Modernising Medical Careers: A Human Resource Management Perspective
14
Assignment II: Modernising Medical Careers: A Human Resource Management Perspective Sadia M. Rajput Submitted for deadline 8 th March 2015 A report submitted in fulfilment of the requirements for Course MBAN-690DE, Masters of Business Administration in Management, University of Nicosia-online.
-
Upload
universityofnicosia-online -
Category
Documents
-
view
4 -
download
0
Transcript of Modernising Medical Careers: A Human Resource Management Perspective

Assignment II: Modernising Medical Careers: A Human Resource Management
Perspective
Sadia M. Rajput
Submitted for deadline 8th March 2015
A report submitted in fulfilment of the requirements for Course MBAN-690DE, Masters of
Business Administration in Management, University of Nicosia-online.
An overall view of MMC’s HRM strategy and practices.
Modernising Medical Careers (MMC) is an online based programme set up to assist
postgraduate medical students find placements in hospitals for their medical training before
becoming specialised medical professional and practitioners. It is based on “seven pillars” to
enhance the medical care delivered to patients by providing doctors with necessary skills. The
new training system was intended to be “trainee-centred; competency assessed; service-based;
quality-assured; flexible; coached; and structured and streamlined” (DHET, 2004: 2-3). This
essay will draw on the article published by the DHET MMC: the next step in order to ascertain
the Human Resource Management (HRM) strategy and practices.
The medical training framework was intended to resolve outstanding issues with the medical
education in the UK and to support the medical work force. Some of these challenges were
arguably caused by the new deal and work time derivative set up many years prior and more
specifically to resolve the issue of the “lost tribe” of Senior House Officer (SHO) grade
(Executive, 2002). The SHO grade consists of postgraduate medical students who are
undergoing training in a specific area of specialisation in medicine under the supervision of an
existing consultant or registrar (Executive, 2002). This type of training was similar to an
apprenticeship that lasted at least two years if not more. The SHO grade were coined the “lost
tribe” prior to the reform because some doctors that did not specialise in fields recognised by
the Deanery, remain unaccounted for in the medical work force and others never moved out of
the SHO grade into any particular specialities (Executive, 2002).
Diliner (1993) has argued that this grade has the largest number of doctors however, there is
no distinct role that they play in hospitals as it is unclear what skills they have. With the
introduction of the work time derivative, a regulation on the working hours and training hours
of junior doctors, it became hard to ignore that there was a problem that needed to be resolved
within this grade (Diliner, 1993: 1550).
In light of this MMC was meant to reform specific aspects of the SHO as argued by the Scottish
Executive (2002). These were; the poor job structure of the SHO. The reason the SHO job
structure was poor was due to the fact that not all SHO’s are part of a training programme and
if they are, they have short term appointments (Executive, 2002: 4). Secondly, the training is
poorly defined. There are no clear objectives and thus no clear career path for SHO’s
(Executive, 2002: 4). Thirdly, the way junior doctors are selected and recruited is not done in
a standardised manner. The procedures do not establish whether a candidate possesses adequate
skills. As a result, most SHOs are overworked, are not given structured career advice or
appraisal and assessment (Executive, 2002: 4). Finally it can be argued that their training may
not be relevant to the Royal College examinations which are sat for after their training
(Executive, 2002: 4). Therefore, doctors in the SHO grade do not meet a satisfactory level of
competency necessary to deliver world class health care to patients.
Three HRM strategies can be identified within MMC and these are the revamping of the;
recruitment, selection and training processes. These strategies were restructured to address the
issues outlined in the paragraph above. This section will describe how each
strategy was carried. To begin with, the training structure was revised as follows.
Firstly, the previous pre-registration house officer (PRHO) grade after medical school and the
first year of SHO will be combined and compulsory for all post graduate students and will be
called the foundation programme (Executive, 2002: 5). The aim of this foundation programme
is to augment skills such as “team-working, communication, ability to produce high standards
of clinical governance and patient safety, expertise in accessing, appraising and using evidence
as well as time management skills” (Executive, 2002: 5).
Thereafter, doctors can enter into the second band of trainees, which is a broad, time specific
basic specialist training in one of eight areas. There are two options available for doctors here.
Doctors wishing to pursue general practitioner posts will carry out their specialised training for
three years and those who wish to become consultants will train in specialisation for six years
(Executive, 2002: 5). Unlike the previous SHO training, there will be individual programmes
available to junior doctors who feel that they need specific training in a different area other
than the eight broad areas of medicine (Executive, 2002: 5). Therefore, this reform would be
suitable to meet the needs of more doctors.
