
Effect of transdermally delivered aspirin on blood coagulation parameters

JOURNAL OF OCULAR PHARMACOLOGY AND THERAPEUTICSVolume 22, Number 3, 2006© Mary Ann Liebert, Inc.
Ocular Hypotensive Effects of an IntratracheallyDelivered Liposomal !9-Tetrahydrocannabinol
Preparation in Rats
ANNA-MARIA SZCZESNIAK,1 MELANIE E.M. KELLY,1 SARA WHYNOT,1PANG N. SHEK,2 and ORLANDO HUNG1
ABSTRACT
This study investigated the effect of an intratracheal (i.t.) administration of a liposome-en-trapped !9-tetrahydrocannabinol (LTHC) preparation on intraocular pressure (IOP) innonanaesthetized Brown Norway rats. The ocular hypotensive effects of i.t. LTHC were com-pared to that of intraperitoneal (i.p.) LTHC administration.
All i.t. LTHC doses !0.05 mg/kg significantly decreased IOP (P " 0.05) within 30 min ofadministration, and doses of i.t. LTHC !0.1 mg/kg decreased IOP within 15 min of adminis-tration. A maximal reduction in IOP of 2.32 " 0.27 mmHg (n # 4) was seen with 1.0 mg/kg ofi.t. LTHC. In comparison, no significant IOP drop was apparent prior to 30 min with all doses(0.01–1.0 mg/kg) of i.p. LTHC tested, although a similar maximum drop in IOP (2.15 " 0.12mmHg; n # 8) was obtained with 1.0 mg/kg of LTHC. The ED50 for i.t. and i.p. LTHC was0.08 mg/kg and 0.12 mg/kg, respectively. The IOP-lowering effects of i.p. LTHC (0.2 mg/kg)were reduced by 14% and 80% by 0.25 mg/kg (n # 6) and 2.5 mg/kg (n # 6), respectively, ofthe CB1R antagonist, SR141716A.
In conclusion, i.t. LTHC was superior to i.p. LTHC in producing a more rapid and potentdecrease in IOP. The IOP-lowering effect of LTHC was blocked by the CB1R-selective an-tagonist, SR141716A, suggesting that CB1Rs contribute to the ocular hypotensive effect of !9-tetrahydrocannabinol.
INTRODUCTION
#9-TETRAHYDROCANNABINOL (LTHC) is one ofthe main active constituents of marijuana
(Cannabis sativa). In addition to psychotropic,analgesic, and antiemetic activities, smoking mar-ijuana has been reported to decrease intraocularpressure (IOP) in the human and mammalianeye.1–3 The ocular hypotensive action of mari-juana was first reported in human subjects by
Hepler and Frank.4 Since then, a number of stud-ies on human and animal models have confirmedthe ability of cannabinoid drugs, including theendogenous endocannabinoid, anandamide, todirectly decrease IOP.5,6
Endogenous and synthetic cannabinoids exerttheir action through the activation of cannabinoidreceptors. Two receptors, CB1 and CB2, havebeen cloned. CB1 receptors (CB1Rs) are ex-pressed, and were discovered first, in the central
1Departments of Pharmacology, Ophthalmology and Anaesthesiology, Dalhousie University, Halifax, Nova Sco-tia, Canada.
2Operational Medicine Section, Defence Research and Development Canada (DRDC), Toronto, Ontario, Canada.
160

nervous system (CNS) but have also been iden-tified in peripheral tissues, particularly inadipocytes.7 CB2 receptors are prevalent in pe-ripheral tissues and cells.8 Both cannabinoid re-ceptors are Gi protein–coupled receptors andtheir stimulation causes the activation of down-stream signaling pathways, such as adenyl cy-clase inhibition, MAP kinase activation, the inhi-bition of voltage-gated calcium channels, and thepotentiation of inwardly rectifying potassiumcurrents.9 CB1Rs are present in ocular tissue,10,11
and the ocular hypotensive actions of cannabi-noids have been attributed to the activation ofCB1Rs localized to the anterior structures of theeye, which are associated with aqueous humorproduction and outflow.5,6,12,13
It has been suggested that !9-THC andcannabinoid drugs may have potential in thetreatment of glaucoma.2,3,14 In glaucoma, loss ofvision is ultimately caused by the death of reti-nal ganglion cells (RGCs) through apoptosis.15
Apoptosis of RGCs may be multifactorial owingto axon injury at the optic nerve head, arisingfrom mechanical or ischemia insults and involv-ing glutamate receptors and excitotoxicity. In-creased IOP is the principal modifiable risk fac-tor in glaucoma, and drugs that decrease IOP—byeither decreasing aqueous humor secretion or in-creasing outflow—have been shown to slow theprogression of glaucoma.16
Recent studies have suggested, in addition totheir IOP-lowering properties, that cannabinoidsmay be neuroprotective: !9-THC, cannabidiol,the nonpsychotropic component of marijuana, as well as the synthetic cannabinoid agonist, HU-211, decrease glutamate- or NMDA-inducedretinal neuron death in cell-culture models, aswell as in experimental models of NMDA-induced retinal neurotoxicity17 and optic axot-omy.18 In addition, !9-THC and HU-211 havebeen shown to have antioxidant properties thatare independent of CB1Rs and may provide neu-roprotection by acting as scavengers for toxic reactive oxygen species, which are produced fol-lowing excitotoxic insult.19,20 Thus, the combina-tion of both an ocular hypotensive action coupledto retinal neuroprotection would be attractive forthe development of novel cannabinoid drugs fortherapeutic use in glaucoma, as well as other neu-rodegenerative retinal diseases.
