Obstacles to and future goals of ten comprehensive community health promotion projects
16
Journal of Community Health Vol. 16, No. 6, December 1991 OBSTACLES TO AND FUTURE GOALS OF TEN COMPREHENSIVE COMMUNITY HEALTH PROMOTION PROJECTS David G. Altman, PhD; Jerry Endres, MSW; Juliette Linzer, MS; Kate Lorig, DrPH; Beth Howard-Pitney, PhD; Todd Rogers, PhD ABSTRACT: Over 100 project staff, community coalition members, and other representatives from 10 comprehensive community health promotion projects in the western United States were surveyed two years into a three year funding cycle about: (1) the problems or obsta- cles they judged as preventing successful completion of their current goals and objectives, and (2) future goals and objectives they envi- sioned for their projects. The key issues confronting respondents were diverse, although issues around the process of implementing commu- nity health promotion programs were cited more frequently than is- sues related to the content of health promotion. When respondents were asked to prioritize Future Goals in the second survey, consensus across communities was obtained despite broad differences in the type of community surveyed and the health problem targeted. This study identifies the common organizational and community development problems faced by newly emerging community health promotion pro- grams and has implications for other communities involved in design- ing, implementing, and evaluating community-wide health promotion programs. INTRODUCTION Community development can be described as the organization of persons and institutions for the purpose of confronting and resolving community problems and challenges. A necessary component of com- munity development is organizational development. Organizational de- Drs. Altman (Associate Director), Howard-Pitney (Evaluation Director), Rogers (Director) and Mr. Endres (Community Organizer) are with the Health Promotion Resource Center, Stanford Center for Research in Disease Prevention, Stanford University School of Medicine. At the time this paper was written, Ms. Linzer was a graduate student at the Harvard School of Public Health, Boston, Massachusetts, Kate Lorig, Dr.P.H., is Senior Research Scientist in the Department of Immunology and Rhenmatology at the Stanford University School of Medicine. This research was partially supported by grants from the Henry J. Kaiser Family Foun- dation, Menlo Park, California and the Pew Memorial Trust, Philadelphia, Pennsylvania. Requests for reprints should be addressed to: David G. Altman, Stanford Center for Research in Disease Prevention, Stanford University School of Medicine, 1000 Welch Road, Palo Alto, California 94304-1885. 415-723-1000. © 1991 Human Sciences Press, Inc. 299
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Obstacles to and future goals of ten comprehensive community health promotion projects

Journal of Community Health Vol. 16, No. 6, December 1991
OBSTACLES TO AND FUTURE GOALS OF TEN COMPREHENSIVE COMMUNITY
HEALTH PROMOTION PROJECTS
David G. Altman, PhD; Jerry Endres, MSW; Juliette Linzer, MS; Kate Lorig, DrPH; Beth Howard-Pitney, PhD; Todd Rogers, PhD
ABSTRACT: Over 100 project staff, community coalition members, and other representatives from 10 comprehensive community health promotion projects in the western United States were surveyed two years into a three year funding cycle about: (1) the problems or obsta- cles they judged as preventing successful completion of their current goals and objectives, and (2) future goals and objectives they envi- sioned for their projects. The key issues confronting respondents were diverse, although issues around the process of implementing commu- nity health promotion programs were cited more frequently than is- sues related to the content of health promotion. When respondents were asked to prioritize Future Goals in the second survey, consensus across communities was obtained despite broad differences in the type of community surveyed and the health problem targeted. This study identifies the common organizational and community development problems faced by newly emerging community health promotion pro- grams and has implications for other communities involved in design- ing, implementing, and evaluating community-wide health promotion programs.
I N T R O D U C T I O N
Community development can be described as the organization of persons and institutions for the purpose of confronting and resolving community problems and challenges. A necessary component of com- munity development is organizational development. Organizational de-
Drs. Altman (Associate Director), Howard-Pitney (Evaluation Director), Rogers (Director) and Mr. Endres (Community Organizer) are with the Health Promotion Resource Center, Stanford Center for Research in Disease Prevention, Stanford University School of Medicine. At the time this paper was written, Ms. Linzer was a graduate student at the Harvard School of Public Health, Boston, Massachusetts, Kate Lorig, Dr.P.H., is Senior Research Scientist in the Department of Immunology and Rhenmatology at the Stanford University School of Medicine.
This research was partially supported by grants from the Henry J. Kaiser Family Foun- dation, Menlo Park, California and the Pew Memorial Trust, Philadelphia, Pennsylvania.
Requests for reprints should be addressed to: David G. Altman, Stanford Center for Research in Disease Prevention, Stanford University School of Medicine, 1000 Welch Road, Palo Alto, California 94304-1885. 415-723-1000.
