
Comorbidity of attention Deficit Hyperactivity Disorder and Post-Traumatic Stress Disorder
Upload
khangminh22Category
view
1download
0
THE EFFICACY OF A HOMOEOPATHIC COMPLEX (t.r.s 200C ®)
ON THE SYMPTOMS OF POST TRAUMATIC STRESS DISORDER IN WOMEN
A mini-dissertation presented to the
Faculty of Health Sciences, University of Johannesburg,
As partial fulfilment towards the Masters Degree in Technology:
Homoeopathy
By:
Mohsina Rashid Honnorat
Student Number: 802038979
Supervisor: _____________________________ ________________
Dr E.M. Solomon Date
HD.ND.DO.BA
Co-Supervisor: _____________________________ ________________
Dr.Anita Fourie Date
M.A.BA(Hons).Phd(UNISA).BM(UJ).
iii
iii
Executive Summary
Post Traumatic Stress Disorder (hereinafter referred to as “PTSD”) is the diagnosis
encompassing a cluster of distressing symptoms which is characterized by re-experiencing
trauma, by avoidance behaviour and by hyper-arousal, symptoms which persist for more than
a month after a traumatic event and may worsen over time (Follette and Pistorello, 2007).
Where traumatic violence presents women easily develop chronic PTSD. The lifetime
prevalence, risk, tendency and persistence to suffer from the disease symptoms of PTSD, is
significantly higher in women compared with men. Women also experience a longer course of
illness and worse quality-of-life outcomes (Seedat S., Stein D. J. and Carey P.D., 2005).
Conventional treatment methods using antidepressants and mood-enhancers, are plagued by
numerous, documented side effects, such as cardiovascular complications, liver impairment,
neuropsychological changes, suicidal tendencies and aggression (Pacher and Kecskemeti,
2004, Gibbons R.D., Brown C. H., Hur, K., Marcus S.M., Bhaumik D.K., J.A., Herings
R.M.C. and Mann J.J. (2007). The homoeopathic complex t.r.s 200C® by Pegasus
Homeopathic is a commercial product which is indicated for the treatment of shock and
trauma, but there has so far been no other research in respect of its effectiveness in the
treatment of PTSD.
The aim of this research was to determine the efficacy of the homeopathic complex Pegasus
t.r.s 200C® on the symptoms of PTSD in women. Symptoms were assessed by means of a
modified DSM-IV criterion.
Thirty females aged eighteen-fifty-five were recruited by means of an advertisement placed at
The Nisaa Institute for Women’s Development (hereinafter referred to as “Nisaa”) (Appendix
A). All the participants were pre-diagnosed with PTSD lasting not longer than two years,
under supervision of a registered psychologist from the institution. Participants on chronic
medication, except for hypertensive medication, on contraceptives, as well as pregnant or
lactating women, were excluded from the study.
This research was done as a pre-test post-test non-equivalent group design with a double-blind
placebo-control (Robson, 1993; Trochim, 2006). Those who met the criteria were supplied
with a general information form (Appendix B), and were asked to sign a consent form
(Appendix C). They also completed a patient information and case-taking form and
underwent a physical examination (Appendix D). Participants subsequently completed a
iv
modified DSM-IV criterion questionnaire (Appendix E) in order to confirm their PTSD status.
The aforesaid step represented the pre-test. Participants were randomly placed in either a
test/experimental or a placebo/control group made up of fifteen participants per group. Both
groups were earmarked to receive trauma counselling at Nisaa once a week.
The Experimental Group was administered Pegasus t.r.s 200C®, while the Control Group was
given a placebo. All the participants were instructed to take five pillules of their
placebo/medication three times weekly for a period of six weeks. All the participants were
furnished with a calendar (Appendix H) for them to sign, the purpose of which was to indicate
when they had taken the medication/placebo. A follow-up consultation took place in weeks
three and six, at which the modified DSM-IV criterion questionnaire (Appendix E) was
completed, as post-test 1 and post-2 respectively.
Data was analysed using the Mann-Whitney U Test, Friedman Analysis of Variance by Ranks
Test and Wilcoxon Signed-Ranks Test (Devey, 2010).
After an analysis of all the results, it can be concluded that there was a significant reduction of
the overall severity and intensity of PTSD symptoms over a six week duration (p=0.011).
Pegasus t.r.s 200C® significantly improved ten specific symptoms of PTSD but it was
especially effective in dealing with two important symptoms of PTSD, namely, re-
experiencing symptom (flashbacks) and hyper-arousal symptom (irritability)
v
I start in the Name of Allah, the All-Merciful, the most Merciful
I send prayers of blessing and salutations of peace on our beloved Prophet Muhammad
(Sallallāhu ‘alayhi wa-Sallam)
DEDICATION
To my dearest family and friends
To my late beloved uncle Ismail Mahomed
Especially to my late beloved aunt Zuleikha Mahomed
For their love, support and immense patience
During the completion
Of this dissertation
And
To
Women
For their inner strength, resilience and incredible ability to bounce back
vi
ACKNOWLEDGEMENTS
My heartfelt thanks and gratitude goes to all the assistance, kindness, generosity and support
provided by the following persons:
Dr Elizabeth Solomon, the Supervisor of this project, for her warmth, guidance and lovely
outbursts of laughter,
Ivy Segoe the health science librarian from the UJ library, for all her help in tracing for me
the information I needed.
Dr Anita Fourie, the Co-Supervisor of the project, for her sparkling ideas, motivation and
encouragement.
Dr Zubeda Dangor, for her sincerity, dedication and inspiring spirit, and to the whole Nisaa
team.
Dr Kathryn Peck for her immense contribution in refining my research
Antonella, Ian and Gayle from Pegasus Homoeopathic, for their generosity and belief in
the worth of this study.
Richard Devey, Jaclyn Mercia Smith, Jurgen Becker and Bianca, the UJ statistical
consulting service, for their patience and reiterated explanations until I eventually grasped
the beneficial points they were seeking to convey to me.
Ahmad Ali Honnorat: My incredible life partner, greatest teacher and challenger. You are
in the middle, close to my heart. I thank you for not stopping me and allowing me to be a
free spirit, even when the journey was really difficult for you. I love you. I am sorry if I
just could not be the canary in my aunt’s cage. I do appreciate you for your goodness and
being. A very special thank you and deep appreciation for your efforts in helping me to
refine my work.
Rashid Ahmed and Rookaya Mahomed, my dear loving parents, whom I just cannot thank
enough. You are the most amazing people I know, with an enormous spirit of love and
generosity. Your love and duas keep me going.
Mustafa, Humaid, Al-Munsif and Awsat, my precious darling children, my challenges and
joy. I thank you for being patient and putting up with my lack of motherly support during
these ten long years. You are my life, and I love you all dearly. You all are uniquely
awesome.
My heartfelt thanks to my mother-in-law Giovanna Honnorat, Cinzia and Fabio, Riccardo
and Micaela, and to my late father-in-law Salvatore Honnorat. I value your support and
kindness.
vii
My brothers and their families, Suleiman and Hajira, Haroun and Saleha, for their
generosity and kind support. Naseeha, Yusrah, Sufyaan, Fatima, Muhammed and Raeesa.,
Safeeya, Nazeera, Muhammad Hamid and Saadia: I thank you for being part of my life.
My Aunt’s and uncles, the late Ismailpapa and late Zuleikha Mahomed (apafooi), for being
my friend and for her incredible kindness and generosity, as well as Zubeida (Gorima), my
late uncle Yusuf and Haleema, for always being on hand, and my late aunt Zuleikha
Amejee (chotifooi) and Goribibi, Fatima Bismillah (gorifooi) and Fawjee, Shaheda and
Nadia, Abba and late Appa, Yunus papa and Gorimamee and late Chotapapa and
Chotimamee and all my uncle and aunts from the Amejee side and Ayeshakala, and all the
marhoomin Grandparents. I cannot forget either all my cousins from both sides of the
families that have touched my life. I give you a big “thank you” for your well-meaning
wishes and duas. You all are very special to my heart, and I could fill pages writing down
all your names.
Shameema and Ebrahim Patel, my very special friends. I cannot thank you enough.
All my teachers since when I was a little girl. I thank you, as I am totally indebted to you.
Shaheda Mahomed and Khudaija Manga, I thank you for all your love and generosity.
My extremely kind neighbours Aunty Sara, Baboo Vania and family, for taking care of
Awsat, and Muhammed , Roldah Khan and family for their kind support.
Fatima Bhamjee, Ayesha (goribhaai) and Rookayabhaai and Bhamjee family. I thank you
for your warmth, love and generosity. You all are very dear to me.
Zarinakala, Tahira, Amina & Nabeela for your weekly messages, Munira for your jokes.
Sue Nel, who said that my eyes sparkled when I spoke about Homoeopathy, and for
picking up the phone to call the University which resulted in my enrolment. I thank you
my friend. Special thanks to Sue & Tom for allowing me to work at their peaceful home.
Haseena and Abdul Qader (Jerry) Smith for all your love, support, books and knowledge
you provided me with.
Sadhna, my dear best friend of over 30years, and Sheetal, for her valuable advice.
Silvia. I thank you for the encouragement and motivation, especially when the going was
tough. Leah and Nina Frank, Fatima and Rabia Rajah, my friends, from whom I draw
strength.
Masha and Hoosein, for keeping the peace, and Dr. Jean Donaldson, for pushing me to
finalize my studies, not forgetting Pam Azvedo for the cake and teas every week.
All my friends, family and souls that have touch my hearts, especially those whose names I
have forgotten to mention. Please forgive me for such omission, and thanks a million.
viii
Special gratitude is reserved for my mentor and dear friend Dr. Nadia Grigorova for
believing in me when even I did not, as well as for Dr. Bulatov, on account of his immense
knowledge in health-related matters.
Philippe, for all your tender kindness, and numerous hours spent by you helping me with
the graphs, tables and layout of this paper. I thank Krikri for her hospitality, and the girls
for allowing you to give up your precious time. I am completely indebted and most grateful
to you. A zillion thanks to you.
Abdus Samad Nana for being a pillar of strength for me and my family in all these years. I
thank you, and in doing so I am not going to forget Shereen for all her kindness and
generosity, as well as Mohammed Patel & Fatima.
Anna Molakeng, my dear friend and helper. I don’t know what I would do without your
assistance: “Baaie Dankie”. Thanks Anna and Maria for keeping my house in order.
Naseem Aboo, for your incredible energy, enthusiasm, immense love and generosity.
Shaykh Tanner Ansari and Shakha Muzayyen: I thank you for opening up the doors, and
for your immense spirit, love and prayers.
Dr. John Matlander from Ecuador: I thank you for sharing some of your valuable
experiences in natural treatment options while you were with Medici Del Mondo.
Carol Hambly: Thank you for your loyalty, trust and valuable advice. My heartfelt
gratitude for the meticulous corrections and proof reading.
Advocate Enrico Honnorat firstly and lastly for your help as a language advisor and
tremendous skill as an international translator. You remind me of Hahnemann.
ix
TABLE OF CONTENTS PG
TITLE PAGE i
AFFIDAVIT ii
EXECUTIVE SUMMARY iii
DEDICATION v
ACKNOWLEDGEMENTS vi
TABLE OF CONTENTS ix
LIST OF APPENDICES xiii
LIST OF TABLES xiv
LIST OF FIGURES xiv
CHAPTER ONE 1
1.1 Problem Statement 1
1.2 Aim of the study 2
CHAPTER TWO 3
2 LITERATURE REVIEW 3
2.1 Introduction to PTSD 3
2.2 Diagnosis of PTSD 3
2.3 History 4
2.4 Epidemiology - Cause and Distribution 4
2.5 PTSD Treatment 5
2.5.1 Psychotherapy 5
2.5.1.1 Trauma Counselling and Debriefing 5
2.5.1.2 Cognitive-behavioural therapy (CBT) 6
2.5.1.3 Eye movement desensitization and reprocessing (EMDR) 6
2.5.1.4 Community agencies as support structures 7
2.5.1.4.1 Nisaa 7
2.5.1.4.2 Emergency Shelter Services (E.S.S) 8
2.5.1.4.3 Telephone lifeline and helpline services 8
2.5.2 Pharmacotherapy 8
2.5.2.1 Antidepressant drugs 9
2.5.2.1.1 Monoamine oxidase inhibitors (MAIO’s) 9
2.5.2.1.2 Selective serotonin reuptake inhibitors (SSRI’s) 9
2.5.2.1.3 Tri-cyclic antidepressants (TCA’s) 10
x
2.5.2.1.4 Selective nor-epinephrine reuptake inhibitors (SNRI’s) 10
2.5.2.2 Anti-anxiety drugs (Busipirone, Benzodiazepines and beta blockers) 10
2.5.2.3 Hypnotics 11
2.5.2.4 Antipsychotic drugs 11
2.5.2.5 Pharmacokinetic and pharmacodynamics of antidepressants and women 12
2.6 Homoeopathy 12
2.6.1 Introduction 12
2.6.2 Principals of Homoeopathy 13
2.6.3 Provings 13
2.6.4 Principals of dilution, potentisation and aggravations 14
2.6.5 The Homoeopathic single remedy 15
2.6.6 The Homoeopathic complex remedy 15
2.6.7 Homeopathic dosage 15
2.7 Bach Flower Remedies 16
2.7.1 Flower remedies 16
2.7.2 Edward Bach philosophy and works 16
2.8 t.r.s. 200C® 17
2.8.1 Aconitum napellus 18
2.8.2 Arnica montana 18
2.8.3 Hypericum perforatum 19
2.8.4 Ignatia amara 19
2.8.5 Opium Papaver somniferum 20
2.8.6 Passiflora incarnate 21
2.8.7 Impatiens 22
2.8.8 Clematis flower 22
2.8.9 Rock rose 23
2.8.10 Star of Bethlehem 23
2.8.11 Cherry plum 24
2.9 Related Research 25

xi
CHAPTER THREE 26
3. RESEARCH METHODOLOGY 26
3.1 Research sample and recruitment 26
3.1.1 Inclusion criterion 26
3.1.2 Exclusion criterion 26
3.2 Research design and procedure 26
3.3 Medicine administration and randomisation of the study 27
3.4 Reliability and validity of the measurement tool 27
3.5 Data collection and analysis 28
3.6 Ethics 28
CHAPTER FOUR 29
4. RESULTS OF STATISTICAL ANALYSIS 29
4.1 Introduction to results 29
4.2 Results 29
4.2.1 Frequency results 29
4.2.1.1 Age frequency 29
4.2.2 Tests for normality 30
4.2.3 Non-parametric tests 30
4.2.3.1 Mann Whitney U Test 30
4.2.3.2 Freidman Analysis of Variance by Ranks Test 31
4.2.3.3 Wilcoxon Signed-Rank Test and Bonferroni Adjustment 31
4.3 Data obtained from participants pre-test (t1) and post-test 1 (t2) and post-
test 2 (t3) questionnaires. 32
4.3.1 Intensity and severity of the re-experiencing symptom such as thoughts, images
and perception 33
4.3.2 Intensity and severity of the re-experiencing symptom such as recurrent
distressing dreams 34
4.3.3 Intensity and severity of the re-experiencing symptom such as flashbacks,
illusions and hallucinations 35
4.3.4 Intensity and severity of the re-experiencing symptom such as psychological
distress at any reminder of the trauma. 36
4.3.5 Intensity and severity of the re-experiencing symptom such as physiological
reactivity at any reminder of the trauma. 37
xii
4.3.6 Intensity and severity of the persistent avoidance symptom such as thoughts,
feelings and conversation of the trauma. 38
4.3.7 Intensity and severity of the persistent avoidance symptoms as in avoiding
people, places and activities regarding the trauma. 39
4.3.8 Intensity and severity of the persistent avoidance symptom such as unable to
recall important aspects of the trauma. 40
4.3.9 Intensity and severity of the persistent avoidance symptoms such as diminished
interest in significant activities after the trauma. 41
4.3.10 Intensity and severity of the persistent avoidance symptoms such as feelings
of detachment or feelings of estrangement after the trauma. 42
4.3.11. Intensity and severity of the persistent avoidance symptoms such as a
restricted range of effect, like unable to have loving feelings, uncaring and emotional
numbness after the trauma. 43
4.3.12 Intensity and severity of the persistent avoidance symptom such as a sense of
a foreshortened future after the trauma 44
4.3.13 Intensity and severity of hyper-arousal symptom such as difficulty falling or
staying asleep after the trauma 45
4.3.14 Intensity and severity of hyper-arousal symptom such as irritability after the
trauma 46
4.3.15 Intensity and severity of hyper-arousal symptom such as outbursts of anger
after the trauma 47
4.3.16 Intensity and severity of hyper-arousal symptom such as difficulty in
concentration after the trauma 48
4.3.17. Intensity and severity of hyper-arousal symptom such as being hyper-vigilant
or extra careful after the trauma 49
4.3.18 Intensity and severity of hyper-arousal symptom such as exaggerated startled
response or easily frightened 50
4.3.19. The average scores of intensity and severity of all PTSD symptoms 51
CHAPTER FIVE 52
5. DISCUSSION 52
5.1 Demographics information on Recruitment and Race 52
5.2 Living conditions 53
5.3 Trauma Counselling 53
5.4 Type of Trauma 53

xiii
5.5 The Homoeopathic Dosage in the study 53
5.6 Medication and compliancy 54
5.7 Discussion of statistical analysis 54
5.7.1 Age frequency in the study 54
5.7.2 Shapiro-Wilk Test 54
5.7.3 Mann- Whitney U Test 55
5.7.4 Freidman Analysis of Variance by Ranks Test 56
5.7.5 Wilcoxon Signed-Rank Test 57
5.8 Limitations of the study 57
CHAPTER SIX 58
6. CONCLUSIONS 58
6.1 RECOMMENDATION 58
ANECDOTAL RESULTS 60
REFERENCES 62
APPENDICES 67
Appendix A 67
Advert for recruiting Participants
Appendix B 68
Participant information form
Appendix C 70
Participant consent form
Appendix D 71
Patient Information and case taking form
Appendix E 72
Modified Diagnostic Statistical Manual (DSM_IV) Criterion Questionnaire
Appendix F 75
Letter of consent from Nisaa
Appendix G 76
Counselling Format
Appendix H 77
Calendar
Appendix I 78
xiv
Tabulated Statistical Results from question 1-18 of all the Symptoms
LIST OF TABLES
Table 4.1 Age frequency 29
Table 4.2 Mann-Whitney U Test on the Age 30
Table 4.3 Intensity and Severity Scale 32
LIST OF FIGURES
Figure 4.1 Thoughts, images and perception 33
Figure 4.2 Recurrent distressing dreams 34
Figure 4.3 Flashbacks, illusions and hallucinations 35
Figure 4.4 Psychological distresses at any reminder of the trauma 36
Figure 4.5 Physiological reactivity at any reminder of the trauma 37
Figure 4.6 Avoid thoughts, feelings and conversation 38
Figure 4.7 Avoid activities, places or people 39
Figure 4.8 Unable to recall important aspects of the trauma 40
Figure 4.9 Diminished interest in significant activities 41
Figure 4.10 Feelings of detachment, or estrangement 42
Figure 4.11 Restricted range of affect, unloving uncaring 43
Figure 4.12 Sense of a foreshortened future 44
Figure 4.13 Difficulty falling or staying asleep after the trauma 45
Figure 4.14 Hyper-arousal: Irritability 46
Figure 4.15 Outbursts of anger 47
Figure 4.16 Difficulty in concentration 48
Figure 4.17 Hyper-arousal, hyper-vigilant or extra careful 49
Figure 4.18 Exaggerated startled response or easily frightened 50
Figure 4.19 The average scores of PTSD symptoms 51

1
CHAPTER ONE
1.1 Problem Statement
Post Traumatic Stress Disorder (PTSD) is a diagnosis encompassing a cluster of distressing
symptoms which is characterized by re-experiencing trauma, avoidance behaviour and hyper-
arousal. These symptoms continue to occur for more than a month after an individual has
experienced a traumatic event. With regard to some people, these symptoms may even worsen
over time (Follette and Pistorello, 2007).
PTSD is a disorder of frequent occurrence which has the tendency of easily turning chronic in
women who are exposed to traumatic events, such as abuse, rape, robbery and high-jacking,
all of such events being considered common experiences in South Africa. Females with a
history of sexual violation show a significant degree of association with a diagnosis of PTSD.
Although men are generally exposed to more violent traumas, the risk of developing PTSD is
significantly higher in women. Women have a higher tendency to develop a lifetime
prevalence and persistence of symptoms related to such disease. Women who experience
PTSD evince a greater symptom burden and a longer course of illness than their male
counterparts (Seedat S., Stein D. J. and Carey P.D., 2005). They also display worse quality-
of-life outcomes than men. Patients affected by PTSD experience greater work impairment
and demonstrate a higher alcohol usage as a coping strategy (Olley B.O., Zeier M.D., Seedat
S. andStein D.J., 2005).
Drugs which are currently on the market as treatments for PTSD have a large number of
adverse side effects (Pacher and Kecskemeti, 2004; Gibbons R.D., Brown C. H., Hur, K.,
Marcus S.M., Bhaumik D.K., J.A., Herings R.M.C. and Mann J.J., 2007). Hormonal
fluctuations, such as the menstrual cycle, menopause, oral contraceptives and hormone
replacement therapy, may alter the pharmacokinetics and pharmacodynamics of conventional
drug therapies (Seedat et al., 2005).
Homoeopathy is considered a safe and natural method of healing, one which allows the body
to stimulate its own innate defence system in its totality, thereby allowing it to cure itself.
Homoeopathic complex prescribing resorts to the use of two or more remedies which are
combined so as to cover a broad range of stress factors or disease symptoms, wherefore the

2
remedies are enabled to deal with a vast number of symptoms in any given condition
(Solomon, 2010; Caroll, 2007).
The homoeopathic complex remedy Pegasus t.r.s 200C® by Pegasus Homeopathics is a
commercial product which is manufactured for the treatment of shock and trauma, although
there has thus far been no research regarding its effectiveness in the treatment of PTSD.
1.2 Aim of the study
The aim of the research is to determine the efficacy of the homeopathic complex t.r.s 200C®
on the symptoms of PTSD in women. Symptoms were assessed by means of a modified
DSM-IV criterion.
3
CHAPTER TWO
LITERATURE REVIEW
2.1 Introduction to PTSD
Post Traumatic Stress Disorder (PTSD) is an anxiety disorder that is triggered by
experiencing or witnessing a traumatic life-threatening event, such as military combat, natural
disasters, terrorist attacks, serious accidents, or violent personal assaults like rape and
domestic violence. In some people, these types of stress reactions do not go away over time,
and might even get worse (Ganfyd, 2006).
In South Africa, exposure to trauma and Post Traumatic Stress Disorder (PTSD) are recorded
by several studies as having an extremely high rate of incidence (Carrey, P.D., Stein, D.J.,
Zungu-Dirwayi, N., and Seedat, S., 2003; Dinan, B.A., McCall, G.J., and Gibson, D., 2004;
Kaminer, 2006).
Women often experience symptoms of Post Traumatic Stress Disorder as a result of extreme
stress resulting from being physically or emotionally abused by their husbands, boyfriends or
other intimate partners (Kubany E.S., McCaig M.A., Laconsay J.R. 2003)
2.2 Diagnosis of PTSD
In order for patients to be classified as having PTSD, they must have experienced an
emotional trauma of a sufficient magnitude for it to have been traumatic for almost every
person. Patients diagnosed as having the disease persistently re-experience the traumatic
event, show a pattern of avoidance and emotional numbing, and are in a fairly constant hyper-
arousal state (Kaplan, H.I., Sadock B.J. and Grebb J.A. 1994). The Diagnostic and Statistical
Manual for Mental Disorder (DSM-IV) stipulates the following criterion for the diagnosis of
PTSD (American Psychiatric Association, 1994):
Traumatic exposure. This is known as the A-criterion and involves experiencing,
witnessing or being confronted with an event that is either life-threatening or involves
serious threat of injury to oneself or to others.
Re-experiencing. The B-criterion involves having persistent intrusive memories, sudden
flashbacks and hallucinations associated with the trauma.
4
Avoidance. The C-criterion includes symptoms of persistent avoidance of stimuli
associated with the trauma, avoidance of thoughts, feelings or memories of the trauma,
and an inability to recall important aspects of it. Emotional numbness and an outright
refusal to acknowledge or discuss the experience fall within the scope of such symptoms.
Hyper-arousal. The D-criterion may manifest as sleep disturbance, irritability,
nervousness, anger outbursts and concentration problems.
The duration of these symptoms must persist for one month or more, and must cause, to
survivors of a serious traumatic event, significant distress or impairment in social,
occupational or other important areas of human functioning (APA, 1994). Patients must have
between one third and one half of the symptoms from the DSM-IV, trauma exposure from
criterion A, one re-experiencing symptom from criterion B, three avoidance symptoms from
criterion C, and two hyper-arousal symptom from criterion D. These symptoms must be
present for at least one month in order for a person to be diagnosed with PTSD (APA, 1994;
Fourie, 2010; Dangor, 2010)
2.3 History
The formal introduction of PTSD into the psychiatric nomenclature only occurred in 1980
with the 3rd edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III).
The predominant view in psychiatric publications was that PTSD consisted of a medical
disorder, characterized by particular psychobiological dysfunction. During the past decade,
this view has evolved, and trauma is presently seen as a highly prevalent occurrence, very
often accompanied by post traumatic distress, and less commonly followed by a persistent
pathological response known as Post Traumatic Stress Disorder (Stein D.J., Seedat S., Iverson
A. and Wessely S., 2007). Hence, in 1994, the DSM-IV, with its revised criterion for PTS,
replaced the DSM-III.
2.4 Epidemiology-Cause and Distribution
In epidemiological studies, Ballenger J.C., Davidson J.R.T., Lecrubier Y., Nutt D.J., Marshall
R.D., Nemeroff C.B., Shalev A.Y., and Yehuda R., (2004) found that most people experience
a traumatic event at least once in their lives. Whereas exposure to trauma is rather common,
PTSD is fairly uncommon. Several community studies have concluded that, in the developed
world, more than 80% of individuals have been exposed to severe trauma, but less than 10%
went on to actually develop PTSD. Although exposure to traumatic stress over a lifetime has
been shown to be lower in women, the incidence of PTSD in women is twice that in men
(Seedat et al., 2005).
5
There are a number of factors which can contribute to the development of PTSD. These
include factors predating the trauma, such as the individual’s genetic constitution, the severity
and duration of the trauma, and the circumstances of the individual in the post-trauma
scenario, including the presence or otherwise of social support systems (Ballenger et.al,
2004). The degree of severity when compared to the type of trauma is a significant risk factor
and determines the intensity and length of the illness. Other risk factors which have been
reported include childhood abuse, previous psychiatric history, and a family history of
psychiatric illness. A personal predisposition cannot be excluded as a major cause of the
disorder (Van Zyl M., Oosthuizen P.P., Seedat S., 2007).
Early life trauma, too, is presently recognized as another significant factor in the development
of PTSD. Ethological research suggests that experiencing trauma during key development
periods might result in persistent changes to brain morphology and function, and lead to
increased vulnerability to subsequent adversities. Neuro-chemical and structural brain
changes resulting from early developmental stress in animal models and in maltreated
children are well documented (Ballenger et al., 2004).
2.5 PTSD Treatment
It is normal to experience some degree of distress after a trauma that is going to find its
natural resolution in most individuals. A combination of psychotherapy and pharmacotherapy
are, currently, available treatment options for PTSD. Despite the fact that many methods of
psychological treatment and types of medication have been used to treat PTSD, little evidence
about their effectiveness has been hitherto produced (Van Zyl et al., 2007). Leading
specialists in the field of PTSD have recommended that all psychiatric interviews, as well as
interviews with patients with unexplained somatic complaints, should include routine
screenings for trauma due to its disturbingly high incidence in our society. It is suggested that
clinicians should specifically ask about traumatic events, inasmuch as most patients will not
spontaneously volunteer such information, because it is painful or else because they think that
it might not be relevant to their current complaint (Van Zyl et al., 2007).
2.5.1 Psychotherapy
2.5.1.1 Trauma Counselling and Debriefing
Trauma counselling is a specific form of counselling which is designed to cater for victims of
crisis. It is a standard form of current treatment. However different psychologists and
6
institutions may vary in the choice of format of their counselling methods (Dangor, 2010;
Fourie, 2010).
Debriefing is a form of trauma counselling which is usually initiated almost immediately after
the trauma, or within the first four weeks following it, in the course of the acute stress
syndrome stage. A debriefing session usually lasts about two hours. Debriefing sessions
typically involve a discussion of the event, the person’s reaction to it, and an examination of
coping strategies. Debriefing is commonly used to help rescue personnel, people who
witnessed a serious accident, hijacking and violent attacks, as well as victims of random
shootings and the like thereof (Fourie, 2010).
It is commonly known that trauma counselling and cognitive behaviour therapy (CBT) which
are initiated soon after the trauma have been associated with lower rates of PTSD symptoms
three to six months after the inception of the treatment (Seedat et al., 2005). This can however
be time consuming and very costly. In South Africa, patient compliancies a relevant factor,
and lack of consistency, which is either due to work constraints, poverty or lack of education,
represents a major problem (Fourie, 2011).
2.5.1.2 Cognitive-behavioural therapy (CBT)
CBT is used as a therapy to modify illogical and unrealistic interpretations of events which
are the source of negative emotional reactions. Cognitive processing therapy is a combination
of CBT and exposure which involves writing a detailed account of the trauma, one that is read
out to the therapist. CBT is sometimes used in conjunction with cognitive processing therapy,
elements of exposure therapy, and stress inoculation (Seedat et al., 2005)
Trauma-focused CBT consisting in combinations of cognitive reprocessing, eye movement
desensitization, exposure and restructuring, has had some measure of success (Ballenger et
al., 1998). The disadvantage of this technique is that CBT must be combined with other
techniques and, in the event that it is commenced soon after the trauma, it is associated with
lower rates of PTSD after three or six months from the commencement of the treatment.
However, it, too, is time consuming and very costly (Ballenger et al., 1998).
2.5.1.3 Eye movement desensitization and reprocessing (EMDR)
The EMDR Institute Inc. (2009) states that EMDR is a specialized form of psychotherapy
which is integrative and comprehensive. This form uses several modalities of
7
psychotherapies, such as psychodynamics, CBT, interpersonal, experiential and body-centred
therapies, in structured protocols which are designed to maximise the effects of treating
PTSD. EMDR is an efficient treatment for PTSD and its associated conditions, including
depression. In twenty controlled-outcome study findings, where Shapiro’s Adaptive
Information Processing model was used together with EMDR, the conjunction of the two
techniques resulted in providing solutions to traumatic memories in people suffering with
PTSD. This model postulates that pathology will emerge as the direct result whenever
distressing experiences are not processed adequately (Shapiro and Maxfield, 2002). The
theory regarding EMDR is that stimulated rapid eye movement may help in the psychological
processing of the trauma. It is believed that whatever we experience during the day, along
with our reactions to it are processed during REM sleep. In controlled EMDR sessions, a
stimulus such as moving light is used to induce rapid eye movement (EMDR Institute Inc,
2009). The disadvantage of this method is represented by the cost and time factor: it is a very
expensive and specialised modality and there are only a few trained specialists in this field,
especially in South Africa (Fourie, 2011).
2.5.1.4 Community agencies as support structures
Community agencies, help-lines, lifeline emergency telephone counselling services and Non-
Governmental Organizations (NGO’s), act as support structures which collectively offer a
very important service to trauma survivors.
2.5.1.4.1 Nisaa
The Nisaa Institute for Women’s Development (Nisaa) is a community-based organisation
which was started by a group of committed women at the end of 1993, in response to the
growing problem of violence against women. Nisaa is a non-profit, non-governmental
organization, which is opposed to all forms of oppression, exploitation and violence against
women. Nisaa offers counselling and shelter services, awareness and advocacy, training,
research and development of local, national, regional and international partnerships. Nisaa
provides counselling to women who have been subjected to trauma (Dangor, 2010). The
advantage of an institute such as Nisaa is that it offers free counselling and shelter services
which are provided by an excellent staff, although, because of limited resources, this type of
institutes does not operate as a 24 hour service or during week-ends.
8
2.5.1.4.2 Emergency Shelter Services (E.S.S.)
Nisaa’s tenth anniversary annual report strecords that shelter services are provided by Nisaa
together with as many as sixty-seven other organizations in the Gauteng region alone.
Emergency Shelter Services act as a temporary safe haven for abused women, who are either
homeless or too traumatized to live in their homes. Shelters are places where women gain
control and autonomy over their lives in a way they deem appropriate. Therapeutic and
supportive counselling is offered on a weekly basis for the women hosted therein and their
children. In crisis situations, immediate group and individual counselling is provided. The
advantage of a shelter environment is that most women improve their state of well being and
are empowered after a sojourn of only eight weeks at one such shelter. The problem, however,
lies in the lack of sufficient financial and human resources to maintain the growing numbers
of women and children who are in need of shelters. The government is called upon by existing
circumstances to play a more active role in fulfilling this need (Dangor, Z., Segwai P.K., Dry
J., Ogunmefun C., 2008).
2.5.1.4.3 Telephone lifeline and helpline services
These services are usually funded privately by the local community, churches or other
religious organizations boasting volunteers with some training in counselling. They offer free
counselling services to the public. This kind of service to the community is essential as a first
line contact for those women who are too afraid to seek formal help. Although they are
helpful to many women, these counsellors lack the training and skills of professional
psychologists who are equipped to deal with PTSD (Fourie, 2011).
2.5.2 Pharmacotherapy
Almost all types of psycho-pharmacological agents have been used for the treatment of
PTSD, with variable evidence of effectiveness. Several types of antidepressants are used to
treat PTSD. Monoamine oxidase inhibitors (MAOIs) reduce nightmares and flashbacks.
Selective serotonin reuptake inhibitors (SSRI’s), the “drugs of choice” for PTSD, are used for
depression, hyper-arousal, avoidance and numbing symptoms. Selective nor-epinephrine re-
uptake inhibitors (SNRIs), administered in high doses, are used for the treatment of intrusive
and hyper arousal symptoms (Seedat et al., 2005).
Common side effects of the drugs range from mild symptoms like nausea, dizziness and dry
mouth, to more serious life-threatening ones, such as permanent liver impairment, bleeding
tendencies, permanent neuropsychological changes, persistent pulmonary hypertension and
9
cardiovascular side effects, neonatal abstinence syndrome and congenital malformations
(Pacher and Kecskemeti, 2004).
2.5.2.1 Antidepressant drugs
Antidepressant drugs are made up of monoamine oxidase inhibitors (MAIO’s), selective
serotonin reuptake inhibitors (SSRI’s), tricyclic antidepressants (TCA’s), and other drugs
such as selective nor-epinephrine re-uptake inhibitors (SNRI’s). These drugs are used for
severe depression accompanied with lethargy, loss of libido, despair and poor appetite.
Antidepressants stimulate brain cells so as to produce more neurotransmitters, as these
become depleted when the individual concerned is depressed (Henry, 2002).
2.5.2.1.1 Monoamine oxidase inhibitors (MAOI’s)
MAOI’s, such as Brofaromine and Phenelzine (Nardil), are antidepressants which inhibit the
enzyme monoamine oxidase from breaking down the neurotransmitters, thereby allowing it to
be reabsorbed more easily by the brain cells. MAOI’s have been shown to be effective in
treating re-experiencing symptoms, e.g. flashbacks and nocturnal frights, and hyper-arousal
symptoms such as violent outbursts and an exaggerated startled response. The main side
effect of MAOI’s is the risk of a hypertensive crisis. This has a potential of producing coma,
fits, disturbed heart rhythm, muscle spasm and death. These inhibitors cannot be taken with
cheese, yeast extracts, meat or red wine. The adverse effects does not encourage the use of
MAOI’S as first or second line agents in PTSD, (together with the dietary and other drug
restrictions). Other side effects include dizziness, drowsiness and a blurred vision (Henry,
2002).
2.5.2.1.2 Selective serotonin reuptake inhibitors (SSRI’s)
SSRI’s, such as Sertraline (Zoloft), Paroxetine and Fluoxetine (Prozac), are common first
choices for the treatment of PTSD. SSRI’s increase the levels of neurotransmitters by
blocking the re-uptake of only one neurotransmitter, namely, serotonin, by the brain cells.
High doses of these broad-spectrum agents are used to ameliorate PTSD symptoms, such as
re-experiencing symptoms of intrusive thoughts, avoidance and numbing, and hyper-arousal
symptoms, such as anger and explosive outbursts. They are also used in disorders which are
commonly co-morbid with PTSD, such as major depression, panic disorder, social phobia and
generalized anxiety disorder (Henry, 2002). Recent studies have resulted in the requirement to
place a black box warning on SSRI’s and other antidepressant medications, due to the
increased risk of suicide and aggression in patients below the age of 24 (Gibbons et al., 2007).
10
Some of the side effects of SSRI’s include tardive dyskinesia, headache, gastrointestinal
discomfort, weakness, loss of libido and sexual dysfunction.
2.5.2.1.3 Tri-cyclic antidepressants (TCA’s)
TCA’s, for instance Clomipramine (Anafranil) and Doxepin (Sinequan), inhibit the re-uptake
of neurotransmitters, such as serotonin and noradranaline, thereby increasing the
neurotransmitters which operate by the receptors. They are effective in reducing hyper-
arousal symptoms of insomnia and dream disturbances, as well as the re-experiencing of
symptoms of anxiety, guilt, flashbacks and depression. Some of the side effects of this range
of drugs are in dry mouth, blurred vision and rapid heartbeat (Henry, 2002).
2.5.2.1.4 Selective nor-epinephrine reuptake inhibitors (SNRI’s)
High doses of SNRI’s, such as Nefazodone (Serzone), which is also an antidepressant,
enhances the action of stimulating neurotransmitters. They are used to control re-experiencing
symptoms such as flashbacks and intrusive symptoms. Dry mouth, nausea, dizziness and
drowsiness are some of the common side effects (Henry, 2002).
In a PTSD-pooled data analysis of six separate open trials of Nefazodone (SNRI’s), treatment
involved ninety-two patients who experienced combat or civilian trauma. The analysis
revealed better response rates in women than in men. These data suggest that women may
respond more favourably to Seratonergic agents (i.e. drugs which increase the synthesis of
serotonin). This is possibly consistent with positron emission tomography (PET) scans
findings of lower rates of serotonin synthesis in females, as it is 52% higher in normal males.
This has been postulated as being secondary to the effects of circulating gonadal hormones
(Seedat, et al 2005).
2.5.2.2 Anti-anxiety drugs (Busipirone, Benzodiazepines and Beta Blockers)
Benzodiazepines and related drugs depress the action of that part of the brain which controls
emotion. The drug promotes the action of the neurotransmitter gama-aminobutyric acid
(GABA). It binds to neurons which block the transmission of electrical impulses, a fact that in
turn reduces communication between brain cells (Henry, 2002). A Busipirone such as BuSpar
is an anti-anxiety agent that has been shown to reduce hyper-arousal symptoms, such as
anxiety, irritability, insomnia and hyper-vigilance. Dependency is a major problem and thus a
strong side effect as well. Diazepam (Valium) and Chlordiazepoxide (Librium) fall within the
category of benzodiazepines. These have a sedative effect and are used to reduce symptoms of
11
acute stress and anxiety, such as panic attacks and phobias. There is however a very high risk
of psychological dependence and physical abuse of the substance. They are, accordingly, not
usually recommended for PTSD, because patients with this kind of disorder are often pre-
disposed to strong addiction (Henry, 2002). Betablockers reduce anxiety symptoms by
blocking the action of norepinephrine, which is a neurotransmitter released by the sympathetic
nerve endings. Norepinephrine stimulates the heart, the digestive system and other organs of
the body, and can produce anxiety (Henry, 2002).
2.5.2.3 Hypnotics
Barbiturates, Benzodiazepines, Chloral Betaine, Chloral Hydrate and other drugs that induce
sleep, such as Zopiclone, Chlormethiazole and Zolpidem, are all drugs that induce sleep
which depress brain function by interfering with the brain chemistry and the nervous system.
They reduce communication between nerve cells, which then slow down brain activity and
promote sleep. This sleep, however, is relatively lighter, and there is less dream activity and a
less deep sleep when compared to normal sleep. This unsatisfactory sleep pattern leads to a
vicious cycle of more medication and dependency (Henry, 2002).
2.5.2.4 Antipsychotic drugs
Antipsychotic drugs, such as Phenothiazine, Butyrophenone, Carbamarzepine, Lithium,
Clozapine and Risperidone, are also used to treat PTSD in severe cases. These drugs affect the
action and production of a chemical called dopamine which is produced in the brain. These
drugs are called major tranquillizers or neuroleptics. They are used to calm and sedate highly
aggressive and nervous people. Anti-psychotics have been used for the treatment of
flashbacks and hyper-arousal symptoms (Henry, 2002). These drugs have not been proven to
be effective in relieving symptoms over the long term, and display in addition serious side
effects. The reduction of dopamine disturbs the balance of acetylcholine. This manifests in
turn as restlessness, muscle tremors, rigidity and spasms, as well as abnormal facial
movements, such as lip smacking and tongue wagging. It also blocks the action of nor-
adrenaline which affects blood pressure, and causes dizziness and sexual dysfunction (Henry,
2002). Lithium has been shown to reduce re-experiencing symptoms such as intrusive
symptoms and hyper-arousal symptoms of irritability. The side effects of Lithium are dry
mouth, blurred vision, and tachycardia (Henry, 2002).
12
2.5.2.5 Pharmacokinetic and pharmacodynamics of antidepressants and women
Positron Emission Tomography (PET) scan findings indicate lower rates of serotonin
synthesis in females (being 52% higher in normal males), which has been postulated as being
secondary to the effects of circulating gonadal hormones (Seedat et al., 2005).
Two studies have demonstrated a more favourable response to SSRI’s and MAOI’s in women
compared to men. Pre-menopausal women respond better to SSRI’s compared to post-
menopausal women (Seedat et al., 2005). In women, hormonal fluctuations (e.g. menstrual
cycle, menopause, oral contraceptives and hormone replacement therapy) may alter the
pharmacokinetics and pharmacodynamics of the antidepressants which are utilized, a fact that
should be borne in mind when treating women (Seedat et al., 2005)
2.6 Homoeopathy
2.6.1 Introduction
In 1810, a book entitled ‘Organon of the Art of Healing’ was published in Torgaou, a small
town in Germany. “Organon” is a Greek word which signifies “the means”, or “the tools”. Its
author, Samuel Hahnemann, was an extremely prominent physician and medical author of the
time. This created an up-roar in the European medical community, insofar as it introduced an
entirely new and radical system of medicine. Hahnemann, the father and founder of this new
medicine, called it homoeopathy, a word taken from the Greek words omeos, meaning
“similar”, and pathos, meaning “suffering” (Vithoulkas, 1980). Homoeopathy is considered a
highly systematic and scientific method of healing. It is based on fixed laws and principles,
and it is also a healing art, which is used to stimulate the body’s own innate ability to cure
itself (Banerjea, 2003).
Thomas Bradford, who was Hahnemann’s first biographer, describes, in his work “Life and
Letters of Dr. S Hahnemann”, how Hahnemann’s father used to lock his son up in the
company of what he called thinking exercises where he was called upon to solve problems.
He thus learned to develop the use of intuition and insight, and came to know the limitations
of intellectual logic (Bradford, 2004). He started tutoring in Greek and Latin from the age of
twelve, and in later years he translated English books to German. Private lessons in French
and German were also given to him. This all contributed to paying for his education as a
medical doctor. He also knew Italian, Latin and Arabic (De Schepper, 2006). He was a
translator of note, a circumstance which allowed him access to unusual and peculiar sources.
For example, he experimented with Aurum metalicum from the knowledge derived from the
13
Arabian and Andalusian physicians Avicenna and Abukassis, who wrote detailed instructions
on how to make gold soluble for medicinal purpose in the beginning of the twelfth century
(Hahnemann, 1835).
2.6.2 Principles of Homoeopathy
In 1779, Hahnemann had a remarkable insight and discovered the “law of similars” while
translating Cullens Materia Medica. Cullen attributed the anti-malarial properties of Cinchona
bark (from which Quinine is made) to its bitter and astringent properties. Hahnemann knew
other, even more bitter herbs which were not active against malaria. He experimented by
personally ingesting the Cinchona bark. He discovered that it induced in him, who was a
healthy person, similar symptoms to those associated with malaria. He also knew from
practice that the Cinchonia bark was effective against malaria. He thus experimented with
other known remedies and explored unfamiliar new ones. This led him to develop the first
principle of Homoeopathy or the law of similars - Similia similbus curentus or ‘Like cures
Like’ (De Schepper, 2006).
According to Hahnemann the vital force is the innate intelligence in the body which directs its
healing process and maintains homeostasis. Hahnemann describes, in aphorism 9, that the
vital force in a healthy individual consists of a spiritual energy or life force which animates
the material body or organism that controls all the bodily sensations and functions and
maintains them in harmonious operation, so that our reasoned gifted mind can be free to
pursue the higher purpose of existence (Hahnemann, 2001). A remedy which can produce
symptoms in a healthy individual acts as an artificial disease that is only capable of acting
powerfully if the symptoms are as closely related as possible to the ones the sick person is
experiencing. The remedy acts more strongly on the patient’s vital force and annihilates the
sickness and the remnants of the artificial disease produced by the remedy (Hahnemann,
2001).
2.6.3 Provings
Provings are the experimentation with the action of substances on healthy people (De
Schepper, 2006). Hahnemann’s logical mind was determined to know the symptoms which
the various drugs created before he knew what symptoms they might cure. He then set himself
the enormous task of proving a large number of remedies (Gunavante, 2003). In aphorism
106, Hahnemann discusses the fact that the full pathogenic effect of a medicine had to be
known and observed in its totality, including all its symptoms and changes in the condition
14
they produced in a healthy individual, before a homeopathic remedy could be selected to treat
natural diseases (Hahnemann, 2001)
Hahnemann proved more than a hundred remedies on himself, so that he could observe their
properties. Later, under his supervision, his pupils, mostly physicians and family members,
experimented with a large number of substances, in the process observing their effects at all
the levels of being, that is, the physical, general, emotional and mental levels. Hahnemann
recorded his provings of the remedies in his extensive Homoeopathic Materia Medica Pura,
which he said “should exclude every supposition, every mere assertion and fiction. Its entire
contents should be the pure language of Nature, uttered in response to careful and faithful
enquiry” (Gunavante, 2003). There are at present many Materia Medica reference books
Homoeopaths refer to. Information about the curative effects of these remedies has been
consistent and confirmed by clinical practice (De Schepper, 2006).
2.6.4 Principles of dilution, potentisation and aggravations
From the outset, Hahnemann made use of much smaller doses of crude remedy substances
compared with the doctors of his time. When he found that even these doses caused violent
aggravations, he was compelled to use smaller and smaller doses. In this way, he found that
this process could actually enhance the effectiveness of the remedy while at the same time
avoiding the violent reactions. Hahnemann experimented with different ways of preparing
medicines, and he developed a process of diluting medicines until barely a trace of the remedy
remained. He then experimented with increasing the medicines dynamic or energetic state by
succession, which is vigorous shaking, or trituration, that is, grinding the curative substance in
a mortar and pestle into a neutral base (De Schepper, 2006; Richardson-Boedler, 2010).
Experimentation showed that this process of potentisation or attenuation added to the healing
power of the remedies (Richardson-Boedler, 2010). Hahnemann, being a methodical and
systematic chemist, recorded the dilution to a definite scale and method. To his great surprise,
he found that the greater the dilution, the greater the power or potency (Gunavante, 2003).
Some homoeopaths assert that if mental symptoms are prominent, e.g. shock and trauma, high
potencies should be considered (De Schepper 2006). In classical prescribing, however, care is
taken when prescribing high potencies, due to the fact that similar aggravations might occur.
A homoeopathic aggravation happens when existing symptoms become more severe, because
of the primary action of the homoeopathic remedy which suppresses the secondary action of
the vital force. This can occur when the right remedy is given too frequently or in a very high
potency (De Schepper, 2006).

