Model-based Angiogenic Inhibition of Tumor Growth using Adaptive Fuzzy Techniques
13
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 j o ur na l ho me pag e: www.intl.elsevierhealth.com/journals/cmpb Model-based angiogenic inhibition of tumor growth using modern robust control method Levente Kovács a,∗ , Annamária Szeles b , Johanna Sápi a , Dániel A. Drexler b , Imre Rudas a , István Harmati b , Zoltán Sápi c a John von Neumann Faculty of Informatics, Óbuda University, Budapest, Hungary b Department of Control Engineering and Information Technology, Budapest University of Technology and Economics, Budapest, Hungary c 1st Department of Pathology and Experimental Cancer Research, Semmelweis University, Budapest, Hungary a r t i c l e i n f o Article history: Received 13 December 2012 Received in revised form 2 January 2014 Accepted 2 January 2014 Keywords: Antiangiogenic therapy Robust control H ∞ method Uncertainty a b s t r a c t Cancer is one of the most destructive and lethal illnesses of the modern civilization. In the last decades, clinical cancer research shifted toward molecular targeted therapies which have limited side effects in comparison to conventional chemotherapy and radiation therapy. Antiangiogenic therapy is one of the most promising cancer treatment methods. The dynamical model for tumor growth under angiogenic stimulator/inhibitor control was posed by Hahnfeldt et al. in 1999; it was investigated and partly modified many times. In this paper, a modified version of the originally published model is used to describe a continuous infusion therapy. In order to generalize individualized therapies a robust control method is proposed using H ∞ methodology. Uncertainty weighting functions are determined based on the real pathophysiological case and simulations are performed on different tumor volumes to demonstrate the robustness of the proposed method. © 2014 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Cancer is in the front line of lethal illnesses which claims the highest number of human lives in modern societies. The latest statistics show that 7.6 million people died worldwide from cancer in 2008 [1], while in the European Union 1.3 million people are estimated to die in 2013 [2]. The rates are slightly lowered year-by-year resulting a 10% fall in men and 7% fall in women from 2007 data. Unfortunately, Hungary is a leading country of the European Union (but also in top ten in the world) in mortality data of all types of cancer [3,4]. Research and treatment of cancer is a very important mis- sion for medicine. Beside classical methods, in the last decade a lot of new targeted molecular therapies appeared including ∗ Corresponding author at: John von Neumann Faculty of Informatics, Óbuda University, H-1034 Budapest, Hungary. Tel.: +36 1 666 5585; fax: +36 1 666 5522. E-mail address: [email protected] (L. Kovács). mathematical model-based ones. Antiangiogenic therapy rep- resents a relatively new targeted molecular therapy as well, which came up in the last decade and its aim is to inhibit angiogenesis (creating a vascular system of the tumor), which leads to the death of the tumor over the critical volume [5]. The main advantage of antiangiogenic therapy over con- ventional treatments (like chemotherapy) is that tumor cells cannot become “classically” resistant toward the antiangio- genic drugs and antiangiogenic therapy can be used with relatively nontoxic concentrations [6,7]. The idea is not to eliminate the whole tumor, but to control and keep it in a given (minimal volume) state, where for example by classical clin- ical methods it can be efficiently eliminated. Consequently, the procedure can be linked to control engineering theory as a model-based control problem. 0169-2607/$ – see front matter © 2014 Elsevier Ireland Ltd. All rights reserved. http://dx.doi.org/10.1016/j.cmpb.2014.01.002
Transcript of Model-based Angiogenic Inhibition of Tumor Growth using Adaptive Fuzzy Techniques

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
j o ur na l ho me pag e: www.int l .e lsev ierhea l th .com/ journa ls /cmpb
Model-based angiogenic inhibition of tumorgrowth using modern robust control method
Levente Kovácsa,∗, Annamária Szelesb, Johanna Sápia, Dániel A. Drexlerb,Imre Rudasa, István Harmatib, Zoltán Sápi c
a John von Neumann Faculty of Informatics, Óbuda University, Budapest, Hungaryb Department of Control Engineering and Information Technology, Budapest University of Technology and Economics,Budapest, Hungaryc 1st Department of Pathology and Experimental Cancer Research, Semmelweis University, Budapest, Hungary
a r t i c l e i n f o
Article history:
Received 13 December 2012
Received in revised form
2 January 2014
Accepted 2 January 2014
Keywords:
Antiangiogenic therapy
a b s t r a c t
Cancer
is one of the most destructive and lethal illnesses of the modern civilization. In the
last decades, clinical cancer research shifted toward molecular targeted therapies which
have limited side effects in comparison to conventional chemotherapy and radiation
therapy. Antiangiogenic therapy is one of the most promising cancer treatment methods.
The dynamical model for tumor growth under angiogenic stimulator/inhibitor control was
posed by Hahnfeldt et al. in 1999; it was investigated and partly modified many times.
In this paper, a modified version of the originally published model is used to describe
Robust control
H∞ method
Uncertainty
a continuous infusion therapy. In order to generalize individualized therapies a robust
control method is proposed using H∞ methodology. Uncertainty weighting functions are
determined based on the real pathophysiological case and simulations are performed on
mes t
(minimal volume) state, where for example by classical clin-
different tumor volu
1. Introduction
Cancer is in the front line of lethal illnesses which claims thehighest number of human lives in modern societies. The lateststatistics show that 7.6 million people died worldwide fromcancer in 2008 [1], while in the European Union 1.3 millionpeople are estimated to die in 2013 [2]. The rates are slightlylowered year-by-year resulting a 10% fall in men and 7% fallin women from 2007 data. Unfortunately, Hungary is a leadingcountry of the European Union (but also in top ten in the world)in mortality data of all types of cancer [3,4].
Research and treatment of cancer is a very important mis-sion for medicine. Beside classical methods, in the last decadea lot of new targeted molecular therapies appeared including
∗ Corresponding author at: John von Neumann Faculty of Informatics, Ófax: +36 1 666 5522.
E-mail address: [email protected] (L. Kovács).0169-2607/$ – see front matter © 2014 Elsevier Ireland Ltd. All rights reshttp://dx.doi.org/10.1016/j.cmpb.2014.01.002
o demonstrate the robustness of the proposed method.
© 2014 Elsevier Ireland Ltd. All rights reserved.
mathematical model-based ones. Antiangiogenic therapy rep-resents a relatively new targeted molecular therapy as well,which came up in the last decade and its aim is to inhibitangiogenesis (creating a vascular system of the tumor), whichleads to the death of the tumor over the critical volume [5].
The main advantage of antiangiogenic therapy over con-ventional treatments (like chemotherapy) is that tumor cellscannot become “classically” resistant toward the antiangio-genic drugs and antiangiogenic therapy can be used withrelatively nontoxic concentrations [6,7]. The idea is not toeliminate the whole tumor, but to control and keep it in a given
buda University, H-1034 Budapest, Hungary. Tel.: +36 1 666 5585;
ical methods it can be efficiently eliminated. Consequently,the procedure can be linked to control engineering theory asa model-based control problem.
erved.

n b i
iwrdSgtcLwsasTca
etrcii
hmlTalc0astch
ntpSotaetp
hTtmilts
n
c o m p u t e r m e t h o d s a n d p r o g r a m s i
The dynamical model for tumor growth under angiogenicnhibitor control was posed by Hahnfeldt et al. in 1999 [8]; itas investigated and partly modified many times. The most
elevant modifications of the original model were done by’Onofrio and Gandolfi [9], and Ergun et al. [10]. Ledzewicz andchättler [11] discussed the optimal scheduling problem of aiven amount of inhibitors in order to minimize the primaryumor volume. d’Onofrio and Gandolfi designed bang–bangontrol [9], while in [10,11] singular controls were designed.edzewicz et al. [12] investigated suboptimal strategies, piece-ise constant protocols. Kassara and Moustafid [13] applied a
et-valued control method. d’Onofrio A. et al. [14] examined multi-control problem, where angiogenic inhibitors werecheduled in combination with a chemotherapeutic agent.hey solved this problem by bang–bang control; the optimalontrol contains a segment where the control signal is singularnd follows a time-varying feedback.