© 1991 Human Sciences Press, Inc. 299

300 JOURNAL OF COMMUNITY HEALTH
velopment in the community context includes the specific processes and methods by which community members and the organizations through which they affiliate apply community philosophies and values in pro- grammatic initiatives. Typical organizational development processes in- clude problem solving strategies such as identifying perceived problems, setting priorities, planning and designing alternatives, implementing ac- tions, and reviewing progress, l
It is generally accepted that the active participation of commu- nity members and various organizational constituencies in organiza- tional problem solving is a critical factor in improving community health promotion services offered, the health status of community members, and the long-term viability of institutionalization of programs and or- ganizations) -~ Indeed, participation is in vogue as a method for enhanc- ing the effectiveness of community health promotion programs yet little data exist on the knowledge, attitudes, beliefs, and actions of health pro- motion program planners. While many funders, researchers, and serv- ice providers advocate broad community participation, the assumptions regarding its impact are built upon an incomplete empirical and con- ceptual base. For example, field experience suggests that coalitions, one vehicle for enhancing community participation, are quite variable in their effectiveness and vulnerable to decline, with mortality rates in some coalitions as high as 50% within their first year of operation. ~
Data from health promotion project staff, coalition members, and community members are needed to identify critical elements, pro- cesses, and challenges in the development of" effective community pro- grams. In this paper, data from a survey of representatives from diverse community projects in the western United States shed light on the criti- cal topics facing organizations engaged in comprehensive health promo- tion programs.
In 1987, the Henry J. Kaiser Family Foundation awarded three year grants to 11 communities in the western U.S. 7 Two additional years of funding at a reduced level were made available in 1990. These 11 communities were selected from over 600 which wrote a letter of intent in response to the initial Request for Proposals (RFP) from the Founda- tion. Survey data reported in this study were derived from nine of these communities as well as one other similar community funded by the Foundation under a separate initiative. A summary of the key charac- teristics of these communities is provided in Table 1.
The RFP sent to communities in the western U.S. ~ outlined the importance of attending to community and organizational development

David G. Altman et al. 301
TABLE 1
Description of Communities
Location Population Size Health Topic
Colorado (State)
Montana (State)
New Mexico (State)
Northwest Arctic Borough, AK
San Francisco, CA
San Ysidro, CA
Solano County, CA
Summit/Wasatch Counties, UT
Tuolumne County, CA
Wind River, WY
3,300,000
826,000
1,300,000
6,500
Cardiovascular Disease, Substance Abuse, Injuries
Adolescent Pregnancy, Adolescent Health
Cardiovascular Disease
General Health
703,000 Senior Injuries
97,000 Nutrition
288,000 Cancer
25,000 Substance Abuse
42,000
5,500
Adolescent Health
Youth Substance Abuse
All projects develop and implement a comprehensive set of interventions using print and electronic media, grassroots community development, worksite and school programs, provider in- tervention, and environmental and policy programs.
issues, particularly those related to the participation of diverse commu- nity constituencies:
Communities will form councils that include representative of groups such as educational institutions, business, labor, media, religious or- ganizations, voluntary health agencies, health departments, and public service organizations. The council members will generate initial broad public interest and participation in the project, identify the most sig- nificant health problems in the community, and develop one or more specific projects to reduce selected b e h a v i o r s . . , that increase the risk of disease. Communities are encouraged to adopt a broad conceptual approach to prevention that recognizes the influence of social norms

302 JOURNAL OF COMMUNITY HEALTH
and peer pressure, as well as policies, laws, regulations, and social practices that are beyond the control of the individual... During the first year of the project, the Foundation will support the community's planning and development activities that are directly related to specific intervention projects.
These western communities received consultation and technical assistance support from the Health Promotion Resource Center at Stan- ford University (HPRC). ~ Support included consultation in community development, organizational development, strategic and intervention planning, health communication, and evaluation.
Although these communities may be distinguished from others because of the availability of free technical assistance and their success in competing for Foundation funding, they do represent a cross section of communities in the western U.S. with respect to demographic, social, and cultural characteristics. For example, six of the communities were located in predominantly rural areas, two in urban areas, and two had both rural and urban populations. Likewise, two focused on American Indian/Alaska Native communities, one on an Hispanic community, three on multi-ethnic communities, and four on predominantly white communities (see Table 1). The projects were about two years into their funding when data reported here were collected.
The focus of the current study was to assess planning and imple- mentation activities across these diverse community health programs so as to identify and understand the common and unique issues facing community coalitions involved in health promotion. Specifically, we sought input from each health promotion program through the opin- ions of coalition/board members, staff, and community members. The project had two primary goals. The first goal was to engage project staff, coalition/board members, and community representatives in an or- ganizational and community analysis. To increase the project's aware- ness of the issues affecting current and future operations, we designed a nominal group process by which people inw)lved in all the projects com- municated with each other about the issues they faced routinely. This process prevented higher-status or persuasive people in each project from dominating. ~° The process included four primary components: (1) two self-administered mailed surveys which queried respondents about obstacles to achieving current goals and objectives and their desired fu- ture goals; (2) a three-day training workshop held at the HPRC for se- nior project staff which included a review of organizational analysis methods and evaluation of responses from their community surveys; (3) a one-day strategic planning retreat held at each community, with assis-
David G. Altman et al. 303
tance from a project director from another community and an HPRC staff person, where survey data were given back to the community and used as a springboard for reviewing past accomplishments and identify- ing goals for the future; and (4) a one-day debriefing of the strategic planning retreats for senior project staff. Results from the two mailed surveys are repor ted in this paper.
