P A R T T W O - Health Research Web
104
P P ART T T WO PROGRAMME PROFILES
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of P A R T T W O - Health Research Web

PP AA RR TT TT WW OO
PP RR OO GG RR AA MM MM EE PP RR OO FF II LL EE SS
TT AA BB LL EE OO FF CC OO NN TT EE NN TT SS
STD/AIDS control programme ------------------------------------------------------------3 National TB Control Programme ----------------------------------------------------------6 National Leprosy Control Programme -------------------------------------------------- 11 Expanded Programme on Immunization------------------------------------------------ 14 Acute respiratory infection control programme---------------------------------------- 17 National Control of Diarrhoeal diseases Programme---------------------------------- 21 National malaria control program ------------------------------------------------------- 24 Primary Eye Care Programme------------------------------------------------------------ 28 National community based rehabilitation programme -------------------------------- 30 Mental Health Programme---------------------------------------------------------------- 34 Nutrition programme---------------------------------------------------------------------- 38 Reproductive health & population programme----------------------------------------- 41 Village Health Worker Programme ------------------------------------------------------ 48 Oral Health Programme------------------------------------------------------------------- 51 Public Health Laboratory------------------------------------------------------------------ 54 Research and epidemiology unit---------------------------------------------------------- 59 Health Management Information System----------------------------------------------- 62 Public health engineering section -------------------------------------------------------- 66 Health Engineering Division ------------------------------------------------------------- 70 Quality Assurance and Standardisation ------------------------------------------------ 73 Continuing Education Programme ------------------------------------------------------ 76 Information, education & communication for health ---------------------------------- 78 Health Telematics Project ----------------------------------------------------------------- 82 Drugs, Vaccines and Equipment Division---------------------------------------------- 85 Royal Institute of Health Sciences ------------------------------------------------------- 90 National Institute of Traditional Medicine --------------------------------------------- 93 National Indigenous Hospital ------------------------------------------------------------ 95 Pharmaceutical and Research Unit ------------------------------------------------------ 97 Jigme Dorji Wangchuk National Referral Hospital-----------------------------------100 Extension of JDWNR Hospital ----------------------------------------------------------103 Extension of Mongar Regional Referral Hospital-------------------------------------104
HHeeaalltthh PPrrooggrraammmmeess
3
STD/AIDS CONTROL PROGRAMME I. Introduction Bhutan initiated National STD/AIDS Control Programme in 1988. Prior to this, Sexually Transmitted Diseases (STDs), though managed through the various health facilities, were not targeted with active prevention measures. The Short Term Plan (STP) developed in 1989 to counter the spread of the global AIDS pandemic had brought STDs under attention. This led to the formulation and implementation of a three year Medium Term Plan (MTP-I) in 1990. And again in 1995, Strategic Medium Term Plan was developed to address the prevention of sexual transmission of HIV. II. Situation Analysis a) Current Situation Assessment
Although only a few HIV infections have so far been detected, but given the HIV/AIDS epidemic situation in the neighbouring countries, the Government as well as private sector in Bhutan are concerned about the future infection from HIV. So far, 22 HIV positive cases have been diagnosed. Despite low prevalence of HIV infection at the moment, the country is at a significant risk of a widespread epidemic if timely interventions are not made. The major factors responsible for this may be liberal sexual mores that is prevalent in most parts of the country. A recent survey has shown that the HBs AG prevalence in a study population (ANC attendants & hospital outpatients) is to the tune of about 20%. These factors are compounded by the increased mobility of the people both within and outside the country. A nagging concern is that commercial sex workers are today not only limited to the bordering areas but also is becoming evident in some other major townships in the country. The problem of intravenous drug use is not a major concern at present. However, emergency of this problem needs to be kept under surveillance as a few stray cases have been reported. A KABP study, conducted in 1989, found that STDs were more common (8.2%) in the urban areas than the rural (6.3%). The study also found that only 8% amongst the 39% that were aware ever used condoms. Another important finding was that STDs were found to be prevalent not only in the Southern regions, as believed, but also in some of the Central and Eastern regions. The disease occurred commonly in the 15-49 age group, in males, and amongst illiterates (those having lower level of education). b) Situation Assessment at the end of the Ninth Plan
• Voluntary Counselling & Testing Unit established in every district • 100% condom available • Drugs for STI and ARV for pregnant women made available
HHeeaalltthh PPrrooggrraammmmeess
4
III. Program objectives/policy objectives 1. Reduce risk of STD and HIV transmission 2. Reduce the morbidity & mortality associated with HIV/AIDS & STI 3. Reduce the social and economic impact of HIV infection & AIDS 4. VCT services and HIV surveillance system established in All Dzongkhags by
2007 IV. Strategies
1. Prevent sexual transmission through multi-sectoral approach and IECH 2. Prevent transmission through blood and blood products 3. Prevent vertical transmission 4. Counseling and care facilities established 5. Program Strengthening and management
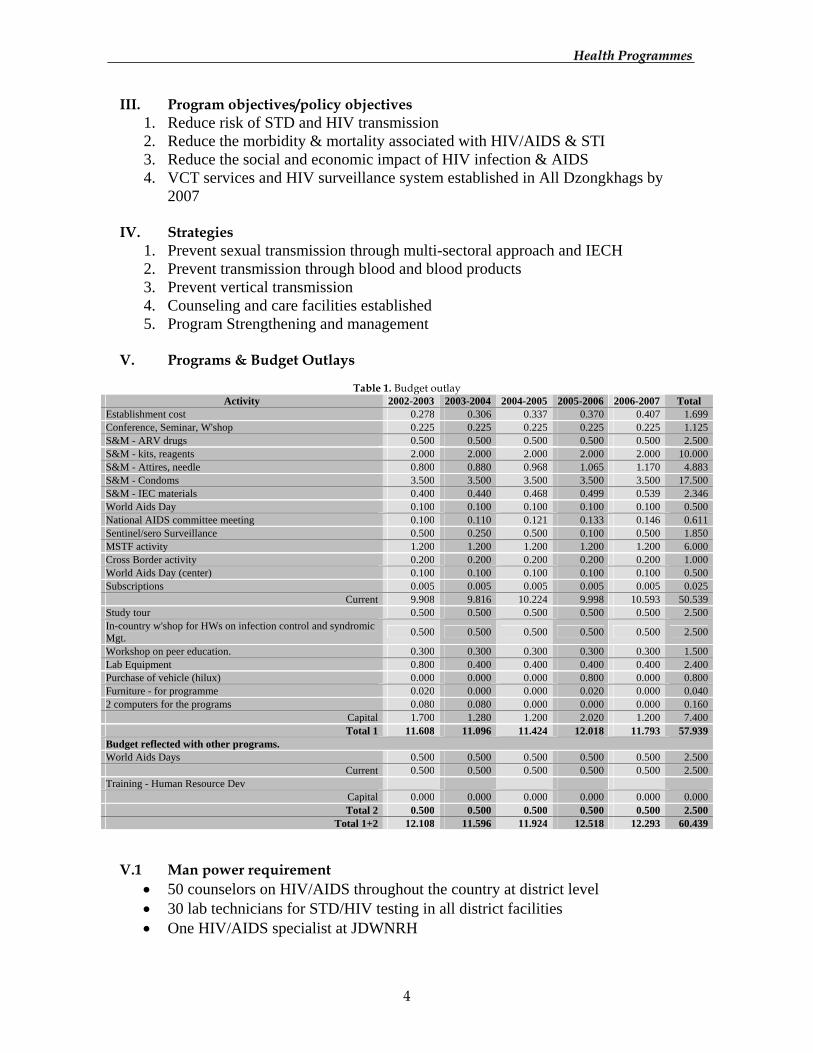
V. Programs & Budget Outlays
Table 1. Budget outlay
Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total Establishment cost 0.278 0.306 0.337 0.370 0.407 1.699Conference, Seminar, W'shop 0.225 0.225 0.225 0.225 0.225 1.125S&M - ARV drugs 0.500 0.500 0.500 0.500 0.500 2.500S&M - kits, reagents 2.000 2.000 2.000 2.000 2.000 10.000S&M - Attires, needle 0.800 0.880 0.968 1.065 1.170 4.883S&M - Condoms 3.500 3.500 3.500 3.500 3.500 17.500S&M - IEC materials 0.400 0.440 0.468 0.499 0.539 2.346World Aids Day 0.100 0.100 0.100 0.100 0.100 0.500National AIDS committee meeting 0.100 0.110 0.121 0.133 0.146 0.611Sentinel/sero Surveillance 0.500 0.250 0.500 0.100 0.500 1.850MSTF activity 1.200 1.200 1.200 1.200 1.200 6.000Cross Border activity 0.200 0.200 0.200 0.200 0.200 1.000World Aids Day (center) 0.100 0.100 0.100 0.100 0.100 0.500Subscriptions 0.005 0.005 0.005 0.005 0.005 0.025
Current 9.908 9.816 10.224 9.998 10.593 50.539Study tour 0.500 0.500 0.500 0.500 0.500 2.500In-country w'shop for HWs on infection control and syndromic Mgt. 0.500 0.500 0.500 0.500 0.500 2.500
Workshop on peer education. 0.300 0.300 0.300 0.300 0.300 1.500Lab Equipment 0.800 0.400 0.400 0.400 0.400 2.400Purchase of vehicle (hilux) 0.000 0.000 0.000 0.800 0.000 0.800Furniture - for programme 0.020 0.000 0.000 0.020 0.000 0.0402 computers for the programs 0.080 0.080 0.000 0.000 0.000 0.160
Capital 1.700 1.280 1.200 2.020 1.200 7.400Total 1 11.608 11.096 11.424 12.018 11.793 57.939
Budget reflected with other programs. World Aids Days 0.500 0.500 0.500 0.500 0.500 2.500
Current 0.500 0.500 0.500 0.500 0.500 2.500Training - Human Resource Dev
Capital 0.000 0.000 0.000 0.000 0.000 0.000Total 2 0.500 0.500 0.500 0.500 0.500 2.500
Total 1+2 12.108 11.596 11.924 12.518 12.293 60.439 V.1 Man power requirement
• 50 counselors on HIV/AIDS throughout the country at district level • 30 lab technicians for STD/HIV testing in all district facilities • One HIV/AIDS specialist at JDWNRH
HHeeaalltthh PPrrooggrraammmmeess
5
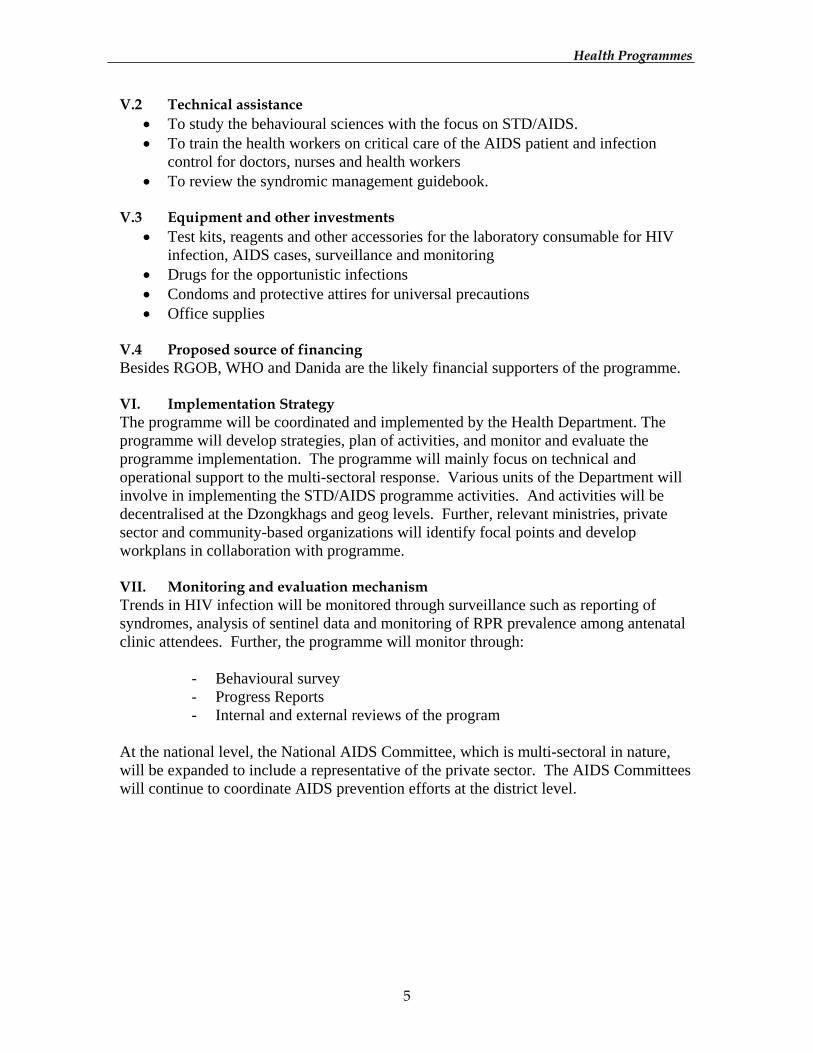
V.2 Technical assistance • To study the behavioural sciences with the focus on STD/AIDS. • To train the health workers on critical care of the AIDS patient and infection
control for doctors, nurses and health workers • To review the syndromic management guidebook.
V.3 Equipment and other investments
• Test kits, reagents and other accessories for the laboratory consumable for HIV infection, AIDS cases, surveillance and monitoring
• Drugs for the opportunistic infections • Condoms and protective attires for universal precautions • Office supplies
V.4 Proposed source of financing Besides RGOB, WHO and Danida are the likely financial supporters of the programme. VI. Implementation Strategy The programme will be coordinated and implemented by the Health Department. The programme will develop strategies, plan of activities, and monitor and evaluate the programme implementation. The programme will mainly focus on technical and operational support to the multi-sectoral response. Various units of the Department will involve in implementing the STD/AIDS programme activities. And activities will be decentralised at the Dzongkhags and geog levels. Further, relevant ministries, private sector and community-based organizations will identify focal points and develop workplans in collaboration with programme. VII. Monitoring and evaluation mechanism Trends in HIV infection will be monitored through surveillance such as reporting of syndromes, analysis of sentinel data and monitoring of RPR prevalence among antenatal clinic attendees. Further, the programme will monitor through:
- Behavioural survey - Progress Reports - Internal and external reviews of the program
At the national level, the National AIDS Committee, which is multi-sectoral in nature, will be expanded to include a representative of the private sector. The AIDS Committees will continue to coordinate AIDS prevention efforts at the district level.
HHeeaalltthh PPrrooggrraammmmeess
6
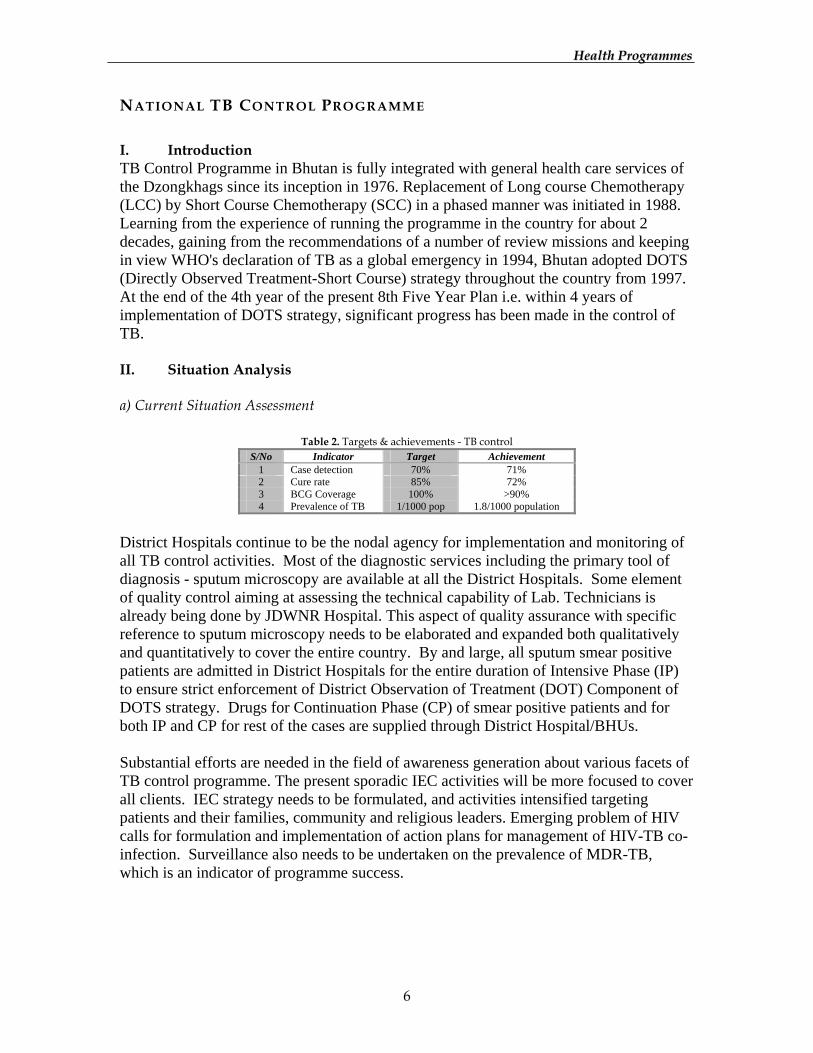
NATIONAL TB CONTROL PROGRAMME I. Introduction TB Control Programme in Bhutan is fully integrated with general health care services of the Dzongkhags since its inception in 1976. Replacement of Long course Chemotherapy (LCC) by Short Course Chemotherapy (SCC) in a phased manner was initiated in 1988. Learning from the experience of running the programme in the country for about 2 decades, gaining from the recommendations of a number of review missions and keeping in view WHO's declaration of TB as a global emergency in 1994, Bhutan adopted DOTS (Directly Observed Treatment-Short Course) strategy throughout the country from 1997. At the end of the 4th year of the present 8th Five Year Plan i.e. within 4 years of implementation of DOTS strategy, significant progress has been made in the control of TB. II. Situation Analysis a) Current Situation Assessment
Table 2. Targets & achievements - TB control S/No Indicator Target Achievement
1 Case detection 70% 71% 2 Cure rate 85% 72% 3 BCG Coverage 100% >90% 4 Prevalence of TB 1/1000 pop 1.8/1000 population
District Hospitals continue to be the nodal agency for implementation and monitoring of all TB control activities. Most of the diagnostic services including the primary tool of diagnosis - sputum microscopy are available at all the District Hospitals. Some element of quality control aiming at assessing the technical capability of Lab. Technicians is already being done by JDWNR Hospital. This aspect of quality assurance with specific reference to sputum microscopy needs to be elaborated and expanded both qualitatively and quantitatively to cover the entire country. By and large, all sputum smear positive patients are admitted in District Hospitals for the entire duration of Intensive Phase (IP) to ensure strict enforcement of District Observation of Treatment (DOT) Component of DOTS strategy. Drugs for Continuation Phase (CP) of smear positive patients and for both IP and CP for rest of the cases are supplied through District Hospital/BHUs. Substantial efforts are needed in the field of awareness generation about various facets of TB control programme. The present sporadic IEC activities will be more focused to cover all clients. IEC strategy needs to be formulated, and activities intensified targeting patients and their families, community and religious leaders. Emerging problem of HIV calls for formulation and implementation of action plans for management of HIV-TB co-infection. Surveillance also needs to be undertaken on the prevalence of MDR-TB, which is an indicator of programme success.
HHeeaalltthh PPrrooggrraammmmeess
7
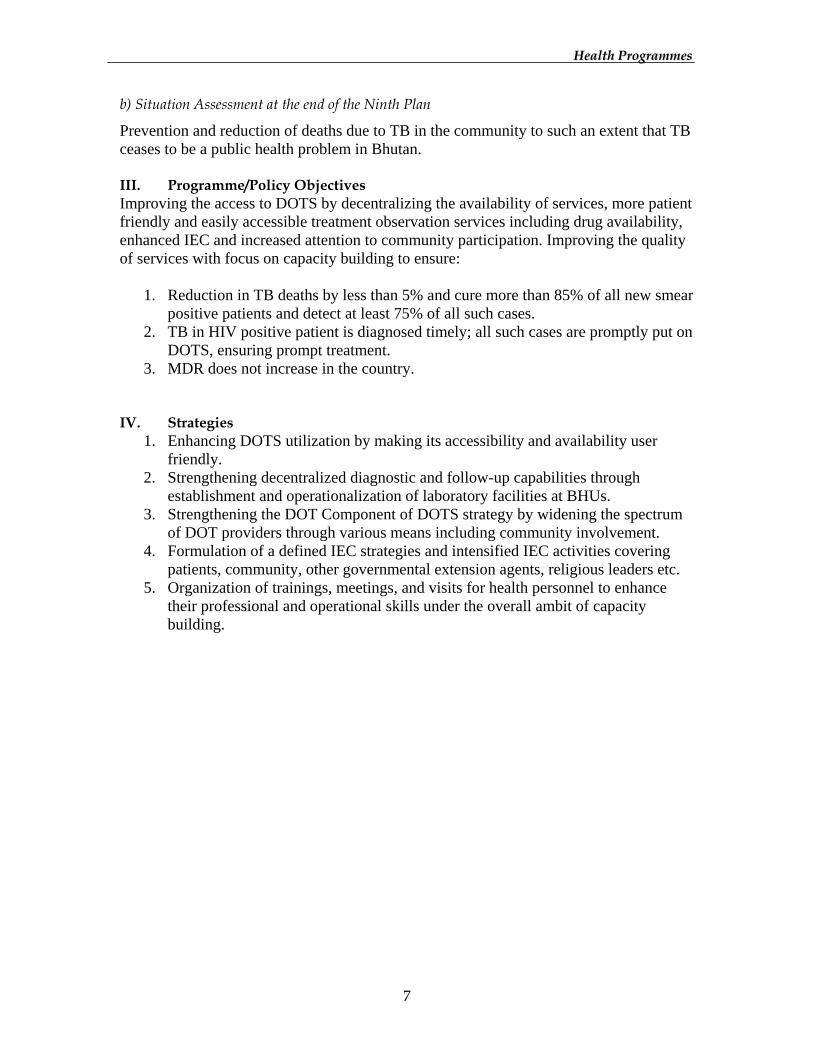
b) Situation Assessment at the end of the Ninth Plan
Prevention and reduction of deaths due to TB in the community to such an extent that TB ceases to be a public health problem in Bhutan. III. Programme/Policy Objectives Improving the access to DOTS by decentralizing the availability of services, more patient friendly and easily accessible treatment observation services including drug availability, enhanced IEC and increased attention to community participation. Improving the quality of services with focus on capacity building to ensure:
1. Reduction in TB deaths by less than 5% and cure more than 85% of all new smear positive patients and detect at least 75% of all such cases.
2. TB in HIV positive patient is diagnosed timely; all such cases are promptly put on DOTS, ensuring prompt treatment.
3. MDR does not increase in the country. IV. Strategies
1. Enhancing DOTS utilization by making its accessibility and availability user friendly.
2. Strengthening decentralized diagnostic and follow-up capabilities through establishment and operationalization of laboratory facilities at BHUs.
3. Strengthening the DOT Component of DOTS strategy by widening the spectrum of DOT providers through various means including community involvement.
4. Formulation of a defined IEC strategies and intensified IEC activities covering patients, community, other governmental extension agents, religious leaders etc.
5. Organization of trainings, meetings, and visits for health personnel to enhance their professional and operational skills under the overall ambit of capacity building.

HHeeaalltthh PPrrooggrraammmmeess
8
V. Programs and Budget Outlay
Table 3. Budget Outlay
Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total Establishment cost 0.369 0.405 0.446 0.490 0.540 2.250IEC material dev 0.500 0.500 0.500 0.500 0.500 2.500Printing and publications 0.300 0.300 0.300 0.300 0.300 1.500Drugs for PHL 0.420 0.420 0.420 0.420 0.420 2.100Anti TB Drugs 2.200 2.420 2.662 2.420 2.229 11.931Text book, stationary 0.400 0.400 0.400 0.400 0.400 2.000Op.Exp-TB days 0.500 0.500 0.500 0.500 0.500 2.500Op.Exp-IECH 0.500 0.500 0.500 0.500 0.500 2.500Op.Exp-Annual risk of infection 0.000 0.500 0.000 0.000 0.000 0.500Op.Exp-drug resistance study 0.000 0.000 0.500 0.000 0.000 0.500Op.Exp-study on DOT's providers 0.000 0.000 0.000 0.500 0.000 0.500Annual TB incharges meetings 0.160 0.160 0.160 0.160 0.160 0.800Conference, Seminar, W'shop 0.090 0.099 0.109 0.120 0.132 0.549
Current 5.439 6.204 6.497 6.310 5.680 30.130Study tour for DOTS program 0.430 0.430 0.430 0.430 0.430 2.150lab material for hospitals 0.580 0.580 0.580 0.580 0.580 2.900X ray for Hospitals 1.000 1.000 1.000 1.000 1.000 5.000Microscopes for BHUs/Hospitals 5.250 0.000 0.000 0.000 0.000 5.2501 vehicle for programme 0.000 0.800 0.000 0.000 0.000 0.8003 van for referral hospitals 0.900 0.000 0.000 0.000 0.000 0.9004 Copiers (3 for Regional) 0.520 0.000 0.000 0.000 0.000 0.5204 LCD Projector (3 for Regional) 0.000 0.800 0.000 0.000 0.000 0.8001 Computers for the program 0.080 0.000 0.000 0.000 0.000 0.080
Capital 8.760 3.610 2.010 2.010 2.010 18.400Total 1 14.199 9.814 8.507 8.320 7.690 48.530
Budget reflected with other programs. Op.Exp-TB days 1.000 1.000 1.000 1.000 1.000 5.000In country w'shop for HWs on TB DOTS. 2.910 2.910 2.910 2.910 2.910 14.550
Current 3.910 3.910 3.910 3.910 3.910 19.550Training - Human Resource Dev 22 two wheelers 0.660 0.000 0.000 0.000 0.000 0.660
Capital 0.660 0.000 0.000 0.000 0.000 0.660Total 2 4.570 3.910 3.910 3.910 3.910 20.210
Total 1+2 18.769 13.724 12.417 12.230 11.600 68.740 V.1 Manpower requirement Three regional supervisors will be posted at Eastern, Central and Western regional hospitals. In the Dzongkhags/Hospitals, TB in-charges will take up the responsibility as a "secondary" duty. The central unit presently manned by a programme manager needs to be strengthened with a full time programme officer with a Statistician/Data Entry Operator. V.2 Technical Assistance Review missions will be required ideally every year, and at the end of the plan period to assess and evaluate the new proposed interventions like community involvement,
HHeeaalltthh PPrrooggrraammmmeess
9
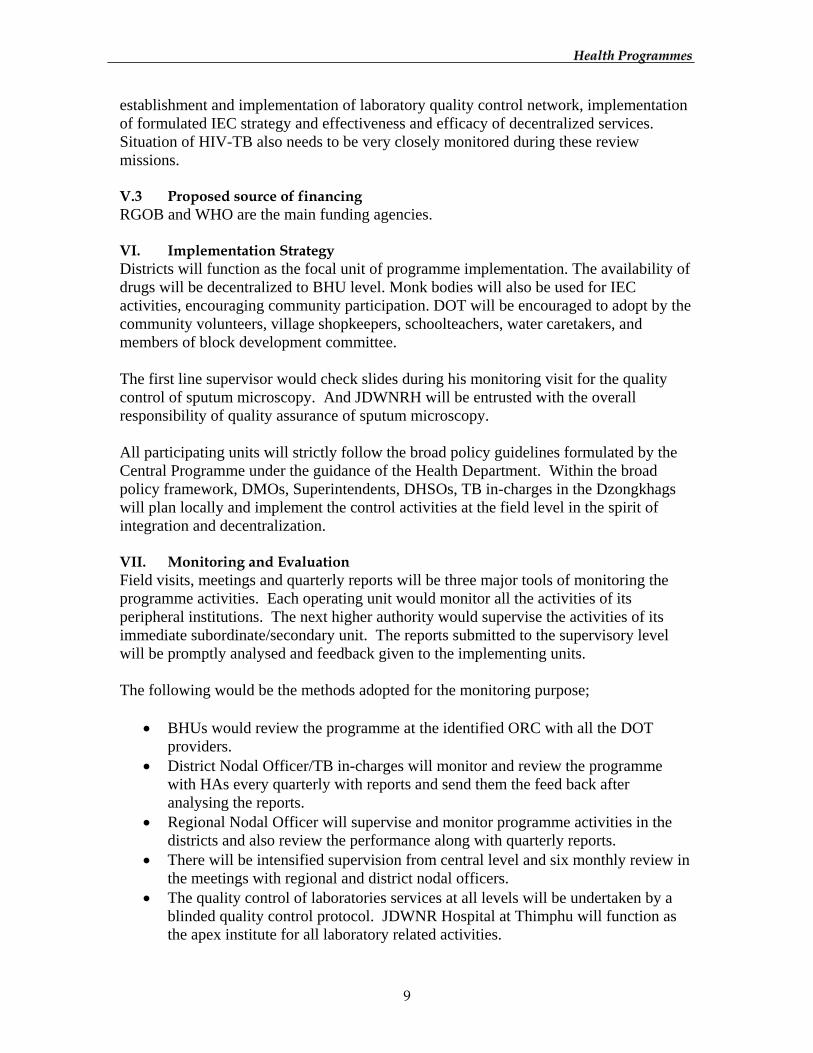
establishment and implementation of laboratory quality control network, implementation of formulated IEC strategy and effectiveness and efficacy of decentralized services. Situation of HIV-TB also needs to be very closely monitored during these review missions. V.3 Proposed source of financing RGOB and WHO are the main funding agencies. VI. Implementation Strategy Districts will function as the focal unit of programme implementation. The availability of drugs will be decentralized to BHU level. Monk bodies will also be used for IEC activities, encouraging community participation. DOT will be encouraged to adopt by the community volunteers, village shopkeepers, schoolteachers, water caretakers, and members of block development committee. The first line supervisor would check slides during his monitoring visit for the quality control of sputum microscopy. And JDWNRH will be entrusted with the overall responsibility of quality assurance of sputum microscopy. All participating units will strictly follow the broad policy guidelines formulated by the Central Programme under the guidance of the Health Department. Within the broad policy framework, DMOs, Superintendents, DHSOs, TB in-charges in the Dzongkhags will plan locally and implement the control activities at the field level in the spirit of integration and decentralization. VII. Monitoring and Evaluation Field visits, meetings and quarterly reports will be three major tools of monitoring the programme activities. Each operating unit would monitor all the activities of its peripheral institutions. The next higher authority would supervise the activities of its immediate subordinate/secondary unit. The reports submitted to the supervisory level will be promptly analysed and feedback given to the implementing units. The following would be the methods adopted for the monitoring purpose;
• BHUs would review the programme at the identified ORC with all the DOT
providers. • District Nodal Officer/TB in-charges will monitor and review the programme
with HAs every quarterly with reports and send them the feed back after analysing the reports.
• Regional Nodal Officer will supervise and monitor programme activities in the districts and also review the performance along with quarterly reports.
• There will be intensified supervision from central level and six monthly review in the meetings with regional and district nodal officers.
• The quality control of laboratories services at all levels will be undertaken by a blinded quality control protocol. JDWNR Hospital at Thimphu will function as the apex institute for all laboratory related activities.

