
Omvårdnad som reflekterande praktik - Luleå tekniska ...
164
DOKTORSAVHANDLING Omvårdnad som reflekterande praktik Att se och använda alternativ till tvång i psykiatrisk vård Git-Marie Ejneborn Looi
-
Upload
khangminh22 -
Category
Documents
-
view
7 -
download
0
Transcript of Omvårdnad som reflekterande praktik - Luleå tekniska ...

DOKTORSAVHANDLING
Institutionen för hälsovetenskapAvdelningen för omvårdnad Omvårdnad som reflekterande praktik
Att se och använda alternativ till tvång i psykiatrisk vård
Git-Marie Ejneborn Looi
ISSN 1402-1544ISBN 978-91-7583-407-8 (tryckt)ISBN 978-91-7583-408-5 (pdf)
Luleå tekniska universitet 2015
Git-M
arie Ejneborn Looi O
mvårdnad som
reflekterande praktik Att se och använda alternativ till tvång i psykiatrisk vård

Omvårdnad som reflekterande praktik
Att se och använda alternativ till tvång i psykiatrisk vård
Git-Marie Ejneborn Looi
Avdelningen för omvårdnad
Institutionen för hälsovetenskap
Luleå tekniska universitet
Sverige
Luleå 2015

Tryck: Luleå tekniska universitet, Grafisk produktion 2015
ISSN 1402-1544 ISBN 978-91-7583-407-8 (tryckt)ISBN 978-91-7583-408-5 (pdf)
Luleå 2015
www.ltu.se
Omslagsbild: Bilden på omslaget föreställer en person som mot sin vilja iförts handskar och
hjälm för att hindras från att skada sig själv. Personer med självskadebeteende som vårdats i
slutenvårdspsykiatrin är kanske de med mest erfarenhet av vad som händer när vårdare inte
längre förmår se en lidande människas behov utan istället ser ett problem som ska hanteras.
Denna avhandling vill motverka sådan självpåtagen maktlöshet och ingjuta hopp hos personal i
psykiatrisk vård genom att visa att det i varje situation finns olika handlingsalternativ. Fotot är
hämtat från Åkerman, S. & Eriksson, T. (2011). Slutstation rättspsyk: om tvångsvårdade kvinnor
som inte dömts för brott. Stockholm: Natur & kultur. Publiceras med tillstånd från författarna.
ISSN

Där konsten tar slut tar våldet vid


Innehåll Abstrakt .............................................................................................................. 1
Delstudier ........................................................................................................... 5
Förord ................................................................................................................ 7
Inledning ............................................................................................................ 9
Bakgrund .......................................................................................................... 11
Tvång ........................................................................................................... 11
Alternativ till tvång ....................................................................................... 14
Självskadebeteende ........................................................................................ 14
Omvårdnadsprocessen ................................................................................... 16
Vetenskapsteoretiskt ramverk ............................................................................ 17
Pragmatism ................................................................................................... 17
Abduktion ................................................................................................ 19
Teori och praktik ...................................................................................... 20
Rational............................................................................................................ 23
Övergripande syfte............................................................................................ 25
Metod .............................................................................................................. 27
Delstudie I .................................................................................................... 27
Deltagare och datainsamling ...................................................................... 27
Analys ....................................................................................................... 29
Metodval och etiska överväganden ............................................................ 29
Delstudie II ................................................................................................... 31
Deltagare och datainsamling ...................................................................... 31
Analys ....................................................................................................... 31
Metodval och etiska överväganden ............................................................ 32

Delstudie III och IV ...................................................................................... 34
Deltagare och datainsamling ...................................................................... 34
Analys delstudie III ................................................................................... 35
Analys delstudie IV ................................................................................... 36
Metodval och etiska överväganden ............................................................ 37
Metasyntes .................................................................................................... 39
Resultat ............................................................................................................ 41
Sammanfattning av resultatet från delstudie I-IV ........................................... 41
Delstudie I ................................................................................................ 41
Delstudie II ............................................................................................... 42
Delstudie III.............................................................................................. 43
Delstudie IV ............................................................................................. 43
Omvårdnad som reflekterande praktik .......................................................... 44
Syntes ....................................................................................................... 44
Relation .................................................................................................... 46
Behov ....................................................................................................... 47
Åtgärd ....................................................................................................... 48
Diskussion och kliniska implikationer ............................................................... 51
Omvårdnadsplanering ............................................................................... 53
Reflektion ................................................................................................ 54
Interaktivt projekt ..................................................................................... 56
Slutsats .............................................................................................................. 59
Jag vill tacka… .................................................................................................. 61
Referenser ........................................................................................................ 63
Summary in English .......................................................................................... 77

Abstrakt Tvångsåtgärder som fastspänning och tvångsmedicinering är vanligt
förekommande inom den psykiatriska vården och motiveras ofta av personal med
att det saknas alternativ. Användandet av tvångsåtgärder tycks vara särskilt vanligt
när det gäller unga kvinnor med självskadebeteende. Dessa kan uppleva
tvångsåtgärder som bestraffning och som ett hinder för att söka vård. Relationen
mellan patient och vårdare har beskrivits som ett kraftfullt verktyg för att minska
användandet av tvångsåtgärder, men det saknas i stor utsträckning forskning om
tvångsvård som fokuserar på patienters perspektiv och alternativ till tvång.
Avhandlingens övergripande syfte har varit att få ökad kunskap och förståelse för
omvårdnad som process i psykiatrisk vård ur patienters, studenters och personals
perspektiv, med särskilt fokus på alternativ till tvång vid självskadebeteende.
Avhandlingen har en pragmatisk utgångspunkt där ambitionen har varit att
resultat ska kunna omsättas i konkreta handlingar. Delstudierna har en kvalitativ
ansats där datamaterial har analyserats med innehållsanalys. Data består av 19
skrivna berättelser från personer som vårdats för självskadebeteende och som har
erfarenhet av tvångåtgärder, 14 loggböcker skrivna av sjuksköterskestudenter
under deras verksamhetsförlagda utbildning inom psykiatrisk vård, samt
fokusgruppsintervjuer med totalt 26 skötare, sjuksköterskor, läkare och
enhetschefer med erfarenhet av att tvångsvårda patienter.
Av berättelserna framkom att personer som vårdats inom psykiatrisk vård hade en
önskan om att mötas av förståelse av personalen, att utveckla tillitsfulla och
ömsesidiga relationer med dem, och att få vård som grundades på vetenskapliga
metoder. Deras faktiska erfarenheter beskrev en vård som var oförutsägbar,
kontraproduktiv och byggd på misstro och distans. Studenterna beskrev i
loggböckerna vikten av att avsätta tid och engagemang för relationsskapande,
1

2
något som beskrevs som en förutsättning för att kunna göra bedömningar och lära
sig förstå patientens individuella tecken på hälsa och ohälsa. De beskrev hur de
identifierade patienters abstrakta behov så som behov av trygghet, empowerment,
självkänsla och hopp. Med dessa som grund individanpassade de åtgärder och
förhållningssätt och synliggjorde samt tog tillvara patienternas förmågor. I
fokusgruppsintervjuerna framkom hur personal med utgångspunkt i utmanande
situationer i psykiatrisk slutenvård resonerade kring möjliga åtgärder med fokus
antingen på personalens behov, patientens upplevelse, att följa rutiner eller att
uppfostra patienter. Beroende på fokus skiljde sig förhållningssätt och utformning
av åtgärder markant åt. I fokusgruppsintervjuerna framkom även personalens syn
på samarbete utifrån olika professionella roller. Utmärkande var att skötarna, trots
att de hade lägst formell kompetens, var den yrkesgrupp med störst inflytande vid
beslut om tvångsåtgärder eftersom de arbetade närmast patienterna och därför
hade förstahandsinformation om dem.
Resultaten visade en stor överenstämmelse mellan patienters, studenters och
personals perspektiv. En metasyntes av de olika delstudiernas resultat beskriver
omvårdnad som en reflektiv praktik. Att vårdaren har förmågan att bygga upp en
tillitsfull relation till patienten är en förutsättning för en relevant bedömning.
Bedömningen innebär att patientens individuella behov och förmågor identifieras
och ligger till grund för val av åtgärd och förhållningsätt med målet att minska
lidande och öka välbefinnande. Vägen till åtgärden är inte statisk, till en början
kan åtgärder enbart ha ett relationskapande syfte, behov kan förändras, åtgärder
behöva modifieras liksom att tilliten i relationen kan påverkas av olika faktorer.
Detta innebär att vägen till åtgärden inte bör ses som ett linjärt förlopp utan bättre
förstås som en dynamisk process som förutsätter ett reflekterande förhållningssätt
med relationen som grund, med det övergripande målet att stärka patientens
förutsättningar till återhämtning och välbefinnande.

3
Den övergripande slutsats som kan dras är att om vårdarna lyckas skapa en
ömsesidig, tillitsfull relation till patienten, kan förstå dennes utryckta behov och
outtalade tecken samt arbetar proaktivt, i samarbete med patienten, med åtgärder
och medvetna förhållningssätt, så finns sällan behov av tvångsåtgärder. För detta
krävs att vårdarna får stöd i att utveckla sin reflektiva förmåga och även i att få ta
eget ansvar för varje situation och därigenom bygga upp en tillit till sin egen
förmåga.
Nyckelord: Alternativ till tvångsåtgärder, omvårdnad, process, psykiatrisk vård,
självskadebeteende, pragmatism, kvalitativ innehållsanalys

4

5
Delstudier Denna avhandling bygger på nedanstående artiklar vilka refereras till i texten med
dess romerska numrering.
I Looi, G. E., Engström, Å., & Sävenstedt, S. (2015). A self-destructive care:
Self-reports of people who experienced coercive measures and their
suggestions for alternatives. Issues in Mental Health Nursing, 36(2), 96-103.
doi:http://dx.doi.org/10.3109/01612840.2014.951134
II Looi, G. E., Sävenstedt, S., & Engström, Å. (accepted). Easy but not simple –
Nursing students’ descriptions of the process of care in a psychiatric context.
Issues in Mental Health Nursing.
III Looi, G. E., Gabrielsson, S., Sävenstedt, S., & Zingmark, K. (2014). Solving
the staff's problem or meeting the patients’ needs: Staff members’ reasoning
about choice of action in challenging situations in psychiatric inpatient care.
Issues in Mental Health Nursing, 35(6), 470-479.
doi:http://dx.doi.org/10.3109/01612840.2013.879629
IV Gabrielsson, S., Looi, G. E., Zingmark, K., & Sävenstedt, S. (2014).
Knowledge of the patient as decision-making power: Staff members'
perceptions of interprofessional collaboration in challenging situations in
psychiatric inpatient care. Scandinavian Journal of Caring Sciences, 28(4), 784-
792. doi:http://dx.doi.org/10.1111/scs.12111
Originalartiklar publiceras med tillstånd av tidskrifternas utgivare.

6
7
Förord En morgon i mina yngre tonår vaknade jag med en stark känsla för att det var
inom psykiatrin jag i framtiden skulle arbeta. Att jag inte hade någon tidigare
erfarenhet inom området spelade ingen roll, jag var fast övertygad om vad som
var mitt blivande yrke. Några år senare, 1985, avslutade jag min skötarutbildning
och kommande år arbetade jag som stolt skötare inom olika områden av
psykiatrin.
Genom åren har jag mött många människor med psykisk ohälsa, och dessa möten
har fungerat som källor för såväl inspiration som kunskap. Jag har fått ta del av
människors livsberättelser och erfarenheter, vilket har gett mig ökad kunskap,
inblick och förståelse för deras behov och situation.
En tid som varit särskilt betydelsefull för min yrkesmässiga utveckling är mina år,
i början av 90-talet, då jag arbetade med personer som nyinsjuknat i psykos på ett
utrednings- och behandlingshem. Jag ingick i en personalgrupp som fick
förtroendet att både planera och bygga upp en helt ny typ av verksamhet som
hade ett uppdrag att utreda, behandla och vid behov även rehabilitera unga vuxna
med misstänkt psykossjukdom. Idag kan jag titta tillbaka och konstatera att vi
framförallt stöttade de unga vuxna i deras återhämtningsprocess. Något som
väckte reaktioner var att vi tidigt i planeringsprocessen fattade beslutet att
behandlingshemmet skulle bedrivas under frivilliga former, eftersträva så hög
patientdelaktighet som möjligt och att vi inte skulle ha tillgång till tvångsåtgärder.
Många olyckskorpar kraxade, men detta var ett upplägg som skulle visa sig
fungera mycket bra. Åren på behandlingshemmet blev bland de mest lärorika i
min yrkeskarriär, och jag arbetade på behandlingshemmet fram till dess en ny
ledning tillsattes.

8
Jag valde då att gå vidare och skaffa mig nya erfarenheter från andra delar av
psykiatrin, och det var i samband med detta som jag började få inblick i de brister
som på många sätt påverkade den psykiatriska vården. Frustrationen jag kände
över den hopplöshet och maktlöshet som jag tyckte genomsyrade många
arbetsplatser inom psykiatrin, ledde till att jag bestämde mig för att öka mina
möjligheter att kunna påverka vårdkvaliteten i positiv riktning och jag utbildade
mig till specialistsjuksköterska i psykiatrisk vård. Som färdigutbildad
specialistsjuksköterska fick jag sedan chansen att under några år bedriva ett
utvecklingsprojekt på en akutpsykiatrisk avdelning, ett uppdrag som inspirerade
och övertygade mig på samma sätt som arbetet på behandlingshemmet hade gjort
15 år tidigare. Även här visade det sig att det med relativt små medel är möjligt
att bedriva psykiatrisk vård som bygger på ömsesidighet och samarbete mellan
patient och vårdare, och där tvångsåtgärder i de flesta fall går att undvika.
Mina positiva erfarenheter blev sedan min startpunkt när jag slutligen blev
antagen som doktorand med möjligheten att utforma mitt projekt. Tron på att
förändring är möjligt är min självklara drivkraft.

9
Inledning Den här avhandlingen handlar om förståelse för omvårdnad som process i
psykiatrisk vård med ett särskilt fokus på alternativ till tvång. Tvång motiveras
ofta med att det är nödvändigt för patienten när vårdare inte ser några andra
alternativ (Muir-Cochrane, Baird & McCann, 2015). Studier som beskriver
upplevelsen av tvång från patientens perspektiv är relativt få och de som finns
visar att tvång ofta upplevs som en strategi för kontroll och övervakning istället
för att möta deras behov (Hörberg, Sjögren & Dahlberg, 2012; Meehan,
McIntosh & Bergen, 2006 ). Ett sätt att arbeta med omvårdnad som en process, i
den psykiatriska vården illustreras i följande fallbeskrivning. Den är hämtad från
en sjuksköterskestudents loggbok som hon skrev i samband med att hon gick en
verksamhetsförlagd kurs med placering på en sluten psykiatrisk avdelning.
Fallbeskrivning: Patienten är en medelåldersman som tvångsvårdats många gånger på
avdelningen på grund av paranoida vanföreställningar och då vid upprepade tillfällen blivit
lagd i bälte. Under rapporten framkommer att mannen uppträder aggressivt, sover inte,
vandrar runt i korridoren och vägrar att vistas på sitt enskilda patientrum. Studenten
försöker att finnas i närheten av mannen utan att tränga sig på och efter en stund ber
patienten studenten om hjälp med några praktiska göromål och på det sättet så påbörjas ett
relationsskapande. När mannen tar kontakt så förmedlar studenten att hon tar sig tid, är
närvarande, lyssnar och tar mannen på allvar. När studenten lyssnar till mannens
beskrivning av sin situation så framkommer det att han är rädd och tycker att det är
obehagligt att vara på rummet på grund av möblernas placering. Studenten frågar då hur
han skulle vilja ha det istället och hur det ser ut hemma hos honom. Han beskriver bland
annat att han vill ha uppsikt över dörren både när han sitter vid skrivbordet och när han
sover. Utifrån mannens beskrivning av sin situation bedömer studenten att han har behov
av sömn, trygghet, tillit och ökad empowerment.

10
För att mannen ska känna sig trygg och kunna visats och kunna sova i sitt rum så väljer
studenten som en första åtgärd att tillsammans med patienten möblera om patientrummet.
Studenten har ett medvetet förhållningssätt där hon bekräftar mannen och uppmuntrar till
medbestämmande och delaktighet för att han ska känna att han har en viss makt och
kontroll över sin situation.
Studentens utvärdering, citat från loggboken: För mig kan man säga att denna åtgärd
var en lätt handling, men den inlevelse patienten hade visar att det var något som betydde
jättemycket för honom. Han fick ha kontrollen och bestämma och jag lyssnade på hans
önskemål och visade att det var viktigt det vi gjorde. Patienten sa att han kände sig mycket
tryggare inne på sitt rum och han fick mer ro att skriva och läsa. Jag och min handledare
kom fram till att han verkade både lugnare och gladare och på läkarronden idag fick jag
höra av överläkaren att denna patient är den sjukaste patient som de har.

11
Bakgrund
Tvång
Under 2013 vårdades ca 12 500 patienter i Sverige under någon av de två
kompletterande psykiatriska tvångslagarna, lagen (SFS,1991:1129) om
rättspsykiatrisk vård [LRV] eller lagen (SFS, 1991:1128) om psykiatrisk
tvångsvård [LPT] (Socialstyrelsens statistikdatabas). Föreskrifterna i hälso- och
sjukvårdslagen (1982:763) gäller all psykiatrisk vård, tvångsvårdslagstiftningen är
enbart ett komplement. Enligt lagen ska tvångsvården syfta till att patienten
frivilligt ska kunna medverka till nödvändig vård och ta emot det stöd som han
eller hon behöver. För att tvångsvård ska vara aktuellt måste tre förutsättningar
vara uppfyllda: (1) patienten ska lida av en allvarlig psykisk störning, till exempel
psykos eller depression med suicidrisk; (2) patienten ska vara i
oundgängligt behov av psykiatrisk heldygnsvård; (3) patienten motsätter sig
vården eller det finns grundad anledning att anta att vården inte kan ges med
patientens samtycke (SFS, 1991:1128).
Fram till 1929 var tvångsvård den enda vårdform som erbjöds till personer med
psykiska funktionshinder (Björkman, 2001). Dagens tvångsvårdslagstiftning
tillkom 1992 och ersatte Lagen om sluten psykiatrisk vård i vissa fall [LSPV].
Syftet med den nya lagstiftningen, LPT, var att minska användandet av tvång och
att stärka patientens autonomi och rättsäkerhet, psykiatrisk vård skulle ges under
frivilliga former i så stor utsträckning som möjligt. Det primära
bedömningskriteriet skulle vara vårdbehovet, inte skyddet för omgivningen
(Socialstyrelsen 1991:9). Trots goda intentioner visar studier att den nya
lagstiftningen inte haft avsedd effekt. Patienterna upplevde inte någon ökad
autonomi, fler patienter hade utsatts för tvångsåtgärder (Wallsten & Kjellin, 2004;
Wallsten, Östman, Sjöberg & Kjellin, 2008) och många frivilligt vårdade

12
patienter uppgav att de utsatts för tvångsåtgärder under vårdtiden (Kjellin et al.,
2004). Det framkommer även en stor diskrepans mellan dokumentation av
tvångsåtgärder och patienternas beskrivningar, i 42 procent av fallen där
patienterna uppgett att de utsatts för tvång fanns inte åtgärderna dokumenterade i
journalen (Wallsten, Kjellin & Sjöberg, 2008).
I denna avhandling definieras tvång utifrån patientens upplevelse. Tvångsåtgärder
får enligt lag (SFS, 1991:1128) endast användas om de står i rimlig proportion till
syftet med åtgärden och ska utövas så skonsamt som möjligt och med största
möjliga hänsyn till patienten. Tvångsåtgärder får endast användas om patienten
inte, genom en individuellt anpassad information, kan förmås att frivilligt
medverka till att ta emot vård (SFS, 1991:1128). Raboch et al. (2010) har
studerat tvångsåtgärder i tio Europiska länder och funnit att typ av åtgärd och
frekvens varierar stort. Diagnos och svåra symtom var faktorer som generellt gick
att koppla till användning av tvångåtgärder men Raboch et al. menar på att den
stora variationen mellan länderna kan bero på landets sociokulturella traditioner
och vårdkulturer. Som tidigare framkommit förekommer även en stor diskrepans
mellan vad vårdare och patient anser vara tvång och det juridiska tvånget
överensstämmer inte alltid med det upplevda.
Att vårda en person mot dennes vilja ställer särskilt höga krav på vårdgivaren och
patienten ska kunna erbjudas ett varierat och individanpassat vårdutbud
(Socialstyrelsen, 2009). Dock framkommer i socialstyrelsens inventering att den
vård som erbjuds är ensidig och den vanligaste åtgärden är medicinska insatser.
Rapporten visar vidare på att den psykiatriska tvångsvården behöver utvecklas för
att kunna erbjuda en vård av hög kvalitet. Föreslagna åtgärder är bland annat att
stärka personalens kompetens så att ett varierat och behovsanpassat vårdinnehåll
kan erbjudas (Socialstyrelsen, 2009).

13
Patienter som tvångsvårdats beskriver dock en organisation som präglas av rigida
regelsystem där de kan bemötas av vårdare som har en arrogant attityd, uttalar
provocerande kommentarer och som har fokus på kontroll och övervakning
istället för vård (Hörberg et al., 2012; Meehan et al., 2006). Enligt Meehan et al.
så var medicineringssituationen den största utlösande faktorn för aggressivitet och
patienterna upplevde att syftet med medicineringen snarare handlade om
beteendekontroll och straff än behandling för deras sjukdom. Enligt en
forskningsöversikt (Jarrett, Bowers & Simpson, 2008) sker tvångsmedicinering
ofta slentrianmässigt och kan inte betraktas som en evidensbaserad
behandlingsmetod, då det råder brist på forskning inom området. I studierna
framkom inga beskrivningar av alternativ till tvång och endast ett fåtal artiklar
beskrev utlösande faktorer till tvångsåtgärden. Jarrett et al. anser bland annat att
personalens attityder, preventiva insatser och alternativ till tvångsåtgärder är
faktorer som bör undersökas vidare.
I en nyligt publicerad översiktsartikel om tvångsvård visar van den Hooff och
Goossensen (2014) att det genomgående starkaste önskemålet, från ett
patientperspektiv, var att personalen lyssnade och tog patienten på allvar, men
patienternas erfarenheter var ofta de motsatta. Ser man till den aktuella
forskningen inom området så är det fortfarande ett stort fokus på säkerhet/risk,
personal och organisatoriska faktorer (Bak et al., 2015; Björkdahl, Hansebo &
Palmstierna, 2013; Bowers et al., 2009; Bowers et al., 2015; De Benedictis et al.,
2011; Fluttert, van Meijel, Nijman, Bjørkly & Grypdonck, 2010 m.fl.) och
mindre fokus på patientens perspektiv och den flexibla och behovsanpassade
tvångsvården som socialstyrelsen efterlyser.

14
Alternativ till tvång
Ett flertal studier visar på att sjuksköterskor kan se på tvångsåtgärder som en
självklar och nödvändig arbetsuppgift utan andra acceptabla alternativ (Haglund,
von Knorring & von Essen, 2003; Jarrett et al., 2008; Marangos-Frost & Wells,
2000; Muir-Cochrane et al., 2015; Olofsson, 2005; Olofsson, Gilje, Jacobson &
Norberg, 1998). Att utföra tvångsåtgärder innebär dock ofta en inre konflikt för
sjuksköterskor då de vill se sig själva och sina kollegor som goda vårdare medan
tvångsåtgärder inte ses som en del av den goda vården (Olofsson et al., 1998).
Det finns kliniska exempel som visar att det är möjligt att kraftigt reducera
behovet av tvångsåtgärder i psykiatrisk vård (Ashcraft & Anthony, 2008; Barker
& Buchanan-Barker, 2010; Barton, Johnson & Price, 2009; Georgieva, de Haan,
Smith & Mulder, 2010; Hejlskov Elvén & Abild, 2015 m.fl.). Gemensamma
faktorer som bidrog till ett minskat behov av tvångsåtgärder, utifrån exemplen
ovan, var att vårdarna aktivt eftersträvade en nära relation till patient och hade
fokus på hopp och empowerment istället för kontroll och korrigering. Detta
bekräftas även i intervjustudier som beskriver att relationen mellan patient och
vårdare är ett kraftfullt verktyg för att förhindra tvångsåtgärder (Haglund et al.,
2003; Olofsson & Norberg, 2001; Vuckovich, 2009 m.fl.). Andra studier lyfter
även upp ledarskapet och organisationens betydelse (Huckshorn, 2004),
vårdmiljön (Muir-Cochrane et al., 2015) samt personalutbildning och reducering
av avdelningsregler (Huckshorn, 2014).
Självskadebeteende
I Sverige är personer med självskadebeteende överrepresenterade i statistiken över
tvångsåtgärder (Holm, Björkdahl & Björkenstam, 2011). Det är inget klart
definierat begrepp och det saknas konsensus om vad som ska räknas som
självskadebeteende (Mangnall & Yurkovich, 2008). I denna avhandling har det
15
varit upp till deltagaren själv att avgöra om de anser sig ha ett självskadebeteende,
då rekryteringen av dessa deltagare skett helt anonymt (delstudie I).
Självskadebeteende har beskrivits som en samsjuklighetsproblematik till andra
diagoser och även i vissa fall kopplats till barndomstrauman (Mangnall &
Yurkovich, 2008; McAllister, 2003). I den senaste versionen av diagnosmanualen
DSM-V har dock icke suicidalt självskadebeteende (non-suicidal self-injury
[NSSI]) för första gången kommit med som förslagen oberoende diagnos
(American Psychiatric Association, 2013).
I en nyutkommen rapport (SBU, 2015) framkommer att personer med
självskadebeteende utsätts för dömande attityder från vårdpersonal. De känner sig
även maktlösa och upplever att tvångsåtgärder kan förekomma i straffande syfte,
de negativa vårderfarenheterna bidrar till att de inte söker vård. McAllister (2003)
visar på att självskadandet kan ha många olika orsaker och fylla olika syften för
personen som skadar sig. McAllister drar då slutsaten att vårdarna måste vara
flexibla och kunna erbjuda olika individuella lösningar för att kunna bryta det
traditionellt negativa diskurserna som ofta förekommer i den psykiatriska vården.
En nyligt publicerad litteraturöversikt (Karman, Kool, Poslawsky & van Meijel,
2015) visar att personalens bemötande och attityder har stor påverkan på
patientens välbefinnande och upplevelser av vårdens kvalitet. Resultatet visar
även på att det är vanligt att sjuksköterskor har negativa attityder till personer
med självskadebeteende.
Patienter vill bemötas som kompetenta unika individer och kunna känna att
personalen ser deras individuella behov (Lindgren, Öster, Åström & Hällgren
Graneheim, 2011). Tofthagen, Talseth och Fagerström (2014) visar på att
sjuksköterskor kan främja patienternas välbefinnande genom att skapa
förutsättningar för en ömsesidig relation och initiera personcentrerade
interventioner. Lindgren och Hällgren Graneheim (2015) lyfter också vikten av
det genuina mötet som en förutsättning för patientens återhämtning men visar

16
även på att arbetet med personer som skadar sig själva kan vara både utmanade
och oförutsägbart vilket innebär att vårdaren har behov av kunskap, stöd och av
att få tid för reflektion för att kunna göra ett bra arbete. Detta stöds även av
Karman et al. (2015) som dessutom betonar möjligheten att arbeta nära patienten
samt stöd från kollegor som viktigt faktorer för att kunna förändra
sjuksköterskornas negativa attityder till patienter med självskadebeteende.
Omvårdnadsprocessen
I detta avhandlingsarbete beskrivs omvårdnadsarbete utifrån the process of care (se
delstudie II) eller omvårdnad som process och består av de tre delarna relation och
relationsskapandet, behov och behovsbedömning och åtgärder och förhållningssätt.
Både patienter och sjuksköterskor beskriver att en personlig relation är grunden
för en vårdande allians (Halldorsdottir, 1996; Jormfeldt, Svedberg, & Arvidsson,
2003; Svedberg, Jormfeldt, & Arvidsson, 2003 m.fl.). Relationen stärker
förutsättningarna för att se patienten som en unik individ med unika behov,
vilket är en nödvändighet för att främja hälsoprocessen. Omvårdnadsåtgärder som
fokuserar på respekt, delaktighet och empowerment är betydelsefulla för
patienternas upplevelse av hälsa (Svedberg et al., 2003). Detta står dock i kontrast
till hur omvårdnadsprocessen traditionellt beskrivs, där vare sig relationens
betydelse eller relationsskapande faktorer är synliggjorda. Omvårdnadsprocessen
beskrivs som en problemlösningsmodell som startar med datainsamling och går
sedan vidare med planering, utförande av intervention och avslutas med
utvärdering (Yura & Walsh, 1988) och i vissa fall så läggs även
omvårdnadsdiagnostisering till processen (Carnevali, 1983; Gordon, 2002 m.fl).
Eriksson (2014) beskriver relationen mellan patient och vårdare som kärnan i
vårdprocessen. Dock synliggör inte heller Eriksson relationen utan processen inleds
med patientanalys, som till stor del påminner om omvårdnadensprocessens
beskrivning av datainsamlingen.

17
Vetenskapsteoretiskt ramverk Min vetenskapsteoretiska utgångspunkt är pragmatismen, vilket innebär att jag
har haft ambitionen att omsätta delstudiernas resultat till praktiska handlingar. Det
innebär att mitt fokus inte i första hand varit att förstå hur en patient upplever
tvångsåtgärder utan att söka efter konkreta handlingsalternativ där patientens
behov kan mötas utan att tvång används. Ytterligare en viktig aspekt utifrån detta
handlingsperspektiv har för mig varit att försöka förstå vad vårdare grundar sina
val av handlingar på.
Min långa erfarenhet inom psykiatrin kan innebära en risk för att jag blivit
begränsad i min förmåga att se olika möjligheter (jmf Hellzén, Kristiansen &
Norbergh, 20031), och jag har därför strävat efter en att ha en bred ansats och
utgått ifrån flera perspektiv. Konkret har det inneburit att jag samlat kunskap och
erfarenheter från både patienter, studenter och personal. Detta har hjälpt mig att
se fler möjligheter och handlingsalternativ. Dessutom har jag haft förmånen att i
vissa delar ha ett nära samarbete med en annan doktorand, vilket har varit mycket
berikande och stimulerat till kritisk reflektion och nya infallsvinklar.
Pragmatism
Pragmatismen formulerades i slutet av 1800-talet av Charles S Peirce och
kännetecknas av att den värderar en metod eller teori enligt dess funktion,
tillämpning och användbarhet (Peirce, 1990). Det finns ett antal filosofer som
utgått från Peirces teorier, och jag har i denna avhandling främst använt Richard
Rorty och John Deweys tankar som grund för mina reflektioner. Dewey är
filosof och har producerat en mängd teorier inom olika områden så som
1 Hellzén et al. visar på att lång erfarenhet kan vara en belastning då känsligheten i relation till brukarna minskade och de med lång erfarenhet hade sämre attityd.

18
pedagogik, moral, demokrati och socialpsykologi. I denna avhandling refereras till
delar av Deweys teorier utifrån professorerna i pedagogik John Hartman och Gert
Biestas bearbetningar och tolkningar av Deweys texter (Biesta, 2004; Hartman,
2003).
Denna avhandling har ett fokus på alternativ till tvång, det vill säga ett
handlingsperspektiv. Utgångspunkten har varit personers erfarenheter av
psykiatrisk vård, från olika perspektiv. Inom pragmatismen finns det inte någon
platonsk önskan om att urskilja skenet från verklighetens innersta natur eller en
tro på att tingen verkligen är på ett visst sätt utan det anses mer meningsfullt att
utgå från att det finns mer eller mindre användbara beskrivningar av världen
(Rorty, 2003). Dewey ställde sig kritiskt till det dualistiska tänkandet2 och
utarbetade en handlingsteori som utgår från våra erfarenheter. Han menar på, i
motsats till många andra filosofer, att vi alltid är i kontakt med världen (Biesta,
2004). Enligt pragmatismen så är det inte meningsfullt att beskriva kunskap som
ett sätt att representera verkligheten, då sanningssökandet inte fyller någon
funktion i sig, istället bör forskningen ses som ett sätt att använda verkligheten
(Rorty, 2003). Det innebär, enligt Rorty, att sökande efter kunskap inte är ett
mål i sig utan bara ett av många medel för strävan efter mänsklig lycka.
I delstudierna finns det beskrivningar från flera olika typer av verksamheter, vilket
kan anses vara ett problem om man söker efter homogenitet eller sanningar. I
denna avhandling har ambitionen varit att visa att det finns många olika val
snarare än att identifiera den ”perfekta” tvångsfria vården eller att fastslå att
tvångsåtgärder är förkastligt. Därför tänker jag att beskrivningar från olika
2 Biesta (2004) beskriver att dualismen särskiljer delar exempelvis kropps – själ, stimuli – respons etc. medan Dewey anser att vi bör se delarna som funktionella faktorer inom en konkret helhet, inte som existentiella olikheter som dualismen förespråkar. Jag tolkar det som att det centrala är faktorers ömsesidiga påverkan, det vill säga processen, och inte hur faktorer står i relation till varandra.

19
kontexter kan berika datainsamlingen och öppna upp för fler alternativ till
tvångsåtgärder. Sammanfattningsvis så har jag inte haft ambitionen att identifiera
ett rätt eller fel sätt att handla utan visa på möjligheter att välja olika alternativ för
att skapa hopp och tillfredställelse i vården både för patienter och för vårdare.
Abduktion
I mina resonemang har jag utgått från abduktion som är den bevisföringsform
som pragmatismen grundar sig på. Abduktion kan enkelt förklaras som att
hypoteser formuleras utifrån den erfarenhet vi har, kreativa hypoteser. Hypoteserna
testas empiriskt för att eventuellt formulera en ny hypotes som prövas, detta
fortsätter till dess att vi kan anta att vi nått den bästa förklaringen, tills vidare
(Harman, 1965; Peirce, 1990). Abduktionen öppnar upp för och stimuleras av
skilda perspektiv, kreativitet och associationsrikedom (Svensson, 2002a). Enligt
Svensson (2002a) handlar abduktion om att pendla mellan del och helhet för att
få en fördjupad förståelse och ökad insikt så att en ny innebörd kan uppstå till det
som redan är känt. En kritik mot abduktionen har varit att den inte följer samma
traditionellt stringenta regelverk som de övriga bevisföringsformerna, det vill säga
induktion, deduktion och hypotetisk deduktion. Samtidigt anser Birkler (2008)
att styrkan med abduktionen istället är att den är mycket tillämpbar.
Abduktionen skiljer sig från induktion som är den traditionella
bevisföringsformen inom den kvalitativa omvårdnadsforskningen (Bergdahl &
Berterö, 2015). I ett induktivt förhållningssätt utgår forskaren från en öppen och
förutsättningslös utgångspunkt och går mot en generalisering (Kvale &
Brinkmann, 2014). I en strikt tillämpning innebär det att tidigare erfarenheter
och kunskaper sätts åt sidan och att forskaren strävar mot ett öppet
förhållningssätt till det fenomen som studeras. Ett exempel på kritik mot ett
induktivt förhållningssätt är Bergdahl och Berterö (2015) som är starkt kritiska till
hur dagens omvårdnadsforskning generellt ser ut där de anser att den är för
20
ospecifik och allmän. De anser vidare att det är viktigt att inte bara generera
allmänna teorier utan även kritiskt granska och utveckla teorierna genom att
hypotestesta och se om de är praktiskt tillämpbara. Eriksson och Lindström
(1997) stödjer ett sådant resonemang och menar att ett abduktivt förhållningssätt
kan vara en konstruktiv väg för att utveckla och förnya arbetssätt inom vården.
För att omsätta det abduktiva resonemanget till mitt forskningsprojekt så utgick
jag från mina egna erfarenheter av att vårda vid tvångsvård och mina erfarenheter
av att använda andra alternativ än tvångsåtgärder. Dessutom studerade jag tidigare
forskning som beskriver olika erfarenheter av tvångsåtgärder och alternativ till
tvång. Dessa utgångspunkter fanns sedan med i planeringen och utformningen av
de delstudier och analyser som ingår i avhandlingen. I forskningsprojekt har jag
utgått ifrån två övergripande hypoteser: det finns alternativ till tvångsåtgärder och
personal vill använda alternativ om de kan. Då jag insåg att delstudiernas resultat hade
många gemensamma skärningspunkter så genomförde jag även en metasyntes (jmf
Walsh & Downe, 2005). Detta innebär att de fyra resultaten sammanfördes och
tolkades (Graneheim & Lundman, 2004) till ett sammantaget femte resultat (se
resultat) som förväntas ligga till grund för en konkret arbetsmodell.
Teori och praktik
Att överbrygga klyftan mellan teori och praktik och implementera nya teorier
och metoder inom vården är inte helt enkelt (jmf Gask & Coventry, 2012;
Maben, Latter & Clark, 2006; Thorne et al., 1998). Enligt Biesta, så anser Dewey
att kunskap alltid handlar om relationen mellan våra handlingar och dess
konsekvenser, det vill säga att vi får kunskap om världen via våra handlingar.
Dewey ser inte människan som åskådare av ett färdigt universum utan menar att
vi är deltagare i ett ständigt utvecklande av ett oavslutat universum. Han menar
vidare att det krävs en process där vi gör kunskap, ”kunskapande”, något som
enligt Dewey är nödvändigt för att att få insikt om kunskapen (Biesta, 2004).