T h e organizational development assessment process utilized in this project was designed to:
1. Create a shared sense of planning; 2. Increase control over organizational development within limits
established by the community and funders; 3. Prepare for upcoming site visits by current and potential
funders; 4. Motivate community members to examine actively the project
from a new perspective and take responsibility for project activ- ities; and
5. Provide training to project staff on methods of community and organizational development.
Principles of action research, defined operationally as the merger of the provision of technical assistance and the collection of data on project functioning, guided this project. '''1~
M E T H O D S
A nominal group process conducted with representatives of 10 commu- nity projects was used to generate a list of current problems and obstacles and to set priorities for future goals for the project. The names and addresses of all coalition/board members, staff, and up to five key people from the community population were identified and subsequently contacted by project directors for participation in the project. The 271 people identified in the 10 diverse sites projects were then sent two waves of surveys. The number of people identified in each of the 10 communities ranged from 11-52 with a mean of 27. Of these 271, 109 (40%) returned the first survey (range by community = 3% to 83%). Responses to the second survey were received from only nine communities because staff turnover in one community resulted in their inability to monitor data collection in their isolated rural area. Ninety-five people (37 percent) from nine communities returned the second survey (range by community = 6% to 68%. No follow-up reminders were mailed to non-respondents. We are unable to compare differences between respondents and non-respondents because

304 JOURNAL OF COMMUNITY HEALTH
survey responses were kept anonymous and confidential. Each response was given equal weight in the analysis.
Survey Instruments
Two surveys were designed. Survey 1 contained three questions. Re- spondents were asked to list up to 11: (a) problems or obstacles they thought prevented the successful implementation of current project goals and objectives (hereafter referred to as "Current Obstacles"); (b) future goals and objectives they would like to see their project achieve regarding its internal management and structure; and (c) future goals and objectives they would like to see their project achieve within the community. Several thousand separate responses to these three questions were received. Responses to questions about future goals and objectives within the community and within the management and structure were subsequently merged into a single category hereafter referred to as "Fu- ture Goals" because there was significant overlap between responses. Responses to each question were clustered initially by three HPRC staff into one of 32 subheadings.
Survey 2, comprised of the 32 subheadings and individual responses from Survey 1, were sent back to all 271 people who received the first survey. Respondents were asked to select the one individual response most relevant to their proiect in each of the 32 subheadings and to rank the overall importance of each subheading on a scale ti-om 0-100, with 0 indicating no importance and 100 indicating greatest importance. The scores assigned to the individual re- sponses were considered to be reflective of the overall importance of the sub- heading at-large.
The mean rating across respondents in each community was calculated and rank ordered using the 0-100 importance score. Seven of the 32 subhead- ings were combined during data analysis because of their conceptual overlap, resulting in 25 subheadings, 12 for Current Obstacles and 13 for Future Goals. The top five rank-ordered subcategories were considered the top community priorities. In the case of a tie for the fifth ranking, all subheadings with the same score were included. Scoring was not used to differentiate the differences in the importance of the top five issues because many of the mean differences between subheadings were small. Rather, the five top priorities were treated equally during the subsequent analysis in order to obtain a broad representa- tion of the high priority issues.
