Mutations of human TMHS cause recessively inherited non-syndromic hearing loss
7
ORIGINAL ARTICLE Mutations of human TMHS cause recessively inherited non-syndromic hearing loss M I Shabbir*, Z M Ahmed*, S Y Khan, Saima Riazuddin, A M Waryah, S N Khan, R D Camps, M Ghosh, M Kabra, I A Belyantseva, T B Friedman, Sheikh Riazuddin ............................................................................................................................... See end of article for authors’ affiliations ....................... Correspondence to: ProfessorSheikhRiazuddin, National Centre of Excellence in Molecular Biology, University of the Punjab, 87 West Canal Bank Road, Thokar Niaz Baig, Lahore 53700, Pakistan; riaz@lhr. comsats.net.pk Received 24 November 2005 Revised version received 19 January 2006 Accepted for publication 24 January 2006 Published Online First 3 February 2006 ....................... J Med Genet 2006;43:634–640. doi: 10.1136/jmg.2005.039834 Background: Approximately half the cases of prelingual hearing loss are caused by genetic factors. Identification of genes causing deafness is a crucial first step in understanding the normal function of these genes in the auditory system. Recently, a mutant allele of Tmhs was reported to be associated with deafness and circling behaviour in the hurry-scurry mouse. Tmhs encodes a predicted tetraspan protein of unknown function, which is expressed in inner ear hair cells. The human homologue of Tmhs is located on chromosome 6p. Objective: To determine the cause of deafness in four consanguineous families segregating recessive deafness linked to markers on chromosome 6p21.1-p22.3 defining a novel DFNB locus. Results: A novel locus for non-syndromic deafness DFNB67 was mapped in an interval of approximately 28.51 cM on human chromosome 6p21.1-p22.3. DNA sequence analysis of TMHS revealed a homozygous frameshift mutation (246delC) and a missense mutation (Y127C) in affected individuals of two families segregating non-syndromic deafness, one of which showed significant evidence of linkage to markers in the DFNB67 interval. The localisation of mTMHS in developing mouse inner ear hair cells was refined and found to be expressed briefly from E16.5 to P3. Conclusions: These findings establish the importance of TMHS for normal sound transduction in humans. T here are approximately 100 genes that are associated with hearing loss in the mouse. 1 In humans, more than 47 deafness loci have been mapped and 21 of the corresponding genes have been identified. 23 Because of the similarities in the morphology of their auditory systems, deaf mice have provided a valuable resource for understanding the pathophysiology of human hereditary hearing disorders and the normal functions of these genes. Molecular genetic studies of deaf mice have been instrumental in identifying six orthologous deafness genes in humans, including MYO7A (USH1B), MYO15 (DFNB3), TMIE (DFNB6), PCDH15 (DFNB23/USH1F), WHRN (DFNB31), and SANS (USH1G). 4–15 When a novel human deafness locus is mapped, the question arises as to whether or not there is a strain of deaf mouse that carries a mutated gene at a chromosomal map position suggesting conserved synteny with a human locus for deafness. Positional cloning in the mouse or phenotypic rescue using a BAC transgene 13 16 can lead to gene identifica- tion more quickly than sequencing human genes in a large chromosomal interval of a deafness locus. 17 Alternatively, identification of a gene responsible for deafness in a mouse may suggest a candidate human chromosomal location to screen for linkage of deafness segregating in large families that have a structure suitable for providing significant evidence of linkage. 18 A combination of two of these strategies was used to identify mutations of TMHS (MIM_609427) as the gene on human chromosome 6p21.1- p22.3 responsible for non-syndromic deafness DFNB67, segregating in two consanguineous families. METHODS Family enrolment Approval for the study was obtained from the institutional review board at the National Centre of Excellence in Molecular Biology, Lahore, Pakistan (FWA00001758), the NIDCD/NINDS IRB at the National Institutes of Health, Bethesba, Maryland, USA (OH-93-N-016) and the institu- tional review board at the All India Institute of Medical Sciences, Delhi, India (FWA00001997). Written informed consent was obtained from all the participants. Families PKDF374, PKDF619, and PKDF638 were ascertained from Sindh, Pakistan and family HTN-09 lives in Chennai, India. The inheritance patterns of deafness segregating in families PKDF374, PKDF619, PKDF638, and HTN-09 are consistent with an autosomal recessive trait (fig 1). Clinical evaluation All participating members of these families were evaluated by a physician to rule out obvious extra-auditory phenotypes associated with common syndromic forms of deafness. Air conduction pure tone audiometry tests were carried out under quiet ambient conditions at octave frequencies ranging from 250 to 8000 Hz. Vestibular function was evaluated by tandem gait and Romberg testing. Linkage analysis Genomic DNA was extracted from peripheral venous blood samples by a standard protocol. 19 Samples were genotyped for markers flanking known DFNB loci, using marker informa- tion provided by the Hereditary Hearing Loss Homepage (as of August 2004 http://webhost.ua.ac.be/hhh/). For genome- wide screens, we used the ABI Prism v2.5 Linkage Mapping Set (panels 1 to 27; Applied Biosystems, Foster City, California, USA) containing 388 fluorescently labelled micro- satellite markers spaced at an average interval of 10 cM. Short tandem repeat polymorphisms (STRPs) were amplified by polymerase chain reaction (PCR), alleles were assigned using Genescan 3.7 and Genotyper 3.7 (Applied Biosystems), and LOD scores were calculated using LINKMAP as described. 9 20 21 634 www.jmedgenet.com
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Mutations of human TMHS cause recessively inherited non-syndromic hearing loss

ORIGINAL ARTICLE
Mutations of human TMHS cause recessivelyinherited non-syndromic hearing lossM I Shabbir*, Z M Ahmed*, S Y Khan, Saima Riazuddin, A M Waryah, S N Khan,R D Camps, M Ghosh, M Kabra, I A Belyantseva, T B Friedman, Sheikh Riazuddin. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
See end of article forauthors’ affiliations. . . . . . . . . . . . . . . . . . . . . . .
