
Mothers’ Beliefs about Infant Care Practices in a South Indian Village: The Role of Maternal...
34
Mothers’ Beliefs about Infant Care Practices in a South Indian Village: The Role of Maternal Education in Child Survival Pamela Rao, PhD Correspondence information: Pamela Rao, PhD 1514 17 th St, NW, #212 Washington, DC 20036 Phone: 336-287-1189 E-mail: [email protected]
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Mothers’ Beliefs about Infant Care Practices in a South Indian Village: The Role of Maternal...

Mothers’ Beliefs about Infant Care Practices in a South Indian Village:
The Role of Maternal Education in Child Survival
Pamela Rao, PhD Correspondence information: Pamela Rao, PhD
1514 17th St, NW, #212 Washington, DC 20036 Phone: 336-287-1189 E-mail: [email protected]
Mothers’ Beliefs about Infant Care Practices in a South Indian Village:
The Role of Maternal Education in Child Survival
Infant and child mortality rates remain high in many parts of the world despite the existence of
inexpensive, easily implemented interventions. Maternal education has been linked with under-5
mortality rates, but the pathway of influence is unclear. I investigated the relationship between
maternal education and beliefs about survival-promoting reproductive and childcare practices.
Women, regardless of education, reported survival-promoting beliefs concerning practices
targeted by government health education programs, e.g., breastfeeding, immunizations.
However, better-educated women were more likely to report survival-promoting beliefs about
socioculturally or economically constrained practices, e.g., age at marriage, birth setting.
Alternative approaches are needed to influence socioculturally- and economically-moderated
beliefs and behaviors effecting child survival for less-educated mothers.
[child survival, human development, maternal education, childcare practices, India]
Acknowledgement
This project was funded by Grant No. 8584 from the Wenner-Gren Foundation for
Anthropological Research.
1
Mothers’ Beliefs about Infant Care Practices in a South Indian Village:
The Role of Maternal Education in Child Survival
INTRODUCTION
Child survival, generally operationalized as the overall infant and child mortality
rates for a region for research and policy purposes, is considered a fundamental indicator
of the overall human development of a population (United Nations Development
Programme [UNDP], 2002). Infant mortality rates (IMR) are sensitive indicators of
socio-economic development, health conditions, and the status of women in a region
(Jain and Visaria, 1988a; Mahadevan, et al., 1985; Misra, et al., 1993; Singh, et al.,
1991). Despite impressive improvements in worldwide health measures, preventable
illnesses and “diseases of poverty” continue to contribute to the deaths of thousands of
children every day throughout the world. Yet many of these deaths could have easily
been prevented using existing interventions that are affordable and accessible even in
relatively resource-poor countries (Jones, et al., 2003; Bryce, et al., 2003; The Bellagio
Study Group, 2003).
Numerous research studies have been conducted worldwide to identify
determinants of infant and child survival at all levels, from the socio-political milieu to
household characteristics to individual behaviors (e.g., Mosley and Chen, 1984; Visaria,
et al., 1997; Scheper-Hughes, 1987). Maternal education has been identified in studies
around the world as the strongest predictor of child survival worldwide, even more so
than access to health care or father’s occupation. Although education may be only a
proxy for a straightforward socio-economic underpinning for child survival, other, more
2
subtle, interactions between mother’s education and children’s health outcomes are being
pinpointed (Visaria, et al., 1997). A clearer understanding of the ways in which maternal
education influences child survival is necessary if this important finding is to lead to
reductions in infant and child mortality—a fundamental component of the development
initiatives of many countries.
The case of India deserves special attention because of its large population, which
magnifies the effect of the IMR beyond its rank in the world (Black, et al., 2003), as well
as the low educational and literacy attainment of large segments of the female population
(Government of India, 2004a, 2004b). Despite the implementation of a variety of child
health and women’s development initiatives, rates of infant and child mortality remain
unacceptably high in many parts of the country. The research upon which this paper is
based sought to identify pathways by which mother’s education influences child health in
India (Rao, 1999). This paper describes the results of a component of the study that
assessed the relationship of maternal educational attainment with variations in infant and
young child care practices known to influence child survival (Black, et al., 2003; Jansen,
et al., 1993; UNICEF, 1990).
Child Survival in India
Since gaining independence in 1947, a national goal of the Government of India
has been to improve the health status of its citizens (Jain and Visaria, 1988b). Substantial
research on child health issues has already been conducted, and government health care is
comparatively available and accessible. As a result, infant and child mortality rates
declined substantially during the last half century. The all-India IMR in 2001 was about
3
67 per 1000 and the under-5 mortality rate was 93 (UNDP, 2003). IMRs for individual
Indian states ranged from 11 in Kerala to 90 in Orissa (Government of India, 2002).
These rates are high in comparison to the industrialized areas of the world, where IMRs
are below 4 per 1000 in northern Europe and Japan. However, they compare favorably
with IMRs in other less developed regions such as sub-Saharan Africa, where rates are as
high as 180 per 1000 live births. The situation is similar with India’s under-5 mortality
rates in comparison with rates from 3 to over 300 per 1000 worldwide (UNDP, 2003).
As in the rest of the world, mother’s education has emerged as a leading predictor
of child health outcomes influencing survival rates in India (Ashraf, 1990; Beenstock and
Sturdy, 1990; Daga and Daga, 1993; Das Gupta, 1990; Gandotra, et al., 1989; Goodburn,
et al., 1990; Kutty, 1989; Mahadevan, et al., 1985; Mukhopadhyay and Seymour, 1993;
Shariff, 1987; Ware, 1984). The National Family Health Survey of India shows
statistically significant differences in infant mortality based on mother‘s literacy status
(literate versus illiterate) even when adjusted for a variety of socioeconomic factors
(Pandey, 1998). A significant gender gap in educational attainment still exists in India
(Kingdon, 2002). Only 65 girls for every 100 boys were enrolled in secondary school
during 2001 (Government of India, 2004a) and the literacy rate was 75.3% for males as
opposed to 53.7% for females (Government of India, 2004b). These data point to an
important and useful point of convergence for child health and women’s development
interventions.
The Government of India’s Integrated Child Development Service (ICDS) is one
of the most extensive child survival and women’s development initiatives in the world
4
(Tandon, 1997; Rattan, 1997a). Services such as preschool education, supplemental
nutrition for children and nursing mothers, and infant care training are offered by lay
health workers in more than 400,000 village service sites known as anganwadi centers
(Rattan, 1997a, 1997b). While the ICDS program’s successes have been somewhat
uneven, it has nonetheless produced many positive outcomes (Tandon, 1997), and it
remains an important component of the Government of India’s long-term development
program.