HHeeaalltthh PPrrooggrraammmmeess
10
HHeeaalltthh PPrrooggrraammmmeess
11
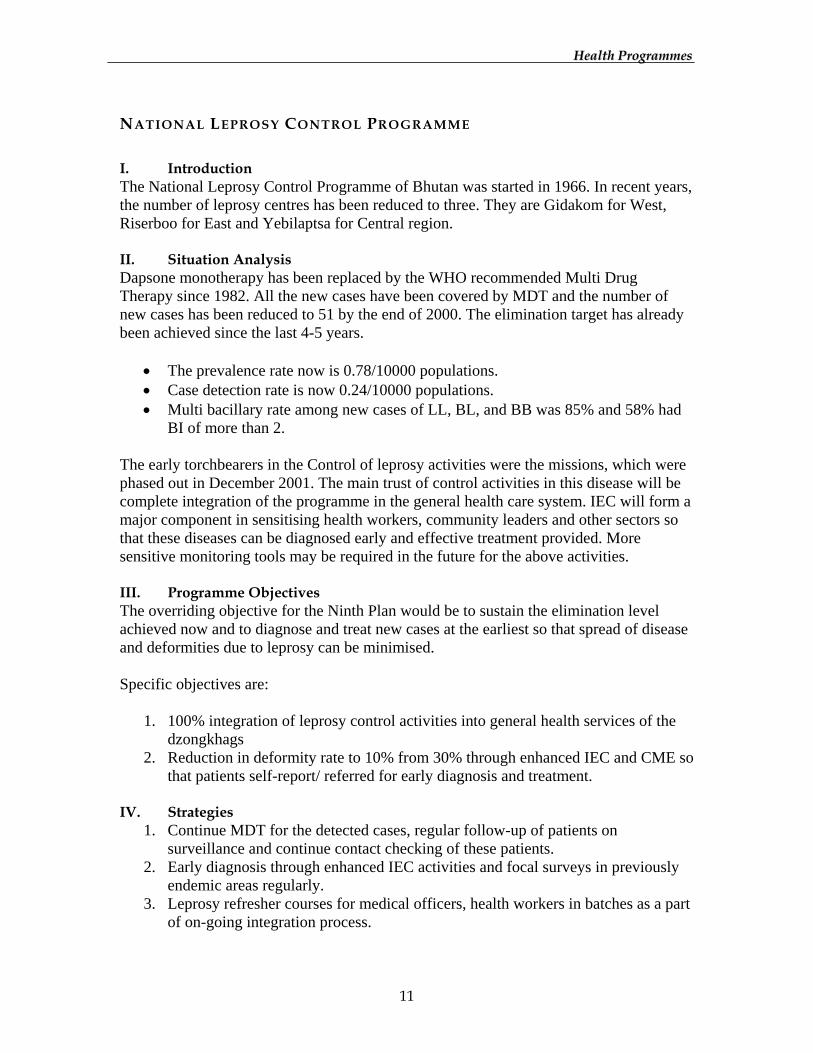
NATIONAL LEPROSY CONTROL PROGRAMME I. Introduction The National Leprosy Control Programme of Bhutan was started in 1966. In recent years, the number of leprosy centres has been reduced to three. They are Gidakom for West, Riserboo for East and Yebilaptsa for Central region. II. Situation Analysis Dapsone monotherapy has been replaced by the WHO recommended Multi Drug Therapy since 1982. All the new cases have been covered by MDT and the number of new cases has been reduced to 51 by the end of 2000. The elimination target has already been achieved since the last 4-5 years.
• The prevalence rate now is 0.78/10000 populations. • Case detection rate is now 0.24/10000 populations. • Multi bacillary rate among new cases of LL, BL, and BB was 85% and 58% had
BI of more than 2. The early torchbearers in the Control of leprosy activities were the missions, which were phased out in December 2001. The main trust of control activities in this disease will be complete integration of the programme in the general health care system. IEC will form a major component in sensitising health workers, community leaders and other sectors so that these diseases can be diagnosed early and effective treatment provided. More sensitive monitoring tools may be required in the future for the above activities. III. Programme Objectives The overriding objective for the Ninth Plan would be to sustain the elimination level achieved now and to diagnose and treat new cases at the earliest so that spread of disease and deformities due to leprosy can be minimised. Specific objectives are:
1. 100% integration of leprosy control activities into general health services of the
dzongkhags 2. Reduction in deformity rate to 10% from 30% through enhanced IEC and CME so
that patients self-report/ referred for early diagnosis and treatment. IV. Strategies
1. Continue MDT for the detected cases, regular follow-up of patients on surveillance and continue contact checking of these patients.
2. Early diagnosis through enhanced IEC activities and focal surveys in previously endemic areas regularly.
3. Leprosy refresher courses for medical officers, health workers in batches as a part of on-going integration process.
HHeeaalltthh PPrrooggrraammmmeess
12
4. Continue specialised deformity and disability care to rehabilitate the disabled to ensure that they lead a healthy and productive life.
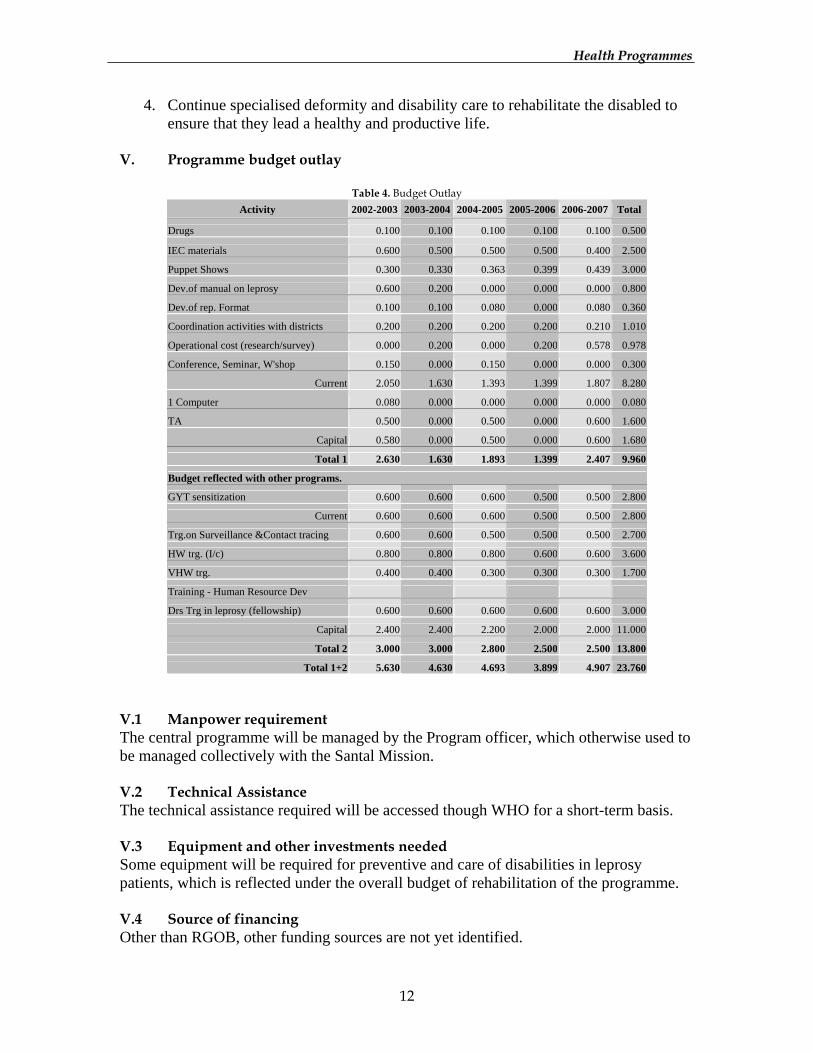
V. Programme budget outlay
Table 4. Budget Outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Drugs 0.100 0.100 0.100 0.100 0.100 0.500
IEC materials 0.600 0.500 0.500 0.500 0.400 2.500
Puppet Shows 0.300 0.330 0.363 0.399 0.439 3.000
Dev.of manual on leprosy 0.600 0.200 0.000 0.000 0.000 0.800
Dev.of rep. Format 0.100 0.100 0.080 0.000 0.080 0.360
Coordination activities with districts 0.200 0.200 0.200 0.200 0.210 1.010
Operational cost (research/survey) 0.000 0.200 0.000 0.200 0.578 0.978
Conference, Seminar, W'shop 0.150 0.000 0.150 0.000 0.000 0.300
Current 2.050 1.630 1.393 1.399 1.807 8.280
1 Computer 0.080 0.000 0.000 0.000 0.000 0.080
TA 0.500 0.000 0.500 0.000 0.600 1.600
Capital 0.580 0.000 0.500 0.000 0.600 1.680
Total 1 2.630 1.630 1.893 1.399 2.407 9.960
Budget reflected with other programs.
GYT sensitization 0.600 0.600 0.600 0.500 0.500 2.800
Current 0.600 0.600 0.600 0.500 0.500 2.800
Trg.on Surveillance &Contact tracing 0.600 0.600 0.500 0.500 0.500 2.700
HW trg. (I/c) 0.800 0.800 0.800 0.600 0.600 3.600
VHW trg. 0.400 0.400 0.300 0.300 0.300 1.700
Training - Human Resource Dev
Drs Trg in leprosy (fellowship) 0.600 0.600 0.600 0.600 0.600 3.000
Capital 2.400 2.400 2.200 2.000 2.000 11.000
Total 2 3.000 3.000 2.800 2.500 2.500 13.800
Total 1+2 5.630 4.630 4.693 3.899 4.907 23.760 V.1 Manpower requirement The central programme will be managed by the Program officer, which otherwise used to be managed collectively with the Santal Mission. V.2 Technical Assistance The technical assistance required will be accessed though WHO for a short-term basis. V.3 Equipment and other investments needed Some equipment will be required for preventive and care of disabilities in leprosy patients, which is reflected under the overall budget of rehabilitation of the programme. V.4 Source of financing Other than RGOB, other funding sources are not yet identified.
HHeeaalltthh PPrrooggrraammmmeess
13
VI. Implementation strategy The programme manager under the Public Health Department will be responsible for planning policies, making yearly and five-yearly plans and supporting the Dzongakhgs technically. The overall implementation will be carried out by the dzongkhags and fine-tuning of this in the philosophy of integration and decentralization will take sometime till middle of this plan period. VII. Monitoring and evaluation mechanism Through HMIS and reporting systems directly related to the programme, monitoring will be carried out by the programme at PHD. In essence, over the years, individual Dzongkhags/regions will be empowered to monitor and evaluate the activities. The external assistance might also be required to evaluate the programme by the final year of the programme implementation.
HHeeaalltthh PPrrooggrraammmmeess
14
EXPANDED PROGRAMME ON IMMUNIZATION I. Introduction The EPI was launched in the country on 15th Nov. 1979 coinciding with International Year of Child with an objective of reducing the seven vaccine preventable diseases, (TB, Diphtheria, Pertussis, Tetanus, Polio, Measles & Hep.B). In December 1994, the Tetanus Toxoid vaccine for pregnant woman was also introduced into the programme. In mid 1996 Hep.B vaccine for children under one year of age was introduced as an integral component of EPI. The EPI services have been fully integrated into the general health services and mainly with MCH/FP in particular. It is delivered through existing Hospitals, BHUs and ORCs. Overall Immunization services are aimed for effective coverage with all seven antigens aimed at all infants under one year of age and to all pregnant women and women in child bearing age. II. Situation Analysis a) Current Situation Assessment
Since declaration of UCI in the year 1991, Bhutan has been successful in sustaining above 85% coverage of children under 1 year of age by all EPI antigens. With AFP surveillance established in 1997, no polio cases have been detected to date. So far a total of 10 AFP cases has been tested and all were found negative and Bhutan is strongly committed to eradication of poliomyelitis by the year 2005. There is a decreasing trend in measles coverage and rise in the incidence of measles cases (840 cases in 2000 compared to 84 cases in 1999). There is also a lack of confirmatory investigation on reported measles cases. b) Situation Assessment at the end of the Ninth Plan
EPI activities on all EPI disease will be intensified and universal child immunisation coverage maintained. A baseline study on Haemophilus influenza (Hip) infection will be carried out, and if the prevalence rate is high then the vaccine will be introduced along with other EPI vaccines. Nation wide EPI coverage review and cold chain system will be undertaken to determine the achievements, problem and future needs to guide the programme. III. Program Objectives/Policy Objectives for 9FYP Overall objective of the programme is to reduce the seven vaccine preventable diseases to a level at which they are no longer a public health problem. Specific Objectives are:

HHeeaalltthh PPrrooggrraammmmeess
15
1. To sustain the high national immunization coverage level at or above 90% for children of one year of age.
2. To achieve polio certification by 2005. 3. 90% reduction of measles cases. 4. To eliminate Neo-natal Tetanus by 2005. 5. To increase the safety of injection used for all EPI vaccines through the use of
auto-disable syringe for all injection by end of 2004. 6. To develop sustainability in the EPI programme through national capacity
building. IV. Strategies
1. Immunization for the un-reached and low-reach group 2. Ensuring quality and vaccination safety 3. Minimising missed opportunity 4. Provision of required vaccines and vaccination supplies 5. Establishing and strengthening surveillance for EPI disease 6. Community mobilization 7. National capacity development for ensuring sustainability
V.1 Programme Budget Outlay
Table 5. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 1.082 1.191 1.310 1.441 1.585 6.608 Conference, Seminar, W'shop 0.100 0.000 0.100 0.000 0.100 0.300 Vaccines supply 2.440 2.575 2.669 2.765 2.857 13.306Hep B vaccines 1.700 1.800 1.800 1.900 2.000 9.200 Hib Vaccines 1.700 1.800 1.800 1.900 2.000 9.200 Vit A during SNID 0.048 0.048 0.048 0.048 0.048 0.240 Lab reagent for screening Hep B 0.650 0.715 0.787 0.865 0.952 3.968 Auto destruct syringes 0.476 0.492 0.507 0.523 0.539 2.537 Maintenance of cold room 0.096 0.096 0.096 0.096 0.096 0.480 EPI -IEC though radio 0.240 0.264 0.288 0.312 0.336 1.440 IEC advocacy 1.000 1.000 1.000 1.000 1.000 5.000 Hib burden study 0.240 0.000 0.000 0.000 0.000 0.240 EPI Survey 0.000 0.000 0.000 1.500 0.000 1.500 Interagency Coordination Meeting 0.048 0.048 0.048 0.048 0.048 0.240 Review/update EPI pillory guidelines 0.480 0.000 0.000 0.000 0.000 0.480 Reporting formats, AFP surveillance 0.480 0.144 0.144 0.144 0.144 1.056 SNID operational cost 8.160 8.976 9.874 10.861 11.860 49.731SNID with TT 0.000 3.168 0.000 0.000 0.000 3.168 SNID with Measles 0.000 0.000 3.168 0.000 0.000 3.168 Study of injection safety equipment 0.240 0.000 0.000 0.000 0.000 0.240 Measles, polio, & MNT surveillance 0.480 0.480 0.480 0.480 0.480 2.400
Current 19.660 22.797 24.118 23.883 24.044 114.502Trg of pry health care workers on revised policy guidelines 0.400 0.400 0.400 0.400 0.400 2.000 Project monitoring and management 0.000 0.240 0.000 0.000 0.000 0.240 Cold chain equipment 2.230 2.139 2.132 1.876 1.732 10.109Vaccination equipments 0.369 2.583 2.678 2.837 2.903 11.3702 Hilux for the programme 0.800 0.000 0.800 0.000 0.000 1.600 1 computer 0.000 0.080 0.000 0.000 0.000 0.080
Capital 3.799 5.442 6.010 5.113 5.035 25.399Total 1 23.459 28.239 30.128 28.996 29.079 139.901
HHeeaalltthh PPrrooggrraammmmeess
16
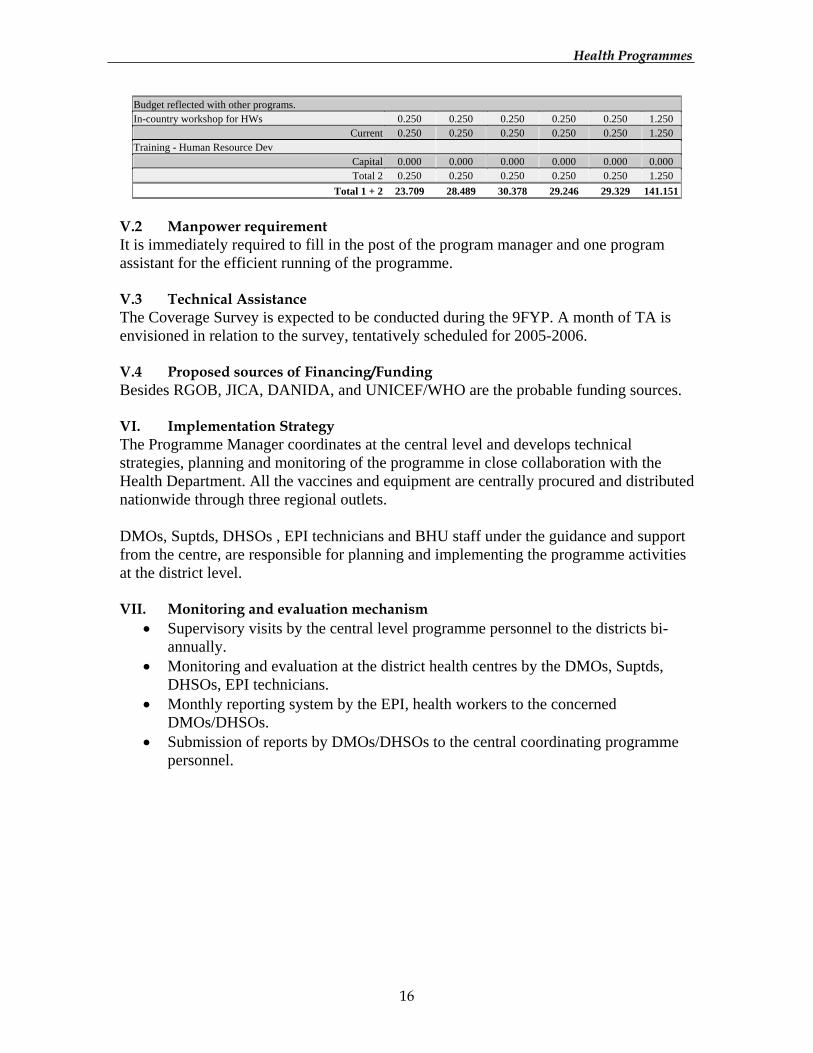
Budget reflected with other programs. In-country workshop for HWs 0.250 0.250 0.250 0.250 0.250 1.250
Current 0.250 0.250 0.250 0.250 0.250 1.250 Training - Human Resource Dev
Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.250 0.250 0.250 0.250 0.250 1.250
Total 1 + 2 23.709 28.489 30.378 29.246 29.329 141.151
V.2 Manpower requirement It is immediately required to fill in the post of the program manager and one program assistant for the efficient running of the programme. V.3 Technical Assistance The Coverage Survey is expected to be conducted during the 9FYP. A month of TA is envisioned in relation to the survey, tentatively scheduled for 2005-2006. V.4 Proposed sources of Financing/Funding Besides RGOB, JICA, DANIDA, and UNICEF/WHO are the probable funding sources. VI. Implementation Strategy The Programme Manager coordinates at the central level and develops technical strategies, planning and monitoring of the programme in close collaboration with the Health Department. All the vaccines and equipment are centrally procured and distributed nationwide through three regional outlets. DMOs, Suptds, DHSOs , EPI technicians and BHU staff under the guidance and support from the centre, are responsible for planning and implementing the programme activities at the district level. VII. Monitoring and evaluation mechanism
• Supervisory visits by the central level programme personnel to the districts bi-annually.
• Monitoring and evaluation at the district health centres by the DMOs, Suptds, DHSOs, EPI technicians.
• Monthly reporting system by the EPI, health workers to the concerned DMOs/DHSOs.
• Submission of reports by DMOs/DHSOs to the central coordinating programme personnel.
HHeeaalltthh PPrrooggrraammmmeess
17
ACUTE RESPIRATORY INFECTION CONTROL PROGRAMME I. Introduction ARI Programme is an ongoing integrated health activity. It is being decentralised right down to the BHU level. There are now 1200 active VHWs delivering services at the village level in collaboration with health workers. The ARI activity was initially integrated since 1987 during in-service training of health workers on Mid- level Management Course on EPI, CDD conducted at NIFH Galegphu. The ARI Program activities were intensified since 1993, as it was still then the leading cause of morbidity among communicable disease in the BHUs and hospitals. It is being noted that ARI has overtaken other communicable diseases since early 1990. However, there is no clear data of the mortality that it causes, and it is believed to contribute quite significantly. For these reason now the Government has accepted the introduction of IMCI strategy in the health, which would further strengthen the control activities of ARI/CDD/EPI to bring down the morbidity and mortality of pneumonia, diarrhoea, measles and the malnutrition related diseases in the country. Early Childhood Care for Development (ECCD) will be included with IMCI looking into prevention of morbidity and mortality due to common illness like ARI and CDD during 9 FYP. II. Situation Analysis: a) Current Situation Assessment
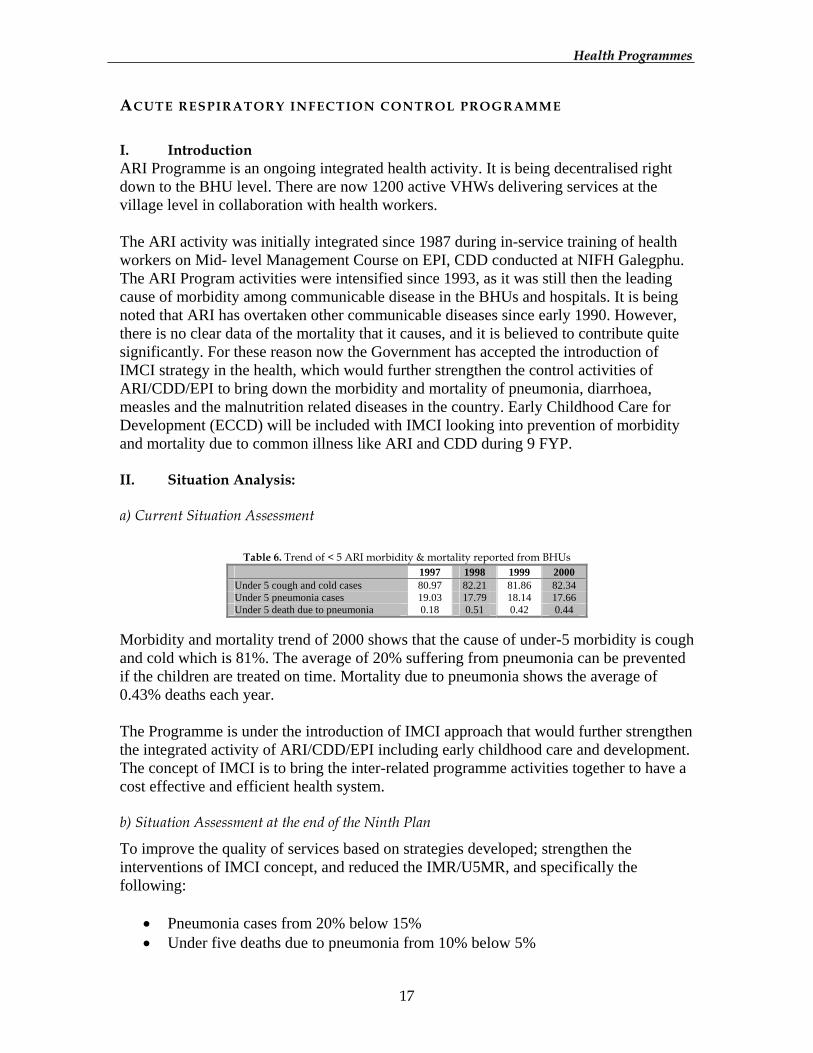
Table 6. Trend of < 5 ARI morbidity & mortality reported from BHUs
1997 1998 1999 2000 Under 5 cough and cold cases 80.97 82.21 81.86 82.34 Under 5 pneumonia cases 19.03 17.79 18.14 17.66 Under 5 death due to pneumonia 0.18 0.51 0.42 0.44
Morbidity and mortality trend of 2000 shows that the cause of under-5 morbidity is cough and cold which is 81%. The average of 20% suffering from pneumonia can be prevented if the children are treated on time. Mortality due to pneumonia shows the average of 0.43% deaths each year. The Programme is under the introduction of IMCI approach that would further strengthen the integrated activity of ARI/CDD/EPI including early childhood care and development. The concept of IMCI is to bring the inter-related programme activities together to have a cost effective and efficient health system. b) Situation Assessment at the end of the Ninth Plan
To improve the quality of services based on strategies developed; strengthen the interventions of IMCI concept, and reduced the IMR/U5MR, and specifically the following:
• Pneumonia cases from 20% below 15% • Under five deaths due to pneumonia from 10% below 5%

HHeeaalltthh PPrrooggrraammmmeess
18
• ARI episodes below 3% Besides, the existing MCH clinic would have expanded to “well-child clinic” to promote childcare practice to children under five, and parents and caretakers encouraged to take children to the Well-child clinic even after the completion of the immunisation schedule. III. Programme/Policy Objectives
• IMCI approach applied 100% • Reduction of ARI episode to below 3% • Reduction of under 5 pneumonia cases from 20% to below 15%. • Reduction of under 5 deaths due to pneumonia from 10% to < 5% • Over all reduction of IMR & U5MR by 20% of 2000 status.
IV. Strategies
1. Strengthening the capacity building: • Continuing education for health workers to ensure the quality of
services. • Training on IMCI for DMOs/DHSOs and health workers.
2. Strengthening the provision of Supplies:
Reinforcement of adequate supply of appropriate basic neonatal/paediatric equipment and ARI drugs to the health facilities
3. Community participation:
Education and training for VHWs, DYT/GYT member-mothers on the Prevention and Control of household dust and smoke through the grass-root level orientation.
4. Research activity:
To determine the under-five morbidity and mortality rates and other social factors affecting them, survey/research on IMCI activity impact will be carried out so as to identify an appropriate intervention for the growing problem.

HHeeaalltthh PPrrooggrraammmmeess
19
V.1 Programme and Budget Outlays
Table 7. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.127 0.139 0.153 0.168 0.185 0.772 IEC materials 0.150 0.165 0.182 0.200 0.220 0.916 Survey 1.000 0.000 0.000 0.000 0.000 1.000 IMCI monitoring in districts 0.300 0.300 0.300 0.200 0.307 1.407 Conference, Seminar, W'shop 0.150 0.000 0.150 0.000 0.150 0.450
Current 1.727 0.604 0.785 0.568 0.862 4.545 Pediatric equipment 1.000 1.000 1.000 1.000 1.000 5.000 Furniture for the program 0.040 0.000 0.000 0.000 0.020 0.060 Office equipment 0.170 0.000 0.000 0.000 0.020 0.190 1 Computer 0.000 0.080 0.000 0.000 0.000 0.080
Capital 1.210 1.080 1.000 1.000 1.040 5.330 Total 1 2.937 1.684 1.785 1.568 1.902 9.875
Budget reflected with other programs. S&M, medicines 1.000 1.000 1.000 1.000 1.000 5.000
Current 1.000 1.000 1.000 1.000 1.000 5.000 Training - Human Resource Dev In country trg for Health Workers 0.300 0.330 0.363 0.399 0.439 1.832 Trg of mothers 1.000 1.100 1.210 1.331 1.464 6.105
Capital 1.300 1.430 1.573 1.730 1.903 7.937 Total 2 2.300 2.430 2.573 2.730 2.903 12.937
Total 1 + 2 5.237 4.114 4.358 4.298 4.805 22.812 V.2 Manpower requirement Introduction of the IMCI concept is still premature and a full time technical focal person is required to guide the integrated programs at the central level. However, the programme activities are fully integrated within general health services integrating ARI, CDD and EPI. V.3 Technical Assistance Technical assistance will be sought to conduct a research on ARI caseload and type as to track down the causes of its high morbidity and mortality. V.4 Equipment and other investment needed: i) Nebulizer (3nos), ii) Oxygenconcentrator (3nos), iii) Otoscope (3nos), iv) Paediatric ECH (3nos), v) Pulse Oximeter (3nos), vi) Infusion pump (3nos), vii) Heat radiator (3nos), viii) Neonatal weighing machine (3nos), ix) Neonatal Resuscitation table and overhead radiant warmer (3nos), x) Paediatric CP Monitor (3nos), xi) Paediatric ventilator (3nos), xii) campaign equipment V.5 Proposed source of Financing RGOB, UNICEF and WHO are the likely financial supporters for this program in the 9FYP. VI. Implementation Strategy: The Programme Manager will coordinate at the central level and develop technical strategy, planning and monitoring of the programme in close collaboration with the Health Department. All the vaccines and equipment are centrally procured and distributed
HHeeaalltthh PPrrooggrraammmmeess
20
nationwide through three regional outlets. While Dzongkhag Health Services will be responsible for planning, implementing and monitoring of the programme activities at the district level. VII. Monitoring and evaluation mechanism:
• Survey for data collection/analysis and assess the causes of ARI. • Supervisory visits biannually from Programme to the districts. • Monitoring and evaluation at the district health centres by the DMOs DHSOs. • Monthly reporting system from the health facilities to DMOs/DHSOs. • Submission of reports by DMOs/DHSOs to the Central programme. • Regular information feedback mechanisms between the central and districts.

HHeeaalltthh PPrrooggrraammmmeess
21
NATIONAL CONTROL OF DIARRHOEAL DISEASES PROGRAMME I. Introduction. The National Control of Diarrhoeal Diseases Program was initiated in 1982 and became operational in 1984, as there was high morbidity and mortality due to diarrhoeal diseases in the Country. Diarrhoeal diseases still continue to be a major health problem affecting the well being of the children in the country. It stands second in trend among the 10 commonest morbidity. Concerted effort is required to ensure the continuance and effectiveness of public awareness and education campaign. This is necessary to complement the training for health workers, mothers, and VHWs on proper management of the diarrhoeal diseases. The provision of ORT needs to be continued especially for reaching the un-reached population where diarrhoeal diseases remain the main cause of morbidity. II. Situation analysis. a) Current Situation Assessment
Of the total morbidity and mortality reported from the hospitals and BHUs in the country, the contribution from diarrhoea/dysentery is substantially high as indicated below;
Table 8. Mortality and Morbidity cases from diarrhoea/dysentery 1. Total incidence rate due to diarrhoea/dysentery (2000) 11.14 2. Under five incidence due to diarrhoea/dysentery (2000) 21.17 3. Total mortality due to diarrhoea/dysentery (all age group, 2000) 6.6 4. Under five years mortality due to diarrhoea/dysentery (2000) 13.3
Source: - National Health Survey 2000 and Annual Health Bulletin 1999
Table 9. Diarrhoea & Dysentery cases reported from Hospitals & BHUs (1996 – 2000) Year Diarrhoea cases under
5 yrs. of age Dysentery cases under
5 yrs. Diarrhoea cases 5 yrs.
& above Dysentery cases 5
yrs. & above Total
1996 34,334 9,475 64,140 16,413 1,24,362 1997 26,700 6,529 61,321 14,311 10,8,861 1998 24,020 11,236 56,783 32,609 1,24,648 1999 21,388 11,458 49,474 32,168 1,14,488 2000 21,991 12,170 50,812 34,967 1,19,940
Although the Program in co-ordination with the Dzongkhags had put its effort to bring down the morbidity & mortality through training of health workers, mothers, VHWs on proper case management including promotion of proper feeding, sanitation & hygiene practices in the areas, the morbidity pattern still remains static which really is a concern. However, the mortality due to diarrhoea had drastically reduced. With the introduction & exploration of new strategy on ECCD & IMCI, the program would expect to observe further changes with the application of holistic approach to childcare services in the future.
HHeeaalltthh PPrrooggrraammmmeess
22
b) Situation Assessment at the end of the Ninth Plan
There is a knowledge, attitude, behaviour and practices gap on the various health activities and this needs to be evaluated at the end of the 9th five year plan, including health workers, mothers/care givers and VHWs on proper management of diarrhoeal diseases, sanitation, hygiene practices, correct feeding practices during the illness, recognition of danger signs in the sick children, correct use of Oral Rehydration Therapy (ORT), correct preparation of ORS etc. III. Program /policy objectives for the 9FYP To reduce morbidity & mortality due to diarrhoeal diseases, through promotion of sanitation, hygiene & proper case management practices. Specific Objectives:-
1. To reduce deaths due to diarrhoea in children under five from 13.3% to less than
5%. 2. To reduce diarrhoeal incidence rate amongst five years of age from 21% to 10%. 3. To reduce number of episodes from 3.9 per year to less than 3 per year. 4. To enable people to become more self-reliant in prevention and management of
diarrhoeal diseases. IV. Strategies
1. Timely distribution /supply of CDD drugs & equipment. 2. Strengthen capacity building for health workers through in-service training. 3. Investigation of outbreak & use of containment measures, mainly for cholera &
gastroenteritis. 4. Strengthen & integrate ECCD into health intervention through communities &
families with knowledge & skills required for childcare. 5. Strengthen monitoring, supervision & evaluation capacity. . 6. Improve quality services
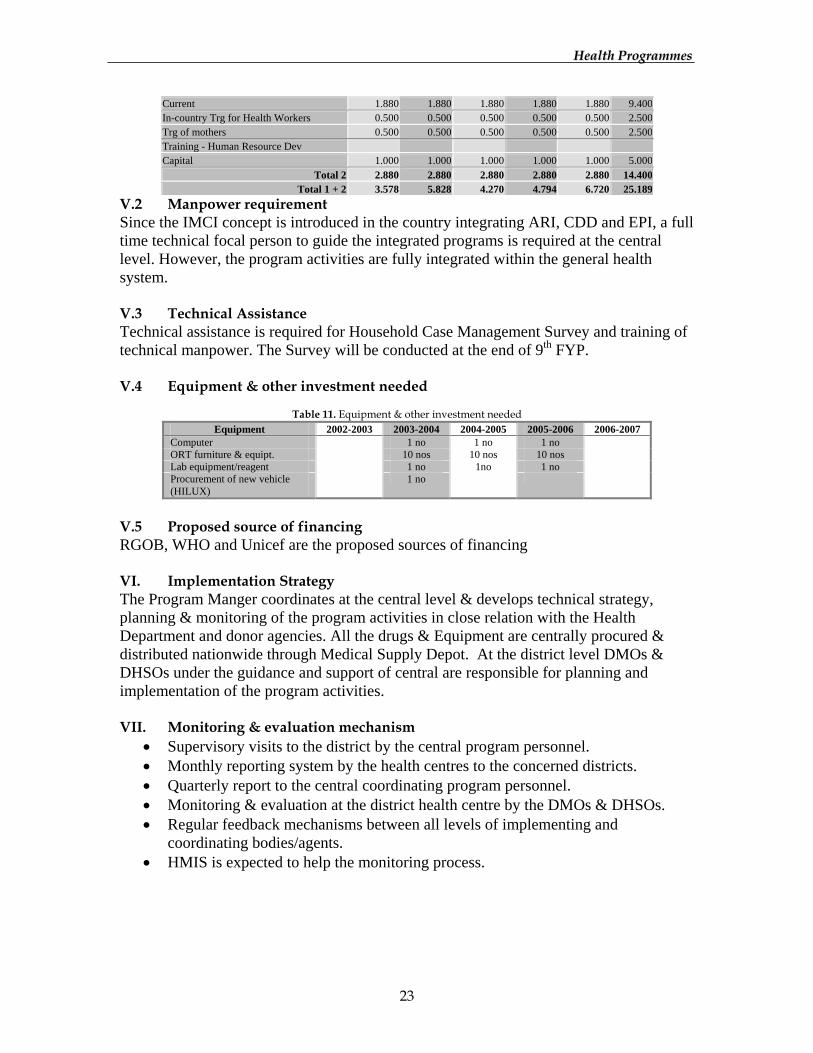
V.1 Programs Budget Outlays
Table 10. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.198 0.218 0.240 0.264 0.290 1.209 Conference, Seminar, W'shop 0.150 0.000 0.150 0.000 0.000 0.300 IEC materials 0.000 0.400 0.000 0.400 0.400 1.200 Std.trg manual printing 0.000 0.300 0.000 0.300 0.000 0.600 Dev of trg. manual on ECCD/IMCI 0.000 0.200 0.000 0.000 0.000 0.200 CDD Messages through Media 0.150 0.150 0.150 0.150 0.150 0.750 Operational cost /survey/emergency 0.200 0.300 0.300 0.250 3.000 4.050 Current 0.698 1.568 0.840 1.364 3.840 8.309 Plant and Equipment 0.000 0.500 0.500 0.500 0.000 1.500 1hilux for the program 0.000 0.800 0.000 0.000 0.000 0.800 ORT furniture for new BHUs 0.000 0.080 0.050 0.050 0.000 0.180 Capital 0.000 1.380 0.550 0.550 0.000 2.480
Total 1 0.698 2.948 1.390 1.914 3.840 10.789 Budget reflected with other programs. S&M, medicines 1.880 1.880 1.880 1.880 1.880 9.400
HHeeaalltthh PPrrooggrraammmmeess
23
Current 1.880 1.880 1.880 1.880 1.880 9.400 In-country Trg for Health Workers 0.500 0.500 0.500 0.500 0.500 2.500 Trg of mothers 0.500 0.500 0.500 0.500 0.500 2.500 Training - Human Resource Dev Capital 1.000 1.000 1.000 1.000 1.000 5.000
Total 2 2.880 2.880 2.880 2.880 2.880 14.400 Total 1 + 2 3.578 5.828 4.270 4.794 6.720 25.189
V.2 Manpower requirement Since the IMCI concept is introduced in the country integrating ARI, CDD and EPI, a full time technical focal person to guide the integrated programs is required at the central level. However, the program activities are fully integrated within the general health system. V.3 Technical Assistance Technical assistance is required for Household Case Management Survey and training of technical manpower. The Survey will be conducted at the end of 9th FYP. V.4 Equipment & other investment needed
Table 11. Equipment & other investment needed
Equipment 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Computer 1 no 1 no 1 no ORT furniture & equipt. 10 nos 10 nos 10 nos Lab equipment/reagent 1 no 1no 1 no Procurement of new vehicle (HILUX)
1 no
V.5 Proposed source of financing RGOB, WHO and Unicef are the proposed sources of financing VI. Implementation Strategy The Program Manger coordinates at the central level & develops technical strategy, planning & monitoring of the program activities in close relation with the Health Department and donor agencies. All the drugs & Equipment are centrally procured & distributed nationwide through Medical Supply Depot. At the district level DMOs & DHSOs under the guidance and support of central are responsible for planning and implementation of the program activities. VII. Monitoring & evaluation mechanism
• Supervisory visits to the district by the central program personnel. • Monthly reporting system by the health centres to the concerned districts. • Quarterly report to the central coordinating program personnel. • Monitoring & evaluation at the district health centre by the DMOs & DHSOs. • Regular feedback mechanisms between all levels of implementing and
coordinating bodies/agents. • HMIS is expected to help the monitoring process.