RESULTS
Survey 1
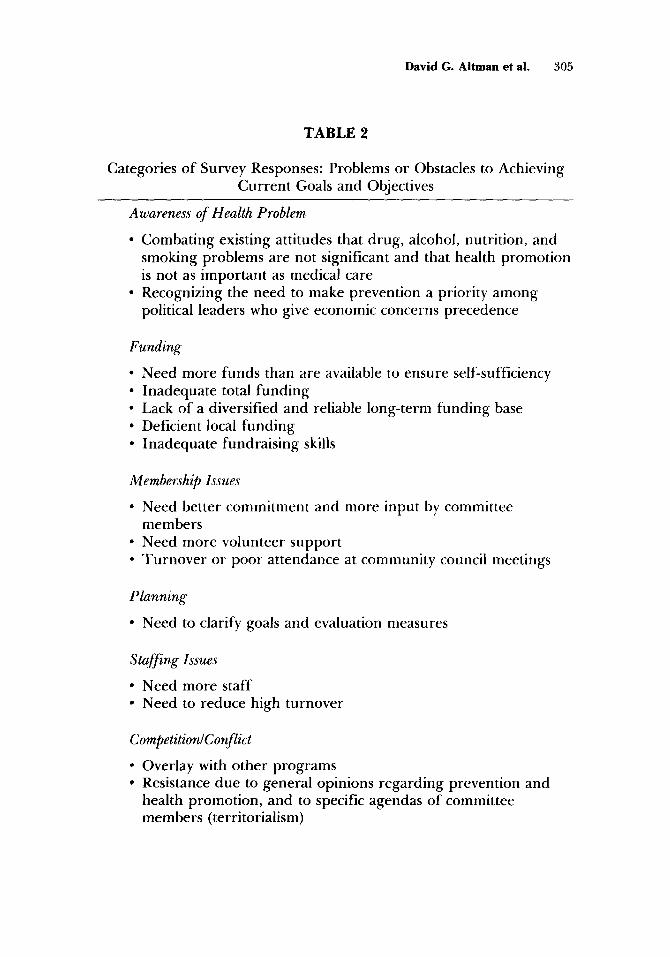
Tab le 2 (Cur ren t Obstacles) and "Fable 3 (Fu ture Goals) list the major categories and show examples o f some o f the typical responses to
David G. Al tman et al. 305
TABLE 2
Categories o f Survey Responses: Problems or Obstacles to Achieving Cur ren t Goals and Objectives
Awareness of Health Problem
• Combat ing existing att i tudes that drug , alcohol, nutr i t ion, and smoking problems are not significant and that health p romot ion is not as impor tan t as medical care
• Recognizing the need to make prevent ion a priority a m o n g political leaders who give economic concerns precedence
Funding
• Need more funds than are available to ensure self-sufficiency • Inadequa te total f und i ng • Lack of a diversified and reliable long-term fund ing base • Deficient local f und i ng • Inadequa te fundra is ing skills
Membership Issues
• Need better c o m m i t m e n t and more inpu t by commit tee member s
• Need more volunteer suppor t • T u r n o v e r or poor a t tendance at communi ty council meet ings
Planning
• Need to clarify goals and evaluation measures
Staffing Issues
• Need more staff • Need to reduce high tu rnover
Competition~Conflict
° Overlay with o ther p rograms • Resistance due to general opinions regard ing prevent ion and
heal th p romot ion , and to specific agendas o f commit tee member s (territorialism)
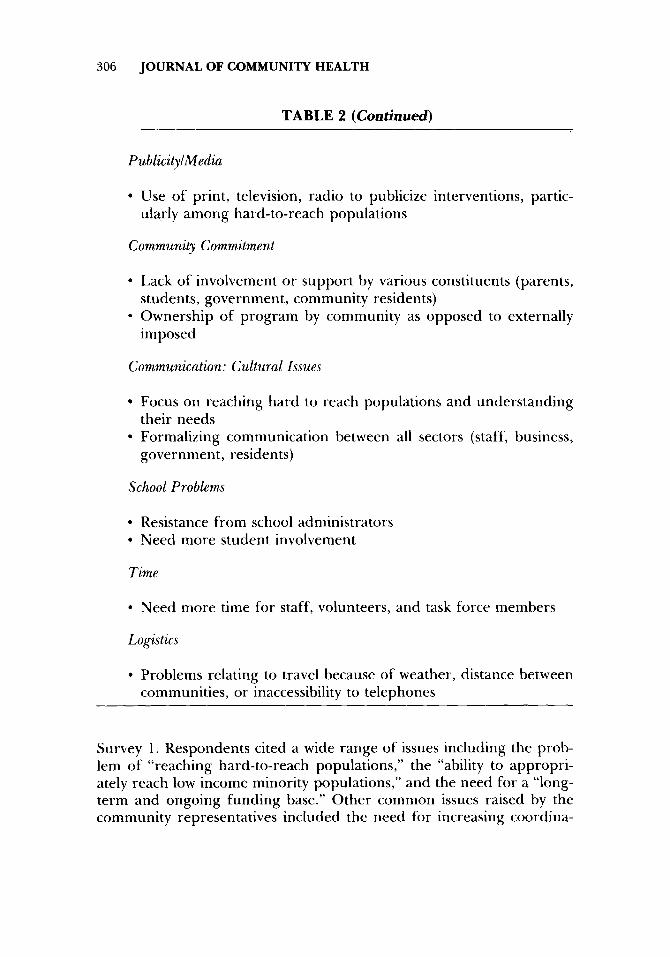
306 JOURNAL OF COMMUNITY HEALTH
T A B L E 2 (Continued)
Publicity~Media
• Use of print, television, radio to publicize interventions, partic- ularly among hard-to-reach populations
Community Commitment
• Lack of involvement or support by various constituents (parents, students, government, community residents)
• Ownership of program by community as opposed to externally imposed
Communication: Cultural Issues
• Focus on reaching hard to reach populations and unders tanding their needs
• Formalizing communication between all sectors (staff, business, government, residents)
School Problems
• Resistance from school administrators • Need more student involvement
Time
• Need more time tbr staff, volunteers, and task force members
Logistics
• Problems relating to travel because of weather, distance between communities, or inaccessibility to telephones
Survey 1. Respondents cited a wide range of issues including the prob- lem of "reaching hard-to-reach populations," the "ability to appropri- ately reach low income minority populations," and the need for a "long- term and ongoing funding base." Other common issues raised by the community representatives included the need for increasing coordina-
David G. Altman et al. 307
TABLE 3
Categories of Survey Responses: Future Goals and Objectives
Community Involvement~Community Support
