Routinely recorded versus dedicated time registrations during trauma work-up
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Organisational quality, nurse staffing and the quality of chronic diseasemanagement in primary care: Observational study using routinelycollected data
Peter Griffiths a,*, Jill Maben b, Trevor Murrells b
a University of Southampton, Faculty of Health Sciences, Building 67, Southampton SO17 1BJ, United Kingdomb King’s College London, National Nursing Research Unit, School of Nursing and Midwifery, 57 Waterloo Road, London SE1 8WA, United Kingdom
What is already known about the topic?
� Higher levels of nurse staffing have been associated withhigher quality of care in hospitals and primary care.
International Journal of Nursing Studies 48 (2011) 1199–1210
A R T I C L E I N F O
Article history:
Received 20 January 2011
Received in revised form 4 March 2011
Accepted 27 March 2011
Keywords:
Workforce
Primary care
Practice nurses
Quality of care indicators
Performance
Staffing levels
Organisational factors
Multivariate analysis
A B S T R A C T
Background: An association between quality of care and staffing levels, particularly
registered nurses, has been established in acute hospitals. Recently an association
between nurse staffing and quality of care for several chronic conditions has also been
demonstrated for primary care in English general practice. A smaller body of literature
identifies organisational factors, in particular issues of human resource management, as
being a dominant factor. However the literature has tended to consider staffing and
organisational factors separately.
Aims and objectives: We aim to determine whether relationships between the quality of
clinical care and nurse staffing in general practice are attenuated or enhanced when
organisational factors associated with quality of care are considered. We further aim to
determine the relative contribution and interaction between these factors.
Method: We used routinely collected data from 8409 English general practices. The data,
on organisational factors and the quality of clinical care for a range of long term conditions,
is gathered as part of ‘‘Quality and Outcomes Framework’’ pay for performance system.
Regression models exploring the relationship of staffing and organisational factors with
care quality were fitted using MPLUS statistical modelling software.
Results: Higher levels of nurse staffing, clinical recording, education and reflection on the
results of patient surveys were significantly associated with improved clinical care for
COPD, CHD, Diabetes and Hypothyroidism after controlling for organisational factors.
There was some evidence of attenuation of the estimated nurse staffing effect when
organisational factors were considered, but this was small. The effect of staffing interacted
significantly with the effect of organisational factors. Overall however, the characteristics
that emerged as the strongest predictors of quality of clinical care were not staffing levels
but the organisational factors of clinical recording, education and training and use of
patient experience surveys.
Conclusions: Organisational factors contribute significantly to observed variation in the
quality of care in English general practices. Levels of nurse staffing have an independent
association with quality but also interact with organisational factors. The observed
relationships are not necessarily causal but a causal relationship is plausible. The benefits
and importance of education, training and personal development of nursing and other
practice staff was clearly indicated.
� 2011 Published by Elsevier Ltd.
* Corresponding author. Tel.: +44 023 8059 7979.
E-mail address: [email protected] (P. Griffiths).
Contents lists available at ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
0020-7489/$ – see front matter � 2011 Published by Elsevier Ltd.
doi:10.1016/j.ijnurstu.2011.03.011

Author's personal copy
� Various organisational factors have also been associatedwith improved quality of care in hospitals.� Few studies have examined staffing and organisational
factors simultaneously to assess their relative contribu-tion.
What this paper adds
� Both nurse staffing and organisational factors wereassociated with the quality of care for a range of chronicconditions in UK general practices.� The association between quality and organisation was
much stronger than the association with nurse staffing.� There was an interaction between staffing and organisa-
tion which suggested that the adverse effects of thelowest levels of nurse staffing were mitigated byorganisational quality.
There is a large literature exploring the associationbetween quality, as measured by patient safety outcomes,and health care staffing levels, particularly registerednurses, in acute hospitals (Kane et al., 2007). A smaller butsignificant body of literature identifies organisationalfactors, in particular issues of human resource manage-ment, as being a dominant factor in care quality (Kazanjianet al., 2005). However this literature has tended to considerstaffing and management factors separately. In addition tobeing limited to acute care settings this literature hasrarely considered positive impacts on quality of care,focussing instead on safety. In this study we explore theassociations between staffing levels, organisation andmanagement factors and quality of care concurrently ina primary care setting.
In acute care, the term ‘magnet hospital’ has been usedto describe hospitals where a number of organisationalcharacteristics including leadership and management ofthe clinical (nursing) team, relationships with doctors(physicians) and support for education and training ofnursing staff (Aiken et al., 1994) are associated with bothbetter staffing and better patient outcomes. Because of thisconfounding it is unclear if there is an independent andcausal effect of staffing despite the large number of studiessuggesting that higher nurse staffing is associated withbetter outcomes (Kane et al., 2007). Some studies havedirectly assessed the effect of organisational character-istics. A systematic review identified the existence ofassociations between the work environment (autonomy,nursing workload, inter-professional relations, nursingmanagement, nursing standards and professional devel-opment) and patient mortality in acute care (Kazanjianet al., 2005). However, most of this research did notconsider staffing levels, which leaves open the possibilitythat positive organisational characteristics may be moreimportant than staffing levels, or, conversely may simplybe a product of well-resourced teams and increasedcapacity, and thus the precise organisational forms arenot relevant to delivering good quality care.
One of the few studies to consider staffing andorganisational factors concurrently undertaken by Westand colleagues (West et al., 2002) did find strongassociations between appraisal, training and team workingand mortality after controlling for levels of medical
staffing. However this research did not consider the levelof nurse staffing which is the most researched staffingvariable and one whose significance is well established(Kane et al., 2007). More recently (Aiken et al., 2008) foundthat the nursing work environment, which includes itemsexploring organisational factors such as staff developmentand quality management relationships, is more stronglyassociated with both nurse and patient outcomes in acutecare settings than is nurse staffing.
The question of the relationship between quality of careand nurse staffing is particularly pertinent in primary care,since the contribution of nurses to clinical care in this areais hotly contested. In some countries the increased use ofnurses in primary care has been driven by difficultyrecruiting physicians or as a way of saving money (Pearceet al., 2010; Sox, 2000). In England increases in the use ofnurses has been associated with the introduction of a ‘payfor performance’ system, the Quality and OutcomesFramework (QOF), for general practice. This systemmeasures performance of the practice in clinical care fora number of disease areas (e.g. diabetes, coronary heartdisease) and in terms of a number of organisationalcharacteristics (e.g. length of appointments, personallearning plans for practice employed nurses) many ofwhich are thought to support high quality care.
Much of the work involved in delivering the perfor-mance measured by the Quality and Outcomes Frameworkhas been delegated by GPs to nurses (Leese, 2006) and overrecent years there has been a steady increase in both thenumber of nurses employed in general practice and theproportion of consultations that are undertaken by them(Hippisley-Cox et al., 2007; The Information Centre, 2008).But concerns are consistently raised about the progressionof the nursing role in primary care and the quality andsafety of the care that nurses can give (Bagley et al., 2000;Burke, 2009; Knight, 2008). The contribution of nurses tomeeting the Quality and Outcomes Framework targets inthe UK has been dismissed as being essentially an exercisein form filling with no real contribution to the quality ofcare (Dr Crippen, 2010; Anon, 2007). If that was the casethen once organisational factors were taken into account,for example systems for record keeping, then one wouldexpect that the effect of nurse staffing would disappear ordiminish.
Our previous paper showed a positive associationbetween registered nurse staffing and the quality of carein English general practice (Griffiths et al., 2010a,b). A highlevel of nurse staffing (fewer patients per full timeequivalent practice employed nurse) was significantlyassociated with better performance in a number of clinicalconditions (e.g. chronic obstructive pulmonary disease(COPD) and Diabetes) suggesting that nurse staffing wasassociated with real differences in patient condition andnot simply superficial compliance with processes. Thisreflects the research in hospital settings. However, inneither case is it clear whether the relationship observed isa causal one or whether the association with nurse staffingwould remain once other factors are taken into account.
In this paper we determine whether relationshipsbetween the quality of clinical care and nurse staffingpreviously observed were attenuated when organisational
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–12101200

Author's personal copy
factors pertinent to care in general were considered added tothe model. We also explored the potential interactionbetween nurse staffing levels and organisational factors todetermine if the effects of these factors varied depending onlevels of staffing (or vice versa). In order to do this we useddata on organisational factors from the Quality andOutcomes Framework to see what impact these had onthe relationship between quality of care for the Quality andOutcomes Framework clinical conditions and nurse staffing.
