriamycin, cyclophosphamide,vincristine solumedrol; MINE: mesna, ifosphamide, novatrone,etoposide.
* ASHAP/MBACOS/MINE is considered one regimen.
doses consisted of cyclophosphamide at a dose of 700 mg/m2/d and a total paclitaxel dose of 125 mg/m2 over 72 h.Treatment was stopped if grade IV non-haematologicaltoxicity developed.
Response criteria. A CR was defined as normalizationof radiological, physical and bone marrow findings for atleast 4 weeks, or stable residual radiographic abnormalitieswith no gallium uptake for at least 8 weeks. A partialresponse (PR) was defined as at least a 50% reduction inthe sum of the products of the greatest cross-sectionaldiameters of measurable lesions without evidence of newlesions.
RESULTS
Patient characteristicsBetween April 1995 and December 1996, 77 patients wereeligible for the study. Two patients withdrew consent and onepatient received one course and was lost to follow-up.Therefore 74 patients (96%) were evaluable for treatmentresponse and toxicity, of whom 72% had diffuse large B-cellNHL and 16% had transformed NHL (Table I). All patientshad received prior combination chemotherapy, and 22patients (23%) received radiation therapy. 41 patients(55%) had primary refractory disease (never achieved a CRwith histologic evidence of active disease or persistentgallium activity) and 12 patients (16%) had a resistantrelapse (Table I).
The median age of the patients was 59 years (range24–75 years). 21 patients (28%) were >65 years and 36patients (49%) were >60 years. 56 patients (76%) hadelevated lactate dehydrogenase (LDH) values. The pretreat-ment B2 microglobulin level was determined in 44 patients,15 of whom (36%) had elevated levels (>3 mg/l).
Treatment responseThirty-three patients achieved a PR or CR for an overallresponse rate of 45% (95% CI 33–57%). The response rates
q 1998 Blackwell Science Ltd, British Journal of Haematology 103: 678–683
680 Anas Younes et alTable II. Treatment responses.
Response to cyclophosphamide þ paclitaxelNo. ofpatients CR PR % CR þ PR
Disease categoryRelapsed disease 33 11 (33%) 13 (39%) 73%
Relapse from CR 21 8 (38%) 9 (43%) 81%Reistant relapse 12 3 (35%) 4 (33%) 58%
Primary refractory 41 1 (2%) 8 (20%) 22%Total 74 12 (16%) 21 (28%) 45%
Prior treatmentPrior ara-C/platinum 38 7 11 18 (47%)
Ara-C/platinum sensitive 17 6 6 12 (71%)Ara-C/platinum resistant 21 1 5 6 (29%)
No prior ara-C/platinum 36 5 11 16 (44%)
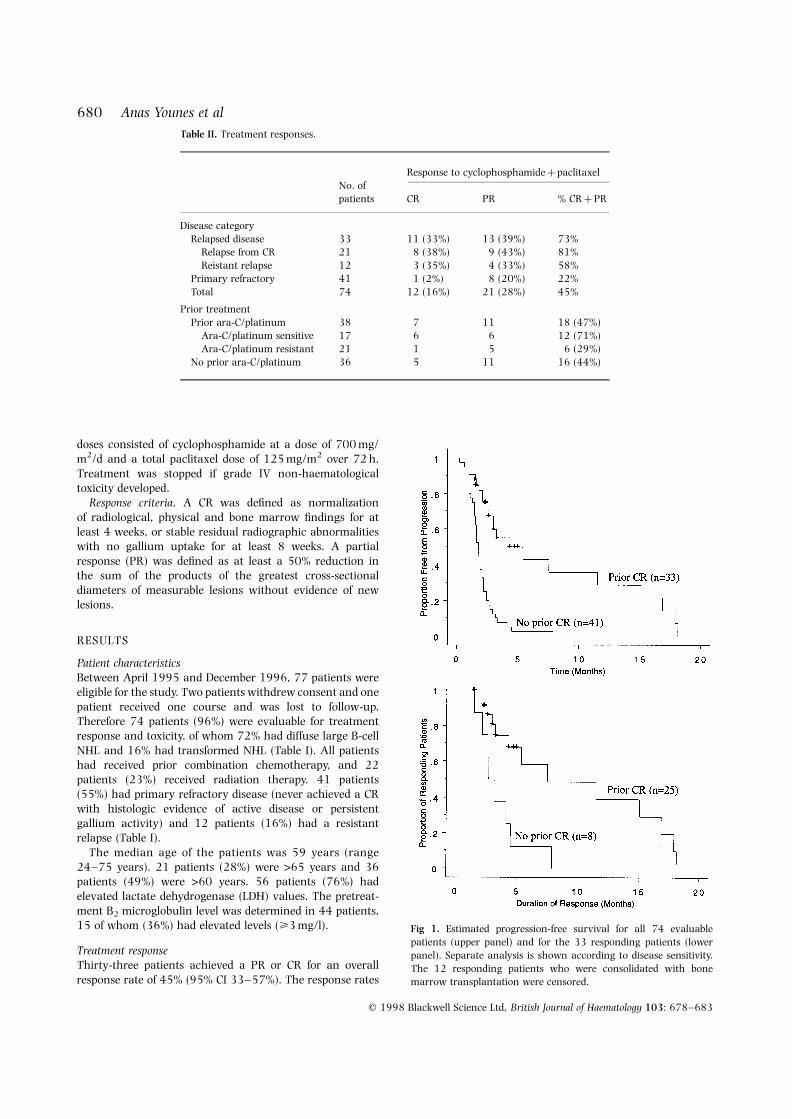
