Microsoft Outlook - Queensland Parliament
76
1 From: Martin Milne Sent: Friday, 25 February 2022 2:42 PM To: Mental Health Select Committee Subject: Mental Health Select Committee - Questions on notice Attachments: QLD_QonNotice.docx; QLD_FloorPrice.docx; MUP International and Domestic Experience.docx; MUP_FAQs_Stockwell_Academic_May21.docx; CommonCause Message Guide Drug Stigma.pdf; ADF_Stigma_background_paper.pdf; List of Queensland LDATs.pdf Dear Amanda Please find attached our answers to the questions on notice from last week’s committee hearing. The first document contains information on drink and other drugs consumption during COVID, drug driving and risky drinking. Also attached is a collection of documents on Minimum Unit Pricing(MUP)/floor pricing, along with information on stigma. Finally, there is a list of Queensland LDATs. I will send a copy of our LDAT Highlights Report in a separate email as it is a large document. Yours sincerely Martin Milne | State Manager - Queensland he/him/his T M W adf.org.au Suite 1001, Level 10 490 Upper Edward Street, Spring Hill, QLD 4000 The Alcohol and Drug Foundation acknowledges Traditional Owners of Country throughout Australia. We pay our respects to Aboriginal and Torres Strait Islander cultures; and to Elders past, present and emerging. The ADF is committed to a safe and inclusive environment for all. This email and any attachments may contain legally privileged or confidential information and may be protected by copyright. You must not use or disclose them other than for the purposes for which they were supplied. The privilege or confidentiality attached to this message and attachments is not waived by reason of mistaken delivery to you. If you are not the intended recipient, you must not use, disclose, retain, forward or reproduce this message or any attachments. If you receive this message in error please notify the sender by return email or telephone and destroy and delete all.
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of Microsoft Outlook - Queensland Parliament

1
From: Martin Milne Sent: Friday, 25 February 2022 2:42 PMTo: Mental Health Select CommitteeSubject: Mental Health Select Committee - Questions on noticeAttachments: QLD_QonNotice.docx; QLD_FloorPrice.docx; MUP International and Domestic
Experience.docx; MUP_FAQs_Stockwell_Academic_May21.docx; CommonCause Message Guide Drug Stigma.pdf; ADF_Stigma_background_paper.pdf; List of Queensland LDATs.pdf
Dear Amanda
Please find attached our answers to the questions on notice from last week’s committee hearing.
The first document contains information on drink and other drugs consumption during COVID, drug driving and risky drinking.
Also attached is a collection of documents on Minimum Unit Pricing(MUP)/floor pricing, along with information on stigma.
Finally, there is a list of Queensland LDATs. I will send a copy of our LDAT Highlights Report in a separate email as it is a large document.
Yours sincerely Martin Milne | State Manager - Queensland he/him/his
T M
W adf.org.au
Suite 1001, Level 10 490 Upper Edward Street, Spring Hill, QLD 4000
The Alcohol and Drug Foundation acknowledges Traditional Owners of Country throughout Australia. We pay our respects to Aboriginal and Torres Strait Islander cultures; and to Elders past, present and emerging.
The ADF is committed to a safe and inclusive environment for all.
This email and any attachments may contain legally privileged or confidential information and may be protectedby copyright. You must not use or disclose them other than for the purposes for which they were supplied. Theprivilege or confidentiality attached to this message and attachments is not waived by reason of mistaken deliveryto you. If you are not the intended recipient, you must not use, disclose, retain, forward or reproduce this message or any attachments. If you receive this message in error please notify the sender by return email or telephone anddestroy and delete all.
2
Disclaimer
The information contained in this communication from the sender is confidential. It is intended solely for use by the recipient and others authorized to receive it. If you are not the recipient, you are hereby notified that any disclosure, copying, distribution or taking action in relation of the contents of this information is strictly prohibited and may be unlawful. This email has been scanned for viruses and malware, and may have been automatically archived by Mimecast, a leader in email security and cyber resilience. Mimecast integrates email defenses with brand protection, security awareness training, web security, compliance and other essential capabilities. Mimecast helps protect large and small organizations from malicious activity, human error and technology failure; and to lead the movement toward building a more resilient world. To find out more, visit our website.

Alcohol and other drugs stigmas • 01
Alcohol and other drugs: Stigma
adf.org.au
A background paper

© Alcohol and Drug Foundation 2019
Disclaimer: The Alcohol and Drug Foundation has used its best endeavours to ensure that material contained in this publication was correct at the time of printing. The Alcohol and Drug Foundation gives no warranty and accepts no responsibility for the accuracy or completeness of information and reserves the right to make changes without notice at any time in its absolute discretion.

Contents
Stigma: An introduction 3
Why does stigma matter? 4
What is stigma? 5
What impact does stigma have? 8
What can we do about stigma? 9
Let’s start with a conversation 11
References 12

2

Alcohol and other drugs: Stigma • 3
Stigma An introduction
For people who use alcohol and other drugs (AOD), stigma is a real problem. Other people’s actions and language can make them feel unwelcome and unsafe. That can stop them from seeking the services they need, which can negatively impact their health, wellbeing, employment and social outcomes.
Stigma is a complex and powerful social phenomenon that manifests as strong feelings of disapproval.
The World Health Organization has ranked illegal drug dependence as the most stigmatised health condition globally. Alcohol dependence is listed at number four.1
By reducing stigma overall outcomes can be improved by increasing rates of help-seeking and decreasing negative impacts on individuals.
To sustainably tackle the stigma around illicit drug use and alcohol and other drug (AOD) dependence – and minimise its impact on people’s physical and mental health – stigma needs to be better understood. It also needs to be addressed holistically with initiatives targeted at the three types of stigma: social, structural and self-stigma.
This paper provides an evidence-based review of the stigma associated with illicit drug use and AOD dependence. It also calls for a much-needed course of action for public health intervention. This paper is not designed to be the solution, but it will hopefully start the conversation.
4
Why does stigma matter?Stigma associated with alcohol and other drug (AOD) contributes to health inequalities and adverse health outcomes.2,3
Impacts of stigma can include increased stress, reinforced differences in socio–economic status, delays in seeking support/treatment and people leaving support/treatment.
Research and user experience surveys suggest that experience of stigma could be considered as a social determinant of health.4
Stigma has been shown to worsen stress, reinforce differences in socio-economic status and delay help-seeking. It can also lead to people leaving treatment and support services.
It’s difficult to estimate the exact number of people who are affected by AOD-related stigma or to quantify the harms they experience because of it. Some of the most at-risk people who use illicit drugs or experience a dependence on AOD may also experience homelessness or unstable living.
Many people affected by stigma are silent or lack a space in which to voice their experience. Others are reticent to interact with researchers.
While the impact of stigma may be more damaging in already marginalised communities, discrimination and prejudice can affect anyone. The Australian Government’s 2017–26 National Drug Strategy notes:
Approaches and policy responses aimed at reducing alcohol, tobacco and other drug harms in priority populations should be informed by evidence as it develops and should be reviewed regularly. It is also important that any responses do not inadvertently or unintentionally further marginalise or stigmatise people who are at higher risk of experiencing alcohol, tobacco and other drug related harm.

Alcohol and other drugs: Stigma • 5
What is stigma?Stigma is a social process that occurs when a person is deemed by others to possess a trait or status that makes them less acceptable.
Being stigmatised can reduce someone “from a whole and usual person to a tainted, discounted one”.5
Stigma marginalises and alienates the people who are subjected to it.
Stigma comes from the social process of labelling, judging and stereotyping. We categorise and label5 naturally because it is an efficient way to process new experiences quickly. Because of our experiences, biases, influencing factors and social norms, we then often attach judgments and stereotypes to these labels.
Stigma associated with AODPeople who use illicit drugs or are experiencing a dependence on AOD tend to be subjected to greater stigma than those with other health conditions, including people with a mental illness.
Other key factors that contribute to stigmatisation include perceived danger, insufficient information, perceived level of responsibility, age, lack of contact and cultural factors.
Although alcohol is a drug, the general social acceptability of alcohol use means people who use alcohol, but are not dependent on it, tend to be less stigmatised.
The stigma associated with a drug typically increases with a lack of understanding about the drug and how it works, as well as its legal status and social acceptability. This is evidenced by a 2014 Australian study that found that people are generally more comfortable if they encounter an alcohol dependent person than a person dependent on heroin.6
Stigma is sometimes used as a social tool to discourage and marginalise certain behaviours and, by extension, the people who engage in them.
The varying levels of stigma associated with different drugs is also reflected in public approval of policy approaches. For example, more people support coerced treatment for people with a dependence on heroin and fewer people support coerced treatment for people with a dependence on alcohol.3
Varying degrees of stigmaThe regularity of drug use influences the degree of stigma that may be experienced. For instance, a person who uses cannabis a few times a year may be viewed very differently to someone who uses cannabis daily.
The type of drug also impacts the degree of stigma. For example, the stigma – including self-stigma – associated with heroin use is higher than that associated with cannabis use.7
Stigma also varies with different methods of consumption. Intravenous drug use carries significantly greater stigma than smoking, snorting or swallowing drugs.8 People who inject drugs are often seen as ‘irresponsible and dangerous’ and stereotyped as engaging in criminal behaviour to pay for drug use.9,10,11 Internalised shame, or self-stigma, is also commonly reported amongst people who inject drugs.8 This can increase risk-taking behaviour (such as sharing needles and self-harm).11 It can also impact mental health and self-esteem, leading to a greater potential for increased severity of dependence.8,10

6
Types of stigmaStigma manifests in three primary forms:12
Causes of stigmaFactors that contribute to stigma are complex. However, there are three main problem types: knowledge, attitude and behaviour.
Type Cause Impact
Problem of knowledge: Ignorance
A lack of understanding creates fear about illicit drug use and dependence on AOD. Media coverage also has a key role to play in either increasing or decreasing stigma related to AOD.
This can deepen societal distrust of people who use illegal drugs as it reinforces stigmatising labels and perceptions.
Problem of attitude: Prejudice
Some people blame people who use AOD for other health, economic, and social issues they have. This is because they believe the behaviour is a personal decision.Another issue is social perceptions of controllability. Language is also important in forming attitudes. It can also affect how a person is treated by medical professionals in a clinical setting.
The lack of understanding about AOD and their effects, and why people use them, can lead to inaccurate generalisations, antipathy, hostility, negative attitudes and prejudices.13
Problem of behaviour: Discrimination
Discrimination may arise because of behaviour at an interpersonal level, but also because of established rules and systems.
This discrimination can lead to restricted access to resources or opportunities or render the group powerless.14,15
Self-stigma
Internalised feelings of shame,
low self-esteem and low self-
efficacy. Structural stigma
Prejudice and discrimination by
policies, laws and institutions.
Social/public stigma
Stereotypes, prejudices and discrimination endorsed by
general population.

Alcohol and other drugs: Stigma • 7
More than one stigmaPeople who use alcohol and other drugs (AODs) can be subject to additional stigmas, resulting in overlapping layers of discrimination.
Additional stigmas can stem from an individual’s perceived social identity. Social identity comes from characteristics such as class, gender identity, sexual orientation, ethnicity, age, history of interactions with the justice or child protection systems, religious or spiritual beliefs, mental health status, dis/ability, body type, literacy and numeracy, and educational qualifications. All these characteristics can have varying degrees of stigma attached to them.
When a person has multiple social identities that are stigmatised, their experience of stigma, discrimination and exclusion can be intensified.
For example, a person who has a dependence on AOD may be stigmatised for their dependence. If that person is also non-literate in English, they may be further stigmatised because of that. That person’s experience of exclusion may be further compounded if they also have poor mental health.
Stigma and social identities are complex. Because of this, there are no hard and fast rules about what an individual’s experience is going to be.
Language is important in forming attitudes. There are obvious discriminatory and dehumanising words that are used to denigrate and insult people who use illicit drugs or experience a dependence on AOD. These can create an alienating “us” and “them” mindset. There are also more subtle language issues where words have negative connotations, such as referring to someone who is no longer using illicit drugs as being “clean”.
Language can also affect how a person is treated by medical professionals in a clinical setting. A 2009 study demonstrated that even highly trained mental health professionals, when exposed to a subtle shift in language (“substance abuser” versus “substance user”), applied different judgments and attitudes in their response.1 Advocates of person-first language recognise that the order of the words, not just the words used, affects the images that are generated about the person or group being described.16
Communication structures and procedures in the health system (e.g. triage systems) have been found to increase the stigmatisation of people who use drugs. This was demonstrated in a study which included people with a positive diagnosis of hepatitis C. Having that diagnosis changed the way a person experienced the health system. As part of that study, several members of an emergency department staff admitted that they maintained a list of the names of people they suspected of drug seeking. They acknowledged that when they recognised the name of a patient as a drug seeker, they tended to discount the patient’s symptoms.17
• • • • • •
8
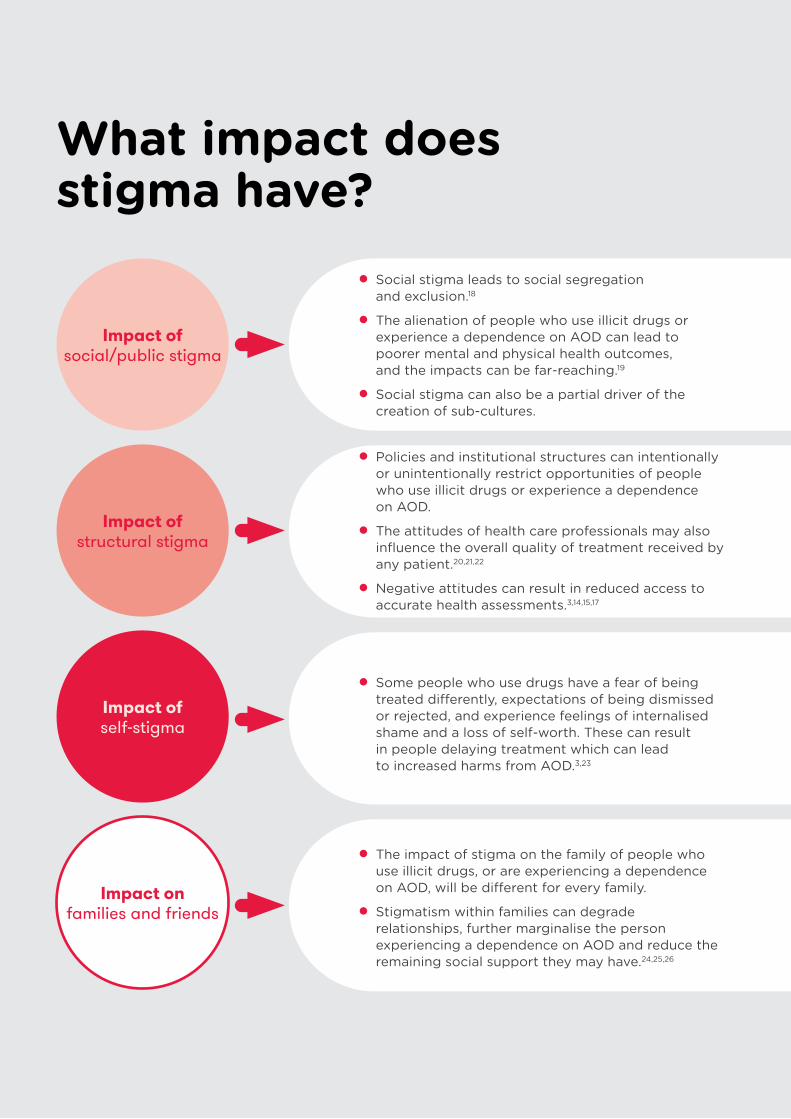
What impact does stigma have?
Impact of social/public stigma
Impact of structural stigma
Impact of self-stigma
Impact on families and friends
• Social stigma leads to social segregationand exclusion.18
• The alienation of people who use illicit drugs orexperience a dependence on AOD can lead topoorer mental and physical health outcomes,and the impacts can be far-reaching.19
• Social stigma can also be a partial driver of thecreation of sub-cultures.
• Policies and institutional structures can intentionallyor unintentionally restrict opportunities of peoplewho use illicit drugs or experience a dependenceon AOD.
• The attitudes of health care professionals may alsoinfluence the overall quality of treatment received byany patient.20,21,22
• Negative attitudes can result in reduced access toaccurate health assessments.3,14,15,17
• Some people who use drugs have a fear of beingtreated differently, expectations of being dismissedor rejected, and experience feelings of internalisedshame and a loss of self-worth. These can resultin people delaying treatment which can leadto increased harms from AOD.3,23
• The impact of stigma on the family of people whouse illicit drugs, or are experiencing a dependenceon AOD, will be different for every family.
• Stigmatism within families can degraderelationships, further marginalise the personexperiencing a dependence on AOD and reduce theremaining social support they may have.24,25,26

Alcohol and other drugs: Stigma • 9
What can we do about stigma?There are three primary problems that lead to stigma. They are attitudes, knowledge and behaviour.
These problems interact with and influence each other in complex ways. Changing one of these may or may not change the others.
Knowledge, attitudes, and behaviour also occur in, and are shaped by, the context of external environmental factors, such as laws, policies and social norms (Figure 1). The individual characteristics of knowledge, attitudes and behaviour also influence those external factors. Changes in public attitude towards cannabis use, for example, have resulted in decriminalisation and legalisation in several countries. Drug laws also strongly influence societal perceptions about different drugs, and by extension the people who use them.
Given the interaction between knowledge, attitudes, behaviour and environment, a long-term, holistic approach is likely to demonstrate the greatest impact in reducing stigma. Such an approach could involve simultaneously:• changing the environment
(social norms, policies and public discourse)• increasing knowledge (reducing ignorance)• shifting attitudes (reducing prejudice)
to change behaviours (reducing discrimination).
Figure 1. The model of change addresses the key stigma factors.
Stigma
Knowledge
AttitudeBehaviour
Laws/policies/social normsEnvironment

10
Key opportunities for action in Australia include:01. Research to identify the drivers of stigma
> Explore the key drivers of stigma, including knowledge, attitudes and behaviours, and how people who use AOD or have a dependence may experience stigma
> Identify key audience segments where these drivers are particularly relevant
> Identify the types of activities which may be most appropriate to key audience segments.
02. Improve knowledge and understanding among the general public and dispel myths about AOD use and dependence > Ensure provision of accurate, factual, objective and unbiased information about drugs and their effects to the public – this information should be accessible in multiple languages and dispel commonly held myths
> Influence and improve the way media uses language and reports on AOD issues by leveraging existing guidelines
> Provide evidence-based education programs in schools to enhance knowledge and reduce stigma
> Identify evidence of previous effective and unsuccessful stigma reduction campaign approaches to inform the development of future campaigns designed to reduce AOD-specific stigma.
03. Strengthen training and workforce development across the range of professionals who work with people who use drugs > Embed AOD-specific training in health professional and emergency services curriculum
> Investigate opportunities to embed contact-based programs that involve direct involvement with people experiencing AOD issues, within undergraduate, post-graduate and professional development training opportunities, to determine their feasibility and potential utility.
04. Support and promote help-seeking behaviour within a framework that recognises some members of every segment of society use AOD, and the experience of dependence varies between individuals > Ensure a variety of treatment and support options are available, including peer-based recovery support services and groups, contact with peer role models, self-help support groups for family members, as well as harm reduction
> Support people who are seeking help with alcohol or other drugs issues to access and choose a treatment pathway most appropriate for them.
05. Investigate and implement opportunities to decrease structural stigma > This would include legislative and administrative restrictions within society including facilities that provide support and treatment to people who use drugs.