Correspondence to:ProfessorSheikhRiazuddin,National Centre ofExcellence in MolecularBiology, University of thePunjab, 87 West CanalBank Road, Thokar NiazBaig, Lahore 53700,Pakistan; [email protected]
Received24 November 2005Revised version received19 January 2006Accepted for publication24 January 2006Published Online First3 February 2006. . . . . . . . . . . . . . . . . . . . . . .
J Med Genet 2006;43:634–640. doi: 10.1136/jmg.2005.039834
Background: Approximately half the cases of prelingual hearing loss are caused by genetic factors.Identification of genes causing deafness is a crucial first step in understanding the normal function of thesegenes in the auditory system. Recently, a mutant allele of Tmhs was reported to be associated withdeafness and circling behaviour in the hurry-scurry mouse. Tmhs encodes a predicted tetraspan protein ofunknown function, which is expressed in inner ear hair cells. The human homologue of Tmhs is located onchromosome 6p.Objective: To determine the cause of deafness in four consanguineous families segregating recessivedeafness linked to markers on chromosome 6p21.1-p22.3 defining a novel DFNB locus.Results: A novel locus for non-syndromic deafness DFNB67 was mapped in an interval of approximately28.51 cM on human chromosome 6p21.1-p22.3. DNA sequence analysis of TMHS revealed ahomozygous frameshift mutation (246delC) and a missense mutation (Y127C) in affected individuals oftwo families segregating non-syndromic deafness, one of which showed significant evidence of linkage tomarkers in the DFNB67 interval. The localisation of mTMHS in developing mouse inner ear hair cells wasrefined and found to be expressed briefly from E16.5 to P3.Conclusions: These findings establish the importance of TMHS for normal sound transduction in humans.
There are approximately 100 genes that are associatedwith hearing loss in the mouse.1 In humans, more than47 deafness loci have been mapped and 21 of the
corresponding genes have been identified.2 3 Because of thesimilarities in the morphology of their auditory systems, deafmice have provided a valuable resource for understanding thepathophysiology of human hereditary hearing disorders andthe normal functions of these genes. Molecular geneticstudies of deaf mice have been instrumental in identifying sixorthologous deafness genes in humans, including MYO7A(USH1B), MYO15 (DFNB3), TMIE (DFNB6), PCDH15(DFNB23/USH1F), WHRN (DFNB31), and SANS (USH1G).4–15
When a novel human deafness locus is mapped, thequestion arises as to whether or not there is a strain of deafmouse that carries a mutated gene at a chromosomal mapposition suggesting conserved synteny with a human locusfor deafness. Positional cloning in the mouse or phenotypicrescue using a BAC transgene13 16 can lead to gene identifica-tion more quickly than sequencing human genes in a largechromosomal interval of a deafness locus.17 Alternatively,identification of a gene responsible for deafness in a mousemay suggest a candidate human chromosomal location toscreen for linkage of deafness segregating in large familiesthat have a structure suitable for providing significantevidence of linkage.18 A combination of two of thesestrategies was used to identify mutations of TMHS(MIM_609427) as the gene on human chromosome 6p21.1-p22.3 responsible for non-syndromic deafness DFNB67,segregating in two consanguineous families.
METHODSFamily enrolmentApproval for the study was obtained from the institutionalreview board at the National Centre of Excellence inMolecular Biology, Lahore, Pakistan (FWA00001758), the
NIDCD/NINDS IRB at the National Institutes of Health,Bethesba, Maryland, USA (OH-93-N-016) and the institu-tional review board at the All India Institute of MedicalSciences, Delhi, India (FWA00001997). Written informedconsent was obtained from all the participants. FamiliesPKDF374, PKDF619, and PKDF638 were ascertained fromSindh, Pakistan and family HTN-09 lives in Chennai, India.The inheritance patterns of deafness segregating in familiesPKDF374, PKDF619, PKDF638, and HTN-09 are consistentwith an autosomal recessive trait (fig 1).
Clinical evaluationAll participating members of these families were evaluated bya physician to rule out obvious extra-auditory phenotypesassociated with common syndromic forms of deafness. Airconduction pure tone audiometry tests were carried outunder quiet ambient conditions at octave frequencies rangingfrom 250 to 8000 Hz. Vestibular function was evaluated bytandem gait and Romberg testing.
