Habit reversal versus supportive psychotherapy in Tourette's disorder: A randomized controlled trial...
12
Behaviour Research and Therapy 44 (2006) 1079–1090 Habit reversal versus supportive psychotherapy in Tourette’s disorder: A randomized controlled trial and predictors of treatment response Thilo Deckersbach , Scott Rauch, Ulrike Buhlmann, Sabine Wilhelm OCD Clinic/Psychiatric Neuroscience Division, Department of Psychiatry, 149-2611, Massachusetts General Hospital, Bldg. 149, 13th St. Charlestown, MA 02129, USA Received 7 March 2005; received in revised form 4 August 2005; accepted 15 August 2005 Abstract Tourette syndrome (TS) is characterized by chronic motor and vocal tics. Habit reversal therapy (HR) is a behavioral treatment for tics which has received recent empirical support. The present study compared the efficacy of HRT in reducing tics, improving life-satisfaction and psychosocial functioning in comparison with supportive psychotherapy (SP) in outpatients with TS. In addition, we investigated whether impairments in response inhibition in patients with TS predict response to HR treatment which specifically aims to inhibit tics. Thirty adult outpatients with DSM-IV TS were randomized to 14 individual sessions of HR (n ¼ 15); or SP (n ¼ 15). HR but not SP reduced tic severity over the course of the treatment. Both groups improved in life-satisfaction and psychosocial functioning during active treatment. Reductions in tic severity (HR) and improvements in life-satisfaction and psychosocial functioning (HR and SP) remained stable at the 6-month follow-up. The extent of pre-treatment response inhibition impairment in the HR group predicted reductions in tic-severity from pre- to post-treatment. Our results suggest that HR has specific tic-reducing effects although SP is effective in improving life-satisfaction and psychosocial functioning. Assessments of response inhibition may be of value for predicting treatment response to HR. r 2005 Elsevier Ltd. All rights reserved. Keywords: Tourette’s disorder; Tics; Habit reversal; Treatment outcome; Predictors of treatment response Introduction Tourette’s disorder, also called Tourette syndrome (TS), is characterized by both motor and vocal tics that often interfere substantially with social or occupational functioning (APA, 1994) and frequently result in embarrassment, as well as low rates of self-esteem and life-satisfaction (e.g. Horn, 2001; Riddle & Carlson, 2001). Tics are recurrent, non-rhythmic, stereotyped motor movements or vocalizations that typically involve the head, torso and upper and lower limbs (APA, 1994). Common motor tics include eye blinking, touching, ARTICLE IN PRESS www.elsevier.com/locate/brat 0005-7967/$ - see front matter r 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.brat.2005.08.007 Corresponding author. +1 617 724 6300x1340183; fax: +1 617 726 4078. E-mail address: [email protected] (T. Deckersbach).
-
Upload
massgeneral -
Category
Documents
-
view
0 -
download
0
Transcript of Habit reversal versus supportive psychotherapy in Tourette's disorder: A randomized controlled trial...
ARTICLE IN PRESS
0005-7967/$ - se
doi:10.1016/j.br
�CorrespondE-mail addr
Behaviour Research and Therapy 44 (2006) 1079–1090
www.elsevier.com/locate/brat
Habit reversal versus supportive psychotherapy in Tourette’sdisorder: A randomized controlled trial and predictors of
treatment response
Thilo Deckersbach�, Scott Rauch, Ulrike Buhlmann, Sabine Wilhelm
OCD Clinic/Psychiatric Neuroscience Division, Department of Psychiatry, 149-2611, Massachusetts General Hospital,
Bldg. 149, 13th St. Charlestown, MA 02129, USA
Received 7 March 2005; received in revised form 4 August 2005; accepted 15 August 2005
Abstract
Tourette syndrome (TS) is characterized by chronic motor and vocal tics. Habit reversal therapy (HR) is a behavioral
treatment for tics which has received recent empirical support. The present study compared the efficacy of HRT in
reducing tics, improving life-satisfaction and psychosocial functioning in comparison with supportive psychotherapy (SP)
in outpatients with TS. In addition, we investigated whether impairments in response inhibition in patients with TS predict
response to HR treatment which specifically aims to inhibit tics. Thirty adult outpatients with DSM-IV TS were
randomized to 14 individual sessions of HR (n ¼ 15); or SP (n ¼ 15). HR but not SP reduced tic severity over the course of
the treatment. Both groups improved in life-satisfaction and psychosocial functioning during active treatment. Reductions
in tic severity (HR) and improvements in life-satisfaction and psychosocial functioning (HR and SP) remained stable at the
6-month follow-up. The extent of pre-treatment response inhibition impairment in the HR group predicted reductions in
tic-severity from pre- to post-treatment. Our results suggest that HR has specific tic-reducing effects although SP is
effective in improving life-satisfaction and psychosocial functioning. Assessments of response inhibition may be of value
for predicting treatment response to HR.
r 2005 Elsevier Ltd. All rights reserved.
Keywords: Tourette’s disorder; Tics; Habit reversal; Treatment outcome; Predictors of treatment response
Introduction
Tourette’s disorder, also called Tourette syndrome (TS), is characterized by both motor and vocal tics thatoften interfere substantially with social or occupational functioning (APA, 1994) and frequently result inembarrassment, as well as low rates of self-esteem and life-satisfaction (e.g. Horn, 2001; Riddle & Carlson,2001). Tics are recurrent, non-rhythmic, stereotyped motor movements or vocalizations that typically involvethe head, torso and upper and lower limbs (APA, 1994). Common motor tics include eye blinking, touching,
e front matter r 2005 Elsevier Ltd. All rights reserved.
at.2005.08.007
ing author. +1 617 724 6300x1340183; fax: +1 617 726 4078.
ess: [email protected] (T. Deckersbach).
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–10901080
squatting or knee bends. Vocal tics often include uttering sounds or words such as grunts, yelps, sniffs, orthroat clearing (Leckman, Peterson, King, Scahill, & Cohen, 2001).
To date, pharmacotherapy has been considered the treatment of choice for TS. Its efficacy has beendemonstrated in placebo-controlled trials (Leckman et al., 1991; Sallee, Nesbitt, Jackson, Sine, & Sethuraman,1997; Scahill, Leckman, Schultz, Katsovich, & Peterson, 2003; Shapiro et al., 1989). This includes randomizedtrials documenting the efficacy of haloperidol, pimozide, risperidone and clonidine (Leckman et al., 1991;Sallee et al., 1997; Scahill et al., 2003; Shapiro et al., 1989). However, many patients refuse or discontinuemedication because of unwanted side effects; others are unresponsive to medication or suffer from residual ticsdespite pharmacotherapy. As a result, a behavioral treatment called habit reversal is becoming increasinglypopular as a non-pharmacologic treatment alternative or adjunct to pharmacological treatments. Briefly, inHR patients learn to apply antagonistic, competing movements to inhibit the occurrence of tics. Althoughdeveloped over 30 years ago (Azrin & Nunn, 1973), it’s effectiveness has mostly been tested in studies usingsingle-subject designs. To our knowledge, to date, there are only four randomized controlled trials that haveinvestigated the effectiveness of HR in a controlled fashion. Using a waitlist-control design, Azrin andPeterson (1990) reported a 93% tic reduction in a group of patients treated with HR compared with noimprovement of patients on a waiting list. O’Connor et al. (2001), who also used a waitlist-control design,found significant reductions in tic-frequency and intensity compared to waitlist in 47 patients with chronic ticdisorder following a treatment that included HR. Wilhelm et al. (2003) conducted a randomized controlledtrial comparing the effectiveness of HR with supportive psychotherapy (SP) in patients with TS. They foundthat HR but not SP significantly reduced tic severity following 14 individual sessions of HR. Follow-up dataindicated that patients remained significantly improved at the 10-month follow-up. Recently, Verdellen,Keijsers, Cath, and Hoogduin (2004) compared the effectiveness of 10-session individual HR to exposure andresponse prevention therapy in patients with TS. They found that both HR and exposure treatment areeffective in reducing tic severity.