Alcohol and other drugs: Stigma • 11
Let’s start with a conversationTo reduce stigma, it’s necessary to recognise and understand why ignorance, prejudice and discrimination towards people who use AOD exists. It is also necessary to identify the extent of the problem and the impact that it has on the lives of people.
Stigma must be addressed holistically with a multi-pronged approach. This approach should feature initiatives targeted at social, structural and self-stigma. Such an approach will create the greatest and most sustainable impact.
Illicit drug use, and experience of dependence on AOD, are emotional and value-laden topics. Many people hold strong opinions about them. The messaging of any initiatives to change knowledge and attitudes must be carefully constructed so that attitudes will shift.
Information and evidence alone are not enough to change attitudes and behaviours.27 Strategies also need to be developed for different target populations. For example, providing young people with evidence-based AOD education in school
may help address the problem of knowledge (ignorance) by equipping them with facts from a young age. This is a useful element of a long-term strategy to reduce stigma. However, addressing the existing problems of knowledge (ignorance) and attitudes (prejudice) in adults, who may have firmly held beliefs and attitudes about the issue, requires a more nuanced approach.
One thing is certain: it’s going to take many conversations.

12
References1. Kelly JF, Westerhoff CM. Does it matter how we refer
to individuals with substance-related conditions? A randomized study of two commonly used terms. International Journal of Drug Policy. 2010 May 1;21(3):202–7.
2. Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. American Journal of Public Health. 2013 May;103(5):813–21.
3. Lancaster K, Seear K, Ritter A. Reducing stigma and discrimination for people experiencing problematic alcohol and other drug use. Sydney: UNSW, 2017.
4. Liamputtong P, Kitisriworapan S. Deviance, difference, and stigma as social determinants of health. Health, illness, and well-being: Perspectives and social determinants. 2012:242–56.
5. Goffman, E. Stigma: Notes on the Management of a Spoiled Identity. New York: Prentice Hall, 1963.
6. Meurk C, Carter A, Partridge B, Lucke J, Hall W. How is acceptance of the brain disease model of addiction related to Australians’ attitudes towards addicted individuals and treatments for addiction? BMC psychiatry. 2014 Dec;14(1):373.
7. Brown SA. Stigma towards marijuana users and heroin users. Journal of Psychoactive Drugs. 2015 May 27;47(3):213–20.
8. Paquette CE, Syvertsen JL, Pollini RA. Stigma at every turn: Health services experiences among people who inject drugs. International Journal of Drug Policy. 2018 Jul 31;57:104–10.
9. Conrad S, Garrett LE, Cooksley WG, Dunne MP, MacDonald GA. Living with chronic hepatitis C means you just haven’t got a normal life any more. Chronic Illness. 2006 Jun;2(2):121–31.
10. Cama E, Brener L, Wilson H, von Hippel C. Internalized stigma among people who inject drugs. Substance use & misuse. 2016 Oct 14;51(12):1664–8.
11. von Hippel C, Brener L, Horwitz R. Implicit and explicit internalized stigma: Relationship with risky behaviors, psychosocial functioning and healthcare access among people who inject drugs. Addictive behaviors. 2018 Jan 1;76:305–11.
12. Livingston JD, Milne T, Fang ML, Amari E. The effectiveness of interventions for reducing stigma related to substance use disorders: a systematic review. Addiction. 2012 Jan;107(1):39–50.
13. Lloyd C. Sinning and sinned against: The stigmatisation of problem drug users. London: UK. 2010.
14. Thornicroft G, Rose D, Kassam A, Sartorius N. Stigma: ignorance, prejudice or discrimination? The British Journal of Psychiatry. 2007 Mar;190(3):192–3.
15. Beyond Blue. Beyondblue Position Statement: Stigma and Discrimination. n/d.
16. Blaska J. The power of language: Speak and write using “person first”. Perspectives on disability. 1993:25–32.
17. Paterson B, Hirsch G, Andres K. Structural factors that promote stigmatization of drug users with hepatitis C in hospital emergency departments. International Journal of Drug Policy. 2013 Sep 1;24(5):471–8.
18. Blendon RJ, Young JT. The public and the war on illicit drugs. Jama. 1998 Mar 18;279(11):827–32.
19. Lancaster K, Santana L, Madden A, Ritter A. Stigma and subjectivities: Examining the textured relationship between lived experience and opinions about drug policy among people who inject drugs. Drugs: Education, Prevention and Policy. 2015 May 4;22(3):224–31.
20. Van Boekel LC, Brouwers EP, Van Weeghel J, Garretsen HF. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: systematic review. Drug and Alcohol Dependence. 2013 Jul 1;131(1–2):23–35.
21. McGillion J, Wanigaratne S, Feinmann C, Godden T, Byrne A. GPs’ attitudes towards the treatment of drug misusers. Br J Gen Pract. 2000 May 1;50(454):385–6.
22. Skinner N, Feather NT, Freeman T, Roche A. Stigma and discrimination in healthcare provision to drug users: The role of values, affect, and deservingness judgments. Journal of Applied Social Psychology. 2007 Jan;37(1):163–86.
23. Lloyd C. The stigmatization of problem drug users: A narrative literature review. Drugs: Education, Prevention and Policy. 2013 Apr 1;20(2):85–95.
24. Earnshaw V, Smith L, Copenhaver M. Drug addiction stigma in the context of methadone maintenance therapy: an investigation into understudied sources of stigma. International Journal of Mental Health and Addiction. 2013 Feb 1;11(1):110–22.
25. Marshall O. Associative stigma among families of alcohol and other drug users. 2013.
26. Tamutiene I, Laslett AM. Associative stigma and other harms in a sample of families of heavy drinkers in Lithuania. Journal of Substance Use. 2017 Jul 4;22(4):425–33.
27. Kahan DM, Braman D. Cultural cognition and public policy. Yale L. & Pol’y Rev. 2006;24:149.

Alcohol and other drugs stigmas • 13

Alcohol and other drugs stigmas • 14
adf.org.auDrug Info line: 1300 85 85 84

This message guide has been written for people who talk about drugs and drugs policy in Australia, including those who use drugs themselves, and are concerned about the high levels of stigma associated with the issue.
The guide was commissioned by the Alcohol and Drug Foundation, Uniting NSW.ACT and the New Zealand Drug Foundation and developed by Common Cause Australia in consultation with a range of diverse range of stakeholders including people with lived experience of drug use and drug stigma.
Why we developed this guide
Stigma is a common and complex problem for people who consume drugs and is a key challenge in minimising the harms associated with drug use.
Stigma can make people feel unwelcome and unsafe, and may prevent them from seeking health and support services. It can have negative impacts on a person’s wellbeing, employment and social outcomes.
Stigma can also intentionally or unintentionally impact on policies and systems, which can restrict opportunities for people who use illicit drugs or experience dependence. It can hinder efforts to reduce drug-related harms and result in reduced access to health services.
The way we talk about illicit drug use and people who consume drugs plays an important role in helping to reduce stigma.
Whether you work in a drug treatment service or are lobbying for drug policy reform, the recommendations in this guide should prove useful to you in both reducing discriminatory attitudes and behaviours towards people who use drugs, while boosting public support for policy reform and increased funding for drug treatment.
It is our hope, that this new narrative will also motivate our existing supporters to speak more openly, honestly and persuasively to the people in their circle of influence about drug use and drug policy.
ApproachThe research and recommendations outlined in this guide are based on the Common Cause approach to community engagement. This approach is based on decades of research from the fields of social psychology, cognitive linguistics and behavioural economics.
A key finding of this research is that most people are able to think about any issue from multiple and often conflicting perspectives. Importantly, these different perspectives operate mostly at a subconscious and emotive level, which means people’s attitudes and behaviours are often driven by factors beyond their conscious awareness.
In our research on drug stigma, our focus was on identifying perspectives (also known as frames) which make people feel at a gut level that people who use drugs deserve the same level of respect, care and support as everyone else. We also sought to understand which frames moved people into an oppositional mindset in which people who use drugs deserve to be punished and shamed. Identifying these unhelpful frames is critical, as it tells us what frames we need to be careful to avoid in all our messaging.
MethodologyIn order to identify the dominant frames people in Australia use to reason about drugs and the people who use them, we conducted a nation-wide frames analysis. This involved collecting and coding over 17,000 words of language data from dozens of publicly available sources of discourse on the topic of drugs - including media articles, political debate, social media discussions and popular culture.
MESSAGE GUIDE DRUG STIGMA

In addition, we conducted 15 one-on-one interviews with advocates concerned about drug stigma in Australia – including treatment providers, policy advocates, doctors, lawyers, politicians and people with experience of being stigmatised because of their use of drugs.
This language data was then coded and analysed based on key metaphors, values and story logic in order to identify the dominant supportive and oppositional frames used by Australians to think and talk about the topic.
These findings were then tested using an online survey of more than 1,400 Australians1. The 20-minute survey included a range of question formats - including forced choice2 and split sample3 questions. We also tested five 30-second audio-recorded messages in which participants moved a dial up and down on their screens as they listened to the messages to indicate their level of agreement with what they were hearing in that moment. This provided us with a moment-by-moment view of the persuasive effect of the messages we tested and allowed us to isolate specific words and phrases that most resonated with audiences.
Segmentation Our research identified three key attitudinal groups related to drug stigma:
• Supporters: people who strongly agree with messages suggesting people who use drugs deserve the same respect and care as everyone else and should not be punished
• Persuadables: people who hold weaker attitudes overall and tend to move between oppositional and supporter perspectives.
• Opponents: people who strongly agree with messages suggesting people who use drugs need to be punished and shamed
Our survey found that supporters and opponents each represent less than one-fifth of Australians, while the remaining two-thirds of the population is persuadable.
We analysed the results of our survey based on the responses of these three groups to each of the questions and messages. Messages that appealed strongly to supporters and also shifted persuadables were identified as most useful for future messaging. These are messages that move persuadables into a supporter mindset. On the flip side, messages that appealed strongly to both opponents and persuadables were identified as harmful messages because they move the latter into an oppositional frame of mind.
Guide structureIn what follows, we provide a number of tips on how to talk about drugs and drug policy in ways that reduce stigma towards people who use drugs. This is followed by a suggested story structure comprised of messaging elements that tested well in our research. Finally, we provide some guidance on common words and phrases we should either replace or embrace.
1 The sample of 1474 respondents was drawn from a panel and weighted to be representative of the Australian population by age, state and gender.2 Forced choice questions force respondents to choose between one of two statements with no option to skip or opt out of the question. This allows us to assess
the strength of opposing frames relative to each other – for example, to assess whether a promising advocate message is more or less powerful than a common opposition message.
3 Split sample questions split the entire sample into two random groups and present each with different versions of the question. These questions are used to assess the impact of using different words or frames on people’s responses.
18% 16%66%
TOP TIPSFIRST, DO NO HARMThe dominant narrative around illicit drugs in Australia is extremely unhelpful. Many journalists and public commentators frame drugs as evil, dirty and dangerous. Far too often, these characteristics are then carried over and applied to the people who use these substances. Reducing the stigma our society places on people who use drugs requires us, therefore, to avoid messaging that reinforces this unhelpful narrative about drugs.
Unfortunately, our discourse analysis suggests that advocates often use language and framing that, whether intentional or not, panders to this dominant narrative. The following suggestions will help you avoid these common messaging mistakes in your future communications.
#1: Don’t scare people
One of the key characteristics of the opposition segment in our research is the degree to which they believe illicit drugs are dangerous, dirty and addictive. In other words, heightened fear and disgust around drugs correlates with higher levels of stigmatising attitudes towards people who use them. This closely mirrors findings from previous research that fear and disgust-based messaging can increase people’s discriminatory attitudes and behaviours.
In our communications, therefore, we should avoid messaging that dials up people’s fear of drugs and those who use them. This includes stories that focus exclusively on the worst possible outcomes of drug use – addiction, devastation and death. Similarly, referring to drugs as a crisis or ‘pandemic’ is not helpful nor are stories and imagery which associates drug use with dirtiness or disease. While this framing is likely to attract the interest of media and others, it is also likely to activate a stigmatising mindset in some audiences.
Another subtle way in which advocates may be pandering to an irrationally heightened level of fear around drugs is by implying that our primary concern is ending drug use. When we interviewed advocates, almost all said their primary concern was ending the harms associated with punitive drug policies and the discrimination people who use drugs face in all walks of life. However, in the public discourse, advocates often failed to make this clear and either implicitly or explicitly accepted the dominant frame that ending drug use should be our ultimate goal.
Similarly, implying that everyone who uses drugs needs treatment or would benefit from reducing or stopping their consumption of drugs panders to the unhelpful notion that drug use is inherently harmful and/or addictive.
IN SHORT: Avoid messaging that activates fear and disgust or implies that all drug use is necessarily
problematic.
#2: Avoid Law & Order framing
In our testing, we found references to legality or crime tended to reduce support rates from persuadable audiences. Indeed, law and order appears to be a key element of the opposition mindset4. This suggests that when people think about drugs from the perspective of maintaining law and order or reducing crime, they are more likely to stigmatise people who use drugs.
4 The opposition was the only segment to nominate ‘law and order’ among their top three concerns for Australia.

In our messaging, therefore, it is important we do not imply that drug policy reform or treatment services are necessary in order to reduce crime. This is something many advocates have done previously in an attempt to appeal to audiences concerned about crime. This research suggests, however, that framing our solutions in terms of crime or community safety5 has the opposite effect of increasing people’s judgement of those who break the law by using illegal drugs.
Similarly, in calling for policy reform, some advocates point to the fact that the criminalisation of drugs means that they are produced in unregulated environments and are sold on the black market. This both increases the risks of drug use and creates a profitable underworld market. However, reminding people of this fact only builds our audiences association between drugs and crime. Indeed, this message was strongly endorsed by our opposition – a clear sign that it fails to toggle audiences out of a stigmatising mindset.
IN SHORT: Avoid justifying drug policy reform or drug treatment services from the perspective of reducing
crime or increasing community safety.
#3: Don’t mythbust
One of the most common messaging mistakes made by advocates is mythbusting – using facts and figures to show how a common fallacy around drugs or drug use is wrong. While the desire to correct myths is both natural and strong (especially on an issue like drugs where misconceptions are common), when you mythbust you mythbuild.
Research shows that every time we are exposed to a concept (even when framed as untrue) it is strengthened as a frame in our minds. It’s also more likely to be activated next time we think about that issue. Mythbusting, therefore, has the counterproductive effect of activating and strengthening the very same ideas we are trying to dispel.
Similarly, advocates have an unhelpful tendency to remind people of what we don’t want them to believe at the same time as telling them what we do want them to believe. We say things such as: “Drugs are a health issue, not a criminal issue” and “We should treat people as human beings, not criminals” and “We want treatment, not punishment”. Our testing confirmed this only weakens our message by activating unhelpful ideas in our persuadable audiences.
IN SHORT: Stop reminding people of unhelpful ideas and tell your story instead.
#4: Abandon the war on drugs
Advocates often talk about the war on drugs having failed and the need, therefore, for ‘a new approach’. Unfortunately, reminding people of the war on drugs – even to say it has failed – does nothing to shift the frame for drugs as an issue. In fact, it locks us into the very frame we most need to escape.
In addition, our research suggests the failure of the ‘war’ means different things to different people. For supporters, it is evidence that punishment and criminalisation do not work. But for the opposition it just means we failed to punish and enforce enough! This is not a strong foundation from which to build a new story to move persuadable audiences. In fact, in our dial testing, the message we tested that referenced the failed war on drugs was the least convincing message for persuadable audiences.
IN SHORT: Stop talking about the failed war on drugs. It traps us in an unhelpful frame and fails to move
persuadable audiences.
5 In our messaging, we need to be careful not to imply that we should only care about the lives of people who use drugs if it negatively affects others. Therefore, framing treatment services or drug policy reform from the perspective of improving community safety is unhelpful. Talking about the health, wellbeing and safety of people who use drugs, however, is helpful as it implies they have inherent worth.