Linkage analysisGenomic DNA was extracted from peripheral venous bloodsamples by a standard protocol.19 Samples were genotyped formarkers flanking known DFNB loci, using marker informa-tion provided by the Hereditary Hearing Loss Homepage (asof August 2004 http://webhost.ua.ac.be/hhh/). For genome-wide screens, we used the ABI Prism v2.5 Linkage MappingSet (panels 1 to 27; Applied Biosystems, Foster City,California, USA) containing 388 fluorescently labelled micro-satellite markers spaced at an average interval of 10 cM.Short tandem repeat polymorphisms (STRPs) were amplifiedby polymerase chain reaction (PCR), alleles were assignedusing Genescan 3.7 and Genotyper 3.7 (Applied Biosystems),and LOD scores were calculated using LINKMAP asdescribed.9 20 21
634
www.jmedgenet.com

Candidate gene screeningCandidate genes were identified using the UCSC GenomeBioinformatics web browser (http://genome.ucsc.edu/) andselected for mutation screening on the basis of their potentialrole in the inner ear. Primers used for PCR amplification andsubsequent sequencing of COL11A2 and TMHS exons weredesigned using the Primer3 Web site (http://frodo.wi.mit.edu/cgi-bin/primer3/primer3_www.cgi). PCR primers are fromsequence flanking each exon (supplementary tables 1 and 2;the supplementary tables can be seen on the journal website:http://www.jmedgenet.co/supplemental). Amplification,sequencing reactions, and mutation analysis were carriedout as described.8
ImmunocytochemistryIn order to characterise in greater detail the cellular localisa-tion and developmental profile of TMHS with immunofluor-escence confocal microscopy, we used a previously reported
affinity purified rabbit polyclonal antiserum generouslyprovided by Ken Johnson.22 Immunostaining was carried outas described.11 23 After fixation in 4% paraformaldehyde fortwo hours at room temperature, organs of Corti and vestibularend organs of mice were dissected in phosphate bufferedsaline (PBS). Samples were permeabilised in 0.5% Triton X-100 for 30 minutes and then washed in PBS. Non-specificbinding sites were blocked using 5% normal goat serum (LifeTechnologies, Gaithersburg, Maryland, USA) and 2% bovineserum albumin (ICN, Aurora, Ohio, USA) in PBS. Sampleswere incubated for two hours in the anti-mTMHS antiseraat a concentration of approximately 5 mg/ml in blockingsolution. After three rinses in PBS, samples were incubatedin a 1:200 dilution of the FITC conjugated anti-rabbit IgG for30 minutes, washed again three times with PBS, mountedusing the ProLong Antifade kit (Molecular Probes, Eugene,Oregon, USA), and viewed with a LSM510 Zeiss confocalmicroscope.23
1 2I PKDF374
1 2II
3 4
1 2
13211113
40.1444.4148.2648.2649.5060.4466.3768.65
cMD6S1660D6S276D6S439D6S1645D6S291D6S1575D6S282D6S1650
Marker22132224
III31323331
32132222
1 6
22132224
40.1444.4148.2648.2649.5060.4466.3768.65
cMD6S1660D6S276D6S439D6S1645D6S291D6S1575D6S282D6S1650
Marker32132222
IV 5
13211113
31323331
22132224
31323331
4
22132224
32132222
3
32132222
2
22132224
32132222
22132224
1 2I HTN-09
1 2II
3 4
3 4
231412
44.4148.2648.2649.5060.4461.86
cMD6S276D6S439D6S1645D6S291D6S1575D6S1549
Marker313245
III5
313245
44.4148.2648.2649.5060.4461.86
cMD6S276D6S439D6S1645D6S291D6S1575D6S1549
Marker
cMMarker
313245
313245
313245
313245
313245
313245
121321
121321
313245
1 4IV 32
1 2I PKDF638
1 2II
3 4
1 2
211112
29.3035.6640.1444.4147.1048.26
cMD6S289D6S422D6S1660D6S276D6S1611D6S439
Marker121311
III
211112
29.3035.6640.1444.4147.7148.26
cMD6S289D6S422D6S1660D6S276D6S1611D6S439
Marker211111
12123113
29.3035.6640.1444.4147.7148.2649.5053.81
D6S289D6S422D6S1660D6S276D6S1611D6S1645D6S291D6S1610
22123112
21211111
29.3035.6640.1444.4147.1048.2649.5053.81
D6S289D6S422D6S1660D6S276D6S1611D6S1645D6S291D6S1610
12123113
12123113
22123112
12123113
22123112
211112
211112
211112
111112
211112
212211
211112
121311
211112
121311
1 6IV 5432
1 2I PKDF619
1 2 3 4
1 2III
II
1 2IV
1V 2
22123113
12332121
4
12123113
12332121
53
21211111
12332121
6
3
4 2
22
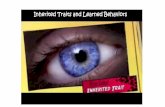
Figure 1 Chromosome 6 markers that co-segregate with deafness in families PKDF374, PKDF619, PKDF638, and HTN-09. STR marker positionsare in cM according to the Marshfield human genetic map (http://research.marshfieldclinic.org/genetics/). The linked haplotypes are boxed.Filled symbols denote profound sensorineural hearing loss. The DFNB67 interval is defined by meiotic breakpoints in family PKDF374. Multipointlinkage analyses provided Zmax (maximum LOD scores) of 3.2 for family PKDF374 (markers D6S439 and D6S1645), 1.80 for family HTN-09(markers D6S439 and D6S1645), 2.35 for family PKDF638 (markers D6S276 and D6S1611), and 2.80 for family PKDF619 (markers D6S1660and D6S276).