Refocusing Child Survival Research
Infant or child mortality rates are problematic as measures of unmet need for
infant health and well-being since in effect they represent lost opportunities to influence
outcomes (Jansen, et al., 1993). During the 1990 World Summit on Children, a set of
specific infant care factors were identified as having the greatest impact on child health
outcomes (United Nations Children’s Fund [UNICEF], 1990), including birth spacing,
childbirth practices, breastfeeding, immunizations, infant growth, and diarrheal disease
management. The Child-at-Risk Index (or CAR) was developed by researchers at WHO
in order to shift the focus on child survival research to these indicators that could be
assessed with respect to currently living children (Jansen, et al., 1993). Criteria for
inclusion in the index were:
… their usefulness in program management; a documented relationship to
mortality change; sensitivity to change over time and program
intervention; reliable measurement even with limited resources for
5
monitoring and evaluation; and consistency with indicators used by other
donors and in terms of data collection methodology (Jansen, 1993:3).
The specific indicators and related measures are:
1. Birth order and spacing: A healthy reproductive pattern depends on a combination of
factors for both the mother and her children. A younger age at marriage implies a
younger age at first pregnancy, which is a risk factor for infant and child mortality, as
well as poorer health outcomes in surviving children (Mehra and Agrawal, 2004;
Phipps and Sowers, 2002). A belief in the likelihood of one or more children dying in
a family tends to result in larger family sizes, resulting in a decrease in the resources
and attention available per child in the family (Azuh, 1994).
2. Safe delivery care: In the CAR Index, safe delivery is defined by whether or not a
medically-trained person attended the birth. At issue is the proximity of or access to
an individual equipped to handle medical emergencies should they arise. Traditional
birth practices that increase the risk of neonatal tetanus, such as the application of
cow dung to the umbilicus, are still practiced by some non-medically trained birth
attendants. In India, the use of traditional birth attendants is common for economic
reasons (they are much less expensive), and because children are frequently born at
home rather than in a hospital or clinical setting.
3. Exclusive period of breastfeeding: The positive impact of breastfeeding for child
health and survival, particularly in developing countries, is well established.
Research has shown it to be protective against certain childhood illnesses such as ear
and respiratory infections (Bonuck, et al., 2002, Pugh, et al., 2002). In situations
6
where the risk of contamination, spoilage or excessive dilution of formula is high, it
can reduce the risk of infection and undernutrition (Wilmoth and Elder, 1995; Rogers,
et al., 1997a, 1997b; Pugh, et al., 2002). Other benefits include suppressed fertility
(natural birth spacing), mother-child bonding, and financial savings to the household
(Wilmoth and Elder, 1995). Although colostrum is generally considered beneficial to
children’s health, in some developing countries it is customarily withheld, which
delays breastfeeding initiation for a day or more after birth (Rogers, et al., 1997a).
4. Diarrheal disease management: Diarrheal disease is an important cause of infant
mortality and morbidity, especially in areas with polluted water supplies, as is often
the case in crowded villages with limited sanitation facilities (Waterston, 2003).
However, while diarrheal disease can be difficult to avoid, it is easily managed with
oral rehydration therapy (ORT). Oral rehydration salt mixes are readily available
from anganwadi workers and Primary Health Centres. Because time is of the essence
in treating diarrhea, knowledge, access, and willingness to use ORT are important
factors in reducing mortality.
5. Immunization status: Immunization programs have been successful in reducing the
incidence of childhood illnesses worldwide and are believed to have eradicated some
such as smallpox (Greenough, 1995; Wright, 1995). In India, programs for
promoting the vaccination of children have been an integral part of all health care
delivery systems, including the ICDS program (Streefland, 1995).
6. Nutritional status: Determination of adequate growth is based on the international
reference population established by the National Center for Health Statistics and

7
endorsed by the World Health Organization. Adequate weight gain depends upon,
among other variables, when supplemental nutrition is initiated and the types of food
that are introduced (Wilmoth and Elder, 1995; Rogers, et al., 1997b). Adequate
growth is crucial for proper physical and cognitive development, as well as for
reducing vulnerability to risks from a variety of environmental hazards (Engle, et al.,
1996).
THE STUDY: MATERNAL BELIEFS ABOUT INFANT CARE
This paper reports the results of one part of a larger research project to investigate
intracultural differences in beliefs about infant and early childhood care on the basis of
mother's educational level (Rao, 1999). Besides its identification as a crucial predictor of
child health outcomes, maternal educational attainment is a useful independent variable
for research purposes because it is more stable and measurable than most predictive
factors, such as prenatal care or nutritional status during pregnancy, or than
socioeconomic variables, such as income or caste. It is also more easily quantified than
literacy rates, which vary depending on definition. Furthermore, improving educational
levels of women in developing countries is a fundamental component of most human
development programs. The potential synergy from linking child survival and maternal
education initiatives further strengthens the case for including both in development plans.
Study Site
a village in southeastern India in the state of Andhra Pradesh (AP). Gramamu
(Telugu pseudonym, literally “village”), located in a coastal district of AP, was selected
because it is a typical ICDS village with a range of socioeconomic situations and at least
8
some relatively well-educated women. It is a fairly large village by Indian standards,
with about 7,000 people living in around 1,400 households. Primary means of livelihood
include agricultural field work (principally rice and peanuts), handloom weaving (for
both export and domestic distribution) and fishing. Handloom weaving for export is the
village’s main source of income; the Padmasali weaver caste makes up the second largest
occupation group after hired farm labor.
In some respects, Gramamu might be considered a "forward" or economically
advantaged village: it has year-round bus connections to a significant town, a large
proportion of homes have electricity and access to clean water, and it has several primary
and high schools. However, it is classified as "backward," or disadvantaged, by the
Government of India because most of its inhabitants are engaged in low-paying
occupations or belong to castes traditionally considered disadvantaged, specifically the
Padmasali weavers, Jalari fishers, and Sri Yanadalu farm laborers. The various
caste/occupational groups live in segregated areas of the village, known locally as
colonies. Despite the presence of numerous educational facilities, rates of female
education are generally low in Gramamu. The lowest rates are found among the Jalari
fishers, who are also the most poor. The few educated women living in the Jalari areas
are married to schoolteachers or to other educated men brought in to work in the newly-
developing aquaculture (prawn) industry.
Sample Selection
A series of interviews were conducted with 130 mothers of children between the
ages of 12 and 72 months. The sampling frame was created by compiling a list of the
9
households in the village from the records maintained by the anganwadi teachers, village
level health workers of the ICDS program. Anganwadi teachers are expected to conduct
a quarterly census of the households in their assigned areas of the village, during which
they record any changes (e.g., births, marriages) that have occurred during the previous
three months. Details on all homes were recorded on this list, including number and sex
of residents, caste, occupation of head of household, income, ages of all females who
might have children (of any age), and dates of birth of all children in the target range (up
to 72 months). Registered households that did not list any females who had attained
childbearing age were omitted from the compilation.