• Increase involvement with children, seniors, parents, minority groups, businesses, volunteers, students, local agencies, and the legislature
• Need a sense of ownership of programs
Promotion~Reach
° Create a market strategy to increase visibility and awareness of problems as well as intervention and prevention programs through use of media sources
• Try to reach low income and minority populations
Funding
• Obtain additional resources-- in-kind, mini-grants, corporate loaned executive
• Develop ongoing resources to ensure self-sufficiency of program
Coalition Building
• Improve communicat ion and coordination, and formalize partnerships among those involved--government , business, schools
• Need broader support among power structure within community
Interventions~Program Quality
• Increase support of education, services, and events regarding health problems
• Provide strong leadership that works toward comprehensive health education programs
• Decentralize control over program • Integrate all sectors within and between communities • Increase networking
308 JOURNAL OF COMMUNITY HEALTH
T A B L E 3 (Continued)
Mission~Strategic Planning
• Clarify mission and def ine goals/objectives • Maintain long-range strategic plan • Set long-range plan with con t inued evaluation of goals and objec-
tives
Institutionalization
• In tegra te p r o g r a m into communi ty such that health p romot ion does not end when fund ing does
Evaluation~Needs Assessment
• Pe r fo rm needs assessment • Look at long- te rm effects • Develop effective ongo ing evaluation with upda t ed informat ion • Ensure representa t ion and involvement of all sectors of the com-
muni ty
Helping Youth: Programs
• Expand p rog rams to include K-12 • Inc lude physical activity, awareness o f health risks, sex educat ion,
pa ren t ing
Training
• Develop local heal th p romot ion expert ise • Maintain ability to access and provide technical assistance
Facilities
• Design commun i ty center according to needs o f communi ty and make it accessible to all
Legislation
• Keep abreast of pe r t inen t legislative issues • Increase involvement and communica t ion with legislature
David G. Altman et al. 309
Staffing
• Increase staff size to include specialists and volunteers with a ra- cial/ethnic balance
tion, cooperation, commitment, communication, and involvement of project staff, parents, schools, board members, legislature, local agen- cies/clubs, businesses; the importance of increasing community aware- ness of health promotion and disease prevention programs; obtaining sufficient and committed volunteer and paid staff; clarifying goals; and establishing a long-range strategic plan.
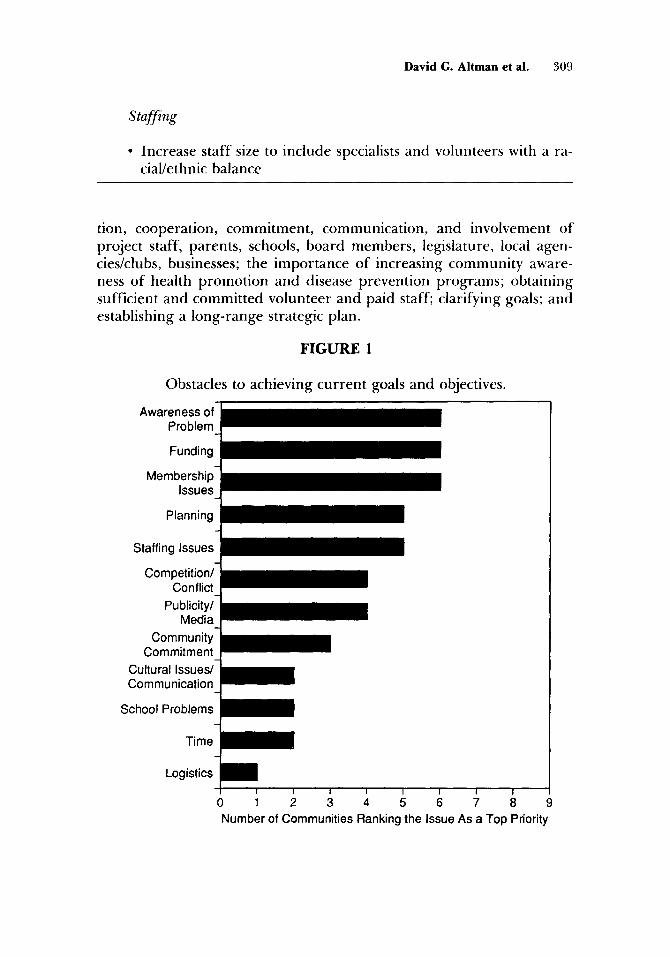
F I G U R E 1
Obstacles to achieving current goals and objectives.
