MRI From Picture to Proton
11
MRI From Picture to Proton Donald W. McRobbie Elizabeth A. Moore Martin J. Graves and Martin R. Prince
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of MRI From Picture to Proton

MRI From Picture to Proton
Donald W. McRobbie
Elizabeth A. Moore
Martin J. Graves and
Martin R. Prince

The Pitt Building, Trumpington Street, Cambridge, United Kingdom
The Edinburgh Building, Cambridge CB2 2RU, UK
40 West 20th Street, New York, NY 10011-4211, USA
477 Williamstown Road, Port Melbourne, VIC 3207, Australia
Ruiz de Alarcón 13, 28014 Madrid, Spain
Dock House, The Waterfront, Cape Town 8001, South Africa
http://www.cambridge.org
© Donald W. McRobbie, Elizabeth A. Moore, Martin J. Graves and
Martin R. Prince 2003
This book is in copyright. Subject to statutory exception
and to the provisions of relevant collective licensing agreements,
no reproduction of any part may take place without the written
permission of Cambridge University Press.
First published 2003
Printed in the United Kingdom at the University Press, Cambridge
Typeface Utopia 8.5/12 System QuarkXPress® [ ]
A catalogue record for this book is available from the British Library
Library of Congress Cataloguing in Publication data
MRI from picture to proton / Donald W. McRobbie . . . [et al.].
p. cm.
Includes bibliographical references and index.
ISBN 0 521 52319 2
1. Magnetic resonance imaging. I. McRobbie, Donald W., 1958–
RC78.7.N83 M756 2003
616.07�548–dc21 2002067238
ISBN 0 521 81859 1 hardback
ISBN 0 521 52319 2 paperback

Contents
Acknowledgements xi
1 MR: What’s the attraction? 11.1 It’s not rocket science, but I like it 11.2 A brief history of medical imaging 21.3 How to use this book 4Further reading 6
Part A The basic stuff
2 Early daze: your first week in MR 92.1 Introduction 92.2 Welcome to the MR unit 92.3 Safety first 132.4 The patient’s journey 152.5 Basic clinical protocols 172.6 A week in the life of an MRI
radiographer 23Further reading 25
3 Seeing is believing: introduction to imagecontrast 273.1 Introduction 273.2 Some basic stuff 273.3 T1-weighted images 303.4 T2-weighted images 313.5 PD-weighted images 343.6 Gradient-echo T1-weighted images 353.7 Gradient-echo T 2
*-weighted images 363.8 Gradient-echo PD-weighted images 393.9 STIR images 393.10 FLAIR images 40
vii

3.11 Contrast agents 413.12 Angiographic images 44Further reading 45
4 The devil’s in the detail: pixels, matricesand slices 464.1 Introduction 464.2 Digital and analogue images 464.3 Matrices, pixels and an introduction to
resolution 514.4 Displaying images 554.5 What do the pixels represent? 564.6 From 2D to 3D 58Further reading 62
5 What you set is what you get: basicimage optimization 635.1 Introduction 635.2 Looking on the bright side: what are we
trying to optimize? 635.3 Trading places: resolution, SNR and
scan time 675.4 Ever the optimist: practical steps to
optimization 71Further reading 76
6 Improving your image: how to avoidartefacts 776.1 Introduction 776.2 Keep still please: gross patient
motion 776.3 Physiological motion 786.4 Motion artefacts from flow 846.5 Lose the fat! 866.6 Partial volume artefact and cross-talk 946.7 Phase sampling artefacts 966.8 Susceptibility and metal artefacts 996.9 Equipment artefacts 1016.10 What’s causing this artefact? 105Further reading 105
7 Spaced out: spatial encoding 1067.1 Introduction 1067.2 Anatomy of a pulse sequence 1067.3 From Larmor to Fourier via gradients 107
7.4 Something to get excited about: theimage slice 112