Individuals with TS often report that tics cause marked embarrassment and are associated with low self-esteem and decreased life-satisfaction. To date, behavioral treatments of TS have exclusively focused on tic-reducing effects while improvements in psychosocial functioning and life-satisfactions have not been assessed.Although supportive psychotherapy may not have tic-reducing effects, it is conceivable to hypothesize that atreatment that is aimed at providing support for coping with TS may improve self-esteem and psychosocialfunctioning despite persisting occurrence of tics. The present study was in part designed to test this hypothesisby comparing the effectiveness of HR and SP on separate measures of tic frequency, psychosocial functioning,and life-satisfaction in individuals with TS.
From a neurobiological perspective, tics are believed to be a result of dysregulation of cortical-subcorticalcircuits (Mink, 2001; Graybiel & Canales, 2001). More specifically, tics are presumably due to failed inhibitionwithin cortico-striato-thalamo-cortical circuits. Consistent with this view, there is converging evidence fromneuropsychological studies that individuals with TS exhibit impairments in response inhibition (e.g., Johanneset al., 2001, 2003; Swerdlow, Magulac, Filion, & Zinner, 1996). For example, Swerdlow et al. (1996) used avisuospatial priming paradigm to investigate inhibitory and facilitatory effects of a pre-signal (prime) onsubsequent reaction times to a probe. They found that, in comparison to healthy control participants,individuals with TS were characterized by reduced inhibitory effects in relation to increased facilitatorypriming effects. Similarly, Johannes et al. (2001, 2003) reported that responses to the interference condition ofthe Stroop paradigm and a Go-NoGo paradigm were associated with enhanced frontal negativity as assessedby EEG in individuals with TS compared to healthy controls. Although the exact nature of the link betweenimpairments in response inhibition and tics in individuals with TS remains to be elucidated, we hypothesizedthat impairments in response inhibition may be a predictor of response to HR which specifically teachesparticipants to withhold (or inhibit) tics via competing responses. More specifically, we hypothesized thatindividuals with greater impairment in response inhibition (or facilitation) in a visuospatial priming paradigmwould exhibit a less favorable response to HR treatment.
In summary, the purpose of the study was threefold: (1) To replicate our previous findings (Wilhelm et al.,2003) of tic-reducing effects of HR compared to SP in a randomized controlled trial; (2) to extend our previoustrial by investigating the impact of HR and SP on psychosocial functioning and life-satisfaction and (3) toinvestigate performance on a visuospatial priming task as a predictor of tic-reduction following HR.

ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–1090 1081
Method
Patients
Study participants were 35 individuals who met DSM-IV criteria for TS (13 females). TS participants wererecruited through the OCD Clinic at the Massachusetts General Hospital (MGH). All participants providedwritten informed consent prior to participation. Exclusion criteria for TS patients were psychotic disorder,substance abuse or dependence, organic mental disorder, suicidal and/or severe major depression, verbal IQbelow 80 and the presence of a neurologic condition other than TS. Patients who took psychotropicmedications for tics were included in the trial if the present dosage of all psychotropic medications had beenstable for at least three months, and if patients agreed to no dose or medication change and no new medicationduring the study. Diagnoses of TS patients were determined by the first author using the Structured ClinicalInterview for DSM-IV (First, Spitzer, Gibbon, & Williams, 1995) which included a TS DSM-IV module. Atotal of 28 patients completed the study (HR: n ¼ 13, 6 females; SP: n ¼ 15, 7 females). Three patientswithdrew from the study after completing the screening visit and before randomization due to concerns abouttime related to traveling to the treatment visits. Two patients (HR, n ¼ 1, SP, n ¼ 1) withdrew/dropped fromthe study after session 2 (SP) and 3 (HR) respectively. Both patients dropped from the study due to concernsabout the time investment associated with the study. Two patients (HR, n ¼ 2, both males) dropped out aftersession 8 and 10, respectively, after substantial reduction of tic severity.
All patients but one were medically healthy by self-report. One patient was treated with athenolol forhypertension at the time of the study. The mean age of the patient sample was 35.1 years (SD ¼ 12.2; HR:M ¼ 36.6, SD ¼ 13.0; SP: M ¼ 33.6, SD ¼ 11.6). Mean age at onset was 7.5 years (SD ¼ 3.2; HR: M ¼ 7.7;SD ¼ 3.5; SP: M ¼ 7.2, SD ¼ 2.9). Patients had a mean of 14.9 years of education (SD ¼ 2.63; HR:M ¼ 14.7; SD ¼ 2.5; SP: M ¼ 15.2, SD ¼ 2.8) and a mean verbal IQ of 110.7 (SD ¼ 12.5; HR: M ¼ 109.4;SD ¼ 12.0; SP: M ¼ 112.0, SD ¼ 13.2). Sixteen patients were taking medication to reduce tics (HR: n ¼ 7, SP:n ¼ 9). These included antipsychotics (n ¼ 4, risperidone n ¼ 3, haldoperidol, n ¼ 1), clonidine (n ¼ 6) orselective serotonin reuptake inhibitors (SSRI; n ¼ 6). All non-medicated patients had taken TS medications inthe past but had discontinued medications either due to lack of effect on tics or intolerable side effects. Forthese patients, past TS medication trials included antipsychotics, clonidine and SSRIs. Fifteen of the 28patients who completed the study had comorbid DSM-IV disorders in addition to TS (HR ¼ 7; SP ¼ 8). Thisincluded mild major depression (HR: n ¼ 2, SP: n ¼ 1), OCD (HR: n ¼ 4, SP: n ¼ 5), social phobia HR:n ¼ 1, SP: n ¼ 1), and panic disorder (SP: n ¼ 1). The two patients in the HR group who dropped out aftersession 8 were comorbidity-free. HR and SP patients did not differ in their age of onset (F ð1:28Þ ¼ 0:21,p ¼ 0:65), the number of nonmedicated patients (w2ð1Þ ¼ 0:54, p ¼ 0:46) and the number of comorbidity-freepatients (w2ð1Þ ¼ 0:13, p ¼ 0:72).
Controls
To investigate the degree of response inhibition impairment in TS patients (see Measurements, Visuospatialpriming task), a group of 20 normal control participants (‘‘non-TS control participants’’, 8 females) wasrecruited through bulletin board notices at MGH. All non-TS control participants were medically healthy, hadno current or past Axis I disorder (as confirmed by SCID) and had no history of significant head injury,seizure, neurologic condition, or current major medical condition by report. All non-TS controls wereunrelated to TS patients. Non-TS control participants had a mean age of 34.3 years (SD ¼ 8.8), a mean yearsof education of 14.5 years (SD ¼ 2.7) and a mean verbal IQ of 110.5 (SD ¼ 10.6). HR and SP patients andcontrol participants did not differ with regard to age (F ð2:47Þ ¼ 0:31, p ¼ 0:73), sex (w2ð1Þ ¼ 0:19, p ¼ 0:91),years of education (F ð2:47Þ ¼ 0:30, p ¼ 0:74) or estimated verbal IQ (F ð2:47Þ ¼ 0:19; p ¼ 0:82).
