Multisystemic therapy with violent and chronic juvenile offenders and their families: The role of...
13
Journal of Consulting and Clinical Psychology IW.Vol. 65, No. 5, 821-833 Copyright 1997 by the American Psychological Association, Inc. 0022-006X797/S3.00 Multisystemic Therapy With Violent and Chronic Juvenile Offenders and Their Families: The Role of Treatment Fidelity in Successful Dissemination Scott W. Henggeler Medical University of South Carolina Gary B. Melton University of South Carolina Michael J. Brondino Medical University of South Carolina David G. Scherer University of New Mexico Jerome H. Hanley South Carolina Department of Mental Health The effects of multisystemic therapy (MST) in treating violent and chronic juvenile offenders and their families in the absence of ongoing treatment fidelity checks were examined. Across 2 public sector mental health sites, 155 youths and their families were randomly assigned to MST versus usual juvenile justice services. Although MST improved adolescent symptomology at posttreatment and decreased incarceration by 47% at a 1.7-year follow-up, findings for decreased criminal activity were not as favorable as observed on other recent trials of MST. Analyses of parent, adolescent, and therapist reports of MST treatment adherence, however indicated that outcomes were substantially better in cases where treatment adherence ratings were high. These results highlight the importance of maintaining treatment fidelity when disseminating complex family-based services to community settings. The management of violent and chronic juvenile offenders has become an important issue on the nation's social policy agenda, largely because of the considerable social and economic costs exacted by these youths. For example, chronic juvenile offenders are at high risk for mental health problems, substance abuse, poor physical health, low educational and vocational pro- ductivity, and interpersonal difficulties (Farrington, 1991; Laub & Sampson, 1994). Likewise, the financial cost of violent crime is staggering, with costs pertaining to victimization (i.e., Scott W. Henggeler and Michael J. Brondino, Department of Psychia- try and Behavioral Sciences, Medical University of South Carolina; Gary B. Melton, Institute for Families in Society, University of South Carolina; David G. Scherer, College of Education, University of New Mexico; Jerome H. Hanley, Division of Children, Adolescents, and Their Families, South Carolina Department of Mental Health. Preparation of this article was supported by Grant R18MH48136 originally from the National Institute of Mental Health and later trans- ferred to the Center for Mental Health Services, Substance Abuse and Mental Health Services Administration. Special thanks go to Joseph Bevilacqua, Ida Wannamaker, Bessie Abraham, and Gary Moneypenny of the South Carolina Department of Mental Health; Mary Jane Sanders, Dottie Reynolds, James Lucas, and Margaret Barber of the South Caro- lina Department of Juvenile Justice; and the therapists and research assistants without whose help the project would not have been possible. Correspondence concerning this article should be addressed to Scott W. Henggeler, Family Services Research Center, Department of Psychia- try and Behavioral Sciences, 171 Ashley Avenue, Medical University of South Carolina, Charleston, South Carolina 29425. health related, lost productivity, reduced quality of life), law enforcement, and the maintenance and expansion of the correc- tional system (Cohen, Miller, & Rossman, 1994). Compounding the problems posed by violent and chronic juvenile offenders is the general lack of success that mental health and juvenile justice services have had in ameliorating the serious antisocial behavior of youth (Melton & Pagliocca, 1992; Tate, Reppucci, & Mulvey, 1995). Recently, however, an innova- tive family- and home-based treatment (multisystemic therapy; Henggeler & Borduin, 1990; Henggeler, Schoenwald, Borduin, Rowland, & Cunningham, in press) has documented long-term reductions in the criminal activity of serious juvenile offenders in two randomized trials. With a sample of violent and chronic juvenile offenders at imminent risk of incarceration, Henggeler and his colleagues (Henggeler, Melton, & Smith, 1992; Heng- geler, Melton, Smith, Schoenwald, & Hanley, 1993) showed that multisystemic therapy (MST) improved family functioning at posttreatment, reduced incarceration at a 59-week follow-up, and reduced rearrest at a 2.4-year follow-up. Importantly, such outcomes for MST were achieved at considerable cost savings. Similarly, with a sample of chronic juvenile offenders, Borduin et al. (1995) showed that MST unproved individual and family functioning at posttreatment and greatly reduced violent and other criminal activity at a 4-year follow-up. The success of MST has been attributed to several characteris- tics that differentiate this treatment model from other empiri- cally based treatment approaches (Henggeler, Schoenwald, & Pickrel, 1995). First, MST addresses the multiple known deter- 821
Transcript of Multisystemic therapy with violent and chronic juvenile offenders and their families: The role of...

Journal of Consulting and Clinical PsychologyIW.Vol. 65, No. 5, 821-833
Copyright 1997 by the American Psychological Association, Inc.0022-006X797/S3.00
Multisystemic Therapy With Violent and Chronic Juvenile Offendersand Their Families: The Role of Treatment Fidelity
in Successful Dissemination
Scott W. HenggelerMedical University of South Carolina
Gary B. MeltonUniversity of South Carolina
Michael J. BrondinoMedical University of South Carolina
David G. SchererUniversity of New Mexico
Jerome H. HanleySouth Carolina Department of Mental Health
The effects of multisystemic therapy (MST) in treating violent and chronic juvenile offenders andtheir families in the absence of ongoing treatment fidelity checks were examined. Across 2 publicsector mental health sites, 155 youths and their families were randomly assigned to MST versususual juvenile justice services. Although MST improved adolescent symptomology at posttreatmentand decreased incarceration by 47% at a 1.7-year follow-up, findings for decreased criminal activitywere not as favorable as observed on other recent trials of MST. Analyses of parent, adolescent, andtherapist reports of MST treatment adherence, however indicated that outcomes were substantiallybetter in cases where treatment adherence ratings were high. These results highlight the importanceof maintaining treatment fidelity when disseminating complex family-based services to communitysettings.
The management of violent and chronic juvenile offendershas become an important issue on the nation's social policyagenda, largely because of the considerable social and economiccosts exacted by these youths. For example, chronic juvenileoffenders are at high risk for mental health problems, substanceabuse, poor physical health, low educational and vocational pro-ductivity, and interpersonal difficulties (Farrington, 1991;Laub & Sampson, 1994). Likewise, the financial cost of violentcrime is staggering, with costs pertaining to victimization (i.e.,
Scott W. Henggeler and Michael J. Brondino, Department of Psychia-try and Behavioral Sciences, Medical University of South Carolina; GaryB. Melton, Institute for Families in Society, University of South Carolina;David G. Scherer, College of Education, University of New Mexico;Jerome H. Hanley, Division of Children, Adolescents, and Their Families,South Carolina Department of Mental Health.
Preparation of this article was supported by Grant R18MH48136originally from the National Institute of Mental Health and later trans-ferred to the Center for Mental Health Services, Substance Abuse andMental Health Services Administration. Special thanks go to JosephBevilacqua, Ida Wannamaker, Bessie Abraham, and Gary Moneypennyof the South Carolina Department of Mental Health; Mary Jane Sanders,Dottie Reynolds, James Lucas, and Margaret Barber of the South Caro-lina Department of Juvenile Justice; and the therapists and researchassistants without whose help the project would not have been possible.
Correspondence concerning this article should be addressed to ScottW. Henggeler, Family Services Research Center, Department of Psychia-try and Behavioral Sciences, 171 Ashley Avenue, Medical University ofSouth Carolina, Charleston, South Carolina 29425.
health related, lost productivity, reduced quality of life), lawenforcement, and the maintenance and expansion of the correc-tional system (Cohen, Miller, & Rossman, 1994).
Compounding the problems posed by violent and chronicjuvenile offenders is the general lack of success that mentalhealth and juvenile justice services have had in ameliorating theserious antisocial behavior of youth (Melton & Pagliocca, 1992;Tate, Reppucci, & Mulvey, 1995). Recently, however, an innova-tive family- and home-based treatment (multisystemic therapy;Henggeler & Borduin, 1990; Henggeler, Schoenwald, Borduin,Rowland, & Cunningham, in press) has documented long-termreductions in the criminal activity of serious juvenile offendersin two randomized trials. With a sample of violent and chronicjuvenile offenders at imminent risk of incarceration, Henggelerand his colleagues (Henggeler, Melton, & Smith, 1992; Heng-geler, Melton, Smith, Schoenwald, & Hanley, 1993) showed thatmultisystemic therapy (MST) improved family functioning atposttreatment, reduced incarceration at a 59-week follow-up,and reduced rearrest at a 2.4-year follow-up. Importantly, suchoutcomes for MST were achieved at considerable cost savings.Similarly, with a sample of chronic juvenile offenders, Borduinet al. (1995) showed that MST unproved individual and familyfunctioning at posttreatment and greatly reduced violent andother criminal activity at a 4-year follow-up.
The success of MST has been attributed to several characteris-tics that differentiate this treatment model from other empiri-cally based treatment approaches (Henggeler, Schoenwald, &Pickrel, 1995). First, MST addresses the multiple known deter-
821

822 HENGGELER, MELTON, BRONDINO, SCHERER, AND HANLEY
minants of serious antisocial behavior (i.e., individual, family,
peer, school, and community factors; Elliott, 1994; Thornberry,
Huizinga, & Loeber, 1995; Tolan & Guerra, 1994) in a compre-
hensive, yet individualized, fashion. Second, identified problems
are treated in the natural ecology of the youth and his or her
family. The provision of services in home, school, and other
community locations overcomes barriers to service access and
largely negates problems of treatment generalization. Third, the
MST therapist training protocol brings a level of clinical rigor
to community settings that is similar in intensity to that used in
clinical trials conducted in university settings (Weisz, Donen-
berg, Weiss, & Han, 1995). This training protocol includes four
components: 5 days of orientation to MST principles, quarterly
booster training, weekly on-site supervision consistent with the
MST model, and weekly treatment integrity checks through
consultation with an expert in MST.