HHeeaalltthh PPrrooggrraammmmeess
24
NATIONAL MALARIA CONTROL PROGRAM I. Introduction The National Malaria Control Program (NMCP) was established in 1964 with the scheme aimed at eradicating malaria in the country. The main prevention and control strategy, then, was active surveillance, case management, and vector control by Indoor Residual Spraying (IRS) with DDT. However, DDT was substituted by Deltramethrine in 1994 and this change in insecticide brought dramatic reduction in malaria morbidity and mortality. In compliance with Global Roll Back malaria strategy, IRS was discontinued in favour of Insecticide Treated Bed Net (ITBN) Program. Presently, ITBN coverage is between 70 to 80 percent. The implementation of the revised control strategy has further reduced malaria disease burden in the country with Annual Parasite Incidence for 2000 at 16.1 (111.1 in 1994) and annual case reduction rate over 80%. Although NMCP started as a vertical program, it is now integrated into the general health services. Further decentralization of the program activities, highly technical in nature, is envisaged on need basis. All health centres in malaria endemic areas are provided with facilities for early diagnosis and prompt treatment. II. Situation Analysis a) Current situation assessment
Malaria awareness among general population is quite poor. Therefore, IEC advocacy activities need to be intensified and sustained in order to improve on early case detection and timely treatment. The IEC campaign will also bring about marked increase in ITBN coverage. One area that program failed to make much headway is in inter-sector collaboration. Attempts have been made to initiate collaborative activities in the control program but failed to obtain desired outcome. So there is a need to involve the relevant stakeholders in the program activities. NMCP has received generous funding support from Government of India (GOI) in the 8th Five Year Plan period (Nu.4.000 million per annum). The fund was used mainly for the procurement of insecticides, which incurs major expenditure. Program is also supported by WHO in terms of training and equipment supplies. b) Situation Assessment at the end of the Ninth Plan
The National Malaria Control Program strategies of 9FYP will be implemented and maintained as per the program guidelines. III. Program /Policy Objectives Reduce malaria disease burden and help enhance socio-economic development process of the people living in malaria endemic areas.
HHeeaalltthh PPrrooggrraammmmeess
25
Specific Objectives are as follows; 1. Reduce malaria mortality to less than 25% as compared to 2001, 2. Ensure Early Diagnosis and Prompt Treatment (EDPT) facilities in all malaria
transmission areas, 3. Intensify malaria IEC campaigns, and create basic awareness on prevention and
control of malaria in over 95% of the population in endemic areas, 4. Ensure Insecticide Treated Bed Net (ITBN) program implemented status with
coverage of over 90% of rural population, 5. Strengthen Entomological and Drug Research Units with the required facilities
and skills to meet the growing research needs of the program, 6. Initiate inter-sector collaborative control activities in endemic Dzongkhags, 7. Strengthen Dzongkhag’s implementation capacity for decentralized malaria
control activities. IV. Strategies
1. Provision of microscopy diagnostic facility and anti-malarial drugs in all health centers in the endemic areas for facilitating EDPT.
2. Decentralization of malaria microscopy and case management refresher courses. 3. Selective and comprehensive use of insecticides for control of adult and larval
vectors as determined by the endemicity and intensity of transmission areas, and susceptibility status.
4. Awareness creation about primary prevention and control of malaria in the communities through enhanced IEC advocacy program, and community participation in the control program with primary focus to make ITBN program self-sustainable.
5. Initiation of inter-sector collaborative efforts in the malaria control program through introduction of mosquito proof engineering designs, and environmental management, especially the sectors involved in the major construction projects.
6. Use of epidemiological and other parameters to predict epidemic, and institution of rapid response mechanism to manage epidemics.
7. Capacity development both in terms of infrastructure and human resource by strengthening research units with equipment, furniture and appropriate expertise for carrying out operational researches.
8. Intensify research activities on drug sensitivity studies in all high risk endemic Dzongkhags and sustain and strengthen entomological surveillance system.

HHeeaalltthh PPrrooggrraammmmeess
26
V.1 Program budget outlay
Table 12. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 5.506 6.056 6.662 7.328 8.061 14.722 IEC for southern Dzongkhags 0.400 0.440 0.484 0.532 0.586 2.442 IEC for NMCP Head quarters 0.230 0.253 0.278 0.306 0.337 17.164 S&M-chemicals 7.583 8.306 9.108 12.666 13.830 51.493 S&M-animal feeds 0.190 0.209 0.230 0.253 0.278 1.160 Conference, Seminar, W'shop 0.117 0.129 0.142 0.156 0.171 0.313 Uniforms 0.750 0.000 0.000 0.000 0.950 1.700
Current 14.776 15.393 16.903 21.241 24.212 92.525 Study tour on vector borne disease 0.000 0.560 0.500 0.000 0.000 1.060 Plant-telecom 0.104 0.500 0.000 0.000 0.000 0.604 Plant-tools 6.600 6.600 6.600 6.600 6.600 33.000 2 Generators 0.000 0.200 0.000 0.000 0.000 0.200 2 Hiluxes 0.800 0.000 0.000 0.800 0.000 1.600 Furniture 0.000 0.000 0.000 2.000 0.000 2.000 Office equipment 0.450 0.000 0.000 0.000 0.351 0.801 8 Computers 0.000 0.640 0.000 0.000 0.000 0.640 Professional Services (STC) 0.150 0.000 0.150 0.515 0.150 0.965
Capital 8.104 8.500 7.250 9.915 7.101 40.870 Total 1 22.880 23.893 24.153 31.156 31.313 133.395
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Training of Health Workers 0.190 0.209 0.230 0.253 0.278 1.160
Capital 0.190 0.209 0.230 0.253 0.278 1.160 Total 2 0.190 0.209 0.230 0.253 0.278 1.160
Total 1 + 2 23.070 24.102 24.383 31.409 31.592 134.555 V.2 Manpower requirement The posts for an Entomologist, Epidemiologist and Research Officer that are lying vacant presently need to be filled. V.3 Technical assistance For improving quality services, technical support will be sought from the Department and WHO whenever required during the plan period. V.4 Equipment and other investment needed The research activities of Entomology Unit and Drug Research Unit entail visits to all malaria endemic areas of the country. Each unit genuinely requires one vehicle attached to the unit to facilitate their activities. One priority transport need is the distribution of drugs and other supplies to all the health centers in the country. V.5 Proposed source of financing Besides RGOB, GIO, WHO and Danida are the likely financial supporters for the program. VI. Implementation Strategy The Program Manager coordinates at the central level and develops program strategies, training manuals, guidelines etc. The planning at the national level is done in consultation

HHeeaalltthh PPrrooggrraammmmeess
27
with the collaborating partners. The central program will also provide technical and logistic support to the Dzongkhags, besides supplies of anti-malarial drugs, rapid diagnostic test kits, insecticides, bed nets and forms & formats. The Dzongkhag health authorities are fully responsible for the malaria control program in the their respective Dzongkhags. VII. Monitoring and evaluation mechanism
1. Technical supervisory visits to malaria centres to assess the situation in the fields 2. Cross checking of BSE to assess the skills of health workers 3. Collection, compilation & analysis of the data 4. Conduct entomological and drug sensitivity studies 5. Supervision by DMOs and DHSOs Data collection and analysis 6. The annual review-cum-planning & coordination workshops
HHeeaalltthh PPrrooggrraammmmeess
28
PRIMARY EYE CARE PROGRAMME I. Introduction Primary Eye Care Programme is an ongoing programme to prevent and control major available causes of blindness and to make eye care services to all with active financial support from the Himalayan Cataract Project. II. Programme Objectives and strategies
1. Eye Health Education: the education on eye care will be provided to community and school children. Health education materials, pamphlets, posters and audio-visual aid will be developed and distributed.
2. Strengthening of services: the services for eye care deliver will be strengthened at
different levels of health care system. 3. Man Power Development: to meet the acute shortage of trained manpower, three
national doctors will be trained during this plan period. The services of expatriate Ophthalmologist will be continued as an interim measure.
4. Out Reach Services: School eye health programme will be strengthened and
free/subsidised spectacles will be provided to students for those who are in need. Operative eye camps and outreach clinics will be enhanced to reach the eye services to remote areas and to clear the cataract backlog.
5. Development of appropriate information system: information system will be
developed as an integral part of national information system to facilitate the monitoring and evaluation of the planned activities.
6. Specific disease control programme: clearing of cataract backlog and prevention
of corneal ulcer/trauma will be given high priority during this plan. III. Proposed source of financing Other then RGOB for the recurrent cost, the Himalayan Cataract Project is the probable financial supporter of this programme.
HHeeaalltthh PPrrooggrraammmmeess
29
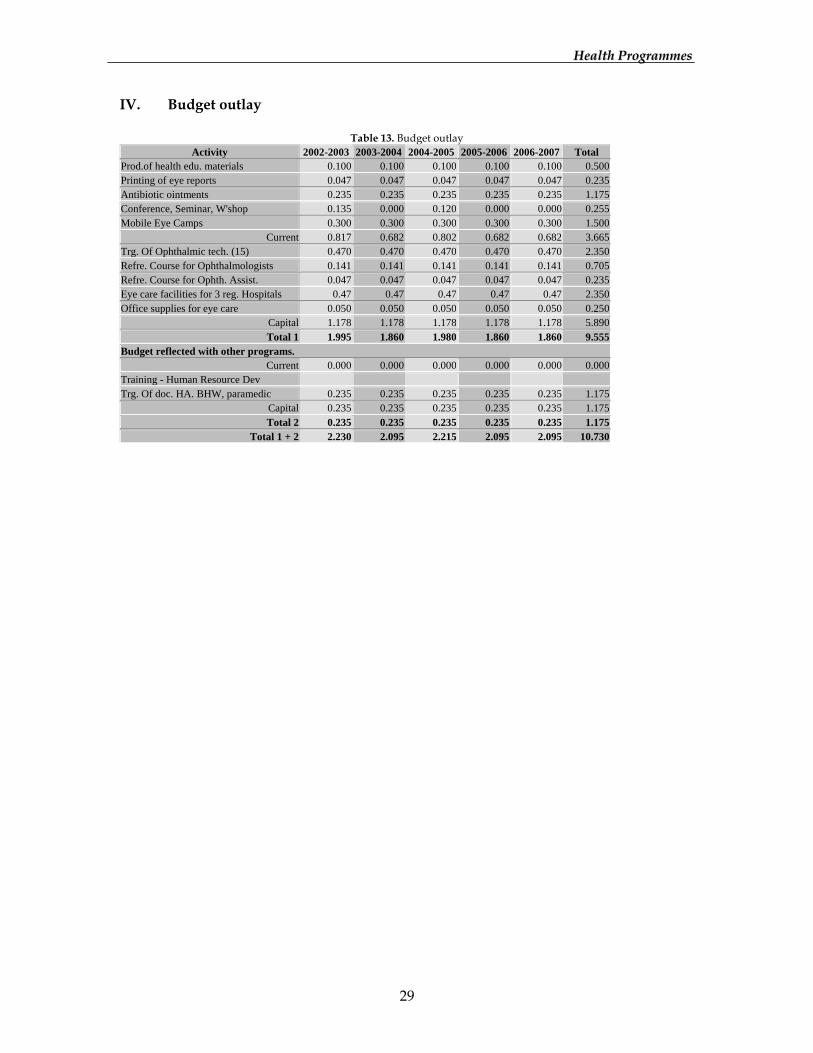
IV. Budget outlay
Table 13. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Prod.of health edu. materials 0.100 0.100 0.100 0.100 0.100 0.500 Printing of eye reports 0.047 0.047 0.047 0.047 0.047 0.235 Antibiotic ointments 0.235 0.235 0.235 0.235 0.235 1.175 Conference, Seminar, W'shop 0.135 0.000 0.120 0.000 0.000 0.255 Mobile Eye Camps 0.300 0.300 0.300 0.300 0.300 1.500
Current 0.817 0.682 0.802 0.682 0.682 3.665 Trg. Of Ophthalmic tech. (15) 0.470 0.470 0.470 0.470 0.470 2.350 Refre. Course for Ophthalmologists 0.141 0.141 0.141 0.141 0.141 0.705 Refre. Course for Ophth. Assist. 0.047 0.047 0.047 0.047 0.047 0.235 Eye care facilities for 3 reg. Hospitals 0.47 0.47 0.47 0.47 0.47 2.350 Office supplies for eye care 0.050 0.050 0.050 0.050 0.050 0.250
Capital 1.178 1.178 1.178 1.178 1.178 5.890 Total 1 1.995 1.860 1.980 1.860 1.860 9.555
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Trg. Of doc. HA. BHW, paramedic 0.235 0.235 0.235 0.235 0.235 1.175
Capital 0.235 0.235 0.235 0.235 0.235 1.175 Total 2 0.235 0.235 0.235 0.235 0.235 1.175
Total 1 + 2 2.230 2.095 2.215 2.095 2.095 10.730
HHeeaalltthh PPrrooggrraammmmeess
30
NATIONAL COMMUNITY BASED REHABILITATION PROGRAMME I. Introduction After Bhutan became signatory to ESCAP Commission on Disability in 1993 there has been increased concern for disability prevention, rehabilitation and providing equal opportunities for the disabled. The Community Based Rehabilitation (CBR) Programme was first initiated in 1997 as a pilot programme in Khaling, Trashigang, by using Primary Health Care infrastructure. WHO initially and Danida in 1999 provided technical and financial support. Pilot programme was extended to Mewang, Thimphu in 2000. II. Situation analysis a) Current Situation Assessment
Disability is not a well-defined condition in Bhutan, and there are many terminology and conceptual differences. The number of people with disabilities in Bhutan, according to the pilot programmes, is about 21,000 (3.5% of the total population). But there will be a nation-wide survey to correctly assess the extent, coverage and degree of disability. Nonetheless, this pilot Programme serves as a starting point of delivery of rehabilitation service in rural areas. Health Department alone cannot rehabilitate the disabled people. Other sectors like education, vocational and social services can equally contribute. Thus, a National Co-ordination Committee on Disability (NCCD) was formed to rope in these different sectors. Education for instance has started developing policy for special education for people with disabilities. Few disabled children have been enrolled in normal schools. b) Situation Assessment at the end of the Ninth Plan
The vision statement is that “All Persons with Disabilities are able to attain the fullest potentials, become self reliant within their limitations and be active contributors in nation building to the extent possible”. At the end of 9FYP, the following would have been achieved:
• Recognition and inclusion of disability prevention and rehabilitation as an integral
part of primary health care in all 20 dzongkhags • Provision of medical rehabilitation for all types of disabilities • Promoting integration of children with disabilities into normal schools • Promoting activities for vocational rehabilitation of disabled adults and • Community awareness and social integration of people with disabilities in
community activities. III. Programme /Policy objectives for the 9 FYP To improve the quality of life of disabled people with a view of reaching their full social integration and participation, the following objectives have been adopted;
HHeeaalltthh PPrrooggrraammmmeess
31
1. To introduce the community-oriented disability prevention and rehabilitation services and making it as an integral part of the comprehensive primary health care delivery system in all remaining Dzongkhags
2. To undertake human resource development in rehabilitation professional and in the knowledge of community rehabilitation at all levels.
3. To develop/establish a National Rehabilitation Centre for the country. 4. To diminish the overall impact of disability 5. To undertake research into methods of CBR delivery system. 6. To facilitate and co-ordinate the involvement of other sectors in disability
prevention and rehabilitation programmes through the multi-sectoral approach.
IV. Strategies
1. The overall guiding strategy is to develop a community-based model with the main features being the grass-root participation in development
2. Disability prevention and rehabilitation programmes will be integrated from the process of planning to the delivery of services. It will mobilise traditional family units and social structures, supportive traditional practices to create a sustainable network to improve the quality of life of people with disabilities.
3. Complementary programmes and strategies will be developed and implemented to meet the goals. Systems will be put in place to ensure quality of services to meet the needs of people with disabilities and their families. Cost-effectiveness will be promoted through efficient and effective use of resources available to increase access for people with disabilities. The Programme adopts the following strategies:
• Expansion of CBR Programme to all remaining Dzongkhags through the
existing PHC approach. • Training of undergraduates in the field of rehabilitation and health
workers/physiotherapy technicians in CBR methodology. • Developing diagnostic and production capabilities through establishment
of National Rehabilitation Centre and establishment of other units in selected district hospitals.
• Enhanced IEC activities in disability prevention and raise awareness of the Programme.
• Effective intersectional collaboration and community participation at all levels to address the issues of disability.
HHeeaalltthh PPrrooggrraammmmeess
32
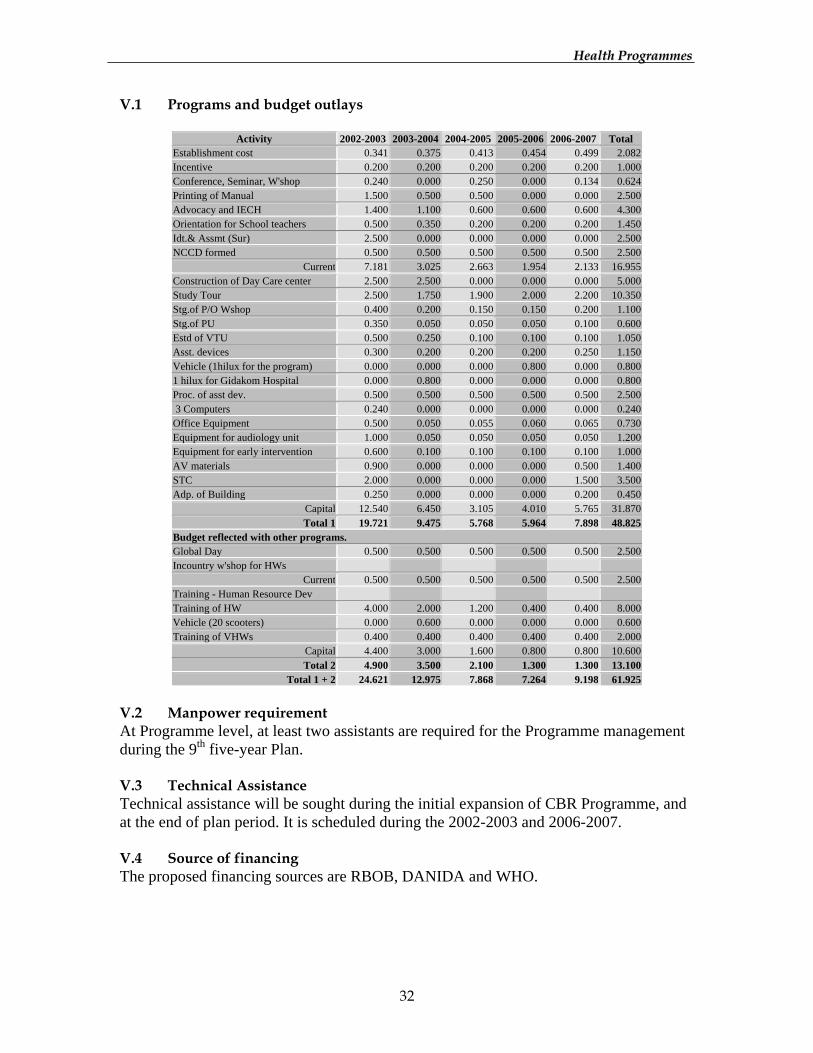
V.1 Programs and budget outlays
Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total Establishment cost 0.341 0.375 0.413 0.454 0.499 2.082 Incentive 0.200 0.200 0.200 0.200 0.200 1.000 Conference, Seminar, W'shop 0.240 0.000 0.250 0.000 0.134 0.624 Printing of Manual 1.500 0.500 0.500 0.000 0.000 2.500 Advocacy and IECH 1.400 1.100 0.600 0.600 0.600 4.300 Orientation for School teachers 0.500 0.350 0.200 0.200 0.200 1.450 Idt.& Assmt (Sur) 2.500 0.000 0.000 0.000 0.000 2.500 NCCD formed 0.500 0.500 0.500 0.500 0.500 2.500
Current 7.181 3.025 2.663 1.954 2.133 16.955 Construction of Day Care center 2.500 2.500 0.000 0.000 0.000 5.000 Study Tour 2.500 1.750 1.900 2.000 2.200 10.350 Stg.of P/O Wshop 0.400 0.200 0.150 0.150 0.200 1.100 Stg.of PU 0.350 0.050 0.050 0.050 0.100 0.600 Estd of VTU 0.500 0.250 0.100 0.100 0.100 1.050 Asst. devices 0.300 0.200 0.200 0.200 0.250 1.150 Vehicle (1hilux for the program) 0.000 0.000 0.000 0.800 0.000 0.800 1 hilux for Gidakom Hospital 0.000 0.800 0.000 0.000 0.000 0.800 Proc. of asst dev. 0.500 0.500 0.500 0.500 0.500 2.500 3 Computers 0.240 0.000 0.000 0.000 0.000 0.240 Office Equipment 0.500 0.050 0.055 0.060 0.065 0.730 Equipment for audiology unit 1.000 0.050 0.050 0.050 0.050 1.200 Equipment for early intervention 0.600 0.100 0.100 0.100 0.100 1.000 AV materials 0.900 0.000 0.000 0.000 0.500 1.400 STC 2.000 0.000 0.000 0.000 1.500 3.500 Adp. of Building 0.250 0.000 0.000 0.000 0.200 0.450
Capital 12.540 6.450 3.105 4.010 5.765 31.870 Total 1 19.721 9.475 5.768 5.964 7.898 48.825
Budget reflected with other programs. Global Day 0.500 0.500 0.500 0.500 0.500 2.500 Incountry w'shop for HWs
Current 0.500 0.500 0.500 0.500 0.500 2.500 Training - Human Resource Dev Training of HW 4.000 2.000 1.200 0.400 0.400 8.000 Vehicle (20 scooters) 0.000 0.600 0.000 0.000 0.000 0.600 Training of VHWs 0.400 0.400 0.400 0.400 0.400 2.000
Capital 4.400 3.000 1.600 0.800 0.800 10.600 Total 2 4.900 3.500 2.100 1.300 1.300 13.100
Total 1 + 2 24.621 12.975 7.868 7.264 9.198 61.925 V.2 Manpower requirement At Programme level, at least two assistants are required for the Programme management during the 9th five-year Plan. V.3 Technical Assistance Technical assistance will be sought during the initial expansion of CBR Programme, and at the end of plan period. It is scheduled during the 2002-2003 and 2006-2007. V.4 Source of financing The proposed financing sources are RBOB, DANIDA and WHO.
HHeeaalltthh PPrrooggrraammmmeess
33
VI. Implementation Strategy Public Health Department will support the Programme in the implementation of disability prevention, rehabilitation and equalisation of opportunities of people with disabilities. The Programme Manager will be responsible for developing technical strategies, policy guidelines, and in mobilising the resources. The close consultation with the National Co-ordination Committee on Disability (NCCD) will be carried out whenever required. The DMOs, Superintendents, DHSOs, Physiotherapist/Physiotherapy Technicians and HAs, Community Members, People with Disabilities and their families in the Dzongkhags will plan and implement in the spirit of integration, decentralisation and empowerment. VII. Monitoring and evaluation mechanism
• Within the standard procedures and through the HMIS, the CBR Programme will identify the priority information to be gathered. A combination of site visits, staff meetings and report review will be used.
• Monthly, quarterly and annual summaries of the rehabilitation activities at different levels will be reported to the district and national level. This will be done to see the implementation of the activities and any deviation thereof, so that modification of activities or adjustment in the plan can be decided upon.
• The Programme personnel shall participate in the monitoring of the CBR Programme.
• An appropriate evaluation system shall be developed. This will probably be a review of the Programme to determine whether objectives have been met. This review will also see whether CBR Programme Bhutan could be implemented as a component of PHC. A selected team of internal and external representatives will do the review
HHeeaalltthh PPrrooggrraammmmeess
34
MENTAL HEALTH PROGRAMME I. Introduction The Royal Government of Bhutan formulated a National Community Mental Health Program in 1997 coinciding with the beginning of the 8th five-year plan of development with the primary objective of sensitising health personnel at all levels to be able to provide mental health care along with general health care and reduce problems related to alcohol, drug dependence and mental and neurological disorders. A WHO consultant psychiatrist recruited from Myanmar worked on a manual on mental health for primary medical officers, and some IEC materials on mental health were developed. A Bhutanese National psychiatrist started regular psychiatric out patient department and inpatient service along with an expatriate psychiatrist from Myanmar in 1999. II. Situation Analysis a) Current Situation Assessment
Mental health problem is one of the emerging health problems in Bhutan. Until recently, there was no separate system of collecting information and data on mental health and substance abuse. Some small random studies showed that depression and anxiety are the most common mental disorder, which constitutes 80% of the mental disorders. Depression is more common in women than men, although both sexes are in the active adult age group. Depression is expected to rise with increasing stress caused by rapid modernization and other social changes. Alcohol is another major problem in Bhutan. It was number one cause of death in JDWNR Hospital in 2000. The World Bank and WHO estimate that 11% of the global burden of disease in 1998 was attributable to mental disorders and neurological disease. And depression had become the single largest cause of disability worldwide. In Bhutan, where general knowledge about mental health is limited, emotional and psycho-social problems often manifest physically in multiple bodily complaints which often result in being misdiagnosed and inadequately treated thereby wasting resources and time. It is expected that because of lack of awareness on mental health, people have certain myths, belief, stigma and negative attitude towards mental disorders, which stop them in seeking help from the health facilities, while ill persons and their families suffer in silence. Until recently, disease burden has been measured based on death statistics. It did not take into account non-fatal conditions, including measuring mental illness and neurological conditions such as epilepsy and severe mental retardation. But when disease burden measurement includes time lived with a disability, several of these illness become a leading cause of burden. Since its commencement, Mental Health Programme had carried out a series of groundwork activities, particularly on sensitising and creating awareness to both health

HHeeaalltthh PPrrooggrraammmmeess
35
workers and general public. Following are the major initiatives undertaken during the past years of development.
1. Developed a core mental health team; 2. Establishing of regular psychiatric OPD clinic at JDWNR Hospital. 3. Introduction of mental health care for trainees at RIHS. 4. Enhancement of essential drug list to include psychiatric drugs at health care
centres 5. Activities with education sector for student counselling. 6. Orienting the doctors, nurses & health workers in basic psychiatric nursing.
b) Situation Assessment at the end of the Ninth Plan
The Programme would have gradually covered the entire country with health staff oriented to provide basic mental health care at community level. Advocacy and IEC activities on mental health care for community leaders, clergy, and traditional healers would have been intensified. III. Program Objective/Policy Objectives for 9thFYP.
• To reduce the burden of mental, neurogical diseases, alcohol and drug dependence.
• To determine the prevalence of severe mental disorders in the country. • Provision of basic mental health care covering all dzongkhags by the end of 2007
though integration of mental health care into the primary health care delivery system.
• To involve traditional and indigenous system of medicine in the mental health care.
IV. Strategies
1. Identification of mental health problems and carry out activities at different levels of health system.
2. Introduction and integration of meditation and yoga in mental health care. 3. Promotion of mental health through advocacy and IEC activities and education of
general public, community leaders, religion community and traditional practitioners.
4. Community based rehabilitation for mentally disabled 5. Initiate innovative traditional approaches to mental health care and appropriate
training for indigenous and religious practitioners. 6. Referral support in terms of logistics and software for training, research, treatment
and rehabilitation to support community mental health care. 7. Intersectoral co-ordination with important sectors such as education, law & order,
armed forces and social welfare organizations to promote mental health. 8. Development of professional capacity to support training of health workers and
non-health workers.
HHeeaalltthh PPrrooggrraammmmeess
36
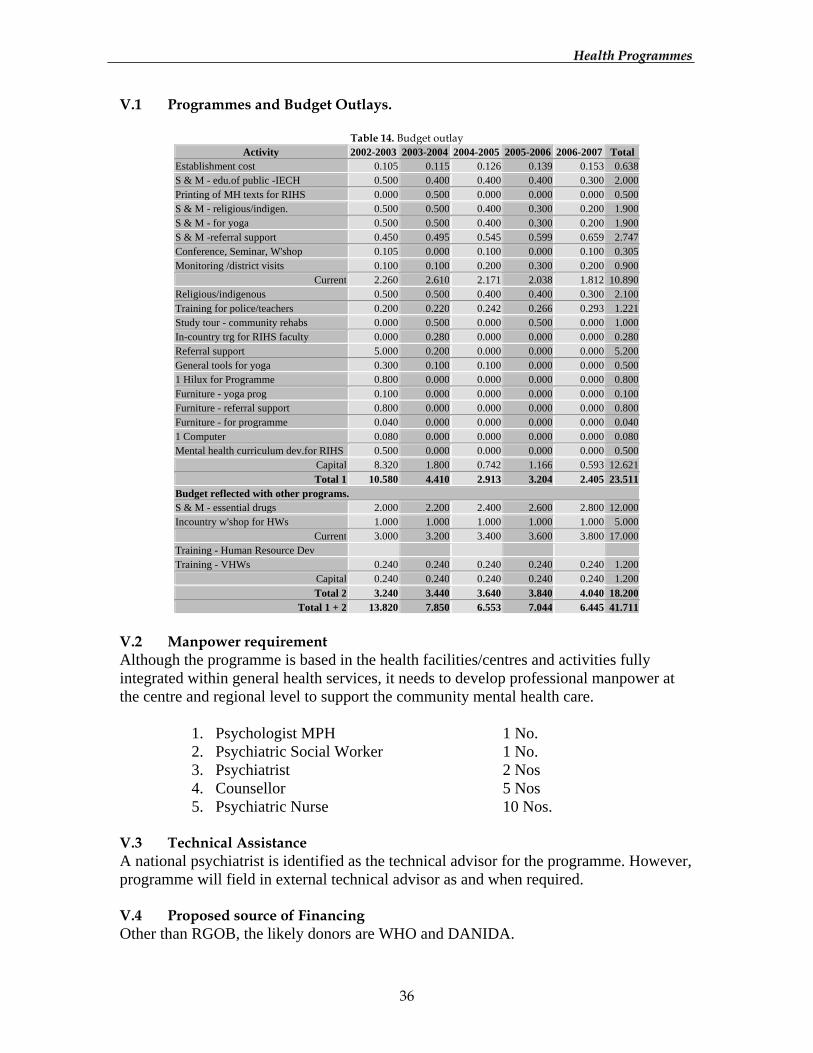
V.1 Programmes and Budget Outlays.
Table 14. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.105 0.115 0.126 0.139 0.153 0.638 S & M - edu.of public -IECH 0.500 0.400 0.400 0.400 0.300 2.000 Printing of MH texts for RIHS 0.000 0.500 0.000 0.000 0.000 0.500 S & M - religious/indigen. 0.500 0.500 0.400 0.300 0.200 1.900 S & M - for yoga 0.500 0.500 0.400 0.300 0.200 1.900 S & M -referral support 0.450 0.495 0.545 0.599 0.659 2.747 Conference, Seminar, W'shop 0.105 0.000 0.100 0.000 0.100 0.305 Monitoring /district visits 0.100 0.100 0.200 0.300 0.200 0.900
Current 2.260 2.610 2.171 2.038 1.812 10.890 Religious/indigenous 0.500 0.500 0.400 0.400 0.300 2.100 Training for police/teachers 0.200 0.220 0.242 0.266 0.293 1.221 Study tour - community rehabs 0.000 0.500 0.000 0.500 0.000 1.000 In-country trg for RIHS faculty 0.000 0.280 0.000 0.000 0.000 0.280 Referral support 5.000 0.200 0.000 0.000 0.000 5.200 General tools for yoga 0.300 0.100 0.100 0.000 0.000 0.500 1 Hilux for Programme 0.800 0.000 0.000 0.000 0.000 0.800 Furniture - yoga prog 0.100 0.000 0.000 0.000 0.000 0.100 Furniture - referral support 0.800 0.000 0.000 0.000 0.000 0.800 Furniture - for programme 0.040 0.000 0.000 0.000 0.000 0.040 1 Computer 0.080 0.000 0.000 0.000 0.000 0.080 Mental health curriculum dev.for RIHS 0.500 0.000 0.000 0.000 0.000 0.500
Capital 8.320 1.800 0.742 1.166 0.593 12.621 Total 1 10.580 4.410 2.913 3.204 2.405 23.511
Budget reflected with other programs. S & M - essential drugs 2.000 2.200 2.400 2.600 2.800 12.000 Incountry w'shop for HWs 1.000 1.000 1.000 1.000 1.000 5.000
Current 3.000 3.200 3.400 3.600 3.800 17.000 Training - Human Resource Dev Training - VHWs 0.240 0.240 0.240 0.240 0.240 1.200
Capital 0.240 0.240 0.240 0.240 0.240 1.200 Total 2 3.240 3.440 3.640 3.840 4.040 18.200
Total 1 + 2 13.820 7.850 6.553 7.044 6.445 41.711
V.2 Manpower requirement Although the programme is based in the health facilities/centres and activities fully integrated within general health services, it needs to develop professional manpower at the centre and regional level to support the community mental health care.
1. Psychologist MPH 1 No. 2. Psychiatric Social Worker 1 No. 3. Psychiatrist 2 Nos 4. Counsellor 5 Nos 5. Psychiatric Nurse 10 Nos.
V.3 Technical Assistance A national psychiatrist is identified as the technical advisor for the programme. However, programme will field in external technical advisor as and when required. V.4 Proposed source of Financing Other than RGOB, the likely donors are WHO and DANIDA.
HHeeaalltthh PPrrooggrraammmmeess
37
VI. Implementation Strategy The programme will be totally integrated into the general health services with only a central programme which will be co-ordinated by a programme manager who will be responsible to plan, supervise, monitor and co-ordinate mental health activities. The program would emphasize on community based mental health care strategy and at the same time a specialized mental health facility will also be developed to provide back-up support for preventive and curative requirements. VII. Monitoring and evaluation mechanism
• Supervisory visit by the central level programme personnel to the districts • Monitoring and evaluation at the districts health centres by the DMOs & DHSOs. • Six monthly reporting system by DMOs/DSHOs/Incharge of the health centers to
the central coordinating programme personnel. • Regular information feedback mechanism between all levels of implementing and
co- coordinating bodies.