7.5 In-plane localization 1177.6 Consequences of Fourier imaging 1287.7 Speeding it up 1327.8 3D FT 133Further reading 134
8 Getting in tune: resonance andrelaxation 1358.1 Introduction 1358.2 Spinning nuclei 1358.3 Measuring the magnetic moment 1388.4 Creating echoes 1418.5 Relaxation times 1468.6 Relaxation time mechanisms 1528.7 Measuring relaxation times in vivo 1578.8 Contrast agent theory 160Further reading 163
9 Let’s talk technical: MR equipment 1649.1 Introduction 1649.2 Magnets 1649.3 Gradients 1709.4 Radiofrequency system 1749.5 Computer systems 1859.6 Open MRI systems 1859.7 Siting and installation 187Further reading 188
10 But is it safe? Bio-effects 18910.1 Introduction 18910.2 Radiofrequency effects 18910.3 Gradient effects 19110.4 Static field effects 193Further reading 197
Part B The specialist stuff
11 Ghosts in the machine: quality control 20111.1 Introduction 20111.2 The quality cycle 20111.3 Signal parameters 20211.4 Geometric parameters 209
Contents
viii

11.5 Relaxation parameters 21411.6 Artefacts 21511.7 Spectroscopic QA 216Further reading 217
12 Acronyms anonymous: a guide to thepulse sequence jungle 21812.1 Introduction 21812.2 Getting above the trees: a sequences
overview 21812.3 RARING to go: spin-echo-based
techniques 22012.4 Spoiled for choice: gradient echo 23212.5 Ultra-fast GE imaging 24512.6 Pulse sequence conversion chart 252Further reading 252
13 Go with the flow: MR angiography 25513.1 Introduction 25513.2 Effect of flow in conventional imaging
techniques 25513.3 Time-of-flight MR angiography 26013.4 Phase-contrast angiography 26413.5 Contrast-enhanced MR angiography 26913.6 Novel contrast agents 273Further reading 277
14 A heart to heart discussion: cardiac MRI 27814.1 Introduction 27814.2 Artefact challenges 27814.3 Morphological imaging 28114.4 Functional imaging 28114.5 Cine phase-contrast velocity mapping 29314.6 Myocardial perfusion imaging 29514.7 Myocardial viability 29714.8 Coronary artery imaging 297Further reading 299
15 It’s not just squiggles: in vivospectroscopy 30015.1 Introduction 30015.2 Some basic chemistry 30115.3 Single-voxel spectroscopy 30415.4 Processing of single-voxel spectra 31015.5 Chemical shift imaging 31215.6 Phosphorus spectroscopy 31315.7 Other nuclei 315Further reading 316
16 To BOLDly go: new frontiers 31716.1 Introduction 31716.2 EPI acquisition methods 31716.3 Diffusion imaging 32216.4 Perfusion imaging 32816.5 Brain activation mapping using the
BOLD effect 33316.6 Hyperpolarized gases 33716.7 New reconstruction methods 33916.8 The final frontier 342Further reading 342
Appendix: maths revision 343A.1 Vectors 343A.2 Sine and cosine waves 344A.3 Exponentials 345A.4 Complex numbers 345A.5 Simple Fourier analysis 346A.6 Some useful constants 347
Index 348
Colour plates between pages 324 and 325.
Contents
ix

1.1 It’s not rocket science, but I like it
How would you impress a stranger you meet at a partywith your intelligence? You might claim to be a brainsurgeon or a rocket scientist. Well Magnetic Resonance(MR) is not rocket science, it’s better than that. MRinvolves an amazing combination of advanced scienceand engineering, including the use of superconductiv-ity, cryogenics, quantum physics, digital and computertechnology – and all within the radiology department ofyour local hospital. MR imaging has evolved fromunpromising beginnings in the 1970s to become nowa-days the imaging method of choice for a large propor-tion of radiological examinations and the ‘jewel in thecrown’ of medical technology. A modern MRI scanner isshown in figure 1.1.