With the documented success of MST when implemented
by therapists working in community (Henggeler et al., 1992;
Henggeler et al., 1993) and university (Borduin et al., 1995)
settings, important directions in the further validation of this
treatment model pertain to the parameters of its successful dis-
semination. The purpose of this study, therefore, was to deter-
mine whether the effectiveness of MST could be maintained in
community mental health settings when experts in MST did not
provide significant clinical oversight. In previous clinical trials
of MST (Borduin et al., 1995; Brunk, Henggeler, & Whelan,
1987; Henggeler et al., 1991; Henggeler et al., 1992; Henggeler,
Pickrel, & Brondino, 1997; Henggeler et al., 1986), an MST
expert hired or consulted with regard to the hiring of therapists
and provided weekly expert consultation to therapists to enhance
treatment fidelity. Such extensive involvement of an MST expert
might constitute financial and administrative barriers to the
broader dissemination of MST; that is, weekly consultation with
an MST expert adds an additional cost to a project for both the
therapists' and consultant's time, relatively few MST experts are
available to provide such consultation, and many experienced
therapists and administrators are reluctant to embrace a form
of oversight that emphasizes program features that may conflict
with current practices (e.g., MST emphasizes program account-
ability for clinical outcomes).
[n consideration of these financial and administrative barriers,
the present public-academic collaboration (Bray & Bevilacqua,
1993) examined the effectiveness of MST under conditions that
reflect one real-world (and convenient) option for the dissemi-
nation of MST. Program administrators at two public community
mental health center sites had primary authority for hiring thera-
pists to deliver MST home-based services. In addition, an MST
expert did not provide weekly integrity checks and consultation
to project therapists and supervisors. Thus, the MST training
protocol took the form of the types of clinical training that are
typically provided in community mental health settings: in-
tensive workshops with little follow-up to monitor treatment
adherence.
In summary, the present study examined whether MST effects
with violent and chronic juvenile offenders could be maintained
when MST training and fidelity checks were similar to prevailing
clinical practices (i.e., workshop training, minimal attention to
treatment adherence). If the treatment effects could be main-tained, the effective dissemination of this complex treatment
model could be greatly expedited. On the other hand, if treatment
effects similar to previous studies were not observed, such fail-
ure to replicate could be due to difficulties in therapist adherence
to the MST treatment protocol. In anticipation of this possibility,
parent, adolescent, and therapist ratings of MST treatment adher-
ence were assessed, and associations between adherence and
clinical outcomes are reported.
Method
Design
The study followed a 2 X 2 X 2 Condition (MST vs. usual services
[US]) X Time (pretest vs. posttest) x Site (Site 1 [SI] vs. Site 2 [S2])
mixed factorial design, with families randomly assigned to treatment
conditions (WMST = 82, raus = 73). In addition to the pretest and posttest
data reported here, we conducted a 1.7-year follow-up to examine arrest
and incarceration rates. To further control for historical and related
threats to validity, we temporally yoked the families assigned to receive
MST services with families assigned to receive the usual services af-
forded to offending youths by the South Carolina Department of Juvenile
Justice (DJJ). Because families were referred by the DJJ staff in a
family's county of residence and rates of referral were very low at certain
times of the year in the more rural and sparsely populated counties, four
of the families in the MST condition could not be yoked to a comparison
family. An additional five MST families were not yoked, either because
of a family's acceptance at the end of the project, when there remained
insufficient time to recruit a comparison family, or because of participant
attrition as is described later.
As a precondition for locating the project at each of the sites, the
judges and solicitors agreed that project participants (chronic or violent
juvenile offenders) would be initially placed on probation rather than
removed from the community as part of the research design. As part of
this arrangement, a judge's consent to remain in the community was
obtained by project staff for each youth recruited in the study. %uths
were randomly assigned to a treatment condition only after the court's
consent was obtained. Moreover, the judges, solicitors, public defenders,
and other court-related personnel were kept unaware of the treatment
condition of the youth through a process agreed on by all parties before
the project's inception.
Sites
The two sites were chosen to achieve representation of racial group
and urban and rural settings. Each site covered a three county area. The
first, SI, encompassed urban and rural areas and had a majority Cauca-
sian population (77.8%; U.S. Bureau of the Census, 1993). S2 was
predominantly rural and majority African American (58.4%; U.S. Bu-
reau of the Census, 1993). Each site was staffed by a therapy team
consisting of two full-time therapists and a therapist supervisor who
were housed in a regional community mental health center of the South
Carolina Department of Mental Health or in one of the center's satellite
offices.
Participants
Participants were 155 violent or chronic juvenile offenders and their
primary caregivers. To be included, the adolescents had to (a) be between
11 and 17 years of age, (b) have committed a serious criminal offense
or have at least three prior criminal offenses other than status offenses,
and (c) be at imminent risk of being placed outside the home because
of serious criminal involvement. At the time of referral, the 155 youths
ranged in age from 10.4 to 17.6 years (M = 15.22), 81.9% were male,
80.6% were African American, and 19.4% were Caucasian. Approxi-

THE ROLE OF TREATMENT FIDELITY 823
mately 40% of the age-eligible adolescents reported being employed
full-time or part-time, and 79% of the sample were in school. The
majority of the youths were from single-parent homes (38.1%) or lived
with their biological mother and another adult who was not their biologi-
cal father (31.6%). The youths averaged 3.07 prior arrests (SD = 2.07),
40% had at least one prior arrest for a violent crime, and 59% had at
least one previous incarceration. The youths' pre-entry offenses averaged
8.8 (SD = 2.21) on a 17-point Seriousness scale (Hanson, Henggeler,
Haefele, & Rodick, 1984) on which low scores were characterized by
status offenses; midrange values by crimes such as assault and battery,
breaking and entering, and carrying a dangerous weapon; and high scores
by armed robbery and criminal sexual conduct.
Primary caregivers ranged in age from 25,5 to 75.5 years (M =
41.30) and were predominantly female (92.2%) and African American
(80.6%). Mothers were overwhelmingly represented as primary caregiv-
ers (n = 136), although the sample also included 10 grandmothers, 3
fathers, 4 other family members (e.g., aunts, sisters, etc.), and 2 foster
parents as primary caregivers. Approximately 50% of the youths lived
in two-parent households, although only 15% lived with two biological
parents. The average family had 5.0 family members (SD = 2.18). Only
14.2% of the adolescents' mothers and 3.2% of fathers had attended
college or were college graduates, and most of the mothers (55.6%) and
many of the fathers (38.1%) had not completed high school. Consistent
with relatively low levels of parental education, the median family in-
come was between $5,000 and $10,000 per year. Moreover, the sample
was quite mobile, with 25.2% having moved at least once in the year
before the pretest and 16.1% having made two or more moves during
the same period. The aforementioned demographic characteristics did
not differ between site or treatment conditions.
Treatment Conditions
MST. The conceptual foundation of MST is Bronfenbrenner's
(1979) theory of social ecology in which the process of human develop-
ment is viewed as a reciprocal interchange between the individual and
interconnected systems including, but not limited to, the family, extended
family, peer, school, work, community, and cultural contexts. From this
perspective, and consistent with findings from the delinquency causal-
modeling literature (Henggeler, 1991), problem behaviors are under-
stood to be multidetermined and linked with the multiple systems in
which youths and families are embedded. Thus, the scope of MST
interventions is not limited to the individual adolescent or the family
system, but includes difficulties between other systems such as the fam-
ily-peer and family-school mesosystems.
Because of the varying demands of each case, MST therapists must
be capable of applying a range of empirically based therapeutic ap-
proaches (e.g., structural family therapy, cognitive behavior therapy) and
tailoring interventions to the unique needs and strengths of each family.
Consistent with family preservation models of treatment delivery, MST
services are most often provided in the home at times that are convenient
for the families—although it is not unusual for meetings to be held in
schools, neighborhood settings, social service agencies, and elsewhere
in the community. MST treatment goals are family driven, rather than
therapist driven, and family members are viewed as full partners and
collaborators in the treatment process. Given the complexity of interven-
tions involving MST, the behavior of the therapists is governed by a set
of nine treatment principles (see Appendix A), rather than explicitly
delineated as a set of sequential and invariant steps or techniques. These
principles are delineated in a treatment manual (Henggeler et al., 1994)
and volume (Henggeler et al., in press), and extensive clinical descrip-
tions are provided by Henggeler and Borduin (1990). Therapist adher-
ence to these treatment principles serves to operationalize MST treatment
fidelity.
Ten MST therapists participated (five per site over the course of the
project), and all were masters-level mental health professionals with
backgrounds in social work or pastoral counseling. Prior clinical experi-
ence varied considerably, ranging from 1 to 15 years of direct service
provision. Supervisory therapists were required to have had at least 2
years of clinical experience. Despite considerable effort to recruit thera-
pists at each site to achieve mixed gender and racial representation,
balance was achieved only for gender; with three male therapists and
two female therapists in each site. The applicant pools in each site
corresponded to the majority racial group in that region, with the result
that all the therapists and therapist supervisors were African American
in S2 and all were Caucasian in SI.
The therapists were trained in MST using one of two training proto-
cols. The first group of therapists (n = 6) was provided with 6 days of
intensive didactic and experiential training that included role playing,
critical analysis of cases, and problem solving exercises. These training
sessions were videotaped in full, and the videotapes were used as the
principal instructional modality for a second group (n = 4) of therapists.
This second group comprised one late hire in SI and replacement thera-
pists from both sites because of staff turnover. Both groups were pro-
vided with a copy of a treatment manual describing MST.
Treatment integrity was supported by means of direct therapist super-
vision provided by the therapist supervisors in individual sessions held
once each week and in weekly staffings that included the therapist super-
visor; the coordinator of child, adolescent, and family services from
each regional mental health center; and the program coordinator. The
families averaged 122.6 days (SD = 32.6 days, range = 68-226 days)
and 116.6 days (SD = 39.8 days, range = 60-286 days) in treatment
in SI and S2, respectively. In addition, quarterly booster trainings were
held to discuss current cases and increase the therapists' overall under-
standing of MST. However, as noted previously and in contrast with
other evaluations of MST, the therapists did not have weekly access to
consultation with an expert in MST.