#5: Don’t build empathy through enjoyment
In our interviews, many advocates suggested we should talk more about the enjoyment people derive from using drugs. They suggested this might help build greater empathy and understanding from people who do not use drugs.
Our message testing, however, found that people who hold highly stigmatising attitudes towards people who use drugs already strongly agree with the statement that “people take prohibited drugs because they enjoy how it makes them feel”. Repeating this message, therefore, does not appear to help us tell a more helpful story.
IN SHORT: Framing drugs as enjoyable does not build empathy for people who use drugs.
TELL A NEW STORYIf we want to change the way Australians think about people who use drugs, we need to tell a different story about drugs and the people who use them. The following recommendations are designed to help you tell that new story. They are based on messages that tested well in our research and toggled persuadable audiences into a more supportive and compassionate mindset.
#6: Frame by values
To shift the narrative on drugs and change the way persuadable people feel about those who use them, we need to embed altruistic and open-minded values at the heart of our messaging. In our testing, we found messages based around altruistic and community oriented values including honesty, helpfulness and equality, were significantly more effective at activating supportive attitudes in persuadable audiences than purely fact-based messages.
Indeed, framing the issue of drug stigma around openness and honesty was particularly effective and is a key recommendation for the story structure outlined in this guide (see “Story Structure” below). Combining this with messages around love and support for people who need it, worked particularly well.
Finally, while the messages we tested didn’t explore openness to change values such as freedom, choice, creativity and curiosity in any depth, these were central values for our supporter segment. This suggests these values may provide fruitful territory for our messaging if we can prime them in persuadable audiences.
IN SHORT: Use messaging that connects strongly to altruistic and open-minded values.
#7: Put people who perpetuate stigma in the frame
In order to tell a new story, we need to shift focus and blame away from people who use drugs and onto external actors. This means shifting the problem from ‘drug use’ over to ‘drug stigma’ and the people who perpetuate it.
Framing the community as a whole as the cause of stigma is not helpful as this activates defensiveness in persuadable audiences. Instead, it is more persuasive to shift the focus onto prominent people who support punitive policies and sensationalist media coverage. Our message testing found most persuadable audiences agreed the legality of drugs had more to do with politics than levels of harm, and that we need more facts and less sensationalism in media coverage of drugs.
IN SHORT: To shift the focus off people who use drugs, frame those who use perpetuate drug stigma as the
problem.

#8: Paint a new picture of people who use drugs
It is easier to stigmatise a group of people who don’t look like ‘us’. Painting a more realistic and diverse picture of the people who use illicit drugs in Australia is, therefore, an important step to breaking down unhelpful stereotypes.
One way to do this is to ensure that the stories we tell of people who use drugs, reflects a diversity of occupations, ages, social status and outcomes.
IN SHORT: Point to the diversity of people who use drugs in Australia to undermine simplistic stereotypes
#9: Point out that preventing all drug use is unrealistic
One way to shift the conversation from preventing drug use to improving the health and wellbeing of those who do, is to point out that stopping all use of illicit drugs is unrealistic. This is common sense to most persuadable people and, therefore, a useful element to include in our messaging to establish common ground.
It is important to note, however, that this message does not, by itself, set a new frame for the issue. It is possible to agree that drug use can never be stopped entirely, but that it should be minimised as far as possible by any means necessary – including harsh punishments for people who use them. Make sure, therefore, to couch this message within the broader context of the need for more openness and honesty around drug use and the ways in which we can support the health and wellbeing of those who do. In other words, treat this message as a throwaway line rather than a core framing device. An example of this is provided in our suggested message later in the guide.
IN SHORT: Remind people that stopping all drug use is unrealistic
#10: Bring alcohol into the frame
One of the key differences between supporters and opponents in our research was the degree to which they believed the legality of drugs is related to the harms they cause. Indeed, supporters rank alcohol as the most harmful drug in Australia, while our opponents rank it among the least harmful.
Reminding persuadable audiences that alcohol is a harmful drug, therefore, is one way to activate a supporter mindset, by demonstrating subtly that the legality of drugs is not a reliable indicator of the harms they cause. It also serves to expand the definition of ‘drug users’ to a much larger portion of the population – challenging simplistic stereotypes.
Similarly, making references to ‘alcohol and other drugs’, as opposed to just ‘drugs’, helps to associate the two concepts in people’s minds and in our testing toggled persuadable audiences into more of a supporter mindset. Of course, this won’t always be appropriate - for example, when you’re referring specifically to illicit drugs. But connecting the two concepts whenever possible to do so, will help shift this frame over time.
IN SHORT: Remind people that alcohol is a drug that causes significant harm in Australia

#11: Frame dependence as a symptom
The vast majority of the supporters in our research believed that substance dependence was a symptom, not the source, of people’s problems. While the opposition disagreed, persuadables were marginally more likely to agree with supporters on this part of the narrative.
That said, most persuadables also agreed that ‘people who use prohibited drugs will most likely become addicted’. Therefore, it is important in our messaging that we frame substance dependence as an outcome of other life challenges, rather than something caused by the drug itself.
Similarly, when talking about support services, we should be careful not to imply that everyone who uses drugs requires treatment. For example, instead of talking about drugs being a health issue (which implies that everyone who uses drugs is unhealthy), we would talk about drug dependence being a health issue.
IN SHORT: Explain why substance dependence happens rather than imply it can happen to anyone.

STORY STRUCTUREMore than anything else, it is stories that persuade human beings. If the story you’re telling doesn’t make logical sense at an intuitive level or doesn’t connect with their values, they’ll walk away either unconvinced or unconcerned. In either case, you’ve wasted your time.
To tell a persuasive story, we need to be clear about the vision of what we want and the values at stake, the barrier to achieving that vision, and the solution required. Using the below vision-barrier-action story framework will help you tell a values-driven story in which our solutions make sense to persuadable audience.
Our recommendations are based on story elements that tested well in our research and work together to tell a logical story that supports the solutions most advocates support. Although this story is no silver bullet to drug stigma, it incorporates evidence-based messages that will shift most persuadable people into a more supportive mindset.
VISION:
• Emphasise the importance of openness and honesty• Paint a diverse picture of people who use drugs
BARRIER:
• Point to politics and media sensationalism as a barrier to honesty and enablers of stigma• Explain how secrecy and stigma harms people
ACTION:
• Frame your solution as an innovative approach to drugs based on openness and honesty• Call for more compassion and support for people who need help
Example message:
Below is an example of how our recommended story structure could be executed as a complete message, while also incorporating the messaging tips included in this guide.
As a community, we should be able to have more honest and open conversations about alcohol and other drugs. Pretending we can stop all use of drugs is simply not realistic. We know a lot of people, from lawyers to mechanics to office workers, use prohibited drugs and lead otherwise normal lives.
Yet in Australia, most people agree our attitudes and laws around alcohol and other drugs are based more on politics than common sense. Not only do some media outlets use sensationalism more than facts to shame and dehumanise people who use drugs, but our harsh and outdated approach to drugs prevents people who use them from being honest about their experiences.
This stops those who do need help, from seeking it, because they feel rejected and alone.
Indeed, for people who do have issues with their use of alcohol or other drugs this often has more to do with other challenges they’re facing than the drugs themselves, which they use as an imperfect solution to their pain. In these situations, our role as a community is to help people find better solutions, not dish out judgement and shame.
Meanwhile, we know that innovative approaches that encourage people to be honest and open about drugs, like pill testing at music festivals and medically supervised injecting rooms, keep people safe from easily preventable harms.
While not everyone has a problem with their use of drugs, for those that do, our first response as a caring community should always be to provide the love, support and treatment people need to stay healthy and well.

Words to replace and embraceMany of the common words and phrases we use when talking about drugs and the people who use them reinforce unhelpful narratives that contribute to stigma. Below is a list of words and phrases to replace with alternatives you can embrace.
In addition to the below list, we recommend you reference the Power of Words guide, which includes more detailed recommendations for healthcare and other professionals on how to avoid stigmatising language around drugs.
Replace Embrace Why
Drugs* Alcohol and other drugs Where applicable, reference alcohol together with drugs in order to challenge people’s preconceptions of ‘drugs’ and ‘people who use drugs’.
*Where you are referring specifically to illicit drugs, saying “drugs” alone is perfectly fine.
Drug users People who use drugs Putting people’s humanity first and framing drug use as a behaviour, rather than a characteristic elicits more empathy and avoids defining people by one aspect of their lives.
Problematic drug users People who have issues with their use alcohol or other drugs
People experiencing dependence on alcohol or other drugs
Use person centred language to avoid labelling the individuals themselves as “problematic”.
People who need treatment People who think they need treatment
Don’t imply that others know what is best for people who use drugs.
End drug harms Keep people who use drugs happy, healthy and safe
Avoid implying that drugs are inherently harmful. Focus instead on your positive vision for people’s health and wellbeing.
The war on drugs has failed We need to have a more open and honest conversation about drugs
People who use drugs should be treated with the same compassion and respect as everyone else in our community.
Referring to the ‘war on drugs’ traps us within the dominant unhelpful frame for drugs. Instead of negating this unhelpful frame, tell a new story about drugs and the values that should guide our treatment of them and people who use them.

Drug dependence should be treated as a health issue, not a criminal issue.
We need treatment, not punishment
Drug dependence should be treated as a health issue.
We need better treatment options for those who think they need it.
Reminding people of ideas we would rather they forget only dilutes our message. Stick to talking about what we do want without mentioning what we don’t want.
There is no safe level of drug use. Use of any drug always carries some risk
While most people who use drugs do not suffer serious harms, the use of any drug, whether legal or not, always carries risk. [Followed by articulation of the contexts that cause risk that can be altered through reduced stigma and policy change]
Paint a more realistic picture of drug harms and point out how context plays an important role in determining risk. This turns the conversation from “what bad things do drugs cause” to “how can we alter the context in which people take drugs to make them more safe”.

LDAT Name Lead Org NameLGA Name (This may not be the
same as delivery location)State Electorate
NamePriority Population
A brighter future for CALD youthEthnic Communities Council of Queensland (ECCQ) Brisbane (C) South Brisbane Culturally and linguistically diverse
ADRA Logan Local Drug Action Team
Adventist Development and Relief Agency Australia Logan (C) Woodridge
Bowen Youth Network GroupQueensland Police-Citizens Welfare Association (PCYC) Whitsunday (R) Burdekin
Brisbane North School-Community Partnership Community Living Association, Inc. Brisbane (C) NudgeeBundaberg LDAT YMCA Of Bundaberg Inc Bundaberg (R) BundabergCALD Community Action for a Healthy Society
Ethnic Communities Council of Queensland (ECCQ) Brisbane (C) South Brisbane Culturally and linguistically diverse
Centacare FNQ Centacare FNQ Cairns (R) Cairns Culturally and linguistically diverseCentral Queensland Local Drug Action Team
Queensland Blue Light Association Incorporated Brisbane (C) Chatsworth
Central West Suicide Prevention Network Lives Lived Well Mackay (R) MackayCharleville LDAT Queensland Police Service Moreton Bay (R) RedcliffeCharters Towers Health and Welfare Network PCYC Charters Towers Charters Towers (R) TraegerGladstone LDAT Community Focus National Limited Gladstone (R) Gladstone
Gold Coast LDAT PCYC Gold Coast Gold Coast (C) Surfers ParadiseGoondiwindi Local Drug Action Team - Community Response Care Goondiwindi Association Inc Goondiwindi (R) Southern DownsGungarde Community Centre Aboriginal Corporation
Gungarde Community Centre Aboriginal Corporation Cook (S) Cook Aboriginal and/or Torres Strait Islanders
Healthy Lives: Healthy Children LDAT Nambour Community Centre Sunshine Coast (R) Nicklin
Hervey Bay LDATHervey Bay Neighbourhood Centre (HBNC) Inc Fraser Coast (R) Hervey Bay

Inglewood LDATInglewood Community Welfare Group Inc Goondiwindi (R) Southern Downs
Ipswich LDATQueensland Police Service, Ipswich District Crime Prevention Unit Ipswich (C) Ipswich West
Isaac RegionNorthern Australia Primary Health Limited Townsville (C) Mundingburra
LDAT Winton Winton Neighbourhood Centre Winton (S) GregoryLeichhardt LDAT Ngaran Goori Ltd. Ipswich (C) Ipswich West Aboriginal and/or Torres Strait Islanders'Life', its in your hands Queensland Police Service Moreton Bay (R) RedcliffeLogan Youth at Work LDAT YFS Ltd Logan (C) WaterfordLove your Hood '77 Inala Youth Care Community Inc Brisbane (C) Inala
Mackay LDATNorthern Australia Primary Health Limited Townsville (C) Mundingburra
Maranoa Region Drug Action Team
Lifeline Darling Downs & South West Queensland Ltd Western Downs (R) Warrego
Maryborough LDAT Maryborough Neighbourhood Centre Fraser Coast (R) Maryborough
Mentoring MattersCunnamulla Aboriginal Corporation for Health Paroo (S) Warrego Aboriginal and/or Torres Strait Islanders
Mount IsaYoung People Ahead Youth and Community Services Inc. Mount Isa (C) Traeger Aboriginal and/or Torres Strait Islanders
Nalinah Balin (Our Youth)
Aboriginal and Torres Strait Islander Corporation for Welfare Resource Housing Gold Coast (C) Currumbin Aboriginal and/or Torres Strait Islanders
New Children's Pathways Lowood/Coominya LDAT New Childrens Pathways Inc Brisbane (C) Moggill
Our Youth Matters Project LDAT
Queensland Program of Assistance to Survivors of Torture and Trauma (QPASTT) Inc Brisbane (C) South Brisbane Culturally and linguistically diverse
Queensland Blue Light FNQ LDATQueensland Blue Light Association Incorporated Brisbane (C) Chatsworth
Queensland Blue Light LDATQueensland Blue Light Association Incorporated Brisbane (C) Chatsworth

Redcliffe Local Drug Action TeamQueensland Police-Citizens Youth Welfare Association ? Redcliffe Branch Brisbane (C) Chatsworth
Redlands Local Drug Action Team The Cage Youth Foundation Redland (C) Redlands
SarinaNorthern Australia Primary Health Limited Townsville (C) Mundingburra
SCHEMA Action Team SCHEMA Collective Brisbane (C) StaffordSouth Burnett LDAT South Burnett PCYC South Burnett (R) NanangoSt George QLD LDAT Care Balonne Assoc Inc Balonne (S) WarregoStrong Aboriginal Families in Eidsvold LDAT
Stepping Black Indigenous Corporation Australia Bundaberg (R) Bundaberg Aboriginal and/or Torres Strait Islanders
Strong Sisters Program Lockhart River Tribal Voice Connections Cairns (R) Cairns Aboriginal and/or Torres Strait Islanders
Stronger Foundations Carbal Medical Services Toowoomba (R)Toowoomba North
Tablelands Drug Action Alliance Better Together Community Support Inc Tablelands (R) HillThe Ridge Collective The Ridge YMCA (Y-Care SE QLD Inc.) Brisbane (C) Algester
Toowoomba YP LDAT Civic Assist Toowoomba (R)Toowoomba South
Uncle Alfred Mens Group Uncle Alfred Mens Group Townsville (C) Mundingburra Aboriginal and/or Torres Strait Islanders
Walking Strong LDATThe Institute for Urban Indigenous Health Brisbane (C) Clayfield Aboriginal and/or Torres Strait Islanders
Western Downs LDAT Chinchilla Community Centre Western Downs (R) Callide
Zenadth Kes Gulags LDAT One Blood Hidden Image Entertainment Group Torres (S) Cook Aboriginal and/or Torres Strait Islanders
LDATs prevously operated in these areas
Cape York Remote Communities QPS Torres (S) Cook Aboriginal and/or Torres Strait IslandersDoomadgee LDAT QPS Mount Isa (C) Traeger Aboriginal and/or Torres Strait Islanders

