Neurosurgical treatment of tourette's syndrome: A critical review
16
Neurosurgicai Treatment of Tourette's Syndrome: A Critical Review Scott L. Rauch, Lee Baer, G. Rees Cosgrove, and Michael A. Jenike Some patients with Tourette's syndrome (TS) remain disabled despite conventional treatment. Recently, neurosurgical procedures have been reported to be potentially effective interventions for such intractable cases. Clinicians are now being asked to make recom- mendations to patients about these candidate opera- tions. This review explores the reported experience with neurosurgical treatment of TS to assess critically the evidence regarding risks and benefits. Toward that end, the rationale for the various procedures and the relevant neuroanatomy are outlined and recommenda- tions for patient selection and management of future cases are discussed. We reviewed all available pub- lished reports on this subject and two unpublished cases, totaling 36 patients. Although a variety of operations have been used to treat TS, there is limited evidence pertaining to the risks or benefits of any surgical procedure. Neurosurgical treatment of TS remains experimental, since there is only anecdotal experience with these operations. Furthermore, there is no compelling evidence that any neurosurgical pro- cedure is superior to all others. If these experimental neurosurgeries are to continue, guidelines should be developed regarding patient and operation selection, and interdisciplinary assessment committees should implement such guidelines at institutions where these operations are performed. Moreover, future cases should be prospectively studied using contemporary technologies to assess lesion placement and size and validated clinical instruments to characterize patients and assess outcome, including adverse effects. Copyright © 1995 by W.B. Saunders Company T OURETTE'S SYNDROME (TS), or To- urette's disorder, is a neuropsychiatric con- dition characterized by motor and vocal tics, lasting longer than 1 year and emerging before age 21. I The estimated prevalence of TS is approximately 0.5%, with a preponderance in males versus females of at least 3:1. 2,3 The motor movements and vocalizations can often be temporarily suppressed, although the occur- rence of tics, especially in public, can be humili- ating and socially and vocationally debilitating. Pharmacotherapy has been the mainstay of treatment. Antidopaminergic agents such as haloperidol and pimozide, 24 the e~2-adrenergic agonist clonidine, 3,6,7 and the benzodiazepine clonazepam 3,6 have all been demonstrated to be beneficial for some TS patients. One recent study suggested that the behavior-therapy tech- nique of habit reversal can also be effective.8 Despite adequate trials of these conventional therapies, some TS patients have residual debili- tating symptoms. Neurosurgical treatments have been at- tempted in a few treatment-refractory TS pa- tients. Recently, patients and clinicians have become increasingly interested in these surgical procedures as anecdotal successes have been publicized. However, important unanswered questions remain regarding the scientific ratio- nale, clinical evaluation, patient selection, safety, efficacy and ethics surrounding such surgical procedures. The present review examines the reported experience with neurosurgical treatment of TS. Case report data are presented first, followed by discussion of relevant neuroanatomy and clini- cal considerations. Recommendations regard- ing future study of these controversial opera- tions are presented, based in part on the authors' experience with neurosurgical treatment of ob- sessive-compulsive disorder (OCD). 9 NEUROSURGICAL PROCEDURES USED IN TS A variety of neurosurgical procedures have been performed in attempts to treat TS (Fig 1). Reports to date have described (1) frontal lobe operations (i.e., frontal lobotomy and bimedial frontal leukotomy), (2) limbic system opera- tions (i.e., anterior cingulotomy, limbic leu- kotomy), (3) a novel multisite operation (i.e., anterior cingulotomy combined with infratha- lamic lesions), (4) thalamic operations (i.e., bilateral coagulation of rostral intralaminar and medial thalamic nuclei, and ventral-tier tha- lamic lesions), and (5) a cerebellar operation (i.e., bilateral cerebellar dentatotomy). From the Obsessive Compulsive Disorders Clinical and Research Unit, Department of Psychiatry, and Department of Neurosurgery, Massachusetts General Hospital and Harvard Medical School, Boston, MA. Address reprint requests to Scott L. Rauch, M.D., Depart- ment of Psychiatry, OCD Unit, 9th Floor, Massachusetts General Hospital-East, 149 Thirteenth St, Charlestown, MA 02129. Copyright © 1995 by W.B. Saunders Company 0010-440X/95/3602-0001503.00/0 Comprehensive Psychiatry, Vol. 36, No. 2 (March/April), 1995: pp 141-156 141
Transcript of Neurosurgical treatment of tourette's syndrome: A critical review

Neurosurgicai Treatment of Tourette's Syndrome: A Critical Review
Scott L. Rauch, Lee Baer, G. Rees Cosgrove, and Michael A. Jenike
Some patients with Tourette's syndrome (TS) remain disabled despite conventional treatment. Recently, neurosurgical procedures have been reported to be potentially effective interventions for such intractable cases. Clinicians are now being asked to make recom- mendations to patients about these candidate opera- tions. This review explores the reported experience with neurosurgical treatment of TS to assess critically the evidence regarding risks and benefits. Toward that end, the rationale for the various procedures and the relevant neuroanatomy are outlined and recommenda- tions for patient selection and management of future cases are discussed. We reviewed all available pub- lished reports on this subject and two unpublished cases, totaling 36 patients. Although a variety of operations have been used to treat TS, there is limited
evidence pertaining to the risks or benefits of any surgical procedure. Neurosurgical treatment of TS remains experimental, since there is only anecdotal experience with these operations. Furthermore, there is no compelling evidence that any neurosurgical pro- cedure is superior to all others. If these experimental neurosurgeries are to continue, guidelines should be developed regarding patient and operation selection, and interdisciplinary assessment committees should implement such guidelines at institutions where these operations are performed. Moreover, future cases should be prospectively studied using contemporary technologies to assess lesion placement and size and validated clinical instruments to characterize patients and assess outcome, including adverse effects. Copyright © 1995 by W.B. Saunders Company
T OURETTE'S SYNDROME (TS), or To- urette's disorder, is a neuropsychiatric con-
dition characterized by motor and vocal tics, lasting longer than 1 year and emerging before age 21. I The estimated prevalence of TS is approximately 0.5%, with a preponderance in males versus females of at least 3:1. 2,3 The motor movements and vocalizations can often be temporarily suppressed, although the occur- rence of tics, especially in public, can be humili- ating and socially and vocationally debilitating. Pharmacotherapy has been the mainstay of treatment. Antidopaminergic agents such as haloperidol and pimozide, 24 the e~2-adrenergic agonist clonidine, 3,6,7 and the benzodiazepine clonazepam 3,6 have all been demonstrated to be beneficial for some TS patients. One recent study suggested that the behavior-therapy tech- nique of habit reversal can also be effective. 8 Despite adequate trials of these conventional therapies, some TS patients have residual debili- tating symptoms.
Neurosurgical treatments have been at- tempted in a few treatment-refractory TS pa- tients. Recently, patients and clinicians have become increasingly interested in these surgical procedures as anecdotal successes have been publicized. However, important unanswered questions remain regarding the scientific ratio- nale, clinical evaluation, patient selection, safety, efficacy and ethics surrounding such surgical procedures.
The present review examines the reported
experience with neurosurgical treatment of TS. Case report data are presented first, followed by discussion of relevant neuroanatomy and clini- cal considerations. Recommendations regard- ing future study of these controversial opera- tions are presented, based in part on the authors' experience with neurosurgical treatment of ob- sessive-compulsive disorder (OCD). 9
NEUROSURGICAL PROCEDURES USED IN TS
A variety of neurosurgical procedures have been performed in attempts to treat TS (Fig 1). Reports to date have described (1) frontal lobe operations (i.e., frontal lobotomy and bimedial frontal leukotomy), (2) limbic system opera- tions (i.e., anterior cingulotomy, limbic leu- kotomy), (3) a novel multisite operation (i.e., anterior cingulotomy combined with infratha- lamic lesions), (4) thalamic operations (i.e., bilateral coagulation of rostral intralaminar and medial thalamic nuclei, and ventral-tier tha- lamic lesions), and (5) a cerebellar operation (i.e., bilateral cerebellar dentatotomy).
From the Obsessive Compulsive Disorders Clinical and Research Unit, Department of Psychiatry, and Department of Neurosurgery, Massachusetts General Hospital and Harvard Medical School, Boston, MA.
Address reprint requests to Scott L. Rauch, M.D., Depart- ment of Psychiatry, OCD Unit, 9th Floor, Massachusetts General Hospital-East, 149 Thirteenth St, Charlestown, MA 02129.
Copyright © 1995 by W.B. Saunders Company 0010-440X/95/3602-0001503.00/0
Comprehensive Psychiatry, Vol. 36, No. 2 (March/April), 1995: pp 141-156 141