HHeeaalltthh PPrrooggrraammmmeess
38
NUTRITION PROGRAMME I. Introduction The Nutrition Programme was established in 1985. Since then it has been working in collaboration with other sectors in order to improve the nutritional status of the population in the country. Unicef is the main financial supporter of the programme. Primary focus of the nutrition intervention is to reduce the protein energy malnutrition (PEM) and micronutrient deficiencies among the population. II. Situation Analysis a) Current Situation Assessment
The first nationwide assessment in 1988 indicated 38% of children under-five were malnourished and that 56% stunted. The second assessment in 1999 indicated 19% of children under-five underweight and 40% stunted. The 19% reduction in underweight and 16% reduction in stunting cases indicate the substantial improvement in the nutritional health of the under-five children in the last one-decade. Community participation in the intervention to combat malnutrition has been addressed through Community based nutrition program. It has been initiated in the region with food insecure with future prospective of expanding it to the whole nation. The total Goiter Rate was 65% and Salt Iodination almost zero in 1983. Today the TGR stands at 14%, universal Salt Iodination stands close to 100% and salt samples with required amount of iodine at the household level is 82%. The cyclic monitoring initiated in 1997 also monitors and evaluates the IDDCP, thereby identifying timely interventions to further reduce the IDD prevalence. Nationwide Vitamin-A deficiency study conducted in 2000 revealed sub-clinical Vitamin-A prevalence of 2.6%. And Iron deficiency anemia is still considered a major public health problem in Bhutan. The first time study on the iron compliance among pregnant women had been undertaken, which will give an idea about the accessibility of the iron tablet to the pregnant woman and regularity of tablet intake by them and can determine the factors dominating the issue of iron compliance. b) Situation Assessment at the end of the Ninth Plan
Ensuring healthy physical and mental development of the women and children through adequate nutrition and avoiding premature death or disability from diet related chronic disease and progressing into fit and healthy old age. III. Programme/Policy objectives
1. To reduce the prevalence of protein energy malnutrition in under five children from 40% to 15%.
HHeeaalltthh PPrrooggrraammmmeess
39
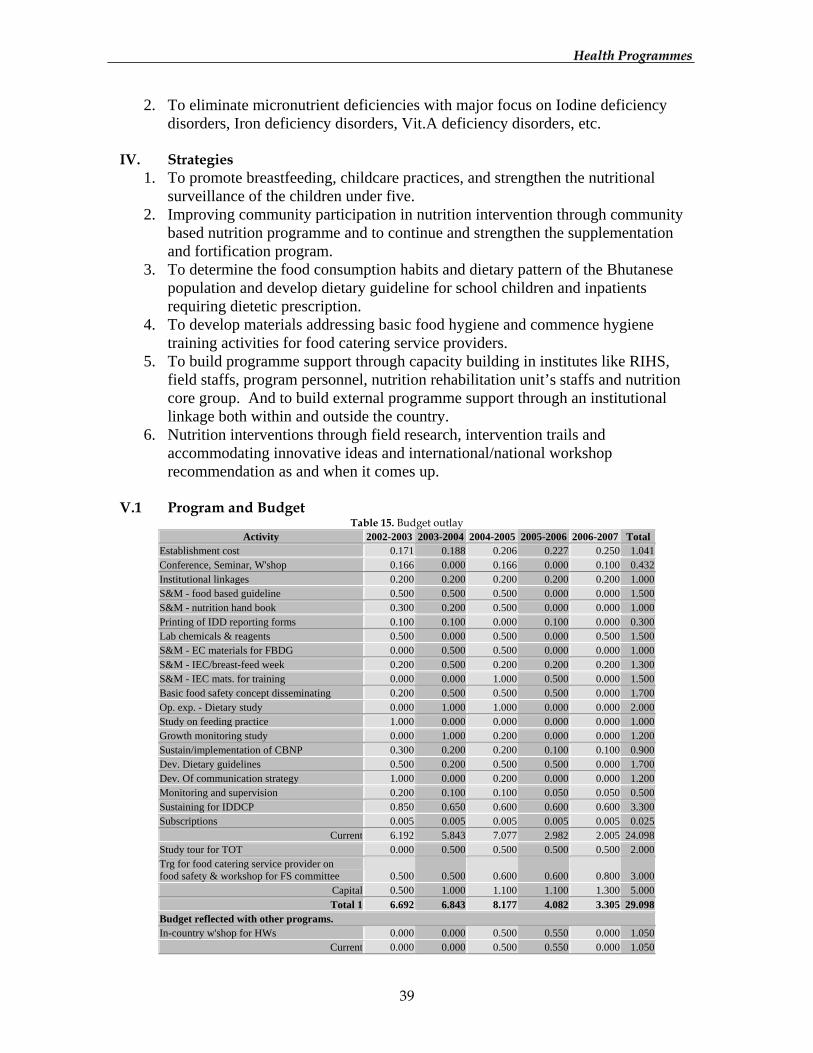
2. To eliminate micronutrient deficiencies with major focus on Iodine deficiency disorders, Iron deficiency disorders, Vit.A deficiency disorders, etc.
IV. Strategies
1. To promote breastfeeding, childcare practices, and strengthen the nutritional surveillance of the children under five.
2. Improving community participation in nutrition intervention through community based nutrition programme and to continue and strengthen the supplementation and fortification program.
3. To determine the food consumption habits and dietary pattern of the Bhutanese population and develop dietary guideline for school children and inpatients requiring dietetic prescription.
4. To develop materials addressing basic food hygiene and commence hygiene training activities for food catering service providers.
5. To build programme support through capacity building in institutes like RIHS, field staffs, program personnel, nutrition rehabilitation unit’s staffs and nutrition core group. And to build external programme support through an institutional linkage both within and outside the country.
6. Nutrition interventions through field research, intervention trails and accommodating innovative ideas and international/national workshop recommendation as and when it comes up.
V.1 Program and Budget
Table 15. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.171 0.188 0.206 0.227 0.250 1.041Conference, Seminar, W'shop 0.166 0.000 0.166 0.000 0.100 0.432Institutional linkages 0.200 0.200 0.200 0.200 0.200 1.000S&M - food based guideline 0.500 0.500 0.500 0.000 0.000 1.500S&M - nutrition hand book 0.300 0.200 0.500 0.000 0.000 1.000Printing of IDD reporting forms 0.100 0.100 0.000 0.100 0.000 0.300Lab chemicals & reagents 0.500 0.000 0.500 0.000 0.500 1.500S&M - EC materials for FBDG 0.000 0.500 0.500 0.000 0.000 1.000S&M - IEC/breast-feed week 0.200 0.500 0.200 0.200 0.200 1.300S&M - IEC mats. for training 0.000 0.000 1.000 0.500 0.000 1.500Basic food safety concept disseminating 0.200 0.500 0.500 0.500 0.000 1.700Op. exp. - Dietary study 0.000 1.000 1.000 0.000 0.000 2.000Study on feeding practice 1.000 0.000 0.000 0.000 0.000 1.000Growth monitoring study 0.000 1.000 0.200 0.000 0.000 1.200Sustain/implementation of CBNP 0.300 0.200 0.200 0.100 0.100 0.900Dev. Dietary guidelines 0.500 0.200 0.500 0.500 0.000 1.700Dev. Of communication strategy 1.000 0.000 0.200 0.000 0.000 1.200Monitoring and supervision 0.200 0.100 0.100 0.050 0.050 0.500Sustaining for IDDCP 0.850 0.650 0.600 0.600 0.600 3.300Subscriptions 0.005 0.005 0.005 0.005 0.005 0.025
Current 6.192 5.843 7.077 2.982 2.005 24.098Study tour for TOT 0.000 0.500 0.500 0.500 0.500 2.000Trg for food catering service provider on food safety & workshop for FS committee 0.500 0.500 0.600 0.600 0.800 3.000
Capital 0.500 1.000 1.100 1.100 1.300 5.000Total 1 6.692 6.843 8.177 4.082 3.305 29.098
Budget reflected with other programs. In-country w'shop for HWs 0.000 0.000 0.500 0.550 0.000 1.050
Current 0.000 0.000 0.500 0.550 0.000 1.050
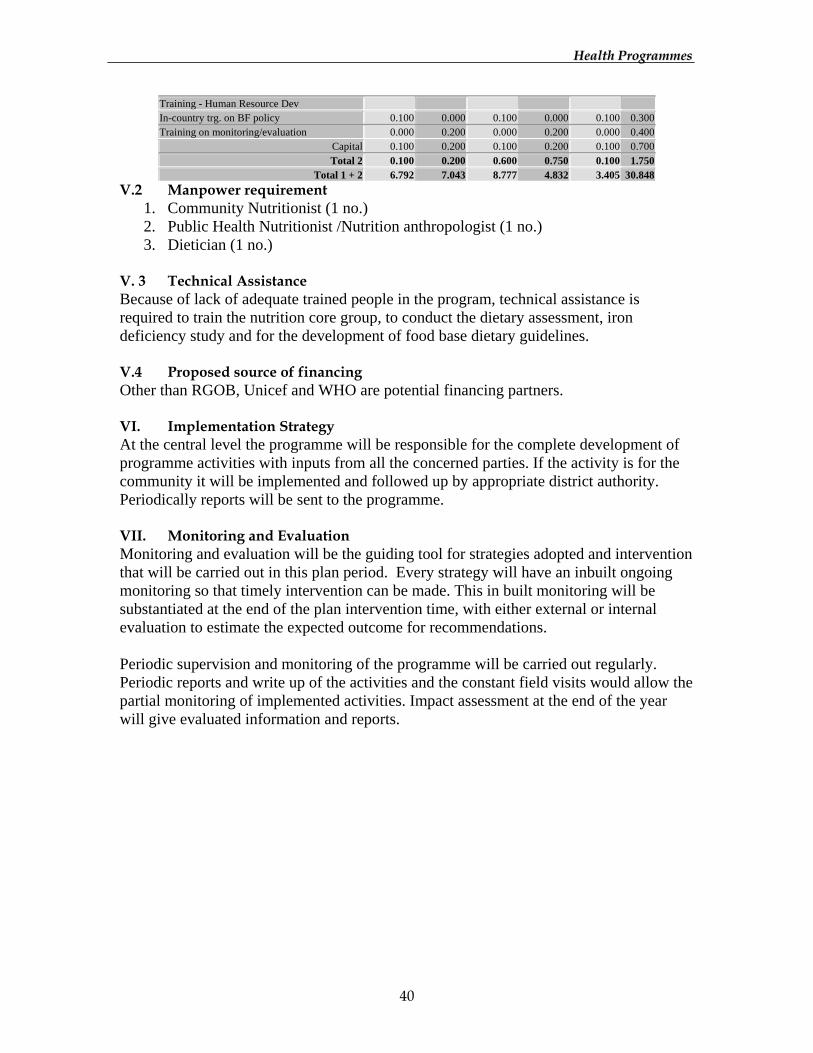
HHeeaalltthh PPrrooggrraammmmeess
40
Training - Human Resource Dev In-country trg. on BF policy 0.100 0.000 0.100 0.000 0.100 0.300Training on monitoring/evaluation 0.000 0.200 0.000 0.200 0.000 0.400
Capital 0.100 0.200 0.100 0.200 0.100 0.700Total 2 0.100 0.200 0.600 0.750 0.100 1.750
Total 1 + 2 6.792 7.043 8.777 4.832 3.405 30.848V.2 Manpower requirement
1. Community Nutritionist (1 no.) 2. Public Health Nutritionist /Nutrition anthropologist (1 no.) 3. Dietician (1 no.)
V. 3 Technical Assistance Because of lack of adequate trained people in the program, technical assistance is required to train the nutrition core group, to conduct the dietary assessment, iron deficiency study and for the development of food base dietary guidelines. V.4 Proposed source of financing Other than RGOB, Unicef and WHO are potential financing partners. VI. Implementation Strategy At the central level the programme will be responsible for the complete development of programme activities with inputs from all the concerned parties. If the activity is for the community it will be implemented and followed up by appropriate district authority. Periodically reports will be sent to the programme. VII. Monitoring and Evaluation Monitoring and evaluation will be the guiding tool for strategies adopted and intervention that will be carried out in this plan period. Every strategy will have an inbuilt ongoing monitoring so that timely intervention can be made. This in built monitoring will be substantiated at the end of the plan intervention time, with either external or internal evaluation to estimate the expected outcome for recommendations. Periodic supervision and monitoring of the programme will be carried out regularly. Periodic reports and write up of the activities and the constant field visits would allow the partial monitoring of implemented activities. Impact assessment at the end of the year will give evaluated information and reports.
HHeeaalltthh PPrrooggrraammmmeess
41
REPRODUCTIVE HEALTH & POPULATION PROGRAMME I. Introduction High Maternal death ratio (MMR), high infant and under five deaths (IMR), high fertility rate and high natural growth rate are some of the concerns the Government has recognised as early as early seventies. Integrated Maternal and child Health (MCH) programme was started to address the problem of high maternal and infant deaths rate as early as 1978. This programme included Antenatal Care, Care during delivery, postnatal care and care of the children up to 5 years of age. Infant immunisation and immunisation of Mother with tetanus toxoid has become an important component of the programme. The child immunisation programme was further expanded both in geographical coverage and number of Antigen content. The Family Planning programme is now an integrated part of the Primary Health care delivery system. The need to address the other aspects of reproductive health of men and women has resulted in the adoption of Reproductive Health concept in 1997. Considering the prevailing health conditions, infrastructure and available human resource, the following were identified as priority elements of Reproductive Health – Family planning, Safe Motherhood, Prevention and Management of complicated abortion, RTI/STD/HIV, Prevention and management of infertility, Adolescent reproductive health, childcare, and Reproductive tract and breast cancer. High-level political commitment in improving Reproductive Health has been achieved. Her Majesty Ashi Sangay Choden Wangchuck, the UNFPA Good-will Ambassador, played an active role in advocating Safe Motherhood, Adolescent Health, Family Planning, Sanitation, STD/AIDs and teenage Pregnancies and abortion with special focus on schools and armed forces and un-reached communities in the remote areas. II. Situation Analysis a) Current Situation Assessment
1. Family Planning:
The following methods of contraceptive are being provided at different levels of Health care delivery System.
1. Oral Contraceptives Pills, 2. Injectable Depot Medroxy Progesteron Acetate 3. Male Condom, 4. Intra uterine device, 5. Male sterilisation, 6. Female sterilisation
HHeeaalltthh PPrrooggrraammmmeess
42
DMPA is the most widely used method of Contraceptives. Contraceptive prevalence rate (CPR) has increased from 18.5% to 30.5% and this has contributed significantly in reduction of growth rate from 3.1% to 2.6%. 2. Safe Motherhood:
• Antenatal care: Approximately 20,000 women are expected to become pregnant every year. 51% of these women attend Antenatal clinic at least for one time during a pregnancy. In an average, women make 2.46% visits to the clinic during the pregnancy. Some common complications encountered during pregnancy are anaemia, antepartum haemorrhage, abortion with or without complications etc.
• Intranatal care: At present 78.3% of deliveries take place at home and the rest in hospitals and BHUs. Trained birth attendance still remains low at 23.66%. About 98% of the trained deliveries result in live birth and the rest 2% (approx.) in still birth. Major intra-partum complications encountered are obstructed labour, prolonged labour, malpresentation, abnormal lie, Hypertensive disease, premature by birth and others.
• Postnatal Care: In 2000 about 80% of the ANC attendees attended postnatal clinic at least once. In an average, women make 1.25 visit during the postnatal period. And the major complications reported are Postpartum Haemorrhage, Retained Placenta, PPH with Retained placenta, Pyrexia and Others.
• Maternal deaths: Maternal deaths ratio (MMR) estimated at 2.55/1000 live birth,though significantly improved from past, is one of the highest in the region.
Table 16: Trends in Maternal Mortality ratio (MMR) Year Estimated rate 1984 7.7. per thousand live birth 1994 per thousand live birth 2000 per thousand live birth
There is no existing mechanism to monitor the causes of maternal deaths, as institute births are only quarters of the total births in the country.
• Prevention and management of complication of abortion: - Actual incidence of abortion and its complication are not known. In the Need Assessment survey conducted in 2000, 71 cases were admitted for abortion and its complication. Case fatality rate for abortion complication, which includes induced septic abortion, is one of the highest (1.41%) among obstetric complication. Incidence of ectopic pregnancy appeared to be quite high though no maternal deaths were reported in the survey.
• RTI/STD/HIV:

HHeeaalltthh PPrrooggrraammmmeess
43
Reproductive tract infection can have serious consequences including infertility, ectopic pregnancy, chronic pelvis pain, abortion and increased risk of HIV transmission. The most common RTIs are Candidiasis, Bacterial Vaginosis, PID, Gonorrhoea, Syphilis, Chlamdia, Hepatitis B etc. Incidence of HIV infection is gradually increasing especially in men and women of reproductive age.
• Prevention and management of infertility: The reproductive Health Unit of JDWNRH has recorded 72 infertility couples in the span of 1 year. Prevalence of STD, Unsafe abortion, Unhygienic delivery increased acceptance of permanent method of family planning influence the prevalence of infertility directly or indirectly. Investigation and management for both male and female infertility are well developed at JDWNRH hospital.
• Adolescent reproductive Health: Adolescent reproductive health is directly dependent upon their sexual behaviour, pregnancy and child bearing. Available fertility data in clinic suggested that there is a sizeable proportion (approx. 15%) teenage mother. This indicates that heterosexual behaviour among teenage females is quite common. Irrespective of their marital status only 2.4% of women between 10-19 years of age are using some form of contraceptives.
• Child survival including Neonatal Care: Estimated 15.6% of institutional births are low birth weight babies. These groups of babies need special care. Approximately 3/4 of deliveries take place at home, therefore, birth weights of this group of babies are not known. Neonatal deaths rate, through never estimated, is assumed to be high and contributed a major portion of infant deaths rate.
• Infant & < 5 Care: Approximately 70-70% infant attended clinic at least 4 times. Primary immunisation against 7 EPI target diseases, Growth Monitoring, Vit. A supplementation is some of the services that are provided by the clinics. Since the achievement of the UCI in 1990, more than 85% EPI coverage of infant is maintained.
• Cancer of the Reproductive tract and Breast: Cancer of the uterus is the second commonest of all malignancies encountered in the country. Major risk factors identified are early initiation of sexual intercourse, multiple sexual partners, and STDs. Actual prevalence of Breast cancer in the Country is not known. At present, emphasis is being given on early Detection through Breast Self Examination and appropriate management to increase the 5-year survival rate. b) Situation Assessment at the end of the Ninth Plan
1. Family Planning.
More women and men of reproductive age would accept the family planning method. And there would be increase in contraceptive prevalence rate, reduction of fertility rate, reduction of maternal deaths and reduction in infant mortality rate.
HHeeaalltthh PPrrooggrraammmmeess
44
2. Safe Motherhood and Child Survival:
General Health for the mother and the child improved, through provision of quality care to all women during pregnancy, labour and lactation, adolescent and children especially at the end of the plan period. 3. Abortion and its complication:
Substantial deduction on unwanted pregnancies induced septic abortion and their complication. 4. RTI/STD/HIV:
All cases of RTIs/STDs would have been managed appropriately and community awareness about their transmission and prevention of STDs/HIV improved 5. Adolescent Reproductive Health:
Reduction in the number of teenage pregnancy and its complication and increase in the contraceptive use among 15-19 years age group of women population. 6. Cancer of the Reproductive tract and breast:
Cervical cancer screening facilities expanded to cover at least 50% of the population and mortality due to breast cancer reduced. 7. Infertility:
All infertility couples received necessary investigation and appropriate management. III. Program / policy objectives for the Ninth Plan To improve the quality of Reproductive life of men, women and adolescents by establishing an high quality reproductive Health services at all levels, thereby contributing significantly to achieve the over all National goal of Gross National Happiness.
1. To reduce maternal mortality from 255 to 1.63/1000 live birth. 2. To increase family planning knowledge from 94% to 100% among women of
child bearing age. 3. To reduce anaemia in pregnant women from 60% to 30% 4. To increase contraceptive prevalence rate from 30.7 to 60% 5. To reduce infant mortality from 50/1000 Live birth to 30/1000 live births. 6. To reduce neonatal mortality 7. To reduce growth rate from 2.6 to 2% 0r less. 8. Increase Ante natal visit from 51% to 100% 9. Increase trained birth attendance from 24% to 50% 10. Increase post natal clinic attendance from 48% to 100% 11. Reduce Total fertility rate from 4.7 to 3 or less 12. Cervical cancer screening facilities extended to 50% of target population
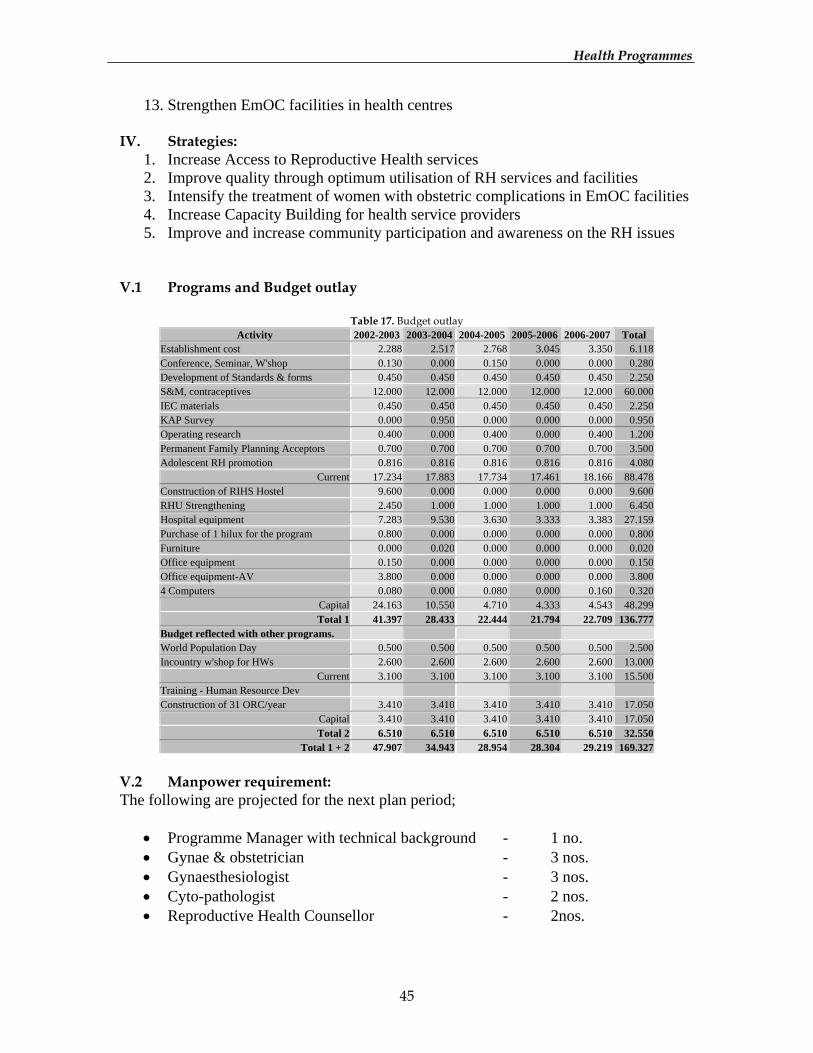
HHeeaalltthh PPrrooggrraammmmeess
45
13. Strengthen EmOC facilities in health centres IV. Strategies:
1. Increase Access to Reproductive Health services 2. Improve quality through optimum utilisation of RH services and facilities 3. Intensify the treatment of women with obstetric complications in EmOC facilities 4. Increase Capacity Building for health service providers 5. Improve and increase community participation and awareness on the RH issues
V.1 Programs and Budget outlay
Table 17. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 2.288 2.517 2.768 3.045 3.350 6.118 Conference, Seminar, W'shop 0.130 0.000 0.150 0.000 0.000 0.280 Development of Standards & forms 0.450 0.450 0.450 0.450 0.450 2.250 S&M, contraceptives 12.000 12.000 12.000 12.000 12.000 60.000 IEC materials 0.450 0.450 0.450 0.450 0.450 2.250 KAP Survey 0.000 0.950 0.000 0.000 0.000 0.950 Operating research 0.400 0.000 0.400 0.000 0.400 1.200 Permanent Family Planning Acceptors 0.700 0.700 0.700 0.700 0.700 3.500 Adolescent RH promotion 0.816 0.816 0.816 0.816 0.816 4.080
Current 17.234 17.883 17.734 17.461 18.166 88.478 Construction of RIHS Hostel 9.600 0.000 0.000 0.000 0.000 9.600 RHU Strengthening 2.450 1.000 1.000 1.000 1.000 6.450 Hospital equipment 7.283 9.530 3.630 3.333 3.383 27.159 Purchase of 1 hilux for the program 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.000 0.020 0.000 0.000 0.000 0.020 Office equipment 0.150 0.000 0.000 0.000 0.000 0.150 Office equipment-AV 3.800 0.000 0.000 0.000 0.000 3.800 4 Computers 0.080 0.000 0.080 0.000 0.160 0.320
Capital 24.163 10.550 4.710 4.333 4.543 48.299 Total 1 41.397 28.433 22.444 21.794 22.709 136.777
Budget reflected with other programs. World Population Day 0.500 0.500 0.500 0.500 0.500 2.500 Incountry w'shop for HWs 2.600 2.600 2.600 2.600 2.600 13.000
Current 3.100 3.100 3.100 3.100 3.100 15.500 Training - Human Resource Dev Construction of 31 ORC/year 3.410 3.410 3.410 3.410 3.410 17.050
Capital 3.410 3.410 3.410 3.410 3.410 17.050 Total 2 6.510 6.510 6.510 6.510 6.510 32.550
Total 1 + 2 47.907 34.943 28.954 28.304 29.219 169.327
V.2 Manpower requirement: The following are projected for the next plan period;
• Programme Manager with technical background - 1 no. • Gynae & obstetrician - 3 nos. • Gynaesthesiologist - 3 nos. • Cyto-pathologist - 2 nos. • Reproductive Health Counsellor - 2nos.
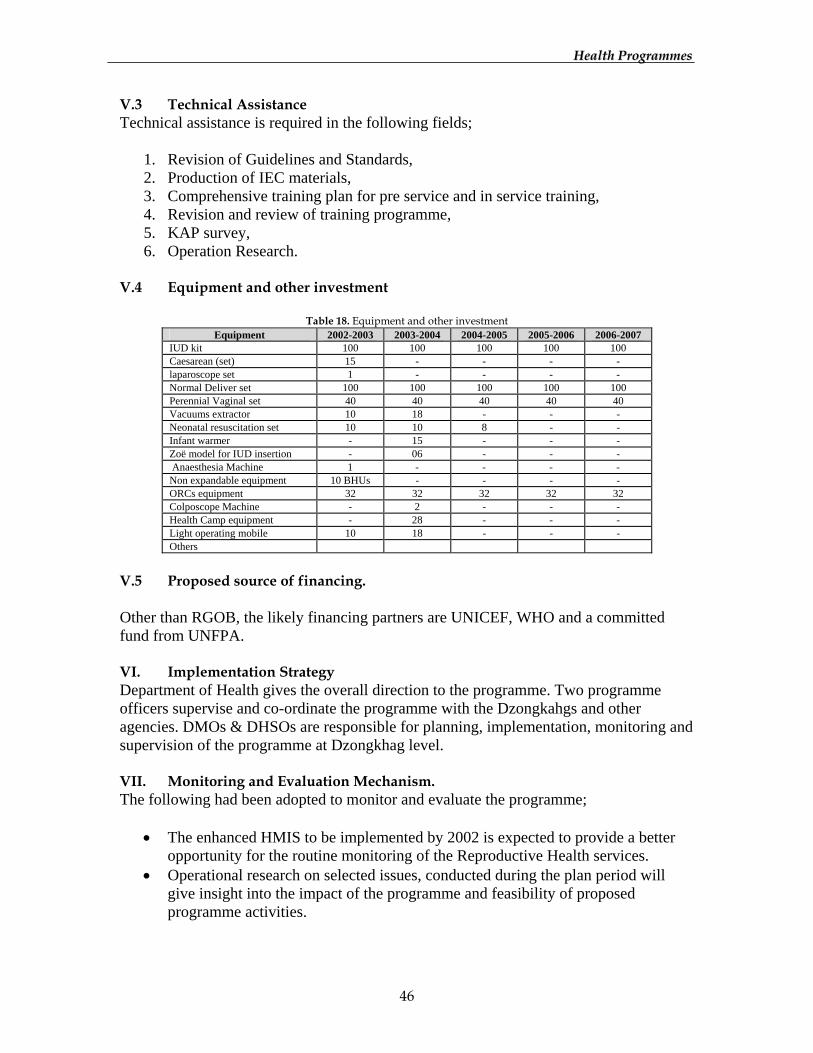
HHeeaalltthh PPrrooggrraammmmeess
46
V.3 Technical Assistance Technical assistance is required in the following fields;
1. Revision of Guidelines and Standards, 2. Production of IEC materials, 3. Comprehensive training plan for pre service and in service training, 4. Revision and review of training programme, 5. KAP survey, 6. Operation Research.
V.4 Equipment and other investment
Table 18. Equipment and other investment Equipment 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007
IUD kit 100 100 100 100 100 Caesarean (set) 15 - - - - laparoscope set 1 - - - - Normal Deliver set 100 100 100 100 100 Perennial Vaginal set 40 40 40 40 40 Vacuums extractor 10 18 - - - Neonatal resuscitation set 10 10 8 - - Infant warmer - 15 - - - Zoë model for IUD insertion - 06 - - - Anaesthesia Machine 1 - - - - Non expandable equipment 10 BHUs - - - - ORCs equipment 32 32 32 32 32 Colposcope Machine - 2 - - - Health Camp equipment - 28 - - - Light operating mobile 10 18 - - - Others
V.5 Proposed source of financing. Other than RGOB, the likely financing partners are UNICEF, WHO and a committed fund from UNFPA. VI. Implementation Strategy Department of Health gives the overall direction to the programme. Two programme officers supervise and co-ordinate the programme with the Dzongkahgs and other agencies. DMOs & DHSOs are responsible for planning, implementation, monitoring and supervision of the programme at Dzongkhag level. VII. Monitoring and Evaluation Mechanism. The following had been adopted to monitor and evaluate the programme;
• The enhanced HMIS to be implemented by 2002 is expected to provide a better opportunity for the routine monitoring of the Reproductive Health services.
• Operational research on selected issues, conducted during the plan period will give insight into the impact of the programme and feasibility of proposed programme activities.