In this village of approximately 7,000 people, around 90 women had attended
between one and six years of school, approximately 60 had attended between six and ten
years, but only 20 mothers had been educated beyond the 10th standard. Because the
study was intended to focus on mothers with children in the child survival age group, the
sample was further limited to mothers with children between the ages of 12 and 72
months. After this additional eligibility criterion was applied, the result was a stratified
sample of approximately 30 mothers in each of the lower two educational categories.
Since there were so few mothers with more than ten years of education, all women who
were available were invited to participate regardless of whether they had children in the
target age range. The remaining 46 mothers, who never attended school, included
women from all eight colonies. The number of mothers recruited from each colony was
proportionate with the size of its population in the village as a whole.
10
Data Collection
A questionnaire was developed with questions addressing the CAR variables by
asking about beliefs and attitudes towards child rearing issues relevant to each concept.
Each CAR variable was expanded into a set of questions that addressed various aspects in
order to understand how mothers conceptualize those aspects of child rearing most likely
to influence health outcomes. For example, questions were asked about practices
affecting weight-for-age, such as the age at which supplemental feeding should begin and
the types of foods that should be introduced. A list of the questions is provided in the
Appendix.
Date were collected over the course of two interviews and one follow up visit.
All interviews were conducted in the participant’s home in her native language, Telugu,
with the aid of an interpreter. Responses were recorded on paper in English in as direct a
translation from Telugu as was reasonable. Concepts that could not be readily translated
into English were recorded in Telugu, and the meaning was later negotiated with several
native Telugu speakers who are also fluent in English. During the first interview,
background information was gathered on the mother, children, and the household; one or
two children in the target age range (12 to 72 months) were weighed; and the mother and
her children were photographed. During the second interview, which took place
approximately three months later, the CAR questionnaire was administered and the target
children were weighed again. At the end of the field period, a third visit was made to all
informants in order to thank them for participating, give them a copy of the photograph
that was taken during the first interview, and to fill in any gaps in the questionnaire data.
11
Results
Responses were analyzed using nonparametric techniques (chi-square). A
summary of the results is provided in Table 1.
[TABLE 1 ABOUT HERE.]
Birth Spacing: a function of the index child's order within the family's children and the
number of months separating that child from older and younger siblings. To obtain an
idea of what mothers in the village consider to be a preferable childbearing strategy,
questions were asked about practices that affect their own reproductive health as well
their children’s survival, such as age at marriage (which influences age at first
pregnancy), the ideal number of children, knowledge of birth spacing methods, and
attitudes towards using them. Ideal age at marriage showed a distinct positive trend
(Table 2), i.e., higher education was associated with later age at marriage. The range of
responses was also narrower for more educated women. The average preferred age at
marriage by less-educated mothers was 16.6 years of age (range 12 to 21 years).
Conversely, mothers with the most education preferred an average age of 19.9 years of
age (range 17 to 21 years). The vast majority of mothers considered two to be the
preferred number of children, and many noted that the ideal family includes one male
and one female child. Less-educated mothers were slightly more likely to suggest that
the ideal number of children is three (Table 2). The majority of mothers indicated that
the ideal number of years between pregnancies (i.e., birth spacing) should be about three
years, but overall, the responses did not demonstrate a strong trend by maternal education
(Table 2). Mothers who had never attended school recommended the highest mean
12
number of years between children (3.4 years; range 2 to 6 years), while the lowest mean
response was given by mothers in the second-lowest educational group (2.8 years; range
1 to 5 years).
A surprising number of mothers, including highly literate ones, either responded
that they were not aware of methods for delaying pregnancy for purposes of birth spacing
or refused to discuss the topic (Table 2). Some mothers claimed they simply did not
know about methods of contraception, while others observed that it was not an
appropriate topic of conversation to have with the unmarried researchers. Even well
educated mothers were concerned that admitting knowledge of family planning methods
would be seen by their husbands or in-laws as evidence that they are women of low
morals. Overall, however, less-educated mothers were statistically significantly more
likely to report lack of knowledge of spacing methods.
The last question asked on this topic addressed the mother’s perception of the risk
of children dying. While the risk of infant death was thought to be low in Gramamu, the
responses did reveal a statistically significant trend among less-educated mothers to
believe it was a concern (Table 2). One respondent with no education reported that every
mother in her family had experienced at least one child death.
[TABLE 2 ABOUT HERE]
Safe Delivery: the presence of a trained medical attendant at the index child's birth.
Mothers were asked where children should be born and who should be present during
labor and delivery. There was overwhelming agreement that the delivery attendant
should be female, regardless of whether she is a physician (“daktar-amma,” literally “lady
13
doctor”), a traditional birth attendant, or a female relative. The stated preference for
delivery location tracked closely with the preference for type of birth attendant. Mothers
who preferred hospital deliveries also preferred medical attendants, while traditional birth
attendants were fine for home deliveries. Both variables were statistically significant
with respect to mother’s education, with less-educated mothers more likely to prefer a
traditional birth attendant and home delivery (Table 3).
[TABLE 3 ABOUT HERE]
Exclusive Breastfeeding: the number of months the child was exclusively breastfed before
any kind of supplemental nutrition was introduced. Mothers in the study were asked
about when breastfeeding should be initiated, when solid or other foods should be
introduced (ending the period of exclusive breastfeeding) and when the child should be
weaned completely. Most mothers indicated that breastfeeding should be initiated on the
day the child is born and that all the milk, including the colostrum, should be given. A
few mothers indicated that the first day’s milk is bad and should not be given to children,
but others noted that although they used to hold that belief, they were now better
educated on the matter and knew the importance of giving all the milk.
Most mothers said that supplemental feeding, usually rice, should be introduced
around 6 months. In India, the introduction of solid food, specifically rice, is culturally
mandated to take place in the child’s sixth month in a “first rice” ceremony
(“annaprasanam,” literally “offering rice”). This important ceremony is observed by
Indians of all socio-economic groups and tends to correspond with the generally
recommended age for the introduction of other foods. A preference for a longer duration
14
of breastfeeding by less-educated mothers is evident in the responses to question
regarding the age at which children should be weaned. The mean age at weaning
recommended by uneducated mothers (34.3 months) was over twice as long as that
recommended by the most educated mothers (14.3 months). This is the only variable that
showed a negative trend with respect to mother’s education (Table 4).