In these studies the applied control strategies are nonlin-ar, and their practical feasibility is not discussed. In [11,12],he control strategy is based on the tumor volume and the car-ying capacity, however in clinical practice, only tumor volumean be measured. The control strategy presented in this papers linear and was designed based on the tumor volume whichs a measurable quantity, e.g. using medical imaging.
The model of the system to be controlled is nonlinear,owever the applied controller is linear; thus, a linear systemodel is needed in order to carry out the controller design. The
inear model is acquired using operating point linearization.he linearized model is then used for the controller design,nd the resulting controller is evaluated on the original non-inear model. Since the applied control strategy is set pointontrol, the difference between the reference signal (which is
mm3 of tumor volume in our case, since the aim of the ther-py is to eliminate the tumor) and the actual output of theystem may be large at the beginning of the control transient;herefore, large control inputs may be present. However, theseontrol inputs are physiologically unfeasible, thus saturationas to be applied on the controller output.
Choosing the right linear control strategy for the problem isot straightforward. Because of the nonlinearities of the sys-
em, certain linear controllers designed at a specific operatingoint may not be suitable for the original nonlinear system.imple controllers, like PID control fails in a sense that theutput of the controller is unfeasibly high for clinical applica-ions, even if the system is close to the operating point usedt linearization. Control techniques based on state feedback,.g. pole-placement, LQ control are more suitable for the task;hey give physiologically feasible control signals for the wholeeriod, except for the high initial transient.
Application of controllers like pole-placement or LQ controlas already been examined previously by the authors [15,16].he characteristics of the control input are typical: the con-
rol input is saturated at the initial phase, and decreases to ainimum value later in the therapy. If the controller design
s correct, this minimal value is the minimal inhibitor serumevel that is needed to keep the tumor in the avascular state
hat can be calculated from the steady-state equations of theystem.The main issue in the application of state-feedback tech-iques for therapeutic design is minimizing the amount of
o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 e99
inhibitor needed for the therapy. Since previously applied lin-ear controllers are designed in a specific operating point, butapplied to the nonlinear model, this may lead to unmod-elled behavior of the closed-loop system. Simulation resultsin [15,16] showed that the stability of the closed-loop systemis not harmed; however, the amount of inhibitor used duringtherapy may be higher than required in reality. Performanceof state-feedback strategy can be improved by applying H∞control strategy.
Linear H∞ control syntheses are promising methods onthe palette of the robust control systems. This postmod-ern technique was elaborated in the 1980s [17]. Progressively,it gains ground by more and more powerful computationalsoft- and hardware [18,19]. One of the biggest advantages ofthese methodologies (beyond the well-defined mathematicalbackgrounds) might be the robustness itself, against modelmismatches and disturbances.
The aim of the manuscript is to elaborate modernrobust control techniques on a tumor model based on miceexperiments [8], and many times investigated since 1999[10,14,15,20,21]. The current paper presents how control opti-mization can be carried out using H∞ methodologies – designin a worst-case sense. The control strategy is analyzed fromdifferent point of views. The effect of different saturation lev-els and different initial tumor volumes on the total inhibitorinlet and on the speed of tumor regression is investigated.Realization issues like low sampling frequency, high mea-surement noise and parameter perturbations are discussed indetail in a separate section.
The paper is organized as follows. Section 2 gives a shortreview of conventional and targeted molecular therapies,while Section 3 presents the tumor model of our investiga-tions, and does a brief analysis of the model used. In Section4 the H∞ design is summarized, while simulation results, andcontrol strategies accordingly, are presented in Section 5. Real-ization issues are discussed in Section 6. Finally, the paperends with the conclusions and future work aspects in Section7.
2. Biomedical background
Conventional cancer therapies are surgical oncology [22,23],radiotherapy [24,25] and chemotherapy [26,27]. Using surgicaloncology the tumor cells can be totally removed (zero-orderkinetics), in contrast to using chemotherapy or radiationtherapy where only a fraction of tumor cells are killed (first-order kinetics). When a cancer has been removed by surgery,chemotherapy or radiotherapy may be used to keep the cancerfrom coming back (adjuvant therapy). However, chemotherapyand radiotherapy have significant side effects (anemia, alope-cia, nausea and vomiting, nerve problems, skin problems [28])and these treatments are toxic to all cells, because not onlycancer cells are dividing rapidly, there are also highly prolife-rative normal tissues.
Treatments, which are based on specific molecules that tar-
get a signaling pathway in the growth and development ofa tumor cell are called targeted molecular therapies (TMTs).Some of these specific molecules may be present in nor-mal tissues, but in tumor cells they are often mutated or
s i n
e100 c o m p u t e r m e t h o d s a n d p r o g r a moverexpressed [29]. The main differences between conven-tional cancer therapies and targeted molecular therapies arenot only the acting ways, but also the goals. The goal of con-ventional cancer therapies is to eliminate the tumor mass,but if this has happened, the tumor may recrudesce and givemetastasis. The new approach is targeted therapy: acting inspecific molecular ways, where the goal is to prevent tumorcells from growing and developing; ergo, prevent toxicity. Thisis more important than eliminating the tumor mass – for thepatients, there is a better chance of survival if they have inac-tive tumor mass than if they do not have tumor for a while,but there is the risk of recurrence.
A promising field in TMTs is antiangiogenic therapy [5].Angiogenesis is the process of forming new blood vessels,which occurs normally in the human body at specific times(during embryogenesis and infrequently in adults); it is pre-cisely controlled by proangiogenic and antiangiogenic factors,so as a result there is angiogenic balance in the body. Whentumor proliferation begins, a small sized tumor can pick upenough oxygen from nearby capillaries, but after a certainsize (1–2 mm diameter) tumor development stops, becausethe diffusion of oxygen through tissues is limited. A tumorneeds its own blood vessels to grow; however, forming newvessels is inhibited by the antiangiogenic factors of the body.Tumors have to break through this strict control – the processwhen the tumor becomes able to form own blood vessels iscalled angiogenic switch [30]. If the tumor can be kept in anavascular dormant state when the cellular proliferation rateis balanced by the apoptotic rate, the tumor will be unable togrow in size beyond a few millimeters [6]. As a result, the aimof antiangiogenic cancer therapy is to prevent tumors fromforming new blood vessels, because without angiogenesistumor growth is inhibited.
Several angiogenic inhibitors are known in medicalpractice, for example endostatin [31] or bevacizumab [32]. Con-trary to conventional treatments, using antiangiogenic ther-apy tumor cells cannot become “classically” resistant towardthe antiangiogenic drugs [6] and antiangiogenic drugs are rel-atively nontoxic [33]. However, due to high costs of the antian-giogenic drugs, their optimal usage is preferred which gives anideal field for model-based and optimal control theory.
3. Dynamical model of tumor growth
In 1999, Hahnfeldt et al. posed the model formulation fortumor growth control under the actions of angiogenic stim-ulation and inhibition [8].