1. Method
1.1. Data sources and sample
We used Quality and Outcomes Framework data for2005/2006 obtained from the NHS Information Centre atLeeds (United Kingdom) as a source of data on bothorganisational factors and the quality of clinical care for arange of long term conditions: asthma, chronic obstructivepulmonary disease, coronary heart disease, diabetes,hypertension, hypothyroidism, severe long term mentalhealth problems, and stroke. These data were matched topractice and population data. An estimate of the number offull-time equivalent (FTE) practice nurses employed by eachpractice was obtained using headcount data from Binleys, ahealth information specialist who have staffing informationon every UK practice, and area data on full time equivalentnumbers of nurses employed at the primary care trust levelwas obtained from the NHS Information Centre1. Thesesources of data are described in detail elsewhere (Griffithset al., 2010a,b). The dataset contains information from 8409practices. We excluded small practices (<1000 patients),practices without condition registers or no patients on theregister, where registers were half the size of denominatorsused to calculate indicator specific achievement reportingand practices where an estimate of practice nurse staffingwas not available. This reduced the number of practices tobetween 7431 and 7456 depending on the condition beingstudied.
The Quality and Outcomes Framework 2005/2006comprises four domains (clinical, organisational, patientexperience and additional services). We used the data onclinical care quality from the clinical domains as ourdependant variables to measure the quality of clinical careand used organisational factors derived from the organisa-tional and patient experiences domains as independentvariables. We did not consider ‘additional services’ as theseare generally services provided by the practice which donot impact upon the clinical conditions covered by theQuality and Outcomes Framework.
1.2. Variables
The Quality and Outcomes Framework clinical domainprovides information on the quality of care for tenconditions. For each condition there is a set of indicatorsmeasuring process and intermediate outcomes: asthma
(7), cancer (2), chronic obstructive pulmonary disease (8),coronary heart disease (CHD) (15), diabetes (18), epilepsy(4), hypertension (5), hypothyroidism (2), severe long termmental health (5), and stroke (10).
As this data is used as part of a pay for performancesystem and is not collected for research purposes there is asignificant risk of bias. Achievement on the indicators canbe expressed as reported achievement, used in the pay forperformance system, where practices can exclude somepatients from the denominator because they believe thatthe indicator does not apply. As this is open to manipula-tion by the practice we used the size of the conditionregister for the practice as the denominator and calculatedpopulation achievement instead, that is how many peoplein the entire population with the disease met the targetspecified in the indicator. Population achievement can onlybe calculated for those indicators that apply to all patientson the register. None of the indicators for cancer andepilepsy applied to all patients on this register so these twoclinical conditions were omitted from the analysis. Acomposite score of weighted indicators was generated foreach of these clinical conditions (Doran et al., 2006).
The patient experience domain comprises two ele-ments related to how the practice manages patientexperience. The first is the length of appointments offered(1 = routine booked appointments with doctors of not lessthan 10 minutes, 0 = length of consultation requirementnot met). The second considers the practice’s use of patientsurveys. The three patient survey items were used toconstruct an ordinal variable that measures to what degreeeach practice utilised the survey (0 = not conducted,1 = survey undertaken, 2 = survey undertaken, resultsreflected upon, changes proposed, 3 = survey undertaken,results discussed as a team, with a patient group/non-executive director of the primary care organisation,changes proposed and evidence these have been enactedupon).
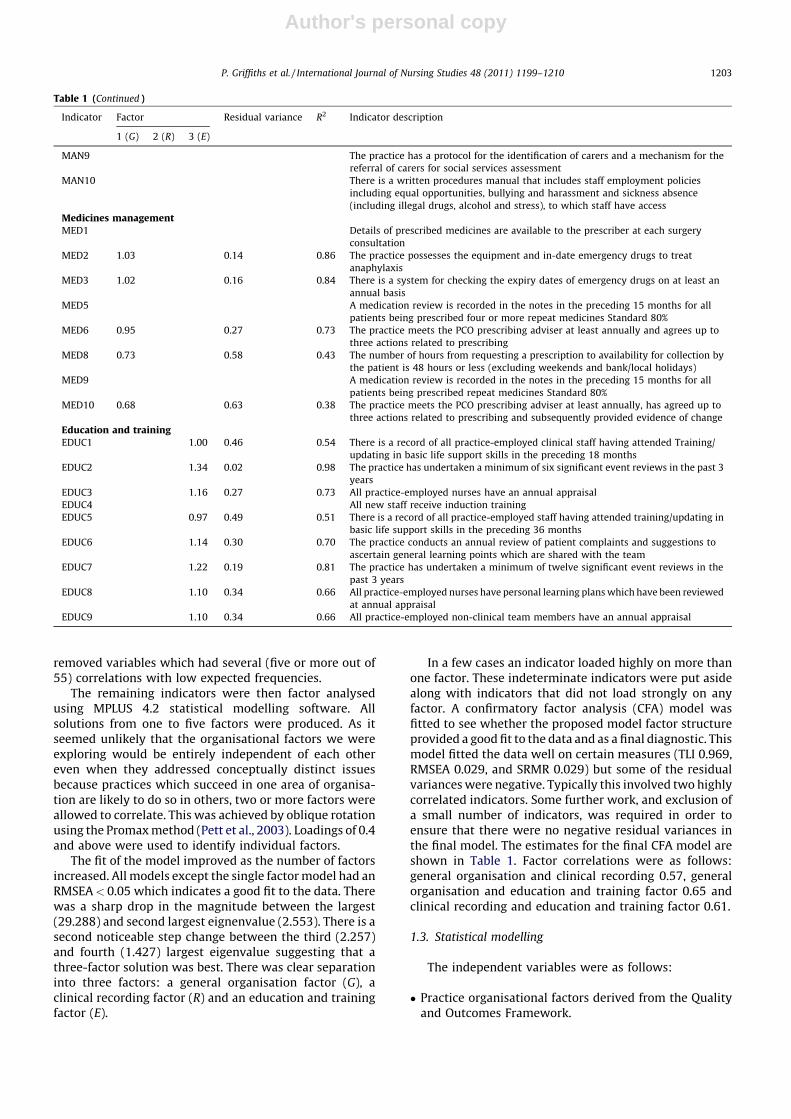
The organisational domain consists of five areas. Eachorganisational area is represented by a set of indicators(Table 1): records and information about patients (19),patient communication (8), education and training (9),practice management (10), medicines management (10).Most of the time practices achieved the maximum score foreach indicator because the standard was met (e.g. details ofprescribed medicines are available to the prescriber at eachsurgery). For analysis purposes we collapsed the indicatorsinto two categories (1 = met/maximum score 0 = not met/less than maximum score).
We undertook a factor analysis to identify underlyingfactors in the large number of individual organisationalitems. As the collapsed organisational indicator data arenot continuous and do not conform to conventional(normal) distributional assumptions we used approachesbased on tetrachoric correlations (a measure of correlationbetween two unobserved continuous variables), whereeach unobserved variable is represented by an observeddichotomous variable (Muthen, 1989). Tetrachoric corre-lations are calculated using a two stage proceduredescribed in Brown and Benedetti (1977). Tetrachoriccorrelations are subject to increasing bias when expectedcell frequencies in the bivariate table fall below 5 and so we
1 Primary care trusts (PCTs) in England provide some health services
and commission others for local areas comprising about 300,000 people.
A PCT would typically include approximately 50 practices.
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–1210 1201

Author's personal copy
Table 1
Confirmatory factor analysis–final model loadings and ancillary statistics.