US. Youths in the US condition were, without exception, placed on
probation for a minimum of 6 months and, depending on the nature of
the adolescent's offenses, were often further instructed by the courts to
make restitution. During probation, the youth was typically seen by his
or her probation officer at least once per month, although in some cases
a youth may have been seen as frequently as once per week. The youth's
school attendance was monitored during this time, and he or she was
referred to other social service agencies (e.g., the Department of Mental
Health, alcohol and drug abuse programming, vocational counseling
or training) for help in particular problem areas. Youth experiencing
difficulties in school were occasionally placed in alterative schooling or
referred to special programs for school dropouts. If progress was not
noted in the case during the probation period, DJJ had the option of
initiating an out-of-home placement.
Research Procedures
Participants were referred to the project by DJJ intake officers in the
family's county of residence following the juvenile's arrest for a criminal
offense. When an opening occurred in the project, a list of names of all
adolescents meeting the eligibility criteria at that time was compiled by
the intake personnel at the local DJJ offices. A research assistant at each
site then randomly selected a number of families equal to the number
of openings (plus two alternates in case of refusals) from the list. These
families were approached by a project staff member either at the local
DJJ office or in the family home, the project was explained in full, and
the families were asked to participate in the study. Over the course of
the project, only 6.6% of the families approached refused to participate.
After we received written informed consent, the family was randomly
assigned to a treatment condition, and the initial assessment made within
3 days of consent but before the beginning of therapy for the MST
condition. The identical assessment battery was administered to an MST

824 HENGGELER, MELTON, BRONDDSKX SCHERER, AND HANLEY
family and its yoked comparison within 72 hr of the termination of the
MST family from therapy. Families were paid $50 for each completed
assessment battery. In addition to the outcome measures, families in the
MST condition were asked to complete treatment adherence measures
following two randomly selected therapy sessions during the fourth and
eighth weeks of therapy.
Measures
The assessment battery was developed to tap key constructs represent-
ing instrumental and ultimate outcomes. An emphasis was placed on
measuring the constructs from multiple perspectives. Ultimate outcomes
tapped the adolescents' criminal activity and incarceration rates and the
primary caregivers' and adolescents* emotional-behavioral functioning.
Instrumental outcomes included changes in family functioning and the
adolescents' peer relations. In addition, parents, youths, and therapists
in the MST condition completed a treatment adherence questionnaire at
two intervals during treatment.
Individual emotional adjustment and adolescent behavior problems.
Primary caregiver and adolescent psychological distress were assessed
by the Global Severity Index (GSI) of the Brief Symptom Inventory
(BSI; Derogatis, 1993), which is a short form of the Symptom Check-
list—90—Revised. The 53 self-report items of the BSI are rated on a
scale ranging from 0 (not bothered in the previous week by the symptom)
to 4 (extremely bothered by that symptom). The GSI is considered the
best single index of respondent emotional distress and is formed by
summing scores across the items and dividing by the total number of
items. Coefficient alphas for the BSI subscales range from .71 to .85,
test-retest reliability is .90 for the GSI, and the subscale scores correlate
.90 or above with those of the SCL-90-R subscales. As described in
the manual (Derogatis, 1993), numerous studies have supported the
convergent, discriminant, and predictive validity of the BSI. A sample
item is, "How much are you bothered by feelings that others are to
blame for most of your troubles?"
Adolescent behavior problems were assessed through caregiver re-
ports (total score) on the 89-item Revised Problem Behavior Checklist
(RBPC; Quay & Peterson, 1987). The RBPC has strong psychometric
properties (McMahon & Forehand, 1988) and has predicted serious
offense history in delinquents (Hanson et al., 1984). Item scores range
from 0 (no problem) to 2 (severe problem), and caregivers are asked
to indicate how much, for example, "staying out late" and "stealing in
company of others" has been a problem for their child.
Criminal activity. Adolescent responses on the Self-Report Delin-
quency Scale (3RD; Elliott, Ageton, Huizinga, Knowles, & Canter,
1983) were used to assess youth reports of criminal activity during the
previous 3 months. The 40-item SRD, used in the National \buth Survey,
is probably the best validated of the self-report delinquency scales1
(Henggeler, 1989) and includes a General Delinquency scale that pro-
vides a summary measure of criminal offenses and an Index Offense
scale that includes only relatively serious offenses. Elliott et al. (1983)
reported test-retest reliabilities for SRD subscales to range from .80-
.99, and the discriminant validity and predictive validity have been
supported with chronic offenders (Dunford & Elliott, 1984) and serious
offenders (Elliott, Huizinga, & Ageton, 1985). Moreover, the SRD has
been sensitive to MST treatment effects in a previous clinical trial (Heng-
geler et al., 1992). A sample item is, "How many times in the past 3
months have you stolen (or tried to steal) a motor vehicle, such as a
car or motorcycle?"
Arrest and incarceration histories of the adolescents were obtained
from a database maintained by the DJJ that includes offense, arrest,
adjudication, and incarceration histories. These data were collected ap-
proximately 1.7 years from the project's ending date for all participants.
Offenses were coded as to their severity using the Seriousness Index
developed by Hanson et al. (1984). In the analyses that follow, a time
point 100 days past the adolescent's 17th birthday or the date of the
final data collection was used as a cutpoint because DJJ records do not
extend past the 17th birthdate of a client. The additional 100 days
allowed us to take into account the lag in reporting that usually takes
place in service systems.
Family relations. The Family Adaptability and Cohesion Evaluation
Scales (FACES-III; Olson, Portner, & Lavee, 1985) and Family Assess-
ment Measure (FAM-JJI; Skinner, Steinhauer, & Santa-Barbara, 1983)
were used to assess family functioning with separate reports being made
by the primary caregiver and the adolescent. The 20 items on the FACES-
III (Olson et al., 1985) assess family adaptability and cohesion. The
validity of this self-report instrument has been supported in previous
research on delinquency (Rodick, Henggelei; & Hanson, 1986) and with
violent juvenile offenders (Blaske, Borduin, Henggeler, & Mann, 1989).
Internal consistency has been estimated to be .67 for the Adaptability
subscale and .77 for the Cohesion subscale. The Lifcert-type items are
rated on a scale from 1 (almost never) to 5 (almost always). Consistent
with the recommendations of Henggeler, Burr-Harris, Borduin, and
McCallum (1991), the Cohesion subscale and Adaptability subscale
scores were treated as linear in the analyses. A sample item is, "Family
members feel closer to other family members than to people outside of
the family." The FAM-III is a 50-item self-report measure that covers
the areas of task accomplishment, role performance, communication,
affective involvement, and control. Responses to items are made on a
scale ranging from 1 (strongly agree) to 4 (strongly disagree). The
General Index provides an overall measure of family functioning and is
derived by summing across the 50 items. Low scores on the FAM-III
indicate low rates of problems and high scores indicate increased prob-
lems. Internal consistency for the General Scale has been estimated to
be .93 for adults and .94 for children. A sample item is, "We are as
well adjusted as any family could possibly be."
Parental monitoring. The parent version of the Monitoring Index
(Patterson &. Dishion, 1985) contains 17 items representing aspects of
monitoring behavior (e.g., the parents' direct supervision of, control of,
and trust in the child; the number of hours per day that the child is
un supervised; and a dichotomous item indicating whether the child wan-
ders from home in the evening unsupervised). Factor scores were formed
using the scoring procedures originally developed for the measure. An
overall monitoring index was created by summing the factor scores
associated with parental control and direct supervision and adjusting
these scores through subtraction for leaving the child unsupervised and
allowing the child to wander. The adolescent version of the Monitoring
Index was formed by summing across the factors on the 14-item adoles-
cent version of the scale. Information on the reliability and validity of
the indices reported here are not currently available, but over a decade
of research has examined the associations between composites of these
items and measures of antisocial behavior in children (Patterson, Reid, &
Dishion, 1992). The following sample item was taken from the parent
version: "If s/he tells you that s/he is going to a friend's house, how
often do you think that s/he will be there?"
Peer relations. Adolescent peer relations were assessed using pri-
mary caregiver and adolescent reports on the 13-item Missouri Peer
Relations Inventory (MPRJ; Borduin, Blaske, Cone, Mann, & Hazelrigg,
1989) and adolescent responses to the 14-item Parent Peer Conformity
Inventory (PPC1; Berndt, 1979). Results of factor analyses indicate that
the items on the MPRI represent three dimensions of adolescent peer
relationships: emotional bonding, aggression, and social maturity. This
three-dimensional factor structure has been replicated, and the subscales
have been demonstrated to have acceptable internal consistency (.65-
.82) and test-retest reliability (.71-.94) over a two week interval
(Blaske, Borduin, Henggeler, & Mann, 1989). A sample item is, "Please
circle the number on the 5-point scale that best describes your child's:
temper: lack of impulse control with friends." The PPCI was used to
measure prosocial and antisocial peer conformity. This instrument pro-

THE ROLE OF TREATMENT FIDELITY 825
vides the respondent with a brief description of a scenario such as being
in a position to cheat off a copy of an exam accidentally dropped by a
teacher. The adolescent is then asked to tell what he or she would dounder those circumstances. A difference score created by subtracting thescore on the Antisocial Behavior subscale from that of the Prosocial
subscale provides an index of reported antisocial peer conformity. Relia-bility is satisfactory for antisocial conformity (.81) but poor for proso-
cial conformity (Berndt, 1979). The validity of the PPCI has beensupported in a study of adolescent drug use and criminal behavior(Brown, Clasen, & Eicher, 1986).
MST treatment adherence. The MST Adherence Measure (Heng-geler & Borduin, 1992) is a 26-item Likert-format questionnaire de-signed to measure family and therapist behaviors specific to the practiceof MST. MST is specified through therapist adherence to nine treatment
principles (Appendix A), and, as such, items were developed by expertconsensus to reflect these principles (Appendix B). The adherence mea-sures were completed by the parents (n = 62), adolescents (n = 67),
and therapists (n = 77) after randomly selected therapy sessions duringthe fourth and eighth weeks of therapy for each family in the MST
condition.