In their experiments, mice were injected with Lewis lungcarcinoma cells. According to their observations, the nonlin-ear model of tumor growth under angiogenic inhibition isdefined by the following equations:
x1 = −�1x1 ln(
x1
x2
)x2 = bx1 − dx1
2/3x2 − ex2x3t∫ (1)
x3 =0
u(t′)e−�3(t−t′)dt′
y = x1
b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
where x1 is the tumor volume (mm3), x2 is the supportingvasculature volume (mm3), x3 is the inhibitor serum level(mg/kg), and u is the inhibitor administration rate (mg/kg/day).From this model one can derive the following second-ordersystem:
x1 = −�1x1 ln(
x1
x2
)x2 = bx1 − dx1
2/3x2 − ex2u
y = x1
(2)
where x1 is the tumor volume (mm3), x2 is the vasculaturevolume (mm3), and u is the serum level of the inhibitor(mg/kg). The parameters characteristic for the Lewis lung car-cinoma and the mice used in the experiment are the growthparameter �1 = 0.192 (day−1), the vascular endothelial fac-tor b = 5.85 (day−1), and the endothelial cell death d = 0.00873(day−1 mm−2). The parameter characteristic for the appliedinhibitor (endostatin) is the vascular inactivation rate e = 0.66(day−1 (mg/kg)−1).
The first equation in (2) describes the phenomenology oftumor growth slowdown, as the tumor grows and resorts itsavailable support. In the second equation of (2), the first termrepresents the stimulatory capacity of the tumor upon theinducible vasculature (bx1), the second term represents theendogenous inhibition of previously generated vasculature(−dx
2/31 x2) and the third term describes inhibition of tumor
vasculature due to applied inhibition (−ex2u). The third (out-put) equation in (2) shows that dosage control is performedbased on the tumor volume measurement.
This simplified model uses zero-order pharmacokinetics,instead of the first-order pharmacokinetics of the originalmodel defined by the third equation in (1) [34]; hence, theinput of the simplified model is the serum level of the inhibitor(that is x3 in the original model). It follows that the clearanceof the inhibitor (parameter �3 in (1)) is not considered in thismodel.
In the remainder of this paper, equations in (2) will be usedas the tumor growth model. Note that this model is usuallyused when control engineering aspects of antiangiogenic ther-apy are addressed [9,21].
3.1. Steady-states of the tumor growth model
Steady-state analysis can bring two important results that cor-respond to the physiological characteristics of the system. Thefirst equation in (2) describes a Gompertzian growth, i.e. thetumor growth saturates at a maximal tumor volume, whenthe tumor volume and the endothelial volume are equal (i.e.x1 = x2). The tumor volume cannot grow beyond this value,however metastasis can occur (new tumor starts to grow ata different part of the body). The other extreme is when the
tumor is avascular, i.e. there is no endothelial volume, and thetumor volume is minimal. Using the steady-state analysis, onecan derive the amount of inhibitor that is needed to maintainthis avascular tumor state.
n b i o
e
iftia
x
ue
i
s
u
tgict
3
ItlCslbfo
�
sm
D
system, deriving a linear model is necessary, as the H∞ controldesign requires a linear nominal model. The linear model is
0 10 20 30 40 50 60 70 80 90 1000
5000
10000
15000
Tumor growth without angiogenic inhibitito n
Time (day)
Tum
or s
ize
(mm
3 )
Tumor volumeTumor vasculature volume
0
5000
10000
15000
Tumor regression under angiogenic inhibition (5 mg/kg endostatin )
Tum
or s
ize
(mm
3 ) Tumor volumeTumor vasculature volume
c o m p u t e r m e t h o d s a n d p r o g r a m s i
The equilibrium points, where the derivatives of x1 and x2
qual zero, satisfy the following system of equations:
0 = −�1x10 ln(
x10
x20
)0 = bx10 − dx
2/310 x20 − ex20u0
(3)
The trivial solution means that no tumor is developed,.e. x10 = 0 mm3, x20 = 0 mm3. The non-trivial solution derivesrom the first equation in (3), i.e. x10 = x20. By substitutinghis expression into the second equation in (3), and express-ng the steady-state tumor volume, the following equation iscquired:
10 =(
b − eu0
d
)3/2
(4)
Substituting u0 = 0 mg/kg, the maximal tumor volume ofncontrolled tumor growth is derived in terms of the param-ters b and d as:
x10|u0=0 =(
b
d
)3/2
(5)
This value is 17,340 mm3 with the parameter values givenn the previous subsection.
Expressing u0 from (4) and taking x10 → 0 mm3, the inhibitorerum level needed to maintain the avascular state is:
0,av = b
e(6)
The value of the inhibitor serum level needed to main-ain the avascular state is 8.8 mg/kg with the parameter valuesiven in the previous subsection. In practice, this means thatt is unnecessary applying higher doses than u0,av to an avas-ular tumor; however, applying lower dose leads to undesiredumor growth.
.2. Controllability of the tumor growth model
n [20], controllability of the system is proved only in case ofhe linearized system. The present work derives the control-ability of the nonlinear system using the Lie Algebra Rankondition (LARC) [35]. In this case, the system has only twotate variables, thus the distribution � for checking control-ability is created from the control vector field g and the Lieracket [35] of the control vector field and the drift vector field
as � = {g,[f, g]}. The state-dependent matrix representationf � is:
=[
0 −�1ex1
−ex2 bex1
](7)
According to the LARC, the system is controllable in a giventate, if the matrix (7) is full rank. The determinant D of the
atrix is:= −�1e2x1x2 (8)
m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 e101
It can be easily verified that the matrix in (7) is singular inthe following cases:
• x1 = 0 mm3, x2 arbitrary. In this case, the tumor volume iszero, thus there is no tumor to be controlled.
• x1 /= 0 mm3 and x2 = 0 mm3. In this case, there is no sup-porting vasculature, thus the tumor is avascular. The controlstrategy to be applied is based on the results of thesteady-state analysis, i.e. if the u0,av serum inhibitor levelis maintained, the tumor can be kept in the avascularstate.
In any other cases (x1 /= 0 mm3 and x2 /= 0 mm3) the sys-tem is controllable, and the control strategy described belowcan be applied.
In [15], the controllability analysis has been carried out tothe tumor growth model with three state variables, and leadto similar results.
3.3. Operating point linearization of the tumor growthmodel
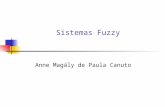
Fig. 1 shows the tumor growth slowdown and asymptoticlimit (17,340 mm3) of Lewis lung tumor size that would hypo-thetically be reached if this size of tumor were compatiblewith the life of the animal (upper part of Fig. 1, being equiv-alent of an open-loop therapy; this is also equivalent toa lethal steady-state case). Under antiangiogenic treatment(constant 5 mg/kg endostatin), initiated from the largest tumorvolume, tumor size is projected to plateau as a result ofparallel plateauing of available vascular support. Angiogenicinhibitors act to generate lower plateau points (lower part ofFig. 1).
Since the aim of this work is to design robust control for the
0 10 20 30 40 50 60 70 80 90 100Time (day)
Fig. 1 – Tumor growth without and under angiogenicinhibition.

e102 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
inte
Fig. 2 – The closed-loopacquired by operating point linearization. The symbolic formof the linearization is:
x1 =(
−�1x10 ln(
x10
x20
)− �1
)x1 + �1
x10
x20x2
x2 =(
b − 23
dx−1/310 x20
)x1 + (−dx2/3
10 − eu0)x2 − ex20u
y = x1
(9)
The non-trivial equilibrium points of the linearized modelcan be calculated from (3), i.e. x10 = x20. The assessed operatingpoint is x10 = x20 = 100 mm3, which is a small value in the entiretumor volume range, with u0 = 5 mg/kg [20]. The eigenvaluesof the linearized system are p1 = 0.1 and p2 = −3.7. p1 is on theright-half plane, thus the system is unstable, correspondingto the pathophysiological case. After evaluating the controlla-bility and the observability criteria, one gets that the systemis controllable and observable.