Procedure
Following the screening visit (SCID, inclusion/exclusion criteria), patients completed a pre-treatmentassessment which included measures of TS severity, severity of depression, obsessive-compulsive and attention
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–10901082
deficit hyperactivity symptoms, as well as measures of psychosocial functioning and verbal IQ (seeMeasurements). In addition, at the pre-treatment assessment visit, all patients completed the VisuospatialPriming task (VSP) as a measure of response inhibition and predictor of treatment response. Patients wererandomized to 14 individual sessions of either HR or SP. Patients also completed a mid-treatment clinicalassessment (session 8), a post-treatment clinical assessment at the end of treatment (after session 14) and a6-month follow-up assessment using a subset of clinical scales and questionnaires administered at the pre-treatment assessment. Twenty-three (HR: n ¼ 11; SP: n ¼ 12) of the 28 treatment completers also completedthe 6-month follow-up assessment. None of the patients who withdrew or dropped out before the end oftreatment returned for the follow-up assessment. Patients who dropped out of treatment before session 3 andpatients who did not return to the follow-up did not differ from patients who completed the study in terms ofdemographic measures and tic-severity (all p40.35). Patients in the SP group who did not respond totreatment were offered HRT free of charge. All patients were treated and assessed in the OCD Clinic at MGHby the first author (a doctoral level clinician with extensive experience in clinical assessments of TS as well astreatment with HR and SP; Wilhelm et al., 2003). Non-TS control participants completed the VSP task andmeasures for estimating verbal IQ as part of a single visit.
Treatments
For patients, both treatment conditions consisted of 14 individual 50min treatment sessions conducted overfive months. For the first two months, treatment sessions were held weekly (session 1–8) followed by bi-weeklysessions for the next two months (sessions 9–12). To prevent relapse, active treatment was then tapered overthe next two months with two visits spaced apart over four weeks (sessions 13 and 14).
HR consisted of a manualized treatment for tics (based on the strategies described in Azrin & Nunn, 1973;Azrin & Peterson, 1990; Wilhelm et al., 2003). HR consisted of (1) self-monitoring, (2) competing responses,(3) relaxation training and (4) contingency management. Self-monitoring was conducted to increase patient’sawareness of the early sensations or urges preceding tics and to obtain detailed descriptions of the physicaltopography of tics. Patients were provided with charts in which they recorded the occurrence of tics, precedingsensations/urges and the muscles and movements involved in a tic. Competing response training involveddesign and implementation of movements/behaviors that were incompatible with tics, thereby preventing theiroccurrence. Patients were trained to implement competing responses contingent on early sensations/urgespreceding a tic or (if preceding sensations/urges could not be identified) after the first occurrence of the tic. Forcomplex tics or tics occurring in sequences or bouts, competing responses for individual components weredeveloped first (shaped) and then chained. In addition, patients were also trained in diaphragmatic breathingand relaxation techniques and learned to set goals for tic reduction and to positively reinforce themselves.Patients practiced self-monitoring, competing responses, breathing and relaxation techniques in sessions andat home in-between sessions. Treatment would typically start with the most bothersome tic(s) unless thepatient and clinician determined that competing responses for a less bothersome tic would be easier toimplement before moving on to a more bothersome/severe/complex tic.
SP involved treatment components that are commonly used in this treatment modality for patients with avariety of psychiatric or chronic medical problems (Pinsker, Pinsker & Rosenthal, 1988). The goal of SP wasto improve self-esteem, life-satisfaction and psychosocial functioning (related and unrelated to tics) byreducing distress and increasing patients’ coping skills (Pinsker, 1997; Novalis, Rojcewicz, & Peele, 1993).Treatment components included encouragement, reassurance, reframing (to change the patient’s perspective),clarification, ventilation (allowing the patient to express intense feelings), as well as the modeling ofappropriate, mature behavior, absolution (i.e., normalizing minor inadequacies to eliminate guilt) and advicegiving (Pinsker, 1997; Novalis et al., 1993). No HR techniques for reducing tics were used in the SP treatmentcondition.
Measurements
Clinical scales and self-report questionnaires completed by patients at pre-treatment, mid-treatment, post-treatment and at the 6-month follow-up included the Yale Global Tic Severity Scale (YGTSS; Leckman et al.,
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–1090 1083
1989), the Clinical Global Impression-Improvement (CGI-I; Guy, 1976), the Beck Depression Inventory (BDI;Beck & Steer, 1987), the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS; Goodman et al., 1989); and theADHD symptom checklist (Barkley, 1990; DuPaul, 1990). Psychosocial functioning and life-satisfaction wereassessed with the Sheehan Disability Inventory (Leon, Shear, Portera, & Klerman, 1992) and the SchwartzOutcome Scale (SOS-10; Blais et al., 1999). In addition, all participants completed the Visuospatial priming(VSP; Swerdlow et al., 1996) task as a measure of response inhibition. Verbal IQ was estimated using thesubtests information, vocabulary and similarities from the Wechsler Adult Intelligence Scale-Revised(Wechsler, 1981).
Tic-severity. The primary outcome measure of the study was the YGTSS. The YGTSS is a well-establishedsemi-structured clinical rating scale with good convergent and discriminant validity and interrater reliability(Leckman et al., 1989; Walkup, Rosenberg, Brown, & Singer, 1992). For the week preceding the interview,information on tic severity is acquired for motor and vocal tics. The number, frequency, intensity, complexityand interference of all motor and vocal tics (as a group) is rated from 0 to 5 with higher scores indicating moretics, higher frequency, etc. These ratings are then summed up to the Total Tic Score which reflects tic severity(0 ¼ no tics; 50 ¼ most severe tics). In addition, improvement in tic-severity is rated using the CGI-I whichcompares current severity to baseline (Conners & Barkley, 1985; Guy, 1976). A score of 1or 2 corresponds tovery much improved and much improved, respectively; a score of 3 indicates minimal change and a score of 4reflects no change. The rating of the CGI-I was made based on changes in tic-severity. All clinical ratings(YGTSS and CGI-I) were conducted by the first author (T.D.). A rating of much improved or very muchimproved was regarded as a positive response ( ¼ responder).
Psychosocial functioning. It was assessed using the Sheehan disability inventory (Leon et al., 1992). This4-item self-report scale measures work, social and family disability on 10-point scales. The overall work andsocial disability is then integrated in a single 5 point scale rating ranging from no symptoms (1) to symptomsradically change or prevent normal work or social life (5) with intermediate steps indicating markedinterference (4), minor interference (3) or no interference despite presence of symptoms (2).
Life satisfaction. It was assessed using the Schwartz outcome scale (SOS-10; Blais et al., 1999). It consists of10 items assessing general life satisfaction (e.g. ‘‘I am generally satisfied with my psychological health’’). Eachitem is rated on a 6-point rating scale from ‘‘never’’ (0) to ‘‘all the time or nearly all the time’’ (6) resulting in apossible range of scores between 0 and 60.