To delineate the central constructs tapped by the adherence measureand to reduce the number of variables for use in the data analyses,
separate exploratory factor analyses using a maximum likelihood (ml)extraction method and nonorthogonal rotations were completed for eachgroup of respondents. Input data matrices were constructed by averaging
the four and eight week ratings on the adherence measures. As an initial
step in the factor analyses for each group, a principal components analy-sis was run and a scree plot was output from the analysis. On the basis
of the scree plot and using the criterion of the number of eigenvaluesgreater than 1.0, a starting point for the optimal number of factors wasidentified for the analysis of the data for each group of respondents.
Factor analyses were then conducted for the parent, adolescent, andtherapist groups with solutions obtained for ±2 factors around the ini-tially identified optimum number of factors. The final choice of solutions
was based on the criterion of the interpretability of the results.
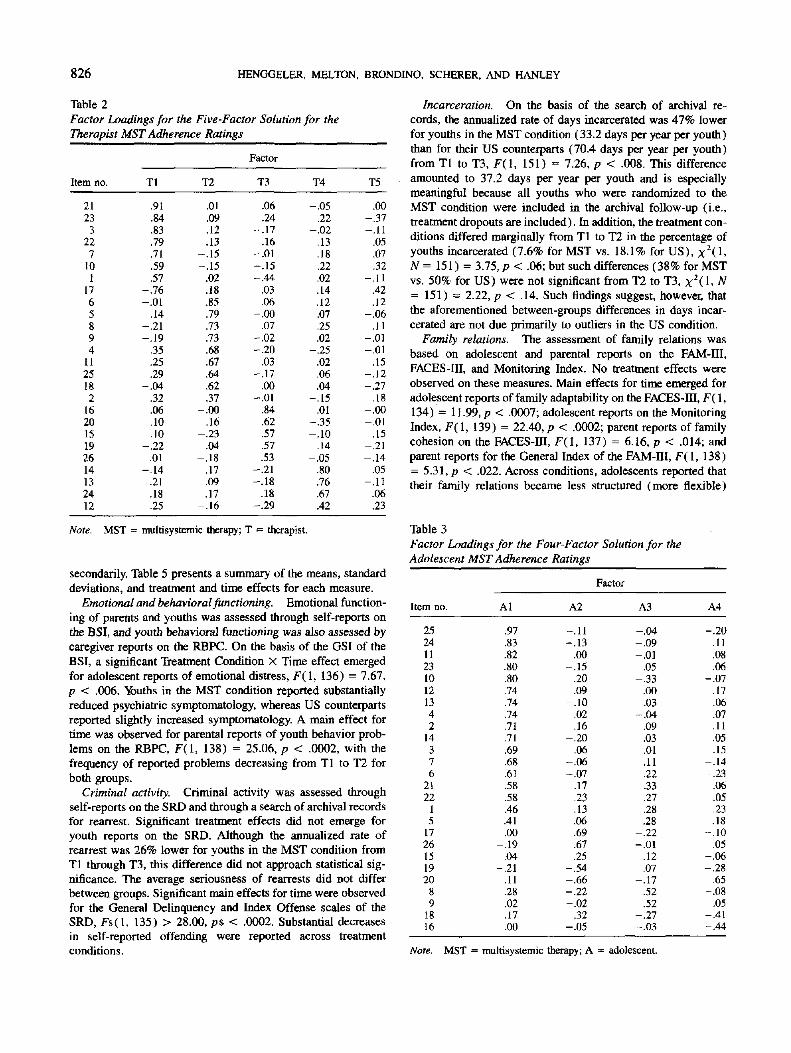
From these analyses, we selected a six-factor solution for the parentdata, a five-factor solution for the therapist data, and a four-factor solu-
tion for the adolescent data as most interpretable. Table 1, Table 2, and
Table 3 list the items and factor loadings for each group of respondents,and the interfactor correlations are provided in Table 4. The six-factor
solution for the parent ratings included factors representing: therapistadherence to the MST treatment principles, the degree to which thesessions were nonproductive, the effort by the family and therapist tosolve the family's problems, therapist attempts to change the family's
interactions within the family and with persons outside of the family, alack of therapeutic direction in the session, and the degree of family-therapist consensus. The five dimensions characterizing the therapist
ratings included factors representing: engagement of the family, adher-ence to the MST principles, the degree to which the sessions werenonproductive, the need of the therapist to focus on the family's noncom-
pliance, and the degree of family-therapist conflict. For the adolescentdata, the following factors were represented: therapist adherence to theMST principles, therapist focus on the family's noncompliance, lack ofdirection in the sessions, and level of productivity of the sessions,
Table 1
Factor Loadings for the Six-Factor Solution for the Primary
Caregiver MST Adherence Ratings
Results
Attrition
Between pretest and posttest, 9.7% (n = 15) of the families
were lost from the study because of their having moved out of
South Carolina, death, or voluntary withdrawal from the re-
search protocol. Differences between the project dropouts («MST
= 7, nus = 8) and project completers (n = 140) were examined
Factor
Item no.
232565
112113122
221424
1171526163498
1819207
10
PI
.94
.91
.88
.88
.82
.82
.79
.78
.74
.71
.61
.58
.45-.06
.10
.01-.09
.18
.25
.00
.06
.06-.01-.09
.55
.22
P2
-.09.07
-.07.02
-.14.00.03
-.10.20
-.11.12.10.27.77.72.46.39.08.02
-.09.14
-.08.22
-.02-.02-.04
P3
-.01.01
-.06-.02
.05
.06-.05-.19
.22
.21-.03
.01
.03
.04-.09
.07
.17
.75
.71
.08-.08
.08-.08
.16
.31
.39
P4
.08-.05-.03-.14
.00
.03-.05-.01-.11
.06.11.19.13
-.09.10.27
-.14.04.04.79.75.20.06.26
-.06-.02
P5
.03
.05
.23
.21
.21-.09-.16-.03-.13-.02-.17-.11-.24
.40
.00
.03-.07-.02
.12
.18
.11
.67
.60
.25
.07
-.14
P6
-13-.00
.14-.07
.10-.02
.41
.48-.21
.09.30.19.01.21
-.05-.02-.12
.09
.09
.04-.09-.08-.09
.02
.49
.46
Note. MST = multisystemic therapy; P = primary caregiver.
using univariate analyses of variance (ANOVAs) on pretest
scores on demographic and dependent measures. Dropouts were
denned as any participant who, for any reason, refused or was
unable to continue in the project. Primary caregiver reports
indicated that the mothers in the dropout group were slightly
better educated than were the completers, F(l, 153) = 6.81, p
< .02 (Md™,™,, = 12.29, Mcorop,̂ = 10.55). No other between-
groups differences were observed. The small number and some-
what equal distribution of dropouts across treatment conditions
in conjunction with the finding of no differences outside of the
mother's educational status suggests that participant attrition
should have little impact on the interpretation of the results
reported subsequently.
Treatment Effects
We conducted a series of 2 X 2 X 2 Time (pretreatment [Tl]
vs. posttreatment [T2]) X Treatment Condition (MST vs. US)
X Site (SI vs. S2) ANOVAs on the psychosocial measures
collected during the pretreatment and posttreatment assessments.
In addition, 2 x 2 (Treatment Condition X Site) ANCAfts were
used to evaluate longer term outcomes for rearrest and incarcera-
tion through the 1.7-year follow-up (T3). The following presen-
tation of outcomes focuses on treatment-related effects, as the
examination of such effects is the major thrust of the study.
Main effects for time- and site-related effects are presented
826 HENGGELER, MELTON, BRONDINO, SCHERER, AND HANLEY
Table 2
Factor Loadings for the Five-Factor Solution for the
Therapist MST Adherence Ratings
Item no.
21233
227
101
1765S94
1125182
162015192614132412
Tl
.91
.84
.83
.79
.71
.59
.57-.76-.01
.14-.21-.19
.35
.25
.29-.04
.32
.06
.10
.10-.22
.01-.14
.21
.18
.25
T2
.01
.09
.12
.13-.15-.15
.02
.18
.85
.79
.73
.73
.68
.67
.64
.62
.37-.00
.16-.23
.04-.18
.17
.09
.17-.16
Factor
T3
.06
.24-.17
.16-.01-.15-.44
.03
.06-.00
.07-.02-.20
.03-.17
.00-.01
.84
.62
.57
.57
.53-.21-.18
.18-.29
T4
-.05.22
-.02.13.18.22.02.14.12.07.25.02
-.25.02.06.04
-.15.01
-.35-.10
.14
-.05.80.76.67.42
T5
.00-.37-.11
.05
.07
.32-.11
.42
.12-.06
.11-.01-.01
.15-.12-.27
.18-.00-.01
.15-.21-.14
.05-.11
.06
.23
Note. MST = multisystemic therapy; T = therapist.
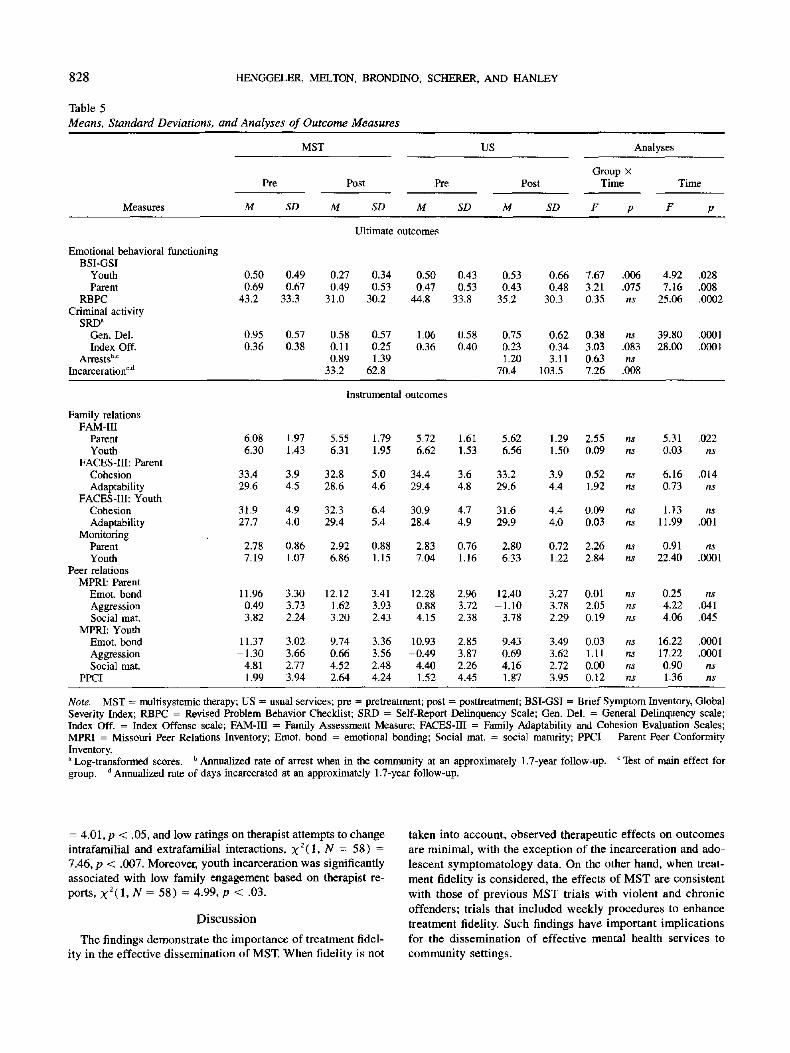
secondarily. Table 5 presents a summary of the means, standard
deviations, and treatment and time effects for each measure.