HHeeaalltthh PPrrooggrraammmmeess
47
• KAP survey is expected to bring into focus the existing problems and give direction to address them.
• All Maternal deaths will be investigated, reviewed by the Committee and feed back be provided to the individual dzongkhags.
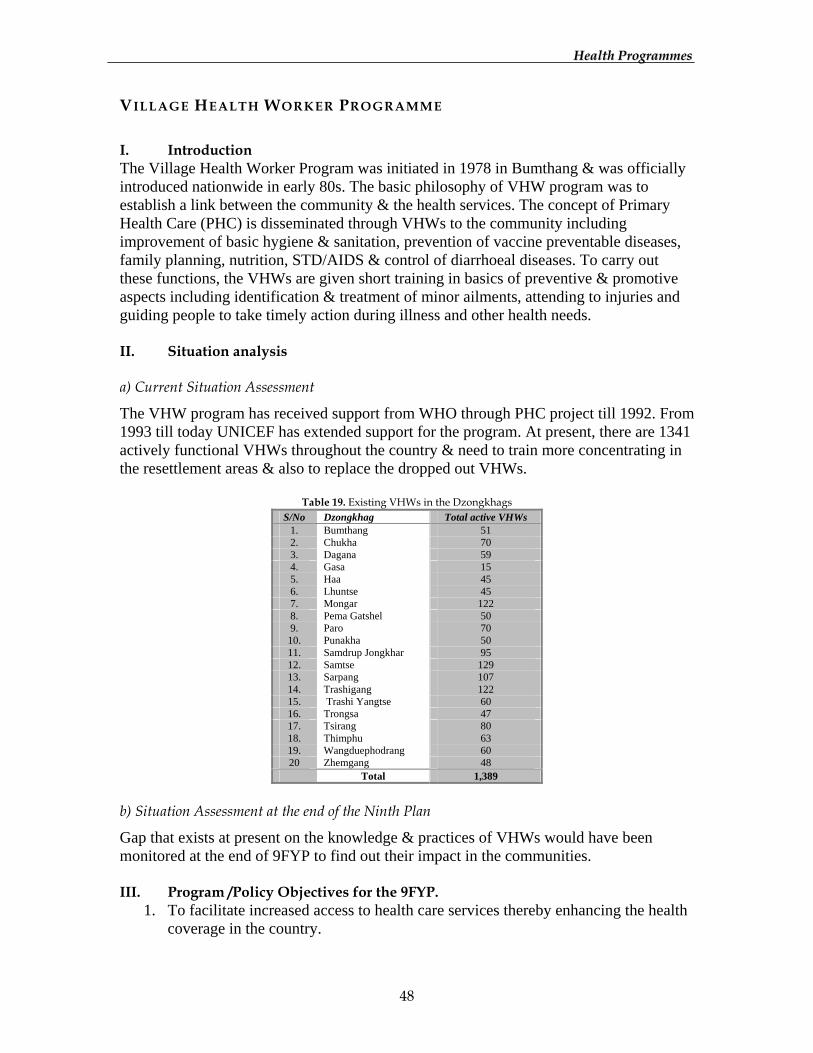
HHeeaalltthh PPrrooggrraammmmeess
48
VILLAGE HEALTH WORKER PROGRAMME I. Introduction The Village Health Worker Program was initiated in 1978 in Bumthang & was officially introduced nationwide in early 80s. The basic philosophy of VHW program was to establish a link between the community & the health services. The concept of Primary Health Care (PHC) is disseminated through VHWs to the community including improvement of basic hygiene & sanitation, prevention of vaccine preventable diseases, family planning, nutrition, STD/AIDS & control of diarrhoeal diseases. To carry out these functions, the VHWs are given short training in basics of preventive & promotive aspects including identification & treatment of minor ailments, attending to injuries and guiding people to take timely action during illness and other health needs. II. Situation analysis a) Current Situation Assessment
The VHW program has received support from WHO through PHC project till 1992. From 1993 till today UNICEF has extended support for the program. At present, there are 1341 actively functional VHWs throughout the country & need to train more concentrating in the resettlement areas & also to replace the dropped out VHWs.
Table 19. Existing VHWs in the Dzongkhags S/No Dzongkhag Total active VHWs
1. Bumthang 51 2. Chukha 70 3. Dagana 59 4. Gasa 15 5. Haa 45 6. Lhuntse 45 7. Mongar 122 8. Pema Gatshel 50 9. Paro 70 10. Punakha 50 11. Samdrup Jongkhar 95 12. Samtse 129 13. Sarpang 107 14. Trashigang 122 15. Trashi Yangtse 60 16. Trongsa 47 17. Tsirang 80 18. Thimphu 63 19. Wangduephodrang 60 20 Zhemgang 48
Total 1,389
b) Situation Assessment at the end of the Ninth Plan
Gap that exists at present on the knowledge & practices of VHWs would have been monitored at the end of 9FYP to find out their impact in the communities. III. Program /Policy Objectives for the 9FYP.
1. To facilitate increased access to health care services thereby enhancing the health coverage in the country.
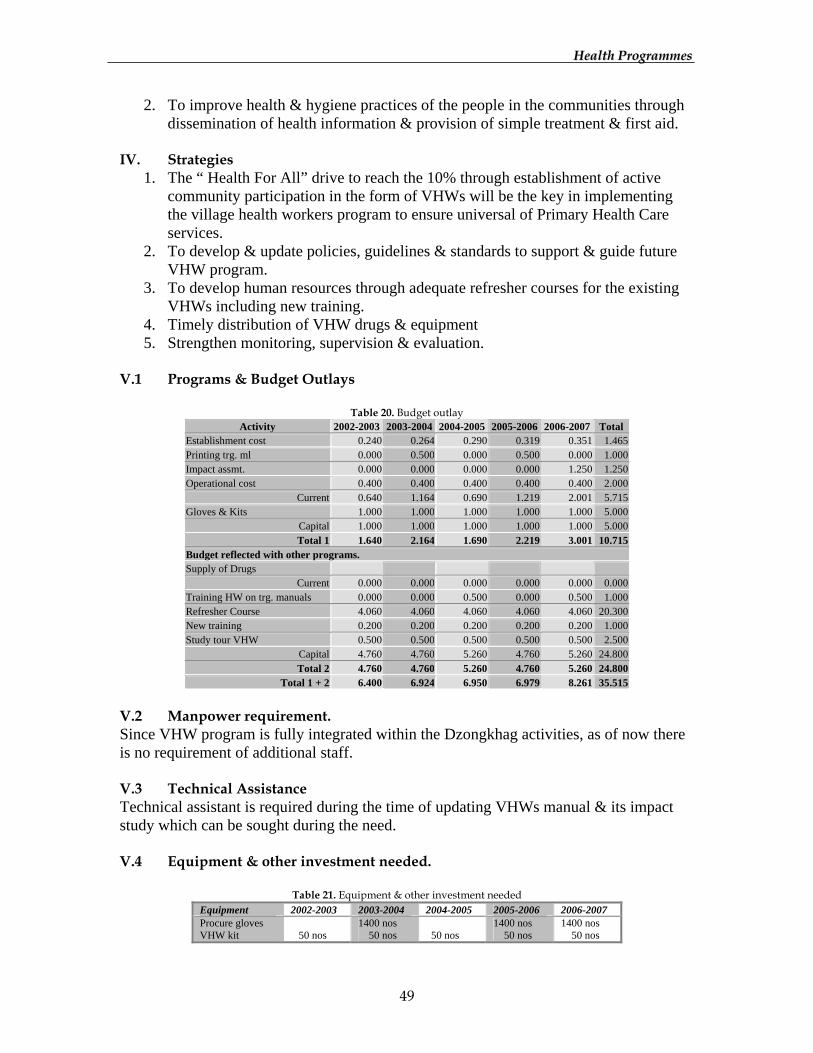
HHeeaalltthh PPrrooggrraammmmeess
49
2. To improve health & hygiene practices of the people in the communities through dissemination of health information & provision of simple treatment & first aid.
IV. Strategies
1. The “ Health For All” drive to reach the 10% through establishment of active community participation in the form of VHWs will be the key in implementing the village health workers program to ensure universal of Primary Health Care services.
2. To develop & update policies, guidelines & standards to support & guide future VHW program.
3. To develop human resources through adequate refresher courses for the existing VHWs including new training.
4. Timely distribution of VHW drugs & equipment 5. Strengthen monitoring, supervision & evaluation.
V.1 Programs & Budget Outlays
Table 20. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.240 0.264 0.290 0.319 0.351 1.465 Printing trg. ml 0.000 0.500 0.000 0.500 0.000 1.000 Impact assmt. 0.000 0.000 0.000 0.000 1.250 1.250 Operational cost 0.400 0.400 0.400 0.400 0.400 2.000
Current 0.640 1.164 0.690 1.219 2.001 5.715 Gloves & Kits 1.000 1.000 1.000 1.000 1.000 5.000
Capital 1.000 1.000 1.000 1.000 1.000 5.000 Total 1 1.640 2.164 1.690 2.219 3.001 10.715
Budget reflected with other programs. Supply of Drugs
Current 0.000 0.000 0.000 0.000 0.000 0.000 Training HW on trg. manuals 0.000 0.000 0.500 0.000 0.500 1.000 Refresher Course 4.060 4.060 4.060 4.060 4.060 20.300 New training 0.200 0.200 0.200 0.200 0.200 1.000 Study tour VHW 0.500 0.500 0.500 0.500 0.500 2.500
Capital 4.760 4.760 5.260 4.760 5.260 24.800 Total 2 4.760 4.760 5.260 4.760 5.260 24.800
Total 1 + 2 6.400 6.924 6.950 6.979 8.261 35.515 V.2 Manpower requirement. Since VHW program is fully integrated within the Dzongkhag activities, as of now there is no requirement of additional staff. V.3 Technical Assistance Technical assistant is required during the time of updating VHWs manual & its impact study which can be sought during the need. V.4 Equipment & other investment needed.
Table 21. Equipment & other investment needed Equipment 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Procure gloves 1400 nos 1400 nos 1400 nos VHW kit 50 nos 50 nos 50 nos 50 nos 50 nos
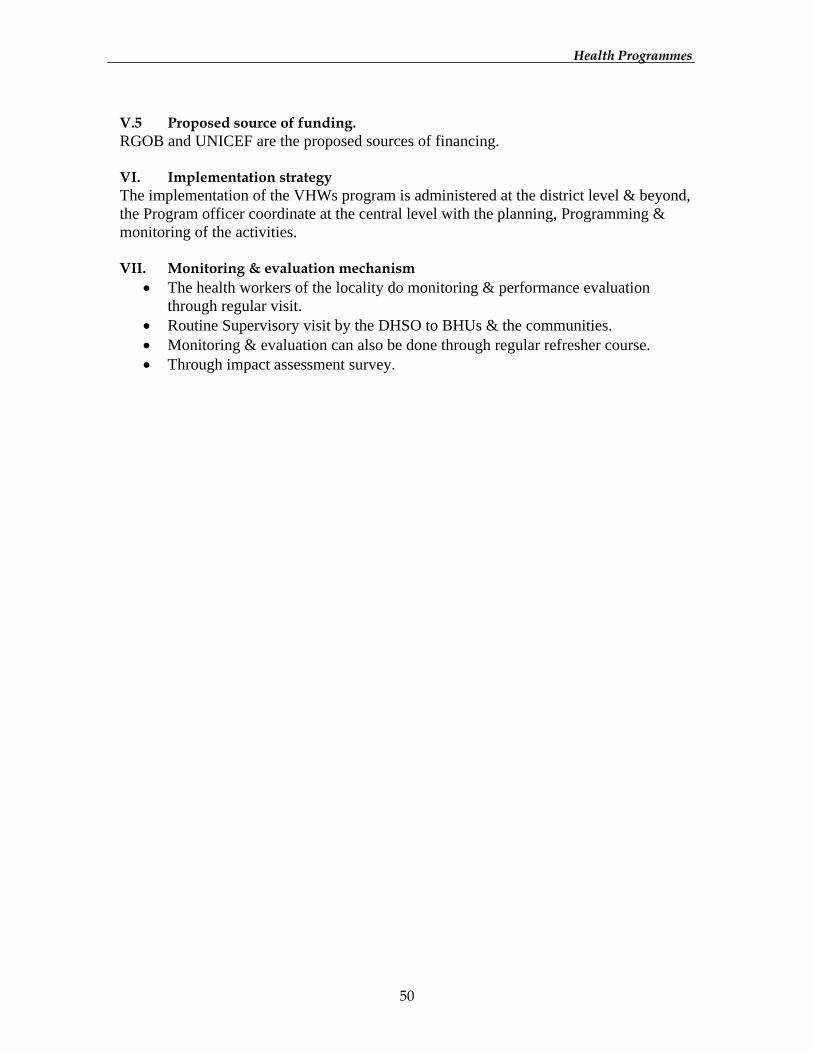
HHeeaalltthh PPrrooggrraammmmeess
50
V.5 Proposed source of funding. RGOB and UNICEF are the proposed sources of financing. VI. Implementation strategy The implementation of the VHWs program is administered at the district level & beyond, the Program officer coordinate at the central level with the planning, Programming & monitoring of the activities. VII. Monitoring & evaluation mechanism
• The health workers of the locality do monitoring & performance evaluation through regular visit.
• Routine Supervisory visit by the DHSO to BHUs & the communities. • Monitoring & evaluation can also be done through regular refresher course. • Through impact assessment survey.

HHeeaalltthh PPrrooggrraammmmeess
51
ORAL HEALTH PROGRAMME I. Introduction Oral health programme was initiated in late 1980s, but always faced financial and manpower constraints to implement major activities. It was only quite sometime later in 1998 that oral health was given due recognition as a separate programme and was put under the umbrella of WHO assisted programmes. Since then programme had carried out number of both preventive and curative activities. II. Situation Analysis a) Current Situation Assessment
While achieving many targets in preventive coverage of some of the communicable diseases, non-communicable diseases like oral and dental diseases had been receiving equal recognition as a public health problem. It is because of the magnitude and wide spread nature of the oral diseases ranging amongst all age groups of both sexes for which recognition as a major public health problem is of paramount importance. The basic oral health preventive, curative and educative services are integrated within the primary health care system and its accessibility is being made far and wide across the country. There are only five hospitals with dental surgeons, while other hospitals have primary health care workers/dental hygienists. Oral diseases have a high morbidity in all the hospitals. It is one of the first top ten morbidities in the country. And so far no nation wide survey has been carried out. Oral health and oral diseases awareness is yet to reach the grass root community mass and monastic schools. There is lack of preventive activities at the community level. But at the curative level, there is need to regularize standardization of equipments and materials for a uniform and safe delivery of services. With rising trend of HIV/AIDS and hepatitis, promotion on safe dental health services and proper sterilization as per international norms need to be given priority and emphasised in all the health centres. Oral health has a tremendous task ahead in promoting preventive programmes at the community level, education and monastic institutes. The concept of primary health care services with an educational approach and emphasis on community involvement needs gearing up. b) Situation assessment at the end of the Ninth Plan
• All 20 Dzongkahgs to be covered by primary preventive programmes • General awareness to reach to the grass root level and community involvement
initiated • National data on common oral diseases established • Educative, promotive and basic curative services made accessible to every
community • Uniform and safe oral health care delivery systems rendered through all district
health facilities

HHeeaalltthh PPrrooggrraammmmeess
52
• More specialised services introduced at national referral hospital as per the rising demand of the community
• Promotion of user fees in other areas emphasised and avenues of the means of sustainability studied and approached.
III. Program/policy objectives The broad objective of the programme is to promote and strengthen preventive primary oral health programmes within the context of Primary Health Care System in the country. Specific objectives are as follows:
1. To generate 90% community awareness on oral health diseases and common
preventive measures 2. To establish school oral health programme in all schools of the country, including
monastic schools 3. To achieve accessibility of basic preventive, educative and curative services to at
least 80% of community by the end of 9FYP. 4. To achieve 100% safe oral health care delivery system in all the district hospitals 5. Introduction of specialised oral health services in district hospitals
IV. Strategies
1. Training of VHWs on oral health at community level. 2. Introduction of oral health, common diseases and their prevention in primary
school curriculum. 3. Updating training curriculum for training of primary oral health workers at RIHS. 4. Standardising procurement and distribution of dental equipments in coordination
with DEVD. 5. Promotion and strengthening of CME at all levels both in- and out-country. 6. Meet manpower requirement at primary level by training more primary oral
health workers in coordination with RIHS V.1 Programme budget outlay
Table 22. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Vehicle hiring for district activity 0.036 0.036 0.036 0.036 0.280 0.424 Medicines and Lab consumables 0.900 0.900 0.900 0.900 0.900 4.500 Maintenance of medical equipment 0.500 0.500 0.500 0.500 0.576 2.576 Review & update trg curricula for RIHS 0.200 0.200 0.000 0.000 0.000 0.400 Conference, Seminar, W'shop 0.120 0.000 0.180 0.000 0.000 0.300
Current 1.756 1.636 1.616 1.436 1.756 8.200 In-country trg for oral health workers 0.300 0.800 0.300 0.800 0.000 2.200 1 Computer 0.080 0.000 0.000 0.000 0.000 0.080 Professional services 0.000 0.500 0.500 0.500 0.500 2.000
Capital 0.380 1.300 0.800 1.300 0.500 4.280 Total 1 2.136 2.936 2.416 2.736 2.256 12.480
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Hospital and Lab Equipments 7.920 8.000 0.000 0.000 5.000 20.920 2 sirona siemens for JDWNRH,

HHeeaalltthh PPrrooggrraammmmeess
53
5 dental chairs for 5 dist.hospitals 1 OPG X- ray machine for Mongar 10 autoclaves with accessories
Capital 7.920 8.000 0.000 0.000 5.000 20.920 Total 2 7.920 8.000 0.000 0.000 5.000 20.920
Total 1 + 2 10.056 10.936 2.416 2.736 7.256 33.400 V.2 Manpower requirement Although it is integrated in the general health services, additional manpower at doctor’s level is required to cover at least 10 districts for uniform quality care. And there is a need of Assistant Program officer and computer programmer at the central level. V.3 Technical assistance Technical assistance/consultants may be required for survey and analysis of oral health data and initiate research activities at the end of 9FYP. V.4 Equipments and other investments needed
1) 3 nos of sirona siemen chains for JDWNRH, 2) 5 dental chairs for districts hospitals 3) OPG x-ray machine for MRRH, 4) Auto claves & accessories for Sibsoo & Dewathang
hospitals, 5) one computer for the programme.
V.5 Proposed source of funding RGOB / Danida/ WHO may be fund this programme. VI. Implementation strategy The programme manager coordinates at the central level and develops technical strategies, planning, resource mobilization and monitoring for the programme activities in close collaboration with the Department of Public Health. All preventive programmes at the school and community level are being decentralised to respective district hospitals under the guidance of DMOs and DHSOs. VII. Monitoring and evaluation mechanism
• Annual supervision of districts by the central program personnel • Monitoring and evaluation at the district level will be carried out by respective
DHSO/DMO • Monthly reporting system by oral health workers to district head, concerned
department and the central programme. • Submission of annual reports by DMO/DHSO to the central programme • Regular information as and when required and sharing resources.
HHeeaalltthh PPrrooggrraammmmeess
54
PUBLIC HEALTH LABORATORY I. Introduction The Public Health laboratory was established in July 1989, to carry out Water Quality monitoring, Food and Drug analysis. While water quality monitoring was started, food analysis never received the priority it required. Sending samples of pharmaceutical drugs abroad for analysis of quality was felt to be much more economical and drug analysis was never considered. II. Situation Analysis a) Current situation assessment Currently the Public Health Laboratory carries out the following activities:
1. Water quality monitoring both bacteriological and chemical analysis 2. Monitoring of iodine in salt nation-wide by analyzing salt samples every quarter
at salt plant, retailer and household level and conducts yearly cyclic monitoring surveys to strengthened Iodine Deficiency Control Programme (IDDPC) in the country.
3. Diagnosis of Tuberculosis through Direct microscopy and culture. 4. Diagnosis and screening of HIV and STDs, in patients, for blood transfusion
screening and surveillance in the country. 5. Besides the above activities the PHL also carry out basic food microbiology,
investigation of epidemic/out-breaks, conduct surveys in collaboration with programs, and conduct training of various health programs on diagnostic procedures for students in RIHS and in-services staff.
PHL needs to focus on issues of importance to strengthen the health services in the country by setting up analytical facilities for the following activities:
1. Food Safety - To carry out complete microbiological and chemical analysis of food. Surveillance of food-borne diseases can be carried out and appropriate control measures initiated to combat these diseases.
2. Environmental Monitoring – Currently water quality monitoring in urban areas are done. However, environmental changes will continue to occur with the accelerated pace of development. In this regard air pollution, river and wastewater need to be monitored to study their effect on human health.
3. Poison information and control centre – Information on all toxic chemicals in the country would be maintained so that if an incidence of chemical or biological poisoning arises a quick response can be initiated.
4. Forensics Unit – Samples from medico-legal cases are sent out of the country due to lack of analytical capacity at PHL. The results take about 6-8 months and in many cases results are doubtful. Therefore, if a separate Forensic laboratory is set up, the PHL could carry out forensic analysis. A toxicology unit would also be needed in this connection.
HHeeaalltthh PPrrooggrraammmmeess
55
5. Communicable disease surveillance – surveillance of gastrointestinal diseases, including food poisoning and water borne diseases, respiratory diseases, esp. tuberculosis and pneumonia, other bacteraemias, zoonoses and nosocomial infection, HIV and STD’s need to be improved so that proper data can be generated to study the trend of diseases.
6. Reference centre in Quality Assurance Programme for the country – Quality Assurance Programs plays a vital role in assessing all level of diagnostic procedures in various disciplines of laboratory services both at national and international level. This ensures the quality of service and minimizes wrong results. QA programs have therefore, come to play a very important role in any institution for proper delivery of services.
7. National Surveillance of immunization programmes – Bhutan has made a lot of stride in childhood immunization coverage of vaccine preventable diseases like measles, diphtheria and polio. However, there is no mechanism for monitoring the uptake, safety and efficacy of vaccine in routine use. The study of these parameters is required to ensure the safety and effectiveness of old and new vaccine alike. Also, surveillance of such disease have become very important for their prevention and control, especially, measles, polio, etc.
8. Research and development – studies into the prevalence and incidences of many diseases in Bhutan through laboratory diagnosis are necessary to generate proper data and for initiating control measures. For example, Prevalence of Streptococcus Group A in the population (control of rheumatic heart diseases), prevalence of Helicobacter pylori and its control and studies in non-communicable diseases. Such research could be carried out in the PHL.
Bhutan has achieved above 90% coverage of adequately iodised salt in the country and the Health Department will be applying for the certification of IDD elimination by the end of 2001, which would be one of the most important achievements of the Health services. PHL would contribute towards reducing morbidity and mortality among the general public in relation to communicable diseases, food and water borne diseases and improved overall public health in the country. The Public Health Laboratory is involved in overall delivery of quality health services through diagnosis, prevention and control of diseases of public health concern. Also involved in study of the trend of diseases and development of the strategies for prevention in the country. PHL at present supports different programmes like STD/AIDS programme, TB control programme, Nutrition programme, Food safety, EPI programme, CDD programme. b) Situation assessment at the end of 9FYP
In addition to strengthening the current activities, food safety would have ensured, environmental monitoring started, quality assurance system for laboratory diagnostic procedures in the country intensified, Forensics unit and Poison information and control centre established, and communicable diseases surveillance and research initiated.
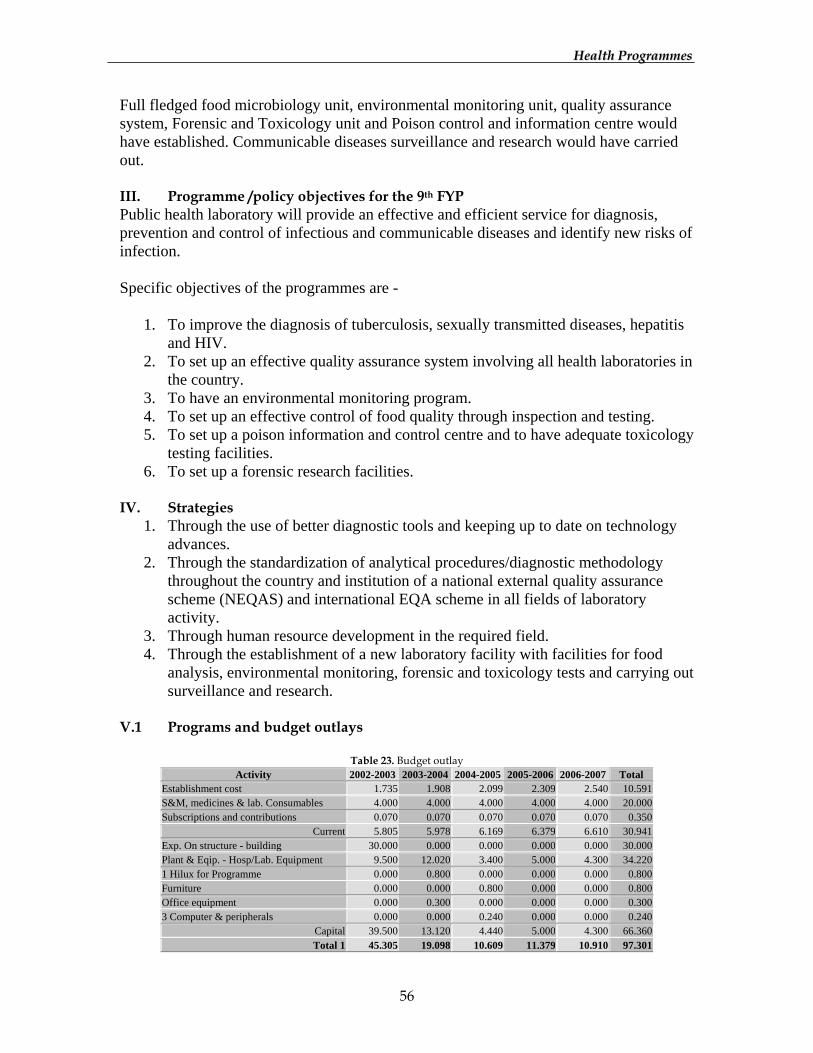
HHeeaalltthh PPrrooggrraammmmeess
56
Full fledged food microbiology unit, environmental monitoring unit, quality assurance system, Forensic and Toxicology unit and Poison control and information centre would have established. Communicable diseases surveillance and research would have carried out. III. Programme /policy objectives for the 9th FYP Public health laboratory will provide an effective and efficient service for diagnosis, prevention and control of infectious and communicable diseases and identify new risks of infection. Specific objectives of the programmes are -
1. To improve the diagnosis of tuberculosis, sexually transmitted diseases, hepatitis
and HIV. 2. To set up an effective quality assurance system involving all health laboratories in
the country. 3. To have an environmental monitoring program. 4. To set up an effective control of food quality through inspection and testing. 5. To set up a poison information and control centre and to have adequate toxicology
testing facilities. 6. To set up a forensic research facilities.
IV. Strategies
1. Through the use of better diagnostic tools and keeping up to date on technology advances.
2. Through the standardization of analytical procedures/diagnostic methodology throughout the country and institution of a national external quality assurance scheme (NEQAS) and international EQA scheme in all fields of laboratory activity.
3. Through human resource development in the required field. 4. Through the establishment of a new laboratory facility with facilities for food
analysis, environmental monitoring, forensic and toxicology tests and carrying out surveillance and research.
V.1 Programs and budget outlays
Table 23. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 1.735 1.908 2.099 2.309 2.540 10.591 S&M, medicines & lab. Consumables 4.000 4.000 4.000 4.000 4.000 20.000 Subscriptions and contributions 0.070 0.070 0.070 0.070 0.070 0.350
Current 5.805 5.978 6.169 6.379 6.610 30.941 Exp. On structure - building 30.000 0.000 0.000 0.000 0.000 30.000 Plant & Eqip. - Hosp/Lab. Equipment 9.500 12.020 3.400 5.000 4.300 34.220 1 Hilux for Programme 0.000 0.800 0.000 0.000 0.000 0.800 Furniture 0.000 0.000 0.800 0.000 0.000 0.800 Office equipment 0.000 0.300 0.000 0.000 0.000 0.300 3 Computer & peripherals 0.000 0.000 0.240 0.000 0.000 0.240
Capital 39.500 13.120 4.440 5.000 4.300 66.360 Total 1 45.305 19.098 10.609 11.379 10.910 97.301
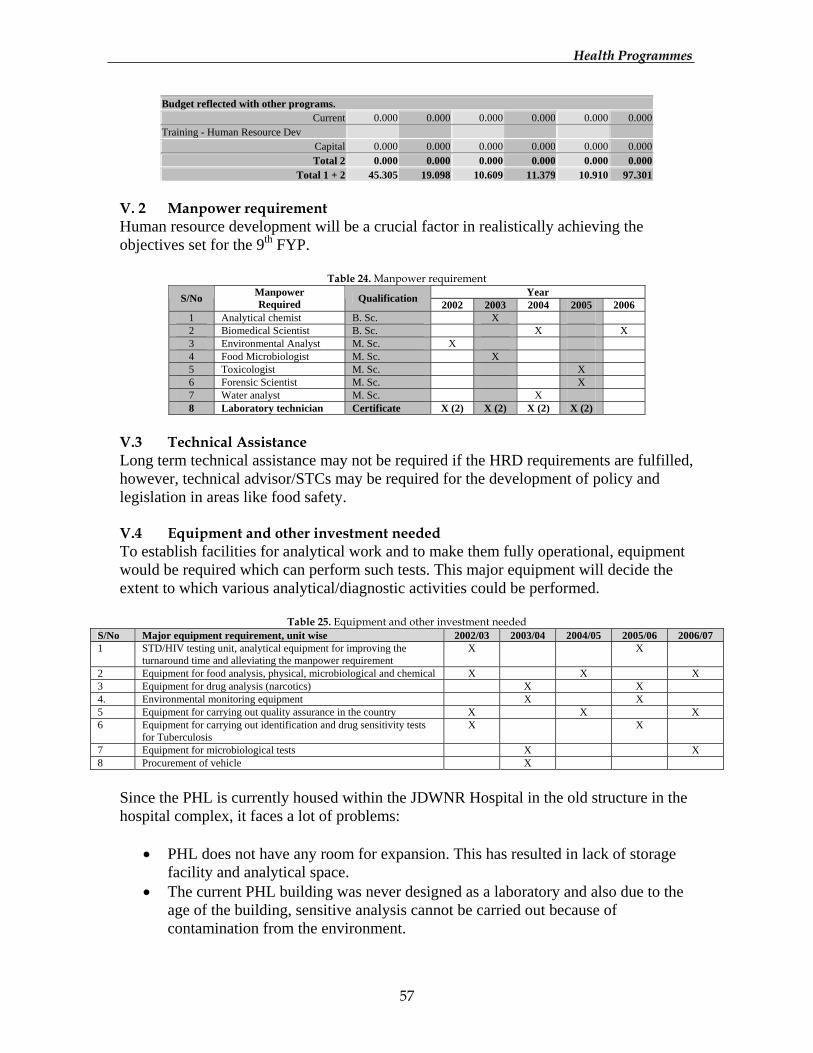
HHeeaalltthh PPrrooggrraammmmeess
57
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 45.305 19.098 10.609 11.379 10.910 97.301 V. 2 Manpower requirement Human resource development will be a crucial factor in realistically achieving the objectives set for the 9th FYP.
Table 24. Manpower requirement Year S/No Manpower
Required Qualification 2002 2003 2004 2005 2006 1 Analytical chemist B. Sc. X 2 Biomedical Scientist B. Sc. X X 3 Environmental Analyst M. Sc. X 4 Food Microbiologist M. Sc. X 5 Toxicologist M. Sc. X 6 Forensic Scientist M. Sc. X 7 Water analyst M. Sc. X 8 Laboratory technician Certificate X (2) X (2) X (2) X (2)
V.3 Technical Assistance Long term technical assistance may not be required if the HRD requirements are fulfilled, however, technical advisor/STCs may be required for the development of policy and legislation in areas like food safety. V.4 Equipment and other investment needed To establish facilities for analytical work and to make them fully operational, equipment would be required which can perform such tests. This major equipment will decide the extent to which various analytical/diagnostic activities could be performed.
Table 25. Equipment and other investment needed S/No Major equipment requirement, unit wise 2002/03 2003/04 2004/05 2005/06 2006/07 1 STD/HIV testing unit, analytical equipment for improving the
turnaround time and alleviating the manpower requirement X X
2 Equipment for food analysis, physical, microbiological and chemical X X X 3 Equipment for drug analysis (narcotics) X X 4. Environmental monitoring equipment X X 5 Equipment for carrying out quality assurance in the country X X X 6 Equipment for carrying out identification and drug sensitivity tests
for Tuberculosis X X
7 Equipment for microbiological tests X X 8 Procurement of vehicle X
Since the PHL is currently housed within the JDWNR Hospital in the old structure in the hospital complex, it faces a lot of problems:
• PHL does not have any room for expansion. This has resulted in lack of storage
facility and analytical space. • The current PHL building was never designed as a laboratory and also due to the
age of the building, sensitive analysis cannot be carried out because of contamination from the environment.
HHeeaalltthh PPrrooggrraammmmeess
58
V.5 Proposed source of financing RGOB, Danida and WHO are the proposed sources of financing VI. Implementation strategy The head of the Public Health Laboratory will coordinate and plan all activities in close consultation with the concerned Programmes and the Health Dept. Procurement of supplies will be carried out through the DVED and trainings coordinated through the AFD. Infrastructure development will be carried out in consultation and managed by the Health Engineering Division. WHO assistance will be sought in implementation of quality assurance schemes and for laboratory accreditation if necessary. VII. Monitoring and evaluation mechanism Monitoring will be carried out by the Dept. through the monthly/quarterly/annual reports of activities carried out in the PHL, submitted to the Dept. and evaluation will be carried out through the progress reports, periodic reviews and evaluation visits to the PHL.
HHeeaalltthh PPrrooggrraammmmeess
59
RESEARCH AND EPIDEMIOLOGY UNIT I. Introduction All sources of information and data indicate that health service coverage is about 90%. Yet demand for health services is increasing rapidly and prioritisations and sound investments are key to further success in this milieu of increasing demands and decreasing resources. To use the resources optimally, it is necessary to evaluate, re-assess, and prioritise so that more is achieved with less. And one of the most effective tools for such approach is research. Research is necessary to understand the problems and to seek for appropriate and cost effective solutions. With this rationality, Ministry of Health & Education established the Health Research & Epidemiology Unit on July 10, 1995. II. Situation Analysis a) Current Situation Assessment
About ten small including few nation wide researches were conducted so far. Most of the planned studies couldn’t be carried out because of lack of skilled manpower. b) Situation Assessment at the end of the Ninth Plan
The strategic decisions in the health would be increasingly based on the sound and systematically collected and analysed information both at the central as well as the Dzongkhag levels.
The Unit would have coordinated all health researches undertaken by programs while it being the apex centre for resources in health research, having consultative functions for research design, database management, statistical analysis, and interpretation of results. The research skills would have promoted and imparted to the health workers, contributing to national self-reliance in the field. III. Programme/Policy Objectives for the 9FYP
1. While biomedical research and epidemiological research are important and cannot be excluded totally, the major emphasis will be on the strengthening of health systems research.
2. To identify health problems peculiar to our geographic and socio-cultural settings and to seek for solutions that are cost effective/efficient and acceptable to the population
3. To make research an important tool for informed policy decisions for appropriate prioritisation for sound investment.
4. To further enhance the epidemiological services done through the regular reporting system (HMIS) by doing field research.
5. To link national, regional and international research partners and to network to tap on the resources and expertise to enhance and build national competence in research.
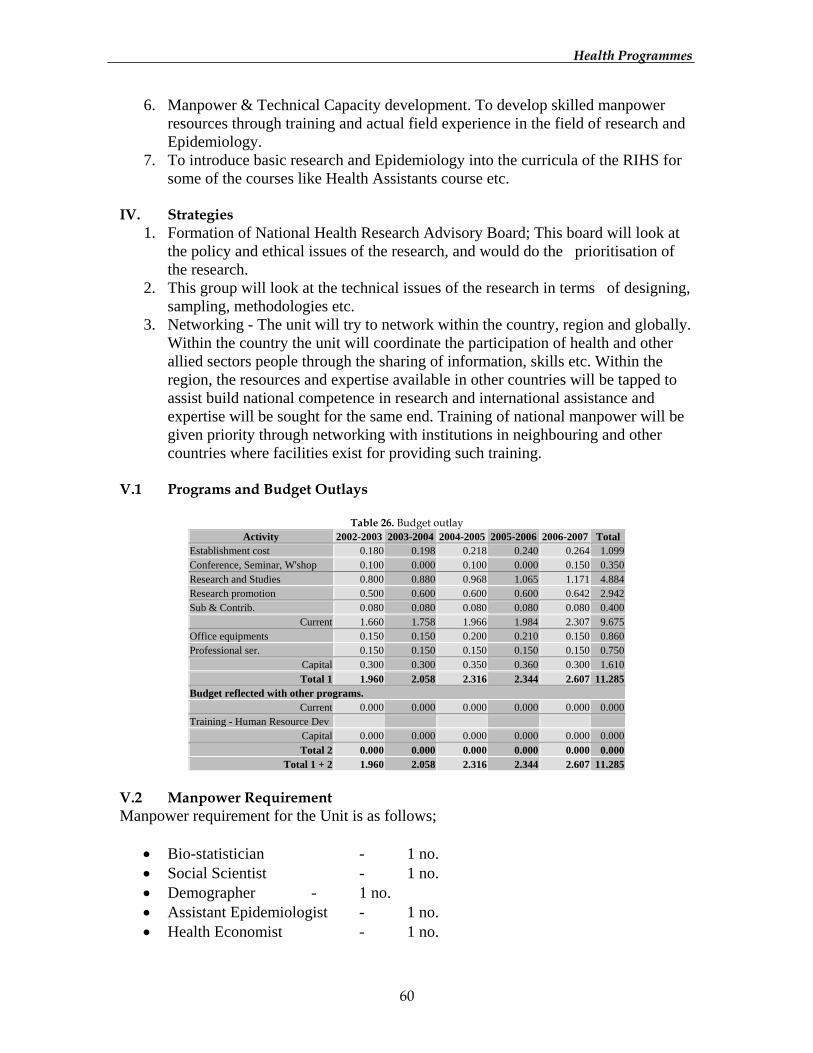
HHeeaalltthh PPrrooggrraammmmeess
60
6. Manpower & Technical Capacity development. To develop skilled manpower resources through training and actual field experience in the field of research and Epidemiology.
7. To introduce basic research and Epidemiology into the curricula of the RIHS for some of the courses like Health Assistants course etc.
IV. Strategies
1. Formation of National Health Research Advisory Board; This board will look at the policy and ethical issues of the research, and would do the prioritisation of the research.
2. This group will look at the technical issues of the research in terms of designing, sampling, methodologies etc.
3. Networking - The unit will try to network within the country, region and globally. Within the country the unit will coordinate the participation of health and other allied sectors people through the sharing of information, skills etc. Within the region, the resources and expertise available in other countries will be tapped to assist build national competence in research and international assistance and expertise will be sought for the same end. Training of national manpower will be given priority through networking with institutions in neighbouring and other countries where facilities exist for providing such training.
V.1 Programs and Budget Outlays
Table 26. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.180 0.198 0.218 0.240 0.264 1.099 Conference, Seminar, W'shop 0.100 0.000 0.100 0.000 0.150 0.350 Research and Studies 0.800 0.880 0.968 1.065 1.171 4.884 Research promotion 0.500 0.600 0.600 0.600 0.642 2.942 Sub & Contrib. 0.080 0.080 0.080 0.080 0.080 0.400
Current 1.660 1.758 1.966 1.984 2.307 9.675 Office equipments 0.150 0.150 0.200 0.210 0.150 0.860 Professional ser. 0.150 0.150 0.150 0.150 0.150 0.750
Capital 0.300 0.300 0.350 0.360 0.300 1.610 Total 1 1.960 2.058 2.316 2.344 2.607 11.285
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 1.960 2.058 2.316 2.344 2.607 11.285 V.2 Manpower Requirement Manpower requirement for the Unit is as follows;
• Bio-statistician - 1 no. • Social Scientist - 1 no. • Demographer - 1 no. • Assistant Epidemiologist - 1 no. • Health Economist - 1 no.
HHeeaalltthh PPrrooggrraammmmeess
61
• Data Enumerators - 3 nos. • Computer programmer - 1 no.
V.3 Technical Assistance As long as the above manpower is not fulfilled, the unit will keep on having technical assistance as and when required. The technical assistance for the unit will be mainly in terms of development of study protocol and in the analysis of data. V.4 Equipments and other investments The equipment requirements are the strengthening of laboratory services in the country by equipping with basic essential equipments, reagents and chemicals so that laboratories can provide the essential backup for health research. The unit also needs to keep updated with latest statistical software’s in the market so that it is compatible with other institutes and organizations once the unit gets networked. V.5 Proposed Source of Funding Apart from RGB, DANIDA and WHO are the likely financing supporters for the Ninth Plan. However, in the near future the unit looks upon Health Trust Fund to grant funds to carry out researches screened by Scientific Advisory Committee and Research Advisory Board. VI. Implementing Strategy The unit is planning to enhance the research skills in the dzongkhag along with the HMIS. Once this is done small-scale research specific to their dzongkhag will be implemented at the dzongkhag level. However, by and large this will remain as a centrally executed activity. The monitoring and evaluation part of the research can be fully decentralized to the dzongkhag level once there is adequate capacity in the district. VII. Monitoring and evaluation mechanism The immediate outcome of any research is to see whether any research findings have resulted into action. The other way is look at how many research findings are published in reputed journals within the country, within the region and even in the international journals. The number of research conducted can also be an indicator for monitoring and evaluation purpose.