Indicator Factor Residual variance R2 Indicator description
1 (G) 2 (R) 3 (E)
Records and information about patientsREC1 1.00 0.19 0.81 Each patient contact with a clinician is recorded in the patient’s record, including
consultations, visits and telephone advice
REC2 0.83 0.45 0.56 Entries in the records are legible
REC3 1.08 0.06 0.95 The practice has a system for transferring and acting on information about patients
seen by other doctors out of hours
REC5 1.07 0.08 0.93 The practice has a system for dealing with any hospital report or investigation result
which identifies a responsible health professional, and ensures that any necessary
action is taken
REC6 1.08 0.05 0.95 There is a system for ensuring that the relevant team members are informed about
patients who have died
REC7 1.10 0.03 0.97 The medicines that a patient is receiving are clearly listed in his or her record
REC8 1.07 0.08 0.92 There is a designated place for the recording of drug allergies and adverse reactions in
the notes and these are clearly recorded
REC9 0.54 0.77 0.24 For repeat medicines, an indication for the drug can be identified in the records (for
drugs added to the repeat prescription with effect from 1 April 2004). Minimum
Standard 80%
REC12 1.00 0.20 0.81 When a member of the team prescribes a medicine, there is a mechanism for that
prescription to be entered into the patient’s general practice record
REC13 0.91 0.34 0.67 There is a system to alert the out-of-hours service or duty doctor to patients dying at
home
REC14 1.02 0.15 0.85 The records, hospital letters and investigation reports are filed in date order or
available electronically in date order
REC15 1.00 0.51 0.49 The practice has up-to-date clinical summaries in at least 60% of patient records
REC16 1.13 0.36 0.64 The smoking status of patients aged from 15 to 75 is recorded for at least 75% of
patients
REC17 0.91 0.59 0.41 The blood pressure of patients aged 45 and over is recorded in the preceding 5 years
for at least 75% of patients
REC18 The practice has up-to-date clinical summaries in at least 80% of patient records
REC19 1.15 0.35 0.65 80% of newly registered patients have had their notes summarised within 8 weeks of
receipt by the practice
Patient communicationINF1 1.00 0.20 0.81 The practice has a system to allow patients to contact the out-of-hours service by
making no more than two telephone calls
INF2 0.50 0.80 0.20 If an answering system is used out of hours, the message is clear and the contact
number is given at least twice
INF3 1.05 0.11 0.90 The practice has arrangements for patients to speak to GPs and nurses on the
telephone during the working day
INF4 0.95 0.28 0.72 If a patient is removed from a practice’s list, the practice provides an explanation of
the reasons in writing to the patient and information on how to find a new practice,
unless it is perceived that such an action would result in a violent response by the
patient
INF5 1.00 0.19 0.81 The practice supports smokers in stopping smoking by a strategy which includes
providing literature and offering appropriate therapy
INF6 0.82 0.46 0.54 Information is available to patients on the roles of the GP, community midwife, health
visitor and hospital clinics in the provision of ante-natal and post-natal care
INF7 Patients are able to access a receptionist via telephone and face to face in the practice,
for at least 45 hours over 5 days, Monday to Friday, except where agreed with the PCO
INF8 The practice has a system to allow patients to contact the out-of-hours service by
making no more than one telephone call
Practice managementMAN1 0.98 0.23 0.77 Individual healthcare professionals have access to information on local procedures
relating to Child Protection
MAN2 0.98 0.22 0.78 There are clearly defined arrangements for backing up computer data, back-up
verification, safe storage of back-up tapes and authorisation for loading programmes
where a computer is used
MAN3 0.69 0.62 0.38 The Hepatitis B status of all doctors and relevant practice-employed staff is recorded
and immunisation recommended if required in accordance with national guidance
MAN4 0.72 0.59 0.41 The arrangements for instrument sterilisation comply with national guidelines as
applicable to primary care
MAN5 0.91 0.33 0.68 The practice offers a range of appointment times to patients, which as a minimum
should include morning and afternoon appointments five mornings and four
afternoons per week, except where agreed with the PCO
MAN6 0.89 0.36 0.64 Person specifications and job descriptions are produced for all advertised vacancies
MAN7 0.79 0.50 0.50 The practice has systems in place to ensure regular and appropriate inspection,
calibration, maintenance and replacement of equipment
MAN8 The practice has a policy to ensure the prevention of fraud and has defined levels of
financial responsibility and accountability for staff undertaking financial transactions
(accounts, payroll, drawings, payment of invoices, signing cheques, petty cash
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–12101202
Author's personal copy
removed variables which had several (five or more out of55) correlations with low expected frequencies.
The remaining indicators were then factor analysedusing MPLUS 4.2 statistical modelling software. Allsolutions from one to five factors were produced. As itseemed unlikely that the organisational factors we wereexploring would be entirely independent of each othereven when they addressed conceptually distinct issuesbecause practices which succeed in one area of organisa-tion are likely to do so in others, two or more factors wereallowed to correlate. This was achieved by oblique rotationusing the Promax method (Pett et al., 2003). Loadings of 0.4and above were used to identify individual factors.
The fit of the model improved as the number of factorsincreased. All models except the single factor model had anRMSEA < 0.05 which indicates a good fit to the data. Therewas a sharp drop in the magnitude between the largest(29.288) and second largest eignenvalue (2.553). There is asecond noticeable step change between the third (2.257)and fourth (1.427) largest eigenvalue suggesting that athree-factor solution was best. There was clear separationinto three factors: a general organisation factor (G), aclinical recording factor (R) and an education and trainingfactor (E).
In a few cases an indicator loaded highly on more thanone factor. These indeterminate indicators were put asidealong with indicators that did not load strongly on anyfactor. A confirmatory factor analysis (CFA) model wasfitted to see whether the proposed model factor structureprovided a good fit to the data and as a final diagnostic. Thismodel fitted the data well on certain measures (TLI 0.969,RMSEA 0.029, and SRMR 0.029) but some of the residualvariances were negative. Typically this involved two highlycorrelated indicators. Some further work, and exclusion ofa small number of indicators, was required in order toensure that there were no negative residual variances inthe final model. The estimates for the final CFA model areshown in Table 1. Factor correlations were as follows:general organisation and clinical recording 0.57, generalorganisation and education and training factor 0.65 andclinical recording and education and training factor 0.61.
1.3. Statistical modelling
The independent variables were as follows:
� Practice organisational factors derived from the Qualityand Outcomes Framework.
Table 1 (Continued )
Indicator Factor Residual variance R2 Indicator description
1 (G) 2 (R) 3 (E)
MAN9 The practice has a protocol for the identification of carers and a mechanism for the
referral of carers for social services assessment
MAN10 There is a written procedures manual that includes staff employment policies
including equal opportunities, bullying and harassment and sickness absence
(including illegal drugs, alcohol and stress), to which staff have access
Medicines managementMED1 Details of prescribed medicines are available to the prescriber at each surgery
consultation
MED2 1.03 0.14 0.86 The practice possesses the equipment and in-date emergency drugs to treat
anaphylaxis
MED3 1.02 0.16 0.84 There is a system for checking the expiry dates of emergency drugs on at least an
annual basis
MED5 A medication review is recorded in the notes in the preceding 15 months for all
patients being prescribed four or more repeat medicines Standard 80%
MED6 0.95 0.27 0.73 The practice meets the PCO prescribing adviser at least annually and agrees up to
three actions related to prescribing
MED8 0.73 0.58 0.43 The number of hours from requesting a prescription to availability for collection by
the patient is 48 hours or less (excluding weekends and bank/local holidays)
MED9 A medication review is recorded in the notes in the preceding 15 months for all
patients being prescribed repeat medicines Standard 80%
MED10 0.68 0.63 0.38 The practice meets the PCO prescribing adviser at least annually, has agreed up to
three actions related to prescribing and subsequently provided evidence of change
Education and trainingEDUC1 1.00 0.46 0.54 There is a record of all practice-employed clinical staff having attended Training/
updating in basic life support skills in the preceding 18 months
EDUC2 1.34 0.02 0.98 The practice has undertaken a minimum of six significant event reviews in the past 3
years
EDUC3 1.16 0.27 0.73 All practice-employed nurses have an annual appraisal
EDUC4 All new staff receive induction training
EDUC5 0.97 0.49 0.51 There is a record of all practice-employed staff having attended training/updating in
basic life support skills in the preceding 36 months
EDUC6 1.14 0.30 0.70 The practice conducts an annual review of patient complaints and suggestions to
ascertain general learning points which are shared with the team
EDUC7 1.22 0.19 0.81 The practice has undertaken a minimum of twelve significant event reviews in the
past 3 years
EDUC8 1.10 0.34 0.66 All practice-employed nurses have personal learning plans which have been reviewed
at annual appraisal
EDUC9 1.10 0.34 0.66 All practice-employed non-clinical team members have an annual appraisal
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–1210 1203

Author's personal copy
� Geographic area and deprivation (density, Index ofMultiple Deprivation).� Patients characteristics (percent whose health was good,
percent aged �15 years, percent who were female,percent aged �65 years, percent from a racial or ethnicminority).� Practice characteristics (size, list size per full time
equivalent (FTE) General Practitioner (medical doctor),single-handed practice, primary medical services con-tract).� General practitioner characteristics (percent aged �45
years, percent female, percent qualified in the UK).� Condition Prevalence� Practice nurse staffing (practice list size per FTE practice
nurses grouped into quintiles (�3038.01, 3038.02–3901.48, 3901.49–4823.44, 4823.45–6210.68, and�6210.69)) with a sixth category for practices withouta nurse.