21
Hartman (2003) beskriver Deweys tankar som att tanke och handling inte kan
åtskiljas på samma sätt som att teori och praktik är varandras förutsättningar, utan
inbördes rangordning. Han anser vidare att reflektion måste ha förankring i
handling och praktiska handlingar genererar ingen erfarenhet utan reflektion.
Detta innebär att om tanke och handling är synkrona så finns ett etiskt krav på
människan att leva som man lär och i det ingår att reflektera över sina handlingar,
vilket Dewey benämner som intelligent action (Hartman, 2003).
Aktionsforskningen är en forskningsmetod som bygger på pragmatismen och
Deweys teorier har fått ligga till grund för bland annat beskrivningen av
begreppet outcome validity (workability). Outcome validity är ett kvalitetsmått och
handlar om att mäta om forskningen lett till några reella förändringar, det vill säga
löst problemet, vilket är ett viktigt mål inom metoden (Herr & Andersson, 2014).
Även om de forskningsmetoder som jag använt inte varit inom ramen för
aktionsforskning så finns det delar i metoden som jag har inspirerats av. Jag har
haft ambitionen att skriva artiklar som är vetenskapligt välgrundade och samtidigt
lättlästa och omsättningsbara för att de ska kunna användas i verksamheterna till
stöd för reella förändringar. Dessutom har jag valt att skriva kappan på svenska
och eftersträvat att ha ett mer direkt tilltal med förhoppningen att den ska bli
intressant för en bred läsargrupp. Som stöd i utormningen av kappan, förutom
den traditionella akademiska processen, så har jag haft en referensgrupp bestående
av patient- närstående - och personalrepresentanter som fått läsa och ge
synpunkter på framförallt språkbruk, begriplighet och omsättningsbarhet. Jag
tänker att denna process delvis skulle kunna svara upp mot det Herr och
Andersson (2014) beskriver som democratic validity där de förespråkar vikten av att
personerna som forskningen berör bör vara involverade utifrån ett etiskt och
socialt rättighetsperspektiv.

22
23
Rational Utifrån litteratur och mina egna erfarenheter tycks det finnas alternativ till tvång
men tvångsåtgärder är fortfarande vanligt förekommande inom den psykiatriska
vården och dessa motiveras ofta av personal med att det saknas alternativ.
Omvårdnadsforskning beskriver betydelsen av relationer, hur bedömningar av
behov kan genomföras och interventioner som kan fungera som alternativ till
tvång.
I det forskningsprojekt som ligger till grund för denna avhandling har jag utgått
ifrån två övergripande hypoteser: det finns alternativ till tvångsåtgärder och personal
vill använda alternativ om de kan. Hypoteserna har funnits med som grundläggande
antagande i planeringen och genomförandet av alla studier.
Omvårdnad kan beskrivas som en process med tre tydligt avgränsade områden
som i sig är beroende av varandra: skapandet av en relation, identifiering av
behov, samt åtgärder och förhållningssätt. En genomgång av litteraturen visar att
det finns forskning om tvång i psykiatrisk vård som beskriver delarna i processen,
men begränsat med forskning kring hur delarna kan knytas ihop till en helhet.
Jag har haft ambitionen att ta steget från kunskap om delar av den komplexa
verklighet som påverkar vården av personer med psykisk ohälsa till praktiska
handlingar som kan användas i omvårdnadsarbetet. Det innebär att mitt fokus
inte i första hand varit att förstå hur en patient upplever tvångsåtgärder utan att
söka efter konkreta handlingsalternativ där patientens behov kan mötas utan att
tvång används. Ur ett handlingsperspektiv har det för mig också varit viktigt att
försöka förstå vad personalen grundar sina val av handlingar på.

24
Jag hoppas att denna avhandling ska bidra till ny kunskap genom att synliggöra
och visa på hur de olika delarna, relation, behov och åtgärd, kan sättas ihop till en
helhet. På det sättet kan innehållet i omvårdnadsarbetet konkretiseras för både
personal och patienter vilket förhoppningsvis ger dem nya och bättre verktyg att
hantera en svår situation.

25
Övergripande syfte Baserat på mina utgångspunkter och argumentationen i rationalen är därför det
övergripande syftet att få ökad kunskap och förståelse för omvårdnad som process
i psykiatrisk vård ur patienters, studenters och personals perspektiv, med särskilt
fokus på alternativ till tvång vid självskadebeteende.

26

27
Metod Alla fyra delstudierna analyserades inom ramen för kvalitativ innehållsanalys men
tillvägagångssättet varierade beroende på typ av data (fokusgruppsintervjuer,
självskrivna patientskildringar och loggböcker). Innehållsanalys är en flexibel
metod som är användbar för att analysera olika typer av textmaterial (Graneheim
& Lundman, 2004). Enligt Krippendorff (2013) har en text flera olika meningar
då den kan läsas ur flera olika perspektiv beroende på vilken utgångspunkt och
erfarenhet forskaren har. Detta är förenligt med den abduktiva processen där
forskaren använder sin erfarenhet i analysen och pendlar mellan praktik och teori
(Krippendorff , 2013). Krippendorff anser vidare att en text inte har en
förutbestämd mening som ska identifieras utan betydelsen i texten arbetas
succesivt fram och synliggörs av forskaren under tolkningsprocessen. Med stöd av
innehållsanalysen så kan texter bearbetas på ett systematiskt sätt så att trovärdiga
slutsatser kan dras (Krippendorff, 2013). En sammanställning av delstudiernas
syften, deltagare, datainsamlings- samt analysmetod visas i Tabell 1.
Delstudie I
Deltagare och datainsamling
Potentiella deltagare kontaktades via sociala medier och brukarorganisationers
hemsidor. Via dessa kanaler gavs en kort information och en länk till en hemsida
där de potentiella deltagarna fick utförlig information om studien.
Inklusionskriterierna var att personen hade vårdats för ett självskadebeteende och
hade erfarenheter av tvångsåtgärder/av situationer där tvångsåtgärder kunnat
undvikas samt vara minst 18 år. På hemsidan fanns ett webbformulär, med
instruktionen ”skriv din berättelse här”, där deltagarna helt anonymt kunde
beskriva sina erfarenheter i fritext. Datainsamlingen pågick under ca tre månader

28
Tabell 1. Sammanställning av delstudiernas (I-IV) syften, deltagare, datainsamlingsmetod och
analysmetod.
Studie Syfte Deltagare Datainsamling Dataanalys
I Beskriva vilka uppfattningar personer med självskadebeteende har om alternativ till tvång i förhållande till deras erfarenheter av psykiatrisk slutenvård
19 personer Skrivna berättelser inlämnade anonymt via hemsida
Kvalitativ innehållsanalys
II Undersöka omvårdnad som process genom att beskriva sjuksköterskestudenters resonemang och erfarenheter av relationsskapande, behovsbedömningar och val av åtgärder i psykiatrisk vård.
14 sjuksköterske-studenter
Skrivna webbaserade loggböcker
Kvalitativ innehållsanalys
III Beskriva personals resonemang kring val av åtgärder i utmanande situationer i psykiatrisk slutenvård
8 skötare 10 sjuk-sköterskor 4 enhets- chefer 4 läkare
Fokusgruppsintervjuer Kvalitativ innehållsanalys
IV Beskriva personals uppfattningar av interprofessionellt samarbete i utmanande situationer i psykiatrisk slutenvård
8 skötare 10 sjuk-sköterskor 4 enhets-chefer 4 läkare
Fokusgruppsintervjuer Kvalitativ innehållsanalys
29
och genererade nitton berättelser. Det fanns inga frågor om
bakgrundsinformation men i berättelserna framkom att bland deltagarna fanns
både kvinnor och män i varierande åldrar samt att vissa hade erfarenhet från
rättspsykiatrin. Flera av deltagarna beskrev även tidigare erfarenheter från vård
inom barnpsykiatrin.
Analys
Analysen inleddes med att alla berättelserna sattes ihop till en text och lästes för
att få en förståelse för innehållet. Efter att ha läst berättelserna upprepade gånger
så utvecklades en analysstrategi som innebar att texten delades upp i två olika
grupper. En grupp bestod av kondenserade meningsenheter som beskrev
generella erfarenheter vården och den andra gruppen bestod av beskrivningar av
erfarenheter av alternativ till tvångsåtgärder samt önskningar och förslag till
alternativ. Texten i respektive grupp lästes på nytt och tre innehållsområden (jmf
Graneheim & Lundman, 2004) identifierades. I nästa steg anlyserades texten
genom att först sortera in textenheterna under respektive innehållsområde och
sedan kategorisera dem i flera steg. Respektive grupp genererade tre
subkategorier som låg till grund för de tre slutkategorierna som beskriver
önskningar i förhållande till reella erfarenheter.
Metodval och etiska överväganden
Jag övervägde under lång tid om forskningsprojektet gynnades av att fokusera på
en speciell patientgrupp. Mitt dilemma handlade om hur jag trodde att
avhandlingen skulle uppfattas. Valet att fokusera på en patientgrupp kunde bidra
till att avhandlingen uppfattades fokusera på en patientgrupps problematik i stället
för alternativ till tvång, samtidigt kunde valet att ha fokus på en patientgrupp
synliggöra det jag ville säga på ett tydligare sätt. Till slut så bestämde jag mig för
att det kunde vara mer meningsfullt att utgå från personer med
självskadebeteende. Beslutet grundades dels utifrån min yrkesmässiga erfarenhet
30
av att tvångsåtgärder sällan var nödvändigt för denna patientgrupp, men trots
detta användes frekvent. Samt att vid tidpunkten för revideringen av etikansökan
publicerades en artikel med aktuell statistik som visade på att tvångsåtgärder
ökade mest för gruppen unga kvinnor och att sjukhusvård efter självmordsförsök
eller avsiktlig självskada fördubblats för samma grupp under den senaste 15-års
perioden (Holm et al., 2011). Sammantaget kändes valet av grupp naturlig för att
företräda problematiken, så tanken är inte att arbetssättet är specifikt för just
denna patientgrupp, utan det var en grupp som var representativ utifrån syftet.
Att utsättas för tvångsåtgärder kan upplevas mycket traumatiskt och kan även
återuppväcka andra svåra minnen (Bonner, Lowe, Rawcliffe & Wellman, 2002).
Att berätta om dessa erfarenheter kan givetvis riskera att skapa ett ytterligare
lidande. Utifrån denna vetskap så övervägde jag studien och formen för
datainsamling noggrant. Kom dock fram till att det möjligen kan vara så att det
finns risk för att det blir en paternalistisk omtanke som innebär att personer som
har erfarenhet av att tvångvårdas inte alls kommer till tals. Det råder mycket stor
brist på studier som beskriver vårderfarenheter ur ett patientperspektiv men det
finns desto fler studier som beskriver personalens uppfattningar om och
erfarenheter av att vårda personer med självskadebeteende (James, Stewart &
Bowers, 2012). På hemsidan fanns information om studien och tydliga
uppmaningar om att inte delta i studien om personen trodde att deltagandet
kunde bidra till att de började må sämre. Jag hade kunnat välja att göra intervjuer
istället, för att kunna följa upp deltagarna på ett bättre sätt, men jag hade då missat
möjligheten till spridning av deltagare över hela landet. Genom den geografiska
spridningen så minskar risken för att berättelserna skulle vara beskrivningar från
samma enhet. Anonymiteten kan även skapa trygghet och bidra till mer
frispråkiga svar (O’Connor, Madge, Shaw & Wellens, 2008).

31
Delstudie II
Deltagare och datainsamling
Deltagarna i denna delstudie bestod av 14 före detta sjuksköterskestudenter som
under sin sjuksköterskeutbildning genomfört en fyra veckor lång kurs som var
verksamhetsförlagd inom olika typer av psykiatriska verksamheter. Kontinuerligt
under kursens gång skrev de loggbok där de beskrev sina reflektioner och sitt
arbete med en utvald patient. Urvalet skedde genom att loggböcker där studenter
fått betyget väl godkänd lästes i syfte att identifiera de studenter som lyckats
synnerligen väl med att skapa tillitsfulla relationer till utmanande patienter.
Ytterligare inklusionskriterium var att studenten arbetat självständigt och fått
sparsamt med feedback från läraren samt att läraren hade verifierat studentens
beskrivningar med handledare eller klinisk adjunkt.
Studenterna hade en studieuppgift i kursen som gick ut på att de skulle arbeta
med en patient över tid och med denne försöka skapa en tillitsfull relation,
identifiera behov och planera, utföra samt utvärdera de valda åtgärderna.
Fortlöpande skulle studenterna dokumentera sitt eget arbete i en webbaserad
loggbok, de skulle även genomgående reflektera över och argumentera för sina
bedömningar och val. De fick även vid några tillfällen feedback från lärare. Det
var enbart de själva och läraren som hade tillgång till loggboken. Studenterna var
inte medvetna om att deras texter skulle ingå i någon studie när de skrev
loggarna. De utvalda loggböckerna innehöll 5 000-15 000 ord vardera.
Analys
Analysen inleddes med att loggböckerna lästes igenom noggrant och texten
sorterades sedan in under tre innehållsområden (jmf Graneheim & Lundman,
2004), relation, behov och åtgärd, utifrån strukturen på studieuppgiften. Därefter
lästes texten inom respektive innehållsområde förutsättningslöst och analyserades
32
genom att meningsenheter identifierades som beskrev vad studenterna gör, hur
de gör det och med vilka argument/vilket syfte. Meningsenheterna
kategoriserades sedan i flera steg. Analysen resulterade i sex subkategorier och tre
huvudkategorier.
Metodval och etiska överväganden
Utifrån det övergripande syftet med avhandlingen så har denna delstudie utgått
från hypotesen, om man inte har tillgång till tvångsåtgärder och får stöd i att reflektera så
blir man mer kreativ i sitt vårdande och hittar alternativa lösningar. I min roll som lärare
så har jag inspirerats av filosofen och pedagogen John Deweys syn på lärande,
vilket också har påverkat forskningsprojektet. Enligt Biesta (2004), anser Dewey
att kunskap alltid handlar om relationen mellan handlingar och dess
konsekvenser, det vill säga tanke och handling kan inte åtskiljas på samma sätt
som teori och praktik är varandras förutsättningar. Att använda studenternas
loggböcker kändes utifrån detta perspektiv helt självklart. Det fanns en stor väl
bearbetad kunskapskälla i deras texter där Deweys resonemang kring sambandet
mellan teori, praktik och reflektion, kunde tillämpas och där studenternas
erfarenheter kunde tillvaratas.
Lärarens feedback till studenterna kan ha påverkat innehållet i loggböckerna och
därmed resultatet. Jag har dock tagit hänsyn till detta i urvalet så enbart
loggböcker där det förekommit sparsamt med feedback valdes ut. Feedbacken
lämnades kvar i det första analyssteget för att medförfattarna skulle kunna göra en
bedömning av lärarens eventuella påverkan. Det fanns även risk för att
studenterna idealiserat sina egna insatser, då studenten är i beroendeställning och
ska bedömas och betygsättas. Läraren hade en kontinuerlig kontakt med
handledare och kliniska adjunkter som bekräftade studenternas beskrivningar och
det verkade främst föreligga en risk för att studenterna tonat ner sin egen
betydelse och insats.

33
Det kan även anses problematiskt att studenterna läste kurslitteratur och utförde
studieuppgifter parallellt med skrivandet i loggboken samt att analysen utgick från
en studieuppgift. Då innehållet i datamaterialet blev styrt mot vissa teorietiska
utgångspunkter och givna ramar. Det fanns dock även en öppen ansats senare i
analysprocessen när studenternas beskrivningar av deras arbete och individuella
val inom respektive innehållsområde analyserades. Detta tillvägagångssätt
överensstämer väl med den abduktiva ansatsen då det är möjligt att växla mellan
teori och empiri för att succesivt öka förståelsen (Peirce, 1990). Innehållsanalys
beskrivs som en flexibel metod som kan användas i syfte att ge förslag på
praktiska, utbildnings och forskningsmässiga implikationer (Krippendorf, 2013),
vilket stöds av det pragmatiska förhållningssättet.
Att analysera en skriven, processad och reflekterad text skiljer sig en del från att
analysera en fenomenologisk kvalitativ intervju (jmf Kvale & Brinkmann, 2014),
även den fenomenologiska synen på kunskap skiljer sig från den pragmatiska.
Ricoeurs kunskapssyn utgår från ett empiriskt-holistiskt paradigm och har därmed
ett induktivt förhållningssätt (Thompson, 1981). Ricoeur (1976) menar på att
text inte är tal och skillnaden består i att tal är spontant och en text är tillrättalagd.
Ricoeur anser vidare att en berättelse ska vara så fri som möjligt från
teoretiserande och reflekterande för att nå ett djup i intervjun. Jag anser att texten
i loggböckerna har en annan typ av djup, även om tolkningsgraden inte är lika
hög, tack vare att studenterna har haft möjlighet att pröva, reflektera och
ompröva under en längre tid. Studenternas texter är reflekterade i en process i
flera steg och även till viss del bearbetade och teoretiserad mot kurslitteratur och
vetenskapliga artiklar. Först därefter startar den vetenskapliga analysprocessen där
det krävs ytterligare bearbetning och reflektion för att sammanställa innehållet i
texterna och formulera ett trovärdigt resultat av hög kvalitet. Jag jämför och

34
finner stöd för min argumentation om processen utifrån Herr och Anderssons
(2014) resonemang beträffande process validity. Enligt Herr och Andersson är
processtänkandet inte enbart begränsat till metoden utan bör vara ett
genomgående kvalitetskriterium och poängterar att det är viktigt att
bearbetningen inte stannar på ett ytligt plan utan är reflekterad på flera nivåer.
Med hänsyn till studenternas ringa erfarenhet så kan det diskuteras om studenter
var det bästa valet av deltagare, utifrån syftet med studien. Valet av deltagare till
denna delstudie utgick främst från det övergripande syftet då studenter är den
enda kategori vårdare, i patientnära arbete, som inte har tillgång till
tvångsåtgärder och därmed varit nödgade att utveckla andra alternativ. Dessutom
valdes endast de studenter som, enligt min bedömning, lyckats ovanligt bra med
att skapa relationer till uttalat ”svåra” patienter. Utifrån detta resonemang anser
jag att deltagarna i studien var bäst lämpade för att besvara forskningsfrågan men
inte i första hand för att de var studenter.
Delstudie III och IV
Deltagare och datainsamling
Alla skötare och sjuksköterskor (ca 50 personer) som arbetade på en
akutpsykiatrisk avdelning samt samtliga läkare och enhetschefer (ca 10 personer),
med erfarenhet av tvångsvård, som arbetade inom verksamhetsområdet tillfrågdes
om deltagande i studierna. Tjugoåtta tackade ja och tjugosex deltog slutligen i
fokusgruppsintervjuerna. Deltagarna fördelades i sex grupper utifrån
yrkestillhörighet (skötare, sjuksköterskor, enhetschefer och läkare) och erfarenhet
(mer eller mindre än 5 års erfarenhet av arbete inom psykiatrisk vård).
Datainsamling genom fokusgruppintervjuer ger möjlighet att ta del av
resonemang om ett givet ämne och genom interaktionen i gruppen belysa
komplexa beteenden och motiv (Morgan, 1997). Intervjuerna fokuserade på
35
synen på begränsande åtgärder och utgick från en vinjett (se nedan). Intervjun
inleddes med en öppen fråga ”Vad händer sen?” som följdes upp av frågan ”Vad
gör du?” Även klargörande frågor ställdes samt uppmuntrande kommentarer för
att utveckla olika resonemang. Ett protokoll användes för att kontrollera och
säkerställa att alla grupper diskuterade de förvalda områdena (bältesläggning,
extravak, ansvar och professionella roller) utifrån syftet. Under intervjuerna
deltog en moderator som ledde intervjun och en observatör vars uppgift var att
säkerställa att alla områden bearbetats och följa upp eventuella ”trådar” som
intervjuaren missade samt sköta inspelningen. I de grupper där någon deltagare
var mindre aktiv bjöd moderatorn in deltagaren i samtalet genom att ställa någon
fråga direkt till personen.
Vinjett: På avdelningen vårdas sedan en vecka en ung kvinnlig patient. Hon har tidigare
vårdats inneliggande vid ett flertal tillfällen och vårdas nu enligt lagen om psykiatrisk
tvångsvård efter en paracetamolintox i oklart syfte. Vid upprepade tillfällen har begränsande
åtgärder vidtagits i samband med att hon skadat sig själv eller andra inne på avdelningen.
Hela personalgruppen (skötare, sjuksköterskor, läkare, enhetschef) sitter och dricker
morgonkaffe. Personalen ser från fikarummet hur patienten springer genom korridoren fram
till ett kvarglömt dricksglas. Hon plockar upp glaset och slänger det i golvet så att det går
sönder, plockar upp en stor glasskärva och börjar skära sig i djupt i armen samtidigt som
hon skriker: - Släpp ut mig!
Analys delstudie III
Analysen inleddes med att alla intervjuer lästes som en helhet och utifrån syftet så
formulerades tre frågor som stöd för att strukturera upp analysen. Den första
frågan var ”varför väljer deltagarna att göra som de gör?” och meningsenheter
som beskrev resonemang kring val av åtgärder sorterdes ut och fyra olika
skäl/anledningar till deras val identifierades. Meningsenheterna kondenserades
och deltagarnas resonemang runt dessa skäl/anledningar lästes på nytt och

36
tolkades sedan vidare tills fyra fokus som karaktäriserade deras resonemang kunde
formuleras. Den andra frågan ”Vilka olika åtgärder väljer deltagarna?” besvarades
genom att identifiera vilka typer av åtgärder som beskrevs i de befintliga
meningsenheterna, vilket resulterade i att åtta åtgärder identifierades. För att
identifiera hur deltagarna förhöll sig till patienten vid utförande av åtgärden
ställdes en tredje fråga ”Hur utfördes åtgärden?”. För att besvara den frågan
sammanfördes resonemangen om fokus med åtgärd, till exempel alla resonemang
som tolkats som rutinmässiga (fokus) och handlade om samtal (åtgärd) bildade en
grupp etcetera. Genom att sedan upprepade gånger läsa de olika resonemangen
som gick att koppla till respektive åtgärd så identifierades 26 olika förhållningssätt
som var karaktäristiska utifrån resonemangen och i förhållande till varje åtgärd.
Under hela processens gång så skedde omvärderingar och korrigeringar utifrån
diskussioner i forskargruppen. Avslutningsvis ställdes den övergripande frågan
”Hur kan deltagarnas resonemang om val av åtgärder beskrivas?” Den frågan
besvarades genom att hela texten lästes på nytt och ställdes i förhållande till
resultatet. Det tolkade svaret formulerades och bildade det övergripande temat.
Analys delstudie IV
Även i denna analys lästes den utskrivna intervjutexten som en helhet. Utifrån
syftet valdes meningsenheter ut, kondenserades och sorterades upp utifrån grupp
och profession. I ett första steg identifierades och formulerades föreställningar
kring yrkesspecifika förhållningssätt som framkommit om respektive
profession/yrkesgrupp. För att urskilja hur deltagarna ser på arbetet i teamet och
det gemensamma ansvaret bearbetades och tolkades meningsenheterna på nytt,
oberoende av yrkesgrupp, och fyra typer av förväntningar identifierades och
formulerades. I det tredje steget så sorterades de yrkesspecifika meningsenheterna
ut för att få svar på hur deltagarna såg på det yrkesspecifika ansvaret.
Avslutningsvis tolkades hela resultatet som en helhet och ett gemensamt tema
identifierades.

37
Metodval och etiska överväganden
Tvångsåtgärder kan upplevas svåra att prata om då personal kan känna sig
ifrågasatta och sårbara när de ska beskriva arbetsuppgifter kopplade till tvång
(Olofsson, 2005). Lützén och Schreiber (1998) menar dock att fokusgrupper kan
vara att föredra när intervjuer ska genomföras inom psykiatrisk vård med
motiveringen att psykiatrisk omvårdnad är en kommunikativ och interagerande
verksamhet där personalen är van att diskutera vårdrelaterade frågor i formella
och informella grupper.
Uppgiften att vara moderator alternerades med en av medförfattarna 3. Vi
reflekterade över vem av oss som skulle vara lämpligast till att göra intervjuerna i
respektive grupp. Vi kom fram till att jag som varit skötare i många år skulle
ansvara för intervjuerna med skötarna. Jag hade även arbetat med några av dem
och hade då varit en ”insider” men i forskarrollen blev jag nu en ”outsider”.
Vilket kan jämföras med Herr och Anderssons (2014) resonemang kring
positionering utifrån etnicitet, kön, tidigare yrkesroll etcetera. Herr och
Andersson menar att positionering kan vara på olika nivåer. I detta fall så hade vi
en gemensam bakgrund utifrån både yrkesroll och i vissa fall personlig kännedom
så då kunde jag eventuellt ha en fördel och till viss del bli en insider. Vårt
resonemang utgick ifrån att de kanske kände en större tillit och trygghet till mig
då jag har varit ”en av dem”, jämfört med min kollega som de endast kände till i
yrkesrollen som sjuksköterska och forskare.
3 Deltstudierna III och IV genomfördes i samarbete med doktorand Sebastian Gabrielsson och finns även inkluderade i dennes avhandling "A moral endeavour in a demoralizing context: Psychiatric inpatient care from the perspective of professional caregivers".

38
När vi diskuterade val av moderator till läkargruppen så blev det istället en
genusfråga. Vårt resonemang utgick från att de flesta läkarna var män och att de
eventuellt skulle känna en större samhörighet (jmf Herr & Anderssons
resonemang ovan) och respekt för min kollega då han också var man. Möjligen
var detta resonemang bara ett uttryck för våra stereotypa fördomar, men så
resonerade vi. Gunnarsson (2007) hänvisar till Haavinds koncept om den relativa
underordningen av kvinnor och Gunnarsson menar att det är viktigt att reflektera
över och synliggöra makt (o)balanser under forskningsprocessens gång. I detta fall
så tänker jag att vi nyttjade eventuella fördelar med att min kollega var man för
att gynna vårt eget mål om att få så innehållsrika intervjuer som möjligt, utifrån
syftet i studien. Resterande grupper delades upp utifrån att modererandet skulle
fördelas jämt, det vill säga min kollega var moderator för sjuksköterskorna och jag
var moderator i fokusgruppsintervjun med enhetscheferna.
Vi upplevde inga svårigheter med att få deltagarna att diskutera men i vissa
grupper var det någon deltagare som var lite lågmäld. Vi hade kunnat få andra
typer av diskussioner om vi valt att ha yrkesmässigt blandade grupper, men ansåg
att det möjligen kändes tryggare att samtala om ansvar och roller inom sin egen
yrkeskår. Dessutom så kunde möjligen en chefs närvaro, i blandade grupper, ha
en hämmande inverkan (Morgan, 1997). Det var ett procentuellt större bortfall i
skötargruppen som var den största yrkeskategorin på avdelningen. En tänkbar
anledning kan vara att många av skötarna arbetade enbart nattskift och de hade
inte möjlighet att delta i intervjuerna under sin ordinarie arbetestid.
Vinjetten beskriver en situation där en person skadar sig själv men i övrigt finns
ingen djupare beskrivning av patientens problematik och diagnos, vilket var ett
medvetet val, då vi vill att fokus skulle vara på hur personal resonerar och agerar
utifrån en situation som kunde anses som utmanande.
39
Metasyntes I syfte att få ytterligare kunskap och förståelse för omvårdnad som process i
psykiatrisk vård genomfördes en metasyntes av delstudiernas resultat. Walsh och
Downe (2005) menar att i en metasyntes integreras resultat från ett antal olika,
men inbördes relaterade, kvalitativa studier i ett tolkande syfte.
Datamaterialet var förutbestämt och begränsat och metasyntesen genomfördes
med stöd av metoder beskrivna i kvalitativ innehållsanalys (Graneheim &
Lundman, 2004). Analysen utgick ifrån omvårdnad som process med tre tydligt
avgränsade områden, relation, behov, samt åtgärder och förhållningssätt och dessa
områden skapade strukturen för analysen. Analysprocessen inleddes med att
resultattexten från delstudierna I-IV lästes upprepade gånger och text som beskrev
relation och relationsskapandet, behov och bedömningar och åtgärd och
förhållningssätt identifierades och sorterades upp i tre grupper. Därefter
formulerades meningsenheter under respektive innehållsområde (jmf Graneheim
& Lundman, 2004) och liknande beskrivningar sammanställdes med utgångspunkt
i vad som minskar respektive ökar risken för tvångsåtgärder. Slutligen
identifierades nyckelord och meningar från respektive innehållsområde som
sammanställdes i en figur (figur 1) som ska symbolisera en dynamisk process och
visa på respektive områdes centrala innehåll. Resultatet presenteras utifrån
respektive innehållsområde (relation, behov, åtgärd). Hänvisning till respektive
delstudie finns angiven inom parentes med romerska siffror.

40
41
Resultat
Sammanfattning av resultatet från delstudie I-IV
Delstudie I
Resultatet bygger på beskrivningar från 19 personer med erfarenhet av att ha
vårdats på en psykiatrisk enhet för ett självskadebeteende. Analysen resulterade i
tre kategorier. Genomgående så fanns en stor diskrepans mellan deltagarnas
önskemål och deras reella erfarenheter. De beskrev en önskan om att vårdarna
skulle se och förstå deras behov och att de skulle blir bli sedda och lyssnade till.
Deras erfarenhet var dock att de ofta blev negligerade och kände då en stor
maktlöshet. När de kände sig övergivna av vårdarna så sökte de egna
copingstrategier för att hantera sin ångest vilket i sin tur ofta resulterade i
tvångsåtgärder. I de fall som vårdarna kunde tolka deras signaler och förstå
situationen utifrån deras perspektiv så gick det att hitta individuella lösningar för
att möta deras behov, och tvångsåtgärder var inte nödvändiga. Deltagarna
önskade också en ömsesidig relation med vårdarna men möttes ofta med misstro.
Deltagarna beskrev ifrågasättande distanserade vårdare som hotade med
tvångsåtgärder, vilket ledde till att vårdarna upplevdes som fienden. Vårdarnas
fokus var ofta på att minimera risker för självskada genom olika begränsningar
istället för att försöka bygga en tillitsfull relation som beskrevs som den viktigaste
faktorn för att öka välbefinnandet och minska risken för självskada. I den
avslutande kategorin beskrev deltagarna att de vill ha en professionell vård men
deras erfarenheter var att vården ofta var kontraproduktiv. Övervakning och
disciplinering i en rigid och kaotisk vårdmiljö var vanliga beskrivningar, vilket
medfört att många av deltagarna helt förlorat tilltron till vården. Deltagarna
beskrev att i en professionell vård ingick bland annat flexibla individuella
42
vårdplaner som upprättades i samarbete med patienten, vårdpersonal med rätt
kompetens och möjlighet att få prata med en läkare som känner patientenen.
Delstudie II
Resultatet i delstudie två utgick från 14 sjuksköterskestudenters loggböcker och
resulterade i tre kategorier som beskriver resonemang och utförande av
relationskapande, behovsbedömning och utförande av åtgärderer som
sammantaget bildar ”the process of care”. I första kategorin beskrivs vikten av att
ha tillit till den tillitsfulla relationen. Med tillitsfull avsågs att patienten kände sig
trygg i studentens sällskap och hade tillräcklig tillit för att kunna uttrycka sina
tankar och upplevelser om sin aktuella situation. Utan en tillitsfull relation så
menade studenterna på att det fanns en uppenbar risk för felbedömningar och att
behov förbisågs eller att patienten tillskrevs behov de inte hade. Tillgänglighet,
bekräftelse, genuint engagemang, respekt, samhörighet och ärlighet var faktorer
som ansågs viktiga för relationsskapandet. Hinder för relationskapandet kunde
vara fördomar om och etikettering av patienter men även patienternas symtom.
Behovsbedömningarna handlade framförallt om att ge röst åt de outtalade
behoven. Detta gjordes genom att studenterna var mycket receptiva för att
försöka förstå och tolka tecken hos patienter som inte hade förmågan att själva
uttrycka sina behov. De identifierad basala behov så som sömn och nutrition men
framförallt såg de mer abstrakta behov som hopp, stärkt självkänsla och
empowerment. Utförande av åtgärder handlade till stor del om att balansera
mellan ett utförande av åtgärden och ett medvetet förhållningssätt. Åtgärderna
syftade till att tillgodose individuella behov och ta tillvara patientens förmågor för
att främja en positiv återhämtningsprocess.

43
Delstudie III
Resultatet utgår från olika personalgruppers resonemang kring val av åtgärder vid
utmanande situationer. Utifrån resonemangen identifierades åtta olika val av
åtgärder: agera (akut), samtala, vara med, aktivera, bälteslägga, övervaka,
tvångsmedicinera samt utskrivning, som utfördes med fokus antingen på
personalens behov, patientens upplevelse, att följa rutiner eller att uppfostra
patienter. Beroende på fokus identifierades 26 olika förhållningsätt vid utförandet
av de olika åtgärderna. Som exempel kan nämnas att vid samtal som utgick från
fokus på patientens upplevelse så hade vårdarna ett förhållningssätt där de visade
på att de var intresserade av att lyssna och försöka förstå patientens situation och
behov. Vilket kan jämföras med ett uppfostringsfokus där samtalet istället var av
klargörande karaktär och vårdarna hade då ett förhållningsättet med fokus på att
patienten skulle förstå ”vad som gäller”. Det övergripande temat visar på
spänningen mellan att lösa personalens problem eller att tillgodose patientens
behov.
Delstudie IV
Resultatet bygger på samma fokusgruppsintervjuer som delstudie III men syftar
till att beskriva personalens syn på samarbete utifrån olika professionella roller.
Läkaren beskrivs som den distanserade beslutsfattaren, enhetscheferna som
misstänksamma övervakare, sjuksköterskorna som förmedlande dämpare och
skötarna som informerade utförare. De olika yrkesgrupperna beskriver att de har
gemenamma ansvarsområden men också ett yrkesspecifikt ansvar i samband med
utmanade situationer. Utmärkande var att skötarna, trots att de hade lägst formell
kompetens, var den yrkesgrupp med störst inflytande vid beslut om
tvångsåtgärder eftersom de arbetade närmast patienterna och därför hade
förstahandsinformation om dem.
44
Omvårdnad som reflekterande praktik
Resultatet som presenteras nedan är en tolkad sammanställning av delstudiernas
resultat utifrån delarna relation, behov och åtgärder, i omvårdnad som process. I
metasyntesen framkommer att reflektion verkar vara en avgörande faktor för
vilken typ av bedömningar och vilka val vårdare gör. Resultatet förstås och
omsätts i diskussionen utifrån bland annat Schöns (1983) teori om reflection-in-
action och reflection-on-action, vilket innebär att reflektion över handling bör ske
både i den aktuella situationen såväl som efter. Olika former av stöd till reflektion
bedöms vara ett meningsfullt verktyg i det arbetssätt som här benämns som
omvårdnad som reflekterande praktik. Resultatet inleds med en övergripande
beskrivning av syntesen med dess centrala innehåll om procesen, vilket också
illustreras med en figur (figur 1). Därefter beskrivs innehållet i varje del av
processen mera ingående.
Syntes
Tolkningen av de sammanvägda resultaten visar att varje del av processen bygger
på och är beroende av varandra. Att vårdaren har förmågan att bygga upp en
tillitsfull relation till patienten är en förutsättning för en relevant
behovsbedömning och identifiering av patientens förmågor. Bedömning av
individuella behov är i sin tur utgångspunkten för val av åtgärd och
förhållningsätt med målet att minska lidande och öka välbefinnande. Vägen till
åtgärden är i denna process dock inte statisk eller linjär, till en början kan
exempelvis åtgärder enbart ha ett relationskapande syfte, behov kan förändras,
åtgärder behöva modifieras liksom att tilliten i relationen kan påverkas av olika
faktorer. Detta innebär att vägen till åtgärden bör förstås som en dynamisk process
som förutsätter ett reflekterande förhållningssätt med relationen som grund, med
det övergripande målet att stärka patientens förutsättningar till återhämtning och
välbefinnande.