142 RAUCH ET AL
/ / / / / z t/.- /~'. / / / / " . j 1 1 . . , . , , ,
/ . A n t e r i o r - . . . . ;, : ; ....... "--.~
/ , - , I , ~ . . . . . . . . . . . . . . . . ; . ..~ :. / ....... ,~ . ~,, " .., , . ',,,
' ' / / / C ~ g u l ~ i / C ° r t e x ~'""//~i~i' mus"~~a~i "~~/'/', o
Cal losum-~, , , ,,,,. \
: . ".. ,,,,,,. ~ ,, \ ". d ; "; / ':
.. ......... , ...... ... ..,,,,,,, : ...
~,,,,,, .......... , .... .. ''., .......... ,,. ".. !.,,.,,..,,<,, ; ........... ,,~ ~
/,---- -~ z,.. ,;~,:
O r b i t o f f o n t a l C o r t e x '~ ~ I . . . . . ,
I n f r a t h a l a i n i c ' ~->~:~ .............. m e d i I ~" ;, ,...: : " . - - , ~ - C e r e b e l l u m Bi] L e i o n s ,~ ;~, ~ /
F r o n t a l "'%,,,~ \ !~ , L e u c o t o m y ~. ; ",,~ ,
C e r e b e l l a r D e n t a t o t o m y
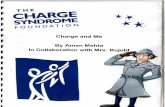
Fig 1. Relevant neuroanatomy and approximate locations of different lesion target sites for the various neurosurgical procedures are depicted in a highly schematized illustration of the brain in parasagittal section. The exact method, size, and placement of lesions have evolved for a number of these surgeries. In particular, whereas bimedial frontal leukotomy and cingulotomy were at one time performed as freehand procedures, these are now performed with greater precision via stereotactic placement of lesions. Note that limbic leukotomy entails combining the stereotactic lesions of anterior cingulotomy and bimedial frontal leukotomy. D.E. Richardson's novel procedure entails combining infrathalamic lesions and anterior cingulotomy. The lesions of frontal Iobotomy (a gross freehand procedure) are not shown.
C A S E R E P O R T S : N E U R O S U R G E R Y FOR T S
Table 1 lists all cases of neurosurgery for TS reviewed herein (N = 36). Cases appearing in peer-reviewed litera- ture were identified via a search conducted using Paper Chase (Paper Chase, Boston, MA). Non-peer-reviewed sources were identified by cross-referencing from the bibli- ographies of peer-reviewed sources, and well-known neuro- surgical texts. Data from additional unpublished cases were communicated to us by colleagues with relevant experience. The case summaries that follow are organized according to the type of operation performed. The degree of detail provided in the case reviews reflects that available from the original reports. For some cases, only summary data are available.
Frontal Lobe Operations (two cases) In 1964, Stevens reported a case of transorbital (frontal)
lobotomy performed in 1955 by Dr. James Watts on a 37-year-old man suffering from TS. 1° The patient was
educated through age 15, had no employment history, and remained dependent on his parents throughout adulthood. At age 8, he developed a motor tic followed by vocal tics, including coprolalia. His repertoire of tics varied, as did the intensity. Motor tics primarily consisted of rhythmic head movements, throwing out his arms, and "a violent general- ized shudder" that was combined with copralalic utter- ances. Later, he developed echolalia and echopraxia. His tics occasionally led to bumping his head, and his barking kept his family awake at night. The tics were reported to occur at a frequency of five to seven per minute when he was relaxed. The severity and persistence of his symptoms left him debilitated. There was no other significant medical history. Family history was "negative." He had been exam- ined by several renowned physicians of the era (including Adolph Meyer and Sir Henry Head) and had received psychotherapy and occupational therapy to no avail. He was noted to be pleasant and cooperative but "childish" on psychiatric examination. No other abnormalities were noted

NEUROSURGERY FOR TOURETTE'S SYNDROME 143
on neurologic examination. An electroencephalogram (EEG) and a pneumoencephalogram were normal.
Stevens noted, "He not only recognized the absurdity and impropriety of his verbal explosions but found it increas- ingly intolerable and was desperate for help . . . . In the light of the patient's incapacity, the prolonged duration and prospect of further progression, a transorbital lobotomy was performed.. . , ,m
By report, he became more relaxed in the postoperative period and continued to improve over the next several weeks, although these observations were confounded by the addition of chlorpromazine (100 mg/d) during this time. (No mention was made of preoperative pharmacologic interventions.) He was, for the first time, able to attend social events without being disruptive.
Two years of follow-up evaluation found a marked decrease in frequency, duration, and amplitude of tics, and at 9 years these gains persisted. There were no reported adverse psychiatric or neurologic sequelae, although no formal testing was described. The researcher did allude to postoperative obesity, another observation confounded by addition of neuroleptic therapy.
Stevens provided no theoretic justification for the poten- tial efficacy of frontal lobotomy. This anecdotal report was uncontrolled, and most glaring is the confounding influence of neuroleptic treatment in the postoperative period. No formal preoperative or postoperative testing was performed to gauge clinical improvement or adverse effects. The potential adverse effects of frontal lobotomy have subse- quently become well known.
In 1962, Baker jl described a bimedial frontal leukotomy performed on a 22-year-old man with TS. The patient had suffered birth trauma in conjunction with a 3-day labor. Hypotonicity, a "deformed head," and an inability to cry or suckle were evident at birth. Developmental delays in- cluded slow motor development with "weakness and incoor- dination" and failure to speak until 30 months. He suffered grand mal seizures at 3 and 5 years of age. Motor and vocal tics were noted at age 9 and gradually worsened. He was also enuretic until age 12. At age 16, he was dismissed from school due to TS symptoms, despite otherwise good aca- demic performance. Panic symptoms emerged at age 20, and he became progressively hopeless thereafter while suffering from intrusive violent and sexual fantasies.
Neuropsychiatric treatment throughout childhood was of little benefit. Pharmacologic treatment with chlorpromazine (up to 700 mg/d) "afforded a slight reduction of the tic," but had no effect on panic.
Preoperatively, his repertoire of tics consisted of a variety of motor tics and a frequent neck jerk accompanied by a cupping of his hand over one ear while shouting out "eh!". He also exhibited occasional coprolalia. His tic frequency during a teaching rounds was 14 per minute (although this was coincident with a period of chlorpromazine with- drawal). His mental status was otherwise unremarkable on examination. His 1Q was said to be 110, and "personality tests" were interpreted as suggestive of "obsessional person- ality." Physical examination showed pallor of the right optic disk (he had undergone surgery for a right esotropia) and left-sternocleidomastoid hypertrophy (attributed to his tor-
ticollic tics). Spinal fluid analysis, EEG, air encephalogram, and right-carotid arteriogram were all normal.
His operation was complicated by a staphylococcal fron- tal abscess with grand mal seizures, which was relieved by aspiration and treatment with antibiotics and (unspecified) anticonvulsants. Additional details pertaining to the opera- tion were not provided.
During the 14-month postoperative follow-up period, his tics and panic were reported to be "markedly reduced" and he was successfully attending night school. When he was again presented at teaching rounds, only two tics were observed during a 30-minute period. The medical regimen at the time of that assessment was not specified. He was discharged on treatment with chlorpromazine (up to 800 mg/d) and phenytoin (which when given preoperatively had no effect on his tics). The "destructive fantasies" abated, but he continued to exhibit a short attention span and avoidance of social situations. His IQ was subsequently measured at 115.
Baker's TS patient suffered from concurrent symptoms reminiscent of depression, OCD, panic disorder, and atten- tional deficits, and all but the attentional deficits were observed to remit postoperatively. According to Baker, the indications for the frontal lobe procedure were the patient's hopelessness (possibly a depressive symptom), destructive thoughts (possibly obsessions), and panic; the response with regard to tics was to some extent unanticipated.
Limbic System Surgery (five cases) Robertson et al. 12 reported in 1990 the case of a 19-year-
old man with TS and self-injurious behaviors who was treated by limbic leukotomy. A cesarean delivery precipi- tated by placenta previa complicated the patient's birth and necessitated a 4-day postpartum hospital stay. His develop- ment proceeded normally until age 5 and a half, when facial tics emerged. Over the subsequent 10 years he exhibited a wide variety of motor tics, and at age 15 he developed symptoms of OCD including repeating and checking compul- sions and "distasteful" and "lurid" intrusive thoughts. At age 16 he developed grunts, which at 17 evolved into coprolalia and were accompanied by a variety of self- injurious behaviors (e.g., lip-biting, head-banging, and self- burning with cigarettes). He became obsessed with the notion that he might jump off a building, developed an irresistible urge to touch the back of his eye, and caused repeated injury to his cornea.
Preoperatively, his physical examination was otherwise normal. A brain computed tomography (CT) scan and EEG were normal. A magnetic resonance imaging (MRI) scan showed a high-signal focus in the region of the right globus pallidus. Neuropsychologic testing found a verbal IQ of 117 and performance IQ of 114.
Initially, pharmacologic treatment with sulpride (200 mg twice daily) abolished the motor tics, but despite an increase in the dose (up to 1 g/d), the self-injurious behavior persisted. He was hospitalized due to increasing risk of self-enueleation, and at that time he evidenced symptoms of major depression. Additional interventions with chlorpro- thixene (a dopamine antagonist; 500 mg/d) and clomipra- mine (an antiobsessional/antidepressant; 200 mg/d) along with behavioral response-prevention techniques "led to