Western QLD LDATQueensland Rugby Football League Central Division Rockhampton (R) Rockhampton

MUP Briefing
International and domestic experience
What did they do What happened
Scotland Scotland was the first country to introduce a MUP in the EU. The bill was initially passed in 2012 but challenged by the alcohol industry through legal action from 2013-2017. Courts in Scotland, the EU and UK were involved with an eventual ruling that the legislation did not breach EU law and is appropriately targeted, lawful and proportionate.
In April 2018, the Scottish Parliament unanimously approved the Alcohol (Minimum Price per Unit)(Scotland) Order setting the minimum price at 50p per unit.
The Scottish Government committed to a review of the minimum price for alcohol after two full years of implementation (1st May 2020) and the MUP legislation includes a ‘sunset clause’, meaning that it will expire after the sixth year of implementation (30 April 2024). To inform this decision there is a ‘review clause’ requiring that the Minister present a review report to parliament on the impact of MUP after five years of its operation.
Formal evaluation is happening with a final report due late 2023.
Modelling
Scotland led the way in undertaking modelling to understand the impacts and appropriate price point for MUP. They commissioned work from the University of Sheffield which estimated that a 50p per unit minimum price would lead to a 3.5% reduction in alcohol consumption (7% for harmful
• alcohol consumption fell by 3.6% after MUP was introduced compared with a 3.2% increase in alcohol consumption in neighbouring England (Health Scotland, 2020).
• significant 10% reduction in alcohol-related deaths, the first in seven years (Alcohol Focus Scotland, 2021).
• very few consumers travelled south to England specifically to purchase alcohol, only 3% reported doing so in one sample.
• Scottish alcohol retailers just north of the border experienced no economic hardship after MUP was introduced with no noticeable impact on their businesses (Health Scotland, 2020).
Medium term impacts
• In Scotland, MUP has not been associated with increased expenditure on alcohol by households that generally bought small amounts of alcohol, particularly those with low incomes.1
• The difference between Scotland and northern England in 2020 was a 7.6% price increase and a 7.7% decrease in purchases per adult per household per day on a day that an alcohol purchase was made.
1 Peter Anderson, Amy O’Donnell, Eileen Kaner, Eva Jane Llopis, Jakob Manthey & Jurger Rehm. Impact of minimum unit pricing on alcohol purchases in Scotland and Wales: controlled interrupted time series analyses Lancet Public Health 2021 Published Online May 28, 2021 https://doi.org/10.1016/ S2468-2667(21)00052-9

drinkers), preventing around 60 alcohol related deaths and 1,300 hospital admissions in the first year alone.
The modelling demonstrated that at full effect of the policy (year 20) would result in:
• Around 120 fewer deaths related to alcohol per year17
• Around 2,000 fewer hospital admissions related to alcohol per year17
• Around 3,500 fewer crimes per year
Northern Territory
The NT experiences some of the highest alcohol related harm in the country.
Recognising the need to address the serious negative social, health, and economic impacts on the Territory community, in 2017, the NT govt announced a review of the NT’s alcohol policies and legislation. The Alcohol Policies and Legislation Review Final Report (also called the Riley Review) was completed in October 2017. The NT Government ‘supported’ 187 of the review’s recommendations and ‘supported in-principle’ 32 recommendations (the only recommendation the Government did not support was the recommendation that all takeaway sales be banned on Sundays).
Research provided to the Riley Review showed that the heaviest consumers of alcohol and individuals at risk of harm disproportionately depend on the cheapest alcohol. Young drinkers were identified as being particularly sensitive to the price of alcohol. The research also showed that at risk and dependent drinkers are more price sensitive than moderate drinkers. The evidence strongly suggested that the introduction of a MUP would be effective in reducing the harms of excessive drinking through the closer targeting of access and cost of products.
The NT Govt released an Alcohol Harm Minimisation Plan for 2018-2019 and introduced a bill to introduce a minimum floor price in May 2018 which passed in August 2018, commencing 1 October 2018. The price was set at $1.30 per 10 g unit of ethanol (i.e. standard drink).
Evaluation report released in 2020
• MUP legislation has been associated with significant declines in:
o alcohol-related assault offences o alcohol-related road traffic crashes (resulting in
injury or fatality) o the number of child protection notifications,
protection orders, and out-of-home care cases. o alcohol-related ambulance attendances o alcohol-related emergency department (ED)
presentations o total alcohol wholesale supply per capita o protective custody episodes o Sobering Up Shelter admissions
• The introduction of the MUP legislation has been associated with no significant changes in:
o Number of liquor licences across the NT o Tourism number and expenditure
Further research demonstrated that overall consumption of alcohol decreased in some regions with particularly large

The price point of $1.30 was selected as it didn’t affect the price of most beers but did target the problem alcohol at the time, namely cheap wine and port. Industry was assured by profits remaining with retailers rather than going to government.
The legislation states that the Minister must review the MUP every 3 years. This review is due to commence in October 2021.
Implementation
The NT Govt developed a website with more information for retailers and the public about what the change meant and how to implement it in various settings. Promotional materials that retailers could use and information for interstate retailers delivering into the NT was also provided.
An Alcohol Review Implementation Taskforce was established to manage stakeholder relations and were very proactive in pulling together and managing a strategically selected industry reference group and other key stakeholders. A dedicated resource for communications and stakeholder relations was put in place early and stakeholders were updated regularly via email, briefings and pre-release reporting etc of major happenings. Following anecdotes of price hiking at point of sale the ACCC was engaged (this would be a learning, bringing this risk under control earlier).
The NT government committed to reporting regularly on progress through an agreed set of indicators. They funded research groups to undertake additional research on the policy measures implemented. All outlined here. In March 2020 they released an evaluation of the MUP in the NT.
decreases in the sales of cheap cask wine which fell by 50% across the territory (Taylor et al., 2021).
Republic of Ireland
MUP was included in the Public Health (Alcohol) Act 2018. The Act had its genesis in the 2012 report of the National Substance Misuse Strategy which was a wide ranging report in Ireland. This led to a government decision in 2013 to put forward legislation which for the first time took a public health approach to alcohol control measures.
The legislation had a very long progress through the parliament as, in addition to MUP, it contained a number of reforms that were contentious in the
Commences Jan 2022

industry, including health information labelling of alcohol products, restrictions on alcohol advertising, sports marketing, and a role for the Health Service in the granting of alcohol sale licenses.
Although the MUP measure was passed by parliament in 2018, it was not commenced until May 2021 and will come into force from Jan 2022. The price has been set at $1.00 per standard drink (10c per 1 gm alcohol).
Modelling
The Irish Government commissioned modelling from the University of Sheffield for a MUP ranging from 40c to 120c. The findings demonstrated MUP would be effective in reducing alcohol consumption, alcohol-related harms (including alcohol-related deaths, hospitalisations, crimes and workplace absences) and the costs associated with those harms.
Stakeholders
Public Health groups supported messaging with key spokespeople including health practitioners, community groups and people with lived experience. They also undertook regular price surveys demonstrating the limited range of products that would be affected. A website was established that provided price calculators for the public to reinforce the small impact on most products.
Industry was divided, with key opponents being the supermarkets. However, smaller retailers, and many producers and hoteliers supported the reform, as they were at times being priced out of the industry by the very cheap wholesale prices offered by supermarket owned retailers.
Alcohol Action Ireland also mobilised individuals at a local level to meet with MPs who were supportive and/or opponents of the policy, responding to action from Industry which targeted local MPs around local impacts. A consistent message relating to harm was used by all community advocates.
Northern Ireland
Minimum pricing for alcohol had cross-party support in the Northern Ireland Assembly before it was suspended in March 2017.

Wales Wales introduced a minimum unit price for alcohol through the Public Health (Minimum Price for Alcohol) (Wales) Act 2018. The bill was introduced in October 2017 and passed in June 2019. A 50p per unit minimum price was implemented from 2 March 2020. The Welsh legislation also includes a 5 year ‘sunset clause’ requiring the government to re-authorise the legislation.
Modelling
The Welsh government commissioned the University of Sheffield to do their own modelling specific to Wales.
Stakeholders
The Welsh government undertook several consultations with stakeholders: first in 2014 following its proposal to adopt MUP, second, between July and December 2015 to discuss design, and finally in 2018 after the passage of the legislation to consult on pricing level.
The Welsh government had limited capacity to understand alcohol policy in-house so commissioned a lot of the policy work to Alcohol Concern Wales and other expert groups. The Scottish experience, occurring in parallel, also informed the thinking and actions.
Public health bodies were critical in coordinating experts and providing a voice for the policy. Although policymakers anticipated resistance, interview data and media coverage between 2014 and 2017 suggest industry opposition was relatively muted and less prominent in the process than in Scotland and England2
Short term impacts
• In Wales in the introduction of MUP led to a decrease in purchases compared to western England. in the first half of 2020 there was an 8.6% reduction in purchase per adult per household per day on a day that an alcohol purchase. 3
Canada All 13 Canadian provinces and territories have some form of minimum pricing, some with higher minimum prices for drinks sold in bars and restaurants than for alcohol sold in off premise outlets (Vallance et al, 2021). In some
2 : Matthew Lesch & Jim McCambridge (2021): Policy communities, devolution and policy transfer: The case of alcohol pricing in Wales, Regional & Federal Studies, DOI: 10.1080/13597566.2021.1934454 3 Peter Anderson, Amy O’Donnell, Eileen Kaner, Eva Jane Llopis, Jakob Manthey & Jurger Rehm. Impact of minimum unit pricing on alcohol purchases in Scotland and Wales: controlled interrupted time series analyses Lancet Public Health 2021 Published Online May 28, 2021 https://doi.org/10.1016/ S2468-2667(21)00052-9

provinces, minimum pricing has been in place for almost a century e.g., Ontario.
Saskatchewan
In Saskatchewan, this was done for wines and sherries above 15% alcohol by volume and beers above 8.5% alcohol by volume. This approach still falls short of the MUP ideal of a precise sliding scale of minimum prices according to exact alcoholic strength (Stockwell et al., 2012).
British Columbia
The prices of different products (e.g., wine, beer) changed at different times and amounts over a 20 year period. Researchers took advantage of this as a ‘natural experiment’ and examined quarterly alcohol sales, quarterly alcohol prices and both quarterly and annual economic indicators in order to estimate the causal effects of minimum unit pricing on consumption (Stockwell et al., 2012a).
Further studies have examined other aspects of minimum unit price impacts, such as effect variance depending on socio-economic area, hospital admissions, alcohol attributable deaths, assaults, and impaired driving.
Quebec (modelling only)
Researchers have undertaken modelling to understand impacts of changes to MUP in some Canadian provinces.
Researchers with access to comprehensive data on prices, strengths and sales volumes of individual products in Quebec calculated that a minimum unit price between CAD$1.50 and $1.75 would substantially reduce the alcohol-caused burden of disease.
Saskatchewan
A 10% increase in minimum prices was associated with an 8.43% decrease in total alcohol consumption (Stockwell et al., 2012b). This difference is at least partly likely to be due to Saskatchewan having minimum prices that were closer to the MUP ideal.
Consumption of high strength beer (greater than 6.8% alcohol/volume) and fortified wine declined the most, relative to lower strength beverages (Stockwell et al, 2012b).
British Columbia
A 10% increase in average minimum prices across all beverages was estimated to be associated with a 3.4% reduction in total alcohol consumption (Stockwell et al., 2012a).
A later study looking at different effects of a minimum unit price depending on socio-economic status of communities found a 10% increase in average minimum prices was associated with a 35% decrease in acute alcohol-related hospital admissions in low-income regions, but with only a 6% to 8% decrease in higher income regions (Zhao and Stockwell, 2017).
The increase in minimum price has been accompanied by decreases in hospital admissions (Stockwell et al., 2013), deaths (Zhao et al., 2013), assaults and impaired driving (Stockwell et al., 2015).

It was estimated that the lower minimum unit price of CAD$1.50 could reduce:
• alcohol-attributable deaths by 5.9% • alcohol-attributable hospital stays by 8.4%.
It was further estimated that the higher minimum unit price of CAD$1.75 could reduce:
• alcohol-attributable deaths by 11.5% • alcohol-attributable hospital stays by 16.3%,
(Sherk et al, 2020).
US In April 2021 the Oregon Liquor Control Commission introduced a limited MUP for spirit products, so becoming the first US state to set some form of minimum pricing (KTVZ News, 2021).
Eastern Europe
In some other countries, "minimum pricing" has been used by governments to set floor prices for alcoholic drinks in order to stabilise markets and, in particular, protect them from cheap imports (Stockwell et al., 2014). However, the rates set for these minimum prices do not relate to a fixed "unit" of alcohol but rather to a volume of beverage (e.g. litre) no matter its strength. From a health and safety perspective, this is an undesireable limitation because it means minimum prices of a low strength product (e.g. 3% strength beer) can be the same as those for a high-strength equivalent (e.g. a 9% strength beer) and so there is no incentive for consumers to choose lower strength products.
Many former Soviet bloc countries such as Kazakhstan, Moldova, Belarus, Ukraine, Russia, Uzbekistan, Armenia and Kyrgyzstan have introduced minimum prices for alcohol over the past two decades, but these are based on the price per litre and so do not meet the ideal of MUP. Armenia has a comprehensive MUP for all products while Ukraine does only for spirits.

References
Coomber K., Miller P., Taylor N., Livingston M., Smith J., Buykx P., Clifford R., Scott D., CliffordS., Chikritzhs T., Nambiar D., & Moayeri F. (2020) Investigating the introduction of the alcohol minimum unit price in the Northern Territory. Summary Report. Deakin University, Geelong, Australia. Prepared for the Northern Territory Department of Health.URL: https://alcoholreform.nt.gov.au/__data/assets/pdf_file/0009/818280/investigating-introduction-of-alcohol-minimum-unit-price-nt-summary-report.pdf .
Alcohol Focus Scotland (2021) Alcohol Deaths and Minimum Unit Pricing. Alcohol Focus Scotland, Edinburgh, Scotland. URL: https://www.alcohol-focus-scotland.org.uk/news/alcohol-deaths-and-minimum-unit-pricing/ .
Public Health Scotland (2020) Public Attitudes to Minimum Unit Pricing in Scotland. Public Health Scotland. URL: https://publichealthscotland.scot/news/2020/september/public-attitudes-to-minimum-unit-pricing-in-scotland/ .
Holmes J, Meng Y, Meier PS, Brennan A, Angus C, Campbell-Burton A, et al. (2014) Effects of minimum unit pricing for alcohol on different income and socioeconomic groups: a modelling study. Lancet, 383(9929):1655-64.
National Alcohol Strategy Advisory Committee (2015). Social reference prices for alcohol: A tool for Canadian governments to promote a culture of moderation. National Alcohol Strategy Advisory Committee. Canadian Centre on Substance Abuse, Ottawa, ON.
NHMRC (2020) Australian guidelines to reduce health risks from drinking alcohol. National Health and Medical Research Council, Canberra, Australia. URL: https://www.nhmrc.gov.au/health-advice/alcohol .
Zhao, J., & Stockwell, T. (2017). The impacts of minimum alcohol pricing on alcohol attributable morbidity in regions of British Colombia, Canada with low, medium and high mean family income. Addiction, 112, 1942-1951. http://onlinelibrary.wiley.com/doi/10.1111/add.13902/epdf .
Stockwell, T. (2014). Minimum unit pricing for alcohol. British Medical Journal, 349:g5617. http://www.bmj.com/content/349/bmj.g5617 .
Stockwell, T., Zhao, J., Martin, G., Macdonald, S., Vallance, K., Treno, A., Ponicki, W., Tu, A., & Buxton, J. (2013). Minimum alcohol prices and outlet densities in British Columbia, Canada: Estimated impacts on alcohol-attributable hospital admissions. American Journal of Public Health, 103(11) 2014-2020. http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2013.301289 .
Zhao, J., Stockwell, T., Martin, G., Macdonald, S., Vallance, K., Treno, A., Ponicki, W., Tu, A. and Buxton, J. (2013). The relationship between changes to minimum alcohol price, outlet densities and alcohol-related death in British Columbia, 2002-2009. Addiction, 108(6) 1059-1069 URL:http://onlinelibrary.wiley.com/doi/10.1111/add.12139/pdf .
Stockwell T, Auld MC, Zhao JH, Martin G. (2012a) Does minimum pricing reduce alcohol consumption? The experience of a Canadian province. Addiction, 107(5): 912-20. http://onlinelibrary.wiley.com/doi/10.1111/j.1360-0443.2011.03763.x/epdf .
Vallance, K., Stockwell, T., Giesbrecht, N., Wettlaufer, A., Chow, C., April, N., Asbridge, M., Callaghan, R., Cukier, S., Hynes, G., Mann, R., Solomon, R., Thomas & G. Thompson, K. Stockwell, T.(2021) The Canadian Alcohol Policy Evaluation (CAPE) project: findings from a review of provincial and territorial alcohol policies. Drug and Alcohol Review, URL: https://onlinelibrary.wiley.com/toc/14653362/0/0 .
Stockwell T, Zhao J, Giesbrecht N, Macdonald S, Thomas G, Wettlaufer A. (2012b). The raising of minimum alcohol pricMinimum Unites in Saskatchewan, Canada: impacts on consumption and

