
mHealth adoption in low-resource environments: A review of the use of mobile healthcare in...
55
This article was downloaded by: [155.69.107.234] On: 28 March 2014, At: 02:09 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Health Communication: International Perspectives Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/uhcm20 mHealth Adoption in Low-Resource Environments: A Review of the Use of Mobile Healthcare in Developing Countries Arul Chib a , Michelle Helena van Velthoven b & Josip Car a b a Nanyang Technological University , Singapore b Global eHealth Unit, Department of Primary Care and Public Health , Imperial College London , London , United Kingdom Published online: 27 Mar 2014. To cite this article: Arul Chib , Michelle Helena van Velthoven & Josip Car (2014): mHealth Adoption in Low-Resource Environments: A Review of the Use of Mobile Healthcare in Developing Countries, Journal of Health Communication: International Perspectives, DOI: 10.1080/10810730.2013.864735 To link to this article: http://dx.doi.org/10.1080/10810730.2013.864735 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Transcript of mHealth adoption in low-resource environments: A review of the use of mobile healthcare in...

This article was downloaded by: [155.69.107.234]On: 28 March 2014, At: 02:09Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Health Communication:International PerspectivesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/uhcm20
mHealth Adoption in Low-ResourceEnvironments: A Review of the Useof Mobile Healthcare in DevelopingCountriesArul Chib a , Michelle Helena van Velthoven b & Josip Car a ba Nanyang Technological University , Singaporeb Global eHealth Unit, Department of Primary Care and PublicHealth , Imperial College London , London , United KingdomPublished online: 27 Mar 2014.
To cite this article: Arul Chib , Michelle Helena van Velthoven & Josip Car (2014): mHealth Adoptionin Low-Resource Environments: A Review of the Use of Mobile Healthcare in Developing Countries,Journal of Health Communication: International Perspectives, DOI: 10.1080/10810730.2013.864735
To link to this article: http://dx.doi.org/10.1080/10810730.2013.864735
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

1
Journal of Health Communication, 0:1–53, 2014Copyright © Taylor & Francis Group, LLCISSN: 1081-0730 print/1087-0415 onlineDOI: 10.1080/10810730.2013.864735
Arul Chib and Michelle Helena van Velthoven are co–first authors.Address correspondence to Arul Chib, Nanyang Technological University, 31 Nanyang
Link, WSCI Building, Singapore 637718. E-mail: [email protected]
mHealth Adoption in Low-Resource Environments: A Review of the Use of Mobile Healthcare
in Developing Countries
ARUL CHIB
Nanyang Technological University, Singapore
MICHELLE HELENA VAN VELTHOVEN
Global eHealth Unit, Department of Primary Care and Public Health, Imperial College London, London, United Kingdom
JOSIP CAR
Nanyang Technological University, Singapore, and Global eHealth Unit, Department of Primary Care and Public Health, Imperial College London, London, United Kingdom
The acknowledged potential of using mobile phones for improving healthcare in low-resource environments of developing countries has yet to translate into significant mHealth policy investment. The low uptake of mHealth in policy agendas may stem from a lack of evidence of the scalable, sustainable impact on health indicators. The mHealth literature in low- and middle-income countries reveals a burgeoning body of knowledge; yet, existing reviews suggest that the projects yield mixed results. This article adopts a stage-based approach to understand the varied contributions to mHealth research. The heuristic of inputs-mechanism-outputs is proposed as a tool to categorize mHealth studies. This review (63 articles comprising 53 studies) reveals that mHealth studies in developing countries tend to concentrate on specific stages, principally on pilot projects that adopt a deterministic approach to technological inputs (n = 32), namely introduction and implementation. Somewhat less studied were research designs that demonstrate evidence of outputs (n = 15), such as improvements in healthcare processes and public health indicators. The review finds a lack of empha-sis on studies that provide theoretical understanding (n = 6) of adoption and appro-priation of technological introduction that produces measurable health outcomes. As a result, there is a lack of dominant theory, or measures of outputs relevant to making policy decisions. Future work needs to aim for establishing theoretical and measure-ment standards, particularly from social scientific perspectives, in collaboration with researchers from the domains of information technology and public health. Priorities should be set for investments and guidance in evaluation disseminated by the scientific community to practitioners and policymakers.
The growing evidence for the use of mobile information and communication tech-nologies and mobility of information in healthcare (called mobile health or mHealth) has attracted the attention of practitioners, researchers and policymakers globally
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

2 A. Chib et al.
(Free et al., 2010; Leslie, Sherrington, Dicks, Gray, & Chang, 2011; Vodafone, 2006; Waegemann, 2010). Mobile phones have the potential to revolutionize healthcare, par-ticularly in low-resource settings of low- and middle-income countries where health-care infrastructure and services are often insufficient (Kahn, Yang, & Kahn, 2010).
Pilot mHealth projects have shown that, particularly in developing countries, mobile phones improve communication and information-delivery and information-retrieval processes over vast distances between healthcare service providers and patients (Tamrat & Kachnowski, 2012). Mobiles provide remote access to healthcare facilities, facilitate trainings for, and consultations among, health workers, and allow for remote monitoring and surveillance to improve public health programs. This phe-nomenon has the potential to lead to an overall increase in the efficiency and effective-ness of under-resourced health infrastructures, ultimately translating into benefits for patients (Bloch, 2010; Ranck, 2011).
In general, however, the scalability of mHealth projects from pilot projects to large-scale nationwide implementation has been low (Ping, Wu, Yu, & Xiao, 2006; World Health Organization, 2011b) with the available evidence proving insufficient to persuade key policymakers and health practitioners (Mechael et al., 2010). Among the reasons for this state of affairs are first, the lack of an ample evidence base, which is understandable for a nascent discipline; and second, a lack of clarity in organiz-ing the evidence to distinguish particular investigative approaches to mHealth, chief among which are the broad domains of technology development, social science, and public health. To resolve these issues, this article aims to investigate prior mHealth reviews and conduct a comprehensive literature review, organizing the studies in a logical framework. In the next paragraph of this section, we provide an overview of the prior mHealth reviews, and then in the Methods and Results section of this article, we describe the assessment of individual studies.
Review of Literature
Recent reviews of mHealth provide a range of analyses focusing on particular techno-logical features, process improvements in healthcare service delivery, and behavior change and healthcare outcomes. As background to this review, we examine these mHealth reviews, noting the number of studies included in parentheses (n) as a measure of scope.
The mHealth literature focusing on developing countries has certainly flourished in recent years. While the mHealth field may no longer comprehensively suffer from Kaplan’s (2006) accusation of having “almost no literature on using mobile telephones as a healthcare intervention [in developing countries]” ; also see SMS literature sub-sequently cited); more recent reviews point to similar concerns (Gurman, Rubin, & Roess, 2012 [n = 16]; Mechael, et al., 2010 [n = 145]).
From a thematic perspective, overview studies and reviews of mHealth globally have developed lists of notable technological features of project implementation (Fjeldsoe, Marshall, & Miller, 2009 [n = 14]; Gurman et al., 2012 [n = 16]; Klasnja & Pratt, 2012 [total number unstated]; Patrick, Griswold, Raab, & Intille, 2008 [total number unstated]), or process improvements such as healthcare service delivery (Blynn & Aubuchon, 2009 [total number unstated]; Mechael et al., 2010 [n = 145]). However, making the theoretical link to effectiveness, namely behavior change or health outcomes, has been less explicit.
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 3
A subset of mHealth reviews focus on SMS, or mobile texting, yet find little rigorous evidence of effectiveness (Fjeldsoe et al., 2009 [n = 14]; Lim, Hocking, Hellard, & Aitken, 2008 [n = 9]), with a few more recent studies focusing on developing coun-tries (Cole-Lewis & Kershaw, 2010 [n = 12]; Deglise, Suggs, & Odermatt, 2012 [n = 34]). Despite lack of evaluation of effectiveness, these earlier reviews suggest partial posi-tive evidence of the effect of text messages. Recent ones are more mixed, noting both substantial (Guy et al., 2012 [n = 18]; Krishna, Boren, & Balas, 2009 [n = 25]), and limited effects on improving healthcare service delivery (de Jongh, Gurol-Urganci, Vodopivec-Jamsek, Car, & Atun, 2012 [n = 4]; Gurol-Urganci, de Jongh, Vodopivec-Jamsek, Car, & Atun, 2012 [n = 1]), and patient care (de Tolly, Skinner, Nembaware, & Benjamin, 2012 [n = 2]; van Velthoven, Brusamento, Majeed, & Car, 2013 [n = 21]). Overall, we conclude that technology introduction and implementation and health-care process improvements have been emphasized in the scientific literature. Less well understood in comparison are mechanisms of adoption and appropriation of technol-ogy at individual and sociocultural levels of analysis.
Researchers have regularly called for theoretically based interventions, suggest-ing the increased likelihood of meeting success criteria (Krishna et al., 2009), yet few reviews examine the role of theory in mHealth projects. A majority of the reviews chose to use methodological standards as an exclusion criteria, limiting the reviews to randomized control trials found within the peer-reviewed literature, mostly upheld as the gold standard, sometimes adding experimental/quasi-experimental research designs. Others used broader inclusion criterion, including all methodologies, as well as drawing from the grey literature.
Aim of This Review
Our overview of reviews showed that though the body of mHealth knowledge is grow-ing and studies have shown potential to improve healthcare, the current evidence is not convincing enough for policymakers. The reviews found mixed results and lack the ability to show robust evidence. The main focus of studies has been on inputs, while research in mechanism factors and underlying theory is missing. Therefore, the fundamental aim of this review is to identify, define, and examine factors of inputs, mechanisms, and outputs, of mobile phones for healthcare workers and patients in low- and middle-income countries. Our objectives were to determine the relative value of research approaches within this linear model, propose recommendations that allow for collaborative research, as well as foster discussion and debate about the relative value of specific approaches to influencing practice and policy. We do this by investi-gating a large number of studies, covering inputs, mechanism, and outputs, and incor-porate both quantitative and qualitative evidence.
Method
Approach
This review article used a deductive approach addressing some of the issues outlined. First, we demarcated the boundaries of the investigation to mHealth studies con-ducted within developing countries, aiming, however, to cover a broader spectrum of articles than those found previously. Second, we focused on all aspects, inputs, mechanism and outputs, as we argued that the investigation of the mechanisms of
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

4 A. Chib et al.
adoption and appropriation of technology using social scientific methods is equally important as evidence for effective technology introduction and implementation, and public health outputs, such as process improvements and patient healthcare indica-tors. Last, given the call for more nuanced methodological approaches (Mechael et al., 2010), we broadened the review to multiple methods of investigation of the mHealth phenomenon.
We propose a pathway of research focus for mHealth studies as a heuristic within which to situate this review (Klasnja & Pratt, 2012; Thomas & Harden, 2008). We cat-egorized the studies under the inputs-mechanism-outputs pathway shown in Figure 1, mapping onto a linear system of investigation within the mHealth field, which are often conflated.
Inputs include factors such as technology access and use vital to technology devel-opers and practitioners who implement mHealth projects within beneficiary commu-nities. Mechanism factors such as psychosocial influences and individual preferences offer explanatory value to understand technology adoption. Last, Outputs include healthcare process factors, including efficiency measures within the health system such as data-management and treatment adherence; and effectiveness measures of patient healthcare factors, defined as behavior change or public health indicators within the beneficiary population. While the silos of technology development-social science-public health domains introduced earlier might seem to map onto this categorization simplistically, such a framework does allow for determining the relative focus of prior research investigations in the field.
Inclusion and Exclusion Criteria
We included research articles fulfilling the following inclusion criteria: those that studied the use of mobile phones in healthcare, focused on patients or healthcare workers, and were undertaken in low-income and low- and upper-middle-income countries as categorized by the World Bank (2012). We included peer-reviewed and non–peer reviewed literature. We considered articles in all languages, but we only found articles in the English language. We excluded research which studied other mobile devices than mobile phones, did not focus on health or was undertaken in high-income countries.
Review Methods
We based our methods on the Cochrane Collaboration systematic review method-ology (Higgins & Green, 2011) and qualitative review methodology (Ring, Ritchie, Mandava, & Jepson, 2010; Sandelowski & Barroso, 2002; Thomas & Harden, 2008). Briefly summarized, this includes defining the review question and developing criteria for inclusion and exclusion of studies, a high sensitivity search for studies, selection and data extraction using a standardized form, and considering meta-analysis when appropriate or a narrative assessment.
Search Methods
One author (M. H. van Velthoven) used mHealth related search terms (phon*, mobil*, mhealth, m-health, ‘m health,’ ehealth, telemedicine and telehealth) to search a number of electronic databases (The Cochrane Central Register of Controlled Trials [CENTRAL, The Cochrane Library, latest issue], PubMed, EMBASE, World
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 5
Health Organization Global Health Library regional index [latest issue], PsycINFO, Web of Science, Mobile Active [http://www.mobileactive.org], KIT Information Portal; mHealth in Low-Resource Settings [http://www.mhealthinfo.org]). The author searched the databases from October 2010 onwards as extensive searches for our pre-vious mHealth systematic reviews (including 32.399 citations) covered the literature before this date. Reference lists of relevant studies and personal collections of articles were also searched. Documents published before 2000 were not included as mobile phones were not widely available in low- or middle- income countries at the time.
One strength of this review is the extensive search of references from which the studies were selected. Because of limited resources, a single author undertook the review process. We acknowledge that the typology is used as a heuristic. The review is intended to be an illustration of the pathway, and not a systematic review of all mHealth studies in developing countries.
Data Extraction and Analysis
The author merged search results across databases, removed duplicates and screened citations against inclusion criteria. Data were extracted using a standardized form including descriptives, inputs, mechanism factors, and outputs. Statistical pooling of results was not possible due to extensive heterogeneity of the study methods.
The articles were further categorized according to the type of the main interven-tion. Certain studies focused on factors falling under more than one category; we chose to concentrate on the main intent of each study. Where studies exhibited more than one category in a significant manner, we examined the linkages.
Results
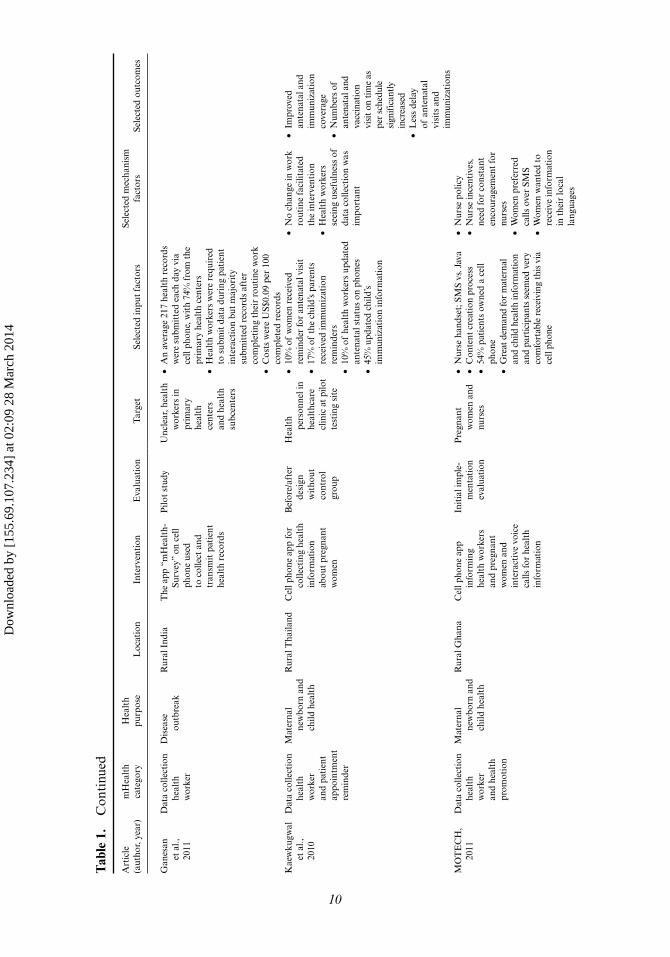
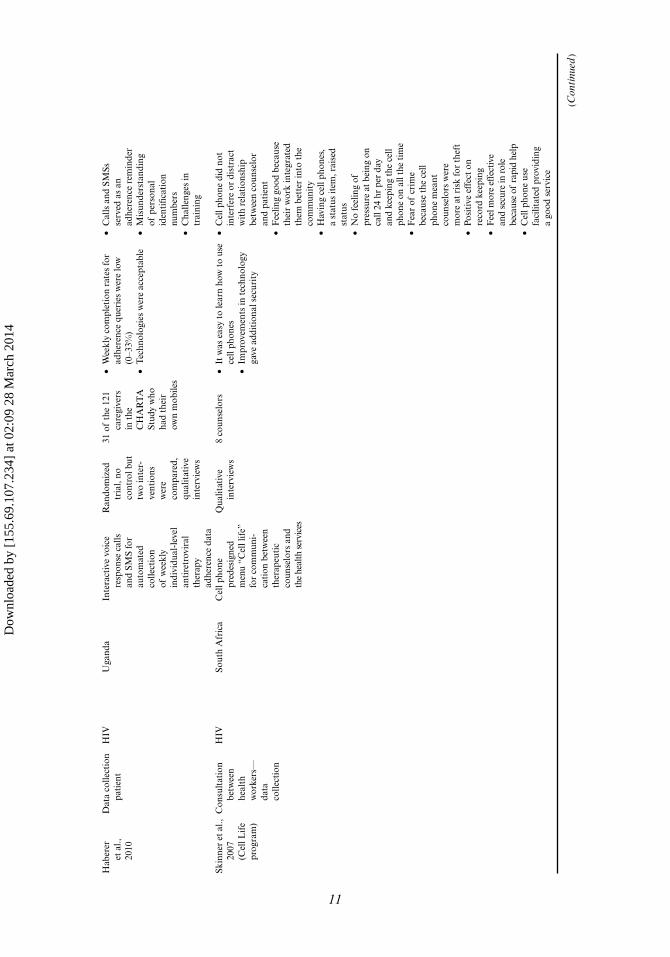
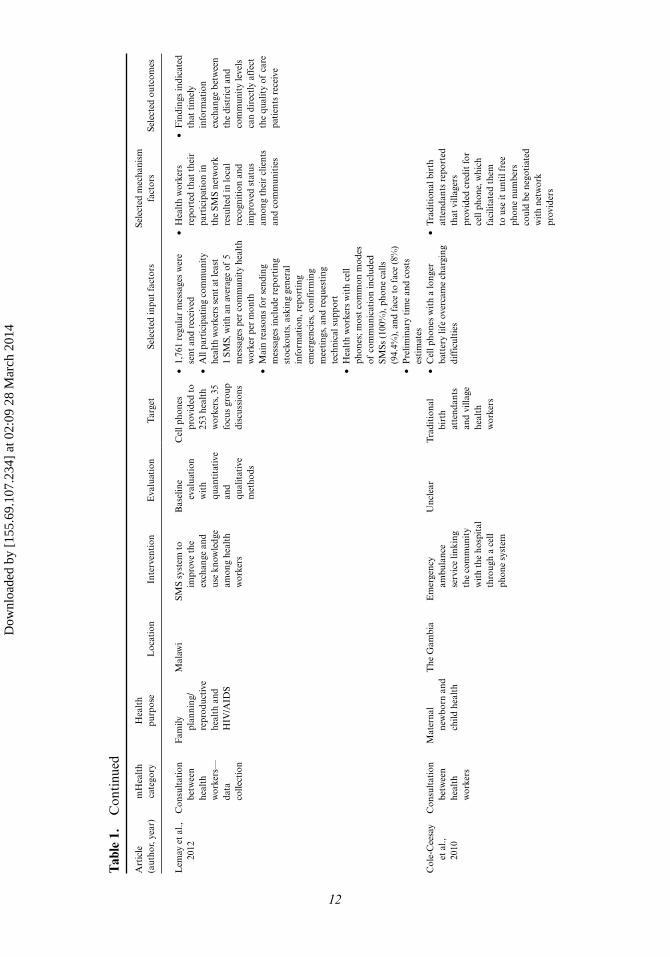
We found 53 studies (represented by 63 articles) addressing one of the three stages of the pathway, inputs-mechanism-outputs, shown in Figure 1. The main types of interventions studied were related to data collection (Alam, Khanam, Khan, Raihan, & Chowdhury, 2010; Andreatta, Debpuur, Danquah, & Perosky, 2011; Asiimwe et al., 2011; Barrington, Wereko-Brobby, Ward, Mwafongo, & Kungulwe, 2010; Ganesan et al., 2011; Haberer, Kiwanuka, Nansera, Wilson, & Bangsberg, 2010; Kaewkungwal et al., 2010; MOTECH, 2011; Rajatonirina et al., 2012; Svoronos et al., 2010; Zhang et al., 2012 [n = 11]), and consultation between health workers (Chandhanayingyong, Tangtrakulwanich, & Kiriratnikom, 2007; Chang et al., 2011; Chib & Chen, 2011; Chib, Cheong, et al., 2012; Cole-Ceesay et al., 2010; Lemay, Sullivan, Jumbe, & Perry, 2012; Macrohon &
Figure 1. The mHealth pathway: Proposed pathway of research focus for mHealth studies as a heuristic within which this review is situated. The blue boxes indicate the three categories of the pathway; the white boxes give examples of factors belonging to those categories.
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

6 A. Chib et al.
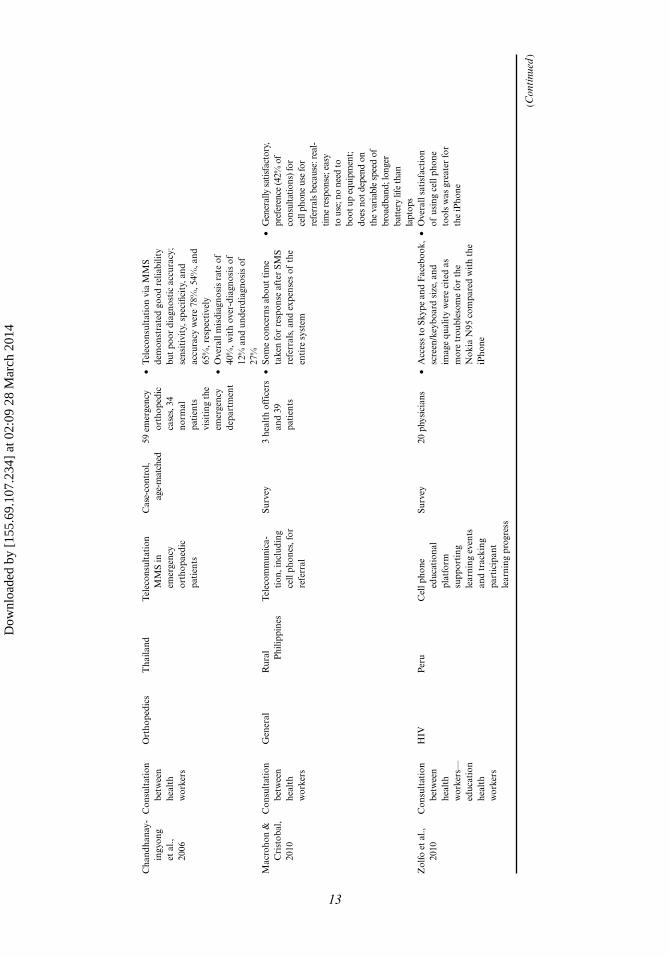
Cristobal, 2011; Skinner, Rivette, & Bloomberg, 2007; Zolfo et al., 2010; Zurovac et al., 2011 [n = 11]).
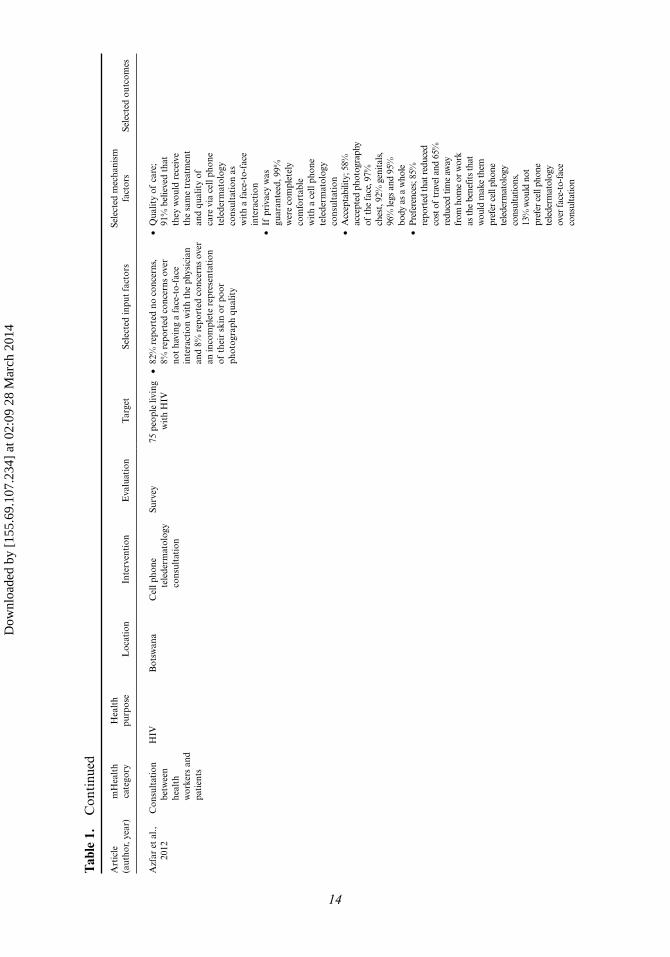
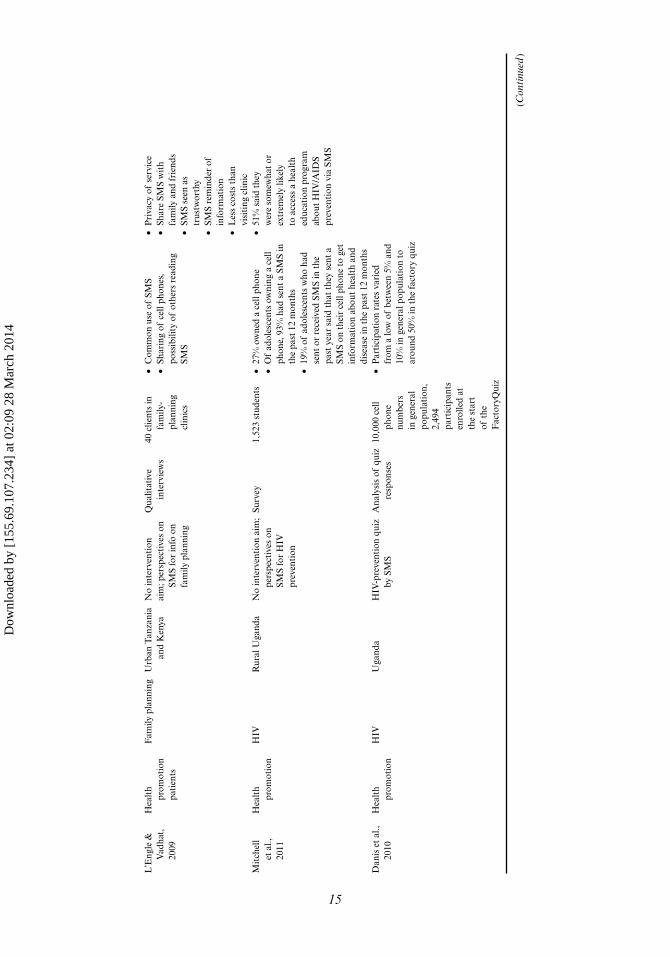
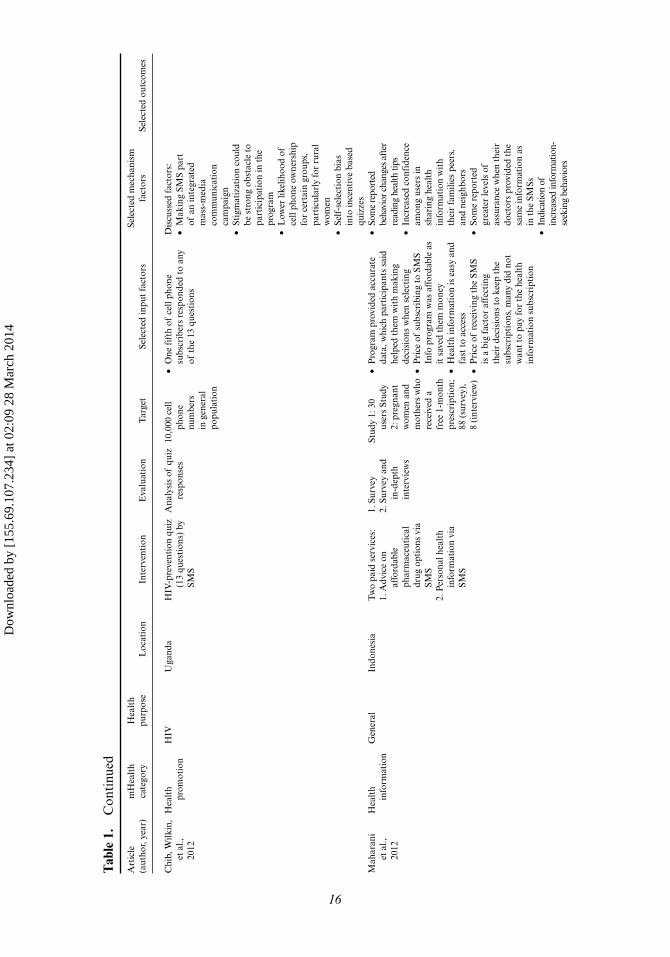
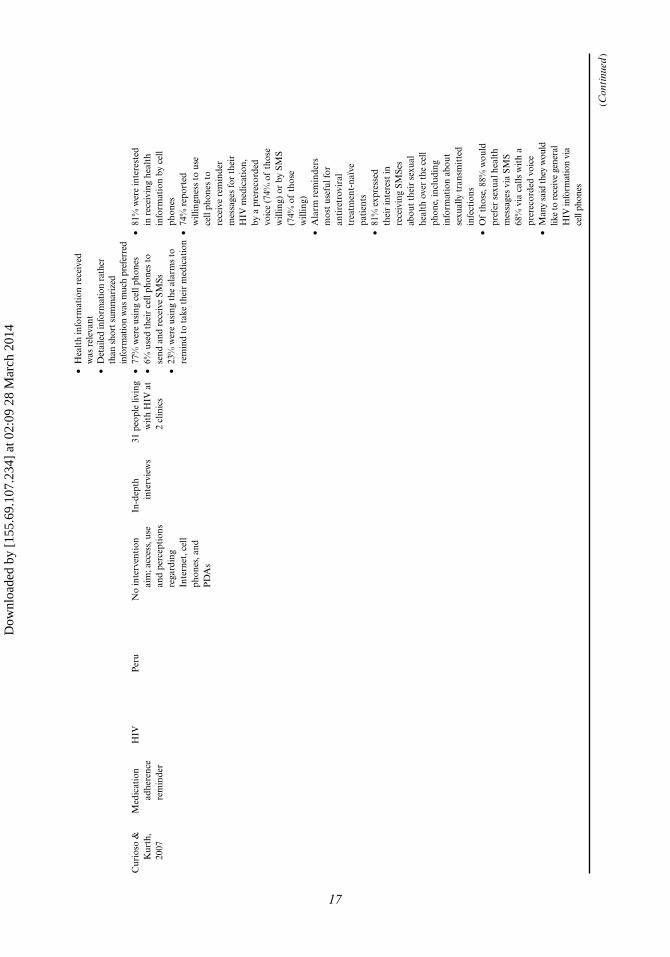
We categorized the articles by the main type of intervention; data collection (Alam et al., 2010; Andreatta et al., 2011; Asiimwe et al., 2011; Barrington et al., 2010; Ganesan et al., 2011; Haberer et al., 2010; Kaewkungwal et al., 2010; MOTECH, 2011; Rajatonirina et al., 2012; Svoronos et al., 2010; Zhang et al., 2012 [n = 11]), consultation between health workers (Chandhanayingyong et al., 2007; Chang et al., 2011; Chib & Chen, 2011; Chib, Cheong, et al., 2012; Chib, Law, Ahmad, & Ismail, 2012; Cole-Ceesay et al., 2010; Lemay et al., 2012; Macrohon & Cristobal, 2011; Skinner et al., 2007; Zolfo et al., 2010; Zurovac et al., 2011 [n = 11]), appointment reminders for health workers (Derenzi et al., 2012 [n = 1]), and patients; health promotion (Chib, Wilkin, Leow, Hoefman, & van Bejima, 2012; Danis et al., 2010; de Tolly et al., 2012; Hamilton, 2010; Jareethum et al., 2008; L’Engle & Vadhat, 2009; K. J. Mitchell, Bull, Kiwanuka, & Ybarra, 2011 [n = 7]), medication reminders (Curioso et al., 2009; Curioso & Kurth, 2007; Lester et al., 2010; Mbuagbaw, Bonono-Momnougui, & Thabane, 2012; Pop-Eleches et al., 2011; Shet et al., 2010; Sidney et al., 2012 [n = 7]), appointment remind-ers (Chen, Fang, Chen, & Dai, 2008; Crankshaw et al., 2010; da Costa, Salomão, Martha, Pisa, & Sigulem, 2010; Kunutsor et al., 2010; Leong, Chen, & Leong, 2006; Liew et al., 2009; Prasad & Anand, 2012 [n = 7]), and health information for patients (Ashraf, Ansari, Tahseen Malik, & Rashid, 2010; Azfar et al., 2011; Maharani, Rosanna, & Liesman, 2012; Odigie et al., 2011; Piette et al., 2011 [n = 5]), test remind-ers (Seidenberg et al., 2012; Wolpaw et al., 2011 [n = 2]), while two studies did not focus on any specific intervention (Faisal, 2011; Hwabamungu & Williams, 2010).