The clinical use of cannabinoid drugs, how-ever, is constrained by problems associated withformulating stable and effective drug delivery
systems that can deliver measured doses. Cur-rently, medical use of !9-THC is primarily reliantupon smoking the marijuana plant. Whereas theinhalation of marijuana results in a rapid deliv-ery of systemic doses of !9-THC and avoids he-patic first-pass metabolism, this route of admin-istration is associated with a significant exposureto mutagens, carcinogens, and other toxic prod-ucts of pyrolysis.21 Although topical drug deliv-ery systems would minimize possible adversesystemic side-effects, the low aqueous solubilityof cannabinoid compounds poses a challenge forthis route of administration.2 Thus, there is a needto continue to develop and test alternative drugdelivery systems for !9-THC and other novelcannabinoid drugs currently under development.A more effective drug delivery system will im-prove the drug profile for treating a variety ofchronic CNS pathologies, including glaucomaand retinal ischemia.
We have developed a liposome-encapsulated!9-THC formulation (LTHC) suitable for pul-monary delivery. The incorporation of !9-THCinto liposomes has a number of advantages overthe existing delivery systems. !9-THC is a highlyviscous, insoluble compound, and the incorpora-tion of !9-THC in liposomes facilitates its ad-ministration. In this study, we compared the oc-ular hypotensive actions of intratracheal (i.t.)LTHC, administered as an aerosol through i.t. in-stillation, to that of intraperitoneal (i.p.) LTHC. Inaddition, we determined whether the IOP-lower-ing effects of LTHC were mediated largely byCB1Rs, using the CB1R antagonist, SR141716A.
METHODS
Measurement of IOP
Brown Norway rats (300 g) were used for allexperiments. Animals were housed under a 12-hlight/dark cycle and maintained on rat chow andwater at libitum, except during experiments. Allanimals were treated in accordance with the stan-dards and procedures set forth by the CanadianCouncil on Animal Care (www.ccac.ca). In doingso, efforts were made to ensure that the animalsexperienced minimal suffering and pain and thatthe experimental design used the smallest num-ber of animals required to obtain valid data.
IOP was measured in the rat eye with a non-invasive method using a tonometer (Tono-
EFFECT OF LIPOSOME-ENCAPSULATED !9-THC ON IOP 161

Pen®XL, Solan Ophthalmic Products; Jackson-ville, FL). Previous experiments, using BrownNorway rats, have shown an excellent correlationbetween IOP measurements made with a Tono-PenXL and transducer-measured IOP.22 Prior totaking IOP measurements, the animals received1 drop (40 !L) of 0.05% tetracaine eye drops(Dioptic Laboratories; Markham, Ontario,Canada) applied topically for local anesthesia.Animals were then placed on a fixed bench andlightly restrained. For IOP measurements, thetonometer was placed gently against the anes-thetized surface of the cornea. For each timepoint, IOP was measured 10 times, with the meanvalue reported. Baseline or control IOP was mea-sured before drug administration, and all otherIOP measurements were made at timed intervalspostdrug administration (see below). All the ex-periments were carried out at the same time inthe morning in order to ensure that any changesin IOP readings were not related to diurnal vari-ations in IOP. To achieve reliable IOP readingsand to minimize stress, animals were handledand exposed to the IOP measurement proceduredaily for at least 5 days prior to the experiments.
Drug preparation and administration
Composition of the liposome preparation wasbased on previous work utilizing liposome-en-capsulated drugs for inhalation, where the rate ofdrug release was determined by the phospho-lipid/cholesterol ratio and hydrophilic/lipophilicproperties of all active ingredients.23–25 LTHC wasprepared by entrapping !9-THC in liposomescomposed of dipalmitoylphosphatidylcholine andcholesterol (Avanti Polar Lipids; Alabaster, AL) ina 7:3 molar ratio. Briefly, the lipids were dissolvedin a minimal volume of chloroform in a round-bot-tomed glass vessel, followed by the addition of adefined amount of !9-THC (Sigma-AldrichCanada, Ltd.; Oakville, Ontario, Canada). Chloro-form was evaporated under a stream of helium at40°C, and the glass vessel was placed under vac-uum for 12 h to remove any residual solvent. Thedried lipid-cannabinoid mixture was hydrated at51°C in phosphate-buffered saline (PBS; 0.15 M,pH 7.2) and kept at this temperature with periodicvortexing for 30 min to form multilamellar vesi-cles. The liposomes with entrapped cannabinoidwere extruded 10 times with a thermobarrel ex-truder (Lipex Biomembranes; Vancouver, BritishColumbia, Canada) fitted with doubly stacked
polycarbonate filters of 400-nm pore size, using ahelium pressure of 100-200 pounds (psi). persquare inch. The extrusion process produced apreparation with a homogeneous liposome-sizedistribution approximately 400 nm, using a Coul-ter N4SD particle-size analyzer (Hialeah, FL). Theliposomal !9-THC was stored as a lyophilizedpowder prior to its use for administration to ani-mals. The lyophilized preparation was reconsti-tuted in PBS (0.15 M, pH 7.2) and adjusted to con-tain 600 !g of !9-THC in 100 mg of lipid per mL.The drug entrapment efficiency of LTHC was de-termined to be greater than 90%.