144 RAUCH ET AL
minor improvements." Addition of L-tryptophan proved unsuccessful. He developed other self-injurious behaviors, causing damage to his nose, and also began to perform the Valsalva maneuver so violently that he caused "extensive" petechial hemorrhages (location not specified).
After detailed discussion with the patient, his family, and two consultant psychiatrists, as well as consideration by an independent Mental Health Review Tribunal, he was re- ferred for neurosurgical treatment. The procedure per- formed was a stereotactic bilateral limbic leukotomy, entail- ing bilateral lesions of the lower middle quadrants of the frontal lobes, as well as the anterior cingulum. Placement of lesions was confirmed by MRI postoperatively. The patient was reported to exhibit some agitation initially, which resolved spontaneously, resulting in an otherwise "unevent- ful" postoperative course.
After the operation, he transiently displayed "mild apa- thy, a mild degree of intellectual impairment, and some minor organizational problems and difficulties in concentra- tion." By 2 days postoperatively, compulsions had markedly decreased, and by 6 weeks had resolved entirely. Thereaf- ter, he continued a course of behavioral therapy. His improvement in OCD symptom severity was quantified via the Leyton Obsessional Scale 13 from 17 to 8 and the Maudsley Compulsion Checklist 14 from unspecified preop- eratively to 1. His Beck Depression Inventory (BDI) J5 score remained unchanged at 4. He was discharged from an inpatient setting 2 months after the surgery, and between 2 and 4 months postoperatively he continued to make func- tional progress, entered a training program, and later attained gainful employment.
At 2 years' follow-up evaluation, while being maintained on sulpride (1,600 nag/d), the manifestations of his TS were limited to a single shoulder tic (improvement estimated at 75% from baseline). He was free of self-destructive behav- ior, but continued with "bouts of verbal aggression and periods of self-doubt and anxiety."
Noting the overlap between OCD and TS, Robertson et al. 12 suggested that self-injurious behaviors may represent a unique brand of compulsion, more common in TS than in primary OCD. Their rationale for choosing limbic leu- kotomy rested on the theoretic role of the cingulate cortex in modulating emotionally charged language and stereo- typed movements, as well as its anatomic relationship with midbrain dopaminergic systems, which have been impli- cated in the pathophysiology of TS. 12,16 They further cited positron-emission tomography (PET) studies 17 implicating metabolic abnormalities in the cingulate cortex of TS subjects.
Robertson et al. also referenced an abstracted case report 18 that was later published as an original article by Kurlan et al. 19 in 1990 reporting a series of two patients with TS and comorbid OCD treated with bilateral radiofre- quency anterior cingulotomy. The first of their 19 cases was a 28-year-old man who developed facial tics at age 5 that lasted several months and then spontaneously remitted, only to have recurrence at age 13 of symptoms consisting of truncal tics and violent obsessive thoughts. Since age 12, he had exhibited mood swings and was diagnosed with bipolar disorder. His affective symptoms were well controlled with lithium (2,100 mg/d). At 19, he developed echopraxia along
with vocal tics in the form of echolalia and palilalia, as well as additional symptoms of OCD (e.g., repetitive standing and sitting, touching of door frames, and preoccupation with odd and even numbers). The OCD symptoms were debilitating: he had difficulty with daily activities and was socially isolated and unemployed. Pharmacologic treat- ments, including imipramine, tranylcypromine, clonidine, trazodone, several neuroleptics, and carbamazepine, were ineffective. The combination of haloperidol (3 mg/d) and benztropine (4 mg/d) led to mild improvement.
At age 21, he had a psychotic episode that responded to treatment with lithium and trifluoperazine. At 24, motor and vocal tics returned, with variable repertoire (including coprolalia) and intensity.
Preoperative physical examination was unremarkable, other than the multiple tics observed. EEG was "mildly abnormal" with "bursts of high-voltage sharp theta waves posteriorly without clinical accompaniment," and a CT scan of the brain was noncontributory.
The decision to proceed with the operation was appar- ently based on the patient's severe disability and failure to respond to an extensive array of other treatments. The operation and immediate postoperative period were uncom- plicated. No postoperative neuroimaging was performed to confirm lesion placement or size.
At the 2-year follow-up evaluation, the patient was noted to have "persistent although modest improvement in his ritualistic activities, obsessions, and functional abilities." These gains were not quantified by validated rating scales, but were globally estimated at "25% to 30% improved." The progress in OCD symptoms was confounded by postop- erative addition of clomipramine (225 mg/d) and clonaz- epam (1 mg/d) to his previous maintenance regimen of haloperidol and lithium. Kurlan et al. stated clearly that "no effects on tics or coprolalia were noted following surgery."
Case no. 2 of their series 19 was a 22-year°old man with a history of developmental speech and motor delays who developed vocal tics and ritualistic behaviors (e.g., a preoc- cupation with the color green, wearing and using items only of that color). At age 10, motor tics emerged and the diagnosis of TS was made. A trial of haloperidol (2 mg/d) resulted in "mild improvement" of the tics. Since some facial movements were correlated with right-temporal sharp- wave activity on EEG, a trial of mephobarbital (300 mg/d) was also begun. From age 13 to 16, he developed a broad repertoire of motor and vocal tics. Treatment with haloperi- dol eventually precipitated a catatonic state, which resolved within 1 month in response to medication discontinuation. After medication withdrawal, his tics gradually improved, only to worsen again after a few months. At age 16, he required hospitalization and suffered weight loss (other symptoms of depression are not mentioned). During the ensuing 15 months, he underwent a variety of medication trials (i.e., haloperidol, imipramine, clonidine, clonazepam, and tranylcypromine), as well as a course of electroconvul- sive therapy (details not available).
Due to his degree of debility and failure to respond to an exhaustive array of conventional therapies, a bilateral radio- frequency stereotactic anterior cingulotomy was performed. A 10-day postoperative period was marked by "improve- ment in spontaneous movements and ability to perform

NEUROSURGERY FOR TOURETTE'S SYNDROME 145
daily activities." However, by 2 months' follow-up, symp- toms had returned to preoperative severity.
Eight months postoperatively, he continued to exhibit motor and vocal tics. A second cingulotomy procedure was performed to enlarge the lesions. No neuroimaging proce- dures were performed postoperatively to document lesion size or location, nor were formal rating scales used to quantify changes in clinical severity.
Two months after the second cingulotomy, he was noted to show "moderate improvement in ritualistic behavior but continued to need assistance with daily activities." Subse- quent pharmacologic trials included trazodone, trihexyphe- nidyl hydrochloride, and lithium, without benefit. Three months after the operation, a trial of reserpine (2.5 mg/d) led to "moderate functional improvement" and increasing independence. By 1 year postoperatively, he was attending school and living independently in a residential facility. Motor and vocal tics persisted postoperatively, although their character, variety, and severity were neither quantified nor explicitly compared with the preoperative state. How- ever, in their summary, Kurlan et al. pointed out that "tics were not alleviated by cingulotomy in our patients or in the case reports by Robertson et al."
Subsequently, Baer et al. 2° reported an additional case of anterior cingulotomy for OCD in a 35-year-old man with concomitant TS. This patient's experience is instructive because OCD symptoms improved after cingulotomy, whereas tics were unchanged or slightly worse. He had onset of both OCD and TS symptoms at age 5, characterized by a wide variety of counting, repeating, and touching rituals along with urges to blurt out obscenities and numerous motor and vocal tics numbering in the hundreds per day. These symptoms persisted into adulthood. Interestingly, he reported that he was easily able to distinguish between his OCD and TS symptoms based on his subjective experience. When assessed via structured clinical interview, he met criteria for OCD, TS, major depression, dysthymia, and alcohol abuse (which he reported was the only treatment that helped control his tics), with an axis II diagnosis of mixed personality disorder. His OCD symptoms had failed to respond to trials of behavioral therapy and adequate trials of clomipramine, fluoxetine, haloperidol, pimozide, and clonidine. Therefore, in the context of severe and treatment-refractory OCD, he was referred for cingu- lotomy.
Immediately before his first cingulotomy, while taking fluoxetine (60 mg/d), the patient's score on the Yale-Brown Obsessive-Compulsive Scale (YBOCS) 21 was 26 and his score on the BDI was 28. (The YBOCS is a validated measure of OCD symptom severity. Obsessions and compul- sions are each rated along five separate dimensions on a 0 to 4-point scale, yielding a maximum score of 20 for obsessions, 20 for compulsions, and 40 total. Entry criteria for OCD treatment studies, for example, typically require a total YBOCS score > 15, which is equated with at least moderate symptom severity.)
He underwent a bilateral thermal radiofrequency stereo- tactic cingulotomy via bur holes in 1989 with an uncompli- cated postoperative course. At 3 months' follow-up evalua- tion, on the same medication, he reported a decrease in urges to touch and break things, but his tics were minimally
increased (with reported emergence of a new vocal tic). His YBOCS score was 12 and BDI score was 15, and Clinical Global Improvement (CGI) 9 reflected that his OCD, depres- sion, and anxiety were "slightly better." At 18 months after the first operation, he returned for evaluation before a second cingulotomy. His YBOCS score was 22 and BDI score was 10. Compared with baseline, on CG1 he reported that his depression and anxiety were "much improved," but that his OCD and tics were "not improved."
In 1991, he underwent a second bilateral anterior cingu- lotomy to extend the original lesions. Again, the immediate postoperative course was unremarkable. At the most recent follow-up evaluation, 13 months after the second operation, his YBOCS score was 1 I, and on CGI, his OCD and anxiety were "much improved," depression was "very much im- proved," and tics were "minimally worse."
This patient apparently experienced improvement in OCD, anxiety, and depression after cingulotomy, whereas his tics were minimally worse. Although this patient was evaluated prospectively, the follow-up evaluation empha- sized OCD symptoms because OCD was the indication for his procedure and TS had not been the focus of the team's prospective research effort.
Finally, Sawle et al. 22 reported the case of a 45-year-old man with comorbid TS and OCD who underwent a limbic leukotomy. The patient had developed motor tics at age 7 years, with emergence at age 10 of "urges" to break things, expose himself, burn money, and destroy clothes. At 35, in addition to persisting motor tics, he developed echolalia, coprolalia, self-injurious compulsions, contamination obses- sions, hoarding, and obsessional slowness. This constella- tion of symptoms led to legal difficulties and loss of employment. Psychiatric and neurologic evaluations at that time showed no abnormalities other than TS and OCD. Specifically, a brain MRI scan was normal and neuropsycho- logic testing yielded a verbal IQ of 108 and performance IQ of 104. The patient underwent a broad array of conventional treatments for OCD and TS. Behavioral therapy met with initial success, but within 2 months his condition had relapsed to pretreatment levels of symptom severity. Phar- macologic trials included carbamazepine, chlorpromazine, clomipramine, clonazepam, fluvoxamine, haloperidol, pimo- zide, procyclidine, propranolol, and sulpride "without sus- tained benefit." Doses and durations of treatment were not specified. The patient was deemed totally disabled by his OCD and TS symptoms. In the face of his treatment refractoriness, he was approved for neurosurgical treatment by the Mental Health Commission and referred for surgery.
Of note, in the original report the operation was correctly termed a limbic leukotomy, but was described as entailing anterior cingulotomy plus anterior hypothalamic lesions. 22 Subsequently, it has been confirmed that the actual targets were those of conventional limbic leukotomy, i.e., anterior cingulate plus frontothalamic fibers (personal communica- tion, G.V. Sawle, July 1994). Postoperatively, the patient exhibited a striking and progressive improvement in both TS and OCD symptoms. There is no mention of postoperative complications or adverse effects. Specifically, at the 1-month follow-up evaluation, repeat neuropsychologic testing dem- onstrated a verbal IQ of 114 and performance IQ of 97. At 3 months postoperatively, reduction of OCD symptoms was