4. H∞ control design
The objective of the paper is to design a linear, robust con-troller, which achieves good tracking property, takes intoaccount the model uncertainties and limits the magnitude ofthe control input and the effect of sensor noise. Fig. 2 repre-sents the closed-loop structure of the proposed problem.
The signals of the system are the following: r is thereference, u is the control input, y is the output, n is the mea-surement noise, e is the modeling error, d is the disturbancecaused by the uncertainty of the model, zu is the penalizedcontrol input, whereas ze is the deviation of the output fromthe required one.
The closed-loop system includes the feedback structure ofthe nominal model Gn and the two-degree of freedom con-troller K, which is partitioned in two parts: Ky is the feedbackpart to meet the requirements of internal and robust stability,disturbance rejection, measurement noise attenuation, andsensitivity minimization, while Kr is the prefilter part, whichoptimizes the response of the overall system to the commandinput such that the output of the system would be near to that
of the chosen ideal system.The input multiplication uncertainty Wunc takes into con-sideration the differences between the nominal model andthe real plant. The weighting function Wn stands for the
rconnection structure.
limitation of sensor noise. The limitation of the control inputis achieved by the weighting function Wu which penalizeslarger deflections. The model matching function Tid describesthe ideal transfer function of the plant. Since the designedcontroller should affect tumor regression even in the worstcase, the reference model, Tid describes fast regression fromthe maximal tumor volume predicted by the model. Finally,the weighting function Wperf penalizes tracking character-istics. These weighting functions determine the frequencycharacteristics of the controller and the closed-loop system.Thus, non-modeled dynamics captured by these weightingfunctions do not influence stability and performance in theclosed-loop system. This is a significant advantage of worst-case design [18].
4.1. Sensitivity analysis
Starting from the formal definition of the multiplicative uncer-tainty, parametric sensitivity analysis was performed on thenonlinear model to determine Wunc. The idea was partiallyadapted and modified from [36,37] in order to incorporateuncertain parameters into the design process. Ranges areassociated with these selected parameters. By taking everysingle extremal combination of the parameters, linearizationis performed. Finally, the frequency content of the perturbedand linearized model is compared and relative difference iscomputed. Instead of using the extremal values, a griddingtechnique is proposed. Consequently, we consider the combi-nation of the selected parameters in a multiplicative manner.
A ±5% variability of the Lewis lung carcinoma parametersand a ±10% variability of the vascular inactivation rate wereassumed [8]. For the Lewis lung carcinoma parameters, factorsf1, f2 and f3 were chosen from a (+5%, +2.5%, 0, −2.5%, −5%)grid, and for the vascular inactivation rate, factor f4 was takenfrom a (+10%, +5%, −5%, −10%) grid. The perturbed nonlinearmodel is:
x1 = −�1x1 ln(
x1
x2
)x2 = bx1 − dx
2/31 x2 − ex2g
y = x1
(10)
where �1 = (1 + f1)�1, b = (1 + f2)b, d = (1 + f3)d and e = (1 +f4)e. For each possible combination, the nonlinear model waslinearized at the operating point described in Section 3, and

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 e103
0.001 0.01 0. 1 1 10 1000
0.2
0.4
0.6
0.8
1
1.2
1.4Sensitivity analysi s
Mul
tiplic
ativ
e m
agni
tude
err
or
Frequency (rad/day)
Fig. 3 – Relative modeling error functions (perturbedsystem compared to the nominal model) in frequencyd
tsr
W
wi1b
s
fsdwtt(bvd
wq
W
4
Sa
10−3
10−2
10−1
100
10 1
10 2
10−6
10−5
10−4
10−3
10−2
10−1
Weighting functions
Frequency (rad/day)
Mag
nitu
de Wunc − Uncertainty weighting functionWperf − Performance weighting functio nWu − Control input weighting functionWn − Sensor noise weighting functio n
The closed loop structure in Fig. 2 can be reorganized as in
omain and uncertainty upper bound (dashed line).
he obtained linear model was used to determine parametricensitivity by determining supWrel of the relative uncertaintyelation [20]:
rel(ω) =∣∣∣∣Gp(ω) − Gn(ω)
Gn(ω)
∣∣∣∣ (11)
here Gp stands for the perturbed model and Gn for the nom-nal model. The frequency domain of interest was ω ∈ [0.001,00] rad/day. The determined parametric sensitivity was upperounded (Fig. 3):
upWrel = 0.47s + 8s + 2
(12)
The results of the sensitivity analysis show that in lowerrequency domain, ω ∈ [0.001, 0.1] rad/day, the model is lessensitive for parameter perturbation than in higher frequencyomain, ω ∈ [0.1, 100] rad/day. In the low frequency domainhich is characteristic for tumor growth dynamics, the uncer-
ainty upper bound allows 125% deviation in the gain of theransfer function relative to the nominal transfer functionFig. 3) instead of the 65% deviation resulted from the pertur-ation of the parameters. This means that significantly largerariance of the parameters is allowed in the low frequencyomain, regardless of their dynamical characteristics.
The obtained uncertainty weighting function Wunc shouldork as a high pass filter to reduce disturbance at low fre-uency, and to avoid strong restrictions at high frequency:
unc = 0.01s + 2s + 8
(13)
.2. Weighting functions
ensor-noise, as a wide-band signal, can be modeled with constant value. During the design process, Wn anticipates
Fig. 4 – Weighting functions in frequency domain.
5% measurement noise for volume measurements. This is inaccordance with the measurement noise used in [8].
The control input is limited implicitly (no hard constraint orsaturation can be considered in the design phase) and is penal-ized by the weighting function Wu. The larger the weight, thesmaller the deflections; therefore, the control activity can bereduced. The weight on endostatin inlet is defined to be con-stant over the entire frequency domain and with a magnitudeequal to the inverse of the maximal inhibitor level. Becauseof physiological reasons, the inhibitor level was maximized in100 mg/kg (since high doses are not desirable).
The performance weighting function Wperf chosen fortracking errors should be large in the frequency range wheresmall errors are desired and small where larger errors can betolerated. In other words, to achieve good tracking Wperf shouldbe larger at low frequency to imitate an integrator and lowerat high frequency. The optimal performance weighting func-tion was chosen in two steps: first, using exact formulationto determine its behavior in the frequency domain, second,tuning its amplification based on expertize. The pole of theweighting function was chosen by virtue of the sensitivityanalysis, as a limit frequency of significant disturbances. Thezero of the weighting function was chosen based on the uncer-tainty weighting function to form the desired “cone” shape inthe frequency domain (Fig. 4). The amplification was set tocompensate the amplification of the model-matching func-tion and to minimize oscillation in constant reference signaltracking:
Wperf = 6.5 × 10−7 s + 8s + 1
(14)
The chosen weighting functions are summarized in Fig. 4.
4.3. Robust control design procedure
Fig. 5 to form the generalized structure of H∞ control designthat is called the �–P–K structure (a compact form of the gen-eralized structure is shown in Fig. 6). As signals, w∗ = [ r n ]

e104 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
erco
Fig. 5 – Reorganization of the closed loop intdenotes the external inputs, z∗ = [ ze zu ] represents the out-put signals to be minimized or penalized (also called theperformance outputs). The closed-loop function M can bederived as the lower linear fractional transformation of thepair (P, K) [18]. The transfer function M can be partitionedaccording to the input and output signals as:
[e
z∗
]=
[M11 M12
M21 M22
][d
w∗
](15)
Fig. 6 – The generalized �–P–K structure.
nnection structure into the �–P–K structure.