Mutations of TMHS and hearing loss 635
www.jmedgenet.com

RESULTSPhenotypeAffected individuals in families PKDF374, PKDF619,PKDF638, and HTN-09 had congenital bilateral profoundhearing loss. Although, we cannot rule out a mixed hearingloss, the expression pattern of TMHS in the inner ear suggestsa sensorineural deficit. No vestibular dysfunction wasdetected using tandem gait or Romberg testing. Clinicalevaluation revealed no ophthalmological, skin, or renalanomalies. Fundoscopic examination of IV:2 (22 years) andIV:4 (35 years) from family PKDF374 (fig 1) showed no signsof retinitis pigmentosa.
Mapping of DFNB67Over 600 families segregating profound congenital deafnesswere ascertained in Pakistan and were suitable for geneticlinkage analyses. After excluding linkage to known DFNBloci,3 a genome-wide linkage analysis was initially under-taken using DNA samples from four affected and fourunaffected members of family PKDF374. Initial evidence of
linkage was on chromosome 6p21.1-p22.3. Additional shorttandem repeat (STR) markers were genotyped for all theparticipating family members, and haplotype analysisrevealed a region of homozygosity of approximately 29centi-Morgans (cM) delimited by markers D6S1660(40.14 cM) and D6S1650 (68.65 cM) (fig 1). Multipointlinkage analysis provided a Zmax (maximum LOD score) of3.2 for the markers D6S439 (48.26 cM) and D6S1645(48.26 cM). We then discovered three additional families(PKDF619, PKDF638, and HTN-09) segregating deafnessconsistent with linkage to markers in the 6p21.1-p22.3interval (fig 1). The Human Genome Organization (HUGO)(http://www.gene.ucl.ac.uk/hugo) nomenclature committee24
assigned DFNB67 as the designation for this locus for non-syndromic deafness.
Genetic and physical mapA genetic and physical map of the DFNB67 interval is shownin fig 2. This interval has more than 70 annotated genes andapproximately 100 predicted genes (UCSC Genome
PKDF374
6p22
.36p
22.2
6p22
.16p
21.3
16p
21.2
Chr
omos
ome
6
6p21
.1
DFN
B67
Crit
ical
Inte
rval
(~ 2
8.51
cM
)
6p21
.33
6p21
.32
D6S1650 (44.23)68.65
D6S282 (43.34)66.37
D6S1549 (41.49)61.86D6S1575 (41.25)60.44
D6S1610 (39.37)53.81
D6S291 (36.37)49.50D6S1645 (35.69)48.26D6S439 (35.26)48.26
D6S1611 (35.48)47.71
D6S276 (24.29)44.41
D6S1660 (23.42)40.14
D6S422 (20.48)35.66
D6S289 (15.39)29.30cM Mb
HTN-09
PKDF619
Overlappingdeafness loci
Candidategenes
PKDF638
DFNB66
DFNB53 DFNA31 DCDC2 (24.28)SLC17A4 (25.86)SLC17A1 (25.89)SLC17A3 (25.95)SLC17A2 (26.02)
GABBR1 (29.68)
POU5F1 (31.24)
COL11A2 (33.24)SLC39A7 (33.28)
TMHS (35.88)SLC26A8 (36.02)
FGD2 (37.08)KCNK5 (39.26)
KCNK17 (39.37)KCNK16 (39.39)
FOXP4 (41.62)
VMP (24.23)Mb
DFNA13
DFNA21
Figure 2 Chromosome 6p21.1-p22.3 showing the linkage interval of DFNB67. Short tandem repeat (STR) markers are represented by filled circles.The sex-averaged recombination distances in cM and in Mb are indicated along with STR markers. The DFNB67 interval is based on the meioticbreakpoints in family PKDF374. Linkage regions of five overlapping autosomal deafness loci (DFNB53, DFNB66, DFNA13, DFNA21, and DFNA31)are also illustrated. Cytogenetic locations of several candidate genes are indicated. The Mb positions of the markers and the genes are according to theMay 2004 NCBI build 35 of the human genome browser assembly (http://genome.cse.ucsc.edu/cgi-bin/hgGateway).
636 Shabbir, Ahmed, Khan, et al
www.jmedgenet.com

Bioinformatics: http://genome.ucsc.edu). COL11A2 was acandidate in these families, as allelic variants of this geneare associated with recessive deafness DFNB5325 and non-ocular Stickler syndrome.3 However, DNA sequence analysisof the 66 exons of COL11A2 from two affected individualsfrom each of the four DFNB67 families did not reveal anydisease associated variants.
Identification of DFNB67 geneTMHS was also a candidate gene for DFNB67 (fig 2) as amissense mutation of the mouse orthologue, Tmhs, wasreported to cause deafness and vestibular dysfunction in thehurry-scurry (hscy) mouse, and TMHS is expressed in theinner ear hair cell stereocilia of mice.22 Like Tmhs, humanTMHS has four exons (NM_182548), which encode a 2162base pair mRNA. The deduced translation of this cDNA yieldsa protein of 219 amino acids that has four predictedtransmembrane helices. We screened the protein codingsequence, adjacent intronic sequence, and the 59 and 39 UTRsof TMHS in two affected individuals from each of the DFNB67linked families. Affected individuals of family PKDF374 hada homozygous deletion of a single nucleotide at position 246(246delC) in the first exon of TMHS (fig 3A), which co-segregated with the hearing loss. This mutant allele ispredicted to cause a frameshift and a subsequent truncationof the deduced protein at amino acid position 84 (P83fsX84;fig 3B). A homozygous missense mutation (380ARG) wasfound in all the affected individuals of family HTN-09(fig 3A). This allele results in an amino acid substitution ofa conserved tyrosine residue at position 127 (Y127C; fig 3,panels B and C). These two mutations (246delC and380ARG) were not found in 200 chromosomes fromethnically and geographically matched normally hearingindividuals from Sindh province of Pakistan and Chennai,India.