Additionally, there are five principles that govern the training strategy to ensure that the reform
achieves the objective of improving training and the quality of health care. The training should
begin with all postgraduate medical students and will firstly be based on a programme, tailored
as per the needs of a trainee, carried out within a specific time frame and finally, it should be
flexible enough to allow junior doctors to take a research or career break and resume training
when necessary. This concludes the training strategy and practices.
This next section will outline the recruitment and selection strategy and practices carried out
by MMC. The new strategy was to have postgraduate medical deans responsible for the
programmes with regards to training support, placement and appointment of junior doctors.
The recruitment and selection process of junior doctors was implemented by Medical Training
Application Service (MTAS). The system was designed to centrally receive and process
applications from doctors around the United Kingdom in the most efficient way possible
(House of Commons, 2007).
The selection process was based on an online application submission of 150 word responses to
a series of questions. All applicants were allowed to make four separate applications through
the online portal. The answers that the junior doctors wrote were then allocated score points in
order to shortlist candidates for the interview. The score points would indicate to the
consultants whether the candidate had qualities, attributes and attitudes they were looking for
to fill the posts (House of Commons, 2007).
Thereafter, shortlisted candidates would be interviewed by answering a series of questions that
were marked according to a rubric. The point of the interview was to assess whether the
applicant acquired specific traits. All successful applicants were then taken through a second
round of interviews before being accepted, confirmed and placed for training with a specific
hospital, depending on their speciality (House of Commons, 2007).
In conclusion, this essay has provided an outline of MMC HRM strategy and practices as set
out by the NHS and the Department of health. Three HRM strategies namely recruitment,
selection and training have been described.
Factors that may have contributed to the failure of MMC
In order to decide which factors affected MMC from being successful, this essay will draw on
the conclusions of stakeholders who were directly affected by the implementation of MMC.
The main stakeholders are the “trainee doctors, workforce planners, NHS employers, the
government, and patients” (Maddon and Maddon, 2007: 426). The reason there is an uproar of
failures is because impact of the failure of MMC to one stakeholder such as the junior doctors
has had a compounding rippling consequence to the other.
Maddon and Maddon (2007) argue that MMC has failed because it seems to have evolved into
something that stakeholders feel does not address the issues it was set out to resolve. It should
be noted that different stakeholders were affected by different factors. With regards to the
junior doctors, MMC failed to satisfy the “five principles” for reform. For example, one of the
principles that MMC failed to satisfy was a broad programme that is flexible. In addition, once
MMC kicked off the notion of a tailored program to suit an individual’s preference was
abandoned (Maddon and Maddon, 2007: 428).
The second aspect that MMC failed at was that it did not efficiently restructure the programme
so that it was producing consultants and general practitioners any faster that the old system. In
fact, they MMC was directly resolving the issue of having a large pool of SHO grade doctors
but the consequence of this meant that hospitals has fewer flexible doctors (Maddon and
Maddon, 2007: 428). With the additional pressure of the work time derivative (WTD) this
results in poor workforce planning.
Maddon and Maddon (2007) further argue that the effects on patients will not be favourable as
the doctors have less experience that previously trained doctors and this is a challenge as
patients’ needs are becoming more complex. However, there is no evidence to suggest how
significant this factor is as the difference in training between the previous consultants and is
between 1-2 years. This coupled with the advancement in technology and research available to
the doctors may cushion the extent to which this is a factor that caused MMC to fail.
An alternative perspective would be to look at the recruitment and selection carried out by
MTAS in conjunction with the security breach of the IT system which heightened the tension.
In addition to this, the organisation structure of MMC could be likened to a cobweb and the
move to allow foreign doctors to compete for a training place. These perspective have been
outline by the House of Commons (HC) over three volumes and will be discussed in detail
below.
According to a review by the HC in 2007, the fundamental triggers that led to MMC crisis was
the overall failure of the MTAS national recruitment system. They outline the combination of
the most significant failings as the shortlisting process, excess eligible applicants, design flaws
in the MTAS and MMC (House of Commons, 2007: 43). It can be argued that the shortlisting
process was designed to function as follows. Applicants had to submit their applications on a
web portal and wait to get called in for an interview, if they passed the first round, they would
be shortlisted and called in for a second round of interviews (House of Commons, 2007: 443-
44). However, due to poor MTAS design and lack of sufficient training given to consultants
and not enough time before going live, the selection process was disorganised and led to
devastating consequences.