15
2.6.5 The Homoeopathic single remedy
Administering a single remedy at a time was advocated by Hahnemann as a natural
consequence of the fact that the Materia Medica contains the symptomatology of single
remedies (Gunavante, 2003).
2.6.6 The Homoeopathic complex remedy
In complex prescribing, two or more remedies known to cause a particular disease picture are
combined so as to cover a broad range of the disease symptoms. In prescribing a single
remedy the characteristic reactions of an individual are taken into high account, whereas in
complex prescribing the complex is aimed at a disease condition and therefore can apply to
many people (Solomon, 2010; Caroll, 2007).
Various schools within the field of homoeopathy have prescribed combinations of
homoeopathic remedies with a view to tackling specific disease states (Richardson- Boedler,
2010). Dr Hans Heinrich Reckeweg postulated from the results of years of experiments that
the action of homoeopathic remedies whether single or complex in no way loses its healing
capacity. He also argued that multiple potencies of the same substance in one remedy can
retain its own individual action. These multi-potency remedies, also called a “homoccord,”
potentially allowed the patient’s system to utilise not only the remedy it needed, but also its
optimal potency. (Reckeweg, 1983)
2.6.7 Homeopathic dosage
In Hahnemannian homoeopathy, the question of dose (potency) depends on several factors,
such as the depth of action of the remedy, the degree of chronicity or acuteness of the disease,
the susceptibility of the patient, and the plane of action which is expected from the remedy
(Gunavante, 2003).
The frequency of the dosage is affected by the potency and the same criteria as above.
Hahnemann laid down a general rule that repetition of a dose should depend on a patient’s
reaction, and that the dose of the carefully selected remedy should be allowed to act as long as
it is accomplishing its effect, in order not to disturb the process of recovery. Medicines do not
cure but they only stimulate the curative action of the patient. The repetition can only be the
renewed call of symptoms (De Schepper, 2006; Gunavante, 2003)

16
Pegasus t.r.s 200C® was created in the 200CH potency because of the 200th’s known dynamic
spectrum in curing mental emotional states with regard to trauma and shock. Because the
200th potency action is for a time, therefore it was repeated only three times per week.
2.7 Bach Flower Remedies
2.7.1 Flower remedies
Bach flower remedies are remedies which are prepared from flowers themselves. Dr. Edward
Bach, the founder of Bach flower remedies, believed that the flower petals stored the purest
healing energy from the plant kingdom, and that such energy corresponded to the higher and
subtler vibrations of man’s higher consciousness. Saying that “Flowers represent the “head”
of the plant, just as the head is to man because of its cognitive perception, consciousness and
personality, as well as the fruits to regeneration, growth and procreation.” The flower essence
yields fruits of renewed consciousness in man (Richardson-Boedler, 2010). The Bach flower
remedies are all prepared from the flowers of wild plants, bushes or trees. They are neither
harmful nor addictive (Chancellor, 1974).
2.7.2 Edward Bach philosophy and works
Bach flower remedies were developed by Edward Bach, a medical doctor from Wales. He
was of the opinion that physical disease was the result of a negative mental state. He was
influenced by Hahnemann’s philosophy (Howard, 1991). Bach was inspired by Hahnemann in
using a safe and gentle approach to healing, as well as in using natural medicinal substances,
to be searched for in plants from nature, which would have a similar healing effect
(Richardson- Boedler, 2010). Edward Bach was a renowned physician who practiced as a
bacteriologist for twenty years in Harley Street, London. He became famous in Homeopathic
circles after he developed the seven Bach Bowel Nosodes (Chancellor, 1974). Nosodes are
remedies made from diseased substances. Bach developed seven vaccines (nosodes) from
bacteria of the intestinal flora, and matched them to seven different types of personalities in
his patients. He used them successfully in treatment. He hypothesised that all chronic diseases
have their original seat in the mind and emotions. He envisaged that physical suffering could
be prevented if remedies were made from a plant source which is purer than from a diseased
source such as the nosodes. His prescriptions aimed at re-establishing harmony in the mental
and emotional states (Richardson- Boedler, 2010). In 1930, he gave up his lucrative practice
and research so as to devote himself totally to the finding of the flower remedies and the
perfecting of his method of flower healing. Bach wrote in his book, “The Twelve Healers and
17
Other Remedies” (1973, p 3-4), “in treating cases with these remedies, no notice is taken of
the nature of the disease. The individual is treated, and as he becomes well, the disease goes,
having being cast off by the increase of health”. He also stated that “the mind being the most
delicate and sensitive part of the body, shows the onset and the course of a disease much more
definitely than the body. Accordingly, the outlook of the mind is chosen as the guide
concerning of which remedy or remedies should be deemed necessary” (Bach, 1973; p 3-4.,
Wheeler, 1982, p 3-5). In the Bach Remedies Repertory, F.J. Wheeler (1982) states that Dr.
Bach was of the opinion that the basis of a disease was to be found in the existence of
disharmony between the spiritual and mental aspects of a human being. Bach also enjoined
the following: “Take no notice of the disease, think only of the outlook on life of the one in
distress” (Bach, 1973, p 3-4; Chancellor, 1974, p II).
2.8 Pegasus t.r.s. 200C®
The homoeopathic complex Pegasus t.r.s 200C® “(trauma, rescue, shock) is a complex
remedy, manufactured by Pegasus Homeopathics (2007), which is a complex of
homoeopathic and Bach flower remedies, (Rescue Remedy in particular) and is indicated to
be clinically suitable for trauma and shock. All the homoeopathic remedies were prepared in
the 200C potency, while the Rescue Remedy was prepared in its normal manner without any
potentising. Pegasus t.r.s 200C® consists of the following homoeopathic remedies: Aconitum
napellus 200CH, Arnica montana 200CH, Hypericum perforatum 200CH, Ignatia amara
200CH, Opium 200CH, Passiflora incarnate 200CH; and of the Bach Flower Rescue
Remedies: Impatiens, Clematis, Rock Rose, Star of Bethlehem and Cherry Plum (Pegasus
Homeopathics, 2007). The product is commercially available, and it is generally found in
most pharmacies and health stores in South Africa.
The combination of Homoeopathic remedies and Bach flower remedies is reported to be most
effective by virtue of the fact that they complement each other in treating diseases having
their origin in a mental and emotional imbalance. Mental and emotional imbalances, which
are caused by shock, accidents and trauma, occasion deep feelings of powerlessness,
hopelessness, anger and denial. According to Richardson-Boedler While the Bach flower
remedies act on the mental and emotional impediments, they free the consciousness of the
person, so that the curative process of the body is enabled to let the homeopathic remedies
function at their best (Richardson-Boedler, 2010).
18
Rescue Remedy is a composite remedy which Dr. Bach formulated for use in emergency,
trauma and shock. It is composed by five remedies: Star of Bethlehem for shock, Rock Rose
for terror and panic, Impatiens for mental stress and tension, Cherry Plum for desperation, and
Clematis for the bemused, far away, out-of-the-body feeling which often precedes fainting or
loss of consciousness. Rescue Remedy is used in situations in which one can detect panic,
shock, mental numbness, great fear and hysteria (Chancellor, 1974; Vlamis, 1994).
2.8.1 Aconitum napellus
Aconitum napellus, commonly known as Monkshood, is a garden plant with blue flowers
which look like a hood, whence the name Monkshood. It belongs to the Natural order
Ranunculaceae. The natural habitat of Aconitum napellus consists in the wet, shady, hilly
places in the high altitudes of Europe and Siberia, and it is cultivated in the mountainous
regions of the Pacific coast of the Americas. The tincture is prepared from the whole plant, as
gathered at the time of flowering. The plant is highly poisonous, especially its roots, and the
results of repeated experiments show the root to possess the strength of the leaves multiplied
by nine (AIH, 1897)
This remedy acts predominantly upon the cerebro-spinal nervous system, by producing a
stimulatory activity on the arterial circulation and paralyzing the arterial capillaries. It also
affects the sensory nerves before the motor nerves (Cowperthwaite, 2004).Typically, the
mental symptom picture produced by Aconitum napellus is one of intense fear, along with
anguish of one’s mind and body. There is intense physical and mental restlessness, which is a
strong hyper-arousal symptom of PTSD. The symptoms of anxiety are acute, sudden and
violent, similar to panic attacks. There is a feeling of foreboding and fear of death. There is a
conviction that death is imminent and a sensation of a foreshortened future. That, too, is one
of the PTSD symptoms. There is a tendency to start or experience an exaggerated startled
response, yet another PTSD symptom. One additionally discerns a feeling that what had just
occurred was but a dream. This denotes an avoidance symptom (Banerjee, 2003).
2.8.2 Arnica montana
Arnica montana is also commonly known as Leopards Bane. It belongs to the natural order of
Compositae/Asteraceae. Arnica montana is a perennial herb which comes from the
mountainous districts of the northern hemisphere. The relevant healing tincture is prepared
from the roots, rhizomes, leaves and flowers thereof (Cowperthwaite, 2004).

19
Arnica montana is predominantly used to treat all types of trauma due to shock, grief, remorse
and mental strain. Patients it is administered to are individuals who have experienced a sore,
lame, bruised feeling, mentally, emotionally and physically. The re-experiencing symptoms
which Arnica montana engenders are nightmares and dreadful dreams. People treated with it
dream of previous traumas, eg. Accidents and robbers. That is accompanied by a sudden,
sharp fear of dying. They have deep anguish and suffer violent attacks of anxiety of a
hypochondriac nature. They rise up at night with a fear of sudden death, with an expression of
terror, and with a picture of the horrors produced by the flashbacks which are repeated. The
hyper-arousal symptoms of the Arnica montana patients include their morose attitude, the fact
they want to be left alone, their irritability, and their desire not to be talked to or approached.
There is also in them a lack of memory and concentration, as well as agoraphobia,
nervousness and inability to bear pain. They experience low energy, and lack the ability to
perform active work continuously (Boerike, 2000; Kent, 1966).
2.8.3 Hypericum perforatum
Hypericum perforatum is also commonly known as St Johns’s-Wort. The natural order
Hypericum perforatum belongs to is Hypericaceae. Hypericum perforatum’s habitat is
woodlands, roadside verges and waste ground. It grows abundantly in Europe, America,
China, Russia, India and Turkey. The tincture is prepared from the whole, fresh, complete,
flowering plant which is chopped into fine pieces. The primary, active ingredient in
Hypericum perforatum is hypericine, a glycoside which is regaled with sedative and anti-
depressive properties. This is, therefore, what made Hypericum perforatum famous for the
effectiveness of its herbal preparation in treating depression. Historically, this herb has been
known since the times of Dioscorides. During the middle ages, it was believed to cast out
demons (Schauenberg & Paris, 1977).
Hypericum perforatum has an effect on the nervous system. That fact affects the cerebro-
spinal system in its sensory function. It has a strong effect on the vascular system, which
affects the nerves, especially when there is inflammation. It produces an irritated and highly
sensitive condition of those parts freely supplied with nerves, especially sharp pain that shoots
upwards. In its homoeopathic form, it is considered effective in dealing with the after effects
of shock, mental agony with constant drowsiness. The homoeopathic preparation is also
beneficial to people who are vulnerable to becoming depressed, scared or traumatized,
particularly in the aftermath of an accident or injury of any kind. Such persons can become
panicky or lethargic. The most obvious symptoms they experience are weakness of memory
20
and a great nervous depression, particularly in the event that wounds are present. They feel as
if they are lifted high in the air. They experience anxiety and melancholia which are PTSD
symptoms (Vermeulen, 2001).
2.8.4 Ignatia amara
Ignatia amara, commonly known as St Ignatius Bean, has a synonym known as Strychnos
Ignatii. The said synonym is so-called because it contains strychnine, which is a powerful
poison that acts on the nervous system when ingested. It belongs to the natural order Logani-
aceae. Ignatia amara’s natural habitat is the Philippine Islands and Cochin China. It is
prepared as a tincture from either the triturated powdered seeds or beans. It is named after the
founder of the order of the Spanish Jesuits who introduced the seeds to Europe from the
Philippines in the 17th century. The natives used the beans as amulets (AIH, 1897).
It acts on the medulla oblongata, the spinal nervous system, as well as on the entire central
nervous system. One can detect an intense sensitivity, acuteness and excitement of the sense
nerves, a special sensation, and an increased susceptibility to external impressions, both
mental and physical. The Homoeopathic remedy Ignatia amara was proved and published in
(1821-1834) by Hahnemann in his Materia Medica Pura (AIH, 1897). The main symptom of
Ignatia amara is a finely sensitive mood, with an inclination to sadness and anger followed by
silent grief or disappointment. People treated with it are continually brooding over imaginary
troubles. Strong emotional problems such as separation or death produce acute grief. They
suffer from the effects of grief and worry. They experience tremendous exhaustion due to
concentrated grief. They have changeable moods, a tendency towards involuntary sighing and
sobbing, as well as memory loss. They are introspective, silently brooding, melancholic, sad,
tearful and not very communicative. They are often impatient, fearful, indifferent to
everything and restless. Some re-experiencing, avoidance and hyper-arousal symptoms of
PTSD are prominent in patients treated with this remedy (Banerjea, 2003; Boericke, 2000).
2.8.5 Opium
Papaver somniferum is most commonly known as Opium. It is also called the white poppy. Its
natural order is Papaveraceae. It is a plant which is native to Asia and is extensively
cultivated in Europe, North and South America. The homoeopathic remedy opium is
produced from the white juices of the opium poppy plant, which abound in the capsules
containing the seed. A tincture is prepared from its juices. The homoeopathic preparation does
not contain any trace or attributes of raw opium, and it is safer than its chemical derivatives,
21
such as codeine and morphine, which are extensively used in conventional medicine, as the
latter are characterized by very strong addictive tendencies. Opium has been used for its
analgesic, euphoric and narcotic properties since the age of the ancient Greeks and Romans,
from as early as the third century BC (AIH, 1897).
Opium acts on the cerebro-spinal and sympathetic nervous system by producing brief
excitation, which is rapidly followed by depression and a paralysis of all functional activity.
Opium is a valuable remedy for a gamut of ailments ranging from fright or post-fright
emotion to fear of flashbacks of the trauma and subsequent effects. Kent (1966) mentions that
fear is a strong characteristic of Opium, along with the side effects of the mental state which is
occasioned by fear. When complaints due to fear, where the cause of the fear is constantly re-
experienced, arise, people affected by such state experience hallucinations such as frightful
images of fire, ghosts, murder, the sight of someone carrying the victim off, and visions of
devils. One can observe in Opium patients an insensibility of the nervous system, depressive
drowsy stupor, painlessness, torpor, general sluggishness and a lack of vital reaction. Patients
have no desires. Opium lessens voluntary movements, contracts pupils, and slows the higher
intellectual powers. It reduces self-control, power of concentration and judgment. It stimulates
the imagination by causing frightful fancies. Opium is very effective for the re-experiencing
system of flashbacks and hallucination symptoms of PTSD (Boerike, 2000; Kent, 1966).
2.8.6 Passiflora incarnata
Passiflora incarnata is also known as purple passion flower, maypop, wild passion-vine and
wild apricot. It belongs to the natural order of Passifloraceae. The natural habitat of
Passiflora incarnata lies in the Southern and South-eastern regions of the United States, as
well as Tennessee (AIH, 1897; Schauenberg & Paris, 1977).
It was introduced into Homoeopathic practice by Dr. Hall in 1875, and is effective in treating
hyper-arousal symptoms, such as insomnia, sleeplessness, nervousness, anxiety of a nervous
type, insomnia caused by mental fatigue, and exaggerated startled response. People who
suffer from stress and anxiety are not mentally awake during their sleep, That occurs when
deep sleep and dream sleep are insufficient within the sleep cycle, a fact which makes them
more wakeful during sleep). Passiflora incarnata is soothing on the nervous system, promotes
normal sleep, and is resorted to for the treatment of hysteria and acute mania. The symptoms
of passiflora incarnata worsen when noise is present, and conversely improve when the
environment is peaceful and tranquil (Vermeulen, 2001).

22
2.8.7 Impatiens
Impatiens noli-tangere is commonly known as touch-me-nots, busy lizzie, jewelweeds and
impatiens. They belong to the natural order of the Balsaminaceae family. Their natural habitat
is situated in the lower foothills of mountains, hills, ravines, damp areas and open scrublands
(Schauenberg & Paris, 1977).
This remedy is indicated for people who are impatient and irritable, bad tempered, and prone
to outbursts of anger. They are also accident-prone, and get injured out of their own
impetuousness. This is the remedy for all manifestations of pain caused by tension, such as
cramps, pain spastic conditions or other complaints brought about by their irritable nature
(Bach, 1973; Chancellor, 1974). Mind symptoms of a sensation of internal mental agitation,
restlessness, short temper, being intimidated and reeling under the effects of a tense, wound
up mind, are the characteristic symptoms of Impatiens. Their common emotional experiences
are anger, frustration, dissatisfaction and irritability Richardson-Boedler, 2010).
The keywords for the Impatiens remedy are impatience, irritability and extreme mental
tension, all of which represent hyper-arousal symptoms associated with PTSD (Bach, 1973;
Chancellor, 1974).
2.8.8 Clematis flower
Clematis vita alba is commonly known as old man’s beard, traveller’s joy and Clematis. It
comes from the natural order of the Ranunculaceae family. Its habitat is common along the
edges of woodlands and clearings gifted with a soil rich in lime (Schauenberg & Paris, 1977).
Dr.Bach said that the following symptoms were common, though in varying degrees, in the
Clematis type: A vacant faraway look, no great interest in life, dreamy, inattentiveness, pre-
occupation, drowsiness, not being fully awake, and unconsciousness. People belonging to this
type are heavy sleepers, absent minded individuals with a marked pallor and a lack of
concentration caused by their half-hearted interest in life and the present. They avoid
difficulties or unpleasantness by allowing their attention to wander and by withdrawing into a
world of illusion and unreality. Whenever they become ill, they make little or no effort to get
well. It is almost as if they wish to leave this earth, perhaps to join some loved one who is
dead, or because life does not come up to their expectations. This lack of co-operation or
effort to get well was called by Dr. Bach “a polite form of suicide”. Clematis symptoms
correspond with the PTSD symptoms of numbness and lack of concentration (Bach, 1973;
23
Chancellor, 1974). Mind symptoms include a sensation of unreality, dreaminess, drowsiness,
a sleepy, light-headed nature, a hazy and veiled mind, daydreaming and absent mindedness.
All of them are symptoms characterizing Clematis. Common emotional experiences are
loneliness, sadness and longing for a hopeful, better life, together with disillusionment
(Richardson-Boedler, 2010).
The keywords of Clematis are indifference, dreaminess, inattention, and unconsciousness, an
array of aspects which are reflected in the avoidance symptoms of PTSD (Bach, 1973;
Chancellor, 1974).
2.8.9 Rock Rose
Helianthemum nummularium is commonly known as Rock Rose or Sun Rose. It belongs to
the natural order of the Cistaceae family. The natural habitat is found in grasslands, sunny
places, cultivated gardens and well drained soil. It is found throughout Europe, North and
South America, Mediterranean basin and Western Asia (Schauenberg & Paris, 1977).
Rock rose is the remedy to be given whenever an individual experiences fear and terror. The
remedy is used for acute trauma, such as one arising from an accident or a near escape (Bach,
1973; Chancellor, 1974). Mind symptoms of fight or flight due to trauma, anxiety, a sensation
of internal agitation and nervousness, nightmares, phobias and panic attacks with inner
trembling, fixations and obsessions, are characteristic symptoms of Rock Rose. Common
emotional experiences are anger, hatred, impatience, helplessness, despair, irrational
resentment and aggression (Richardson-Boedler, 2010).
The keywords of Rock Rose are terror, panic, extreme fright due to exposure to trauma and
nightmares, all of which are symptoms of PTSD (Bach, 1973; Chancellor, 1974).
2.8.10 Star of Bethlehem
Ornithogalum umbellatum is commonly known as Star-of-Bethlehem or grass lily. It is from
the natural order Asparagales in the family of Asperagaceae or Hyacinthaceae. The natural
habitat of the Star of Bethlehem is Central and Eastern Europe as well as parts of the Middle
East (Schauenberg & Paris, 1977).
Star of Bethlehem is given to anyone exposed to shock in any form. There is great distress
and unhappiness due to the traumatic event. It is always used in every case of an accident or