Doses of LTHC (0.01–1.0 mg/kg) or placebo li-posomes (control) were administered by i.t. in-stillation, using a hydraulic microsprayer thatgenerated an aerosol with an MMD of 18 !m, atan operating pressure of 2000 psi (PennCentury™Microsprayer; Philadelphia, PA). The Micro-sprayer allows for the local pulmonary deliveryof the drug with close to 100% efficiency26 andhas been used successfully in rodents toward in-ducing minimal respiratory distress.27–29
In order to determine the plasma concentrationof !9-THC, rats were anesthetized underhalothane anesthesia (Halocarbon Laboratories;Diver Edge, NJ), and were administered 0.2mg/kg of i.t. LTHC. While under anesthesia, 3 mL of blood per animal was obtained by car-diac puncture at 15-, 30-, 45-, 60-, and 120-mintime points, followed by immediately sacrificingthe animals immediate sacrifice by cervical dis-location. Plasma !9-THC concentrations of ani-mals receiving inhaled LTHC were determinedusing a modified gas chromatography–massspectrometry technique, as described by Freder-ick and Fowler.30 Analysis of plasma !9-THCdemonstrated that an i.t. LTHC dose of "0.2mg/kg produced a rapid increase in plasma CTHCwithin 5–10 min, and CTHC was maintained abovethe therapeutic range (1–2 ng.mL#1) for 2 h fol-lowing pulmonary administration in rats (datanot shown).
Initial predose control (time-zero) IOP mea-surements were made in fully conscious, unanes-thetized animals. Following this measurement,animals were anesthetized using halothane(Halocarbon Laboratories) to allow for the i.t. in-stillation of LTHC. Inhalation anesthetic was ad-ministered using a manifold for nose-only expo-sure with a 1.5-L/min#1 O2/4.5% halothane forinduction and 1.5-L/min#1 O2/ 2.5% halothanefor maintenance of anesthesia. Instillations were
SZCZESNIAK ET AL.162
carried out immediately following satisfactoryanesthesia (loss of foot reflex); then, the full doseof LTHC or placebo liposomes was administeredin one instillation. Immediately after dosing, the en-dotracheal tube was removed, allowing the ani-mals to recover. Rats were fully conscious and mobile within 5 min after the administration pro-cedure. The first IOP reading was made at 15 minafter drug administration, followed by additionalIOP measurements at 30, 45, 60, 75, 90, 105, and 120min. For i.p. delivery, after control IOP measure-ments were taken (time zero), animals were in-jected with either 0.01–1.0 mg/kg of LTHC orplacebo liposomes, following which IOP measure-ments were made at the same time intervals de-tailed above for i.t. delivery of LTHC. The CB1Rantagonist, SR141716A, was kindly provided bySanofi-Synthelabo Recherche (Montpellier, France)and was dissolved in 45% 2-hydroxypropyl-"-cy-clodextrin. Animals were injected i.p. with 0.25mg/kg and 2.5 mg/kg of SR141716A 30 min priorto the administration of LTHC.
Data analysis and statistics
The data were analyzed using one-way analy-sis of variance (ANOVA) analysis with post-hocmultiple comparison, using a Tukey or Dunnettest. P $ 0.05 was considered statistically signifi-cant. The data presented in all the figures repre-sent mean % standard error of the mean. ED50,the dose of agonist producing 50% maximalchange in IOP (!IOP), was calculated by fittingdose-response data for the maximum change inIOP (!IOP) with a variable Hill slope given byparameter “p” where:
y & A1 ' (A2 # A1)/1 ' 10(logXo-x)p
where A1 & !IOP with liposomes or vehicle con-trol, A2 & !IOP with maximal dose of agonisttested, logXo & 50% of A2 (EC50), and p & hillslope.
RESULTS
Effects of i.t. administration of LTHC on IOP
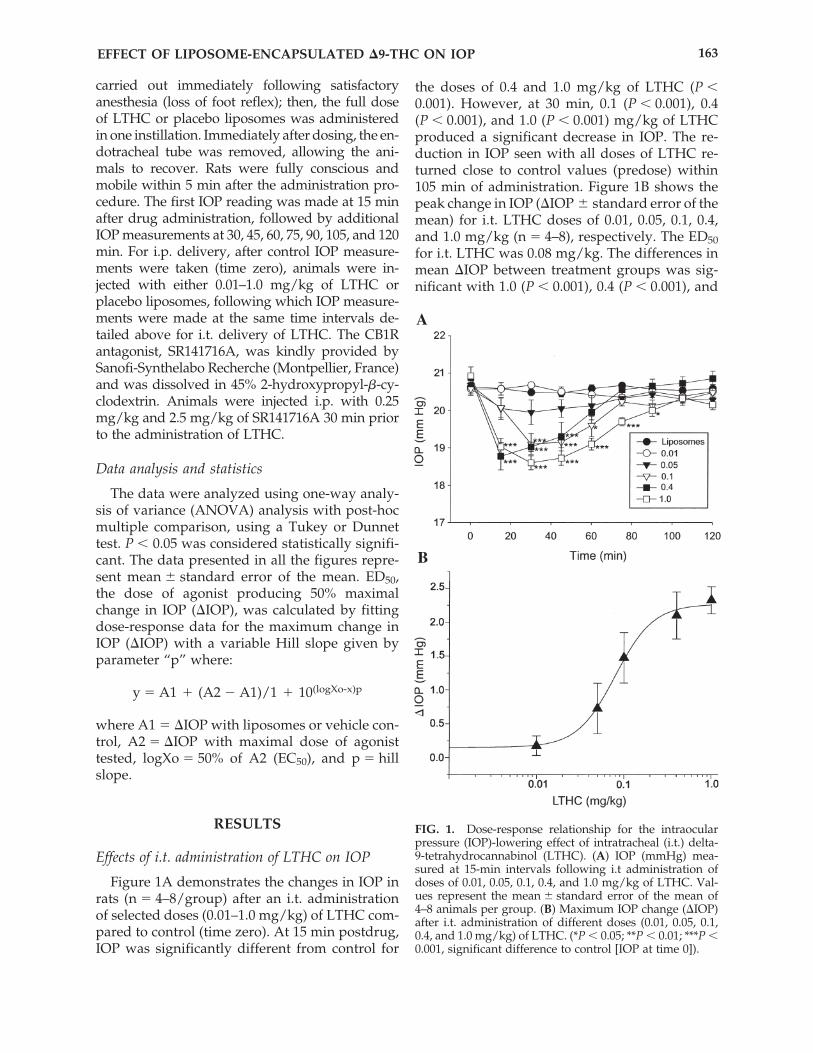
Figure 1A demonstrates the changes in IOP inrats (n & 4–8/group) after an i.t. administrationof selected doses (0.01–1.0 mg/kg) of LTHC com-pared to control (time zero). At 15 min postdrug,IOP was significantly different from control for
the doses of 0.4 and 1.0 mg/kg of LTHC (P $0.001). However, at 30 min, 0.1 (P $ 0.001), 0.4(P $ 0.001), and 1.0 (P $ 0.001) mg/kg of LTHCproduced a significant decrease in IOP. The re-duction in IOP seen with all doses of LTHC re-turned close to control values (predose) within105 min of administration. Figure 1B shows thepeak change in IOP (!IOP % standard error of themean) for i.t. LTHC doses of 0.01, 0.05, 0.1, 0.4,and 1.0 mg/kg (n & 4–8), respectively. The ED50for i.t. LTHC was 0.08 mg/kg. The differences inmean !IOP between treatment groups was sig-nificant with 1.0 (P $ 0.001), 0.4 (P $ 0.001), and
EFFECT OF LIPOSOME-ENCAPSULATED !9-THC ON IOP 163
FIG. 1. Dose-response relationship for the intraocularpressure (IOP)-lowering effect of intratracheal (i.t.) delta-9-tetrahydrocannabinol (LTHC). (A) IOP (mmHg) mea-sured at 15-min intervals following i.t administration ofdoses of 0.01, 0.05, 0.1, 0.4, and 1.0 mg/kg of LTHC. Val-ues represent the mean % standard error of the mean of4–8 animals per group. (B) Maximum IOP change (!IOP)after i.t. administration of different doses (0.01, 0.05, 0.1,0.4, and 1.0 mg/kg) of LTHC. (*P $ 0.05; **P $ 0.01; ***P $0.001, significant difference to control [IOP at time 0]).
A
B
0.1 (P $ 0.05) mg/kg of LTHC significantly dif-ferent from 0.01 mg/kg of LTHC, and 1.0 mg/kgof LTHC significantly different compared to 0.05mg/kg of i.t. LTHC (P $ 0.005).
Effects of i.p. administration of LTHC on IOP
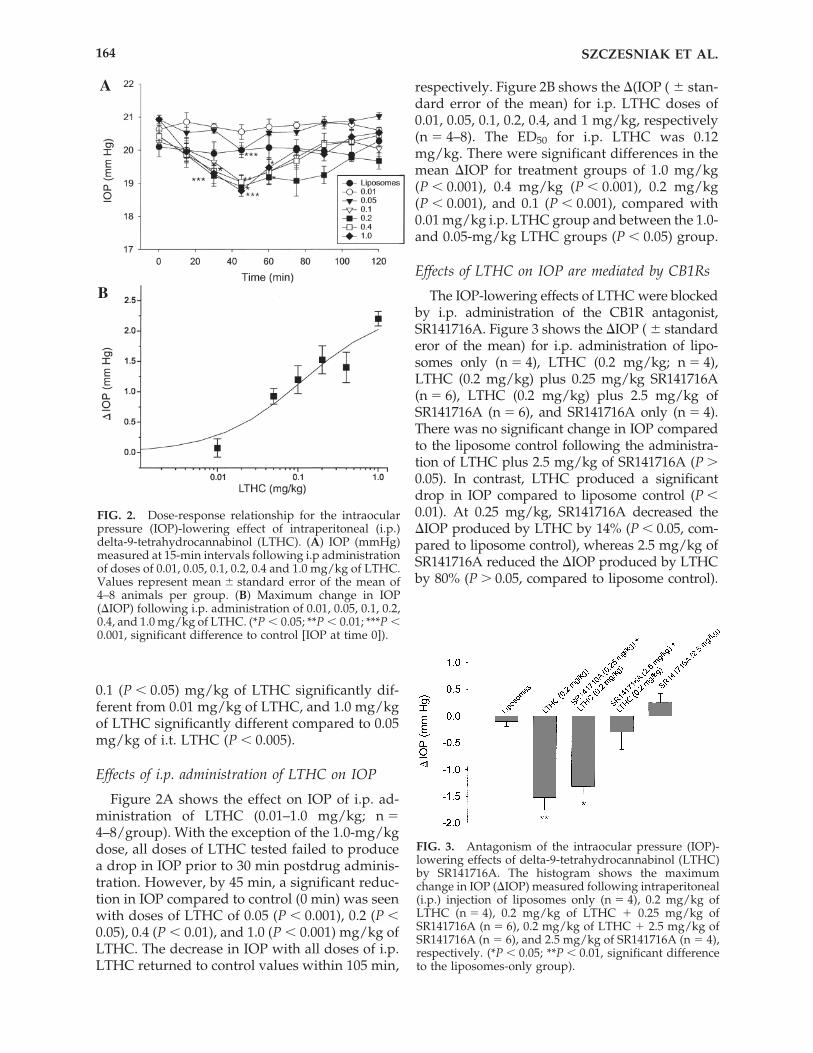
Figure 2A shows the effect on IOP of i.p. ad-ministration of LTHC (0.01–1.0 mg/kg; n &4–8/group). With the exception of the 1.0-mg/kgdose, all doses of LTHC tested failed to producea drop in IOP prior to 30 min postdrug adminis-tration. However, by 45 min, a significant reduc-tion in IOP compared to control (0 min) was seenwith doses of LTHC of 0.05 (P $ 0.001), 0.2 (P $0.05), 0.4 (P $ 0.01), and 1.0 (P $ 0.001) mg/kg ofLTHC. The decrease in IOP with all doses of i.p.LTHC returned to control values within 105 min,
respectively. Figure 2B shows the !(IOP ( % stan-dard error of the mean) for i.p. LTHC doses of0.01, 0.05, 0.1, 0.2, 0.4, and 1 mg/kg, respectively(n & 4–8). The ED50 for i.p. LTHC was 0.12mg/kg. There were significant differences in themean !IOP for treatment groups of 1.0 mg/kg(P $ 0.001), 0.4 mg/kg (P $ 0.001), 0.2 mg/kg(P $ 0.001), and 0.1 (P $ 0.001), compared with0.01 mg/kg i.p. LTHC group and between the 1.0-and 0.05-mg/kg LTHC groups (P $ 0.05) group.