TMHS is expressed transiently in inner ear hair cellstereocil iary bundlesFor the developmental profile of the expression pattern ofTMHS, we immunostained the inner ears from P0, P3, andP10 mice. TMHS immunoreactivity was detected in the organof Corti and vestibular hair cells of C57BL/6 mouse as well asin the other cell types such as supporting cells of cochlear andvestibular sensory epithelia, and internal and external sulcuscells of the organ of Corti (fig 4 and data not shown). At highresolution, TMHS immunoreactivity was detected in thekinocilium and along the length of P0 cochlear hair cellstereocilia and appeared to be more concentrated toward thetips (fig 4, panels A to C). A similar pattern was observed inhair cells of the saccular (fig 4, panels D to F) and utricularmaculae (fig 4, panels G to I). The amount of TMHSimmunoreactivity in the stereocilia appears to vary amongdifferent hair bundles. Hair cells with immature stereociliarybundles have a strong TMHS signal but as the hair cellsmature there is a gradual reduction in immunoreactivity(fig 4, panels D and G), consistent with the report by Longo-Guess and co-workers.22 TMHS immunoreactivity in hair cellstereocilia and kinocilia appears at approximately E16.5 andrapidly disappears by P3, after which we could not detect asignal in stereocilia or in kinocilia except in the vestibularsensory epithelium associated with immature hair cells andin the non-sensory cells (fig 4, panels J to L).
DISCUSSIONIn the hscy mouse, a mutation of Tmhs causes deafness andvestibular dysfunction manifested by circling behaviour.22
The identification of recessive mutations of TMHS indicatesan essential role for TMHS in the human auditory system.There are at least two possibilities to explain the discrepancybetween the loss of vestibular function in Tmhs mutant mice22
but not in humans. TMHS may be required for normal
Figure 3 TMHS mutations. (A) Wild type and mutant alleles from unaffected and affected members of families PKDF374 and HTN-09, respectively. (B)Schematic representation of the predicted TMHS structure (modified from Longo-Guess et al22) showing the stop codon P83fsX84 (which is caused bythe 246delC frameshift mutation) in the sequence encoding the first extracellular loop. The missense mutation Y127C is located in the predicted thirdtransmembrane domain. The location of C161F reported for the hscy mouse22 is indicated by an arrowhead. (C) Alignment of TMHS amino acids fromvarious species shows that Y127 (arrow) is conserved (shaded background, similar amino acids; light background, non-conserved amino acids).
Mutations of TMHS and hearing loss 637
www.jmedgenet.com

development of mouse vestibular hair cells but is not requiredfor development of human vestibular hair cells. Alternatively,unlike mice, humans may be better able to compensatepartially for loss of vestibular dysfunction by somatosensoryand visual input. Subjects in our study were examined in thefield only by tandem gait and Romberg testing, whichprobably excludes severe bilateral vestibular failure but mayhave missed a more subtle compensated vestibular disorder.More sensitive and informative vestibular testing usingposturography was not available to us in India and Pakistan.
The protein encoded by TMHS is a member of a superfamilyof tetraspan proteins, which includes the claudin tightjunction proteins, gap junction proteins, peripheral myelin,and epithelial membrane proteins as well as calciumchannel-like proteins. Several genes of this superfamily havebeen reported to be necessary for hearing in either humans ormice, or both.1 3 The predicted structure of TMHS consists offour transmembrane helices with two extracellular loops.22
The missense mutation (C161F) previously reported in hscymice may disrupt a disulphide bond present in the secondextracellular loop and destabilise the secondary structure.22
The frameshift mutation that we found in family PKDF374(246delC; P83fsX84) is predicted to introduce a stop codon in
the first extracellular loop (fig 3B). In vivo, the mutantmRNA would either be translated into a truncated TMHSprotein with only one transmembrane domain or be degradedby nonsense mediated decay (NMD).26 The Y127C missensemutation (380ARG) found in family HTN-09 causes asubstitution of the second residue of the third transmem-brane domain of TMHS (fig 3B). Tyrosine is a relatively non-polar hydrophobic amino acid with an aromatic side chain,whereas cysteine is a weakly polar hydrophilic amino acidwith a thiol side chain. The large difference between the twoamino acids may cause disruption of the third transmem-brane domain and may lead to mislocalisation of the encodedprotein.