Emotional and behavioral functioning. Emotional function-
ing of parents and youths was assessed through self-reports on
the BSI, and youth behavioral functioning was also assessed by
caregiver reports on the RBPC. On the basis of the OS I of the
BSI, a significant Treatment Condition x Time effect emerged
for adolescent reports of emotional distress, F( 1, 136) = 7.67,
p < .006. \ouths in the MST condition reported substantially
reduced psychiatric symptomatology, whereas US counterparts
reported slightly increased symptomatology. A main effect for
time was observed for parental reports of youth behavior prob-
lems on the RBPC, F(\, 138) = 25.06, p < .0002, with the
frequency of reported problems decreasing from Tl to T2 for
both groups.
Criminal activity. Criminal activity was assessed through
self-reports on the SRD and through a search of archival records
for rearrest. Significant treatment effects did not emerge for
youth reports on the SRD. Although the annualized rate of
rearrest was 26% lower for youths in the MST condition from
Tl through T3, this difference did not approach statistical sig-
nificance. The average seriousness of rearrests did not differ
between groups. Significant main effects for time were observed
for the General Delinquency and Index Offense scales of the
SRD, Fs(l, 135) > 28.00, ps < .0002. Substantial decreases
in self-reported offending were reported across treatment
conditions.
Incarceration. On the basis of the search of archival re-
cords, the annualized rate of days incarcerated was 47% lower
for youths in the MST condition (33.2 days per year per youth)
than for their US counterparts (70.4 days per year per youth)
from Tl to T3, F(l, 151) = 7.26, p < .008. This difference
amounted to 37.2 days per year per youth and is especially
meaningful because all youths who were randomized to the
MST condition were included in the archival follow-up (i.e.,
treatment dropouts are included). In addition, the treatment con-
ditions differed marginally from Tl to T2 in the percentage of
youths incarcerated (7.6% for MST vs. 18.1% for US), x2O,
N = 151) = 3.75, p < .06; but such differences (38% for MST
vs. 50% for US) were not significant from T2 to T3, x2(l , N
= 151) = 2.22, p < .14. Such findings suggest, however, that
the aforementioned between-groups differences in days incar-
cerated are not due primarily to outliers in the US condition.
Family relations. The assessment of family relations was
based on adolescent and parental reports on the FAM-III,
FACES-HI, and Monitoring Index. No treatment effects were
observed on these measures. Main effects for time emerged for
adolescent reports of family adaptability on the FACES-III, F( \,
134) = 11.99, p < .0007; adolescent reports on the Monitoring
Index, F( 1, 139) = 22.40, p < .0002; parent reports of family
cohesion on the FACES-III, F(l, 137) = 6.16,p < .014; and
parent reports for the General Index of the FAM-III, F( 1, 138)
= 5.31, p < .022. Across conditions, adolescents reported that
their family relations became less structured (more flexible)
Table 3
Factor Loadings for the Four-Factor Solution for the
Adolescent MST Adherence Ratings
Factor
Item no.
2524112310121342
14376
2122
15
1726151920
89
1816
Al
.97
.83
.82
.80
.80
.74
.74
.74
.71
.71
.69
.68
.61
.58
.58
.46
.41
.00-.19
.04-.21
.11
.28
.02
.17
.00
A2
-.11-.13
.00-.15
.20
.09-.10
.02
.16-.20
.06-.06-.07
.17
.23
.13
.06
.69
.67
.25-.54-.66-.22-.02
.32-.05
A3
-.04-.09-.01
.05-.33
.00
.03-.04
.09
.03
.01
.11
.22
.33
.27
.28
.28-.22-.01
.12
.07-.17
.52
.52-.27-.03
A4
-.20-.11
.08-.06-.07
.17
.06
.07
.11
.05
.15-.14-.23
.06
.05
.23
.18-.10
.05-.06-.28
.65-.08
.05-.41-.44
Note. MST = multisysffimic therapy; A = adolescent.

THE ROLE OF TREATMENT FIDELITY 827
Table 4
Inter/actor Correlations for Adherence Factors by Respondent Group
Factor
Group and factor 3 4 5
Primary caregiver
PI. AdherenceP2. Nonproductive session
P3. Therapist-family problem solving effortP4. Therapist attempts to change interactionsP5. Lack of direction
P6. Family-therapist consensus
—.16.49.29.06.16
—.03.25.06
-.01
—.15.01
-.06
—.10 —.01 .05 —
Therapist
Tl. Engagement
T2. Therapist adherenceT3. Nonproductive session
T4. Need to focus on noncomplianceT5. Family-therapist conflict
—.49
-.35
.32
.43
—-.30
.38
.30
—-.29 —-.32 .18 —
Al. Adherence
A2. Family-therapist task-oriented sessionA3. Lack of directionA4. Nonproductive session
Adolescent
.10
.40
.23-.06
.10 .14 —
Note. P = primary caregiver; T = therapist; A = adolescent.
from Tl to T2 and that their parents monitored and supervised
them less. Parents reported that family cohesion decreased and
overall family functioning improved from Tl to T2.
Peer relations. The assessment of peer relations was based
on parent and youth reports on the MPRI and youth reports on
the PPCI. Treatment effects were not observed for either of these
instruments. On the MPRI, main effects for time emerged for
parental reports of youth aggression with peers, F(l, 137) =
4.22, p < .041, and social maturity with peers, F(l, 137) =
4.06, p < .045. Main effects for time also emerged for adoles-
cent reports of emotional bonding with peers, F(l, 136) =
16.22, p < .0001, and aggression with peers, F(l, 136) =
17.22, p < .0001. Adolescents reported increased aggression
and decreased emotional bonding with peers, whereas parents
reported decreased aggression and social maturity with peers.
MST Adherence and Ultimate Outcomes
As indicated above, MST had significant effects on two im-
portant ultimate outcomes (incarceration, adolescent symptom-
atology), but no significant effects on several other measures
of ultimate outcome. To investigate the possibility that outcomes
in the MST condition were associated with treatment adherence,
hierarchical multiple regression analyses were conducted in
which the T2 measures of ultimate outcome (BSI, RBPC, and
SRD) served as the dependent variables and the Tl measure of
the respective dependent variable and the treatment adherence
factors, per respondent, served as the independent variables. To
assess for adherence effects on rearrest and incarceration, the
T1-T3 archival indices were used as the dependent variables.
The results of these analyses are presented in Table 6.
BSI, adolescent. Several MST fidelity measures were sig-
nificantly associated with changes in the adolescents' symptom-
atology from Tl to T2. On the basis of parental reports of
treatment adherence, poor outcomes for adolescent symptom-
atology were associated with low emphasis of the therapist on
changing intrafamilial and extrafamilial interactions, F(l, 48)
= 5.90, p < .02; a lack of direction in therapy, F(l, 48) =
5.29, p < .03; and low family-therapist consensus, F(l, 48)
= 5.52, p < .03. Similarly, on the basis of therapists' reports
of treatment fidelity, poor outcomes for adolescent symptomatol-
ogy were associated with nonproductive sessions, F(l, 65) =
8.35, p < .006; and high family-therapist conflict during ses-
sions, F(1, 65) = 6.66, p < .02.
BSI, parent. On the basis of parental reports of MST treat-
ment fidelity, high ratings of parental emotional distress were
significantly associated with high emphasis of the therapist on
changing intrafamilial and extrafamilial interactions, F(l, 49)
= 4.54, p < .03.
SRD. From the therapists' perspective, high adolescent re-
ports of index offenses were significantly associated with low
therapist adherence to MST principles, F(l, 65) = 5.40, p
< .03.
Arrests. On the basis of parental reports of MST fidelity,
high rates of rearrest after Tl were significantly associated with
low therapist adherence to MST principles, F( 1, 51) = 9.55, p
< .004, and low emphasis of the therapist on changing intra-
familial and extrafamilial relations, F(l, 51) = 4.41, p < .05.
Incarceration. On the basis of parental reports of MST fi-
delity, subsequent incarceration of youths was associated sig-
nificantly with nonproductive treatment sessions, x 2 ( l , A f = 5 8 )
828 HENGGELER, MELTON, BRONDINO, SCHERER, AND HANLEY
Table 5
Means, Standard Deviations, and Analyses of Outcome Measures
MST US Analyses
Pre Post Pre PostGroup X
Time Time
Measures M SD SD M SD
Ultimate outcomes
Emotional behavioral functioningBSI-GSI
YouthParent
RBPCCriminal activity
SRD"Gen. Del.Index Off.