45
Relation
Tillit Ömsesidighet
Ärlighet Bekräftelse
Respekt
Behov
Lyssna och förstå Identifiera basala
och abstrakta behov
Åtgärd
Öka välbefinnande och minska lidande Tillvarata förmågor
och resurser Medvetet förhållnings-
sätt Flexibilitet
Figur 1. Översikt över resultatet av metasyntesen. Med utgångspunkt i en förstå-
else av omvårdnad som process beskrivs omvårdnad i psykiatrisk vård som en re-
flekterande praktik där de olika delarna i processen är beroende av och samspelar
med varandra.
46
Relation Resultaten visar på att tillit är grunden i relationsskapandet (I,II,III) och
förutsättningar för tillit skapas via ömsesidighet, ärlighet, bekräftelse samt att
lyssna och genuint försöka förstå patientens situation (I,II). Relationen anses
tillitsfull när patienten känner sig tillräcklig trygg i vårdarens4 sällskap så att denne
vågar uttrycka sina tankar och upplevelser om sin aktuella situation (II). En
tillitsfull och ömsesidig relation mellan patient och vårdare är den enskilt
viktigaste faktorn till att patienterna känner ökat välbefinnande under vårdtiden
(I) och en förutsättning för att kunna identifiera patientens behov och förmågor
(II). Om patienterna känner tillit till personalen så är tvångsåtgärder5 oftast
överflödiga (I,II,III). I vissa fall kan tvångsåtgärder accepteras av patienten om
syftet med åtgärden är välmotiverat och utförs av vårdare som patienten känner
tillit till (I). Om tvångsåtgärder utförs på ett empatiskt och respektfullt sätt, även
om åtgärden går emot mot patientens önskan, så behöver inte ingripandet
påverka relationen negativt (II,III) men det kan också i vissa situationer vara värt
att gå emot verksamhetens regler och rutiner för att undvika att skada en tillitsfull
relation till patienten (II,III). Svåra symtom hos patienter, som paranoida
vanföreställningar och djup melankoli, (II) samt vårdarnas distansering från och
fördomar om patienterna är faktorer som försvårar relationskapandet (I,II). När
patienten inte känner tillit till vårdarna drar sig patienten undan på avdelningen
och undviker att berätta om hur de mår (I,II) och kan sedan avstå från att söka
hjälp trots svårt lidande och akuta vårdbehov (I).
4 Med vårdare avses generellt de som arbetat med patienten (både professionella och studenter) när resultatet är professionsspecifikt så anges den yrkestitel som avses
5 Med tvångsåtgärd avses alla handlingar som går emot patientens önskningar och vilja

47
Behov
För att kunna göra en individuell bedömning av patientens behov krävs det att
vårdaren tar sig tid att lyssna till och försöka förstå det patienten vill berätta men
minst lika viktigt i bedömningen är att försöka identifiera behov som patienten
inte kan kommunicera verbalt. Dessa outtalade behov kan istället uttryckas via
individuella eller mer generella tecken och beteenden exempelvis självskada
(I,II,III). De flesta behoven är inte så påtagliga utan av mer abstrakt karaktär (II).
Att identifiera och ta tillvara patienternas förmågor och resurser är också
grundläggande i en individuell vårdplanering (I,II,III). Det är viktigt att utgå från
patientens perspektiv och att patienten ges möjlighet till aktivt deltagande vid
planeringen och utformningen av vården (I,II,III). När vårdarna är tillgängliga, lär
sig att tolka patientens tecken och tillsammans med patienten identifierar
individuella lösningar för att tillgodose både basala och abstrakta6 behov så kan
tvångsåtgärder undvikas eller avstyras (I,II,III). Bedömningar och ordinationer på
tvångsåtgärder som inte överensstämmer med patienternas behov och strider mot
patientens bästa kan ifrågasättas och även ignoreras (III,IV). Om patienten inte
känner tillit till vården och vårdarna och därför inte vågar uttrycka hur de mår så
är det inte heller möjligt att göra en individuell bedömning av patientens behov
(I,II).
Andra faktorer som försvårar bedömningen och ökar risken för tvångsåtgärder
kan vara att vårdarna inte lyssnar eller tror på patienten eller inte förstår vad
patientens beteende står för (I,II). Bedömningarnas kvalitet kan också påverkas av
personalbrist, överbeläggningar, hög personalomsättning (III), osäkra läkare (IV)
och slentrianmässigt tänkande, till exempel ”hopplösa patienter” (I,II,III).
Bedömningarna kan även ha sin utgångspunkt i föreställningen att patienten
simulerar eller inte förstår sitt eget bästa (I,III). Andra vanliga uppfattningar är att
6 Med abstrakta behov avses här patientens behov som inte är påtagliga (synliga) eller objektivt mätbara som till exempel hopp, självkänsla, empowerment och initiativförmåga

48
patienten bara vill ha uppmärksamhet, och därför inte ska få det, eller att
beteendet hör till sjukdomsbilden samt att fokus ligger på problem istället för
förmågor och möjligheter (II,III). Beslutsmakten är kopplad till skötarna som
arbetar närmast patienten (IV), i vissa fall sammanfaller det med en tillitsfull
relation vilket höjer kvaliteten på bedömningen men i andra fall baseras
bedömningarna enbart på distanserade observationer och tolkningar från
vårdarnas perspektiv (I,III,IV). När bedömningarna fallerar och patientens
individuella behov inte identifierades så känner sig patienten övergiven (I) och
upplever en känsla av hopp- och maktlöshet (I,II). För att klara av vården
använder/utvecklar patienten coping strategier som ur vårdarnas perspektiv ses
som destruktiva. Vårdarna förstår inte patientens tecken och bedömer då
beteendena som oacceptabla utspel (I,II,III), vilket i sin tur ofta leder till
tvångsåtgärder eller utskrivning (I,III).
Åtgärd
Valet av åtgärder7 bör präglas av öppenhet och flexibilitet samt utfromingen av
åtgärden av individanpassning och patientdelaktighet. De åtgärder som patienten
ska erbjudas under vårdtiden, om möjligt utifrån patientens egna förslag,
dokumenteras (I,II,III). Speciellt viktigt är det att formulera vilka åtgärder som
ska vidtas vid tecken på försämring för att kunna arbeta preventivt (I,II,III). En
åtgärd kan vara ett samtal eller en promenad (II,III) men också att läsa dikter,
jonglera, rensa avlopp eller möblera om patientsalar (II). Kvaliteten på utförandet
av varje åtgärd är beroende av vårdarens förhållningssätt. Förhållningsätt som
utgår från bedömningen av de individuella behoven och förmågorna kan vara
exempelvis stärkande, bekräftande, uppmuntrande, stödjande, lugnade, etcetera
(II, III). Om vårdaren har ett medvetet individuellt anpassat förhållningssätt med
7 Med åtgärd avses alla handlingar som utförts utifrån en bedömning av individuella behov med målet att lindra lidande och
öka välbefinnande.

49
hänsyn till patientens behov så ökar patientens förutsättningar att komma vidare i
sin återhämtningsprocess (I,II,III). Andra förhållningssätt som distansering och att
ignorera patientens behov skapar istället ett lidande hos patienten (I) även en
uppfostrande approach med fokus på kontroll, beteende korrigering och straff är
vanligt förkommande (I,II,III) vilket medför att patienten inte vågar berätta för
vårdarna hur de mår och förebyggande åtgärder kan därmed inte vidtas (I).
Extravak är en vanlig åtgärd som innebär en stor påfrestning för både patient och
vårdare (I,III). Extravak innebär också att en vårdare kan avsätta all sin tid till en
patient och har en unik möjlighet att tillgodose behov och stärka och stödja
patientens förutsättningar (II). Dock är uppfostrande och distanserad
förhållningssätt vanliga vid extravak (I,III) utifrån argumentet att det är viktigt att
patienter som vill ha uppmärksamhet inte ska få det (III).
Att läkaren kontinuerligt träffar patienten för utvärdering och samtal är en viktig
förutsättning för att patienten ska kunna vara delaktig i sin vård istället för att
skötare för patientens talan med läkaren (I, IV). En individuell vårdplan som
präglas av kontinuitet, förutsägbarhet, individanpassning och flexibilitet är ett
värdefullt verktyg för att minska risken för tvångsåtgärder medan generella regler i
verksamheten komplicerar arbetet (I,II,III). När vårdare använder förhållningssätt
och åtgärder som är stärkande och ger stöd till patienten så behöver sällan
tvångsåtgärder användas (I,II,III). Däremot är tvångsåtgärder frekvent
förekommande i situationer där patienter anses vara i behov av
beteendekorrigering och bestraffning eller är övergivna av vårdarna. Likaså finns
tillfällen då vårdarna provocerar fram situationer för att få en anledning att
använda tvångsåtgärder (I,III) liksom att det finns tillfällen där vårdarna går emot
kollegornas bedömning för att kunna utföra åtgärder för att tillgodose patientens
behov (I,II,III).

50
51
Diskussion och kliniska implikationer I litteraturgenomgången har jag hittat gott stöd för vikten av en god relation i
omvårdnadsarbetet (Cleary, Hunt, Horsfall & Deacon, 2012; Halldorsdottir,
2008; Shattell, 2004; Shattell, Starr, & Thomas, 2007; Zugai, Stein-Parbury, &
Roche, 2015 m.fl.) och en hel del erfarenheter och utvärderingar av olika
interventioner och arbetssätt, till exempel personcentrering i psykiatrisk vård
(Beckett et al., 2013; Gabrielsson, Sävenstedt & Zingmark, 2015; Jormfeldt,
Rask, Brunt, Bengtsson & Svedberg, 2012; Matthias, Salyers, Rollins & Frankel,
2012 m.fl.). Sedan hittade jag även ett starkt stöd för de delar av mitt resultat som
visar på att vården ofta inte fungerar på ett sådant sätt att en god relation med
patienten prioriteras (Enarsson, Sandman & Hellzén, 2011; Hörberg, Sjögren &
Dahlberg, 2012; Lindgren, Aminoff & Hällgren Graneheim, 2015; Lindström,
1995; Örmon, Torstensson-Levander, Sunnqvist, & Bahtsevani, 2014 m.fl.).
Dessutom beskriver vårdare olika svårigheter med att bedriva en god vård så som
tidsbrist, vårdkultur, regler samt avsaknad av stöd och ledning (Delaney &
Johnson, 2014; Enarsson, Sandman & Hellzén, 2008; Looi & Hellzén, 2006
m.fl.). Andra studier visar på att det finns svårigheter med att omsätta teorier till
praktisk handling (Carlyle, Crowe & Deering, 2012; Gask & Coventry, 2012;
Jormfeldt, Svedberg, Fridlund & Arvidsson, 2007; McCance, McCormack &
Dewing, 2011; O`Donovan, 2007 m.fl.). Sammanfattningsvis kan man med stöd
i litteraturen hävda att vi vet hur god omvårdnad inom den psykiatriska vården
borde vara men inte så mycket om dess konkreta innehåll och hur man gör för
att realisera kunskapen i praktiken (jmf Barker & Buchanan-Barker, 2011)8.
8 Barker och Buchanan-Barker anser att ”mental health nursing” fortfarande är en myt, då sjuksköterskor (även lärare och forskare inom området) tycker att ”mental health nursing” är bra och viktigt men få kan definiera och konkretisera vad som är syftet och innehållet i begreppet.

52
Min intention är att kunna ge ett bidrag till den senare delen genom att diskutera
mitt sammantagna resultat mot, enligt mig, för ändamålet relevanta teorier. Jag
har ambitionen att utifrån beskrivningen av omvårdnad som reflekterande praktik
formulera ett arbetssätt som ska vara lätt att implementera och tillämpa.
Arbetssättet ska förhoppningsvis kunna bidra till en minskat behov av
tvångsåtgärder och ökad kvalitet i vården samt erbjuda personal konkreta och
flexibla verktyg i det patientnära arbetet. Ett möjligt sätt för att utvärdera
arbetssättet, som även skulle kunna bidra till att överbrygga klyftan mellan teori
och praktik, kunde vara projekt som utgår från en interaktiv forskningsmetodik
som exempelvis aktionsforskning.
Jag anser att det finns en allvarlig missuppfattning i den psykiatriska vården idag.
När vi identifierar brister så ropar många efter mer rutiner och när misstag begåtts
så är det rutinerna som brustit, men en rutin blir aldrig bättre än det innehåll som
den vilar på. Patienter suiciderar inte mindre för att det görs suicidbedömningar
eller för att det skrivs vårdplaner om inte den enskilde vårdaren och
organisationen tar ett ansvar för innehållet i vården. Det framgick tydligt, ur alla
tre perspektiven, att användningen av tvångsåtgärder inte minskade när vårdarna
följde rutinerna utan tvärtom så var det när vårdarna lyckades förstå patientens
behov och hade frihet/mod att ”tänka utanför boxen” och hitta individuella
lösningar som tvångsåtgärder kunde undvikas. För att höja kvaliteten på vården
måste vårdarna erbjudas en möjlighet att ge god vård och för det krävs att
vårdarna har kunskap, självkännedom och framförallt mod att förändra. För att
uppnå detta krävs både personligt och organisatoriskt stöd och konkreta verktyg
som kan stödja personalen.
Resultatet i denna avhandling visar tydligt på att en ömsesidig och tillitsfull
relation mellan patient och vårdare är helt avgörande för vårdens kvalitet. Zugai
et al. (2015) översikt visar på att acceptans, ärlighet, respekt, förståelse och en icke
dömande attityd är exempel på faktorer som kan bidra till en god relation, vilket
53
överensstämmer väl med våra resultat. Zugai et al. menar vidare att reflektion,
kunskap och självkännedom är viktiga förutsättningar för att utveckla sin
relationsskapande förmåga (Zugai et al., 2015). För patienterna räcker det inte
med att ”bara” ha en tillitsfull relation till vårdaren utan det är också viktigt att
komma vidare och se deras behov och arbeta med konkreta åtgärder (Shattell et
al., 2007). Detta anser jag ger stöd för vikten av att se relationsskapandet som en
självklar och avgörande del i det konkreta omvårdnadsarbete men även att
relationen ingår i en större dynamisk individanpassad process som även omfattar
behovsbedömningar och åtgärder med målet att främja hälsa och välbefinnande
(jmf Svedberg, Jormfeldt, Fridlund & Arvidsson, 2004)9. Detta medför att
omvårdnadasarbetet blir ett komplext arbete som kräver kunskap men framförallt
flexibelitet och förståelse.
Omvårdnadsplanering
Resultatet i denna avhandling beskriver en översiktlig struktur för
omvårdnadsarbetet som betonar relationen, behov och åtgärder. Detta skiljer sig
från en vanligt använd modell där omvårdnadsprocessen beskrivs som en
problemlösningsmodell (Yura & Walsh, 1988) med fokus på datainsamling,
diagnostik och interventioner (Carnevali, 1983; Gordon, 2002).
En omvårdnadsplanering blir aldrig bättre än den bedömning den stödjer sig på
därför är det viktigt att bygga en god grund för bedömningen via en tillitsfull
relation. Vidare för att kunna göra en relevant vårdplan så ska en aktiv
patientdelaktighet eftersträvas för att skapa en atmosfär som stimulerar till
ömsesidigt kunskapsutbyte i samarbetet mot det gemensamma övergripande målet
om återhämtning. Relationsskapandet bör tydligt lyftas fram och dokumenteras
både till innehåll (relationsskapande åtgärder) och till progress (utvärdering av
9 Svedberg et al. argumenterar för vikten av en mer processfokuserad omvårdnad med hälsa som ett tydligt uppsatt mål för varje omvårdnadsintervention

54
tillit). Vid behovsbedömningen ska både basala och abstrakta behov samt
förmågor identifieras liksom patientens beskrivning av sin situation och vilka
tecken som vårdarna bör känna igen och vara uppmärksamma på. I planering av
åtgärder så ska patientens förmågor och resurser vara utgångspunkten. Åtgärden
ska tydligt gå att koppla ihop med patientens individuella önskemål (om möjligt)
och behov och därmed bör det finnas en stor flexibilitet och öppenhet såväl till
val av åtgärd som till utformning och till vårdarens förhållningssätt. Rigida regler,
distanserade förhållningsätt och ett beteendekorrigerande synsätt är exempel på
faktorer som ökar risken för tvångsåtgärder.
Reflektion
För att vårdare ska kunna arbeta på ett sätt som beskrivs ovan krävs att de får
relevanta förutsättningar. Det framkommer tydligt i resultatet att de vårdare som
förstått den unika individens behov och både kunnat och vågat individanpassa
åtgärderna inte har haft något behov av att använda tvångsåtgärder. Enligt Schön
(1983) har varje arbetsrelaterad situation unika inslag, inte minst inom vården,
och därför blir det svårt att utgå från generella teorier, mallar och rutiner. Schön
anser, utifrån sin teori om reflection-in-action och reflection-on-action, att det
istället är mer meningsfullt att reflektera över varje aktuell situations egenheter
och komma fram till en för situationen/individen anpassad handlingsplan. Liksom
Dewey (1938) anser Schön att tanke och handling är sammanvävda och Schön
menar på att reflektion är svar på en störning och genom att stanna upp så kan en
skicklig praktiker se nya infallsvinklar och har då möjlighet att ompröva sina
bedömningar (Schön, 1983).
För att anamma ett sådant arbetssätt behöver vårdarna både tid och stöd för att
utveckla en professionell trygghet och självkänsla så att de har mod att ifrågasätta

55
och frångå regler och rutiner när det behövs (jmf Huckshorn, 2014)10. Samtidigt
som de behöver utrymme för kontinuerlig reflektion och utvärdering utifrån
konkreta situationer för att utveckla sin bedömningsförmåga och professionella
kompetens (jmf Thorne & Hayes, 1997)11. Vårdarna behöver även en tydlig
vetenskaplig ram att förhålla sig till, vilket i detta fall skulle vara
omvårdnadsperspektivet (Meleis, 2011)12 samtidigt som omedvetna ramar 13
(begränsningar) synliggörs och ifrågasätts (Schön, 1983). Thorne och Hayes
(1997) har också anammat Schöns tankar och menar på att både reflection-in-
action och reflection-on-action gör vårdaren både mer uppmärksam i situation
men det ökar också den professionella medveten och därmed utvecklingen av
praktiken genom att stimulera till att ”tänka omvårdnad”.
Huckshorn (2014) menar att utbildning och förebyggande arbete är viktiga
faktorer för att minska behovet av tvångåtgärder men en minst lika viktig faktor
är att minimera antalet regler på avdelningen för att därigenom minska
förekomsten av konfliktsituationer. Detta synsätt stämmer väl överens med
Hejlskov Elvéns och Abilds (2015) beskrivning av lågeffektivt bemötande som kan
vara ett lämpligt förhållningssätt inom psykiatrin för att minska behovet av
tvångsåtgärder. Det finns mycket att vinna på att hitta arbetssätt som minimerar
tvångsåtgärder då åtgärderna upplevs traumatiserande både för patienter och för
personal. Tvångsingripanden kan skada den vårdande relationen och vården
bidrar då inte till återhämtning (Huckshorn, 2004). Min tanke är att figur 2 kan
utgöra en grund för utbildning och ett stöd för reflektion både i handling och
10 Huckshorn intervjuade personal om deras erfarenheter av hur de hade kunnat minska behovet av tvångsåtgärder och en viktig faktor var att de hade minskat antalet konfliktsituationer genom att minimera avdelningens regler.
11 Thorne och Hayes beskriver omvårdnad ett individualiserat, reflexivt och kontextberoende fenomen.
12 Enligt Meleis omfattas omvårdnadsperspektivet av fyra hörnstenar humanvetenskaplig utgångspunkt, praktisk inriktning, omsorgstradition och hälsoorientering.
13 Till exempel icke vårdande vårdkulturer, regler och rigida rutiner.
56
över handling (fritt översatt från Schön, 1983) och därigenom även stimulera till
kontinuerlig bearbetning av rutiner och arbetssätt.
Interaktivt projekt
Ett viktigt nästa steg är att testa och utvärdera arbetssättet och nedan följer en
tänkt ram för ett utvärderingsprojekt. Jag anser att en hög och aktiv samverkan
mellan patient, vårdare och forskare är en viktig förutsättning för att kunna
utveckla innehållet i arbetssättet. När även mottagare och utövare är med i
forskningsprocessen, utifrån sina olika perspektiv, så tillför det ytterligare
dimensioner (Herr & Andersson, 2014). Aktionsforskningsmetodik kan vara en
lämplig approach för att utvärdera omvårdnadsarbete (Thorne & Hayes, 1997),
eller interaktiv forskning som också är en utvecklingsstödjande och interaktiv
metod men där tyngdpunkten ligger på ett kritiskt perspektiv och mer långsiktig
teoriutveckling (Svensson, 2002b).
Ett projekt skulle kunna inledas med att forskarna bjuder in brukarrepresentanter
från olika brukarorganisationer och vårdare från den enhet som utvärderingen ska
genomföras på, till en inledande träff. Syftet med träffen bör vara både att
presentera arbetssättet, i sin ursprungsform, och grundtankarna för
aktionsforskning samt lyssna in farhågor, önskemål och förslag samt se om intresse
finns för att hjälpa till med att utvärdera och utveckla arbetssättet. När det finns
intresserade personer så görs gemensamt en plan för hur projektet ska genomföras
och utvärderas. Därav är det inte möjligt att detaljplanera projektet i detta läge.
Det finns dock vissa hörnstenar som är viktiga förutsättningar, bland annat en
inledande introducerande utbildningsinsats där omvårdnad som reflekterande
praktik ska bearbetas genom olika interaktiva inslag, till exempel fallbearbetning
som ska stimulera till lärande och kritisk reflektion (jmf Dewey, 1938; Schön,
1983).

57
Projektet i stort ska givetvis genomsyras av samma grundtankar som präglar
arbetssättet, det vill säga flexibilitet, tillit, bekräftelse, utgå från förmågor, respekt
för varandras erfarenheter och kunskaper etcetera. Genomförandet bör bestå av
olika interventioner som ska ge konkret stöd och coachning till personal i
självständig reflektion i situationen men även möjlighet till individuell reflektion
över olika bedömningar och val, möjligen i nätbaserad loggboksform, samt
reflektion i grupp. I detta arbete kan ett reflektionsunderlag, se figur 2, vara ett
bra verktyg. Stödet bör även innehålla individanpassad omvårdnadshandledning
med fokus på relationsskapande faktorer, behovsbedömning och
handlingsalternativ, möjligen i form av omvårdnadskonferenser där vårdplaner
kan bearbetas. I förlängning ska ett antal sjuksköterskor kunna känna sig
tillräckligt trygga med arbetssättet så att de kan ta över stödet och
omvårdnadshandledning till personalgruppen.
Formen för utvärdering bör utformas tillsammans med de andra deltagarna i
projektet, men en möjlig väg skulle kunna vara fokusgruppsintervjuer med
antingen mottagare och utövare av arbetsmodellen åtskilda eller i mixade
grupper. Deltagarna skulle kunna utvärdera de erfarenheter de har utifrån sitt
perspektiv men också tillföra nya förslag som skulle kunna implementeras och
sedan utvärdera på nytt, i enlighet med ett abduktivt förhållningssätt (Harman,
1965; Peirce, 1990). Det skulle också vara meningsfullt att mäta exempelvis
tvångsåtgärder, hot/våldsituationer, självskadebeteende eller andra mätbara
händelser som kan anses relevanta. Efter att arbetssättet testats och utvärderats på
antal enheter, gärna med olika vårdformer exempelvis rättspsykiatri,
kommunpsykiatri, akutpsykiatri etcetera., så skulle det kunna vara möjligt att
sammanställa resultaten och eventuellt kunna formulera en modell för
kontinuerlig omvårdnadsutveckling i psykiatrisk vård.

58
Har du en relation
till patienten?
Tillit Ömsesidighet
Ärlighet Bekräftelse
Respekt
Har du identifierat
patientens behov?
Lyssna och förstå Identifiera basala
och abstrakta behov
Utgår åtgärden
från patientens
behov?
Öka välbefinnande och minska lidande Tillvarata förmågor
och resurser Medvetet förhållnings-
sätt Flexibilitet
Figur 2. Förslag på underlag för reflektion kring val av omvårdnadsåtgärd i psykia-
trisk vård. Respektive fråga besvaras med utgångspunkt i de efterföljande ledor-
den. Om någon eller några av frågorna besvaras med ”nej” föreligger en risk för
att en tänkt åtgärd inte svarar mot den individuella patientens behov.

59
Slutsats Sammanfattningsvis om vårdarna lyckas skapa en ömsesidig, tillitsfull relation till
patienten, kan förstå dennes utryckta behov och outtalade tecken samt arbetar
proaktivt, i samarbete med patienten, med åtgärder och medvetna
förhållningssätt, så finns sällan behov av tvångsåtgärder. För detta krävs att
vårdarna får stöd i att utveckla sin reflektiva förmåga och även i att få ta eget
ansvar för varje situation och därigenom bygga upp en tillit till sin egen förmåga.

60

61
Jag vill tacka… … i första hand alla deltagare i studierna som anförtrott mig era tankar och
erfarenheter och gjort denna avhandling möjlig
… Mai Lindstöm och Institutionen för hälsovetenskap som valt att satsa
kompetensutvecklingsmedel på mig
… Siv Söderberg för att du övertalade mig att ta steget till att bli doktorand
… min handledare Rolf Adolfsson som på distans men troget följt med från
början till slut på denna ibland lite ”guppiga” resa och att jag har fått ”plocka upp
dig från byrålådan” när jag behövt
… min handledare Stefan Sävenstedt för att du gjort motstånd men inte försökt
säga hur jag ska tänka, och för att du har haft mod att låta mig ta egna beslut
… Karin Zingmark för att du vågade tro på mig
… min huvudhandledare Åsa Engström för ditt lugn, uppmuntran och din
övertygelse samt för ditt handfasta stöd när jag behövt det - och så har jag ju
hittat en artfrände
… mina döttrar Ida-Maria och Jennie och ponnyerna Thor och Armani för att ni
varje dag påminner mig om vad som är viktigt i livet!
… min man Jimmy och lilla hunden Bamse för att ni finns och fixar där hemma
så att det alltid känns trivsamt att komma hem!
… alla mina nuvarande och tidigare arbetskamrater för otaliga intressanta och
utvecklande diskussioner om psykiatri och omvårdnad
… till alla som hjälpt mig med korrekturläsning och gett mig synpunkter på
kappans innehåll

62
… Sofia Åkerman och Thérèse Eriksson för uppmuntran och hjälp med
datainsamling och för att jag fick låna omslagsbilden
… Shedo för hjälp med datainsamling.
Störst tack till Sebastian Gabrielsson som förutom att du bidragit till att jag blivit
mer kritisk och eftertänksam, mindre naiv och generellt klokare ;) så har du varit
en avgörande förutsättning för att denna avhandling över huvudtaget blev
skriven!

63
Referenser
American Psychiatric Association. DSM-5 Task Force. (2013). Diagnostic and
statistical manual of mental disorders: DSM-5. (5. ed.) Arlington, Va.: American
Psychiatric Association.
Ashcraft, L., & Anthony, W. (2008). Eliminating seclusion and restraint in
recovery-oriented crisis services. Psychiatric Services, 59(10), 1198-1202.
doi:http://dx.doi.org/10.1176/appi.ps.59.10.1198
Bak, J., Zoffmann, V., Sestoft, D. M., Almvik, R., Siersma, V. D., & Brandt-
Christensen, M. (2015). Comparing the effect of non-medical mechanical
restraint preventive factors between psychiatric units in denmark and norway.
Nordic Journal of Psychiatry, 69(6), 433-443.
doi:http://dx.doi.org/10.3109/08039488.2014.996600
Barker, P., & Buchanan-Barker, P. (2010). The tidal model of mental health
recovery and reclamation: Application in acute care settings. Issues in Mental
Health Nursing, 31(3), 171-180.
doi:http://dx.doi.org/10.3109/01612840903276696
Barker, P., & Buchanan-Barker, P. (2011). Myth of mental health nursing and
the challenge of recovery. International Journal of Mental Health Nursing, 20(5),
337-344. doi:http://dx.doi.org/10.1111/j.1447-0349.2010.00734.x
Barton, S. A., Johnson, M. R., & Price, L. V. (2009). Achieving restraint-free on
an inpatient behavioral health unit. Journal of Psychosocial Nursing and Mental
Health Services, 47(1), 34-40. doi:http://dx.doi.org/10.3928/02793695-
20090101-01
64
Beckett, P., Field, J., Molloy, L., Yu, N., Holmes, D., & Pile, E. (2013). Practice
what you preach: Developing person-centred culture in inpatient mental
health settings through strengths-based, transformational leadership. Issues in
Mental Health Nursing, 34(8), 595-601.
doi:http://dx.doi.org/10.3109/01612840.2013.790524
Bergdahl, E., & Berterö, C.M. (2015). The myth of induction in qualitative
nursing research. Nursing Philosophy : An International Journal for Healthcare
Professionals, 16(2), 110-120. doi:http://dx.doi.org/10.1111/nup.12073
Biesta, G. (2004). Kunskapande som ett sätt att handla. John Deweys
transaktionella teori om kunskapande. Utbildning och demokrati, 13(1), 41-64.
Birkler, J. (2008). Vetenskapsteori – en grundbok. Stockholm: Liber.
Björkdahl, A., Hansebo, G., & Palmstierna, T. (2013). The influence of staff
training on the violence prevention and management climate in psychiatric
inpatient units. Journal of Psychiatric and Mental Health Nursing, 20(5), 396-404.
doi:http://dx.doi.org/10.1111/j.1365-2850.2012.01930.x
Björkman, J. (2001). "Vård för samhällets bästa. Debatten om tvångsvård i svensk
lagstiftning 1850–1970". (Doktorsavhandling, Uppsala universitet).
Bonner, G., Lowe, T., Rawcliffe, D., & Wellman, N. (2002). Trauma for all: A
pilot study of the subjective experience of physical restraint for mental health
inpatients and staff in the UK. Journal of Psychiatric and Mental Health Nursing,
9(4), 465-465.
Bowers, L., Allan, T., Simpson, A., Jones, J., Van, D. M., & Jeffery, D. (2009).
Identifying key factors associated with aggression on acute inpatient
psychiatric wards. Issues in Mental Health Nursing, 30(4), 260-271.
doi:http://dx.doi.org/10.1080/01612840802710829

65
Bowers, L., James, K., Quirk, A., Simpson, A., Stewart, D., & Hodsoll, J. (2015).
Reducing conflict and containment rates on acute psychiatric wards: The
safewards cluster randomised controlled trial. International Journal of Nursing
Studies, 52(9), 1412-1422.
doi:http://dx.doi.org/10.1016/j.ijnurstu.2015.05.001
Carlyle, D., Crowe, M., & Deering, D. (2012). Models of care delivery in
mental health nursing practice: A mixed method study. Journal of Psychiatric
and Mental Health Nursing, 19(3), 221-230.
http://dx.doi.org/10.1111/j.1365-2850.2011.01784.x
Carnevali, D.L. (1983). Nursing care planning: Diagnosis and management. (3rd ed.)
London: Lippincott.
Cleary, M., Hunt, G. E., Horsfall, J., & Deacon, M. (2012). Nurse-patient
interaction in acute adult inpatient mental health units: A review and
synthesis of qualitative studies. Issues in Mental Health Nursing, 33(2), 66-79.
doi:http://dx.doi.org/10.3109/01612840.2011.622428
Dewey, J. (1938). Experience and education. New York: Macmillan.
De Benedictis, L., Dumais, A., Sieu, N., Mailhot, M., Létourneau, G., Tran, M.
M., . . . Lesage, A. D. (2011). Staff perceptions and organizational factors as
predictors of seclusion and restraint on psychiatric wards. Psychiatric Services,
62(5), 484-491. doi:http://dx.doi.org/10.1176/appi.ps.62.5.484
Delaney, K. R., & Johnson, M. E. (2014). Metasynthesis of research on the role
of psychiatric inpatient nurses: What is important to staff? Journal of the
American Psychiatric Nurses Association, 20(2), 125-137.
doi:http://dx.doi.org/10.1177/1078390314527551

66
Enarsson, P., Sandman, P., & Hellzén, O. (2008). “Being good or evil”:
Applying a common staff approach when caring for patients with psychiatric
disease. International Journal of Qualitative Studies on Health and Well-being, 3(4),
219-229. doi:http://dx.doi.org/10.1080/17482620802042297
Enarsson, P., Sandman, P., & Hellzen, O. (2011). "They can do whatever they
want": Meanings of receiving psychiatric care based on a common staff
approach. International Journal of Qualitative Studies on Health and Well-being,
6(1).
Eriksson, K. (2014). Vårdprocessen. (5. uppl.) Stockholm: Liber.
Eriksson, K., & Lindström, U.A. (1997). Abduction - a way to deeper
understanding of the world of caring. Scandinavian Journal of Caring Sciences,
11(4), 195-198.
Fluttert, F. A. J., van Meijel, B., Nijman, H., Bjørkly, S., & Grypdonck, M.
(2010). Preventing aggressive incidents and seclusions in forensic care by
means of the 'early recognition method'. Journal of Clinical Nursing, 19(11-
12), 1529-1537. doi:http://dx.doi.org/10.1111/j.1365-2702.2009.02986.x
Gabrielsson, S., Sävenstedt, S., & Zingmark, K. (2015). Person-centred care:
Clarifying the concept in the context of inpatient psychiatry. Scandinavian
Journal of Caring Sciences, 29(3), 555-562.
doi:http://dx.doi.org/10.1111/scs.12189
Gask, L., & Coventry, P. (2012). Person-centred mental health care: The
challenge of implementation. Epidemiology and Psychiatric Sciences, 21(2), 139-
144. doi:http://dx.doi.org/10.1017/S2045796012000078
67
Georgieva, I., de Haan, G., Smith, W., & Mulder, C. L. (2010). Successful
reduction of seclusion in a newly developed psychiatric intensive care unit.
Journal of Psychiatric Intensive Care, 6(1), 31-38.
doi:http://dx.doi.org/10.1017/S1742646409990082
Gordon, M. (2002). Manual of nursing diagnosis: including all diagnostic categories
approved by the North American Nursing Diagnosis Association. (10. ed.) St. Louis,
Mo.: Mosby.
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in
nursing research: Concepts, procedures and measures to achieve
trustworthiness. Nurse Education Today, 24(2), 105-112.
Gunnarsson, E. (2007). Other sides of the coin. A feminist perspective on
robustness in science and knowledge production. International journal of action
research, 3(3), 349-363.
Haglund, K., von Knorring, L., & von Essen, L. (2003). Forced medication in
psychiatric care: patient experiences and nurses perceptions. Journal of
Psychiatric and Mental Health Nursing, 10, 65-72.
doi:http://dx.doi.org/10.1046/j.1365-2850.2003.00555.x
Halldorsdottir, S. (1996). Caring and uncaring encounters in nursing and health
care: developing a theory. (Doctoral Dissertation, Linköpings Universitet).
Halldorsdottir, S. (2008). The dynamics of the nurse-patient relationship:
Introduction of a synthesized theory from the patient's perspective.
Scandinavian Journal of Caring Sciences, 22(4), 643-652.
doi:http://dx.doi.org/10.1111/j.1471-6712.2007.00568.x
Harman, G. H. (1965). The inference to the best explanation. The Philosophical
Review, 74(1)88-95. http://dx.doi.org/10.2307/2183532

68
Hartman, S. (2003). Läraren från Oil City – inför det nyväckta intresset för John
Dewey. I S. Hartman, K. Roth & N. Rönnström. John Dewey: om reflektivt
lärande i skola och samhälle (s. 7-31). Stockholm: HLS förl.
Hejlskov Elvén, B. & Abild, S. (2015). Beteendeproblem i psykiatrisk vård: [om
lågaffektivt bemötande]. Stockholm: Natur & Kultur.
Hellzen, O., Kristiansen, L., & Norbergh, K. G. (2003). Nurses' attitudes towards
older residents with long-term schizophrenia. Journal of Advanced Nursing,
43(6), 616-622.
Herr, K. & Anderson, G.L. (2014). The action research dissertation: a guide for
students and faculty. Thousand Oaks, Calif.: Sage.
Holm, H., Björkdahl, A., & Björkenstam, E. (2011). Tvångsvård med
frågetecken. Läkartidningen, 108(34), 1544-1545.
Huckshorn, K. A. (2014). Reducing seclusion and restraint use in inpatient
settings. Journal of Psychosocial Nursing and Mental Health Services, 52(11), 40-
47. doi:http://dx.doi.org/10.3928/02793695-20141006-01
Huckshorn, K. A. (2004). Reducing seclusion restraint in mental health use
settings: Core strategies for prevention. Journal of Psychosocial Nursing and
Mental Health Services, 42(9), 22-33.
Hörberg, U., Sjögren, R., & Dahlberg, K. (2012). To be strategically struggling
against resignation: The lived experience of being cared for in forensic
psychiatric care. Issues in Mental Health Nursing, 33(11), 743-751.
doi:http://dx.doi.org/10.3109/01612840.2012.704623
69
James, K., Stewart, D., & Bowers, L. (2012). Self-harm and attempted suicide
within inpatient psychiatric services: A review of the literature. International
Journal of Mental Health Nursing, 21(4), 301-309.
doi:http://dx.doi.org/10.1111/j.1447-0349.2011.00794.x
Jarrett, M., Bowers, L., & Simpson, A. (2008). Coerced medication in psychiatric
inpatient care: literature review. Journal of Advanced Nursing, 64, (6), 538-548.
doi:http://dx.doi.org/10.1111/j.1365-2648.2008.04832.x
Jormfeldt, H., Rask, M., Brunt, D., Bengtsson, A., & Svedberg, P. (2012).
Experiences of a person-centred health education group intervention-A
qualitative study among people with a persistent mental illness. Issues in
Mental Health Nursing, 33(4), 209-216.
doi:http://dx.doi.org/10.3109/01612840.2011.653041
Jormfeldt, H., Svedberg, P., & Arvidsson, B. (2003). Nurses` conceptions of how
health processes are promoted in mental health nursing. Journal of Psychiatric
and Mental Health Nursing, 10, 608-615.
Jormfeldt, H., Svedberg, P., Fridlund, B., & Arvidsson, B. (2007). Perceptions of
the concept of health among nurses working in mental health services: A
phenomenographic study. International Journal of Mental Health Nursing, 16(1),
50-56. doi:http://dx.doi.org/10.1111/j.1447-0349.2006.00444.x
Karman, P., Kool, N., Poslawsky, I. E., & Meijel, B. (2015). Nurses' attitudes
towards self‐harm: A literature review. Journal of Psychiatric and Mental Health
Nursing, 22(1), 65-75. doi:http://dx.doi.org/10.1111/jpm.12171

70
Kjellin, L., Andersson, K., Bartholdson, E., Candefjord, I.-L., Holmström, H.,
Jacobsson, L., Sandlund, M., Wallsten, T., & Östman, M. (2004). Coercion
in psychiatric care – patients` and relatives` experiences from four Swedish
psychiatric services. Nordic Journal of Psychiatry, 58, 153-159.
doi:http://dx.doi.org/10.1080/08039480410005549
Krippendorff, K. (2013). Content analysis: an introduction to its methodology (3rd ed.)
Thousand Oaks, Calif.: SAGE.
Kvale, S. & Brinkmann, S. (2014). Den kvalitativa forskningsintervjun. (3. uppl.)
Lund: Studentlitteratur
Lindgren, B-M., Aminoff, C., & Hällgren Graneheim, U. (2015). Features of
everyday life in psychiatric inpatient care for self-harming: An observational
study of six women. Issues in Mental Health Nursing, 36(2), 82-88.
doi:http://dx.doi.org/10.3109/01612840.2014.941077
Lindgren, B., & Hällgren Graneheim, U. (2015). Meanings of caring for people
who self-harm as disclosed in narratives of dialectical behaviour therapy
professionals. Journal of Psychiatric and Mental Health Nursing, 22(6), 371-378.
doi:http://dx.doi.org/10.1111/jpm.12196
Lindgren, B., Öster, I., Åström, S., & Hällgren Graneheim, U. (2011). ‘They
don’t understand . . . you cut yourself in order to live.’ interpretative
repertoires jointly constructing interactions between adult women who self-
harm and professional caregivers. International Journal of Qualitative Studies on
Health and Well-being, 6(3), 1-13.
doi:http://dx.doi.org/10.3402/qhw.v6i3.7254

71
Lindström, U. Å. (1995). Ensamhetskänslan sviker inte: en kvalitativ studie rörande
patienters upplevelser av vårdkultur och vårdrelation på psykiatriskt sjukhus.
(Doktorsavhandling, Åbo Akademi).
Looi, G. E., & Hellzén, O. (2006). Nurses' perception of the relationship
between themselves and the long-term psychiatric client – An interview
study. Primary Care and Community Psychiatry, 11(4), 185-192.
doi:http://dx.doi.org/10.1185/135525707183058
Lützén, K., & Schreiber, R. (1998). Moral survival in a nontherapeutic
environment. Issues in Mental Health Nursing, 19, 303-315.
Maben, J., Latter, S., & Clark, J. M. (2006). The theory-practice gap: Impact of
professional-bureaucratic work conflict on newly-qualified nurses. Journal of
Advanced Nursing, 55(4), 465-477. doi:http://dx.doi.org/10.1111/j.1365-
2648.2006.03939.x
Mangnall, J., & Yurkovich, E. (2008). A literature review of deliberate self-harm.
Perspectives in Psychiatric Care, 44(3), 175-84.
Marangos-Frost, S., & Wells, D. (2000). Psychiatric nurses` thoughts and feelings
about restraint use: a decision dilemma. Journal of Advanced Nursing, 31(2),
362-369.
Matthias, M. S., Salyers, M. P., Rollins, A. L., & Frankel, R. M. (2012).
Decision making in recovery-oriented mental health care. Psychiatric
Rehabilitation Journal, 35(4), 305-314.
doi:http://dx.doi.org/10.2975/35.4.2012.305.314
72
McAllister, M. (2003). Multiple meanings of self harm: A critical review.
International Journal of Mental Health Nursing, 12(3), 177-185.
McCance, T., McCormack, B., & Dewing, J. (2011). An exploration of person-
centredness in practice. Online Journal of Issues in Nursing, 16(2), 1.
Meehan, T., McIntosh, W., & Bergen, H. (2006). Aggressive behaviour in the
high-secure forensic setting: the perceptions of patients. Journal of Psychiatric
and Mental Health Nursing, 13, 19-25.
Meleis, A.I. (2011). Theoretical nursing: development and progress. (5. ed.)
Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Morgan, D.L. (1997). Focus groups as qualitative research (2d ed). Thousand Oaks
CA: Sage.
Muir-Cochrane, E., Baird, J., & McCann, T. V. (2015). Nurses' experiences of
restraint and seclusion use in short-stay acute old age psychiatry inpatient
units: A qualitative study. Journal of Psychiatric and Mental Health Nursing,
22(2), 109-115. doi:http://dx.doi.org/10.1111/jpm.12189
O’Connor, H., Madge, C., Shaw, R., & Wellens, J. (2008). Internet-based
interviewing. In N. Fielding, R. M. Lee & G. Blank (ed.), The SAGE
Handbook of Online Research Methods (pp. 271-289). Los Angeles: SAGE.
O'Donovan, A. (2007). Patient-centred care in acute psychiatric admission units:
Reality or rhetoric? Journal of Psychiatric and Mental Health Nursing, 14(6),
542-548.