Awareness of Problem
Funding
Membership- Issues
Planning
Staffing Issues
Competition/- Conflict
Publicity/- Media
Community- Commitment
Cultural Issues/- ~ Communication
School Problems ~
Time
Lo I I I I I i I
0 1 2 3 4 5 6 7 8 9 Number of Communities Ranking the Issue As a Top Priority
3 lO JOURNAL OF COMMUNITY HEALTH
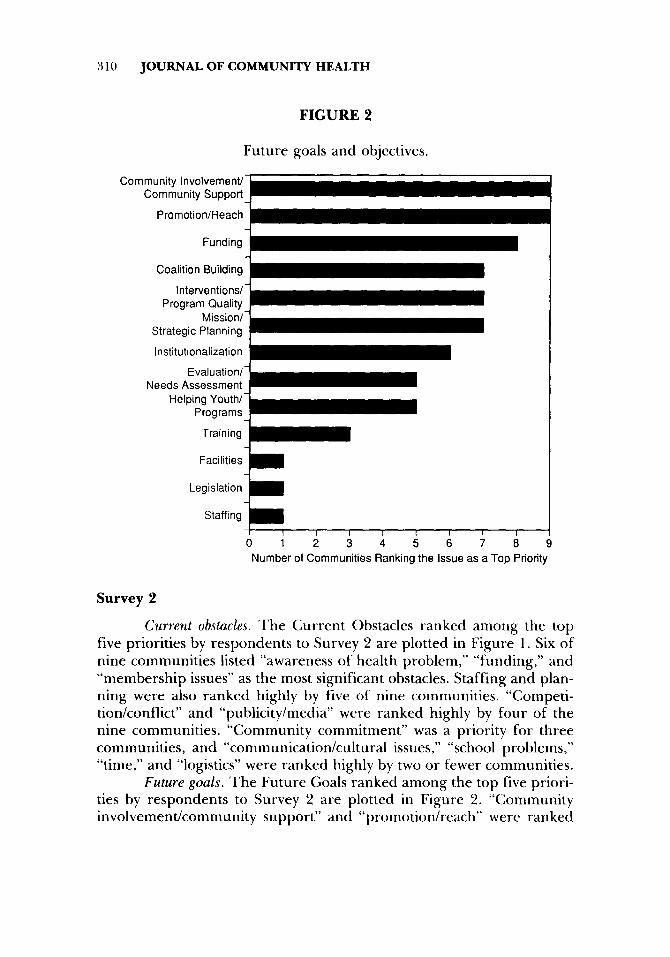
FIGURE 2
Future goals and objectives.
Community Involvement/ Community Support
Promotion/Reach
Funding
Coalition Building
Interventions/- Program Quality
Mission/- Strategic Planning
Institutionalization
Evaluation/- Needs Assessment
Helping Youth/- Programs
Training
Facilities
Legislation ~ i
Staffing I I I [ I I I I
0 1 2 3 4 5 6 7 8 Number of Communities Ranking the Issue as a Top Priority
Survey 2
Current obstacles. The Current Obstacles ranked among the top five priorities by respondents to Survey 2 are plotted in Figure 1. Six of nine communities listed "awareness of health problem," "funding," and "membership issues" as the most significant obstacles. Staffing and plan- ning were also ranked highly by five of nine communities. "Competi- tion/conflict" and "publicity/media" were ranked highly by four of the nine communities. "Community commitment" was a priority for three communities, and "communication/cultural issues," "school problems," "time," and "logistics" were ranked highly by two or fewer communities.