The outcome was that it was difficult to assess a candidates competencies based on what they
had submitted on their application because there was no CV to verify their achievements
(House of Commons, 2007: 43-45). In addition to this, the scoring method for competencies
was flawed because for one, candidates of different levels of training were scored with the
same methodology and secondly, points were awarded to short answers rather than
qualifications (House of Commons, 2007: 43-45). Furthermore, there was a general weakness
in the IT system which consisted of not being able to cope with the demand as it would crash
often and finally there was a security breach on the website which immediately stripped MTAS
of any credibility (House of Commons, 2007: 43-45).
Moreover, Bach (2001) would argue that the scope of the HRM for MMC was too narrow only
focusing on workforce planning and the training. He argues that the role of HRM should be
widened and should include the external fit and internal fit i.e. alignment of MMC’s objectives
and the correct allocation of resources to ensure that the most effective outcome of the reform
is achieved (Bach, 2001). Since healthcare reform is driven by political and economic motives
and is aimed at solving macroeconomic issues and it is evident that the department of health
does not have the necessary skills or capacity to manage people, the implications on healthcare
reform is brittle (Bach. 2001: 2). Therefore it could be the lack of scope of the HR function that
caused MMC to fail.
Finally, the last perspective that will be assessed is the overall governance structure that had
multiple stakeholders and committees to review different aspects of the reform. This structure
was very complicated and disorganised. There were different boards and groups appointed to
handle different aspects of the reform, each with its own mandate. Most groups or individuals
reported to MMC strategy group who should have been accountable for the decisions made for
the reform, yet when the House of Commons did a review, no one was willing to take
ownership. Furthermore, there were a number of senior resignation on MMC side of the table
when the crisis broke out. This indicates that there is poor governance and this without a doubt
was the first sign of trouble for MMC (House of Commons, 2007). Below is a diagram to
illustrate the structures put in place.
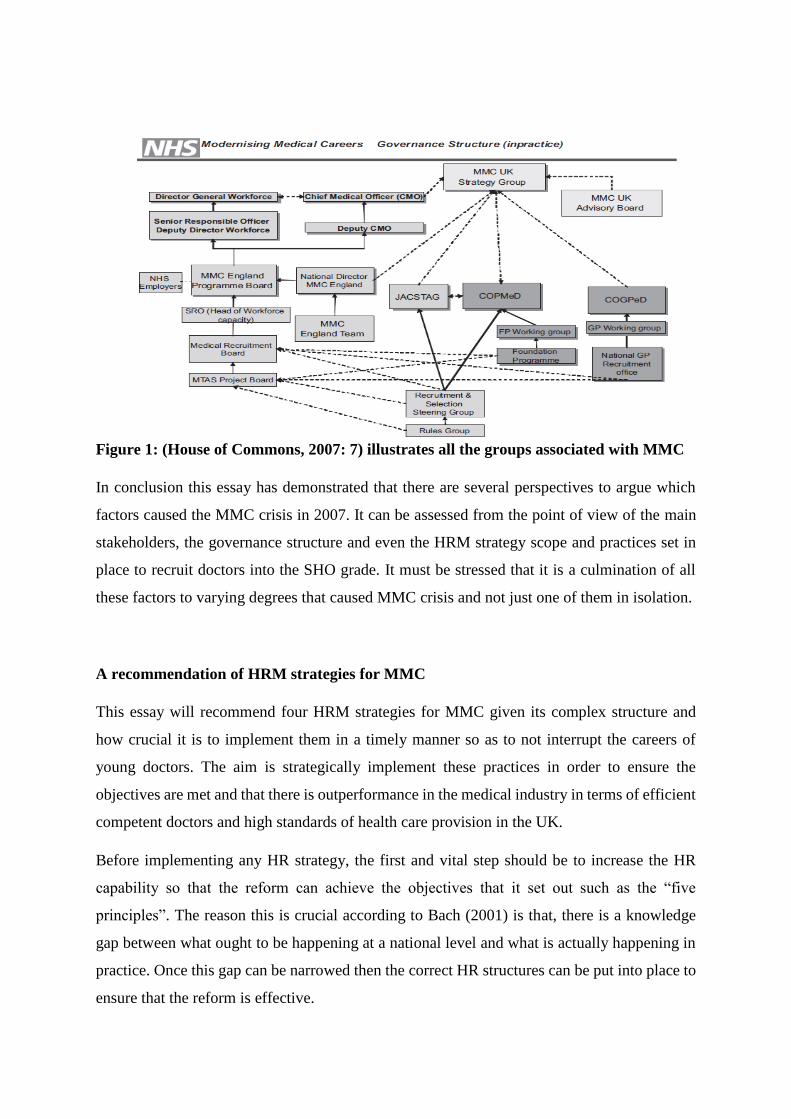
Figure 1: (House of Commons, 2007: 7) illustrates all the groups associated with MMC
In conclusion this essay has demonstrated that there are several perspectives to argue which
factors caused the MMC crisis in 2007. It can be assessed from the point of view of the main
stakeholders, the governance structure and even the HRM strategy scope and practices set in
place to recruit doctors into the SHO grade. It must be stressed that it is a culmination of all
these factors to varying degrees that caused MMC crisis and not just one of them in isolation.