Visuospatial priming (VSP) task. The VSP task (Swerdlow et al., 1996) assesses facilitatory and inhibitoryeffects of a visual pre-signal (priming) on the speed of reaction to a target cue displayed on a computer screen.That is, if the priming directs the attention towards the location of the target cue, the reaction is typicallyfacilitated (i.e. becomes faster; facilitatory priming). If the priming directs the attention away from the locationof the target cue, the reaction is inhibited (i.e. becomes slower; inhibitory priming).
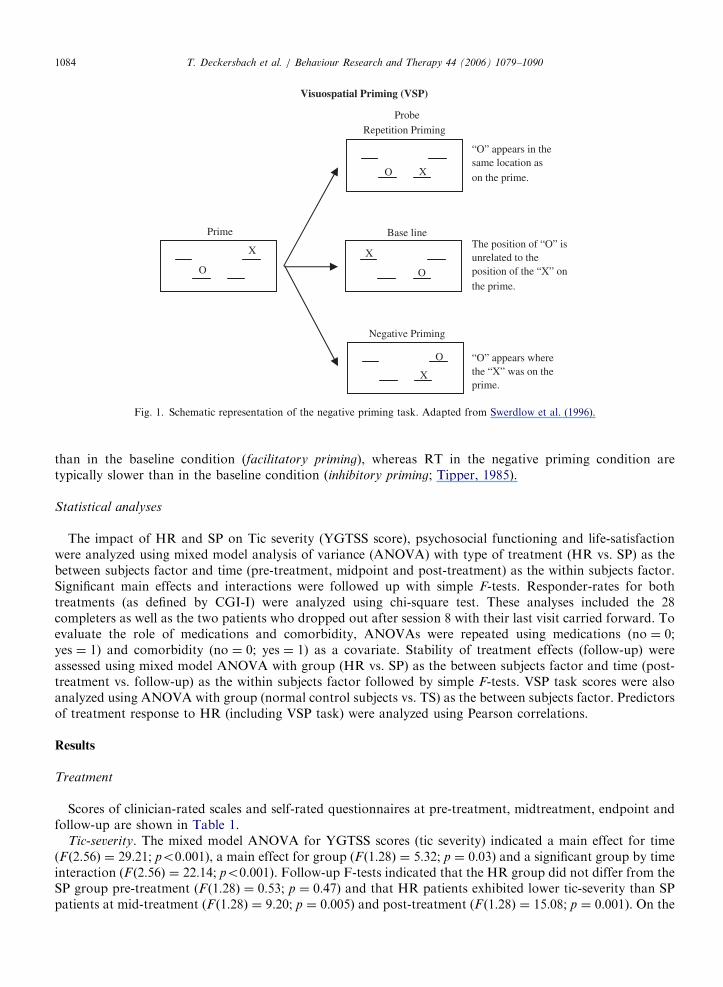
In the VSP task, each trial consists of a probe and a prime (see Fig. 1). The probe entails the simultaneouspresentation of two visual cues (O and X) at four possible spatial locations on a computer screen (see Fig. 1).Subjects are instructed to respond as quickly and accurately as possible to the target cue (O) by pressing one offour keys that correspond to the four possible locations on the screen while ignoring the distractor cue (X).Each probe is preceded by a visual prime. The prime also involves the simultaneous presentation of boththe target cue (O) and the distractor stimulus (X) in the array of the four possible locations on the screen(see Fig. 1).
There are three potential relationships between the prime and the probe in each trial (see Fig. 1): (1) In thebaseline condition, the positions of the target and distractor letters in the probe are unrelated to their positionsin the prime. In the positive (repetition) priming condition, the position of the target remains the same in primeand probe. In the negative priming condition, the target in the probe appears in the location where thedistractor was in the prime. Hence, to respond correctly to the location of the target in the probe, a participantmust attend to a spatial location that he or she has just ignored.
The two main dependent measures in the VSP paradigm are (a) facilitatory priming reaction time: thedifference between the baseline reaction time and the reaction time (RT) to probe targets in the repetitionpriming condition (base RT minus repetition RT), and (b) inhibitory priming reaction time: the differencebetween the baseline RT and the RT to probe targets in the negative priming condition (negative priming RTminus base RT). For healthy individuals, RT to the probe target in the repetition condition are typically faster
ARTICLE IN PRESS
Visuospatial Priming (VSP)
Base line
X
O
The position of “O” isunrelated to theposition of the “X” on the prime.
ProbeRepetition Priming
X O
“O” appears in the same location ason the prime.
Negative Priming
X
O “O” appears wherethe “X” was on theprime.
X
O
Prime
Fig. 1. Schematic representation of the negative priming task. Adapted from Swerdlow et al. (1996).
T. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–10901084
than in the baseline condition (facilitatory priming), whereas RT in the negative priming condition aretypically slower than in the baseline condition (inhibitory priming; Tipper, 1985).
Statistical analyses
The impact of HR and SP on Tic severity (YGTSS score), psychosocial functioning and life-satisfactionwere analyzed using mixed model analysis of variance (ANOVA) with type of treatment (HR vs. SP) as thebetween subjects factor and time (pre-treatment, midpoint and post-treatment) as the within subjects factor.Significant main effects and interactions were followed up with simple F-tests. Responder-rates for bothtreatments (as defined by CGI-I) were analyzed using chi-square test. These analyses included the 28completers as well as the two patients who dropped out after session 8 with their last visit carried forward. Toevaluate the role of medications and comorbidity, ANOVAs were repeated using medications (no ¼ 0;yes ¼ 1) and comorbidity (no ¼ 0; yes ¼ 1) as a covariate. Stability of treatment effects (follow-up) wereassessed using mixed model ANOVA with group (HR vs. SP) as the between subjects factor and time (post-treatment vs. follow-up) as the within subjects factor followed by simple F-tests. VSP task scores were alsoanalyzed using ANOVA with group (normal control subjects vs. TS) as the between subjects factor. Predictorsof treatment response to HR (including VSP task) were analyzed using Pearson correlations.
Results
Treatment
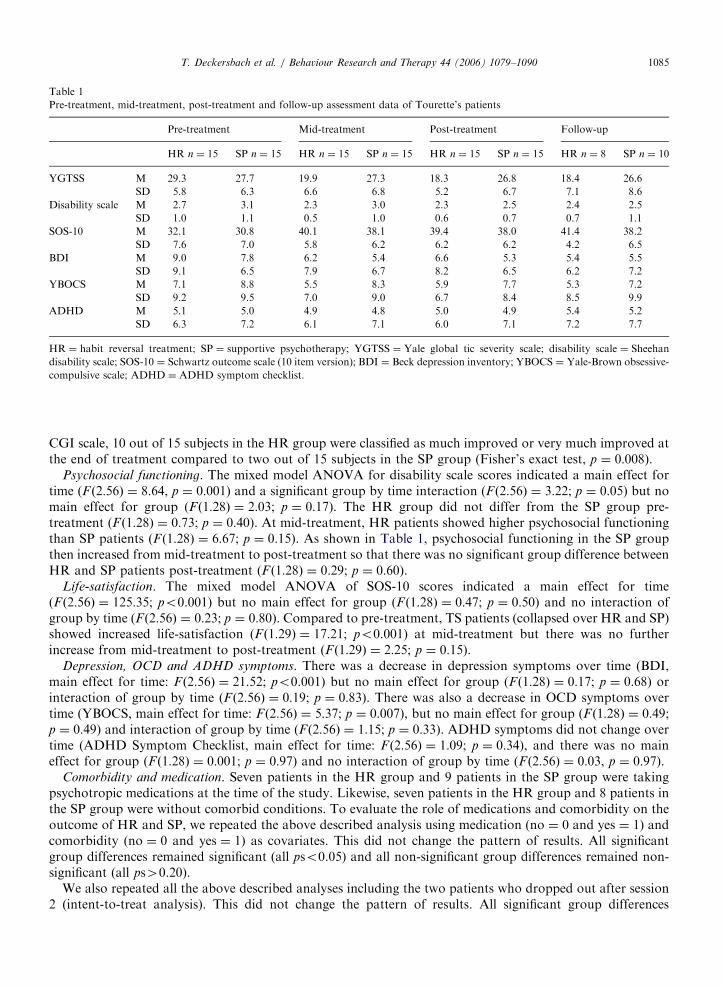
Scores of clinician-rated scales and self-rated questionnaires at pre-treatment, midtreatment, endpoint andfollow-up are shown in Table 1.