The disappearance of TMHS from hair cell stereociliarybundles at P3 occurs just before the gradual loss of cadherin23 from stereocilia, which appears to be complete at P16.27 28
A role for TMHS in organising a transient cytoskeleton–membrane interaction in sensory hair cells would beconsistent with the stereociliary pathology found in hscymice22 and the developmental expression profile of TMHS(fig 4).22
We found no disease associated mutations in TMHS orCOL11A2 in affected members of families PKDF619 and
Figure 4 Immunolocalisation of TMHSin the organ of Corti and vestibularsensory epithelia of a P0 C57BL/6mouse. (A to C) Localisation of TMHS incochlear hair cell stereocilia. (A) Anti-TMHS antibody staining (greenchannel). Arrowhead indicates thestaining of kinocilia. (B) Rhodamine-phalloidin staining of filamentous actinin stereocilia of one row of inner haircells and three rows of outer hair cells(red channel). (C) Merged image forTMHS and F-actin (green and red,respectively). (D to F) TMHS wasdetected predominantly in immaturestereociliary bundles of saccular haircells and its expression level decreasesas bundles mature, as previouslyreported.22 The arrowheads in panel Findicate kinocilia labelling of maturestereociliary bundles and residualstaining of the upper portion ofstereociliary bundles. (G to I) In P0utricular hair cells the pattern ofstereociliary staining with anti-TMHSantibody was similar to that of saccularhair cell stereocilia. The arrowheadspoint to intensely stained immature haircell stereociliary bundles and an arrowpoints to a mature hair cell with stainingin the upper portion of the stereociliarybundle. (J to L) In P10 saccule onlyimmature hair cell stereociliary bundles(arrowheads) and non-sensory cells,such as supporting cells (arrow), arestained with anti-TMHS antibodies,while no staining was observed instereociliary bundles of mature haircells. Scale bar in (C), (F), (I), and (L) is5 mm.
638 Shabbir, Ahmed, Khan, et al
www.jmedgenet.com

PKDF638. The linkage interval defined by these two families(PKDF619, PKDF638) is approximately 19cM delimited bymarkers D6S289 (29.30cM) and D6S439 (48.26). It is possiblethat these individuals harbour mutations of cis actingregulatory elements of either COL11A2 or TMHS. The deafnesslinked haplotype of affected individuals in family PKDF638excludes the protein coding region of TMHS (fig 2).
There are three additional loci for hearing loss defined bydominant mutant alleles (DFNA13, DFNA21, and DFNA31) atchromosome 6p21.2-p22.3 and two recessive deafness loci(DFNB53 and DFNB66) in this interval (fig 2). In the singlefamily used to map DFNB66, TMHS was screened formutations and none was found.29 It seems plausible that amutation of a second gene in this interval is associated withhearing loss in families PKDF619 and PKDF638. Othercandidates in the 6p21.2-p22.3 interval include five solutecarrier family members (SLC17A1, SLC17A2, SLC17A3,SLC17A4, and SLC39A7), POU5F1, a POU domain containingtranscription factor and c-aminobutyric acid B receptor 1(GABBR1). Genes encoding SLCs and POU domain transcrip-tion factors are important for normal hearing.3 30 Anotherpossibility for not finding mutations in TMHS in two of thefour families (fig 1) is that the LOD scores for deafnesssegregating in PKDF619 and PKDF638 (Zmax 2.80 and 2.35,respectively) do not rise to the level of statistical significancefor linkage, and thus there may be spurious association ofdeafness segregating in these two families with STRs onchromosome 6p. The actual deafness-causing mutations infamilies PKDF619 and PKDF638 may be somewhere else inthe genome.
In summary, we have mapped a new non-syndromicrecessive deafness locus DFNB67 on chromosome 6p21.1-p22.3. In two consanguineous families, we have identifiedtwo likely pathogenic mutations of TMHS that co-segregatewith deafness.
ACKNOWLEDGEMENTSWe are grateful to the members of the four families for theirparticipation in this study and to K Johnson for generously providinganti-TMHS antisera. We also thank Dennis Drayna, Andrew Griffith,Karen Friderici, Shin-ichiro Kitajiri, Rob Morell, Julie Schultz, SabihaNazli, and Saeeda Kalsoom for their suggestions in relation to themanuscript. The study was supported by the Higher EducationCommission, Islamabad, Pakistan; Ministry of Science andTechnology, Islamabad, Pakistan; the International Centre forGenetic Engineering and Biotechnology, Trieste, Italy under projectCRP/PAK02-01 (contract No 02/013); and intramural funds from theNational Institute on Deafness and Other Communication Disorders(1 ZO1 DC000035-07 and 1 ZO1 DC000039-07).
The supplementary tables are accessible on the journalwebsite: http://www.jmedgenet.co/supplemental
Authors’ affiliations. . . . . . . . . . . . . . . . . . . . .
M I Shabbir*, S Y Khan, A M Waryah, S N Khan, Sheikh Riazuddin,National Centre of Excellence in Molecular Biology, Punjab University,Lahore, PakistanZ M Ahmed*, Saima Riazuddin, R D Camps, I A Belyantseva,T B Friedman, Section on Human Genetics, Laboratory of MolecularGenetics, National Institutes on Deafness and Other CommunicationDisorders, National Institutes of Health, Rockville, Maryland, USAM Ghosh, M Kabra, Genetic Unit, Department of Paediatrics, All IndiaInstitute of Medical Sciences, New Delhi, India
*These two authors contributed equally to the work
Conflicts of interest: none declared
REFERENCES1 Anagnostopoulos AV. A compendium of mouse knockouts with inner ear
defects. Trends Genet 2002;18:499.2 Finsterer J, Fellinger J. Nuclear and mitochondrial genes mutated in
nonsyndromic impaired hearing. Int J Pediatr Otorhinolaryngol2005;69:621–7.