Effects of LTHC on IOP are mediated by CB1Rs
The IOP-lowering effects of LTHC were blockedby i.p. administration of the CB1R antagonist,SR141716A. Figure 3 shows the !IOP ( % standarderor of the mean) for i.p. administration of lipo-somes only (n & 4), LTHC (0.2 mg/kg; n & 4),LTHC (0.2 mg/kg) plus 0.25 mg/kg SR141716A(n & 6), LTHC (0.2 mg/kg) plus 2.5 mg/kg ofSR141716A (n & 6), and SR141716A only (n & 4).There was no significant change in IOP comparedto the liposome control following the administra-tion of LTHC plus 2.5 mg/kg of SR141716A (P (0.05). In contrast, LTHC produced a significantdrop in IOP compared to liposome control (P $0.01). At 0.25 mg/kg, SR141716A decreased the!IOP produced by LTHC by 14% (P $ 0.05, com-pared to liposome control), whereas 2.5 mg/kg ofSR141716A reduced the !IOP produced by LTHCby 80% (P ( 0.05, compared to liposome control).
SZCZESNIAK ET AL.164
A
B
FIG. 2. Dose-response relationship for the intraocularpressure (IOP)-lowering effect of intraperitoneal (i.p.)delta-9-tetrahydrocannabinol (LTHC). (A) IOP (mmHg)measured at 15-min intervals following i.p administrationof doses of 0.01, 0.05, 0.1, 0.2, 0.4 and 1.0 mg/kg of LTHC.Values represent mean % standard error of the mean of4–8 animals per group. (B) Maximum change in IOP(!IOP) following i.p. administration of 0.01, 0.05, 0.1, 0.2,0.4, and 1.0 mg/kg of LTHC. (*P $ 0.05; **P $ 0.01; ***P $0.001, significant difference to control [IOP at time 0]).
FIG. 3. Antagonism of the intraocular pressure (IOP)-lowering effects of delta-9-tetrahydrocannabinol (LTHC)by SR141716A. The histogram shows the maximumchange in IOP (!IOP) measured following intraperitoneal(i.p.) injection of liposomes only (n & 4), 0.2 mg/kg ofLTHC (n & 4), 0.2 mg/kg of LTHC ' 0.25 mg/kg ofSR141716A (n & 6), 0.2 mg/kg of LTHC ' 2.5 mg/kg ofSR141716A (n & 6), and 2.5 mg/kg of SR141716A (n & 4),respectively. (*P $ 0.05; **P $ 0.01, significant differenceto the liposomes-only group).

Administration of 2.5 mg/kg of SR141716A aloneresulted in a small increase in IOP, compared to theliposomal control group (P $ 0.05).
DISCUSSION
This present study evaluated the ability of a li-posome-entrapped preparation of !9-THC to deliver a pharmacologically sufficient dose of !9-THC through the lungs in rats. The pharmaco-logical action of !9-THC to decrease IOP providedan objective measure of its pharmacodynamic drugaction. The hypothesis of this study was that theintratracheal route of administration would be su-perior to that of parenteral administration for thedelivery of lipsome-encapsulated !9-THC. Our re-sults indicate that i.t. LTHC delivery is more effi-cacious in promoting drug delivery than i.p. LTHC;the i.t. route produced a more rapid decrease inIOP, which was likely owing to a rapid absorptionof the drug from the alveoli into the systemic cir-culation. Furthermore, estimates of ED50 suggestedthat i.t. LTHC was more potent than i.p. LTHC, al-though the maximal efficacy was comparable be-tween both routes of LTHC administration.