Fig 1. Estimated progression-free survival for all 74 evaluablepatients (upper panel) and for the 33 responding patients (lowerpanel). Separate analysis is shown according to disease sensitivity.The 12 responding patients who were consolidated with bonemarrow transplantation were censored.

681Paclitaxel plus Cyclophosphamide in NHL
q 1998 Blackwell Science Ltd, British Journal of Haematology 103: 678–683
varied according to how the disease responded to priortreatments. Patients who were treated after relapsing from aCR had a response rate of 81% (38% CRs and 43% PRs).Patients who had primary refractory disease (never achieveda CR) or resistant relapses (relapsed patients who failed torespond to their last therapy) had response rates of 22% and58%, respectively (Table II). Patients with non-primaryrefractory disease had a median time to treatment failure of4·8 months and a median duration of response of 6·5months (range 2–18 months) (Fig 1). Of the 33 respondingpatients, 12 were consolidated with high-dose chemother-apy and autologous stem-cell transplantation (eight patientswere transplanted while in PR after two courses). Theremaining 21 patients were either not eligible for or refusedstem cell transplantation, and were observed until diseaseprogression.
Responses were similar in patients who had received priorara-C/platinum-based therapy and in those who had not(47% and 44%, respectively). Patients whose diseaseresponded to prior ara-C/platinum therapy had a responserate of 71% compared with a response rate of 29% for thosewhose disease was refractory to ara-C/platinum (Table II).
ToxicityA total of 178 courses were administered to 74 patients. 14patients (19%) received only once course (they did notcontinue because their disease rapidly progressed), 33 (45%)received only two courses (because of either lack of responseor they were crossed over to bone marrow transplantation),10 patients (14%) received three courses, and 17 patients(23%) received four courses. Therefore 60 patients (81%)received at least two courses. In 27 courses (15%) the doseswere reduced because of toxicities. All patients had alopecia.The most common toxicities were nausea, stomatitis and
vomiting (Table III). Neutropenic fever of grade >2 wasobserved after 18% of the courses, and stomatitis of grade >2was seen in 25% after 10% of the courses (Table III).
Thrombocytopenia and neutropenia were not cumulative.20% of the patients had a platelet count <20 × 109/l and35% of the patients had an ANC <0·1 × 109/l. Notreatment-related deaths were observed, but treatmentwas discontinued in 8% of the patients because of grade IVnon-haematological toxicity (Table III).