73
Olofsson, B. (2005). Opening up: psychiatric nurses’ experiences of participating
in reflection groups focusing on the use of coercion. Journal of Psychiatric and
Mental Health Nursing, 12(3), 259-267. http://dx.doi.org/10.1111/j.1365-
2850.2005.00827.x
Olofsson, B., Gilje, F., Jacobson, L., & Norberg, A. (1998). Nurses` narratives
about using coercion in psychiatric care. Journal of Advanced Nursing, 28, (1),
45-53.
Olofsson, B., & Norberg, A. (2001). Experiences of coercion in psychiatric care
as narrated by patients, nurses and physicians. Journal of Advanced Nursing, 33,
(1), 89-97.
Peirce, C.S. (1990). Pragmatism och kosmologi. Göteborg: Daidalos.
Raboch, J., Kališová, L., Nawka, A., Kitzlerová, E., Onchev, G., Karastergiou,
A., ... & Kallert, T. (2010). Use of coercive measures during involuntary
hospitalization: Findings from ten European countries. Psychiatric Services,
61(10), 1012-1017. doi:http://dx.doi.org/10.1176/appi.ps.61.10.1012
Ricoeur, P. (1976). Interpretation theory: discourse and the surplus of meaning. Fort
Worth, Tex.: Texas Christian University Press.
Rorty, R. (2003). Hopp istället för kunskap. Göteborg: Daidalos.
Schön, D.A. (1983). The reflective practitioner: how professionals think in action. New
York: Basic Books.
SBU. Erfarenheter och upplevelser av bemötande och hjälp bland personer med
självskadebeteende. Stockholm: Statens beredning för medicinsk utvärdering
(SBU); 2015. SBU Alert-rapport nr 2015-04. ISSN 1652-7151.

74
Shattell, M. (2004). Nurse-patient interaction: A review of the literature. Journal
of Clinical Nursing, 13(6), 714-722.
Shattell, M. M., Starr, S. S., & Thomas, S. P. (2007). 'Take my hand, help me
out': Mental health service recipients' experience of the therapeutic
relationship. International Journal of Mental Health Nursing, 16(4), 274-284.
doi:http://dx.doi.org/10.1111/j.1447-0349.2007.00477.x
SFS 1982:763. Hälso- och sjukvårdslagen. Stockholm: Riksdagen.
SFS 1991:1128. Lagen om psykiatrisk tvångsvård. Stockholm: Riksdagen.
SFS 1991:1129. Lagen om rättspsykiatrisk vård. Stockholm: Riksdagen.
Socialstyrelsen 1991:9. (1991). Tillämpning av lagen om psykiatrisk tvångsvård.
Stockholm: Socialstyrelsen.
Socialstyrelsen (2009). Innehållet i den psykiatriska tvångsvården. Stockholm:
Socialstyrelsen.
Socialstyrelsens statistikdatabas. Hämtad 150909 från
http://www.socialstyrelsen.se/statistik/statistikdatabas/psykiatrisktvangsvard
Svedberg, P., Jormfeldt, H., & Arvidsson, B. (2003). Patients` conceptions of
how health processes are promoted in mental health nursing. Journal of
Psychiatric and Mental Health Nursing, 10, 448-456.
doi:http://dx.doi.org/10.1046/j.1365-2850.2003.00633.x
Svedberg, P., Jormfeldt, H., Fridlund, B., & Arvidsson, B. (2004). Perceptions of
the concept of health among patients in mental health nursing. Issues in
Mental Health Nursing, 25(7), 723-736.

75
Svensson, L. (2002a). En analys och blick framåt. I Ö. Widegren (Red.),
Interaktiv forskning-för utveckling av teori och praktik (s.173-207). Stockholm:
Arbetslivsinstitutet.
Svensson, L. (2002b). Bakgrund och utgångspunkter. I Ö. Widegren (Red.),
Interaktiv forskning-för utveckling av teori och praktik (s.1-22). Stockholm:
Arbetslivsinstitutet.
Thompson, J. B. (1981). Paul Ricoeur Hermeneutics and the human sciences: essays on
language, action and interpretation. Cambridge: Cambridge university press.
Thorne, S., Canam, C., Dahinten, S., Hall, W., Henderson, A., & Kirkham, S.
R. (1998). Nursing's metaparadigm concepts: Disimpacting the debates.
Journal of Advanced Nursing, 27(6), 1257-1268.
Thorne, S.E. & Hayes, V.E. (red.) (1997). Nursing praxis: knowledge and action.
Thousand Oaks, Calif.: Sage.
Tofthagen, R., Talseth, A., & Fagerström, L. (2014). Mental health nurses'
experiences of caring for patients suffering from self-harm. Nursing Research
and Practice, 2014, 905741. doi:http://dx.doi.org/10.1155/2014/905741
van den Hooff, S., & Goossensen, A. (2014). How to increase quality of care
during coercive admission? A review of literature. Scandinavian Journal of
Caring Sciences, 28(3), 425-434. doi:http://dx.doi.org/10.1111/scs.12070
Vuckovich, P. K. (2009). Strategies nurses use to overcome medication refusal by
involuntary psychiatric patients. Issues in Mental Health Nursing, 30(3), 181-
187. doi:http://dx.doi.org/10.1080/01612840802694478

76
Wallsten, T., & Kjellin, L. (2004). Involuntarily and voluntarily admitted patients'
experiences of psychiatric admission and treatment - a comparison before and
after changed legislation in Sweden. European Psychiatry, 19, 464-468.
Wallsten, T., Kjellin, L., & Sjöberg, R.L. (2008). The diagnostic accuracy of
questions about past experiences of being mechanically restrained in a
population of psychiatric patients. Memory, 16, (5), 548-555.
doi:http://dx.doi.org/10.1080/09658210802010471
Wallsten, T., Östman, M., Sjöberg, R.L., & Kjellin, L. (2008). Patients and next
of kins’ attitudes towards compulsory psychiatric care. Nordic Journal of
Psychiatry, 62, (6), 444-449.
doi:http://dx.doi.org/10.1080/08039480801984248
Walsh, D., & Downe, S. (2005). Meta-synthesis method for qualitative research:
A literature review. Journal of Advanced Nursing, 50(2), 204-211.
Yura, H. & Walsh, M.B. (1988). The nursing process: Assessing, planning,
implementing, evaluating. (5th ed.). Norwalk: Appleton & Lange.
Zugai, J. S., Stein-Parbury, J., & Roche, M. (2015). Therapeutic alliance in
mental health nursing: An evolutionary concept analysis. Issues in Mental
Health Nursing, 36(4), 249-257.
doi:http://dx.doi.org/10.3109/01612840.2014.969795
Örmon, K., Torstensson-Levander, M., Sunnqvist, C., & Bahtsevani, C. (2014).
The duality of suffering and trust: Abused women's experiences of general
psychiatric care—An interview study. Journal of Clinical Nursing, 23(15-16),
2303-2312. doi:http://dx.doi.org/10.1111/jocn.12512

77
Summary in English Nursing as a reflective practice: Identifying and applying alternatives to coercion in
psychiatric care
Coercive measures such as restraints and forced medication are commonly used
in psychiatric care. This practice is often explained by staff as resulting from a lack
of valid alternatives. Coercive measures seem especially common in the care of
young women who self-harm, who are reported to perceive the use of coercive
measures as punishment and a barrier for seeking help.
The overall aim of this thesis was to gain further knowledge and a deeper
understanding of nursing as a process in psychiatric care from the perspective of
patients, students, and professional caregivers, with a particular focus on
alternatives to coercions in the care of persons who self-harm.
This thesis takes a pragmatic stance with the ambition of producing results that
may be put to practical use. The separate studies apply a qualitative approach in
which materials have been analyzed using content analysis. Data consists of 19
written accounts by persons with experience of being treated for self-harm and
being subject to coercive measures, 14 online reflective journals written by
student nurses during clinical placement in psychiatric care, and focus group
interviews with a total of 26 professional caregivers including nurse assistants,
nurses, physicians and ward managers experienced in compulsory psychiatric care.
The written accounts showed that persons treated in psychiatry had a wish to be
met with understanding by staff members, to develop trusting and mutual
relationships with them, and to receive care based on methods grounded in
research. Their actual experiences described care as unpredictable,
counterproductive, and based on mistrust and distance. In the online reflective
78
journals students highlighted a need to dedicate time and commit to relationship-
building, which was described as a precondition for being able to make
assessments and learn to understand patient’s individual signs of health and illness.
They described how they identified patients’ abstract needs such as the need for
security, empowerment, self-esteem and hope. Based on these, students would
individualize actions and approaches and bring forth and make use of patients’
abilities. The focus group interviews revealed how staff members, with a starting
point in challenging situations in psychiatric care, discussed possible actions
focusing either on the needs of the staff, the patient’s experience, to follow
routines or to discipline patients. Approaches and the qualities of actions would
differ distinctly depending on focus. The focus groups interviews also revealed
the staff’s perceptions of interprofessional collaboration following their
professional roles. Findings depicted how nurse assistants, despite having the least
formal competence, were the ones wielding the most power over decisions on
the use of coercive measures, due to them being closest to the patients and thus
possessing first-hand information about them.
Findings show that the perspectives of patients, students, and professional
caregivers align and converge. A meta-synthesis of the separate findings describes
nursing as a reflexive practice. Professional caregivers’ ability to establish a
trusting relationship with the patient forms the basis for a relevant assessment of
patients’ needs. This assessment of needs is the starting point for choices of
actions and approaches and for building on patients’ abilities and resources in
order to alleviate suffering and promote well-being. But the path to choosing a
specific action is not static; actions may have a mere relationship-establishing
intent to begin with, needs may develop and change over time, actions may need
to be modified, and trust may be affected by various circumstances. This implies
that the path leading to an action is not to be understood as fixed, but rather as a
dynamic process presupposing a reflexive approach, building on interpersonal

79
relationships, and aiming to strengthen patients’ capacity for recovery and well-
being.
It may be concluded that coercive measures are uncalled-for when professional
caregivers succeed in establishing mutual, trusting relationships with patients, are
able to identify their needs and work together applying pro-active, supportive
and empowering actions and approaches.
Key words: alternatives to coercion, nursing, process, psychiatric care, self-harm,
pragmatism, qualitative content analysis


Delstudie I


Issues in Mental Health Nursing, 36:96–103, 2015Copyright © 2015 Informa Healthcare USA, Inc.ISSN: 0161-2840 print / 1096-4673 onlineDOI: 10.3109/01612840.2014.951134
A Self-Destructive Care: Self-Reports of PeopleWho Experienced Coercive Measures and theirSuggestions for Alternatives
Git-Marie Ejneborn Looi, RN, RPN, MSc, and Asa Engstrom, RN, CCN, PhDDepartment of Health Sciences, Lulea University of Technology, Lulea, Sweden
Stefan Savenstedt, RN, PhDDepartment of Health Sciences, Lulea University of Technology and Department of Researchand Development, Norrbotten County Council, Lulea, Sweden
Coercive measures are commonly used as a method of inter-vention, despite insufficient evidence for their effectiveness andbenefits. The aim of this study was to describe how people whoself-harm perceive alternatives to coercive measures in relation toactual experiences of psychiatric care. A total of 19 self-reportshave been analysed with qualitative content analysis, resulting inthree categories: a wish for understanding instead of neglect; a wishfor mutual relation instead of distrust; a wish for professionalisminstead of a counterproductive care. In conclusion, if the caregiverscan understand and collaborate with the patient, there is seldomany need for coercive measures.
INTRODUCTIONCoercive measures remain common interventions in acute
psychiatric wards (Knutzen et al., 2014). Reviews of existingliterature show that, although some research exists on outcomesof involuntary hospitalisations and the use of coercive methods,few studies take an inside perspective allowing the patient to beheard (Hooff & Goossensen, 2013; Jarret, Bowers, & Simpson,2008; Katsakou & Priebe, 2006). This paper focusses on peoplewith experiences of psychiatric inpatient care, coercion and self-harm. Listening to people’s experiences is essential to developa person-centred care where alternatives to coercive measuresare identified, tested and evaluated.
The empirical evidence regarding outcomes and impactsof involuntary hospitalisations is inconsistent and insufficient(Katsakou & Priebe, 2006). The same goes for the effectivenessand benefits of containment measures (Jarret et al., 2008;Muralidharan & Fenton, 2006; Sailas & Fenton, 2000). At thesame time, there is a considerable amount of research describing
Address correspondence to Git-Marie Ejneborn Looi, Departmentof Health Sciences, Lulea University of Technology, Lulea, 97187Sweden. E-mail: [email protected]
harmful physical and psychological effects on patients and stafffollowing the use of coercive measures (Bonner, Lowe, Raw-cliffe, & Wellman, 2002; Fisher, 1994). This implies that thereis an urgent need for additional research to clarify the manyissues in this field (Jarret et al., 2008; Nelstrop et al., 2006). Al-though coercive measures are common in European psychiatricwards, differences between the countries exist (Raboch et al.,2010). Nurses tend to view coercive measures as necessary andunavoidable, believing they have no alternatives (Haglund, vonKnorring, & von Essen, 2003; Marangos Frost & Wells, 2000).According to a literature review (Jarrett et al., 2008) concerningcoerced medications, there was a notable lack of considerationof events leading to coercion and a complete absence ofinvestigation of an alternative. Coerced medication seems likeit is a ‘taken-for-granted’ practice in inpatient psychiatric carein countries such as Sweden, site of the present study.
People with experience of psychiatric care describe episodesin which they saw involuntary admission as necessary to keepthemselves or others safe while other testimonies describe thisas an unnecessary overreaction and a practice in need of revision(Katsakou et al., 2012; Sibitz et al., 2011). Research focussed onpatients’ experiences of coercive measures (Kontio et al., 2012;Soininen et al., 2013) reveals that patients are dissatisfied withthe lack of interaction with staff and think that coercive measuresare hardly necessary at all. They suggested that alternativesshould have been offered first. It is important to find alternativesto coercion, as this type of intrusive intervention could leadto greater morbidity and mortality than alternative approaches(Muralidharan & Fenton, 2006; Sailas & Fenton, 2000).
An analysis of official statistics concerning involuntary psy-chiatric care in Sweden (Holm, Bjorkdahl, & Bjorkenstam,2011) showed that involuntary hospitalisations and the use ofmechanical restraint increase dramatically in the group of youngwomen with self-harm behaviour. Patients who self-harm de-scribe how they never feel as lonely as when they are inpatients
96

SELF-REPORTS OF COERCIVE MEASURES AND SUGGESTIONS FOR ALTERNATIVES 97
in psychiatric care and their needs are neither seen nor met(Lindgren, Wilstrand, Gilje, & Olofsson, 2004).
Recent studies (Stewart, Van der Merwe, Bowers, Simpson,& Jones, 2010; Bowers et al., 2012) show that it is possibleto use alternatives to coercive measures, even if the standardof the evidence is poor. Stewart et al. (2010) argue that moreattention should be directed towards understanding how careinterventions can reduce the need for coercive measures, an is-sue that is mainly overlooked. One important aspect of such anunderstanding concerns listening to the patients’ perceptions, in-cluding their wishes and thoughts, about their own care. This isemphasised by James, Stewart and Bowers (2012) who claimedthat there is an urgent need for more research to provide mean-ingful care for people who self-harm, especially studies thatconsult service users about their experiences. In this study, wewant to contribute to this line of research and provide an oppor-tunity for people who self-harm to report on their wishes andexperiences in relation to inpatient psychiatric care.
The aim of this study was to describe how people who self-harm perceive alternatives to coercive measures in relation toactual experiences of psychiatric care.
METHODThis study applies a qualitative approach and is based on
self-reports written by persons with experiences of self-harmand being admitted to psychiatric inpatient care where coercivemeasures were used.
Participants, Data Collection and ProcedureThe participants were recruited during 2013 through mes-
sages posted in social media (Twitter, Facebook, blogs and per-sonal websites) asking potential participants in Sweden to visita homepage where they were given information about the studyand asked to participate. The requirement was that they were≥18 years of age and had experience of self-harm and of beingtreated in psychiatric inpatient care. They were asked to writea self-report in Swedish or English using an electronic form onthe website. The report should cover their experiences of thecare they had received and their perception of alternative to co-ercive treatment methods and the direct instruction was ‘writeyour story here’. The report was anonymous and no informationabout the participant was required. In all, 19 self-reports wereincluded in the study. All the reports were written in Swedish.The reports varied in length from a couple of paragraphs to sev-eral pages, most of them were one page with about 700 words.
Although no personal data was required, the information pro-vided spontaneously gave some insights regarding participants’characteristics. In some cases, the participants signed with theirnames, which suggested that there were both men and women.Several participants indicated that they had extensive experiencewith psychiatric inpatient care. The sample’s countries of originare unknown, but all self-reports indicated that they were fromSweden.
AnalysisThe texts of the self-reports were analysed in a systematic
way using a method for qualitative content analysis, allowingreplicable and valid inferences from the texts (Krippendorff,2013). Following Krippendorff, the understanding of the contentwas developed during the process of reading and analysing thetext where it was continuously reconceptualised, thus directingand redirecting the analysis.
In the process of analysis, all written self-reports were firstput together and treated as one text and read several times inorder to get an initial understanding of the content. No textwas excluded. Based on this reading, an analysis strategy wasdeveloped; text units that described the participant’s general ex-perience of psychiatric inpatient care were identified, condensedand placed in a separate group, while text units that describedexperience and perception of alternatives to coercive methodswere condensed and grouped separately. In this process, the textunits were systematically coded to facilitate tracing them backto the original text (Graneheim & Lundman, 2004).
The categorising of the content started with an analysis of thetext units belonging to the group that described experience andperception of alternative to coercive methods and then contentareas were formulated. This process was carried out step-wisetowards higher levels of abstraction until three sub-categorieswere formulated (Graneheim & Lundman, 2004). The remain-ing text units were thereafter categorised and grouped accordingto the three first identified sub-categories to connect the contentdescribing experience of coercive methods in psychiatric inpa-tient care with the perception and experience of alternative treat-ments. Finally, the whole process was reviewed and each stepdiscussed between the authors until an agreement was reachedon the formulation of three content areas and three categories.
Ethical ConsiderationsPrior to conducting the study, ethical approval was granted
from the regional ethics committee in Umea (2010-4-31M). Thecommittee was also informed of and approved alterations to theoriginal design (2012-315-32M).
RESULTSThe results of the content analysis are presented as three
categories belonging to three different content areas (Table 1).The categories describe the contrast between the participants’wishes and their experience of care.
A Wish for Understanding Instead of NeglectIn the descriptions of encounters with staff, there was often
a significant gap between what the participants hoped for andwhat they had experienced. A common thread was a wish tobe understood, confirmed and met in an open way and wherethe participants felt that they as persons were listened to in aserious way. A wish to be understood related to a hope that thestaff in the encounters could look behind their behaviour and

98 G.-M. EJNEBORN-LOOI ET AL.
TABLE 1Overview of content areas and categories
Content areas Category
Encounters A wish for understanding instead ofneglect
Relation A wish for mutual relation instead ofdistrust
Care A wish for professionalism instead of acounterproductive care
understand what they were trying to communicate. These wisheswere often in sharp contrast to the experience of encounters withthe staff, which predominantly were characterised by neglect ora fostering approach focussing on correction of their behaviour.
The experience of neglect was based on staff members’ lackof interest in realising the participants’ needs. Instead, partici-pants often felt as though they were questioned and belittled ina degrading way. Some describe feeling that the staff membersconveyed a message that they were not interested in understand-ing their problems and listening to their needs, which enhancedthe participants’ feelings of being abandoned. The presence of astaff member when restricted to constant observation did not al-ways help, since the priority often seemed more geared towardscontrol than communication and interaction.
Still I started to scratch myself, when the staff member discovering itshe got angry, arguing that I could not treat her in that way. She wasvery strong and managed to hold both my hands with only one hand,which was hurting a lot considering my wrist wounds, while she atthe same time was reading a magazine. I felt completely powerlessand neglected, especially considering that I earlier the same day hadexplained in what way they could help me. (Report 10)
Some of the participants described how the lack of under-standing from the staff and their paternalistic approach couldmake them indifferent to what happened to them, while for oth-ers, it could lead to frustration and feelings of shame. Lack ofunderstanding meant that the participants had to use differentcoping strategies, such as beating and scratching themselves,kicking a wall or doing something else that made the feeling ofpain overrun the anxiety. In these situations, the staff responseswere often coercive measures.
I was calm for a while and nobody [had two staff members as specialobservers] even tried to talk to me. I tried to stay calm but wasnot successful when not given any support. I started beating myselfagain, as a response they held down my arms. The nurse entered andwhen she realised what was going on she called the doctor and veryfast the order was, put her in the belt. (Report 13)
The feeling of powerlessness was enforced by being ignoredand not listened to. This feeling was especially enhanced whenparticipants were ignored in situations where they were undergreat emotional stress and needed support. Another contributingfactor was to experience the alertness of the staff when the
same situation escalated and coercive measures were deemednecessary.
The wish for understanding and to be listened to was en-hanced by positive experience of encounters with staff, such assituations where they just sat down next to them and talked aboutthe prevailing feelings and thoughts. Several of the participantshad the view that there was no need for coercive measures if thestaff members had listened to them, seen their needs and triedto understand their problem.
they pressed the alarm and 10 staffers came running and jumpedon me. Since I’m afraid of being restrained I fought for my life. Atsome of these occasions, a guy would come running from anotherward. Although he would only meet me under these circumstances,he would order all others out of my room and hold me like a childuntil I was calm. When he came I would calm down in like an hour.He did exactly the right thing for me. He understood that I onlyneeded someone to hold me. (Report 3)
In the participants’ wish for understanding it was importantthat the staff members could interpret their signals, see the sit-uation from their perspective and not forget the strong powerthe staff had. When staff members manage to understand thepatients’ situation, the perception was that they were able tofind individual solutions to meet the patients’ needs.
A Wish for Mutual Relation Instead of DistrustThe perceptions presented in the self-reports were that a
mutual trustful relation between the patient and staff memberscould prevent the need for coercive measures. A trustful relationwas, according to the participants, built and maintained throughhonesty and mutuality. Trust and confidence were described asthe most important conditions to improve their wellbeing. Ina trustful relation, the patient has the confidence to open upand admit to having periods of anxiety and a need for supportand comfort from the staff member. The described experienceof distrust and animosity was on the other hand destructive forbuilding and maintaining relations. In the absence of a mutualrelation, there was often a questioning of the patient and useof threats and coercive measures. As a consequence of the mu-tual mistrust, the patients tended to view the staff members asunpredictable and unreliable enemies.
I believe in trust when it comes to reducing the use of coercivemeasures. If I had felt trust instead of hatred I would have been ableto tell them how I feel instead of harming myself or getting angry(which gets you in restraints immediately). (Report 12)
The self-reports contained descriptions of how the partic-ipants experienced an atmosphere of distrust in their relationwith staff members. There was often a threat present and sim-ply the suspicion that they might consider hurting themselvescould lead to such punishment as mechanical restraint. Therewere also descriptions of broken agreements and changed con-ditions that contributed to the distrust between the patients andstaff. Sometimes it was as though the staff wanted to provokefrustration to justify the use of coercive measures.

SELF-REPORTS OF COERCIVE MEASURES AND SUGGESTIONS FOR ALTERNATIVES 99
When I heard the doctor’s order, I panicked and tried to pull thestraps to make me free at the same time as I shouted – You toldme that I didn’t have to take the injection if I accepted to takethe anti-psychotic pill. He answered – but you are still not calmand I replied – I was calm until now when you gave the order. Hejust turned around and walked away and I could not do anything.(Report 13)
There were several self-reports describing how the partic-ipants had been blamed, questioned and mistrusted in theirtalks with the doctor. They appealed for help and were in deepneed of support but were treated with mistrust and disrespectfulcomments.
The doctor told me that he pitied my parents that they had got me astheir daughter. Another claimed that I had invented and lied aboutthe sexual assaults I claimed I have been through between the age of6–12. (Report 5)
Staff members were often described as having a distancingapproach and not being engaged in the care. The participantsexperienced often that the main concern of staff was more onminimising the risk of self-harm in the wards and less on build-ing a trustful relation.
I wish to meet engaged and involved staff members and not meanwhite coats that threaten me with coercive measures. Today Iwould rather kill myself than turn to the psychiatric care for help.(Report 12)
Hearing staff members discussing and commenting on themand other patients in a disrespectful way also enhanced theatmosphere of distrust. It was also discouraging to watch howother patients were treated and how they had to endure coercivemeasures.
I have seen people been battered for no other reason than they wantedto use the toilet in the night, it is awful. (Report 11)
In contrast to the described experiences, the self-reports re-veal a clear wish to cooperate with staff members and to build atrustful relation with them. The participants had turned to psy-chiatric care to receive help and care and wished that the carecould be built on mutual trust.
I was motivated to quit with my behaviour and if the staff had setaside time and effort to build a trustful relation with me I could havetold them . . . I want to quit this shit. (Report 7)
A Wish for Professionalism Instead of aCounterproductive Care
The participants had a strong wish to be met by profession-alism. That included a wish to be cared for by staff memberswho had a competence and knowledge about their problems andneeds, used personal care plans and used interventions that wereknowledge-based. This included also an understanding that insome rare difficult situations, it could be acceptable to use co-ercive methods. In contrast, most of the participants describedexperiences of a self-defeating care, where the main focus was
on following general rules and disciplinary actions. This sug-gested the goal of the care was to minimise the time of careand prevent further admissions to inpatient psychiatric care. Inseveral of the self-reports, the inpatient psychiatric care wasdescribed as counterproductive in the sense that they had moreproblems when they left the ward than when they entered it.
There was an experience among the participants that itseemed the primary aim of the care was to keep them in cus-tody, deny their wishes, monitor them and make corrections oftheir behaviour by disciplining them. They described the careenvironment as chaotic and frightening and they had to arguefor what they felt were obvious correct care approaches, suchas not having to share a room with violent and suicidal patients,to be cared for by a female staff instead of a male when havingexperienced sexual abuse, or to see the doctor.
One day she [roommate] tries to commit suicide three times, thesecurity guards show up because she is going to be put in restraints. Ipanic and run out terrified and afflicted by the violence in there. [. . .]and then the suicidal patient is gone and I have my old roommate back(as I had asked for to start with). This whole mess just because theywouldn’t think things through to begin with. This was distressingand adding feelings of hopelessness and thoughts on killing myself.It is so unnecessary! (Report 17)
Some participants experienced that one staff member some-times tried to argue for a caring approach but was often over-ruled by the staff that wanted to use the coercive measures.Mechanical restraints were frequently described as a traumatis-ing experience connected to feelings of having to fight for theirlife. This feeling was emphasised by the fact that there oftenwere many staff members involved in the holding and some-times also policemen and they usually had bruises as a result ofthose incidents.
When I did some self-harming activity they fired off the alarm and10 staff members came running and jumped on me . . . It gave mescars in my soul. When I met my boyfriend I often became scaredwhen he tried to hold me even if I perceived it was out of love forme. (Report 3)
The use of coerced medication of sedative drugs was seldomperceived as logical. The experience of overmedication, the useof non-effective drugs and the experience of bad side-effectswere described by most of the participants.
They gave me Risperdal [anti-psychotic medicine] for 3 years. Laterwhen I did some reading on the effectiveness of Risperdal I didn’t findmuch evidence. What I did experience was disturbing side-effects,I got tired and slow-minded. When I didn’t want it they grabbedme and forced the medicine into me in a physically very offensivemanner . . . A lot of coercive measures can be performed with only theparents’ approval, without any support in the law . . . The psychiatriccare should protect children from their parents’ wish to use measuresas forced feeding, being locked in and coerced medication, in thesame way as the law protects children from maltreatment. (Report 9)
Some of the participants described the informal coercion asthe most difficult to stand and most offensive. There were severalreports of situations where they had been admitted to psychiatric

100 G.-M. EJNEBORN-LOOI ET AL.
inpatient care voluntarily but still daily had to endure situationswhere different coercive measures were used. Some participantsdescribe that they do not tell how they feel and hide their self-harm behaviour to avoid punishment.
Finally I decided to hide my anxiety and pretend that everythingwas alright. Instead I self-harm during the night, hidden in my bed.(Report 10)
Some of the participants describe that they had totally lostall their hope for support from the care system and thereforealso their hope for recovery. They did not make contact with thepsychiatric healthcare system even in situations of acute needof care and treatment. Others used their own coping strategiesin order to get the care they wanted and needed.
I came to the conclusion that if I was in really bad shape and wantedto be admitted I first have to harm myself and then say that I didn’twant to be admitted. That’s the most efficient way. There’s no use inasking for help before harming oneself. (Report 4)
There were many descriptions of discontinuity in the careplans. One participant described an incident prior to being ad-mitted in which a new senior doctor had questioned her. He hadasked her if she believed that the ward was a hotel, claimingthat she was spoiled and lived a life of luxury. For the partic-ipant, it was just unbelievable how anyone could associate aninpatient psychiatric ward with a luxury hotel, ‘It is rude, veryunprofessional and not confidence building’. There were alsodescriptions of solid care plans being disrupted because of lackof continuity among the doctors. Every doctor has an individualview of what the care should look like and when the participantshad tried to argue to maintain the care plan, they were met withcontemptuous treatment and discharged from the ward with nofurther support.
The final words I will never forget, it hits me deep in my soul andsends shivers up my spine. The psychiatrist said, “you will be suicidalall your life and that’s no reason for being admitted”. Psychiatry issupposed to be there when you need it and inspire hope. Where wasthat in those words he gave me? (Report 17)
There were several concrete suggestions in the self-reports onhow to improve the care. The participants felt that it is importantto not mix people with totally different types of diagnosis andnot place people in locked wards when it was not necessary. Thecare should be based on flexibility and individualised solutionsand the care plans should be formed in cooperation with thepatient. That included an insight that there can be situationswhere coercive methods are necessary due to the patient’s severeconditions.
My clothes were taken, they change the bedclothes, remove the lightbulb and keep the light on all night. The suicide-watch sat besideme. At that point they probably did everything possible to avoidmechanical restraints, I don’t know if it would have come to that,but there wasn’t much else to do. (Report 15)
Another important suggestion was to have committed regularstaff with the right professional competence on the ward. That
includes the opportunity to talk regularly with a psychiatrist whoknows the patient and use of drug treatments only when there isevidence that they are the best alternative.
My wish is that there will be less coercive measures and more ofcare in the future. More talks with the patients about why they harmthemselves, how they want to be helped and how to change theirmindset. (Report 8)
DISCUSSIONThe results show that there is a considerable gap between par-
ticipants’ wishes and their actual experiences of psychiatric care.They did not ask for miracle treatment but asked to be listenedto, understood and met in a mutual relation with professionalcaregivers in an adapted environment. This description of partic-ipants’ negative experiences of inpatient psychiatric care is con-sistent with earlier research findings (Carlsson, Dahlberg, Eke-bergh, & Dahlberg, 2006; Lindgren, Oster, Astrom, & HallgrenGraneheim, 2011; O’Donovan, 2007; Koekkoek et al., 2010).Lindgren et al. (2011) describe that the dominant approach forpatients who self-harm was the ‘fostering repertoire’ in whichthe caregivers try to motivate the patients by putting up rules andthe patients have to earn obvious rights by following these rules.O’Donovan (2007) also found that strict enforcement of rules,lack of choices, coercion and threats, are typical responses whencaregivers describe their practice for patients who self-harm.The participants’ wishes and perceptions correspond to an un-derstanding of care that might be described as person-centredand recovery-oriented (Barker, 2001). It can be argued that pro-fessional caregivers should strive to meet the needs and wantsof these patients in a person-centred care approach to offer acare with a limited use of coercive measures.
People who self-harm are perceived as a difficult categoryof patients in psychiatric care from the staffs’ point of view(Koekkoek, van Meijel, & Hutschemaekers, 2006; Thompson,Powis, & Carradice, 2008). One way of understanding the par-ticipants’ negative experiences of the care can be by acknowl-edging that patients who self-harm evoke strong feelings inprofessional caregivers, as well as admitting that nurses ap-parently are having trouble correctly interpreting patient be-haviour. As a result, nurses may respond to the behaviours andneeds of people that self-harm with a variety of utterly dif-ferent interventions (Lindgren et al., 2011; Lindsey, 2009). Itseems credible that patients who self-harm will have stricterrules and restrictions imposed upon them than other groups ofpatients and also face the risk of discharge without follow-upas a consequence of their symptoms (e.g. self-harm) (Koekkoeket al., 2010; Looi, Gabrielsson, Savenstedt, & Zingmark, 2014;O’Donovan, 2007). According to Lindsey (2009), nurses’ de-cisions to restrain may be influenced by their own personallevel of tolerance towards the patient’s behaviour and there isa general inconsistency in their pattern of intervention choice.Koekkoek et al. (2006) show that this group of patients are lack-ing sufficient support from effective treatment strategies. This