Tic-severity. The mixed model ANOVA for YGTSS scores (tic severity) indicated a main effect for time(F ð2:56Þ ¼ 29:21; po0.001), a main effect for group (F ð1:28Þ ¼ 5:32; p ¼ 0:03) and a significant group by timeinteraction (F ð2:56Þ ¼ 22:14; po0.001). Follow-up F-tests indicated that the HR group did not differ from theSP group pre-treatment (F ð1:28Þ ¼ 0:53; p ¼ 0:47) and that HR patients exhibited lower tic-severity than SPpatients at mid-treatment (F ð1:28Þ ¼ 9:20; p ¼ 0:005) and post-treatment (F ð1:28Þ ¼ 15:08; p ¼ 0:001). On the
ARTICLE IN PRESS
Table 1
Pre-treatment, mid-treatment, post-treatment and follow-up assessment data of Tourette’s patients
Pre-treatment Mid-treatment Post-treatment Follow-up
HR n ¼ 15 SP n ¼ 15 HR n ¼ 15 SP n ¼ 15 HR n ¼ 15 SP n ¼ 15 HR n ¼ 8 SP n ¼ 10
YGTSS M 29.3 27.7 19.9 27.3 18.3 26.8 18.4 26.6
SD 5.8 6.3 6.6 6.8 5.2 6.7 7.1 8.6
Disability scale M 2.7 3.1 2.3 3.0 2.3 2.5 2.4 2.5
SD 1.0 1.1 0.5 1.0 0.6 0.7 0.7 1.1
SOS-10 M 32.1 30.8 40.1 38.1 39.4 38.0 41.4 38.2
SD 7.6 7.0 5.8 6.2 6.2 6.2 4.2 6.5
BDI M 9.0 7.8 6.2 5.4 6.6 5.3 5.4 5.5
SD 9.1 6.5 7.9 6.7 8.2 6.5 6.2 7.2
YBOCS M 7.1 8.8 5.5 8.3 5.9 7.7 5.3 7.2
SD 9.2 9.5 7.0 9.0 6.7 8.4 8.5 9.9
ADHD M 5.1 5.0 4.9 4.8 5.0 4.9 5.4 5.2
SD 6.3 7.2 6.1 7.1 6.0 7.1 7.2 7.7
HR ¼ habit reversal treatment; SP ¼ supportive psychotherapy; YGTSS ¼ Yale global tic severity scale; disability scale ¼ Sheehan
disability scale; SOS-10 ¼ Schwartz outcome scale (10 item version); BDI ¼ Beck depression inventory; YBOCS ¼ Yale-Brown obsessive-
compulsive scale; ADHD ¼ ADHD symptom checklist.
T. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–1090 1085
CGI scale, 10 out of 15 subjects in the HR group were classified as much improved or very much improved atthe end of treatment compared to two out of 15 subjects in the SP group (Fisher’s exact test, p ¼ 0:008).
Psychosocial functioning. The mixed model ANOVA for disability scale scores indicated a main effect fortime (F ð2:56Þ ¼ 8:64, p ¼ 0:001) and a significant group by time interaction (F ð2:56Þ ¼ 3:22; p ¼ 0:05) but nomain effect for group (F ð1:28Þ ¼ 2:03; p ¼ 0:17). The HR group did not differ from the SP group pre-treatment (F ð1:28Þ ¼ 0:73; p ¼ 0:40). At mid-treatment, HR patients showed higher psychosocial functioningthan SP patients (F ð1:28Þ ¼ 6:67; p ¼ 0:15). As shown in Table 1, psychosocial functioning in the SP groupthen increased from mid-treatment to post-treatment so that there was no significant group difference betweenHR and SP patients post-treatment (F ð1:28Þ ¼ 0:29; p ¼ 0:60).
Life-satisfaction. The mixed model ANOVA of SOS-10 scores indicated a main effect for time(F ð2:56Þ ¼ 125:35; po0.001) but no main effect for group (F ð1:28Þ ¼ 0:47; p ¼ 0:50) and no interaction ofgroup by time (F ð2:56Þ ¼ 0:23; p ¼ 0:80). Compared to pre-treatment, TS patients (collapsed over HR and SP)showed increased life-satisfaction (F ð1:29Þ ¼ 17:21; po0.001) at mid-treatment but there was no furtherincrease from mid-treatment to post-treatment (F ð1:29Þ ¼ 2:25; p ¼ 0:15).
Depression, OCD and ADHD symptoms. There was a decrease in depression symptoms over time (BDI,main effect for time: F ð2:56Þ ¼ 21:52; po0.001) but no main effect for group (F ð1:28Þ ¼ 0:17; p ¼ 0:68) orinteraction of group by time (F ð2:56Þ ¼ 0:19; p ¼ 0:83). There was also a decrease in OCD symptoms overtime (YBOCS, main effect for time: F ð2:56Þ ¼ 5:37; p ¼ 0:007), but no main effect for group (F ð1:28Þ ¼ 0:49;p ¼ 0:49) and interaction of group by time (F ð2:56Þ ¼ 1:15; p ¼ 0:33). ADHD symptoms did not change overtime (ADHD Symptom Checklist, main effect for time: F ð2:56Þ ¼ 1:09; p ¼ 0:34), and there was no maineffect for group (F ð1:28Þ ¼ 0:001; p ¼ 0:97) and no interaction of group by time (F ð2:56Þ ¼ 0:03, p ¼ 0:97).
Comorbidity and medication. Seven patients in the HR group and 9 patients in the SP group were takingpsychotropic medications at the time of the study. Likewise, seven patients in the HR group and 8 patients inthe SP group were without comorbid conditions. To evaluate the role of medications and comorbidity on theoutcome of HR and SP, we repeated the above described analysis using medication (no ¼ 0 and yes ¼ 1) andcomorbidity (no ¼ 0 and yes ¼ 1) as covariates. This did not change the pattern of results. All significantgroup differences remained significant (all pso0.05) and all non-significant group differences remained non-significant (all ps40.20).
We also repeated all the above described analyses including the two patients who dropped out after session2 (intent-to-treat analysis). This did not change the pattern of results. All significant group differences
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–10901086
remained significant (all pso0.05) and all non-significant group differences remained non-significant (allps40.16).