146 RAUCH ET AL
"considerable"; at 6 months, he showed "overall 70% improvement"; and at 19 months, "he was living indepen- dently with no clinical signs of [TS]" and his OCD contin- ued "substantially improved."
The case reported by Sawle et al. 22 is most valuable in that the investigators present the results of PET studies per- formed before and after surgery. Normalized cerebral metabolic rates of oxygen consumption decreased substan- tially from preoperative to postoperative studies in the caudate, anterior cingulate, medial frontal cortex, and thalamus. These findings, although anecdotal, are conver- gent with recent PET studies of OCD symptom provoca- tion 23 and OCD symptom improvement, z4,25 Implications of PET data with respect to TS are difficult to interpret, given the confounding factor of OCD comorbidity. Nonetheless, the apparent changes in brain oxygen metabolism that accompany symptomatic improvement of OCD and TS in conjunction with limbic leukotomy are intriguing.
Novel Multisite Surgery: Cingulotomy Plus Infrathalamic Lesions (three cases)
There have been three cases of a novel combined surgery for TS entailing anterior cingulotomy plus infrathalamic lesions, performed by Dr. Donald E. Richardson, 26 (per- sonal communication, December 1991 and November 1992). First, Dr. Richardson provided us with a videotape includ- ing preoperative, intraoperative, and postoperative excerpts illustrating the progress of a 34-year-old woman with severe TS, OCD, and bipolar disorder, treated with bilateral anterior cingulotomy in combination with lesioning of the left infrathalamic area. This patient displayed numerous motor and vocal tics (including coprolalia). Upon reviewing the preoperative segment, we counted 18 tics per minute during a randomly selected 5-minute epoch.
Intraoperatively, the video showed the neurosurgeon stimulating the left infrathalamic area, during which the patient's tics increased in intensity and frequency. In fact, the patient requested that the stimulation be discontinued because of the feeling that it caused. Subsequently, a lesion of the infrathalamic area was made and the patient's tics rapidly subsided.
A 10-minute excerpt from a postoperative interview showed the patient to be more relaxed and nearly free of tics (timing of follow-up period from operative date not speci- fied). We counted a total of only 18 tics in 10 minutes of videotape and only two tics per minute during a random 5-minute epoch. She stated that the intraoperative stimula- tion of her infrathalamic area had re-created the same feeling of tension that typically preceded her tics. Further- more, she reported that postoperatively she was much improved without complications or new complaints. She had been maintained on lithium throughout the course chronicled by the videotape (dose and duration not speci- fied), and no other treatments were described.
Although these videotaped interviews are compelling, they are excerpts and include no assessment of symptom severity with accepted clinical rating scales. Much crucial information was lacking. Fluctuation in the severity of her symptoms preoperatively was not documented. Nor was there any information suggesting that preoperative and postoperative examinations (e.g., neuropsychologic testing)
had been performed to assess whether changes in other functions had occurred as a consequence of the operation.
Dr. Richardson further reported to us that two other patients undergoing this same procedure had far poorer outcomes (personal communication, November 1992). The second case, a 40-year-old man with forceful, self-injurious motor tics, coprolalia, and OCD, has been described in detail via a published case report. 26 The patient had a broad array of motor tics that first developed at age 3 and vocal tics that emerged at age 11 and progressed to include coprolalia. He had an extended period of mild symptom severity during his twenties, with reemergence of more severe illness by age 29, when he presented to the Yale Child Study Center for care. At that time, clinical evaluation showed that in addition to numerous motor and vocal tics (including coprolalia), he had developed self-injurious tics that en- tailed striking the side of his face with his fist and biting his hand, as well as OCD (characterized by repetitive touching, checking, and cleaning). His past history was remarkable for attention deficit hyperactivity disorder and major depres- sion. The family history was positive for tic disorders (father and sister) and OCD (father).
During the subsequent decade, he underwent an exhaus- tive array of pharmacologic trials, including haloperidol, pimozide, clonidine, naltrexone, nifedipine, fluoxetine, and desipramine. Although some of these trials resulted in symptomatic improvement, his self-injurious tics remained refractory and led to left-retinal detachment.
Preoperatively in 1991, without neuroleptic therapy, his tics were considered "severe" to "extremely severe." His Yale Global Tic Severity Scale (YGTSS) 27 scores were 22 for motor tics and 20 for phonic tics, with a global severity score of 90; his OCD symptoms were "moderate" to "marked," with a YBOCS score of 22. (The YGTSS is an instrument for quantification of tic severity. The severities of motor and phonic tics are rated along five separate dimensions on a 0 to 5-point scale, and overall impairment is rated on a 0 to 50-point scale. Thus, the maximum scores, denoting maximal symptom severity, are 25 points for each of the motor and phonic scales and 50 points for the overall impairment scale, yielding a combined maximum of 100. 27)
In the summer of 1991, bilateral anterior cingulotomy and bilateral lesions of the infrathalamic region were per- formed. OCD and some of the patient's motor tics were said to be improved postoperatively. A repeat procedure was performed less than 3 weeks later to extend the lesions on the left because of severe residual tics.
Immediately after the surgery, the patient was noted to be dysarthric, with difficulty swallowing. The immediate postop- erative course was further complicated by "sepsis of un- known etiology," which responded to antibiotics and cortico- steroids.
The patient was evaluated at 4 and 8 months and found to be in similar clinical condition at both time points: At the 8-month evaluation, YGTSS scores were 15 for motor tics and 9 for phonic tics, with a global severity score of 69; the YBOCS score was 7. Despite this estimated 30% to 45% improvement in tics and 68% improvement in OCD, self- injurious behaviors persisted and the patient was left with severe residual neurologic deficits. He suffered apparently irreversible damage affecting his speech, phonation, swallow-

NEUROSURGERY FOR TOURETTE'S SYNDROME 147
ing, handwriting (with micrographia), extraocular move- ments, and gait. At 16 months' follow-up evaluation, the patient remained severely debilitated by these neurologic sequelae to the surgery. Despite moderate OCD and TS symptom improvement, the intervention failed to alleviate the self-injurious tics for which the procedure had been deemed indicated and produced a catastrophic constella- tion of adverse effects.
There is scant information available to us regarding a third case (D.E. Richardson, personal communication, November 1992) involving a young man with TS and comorbid polysubstance abuse who underwent this same neurosurgical intervention without improvement of his TS. His course was further complicated by a serious postopera- tive motor vehicle accident of uncertain cause, in the context of continued substance abuse.
Thalamic Surgery (25 cases) In 1962, Cooper reported a series of 50 cases character-
ized by various forms of dystonia, which were treated with a number of different kinds of operations targeting the basal ganglia. 28 Of these, one case involved bilateral chemothala- mectomy of a 16-year-old girl with TS. The patient was neurologically normal until age 9, when she developed facial motor and simple phonic tics. The motor tics gradually migrated to include all her extremities and much of her torso. The tics were worse in the company of others and she became progressively anxious, although no anxiety disorder diagnosis was noted. From ages 12 to 16, she underwent psychotherapy, as well as hypnosis, and sedative medication trials (dose, duration, and compound unspecified) without benefit. By age 16, she had become a recluse and "virtually incapacitated," with constant involuntary muscle move- ments and loud, explosive grunts. In the autumn of 1960, she underwent a left chemothalamectomy, targeting the ventro- lateral nucleus. Postoperatively, there was immediate cessa- tion of vocal tics and motor tics on the right side of the body and face. Left-sided tics persisted, but the postoperative course was otherwise uncomplicated. Two months later, remission of right motor tics continued, with 50% resur- gence of the vocal tic and persistent left-sided motor tics. Four months after the original surgery, a right chemothala- mectomy was performed. This time, there was immediate improvement of right-sided motor tics. At discharge, the patient was essentially without motor or phonic tics. Six years after the second operation, reevaluation showed a mild return of right-sided motor tics involving the face, extremities, and trunk, as well as complaints of a right-sided sensation of tightness (akin to a premonitory sensation). Therefore, she underwent an additional left cryothalamec- tomy, which was tolerated without sequelae but did not yield any additional benefit.
In summary, this patient sustained an estimated 90% improvement in motor tics and complete irradication of vocal tics without adverse sequelae. As a consequence of her symptomatic improvement, she was able to graduate high school and establish gainful employment in a secre- tarial capacity.
In 1969, in Dr. Cooper's textbook on involuntary move- ment disorders, he again described the above-mentioned case and alluded to five others. 29 Although he noted that the
former was typical of the six cases his group had seen and treated in this manner, we have been unable to locate any detailed published account of the other five cases.
In 1970, Hassler and Dieckmann 3° reported three TS patients who were treated with bilateral coagulation of the rostral intralaminar and medial thalamic nuclei. These three patients' tics were noted to improve by 70%, 90%, and 100% (including irradication of coprolalia), respectively. Their rationale for selecting this procedure was based on their previous positive experience in patients suffering from OCD, as well as their understanding of the relevant neuro- anatomy. 31,32 They concluded that "this therapeutic effect confirms the hypothesis that the symptoms of generalized tic disease are motor compulsions," and that the obsessive component is eliminated by lesioning the medial nuclei and the compulsive component responds to intralaminar le- sions.
Via book chapters on related topics, 31,32 they summarized their updated experience with this operation for TS. In all, they have reported on 15 cases. Although detailed case reports were not furnished for the majority of these cases, outcome in terms of efficacy was tabulated for nine of the cases as follows: four patients improved 90% to 100% and five patients improved 50% to 80%, whereas two patients (both from the 50%- to 80%-improved group) suffered unspecified adverse effects. They acknowledged that this procedure, when performed for other indications, has resulted in psychomotor akinesia and amnesia. A review of their contributions also reveals an evolving and complicated theory regarding the functional anatomy involving substruc- tures within the thalamus. 31,32
In 1977, Divitiis et al. 33 reported the cases of three patients with "multiple tics, motor compulsions, and copro- lalia," consistent with a TS diagnosis, who were likewise treated with thalamotomy. Each had previously undergone psychotherapy without benefit, although no mention is made of prior medication trials. Radiofrequency-coagula- tion lesions of the dorsal medial and intralaminar nuclei of the thalamus were performed unilaterally on the right, with no complications noted. Postoperatively, Divitiis et al. observed "complete remission in two patients, while the third had a small reduction in symptomatology." The third patient returned after 9 months with no clinical change from his preoperative status. He then underwent a second, contralateral procedure, again without benefit. The other two patients had remission of their symptoms for over 1 year, but in both cases TS symptoms returned. In one case, the reemergence of tics occurred after "a prolonged period of mental confusion"; in the other, tics recurred gradually. Both patients refused the contralateral procedure. Based on these three patients, Divitiis et al. concluded that "this procedure is not successful in treating the Gilles de la Tourette syndrome. 33''
Finally, in 1991, Korzen et al. 34 reported a case of a 19-year-old man with TS who underwent bilateral cryode- struction of the ventrolateral thalamic nuclei. The patient developed motor tics at age 5, as well as phobic anxiety symptoms. At 10 years of age, vocal tics emerged and progressed to coprolalia. His condition worsened during puberty. A trial of pimozide was initially helpful in reducing tics, but TS symptoms returned to their full severity while