SELF-REPORTS OF COERCIVE MEASURES AND SUGGESTIONS FOR ALTERNATIVES 101
might be explained by how a lack of strategies result in ad hocnursing care leaving nurses stressed, disempowered and lackinghope when caring for patients who self-harm (Thompson et al.,2008; Wilstrand, Lindgren, Gilje, & Olofsson, 2007). Accord-ing to Knutzen et al. (2014) the risk for frequent use of restraintscan be better explained by professional caregivers’ inadequateresponse to patient behaviour and symptoms than by patientcharacteristics.
The results showed that the participants want to be listened to.They wish that the staff members put their own preconceptionsaside and open-up to their experience and truly listen, tryingto understand what the patient needs. Koekkoek et al. (2010)confirmed that patients stress the importance of listening be-ing based on true interest and authenticity, not just professionalcourtesy. According to Barker (2001), it is crucial to allow pa-tients to verbalise their experiences and perceived meanings inorder to gain a common understanding. To achieve that kind ofnursing care, Barker advocates a narrative-based form of carepractice. Barker (2001) argues, as the results of this study alsoshow, that the process of psychiatric care can reinforce a feelingof disempowerment. Patients testify that professional caregiversoften concentrate on what patients cannot do instead of shiftingfocus and building on what they can do (Koekkoek et al., 2010).
An important aspect of listening, which was emphasised inthe results, is to respect that the patient may have differentoptions and be willing to let go some of your own power (Lind-gren et al., 2011). It is important to see the patient as a personwith strengths and knowledge. This will shift attention towardshow the patient can utilise these resources in their own care.Lloyd (2007) interviewed acute mental health nurses about howthey use empowerment and found four important componentsto achieve an empowering practice: using responsibility wisely;understanding of mental illness; working in a team; and devel-oping relationships. This means that rigid general rules are notcompatible with individualistic person-centred care and empow-ering approaches. This is not to say that everything the patientwishes for is to be accepted by staff. Sometimes, nurses mustuse their power, assume responsibility and temporarily violatethe patient’s autonomy. But if that happens, measures must betaken to restore the power balance, e.g. have a debriefing sessionas soon as possible to restore the power balance (Lloyd, 2007).
It is well known that patients in Swedish inpatient psychiatrywish for a closeness and attention of staff members but expe-rience feelings of abandonment, futility and distrust (Carlssonet al., 2006; Horberg, Sjogren, & Dahlberg, 2012; Olofsson &Jacobsson, 2001). In the results, participants described not onlyhow they long for help and support, but also how they possessabilities and knowledge that they would like to utilise in collab-oration with caregivers. Professional caregivers might perceivethis as contradictory, as patients who self-harm are traditionallyperceived as manipulative and lacking the capacity to under-stand what is best for them; a view resulting in paternalisticcare characterised by rules and containment (Lindgren et al.,2011; O’Donovan, 2007; Thompson et al., 2008). Consistent
with these views on patients who self-harm is a constant dis-trust among professional caregivers towards the patient and asa result, patients that are able to articulate their needs and seekhelp before harming themselves are assessed as not in need ofcare (Koekkoek et al., 2010).
Professional caregivers might also perceive self-harm be-haviour as intentionally directed towards persons close to them.They fear that the patient might commit suicide and then conse-quently focus on risk-reduction instead of providing support tothe person who self-harms (Thompson et al., 2008; Wilstrandet al., 2007), a finding supported by the results of this study.We suggest that both caregivers’ fear being manipulated and thepotential risk for the patient to commit suicide counteracts col-laboration and flexible care of the patient. Instead, it promotesa care based on confrontation, rules, intimidation and coercion.It would seem that skilled and confident professional caregiverswith the ability to uphold mutual, trusting relationships withpatients are better off when it comes to providing restraints-free care. Baker, Bowers and Owiti (2009) suggest that fewerrestrictions may promote better treatment acceptance and saferoutcomes. Several other studies support the notion that it is pos-sible to reduce or minimise the need for coercive measuresin inpatient psychiatry (Huckshorn, 2004; McCue, Urcuyo,Lilu, Tobias, & Chambers, 2004; Salzmann-Erikson, Lutzen,Ivarsson, & Eriksson, 2008; Stewart et al., 2010).
However, the results of this study suggest some commonwishes that might support professional caregivers in making acollaborative effort with the patient. This might lead towardsan individualised care, in which caregiver and patient cometogether without preconceptions and the patient is seen as aperson, resulting in a mutual and trusting relationship and a carepractice built on knowledge instead of a limiting fear.
LimitationsThis delimited qualitative study provides knowledge that can
increase the understanding of how patients can experience co-ercive measures and alternatives that can be used, but the studyis based on a rather small sample (n = 19). This type ofdata collection is not dependent on where the participant stays,so the accounts in this study cannot be explained by a uniquecare culture in one hospital. It has also been found that theanonymity allows far more candid answers (O’Connor, Madge,Shaw, & Wellens, 2008). A weakness with this type of self-report is that you are not able to follow-up important threadsor contact the informants for clarifying questions. As data werecollected through self-reports from a homepage, we have nobackground data about the participants, but found it not to benecessary for this study. All self-reports who offered a statementand all text in each report was included. Most of the reports werereally homogenous and very rich in content. The richness canbe explained by the time the participants had to reflect on theiranswers. Under some circumstances, it can be important to getmore spontaneous answers and then this type of data collection

102 G.-M. EJNEBORN-LOOI ET AL.
is not suitable (O’Connor et al., 2008), but in this study that wasnot the aim. Another weakness with self-reports via social me-dia is that we do not know why some chose to write their story,while others do not and if the participants who chose to partic-ipate might have, e.g. significantly bad experiences. However,most of the reports included both good and bad experiences. Thetrustworthiness of the results is also supported by the system-atic and structured work with the analysis of data by the authors(Graneheim & Lundman, 2004).
CONCLUSIONS AND IMPLICATIONSThis study indicates a paradoxical situation in inpatient psy-
chiatric care putting persons who self-harm in a catch-22 sit-uation. If they do not say what they need they will not get it,but if they say what they need they are denied it. The logicbehind this is that caregivers believe patients who self-harm tobe manipulative. This is in contrast to the results of this study,which suggest that patients are actually forced to behave in a‘manipulative’ way as a response to caregivers’ disbelief. Asa result, the care will not be in line with the patient’s wishesand needs and the distrustful approach creates a psychiatric carethat is counterproductive for its own purposes and could bestbe described as self-destructive. The self-destructive care re-inforces and triggers destructive means of communication inpersons who self-harm. Patients are left feeling misunderstood,abandoned and violated. As a consequence, many of them tryby all means to avoid contact with the psychiatric care system,which often in the end results in involuntarily hospitalisationand coercive measures.
Much is to be gained if caregivers were to listen to thepatients. Starting with the descriptions offered in this study,it would seem that providing a flexible, person-centred care,adapted to a patient’s individual needs, is not that difficult. Itwould make life on the ward easier for both patients and care-givers, resulting in quality care, in which the need for coercivemeasures is minimised.
• Work proactively – pay attention to signs of deteri-oration in time and put in agreed actions as soon aspossible
• Listen, try to understand and assume that what thepatient says is true
• Implement a care plan that is individualised and flexi-ble – reject the general rules, threats and consequences
• Share your power with the patient and strive for mu-tual cooperation, both around the planning of care anddischarge
• Avoid self-harm by building a trusting relationship – asafer tool than limiting the care environment
• Achieve the patients’ needs during the hospital stayso the patient has strengthened potential at discharge,needs can relate to hope, self-esteem or empowerment
• Avoid coercion measures but never make it an overar-ching goal; it may in some cases be a justifiable actionbased on specific individual needs.
Declaration of Interest: The authors report no conflicts ofinterest. The authors alone are responsible for the content andwriting of the paper.
REFERENCESBaker, J. A., Bowers, L., & Owiti, J. A. (2009). Wards’ features associated with
high rates of medication refusal by patients: A large multi-centred survey.General Hospital Psychiatry, 31(1), 80–89.
Barker, P. (2001). The tidal model: Developing an empowering, person-centredapproach to recovery within psychiatric and mental health nursing. Journalof Psychiatric and Mental Health Nursing, 8(3), 233–240.
Bonner, G., Lowe, T., Rawcliffe, D., & Wellman, N. (2002). Trauma for all: Apilot study of the subjective experience of physical restraint for mental healthinpatients and staff in the UK. Journal of Psychiatric and Mental HealthNursing, 9(4), 465–465.
Bowers, L., Ross, J., Owiti, J., Baker, J., Adams, C., & Stewart, D. (2012).Event sequencing of forced intramuscular medication in England. Journal ofPsychiatric and Mental Health Nursing, 19(9), 799–806.
Carlsson, G., Dahlberg, K., Ekebergh, M., & Dahlberg, H. (2006). Patientslonging for authentic personal care: A phenomenological study of violentencounters in psychiatric settings. Issues in Mental Health Nursing, 27(3),287–305.
Fisher, W. A. (1994). Restraint and seclusion: A review of the literature. Amer-ican Journal of Psychiatry, 151(11), 1584–1591.
Graneheim, U. H. & Lundman, B. (2004). Qualitative content analysis in nurs-ing research: Concepts, procedures and measures to achieve trustworthiness.Nurse Education Today, 24(2), 105–112.
Haglund, K., von Knorring, L., & von Essen, L. (2003). Forced medicationin psychiatric care: Patient experiences and nurse perceptions. Journal ofPsychiatric and Mental Health Nursing, 10(1), 65–72.
Holm, H., Bjorkdahl, A., & Bjorkenstam, E. (2011). Tvangsvard medfragetecken [Compulsory care with a question mark]. Lakartidningen,108(34), 1544–1545.
Hooff, S. & Goossensen, A. (2013). How to increase quality of care duringcoercive admission? A review of literature. Scandinavian Journal of CaringSciences, 28(3), 425–434.
Huckshorn, K. A. (2004). Reducing seclusion restraint in mental health usesettings: Core strategies for prevention. Journal of Psychosocial Nursing andMental Health Services, 42(9), 22–33.
Horberg, U., Sjogren, R., & Dahlberg, K. (2012). To be strategically strug-gling against resignation: The lived experience of being cared for inforensic psychiatric care. Issues in Mental Health Nursing, 33(11), 743–751.
James, K., Stewart, D., & Bowers, L. (2012). Self-harm and attempted suicidewithin inpatient psychiatric services: A review of the literature. InternationalJournal of Mental Health Nursing, 21(4), 301–309.
Jarrett, M., Bowers, L., & Simpson, A. (2008). Coerced medication in psychi-atric inpatient care: Literature review. Journal of Advanced Nursing, 64(6),538.
Katsakou, C. & Priebe, S. (2006). Outcomes of involuntary hospital admission–areview. Acta Psychiatrica Scandinavica, 114(4), 232–241.
Katsakou, C., Rose, D., Amos, T., Bowers, L., McCabe, R., Oliver, D., et al.(2012). Psychiatric patients’ views on why their involuntary hospitalisationwas right or wrong: A qualitative study. Social Psychiatry and PsychiatricEpidemiology, 47(7), 1169–1179.
Knutzen, M., Bjørkly, S., Eidhammer, G., Lorentzen, S., Mjøsund, N. H.,Opjordsmoen, S., et al. (2014). Characteristics of patients frequently

SELF-REPORTS OF COERCIVE MEASURES AND SUGGESTIONS FOR ALTERNATIVES 103
subjected to pharmacological and mechanical restraint – a register studyin three Norwegian acute psychiatric wards. Psychiatry Research, 215(1),127–133.
Koekkoek, B., van Meijel, B., & Hutschemaekers, G. (2006). Difficult patientsin mental health care: A review. Psychiatric Services, 57(6), 795–802.
Koekkoek, B., van Meijel, B., van Ommen, J., Pennings, R., Kaasenbrood, A.,Hutschemaekers, G., et al. (2010). Ambivalent connections: A qualitativestudy of the care experiences of non-psychotic chronic patients who areperceived as ‘difficult’ by professionals. BMC Psychiatry, 10(1), 96.
Kontio, R., Joffe, G., Putkonen, H., Kuosmanen, L., Hane, K., Holi, M., et al.(2012). Seclusion and restraint in psychiatry: Patients’ experiences and practi-cal suggestions on how to improve practices and use alternatives. Perspectivesin Psychiatric Care, 48(1), 16–24.
Krippendorff, K. (2013). Content analysis: an introduction to its methodology(3rd ed.) Thousand Oaks, CA: Sage.
Lindgren, B., Wilstrand, C., Gilje, F., & Olofsson, B. (2004). Struggling forhopefulness: A qualitative study of Swedish women who self-harm. Journalof Psychiatric and Mental Health Nursing, 11(3), 284–291.
Lindgren, B., Oster, I., Astrom, S., & Hallgren Graneheim, U. (2011). ‘Theydon’t understand . . . you cut yourself in order to live.’ Interpretative reper-toires jointly constructing interactions between adult women who self-harmand professional caregivers. International Journal of Qualitative Studies onHealth and Well-Being, 2011, 6.
Lindsey, P. L. (2009). Psychiatric nurses’ decision to restrain. Journal of Psy-chosocial Nursing and Mental Health Services, 47(9), 41–49.
Lloyd, M. (2007). Empowerment in the interpersonal field: Discourses of acutemental health nurses. Journal of Psychiatric and Mental Health Nursing,14(5), 485–494.
Looi, G. E., Gabrielsson, S., Savenstedt, S., & Zingmark, K. (2014). Solvingthe staff’s problem or meeting the patients’ needs: Staff members’ reasoningabout choice of action in challenging situations in psychiatric inpatient care.Issues in Mental Health Nursing, 35(6), 470–479.
Marangos Frost, S. & Wells, D. (2000). Psychiatric nurses’ thoughts and feelingsabout restraint use: A decision dilemma. Journal of Advanced Nursing, 31(2),362–369.
McCue, R. E., Urcuyo, L., Lilu, Y., Tobias, T., & Chambers, M. J. (2004).Reducing restraint use in a public psychiatric inpatient service. Journal ofBehavioural Health Services & Research, 31(2), 217–224.
Muralidharan, S. & Fenton, M. (2006). Containment strategies for peoplewith serious mental illness. Cochrane Database of Systematic Reviews, 3,CD002084.
Nelstrop, L., Chandler-Oatts, J., Bingley, W., Bleetman, T., Corr, F., Cronin-Davis, J., et al. (2006). A systematic review of the safety and effectivenessof restraint and seclusion as interventions for the short-term management ofviolence in adult psychiatric inpatient settings and emergency departments.Worldviews on Evidence-based Nursing, 3(1), 8–18.
O’Connor, H., Madge, C., Shaw, R., & Wellens, J. (2008). Internet-based inter-viewing. In N. Fielding, R. M. Lee, & G. Blank (Eds), The SAGE handbookof online research methods (pp. 271–289). Thousand Oaks, CA: Sage.
O’Donovan, A. (2007). Patient-centred care in acute psychiatric admission units:Reality or rhetoric? Journal of Psychiatric and Mental Health Nursing, 14(6),542–548.
Olofsson, B. & Jacobsson, L. (2001). A plea for respect: Involuntarily hos-pitalised psychiatric patients’ narratives about being subjected to coercion.Journal of Psychiatric and Mental Health Nursing, 8(4), 357–366.
Raboch, J., Kalisova, L., Nawka, A., Kitzlerova, E., Onchev, G., Karastergiou,A., et al. (2010). Use of coercive measures during involuntary hospitalisa-tion: Findings from ten European countries. Psychiatric Services, 61(10),1012–1017.
Sailas, E. & Fenton, M. (2000). Seclusion and restraint for people with seriousmental illnesses. Cochrane Database of Systematic Reviews, (2):CD001163.
Salzmann-Erikson, M., Lutzen, K., Ivarsson, A. B., & Eriksson, H. (2008).The core characteristics and nursing care activities in psychiatric intensivecare units in Sweden. International Journal of Mental Health Nursing, 17(2),98–107.
Sibitz, I., Scheutz, A., Lakeman, R., Schrank, B., Schaffer, M., & Amering, M.(2011). Impact of coercive measures on life stories: Qualitative study. BritishJournal of Psychiatry, 199(3), 239–244.
Soininen, P., Valimaki, M., Noda, T., Puukka, P., Korkeila, J., Joffe, G., et al.(2013). Secluded and restrained patients’ perceptions of their treatment. In-ternational Journal of Mental Health Nursing, 22(1), 47–55.
Stewart, D., Van der Merwe, M., Bowers, L., Simpson, A., & Jones, J. (2010). Areview of interventions to reduce mechanical restraint and seclusion amongadult psychiatric inpatients. Issues in Mental Health Nursing, 31(6), 413–424.
Thompson, A. R., Powis, J., & Carradice, A. (2008). Community psychiatricnurses’ experience of working with people who engage in deliberate self-harm. International Journal of Mental Health Nursing, 17(3), 153–161.
Wilstrand, C., Lindgren, B. M., Gilje, F., & Olofsson, B. (2007). Being bur-dened and balancing boundaries: A qualitative study of nurses’ experiencescaring for patients who self-harm. Journal of Psychiatric and Mental HealthNursing, 14(1), 72–78.

Delstudie II


Easy but not simple –
Nursing students’ descriptions of the process of
care in a psychiatric context
Running title:
The process of care in a psychiatric context
Authors: Ejneborn Looi, Git-Marie, RPN, RN, MSc Sävenstedt, Stefan, RN, PhD, Professor Engström, Åsa, RN, CCN, MSc, PhD, Associate Professor Department of Health Sciences, Luleå University of Technology, Luleå, Sweden Corresponding author: Git-Marie Ejneborn-Looi Department of Health Sciences, Luleå University of Technology, 971 87 Luleå, Sweden E-mail: [email protected] Phone: +46703281236 Fax: +46920491399
1

Abstract
The nurse-patient interaction is the cornerstone of psychiatric care, yet the
concept “mental health nursing” is difficult to describe. This paper aims to
address this problem through the experiences of nursing students. Online
journals from 14 nursing students were analyzed using qualitative content
analysis, resulting in three categories: “Trusting the trusting relationship”,
“Voicing the unspoken needs” and “Balancing the dynamics of doing and
being”. The study demonstrates that providing nursing care based on
trusting relationships is not a demanding task, but it takes place in a
complex environment with a tendency to make easy things complicated.
Key words: the process of care, mental health nursing, relationship, need
assessment, interventions
2

Both researchers and clinicians struggle to articulate the content of nursing
practice in psychiatric mental health care. This paper aims to address this
challenge through nursing students’ descriptions of their work with
patients in different types of psychiatric care settings. Their work in this
paper will be called “the process of care” and includes building
relationships, assessing needs and abilities, and implementing interventions
(actions including a conscious approach).
The nursing process traditionally starts with an assessment (data
collection). It continues with planning, implementation of the chosen
nursing intervention, and evaluation (Yura & Walsh, 1988). Others add
making a diagnosis to the process (Carnevali, 1983; Gordon, 2002). In
these descriptions of the nursing process, the nurse-patient relationship is
seldom included or may simply be taken for granted. In contrast,
Halldorsdottir (2008) argues that the nurse-patient relationship is the most
fundamental aspect of professional nursing. If the relationship reaches what
Halldorsdottir calls “a life-giving nurse-patient relationship”, it can
significantly empower the patient and increase his or her feelings of health
and well-being, summarized as empowerment (Halldorsdottir, 2008).
From their literature review, Cleary, Hunt, Horsfall and Deacon (2012)
describe that the nurse-patient interaction continues to be the cornerstone
of psychiatric inpatient care, and mental health nursing, often described as
an empowering process, distinctly stresses the nurse-patient relationship as
an essential factor (Barker & Buchanan-Barker, 2010; Lakeman, 2012;
Svedberg, 2011). However, according to Looi and Hellzén (2006),
insecurity about how nurses are expected to act in a nurse-patient
relationship results in different approaches that are strongly influenced by
each nurse’s personal view of what the “right” caring approach entails.
Barker and Buchanan-Barker (2008; 2011) consider that that the concept
3
“mental health nursing” is still a myth, i.e. many professionals believe in it
and value it highly, yet describing and defining the concept is difficult and
quite vague.
The nursing students who participated in this study formulate and reflect
on the process of care in online journals, e.g. what they are doing, how
they do it, and why they do it. According to Dewey (1938), when a
theory has been tried out in practice, reflecting upon the experience is a
good opportunity to develop knowledge. Using reflective journals as a
pedagogic tool for nursing students during their clinical placement offers
positive experiences (Kok & Chabeli, 2002; Landeen, Byrne, & Brown,
1995). It is also known that a good patient-student relationship can benefit
both the patient’s health and the student’s learning process (Suikkala &
Leino-Kilpi, 2001; 2005). However, using nursing students’ experiences
recorded in reflective online journals doesn’t seem to be common, and it
appears that the process of care, from establishing relationships to the
implementation of an intervention, has not yet been described from their
perspectives.
The students in this study were included due to their successful work with
patients with changeling behavior. The aim of this study is to investigate
the process of care by describing these nursing students’ reasoning and
experiences related to creating relationships, conducting needs assessments,
and choosing interventions in psychiatric care.
4

METHOD
This study applies a qualitative design and has an abductive approach,
which can be suitable for renewing patterns and acquiring a deeper
understanding of caring (Eriksson & Lindström, 1997). The data is based
on nursing students’ descriptions of their work in different psychiatric
inpatient settings as recorded in reflective online journals.
Context
The psychiatric nursing care course took place during the second year of a
three-year university course to become a registered nurse in Sweden. The
nursing students previously had about 10 weeks’ experience of nursing
practice within somatic care. The full-time course was 5 weeks in
duration, and practical skills and theoretical knowledge were combined,
practised and examined. Workplace training was conducted in different
areas of psychiatry: forensic psychiatry (5), municipal psychiatry (2),
addiction unit (1), emergency psychiatry (3), and general psychiatry (3).
The patients for whom the students cared suffered mostly from different
types of schizophrenia, severe depression, neuropsychiatric diagnoses, and
self-harming behaviours. Most were admitted involuntarily.
The nursing students’ assignment was to work with a patient and attempt
to establish a relationship, identify needs, and plan, perform, and evaluate
the chosen interventions. The students continuously documented their
work in reflective online journals; those chosen for this study contained
approximately 5,000–15,000 words each. The students reflected on and
argued for their assessments and choices, and they received feedback from
a lecturer a couple of times during the course.
5
Participants
Seventeen (17) former students (16 women and one man) who had
succeeded in establishing relationships with patients known to be
“challenging” were selected and asked if they were interested in
participating in the study. The requests were sent by post, and students
could respond either by post or email. A lack of a response was interpreted
as a no. Fourteen (14) students, all female, agreed to participate, two did
not respond, and one letter was returned because it had been sent to the
wrong address.
Analysis
The analysis commenced by reading the nursing students’ journals. The
text that described aspects of the care process was sorted into three content
areas (cf. Graneheim & Lundman, 2004): relationships, needs and
interventions. Next, the texts from each content area were divided into
meaning units and were assigned a numerical code so that each meaning
unit could be traced back to each journal. Then, each content area was
analyzed separately, first by reading the text to understand what each
content area was about in more detail, and then to categorize the meaning
units step-wise (cf. Graneheim & Lundman, 2004) to find out what the
students did, how they did it, and for what reason. This process was
discussed and reflected upon by the authors until six sub-categories were
formulated in the three content areas that formed the three final categories
(Table 1).
Methodological considerations
The lectors’ feedback to the nursing students could have affected the
content of the journals and therefore the results. The authors remained
aware of this possibility as they reviewed journals, and only those that
6

received minimal feedback were selected. The feedback was also included
in the initial stages of analysis; this allowed the co-authors to assess the
relationship between the nursing students’ descriptions and the lector’s
feedback, thus reducing the risk that lector would influence the direction
students took. Another risk was that students might have embellished their
work, as they are in a dependent position and will be assessed by the
lector. However, the lector had a continuing dialogue with the supervisor
and clinical lecturer in which they confirmed the descriptions; the risk
seemed mostly to be that they had toned down their own significance and
contributions.
Ethical considerations
Ethical approval was granted by the regional Ethics Committee in Umea
(2010-4-31M), which was also informed of the original design (2012-315-
32M) and approved alterations to it.
7

RESULTS and DISCUSSION
The results were developed from journals written by nursing students who
had successfully managed to create a trusting relationship with patients
who were recognized as “challenging” and who, working with the
patient, had begun a positive health process. The results are shown from
three content areas, categories and sub-categories (Table 1), and together
they form “the process of care”. This involves working with the patient
on different areas (relationships, needs, interventions). The process is not
linear; the nursing students could move back and forth between the
different areas, depending on external and internal factors and renewed
assessments. The same intervention could, in some cases, have the goal of
creating relationships and, in other cases, be chosen with the aim of
satisfying an individual need. However, a trustworthy relationship was
seen as vital to achieving a high quality of nursing care.
------------------------------------- INSERT TABLE 1 ABOUT HERE -------------------------------
Result: Trusting the trusting relationship
The nursing students made a case for a secure and trusting relationship as a
precondition for identifying the patients’ real needs and resources. In
regard to trust, the patients felt secure with the nursing students and had
sufficient confidence to be able to express their thoughts and experiences
about their current situation. Without a trusting relationship, there was a
clear risk of misinterpretation and of needs being overlooked or patients
attributing needs they did not have. All of the nursing students described
that a trusting relationship was a precondition for helping patients feel that
the students were involved in their care.
8

How to support a trusting relationship
By being easily approachable and showing that they had time and an
interest in the patients, the students created opportunities for interactions.
Being confirmatory and showing genuine interest in the patient as an
individual was the most frequently described condition for creating
relationships. Students demonstrated their interest by listening, trying to
understand, and being present in the patient’s pain and suffering, thereby
strengthening the relationship. They also found that it was just as
important to be approachable and to listen when the patient was well and
described his or her interests, wishes and other issues that were important
for the patient to raise. Another important aspect that illustrated their
acknowledgment of patients was that many students described feeling and
clearly showing a sincere and genuine happiness about patients’
improvements and successes.
The nursing students also offered to talk about their own interests and
experiences and to answer patients’ questions. This meant that a feeling of
mutuality could increase if patients and students were close in age or had
similar interests, such as the same tastes in music or sports. Defending a
patient’s integrity and showing respect were described as necessary
prerequisites. These could be achieved in many ways, but in general, the
nursing students considered that it was important to approach the patient
when the patient wanted to be approached and to always ask about the
patient’s preferences. Doing so also strengthened the patient’s autonomy
by encouraging him or her to make as many decisions as possible and trust
his or her own ability.
The staff were totally impressed that I have been able to create such a
good relationship with him in such a short time. By really just being,
9

I try not to stress him but allow him to decide what our meeting will
be like. (Student 9)
Honesty was also an important factor in creating relationships. The
students described being careful to make only promises that they were sure
they could keep. They were also clear about why they were on the ward
and how long they would be there so that patients wouldn’t feel let down
and abandoned. In addition, the nursing students used different kinds of
“tools” to encourage building the relationship; for example, they could
choose to introduce various documents that gave them a reason to follow
up with a patient.
Through the sleep diary, it became easier to create a safe and trusting
relationship when the patient had a reason to sit down with me and
talk about his own self-assessment. The sleep diary itself was not
important, but it was a good thing to have when he took the
initiative to talk to me about it, but in fact we always got on to other
matters. (Student 1)
The nursing students used different conversation techniques. The majority
described using open-ended questions and active listening, while some
said they spoke with a lower pitch or a softer voice. They also reflected on
their body language; for example, they sat down to signal that they had
time and were interested in what the patient had to say. Inviting patients
to play games or engage in conversations where they had opportunities to
demonstrate their knowledge were other measures that the students found
strengthened their relationships with the patients.
10
How to know if it is a trusting relationship
The nursing students clearly described knowing when a trusting
relationship had advanced. They described small, subtle signs such as
smiles and eye contact and more tangible ones, such as the patient turning
to them for companionship or help with a variety of things.
Patients might shake students’ hands or give them a hug, as well as
cooperating in their own care and treatment. The nursing students
considered that these meant a more-trustworthy relationship had been
created.
My patient asked me if it was my last day tomorrow, and then he
wondered if I could give him the injection. So this morning the
patient asked for the injection on his own initiative. The other staff
were surprised that he came and asked for his injection (he was
usually given a forced injection). (Student 6)
What obstacles are encountered in building relationships
The nursing students also identified several obstacles to building
relationships. For instance, they were well aware of the risk that their
prejudices could affect the conditions for creating a relationship, and
several students described hearing reports about patients who had been
labelled as “hopeless” or aggressive”. A strategy that emerged from several
students was that they wanted to get to know patients before they started
to read about their diagnoses and past histories so the information
wouldn’t influence them. Several students also described being afraid of
certain patients initially but quickly changing their opinions, while others
were fearful of doing something “wrong” and therefore hesitated to make
contact with a patient.
11

She felt so alone and lacking support as she sat in the room with the
doctor’s, nurse’s, daughter’s and my eyes on her. I wanted to move
closer and show by touch that she was safe, but I didn’t dare. No one
else made an attempt to do it either, and I think I got scared of being
a bit too forward. I still regret it … (student 10)
In some cases, the students described how a patient’s personality or
symptoms could complicate creating relationships. They described that
some patients didn’t want their company, and then the only response was
to accept their wishes; however, it could also be a question of the patient
being deeply depressed or paranoid.
The nursing students also discussed the risk of harming the relationship by
carrying out treatments that patients didn’t wish to receive. However, this
meant that the relationship could also be strengthened if students managed
to perform their duties in a way that was beneficial for and agreeable to
the patient.
Maybe she’s scared of injections and this might result in our first
meeting not turning out that positively. But, at the same time, if she
is scared, I can try keeping her fear at bay with calmness and
carefulness. (Student 5)
Discussion: Trusting the trusting relationship
In many cases, the nursing students managed in a short time to achieve a
trustworthy relationship with admittedly “challenging” patients where the
staff had “failed”, which was surprising for both staff and nursing students.
To understand the nursing students’ success, we looked at what they were
doing and the approach they were using, but we also considered the
situations that the students had compared to the nurses (and whether those
conditions could be applied organization-wide). One possible reason
12

could be that the patients perceived the students as more trustworthy and
less threatening because they didn’t have the same authority as the nurses.
Students identified trust as the most important quality in the relationship.
However, according to Hem, Heggen and Ruyter (2008), achieving a
trusting relationship between the nurse and the patient is challenging.
Hem et al. argue the need for trusting relationships in psychiatric care, but
achieving them requires radical change. This kind of improvement is not
realized by increasing staff or raising pay; it requires a change in the
professional nursing role that includes developing effective countercultural
skills. This, in turn, calls for professional development in practice,
education and research (Hem et al., 2008). The nursing students had a
clear mission – to learn how to create a trusting relationship with the
patient, and in that learning process they consciously reflected and
evaluated not only their own actions and approaches but also the responses
of patients in order to develop their skills in relationship-building. It is
well known that reflection and self-reflection are important factors for
nursing students’ progress in personal and practical skills (Cameron &
Mitchell, 1993; Kelly, Hager, & Gallagher, 2014). However, reflection
alone is not enough, according to Dewey’s holistic theory of knowing.
Reflection and action must be combined and are interdependent in the
same way theory and practice are (Hartman, 2003). Taken together,
theory, practise and reflection might have given the students a set of tools
to develop skills to be able to think “outside the box” of traditional care
on the ward, which might be compared to Hem et al.’s (2008)
descriptions of countercultural competence and be one of several
explanations for the students high level of success in creating trusting
relationships.
Another difference was related to the nurses’ many responsibilities and
lack of time compared to the nursing students, who needed to care for
13

only one patient at a time. In a review (Cleary et al., 2012) about nurse-
patient interaction, the authors write that showing interest in the patient
and what they call an integrated triad including listening, understanding,
and responding were critical factors from the patients’ perspectives. These
results about what patients want align well with the students’ descriptions
of their work in this study.
However, if the nurse listens but does not try to understand and respond
to the patient, listening could have the opposite effect and cause the
patient to feel rejected (Hem & Heggen, 2004). According to Hem and
Heggen, a nurse’s rejection of a patient can have two causes, internal
factors (for example, unclear roles and responsibilities; cf. Hem et al.,
2008) and external factors such as inadequate staffing (e.g. not enough
time for the patient). A study by Shattell, Andes and Thomas (2008) found
that if the nurse-to-patient ratio is very low, nurses describe having to be
task-oriented and unable to focus on each patient’s needs. We cannot
know about the staff ratio on the different wards, but based on the nursing
students’ experiences and actual research, if we agree that the nurse-
patient relationship is important for the quality of care, then providing
nurses with adequate working conditions regarding both internal and
external factors is critical.
14

Result: Voicing the unspoken needs
The nursing students described different ways of gathering information
about a patient in order to make an assessment of his or her individual
needs, and then being able to choose the appropriate measures. The most
common and frequent description was that, while they were talking to
patients and listening to try to understand their overall situations, students
were also cognizant of the need to attempt to identify patients’ different
resources and abilities. They also talked with staff and, when appropriate,
with relatives of the patients. Reading medical journals and patients’ self-
assessments was also included in gathering information.
How can different behaviours be understood
In addition to the usual data collection as described above, needs
assessments included identifying and interpreting different signs. The
students were very receptive and tried to understand patients’ different
signals and behaviours. For example, in cases where the patients had been
delusional or deeply depressed, the students believed that it was important
to try to understand what the different behaviours meant since the patients
were unable to express their own needs.
Because he doesn’t have an insight into his illness, I can’t ask him
what the problem is or what he wants. His only problem is that he’s
locked up in totally the wrong place, but during observations and
conversations with him, I have the feeling that he is in need of
security, trust and participation. He’s a man who believes that his
surroundings are poisoning him, and he doesn’t trust anyone.
(Student 6)
15
In other cases, the students were told that behaviours were linked to the
clinical picture, such as when it was difficult to get the patient’s attention
and he or she was withdrawn. However, the students were of the opinion
that withdrawal could have a number of causes and purposes. By this, they
meant that some patients withdrew because they had a pointless and dull
existence, whilst others felt abandoned and felt no affinity with the staff.
In other cases, the students interpreted a patient’s distancing himself or
herself as a coping strategy. Therefore, they considered it important to
learn to read how the patient felt and make new assessments daily to
identify an individual balance between closeness and distance in order to
show respect for the patient without abandoning him or her.
Students also met patients who displayed threatening behaviours, but they
interpreted these more as expressions of the patient’s illness and feeling
frustrated.
I know that he can scare both patients and staff with his behaviour,
which is an expression for him feeling ill; he is often misunderstood,
and he has expressed his gratitude because I have dared to meet him
and suppressed the process. (Student 5)
A nursing student described that staff said she should watch out for a
“chronically aggressive woman”, but instead, she saw a woman with a
chaotic life situation and in despair who felt mistrusted and wrongly
judged. Often, students interpreted a patient’s behaviour more positively
and saw opportunities for the patient’s development; they experienced
rigid rules as often making it more difficult to make individual assessments
of a patient’s needs.
16

Staff forbade a young girl with an eating disorder to heat up food
after 8 p.m. because there’d be too much noise. I wonder about the
reasoning then; I would be happy no matter what time of day a
patient with anorexia nervosa wants to eat. (Student 10)
The students also saw numerous small signs they considered extremely
important to take into consideration.
It is difficult to explain, but she gets so happy when she has her hair
plaited and feels pretty. If she had totally given up hope, she
wouldn’t have cared at all, I believe. Deep inside there is a spark of
life that needs to be reawakened. (Student 1)
The students felt it was obvious to prioritize patients who felt unwell and
saw different behaviours as signals that they would try to respond to. They
found it difficult to understand how staff could reach the opposite
assessment and take an opposing action.
Strongly disputing a decision to leave a hyperventilating, crying,
anxiety-ridden young girl whose upbringing has been insecure (and
who’s experienced so many things I don’t even want to think about)
alone so as not to give her unnecessary attention … I think that her
way of saying that she doesn’t feel well is just by sitting in the
corridor. What kind of pain do we then cause her by ignoring her?
Are we not there to pay attention to the patients? A girl who’s been
fighting her whole life for somebody’s attention and not even when
she is genuinely feeling bad does she get the attention … (Student
10)
17