A recommendation of HRM strategies for MMC
This essay will recommend four HRM strategies for MMC given its complex structure and
how crucial it is to implement them in a timely manner so as to not interrupt the careers of
young doctors. The aim is strategically implement these practices in order to ensure the
objectives are met and that there is outperformance in the medical industry in terms of efficient
competent doctors and high standards of health care provision in the UK.
Before implementing any HR strategy, the first and vital step should be to increase the HR
capability so that the reform can achieve the objectives that it set out such as the “five
principles”. The reason this is crucial according to Bach (2001) is that, there is a knowledge
gap between what ought to be happening at a national level and what is actually happening in
practice. Once this gap can be narrowed then the correct HR structures can be put into place to
ensure that the reform is effective.
Secondly, it is likely that the Department of Health does not have the HR expertise and should
therefore consider outsourcing this role to HR professionals who will act as a strategic partner
to guide and recommend effective practices that will help the increase the effectiveness of the
reform. Armstrong (2006) points out that a HR partner is a long term investment as it is likely
that the organisations performance will improve if there is an alignment between HR practises
and MMC objectives.
The first and most important HRM strategy would be to create a workforce plan. Knowing how
many doctors are currently required and how many will be required in the future is essential in
order to carry out a reform. This involves knowing how many doctors at any one time will be
undergoing training and at what stage of the training they are in. Structures need to be put in
place once a clear vision has been depicted by the MMC strategy group. As outline by the
Royal College of Medicine (2011), they stress that workforce planning ensures that we know
what is required in terms of medical services for the next decade or more and what it will take
to become a doctor in a socialist field of medicine.
In order to carry out an effective workforce plan, there needs to be accurate data available of
what the trends over the past have been in order to project for the future. This will also have
implications on the finance side. It will help prepare budgets in order to allocate funds to assist
the growth and refinement through the reform.
Thereafter, the second HRM strategy recommendation would be that MMC has a strategic
recruitment and selection strategy because doctors are the agents that will deliver good health
care and their interests need to be catered for in a professional manner if that is going to be the
outcome. A recruitment and selection strategy is said to be strategic when it is aligned with the
overall objectives of MMC (Stewart and Brown, 2009).
As a result of investing in HR capabilities and relevant practices, it is inevitable that staff will
have to be trained on how to carry out certain functions with competency (Bach, 2001). In the
case of MMC since it is the deans and consultants carrying out the selection process, they will
need to know how to assess the candidate’s competency by implementing a standard in order
for the process to be unbiased and fair.
The third recommendation would be a strategy to manage the quality of patient care given. The
focus should be on the wellbeing of the patient and their needs. Armstrong (2006) would argue
that this is attainable by instilling the value of attaining high quality during the training of the
foundation programme. This is essential because ensuring that there is overall good patient care
is the responsibility of each individual junior doctor. If each doctor takes ownership of his, then
the job will be half done. There are multiple quality management strategies available and a
suitable one will depend on several factors such as the area of specialisation of the doctor and
will need to be tailored accordingly.
The final recommendation would be to ensure that the training programme is centred on the
junior doctors and their careers. This means involving them every step of the way and getting
feedback on what they think of the reform, the restructured training, conducting user
acceptance testing with a sample of junior doctors and deans before going live on I.T systems
for example. The underlying premise of strategic human resource management is that people
are the most valued asset (Armstrong. 2006: 3). This will also serve to motivate the junior
doctors. In order for doctors to deliver high quality patient care, their needs also need to be
catered for as the quality of care they deliver is directly related to their treatment (Bach, 2001).