148 RAUCH ET AL
the patient was still being maintained on a neuroleptic. His symptoms waxed and waned, with a severe exacerbation occurring at age 18. OCD symptoms became prominent in addition to tics, aggressiveness, and social isolation, prompt- ing hospitalization. Neurologic evaluation at that time included a normal CT scan of the brain and abnormalities on EEG that consisted of mild left temporal and occipital slowing. In preparation for the proposed thalamic lesioning procedure, the patient was studied via a series of intraopera- tive electrical stimulations in the vicinity of the thalamus. This surgery culminated in the cryodestruction of the patient's right ventrolateral thalamic nucleus. The postop- erative period was remarkable for a transient loss of speech, which lasted 4 days. Three months later, cryodestructive lesions of the ventrolateral thalamic nuclei were made without complication. Three weeks postoperatively, he was discharged to home, showing "definite improvement" in his
TS. The patient returned for follow-up evaluation 1 year later to be considered as a candidate for additional surgery. It was determined at that time that his motor and vocal tics, including coprolalia, had practically disappeared. He had been maintained on a consistent dose (unspecified) of pimozide, which had been ineffective preoperatively. Since the operation, he was no longer socially isolated, could enjoy traveling on vacations, had established full-time employment, and experienced "normalization of affect." No enduring adverse sequelae of the surgery were noted.
Cerebellar Surgery (one case) In 1972, Nadvornik et al. 35 reported a series of seven
patients with a variety of spastic or myoclonic symptoms treated with stereotactic dentatotomy; the investigators' focus was the description of a new surgical approach. One
Table 1. Neurosurgical Procedures for TS
Primary Secondary No. of Clinical Adverse Type of Operation D iagnos is Diagnoses Patients Response Effects References
Frontal Surgery Bimedial frontal
leukotomy TS
Frontal Iobotomy TS None mentioned Limbic System surgery
Bilateral anterior OCD TS: 1 with psychotic cingulotomy episode
Panic attacks, birth 1 Tics and panic Frontal abscess with Baker, 11 1962 trauma, hopeless- attacks were mark- grand real seizures ness edly reduced, relieved by medi-
socially acceptable cation 1 Improved Obesity Stevens, 1° 1964
Bilateral anterior OCD TS, dysthymia, MDD, cingulotomy alcohol abuse,
mixed personality disorder
Limbic leukotomy TS Severe self-injurious behaviors, MDD
Limbic leukotomy OCD TS
Novel Multisite Surgery Bilateral anterior TS
cingulotomy plus infratha- lamic lesion
Bilateral anterior TS cingulotomy plus infratha- lamic lesion
Attention deficit hyperactivity dis- order, MDD, OCD symptoms
1 with bipolar dis- order
1with polysubstance abuse
2 Rituals improved in 1 Transient aseptic Slowness improved meningitis in 1
in1 No mention of
improvement in tics
1 OCD much improved, MDD very much improved, tics minimally worse
1 Complete and sus- tained resolution of destructive behavior, 75% reduction in tics
1 No signs of TS, OCD substantially improved
Kurlan et al, ls,19 1988, 1990
Tics minimally worse Baer et al, 2° 1994
Mild apathy, intellec- Robertson et al, 12 tual impairment, 1990 and difficulty con- centrating
None mentioned Sawle et al, =2 1993
30%-45% improve- ment in motor and injurious tics, plus phonic tics, 68% dysarthria, dys- improvement in phonia, dysphagia, OCD symptoms ataxia, micro-
9raphia, supra- nuclear palsy
Reemergence of self- Leckman et al, 2e 1993
90% reduction of tics None in 1 case in 1 case 1 case continued
No improvement in 1 substance abuse and had serious auto accident
Richardson (personal communication, December 1991 and November 1992)

NEUROSURGERY FOR TOURETTE'S SYNDROME 149
patient in this series was a 12-year-old boy diagnosed with TS who suffered from "myoclonic movements in the face and diaphragm followed by bark-like sounds." In this patient 's case, a bilateral dentatotomy was performed trans- tentorially via a single right-sided parieto-occipital bur hole, and no operative complications were documented. After the operation, they noted that his "movements decreased" and the "bark-like sounds disappeared."
This report contains no discussion of preoperative or postoperative treatment with medications or behavioral techniques, no mention of preoperative or postoperative assessment with validated clinical rating scales, and no attempt to quantify the improvement described. Nadvornik et al. provided no theoretic justification for the use of this procedure on patients with TS.
C R I T I C A L R E V I E W OF R E P O R T E D C A S E S
The few case reports and personal communi- cations involving 36 patients herein described illustrate that there are very limited data pertain- ing to neurosurgical treatment of TS. A variety of operations have been used, and fewer than 20 patients have received any single procedure
(Table 1). None of the published reports used a prospective design that allowed for valid quanti- tative assessment of clinical improvement in tics or adverse effects over a sizeable cohort. More- over, there is limited information pertaining to the nature of pharmacologic and behavioral treatments provided during preoperative and postoperative periods. Consequently, there is at present no substantial scientific evidence to support the effectiveness of any of these proce- dures in the treatment of TS. Furthermore, there is no compelling evidence to suggest that any one of these candidate procedures is supe- rior to the others, although these anecdotal cases suggest that cingulotomy alone may be particularly ineffective for alleviating tic symp- toms t9,2° and that combined cingulotomy plus infrathalamic lesions may be particularly danger- ous. 26 Consequently, all these procedures must be considered experimental treatments for TS.
Table 1. Neurosurgical Procedures for TS (Cont'd)
Primary Secondary No. of Clinical Adverse Type of Operation D iagnos is Diagnoses Patients Response Effects References
Thalamic Surgery Bilateral chemo- TS None mentioned 6 1 was 90% relieved None mentioned Cooper, 2s.2e 1962,
thalamectomy of of tics, "typical" of 1969
ventrolateral other 5 cases (only nuclei 1 reported in
detail) Bilateral coagula- TS None mentioned 15 4 were 90%-100% 2 with unspecified Hassler and Dieck-
tion of rostral improved adverse effects mann, 30,31 1970,
intralaminar and 5 were 50%-80% (possibly akinesia 1973; Hassler, 32
medial nuclei of improved for and/or amnesia) 1982
thalamus copralalia and motor tics
6 others not
described in detail,
with comparable
outcome Bilateral coagula- TS None mentioned 3 Complete remission Prolonged period of Devitiis et al, 33 1977
tion of rostral in 2, with relapse mental confusion intralaminar and in both after 1 year in 1
medial nuclei of No improvement in 1
thalamus Bilateral cryode- TS
struction of ven-
trolateral tha-
lamic nuclei
Cerebellar Surgery Bilateral cerebellar
dentatotomy
OCD symptoms 1 Near resolution of all Transient speech Korzen et al, 34 1991
tics and copralalia, deficit (resolved
improved social after 4 days)
life, employed for
1st time
TS None mentioned 1 Movements None mentioned Nadvornik et al, 35
decreased, bark- 1972
like sounds disap-
peared

150 RAUCH ET AL
THEORETIC RATIONALE FOR CANDIDATE OPERATIONS
Because of the invasiveness of neurosurgical intervention and the checkered history of neuro- surgical treatments for neuropsychiatric condi- tions, there are necessary concerns about the rationale behind these procedures. Little has been written about the mechanisms by which any of these surgical procedures should allevi- ate TS. In contrast, there are numerous publica- tions about the use of neurosurgical treatment for other neuropsychiatric conditions including OCD, major affective illness, schizophrenia, and chronic pain. 36-46 Of the extensive clinical experience with limbic system operations for other neuropsychiatric indications, most rel- evant to TS is the experience with limbic system surgery for OCD, because of the apparent link between OCD and TS (description follows).
Pathophysiology of TS
The pathophysiology of TS remains poorly understood. Several lines of evidence suggest that tics are mediated via midbrain dopaminer- gic systems and their interactions with the basal ganglia. 3,47 Dopamine antagonists are effective therapies for TS, 3-6 and dopamine agonists reli- ably exacerbate TS. 3,48-5° Functionally excessive dopaminergic transmission, perhaps via recep- tor supersensitivity, has been hypothesized in the pathobiology of TS. 3,51 Dopaminergic in- volvement may not be limited to the nigrostria- tal tracts, but may also include influences from mesolimbic and mesocortical projections. Dopa- minergic projections to limbic striatum have typically been associated with affective illness and psychosis, and may be involved in OCD as well. Furthermore, the efficacy of nondopamin- ergic agents in the treatment of TS, and a growing appreciation for the neurochemical complexity of the basal ganglia suggest that other neurotransmitters also play some role in mediating symptoms.
The role of the basal ganglia in mediating cognitive, affective, and especially motor func- tions is consistent with the notion that it could be a site of pathology in TS. 52 Basal ganglia pathology has been established in a variety of other movement disorders such as Parkinson's disease, Huntington's disorder, and encephali- tis lethargica. One study using PET to measure
regional glucose utilization in TS patients showed hypermetabolism in basal ganglia, fron- tal cortex, and temporal lobes bilaterally. 17 Sub- sequent PET studies have provided data sup- porting theories that corticostriatal circuits, including sensorimotor cortex, putamen, and ventral striatum, play a role in the pathophysiol- ogy of TS. 53-55 Recent morphometric MRI stud- ies of TS converge to suggest abnormal symme- try of the lenticular nuclei. 56-58 In addition, animal studies suggest that the cingulate cortex plays a central role in the neuroanatomy of vocalization. 47 The most comprehensive pub- lished model of OCD acknowledges involve- ment of many of these structures. 59-61 If TS and OCD represent a spectrum disorder, as has been suggested, the underlying pathology may parallel that spectrum topographically. Baxter et al. 6° have hypothesized that patients with TS alone have relative dorsolateral involvement of the striatum, whereas patients with OCD alone have relative ventromedial involvement of the striatum. Indeed, contemporary neurobiologic models of TS focus on the relevant cortico- striato-thalamo-cortical circuits. 55
In summary, the roles of the basal ganglia and the nigrostriatal dopaminergic system have long been central to models of TS pathophysiology. Involvement of frontal cortex, cingulum, and thalamus is now also suspected. The influences of mesolimbic and mesocortical dopaminergic systems, as well as other transmitter systems, require further study.
Relationship Between TS and OCD
TS and OCD are clinically related in several ways: First, there is a high rate of symptom overlap; it has been estimated that 30% to 90% of patients with TS exhibit OCD symptoms. 3,6z,63 Second, there are some symptoms (i.e., repeti- tive rubbing, tapping, and touching behaviors) that lie on the border between tics and compul- sions. 64 Third, family studies have found that TS and OCD may be genetically related, 65,66 and a series of studies have led to the conclusion that in some cases TS and OCD represent different phenotypic expressions of the same genetic abnormality. 65-68 Genetic transmission appears to follow the pattern of an autosomal dominant gene with incomplete penetrance; in the case of