24
trauma, whether severe or light, wherever there is an element of shock connected to the event.
If the shock is neutralized, bodily recuperation is then accelerated to a great degree. Sudden
sad news, a bad fright, and a grievous disappointment, all result in shock and unhappiness. Dr
Bach called this remedy “the comforter and soother of pains and sorrow”. Sometimes, the
effect of mental shock can manifest itself almost immediately in the body, while on other
occasions the effect of shock is repressed. Where there has been shock, there is always an
effect after the shock (Bach, 1973; Chancellor, 1974). Mind symptoms of numbness,
avoidance because the conscious mind cannot accept and cope with the shock, retreat of the
mind due to the trauma, are the characteristic symptoms of Star of Bethlehem. Common
emotional experiences include deep sadness escorted by pain and despair. Hopelessness, fear,
shame, frustration and guilt are also strong emotions that are experienced by the category of
people to whom Star of Bethlehem is administered (Richardson-Boedler, 2010).
The keywords for Star of Bethlehem are after-effect of shock. The function is to neutralize
shock in any form. Shock and Trauma constitute the basic aetiology of PTSD (Bach, 1973;
Chancellor, 1974).
2.8.11 Cherry plum
Prunus cerasifera or Prunus divaricata is also known as morello cherry, sour cherry,
myrobalan plum or cherry plum. It is an angiosperm belonging to the natural order Rosales
and the Rosaceae family. It is a native of Russian Central Asia and Iran, and found through
the Caucasus up to the Baltic peninsula (Schauenberg & Paris, 1977).
This remedy is given for treating desperation and deep depression in individuals who are on
the verge of a nervous breakdown. It is meant for those people who contemplate turning to
suicide as an escape due to despondency, and for those people who undergo prolonged and
continuous mental or physical suffering. The distress is so great that they fear as of their mind
would give way under the strain. They fear that they would lose control of their thoughts and
action and be impelled to do something dreadful, which they would never have thought of
carrying out under normal circumstances (Bach, 1973; Chancellor, 1974). Mind symptoms
include the fact that there is constantly an overstrained, unbalanced mind. The mind is flooded
with undesired thoughts of the trauma, and there is great fear of the flashback symptoms.
Depression and a tendency to commit suicide are also characteristic symptoms of Cherry
Plum. Common emotional experiences are deep anguish, distress, and intense fear of losing
control (Richardson-Boedler, 2010)
25
Key words for Cherry Plum are desperation, fear of losing control of the mind, and dread of
doing something frightful. Re-experiencing symptoms, avoidance and hyper-arousal
symptoms are all present in this remedy (Bach, 1973; Chancellor, 1974).
2.9 Related Research
Several uncontrolled observational homoeopathic studies on anxiety disorders and depression
reported by Pilkington K.; Kirkwood G.; Rampes H.; Fisher P. and Richardson J.(2005; 2006)
showed positive results and included high levels of patient satisfaction. However, due to a
lack of a control group, it was difficult to assess the extent to which any response was due
specifically to the homoeopathic effects.
In two randomized controlled trials which addressed mixed anxiety and depressive disorders,
homoeopathic complexes were reported to be as effective as Benzodiazepine such as
Lorazepam and Diazepam (Pilkington et-al., 2006).
Lankaser (2004) concluded in a similimum study on PTSD that there was a general
improvement in post traumatic stress frequency, severity and intensity in respect of each
patient, as well as improvement in energy levels, sleep patterns, appetite, general well being,
attitude and outlook on life.
26
CHAPTER THREE
3. RESEARCH METHODOLOGY
3.1 Research sample and recruitment
Thirty females between the ages 18-55 were recruited by means of purposive sampling via an
advertisement (Appendix A) placed at Nisaa, with authorization (Appendix F), and by word
of mouth.
3.1.1 Inclusion criterion
All participants had to be diagnosed with PTSD under the supervision of a registered
psychologist.
Symptoms of PTSD had to be in existence for at least one month and not more than two
years before joining the study.
Participants had not received more than four weeks of trauma counselling prior to the
study.
Participants had not taken any medication for their psychological symptoms for four
weeks prior to the start of the study and throughout the duration of the study.
Participants on hypertensive and/or on contraceptives were to continue as normal.
3.1.2 Exclusion criterion
Participants on chronic medication, homoeopathic medication, and other medication taken for
their psychological symptoms, as well as pregnant and lactating women, were excluded from
the study.
3.2 Research design and procedure
This was a pre-test, post-test non-equivalent group design with a double-blind placebo-control
(Trochim, 2006; Robson, 1993). Participants were randomly placed either in an experimental
or in a placebo group, each of them comprising fifteen participants. The research duration was
six weeks. The pre-test, post-test was the preferred method to compare participant groups and
to measure the degree of changes occurring as a result of treatments or interventions.
Recourse to that method allowed for individual differences, and thus provided a sensitive
measure of treatment effects (Robson, 1993; Shuttleworth, 2009). Participants who met the
inclusion criteria were given a full explanation of the research procedures and questionnaires,
27
and were further supplied with a participant information form (Appendix B) and a participant
consent form to sign (Appendix C). They then completed the patient information and case-
taking form (Appendix D), and underwent a relevant physical medical-examination aimed at
checking any obvious pathology (Appendix D). Thereafter, all participants were handed a
modified DSM-IV criterion questionnaire (Appendix E) to complete which rated the
severity/intensity of their symptoms according to a 7-point rating for each of their symptoms.
This stage, which amounted to the pre-test, also confirmed their PTSD status. Both groups
were to receive the standard trauma counselling once a week from Nisaa (Appendix G). In
order to further reduce possible variables, Nisaa recruits experienced the same standards of
trauma counselling, even though different psychologists and institutions differ in their
counselling methods (Dangor, 2010; Fourie, 2010).
The experimental group received Pegasus t.r.s 200C®, while the placebo group received a
placebo three times a week. A follow up consultation took place three weeks later. During it,
the modified DSM-IV questionnaire (Appendix E) was completed as post-test 1. On the last
day of the study on week six, the modified DSM-IV criterion questionnaire (Appendix E) was
repeated as post-test 2.
3.3 Medicine administration and randomisation of the study
The dosage and potency of the remedy were standardized throughout the study. Participants
were required to take five pillules of their placebo or medication, three times weekly on a
Monday, Wednesday and Friday, for a period of six weeks (Appendix H). Medication/placebo
was administered sublingually, fifteen minutes away from food and drinks. Medicine and
placebos were randomly numbered by the supplier. Participants selected a medication or a
placebo randomly from a box which was recorded and which automatically placed them into
either the experimental or the placebo group. Neither the researcher nor the participants knew
who was in which group, since the packaging, appearance and taste of the remedy and
placebo were identical hence, a double blind research. Participants were furnished with a
calendar (Appendix H), which they were required to sign whenever they had taken their
medication. This helped to ensure compliance on the part of the participants
3.4 Reliability and validity of the measurement tool
The DSM-IV is the standard diagnostic criterion for assessing PTSD (APA, 1994). The DSM-
IV criterion (APA, 1994) was modified and simplified in this study and used to assess the
PTSD symptoms of the participants over time.
28
3.5 Data collection and analysis
After the study the suppliers un-blinded the numbers of the remedies and the researcher could
match the numbers to the participants who took the remedy and the placebo. The results from
all the participants were then collected from the data as obtained from the modified PTSD
questionnaire, which was based on the DSM-IV criteria (APA, 1994). The data were then
statistically analysed by means of the SPSS (statistical package for social sciences)
programme version 18. The data was analysed by using the Shapiro-Wilk Test, Mann-
Whitney U Test, Friedman Analysis of Variance by Ranks Test, and Wilcoxon Signed Rank
Test with a Bonferroni adjustment (Pallant, 2007; Robson 1993).
3.6 Ethics
Participants were supplied with an information form and were requested to sign a consent
form relating to the study. No anticipated risks were expected to ensue from the study.
Participants were instructed by the researcher that, in the event they had any concerns, they
were to stop the medication and contact the researcher immediately. Participants would, if
necessary be evaluated by the psychologist supervisor and referred appropriately. Privacy,
anonymity and confidentiality were maintained by not linking personal details to any data.
Participants were able to have access to results on request at the end of the study. All
participants were treated with dignity and respect. All participation was voluntary with no
negative consequences for non-participation. Participants falling within the placebo group
were able to receive six weeks medication of Pegasus t.r.s 200® on completion of the study.
The study was passed by the Higher Degrees Committee of the Faculty of Health Science at
the University of Johannesburg and the Higher Degrees Academic Ethics Committee on 17th
of September 2010 with the reference No. AEC75/01-2010.
29
CHAPTER FOUR
4. RESULTS OF STATISTICAL ANALYSIS
4.1 Introduction to results
On completion of the study, the data was un-blinded and all the data obtained from each
participant were collated and analysed. The severity and intensity of PTSD symptoms were
analysed in the experimental and placebo groups over a six week period. The change in the
symptoms between the experimental and the placebo groups was analysed statistically. Note
should be taken of the fact that, in the tables and charts here under, the experimental group is
sometimes referred to as the test group and the placebo group as the control groups.
4.2 Results
4.2.1 Frequency results
The data were obtained from the patient information form (Appendix B), which the
participants completed at their first consultation. The results analysed included frequency of
age.
4.2.1.1 Age frequency
Table 4.1 illustrates the mean ages, the maximum and minimum age and percentages in the
experimental/test group and the placebo/control group. The test for normality concerning the
ages between the experimental group and the placebo group was normal (table 4.2). The mean
age recruited for the study was thirty-seven years for the experimental group and thirty-eight
years for the placebo group. The p-value was greater than 0.05, and the mean ranks was
38.60, which means that there was no significant difference in the ages between the two
groups.
Table 4.1 Age frequency
Age Cases
Group Youngest
Min Oldest Max
Mean Valid Missing Total
N % N % N % Test 21 53 37 13 86.7 2 13.3 15 100 Control 21 52 38 13 86.7 2 13.3 15 100
30
Table 4.2 illustrates the values of the Mann-Whitney U Test on the Age of the experimental/test and placebo/control groups. Table 4.2 Mann-Whitney U Test on age
Age
Group Z-score P-value N n Sd Mean Ranks Mean -.333 .739 30 37.60
Test 15 8.920 37 Control 15 10.557 38
4.2.2 Tests for normality
The Shapiro-Wilk test was used to test Normality because of the small numbers involved. P
values had to be greater or equal to 0.05 for them to indicate a normal distribution. The
Shapiro-Wilk test results indicated a normal distribution with regard to some of the symptoms
in the experimental and placebo groups. It also indicated a “not normal” or skewed
distribution as far as the other symptoms in both groups were concerned. The total and
average pre-test, p-values of the experimental group were 0.737 and 0.718 respectively. These
results are greater than 0.05, which signifies a normal distribution compared to the total and
average pre-test, p-values of the placebo group, as the latter were 0.013 and 0.013
respectively, thereby signifying a skewed distribution. The total and average post-test 1, p-
values of the experimental group were 0.501 and 0.511 respectively. Such results exceeded n
0.05, which signifies a normal distribution compared to the total and average post-test 1, p-
values of the placebo group that stood at 0.004 and 0.004 respectively and signified a skewed
distribution.The total and average post-test 2, p-values of the experimental group were 0.016
and 0.016 respectively, while the total and average post-test 2, p-values of the placebo group
were 0.014 and 0.014 respectively, i.e. less than 0.05, which signified a skewed distribution
and, accordingly, other than a normal distribution for both groups. The significance of this
final result of the test relating to normality determines the appropriate statistical test which is
needed to analyse the data.
4.2.3 Non-parametric tests
The decision was taken that non-parametric tests would be appropriate because of the small
numbers of participants involved and the lack of normal distribution indicated in the Shapiro-
Wilk Test. The Mann-Whitney U Test, Freidman Analysis of Variance by Ranks Test and
Wilcoxon Signed Rank Test were the necessary tests which were implemented.
4.2.3.1 Mann Whitney U Test
31
In order to test the differences between two independent groups, such as an experimental
group that took a remedy and a placebo group that took a placebo, a Mann Whitney U test
was used. It is a non-parametric test comprising two variables, a categorical variable such as
the two abovementioned groups, being a variable which does not change over time, and a
continuous variable, which consists in the severity and intensity of PTSD symptoms and
which does change over time (Pallant, 2007). The test is used to determine whether, within a
particular time frame, there is a difference in the severity and intensity of PTSD symptoms as
between the experimental group and the placebo group. It is a broad test to determine whether
the remedy did work or not, as compared to the placebo, with regard to all PTSD symptoms.
4.2.3.2 Freidman Analysis of Variance by Ranks Test
The Freidman Analysis of Variance by Ranks Test was performed only on the basis that the
Mann Whitney U test was significant. It represented the second nonparametric test to be
performed. This is a more stringent test, which is used to measure a change in the stress levels
of the experimental and the placebo groups over more than two time periods (Becker, 2011;
Smith, 2011).
This test is used when the same sample of subjects who took the remedy or placebo is tested
on each symptom over three or more time periods and then compared with one another
(Pallant, 2007). In order for this test to be really significant, the p-values of the test group
must be less then or equal to 0.05, and the p-value of the control group must be in greater than
0.05.
4.2.3.3 Wilcoxon Signed-Rank Test and Bonferroni Adjustment
The Wilcoxon Signed Rank Test is designed for use with measurements that are repeated over
at least two time periods (Pallant, 2007). The Wilcoxon Signed-Rank Test was the third non-
parametric statistical test to be implemented. It is done only if the Freidman Analysis of
Variance by Ranks Test indicates positive results. In order to refine the study a bit further, this
test determines where the changes occurred after the participants took the remedy or the
placebo. A comparison is made from the time when the remedy/placebo was taken, which is
week 1 to week 3 for the pre-test (t1) and post-test 1 (t2), and week 1 to week 6 for the pre-
test (t1) and post-test 2 (t3). That was done in order to determine whether the remedy worked
best in the first three weeks or in the last three weeks. One can interpret, in the light of this
test, where exactly the changes occur (Devey, 2010).
Among the intra group post hoc comparisons that were performed, a Bonferroni adjustment
was done to avoid a type one error .This is to avoid reaching a significant result by chance.
32
The alpha level or scale of significant p- value of 0.5 is divided by the number of tests
performed, namely two in this study. This new alpha level becomes the new criterion for
determining significance. The stricter p-value of 0.025 is thus compared to the test results of
the Wilcoxon Signed-Rank Test in order to determine where the difference occurred (Pallant,
2007).
4.3 Data obtained from participants pre-test (t1) and post-test 1 (t2) and post-test 2 (t3)
questionnaires.
The participants were required to complete a questionnaire based on a modified DSM-IV
criteria in order to rate their symptoms according to a seven-point scale, which ranged from
always to never (Table 4.3). The following Figures 1-18 represent bar graphs which illustrate
the mean values of the severity and intensity of the re-experiencing, avoidance and hyper-
arousal symptoms of the participants in both groups, as indicated by the three questionnaires
over the six weeks study period. It also depicts the Mann-Whitney test which compares the
test and the control groups within a time period in terms of an inter-group analysis. The
Friedman test which compares the same two groups over the three time periods, i.e. intra-
group analysis, can also be viewed.
The statistical value of the result of each question is tabulated, with the p-values noted in the
tables below the charts and significant values indicated in bold.
Experimental groups are also called test groups, while placebo group are inter alia known in
this study as control groups.
Pre (t1) = pre-test at day 1 before any medication or placebo was taken
Post 3 (t2) = post-test 1 after three weeks of medication or placebo taken
Post 6 (t3) = post-test 2 after six weeks of medication or placebo taken
Table 4.3 Intensity and Severity Scale
Intensity Frequency Severity
0 Never No symptoms
1 Almost Never No symptoms
2 Very rarely Mild symptoms
3 Rarely Mild symptoms
4 Sometimes Moderate symptoms
5 Often Moderate symptoms
6 Very often Severe Symptoms

33
4.3.1 Intensity and severity of the re-experiencing symptom such as thoughts, images
and perception.
Figure 4.1 Represents a bar graph that illustrates the mean values of severity and intensity of
the re-experiencing symptoms of thoughts, images and perceptions of the participants of both
groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.1 Re-experiencing thoughts, images and perception
A Mann- Whitney U test revealed a significant difference in the severity and intensity of the
re-experiencing symptoms of thoughts, images and perceptions of the participants in the test
group (n = 13, Mean = 3.08, Mean rank = 10.58, Sd = 1.605) compared to the control group
(n = 13, Mean = 4.62, Mean rank = 16.42, Sd = 2.063), (U = 46.500, z = -1.975, p=0.048,) at
post-test 6.
5.8
4.23
3.08
6.13
4.62 4.62
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Re-experiencing thoughts, images and perception
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
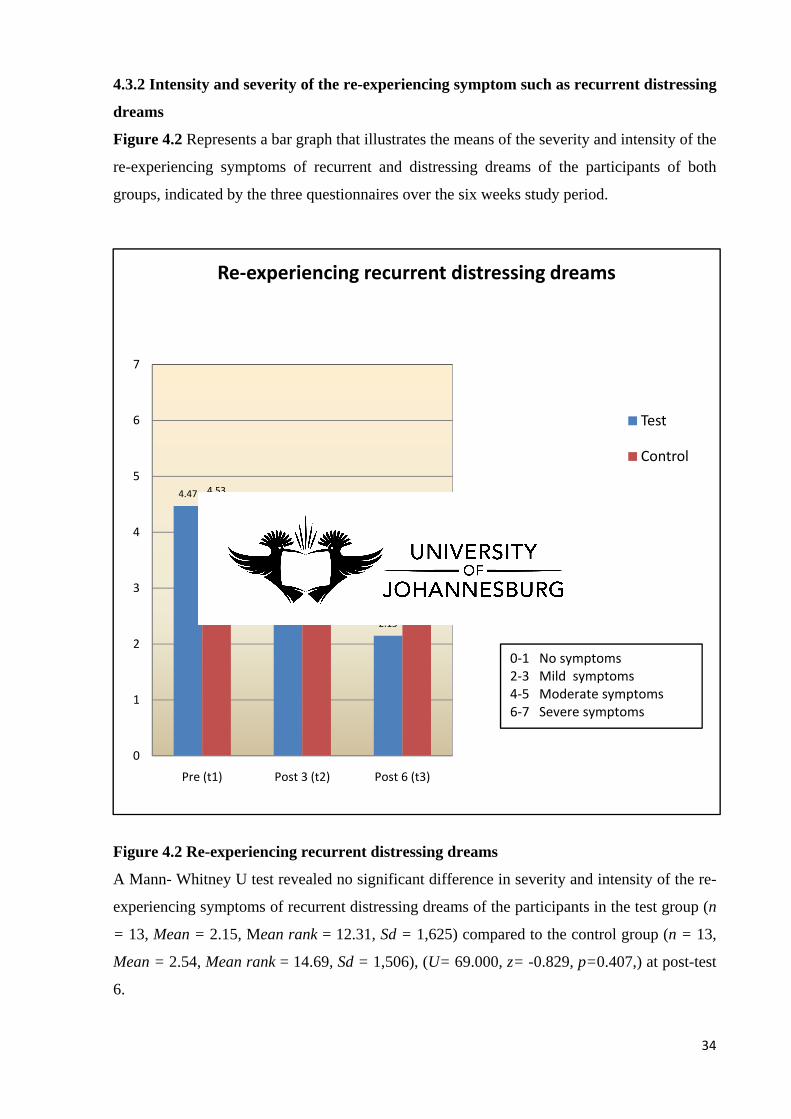
34
4.3.2 Intensity and severity of the re-experiencing symptom such as recurrent distressing
dreams
Figure 4.2 Represents a bar graph that illustrates the means of the severity and intensity of the
re-experiencing symptoms of recurrent and distressing dreams of the participants of both
groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.2 Re-experiencing recurrent distressing dreams
A Mann- Whitney U test revealed no significant difference in severity and intensity of the re-
experiencing symptoms of recurrent distressing dreams of the participants in the test group (n
= 13, Mean = 2.15, Mean rank = 12.31, Sd = 1,625) compared to the control group (n = 13,
Mean = 2.54, Mean rank = 14.69, Sd = 1,506), (U= 69.000, z= -0.829, p=0.407,) at post-test
6.
4.47
3
2.15
4.53
2.772.54
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Re-experiencing recurrent distressing dreams
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
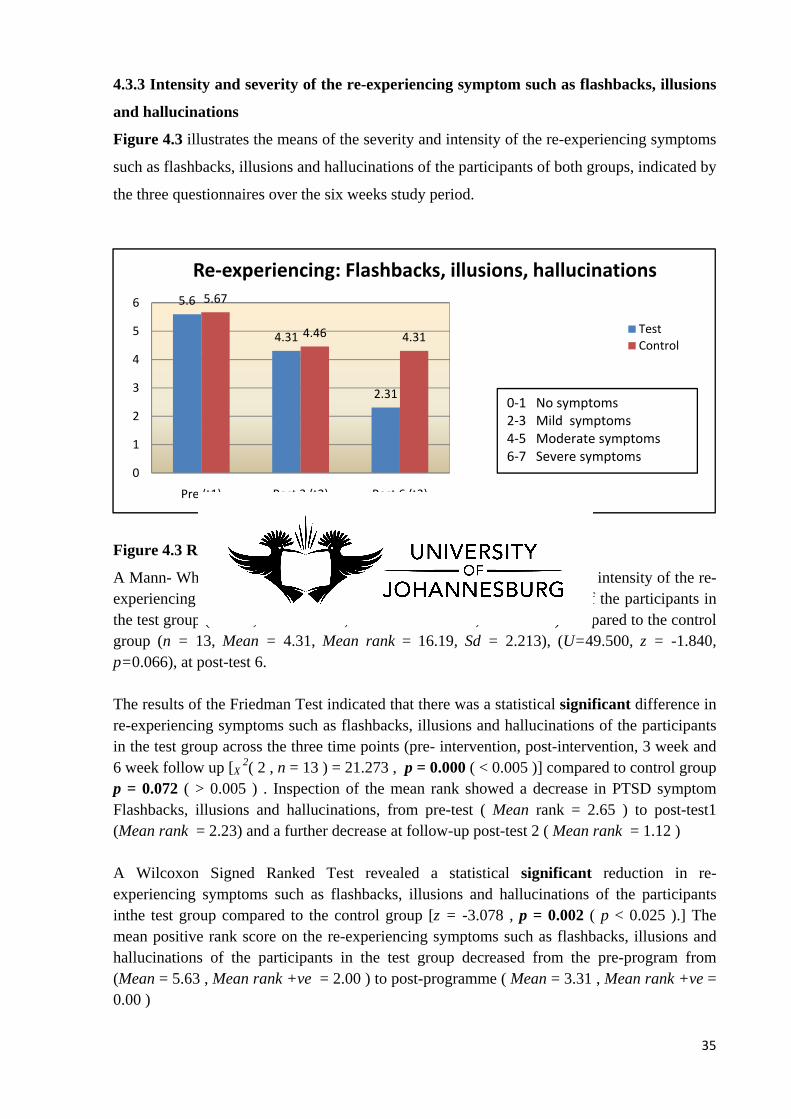
35
4.3.3 Intensity and severity of the re-experiencing symptom such as flashbacks, illusions
and hallucinations
Figure 4.3 illustrates the means of the severity and intensity of the re-experiencing symptoms
such as flashbacks, illusions and hallucinations of the participants of both groups, indicated by
the three questionnaires over the six weeks study period.
Figure 4.3 Re-experiencing: flashbacks, illusions, hallucinations
A Mann- Whitney U test revealed no significant difference in severity and intensity of the re-experiencing symptoms such as flashbacks, illusions and hallucinations of the participants in the test group (n = 13, Mean = 2.31, Mean rank = 10.81, Sd = 1.584) compared to the control group (n = 13, Mean = 4.31, Mean rank = 16.19, Sd = 2.213), (U=49.500, z = -1.840, p=0.066), at post-test 6. The results of the Friedman Test indicated that there was a statistical significant difference in re-experiencing symptoms such as flashbacks, illusions and hallucinations of the participants in the test group across the three time points (pre- intervention, post-intervention, 3 week and 6 week follow up [X
2( 2 , n = 13 ) = 21.273 , p = 0.000 ( < 0.005 )] compared to control group p = 0.072 ( > 0.005 ) . Inspection of the mean rank showed a decrease in PTSD symptom Flashbacks, illusions and hallucinations, from pre-test ( Mean rank = 2.65 ) to post-test1 (Mean rank = 2.23) and a further decrease at follow-up post-test 2 ( Mean rank = 1.12 ) A Wilcoxon Signed Ranked Test revealed a statistical significant reduction in re-experiencing symptoms such as flashbacks, illusions and hallucinations of the participants inthe test group compared to the control group [z = -3.078 , p = 0.002 ( p < 0.025 ).] The mean positive rank score on the re-experiencing symptoms such as flashbacks, illusions and hallucinations of the participants in the test group decreased from the pre-program from (Mean = 5.63 , Mean rank +ve = 2.00 ) to post-programme ( Mean = 3.31 , Mean rank +ve = 0.00 )
5.6
4.31
2.31
5.67
4.46 4.31
0
1
2
3
4
5
6
Pre (t1) Post 3 (t2) Post 6 (t3)
Re-experiencing: Flashbacks, illusions, hallucinations
TestControl
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
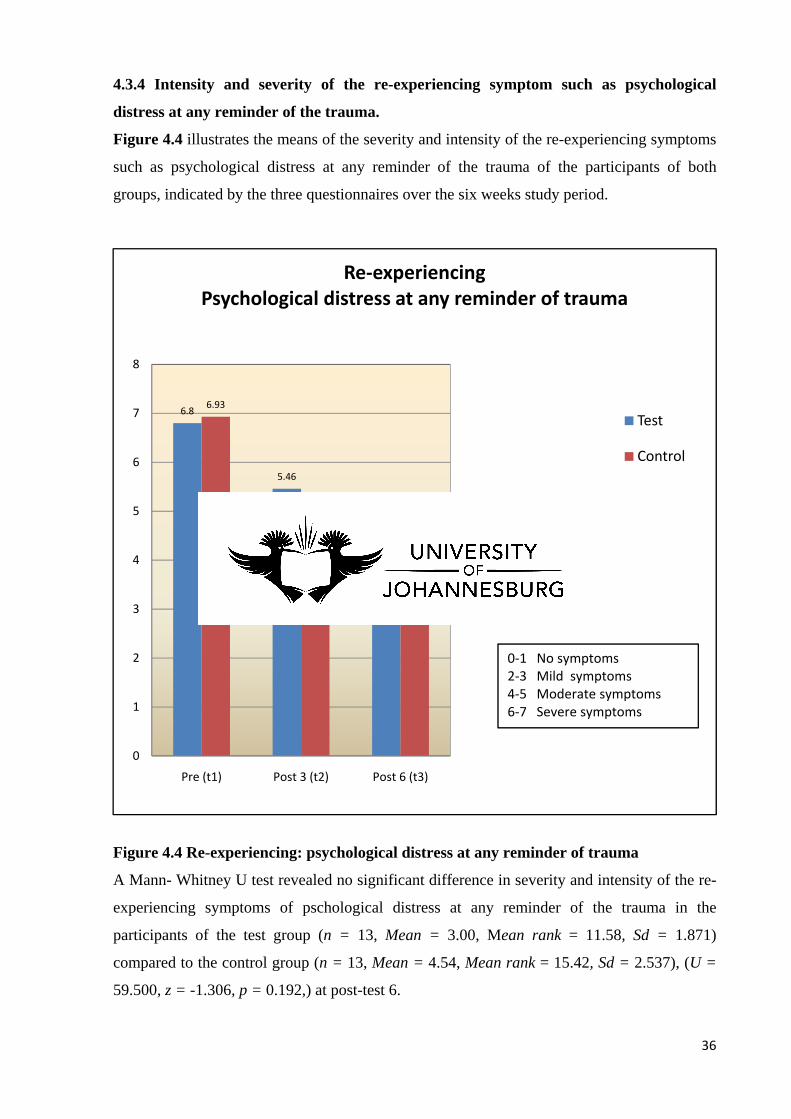
36
4.3.4 Intensity and severity of the re-experiencing symptom such as psychological
distress at any reminder of the trauma.
Figure 4.4 illustrates the means of the severity and intensity of the re-experiencing symptoms
such as psychological distress at any reminder of the trauma of the participants of both
groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.4 Re-experiencing: psychological distress at any reminder of trauma
A Mann- Whitney U test revealed no significant difference in severity and intensity of the re-
experiencing symptoms of pschological distress at any reminder of the trauma in the
participants of the test group (n = 13, Mean = 3.00, Mean rank = 11.58, Sd = 1.871)
compared to the control group (n = 13, Mean = 4.54, Mean rank = 15.42, Sd = 2.537), (U =
59.500, z = -1.306, p = 0.192,) at post-test 6.
6.8
5.46
3
6.93
4.62 4.54
0
1
2
3
4
5
6
7
8
Pre (t1) Post 3 (t2) Post 6 (t3)
Re-experiencingPsychological distress at any reminder of trauma
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
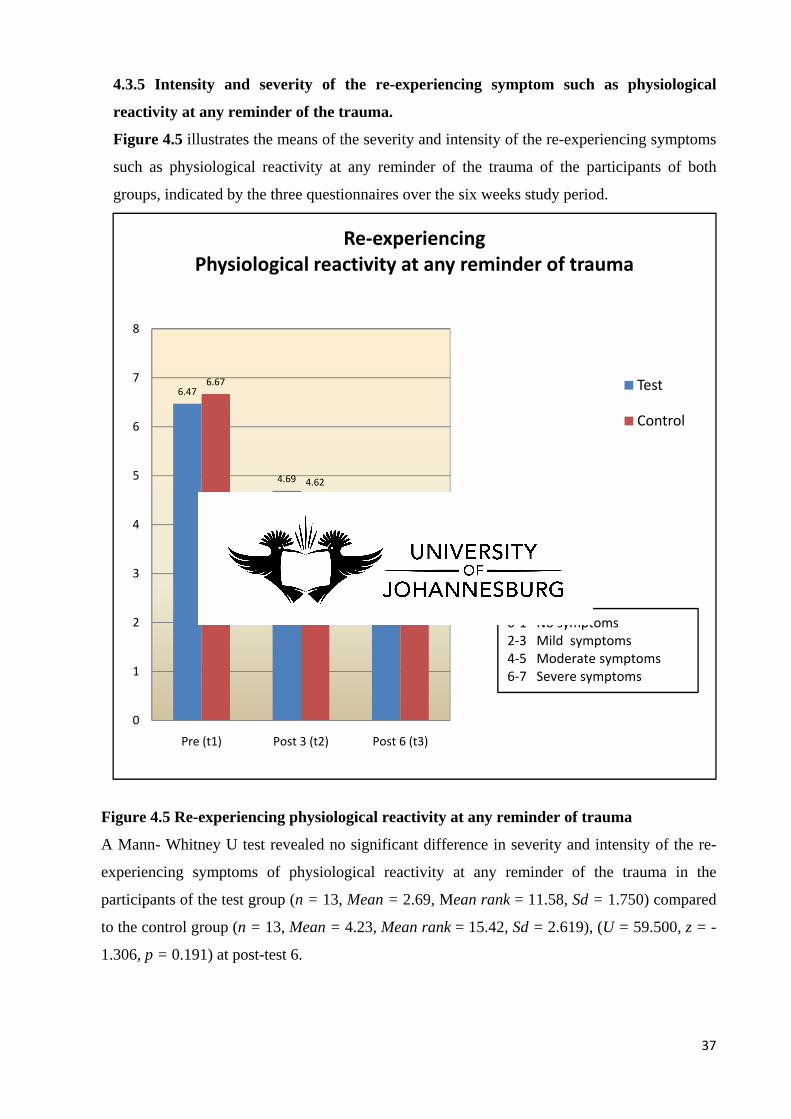
37
4.3.5 Intensity and severity of the re-experiencing symptom such as physiological
reactivity at any reminder of the trauma.
Figure 4.5 illustrates the means of the severity and intensity of the re-experiencing symptoms
such as physiological reactivity at any reminder of the trauma of the participants of both
groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.5 Re-experiencing physiological reactivity at any reminder of trauma
A Mann- Whitney U test revealed no significant difference in severity and intensity of the re-
experiencing symptoms of physiological reactivity at any reminder of the trauma in the
participants of the test group (n = 13, Mean = 2.69, Mean rank = 11.58, Sd = 1.750) compared
to the control group (n = 13, Mean = 4.23, Mean rank = 15.42, Sd = 2.619), (U = 59.500, z = -
1.306, p = 0.191) at post-test 6.
6.47
4.69
2.69
6.67
4.62
4.23
0
1
2
3
4
5
6
7
8
Pre (t1) Post 3 (t2) Post 6 (t3)
Re-experiencingPhysiological reactivity at any reminder of trauma
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
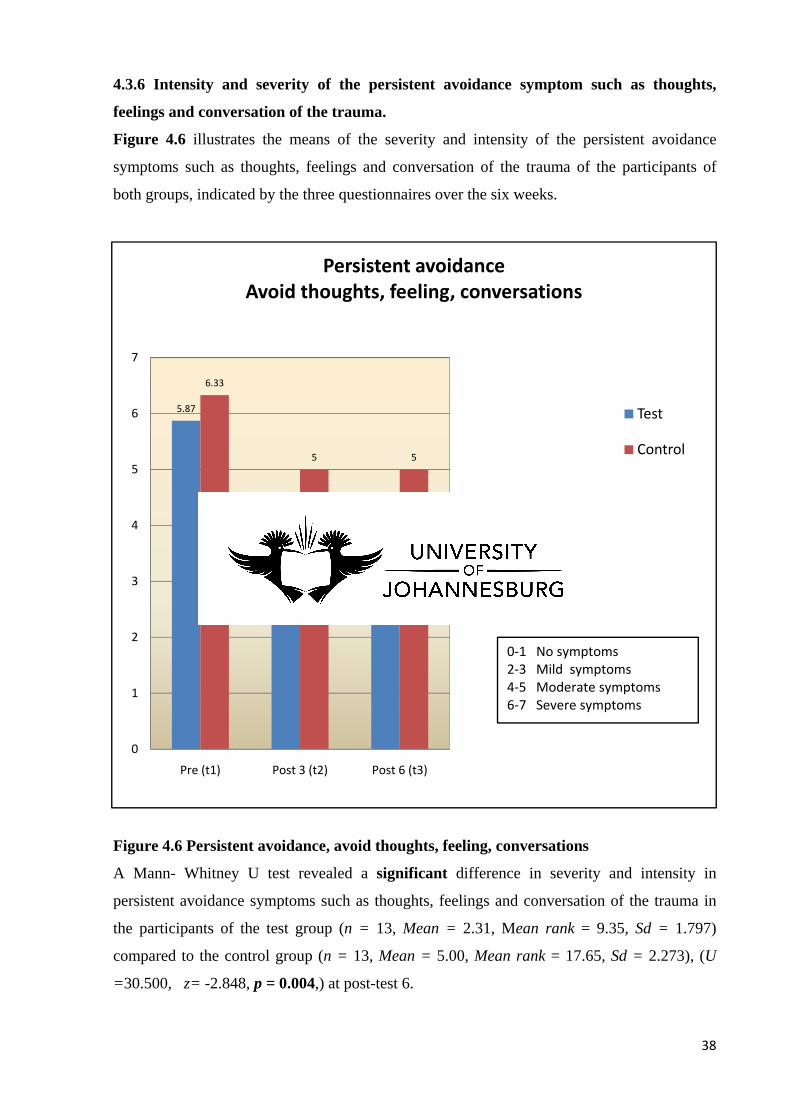
38
4.3.6 Intensity and severity of the persistent avoidance symptom such as thoughts,
feelings and conversation of the trauma.
Figure 4.6 illustrates the means of the severity and intensity of the persistent avoidance
symptoms such as thoughts, feelings and conversation of the trauma of the participants of
both groups, indicated by the three questionnaires over the six weeks.
Figure 4.6 Persistent avoidance, avoid thoughts, feeling, conversations
A Mann- Whitney U test revealed a significant difference in severity and intensity in
persistent avoidance symptoms such as thoughts, feelings and conversation of the trauma in
the participants of the test group (n = 13, Mean = 2.31, Mean rank = 9.35, Sd = 1.797)
compared to the control group (n = 13, Mean = 5.00, Mean rank = 17.65, Sd = 2.273), (U
=30.500, z= -2.848, p = 0.004,) at post-test 6.
5.87
3.69
2.31
6.33
5 5
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Persistent avoidanceAvoid thoughts, feeling, conversations
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
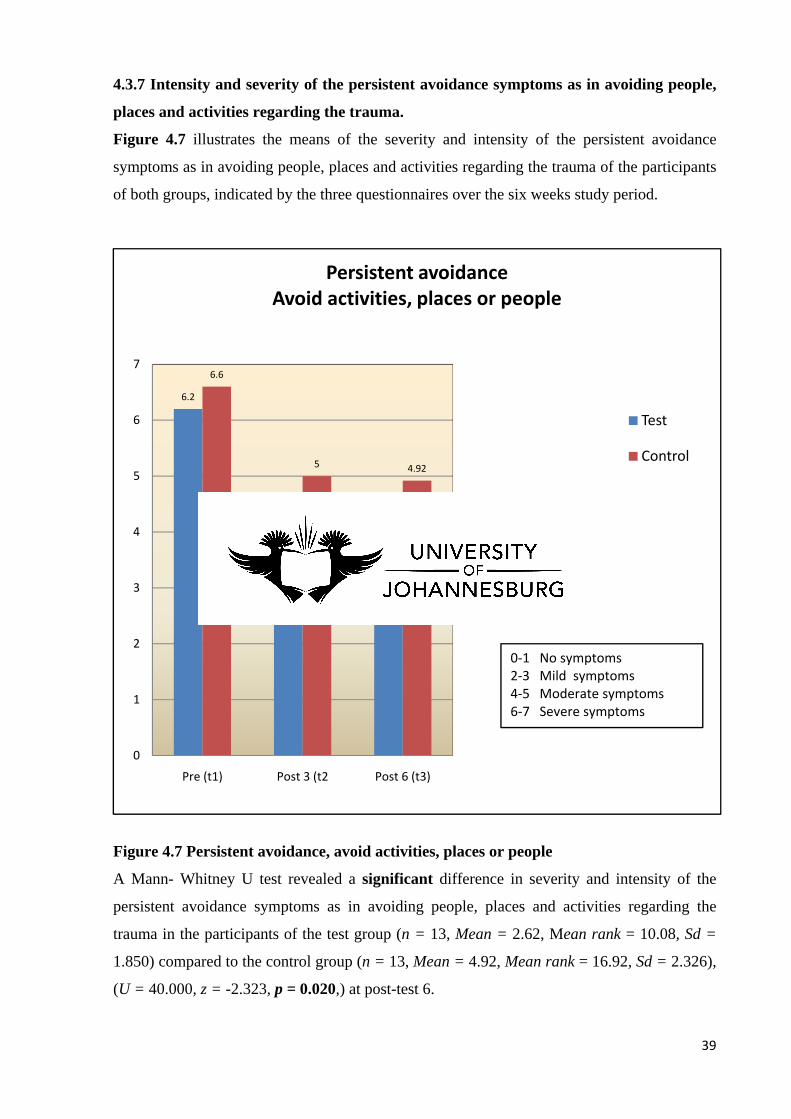
39
4.3.7 Intensity and severity of the persistent avoidance symptoms as in avoiding people,
places and activities regarding the trauma.
Figure 4.7 illustrates the means of the severity and intensity of the persistent avoidance
symptoms as in avoiding people, places and activities regarding the trauma of the participants
of both groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.7 Persistent avoidance, avoid activities, places or people
A Mann- Whitney U test revealed a significant difference in severity and intensity of the
persistent avoidance symptoms as in avoiding people, places and activities regarding the
trauma in the participants of the test group (n = 13, Mean = 2.62, Mean rank = 10.08, Sd =
1.850) compared to the control group (n = 13, Mean = 4.92, Mean rank = 16.92, Sd = 2.326),
(U = 40.000, z = -2.323, p = 0.020,) at post-test 6.
6.2
4.31
2.62
6.6
5 4.92
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2 Post 6 (t3)
Persistent avoidanceAvoid activities, places or people
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms

40
4.3.8 Intensity and severity of the persistent avoidance symptom such as unable to recall
important aspects of the trauma.
Figure 4.8 illustrates the means of the severity and intensity of the persistent avoidance
symptoms such as unable to recall important aspects of the trauma by the participants of both
groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.8 Persistent avoidance, unable to recall important aspects of the trauma
A Mann- Whitney U test revealed a significant difference in severity and intensity of the
persistent avoidance symptoms such as unable to recall important aspects of the trauma in the
participants of the test group (n = 13, Mean = 1.69, Mean rank = 10.15, Sd = 1.316)
compared to the control group (n = 13, Mean = 3.85, Mean rank = 16.85, Sd = 2.444),
(U=41.000, z = -2.390, p = 0.017,) at post-test 6.
4.53
2.38
1.69
5.73
3.77 3.85
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Persistent avoidanceUnable to recall important aspects of the trauma
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
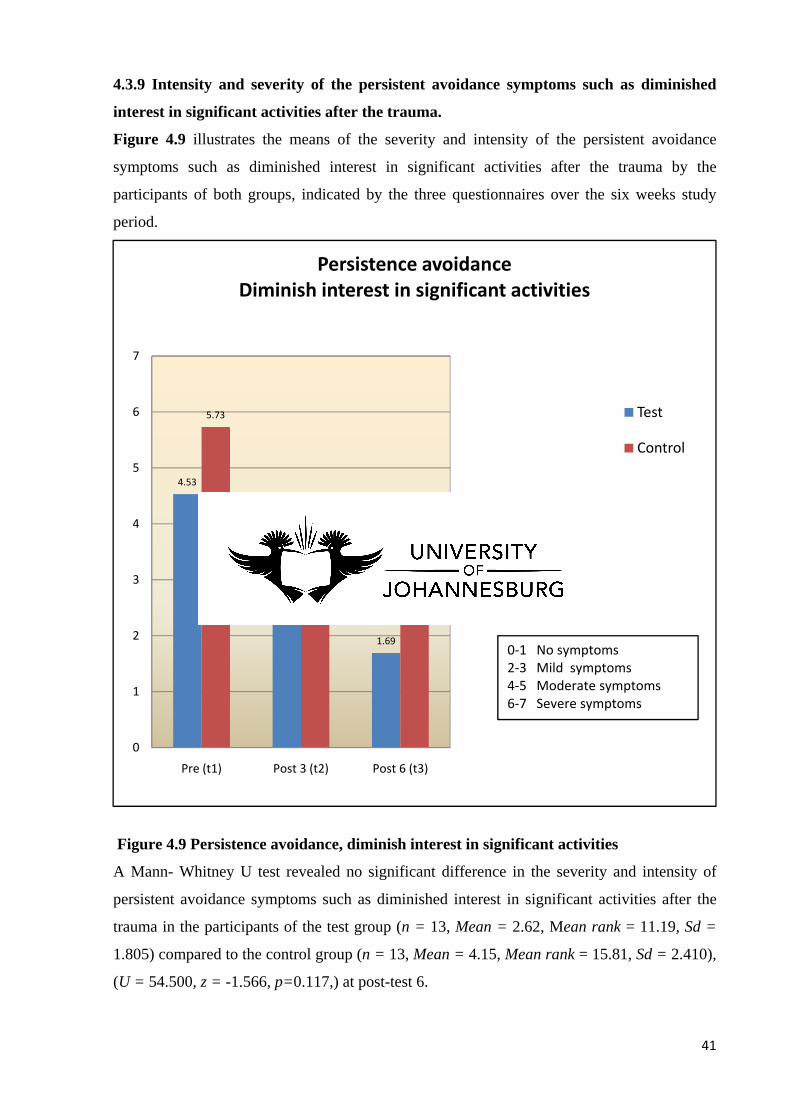
41
4.3.9 Intensity and severity of the persistent avoidance symptoms such as diminished
interest in significant activities after the trauma.
Figure 4.9 illustrates the means of the severity and intensity of the persistent avoidance
symptoms such as diminished interest in significant activities after the trauma by the
participants of both groups, indicated by the three questionnaires over the six weeks study
period.
Figure 4.9 Persistence avoidance, diminish interest in significant activities
A Mann- Whitney U test revealed no significant difference in the severity and intensity of
persistent avoidance symptoms such as diminished interest in significant activities after the
trauma in the participants of the test group (n = 13, Mean = 2.62, Mean rank = 11.19, Sd =
1.805) compared to the control group (n = 13, Mean = 4.15, Mean rank = 15.81, Sd = 2.410),
(U = 54.500, z = -1.566, p=0.117,) at post-test 6.
4.53
2.38
1.69
5.73
3.77 3.85
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Persistence avoidanceDiminish interest in significant activities
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
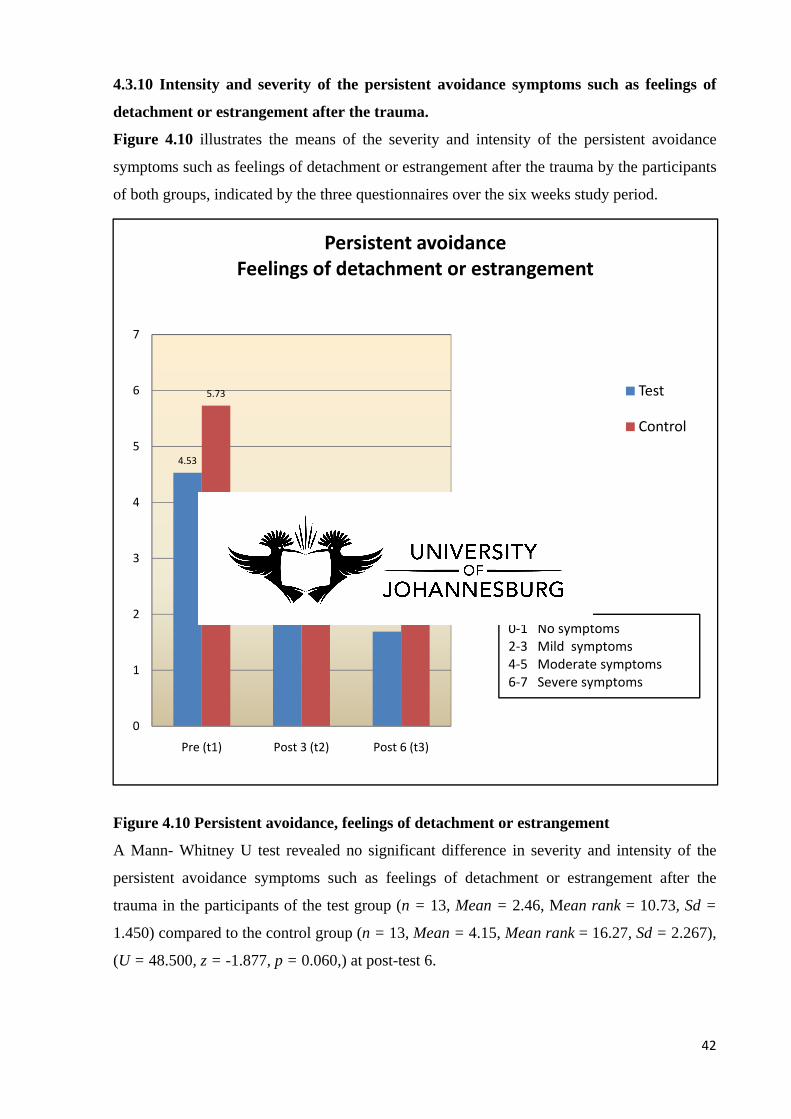
42
4.3.10 Intensity and severity of the persistent avoidance symptoms such as feelings of
detachment or estrangement after the trauma.
Figure 4.10 illustrates the means of the severity and intensity of the persistent avoidance
symptoms such as feelings of detachment or estrangement after the trauma by the participants
of both groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.10 Persistent avoidance, feelings of detachment or estrangement
A Mann- Whitney U test revealed no significant difference in severity and intensity of the
persistent avoidance symptoms such as feelings of detachment or estrangement after the
trauma in the participants of the test group (n = 13, Mean = 2.46, Mean rank = 10.73, Sd =
1.450) compared to the control group (n = 13, Mean = 4.15, Mean rank = 16.27, Sd = 2.267),
(U = 48.500, z = -1.877, p = 0.060,) at post-test 6.
4.53
2.38
1.69
5.73
3.77 3.85
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Persistent avoidanceFeelings of detachment or estrangement
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms

43
4.3.11. Intensity and severity of the persistent avoidance symptoms such as a restricted
range of effect, like unable to have loving feelings, uncaring and emotional numbness
after the trauma.
Figure 4.11 illustrates the means of the severity and intensity of the persistent avoidance
symptoms such as a restricted range of affect, like unable to have loving feelings, uncaring
and emotional numbness after the trauma by the participants of both groups, indicated by the
three questionnaires over the six weeks study period.
Figure 4.11 Persistant avoidance, restricted range of affect, unloving, uncaring A Mann- Whitney U test revealed no significant difference in severity and intensity of the persistent avoidance symptoms such as a restricted range of affect, like unable to have loving feelings, uncaring and emotional numbness after the trauma in the participants of the test group (n = 13, Mean = 2.31, Mean rank = 11.27, Sd = 1.494) compared to the control group (n = 13, Mean = 3.69, Mean rank = 15.73, Sd = 2.323), (U = 55.500, z = -1.529, p = 0.126,) at post-test 6.
5.8
3.85
2.31
5.87
3.853.69
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Persistant avoidanceRestricted range of affect, unloving, uncaring
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms

44
4.3.12 Intensity and severity of the persistent avoidance symptom such as a sense of a
foreshortened future after the trauma
Figure 4.12 illustrates the means of the severity and intensity of the persistent avoidance
symptom such as a sense of a foreshortened future after the trauma by the participants of both
groups, indicated by the three questionnaires over the six weeks study period.
Figure 4.12 Persistent avoidance, sense of a foreshortened future
A Mann- Whitney U test revealed no significant difference in severity and intensity of
persistent avoidance symptom such as a sense of a foreshortened future after the trauma in the
participants of the test group (n = 13, Mean = 2.54, Mean rank = 11.38, Sd = 2.106)
compared to the control group (n = 13, Mean = 4.08, Mean rank = 15.62, Sd = 2.326), (U =
57.000, z = -1.464, p = 0.143,) at post-test 6.
5.07
3.31
2.54
6.13
4.314.08
0
1
2
3
4
5
6
7
Pre (t1) post (t2) Post 6 (t3)
Persistent avoidanceSense of a foreshortened future
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
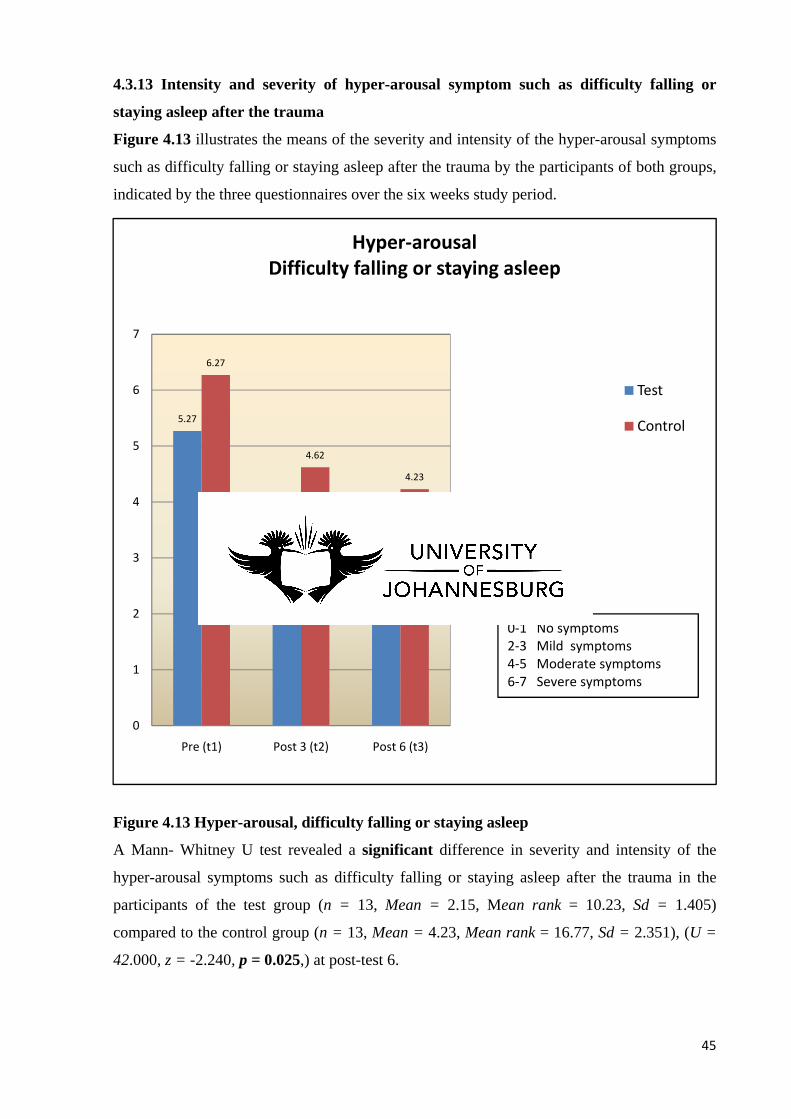
45
4.3.13 Intensity and severity of hyper-arousal symptom such as difficulty falling or
staying asleep after the trauma
Figure 4.13 illustrates the means of the severity and intensity of the hyper-arousal symptoms
such as difficulty falling or staying asleep after the trauma by the participants of both groups,
indicated by the three questionnaires over the six weeks study period.
Figure 4.13 Hyper-arousal, difficulty falling or staying asleep
A Mann- Whitney U test revealed a significant difference in severity and intensity of the
hyper-arousal symptoms such as difficulty falling or staying asleep after the trauma in the
participants of the test group (n = 13, Mean = 2.15, Mean rank = 10.23, Sd = 1.405)
compared to the control group (n = 13, Mean = 4.23, Mean rank = 16.77, Sd = 2.351), (U =
42.000, z = -2.240, p = 0.025,) at post-test 6.
5.27
3.15
2.15
6.27
4.62
4.23
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Hyper-arousalDifficulty falling or staying asleep
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
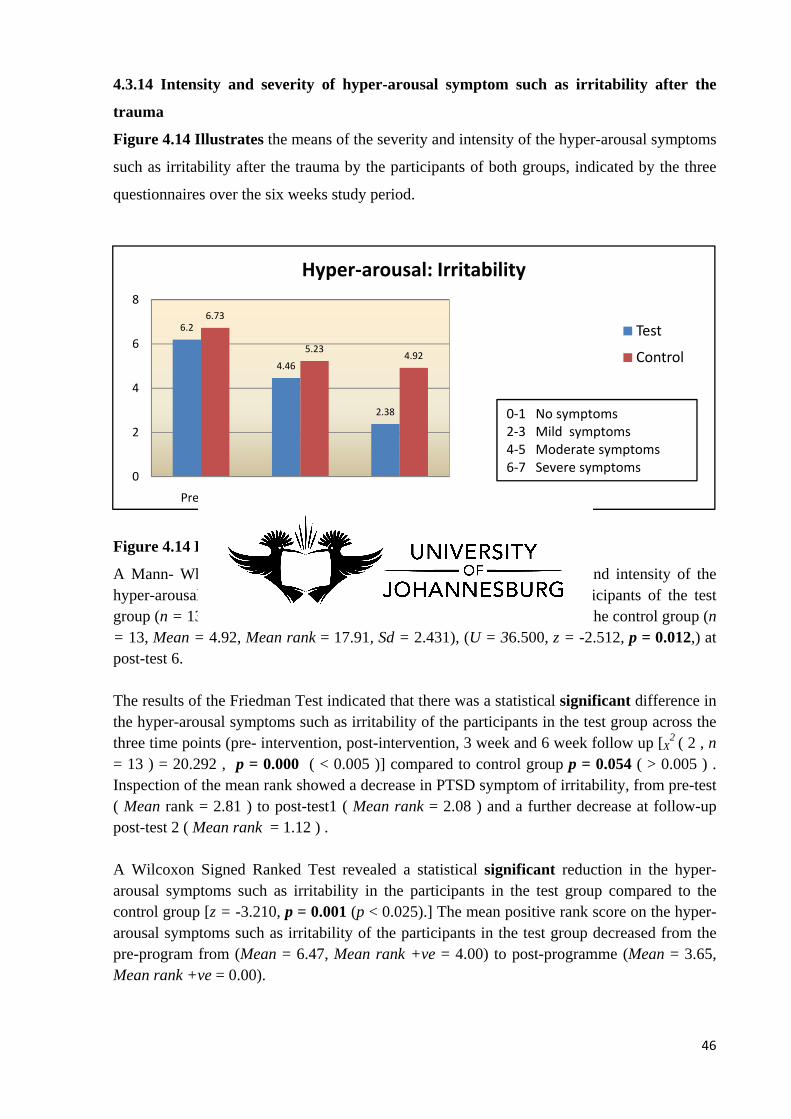
46
4.3.14 Intensity and severity of hyper-arousal symptom such as irritability after the
trauma
Figure 4.14 Illustrates the means of the severity and intensity of the hyper-arousal symptoms
such as irritability after the trauma by the participants of both groups, indicated by the three
questionnaires over the six weeks study period.
Figure 4.14 Hyper-arousal: Irritability
A Mann- Whitney U test revealed a significant difference in severity and intensity of the hyper-arousal symptoms such as irritability after the trauma in the participants of the test group (n = 13, Mean = 2.38, Mean rank = 9.81, Sd = 0.870) compared to the control group (n = 13, Mean = 4.92, Mean rank = 17.91, Sd = 2.431), (U = 36.500, z = -2.512, p = 0.012,) at post-test 6. The results of the Friedman Test indicated that there was a statistical significant difference in the hyper-arousal symptoms such as irritability of the participants in the test group across the three time points (pre- intervention, post-intervention, 3 week and 6 week follow up [X
2 ( 2 , n = 13 ) = 20.292 , p = 0.000 ( < 0.005 )] compared to control group p = 0.054 ( > 0.005 ) . Inspection of the mean rank showed a decrease in PTSD symptom of irritability, from pre-test ( Mean rank = 2.81 ) to post-test1 ( Mean rank = 2.08 ) and a further decrease at follow-up post-test 2 ( Mean rank = 1.12 ) . A Wilcoxon Signed Ranked Test revealed a statistical significant reduction in the hyper-arousal symptoms such as irritability in the participants in the test group compared to the control group [z = -3.210, p = 0.001 (p < 0.025).] The mean positive rank score on the hyper-arousal symptoms such as irritability of the participants in the test group decreased from the pre-program from (Mean = 6.47, Mean rank +ve = 4.00) to post-programme (Mean = 3.65, Mean rank +ve = 0.00).
6.2
4.46
2.38
6.73
5.234.92
0
2
4
6
8
Pre (t1) Post 3 (t2) Post 6 (t3)
Hyper-arousal: Irritability
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
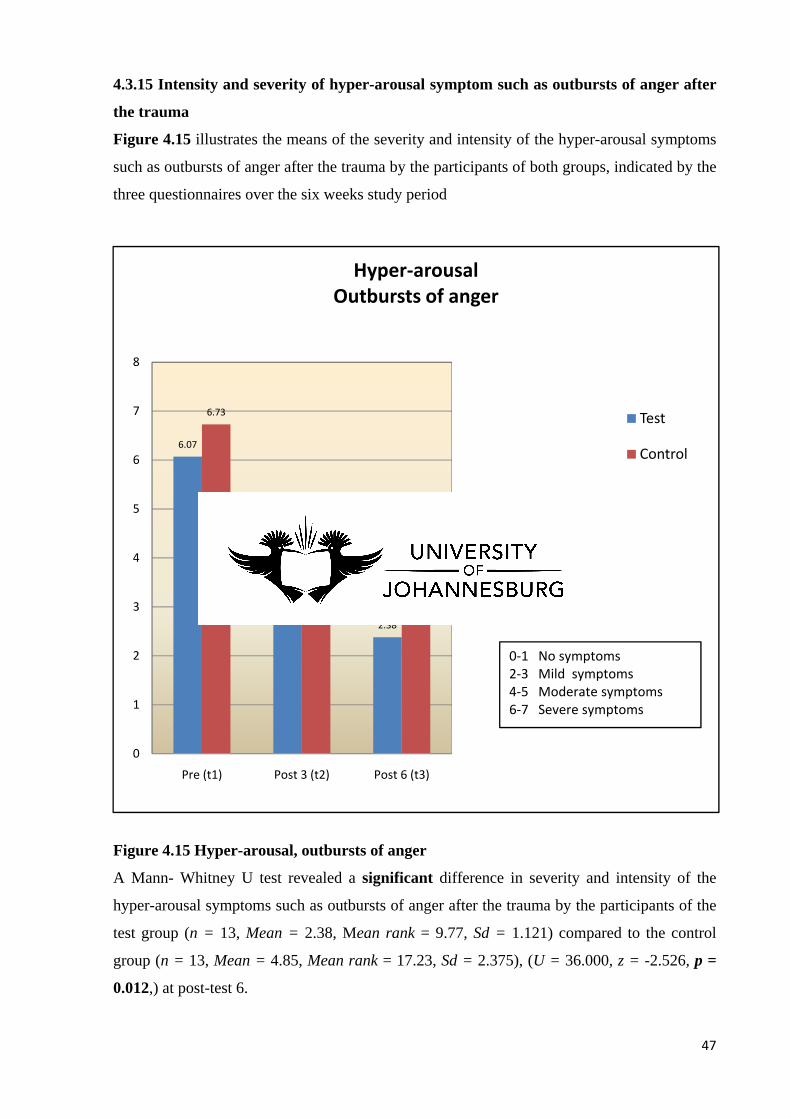
47
4.3.15 Intensity and severity of hyper-arousal symptom such as outbursts of anger after
the trauma
Figure 4.15 illustrates the means of the severity and intensity of the hyper-arousal symptoms
such as outbursts of anger after the trauma by the participants of both groups, indicated by the
three questionnaires over the six weeks study period
Figure 4.15 Hyper-arousal, outbursts of anger
A Mann- Whitney U test revealed a significant difference in severity and intensity of the
hyper-arousal symptoms such as outbursts of anger after the trauma by the participants of the
test group (n = 13, Mean = 2.38, Mean rank = 9.77, Sd = 1.121) compared to the control
group (n = 13, Mean = 4.85, Mean rank = 17.23, Sd = 2.375), (U = 36.000, z = -2.526, p =
0.012,) at post-test 6.
6.07
4.46
2.38
6.73
54.85
0
1
2
3
4
5
6
7
8
Pre (t1) Post 3 (t2) Post 6 (t3)
Hyper-arousalOutbursts of anger
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
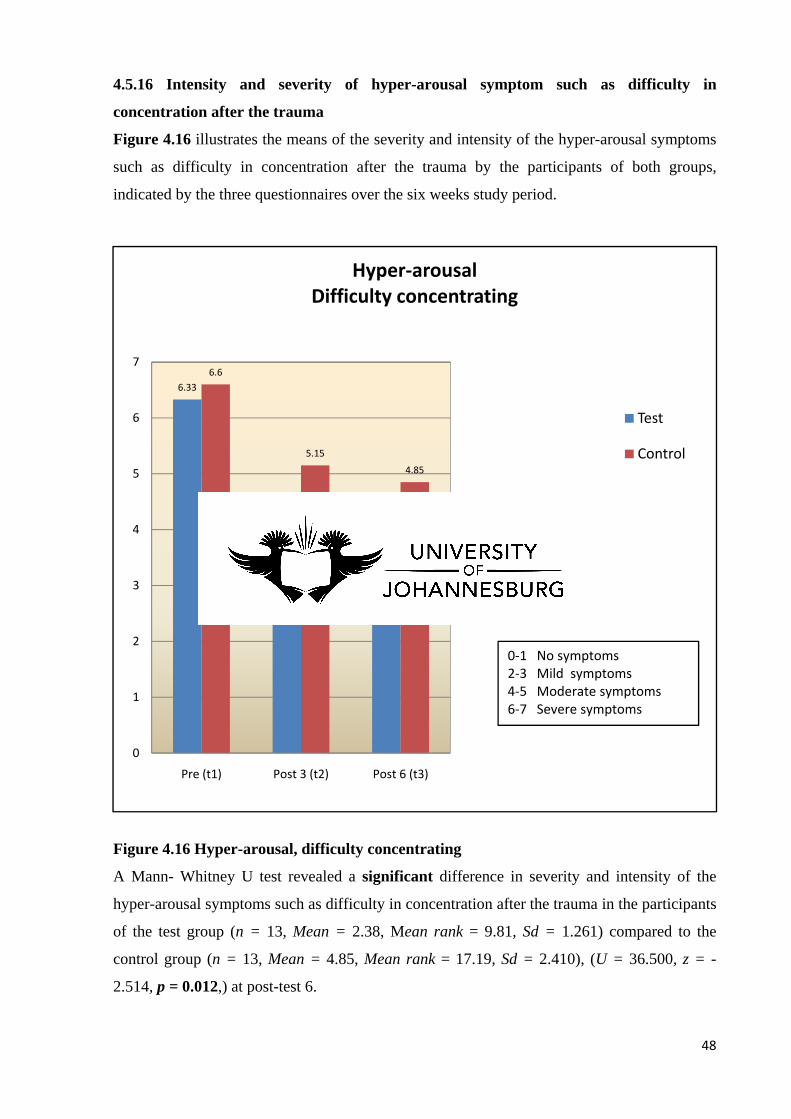
48
4.5.16 Intensity and severity of hyper-arousal symptom such as difficulty in
concentration after the trauma
Figure 4.16 illustrates the means of the severity and intensity of the hyper-arousal symptoms
such as difficulty in concentration after the trauma by the participants of both groups,
indicated by the three questionnaires over the six weeks study period.
Figure 4.16 Hyper-arousal, difficulty concentrating
A Mann- Whitney U test revealed a significant difference in severity and intensity of the
hyper-arousal symptoms such as difficulty in concentration after the trauma in the participants
of the test group (n = 13, Mean = 2.38, Mean rank = 9.81, Sd = 1.261) compared to the
control group (n = 13, Mean = 4.85, Mean rank = 17.19, Sd = 2.410), (U = 36.500, z = -
2.514, p = 0.012,) at post-test 6.
6.33
4.08
2.38
6.6
5.154.85
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Hyper-arousalDifficulty concentrating
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
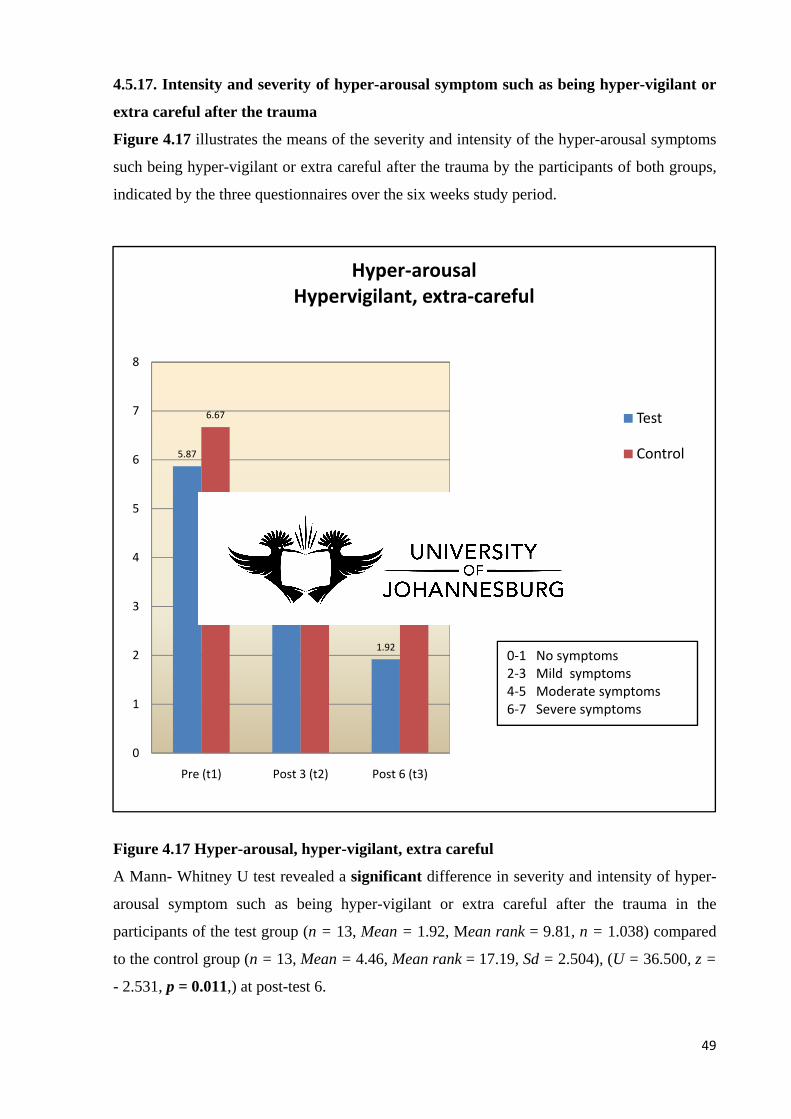
49
4.5.17. Intensity and severity of hyper-arousal symptom such as being hyper-vigilant or
extra careful after the trauma
Figure 4.17 illustrates the means of the severity and intensity of the hyper-arousal symptoms
such being hyper-vigilant or extra careful after the trauma by the participants of both groups,
indicated by the three questionnaires over the six weeks study period.
Figure 4.17 Hyper-arousal, hyper-vigilant, extra careful
A Mann- Whitney U test revealed a significant difference in severity and intensity of hyper-
arousal symptom such as being hyper-vigilant or extra careful after the trauma in the
participants of the test group (n = 13, Mean = 1.92, Mean rank = 9.81, n = 1.038) compared
to the control group (n = 13, Mean = 4.46, Mean rank = 17.19, Sd = 2.504), (U = 36.500, z =
- 2.531, p = 0.011,) at post-test 6.
5.87
3.62
1.92
6.67
4.624.46
0
1
2
3
4
5
6
7
8
Pre (t1) Post 3 (t2) Post 6 (t3)
Hyper-arousalHypervigilant, extra-careful
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
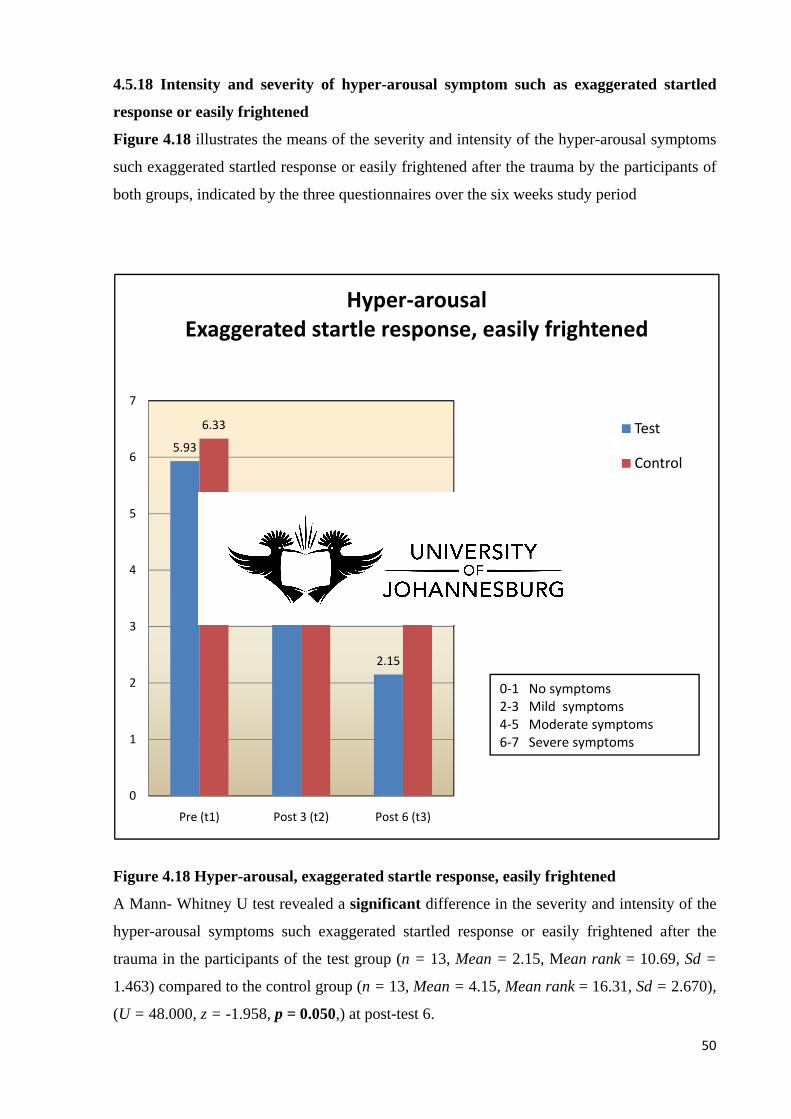
50
4.5.18 Intensity and severity of hyper-arousal symptom such as exaggerated startled
response or easily frightened
Figure 4.18 illustrates the means of the severity and intensity of the hyper-arousal symptoms
such exaggerated startled response or easily frightened after the trauma by the participants of
both groups, indicated by the three questionnaires over the six weeks study period
Figure 4.18 Hyper-arousal, exaggerated startle response, easily frightened
A Mann- Whitney U test revealed a significant difference in the severity and intensity of the
hyper-arousal symptoms such exaggerated startled response or easily frightened after the
trauma in the participants of the test group (n = 13, Mean = 2.15, Mean rank = 10.69, Sd =
1.463) compared to the control group (n = 13, Mean = 4.15, Mean rank = 16.31, Sd = 2.670),
(U = 48.000, z = -1.958, p = 0.050,) at post-test 6.
5.93
4.08
2.15
6.33
4.464.15
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Hyper-arousalExaggerated startle response, easily frightened
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
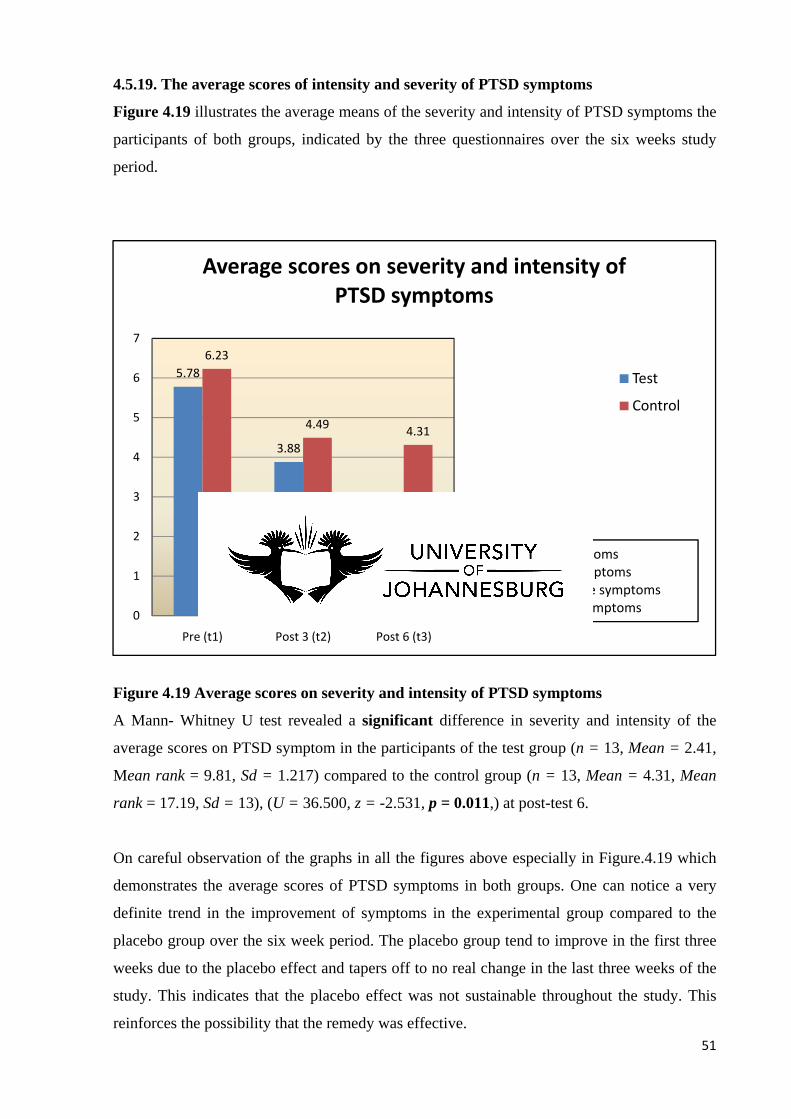
51
4.5.19. The average scores of intensity and severity of PTSD symptoms
Figure 4.19 illustrates the average means of the severity and intensity of PTSD symptoms the
participants of both groups, indicated by the three questionnaires over the six weeks study
period.
Figure 4.19 Average scores on severity and intensity of PTSD symptoms
A Mann- Whitney U test revealed a significant difference in severity and intensity of the
average scores on PTSD symptom in the participants of the test group (n = 13, Mean = 2.41,
Mean rank = 9.81, Sd = 1.217) compared to the control group (n = 13, Mean = 4.31, Mean
rank = 17.19, Sd = 13), (U = 36.500, z = -2.531, p = 0.011,) at post-test 6.
On careful observation of the graphs in all the figures above especially in Figure.4.19 which
demonstrates the average scores of PTSD symptoms in both groups. One can notice a very
definite trend in the improvement of symptoms in the experimental group compared to the
placebo group over the six week period. The placebo group tend to improve in the first three
weeks due to the placebo effect and tapers off to no real change in the last three weeks of the
study. This indicates that the placebo effect was not sustainable throughout the study. This
reinforces the possibility that the remedy was effective.
5.78
3.88
2.41
6.23
4.49 4.31
0
1
2
3
4
5
6
7
Pre (t1) Post 3 (t2) Post 6 (t3)
Average scores on severity and intensity of PTSD symptoms
Test
Control
0-1 No symptoms2-3 Mild symptoms4-5 Moderate symptoms6-7 Severe symptoms
52
CHAPTER FIVE
5. DISCUSSION
The study aimed to determine the efficacy of a homoeopathic complex remedy in the
treatment of post traumatic stress disorder in women. The homoeopathic complex Pegasus
t.r.s 200C® is a complex of homoeopathic and Bach flower remedies, and is indicated to be
clinically suitable for trauma and shock. It consists of homoeopathic remedies: Aconitum
napellus 200CH, Arnica montana 200CH, Hypericum perforatum 200CH, Ignatia amara
200CH, Opium 200CH, Passiflora incarnate 200CH; and Bach Flower Remedies: Impatiens,
Clematis, Rock rose, Star of Bethlehem and Cherry plum (Pegasus Homeopathics, 2007).
5.1 Demographic information on Recruitment and Race
There were thirty-one female participants between the ages of twenty-one to fifty-three who
were recruited by means of purposive sampling for the study. One participant could not be
accepted because she was over fifty-five and on heart medication. Two participants dropped
out because they felt that they had a reaction to the medication and felt worse than before:
One of them was from the experimental group while the other from the placebo group. It is
not clear if the participant from the experimental group had an aggravation due to the
homeopathic remedy, which may cause the existing symptoms to temporarily get worse, or if
such aggravation was influenced by other factors in the same manner as the participant from
the placebo group. One participant from the experimental group threw away her medication
by mistake and had to withdraw from the study. One participant from the placebo group gave
no specific reason for dropping out. Twenty six participants completed the study, thirteen
from each group.
Women from all races were invited to participate in this research. One White woman, one
Coloured woman, nine Black women and twenty Indian women were recruited for the study.
One Indian woman did not fit the criteria. The reason behind the fact that so many Indian
women participated in the study is due to the fact Nisaa is based in Lenasia, which is a
predominantly Indian area created during the apartheid regime. Black women also
participated in the study because of advertisements placed at the Nisaa offices in both Soweto
and Orange Farm. Some participants heard about the study by word of mouth.
53
5.2 Living conditions
Twenty-three of the participants lived in their own homes. Seven lived in the shelter that was
provided by Nisaa. The only participant not accepted into the study was from a shelter and she
received counselling and the necessary protection for her wellbeing. The living conditions
were different with regard to the women participating in the study with some living in a
sheltered environment and others in their home. The impact of this variable on the study is
unknown.
5.3 Trauma Counselling
All participants were instructed to attend trauma counselling at Nisaa. This was meant to be a
back-up especially for those who had placebo instead of a homoeopathic remedy. It was
therefore assumed that all participants from both groups received the standard trauma
counselling once a week from Nisaa (Appendix G).
5.4 Type of Trauma
All the participants had experienced grief of some kind for example the loss or death of
someone dear as a consequence of a hijacking, a shoot-out or a disastrous accident. They had
experienced a loss of dignity and sense of helplessness due to violence or an abusive
relationship. Ten participants had suffered from PTSD due to domestic violence and twenty
participants had suffered due to grief from other experiences. It is difficult to assess whether
the type of trauma concerned, such as trauma due to domestic violence and trauma due to
grief would influence the outcome of the study in any way since the results of both sub-
groups that were included in the experimental group responded favourably to the remedy.
5.5 The Homoeopathic Dosage in the study
The potencies for the homoeopathic remedies in Pegasus t.r.s 200C® are all 200CH except
for the Bach flower remedies. Some homoeopaths assert that in the event if mental symptoms
are prominent, high potencies should be considered (De Schepper 2006). Shock and trauma
respond to high potencies due to the severe mental and emotional symptoms which are
involved. In classical prescribing special care is taken when prescribing high potencies,
inasmuch as similar aggravations can occur. A homoeopathic aggravation happens when
existing symptoms become more severe, because of the primary action of the homoeopathic
remedy which suppresses the secondary action of the vital force. This can occur when the
right remedy is given too frequently or in a very high potency (De Schepper, 2006). In this
54
kind of similar aggravation the participants might start experiencing the very symptoms that
the remedy ought to eradicate.
For this reason the researcher proceeded with great care prescribing the remedy only three
times a week. The dosage of the remedy was very conservative because of its high potency. It
was important to be cautious as no adjustment could be made during the study in the event of
a proving or severe similar aggravation. In homoeopathic practice the patient’s response to the
remedy would be closely monitored and adjusted accordingly to the individual’s need.
Nevertheless some significant results were observed over and above this cautious and
conservative dosage which adds to the credible results.
5.6 Medication and compliancy
There is good reason to believe that the participants that took part in the study were compliant
in taking their medication. Most participants produced their calendars and others who forgot
their calendars re-assured the researcher that medication was taken as instructed.
5.7 Discussion of statistical analysis
5.7.1 Age frequency in the study
The participants recruited for the study were between the ages eighteen and fifty-five years
(Appendix A). The data for the ages were garnered from the patient information and case
taking form (Appendix D). The test for normality relating to the ages between the test group
and control group was normal (Table 4.2). The mean age recruited for the study was thirty-
seven years for the test group and thirty-eight years for the control group. The p-value was
0.739 which is greater than 0.05 and mean ranks was 38.60 which means that there was no
significant difference in the ages between the two groups (Table 4.1). There was an even
distribution between the experimental group and the placebo group. The youngest minimum
age was twenty-one in both groups and the oldest age was fifty-two years and fifty-three3
years in the placebo and experimental group respectively.
5.7.2 Shapiro-Wilk Test
The Shapiro-Wilk test was used to test for normality in each group because of the small
number of participants recruited for in the study. A normal distribution meant that the p-
values had to be greater or equal to 0.05. The Shapiro-Wilk test results indicated a normal
distribution for some of the symptoms in the experimental and placebo groups. It also
55
indicated a “not normal” or skewed distribution for the remainder of the symptoms in both the
groups. Therefore non-parametric tests were performed due to the small numbers of
participants and the lack of normal distribution.
5.7.3 Mann- Whitney U Test
The Mann-Whitney U test was found to be significant for the following ten symptoms of
PTSD
Severity and intensity of the re-experiencing symptoms of thoughts, images and
perceptions in the participants, p =0.048
Severity and intensity in persistent avoidance symptoms such as thoughts, feelings and
conversation of the trauma, p =0.004
Severity and intensity of the persistent avoidance symptoms such as in avoiding people,
places and activities regarding the trauma, p =0.020
Severity and intensity of the persistent avoidance symptoms such as unable to recall
important aspects of the trauma, p =0.017
Severity and intensity of the hyper-arousal symptoms such as difficulty in falling or
staying asleep after the trauma, p =0.025
Severity and intensity of the hyper-arousal symptoms such as irritability after the trauma,
p =0.012
Severity and intensity of the hyper-arousal symptoms such as outbursts of anger after the
trauma, p =0.012
Severity and intensity of the hyper-arousal symptoms such difficulty in concentration
after the trauma, p =0.012
Severity and intensity of hyper-arousal symptoms such as being hyper-vigilant or extra
careful after the trauma, p =0.011
Severity and intensity of the hyper-arousal symptoms such exaggerated startled response
or easily frightened after the trauma, p =0.05
It can thus be said that the Mann-Whitney test was significant on one re-experiencing
symptom, three persistent avoidance symptoms and six hyper-arousal symptoms.
No significant differences were obtained for the following eight symptoms
Severity and intensity of the re-experiencing symptoms such as recurrent distressing
dreams after the trauma, p =0.407
56
Severity and intensity of the re-experiencing symptoms such as flashbacks, illusions and
hallucinations after the trauma, p =0.066
Severity and intensity of the re-experiencing symptoms such as psychological distress at
any reminder of the trauma after the trauma, p =0.192
Severity and intensity of the re-experiencing symptoms such as physiological reactivity at
any reminder of the trauma after the trauma, p =0.0191
Severity and intensity of the persistent avoidance symptoms such as diminished interest
in significant activities after the trauma, p =0.117
Severity and intensity of the persistent avoidance symptoms such as feelings of
detachment or estrangement after the trauma, p =0.06
Severity and intensity of the persistent avoidance symptoms such as a restricted range of
effect, like unable to have loving feelings, uncaring and emotional numbness after the
trauma, p =0.126
Severity and intensity of the persistent avoidance symptoms such as a sense of a
foreshortened future after the trauma, p =0.143
However the total average scores of the intensity and severity of PTSD symptoms had a
significant p =0.011. This indicated an over-all improvement of PTSD symptoms in the
experimental group compared to the placebo group.
5.7.4 Freidman Analysis of Variance by Ranks Test
The ‘Friedman Analysis of Variance by Ranks Test’ test was found to be significant for two
symptoms of PTSD, namely:
The severity and intensity of the re-experiencing symptoms such as flashbacks, illusions
and hallucinations with a significant p = 0.000 in the test group compared to the control
group which had p = 0.072.
The severity and intensity of hyper-arousal symptoms such as irritability with a
significant p = 0.000 in the test group compared to the control group which had a p =
0.054
It can thus be said that the Freidman Analysis of Variance by Ranks Test showed significance
on the re-experiencing symptoms of flashbacks, illusions, hallucinations and the hyper-
arousal symptom of irritability.
57
5.7.5 Wilcoxon Signed-Rank Test
The Wilcoxon Signed-Rank Test indicates where exactly in the time line the changes
occurred. The symptoms in the test group progressively got better between week one and
week six, with a significant difference between week three and week six as can be observed in
figures 1-19. However in the placebo group the improvement is noted in the first three weeks
and then it tapers to a minimal or no real significant change in the last three weeks of the
study. This demonstrates the placebo effect was strongest at the start of the study but then had
no effect. A Bonferroni adjustment was made and p-values were significant for the test group
in the following two symptoms.
The re-experiencing symptoms of flashbacks, illusions, hallucinations which had the
smallest p-value of 0.002 which is less than 0.025 and second smallest p-value of 0.027
which is less than 0.05.
The hyper-arousal symptom of irritability had the smallest p-value of 0.001 which is less
than 0.025 and second smallest p-value of 0.014 which is less than 0.05.
This comparison of the Bonferroni adjustment is a further refinement of the study which was
resorted to in order to avoid statistical errors by chance.
5.8 Limitations of the study
Some of the limitations of the study have already been alluded to in the discussion. There is
no certainty as to how these variables might have impacted on the results obtained.
The living conditions were variable with some participants living in shelters and some at
resided in their homes.
The type of trauma and duration of traumatic suffering was different in respect to each
participant.
Participants were expected to attend trauma counselling, yet the researcher was unable to
confirm that all participants were compliant in this respect. The participants in shelters
had compulsory counselling.
The repetition of the homeopathic remedy Pegasus t.r.s 200® was given very
conservatively at three times weekly, and this may well represent other than the optimal
repetition with regard to all the participants.