Follow-up
Twenty-three patients could be reached for the follow-up assessment 6 months after the last treatmentsession (n ¼ 11 of the completers in the HR group and n ¼ 12 of the completers in the SP group). Five patientshad received psychological treatment after the endpoint of the study. One patient in the HR group (aresponder according to the CGI-I) continued clinically with HR. Two patients in the HR group reportedhaving received supportive-type psychological treatment in between endpoint and 6 month follow-up. Twopatients in the SP group had been treated clinically with HR. HR and SP patients who had receivedpsychological treatment after the endpoint of the study (n ¼ 5) were excluded from the following analyses.
Tic-severity. A mixed model ANOVA for YGTSS scores indicated a main effect for group (HR vs. SP;F ð1:16Þ ¼ 5:71; p ¼ 0:03) but no main effect for time (post-treatment vs. follow-up; F ð1:16Þ ¼ 0:23; p ¼ 0:68)or interaction of group by time (F ð1:16Þ ¼ 0:02; p ¼ 0:88). As shown in Table 1, HR patients continued toshow lower tic severity at the 6-month follow-up compared to the SP group. On the CGI-I, six patients in theHR group and one patient in the SP group were classified as responders at the follow-up (Fisher’s exact test:p ¼ 0:002). The responder in the SP group had received HR in the 6-month follow-up period. All 6 patientswho were classified as responders in the HR condition had responded to treatment at the end of activetreatment.
Psychosocial functioning. The mixed model ANOVA for disability scale scores indicated no main effect fortime (post-treatment vs. follow-up; F ð1:16Þ ¼ 0:31; p ¼ 0:59), no main effect for group (F ð1:16Þ ¼ 0:25;p ¼ 0:63), and no group by time interaction (F ð1:16Þ ¼ 0:03; p ¼ 0:86). As shown in Table 1, both groupsremained improved in psychosocial functioning at the 6-month follow-up.
Life-satisfaction. The mixed model ANOVA of SOS-10 scores indicated no main effect for group(F ð1:16Þ ¼ 1:28; p ¼ 0:29), no main effect for time (post-treatment vs. follow-up; F ð1:16Þ ¼ 1:23; p ¼ 0:28) andno interaction of group by time (F ð1:16Þ ¼ 0:02; p ¼ 0:88). As shown in Table 2, both patient groups remainedimproved in life-satisfaction at the 6-month follow-up.
Depression, OCD and ADHD symptoms. There was no change in depression symptoms between post-treatment and follow-up (BDI; main effect for time: F ð1:16Þ ¼ 0:04; p ¼ 0:85), no main effect for group(F ð1:16Þ ¼ 0:01; p ¼ 0:92) and no interaction of group by time (F ð1:16Þ ¼ 0:14; p ¼ 0:72. There as also nochange in OCD symptoms (YBOCS, main effect for time: F ð1:16Þ ¼ 0:01; p ¼ 0:92), and no main effect forgroup (F ð1:16Þ ¼ 0:07; p ¼ 0:80) and no interaction of group by time (F ð1:16Þ ¼ 0:94; p ¼ 0:35). Likewise,there was no change in ADHD symptoms between post-treatment and follow-up (Symptom Checklist, maineffect for time: F ð1:16Þ ¼ 0:13; p ¼ 0:73), and no main effect for group (F(1,16) ¼ .11; p ¼ .75) and nointeraction of group by time (F ð1:16Þ ¼ 0:57; p ¼ 0:46).
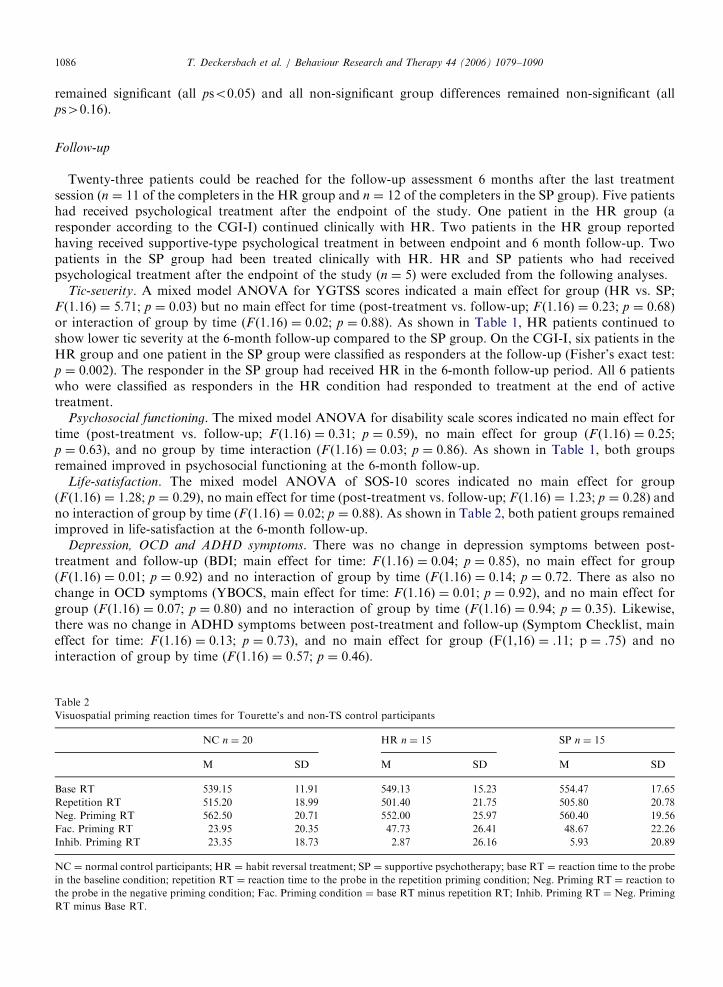
Table 2
Visuospatial priming reaction times for Tourette’s and non-TS control participants
NC n ¼ 20 HR n ¼ 15 SP n ¼ 15
M SD M SD M SD
Base RT 539.15 11.91 549.13 15.23 554.47 17.65
Repetition RT 515.20 18.99 501.40 21.75 505.80 20.78
Neg. Priming RT 562.50 20.71 552.00 25.97 560.40 19.56
Fac. Priming RT 23.95 20.35 47.73 26.41 48.67 22.26
Inhib. Priming RT 23.35 18.73 2.87 26.16 5.93 20.89
NC ¼ normal control participants; HR ¼ habit reversal treatment; SP ¼ supportive psychotherapy; base RT ¼ reaction time to the probe
in the baseline condition; repetition RT ¼ reaction time to the probe in the repetition priming condition; Neg. Priming RT ¼ reaction to
the probe in the negative priming condition; Fac. Priming condition ¼ base RT minus repetition RT; Inhib. Priming RT ¼ Neg. Priming
RT minus Base RT.
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–1090 1087
The above described analyses were repeated using medication (no ¼ 0 and yes ¼ 1) and comorbidity(no ¼ 0 and yes ¼ 1) as covariates. All significant group differences remained significant (po0.05), all non-significant group differences remained non-significant (all ps40.26).
Predictors of treatment response
Tic-severity, age of onset. To explore predictors of treatment response, we correlated pre-treatment ticseverity (YGTSS scores) and age of onset with response to treatment (drop in YGTSS tic severity scores frompre to post treatment) in the HR group. There was no significant correlation between pre-treatment YGTSStic-severity and drop in YGTSS tic severity from pre-to post treatment (r ¼ 0:17, p ¼ 0:55). Age of onset wasnot significantly correlated with drop in YGTSS tic severity from pre- to post-treatment (r ¼ 0:15, p ¼ 0:60).