This formulation shows that the transfer function M11 char-acterizes the error caused by the model uncertainties modeledas the disturbance d, while the transfer function M22 charac-terizes the nominal performance of the closed-loop system.The block matrix can be interpreted as follows: the M22 nom-inal transfer is perturbed by disturbances, which effect iscaptured in transfer function M11, while the performance ofthe closed-loop system is weighted by the transfer functionsM12 and M21 in order to achieve robust performance.
The aim of the suboptimal design is to find a stabilizingcontroller K such that the H∞-norm of the closed-loop functionis less than a given positive number [19], i.e.
‖M‖∞ =∥∥Fl(P, K)
∥∥∞ < � (16)
The scope of the H∞ controller design is to guarantee robustperformance of the system. This can be realized by fulfilling theconditions of robust stability and nominal performance. To guar-antee nominal stability, the system must be internally stable,which means that the created transfer function is stable fromall inputs to all outputs. The robust stability is achieved byfulfilling the ‖M11‖∞ < 1 condition, while the nominal perfor-mance is achieved if the ‖M22‖∞ < 1 performance objective issatisfied. As a result, the condition of the robust performance
is equivalent to the following [20]:∥∥Fu(M, �)∥∥
∞ < 1 (17)

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 e105
10−3
10−2
10−1
100
10 1
10 2
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
0.045
0.05
Frequency (rad/day)
Mag
nitu
de
Stability, Performance
RSNPRP
Fp
s
w
K 9)
K
K
K
5
Td(fiTpCasw
0 5 10 15 20 25 30 35 400
5000
10000
15000
Tumor volume
Vol
ume
(mm
3 )
Time (day)
0 5 10 15 20 25 30 35 400
20
40
60
80
100
Control input
End
osta
tin (
mg/
kg)
Time (day)
Saturation: 100 mg/kgSaturation: 50 mg/kgSaturation: 20 mg/kgSaturation: 10 mg/kg
Saturation: 100 mg/kgSaturation: 50 mg/kgSaturation: 20 mg/kgSaturation: 10 mg/kg
Fig. 8 – Tumor regression under control-initial tumor3
ig. 7 – Evolution of robust stability, nominal and robusterformance.
The controller is realized by the dynamic system with theystem equations:
v = KAv + KB
[r
y
]
u = KCv + KD
[r
y
] (18)
here the matrices are:
A =
⎡⎢⎢⎢⎢⎢⎣
−19.3435 0.1920 0 0 0
−970.6615 −3.5987 0 −0.0009 −53.1008
0 0 −9.5 0 0
0 0 −0.1019 −0.1 0
0.0067 0.0004 0 0 −0.3293
⎤⎥⎥⎥⎥⎥⎦(1
B =
⎡⎢⎢⎢⎢⎢⎣
0 3.1859
0 162.0788
21.8859 0
0 0.0001
0 0
⎤⎥⎥⎥⎥⎥⎦ (20)
C = [ 0.1890 0.0101 0 0.0001 4.8365 ] (21)
D = [ 0 0 ]. (22)
. Simulation results
he frequency domain analysis (Fig. 7) showed that the con-itions of robust stability (||M11||∞ < 1), nominal performance
||M11||∞ < 1) and robust performance (||Fu(M, �)||∞ < 1) are ful-lled, since all the corresponding norms are smaller than 1.he achieved � value was 0.04, and the designed controllerroved to be stable since its poles are on the left-half plane.
onsequently, the designed controller is suitable for practicalpplications. The dominant singular values of the closed-loopystem have shown that the entire system could be modeledith a second order system [38].volume 17,340 mm .
The time domain analysis showed that control input sat-uration is necessary, since the magnitude of the controlleroutput (over 1000 mg/kg) was not acceptable physiologically.The simulation was carried out for the case of different sat-uration levels from different initial tumor volumes. In Fig. 8one can see that tumor volume reaches a steady-state dur-ing the treatment, which is independent of the tumor volumeat which the therapy was initiated, and depends only onhow the ongoing treatment modulates the balance betweenangiogenic stimulators and inhibitors. The authors of [11,12]and [13] carry out optimal control design where the inhibitorconcentration’s upper limit is 75 mg/kg. These studies reacha tumor volume plateau above 1000 mm3 in 50–100 days;our control strategy reaches a tumor volume plateau under100 mm3 in less than 50 days.
The controller was validated with higher noise thanassumed in the control design process (i.e. 20% noise insteadof 5%), the result of the simulation with 50 mg/kg saturationon the control input is presented in Fig. 9. The noise-freecurve represents the tumor volume, while the noisy curve isthe measured tumor volume; based on which control input iscalculated. The result shows that the effect of noise on thetumor regression is negligible; this can be easily verified bycomparing the characteristics of the tumor output withoutnoise (noise-free curve in Fig. 9.) to the typical characteristicsof tumor output shown on Fig. 8 as well. It should be noted thatthe attained plateau is less than 100 mm3 even in the case ofthe noisy measurement.
At the beginning of the treatment the inhibitor serum levelholds a higher constant value and after a while decreases to alower constant value. The higher the maximal possible serumlevel of endostatin, the sooner the reduction of the dose ispossible (Fig. 10). A strongly limited controller output resultsin a less reasonable control strategy, since for more than 22days a constant dose is prescribed and after 30 days from the
beginning of the therapy a lower constant dose is reached;hence, a more dynamical controller is needed to show betterperformance in tumor regression. Weakly limited controller
e106 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
0 5 10 15 20 25 30 35 400
0.5
1
1.5
2
2.5
x 104
Vol
ume
(mm
3 )
Tumor volume
0 5 10 15 20 25 30 35 400
10
20
30
40
50
Control input
End
osta
tin (
mg/
kg)
Time (day)
Output of the nonlinear model with noiseOutput of the nonlinear model
Fig. 9 – Result of the simulation with 50 mg/kg saturationon the control input, and 20% noise (Gaussian white noise)
0 2000 4000 6000 8000 10000 12000 14000 16000 18000300
400
500
600
700
800
900
1000
1100
1200
Initial tumor volume (mm3)
End
osta
tin (
mg/
kg)
Total endostatin inlet
Saturation: 100 mg/kgSaturation: 50 mg/kgSaturation: 20 mg/kgSaturation: 10 mg/kg
Fig. 11 – Inhibitor inlet variation scenarios during the
on the output of the nonlinear tumor growth model.
output decreases from the upper limit dose after the first sixdays; however, these induce a larger strain on the body inthe first ten days. Thus the medium range of the saturationlevel is reasonable, i.e. 30–50 mg/kg. Regarding these facts,control techniques should not exceed the maximal serumlevel of 50 mg/kg. Compared to the results of [13], in whichthe set-valued protocol is efficient only if inhibitor concentra-tions vary between 69 and 75 mg/kg, the performance of theresulting tumor regression is worse in terms of speed thanthe performance of the robust control strategy with maximalserum level of 50 mg/kg.
Besides maximizing the efficiency of the treatment,another challenge is to minimize the strain caused on the body
and the costs of the treatment. The aim of this assessment isto show the variation of the total inhibitor inlet as a functionof the initial tumor volume and the maximal endostatin inlet.20 30 40 50 60 70 80 90 1004
6
8
10
12
14
16
18
20
22
24Maximal period of maximal dose at diverse saturation level s
Saturation (mg/kg)
Tim
e (d
ay)
Fig. 10 – The period of the maximal constant dose atdiverse saturation levels.
entire treatment.
In Fig. 11 one can see how the total inhibitor inlet varies withthe initial tumor volume.