HHeeaalltthh PPrrooggrraammmmeess
62
HEALTH MANAGEMENT INFORMATION SYSTEM I. Introduction The system of recording and reporting of health services existed long before since inception of the Health Department, and is still popularly known as Health Information System (HIS). With the introduction of successive Five Year Plans, new programmes and projects have been created in the Department. As a result, there has been increasing use of information at various levels, both within and outside government agencies/organisation, whereby at times the current Health Information System is no longer in a position to meet these demands. Significant health sector reforms and decentralization system have also changed the information requirements. Use of information is crucial to improve quality of health care services and to assist managers at all levels in the decision making process related to case management, problem identification, performance evaluation, strategic planning, and optimizing the use of limited financial resources. II. Situation Analysis a) Current situation assessment
Feeling the need to streamline the existing system with stronger management support and review the present health information system, the DANIDA funded project with technical assistance from Eurohealth was formulated for a period of 2 years. A phased activity approach has been initiated since January 2000, and major groundwork on review of current recording/reporting system and revised version of manual system have been developed with regard to forms and formats, registers and cards in close consultation with the field staff at district level. It is ultimately aimed at benefiting not only the whole health system but also to greatly reduce the overburdened workload in the periphery, enabling them to concentrate in the quality health services delivery in the community at large. b) Situation Assessment at the end of the Ninth Plan
An urgent need for more research capacity to generate better baseline data and qualitative information for planning has been identified as a priority area to be pursued during the 9th Five Year Plan. Data required for monitoring the essential health indicators would have been produced, summarized and reported in an accurate & timely manner. And the resultant information analyzed and presented in simple, practical and understandable formats to managers in time and kept aware of the current health performance situation, and to be able to detect events or trends that require corrective action. The data and indicators generated and managed by this system should largely satisfy the information required to monitor progress in the health development plan, and against international goals and targets.
HHeeaalltthh PPrrooggrraammmmeess
63
III. Policy/Programme Objectives The general objective is to have an enhanced management information system so that it becomes an efficient tool to support the implementation of health programmes and to identify indicators appropriate for monitoring the progress within the health sector. Specific objectives are:
1. To develop appropriate indicators to help assess the performance of health
programmes in terms of monitoring overall progress within the sector. 2. To assess from time to time the existing health information system to determine
its applicability and utility, including its strengths and weaknesses. 3. To develop additional information requirement to support health services
management, including information requirements for future planning and prioritisation.
4. To ensure full computerisation of health information systems and maintain efficient link up on a national network.
5. Ensure up-to-date requirement of IT features as tools for efficient HMIS. 6. To ensure appropriate and effective feedback system.
IV. Strategies The strengthening and management of national Health Information System is one of the most challenging tasks of the Health Department. Since it is one of the priority areas of health services, strategies are focussed in the strengthening of effective implementation of health services including human resource development.
1. In order that the national health information system fulfils the priority needs of the government and the system managed by a fully functional team of requisite manpower, appropriate capacity development will be a constant effort in line with HRD policy of the Department.
2. The HMIS in collaboration with RIHS and relevant institutes will ensure a regular in-service training as well as refresher courses to update knowledge of relevant health personnel at all levels.
3. The HIU will ensure update of required IT both at central and district level offices and its procurement of supplies and equipment as appropriate.
4. For efficient and effective management of HMIS, required transportation and communication facilities will be provided.
5. Efforts will be made to secure minimum financial resources to support the activities envisaged.
6. At each stage of implementation, monitoring and evaluation will take place as a routine measure on the outcome of activities.
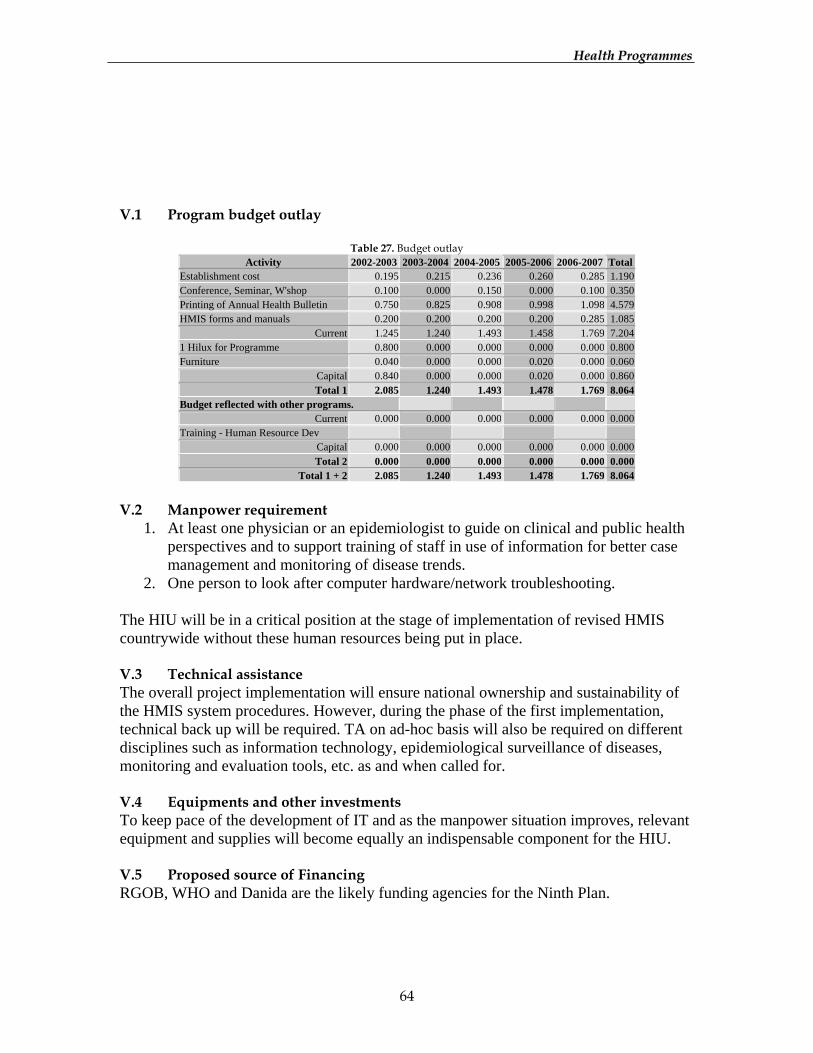
HHeeaalltthh PPrrooggrraammmmeess
64
V.1 Program budget outlay
Table 27. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.195 0.215 0.236 0.260 0.285 1.190 Conference, Seminar, W'shop 0.100 0.000 0.150 0.000 0.100 0.350 Printing of Annual Health Bulletin 0.750 0.825 0.908 0.998 1.098 4.579 HMIS forms and manuals 0.200 0.200 0.200 0.200 0.285 1.085
Current 1.245 1.240 1.493 1.458 1.769 7.204 1 Hilux for Programme 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.040 0.000 0.000 0.020 0.000 0.060
Capital 0.840 0.000 0.000 0.020 0.000 0.860 Total 1 2.085 1.240 1.493 1.478 1.769 8.064
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 2.085 1.240 1.493 1.478 1.769 8.064
V.2 Manpower requirement
1. At least one physician or an epidemiologist to guide on clinical and public health perspectives and to support training of staff in use of information for better case management and monitoring of disease trends.
2. One person to look after computer hardware/network troubleshooting. The HIU will be in a critical position at the stage of implementation of revised HMIS countrywide without these human resources being put in place. V.3 Technical assistance The overall project implementation will ensure national ownership and sustainability of the HMIS system procedures. However, during the phase of the first implementation, technical back up will be required. TA on ad-hoc basis will also be required on different disciplines such as information technology, epidemiological surveillance of diseases, monitoring and evaluation tools, etc. as and when called for. V.4 Equipments and other investments To keep pace of the development of IT and as the manpower situation improves, relevant equipment and supplies will become equally an indispensable component for the HIU. V.5 Proposed source of Financing RGOB, WHO and Danida are the likely funding agencies for the Ninth Plan.
HHeeaalltthh PPrrooggrraammmmeess
65
VI. Implementation strategy The actual implementation of ongoing enhancement project will exactly coincide with the 9th FYP. Dzongkhag health sector and all health facilities including institutions will be directly responsible for the implementation through the coordination from the central programme. VII. Monitoring and evaluation mechanism The HMIS monitoring at the district level will be done by DHSO’s through a set of structured monitoring tools that will be developed by the TA/MSH in collaboration with the task force. The information core group at the central level will be fully in-charge of the national level task of monitoring and evaluation under guidance of the proposed TA that will be available at the initial phase of the implementation period.
HHeeaalltthh PPrrooggrraammmmeess
66
PUBLIC HEALTH ENGINEERING SECTION I. Introduction The Rural Water Supply and Sanitation Programme was started in 1974. During this period, the government and a number of international donors have invested more than Nu.300 million. The Royal Government had transferred the Rural Water Supply and Sanitation Programme, which was with Public Works Division, to Health Department in 1998, in view of the advantageous position Health was in to mobilise funds and accelerate its implementation by involving the health staff at the grass roots level. Above all the transfer was anticipated to have a much greater impact on the health of the people as hardware and software components of water and sanitation can be better coordinated being under the same Division. At mid of 2001, more than 75% of the rural population have been supplied with safe and improved water through the construction of 2300 schemes and about 88% of rural households are estimated to have access to at least a basic level of sanitation. II. Situation analysis a) Current Situation Assessment
PHE’s emphasis had been to provide durable and appropriate technologies to the rural population. However, in 1998 it had been observed that about 30% of the schemes built required rehabilitation. Since then, the programme placed high emphasis on developing software activities that emphasized community ownership and sustainable management of RWSS facilities and as well as their effective use. Community Planning and Monitoring Workshops have been developed over the last three years which give opportunity to people to plan for implementation, monitoring and maintenance of their water and sanitation facilities. There are now trained water caretakers to operate and maintain the water schemes. While the overall health situation has improved, poor personal and home hygiene are leading causes of ill health among Bhutanese children. b) Situation Assessment at the end of the Ninth Plan
All the rural population has access to clean drinking water supply and basic sanitary latrines, which are properly maintained and effectively used. III. Programme/policy objectives for the 9 FYP The long-term aim of the programme is to improve the health of the rural population by reducing the incidence of water borne and related diseases through the provision of safe drinking water and basic sanitary latrines. Specific objectives:
1. To provide universal access to safe drinking water supply to the rural population 2. To promote and ensure use of basic sanitary latrines by all the rural population
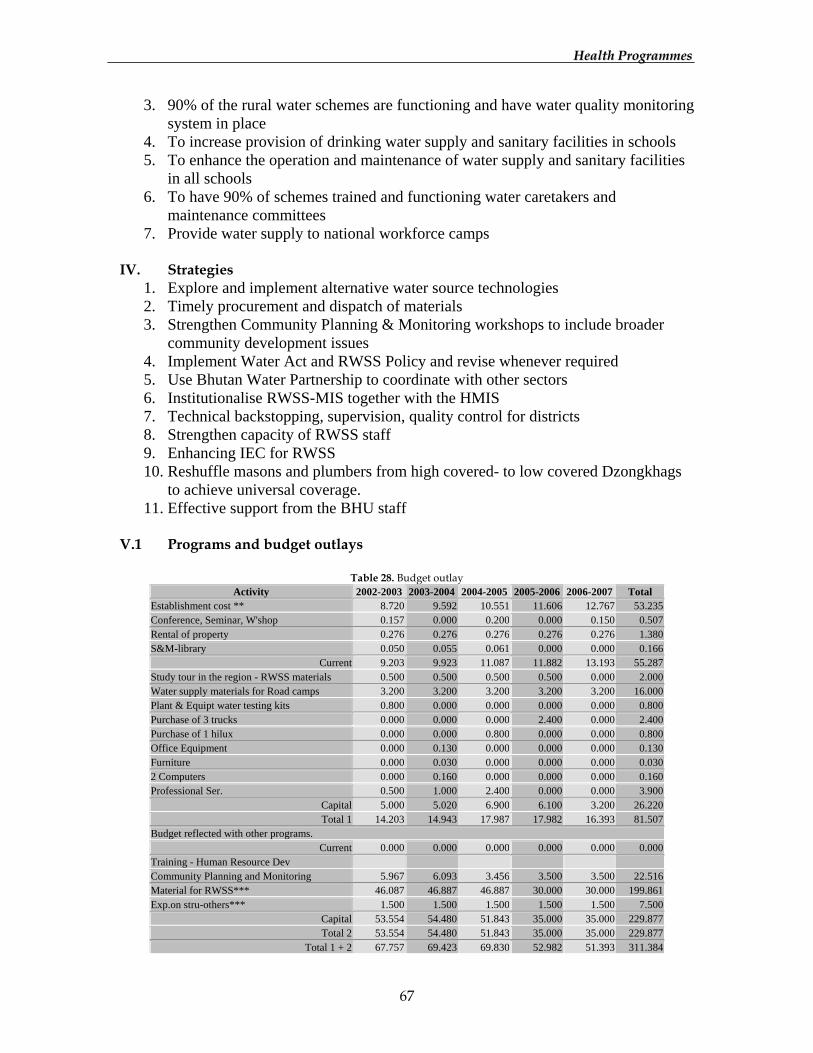
HHeeaalltthh PPrrooggrraammmmeess
67
3. 90% of the rural water schemes are functioning and have water quality monitoring system in place
4. To increase provision of drinking water supply and sanitary facilities in schools 5. To enhance the operation and maintenance of water supply and sanitary facilities
in all schools 6. To have 90% of schemes trained and functioning water caretakers and
maintenance committees 7. Provide water supply to national workforce camps
IV. Strategies
1. Explore and implement alternative water source technologies 2. Timely procurement and dispatch of materials 3. Strengthen Community Planning & Monitoring workshops to include broader
community development issues 4. Implement Water Act and RWSS Policy and revise whenever required 5. Use Bhutan Water Partnership to coordinate with other sectors 6. Institutionalise RWSS-MIS together with the HMIS 7. Technical backstopping, supervision, quality control for districts 8. Strengthen capacity of RWSS staff 9. Enhancing IEC for RWSS 10. Reshuffle masons and plumbers from high covered- to low covered Dzongkhags
to achieve universal coverage. 11. Effective support from the BHU staff
V.1 Programs and budget outlays
Table 28. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost ** 8.720 9.592 10.551 11.606 12.767 53.235Conference, Seminar, W'shop 0.157 0.000 0.200 0.000 0.150 0.507Rental of property 0.276 0.276 0.276 0.276 0.276 1.380S&M-library 0.050 0.055 0.061 0.000 0.000 0.166
Current 9.203 9.923 11.087 11.882 13.193 55.287Study tour in the region - RWSS materials 0.500 0.500 0.500 0.500 0.000 2.000Water supply materials for Road camps 3.200 3.200 3.200 3.200 3.200 16.000Plant & Equipt water testing kits 0.800 0.000 0.000 0.000 0.000 0.800Purchase of 3 trucks 0.000 0.000 0.000 2.400 0.000 2.400Purchase of 1 hilux 0.000 0.000 0.800 0.000 0.000 0.800Office Equipment 0.000 0.130 0.000 0.000 0.000 0.130Furniture 0.000 0.030 0.000 0.000 0.000 0.0302 Computers 0.000 0.160 0.000 0.000 0.000 0.160Professional Ser. 0.500 1.000 2.400 0.000 0.000 3.900
Capital 5.000 5.020 6.900 6.100 3.200 26.220Total 1 14.203 14.943 17.987 17.982 16.393 81.507
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Community Planning and Monitoring 5.967 6.093 3.456 3.500 3.500 22.516Material for RWSS*** 46.087 46.887 46.887 30.000 30.000 199.861Exp.on stru-others*** 1.500 1.500 1.500 1.500 1.500 7.500
Capital 53.554 54.480 51.843 35.000 35.000 229.877Total 2 53.554 54.480 51.843 35.000 35.000 229.877
Total 1 + 2 67.757 69.423 69.830 52.982 51.393 311.384
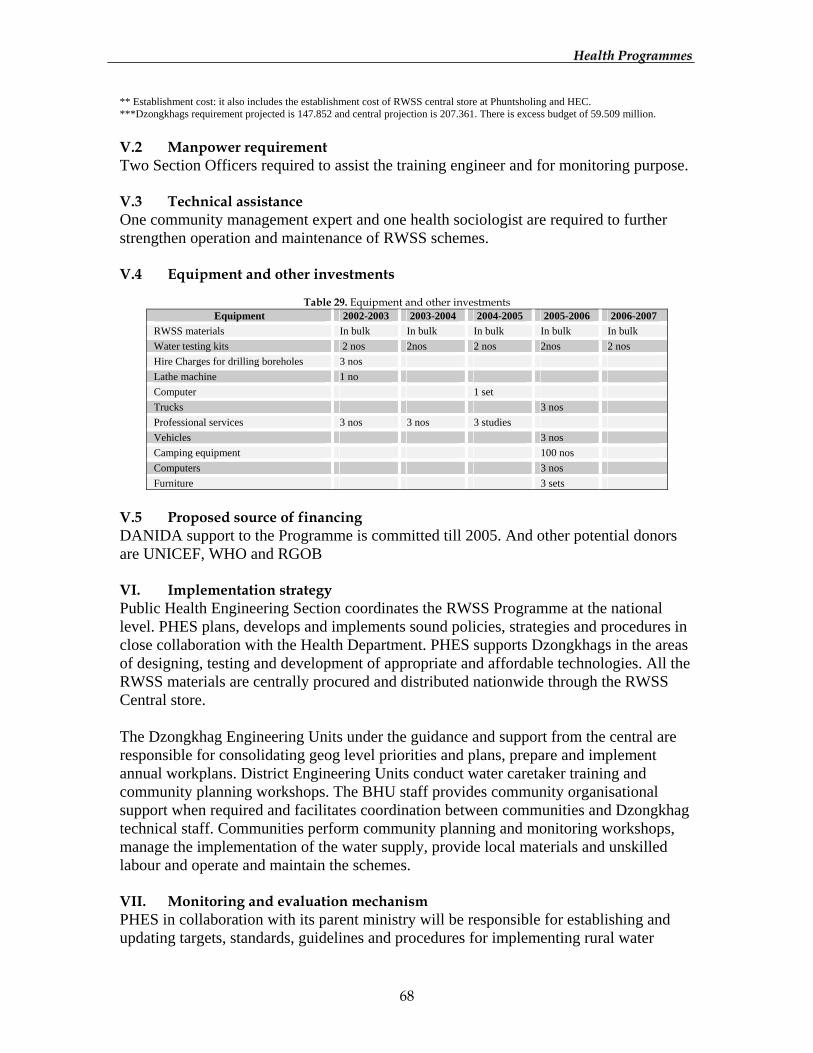
HHeeaalltthh PPrrooggrraammmmeess
68
** Establishment cost: it also includes the establishment cost of RWSS central store at Phuntsholing and HEC. ***Dzongkhags requirement projected is 147.852 and central projection is 207.361. There is excess budget of 59.509 million. V.2 Manpower requirement Two Section Officers required to assist the training engineer and for monitoring purpose. V.3 Technical assistance One community management expert and one health sociologist are required to further strengthen operation and maintenance of RWSS schemes. V.4 Equipment and other investments
Table 29. Equipment and other investments
Equipment 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 RWSS materials In bulk In bulk In bulk In bulk In bulk Water testing kits 2 nos 2nos 2 nos 2nos 2 nos Hire Charges for drilling boreholes 3 nos Lathe machine 1 no Computer 1 set Trucks 3 nos Professional services 3 nos 3 nos 3 studies Vehicles 3 nos Camping equipment 100 nos Computers 3 nos Furniture 3 sets
V.5 Proposed source of financing DANIDA support to the Programme is committed till 2005. And other potential donors are UNICEF, WHO and RGOB VI. Implementation strategy Public Health Engineering Section coordinates the RWSS Programme at the national level. PHES plans, develops and implements sound policies, strategies and procedures in close collaboration with the Health Department. PHES supports Dzongkhags in the areas of designing, testing and development of appropriate and affordable technologies. All the RWSS materials are centrally procured and distributed nationwide through the RWSS Central store. The Dzongkhag Engineering Units under the guidance and support from the central are responsible for consolidating geog level priorities and plans, prepare and implement annual workplans. District Engineering Units conduct water caretaker training and community planning workshops. The BHU staff provides community organisational support when required and facilitates coordination between communities and Dzongkhag technical staff. Communities perform community planning and monitoring workshops, manage the implementation of the water supply, provide local materials and unskilled labour and operate and maintain the schemes. VII. Monitoring and evaluation mechanism PHES in collaboration with its parent ministry will be responsible for establishing and updating targets, standards, guidelines and procedures for implementing rural water

HHeeaalltthh PPrrooggrraammmmeess
69
schemes throughout the country. BHU staff in collaboration with dzongkhag engineering staff will assist PHES in monitoring scheme functionality, contamination risk and use of rural water supply schemes. PHES will maintain a MIS system for the RWSS sector. This system will be consistent with and complement other monitoring and reporting requirements of the sector such as HMIS. Some of the monitoring tools are as follows:
• Quarterly supervisory visits by the central level programme personnel to the districts and construction sites at the villages
• Submission of quarterly progress reports and completion certificate of schemes to the central by the districts
• Self monitoring of the RWSS structures by the communities and reporting to BHU staff
• Monitoring of the RWSS by BHU staff during their regular visits to the villages • Submission of reports by BHUs through districts to the central programme
To improve the flow of information, PHES will issue an annual report including progress and achievements, financial information and other relevant information based on progress and monitoring reports from dzongkhags and health staff, supplemented by periodic studies and evaluations initiated by PHES.
HHeeaalltthh PPrrooggrraammmmeess
70
HEALTH ENGINEERING DIVISION I. Introduction Health Engineering Division, formerly known as Health Engineering Cell, was established in 1993 with assistance from Danida under Public Works Division and later transferred to the Health Department, MHE. II. Situation Analysis a) Current Situation Assessment
The establishment of this division was the reflection of the importance accorded by RGOB on establishing basic health units and hospitals throughout the country, utilizing and developing its own in-house design capacity as part of its commitment to achieving Health-for-all goals. HED manages the designs and supervision of hospital constructions and other health buildings, design basic health units and renders technical assistance to the Dzongkhags as and when required during the constructions. b) Situation Assessment at the end of the Ninth Plan
It is assumed that the division will gradually change from a pure engineering and architectural design office to a maintenance division having adequate capacity to undertake design and supervision of new structures and rehabilitation of existing ones, but at much lower scale. It is further envisaged that a close coordination be established between the new Ministry of Constructions and Health Maintenance Unit. But the HED will continue to be with the Health services. III. Programme/Policy objectives for the 9FYP
1. Undertake the maintenance requirements of all health infrastructures in Bhutan and at the same time being able to undertake the design and supervision of new structures as per the 9FYP.
2. Develop and introduce appropriate construction methods to allow for more hygienic and use-friendly BHUs and hospitals.
3. Set up a well-defined maintenance unit to coordinate with the district engineering cells.
4. Ensure timely maintenance. IV. Strategies
1. To establish an easy, user-friendly and uniform maintenance system 2. To develop a maintenance system that will be line with the overall RGOB policy
on decentralization. 3. To establish a system that will optimise utilization of maintenance.
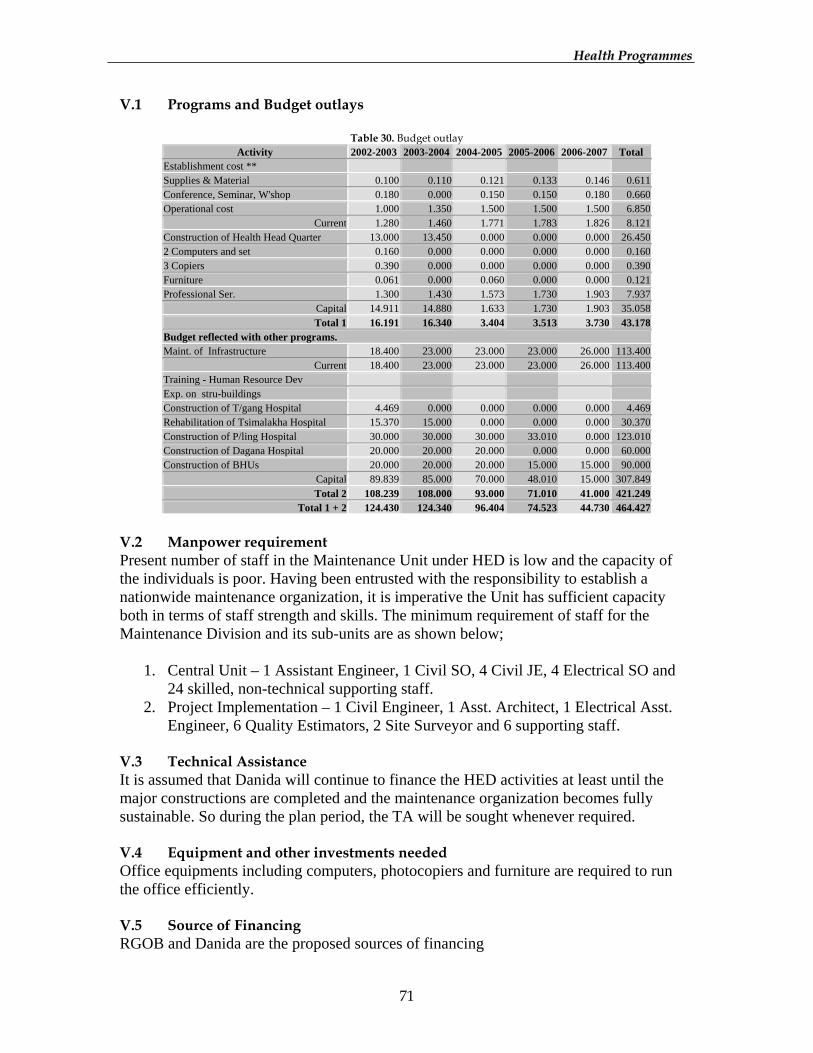
HHeeaalltthh PPrrooggrraammmmeess
71
V.1 Programs and Budget outlays
Table 30. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost ** Supplies & Material 0.100 0.110 0.121 0.133 0.146 0.611 Conference, Seminar, W'shop 0.180 0.000 0.150 0.150 0.180 0.660 Operational cost 1.000 1.350 1.500 1.500 1.500 6.850
Current 1.280 1.460 1.771 1.783 1.826 8.121 Construction of Health Head Quarter 13.000 13.450 0.000 0.000 0.000 26.450 2 Computers and set 0.160 0.000 0.000 0.000 0.000 0.160 3 Copiers 0.390 0.000 0.000 0.000 0.000 0.390 Furniture 0.061 0.000 0.060 0.000 0.000 0.121 Professional Ser. 1.300 1.430 1.573 1.730 1.903 7.937
Capital 14.911 14.880 1.633 1.730 1.903 35.058 Total 1 16.191 16.340 3.404 3.513 3.730 43.178
Budget reflected with other programs. Maint. of Infrastructure 18.400 23.000 23.000 23.000 26.000 113.400
Current 18.400 23.000 23.000 23.000 26.000 113.400 Training - Human Resource Dev Exp. on stru-buildings Construction of T/gang Hospital 4.469 0.000 0.000 0.000 0.000 4.469 Rehabilitation of Tsimalakha Hospital 15.370 15.000 0.000 0.000 0.000 30.370 Construction of P/ling Hospital 30.000 30.000 30.000 33.010 0.000 123.010 Construction of Dagana Hospital 20.000 20.000 20.000 0.000 0.000 60.000 Construction of BHUs 20.000 20.000 20.000 15.000 15.000 90.000
Capital 89.839 85.000 70.000 48.010 15.000 307.849 Total 2 108.239 108.000 93.000 71.010 41.000 421.249
Total 1 + 2 124.430 124.340 96.404 74.523 44.730 464.427
V.2 Manpower requirement Present number of staff in the Maintenance Unit under HED is low and the capacity of the individuals is poor. Having been entrusted with the responsibility to establish a nationwide maintenance organization, it is imperative the Unit has sufficient capacity both in terms of staff strength and skills. The minimum requirement of staff for the Maintenance Division and its sub-units are as shown below;
1. Central Unit – 1 Assistant Engineer, 1 Civil SO, 4 Civil JE, 4 Electrical SO and 24 skilled, non-technical supporting staff.
2. Project Implementation – 1 Civil Engineer, 1 Asst. Architect, 1 Electrical Asst. Engineer, 6 Quality Estimators, 2 Site Surveyor and 6 supporting staff.
V.3 Technical Assistance It is assumed that Danida will continue to finance the HED activities at least until the major constructions are completed and the maintenance organization becomes fully sustainable. So during the plan period, the TA will be sought whenever required. V.4 Equipment and other investments needed Office equipments including computers, photocopiers and furniture are required to run the office efficiently. V.5 Source of Financing RGOB and Danida are the proposed sources of financing

HHeeaalltthh PPrrooggrraammmmeess
72
VI. Implementation Strategy Under the new maintenance division, there will be specification of different management and implementation responsibilities, embedded at the central and de-central levels between the different managing and implementing entities. Further, the process of program implementation will be outlined. VII. Monitoring and evaluation mechanism There will be indicators to be used to assess the output as well as the means of verification. In addition, the responsibilities for collection of data, analysis and reporting and for providing feedback will be clearly spelt out.