Arrests"-'Incarceration°'d
0.500.69
43.2
0.950.36
0.490.67
33.3
0.57
0.38
0.27
0.4931.0
0.580.110.89
33.2
0.340.53
30.2
0.570.251.39
62.8
0.500.47
44.8
1.060.36
0.430.53
33.8
0.580.40
0.53
0.4335.2
0.750.231.20
70.4
0.66
0.4830.3
0.620.34
3.11103.5
7.673.210.35
0.383.03
0.637.26
.006
.075ns
ns.083ns
.008
4.92
7.1625.06
39.8028.00
.028
.008
.0002
.0001
.0001
Instrumental outcomes
Family relations
FAM-mParentYouth
FACES-HI: ParentCohesionAdaptability
FACES-III: YouthCohesionAdaptability
MonitoringParentYouth
Peer relationsMPRI: Parent
Emot. bondAggression
Social mat.MPRI: Youth
Emot. bondAggression
Social mat.PPCI
6.086.30
33.429.6
31.927.7
2.787.19
11.96-0.49
3.82
11.37-1.30
4.811.99
1.97
1.43
3.94.5
4.94.0
0.861.07
3.303.732.24
3.023.66
2.773.94
5.556.31
32.828.6
32.329.4
2.926.86
12.12-1.62
3.20
9.740.664.522.64
1.791.95
5.04.6
6.45.4
0.881.15
3.413.93
2.43
3.363.56
2.484.24
5.726.62
34.429.4
30.928.4
2.837.04
12.28-0.88
4.15
10.93-0.49
4.401.52
1.611.53
3.64.8
4.74.9
0.761.16
2.963.72
2.38
2.853.87
2.264.45
5.626.56
33.2
29.6
31.629.9
2.806.33
12.40-1.10
3.78
9.430.694.161.87
1.291.50
3.94.4
4.44.0
0.721.22
3.273.78
2.29
3.493.62
2.723.95
2.550.09
0.521.92
0.090.03
2.262.84
0.012.050.19
0.031.11
0.000.12
nsns
nsns
nsns
nsns
nsnsns
nsnsnsns
5.310.03
6.160.73
1.1311.99
0.9122.40
0.254.22
4.06
16.2217.22
0.901.36
.022ns
.014ns
ns.001
ns.0001
ns.041
.045
.0001
.0001
nsns
Note. MST = multisystemic therapy; US = usual services; pre = pretreatment; post = posttrearment; BSI-GSI = Brief Symptom Inventory, GlobalSeverity Index; RBPC = Revised Problem Behavior Checklist; SRD = Self-Report Delinquency Scale; Gen. Del. = General Delinquency scale;Index Off. = Index Offense scale; FAM-in = Family Assessment Measure; FACES-III = Family Adaptability and Cohesion Evaluation Scales;MPRI = Missouri Peer Relations Inventory; Emot. bond = emotional bonding; Social mat. — social maturity; PPCI = Parent Peer Conformity
Inventory.a Log-transformed scores. b Annualized rate of arrest when hi the community at an approximately 1.7-year follow-up. c Test of main effect forgroup. d Annualized rate of days incarcerated at an approximately 1.7-year follow-up.
= 4.01, p < .05, and low ratings on therapist attempts to change taken into account, observed therapeutic effects on outcomes
intrafamilial and extrafarailial interactions, X2(l . N = 58) =
7.46, p < .007. Moreover, youth incarceration was significantly
associated with low family engagement based on therapist re-
ports, x2( 1. N = 58) = 4.99, p < .03.
Discussion
The findings demonstrate the importance of treatment fidel-
ity in the effective dissemination of MST. When fidelity is not
are minimal, with the exception of the incarceration and ado-
lescent symptomatology data. On the other hand, when treat-
ment fidelity is considered, the effects of MST are consistent
with those of previous MST trials with violent and chronic
offenders; trials that included weekly procedures to enhance
treatment fidelity. Such findings have important implications
for the dissemination of effective mental health services to
community settings.

THE ROLE OF TREATMENT FIDELITY 829
Table 6
Standardized Regression Coefficients and Significance Levels from the Multiple Regression
Analyses Relating MST Treatment Adherence to Ultimate Outcomes
Adherencefactors
ParentPIP2P3P4P5P6
TherapistTlT2T3T4T5
AdolescentAlA2A3A4
BSI
Adolescent
.04
.10-.22-.31*
.29*-.30*
-.21.07.39**.11.36*
-.01-.18-.22
.02
SRD
Parent
.00
.21
.03
.25*-.01-.18
.01
.07
.17-.04
.10
.03-.07-.01
.03
RBPC
-.01.10
-.06-.06-.04-.19
-.15.05.10
-.10.12
-.12-.13
.08
.13
Gen. Del.
.11
.21-.12-.18
.06-.02
.05-.22
.18
.20
.11
-.02-.12-.06-.10
Index
-.01.03
-.03-.27
.07
.20
.12-.33*
.22
.22
.09
-.02.03
-.03.14
Arrests
-.48**.10.22
-.28*.06.12
-.04.04
-.18-.15-.02
-.21*.01.05.04
Incarceration
.34
.36*-.28-.59**
.19-.11
-.45*-.06-.28
.28-.06
-.29.09.15
-.24
Note. MST = multisystemic therapy; BSI — Brief Symptom Inventory; RBPC = Revised Problem BehaviorChecklist; SRD = Self-Report Delinquency scale; Gen. Del. = General Delinquency scale; Index = IndexOffense scale; P = parent; T = therapist; A = adolescent.*p < .05. **p<.01.
MST Outcomes Irrespective of Treatment Fidelity
In previous randomized trials with violent or chronic juvenile
offenders, in which considerable supervisory resources were
devoted to maintaining treatment fidelity, MST demonstrated
43% (Henggeler et al., 1992) and 64% (Borduin et al., 1995)
reductions in rearrest, a 64% reduction in incarceration (Heng-
geler et al., 1992), a reduction in self-reported offending (Heng-
geler et al., 1992), and a variety of effects for improved family
relations, peer relations, youth behavior problems, and parental
symptomatology. In the present study, MST produced a 26%
reduction in rearrest (not statistically significant), a 47% reduc-
tion in days incarcerated, and a significant improvement in ado-
lescent psychiatric symptomatology. Overall, the improvements
in adolescent symptomatology and the decrease in days incarcer-
ated are consistent with the goals of MST On the other hand,
the lack of significant effects on instrumental outcomes and
criminal activity is disappointing, as such effects are central
goals of MST.
In light of the modest outcomes achieved by MST in this
study and the fact that several factors interacted during the
course of this project to influence therapists' adherence to the
MST treatment protocol, it seems possible that poorer outcomes
in the MST condition were associated with low treatment adher-
ence. As discussed next, treatment adherence played an im-
portant role in achieving desired outcomes.
MST Fidelity and Ultimate Outcomes
Therapist adherence to the MST treatment principles was an
important predictor for key outcomes pertaining to the adoles-
cents' criminal activity and incarceration during the 1.7-year
follow-up. Parent and adolescent ratings of treatment adherence
predicted low rates of rearrest; and therapist ratings of treatment
adherence and treatment engagement predicted decreased self-
reported index offenses and low probability of incarceration,
respectively. These findings support the underlying clinical as-
sumptions of MST that have been operationalized by the nine
MST treatment principles (Henggeler et al., 1994). Importantly,
these assumptions are largely consistent with recommendations
that leading investigators (Gendreau, 1996; Mulvey, Arthur, &
Reppucci, 1993; Tolan & Guerra, 1994) have made regarding
the types of services that are most likely to achieve favorable
results with juvenile offenders (i.e., goal oriented, family based,
structured). Thus, as demonstrated in this and previous studies
of MST, treatment of serious antisocial behavior in juveniles
can be successful when the known determinants of antisocial
behavior are intensively addressed in the natural environment
with youths and families.
A second set of interesting findings pertains to the frequent
link between favorable clinical outcomes and parent reports of
therapeutic attempts to change intrafamilial and extrafamilial
interactions. On the basis of parental reports, therapists' empha-
sis on such change was associated with low rates of rearrest,
incarceration, and adolescent emotional distress. Such findings
are highly consistent with the extensive causal modeling litera-
ture (Henggeler, 1991, 1997) showing that serious antisocial
behavior in youths is linked with key aspects of family relations
(e.g., discipline) and with the child's and family's relations
with important extrafamilial systems (e.g., peers, school,
church, social support system). In contrast with findings that

830 HENGGELER, MELTON, BRONDINO, SCHERER, AND HANLEY
improved adolescent functioning was associated with therapist
attempts to change intrafamilial and extrafamilial interactions,
such therapeutic emphases were associated with increased pa-
rental emotional distress. This finding most likely reflects the
increased stress that parents may experience as they implement
important interventions within the family (e.g., setting curfews,
enforcing limits, addressing personal barriers to effective parent-
ing such as drug abuse) and outside the family (e.g., negotiating
with teachers, disengaging their child from deviant peers). Al-
though therapists attempted to address this stress by building
indigenous support networks, increased parental stress, at least
temporarily, may be an inevitable effect of the types of changes
emphasized by MST.
Finally, several findings suggest that favorable outcomes are
linked with the emphasis of MST as a task-oriented, goal-ori-
ented, and efficient set of interventions, within a collaborative
family-therapist context. On the basis of parental reports, fam-
ily-therapist consensus was associated with decreased adoles-
cent psychiatric symptomatology; a clear direction in treatment
was associated with improved adolescent symptomatology; and
productive sessions were linked with a low probability of adoles-
cent incarceration. From the therapists' perspective, productive
sessions and low family-therapist conflict were linked with
improved adolescent symptomatology. Overall, these findings
support the association between high adherence to MST treat-
ment principles and improved functioning in adolescents who
are serious criminal offenders.
Clinical and Policy Implications
The findings support the view that a lack of treatment fidelity
may be a key reason why mental health treatment approaches
have had more success in research settings than in community
settings (Weisz et al., 1995). In the present study, an important
component of the standard MST protocol for maintaining treat-
ment fidelity was withdrawn: weekly feedback from an expert
regarding treatment adherence. We contend that the elimination
of this component greatly increased variability in following the
MST treatment protocol, which resulted in an overall reduction
in the fidelity of MST. Such a contention is supported by the
modest outcome results of this study in comparison with previ-
ous MST studies that provided such weekly feedback, and by
the compelling findings regarding the linkages between MST
fidelity and favorable outcomes. Assuming that our views are
accurate, a critical goal of future research is to develop and
validate cost-effective strategies for transferring the rigor of
university-based treatment protocols to community settings.