The organisational factors identified by the factoranalysis were treated as latent variables and all othervariables as observed independent variables. A regressionmodel was fitted simultaneously to all quality scores for allclinical conditions using MPLUS version 4.2. The unit ofanalysis was the practice. Although practices are clusteredwithin primary care trusts and regions we did not usemulti-level modelling as our previous work showed thatvariance associated with primary care trust was smallcompared to variance at the practice level (Griffiths et al.,2010a,b) and, furthermore, the multi-level model was notcompatible with modelling multiple dependant variablessimultaneously (the models did not converge). Typicallyvariance associated with the trust was more than ten timessmaller than that associated with practices.
We included geographic, patient, practice and practi-tioner characteristics in the model as several of thesevariables have been shown to have significant associationswith quality of care in previous research. Thus while thesevariables were not of direct interest we needed to controlfor them while exploring those associations that directlyinterested us. Three other patient variables (per centwhose health was good, per cent aged �15 years, per centwho were female) were considered but excluded becauseof collinearity (Griffiths et al., 2010a,b).
Preliminary analysis also provided evidence of colli-nearity between the general organisation factor, clinicalrecording factor and education and training factors that wehad derived from the organisational domain. When fittedindividually, higher scores on each organisational factorwere associated with higher Quality and OutcomesFramework composite scores. However when all threeorganisational factors were fitted simultaneously the signof the b coefficient of the general factor went from positiveto negative for most clinical conditions, indicating thatthere was collinearity. As statistical models typicallyassume that collinearity is not high we therefore droppedthe general organisation factor from the model, as itsspecific meaning was less clear that the other two factors.
The effect of practice nurse staffing was tested bydropping this variable from the model and comparing themodel fit (difference in fit between models). We deter-mined whether the effect of practice nurse staffing was
attenuated by the organisational factors by dropping themfrom the model and examining the differences betweenthe b estimates for models.
To determine whether the effects of organisationalfactors were constant or varied with levels of nurse staffingwe plotted clinical condition quality scores by practicenurse staffing and organisational factor score quintiles forthe clinical recording and education and training factorsand added an interaction term to the regression model. Theglobal model (across all clinical conditions) with theinteraction term failed to converge. We therefore fittedseparate random effect models for each clinical conditionusing a Monte Carlo approach with between 1000 and1500 integration points (Muthen and Muthen, 2007). Mostof these models reached convergence. When convergencefailed, the number of integration points was increased. Theinteraction could be tested for all clinical conditions andorganisational factors except mental health (clinicalrecording), stroke (clinical recording) and COPD(educationand training).
2. Results
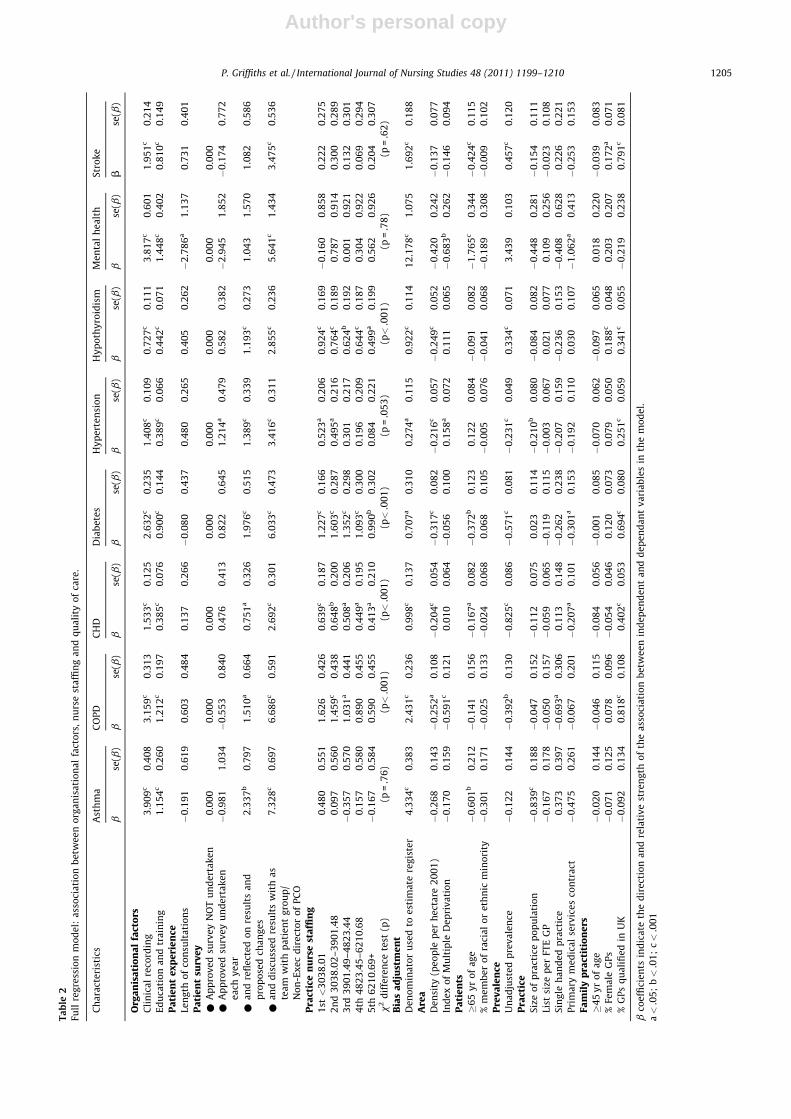
The global effect of practice nurse staffing wasstatistically significant (x2 = 37.43, 6d.f., p < 0.001). Prac-tice nurse staffing was positively and significantly(p < 0.01) associated with quality of care scores for COPD,CHD, Diabetes, and Hypothyroidism (Table 2)2. Theassociation between practice nurse staffing and hyperten-sion was close to significance (p = 0.053). There were nosignificant association between quality of clinical care andlist size per full-time equivalent GP (p > 0.05).
Clinical recording, education and training and makingmore use of the patient survey were significantly(p < 0.001) and positively related to clinical care qualityas measured by Quality and Outcomes Frameworkcomposite scores for all clinical conditions. The effect ofclinical recording was strongest for asthma, COPD andmental health and weakest for hypothyroidism, hyperten-sion and CHD. The effect of education and training wasstrongest for asthma and mental health and weakest forCHD, hypertension and hypothyroidism. Those practicesthat had undertaken a patient survey each year, reflectedon the results, proposed changes and discussed the resultsas a team with a patient group or non-executive directorhad significantly better care for all clinical conditions. Therelationship between the length of consultation indicatorand clinical quality scores was inconsistent and not alwayspositive. For example, not meeting the required consulta-tion length was associated with better scores for mentalhealth (p < 0.05).
Amongst the other characteristics five or more sig-nificant associations were found for population density (5),percent of patients aged 65 and over (5), unadjusted
2 Note degrees of freedom are calculated in a non-conventional way for
difference testing when using the MPLUS WLSMV estimator in models
containing both categorical and continuous dependent variables which
was different to the more conventional approach using the Sartorra–
Bentler method for models with continuous dependent variables only.
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–12101204
Author's personal copy
Ta
ble
2
Full
reg
ress
ion
mo
de
l:a
sso
cia
tio
nb
etw
ee
no
rga
nis
ati
on
al
fact
ors
,n
urs
est
affi
ng
an
dq
ua
lity
of
care
.