Inputs
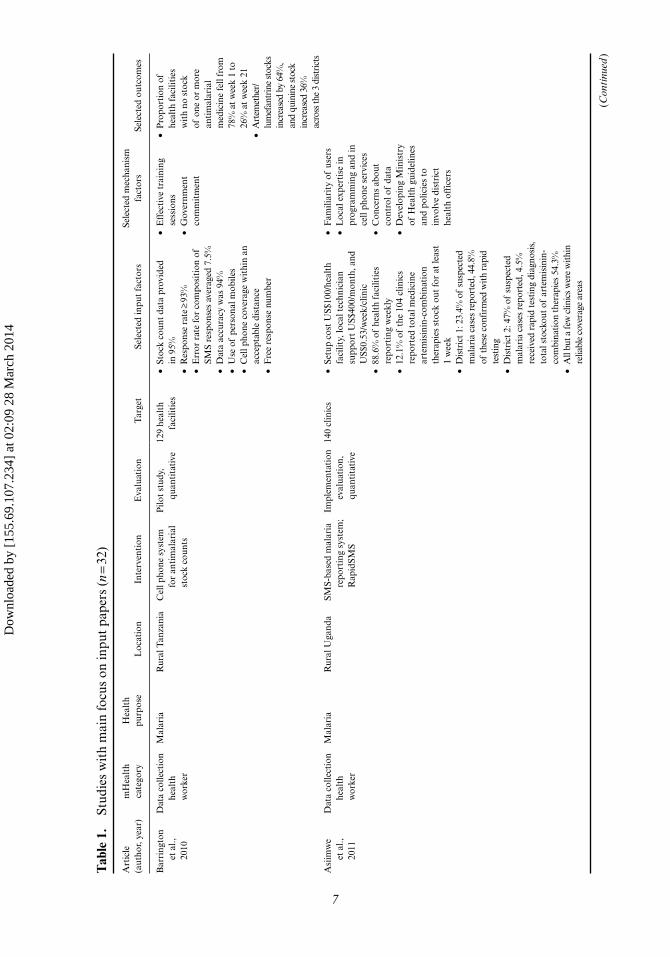
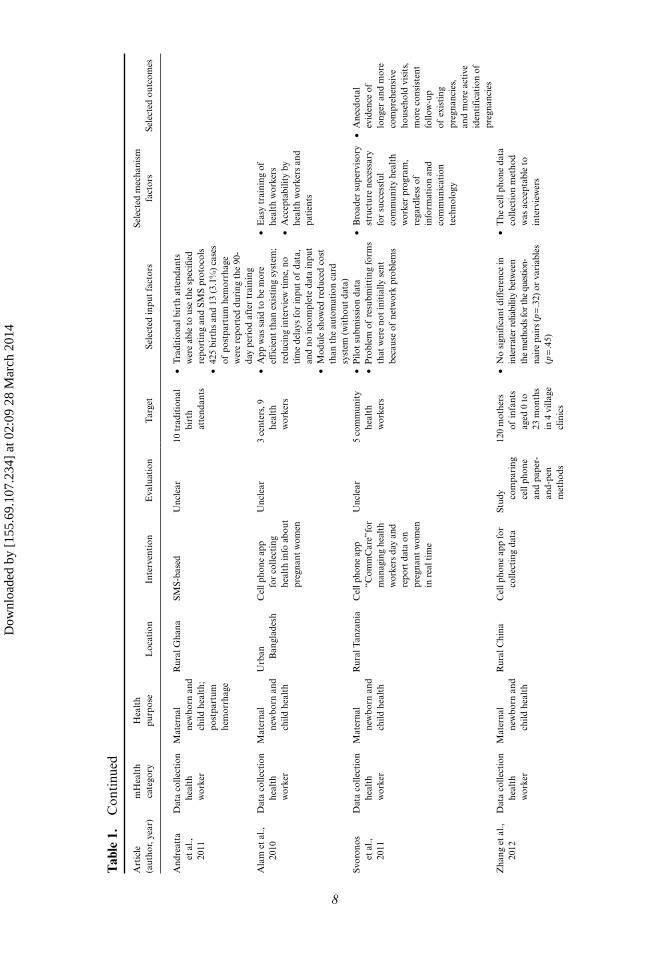
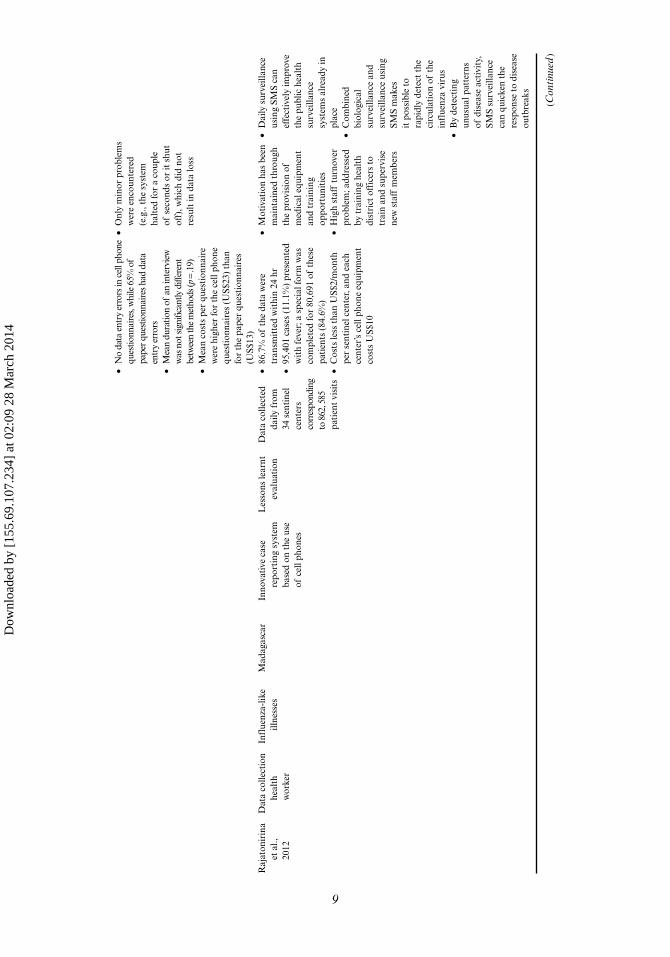
A number of studies (Alam et al., 2010; Andreatta et al., 2011; Asiimwe et al., 2011; Azfar et al., 2011; Barrington et al., 2010; Chandhanayingyong et al., 2007; Chib, Wilkin, et al., 2012; Cole-Ceesay et al., 2010; Crankshaw et al., 2010; Curioso et al., 2009; Curioso & Kurth, 2007; Danis et al., 2010; Derenzi et al., 2012; Faisal, 2011; Ganesan et al., 2011; Haberer et al., 2010; Kaewkungwal et al., 2010; L’Engle & Vadhat, 2009; Lemay et al., 2012; Macrohon & Cristobal, 2011; Maharani et al., 2012; Mbuagbaw et al., 2012; Mitchell et al., 2011; MOTECH, 2011; Rajatonirina et al., 2012; Shet et al., 2010; Sidney et al., 2012; Skinner et al., 2007; Svoronos et al., 2010; Wolpaw et al., 2011; Zhang et al., 2012; Zolfo et al., 2010 [n = 32]) described technological inputs required for mHealth implementation, focusing on technology access and use and on the feasi-bility of the intervention in terms of satisfaction, response rates, data accuracy and error rates and setup costs. These studies were mostly pilot studies, implementation evaluations, and studies with undefined design or interviews. A detailed description can be found in Table 1.
The range of technologies used for data collection ranged from mobile applica-tions (Alam et al., 2010; Ganesan et al., 2011; Kaewkungwal et al., 2010; Svoronos et al., 2010; Zhang et al., 2012), SMS-based mobile applications (Asiimwe et al., 2011; Barrington et al., 2010), to interactive voice calls and SMS (Haberer et al., 2010; Rajatonirina et al., 2012). For consultation between health workers, SMS (Lemay et al., 2012; Macrohon & Cristobal, 2011), or MMS (Azfar et al., 2011; Chandhanayingyong et al., 2007) was used. Other studies used calls and SMS for reminding patients (Wolpaw et al., 2011), or health workers (Derenzi et al., 2012) of their appointments,
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Bar
ring
ton
et a
l.,
2010
Dat
a co
llect
ion
heal
th
wor
ker
Mal
aria
Rur
al T
anza
nia
Cel
l pho
ne s
yste
m
for
anti
mal
aria
l st
ock
coun
ts
Pilo
t st
udy,
qu
anti
tati
ve12
9 he
alth
fa
cilit
ies
• St
ock
coun
t da
ta p
rovi
ded
in 9
5%•
Res
pons
e ra
te ≥
93%
• E
rror
rat
e fo
r co
mpo
siti
on o
f SM
S re
spon
ses
aver
aged
7.5
%•
Dat
a ac
cura
cy w
as 9
4%•
Use
of
pers
onal
mob
iles
• C
ell p
hone
cov
erag
e w
ithi
n an
ac
cept
able
dis
tanc
e•
Fre
e re
spon
se n
umbe
r
• E
ffec
tive
tra
inin
g se
ssio
ns•
Gov
ernm
ent
com
mit
men
t
• P
ropo
rtio
n of
he
alth
faci
litie
s w
ith
no s
tock
of
one
or
mor
e an
tim
alar
ial
med
icin
e fe
ll fr
om
78%
at w
eek
1 to
26
% a
t wee
k 21
• A
rtem
ethe
r/lu
mef
antr
ine
stoc
ks
incr
ease
d by
64%
, an
d qu
inin
e st
ock
incr
ease
d 36
%
acro
ss th
e 3
dist
rict
sA
siim
we
et a
l.,
2011
Dat
a co
llect
ion
heal
th
wor
ker
Mal
aria
Rur
al U
gand
aSM
S-ba
sed
mal
aria
re
port
ing
syst
em;
Rap
idSM
S
Impl
emen
tati
on
eval
uati
on,
quan
tita
tive
140
clin
ics
• Se
tup
cost
US$
100/
heal
th
faci
lity,
loca
l tec
hnic
ian
supp
ort
US$
400/
mon
th, a
nd
US$
0.53
/wee
k/cl
inic
• 88
.6%
of
heal
th f
acili
ties
re
port
ing
wee
kly
• 12
.1%
of
the
104
clin
ics
repo
rted
tot
al m
edic
ine
arte
mis
inin
-com
bina
tion
th
erap
ies
stoc
k ou
t fo
r at
leas
t 1
wee
k•
Dis
tric
t 1: 2
3.4%
of
susp
ecte
d m
alar
ia c
ases
rep
orte
d, 4
4.8%
of
thes
e co
nfir
med
with
rap
id
test
ing
• D
istr
ict 2
: 47%
of
susp
ecte
d m
alar
ia c
ases
rep
orte
d, 4
.5%
re
ceiv
ed r
apid
test
ing
diag
nosi
s,
tota
l sto
ckou
t of
arte
mis
inin
-co
mbi
nati
on th
erap
ies
54.3
%•
All
but a
few
clin
ics
wer
e w
ithin
re
liabl
e co
vera
ge a
reas
• F
amili
arit
y of
use
rs•
Loc
al e
xper
tise
in
prog
ram
min
g an
d in
ce
ll ph
one
serv
ices
• C
once
rns
abou
t co
ntro
l of
data
• D
evel
opin
g M
inis
try
of H
ealt
h gu
idel
ines
an
d po
licie
s to
in
volv
e di
stri
ct
heal
th o
ffic
ers
(Con
tinu
ed)
Tab
le 1
. St
udie
s w
ith
mai
n fo
cus
on in
put
pape
rs (
n = 32
)
7
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
And
reat
ta
et a
l.,
2011
Dat
a co
llect
ion
heal
th
wor
ker
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth;
po
stpa
rtum
he
mor
rhag
e
Rur
al G
hana
SMS-
base
d U
ncle
ar10
tra
diti
onal
bi
rth
atte
ndan
ts
• T
radi
tion
al b
irth
att
enda
nts
wer
e ab
le t
o us
e th
e sp
ecifi
ed
repo
rtin
g an
d SM
S pr
otoc
ols
• 42
5 bi
rths
and
13
(3.1
%)
case
s of
pos
tpar
tum
hem
orrh
age
wer
e re
port
ed d
urin
g th
e 90
-da
y pe
riod
aft
er t
rain
ing
Ala
m e
t al
., 20
10D
ata
colle
ctio
n he
alth
w
orke
r
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth
Urb
an
Ban
glad
esh
Cel
l pho
ne a
pp
for
colle
ctin
g he
alth
info
abo
ut
preg
nant
wom
en
Unc
lear
3 ce
nter
s, 9
he
alth
w
orke
rs
• A
pp w
as s
aid
to b
e m
ore
effi
cien
t th
an e
xist
ing
syst
em;
redu
cing
inte
rvie
w t
ime,
no
tim
e de
lays
for
inpu
t of
dat
a,
and
no in
com
plet
e da
ta in
put
• M
odul
e sh
owed
red
uced
cos
t th
an t
he a
utom
atio
n ca
rd
syst
em (
wit
hout
dat
a)
• E
asy
trai
ning
of
heal
th w
orke
rs•
Acc
epta
bilit
y by
he
alth
wor
kers
and
pa
tien
ts
Svor
onos
et
al.,
20
11
Dat
a co
llect
ion
heal
th
wor
ker
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth
Rur
al T
anza
nia
Cel
l pho
ne a
pp
“Com
m C
are”
for
man
agin
g he
alth
w
orke
rs d
ay a
nd
repo
rt d
ata
on
preg
nant
wom
en
in r
eal t
ime
Unc
lear
5 co
mm
unit
y he
alth
w
orke
rs
• P
ilot
subm
issi
on d
ata
• P
robl
em o
f re
subm
itti
ng fo
rms
that
wer
e no
t in
itia
lly s
ent
beca
use
of n
etw
ork
prob
lem
s
• B
road
er s
uper
viso
ry
stru
ctur
e ne
cess
ary
for
succ
essf
ul
com
mun
ity
heal
th
wor
ker
prog
ram
, re
gard
less
of
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gy
• A
necd
otal
ev
iden
ce o
f lo
nger
and
mor
e co
m pr
ehen
sive
ho
useh
old
visi
ts,
mor
e co
nsis
tent
fo
llow
-up
of e
xist
ing
preg
nanc
ies,
an
d m
ore
acti
ve
iden
tifi
cati
on o
f pr
egna
ncie
sZ
hang
et
al.,
2012
Dat
a co
llect
ion
heal
th
wor
ker
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth
Rur
al C
hina
Cel
l pho
ne a
pp fo
r co
llect
ing
data
St
udy com
pari
ng
cell
phon
e an
d pa
per-
and-
pen
met
hods
120
mot
hers
of
infa
nts
aged
0 t
o 23
mon
ths
in 4
vill
age
clin
ics
• N
o si
gnif
ican
t di
ffer
ence
in
inte
rrat
er re
liabi
lity
bet w
een
the
met
hods
for t
he q
uest
ion-
nair
e pa
irs
(p =
.32)
or
vari
able
s (p
= .4
5)
• T
he c
ell p
hone
dat
a co
llect
ion
met
hod
was
acc
epta
ble
to
inte
rvie
wer
s
8
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
• N
o da
ta e
ntry
err
ors i
n ce
ll ph
one
ques
tionn
aire
s, w
hile
65%
of
pape
r que
stio
nnai
res h
ad d
ata
entr
y er
rors
• M
ean
dura
tion
of a
n in
terv
iew
w
as n
ot si
gnifi
cant
ly d
iffer
ent
betw
een
the
met
hods
(p =
.19)
• M
ean
cost
s pe
r qu
esti
onna
ire
wer
e hi
gher
for
the
cell
phon
e qu
esti
onna
ires
(U
S$23
) th
an
for
the
pape
r qu
esti
onna
ires
(U
S$13
)
• O
nly
min
or p
robl
ems
wer
e en
coun
tere
d (e
.g.,
the
syst
em
halt
ed fo
r a
coup
le
of s
econ
ds o
r it
shu
t of
f), w
hich
did
not
re
sult
in d
ata
loss
Raj
aton
irin
a et
al.,
20
12
Dat
a co
llect
ion
heal
th
wor
ker
Infl
uenz
a-lik
e ill
ness
esM
adag
asca
rIn
nova
tive
cas
e re
port
ing
syst
em
base
d on
the
use
of
cel
l pho
nes
Les
sons
lear
nt
eval
uati
onD
ata
colle
cted
da
ily f
rom
34
sen
tine
l ce
nter
s co
rres
pond
ing
to 8
62, 5
85
pati
ent
visi
ts
• 86
.7%
of
the
data
wer
e tr
ansm
itte
d w
ithi
n 24
hr
• 95
,401
cas
es (
11.1
%)
pres
ente
d w
ith
feve
r; a
spe
cial
form
was
co
mpl
eted
for
80,6
91 o
f th
ese
pati
ents
(84
.6%
)•
Cos
ts le
ss t
han
US$
2/m
onth
pe
r se
ntin
el c
ente
r, an
d ea
ch
cent
er’s
cell
phon
e eq
uipm
ent
cost
s U
S$10
• M
otiv
atio
n ha
s be
en
mai
ntai
ned
thro
ugh
the
prov
isio
n of
m
edic
al e
quip
men
t an
d tr
aini
ng
oppo
rtun
itie
s•
Hig
h st
aff
turn
over
pr
oble
m; a
ddre
ssed
by
tra
inin
g he
alth
di
stri
ct o
ffic
ers
to
trai
n an
d su
perv
ise
new
sta
ff m
embe
rs
• D
aily
sur
veill
ance
us
ing
SMS
can
effe
ctiv
ely
impr
ove
the
publ
ic h
ealt
h su
rvei
llanc
e sy
stem
s al
read
y in
pl
ace
• C
ombi
ned
biol
ogic
al
surv
eilla
nce
and
surv
eilla
nce
usin
g SM
S m
akes
it
pos
sibl
e to
ra
pidl
y de
tect
the
ci
rcul
atio
n of
the
in
flue
nza
viru
s•
By
dete
ctin
g un
usua
l pat
tern
s of
dis
ease
act
ivit
y,
SMS
surv
eilla
nce
can
quic
ken
the
resp
onse
to d
isea
se
outb
reak
s
( Con
tinu
ed)
9
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Gan
esan
et
al.,
20
11
Dat
a co
llect
ion
heal
th
wor
ker
Dis
ease
ou
tbre
akR
ural
Ind
iaT
he a
pp “
mH
ealt
h-Su
rvey
” on
cel
l ph
one
used
to
col
lect
and
tr
ansm
it p
atie
nt
heal
th r
ecor
ds
Pilo
t st
udy
Unc
lear
, hea
lth
wor
kers
in
prim
ary
heal
th
cent
ers
and
heal
th
subc
ente
rs
• A
n av
erag
e 21
7 he
alth
rec
ords
w
ere
subm
itte
d ea
ch d
ay v
ia
cell
phon
e, w
ith
74%
fro
m t
he
prim
ary
heal
th c
ente
rs•
Hea
lth
wor
kers
wer
e re
quir
ed
to s
ubm
it d
ata
duri
ng p
atie
nt
inte
ract
ion
but
maj
orit
y su
bmit
ted
reco
rds
afte
r co
mpl
etin
g th
eir
rout
ine
wor
k•
Cos
ts w
ere
US$
0.09
per
100
co
mpl
eted
rec
ords
Kae
wku
gwal
et
al.,
20
10
Dat
a co
llect
ion
heal
th
wor
ker
and
pati
ent
appo
intm
ent
rem
inde
r
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth
Rur
al T
haila
ndC
ell p
hone
app
for
colle
ctin
g he
alth
in
form
atio
n ab
out
preg
nant
w
omen
Bef
ore/
afte
r de
sign
w
itho
ut
cont
rol
grou
p
Hea
lth
pers
onne
l in
heal
thca
re
clin
ic a
t pilo
t te
stin
g si
te
• 10
% o
f w
omen
rec
eive
d re
min
der
for
ante
nata
l vis
it•
17%
of
the
child
’s pa
rent
s re
ceiv
ed im
mun
izat
ion
rem
inde
rs•
10%
of
heal
th w
orke
rs u
pdat
ed
ante
nata
l sta
tus
on p
hone
s•
45%
upd
ated
chi
ld’s
imm
uniz
atio
n in
form
atio
n
• N
o ch
ange
in w
ork
rout
ine
faci
litat
ed
the
inte
rven
tion
• H
ealt
h w
orke
rs
seei
ng u
sefu
lnes
s of
da
ta c
olle
ctio
n w
as
impo
rtan
t
• Im
prov
ed
ante
nata
l and
im
mun
izat
ion
cove
rage
• N
umbe
rs o
f an
tena
tal a
nd
vacc
inat
ion
visi
t on
tim
e as
pe
r sc
hedu
le
sign
ific
antly
in
crea
sed
• L
ess
dela
y of
ant
enat
al
visi
ts a
nd
imm
uniz
atio
ns
MO
TE
CH
, 20
11D
ata
colle
ctio
n he
alth
w
orke
r an
d he
alth
pr
omot
ion
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth
Rur
al G
hana
Cel
l pho
ne a
pp
info
rmin
g he
alth
wor
kers
an
d pr
egna
nt
wom
en a
nd
inte
ract
ive
voic
e ca
lls fo
r he
alth
in
form
atio
n
Init
ial i
mpl
e-m
enta
tion
ev
alua
tion
Pre
gnan
t w
omen
and
nu
rses
• N
urse
han
dset
; SM
S vs
. Jav
a•
Con
tent
cre
atio
n pr
oces
s•
54%
pat
ient
s ow
ned
a ce
ll ph
one
• G
reat
dem
and
for
mat
erna
l an
d ch
ild h
ealt
h in
form
atio
n an
d pa
rtic
ipan
ts s
eem
ed v
ery
com
fort
able
rec
eivi
ng th
is v
ia
cell
phon
e
• N
urse
pol
icy
• N
urse
ince
ntiv
es,
need
for
cons
tant
en
cour
agem
ent
for
nurs
es•
Wom
en p
refe
rred
ca
lls o
ver
SMS
• W
omen
wan
ted
to
rece
ive
info
rmat
ion
in t
heir
loca
l la
ngua
ges
10
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Hab
erer
et
al.,
20
10
Dat
a co
llect
ion
pati
ent
HIV
Uga
nda
Inte
ract
ive
voic
e re
spon
se c
alls
an
d SM
S fo
r au
tom
ated
co
llect
ion
of w
eekl
y in
divi
dual
-lev
el
anti
retr
ovir
al
ther
apy
adhe
renc
e da
ta
Ran
dom
ized
tr
ial,
no
cont
rol b
ut
two
inte
r-ve
ntio
ns
wer
e co
mpa
red,
qu
alit
ativ
e in
terv
iew
s
31 o
f th
e 12
1 ca
regi
vers
in
the
C
HA
RT
A
Stud
y w
ho
had
thei
r ow
n m
obile
s
• W
eekl
y co
mpl
etio
n ra
tes
for
adhe
renc
e qu
erie
s w
ere
low
(0
–33%
)•
Tec
hnol
ogie
s w
ere
acce
ptab
le
• C
alls
and
SM
Ss
serv
ed a
s an
ad
here
nce
rem
inde
r•
Mis
unde
rsta
ndin
g of
per
sona
l id
enti
ficat
ion
num
bers
• C
halle
nges
in
trai
ning
Skin
ner
et a
l.,
2007
(C
ell L
ife
prog
ram
)
Con
sult
atio
n be
twee
n he
alth
w
orke
rs—
data
co
llect
ion
HIV
Sout
h A
fric
aC
ell p
hone
pr
edes
igne
d m
enu
“Cel
l lif
e”
for
com
mun
i-ca
tion
bet
wee
n th
erap
euti
c co
unse
lors
and
th
e he
alth
serv
ices
Qua
litat
ive
inte
rvie
ws
8 co
unse
lors
• It
was
eas
y to
lear
n ho
w t
o us
e ce
ll ph
ones
• Im
prov
emen
ts in
tec
hnol
ogy
gave
add
itio
nal s
ecur
ity
• C
ell p
hone
did
not
in
terf
ere
or d
istr
act
wit
h re
lati
onsh
ip
betw
een
coun
selo
r an
d pa
tien
t•
Fee
ling
good
bec
ause
th
eir
wor
k in
tegr
ated
th
em b
ette
r in
to t
he
com
mun
ity
• H
avin
g ce
ll ph
ones
, a
stat
us it
em, r
aise
d st
atus
• N
o fe
elin
g of
pr
essu
re a
t bei
ng o
n ca
ll 24
hr
per
day
and
keep
ing
the
cell
phon
e on
all
the
tim
e•
Fea
r of
cri
me
beca
use
the
cell
phon
e m
eant
co
unse
lors
wer
e m
ore
at r
isk
for
thef
t•
Posi
tive
eff
ect
on
reco
rd k
eepi
ng•
Fee
l mor
e ef
fect
ive
and
secu
re in
role
be
caus
e of
rap
id h
elp
• C
ell p
hone
use
fa
cilit
ated
pro
vidi
ng
a go
od s
ervi
ce
(Con
tinu
ed)
11
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Lem
ay e
t al
., 20
12C
onsu
ltat
ion
betw
een
heal
th
wor
kers
—da
ta
colle
ctio
n
Fam
ily
plan
ning
/re
prod
ucti
ve
heal
th a
nd
HIV
/AID
S
Mal
awi
SMS
syst
em t
o im
prov
e th
e ex
chan
ge a
nd
use
know
ledg
e am
ong
heal
th
wor
kers
Bas
elin
e ev
alua
tion
w
ith
quan
tita
tive
an
d qu
alit
ativ
e m
etho
ds
Cel
l pho
nes
prov
ided
to
253
heal
th
wor
kers
, 35
focu
s gr
oup
disc
ussi
ons
• 1,
761
regu
lar
mes
sage
s w
ere
sent
and
rec
eive
d•
All
part
icip
atin
g co
mm
unit
y he
alth
wor
kers
sen
t at l
east
1
SMS,
wit
h an
ave
rage
of
5 m
essa
ges
per
com
mun
ity
heal
th
wor
ker
per
mon
th•
Mai
n re
ason
s fo
r se
ndin
g m
essa
ges
incl
ude
repo
rtin
g st
ocko
uts,
ask
ing
gene
ral
info
rmat
ion,
rep
orti
ng
emer
genc
ies,
con
firm
ing
mee
ting
s, a
nd r
eque
stin
g te
chni
cal s
uppo
rt•
Hea
lth
wor
kers
wit
h ce
ll ph
ones
; mos
t co
mm
on m
odes
of
com
mun
icat
ion
incl
uded
SM
Ss (
100%
), p
hone
cal
ls
(94.