The nursing students also thought that behaviours they interpreted as
positive signs could, in the staff’s assessment, be used instead against the
patient; students felt these signs could be significant, for example, for a
diagnosis or for the patient being discharged.
“It can’t be true that she’s so depressed because she sits on the sofa
and sometimes smiles.” It’s great that she can smile! But that doesn’t
tell the whole truth about how people feel. (Student 5)
How can a patient’s needs be assessed
The nursing students identified a number of patient needs, some very
specific but most more abstract in nature. The students were of the
opinion that the need for increased self-esteem could express itself through
the patient not demanding anything or having no confidence in his or her
abilities. Some nursing students connected low self-esteem to a patient’s
unkempt appearance, arguing that this could indicate the patient believed
he or she was unworthy of being clean and looking nice. Because many
patients had experienced a number of failures in life, the students reasoned
that the care often focused on the patient’s shortcomings and problems.
I noted that he was looking for some kind of praise or
acknowledgement. Then afterwards I thought about this as he gets a
lot of negative comments because he’s filthy, his clothes are dirty or
his sheets are soiled with snuff. He doesn’t get many positive
comments. (Student 13)
The students felt that many needs were connected, and if they were
successful in satisfying one need, this could contribute to reinforcing other
needs, and hope was a normal positive “side effect”. The need for
increased hopefulness was identified in essentially all patients. The students
argued that many patients described having no belief in the future; they
18
had no energy to fight because “there is no point” and felt that their
existence was pointless. The nursing students argued that patients had a
need for increased participation and empowerment based on that they
rarely participated in decisions concerning their care. The students also
thought that the patients often had insufficient knowledge and
information about their own illness and treatment and lacked coping
strategies for different symptoms such as anxiety, uneasiness, and
restlessness, which the students considered as decreasing patients’ feelings
of empowerment and control over their situation.
Motivation and the need to take the initiative were other common
assessments. Nevertheless, most of the students were very careful when
distinguishing these needs. One student described that it was important to
meet the patient’s need to strengthen his or her sense of initiative “… for
him to get started and do all the things he is motivated to do and that he thinks are
fun and that makes him feel good”. Students also argued that, when they saw
that a patient had received adequate support, he or she was successful in
carrying out different activities; they felt this indicated that the patient had
the will and motivation but lacked the power and ability to get started.
They inferred that, if motivation was lacking, patients might have had the
ability to begin and carry out an activity but lacked the desire and interest
to do so.
It’s not possible to design interventions that motivate the patient to
achieve our goals. It’s important to work out the goals together; we
have listened to what the patient wants to achieve and that the
patient feels involved and motivated to achieve these goals.
Otherwise, we’ll never reach these goals, and it’s also good because
they aren’t the patient’s goals. (Student 1)
19

Trust and confidence were also frequently occurring needs identified by
the students. They were of the opinion that lack of trust could be
manifested by patients not saying how they really felt or being fearful
about eating food or taking their medication. A patient could also
experience the environment as unsafe and frightening. In other cases,
examinations and treatments could be sources of insecurity or the fear that
they wouldn’t have a secure existence when they were discharged.
Discussion: Voicing the unspoken needs
In this study, the nursing students often saw signs and conducted
assessments different from those of staff. This could be for a number of
reasons, and one that is obvious is the students’ lack of experience
compared to most of the nurses. Another is that the students appear to
have focused on patients’ abilities and had a more salutogenic perspective
compared to the nurses, whose perspective could have been more
pathogenic (cf. Jormfeldt, 2011; Svedberg, 2011). Jormfeldt (2011) argues
that promoting health is important in supporting the patient’s self-esteem
and empowerment. Empowerment appears to be the most important
intervention in health promotion from both the patient and staff
perspective (Svedberg, Hansson, & Svensson, 2009). The nursing students’
descriptions are similar to what Svedberg et al. call an empowerment
approach, and this is described additionally when students attempt to
improve relationships with patients and implement interventions.
Furthermore, when they assess a patient, they often identify a need for
enhanced empowerment and improved self-esteem. Research results show
that while low self-esteem should be seen as a risk factor, improved self-
esteem can have a protective function in both physical and mental health
care (Mann, Hosman, Schaalma, & de Vries, 2004).
20
In nursing theories, experience is defined as an important factor for the
quality of care (Benner, 2001; Haldordottir, 2008), but most of the
students had no psychiatric care experience. However, in the psychiatric
context, it sometimes appears that many years of experience can be a
impediment because experienced nurses can be less sensitive in regard to
patients’ needs and may have a more symptom-oriented approach
(Hellzén, Kristiansen, & Norbergh, 2003). In another study, Hellzén
(2004) found that the main factor in regard to how much time a nurse
spent with a patient depended on whether the nurse liked the patient or
not. The students’ lack of experience could have exerted a positive effect,
in the sense that they did not know patients or have much knowledge
about their psychiatric diagnoses. Instead, they have as their assignment
the clear instruction to focus on understanding patients’ needs. Another
possible difficulty for staff as opposed to students is that staff have to deal
with the caring culture, and a common staff approach can lead to a
personal conflict between a focus on relationships with one’s colleagues
versus a patient’s situation and needs (Enarsson, Sandman, & Hellzén,
2008; Looi, Gabrielsson, Sävenstedt, & Zingmark, 2014). Some students
were also critical about the staff’s assessments and argued that some rules
and treatments could have been harmful to patients. The students’ critical
reflections conform to patients’ experiences (Looi, Engström, &
Sävenstedt, 2015).
A third difference between the registered nurses and the nursing students
involved responsibilities. Sometimes patients are assessed as violent, and
assessing the potential for violence is an important task for nurses so that
preventive interventions can be implemented (Björkdahl, Olsson, &
Palmstierna, 2006). The nursing students had no responsibilities in regard
to this kind of task, but when a student met a patient who was considered
aggressive, the student often interpreted the aggressive behaviour
21

differently, and the patient did not express any aggressive behaviours
towards the nursing student. Carlsson, Dahlberg, Ekebergh and Dahlberg
(2006) argue that it is possible to prevent violent encounters with
“authentic personal” and “undisguised” care, approaches similar to what
the nursing students described.
Thus, it seems like the nursing students’ basis for assessments was
understanding and respect for each patient’s own story, “positive”
understanding of patients’ behaviours, and a focus on their capabilities.
Students’ lack of experience can, to some extent, be compensated by not
having been influenced by the caring culture within the institution/ward.
The nursing students had no preconceived opinions and didn’t have to
take the caring culture into account, which might have helped them to
see needs from the patient’s perspective (cf. Looi et al., 2014).
22

Result: Balancing the dynamics of doing and being
The nursing students carried out different types of interventions to meet
individual needs and take advantage of patients’ abilities and resources.
Their descriptions of planning and carrying out interventions described an
approach and an action. It was important that both were included and
visible in the interventions.
What to do, how to do it, and how to be
The nursing students demonstrated that it wasn’t possible to decide on a
specific action in order to address a specific need; rather, different types of
actions were used to address the same needs and vice versa. Conversely,
several approaches were described for more specific needs. For example,
the students were deliberate about listening to and acknowledging the
patients and their abilities to strengthen their self-esteem and intrinsic
value. It was also about providing them with the space and opportunity to
give something back to the nursing students, which was seen as important
for strengthening patients’ self-esteem. Examples of steps taken to
strengthen self-esteem, motivation, and hopefulness include letting
patients teach the students something they were good at, like playing an
instrument, needlework, or a sport.
I’ll let the patient teach me to play a song on the piano; this can
improve his self-esteem when he feels that he is really good at
something and has skills that he can share with others, but also the
feeling of other’s appreciation when he shares his skills and plays
beautifully on the piano. (Student 1)
Sometimes the tables were turned, and a nursing student taught the
patient something, for example, to play a game or make jewellery. The
nursing students could also take excursions with patients, going for coffee
23

or visiting the library with the aim of motivating the patient, breaking the
isolation, and promoting hopefulness. Further steps that the nursing
students mentioned for promoting hope and self-esteem were showing
interest in some of the items patients had created, for example, paintings
and poems. This could also entail the student helping the patient to plait
her hair or put on makeup or giving a massage. Some measures were
clearly connected to tangible needs like hygiene, nutrition or sleep, but
the students added factors that could also satisfy other, more abstract
needs.
After showering I saw that she had very dry skin, so I carefully
rubbed cream onto her, and her husband said that she likes to have a
massage so I took the opportunity to carefully massage the lotion onto
her legs, also with the aim to increase blood circulation, considering
her immobilization, as well as to increase well-being and self-esteem.
(Student 5)
Conversations and walks were frequently occurring measures described by
the nursing students, but in some cases the students chose unique measures
to satisfy individual needs.
Yesterday a male opiate addict and I were taking the drainpipe away
from the sink to clean it. We had fun together, and he enjoyed
having something to do despite the fact that it was a pretty disgusting
task. Otherwise, he only walked around nervously waiting for his
medication. (Student 7)
Rearranging the furniture in a patient’s room was a measure aimed to
create a sense of safety for a paranoid patient who didn’t dare to be in the
room. Teaching the patient different coping strategies to handle worry,
anger, and anxiety was also a common measure aimed at strengthening the
24

patient’s feeling of control and empowerment and thereby contributing to
a sense of security.
The approaches that the nursing students described to encourage
participation and empowerment might include the patient being able to
choose between different activities and decide both the design and time of
the activity, with the aim of encouraging and respecting the patient’s
autonomy and participation in decision-making. The students could also
choose some unusual approaches to traditional steps, for example, not only
giving information but also satisfying abstract needs.
The schedule that he now has is a piece of A4 with times and it
doesn’t work. I thought that you could draw a clock on the
whiteboard in his room and at every specific time, he can write what
he will do during the day. Then he will get the visual part with the
clock and through that it might be easier for him to remember, and
besides, if he writes it down himself he needs to think what he will
do and to memorize it and to write down the information himself
too. The combination of several senses, I believe, will make it easier
for him to remember the things he needs to do, which in turn will
increase his self-esteem and empowerment. (Student 9)
To strengthen the patient’s ability for initiative, the student could “push”
the patient in an encouraging and supportive way both verbally and
physically, for example, by laying out things the patient needed and
guiding the patient step by step or gradually handing over the
responsibility for different tasks to the patient. They described it as
important for them to ensure that the demands on the patients were at a
reasonable level so they would feel competent and not experience failure.
Some steps could also be connected to satisfying many abstract needs at
the same time.
25
The conversation that was created around the sleep diary makes him
feel that someone has time for him, listening to him, and really takes
him seriously, which also strengthens his participation and self-
esteem; self-esteem is also strengthened by him feeling that he can
manage the task; also, his ability to take the initiative is strengthened
when he has the responsibility to take initiative to fill in his sleep
diary on a daily basis. (Student 1)
The nursing students were generally given the freedom to try out different
interventions, but in some cases, they were forced to break the ward’s
rules to show that they took the patient’s suffering seriously and could
take measures to strengthen the patient and help him or her to feel secure
or to encourage a sense of well-being.
Discussion: Balancing the dynamics of doing and being
The nursing students carried out many interventions with the patients;
some of the activities were common ones in a psychiatric ward, such as
talking and going for a walk. However, the nursing students were always
aware of the patients’ needs for planning and working together
collaboratively towards a mutual goal that aligned well with the patient’s
wishes about how care should be conducted (Looi et al., 2015). Aiming to
individualize the intervention, they made evaluations continuously and
were open to altering the intervention and their own approach. Most of
the interventions began with the patient’s abilities or focused on support
or developing the patient’s skills. This way of working is in agreement
with Svedberg’s (2011) model of the process-oriented health promotion
intervention in mental health care; alliance, empowerment, and educational
and practical support are essential concepts of this model.
26

Most of the patients that the students worked with have experienced
coercive measures. A significant difference between the student and the
staff was that the students didn’t have access to coercive measures that
could possibly have a vital significance in the whole process. In planning
and implementing interventions, the students based their decisions on the
patient’s individual needs instead of focusing on correcting behaviours and
solving problems using coercive measures, which can be common
strategies, especially if the nursing staff is under pressure (Looi et al., 2014)
or lack knowledge and hope about the patient’s recovery (Ashcraft &
Anthony, 2008).
The lack of coercive measures may have contributed to the students
having to use alternatives; thus, they developed their repertoire of care
based on mutual cooperation with the patient instead of confrontation (cf.
Ashcraft & Anthony, 2008). This could have contributed to their
successful results in stimulating positive health processes.
Conclusion
One may wonder whether students are the best choice of participants to
answer the research question. In this case, the sample was a few students
who managed surprisingly well with their work with patients with
challenging behaviour. Because they were students they had good
prerequists such as time and opportunity to prioritize a patient. They had
no access to coercive measures which might have created security for the
patient. The students did not know the workplace and were not part of
the regular staff group which meant that they had no knowledge of or
needed to relate to the current health care culture. Students have limited
professional experiences and are therefore not the best choice to describe
the experience of caring for patients in a psychiatric ward, but they have
27

other conditions which can be suitable based on their unique work
situation.
The expression “simple but not easy” is sometimes used to describe a
basically uncomplicated task that still requires considerable effort to
accomplish. The results of this study, however, suggest a situation that can
be characterized as “easy but not simple”. Providing high-quality nursing
care based on trusting relationships is basically not a demanding task, but it
takes place in a complex environment with a tendency to make easy
things complicated.
Clinical implications and further research
The description of the process of care in this paper is not supposed to be
seen as a manual to follow step by step. Rather, it is a framework for those
who work from a nursing perspective where relationships, needs and
interventions are key elements in the planning and design of patient care.
The results show the importance of the nurses has knowledge of,
understand and prioritise the relationship-building in order to lay the
foundations for nursing quality work. This means that the patient nursing
relationship should have plenty of space and priority in nursing education.
As further research it would be interesting to have the patients' perspective
based on the factors they value on the basis of particularly good care
experiences with students as carers.
Declaration of interest: The authors report no conflicts of interest. The
authors alone are responsible for the content and writing of the paper.
28

REFERENCES
Ashcraft, L., & Anthony, W. (2008). Eliminating seclusion and restraint in
recovery-oriented crisis services. Psychiatric Services, 59(10), 1198-1202.
Barker, P., & Buchanan-Barker, P. (2008). Mental health in an age of
celebrity: The courage to care. Medical Humanities, 34(2), 110-114.
Barker, P., & Buchanan-Barker, P. (2010). The tidal model of mental
health recovery and reclamation: Application in acute care settings. Issues
in Mental Health Nursing, 31(3), 171-180.
Barker, P., & Buchanan-Barker, P. (2011). Myth of mental health nursing
and the challenge of recovery. International Journal of Mental Health Nursing,
20(5), 337-344.
Benner, P. E. (2001). From novice to expert: Excellence and power in clinical
nursing practice. (Commemorative ed.). Upper Saddle River, NJ: Prentice
Hall.
Björkdahl, A., Olsson, D., & Palmstierna, T. (2006). Nurses' short-term
prediction of violence in acute psychiatric intensive care. Acta Psychiatrica
Scandinavica, 113(3), 224-229.
Cameron, B. L., & Mitchell, A. M. (1993). Reflective peer journals:
Developing authentic nurses. Journal of Advanced Nursing, 18(2), 290-297.
Carlsson, G., Dahlberg, K., Ekebergh, M., & Dahlberg, H. (2006).
Patients longing for authentic personal care: A phenomenological study of
violent encounters in psychiatric settings. Issues in Mental Health Nursing,
27(3), 287-305.
Carnevali, D.L. (1983). Nursing care planning: Diagnosis and management.
(3rd ed.) London: Lippincott.
29
Cleary, M., Hunt, G. E., Horsfall, J., & Deacon, M. (2012). Nurse-patient
interaction in acute adult inpatient mental health units: A review and
synthesis of qualitative studies. Issues in Mental Health Nursing, 33(2), 66-
79.
Dewey, J. (1938). Experience and education. New York: Macmillan.
Enarsson, P., Sandman, P., & Hellzén, O. (2008). “Being good or evil”:
Applying a common staff approach when caring for patients with
psychiatric disease. International Journal of Qualitative Studies on Health and
Well-being, 3(4), 219-229.
Eriksson, K., & Lindström, U. A. (1997). Abduction – A way to deeper
understanding of the world of caring. Scandinavian Journal of Caring
Sciences, 11(4), 195-198.
Gordon, M. (2002). Manual of nursing diagnosis: including all diagnostic
categories approved by the North American Nursing Diagnosis Association. (10.
ed.) St. Louis, Mo.: Mosby.
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in
nursing research: Concepts, procedures and measures to achieve
trustworthiness. Nurse Education Today, 24(2), 105-112.
Halldorsdottir, S. (2008). The dynamics of the nurse-patient relationship:
Introduction of a synthesized theory from the patient's perspective.
Scandinavian Journal of Caring Sciences, 22(4), 643-652.
Hartman, S. (2003). Läraren från Oil city – inför det nyväckta intresset för
John Dewey [The teacher from Oil City - faced with the resurgence of
the John Dewey]. In S. G. Hartman, K. Roth & N. Rönnström John
Dewey: om reflektivt lärande i skola och samhälle [John Dewey: on
reflective learning in school and society]. Stockholm: HLS Förlag.
30

Hellzen, O. (2004). Nurses' personal statements about factors that
influence their decisions about the time they spend with residents with
long-term mental illness living in psychiatric group dwellings. Scandinavian
Journal of Caring Sciences, 18(3), 257-263.
Hellzén, O., Kristiansen, L., & Norbergh, K. G. (2003). Nurses' attitudes
towards older residents with long-term schizophrenia. Journal of Advanced
Nursing, 43(6), 616-622.
Hem, M. H., & Heggen, K. (2004). Rejection – A neglected
phenomenon in psychiatric nursing. Journal of Psychiatric and Mental Health
Nursing, 11(1), 55-63.
Hem, M. H., Heggen, K., & Ruyter, K. W. (2008). Creating trust in an
acute psychiatric ward. Nursing Ethics, 15(6), 777-788.
Jormfeldt, H. (2011). Supporting positive dimensions of health, challenges
in mental health care. International Journal of Qualitative Studies on Health
and Well-being, 6(2).
Kelly, M. A., Hager, P., & Gallagher, R. (2014). What matters most?
Students’ rankings of simulation components that contribute to clinical
judgment. Journal of Nursing Education, 53(2), 97-101.
Kok, J., & Chabeli, M. M. (2002). Reflective journal writing: How it
promotes reflective thinking in clinical nursing education: A students'
perspective. Curationis, 25(3), 35-42.
Lakeman, R. (2012). What is good mental health nursing? A survey of
Irish nurses. Archives of Psychiatric Nursing, 26(3), 225-231.
Landeen, J., Byrne, C., & Brown, B. (1995). Exploring the lived
experiences of psychiatric nursing students through self-reflective journals.
Journal of Advanced Nursing, 21(5), 878-885.
31
Looi, G. E., Engström, Å., & Sävenstedt, S. (2015). A self-destructive
care: Self-reports of people who experienced coercive measures and their
suggestions for alternatives. Issues in Mental Health Nursing, 36(2), 96-103.
Looi, G. E., Gabrielsson, S., Sävenstedt, S., & Zingmark, K. (2014).
Solving the staff's problem or meeting the patients' needs: Staff members'
reasoning about choice of action in challenging situations in psychiatric
inpatient care. Issues in Mental Health Nursing, 35(6), 470-479.
Looi, G. E., & Hellzén, O. (2006). Nurses' perception of the relationship
between themselves and the long-term psychiatric client – An interview
study. Primary Care and Community Psychiatry, 11(4), 185-192.
Mann, M., Hosman, C. M. H., Schaalma, H. P. & de Vries, N. K.,
(2004). Self-esteem in a broad-spectrum approach for mental health
promotion. Health Education Research, 19(4), 357-372.
Shattell, M. M., Andes, M., & Thomas, S. P. (2008). How patients and
nurses experience the acute care psychiatric environment. Nursing Inquiry,
15(3), 242-250.
Suikkala, A., & Leino-Kilpi, H. (2001). Nursing student-patient
relationship: A review of the literature from 1984 to 1998. Journal of
Advanced Nursing, 33(1), 42-50.
Suikkala, A., & Leino-Kilpi, H. (2005). Nursing student-patient
relationship: Experiences of students and patients. Nurse Education Today,
25(5), 344-354.
Svedberg, P. (2011). In what direction should we go to promote health in
mental health care? International Journal of Qualitative Studies on Health and
Well-being, 6(2).
32

Svedberg, P., Hansson, L., & Svensson, B. (2009). The attitudes of
patients and staff towards aspects of health promotion interventions in
mental health services in Sweden. Health Promotion International, 24(3),
269-276.
Yura, H. & Walsh, M.B. (1988). The nursing process: Assessing, planning,
implementing, evaluating. (5th ed.). Norwalk: Appleton & Lange.
33

Tab
le 1
. O
verv
iew
of co
nten
t ar
eas
(n=
3),
cate
gori
es (
n=3)
and
sub
-cat
egor
ies
(n=
6)
Conte
nt
C
ateg
ory
S
ub-c
ateg
ory
area
s
Rel
atio
n
Tru
stin
g th
e tr
ustin
g re
latio
nshi
p
How
to
supp
ort
a tr
ustin
g re
latio
nshi
p H
ow t
o kn
ow if
it is
a t
rust
ing
rela
tions
hip
Wha
t ob
stac
les
are
enco
unte
red
in b
uild
ing
rela
tions
hips
N
eeds
Voi
cing
the
uns
poke
n ne
eds
H
ow c
an d
iffer
ent
beha
viou
rs b
e un
ders
tood
H
ow c
an a
pat
ient
’s ne
eds
be a
sses
sed
Inte
rven
tions
B
alan
cing
the
dyn
amic
s of
doi
ng a
nd b
eing
W
hat
to d
o, h
ow t
o do
it a
nd h
ow t
o be

Delstudie III


Issues in Mental Health Nursing, 35:470–479, 2014Copyright © 2014 Informa Healthcare USA, Inc.ISSN: 0161-2840 print / 1096-4673 onlineDOI: 10.3109/01612840.2013.879629
Solving the Staff’s Problem or Meeting the Patients’ Needs:Staff Members’ Reasoning about Choice of Actionin Challenging Situations in Psychiatric Inpatient Care
Git-Marie Ejneborn Looi RPN, RN, MSc and Sebastian Gabrielsson, RPN,RN, MScLulea University of Technology, Department of Health Sciences, Lulea, Sweden
Stefan Savenstedt, RN, PhDLulea University of Technology, Department of Health Sciences, Lulea, Sweden, and Norrbotten CountyCouncil, Department of Research and Development, Lulea, Sweden
Karin Zingmark, RN, PhDNorrbotten County Council, Department of Research and Development, Lulea, Sweden, and LuleaUniversity of Technology, Department of Health Sciences, Lulea, Sweden
Coercion in challenging situations is often seen as a necessarycomponent of psychiatric care. This study aims to describe staffmembers’ reasoning about their choice of action in challenging sit-uations in inpatient psychiatric care. Focus group interviews with26 staff members were analyzed using qualitative content analy-sis. The results provide an overview of the integrated structure ofparticipants’ reasoning and suggest that staff members’ reasoningabout choice of action can be described as a matter of either solvingthe staff’s problems or meeting the patients’ needs. These resultscan be of use in further research, educational interventions, andstaff development activities.
In response to challenging patient-related situations in psy-chiatric settings, staff members choose from a number of pos-sible actions. To date, scant research has focused on the pro-cess of clinical reasoning and decision-making in the contextof challenging situations within psychiatric inpatient care set-tings. Marangos-Frost and Wells (2000) studied how nurses’emotional reactions to violent patients affected the use of re-striction; they found the use of restraints to be complex and thatnormative-affective factors influence nurses’ decisions. Larue,Dumais, Ahern, Bernheim, and Mailhot (2009) presented acategorization of influential factors and suggested a model ofdecision-making that regarded seclusion as centred on the bi-directional relationship of patients and staff as influenced by
Address correspondence to Git-Marie Ejneborn Looi, Lulea Uni-versity of Technology, Department of Health Sciences, Lulea, 97187Sweden. E-mail: [email protected]
environmental and organizational factors, with the team alsobeing a factor. Laiho et al. (2012) conducted a literature reviewto describe factors influencing the decision to use seclusion orrestraints. They concluded that making such a decision is a dy-namic process that consists of evaluating the patient’s behaviour,assessing risk, and implementing de-escalating interventions. Inthis process, staff members take into account the risk towardsthe patient, other patients, and themselves, as well as the needto maintain a therapeutic ward milieu.
For the purpose of this study, a challenging situation is un-derstood to be a patient-related situation that may interfere withthe ability of staff members to deliver quality care and achievedesirable outcomes. Possible responses include the use of co-ercion, which is an area of psychiatric care in need of qualityimprovement (Hooff & Goossensen, 2013). Currently, Swedishlaws regulating compulsory psychiatric care stipulate that coer-cive measures (i.e., mechanical restraints, seclusion, and forcedmedication) may be used only to the extent necessary to impelthe patient to participate voluntarily in his or her care. If suffi-cient, less-intrusive measures should be used. Holm, Bjorkdahl,and Bjorkenstam (2011) analysed official statistics regardingcompulsory psychiatric care in Sweden and found that everythird person subjected to mechanical restraints is a female be-tween 18 to 34 years of age, a group they believed to be diag-nosed predominantly with personality disorder and displayingsuicidal or self-harm behaviours. Among the many negative ex-periences associated with coercive measures and reported bystaff and patients, perhaps the most troubling are reports of co-ercive measures that traumatize patients (Sibitz et al., 2011) and
470
.

CHOICE OF ACTION IN INPATIENT PSYCHIATRIC CARE 471
descriptions of coercion as acts of re-traumatization of already-traumatized persons (Bonner, Lowe, Rawcliffe, & Wellman,2002). The use of containment measures is reportedly based ontradition and common sense rather than on research-based evi-dence (Jarrett, Bowers, & Simpson, 2008; Muralidharan & Fen-ton, 2006; Sailas & Fenton, 2000), and nurses have been shownto be inconsistent in the use of coercive measures (Huckshorn,2004; Lindsey, 2009). Nurses tend to regard the use of coer-cive measures as a necessary component of psychiatric care forwhich there are no alternatives (Haglund, von Knorring, & vonEssen, 2003; Happell & Harrow, 2010; Marangos-Frost & Wells,2000). Levels of conflict behaviour and the use of containmentmeasures on psychiatric wards have been shown to be interre-lated and affected by organizational features; wards with effec-tive leadership, teamwork, structure, positive attitudes towardpatients, and low burnout rates among staff have lower rates ofcontainment events (Bowers, Nijman, Simpson, & Jones, 2011).The use of seclusion and restraint can be dramatically reducedwhen these latter characteristics are made a priority, even insettings perceived as hopeless, such as the inpatient care of per-sons who self-harm (Georgieva, de Haan, Smith, & Mulder,2010).
While the reasoning and decision-making of staff membersin this context have attracted little attention from researchers, abetter understanding of why and how staff members choose touse or not use coercion in challenging situations has the potentialto facilitate the use of alternatives to coercion. The aim of thisstudy is to describe staff members’ reasoning on their choiceof action in challenging situations in inpatient psychiatric caresettings.
MATERIALS AND METHODSIn order to describe the reasoning used by staff members as
they chose their actions in challenging situations, focus groupinterviews were conducted with staff members experienced inacute psychiatric inpatient care; the interviews were transcribedverbatim and analysed using qualitative content analysis. Theresults of a second analysis, describing staff members’ percep-tions of interprofessional collaboration, are reported elsewhere.
Participants and ProcedureStaff members working at a psychiatric clinic in Northern
Sweden were asked to participate in the study. The care climateat this clinic was considered to be representative of Swedishinpatient psychiatry in general, and thus the setting was deemedsuitable for this study. The clinic consisted of several outpatientunits and one general psychiatry inpatient unit with a 24-bedlocked ward and a 24-hour admittance and consultancy service.
A majority of nursing staff at the inpatient unit were nurs-ing assistants with training at the secondary level, followed bypsychiatric nurses (registered nurses with or without psychiatricspecialist training) with undergraduate degrees. Physicians wereexpected to function in both inpatient and outpatient care set-
tings. The ward manager primarily responsible for the inpatientunit, a psychiatric nurse, functioned as part of the clinic’s man-agement team and also had managerial responsibilities outsidethe ward. Policy required a minimum staffing of two psychi-atric nurses and three nursing assistants (at night, the mini-mum staffing requirement was one psychiatric nurse and threenursing assistants), a junior physician in close proximity to theward, and an on-call psychiatrist who was available by phone.The inpatient unit would admit adult persons presenting acutemental health problems on a voluntary or compulsory basis.The premises allowed for the use of mechanical restraints ina designated room and the possibility to secure parts of theward using locked doors. Inpatient treatment options includedpharmacological therapy and electroconvulsive therapy (ECT).Containment measures used on the ward included physical re-straint (staff members holding a patient), mechanical restraint(restricting a patient’s ability to move by using straps), specialobservations (constant and intermittent), time out (the patient isasked to stay in his or her room or another specified area), open-area seclusion (the patient is isolated in a locked section of theward and accompanied by staff), and compulsory intramuscularsedation.
A total of 26 participants including 8 nursing assistants, 10psychiatric nurses, 4 ward managers, and 4 physicians tookpart in the study. Their combined years of work experience inpsychiatric care averaged 10.5 years, with a minimum of 2 yearsof experience working in this field and a maximum of 18 years.There were 12 male and 14 female participants, with an averageage of 44.5 years and an age range from 24 to 66 years of age.The criteria for inclusion in the study were experience workingin psychiatric inpatient care and a willingness to participate.Staff members were informed about the study at staff meetingsby the first and second authors (G-MEL and SG), and they weregiven the opportunity to ask questions. Approximately 50 staffmembers received information about the study; 28 gave theirwritten informed consent to participate; two failed to attend theinterviews.
Data CollectionThe 26 participants were grouped into six focus groups with
four to six participants in each group and were divided accord-ing to profession and number of years of work experience (cf.Morgan, 1997), thus forming one group of experienced nursingassistants and one group with less experience, one group of ex-perienced psychiatric nurses and one group with less experience,and one group of ward managers and one of physicians. For thepurposes of this study, participants with fewer than five yearsof experience in inpatient psychiatry were considered “less ex-perienced.” The interviews were conducted at the participants’workplace between October 2010 and January 2011. Interviewslasted an average of 70 minutes and ranged from 42 minutes(in the case of physicians) to 87 minutes (in the case of wardmanagers). The first and second authors took turns acting as
.

472 G-M. E. LOOI ET AL.
moderators during the interviews. Two senior researchers tookturns acting as assistants to keep track of time and ask addi-tional questions. The interviews were recorded and transcribedverbatim.
As a basis for the focus group interview, the moderator reada vignette describing an act of self-harm:
A young female patient has been cared for at the ward for a week. Shehas been subject to inpatient care several times before. She is nowinvoluntarily admitted after intoxicating herself with paracetamolfor unknown purposes. On several occasions, containment measureshave been taken when she has harmed herself or others at the ward.All staff members (nursing assistants, psychiatric nurses, physicians,ward manager) are sitting down having their morning coffee. Fromthe staff room, they observe the patient running through the hallwaytowards a drinking glass that has been left behind. She picks theglass up, and it breaks as she throws it to the floor. She picks up alarge piece of glass and starts cutting herself deeply in the arm asshe shouts, “Let me out!”
Following the vignette, participants were asked the broadquestion “What happens next?” and later were asked a more spe-cific question, “What would you do?” Participants were asked todiscuss these questions among themselves, and the researcherssummarised the discussions and asked encouraging and clarify-ing questions. To make sure that certain areas of interest werecovered in all groups, an interview guide was used that includedthe following pre-defined topics: mechanical restraints, specialobservation, and professional roles and responsibilities.
AnalysisThe transcribed interviews were analysed using qualitative
content analysis. This is a method of analysing written and ver-bal communication in a systematic way and making replicableand valid inferences from texts (Krippendorff, 2013). FollowingKrippendorff, the content was not understood as a pre-existingentity inherent in the text, but rather as content created duringthe process of reading and analysing the text in a specific contextthat is continuously reconceptualised as the analysis proceeds,thus directing and redirecting the analysis. The context of thisanalysis was understood to be the authors’ understanding ofstaff members’ reasoning on their choice of action in challeng-ing situations. Thus, the analysis can be described as a processin which the authors’ understanding interacted with the text,the outcome being the authors’ reformulated understanding ex-pressed as descriptions and interpretations of the content of thetext.
The analytical process was carried out systematically andstepwise. The text was read as a whole with the aim in mind.Based on this reading of the text, analytical questions corre-sponding to the aim of the study were formulated to guide theanalysis (see Table 1). The analytic process aimed to describepatterns and structures in participants’ reasoning by reviewingthe answers to these questions, thus providing a description of
TABLE 1Analytical Questions Formulated to Guide the Analysis inOrder to Describe Staff Members’ Reasoning on Choice of
Action in Challenging Situations in Psychiatric Inpatient Care
Overarching Question Specific Questions
“How can participants’reasoning on choice ofaction be described?”
1. “Why do participantsconsider certain actions?”
2. “What actions areconsidered byparticipants?”
3. “How are actionsconsidered by participantsdescribed?”
participants’ reasoning on different levels of abstraction andinterpretation (cf. Graneheim & Lundman, 2004).
The analytic process started by answering specific questions.The question, “Why do participants consider certain ac-
tions?”, was answered in several steps. First, meaning unitsin the interview text containing participants’ reasoning on theirchoice of action were identified. These were read, and fourreasons for choosing a particular action were formulated. Par-ticipants’ different reasons for their choice of action were furtheranalysed to distinguish four different focuses that characterisedtheir reasoning.
The second specific question, “What actions are consideredby participants?”, was answered by coding the meaning unitsrelated to participants’ reasoning on their choice of action ac-cording to the type of action they took. In that analysis, eighttypes of actions were identified.
The specific question, “How are the actions considered byparticipants described?”, was answered by grouping meaningunits that previously had been coded for a special action anda special reason for choosing an action together and readingthem repeatedly. The content of each group was analysed, and26 approaches were formulated that simultaneously reflectedqualities of each type of action and the consequences of thedifferent reasons for choosing an action.
As a final step, the overarching question “How can partic-ipants’ reasoning on choice of action be described?”, was an-swered by viewing the text as a whole and considering the resultsof the analysis of the specific questions. In this last step of theanalysis, a theme was identified describing modes of reasoning.
Making replicable and valid inferences from texts in eachstep of answering the analytical questions was ensured througha rigorous process (cf. Krippendorff, 2013). In this process, theformation of different results was constantly cross-reviewed,reformulated, and regularly checked against what was stated inthe original text. All study authors took part in the process ofanalysing the text, and each step was discussed until agreementwas reached (cf. Graneheim & Lundman, 2004).
.