[TABLE 4 ABOUT HERE]
Diarrheal Disease Management: the use of oral rehydration therapy for the index child's
most recent episode of diarrheal disease. Mothers were asked what they believed to be
the cause of diarrhea and what treatments were available and preferred. Diarrhea was
attributed to a wide range of causes, including teething, playing in mud, digestion
problems, contaminated food or water, changes in food or water, and lack of
environmental cleanliness. It was also observed that foods that have the humoral
property of producing “heat,” such as buffalo milk, chilies, pickles and wheat flour, can
cause diarrhea, whether ingested directly by the child or indirectly through the mother’s
milk. Change in the weather (particularly the onset of summer) was another oft-
mentioned cause, as was poor health in general.
Twenty-five percent of mothers across all educational levels included oral
rehydration therapy on the list of possible treatments for diarrhea (data not presented).
Alternative therapies included giving the child syrups, drops or tonics obtained from the
village’s Registered Medical Practitioner (RMP), or taking him/her to the hospital or
doctor for injections or prescription medicines. A few mothers recommended traditional
treatments, including coconut water, buttermilk, pomegranate juice, dry ginger, and a
15
homemade medicine comprised of leaves of a locally common tree (wapu), ginger and
honey. Diarrhea could also be treated by feeding the child foods with the proper humoral
properties, such as leafy vegetables (which are “cold” foods) to balance and treat diarrhea
(a “hot” condition).
Immunization: the percentage of recommended immunizations received. Mothers in this
study were asked about their knowledge of recommended vaccinations for children and
about their purpose. All mothers in the study indicated that they knew the value of
immunizations for children, although one relatively well-educated mother chose not to
allow her younger children to receive the polio vaccination after her oldest daughter
developed polio after receiving it. Those mothers who were familiar with the purpose of
immunizations were most likely to mention polio, measles, tetanus, tuberculosis, and
whooping cough. Other diseases mentioned included cholera, malaria, chicken pox, and
goiter. A surprising number of mothers believed that brain tumors (“meda wapu”) could
be prevented by immunization. They had heard claims that ayurvedic medicine could
prevent brain tumors and assumed by extension that allopathic medicine could do
likewise. Responses to these questions did not vary by mother’s education (data not
presented).
Nutritional Status: numerical score reflecting relative weight-for-age. Mothers were
asked when supplemental feeding should begin, and what types of foods are
recommended. There was very little variation in the recommended age at first feeding,
with responses tending towards the timing of the annaprasanam ceremony (6 months).
The least educated mothers recommended waiting the longest, an average of around 5.1
16
months. Mothers educated between one and five years averaged 5.3 months, between six
and ten years averaged 5.0 months, and over eleven years averaged 4.3 months.
Although not a strong trend, there was the appearance of a relationship in which mothers
with less than eleven years of education generally recommended later introduction of
supplemental feeding. Suitable foods included bananas and other soft fruits, biscuits
(similar to bland cookies or crackers), boiled carrots or potatoes, various types of
porridge (rava, ragi, paisam), rice diluted with water or curds, and an extensive selection
of commercial infant formulas (e.g., Nestam, Cerelac, Farex, Complan), as well as
powdered mixes normally intended for adults (e.g., Horlicks, Bornvita).
DISCUSSION
Inspection of the trends listed in Table 1 reveals that responses to about half of the
Child-At-Risk Index questions have the hypothesized relationship with mother’s
education, that is, higher education is associated with infant and child care beliefs and
practices that generally predict better health outcomes. Of those, responses to four
questions were statistically significant. Only one variable showed a negative trend, and
the remainder showed no discernible trend with respect to mother’s education. Because
the questions in this portion of the study were intended to elicit beliefs about particular
child rearing practices, rather than actual behaviors, responses tended to cluster around
certain locally observed or culturally directed patterns, weakening any statistically
significant variation with respect to mother’s education. Definite trends are nonetheless
evident in the results, and several variables did show statistically strong correlations with
mother’s education.
17
Direct association: knowledge of birth spacing methods, preferred birth location and
attendant, and belief about the risk of child mortality
Family planning has been a major preoccupation of the Indian Government’s
population control and women’s health programs since the 1960s. Numerous programs
to promote the use of spacing methods and to encourage permanent methods after the
second child is born have been implemented with varying results. Given the ubiquity of
the family planning messages, which can be seen on seemingly every building beam and
sign post in rural and urban India and heard on television and radio announcements, it is
hard to imagine that anyone could be unaware of the suggested methods or the goal of the
programs regardless of literacy status. However, women must be very careful to
maintain their own and their families good names by not giving the impression of
impropriety that a public admission of knowledge might indicate. It is to be expected that
women from the groups that restrict women’s education would be even more reluctant to
admit knowing about birth spacing methods. Delaying and spacing child bearing can be
difficult in a situation where “lack” of knowledge of birth control is culturally sanctioned.
Ideally, it should be more acceptable for educated girls to know about birth
control methods, however, women were reluctant to demonstrate in public, e.g., under the
watchful eye of friends and relatives during an interview, that they were familiar with
birth control methods. This last finding may indicate a need for attention to the attitudes
of men as much as those of women on the subject of birth control and spacing. Perhaps if
men were more familiar with the available alternatives, their minimal risk to health and
fertility, and the benefits to parents and children of properly spaced births, they would be
18
more inclined to participate in those decisions, and women would feel more free to learn
about, obtain, and use them.
A related question, ideal age at marriage, also showed a positive trend with
mother’s education, although not a statistically significant one. Since later age at
marriage, and thus at first pregnancy, is associated with better birth outcomes and lower
rates of maternal mortality, the educational process itself indirectly effects birth and
health outcomes by delaying marriage, and consequently, age at first delivery. Less-
educated mothers are often expected by their extended families to arrange daughters’
marriages at a relatively young age (between 12 and 16). These mothers usually belong
to castes that do not traditionally educate daughters because it is expected that they will
leave home immediately after marriage and never contribute economically to their natal
family. Moreover, they represent a financial burden while they are living there unless
they are working, which precludes attending school. Conversely, mothers who belong to
castes that believe in educating their daughters will delay arranging their marriages until
after they reach their expected level of education. These are more likely to be the case
with mothers who are themselves more educated.
Economic realities influence preferred behaviors in many of the decisions made
by mothers and families. The traditional preference that a mother’s first delivery take
place in her natal home (i.e., with her own mother and perhaps sisters in attendance), with
later births taking place in her marital home means that many births do not occur in
hospitals. It would therefore be unrealistic to expect them to be attended by a
biomedically-trained physician. The stated preference of less-educated mothers for a
19
non-medical delivery setting was explained by several mothers as stemming from
concern about the expense of a hospital delivery, as well as a desire to avoid the
possibility of a surgical delivery. However, many mothers also specified that home
deliveries were only appropriate in the case of a normal delivery. Giving birth in a
hospital is still relatively uncommon, although if there was any possibility of a difficult or
complicated delivery, it was preferable. The generally later age at the introduction of
supplemental feeding recommended by mothers with less education may also have
economic significance since they may not have the access to resources to initiate
supplemental feeding at a younger age. Finally, beliefs about the risk of child mortality
may also stem from economic realities. Educated mothers who are generally from
wealthier families are less likely to experience child death and may therefore perceive
themselves as having more control over the possibility. Conversely, a mother who is
restricted by both lack of literacy and of resources is more at the mercy of her
environment and circumstances and may feel she has little or no control over her own
(and her children’s) fate.