implications for public health. American Journal of Public Health. 102(12): e103-10. URL: http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2012.301094 .
Stockwell, T., Wettlaufer, A., Vallance, K., Chow, C., Giesbrecht, N., et al. (2019). Strategies to Reduce Alcohol-Related Harms and Costs in Canada: An Evaluation of Provincial and Territorial Policies. Victoria, BC: Canadian Institute for Substance Use Research, University of Victoria. URL:https://www.uvic.ca/research/centres/cisur/assets/docs/report-cape-pt-en.pdf .
KTVZ News (2021) Oregon high-proof, low-cost spirits to rise in price; Bend distiller sees little impact. URL: https://ktvz.com/news/central-oregon/2021/04/12/olcc-raises-pricimg-on-high-proof-low-cost-spirits-to-increase-in-cost/ ).
Health Scotland (2020) Sales-based consumption: a descriptive analysis of one year post-MUP off-trade alcohol sales data – briefing paper. Health Scotland, Edinburgh, Scotland. URL: http://www.healthscotland.scot/media/2953/c-users-kims-desktop-mup-sales-based-consumption-plain-english-briefing.pdf .
Taylor, N., Miller, P., Coomber, K., Livingston,M., Scott, D., Buykx, P. and Chikritzhs, T. (2021) The impact of a minimum unit price on wholesale alcohol supply trends in the Northern Territory, Australia. Australian and New Zealand Journal of Public Health. URL: https://doi.org/10.1111/1753-6405.13055 .
Stockwell, T., Zhao, J., Marzell, M., Gruenewald, P., Macdonald, S., Ponicki, W. & Martin, G. (2015). Relationships between minimum alcohol pricing and crime during the partial privatization of a Canadian government alcohol monopoly. Journal of Studies on Alcohol and Drugs, 76(4), 628-634. http://www.jsad.com/doi/abs/10.15288/jsad.2015.76.628 .
Sherk, A., Stockwell, T., April, N., Churchill, S., Sorge, J., & Gamache, P. (2020) The potential health impact of an alcohol minimum unit price in Québec: An application of the International Model of Alcohol Harms and Policies. Journal of Studies on Alcohol and Drugs, 81, 631–640. doi:10.15288/jsad.2020.81.631.
Griffith, R., O'Connell, M. and Smith, K. (2020) Tackling heavy drinking through tax reform and minimum unit pricing. Institute for Fiscal Studies, London, UK. URL: https://www.ifs.org.uk/publications/15183 .
Erickson, R., Stockwell, T., Pauly, B., Chow, C., Roemer, A., Zhao, J., Vallance, K. & Wettlaufer, A. (2018). How do people with homelessness and alcohol dependence cope when alcohol is unaffordable? A comparison of residents of Canadian Managed Alcohol Programs (MAPs) and locally recruited controls. Drug Alcohol Review, 37(S1), S174 – S183. URL:https://onlinelibrary.wiley.com/doi/abs/10.1111/dar.12649 .
Falkner, C., Christie, G., Zhou, L. and JKing, J. (2015) The effect of alcohol price on dependent drinkers’ alcohol consumption. New Zealand Medical Journal, Vol 128 No 1427: 18. URL: https://www.nzma.org.nz/journal-articles/the-effect-of-alcohol-price-on-dependent-drinkers-alcohol-consumption .
Gruenewald PJ, Ponicki WR, Holder HD, Romelsjo A. (2006) Alcohol prices, beverage quality, and the demand for alcohol: quality substitutions and price elasticities. Alcoholism, Clinical and Experimental Research. 30(1):96-105.
Wagenaar A, Tobler A, Komro K. (2010) Effects of alcohol tax and price policies on morbidity and mortality: A systematic review. American Journal of Public Health, 100, 2270-8.
Canadian Substance Use Costs and Harms Scientific Working Group (2020) Canadian substance use costs and harms (2007–2017). Prepared by the Canadian Institute for Substance Use Research
and the Canadian Centre on Substance Use and Addiction. Canadian Centre on Substance Use and Addiction: Ottawa, ON.
Ng Fat, L. and Shelton, N. (2012) Associations between self-reported illness and non-drinking in young adults. Addiction, 107(9): 1612-20.
Bellis, M., Hughes, K., Nicholls, J., Sheron, N., Gilmore, I., Jones, L. (2016). The alcohol harm paradox: using a national survey to explore how alcohol may disproportionately impact health in deprived individuals. BMC Public Health 16.111.
Health Scotland (2020) Minimum Unit Pricing of Alcohol. Evaluating the impacts on the alcoholic drinks industry in Scotland: baseline evidence and initial impacts. A report from Frontier Economics.
URL: http://www.healthscotland.scot/media/2810/frontier-economics-mup-evaluating-the-impacts-on-the-alcoholic-drinks-industry-in-scotland.pdf .
Stockwell, T., Sherk, A., Norstrom, T., Angus, C., Ramstedt, M., Andreasson, S., Chikritzhs T., Gripenberg, J., Holder, H., Holmes, J., Makela, P. (2018) Estimating the public health impact of disbanding a government alcohol monopoly: Application of new methods to the case of Sweden. BMC Public Health, 2018; 18: 1400. doi: 10.1186/s12889-018-6312-x.
Ye, Y. and Kerr, W. (2016) Estimated increase in cross‐border purchases by Washington residents following liquor privatization and implications for alcohol consumption trends. Addiction, 111 (11).

MUP FAQs
1. What is MUP?
Minimum Unit Pricing (MUP) is a new approach to reducing the health and social harms from alcohol use by raising the price of cheap, high-strength drinks that are often favoured by heavy drinkers. MUP sets a floor price for a fixed amount or "unit" of pure alcohol below which it cannot be sold. Usually, a "unit of alcohol" is the same as a "standard drink" which in Australia is defined as 10 g or 12.66 mL of pure alcohol, or roughly the amount of alcohol in a 375mL can or bottle of 3.5% beer, a 30 mL nip of 40% spirits or a small 100mL glass of 13% wine (NHMRC, 2020). For example, in October 2018 the Northern Territory introduced an MUP of $1.30 for a standard drink of any alcoholic beverage as a strategy to reduce harmful drinking.
2. What are the benefits of MUP?
The main benefits of MUP are reductions in the health and social harms caused by alcohol use, whether experienced directly by drinkers, by their friends and family members or the wider community. MUP is a highly targeted strategy which hits the pockets of heavy drinkers particularly, resulting in many people drinking less and so being at lower risk of injuries (e.g. from car crashes and violence) and serious illnesses (e.g. liver disease and cancers). The introduction of the $1.30 MUP in the Northern Territory was followed by significant reductions in alcohol-related ambulance callouts, emergency department presentations, assaults, arrests, road crashes and child protection cases (Coomber et al, 2020). In Scotland, a 50p MUP was followed by a significant reduction in alcohol-related deaths, the first in seven years (Alcohol Focus Scotland, 2020).
MUP has other significant benefits when compared with other ways of using price increases to reduce alcohol-related harm. Firstly, MUP is more popular with the public than across-the-board tax increases. For example, in Scotland, the popularity of MUP increased after it was implemented and the benefits had become clear. About half of those polled in 2020 were in support and only a quarter were opposed (Public Health Scotland, 2020). One reason MUP is more popular than increased alcohol taxes is that MUP mostly effects the price of cheap, high-strength products and has relatively little impact on products preferred by light or moderate drinkers (Holmes et al., 2014).
Another practical benefit of MUP is that it protects the profits of businesses involved in the sale of alcohol by allowing them to make more money while selling less alcohol. As an indication of this, Canadian producers of beer, wine and spirits often lobby for increases in the minimum prices set for their products by provincial government regulators (Stockwell et al., 2015). While some industry groups oppose any perceived government interference in their marketplace, others see the commercial benefits of setting minimum prices and so are less likely to oppose them.
A major benefit of MUP is that it produces greater improvements in health outcomes for people on low incomes. People on low incomes are less likely to drink alcohol than people on high incomes but when they drink heavily they are more likely to experience serious harms (Zhao et al, 2017). However, it has been shown there are also greater reductions in hospital admissions among people on low income when minimum prices increase (Zhao and Stockwell, 2017).
3. Where has it been used and has it worked?
The purest examples of MUP are the 50p per 8 g unit of ethanol introduced by Scotland in May 2018 and the $1.30 per 10 g unit of ethanol (i.e. standard drink) by Australia's Northern Territory in October, 2018. In some other countries, "minimum pricing" has been used by governments to set floor prices for alcoholic drinks in order to stabilise markets and, in particular, protect them from cheap imports (Stockwell et al., 2014). However, the rates set for these minimum prices do not relate to a fixed "unit" of alcohol but rather to a volume of beverage (e.g. litre) no matter its strength. From a health and safety perspective, this is an important limitation because it means

minimum prices of a low strength product (e.g. 3% strength beer) can be the same as those for a high-strength equivalent (e.g. a 9% strength beer) and so there is no incentive for consumers to choose lower strength products. However, there is evidence from Canada that this kind of less perfect minimum pricing can still be effective at reducing harmful alcohol use (e.g. Stockwell et al., 2013; Zhao et al, 2013). All 13 Canadian provinces and territories have some form of minimum pricing, some with higher minimum prices for drinks sold in bars and restaurants than for alcohol sold in off premise outlets (Vallance et al, 2021). In some provinces, minimum pricing has been in place for almost a century e.g. Ontario. More recently some Canadian provinces have set higher minimum prices for some higher strength drinks in order to more effectively reduce harmful drinking. In Saskatchewan, for example, this was done for wines and sherries above 15% and beers above 8.5% alcohol by volume. This approach still falls short of the MUP ideal of a precise sliding scale of minimum prices according to exact alcoholic strength (Stockwell et al., 2012). In Manitoba, the government-owned alcohol distributor sets increasing minimum prices for every 1% increase in the alcohol content of all alcoholic drinks, however they also have discounts for bulk purchases so this approach also falls short of the MUP ideal (Stockwell et al., 2019).
Many former Soviet bloc countries such as Kazakhstan, Moldova, Belarus, Ukraine, Russia, Uzbekistan, Armenia and Kyrgyzstan have introduced minimum prices for alcohol over the past two decades, but again these are mostly set at rates per litre of beverage and so do not quite meet the ideal of MUP. Armenia has a comprehensive MUP for all products while Ukraine does only for spirits. Finally, in April 2021 the Oregon Liquor Control Commission introduced a limited MUP for spirit products, so becoming the first US state to set some form of minimum pricing (KTVZ News, 2021).
There is a growing body of evidence showing that minimum pricing in general and MUP in particular effectively reduce alcohol consumption and related harms. The Scottish government reported that alcohol consumption fell by 3.6% after MUP was introduced compared with a 3.2% increase in alcohol consumption in neighbouring England (Health Scotland, 2020). In the Northern Territory, overall consumption of alcohol decreased in some regions with particularly large decreases in the sales of cheap cask wine which fell by half across the territory (Taylor et al., 2021). In Canada, a 10% change in average minimum prices across all beverages was estimated to be associated with a 3.4% change in total consumption in the opposite direction (Stockwell et al., 2012a). However, in Saskatchewan where minimum prices were closer to MUP, a 10% change in minimum prices was associated with an 8.4% opposite change in total alcohol consumption (Stockwell et al., 2012b). This difference is at least partly likely to be due to Saskatchewan having minimum prices that were closer to the MUP ideal.
There is also direct evidence that minimum pricing effectively reduces alcohol-related harms. The introduction of the $1.30 MUP in the Northern Territory was followed by significant reductions in alcohol-related ambulance callouts, emergency department presentations, assaults, arrests, road crashes and child protection cases (Miller et al, 2020). In Scotland, a 50p MUP was followed by a significant 10% reduction in alcohol-related deaths, the first in seven years (Alcohol Focus Scotland, 2021). In Canada, increases in minimum prices have been accompanied by decreases in hospital admissions (Stockwell et al., 2013), deaths (Zhao et al., 2013), assaults and impaired driving (Stockwell et al., 2015) – and decreases in minimum prices were associated with significant increases in these harms.
4. How much does it increase the cost of alcohol by?
MUP works by increasing the cost of the cheapest alcohol products available. The increase in the cost of these products depends completely on their price per "unit" or standard drink before the measure takes place. In Australia, there are more than 10,000 individual alcohol products available for sale somewhere at any time. The increase in cost can be defined in different ways, for example: (i) the number and percentage of available products that go up in price, or (ii) the average price

increase for all cheap products affected by the new MUP. As an example, researchers with access to comprehensive data on prices, strengths and sales volumes of individual products in Canada calculated that an MUP of $1.50 would increase the price of just 2.5% of 960 of the 18,914 products available for sale in Québec in 2014. Because heavy drinkers prefer these cheap products, this actually increased the price of 24% of all total alcohol sales. The average price increase for these affected products was 13% (Sherk et al, 2020). The higher the MUP then the more products are affected and the greater the change in average price – and, in turn, the greater impact on alcohol-related harm.
In short, the increase in alcohol prices caused by an MUP can be as little or as large as policymakers choose after taking into account the extent of health benefits desired and, perhaps, the acceptability of the price rise.
5. Does MUP mean consumers pay a lot more for alcohol?
Most consumers would not notice any difference in price at all with an MUP because they only impact on a small percentage of all available products. Light and moderate drinkers rarely drink the very cheapest products and, even if they do, would be spending very little extra because they do not drink much. A careful analysis conducted in the UK showed that an MUP of 45p would result in moderate drinkers spending just 4p more per year on alcohol if they had low income and £1.86 more per year if they had a high income. "Harmful" or heavy drinkers would actually spend £34.63 less per year on alcohol if they had a low income, while heavy drinkers on a high income would spend £16.35 more across the whole year (Holmes et al, 2014).
6. Who gets the profits – won’t it just make Industry richer?
The introduction of an MUP for alcohol in Australia would help alcohol producers, distributors and retailers be more profitable while selling less alcohol. This is because when prices go up on alcohol, consumption goes down - but consumption goes down by a smaller percentage than prices go up resulting in increased profits overall. Most alcohol industry sectors would make more money from selling very cheap, high strength drinks while selling lower volumes of these especially problematic products. Some consumers would shift their consumption to lower alcohol content brands which usually have higher profit margins. For similar reasons, the federal government would collect more revenue from the 10% GST and also from wine taxes. The government would make less money, however, from excise taxes on beer and spirits because these are fixed on the amount of pure alcohol sold not the volume of beverage. For the UK, it has been calculated that an MUP results in slightly lower tax revenues overall (Griffith et al, 2020) so these authors recommend increasing alcohol excise taxes alongside MUP to share the proceeds between the private and public sectors.
That some sectors of the alcohol industry can benefit from MUP helps with the feasibility of the policy because it means there will usually be less opposition to this effective harm reduction strategy from a powerful lobby group - in Canada and the US some alcohol industry sectors have actively supported MUP for this reason. If there is concern that MUP would make the industry too profitable, the federal government always has the opportunity to raise excise taxes a little so that the increased profits are shared.
7. Who is most impacted by MUP?
The people who are most directly impacted by MUP are those who like to drink the cheap, high-strength alcoholic beverages that would go up in price. This group primarily includes heavy and dependent drinkers but also anyone drinking on a budget, such as young people and people on low incomes. Research from Canada (Erickson et al, 2018), New Zealand (Falkner et al, 2015) and the UK (Holmes et al, 2014) has shown that heavy drinkers and people with alcohol use disorders on low incomes will actually reduce both how much they drink and how much they spend on alcohol, resulting in substantial health and safety benefits for this group. UK researchers estimated that an MUP of 45p would result in moderate drinkers on low incomes would spend just 4p more per year on alcohol high income moderate drinkers just £1.86 more per year (Holmes et al, 2014).