Visuospatial priming. All TS patients and control participants completed the VSP task. Mean reaction timesin the VSP task for HR, SP and non-TS control participants are shown in Table 2.
To explore whether TS patients were impaired in the VSP task, VSP facilitation and inhibitory prime RTwere entered into an analysis of variance with group (TS [collapsed over HR and SP] and non-TS controls) asthe between subjects factor and baseline RT as a covariate. TS participants showed more facilitatory priming(i.e. faster RT to repetition primes compared to baseline) compared to non-TS control participants(F ð2:47Þ ¼ 5:65; p ¼ 0:02). TS participants also showed less inhibitory priming (i.e. less slowing of RT innegative priming trials compared to baseline) than non-TS control participants (F ð1:47Þ ¼ 4:13; p ¼ 0:05; seeTable 2). Compared to non-TS controls, both TS groups had comparable effect sizes for facilitation primingRT (HR: Cohen’s d ¼ 1.02; SP: Cohen’s d ¼ 1:16) and inhibitory priming RT (HR: Cohen’s d ¼ 0:91, SP:Cohen’s d ¼ 0:88). In the HR group, there was no significant correlation between facilitatory priming RT andYGTSS pre-treatment tic severity (r ¼ �0:11, p ¼ 0:70). There was a small but non-significant negativecorrelation between inhibitory priming RT and pre-treatment YGTSS tic-severity scores (r ¼ �0:26,p ¼ 0:35). On the other hand, facilitatory priming RT were negatively correlated with the observed decreasein YGTSS tic severity from pre- to post treatment (r ¼ �0:66, p ¼ 0:008). Patients with more facilitatorypriming showed less of a decrease in the YGTSS tic severity score from pre-to post treatment. Likewise,inhibitory priming RT were positively correlated with the magnitude of decrease in YGTSS tic severity frompre-to post treatment (r ¼ 0:60, p ¼ 0:02). Patients with slower inhibitory RT showed higher decreases inYGTSS severity from pre-to post treatment.
Discussion
We set out to investigate the effectiveness of HR compared to supportive psychotherapy for reducing ticseverity and improving psychosocial functioning and life-satisfaction in adult outpatients with TS. Patientswho received habit reversal treatment, but not those who underwent supportive psychotherapy, showedsignificant and clinically meaningful reductions in tic severity as measured by the YGTSS and CGI.Furthermore, reductions in tic severity observed at the end of active treatment remained relatively stable asindicated by reduced tic severity at the 6-month follow-up in the HR group compared to patients who receivedsupportive psychotherapy. This finding is consistent with our previous randomized controlled trial in patientswith TS which compared the effectiveness of HR and SP in a similarly large sample of TS patients. However, itshould be noted, that the rater who judged tic severity and clinical improvement (CGI) was aware of thetreatment conditions to which the patients had been assigned. Thus, it cannot be ruled out that rater bias mayin part account for our findings. Including medication and comorbidity as covariates did not change thepattern of results, suggesting that patients taking medications and those with comorbid conditions benefitedfrom HR treatment to the same extent as non-medicated patients or patients without comorbid psychiatricconditions. However, all non-medicated patients in the present sample had previously taken medications forTS. Thus, our results suggest that HR appears to be effective for pharmacotherapy failures, partial-responders, patients who relapsed after pharmacotherapy, and may be a behavioral treatment alternative topharmacotherapy. Patients in this study completed a mid-treatment assessment in addition to assessmentsconducted at post-treatment and follow-up. This indicated that HR patients achieved most of their overallreduction in tic severity within the first 8 sessions with relatively modest gains thereafter. This suggests that a
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–10901088
shorter course of HR (e.g., eight individual sessions) may produce equal gains compared to a longer and morecost-intensive course of HR (i.e., 14 sessions).
The present study was designed to investigate multiple aspects of treatment response including effectsof HR and SP on psychosocial functioning and life-satisfaction. Both patient groups experienced increasesin life-satisfaction as measured by the SOS-10 from pre-treatment to mid-treatment. These gains remainedstable to the end of treatment and were also observed at the 6-month follow-up. However, effects of HRand SP on psychosocial functioning followed a different time pattern. HR patients improved inpsychosocial functioning from pre-treatment to mid-treatment and remained stable thereafter, while patientsin the SP group showed improvements in psychosocial functioning from mid-treatment to the end oftreatment. It is possible that for HR patients more control over the occurrence of tics (i.e. competingresponses) contributes to improvements in life-satisfaction and psychosocial functioning. For SP patients,improvements in self-esteem (e.g., being less embarrassed about their tics) may be a precursor for improvedpsychosocial functioning, thereby accounting for the lag in improvement in psychosocial functioning in the SPgroup compared to HR. In summary, our study suggests that compared to SP, HR appears to be superior withrespect to reducing tic severity but both treatments improve life-satisfaction and psychosocial functioning.Future research is needed to examine the mechanisms of change which underlie those treatment effects.Nevertheless, for achieving more life-satisfaction and higher psychosocial functioning, SP may be an effectivealternative or adjunct treatment for individuals with TS, and especially for those who do not achieve ticreduction with HR.
Our study was designed to investigate whether the degree of impairment in response inhibition predictsresponse to HR. TS patients in our study were characterized by increased facilitatory priming and reducedinhibitory priming. This finding is largely consistent with the results of a previous study using the VSP task(Swerdlow et al., 1996) that also found that TS patients are characterized by increased facilitatory priming, inrelation to inhibitory priming, in children as well as adults with TS.
Our study suggests that individuals with greater deficits in response inhibition (or facilitatory priming)do not necessarily have more severe tics but will respond less well to habit reversal treatment. Overall,this finding should be considered preliminary given the modest sample size in our study and thereforewarrants replication in a larger sample. One of the active components of HR is the capacity to performcompeting responses that are contingent on premonitory sensations or urges and are held until the urgeto perform a certain tic has subsided. This typically results in negative reinforcement of tics and areduced likelihood for subsequent occurrence of the same tic. Competing responses aim to interrupt thiscycle by performing movements that are antagonistic to the tic. Premonitor sensations/urges in indivi-duals with TS may reflect impairments in inhibitory processes that are an integral part of normal sensori-motor gating processes. Largely consistent with this view, in tic suppression studies, individuals with moreattentional problems had more difficulties suppressing tics (Peterson et al., 1998; Himle & Woods, 2005).Future HRT studies may utilize pre-treatment neuroimaging (e.g. fMRI) to investigate the func-tional neuroanatomy associated response inhibition impairment in TS. In summary, individuals with moreimpaired inhibition (as assessed by the VSP task or other tasks) may experience stronger or more durableurges which may make it more difficult to implement competing responses thereby accounting for lowerresponse to HR.
Acknowledgements
We thank Laura A. Cook for her helpful comments on earlier versions of this manuscript. This research wassupported by the Tourette Syndrome Association post-doctoral fellowship grant to Thilo Deckersbach.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Azrin, N. H., & Nunn, R. G. (1973). Habit reversal: A method of eliminating nervous habits and tics. Behaviour Research and Therapy, 11,
619–628.