A higher saturation level can be beneficial if the goal isfast tumor regression. According to the simulation results, incase of lower saturation level, tumor regression to the finalset point was reached after 35–70 days of treatment. In case ofhigher saturation level, tumor regression to the final set pointwas reached after 16–20 days of treatment (Fig. 10). However,higher daily inhibitor dose infers higher total inlet of endo-statin (Fig. 11), which has to be taken into consideration; thus,the optimal maximal serum level was chosen to be 50 mg/kg.
Ref. [16] investigates the total inhibitor inlet. The total inletneeded by the LQ optimal control was 1202 mg/kg, and thetotal inlet needed by state-feedback with pole placement was1207 mg/kg. In our case, by beginning the therapy from thesame initial tumor volume (17,340 mm3) with 50 mg/kg satu-ration level, the total inhibitor consumed becomes 865 mg/kgwhich is a significant amelioration. Ref. [13] does not pub-lish the total inhibitor inlet numerically; however, it operateswith inhibitor serum levels over 65 mg/kg which results in arelatively high total inhibitor inlet (over 5000 mg/kg).
An interesting aspect is to investigate the properties of theclosed-loop system if the tumor growth model is linearized atdiverse operating points and the controller design is imple-mented on the latter models, as nominal models. The setpoint attained by the ongoing treatment and the constantinhibitor serum level necessary to retain the tumor volumeat a lower level are functions of the operating point of thelinearization (Fig. 12). It can be seen that the higher theoperating point of the linearization, the higher the plateauattained, and the lower the angiogenic inhibitor serum levelrequired obtaining balance between angiogenic stimulatorsand inhibitors. In other words, controllers designed at higheroperating points are not efficient in tumor regression, sincethe maximal controller output is less than 10 mg/kg (Fig. 13).
3
Thus, the tumor reaches the steady state at over 10,000 mm ,and the constant inhibitor level to maintain this steady stateis less than 2 mg/kg, as shown in Fig. 12. Controllers designedat smaller operating points can generate controller outputs
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 e107
0 2000 4000 6000 8000 10000 12000 14000 160000
0.5
1
1.5
2x 10
4 Minimal volume of the tumor at the end of the treatment
Tum
or v
olum
e(m
m3 )
0 2000 4000 6000 8000 10000 12000 14000 160000
2
4
6
8
10Constant inhibitor level to reach minimal volume
Working point of the linearization (mm3)
End
osta
tin(m
g/kg
)
Fig. 12 – Minimal tumor volume attained by the treatmenta
oe1clt
oopodoul
a
Fo
0 5 10 15 20 25 30 35 400
0.5
1
1.5
2
2.5x 10
4 Tumor volume
Vol
ume
(mm
3 ) Sample time: 1 hourSample time: 6 hoursSample time: 1 daySample time: 3 days
0 5 10 15 20 25 30 35 400
0.5
1
1.5
2
2.5x 10
4 Measured tumor volume
Vol
ume
(mm
3 ) Sample time: 1 hourSample time: 6 hoursSample time: 1 daySample time: 3 days
0 5 10 15 20 25 30 35 400
20
40
Control input
End
osta
tin (
mg/
kg)
Time (day)
Sample time: 1 hourSample time: 6 hoursSample time: 1 daySample time: 3 days
Fig. 14 – The performance of the control strategy usingdifferent measurement frequencies. The curves are thefollowing: the actual tumor volume (green), the measuredtumor volume (blue) – with 25% measurement noise – andthe control input calculated based on tumor volumemeasurements (red). (For interpretation of the references tocolor in this figure legend, the reader is referred to the web
nd control input required at the plateau.
ver 1000 mg/kg. In these cases saturation is needed; how-ver, these are able to decrease the tumor volume under00 mm3, and maintain the tumor in the avascular state withonstant inhibitor levels between 8 mg/kg and 8.8 mg/kg, theatter being the maximal serum level to maintain tumors inhe avascular state.
A controller, which is able to switch between differentperating points, could achieve good performance at lowerperating points; though, it could not significantly exceed theerformance of the controller presented in the entire domainf interest. Additionally, at higher operating points strongeterioration can be expected. Controllers designed at higherperation points show deficiency in diminution of tumor vol-me, because the magnitude of the control signal is notably
imited (Fig. 13).Consequently, good performance, fast tumor regression
nd low final tumor size can be achieved, if the controller
0 2000 4000 6000 8000 10000 12000 14000 16000
100
101
102
103
104
Maximal output of the controller
Working point of the linearization (mm3)
End
osta
tin(m
g/kg
)
ig. 13 – Maximal output of the controller at diverseperating points.
version of this article.)
design is performed on a nominal model linearized at lowoperating point, and the controller output is weakly saturated(50–100 mg/kg). From a physiological aspect, moderately sat-urated (30–50 mg/kg) inhibitor level is reasonable. Hence, theduration of the treatment is not extremely long, and neitherthe inhibitor serum level nor the total inlet exceeds an accept-able limit.
6. Realization issues
In this section, we discuss the application of the controllerin clinically feasible scenarios. The effects of low samplingfrequency, measurement noise and parametric perturbationon the performance of the closed-loop system are analyzed.
In the previous sections, we supposed that tumor volumemeasurements can be done at a relatively high frequency.However, in clinical practice tumor volume measurements areusually done at a lower frequency (<1 days−1). The closed-loopsystem is simulated using the designed continuous-time con-troller and the continuous-time nonlinear model. However,both the output of the controller and the output of the modelare sampled with a zero-order hold.
In Fig. 14 the performance of the control strategy is shownusing sample times of 1 h, 6 h, 1 day and 3 days. There are twosignificant effects of low sampling frequency that need to be
discussed. On the one hand, the low sampling time impliestime delay; thus, tumor regression begins later and serumlevel has to be held on higher levels for longer periods. On
e108 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
0 5 10 15 20 25 30 35 400
5000
10000
15000
Tumor volume
Vol
ume
(mm
3 )
0 5 10 15 20 25 30 35 400
10
20
30
40
50
Control input
End
osta
tin (
mg/
kg)
Time (day)
Transient between days 5−10Transient between days 10−15Transient between days 15−20
Transient between days 5−10Transient between days 10−15Transient between days 15−20
Fig. 15 – Characteristics of tumor regression and controlinput in case of different perturbation scenarios –parameters change between the 5th and 10th day (blue),the 10th and 15th day (red) and the 15th and 20th day(green), each model parameter is perturbed independentlywith a variability of ±25%. (For interpretation of thereferences to color in this figure legend, the reader is
5−10 10−15 15−20700
750
800
850
900
950
1000Total inhibitor inlet in case of transient behavior
Tot
al in
hibi
tor
inle
t (m
g/kg
)
Days of transient
Fig. 16 – The total inhibitor inlet in case of differentperturbation scenarios – parameters change between the5th and 10th day (blue), the 10th and 15th day (red) and the15th and 20th day (green), each model parameter isperturbed independently with a variability of ±25%. (Forinterpretation of the references to color in this figure legend,
referred to the web version of this article.)
the other hand, because of high degree of measurement noisethe control input oscillates in the steady-state where the min-imal tumor volume is reached; thus, it is more reasonable tohold a given constant serum level (e.g. the theoretical limit8.8 mg/kg) instead of using the serum levels calculated by thecontroller. However, no significant deterioration of control wasfound, since the controller was able to secure tumor regressionand to follow the tumor volume changes in spite of the highlevel measurement noise.
Figs. 15 and 16 demonstrate the effect of parametric pertur-bation on the closed-loop system. In this scenario, there is nomeasurement noise, and the measurements are taken contin-uously. The parameters are perturbed independently (b, d, �1,e) with a variability of ±25% in three different time intervals:
• between the 5th and 10th day,• between the 10th and 15th day,• between the 15th and 20th day.