DISCUSSION
The activity of paclitaxel in patients with relapsed andrefractory NHL has been studied by three independentgroups using different doses and infusion schedules (Presset al, 1998; Wilson et al, 1995; Younes et al, 1997a). Inpatients with non-primary refractory aggressive NHL,paclitaxel induced a response rate of 25–50%, with higherand more complete responses were observed when higherdoses of paclitaxel were infused over a shorter period of time(Press et al, 1998; Younes et al, 1997a). In this report wedescribe our experience with the first paclitaxel-basedcombination for the treatment of relapsed and refractoryaggressive NHL.
The overall response rate in the current study was 45%,but patients who did not have a primary refractory diseasehad a response rate of 73% (33% CRs). Because respondingpatients were allowed to be consolidated with high-dosetherapy and bone marrow transplantation after only twocourses, the CR rate and response duration in this study mayhave been underestimated. In fact, eight patients wereconsolidated with stem cell/bone marrow transplantationafter achieving PRs after only two courses of therapy.Although only 12 patients were treated in a setting ofresistant relapse (did not respond to their last salvagetherapy), it is interesting to note that 58% of these patientsresponded (25% CRs). However, consistent with previousobservations, patients with primary refractory diseasecontinue to be poor responders. It is for this reason thatresponse rates should be reported separately for patientswith primary refractory and non-primary refractory disease.Thus, trials that include high number of patients withprimary refractory NHL are expected to have a lower overallresponse rate. Therefore the activity of a new drug orregimen should not be judged based on the overall responserate because such analysis may lead to excluding potentiallyactive agents prematurely. On the other hand, a regimen thatcan induce a high response rate in NHL patients whosedisease was not refractory to induction therapy should betested in newly diagnosed patients with poor-risk featuresbecause these patients are infrequently cured with CHOPchemotherapy (Shipp et al, 1993).
One important aspect of this programme was its ability toinduce responses in patients who had previously receivedara-C/platinum-based therapy, which is frequently used as afirst-line salvage therapy. Although several other salvageprogrammes have been used to treat relapsed NHL, theywere mainly aimed at CHOP or CHOP-equivalent failures andincluded patients with variable histologies (Rodriguez et al,
Table III. Toxicity of cyclophosphamide plus paclitaxel in NHLpatients.
National Cancer Institute grade
Toxicity 1 2 3 4
Proportion of 74 patientsAlopecia 100%Diarrhoea 5% 14% 4% –Nausea 64% 14% 5% –Vomiting 30% 16% 4% –Stomatitis 23% 23% 18% 7%Sensory neuropathy 16% 5% 4% –Motor neuropathy 1% 3% 5% –Cardiac arrhythmia – 3% 1% 1%Haemorrhagic cystitis – 1% – –
Proportion of 178 coursesNeutropenic fever 4% 13% 16% 2%Diarrhoea 2% 7% 2% –Nausea 26% 6% 2% –Vomiting 12% 7% 2% –Stomatitis 10% 10% 7% 3%

1995; Velasquez et al, 1994; Wilson et al, 1993). Thesesalvage programmes have also varied in the number ofpatients included with refractory disease, the number ofprior treatment regimens, the median age, and LDH levels.Therefore it is difficult to compare the activities of thesedifferent programmes (Table IV). In this study the patientswere more homogenous because only those with aggressivehistologies were included.
In this study, treatment was reasonably well tolerateddespite the fact that the median patient age was 59 years andthat the patients were heavily pretreated. Dose reduction wasdone after only 15% of the courses. Although cardiacarrhythmia was noted in four patients, no treatment-relateddeaths occurred.
Based on this study, the combination of paclitaxel andcyclophosphamide seems to be active in the treatment ofpatients with relapsed aggressive NHL. Because 81% of thepatients who had a relapse following a CR responded to thiscombination, it is possible that even more favourable activityand less toxic effects could be observed in less heavilypretreated patients. Because the combination of paclitaxeland cyclophosphamide plus G-CSF was reported to ade-quately mobilize stem cells into the peripheral blood(Demirer et al, 1995; Fennelly et al, 1995), this combinationcan be used prior to high-dose chemotherapy and auto-logous stem-cell infusion. The real test of the activity of thisregimen can only be determined in newly diagnosed patientswith poor prognostic features.
ACKNOWLEDGMENTS
Anas Younes is the recipient of an American Cancer SocietyClinical Oncology Career Development Award. This workwas supported in part by grants from Bristol-Myers SquibbPharmaceutical and Amgen.