Ch
ara
cte
rist
ics
Ast
hm
aC
OP
DC
HD
Dia
be
tes
Hy
pe
rte
nsi
on
Hy
po
thy
roid
ism
Me
nta
lh
ea
lth
Str
ok
e
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
Org
an
isa
tio
na
lfa
cto
rsC
lin
ica
lre
cord
ing
3.9
09
c0
.40
83
.15
9c
0.3
13
1.5
33
c0
.12
52
.63
2c
0.2
35
1.4
08
c0
.10
90
.72
7c
0.1
11
3.8
17
c0
.60
11
.95
1c
0.2
14
Ed
uca
tio
na
nd
tra
inin
g1
.15
4c
0.2
60
1.2
12
c0
.19
70
.38
5c
0.0
76
0.9
00
c0
.14
40
.38
9c
0.0
66
0.4
42
c0
.07
11
.44
8c
0.4
02
0.8
10
c0
.14
9
Pa
tie
nt
ex
pe
rie
nce
Len
gth
of
con
sult
ati
on
s�
0.1
91
0.6
19
0.6
03
0.4
84
0.1
37
0.2
66
�0
.08
00
.43
70
.48
00
.26
50
.40
50
.26
2�
2.7
86
a1
.13
70
.73
10
.40
1
Pa
tie
nt
surv
ey
*A
pp
rov
ed
surv
ey
NO
Tu
nd
ert
ak
en
0.0
00
0.0
00
0.0
00
0.0
00
0.0
00
0.0
00
0.0
00
0.0
00
*A
pp
rov
ed
surv
ey
un
de
rta
ke
n
ea
chy
ea
r
�0
.98
11
.03
4�
0.5
53
0.8
40
0.4
76
0.4
13
0.8
22
0.6
45
1.2
14
a0
.47
90
.58
20
.38
2�
2.9
45
1.8
52
�0
.17
40
.77
2
*a
nd
refl
ect
ed
on
resu
lts
an
d
pro
po
sed
cha
ng
es
2.3
37
b0
.79
71
.51
0a
0.6
64
0.7
51
a0
.32
61
.97
6c
0.5
15
1.3
89
c0
.33
91
.19
3c
0.2
73
1.0
43
1.5
70
1.0
82
0.5
86
*a
nd
dis
cuss
ed
resu
lts
wit
ha
s
tea
mw
ith
pa
tie
nt
gro
up
/
No
n-E
xe
cd
ire
cto
ro
fP
CO
7.3
28
c0
.69
76
.68
6c
0.5
91
2.6
92
c0
.30
16
.03
3c
0.4
73
3.4
16
c0
.31
12
.85
5c
0.2
36
5.6
41
c1
.43
43
.47
5c
0.5
36
Pra
ctic
en
urs
est
affi
ng
1st<
30
38
.01
0.4
80
0.5
51
1.6
26
0.4
26
0.6
39
c0
.18
71
.22
7c
0.1
66
0.5
23
a0
.20
60
.92
4c
0.1
69
�0
.16
00
.85
80
.22
20
.27
5
2n
d3
03
8.0
2–
39
01
.48
0.0
97
0.5
60
1.4
59
c0
.43
80
.64
8b
0.2
00
1.6
03
c0
.28
70
.49
5a
0.2
16
0.7
64
c0
.18
90
.78
70
.91
40
.30
00
.28
9
3rd
39
01
.49
–4
82
3.4
4�
0.3
57
0.5
70
1.0
31
a0
.44
10
.50
8a
0.2
06
1.3
52
c0
.29
80
.30
10
.21
70
.62
4b
0.1
92
0.0
01
0.9
21
0.1
32
0.3
01
4th
48
23
.45
–6
21
0.6
80
.15
70
.58
00
.89
00
.45
50
.44
9a
0.1
95
1.0
93
c0
.30
00
.19
60
.20
90
.64
4c
0.1
87
0.3
04
0.9
22
0.0
69
0.2
94
5th
62
10
.69
+�
0.1
67
0.5
84
0.5
90
0.4
55
0.4
13
a0
.21
00
.99
0b
0.3
02
0.0
84
0.2
21
0.4
99
a0
.19
90
.56
20
.92
60
.20
40
.30
7
x2
dif
fere
nce
test
(p)
(p=
.76
)(p<
.00
1)
(p<
.00
1)
(p<
.00
1)
(p=
.05
3)
(p<
.00
1)
(p=
.78
)(p
=.6
2)
Bia
sa
dju
stm
en
tD
en
om
ina
tor
use
dto
est
ima
tere
gis
ter
4.3
34
c0
.38
32
.43
1c
0.2
36
0.9
98
c0
.13
70
.70
7a
0.3
10
0.2
74
a0
.11
50
.92
2c
0.1
14
12
.17
8c
1.0
75
1.6
92
c0
.18
8
Are
aD
en
sity
(pe
op
lep
er
he
cta
re2
00
1)
�0
.26
80
.14
3�
0.2
52
a0
.10
8�
0.2
04
c0
.05
4�
0.3
17
c0
.08
2�
0.2
16
c0
.05
7�
0.2
49
c0
.05
2�
0.4
20
0.2
42
�0
.13
70
.07
7
Ind
ex
of
Mu
ltip
leD
ep
riv
ati
on
�0
.17
00
.15
9�
0.5
91
c0
.12
10
.01
00
.06
4�
0.0
56
0.1
00
0.1
58
a0
.07
20
.11
10
.06
5�
0.6
83
b0
.26
2�
0.1
46
0.0
94
Pa
tie
nts
�6
5y
ro
fa
ge
�0
.60
1b
0.2
12
�0
.14
10
.15
6�
0.1
67
a0
.08
2�
0.3
72
b0
.12
30
.12
20
.08
4�
0.0
91
0.0
82
�1
.76
5c
0.3
44
�0
.42
4c
0.1
15
%m
em
be
ro
fra
cia
lo
re
thn
icm
ino
rity
�0
.30
10
.17
1�
0.0
25
0.1
33
�0
.02
40
.06
80
.06
80
.10
5�
0.0
05
0.0
76
�0
.04
10
.06
8�
0.1
89
0.3
08
�0
.00
90
.10
2
Pre
va
len
ceU
na
dju
ste
dp
rev
ale
nce
�0
.12
20
.14
4�
0.3
92
b0
.13
0�
0.8
25
c0
.08
6�
0.5
71
c0
.08
1�
0.2
31
c0
.04
90
.33
4c
0.0
71
3.4
39
0.1
03
0.4
57
c0
.12
0
Pra
ctic
eS
ize
of
pra
ctic
ep
op
ula
tio
n�
0.8
39
c0
.18
8�
0.0
47
0.1
52
�0
.11
20
.07
50
.02
30
.11
4�
0.2
10
b0
.08
0�
0.0
84
0.0
82
�0
.44
80
.28
1�
0.1
54
0.1
11
List
size
pe
rFT
EG
P�
0.1
67
0.1
78
�0
.05
00
.15
7�
0.0
59
0.0
65
�0
.11
90
.11
5�
0.0
03
0.0
67
0.0
21
0.0
77
0.1
09
0.2
56
�0
.02
30
.10
8
Sin
gle
ha
nd
ed
pra
ctic
e0
.37
30
.39
7�
0.6
93
a0
.30
60
.11
30
.14
8�
0.2
62
0.2
38
�0
.20
70
.15
9�
0.2
36
0.1
53
�0
.40
80
.62
80
.22
60
.22
1
Pri
ma
rym
ed
ica
lse
rvic
es
con
tra
ct�
0.4
75
0.2
61
�0
.06
70
.20
1�
0.2
07
a0
.10
1�
0.3
01
a0
.15
3�
0.1
92
0.1
10
0.0
30
0.1
07
�1
.06
2a
0.4
13
�0
.25
30
.15
3
Fa
mil
yp
ract
itio
ne
rs�
45
yr
of
ag
e�
0.0
20
0.1
44
�0
.04
60
.11
5�
0.0
84
0.0
56
�0
.00
10
.08
5�
0.0
70
0.0
62
�0
.09
70
.06
50
.01
80
.22
0�
0.0
39
0.0
83
%Fe
ma
leG
Ps
�0
.07
10
.12
50
.07
80
.09
6�
0.0
54
0.0
46
0.1
20
0.0
73
0.0
79
0.0
50
0.1
88
c0
.04
80
.20
30
.20
70
.17
2a
0.0
71
%G
Ps
qu
ali
fie
din
UK
�0
.09
20
.13
40
.81
8c
0.1
08
0.4
02
c0
.05
30
.69
4c
0.0
80
0.2
51
c0
.05
90
.34
1c
0.0
55
�0
.21
90
.23
80
.79
1c
0.0
81
bco
effi
cie
nts
ind
ica
teth
ed
ire
ctio
na
nd
rela
tiv
est
ren
gth
of
the
ass
oci
ati
on
be
twe
en
ind
ep
en
de
nt
an
dd
ep
en
da
nt
va
ria
ble
sin
the
mo
de
l.
a<
.05
;b<
.01
;c<
.00
1
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–1210 1205
Author's personal copy
prevalence (7) and percent GPs qualified in the UK (6) (seeTable 2 for full results).