So what is it? It is an imaging method based princi-pally upon sensitivity to the presence and properties ofwater, which makes up 70% to 90% of most tissues. Theproperties and amount of water in tissue can alter dra-matically with disease and injury which makes MR verysensitive as a diagnostic technique. MR detects subtlechanges in the magnetism of the nucleus, the tiny entitythat lies at the heart of the atom. This is probing deeperthan X-rays, which interact with the clouds or shells ofthe electrons that orbit the nucleus. MR is a truly pow-erful modality. At its most advanced, MR can be usednot just to image anatomy and pathology but to inves-tigate organ function, to probe in vivo chemistry andeven to visualize the brain thinking.
In the early days, the scanners were the domain of thephysicists and engineers who invented and built them,and the technique was called NMR imaging (NMR
stands for nuclear magnetic resonance). The cynicsmay say that the technique really took off clinicallywhen the ‘N-word’ was dropped. This was sensible asthe term ‘nuclear’, although scientifically accurate,implied a connection with nuclear energy and, in thelast of the cold war years, resonated in the public’s mindwith the spectre of nuclear weapons.
Because of the diversity of sciences and technologiesthat gave birth to and continue to nurture MR, it is anextremely hard subject to learn. A lifetime is not enoughto become expert in every aspect. Clinicians, technolo-gists and scientists all struggle with the study of thesubject. The result is sometimes an obscurity of under-standing or a dilution of scientific truth resulting in mis-conceptions. This is why we have chosen to write thisbook. Our aim is to introduce you to MR as a tool –
1
1
MR: What’s the attraction?
Figure 1.1 Modern superconducting MR system. Courtesy of
Philips Medical Systems.

rather like learning to drive a car. Once you are confi-dent on the road, we can then start to learn how theengine works.
1.2 A brief history of medical imaging
Radiology began after the accidental discovery of ‘X-rays’ by Roentgen in 1895. At about the same time(1896) Becquerel and the Curies were discovering radio-activity and radium and making possible the futuredevelopment of nuclear medicine. Within a couple ofyears most of the basic techniques of radiography wereestablished, e.g. the use of fluorescent screens (Pupin1896), contrast media (Lindenthal 1896), even the prin-ciple of angiography. Early fluoroscopy entailed directviewing from a fluorescent plate, i.e. putting your headin the main beam, a practice frowned upon today!Unfortunately radiation protection followed slightlytoo late for the pioneers of radiology. The next real tech-nical breakthrough was the development of the imageintensifier in the 1950s, but the basis of conventionalradiography remained the same until the recent IT anddigital revolutions. Computed Tomography (CT) was ahuge breakthrough earning Hounsfield and Cormackthe Nobel Prize for medicine and physiology in 1979. X-ray CT was unique in producing tomographic images orslices of the living human body for the first time andwith a higher contrast than achievable by conventionalplanar techniques. The combination of a moving X-raygantry and the computing power necessary to recon-struct from projections made CT possible.
In nuclear medicine a similar evolution was occur-ring, from the development of the gamma camera byAnger in 1958 to tomographic imaging in the form ofSingle Photon Emission Computed Tomography(SPECT) and Positron Emission Tomography (PET)which is ongoing today. Even now PET is not incommon clinical use although its ability to imageminute concentrations of metabolites is unique andmakes it a powerful research tool in the aetiology ofdisease and effect of drugs.
Ultrasound was developed in the 1950s following thedevelopment of SONAR in World War II and was uniquein involving no ionizing radiation and offering the pos-
sibility of safe, noninvasive imaging. Its ability to imagein real time and its sensitivity to flow, through theDoppler effect, have been key factors in its widespreadrole in obstetrics, cardiology, vascular disease and forreal-time biopsy guidance and minimally invasivesurgery.