REFERENCES
Armitage, J.O. (1992) Chemotherapy for non-Hodgkin’s lymphoma.Current Opinion in Oncology, 4, 840–846.
Armitage, J.O. (1993) Treatment of non-Hodgkin’s lymphoma. NewEngland Journal of Medicine, 328, 1023–1030.
Demirer, T., Rowley, S., Buckner, C.D., Appelbaum, F.R., Lilleby, K.,Storb, R., Schiffman, K. & Bensinger, W.I. (1995) Peripheral-bloodstem-cell collections after paclitaxel, cyclophosphamide, andrecombinant human granulocyte colony-stimulating factor inpatients with breast and ovarian cancer. Journal of ClinicalOncology, 13, 1714–1719.
Fennelly, D., Schneider, H., Spriggs, D., Bengala, C., Hakes, T.,Reich, L., Barakat, R., Curtin, J., Moore, M.A., Hoskins, W.,Norton, L. & Crown, J. (1995) Dose escalation of paclitaxel withhigh-dose cyclophosphamide, with analysis of progenitor-cellmobilization and hematologic support of advanced ovariancancer patients receiving rapidly sequenced high-dose carbo-platin/cyclophosphamide courses. Journal of Clinical Oncology, 13,1160–1166.
Fisher, R.I., Gaynor, E.R., Dahlberg, S., Oken, M.M., Grogan, T.M.,Mize, E.M., Glick, J.H., Coltman, C.A., Jr & Miller, T.P. (1993)Comparison of a standard regimen (CHOP) with three intensivechemotherapy regimens for advanced non-Hodgkin’s lymphoma.New England Journal of Medicine, 328, 1002–1006.
Harris, N.L., Jaffe, E.S., Stein, H., Banks, P.M., Chan, J.K., Cleary, M.L.,Delsol, G., De Wolf-Peeters, C., Falini, B., Gatter, K.C., Grogan,T.M., Isaacson, P.G., Knowles, D.M., Mason, D.Y., Muller-Hermelink, H.-K., Pileri, S.A., Piris, M.A., Ralfkiaer, E. &Warnke, R.A. (1994) A revised European–American classificationof lymphoid neoplasms: a proposal from the InternationalLymphoma Study Group. Blood, 84, 1361–1392.
Hryniuk, W. (1993) CHOP versus m-BACOD in non-Hodgkin’slymphoma. (Letter). New England Journal of Medicine, 328, 581.
Press, O., Leblanc, M., O’Rourke, T., Gagnet, S., Chapman, R.,Blacerzak, S. & Fisher, R. (1998) Phase II trial of paclitaxel by 24-hour continuous infusion for relapsed non-Hodgkin’s lymphoma:Southwest Oncology Group Trial 9246. Journal of Clinical Oncology,16, 574–578.
Rodriguez, M.A., Cabanillas, F.C., Velasquez, W., Hagemeister, F.B.,McLaughlin, P., Swan, F. & Romaguera, J.E. (1995) Results of asalvage treatment program for relapsing lymphoma: MINEconsolidated with ESHAP. Journal of Clinical Oncology, 13, 1734–1741.
Shipp, M.A., Harrington, D.P., Anderson, J.R., Armitage, J.O.,Bonadonna, G., Brittinger, G., Cabanillas, F., Canellos, G.P., Coiffier,B., Connors, J.M., Cowan, R.A., Crowther, D., Dahlberg, S.,Engelhard, M., Fisher, R.I., Gisselbrecht, C., Horning, S.J., Lepage,E., Lister, T.A., Meerwaldt, J.H., Montserrat, E., Nissen, N.I., Oken,M.M., Peterson, B.A., Tondini, C., Velasquez, W.A. & Yeap, B.Y.(1993) A predictive model for aggressive non-Hodgkin’s lym-phoma. The International Non-Hodgkin’s Lymphoma PrognosticFactors Project. New England Journal of Medicine, 329, 987–994.