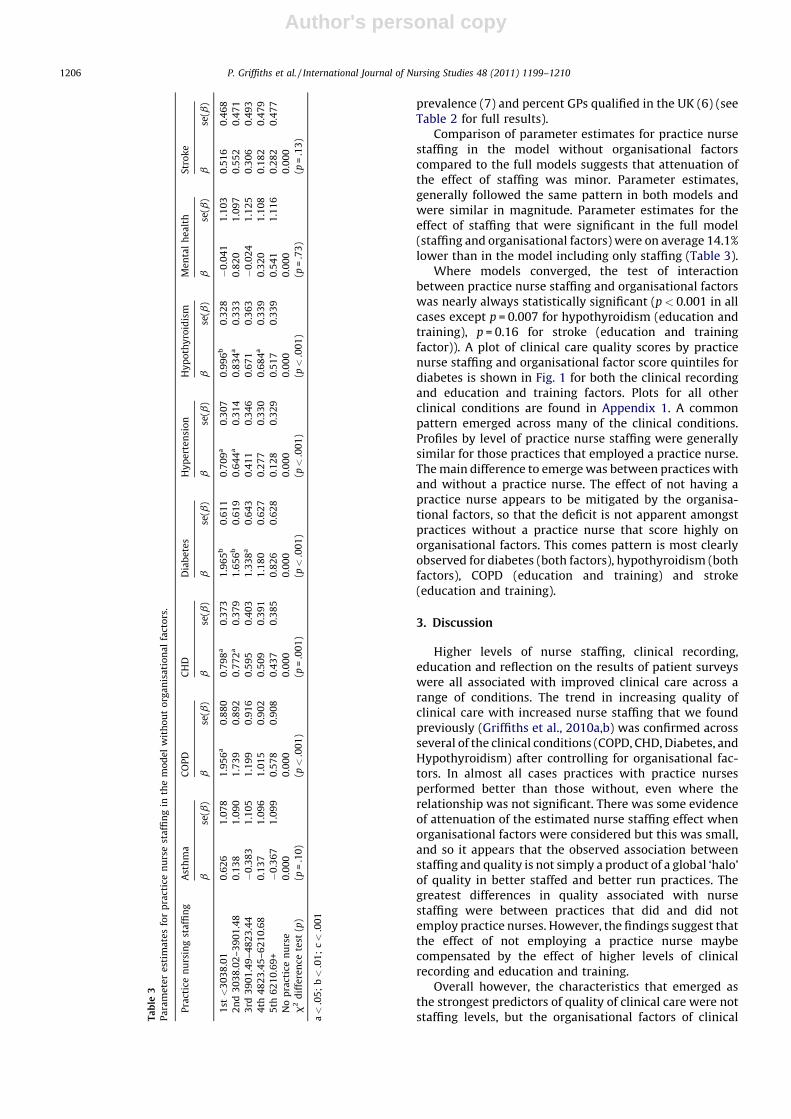
Comparison of parameter estimates for practice nursestaffing in the model without organisational factorscompared to the full models suggests that attenuation ofthe effect of staffing was minor. Parameter estimates,generally followed the same pattern in both models andwere similar in magnitude. Parameter estimates for theeffect of staffing that were significant in the full model(staffing and organisational factors) were on average 14.1%lower than in the model including only staffing (Table 3).
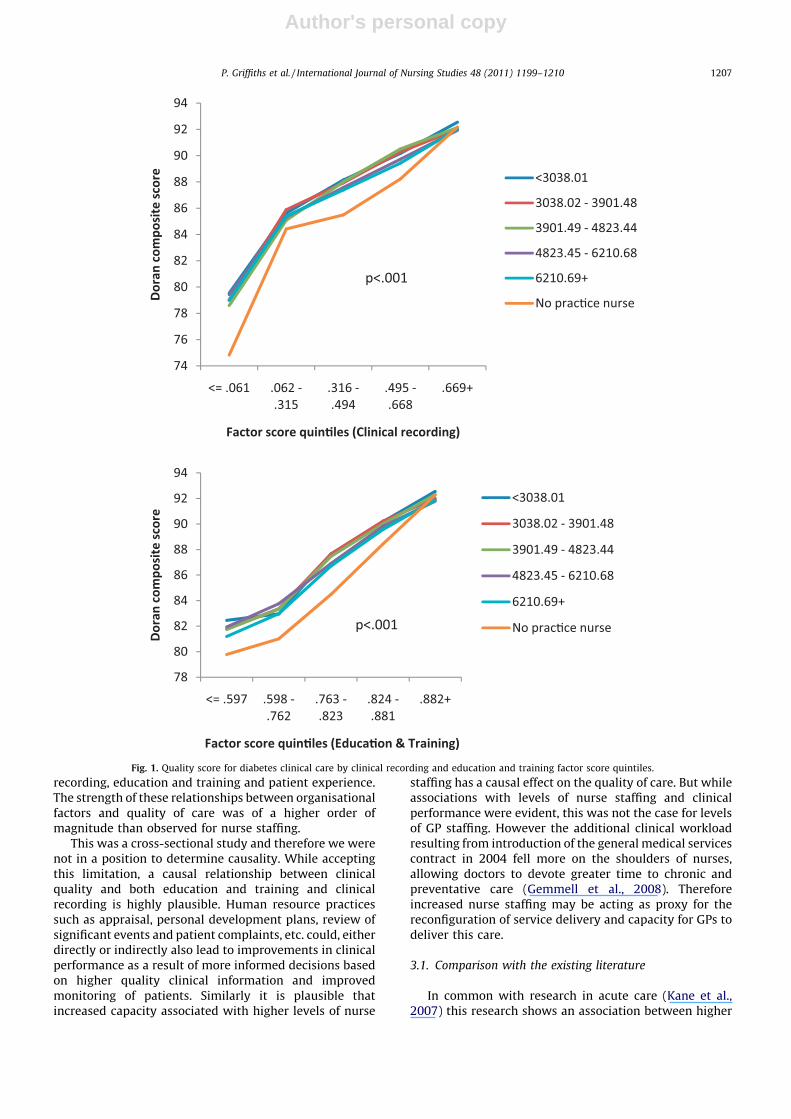
Where models converged, the test of interactionbetween practice nurse staffing and organisational factorswas nearly always statistically significant (p < 0.001 in allcases except p = 0.007 for hypothyroidism (education andtraining), p = 0.16 for stroke (education and trainingfactor)). A plot of clinical care quality scores by practicenurse staffing and organisational factor score quintiles fordiabetes is shown in Fig. 1 for both the clinical recordingand education and training factors. Plots for all otherclinical conditions are found in Appendix 1. A commonpattern emerged across many of the clinical conditions.Profiles by level of practice nurse staffing were generallysimilar for those practices that employed a practice nurse.The main difference to emerge was between practices withand without a practice nurse. The effect of not having apractice nurse appears to be mitigated by the organisa-tional factors, so that the deficit is not apparent amongstpractices without a practice nurse that score highly onorganisational factors. This comes pattern is most clearlyobserved for diabetes (both factors), hypothyroidism (bothfactors), COPD (education and training) and stroke(education and training).
3. Discussion
Higher levels of nurse staffing, clinical recording,education and reflection on the results of patient surveyswere all associated with improved clinical care across arange of conditions. The trend in increasing quality ofclinical care with increased nurse staffing that we foundpreviously (Griffiths et al., 2010a,b) was confirmed acrossseveral of the clinical conditions (COPD, CHD, Diabetes, andHypothyroidism) after controlling for organisational fac-tors. In almost all cases practices with practice nursesperformed better than those without, even where therelationship was not significant. There was some evidenceof attenuation of the estimated nurse staffing effect whenorganisational factors were considered but this was small,and so it appears that the observed association betweenstaffing and quality is not simply a product of a global ‘halo’of quality in better staffed and better run practices. Thegreatest differences in quality associated with nursestaffing were between practices that did and did notemploy practice nurses. However, the findings suggest thatthe effect of not employing a practice nurse maybecompensated by the effect of higher levels of clinicalrecording and education and training.
Overall however, the characteristics that emerged asthe strongest predictors of quality of clinical care were notstaffing levels, but the organisational factors of clinicalT
ab
le3
Pa
ram
ete
re
stim
ate
sfo
rp
ract
ice
nu
rse
sta
ffin
gin
the
mo
de
lw
ith
ou
to
rga
nis
ati
on
al
fact
ors
.