With regard to the duration of action, theIOP-lowering effect of both i.t. and i.p. LTHCreturned to baseline levels approximately 1.5–2h after drug administration. !9-THC is a highlylipophilic drug with a large volume of distri-bution. An average estimated volume of 3.4 L/kg(or 236 L for a 70-kg subject) has been reported.1The short duration of LTHC drug effect can, inpart, be explained by the rapid redistribution of!9-THC to other tissues. At this point, it shouldbe mentioned that the liposomes containing en-trapped !9-THC were of approximately uni-form size (368 % 42 nm from the Coulter N4SDparticle-size analyzer), and, therefore, it is likelythat the !9-THC was released at the same ratefrom all liposomes. We anticipate that the dura-tion of action of LTHC could be prolonged by theinclusion of a mixed population of liposomesizes.31,32 It may also be possible to increase thecirculation time of liposomes by incorporation ofdistearoylglycerophosphoethanolamine metho-xylpolyethyleneglycol 2000 (DSPE-MPEG), whichreduces the removal of liposomes by the retic-uloendothelial system.33
Whereas this report describes the first study,where liposome-entrapped !9-THC was used for i.t. delivery in rodents, the administration ofaerosolized cannabinoids, including !9-THC,
have been examined in mice. Lichtman and col-leagues34 used a small-particle aerosol generator(SPAG) nebulizer to generate an aerosol with anoutput of 0.154 mg/L of aerosolized !9-THC,with particles less than 5.0 !m in diameter. In thisstudy, !9-THC was formulated in a vehicle consisting of 1:1:18 ethanol/emulphor/saline. In-halation exposure of the !9-THC aerosol in micewas able to elicit antinociceptive effects that weredependent on dose and time of exposure. The on-set of antinociceptive effects, with an estimated1.8 mg/kg of !9-THC, occurred within 5 min,lasted approximately 40 min, and were blockedby the CB1R antagonist, SR141716A.
Our observation that the IOP-lowering effects ofLTHC can be obviated by SR1416716A, an antago-nist that has been shown to discriminate CB1R-spe-cific effects,1,5,6,8 provides support for a CB1R-spe-cific mode of action accounting for the acute ocularhypotensive actions of !9-THC. The distribution ofCB1Rs in different eye tissues involved in aqueoushumor inflow and outflow, including ciliary body,trabecular meshwork, and Schlemm’s canal, sug-gests that endogenous cannabinoids may be in-volved in the regulation of IOP by acting at multi-ple ocular sites.2,10–12,14,35–37
Pharmacological studies examining alternate de-livery systems, to smoking, for cannabinoids in hu-mans and animals, have primarily examined oral,rectal, and topical formulations. Dronabinol (Mari-nol®), a synthetic !9-THC, has been used to relievenausea and vomiting related to cancer chemother-apy and to stimulate appetite in patients with ac-quired immunodeficiency disease (AIDS).38 How-ever, when taken orally, !9-THC undergoessignificant first-pass metabolism, resulting in an er-ratic, unpredictable absorption ($15%) and a de-layed onset of action.1,39,40 Whereas rectal applica-tion can avoid the hepatic first-pass effect withhigher bioavailability than oral administration, thebioavailability through this route varied with dif-ferent formulations.41 Most ophthalmic studies oftopical !9-THC and cannabinoid drugs in humanswith glaucoma and in animal models have em-ployed the use of vehicles such as light mineraloil,42 cyclodextrin, or hydroxypropylmethylcellu-lose.14,43,44 Despite an IOP-lowering effect, topicalapplication to the cornea has resulted in limitedbioavailability and, in some cases, ocular irritationand toxicity.1,2,43 Recently, the results of a phase Istudy evaluating safety and tolerability of a one-time dose of pulmonary dronabinol found that thisformulation of synthetic !9-THC, delivered with apressurized metered dose inhaler, provided rapid
EFFECT OF LIPOSOME-ENCAPSULATED !9-THC ON IOP 165
systemic absorption, which was well tolerated inboth young and elderly subjects. A proof-of prin-cipal clinical trial is now underway to evaluatethe efficacy, safety, and tolerability of pulmonarydronabinol for the acute treatment of migraineheadache.45
CONCLUSIONS
Our study indicates that the administration of aliposome-entrapped !9-THC can provide an ef-fective means of delivering pharmacologically ac-tive cannabinoids. Furthermore, liposome-encap-sulated drugs delivered through the respiratorysystem have been demonstrated to be well toler-ated in both animal models and in humans.46–47
With the emerging impetus to develop cannabi-noids for therapeutic use in chronic neurodegen-erative conditions, the use of liposomes as a drug-carrying vehicle can facilitate the delivery of thesehighly lipophylic drugs, thus allowing for alter-native drug delivery routes to be employed.Whereas our study compared i.t. versus i.p. routesof LTHC administration, it is conceivable that top-ical applications of LTHC will also prove to be ef-fective, possibly mediating a better corneal pene-tration, less toxicity, and a longer drug half-lifethan previously tested formulations. The avail-ability of alternative delivery systems for cannabi-noid drugs may lead to further utility of thesedrugs in the treatment of chronic eye disease.
ACKNOWLEDGMENTS
This work was supported by the Nova ScotiaHealth Research Foundation (NSHRF), the Cana-dian Institute of Health Research (CIHR) grantIAO-13484 (MEMK), and Defense Research andDevelopment Canada (DRDC). The authors wishto thank Doug Saunders of DRDC for the prepa-ration of liposomal formulations.