CHOICE OF ACTION IN INPATIENT PSYCHIATRIC CARE 473
Ethical ConsiderationsPrior to conducting the study, ethical approval was granted
by the regional ethics committee in Umea (2010-4-31M), whichalso was informed of the original design (2012-315-32M) andapproved alterations to it.
RESULTSParticipating staff members’ reasoning on the type of action
they took is presented as integrated results where the answer tothe overarching question, “How can participants’ reasoning onchoice of action be described?” is first presented as a theme.Thereafter, the integrated results of the specific questions arepresented from the bases of identified focuses of reasoning.The integrated structure of participants’ reasoning is shown inFigure 1. The results aim to describe patterns and structures inparticipants’ reasoning rather than the experiences and views ofindividual participants or groups of participants.
Modes of Reasoning: Solving the Staff’s Problemsor Meeting the Patients’ Needs
Underlying threads in the participating staff members’ rea-soning formed a theme that described participants’ reasoning asa matter of solving the staff’s problems or meeting the patients’needs. This was understood as a duality of two basic modes ofreasoning that was present throughout their discussions. In theirreasoning, participants would, on one hand, emphasise their ownperspectives and safety at the expense of the individual patient’sneeds, thus making it a priority to solve the staff’s problems.This prioritization was often described as a necessity because ofthe everyday limitations on the ward in terms of overcrowdingand staff shortages, but also as a consequence of staff possess-ing superior knowledge, and patients not knowing what’s bestfor them. On the other hand, participants expressed a desire todeliver high-quality care to patients and a need to understandpatients’ perspectives. They strived to be flexible in order tomeet the needs of individual patients, even if this occasionallymeant taking a stance contrary to the opinions of their superiorsand colleagues. Figure 1 provides a visualisation of the inte-grated structure of the content of participating staff members’reasoning.
Staff-Focused ReasoningOne reason for the choice of action described in the partici-
pating staff members’ discussions was that staff members would“look out for themselves.” Types of actions considered by par-ticipants on the basis of this included responding to the situation,talking with the patient, being with the patient, restraining thepatient, and observing the patient. Approaches described byparticipants that reflected qualities of these types of actions andthe consequences of this staff-focused reasoning are presentedbelow.
In reasoning understood to be staff-focused, participants intheir discussions emphasized the importance of keeping staff
safe when responding to the situation described in the vignette.This could mean physically restraining a patient in order to pro-tect themselves and other staff members. One participant statedthat staff would “react quite instinctively and protect themselvesand try to protect the patient if possible.” In reasoning under-stood to be staff-focused, the action of talking to the patient wasaimed at calming the patient and reducing aggression, thus mak-ing it easier to control the situation without using mechanicalrestraints. Participants described how, if mechanical restraintshad to be used, talking with the patient could “play down theincident” and, it was hoped, cause the patient to “forgive andforget.” In this type of reasoning, being able to keep one’s cooland control one’s temper when with the patient was consideredimportant, since a staff member’s losing his or her temper couldbackfire and provoke the patient. Participants stated that staffmembers who manage to appear calm seldom need to be afraid.Another strategy mentioned for protecting staff members wasnot to be alone; for example, staff members accompanied physi-cians when meeting patients. Using mechanical restraints wasdescribed as another way of protecting staff members and, indoing so, the need to gain and maintain control was empha-sized. Participants perceived that the risk for using mechanicalrestraints increases as staff members become tired and weary,since fatigue causes staff members to desire peace and quiet onthe ward, as illustrated by the following quote:
but the danger is, you have to see how it is here at the ward, becauseunfortunately it’s a downward spiral, because, I mean, it’s only lifesupport really what we’re doing here today, and staff can only copefor so long, so you can only stress it that far and try to calm, andcalm, and calm, and calm, and calm, and give and take and try stuff,like it’s good if we work together towards this goal to try to make youfeel better. You can only manage that for so long with the workloadand shortage of staff we have here, so the danger is that there will bemore coercive measures just to keep it safe.
Accounts also were given of how some staff members actu-ally enjoyed violence and had a wish to become the centre ofattention. Participants described how this would lead them toprovoke patients, resulting in the use of mechanical restraints.Finally, staff-focused reasoning on observing patients using spe-cial observations centred on making it convenient for staff. Inparticular, participants described how they sought to minimizetime spent with especially demanding patients. One participantstated that constant observation can be “very demanding, so youtend to avoid it,” and that this method can be used when physi-cians lack knowledge about a particular patient, since “it’s easyto play it safe.”
Experience-Focused ReasoningThe analysis suggested that another reason for choosing a
particular action was that the patient “needed it.” Types of ac-tions considered by participants on the basis of this reason werethe same as in the reasoning described above, with the additionof engaging the patient in activities and medicating the patient.Approaches discussed in relation to these types of actions when
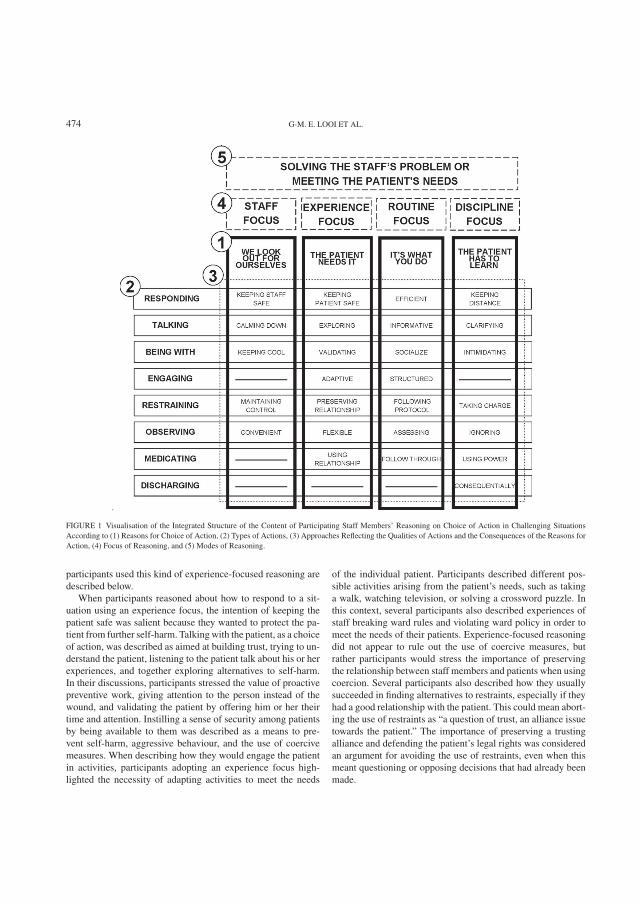
474 G-M. E. LOOI ET AL.
FIGURE 1 Visualisation of the Integrated Structure of the Content of Participating Staff Members’ Reasoning on Choice of Action in Challenging SituationsAccording to (1) Reasons for Choice of Action, (2) Types of Actions, (3) Approaches Reflecting the Qualities of Actions and the Consequences of the Reasons forAction, (4) Focus of Reasoning, and (5) Modes of Reasoning.
participants used this kind of experience-focused reasoning aredescribed below.
When participants reasoned about how to respond to a sit-uation using an experience focus, the intention of keeping thepatient safe was salient because they wanted to protect the pa-tient from further self-harm. Talking with the patient, as a choiceof action, was described as aimed at building trust, trying to un-derstand the patient, listening to the patient talk about his or herexperiences, and together exploring alternatives to self-harm.In their discussions, participants stressed the value of proactivepreventive work, giving attention to the person instead of thewound, and validating the patient by offering him or her theirtime and attention. Instilling a sense of security among patientsby being available to them was described as a means to pre-vent self-harm, aggressive behaviour, and the use of coercivemeasures. When describing how they would engage the patientin activities, participants adopting an experience focus high-lighted the necessity of adapting activities to meet the needs
of the individual patient. Participants described different pos-sible activities arising from the patient’s needs, such as takinga walk, watching television, or solving a crossword puzzle. Inthis context, several participants also described experiences ofstaff breaking ward rules and violating ward policy in order tomeet the needs of their patients. Experience-focused reasoningdid not appear to rule out the use of coercive measures, butrather participants would stress the importance of preservingthe relationship between staff members and patients when usingcoercion. Several participants also described how they usuallysucceeded in finding alternatives to restraints, especially if theyhad a good relationship with the patient. This could mean abort-ing the use of restraints as “a question of trust, an alliance issuetowards the patient.” The importance of preserving a trustingalliance and defending the patient’s legal rights was consideredan argument for avoiding the use of restraints, even when thismeant questioning or opposing decisions that had already beenmade.
.

CHOICE OF ACTION IN INPATIENT PSYCHIATRIC CARE 475
You can’t, just to please the physician, disregard the patient; like ifyou find another method I can’t just be thinking that I must please myphysician; then I would be guilty of misconduct as a nurse towardsmy patient.
Participants also made arguments for the use of mechani-cal restraints, which they viewed, in some cases, as a betteralternative than having several staff members manually restrainan aggressive patient or medicating the patient by force. Whentalking about observing the patient, participants with a focus onexperience stressed the importance of being flexible. Respect-ing a patient’s request for a specific staff member to carry outobservations was perceived as important. In experience-focusedreasoning, participants stressed the importance of building onthe relationship established with patients. For example, the riskof having to hold the patient by force to administer medicationwas thought to be minimized by letting the staff member withthe best relationship with the patient try talking to him or herfirst.
Routine-Focused ReasoningIn participants’ discussions, a third reason for choosing an
action was simply because “it’s what you do.” The types ofactions considered in relation to this reason were the same asfor experience-focused reasoning, but, as explained below, theapproaches described differed when participants’ reasoning wasroutine focused.
Participants adopting a routine focus stressed the importanceof being efficient in responding to patients’ behaviours. In ref-erence to the vignette described previously, for example, par-ticipants stated that running to the patient, holding her, andremoving the piece of broken glass should be done quickly andefficiently, and that, as one participant put it, what happens af-terwards was “in a way, not relevant.” Participants described theaction of talking to the patient as primarily a matter of beinginformative, the purpose being to establish rapport so they couldinform, offer an explanation, and assess the patient. Participantsusing routine-focused reasoning described being with the pa-tient primarily as a matter of socializing. Participants describedhow staff keep patients company by lingering for a moment, orthat they might order nursing observations until the patient hascalmed down. Thus, a routine focus seemed to allow for the in-tensity of staff presence to be negotiated with the patient. Whentalking about engaging the patient in activities, the participantsdescribed using structured activities, such as chain analysis andrating scales, and making formalized agreements with the pa-tients. When discussing restraining a patient using mechanicalrestraints, participants who adopted a routine focus stressed theimportance of following protocol using clear-cut coordinationand frequent assessments, as well as informing and assisting thepatient.
If you’re to bring someone to the restraining room, then maybe twopeople have to hold the person, and then someone has to open thedoor, and there’s things to be produced so you have a little strategy
to make things run as smoothly as possible so you don’t have tohustle the patient, but you get them there as swiftly and painlesslyas possible.
Some participants argued that it was not always necessary totalk to the patient and that orders should be followed through,even if alternatives existed, because “if a physician says me-chanical restraints, then mechanical restraints it is.” In acutesituations, it may not be possible to wait for a physician’s or-ders, and staff agreed that sometimes they needed to act inself-defence and apply mechanical restraints without orders.Routine-focused observing using special observations was pri-marily about assessing the patient, as the importance of observ-ing and registering mood changes in the patients was the startingpoint for some participants’ reasoning. This made it possibleto assess whether special observations in the form of constantobservation should continue, be terminated (preferably), or bereplaced by intermittent observations. When talking about med-icating the patient, participants using a routine focus thoughtit important to be decisive and to follow through. Forced med-ication could be given without a physician seeing the patientfirst, even when patients explicitly requested to see a doctor. Noroutine-focused reasoning considered discharging the patient arelevant choice of action.
Discipline-Focused ReasoningFinally, participants sometimes described how actions were
chosen because the patient “has to learn.” The types of actionsconsidered by participants on the basis of this reason includedresponding to the situation, talking with the patient, being withthe patient, engaging the patient in activities, restraining thepatient, observing the patient, medicating the patient, and alsodischarging the patient. The approaches reflecting qualities ofthese types of actions and the consequences of this type ofreasoning, which is understood to be discipline-focused, aredescribed as follows.
Staff members responding to patients on the basis ofdiscipline-focused reasoning were characterized as keeping adistance from patients. Participants described how staff mightchoose not to respond to certain patient behaviours at all bylooking the other way or choosing not to pay attention to them.Talking to the patient meant clarifying things for him or her (e.g.,telling the patient “this is unacceptable; you are not allowed todo this”). Participants described how staff would explain tothe patients that their behaviour was unacceptable and that fur-ther self-harm would lead to consequences. Patients also couldbe informed upon admission that if they hurt themselves, theywould be discharged. They might also be told to clean up theirown messes. Discipline-focused reasoning for being with thepatient stressed the need for intimidating patients. Participantsdescribed how they could choose to be present when patientstalked to the doctor, so that the patient would not dare to simulateillness or lie to the physician. When restraining patients usingmechanical restraints, participants noted that taking charge of
.

476 G-M. E. LOOI ET AL.
the situation was important. Participants described that the riskfor coercive measures increased if the patient had been frus-trated and boisterous, and mechanical restraints might be usedas punishment.
The harshest punishment I’ve experienced regarding patients andmechanical restraints is a patient who set his room on fire at 9 a.m.,and at 3 p.m., mechanical restraints are ordered and there was noother intention; it was pure punishment.
Participants also described how patients who do not accepthelp that is offered might be perceived as ungrateful, whichmight provoke staff and lead to mechanical restraints beingused.
. . . it can also become so provocative toward staff that you becomesomewhat angry at the whole situation, and you think you have triedto make it a little better for the patient and maybe she can’t accept itbut chooses her own measures instead; it can become provoking forstaff and then maybe you don’t think like [name of other informant]you just drag her in to the restraints room.
Concerning observing patients, discipline-focused reasoningstressed the importance of ignoring the patient during special ob-servations. Participants adopting a discipline focus consideredit important not to offer the patient their attention if that waswhat the patient wanted. They also described incidents of staffmembers leaving a patient alone during constant observations.When medicating patients by administering forced medication,participants using discipline-focused reasoning considered theuse of power to be important. Participants described how staffbeing subjected to violence during the use of restraints couldaffect the assessment of the patient and result in increased useof medication. Discipline-focused reasoning was the only typeof reasoning that entailed discharging the patient as a possiblechoice of action, warranted by a desire to act consequentially,since discipline-focused participants perceived self-harm as aviolation of ward rules and saw it as “completely justified todischarge patients who violate rules.” One participant describedthe consequence of discharge to a patient by stating that, “thenshe would have learned that if you cut yourself on the ward,then you get discharged.” Participants stressed the importanceof a routine in which an agreement is signed, with the patient,stating that self-harm will lead to discharge, so that the patientlearns not to self-harm.
DISCUSSIONThe results show that the content of staff’s reasoning on their
choice of action in challenging situations in inpatient psychi-atric care settings can be described in terms of different modesand different focuses. We propose that each focus of reason-ing described in the results can be viewed as representing oneextreme of a continuum, the endpoints of which constitute themodes of reasoning either directed at solving the staff’s prob-lem or directed at meeting the patients’ needs. The proposedrelationships between modes of reasoning and focus of reason-ing are visualised in Figure 2 and discussed here. We would
FIGURE 2 Mind Map Visualising the Duality of the Two Modes of Reasoningof Psychiatric Inpatient Staff.
like to stress that this Figure and the duality it illustrates isbased on a description of patterns and structure in participants’reasoning. It depicts various possible trails of reasoning thatpsychiatric inpatient staff members might embark on and is notto be understood as a representation of individual staff mem-bers’ perceptions of care or actual praxis. Potential relationshipsamong modes of reasoning, focus of reasoning, and the realityof inpatient psychiatric care are discussed here. Each of the fourdescribed focuses of reasoning (staff, experience, routine, anddiscipline) is discussed, building a case for the relevance of theproposed modes of reasoning (solving the staff’s problems ormeeting the patients’ needs) for psychiatric nursing knowledgeand practices. These are then compared to other concepts ofpsychiatric nursing care and conclusions are made.
The results showed that one way of reasoning was staff-focused reasoning, where staff members take particular actionsprimarily because they look out for themselves in terms of safetyand comfort; at the same time, this does not necessarily omitbeing concerned for the patient. This way of reasoning can be un-derstood in terms of risk management and the identification andavoidance of unfavourable outcomes. Concerns have been ex-pressed that an increased focus on risk management might havenegative consequences (Buchanan-Barker & Barker, 2005). Itcan be argued that risk management, although undertaken in thename of altruism, functions as an instrument of social control(O’Byrne, 2008), serving the interests of those performing itand thus reflecting a staff-focused reasoning in psychiatric care.In order to focus on the needs of individual patients, a shiftfrom risk management and observing the patient′s behaviour tounderstanding the patient’s experience is needed.
In the results, understanding the patient′s experience was seenas a possible focus of reasoning where it was important to listento and value the patient’s perspective. People who self-harm con-stitute a heterogeneous group needing individual considerations
.

CHOICE OF ACTION IN INPATIENT PSYCHIATRIC CARE 477
in treatment (Hume & Platt, 2007). They need to be listened toand to have their experiences acknowledged and respected (Har-ris, 2000; Lindgren, Wilstrand, Gilje, & Olofsson, 2004; Weber,2002). Self-harm can be understood as a means to communicate(Harris, 2000), a coping strategy to deal with inner pain (Har-ris, 2000; Schoppmann, Schrock, Schnepp, & Buscher, 2007;Sinclair & Green, 2005), and, paradoxically, a survival strategy(Lindgren, Oster, Astrom, & Graneheim, 2011). To focus onthe subjective experience of patients is to have a person-centredapproach to psychiatry and psychiatric nursing, which also re-quires a shift from rigidly following routines to being flexibleand adapting to the situation at hand.
An additional way of reasoning was described in the resultsas a focus on routine where you do certain things because that’show they are done or have been done in the past. Routines canbe manifested as policy documents, as standardized care plans,and as informal ward rules in a ward culture. However they aremanifested, the key role of routines in this way of reasoning is toprovide a strategy for dealing with conflict. This preparednessis likely to promote rigidity rather than flexibility in staff inter-actions with patients. Enarsson, Sandman, and Hellzen (2007)describe how routines are often developed without patient inputin order to deal with disturbing events for which no routine re-sponse exists and to achieve unity and security among nurses.Routines can be seen as a covert exercise of power, afflict-ing patients who feel afraid, powerless, and compelled to obey(Enarsson, Sandman, & Hellzen, 2011). One argument in staffmembers’ reasoning for a routine focus and structure in the man-agement of patient care is that it is highly effective, and indeedthere is compelling evidence that an efficient ward structure isassociated with lower levels of conflict behaviour and contain-ment measures (Bowers et al., 2011). However, it can be arguedthat it is important to distinguish between working by rules andworking by principles when building structure. The relation-ship between rules and principles can be described as a choicebetween “binding rules interpreted by non-binding principlesand non-binding rules backed by binding principles” (Braith-waite, 2002, p. 47). In this, it is apparent that the staff memberswho focused on routine in their reasoning put a greater empha-sis on binding rules than on binding principles, which limitstheir ability to use a flexible and adaptive approach to situa-tions that arise. Shifting the focus away from routines calls forprinciples rather than rules as a basis for actions and would notnecessarily result in less structure. When the goal is to meetpatients’ individual needs, a shift from discipline to empow-erment as a guiding principle for psychiatric inpatient care isimportant.
Reasoning that focuses on discipline means that an action istaken because the patient “has to learn.” Lindgren et al. (2011)described how taking a fostering approach toward women whoself-harm restricts a staff’s ability to act because, in an author-itative position, they define acceptable behaviour and imposedemands and limits. In the context of forensic care, Horberg,Sjogren, and Dahlberg (2012) describe patients’ experiences of
adapting to staff demands as characterized by loneliness and fearof punishment. As an alternative, the results of Lindgren et al.(2011) suggest that supportive staff interacting with patientsmight render a positive experience in which the patient is metwith respect as an individual. Andreasson and Skarsater (2012)described how taking advantage of patient’s resources can pre-vent traumatization during compulsory treatment and suggestedthat spending time with help-seeking patients can prevent the useof coercive measures. We suggest that a focus on empowermentinstead of discipline might result in a shift away from seeingpatients as individuals to be corrected towards seeing them ascompetent experts in need of support and empowerment.
A mode of reasoning aimed at identifying and meeting pa-tients’ needs corresponds to such person-centred conceptionsof psychiatric nursing as those described by Peplau (1991) andBarker (2001); the problem-solving mode of reasoning mightbetter align with a more custodial approach to psychiatric carethat aims to control patient behaviour.
Describing caring approaches of nurses in acute psychi-atric intensive care wards, Bjorkdahl, Palmstierna, and Hansebo(2010) used the metaphor of a ballet dancer to illustrate a person-centred caring approach while a bulldozer represented a pater-nalistic and potentially uncaring approach. Our results, describ-ing two modes of reasoning, might, to some extent, reflect andhelp to further understand the complexity of these approaches.
Bjorkdahl et al. describe how nurses, when adopting a balletdancer approach, would signal a caring approach, put them-selves in the patient’s shoes and use themselves as finely tunedinstruments. This approach can be compared to the mode of rea-soning directed towards meeting the patients’ needs describedin our study: Meeting the patient’s needs meant solving theproblem as affecting the patient (patient focus) and as perceivedby the patient (experience focus), in the best-possible manner(situation focus), for the purpose of strengthening the patient’sability to manage the problem (empowerment focus).
Bjorkdahl et al. described the bulldozer approach as em-phasizing guarding the ward against chaos, ensuring sufficientpower and justifying the use of controlling actions, but alsokeeping a critical mind and allowing for feelings. The bulldozerapproach can be compared with the mode of reasoning we de-scribe as directed towards solving the staff’s problem: Solvingthe staff’s problem means solving the problem as it affects staff(staff focus) and as perceived by staff (behaviour focus), ina manner agreed upon amongst staff (routine focus), for thepurpose of preventing a recurrence of the problem (disciplinefocus). Bjorkdahl et al. argue that the bulldozer approach, aimedat keeping the ward safe and orderly, is associated with a risk ofuncaring and harmful actions while at the same time encompass-ing a potential for caring. We suggest that our results provide anunderstanding of how staff members, when aware of the signifi-cance of meeting the patients’ needs and not merely content withsolving the staff’s problem, are not only more likely to adopt aperson-centred, caring approach, but also to achieve the caringpotential of a paternalistic approach. Thus, understanding staff
.

478 G-M. E. LOOI ET AL.
members’ modes of reasoning might be useful for promotingperson-centred care.
LimitationsThis study employed a qualitative design, and therefore the
results are not generalizable. They do, however, provide knowl-edge that might promote an increased understanding of staff’sreasoning and choice of action, and facilitate such an under-standing through critical reflection (cf. Sandelowski, 1997).Preliminary findings were presented and reflected upon withstaff members in a similar setting. They found the findings to befamiliar and expressed that addressing situations using differ-ent focuses was a meaningful exercise that might help furtherdevelop the psychiatric nursing practice. It is obvious from ourclinical experience and review of the literature that the contentof staff reasoning described in this study is not unusual and hasbeen, in part, described by other researchers. The trustworthi-ness of the results also is supported by the richness of the dataand the structured and rigorous method of working with theanalysis of data (cf. Graneheim & Lundman, 2004).
CONCLUSIONTo facilitate the use of alternatives to coercive measures in
inpatient psychiatric care settings, the objective must be to iden-tify and meet patients’ individual needs and not merely to solvethe staff’s problems through the use of short-term solutions. Anunderstanding of focuses and modes in staff’s reasoning in psy-chiatric care can form a basis for further research and can leadto educational interventions aimed at better understanding howpsychiatric inpatient care can become more person-centred. Wesuggest that the results of this study be used as a pedagogicaltool in the visualisation of reasoning on choice of action in orderto facilitate critical reflection on psychiatric nursing practice ineducation and professional staff-development activities.
Declaration of Interest: The authors report no conflicts ofinterest. The authors alone are responsible for the content andwriting of the paper.
REFERENCESAndreasson, E., & Skarsater, I. (2012). Patients treated for psychosis and
their perceptions of care in compulsory treatment: Basis for an actionplan. Journal of Psychiatric and Mental Health Nursing, 19(1), 15–22. doi:http://dx.doi.org/10.1111/j.1365-2850.2011.01748.x
Barker, P. (2001). The tidal model: Developing an empowering, person-centredapproach to recovery within psychiatric and mental health nursing. Journalof Psychiatric and Mental Health Nursing, 8(3), 233–240.
Bjorkdahl, A., Palmstierna, T., & Hansebo, G. (2010). The bulldozer and theballet dancer: Aspects of nurses’ caring approaches in acute psychiatric inten-sive care. Journal of Psychiatric and Mental Health Nursing, 17(6), 510–518.doi: http://dx.doi.org/10.1111/j.1365-2850.2010.01548.x
Bonner, G., Lowe, T., Rawcliffe, D., & Wellman, N. (2002). Trauma for all: Apilot study of the subjective experience of physical restraint for mental health
inpatients and staff in the UK. Journal of Psychiatric and Mental HealthNursing, 9(4), 465–465.
Bowers, L., Nijman, H., Simpson, A., & Jones, J. (2011). The relation-ship between leadership, teamworking, structure, burnout and attitude topatients on acute psychiatric wards. Social Psychiatry and PsychiatricEpidemiology, 46(2), 143–148. doi: http://dx.doi.org/10.1007/s00127-010-0180-8
Braithwaite, J. (2002). Rules and principles: A theory of legal certainty. Aus-tralian Journal of Legal Philosophy, 27, 47–82.
Buchanan-Barker, P., & Barker, P. (2005). Observation: The original sinof mental health nursing? Journal of Psychiatric and Mental HealthNursing, 12(5), 541–549. doi: http://dx.doi.org/10.1111/j.1365-2850.2005.00876.x
Enarsson, P., Sandman, P., & Hellzen, O. (2007). The preservation of or-der: The use of common approach among staff toward clients in long-term psychiatric care. Qualitative Health Research, 17(6), 718–729. doi:http://dx.doi.org/10.1177/1049732307302668
Enarsson, P., Sandman, P., & Hellzen, O. (2011). “They can do whatever theywant”: Meanings of receiving psychiatric care based on a common staffapproach. International Journal of Qualitative Studies on Health and Well-Being, 6(1). doi: http://dx.doi.org/10.3402/qhw.v6i1.5296
Georgieva, I., de Haan, G., Smith, W., & Mulder, C. L. (2010). Successfulreduction of seclusion in a newly developed psychiatric intensive care unit.Journal of Psychiatric Intensive Care, 6(1), 31–38. doi: http://dx.doi.org/10.1017/S1742646409990082
Graneheim, U. H., & Lundman, B. (2004). Qualitative content analysis in nurs-ing research: Concepts, procedures and measures to achieve trustworthiness.Nurse Education Today, 24(2), 105–112.
Haglund, K., von Knorring, L., & von Essen, L. (2003). Forced medication inpsychiatric care: Patient experiences and nurse perceptions. Journal of Psy-chiatric and Mental Health Nursing, 10(1), 65–72. doi: http://dx.doi.org/10.1046/j.1365-2850.2003.00555.x
Happell, B., & Harrow, A. (2010). Nurses’ attitudes to the use of seclu-sion: A review of the literature. International Journal of Mental HealthNursing, 19(3), 162–168. doi: http://dx.doi.org/10.1111/j.1447-0349.2010.00669.x
Harris, J. (2000). Self-harm: Cutting the bad out of me. Qualitative HealthResearch, 10(2), 164–173.
Holm, H., Bjorkdahl, A., & Bjorkenstam, E. (2011). Tvangsvard medfragetecken [Compulsory care with a question mark]. Lakartidningen,108(34), 1544–1545.
Hooff, S., & Goossensen, A. (2013). How to increase quality of care duringcoercive admission? A review of literature. Scandinavian Journal of CaringSciences. doi: http://dx.doi.org/10.1111/scs.12070
Horberg, U., Sjogren, R., & Dahlberg, K. (2012). To be strategically strug-gling against resignation: The lived experience of being cared for in forensicpsychiatric care. Issues in Mental Health Nursing, 33(11), 743–751. doi:http://dx.doi.org/10.3109/01612840.2012.704623
Huckshorn, K. A. (2004). Reducing seclusion restraint in mental health usesettings: Core strategies for prevention. Journal of Psychosocial Nursing andMental Health Services, 42(9), 22–33.
Hume, M., & Platt, S. (2007). Appropriate interventions for the prevention andmanagement of self-harm: A qualitative exploration of service-users’ views.BMC Public Health, 7, 9.
Jarrett, M., Bowers, L., & Simpson, A. (2008). Coerced medicationin psychiatric inpatient care: Literature review. Journal of AdvancedNursing, 64(6), 538–548. doi: http://dx.doi.org/10.1111/j.1365-2648.2008.04832.x
Krippendorff, K. (2013). Content analysis: An introduction to its methodology(3rd ed.) Thousand Oaks, CA: Sage.
Laiho, T., Kattainen, E., Astedt-Kurki, P., Putkonen, H., Lindberg, N., & Kylma,J. (2012). Clinical decision making involved in secluding and restrainingan adult psychiatric patients: An integrative literature review. Journal ofPsychiatric and Mental Health Nursing, 20(9), 830–839.
.

CHOICE OF ACTION IN INPATIENT PSYCHIATRIC CARE 479
Larue, C., Dumais, A., Ahern, E., Bernheim, E., & Mailhot, K. (2009). Fac-tors influencing decisions on seclusion and restraint. Journal of Psychiatricand Mental Health Nursing, 16(5), 440–446. doi: http://dx.doi.org/10.1111/j.1365-2850.2009.01396.x
Lindgren, B., Oster, I., Astrom, S., & Graneheim, U. H. (2011). “They don’t un-derstand . . . you cut yourself in order to live”: Interpretative repertoires jointlyconstructing interactions between adult women who self-harm and profes-sional caregivers. International Journal of Qualitative Studies on Health andWell-Being, 6(3). doi: http://dx.doi.org/10.3402/qhw.v6i3.7254
Lindgren, B., Wilstrand, C., Gilje, F., & Olofsson, B. (2004). Strugglingfor hopefulness: A qualitative study of Swedish women who self-harm.Journal of Psychiatric and Mental Health Nursing, 11(3), 284–291. doi:http://dx.doi.org/10.1111/j.1365-2850.2004.00712.x
Lindsey, P. L. (2009). Psychiatric nurses’ decision to restrain. Journal of Psy-chosocial Nursing and Mental Health Services, 47(9), 41–49.
Marangos-Frost, S., & Wells, D. (2000). Psychiatric nurses’ thoughts and feel-ings about restraint use: A decision dilemma. Journal of Advanced Nursing,31(2), 362–369.
Morgan, D. L. (1997). Focus groups as qualitative research (2nd ed.) ThousandOaks, CA: Sage.
Muralidharan, S., & Fenton, M. (2006). Containment strategies for peo-ple with serious mental illness. The Cochrane Database of System-atic Reviews, 3. Retrieved from http://search.proquest.com/docview/68649534?accountid=27917
O’Byrne, P. (2008). The dissection of risk: A conceptual analysis. Nurs-ing Inquiry, 15(1), 30–39. doi: http://dx.doi.org/10.1111/j.1440-1800.2008.00372.x
Peplau, H. E. (1991). Interpersonal relations in nursing: A conceptual frameof reference for psychodynamic nursing. New York, NY: Springer. (Originalwork published 1952)
Sailas, E., & Fenton, M. (2000). Seclusion and restraint for people with seriousmental illnesses. Cochrane Database of Systematic Reviews, 2.
Sandelowski, M. (1997). “To be of use”: Enhancing the utility of qualitativeresearch. Nursing Outlook, 45(3), 125–132.
Schoppmann, S., Schrock, R., Schnepp, W., & Buscher, A. (2007). “Then Ijust showed her my arms. . .”: Bodily sensations in moments of alienationrelated to self-injurious behaviour. A hermeneutic phenomenological study.Journal of Psychiatric and Mental Health Nursing, 14(6), 587–597. doi:http://dx.doi.org/10.1111/j.1365-2850.2007.01150.x
Sibitz, I., Scheutz, A., Lakeman, R., Schrank, B., Schaffer, M., & Amering, M.(2011). Impact of coercive measures on life stories: Qualitative study. TheBritish Journal of Psychiatry, 199(3), 239–244.
Sinclair, J., & Green, J. (2005). Understanding resolution of deliberate selfharm: Qualitative interview study of patients’ experiences. British MedicalJournal, 330(7500), 1112–1115.
Weber, M. T. (2002). Triggers for self-abuse: A qualitative study. Archivesof Psychiatric Nursing, 16(3), 118–124. doi: http://dx.doi.org/10.1053/apnu.2002.32948
.

Delstudie IV

EMP IR ICAL STUD IES
Knowledge of the patient as decision-making power: staffmembers’ perceptions of interprofessional collaboration inchallenging situations in psychiatric inpatient care
Sebastian Gabrielsson RPN, RN, MSc (PhD Student)1, Git-Marie E. Looi RPN, RN, MSc (PhD Student)1,
Karin Zingmark RN, PhD (Associate Professor)1,2 and Stefan S€avenstedt RN, PhD (Associate Professor)1,2
1Department of Health Sciences, Lule�a University of Technology, Lule�a, Sweden and 2Department of Research and Development,
Norrbotten County Council, Lule�a, Sweden
Scand J Caring Sci; 2014; 28; 784–792
Knowledge of the patient as decision-making power:
staff members’ perceptions of interprofessional
collaboration in challenging situations in psychiatric
inpatient care
Challenging situations in psychiatric inpatient settings
call for interprofessional collaboration, but the roles and
responsibilities held by members of different professions
is unclear. The aim of this study was to describe staff
members’ perceptions of interprofessional collaboration
in the context of challenging situations in psychiatric
inpatient care. Prior to the study taking place, ethical
approval was granted. Focus group interviews were con-
ducted with 26 physicians, ward managers, psychiatric
nurses, and nursing assistants. These interviews were
then transcribed and analysed using qualitative content
analysis. Results described participants’ perceptions of
shared responsibilities, profession-specific responsibilities
and professional approaches. In this, recognising knowledge
of the patient as decision-making power was understood to
be a recurring theme. This is a delimited qualitative study
that reflects the specific working conditions of the partici-
pants at the time the study was conducted. The findings
suggest that nursing assistants are the most influential
professionals due to their closeness to and first-hand
knowledge of patients. The results also point to the possi-
bility of other professionals gaining influence by getting
closer to patients and utilising their professional knowl-
edge, thus contributing to a more person-centred care.
Keywords: interprofessional collaboration, challenging
situations, focus groups, professional practice, psychiatric
inpatient care.
Submitted 11 September 2013, Accepted 9 December 2013
Introduction
Psychiatric staff members working in inpatient settings
face challenging patient-related situations in which they
are to some extent dependent upon each other and
required to collaborate interprofessionally. Teamwork has
been described as the main context in which collabora-
tive patient-centred care is provided (1), and the team
has been suggested as the heart of decision-making in
challenging situations (2). Still, the nature of interprofes-
sional roles and responsibilities and the functioning and
utility of interprofessional teams in psychiatric inpatient
settings are unclear, and it has been suggested that the
ambitions of interdisciplinary teamwork in inpatient psy-
chiatric care have not been realised (3).
Bowers et al. have shown how the use of containment
measures in psychiatric inpatient care are closely linked
to the occurrence of conflict behaviour and that both
conflict and containment are affected by organisational
features; wards with good leadership, teamwork, struc-
ture, and attitudes towards patients and low burnout
have low rates of containment events (4). Organisational
factors such as effective managers, strong nurse-physician
relationships and higher nurse-patient staffing ratios have
been associated with lower levels of nurse burnout as
well as lower levels of adverse advents which suggests
that nurses’ work environment could have a positive
effect on psychiatric nurses’ capacity to sustain a safe and
effective care environment by enabling them to utilise
their skills and achieve their goals in caring for the
patients (5, 6).
Few studies focus on analysing, describing, or prob-
lematising interprofessional variations or relations in
challenging situations. Research describing a staff
perspective, including qualitative data from multiple
Correspondence to:
Sebastian Gabrielsson, Department of Health Sciences, Lule�a
University of Technology, 971 87 Lule�a, Sweden.
E-mail: [email protected]
784 © 2014 Nordic College of Caring Science
doi: 10.1111/scs.12111

professions, report little variation on behalf of profes-
sion and give only limited insight into interprofessional
aspects. When Olofsson and Norberg (7) interviewed
physicians, nurses and patients about experiences of
actual coercive events, the results described few varia-
tions between professions and only random illumina-
tions of the relationships and interactions between
physicians and nurses. Physicians described the purpose
of coercive actions as making nurses feel safe, and a
lack of agreement between nurses and physicians was
perceived as troublesome. Kontio et al. (8) conducted
separate focus groups interviews with physicians and
nurses but found data from the different professions to
be mainly similar. Following a second analysis of the
same material, a few insights on profession-specific
roles and responsibilities can be gained, as it described
how nurses felt uncertain about their own decisions
when they were made quickly with no time for discus-
sion with other staff members, and physicians
experienced ethical dilemmas when having to make ad
hoc or post hoc decisions on information received from
nurses (9).
The successful management of challenging situations
in psychiatric inpatient settings is reliant on interprofes-
sional collaboration. The review of literature indicates
that there is a need for more research on the variations
and relations of different professions. The aim of this
study was therefore to describe staff members’ percep-
tions of interprofessional collaboration in the context of
challenging situations in psychiatric inpatient care.
Materials and methods
Focus group interviews were conducted with staff mem-
bers experienced in acute psychiatric inpatient care, tran-
scribed verbatim and analysed using qualitative content
analysis. The results of a second analysis of the same
data, describing staff members’ reasoning on choice of
action, are reported elsewhere.
Participants and procedure
The criteria for inclusion were experience of working in
psychiatric inpatient care and willingness to participate.
Participants were recruited among members of staff at a
psychiatric clinic in northern Sweden consisting of sev-
eral outpatient units and one inpatient unit with a
24-bed locked ward and a 24-hour admittance and con-
sultancy service. At the time the study was conducted,
the inpatient ward employed approximately 50 nursing
staff and was headed by two ward managers. The ward
managers shared managerial duties at the clinic with a
group of managers who would, at times, fill in for each
other. All physicians regularly and temporarily employed
at the clinic also worked at the ward interchangeably
with other responsibilities. A total of approximately 50
nursing staff members at the inpatient ward and ward
managers and physicians at the clinic were asked to par-
ticipate. Of these, 28 agreed to participate, two of which
failed to attend the interviews. Characteristics of the par-
ticipants and focus groups are presented in Table 1.
Data collection
The interviews were conducted at the participants’ work-
place between October 2010 and January 2011. The 26
participants were grouped into six focus groups with four
to six participants and divided according to profession
and length of work experience, cf Morgan (10). In the
context of this paper, the term physician refers to psychia-
trists as well as physicians in training to become psychia-
trists, while the term ward manager refers to
nonphysicians with primarily managerial responsibilities.
Psychiatric nurse refers to registered nurses with higher
education, with or without specialist psychiatric training,
and nursing assistant refers to nursing staff with second-
ary-level education, with or without specialist psychiatric
training. Characteristics of the interviews are presented
in Table 1. Authors one and two took turns acting as
Table 1 Participant and focus group characteristics
Group
no.
Profession of
participants
Number of
participants
Length of interview
(minutes)
Mean experience in
profession (years)
Mean experience in inpatient
psychiatry (years)
Gender (male/
female)
1 Psychiatric
nurses
4 72 17.625 17.375 1/3
2 Psychiatric
nurses
6 79 2.25 2.33 3/3
3 Nursing
assistants
4 79 14.25 12.75 3/1
4 Nursing
assistants
4 61 3.25 2.875 2/2
5 Ward managers 4 87 11.75 20.5 1/3
6 Physicians 4 42 13.75 5.375 2/2
Knowledge of the patient as power 785
© 2014 Nordic College of Caring Science

moderators during the interviews. Two senior researchers
took turns acting as assistants, keeping track of time and
asking additional questions. The interviews were
recorded and transcribed verbatim.
Each focus group interview began with the moderator
reading a vignette describing a challenging situation with
many possible choices of actions and responses. The vign-
ette, designed to depict a realistic and well-known sce-
nario, was developed on the basis of the first two
authors’ familiarity with psychiatric care. Before being
used in the focus group interviews, nurses experienced in
inpatient psychiatry were asked to read and comment on
drafts of the vignette, whereupon minor alterations were
made, thus ensuring the credibility and relevance of the
scenario.
Vignette: A young female patient has been cared for at the
ward for a week. She has been subject to inpatient care sev-
eral times before. She is now involuntarily admitted after
intoxicating herself with paracetamol for unknown purposes.
On several occasions, containment measures have been taken
when she has harmed herself or others at the ward. All staff
members (nursing assistants, psychiatric nurses, physicians,
ward manager) are sitting down having their morning coffee.
From the staff room, they observe how the patient runs
through the hallway towards a left-behind drinking glass.
She picks the glass up and it breaks as she throws it to the
floor. She picks up a large piece of glass and starts cutting
herself deep in the arm as she shouts: ‘Let me out!’
After reading and listening to the vignette, participants
were asked a broad question (‘What happens next?’), fol-
lowed later by a more specific question (‘What would
you do?’). Participants were asked to freely discuss these
questions; summaries were made, and encouraging and
clarifying questions were asked. To make sure that cer-
tain areas of interest were covered in all groups, an inter-
view guide with the following predefined topics were
used: mechanical restraints, special observation, and pro-
fessional roles and responsibilities. To ensure sufficient
variation in participants’ reasoning, all participants were
actively encouraged by the moderator to participate in
the discussion, and the moderator did not end the inter-
view until participants stated that they had nothing more
to add.
Analysis
The transcribed interviews were analysed using qualita-
tive content analysis in order to describe participants’
reasoning. For the purpose of this study, only the ver-
bal content of the interviews was analysed. Krippendorf
(11) describes content analysis as a method of analy-
sing written and verbal communication in a systematic
way and making replicable and valid inferences from
texts. This makes qualitative content analysis a method
suitable for describing the content of written text in a
systematic and trustworthy manner, cf Graneheim and
Lundman (12). The analytical process was carried out
systematically and step-wise and involved the simulta-
neous emergence of multiple, inter-related categories of
content.
The text was read as whole. Meaning units relevant
for the purpose of this study were extracted and sorted
according to the focus group from which they originated
and the profession they concerned. A preliminary set of
categories describing the perceptions of each profession
was formulated. Categories were compared across profes-
sions, and new levels of categories describing an under-
standing of shared responsibilities were formulated.
Categories and meaning units for each profession were
once again reviewed, resulting in a new level of catego-
ries describing profession-specific approaches. Finally, the
categories and their content were viewed as a whole, and
a common thread was identified.
Ethical considerations
Prior to the study taking place, ethical approval was
granted from the regional ethics committee in Ume�a
(2010-4-31M). Due to the richness of gathered data,
multiple analyses were performed, an alteration to the
original design of which the committee was informed
and approved of (2012-315-32M). All participants gave
their written informed consent to participate in the
study.
Results
Following the analysis of the staff members’ focus
group discussions, it was found that their perceptions
of interprofessional collaboration in relation to the chal-
lenging situation presented in the vignette could be
divided into areas of shared responsibilities and profes-
sion-specific responsibilities. In these areas, professional
approaches were identified, as physicians could be
described as distant decision-makers, ward manager as sus-
picious supervisors, psychiatric nurse as mediating modera-
tors, and nursing assistant as informed performers (Fig. 1).
Common expectations of psychiatric professionals
expressed in the interviews included the capacity to
talk to each other, to control the situation, to know the
patient and to set the stage. These skills were important
for all different professionals, but the specific contribu-
tion in these areas showed some variation depending
on profession. Looking at a comprehensive analysis of
the results, a theme emerged as a common thread that
was described as recognising knowledge of the patient as
decision-making power.
786 S. Gabrielsson et al.
© 2014 Nordic College of Caring Science