Pra
ctic
en
urs
ing
sta
ffin
gA
sth
ma
CO
PD
CH
DD
iab
ete
sH
yp
ert
en
sio
nH
yp
oth
yro
idis
mM
en
tal
he
alt
hS
tro
ke
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
bse
(b)
1st<
30
38
.01
0.6
26
1.0
78
1.9
56
a0
.88
00
.79
8a
0.3
73
1.9
65
b0
.61
10
.70
9a
0.3
07
0.9
96
b0
.32
8�
0.0
41
1.1
03
0.5
16
0.4
68
2n
d3
03
8.0
2–
39
01
.48
0.1
38
1.0
90
1.7
39
0.8
92
0.7
72
a0
.37
91
.65
6b
0.6
19
0.6
44
a0
.31
40
.83
4a
0.3
33
0.8
20
1.0
97
0.5
52
0.4
71
3rd
39
01
.49
–4
82
3.4
4�
0.3
83
1.1
05
1.1
99
0.9
16
0.5
95
0.4
03
1.3
38
a0
.64
30
.41
10
.34
60
.67
10
.36
3�
0.0
24
1.1
25
0.3
06
0.4
93
4th
48
23
.45
–6
21
0.6
80
.13
71
.09
61
.01
50
.90
20
.50
90
.39
11
.18
00
.62
70
.27
70
.33
00
.68
4a
0.3
39
0.3
20
1.1
08
0.1
82
0.4
79
5th
62
10
.69
+�
0.3
67
1.0
99
0.5
78
0.9
08
0.4
37
0.3
85
0.8
26
0.6
28
0.1
28
0.3
29
0.5
17
0.3
39
0.5
41
1.1
16
0.2
82
0.4
77
No
pra
ctic
en
urs
e0
.00
00
.00
00
.00
00
.00
00
.00
00
.00
00
.00
00
.00
0
x2
dif
fere
nce
test
(p)
(p=
.10
)(p<
.00
1)
(p=
.00
1)
(p<
.00
1)
(p<
.00
1)
(p<
.00
1)
(p=
.73
)(p
=.1
3)
a<
.05
;b<
.01
;c<
.00
1
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–12101206
Author's personal copy
recording, education and training and patient experience.The strength of these relationships between organisationalfactors and quality of care was of a higher order ofmagnitude than observed for nurse staffing.
This was a cross-sectional study and therefore we werenot in a position to determine causality. While acceptingthis limitation, a causal relationship between clinicalquality and both education and training and clinicalrecording is highly plausible. Human resource practicessuch as appraisal, personal development plans, review ofsignificant events and patient complaints, etc. could, eitherdirectly or indirectly also lead to improvements in clinicalperformance as a result of more informed decisions basedon higher quality clinical information and improvedmonitoring of patients. Similarly it is plausible thatincreased capacity associated with higher levels of nurse
staffing has a causal effect on the quality of care. But whileassociations with levels of nurse staffing and clinicalperformance were evident, this was not the case for levelsof GP staffing. However the additional clinical workloadresulting from introduction of the general medical servicescontract in 2004 fell more on the shoulders of nurses,allowing doctors to devote greater time to chronic andpreventative care (Gemmell et al., 2008). Thereforeincreased nurse staffing may be acting as proxy for thereconfiguration of service delivery and capacity for GPs todeliver this care.
3.1. Comparison with the existing literature
In common with research in acute care (Kane et al.,2007) this research shows an association between higher
74
76
78
80
82
84
86
88
90
92
94
<= .06 1 .062 -.31 5
.316 -.49 4
.495 -.66 8
.669+
Dor
an c
ompo
site
sco
re
Factor score quin�les (Clinical recording)
<3038.01
3038.02 - 3901.4 8
3901.49 - 4823.4 4
4823.45 - 6210.6 8
6210.69+
No prac�ce nurse
p<.001
78
80
82
84
86
88
90
92
94
<= .59 7 .598 -.76 2
.763 -.82 3
.824 -.88 1
.882+
Dor
an c
ompo
site
sco
re
Factor score quin�les (Educa�on & Training)
<3038.01
3038.02 - 3901.4 8
3901.49 - 4823.4 4
4823.45 - 6210.6 8
6210.69+
No prac�ce nursep<.001
Fig. 1. Quality score for diabetes clinical care by clinical recording and education and training factor score quintiles.
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–1210 1207

Author's personal copy
levels of nurse staffing and quality of care. Unlike most ofthe research from these settings this study has also shownthat the association remains even, when controlling for thenumbers of doctors and organisational factors, both ofwhich have been shown to be associated with quality inacute care (Jarman et al., 1999; West et al., 2006).Systematic reviews (Gemmell et al., 2008) have shownthat nurses can provide high quality care to patients withlong-term conditions which is supported by this study.
However, the measures of quality used in the Qualityand Outcomes Framework are primarily based on pro-cesses of care and intermediate outcomes, such as controlof blood pressure. When examining hospital admissionsthe relationship between nurse staffing in primary careand quality is less clear. While higher nurse staffing ingeneral practice is associated with fewer admissions forAsthma and COPD, it is associated with more admissionsfor diabetes (Griffiths et al., 2010a,b). Although thecomplexity of diabetes care raises doubts about the useof diabetes admissions as an indicator of quality in primarycare, results such as this should serve as a reminder thatcausal inference remains problematic.
Organisational factors have been identified as signifi-cant predictors of quality in acute care. In hospital settingsthe extent of team working and training strategies havebeen linked to positive performance (West et al., 2002).Perceived quality of nurses’ working environment, whichincluded aspects of staff development as well as leadershipand teamwork between nurses and doctors, has also beenshown to be associated with mortality in acute care (Aikenet al., 2008). There is clearly more potential for teamworking in practices which employ nurses and it may bethat the benefits associated with higher nurse staffinglevels which we observed, which are mostly derived fromemploying any nurses, result from the increased potentialfor teamwork. Our study found that there were a smallnumber of practices that did not employ a nurse whoperformed well when this was accompanied by high levelsof clinical recording, suggesting that other organisationalfactors can compensate for this deficit. However, ourdataset contained no direct measure of team working andso we were unable to explicitly explore this factor.
The evidence on staffing and outcome relationships inacute care has been used to advocate for mandatorystaffing levels (Buchan, 2005). The argument for this isprimarily based on concerns about patient safety in acutecare settings and there are concerns that any minimumratio could come to be regarded as a ‘target’ which did notadequately meet the needs of some patient groups (Spetzet al., 2009). It has also been suggested that legislatingratios for nurse staffing can be stifling for management andlimit innovation (Buchan, 2005; Spetz et al., 2009). A moresystematic approach to HR practices that goes beyondsimply changing the skill mix through numbers of staff isrequired (Dubois and Singh, 2009).
While it is unlikely that similar proposals on staffingwill emerge in primary care, it has been argued thatpractice nurses can provide care equal to or better thandoctors (Burke, 2009) resulting in calls for furtherexpansion of the nursing role. Efficiency gains arepredicted if doctors withdraw from tasks that nurses can
perform, to focus on the tasks only doctors can perform(Sibbald, 2008), which potentially leads to an increaseddemand for nurses. Concerns however remain about thelevel of training that practice nurses receive which, unlikedoctors, is not regulated and therefore key competenciesare not guaranteed. This study underlines the crucialimportance of education and training of practice staff inensuring that quality of care is maintained and enhanced.Getting practices to aspire to a rich mix of skilled staffworking as a team is potentially less contentious thanidentifying a requirement for more of a specific staff group.In a similar vein, Dubois and Singh (2009) have suggestedmoving the human resource management focus away fromskill-mix to skill management. The focus then becomes lessabout numbers of staff and more about the individual’sabilities to adapt and adjust to the changing circumstances.This leads into discussions about aspects of healthcare staffroles (enhancement, enlargement, delegation, substitu-tion) set in the context of patient need and organisationaland institutional factors.
3.2. Strengths and limitations of the study
This study used data collected on all English GPpractices. About 11% of practices had to be excluded ongrounds of data quality and lack of available data tocalculate nurse staffing estimates. Full time equivalentnurse staffing had to be estimated from headcount(number of employees) because data on full timeequivalence is not routinely collected in the UK at thepractice level, although this estimate appears robust(Griffiths et al., 2010a,b).
The organisational factors that we studied weredetermined by the available data. Performance on Qualityand Outcomes Framework organisational indicators (andclinical domain indicators) was, and still is, used todetermine payment to GP practices. How well theyrepresent all the potential organisational factors thatmight impact on quality of care and whether they remain‘‘fit for purpose’’ is open to question. Many of those used in2005/2006 are still in use today, which suggests a degree ofrobustness, and they were selected for a specific purpose inmind; to improve clinical outcomes. However importantfactors, such as team work, could not be studied. Ourmodel also lacked measures of staff wellbeing andperceptions of the organisational climate which, have alsobeen identified as significant in other settings. Thesedisadvantages should be set against the benefit of apopulation sample with very low unit (practice) and item(indicator) non response.
Certain assumptions underpin the factor analysis ofdichotomous items that we performed. The approachproposed by (Muthen, 1989) appears to be robust topotential violations. The analysis was made more robust byremoving a small number of indicators that produced lowfrequency counts when cross-tabulated with other indi-cators. The final factor structure is unlikely to have beenaffected greatly by their exclusion. We were unable tocompute multi-level models to account for clustering ofpractices in primary care trusts. Other studies suggest thatfailure to account for clustering when the variance
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–12101208

Author's personal copy
associated with the cluster is low makes no substantivechange to conclusions, although estimation can beimproved (Park and Lake, 2005). Furthermore the PrimaryCare Trust is primarily a geographical cluster andgeographical factors (such as deprivation and urbanicity)were included in the model.