Therefore, the HRM recommendations offered to MMC have been focused on firstly ensuring
that there is a workforce plan, having a strategic recruitment and selection plan, delivering
quality patient care, and addressing the doctor’s needs because they are the individuals that will
provide the health care services. However, before jumping the gun, it is imperative that MMC
has a functional HR partner that it recognises as a strategic partner to help achieve an effective
reform of the medical workforce.
HRM practices that are likely to improve the function and publicity of MMC
This section will outline three specific HRM practices that will help improve the way the MMC
is viewed and how effective it is in establishing a career path for doctors. It will draw on
recommendations made by several inquirers in light of MCCs crisis such as the Tooke (2008)
inquiry and the inquiry made by the House of Commons (2007). This is not to say that these
are the only practices that will help, but they will definitely make a significant impact.
The first structural adjustment will have to begin with the governance structure of the MMC.
As argued in the House of Commons (2007) report, it was established that one of the ways to
save the MMC’s disaster was to fix what the crux of the problem was. As mentioned earlier
about the governance structure being complex and lacking accountability, the house of
commons ruled that “the governance systems for MMC have been simplified and improved
and a single line of accountability established” (House of Commons, 2007: 125).
This simply meant that the organizational layout needed to be simplified which involves a
number of realigning and streamlining activities of the different organisations and boards
involved in the reform. Tooke (2008) recommends there is a need to revisit the initial concept
of reforming the medical profession and reconstructing the framework form the basic principles
underline in Unfinished Business. These changes would improve the function of the MMC to
the extent that channels of communication would be simplified and thus making decisions
would be less bureaucratic. In addition to this, it would be easier to track which board is in
charge of what decision making processes. Therefore, it is likely the publicity of the MMC is
likely to positively benefit if people have faith in the governance structure.
Secondary to the above, but the most significant factor are the doctors themselves and what
they want out of their medical careers. A lot of the reform was centralised around the different
stakeholders and their interests but what was most striking was that decisions about the
specialist training and a doctor’s career was never consulted with the actual doctors themselves.
The underlying premise of HRM is that people are an organisations most valuable asset
(Armstrong, 2006: 3). Therefore the doctors should be at the centre of the reform and they
should be engaged with matters concerning medical reform. After all, they are the ones who
will determine the extent to which MMC is a failure or a success.
To demonstrate the relevance of the above argument, this paper will draw on a survey
conducted by Allen (2008) at the University of Manchester that tried to establish the factors
that influence a medical student career choice. The results were simply that the MMC reform
had made career choice issues an important factor to look at. What they discovered was that.
The “views of undergraduates are important as they are trained to be doctors of the future”
(Allen, 2008: 166). Such findings are crucial because they highlight the fact the doctors will
determine or at least try to dictate the terms of their career and therefore the MMC should use
such information to reform the medical profession. This would have been useful had this
approach been implemented in the beginning however, a doctor’s medical career must continue
and hence the second recommendation entails involving the young doctors in reform decisions
for an effective outcome. In support of this view, they concluded that “continuing research and
exploring the needs and expectations of our future doctors are likely to be essential tools during
this period of uncertainty and transition in medical training” (Allen, 2008: 166). This is also
one of recommendation offered by Tooke (2008). It is therefore without a doubt that such an
approach can restore the publicity and functioning of the MMC.
Moreover, the third and final recommendation is to restructure workforce planning. This entails
understanding the capacity and capabilities of the current medical workforce and making
provisions for the future and also using information of the past trends in order to make informed
decisions about the future of workforce planning. The Tooke (2008) report gives a number of
ground-breaking recommendations that will be discussed in the section below.
The Tooke (2008) report highlights the fact that the MMC reform was never going to resolve
the current issues of the “lost tribe” with the framework it was operating under because it was
not based on a model of workforce supply that was relevant to the current situation and the
future requirements of the medical profession. A quick fix is not the solution to the
longstanding structural problems of the medical profession. The report therefore makes the
following recommendations.
Firstly, there should be a model of workforce planning and this can be derived by seeking the
assistance and expertise of universities, in particular health economist and epidemiologist
modellers for example and regular reviewing their projections in order to make informed
decisions (Tooke, 2008: 26). Furthermore, the MMC would have to publicly declare and the
eligibility of foreign students for the postgraduate training and use this supply of doctors to
compensate for the gaps rather than have this group compete against local doctors (Tooke,
2008: 25). Lastly, the Department of Health should invest in having a database of the existing
skills and certifications of all the doctors in different regions. This will be useful in determine
what specialities have less doctors and what needs to be done to increase those numbers but
more importantly to the medical students to make informed career decisions (Tooke, 2008: 26).