Typically, such rigor includes the training of therapists to speci-
fied adherence criteria, followed by consistent monitoring oftherapist behavior and feedback aimed at maximizing treatment
fidelity. Although such training and intensive supervision
increase program cost, the incremental costs are minimal whencompared with the costs of providing services that are
ineffective.
Yet, even when effective training and supervisory protocols
are developed, many potential barriers must be overcome for thesuccessful dissemination of an innovative treatment technology
(Gendreau, 1995). Regarding MST, for example, therapist, ad-
ministrative, and fiscal barriers may attenuate the effectiveness
of dissemination. Therapist characteristics that hinder treatment
fidelity include clinical belief systems that are nonecological,
pejorative attitudes toward parents of youths who have signifi-
cant problems, reluctance to assume accountability for out-
comes, and difficulty in viewing families as full collaborators
in all aspects of treatment. Likewise, a lack of administrative
support of therapists regarding issues such as scheduling, travel,
salary, and clinical support can undermine program integrity, as
can fiscal incentives for moving children to out-of-home place-
ments rather than providing the intensive community-based ser-
vices that may be needed to maintain a child with his or her
family. Thus, to disseminate effectively to community settings,
a broad, complex, and multifaceted set of issues must be ad-
dressed (Schoenwald & Henggeler, in press).
At the policy level, perhaps the most persuasive argument for
the dissemination of family- and community-based alternatives
to out-of-home placements is the potential cost savings and cost-
effectiveness. The present study supports the fiscal viability of
MST as a treatment of serious juvenile offenders and their fami-
lies. Through the first 1.7 years of follow-up, MST reduced
incarceration by an average of 37.2 days per year. Assuming
that this rate of reduced incarceration was maintained for 2.0
years and that 1 day of incarceration costs $100, a savings of
57,440 would be realized for each youth receiving MST. This
savings compares favorably to the per-adolescent program costs
of approximately $4,000 for this study. Tb conclude with greater
confidence that the MST programs in the present study were less
costly than usual services, however, we need a comprehensive
examination of service utilization across service sectors (e.g.,
social welfare, mental health, juvenile justice, primary care) to
more fully explicate the types of services received by the youth
and to explore the possibilities of cost shifting. Nevertheless, a
recent cost analysis of MST with substance-abusing and depen-
dent delinquents has shown no evidence of cost shifting
(Schoenwald, Ward,Henggeler, Pickrel, & Patel, 1996). Indeed,
the incremental costs of MST in that study were nearly offset
by the savings incurred as a result of reductions in days of out-
of-home placement during the first year after referral.
In conclusion, the results of this study highlight the impor-
tance of maintaining treatment fidelity in the dissemination of
complex interventions to community settings. Moreover, the out-
comes further support the view that intensive family- and com-
munity-based services can serve as viable alternatives to out-
of-home placement of youths presenting serious antisocial be-
havior. Such services, however, must be delivered with fidelity
and have the capacity to attend to the multiple known determi-
nants of serious clinical problems and to provide services with
high ecological validity (Henggeler et al., 1995).
References
Berndt, T. J. (1979). Developmental changes in conformity to peers and
parents. Developmental Psychology, 15, 608-616.
Blaske, D. M., Borduin, C. M., Henggeler, S. W., & Mann, B. J. (1989).
Individual, family and peer characteristics of adolescent sex offenders
and assaultive offenders. Developmental Psychology, 25, 846-855.
Borduin, C. M, Blaske, D. M., Cone, L., Mann, B. J., & Hazelrigg,
M. D. (1989). Development and validation of a measure of peer
relations: The Missouri Peer Relations Inventory. Unpublished manu-
script, Department of Psychology, University of Missouri—Columbia.

THE ROLE OF TREATMENT FIDELITY 831
Borduin, C. M., Mann, B. J., Cone, L. T., Henggeler, S. W., Fucci, B. R.,
Blaske, D. M., & Williams, R. A. (1995). Multisystemic treatment
of serious juvenile offenders: Long-term prevention of criminality and
violence. Journal of Consulting and Clinical Psychology, 63, 569-
578.
Bray, J. D., & Bevilacqua, J. J. (1993). A multidisciplinary public-aca-
demic liasion to improve public mental health services in South Caro-
lina. Hospital and Community Psychiatry, 44, 985-990.
Bronfenbrenner, U. (1979). The ecology of human development: Experi-
ments by nature and design. Cambridge, MA: Harvard University
Press.
Brown, B. B., Clasen, D. R., & Eicher, S. A. (1986). Perceptions of
peer pressure, peer conformity dispositions, and self-reported behav-
ior among adolescents. Developmental Psychology, 22, 521-530.
Brunk, M., Henggeler, S. W., & Whelan, J. P. (1987). A comparison of
multisystemic therapy and parent training in the brief treatment of
child abuse and neglect. Journal of Consulting and Clinical Psychol-
ogy, 55, 311-318.
Cohen, M. A., Miller, T. R., & Rossman, S. B. (1994). The costs and
consequences of violent behavior in the United States. In A. J. Reiss,
Jr., & J. A. Roth (Eds.), Understanding and preventing violence (pp.
67-166). Washington, DC: National Research Council, National
Academy Press.
Derogatis, L. R. (1993). Brief Symptom Inventory: Administration,
scoring, and procedures manual. Minneapolis, MN: National Com-
puter Systems, Inc.
Dunford, F. W., & Elliott, D. S. (1984). Identifying career offenders
using self-reported data. Journal of Research in Crime and Delin-
quency, 21, 57-86.
Elliott, D. S. (1994). Youth violence: An overview. Boulder: University
of Colorado, Center for the Study and Prevention of Violence, Institute
for Behavioral Sciences, University of Colorado.
Elliott, D. S., Ageton, S. S., Huizinga, D., Knowles, B. A., & Canter,
R. J. (1983). The prevalence and incidence of delinquent behavior:
1976-1980 (National Youth Survey Project Report No. 26). Boulder,
CO: Behavioral Research Institute.
Elliott, D. S., Huizinga, D., & Ageton, S. S. (1985). Explaining delin-
quency and drug use. Beverly Hills, CA: Sage.
Farrington, D. P. (1991). Childhood aggression and adult violence: Early
precursors and later-life outcomes. In D. J. Pepler & K. H. Rubin
(Eds.), The development and treatment of childhood aggression (pp.
5-29). Hillsdale, NJ: Erlbaum.
Gendreau, P. (1995). Technology transfer in the criminal justice field.
InT. E. Backer, S. L. David, & G. Soucy (Eds.), Reviewing the behav-
ioral science knowledge base on technology transfer (NIH Publication
No. 95-4035, pp. 198-208). Rockville, MD: National Institute onDrug Abuse.
Gendreau, P. (1996). Offender rehabilitation: What we know and whatneeds to be done. Criminal Justice and Behavior, 23, 144-161.
Hanson, C. L., Henggeler, S. W., Haefele, W. F., & Rodick, J. D. (1984).
Demographic, individual, and family relationship correlates of serious
and repeated crime among adolescents and their siblings. Journal of
Consulting and Clinical Psychology, 52, 528-538.
Henggeler, S. W. (1989). Delinquency in adolescence. Newbury Park,
CA: Sage.
Henggeler, S. W. (1991). Multidimensional causal models of delinquent
behavior and their implications for treatment. In R. Cohen & A. Siegel
(Eds.), Context and development (pp. 161-181). Hillsdale, NJ:Erlbaum.
Henggeler, S. W. (1997). The development of effective drug abuse ser-
vices for youth. In J. A. Egertson, D. M. Fox, & A. I. Leshner (Eds.),
Treating drug abusers effectively (pp. 253-279). New York: Black-
well Publishers.
Henggeler, S. W., & Borduin, C. M. (1990). Family therapy and beyond:
A multisystemic approach to treating the behavior problems of chil-
dren and adolescents. Pacific Grove, CA: Brooks/Cole.
Henggeler, S. W., & Borduin, C. M. (1992). Multisystemic therapy ad-
herence scales. Unpublished instrument. Department of Psychiatry
and Behavioral Sciences, Medical University of South Carolina.
Henggeler, S. W, Borduin, C. M., Melton, G. B., Mann, B. J., Smith,
L., & Hall, J. A., Cone, L., & Fucci, B. R. (1991). Effects of multisys-
temic therapy on drug use and abuse in serious juvenile offenders: A
progress report from two outcome studies. Family Dynamics of Addic-
tion Quarterly, 1, 40-51.
Henggeler, S. W, Burr-Harris, A. W, Borduin, C. M., & McCallum, G.
(1991). Use of the Family Adaptability and Cohesion Evaluation
Scales in child clinical research. Journal of Abnormal Child Psychol-
ogy, 19, 53-63.
Henggeler, S. W., Melton, G. B., & Smith, L. A. (1992). Family preser-
vation using multisystemic therapy: An effective alternative to incar-
cerating serious juvenile offenders. Journal of Consulting and Clinical
Psychology, 60, 953-961.
Henggeler, S. W., Melton, G. B., Smith, L. A., Schoenwald, S. K., &
Hanley, J. H. (1993). Family preservation using multisystemic ther-
apy: Long-term follow-up to a clinical trial with serious juvenile
offenders. Journal of Child and Family Studies, 2, 283-293.
Henggeler, S. W., Pickrel, S. G., & Brondino, M. J. (1997). Multisys-
temic treatment of substance abusing/dependent delinquents: Out-
comes for drug use, criminality, and out-of-home placement at
posttreatment and 6-month follow-up. Manuscript submitted for
publication.
Henggeler, S. W., Rodick, J. D., Borduin, C. M., Hanson, C. L., Watson,
S. M., & Urey, J. R. (1986). Multisystemic treatment of juvenile of-
fenders: Effects on adolescent behavior and family interactions. Devel-
opmental Psychology, 22, 132-141.