3.3. Implications for clinical practice and future research
The economic rationale for using more nurses is thatthey are cheaper to employ. This study shows that they canalso be associated with improved quality of care but theyshould be deployed in areas where there is consistentevidence of equivalent or superior care to doctors (Sibbaldet al., 2006). Salary savings could quite easily be lost bylower productivity (Goryakin et al., in press). Thereforerole changes should be carefully targeted towards thoseareas where benefit has clearly been demonstratedpreviously or where there is a high level of confidencethat benefits will result. This reallocation of activity fromdoctors to nurses can result in other benefits, for exampleallowing doctors to focus on more complex care. Thereforeincreased nurse staffing can result in both direct andindirect effects.
Although we should be wary of assuming that the crosssectional relationships we observed are causal, causality ishighly plausible. These results highlight how important isthe organisation and management of care, includinghuman resource management, in delivering high qualityclinical care in general practice. While nurse staffing levelswere significant predictors of quality in several conditionsthe main effect was associated with having any practicenurses, which suggests that the benefit might derive frommulti-disciplinary teams. The benefits of education,training and personal development of nurses in generalpractice were clearly indicated. In this research, themeasurement of these organisational variables is coarseand there is ample scope for considerable variation in thequantity and quality of training and support provided to bemasked. Further work should consider exploring theadvantages of specific training for managing specificconditions (e.g. specialist courses in diabetes). Generalpractice should recognise the potential advantages thatderive from organisational development and investment insupport for existing staff compared to the relativelymodest benefits that derive from investing in more staffin isolation.
Conflict of interest
None declared.
Funding
This research was funded by a ‘Policy ResearchProgramme in the Department of Health in England’.
Ethical approval
Not required.
Acknowledgements
This is an independent report commissioned andfunded by the Policy Research Programme in the Depart-
ment of Health in England. The views expressed are notnecessarily those of the Department.
Appendix A. Supplementary data
Supplementary data associated with this article canbe found, in the online version, at doi:10.1016/j.ijnurstu.2011.03.011.
References
Aiken, L., Clarke, S., Sloane, D., Lake, E., Cheney, T., 2008. Effects of hospitalcare environment on patient mortality and nurse outcomes. TheJournal of Nursing Administration 38 (5), 223.
Aiken, L.H., Smith, H.L., Lake, E.T., 1994. Lower Medicare mortality amonga set of hospitals known for good nursing care. Medical Care 32 (8),771–787.
Anon, 2007. QOF nurse survey—Are targets damaging patient care?Independent Nurse http://www.internurse.com/cgi-bin/go.pl/library/abstract.html?uid=75435, [accessed 03/05/2011]
Bagley, B., Chan-Tack, K.M., Hicks, P., Rayburn, K., Nasir, L., Willems, J.P.,Kim, C., Poplin, C.M., Mundinger, M.O., Kane, R.L., Sox, H.C., 2000.Health outcomes among patients treated by nurse practitioners orphysicians. JAMA 283 (19), 2521–2524.
Brown, M.B., Benedetti, J.K., 1977. On the mean and variance of thetetrachoric correlation coefficient. Psychometrika 42 (3), 347–355.
Buchan, J., 2005. A certain ratio? The policy implications of minimumstaffing ratios in nursing. Journal of Health Services Research andPolicy 10 (4), 239–244.
Burke, L., 2009. Nurse practitioners and general practitioners, is there anydifference? InnovAiT 2 (11), 687–688.
Dr Crippen, 2010. Dr Crippen: Only in Our Points-Obsessed System couldNurses be ‘better’ than Doctors. Guardian, London, pp. 15.
Doran, T., Fullwood, C., Gravelle, H., Reeves, D., Kontopantelis, E., Hiroeh, U.,Roland, D.M., 2006. Pay-for-performance programs in family practicesin the United Kingdom. New England Journal of Medicine 355, 375–384.
Dubois, C.-A., Singh, D., 2009. From staff-mix to skill-mix and beyond:towards a systemic approach to health workforce management.Human Resources for Health 7 (1), 87.
Gemmell, I., Campbell, S., Hann, M., Sibbald, B., 2008. Assessing workloadin general practice in England before and after the introduction of thepay-for-performance contract. Journal of Advanced Nursing 65 (3),509–515.
Goryakin, Y., Griffiths, P., Maben, J., in press. Economic evaluation of nursestaffing and nurse substitution in health care: a scoping review. Inter-national Journal of Nursing Studies, doi:j.ijnurstu.2010.1007.1018.
Griffiths, P., Murrells, T., Dawoud, D., Jones, S., 2010a. Hospital admissionsfor asthma, diabetes and COPD: is there an association with practicenurse staffing? A cross sectional study using routinely collected data.BMC Health Services Research 10, 276, doi:10.1186/1472-6963-1110-1276.
Griffiths, P., Murrells, T., Maben, J., Jones, S., Ashworth, M., 2010b. Nursestaffing and quality of care in UK general practice: cross-sectionalstudy using routinely collected data. British Journal of General Prac-tice 60 (1), e36–e48.
Hippisley-Cox, J., Fenty, J., Heaps, M., 2007. Trends in Consultation Ratesin General Practice 1995 to 2006: Analysis of the QRESEARCH data-base. NHS Information Centre.
Jarman, B., Gault, S., Alves, B., Hider, A., Dolan, S., Cook, A., Hurwitz, B.,Iezzoni, L.I., 1999. Explaining differences in English hospital deathrates using routinely collected data. BMJ 318 (7197), 1515–1520.
Kane, R., Shamliyan, T., Mueller, C., Duval, S., Wilt, T., 2007. The associationof registered nurse staffing levels and patient outcomes: systematicreview and meta-analysis. Medical Care 45 (12), 1195–1204.
Kazanjian, A., Green, C., Wong, J., Reid, R., 2005. Effect of the hospitalnursing environment on patient mortality: a systematic review.Journal of Health Services Research and Policy 10, 111–117A.
Knight, R., 2008. Should primary care be nurse led? BMJ 337, a1169.Leese, B., 2006. New opportunities for nurses and other healthcare
professionals? A review of the potential impact of the new GMScontract on the primary care workforce. Journal of Health Organisa-tion and Management 20 (6), 525–536.
Muthen, B., 1989. Dichotomous factor analysis of symptom data. Socio-logical Methods and Research 18 (1), 19–65.
Muthen, L.K., Muthen, B.O., 2007. Mplus User’s Guide. Muthen & Muthen,Los Angeles, CA.
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–1210 1209

Author's personal copy
Park, S.E., Lake, T., 2005. Multilevel modeling of a clustered continuousoutcome: nurses’ work hours and burnout. Nursing Research 54 (6),406.
Pearce, C., Hall, S., Phillips, C., 2010. When policy meets the personal:general practice nurses in Australia. Journal of Health ServicesResearch and Policy, doi:10/1016/j.hsrp.2009.009099.
Pett, M.A., Lackey, N.R., Sullivan, J.J., 2003. Making Sense of Factor Ana-lysis: the Use of Factor Analysis for Instrument Development inHealth Care Research. Sage, Thosand Oaks, CA.
Sibbald, B., 2008. Should primary caare be nurse led? BMJ 337, a1157.Sibbald, B., Laurant, M.G., Reeves, D., 2006. Advanced nurse roles in UK
primary care. The Medical Journal of Australia 185 (1), 10–12.Sox, H.C., 2000. Independent primary care practice by nurse practitioners.
JAMA 283 (1), 106–108.
Spetz, J., Chapman, S., Herrera, C., Kaiser, J., Seago, J., Dower, C., 2009.Assessing the Impact of California’s Nurse Staffing Ratios on Hospitalsand Patient Care. California Health Care Foundation Issue Brief (Feb-ruary), pp. 1–10.
The Information Centre, 2008. General and Personal Medical ServicesEngland 1997–2007. The Information Centre.
West, M.A., Borrill, C., Dawson, J., Scully, J., Carter, M., Anelay, S., Patterson,M., Waring, J., 2002. The link between the management of employeesand patient mortality in acute hospitals. The International Journal ofHuman Resource Management 13 (8), 1299–1310.
West, M.A., Guthrie, J.P., Dawson, J.F., Borrill, C.S., Carter, M., 2006.Reducing patient mortality in hospitals: the role of humanresource management. Journal of Organizational Behavior 27(7), 983–1002.
P. Griffiths et al. / International Journal of Nursing Studies 48 (2011) 1199–12101210
Copyright © 2022 FDOKUMEN