3 Friedman TB, Griffith AJ. Human nonsyndromic sensorineural deafness. AnnuRev Genomics Hum Genet 2003;4:341–402.
4 Weil D, Blanchard S, Kaplan J, Guilford P, Gibson F, Walsh J, Mburu P,Varela A, Levilliers J, Weston MD, et al. Defective myosin VIIA generesponsible for Usher syndrome type 1B. Nature 1995;374:60–1.
5 Friedman TB, Liang Y, Weber JL, Hinnant JT, Barber TD, Winata S, Arhya IN,Asher JH. A gene for congenital, recessive deafness DFNB3 maps to thepericentromeric region of chromosome 17. Nat Genet 1995;9:86–91.
6 Wang A, Liang Y, Fridell RA, Probst FJ, Wilcox ER, Touchman JW, Morton CC,Morell RJ, Noben-Trauth K, Camper SA, Friedman TB. Association ofunconventional myosin MYO15 mutations with human nonsyndromic deafnessDFNB3. Science 1998;280:1447–51.
7 Fukushima K, Ramesh A, Srisailapathy CR, Ni L, Wayne S, O’Neill ME, VanCamp G, Coucke P, Jain P, Wilcox ER, et al. An autosomal recessivenonsyndromic form of sensorineural hearing loss maps to 3p-DFNB6.Genome Res 1995;5:305–8.
8 Naz S, Giguere CM, Kohrman DC, Mitchem KL, Riazuddin S, Morell RJ,Ramesh A, Srisailpathy S, Deshmukh D, Riazuddin S, Griffith AJ, Friedman TB,Smith RJ, Wilcox ER. Mutations in a novel gene, TMIE, are associated withhearing loss linked to the DFNB6 locus. Am J Hum Genet 2002;71:632–6.
9 Ahmed ZM, Riazuddin S, Bernstein SL, Ahmed Z, Khan S, Griffith AJ,Morell RJ, Friedman TB, Riazuddin S, Wilcox ER. Mutations of theprotocadherin gene PCDH15 cause Usher syndrome type 1F. Am J HumGenet 2001;69:25–34.
10 Alagramam KN, Yuan H, Kuehn MH, Murcia CL, Wayne S, Srisailpathy CR,Lowry RB, Knaus R, Van Laer L, Bernier FP, Schwartz S, Lee C, Morton CC,Mullins RF, Ramesh A, Van Camp G, Hageman GS, Woychik RP, Smith RJ.Mutations in the novel protocadherin PCDH15 cause Usher syndrome type 1F.Hum Mol Genet 2001;10:1709–18.
11 Ahmed ZM, Riazuddin S, Ahmad J, Bernstein SL, Guo Y, Sabar MF, Sieving P,Riazuddin S, Griffith AJ, Friedman TB, Belyantseva IA, Wilcox ER. PCDH15 isexpressed in the neurosensory epithelium of the eye and ear and mutantalleles are responsible for both USH1F and DFNB23. Hum Mol Genet2003;12:3215–23.
12 Mustapha M, Chouery E, Chardenoux S, Naboulsi M, Paronnaud J,Lemainque A, Megarbane A, Loiselet J, Weil D, Lathrop M, Petit C. DFNB31,a recessive form of sensorineural hearing loss, maps to chromosome 9q32–34. Eur J Hum Genet 2002;10:210–12.
13 Mburu P, Mustapha M, Varela A, Weil D, El-Amraoui A, Holme RH, Rump A,Hardisty RE, Blanchard S, Coimbra RS, Perfettini I, Parkinson N, Mallon AM,Glenister P, Rogers MJ, Paige AJ, Moir L, Clay J, Rosenthal A, Liu XZ,Blanco G, Steel KP, Petit C, Brown SD. Defects in whirlin, a PDZ domainmolecule involved in stereocilia elongation, cause deafness in the whirlermouse and families with DFNB31. Nat Genet 2003;34:421–8.
14 Weil D, El-Amraoui A, Masmoudi S, Mustapha M, Kikkawa Y, Laine S,Delmaghani S, Adato A, Nadifi S, Zina ZB, Hamel C, Gal A, Ayadi H,Yonekawa H, Petit C. Usher syndrome type I G (USH1G) is caused bymutations in the gene encoding SANS, a protein that associates with theUSH1C protein, harmonin. Hum Mol Genet 2003;12:463–71.
15 Mustapha M, Chouery E, Torchard-Pagnez D, Nouaille S, Khrais A,Sayegh FN, Megarbane A, Loiselet J, Lathrop M, Petit C, Weil D. A novellocus for Usher syndrome type I, USH1G, maps to chromosome 17q24-25.Hum Genet 2002;110:348–50.
16 Probst FJ, Fridell RA, Raphael Y, Saunders TL, Wang A, Liang Y, Morell RJ,Touchman JW, Lyons RH, Noben-Trauth K, Friedman TB, Camper SA.Correction of deafness in shaker-2 mice by an unconventional myosin in aBAC transgene. Science 1998;280:1444–7.
17 Johnson KR. Mouse models of human hearing disorders. Curr Genom2001;2:55–69.
18 Steel KP, Kros CJ. A genetic approach to understanding auditory function.Nat Genet 2001;27:143–9.
19 Grimberg J, Nawoschik S, Belluscio L, McKee R, Turck A, Eisenberg A. Asimple and efficient non-organic procedure for the isolation of genomic DNAfrom blood. Nucleic Acids Res 1989;17:83–90.