4%),
and
fac
e to
fac
e (8
%)
• P
relim
inar
y ti
me
and
cost
s es
tim
ates
• H
ealt
h w
orke
rs
repo
rted
tha
t th
eir
part
icip
atio
n in
th
e SM
S ne
twor
k re
sult
ed in
loca
l re
cogn
itio
n an
d im
prov
ed s
tatu
s am
ong
thei
r cl
ient
s an
d co
mm
unit
ies
• F
indi
ngs
indi
cate
d th
at t
imel
y in
form
atio
n ex
chan
ge b
etw
een
the
dist
rict
and
co
mm
unit
y le
vels
ca
n di
rect
ly a
ffec
t th
e qu
alit
y of
car
e pa
tien
ts r
ecei
ve
Col
e-C
eesa
y et
al.,
20
10
Con
sult
atio
n be
twee
n he
alth
w
orke
rs
Mat
erna
l ne
wbo
rn a
nd
child
hea
lth
The
Gam
bia
Em
erge
ncy
ambu
lanc
e se
rvic
e lin
king
th
e co
mm
unit
y w
ith
the
hosp
ital
th
roug
h a
cell
phon
e sy
stem
Unc
lear
Tra
diti
onal
bi
rth
atte
ndan
ts
and
villa
ge
heal
th
wor
kers
• C
ell p
hone
s w
ith
a lo
nger
ba
tter
y lif
e ov
erca
me
char
ging
di
ffic
ulti
es
• T
radi
tion
al b
irth
at
tend
ants
rep
orte
d th
at v
illag
ers
prov
ided
cre
dit
for
cell
phon
e, w
hich
fa
cilit
ated
the
m
to u
se it
unt
il fr
ee
phon
e nu
mbe
rs
coul
d be
neg
otia
ted
wit
h ne
twor
k pr
ovid
ers
12
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Cha
ndha
nay-
ingy
ong
et a
l.,
2006
Con
sult
atio
n be
twee
n he
alth
w
orke
rs
Ort
hope
dics
Tha
iland
Tel
econ
sult
atio
n M
MS
in
emer
genc
y or
thop
aedi
c pa
tien
ts
Cas
e-co
ntro
l, ag
e-m
atch
ed59
em
erge
ncy
orth
oped
ic
case
s, 3
4 no
rmal
pa
tien
ts
visi
ting
the
em
erge
ncy
depa
rtm
ent
• T
elec
onsu
ltat
ion
via
MM
S de
mon
stra
ted
good
rel
iabi
lity
but
poor
dia
gnos
tic
accu
racy
; se
nsit
ivit
y, s
peci
ficit
y, a
nd
accu
racy
wer
e 78
%, 5
4%, a
nd
65%
, res
pect
ivel
y•
Ove
rall
mis
diag
nosi
s ra
te o
f 40
%, w
ith
over
-dia
gnos
is o
f 12
% a
nd u
nder
diag
nosi
s of
27
%M
acro
hon
&
Cri
stob
al,
2010
Con
sult
atio
n be
twee
n he
alth
w
orke
rs
Gen
eral
Rur
al
Phi
lippi
nes
Tel
ecom
mun
ica-
tion
, inc
ludi
ng
cell
phon
es, f
or
refe
rral
Surv
ey3
heal
th o
ffic
ers
and
39
pati
ents
• So
me
conc
erns
abo
ut t
ime
take
n fo
r re
spon
se a
fter
SM
S re
ferr
als,
and
exp
ense
s of
the
en
tire
sys
tem
• G
ener
ally
sat
isfa
ctor
y,
pref
eren
ce (4
2% o
f co
nsul
tatio
ns) f
or
cell
phon
e us
e fo
r re
ferr
als
beca
use:
real
-tim
e re
spon
se; e
asy
to u
se; n
o ne
ed to
bo
ot u
p eq
uipm
ent;
do
es n
ot d
epen
d on
th
e va
riab
le s
peed
of
broa
dban
d; lo
nger
ba
tter
y lif
e th
an
lapt
ops
Zol
fo e
t al
., 20
10C
onsu
ltat
ion
betw
een
heal
th
wor
kers
—ed
ucat
ion
heal
th
wor
kers
HIV
Per
uC
ell p
hone
ed
ucat
iona
l pl
atfo
rm
supp
orti
ng
lear
ning
eve
nts
and
trac
king
pa
rtic
ipan
t le
arni
ng p
rogr
ess
Surv
ey20
phy
sici
ans
• A
cces
s to
Sky
pe a
nd F
aceb
ook,
sc
reen
/key
boar
d si
ze, a
nd
imag
e qu
alit
y w
ere
cite
d as
m
ore
trou
bles
ome
for
the
Nok
ia N
95 c
ompa
red
wit
h th
e iP
hone
• O
vera
ll sa
tisf
acti
on
of u
sing
cel
l pho
ne
tool
s w
as g
reat
er fo
r th
e iP
hone
( Con
tinu
ed)
13
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Azf
ar e
t al
., 20
12C
onsu
ltat
ion
betw
een
heal
th
wor
kers
and
pa
tien
ts
HIV
Bot
swan
aC
ell p
hone
te
lede
rmat
olog
y co
nsul
tati
on
Surv
ey75
peo
ple
livin
g w
ith
HIV
• 82
% r
epor
ted
no c
once
rns,
8%
rep
orte
d co
ncer
ns o
ver
not
havi
ng a
fac
e-to
-fac
e in
tera
ctio
n w
ith
the
phys
icia
n an
d 8%
rep
orte
d co
ncer
ns o
ver
an in
com
plet
e re
pres
enta
tion
of
the
ir s
kin
or p
oor
phot
ogra
ph q
ualit
y
• Q
ualit
y of
car
e;
91%
bel
ieve
d th
at
they
wou
ld r
ecei
ve
the
sam
e tr
eatm
ent
and
qual
ity
of
care
via
cel
l pho
ne
tele
derm
atol
ogy
cons
ulta
tion
as
wit
h a
face
-to-
face
in
tera
ctio
n•
If p
riva
cy w
as
guar
ante
ed, 9
9%
wer
e co
mpl
etel
y co
mfo
rtab
le
wit
h a
cell
phon
e te
lede
rmat
olog
y co
nsul
tati
on•
Acc
epta
bilit
y; 5
8%
acce
pted
pho
togr
aphy
of
the
face
, 97%
ch
est,
92%
gen
itals,
96
% le
gs a
nd 9
5%
body
as
a w
hole
• P
refe
renc
es; 8
5%
repo
rted
that
redu
ced
cost
of
trav
el a
nd 6
5%
redu
ced
time
away
fr
om h
ome
or w
ork
as th
e be
nefit
s th
at
wou
ld m
ake
them
pr
efer
cel
l pho
ne
tele
derm
atol
ogy
cons
ulta
tions
, 13
% w
ould
not
pr
efer
cel
l pho
ne
tele
derm
atol
ogy
over
face
-to-
face
co
nsul
tatio
n
14
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
L’E
ngle
&
Vad
hat,
20
09
Hea
lth
prom
otio
n pa
tien
ts
Fam
ily p
lann
ing
Urb
an T
anza
nia
and
Ken
yaN
o in
terv
enti
onai
m; p
ersp
ecti
ves
on
SMS
for
info
on
fam
ily p
lann
ing
Qua
litat
ive
inte
rvie
ws
40 c
lient
s in
fa
mily
-pl
anni
ng
clin
ics
• C
omm
on u
se o
f SM
S•
Shar
ing
of c
ell p
hone
s,
poss
ibili
ty o
f ot
hers
rea
ding
SM
S
• P
riva
cy o
f se
rvic
e•
Shar
e SM
S w
ith
fam
ily a
nd f
rien
ds•
SMS
seen
as
trus
twor
thy
• SM
S re
min
der
of
info
rmat
ion
• L
ess
cost
s th
an
visi
ting
clin
icM
itch
ell
et a
l.,
2011
Hea
lth
prom
otio
nH
IVR
ural
Uga
nda
No
inte
rven
tion
aim
; pe
rspe
ctiv
es o
n SM
S fo
r H
IV
prev
enti
on
Surv
ey
1,52
3 st
uden
ts•
27%
ow
ned
a ce
ll ph
one
• O
f ad
oles
cent
s ow
ning
a c
ell
phon
e, 9
3% h
ad s
ent
a SM
S in
th
e pa
st 1
2 m
onth
s•
19%
of
adol
esce
nts
who
had
se
nt o
r re
ceiv
ed S
MS
in t
he
past
yea
r sa
id t
hat
they
sen
t a
SMS
on t
heir
cel
l pho
ne t
o ge
t in
form
atio
n ab
out
heal
th a
nd
dise
ase
in t
he p
ast
12 m
onth
s
• 51
% s
aid
they
w
ere
som
ewha
t or
ex
trem
ely
likel
y to
acc
ess
a he
alth
ed
ucat
ion
prog
ram
ab
out
HIV
/AID
S pr
even
tion
via
SM
S
Dan
is e
t al
., 20
10H
ealt
h pr
omot
ion
HIV
Uga
nda
HIV
-pre
vent
ion
quiz
by
SM
SA
naly
sis
of q
uiz
resp
onse
s10
,000
cel
l ph
one
num
bers
in
gen
eral
po
pula
tion
, 2,
494
part
icip
ants
en
rolle
d at
th
e st
art
of t
he
Fac
tory
Qui
z
• P
arti
cipa
tion
rat
es v
arie
d fr
om a
low
of
betw
een
5% a
nd
10%
in g
ener
al p
opul
atio
n to
ar
ound
50%
in t
he f
acto
ry q
uiz
( Con
tinu
ed)
15
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Chi
b, W
ilkin
, et
al.,
20
12
Hea
lth
prom
otio
nH
IVU
gand
aH
IV-p
reve
ntio
n qu
iz
(13
ques
tion
s) b
y SM
S
Ana
lysi
s of
qui
z re
spon
ses
10,0
00 c
ell
phon
e nu
mbe
rs
in g
ener
al
popu
lati
on
• O
ne f
ifth
of
cell
phon
e su
bscr
iber
s re
spon
ded
to a
ny
of t
he 1
3 qu
esti
ons
Dis
cuss
ed f
acto
rs:
• M
akin
g SM
S pa
rt
of a
n in
tegr
ated
m
ass-
med
ia
com
mun
icat
ion
cam
paig
n•
Stig
mat
izat
ion
coul
d be
str
ong
obst
acle
to
part
icip
atio
n in
the
pr
ogra
m•
Low
er li
kelih
ood
of
cell
phon
e ow
ners
hip
for
cert
ain
grou
ps,
part
icul
arly
for
rura
l w
omen
• Se
lf-s
elec
tion
bia
s in
to in
cent
ive
base
d qu
izze
sM
ahar
ani
et a
l.,
2012
Hea
lth
info
rmat
ion
Gen
eral
Indo
nesi
aTw
o pa
id s
ervi
ces:
1. A
dvic
e on
af
ford
able
ph
arm
aceu
tica
l dr
ug o
ptio
ns v
ia
SMS
2. P
erso
nal h
ealt
h in
form
atio
n vi
a SM
S
1. S
urve
y2.
Sur
vey
and
in-d
epth
in
terv
iew
s
Stud
y 1:
30
user
s St
udy
2: p
regn
ant
wom
en a
nd
mot
hers
who
re
ceiv
ed a
fr
ee 1
-mon
th
pres
crip
tion
; 88
(su
rvey
),
8 (i
nter
view
)
• P
rogr
am p
rovi
ded
accu
rate
da
ta, w
hich
par
tici
pant
s sa
id
help
ed t
hem
wit
h m
akin
g de
cisi
ons
whe
n se
lect
ing
• P
rice
of
subs
crib
ing
to S
MS
Info
pro
gram
was
aff
orda
ble
as
it s
aved
the
m m
oney
• H
ealt
h in
form
atio
n is
eas
y an
d fa
st t
o ac
cess
• P
rice
of
rece
ivin
g th
e SM
S is
a b
ig f
acto
r af
fect
ing
thei
r de
cisi
ons
to k
eep
the
subs
crip
tion
s, m
any
did
not
wan
t to
pay
for
the
heal
th
info
rmat
ion
subs
crip
tion
• So
me
repo
rted
be
havi
or c
hang
es a
fter
re
adin
g he
alth
tips
• In
crea
sed
conf
iden
ce
amon
g us
ers
in
shar
ing
heal
th
info
rmat
ion
wit
h th
eir
fam
ilies
pee
rs,
and
neig
hbor
s•
Som
e re
port
ed
grea
ter
leve
ls o
f as
sura
nce
whe
n th
eir
doct
ors
prov
ided
the
sa
me
info
rmat
ion
as
in t
he S
MSs
• In
dica
tion
of
incr
ease
d in
form
atio
n-se
ekin
g be
havi
ors
16
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
• H
ealt
h in
form
atio
n re
ceiv
ed
was
rel
evan
t•
Det
aile
d in
form
atio
n ra
ther
th
an s
hort
sum
mar
ized
in
form
atio
n w
as m
uch
pref
erre
dC
urio
so &
K
urth
, 20
07
Med
icat
ion
adhe
renc
e re
min
der
HIV
Per
uN
o in
terv
enti
on
aim
; acc
ess,
use
an
d pe
rcep
tion
s re
gard
ing
Inte
rnet
, cel
l ph
ones
, and
P
DA
s
In-d
epth
in
terv
iew
s31
peo
ple
livin
g w
ith
HIV
at
2 cl
inic
s
• 77
% w
ere
usin
g ce
ll ph
ones
• 6%
use
d th
eir
cell
phon
es t
o se
nd a
nd r
ecei
ve S
MSs
• 23
% w
ere
usin
g th
e al
arm
s to
re
min
d to
take
thei
r m
edic
atio
n
• 81
% w
ere
inte
rest
ed
in r
ecei
ving
hea
lth
info
rmat
ion
by c
ell
phon
es•
74%
rep
orte
d w
illin
gnes
s to
use
ce
ll ph
ones
to
rece
ive
rem
inde
r m
essa
ges
for
thei
r H
IV m
edic
atio
n,
by a
pre
reco
rded
vo
ice
(74%
of
thos
e w
illin
g) o
r by
SM
S (7
4% o
f th
ose
will
ing)
• A
larm
rem
inde
rs
mos
t us
eful
for
anti
retr
ovir
al
trea
tmen
t-na
ïve
pati
ents
• 81
% e
xpre
ssed
th
eir
inte
rest
in
rece
ivin
g SM
Ses
abou
t the
ir s
exua
l he
alth
ove
r th
e ce
ll ph
one,
incl
udin
g in
form
atio
n ab
out
sexu
ally
tran
smit
ted
infe
ctio
ns•
Of
thos
e, 8
8% w
ould
pr
efer
sex
ual h
ealt
h m
essa
ges
via
SMS
68%
via
cal
ls w
ith
a pr
erec
orde
d vo
ice
• M
any
said
they
wou
ld
like
to r
ecei
ve g
ener
al
HIV
info
rmat
ion
via
cell
phon
es
( Con
tinu
ed)
17
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
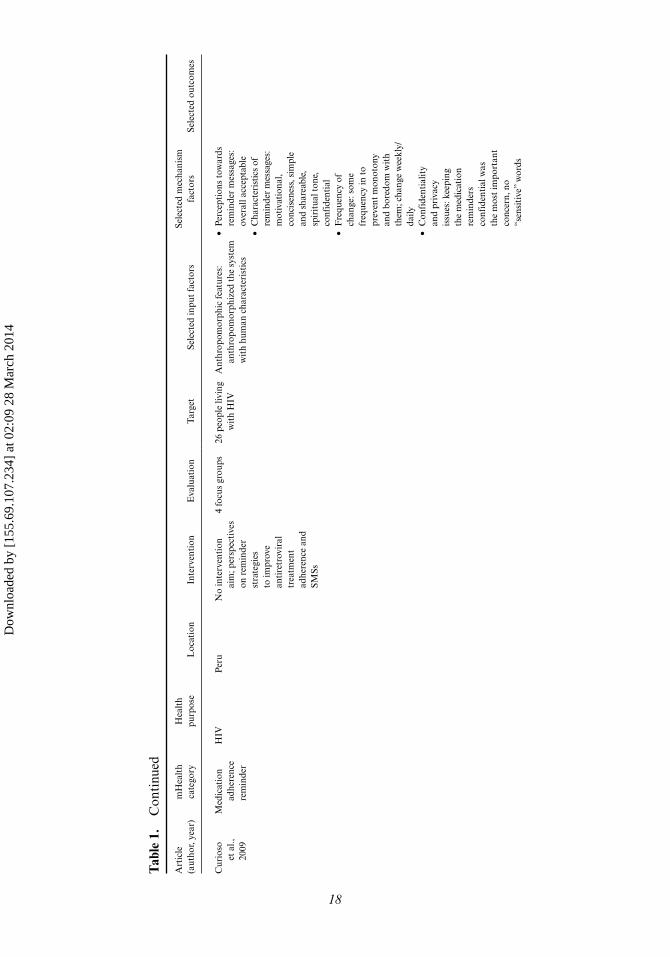
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Cur
ioso
et
al.,
20
09
Med
icat
ion
adhe
renc
e re
min
der
HIV
Per
uN
o in
terv
enti
on
aim
; per
spec
tive
s on
rem
inde
r st
rate
gies
to
impr
ove
anti
retr
ovir
al
trea
tmen
t ad
here
nce
and
SMSs
4 fo
cus
grou
ps26
peo
ple
livin
g w
ith
HIV
Ant
hrop
omor
phic
fea
ture
s:
anth
ropo
mor
phiz
ed th
e sy
stem
w
ith
hum
an c
hara
cter
isti
cs
• P
erce
ptio
ns t
owar
ds
rem
inde
r m
essa
ges:
ov
eral
l acc
epta
ble
• C
hara
cter
isti
cs o
f re
min
der
mes
sage
s:
mot
ivat
iona
l, co
ncis
enes
s, s
impl
e an
d sh
area
ble,
sp
irit
ual t
one,
co
nfid
enti
al•
Fre
quen
cy o
f ch
ange
: som
e fr
eque
ncy
in t
o pr
even
t m
onot
ony
and
bore
dom
wit
h th
em; c
hang
e w
eekl
y/da
ily•
Con
fide
ntia
lity
and
priv
acy
issu
es: k
eepi
ng
the
med
icat
ion
rem
inde
rs
conf
iden
tial
was
th
e m
ost
impo
rtan
t co
ncer
n, n
o “s
ensi
tive
” w
ords
18
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
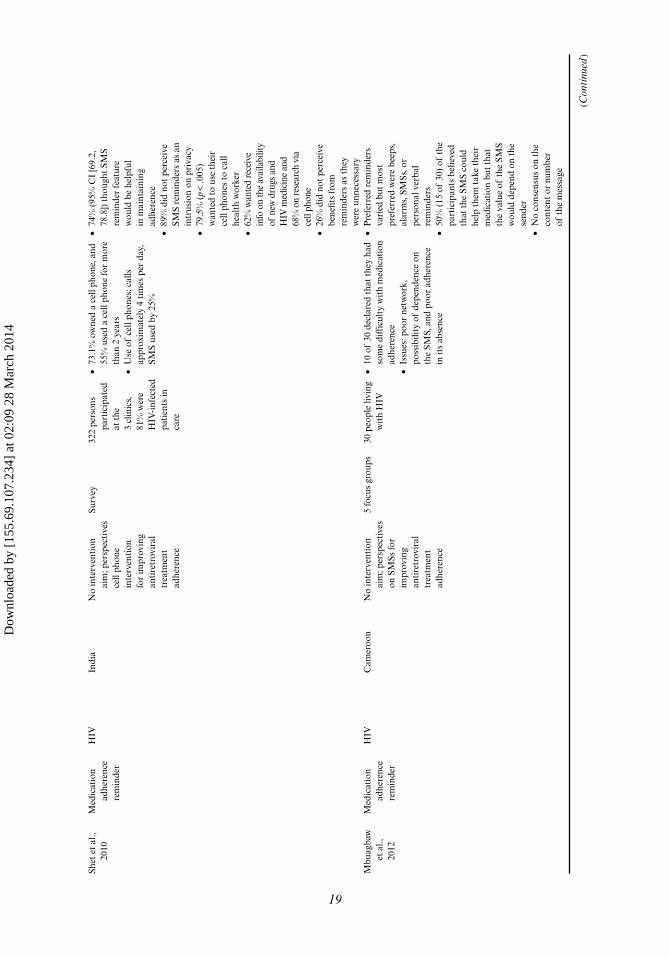
Shet
et
al.,
2010
Med
icat
ion
adhe
renc
e re
min
der
HIV
Indi
aN
o in
terv
enti
on
aim
; per
spec
tive
s ce
ll ph
one
inte
rven
tion
fo
r im
prov
ing
anti
retr
ovir
al
trea
tmen
t ad
here
nce
Surv
ey32
2 pe
rson
s pa
rtic
ipat
ed
at t
he
3 cl
inic
s,
81%
wer
e H
IV-i
nfec
ted
pati
ents
in
care
• 73
.1%
ow
ned
a ce
ll ph
one,
and
55
% u
sed
a ce
ll ph
one
for
mor
e th
an 2
yea
rs•
Use
of
cell
phon
es; c
alls
ap
prox
imat
ely
4 ti
mes
per
day
, SM
S us
ed b
y 25
%
• 74
% (
95%
CI
[69.
2,
78.8
]) t
houg
ht S
MS
rem
inde
r fe
atur
e w
ould
be
help
ful
in m
aint
aini
ng
adhe
renc
e•
89%
did
not
per
ceiv
e SM
S re
min
ders
as
an
intr
usio
n on
pri
vacy
• 79
.5%
(p
< .0
05)
wan
ted
to u
se t
heir
ce
ll ph
ones
to
call
heal
th w
orke
r•
62%
wan
ted
rece
ive
info
on
the
avai
labi
lity
of n
ew d
rugs
and
H
IV m
edic
ine
and
68%
on
rese
arch
via
ce
ll ph
one
• 26
% d
id n
ot p
erce
ive
bene
fits
from
re
min
ders
as
they
w
ere
unne
cess
ary
Mbu
agba
w
et a
l.,
2012
Med
icat
ion
adhe
renc
e re
min
der
HIV
Cam
eroo
nN
o in
terv
enti
on
aim
; per
spec
tive
s on
SM
Ss fo
r im
prov
ing
anti
retr
ovir
al
trea
tmen
t ad
here
nce
5 fo
cus
grou
ps30
peo
ple
livin
g w
ith
HIV
• 10
of
30 d
ecla
red
that
the
y ha
d so
me
diff
icul
ty w
ith
med
icat
ion
adhe
renc
e•
Issu
es: p
oor
netw
ork,
po
ssib
ility
of
depe
nden
ce o
n th
e SM
S, a
nd p
oor
adhe
renc
e in
its
abse
nce
• P
refe
rred
rem
inde
rs
vari
ed b
ut m
ost
pref
erre
d w
ere
beep
s,
alar
ms,
SM
Ss, o
r pe
rson
al v
erba
l re
min
ders
• 50
% (
15 o
f 30
) of
the
pa
rtic
ipan
ts b
elie
ved
that
the
SM
S co
uld
help
the
m t
ake
thei
r m
edic
atio
n bu
t th
at
the
valu
e of
the
SM
S w
ould
dep
end
on t
he
send
er•
No
cons
ensu
s on
the
co
nten
t or
num
ber
of t
he m
essa
ge
( Con
tinu
ed)
19
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
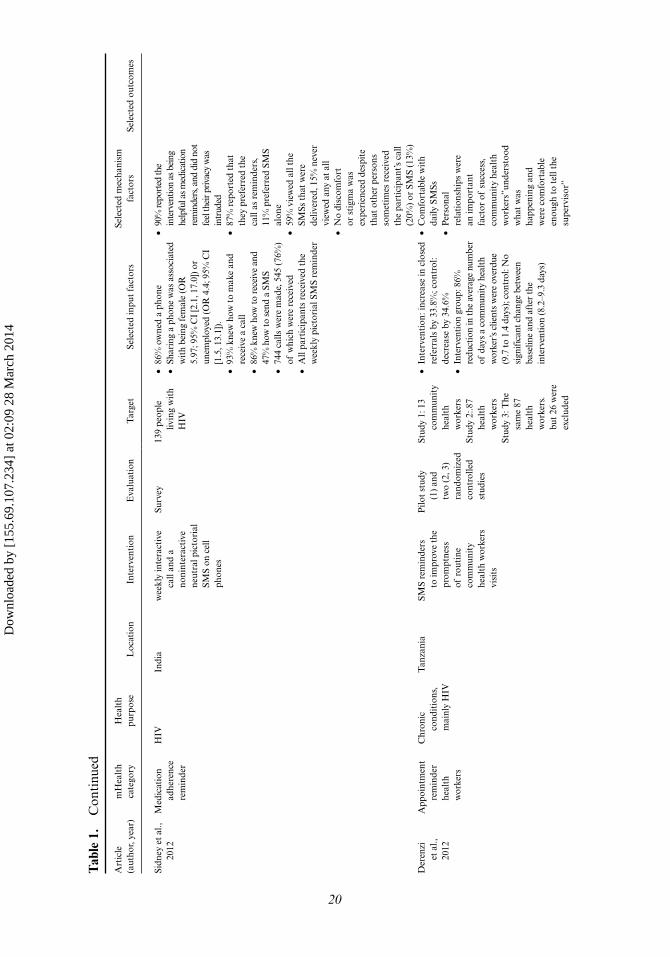
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Sidn
ey e
t al
., 20
12M
edic
atio
n ad
here
nce
rem
inde
r
HIV
Indi
aw
eekl
y in
tera
ctiv
e ca
ll an
d a
noni
nter
acti
ve
neut
ral p
icto
rial
SM
S on
cel
l ph
ones
Surv
ey13
9 pe
ople
liv
ing
wit
h H
IV
• 86
% o
wne
d a
phon
e•
Shar
ing
a ph
one
was
ass
ocia
ted
wit
h be
ing
fem
ale
(OR
5.