q 1998 Blackwell Science Ltd, British Journal of Haematology 103: 678–683
682 Anas Younes et alTable IV. Salvage programmes for aggressive NHL.
Response (%) % of patients with:
No. of Prior PrimaryRegimen/reference patients PR CR PR þCR ara-C/platinum refractory disease
DHAP (Velasquez et al, 1998) 68 16 (24%) 24 (33%) 40 (59%) 0% Not specifiedESHAP (Velasquez et al, 1994) 85 17 (20%) 32 (38%) 49 (58%) 0% Not specifiedMINE/ESHAP (Rodriguez et al, 1992) 56 13 (23%) 23 (41%) 36 (64%) 0% Not specifiedEPOCH (Wilson et al, 1993) 53 26 (49%) 18 (34%) 44 (83%) 0% 45%Cyclophosphamide þ paclitaxel (this study) 74 21 (28%) 12 (16%) 33 (45%) 51% 55%
DHAP: dexamethasone, high-dose ara-C, platinum; ESHAP: DHAP þetoposide; MINE: mesna, ifosphamide, novantrone, etoposide; EPOCH:etoposide, prednisone, vincristine, cyclophosphamide, hydroxydoxorubicin.

683Paclitaxel plus Cyclophosphamide in NHL
q 1998 Blackwell Science Ltd, British Journal of Haematology 103: 678–683
Tolcher, A.W., Cowan, K.H,., Noone, M.H., Denicoff, A.M.,Kohler, D.R., Goldspiel, B.R., Barnes, C.S., McCabe, M.,Gossard, M.R., Zujewski, J. & O’Shaughnessy, J.A. (1996) PhaseI study of paclitaxel in combination with cyclophosphamide andgranulocyte colony-stimulating actor in metastatic breast cancerpatients. Journal of Clinical Oncology, 14, 95–102.
Velasquez, W.S., Cabanillas, F., Salvador, P., McLaughlin, P.,Fridrik, M., Tucker, S., Jagannath, S., Hagemeister, F.B.,Redman, J.R., Swan, F. & Barlogie, B. (1988) Effective salvagetherapy for lymphoma with cisplatin in combination with high-dose Ara-C and dexamethasone (DHAP). Blood, 71, 117–122.
Velasquez, W.S., McLaughlin, P., Tucker, S., Hagemeister, F.B., Swan,F., Rodriguez, M.A., Romaguera, J., Rubenstein, E. & Cabanillas, F.(1994) ESHAP – an effective chemotherapy regimen in refractoryand relapsing lymphoma: a 4-year follow-up study. Journal ofClinical Oncology, 12, 1169–1176.
Wilson, W.H., Bryant, G., Bates, S., Fojo, A., Wittes, R.E,
Steinberg, S.M., Kohler, D.R., Jaffe, E.S, Herdt, J., Cheson, B.D. &Chabner, B.A. (1993) EPOCH chemotherapy: toxicity and efficacyin relapsed and refractory non-Hodgkin’s lymphoma. Journal ofClinical Oncology, 11, 1573–1582.
Wilson, W.H., Chabner, B.A., Bryant, G., Bates, S., Fojo, A., Regis, J.,Jaffe, E., Steinberg, S.M., Goldspiel, B.R., Cheson, B. & Wittes, R.E.(1995) Phase II study of paclitaxel in relapsed non-Hodgkin’slymphomas. Journal of Clinical Oncology, 13, 381–386.
Younes, A., Ayoub, J.P., Sarris, A., Hagemeister, F., North, L., Pate, O.,McLaughlin, P., Rodriguez, M.A., Romaguera, J., Kurzrock, R.,Preti, A., Bachier, C., Smith, T. & Cabanillas, F. (1997a) Paclitaxelactivity for the treatment of non-Hodgkin’s lymphoma: final reportof a phase II trial. British Journal of Haematology, 96, 328–332.
Younes, A., Ayoub, J.P., Sarris, A., North, L., Pate, O., McLaughlin, P.,Rodriguez, A., Romaguera, J., Hagemeister, F., Bachier, C., Preti, A.& Cabanillas, F. (1997b) Paclitaxel (Taxol(R)) for the treatment oflymphoma. Annals of Oncology, 8, 129–131.




