Parameter perturbation does not affect tumor regressionbefore the 5th day because of the applied saturation. Afterthe 20th day, steady-state is achieved and the tumor volumeis nearly minimal; thus, perturbations do not change signifi-cantly the performance of the controller.
If the condition of the patient changes after the 10th dayof the therapy, the speed of tumor regression does not changeremarkably, total inhibitor inlet varies between 815.8 mg/kgand 916.4 mg/kg (Fig. 16). Parameter perturbation between the5th and 10th day can cause both deterioration and amelio-
ration with regard to the speed of tumor regression, dailyand total inhibitor inlet (Fig. 15). The total inhibitor inletvaries between 742.9 mg/kg and 964.9 mg/kg (Fig. 16). Thesethe reader is referred to the web version of this article.)
simulations demonstrated that the designed controller reactsto parametric changes very pliantly, as expected from robustcontrol methodology.
Regardless of the good performance under certain real-ization limitations, the designed controller is continuous;thus, continuous tumor measurements are required for properoperation. However, in clinical practice tumor volume mea-surement is not feasible for real-time closed-loop control,since measurements are based on medical imaging tech-niques, like X-ray. Sensors and actuators for continuous-timetumor control are not yet developed. Thus, the application ofthis technique will be in experimental phase for a long timeto come.
7. Conclusions
In the course of H∞ design robust stability, nominal perfor-mance and robust performance were achieved. The propertiesof the closed-loop system were investigated by varying thetumor volume at which the nominal model used by thecontroller design was linearized. Tumor regression and totalinhibitor inlet were analyzed at different saturation levels ofthe controller output. The most important characteristics ofcontrollers designed at different operating points were com-pared according to the steady-states reached (with regardto tumor volume plateau and inhibitor serum level) andmaximal magnitude of controller output. The controllers,designed at low operating points, showed robustness of a highdegree against the nonlinearities of the system. Good per-
formance, fast tumor regression and small final tumor sizewere achieved, as presented in the manuscript. Moderatelysaturated controllers (saturation levels between 30–50 mg/kg)
n b i o
sshbut
tipaelatfa
ocmrv
A
T2sHp“ipb
r
c o m p u t e r m e t h o d s a n d p r o g r a m s i
howed the best results; namely, relatively fast tumor regres-ion using low serum levels. The controllers, designed atigh operating points could not decrease the tumor volume,ecause the maximal magnitude of the controller output wasnder the value needed to achieve the avascular state of theumor (8.8 mg/kg).
The best achieved controller was compared to other con-rol strategies applied by the authors and other researchersdentified in the literature. The H∞ controller outperformedreviously applied control strategies in terms of total inletnd daily inlet of inhibitor, and tumor regression speed. Theffect of some aspects of physiologically realistic scenarios,ike low measurement frequency, high measurement noise,nd parametric perturbation were also discussed. We showedhat parametric perturbation has significant effect on the per-ormance only if the perturbation takes place between the 5thnd 10th day of the treatment.
Further work will be related to other robust control meth-ds like �-synthesis design, but also to the use of nonlinearontrol methods and optimal control [39,40]. Higher orderodel synthesis will be also performed. A further aim of
esearch is modeling and controlling combined therapy andalidation on animal experiments.
cknowledgments
his work was supported by the TÁMOP-4.2.1/B-09/1/KMR-010-0002 grant. The first author, Levente Kovács was alsoupported by the János Bolyai Research Scholarship of theungarian Academy of Sciences. Annamária Szeles is sup-orted in the frames of TÁMOP 4.2.4.A/1-11-1-2012-0001National Excellence Program-Elaborating and operating annland student and researcher personal support system”. Theroject was subsidized by the European Union and co-financedy the European Social Fund.
e f e r e n c e s
[1] World Health Organization (WHO), Cancer,http://www.who.int/cancer/en/
[2] M. Malvezzi, P. Bertuccio, F. Levi, C. La Vecchia, E. Negri,European cancer mortality predictions for the year 2013,Annals of Oncology (2013) 1–9.
[3] WHO, International Agency of Research on Cancer,http://www-dep.iarc.fr/
[4] WHO, Global Health Observatory,http://www.who.int/gho/en/
[5] J.M. Pluda, Tumor-associated angiogenesis: mechanisms,clinical implications, and therapeutic strategies, Seminarsin Oncology 24 (2) (1997) 203–218.
[6] R. Kerbel, A cancer therapy resistant to resistance, Nature390 (1997) 335–336.
[7] Y.Y. Qian, H. Zhang, Y. Hou, L. Yuan, G.Q. Li, S.Y. Guo, H.Tadashi, Y.Q. Liu, Celastrus orbiculatus extract inhibits tumorangiogenesis by targeting vascular endothelial growth factorsignaling pathway and shows potent antitumor activity inhepatocarcinomas in vitro and in vivo, Chinese Journal of
Integrative Medicine 18 (10) (2011) 752–760.[8] P. Hahnfeldt, D. Panigrahy, J. Folkman, L. Hlatky, Tumordevelopment under angiogenic signaling: a dynamicaltheory of tumor growth, treatment response, and
m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110 e109
postvascular dormancy, Cancer Research 59 (1999)4770–4775.
[9] A. d’Onofrio, A. Gandolfi, Tumour eradication byantiangiogenic therapy: analysis and extensions of themodel by Hahnfeldt et al., Mathematical Biosciences 191(2004) 159–184.
[10] A. Ergun, K. Camphausen, L.M. Wein, Optimal scheduling ofradiotherapy and angiogenic inhibitors, Bulletin ofMathematical Biology 65 (2003) 407–424.
[11] U. Ledzewicz, H. Schättler, Anti-angiogenic therapy incancer treatment as an optimal control problem, SIAMJournal on Control and Optimization 46 (2007) 1052–1079.
[12] U. Ledzewicz, J. Marriott, H. Maurer, H. Schättler, Realizableprotocols for optimal administration of drugs inmathematical models for anti-angiogenic treatment,Mathematical Medicine and Biology 27 (2) (2010) 157–179.
[13] K. Kassara, A. Moustafid, Angiogenesis inhibition andtumor–immune interactions with chemotherapy by acontrol set-valued method, Mathematical Biosciences 231(2) (2011) 135–143.
[14] A. d’Onofrio, U. Ledzewicz, H. Maurer, H. Schättler, Onoptimal delivery of combination therapy for tumors,Mathematical Biosciences 222 (1) (2009) 13–26.
[15] D.A. Drexler, L. Kovács, J. Sápi, I. Harmati, Z. Benyo,Model-based analysis and synthesis of tumor growth underangiogenic inhibition: a case study, in: Proc. of 18th WorldCongress of the International Federation of AutomaticControl, Milano, Italy, 2011, pp. 3753–3758.
[16] J. Sápi, D.A. Drexler, I. Harmati, Z. Sápi, L. Kovács, Linearstate-feedback control synthesis of tumor growth control inantiangiogenic therapy, in: Proc. of the 16th InternationalSymposium on Applied Machine Intelligence andInformatics, Herlany, Slovakia, 2012, pp. 143–148.
[17] J.C. Doyle, K. Glover, P.P. Khargonekar, B.A. Francis,State-space solutions to standard H2 and H∞ controlproblems, IEEE Transactions on Automatic Control 34 (8)(1989) 831–847.
[18] K. Zhou, Robust and Optimal Control, Prentice Hall, NewJersey, 1996.
[19] D.W. Gu, P.H. Petkov, M.M. Konstantinov, Robust ControlDesign with MATLAB, Springer, London, 2005.