97; 9
5% C
I [2
.1, 1
7.0]
) or
unem
ploy
ed (O
R 4
.4; 9
5% C
I [1
.5, 1
3.1]
).•
93%
kne
w h
ow t
o m
ake
and
rece
ive
a ca
ll•
86%
kne
w h
ow to
rec
eive
and
47
% h
ow to
sen
d a
SMS
• 74
4 ca
lls w
ere
mad
e, 5
45 (
76%
) of
whi
ch w
ere
rece
ived
• A
ll pa
rtic
ipan
ts r
ecei
ved
the
wee
kly
pict
oria
l SM
S re
min
der
• 90
% re
port
ed th
e in
terv
entio
n as
bei
ng
help
ful a
s med
icat
ion
rem
inde
rs, a
nd d
id n
ot
feel
thei
r priv
acy
was
in
trud
ed•
87%
rep
orte
d th
at
they
pre
ferr
ed t
he
call
as r
emin
ders
, 11
% p
refe
rred
SM
S al
one
• 59
% v
iew
ed a
ll th
e SM
Ss t
hat
wer
e de
liver
ed, 1
5% n
ever
vi
ewed
any
at
all
• N
o di
scom
fort
or
sti
gma
was
ex
peri
ence
d de
spit
e th
at o
ther
per
sons
so
met
imes
rec
eive
d th
e pa
rtic
ipan
t’s c
all
(20%
) or
SM
S (1
3%)
Der
enzi
et
al.,
20
12
App
oint
men
t re
min
der
heal
th
wor
kers
Chr
onic
co
ndit
ions
, m
ainl
y H
IV
Tan
zani
aSM
S re
min
ders
to
impr
ove
the
prom
ptne
ss
of r
outi
ne
com
mun
ity
heal
th w
orke
rs
visi
ts
Pilo
t st
udy
(1)
and
two
(2, 3
) ra
ndom
ized
co
ntro
lled
stud
ies
Stud
y 1:
13
com
mun
ity
heal
th
wor
kers
Stud
y 2:
.87
heal
th
wor
kers
Stud
y 3:
The
sa
me
87
heal
th
wor
kers
. bu
t 26
wer
e ex
clud
ed
• In
terv
enti
on: i
ncre
ase
in c
lose
d re
ferr
als
by 3
3.8%
; con
trol
: de
crea
se b
y 34
.6%
• In
terv
entio
n gr
oup:
86%
re
duct
ion
in th
e av
erag
e nu
mbe
r of
day
s a
com
mun
ity h
ealth
w
orke
r’s c
lient
s w
ere
over
due
(9.7
to 1
.4 d
ays)
; con
trol
: No
sign
ifica
nt c
hang
e be
twee
n ba
selin
e an
d af
ter
the
inte
rven
tion
(8.2
–9.3
day
s)
• C
omfo
rtab
le w
ith
daily
SM
Ss•
Per
sona
l re
lati
onsh
ips
wer
e an
impo
rtan
t fa
ctor
of
succ
ess,
co
mm
unit
y he
alth
w
orke
rs”u
nder
stoo
d w
hat
was
ha
ppen
ing
and
wer
e co
mfo
rtab
le
enou
gh t
o te
ll th
e su
perv
isor
”
20
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
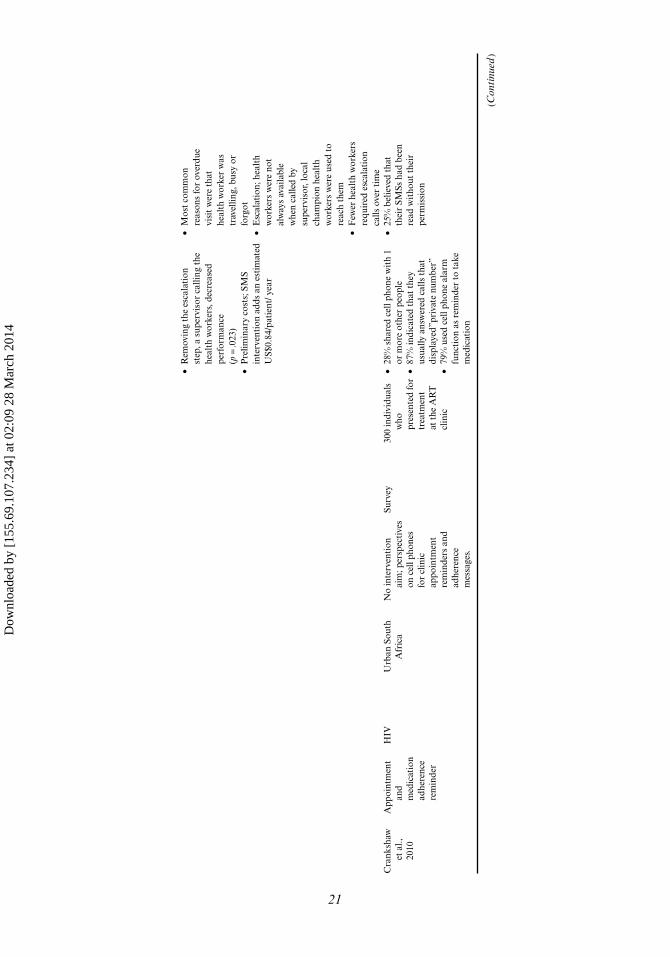
• R
emov
ing
the
esca
lati
on
step
, a s
uper
viso
r ca
lling
the
he
alth
wor
kers
, dec
reas
ed
perf
orm
ance
(p
= .0
23)
• P
relim
inar
y co
sts;
SM
S in
terv
enti
on a
dds
an e
stim
ated
U
S$0.
84/p
atie
nt/ y
ear
• M
ost
com
mon
re
ason
s fo
r ov
erdu
e vi
sit
wer
e th
at
heal
th w
orke
r w
as
trav
ellin
g, b
usy
or
forg
ot•
Esc
alat
ion;
hea
lth
wor
kers
wer
e no
t al
way
s av
aila
ble
whe
n ca
lled
by
supe
rvis
or, l
ocal
ch
ampi
on h
ealt
h w
orke
rs w
ere
used
to
reac
h th
em•
Few
er h
ealt
h w
orke
rs
requ
ired
esc
alat
ion
calls
ove
r ti
me
Cra
nksh
aw
et a
l.,
2010
App
oint
men
t an
d m
edic
atio
n ad
here
nce
rem
inde
r
HIV
Urb
an S
outh
A
fric
aN
o in
terv
enti
on
aim
; per
spec
tive
s on
cel
l pho
nes
for
clin
ic
appo
intm
ent
rem
inde
rs a
nd
adhe
renc
e m
essa
ges.
Surv
ey30
0 in
divi
dual
s w
ho
pres
ente
d fo
r tr
eatm
ent
at t
he A
RT
cl
inic
• 28
% s
hare
d ce
ll ph
one
wit
h 1
or m
ore
othe
r pe
ople
• 87
% in
dica
ted
that
the
y us
ually
ans
wer
ed c
alls
tha
t di
spla
yed”
priv
ate
num
ber”
• 79
% u
sed
cell
phon
e al
arm
fu
ncti
on a
s re
min
der
to t
ake
med
icat
ion
• 25
% b
elie
ved
that
th
eir
SMSs
had
bee
n re
ad w
itho
ut t
heir
pe
rmis
sion
(Con
tinu
ed)
21
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
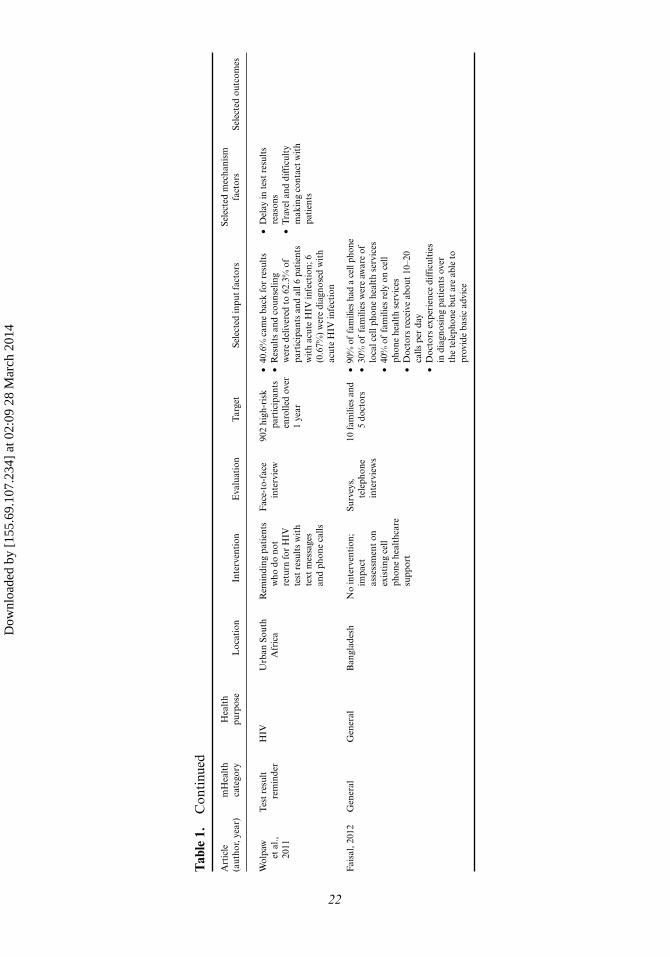
Tab
le 1
. C
onti
nued
Art
icle
(a
utho
r, ye
ar)
mH
ealt
h ca
tego
ryH
ealt
h pu
rpos
eL
ocat
ion
Inte
rven
tion
Eva
luat
ion
Tar
get
Sele
cted
inpu
t fa
ctor
sSe
lect
ed m
echa
nism
fa
ctor
sSe
lect
ed o
utco
mes
Wol
paw
et
al.,
20
11
Tes
t re
sult
re
min
der
HIV
Urb
an S
outh
A
fric
aR
emin
ding
pat
ient
s w
ho d
o no
t re
turn
for
HIV
te
st r
esul
ts w
ith
text
mes
sage
s an
d ph
one
calls
Fac
e-to
-fac
e in
terv
iew
90
2 hi
gh-r
isk
part
icip
ants
en
rolle
d ov
er
1 ye
ar
• 40
.6%
cam
e ba
ck fo
r re
sult
s•
Res
ults
and
cou
nsel
ing
wer
e de
liver
ed t
o 62
.3%
of
part
icip
ants
and
all
6 pa
tien
ts
wit
h ac
ute
HIV
infe
ctio
n; 6
(0
.67%
) w
ere
diag
nose
d w
ith
acut
e H
IV in
fect
ion
• D
elay
in t
est
resu
lts
reas
ons
• T
rave
l and
diff
icul
ty
mak
ing
cont
act
wit
h pa
tien
ts
Fai
sal,
2012
Gen
eral
Gen
eral
Ban
glad
esh
No
inte
rven
tion
; im
pact
as
sess
men
t on
ex
isti
ng c
ell
phon
e he
alth
care
su
ppor
t
Surv
eys,
te
leph
one
inte
rvie
ws
10 f
amili
es a
nd
5 do
ctor
s•
90%
of
fam
ilies
had
a c
ell p
hone
• 30
% o
f fa
mili
es w
ere
awar
e of
lo
cal c
ell p
hone
hea
lth
serv
ices
• 40
% o
f fa
mili
es r
ely
on c
ell
phon
e he
alth
ser
vice
s•
Doc
tors
rec
eive
abo
ut 1
0–20
ca
lls p
er d
ay•
Doc
tors
exp
erie
nce
diff
icul
ties
in
dia
gnos
ing
pati
ents
ove
r th
e te
leph
one
but
are
able
to
prov
ide
basi
c ad
vice
22
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 23
and SMS quizzes for health promotion (Chib, Wilkin, et al., 2012; Danis et al., 2010), providing health information (Maharani et al., 2012), and an application for health worker’s learning (Zolfo et al., 2010). A diverse set of standards was applied, with no evidence provided for interoperability.
Other studies researched the possibility of an SMS intervention for family plan-ning (L’Engle & Vadhat, 2009), HIV prevention (J. R. Mitchell et al., 2011), or antiret-roviral therapy reminders (Curioso et al., 2009; Mbuagbaw et al., 2012; Shet et al., 2010). The use of mobiles was studied in general (Faisal, 2011), for clinic appointment reminders and adherence messages (Crankshaw et al., 2010; Shet et al., 2010), and the use of information and communication technology in general for people living with HIV (Curioso & Kurth, 2007).
It is worth noting that this group of studies were more relevant to practitioners yet lacked explicit theoretical support and largely failed to address outputs. However, we found factors for technology adoption in these articles such as perceived facili-tators and barriers and preferences (Alam et al., 2010; Asiimwe et al., 2011; Azfar et al., 2011; Barrington et al., 2010; Chib, Wilkin, et al., 2012; Cole-Ceesay et al., 2010; Crankshaw et al., 2010; Curioso et al., 2009; W. H. Curioso & A. E. Kurth, 2007; Derenzi et al., 2012; Faisal, 2011; Haberer et al., 2010; Kaewkungwal et al., 2010; L’Engle & Vadhat, 2009; Lemay et al., 2012; Macrohon & Cristobal, 2011; Mbuagbaw et al., 2012; J. R. Mitchell et al., 2011; MOTECH, 2011; Rajatonirina et al., 2012; Shet et al., 2010; Skinner et al., 2007; T. Svoronos et al., 2010; Wolpaw et al., 2011; Zhang et al., 2012). Some of these studies provided some evidence of potential impact (Barrington et al., 2010; Kaewkungwal et al., 2010; Lemay et al., 2012; Rajatonirina et al., 2012; T. Svoronos et al., 2010). Two studies in rural Tanzania showed impact: increases in the numbers of antimalarial medicines stocks (Barrington et al., 2010), and anecdotal evidence of improved management of antenatal care (Svoronos et al., 2010). A study in rural Thailand reported improved antenatal and immunization cov-erage (Kaewkungwal et al., 2010).
Mechanism
A second and smaller number of studies (Ashraf et al., 2010; Chib & Chen, 2011; Chib, Cheong, et al., 2012; Chib, Law, et al., 2012; Hamilton, 2010; Hwabamungu & Williams, 2010 [n = 6]) investigated the reasons for technology adoption, using theoret-ical models for explanation or validation of the findings. These studies are described in detail in Table 2.
Four of these studies (Chib & Chen, 2011; Chib, Law, et al., 2012; Hamilton, 2010; Hwabamungu & Williams, 2010) used theory to explain the potential for mobile phones in addressing health problems. The ICT4 healthcare develop-ment model, was used by community healthcare workers for accessing informa-tion by mobile phones in rural India (Chib, Cheong, et al., 2012). Spatiotemporal arguments (Castells, 1989) were used in rural Nepal to structure the potential of mobile phones for rural communities (Chib, Law, et al., 2012). The Technology Acceptance Model (Davis, 1986) was adapted to study views of people living with HIV and healthcare workers on usability of mobile phone applications for health-care in South Africa. However, the exact constructs of the theories studied were not described (Hwabamungu & Williams, 2010). Social marketing theory (Hastings, 2007) was used in rural Kenya for studying the use of mobile phones for health promotion (Hamilton, 2010).
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
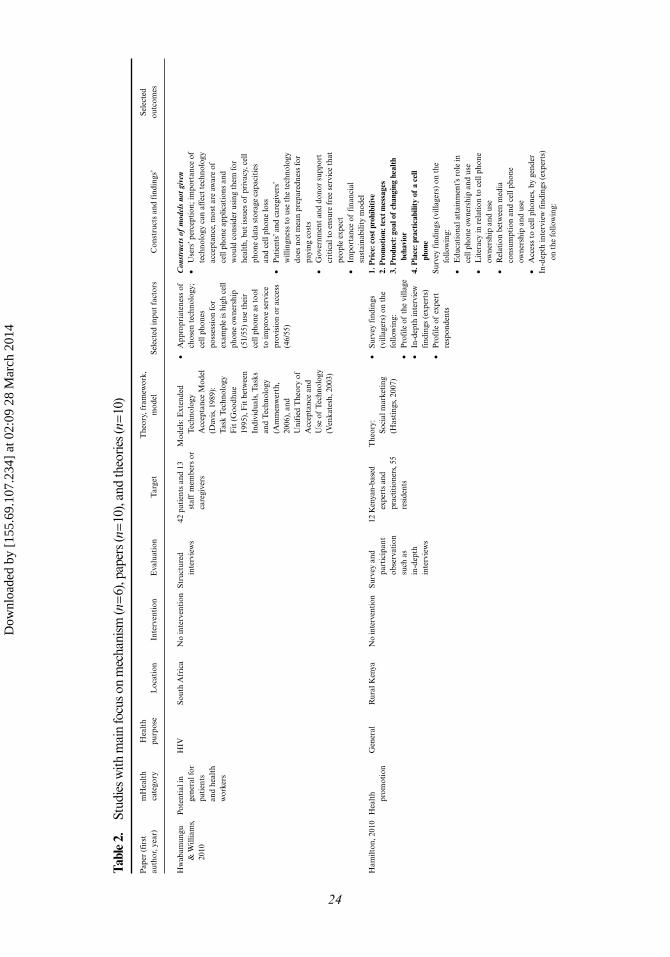
Tabl
e 2.
St
udie
s with
mai
n fo
cus o
n m
echa
nism
(n =
6), p
aper
s (n =
10),
and
theo
ries
(n =
10)
Pap
er (
firs
t au
thor
, yea
r)m
Hea
lth
cate
gory
Hea
lth
purp
ose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tT
heor
y, f
ram
ewor
k,
mod
elSe
lect
ed in
put
fact
ors
Con
stru
cts
and
find
ings
’Se
lect
ed
outc
omes
Hw
abam
ungu
&
Will
iam
s,
2010
Pote
ntia
l in
gene
ral f
or
pati
ents
an
d he
alth
w
orke
rs
HIV
Sout
h A
fric
aN
o in
terv
enti
onSt
ruct
ured
in
terv
iew
s42
pat
ient
s an
d 13
st
aff
mem
bers
or
care
give
rs
Mod
els:
Ext
ende
d T
echn
olog
y A
ccep
tanc
e M
odel
(D
avis
, 198
9):
Tas
k T
echn
olog
y F
it (
Goo
dhue
19
95),
Fit
bet
wee
n In
divi
dual
s, T
asks
an
d T
echn
olog
y (A
mm
enw
erth
, 20
06),
and
U
nifi
ed T
heor
y of
A
ccep
tanc
e an
d U
se o
f T
echn
olog
y (V
enka
tesh
, 200
3)
• A
ppro
pria
tene
ss o
f ch
osen
tec
hnol
ogy;
ce
ll ph
ones
po
sses
sion
for
exam
ple
is h
igh
cell
phon
e ow
ners
hip
(51/
55)
use
thei
r ce
ll ph
one
as t
ool
to im
prov
e se
rvic
e pr
ovis
ion
or a
cces
s (4
6/55
)
Con
stru
cts
of m
odel
s no
t giv
en•
Use
rs’ p
erce
ptio
n; im
port
ance
of
tech
nolo
gy c
an a
ffec
t te
chno
logy
ac
cept
ance
, mos
t ar
e aw
are
of
cell
phon
e ap
plic
atio
ns a
nd
wou
ld c
onsi
der
usin
g th
em fo
r he
alth
, but
issu
es o
f pr
ivac
y, c
ell
phon
e da
ta s
tora
ge c
apac
itie
s an
d ce
ll ph
one
loss
• P
atie
nts’
and
car
egiv
ers’
w
illin
gnes
s to
use
the
tec
hnol
ogy
does
not
mea
n pr
epar
edne
ss fo
r pa
ying
cos
ts•
Gov
ernm
ent
and
dono
r su
ppor
t cr
itic
al t
o en
sure
fre
e se
rvic
e th
at
peop
le e
xpec
t•
Impo
rtan
ce o
f fi
nanc
ial
sust
aina
bilit
y m
odel
H
amilt
on, 2
010
Hea
lth
prom
otio
n G
ener
alR
ural
Ken
yaN
o in
terv
entio
nSu
rvey
and
pa
rtic
ipan
t ob
serv
atio
n su
ch a
s in
-dep
th
inte
rvie
ws
12 K
enya
n-ba
sed
expe
rts
and
prac
titio
ners
, 55
resi
dent
s
The
ory:
Soci
al m
arke
ting
(H
asti
ngs,
200
7)
• Su
rvey
fin
ding
s (v
illag
ers)
on
the
follo
win
g:•
Pro
file
of
the
villa
ge•
In-d
epth
inte
rvie
w
find
ings
(ex
pert
s)•
Pro
file
of
expe
rt
resp
onde
nts
1. P
rice
: cos
t pro
hibi
tive
2. P
rom
otio
n: te
xt m
essa
ges
3. P
rodu
ct: g
oal o
f ch
angi
ng h
ealt
h be
havi
or4.
Pla
ce: p
ract
icab
ility
of
a ce
ll ph
one
Surv
ey f
indi
ngs
(vill
ager
s) o
n th
e fo
llow
ing:
• E
duca
tion
al a
ttai
nmen
t’s r
ole
in
cell
phon
e ow
ners
hip
and
use
• L
iter
acy
in r
elat
ion
to c
ell p
hone
ow
ners
hip
and
use
• R
elat
ion
betw
een
med
ia
cons
umpt
ion
and
cell
phon
e ow
ners
hip
and
use
• A
cces
s to
cel
l pho
nes,
by
gend
erIn
-dep
th in
terv
iew
fin
ding
s (e
xper
ts)
on t
he fo
llow
ing:
24
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
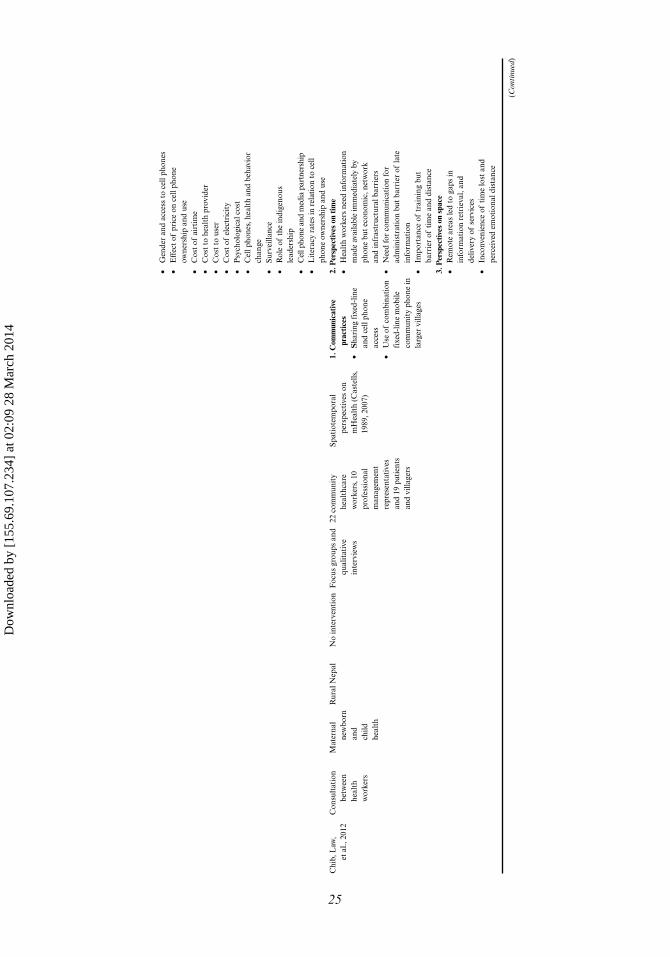
• G
ende
r an
d ac
cess
to
cell
phon
es•
Eff
ect
of p
rice
on
cell
phon
e ow
ners
hip
and
use
• C
ost
of a
irti
me
• C
ost
to h
ealt
h pr
ovid
er•
Cos
t to
use
r•
Cos
t of
ele
ctri
city
• P
sych
olog
ical
cos
t•
Cel
l pho
nes,
hea
lth
and
beha
vior
ch
ange
• Su
rvei
llanc
e•
Rol
e of
the
indi
geno
us
lead
ersh
ip•
Cel
l pho
ne a
nd m
edia
par
tner
ship
• L
iter
acy
rate
s in
rel
atio
n to
cel
l ph
one
owne
rshi
p an
d us
eC
hib,
Law
, et
al.,
201
2C
onsu
ltat
ion
betw
een
heal
th
wor
kers
Mat
erna
l ne
wbo
rn
and
child
he
alth
Rur
al N
epal
No
inte
rven
tion
Foc
us g
roup
s an
d qu
alit
ativ
e in
terv
iew
s
22 c
omm
unit
y he
alth
care
w
orke
rs, 1
0 pr
ofes
sion
al
man
agem
ent
repr
esen
tati
ves
and
19 p
atie
nts
and
villa
gers
Spat
iote
mpo
ral
pers
pect
ives
on
mH
ealt
h (C
aste
lls,
1989
, 200
7)
1. C
omm
unic
ativ
e pr
acti
ces
• S
hari
ng f
ixed
-lin
e an
d ce
ll ph
one
acce
ss•
Use
of
com
bina
tion
fi
xed-
line
mob
ile
com
mun
ity
phon
e in
la
rger
vill
ages
2. P
ersp
ectiv
es o
n ti
me
• H
ealt
h w
orke
rs n
eed
info
rmat
ion
mad
e av
aila
ble
imm
edia
tely
by
phon
e bu
t ec
onom
ic, n
etw
ork
and
infr
astr
uctu
ral b
arri
ers
• N
eed
for
com
mun
icat
ion
for
adm
inis
trat
ion
but
barr
ier
of la
te
info
rmat
ion
• Im
port
ance
of
trai
ning
but
ba
rrie
r of
tim
e an
d di
stan
ce3.
Per
spec
tives
on
spac
e•
Rem
ote
area
s le
d to
gap
s in
in
form
atio
n re
trie
val,
and
deliv
ery
of s
ervi
ces
• In
conv
enie
nce
of t
ime
lost
and
pe
rcei
ved
emot
iona
l dis
tanc
e
(Con
tinu
ed)
25
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
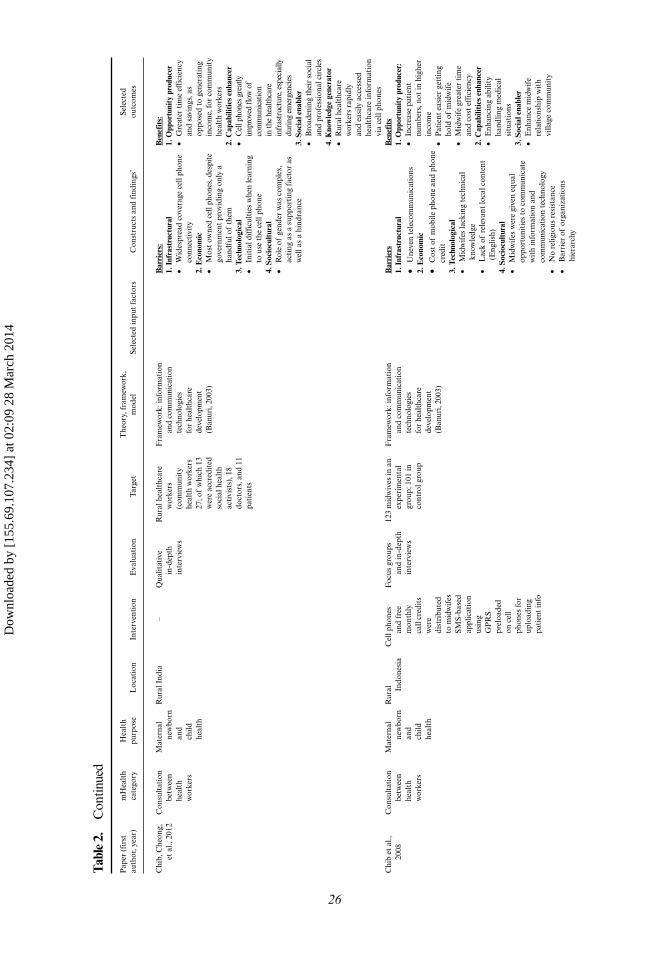
Tabl
e 2.
C
ontin
ued
Pap
er (
firs
t au
thor
, yea
r)m
Hea
lth
cate
gory
Hea
lth
purp
ose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tT
heor
y, f
ram
ewor
k,
mod
elSe
lect
ed in
put
fact
ors
Con
stru
cts
and
find
ings
’Se
lect
ed
outc
omes
Chi
b, C
heon
g,
et a
l., 2
012
Con
sult
atio
n be
twee
n he
alth
w
orke
rs
Mat
erna
l ne
wbo
rn
and
child
he
alth
Rur
al I
ndia
–Q
ualit
ativ
e in
-dep
th
inte
rvie
ws
Rur
al h
ealt
hcar
e w
orke
rs
(com
mun
ity
heal
th w
orke
rs
27; o
f w
hich
13
wer
e ac
cred
ited
so
cial
hea
lth
acti
vist
s), 1
8 do
ctor
s, a
nd 1
1 pa
tien
ts
Fra
mew
ork:
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gies
fo
r he
alth
care
de
velo
pmen
t (B
anur
i, 20
03)
Bar
rier
s:1.
Inf
rast
ruct
ural
• W
ides
prea
d co
vera
ge c
ell p
hone
co
nnec
tivi
ty2.
Eco
nom
ic•
Mos
t ow
ned
cell
phon
es, d
espi
te
gove
rnm
ent
prov
idin
g on
ly a
ha
ndfu
l of
them
3. T
echn
olog
ical
• In
itia
l diff
icul
ties
whe
n le
arni
ng
to u
se t
he c
ell p
hone
4. S
ocio
cult
ural
• R
ole
of g
ende
r w
as c
ompl
ex,
acti
ng a
s a
supp
orti
ng f
acto
r as
w
ell a
s a
hind
ranc
e
Ben
efit
s:1.
Opp
ortu
nity
pro
duce
r•
Gre
ater
tim
e ef
fici
ency
an
d sa
ving
s, a
s op
pose
d to
gen
erat
ing
inco
me,
for
com
mun
ity
heal
th w
orke
rs2.
Cap
abili
ties
enh
ance
r•
Cel
l pho
nes
grea
tly
impr
oved
flow
of
com
mun
icat
ion
in th
e he
alth
care
in
fras
truc
ture
, esp
ecia
lly
duri
ng e
mer
genc
ies
3. S
ocia
l ena
bler
• B
road
enin
g th
eir
soci
al
and
prof
essi
onal
cir
cles
4. K
now
ledg
e ge
nera
tor
• R
ural
hea
lthc
are
wor
kers
rap
idly
an
d ea
sily
acc
esse
d he
alth
care
info
rmat
ion
via
cell
phon
esC
hib
et a
l.,
2008
Con
sult
atio
n be
twee
n he
alth
w
orke
rs
Mat
erna
l ne
wbo
rn
and
child
he
alth
Rur
al
Indo
nesi
aC
ell p
hone
s an
d fr
ee
mon
thly
ca
ll cr
edit
s w
ere
dist
ribu
ted
to m
idw
ifes
SM
S-ba
sed
appl
icat
ion
usin
g G
PR
S pr
eloa
ded
on c
ell
phon
es fo
r up
load
ing
pati
ent
info
Foc
us g
roup
s an
d in
-dep
th
inte
rvie
ws
123
mid
wiv
es in
an
expe
rim
enta
l gr
oup;
101
in
cont
rol g
roup
Fra
mew
ork:
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gies
fo
r he
alth
care
de
velo
pmen
t (B
anur
i, 20
03)
Bar
rier
s1.