Many people would also be indirectly impacted by MUP. Alcohol manufacturers and retailers would take slightly more profit from their trade. Families of people with drink problems would be less likely to experience violence. People working in Emergency Departments would have fewer people to treat for injuries caused by their drinking. In general, there would also be broad societal benefits because of reductions in crime, hospital admissions, work absenteeism and premature death.
8. Does MUP penalise everyone for the problems of a few?
MUP is a highly targeted strategy with barely any direct effects on the majority of drinkers, especially on those who drink moderately. In Québec, Canada it was estimated that an MUP of as much as $1.50 per standard drink would only affect the prices of 2.5% of all products available for sale in that province (Sherk et al, 2020). In Saskatchewan, Canada when an MUP-like pricing policy was increased and applied to all alcoholic beverages, the price of 8.5% of all alcohol products was increased (Stockwell et al, 2012b). Many people experience the health and safety benefits from MUP. Those who drink the most of the cheap, high strength products that increase in price experience the greatest health and safety benefits. Safer roads and streets, more productive workplaces and fewer economic costs from alcohol are among the broad societal benefits that would be experienced by the "many” from an MUP.
9. Are some alcohol products more affected than others by MUP?
MUP mostly affects the prices of the cheap, high strength products. In the Northern Territory, the $1.30 MUP had a particularly significant impact on cask wine sales which went down by approximately 50% (Taylor et al., 2020). In Canada, products particularly affected have been found to be high strength beers (e.g. greater than 8.5% alcohol/volume) and fortified wines (Stockwell et al, 2012b). The Northern Territory MUP also had a major impact on fortified wines with an average price rise of over one third being observed (Taylor et al., 2020). While there is a great range of prices per standard drink for all types of alcoholic beverage, in general beer and distilled spirits prices tend to be the lowest per standard drink and prices of table wine the highest. A detailed Canadian analysis found that a CAD$1.50 MUP would result in price increases for 14% of spirit products, 6% of beers and only 3% of wines (Sherk et al., 2020).
10. Won’t heavy drinkers find others things to drink or switch to using drugs?
When alcohol prices rise drinkers will sometimes seek out cheaper, lower quality alternatives. However, when it is already the price of the cheapest alcohol that has increased there are few alternatives short of making one's own alcohol or being prepared to drink non-beverage alcohol, which very drinkers are prepared to do (Falkner et al, 2015; Erickson et al, 2018; Gruenewald et al., 2006). It has been very well established by studies from around the world that alcohol price increases lead to reduced harms such as lower rates of liver disease and alcohol-related deaths (Wagenaar et al, 2010; Zhao et al, 2013). These benefits would not be possible if drinkers completely substituted their preferred alcohol brands with cheaper alternatives when prices rise. Detailed studies of how dependent drinkers cope when alcohol is unaffordable (Falkner et al, 2015; Erickson et al, 2018) find that most common strategies reported involved drinking less e.g. waiting for the next welfare check, making existing supplies last longer or going into treatment. Very few members of this vulnerable group reported being prepared to resort to drinking non-beverage alcohol or committing crimes to access more money. While some people did switch to other drugs when they could not afford alcohol, mostly they just substituted cannabis for alcohol, a much safer alternative for a heavy drinker (CSUCH, 2020; Erickson et al., 2018).
11. Won’t MUP adversely affect those who are already worse off?
MUP has been shown to have especially positive impacts for people on low incomes who drink heavily. People with less income are also less likely to drink heavily and are more likely to abstain

(Ng Fat and Sheldon, 2012). However, those who do drink heavily are more likely to become ill, be injured or die prematurely from alcohol-related reasons (reference). Minimum pricing has been found to be particularly effective for this group. A Canadian study found that a 10% increase in average minimum prices was associated with a 35% decrease in acute alcohol-related hospital admissions in low income regions but with only a 6% to 8% decrease in higher income regions (Zhao and Stockwell, 2017). This outcome was also predicted on theoretical grounds in a landmark UK modelling study which estimated that MUP would reduce alcohol spending by heavy drinkers on low incomes and that they would experience the greatest health benefits from reduced alcohol intake (Holmes et al., 2014).
Studies of how dependent drinkers on low incomes cope when alcohol prices rise from New Zealand (Falkner et al, 2015) and Canada (Erickson et al, 2018) find that “positive” strategies are the most commonly reported e.g. collecting bottles and cans from the streets to cash in for container, not drinking and waiting for the next welfare check, making existing supplies last longer or going into treatment. Very few members of these most vulnerable groups report being prepared to resort to drinking non-beverage alcohol or committing crimes to access more money. While some people did switch to other drugs when they could not afford alcohol, most reported substituting cannabis for alcohol, a much safer alternative for a heavy drinker (CSUCH, 2020; Erickson et al., 2018).
12. Won’t MUP unfairly impact those who are light or moderate drinkers?
Light and moderate drinkers are hardly affected by MUP policies because they rarely drink the cheapest beverages that would increase in price and, even when they do drink these beverages they spend so little on alcohol that they would be paying very little extra. They would, however, experience benefits from safer roads and safer streets at night along with greater access to healthcare because of reductions in people attending Emergency Departments and hospitals for injuries and illnesses caused by alcohol use. A detailed analysis conducted by UK researchers found that an MUP of 45p would result in moderate drinkers spending just 4p more per year on alcohol if they had low income and £1.86 more per year if they had a high income (Holmes et al, 2014).
13. Will people travel across borders to access cheap alcohol potentially causing more harm?
Cross-border shopping has been shown to have very little impact on the effectiveness of MUP. In Scotland, a detailed study of the economic impact of MUP found that very few consumers travelled south to England specifically to purchase alcohol, only 3% reported doing so in one sample. Furthermore, Scottish alcohol retailers just north of the border experienced no economic hardship after MUP was introduced with no noticeable impact on their businesses (Health Scotland, 2020).
The fact that minimum pricing and MUP have both been shown to reduce consumption and alcohol-related harms means that cross-border shopping does not substantially undermine these policies. There have been several studies around the world of cross-border shopping. In Sweden, there is a substantial cross-border trade with neighbouring European countries e.g. Estonia and Denmark amounting to almost 20% of total per capita alcohol consumption. However, it has been shown that pricing increases for the domestic alcohol market still reduce overall consumption and related harms with only small compensating increases in cross-border trade (Stockwell et al., 2018). A US study looked at the extent to which a tax increase in Washington state led to increased cross-border sales in Oregon and found only very small effects (Ye and Kerr, 2016).
14. What about granny who has a glass of port each night?
Most likely Granny will be drinking a glass of port or sherry that would not be affected by MUP in the slightest. If she was to be drinking a glass of a cheap fortified wine every night, she might be able purchase highly discounted cheap fortified wines, for example at $6.50 per bottle for a port with 18.5% alcohol by volume (the cheapest example identified in an Internet search for members of a

wine club). While most ports retail in the range of between $15 and $30 per bottle, this $6.50 per bottle example would contain almost 11 Australian standard drinks at a value of about $0.59 each. Assuming Granny has one standard drink of port per night and an MUP of $1.30 was to be introduced, she would be spending an extra $0.71 per day or $3.57 extra per week. However, among the many hundred varieties of ports and sherries on the market, only a tiny percentage are available at such low prices and their quality is extremely low.
Granny may also be happy to be paying a tiny bit extra for her nightly drink if she understood that the MUP policy responsible for this was also preventing serious injury and illness in the wider community and was also saving lives.
References
Coomber K., Miller P., Taylor N., Livingston M., Smith J., Buykx P., Clifford R., Scott D., CliffordS., Chikritzhs T., Nambiar D., & Moayeri F. (2020) Investigating the introduction of the alcohol minimum unit price in the Northern Territory. Summary Report. Deakin University, Geelong, Australia. Prepared for the Northern Territory Department of Health.URL: https://alcoholreform.nt.gov.au/__data/assets/pdf_file/0009/818280/investigating-introduction-of-alcohol-minimum-unit-price-nt-summary-report.pdf . Alcohol Focus Scotland (2021) Alcohol Deaths and Minimum Unit Pricing. Alcohol Focus Scotland, Edinburgh, Scotland. URL: https://www.alcohol-focus-scotland.org.uk/news/alcohol-deaths-and-minimum-unit-pricing/ .
Public Health Scotland (2020) Public Attitudes to Minimum Unit Pricing in Scotland. Public Health Scotland. URL: https://publichealthscotland.scot/news/2020/september/public-attitudes-to-minimum-unit-pricing-in-scotland/ . Holmes J, Meng Y, Meier PS, Brennan A, Angus C, Campbell-Burton A, et al. (2014) Effects of minimum unit pricing for alcohol on different income and socioeconomic groups: a modelling study. Lancet, 383(9929):1655-64.
National Alcohol Strategy Advisory Committee (2015). Social reference prices for alcohol: A tool for Canadian governments to promote a culture of moderation. National Alcohol Strategy Advisory Committee. Canadian Centre on Substance Abuse, Ottawa, ON.
NHMRC (2020) Australian guidelines to reduce health risks from drinking alcohol. National Health and Medical Research Council, Canberra, Australia. URL: https://www.nhmrc.gov.au/health-advice/alcohol .
Zhao, J., & Stockwell, T. (2017). The impacts of minimum alcohol pricing on alcohol attributable morbidity in regions of British Colombia, Canada with low, medium and high mean family income. Addiction, 112, 1942-1951. http://onlinelibrary.wiley.com/doi/10.1111/add.13902/epdf . Stockwell, T. (2014). Minimum unit pricing for alcohol. British Medical Journal, 349:g5617. http://www.bmj.com/content/349/bmj.g5617 . Stockwell, T., Zhao, J., Martin, G., Macdonald, S., Vallance, K., Treno, A., Ponicki, W., Tu, A., & Buxton, J. (2013). Minimum alcohol prices and outlet densities in British Columbia, Canada: Estimated impacts on alcohol-attributable hospital admissions. American Journal of Public Health, 103(11) 2014-2020. http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2013.301289 . Zhao, J., Stockwell, T., Martin, G., Macdonald, S., Vallance, K., Treno, A., Ponicki, W., Tu, A. and Buxton, J. (2013). The relationship between changes to minimum alcohol price, outlet densities and alcohol-related death in British Columbia, 2002-2009. Addiction, 108(6) 1059-1069 URL:http://onlinelibrary.wiley.com/doi/10.1111/add.12139/pdf .
Stockwell T, Auld MC, Zhao JH, Martin G. (2012a) Does minimum pricing reduce alcohol consumption? The experience of a Canadian province. Addiction, 107(5): 912-20. http://onlinelibrary.wiley.com/doi/10.1111/j.1360-0443.2011.03763.x/epdf . Vallance, K., Stockwell, T., Giesbrecht, N., Wettlaufer, A., Chow, C., April, N., Asbridge, M., Callaghan, R., Cukier, S., Hynes, G., Mann, R., Solomon, R., Thomas & G. Thompson, K. Stockwell, T.(2021) The Canadian Alcohol Policy Evaluation (CAPE) project: findings from a review of provincial and territorial alcohol policies. Drug and Alcohol Review, URL: https://onlinelibrary.wiley.com/toc/14653362/0/0 .
Stockwell T, Zhao J, Giesbrecht N, Macdonald S, Thomas G, Wettlaufer A. (2012b). The raising of minimum alcohol pricMinimum Unites in Saskatchewan, Canada: impacts on consumption and implications for public health. American Journal of Public Health. 102(12): e103-10. URL: http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2012.301094 . Stockwell, T., Wettlaufer, A., Vallance, K., Chow, C., Giesbrecht, N., et al. (2019). Strategies to Reduce Alcohol-Related Harms and Costs in Canada: An Evaluation of Provincial and Territorial Policies. Victoria, BC: Canadian Institute for Substance Use Research, University of Victoria. URL:https://www.uvic.ca/research/centres/cisur/assets/docs/report-cape-pt-en.pdf .
KTVZ News (2021) Oregon high-proof, low-cost spirits to rise in price; Bend distiller sees little impact. URL: https://ktvz.com/news/central-oregon/2021/04/12/olcc-raises-pricimg-on-high-proof-low-cost-spirits-to-increase-in-cost/ ).
Health Scotland (2020) Sales-based consumption: a descriptive analysis of one year post-MUP off-trade alcohol sales data – briefing paper. Health Scotland, Edinburgh, Scotland. URL: http://www.healthscotland.scot/media/2953/c-users-kims-desktop-mup-sales-based-consumption-plain-english-briefing.pdf .
Taylor, N., Miller, P., Coomber, K., Livingston,M., Scott, D., Buykx, P. and Chikritzhs, T. (2021) The impact of a minimum unit price on wholesale alcohol supply trends in the Northern Territory, Australia. Australian and New Zealand Journal of Public Health. URL: https://doi.org/10.1111/1753-6405.13055 . Stockwell, T., Zhao, J., Marzell, M., Gruenewald, P., Macdonald, S., Ponicki, W. & Martin, G. (2015). Relationships between minimum alcohol pricing and crime during the partial privatization of a Canadian government alcohol monopoly. Journal of Studies on Alcohol and Drugs, 76(4), 628-634. http://www.jsad.com/doi/abs/10.15288/jsad.2015.76.628 .
Sherk, A., Stockwell, T., April, N., Churchill, S., Sorge, J., & Gamache, P. (2020) The potential health impact of an alcohol minimum unit price in Québec: An application of the International Model of Alcohol Harms and Policies. Journal of Studies on Alcohol and Drugs, 81, 631–640. doi:10.15288/jsad.2020.81.631.
Griffith, R., O'Connell, M. and Smith, K. (2020) Tackling heavy drinking through tax reform and minimum unit pricing. Institute for Fiscal Studies, London, UK. URL: https://www.ifs.org.uk/publications/15183 .
Erickson, R., Stockwell, T., Pauly, B., Chow, C., Roemer, A., Zhao, J., Vallance, K. & Wettlaufer, A. (2018). How do people with homelessness and alcohol dependence cope when alcohol is unaffordable? A comparison of residents of Canadian Managed Alcohol Programs (MAPs) and locally recruited controls. Drug Alcohol Review, 37(S1), S174 – S183. URL:https://onlinelibrary.wiley.com/doi/abs/10.1111/dar.12649 .
Falkner, C., Christie, G., Zhou, L. and JKing, J. (2015) The effect of alcohol price on dependent drinkers’ alcohol consumption. New Zealand Medical Journal, Vol 128 No 1427: 18. URL: https://www.nzma.org.nz/journal-articles/the-effect-of-alcohol-price-on-dependent-drinkers-alcohol-consumption .

Gruenewald PJ, Ponicki WR, Holder HD, Romelsjo A. (2006) Alcohol prices, beverage quality, and the demand for alcohol: quality substitutions and price elasticities. Alcoholism, Clinical and Experimental Research. 30(1):96-105. Wagenaar A, Tobler A, Komro K. (2010) Effects of alcohol tax and price policies on morbidity and mortality: A systematic review. American Journal of Public Health, 100, 2270-8. Canadian Substance Use Costs and Harms Scientific Working Group (2020) Canadian substance use costs and harms (2007–2017). Prepared by the Canadian Institute for Substance Use Research and the Canadian Centre on Substance Use and Addiction. Canadian Centre on Substance Use and Addiction: Ottawa, ON. Ng Fat, L. and Shelton, N. (2012) Associations between self-reported illness and non-drinking in young adults. Addiction, 107(9): 1612-20. Bellis, M., Hughes, K., Nicholls, J., Sheron, N., Gilmore, I., Jones, L. (2016). The alcohol harm paradox: using a national survey to explore how alcohol may disproportionately impact health in deprived individuals. BMC Public Health 16.111. Health Scotland (2020) Minimum Unit Pricing of Alcohol. Evaluating the impacts on the alcoholic drinks industry in Scotland: baseline evidence and initial impacts. A report from Frontier Economics. URL: http://www.healthscotland.scot/media/2810/frontier-economics-mup-evaluating-the-impacts-on-the-alcoholic-drinks-industry-in-scotland.pdf . Stockwell, T., Sherk, A., Norstrom, T., Angus, C., Ramstedt, M., Andreasson, S., Chikritzhs T., Gripenberg, J., Holder, H., Holmes, J., Makela, P. (2018) Estimating the public health impact of disbanding a government alcohol monopoly: Application of new methods to the case of Sweden. BMC Public Health, 2018; 18: 1400. doi: 10.1186/s12889-018-6312-x. Ye, Y. and Kerr, W. (2016) Estimated increase in cross‐border purchases by Washington residents following liquor privatization and implications for alcohol consumption trends. Addiction, 111 (11).