HHeeaalltthh PPrrooggrraammmmeess
73
QUALITY ASSURANCE AND STANDARDISATION I. Introduction: The Ministry of Health and Education in cognisance of the government's priorities established the Quality Assurance and Standardisation Section under the new Health Care Division, as part of the overall restructuring exercise of the government machinery. The Division itself started functioning in the early months of 2001. The QA and S program under the Division will initiate a process of review and analysis of the status of our services and try to generate a series of activities leading to the development and implementation of a national guide-lines to guide service delivery in all the health care centres. II. Situation Analysis: a) Current Situation Assessment
The Ministry and the Health Department deliberate opportune initiatives that the Royal Government's 9th Five Year Plan includes quality assurance and standardisation (QA&S), consolidation, decentralisation, community involvement and sustainability as the cornerstones of the Plan. With the establishment of this programme, the emphasis is to improve the quality of services and further consolidate the infrastructure. b) Situation Assessment at the end of the Ninth Plan
By the end of the 9th Five Year Plan, there will be a Nation-wide Quality Assurance System having clear policies with authorised and participatory leadership, and indicators that are practical and realistic. There will be wide spread awareness in the community of the need for quality in health services and all health personnel will be aware of and feel the need for quality assurance as reflected in their attitude and behaviour. III. Programme objectives:
1. To establish structures and processes in the ministry of health to ensure continuous improvement in the quality of health cares and appropriate development and use of health technologies
2. To establish a Quality Assurance and Standardisation (QA&S) organisation and system.
3. To plan QA&S outputs and activities to be implemented in the 9th FYP (2002-2007)
IV. Strategies
1. A detailed Program Policy Strategy developed and approved 2. Review and analyse the service/supply status in all the Health care centres. 3. QA workshop for different categories of health personnel in all the districts 4. QA guidelines available in all health care centres 5. Conduct and coordinate regular QA supportive supervisory visits 6. Insititute QA concept in pre service training. 7. QA & S well established in all the health care centres.
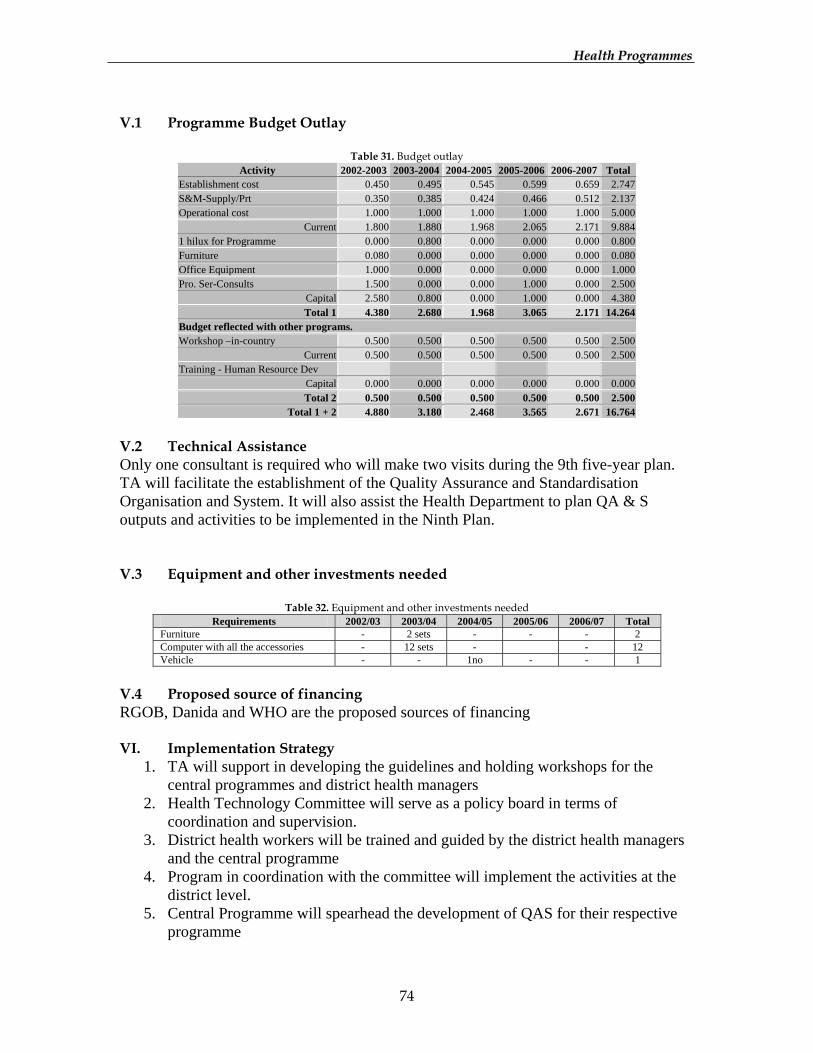
HHeeaalltthh PPrrooggrraammmmeess
74
V.1 Programme Budget Outlay
Table 31. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.450 0.495 0.545 0.599 0.659 2.747 S&M-Supply/Prt 0.350 0.385 0.424 0.466 0.512 2.137 Operational cost 1.000 1.000 1.000 1.000 1.000 5.000
Current 1.800 1.880 1.968 2.065 2.171 9.884 1 hilux for Programme 0.000 0.800 0.000 0.000 0.000 0.800 Furniture 0.080 0.000 0.000 0.000 0.000 0.080 Office Equipment 1.000 0.000 0.000 0.000 0.000 1.000 Pro. Ser-Consults 1.500 0.000 0.000 1.000 0.000 2.500
Capital 2.580 0.800 0.000 1.000 0.000 4.380 Total 1 4.380 2.680 1.968 3.065 2.171 14.264
Budget reflected with other programs. Workshop –in-country 0.500 0.500 0.500 0.500 0.500 2.500
Current 0.500 0.500 0.500 0.500 0.500 2.500 Training - Human Resource Dev
Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.500 0.500 0.500 0.500 0.500 2.500
Total 1 + 2 4.880 3.180 2.468 3.565 2.671 16.764
V.2 Technical Assistance Only one consultant is required who will make two visits during the 9th five-year plan. TA will facilitate the establishment of the Quality Assurance and Standardisation Organisation and System. It will also assist the Health Department to plan QA & S outputs and activities to be implemented in the Ninth Plan. V.3 Equipment and other investments needed
Table 32. Equipment and other investments needed Requirements 2002/03 2003/04 2004/05 2005/06 2006/07 Total
Furniture - 2 sets - - - 2 Computer with all the accessories - 12 sets - - 12 Vehicle - - 1no - - 1
V.4 Proposed source of financing RGOB, Danida and WHO are the proposed sources of financing VI. Implementation Strategy
1. TA will support in developing the guidelines and holding workshops for the central programmes and district health managers
2. Health Technology Committee will serve as a policy board in terms of coordination and supervision.
3. District health workers will be trained and guided by the district health managers and the central programme
4. Program in coordination with the committee will implement the activities at the district level.
5. Central Programme will spearhead the development of QAS for their respective programme

HHeeaalltthh PPrrooggrraammmmeess
75
VII. Monitoring and Evaluation Mechanism
1. Periodic supervisory visits by the programme and the committee 2. Monitoring and Evaluation quarterly 3. 3. Regular information feedback through monthly reporting system
HHeeaalltthh PPrrooggrraammmmeess
76
CONTINUING EDUCATION PROGRAMME I. Introduction: The Health Department initiated a Training Section under the Human Resource Unit with the responsibility to plan and execute a needs assessment, co-ordinate and package all training activities and to institute a proper evaluation mechanism. With the institution of the restructuring exercise in 2000, a continuing Education Section has been established under the Health Care Division. It is also forecasted that that when the Ministry of Health is established in 2002, the Department of Medical Education will be responsible for such activities. These are landmark developments for continuing education programme for the health services and therefore it is important for the Health Department to clearly understand the needs and project a strategy for developing an effective programme right now. II. Situation Analysis a) Current Situation Assessment
The form of Continuing Education as implemented till now is mainly through workshops, seminars, meetings, courses, and study tours, supervisory visits and through written materials. With this diversity of approach it is not surprising that the effectiveness and outlook for continuing education should be variable. It is now important for the Health Department to design our own system, by taking into account the way in which our Health Care is organised, the local culture and economic situation, the demand for continuing education and the constraints and resources available. This becomes even more critical with the focus on quality assurance in service delivery in the 9th plan and onwards. b) Situation Assessment at the end of the Ninth Plan
• By the end of the 9th FYP, the Continuing Education System will be widely developed in the country.
• The health workers will have improved new skills and competence in health needs and health care policies.
• A continuing education management structure established in the centre with close linkage with RIHS, ITMS and the Referral Hospitals.
• A Training master plan with a systematic approach for training needs assessment, training standardisation and evaluation institutionalised.
III. Programme/Policy objectives To develop a strategic continuing education system for that is responsive to the local needs and changing health care technology.
1. Coordinate all human resource development 2. Under take TNA and prioritise continuing education needs
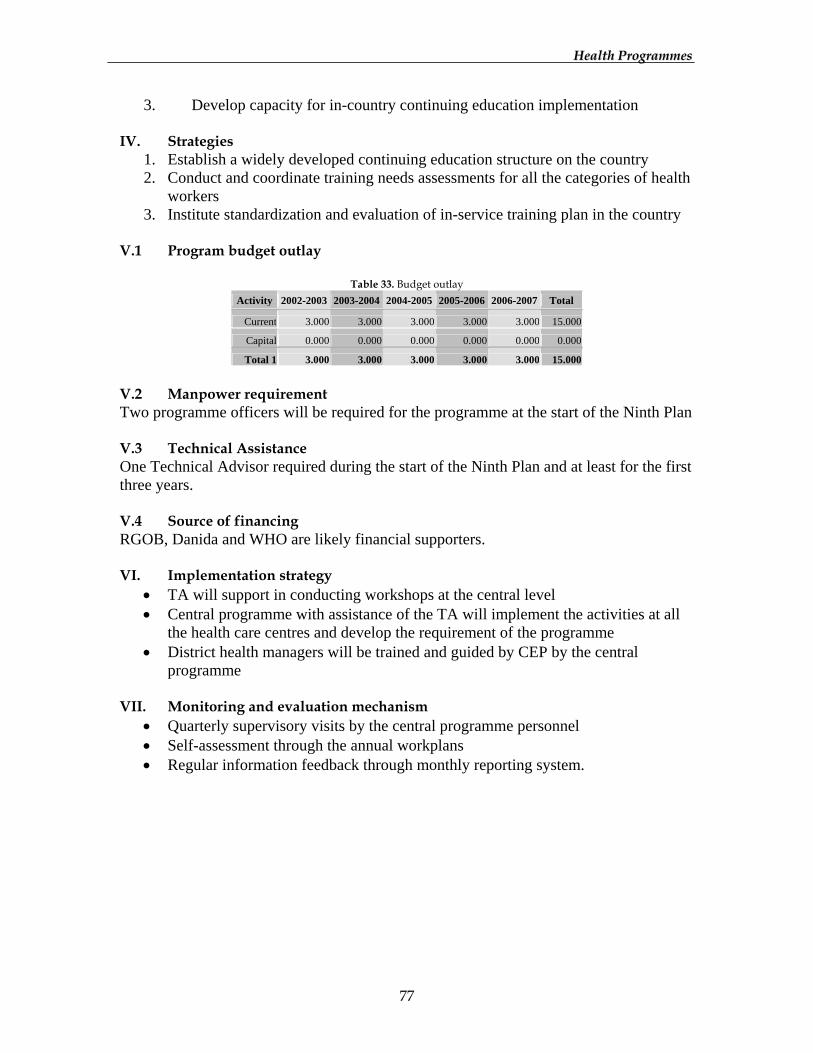
HHeeaalltthh PPrrooggrraammmmeess
77
3. Develop capacity for in-country continuing education implementation IV. Strategies
1. Establish a widely developed continuing education structure on the country 2. Conduct and coordinate training needs assessments for all the categories of health
workers 3. Institute standardization and evaluation of in-service training plan in the country
V.1 Program budget outlay
Table 33. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Current 3.000 3.000 3.000 3.000 3.000 15.000
Capital 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 3.000 3.000 3.000 3.000 3.000 15.000
V.2 Manpower requirement Two programme officers will be required for the programme at the start of the Ninth Plan V.3 Technical Assistance One Technical Advisor required during the start of the Ninth Plan and at least for the first three years. V.4 Source of financing RGOB, Danida and WHO are likely financial supporters. VI. Implementation strategy
• TA will support in conducting workshops at the central level • Central programme with assistance of the TA will implement the activities at all
the health care centres and develop the requirement of the programme • District health managers will be trained and guided by CEP by the central
programme VII. Monitoring and evaluation mechanism
• Quarterly supervisory visits by the central programme personnel • Self-assessment through the annual workplans • Regular information feedback through monthly reporting system.
HHeeaalltthh PPrrooggrraammmmeess
78
INFORMATION, EDUCATION & COMMUNICATION FOR HEALTH I. Introduction Information, Education and Communication for Health (IECH) Division was established in 1991 as a means to further strengthen Primary Health Care in the Kingdom through Danish Assistance under HSSP I. Impressive achievements have been made since its establishment. The capacity of the Division both in terms of physical and human resource in the area of material development has been strengthened. II. Situation analysis a) Current Situation Assessment
Based on the findings of IECH Impact study carried out in 2001, the Knowledge, Practice and Media Preference status stand as follows:
a. Knowledge on Diseases: Percent of people that are aware and known at least about the major causes of some diseases; i) 71% in ARI, ii) 36 in TB, iii) 72% in CDD, iv) 71% in STD/AIDS, v) 26% in Malaria, vi) 47% in Skin Infections, vii) 43% in Eye Infections, viii) 29% in Ear Infections
b. Health Practices:
i. 45% brush their teeth daily ii. 98% wash their hands before eating
iii. 36% wash their hands before handling food iv. 10% wash their hands after defecation v. 79% take bath atleast once a week
vi. 90% use soap for bathing vii. 95% use soap for washing hands
viii. 40% chew doma with 17% chewing daily ix. 8% use tobacco for either chewing or sniffing x. 1% smoke either bidi or cigarette
xi. 45% drink alcohol with 31% drinking more than a bottle per week xii. 91% eat fruits and green leafy vegetables often
xiii. 73% feed colostrum to the baby xiv. 96% use iodised salt xv. 42% receive/give special diet to pregnant women
xvi. 87% of household has a Kitchen Garden xvii. 64% of household has some form of drainage system
xviii. 79% of household had garbage pit xix. 66% of household keep animals away from the house xx. 74% of household has access to tap water
xxi. 95% of household has a latrine installed
HHeeaalltthh PPrrooggrraammmmeess
79
c. Media Preference:
i. 67% listen to Radio ii. 98.85% of Radio listener listen to BBS iii. 34.2% of BBS listener generally listen to health information iv. 15% watch TV v. 15% read Newspaper
4) Recall of IECH materials
i. 71% for Calendar ii. 65% for Posters iii. 45% for AV iv. 14% for pamphlets/leaflets v. 13% for flip chart vi. 10% for Banners
The areas that need further strengthening and improvement as identified through reviews and technical assistance are as follows;
1. The capacity of the Division is limited to undertake well-planned strategic approach due to lack of staff with effective communication and technical background. Unless the Division is able to recruit additional professional staff, the quality and effectiveness would be always be at stake.
2. Coordination with public health programmes is weak. 3. Adoption of strategies because of all kinds of demands placed on the Division is
proving to be a less effective approach in bringing desired behavioural changes. There is a need to identify priority areas of health to focus and undertake a campaign approach.
4. Research, Monitoring and Evaluation remains an area of weakness due to lack of adequate capacity within the Division. This area needs to be internalised within the Division for better understanding of health issues and for effective planning of IECH activities.
b) Situation Assessment at the end of the Ninth Plan
By the end of the 9FYP, the IECH Division will be a fully developed institution with: a. Professional capacity, to plan and carry out IEC activities. b. Tech. capacity to design and produce quality IEC materials.
III. Programme/Policy objectives
1. To increase the level of health awareness and knowledge to the community to induce desired behavioural changes.
2. To improve the quality and effectiveness of IEC services provided. 3. To support the programmes and districts in formulating IEC strategies and
production of IEC materials. 4. To strengthen advocacy efforts at all levels for priority health issues.
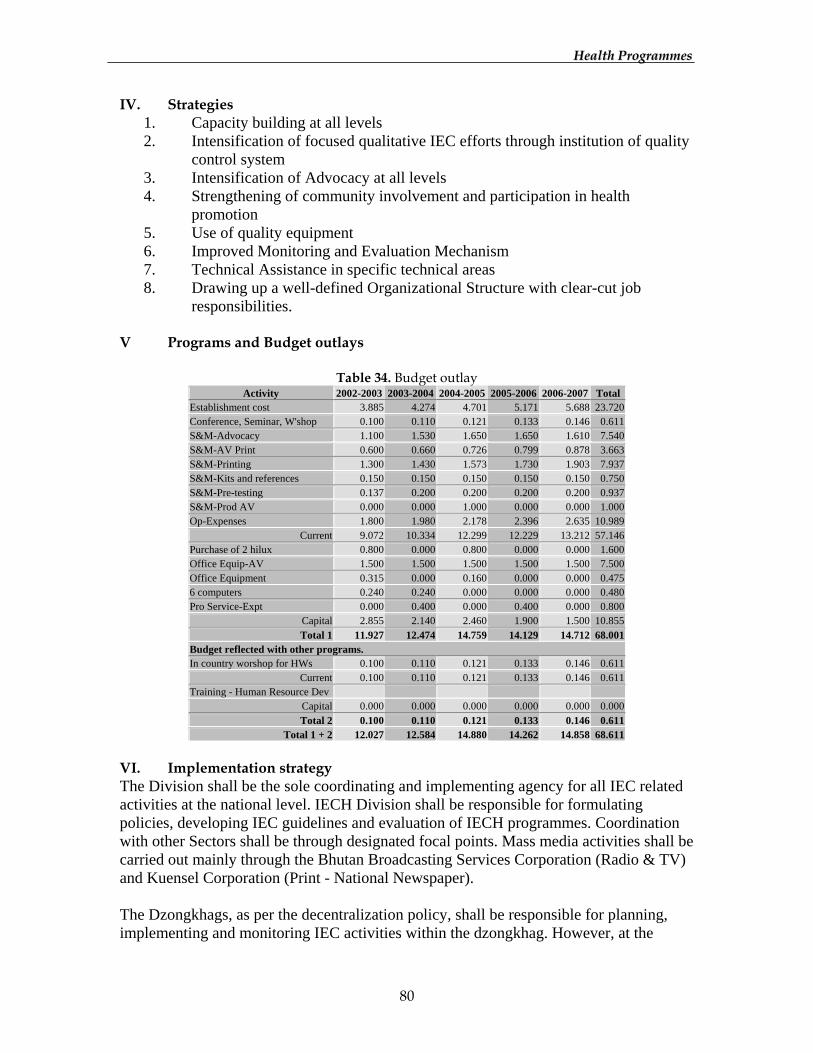
HHeeaalltthh PPrrooggrraammmmeess
80
IV. Strategies 1. Capacity building at all levels 2. Intensification of focused qualitative IEC efforts through institution of quality
control system 3. Intensification of Advocacy at all levels 4. Strengthening of community involvement and participation in health
promotion 5. Use of quality equipment 6. Improved Monitoring and Evaluation Mechanism 7. Technical Assistance in specific technical areas 8. Drawing up a well-defined Organizational Structure with clear-cut job
responsibilities. V Programs and Budget outlays
Table 34. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 3.885 4.274 4.701 5.171 5.688 23.720 Conference, Seminar, W'shop 0.100 0.110 0.121 0.133 0.146 0.611 S&M-Advocacy 1.100 1.530 1.650 1.650 1.610 7.540 S&M-AV Print 0.600 0.660 0.726 0.799 0.878 3.663 S&M-Printing 1.300 1.430 1.573 1.730 1.903 7.937 S&M-Kits and references 0.150 0.150 0.150 0.150 0.150 0.750 S&M-Pre-testing 0.137 0.200 0.200 0.200 0.200 0.937 S&M-Prod AV 0.000 0.000 1.000 0.000 0.000 1.000 Op-Expenses 1.800 1.980 2.178 2.396 2.635 10.989
Current 9.072 10.334 12.299 12.229 13.212 57.146 Purchase of 2 hilux 0.800 0.000 0.800 0.000 0.000 1.600 Office Equip-AV 1.500 1.500 1.500 1.500 1.500 7.500 Office Equipment 0.315 0.000 0.160 0.000 0.000 0.475 6 computers 0.240 0.240 0.000 0.000 0.000 0.480 Pro Service-Expt 0.000 0.400 0.000 0.400 0.000 0.800
Capital 2.855 2.140 2.460 1.900 1.500 10.855 Total 1 11.927 12.474 14.759 14.129 14.712 68.001
Budget reflected with other programs. In country worshop for HWs 0.100 0.110 0.121 0.133 0.146 0.611
Current 0.100 0.110 0.121 0.133 0.146 0.611 Training - Human Resource Dev
Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.100 0.110 0.121 0.133 0.146 0.611
Total 1 + 2 12.027 12.584 14.880 14.262 14.858 68.611 VI. Implementation strategy The Division shall be the sole coordinating and implementing agency for all IEC related activities at the national level. IECH Division shall be responsible for formulating policies, developing IEC guidelines and evaluation of IECH programmes. Coordination with other Sectors shall be through designated focal points. Mass media activities shall be carried out mainly through the Bhutan Broadcasting Services Corporation (Radio & TV) and Kuensel Corporation (Print - National Newspaper). The Dzongkhags, as per the decentralization policy, shall be responsible for planning, implementing and monitoring IEC activities within the dzongkhag. However, at the
HHeeaalltthh PPrrooggrraammmmeess
81
community level, BHU shall be responsible for coordination and conduct of IEC activities. VII. Monitoring & evaluation Monitoring shall be carried out in line with the guidelines issued by the Planning and Policy Division of the Ministry. Within the Division, it will be done through the regular meetings and reports submitted. Programme Evaluation shall be carried out towards the end of the plan period.
HHeeaalltthh PPrrooggrraammmmeess
82
HEALTH TELEMATICS PROJECT I. Introduction To overcome the remoteness of various BHUs due to the harsh topographical nature, a radiotelephonic linkage was started in the Seventh Plan with the help of WHO and later with Danida. Such linkage had been of immense benefit in improving the quality of medical consultations and also improving the referrals from the BHUs. The then Director General of WHO and Representative of WHO to Bhutan received an audience from His Majesty the King in 1997, and it was then that the issue of possibility of introducing telematics as a cost effective alternative to ensure effective health care delivery service for the scattered population of Bhutan was raised by His Majesty himself. Since then with the support of WHO, various technical assistance was fielded in to explore the avenues for such an alternative. The tele-linkage between JDWNR Hospital and Mongar Regional Referral Hospital is now established and functioning fully through lease line Internet connections. II. Situation Analysis The human resources are chronically short in the health facilities. The Doctor to Population ration is almost 1: 5505 which by any standard is quite poor. The shortage of specialised physicians particularly poses a daunting task in the improvement of the quality of health and medical services. About 78% of the Bhutanese are within 3 hour walking distance from the nearest health facility, while the remaining groups of population have difficulty in accessing the health services due to longer distance. The low diagnostic capacity of the district hospitals has also resulted in heavy patient referrals. Further topographical difficulty involving quite a distance between the district hospitals and the bigger referral hospitals has always been one of the major obstacles in saving most of the critical lives. In addition, lack of critical amenities like road, transport facilities and telecommunication facilities particularly in the rural areas have aggravated the situation in most of the instances. In order to overcome some of the difficulties and constraints that the health sector is facing, telemedicine is looked upon as a cost effective mechanism to ensure quality health care services to the Bhutanese at large. III. Program/ Policy objectives The overall long-term objective is to improve the quality of life of the people in remote areas. Specific objectives are as follows;
1. To improve diagnostic services of district hospitals 2. To reduce patient referrals 3. To provide a forum for Continuing Medical Education (CME) in hospitals
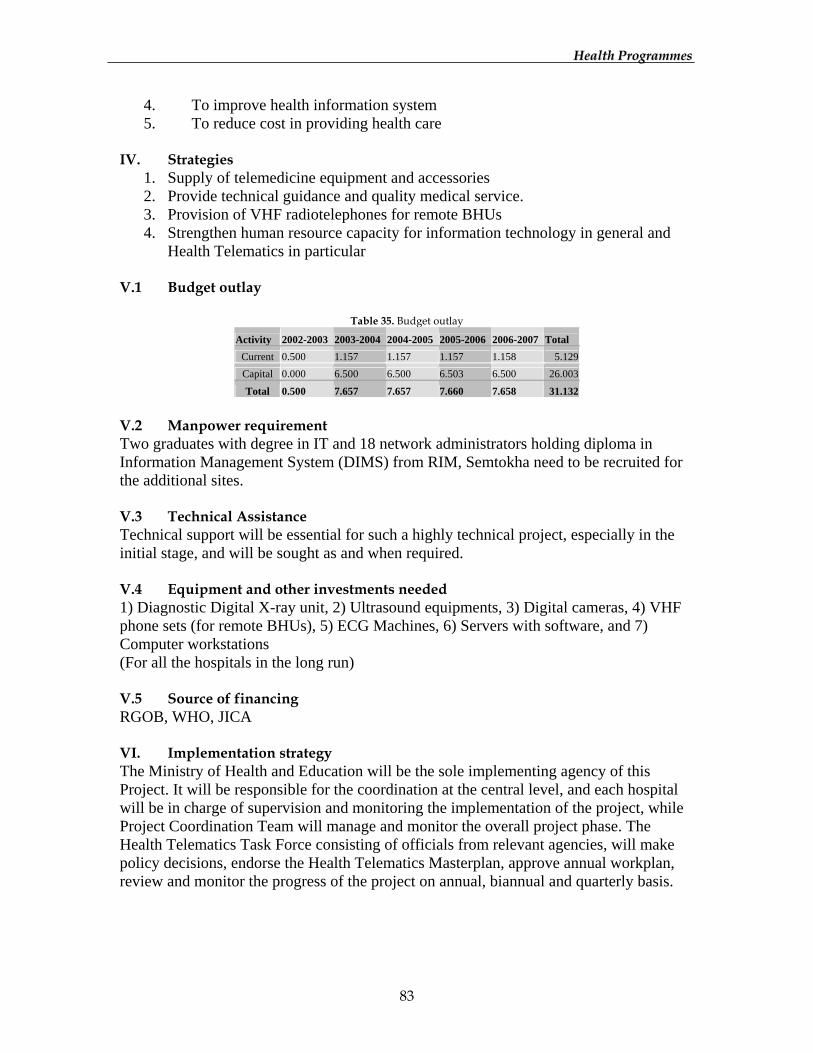
HHeeaalltthh PPrrooggrraammmmeess
83
4. To improve health information system 5. To reduce cost in providing health care
IV. Strategies
1. Supply of telemedicine equipment and accessories 2. Provide technical guidance and quality medical service. 3. Provision of VHF radiotelephones for remote BHUs 4. Strengthen human resource capacity for information technology in general and
Health Telematics in particular V.1 Budget outlay
Table 35. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Current 0.500 1.157 1.157 1.157 1.158 5.129 Capital 0.000 6.500 6.500 6.503 6.500 26.003
Total 0.500 7.657 7.657 7.660 7.658 31.132
V.2 Manpower requirement Two graduates with degree in IT and 18 network administrators holding diploma in Information Management System (DIMS) from RIM, Semtokha need to be recruited for the additional sites. V.3 Technical Assistance Technical support will be essential for such a highly technical project, especially in the initial stage, and will be sought as and when required. V.4 Equipment and other investments needed 1) Diagnostic Digital X-ray unit, 2) Ultrasound equipments, 3) Digital cameras, 4) VHF phone sets (for remote BHUs), 5) ECG Machines, 6) Servers with software, and 7) Computer workstations (For all the hospitals in the long run) V.5 Source of financing RGOB, WHO, JICA VI. Implementation strategy The Ministry of Health and Education will be the sole implementing agency of this Project. It will be responsible for the coordination at the central level, and each hospital will be in charge of supervision and monitoring the implementation of the project, while Project Coordination Team will manage and monitor the overall project phase. The Health Telematics Task Force consisting of officials from relevant agencies, will make policy decisions, endorse the Health Telematics Masterplan, approve annual workplan, review and monitor the progress of the project on annual, biannual and quarterly basis.
HHeeaalltthh PPrrooggrraammmmeess
84
VII. Monitoring and evaluation mechanism 1. The project managers will report to the Project Coordinator on scheduling,
casting, testing and the overall status of the project and other issues on a scheduled weekly basis.
2. Call on meetings to resolve any issues or urgent items. 3. Timely delivery of agreed deliverables will be monitored by the Project
Coordinator and Team as per the development and implementation schedule. 4. The Task Force will assess the outcomes of the project and deliverables at the end
of the implementation and during the post implementation period.
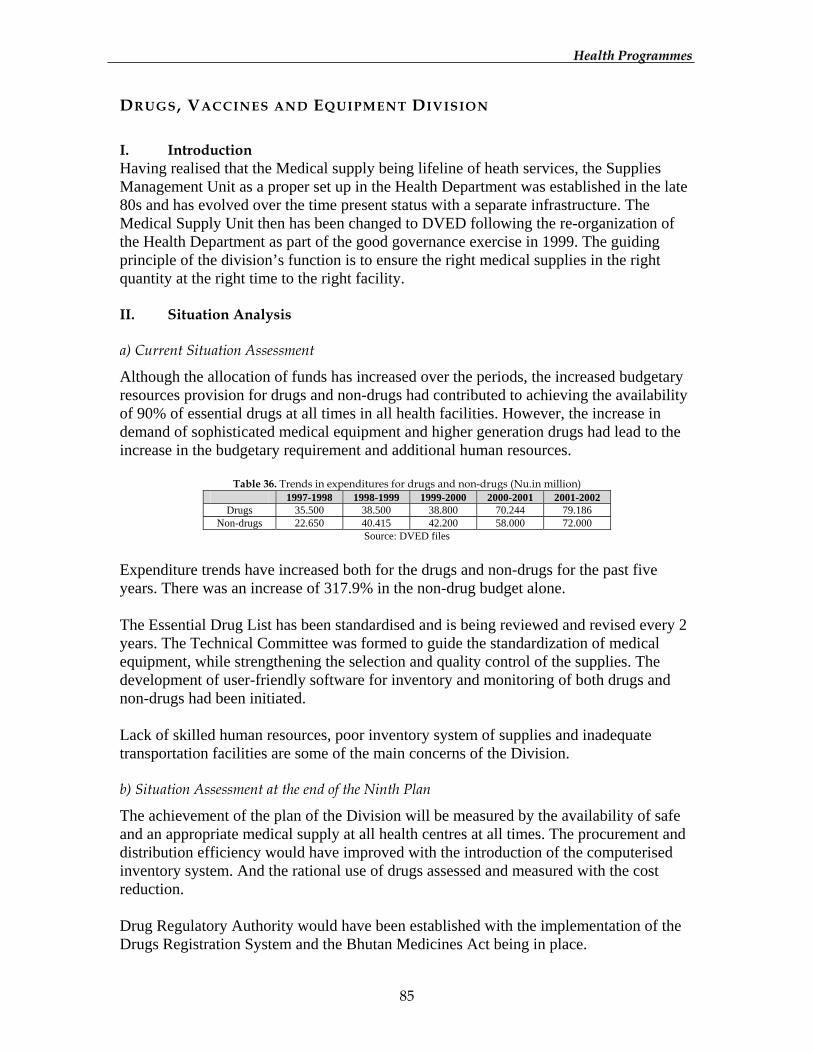
HHeeaalltthh PPrrooggrraammmmeess
85
DRUGS, VACCINES AND EQUIPMENT DIVISION I. Introduction Having realised that the Medical supply being lifeline of heath services, the Supplies Management Unit as a proper set up in the Health Department was established in the late 80s and has evolved over the time present status with a separate infrastructure. The Medical Supply Unit then has been changed to DVED following the re-organization of the Health Department as part of the good governance exercise in 1999. The guiding principle of the division’s function is to ensure the right medical supplies in the right quantity at the right time to the right facility. II. Situation Analysis a) Current Situation Assessment
Although the allocation of funds has increased over the periods, the increased budgetary resources provision for drugs and non-drugs had contributed to achieving the availability of 90% of essential drugs at all times in all health facilities. However, the increase in demand of sophisticated medical equipment and higher generation drugs had lead to the increase in the budgetary requirement and additional human resources.
Table 36. Trends in expenditures for drugs and non-drugs (Nu.in million) 1997-1998 1998-1999 1999-2000 2000-2001 2001-2002
Drugs 35.500 38.500 38.800 70.244 79.186 Non-drugs 22.650 40.415 42.200 58.000 72.000
Source: DVED files Expenditure trends have increased both for the drugs and non-drugs for the past five years. There was an increase of 317.9% in the non-drug budget alone. The Essential Drug List has been standardised and is being reviewed and revised every 2 years. The Technical Committee was formed to guide the standardization of medical equipment, while strengthening the selection and quality control of the supplies. The development of user-friendly software for inventory and monitoring of both drugs and non-drugs had been initiated. Lack of skilled human resources, poor inventory system of supplies and inadequate transportation facilities are some of the main concerns of the Division. b) Situation Assessment at the end of the Ninth Plan
The achievement of the plan of the Division will be measured by the availability of safe and an appropriate medical supply at all health centres at all times. The procurement and distribution efficiency would have improved with the introduction of the computerised inventory system. And the rational use of drugs assessed and measured with the cost reduction. Drug Regulatory Authority would have been established with the implementation of the Drugs Registration System and the Bhutan Medicines Act being in place.
HHeeaalltthh PPrrooggrraammmmeess
86
III. Programme/Policy objectives Ensuring delivery of safe, effective and quality medical supplies at all times to all health facilities is the overriding objective of the programme. Specific objectives:
1. Maintain availability of medical supplies in health facilities at 90% 2. To improve the quality of drugs and standardization of other medical supplies 3. Develop appropriate human resources for the management of medical supplies 4. Enact Bhutan Medicine Act and develop legislation for implementation 5. Promote and improve rational use of drugs
IV. Strategies 1) Maintain availability of appropriate medical supplies at 90%
While the availability of the medical supplies has improved, the selection and procurement of supplies system will be further strengthened during the 9th Plan. An appropriate mechanism for timely distribution of medical supplies will be given focus, while provision of proper storage facilities for the drugs, vaccines and equipment in all health facilities must receive equal emphasis. A monitoring mechanism will be put in place with the computerised inventory system developed and networked to the MSD and some bigger hospitals. A provision of adequate transport facilities will be endured for timely delivery of supplies. 2) Quality control of drugs and standardization of drugs and other medical supplies
In order to achieve the cost effectiveness of the supplies the quality assurance and standardization of medical supplies will be given attention. The present system of drug quality testing at the WHO collaborating drug quality control laboratories will be strengthened through development of proper guideline. As a part of quality assurance, the division will implement the Drug Registration System. This will not only ensure the quality of the drugs procured by division but also put a control over the quality of drugs procured by the private firms and further, control the counterfeit drugs. In the light of maintaining the quality of supplies, improved storage facilities will be constructed. 3) Develop appropriate Human Resources for the management of medical supplies
Adequate skilled manpower will be strengthened both at DVED and MSD to meet the growing need for competent and efficient work. Continuing Education for all categories of health workers will be continued on the good stores management and rational use of drugs. The respective relevant people will be trained in quality control, drug regulatory, drug registration and other pharmaceutical fields to equip them to establish the new activities.
HHeeaalltthh PPrrooggrraammmmeess
87
4) Enact Bhutan Medicines Act and develop legislation for implementation
Revision of draft BMA will be carried out and addressed during the National Assembly to be passed. The training of inspection, licensing will be an important area to be considered during the plan period. 5) Promote and improve rational use of drugs
Promotion of rational use of drugs by the prescriber will continue to be the focus of the plan to ensure the safe and cost effective treatment to the patients. Operational research on drug availability and drug utility will form an important activity. The hospital therapeutics will be established to strengthen the clinical excellence and provide information on risk-benefit aspects of the treatment. V.1 Programs and Budget Outlays
Table 37. Budget outlay (DVED) Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total Establishment cost 5.587 6.146 6.760 7.436 8.180 34.109Conference, Seminar, W'shop 0.124 0.136 0.150 0.150 0.150 0.710Office supplies,printg. Publications 1.808 2.008 0.000 0.000 0.421 4.237Medicines & Lab.consum/Drugs** 34.037 41.715 45.195 54.860 65.196 241.003Medicines & expandi materials** 19.153 19.977 22.324 23.250 29.809 114.513Hospi/Lab. Non-expandable equipt.** 19.471 20.485 18.828 19.530 18.886 97.200Other supplies and cons 2.100 2.210 2.331 2.464 2.611 11.716Subscriptions 0.050 0.055 0.061 0.067 0.073 0.305
Current 82.329 92.732 95.648 107.757 125.326 503.792Tools and equip 12.650 13.498 13.997 13.190 13.416 66.751Office equipment 0.130 0.000 0.100 0.100 0.000 0.3307 Computers & peripherals 0.000 0.160 0.160 0.000 0.000 0.320
Capital 12.780 13.658 14.257 13.290 13.416 67.401Total 1 95.109 106.390 109.905 121.047 138.741 571.192
Budget reflected with other programs. Medicines & Lab.consum/Drugs** 26.134 26.395 26.659 26.925 27.195 133.308Medicines & Lab.consum/Drugs** 0.670 0.677 0.683 0.690 0.697 3.417Medicines & Lab.consum/Drugs** 10.815 10.924 11.033 11.143 11.255 55.170Medicines & Lab.consum/Drugs** 0.268 0.271 0.274 0.276 0.279 1.368Medicines & Lab.consum/Drugs** 0.625 0.631 0.637 0.643 0.650 3.186Medicines & Lab.consum/Drugs** 0.292 0.295 0.298 0.301 0.304 1.490Medicines & Lab.consum/Drugs** 1.005 1.015 1.025 1.035 1.046 5.126Expendable and non expandable 41.409 41.823 42.241 42.664 43.090 211.227Expendable and non expandable 2.822 2.850 2.878 2.907 2.936 14.393Expendable and non expandable 25.025 25.275 25.528 25.783 26.041 127.652Expendable and non expandable 2.822 2.850 2.878 2.907 2.936 14.393Expendable and non expandable 0.856 0.864 0.873 0.882 0.891 4.366Expendable and non expandable 0.622 0.628 0.634 0.640 0.647 3.171Expendable and non expandable 0.622 0.628 0.634 0.640 0.647 3.171Workshop -incountry 0.500 0.500 0.500 0.500 0.500 2.500
Current 114.487 115.626 116.775 117.936 119.114 583.938Training - Human Resource Dev
Capital 0.000 0.000 0.000 0.000 0.000 0.000Total 2 114.487 115.626 116.775 117.936 119.114 583.938
Total 1 + 2 209.596 222.016 226.680 238.983 257.855 1155.130