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–1090 1089
Azrin, N. H., & Peterson, A. L. (1990). Treatment of Tourette syndrome by habit reversal: A waiting-list control group comparison.
Behavior Therapy, 21, 305–318.
Barkley, R. A. (1990). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York, NY: Guilford Press.
Beck, A. T., & Steer, R. A. (1987). Beck depression inventory manual. San Antonio, TX: The Psychological Corporation.
Blais, M. A., Lenderking, W. R., Baer, L., deLorell, A., Peets, K., Leahy, L., & Burns, C. (1999). Development and initial validation of a
brief mental health outcome measure. Journal of Personality Assessment, 73, 359–373.
Conners, C. K., & Barkley, R. A. (1985). Rating scales and checklist for child psychopharmacology. Psychopharmacology Bulletin, 21,
809–852.
DuPaul, G. (1990). The ADHD rating scale: Normative data, reliability, and validity. Unpublished manuscript of the University of
Massachusetts Medical School.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1995). Structured Clinical Interview for DSM-IV Axis I Disorders-Patient
Edition. New York: Biometrics Research Department, New York Psychiatric Institute.
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L., Heninger, G. R., & Charney, D. S. (1989).
The Yale-Brown Obsessive-Compulsive Scale (Y-BOCS). Archives of General Psychiatry, 46, 1006–1011.
Graybiel, A. M., & Canales, J. J. (2001). The neurobiology of repetitive behaviors: Clues to the neurobiology of Tourette syndrome.
Advances in Neurology, 85, 123–131.
Guy, W. (1976). ECDEU assessment manual for psychopharmacology. Rev. Rockville, Md: National Institute of Mental Health. (DHEW
publication no. (ADM) 76-338).
Himle, M. B., & Woods, D. W. (2005). An experimental evaluation of tic suppression and the tic rebound effect. Behaviour Research and
Therapy, 43, 1443–1451.
Horn, S. (2001). Gilles de la Tourette syndrome. Clinical Neuropharmacology, 24, 125–128.
Johannes, S., Wieringa, B. M., Mantey, M., Nager, W., Rada, D., Muller-Vahl, K. R., Emrich, H. M., Dengler, R., Munte, T. F., &
Dietrich, D. (2001). Altered inhibition of motor responses in Tourette Syndrome and Obsessive-Compulsive Disorder. Acta
Neurologica Scandinavica, 104, 36–43.
Johannes, S., Wieringa, B. M., Nager, W., Rada, D., Muller-Vahl, K. R., Emrich, H. M., Dengler, R., Munte, T. F., & Dietrich, D. (2003).
Tourette syndrome and obsessive-compulsive disorder: Event-related brain potentials show similar mechanisms [correction of
mechansims] of frontal inhibition but dissimilar target evaluation processes. Behavioural Neurology, 14, 9–17.
Leckman, J. F., Hardin, M. T., Riddle, M. A., Stevenson, J., Ort, S. I., & Cohen, D. J. (1991). Clonidine treatment of Gilles de la
Tourette’s syndrome. Archives of General Psychiatry, 48, 324–328.
Leckman, J. F., Peterson, B. S., King, R. A., Scahill, L., & Cohen, D. J. (2001). Phenomenology of tics and natural history of tic disorders.
Advances in Neurology, 85, 1–14.
Leckman, J. F., Riddle, M. A., Hardin, M. T., Ort, S. I., Swartz, K. L., Stevenson, J., & Cohen, D. J. (1989). The Yale global tic severity
scale (YGTSS): Initial testing of a clinician-rated scale of tic severity. Journal of the American Academy of Child and Adolescent
Psychiatry, 28, 566–573.
Leon, A. C., Shear, M. K., Portera, L., & Klerman, G. L. (1992). Assessing impairment in patients with panic disorder: The Sheehan
disability scale. Social Psychiatry and Psychiatric Epidemiology, 27, 78–82.
Mink, J. W. (2001). Neurobiology of basal ganglia circuits in Tourette syndrome: Faulty inhibition of unwanted motor patterns? Advances in
Neurology, 85, 113–122.
Novalis, P. N., Rojcewicz, S. J., & Peele, R. (1993). Clinical manual of supportive psychotherapy. Washington, DC: American Psychiatric
Press.
O’Connor, K. P., Brault, M., Robillard, S., Loiselle, J., Borgeat, F., & Stip, E. (2001). Evaluation of a cognitive-behavioural program for
the management of chronic tic and habit disorders. Behaviour Research and Therapy, 39, 667–681.
Peterson, B. S., Skudlarski, P., Anderson, A. W., Zhang, H., Gatenby, J. C., Lacadie, C. M., Leckman, J. F., & Gore, J. C. (1998).
A functional magnetic resonance imaging study of tie suppression in Tourette syndrome. Archives of General Psychiatry, 55,
326–333.
Pinsker, H. (1997). A primer of supportive psychotherapy. Hillsdayle, NJ: The Analytic Press.
Pinsker, H., & Rosenthal, R. (1988). Beth Israel Medical Center Supportive psychotherapy manual. Social and Behavior Science
Documents, 18, 57.
Riddle, M. A., & Carlson, J. (2001). Clinical psychopharmacology for Tourette syndrome and associated disorders. Advances in
Neurology, 85, 343–354.
Sallee, F. R., Nesbitt, L., Jackson, C., Sine, L., & Sethuraman, G. (1997). Relative efficacy of haloperidol and pimozide in children and
adolescents with Tourette’s disorder. American Journal of Psychiatry, 154, 1057–1062.
Scahill, L., Leckman, J. F., Schultz, R. T., Katsovich, L., & Peterson, B. S. (2003). A placebo-controlled trial of risperidone in Tourette
syndrome. Neurology, 60, 1130–1135.
Shapiro, E., Shapiro, A. K., Fulop, G., Hubbard, M., Mandeli, J., Nordlie, J., & Phillips, R. A. (1989). Controlled study of haloperidol,
pimozide and placebo for the treatment of Gilles de la Tourette’s syndrome. Archives of General Psychiatry, 46, 722–730.
Swerdlow, N. R., Magulac, M., Filion, D., & Zinner, S. (1996). Visuospatial priming and latent inhibition in children and adults with
Tourette’s disorder. Neuropsychology, 10, 485–494.
Tipper, S. P. (1985). The negative priming effect: Inhibitory effects on ignoring primes. Quarterly Journal of Experimental Psychology,
37A, 571–590.
Verdellen, C. W., Keijsers, G. P., Cath, D. C., & Hoogduin, C. A. (2004). Exposure with response prevention versus habit reversal in
Tourettes’s syndrome: a controlled study. Behaviour Research and Therapy, 42, 501–511.
ARTICLE IN PRESST. Deckersbach et al. / Behaviour Research and Therapy 44 (2006) 1079–10901090
Walkup, J. T., Rosenberg, L. A., Brown, J., & Singer, H. S. (1992). The validity of instruments measuring tic severity in Tourette’s
syndrome. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 472–477.
Wechsler, D. (1981). Wechsler intelligence scale-revised. Cleveland, OH: The Psychological Corporation.
Wilhelm, S., Deckersbach, T., Coffey, B. J., Bohne, A., Peterson, A. L., & Baer, L. (2003). Habit reversal versus supportive psychotherapy
for Tourette’s disorder: A randomized controlled trial. American Journal of Psychiatry, 160, 1175–1177.