NEUROSURGERY FOR TOURE'I-'I'E'S SYNDROME 151
TS, its expression is sex-influenced with male preponderance. 65-6s
Clinical and genetic relationships between TS and OCD may also extend to models of patho- physiology. In both cases, the basal ganglia have been implicated as potential sites of abnormal- ity, although current theories of pathophysiol- ogy in OCD emphasize the role of the fronto- striato-pallido-thalamo-ffontal (FSPTF) loop and the Papez circuit. 4°,59-61,69
Investigations of neurotransmitter dysregula- tion in OCD have focused on serotonergic systems, because of the clinical efficacy of sero- tonergic medications in treating O C D . 61 Antido- paminergic agents that are efficacious for TS are typically not beneficial for OCD, although they may be effective as augmenting agents in the face of concurrent tics. 7° Conversely, the serotonergic agents that represent the first line of therapy for OCD are not typically helpful in treatment of the tics of TS. Thus, despite clinical similarities in the two disorders, this disparity in treatment response exemplifies the fact that effective treatments for OCD are not necessarily effective for TS, or vica versa.
Neuroanatomy Relevant to TS and OCD
Although a comprehensive review of neuro- anatomy is beyond the scope of this article, detailed accounts are available elsewhere. 52,71,72
Neurosurgical lesions may be conceptualized as influencing neural systems, rather than as simply ablating target structures. There are several relevant circuits whose functional neuro- anatomy must be appreciated to comprehend the potential impact of the candidate neurosur- geries.
The frontal cortex sends projections via white matter tracts (1) to cingulate cortex and other limbic structures, (2) directly to thalamic nuclei, and (3) indirectly to thalamic nuclei via integra- tive relays at the level of the striatum and globus pallidus. Sensorimotor cortex also has projec- tions to the thalamus via the striatum (predomi- nately the putamen) to ventral-tier thalamic nuclei. The thalamus sends reciprocal projec- tions to frontal cortex, as well as to other cortical regions including cingulate, sensorimo- tor, and premotor cortex. It is suspected that the frontothalamic axis is a mutually excitatory reverberating loop modulated by inputs from
the cingulate cortex and the basal ganglia (i.e., the striatum and globus pallidus). The sensori- motor corticothalamic circuit represents a segre- gated parallel pathway mediated via the puta- men. Modulatory influences on these corticostriatal systems may include (1) connec- tions from the subthalamus to the thalamus via the globus pallidus; (2) dopaminergic projec- tions from the substantia nigra to the striatum; (3) dopaminergic projections from the ventral tegmentum to frontal cortex and limbic struc- tures, including the limbic striatum (i.e., nucleus accumbens); and (4) diffuse serotonergic projec- tions from the raphe nuclei.
The respective roles of the different struc- tures in these circuits are not fully understood. One theory suggests that the frontothalamic positive-feedback circuit mediates behavioral drives (i.e., urges associated with tics or compul- sions), whereas the FSPTF pathway provides modulatory feedback, which functionally inhib- its or "controls" those drives. 59 Presumably, limbic circuits, including inputs from cingulate cortex and limbic striatum, mediate the affec- tive valence of drives and behaviors. Cortico- striato-thalamic pathways originating in sensori- motor cortex may be of unique importance in TS by mediating the fundamental motor compo- nent of tics or associated sensory premonitory urges . 55,73
All the reported candidate neurosurgeries impact the circuits described above.
Pathophysiology and Neurosurgical Treatment of OCD
The rationale for limbic system operations (i.e., anterior capsulotomy, anterior cingu- lotomy, subcaudate tractotomy, and limbic leu- kotomy) and thalamotomy for OCD has been reviewed elsewhere. 4° In short, the FSPTF cir- cuit and its connections with the Papez circuit 69 have been hypothesized to mediate OCD symp- toms. 4°,59 The lesions of limbic system surgery theoretically interrupt those circuits, thereby disrupting cyclic feedback and alleviating un- wanted symptoms. Although this theory re- mains crude and poorly tested, an impressive body of data has accumulated that demon- strates the relative safety of limbic system surger- ies. 36,37,40'74 Their efficacy in the treatment of OCD, although supported by many case reports

152 RAUCH ET AL
and open trials, remains incompletely studied, since few prospective and no double-blind stud- ies with sham operations and random assign- ment have been conducted. 9,4°
Functional Neuroanatomy of Candidate Surgeries for TS
Frontal lobotomy entails a crude severing of connections between prefrontal cortex and the rest of the brain. Not only are the frontotha- lamic axis, FSPTF loop, and the frontocingulate connections severed, but also communication between frontal cortex and other areas of asso- ciation cortex. Consequently, frontal lobotomy not only interrupts the frontothalamic axis- associated drives, it also blocks the inhibitory- feedback circuit and results in a well-docu- mented frontal syndrome. 75,76
Bimedial frontal leukotomy entails a more limited and precise interruption of the medial white matter tracts that primarily carry fronto- thalamic connections, specifically from orbito- frontal cortex to the medial thalamic nuclei (Fig 1). This distinction is important, since these medial orbitothalamic tracts have been impli- cated in the pathophysiology of OCD.59
Anterior cingulotomy entails lesioning of an- terior cingulate cortex, as well as the anterior cingulate bundle, which consists of white matter tracts intrinsic to the Papez circuit coursing adjacent to cingulate cortex. Limbic leukotomy entails combined lesions of the orbitothalamic tracts with bilateral anterior cingulotomy. Ante- rior capsulotomy and subcaudate tractotomy (neurosurgical procedures for OCD that have not, to date, been applied in the treatment of TS) sever frontothalamic connections further downstream, as well as frontostriatal projec- tions. All these limbic system surgeries have been reported to reduce the symptoms of OCD. 4°
Anterior cingulotomy plus infrathalamic le- sioning combines cingulotomy with a lesion of the infrathalamic area. This infrathalamic re- gion is adjacent to the ventral tier of thalamic nuclei and encompasses fibers of passage be- tween thalamus, subthalamic nucleus, and pall- idum. Lesions of the infrathalamic region can influence ventral-tier thalamic input and out- put. It is not clear, based on the functional neuroanatomy of this region, whether the net
effects of such a lesion should improve or exacerbate symptoms of a movement disorder.
The thalamus is a complex structure with several discrete divisions, each with its unique input and output profile. The medial thalamic nucleus, also known as the dorsal medial nucleus, receives input from other thalamic nuclei, lim- bic structures, and prefrontal (including orbito- frontal) cortex. The medial thalamic nucleus sends its projections primarily to prefrontal cortex in a reciprocal manner. The intralaminar nuclei are several small nuclei scattered through- out the intralaminar connective tissue, which separates the various subdivisions of the thala- mus. The intralaminar nuclei receive input dif- fusely from the other thalamic nuclei, as well as the reticular formation and the basal ganglia. The intralaminar nuclei send their output dif- fusely to cortex, including frontal, motor, and premotor cortex. In this way, the medial tha- lamic nucleus and the intralaminar nuclei corre- spond to the thalamic relay sites of the hypoth- esized FSPTF circuit. 59 Therefore, operations that lesion the medial thalamic and intralami- nar nuclei bilaterally can be conceptualized as interrupting the frontothalamic axis within the thalamus while leaving other thalamic nuclei relatively intact.
The ventral-tier nuclei of the thalamus serve as the principal relay nuclei for the sensory and motor systems. In this manner, lesions of ventral- tier nuclei can be conceptualized as interrupt- ing the sensorimotor cortico-striato-thalamo- cortical circuit within the thalamus.
The cerebellum also influences the motor system via communication with the thalamus. The dentate nucleus, one of the deep nuclei of the cerebellum, sends its projections via the superior cerebeUar peduncle to the ventral-tier nuclei of the thalamus. These efferents contrib- ute to the thalamic fasciculus, which courses through the infrathalamic region. The ventral- tier nuclei of the thalamus also integrate input from the basal ganglia and in turn send projec- tions to motor and premotor cortex. This path- way is theorized to play a role in preparation, learning, and execution of motor movements. Consequently, lesions of the dentate nuclei of the cerebellum would be expected to interrupt this contribution to motor movement. As dis- cussed earlier, dentatotomy has also been re-