20 Ahmad J, Khan SN, Khan SY, Ramzan K, Riazuddin S, Ahmed ZM,Wilcox ER, Friedman TB, Riazuddin S. DFNB48, a new nonsyndromicrecessive deafness locus, maps to chromosome 15q23-q25.1. Hum Genet2005;116:407–12.
21 Ramzan K, Shaikh SR, Ahmad J, Khan SN, Riazuddin S, Ahmed ZM,Friedman TB, Wilcox ER, Riazuddin S. A new locus for nonsyndromicdeafness DFNB49 maps to chromosome 5q12.3-q14.1. Hum Genet2005;116:17–22.
22 Longo-Guess CM, Gagnon LH, Cook SA, Wu J, Zheng OY, Johnson KR. Amissense mutation in the previously undescribed gene Tmhs underlies deafnessin hurry-scurry (hscy) mice. Proc Natl Acad Sci USA 2005;102:7894–9.
23 Belyantseva IA, Boger ET, Naz S, Frolenkov GI, Sellers JR, Ahmed ZM,Griffith AJ, Friedman TB. Myosin-XVa is required for tip localization of whirlinand differential elongation of hair-cell stereocilia. Nat Cell Biol2005;7:148–56.
24 Povey S, Lovering R, Bruford E, Wright M, Lush M, Wain H. The HUGO GeneNomenclature Committee (HGNC). Hum Genet 2001;109:678–80.
25 Chen W, Kahrizi K, Meyer NC, Riazulhosseini Y, Van Camp G,Najamabadi H, Smith RJH. Mutation of COL11A2 causes autosomal recessivenon-syndromic hearing loss at DFNB53 locus. J Med Genet 2005;42:e61.
Mutations of TMHS and hearing loss 639
www.jmedgenet.com

26 Maquat LE. Nonsense-mediated mRNA decay: splicing, translation and mRNPdynamics. Nat Rev Mol Cell Biol 2004;5:89–99.
27 Lagziel A, Ahmed ZM, Schultz JM, Morell RJ, Belyantseva IA, Friedman TB.Spatiotemporal pattern and isoforms of cadherin 23 in wild type andwaltzer mice during inner ear hair cell development. Dev Biol2005;280:295–306.
28 Michel V, Goodyear RJ, Weil D, Marcotti W, Perfettini I, Wolfrum U, Kros CJ,Richardson GP, Petit C. Cadherin 23 is a component of the transient lateral
links in the developing hair bundles of cochlear sensory cells. Dev Biol2005;280:281–94.
29 Tlili A, Mannikko M, Charfedine I, Lahmar I, Benzina Z, Ben Amor M, Driss N,Ala-Kokko L, Drira M, Masmoudi S, Ayadi H. A novel autosomal recessivenon-syndromic deafness locus, DFNB66, maps to chromosome 6p21.2-22.3in a large Tunisian consanguineous family. Hum Hered 2005;60:123–8.
30 Petit C, Levilliers J, Hardelin JP. Molecular genetics of hearing loss. Annu RevGenet 2001;35:589–646.
Clinical Evidence—Call for contributors
Clinical Evidence is a regularly updated evidence-based journal available worldwide both asa paper version and on the internet. Clinical Evidence needs to recruit a number of newcontributors. Contributors are healthcare professionals or epidemiologists with experience inevidence-based medicine and the ability to write in a concise and structured way.Areas for which we are currently seeking contributors:
N Pregnancy and childbirth
N Endocrine disorders
N Palliative care
N Tropical diseases
We are also looking for contributors for existing topics. For full details on what these topicsare please visit www.clinicalevidence.com/ceweb/contribute/index.jspHowever, we are always looking for others, so do not let this list discourage you.Being a contributor involves:
N Selecting from a validated, screened search (performed by in-house InformationSpecialists) epidemiologically sound studies for inclusion.
N Documenting your decisions about which studies to include on an inclusion and exclusionform, which we keep on file.
N Writing the text to a highly structured template (about 1500-3000 words), using evidencefrom the final studies chosen, within 8-10 weeks of receiving the literature search.
N Working with Clinical Evidence editors to ensure that the final text meets epidemiologicaland style standards.
N Updating the text every 12 months using any new, sound evidence that becomes available.The Clinical Evidence in-house team will conduct the searches for contributors; your task issimply to filter out high quality studies and incorporate them in the existing text.
If you would like to become a contributor for Clinical Evidence or require more informationabout what this involves please send your contact details and a copy of your CV, clearlystating the clinical area you are interested in, to [email protected].
Call for peer reviewers
Clinical Evidence also needs to recruit a number of new peer reviewers specifically with aninterest in the clinical areas stated above, and also others related to general practice. Peerreviewers are healthcare professionals or epidemiologists with experience in evidence-basedmedicine. As a peer reviewer you would be asked for your views on the clinical relevance,validity, and accessibility of specific topics within the journal, and their usefulness to theintended audience (international generalists and healthcare professionals, possibly withlimited statistical knowledge). Topics are usually 1500-3000 words in length and we wouldask you to review between 2-5 topics per year. The peer review process takes placethroughout the year, and out turnaround time for each review is ideally 10-14 days.If you are interested in becoming a peer reviewer for Clinical Evidence, please complete thepeer review questionnaire at www.clinicalevidence.com/ceweb/contribute/peerreviewer.jsp
640 Shabbir, Ahmed, Khan, et al
www.jmedgenet.com