HHeeaalltthh PPrrooggrraammmmeess
88
Table 38. Budget outlay (HERM) Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 0.880 0.968 1.065 1.171 1.288 5.372 Conference, Seminar, W'shop 0.100 0.000 0.100 0.150 0.090 0.440 Operational cost 0.600 0.800 0.800 0.800 0.721 3.721
Current 1.580 1.768 1.965 2.121 2.099 9.533 General tools, instruments 0.550 0.605 0.666 0.732 2.416 4.969 1 hilux for Programme 0.000 0.800 0.000 0.000 0.000 0.800 2 Computers & peripherals 0.000 0.160 0.000 0.000 0.000 0.160 Professional services 1.200 1.320 1.452 1.597 1.757 7.326
Capital 1.750 2.885 2.118 2.329 4.172 13.255 Total 1 3.330 4.653 4.083 4.451 6.272 22.788
Budget reflected with other programs. W'shop -incountry 0.500 0.500 0.500 0.500 0.500 2.500
Current 0.500 0.500 0.500 0.500 0.500 2.500 Training - Human Resource Dev
Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.500 0.500 0.500 0.500 0.500 2.500
Total 1 + 2 3.830 5.153 4.583 4.951 6.772 25.288 V.2 Manpower requirement
Table 39. Manpower requirement
S/No Title Qualification Requirements 1 Procurement officer Master degree/Graduate 3 2 Asstt. Procurement Officer Diploma/Sr.Pharm.tech 5 3 Pharmacist B.Pharm/Master degree 11 4 Pharm Technicians Certificate/Diploma 39 5 Computer programmer Certificate/Diploma 8
6 Store Officer/Incharges Diploma pharm/technicians 10 7 Drug Controller/Dy. DC Master Degree/PG Diploma 2 8 Drug Inspector Diploma Pharm 7 9 Drug analyst/Asstt. DA B.Pharm/Graduate 3+5 10 Adm. Officer Graduate 1 11 Bio-medical engineer/asstt. Graduate/ PG Diploma 1+2 12 Bio-medical section officer Diploma RBP 5 13 Bio-medical techns RTI 15 14 EPI technicians RTI 2 15 Supporting staff 13
V.3 Technical Assistance TA is required in the following activities;
1. Development of inventory software and computer programmes 2. Drug regulation and legislation 3. Drug registration and licensing 4. Quality control laboratory 5. Essential Drugs programme evaluation
V.4 Equipment and other investment needed
1. Advanced and sophisticated hospital equipment for all departments 2. Office equipment-computers and photocopiers 3. Audio-visual teaching aids 4. Vehicles for logistics and medical transportation, storage equipment
HHeeaalltthh PPrrooggrraammmmeess
89
V.5 Proposed source of financing RGOB, UNICEF, WHO and Danida are the main financial supporters for the Ninth Plan. Apart from this, Health Trust Fund will support for Essential Drugs and Vaccines. VI. Implementation Strategy The DVED will implement procurement of Drugs and Medical supplies centrally through the globally tendering system. The National Tender Committee, National Drug Committee and the National Selection Committee will guide the selection, procurement and distribution of medical supplies. Computerised inventory system and the 6 monthly drug report and annual indent of the medical supplies will be the most important tools for monitoring. The division with the existing technical expertise will provide training of the in-service of the health workers and consultant will be recruited as and when necessary. Transport will be improved by providing additional fleet of vehicles so that the availability of medical supplies in the country can be sustained. VII. Monitoring and evaluation mechanism
1. Continue the six monthly drugs report to give a feedback on the availability of the drugs and the annual requirements and to ensure timely mobilization of supplies
2. Strengthen the prescription survey report which will give an indication of the drug utilization status and the division can give necessary interventions if needed.
3. Conduct supervisory visit from the division to the health centres. 4. Collect the samples for random quality resting for quality assurance of supplies 5. Develop computerised inventory of supplies to provide information on status of
supply.
HHeeaalltthh PPrrooggrraammmmeess
90
ROYAL INSTITUTE OF HEALTH SCIENCES I. Introduction The Royal Institute of Health Sciences has been functioning for the last 26 years with the main responsibility to develop human resources for health in different disciples to provide health care services for the people of Bhutan. There are 9 different training Certificate programmes of 2 years duration for Class X pass and a 3 years Diploma in General Nursing and Midwifery for Class XII passed candidates. II. Situation Analysis a) Current Situation Assessment
As of June 2002, the Institute has trained more than 1400 health workers. In addition to the regular pre-service training programmes, it is also responsible to organize and conduct in-service training for the health workers and nurses. There is still shortage of health workers in almost all categories due to expanding infrastructure and services at all levels. To improve the quality of health care would entail an increased intake of trainees in some disciplines during the 9FYP and introduction of some new disciplines as per the need of some clinical departments in the JDWNRH. Faculty development both in terms of quantity and quality would be the priority un order to improve the current training programmes and in preparation for up-gradation into College of Nursing and Health Sciences. At the same time, the existing infrastructure needs to be maintained and upgraded. b) Situation Assessment at the end of the Ninth Plan
It is envision to train about 500 new health workers in different disciplines, and human resource situation in the Health Sector would have greatly improved. The quality of training programs would have improved through trainings and enhancement of qualification of the existing faculty and recruitment of additional qualified trainers. 30 senior GNMs would have completed Bachelor of Nursing conversion course in collaboration with La Trope University of Australia. III. Policy/programme objectives The main objectives for the RIHS will be to strengthen and improve the quality of training programs for all the categories of health workers, to introduce degree program in Nursing and other relevant technical support services. The Institute will also focus more on the continuing education and other in-service training programs to update the health workers and improve the quality of health care services. IV. Strategies
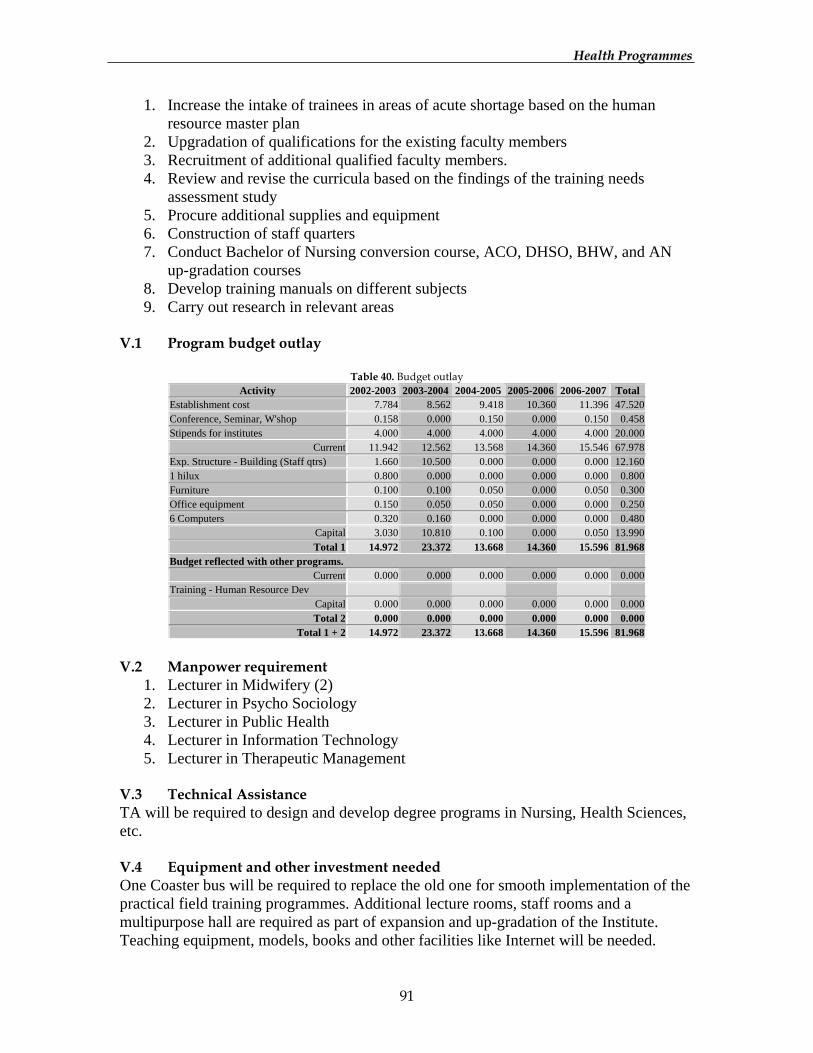
HHeeaalltthh PPrrooggrraammmmeess
91
1. Increase the intake of trainees in areas of acute shortage based on the human resource master plan
2. Upgradation of qualifications for the existing faculty members 3. Recruitment of additional qualified faculty members. 4. Review and revise the curricula based on the findings of the training needs
assessment study 5. Procure additional supplies and equipment 6. Construction of staff quarters 7. Conduct Bachelor of Nursing conversion course, ACO, DHSO, BHW, and AN
up-gradation courses 8. Develop training manuals on different subjects 9. Carry out research in relevant areas
V.1 Program budget outlay
Table 40. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 7.784 8.562 9.418 10.360 11.396 47.520 Conference, Seminar, W'shop 0.158 0.000 0.150 0.000 0.150 0.458 Stipends for institutes 4.000 4.000 4.000 4.000 4.000 20.000
Current 11.942 12.562 13.568 14.360 15.546 67.978 Exp. Structure - Building (Staff qtrs) 1.660 10.500 0.000 0.000 0.000 12.160 1 hilux 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.100 0.100 0.050 0.000 0.050 0.300 Office equipment 0.150 0.050 0.050 0.000 0.000 0.250 6 Computers 0.320 0.160 0.000 0.000 0.000 0.480
Capital 3.030 10.810 0.100 0.000 0.050 13.990 Total 1 14.972 23.372 13.668 14.360 15.596 81.968
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 14.972 23.372 13.668 14.360 15.596 81.968
V.2 Manpower requirement
1. Lecturer in Midwifery (2) 2. Lecturer in Psycho Sociology 3. Lecturer in Public Health 4. Lecturer in Information Technology 5. Lecturer in Therapeutic Management
V.3 Technical Assistance TA will be required to design and develop degree programs in Nursing, Health Sciences, etc. V.4 Equipment and other investment needed One Coaster bus will be required to replace the old one for smooth implementation of the practical field training programmes. Additional lecture rooms, staff rooms and a multipurpose hall are required as part of expansion and up-gradation of the Institute. Teaching equipment, models, books and other facilities like Internet will be needed.
HHeeaalltthh PPrrooggrraammmmeess
92
V.5 Source of financing RGOB, Danida, WHO and Unicef are the potential financial supporters of the institute programs. VI. Implementation strategy The responsibilities for upgrading the qualifications for the existing faculty members and recruitment of additional faculty members and staff support lie with the Department of Health and RCSC. Some of the strategies for strengthening the training programs will be as follows;
• Revision of curriculum based on the actual training needs • Enhancing the knowledge and skills of the faculty members though in-service
trainings • Ensuring adequate supplies and equipment required to implement the training
programmes and strengthening the practical field training programs for the health workers
The RIHS will also be responsible for conducting in-service and up-gradation training programs for the health workers as a part of their continuing education. The Institute will work in collaboration with the Department and other agencies for proper implementation of its programs. VII. Monitoring and Evaluation mechanism The Department of Health Services will monitor all the programme activities carried out by the RIHS through regular meetings, progress reports and visits. At the Institute level, activities will be reviewed on an annual basis and the review published in the form of an Annual Report for the consumption by all stakeholders of the Institute.
HHeeaalltthh PPrrooggrraammmmeess
93
NATIONAL INSTITUTE OF TRADITIONAL MEDICINE I. Introduction Following the endorsement of the 32nd National Assembly in 1968, a Training Unit was established at Dechenchholing. In 1978, the training for the first batch of 15 drungtshos was started with the establishment of National Institute of Traditional Medicine that was expanding the horizons of Indigenous facilities and services in Bhutan. Presently, the following units function at the NITM: Administrative Unit, Indigenous Unit, Training Institute, Pharmaceutical Manufacturing Unit, Research Unit, and Project Management Unit. And there are presently 27 staff members manning the NITM at Thimphu. II. Situation Analysis a) Current Situation Assessment
The Institute was established with aims to develop human resource required to deliver Traditional Medicine Services to the citizens of Bhutan. This is the first National Institute that trains degree level of six years course to become drungtshos equivalent to compounders. The institute is totally run by Bhutanese faculties and has its own capacity of producing human resources, thus promoting self-reliance. Till date it has produced enough drungtshos and sMenpas to reach traditional services to all the corners of the country. b) Situation Assessment at the end of the Ninth Plan
The Institute that has the capacity to provide internationally recognised higher level of education and training in traditional medicine would be further strengthened in order to meet the human resources requirement of the country. III. Programme/Policy Objectives Expansion of traditional medicine services through the production of quality and adequate human resources and promote self-reliance and self-sufficiency in technical manpower.
• Enhancement of technical capability of faculty members and capacity building • Create conducive environment by acquiring appropriate infrastructures • Up-gradation of training facilities and curricula • Introduction of higher level of training (post graduate) and specialised course in
TM IV. Strategies
1. Human Resource Development and capacity building 2. Construction of appropriate infrastructure 3. Acquisition of technology and technological standardization 4. Initiation of postgraduate courses and specialization
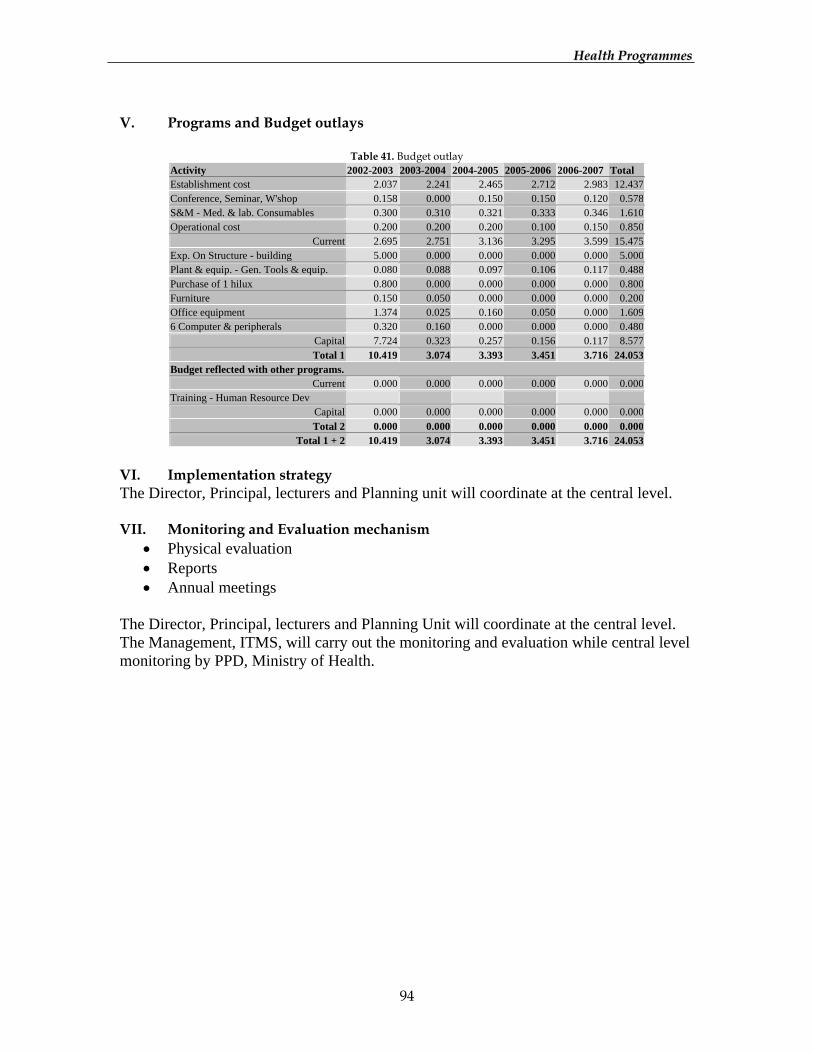
HHeeaalltthh PPrrooggrraammmmeess
94
V. Programs and Budget outlays
Table 41. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total Establishment cost 2.037 2.241 2.465 2.712 2.983 12.437 Conference, Seminar, W'shop 0.158 0.000 0.150 0.150 0.120 0.578 S&M - Med. & lab. Consumables 0.300 0.310 0.321 0.333 0.346 1.610 Operational cost 0.200 0.200 0.200 0.100 0.150 0.850
Current 2.695 2.751 3.136 3.295 3.599 15.475 Exp. On Structure - building 5.000 0.000 0.000 0.000 0.000 5.000 Plant & equip. - Gen. Tools & equip. 0.080 0.088 0.097 0.106 0.117 0.488 Purchase of 1 hilux 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.150 0.050 0.000 0.000 0.000 0.200 Office equipment 1.374 0.025 0.160 0.050 0.000 1.609 6 Computer & peripherals 0.320 0.160 0.000 0.000 0.000 0.480
Capital 7.724 0.323 0.257 0.156 0.117 8.577 Total 1 10.419 3.074 3.393 3.451 3.716 24.053
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 10.419 3.074 3.393 3.451 3.716 24.053
VI. Implementation strategy The Director, Principal, lecturers and Planning unit will coordinate at the central level. VII. Monitoring and Evaluation mechanism
• Physical evaluation • Reports • Annual meetings
The Director, Principal, lecturers and Planning Unit will coordinate at the central level. The Management, ITMS, will carry out the monitoring and evaluation while central level monitoring by PPD, Ministry of Health.
HHeeaalltthh PPrrooggrraammmmeess
95
NATIONAL INDIGENOUS HOSPITAL I. Introduction Traditional Medicine practices exited in Bhutan since 1616 A.D., but the full-fledged system was formally established only in 1968 by Late His Majesty the King Jigme Dorji Wangchuk. II. Situation Analysis a) Current Situation Assessment
The National Indigenous Hospital was established in 1968 with aims to provide traditional medicinal services to the citizens of Bhutan. There are now 1 Indigenous Hospital at Thimphu and 18 Indigenous Units spread across the country. The Hospital functions as a unit under the umbrella of Indigenous Traditional Medicine Services. b) Situation Assessment at the end of the Ninth Plan
A well integrated traditional medicinal services with a forward looking management system, delivering quality services. III. Programme/Policy objectives
1. Improve quality of traditional medical services 2. Strengthen the integration with modern Health 3. Strengthen the managerial and technical capacity at various levels 4. Consolidate existing range of services and initiate new range of services 5. Protection and preservation of traditional knowledge and traditional medical
intervention 6. Consolidation of infrastructure and acquire appropriate technology
IV. Strategies
1. Human Resource Development and capacity enhancement 2. Recruitment of appropriate manpower 3. Short and Long Term Training 4. Integration and institutional linkages 5. Construction of appropriate infrastructure 6. Construction of therapy section 7. Construction of staff quarters 8. Acquisition of technology and technological standardization
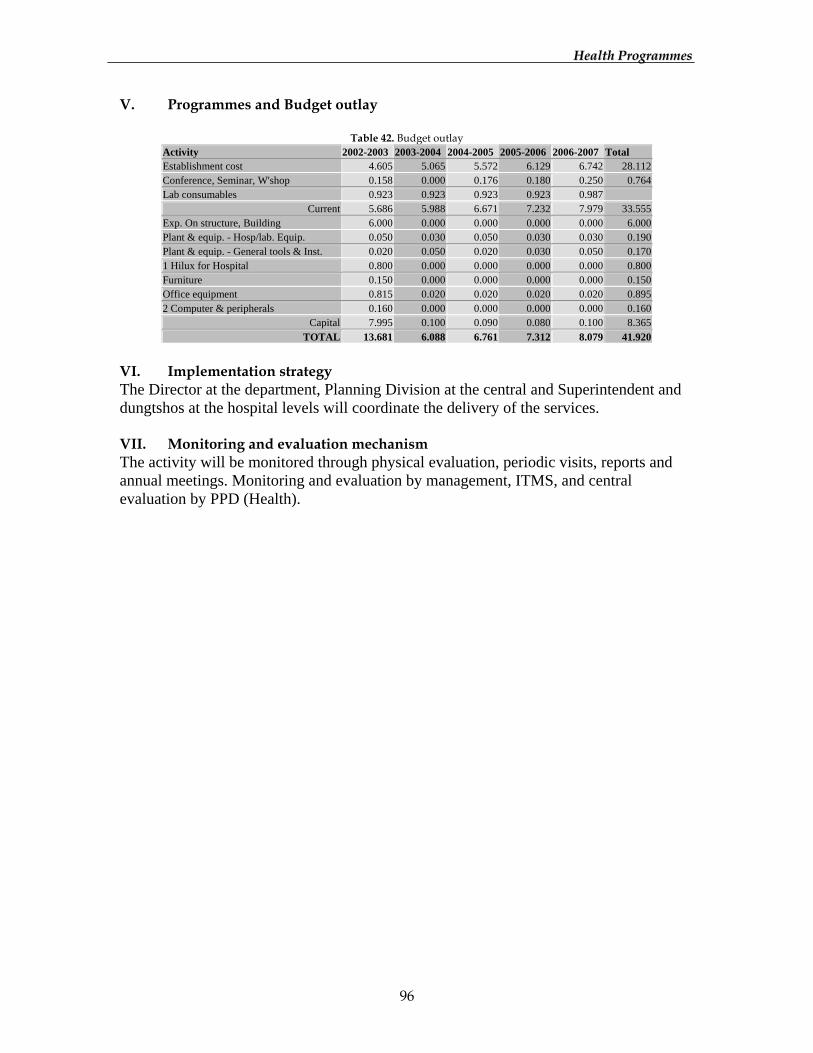
HHeeaalltthh PPrrooggrraammmmeess
96
V. Programmes and Budget outlay
Table 42. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total Establishment cost 4.605 5.065 5.572 6.129 6.742 28.112 Conference, Seminar, W'shop 0.158 0.000 0.176 0.180 0.250 0.764 Lab consumables 0.923 0.923 0.923 0.923 0.987
Current 5.686 5.988 6.671 7.232 7.979 33.555 Exp. On structure, Building 6.000 0.000 0.000 0.000 0.000 6.000 Plant & equip. - Hosp/lab. Equip. 0.050 0.030 0.050 0.030 0.030 0.190 Plant & equip. - General tools & Inst. 0.020 0.050 0.020 0.030 0.050 0.170 1 Hilux for Hospital 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.150 0.000 0.000 0.000 0.000 0.150 Office equipment 0.815 0.020 0.020 0.020 0.020 0.895 2 Computer & peripherals 0.160 0.000 0.000 0.000 0.000 0.160
Capital 7.995 0.100 0.090 0.080 0.100 8.365 TOTAL 13.681 6.088 6.761 7.312 8.079 41.920
VI. Implementation strategy The Director at the department, Planning Division at the central and Superintendent and dungtshos at the hospital levels will coordinate the delivery of the services. VII. Monitoring and evaluation mechanism The activity will be monitored through physical evaluation, periodic visits, reports and annual meetings. Monitoring and evaluation by management, ITMS, and central evaluation by PPD (Health).
HHeeaalltthh PPrrooggrraammmmeess
97
PHARMACEUTICAL AND RESEARCH UNIT I. Introduction The Pharmaceutical and Research Unit was established in 1998 with the purpose of manufacturing traditional medicines and conducting scientific research for quality enhancement of the same. Unlike modern drugs, traditional medicine in Bhutan is purely an indigenous product since its source, processing know-how and the human resource capacity are available in the country. II. Situation Analysis a) Current Situation Assessment
Traditional medicine being an integral part of the national health services, timely supply of effective traditional drugs in sufficient amount plays a crucial role in the delivery of quality health services. With the commissioning of pharmaceutical and research unit, shortage of traditional medicines has been significantly reduced. With production of approx. 5 metric tons of traditional medicines, the requirements for the 18 indigenous units in the districts are sufficiently met. In addition, dozens of its herbal products are marketed in the local market. Since the Unit is the user of medicinal plants and other natural resources, collaboration with the National Conservation Division, National Parks, Bio-diversity program and the RNRRCs in the MoA is being continued. Besides, cooperation and partnerships with farmers and local communities are considered very important. b) Situation Assessment at the end of the Ninth Plan
The Unit becoming a self-sustaining and a dynamic profit centre of the Royal Government with operational autonomy, producing and supplying traditional medicines and herbal products of international quality and standards. III. Programme/Policy Objectives Consolidation and quality enhancement of traditional medicine services through production and supply of high quality traditional medicines.
• Strengthen technical capacity and develop leadership in research and product development
• Create conducive environment to encourage innovation and creativity • Consolidate Quality Assurance System • Increase revenue generation capacity • Preserve ancient wisdom and protect intellectual and Property Rights • Decentralization and transferring the ownership
IV. Strategies
HHeeaalltthh PPrrooggrraammmmeess
98
1) Human Resource Development in key areas
The estimated market for the herbal product in the world is more than 75 billion US dollars with the growth rate of 12%. With this scope in mind, human resource at this Unit needs to be developed and technical competence enhanced. Capacity building through long term and short training in key areas such as phyto-chemistry, phyto-pharmaceuticals, quality assurance, pharmacology and marketing receives high priority. 2) Technological Standardization
Fetching in right technology to keep up the pace with contemporary industries obtaining standards must be regarded as a dynamic process of management. Use IT to boost efficiency. 3) Commercial orientation and operational autonomy
For an industry to survive, it has to produce good quality products/services with competitive pricing structures with their competitive brand or category. This would demand management dynamism, taking risk and making decision. Time must be equated to money. Optimal utilization of both equipment and manpower must be instituted, scale of risk benefit balanced for motivation of staff. This would to strengthening and streamlining of the production system. There will be formation of Inter-Ministerial management board that will empower the Unit to make its own day-to-day functional decisions. 4) Strengthening the marketing operations and explore new markets
At the moment the marketing activities are in infancy and in the true commercial sense only one product (Tsheringma tea) has been launched in the domestic market. Market for this has to be expended both within and outside country. For the development of new products and markets, market studies and research needs to be conducted. 5) Advocacy and Promotion
Coping with the age of information and multi-media communication, the Unit intends to selectively and strategically advocate and promote traditional medicines for both public and our own benefits. In addition, communication through Internet will be explored. 6) Strengthening the research and product development capacity
Purchase of equipment; training of staff; acquiring literature and information; study tours and industrial attachment to relevant industries and institutes for technology transfer. 7) Enhance scientific validation of traditional medicines and documentation
Conducting studies and trials in collaboration with other organizations such as Serbithang Veterinary Vaccine Development Centre.

HHeeaalltthh PPrrooggrraammmmeess
99
8) Raw Material sources and industrial integration and linkages
Workshops and seminars for inter-sectoral collaboration. Feasibility studies and surveys. Study tours and exchange visits. Documentation and exchange of information. 9) Community Participation
Training on collection, post harvest care and packing. Cultivation and buy-back schemes. Printing of manuals and information literature. farmers study tours and community meetings. V. Program Budget outlays
Table 43. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 4.821 5.303 5.834 6.417 7.059 29.435 Conference, Seminar, W'shop 0.100 0.000 0.175 0.000 0.129 0.404 Op. Exp. - processing & Manufacture 0.400 0.520 0.676 0.879 1.142 3.617
Current 5.321 5.823 6.685 7.296 8.329 33.455 Exp. On Structure - building 0.000 12.000 0.000 0.000 10.000 22.000 Plant & equip. - Hosp/lab equipment 4.000 4.600 5.380 6.394 6.712 27.086 Plant & equip. - Gen. Tools & equip. 0.235 0.246 0.259 0.277 0.300 1.317 1 Hilux for Programme 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.050 0.000 0.000 0.050 0.000 0.100 Office equipment 0.075 0.098 0.127 0.165 0.214 0.679 2 Computer & peripherals 0.080 0.080 0.000 0.000 0.000 0.160
Capital 5.240 17.024 5.766 6.886 17.226 52.142 Total 1 10.561 22.847 12.451 14.182 25.555 85.597
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev 0.000 0.000 0.000 0.000 0.000 0.000 Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 10.561 22.847 12.451 14.182 25.555 85.597
VI. Implementation Strategies Responsibilities will be assigned to relevant personnel and section heads for implementation. The Management Board will guide and advise respective sections while implementing the planned activities. Inter-sectoral activities will be implemented through coordination workshop, meetings and seminars. The central level coordination will be done in close consultation with other sections of ITMS, Health Care Division and the Health Department. VII. Monitoring and Evaluation The Management Board will monitor the yearly achievements through the set targets and indicators of the unit. Periodic reporting and meetings will be introduced to keep track of the activities.
HHeeaalltthh PPrrooggrraammmmeess
100
JIGME DORJI WANGCHUK NATIONAL REFERRAL HOSPITAL I. Introduction JDWNR Hospital serves not only as Regional Referral for the western Dzongkhags but also as the National Referral hospital for the whole country. Currently it has facilities in all specialised fields but super-specialised services exist only in hemo-dialysis and vasectomy in reproductive health. II. Situation Analysis a) Current Situation Assessment
The patient attendance and admissions are on the increasing trend every year. The workload of the hospital is increased further as this hospital acts as the Thimphu Dzongkhag hospital at the same time a referral for other district hospitals. Besides, it also a fairly good community health services and conducts 9 out reach clinics. The double burden of both communicable and non-communicable disease, and emerging and re-emerging of communicable disease will demand extra services from this hospital. One way to lower the work burden is the Health Telematic’s proper development and its wider coverage, and strengthening of the regional referral and dzongkahgs hospitals. Patients referred outside Bhutan in last three years are 1679, and the cost incurred is Nu. 131.637 million. The referral outside is high, owing to the shortage of specialists and facilities like CT scan, MRI, Cancer unit etc. b) Situation Assessment at the end of the Ninth Plan
Hospital is expected to have good number of specialised services introduced with the establishment of CT scan facility, Neonatology unit, Casualty Unit, Psychiatric Unit and Cancer Unit. The management of hospital should have improved with training for the management personnel. The supply of timely drugs, equipment and lab reagents also improved within the Plan Period. III. Programme/Policy Objectives The general objective is to provide quality care to all the patients and promote the health of our people and prevent diseases. Specific objectives are:
1. Manpower development at various levels for improvement of services 2. Standardization of equipments and procedures 3. Expansion of hospital facilities in terms of no. of beds, specialised units. 4. Promote research in medical fields 5. Promote infection control and develop a proper waste disposal system
HHeeaalltthh PPrrooggrraammmmeess
101
IV. Strategies 1. Train GDMOs in specialised fields and later for super specialisation 2. Human Resource Development for the existing and new staff 3. Formation of Research Institution Board that will encourage operational
and clinical research 4. Establishment of Task Force to take care of infection control and waste
disposal V. 1 Budget Outlay
Table 44. Budget outlay Activity 2002-2003 2003-2004 2004-2005 2005-2006 2006-2007 Total
Establishment cost 65.010 71.511 78.662 86.528 95.181 396.893 Drugs and non drugs 35.840 36.199 36.561 36.926 37.296 182.822 Conference, Seminar, W'shop 0.158 0.150 0.150 0.150 0.190 0.798
Current 101.008 107.860 115.373 123.604 132.667 580.512 Exp. On structure, Building 2.500 3.000 3.500 4.000 4.500 17.500 Plant & equip. - Power generation 3.420 0.600 0.700 0.700 0.800 6.220 3 Ambulances 1.250 1.250 1.250 0.000 0.000 3.750 Purchase of 1 Hilux 0.800 0.000 0.000 0.000 0.000 0.800 Furniture 0.300 0.300 0.300 0.300 0.300 1.500 1Photocopy, 4 printers, 1 projector 0.400 0.000 0.000 0.000 0.000 0.400 6 Computer 0.240 0.000 0.000 0.240 0.000 0.480
Capital 8.910 5.150 5.750 5.240 5.600 30.650 Total 1 109.918 113.010 121.123 128.844 138.267 611.162
Budget reflected with other programs. Current 0.000 0.000 0.000 0.000 0.000 0.000
Training - Human Resource Dev Capital 0.000 0.000 0.000 0.000 0.000 0.000 Total 2 0.000 0.000 0.000 0.000 0.000 0.000
Total 1 + 2 109.918 113.010 121.123 128.844 138.267 611.162
V.2 Manpower requirement A visionary human resource plan projection for next twenty years is carried out. V.3 Technical assistance HVO program in Orthopedic unit, Interplast program in reconstructive surgery, VSOs in Physiotherapy and JOCV in Lab are ongoing and will need to be continued, while hospital would require TA in occupational therapy unit. V.4 Equipment and other investments needed 1 no. of CT scan machine, 1 ECT machine, and Neonatal unit equipment need to be procured. V.5 Source of financing RGOB/International agencies. VI. Implementation strategy The Superintendent is the administrative head that looks after the overall functioning and management of hospital. Each different medical unit is headed by the Unit Head. Specialised and general doctors/nurses carry out the routine works allotted to them.
HHeeaalltthh PPrrooggrraammmmeess
102
Besides, hospital has to coordinate with various central programmes and supply divisions. VII. Monitoring and evaluation mechanism
1. Critical mass of trained manpower on quality assurance developed 2. Set up national standards and quality indicators 3. JDWNRH accreditation completed 4. Task force formed for infection control and waste disposal 5. RBI formed and standard operating procedures laid down

HHeeaalltthh PPrrooggrraammmmeess
103
EXTENSION OF JDWNR HOSPITAL I. Introduction JDWNR hospital is the apex referral centre in Bhutan. It caters to the specialised secondary and tertiary health care services in the country. With the further expansion of the existing facility along with the introduction of specialised services, many cases of out-side referrals could be avoided, while also rendering services to the growing population of the Dzongkhag. II. Situation analysis The Government of India made commitment to support the construction of the expansion of JDWNR Hospital since the beginning of the 7th Five Year Plan. As of now, a filter clinic, laboratory building, staff quarters, and boundary wall are completed. It is estimated that the construction of the main hospital building, in accordance to the master plan and based on the preliminary estimate prepared by Apollo Consultancy, would be Nu. 670 million. III. Policy Objective Extension of the present 200-bedded to 350 bedded national referral hospital as per the Masterplan developed by Apollo Consultancy. This is the ongoing activity of the 7th and 8th Plans. IV. Strategies Continuation of the ongoing activities V. Budget outlay
Table 45. Budget outlay Current Capital Total estimate
20.000 650.000 Nu. 670.000 milln
Manpower Requirements: Status quo Technical Assistance Requirements: Consultants from Apollo Consultancy may be
required while implementing the Masterplan VI. Implementation strategy The Project is fully managed by the Project Director in close collaboration with the Ministry of Health and the Ministry of Finance. VII. Monitoring and Evaluation The Program and the Ministry will do it jointly during and after the completion of the construction.
HHeeaalltthh PPrrooggrraammmmeess
104
EXTENSION OF MONGAR REGIONAL REFERRAL HOSPITAL I. Introduction MRR Hospital serves as the referral point for the six Eastern Dzongkhags. The expansion of infrastructure is in view of reducing workload for the national referral centre as well as providing immediate referral for the far-away Dzongkhags. II. Situation analysis The construction of Mongar Regional Referral Hospital was initiated during the 7th Five Year Plan with support from the Government of India. The project has made good progress. All staff quarters, extension of wards, nurse duty rooms, guesthouse, boundary fencing works and motorable road have been completed. The rehabilitation of some of the existing services has been carried out so that health services delivery will not be affected during the construction of the main hospital building. III. Policy Objective Extension and up-gradation of the present 60-bedded to 150 bedded regional referral hospital as per the Masterplan developed by Apollo Consultancy. This is the ongoing activity of the 7th and 8th Plans IV. Strategy Continuation of the ongoing activities V. Budget outlay
Table 46. Budget outlay
Current Capital Total estimate 20.000 350.000 Nu. 370.000 milln
Manpower Requirements: Status quo Technical Assistance Requirements: Consultants from Apollo Consultancy may be
required while implementing the Masterplan. VI. Implementation strategy The Project is fully managed by the Project Director in close collaboration with the Ministry of Health and the Ministry of Finance. VII. Monitoring and evaluation The Program and the Ministry will do it jointly during and after the completion of the construction.