Henggeler, S. W., Schoenwald, S. K., Borduin, C. M., Rowland, M. D., &
Cunningham, P. B. (in press). Multisystemic treatment of antisocial
behavior in youth. New "fork: Guilford Press.
Henggeler, S. W., Schoenwald, S. K., & Pickrel, S. G. (1995). Multisys-
temic therapy: Bridging the gap between university- and community-
based treatment. Journal of Consulting and Clinical Psychology, 63,
709-717.
Henggeler, S. W., Schoenwald, S. K., Pickrel, S. G., Brondino, M. J.,
Borduin, C. M., & Hall, J. A. (1994). Treatment manual for family
preservation using multisystemic therapy. Columbia: South Carolina
Health and Human Services Finance Commission.
Laub, J. H., & Sampson, R. J. (1994). Unemployment, marital discord,
and deviant behavior: The long-term correlates of childhood misbe-
havior. In T. Hirschi & M. R. Gottfredson (Eds.), The generality of
deviance (pp. 235-252). New Brunswick, NJ: Transaction.
McMahon, R. J., & Forehand, R. (1988). Conduct disorders. In E. J.
Mash & L. G. Terdal (Eds.), Behavioral assessment of childhood
disorders (2nd ed., pp. 105-153). New York: Guilford Press.
Melton, G. B., & Pagliocca, P. M. (1992). Treatment in the juvenile
justice system: Directions for policy and practice. In J. J. Cocozza
(Ed.), Responding to the mental health needs of youth in the juvenile
justice system (pp. 107-139). Miami, FL: The National Coalition
for the Mentally 111 in the Criminal Justice System.
Mulvey, E. P., Arthur, M. W, & Reppucci, N. D. (1993). The prevention
and treatment of juvenile delinquency: A review of the research. Clini-cal Psychology Review, 13, 133-167.
Olson, D. H., Portner, J., & Lavee, Y. (1985). FACES-IH. St Paul: De-
partment of Family Social Science, University of Minnesota.
Patteison, G. R., & Dishion, T. J. (1985). Contributions of family and
peers to delinquency. Criminology, 23, 63-79.
Patterson, G. R., Reid, J. B., & Dishion, T. J. (1992). Antisocial hoys.
Eugene, OR: Castalia.

832 HENGGELER, MELTON, BRONDINO, SCHERER, AND HANLEY
Quay, H. C., & Peterson, D. R. (1987). Manual for the Revised Problem
Behavior Checklist. Coral Gables, FL: University of Miami.
Rodick, J. D., Henggeler, S. W., & Hanson, C. L. (1986). An evaluation
of the Family Adaptability and Cohesion Evaluation Scales and the
circumplex model. Journal of Abnormal and Child Psychology, 14,
77-87.
Schoenwald, S. K., & Henggeler, S. W. (in press). Services research and
family based treatment. In H. Liddle, G. Diamond, R. Levant, & S.
Bray (Eds.), Family psychology intervention science. Washington,
DC: American Psychological Association.
Schoenwald, S. K., Ward, D. M., Henggeler, S. W., Pickrel, S. G., &
Patel, H. (1996). MST treatment of substance abusing or dependent
adolescent offenders: Costs of reducing incarceration, inpatient, and
residential placement. Journal of Child and Family Studies, 4, 431-
444.
Skinner, H. A., Steinhauer, P. D., & Santa-Barbara, J. (1983). The Fam-
ily Assessment Measure. Canadian Journal of Community Mental
Health, 2, 91-105.
Tate, D. C., Reppucci, N. D., & Mulvey, E. P. (1995). Violent juvenile
delinquents: Treatment effectiveness and implications for future ac-
tion. American Psychologist, 50, 777-781.
Thornberry, T. P., Huizinga, D., & Loeber, R. (1995). The prevention
of serious delinquency and violence: Implications from the program
of research on the causes and correlates of delinquency. In J. C. How-
ell, B. Krisberg, J. D. Hawkins, & J. J. Wilson (Eds.), A sourcebook:
Serious, violent, & chronic juvenile offenders (pp. 213-237). New-
bury Park, CA: Sage.
Tolan, P., & Guerra, N. (1994). What works in reducing adolescent
violence: An empirical review of the field. Boulder: Center for the
Study and Prevention of Violence, Institute for Behavioral Sciences,
University of Colorado.
U. S. Bureau of the Census. (1993). 1990 census of population. Social
and economic characteristics: South Carolina. Washington, DC: U.S.
Government Printing Office.
Weisz, J. R., Donenberg, G. R., Weiss, B., & Han, S. S. (1995). Bridging
the gap between laboratory and clinic in child and adolescent psycho-
therapy. Journal of Consulting and Clinical Psychology, 63, 688-
701.
Appendix A
MST Treatment Principles
1. The primary purpose of assessment is to understand the fit between
the identified problems and their broader systemic context.
2. Therapeutic contacts should emphasize the positive and should use
systemic strengths as levers for change.
3. Interventions should be designed to promote responsible behavior
and decrease irresponsible behavior among family members.
4. Interventions should be present-focused and action-oriented, targeting
specific and well-defined problems.
5. Interventions should target sequences of behavior within or between
multiple systems that maintain identified problems.
6. Interventions should be developmentally appropriate and fit the devel-
opmental needs of the youth.
7. Interventions should be designed to require daily or weekly effort by
family members.
8. Intervention effectiveness is evaluated continuously from multiple
perspectives, with providers assuming accountability for overcoming
barriers to successful outcomes.
9. Interventions should be designed to promote treatment generalization and
long-term maintenance of therapeutic change by empowering care givers
to address famiry members' needs across multiple systemic contexts.
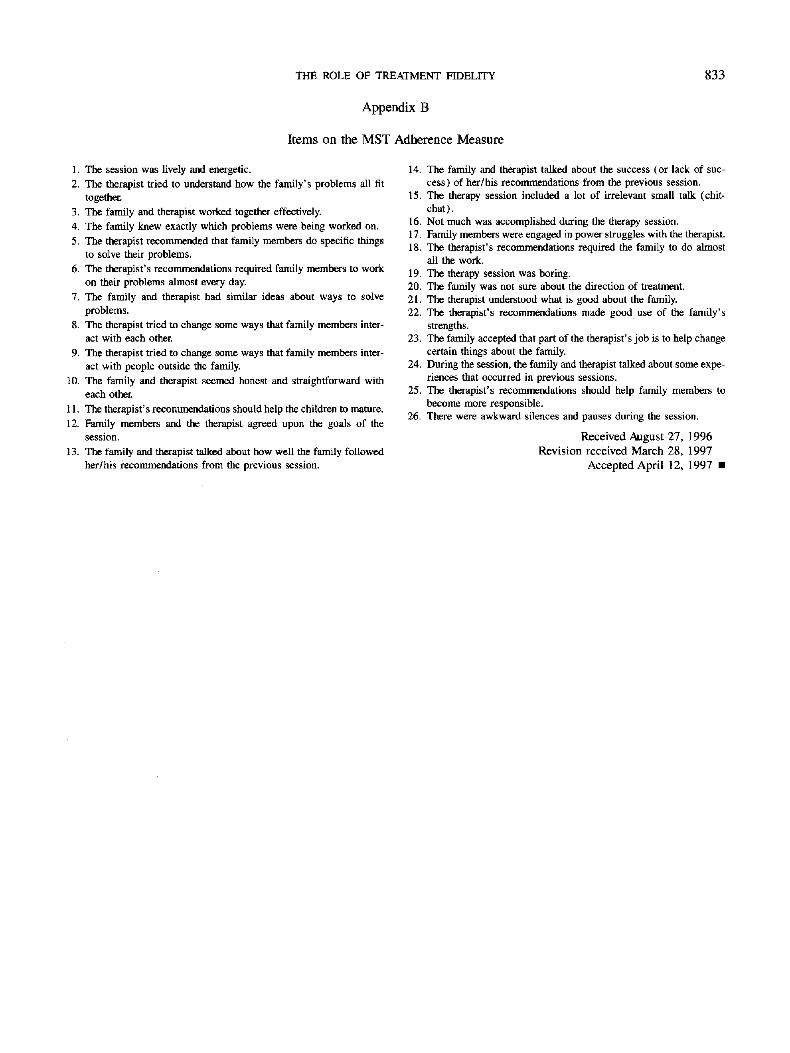
THE ROLE OF TREATMENT FIDELITY 833
Appendix B
Items on the MST Adherence Measure
1. The session was lively and energetic.
2. The therapist tried to understand how the family's problems all fit
together.
3. The family and therapist worked together effectively.
4. The family knew exactly which problems were being worked on.
5. The therapist recommended that family members do specific things
to solve their problems.
6. The therapist's recommendations required family members to work
on their problems almost every day.
7. The family and therapist had similar ideas about ways to solve
problems.
8. The therapist tried to change some ways that family members inter-
act with each other.
9. The therapist tried to change some ways that family members inter-
act with people outside the family.
10. The family and therapist seemed honest and straightforward with
each other.
11. The therapist's recommendations should help the children to mature.
12. Family members and the therapist agreed upon the goals of the
session.
13. The family and therapist talked about how well the family followed
her/his recommendations from the previous session.
14. The family and therapist talked about the success (or lack of suc-
cess) of her/his recommendations from the previous session.
15. The therapy session included a lot of irrelevant small talk (chit-
chat).
16. Not much was accomplished during the therapy session.
17. Family members were engaged in power struggles with the therapist.
18. The therapist's recommendations required the family to do almost
all the work.
19. The therapy session was boring.
20. The family was not sure about the direction of treatment.
21. The therapist understood what is good about the family.
22. The therapist's recommendations made good use of the family's
strengths.
23. The family accepted that part of the therapist's job is to help change
certain things about the family.
24. During the session, the family and therapist talked about some expe-
riences that occurred in previous sessions.
25. The therapist's recommendations should help family members to
become more responsible.
26. There were awkward silences and pauses during the session.
Received August 27, 1996
Revision received March 28, 1997
Accepted April 12, 1997 •