Inf
rast
ruct
ural
• U
neve
n te
leco
mm
unic
atio
ns2.
Eco
nom
ic
• C
ost
of m
obile
pho
ne a
nd p
hone
cr
edit
3. T
echn
olog
ical
• M
idw
ifes
lack
ing
tech
nica
l kn
owle
dge
• L
ack
of r
elev
ant
loca
l con
tent
(E
nglis
h)4.
Soc
iocu
ltur
al•
Mid
wif
es w
ere
give
n eq
ual
oppo
rtun
itie
s to
com
mun
icat
e w
ith
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gy•
No
relig
ious
res
ista
nce
• B
arri
er o
f or
gani
zati
ons
hier
arch
y
Ben
efit
s1.
Opp
ortu
nity
pro
duce
r:•
Incr
ease
pat
ient
nu
mbe
rs, n
ot in
hig
her
inco
me
• P
atie
nt e
asie
r ge
ttin
g ho
ld o
f m
idw
ife
• M
idw
ife
grea
ter
tim
e an
d co
st e
ffic
ienc
y2.
Cap
abili
ties
enh
ance
r•
Enh
anci
ng a
bilit
y ha
ndlin
g m
edic
al
situ
atio
ns3.
Soc
ial e
nabl
er•
Enh
ance
mid
wif
e re
lati
onsh
ip w
ith
villa
ge c
omm
unit
y
26
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
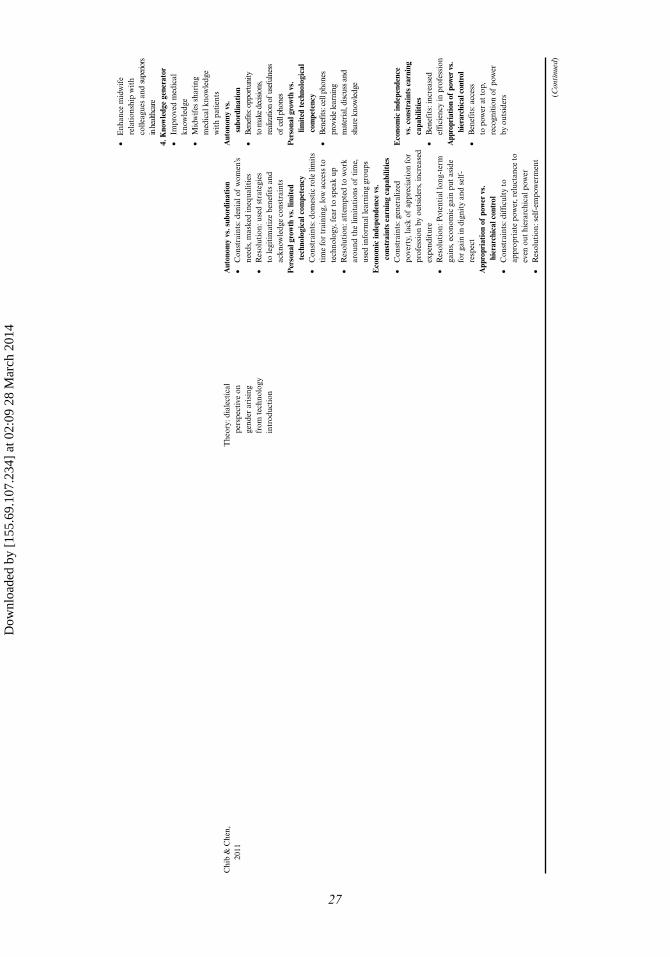
• E
nhan
ce m
idw
ife
rela
tion
ship
wit
h co
lleag
ues
and
supe
riors
in
hea
lthca
re4.
Kno
wle
dge
gene
rato
r•
Impr
oved
med
ical
kn
owle
dge
• M
idw
ifes
sha
ring
m
edic
al k
now
ledg
e w
ith
pati
ents
Chi
b &
Che
n,
2011
The
ory:
dia
lect
ical
pe
rspe
ctiv
e on
ge
nder
ari
sing
fr
om t
echn
olog
y in
trod
ucti
on
Aut
onom
y vs
. sub
ordi
nati
on•
Con
stra
ints
: den
ial o
f w
omen
’s ne
eds,
mas
ked
ineq
ualit
ies
• R
esol
utio
n: u
sed
stra
tegi
es
to le
giti
mat
ize
bene
fits
and
ac
know
ledg
e co
nstr
aint
sP
erso
nal g
row
th v
s. li
mit
ed
tech
nolo
gica
l com
pete
ncy
• C
onst
rain
ts: d
omes
tic
role
lim
its
tim
e fo
r tr
aini
ng, l
ow a
cces
s to
te
chno
logy
, fea
r to
spe
ak u
p•
Res
olut
ion:
att
empt
ed t
o w
ork
arou
nd t
he li
mit
atio
ns o
f ti
me,
us
ed in
form
al le
arni
ng g
roup
sE
cono
mic
inde
pend
ence
vs.
co
nstr
aint
s ea
rnin
g ca
pabi
litie
s
Aut
onom
y vs
. su
bord
inat
ion
• B
enef
its: o
ppor
tuni
ty
to m
ake d
ecisi
ons,
real
izat
ion
of u
sefu
lnes
s of
cell
phon
esP
erso
nal g
row
th v
s.
limit
ed te
chno
logi
cal
com
pete
ncy
• B
enef
its: c
ell p
hone
s pr
ovid
e le
arni
ng
mat
eria
l, di
scus
s and
sh
are
know
ledg
e
• C
onst
rain
ts: g
ener
aliz
ed
pove
rty,
lack
of
appr
ecia
tion
for
prof
essi
on b
y ou
tsid
ers,
incr
ease
d ex
pend
itur
e•
Res
olut
ion:
Pot
enti
al lo
ng-t
erm
ga
ins,
eco
nom
ic g
ain
put
asid
e fo
r ga
in in
dig
nity
and
sel
f-re
spec
tA
ppro
pria
tion
of
pow
er v
s.
hier
arch
ical
con
trol
• C
onst
rain
ts: d
iffic
ulty
to
appr
opri
ate
pow
er, r
eluc
tanc
e to
ev
en o
ut h
iera
rchi
cal p
ower
• R
esol
utio
n: s
elf-
empo
wer
men
t
Eco
nom
ic in
depe
nden
ce
vs. c
onst
rain
ts e
arni
ng
capa
bilit
ies
• B
enef
its:
incr
ease
d ef
fici
ency
in p
rofe
ssio
nA
ppro
pria
tion
of p
ower
vs.
hi
erar
chic
al c
ontr
ol•
Ben
efit
s: a
cces
s to
pow
er a
t top
, re
cogn
itio
n of
pow
er
by o
utsi
ders (C
onti
nued
)
27
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
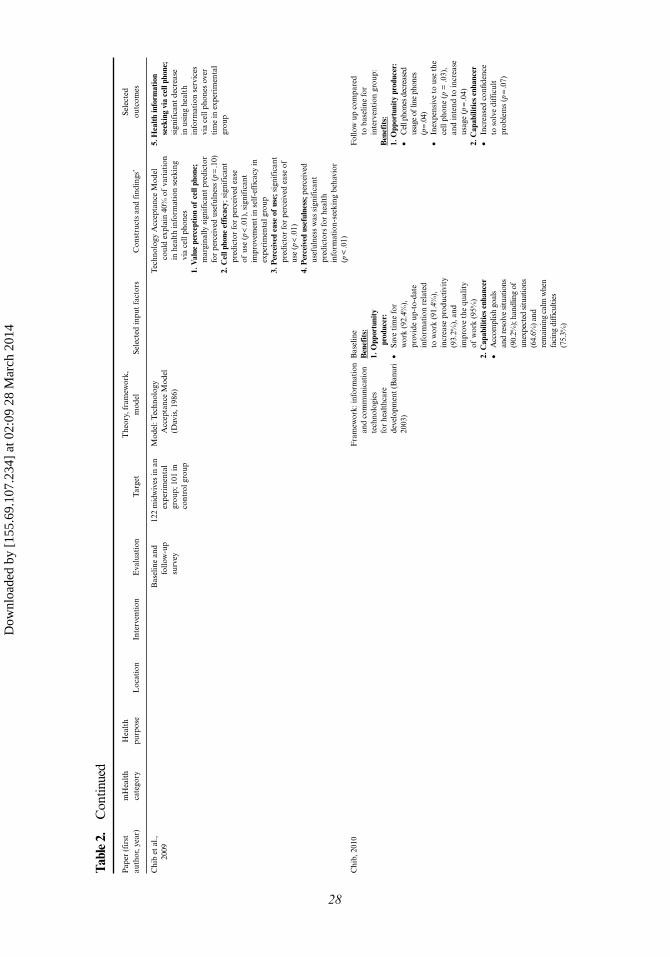
Tabl
e 2.
C
ontin
ued
Pap
er (
firs
t au
thor
, yea
r)m
Hea
lth
cate
gory
Hea
lth
purp
ose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tT
heor
y, f
ram
ewor
k,
mod
elSe
lect
ed in
put
fact
ors
Con
stru
cts
and
find
ings
’Se
lect
ed
outc
omes
Chi
b et
al.,
20
09B
asel
ine
and
follo
w-u
p su
rvey
122
mid
wiv
es in
an
expe
rim
enta
l gr
oup;
101
in
cont
rol g
roup
Mod
el: T
echn
olog
y A
ccep
tanc
e M
odel
(D
avis
, 198
6)
Tec
hnol
ogy
Acc
epta
nce
Mod
el
coul
d ex
plai
n 40
% o
f va
riat
ion
in h
ealt
h in
form
atio
n se
ekin
g vi
a ce
ll ph
ones
1. V
alue
per
cept
ion
of c
ell p
hone
; m
argi
nally
sig
nifi
cant
pre
dict
or
for
perc
eive
d us
eful
ness
(p =
.10)
2. C
ell p
hone
eff
icac
y; s
igni
fica
nt
pred
icto
r fo
r pe
rcei
ved
ease
of
use
(p <
.01)
, sig
nifi
cant
im
prov
emen
t in
sel
f-ef
fica
cy in
ex
peri
men
tal g
roup
3. P
erce
ived
eas
e of
use
; sig
nifi
cant
pr
edic
tor
for
perc
eive
d ea
se o
f us
e (p
< .0
1)4.
Per
ceiv
ed u
sefu
lnes
s; p
erce
ived
us
eful
ness
was
sig
nifi
cant
pr
edic
tors
for
heal
th
info
rmat
ion-
seek
ing
beha
vior
(p
< .0
1)
5. H
ealt
h in
form
atio
n se
ekin
g vi
a ce
ll ph
one;
si
gnif
ican
t de
crea
se
in u
sing
hea
lth
info
rmat
ion
serv
ices
vi
a ce
ll ph
ones
ove
r ti
me
in e
xper
imen
tal
grou
p
Chi
b, 2
010
Fra
mew
ork:
info
rmat
ion
and
com
mun
icat
ion
tech
nolo
gies
fo
r he
alth
care
de
velo
pmen
t (B
anur
i 20
03)
Bas
elin
eB
enef
its:
1. O
ppor
tuni
ty
prod
ucer
:•
Save
tim
e fo
r w
ork
(92.
4%),
pr
ovid
e up
-to-
date
in
form
atio
n re
late
d to
wor
k (9
1.4%
),
incr
ease
pro
duct
ivit
y (9
3.2%
), a
nd
impr
ove
the
qual
ity
of w
ork
(95%
)2.
Cap
abili
ties
enh
ance
r•
Acc
ompl
ish
goal
s an
d re
solv
e si
tuat
ions
(9
0.2%
); ha
ndlin
g of
un
expe
cted
situ
atio
ns
(64.
6%) a
nd
rem
aini
ng c
alm
whe
n fa
cing
diff
icul
ties
(75.
3%)
Fol
low
up
com
pare
d to
bas
elin
e fo
r in
terv
enti
on g
roup
:B
enef
its:
1. O
ppor
tuni
ty p
rodu
cer:
• C
ell p
hone
s dec
reas
ed
usag
e of
line
pho
nes
(p =
.04)
• In
expe
nsiv
e to
use
the
ce
ll ph
one
(p =
.03)
, an
d in
tend
to
incr
ease
us
age
(p =
.04)
2. C
apab
iliti
es e
nhan
cer
• In
crea
sed
confi
denc
e to
sol
ve d
iffic
ult
prob
lem
s (p
= .0
7)
28
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
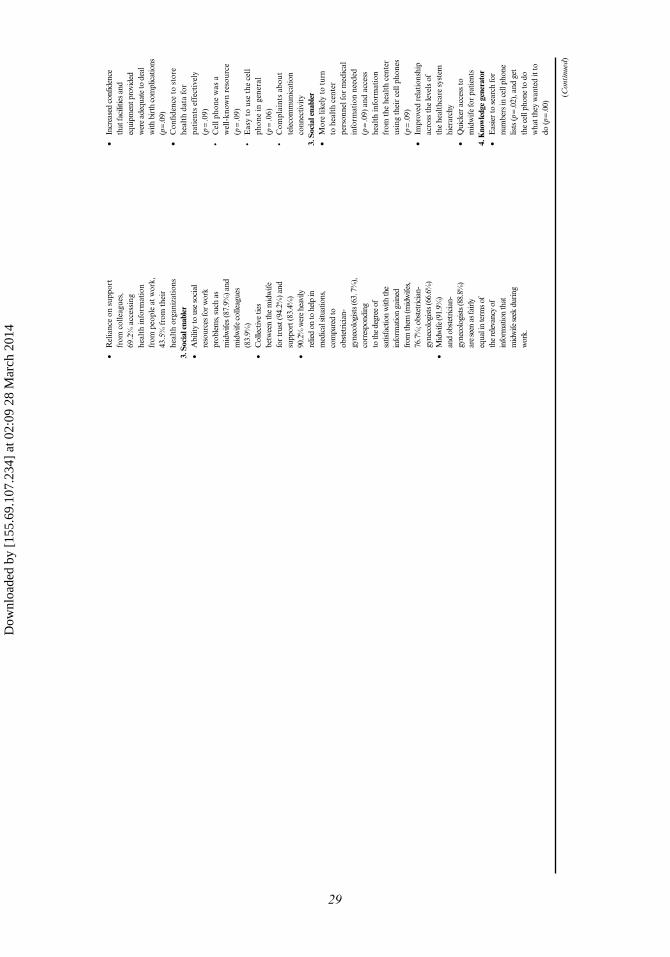
• R
elia
nce
on s
uppo
rt
from
col
leag
ues,
69
.2%
acc
essi
ng
heal
th in
form
atio
n fr
om p
eopl
e at
wor
k,
43.5
% f
rom
the
ir
heal
th o
rgan
izat
ions
3. S
ocia
l ena
bler
• A
bilit
y to
use
soc
ial
reso
urce
s fo
r w
ork
prob
lem
s, su
ch a
s m
idw
ifes
(87.
9%) a
nd
mid
wife
col
leag
ues
(83.
9%)
• C
olle
ctiv
e tie
s be
twee
n th
e m
idw
ife
for
trus
t (94
.2%
) and
su
ppor
t (83
.4%
)•
90.2
% w
ere
heav
ily
relie
d on
to h
elp
in
med
ical
situ
atio
ns,
com
pare
d to
ob
stet
ricia
n-gy
neco
logi
sts (
63. 7
%),
corr
espo
ndin
g to
the
degr
ee o
f sa
tisfa
ctio
n w
ith th
e in
form
atio
n ga
ined
fr
om th
em (m
idw
ifes,
76.7
%; o
bste
tric
ian-
gyne
colo
gist
s (66
.6%
)•
Mid
wife
(91.
9%)
and
obst
etric
ian-
gyne
colo
gist
s (88
.8%
) ar
e se
en a
s fai
rly
equa
l in
term
s of
the
rele
vanc
y of
in
form
atio
n th
at
mid
wife
seek
dur
ing
wor
k.
• In
crea
sed
confi
denc
e th
at fa
cilit
ies a
nd
equi
pmen
t pro
vide
d w
ere
adeq
uate
to d
eal
with
bir
th c
ompl
icat
ions
(p
= .0
9)•
Con
fiden
ce t
o st
ore
heal
th d
ata
for
pati
ents
eff
ecti
vely
(p
= .0
9)•
Cel
l pho
ne w
as a
w
ell-
know
n re
sour
ce
(p =
.09)
• E
asy
to u
se t
he c
ell
phon
e in
gen
eral
(p
= .0
6)•
Com
plai
nts
abou
t te
leco
mm
unic
atio
n co
nnec
tivity
3. S
ocia
l ena
bler
• M
ore
likel
y to
tur
n to
hea
lth
cent
er
pers
onne
l for
med
ical
in
form
atio
n ne
eded
(p
= .0
9) a
nd a
cces
s he
alth
info
rmat
ion
from
the
hea
lth
cent
er
usin
g th
eir
cell
phon
es
(p =
.09)
• Im
prov
ed r
elat
ions
hip
acro
ss th
e le
vels
of
the
heal
thca
re s
yste
m
hier
arch
y•
Qui
cker
acc
ess
to
mid
wife
for
patie
nts
4. K
now
ledg
e ge
nera
tor
• E
asie
r to
sea
rch
for
num
bers
in c
ell p
hone
lis
ts (p
= .0
2), a
nd g
et
the
cell
phon
e to
do
wha
t the
y w
ante
d it
to
do (p
= .0
0)
(Con
tinu
ed)
29
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
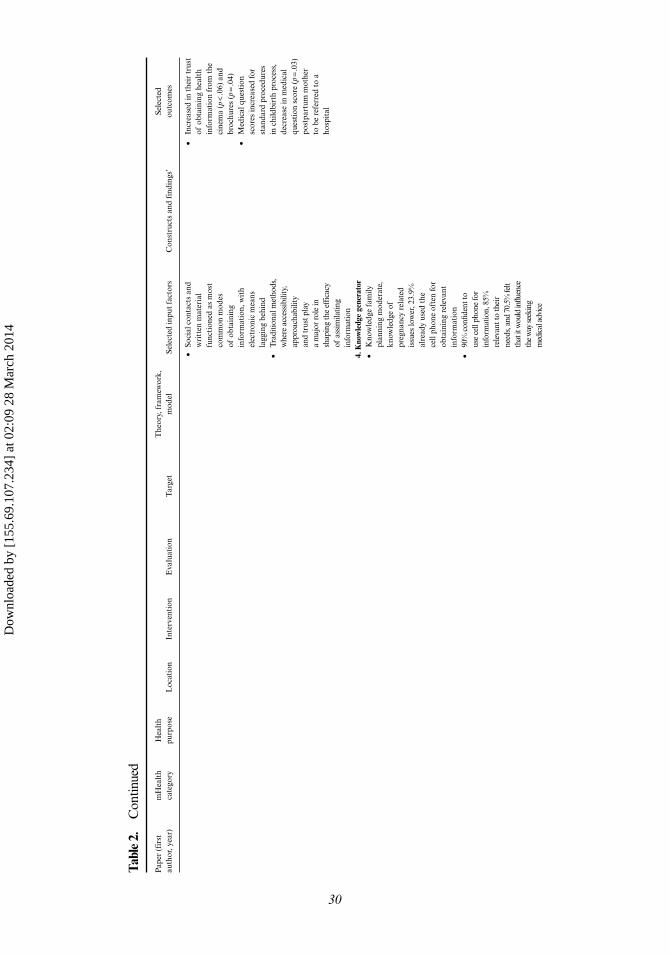
Tabl
e 2.
C
ontin
ued
Pap
er (
firs
t au
thor
, yea
r)m
Hea
lth
cate
gory
Hea
lth
purp
ose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tT
heor
y, f
ram
ewor
k,
mod
elSe
lect
ed in
put
fact
ors
Con
stru
cts
and
find
ings
’Se
lect
ed
outc
omes
•
Soci
al c
onta
cts
and
wri
tten
mat
eria
l fu
ncti
oned
as
mos
t co
mm
on m
odes
of
obt
aini
ng
info
rmat
ion,
wit
h el
ectr
onic
mea
ns
lagg
ing
behi
nd•
Trad
ition
al m
etho
ds,
whe
re a
cces
sibi
lity,
ap
proa
chab
ility
an
d tr
ust p
lay
a m
ajor
role
in
shap
ing
the
effic
acy
of a
ssim
ilatin
g in
form
atio
n
• In
crea
sed
in t
heir
tru
st
of o
btai
ning
hea
lth
info
rmat
ion
from
the
ci
nem
a (p
< .0
6) a
nd
broc
hure
s (p
= .0
4)•
Med
ical
que
stio
n sc
ores
incr
ease
d fo
r st
anda
rd p
roce
dure
s in
chi
ldbi
rth
proc
ess,
de
crea
se in
med
ical
qu
esti
on s
core
(p =
.03)
po
stpa
rtum
mot
her
to b
e re
ferr
ed t
o a
hosp
ital
4. K
now
ledg
e ge
nera
tor
• K
now
ledg
e fa
mily
pl
anni
ng m
oder
ate,
kn
owle
dge
of
preg
nanc
y re
late
d is
sues
low
er, 2
3.9%
al
read
y us
ed t
he
cell
phon
e of
ten
for
obta
inin
g re
leva
nt
info
rmat
ion
• 90
% c
onfid
ent t
o us
e ce
ll ph
one
for
info
rmat
ion,
85%
re
leva
nt to
thei
r ne
eds,
and
70.5
% fe
lt th
at it
wou
ld in
fluen
ce
the
way
seek
ing
med
ical
adv
ice
30
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
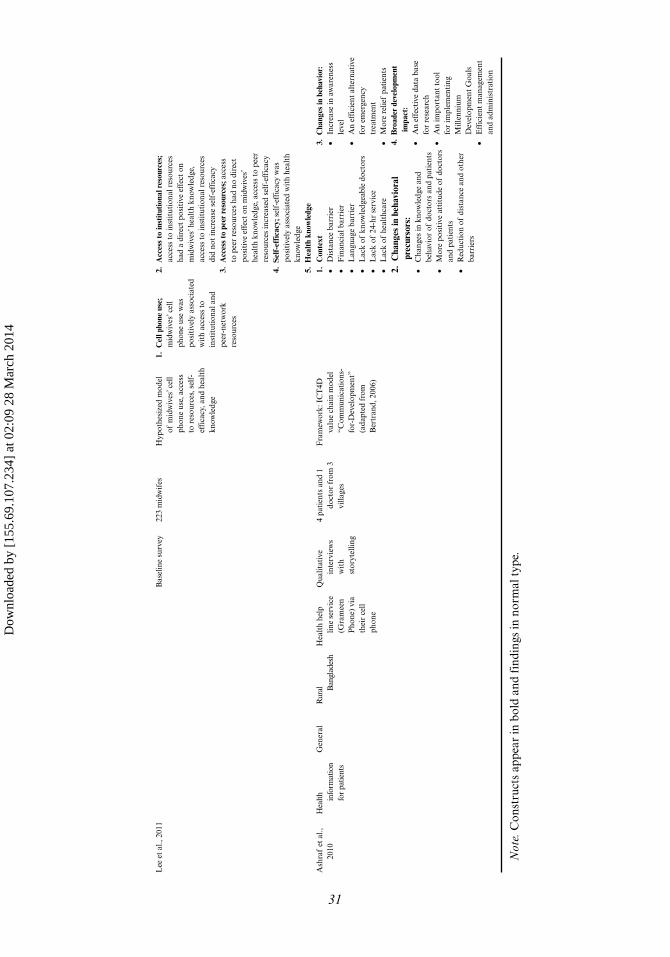
Lee
et
al.,
2011
Bas
elin
e su
rvey
223
mid
wif
esH
ypot
hesi
zed
mod
el
of m
idw
ives
’ cel
l ph
one
use,
acc
ess
to r
esou
rces
, sel
f-ef
fica
cy, a
nd h
ealt
h kn
owle
dge
1. C
ell p
hone
use
; m
idw
ives
’ cel
l ph
one
use
was
po
siti
vely
ass
ocia
ted
wit
h ac
cess
to
inst
itut
iona
l and
pe
er-n
etw
ork
reso
urce
s
2. A
cces
s to
inst
itut
iona
l res
ourc
es;
acce
ss t
o in
stit
utio
nal r
esou
rces
ha
d a
dire
ct p
osit
ive
effe
ct o
n m
idw
ives
’ hea
lth
know
ledg
e,
acce
ss t
o in
stit
utio
nal r
esou
rces
di
d no
t in
crea
se s
elf-
effi
cacy
3. A
cces
s to
pee
r re
sour
ces;
acc
ess
to p
eer
reso
urce
s ha
d no
dir
ect
posi
tive
eff
ect
on m
idw
ives
’ he
alth
kno
wle
dge,
acc
ess
to p
eer
reso
urce
s in
crea
sed
self
-eff
icac
y4.
Sel
f-ef
fica
cy; s
elf-
effi
cacy
was
po
siti
vely
ass
ocia
ted
wit
h he
alth
kn
owle
dge
5. H
ealt
h kn
owle
dge
Ash
raf
et a
l.,
2010
Hea
lth
info
rmat
ion
for
patie
nts
Gen
eral
Rur
al Ban
glad
esh
Hea
lth
help
lin
e se
rvic
e (G
ram
een
Pho
ne)
via
thei
r ce
ll ph
one
Qua
litat
ive
inte
rvie
ws
wit
h st
oryt
ellin
g
4 pa
tien
ts a
nd 1
do
ctor
fro
m 3
vi
llage
s
Fra
mew
ork:
IC
T4D
va
lue
chai
n m
odel
“C
om m
unic
atio
ns-
for-
Dev
elop
men
t”
(ada
pted
fro
m
Ber
tran
d, 2
006)
1. C
onte
xt•
Dis
tanc
e ba
rrie
r•
Fin
anci
al b
arri
er•
Lan
guag
e ba
rrie
r•
Lac
k of
kno
wle
dgea
ble
doct
ors
• L
ack
of 2
4-hr
ser
vice
• L
ack
of h
ealt
hcar
e
3. C
hang
es in
beh
avio
r:•
Incr
ease
in a
war
enes
s le
vel
• A
n ef
fici
ent
alte
rnat
ive
for
emer
genc
y tr
eatm
ent
• M
ore
relie
f pa
tien
ts
2. C
hang
es in
beh
avio
ral
prec
urso
rs:
• C
hang
es in
kno
wle
dge
and
beha
vior
of
doct
ors
and
pati
ents
• M
ore
posi
tive
att
itud
e of
doc
tors
an
d pa
tien
ts•
Red
ucti
on o
f di
stan
ce a
nd o
ther
ba
rrie
rs
4. B
road
er d
evel
opm
ent
impa
ct:
• A
n ef
fect
ive
data
bas
e fo
r re
sear
ch•
An
impo
rtan
t to
ol
for
impl
emen
ting
M
illen
nium
D
evel
opm
ent
Goa
ls•
Eff
icie
nt m
anag
emen
t an
d ad
min
istr
atio
n
Not
e. C
onst
ruct
s ap
pear
in b
old
and
find
ings
in n
orm
al t
ype.
31
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

32 A. Chib et al.
A study in rural Indonesia (represented by five articles: Chib, 2010; Chib & Chen, 2011; Chib, Lwin, Ang, Lin, & Santoso, 2008; Chib, Lwin, & Jung, 2009; Lee, Chib, & Kim, 2011) evaluated an intervention wherein midwifes were provided with mobile phones. Four theories were tested: the ICT4 healthcare model (Banuri, Zaidi, Spanger-Siegfried, Ali, & Zaidi, 2003) in two articles (Chib, 2010; Chib et al., 2008), dialectical perspectives on gender (Baxter & Montgomery, 1996) in one article (Chib & Chen, 2011), the technology acceptance model (Davis, 1985) in one article (Chib et al., 2009), and a hypothesized model of midwives’ mobile phone use, access to resources, self-efficacy, and health knowledge in the last article (Lee et al., 2011). The communication for development framework (Bertrand, O’Reilly, Denison, Anhang, & Sweat, 2006) was used to study a health helpline in rural Bangladesh (Ashraf et al., 2010).
A simple healthcare communication diagram (the study authors came up with this diagram) showing that patients, family, friends and healthcare workers are interconnected, was developed from studying peer health workers’ use of mobile phones to help people living with HIV to adhere to antiretroviral therapy in rural Uganda (as this study focused more on outputs it was categorized accordingly; Chang et al., 2011). The construct of stages of change (Prochaska & DiClemente, 1983) was used in a study obtaining health workers’ perspectives on receiving SMSs, which aimed to improve their malaria case management. Because this study focused more on outputs it was categorized accordingly (Jones et al., 2012; Zurovac et al., 2011).
We found that studies that were based on theory overlapped more with inputs studies than with outputs studies. The mechanism studies aimed to explain the adop-tion of technology using existing theory, or in the rare cases, advancing theory (Chib, 2010; Chib et al., 2009; Lee et al., 2011). However, the selection and contextualization of some theories was questionable, since these rationales were not explicitly stated in all articles (Ashraf et al., 2010; Hwabamungu & Williams, 2010). In three studies, the theoretical investigation concluded with an emphasis on outputs such as improved communication or greater efficiency within the healthcare system (Ashraf et al., 2010; Chib & Chen, 2011; Chib, Cheong, et al., 2012). All of these studies showed the poten-tial of mobile phones, but apart from two (Chang et al., 2011; Zurovac et al., 2011; cat-egorized in the outputs studies), they did not address quantitative effects on healthcare.