58
CHAPTER SIX
6. CONCLUSIONS
It can be concluded that Pegasus t.r.s 200C® significantly improved the overall severity and
intensity of PTSD symptoms over a six week period (p=0.01) and significantly improved ten
specific symptoms of PTSD in the experimental group when compared to the placebo group,
as reflected by the average scores in the Mann-Whitney U Test (p = 0.01). The ten symptoms
were thoughts, images and perceptions; persistent avoidance symptoms such as thoughts,
feelings and conversation of the trauma, avoiding people, places and activities and unable to
recall important aspects of the trauma; difficulty in falling asleep, irritability, outbursts of
anger, difficulty in concentration, hyper-vigilant or extra careful and exaggerated startle
response or easily frightened. Eight symptoms, had no significant results.
It was especially significant in the re-experiencing symptoms of flashbacks, illusions and
hallucinations and the hyper-arousal symptom of irritability. This was indicated by the
Friedman Analysis of Variance by Ranks Test and Wilcoxon Signed-Rank Tests where a
Bonferroni adjustment confirmed aforesaid result.
The remedy Pegasus t.r.s.200C® was administered in this study at a conservative dosage of
three times a week so as to prevent the possible occurrence of homoeopathic aggravations.
While research into the optimal repetition of the dose may be fruitful, in clinical practice the
repetition of the dose can be adjusted to suit the individual needs of the patient.
6.1 RECOMMENDATION
The following recommendations are made for researchers who might consider undertaking
similar studies in the future:
Remedy administration could be made to occur at more regular intervals, such as daily,
twice a day for shorter periods of time like three weeks bolstered by a post-test conducted
at weekly intervals. The aforesaid might lead to a more rapid recovery and also facilitate a
closer monitoring of the participants.
Increase in the sample size, by the inclusion in the study of a larger number of participants.
Results would then be statistically accurate and participants might be recruited from the
police force or paramedics who are exposed to trauma on a daily basis.
59
A cross-gender study or a males only study, would add on to the knowledge of the effect of
the remedy on PTSD symptoms across genders.
A follow-up consultation three-six weeks after the trial might be added to the study in
order to determine if any of the participants experienced a relapse in symptoms.
The remedy could also be researched in relation to the potential treatment of acute stress
syndrome which occurs in the first four weeks after the trauma.
60
ANECDOTAL RESULTS
Anecdotal results are not considered scientific but for the purpose of interest the researcher
has included some observations which arose from the study.
A participant from the test group who had experienced a traumatic hijacking presented severe
symptoms of anxiety which had persisted for more than a year. She was unable to sleep with
the lights off, due to a previous house breaking trauma, and suffered a panic attack every-time
she got into a car after the hijacking experience. She experience some relief to her anxiety
after just three weeks with t.r.s 200C® taken very conservatively only thrice weekly. The
individual started driving lessons three weeks later and now, six weeks later, she sleeps with
the lights off.
Another participant also presented anxiety and hyper-arousal symptoms each evening at 5.30
pm, which was the time her son died in a sudden horrific truck accident. Her symptoms were
especially severe even when her other surviving son happened to be only a bit late in coming
home. She also experienced symptoms of anxiety everytime she passed by a truck on the road.
She was greatly relieved just three weeks into the study, notwithstanding the fact that she had
been experiencing these severe symptoms for nine months prior to the study. Her sister-in law
who also lost her son in the same incident experienced no change since she was given
placebo.
In a traumatic shoot-out, a young man was killed brutally and suddenly. Three survivors of
this event took part in the study six months after the tragic event. One was given a remedy,
while the other two was purely administered placebo. There was no significant change in
symptoms during the study. However they took the remedies after the study and the two
sisters who had received placebo before displayed a marked improvement in hyper-arousal
symptoms after study. The participant who had the remedy and did not show a significant
improvement improved after adjusting the dosage.
Two participants from the same family presented with hyper-arousal symptoms and were
constantly fearful, nervous and edgy after experiencing a traumatic house breaking which
occurred almost two years prior to the study. One had placebo and experienced no change,
whereas the other participant was greatly relieved by the remedy.
61
A mother who lost her son in a possible suicide incident involving a gunshot to the head, she
suffered from severe PTSD symptoms and there was no improvement at all. The boy’s aunt,
who likewise had no difference in PTSD symptoms, also took part in the study.They both had
placebo during the study.
Abused women in the shelters were avoiding their spouses and homes after their traumatic
experiences. They soon develop the courage and confidence and were empowered to face
their partners much earlier then was expected. This was put down to the homoeopathic
remedy they received in the study coupled with the support structure they received from the
shelters.
One has to bear in mind that while these are anecdotes, the study dealt with people who had
vivid and dramatic experiences of real pain, such that even the mere thought of the event
fostered in them anxiety and abundant weeping. These are some examples of situations where
the remedy worked in its clinical capacity. A number of the participants were cleared of some
of the most distressing symptoms of anxiety that they had been suffering over a long period of
time.
62
8. REFERENCES
American Institute of Homeopathy, Committee on Pharmacopeia. (1897). The Homoeopathic
Pharmacopoeia of the United States. Boston: Otis Clapp & Son. p. 71-72, 326-327, 434-435.
American Psychiatric Association. (1994). Diagnostic and Statistical Manual of Mental
Disorders. fourth edition. Washington, DC: American Psychiatric Press, pp 427-429.
Ballenger J.C., Davidson J.R.T., Lecrubier Y., Nutt D.J., Marshall R.D., Nemeroff C.B.,
Shalev A.Y., and Yehuda R., (2004). Consensus Statement Update on Posttraumatic Stress
Disorder From the International Consensus Group on Depression and Anxiety. Available
from http://66.102.1.104/scholar?hl=en&q=cache:0aMO6B7oqqIJ:www.uniovi.es/psiq
(Accessed 20 May 2009)
Bach, E., (1973). The TWELVE HEALERS and Other Remedies. reprinted edition. United
Kingdom: W. Daniel Company LTD. pp.3-4; 9; 13; 16; 20.
Banerjea, S.K., (2003). Synoptic Memorizer of Materia Medica Vol I & II. reprint edition.
New Delhi: B.Jain Publishers (P) LTD. pp. 1-4, 29.
Becker, F., (28 July - 15 September 2011). Statkon, Kingsway campus, UJ. Tel: 559 4406
Personal communication to Honnorat, M.R.
Boerike, W., (2000). New Manual of Homoeopathic Materia Medica and Repertory. second
re-augmented and revised edition based on ninth edition. New Delhi: B. Jain Publishers (P)
LTD. pp. 1-4, 29.
Bradford, T.L., (2004). The Lie and Letters of Dr. Samuel Hahnemann. Reprinted edition.
New Delhi: B.Jain Publishers (P) LTD. pp. 23-24.
Carrey, P.D., Stein, D.J., Zungu-Dirwayi, N., and Seedat, S., (2003). Trauma and
posttraumatic stress disorder in urban Xhosa primary care population: Prevalence, co-
morbidity, and service use patterns. Journal of Nervous and Mental Disease, 191(4), 230-236
Carroll, R.D. (2007). The skeptic’s dictionary, Complex homeopathy, Available from:
http://skepdic.com/complexhomeo.html (Accessed July 2009)

63
Chancellor, P.M., (1974). Handbook of the BACH FLOWER REMEDIES. 3rd edition. London:
The C.W. Daniel Company LTD. pp 237-238.
Cowperthwaite, A.C., (2004). A Text Book of Materia Medica and Theraapeutics,
Characteristics, Analytical and Comparative. 13th edition. New Delhi: B. Jain Publishers (P)
LTD. pp. 1-4, 9-10, 29, 85-86.
Dangor, Z., (15 July 2010). The Nisaa Institute for Women’s Development, Address: 19 Link
street, Lenasia 1827, Tel: 011 852-5082, e-mail address: [email protected] Personal
communication to Honnorat M.R.
Dangor, Z., Segwai P.K., Dry J., Ogunmefun C. (2008), Sheltering Together, Report of the
second Women’s Sheltering Workshop, A publication of Nisaa Institute for Women’s
Development, Lenasia, pp. 15, 21.
De Schepper, L., (2006). Hahnemann Revisited. A Textbook of Classical homeopathy for the
Professional. New Delhi: B. Jain Publishers (P) LTD. pp. 12, 56, 240.
Devey, R., (28 May 2010). Statkon, Kingsway campus, UJ. Tel: 559 4406 Personal
communication to Honnorat, M.R.
Dinan, B.A., McCall, G.J., and Gibson, D., (2007). Community Violence and PTSD in
selected South African townships. Journal of Interpersonal Violence, 19 (6), 727-742.
EMDR Institute, (2009). Information and Clinical applications:http://www.emdr.com/general
information/clinical-applications.html (accessed 25 September 2011)
Follette, V.M., and Pistorello, J., (2007). Finding Life Beyond Trauma: Using Acceptance and
Commitment Therapy to Heal Post traumatic Stress and Trauma-Related Problems. Oakland.
CA : New Harbinger Publications, Inc. p17.
Fourie, A., (20 July 2010, 15 October 2011). PsyCaD,Doorfontein campus, UJ , Tel: 011 559
6833, email-address: [email protected] Personal communication to Honnorat, M.R.
Ganfyd,. (2006). Post Traumatic Stress Disorder. Available from:
http://www.ganfyd.org/index.php?title=post_traumatic_stress_disorder (accessed 25 May
2009)
64
Gibbons R.D., Brown C. H., Hur, K., Marcus S.M., Bhaumik D.K., J.A., Herings R.M.C. and
Mann J.J. (2007). Early Evidence on the effects of Regulator’s Suicidality Warnings on SSRI
Prescriptions and Suicide in Children and Adolescents (Electronic version) Am J Psychiatry,
164:1356-1363
Gunavante, S.M., (2003). Introduction to Homoeopathic Prescribing. Reprint edition. New
Delhi: B.Jain Publishers (P) LTD. pp. 2-3, 6, 12-14.
Hahnemann, S., (2005). The Chronic Diseases. Their peculiar nature and homoeopathic cure.
Translated from German by Professor Louis H Tafel. New Delhi: B.Jain Publishers (P) LTD.
(Originally published in 1835). p. 373.
Hahnemann, S., (2001). Organon of Medicine 5th & 6th Edition, Translated from the fifth
edition with an appendix from German by R.E. Dugeon and William Boericke as per sixth
edition with additions and alterations. reprint edition, Jain Publishers (P) LTD., New Delhi,
pp. 31, 33, 80-81.
Howard, J.R., (1991). The Bach Flower Remedies - Step by Step. Reprint edtion. United
Kingdom: C.W. Daniel Company LTD. pp.5-9.
Henry, J.A., (2002). New Guide to Medicines & drugs. fifth edition. Italy: Dorling Kindersley
Limited. pp. 82-85.
Kaplan, H.I., Sadock B.J. and Grebb J.A. (1994). Synopsis of Psychiatry Behavioral Sciences
Clinical Psychiatry. seventh edition. Maryland, USA: Williams & Wilkins. pp 606-611.
Kaminer D. (2006). Healing processes in trauma narratives: A review (Electronic version)
South African Journal of Psychology, 36(3), pp. 481
Kent, J.T., (1966). Lectures on Homoeopathic Materia Medica. Second Indian edition
(Enlarged). Culcutta: Roy Publishing House. pp. 128, 699.
Kubany E.S., McCaig M.A., Laconsay J.R. (2003) Healing the trauma of Domestic Violence,
A Workbook for Women, New Harbinger Publications, Inc, p11
Lankaser, Y. (2004). The Effect Of The Homeopathic Similimum in Post Traumatic Disorder.
Master’s thesis. Johannesburg: Technikon Witwatersrand, p 183.

65
Nisaa’s Tenth Anniversary Annual Report. ( 2002-2003). P.31
Olley B.O., Zeier M.D., Seedat S., Stein D.J; (2005). Post-traumatic stress disorder among
recently diagnosed patients with HIV/AIDS in South Africa (Electronic version) AIDS Care,
p 550
Pacher, P. and Kecskemeti, V., (2004). Cardiovascular Side Effects of New Antidepressants
and Antipsychotics: New drugs, old concerns? Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2493295/ (Accessed 13 July 2007)
Pallant, J., (2007). SPSS Survival Manual: a Step-by-Step Guide to Data Analysis using SPSS
version. Third edition. Australia: Allen and Unwin. Pp. 206, 220, 223-225, 228-230.
Pegasus Homeopathics. (2007). The blue box homoeopathic treatment kit information
booklet, p 57 Available from www.pegasuskits.com
Pilkington K.; Kirkwood G.; Rampes H.; Fisher P. and Richardson J., (2005). Homeopathy
for depression: a systematic review of the research evidence (Electronic version) Science
direct Homeopathy 94:153-163.
Pilkington, K.; Kirkwood, G.; Rampes, H.; Fisher P. and Richardson J., (2006). Homeopathy
for anxiety and anxiety disorders: A systematic review of the research (Electronic version).
Science direct Homeopathy 95:151-162.
Reckeweg, Hans-Heinrich., (1983). Materia Medica Homoeopathia Antihomotoxica Vol. I, A
selective Pharmocology. First English edition translated from third German edition.Baden-
Baden: Aurelia-Verlag GmBH. p. i
Richardson-Boedler, C., (2010). Applying Bach Flower Therapy to the Healing Profession of
Homeopathy Psychology, Psychiatry Psychosomatic Medicine. Revised second edition. New
Delhi: B.Jain Publishers (P) LTD. pp. xviii, 1-3, 32-45, 233, 245, 268, 290, 301, 333.
Robson, C., (1993). Real world research: A Resource for Social Scientists and Practioner-
Researchers. UK: Blackwell Oxford and USA: Cambridge. p. 89, 102.
Schauenberg, P. and Paris, F., (1977). Guide to medicinal plants. United States: Keats
Publishing, Inc. p. 97, 133, 140-141, 153, 176, 296.
66
Seedat S., Stein D. J. and Carey P.D. (2005). Post Traumatic Stress Disorder in Women
(Electronic version). CNS Drugs 2005; 19 (5) : 411,412,420,423.
Shapiro, F., and Maxfield, L., (2002). EMDR: Information Processing in the treatment of
trauma (Electronic Version) In Session: Journal of Clinical Psychology, Special Issue,
Treatment of PTSD, 58, 933-944
Shuttleworth, M., (2009). Pretest-Posttest Designs-Experimental Research. Available from:
http://www.experiment-resources.com/pretest-posttest-designs.html (Accessed 17 May 2010)
Solomon, E.M., (2010). Department of Homoeopathy, Doornfontein campus, UJ. Tel: 011
559 6262 personal communication to Honnorat M.R. (6 May 2010)
Smith J (15 August-15 September 2011). Statkon, Kingsway campus, UJ. Tel: 011 559 4406
Personal communication to Honnorat, M.R.
Stein D.J., Seedat S., Iverson A. and Wessely S. (2007). Post-traumatic stress disorder:
medicine and politics (Electronic version) Lancet 369:139-141
Trochim, W.M.K. (2006). Research Methods Knowledge Base. Available from:
http://www.socialresearchmethods.net/kb/quasnegd.php (Accessed 17 May 2010)
Van Zyl M., Oosthuizen P.P., Seedat S. (2008). Post traumatic stress disorder: undiagnosed
cases in tertiary inpatient setting (Electronic Version) African Journal of Psychiatry pp. 119-
122 United Kingdom
Vithoulkas, G., (1980). Science of Homoeopathy. USA: Grove Press. pp. 5-6.
Vermeulen, F., (2001). Concordant Materia Medica. Second edition. Netherlands: Emrys, bv.
Publishers. pp. 575
Vlamis, G., (1994). The Healing Power of Bach Flower Rescue Remedy. London: Thorsons,
An Imprint of Harper Collins Publishers, pp 31-33
Wheeler, F.J. (1982). The Bach Remedies Repertory. United Kingdom: C.W Daniel Company
LTD. pp. 3-5.
67
APPENDIX A
RESEARCH ETHICAL CLEARANCE NO. AEC75/01-2010
HAVE YOU EXPERIENCED A TRAUMATIC EVENT WITHIN THE LAST TWO
YEARS?
If you are suffering from persistent memories of the trauma
If you are avoiding to talk or express your feelings regarding the trauma
If you feeling emotional numbness
If you cannot sleep well, are very irritable, get angry very easily or just cannot
concentrate
IF YOU ARE EXPERIECING SOME OF THESE SYMPTOMS,
THEN YOU MAY BE SUFFERING FROM POST TRAUMATIC STRESS
DISORDER.
WOMEN BEWEEN THE AGES 18-55
ARE INVITED TO PARTICIPATE IN THIS RESEARCH STUDY
PLEASE CONTACT
MOHSINA HONNORAT
072 656 0509
68
APPENDIX B
INFORMATION FORM
My name is Mohsina Honnorat and I am conducting research as part of completion of my
Master’s Degree in Homoeopathy as a student in the Faculty of Health Sciences at the
University of Johannesburg.
Post Traumatic Stress Disorder (PTSD) is an anxiety disorder, which affects people who have
been exposed to a traumatic event or events. I understand that the symptoms are distressing
and may occur for more than a month after a traumatic event.
Homoeopathy is a very old method of healing which helps the body to cure illness. It is a
natural therapeutic method of preventing and treating disease.
The purpose of this study is to determine the effect of the homoeopathic remedy (t.r.s 200C® )
on the frequency and severity of post traumatic stress episodes in women.
If you are between the ages 18-55 years old and have been diagnosed with PTSD, you are
invited to take part in the study. If you are taking any medicine for your high blood pressure
or contraception, please continue as usual. Please do not change your lifestyle or take any
other medication for your symptoms while you are on this study. If for some reason you need
to take any medication, please inform me.
The research study will take place over a period of six weeks. I will take your information and
conduct a medical examination. Then you will be given a questionnaire to fill out. I will see
you again after three weeks and then again after six weeks and you will be asked to fill in a
questionnaire on both occasions. During the research study you will receive the usual once a
week counselling at Nisaa.
You are requested to take the pills supplied to you.The pills you receive may contain the
homoeopathic complex remedy or it may be a placebo. A placebo means that it does not
contain any medication. During the study neither, you or I, will know if you are receiving the
medicine or not. After the research study I will supply you with a six week supply of the
homoeopathic remedy if you were taking the placebo during the study.
69
Some of you may experience less severe symptoms. By participating in this study you may be
contributing to scientific knowledge on homoeopathy. We do not expect any risks during the
study but should there be anything that concerns you or if you have any questions, please
contact me at any time. Contact details are provided at the bottom of this form.
You have chosen to participate in this study on a voluntary basis, and you are therefore free to
withdraw from the study at any time. All information received will be confidential and you
will remain anonymous. Your personal detail will not be linked to anything presented in the
research. You may have access to the research findings on request.
Contact Details:
Researcher: Mohsina Honnorat cell: 0726560509
email-address:[email protected]
Supervisor: Dr. Solomon Tel: 011 559 6262
Co-supervisor: Dr. Anita Fourie Tel: 011 559 6833
email-address: [email protected]
70
APPENDIX C
PARTICIPANT CONSENT FORM
The Efficacy of a Homoeopathic complex t.r.s 200C ® on the symptoms of Post Traumatic Stress
Disorder in women
A signed copy of this form will be given to you
I, the voluntary participant, have been completely informed about the procedure of this study. I accept
that I may at any time withdraw my participation in this study. I accept that I am free to enquire about
the research and ask questions, which will be answered by the researcher to the best of their ability.
Signature:____________________________ Date:_____________________
I, the researcher, have given a comprehensive explanation of the intended study procedures and
treatment. I will provide the best explanations that I can with regards to questions posed by the
participants.
Signature:____________________________ Date:_______________________
71
APPENDIX D
PATIENT INFORMATION AND CASE TAKING FORM
Date: ________________________________ Group: ____________________________
Name: ________________________________ ID/D.O.B: __________________________
Gender: _______________________________ Occupation: ________________________
Contact Tel No: ________________________ e-mail: ____________________________
Address: ______________________________ Referred:___________________________
General information
When did you experience your trauma? _________________________________________
Do you suffer from any chronic illness? _________________________________________
Are you pregnant or breastfeeding? ____________________________________________
Do you have any sleep problems/nightmares? ____________________________________
Were you ever hospitalized? __________________________________________________
Do you have difficulty in concentrating/remembering? ____________________________
Are you fearful or afraid for your loved ones? ___________________________________
Do you avoid activities, places or people? _______________________________________
Do you feel sad, irritated, anxious or edgy? _____________________________________
Examination
BP: ___________ RESP RATE: ___________ PULSE: __________ _TEMP: __________
PRIMARY SURVEY:
C A J C O L D

72
APPENDIX E
Modified Diagnostic Statistical Manual (DSM_IV) Criterion Questionnaire
(To be filled out with the help of the researcher)
Scale: 1 = Never
2 = Very rarely
3 = Rarely
4 = Sometimes
5 = Often
6 = Very often
7 = Always
Tick the patient’s response in the appropriate block
Re-experiencing
1. Do you experience recurrent and intrusive distressing recollections of the traumatic event
(thoughts, images or perceptions?
1 2 3 4 5 6 7
2. Do you have recurrent distressing dreams of the event?
1 2 3 4 5 6 7
3. Do you act or feel as if the traumatic event were recurring (flashbacks, reliving the
experience, illusions, and hallucinations)?
1 2 3 4 5 6 7
4. Do you experience any psychological distress (anxiety, sadness, anger, fear) at exposure
to anything that may remind you of the event?
1 2 3 4 5 6 7
5. Do you have any physiological reactivity (sweating, palpitations, increased muscle
tension, increased respiration) at exposure to anything that may remind you of the event?
1 2 3 4 5 6 7
73
Persistent Avoidance:
6. Do you make efforts to avoid thoughts, feelings, or conversations associated with the
trauma?
1 2 3 4 5 6 7
7. Do you avoid activities, places, or people that arouse recollections of the trauma?
1 2 3 4 5 6 7
8. Are you unable to recall important aspects of the trauma?
1 2 3 4 5 6 7
9. Has there been any diminished interest or participation in significant activities (work,
exercise, social activities)?
1 2 3 4 5 6 7
10. Do you experience feelings of detachment or estrangement from others?
1 2 3 4 5 6 7
11. Do you experience restricted range of affect (unable to have loving feelings, uncaring)?
1 2 3 4 5 6 7
12. Do you have a sense of a foreshortened future (do not expect to have a career, marriage,
children, or normal lifespan)?
1 2 3 4 5 6 7
Hyper-arousal :
13. Do you experience any difficulty falling or staying asleep?
1 2 3 4 5 6 7
14. Are you irritable?
1 2 3 4 5 6 7
74
15. Do you experience any outbursts of anger?
1 2 3 4 5 6 7
16. Do you have difficulty concentrating?
1 2 3 4 5 6 7
17. Are you hyper-vigilant (constantly looking over your shoulder, extra careful)?
1 2 3 4 5 6 7
18. Do you experience exaggerated startle response (easily frightened)?
1 2 3 4 5 6 7
File No.: _________________________
Score: ___________________________
Average score: ____________________
Group: __________________________
APP
PENDIX FF
755

APP
PENDIX G
766
77
APPENDIX H
CALENDAR
Directions:
Take five pills, under the tongue three times a week on a Monday, Wednesday and a
Friday.
Take your pills 15 minutes before eating or drinking any food.
After you have taken your pills please sign the calendar I have provided.
This will help me with my record keeping. Thank You.
Note: This calendar is issued at the first consultation and it is very important that you keep it
during the whole study. The researcher will have a copy and keep a record of events. If for
some reason you have not taken your medicine on the Monday, Wednesday or Friday, then it
is possible to move up a day for example, Tuesday, Thursday, Saturday and then go back to
the Monday, Wednesday, Friday routine the following week. Your co-operation and
commitment is highly appreciated. Please bring this calendar with you to your next
consultation.
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Week
1
Date
Week
2
Date
Week
3
Date
Week
4
Date
Week
5
Date
Week
6
Date