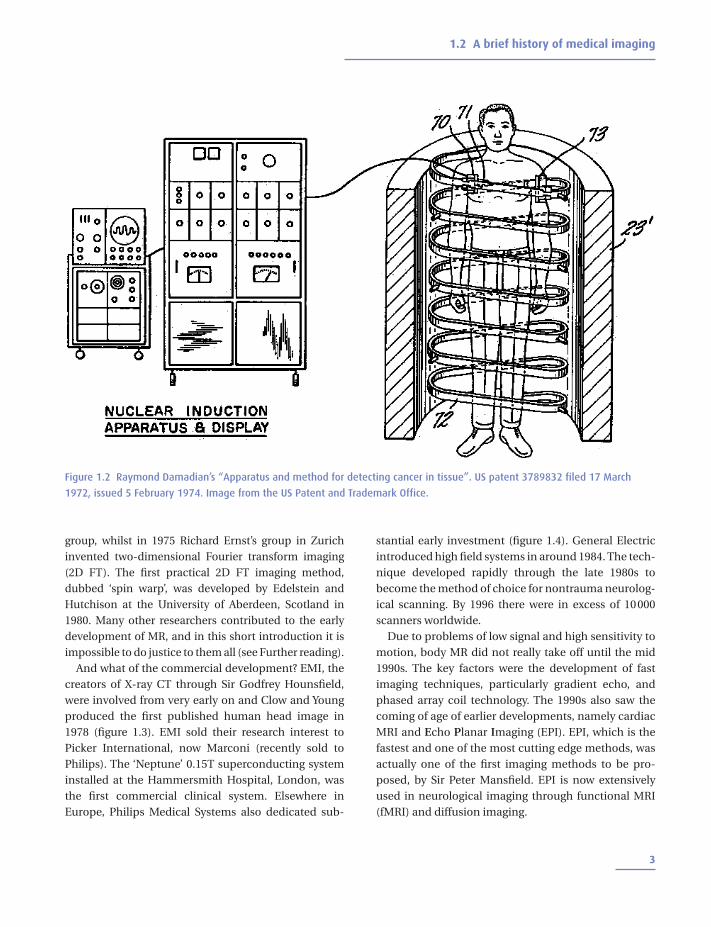
The initial concept for the medical application ofNMR, as it was then called, originated with the discov-ery by Raymond Damadian in 1971 that certain mousetumours displayed elevated relaxation times comparedwith normal tissues in vitro. This exciting discoveryopened the door for a complete new way of imaging thehuman body where the potential contrast betweentissues and disease was many times greater than thatoffered by X-ray technology and ultrasound (figure 1.2).At the same time developments in cryogenics, or thestudy of very low temperatures, made the developmentof whole-body superconducting magnets possible.Damadian and his colleagues at the State University ofNew York, starved of mainstream research funding,went so far as to design and build their own supercon-ducting magnet operating in their Brooklyn laboratoryand the first human body image by NMR is attributed tothem. There is some dispute about who actually is thefounder of modern Magnetic Resonance Imaging(MRI), but one thing is certain, Damadian coined thefirst MR acronym, namely FONAR (Field fOcussedNuclear mAgnetic Resonance). This set a trend, and youcan see the development of the acronym family tree inchapter 12!
In 1973, in an article in Nature, Paul Lauterbur pro-posed using magnetic field gradients to distinguishbetween NMR signals originating from different loca-tions. This is the basis of all modern MRI. UnfortunatelyLauterbur’s brilliant invention was not accompanied bya brilliant acronym; he coined the obscure term ‘zeug-matography’, meaning imaging from a joining together(of the main field and the gradients). In contemporaryMR terms Lauterbur can be said to have invented fre-quency encoding. Whilst the term ‘zeugmatography’sunk without trace, fortunately the technique itdescribed has gone from strength to strength.
Selective excitation, or the sensitization of tomo-graphic image slices, was invented at the University ofNottingham, England in 1974 by Sir Peter Mansfield’s
MR: What’s the attraction?
2
group, whilst in 1975 Richard Ernst’s group in Zurichinvented two-dimensional Fourier transform imaging(2D FT). The first practical 2D FT imaging method,dubbed ‘spin warp’, was developed by Edelstein andHutchison at the University of Aberdeen, Scotland in1980. Many other researchers contributed to the earlydevelopment of MR, and in this short introduction it isimpossible to do justice to them all (see Further reading).