NEUROSURGERY FOR TOURETTE'S SYNDROME 153
ported to be effective in eliminating certain other sudden involuntary movements similar to the tics of TS. 35
RECOMMENDATIONS REGARDING FUTURE EXPERIMENTAL NEUROSURGERY FOR TS
Although controversial, the use of experimen- tal neurosurgery for TS should not necessarily present ethical concerns different from those for intractable pain or seizures. As long as a patient is capable of rendering informed con- sent, such procedures are analogous to any experimental surgical intervention. Unfortu- nately, guidelines for conducting experimental operations are not well established.
There are serious uncertainties regarding any experimental neurosurgical procedure to the extent that such procedures produce irrevers- ible changes, unknown adverse consequences, and questionable benefits. However, in the case of severe, intractable TS, these appropriate concerns must be juxtaposed against the risks of conventional therapies, including tardive dyski- nesia from long-term treatment with neurolep- t ics 77'78 and the morbidity, or in the most ex- treme cases mortality, associated with treatment refractoriness. Patients who suffer from severe TS, are debilitated by their symptoms, and have failed an exhaustive array of conventional phar- macologic and behavioral therapies might rea- sonably arrive at a decision to proceed with an experimental treatment.
However, in addition to informed consent, experimental operations should also require careful patient screening and thoughtful selec- tion of the procedure to be performed. Based on our experience with OCD, we are of the opinion that the appropriateness of a TS pa- tient's candidacy for such a procedure is best assessed by an experienced interdisciplinary committee, taking into account such issues as accuracy of diagnosis, severity of illness, compli- cating influences of comorbid diagnoses, ad- equacy of previous conventional therapies, and ability to render informed consent. Such inter- disciplinary committees already exist for the assessment of candidates seeking neurosurgical interventions for other neuropsychiatric ill- nesses such as intractable cases of OCD, chronic pain, and major affective illness. 37,38
To date, criteria have not been established
regarding appropriate candidacy for neurosurgi- cal treatment of TS. In the case of OCD, our institutional Cingulotomy Assessment Commit- tee has generated criteria for cingulotomy that include standards for "adequate trials of other conventional therapies," as well as contraindica- tions to cingulotomy (e.g., ongoing substance abuse or severe comorbid personality disorder). We suggest that if these experimental surgeries are to continue, such patient criteria for neuro- surgical treatment of TS are essential. Ideally, guidelines pertaining to adequacy of trials using conventional pharmacologic and behavioral therapies, as well as other clinical consider- ations, could be established by a panel of scientific and clinical experts in TS (e.g., the Clinical and Scientific Advisory Boards of the Tourette Syndrome Association). Likewise, the process of selecting candidate operations should proceed thoughtfully.
Moreover, if experimental operations for TS continue to be performed, then it is essential that patients be managed in a manner that enhances the opportunity to learn from the experience and so contribute to the knowledge base from which important future clinical deci- sions can be made.
Ideally, case management should begin with comprehensive preoperative screening, includ- ing clinical assessment by a psychiatrist and a neurologist, as well as by the neurosurgeon. A detailed review of the candidate's history is necessary to confirm the primary diagnosis and severity of illness, as well as to document carefully the adequacy of pharmacologic and behavioral treatment. A validated structured clinical interview instrument should be adminis- tered to confirm the clinical impression of the primary diagnosis, as well as comorbid diag- noses. Validated clinical instruments should be used to characterize quantitatively the severity and repertoire of tics, as well as anxiety, depres- sion, OCD symptoms, and level of social and vocational functioning. Other studies per- formed preoperatively should include EEG, MRI, and neuropsychologic testing. Postopera- tively, quantitative clinical instruments and spe- cial studies should be repeated to document interval changes associated with the operation. In particular, postoperative neuroimaging stud- ies are essential to ascertain the actual location

154 RAUCH ET AL
and extent of the neurosurgical lesions. Clinical assessments should be repeated periodically to gauge long-term efficacy and adverse conse- quences.
CONCLUSIONS
Case reports in the literature provide only anecdotal evidence supporting the efficacy and safety of neurosurgical treatment of TS. Conse- quently, neurosurgical treatment of TS must be considered experimental. There is no compel- ling evidence that any particular neurosurgical procedure is best for TS. Cingulotomy may be particularly ineffective at ameliorating tics, and infrathalamic lesions may be particularly danger- ous. If experimental neurosurgery for TS is to continue, then guidelines should be developed regarding patient and operation selection, and interdisciplinary assessment committees should implement such guidelines. Future cases of neurosurgery for TS should be studied prospec- tively using neuroimaging techniques to assess
placement and extent of surgical lesions, and validated clinical instruments should be admin- istered preoperatively and postoperatively to monitor long-term outcome.
Innovative techniques that allow neurosur- geons to make lesions without opening the cranium (e.g., gamma knife, proton beam, and linear accelerator) increase the potential for performing ethical, controlled studies using ran- domization to sham versus active operations. Results from such studies would be necessary to determine definitively which, if any, of these procedures are effective treatments for TS.
A C K N O W L E D G M E N T
The authors wish to acknowledge the assistance of Dmitry Berdichevsky, M.S., in translating the study re- ported by Korzen et al. in 1991 from Russian to English. We thank Linda Leahy for clerical assistance in processing the manuscript. We also wish to acknowledge the cooperation of Dr. Donald E. Richardson in communicating to us information regarding his experience with the novel mul- tisite neurosurgical procedure described.
REFERENCES
1. American Psychiatric Association. Diagnostic and Sta- tistical Manual of Mental Disorders. Ed. 3. Rev. Washing- ton, DC: American Psychiatric Association, 1987.
2. Shapiro AK, Shapiro ES, Young JG, Feinberg TE. Gilles de la Tourette Syndrome. Ed. 2. New York, NY: Raven, 1988.
3. Singer HS, Walkup JT. Tourette syndrome and other tic disorders: diagnosis, pathophysiology, and treatment. Medicine 1991;70:15-32.
4. Shapiro AK, Shapiro E. Controlled study of pimozide vs placebo in Tourette's syndrome. J Am Acad Child Psychiatry 1984;23:161-173.
5. Shapiro AK, Shapiro E, Fulop G. Pimozide treatment of tic and Tourette disorders. Pediatrics 1987;79:1032-1039.
6. Truong DD, Bressman S, Shale H, Fahn S. Clonaz- epam, haloperidol, and clonidine in tic disorders. South Med J 1988;81:1103-1105.
7. Leckman JF, Hardin MT, Riddle MA, Stevenson J, Ort SI, Cohen DJ. Clonidine treatment of Gilles de la Tourette's syndrome. Arch Gen Psychiatry 1991;48:324-328.
8. Azrin NH, Peterson AL. Treatment of Tourette syn- drome by habit reversal: a waiting-list control group compari- son. Behav Ther 1990;21:305-318.
9. Jenike MA, Baer L, Ballantine HT, Martuza RL, Tynes S, Giriunas I, et al. Cingulotomy for refractory obsessive-compulsive disorder: a long-term follow-up of 33 patients. Arch Gen Psychiatry 1991;48:548-555.
10. Stevens H. The syndrome of Gilles de la Tourette and its treatment. Med Ann DC 1964;33:277-279.
11. Baker EFW. Gilles de la Tourette syndrome treated by bimedial frontal leucotomy. Can Med Assoc J 1962;86:746- 747.
12. Robertson M, Doran M, Trimble M, Lees AJ. The treatment of Gilles de la Tourette syndrome by limbic leucotomy. J Neurol Neurosurg Psychiatry 1990;53:691-694.
13. Cooper J. The Leyton Obsessional Inventory. Psychol Med 1970;1:48-64.
14. Hodgson RJ, Rachman S. Obsessional-compulsive complaints. Behav Res Ther 1977;15:389-395.
15. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychia- try 1961;4:561-571.
16. Talairach J, Bancard J, Geier S, Bordas-Ferrer M, Bonis A, Szilka G. The cingulate gyrus and human behavior. Electroencephalogr Clin Neurophysiol 1973;34:45-52.
17. Chase TN, Foster NL, Fedio P, Brooks R, Mansi L, Kessler R, et al. Gilles de la Tourette syndrome: studies with the fluorine-18-1abeled fluorodeoxyglucose positron emission tomographic method. Ann Neuro11984;15(Suppl): S175.
18. Kurlan R, Caine E, Lichter E. Surgical treatment of severe obsessive-compulsive disorder associated with To- urette's syndrome [abstract]. Neurology 1988;38(Suppl): 203.
19. Kurlan R, Kersun J, BaUantine HT, Caine ED. Neurosurgical treatment of severe obsessive-compulsive disorder associated with Tourette's syndrome. Move Disord 1990;5:152-155.
20. Baer L, Rauch SL, Jenike MA, Cassem NH, Ballan- tine HT, Manzo PA, et al. Cingulotomy in a case of concomitant OCD and Tourette syndrome. Arch Gen Psychiatry 1994;51:73-74.
21. Goodman WK, Price LH, Rasmussen SA, Mazure C, Delgado P, Heninger GR, et al. The Yale-Brown Obsessive-