Outputs
The final set of outputs studies (Chang et al., 2011; Chen et al., 2008; da Costa et al., 2010; de Tolly et al., 2012; Jareethum et al., 2008; Kunutsor et al., 2010; Leong et al., 2006; Lester et al., 2010; Liew et al., 2009; Odigie et al., 2011; Piette et al., 2011; Pop-Eleches et al., 2011; Prasad & Anand, 2012; Seidenberg et al., 2012; Zurovac et al., 2011 [n = 15]) was most relevant to policy, providing some indications of improved patient health outputs, and healthcare process improvements. Table 3 describes these studies in detail. These studies mainly used a randomized (Chen et al., 2008; da Costa et al., 2010; de Tolly et al., 2012; Leong et al., 2006; Lester et al., 2010; Liew et al., 2009; Pop-Eleches et al., 2011) or cluster-randomized (Chang et al., 2011; Zurovac et al., 2011) controlled trial study designs.
Patient outcomes were related to medication adherence (Kunutsor et al., 2010; Lester et al., 2010; Pop-Eleches et al., 2011), HIV counselling and testing (de Tolly et al., 2012; Seidenberg et al., 2012), HIV virology (Chang et al., 2011; Lester et al., 2010), mortality (Chang et al., 2011), retention (Chang et al., 2011), diabetes (Piette
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
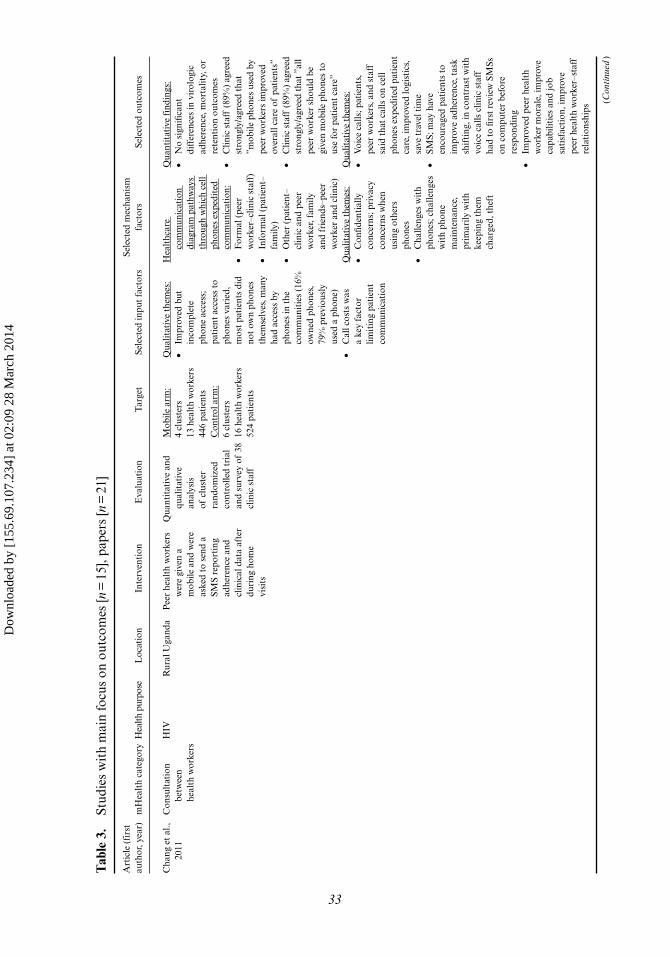
Tab
le 3
. St
udie
s w
ith
mai
n fo
cus
on o
utco
mes
[n =
15]
, pap
ers
[n =
21]
Art
icle
(fi
rst
auth
or, y
ear)
mH
ealt
h ca
tego
ryH
ealth
pur
pose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tSe
lect
ed in
put
fact
ors
Sele
cted
mec
hani
sm
fact
ors
Sele
cted
out
com
es
Cha
ng e
t al
., 20
11C
onsu
ltat
ion
betw
een
heal
th w
orke
rs
HIV
Rur
al U
gand
aP
eer
heal
th w
orke
rs
wer
e gi
ven
a m
obile
and
wer
e as
ked
to s
end
a SM
S re
port
ing
adhe
renc
e an
d cl
inic
al d
ata
afte
r du
ring
hom
e vi
sits
Qua
ntit
ativ
e an
d qu
alit
ativ
e an
alys
is
of c
lust
er
rand
omiz
ed
cont
rolle
d tr
ial
and
surv
ey o
f 38
cl
inic
sta
ff
Mob
ile a
rm:
4 cl
uste
rs13
hea
lth
wor
kers
446
pati
ents
Con
trol
arm
:6
clus
ters
16 h
ealt
h w
orke
rs52
4 pa
tien
ts
Qua
litat
ive
them
es:
• Im
prov
ed b
ut
inco
mpl
ete
phon
e ac
cess
; pa
tien
t ac
cess
to
phon
es v
arie
d,
mos
t pa
tien
ts d
id
not
own
phon
es
them
selv
es, m
any
had
acce
ss b
y ph
ones
in t
he
com
mun
itie
s (1
6%
owne
d ph
ones
, 79
% p
revi
ousl
y us
ed a
pho
ne)
• C
all c
osts
was
a
key
fact
or
limit
ing
pati
ent
com
mun
icat
ion
Hea
lthc
are
com
mun
icat
ion
diag
ram
pat
hway
s th
roug
h w
hich
cel
l ph
ones
exp
edit
ed
com
mun
icat
ion:
•
For
mal
(pe
er
wor
ker–
clin
ic s
taff
) •
Info
rmal
(pa
tien
t–fa
mily
) •
Oth
er (
pati
ent–
clin
ic a
nd p
eer
wor
ker,
fam
ily
and
frie
nds–
peer
w
orke
r an
d cl
inic
)Q
ualit
ativ
e th
emes
:•
Con
fiden
tial
ly
conc
erns
; pri
vacy
co
ncer
ns w
hen
usin
g ot
hers
ph
ones
• C
halle
nges
wit
h ph
ones
; cha
lleng
es
wit
h ph
one
mai
nten
ance
, pr
imar
ily w
ith
keep
ing
them
ch
arge
d, t
heft
Qua
ntit
ativ
e fi
ndin
gs:
• N
o si
gnifi
cant
di
ffer
ence
s in
vir
olog
ic
adhe
renc
e, m
orta
lity,
or
rete
ntio
n ou
tcom
es•
Clin
ic s
taff
(89
%)
agre
ed
stro
ngly
/agr
eed
that
”m
obile
pho
nes
used
by
peer
wor
kers
impr
oved
ov
eral
l car
e of
pat
ient
s”
• C
linic
sta
ff (
89%
) ag
reed
st
rong
ly/a
gree
d th
at ”
all
peer
wor
ker
shou
ld b
e gi
ven
mob
ile p
hone
s to
us
e fo
r pa
tien
t ca
re”
Qua
litat
ive
them
es:
• V
oice
cal
ls; p
atie
nts,
pe
er w
orke
rs, a
nd s
taff
sa
id t
hat
calls
on
cell
phon
es e
xped
ited
pat
ient
ca
re, i
mpr
oved
logi
stic
s,
save
tra
vel t
ime
• SM
S; m
ay h
ave
enco
urag
ed p
atie
nts
to
impr
ove
adhe
renc
e, t
ask
shif
ting
, in
cont
rast
wit
h vo
ice
calls
clin
ic s
taff
ha
d to
firs
t re
view
SM
Ss
on c
ompu
ter
befo
re
resp
ondi
ng•
Impr
oved
pee
r he
alth
w
orke
r m
oral
e, im
prov
e ca
pabi
litie
s an
d jo
b sa
tisf
acti
on, i
mpr
ove
peer
hea
lth
wor
ker–
staf
f re
lati
onsh
ips (C
onti
nued
)
33
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
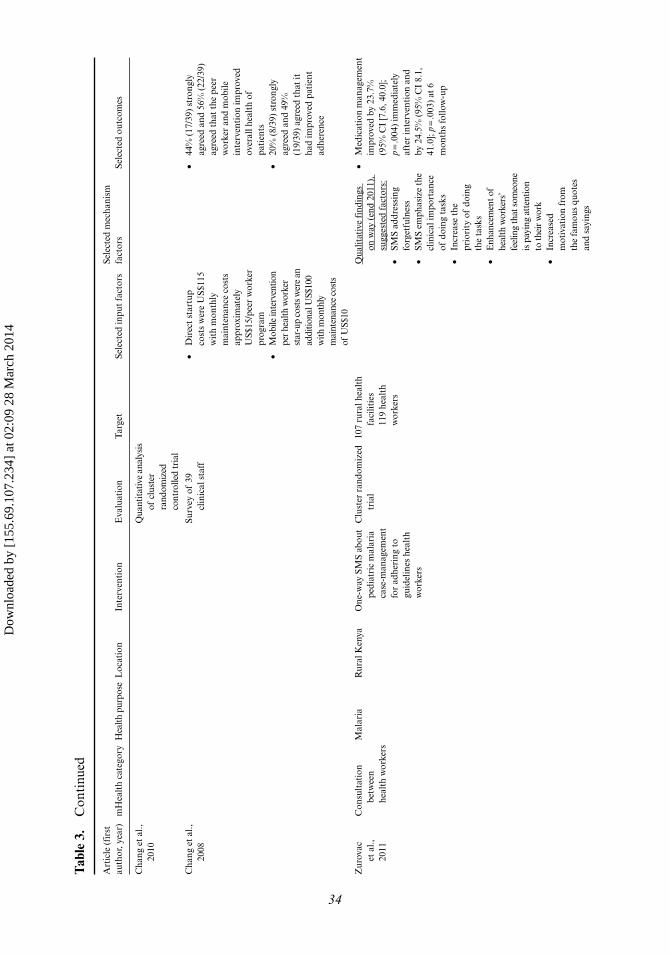
Tab
le 3
. C
onti
nued
Art
icle
(fi
rst
auth
or, y
ear)
mH
ealt
h ca
tego
ryH
ealth
pur
pose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tSe
lect
ed in
put
fact
ors
Sele
cted
mec
hani
sm
fact
ors
Sele
cted
out
com
es
Cha
ng e
t al
., 20
10Q
uant
itat
ive
anal
ysis
of
clu
ster
ra
ndom
ized
co
ntro
lled
tria
l
Cha
ng e
t al
., 20
08Su
rvey
of
39
clin
ical
sta
ff•
Dir
ect
star
tup
cost
s w
ere
US$
115
wit
h m
onth
ly
mai
nten
ance
cos
ts
appr
oxim
atel
y U
S$15
/pee
r w
orke
r pr
ogra
m•
Mob
ile in
terv
entio
n pe
r he
alth
wor
ker
star
-up
cost
s wer
e an
ad
ditio
nal U
S$10
0 w
ith m
onth
ly
mai
nten
ance
cos
ts
of U
S$10
• 44
% (
17/3
9) s
tron
gly
agre
ed a
nd 5
6% (
22/3
9)
agre
ed t
hat
the
peer
w
orke
r an
d m
obile
in
terv
enti
on im
prov
ed
over
all h
ealt
h of
pa
tien
ts•
20%
(8/
39)
stro
ngly
ag
reed
and
49%
(1
9/39
) ag
reed
tha
t it
ha
d im
prov
ed p
atie
nt
adhe
renc
e
Zur
ovac
et
al.,
20
11
Con
sult
atio
n be
twee
n he
alth
wor
kers
Mal
aria
Rur
al K
enya
One
-way
SM
S ab
out
pedi
atri
c m
alar
ia
case
-man
agem
ent
for
adhe
ring
to
guid
elin
es h
ealt
h w
orke
rs
Clu
ster
ran
dom
ized
tr
ial
107
rura
l hea
lth
faci
litie
s 11
9 he
alth
w
orke
rs
Qua
litat
ive
find
ings
on
way
(en
d 20
11),
su
gges
ted
fact
ors:
• SM
S ad
dres
sing
fo
rget
fuln
ess
• SM
S em
phas
ize
the
clin
ical
impo
rtan
ce
of d
oing
tas
ks
• In
crea
se t
he
prio
rity
of
doin
g th
e ta
sks
• E
nhan
cem
ent o
f he
alth
wor
kers
’ fe
elin
g th
at s
omeo
ne
is p
ayin
g at
tent
ion
to th
eir
wor
k•
Incr
ease
d m
otiv
atio
n fr
om
the
fam
ous
quot
es
and
sayi
ngs
• M
edic
atio
n m
anag
emen
t im
prov
ed b
y 23
.7%
(9
5% C
I [7
.6, 4
0.0]
; p =
.004
) im
med
iate
ly
afte
r in
terv
enti
on a
nd
by 2
4.5%
(95
% C
I 8.
1,
41.0
]; p =
.003
) at
6
mon
ths
follo
w-u
p
34
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
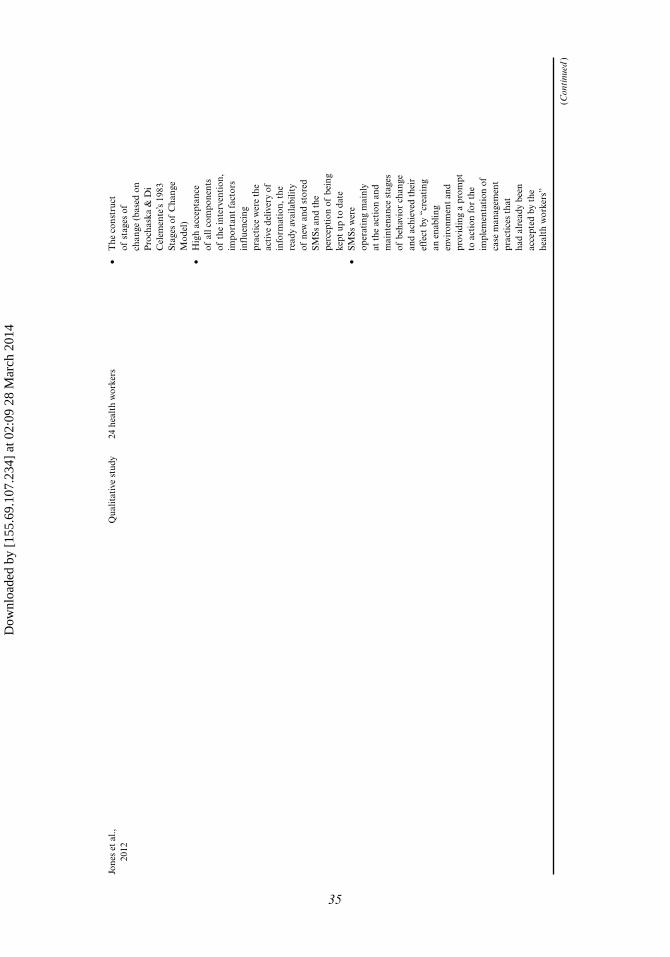
Jone
s et
al.,
20
12Q
ualit
ativ
e st
udy
24 h
ealt
h w
orke
rs•
The
con
stru
ct
of s
tage
s of
ch
ange
(ba
sed
on
Pro
chas
ka &
Di
Cel
emen
te’s
1983
St
ages
of
Cha
nge
Mod
el)
• H
igh
acce
ptan
ce
of a
ll co
mpo
nent
s of
the
inte
rven
tion
, im
port
ant
fact
ors
infl
uenc
ing
prac
tice
wer
e th
e ac
tive
del
iver
y of
in
form
atio
n, t
he
read
y av
aila
bilit
y of
new
and
sto
red
SMSs
and
the
pe
rcep
tion
of
bein
g ke
pt u
p to
dat
e•
SMSs
wer
e op
erat
ing
mai
nly
at t
he a
ctio
n an
d m
aint
enan
ce s
tage
s of
beh
avio
r ch
ange
an
d ac
hiev
ed t
heir
ef
fect
by
“cre
atin
g an
ena
blin
g en
viro
nmen
t an
d pr
ovid
ing
a pr
ompt
to
act
ion
for
the
impl
emen
tati
on o
f ca
se m
anag
emen
t pr
acti
ces
that
ha
d al
read
y be
en
acce
pted
by
the
heal
th w
orke
rs”
(Con
tinu
ed)
35
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
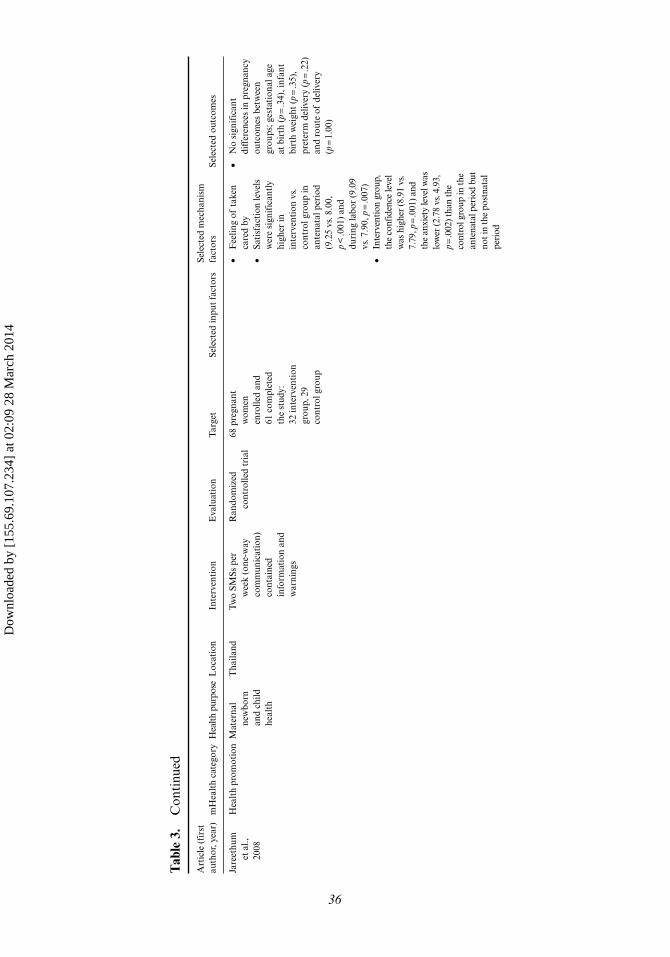
Tab
le 3
. C
onti
nued
Art
icle
(fi
rst
auth
or, y
ear)
mH
ealt
h ca
tego
ryH
ealth
pur
pose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tSe
lect
ed in
put
fact
ors
Sele
cted
mec
hani
sm
fact
ors
Sele
cted
out
com
es
Jare
ethu
m
et a
l.,
2008
Hea
lth
prom
otio
nM
ater
nal
new
born
an
d ch
ild
heal
th
Tha
iland
Two
SMSs
per
w
eek
(one
-way
co
mm
unic
atio
n)
cont
aine
d in
form
atio
n an
d w
arni
ngs
Ran
dom
ized
co
ntro
lled
tria
l68
pre
gnan
t w
omen
en
rolle
d an
d 61
com
plet
ed
the
stud
y:
32 in
terv
enti
on
grou
p, 2
9 co
ntro
l gro
up
• F
eelin
g of
tak
en
care
d by
• Sa
tisf
acti
on le
vels
w
ere
sign
ific
antl
y hi
gher
in
inte
rven
tion
vs.
co
ntro
l gro
up in
an
tena
tal p
erio
d (9
.25
vs. 8
.00,
p
< .0
01)
and
duri
ng la
bor
(9.0
9 vs
. 7.9
0, p
= .0
07)
• In
terv
entio
n gr
oup,
th
e co
nfid
ence
leve
l w
as h
ighe
r (8
.91
vs.
7.79
, p =
.001
) and
th
e an
xiet
y le
vel w
as
low
er (2
.78
vs. 4
.93,
p =
.002
) tha
n th
e co
ntro
l gro
up in
the
ante
nata
l per
iod
but
not i
n th
e po
stna
tal
peri
od
• N
o si
gnif
ican
t di
ffer
ence
s in
pre
gnan
cy
outc
omes
bet
wee
n gr
oups
; ges
tati
onal
age
at
bir
th (
p = .3
4), i
nfan
t bi
rth
wei
ght
(p =
.35)
, pr
eter
m d
eliv
ery
(p =
.22)
and
rout
e of
del
iver
y (p
= 1.
00)
36
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
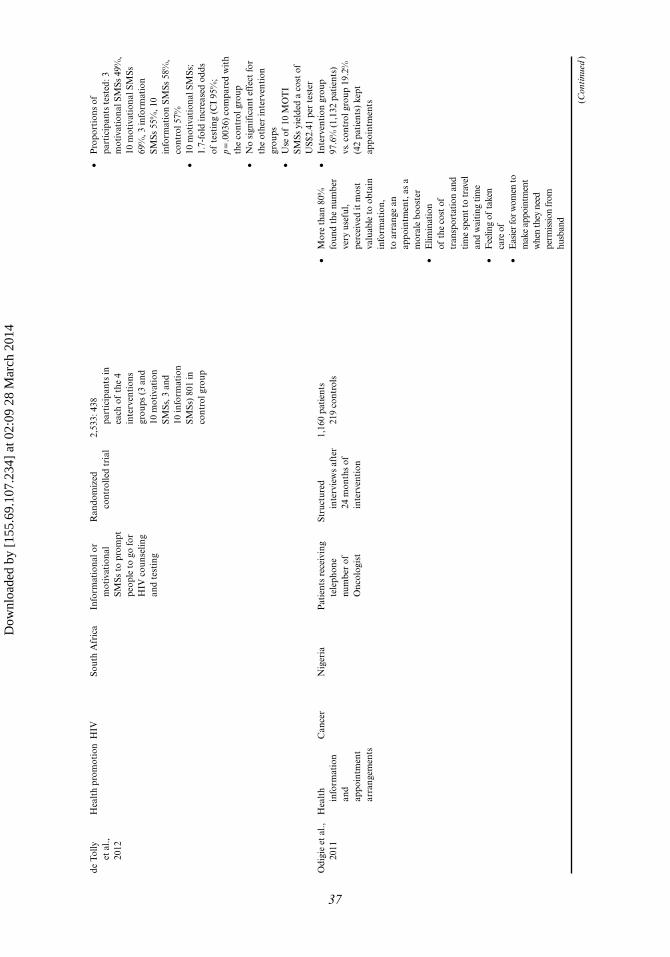
de T
olly
et
al.,
20
12
Hea
lth
prom
otio
nH
IVSo
uth
Afr
ica
Info
rmat
iona
l or
mot
ivat
iona
l SM
Ss t
o pr
ompt
pe
ople
to
go fo
r H
IV c
ouns
elin
g an
d te
stin
g
Ran
dom
ized
co
ntro
lled
tria
l2,
533:
438
pa
rtic
ipan
ts in
ea
ch o
f th
e 4
inte
rven
tion
s gr
oups
(3
and
10 m
otiv
atio
n SM
Ss, 3
and
10
info
rmat
ion
SMSs
) 80
1 in
co
ntro
l gro
up
• P
ropo
rtio
ns o
f pa
rtic
ipan
ts t
este
d: 3
m
otiv
atio
nal S
MSs
49%
, 10
mot
ivat
iona
l SM
Ss
69%
, 3 in
form
atio
n SM
Ss 5
5%, 1
0 in
form
atio
n SM
Ss 5
8%,
cont
rol 5
7%•
10 m
otiv
atio
nal S
MSs
; 1.
7-fo
ld in
crea
sed
odds
of
tes
ting
(C
I 95
%;
p = .0
036)
com
pare
d w
ith
the
cont
rol g
roup
• N
o si
gnif
ican
t ef
fect
for
the
othe
r in
terv
enti
on
grou
ps•
Use
of
10 M
OT
I SM
Ss y
ield
ed a
cos
t of
U
S$2.
41 p
er t
este
r O
digi
e et
al.,
20
11H
ealt
h in
form
atio
n an
d ap
poin
tmen
t ar
rang
emen
ts
Can
cer
Nig
eria
Pat
ient
s re
ceiv
ing
tele
phon
e nu
mbe
r of
O
ncol
ogis
t
Stru
ctur
ed
inte
rvie
ws
afte
r 24
mon
ths
of
inte
rven
tion
1,16
0 pa
tien
ts
219
cont
rols
• M
ore
than
80%
fo
und
the
num
ber
very
use
ful,
perc
eive
d it
mos
t va
luab
le t
o ob
tain
in
form
atio
n,
to a
rran
ge a
n ap
poin
tmen
t, a
s a
mor
ale
boos
ter
• E
limin
atio
n of
the
cost
of
tran
spor
tati
on a
nd
tim
e sp
ent t
o tr
avel
an
d w
aiti
ng ti
me
• F
eelin
g of
take
n ca
re o
f•
Eas
ier f
or w
omen
to
mak
e ap
poin
tmen
t w
hen
they
nee
d pe
rmis
sion
from
hu
sban
d
• In
terv
enti
on g
roup
97
.6%
(1,
132
pati
ents
) vs
. con
trol
gro
up 1
9.2%
(4
2 pa
tien
ts)
kept
ap
poin
tmen
ts (Con
tinu
ed)
37
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
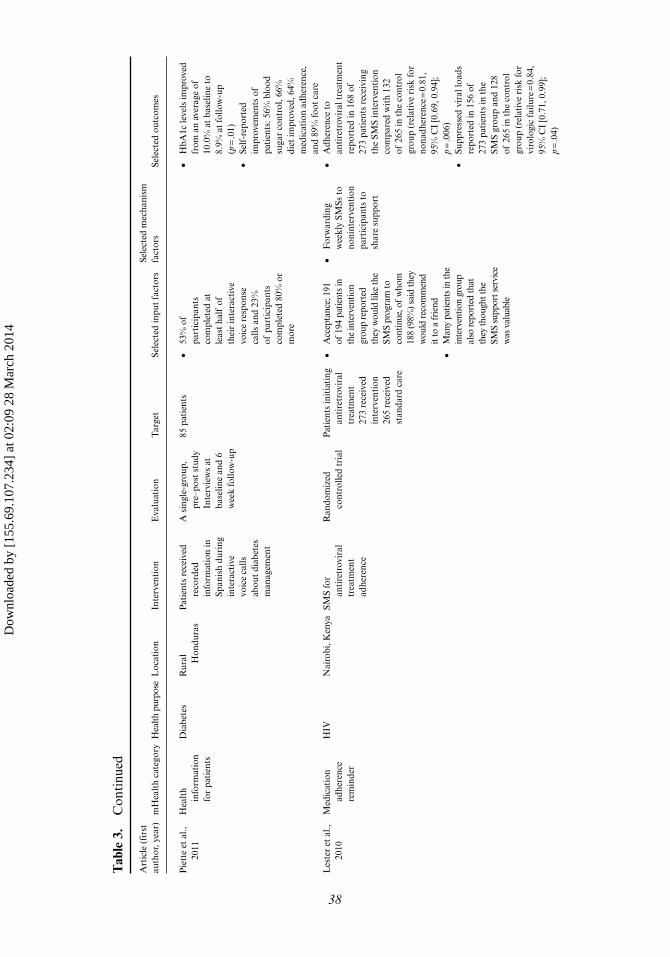
Tab
le 3
. C
onti
nued
Art
icle
(fi
rst
auth
or, y
ear)
mH
ealt
h ca
tego
ryH
ealth
pur
pose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tSe
lect
ed in
put
fact
ors
Sele
cted
mec
hani
sm
fact
ors
Sele
cted
out
com
es
Pie
tte
et a
l.,
2011
Hea
lth
info
rmat
ion
for
pati
ents
Dia
bete
sR
ural
H
ondu
ras
Pat
ient
s re
ceiv
ed
reco
rded
in
form
atio
n in
Sp
anis
h du
ring
in
tera
ctiv
e vo
ice
calls
ab
out
diab
etes
m
anag
emen
t
A s
ingl
e-gr
oup,
pr
e–po
st s
tudy
In
terv
iew
s at
ba
selin
e an
d 6
wee
k fo
llow
-up
85 p
atie
nts
• 53
% o
f pa
rtic
ipan
ts
com
plet
ed a
t le
ast
half
of
thei
r in
tera
ctiv
e vo
ice
resp
onse
ca
lls a
nd 2
3%
of p
arti
cipa
nts
com
plet
ed 8
0% o
r m
ore
• H
bA1c
leve
ls im
prov
ed
from
an
aver
age
of
10.0
% a
t ba
selin
e to
8.