78
Appendix I
Tabulated Statistical Results from question 1-18 of all the Symptoms
I- 1 Q1 Group, Descriptive statistics and Ranks for Mann- Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q1_Pre Total
15 15 30
1.082 0.990 1.033
5.80 6.13 5.97
14.17 16.03
212.50 252.50
Q1_Post 3 Total
1) Test 2) Control
13 13 26
1.536 2.063 1.793
4.23 4.62 4.42
12.08 14.92
157.00 194.00
Q1_Post 6 Total
1) Test 2) Control
13 13 26
1.605 2.063 1.974
3.08 4.62 3.85
10.58 16.42
137.50 213.50
I- 2 Q1 Test statistics for Mann-Whitney U test
Q1_ Pre Q1_ Post 3 Q1_ Post 6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
92.500 -0.872 0.383
66.000 -0.968 0.333
46.500 -1.975 0.048
I- 3 Q1 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q1_Pre Total
1) Test 2) Control
15 15 30
1.082 0.990 1.033
5.80 6.13 5.97
2.69 2.62
4
7
Q1_Post 3 Total
1) Test 2) Control
13 13 26
1.536 2.063 1.793
4.23 4.62 4.42
2.08 1.69
1
7
Q1_Post 6 Total
1) Test 2) Control
13 13 26
1.605 2.063 1.974
3.08 4.62 3.85
1.23 1.69
1
7
I- 4. Q1 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 19.158
2 0.000
13 14.222
2 0.001
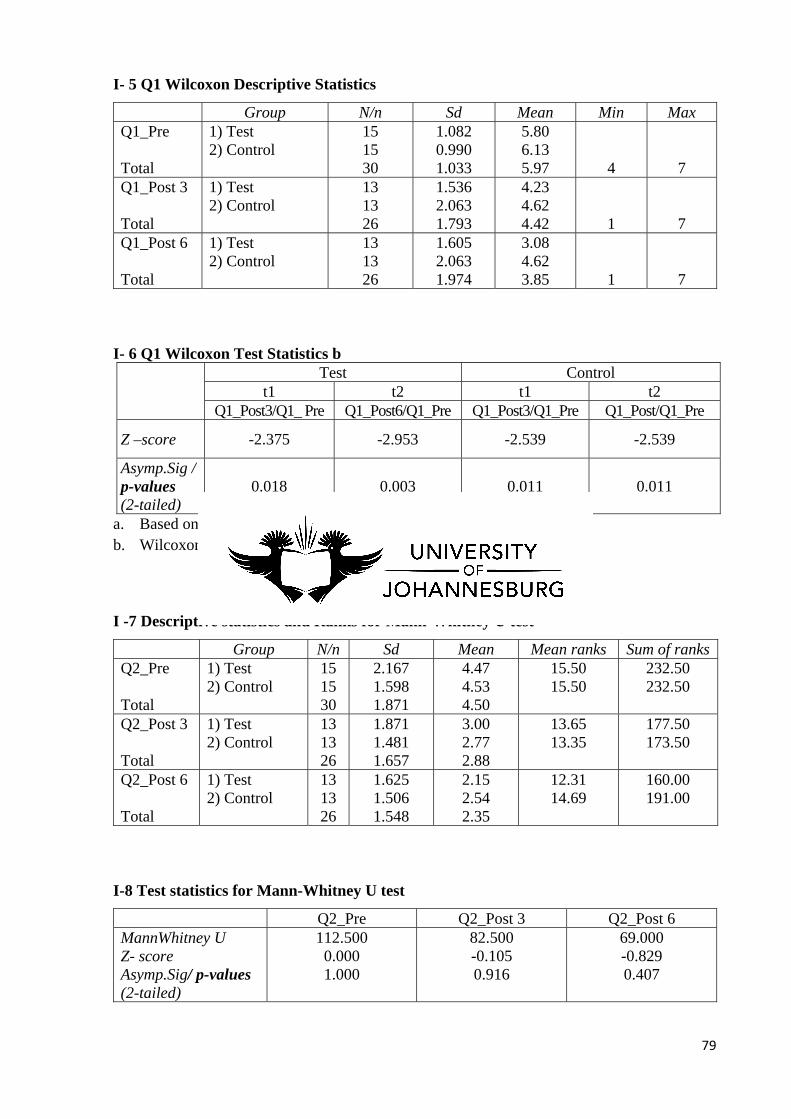
79
I- 5 Q1 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q1_Pre Total
1) Test 2) Control
15 15 30
1.082 0.990 1.033
5.80 6.13 5.97
4
7
Q1_Post 3 Total
1) Test 2) Control
13 13 26
1.536 2.063 1.793
4.23 4.62 4.42
1
7
Q1_Post 6 Total
1) Test 2) Control
13 13 26
1.605 2.063 1.974
3.08 4.62 3.85
1
7
I- 6 Q1 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q1_Post3/Q1_ Pre Q1_Post6/Q1_Pre Q1_Post3/Q1_Pre Q1_Post/Q1_Pre
Z –score -2.375 -2.953 -2.539 -2.539
Asymp.Sig / p-values (2-tailed)
0.018 0.003 0.011 0.011
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I -7 Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranksQ2_Pre Total
1) Test 2) Control
15 15 30
2.167 1.598 1.871
4.47 4.53 4.50
15.50 15.50
232.50 232.50
Q2_Post 3 Total
1) Test 2) Control
13 13 26
1.871 1.481 1.657
3.00 2.77 2.88
13.65 13.35
177.50 173.50
Q2_Post 6 Total
1) Test 2) Control
13 13 26
1.625 1.506 1.548
2.15 2.54 2.35
12.31 14.69
160.00 191.00
I-8 Test statistics for Mann-Whitney U test
Q2_Pre Q2_Post 3 Q2_Post 6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
112.500 0.000 1.000
82.500 -0.105 0.916
69.000 -0.829 0.407
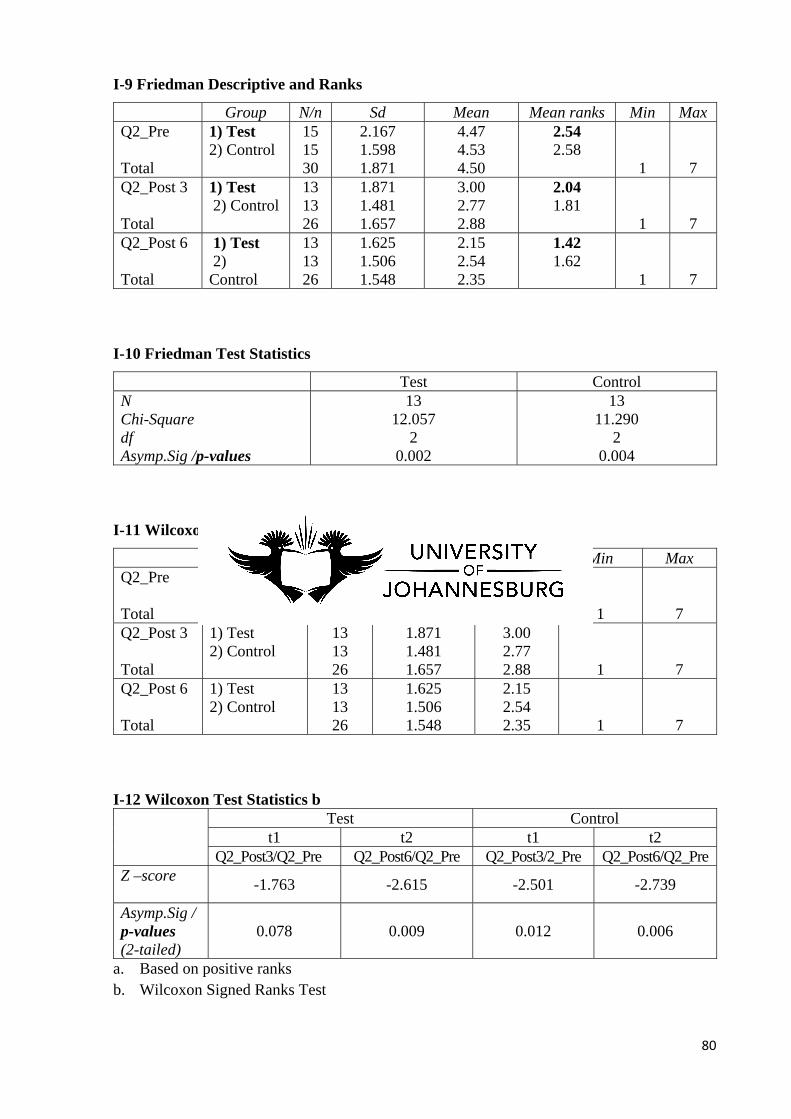
80
I-9 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q2_Pre Total
1) Test 2) Control
15 15 30
2.167 1.598 1.871
4.47 4.53 4.50
2.54 2.58
1
7
Q2_Post 3 Total
1) Test 2) Control
13 13 26
1.871 1.481 1.657
3.00 2.77 2.88
2.04 1.81
1
7
Q2_Post 6 Total
1) Test 2) Control
13 13 26
1.625 1.506 1.548
2.15 2.54 2.35
1.42 1.62
1
7
I-10 Friedman Test Statistics
Test Control N Chi-Square df Asymp.Sig /p-values
13 12.057
2 0.002
13 11.290
2 0.004
I-11 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q2_Pre Total
1) Test 2) Control
15 15 30
2.167 1.598 1.871
4.47 4.53 4.50
1
7
Q2_Post 3 Total
1) Test 2) Control
13 13 26
1.871 1.481 1.657
3.00 2.77 2.88
1
7
Q2_Post 6 Total
1) Test 2) Control
13 13 26
1.625 1.506 1.548
2.15 2.54 2.35
1
7
I-12 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q2_Post3/Q2_Pre Q2_Post6/Q2_Pre Q2_Post3/2_Pre Q2_Post6/Q2_Pre
Z –score
-1.763 -2.615 -2.501 -2.739
Asymp.Sig / p-values (2-tailed)
0.078 0.009 0.012 0.006
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
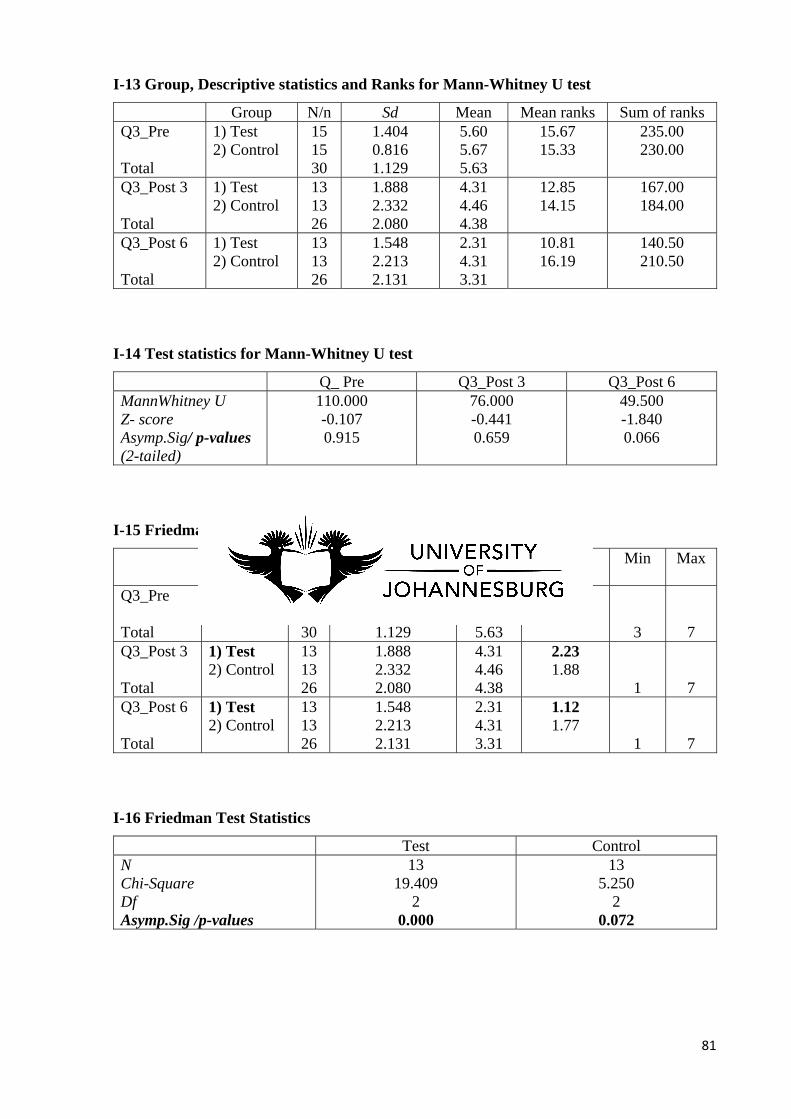
81
I-13 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q3_Pre Total
1) Test 2) Control
15 15 30
1.404 0.816 1.129
5.60 5.67 5.63
15.67 15.33
235.00 230.00
Q3_Post 3 Total
1) Test 2) Control
13 13 26
1.888 2.332 2.080
4.31 4.46 4.38
12.85 14.15
167.00 184.00
Q3_Post 6 Total
1) Test 2) Control
13 13 26
1.548 2.213 2.131
2.31 4.31 3.31
10.81 16.19
140.50 210.50
I-14 Test statistics for Mann-Whitney U test
Q_ Pre Q3_Post 3 Q3_Post 6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
110.000 -0.107 0.915
76.000 -0.441 0.659
49.500 -1.840 0.066
I-15 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks
Min Max
Q3_Pre Total
1) Test 2) Control
15 15 30
1.404 0.816 1.129
5.60 5.67 5.63
2.65 2.35
3
7
Q3_Post 3 Total
1) Test 2) Control
13 13 26
1.888 2.332 2.080
4.31 4.46 4.38
2.23 1.88
1
7
Q3_Post 6 Total
1) Test 2) Control
13 13 26
1.548 2.213 2.131
2.31 4.31 3.31
1.12 1.77
1
7
I-16 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 19.409
2 0.000
13 5.250
2 0.072
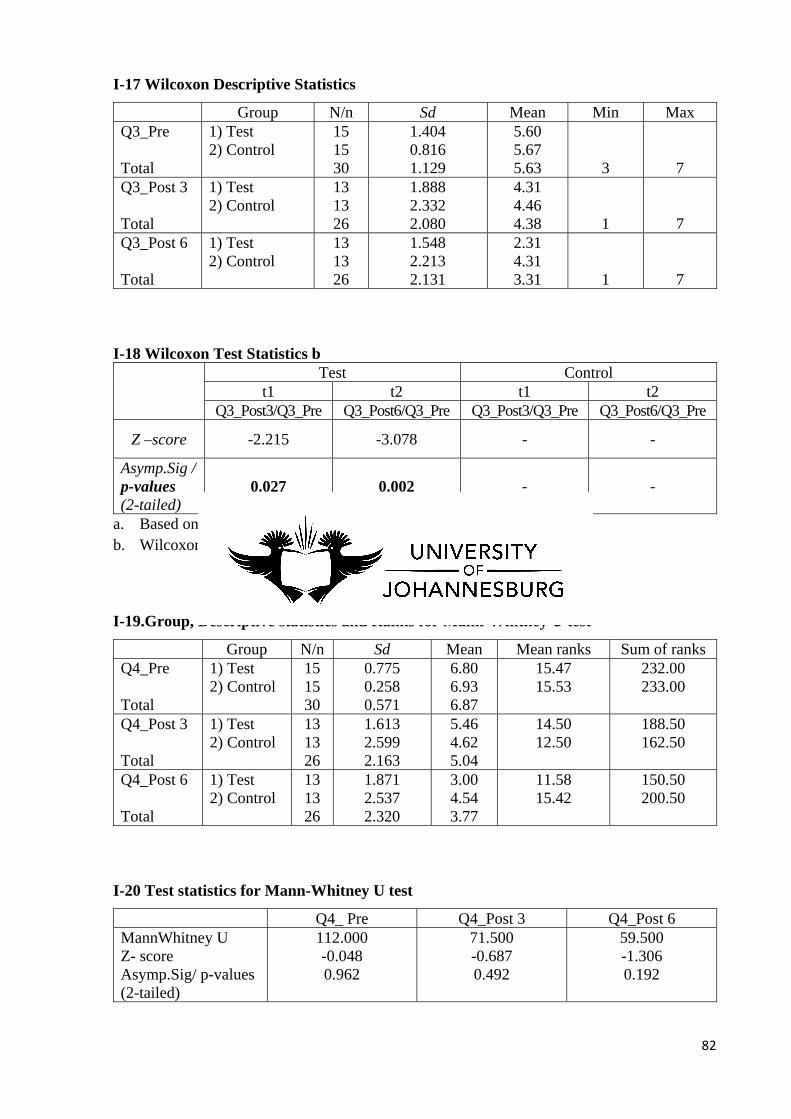
82
I-17 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q3_Pre Total
1) Test 2) Control
15 15 30
1.404 0.816 1.129
5.60 5.67 5.63
3
7
Q3_Post 3 Total
1) Test 2) Control
13 13 26
1.888 2.332 2.080
4.31 4.46 4.38
1
7
Q3_Post 6 Total
1) Test 2) Control
13 13 26
1.548 2.213 2.131
2.31 4.31 3.31
1
7
I-18 Wilcoxon Test Statistics b Test Control
t1 t2 t1 t2 Q3_Post3/Q3_Pre Q3_Post6/Q3_Pre Q3_Post3/Q3_Pre Q3_Post6/Q3_Pre
Z –score -2.215 -3.078 - -
Asymp.Sig / p-values (2-tailed)
0.027 0.002 - -
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-19.Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q4_Pre Total
1) Test 2) Control
15 15 30
0.775 0.258 0.571
6.80 6.93 6.87
15.47 15.53
232.00 233.00
Q4_Post 3 Total
1) Test 2) Control
13 13 26
1.613 2.599 2.163
5.46 4.62 5.04
14.50 12.50
188.50 162.50
Q4_Post 6 Total
1) Test 2) Control
13 13 26
1.871 2.537 2.320
3.00 4.54 3.77
11.58 15.42
150.50 200.50
I-20 Test statistics for Mann-Whitney U test
Q4_ Pre Q4_Post 3 Q4_Post 6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
112.000 -0.048 0.962
71.500 -0.687 0.492
59.500 -1.306 0.192
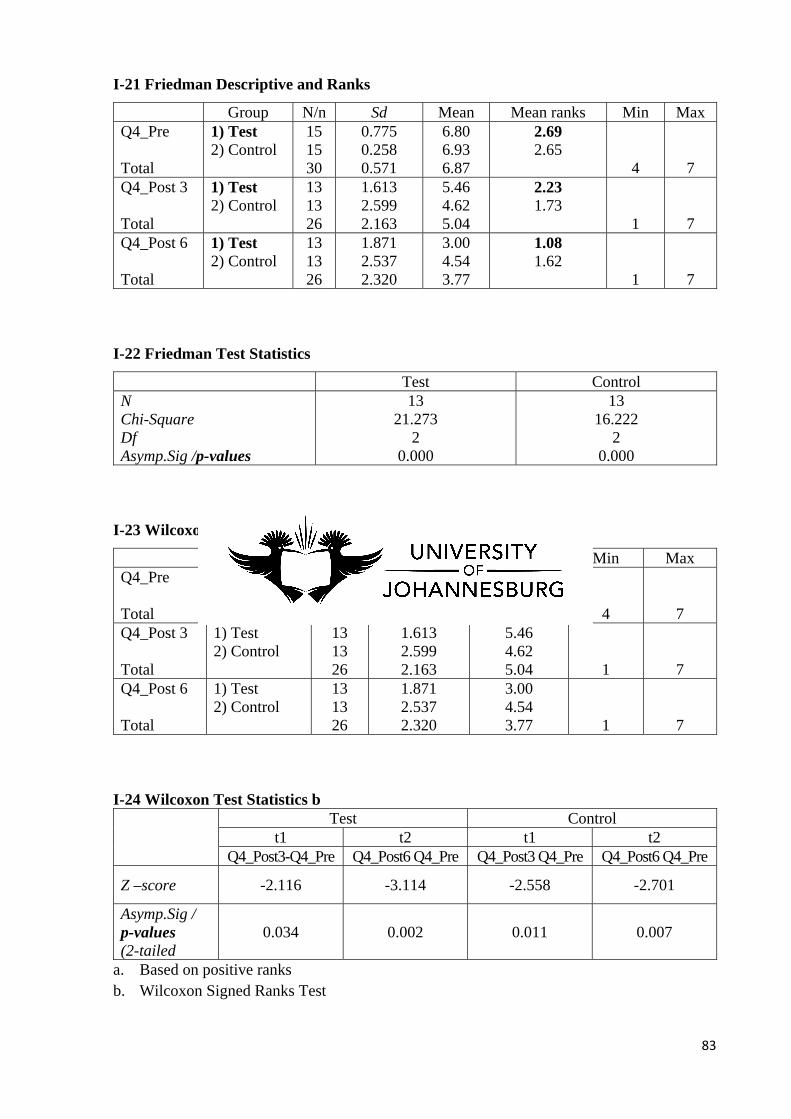
83
I-21 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q4_Pre Total
1) Test 2) Control
15 15 30
0.775 0.258 0.571
6.80 6.93 6.87
2.69 2.65
4
7
Q4_Post 3 Total
1) Test 2) Control
13 13 26
1.613 2.599 2.163
5.46 4.62 5.04
2.23 1.73
1
7
Q4_Post 6 Total
1) Test 2) Control
13 13 26
1.871 2.537 2.320
3.00 4.54 3.77
1.08 1.62
1
7
I-22 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 21.273
2 0.000
13 16.222
2 0.000
I-23 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q4_Pre Total
1) Test 2) Control
15 15 30
0.775 0.258 0.571
6.80 6.93 6.87
4
7
Q4_Post 3 Total
1) Test 2) Control
13 13 26
1.613 2.599 2.163
5.46 4.62 5.04
1
7
Q4_Post 6 Total
1) Test 2) Control
13 13 26
1.871 2.537 2.320
3.00 4.54 3.77
1
7
I-24 Wilcoxon Test Statistics b Test Control
t1 t2 t1 t2 Q4_Post3-Q4_Pre Q4_Post6 Q4_Pre Q4_Post3 Q4_Pre Q4_Post6 Q4_Pre
Z –score -2.116 -3.114 -2.558 -2.701
Asymp.Sig / p-values (2-tailed
0.034 0.002 0.011 0.007
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
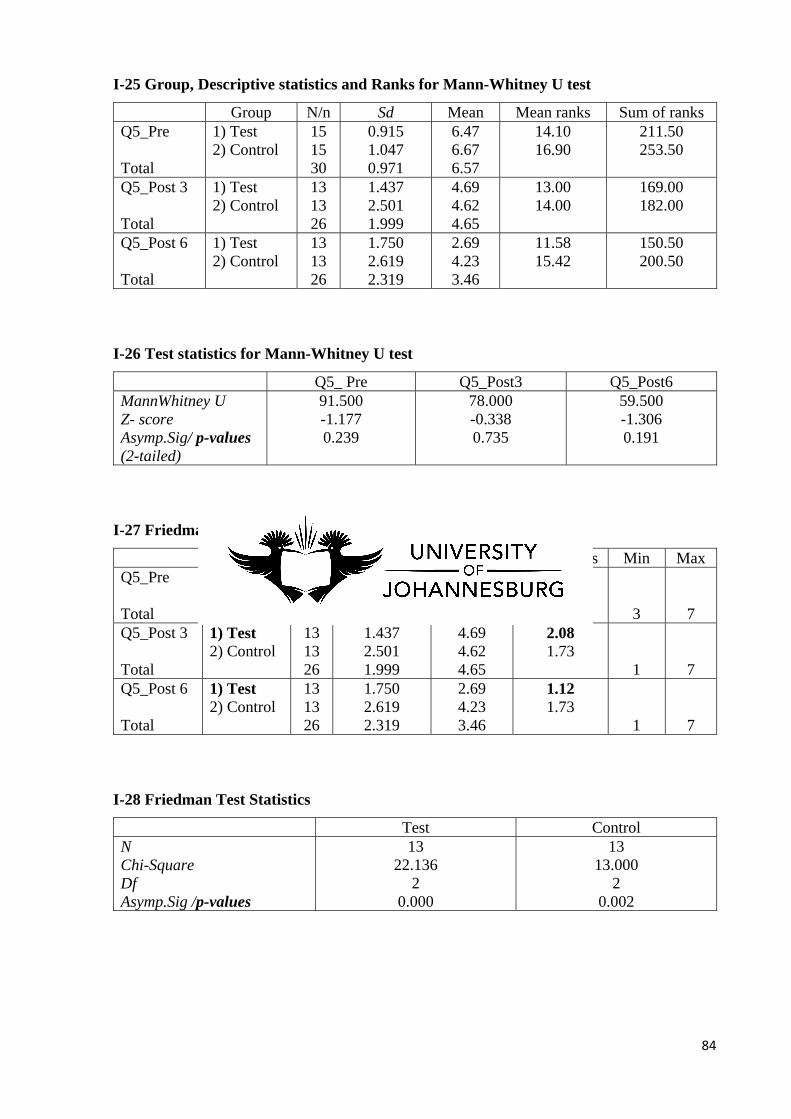
84
I-25 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q5_Pre Total
1) Test 2) Control
15 15 30
0.915 1.047 0.971
6.47 6.67 6.57
14.10 16.90
211.50 253.50
Q5_Post 3 Total
1) Test 2) Control
13 13 26
1.437 2.501 1.999
4.69 4.62 4.65
13.00 14.00
169.00 182.00
Q5_Post 6 Total
1) Test 2) Control
13 13 26
1.750 2.619 2.319
2.69 4.23 3.46
11.58 15.42
150.50 200.50
I-26 Test statistics for Mann-Whitney U test
Q5_ Pre Q5_Post3 Q5_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
91.500 -1.177 0.239
78.000 -0.338 0.735
59.500 -1.306 0.191
I-27 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q5_Pre Total
1) Test 2) Control
15 15 30
0.915 1.047 0.971
6.47 6.67 6.57
2.81 2.58
3
7
Q5_Post 3 Total
1) Test 2) Control
13 13 26
1.437 2.501 1.999
4.69 4.62 4.65
2.08 1.73
1
7
Q5_Post 6 Total
1) Test 2) Control
13 13 26
1.750 2.619 2.319
2.69 4.23 3.46
1.12 1.73
1
7
I-28 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 22.136
2 0.000
13 13.000
2 0.002