Floor price for alcohol A floor price is a proven strategy to reduce the harm caused by the sale of cheap alcohol such as domestic violence, road crashes, and emergency department presentations. A floor price affects the cheapest alcohol being sold in order to protect people who are heavy drinkers from the makers and sellers of cheap alcohol that are targeting them with these products. The alcohol industry knows that the heaviest 10% of drinkers consume more than half of all the alcohol drunk in Australia, and that they are likely to be buying cheap products at the bottom end of the market.1
The cheapest alcohol, despite representing a small fraction of available products, is the cause of a disproportionate amount of alcohol-related harm.
Setting a floor price below which a unit of alcohol may not be sold is identified by the World Health Organisation (WHO) as one of the ‘best buys’ to reduce the harms from alcohol.2 The National Alcohol Strategy includes a floor price under Priority 2 as the responsibility of the state and territory governments.3
Scotland and Australia’s Northern Territory introduced a floor price in 2018, Wales did so in March of 2020, and Ireland’s comes into effect in January 2022. Other countries, such as some Canadian provinces and a number of Eastern European countries, have introduced floor price-like policies, although they fall short of an introducing an ideal floor price.
Research investigating the impacts of the floor price in Scotland, Wales, and the Northern Territory supports maintaining the floor price as an effective measure to reduce harm from alcohol and protect our communities from the harm caused by cheap alcohol.
A floor price has the greatest impact on the heaviest drinkers
The heaviest 10% of drinkers accounted for 54.4% of all alcohol consumed in Australia in 2016, tended to consume cheaper alcohol such as cask wine, and were more likely to drink at home than lighter drinkers.(Livingston)
A floor price helps reduce harm from the cheapest alcohol, such as cask wine, by increasing the lowest prices to reduce consumption.
Research into the impact of the floor price in Scotland and Wales found that, “reductions in purchases of alcohol as a whole were largely confined to households purchasing the largest amount of alcohol.”4
A floor price can reduce harm for individuals and society
The introduction of the floor price in the Northern Territory was followed by significant reductions in alcohol-related ambulance callouts, emergency department presentations, assaults, arrests, road crashes and child protection cases.5
In Scotland, the floor price was followed by a 10% reduction in alcohol-related deaths, the first in seven years, and considering the long-term nature of alcohol-related illness such as cancers and liver disease, the full impact of the floor price will take time to emerge.6

Furthermore, many people other people will experience the health and safety benefits from a floor price for alcohol because reduced alcohol consumption can contribute to safer roads and streets, more productive workplaces, and healthier friends, families, and communities.
Most consumers will not see a price difference
Most consumers will not notice a difference in price because the floor price will only impact the cheapest alcohol - a small percentage of all available products. Light and moderate drinkers rarely drink the very cheapest products and, even if they do, would be spending very little extra because they aren’t drinking much to begin with.(Livingston; Room)
The Scottish floor price was not undermined by neighbouring England’s lack of a floor price
Cross-border shopping has been shown to have very little impact on the effectiveness of a floor price.
Scottish alcohol retailers just north of the border “did not report any significant change in profitability, turnover or employment following the introduction of MUP [floor price].”7
That a floor price has been shown to reduce consumption, particularly in countries smaller than Australia with their close neighbour England lacking a floor price, means that cross-border shopping does not substantially undermine the policy.(Anderson et al.)
A floor price can have positive impacts for people experiencing disadvantage
Alcohol pricing policies may contribute to reducing socioeconomic health inequalities. While people in the most disadvantaged socioeconomic areas tend to drink at less risky levels than those living in the most advantaged, they tend to experience disproportionate harms from that consumption.8,9 Therefore, there are greater potential health gains from reducing alcohol consumption for people experiencing disadvantage who are heavy drinkers.10 The people currently experiencing the greatest amount of harm stand the most to gain from policies to protect them from the makers and sellers of cheap alcohol. A floor price is similar in principle to introducing a ‘sugar tax’, with the goal of increasing price to reduce consumption, and particularly reducing consumption amongst those at the highest risk of experience harm from the product. Tobacco control is another instance of government using price to reduce the consumption of a cancer-causing product. Furthermore, with regard to households that consume light or moderate amounts of alcohol, research examining the impact of the Scottish floor price found that “[t]he introduction of MUP [floor price] was not associated with an increased expenditure on alcohol by households that generally bought small amounts of alcohol and, in particular, those with low incomes.”(Anderson et al)

A floor price can help people who are dependent on alcohol
Because the floor price sets an absolute minimum under which alcohol cannot be sold, there are few alternatives short of making one's own alcohol or being prepared to drink non-beverage alcohol, which very few drinkers are prepared to do.11,12 Studies of how dependent drinkers cope when alcohol is unaffordable find that most common strategies reported involved drinking less, making existing supplies last longer, or going into treatment.(Falkner et al, 2015; Erickson et al, 2018) Very few members of this vulnerable group reported being prepared to resort to drinking non-beverage alcohol or committing crimes to access more money. Reductions in the volume and frequency of alcohol consumed can provide health benefits for people experiencing a dependence and accessing treatment is a best-case response to a rise in the price of the cheapest alcohol.
Australians support a floor price
The National Drug Strategy Household Survey 2019 asked respondents if they supported introducing a minimum unit price (floor price) for alcohol. 39% of respondents supported it while 27% opposed, and 33% neither opposed nor supported it. (NDSHS 2019) A floor price for alcohol may be poorly understood by the public right now, and the global alcohol industry actively works to spread disinformation about the impacts of the policy. Even so, there is support from the Australian public which could be further increased by improving understanding of what a floor price looks like in practice and spreading the truth about what the impacts in other countries have been.

References
1 Livingston M, Callinan S. 2019. Examining Australia's heaviest drinkers. Australian and New Zealand Journal of Public Health; 43:5. 2 World Health Organisation. 2017. Tackling NCDs: 'best buys' and other recommended interventions for the prevention and control of noncommunicable diseases. 3 Commonwealth of Australia. 2019. National Alcohol Strategy 2019-2028. 4 Anderson P, O'Donnell A, Kaner E, Llopis EJ, Manthey J, Rehm J. 2021. Impact of minimum unit pricing on alcohol purchases in Scotland and Wales: controlled interrupted time series analyses. The Lancet Public Health. 5 Coomber K, Miller P, Taylor N, Livingston M, Smith J, Buykx P, et al. 2020. Investigating the introduction of the alcohol minimum unit price in the Northern Territory: Final report. Geelong: Deakin University. 6 Alcohol Focus Scotland. 2021. Alcohol Deaths and Minimum Unit Pricing. Alcohol Focus Scotland, Edinburgh, Scotland. URL: https://www.alcohol-focus-scotland.org.uk/news/alcohol-deaths-and-minimum-unit-pricing/ 7 Health Scotland. 2020. Minimum Unit Pricing of Alcohol. Evaluating the impacts on the alcoholic drinks industry in Scotland: baseline evidence and initial impacts. A report from Frontier Economics. 8 Australian Institute of Health and Welfare. 2020. National Drug Strategy Household Survey 2019. Drug Statistics series no. 32. PHE 270. Canberra AIHW. 9 Roche A, Kostadinov V, Fischer J, Nicholas R. 2015. Evidence review: The social determinants of inequities in alcohol consumption and alcohol-related health outcomes. VicHealth. 10 Jiang H, Room R, Livingston M, Callinan S, Brennan A, Doran C, Thorn M. 2019. The effects of alcohol pricing policies on consumption, health, social and economic outcomes, and health inequality in Australia: a protocol of an epidemiological modelling study. BMJ open; 1:9(6). 11 Falkner, C., Christie, G., Zhou, L. and JKing, J. 2015. The effect of alcohol price on dependent drinkers’ alcohol consumption. New Zealand Medical Journal; 128:1427. 12 Erickson, R., Stockwell, T., Pauly, B., Chow, C., Roemer, A., Zhao, J., Vallance, K. & Wettlaufer, A. 2018. How do people with homelessness and alcohol dependence cope when alcohol is unaffordable? A comparison of residents of Canadian Managed Alcohol Programs (MAPs) and locally recruited controls. Drug Alcohol Review; 37:S1.

Questions on notice for the Queensland Mental Health Commission
Q: AOD trends during COVID, particularly crystal methamphetamine use Note about AOD trends: Because we don’t have Queensland-specific surveys, and the pandemic response (e.g., stay at home orders, density restrictions) was different between states, these trends may not be reflective of the experience in Queensland.
Alcohol
Different surveys produced different numbers, but roughly the same number of people reported either increasing or decreasing their alcohol consumption. The majority reported drinking the same amount.
However, some common reasons for people drinking more (stress, boredom, anxiety) suggest that alcohol was used as a coping mechanism and those may be at increased risk of harm from alcohol if they continue to rely on alcohol to manage similar feelings post-pandemic.
It is also worth noting that alcohol retail turnover for both 2020 and 2021 broke previous records, reaching $15.9 billion in 2021.
Other drugs
Trends in drug use depended on the drug in question. The use of some drugs such as cannabis generally increased during the pandemic, while the use of other drugs such as MDMA and cocaine declined.
Crystal methamphetamine was overall reported to decline by the National Wastewater Drug Monitoring Program however use appears to be slowly returning to pre-pandemic levels.
The ADAPT survey was conducted with people who use drugs at least monthly and found overall declines but some people reporting increases (graph below).

Among the police detainees who participate in the Drug Use Monitoring in Australia (DUMA), people reported both decreasing their use of methamphetamine in 2020 and that the drug market had been impacted by the pandemic. This was corroborated by participants in the ADAPT study, 46% of which reported that crystal methamphetamine was harder to obtain.
It is unclear how quickly drug markets will return to pre-pandemic levels as borders reopen and supply chains resume.
Q: Drug driving – is it increasing, or is testing improving, or both? Regular large-scale drink and drug driving testing was only done intermittently during the pandemic due to health concerns, according to the Queensland police annual report for 2020-21.
However, the 2018-19 report states that,
“QPS conducted more than 70,000 roadside drug tests, with approximately one in five drivers testing positive. This represents an increase of just over 4,000 tests from 2017-18. The QPS also expanded its roadside drug testing capability by increasing the number of officers trained to perform testing to 696. This is a significant increase from 276 officers in 2015-16 and 510 officers in 2016-17.”
This suggests that the likelihood of detection has increased as more officers are trained to perform the testing and more tests are conducted. This does not preclude the possibility of drug driving also increasing.
The dashboard from Austroads showing drug testing numbers and fatalities shows a decline from 2016 in fatal crashes when drivers had drugs in their system, however the data is missing for Queensland so this may not be reflective of the state: https://app.powerbi.com/view?r=eyJrIjoiZTdkODYyN2EtNTI5OS00ZWI1LWFkZjAtMjRiNWZhMGY4ZjNiIiwidCI6ImFhMjFiNjQwLWJhYzItNDU2ZC04NTA1LWYyY2MwN2Y1MTc4NCJ9
The National Drug Driving Working Group states that Australia has the most intensive roadside drug testing program in the world. This is interesting to consider in light of a publication from the Centre for Automotive Safety Research in South Australia which found that mimicking efforts to reduce drink driving for drug driving (methamphetamine specifically) were not effective in reducing cases.
Between 2008 – 2018 in South Australia, there were 28 cases of a fatal crash where the driver tested positive for methamphetamine. The report notes that “while roadside breath testing, legislative changes and increased monitoring have resulted in reduced levels of drunk driving, similar safety countermeasures have had negligible effects on MA [methamphetamine] use in drivers. Continued monitoring of MA use by drivers will, therefore, be necessary to assess the possible effects, or not, of new countermeasures.”
Q: Risky drinking and potential alcohol dependence The National Drug Strategy Household Survey 2019 responses indicate that 4.7 million people were using alcohol in a harmful or hazardous way and 1.6 million people were at high risk or alcohol dependent. Risk of dependence was assessed using questions from a brief alcohol screening tool, ASSIST-Lite.

Local Drug Action Teams Highlights Report 2021.

The Local Drug Action Team (LDAT) program fosters partnerships in communities across Australia, helping build knowledge and skills to address local issues associated with alcohol and other drugs (AOD), including methamphetamine (ice).
LDATs can be a mix of schools, educational institutions, health workers, police, community organisations, businesses and local government who unite to drive a community-led response.
The program emphasises building ‘protective factors’ in the community, working to prevent alcohol and drug issues starting in the first place.
In 2021, the ADF had an overwhelming response during the latest round of applications to enter the Program. There are now approximately 280 LDATs who are supported by the Alcohol and Drug Foundation (ADF) to work with communities and develop a Community Action Plan (CAP) to guide implementation of evidence-based activities to minimise AOD issues.
Although the effects of COVID-19 are still being felt across the nation this year, LDATs have shown incredible resilience, continuing to be a positive force in their communities. Through innovation, creativity and flexibility, they’ve adapted to these unpredictable times, continuing their important alcohol and other drug harm prevention activities.
Strengthening community-led prevention across Australia.
Local Drug Action Teams.
2

Community Hub
The ADF Community Hub has come a long way. What used to be a resource supporting our Local Drug Action Teams has transformed into one that is designed to support a broader range of groups and individuals looking to make a difference in their communities.
The online hub houses a suite of evidence-based information and resources, including toolkits, local government tools and guides, case studies, promotion guidelines and more.
Many people recognise the harms alcohol and other drugs can cause in the community and want to do something about it, but aren’t sure where and how they can start.
That’s why the ADF has made the Community Hub’s evidence-based and simple-to-use resources freely available to all, to help people develop and deliver primary prevention projects in their local area.
community.adf.org.au
279LDATs
91PROGRAM RESOURCES
17 webinars8 resources13 toolkits
3 stakeholder kits50 case studies and stories
11.2mGrant funding
allocated
45%Major citiesof Australia
27%Inner regional
Australia
19%Outer regional
Australia
4%Very remote
5%Remote
320CAPs completed
445CAPs currently being
delivered or completed
1600Partner organisations
1950Total organisations
4949+Media stories
Protective factors
Alcohol and other drug (AOD) issues can change at different stages in people’s lives. Each life stage carries with it different protective factors, which either increase or decrease a person’s chance of developing or being impacted by AOD issues. Local Drug Action Teams work to improve protective factors for their identified target audience in the community.
3

Local Drug Action Teams.
4
Connection To Community. Our Youth Matters LDAT, QLD
Protective factorSense of connectedness to community, school and family
This protective factor is particularly important for people aged between 0 to 17 years old, but applies to all age groups.
Partner organisationsQLD Program of Assistance to Survivors of Torture & Trauma, 99 Steps, MyQ (Multicultural Youth Queensland) and ETHNI.
Target audienceYoung women aged 14 to 25 years from intercultural backgrounds living in Brisbane and its surrounds.
Local challengeRefugees often experience traumas that have long-lasting effects on their lives. Increasing community strength is a vital element of the recovery process. A group of young women, mainly from African backgrounds, approached the LDAT to form a partnership to address issues affecting their communities.
They wanted to be change agents and, together with their peers, gain the skills and confidence to talk to elders, family members and other leaders about topics like healthier relationships, substance use and hygiene. The team’s aim was to build a network of women empowered to act on emerging needs in their communities and support positive cultural change.
SolutionThe LDAT, working with all their partners, were able to support the ‘Girls Leading Our World’ (GLOW) initiative which promotes resilience and social connection in refugee communities through healthy role modelling.
GLOW leaders recruited young women from South Sudan, Burundi, Afghanistan, Sri Lanka and Eritrean backgrounds to participate. Training sessions were held on personal growth, leadership and communications across communities. A workshop facilitated by 99 Steps taught the girls about positive relationships and connection to community as key protective factors against alcohol and other drug harm. They also learnt how to approach school leaders to start up programs on sexual and reproductive
health. Fun picnics in the park encouraged group togetherness and peer support, encouraging and developing young leaders to achieve positive health outcomes.
ImpactThe program delivered five workshops and a camp with 22 peer leaders.
Evaluation showed that participants increased their understanding of the tell-tale signs of toxic versus healthy relationships, both with people and substances. They now can discuss alcohol and other drug issues in an informed way in their communities. The Girl Talk program about sex, relationships and personal identity is being used in a handful of local schools. Links have been made with culturally responsive services that understand the complexities of refugee situations.
The growing GLOW network actively helps refugee communities feel more empowered and connected. More open discussions take place with new ideas put forward to elders and other leaders. Whilst many of the GLOW young women had a voice, they didn’t know where it could take them. With the success of this program, they now know.

5Around Australia Local Drug Action Team snapshots
AfriConnect LDAT, VICThe Ubuntu Peer-to-Peer Leadership Project builds on the work that was delivered by a group of ten young Africans aged 18 to 36 years old during Victoria’s first extended lockdown in 2020. They provided community outreach through phone calls. The peer leaders are now participating in training and workshops to increase their knowledge around AOD and mental health. They’re creating appropriate health messaging for African communities, with the aim of breaking down some of the stigma and barriers that prevent young people from accessing support services.
Broome LDAG LDAT, WAThis LDAT operates in rural WA with cultural camps for Aboriginal and Torres Strait Islander men. Camps are held out on country to provide a culturally safe place for men to discuss key points around current men’s health issues. The camp in partnership with the Looma community had 32 attendees, including the Nyikana-Mangala Kimberley Land Council rangers. The rangers added some much-needed cultural factors to the event with the strong knowledge of country and skill that they passed on to the young men. The Ardyaloon community decided to host the camp at Pender Bay after engaging with the local men’s group during previous visits to the community.
[The program] opened their eyes up to what they can do with their skill set.
Image: AfriConnect mothers group

Local Drug Action Teams.
6
Education. Staying Strong in the City LDAT, SA
Protective factor
Evidence-based drug education
This protective factor positively impacts people aged between 6 to 30 years old.
Partner organisations Flinders University Wellbeing Centre, Iwiri Aboriginal Corporation, WalkAlong Initiative, Department of Education and the Pennington Children’s Centre.
Target audience Children aged 12-17 years and their parents and carers from the Pitjantjatjara-Yankunytjatjara community in Adelaide.
Local challenge Central to Pitjantjatjara-Yankunytjatjara culture is the multi-generational and extensive family unit. In the past few years, families have become dispersed across Adelaide suburbs, leaving them feeling unsupported and isolated. School problems, low self-esteem and rising anxiety have led to young people’s increased risk of alcohol and cannabis use. The community has also experienced family breakdowns between adolescents and their parents or caregivers. In the Pitjantjatjara culture, substances like alcohol and marijuana have no place.
The community wanted a positive approach to addressing the issues with their young people. The challenge was to provide preventative and harm minimisation activities and messages tailored for these young people.
Solution Cultural input from partner organisations helped develop family-centred community building activities including evidence-based drug education. Young people needed reinforcement and exposure to the possibilities of a hopeful future as a means of preventing alcohol and cannabis use.
Forums were held where adolescents spoke about their aspirations and had supported group discussions about their challenges. Parent and caregiver forums discussed parenting as a protective factor and the importance of supporting teenagers during adolescence. Parents also discussed their ambitions for their children and the barriers to overcome. The project culminated in a two-night bush retreat where families were brought back together after a very isolating year in 2020.
Impact The activities educated Pitjantjatjara families about the risks of alcohol and cannabis and, at the same time, enhanced young people’s sense of self-esteem, building cultural identity, and strengthening family connections.
The program was well-received by parents and caregivers who felt it was delivered in a culturally appropriate way.
The bush getaway was very popular with the families who felt they could relax and enjoy being with their children, in contrast to their hectic city lives. With their newly gained knowledge, the program’s participants are potential role models for other families.
Image: Staying Strong in the City family activities

7Around Australia Local Drug Action Team snapshots
Brighton Community Action Group, TAS This Tasmanian LDAT has targeted parents for their AOD education activities. Their most recent Community Action Plan saw the creation of a storybook for parents to use when discussing methamphetamines with young people. Lead partner, Drug Education Network (DEN), has now published the book, making it accessible to a wider audience.
NSW’s Sexuality and Gender Diverse Communities LDAT, NSWHarm reduction training for LGBTIQ+ people is the focus for this team. The training enables participants to attend events and feel connected, without using AOD. The harm reduction training increases their knowledge of AOD effects and issues. Trainees are then able to act as peer support leaders, providing drug education at events.
Once you focus on what is important then your mind can heal.