NEUROSURGERY FOR TOURE3-I-E'S SYNDROME 155
Compulsive Scale: II. Validity. Arch Gen Psychiatry 1989;46: 1012-1016.
22. Sawle GV, Lees AJ, Hymas NF, Brooks D J, Frackow- iak RSJ. The metabolic effects of limbic leucotomy in Gilles de la Tourette syndrome. J Neurol Neurosurg Psychiatry 1993;56:1016-1019.
23. Rauch SL, Jenike MA, Alpert NM, Baer L, Breiter HCR, Savage CR, et al. Regional cerebral blood flow measured during symptom provocation in obsessive-compul- sive disorder using oxygen 15-labeled carbon dioxide and positron emission tomography. Arch Gen Psychiatry 1994;51: 62-70.
24. Baxter LR, Schwartz JM, Bergman KS, Szuba MP, Guze BH, Mazziotta JC, et al. Caudate glucose metabolic rate changes with both drug and behavior therapy for obsessive-compulsive disorder. Arch Gen Psychiatry 1992;49: 681-689.
25. Swedo SE, Pietrini P, Leonard HL, Schapiro MB, Rettew DC, Goldberger EL, et al. Cerebral glucose metabo- lism in childhood-onset obsessive-compulsive disorder: revi- sualization during pharmacotherapy. Arch Gen Psychiatry 1992;49:690-694.
26. Leckman JF, de Lotbiniere AJ, Marek K, Gracco C, Scahill L, Cohen DJ. Severe disturbances in speech, swallow- ing, and gait following stereotactic infrathalamic lesions in Gilles de la Tourette's syndrome. Neurology 1993;43:890- 894.
27. Leckman JF, Riddle MA, Hardin MT. The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry 1989;28:566-573.
28. Cooper IS: Dystonia reversal by operation on basal ganglia. Arch Neurol 1962;7:132-145.
29. Cooper IS: Involuntary Movement Disorders. New York, NY: Harper & Row, 1969:274-279.
30. Hassler R, Dieckmann G. Traitment stereotaxique des tics et cris inarticues ou coprolaliques consideres comme phenomene d'obsession motrice au cours de la maladie de GlUes de la Tourette. Rev Neurol (Paris) 1970;123:89-100.
31. Hassler R, Dieckmann G. Relief of obsessive- compulsive disorders, phobias and tics by stereotactic coagu- lation of the rostral intralaminar and medial-thalamic nu- clei. In: Laitinen LV, Livingston KE (eds): Surgical Approaches in Psychiatry. Proceedings of the Third Interna- tional Congress of Psychosurgery. Baltimore, MD: Univer- sity Park, 1973:206-212.
32. Hassler R. Stereotaxic surgery for psychiatric distur- bances. In: Schaltenbrand G, Walker AE (eds): Stereotaxy of the Human Brain: Anatomical, Physiological, and Clini- cal Applications. Ed. 2. New York, NY: Thieme-Stratton, 1982:570-590.
33. Divitiis E, D'Errico A, Cerillo A. Stereotactic surgery in Gilles de la Tourette syndrome. Acta Neurochir [Suppl] (Wien) 1977;24:73.
34. Korzen AV, Pushkov VV, Kharitonov RA. [Stereo- taxic thalamotomy in the combined treatment]. Zh Nevropa- tol Psikhiatr 1991;3:100-101.
35. Nadvornik P, Sramka M, Lisy L, Svicka I. Experi- ences with dentatotomy. Confin Neurol 1972;34:320-324.
36. Ballantine HT. Neurosurgery for behavioral disor-
ders. In: Wilkens RH, Rengachary SS (eds): Neurosurgery. New York, NY: McGraw-Hill, 1985:2527-2537.
37. BaUantine HT, Bouckoms AJ, Thomas EK, Giriunas IE. Treatment of psychiatric illness by stereotactic cingu- Iotomy. Biol Psychiatry 1987;22:807-819.
38. Ballantine HT, Giriunas IE. Treatment of intractable psychiatric illness and chronic pain by stereotactic cingu- lotomy. In: Schmidek HH, Sweet WH (eds): Operative Neurosurgical Techniques: Indications, Methods and Re- sults. Vol. 2. New York, NY: Harcourt Brace Jovanovich, 1988:1069-1075.
39. Bridges PK, Bartlett JR. Psychosurgery: yesterday and today. Br J Psychiatry 1977;131:249-260.
40. Chiocca EA, Martuza RL. Neurosurgical therapy of obsessive-compulsive disorder. In: Jenike MA, Baer L, Minichiello WE (eds): Obsessive-Compulsive Disorders: Theory and Management. Littleton, MA: Year Book Medi- cal, 1990:283-294.
41. Lewin W. Selective leucotomy: a review. In: Laitinen LV, Livingston KE (eds): Surgical Approaches in Psychia- try. Lancaster, England: Medical and Technical, 1973.
42. Mitchell-Heggs N, Kelly D, Richardson A. Stereotac- tic limbic leucotomy: a follow-up at 16 months. Br J Psychiatry 1976;128:226-240.
43. Kelly D. Anxiety and Emotions: Physiological Basis and Treatment. Springfield, IL: Thomas, 1980;197-300.
44. Rees WL. The value and limitations of psychosurgery in the treatment of psychiatric illness. Psychiatr Neurol Neurochir 1973;76:323-334.
45. Sweet WH, Obrador S, Martin-Rodrigues JG. Neuro- surgical Treatment in Psychiatry, Pain and Epilepsy. Balti- more, MD: University Park, 1977.
46. Tippin J, Henn FA. Modified leukotomy in the treatment of intractable obsessional neurosis. Am J Psychia- try 1982;139:1601-1603.
47. Devinsky O. Neuroanatomy of Gilles de la Tourette's syndrome: possible midbrain involvement. Arch Neurol 1983;40:508-514.
48. Feinberg M, Carrol BJ. Effects of dopamine agonists and antagonists in Tourette's disease. Arch Gen Psychiatry 1979;36:979-985.
49. Golden GS: The relationship between stimulant medi- cation and tics. Pediatr Ann 1988;17:405-408.
50. Klempel K. Gilles de la Tourette symptoms induced by L-dopa. S Afr Med J 1974;48:1379-1380.
51. Wong DF, Pearlson GD, Young LT, Singer H, Villemagne V, Tune L, et al. D2 dopamine receptors are elevated in neuropsychiatric disorders other than schizophre- nia [abstract]. J Cereb Blood Flow Metab 1989;9(Suppl 1):$593.
52. Alexander GE, Crutcher MD, DeLong MR. Basal ganglia-thalamocortical circuits: parallel substrates for mo- tor, oculomotor, "prefrontal" and "limbic" functions. In: Uylings HBM, Van Eden CG, De Bruin JPC, et al. (eds): Progress in Brain Research. Vol. 8. New York, NY: Elsevier Science, 1990:119-146.
53. Chase TN, Godfrey V, Gillespie M. Structural and functional studies of Gilles de la Tourette's syndrome. Rev Neurol (Paris) 1986;142:851-855.
54. Stoetter B, Braun AR, Randolph C, Gernert J, Carson RE, Herscovitch P, et al. Functional neuroanatomy

156 RAUCH ET AL
of Tourette syndrome: limbic-motor interactions studied with PET FDG..Adv Neurol 1992;58:213-226.
55. Leckman JF, Pauls DL, Peterson BS, Riddle MA, -Anderson GM, Cohen DJ. Pathogenesis of Tourette syn- drome: clues from the clinical phenotype and natural history. Adv Neurol 1992;58:15-24.
56. Peterson B, Riddle MA, Cohen D J, Katz LD, Smith JC, Hardin MT, et al. Reduced basal ganglia volumes in Tourette's syndrome using three-dimensional reconstruc- tion techniques from magnetic resonance images. Neurol- ogy 1993;43:941-949.
57. Singer HS, Reiss AL, Brown JE, Aylward EH, Shih B, Chee E, et al. Volumetric MRI changes in basal ganglia of children with Tourette's syndrome. Neurology 1993;43: 950-956.
58. Witelson SF. Clinical neurology as data for basic neuroscience: Tourette's syndrome and the human motor system. Neurology 1993;43:859-861.
59. Modell JG, Mountz JM, Curtis GC, Greden JF. Neurophysiologic dysfunction in basal ganglia/limbic stria- tal and thalamocortical circuits as a pathogenetic mecha- nism of obsessive-compulsive disorder. J Neuropsychiatry 1989;1:27-36.
60. Baxter LR, Schwartz JM, Guze BH, Bergman K, Szuba MP. Neuroimaging in obsessive-compulsive disorder: seeking the mediating neuroanatomy. In: Jenike MA, Baer L, Minichiello WE (eds): Obsessive-Compulsive Disorders: Theory and Management. Littleton, M.A: Year Book Medi- cal, 1990:167-188.
61. Rauch SL, Jenike MA. Neurobiological models of obsessive-compulsive disorder. Psychosomatics 1993;34:20- 32.
62. Frankel M, Cummings JL, Robertson MM, Trimble MR, Hill MA, Benson DF, Obsessions and compulsions in Gilles de la Tourette's syndrome. Neurology 1986;36:378- 382.
63. Pitman RK, Green RC, Jenike MA, Mesulam MM. Clinical comparison of Tourette's disorder and obsessive- compulsive disorder. Am J Psychiatry 1987;144:1166-1171,
64. Holzer JC, Goodman WK, McDougle CJ, Baer L, Boyarsky BK, Leckman JF, et al. Obsessive-compulsive disorder with and without a chronic tic disorder: a compari- son of symptoms in 70 patients. Br J Psychiatry 1994;164:469- 473.
65. Pauls DL, Leckman JF. The inheritance of Gilles de la Tourette's syndrome and associated behaviors: evidence for autosomal dominant transmission. N Engl J Med 1986; 315:993-997.
66. Pauls DL, Towbin KE, Leckman JF, Zahner GEP, Cohen DJ. Gilles de la Tourette syndrome and obsessive- compulsive disorder: evidence supporting a genetic relation- ship. Arch Gen Psychiatry 1986;43:1180-1182.
67. Devor EJ. Untying the Gordian knot: the genetics of Tourette syndrome. J Nerv Ment Dis 1990;178:669-679.
68. Pauls DL, Pakstis AJ, Kurlan R, Kidd KK, Leckman KF, Cohen D J, et al. Segregation and linkage analysis of Tourette's syndrome and related disorders. J Am Acad Child Adolesc Psychiatry 1990;29:195-203.
69. Papez JW. A proposed mechanism of emotion. Arch Neurol Psychiatry 1937;38:725-743.
70. McDougle CJ, Goodman WK, Price LH, Delgado PL, Krystal JH, Charney DS, et al. Neuroleptic addition in fluvoxamine refractory obsessive compulsive disorder. Am J Psychiatry 1990; 147:652-654.
71. Nieuwenhuys R, Voogd J, Huijzen CV. The Human Central Nervous System: .A Synopsis and -Atlas. New York, NY: Springer-Verlag, 1988.
72. Nolte J. The Human Brain. St Louis, MO: Mosby Year Book, 1993.
73. Leckman JF, Walker DE, Cohen DJ. Premonitory urges in Tourette's syndrome. Am J Psychiatry 1993;150:98- 102,
74. Corkin S, Twitchell TE, Sullivan EV. Safety and efficacy of cingulotomy for pain and psychiatric disorders. In: Hitchcock ER, Ballantine HT, Meyerson BA (eds): Modern Concepts in Psychiatric Surgery. New York, NY: Elsevier/North Holland, 1979:253-272.
75. Greenblatt M, Solomon HC. Survey of nine years of lobotomy investigations. Am J Psychiatry 1952;109:262-265.
76. Luria .AR. Higher Cortical Functions in Man. Ed. 2. New York, NY: Basic Books, 1980.
77. Caine E, Polinski R. Tardive dyskinesia in persons with Gilles de la Tourette's disease. Arch Neurol 1981;38: 471-472.
78. Riddle MA, Hardin MT, Towbin KE, Leckman JF, Cohen DJ. Tardive dyskinesia following haloperidol treat- ment for Tourette's syndrome. Arch Gen Psychiatry 1987;44: 98-99.