85
I-29.Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q5_Pre Total
1) Test 2) Control
15 15 30
0.915 1.047 0.971
6.47 6.67 6.57
3
7
Q5_Post 3 Total
1) Test 2) Control
13 13 26
1.437 2.501 1.999
4.69 4.62 4.65
1
7
Q5_Post 6 Total
1) Test 2) Control
13 13 26
1.750 2.619 2.319
2.69 4.23 3.46
1
7
I-30 Wilcoxon Test Statistics b
Test Control t1 t2 t1 t2
Q5_Post3/Q5_Pre Q5_Post6/Q5_Pre Q5_Post3/Q5_Pre Q5_Post6/Q5_Pre
Z -score -2.682 -3.083 -2.546 -2.410
Asymp.Sig p-values (2-tailed)
0.007 0.002 0.011 0.016
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-31 Group, Descriptive statistics and Ranks for Mann- WhitneyU test
Group N/n Sd Mean Mean ranks Sum of ranks Q6_Pre Total
1) Test 2) Control
15 15 30
1.457 1.113 1.296
5.87 6.33 6.10
14.23 16.77
213.50 251.50
Q6_Post 3 Total
1) Test 2) Control
13 13 26
2.097 2.041 2.134
3.69 5.00 4.35
11.19 15.81
145.50 205.50
Q6_Post 6 Total
1) Test 2) Control
13 13 26
1.797 2.273 2.432
2.31 5.00 3.65
9.35 17.65
121.50 229.50
I-32 Test statistics for Mann-Whitney U test
Q6_ Pre Q6_Post3 Q6_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
93.500 -0.894 0.371
54.500 -1.558 0.119
30.500 -2.848 0.004
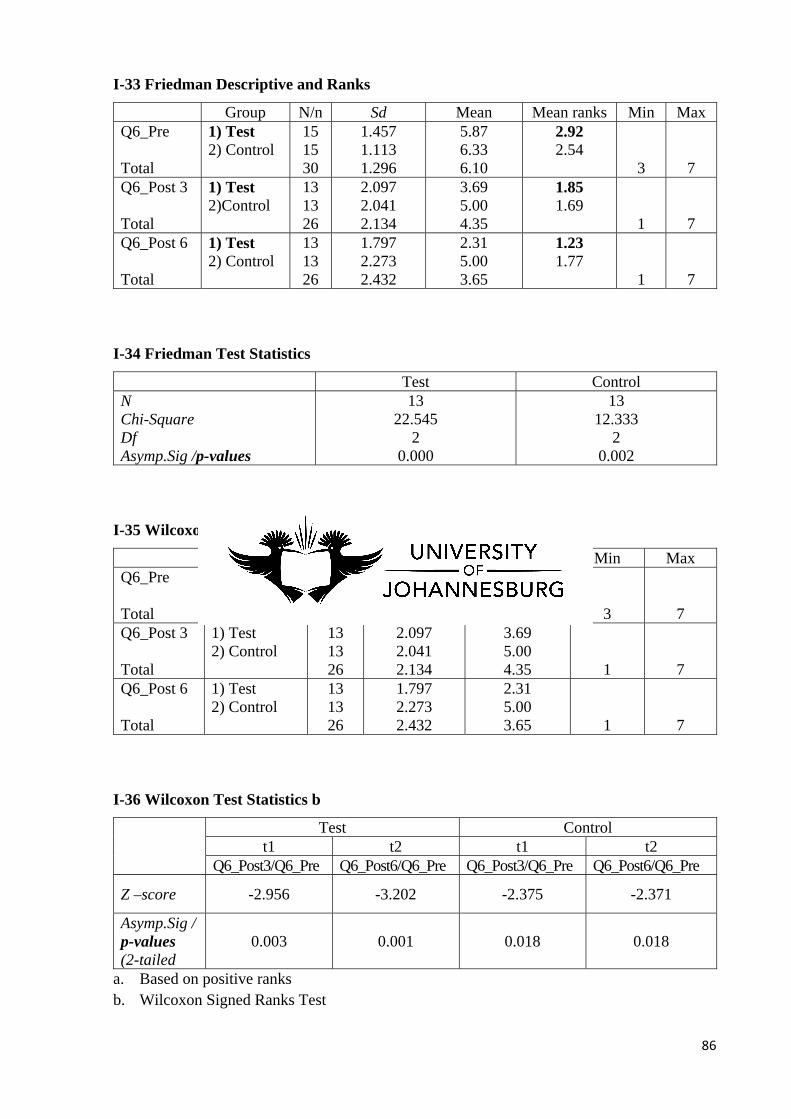
86
I-33 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q6_Pre Total
1) Test 2) Control
15 15 30
1.457 1.113 1.296
5.87 6.33 6.10
2.92 2.54
3
7
Q6_Post 3 Total
1) Test 2)Control
13 13 26
2.097 2.041 2.134
3.69 5.00 4.35
1.85 1.69
1
7
Q6_Post 6 Total
1) Test 2) Control
13 13 26
1.797 2.273 2.432
2.31 5.00 3.65
1.23 1.77
1
7
I-34 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 22.545
2 0.000
13 12.333
2 0.002
I-35 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q6_Pre Total
1) Test 2) Control
15 15 30
1.457 1.113 1.296
5.87 6.33 6.10
3
7
Q6_Post 3 Total
1) Test 2) Control
13 13 26
2.097 2.041 2.134
3.69 5.00 4.35
1
7
Q6_Post 6 Total
1) Test 2) Control
13 13 26
1.797 2.273 2.432
2.31 5.00 3.65
1
7
I-36 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q6_Post3/Q6_Pre Q6_Post6/Q6_Pre Q6_Post3/Q6_Pre Q6_Post6/Q6_Pre
Z –score -2.956 -3.202 -2.375 -2.371
Asymp.Sig / p-values (2-tailed
0.003 0.001 0.018 0.018
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
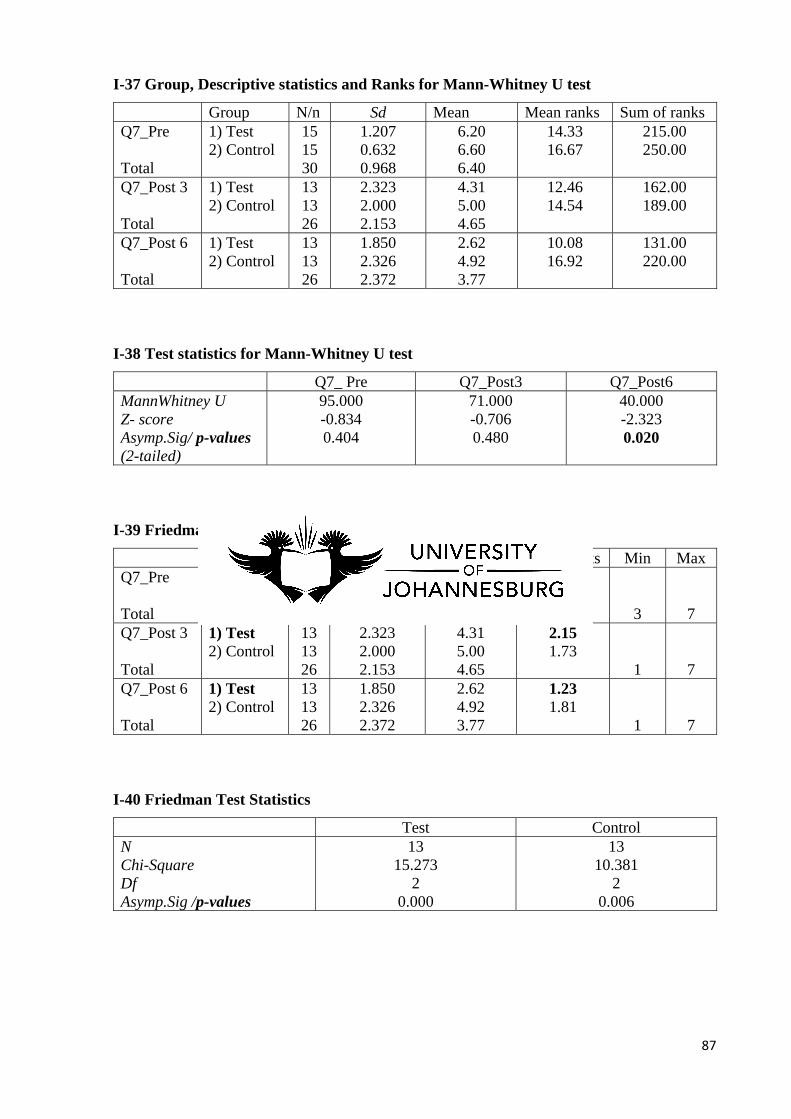
87
I-37 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q7_Pre Total
1) Test 2) Control
15 15 30
1.207 0.632 0.968
6.20 6.60 6.40
14.33 16.67
215.00 250.00
Q7_Post 3 Total
1) Test 2) Control
13 13 26
2.323 2.000 2.153
4.31 5.00 4.65
12.46 14.54
162.00 189.00
Q7_Post 6 Total
1) Test 2) Control
13 13 26
1.850 2.326 2.372
2.62 4.92 3.77
10.08 16.92
131.00 220.00
I-38 Test statistics for Mann-Whitney U test
Q7_ Pre Q7_Post3 Q7_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
95.000 -0.834 0.404
71.000 -0.706 0.480
40.000 -2.323 0.020
I-39 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q7_Pre Total
1) Test 2) Control
15 15 30
1.207 0.632 0.968
6.20 6.60 6.40
2.62 2.46
3
7
Q7_Post 3 Total
1) Test 2) Control
13 13 26
2.323 2.000 2.153
4.31 5.00 4.65
2.15 1.73
1
7
Q7_Post 6 Total
1) Test 2) Control
13 13 26
1.850 2.326 2.372
2.62 4.92 3.77
1.23 1.81
1
7
I-40 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 15.273
2 0.000
13 10.381
2 0.006
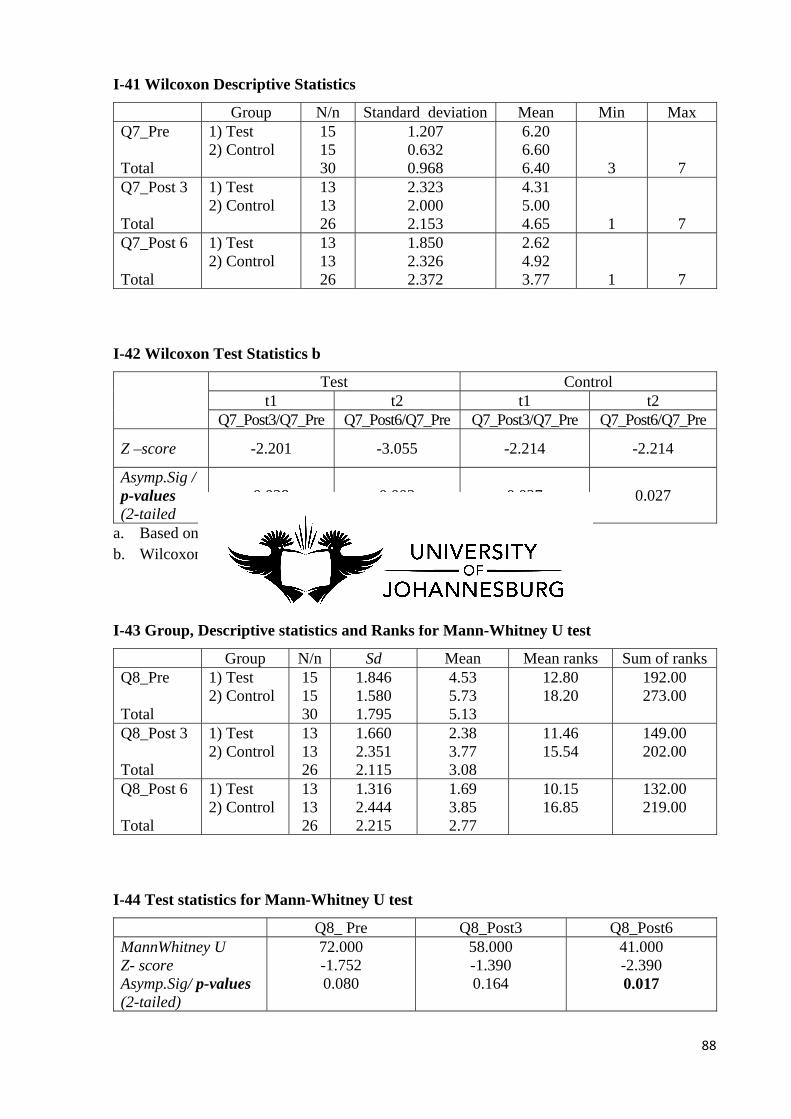
88
I-41 Wilcoxon Descriptive Statistics
Group N/n Standard deviation Mean Min Max Q7_Pre Total
1) Test 2) Control
15 15 30
1.207 0.632 0.968
6.20 6.60 6.40
3
7
Q7_Post 3 Total
1) Test 2) Control
13 13 26
2.323 2.000 2.153
4.31 5.00 4.65
1
7
Q7_Post 6 Total
1) Test 2) Control
13 13 26
1.850 2.326 2.372
2.62 4.92 3.77
1
7
I-42 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q7_Post3/Q7_Pre Q7_Post6/Q7_Pre Q7_Post3/Q7_Pre Q7_Post6/Q7_Pre
Z –score -2.201 -3.055 -2.214 -2.214
Asymp.Sig / p-values (2-tailed
0.028 0.002 0.027 0.027
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-43 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q8_Pre Total
1) Test 2) Control
15 15 30
1.846 1.580 1.795
4.53 5.73 5.13
12.80 18.20
192.00 273.00
Q8_Post 3 Total
1) Test 2) Control
13 13 26
1.660 2.351 2.115
2.38 3.77 3.08
11.46 15.54
149.00 202.00
Q8_Post 6 Total
1) Test 2) Control
13 13 26
1.316 2.444 2.215
1.69 3.85 2.77
10.15 16.85
132.00 219.00
I-44 Test statistics for Mann-Whitney U test
Q8_ Pre Q8_Post3 Q8_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
72.000 -1.752 0.080
58.000 -1.390 0.164
41.000 -2.390 0.017
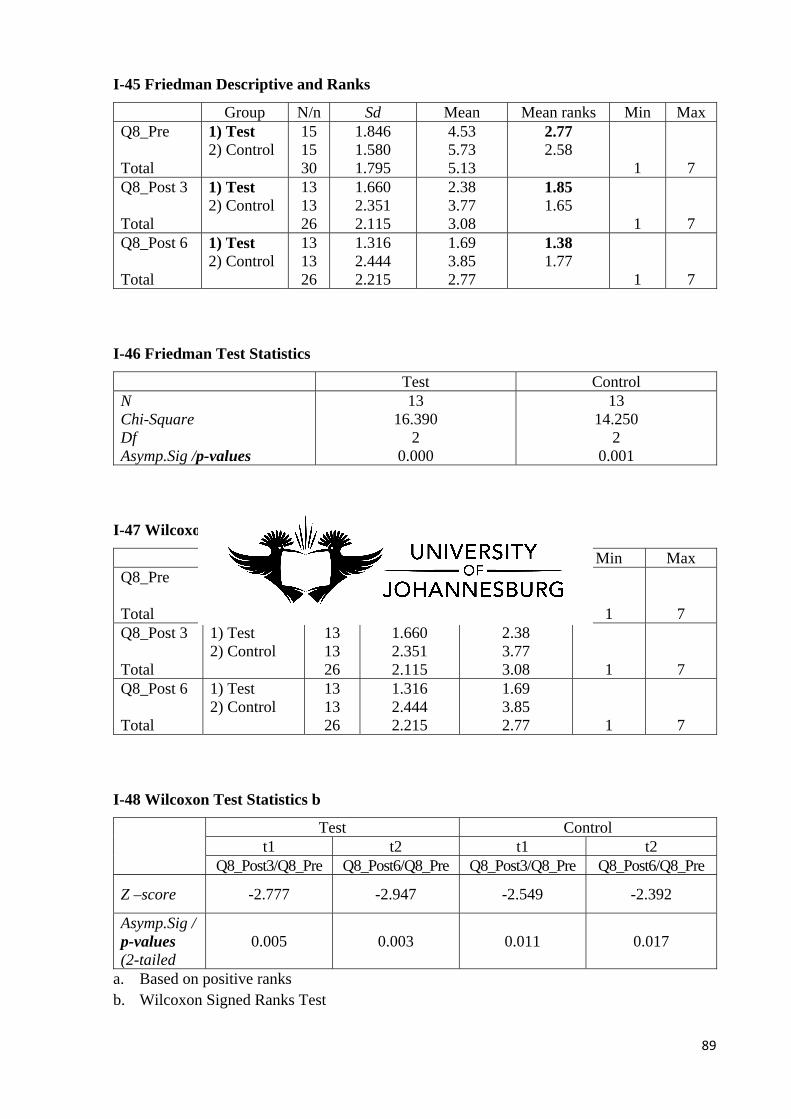
89
I-45 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q8_Pre Total
1) Test 2) Control
15 15 30
1.846 1.580 1.795
4.53 5.73 5.13
2.77 2.58
1
7
Q8_Post 3 Total
1) Test 2) Control
13 13 26
1.660 2.351 2.115
2.38 3.77 3.08
1.85 1.65
1
7
Q8_Post 6 Total
1) Test 2) Control
13 13 26
1.316 2.444 2.215
1.69 3.85 2.77
1.38 1.77
1
7
I-46 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 16.390
2 0.000
13 14.250
2 0.001
I-47 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q8_Pre Total
1) Test 2) Control
15 15 30
1.846 1.580 1.795
4.53 5.73 5.13
1
7
Q8_Post 3 Total
1) Test 2) Control
13 13 26
1.660 2.351 2.115
2.38 3.77 3.08
1
7
Q8_Post 6 Total
1) Test 2) Control
13 13 26
1.316 2.444 2.215
1.69 3.85 2.77
1
7
I-48 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q8_Post3/Q8_Pre Q8_Post6/Q8_Pre Q8_Post3/Q8_Pre Q8_Post6/Q8_Pre
Z –score -2.777 -2.947 -2.549 -2.392
Asymp.Sig / p-values (2-tailed
0.005 0.003 0.011 0.017
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
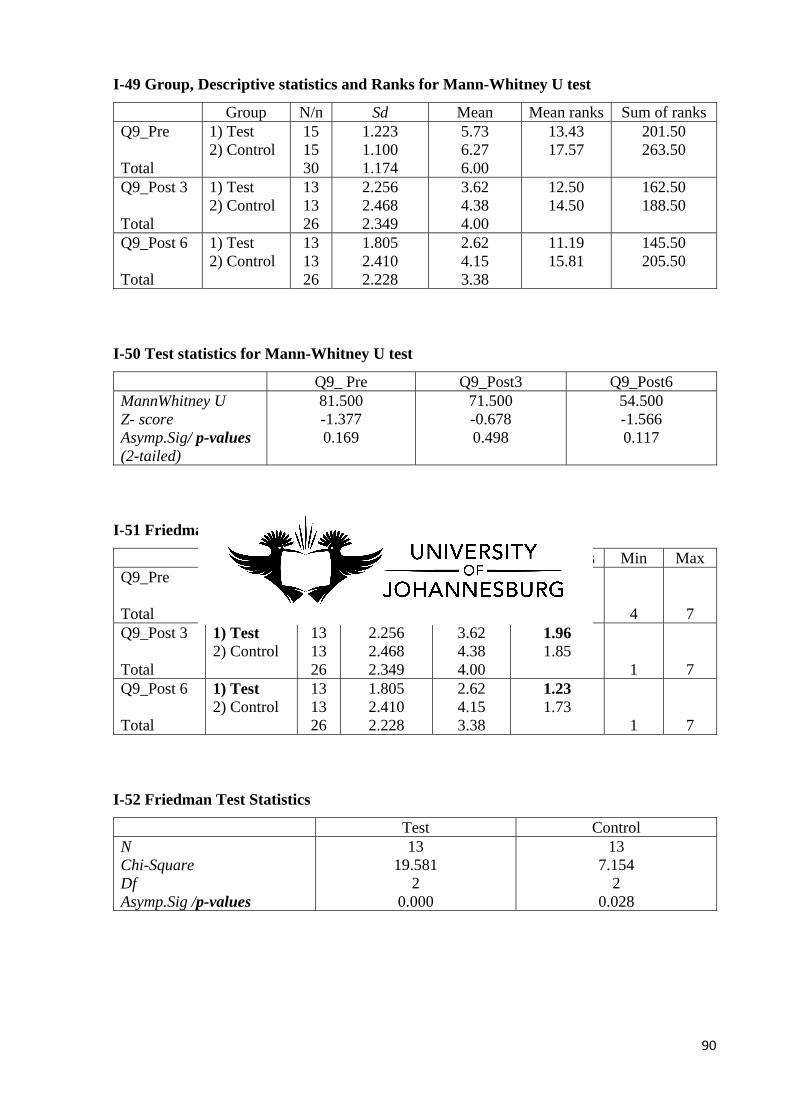
90
I-49 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q9_Pre Total
1) Test 2) Control
15 15 30
1.223 1.100 1.174
5.73 6.27 6.00
13.43 17.57
201.50 263.50
Q9_Post 3 Total
1) Test 2) Control
13 13 26
2.256 2.468 2.349
3.62 4.38 4.00
12.50 14.50
162.50 188.50
Q9_Post 6 Total
1) Test 2) Control
13 13 26
1.805 2.410 2.228
2.62 4.15 3.38
11.19 15.81
145.50 205.50
I-50 Test statistics for Mann-Whitney U test
Q9_ Pre Q9_Post3 Q9_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
81.500 -1.377 0.169
71.500 -0.678 0.498
54.500 -1.566 0.117
I-51 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q9_Pre Total
1) Test 2) Control
15 15 30
1.223 1.100 1.174
5.73 6.27 6.00
2.81 2.42
4
7
Q9_Post 3 Total
1) Test 2) Control
13 13 26
2.256 2.468 2.349
3.62 4.38 4.00
1.96 1.85
1
7
Q9_Post 6 Total
1) Test 2) Control
13 13 26
1.805 2.410 2.228
2.62 4.15 3.38
1.23 1.73
1
7
I-52 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 19.581
2 0.000
13 7.154
2 0.028
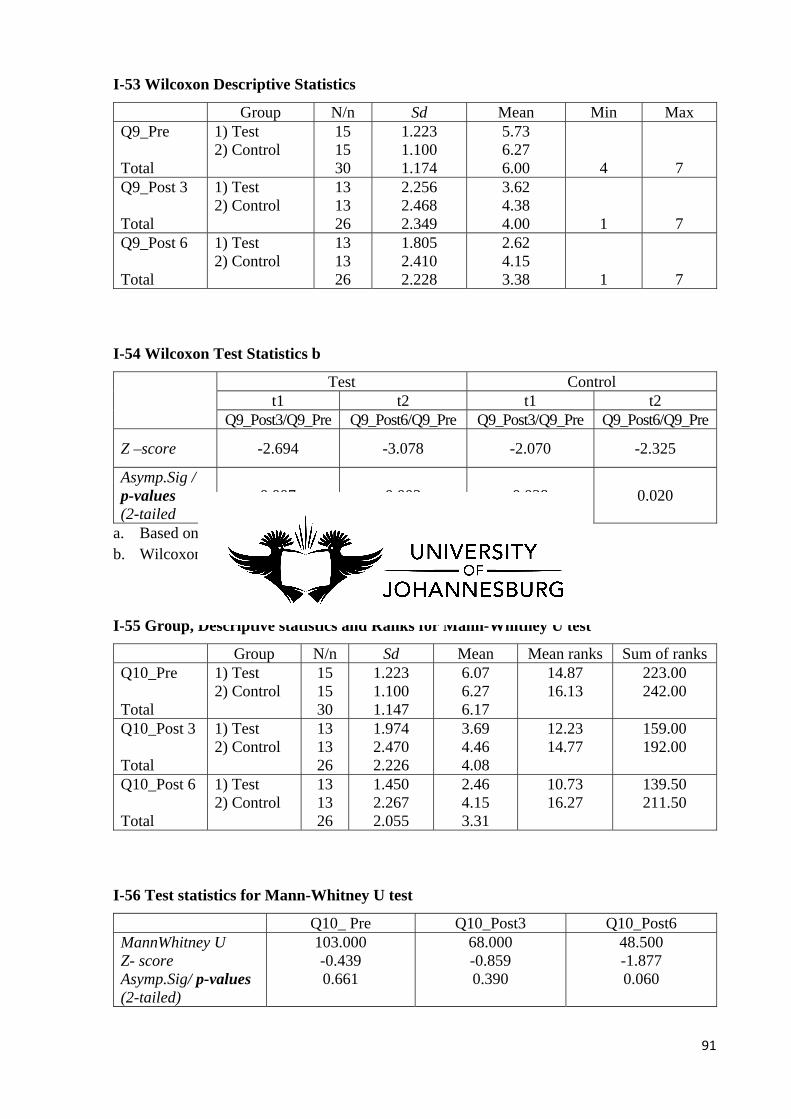
91
I-53 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q9_Pre Total
1) Test 2) Control
15 15 30
1.223 1.100 1.174
5.73 6.27 6.00
4
7
Q9_Post 3 Total
1) Test 2) Control
13 13 26
2.256 2.468 2.349
3.62 4.38 4.00
1
7
Q9_Post 6 Total
1) Test 2) Control
13 13 26
1.805 2.410 2.228
2.62 4.15 3.38
1
7
I-54 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q9_Post3/Q9_Pre Q9_Post6/Q9_Pre Q9_Post3/Q9_Pre Q9_Post6/Q9_Pre
Z –score -2.694 -3.078 -2.070 -2.325
Asymp.Sig / p-values (2-tailed
0.007 0.002 0.038 0.020
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-55 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q10_Pre Total
1) Test 2) Control
15 15 30
1.223 1.100 1.147
6.07 6.27 6.17
14.87 16.13
223.00 242.00
Q10_Post 3 Total
1) Test 2) Control
13 13 26
1.974 2.470 2.226
3.69 4.46 4.08
12.23 14.77
159.00 192.00
Q10_Post 6 Total
1) Test 2) Control
13 13 26
1.450 2.267 2.055
2.46 4.15 3.31
10.73 16.27
139.50 211.50
I-56 Test statistics for Mann-Whitney U test
Q10_ Pre Q10_Post3 Q10_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
103.000 -0.439 0.661
68.000 -0.859 0.390
48.500 -1.877 0.060
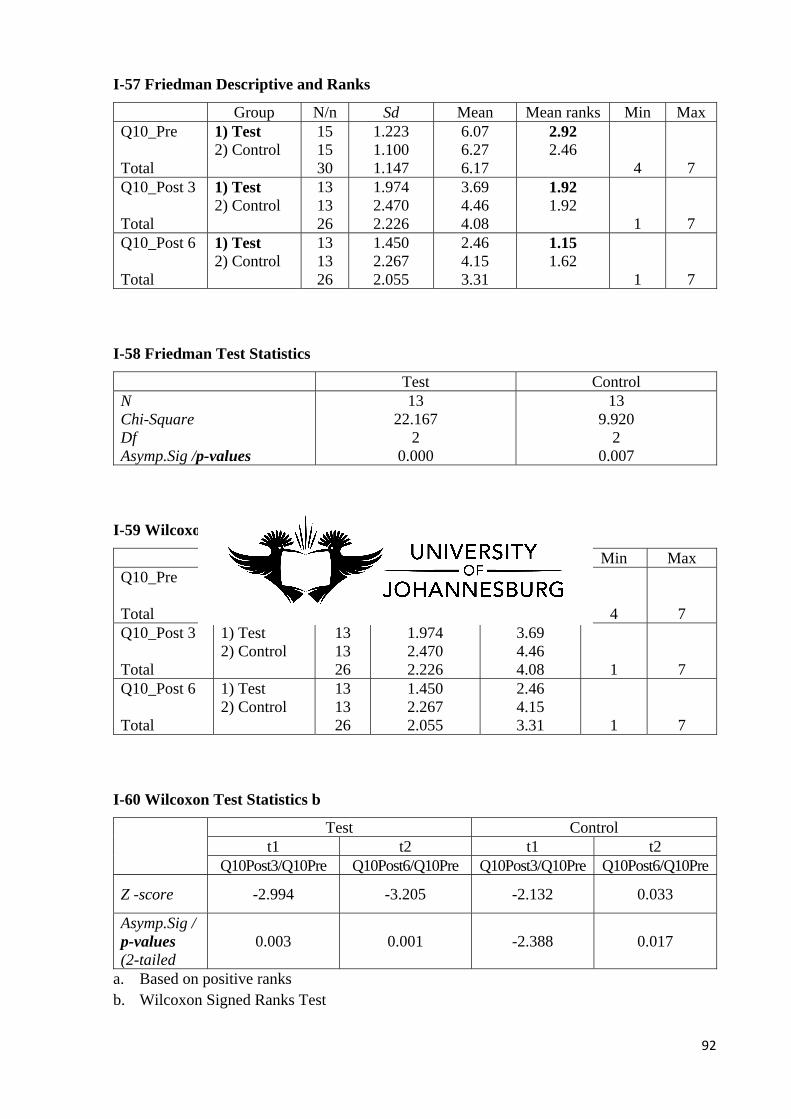
92
I-57 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q10_Pre Total
1) Test 2) Control
15 15 30
1.223 1.100 1.147
6.07 6.27 6.17
2.92 2.46
4
7
Q10_Post 3 Total
1) Test 2) Control
13 13 26
1.974 2.470 2.226
3.69 4.46 4.08
1.92 1.92
1
7
Q10_Post 6 Total
1) Test 2) Control
13 13 26
1.450 2.267 2.055
2.46 4.15 3.31
1.15 1.62
1
7
I-58 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 22.167
2 0.000
13 9.920
2 0.007
I-59 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q10_Pre Total
1) Test 2) Control
15 15 30
1.223 1.100 1.147
6.07 6.27 6.17
4
7
Q10_Post 3 Total
1) Test 2) Control
13 13 26
1.974 2.470 2.226
3.69 4.46 4.08
1
7
Q10_Post 6 Total
1) Test 2) Control
13 13 26
1.450 2.267 2.055
2.46 4.15 3.31
1
7
I-60 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q10Post3/Q10Pre Q10Post6/Q10Pre Q10Post3/Q10Pre Q10Post6/Q10Pre
Z -score -2.994 -3.205 -2.132 0.033
Asymp.Sig / p-values (2-tailed
0.003 0.001 -2.388 0.017
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
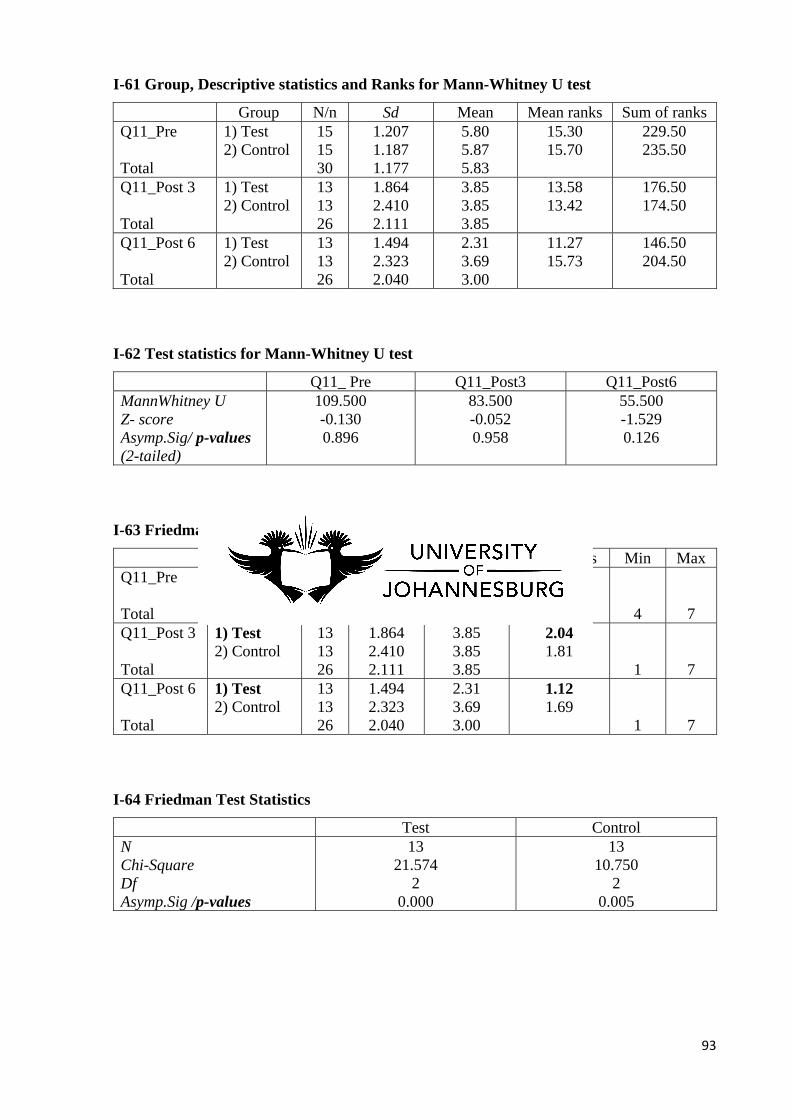
93
I-61 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q11_Pre Total
1) Test 2) Control
15 15 30
1.207 1.187 1.177
5.80 5.87 5.83
15.30 15.70
229.50 235.50
Q11_Post 3 Total
1) Test 2) Control
13 13 26
1.864 2.410 2.111
3.85 3.85 3.85
13.58 13.42
176.50 174.50
Q11_Post 6 Total
1) Test 2) Control
13 13 26
1.494 2.323 2.040
2.31 3.69 3.00
11.27 15.73
146.50 204.50
I-62 Test statistics for Mann-Whitney U test
Q11_ Pre Q11_Post3 Q11_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
109.500 -0.130 0.896
83.500 -0.052 0.958
55.500 -1.529 0.126
I-63 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q11_Pre Total
1) Test 2) Control
15 15 30
1.207 1.187 1.177
5.80 5.87 5.83
2.85 2.50
4
7
Q11_Post 3 Total
1) Test 2) Control
13 13 26
1.864 2.410 2.111
3.85 3.85 3.85
2.04 1.81
1
7
Q11_Post 6 Total
1) Test 2) Control
13 13 26
1.494 2.323 2.040
2.31 3.69 3.00
1.12 1.69
1
7
I-64 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 21.574
2 0.000
13 10.750
2 0.005
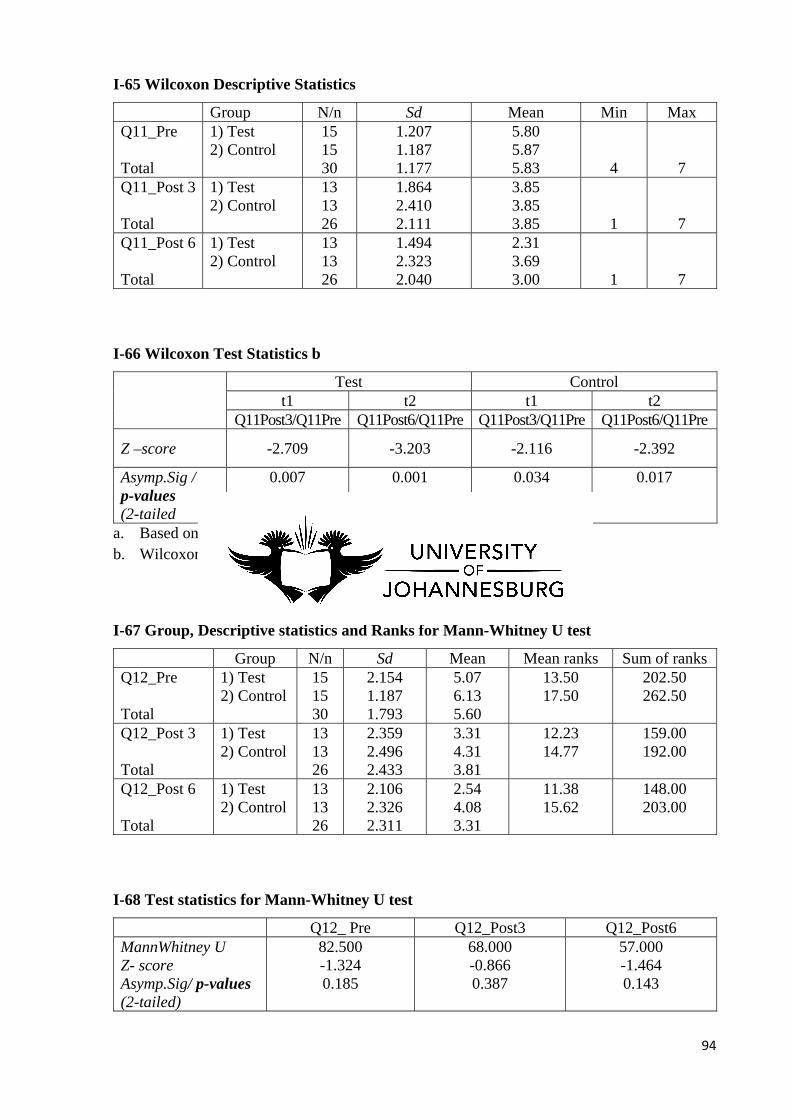
94
I-65 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q11_Pre Total
1) Test 2) Control
15 15 30
1.207 1.187 1.177
5.80 5.87 5.83
4
7
Q11_Post 3 Total
1) Test 2) Control
13 13 26
1.864 2.410 2.111
3.85 3.85 3.85
1
7
Q11_Post 6 Total
1) Test 2) Control
13 13 26
1.494 2.323 2.040
2.31 3.69 3.00
1
7
I-66 Wilcoxon Test Statistics b
Test Control t1 t2 t1 t2
Q11Post3/Q11Pre Q11Post6/Q11Pre Q11Post3/Q11Pre Q11Post6/Q11Pre
Z –score -2.709 -3.203 -2.116 -2.392
Asymp.Sig / p-values (2-tailed
0.007 0.001 0.034 0.017
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-67 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q12_Pre Total
1) Test 2) Control
15 15 30
2.154 1.187 1.793
5.07 6.13 5.60
13.50 17.50
202.50 262.50
Q12_Post 3 Total
1) Test 2) Control
13 13 26
2.359 2.496 2.433
3.31 4.31 3.81
12.23 14.77
159.00 192.00
Q12_Post 6 Total
1) Test 2) Control
13 13 26
2.106 2.326 2.311
2.54 4.08 3.31
11.38 15.62
148.00 203.00
I-68 Test statistics for Mann-Whitney U test
Q12_ Pre Q12_Post3 Q12_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
82.500 -1.324 0.185
68.000 -0.866 0.387
57.000 -1.464 0.143
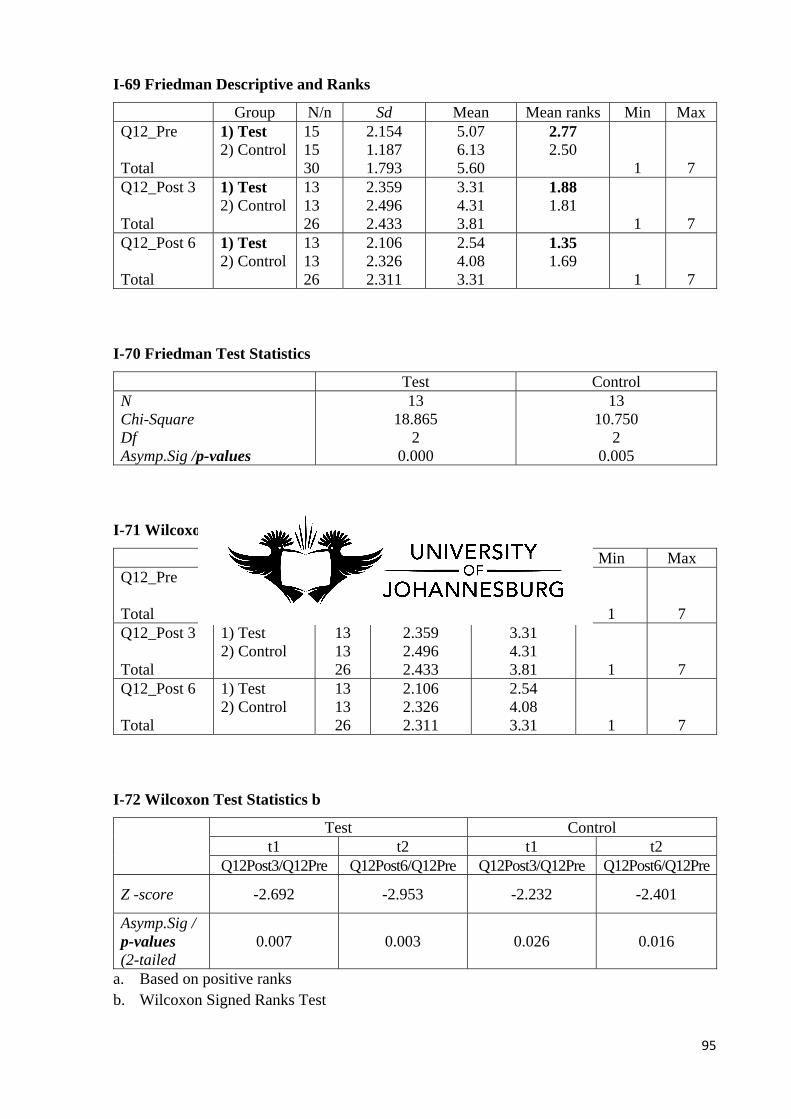
95
I-69 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q12_Pre Total
1) Test 2) Control
15 15 30
2.154 1.187 1.793
5.07 6.13 5.60
2.77 2.50
1
7
Q12_Post 3 Total
1) Test 2) Control
13 13 26
2.359 2.496 2.433
3.31 4.31 3.81
1.88 1.81
1
7
Q12_Post 6 Total
1) Test 2) Control
13 13 26
2.106 2.326 2.311
2.54 4.08 3.31
1.35 1.69
1
7
I-70 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 18.865
2 0.000
13 10.750
2 0.005
I-71 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q12_Pre Total
1) Test 2) Control
15 15 30
2.154 1.187 1.793
5.07 6.13 5.60
1
7
Q12_Post 3 Total
1) Test 2) Control
13 13 26
2.359 2.496 2.433
3.31 4.31 3.81
1
7
Q12_Post 6 Total
1) Test 2) Control
13 13 26
2.106 2.326 2.311
2.54 4.08 3.31
1
7
I-72 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q12Post3/Q12Pre Q12Post6/Q12Pre Q12Post3/Q12Pre Q12Post6/Q12Pre
Z -score -2.692 -2.953 -2.232 -2.401
Asymp.Sig / p-values (2-tailed
0.007 0.003 0.026 0.016
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
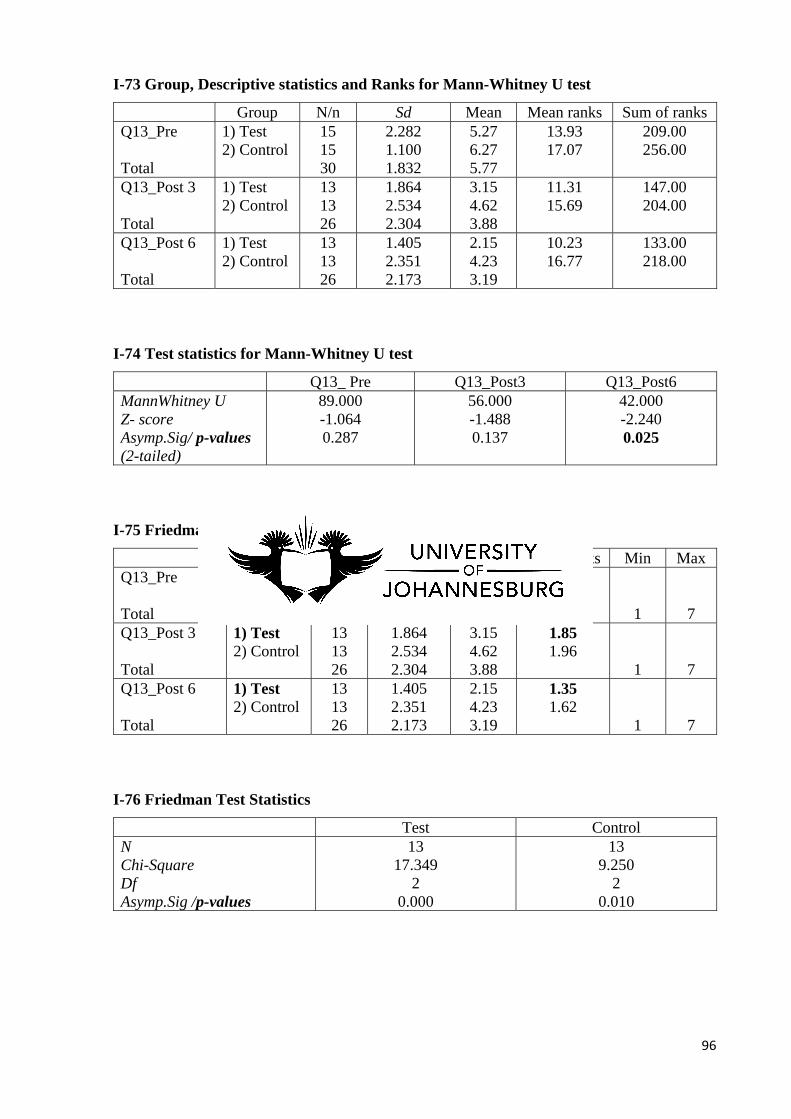
96
I-73 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q13_Pre Total
1) Test 2) Control
15 15 30
2.282 1.100 1.832
5.27 6.27 5.77
13.93 17.07
209.00 256.00
Q13_Post 3 Total
1) Test 2) Control
13 13 26
1.864 2.534 2.304
3.15 4.62 3.88
11.31 15.69
147.00 204.00
Q13_Post 6 Total
1) Test 2) Control
13 13 26
1.405 2.351 2.173
2.15 4.23 3.19
10.23 16.77
133.00 218.00
I-74 Test statistics for Mann-Whitney U test
Q13_ Pre Q13_Post3 Q13_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
89.000 -1.064 0.287
56.000 -1.488 0.137
42.000 -2.240 0.025
I-75 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q13_Pre Total
1) Test 2) Control
15 15 30
2.282 1.100 1.832
5.27 6.27 5.77
2.81 2.42
1
7
Q13_Post 3 Total
1) Test 2) Control
13 13 26
1.864 2.534 2.304
3.15 4.62 3.88
1.85 1.96
1
7
Q13_Post 6 Total
1) Test 2) Control
13 13 26
1.405 2.351 2.173
2.15 4.23 3.19
1.35 1.62
1
7
I-76 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 17.349
2 0.000
13 9.250
2 0.010
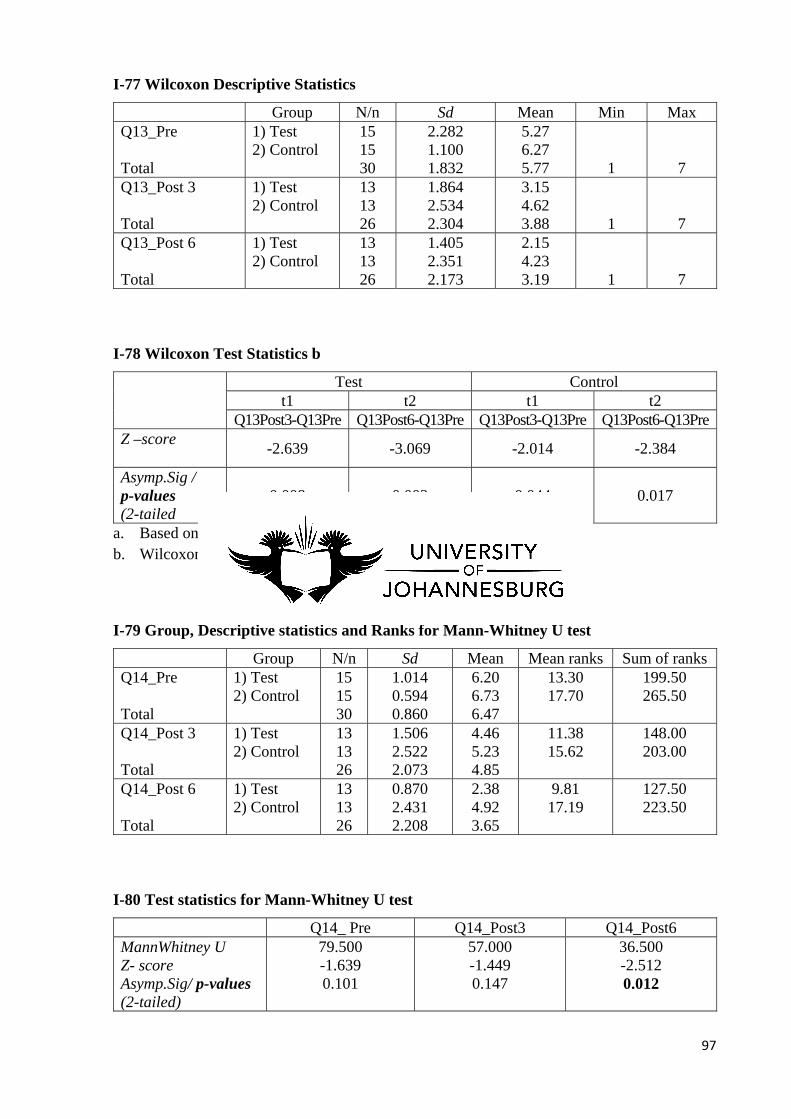
97
I-77 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q13_Pre Total
1) Test 2) Control
15 15 30
2.282 1.100 1.832
5.27 6.27 5.77
1
7
Q13_Post 3 Total
1) Test 2) Control
13 13 26
1.864 2.534 2.304
3.15 4.62 3.88
1
7
Q13_Post 6 Total
1) Test 2) Control
13 13 26
1.405 2.351 2.173
2.15 4.23 3.19
1
7
I-78 Wilcoxon Test Statistics b
Test Control t1 t2 t1 t2
Q13Post3-Q13Pre Q13Post6-Q13Pre Q13Post3-Q13Pre Q13Post6-Q13PreZ –score
-2.639 -3.069 -2.014 -2.384
Asymp.Sig / p-values (2-tailed
0.008 0.002 0.044 0.017
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-79 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q14_Pre Total
1) Test 2) Control
15 15 30
1.014 0.594 0.860
6.20 6.73 6.47
13.30 17.70
199.50 265.50
Q14_Post 3 Total
1) Test 2) Control
13 13 26
1.506 2.522 2.073
4.46 5.23 4.85
11.38 15.62
148.00 203.00
Q14_Post 6 Total
1) Test 2) Control
13 13 26
0.870 2.431 2.208
2.38 4.92 3.65
9.81 17.19
127.50 223.50
I-80 Test statistics for Mann-Whitney U test
Q14_ Pre Q14_Post3 Q14_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
79.500 -1.639 0.101
57.000 -1.449 0.147
36.500 -2.512 0.012