And what of the commercial development? EMI, thecreators of X-ray CT through Sir Godfrey Hounsfield,were involved from very early on and Clow and Youngproduced the first published human head image in1978 (figure 1.3). EMI sold their research interest toPicker International, now Marconi (recently sold toPhilips). The ‘Neptune’ 0.15T superconducting systeminstalled at the Hammersmith Hospital, London, wasthe first commercial clinical system. Elsewhere inEurope, Philips Medical Systems also dedicated sub-
stantial early investment (figure 1.4). General Electricintroduced high field systems in around 1984. The tech-nique developed rapidly through the late 1980s tobecome the method of choice for nontrauma neurolog-ical scanning. By 1996 there were in excess of 10000scanners worldwide.
Due to problems of low signal and high sensitivity tomotion, body MR did not really take off until the mid1990s. The key factors were the development of fastimaging techniques, particularly gradient echo, andphased array coil technology. The 1990s also saw thecoming of age of earlier developments, namely cardiacMRI and Echo Planar Imaging (EPI). EPI, which is thefastest and one of the most cutting edge methods, wasactually one of the first imaging methods to be pro-posed, by Sir Peter Mansfield. EPI is now extensivelyused in neurological imaging through functional MRI(fMRI) and diffusion imaging.
1.2 A brief history of medical imaging
3
Figure 1.2 Raymond Damadian’s “Apparatus and method for detecting cancer in tissue”. US patent 3789832 filed 17 March
1972, issued 5 February 1974. Image from the US Patent and Trademark Office.

1.3 How to use this book
Everyone starts MRI with the same basic problem: it’slike nothing else they’ve learnt in the past. All thatknowledge you have about radioactive isotopes andfilm-screen combinations is useless to you now. Wheredo you start? Most MRI books start at the beginning (avery good place to start, according to the song), andintroduce protons, net magnetization, precession andthe Larmor equation all in the first three pages. We thinkthere is another way, starting at the end with the images
MR: What’s the attraction?
4
Figure 1.3 First ever human head image using MRI at 0.1 T
from EMI Central Research Laboratories. For this image CT
type “back projection” was used. Courtesy of Ian Young.
Figure 1.4 Walker 0.1 T resistive magnet used by Philips in
the early development of MRI. Courtesy of Philips Medical
Systems.
The early history of NMR‘Nuclear induction’, as it was first described, was dis-covered in 1945, soon after the close of World War II,by Bloch and independently by Purcell and Pound.It is said that the development of radio commu-nications in the war effort, to which Purcell hadcontributed scientifically, was one of the factorsunderpinning this important scientific discovery.Another important factor, as in the development ofatomic physics, was the expulsion or fleeing ofEuropean physicists from the Nazi regime, an exodusthat included Bloch and Bloembergen. What didthese MR pioneers discover? That you can detect asignal (a voltage in a coil) when you place a sample ina magnetic field and irradiate it with radiofrequency(RF) energy of a certain frequency, the resonant orLarmor frequency. The signal is produced by theinteraction of the sample nuclei with the magneticfield. The spin echo was ‘stumbled upon’ by Hahn in1949. He discovered that you could get a repeat of theNMR signal at a delayed time by adding a secondburst of RF energy. That’s all you need to know fornow. So what were NMR researchers doing betweenthe forties and the seventies – that’s a long time incultural and scientific terms. The answer: they weredoing chemistry, including Lauterbur, a professor ofchemistry at the same institution as Damadian. NMRdeveloped into a laboratory spectroscopic techniquecapable of examining the molecular structure ofcompounds, until Damadian’s ground-breaking dis-covery in 1971.

that are produced, which is much more useful if you’realready working in the MR unit. After all, you don’texpect to understand how the internal combustionengine works before you learn to drive.
The book is divided into two parts. In part A you willfind everything you need to know about the basics ofMRI, but presented in reverse order. We start with thingsyou can touch and look at: the equipment you find in anMR unit and what the images look like, using terms like‘T1-weighted’ simply as labels. Later on we talk abouthow the images are produced and finally we cover theunderlying physics. By that stage you will be able to linkthese rather difficult concepts back to things whichmatter – the images.