[20] A. Szeles, J. Sápi, D.A. Drexler, I. Harmati, Z. Sápi, L. Kovács,Model-based angiogenic inhibition of tumor growth usingmodern robust control method, in: Proc. of 8th IFACSymposium on Biological and Medical Systems, Budapest,Hungary, 2012, pp. 113–118.
[21] U. Ledzewicz, H. Schätler, A synthesis of optimal controls fora model of tumor growth under angiogenic inhibitors, in:Proc. of the 44th IEEE Conference on Decision and Control,and the European Control Conference, 2005,pp. 934–939.
[22] R.E. Pollock, Advanced Therapy in Surgical Oncology, BCDecker, Hamilton, Ontario, Canada, 2008.
[23] B.W. Feig, D.H. Berger, G.M. Fuhrman, M.D. The, AndersonSurgical Oncology Handbook, 4th ed., Lippincott Williamsand Wilkins, Philadelphia, Pennsylvania, USA, 2006.
[24] P.P. Connell, S. Hellman, Advances in radiotherapy andimplications for the next century: a historical perspective,Cancer Research 69 (2) (2009) 383–392.
[25] M.J. Gazda, R.C. Lawrence, Principles of Radiation Therapy,Cancer Management: A Multidisciplinary Approach, 2001http://www.thymic.org/uploads/reference sub/02radtherapy.pdf/
[26] R. Page, C. Takimoto, Principles of Chemotherapy, CancerManagement: A Multidisciplinary Approach, 2001 http://www.thymic.org/uploads/reference sub/03chemoprinc.pdf/
[27] M.C. Perry, The Chemotherapy Source Book, 4th ed.,Lippincott Williams and Wilkins, Philadelphia,Pennsylvania, USA, 2008.

s i n
e110 c o m p u t e r m e t h o d s a n d p r o g r a m[28] D.J. Samson, T.A. Ratko, B.M. Rothenberg, H.M. Brown, C.J.Bonnell, K.M. Ziegler, N. Aronson, Comparative effectivenessand safety of radiotherapy treatments for head and neckcancer, Comparative Effectiveness Reviews 20 (2012) 1–4.
[29] D.E. Gerber, Targeted therapies: a new generation of cancertreatments, American Family Physician 77 (3) (2008) 311–319.
[30] G. Bergers, L.E. Benjamin, Tumorigenesis and the angiogenicswitch, Nature Reviews Cancer 3 (6) (2003) 401–410.
[31] M.S. O’Reilly, T. Boehm, Y. Shing, N. Fukai, G. Vasios, W.S.Lane, E. Flynn, J.R. Birkhead, B.R. Olsen, J. Folkman,Endostatin: an endogenous inhibitor of angiogenesis andtumor growth, Cell 88 (1997) 277–285.
[32] L.M. Ellis, D.G. Haller, Bevacizumab beyond progression:does this make sense? Journal Clinical Oncology 26 (33)(2008) 5313–5315.
[33] J.S. Pulido, S. Itty, Systemic antiangiogenic therapy: whatgoes around, British Journal of Ophthalmology 93 (4) (2009)420–421.
[34] A. d’Onofrio, P. Cerrai, A bi-parametric model for the tumorangiogenesis and antiangiogenesis therapy, Mathematicaland Computer Modelling 49 (2009) 1156–1163.
[35] A. Isidori, Nonlinear Control Systems, Springer-Verlag,London, 1995.
[36] L. Kovács, B. Kulcsár, A. György, Z. Benyó, Robust servocontrol of a novel type 1 diabetic model, Optimal ControlApplications and Methods 32 (2011) 215–238.
[37] W. Liu, F. Tang, Modeling a simplified regulatory system ofblood glucose at molecular levels, Journal of TheoreticalBiology 252 (2008) 608–620.
[38] A. Szeles, Angiogenic Inhibition of Tumor Growth usingModern Robust Control Methods (M.Sc. thesis), BudapestUniversity of Technology and Economics, 2013.
[39] L.S. Pontryagin, Mathematical Theory of Optimal Processes,Interscience Publishers, New York, USA, 1962.
[40] R.E. Precup, S. Preitl, Optimisation criteria in development offuzzy controllers with dynamics, Engineering Applicationsof Artificial Intelligence 17 (6) (2004) 661–674.
Levente Kovács is associate professor at John von NeumannFaculty of Informatics, Óbuda University. He received MScdegree in electrical engineering from the Politechnica Uni-versity of Timisoara, Romania in 2000, and MSc degree inbiomedical engineering from the Budapest University of Tech-nology and Economics in 2010. He completed his PhD in 2008at the Budapest University of Technology and Economics.His research topic is biomedical and physiological model-ing and control, modern robust control with special interestin diabetic control. He has published more than 200 papers.He is IEEE member from 2009 and IFAC TC 8.2 memberfrom 2010.
Annamária Szeles is MSc student at Department of Control
Engineering and Information Technology, Budapest Universityof Technology and Economics. She received her BSc degreein electrical engineering from Budapest University of Tech-nology and Economics in 2012. Her research interest includesb i o m e d i c i n e 1 1 4 ( 2 0 1 4 ) e98–e110
robust and nonlinear control theory applied on biomedicalsystems.
Johanna Sápi is PhD student at John von Neumann Faculty ofInformatics, Óbuda University. She received her BSc degreein health care management from Semmelweis University,Budapest in 2010 and MSc degree in biomedical engineeringfrom Budapest University of Technology and Economics in2012. Her research interest includes model-based control ofcancer diseases.
Dániel A. Drexler is a research fellow at Department of ControlEngineering and Information Technology, Budapest Universityof Technology and Economics. He received his MSc in elec-trical engineering and MSc in biomedical engineering fromBudapest University of Technology and Economics in 2009 and2011. His research interest includes nonlinear control systems,robot kinematics and physiological control.
Imre Rudas is full professor and rector of the Obuda Univer-sity. He graduated from Bánki Donát Polytechnic, Budapestin 1971, received the MSc in Mathematics from the EötvösLoránd University Budapest in 1977, the PhD in Roboticsfrom the Hungarian Academy of Sciences in 1987, while theDoctor of Science degree from the Hungarian Academy ofSciences in 2004. He received his first Doctor Honoris Causadegree from the Technical University of Kosice, Slovakia andthe second one from “Polytechnica” University of Timisoara,Romania. He is a Fellow of IEEE, Senior Administrative Com-mittee member of IEEE Industrial Electronics Society, memberof Board of Governors of IEEE SMC Society, Chair of IEEEHungary Section, Vice-President of the Hungarian Academy ofEngineering. He is the treasurer of IFSA (International FuzzySystem Association), he had been the President of Hungar-ian Fuzzy Association for ten years. He serves as an associateeditor of several scientific journals. His research topic is inrobotics and control engineering. He has published more than690 papers and received more than 550 independent citationsfor his publications.
István Harmati is associate professor at Department of ControlEngineering and Information Technology, Budapest Univer-sity of Technology and Economics. He received his MSc andPhD degree in electrical engineering from Budapest Univer-sity of Technology and Economics in 1998 and 2004. He wasresearch assistant at the Simon Fraser University, Burnaby, BC,Canada (2000–2001). His research interest includes nonlinearcontrol systems, legged robotic systems, differential and coop-erative games, soft computing methods and adaptive controlsystems.
Zoltán Sápi MD, DSc, is a full professor and deputy headat 1st Department of Pathology and Experimental Cancer
Research, Semmelweis University, Budapest, Hungary. Hisresearch field is tumor genesis including both genetic and epi-genetic changes. He has published more than 90 papers withmore than 100 summed impact factor.