Inverse association: breastfeeding practices
The issues surrounding breastfeeding practices are somewhat more complex to
interpret, since their association with mother’s education differed among questions. On
the one hand, breast milk is a nutritious, convenient, and inexpensive food source for
children, especially in low income households and/or those with a larger number of
children. On the other hand, bottle feeding frees a mother for other activities, and may
appeal to educated mothers because of its apparent air of sophistication. The notion that
20
colostrum is “bad” and should be discarded, as well as the shorter duration of
breastfeeding among educated women in developing countries has been observed in other
studies (Rogers, et al., 1997a). The longer periods of breastfeeding given by the less
educated women probably reflects information received on this topic from the anganwadi
workers, as this is a major focus of ICDS educational activities.
It has been suggested that growth faltering provides a more broad-based indicator
of health status than morbidity or mortality counts (Mosley and Chen, 1984). While it is
widely agreed that breastfeeding is the ideal source of nutrition for infants, it is equally
important that supplemental nutrition be initiated by an appropriate age. This is
especially important for low-income mothers who might be tempted to delay introducing
supplemental foods for economic reasons. Because breast milk is an ideal source of
nutrition and a longer period of exclusive breastfeeding extends the time during which
the child is protected from potentially contaminated food and water, a later age at first
supplemental feeding should be a positive factor. However, there is a point at which the
child’s need for nutrition exceeds that which can be produced by the mother, after which
continued exclusive breastfeeding could put the child at risk for stunted growth. But the
use of contaminated water in infant formulas can cause diarrhea, which also inhibits
growth, a fact noted by several mothers. This issue is highly complex, especially when
considered in the context of the widespread observance of the annaprasanam ceremony,
which skewed the responses of all the educational categories towards introducing
supplemental feeding at six months.
No association: immunization, ORT, number of children, birth spacing, colostrum
21
Immunization, use of oral rehydration therapy, preferred number of children, birth
spacing, and giving the colostrum by initiating breastfeeding on the day of birth, have
been central components of the Government’s family planning and population control for
years. Immunization rates are very high in this village, as is the case throughout much of
India. However, while many mothers could not state the specific purpose of
immunizations other than to keep the children healthy or to prevent disease, their children
were nonetheless fully immunized. The stated preference for medical treatment of
diarrhea rather than the oral rehydration therapy promoted by the public health experts
reflects a general preference for biomedicine (when affordable and available) observed in
other areas of health maintenance, such as immunization coverage. In reality, nearly half
the mothers (48 percent) in another part of this study (Rao, 1999) actually reported using
ORT to treat one or more of their children. Most of those mothers who used ORT were
from the less-educated groups, but there was no statistical significance to the responses
with regards to preferred treatment. The slogan of the family planning program in India
promoting small family size, “We two, our one,” is another ubiquitous campaign of the
central government, and, as noted by one mother, the importance of colostrum has been
emphasized in the ICDS activities. That these variables show no effect by mother’s
education may reflect the success of those programs in this part of India, and throughout
the country as demonstrated by the steadily improving child survival rates.
CONCLUSION
The results of this study generally support the relationship between maternal
education and child survival found in the international literature. More importantly, they
22
also demonstrate that health education programs targeting specific infant care-related
behaviors do indeed benefit mothers with minimal education. Programs such as India’s
ICDS that emphasize low literacy, popular education approaches hold considerable
promise for improving the future of children in developing countries. The women in this
study were clearly not entirely restrained by lack of education or by socially acquired
beliefs about proper infant care practices such as breastfeeding. When the educational
message was received and the necessary resources were available to the mothers, they
were open to new ideas to encourage their children’s health growth and development.
Unfortunately, cultural norms still restrict women’s ability to fully exploit existing
resources with respect to certain messages, such as birth spacing and contraception.
Further research is needed to better understand the situation so that programs can be
tailored to meet the needs of mothers.
The findings of this study are limited by the possible confounding effect of using
education as a proxy for literacy and/or socioeconomic status. Number of years of school
attendance in and of itself does not determine a given person’s literacy level, nor does it
necessarily co-vary with access to other resources that influence child health outcomes.
It is not possible to know with certainty where the mothers in this study learned their
infant care beliefs and practices. It is therefore not possible to know the extent to which
access to education influences their access and receptivity to new information and
knowledge about such practices. Nevertheless, the strength of the trends found in this
relatively small sample suggests that the relationship between maternal education and
23
children’s health outcomes is worth pursuing as a development pathway in many parts of
the world.
A country’s investment in maternal education and children’s health reflects the
importance it places upon human development, and ultimately, its dedication to
improving the future of its people. While current technology and knowledge exist to
make a significant improvements in much of the world, the resources and political will
are not always equally sufficient or available. Encouraging such an emphasis in priorities
of both the public health and international development communities will both benefit the
current population and lay the foundation for healthier populations in the future.
24
APPENDIX:
Infant care Knowledge and Practices Questionnaire
Birth Order and Spacing:
• At what age should women get married?
• At what age should she have her first child?
• How many children is the ideal number?
• How far apart should they be born?
• What can you do to achieve that the time period between births?
• How great is the risk of children dying?
Safe Delivery:
• In what setting should babies be born?
• Who should be with the mother when a child is born?
Breastfeeding:
• What day should it start?
• Should you give all the milk (including colostrum)?
• How long should it be continued?
Nutrition:
• When should you start giving food in addition to milk?
• What foods should you give?
Treatment for Diarrheal disease:
• What causes diarrhea?
• What should be done when a child has diarrhea?
Immunizations:
• What is the purpose of immunizations?
• Should children receive immunizations?

25
REFERENCES
Anand, S., & Sen, A. K. (2000). Human development and economic sustainability. World Development, 28, 2029-2049.
Ashraf, M.S. (1990). Infant Mortality in Rural India: A Diagnostic Study. Lucknow: Print House (India).
Azuh, D. E. (1994). Child Survival Under Threat: A Cross-Sectional Study in India. New Delhi: Vedams Books International.
Beenstock, M., & Sturdy, P. (1990). The determinants of infant mortality in regional India. World Development, 18, 443-453.
Bellagio Study Group on Child Survival (The). (2003). Knowledge into action for child survival. Lancet, 362, 323-27.