REFERENCES
1. Grotenhermen, F. Pharmacokinetics and pharma-codynamics of cannabinoids. Clin. Pharmacokinet.42:327–360, 2003.
2. Järvinen T., Pate, D.W., and Laine, K. Cannabinoidsin the treatment of glaucoma. Pharmacol. Therap.95:203–220, 2002.
3. Tomida, I., Pertwee, R.G., and Azura-Blanco, A.Cannabinoids and glaucoma. Br. J. Ophthalmol. 88:708–713, 2004.
4. Hepler, R.S., and Frank, I.M. Marihuana smoking andintraocular pressure. JAMA 217:1392, 1971.
5. Pate, D.W., Järvinen, K., Urtti, A., et al. Effect of theCB1 receptor antagonist, SR141716A, on cannabinoid-induced ocular hypotension in normotensive rabbits.Life Sci. 48:1881–1893, 1998.
6. Song, Z., and Slowey, C. Involvement of cannabinoidreceptors in the intraocular pressure–lowering effectsof WIN55,212-2. JPET 292:136–139, 2000.
7. Bensaid, M., Gary-Bobo, M., Esclangon, A., et al. Thecannabinoid CB1 receptor antagonist SR141716A in-creases Acrp30 mRNA expression in adipose tissue ofobese fa/fa rats in cultured adipocyte cells. Mol. Phar-macol. 63:908–914, 2003.
8. Howlett, A.C., Breivogel, C.S., Childers, S.R., et al.Cannabinoid physiology and pharmacology: 30 yearsof progress. Neuropharmacology 47(Sl1):345–358, 2004.
9. Rueda, D., Galve-Roperh, I., Haro, A, et al. The CB1cannabinoid receptor is coupled to the activation ofc-Jun N-terminal kinases. Mol. Pharmacol. 58:814–820,2000.
10. Porcella, A., Maxia, C., Gessa, G.L., et al. The humaneye expresses high levels of CB1 cannabinoid recep-tor mRNA and protein. Eur. J. Neurosci. 12:1123–1127,2000.
11. Stamer, W.D., Golightly, S.F., Hosohata, Y., et al.Cannabinoid CB1 receptor expression, activation, anddetection of endogenous ligand in trabecular mesh-work and ciliary process tissues. Eur. J. Pharmacol.431:277–286, 2001
12. Chien, F.Y., Wang, R.F., Mittag, T.W., et al. Effects ofWIN 55212-2, a cannabinoid receptor agonist, onaqueous humor dynamics in monkeys. Arch. Oph-thalmol. 121:87–90, 2003.
13. Mittag, T., and Schmidt, K.G. Mechanisms of neuro-protection against glaucoma. Ophthalmologe 101:1076–1086, 2004.
14. Porcella, A., Maxia, C., Gessa, G.L., et al. The syntheticcannabinoid WIN55,212-2 decreases the intraocularpressure in human glaucoma resistant to conven-tional therapies. Eur. J. Neurosci. 13:409–412, 2001.
15. Quigley, H.A. Neuronal death in glaucoma. Prog.Retin. Eye Res. 18:39–57, 1999.
16. Coleman, A.L., Lerner, F., Bernstein, P., et al. A 3-month, randomized, controlled trial of bimatoprost(LUMIGAN) versus combined timolol and dorzo-lamide (Cosopt) in patients with glaucoma or ocularhypertension. Ophthalmology 110:2362–2368, 2003.
17. El-Remessy, A.B., Khalil, I.E., Matragoon, S., et al.Neuroprotective effect of (#) delta-9-tetrahydro-cannabinol and cannabidiol in N-methyl-D-asparate-induced retinal neurotoxicity: Involvement of perox-ynitre. Am. J. Pathol. 163:1997–2008, 2003.
18. Yoles, E., Belkin, M., and Schwartz, M. HU-211, anonpsychoactive cannabinoid, produces short- andlong-term neuroprotection after optic nerve axotomy.J. Neurotraum. 13:49–57, 1996.
19. Hampson, A.J., Bornheim, L.M., Scanziani, M., et al.Dual effects of anandamide on NMDA receptor-me-diated responses and neurotransmission. J. Neu-rochem. 70:671–676, 1998.
SZCZESNIAK ET AL.166
20. Marsicano, G., Moosmann, B., Hermann, H., et al.Neuroprotective properties of cannabinoids againstoxidative stress: Role of the cannabinoid receptorCB1. J. Neurochem. 80:448–456, 2002.
21. Matthias, P., Tashkin, D.P., Marques-Magallanes, J.A.,et al. Effects of varying marijuana potency on depo-sition of tar and delta-9-THC in the lung during smok-ing. Pharmacol. Biochem. Behav. 58:1145–1150, 1997.
22. Pan, J., Tremblay, F., Archibald, M.L., et al. Nonin-vasive measurement of intraocular pressure in theconscious rat with Tonopen tonometer (ARVO Ab-stract). Inv. Opthalmol. Vis. Sci. 41:S897, Abstract nr4771, 2000.
23. Meisner, D., Pringle, J., and Mezei, M. Liposomal pul-monary drug delivery: In vivo disposition of atropinebase in solution and liposomal form following endo-tracheal installation to the rabbit lung. J. Microencap-sul. 6:379–387, 1989.
24. Hung, O.R., Whynot, S., Varvel, J.R., et al. Pharma-cokinetics of inhaled liposome-encapsulated fentanyl.Anaesthesiology 83:277–284, 1995.
25. Hung, O.R., Zamecnik, T.P., and Shek, P.N. Pul-monary delivery of liposome-encapsulated !9-tetrahydrocannabinol (!9-THC), in United StatesPatent Office. USA, 1999.