9% a
t fo
llow
-up
(p =
.01)
• Se
lf-r
epor
ted
impr
ovem
ents
of
pati
ents
: 56%
blo
od
suga
r co
ntro
l, 66
%
diet
impr
oved
, 64%
m
edic
atio
n ad
here
nce,
an
d 89
% fo
ot c
are
Les
ter
et a
l.,
2010
Med
icat
ion
adhe
renc
e re
min
der
HIV
Nai
robi
, Ken
yaSM
S fo
r an
tire
trov
iral
tr
eatm
ent
adhe
renc
e
Ran
dom
ized
co
ntro
lled
tria
lP
atie
nts
init
iati
ng
anti
retr
ovir
al
trea
tmen
t 27
3 re
ceiv
ed
inte
rven
tion
26
5 re
ceiv
ed
stan
dard
car
e
• A
ccep
tanc
e; 1
91
of 1
94 p
atie
nts
in
the
inte
rven
tion
grou
p re
port
ed
they
wou
ld li
ke th
e SM
S pr
ogra
m to
co
ntin
ue, o
f w
hom
18
8 (9
8%) s
aid
they
w
ould
rec
omm
end
it to
a fr
iend
• M
any
patie
nts
in th
e in
terv
entio
n gr
oup
also
repo
rted
that
th
ey th
ough
t the
SM
S su
ppor
t ser
vice
w
as v
alua
ble
• F
orw
ardi
ng
wee
kly
SMSs
to
noni
nter
vent
ion
part
icip
ants
to
shar
e su
ppor
t
• A
dher
ence
to
anti
retr
ovir
al t
reat
men
t re
port
ed in
168
of
273
pati
ents
rec
eivi
ng
the
SMS
inte
rven
tion
co
mpa
red
wit
h 13
2 of
265
in t
he c
ontr
ol
grou
p (r
elat
ive
risk
for
nona
dher
ence
= 0.
81,
95%
CI
[0.6
9, 0
.94]
; p =
.006
)•
Supp
ress
ed v
iral
load
s re
port
ed in
156
of
273
pati
ents
in t
he
SMS
grou
p an
d 12
8 of
265
in t
he c
ontr
ol
grou
p (r
elat
ive
risk
for
viro
logi
c fa
ilure
= 0.
84,
95%
CI
[0.7
1, 0
.99]
; p =
.04)
38
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
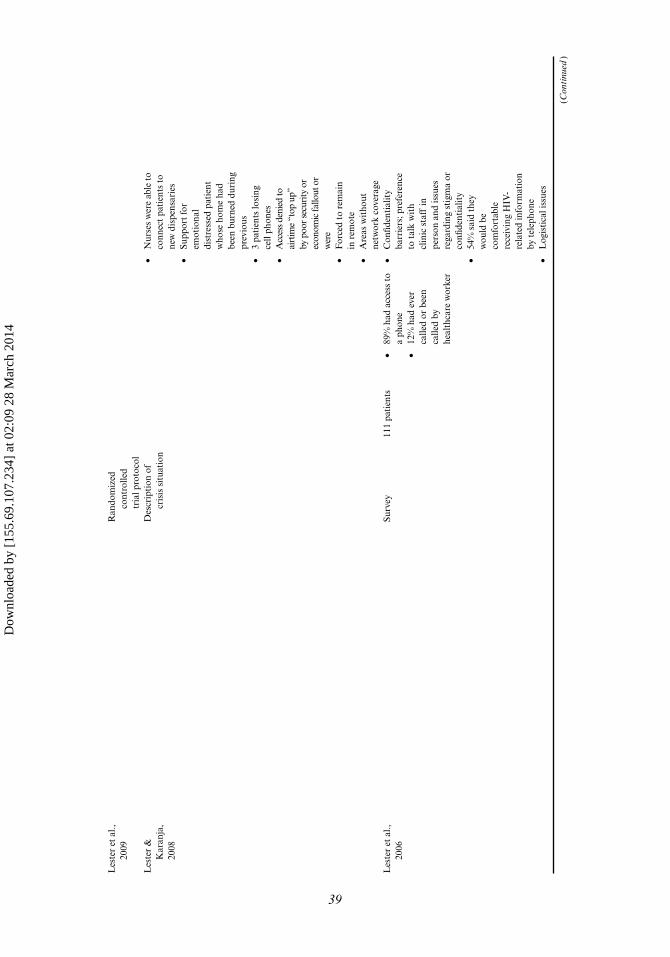
Les
ter
et a
l.,
2009
Ran
dom
ized
co
ntro
lled
tria
l pro
toco
lD
escr
ipti
on o
f cr
isis
sit
uati
on
Les
ter
&
Kar
anja
, 20
08
• N
urse
s w
ere
able
to
conn
ect
pati
ents
to
new
dis
pens
arie
s•
Supp
ort
for
emot
iona
l di
stre
ssed
pat
ient
w
hose
hom
e ha
d be
en b
urne
d du
ring
pr
evio
us•
3 pa
tien
ts lo
sing
ce
ll ph
ones
•
Acc
ess d
enie
d to
ai
rtim
e “t
op u
p”
by p
oor s
ecur
ity o
r ec
onom
ic fa
llout
or
wer
e •
For
ced
to r
emai
n in
rem
ote
• A
reas
wit
hout
ne
twor
k co
vera
geL
este
r et
al.,
20
06Su
rvey
111
pati
ents
• 89
% h
ad a
cces
s to
a
phon
e•
12%
had
eve
r ca
lled
or b
een
calle
d by
he
alth
care
wor
ker
• C
onfid
enti
alit
y ba
rrie
rs; p
refe
renc
e to
tal
k w
ith
clin
ic s
taff
in
pers
on a
nd is
sues
re
gard
ing
stig
ma
or
confi
dent
ialit
y •
54%
sai
d th
ey
wou
ld b
e co
mfo
rtab
le
rece
ivin
g H
IV-
rela
ted
info
rmat
ion
by t
elep
hone
• L
ogis
tica
l iss
ues
(Con
tinu
ed)
39
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
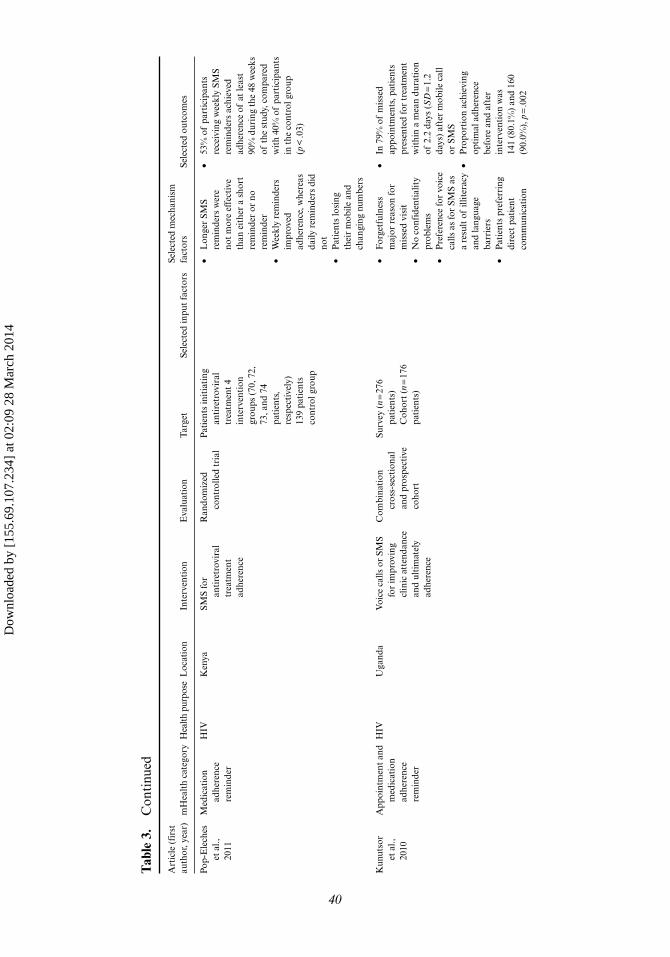
Tab
le 3
. C
onti
nued
Art
icle
(fi
rst
auth
or, y
ear)
mH
ealt
h ca
tego
ryH
ealth
pur
pose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tSe
lect
ed in
put
fact
ors
Sele
cted
mec
hani
sm
fact
ors
Sele
cted
out
com
es
Pop-
Ele
ches
et
al.,
20
11
Med
icat
ion
adhe
renc
e re
min
der
HIV
Ken
yaSM
S fo
r an
tire
trov
iral
tr
eatm
ent
adhe
renc
e
Ran
dom
ized
co
ntro
lled
tria
lP
atie
nts
init
iati
ng
anti
retr
ovir
al
trea
tmen
t 4
inte
rven
tion
gr
oups
(70
, 72,
73
, and
74
pati
ents
, re
spec
tive
ly)
139
pati
ents
co
ntro
l gro
up
• L
onge
r SM
S re
min
ders
wer
e no
t m
ore
effe
ctiv
e th
an e
ithe
r a
shor
t re
min
der
or n
o re
min
der
• W
eekl
y re
min
ders
im
prov
ed
adhe
renc
e, w
here
as
daily
rem
inde
rs d
id
not
• P
atie
nts
losi
ng
thei
r m
obile
and
ch
angi
ng n
umbe
rs
• 53
% o
f pa
rtic
ipan
ts
rece
ivin
g w
eekl
y SM
S re
min
ders
ach
ieve
d ad
here
nce
of a
t le
ast
90%
dur
ing
the
48 w
eeks
of
the
stu
dy, c
ompa
red
wit
h 40
% o
f pa
rtic
ipan
ts
in t
he c
ontr
ol g
roup
(p
< .0
3)
Kun
utso
r et
al.,
20
10
App
oint
men
t an
d m
edic
atio
n ad
here
nce
rem
inde
r
HIV
Uga
nda
Voi
ce c
alls
or
SMS
for
impr
ovin
g cl
inic
att
enda
nce
and
ulti
mat
ely
adhe
renc
e
Com
bina
tion
cr
oss-
sect
iona
l an
d pr
ospe
ctiv
e co
hort
Surv
ey (
n = 27
6 pa
tien
ts)
Coh
ort
(n =
176
pati
ents
)
• F
orge
tful
ness
m
ajor
rea
son
for
mis
sed
visi
t•
No
conf
iden
tial
ity
prob
lem
s•
Pre
fere
nce
for
voic
e ca
lls a
s fo
r SM
S as
a
resu
lt o
f ill
iter
acy
and
lang
uage
ba
rrie
rs
• P
atie
nts
pref
erri
ng
dire
ct p
atie
nt
com
mun
icat
ion
• In
79%
of
mis
sed
appo
intm
ents
, pat
ient
s pr
esen
ted
for
trea
tmen
t w
ithi
n a
mea
n du
rati
on
of 2
.2 d
ays
(SD
= 1.
2 da
ys)
afte
r m
obile
cal
l or
SM
S•
Pro
port
ion
achi
evin
g op
tim
al a
dher
ence
be
fore
and
aft
er
inte
rven
tion
was
14
1 (8
0.1%
) an
d 16
0 (9
0.0%
), p
= .0
02
40
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
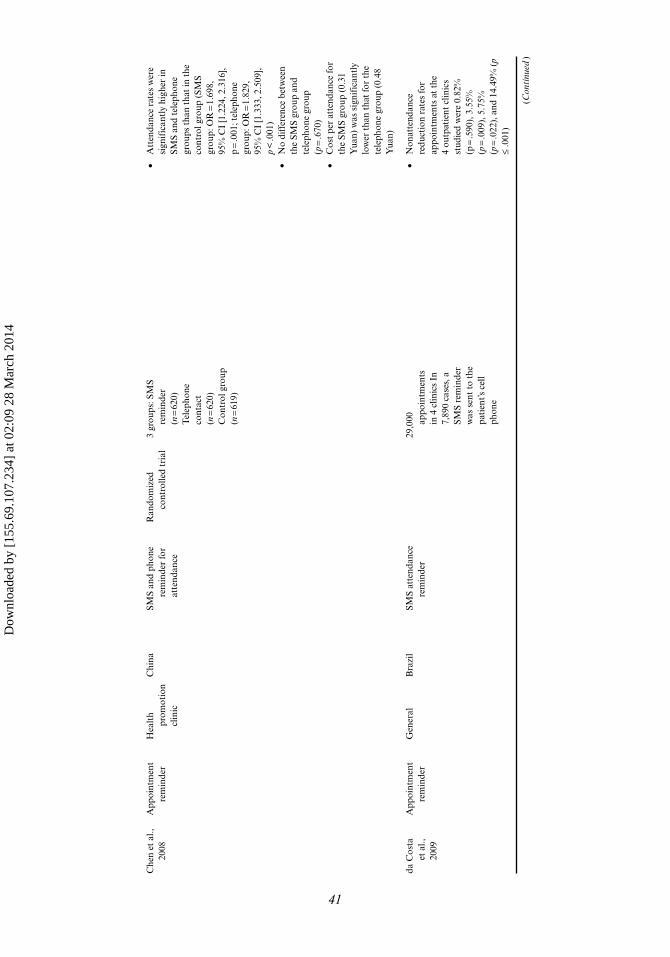
Che
n et
al.,
20
08A
ppoi
ntm
ent
rem
inde
rH
ealt
h pr
omot
ion
clin
ic
Chi
naSM
S an
d ph
one
rem
inde
r fo
r at
tend
ance
Ran
dom
ized
co
ntro
lled
tria
l3
grou
ps: S
MS
rem
inde
r (n
= 62
0)
Tel
epho
ne
cont
act
(n =
620)
Con
trol
gro
up
(n =
619)
• A
tten
danc
e ra
tes
wer
e si
gnif
ican
tly
high
er in
SM
S an
d te
leph
one
grou
ps t
han
that
in t
he
cont
rol g
roup
(SM
S gr
oup:
OR
= 1.
698,
95
% C
I [1
.224
, 2.3
16],
p =
.001
; tel
epho
ne
grou
p: O
R =
1.82
9,
95%
CI
[1.3
33, 2
.509
], p
< .0
01)
• N
o di
ffer
ence
bet
wee
n th
e SM
S gr
oup
and
tele
phon
e gr
oup
(p =
.670
) •
Cos
t pe
r at
tend
ance
for
the
SMS
grou
p (0
.31
Yua
n) w
as s
igni
fica
ntly
lo
wer
tha
n th
at fo
r th
e te
leph
one
grou
p (0
.48
Yua
n)
da C
osta
et
al.,
20
09
App
oint
men
t re
min
der
Gen
eral
Bra
zil
SMS
atte
ndan
ce
rem
inde
r29
,000
ap
poin
tmen
ts
in 4
clin
ics
In
7,89
0 ca
ses,
a
SMS
rem
inde
r w
as s
ent
to t
he
pati
ent’s
cel
l ph
one
• N
onat
tend
ance
re
duct
ion
rate
s fo
r ap
poin
tmen
ts a
t th
e 4
outp
atie
nt c
linic
s st
udie
d w
ere
0.82
%
(p =
.590
), 3
.55%
(p
= .0
09),
5.7
5%
(p =
.022
), a
nd 1
4.49
% (
p ≤
.001
)
(Con
tinu
ed)
41
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
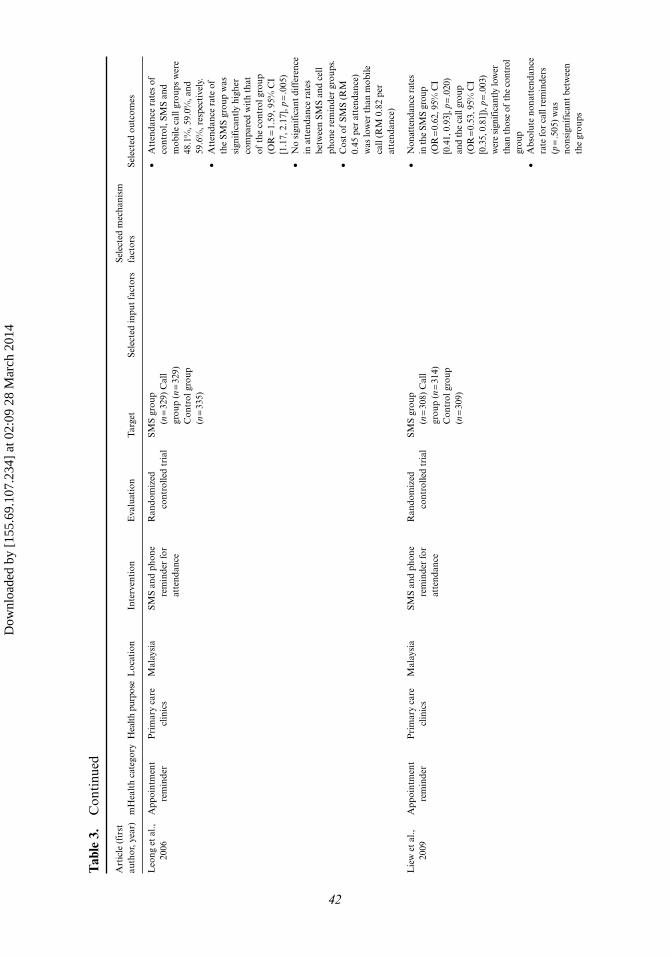
Tab
le 3
. C
onti
nued
Art
icle
(fi
rst
auth
or, y
ear)
mH
ealt
h ca
tego
ryH
ealth
pur
pose
Loc
atio
nIn
terv
enti
onE
valu
atio
nT
arge
tSe
lect
ed in
put
fact
ors
Sele
cted
mec
hani
sm
fact
ors
Sele
cted
out
com
es
Leo
ng e
t al
., 20
06A
ppoi
ntm
ent
rem
inde
rP
rim
ary
care
cl
inic
sM
alay
sia
SMS
and
phon
e re
min
der
for
atte
ndan
ce
Ran
dom
ized
co
ntro
lled
tria
lSM
S gr
oup
(n =
329)
Cal
l gr
oup
(n =
329)
C
ontr
ol g
roup
(n
= 33
5)
• A
tten
danc
e ra
tes
of
cont
rol,
SMS
and
mob
ile c
all g
roup
s w
ere
48.1
%, 5
9.0%
, and
59
.6%
, res
pect
ivel
y.
• A
tten
danc
e ra
te o
f th
e SM
S gr
oup
was
si
gnif
ican
tly
high
er
com
pare
d w
ith
that
of
the
con
trol
gro
up
(OR
= 1.
59, 9
5% C
I [1
.17,
2.1
7], p
= .0
05)
• N
o si
gnif
ican
t di
ffer
ence
in
att
enda
nce
rate
s be
twee
n SM
S an
d ce
ll ph
one
rem
inde
r gr
oups
. •
Cos
t of
SM
S (R
M
0.45
per
att
enda
nce)
w
as lo
wer
tha
n m
obile
ca
ll (R
M 0
.82
per
atte
ndan
ce)
Lie
w e
t al
., 20
09A
ppoi
ntm
ent
rem
inde
rP
rim
ary
care
cl
inic
sM
alay
sia
SMS
and
phon
e re
min
der
for
atte
ndan
ce
Ran
dom
ized
co
ntro
lled
tria
lSM
S gr
oup
(n =
308)
Cal
l gr
oup
(n =
314)
C
ontr
ol g
roup
(n
= 30
9)
•
Non
atte
ndan
ce r
ates
in
the
SMS
grou
p (O
R =
0.62
, 95%
CI
[0.4
1, 0
.93]
, p =
.020
) an
d th
e ca
ll gr
oup
(OR
= 0.
53, 9
5% C
I [0
.35,
0.8
1]),
p = .0
03)
wer
e si
gnifi
cant
ly lo
wer
th
an th
ose
of th
e co
ntro
l gr
oup
• A
bsol
ute
nona
tten
danc
e ra
te fo
r ca
ll re
min
ders
(p
= .5
05)
was
no
nsig
nifi
cant
bet
wee
n th
e gr
oups
42
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
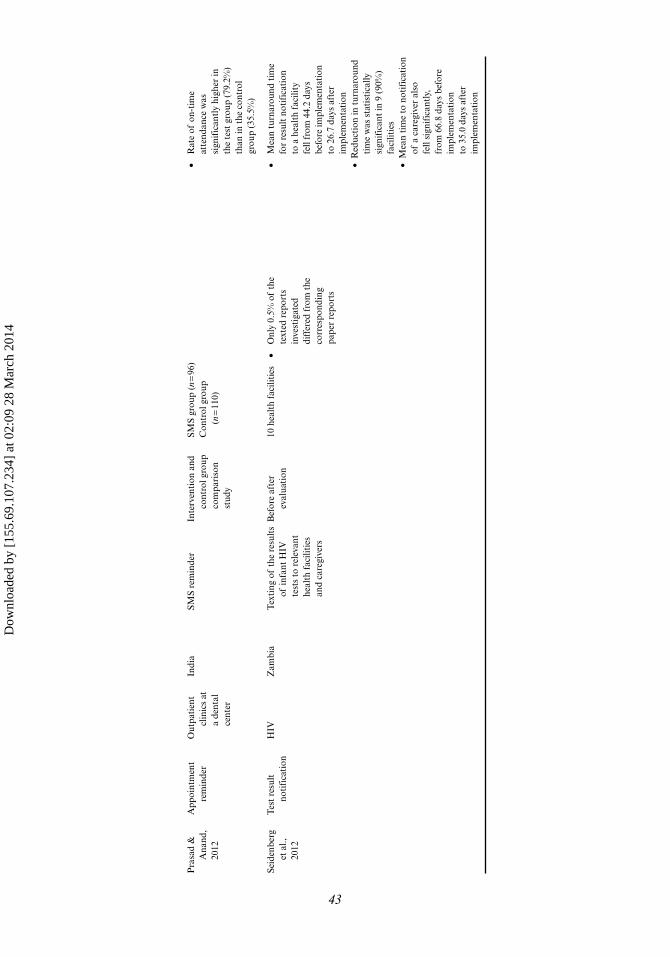
Pra
sad
&
Ana
nd,
2012
App
oint
men
t re
min
der
Out
pati
ent
clin
ics
at
a de
ntal
ce
nter
Indi
aSM
S re
min
der
Inte
rven
tion
and
co
ntro
l gro
up
com
pari
son
stud
y
SMS
grou
p (n
= 96
)C
ontr
ol g
roup
(n
= 11
0)
• R
ate
of o
n-ti
me
atte
ndan
ce w
as
sign
ific
antl
y hi
gher
in
the
test
gro
up (
79.2
%)
than
in t
he c
ontr
ol
grou
p (3
5.5%
)
Seid
enbe
rg
et a
l.,
2012
Tes
t re
sult
no
tifi
cati
onH
IVZ
ambi
aT
exti
ng o
f th
e re
sult
s of
infa
nt H
IV
test
s to
rel
evan
t he
alth
fac
iliti
es
and
care
give
rs
Bef
ore
afte
r ev
alua
tion
10 h
ealt
h fa
cilit
ies
• O
nly
0.5%
of
the
text
ed r
epor
ts
inve
stig
ated
di
ffer
ed f
rom
the
co
rres
pond
ing
pape
r re
port
s
• M
ean
turn
arou
nd t
ime
for
resu
lt n
otif
icat
ion
to a
hea
lth
faci
lity
fell
from
44.
2 da
ys
befo
re im
plem
enta
tion
to
26.
7 da
ys a
fter
im
plem
enta
tion
• R
educ
tion
in t
urna
roun
d ti
me
was
sta
tist
ical
ly
sign
ific
ant
in 9
(90
%)
faci
litie
s•
Mea
n ti
me
to n
otif
icat
ion
of a
car
egiv
er a
lso
fell
sign
ific
antl
y,
from
66.
8 da
ys b
efor
e im
plem
enta
tion
to
35.
0 da
ys a
fter
im
plem
enta
tion
43
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

44 A. Chib et al.
et al., 2011), and pregnancy (Jareethum et al., 2008). The study (represented by three articles) (Chang et al., 2011; Chang et al., 2008; Chang et al., 2010) using the health-care communication (described earlier in mechanism section) found no significant effect on HIV virologic outcomes, adherence to antiretroviral therapy, mortality, or retention (Chang et al., 2011). Two randomized controlled trials in Kenya sent antiretroviral therapy reminder SMSs to people living with HIV, and concluded that recipients significantly improved antiretroviral therapy adherence (Lester et al., 2010; Pop-Eleches et al., 2011), with one study (represented by four articles) (Lester & Karanja, 2008; Lester, Gelmon, & Plummer, 2006; Lester et al., 2009; Lester et al., 2010) also showing improvements in HIV viral load suppression (Lester et al., 2010). Health promotion SMSs for prenatal support found no significant differences in preg-nancy outcomes in Thailand (Jareethum et al., 2008).
Organizational outputs were reported by three randomized controlled trials (Chen et al., 2008; Leong et al., 2006; Liew et al., 2009; Zurovac et al., 2011), and other stud-ies used varied designs (da Costa et al., 2010; Kunutsor et al., 2010; Odigie et al., 2011; Prasad & Anand, 2012; Seidenberg et al., 2012), with evidence of higher appointment attendance rates in the group receiving SMS and/or calls. A cluster randomized con-trolled trial represented by two articles (Jones et al., 2012; Zurovac et al., 2011), sent SMSs on infant malaria case-management to health workers and found that medica-tion management by health workers improved (Jones et al., 2012; Zurovac et al., 2011). Four studies (Chang et al., 2008; Chen et al., 2008; de Tolly et al., 2012; Leong et al., 2006) provided information on costs, but none of the studies reported a full economic cost-effectiveness analysis.
Discussion
This review found 53 mHealth studies in developing countries: 32 inputs studies, 6 mechanism studies, and 15 outputs studies. On the one hand, it is encouraging to see the growing body of evidence related to mHealth in developing countries. On the other, it is evident that social scientific studies explicating processes of technology adoption are less emphasized in this body of research, compared with technology introduction, and improvements in healthcare process and indicators. One result of this emphasis is the relative paucity of critical studies discussing reasons for failure, leading to stances bordering on technological determinism.
We found several gaps in the understanding of mobile interventions in health-care, as conceptualized by the inputs-mechanism-outputs model, for example, of explanatory theory, and of sociological determinants of health outcomes. Few stud-ies used theory or methodological designs (Ashraf et al., 2010; Chib & Chen, 2011; Chib, Cheong, et al., 2012; Chib, Law, et al., 2012; Hamilton, 2010; Hwabamungu & Williams, 2010), to explain why people would use mobile phones for healthcare needs, or link technological inputs to outputs (Chang et al., 2011). When evident, a cross-disciplinary approach led to borrowing of theory from different disciplines, with no dominant theory. The behavior-change theories used failed to account for context (Hwabamungu & Williams, 2010), particularly sociological factors such as culture and gender, essential for evaluating factors influencing how and why interventions work (Svoronos & Mate, 2011). Studies mainly used academically oriented measures (e.g. response rate, data accuracy) rather than measures prescribed by trans-national organ-izations (United Nations or the World Health Organization) such as the Millennium Development Goals indicators.
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 45
Most studies reported one or two stages of the pathway. Three studies (Chang et al., 2011; Lester et al., 2010; Pop-Eleches et al., 2011) attempted to provide informa-tion on the whole pathway, but could not satisfactorily explain the theoretical mecha-nisms for technology adoption. Not a single study was able to provide a theoretical explanation for technology adoption that resulted in a healthcare system outcome. While it might be too early to expect comprehensive studies dealing with the com-plexity of linking concepts across the entire pathway, we expect mHealth scholars to bridge disciplinary boundaries to provide such compelling evidence in the future.
Literature reviews over the past years have shown a lack of data on the effective-ness of mHealth in low- and middle-income countries in general (Blaya, Fraser, & Holt, 2010; Kaplan, 2006), and for specific purposes such as behavior change inter-ventions (Cole-Lewis & Kershaw, 2010; Fjeldsoe et al., 2009), diabetes control (Liang et al., 2011), sexual health (Lim et al., 2008), maternal healthcare (Noordam, Kuepper, Stekelenburg, & Milen, 2011; Tamrat & Kachnowski, 2012), and smoking cessation (Whittaker et al., 2009). Reported improvements of mHealth interventions on estab-lished health indicators were very limited, as were descriptions of cost-effectiveness or adverse effects. Certainly policymakers would expect greater explication of finan-cial feasibility and mitigating factors for possible failures prior to engaging with the discipline.
The literature suggests that some projects are being scaled up to a national level without the necessary evidence from high-quality evaluation (Jordan, Ray, Johnson, & Evans, 2011; Novartis, 2011). It might be too early to do so without a systemic review of the varied mHealth initiatives. Early selection and failure of the wrong initiative, by extension of association, harms the entire field. If policymakers invest in mHealth projects, a fair amount should be reserved for evaluation purposes. Groups such as the mHealth Alliance and World Health Organisation are organizing efforts to ensure mHealth projects are guided by evidence, and avoid duplication (World Health Organization, 2011a).
We found an encouraging growing body of knowledge about mHealth in low-resource setting of developing countries. It is, nonetheless, the appropriate time to acknowledge that the current crop of studies is not delivering the results aimed for. Future work needs to aim for establishing technological, theoretical, and measure-ment standards. There is a need to consider all aspects of the inputs-mechanisms-out-puts pathway to produce a comprehensive picture of how mobile phones can improve healthcare in low- and middle-income countries.
Researchers at the inputs level, primarily information technologists, need to determine the precise problems to be addressed not just from the viewpoint of tech-nological inputs, but rather from both the sociological and healthcare needs per-spectives. Social science researchers should make choices for evaluation in terms of appropriate study design, providing clear evidence of outputs. This group should aim to make their approach relevant to technologists interested in the sociological context within which mHealth projects are conducted. Finally, public health officials need to examine the specific measures identified by policymakers for inclusion in research designs. In conclusion, an obvious recommendation is greater collabora-tion across disciplinary boundaries, or risk fracturing into marginalized silos. The emergent field of mHealth in developing countries is slowly gaining traction, yet can gain credibility and the confidence of practitioners and policymakers with a more organized approach to dissemination of the results. This review offers one such early attempt.
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

46 A. Chib et al.
Funding
The Department of Primary Care & Public Health at Imperial College is grateful for support from the National Institute for Health Research Collaboration for Leadership in Applied Health Research & Care Scheme, the National Institute for Health Research Biomedical Research Centre Scheme, and the Imperial Centre for Patient Safety and Service Quality.