However, Wright and Haggerty (2005) in their research bring out an important argument that
needs to be taken into consideration. They argue that there are three variables: time, cause and
the individual need to be taken into consideration when evaluating the extent to which HRM
affects the organisations performance. More specifically the time lag between coming up with
a policy framework, implementing and then executing training will impact on how successful
the MMC is guaranteed to be. Thus, revisiting the reform is time sensitive and hence a
comprehensive plan needs to be made and executed within the stipulated time frame.

In conclusion this essay has demonstrated 3 possible recommendations for the restoration of
the publicity and functioning of the MMC. These recommendations are not the only options
available but merely a glance into the direction needed and it should be stressed that they are
to be taken in conjunction with one another and any other recommendation. The independent
inquiries done by Sir Tooke (2008) and the House of Commons (2007) to name a few have a
wealth of insight.
Reference List
1. Allen, M. 2008. Modernising medical careers and factors influencing career choices of
medical students. British Journal of Hospital Medicine, Vol. 69 (3): 163 – 166.
2. Armstrong, M. 2006. Strategic Human Resource Management: A Guide to Action.
Third Edition. Kogan Page: London and Philadelphia.
3. Bach, S. 2001. HR and New Approaches to Public Sector Management: Improving
HRM Capacity. In Workshop on Global Health Workforce Strategy. France: 9 – 12.
4. Delamothe, T. 2008. Modernising Medical Careers: Final Report. BMJ: British Medical
Journal, Vol. 336 (7635): 54–55. [Online] Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2190265/ [Accessed February 28th
2015]
5. Diliner, L., 1993. Senior House Officers: The Lost Tribes. BMJ: British Medical
Journal. London. Vol. 307: 1549-1551.
6. Harris, L., and Ogbonna, E. 2001. Strategic human resource management, market
orientation, and organizational performance. Journal of Business Research, Vol. 51:
157 – 166.
7. House of Commons Health Committee. 2008. Modernising medical careers. First
report of session, 2007-08. [Online] Available from:
http://www.publications.parliament.uk/pa/cm200708/cmselect/cmhealth/25/25i.pdf
[Accessed February 15th 2015]
8. House of Commons Health Committee. 2007. Modernising medical careers. Volume II:
Written Evidence, 2007-08. [Online] Available from:
http://www.publications.parliament.uk/pa/cm200708/cmselect/cmhealth/25/25ii.pdf
[Accessed February 15th 2015]
9. House of Commons Health Committee. 2008. Modernising medical careers. Third
report of session, 2007-08. [Online] Available from:
http://www.publications.parliament.uk/pa/cm200708/cmselect/cmhealth/25/25iii.pdf
[Accessed February 15th 2015]
10. Kennedy, J., Knight W., and Rohrer, J. 2007. Myths of MTAS and MMC. Journal of
the Royal Society of Medicine, Vol. 100 (6): 252–254. [Online] Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1885385 [Accessed February 27th
2015]

11. Madden, A., and Madden G. 2007. Has Modernising Medical Careers lost its way?
BMJ: British Medical Journal, Vol. 335 (7617): 426–428.
12. Tooke, J. 2008. Aspiring to Excellence: Findings and Final Recommendations of the
Independent Inquiry into Modernising Medical Careers. [Online] Available from:
http://www.asit.org/assets/documents/MMC_FINAL_REPORT_REVD_4jan.pdf
[Accessed February 15th 2015]
13. Scottish Executive. Edinburgh (United Kingdom). Health Department. 2002.
Unfinished Business: Proposals for Reform of the Senior House Officer Grade Working
together. London: The Stationery Office: 1 – 57.
14. Scottish Executive. Edinburgh (United Kingdom). Health Department. 2004.
Modernising Medical Careers The next steps: The future shape of Foundation,
Specialist and General Practice Training Programmes. London: The Stationery Office:
1 – 22.
15. Stewart, G., and Brown, K. 2009. Human resource management: linking strategy to
practice. Wiley.
16. Wright, P., and Haggerty, J. 2005. Missing Variables in Theories of Strategic Human
Resource Management: Time, Cause, and Individuals. CAHRS: Center for Advanced
Human Resource Studies, Working Paper 5(3).




