Local Drug Action Teams.
8
Knowledge. Communities That Care Alpine LDAT, VIC
Protective factor
Knowledge of harms/health beliefs that support healthy AOD use and the supports available in the AOD space
This protective factor applies to people aged 6 years and up.
Partner organisations Alpine Health, Myrtleford P-12 College and Myrtleford Saints Football Netball Club.
Target audienceClub senior players, coaches, members, administration staff, supporters and the wider Myrtleford community.
Local challengeIn a region hit hard by the Black Summer bushfires and then affected by the COVID-19 pandemic and its economic challenges, it’s no wonder that many Alpine Shire residents were feeling anxious and disconnected.
The local sports community saw that some of its football and netball club members were struggling with their mental health and not seeking help, which is a risk factor for issues with AOD. A prevention approach was needed to normalise discussions
about mental health, reduce its stigma and provide pathways to local services. This would also help to ease the burden on the overstretched local health system.
Solution In a grassroots initiative, the community came together to launch the Myrtleford Football Netball Club (MFNC) Wellbeing Team on World Mental Health Day 2020 via a video message on the club’s Facebook page.
The Wellbeing Team, which consists of club leaders, health professionals and supporters, have all completed Youth Mental Health First Aid training and are skilled up to recognise when someone needs help, including with alcohol and drug issues, and how to encourage them to take action. All wellbeing officers are connected through the club’s Facebook page and can be quickly contacted via FB messenger. Posters and banners around the club help to get people talking about the issue.
With the 2021 season on hold due to COVID-19 restrictions, the club’s wellness activities continue to be front and centre with online quizzes, fitness challenges, monthly communications, videos and use of the hashtag #bekindtoyourmind.
A highlight has been the introduction of a mental health round, now a permanent fixture for the Ovens Murray Football Netball League. This year’s guest speakers were
former AFL player, Glenn Manton, and basketballer and Olympian Lauren Jackson AO. The club has also coordinated wellbeing panel discussions with other community sports clubs.
MFNC was already a member of the Alcohol and Drug Foundation’s Good Sports program, Australia’s largest community sporting health program. The Good Sports mental health support module was an important source of information leading up to the Wellbeing Team’s establishment.
Impact The project has inspired positive change and helped build strong connections, vital to the Myrtleford community’s ongoing recovery and wellbeing.
The overwhelming response to the videos and subsequent conversations has provided all the Wellbeing Team members with opportunities to engage in meaningful conversations.
A sustainable and transferable model has been created through a robust governance structure, capacity building, communications and partnership development. New partnerships developed include local sports schools and GP practices, as a member of the Wellbeing Team is a local GP.
The initiative is attracting increasing interest from other clubs around the state.
Image: MFNC Wellbeing Team

9Around Australia Local Drug Action Team snapshots
Life it’s in Your Hands, QLDThis LDAT brings together at-risk young people into a youth hub, giving them the opportunity to strengthen their community connection and prevent the early uptake of alcohol and other drugs through a range of activities. These activities will use opportunities to connect youth and parents. A strategic plan aiming to open lines of communication, develop referral pathways to support and identify gaps and solutions in service delivery will also be developed through collaborating with community partners.
Brookton Pingelly LDAG LDAT, WABased in the Southern Wheatbelt area of Western Australia, the group runs youth recreation activities with a focus on linking in with mental health services. This increases the young people’s access to, and knowledge of, AOD and mental health support services. The LDAT is running a calendar of subsidised activities to engage young people, free bus transport to activities around the region and is developing a wallet card outlining available support services to be distributed through partner organisations.
It’s taken too long to be able to have these conversations.- Lauren Jackson AO
Olympian and basketballer

Local Drug Action Teams.
10
Belonging. Healthy Glenelg LDAT, VIC
Protective factor
Sense of belonging and engagement with community
This protective factor applies to all age groups.
Partner organisationsWestern District Health Service (Southern Grampians Glenelg Primary Care Partnership), Glenelg Shire Council, Portland District Health, Glenelg Southern Grampians Local Learning and Employment Network, Heywood and District Secondary School and Portland Aluminium.
Target audience Same-sex attracted and gender diverse teens aged 12-17 years living in the Glenelg Shire in south western Victoria.
Local challengeAffected by ongoing COVID-19 restrictions, an LGBTQIA+ youth support group in Portland, called the Skittles, were feeling isolated, disconnected and stigmatised. With high levels of underage drinking in the community, there was an urgent need to boost the group’s social connections, knowledge about mental health and wellbeing and the local support services available. Prejudice and discrimination on the basis of being LGBTQIA+ can reduce a person’s self-esteem and lead to a higher likelihood of mental health problems and risky behaviours with alcohol and other drugs.
SolutionA sense of belonging to a group or community, inclusivity and engagement are essential protective factors for alcohol and other drug use. The Skittles group and their friends were engaged through the Safe and Supported program, a series of online and face-to-face
information sessions on adolescent health and wellbeing which also provided an opportunity to socialise with like-minded teens.
Presenters included local mental health support services, alcohol and other drug services and community guest speakers. Peer-led sessions were the most popular as attendees could relate to the facilitator’s real-life experiences with alcohol dependency. The sessions also aimed to increase the capacity of some Skittles members to present on the topics. By using a peer support model and service providers, there was potential to support connections between young people and also with the service providers.
In 2021, the Skittles continue their good work by taking a rainbow bus around the Shire, organising recreational and other activities for local youth. The messages they carry around include awareness about the importance of mental health, the impacts of alcohol and other drugs, and pathways for accessing support.
Impact on the communityThe program provided an inclusive social environment for same-sex attracted and gender diverse people to feel like they belong. More than 40 young people attended the sessions and reported that they increased their knowledge about help services and alcohol and other drugs, felt socially supported and more competent to facilitate peer-led sessions. Learnings from the program will continue to be spread around the region as the Skittles continue their travels and celebrate diversity and inclusivity.
Images: Skittles picnic

11Around Australia Local Drug Action Team snapshots
Huon Valley LDAT, TASAs part of activities leading up to Tasmanian Youth Week, this LDAT partnered with Huon Valley Council to create a five-minute video that will be part of the Huon Beings series. It’s driven by the Council’s Youth Committee who wanted to share their stories of living in the Valley and talk about their strengths. They identified that they wanted to change the community’s views of young people so that they can be more valued members.
Katherine LDAT, NTThe Katherine LDAT carried out a positive narratives project with Aboriginal and/or Torres Strait Islander young people from Katherine and surrounding communities. A series of storytelling workshops incorporated art, photos, video and social media to share positive stories. The project helped young people in the community to feel heard and gain a stronger sense of belonging.
Image left: Shae Collis from the ADF with Mitch Robson of Huon Valley Council Image right: Katherine LDAT positive narratives project

Local Drug Action Teams.
12
Social Activities. MNC Youth Pathways LDAT, NSW
Protective factor
Participation in positive social activities
This protective factor positively impacts people aged 12 years and up.
Partner organisationsRegional Development Mid North Coast, Arts Mid North Coast, Lifetime Connect, Uniting Care, Nambucca Valley Youth Services, Macksville High School, The Music Station, Cranbourne Music and Headspace.
Target audienceLocal Nambucca Valley teens aged 13 to 17 years old.
Local challengeWhile sport is very popular in small regional and rural towns, young country people passionate about the creative arts often can’t access programs or industry pathways for employment. Youth in Macksville were interested in playing music, which is well known to have positive
effects on mental health and emotional wellbeing. They needed a safe and supported space where they could come together to develop their skills and be guided by trusted adults.
Solution The Ready Set Go Music Youth Mentorship Program was set up to not only teach young people performance skills but introduce them to all aspects of the industry. Held at the Music Station live venue, fortnightly workshops gave 28 young locals the opportunity to tap into the knowledge and networks of local music professionals.
The program covered industry career pathways such as performance, sound production and stage and events management. Through workshops, the participants learnt about having First Aid available at events, how to manage patrons’ alcohol and drug consumption and how to build resilience and support among their peers. Information was provided about support services available in the broader community such as mental health, crisis accommodation and youth services.
Impact All the approaches have contributed to building Macksville youth’s protective factors and including resilience. As well as gaining hands-on experience playing music, participants reported an increase in their confidence and peer support circles and networks. Being able to share their journey with their families and friends at the final music performance increased their positive connection with the wider community.
The guest talks provided insights into careers and job-seeking support services. These connections also formed potential partnerships for future projects.
Media publicity about the program gained the attention of local musicians and regional music events and groups, who have employed some of the teens or provided work experience opportunities.
The program’s participants have now formed the Creative Youth Council and become a partner in the LDAT.
Image: MNC Youth Pathways performance

13Around Australia Local Drug Action Team snapshots
West Belconnen LDAT, ACTFocusing on young people, this LDAT runs regular gardening and cooking projects to involve participants in positive social activities. Gardening and cooking lessons are used as a way to support local Year 6 students to transition to secondary school with increased confidence, self-worth and connection.
Palmerston Youth LDAT, NTCurrently in progress, the LDAT’s Community Action Plan is focused on providing media training for young people in Palmerston to create messages and tell their stories. These stories will be shared through social media platforms with the target audience being young people’s peers, community members and media outlets. The project is open to all local young people, however it has a specific focus on the most vulnerable young people in the community.
I’ve gotten a lot more
comfortable with myself...
and more confident.

Planet Youth in Australia.
Local Drug Action Teams.
14
The Planet Youth model is now being implemented in over 30 countries worldwide. It was developed in Iceland over 20 years ago and has been highly successful in improving wellbeing and reducing rates of alcohol and other drug use amongst young people in Iceland.
The Alcohol and Drug Foundation is working with the Planet Youth Iceland team to trial the evidence-based approach with a small number of LDATs as pilot sites over two-and-a-half years.
The LDATs participating in the Planet Youth pilot in NSW and SA use local findings from the Planet Youth Year
10 surveys to engage with parents, schools, and other community partners. This engagement results in the planning and development of local Community Action Plans that help increase the protective factors in the environment of a young person to prevent the early uptake of alcohol and other drugs.
Known protective factors for the secondary school age group include positive role models, sense of belonging and connectedness to community, school and family, participation in positive activities with adult engagement and involvement in recreational activities.
Image: Limestone Coast LDAT lead Sophie Bourchier

ThenThe need to do something about substance use on the Limestone Coast in South Australia started out with a series of community education forums about crystal methamphetamine (ice) and community resilience in 2018.
With a growing number of teens engaging in risk-taking behaviours in this regional area, the newly formed LDAT recruited secondary schools in five key locations to participate in the evidence-based Climate Schools education program.
Climate Schools works to reinvigorate the school climate around alcohol and drug education, using online health education modules that have been proven to reduce harm and improve wellbeing, setting students up to make positive and informed choices.
Students co-designed presentations for parents on alcohol and other drug harm prevention using their familiar teen language. Older students share knowledge and provide peer leadership to younger students.
The LDAT’s activities have expanded from one council area to seven council areas. All Year 10 students on the Limestone Coast have completed Climate School’s Year 10 module.
NowThis successful partnership approach has taken another step with the LDAT now trialling the Planet Youth model from Iceland, as part of the Alcohol and Drug Foundation’s Australian pilot, which is being executed through seven LDATs in New South Wales and South Australia.
The Limestone Coast pilot kicked off with the Planet Youth student survey to inform community-led action on the ground. Around 270 Year-10 students from four schools responded to questions about substance use, health, mental health, physical activity, family and school experience, internet use and bullying. The data collected showed that the key risk factors for the young people were unsupervised hours and drinking at other homes.
This led to the development of a communications campaign, educating parents about the importance of family time as a protective factor. In addition, all seven Limestone Coast councils and School Parent Governance Groups were engaged around the risk factors from the survey findings and provided with guidelines on building up the protective factors for young people.
Through the Planet Youth model and LDAT activities, the LDAT has seen increased parent and carer involvement and more youth participating in extracurricular activities. While it’s early days, the pilot is demonstrating effectiveness in reducing substance use initiation. Next steps in the trial are more education opportunities and building up parental engagement and networks.
The LDAT is led by Substance Misuse Limestone Coast and the partners are the City of Mount Gambier, District Council of Grant, and Sport and Recreation – Limestone Coast Local Government Association. Through the current Planet Youth engagement, parents and other Limestone Coast councils have expressed an interest in becoming part of the LDAT. Wellbeing SA has contributed funding to support the extension of the trial.
Then and Now. Limestone Coast LDAT, SA 15

Local Drug Action Teams.
16
Welcoming 47 new LDATs in 2021
In early 2021, applications opened for the fifth funding round of the Local Drug Action Team program. There was a high level of interest from across all states and territories, with 99 applications in total received. After a thorough assessment process, 47 new LDATs were accepted into the program. Of these, seven are led by, or have as a partner, Aboriginal and/or Torres Strait Islander organisations.
As the first step in the program, each new LDAT develops and submits a Community Action Plan to address a local concern, which is identified through community consultation. LDATs may receive additional funding to help deliver their prevention activities.
Here’s a sample of some of the fantastic new LDATs who have joined the program.

994707
17
Aboriginal and Torres Strait Islander-led LDATs
Successful LDATs
Applications

Boyup Brook Community Mental Health Action Team Outer regional WAWith the goal of providing ongoing support for the regional community, particularly preventative programs for youth, the LDAT plans to focus on increasing mental health awareness and creating opportunities for social inclusion and connectedness.
A brighter future for CALD youth Metropolitan QLDTackling issues affecting young people from migrant backgrounds, including local and international students, is key for this LDAT. It aims to improve knowledge and reduce stigma by inspiring these young people to create a safe environment to share and reflect on alcohol and drug use in the community and empower them to seek help when needed.
Derwent Valley LDAT Regional TASBuilding on Anglicare Tasmania’s existing partnerships for the My Safe and Strong Families program (which has been operating in the Derwent Valley for five years), the LDAT aims to increase protective factors for families and youth in the community, to prevent and reduce harm from alcohol and drug use.
Celebrating new LDATs in 2021
Local Drug Action Teams.
18

Live4Life Central Goldfields School and Community Partnership Group Regional VICThe Live4Life prevention model will be further rolled out by the LDAT. It focuses on a community partnership, peer-led model which involves positive mental health messaging and education in schools and community groups (recreation, Guides, Scouts, etc.). The model increases protective factors by building the capacity of individuals, their peers, and adults in their lives to support them when in need.
Multicultural Men’s LDAT Metropolitan SAThe local Multicultural Men’s group links to many CALD communities where men are feeling increasingly under pressure and stressed around balancing work, family, and community needs. This group focuses on improving mental health and wellbeing - which includes addressing men that use drugs and alcohol as a coping strategy for their personal challenges. The LDAT will identify issues around youth drinking and a lack of strong role models and protective factors within the community context.
Not So Straight Up Metropolitan ACTThis LDAT will work to help sexuality and gender-diverse people and people with HIV, reduce the harms associated with the use of alcohol and other drugs. It will work with communities and people with lived experience to identify and design primary prevention activities and support services.
Condobolin ‘Men-to-ring’ around us Outer regional NSWThe intention is to develop leadership capacity in the community through a mentoring program, focused on engaging local elders and the community to be trained as mentors. These mentoring relationships will be a tool to help prevent or delay the use of drugs and alcohol in adolescence and young adulthood.
Growing Strongbala Way with the Banatjarl Strongbala Wimun Grup Remote NTThis LDAT will aim to reconnect community to ‘Wanga and Lirriga’, a significant songline corroboree of this region which is specifically focused towards connection and healing on country, as well as healing of people and community. The dances carry cultural law and impart knowledge that gives pathways for cultural healing, strengthening identity and belonging as well as connecting communities.
Hills Flourish Regional SAThe LDAT plans to support the development of protective factors within the community, particularly in young people aged 12+, that will prevent and minimise young people starting to use alcohol and other drugs.
19

Local Drug Action Teams.
20
Alcohol and Drug Foundation
community.adf.org.au
P 03 9611 6100
adf.org.au
twitter.com/AlcoholDrugFdn
facebook.com/AlcoholDrugFdn
Published October 2021