Future goals. The Future Goals ranked among the top five priori- ties by respondents to Survey 2 are plotted in Figure 2. "Community involvement/community support" and "promotion/reach" were ranked
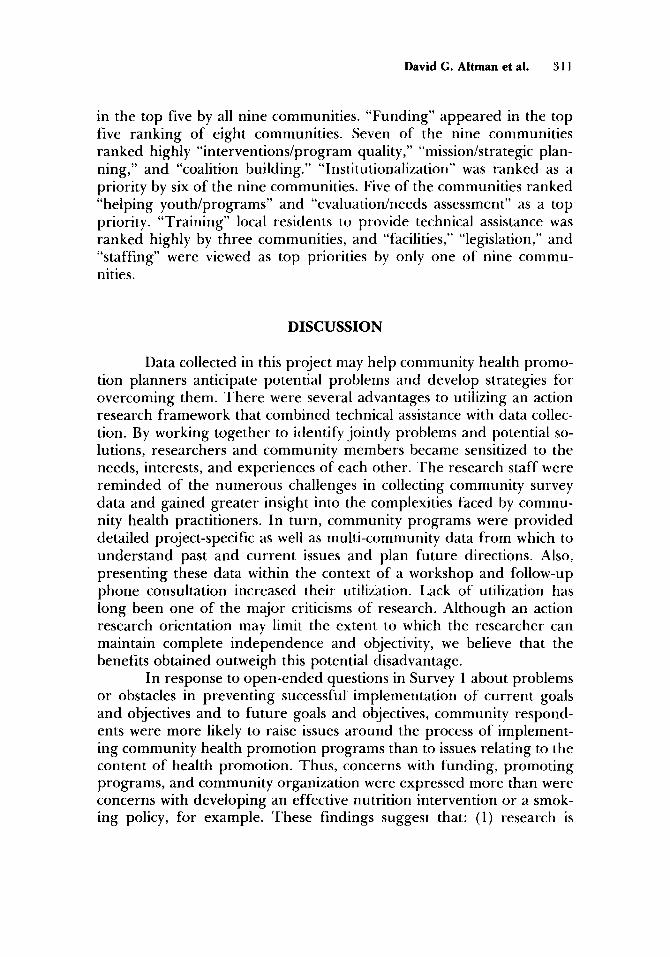
David G. Altman et al. 311
in the top five by all nine communities. "Funding" appeared in the top five ranking of eight communities. Seven of the nine communities ranked highly "interventions/program quality," "mission/strategic plan- ning," and "coalition building." "Institutionalization" was ranked as a priority by six of the nine communities. Five of the communities ranked "helping youth/programs" and "evaluation/needs assessment" as a top priority. "Training" local residents to provide technical assistance was ranked highly by three communities, and "facilities," "legislation," and "staffing" were viewed as top priorities by only one of nine commu- nities.
DISCUSSION
Data collected in this project may help community health promo- tion planners anticipate potential problems and develop strategies for overcoming them. There were several advantages to utilizing an action research framework that combined technical assistance with data collec- tion. By working together to identify jointly problems and potential so- lutions, researchers and community members became sensitized to the needs, interests, and experiences of each other. The research staff were reminded of the numerous challenges in collecting community survey data and gained greater insight into the complexities faced by commu- nity health practitioners. In turn, community programs were provided detailed project-specific as well as multi-community data from which to understand past and current issues and plan future directions. Also, presenting these data within the context of a workshop and follow-up phone consultation increased their utilization. Lack of utilization has long been one of the major criticisms of research. Although an action research orientation may limit the extent to which the researcher can maintain complete independence and objectivity, we believe that the benefits obtained outweigh this potential disadvantage.
In response to open-ended questions in Survey 1 about problems or obstacles in preventing successful implementation of current goals and objectives and to future goals and objectives, community respond- ents were more likely to raise issues around the process of implement- ing community health promotion programs than to issues relating to the content of health promotion. Thus, concerns with funding, promoting programs, and community organization were expressed more than were concerns with developing an effective nutrition intervention or a smok- ing policy, for example. These findings suggest that: (1) research is

312 JOURNAL OF COMMUNITY HEALTH
needed on unders tanding the underlying structural factors that make community change possible, and (2) community health practitioners should be attentive to skills deficits in the non-content areas of commu- nity intervention. Currently, the priority among practitioners and re- searchers seems to be developing more interventions rather than im- proving our unders tanding of and intluence on the context in which existing interventions are delivered.
When communities were asked to prioritize Future Goals in the second survey, consensus emerged as nine of thirteen subheadings were ranked as a priority by five or more communities. The non-consensual i ssuesIs ta f f ing , logistics, facilities, t r a in ing- -were issues int luenced largely by individual community conditions. The consensus in Future Goals was obtained despite broad differences in the type of community surveyed and the health problem targeted. Particularly strong con- sensus emerged a round the importance of community support and in- volvement, community awareness and funding. Again, these are issues that might be considered the essential building blocks of any community health program and are as necessary to address as specific health inter- ventions. These consensual issues are consistent with the related scien- tific literature that stresses the importance to successful community projects of community development, citizen participation, empower- ment, and institutionalization.': '
In contrast to the general consensus on top priorities for Future Goals, there was less consensus on the top five priorities for Curren t Obstacles. No single issue was ranked among the top five priorities by more than six communit ies and only five of twelve issues were ranked as a priority by five or more communities. This may be due to the diversity of communit ies surveyed, the different stages of development of each program, and who responded to the survey from each community. Also, it may be that people can generally agree on a desirable future goal but not on what they have to overcome to achieve it. Also, the wording of the questions, the first focusing on obstacles, the second on future goals and objectives irrespective of obstacles, may have inllu- enced the responses given.