References
Alam, M., Khanam, T., Khan, R., Raihan, A., & Chowdhury, M. (2010). Assessing the scope for use of mobile based solution to improve maternal and child health in Bangladesh: A case study on efficiency of community health workers, automated risk assessment of patients and web based data collection. Presented at the International Conference on Information and Communication Technologies and Development, London, December 13–16. Retrieved from http://www.gg.rhul.ac.uk/ict4d/ictd2010/posters/ICTD2010%20Alam%20et%20al.pdf
Andreatta , P., Debpuur, D., Danquah, A., & Perosky, J. (2011). Using cell phones to collect post-partum hemorrhage outcome data in rural Ghana. International Journal of Gynecology & Obstetrics, 113, 148–151. doi:10.1016/j.ijgo.2010.11.020
Ashraf, M. , Ansari, N. L., Tahseen Malik, B., & Rashid, B. (2010). Evaluating the impact of mobile phone based ‘health help line’ service in rural Bangladesh. Presented at the 2nd International Conference on M4D, Mobile Communication Technology for Development, Kampala, Uganda, November 10–11.
Asiimwe, C., Gelvin, D., Lee, E., Amor, Y., Quinto, Y., Katureebe, C., … Berg, M. (2011). Use of an innovative, affordable, and open-source short message service–based tool to monitor malaria in remote areas of Uganda. American Journal of Tropical Medicine and Hygiene, 85, 26–33.
Azfar, R. S., Weinberg, J. L., Cavric, G., Lee-Keltner, I. A., Bilker, W. B., Gelfand, J. M., & Kovarik, C. L. (2011). HIV-positive patients in Botswana state that mobile teledermatol-ogy is an acceptable method for receiving dermatology care. Journal of Telemedicine and Telecare, 17, 338–340. doi:10.1258/jtt.2011.110115
Banuri, T., Zai di, M., Spanger-Siegfried, E., Ali, K., & Zaidi, S. (2003). Promoting ICT for human development in Asia: Realizing the Millennium Development Goals: Pakistan. Pakintan, Islamabad: UNDP.
Barrington, J., Wereko-Brobby, O., Ward, P., Mwafongo, W., & Kungulwe, S. (2010). SMS for Life: A pilot project to improve anti-malarial drug supply management in rural Tanzania using standard technology. Malaria Journal, 9, 298. doi:10.1186/1475-2875-9-298
Baxter, L., & M ontgomery, B. (1996). Relating: Dialogues and dialectics. New York, NY: Guilford Press.
Bertrand, J. T. , O’Reilly, K., Denison, J., Anhang, R., & Sweat, M. (2006). Systematic review of the effectiveness of mass communication programs to change HIV/AIDS-related behaviors in developing countries. Health Education Research, 21, 567–597. doi:10.1093/her/cyl036
Blaya, J. A., Fra ser, H. S. F., & Holt, B. (2010). E-health technologies show promise in develop-ing countries. Health Affairs, 29, 244–251. doi:10.1377/hlthaff.2009.0894
Bloch, A. (2010). The potential of mobile technologies to positively impact access to essential medicines in low and medium income countries. Washington, DC: mHealth Alliance.
Blynn, E., & Aubuc hon, J. (2009). Piloting mHealth: A research scan. Cambridge, MA: Knowledge Exchange. Retrieved from https://wiki.brown.edu/confluence/download/attachments/9994241/mHealth+Final.pdf
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 47
Castells, M. (1989 ). The informational city: Economic restructuring and urban development. Oxford, England: Blackwell.
Chandhanayingyong, C., Tangtrakulwanich, B., & Kiriratnikom, T. (2007). Teleconsultation for emergency orthopaedic patients using the multimedia messaging service via mobile phones. Journal of Telemedicine and Telecare, 13, 193–196. doi:10.1258/135763307780908049
Chang, L. W., Kagaa yi, J., Arem, H., Nakigozi, G., Ssempijja, V., Serwadda, D., … Reynolds, S. J. (2011). Impact of a mHealth intervention for peer health workers on AIDS care in rural Uganda: A mixed-methods evaluation of a cluster-randomized trial. AIDS Behavior, 15, 1776–1784. doi:10.1007/s10461-011-9995-x
Chang, L. W., Kagaay i, J., Nakigozi, G., Packer, A. H., Serwadda, D., Quinn, T. C., … Reynolds, S. J. (2008). Responding to the human resource crisis: peer health workers, mobile phones, and HIV care in Rakai, Uganda. AIDS Patient Care and STDs, 22, 173–174.
Chang, L. W., Kagaay i, J., Nakigozi, G., Ssempijja, V., Packer, A. H., Serwadda, D., … Reynolds, S. J. (2010). Effect of peer health workers on AIDS care in Rakai, Uganda: a cluster-rand-omized trial. PLoS One, 5, e10923.
Chen, Z. W., Fang, L . Z., Chen, L. Y., & Dai, H. L. (2008). Comparison of an SMS text mes-saging and phone reminder to improve attendance at a health promotion center: A rand-omized controlled trial. Journal of Zhejiang University Science B, 9, 34–38. doi:10.1631/jzus.B071464
Chib, A. (2010). The Aceh Besar midwives with mobile phones project: Design and evaluation perspectives using the information and communication technologies for healthcare devel-opment model. Journal of Computer-Mediated Communication, 15(3), 500–525.
Chib, A., & Chen, V. H. H. (2011). Midwives with mobiles: A dialectical perspective on gen-der arising from technology introduction in rural Indonesia. New Media & Society, 12, 486–501.
Chib, A., Cheong, Y. J., Lee, L. C. L., Ng, C. H. C., Tan, C. K., & Kameswari, V. L.V. (2012). ASHA: The hope of information communication technologies in Indian rural healthcare. Journal of Health Informatics in Developing Countries, 6(1), 406–421.
Chib, A., Law, F., Ahmad, N., & Ismail, N. (2012). Moving mountains with mobiles: Spatio-temporal perspectives on mHealth in Nepal. MedieKultur, Journal of Media and Communication Research, 52, 100–114.
Chib, A., Lwin, M. O., Ang, J., Lin, H., & Santoso, F. (2008). Mobiles and midwives: Improving healthcare communications via mobile phones in Aceh Besar, Indonesia. Asian Journal of Communication, 18, 348–364.
Chib, A., Lwin, M. O., & Jung, Y. (2009). Adoption of mobile phones to enhance health care: A technology acceptance study of maternal care workers in Indonesia. Media Asia, 36(4), 216–222.
Chib, A., Wilkin, H., Leow, X. L., Hoefman, B., & van Bejima, H. (2012). Evaluating the effec-tiveness of a text message HIV/AIDS campaign in North West Uganda. Journal of Health Communication, 17(Suppl 1), 146–157.
Cole-Ceesay, R., Cheri an, M., Sonko, A., Shivute, N., Cham, M., Davis, M., … Southall, D. (2010). Strengthening the emergency healthcare system for mothers and children in The Gambia. Reproductive Health, 7, article 21. doi: 10.1186/1742-4755-7-21.
Cole-Lewis, H., & Kers haw, T. (2010). Text messaging as a tool for behavior change in dis-ease prevention and management. Epidemiologic Reviews, 32, 56–69. doi:10.1093/epirev/mxq004
Crankshaw, T., Corless, I. B., Giddy, J., Nicholas, P. K., Eichbaum, Q., & Butler, L. M. (2010). Exploring the patterns of use and the feasibility of using cellular phones for clinic appoint-ment reminders and adherence messages in an antiretroviral treatment clinic, Durban, South Africa. AIDS Patient Care and STDs, 24, 729–735.
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

48 A. Chib et al.
Curioso, W. H., Alex Qu istberg, D., Cabello, R., Gozzer, E., Garcia, P. J., Holmes, K. K., & Kurth, A. E. (2009). “It’s time for your life“: How should we remind patients to take medicines using short text messages? AMIA Annual Symposium Proceedings, 2009, 129–133.
Curioso, W. H., & Kurth, A . E. (2007). Access, use and perceptions regarding Internet, cell phones and PDAs as a means for health promotion for people living with HIV in Peru. BMC Medical Informatics and Decision Making, 7, 24.
da Costa, T. M., Salomão, P. L., Martha, A. S., Pisa, I. T., & Sigulem, D. (2010). The impact of short message service text messages sent as appointment reminders to patients’ cell phones at outpatient clinics in São Paulo, Brazil. International Journal of Medical Informatics, 79, 65–70. doi:10.1016/j.ijmedinf.2009.09.001
Danis, C. M., Ellis, J. B., Kellogg, W. A., Beijma, H. V., Hoefman, B., Daniels, S. D., & Loggers, J.-W. (2010). Mobile phones for health education in the developing world: SMS as a user inter-face. Paper presented at the First Annual Symposium on Computing for Development, London, United Kingdom, December 17–18. Retrieved from http://dev2010.news.cs.nyu.edu/papers/13-danis.pdf
Davis, F. D. (1985). A tech nology acceptance model for empirically testing new end-user infor-mation systems: theory and results (Unpublished doctoral dissertation). Massachusetts Institute of Technology, Cambridge, MA.
Davis, F. D. (1986). A tech nology acceptance model for empirically testing new end-user infor-mation systems: Theory and results (Unpublished doctoral dissertation). Massachusetts Institute of Technology, Cambridge, MA.
de Tolly, K., Skinner, D., Nembaware, V., & Benjamin, P. (2012). Investigation into the use of short message services to expand uptake of human immunodeficiency virus testing, and whether content and dosage have impact. Telemedicine and e-Health, 18, 18–23. doi:10.1089/tmj.2011.0058.
Deglise, C., Suggs, L. S., & Odermatt, P. (2012). Short message service (SMS) applications for disease prevention in developing countries. Journal of Medical Internet Research, 14, e3. doi:10.2196/jmir.1823
de Jongh, T., Gurol-Urganci, I., Vodopivec-Jamsek, V., Car, J., & Atun, R. (2012). Mobile phone messaging for facilitating self-management of long-term illnesses. Cochrane Database of Systematic Reviews, 12, CD007459. doi:10.1002/14651858.CD007459.pub2
Derenzi, B., Findlater, L., P ayne, J., Birnbaum, B., Mangilima, J., Parikh, T., … Lesh, N. (2012). Improving community health worker performance through automated SMS. Paper presented at the 2012 International Conference on Information and Communication Technologies and Development, Atlanta, Georgia, March 12–15.
Faisal, O. (2011). Mobile ph one-based healthcare in Bangladesh—An impact assessment. Paper presented at the Proceedings of the 11th International Conference on Social Implications of Computers in Developing Countries, Kathmandu, Nepal, May 22–25.
Fjeldsoe, B. S., Marshall, A. L., & Miller, Y. D. (2009). Behavior change interventions delivered by mobile telephone short-message service. American Journal of Preventive Medicine, 36, 165–173. doi:10.1016/j.amepre.2008.09.040
Free, C., Phillips, G., Felix, L., Galli, L., Patel, V., & Edwards, P. (2010). The effectiveness of M-health technologies for improving health and health services: A systematic review pro-tocol. BMC Research Notes, 3, 250.
Ganesan, M., Prashant, S., Pus hpa Mary, V., Janakiraman, N., Jhunjhunwala, A., & Waidyanatha, N. (2011). The use of mobile phone as a tool for capturing patient data in southern rural Tamil Nadu, India Journal of Health Informatics in Developing Countries 5, 219–227.
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 49
Gurman, T. A., Rubin, S. E., & Roess, A. A. (2012). Effectiveness of mHealth behavior change communication interventions in developing countries: A systematic review of the litera-ture. Journal of Health Communication, 17(Suppl. 1), 82–104. doi:10.1080/10810730.2011.649160
Gurol-Urganci, I., de Jongh, T., Vodopivec-Jamsek, V., Car, J., & Atun, R. (2012). Mobile phone messaging for communicating results of medical investigations. Cochrane Database of Systematic Reviews, 6, CD007456. doi:10.1002/14651858.CD007456.pub2
Guy, R., Hocking, J., Wand, H., S tott, S., Ali, H., & Kaldor, J. (2012). How effective are short message service reminders at increasing clinic attendance? A meta-analysis and systematic review. Health Services Research, 47, 614–632. doi:10.1111/j.1475-6773.2011.01342.x
Haberer, J., Kiwanuka, J. E., Nans era, D., Wilson, I., & Bangsberg, D. R. (2010). Challenges in using mobile phones for collection of antiretroviral therapy adherence data in a resource-limited setting. AIDS & Behavior, 14, 1294–1302.
Hamilton, K. (2010). The role of m obile phone technology in health interventions in rural com-munities: A Kenyan exploratory study (Unpublished doctoral dissertation). Howard University, Washington, DC. Available from ProQuest Dissertatio n and Theses database. (UMI No. 3411975)
Hastings, G. (2007). Social marketing: Why should the devil get all the best tunes? Oxford, England: Butterworth-Heinemann.
Higgins, J., & Green, S. (2011). Co chrane handbook for systematic reviews of interventions Version 5.1.0. Cochrane Database of Systematic Reviews.
Hwabamungu, B., & Williams, Q. (20 10). m-Health adoption and sustainability prognosis from a care givers’ and patients’ perspective. Paper presented at the SAICSIT ‘10 2010 Annual Conference of the South African Institute of Computer Scientists and Information Technologists, Bela Bela, South Africa, October 11–13.
Jareethum, R., Titapant, V., Chantra, T., Sommai, V., Chuenwattana, P., & Jirawan, C. (2008). Satisfaction of healthy pregnant women receiving short message service via mobile phone for prenatal support: A randomized controlled trial. Journal of the Medical Association of Thailand, 4, 458–463. Retrieved from http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/295/CN-00640295/frame.html
Jones, C. O., Wasunna, B., Sudoi, R., Githinji, S., Snow, R. W., & Zurovac, D. (2012). “Even if you know everything you can forget“: Health Worker perceptions of mobile phone text-messaging to improve malaria case-management in Kenya. PLoS One, 7, e38636. doi:10.1371/journal.pone.0038636
Jordan, E. T., Ray, E. M., Johnson, P. , & Evans, W. D. (2011). Text4Baby: Using text messag-ing to improve maternal and newborn health. Nursing for Women’s Health, 15, 206–212. doi:10.1111/j.1751-486X.2011.01635.x
Kaewkungwal, J., Singhasivanon, P., Kha msiriwatchara, A., Sawang, S., Meankaew, P., & Wechsart, A. (2010). Application of smart phone in “Better Border Healthcare Program”: A module for mother and child care. BMC Medical Informatics and Decision Making, 10, 69.
Kahn, J. G., Yang, J. S., & Kahn, J. S . (2010). “Mobile” health needs and opportunities in devel-oping countries. Health Affairs, 29, 252–258.
Kaplan, W. A. (2006). Can the ubiquitou s power of mobile phones be used to improve health outcomes in developing countries? Global Health, 2, article 9. doi:10.1186/1744-8603-2-9
Klasnja, P., & Pratt, W. (2012). Healthc are in the pocket: Mapping the space of mobile-phone health interventions. Journal of Biomedical Informatics, 45, 184–198. doi:10.1016/j.jbi.2011.08.017
Krishna, S., Boren, S. A., & Balas, E. A. (2009). Healthcare via cell phones: A systematic review. Telemedicine and e-Health, 15, 231–240. doi:10.1089/tmj.2008.0099
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

50 A. Chib et al.
Kunutsor, S., Walley, J., Katabira, E., Mu churo, S., Balidawa, H., Namagala, E., & Ikoona, E. (2010). Using mobile phones to improve clinic attendance amongst an antiretroviral treat-ment cohort in rural Uganda: A cross-sectional and prospective study. AIDS & Behavior, 14, 1347–1353.
Lee, S., Chib, A., & Kim, J.-N. (2011). Midwives’ mobile phone use and health knowledge in rural communities. Journal of Health Communication, 16, 1006–1023.
Lemay, N. V., Sullivan, T., Jumbe, B., & Per ry, C. P. (2012). Reaching remote health work-ers in Malawi: Baseline assessment of a pilot mHealth intervention. Journal of Health Communication, 17(Suppl. 1), 105–117. doi:10.1080/10810730.2011.649106
L’Engle, K., & Vadhat, H. (2009). Mobile p hone interventions for reproductive health (m4RH): Testing the feasibility of text messaging to improve family planning. Family Health International. Retrieved from http://www.fhi360.org/sites/default/files/media/documents/formative_results_m4rh.pdf
Leong, K. C., Chen, W. S., & Leong, K. W. (20 06). The use of text messaging to improve attend-ance in primary care: A randomized controlled trial. Family Practice, 23, 699–705.
Leslie, I., Sherrington, S., Dicks, D., Gray, N., & Chang, T.-T. (2011). Mobile communications for medical care: A study of current and future healthcare and health promotion applications, and their use in China and elsewhere. Retrieved from http://www.csap.cam.ac.uk/media/uploads/files/1/mobile-communications-for-medical-care.pdf
Lester, R., & Karanja, S. (2008). Mobile phone s: Exceptional tools for HIV/AIDS, health, and crisis management. Lancet Infectious Diseases, 8, 738–739. doi:10.1016/S1473-3099%2808%2970265-2
Lester, R., Gelmon, L., & Plummer, F. A. (2006) . Cell phones: Tightening the communica-tion gap in resource-limited antiretroviral programmes? [Correspondence]. AIDS, 20, 2242–2244. doi:10.1097/QAD.0b013e3280108508
Lester, R., Mills, E. J., Kariri, A., Ritvo, P., Chung, M., Jack, W., & Plummer, F. A. (2009). The HAART cell phone adherence trial (WelTel Kenya1): A randomized controlled trial protocol. Trials, 10, 87. Retrieved from http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/966/CN-00721966/frame.html
Lester, R., Ritvo, P., Mills, E. J., Kariri, A., Karanja, S., Chung, M. H., … Plummer, F. A. (2010). Effects of a mobile phone short message service on antiretroviral treatment adher-ence in Kenya (WelTel Kenya1): A randomised trial. Lancet, 376, 1838–1845. doi:10.1016/s0140-6736(10)61997-6
Liang, X., Wang, Q., Yang, X., Cao, J., Chen, J., Mo, X., … Gu, D. (2011). Effect of mobile phone intervention for diabetes on glycaemic control: A meta-analysis. Diabetes Medicine, 28, 455–463. doi:10.1111/j.1464-5491.2010.03180.x
Liew, S. M., Tong, S. F., Lee, V. K., Ng, C. J., L eong, K. C., & Teng, C. L. (2009). Text messaging reminders to reduce non-attendance in chronic disease follow-up: A clinical trial. British Journal of General Practice, 569, 916–920. Retrieved from http://www.mrw.interscience.wiley.com/cochrane/clcentral/articles/313/CN-00770313/frame.html
Lim, M. S., Hocking, J. S., Hellard, M. E., & Aitke n, C. K. (2008). SMS STI: A review of the uses of mobile phone text messaging in sexual health. International Journal of STD and AIDS, 19, 287–290. doi:10.1258/ijsa.2007.007264
Macrohon, B. C., & Cristobal, F. L. (2011). Rural he althcare delivery using a phone patch service in the teleconsultation program of the Ateneo de Zamboanga University School of Medicine in Western Mindanao, Philippines. Rural Remote Health, 11, 1740. Retrieved from http://www.rrh.org.au
Maharani, A. C., Rosanna, N., & Liesman, T. (2012). The adoption of SMS technology in disseminating health information in Indonesia: A case study on SMS Info Obat Murah
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014
mHealth Adoption in Low-Resource Environments 51
and Nokia Life Healthcare Service. Washington, DC: The Center for Health Market Innovations; Jakarta, Indonesia: Mercy Corps Indonesia. https://www.academia.edu/2357169/Anne_C._Maharani_MPP_Nelty_Rosanna_SKM
Mbuagbaw, L., Bonono-Momnougui, R. C., & Thabane, L. (2012). Considerations in using text messages to improve adherence to highly active antiretroviral therapy: A qualitative study among clients in Yaounde, Cameroon. HIV and AIDS, 4, 45–50. doi:10.2147/hiv.s29954
Mechael, P., Batavia, N., Kaonga, N., Searle, S., Kwan , A., Goldberger, A., … Ossman, J. (2010). Barriers and gaps affecting m-Health in low and middle income countries. Policy White Paper. New York, NY: Center for Global Health and Economic Development, Earth Institute, Columbia University. Retrieved from http://cghed.ei.columbia.edu/sitefiles/file/mHealth-BarriersWhitePaperFINAL.pdf
Mitchell, J. R., Sharma, P., Modi, J., Simpson, M., Th omas, M., Hill, M. D., & Goyal, M. (2011). A smartphone client-server teleradiology system for primary diagnosis of acute stroke. Journal of Medical Internet Research, 13. doi:e3110.2196/jmir.1732
Mitchell, K. J., Bull, S., Kiwanuka, J., & Ybarra, M. L. (2011). Cell phone usage among ado-lescents in Uganda: Acceptability for relaying health information. Health Education Research, 26, 770–781. doi:10.1093/her/cyr022
MOTECH. (2011). Mobile technology for community health in Ghana. Washington, DC: Grameen Foundation. Retrieved from http://www.cs.washington.edu/education/courses/cse490d/12sp/docs/MOTECH.pdf
Noordam, A. C., Kuepper, B. M., Stekelenburg, J., & Mi len, A. (2011). Improvement of mater-nal health services through the use of mobile phones. Tropical Medicine & International Health, 16, 622–626. doi:10.1111/j.1365-3156.2011.02747.x
Novartis. (2011). Vodafone Health Solutions helps SMS f or life to manage drug stocks and save lives in Tanzania. Newbury, Berkshire, United Kingdom: Vodafone Ltd. Retrieved from http://enterprise.vodafone.com/discover_global_enterprise/case_studies/novartis.jsp
Odigie, V. I., Yusufu, L. M. D., Dawotola, D. A., Ejagw ulu, F., Abur, P., Mai, A., & Odigie, E. C. (2011). The mobile phone as a tool in improving cancer care in Nigeria. Psycho-Oncology, 21, 332–335. doi:10.1002/pon.1894
Patrick, K., Griswold, W. G., Raab, F., & Intille, S. S . (2008). Health and the mobile phone. American Journal of Preventive Medicine, 35, 177–181. doi:S0749-3797(08)00407-8 [pii]10.1016/j.amepre.2008.05.001 [doi]
Piette, J., Mendoza-Avelares, M., Ganser, M., Mohamed, M ., Marinec, N., & Krishnan, S. (2011). A preliminary study of a cloud-computing model for chronic illness self-care sup-port in an underdeveloped country. American Journal of Preventive Medicine, 40, 629–632.
Ping, Y., Wu, M. X., Yu, H., & Xiao, G. Q. (2006). The c hallenges for the adoption of m-health. Presented at SOLI ‘06, Service Operations and Logistics, and Informatics, 2006, IEEE International Conference, Shanghai, June 21–23. doi:10.1109/SOLI.2006.329059
Pop-Eleches, C., Thirumurthy, H., Habyarimana, J. P., Ziv in, J. G., Goldstein, M. P., de Walque, D., … Bangsberg, D. R. (2011). Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: A randomized controlled trial of text message reminders. AIDS, 25, 825–834.
Prasad, S., & Anand, R. (2012). Use of mobile telephone s hort message service as a reminder: the effect on patient attendance. International Dental Journal, 62, 21–26. doi:10.1111/j.1875-595X.2011.00081.x
Prochaska, J. O., & DiClemente, C. C. (1983). Stages and pr ocesses of self-change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51, 390–395. doi:10.1037/0022-006X.51.3.390
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

52 A. Chib et al.
Rajatonirina, S., Heraud, J. M., Randrianasolo, L., Orelle, A., Razanajatovo, N. H., Raoelina, Y. N., … Richard, V. (2012). Short message service sentinel surveillance of influenza-like illness in Madagascar, 2008–2012. Bulletin of the World Health Organization, 90, 385–389. doi:10.2471/blt.11.097816
Ranck, J. (2011). Health information and healthcare: the role of technology in unlocking data and wellness—A discussion paper. Washington, DC: United Nations Foundation & Vodafone Foundation Technology Partnership.
Ring, N., Ritchie, K., Mandava, L., & Jepson, R. (2010). A guid e to synthesising qualitative research for researchers undertaking health technology assessments and systematic reviews. Retrieved from http://www.healthcareimprovementscotland.org/programmes/clinical__cost_effectiveness/shtg/synth_qualitative_research.aspx
Sandelowski, M., & Barroso, J. (2002). Finding the findings in qualitative studies. Journal of Nursing Scholarship, 34, 213–219.
Seidenberg, P., Nicholson, S., Schaefer, M., Semrau, K., Bweupe , M., Masese, N., … Thea, D. M. (2012). Early infant diagnosis of HIV infection in Zambia through mobile phone texting of blood test results. Bulletin of the World Health Organization, 90, 348–356. doi:10.2471/blt.11.100032
Shet, A., Arumugam, K., Rodrigues, R., Rajagopalan, N., Shubha, K ., Raj, T., … De Costa, A. (2010). Designing a mobile phone-based intervention to promote adherence to antiretrovi-ral therapy in South India. AIDS & Behavior, 14, 716–721.
Sidney, K., Antony, J., Rodrigues, R., Arumugam, K., Krishnamurth y, S., D’Souza, G., … Shet, A. (2012). Supporting patient adherence to antiretrovirals using mobile phone reminders: patient responses from South India. AIDS Care, 24, 612–617. doi:10.1080/09540121.2011.630357
Skinner, D., Rivette, U., & Bloomberg, C. (2007). Evaluation of use of cellphones to aid compli-ance with drug therapy for HIV patients. AIDS Care, 19, 605–607.
Svoronos, T., & Mate, K. S. (2011). Evaluating large-scale health pr ogrammes at a district level in resource-limited countries. Bulletin of the World Health Organization, 89, 831–837. doi:10.2471/blt.11.088138
Svoronos, T., Mjungub, D., Dhadialla, P., Lukc, R., Zue, C., Jackson, J., & Lesh, N. (2010). CommCare: Automated quality improvement to strengthen community-based health. Retrieved from http://d-tree.org/wp-content/uploads/2010/05/Svoronos-Medinfo-CommCare-safe-pregnancy1.pdf
Tamrat, T., & Kachnowski, S. (2012). Special delivery: An analysis of mHealth in maternal and newborn health programs and their outcomes around the world. Maternal Child Health Journal, 16, 1092–1101. doi:10.1007/s10995-011-0836-3
Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology, 8, 45. doi:10.1186/1471-2288-8-45
van Velthoven, M. H., Brusamento, S., Majeed, A., & Car, J. (2013). Scope and effectiveness of mobile phone messaging for HIV/AIDS care: A systematic review. Psychology, Health & Medicine, 18, 182–202. doi: 10.1080/13548506.2012.701310
Vodafone. (2006). The role of mobile phones in increasing accessibility and efficiency in healthcare (The Vodafone Policy Paper Series). Retrieved from http://www.vodafone.com/content/dam/vodafone/about/public_policy/policy_papers/public_policy_series_4.pdf
Waegemann, C. P. (2010). mHealth: the next generation of telemedicine? Telemedicine and e-Health, 16, 23–25. doi:10.1089/tmj.2010.9990
Whittaker, R., Borland, R., Bullen, C., Lin Ruey, B., McRobbie, H., & Ro dgers, A. (2009). Mobile phone-based interventions for smoking cessation. Cochrane Database of Systematic Review, 2009(4).
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014

mHealth Adoption in Low-Resource Environments 53
World Health Organization. (2011a). Call to action on global eHealth ev aluation. Bellagio, Italy: The Bellagio eHealth Evaluation Group.
World Health Organization. (2011b). mHealth—New horizons for health thr ough mobile technol-ogies. Geneva, Switzerland: Author. Retrieved from http://www.who.int/goe/publications/goe_mhealth_web.pdf
Wolpaw, B. J., Mathews, C., Chopra, M., Hardie, D., Lurie, M. N., & Jenni ngs, K. (2011). Diagnosis and counselling of patients with acute HIV infection in South Africa. Sexually Transmitted Infections, 87, 71–72.
World Bank. (2012). Country and lending groups—Country classification tab le. Retrieved from http://data.worldbank.org/about/country-classifications/country-and-lending-groups
Zhang, S., Wu, Q., van Velthoven, M. H., Chen, L., Car, J., Rudan, … Scherpbier, R. W. (2012). Smartphone versus pen-and-paper data collection of infant feeding practices in rural China. Journal of Medical Internet Research, 14(5), e119.
Zolfo, M., Iglesias, D., Kiyan, C., Echevarria, J., Fucay, L., Llacsahuanga , E., … Lynen, L. (2010). Mobile learning for HIV/AIDS healthcare worker training in resource-limited settings. AIDS Research and Therapy, 7, article 35. doi:10.1186/1742-6405-7-35
Zurovac, D., Sudoi, R. K., Akhwale, W. S., Ndiritu, M., Hamer, D. H., Rowe, A. K., & Snow, R. W. (2011). The effect of mobile phone text-message reminders on Kenyan health workers’ adherence to malaria treatment guidelines: A cluster randomised trial. Lancet, 378, 795–803. doi:10.1016/s0140-6736(11)60783-6
Dow
nloa
ded
by [
155.
69.1
07.2
34]
at 0
2:09
28
Mar
ch 2
014




