Bhutta, Z. A. (2003). Beyond Bellagio: Addressing the challenge of sustainable child health in developing countries. Archives of Disease in Childhood, 89, 483-487.
Black, R. E., Morris, S. S., & Bryce, J. (2003). Where and why are 10 million children dying every year? Lancet, 361, 2226-34.
Bonuck, K., Arno, P. S., Memmott, M. M., Freeman, K., Gold, M., & McKee, D. (2002). State of the art: Breast-feeding promotion interventions: Good public health and economic sense. Journal of Perinatology, 22, 78-81.
Bryce, J., el Arifeen, S., Pariyo, G., Lanata, C. F., Gwatkin, D., Habicht, J.-P., & the Multi-Country Evaluation of IMCI Study Group. (2003). Reducing child mortality: Can public health deliver? Lancet, 362, 159-64.
Daga, A.S., & Daga, S.R. (1990). Health information for primary neonatal care. Journal of Tropical Pediatrics, 36, 141-142.
------. (1993). Epidemiology of perinatal loss in rural Maharashtra. Journal of Tropical Pediatrics, 39, 83-85.
Das Gupta, M. (1990). Death clustering, mother's education and the determinants of child mortality in rural Punjab, India. Population Studies, 44, 489-505.
Dreze, J., & Sen, A. (1997). Indian Development: Selected Regional Perspectives. Delhi: Oxford University Press.
Engle, P. L., Castle, S., & Menon, P. (1996). Child development: vulnerability and resilience. Social Science and Medicine, 43, 621-635.
Gandotra, M.M., Das, N., & Dey, D. (1989). Infant Mortality and Its Causes. Bombay: Himalaya Publishing House.
George, B., Sathy, N., Suguna Bai, N.S., & Atmar, M.E. (1989). Brief Reports: Superstitious beliefs and practices during childhood illnesses. Indian Pediatrics, 26, 936- 938.

26
Goodburn, E., Ebrahim, G.J., & Senapati, S. (1990). Strategies educated mothers use to ensure the health of their children. Journal of Tropical Pediatrics, 36, 235-239.
Greenough, P. (1995). Global immunization and culture: Compliance and resistance in large-scale public health campaigns. Social Science and Medicine, 41, 605-607.
Government of India. (2002). Table 1: Provisional estimates of birth rate, death rate, natural growth rate and infant mortality rate, 2001. Sample Registration System Bulletin 36(2): 1-2. Accessed online at www.censusindia.net on 7/8/04.
-----. (2004a). Table T 00-006: Number of literates and literacy rate by sex. Census of India Basic Population Data. Accessed online at www.censusindia.net/t_00_006.html on 7/8/04.
-----. (2004b). Statement 7.6: Number of girls enrolment per hundred boys enrolled. Department of Education Educational Statistics. Accessed online at www.education.nic.in/htmlweb/edusta_pt2.htm on 7/8/04.
Jain, A. K., & Visaria, P. (eds.). (1988a). Infant Mortality in India: Differentials and Determinants. Newbury Park: Sage Publications.
-----. (1988b). Infant Mortality in India: An Overview. In A. K. Jain & P. Visaria (eds.). Infant Mortality in India: Differentials and Determinants (pp. 23-64). Newbury Park: Sage Publications.
Jansen, W. H., II, Plowman, B. A., & Rock, M. N. (1993). Applying Behavioral Factors to Child Survival Programs. Paper presented at the 92nd Annual Meeting of the American Anthropological Association, Washington, DC.
Jones, G., Steketee, R. W., Black, R. E., Bhutta, Z.A., Morris, S. S., & The Bellagio Child Survival Study Group. (2003). How many child deaths can we prevent this year? Lancet, 362, 65-71.
Kapil, U., Sood, A. K., & Gaur, D. R. (1990). Maternal Beliefs regarding diet during common childhood illnesses. Indian Pediatrics, 27, 595-599.
Kingdon, G. G. (2002). The gender gap in educational attainment in India: How much can be explained? The Journal of Development Studies, 39, 25-53.
Kumar, A. K. S. (1996). Poverty and Human Development in India: Getting Priorities Right. Occasional Paper 30. United Nations Development Programme, Human Development Report Office, New York.
Kutty, V. R. (1989). Women's education and its influence on attitudes to aspects of child-care in a village community in Kerala. Social Science & Medicine, 29, 1299-1303.
Mahadevan, K., Murthy, M.S.R., Reddy, P.R., Reddy, P.J., Gowri, V., & Sivaraju, S. (1985). Infant and Childhood Mortality in India: Bio-social Determinants. Delhi: Mittal Publications.

27
Mehra, S., & Agrawal, D. (2004). Adolescent health determinants for pregnancy and child health outcomes among the urban poor. Indian Pediatrics, 41, 137-145.
Misra, P.K., Thakur, S., Kumar, A., & Tandon, S. (1993). Perinatal Mortality in Rural India With Special Reference to High Risk Pregnancies. Journal of Tropical Pediatrics, 39, 41-44.
Mosley, W. H., & Chen, L. C. (1984). An Analytical Framework for the Study of Child Survival in Developing Countries. In W. H. Mosley & L. C. Chen (eds.). Child Survival: Strategies for Research (pp. 25-45). Cambridge: Cambridge University Press.
Mukhopadhyay, C. C., & Seymour, S. (eds.). (1993). Women, Education and Family Structure in India. Boulder, CO: Westview Press.
Pandey, A., Choe, M. K., Luther, N. Y., Sahu, D., & Chand J. (1998). Infant and Child Mortality in India. National Family Health Survey Subject Reports, Number 11. Mumbai, India: International Institute for Population Sciences.
Pham, H., & Marrow, M. W. (1999). Child survival: A fundamental human right. Minnesota Medicine, 82, 20-26.
Phipps, M. G., & Sowers, M. (2002). Defining early adolescent childbearing. American Journal of Public Health, 92, 125-128.
Pugh, L. C., Milligan, R. A., Frick, K. D., Spatz, D., & Bronner, Y. (2002). Breastfeeding duration, costs, and benefits of a support program for low-income breastfeeding women. Birth, 29, 95-100.
Rao, P. (1999). “Marriage Happens, Children are Born”: Maternal Concepts of Child Rearing in South India. Doctoral dissertation, University of Kentucky, Department of Anthropology.
Rattan, V. (1997a). Women and Child Development and Sustainable Human Development, Vol. 1. New Delhi: S Chand & Company Ltd.
-----. (1997b). Integrated Child Development Services Programme Administration, Vol. 2. New Delhi: S Chand & Company Ltd.
Rogers, I.S., Emmett, P.M., & Golding, J. (1997a). The incidence and duration of breastfeeding. Early Human Development, 49, S45-S74.