Part B contains more advanced topics, such ascardiac MR and spectroscopy, in no particular order.You don’t have to work right through part A before youread these chapters, we just couldn’t fit them neatly intothe reverse order!
1.3 How to use this book
5
The spin doctors: Nobel Laureates’ roll-call(figure 1.5)In 1952 Edward Purcell (Harvard) and Felix Bloch(Stanford) jointly received the Nobel Prize for physics‘for their development of new methods for nuclearmagnetic precision measurements and discoveriesin connection therewith’. Of Purcell’s discovery, theBoston Herald reported that ‘it wouldn’t revolution-ize industry or help the housewife’. Purcell himselfstated that ‘we are dealing not merely with a new toolbut a new subject which I have simply called nuclearmagnetism. If you will think of the history of ordinarymagnetism, the electronic kind, you will rememberthat it has been rich in difficult and provocative prob-lems and full of surprises.’ It seems that the BostonHerald misjudged the importance of NMR!
Bloch, a Swiss-born Jew and friend of quantumphysicist Werner Heisenberg, quit his post in Leipzigin 1933 in disgust at the Nazi’s expulsion of GermanJews (as a Swiss citizen, Bloch himself was exempt).Bloch’s subsequent career at Stanford was crammedwith major contributions to physics and he has beencalled ‘the father of solid state physics’.
Nicolaas Bloembergen, a Dutch citizen, was forcedto hide from the Nazis for the duration of the War,reputedly living on boiled tulip bulbs, until becom-ing Purcell’s first graduate student at Harvard twomonths after the discovery of NMR. With Purcell andRobert Pound he developed the theory of NMR relax-ation, known now by their initials BPP. In 1981 hewon a Nobel Prize for his work in laser spectroscopy.
In 1991 Richard Ernst joined the MRI NobelLaureates ‘for his contributions to the developmentof the methodology of high resolution nuclear mag-netic resonance spectroscopy’. You could sayRichard Ernst achieved the same trick twice: by hisnovel applications of 2D FT in both spectroscopyand imaging.
Other Nobel Laureates associated with NMRinclude Norman Ramsay (1989), a spectroscopypioneer who developed the theory of the chemicalshift, and Isidor Rabi (1944), Ramsey’s PhD mentor,‘for his resonance method for recording the mag-netic properties of atomic nuclei’.
Figure 1.5 Nobel prize-winners in NMR: (a) Purcell
1912–1997, (b) Bloch 1901–1999, (c) Bloembergen b. 1920
and (d) Ernst b. 1933. Courtesy of the Nobel Museum.
(a) (b)
(c) (d)

In all the chapters you will find the most basic infor-mation in the main text. Advanced boxes, shaded inblue, deal with various topics in more detail and areplaced at appropriate places through the text. If you’recompletely new to MR, we suggest you read straightthrough skipping all the advanced boxes. When youneed to understand something a bit better, re-read thechapter this time taking in the blue boxes. The topicscan seem to jump around a bit by splitting them up thisway, but we think it is a good compromise, which allowsus to include enough information for everyone,whether you are a new radiographer hoping to make agood impression in your new job, or a physicist study-ing for a postgraduate degree.
FURTHER READINGChristie DA and Tansey EM (eds) (1996) Making the Human
Body Transparent: The Impact of Nuclear Magnetic
Resonance and Magnetic Resonance Imaging. London:
Wellcome Institute for the History of Medicine. Available
from: http://www.wellcome.ac.uk/en/images/witness_vol2
_pdf_1905.pdf [accessed 24th October 2001]
Mattson J and Simon M (1996) The Pioneers of NMR and
Magnetic Resonance in Medicine: The Story of MRI. Jericho,
NY: Dean Books Co (ISBN: 0961924314)
Thomas AM, Isherwood I and Wells PNT (eds) (1995) Invisible
Light: 100 Years of Medical Radiology. Oxford: Blackwell
Science (ISBN: 0865426279)
MR: What’s the attraction?
6