98
I-81 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q14_Pre Total
1) Test 2) Control
15 15 30
1.014 0.594 0.860
6.20 6.73 6.47
2.81 2.35
4
7
Q14_Post 3 Total
1) Test 2) Control
13 13 26
1.506 2.522 2.073
4.46 5.23 4.85
2.08 1.96
1
7
Q14_Post 6 Total
1) Test 2) Control
13 13 26
0.870 2.431 2.208
2.38 4.92 3.65
1.12 1.69
1
7
I-82 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 20.292
2 0.000
13 5.840
2 0.054
I-83 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q14_Pre Total
1) Test 2) Control
15 15 30
1.014 0.594 0.860
6.20 6.73 6.47
4
7
Q14_Post 3 Total
1) Test 2) Control
13 13 26
1.506 2.522 2.073
4.46 5.23 4.85
1
7
Q14_Post 6 Total
1) Test 2) Control
13 13 26
0.870 2.431 2.208
2.38 4.92 3.65
1
7
I-84 Test Statistics b
Test Control
t1 t2 t1 t2 Q14Post3/Q14Pre Q14Post6/Q14Pre Q14Post3/Q14Pre Q14Post6/Q14Pre
Z –score -2.546 -3.210 - -
Asymp.Sig / p-values (2-tailed
0.014 0.001 - -
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
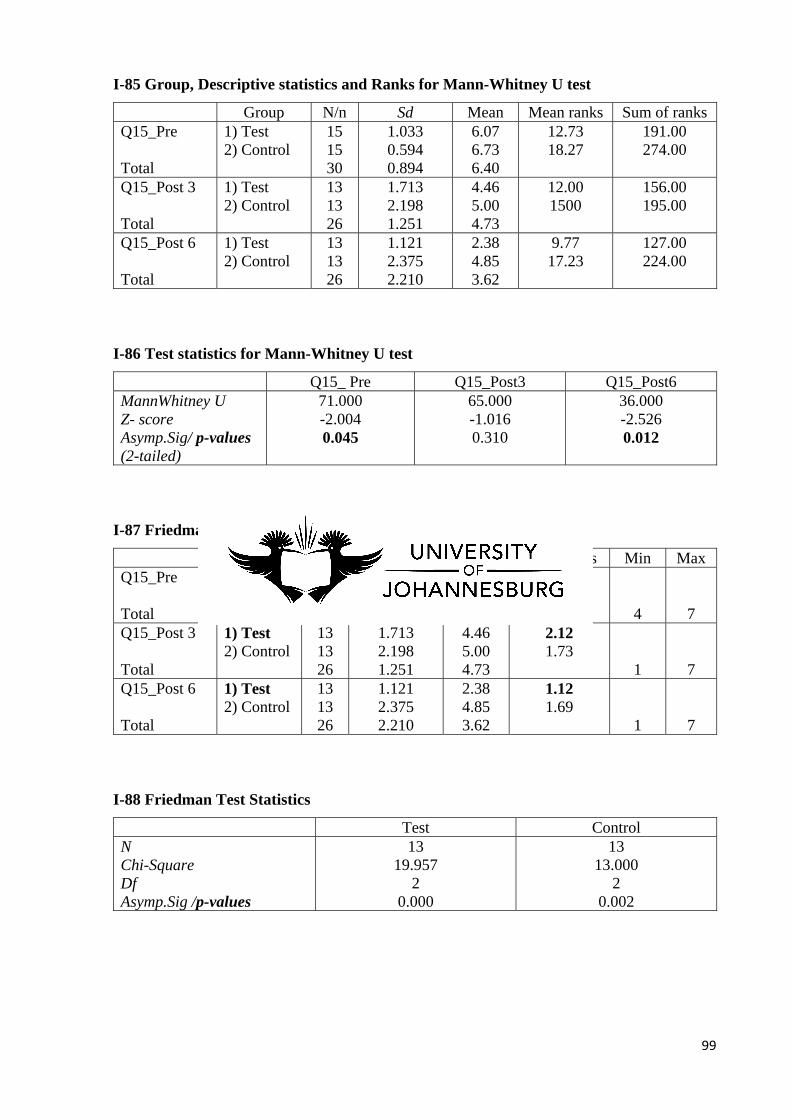
99
I-85 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q15_Pre Total
1) Test 2) Control
15 15 30
1.033 0.594 0.894
6.07 6.73 6.40
12.73 18.27
191.00 274.00
Q15_Post 3 Total
1) Test 2) Control
13 13 26
1.713 2.198 1.251
4.46 5.00 4.73
12.00 1500
156.00 195.00
Q15_Post 6 Total
1) Test 2) Control
13 13 26
1.121 2.375 2.210
2.38 4.85 3.62
9.77 17.23
127.00 224.00
I-86 Test statistics for Mann-Whitney U test
Q15_ Pre Q15_Post3 Q15_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
71.000 -2.004 0.045
65.000 -1.016 0.310
36.000 -2.526 0.012
I-87 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q15_Pre Total
1) Test 2) Control
15 15 30
1.033 0.594 0.894
6.07 6.73 6.40
2.77 2.58
4
7
Q15_Post 3 Total
1) Test 2) Control
13 13 26
1.713 2.198 1.251
4.46 5.00 4.73
2.12 1.73
1
7
Q15_Post 6 Total
1) Test 2) Control
13 13 26
1.121 2.375 2.210
2.38 4.85 3.62
1.12 1.69
1
7
I-88 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 19.957
2 0.000
13 13.000
2 0.002
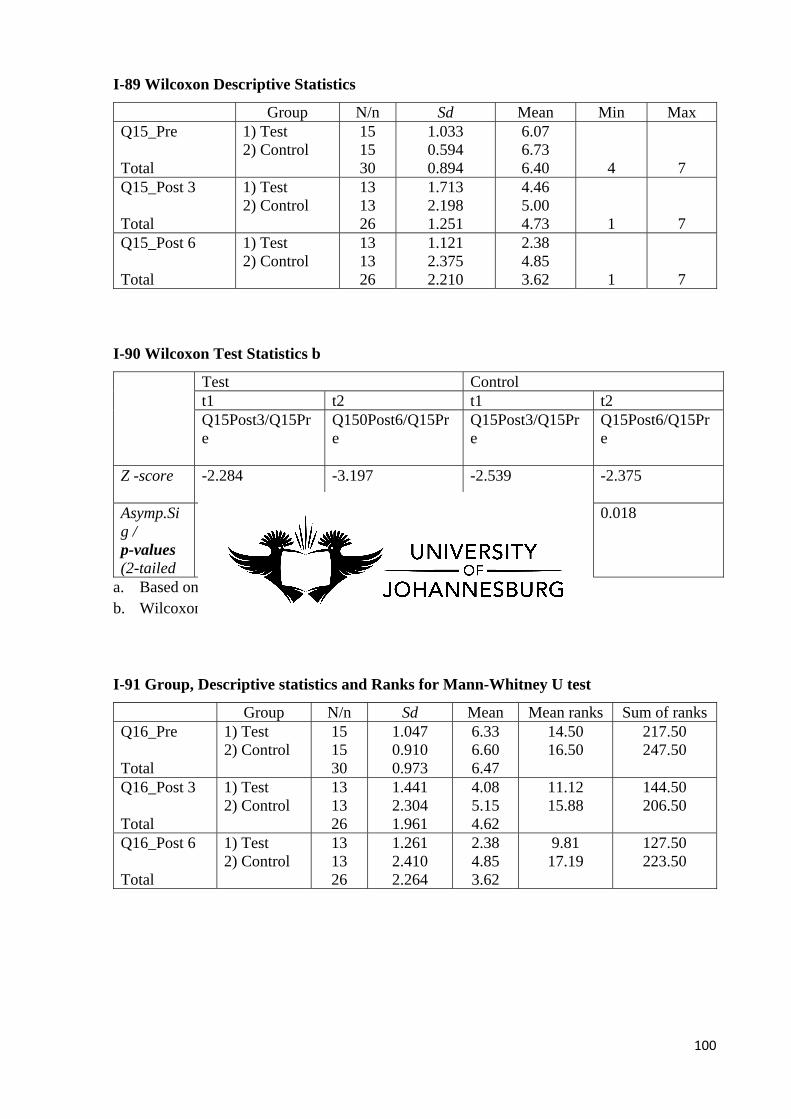
100
I-89 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q15_Pre Total
1) Test 2) Control
15 15 30
1.033 0.594 0.894
6.07 6.73 6.40
4
7
Q15_Post 3 Total
1) Test 2) Control
13 13 26
1.713 2.198 1.251
4.46 5.00 4.73
1
7
Q15_Post 6 Total
1) Test 2) Control
13 13 26
1.121 2.375 2.210
2.38 4.85 3.62
1
7
I-90 Wilcoxon Test Statistics b
Test Control t1 t2 t1 t2 Q15Post3/Q15Pre
Q150Post6/Q15Pre
Q15Post3/Q15Pre
Q15Post6/Q15Pre
Z -score
-2.284 -3.197 -2.539 -2.375
Asymp.Sig / p-values (2-tailed
0.022 0.001 0.011 0.018
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-91 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q16_Pre Total
1) Test 2) Control
15 15 30
1.047 0.910 0.973
6.33 6.60 6.47
14.50 16.50
217.50 247.50
Q16_Post 3 Total
1) Test 2) Control
13 13 26
1.441 2.304 1.961
4.08 5.15 4.62
11.12 15.88
144.50 206.50
Q16_Post 6 Total
1) Test 2) Control
13 13 26
1.261 2.410 2.264
2.38 4.85 3.62
9.81 17.19
127.50 223.50
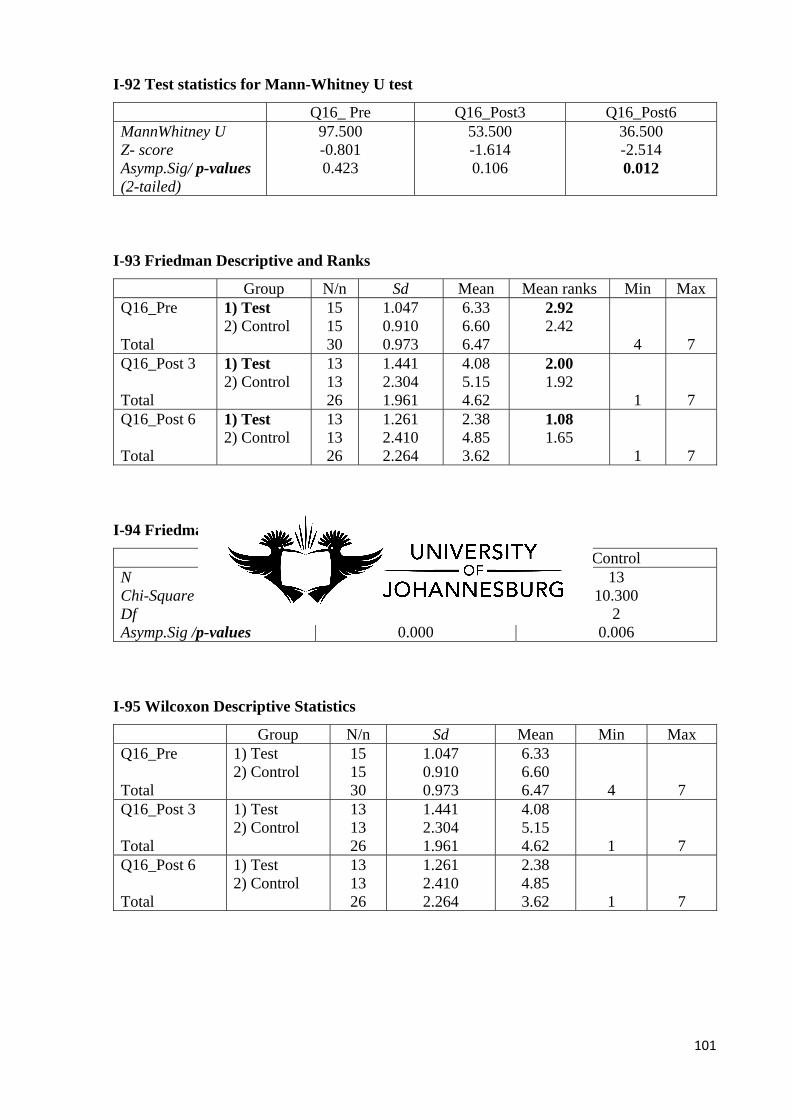
101
I-92 Test statistics for Mann-Whitney U test
Q16_ Pre Q16_Post3 Q16_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
97.500 -0.801 0.423
53.500 -1.614 0.106
36.500 -2.514 0.012
I-93 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q16_Pre Total
1) Test 2) Control
15 15 30
1.047 0.910 0.973
6.33 6.60 6.47
2.92 2.42
4
7
Q16_Post 3 Total
1) Test 2) Control
13 13 26
1.441 2.304 1.961
4.08 5.15 4.62
2.00 1.92
1
7
Q16_Post 6 Total
1) Test 2) Control
13 13 26
1.261 2.410 2.264
2.38 4.85 3.62
1.08 1.65
1
7
I-94 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 24.000
2 0.000
13 10.300
2 0.006
I-95 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q16_Pre Total
1) Test 2) Control
15 15 30
1.047 0.910 0.973
6.33 6.60 6.47
4
7
Q16_Post 3 Total
1) Test 2) Control
13 13 26
1.441 2.304 1.961
4.08 5.15 4.62
1
7
Q16_Post 6 Total
1) Test 2) Control
13 13 26
1.261 2.410 2.264
2.38 4.85 3.62
1
7
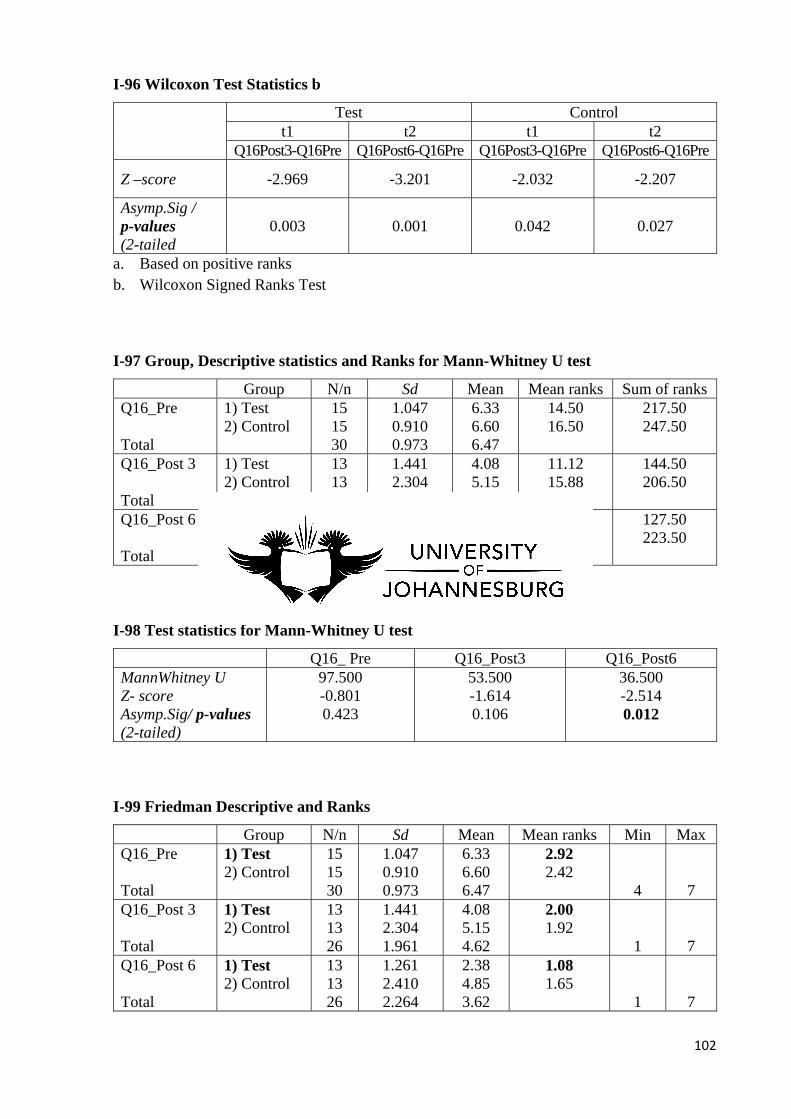
102
I-96 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q16Post3-Q16Pre Q16Post6-Q16Pre Q16Post3-Q16Pre Q16Post6-Q16Pre
Z –score -2.969 -3.201 -2.032 -2.207
Asymp.Sig / p-values (2-tailed
0.003 0.001 0.042 0.027
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-97 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q16_Pre Total
1) Test 2) Control
15 15 30
1.047 0.910 0.973
6.33 6.60 6.47
14.50 16.50
217.50 247.50
Q16_Post 3 Total
1) Test 2) Control
13 13 26
1.441 2.304 1.961
4.08 5.15 4.62
11.12 15.88
144.50 206.50
Q16_Post 6 Total
1) Test 2) Control
13 13 26
1.261 2.410 2.264
2.38 4.85 3.62
9.81 17.19
127.50 223.50
I-98 Test statistics for Mann-Whitney U test
Q16_ Pre Q16_Post3 Q16_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
97.500 -0.801 0.423
53.500 -1.614 0.106
36.500 -2.514 0.012
I-99 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q16_Pre Total
1) Test 2) Control
15 15 30
1.047 0.910 0.973
6.33 6.60 6.47
2.92 2.42
4
7
Q16_Post 3 Total
1) Test 2) Control
13 13 26
1.441 2.304 1.961
4.08 5.15 4.62
2.00 1.92
1
7
Q16_Post 6 Total
1) Test 2) Control
13 13 26
1.261 2.410 2.264
2.38 4.85 3.62
1.08 1.65
1
7
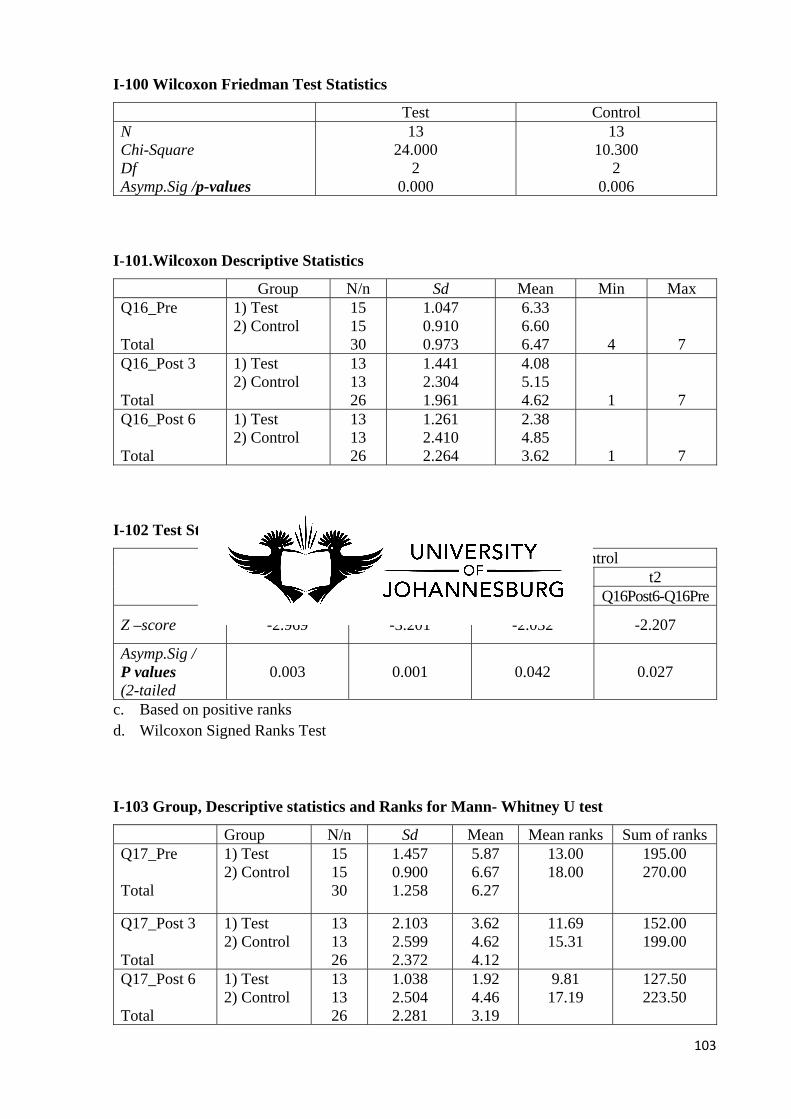
103
I-100 Wilcoxon Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 24.000
2 0.000
13 10.300
2 0.006
I-101.Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q16_Pre Total
1) Test 2) Control
15 15 30
1.047 0.910 0.973
6.33 6.60 6.47
4
7
Q16_Post 3 Total
1) Test 2) Control
13 13 26
1.441 2.304 1.961
4.08 5.15 4.62
1
7
Q16_Post 6 Total
1) Test 2) Control
13 13 26
1.261 2.410 2.264
2.38 4.85 3.62
1
7
I-102 Test Statistics b
Test Control
t1 t2 t1 t2 Q16Post3-Q16Pre Q16Post6-Q16Pre Q16Post3-Q16Pre Q16Post6-Q16Pre
Z –score -2.969 -3.201 -2.032 -2.207
Asymp.Sig / P values (2-tailed
0.003 0.001 0.042 0.027
c. Based on positive ranks d. Wilcoxon Signed Ranks Test
I-103 Group, Descriptive statistics and Ranks for Mann- Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q17_Pre Total
1) Test 2) Control
15 15 30
1.457 0.900 1.258
5.87 6.67 6.27
13.00 18.00
195.00 270.00
Q17_Post 3 Total
1) Test 2) Control
13 13 26
2.103 2.599 2.372
3.62 4.62 4.12
11.69 15.31
152.00 199.00
Q17_Post 6 Total
1) Test 2) Control
13 13 26
1.038 2.504 2.281
1.92 4.46 3.19
9.81 17.19
127.50 223.50
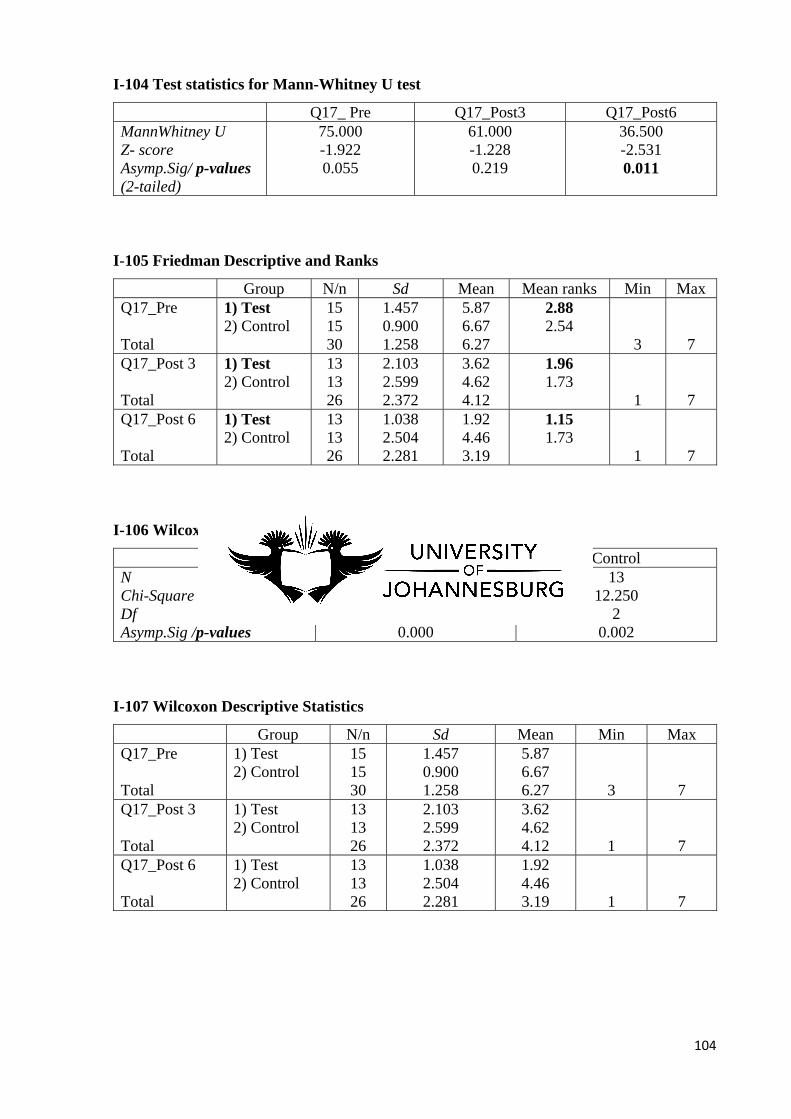
104
I-104 Test statistics for Mann-Whitney U test
Q17_ Pre Q17_Post3 Q17_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
75.000 -1.922 0.055
61.000 -1.228 0.219
36.500 -2.531 0.011
I-105 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q17_Pre Total
1) Test 2) Control
15 15 30
1.457 0.900 1.258
5.87 6.67 6.27
2.88 2.54
3
7
Q17_Post 3 Total
1) Test 2) Control
13 13 26
2.103 2.599 2.372
3.62 4.62 4.12
1.96 1.73
1
7
Q17_Post 6 Total
1) Test 2) Control
13 13 26
1.038 2.504 2.281
1.92 4.46 3.19
1.15 1.73
1
7
I-106 Wilcoxon Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 21.574
2 0.000
13 12.250
2 0.002
I-107 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q17_Pre Total
1) Test 2) Control
15 15 30
1.457 0.900 1.258
5.87 6.67 6.27
3
7
Q17_Post 3 Total
1) Test 2) Control
13 13 26
2.103 2.599 2.372
3.62 4.62 4.12
1
7
Q17_Post 6 Total
1) Test 2) Control
13 13 26
1.038 2.504 2.281
1.92 4.46 3.19
1
7
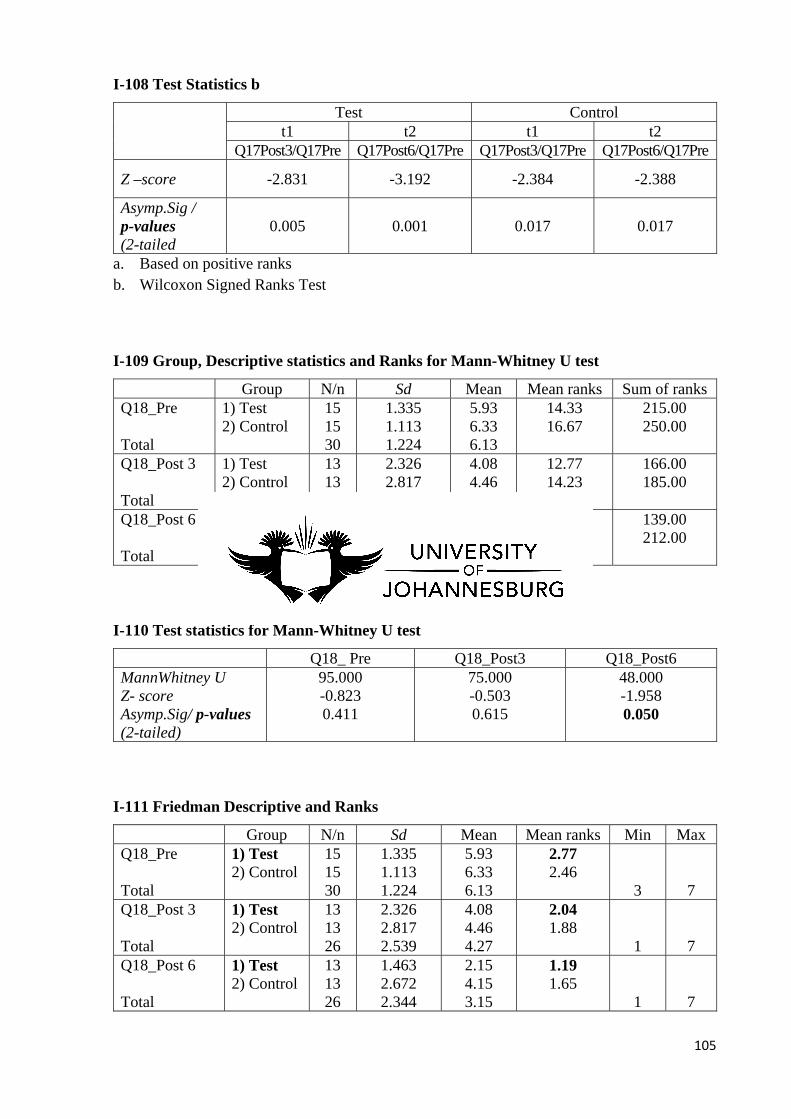
105
I-108 Test Statistics b
Test Control
t1 t2 t1 t2 Q17Post3/Q17Pre Q17Post6/Q17Pre Q17Post3/Q17Pre Q17Post6/Q17Pre
Z –score -2.831 -3.192 -2.384 -2.388
Asymp.Sig / p-values (2-tailed
0.005 0.001 0.017 0.017
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-109 Group, Descriptive statistics and Ranks for Mann-Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Q18_Pre Total
1) Test 2) Control
15 15 30
1.335 1.113 1.224
5.93 6.33 6.13
14.33 16.67
215.00 250.00
Q18_Post 3 Total
1) Test 2) Control
13 13 26
2.326 2.817 2.539
4.08 4.46 4.27
12.77 14.23
166.00 185.00
Q18_Post 6 Total
1) Test 2) Control
13 13 26
1.463 2.672 2.344
2.15 4.15 3.15
10.69 16.31
139.00 212.00
I-110 Test statistics for Mann-Whitney U test
Q18_ Pre Q18_Post3 Q18_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
95.000 -0.823 0.411
75.000 -0.503 0.615
48.000 -1.958 0.050
I-111 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Q18_Pre Total
1) Test 2) Control
15 15 30
1.335 1.113 1.224
5.93 6.33 6.13
2.77 2.46
3
7
Q18_Post 3 Total
1) Test 2) Control
13 13 26
2.326 2.817 2.539
4.08 4.46 4.27
2.04 1.88
1
7
Q18_Post 6 Total
1) Test 2) Control
13 13 26
1.463 2.672 2.344
2.15 4.15 3.15
1.19 1.65
1
7
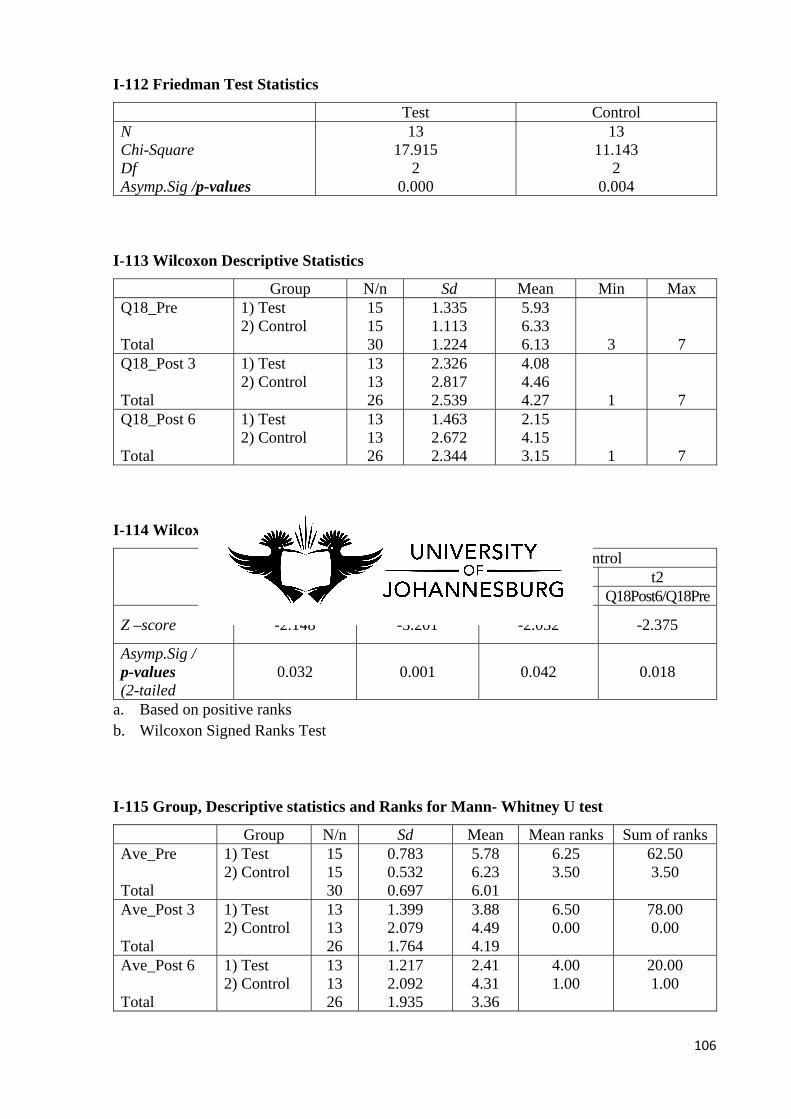
106
I-112 Friedman Test Statistics
Test Control N Chi-Square Df Asymp.Sig /p-values
13 17.915
2 0.000
13 11.143
2 0.004
I-113 Wilcoxon Descriptive Statistics
Group N/n Sd Mean Min Max Q18_Pre Total
1) Test 2) Control
15 15 30
1.335 1.113 1.224
5.93 6.33 6.13
3
7
Q18_Post 3 Total
1) Test 2) Control
13 13 26
2.326 2.817 2.539
4.08 4.46 4.27
1
7
Q18_Post 6 Total
1) Test 2) Control
13 13 26
1.463 2.672 2.344
2.15 4.15 3.15
1
7
I-114 Wilcoxon Test Statistics b
Test Control
t1 t2 t1 t2 Q18Post3/Q18Pre Q18Post6/Q18Pre Q18Post3/Q18Pre Q18Post6/Q18Pre
Z –score -2.148 -3.201 -2.032 -2.375
Asymp.Sig / p-values (2-tailed
0.032 0.001 0.042 0.018
a. Based on positive ranks b. Wilcoxon Signed Ranks Test
I-115 Group, Descriptive statistics and Ranks for Mann- Whitney U test
Group N/n Sd Mean Mean ranks Sum of ranks Ave_Pre Total
1) Test 2) Control
15 15 30
0.783 0.532 0.697
5.78 6.23 6.01
6.25 3.50
62.50 3.50
Ave_Post 3 Total
1) Test 2) Control
13 13 26
1.399 2.079 1.764
3.88 4.49 4.19
6.50 0.00
78.00 0.00
Ave_Post 6 Total
1) Test 2) Control
13 13 26
1.217 2.092 1.935
2.41 4.31 3.36
4.00 1.00
20.00 1.00
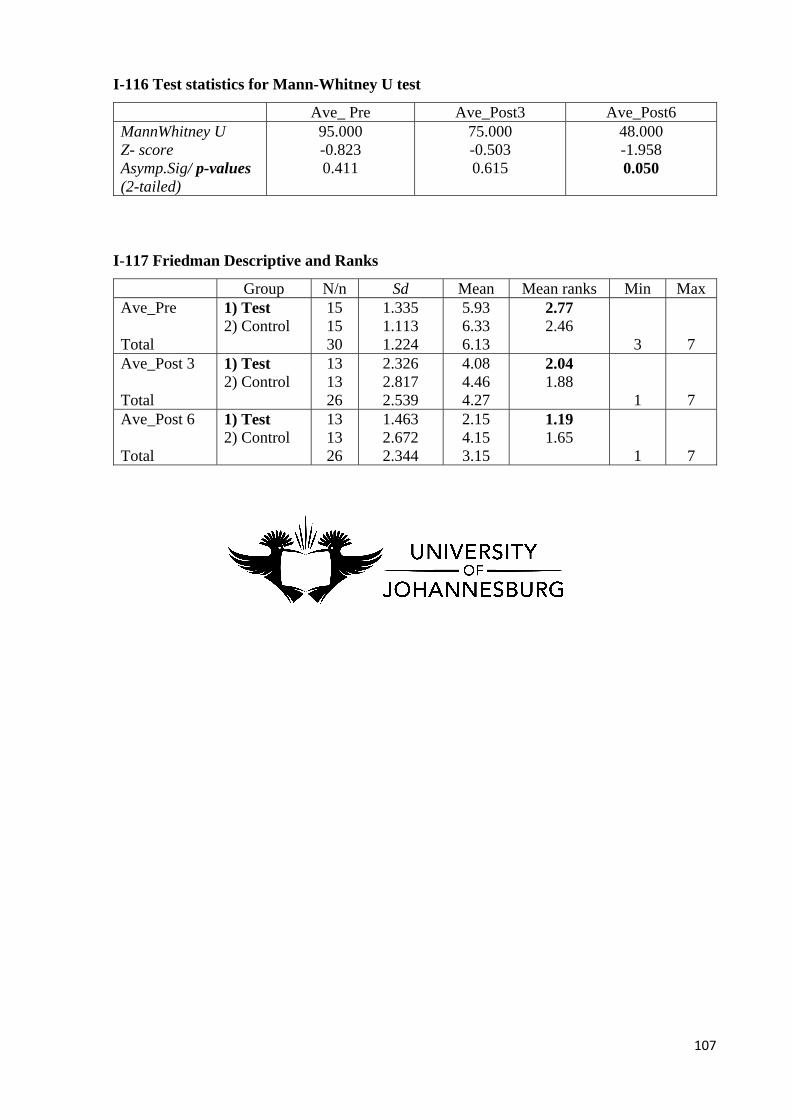
107
I-116 Test statistics for Mann-Whitney U test
Ave_ Pre Ave_Post3 Ave_Post6 MannWhitney U Z- score Asymp.Sig/ p-values (2-tailed)
95.000 -0.823 0.411
75.000 -0.503 0.615
48.000 -1.958 0.050
I-117 Friedman Descriptive and Ranks
Group N/n Sd Mean Mean ranks Min Max Ave_Pre Total
1) Test 2) Control
15 15 30
1.335 1.113 1.224
5.93 6.33 6.13
2.77 2.46
3
7
Ave_Post 3 Total
1) Test 2) Control
13 13 26
2.326 2.817 2.539
4.08 4.46 4.27
2.04 1.88
1
7
Ave_Post 6 Total
1) Test 2) Control
13 13 26
1.463 2.672 2.344
2.15 4.15 3.15
1.19 1.65
1
7
Copyright © 2022 FDOKUMEN




