Physicians – the distant decision-makers
Participants’ perceptions of physicians could be described
by labelling them as distant decision-makers, as they would
only visit the ward when called upon to make evalua-
tions and decisions mainly based on information pro-
vided by others. Physicians were believed to have little
patient contact due to being preoccupied with other
duties.
Control the situation. Physicians were expected to evaluate
and decide. They would keep their distance and usually
attend an acute situation on the ward only when called
upon after the acute problem was solved. Ward managers
did not expect physicians to take the lead unless there
was a medical emergency. Since physical engagement
was thought to affect mental clarity, decision-making and
the possibility of talking to the patient afterwards, physi-
cians would avoid getting directly involved in applying
restraints or ‘wrestling a patient’. Physicians perceived
themselves as the ones deciding which measures to be
taken. Their assessments would primarily concern the
patient’s physical status and the need for medico-surgical
measures, while their evaluations focused on the
patient’s psychiatric status and especially the risk for sui-
cide. In this, they were expected to act professional,
which meant being objective and not letting personal
feelings affect decisions. The physician was seen as an
important person bearing the medical responsibility and
having the ability to give orders to other professionals,
but participants’ views varied as to whether orders
always had to be carried out or could be refused if in the
patient’s best interest. Several nursing staff members
expressed concern that choosing to involve physicians in
a situation would automatically lead to special observa-
tions because the physician either did not know the
patient or because physicians would chose to play it safe,
a concern not expressed by physicians themselves.
Talk to each other. Physicians said they would gather
information primarily by listening to staff members who
knew the patient and the situation. Psychiatric nurses
believed that physicians had no choice but to rely on
the information they were given by the nursing staff,
especially when the physician was new and did not
know the patient, as often was the case because of high
physician turnover. Notably, nursing assistants thought
physicians had to first get to know the nursing staff
before knowing who could be trusted. Nursing assistants
also described how some psychiatrists trusted nursing
staff while others did not, the latter often leading to
more use of special observation. Some less experienced
psychiatric nurses believed that physicians relied too
heavily on information from others, but more experi-
enced psychiatric nurses did not see this as a problem.
Ward managers expected physicians’ decisions to follow
the recommendations of nursing staff, provided they
were given enough information. Some psychiatric nurses
described decision-making as a joint venture, while oth-
ers saw it as the physician making the formal decision
after listening to the nursing staff.
Know the patient. Neither themselves nor other profes-
sionals expected physicians to have much contact with
patients. The way physicians described their relationships
with patients might be characterised as knowing about the
Figure 1 Staff’s perceptions of interprofessional
collaboration in challenging situations in terms of
(1) professional approaches, (2) shared
responsibilities and (3) profession-specific
responsibilities.
Knowledge of the patient as power 787
© 2014 Nordic College of Caring Science

patient rather than knowing the patient in a deeper
sense.
…Yes I believe it’s good when you’re doing rounds
to be able to put a face to a name, maybe you’ve
been around saying hi and seen them in the corridor
and you know who’s behind the name… (Physician
#2)
Physicians described having many other responsibilities
outside of the ward and that, as a psychiatrist, they
would see inpatients once a week at most. Nursing staff
members described the importance of physicians being
familiar with the patients and explained how this could
reduce the use of special observation. Psychiatric nurses
believed that a high physician turnover resulted in a lack
of consistency in decision-making. They wished psychia-
trists were more present on the ward and would see the
patients more often. Lack of patient contact was believed
to have a negative impact on patients’ ability to partici-
pate in their own care. Psychiatric nurses thought physi-
cians should be the one giving patients’ information
about forced medication but reported that they rarely
did.
Set the stage. Physicians believed themselves to influence
ward culture and described how psychiatrists influenced
ward policy and staff members’ thinking and approaches.
Ward managers – the suspicious supervisors
Participants’ perceptions of ward managers could be
described by labelling them as suspicious supervisors. They
were described as occupying a unique position between
and above nursing staff, physicians and patients, from
which they keep a watchful eye on other professionals.
The doings of ward managers as they described them-
selves seemed mainly unknown or unappreciated by
other professionals. Ward managers were described as
having direct contact with all other professionals as well
as patients.
Control the situation. Although ward managers themselves
expressed the possibility of taking the lead in managing
the acute situation, this view was not evident in the dis-
cussions of other professionals. Ward managers thought
they would act as role models by going first, being the
ones telling others what to do, or both. Other profession-
als merely mentioned the possibility of ward managers
helping out if necessary.
… The ward manager is usually first in line, the first
to arrive and stop her from hurting herself, at least
you try to get her aside so you can have a quiet
talk… (Ward manager #4)
Talk to each other. Ward managers described how they
would act as a third party trying to negotiate patient-
friendly agreements between nursing staff and physi-
cians. Ward managers would be approached by nursing
staff reluctant to carry out physicians’ orders or question-
ing physicians’ assessments. Physicians would turn to the
ward manager with questions regarding nursing staff pro-
cedures and responsibilities or seeking advice concerning
patient treatment. Ward mangers took it upon them-
selves to support nursing staff and manipulate or con-
vince physicians to find solutions that would satisfy both
parties and benefit the patients. This negotiating function
of ward managers was not acknowledged by other pro-
fessionals in their discussions.
… I have been called upon many times to talk to
the physician because ‘I don’t want to do this’ and
then I have persuaded the physician… most of the
time it works out just fine… (Ward manager #2)
Know the patient. Ward managers described how they
would verify information they were given by the nursing
staff against other staff members, patient records or by
talking directly to the patient. Experience taught them
which staff members could be trusted to be working in
the patient’s interest and not in the interest of their own
comfort. In evaluating information, ward managers relied
on their own experience of working in psychiatric inpa-
tient care and on their personal knowledge of patients.
Only information deemed trustworthy and relevant was
passed on from nursing staff to physicians. No mentions
of ward managers’ questioning or passing on information
were made by other professionals.
Set the stage. Ward managers themselves gave no accounts
that described how they might contribute in setting the
stage. Psychiatric nurses believed that ward managers
influenced staff attitude and approaches towards patients
through their behaviour. Nursing assistants stated that the
ward manager was responsible for ward structure, for
recruiting apt personnel and for taking action when staff
did not meet set standards of care. Physicians and nursing
assistants expected ward managers to assure that staff
members were given adequate emotional support after
participating in stressful situations.
Psychiatric nurses – the moderating mediators
Participants’ perceptions of psychiatric nurses could best
be described by the label moderating mediators, as they
were described as the ones taking action and delivering
information and, in doing so, using their knowledge to
hinder certain courses of events but facilitating others.
Psychiatric nurses were described as having more patient
contact than physicians but less than nursing assistants.
Like physicians, psychiatric nurses were believed to have
little patient contact due to being preoccupied with other
duties.
788 S. Gabrielsson et al.
© 2014 Nordic College of Caring Science

Control the situation. Psychiatric nurses described how
they would slow things down in acute situations as they
tried to find alternatives to coercion or initiate less intru-
sive measures that do not require a physician to assess
and decide. They would also make assessments prior to
calling the physician to determine the necessity and
avoid special observation if possible, and believed that
sometimes, they were indirectly the ones actually making
physicians’ decisions. Ward managers acknowledged psy-
chiatric nurses as the ones making acute decisions if
aware of the situation, notifying the physician, and, if
necessary, refusing to implement coercive measures.
Nursing assistants expected psychiatric nurses to stand
back and be ready to administer medication when
timely.
Talk to each other. Psychiatric nurses described acting as
messengers delivering information. They described being
highly involved in gathering information and making
assessments of patients, which was described as both
enjoyable andnecessary due to physicians not knowing
the patients. Based on this, they would inform and influ-
ence physicians to make well-informed and desirable
decisions that the nurses believed would benefit the
patient, as illustrated by the following quotes:
… I don’t say that special observations should be ter-
minated if I’m not damned certain… that it’s my
judging and I have a good motivation for it… I don’t
say let’s end special observations we already have
three and there’s a shortage of staff… that’s a lousy
reason to end special observations… then I need a
damn good motivation as for why it should be ended
or I won’t say that it should be… well because I
think if you have special observation then the
patients’ life is in danger, that’s why you have it…
(Inexperienced psychiatric nurse #1)
… but I think when you have been working for a
while and gained some experience that you can
stand up for what you believe and say and think…
in the beginning I think I would listen more to the
nursing assistants that had been working for a long
time and such… but now I can state my own opin-
ion and it’s almost the other way round like in the
beginning I would say ‘end special observation’
because that’s what everybody thought and now I
have more knowledge and now how it can be…
(Inexperienced psychiatric nurse #4)
Nursing assistants expressed concerns that the informa-
tion delivered by psychiatric nurses at rounds and reports
was based solely on the assessments of nursing assistants.
Psychiatric nurses also described being the ones having to
deliver negative responses to the patients because the
physician did not take the time to do it or because they
thought it better that way.
Know the patient. Psychiatric nurses described possessing
knowledge about patients that physicians did not and
took it upon them to expose the patient. This is illustrated
by the following quotes:
… and I’ve been in several talks were I know we’ve
been talking beforehand and the patient’s not well
and she explains what happened and the doctor sits
there talking and it sort of never discloses… and the
session is about to end and you almost panic and
then you have to interrupt and ask how about that
pregnancy you talked about… and the women is like
seventy-five and obviously not pregnant and it all
sort of comes forth… and it’s stuff like that… I
believe it’s our duty to help the physician make the
right assessment, disclose these things and ask the
right questions depending on the patient in front of
you… (Inexperienced psychiatric nurse #2)
… some will put on a show in front of the physician
in order to get to stay on the ward… they get insti-
tutionalised and find it so convenient… nice to stay
on the ward and get meals served and spend time
with other patients and so on… then they might
make things up that aren’t true but if we are there
with them they don’t dare… (Inexperienced nurse
#5)
Psychiatric nurses believed they had relationships with
patients that should be preserved and used when deliver-
ing and obtaining information, but they also felt that
they did not often have enough time to talk to patients
as needed.
Set the stage. Psychiatric nurses described being responsi-
ble for providing structure and for nursing care, a view
shared by nursing assistants. Psychiatric nurses believed
themselves to be role models representing the employer,
with a responsibility to share their knowledge with nurs-
ing assistants and newly employed nurses, adding a
unique nursing perspective. Nursing assistants expressed
a desire for psychiatric nurses to take on a greater
responsibility as nursing leaders. They believed that psy-
chiatric nurses should utilise their nursing knowledge
and thus contribute to the prevention of conflict
situations.
… I mean they talk about having studied nursing,
but to somehow step up and distinguish themselves,
I don’t think they do that … (Experienced nursing
assistant #1)
Nursing assistants – the informed performers
Perceptions of nursing assistants could be described by
assigning them the label informed performers. Nursing
assistants were described as spending time with and get-
ting to know the patients, while at the same time being
Knowledge of the patient as power 789
© 2014 Nordic College of Caring Science
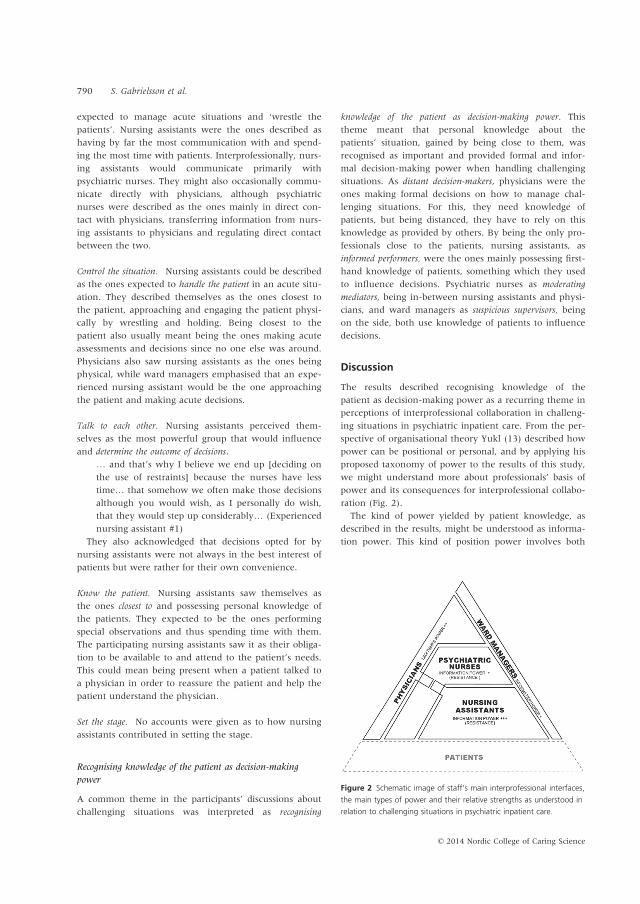
expected to manage acute situations and ‘wrestle the
patients’. Nursing assistants were the ones described as
having by far the most communication with and spend-
ing the most time with patients. Interprofessionally, nurs-
ing assistants would communicate primarily with
psychiatric nurses. They might also occasionally commu-
nicate directly with physicians, although psychiatric
nurses were described as the ones mainly in direct con-
tact with physicians, transferring information from nurs-
ing assistants to physicians and regulating direct contact
between the two.
Control the situation. Nursing assistants could be described
as the ones expected to handle the patient in an acute situ-
ation. They described themselves as the ones closest to
the patient, approaching and engaging the patient physi-
cally by wrestling and holding. Being closest to the
patient also usually meant being the ones making acute
assessments and decisions since no one else was around.
Physicians also saw nursing assistants as the ones being
physical, while ward managers emphasised that an expe-
rienced nursing assistant would be the one approaching
the patient and making acute decisions.
Talk to each other. Nursing assistants perceived them-
selves as the most powerful group that would influence
and determine the outcome of decisions.
… and that’s why I believe we end up [deciding on
the use of restraints] because the nurses have less
time… that somehow we often make those decisions
although you would wish, as I personally do wish,
that they would step up considerably… (Experienced
nursing assistant #1)
They also acknowledged that decisions opted for by
nursing assistants were not always in the best interest of
patients but were rather for their own convenience.
Know the patient. Nursing assistants saw themselves as
the ones closest to and possessing personal knowledge of
the patients. They expected to be the ones performing
special observations and thus spending time with them.
The participating nursing assistants saw it as their obliga-
tion to be available to and attend to the patient’s needs.
This could mean being present when a patient talked to
a physician in order to reassure the patient and help the
patient understand the physician.
Set the stage. No accounts were given as to how nursing
assistants contributed in setting the stage.
Recognising knowledge of the patient as decision-making
power
A common theme in the participants’ discussions about
challenging situations was interpreted as recognising
knowledge of the patient as decision-making power. This
theme meant that personal knowledge about the
patients’ situation, gained by being close to them, was
recognised as important and provided formal and infor-
mal decision-making power when handling challenging
situations. As distant decision-makers, physicians were the
ones making formal decisions on how to manage chal-
lenging situations. For this, they need knowledge of
patients, but being distanced, they have to rely on this
knowledge as provided by others. By being the only pro-
fessionals close to the patients, nursing assistants, as
informed performers, were the ones mainly possessing first-
hand knowledge of patients, something which they used
to influence decisions. Psychiatric nurses as moderating
mediators, being in-between nursing assistants and physi-
cians, and ward managers as suspicious supervisors, being
on the side, both use knowledge of patients to influence
decisions.
Discussion
The results described recognising knowledge of the
patient as decision-making power as a recurring theme in
perceptions of interprofessional collaboration in challeng-
ing situations in psychiatric inpatient care. From the per-
spective of organisational theory Yukl (13) described how
power can be positional or personal, and by applying his
proposed taxonomy of power to the results of this study,
we might understand more about professionals’ basis of
power and its consequences for interprofessional collabo-
ration (Fig. 2).
The kind of power yielded by patient knowledge, as
described in the results, might be understood as informa-
tion power. This kind of position power involves both
Figure 2 Schematic image of staff’s main interprofessional interfaces,
the main types of power and their relative strengths as understood in
relation to challenging situations in psychiatric inpatient care.
790 S. Gabrielsson et al.
© 2014 Nordic College of Caring Science

access to information and control over its distribution,
and it can be used as a source for upwards, downwards
and lateral influence. It would seem that nursing assis-
tants’ positions as the ones closest to the patients gives
them superior access to information in terms of knowl-
edge of patients. The position of psychiatric nurses and
ward managers gives them the possibility to control the
distribution of information but leaves them partially
dependent upon nursing assistants for knowledge of
patients. The distance of the physicians described in the
results leaves them heavily dependent on the informa-
tion of others and thus limiting their decision-making
power. That their decisions are still perceived as impor-
tant seems mainly due to their formal status, indicating
that the physician’s power in the context of challenging
situations is the kind of position power Yukl (13) calls
legitimate power – physicians are listened to and their
orders followed by nursing staff mainly out of respect for
physicians as authorities with certain legal capacities.
Yukl (13) suggests that different types of power are
associated with different outcomes to some extent. Posi-
tion power might invoke compliance or resistance in oth-
ers, while person power might invoke engagement.
Psychiatric nurses or nursing assistants’ refusal to imple-
ment physicians’ orders of restraints might be understood
as an act of resistance in the face of positional power.
This points to an important characteristic of power – it
only works if others believe you have it. Physicians’ legit-
imate power vanishes when others fail to appreciate their
authority. Accordingly, certain information and knowl-
edge only gives power when others perceive this as
important. In the context of challenging situations, our
results suggest that knowledge about patients, not profes-
sional knowledge, is what counts. Psychiatric nurses
would be expected to take on the role of nursing leader-
ship in psychiatric care (14, 15), but our results suggests
this was not the case. Psychiatric nurses were to some
extent acknowledged as having positional power as the
ones responsible for structuring care, and they might pos-
sess some referential power as role models, but, in rela-
tion to nursing assistants, they thoroughly miss out on
acquiring and exercising power of expertise through the
utilisation and sharing of nursing knowledge.
Research indicates the role of the psychiatric nurse in
inpatient psychiatry to be complex and conflicting (16,
17) and to lack clarity (18). Our results also indicate
that the psychiatric nurse is a marginal player in the
interprofessional team, not having the power of infor-
mation from knowing the patient or the power of
expertise from taking on the role of nursing leadership.
If so, nurses might, as has been suggested, give in to
the fact that times have changed and participate in
redefining their role towards that of risk management
assistants (16), or they could abandon humanism alto-
gether (19). This would not presumably contribute to
the making of a person-centred, recovery-oriented inpa-
tient psychiatric care. An alternative course of action,
supposedly more in the interest of the members of the
interprofessional team and patients alike, might be for
psychiatric nurses to position themselves closer to the
patients and reclaim the interpersonal relationship as
the core of psychiatric nursing as well as the raison
d’etre for psychiatric nurses.
It can be argued that interpersonal relationships are at
the core of psychiatric nursing and person-centred care
(20, 21). If the ambition is to deliver person-centred care,
it would seem a prerequisite that physicians as well as
psychiatric nurses have both the desire and the opportu-
nity to get to know and develop first-hand knowledge of
patients, assuming their professional perspectives of med-
icine and nursing, respectively. It would also seem rea-
sonable that all members of the interprofessional team
share their own knowledge and respect others’ knowl-
edge in the pursuit of understanding what is in the
patient’s best interest and how it can best be accom-
plished. This line of arguing corresponds to research on
interprofessional healthcare teamwork, suggesting that
difficulties in collaboration limit the possibility of a holis-
tic understanding of patients’ problems (22).
Limitations
This is a delimited qualitative study. Several of the partic-
ipants expressed that the vignette used indeed described
a familiar situation in the ward, stating that ‘this hap-
pened only yesterday’ or that they knew exactly who the
patient in the scenario was. This indicates that the vign-
ette used as common basis for the focus group discussions
was relevant for psychiatric inpatient care. The results
are however likely to reflect the specific working condi-
tions of the participants at the time the study was con-
ducted and should be handled with caution if transferred
to other settings. Most notably, the results seem to reflect
a lack of continuity in the employment of senior physi-
cians and a high patient-to-staff ratio at the ward in
question. It might be argued, however, that this is more
often than not the reality of contemporary psychiatric
inpatient care.
Conclusions
Our findings suggest that knowledge of patients is an
important means for influencing decision-making that
might need to be considered in future research and
development in the context of inpatient psychiatry. As
nursing assistants are the ones closest to the patients, this
makes them the most influential profession. For psychiat-
ric nurses to realise their potential as nursing leaders
making a substantial contribution to the interprofessional
team in delivering person-centred care, it would seem
Knowledge of the patient as power 791
© 2014 Nordic College of Caring Science

that they need to step up closer to the patients and put
their professional knowledge into action, preferably
accompanied by physicians.
Acknowledgements
Professor Siv S€oderberg and Associate Professor Lisa Sk€ar
participated in the initial planning and data collection.
The authors would like to thank Professor Rolf Adolfsson
of Ume�a University for valuable criticism and support.
Author contributions
Sebastian Gabrielsson and Git-Marie Ejneborn Looi par-
ticipated in the acquisition of data and were responsible
for the study’s original conception and design, which
were then revised with the input of Karin Zingmark and
Stefan S€avenstedt. Sebastian Gabrielsson performed the
analysis with the assistance of Git-Marie Ejneborn Looi
and made initial interpretations of data, which were pre-
sented and repeatedly discussed with the other authors
and revised accordingly. Sebastian Gabrielsson drafted
the manuscript together with Git-Marie Ejneborn Looi,
while Karin Zingmark and Stefan S€avenstedt repeatedly
revised it critically. All authors approved the final version
to be published.
Ethical approval
Ethical approval was granted from the regional ethics
committee in Ume�a (2010-4-31M, 2012-315-32M).
Funding
This study was funded by the Department of Health Sci-
ences at Lule�a University of Technology.
References
1 D’Amour D, Ferrada-Videla M, San
MR, Beaulieu M. The conceptual
basis for interprofessional collabora-
tion: core concepts and theoretical
frameworks. J Interprof Care 2005;
19: 116–31.
2 Larue C, Dumais A, Ahern E, Bern-
heim E, Mailhot M. Factors influenc-
ing decisions on seclusion and
restraint. J Psychiatr Ment Health Nurs
2009; 16: 440–6.
3 Barker PJ, Walker L. Nurses’ percep-
tions of multidisciplinary teamwork
in acute psychiatric settings. J Psychi-
atr Ment Health Nurs 2000; 7: 539–46.
4 Bowers L, Nijman H, Simpson A,
Jones J. The relationship between
leadership, teamworking, structure,
burnout and attitude to patients on
acute psychiatric wards. Soc Psychiatry
Psychiatr Epidemiol 2011; 46: 143–8.
5 Hanrahan NP, Aiken LH, McClaine
L, Hanlon AL. Relationship between
psychiatric nurse work environments
and nurse burnout in acute care
general hospitals. Issues Ment Health
Nurs 2010; 31: 198–207.
6 Hanrahan NP, Kumar A, Aiken LH.
Adverse events associated with orga-
nizational factors of general hospital
inpatient psychiatric care environ-
ments. Psychiatr Serv 2010; 61: 569–74.
7 Olofsson B, Norberg A. Experiences of
coercion in psychiatric care as nar-
rated by patients, nurses, and physi-
cians. J Adv Nurs 2001; 33: 89–97.
8 Kontio R, V€alim€aki M, Putkonen H,
Cocoman A, Turpeinen S, Kuosma-
nen L, Joffe G. Nurses’ and physi-
cians’ educational needs in seclusion
and restraint practices. Perspect Psychi-
atr Care 2009; 45: 198–207.
9 Kontio R, V€alim€aki M, Putkonen H,
Kuosmanen L, Scott A, Joffe G.
Patient restrictions: are there ethical
alternatives to seclusion and restraint?
Nurs Ethics 2010; 17: 65–76.
10 Morgan DL. Focus Groups as Qualita-
tive Research, 2nd edn. 1997, Sage
Publications, Thousand Oaks,
California.
11 Krippendorff K. Content Analysis: An
Introduction to Its Methodology, 3rd
edn. 2013, Sage, Thousand Oaks,
California.
12 Graneheim UH, Lundman B. Quali-
tative content analysis in nursing
research: concepts, procedures and
measures to achieve trustworthiness.
Nurse Educ Today 2004; 24: 105–12.
13 Yukl GA. Leadership in Organizations,
6th edn. 2006, Prentice Hall, Upper
Saddle River, New Jersey.
14 Blegen NE, Severinsson E. Leader-
ship and management in mental
health nursing. J Nurs Manag 2011;
19: 487–97.
15 Holm AL, Severinsson E. The role of
the mental health nursing leader-
ship. J Nurs Manag 2010; 18: 463–71.
16 Fourie WJ, McDonald S, Connor J,
Bartlett S. The role of the registered
nurse in an acute mental health
inpatient setting in New Zealand:
perceptions versus reality. Int J Ment
Health Nurs 2005; 14: 134–41.
17 Seed MS, Torkelson DJ, Alnatour R.
The role of the inpatient psychiatric
nurse and its effect on job satisfac-
tion. Issues Ment Health Nurs 2010;
31: 160–70.
18 Tuvesson H, Wann-Hansson C, Ekl-
und M. The ward atmosphere impor-
tant for the psychosocial work
environment of nursing staff in psy-
chiatric in-patient care. BMC Nurs
2011; 10: 12.
19 Jacob JD, Holmes D, Buus N.
Humanism in forensic psychiatry:
the use of the tidal nursing model.
Nurs Inq 2008; 15: 224–30.
20 Barker P, Jackson S, Stevenson C.
What are psychiatric nurses needed
for? Developing a theory of essential
nursing practice. J Psychiatr Ment
Health Nurs 1999; 6: 273–82.
21 Peplau HE. Interpersonal Relations in
Nursing: A Conceptual Frame of Refer-
ence for Psychodynamic Nursing. 1991
[1988], Springer Publishing Com-
pany, New York.
22 Kvarnstrom S. Difficulties in collabo-
ration: a critical incident study of
interprofessional healthcare team-
work. J Interprof Care 2008; 22: 191–
203.
792 S. Gabrielsson et al.
© 2014 Nordic College of Caring Science


DISSERTATIONS FROM THE DEPARTMENT OF HEALTH SCIENCE, LULEÅ UNIVERSITY OF TECHNOLOGY, SWEDEN Doctoral theses Terttu Häggström. Life-story perspective on caring within cultural contexts: experiences of
severe illness and of caring. (Nursing) 2004. Inger Jacobson. Injuries among female football players. (Physiotherapy) 2006. Karl Elling Ellingsen. Lovregulert tvang og refleksiv praksis. (Health Science and Human
Services) 2006. Annika Näslund. Dynamic ankle-foot orthoses in children with spastic diplegia: interview
and experimental studies. (Physiotherapy) 2007. Inger Lindberg. Postpartum care in transition: parents’ and midwives’ expectations and
experience of postpartum care including the use of videoconferencing. (Nursing) 2007. Åsa Widman. Det är så mycket som kan spela in – en studie av vägar till, genom och från
sjukskrivning baserad på intervjuer med långtidssjukskrivna. (Health Science and Human Services) 2007.
Eija Jumisko. Striving to become familiar with life with traumatic brain injury: experiences of people with traumatic brain injury and their close relatives. (Nursing) 2007.
Gunilla Isaksson. Det sociala nätverkets betydelse för delaktighet i dagliga aktiviteter: erfarenheter från kvinnor med ryggmärgsskada och deras män. (Health Science and Human Services) 2007.
Nina Lindelöf. Effects and experiences of high-intensity functional exercise programmes among older people with physical or cognitive impairment. (Physiotherapy) 2008.
Åsa Engström. A wish to be near: experiences of close relatives within intensive care from the perspective of close relatives, formerly critically ill people and critical care nurses. (Nursing) 2008.
Catrine Kostenius. Giving voice and space to children in health promotion. (Health Science and Human Services) 2008.
Anita Melander Wikman. Ageing well: mobile ICT as a tool for empowerment of elderly people in home health care and rehabilitation. (Physiotherapy) 2008.
Sedigheh Iranmanesh. Caring for dying and meeting death: the views of Iranian and Swedish nurses and student nurses. (Nursing) 2009.
Birgitta Lindberg. When the baby is premature. Experiences of parenthood and getting support via videoconferencing. (Nursing) 2009.
Malin Olsson. Meaning of women’s experiences of living with multiple sclerosis. (Nursing) 2010.
Lars Jacobsson. Long-term outcome after traumatic brain injury. Studies of individuals from northern Sweden. (Health Science) 2010.
Irene Wikman. Fall, perceived fall risk and activity curtailment among older people receiving home-help services. (Physiotherapy) 2011.
Christina Harrefors. God vård och användning av digitala hjälpmedel. Föreställningar hos äldre och vårdpersonal. (Nursing) 2011.
Agneta Larsson. Identifying, describing and promoting health and work ability in a workplace context. (Physiotherapy) 2011.
Lisbeth Eriksson. Telerehabilitation: Physiotherapy at a distance at home. (Physiotherapy) 2011.
Amjad Alhalaweh. Pharmaceutical Cocrystals: Formation mechanisms, solubility behaviour and solid-state properties. (Health Science) 2012.
Katarina Mikaelsson. Fysisk aktivitet, inaktivitet och kapacitet hos gymnasieungdomar. (Physiotherapy) 2012.
Carina Nilsson. Information and communication technology as a tool for support in home care. -Experiences of middle-aged people with serious chronic illness and district nurses. (Nursing) 2012.
Britt-Marie Wällivaara. Contemporary home-based care: encounters, relationships and the use of distance-spanning technology. (Nursing) 2012.
Stina Rutberg. Striving for control and acceptance to feel well. Experiences of living with migraine and attending physical therapy. (Physiotherapy) 2013.
Päivi Juuso. Meanings of women's experiences of living with fibromyalgia. (Nursing) 2013. Anneli Nyman. Togetherness in Everyday Occupations. How Participation in On-Going
Life with Others Enables Change. (Occupational therapy) 2013. Caroline Stridsman. Living with chronic obstructive pulmonary disease with focus on
fatigue, health and well-being. (Nursing) 2013. Ann-Sofie Forslund. A Second Chance at Life: A Study About People Suffering Out-Of-
Hospital Cardiac Arrest. (Nursing) 2014. Birgitta Nordström. Experiences of standing in standing devices: voices from adults, children
and their parents. (Physiotherapy) 2014. Malin Mattsson. Patients’ experiences and patient-reported outcome measures in systemic
lupus erythematosus and systemic sclerosis. (Physiotherapy) 2014. Eva Lindgren. “It’s all about survival”: Young adults’ transitions within psychiatric care from
the perspective of young adults, relatives, and professionals. (Nursing) 2014. Annette Johansson. Implementation of Videoconsultation to Increase Accessibility to Care
and Specialist Care in Rural Areas: - Residents, patients and healthcare personnel´s views. (Nursing) 2015.
Cecilia Björklund. Temporal patterns of daily occupations and personal projects relevant for older persons’ subjective health: a health promotive perspective. (Occupational therapy) 2015.
Ann-Charlotte Kassberg. Förmåga att använda vardagsteknik efter förvärvad hjärnskada: med fokus mot arbete. (Occupational therapy) 2015.
Angelica Forsberg. Patients' experiences of undergoing surgery: From vulnerability towards recovery -including a new, altered life. (Nursing) 2015.
Maria Andersson Marchesoni. “Just deal with it” Health and social care staff´s perspectives on changing work routines by introducing ICT: Perspectives on the process and interpretation of values. (Nursing) 2015.
Sari-Anne Wiklund-Axelsson. Prerequisites for sustainable life style changes among older persons with obesity and for ICT support. (Physiotherapy) 2015.
Anna-Karin Lindqvist. Promoting adolescents' physical activity @ school. (Physiotherapy) 2015.
Ulrica Lundström. Everday life while aging with a traumatic spinal cord injury. (Occupational therapy) 2015.
Sebastian Gabrielsson. A moral endeavour in a demoralizing context: Psychiatric inpatient care from the perspective of professional caregivers. (Nursing) 2015.
Licentiate theses Marja Öhman. Living with serious chronic illness from the perspective ofpeople with serious
chronic illness, close relatives and district nurses. (Nursing) 2003. Kerstin Nyström. Experiences of parenthood and parental support during the child's first
year. (Nursing) 2004.

Eija Jumisko. Being forced to live a different everyday life: the experiences of people with traumatic brain injury and those of their close relatives. (Nursing) 2005.
Åsa Engström. Close relatives of critically ill persons in intensive and critical care: the experiences of close relatives and critical care nurses. (Nursing) 2006.
Anita Melander Wikman. Empowerment in living practice: mobile ICT as a tool for empowerment of elderly people in home health care. (Physiotherapy) 2007.
Carina Nilsson. Using information and communication technology to support people with serious chronic illness living at home. (Nursing) 2007.
Malin Olsson. Expressions of freedom in everyday life: the meaning of women's experiences of living with multiple sclerosis. (Nursing) 2007.
Lena Widerlund. Nya perspektiv men inarbetad praxis: en studie av utvecklingsstördas delaktighet och självbestämmande. (Health Science and Human Services) 2007.
Birgitta Lindberg. Fathers’ experiences of having an infant born prematurely. (Nursing) 2007.
Christina Harrefors. Elderly people’s perception about care and the use of assistive technology services (ATS). (Nursing) 2009.
Lisbeth Eriksson. Effects and patients' experiences of interactive video-based physiotherapy at home after shoulder joint replacement. (Physiotherapy) 2009.
Britt-Marie Wälivaara. Mobile distance-spanning technology in home care. Views and reasoning among persons in need of health care and general practitioners. (Nursing) 2009.
Anita Lindén. Vardagsteknik. Hinder och möjligheter efter förvärvad hjärnskada. (Health Science) 2009.
Ann-Louise Lövgren Engström. Användning av vardagsteknik i dagliga aktiviteter - svårigheter och strategier hos personer med förvärvad hjärnskada. (Health Science) 2010.
Malin Mattsson. Frågeformulär och patientupplevelser vid systemisk lupus erythematosus -en metodstudie och en kvalitativ studie. (Physiotherapy) 2011.
Catharina Nordin. Patients’ experiences of patient participation prior to and within multimodal pain rehabilitation. (Physiotherapy) 2013.
Hamzah Ahmed. Relationship Between Crystal Structure and Mechanical Properties in Cocrystals and Salts of Paracetamol. (Health Science) 2014.
For purchase information: Department of Health Science, Luleå University of Technology, S-971 87 Luleå, Sweden.