26. Beck, S.E., Jones, L.A., Chesnut, K., et al. Repeated de-livery of adeno-associated virus vector to the rabbitairway. J. Virol. 73:9446–9455, 1999.
27. Rees, D.D., and Brain, J.D. Effects of cystic fibrosisairway secretions on rat lung: Role of neutrophil elas-tase. Am. J. Physiol. 269:L195–L202, 1995.
28. Rees, D.D., Rogers, R.A., Cooley, J., et al. Recombi-nant human monocyte/neutrophil elastase inhibitorprotects rat lungs against injury from cystic fibrosisairway secretions. Am. J. Respir. Cell Mol. Biol.20:69–78, 1999.
29. van Helden, H.P., Kuijpers, W.C., Steenvoorden, D.,et al. Intratracheal aerosolization of endotoxin (LPS)in the rat: A comprehensive animal model to studyadult (acute) respiratory distress syndrome. Exp. LungRes. 23:297–316, 1997.
30. Fredrick, D.L., and Fowler, M.W. Comparison of sixcannabinoid metabolite assays. J. Anal. Toxicol.9:116–120, 1985.
31. Torchilin, V.P. Recent advances with liposomes aspharmaceutical carriers. Nat. Rev. 4:145–160, 2005.
32. Nagayasu, A., Uchiyama, K., and Kiwada, H. The sizeof liposomes: A factor which affects their targeting ef-ficiency to tumors and therapeutic activity of liposomalantitumor drugs. Adv. Drug Deliv. Rev. 40:75–87, 1999.
33. Allen, T.M., Hansen, C.B., Martin, F., et al. Liposomescontaining synthetic lipid derivatives of poly(ethyl-ene glycol) show prolonged circulation half-lives invivo. Biochim. Biophys. Acta. 1066:29, 2000.
34. Lichtman, A.H., Peart, J., Poklis, J.L., et al. Pharma-cological evaluation of aerosolized cannabinoids inmice. Eur. J. Pharmacol. 399:141–149, 2000.
35. Straiker, A.J., Maguire, G., Mackie, K., et al. Localiza-tion of the cannabinoid receptors in human anterioreye and retina. Invest. Ophthalmol. Vis. Sci. 40:2442–2448, 1999.
36. Porcella, A., Casellas, P., Gessa, G.L., et al. Cannabi-noid receptor CB1 mRNA is highly expressed in therat ciliary body: Implications for the antiglaucomaproperties of marihuana. Mol. Brain Res. 58:240–245,1998.
37. Sugrue, M.F., Funk, H.A., Leonard, Y., et al. The oc-ular hypotensive effects of synthetic cannabinoids. In-vest. Opthalmol. Vis. Sci. 37:S831, 1996.
38. Rosen, G.H. Pharmacological used for nutritional dis-orders of HIV/AIDS. J. Physicians Assoc. AIDS Care2:30–32, 1995.
39. Lemberger, L., Martz, R., Rodda, B., et al. Compara-tive pharmacology of delta-9-tetrahydrocannabinoland its metabolite, 11-OH-Delta9-tetrahydrocannabi-nol. J. Clin. Invest. 52:2411–2417, 1973.
40. Wall, M.E., and Perez-Reyes, M. The metabolism ofdelta-9-tetrahydrocannabinol and related cannabi-noids in man. J. Clin. Pharmacol. 21:178S–189S, 1981.
41. Brenneisen, R., Egli, A., Elsohly, M.A., et al. The ef-fect of orally and rectally administered delta-9-tetrahydrocannabinol on spasticity: A pilot studywith 2 patients. Int J. Clin. Pharmacol. Ther. 34:446–452,1996.
42. Chiang, C.-W., Barnett, G., and Brine, D. Systemic ab-sorption of !9-tetrahydrocannabinol after ophthalmicadministration to the rabbit. J. Pharm. Sci. 72:136–138,1983.
43. Green, K.A., and Kearse, C.E. Ocular penetration ofdelta-9-tetrahydrocannabinol from rabbit corneal orcul-de-sac application site. Curr. Eye Res. 21:566–570,2000.
44. Laine, K., Järvinen, K., and Järvinen, T. Topically ad-ministered CB2-receptor agonist, JWH-133, does notdecrease intraocular pressure (IOP) in normotensiverabbits. Life Sci. 72:837–842, 2003.
45. Medical News Today. “New synthetic delta-9-THCInhaler offers safe, rapid delivery, Phase 1study.”April 17, 2005. Online document at: www.medical-newstoday.com/medicalnews.php?newsid & 22937Accessed April 17, 2006.
46. Myers, M.A., Thomas, D.A., Straub, L., et al. Pul-monary effects of chronic exposure to liposomeaerosols in mice. Exp. Lung Res. 19:1–19, 1993.
47. Thomas, D.A., Myers, M.A., Wichert, B., et al. Acuteeffects of liposome aerosol inhalation on pulmonaryfunction in healthy human volunteers. Chest99:1268–1270, 1991.
Received: December 15, 2005Accepted: March 14, 2006
Reprint Requests: Orlando HungDepartment of Anaesthesia
Queen Elizabeth II Health Science Centre1278 Tower Road
Halifax, Nova Scotia B3H 2Y9Canada
E-mail: [email protected]
EFFECT OF LIPOSOME-ENCAPSULATED !9-THC ON IOP 167
Copyright © 2022 FDOKUMEN




