-----. (1997b). The Growth and nutritional status of the breast-fed infant. Early Human Development, 49, S157-S174.
Scheper-Hughes, N. (ed.). (1987). Child Survival: Anthropological Perspectives on the Treatment and Maltreatment of Children. Boston: D. Reidel Publishing Company.
Shariff, A. (1987). Child survival: A village-level investigation of some cultural factors associated with morbidity and mortality in South India. Human Organization, 46, 348- 355.
28
Singh, M., Deorari, A. K., Khajuria, R. C., & Paul, V. K. (1991). Perinatal and neonatal mortality in a hospital. Indian Journal of Medical Research, 94, 1-5.
Streefland, P. H. (1995). Enhancing coverage and sustainability of vaccination programs: an explanatory framework with special reference to India. Social Science and Medicine, 41, 647-656.
Tandon, B.N. (1997). ICDS: Past, Present and Future (editorial). Indian Pediatrics, 34, 187-191.
Tandon, B.N., & Kapil U. (1991). ICDS Scheme: A programme for development of mother and child health. Indian Pediatrics, 28, 1425-1428.
United Nations Children’s Fund (UNICEF). (1990). Goals for Children and Development in the 1990s. Available online at www.unicef.org/wsc/goals.htm. Accessed 7/27/04.
United Nations Development Programme (UNDP). (2004). Human Development Report 2004: Cultural Liberty in Today’s Diverse World. New York: Oxford University Press.
-----. (2003). Human Development Report 2003: Millennium Development Goals: A Compact Among Nations to End Human Poverty. New York: Oxford University Press.
-----. (2002). Human Development Report 2002: Deepening Democracy In A Fragmented World. New York: Oxford University Press.
Victoria, C. G., Wagstaff, A., Schellenberg, J. A., Gwatkin, D., Claeson, M., Habicht, J. P. (2003). Applying an equity lens to child health and mortality: More of the same is not enough. Lancet, 362, 233-241.
Visaria, L., Simons, J., & Berman, P. (eds.). (1997) Maternal Education and Child Survival: Pathways and Evidence. New Delhi: Vikas Publishing House Private Limited.
Ware, H. (1984). Effects of Maternal Education, Women's Roles, and Child Care on Child Mortality. In W. H. Mosley & L C. Chen (eds.). Child Survival: Strategies for Research (pp. 191-214). Cambridge: Cambridge University Press.
Waterston, T. (2003 Inequity in child health as a global issue. Pediatrics, 112, 739-741.