Despite the lack of consensus on Current Obstacle priorities, the content of the top three responses to Current Obstacles and Future Goals were similar, awareness of the health problem and promotion; membership and community inw)lvement; and funding. Whether these three issues are seen as obstacles to current goals or as future goals, they clearly were the primary concerns for the community health projects we surveyed two years into their funding. These findings illustrate the im-

David G. Altman et al. 313
portance of planning for the occurrence of these issues from the begin- ning of any community health promotion project and expecting them to resurface over the life of a program. In addition, dealing effectively with these issues is a prerequisite to successful program institutionaliza- tion. The communities surveyed here were sensitized to institutionaliza- tion because of uncertain future funding and because the issue was adopted as a high priority by the primary funder. These data also have implications for funders of community health programs in that address- ing these priority issues and promoting organizational viability requires at a minimum several years of stable funding.
For community health promotion and disease prevention pro- grams to reach their full potential in a cost-effective manner, it is impor- tant to understand the key components that contribute to program suc- cess and the obstacles that may impede achieving such success. This becomes even more salient in the current environment of limited fund- ing for community programs. The experiences of the HPRC in working with many community health promotion programs lead us to suggest that some programs focus considerable attention on intervention design and implementation at the expense of attending to issues of organiza- tional and community development. The latter topics may receive sec- ondary attention because they are not directly connected to the priori- ties of funders, to specific health promotion interventions, or to the ultimate goal of improving community health status. In the long run, however, not attending to these issues may impede the institutionaliza- tion of the program into the community and thus the long-term success of the program. ~
Data from the current study increase our understanding of the key issues faced by health promotion workers on the front line and may ultimately lead to the design, implementation, and maintenance of more effective community programs. In reviewing the organizational analysis project described here with senior project staff, several positive and negative features emerged. On the positive side, it seems to have in- creased understanding of the key components of organizational and community development; team building among project staff, coalition members, and community members; knowledge of project obstacles and goals for the future; and resolve to engage in careful strategic planning. On the negative side, the process was noted by some participants to be too cumbersome and time consuming, probably the reason for the low response rate. Also, some communities had difficulty linking the survey data with the on-site strategic planning retreats, partially a result of the consultants not always using the data during the retreats. Limitations of

314 JOURNAL OF COMMUNITY HEALTH
the survey include the uneven response rates among participating com- munities and the relatively small sample of communities.
Our experiences with this project have several specific implica- tions for other community health promotion programs. First, commu- nity health programs should engage regularly in organizational analysis, even though it can be time-consuming. '3 Second, organizational analysis is a means for achieving desired outcomes, rather than an outcome it- self. Implementation of organizational analysis decisions require exten- sive follow-up and long-term commitment by the organization. We at- tempted to facilitate this follow-up with workshops, retreats, and ongoing technical assistance. Such follow-up also allows adaptation of a general and multi-community organizational analysis process to commu- nity-specific issues and concerns. Third, since insulated analysis leads to misdirected planning, broad community involvement in an organiza- tions' self analysis is critically important to its long-term viability.
REFERENCES
1. Roberts H: Community development: Learning and action. University of Toronto Press, Toronto, 1979.
2. Steckler A & Goodman RM: How to institutionalize health promotion programs. AmJ Health Promotion 3:34-44, 1989.
3. Goodman RM & Steckler A: The life and death of a health promotion program: An institu- tionalization case study. Int Quart Community Health Educ 8:5-21, 1987-88.
4. Goodman RM & Steckler A: A model for the institutionalization of health promotion pro- grams. Family Community Health, 11:63-78, 1989.
5. Cary LJ: Community development ~ a process. University of Missouri Press, Columbia, 1970. 6. Florin P, Chavis D, Wandersman A, & Rich R: A systems approach to understanding and
enhancing grassroots organizations: The Block Booster Project. In R. Levine and H. Fitzgerald (Eds.). Analysis of dynamic psychological systen~g. New York: Plenum, in press.
7. Tarlov AR, Kehrer BH, Hall DP et al.: Foundation work: The health promotion program of the Henry J. Kaiser Family Foundation. Am.] Health Promotion 2:74-80, 1987.
8. HenryJ. Kaiser Family Foundation. The community health promotion grant program: A new community-based grant program to encourage the adoption of healthy lifestyles. Request for Proposal, Henry J. Kaiser Family Foundation, 1987.
9. Rogers T, Altman DG, Howard-Pitney B, et al.: Disseminating health promotion technology: Linkage between university and community. Unpublished manuscript.
10. McKillip, J: Need Analysis: Tools for the Human Services and Education. Sage Publications, New- bury Park, 1987.
1 i. Peters M & Robinson V: The origins and status of action research. J Applied Behavioral Sci 20:113-124, 1984.
12. Susman GI & Evered RD: An assessment o1" the scientific merits of action research. Admin Sci Quart 23:582-603, 1978.
13. KinneJ, Thompson B, Chrisman NJ & HanleyJR: Community organization to enhance deliv- ery of preventive health services. AmerJ Prev Med 5:225-229, 1989.