Wilmoth, T., & Elder, J. P. (1995). An assessment of research on breastfeeding promotion strategies in developing countries. Social Science and Medicine, 41, 579-594.
Wright, P. F. (1995). Global immunization: A medical perspective. Social Science and Medicine, 41, 609-616.

Table 1: Summary of Child At Risk Variables
Statistical Trend with
Mother’s Education
Child At Risk Variable
Positive Trend Preferred Delivery Attendant *
Preferred Delivery Location *
Knowledge of Birth Spacing Methods **
Belief about Risk of Child Mortality **
Ideal age at marriage ***
Mean Age in Months at Introduction of Supplemental Nutrition ***
Negative Trend Mean Age at Weaning
No Significant Trend Preferred number of children
Ideal Birth Interval
Day of Initiation of Breast Feeding
Giving of Colostrum
Preferred Treatment for Diarrhea
Immunization Acceptance
* p < 0.01
** p < 0.05
*** positive trend, not statistically significant
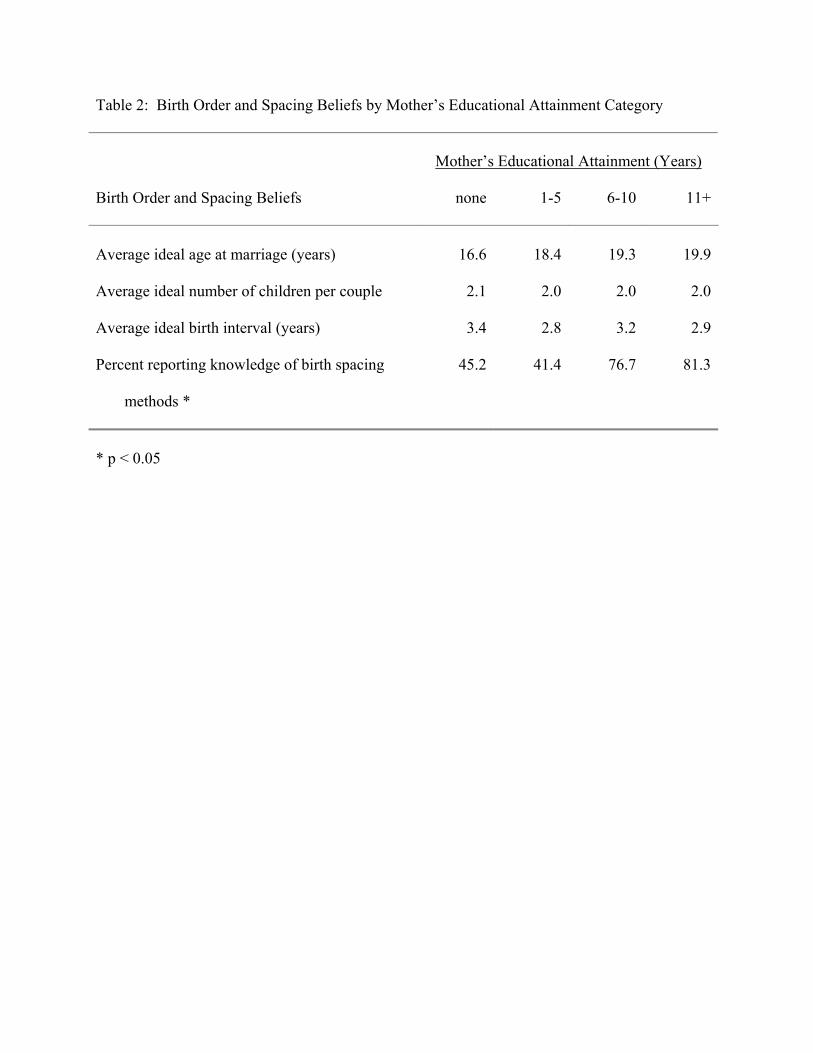
Table 2: Birth Order and Spacing Beliefs by Mother’s Educational Attainment Category
Mother’s Educational Attainment (Years)
Birth Order and Spacing Beliefs none 1-5 6-10 11+
Average ideal age at marriage (years) 16.6 18.4 19.3 19.9
Average ideal number of children per couple 2.1 2.0 2.0 2.0
Average ideal birth interval (years) 3.4 2.8 3.2 2.9
Percent reporting knowledge of birth spacing
methods *
45.2 41.4 76.7 81.3
* p < 0.05
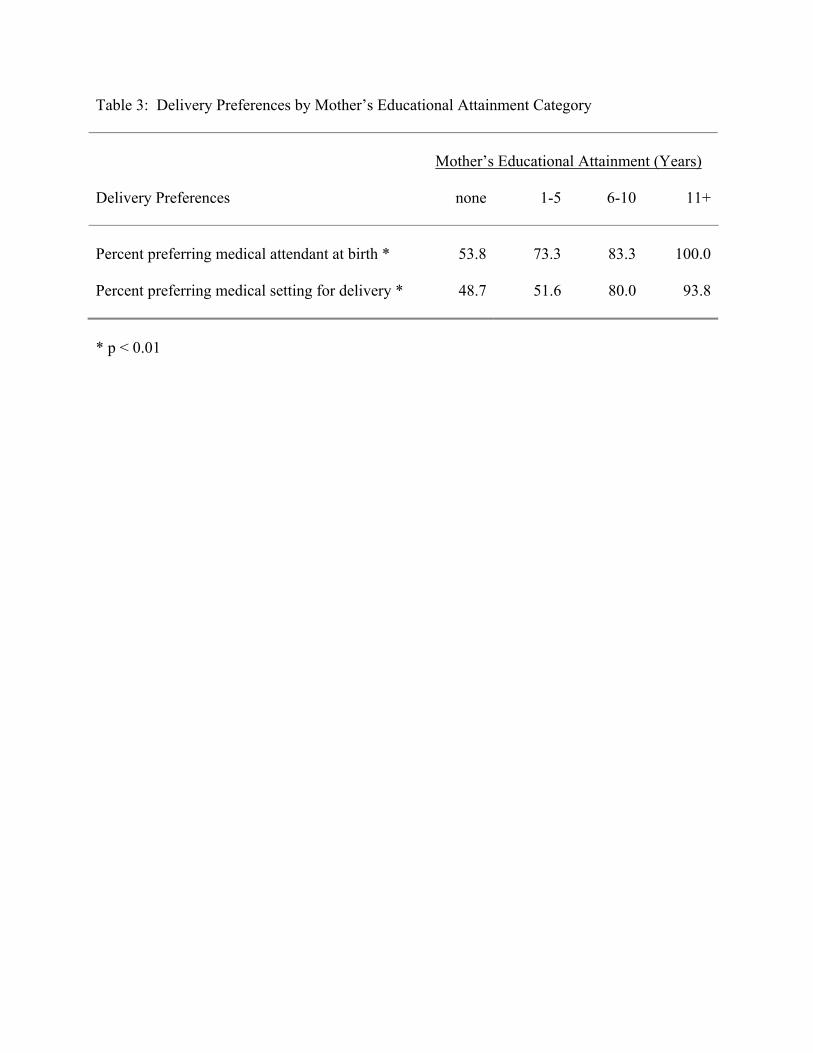
Table 3: Delivery Preferences by Mother’s Educational Attainment Category
Mother’s Educational Attainment (Years)
Delivery Preferences none 1-5 6-10 11+
Percent preferring medical attendant at birth * 53.8 73.3 83.3 100.0 Percent preferring medical setting for delivery * 48.7 51.6 80.0 93.8 * p < 0.01
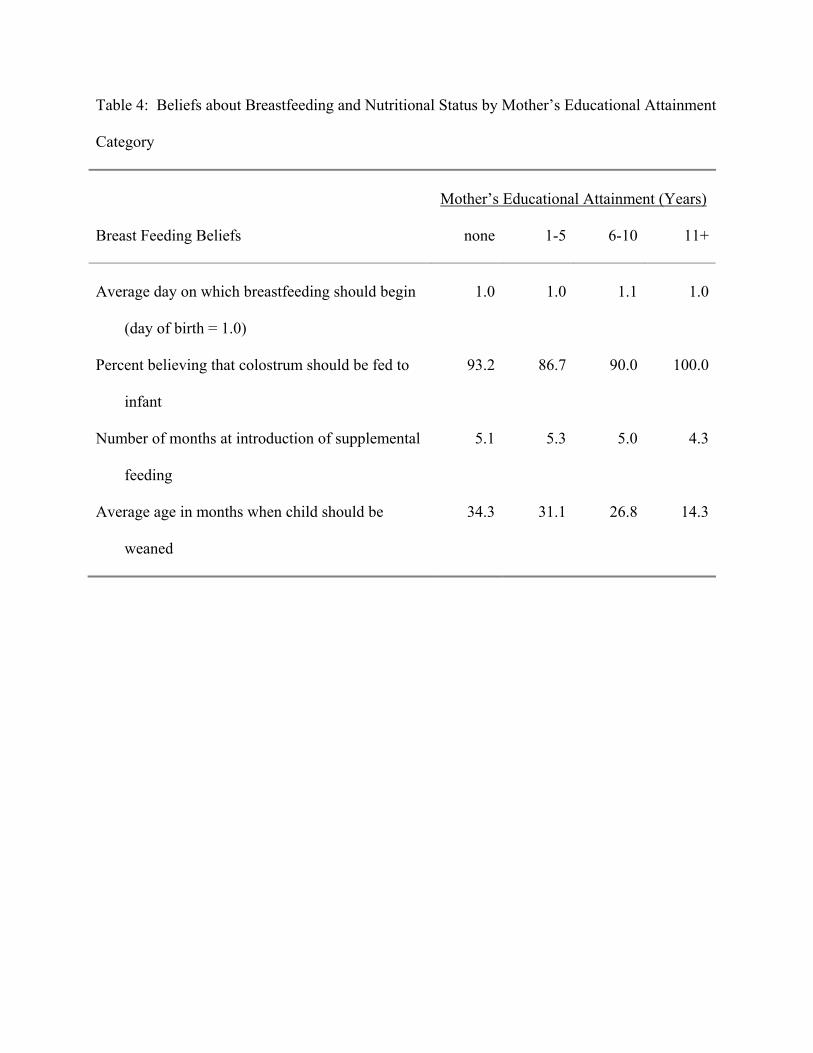
Table 4: Beliefs about Breastfeeding and Nutritional Status by Mother’s Educational Attainment
Category
Mother’s Educational Attainment (Years)
Breast Feeding Beliefs none 1-5 6-10 11+
Average day on which breastfeeding should begin
(day of birth = 1.0)
1.0 1.0 1.1 1.0
Percent believing that colostrum should be fed to
infant
93.2 86.7 90.0 100.0
Number of months at introduction of supplemental
feeding
5.1 5.3 5.0 4.3
Average age in months when child should be
weaned
34.3 31.1 26.8 14.3




















